
9 January 2019 - Case #472 (revised 15 June 2020)
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Week page. To subscribe or unsubscribe to Case of the Week or our other email lists, click here.
Thanks to Dr. V. Pavithra, Sri Ramachandra Medical College & Research Institute Porur, Chennai (India) for contributing this case and Dr. Nat Pernick, PathologyOutlines.com, Inc. for writing the discussion. This case was reviewed in May 2020 by Dr. Jennifer Bennett, University of Chicago and Dr. Carlos Parra-Herran, University of Toronto.

Advertisement
Case of the Week #472
Clinical history:
A 52 year old woman was admitted for multiple itchy, verrucous papules on the vulva. Ruptured papules had a foul smelling discharge. There was no history of fever or trauma.
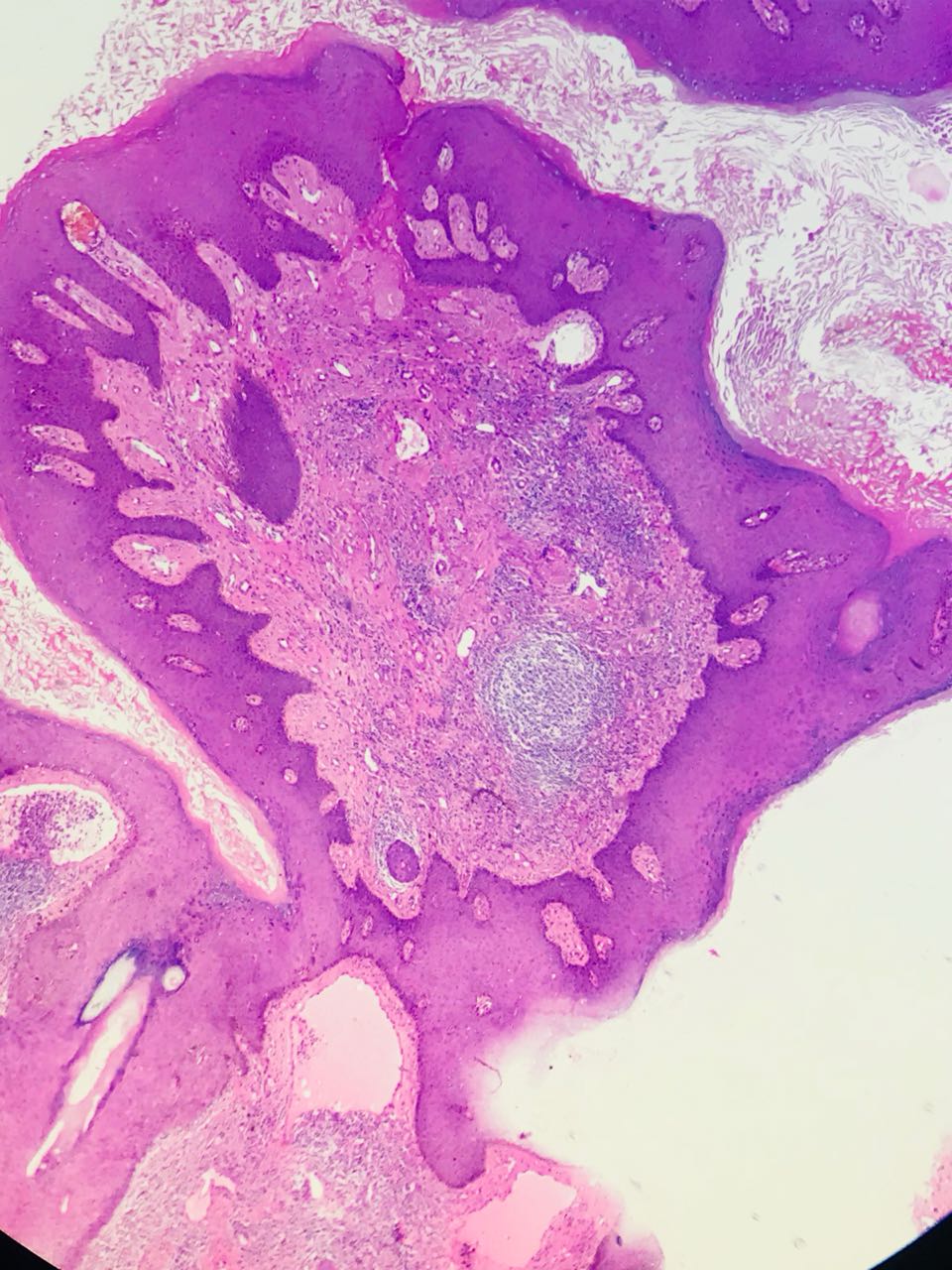
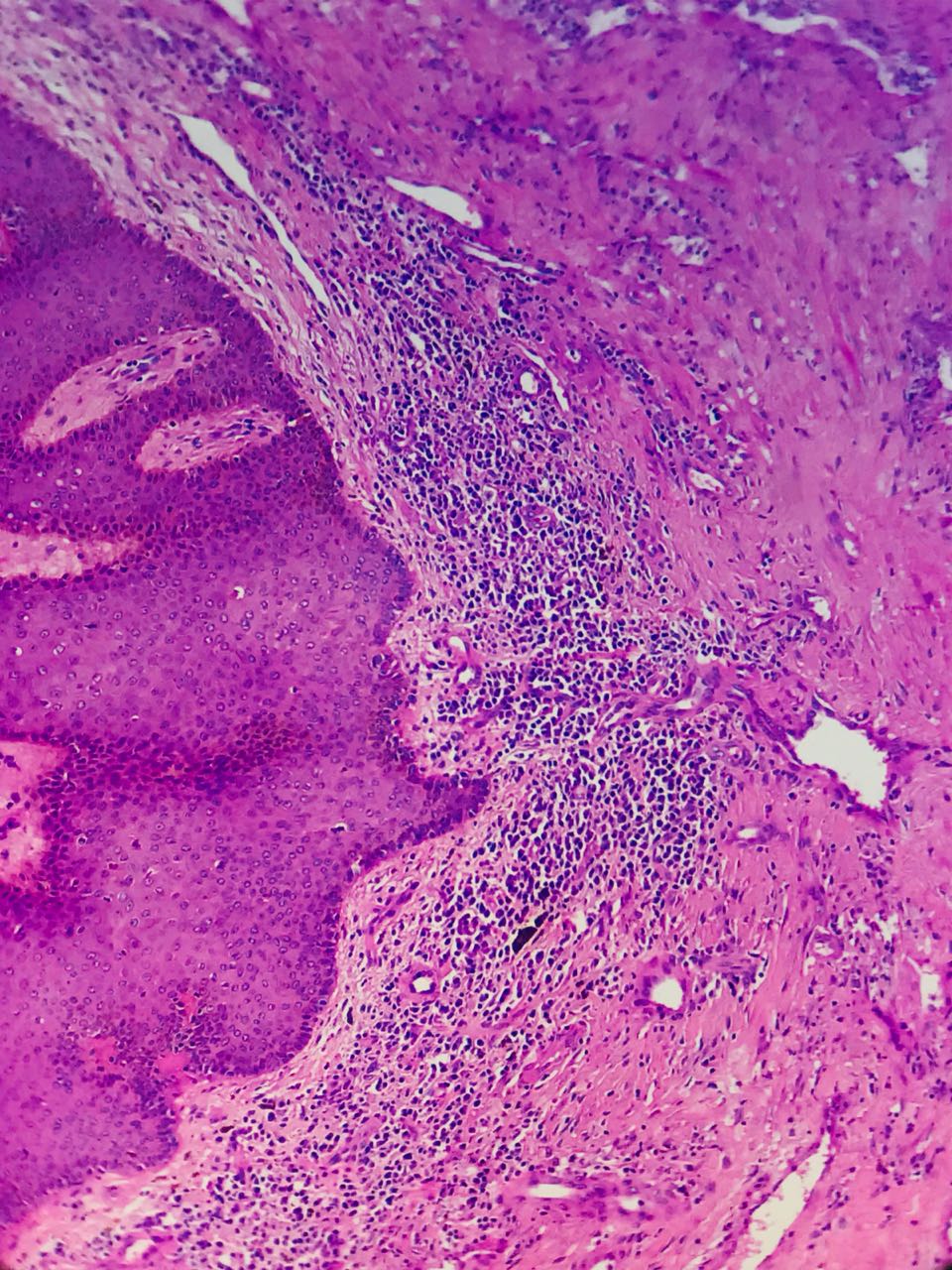
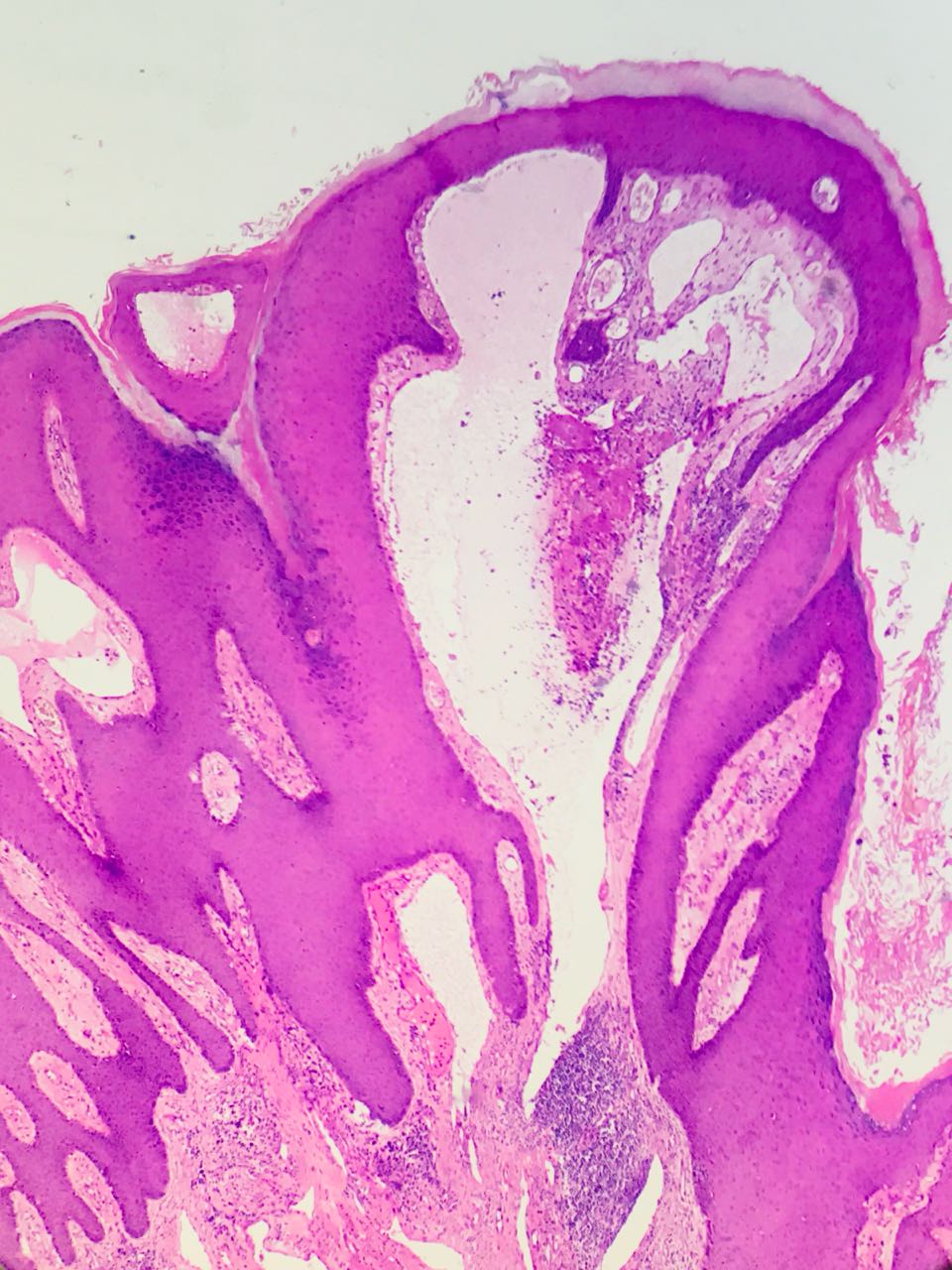
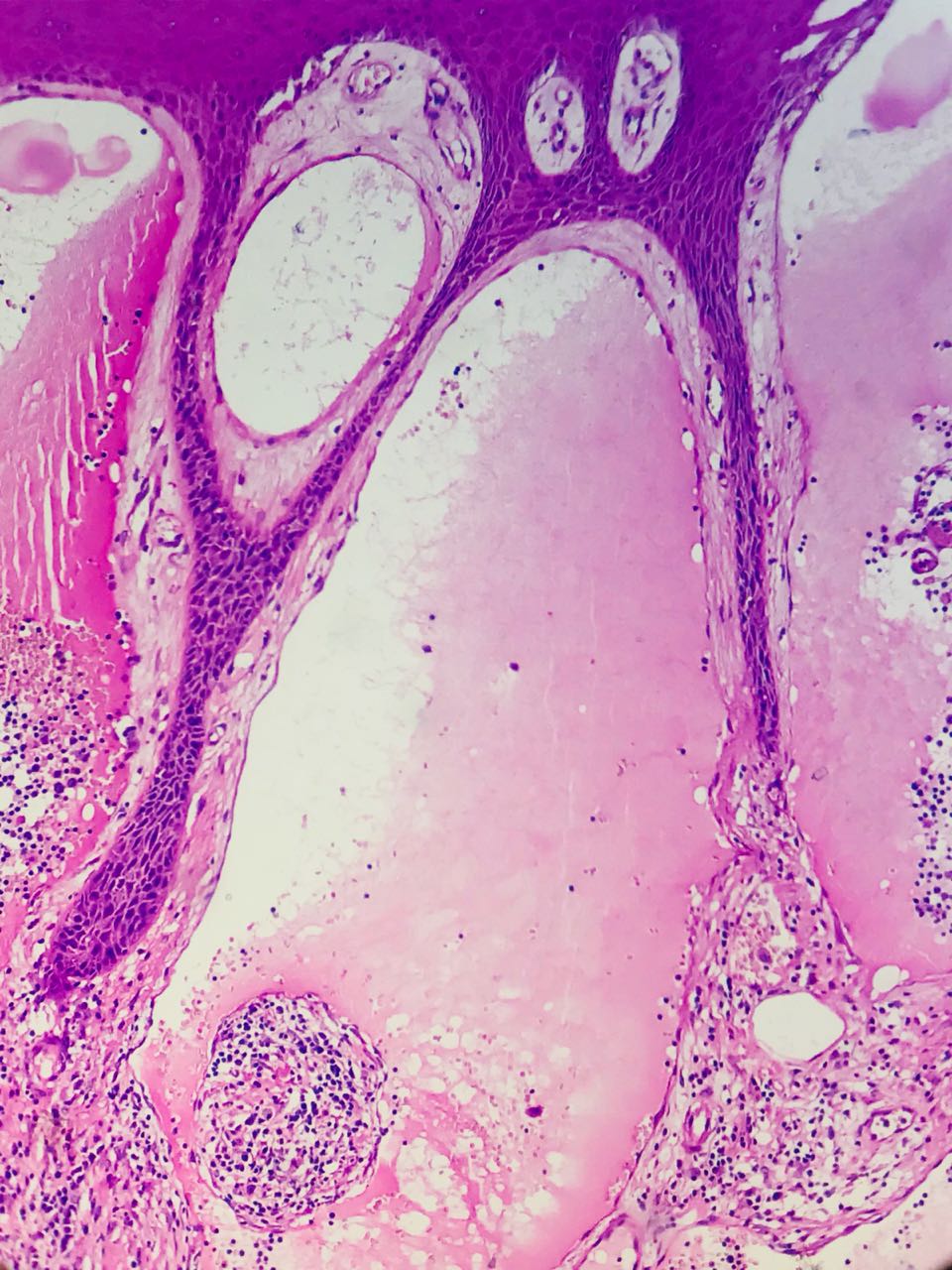
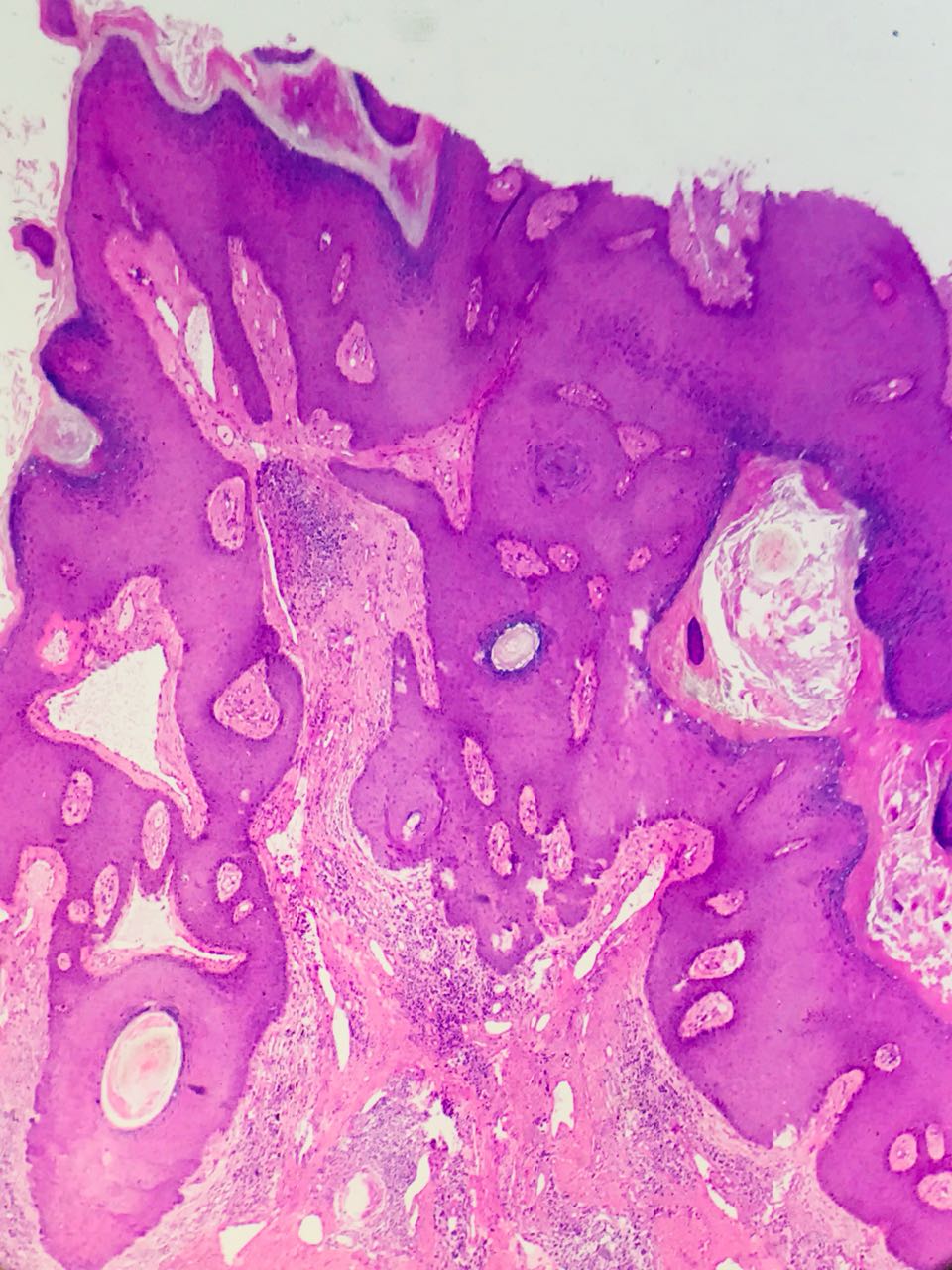
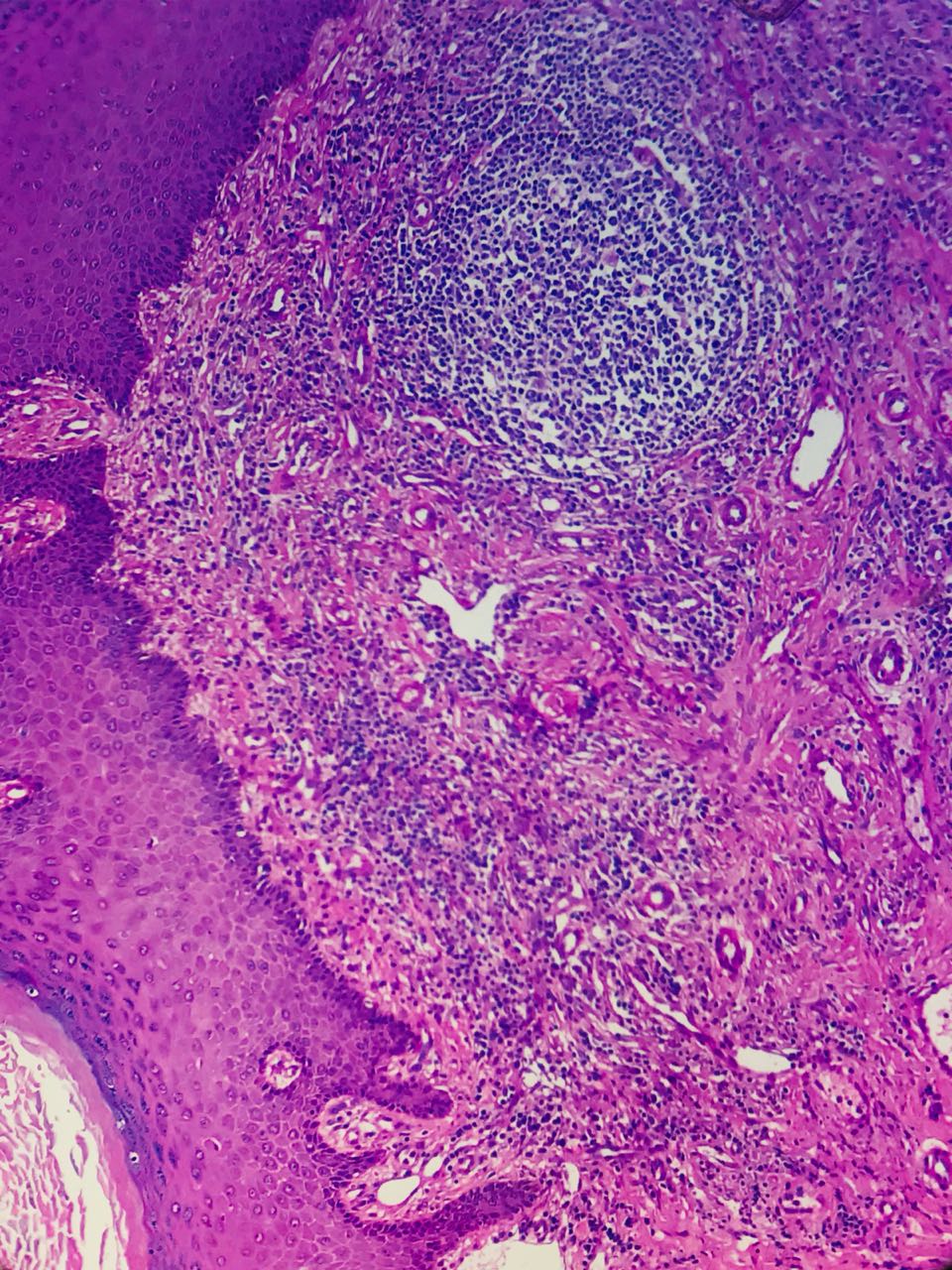
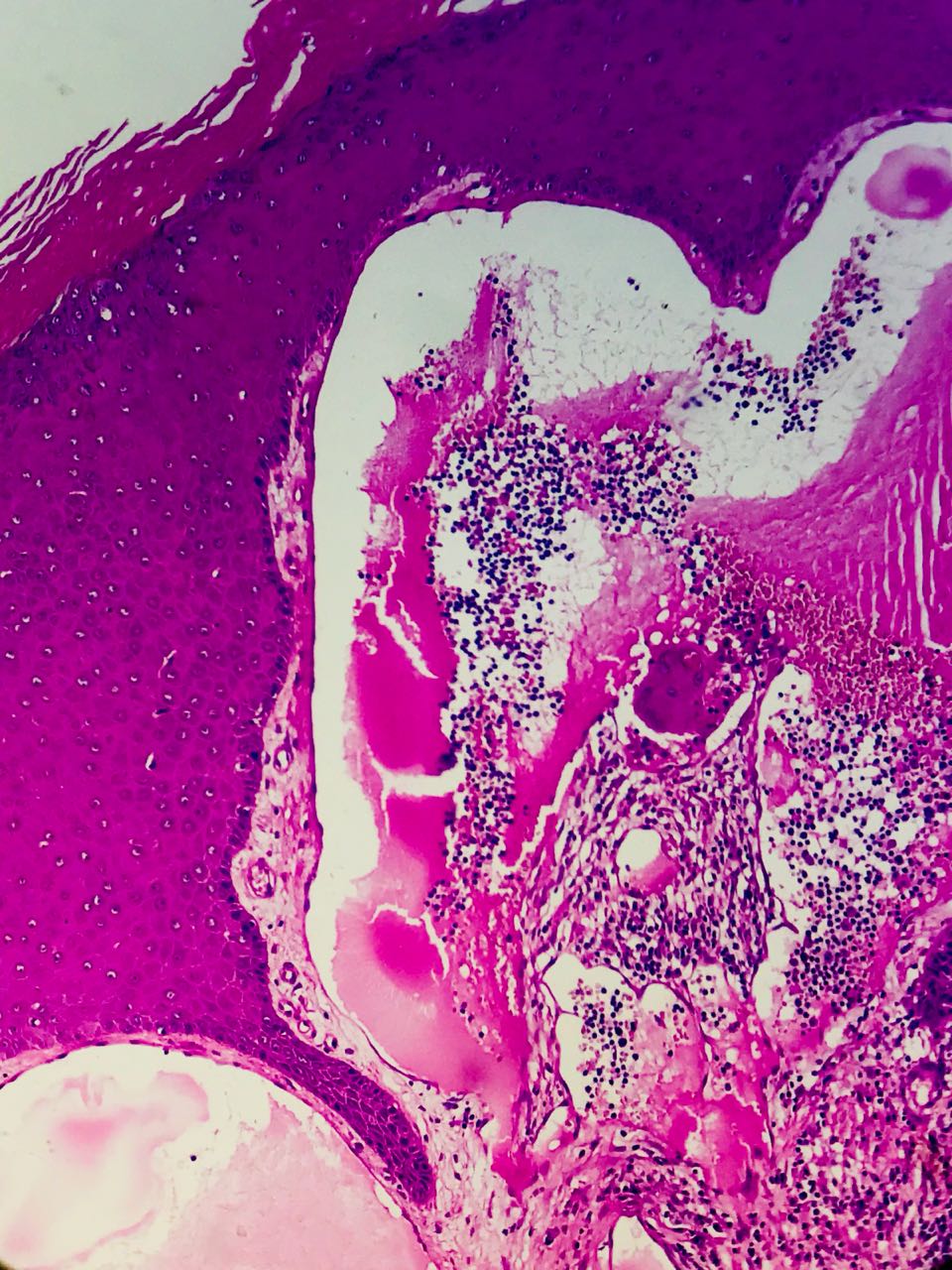
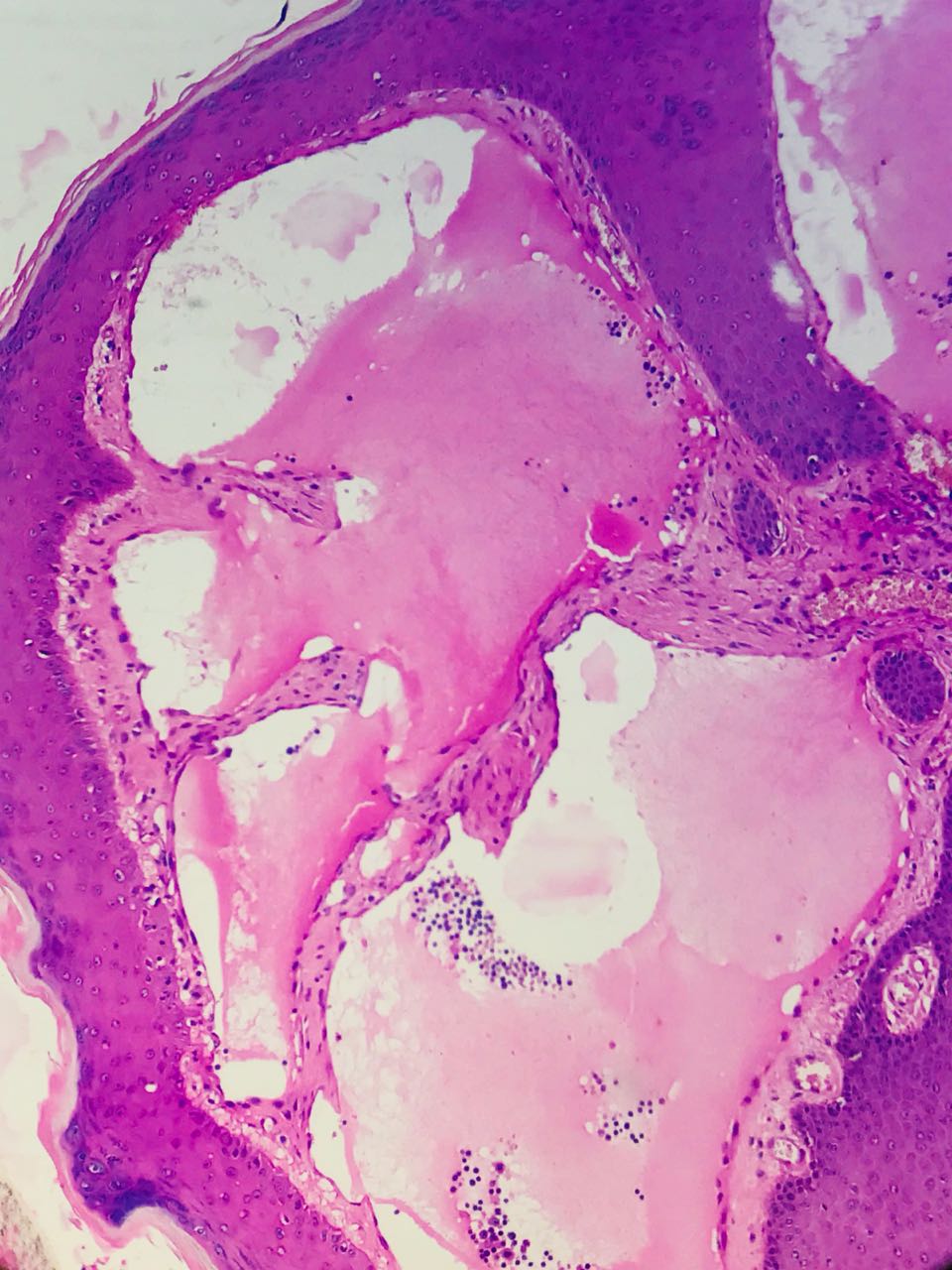
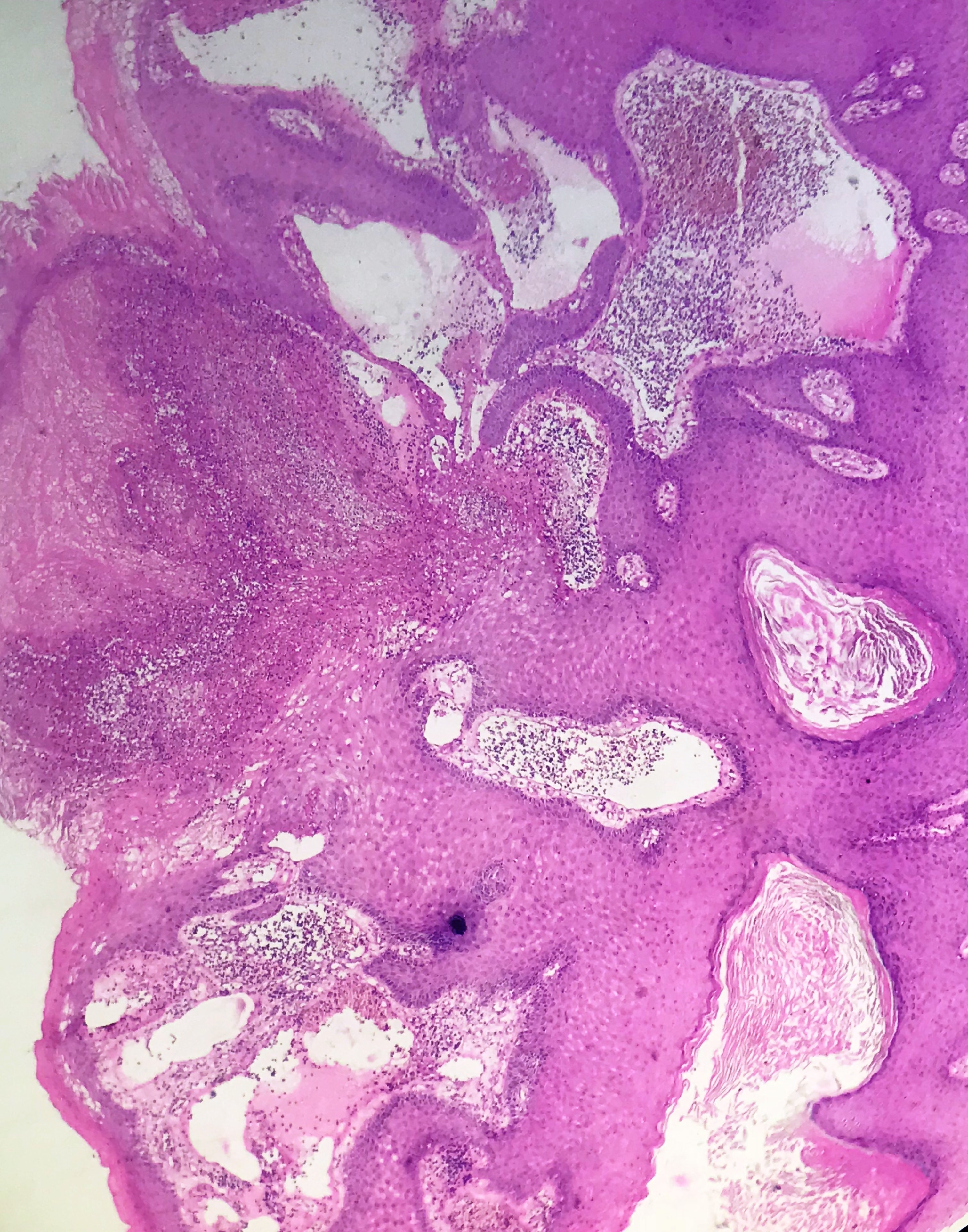
Histopathology images:


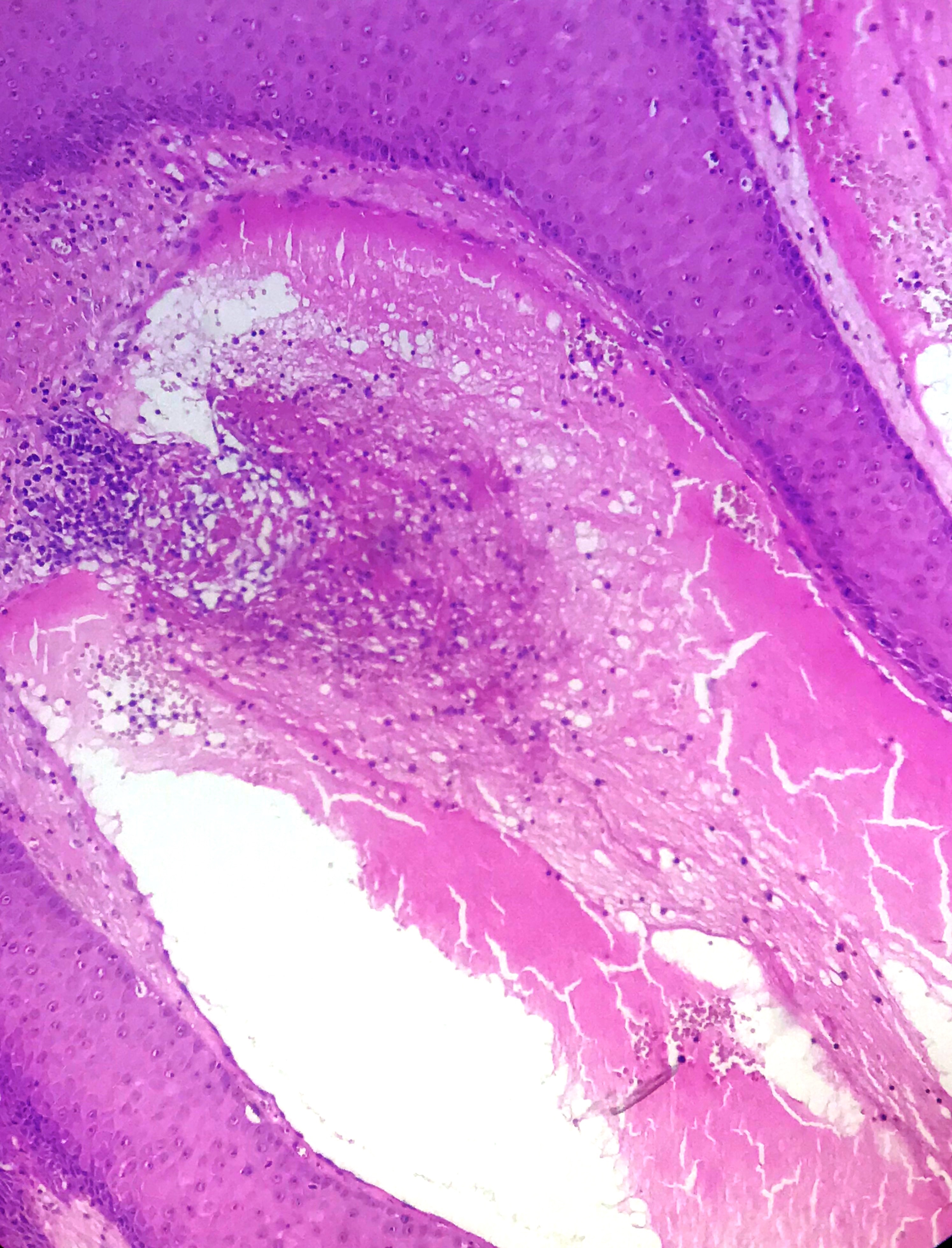

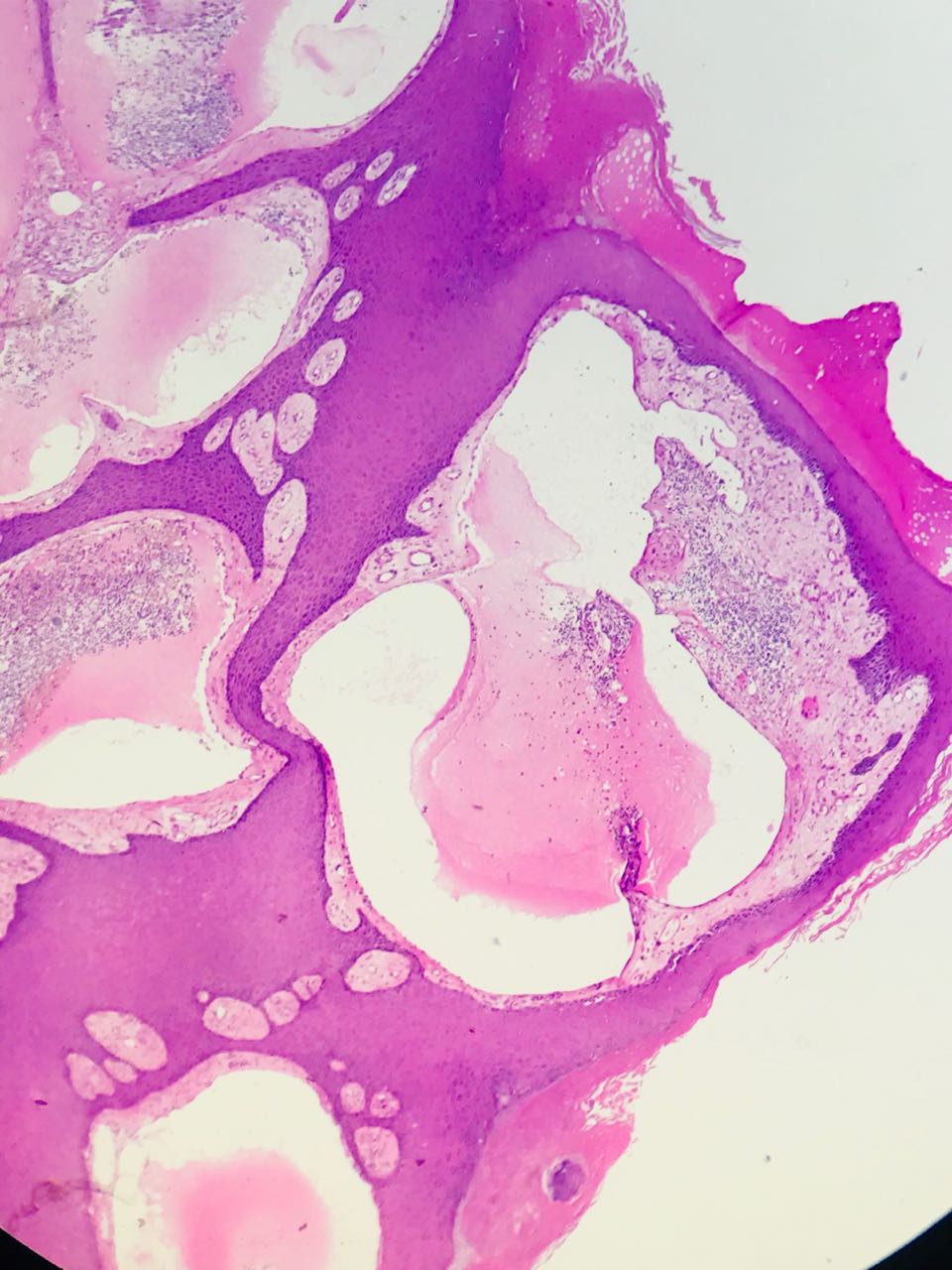
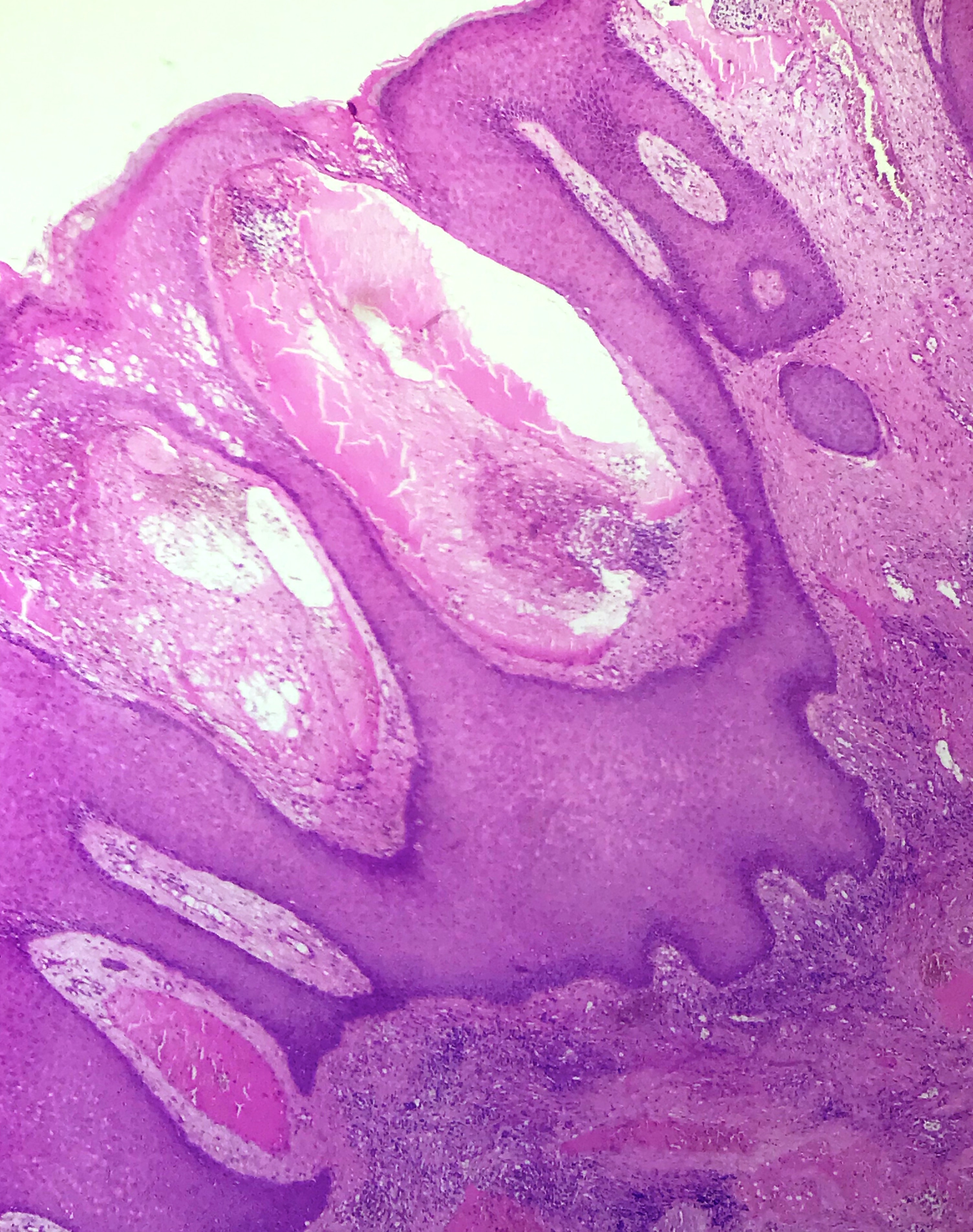
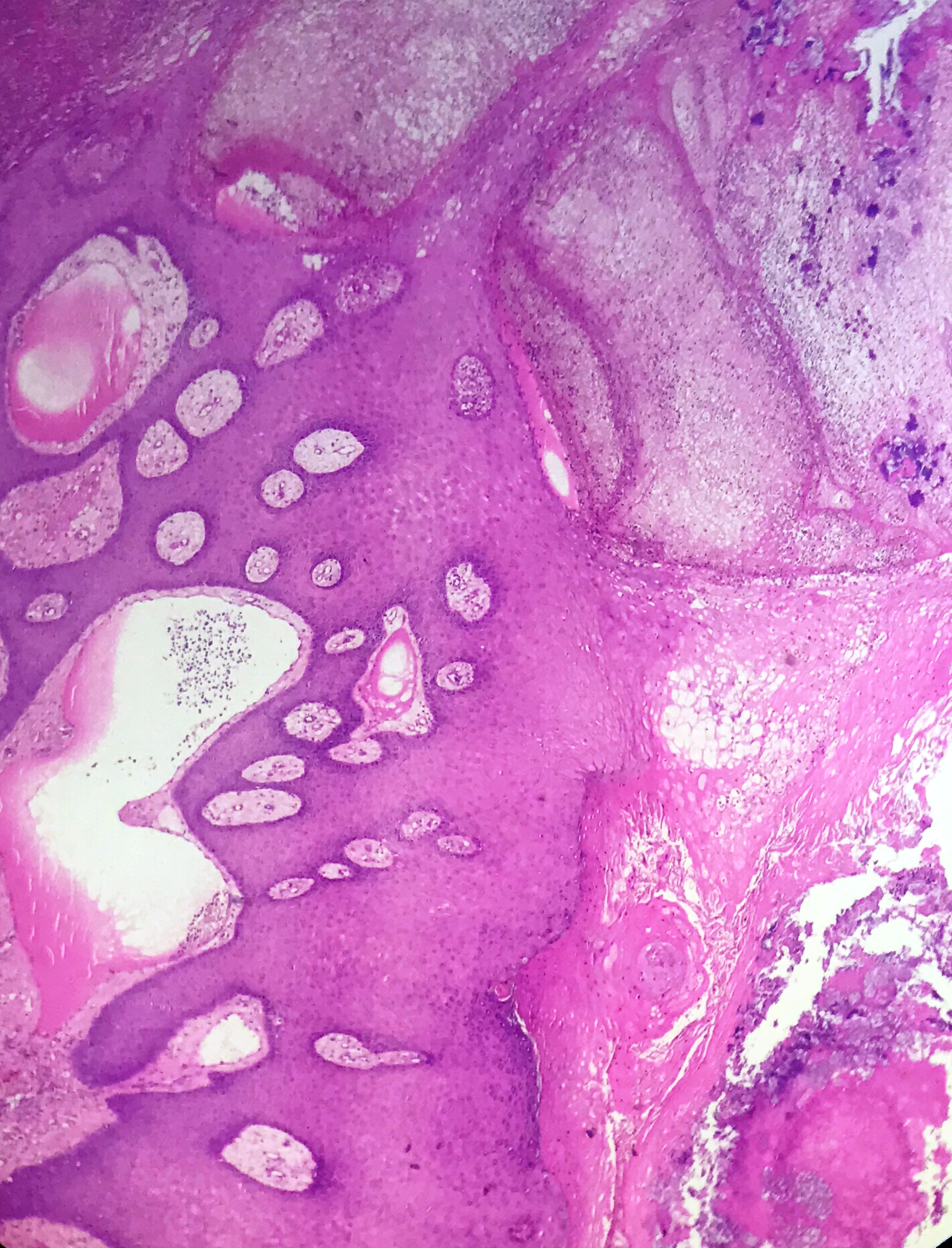
Additional images (not necessary for diagnosis):

What is your diagnosis?
Diagnosis:
Verrucous lymphatic malformation (lymphangioma circumscriptum)
Test question (answer at the end): Which of the following statements is true regarding lymphatic malformations?
A. They typically arise in senior adults.
B. They are unaffected by hormonal changes.
C. They may recur after excision.
D. They are distinctive and unlikely to be confused with other entities.
Discussion:
Lymphatic malformation is the current name (formerly lymphangioma) for congenital malformations of the lymphatic system that are located in the skin and subcutaneous tissue (Semin Pediatr Surg 2014;23:178), see also soft tissue topic. They do not connect with systemic lymphatics. Microcystic lymphatic malformation (lymphangioma circumscriptum) is a common subtype and presents with grouped, clear vesicles less than 2 cm that may appear pink to purple (J Biophotonics 2018;11:e201700124).
Lymphatic malformations account for 4 percent of vascular tumors and 25 percent of benign vascular tumors in children (Medscape: Lymphangioma). Half are evident at birth and most by age 5 years (Int J Dermatol 2009;48:1290). Congenital vulvar lesions can grow extensively at puberty or during pregnancy (J Obstet Gynaecol Res 2018;44:978).
Clinically, the lesion presents as a cluster of small, cutaneous, translucent vesicles which resemble frog spawn. At microscopy, the papillary dermis shows a proliferation of dilated, thin walled lymphatic channels that may communicate with thick walled vessels in the subcutis (Dermatol Online J 2012;18:9). These vessels are filled with lymphatic fluid, and commonly red and white blood cells, although it is unclear how the red blood cells enter the lymphatic system. The epidermis may show hyperkeratosis and acanthosis.
The differential diagnosis of the rare verrucous variation includes lymphangiectasia, metastatic carcinoma, verrucae, molluscum, hemangioma, angiokeratoma and lymphangioendothelioma (Dermatol Online J 2012;18:9). Lymphangiectasia is a rare condition of dilated lymphatics with a history of trauma or disease that obstructs the lymphatics. In the vulva, it may be secondary to pelvic lymphatic obstruction (Int J Dermatol 2016;55:e482). Carcinoma telangiectoides, a rare manifestation of cutaneous metastatic cancer, presents as an erythematous patch with prominent telangiectasias or lymphangioma circumscriptum-like lesions (J Am Acad Dermatol 2009;60:633).
Warts / verrucae, molluscum contagiosum and hemangioma typically have distinct histologic appearances. Angiokeratoma exhibits vascular ectasia of the papillary dermis which may appear to extend into the epidermis. In addition, there is overlying epidermal hyperplasia characterized by acanthosis, elongation of the rete and hyperkeratosis, and often thrombosis within the vascular ectasia. Lymphangioendothelioma is a rare lesion of delicate, thin walled, endothelial lined dilated vascular spaces involving the superficial dermis. Unlike lymphatic malformation, its deeper portion shows vascular space collapse and may dissect collagen bundles.
Treatment options include surgery, sclerotherapy, radiotherapy and laser therapy (Dermatol Surg 2013 ;39:1147, J Cosmet Laser Ther 2018:1), although it may recur.
Test question answer:
C. They may recur after excision. Lymphatic malformations are congenital and usually detected at birth or in the first few years of life. They may be affected by pubertal or pregnancy related hormones. There is a broad differential diagnosis including (acquired) lymphangiectasia, metastatic carcinoma, verrucae, molluscum, hemangioma, angiokeratoma and lymphangioendothelioma.
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Week page. To subscribe or unsubscribe to Case of the Week or our other email lists, click here.
Thanks to Dr. V. Pavithra, Sri Ramachandra Medical College & Research Institute Porur, Chennai (India) for contributing this case and Dr. Nat Pernick, PathologyOutlines.com, Inc. for writing the discussion. This case was reviewed in May 2020 by Dr. Jennifer Bennett, University of Chicago and Dr. Carlos Parra-Herran, University of Toronto.
Advertisement
Case of the Week #472
Clinical history:
A 52 year old woman was admitted for multiple itchy, verrucous papules on the vulva. Ruptured papules had a foul smelling discharge. There was no history of fever or trauma.
Histopathology images:
Additional images (not necessary for diagnosis):
What is your diagnosis?
Diagnosis:
Verrucous lymphatic malformation (lymphangioma circumscriptum)
Test question (answer at the end): Which of the following statements is true regarding lymphatic malformations?
A. They typically arise in senior adults.
B. They are unaffected by hormonal changes.
C. They may recur after excision.
D. They are distinctive and unlikely to be confused with other entities.
Discussion:
Lymphatic malformation is the current name (formerly lymphangioma) for congenital malformations of the lymphatic system that are located in the skin and subcutaneous tissue (Semin Pediatr Surg 2014;23:178), see also soft tissue topic. They do not connect with systemic lymphatics. Microcystic lymphatic malformation (lymphangioma circumscriptum) is a common subtype and presents with grouped, clear vesicles less than 2 cm that may appear pink to purple (J Biophotonics 2018;11:e201700124).
Lymphatic malformations account for 4 percent of vascular tumors and 25 percent of benign vascular tumors in children (Medscape: Lymphangioma). Half are evident at birth and most by age 5 years (Int J Dermatol 2009;48:1290). Congenital vulvar lesions can grow extensively at puberty or during pregnancy (J Obstet Gynaecol Res 2018;44:978).
Clinically, the lesion presents as a cluster of small, cutaneous, translucent vesicles which resemble frog spawn. At microscopy, the papillary dermis shows a proliferation of dilated, thin walled lymphatic channels that may communicate with thick walled vessels in the subcutis (Dermatol Online J 2012;18:9). These vessels are filled with lymphatic fluid, and commonly red and white blood cells, although it is unclear how the red blood cells enter the lymphatic system. The epidermis may show hyperkeratosis and acanthosis.
The differential diagnosis of the rare verrucous variation includes lymphangiectasia, metastatic carcinoma, verrucae, molluscum, hemangioma, angiokeratoma and lymphangioendothelioma (Dermatol Online J 2012;18:9). Lymphangiectasia is a rare condition of dilated lymphatics with a history of trauma or disease that obstructs the lymphatics. In the vulva, it may be secondary to pelvic lymphatic obstruction (Int J Dermatol 2016;55:e482). Carcinoma telangiectoides, a rare manifestation of cutaneous metastatic cancer, presents as an erythematous patch with prominent telangiectasias or lymphangioma circumscriptum-like lesions (J Am Acad Dermatol 2009;60:633).
Warts / verrucae, molluscum contagiosum and hemangioma typically have distinct histologic appearances. Angiokeratoma exhibits vascular ectasia of the papillary dermis which may appear to extend into the epidermis. In addition, there is overlying epidermal hyperplasia characterized by acanthosis, elongation of the rete and hyperkeratosis, and often thrombosis within the vascular ectasia. Lymphangioendothelioma is a rare lesion of delicate, thin walled, endothelial lined dilated vascular spaces involving the superficial dermis. Unlike lymphatic malformation, its deeper portion shows vascular space collapse and may dissect collagen bundles.
Treatment options include surgery, sclerotherapy, radiotherapy and laser therapy (Dermatol Surg 2013 ;39:1147, J Cosmet Laser Ther 2018:1), although it may recur.
Test question answer:
C. They may recur after excision. Lymphatic malformations are congenital and usually detected at birth or in the first few years of life. They may be affected by pubertal or pregnancy related hormones. There is a broad differential diagnosis including (acquired) lymphangiectasia, metastatic carcinoma, verrucae, molluscum, hemangioma, angiokeratoma and lymphangioendothelioma.
