Case contributed by Dr. Julia Braza, Beth Israel Deaconess Medical Center, Boston, Massachusetts (USA), April 2007
An 81 year old woman presented to an outside hospital for syncope, progressive weakness, headaches and unexplained weight loss of 10 pounds, and was transferred to our hospital for further work up.
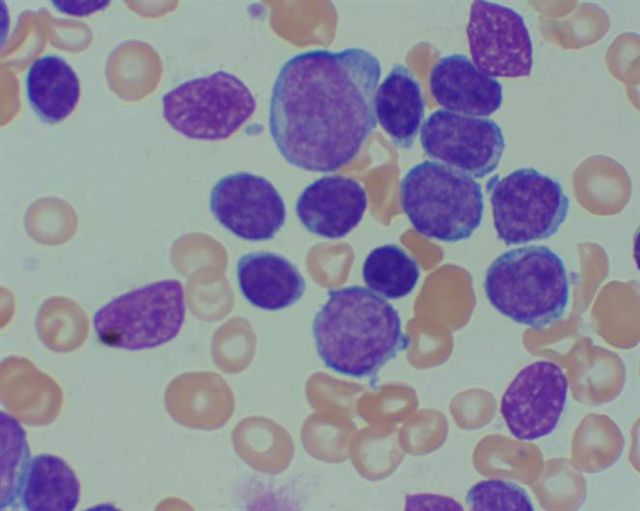
A peripheral blood smear showed WBC = 537,000 with Neutrophils = 3%, Lymphocytes = 95%, Monocytes = 0% and Eosinophils = 2%. The hematocrit was 21 and the platelet count was 221K. Flow Cytometry showed a B-cell population, with a predominant monoclonal Kappa (dim) light chain restricted population, that coexpressed pan-B-cell markers CD19 and CD20, along with CD5 and FMC-7 (dim). They expressed CD38 but were negative for CD23. In addition, they expressed aberrant antigens, including CD4, CD64, CD11c (dim) and CD15.
These findings are consistent with atypical CLL. The differential diagnosis also includes CLL with progression towards CLL / PLL (prolymphocytic leukemia, ruled out by morphology), and mantle cell lymphoma (ruled out by negative FISH studies for t[11;14]).
The expression of myelomonocytic antigens (CD15, CD4, CD64) is unusual, but has been described in a subset of B-CLL.
The patient was treated with prednisone and Chlorambucil and was discharged with no further treatment.
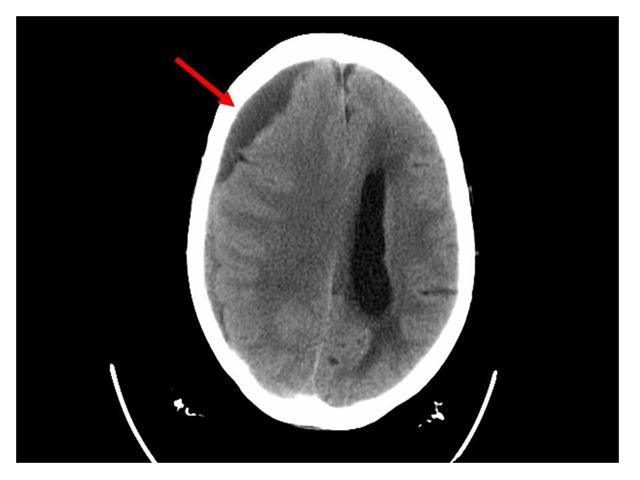
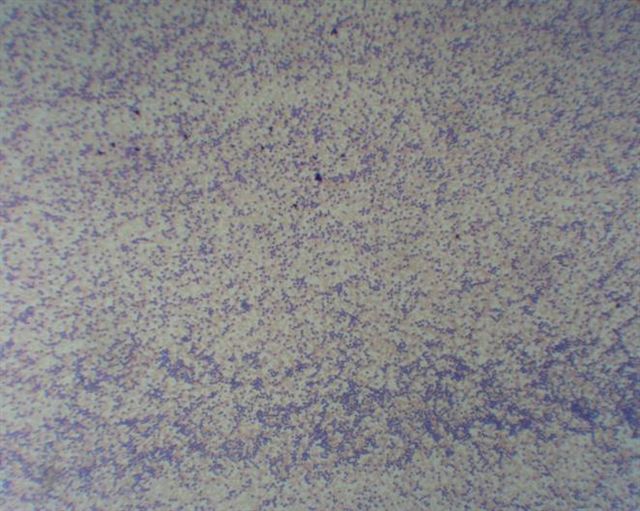
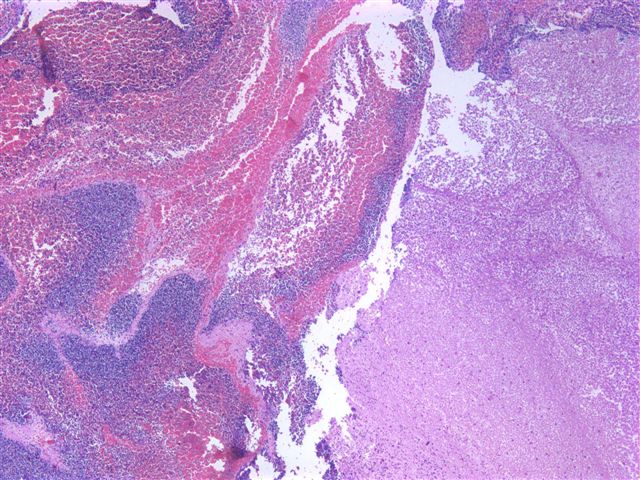
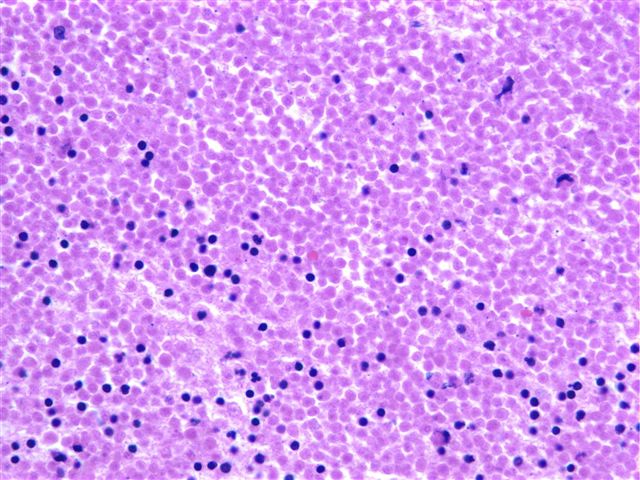
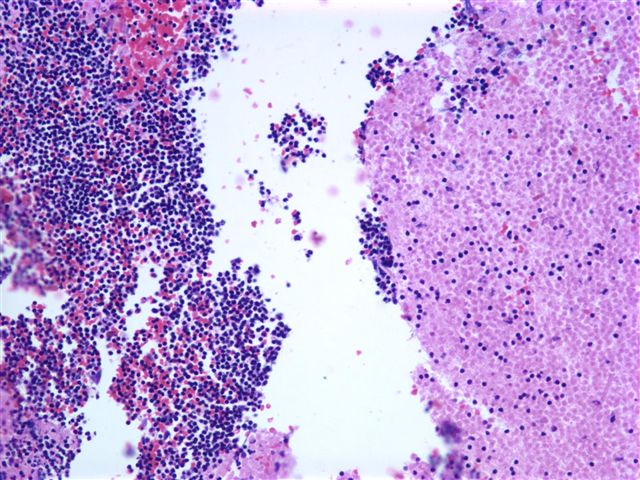
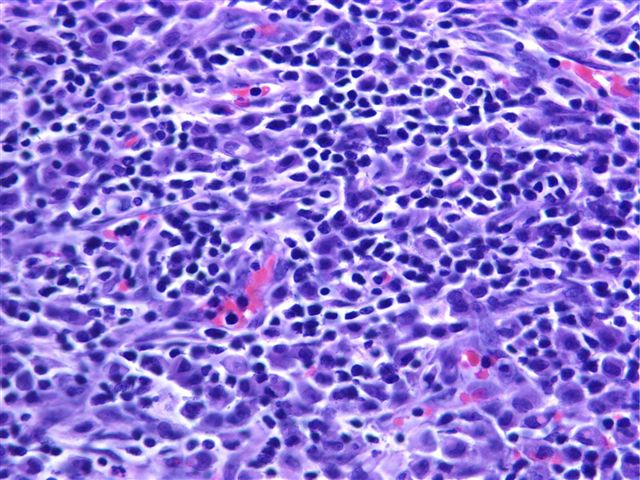
She subsequently returned to our hospital for a fall with a left hip fracture, with progressively worsening lethargy, decreased responsiveness and garbled speech. A head CT showed a large right subdural hemorrhage with associated subfalcine and right uncal herniation (figure 1). The patient underwent a craniotomy to evacuate the subdural hematoma. Peripheral blood smears were obtained (figure 2, figure 3). Smears were also obtained on the evacuated hematoma (figure 4, figure 5, figure 6, figure 7).
Diagnosis: subdural hematoma in the setting of local meningeal infiltration by CLL, see note.
Note: The presence of a tight nodule of small lymphocytes in the vicinity of the thrombus which also contains numerous viable lymphocytes is consistent with preexisting meningeal infiltration by CLL/SLL. After surgery, the patient developed bilateral pneumothorax and acute renal failure. Her family requested comfort measures only. She was extubated, and died shortly thereafter. The family declined autopsy.
-- end --
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}