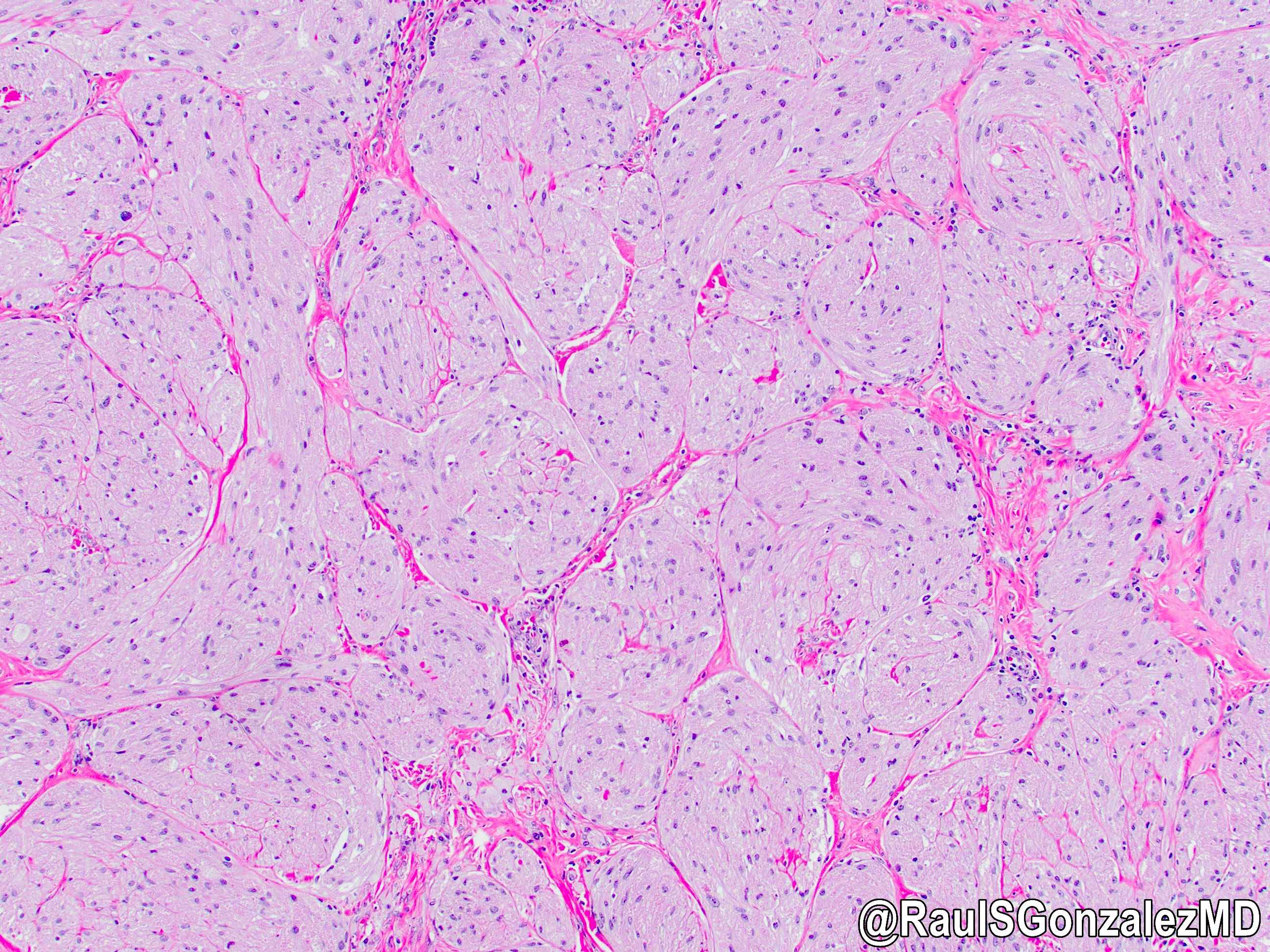
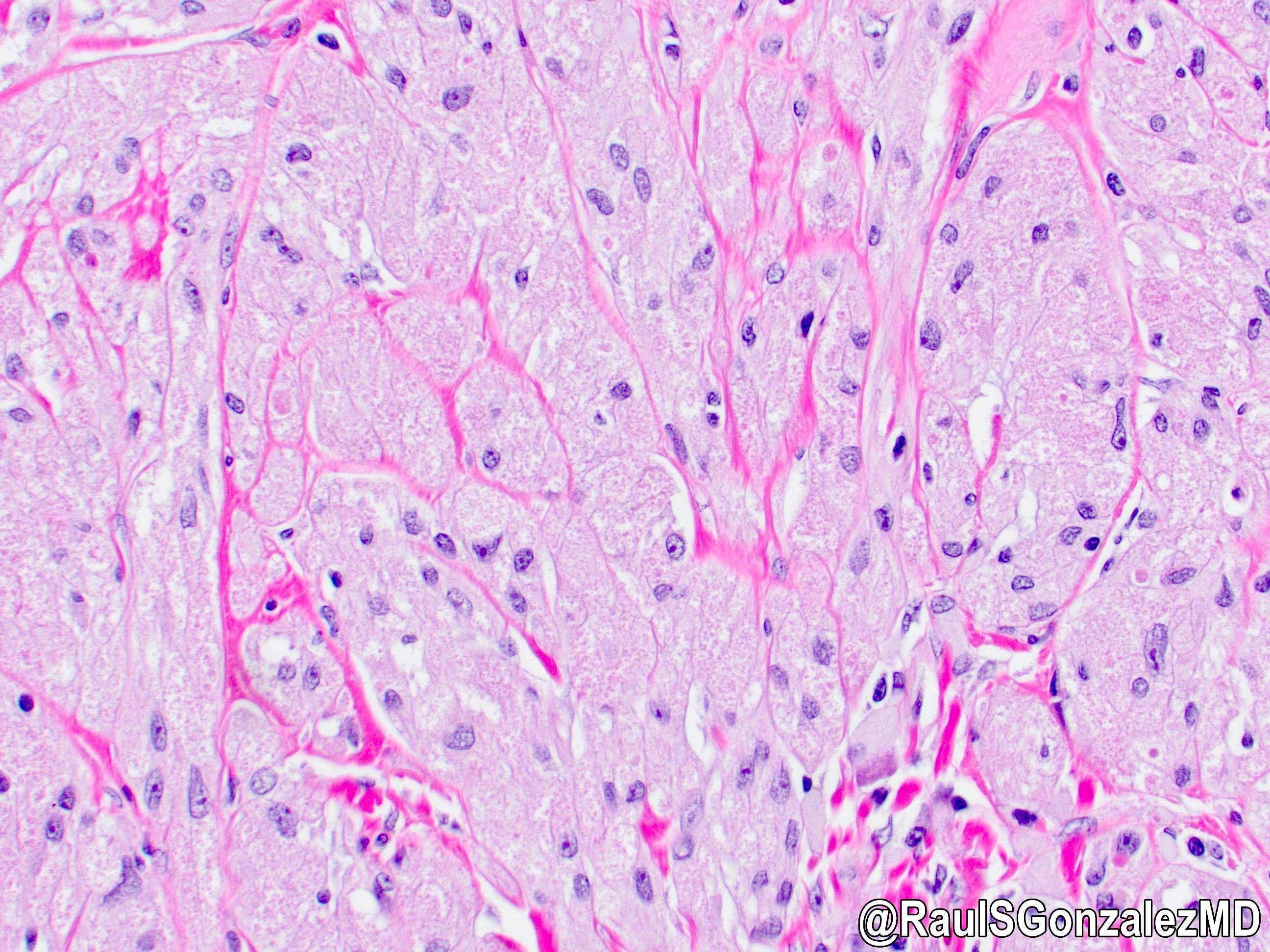
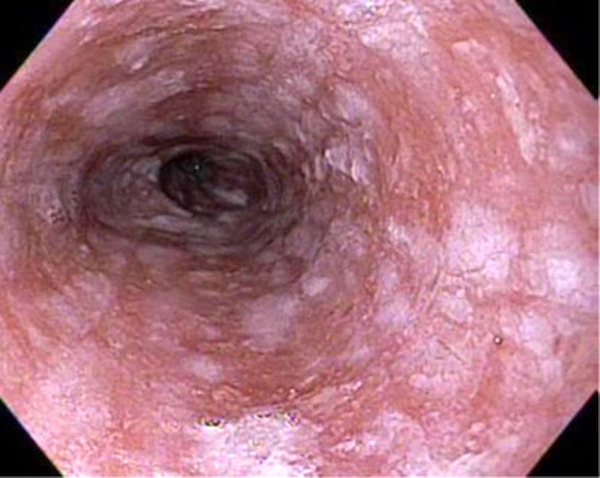
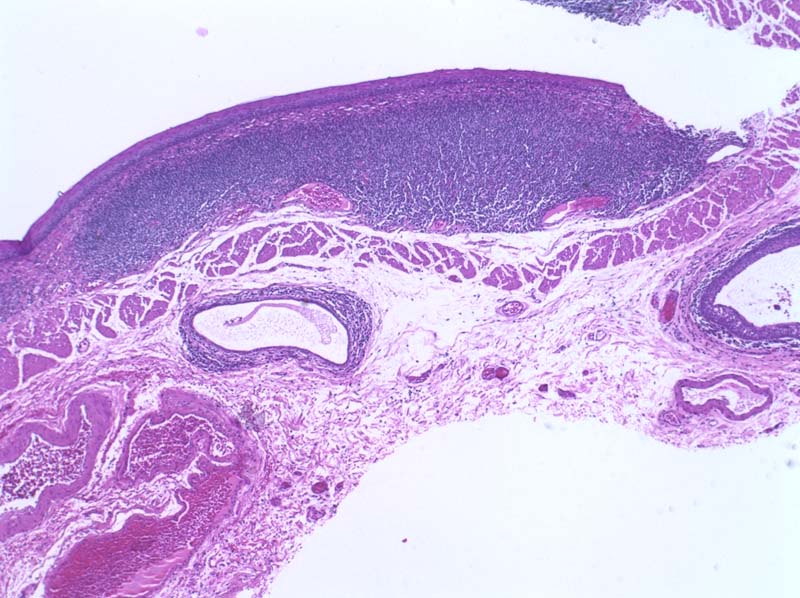
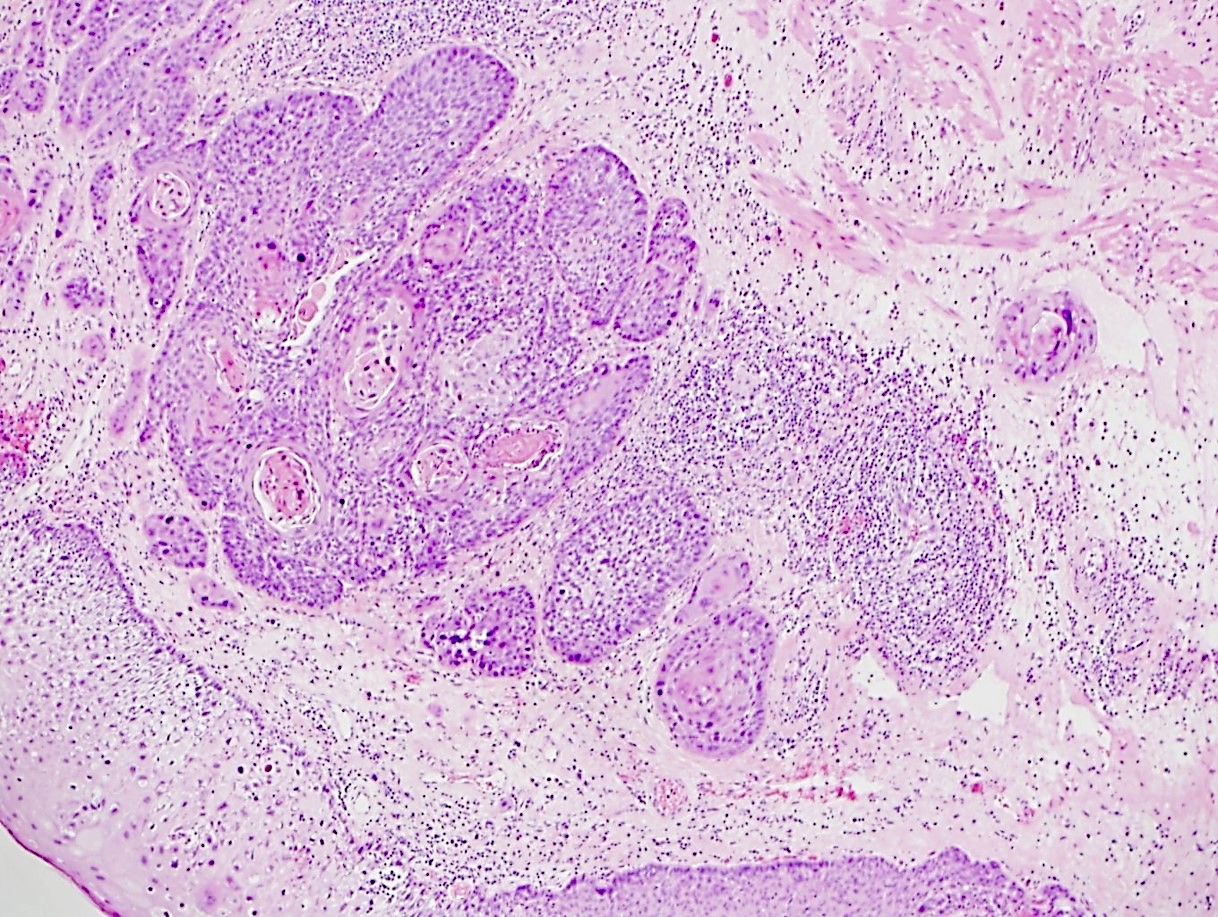
Esophageal motor disorder characterized by lack of progressive peristalsis and partial / incomplete relaxation of lower esophageal sphincter (LES), preventing passage of food into stomach
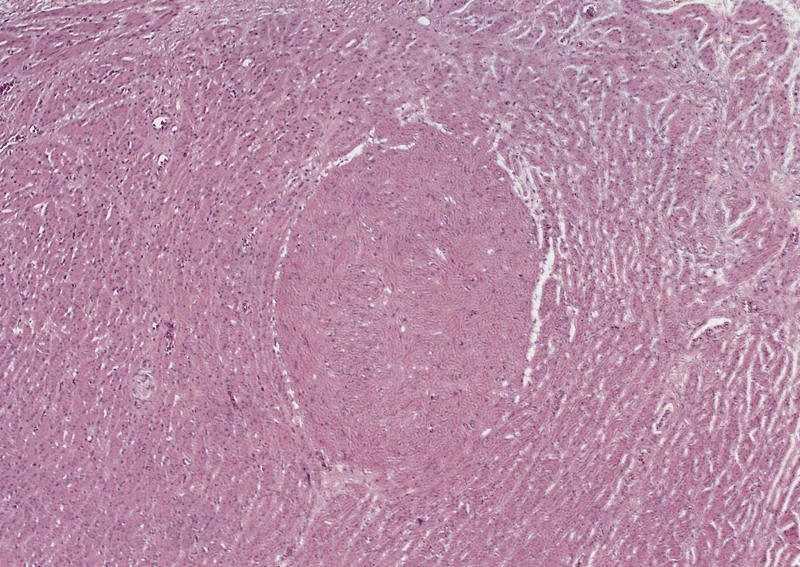
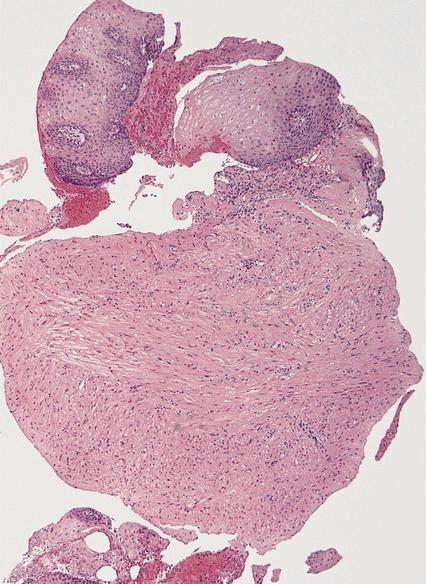
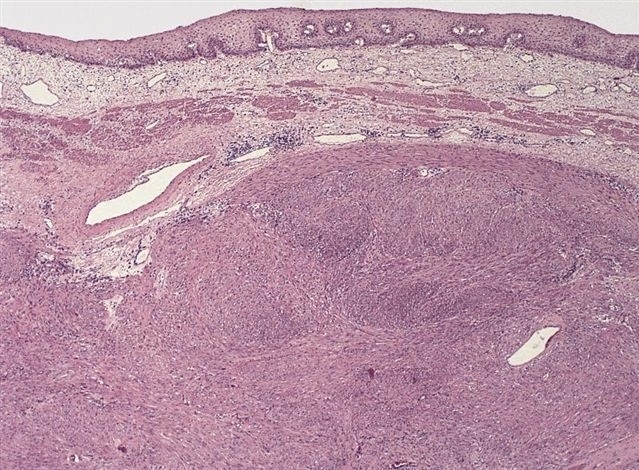
Preferentially involves circular layer of muscularis propria, which is hypertrophied
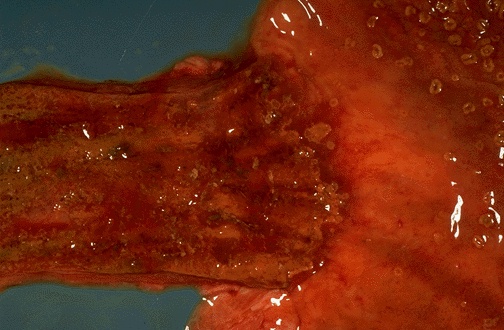
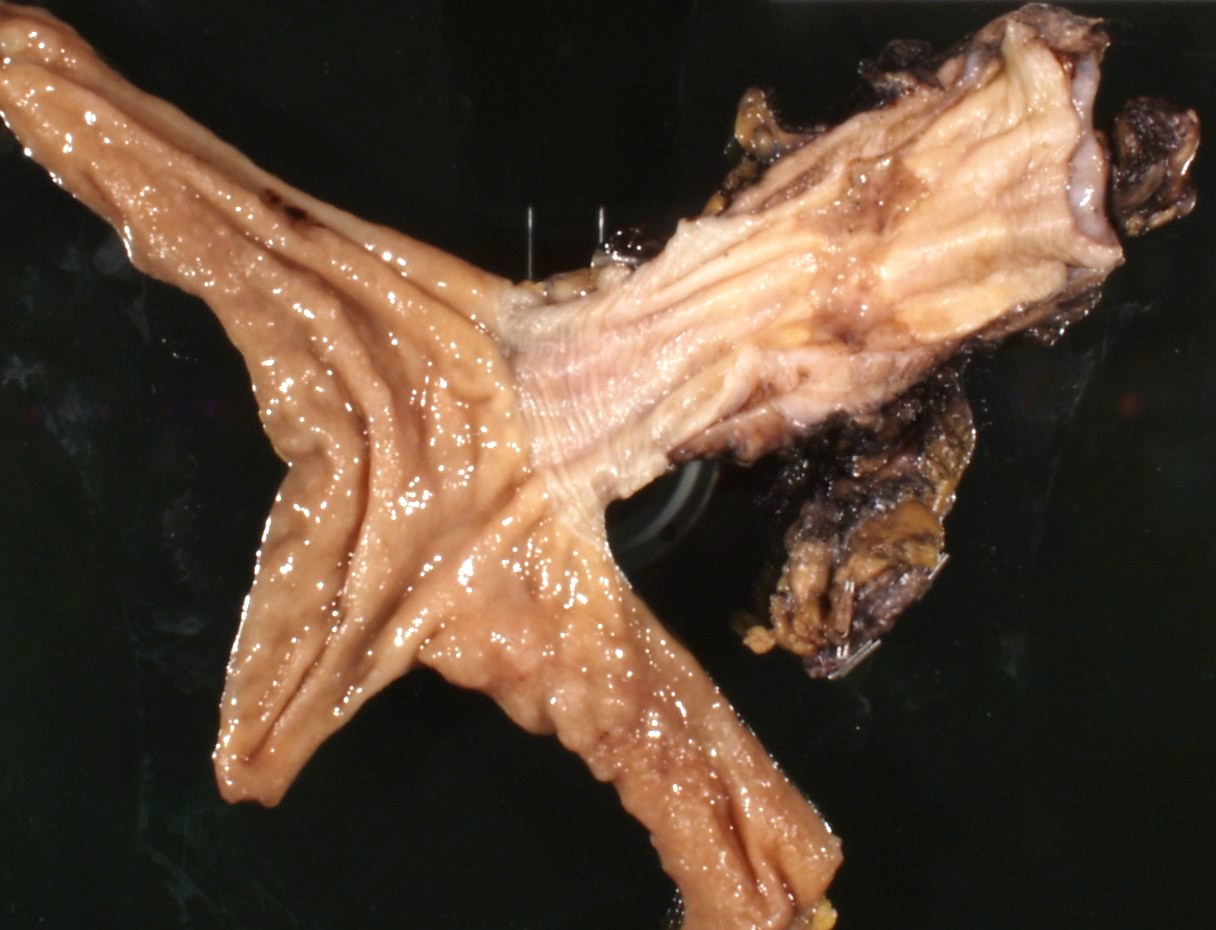
Progressive dilation of esophagus above LES, variable wall thickness
Gross images
Images hosted on other servers:
Dilated esophagus
Microscopic (histologic) description
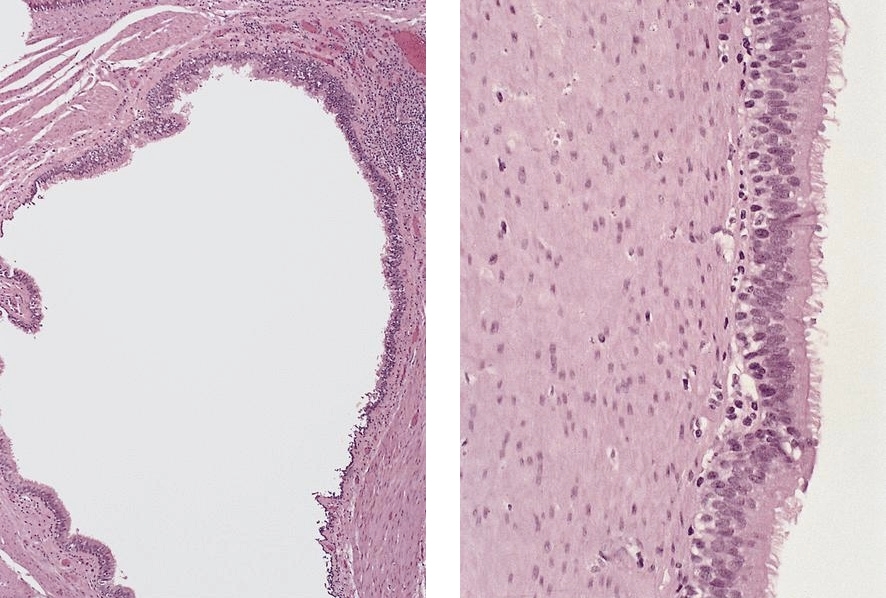
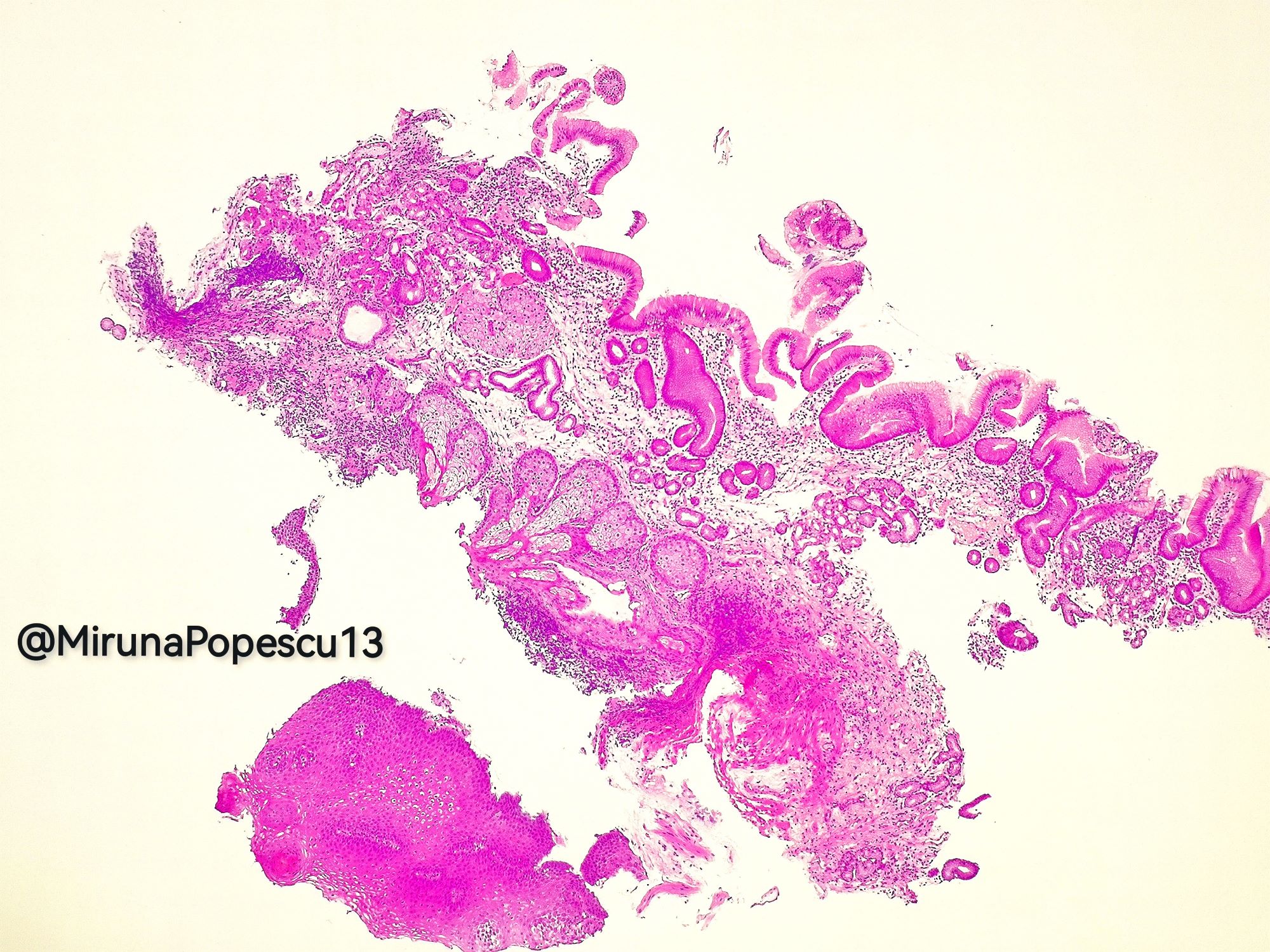
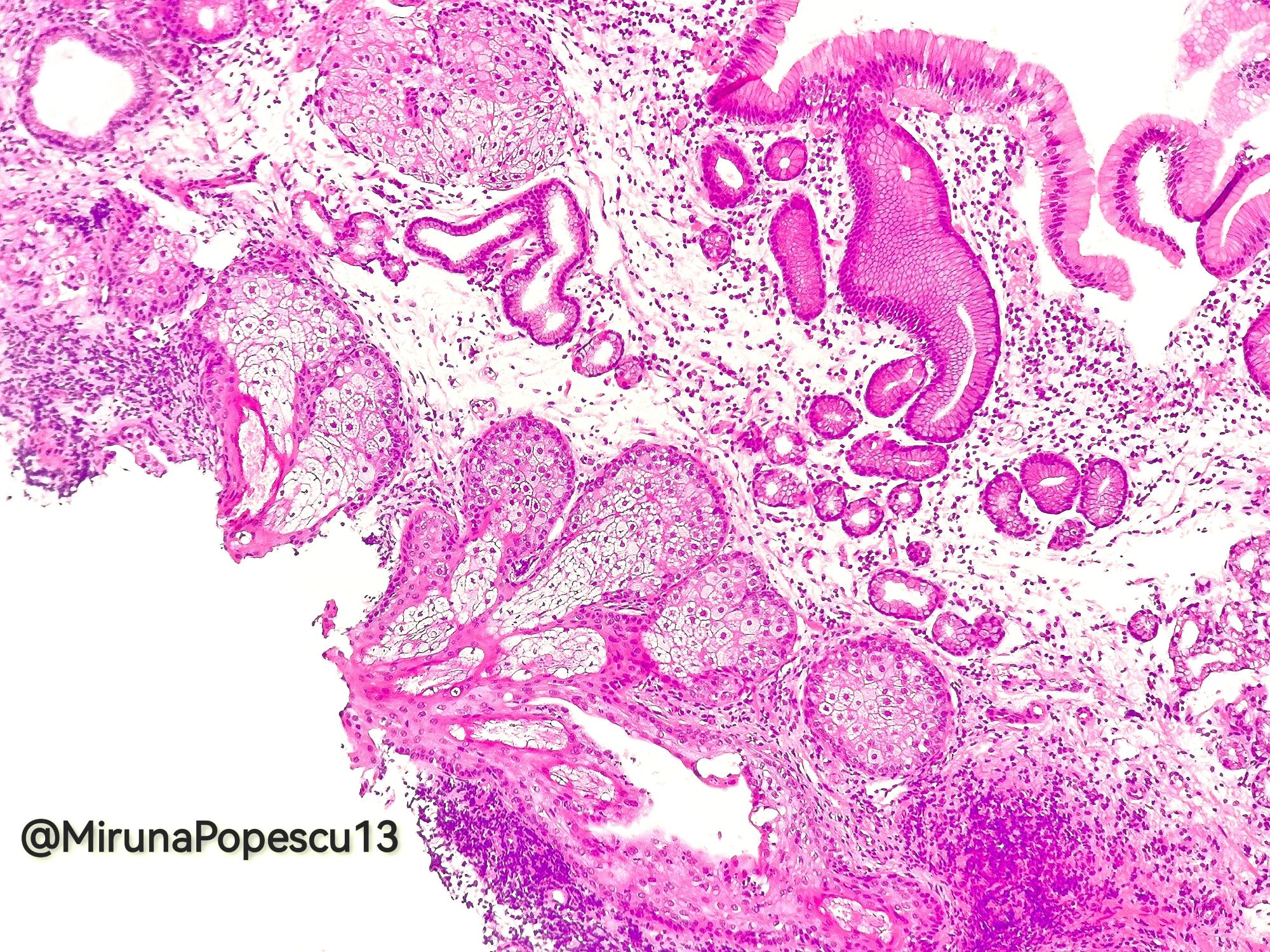
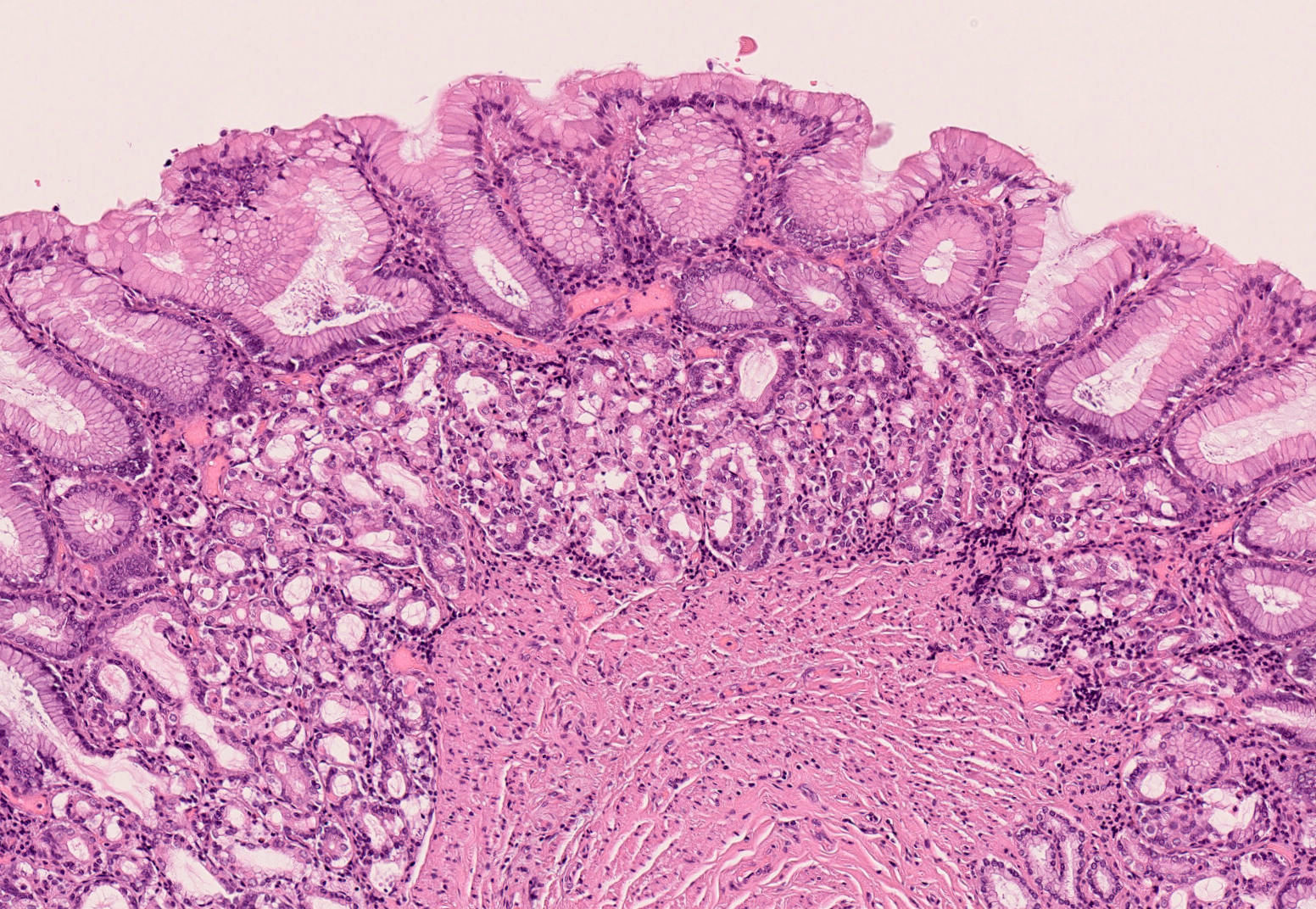
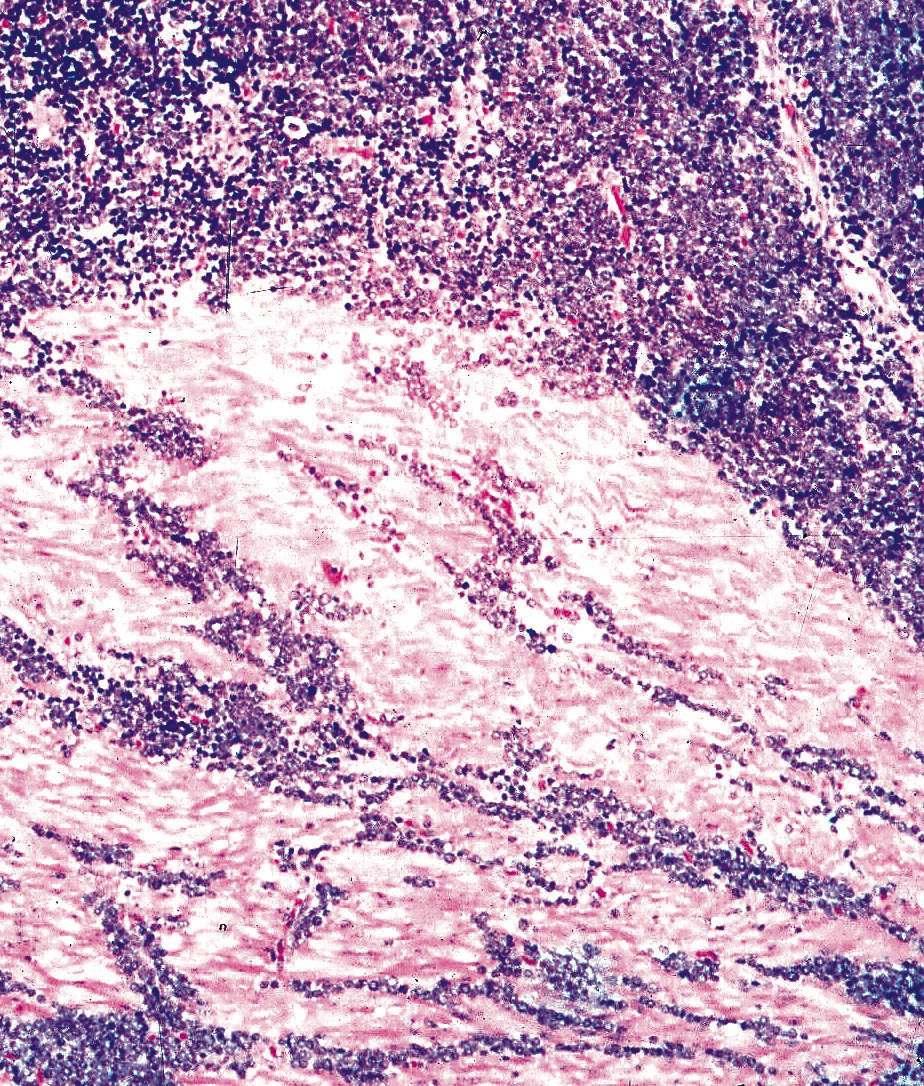
Early: Auerbach / myenteric plexus has lymphocytic inflammation (cytotoxic T cells, eosinophils) with germinal centers and submucosal glandular atrophy
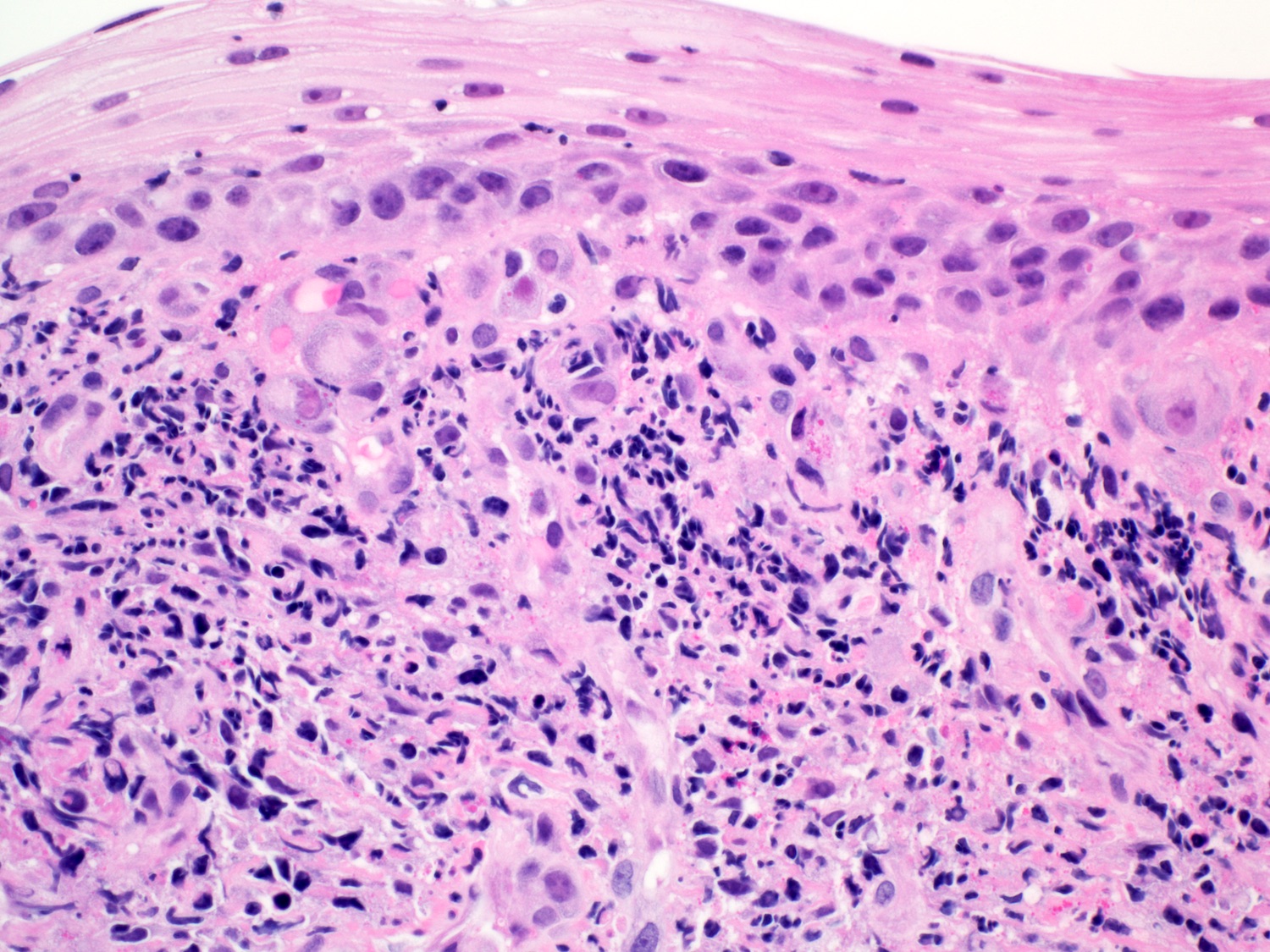
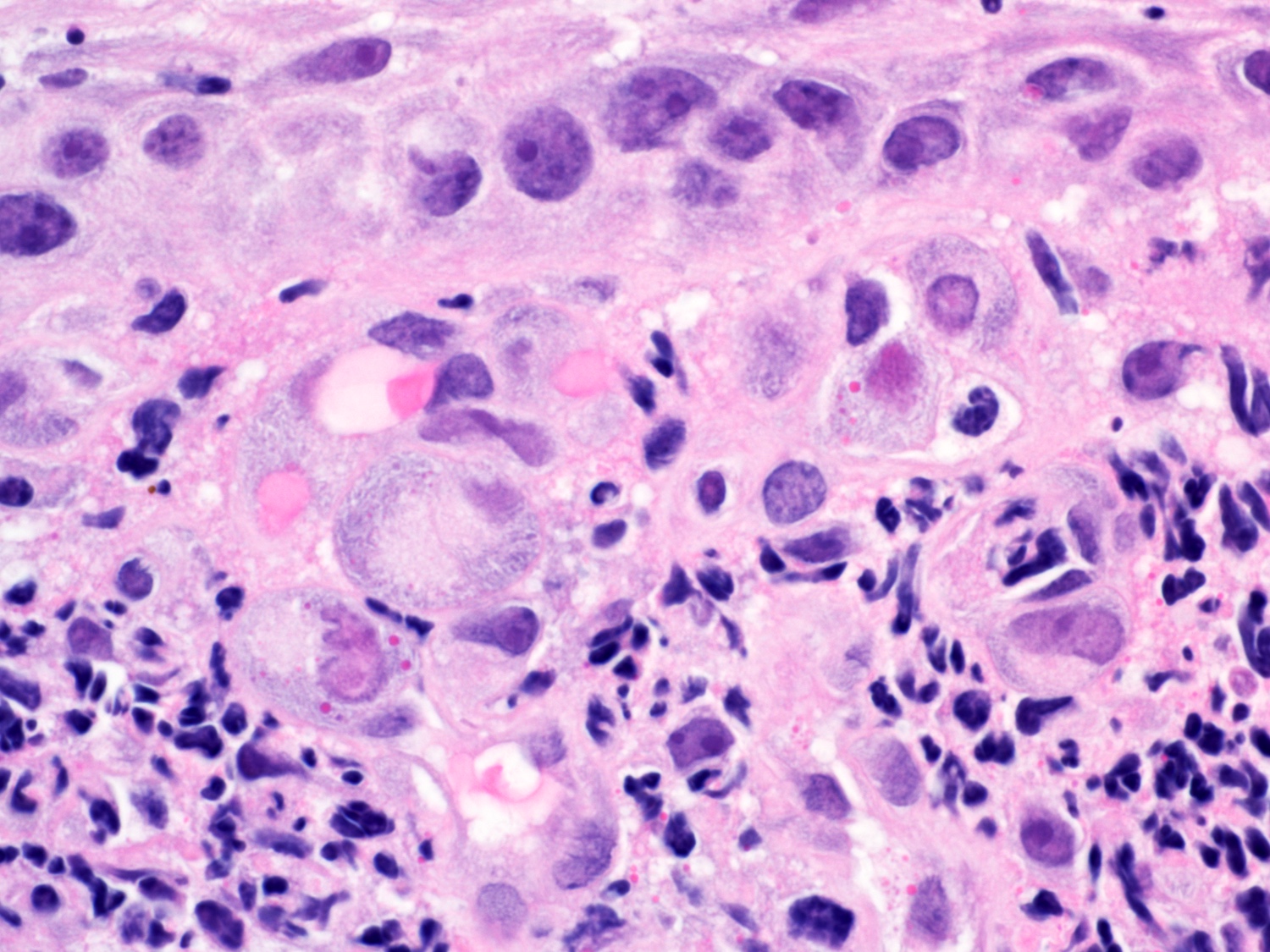
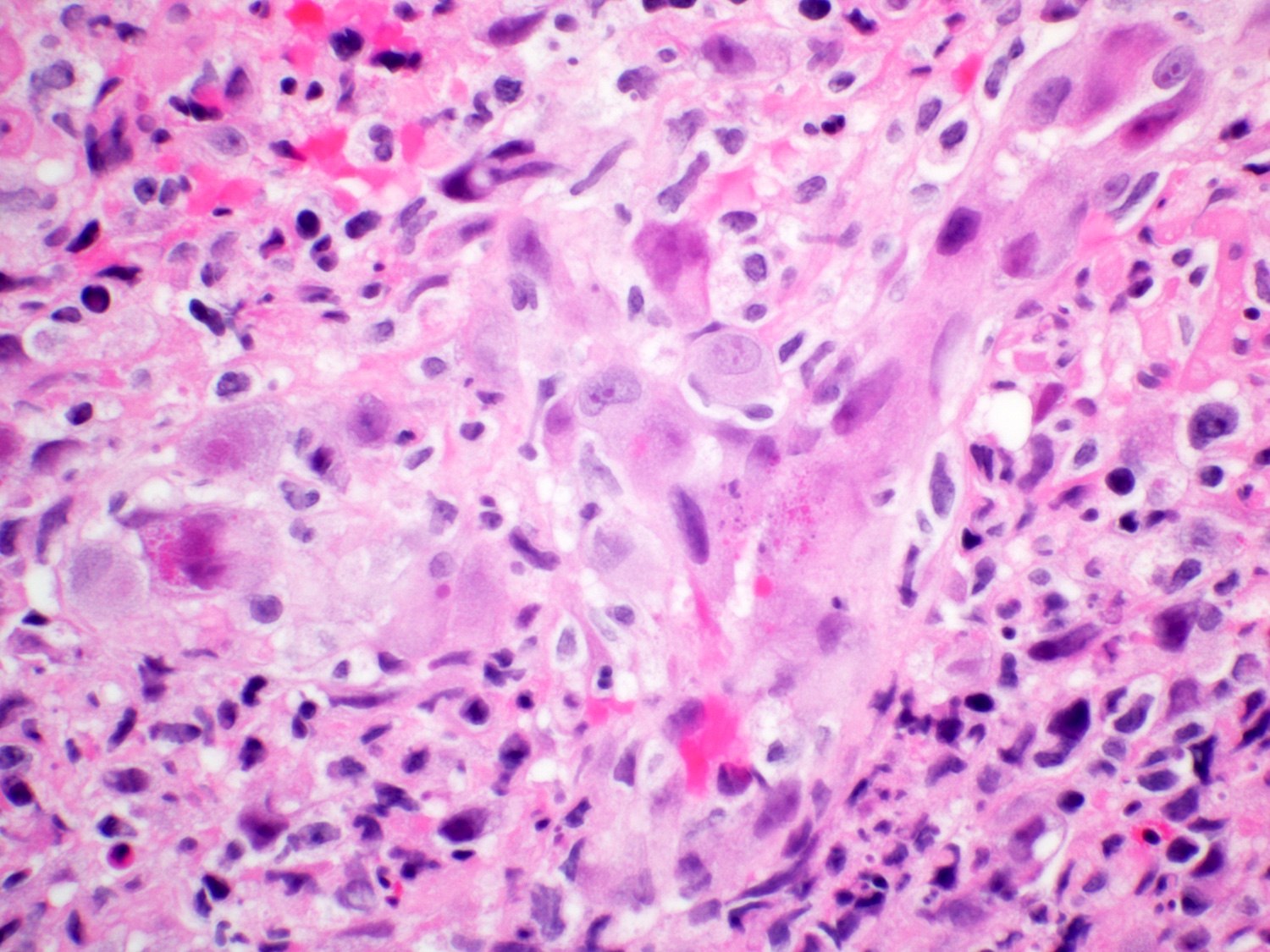
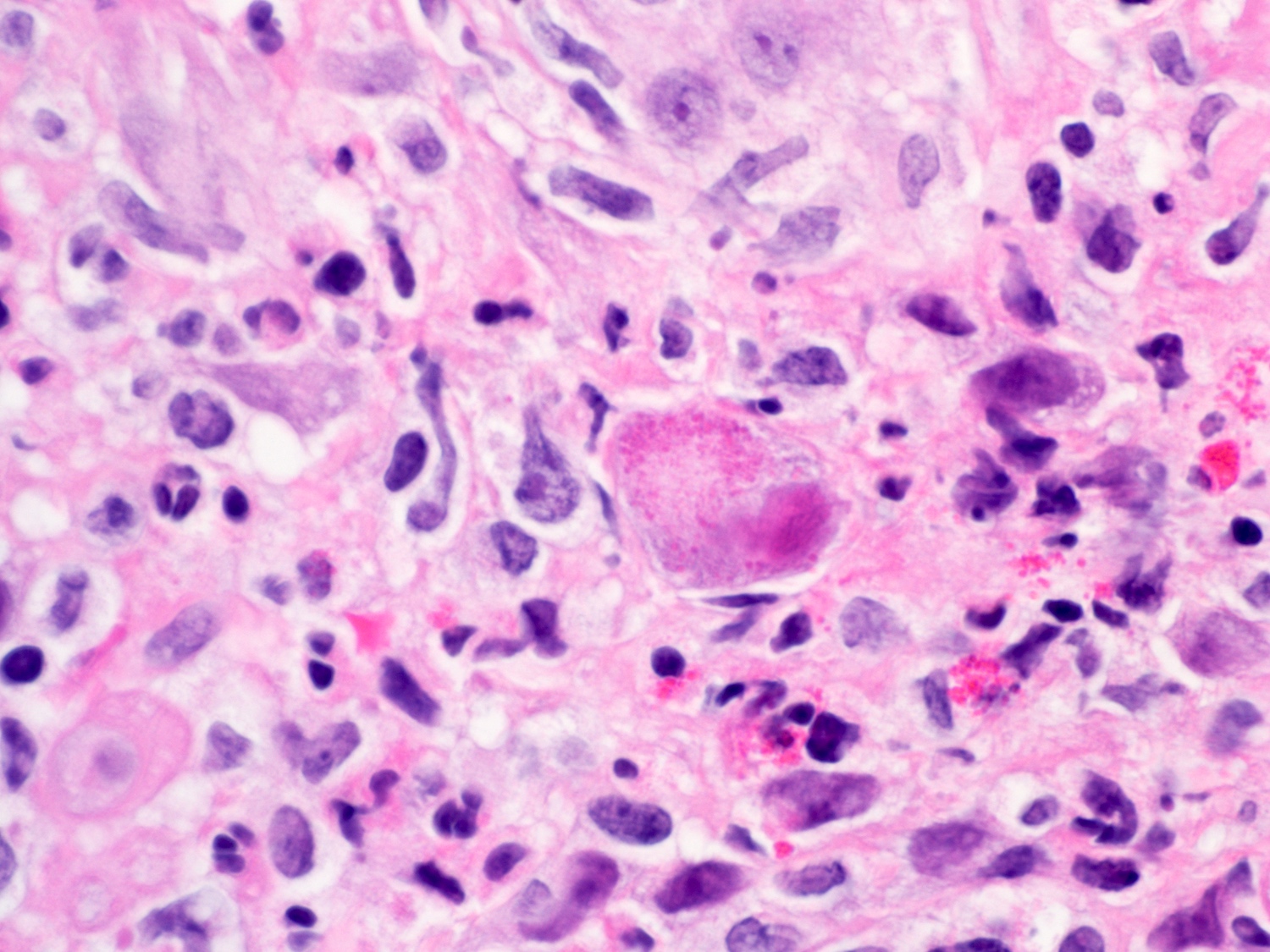
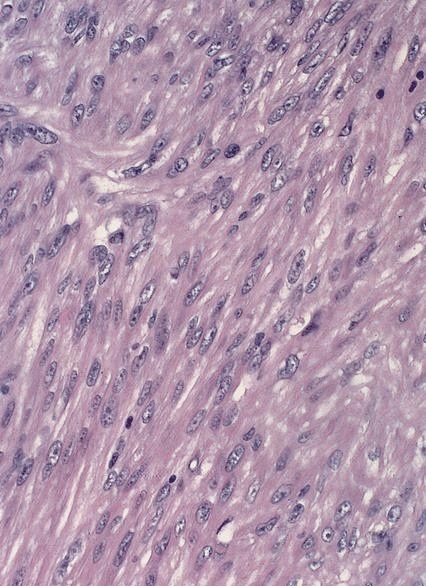
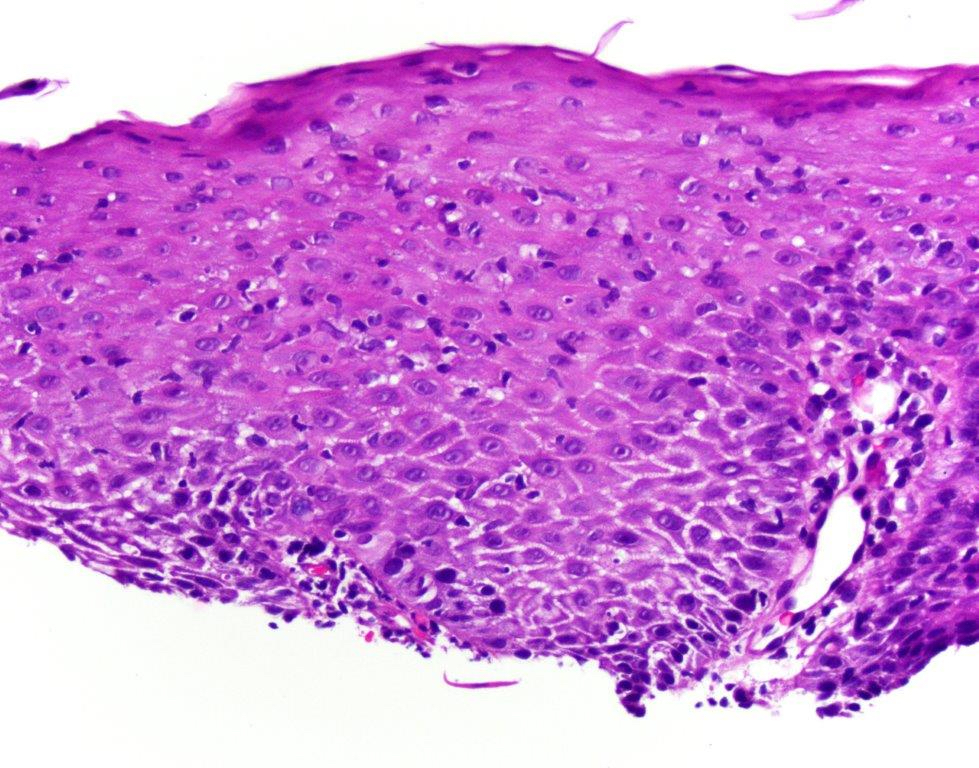
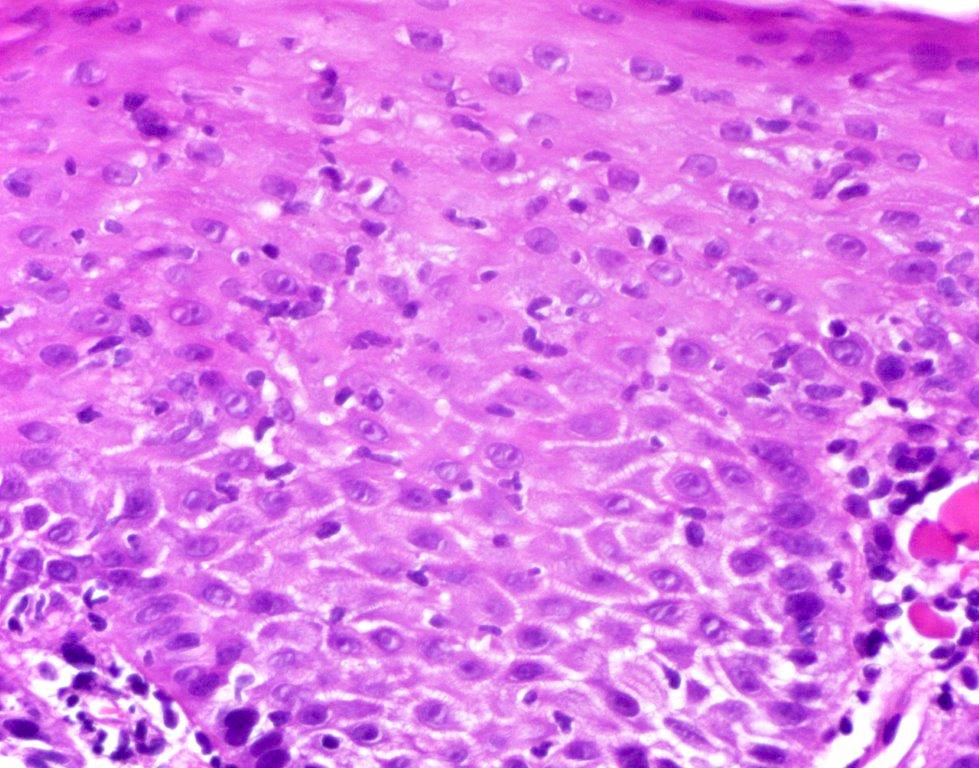
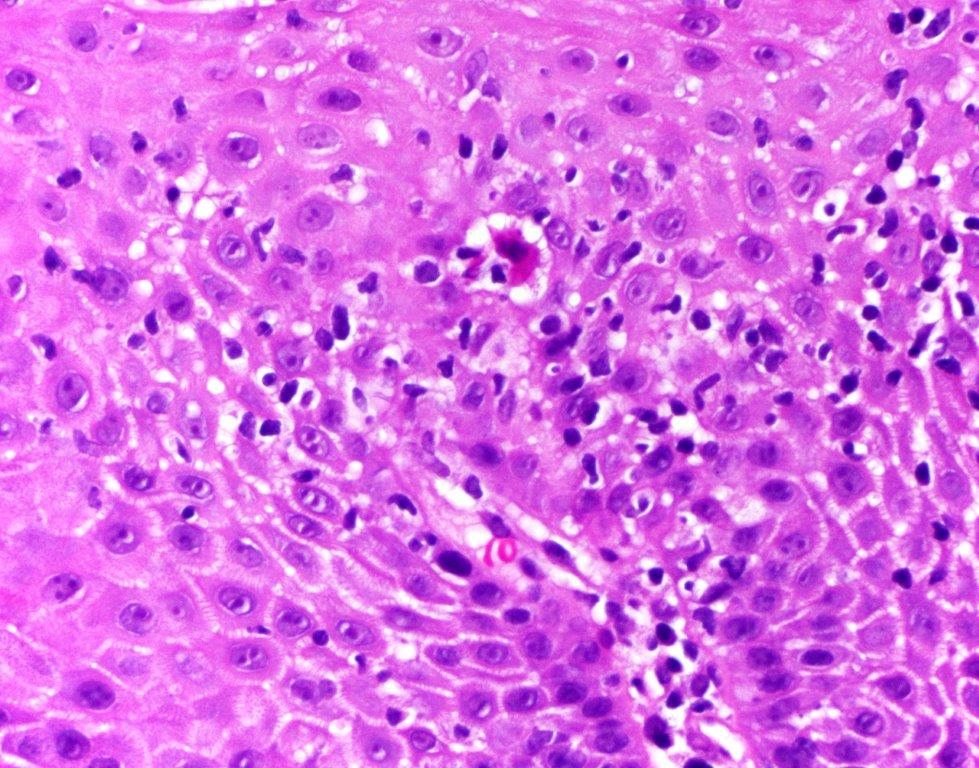
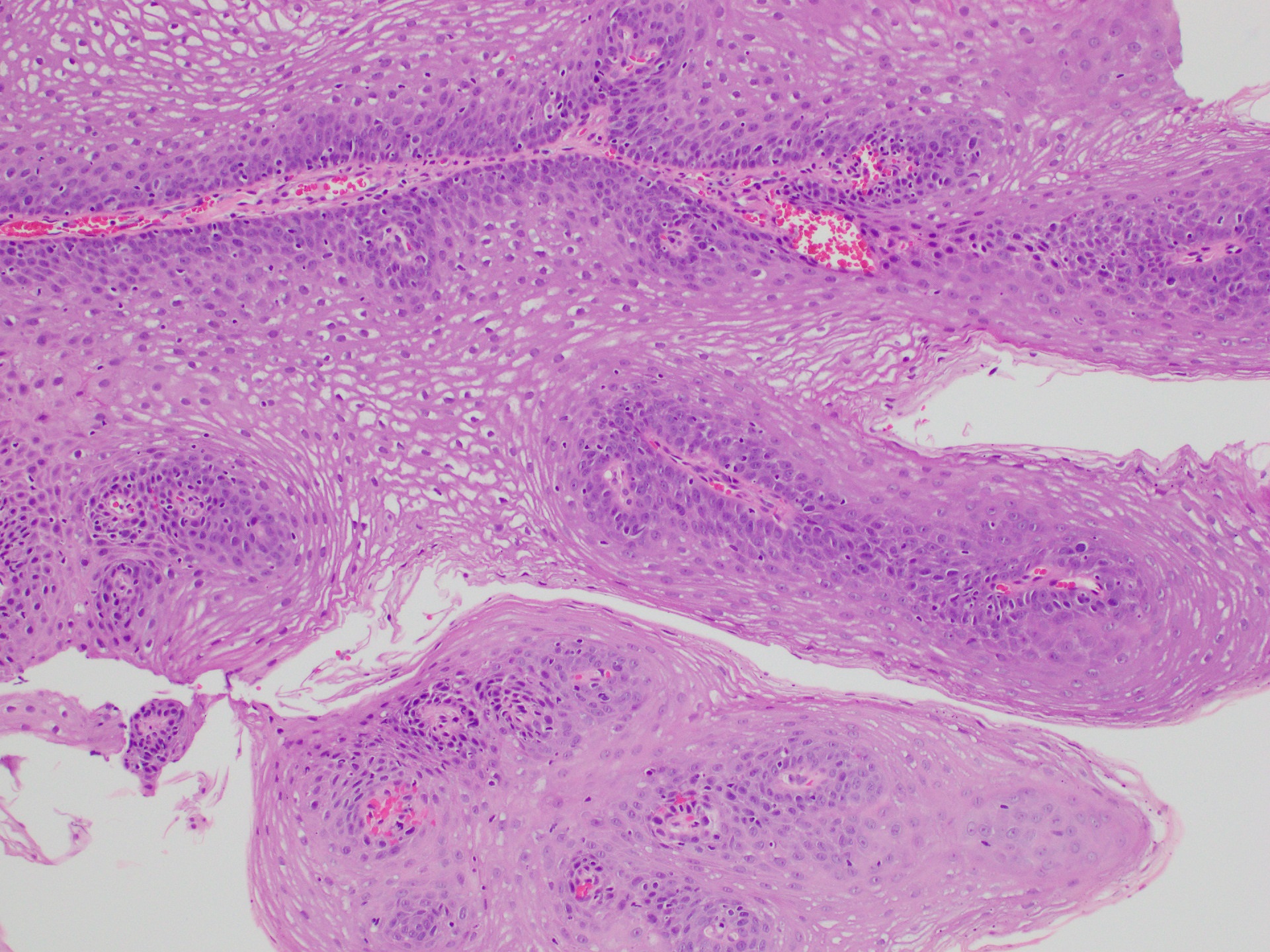
Late: marked depletion / absence of ganglion cells in myenteric plexus (middle of esophagus, may be normal at LES) and replacement of nerves by collagen with muscular hypertrophy; squamous mucosa markedly hyperplastic with papillomatosis and basal cell hyperplasia resembling GERD (J Gastroenterol Hepatol 2006;21:727)
Smooth muscle cells have nuclear and cytoplasmic inclusions, marked loss of small nerve fibers, paucity of granules in nerve fibers; also nonspecific filament disarray, mottling of myocyte fiber density, thick and long cytoplasmic dense bodies, long dense plaques (Am J Clin Pathol 1983;79:319)
Malignant epithelial neoplasm of the esophagus with glandular or mucinous differentiation
Majority of cases occur in the lower esophagus and at the esophagogastric (GE) junction, which is defined endoscopically by the most proximal gastric fold or the distal end of the palisade vessels
Essential features
According to WHO (5th edition), GE junction adenocarcinoma is defined as an adenocarcinoma with an epicenter within 2 cm of the GE junction and extending into the esophagus
Rarely, adenocarcinoma can occur in the middle or upper third of the esophagus; such cases most likely develop from submucosal glands or ectopic columnar epithelium in the esophagus (also known as inlet patches or ectopic gastric mucosa)
Evidence of glandular or mucinous differentiation within an invasive tumor originating in the esophagus and GE junction
Represents 15% of all esophageal cancers worldwide (the majority being esophageal squamous cell carcinoma), with men diagnosed more often than women (Gut 2020;69:1564)
Distinct geographical patterns compared with esophageal squamous cell carcinoma
The majority of adenocarcinoma cases occur in Eastern Asia followed by North America, with China and the U.S. contributing most to the burden on a country level (Gut 2020;69:1564)
Patients with Barrett esophagus have a 10 - 55 fold higher risk of adenocarcinoma (Dig Dis Sci 2018;63:1988)
Rate of progression from Barrett esophagus to adenocarcinoma varies widely in the literature, within 0.07 - 3.6% and 1.5 - 2.5 fold higher when including high grade dysplasia (Gastroenterology 2015;149:577)
Shorter segments (3 cm) of Barrett esophagus have a lower rate of progression to adenocarcinoma than longer segments (≥ 3 cm) (Endoscopy 2019;51:665)
Unclear if proton pump inhibitors (PPI) have a protective effect on decreasing progression to adenocarcinoma (Transl Cancer Res 2021;10:1620)
Almost all cases occur in the lower third of the esophagus and esophagogastric junction
Cases may occur in the upper and middle thirds of the esophagus, most likely developing from submucosal glands or ectopic columnar epithelium in the esophagus (also known as inlet patches or ectopic gastric mucosa)
Pathophysiology
Primarily associated with Barrett esophagus, history of gastroesophageal reflux disease (GERD), obesity, tobacco smoking
51 year old man presented with 2 weeks of reflux, 35 pound weight loss and elevated alpha fetoprotein (AFP) (Clin J Gastroenterol 2017;10:7)
60 year old man presented with epigastric discomfort for one month and a mid esophageal adenocarcinoma arising from a heterotopic pancreas (Thorac Cancer 2022;13:1083)
71 year old man with a history of smoking and Barrett esophagus presenting with dysphagia and weight loss (Anticancer Res 2018;38:5999)
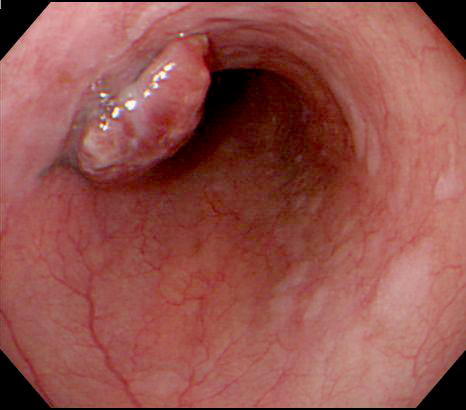
82 year old man presented with a 15 cm incarcerated hiatal hernia and an incidental 3 cm polypoid lesion on endoscopy at the level of the carina (BMJ Case Rep 2020;13:e235802)
Dutch family with clustering of Barrett esophagus and esophageal adenocarcinoma (Fam Cancer 2018;17:435)
Treatment
Dependent on tumor stage and patient's health status
Generally less radiosensitive than esophageal squamous cell carcinoma
Early (T1) lesions may be cured via endoscopic techniques (radiofrequency ablation, endoscopic mucosal resection, endoscopic submucosal dissection)
Preoperative chemoradiation with or without immunotherapy targeting HER2 receptor followed by surgery is the most common treatment protocol for resectable tumors (J Natl Compr Canc Netw 2015;13:194)
Esophagectomy and esophagogastrectomy performed in medically fit patients with localized thoracic esophageal cancer > 5 cm from the cricopharyngeus and in intra-abdominal esophageal and GE junction cancers respectively (J Natl Compr Canc Netw 2015;13:194)
Definitive chemoradiation for cervical and cervicothoracic esophageal cancers within 5 cm of the cricopharyngeus
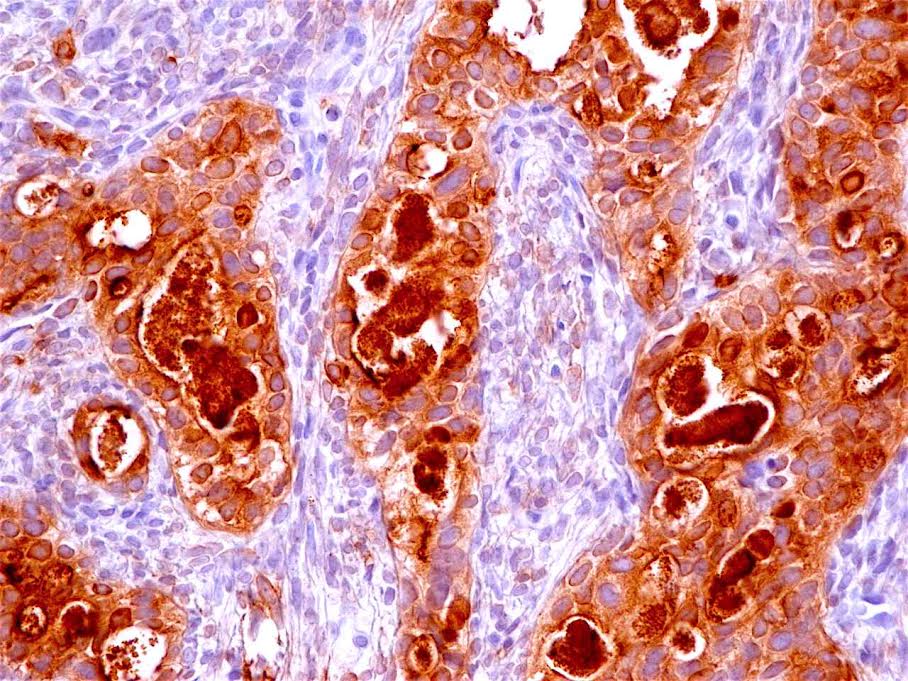
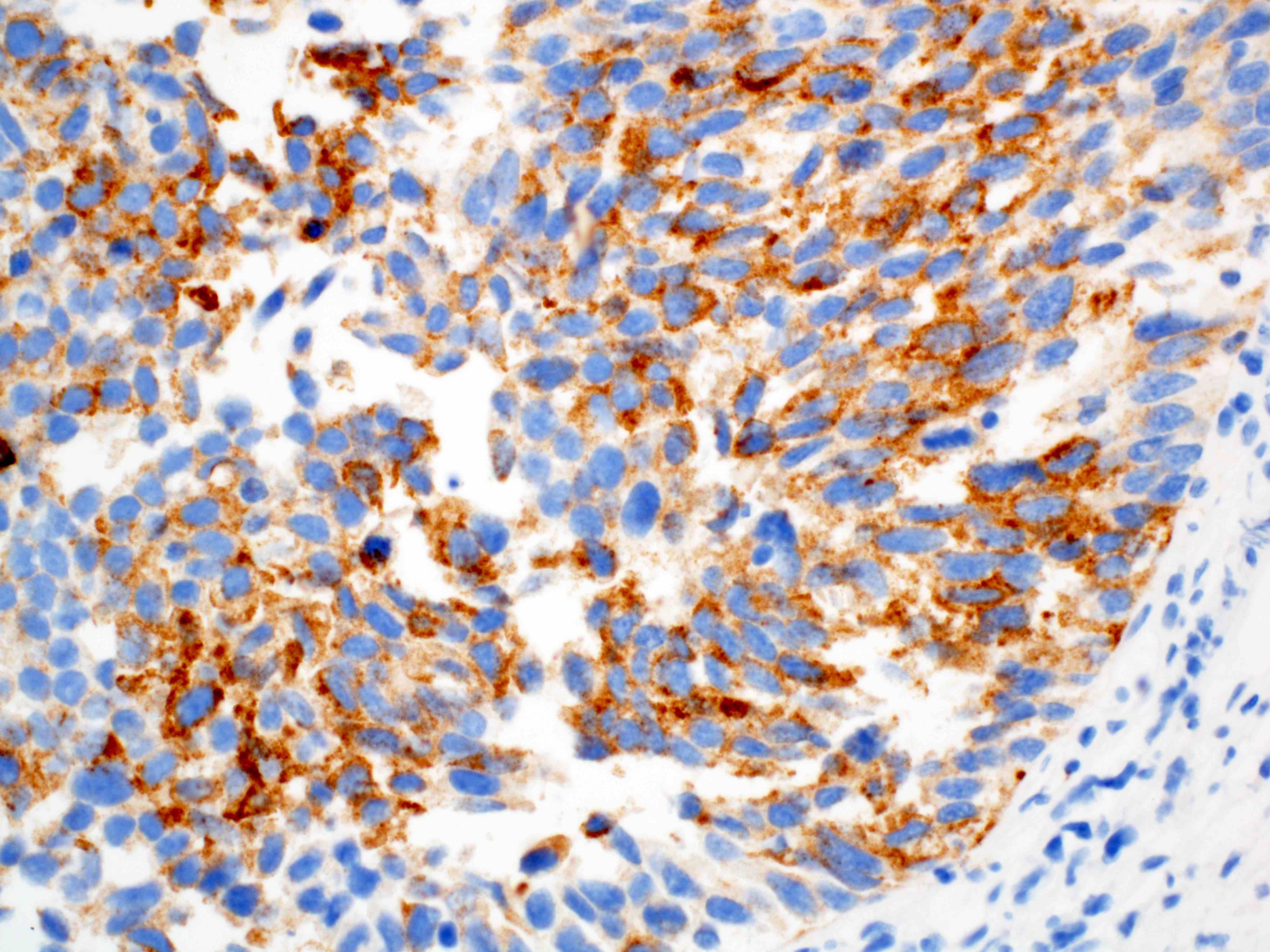
Patients with esophageal adenocarcinoma who had a HER2 score of 3+ or 2+ on immunohistochemistry with positive FISH and treated with trastuzumab plus chemotherapy had a longer median survival compared with patients treated with chemotherapy alone (Lancet 2010;376:687)
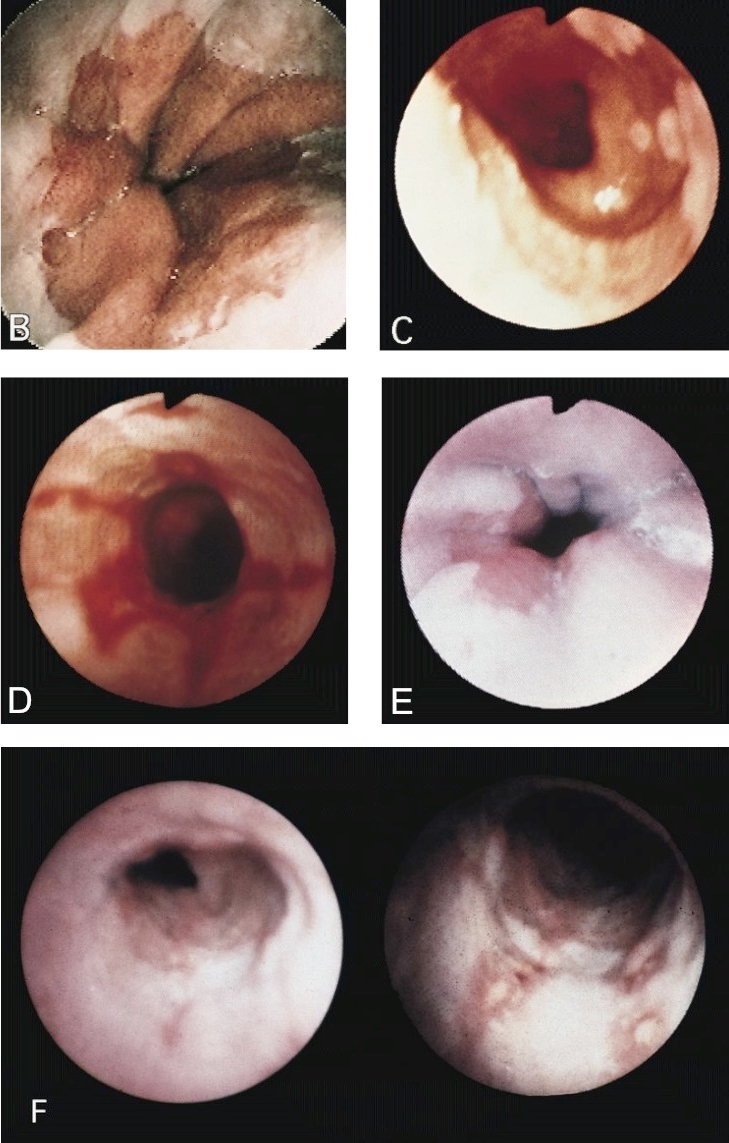
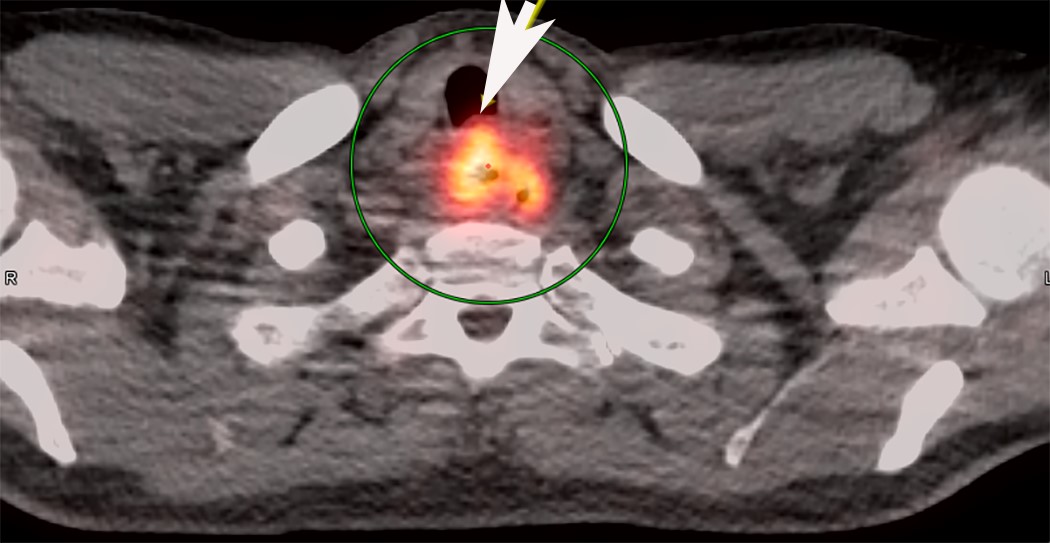
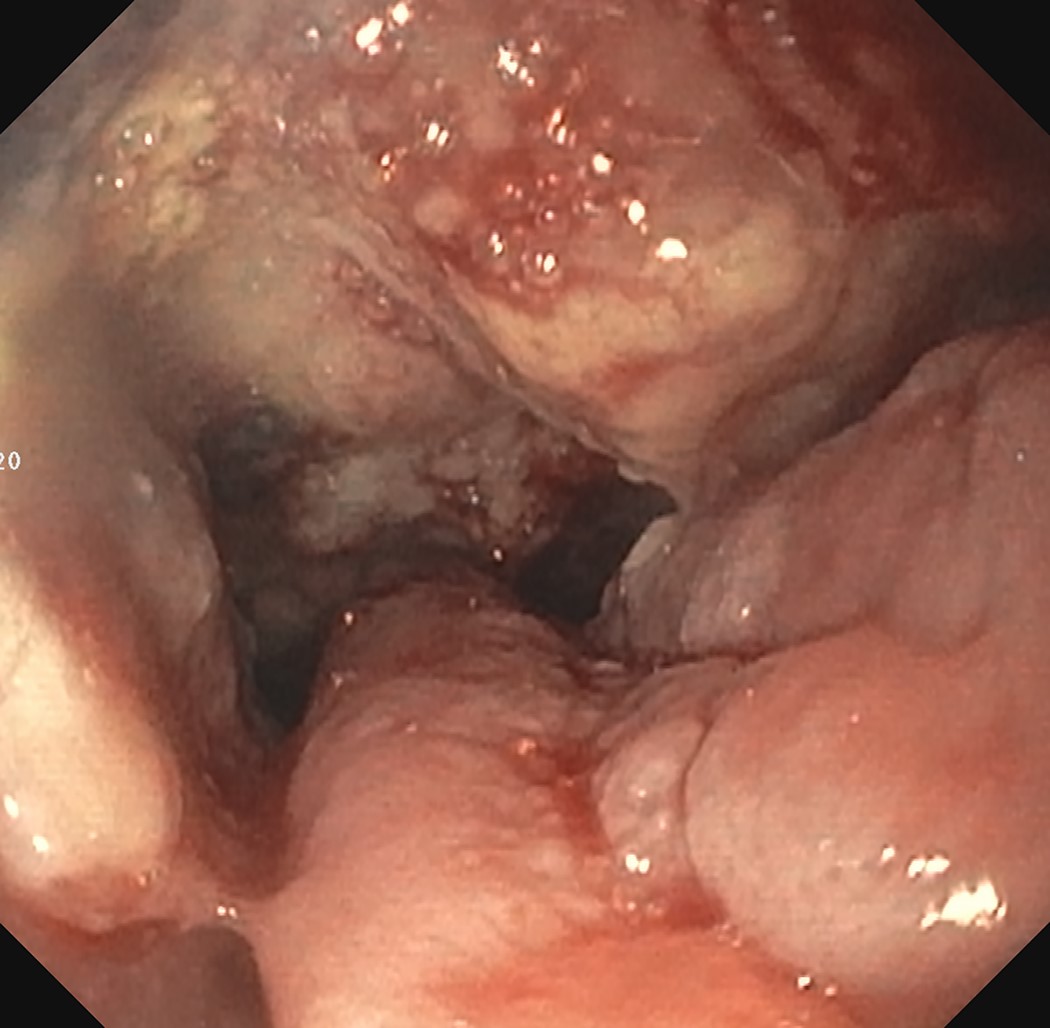
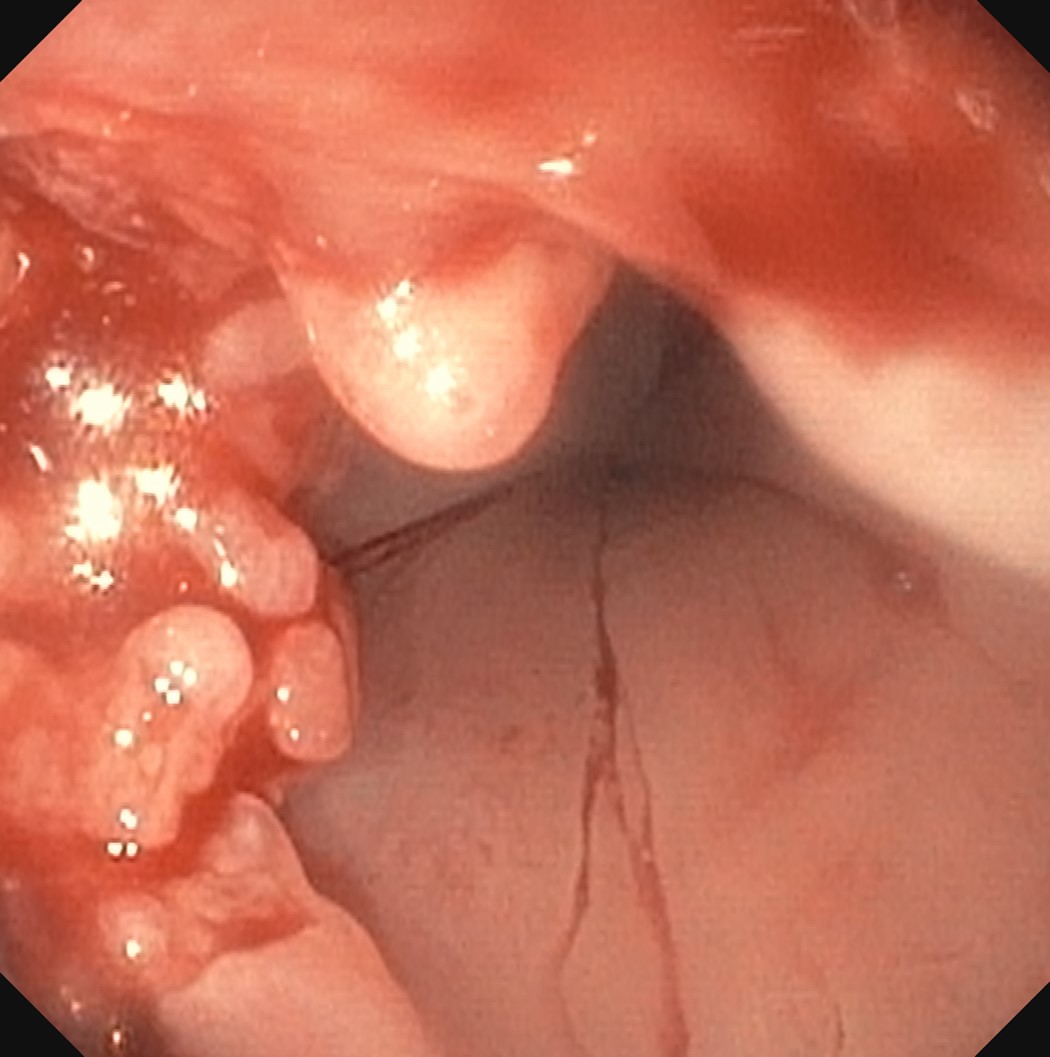
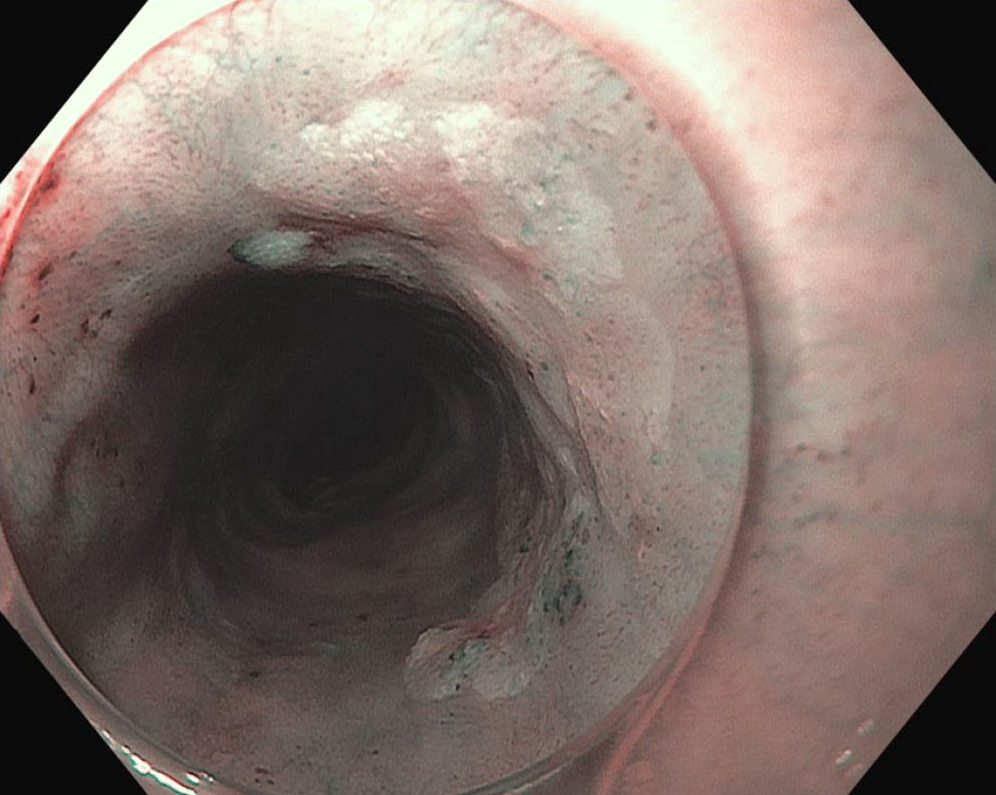
Clinical images
Contributed by Avani Pendse, M.D., Ph.D.
Upper endoscopy
Gross description
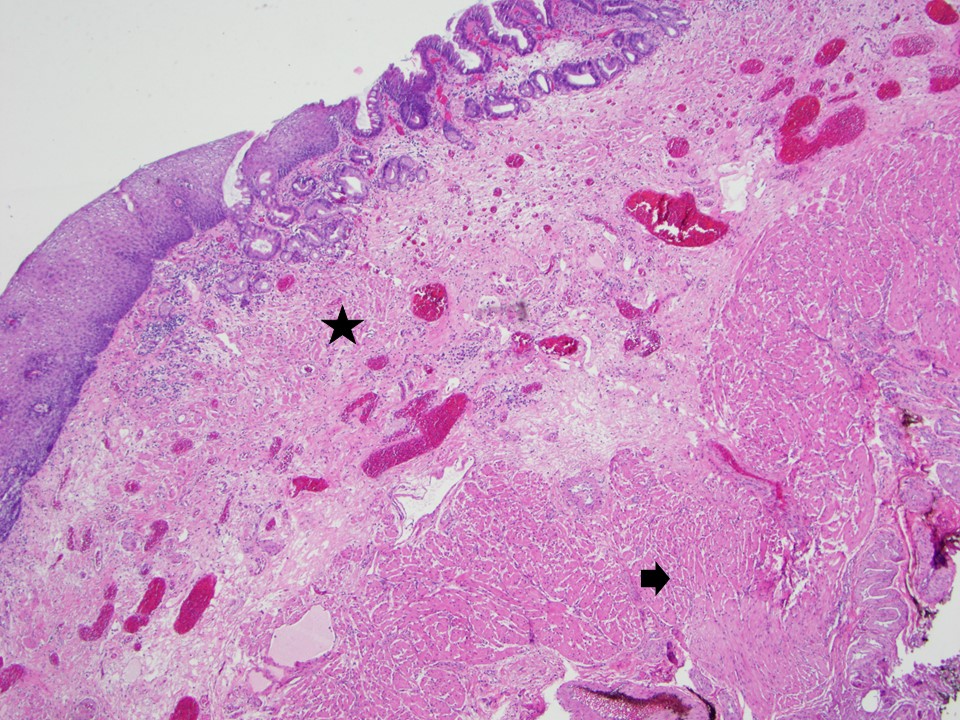
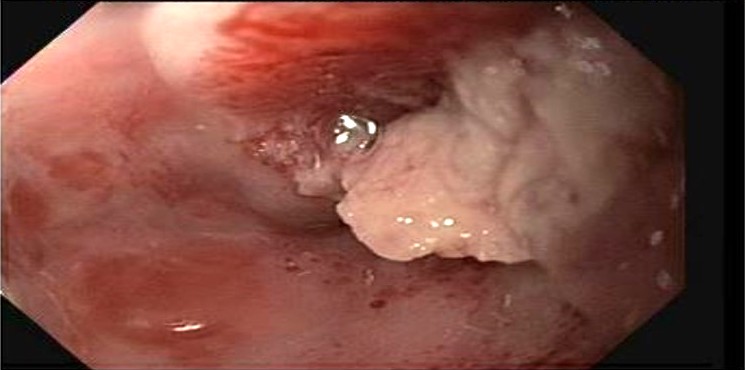
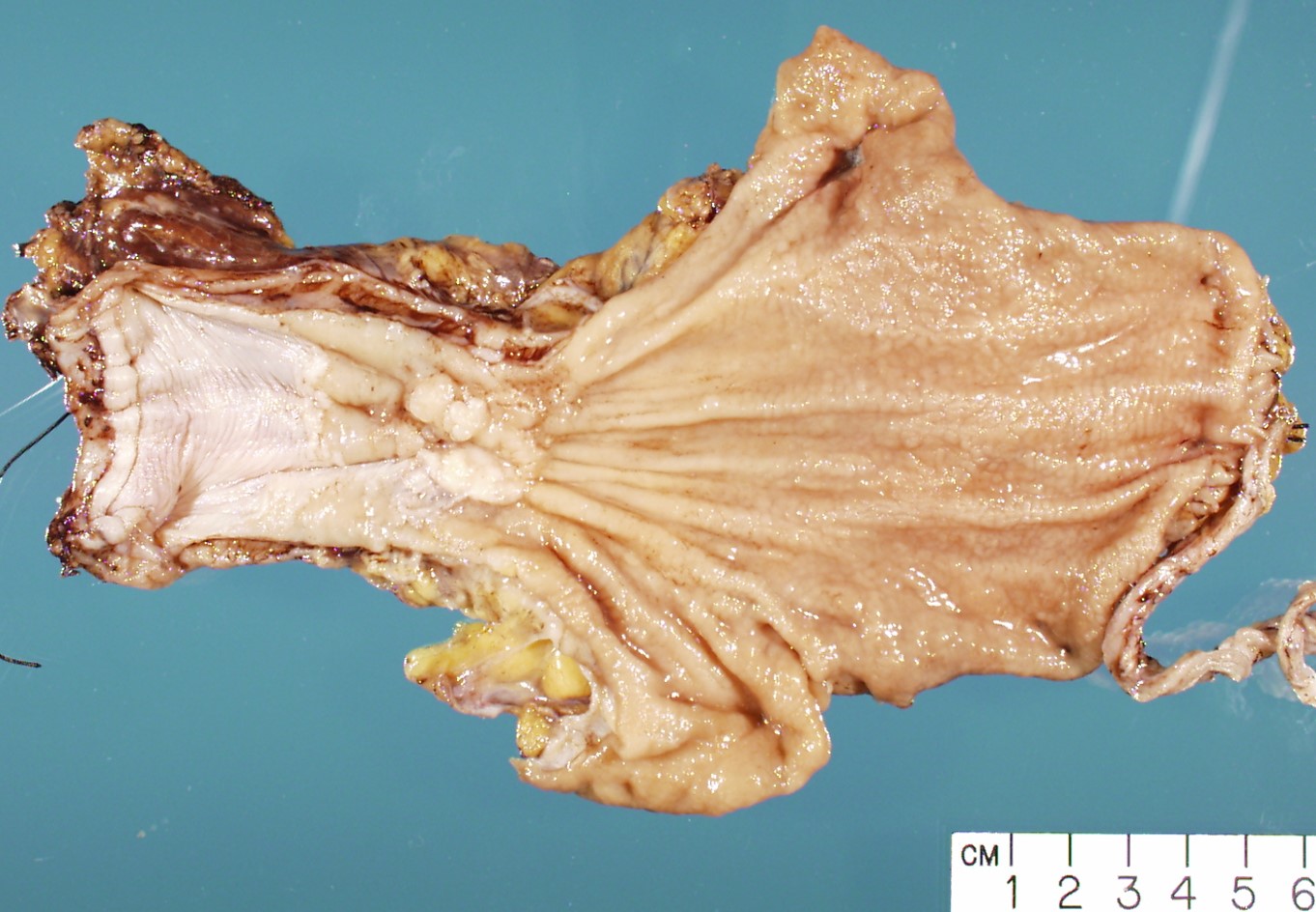
Often appear in advanced stages
May be stricturing, polypoid, fungating, ulcerative or diffusely infiltrative
Gross images
Contributed by Avani Pendse, M.D.
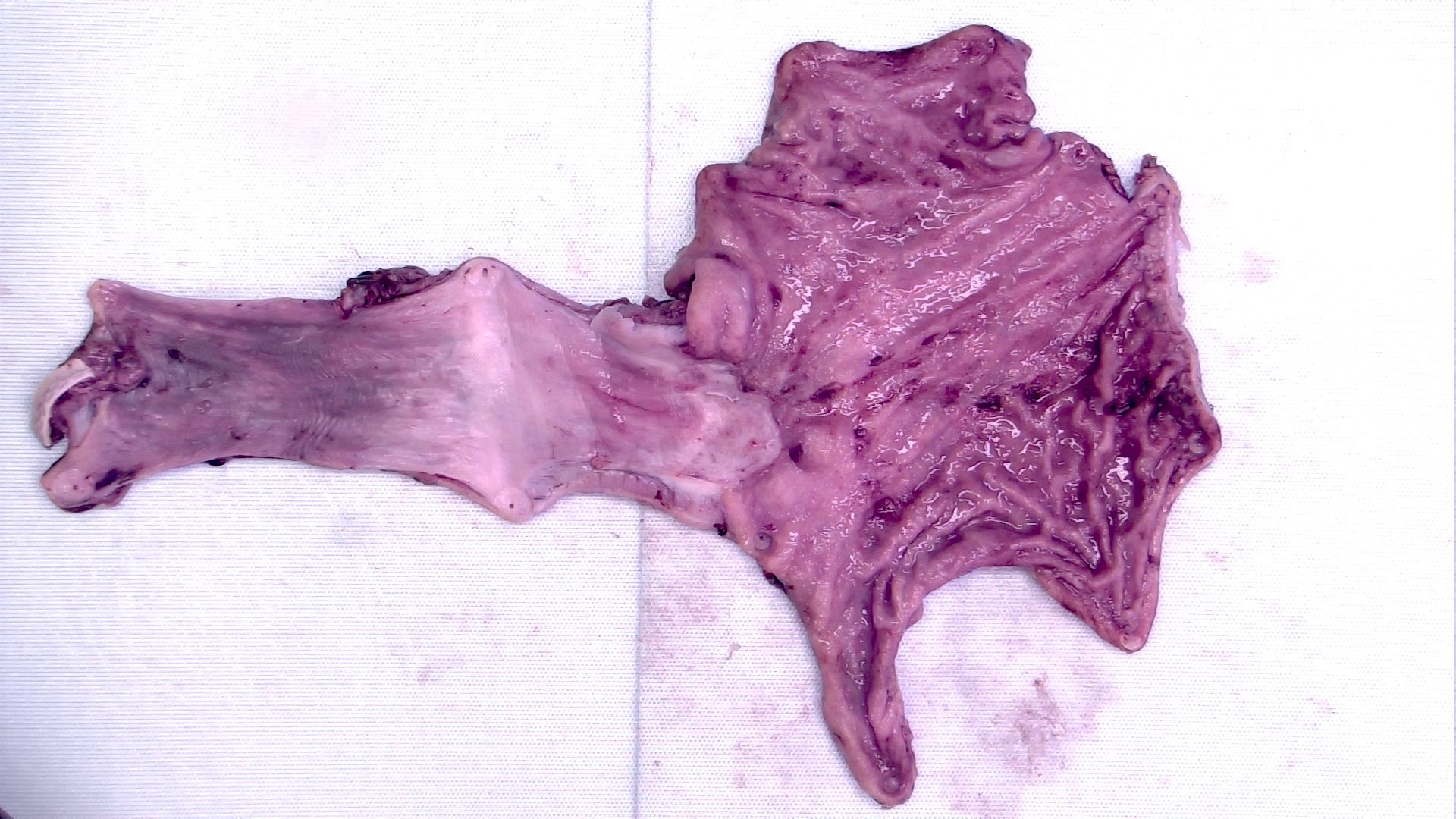
Distal esophagus and GE junction tumor
Ulcer at GE junction
Treated tumor
Frozen section description
Intraoperative frozen section analysis is usually performed for assessment of surgical margin status and to rule out involvement by distant metastases, as surgical management may not be effective if distant metastases are present
Frozen section images
Contributed by Avani Pendse, M.D., Ph.D.
Positive margin, frozen section
Positive margin, permanent
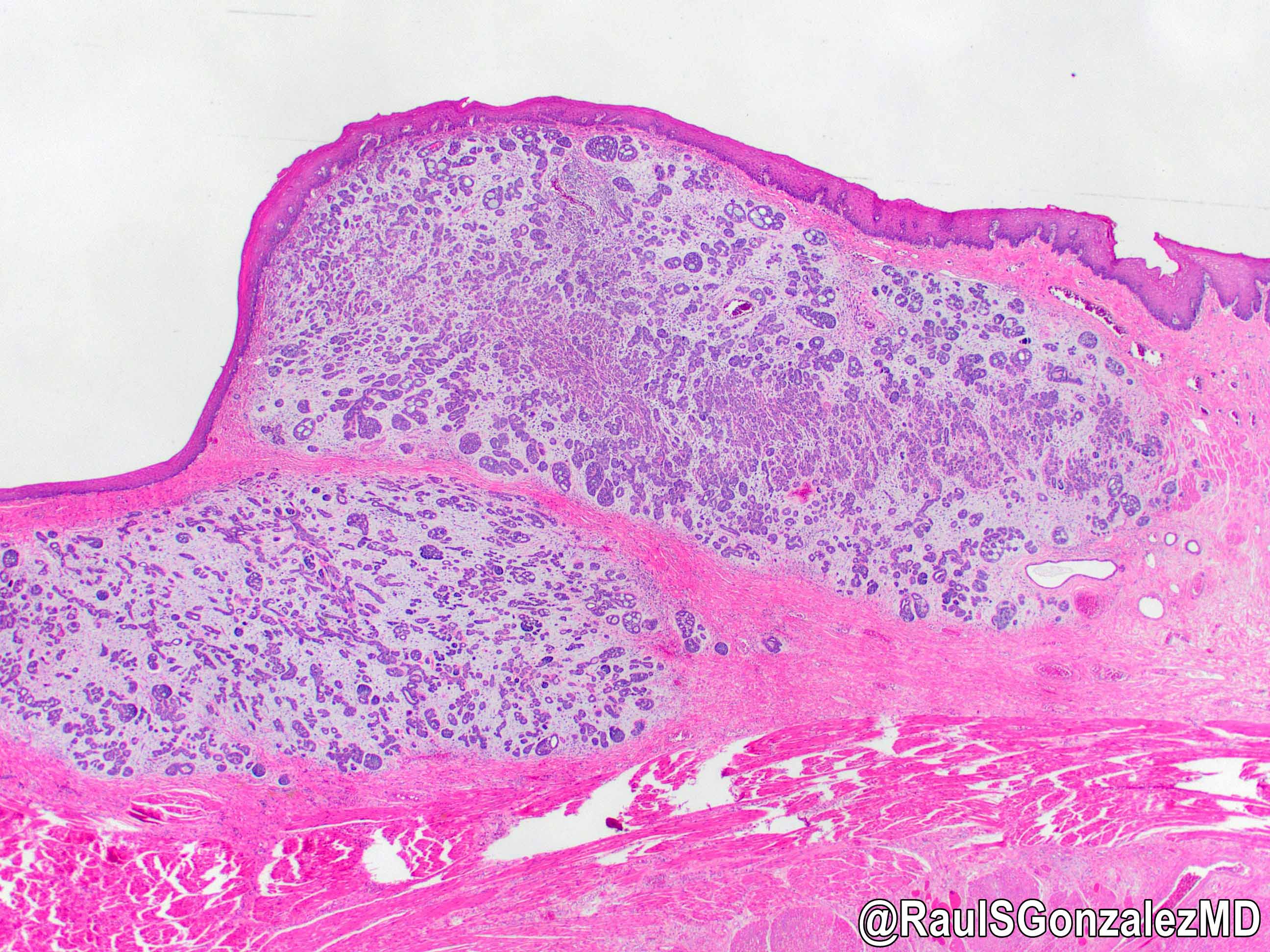
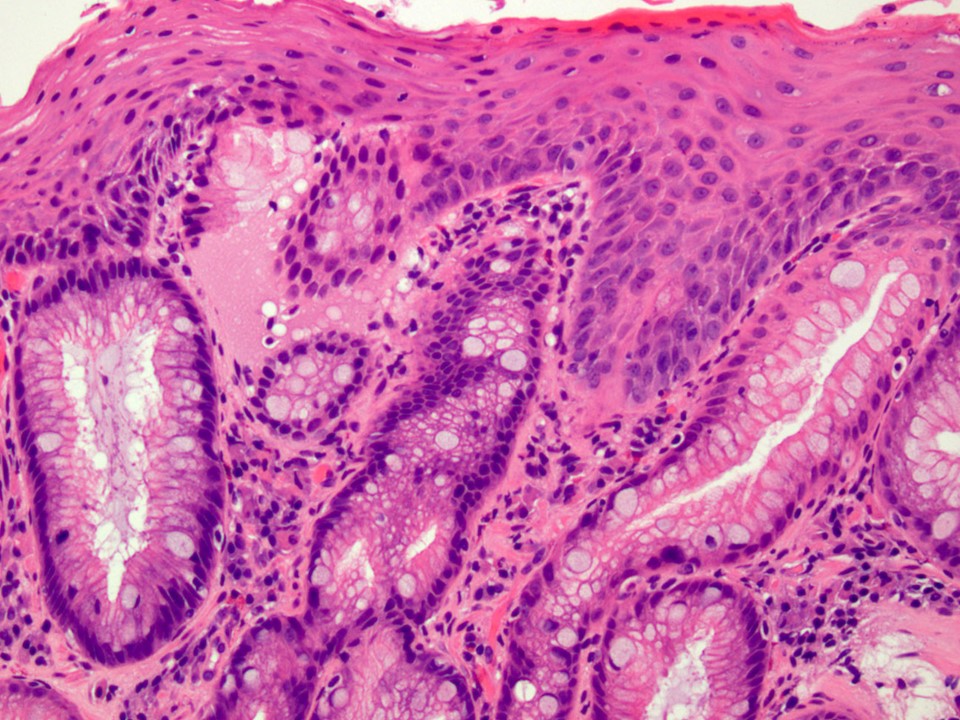
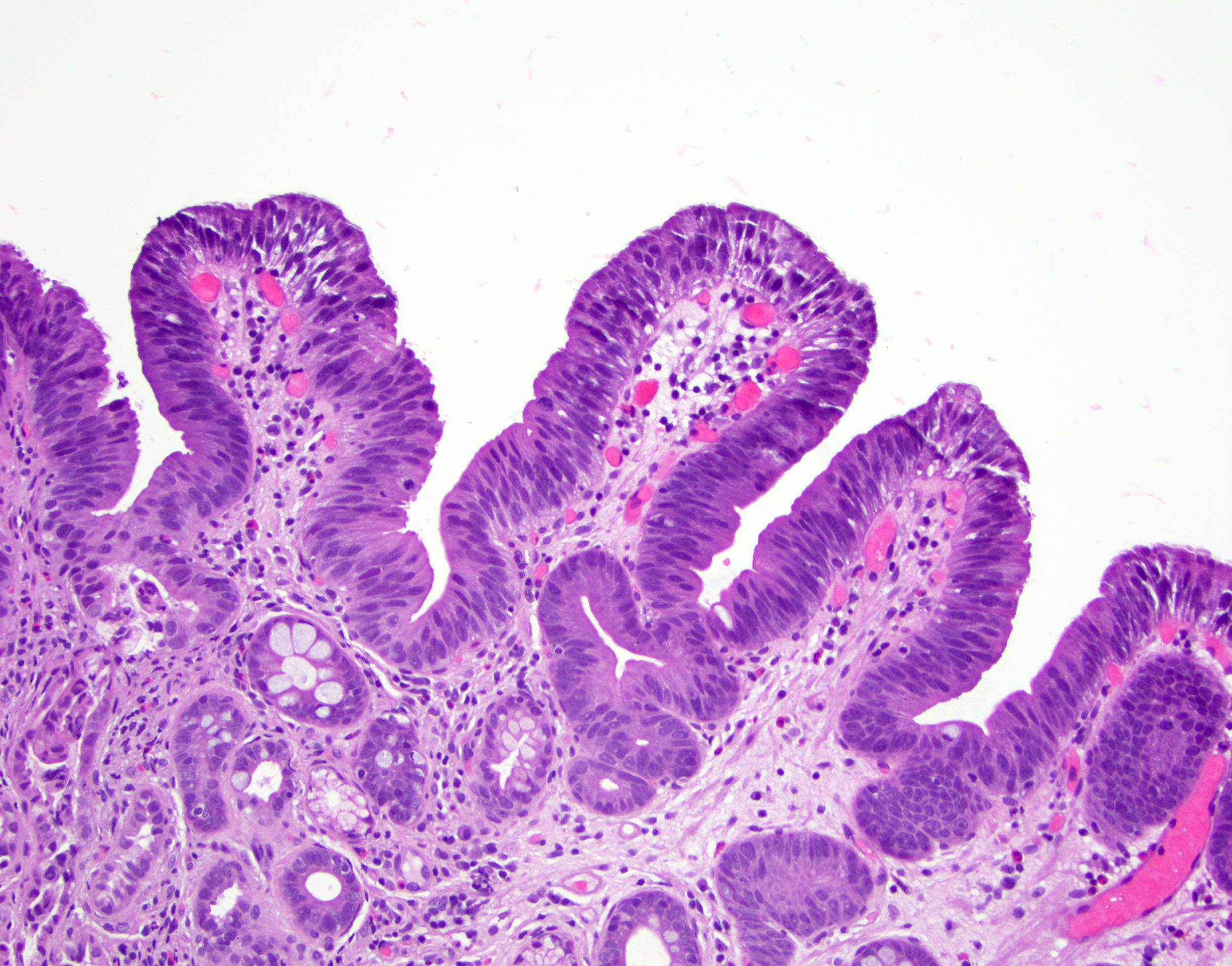
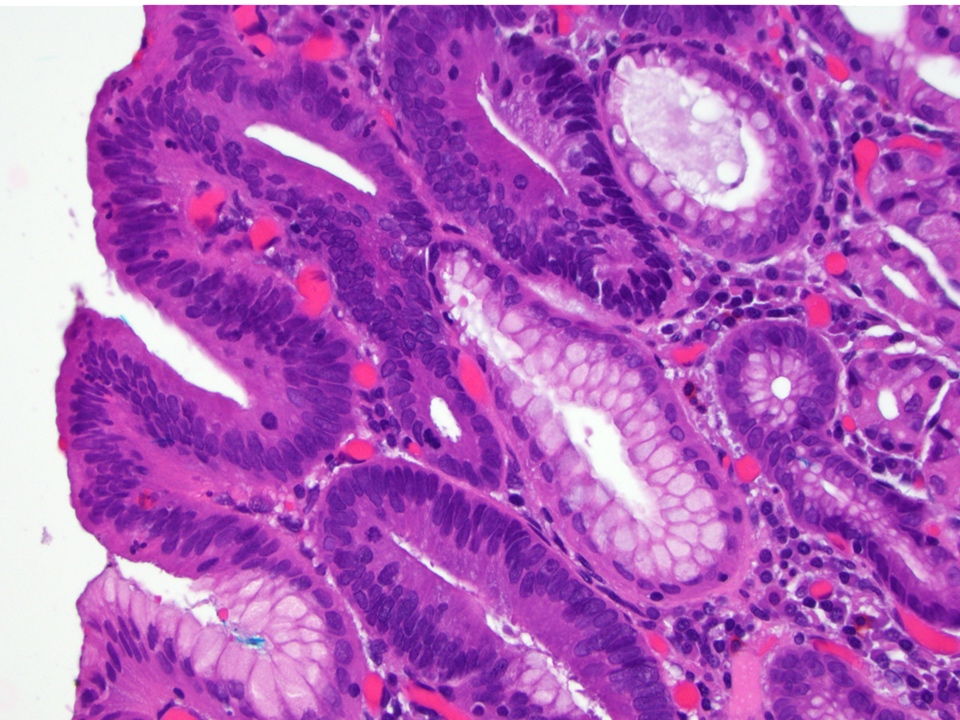
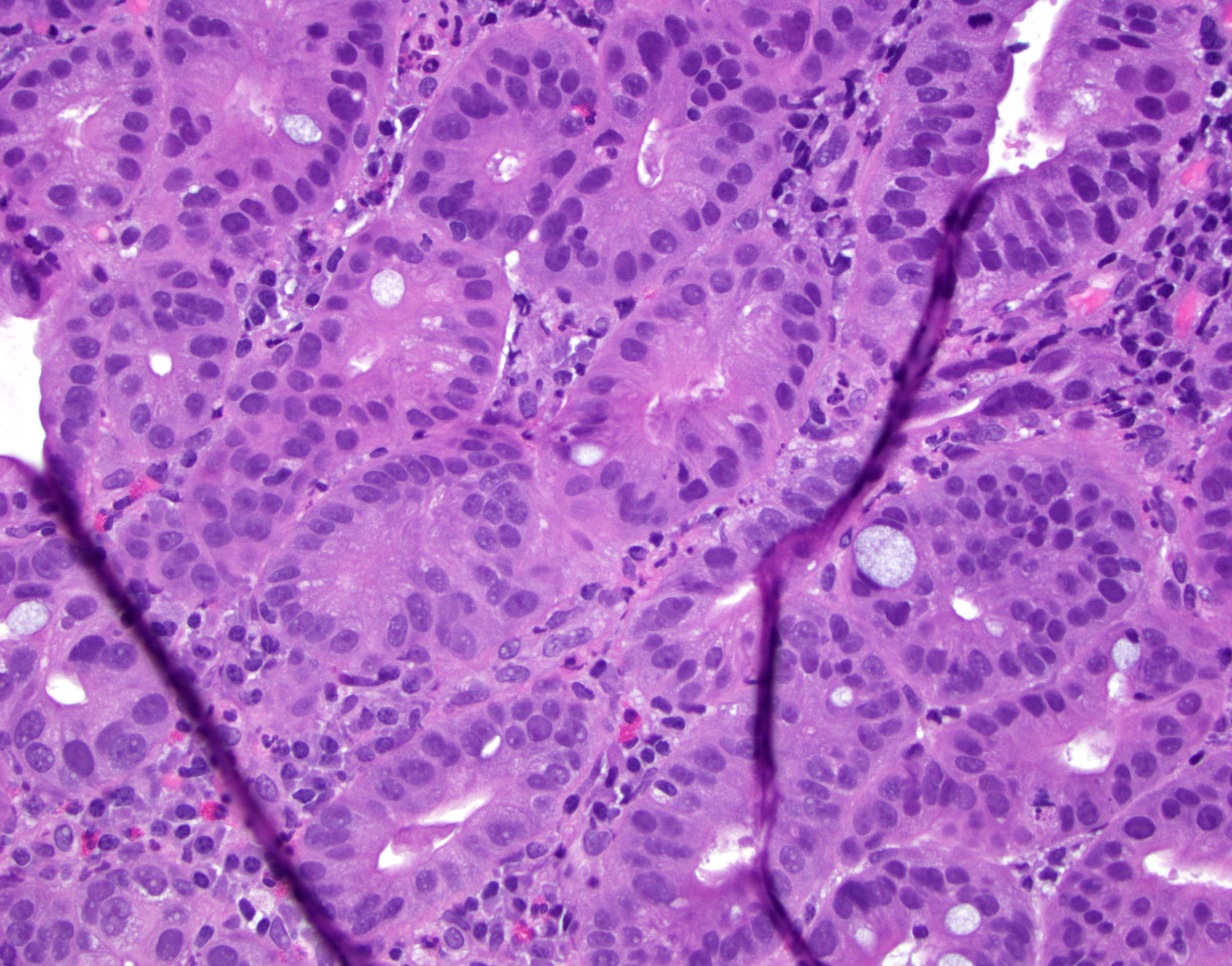
Microscopic (histologic) description
Will show either gastric, intestinal or mixed lineage
If in the lower esophagus, may show adjacent Barrett esophagus with intestinal metaplasia or dysplasia
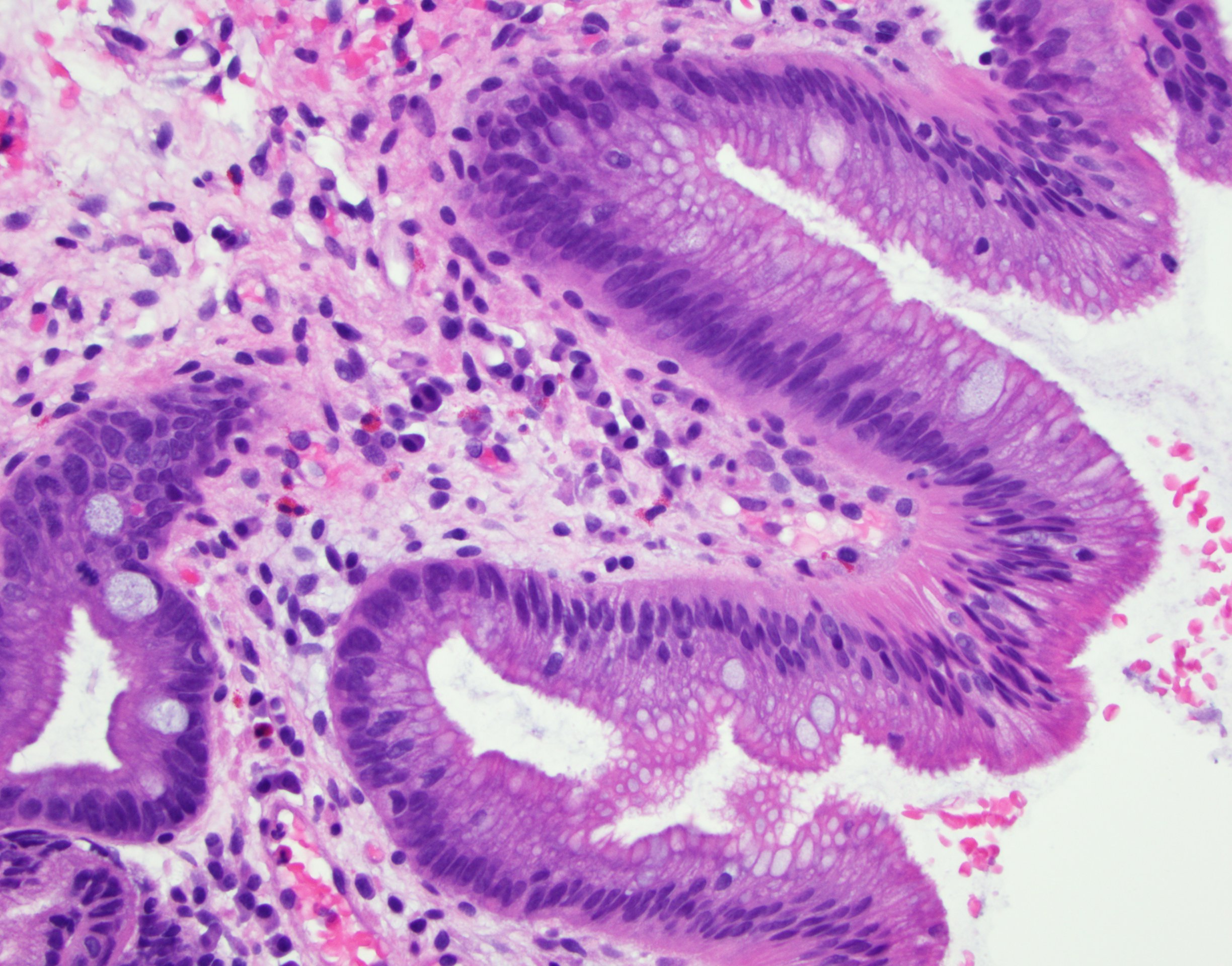
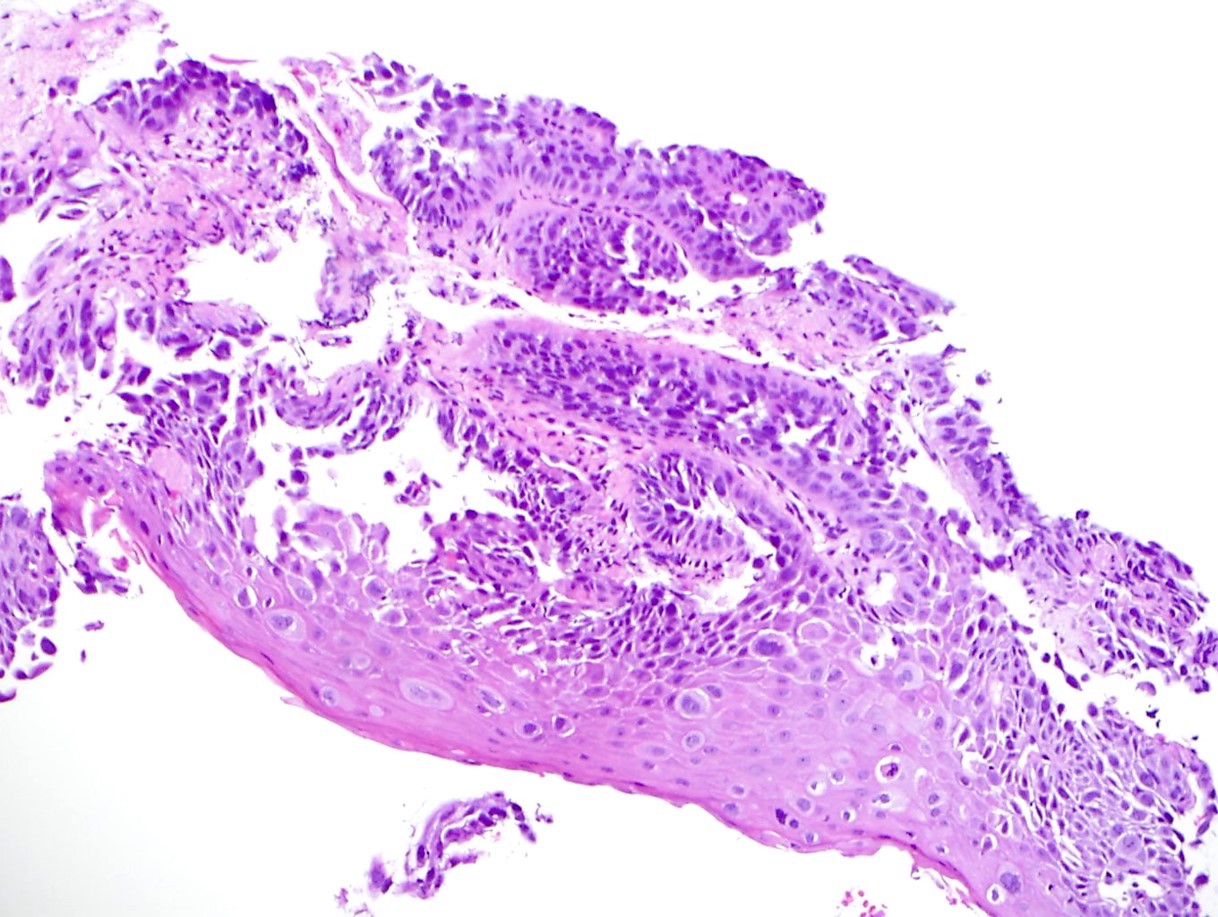
Dysplasia may be low or high grade
Low grade will have cytological atypia but little to no architectural atypia
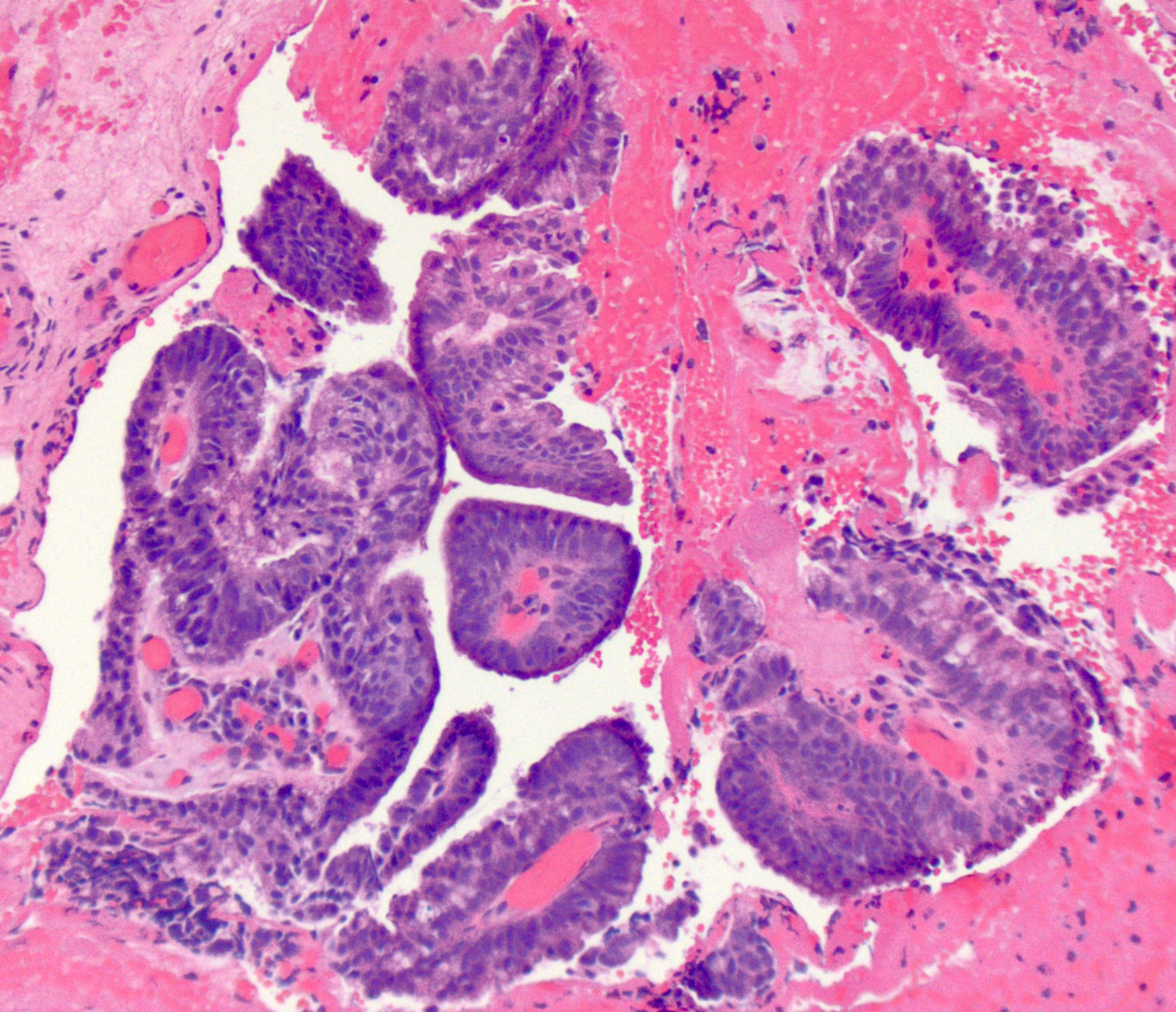
High grade will have increased cytologic atypia and architectural abnormalities but the dysplastic epithelial cells are still limited by basement membrane
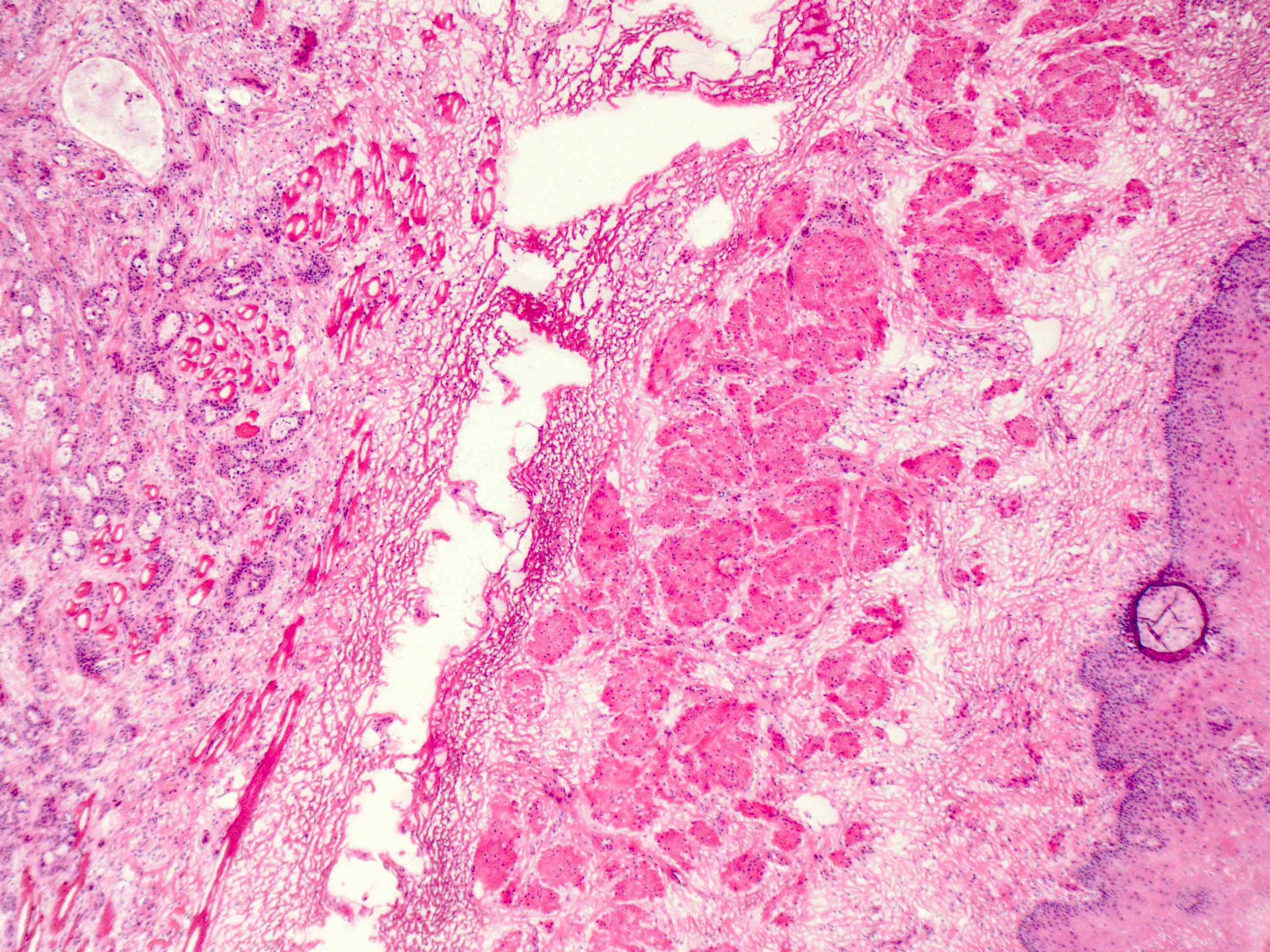
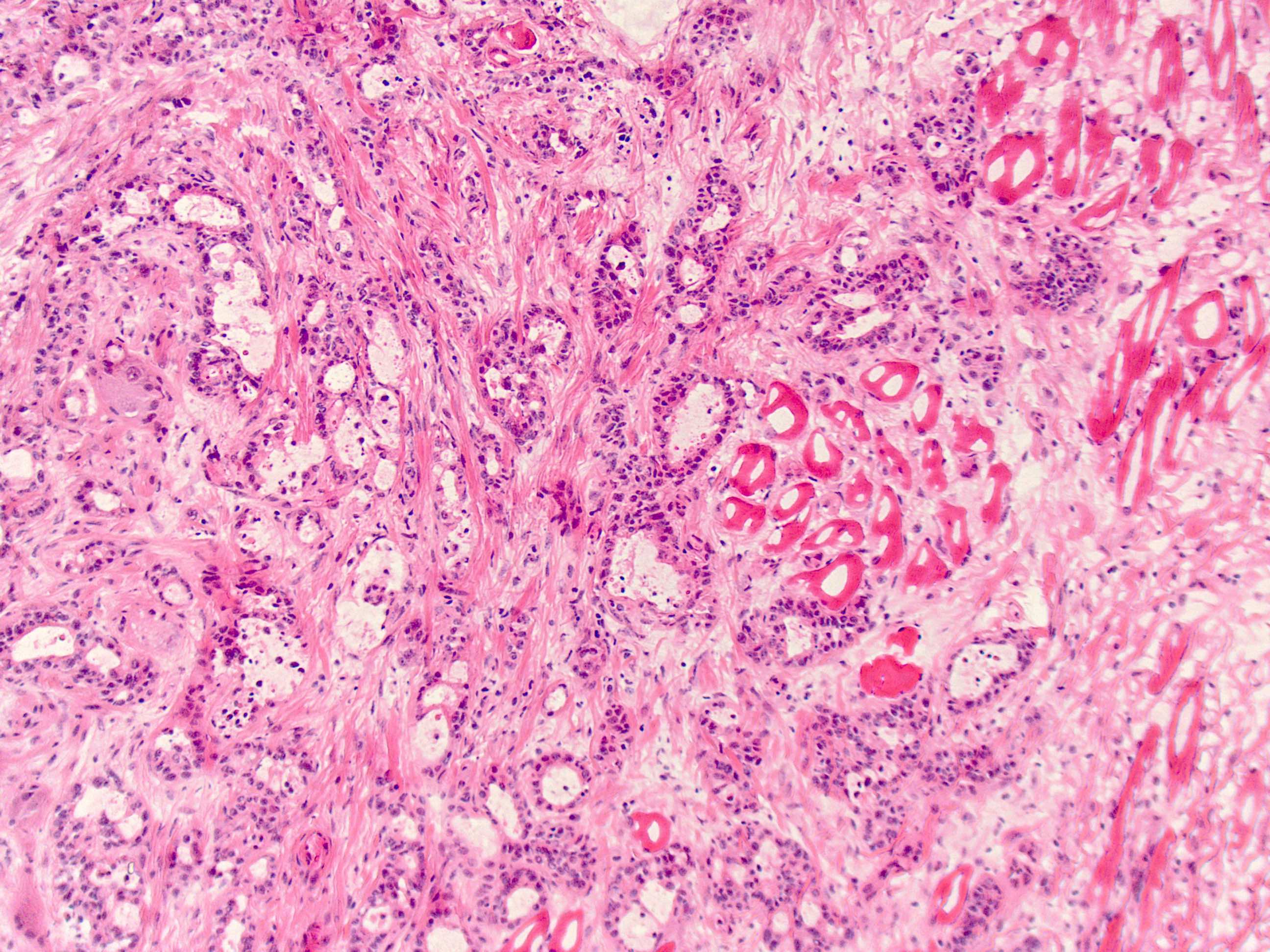
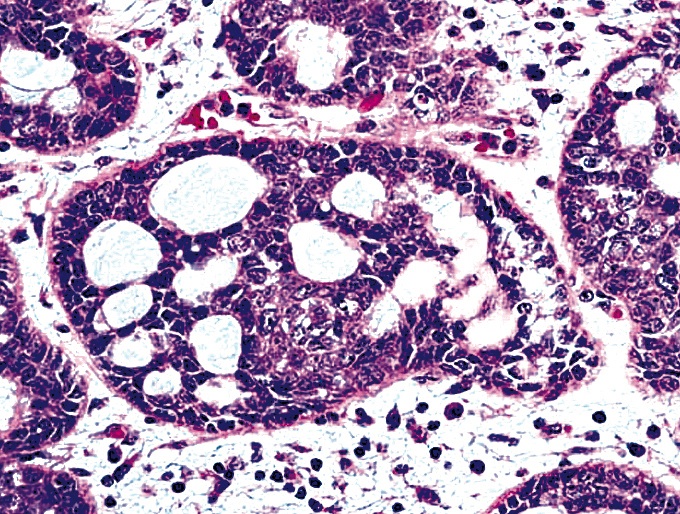
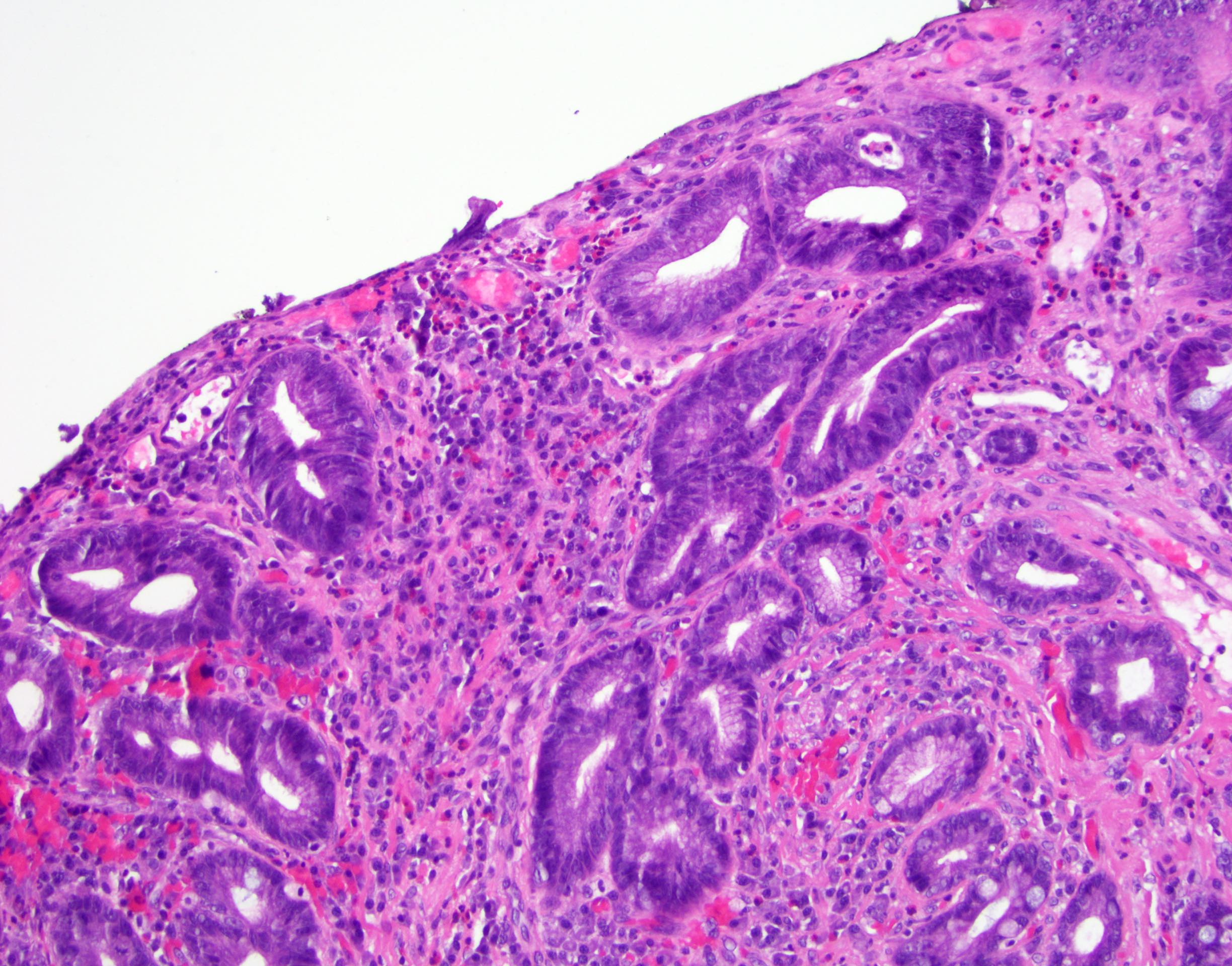
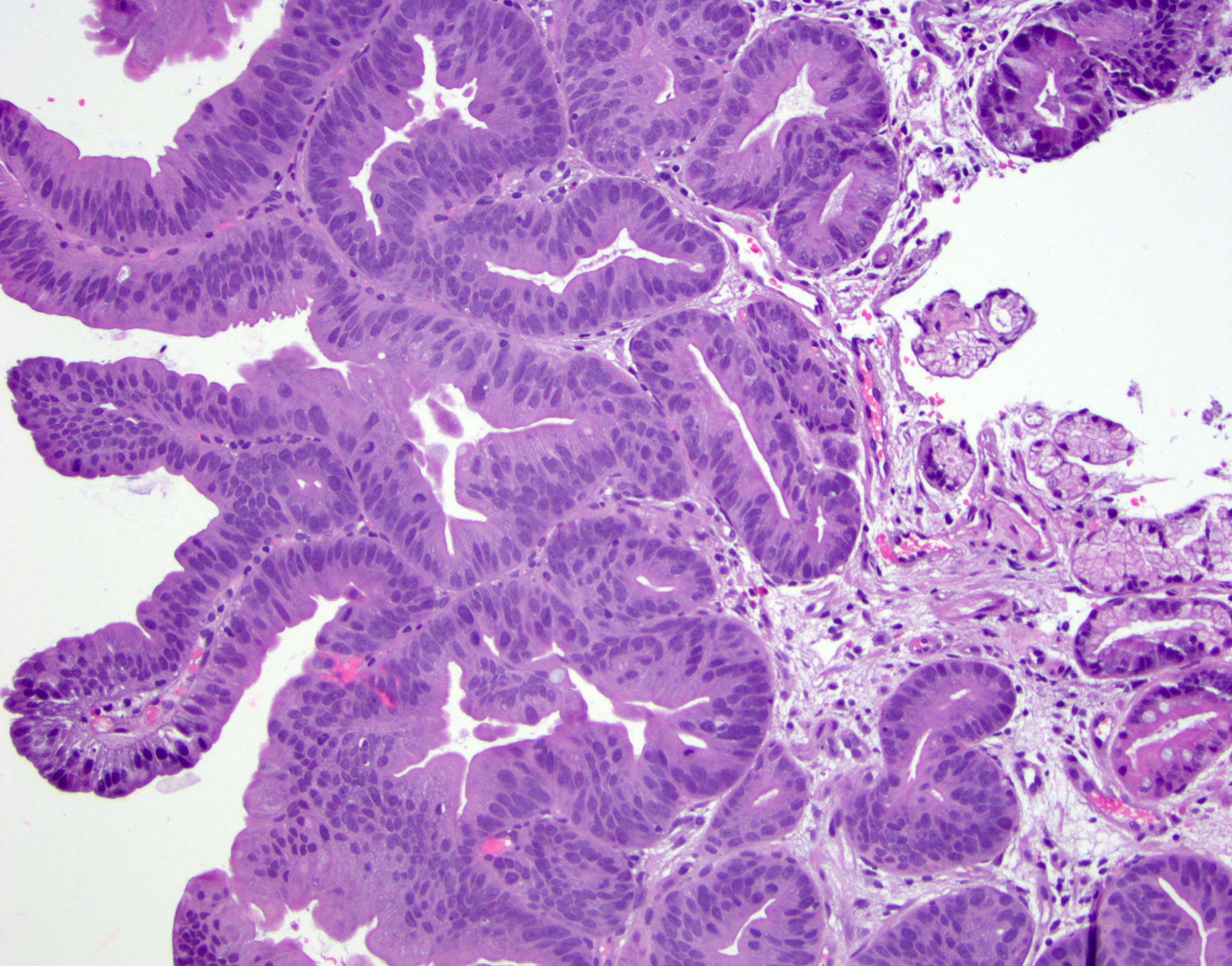
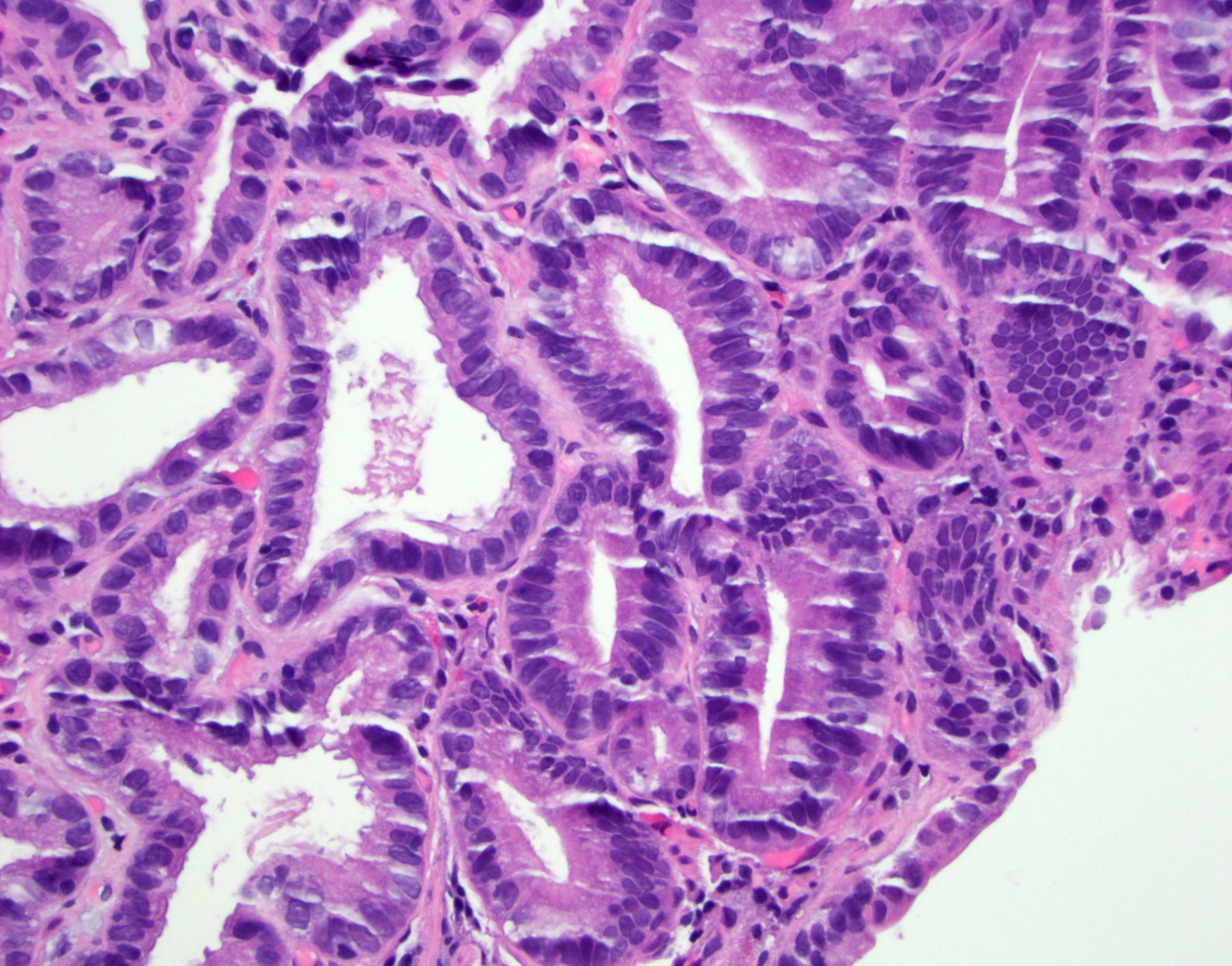
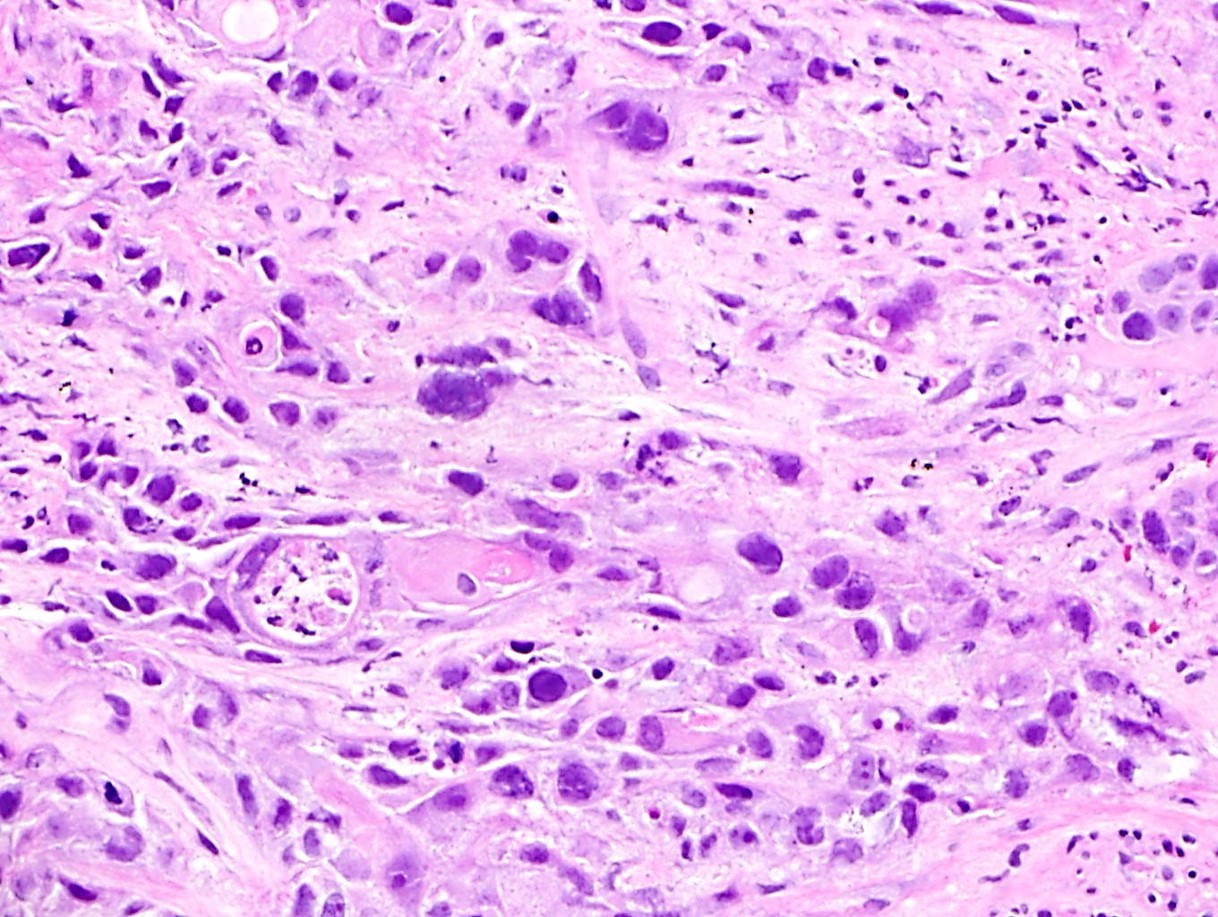
Classified as having tubular, papillary, mucinous and signet ring cell patterns
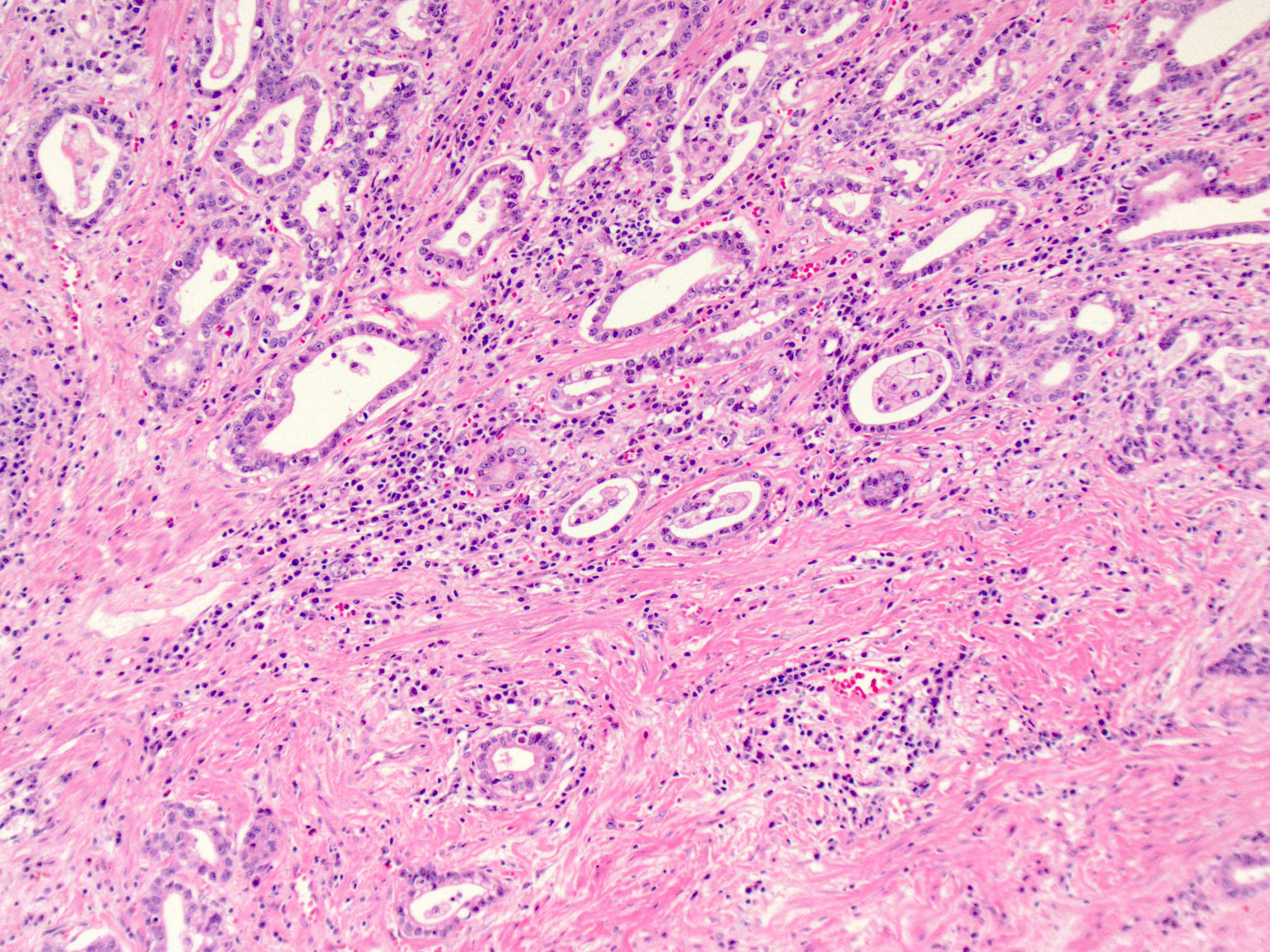
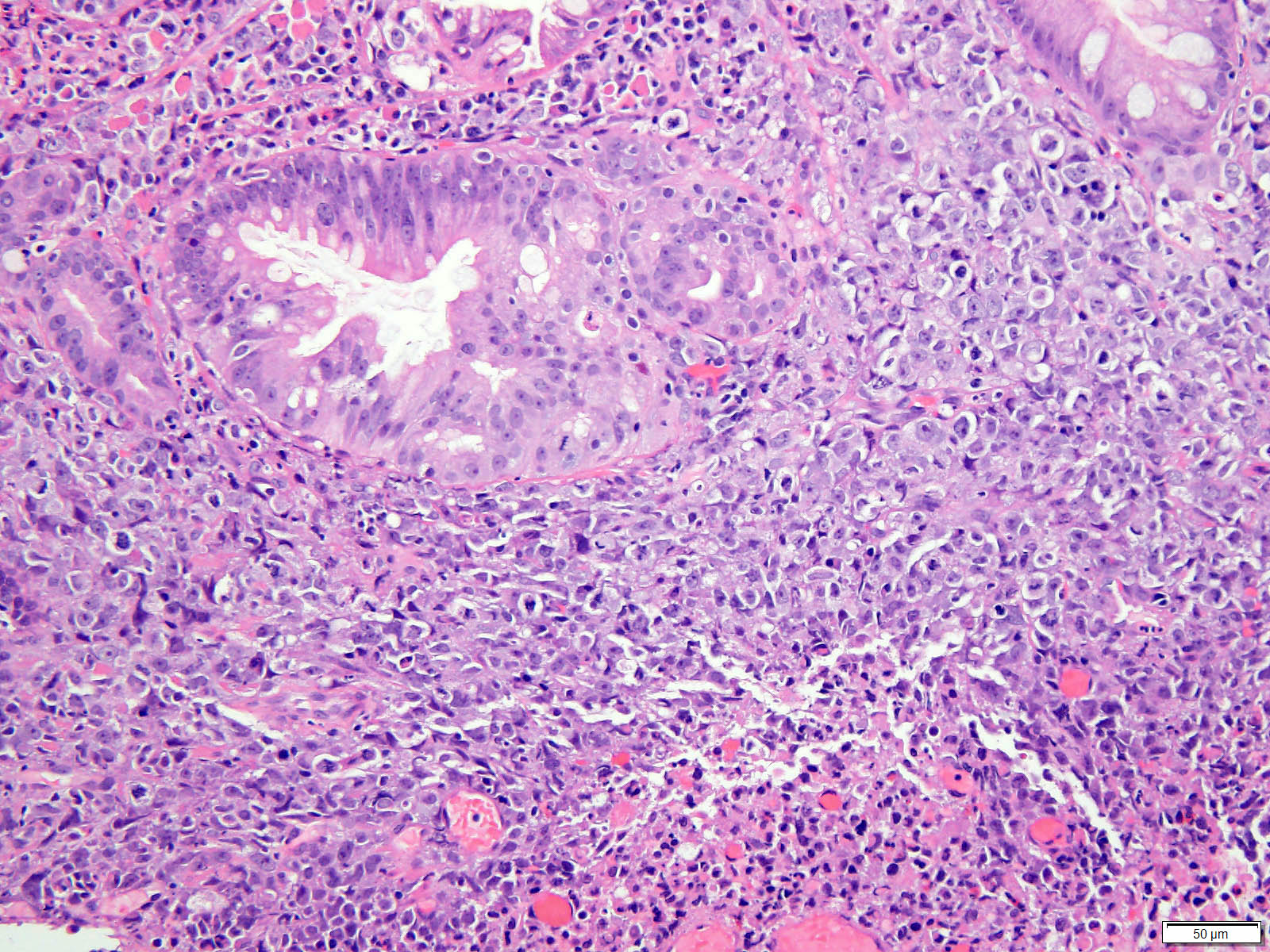
Tubular pattern is most common, with irregular, single or anastomosing tubular glandular structures and a single or stratified layer of malignant epithelium
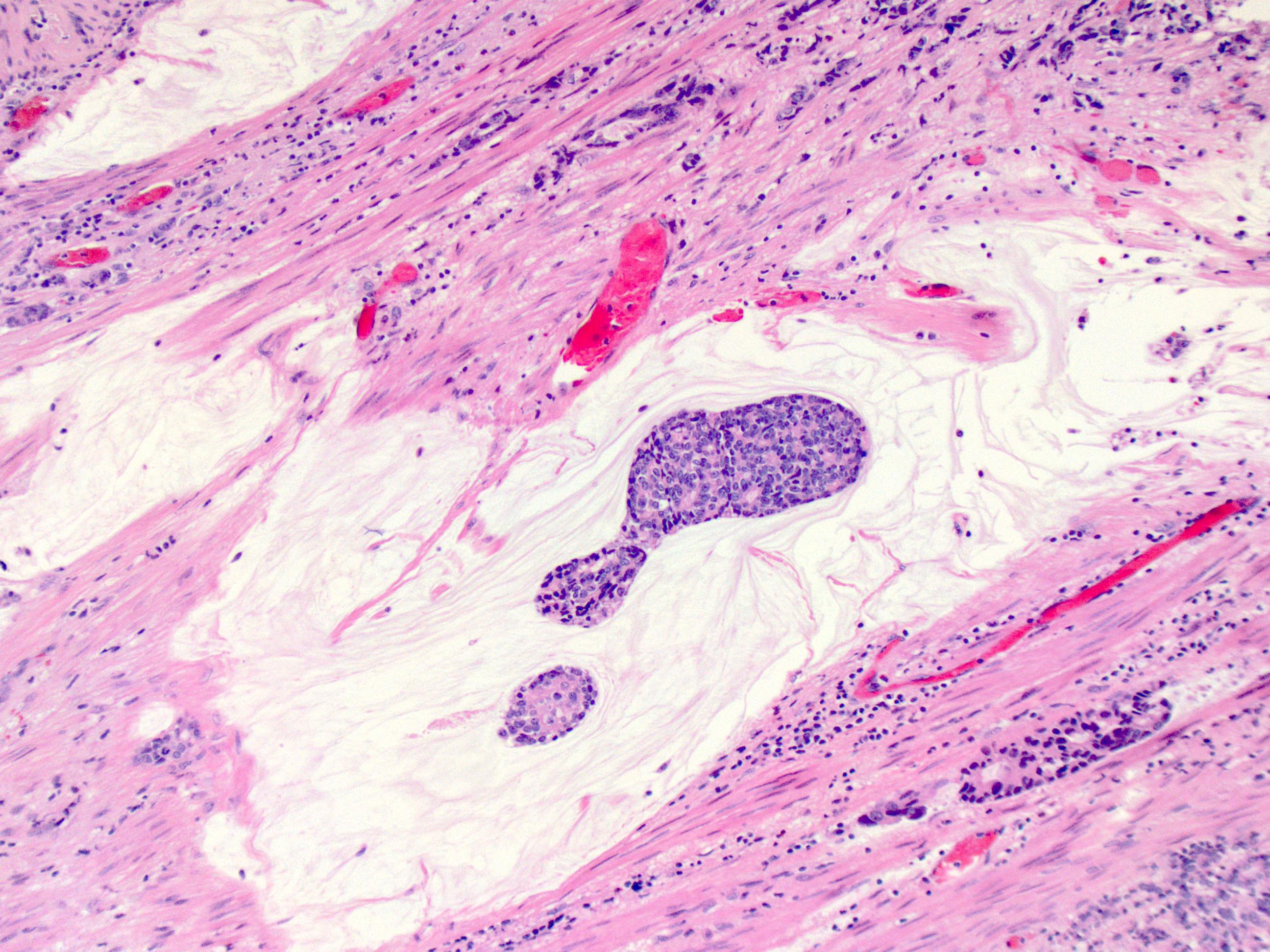
Mucin production is variable
~50% of all esophageal adenocarcinomas are treated preoperatively with chemoradiation and therefore will show histologic changes consistent with treatment effect
These include mucin pools that are acellular or containing small foci of residual adenocarcinoma
Cytologic changes in the treated tumor cells include cytoplasmic eosinophilia, nuclear pyknosis and nuclear karyorrhexis
Only residual viable tumor is considered in the determination of tumor stage and not the acellular mucin
Similarly, lymph nodes with acellular mucin pools and therapy associated fibrosis but without viable tumor cells should be classified as no tumor within the lymph nodes (Mod Pathol 2018;31:4)
Modified Ryan scheme for tumor regression score adapted by the College of American Pathologists (Histopathology 2005;47:141)
0: no viable cells (complete response)
1: single cells or rare groups of cancer cells (near complete response)
2: residual cancer with evident tumor regression but more than single cells or rare groups of cancer cells (partial response)
3: extensive residual cancer with no evidence of regression (poor or no response)
Microscopic (histologic) images
Contributed by Avani Pendse, M.D., Ph.D.
Tubular pattern
Papillary pattern
Mucinous pattern
Signet ring cell pattern
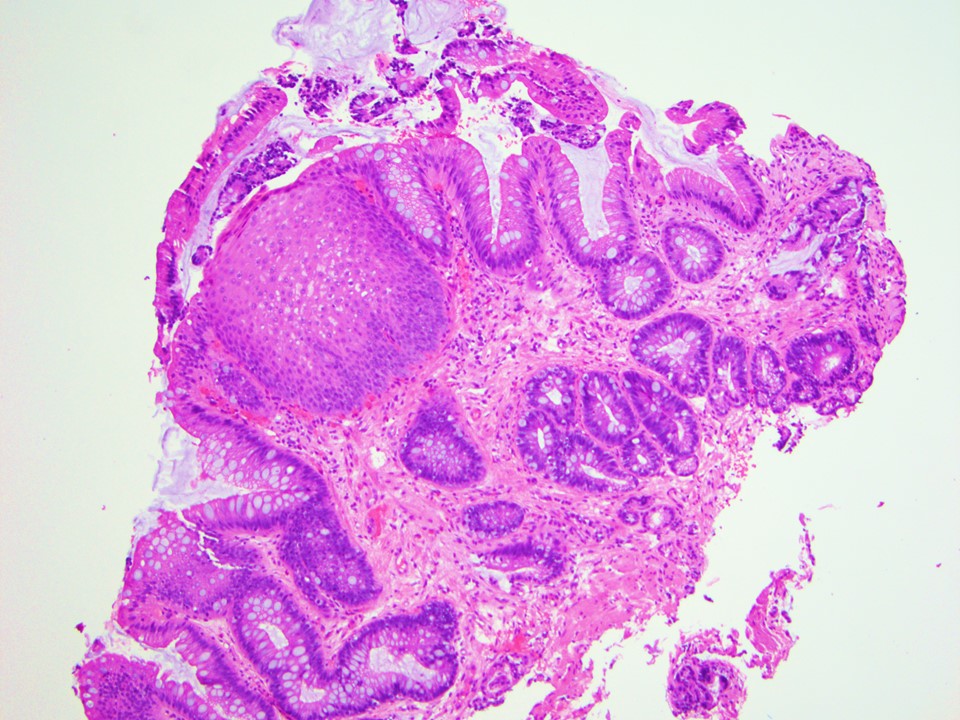
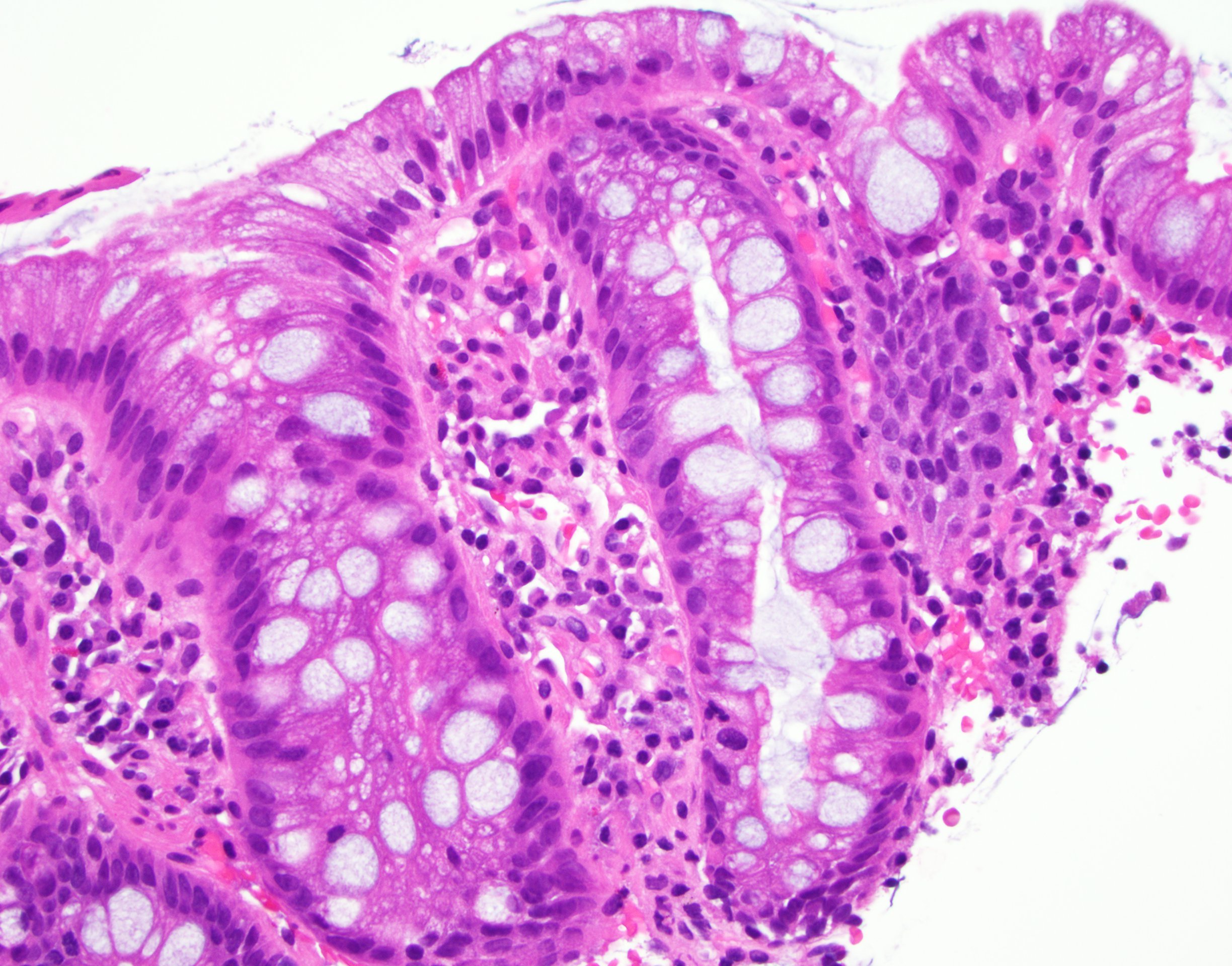
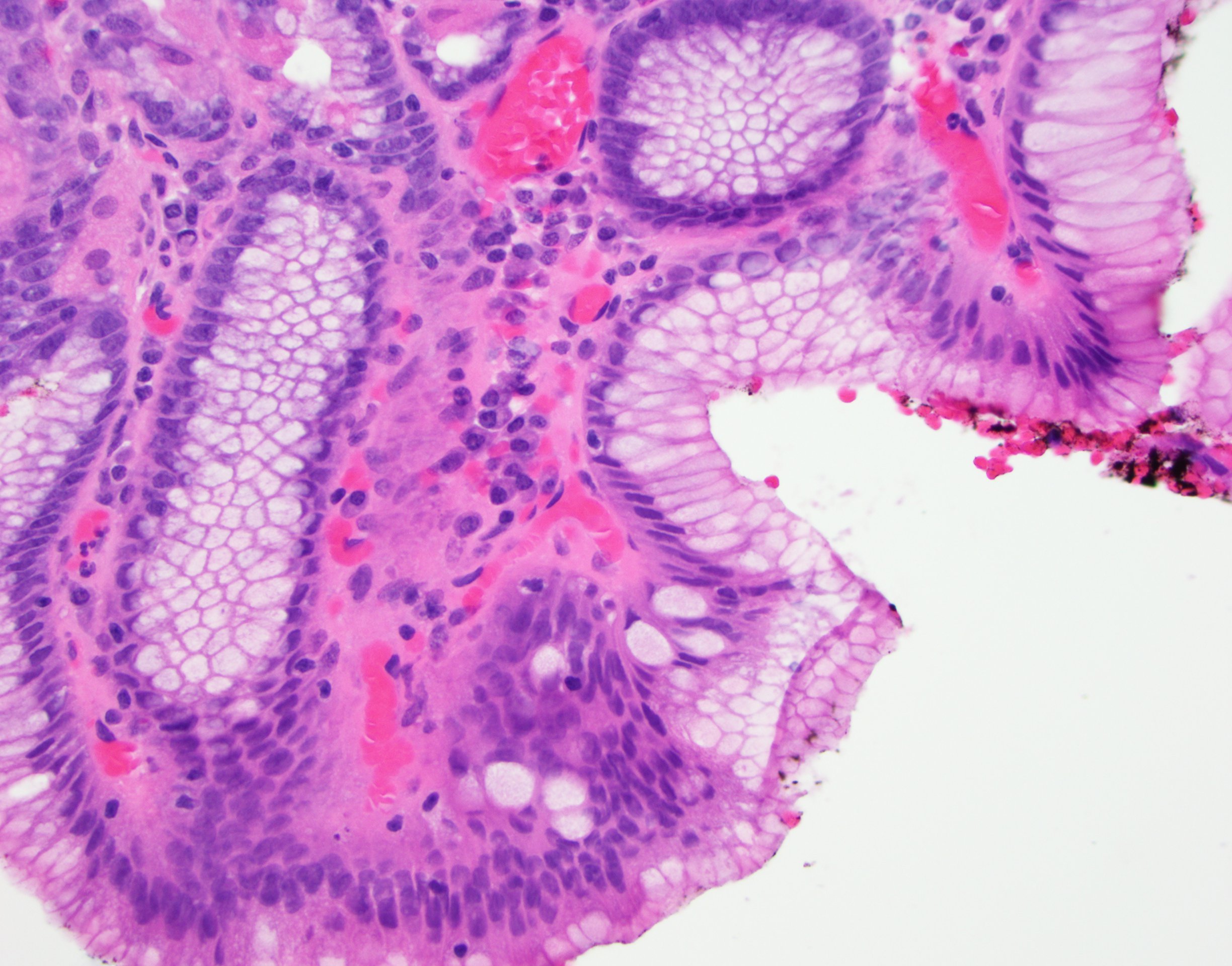
Barrett esophagus
Low grade dysplasia
High grade dysplasia
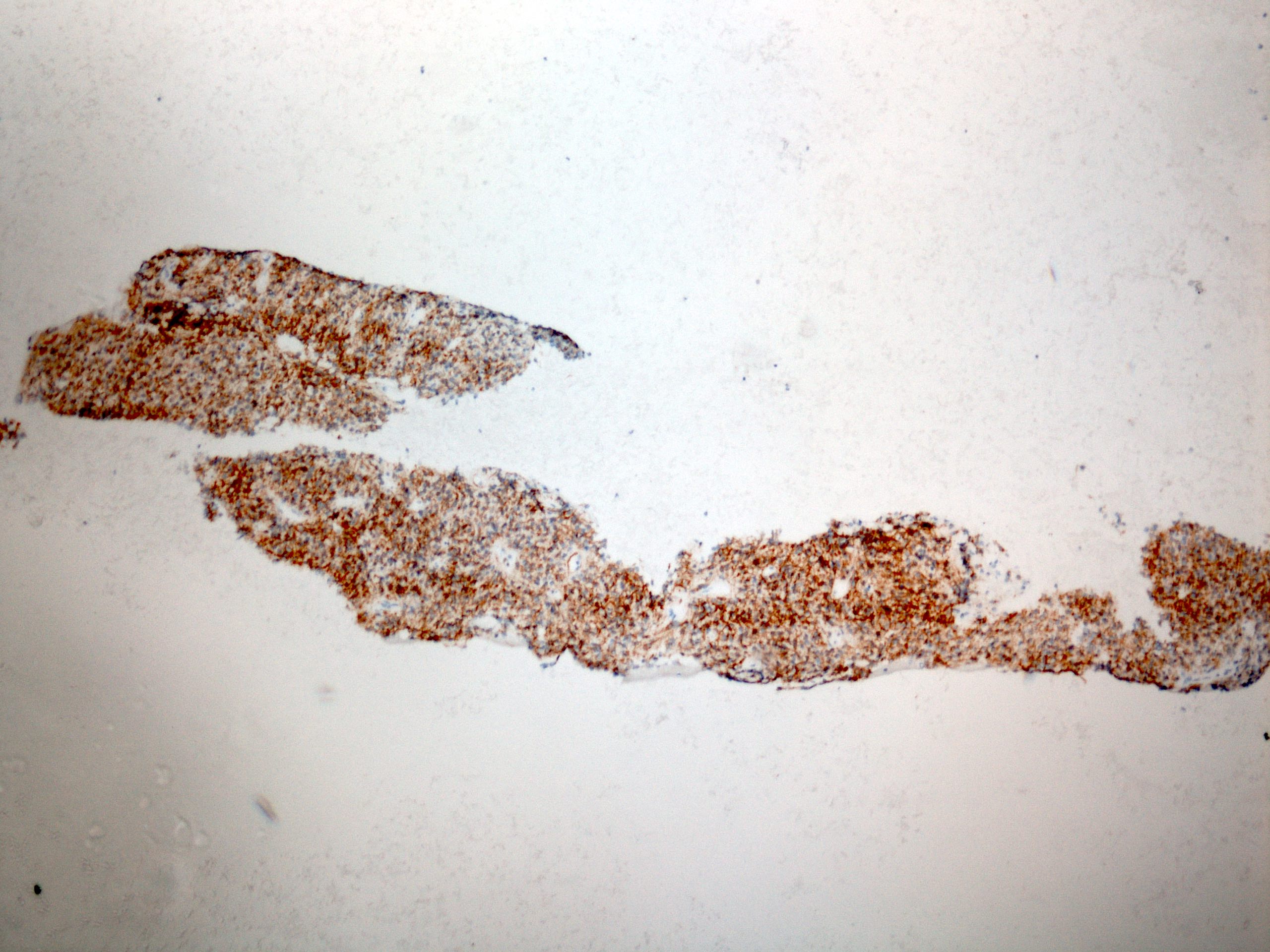
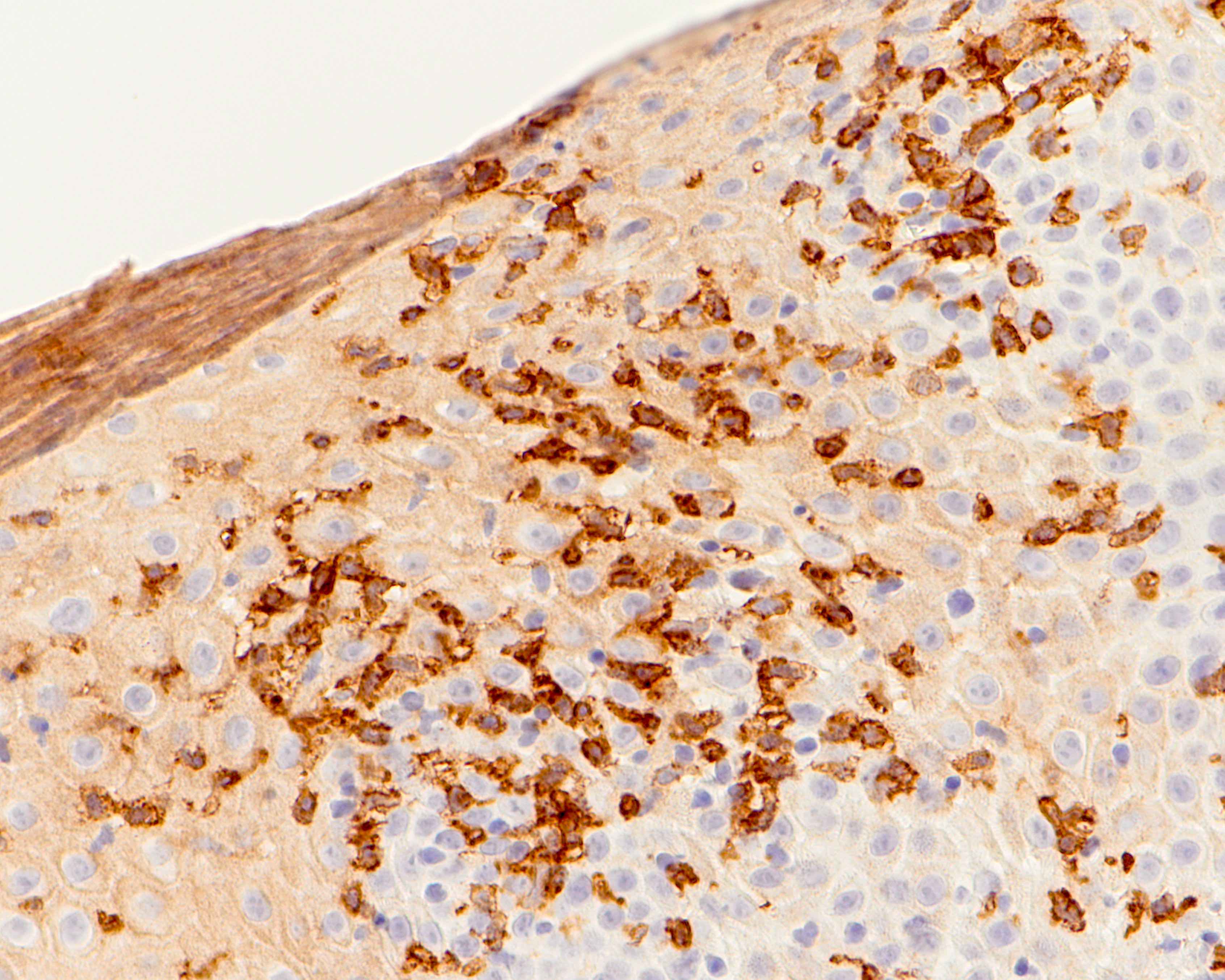
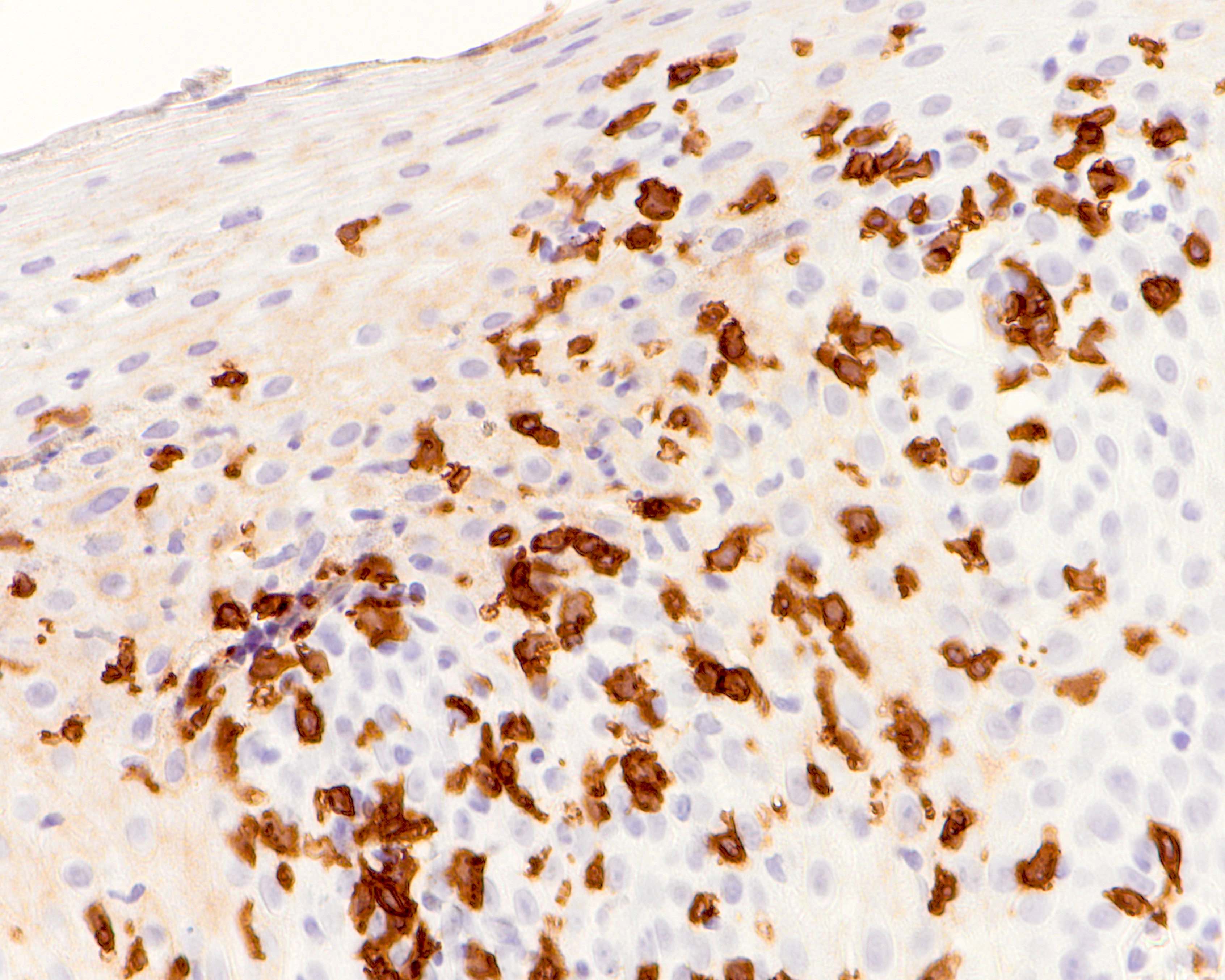
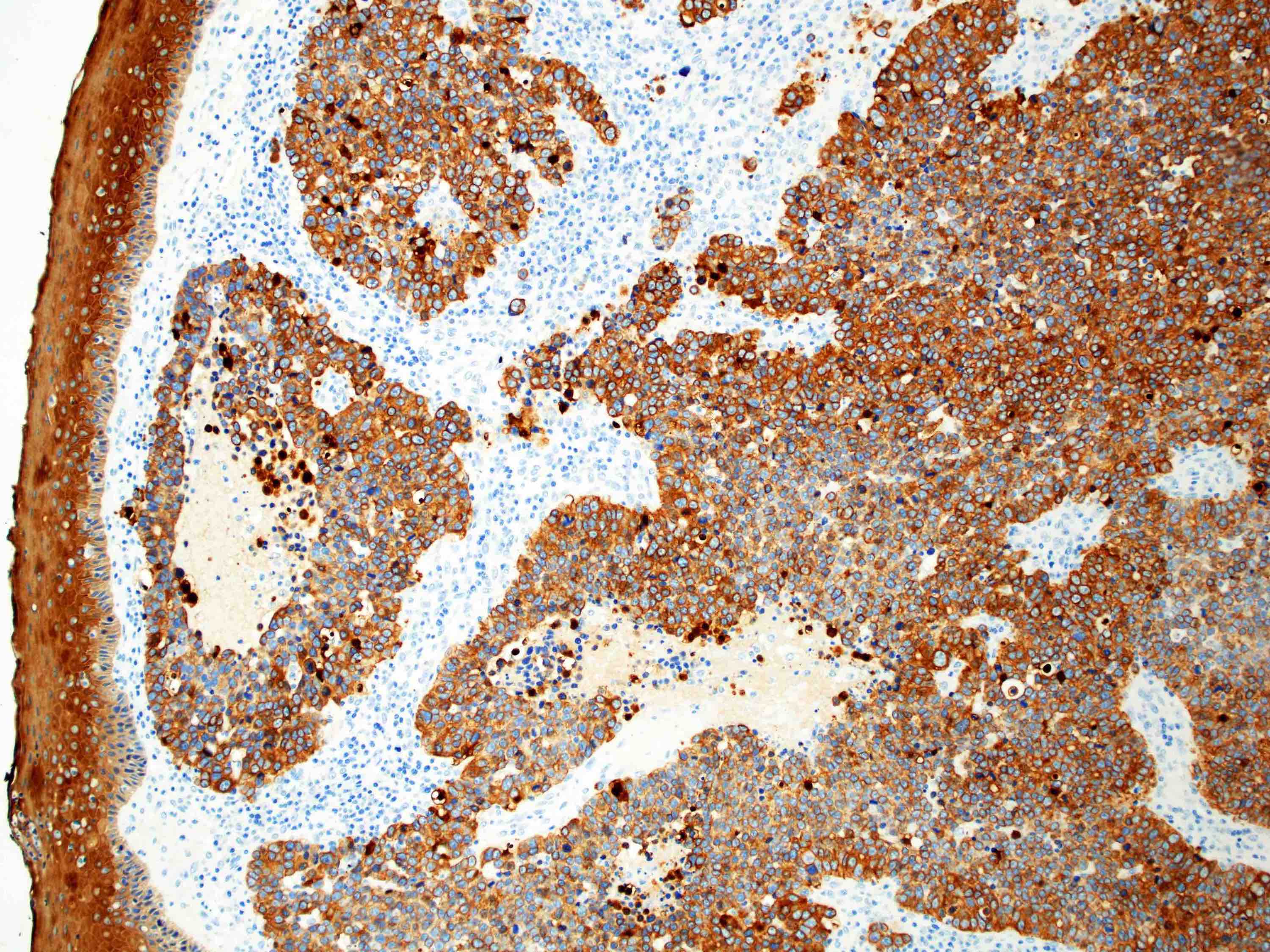
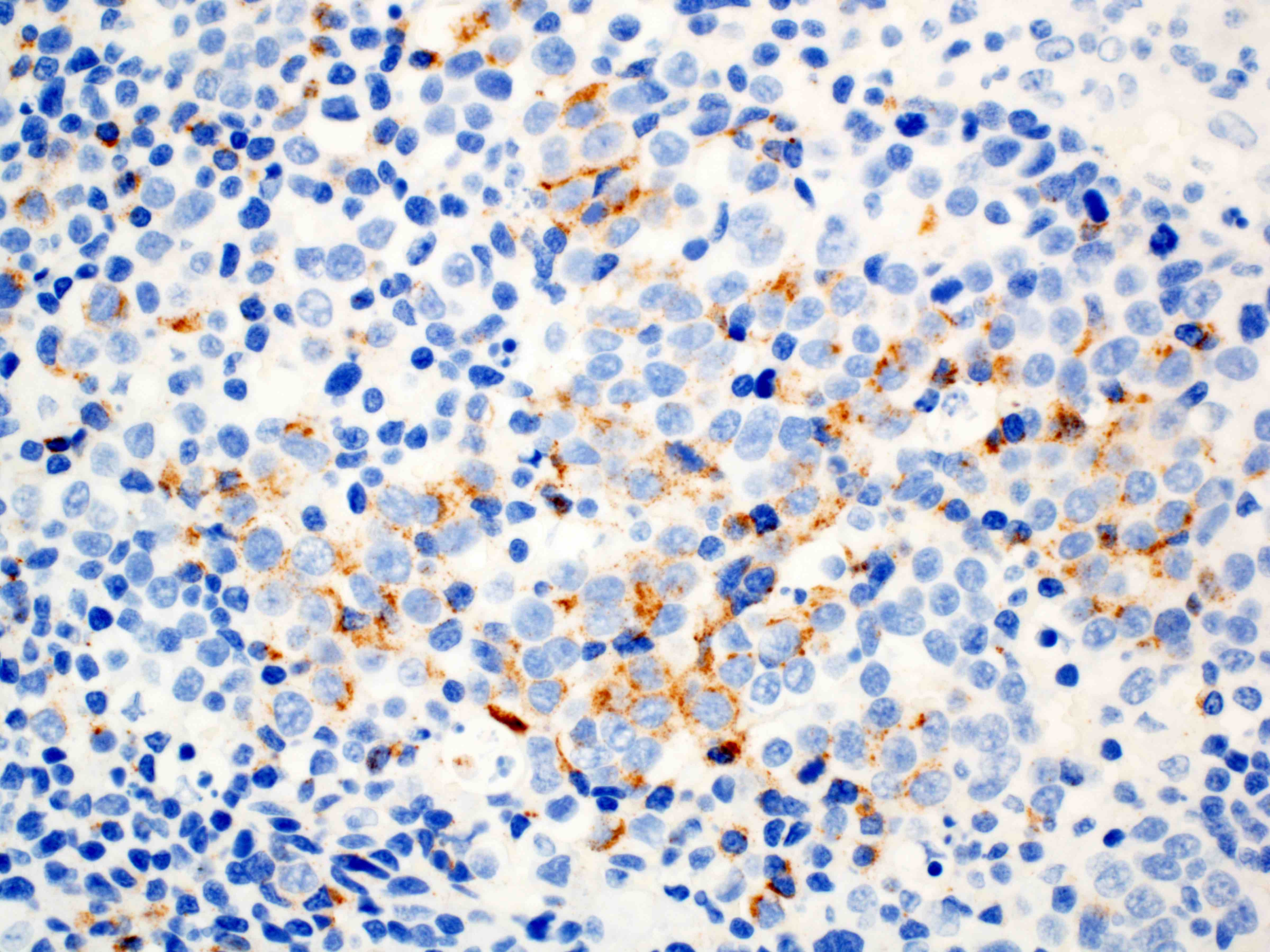
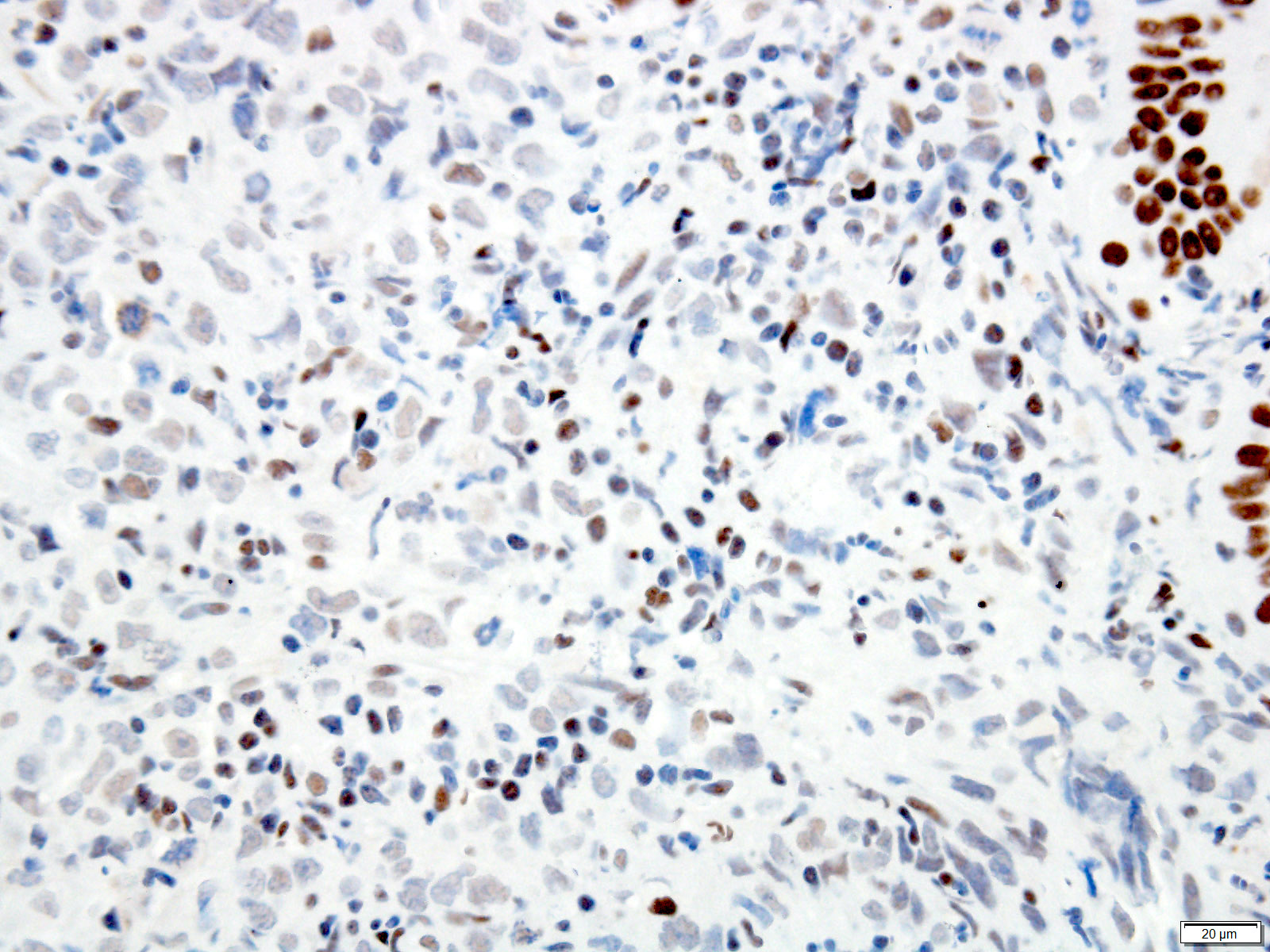
PDL1 positivity
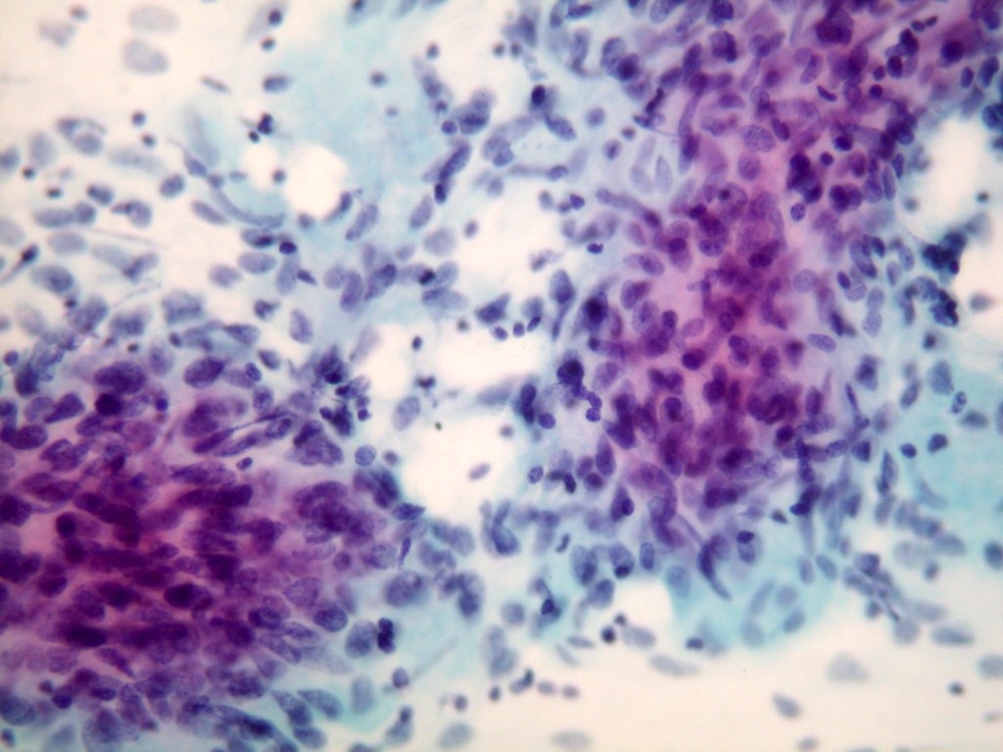
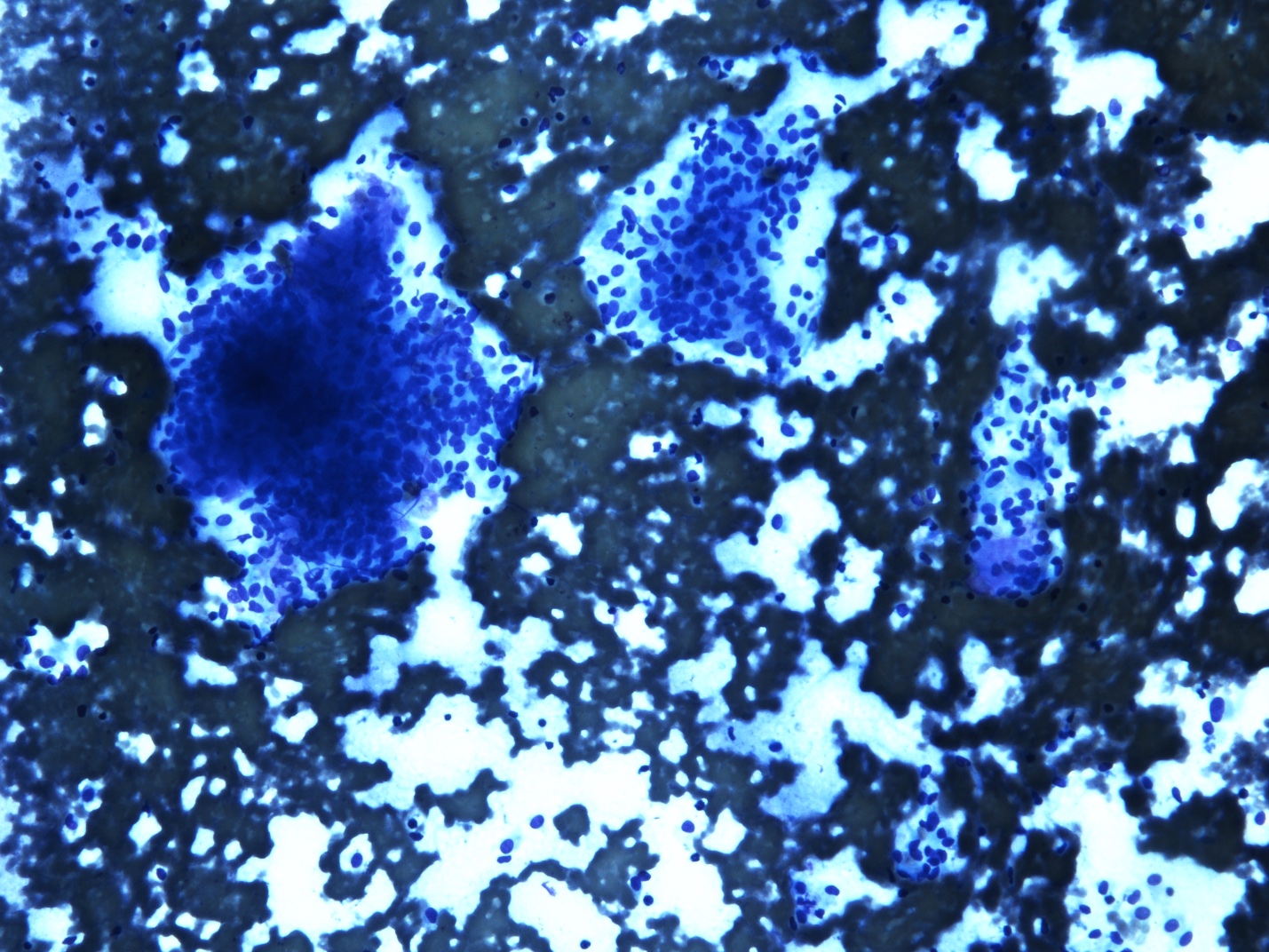
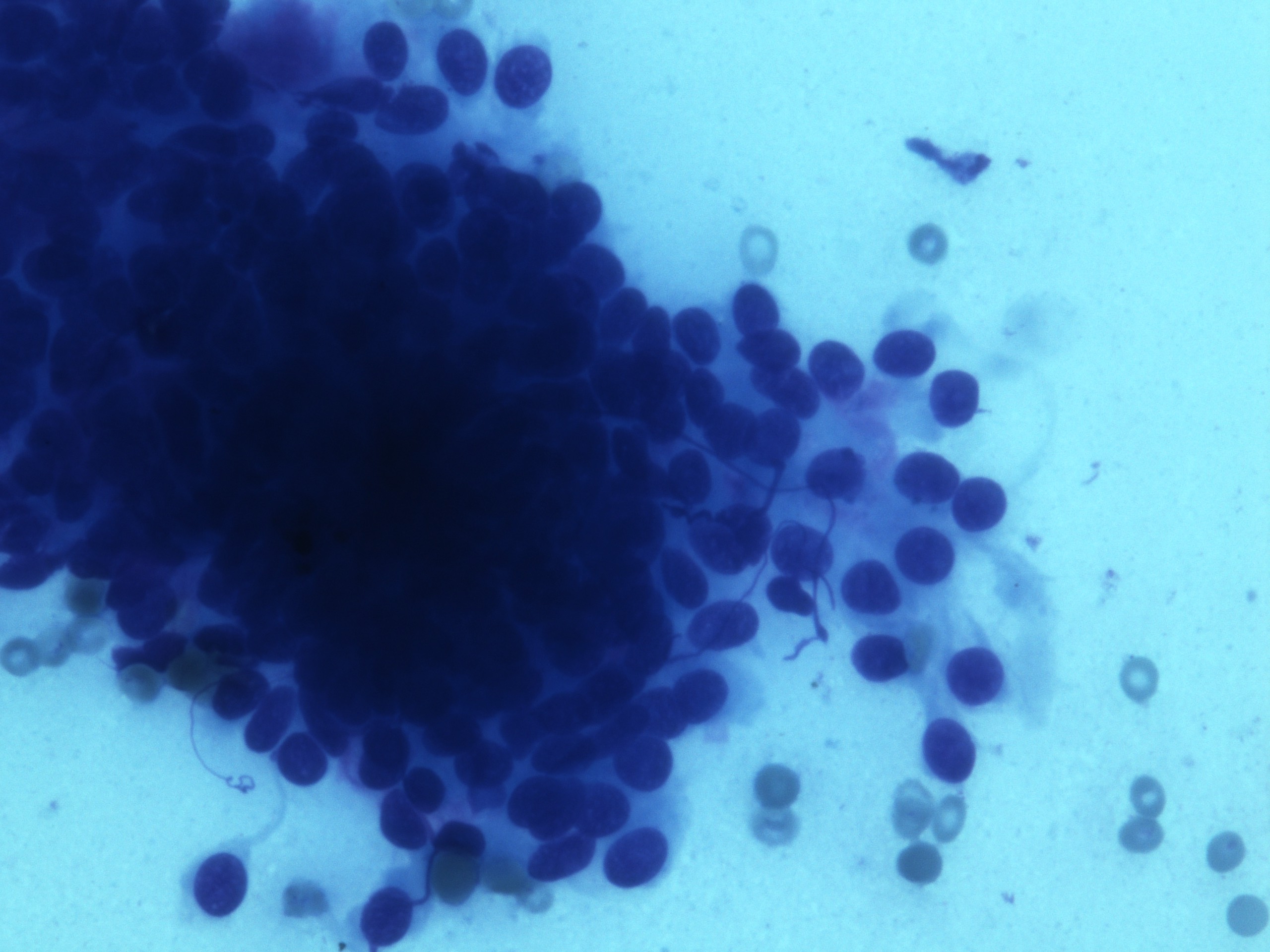
Cytology description
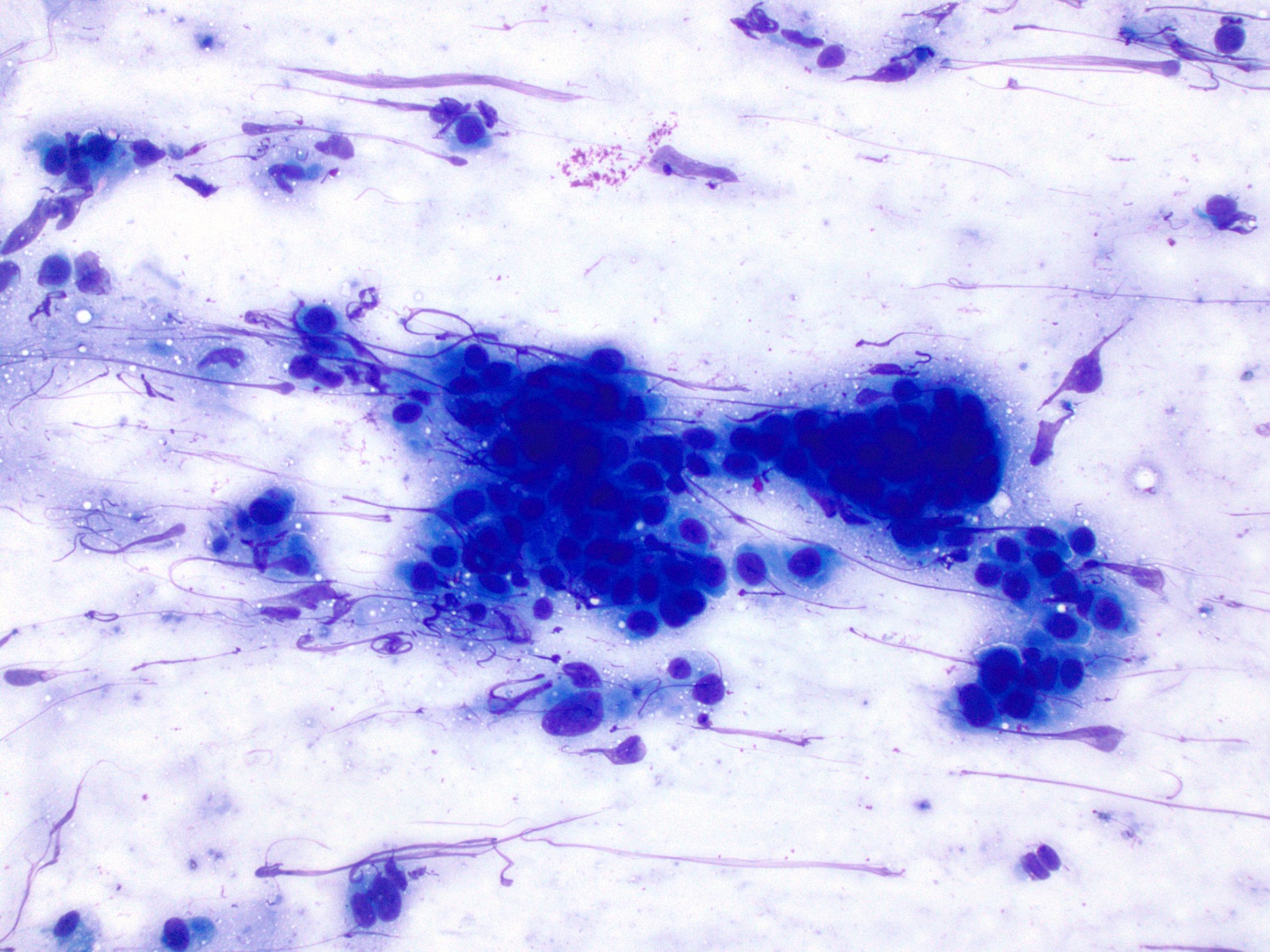
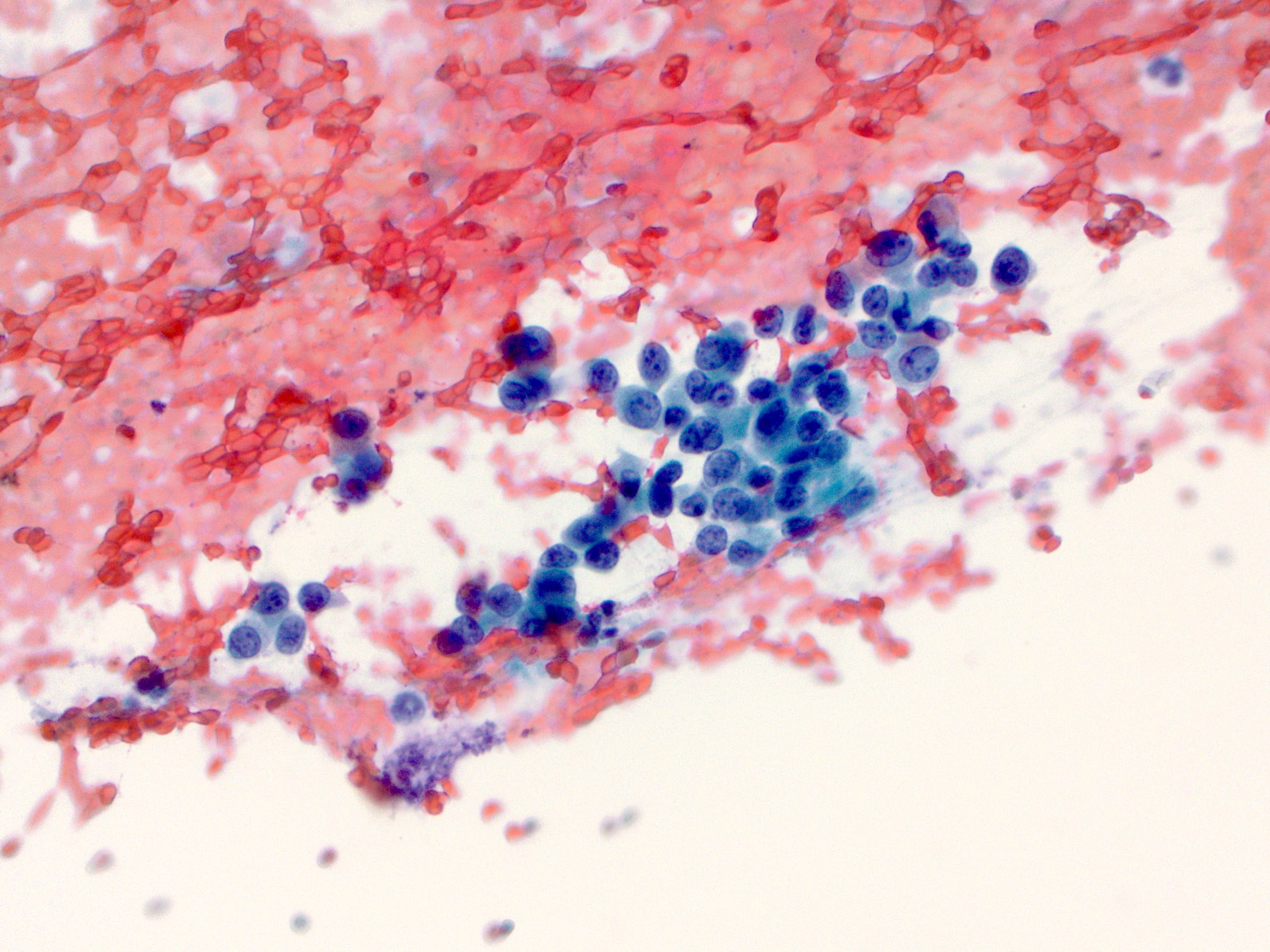
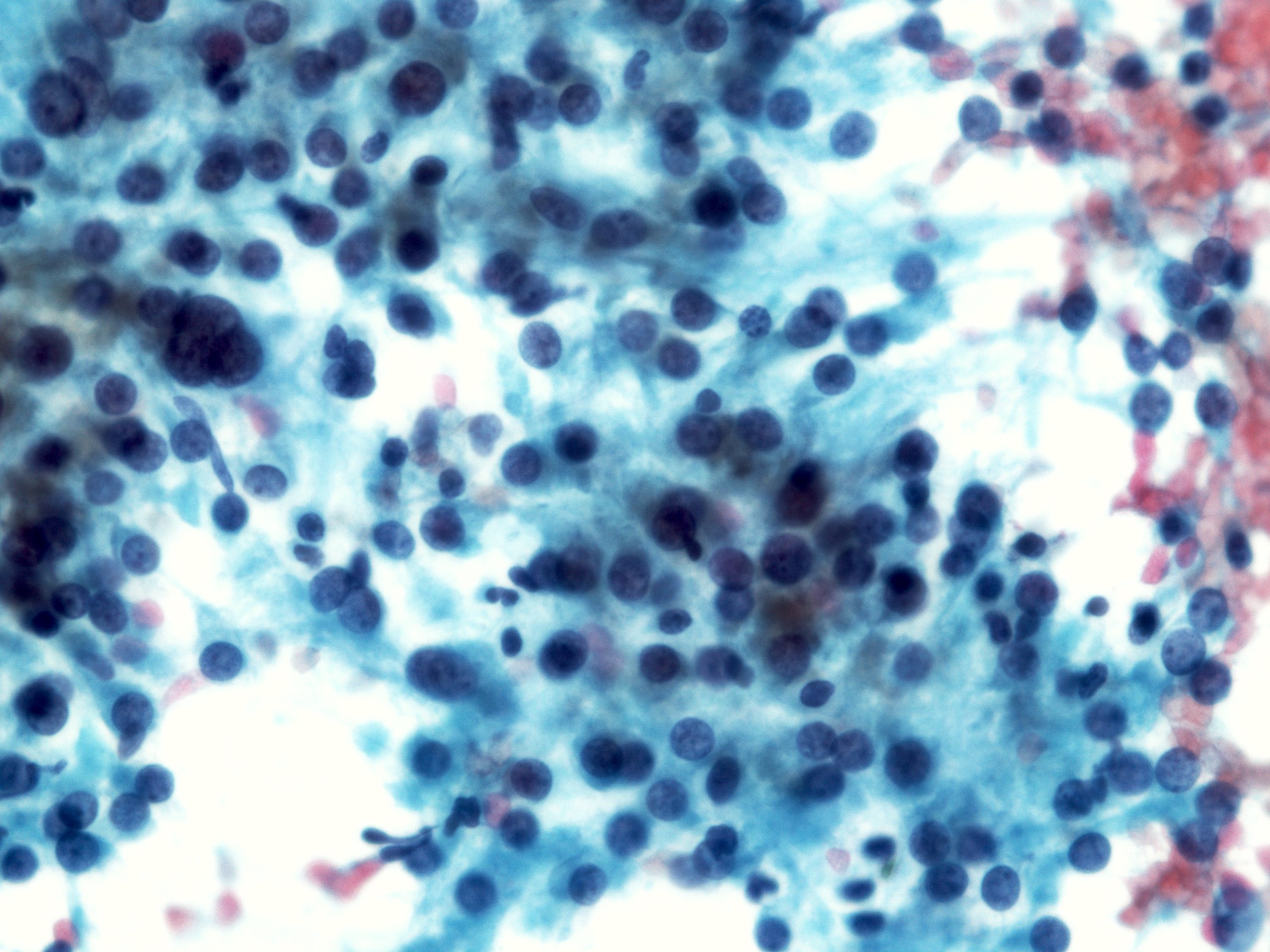
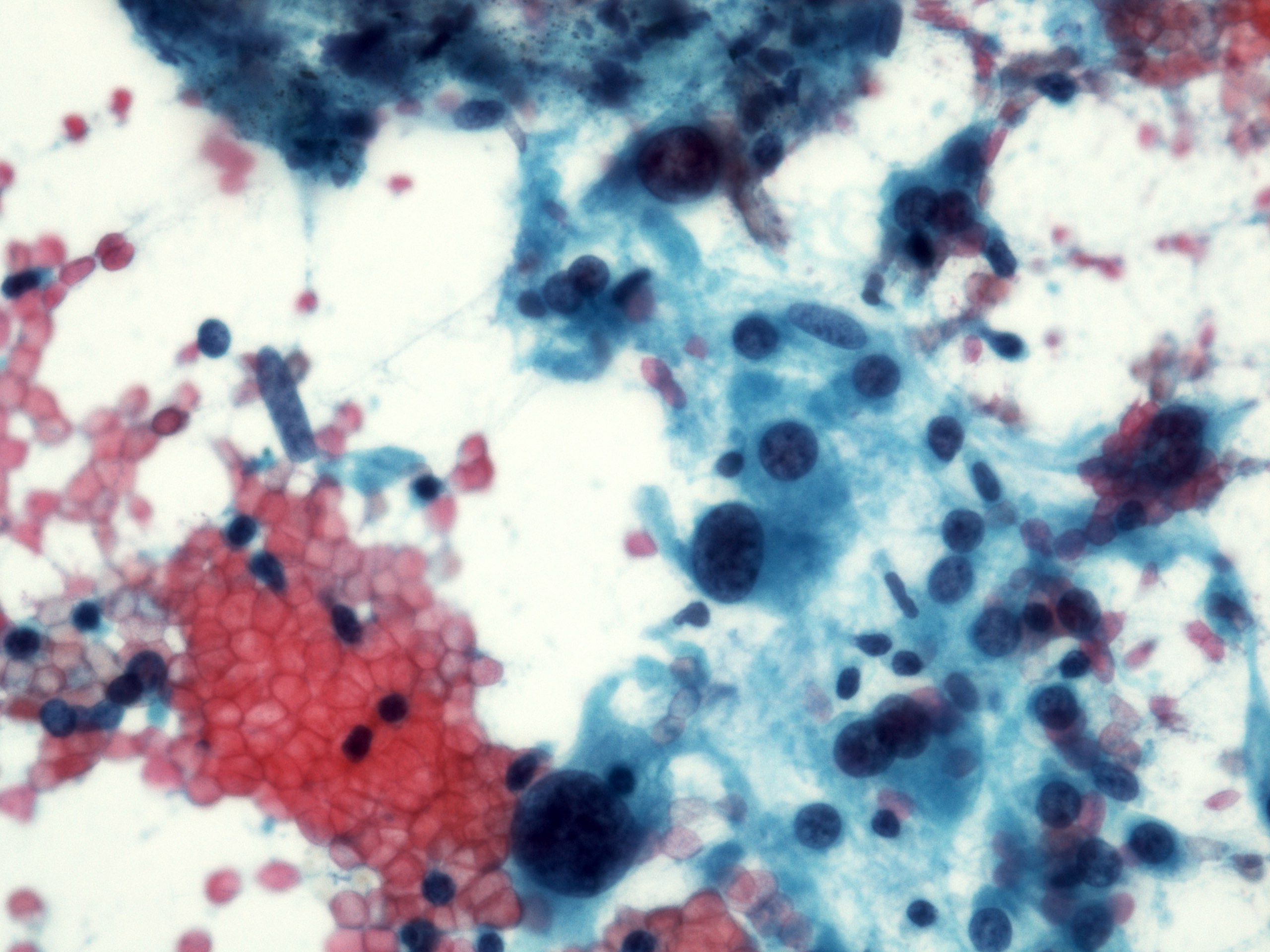
Malignant glandular epithelial cells
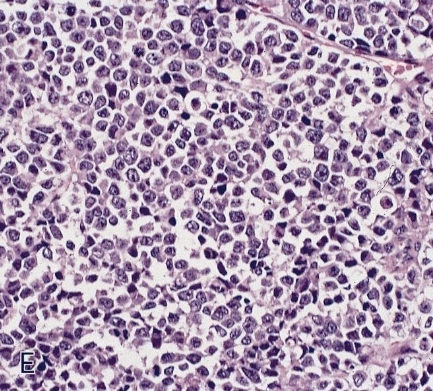
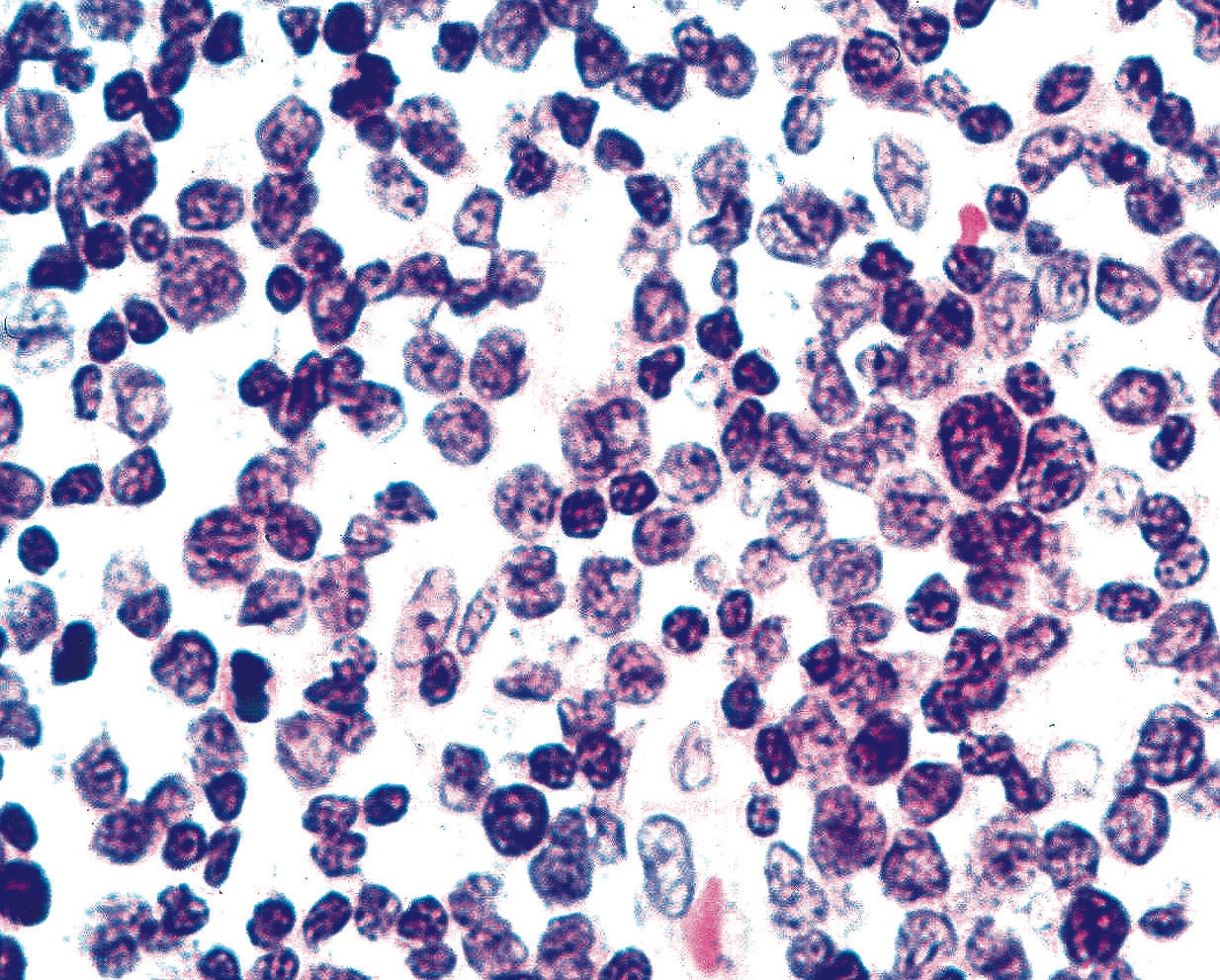
Smears are hypercellular with malignant cell groups showing nuclear enlargement, nuclear pleomorphism, hyperchromasia and irregular nuclear membranes
Background may show tumor diathesis or necrosis
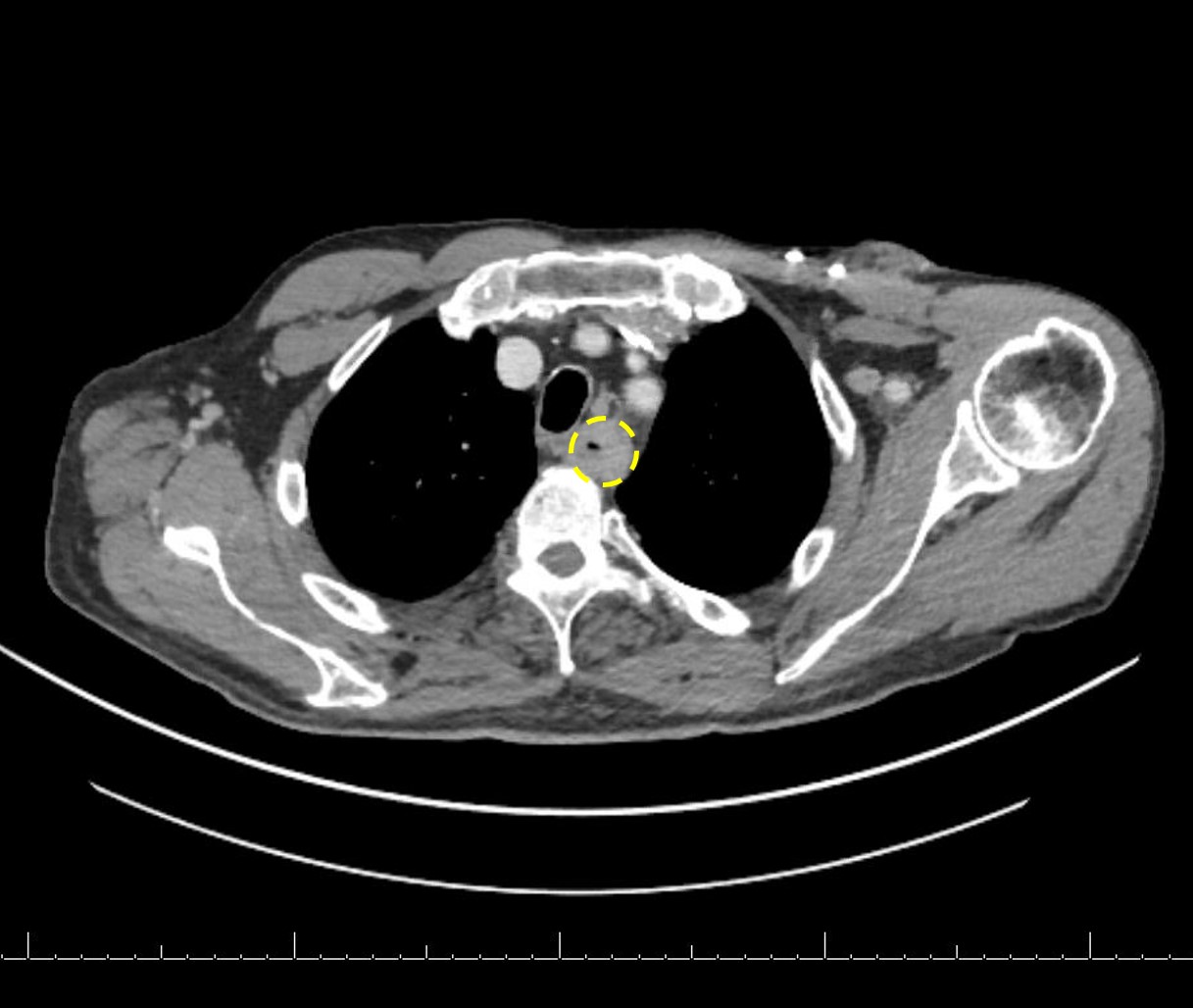
Primary tumor is rarely sampled via cytology but endoscopic ultrasound guided fine needle aspiration (EUS-FNA) and transbronchial FNA sampling may be used to evaluate for paraesophageal and mediastinal / thoracic lymph node metastases (Clinics (Sao Paulo) 2011;66:1579)
Cytology images
Contributed by Avani Pendse, M.D., Ph.D.
Hypercellular smear
Malignant cells on Diff-Quik
Malignant cells on Pap
Positive stains
Immunohistochemistry is rarely needed for a diagnosis
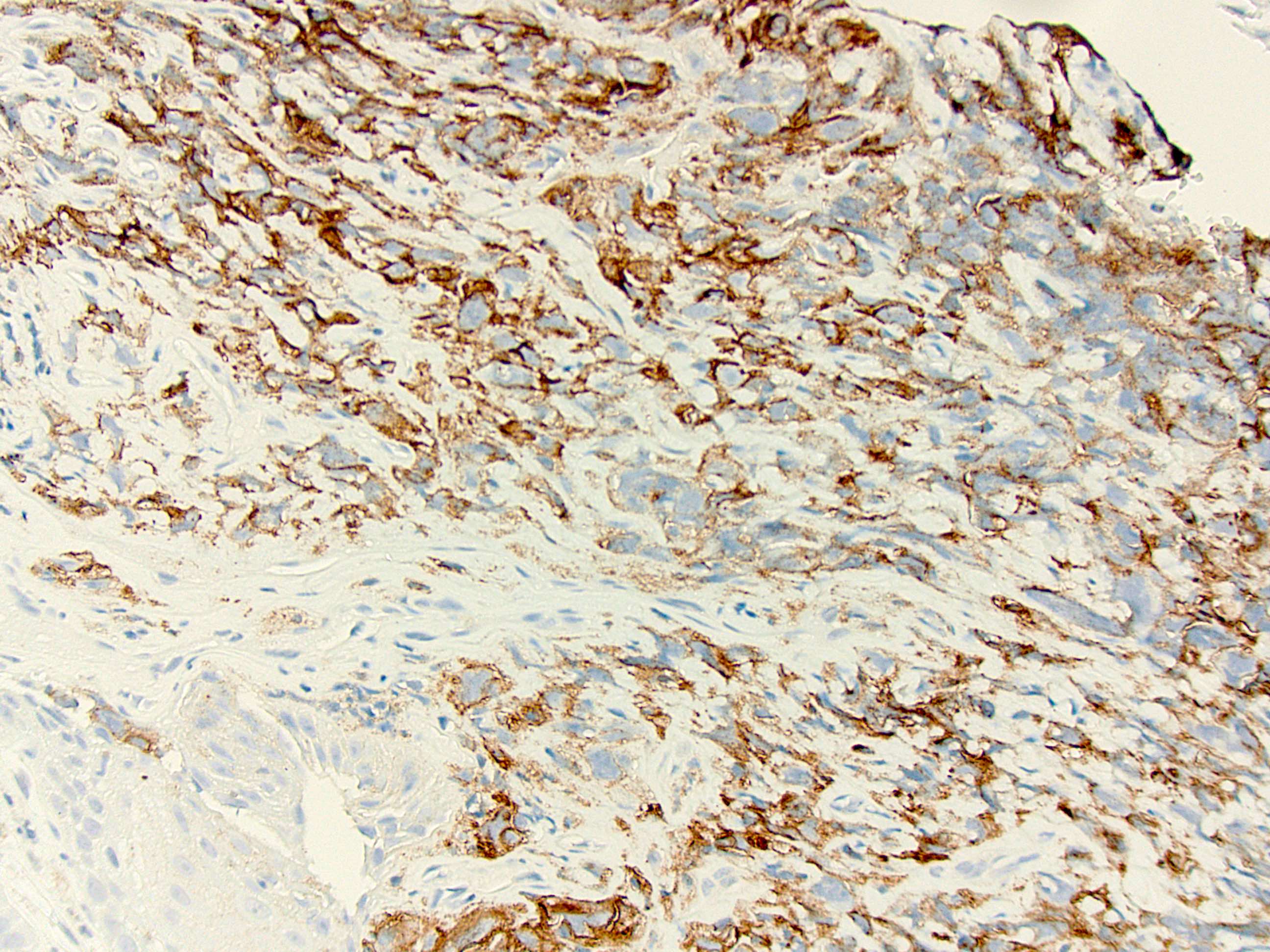
HER2 testing by IHC or FISH is recommended in all patients with metastatic esophagogastric junction carcinoma at diagnosis (J Natl Compr Canc Netw 2015;13:194)
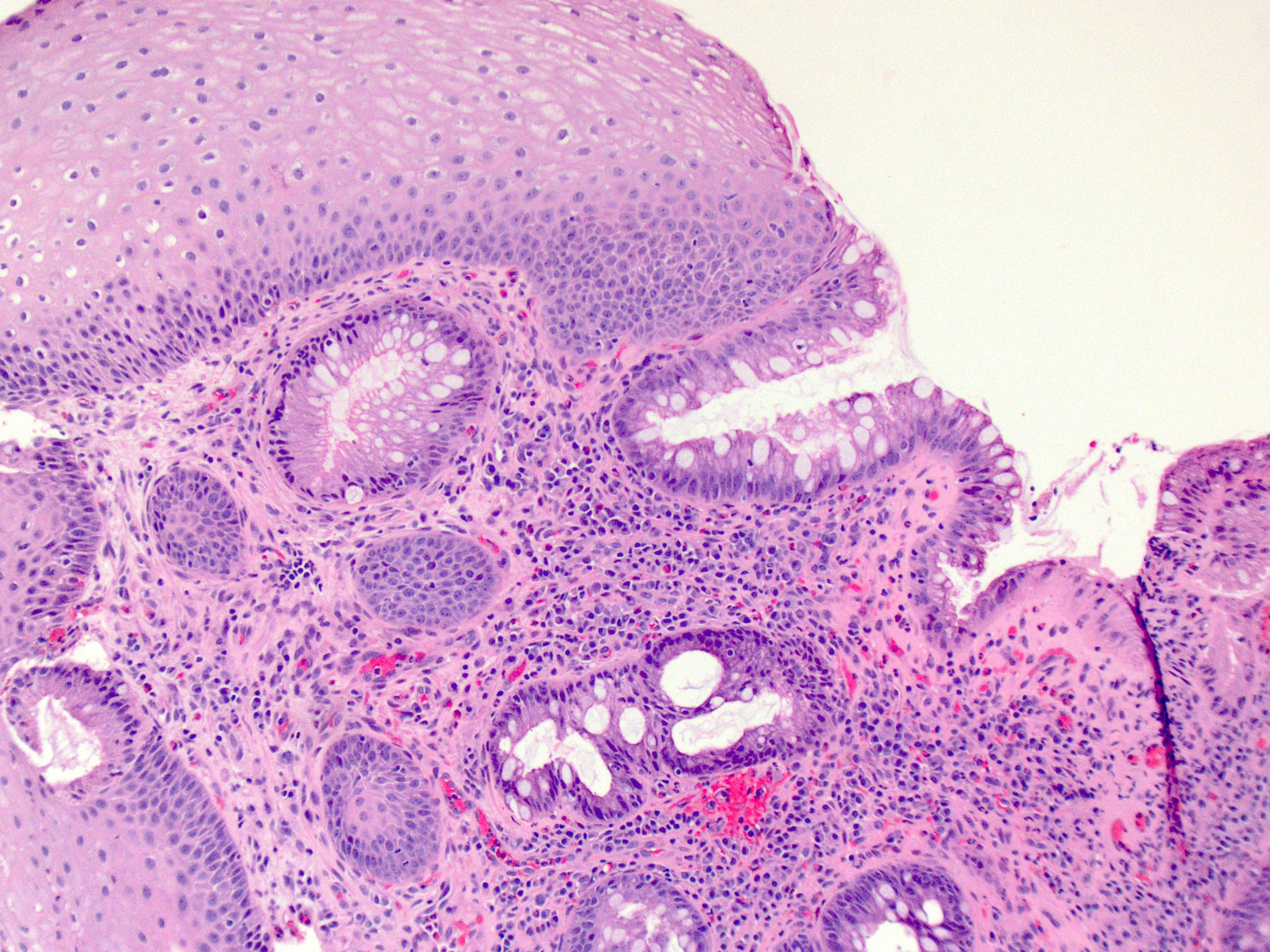
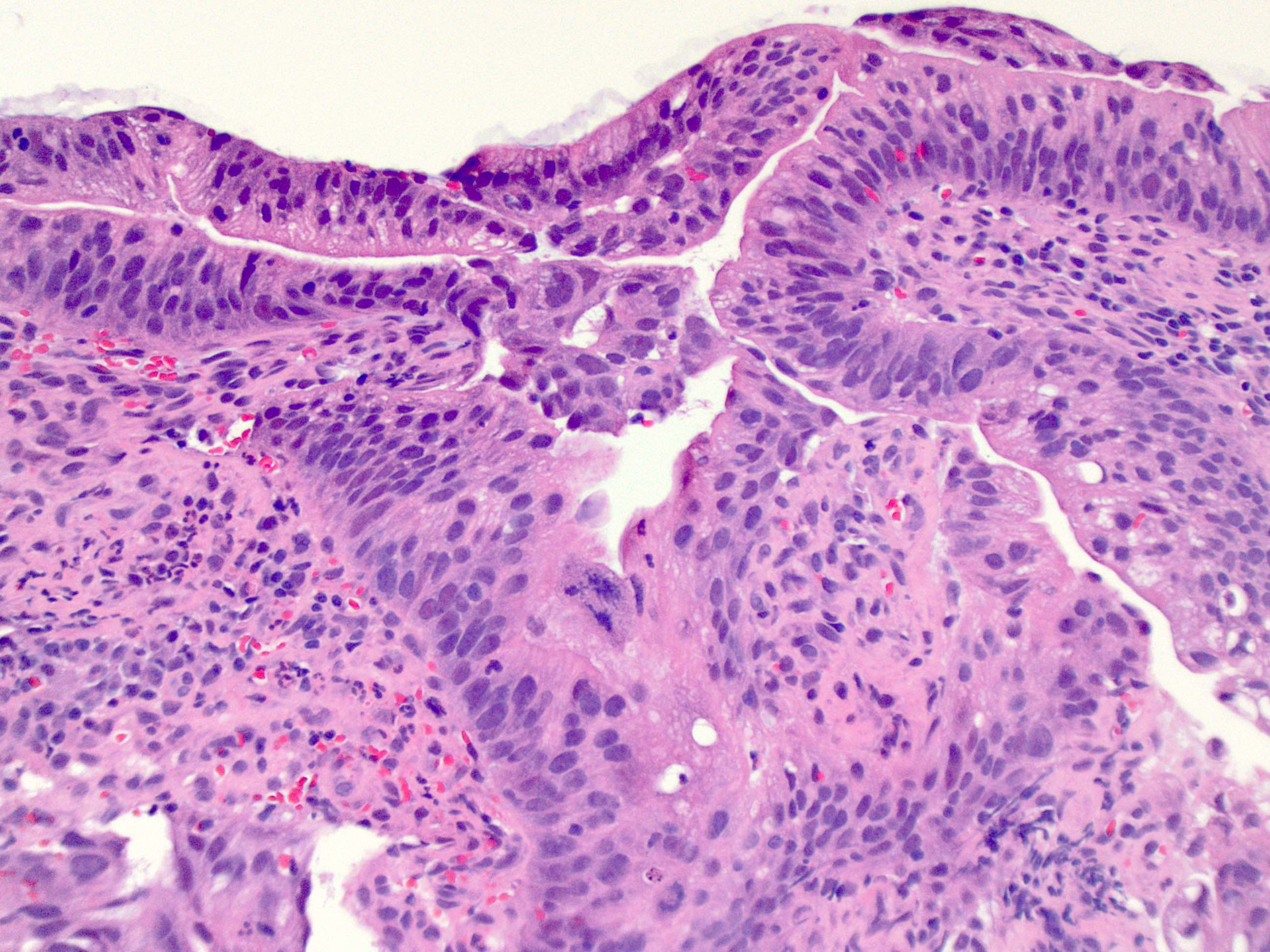
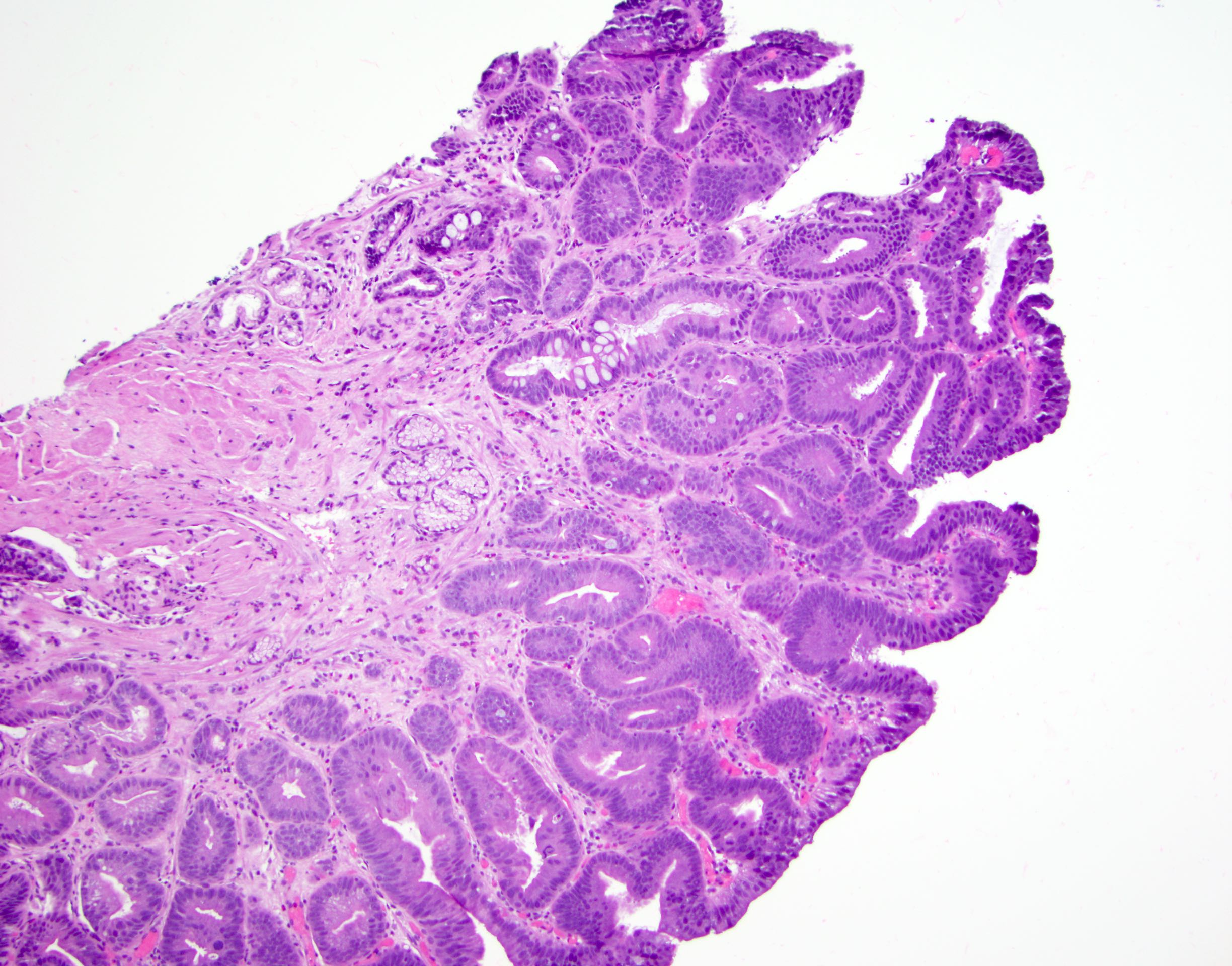
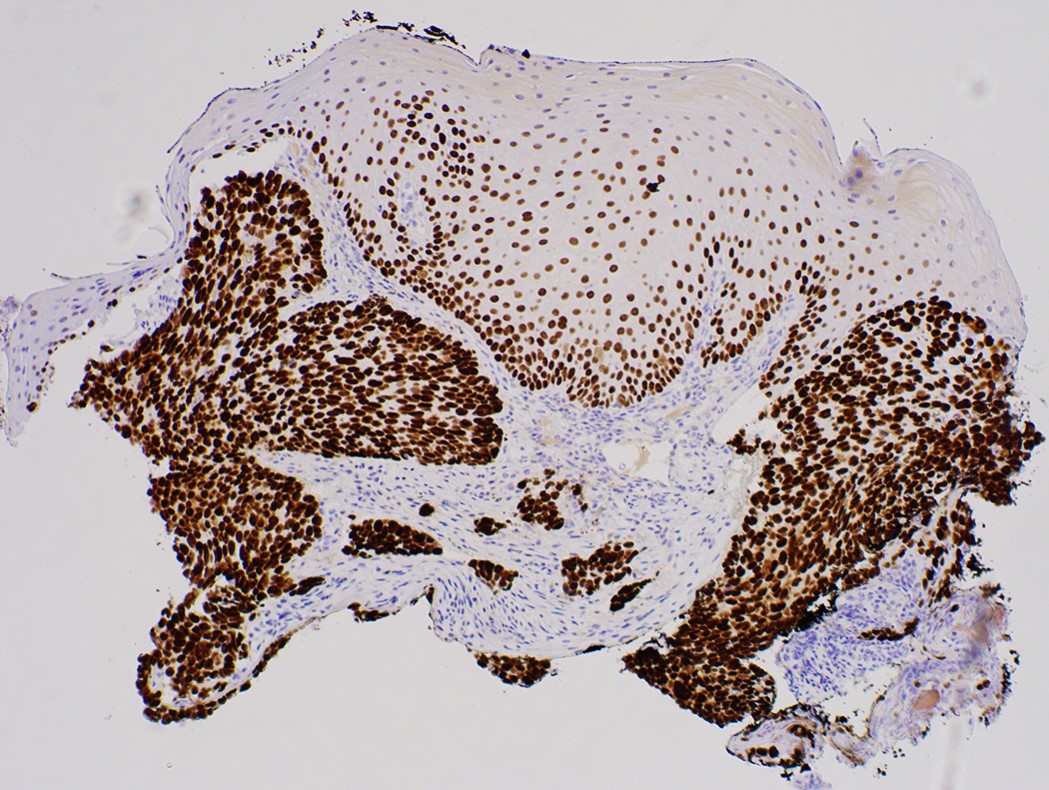
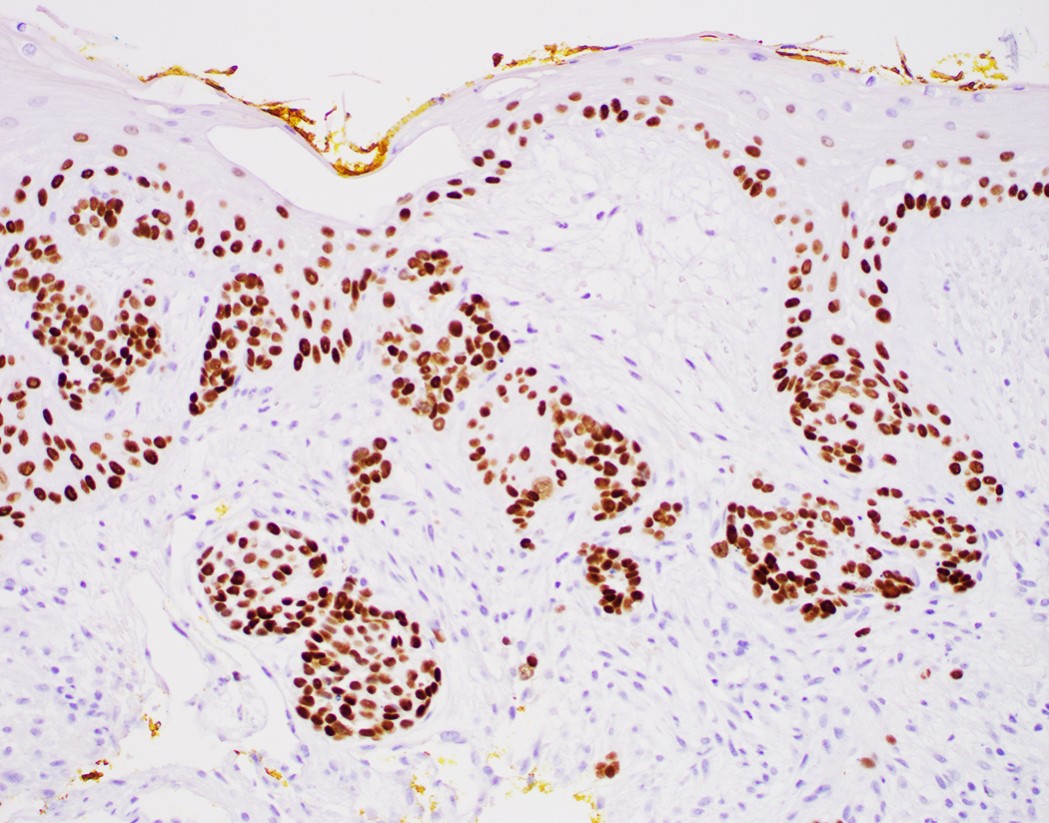
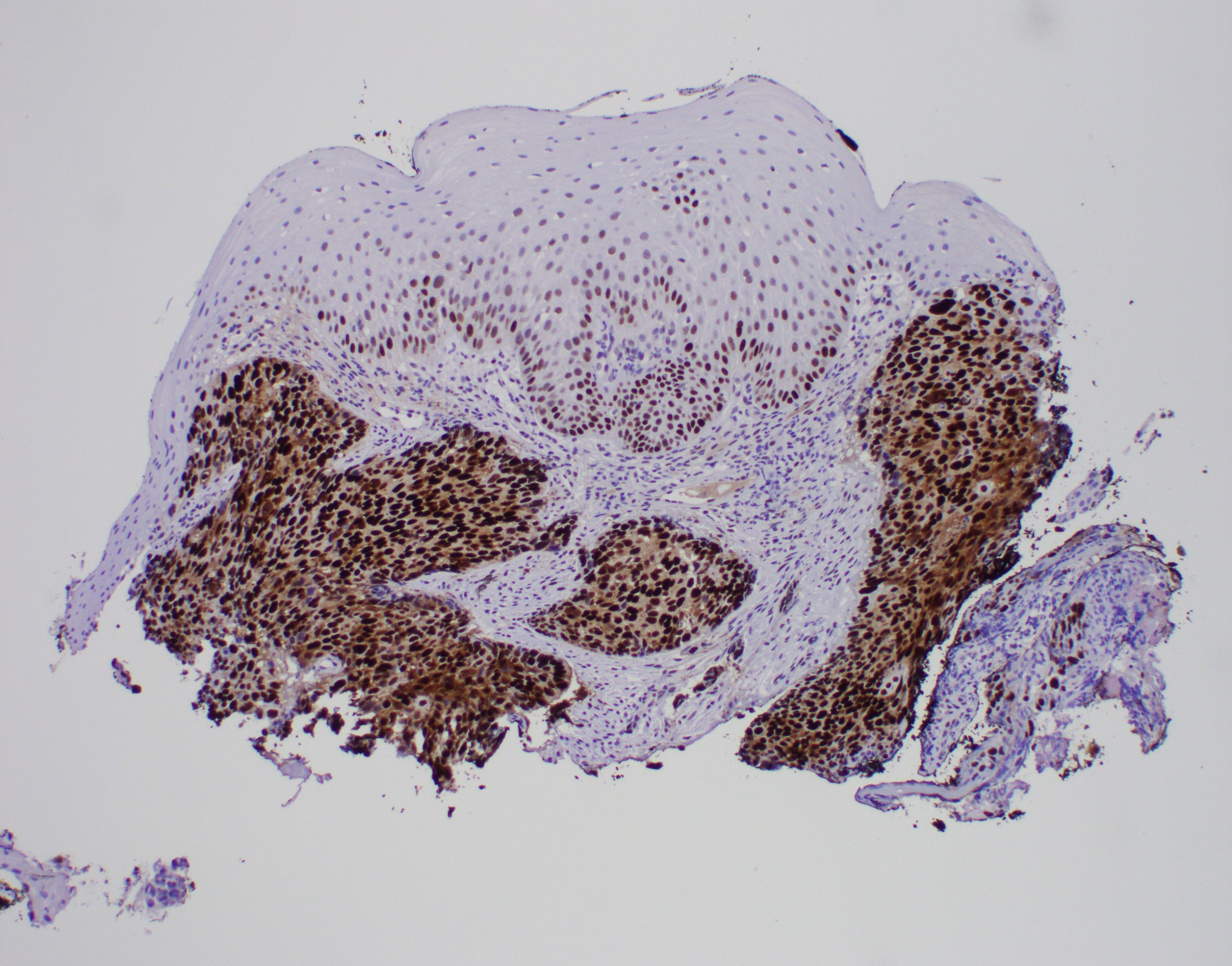
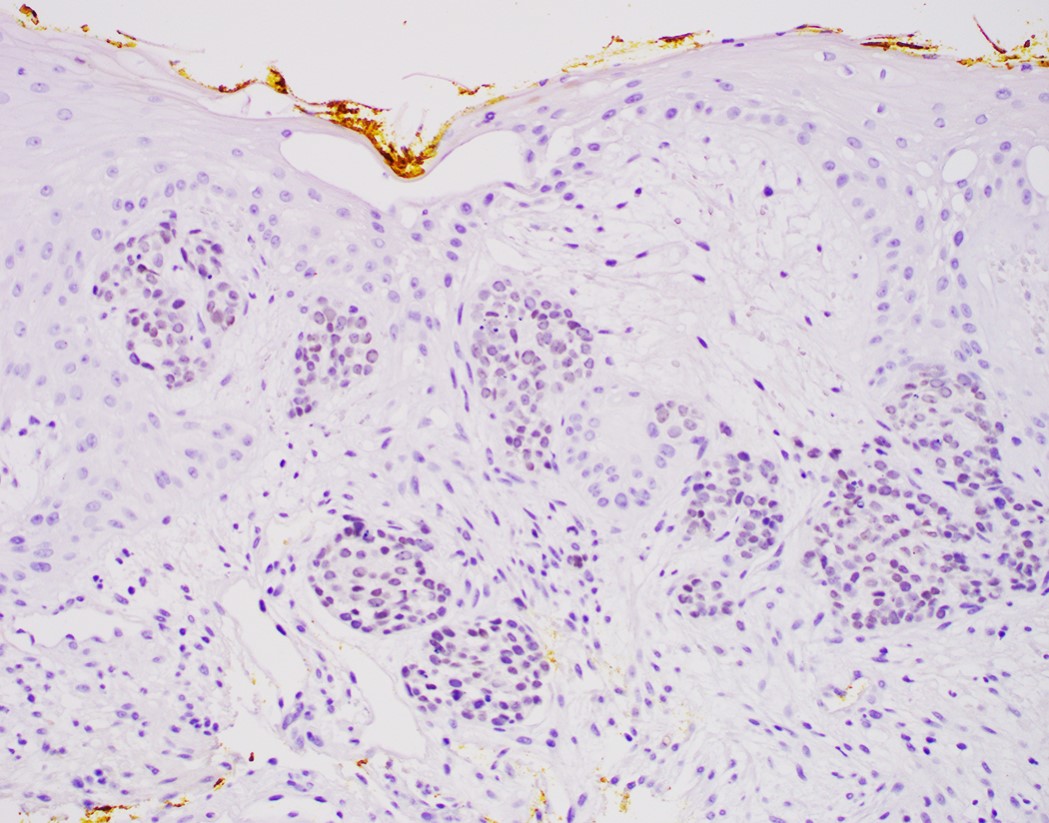
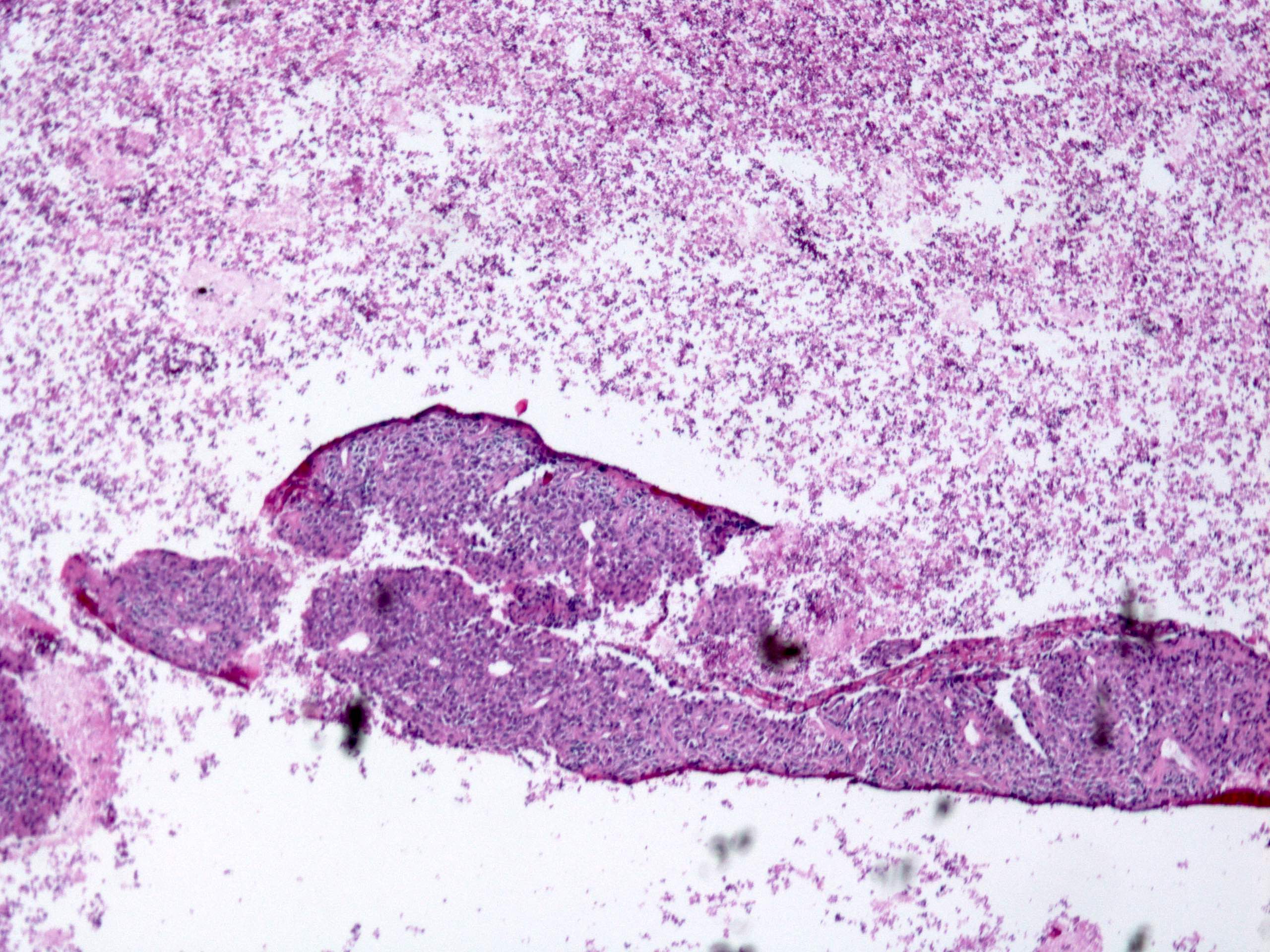
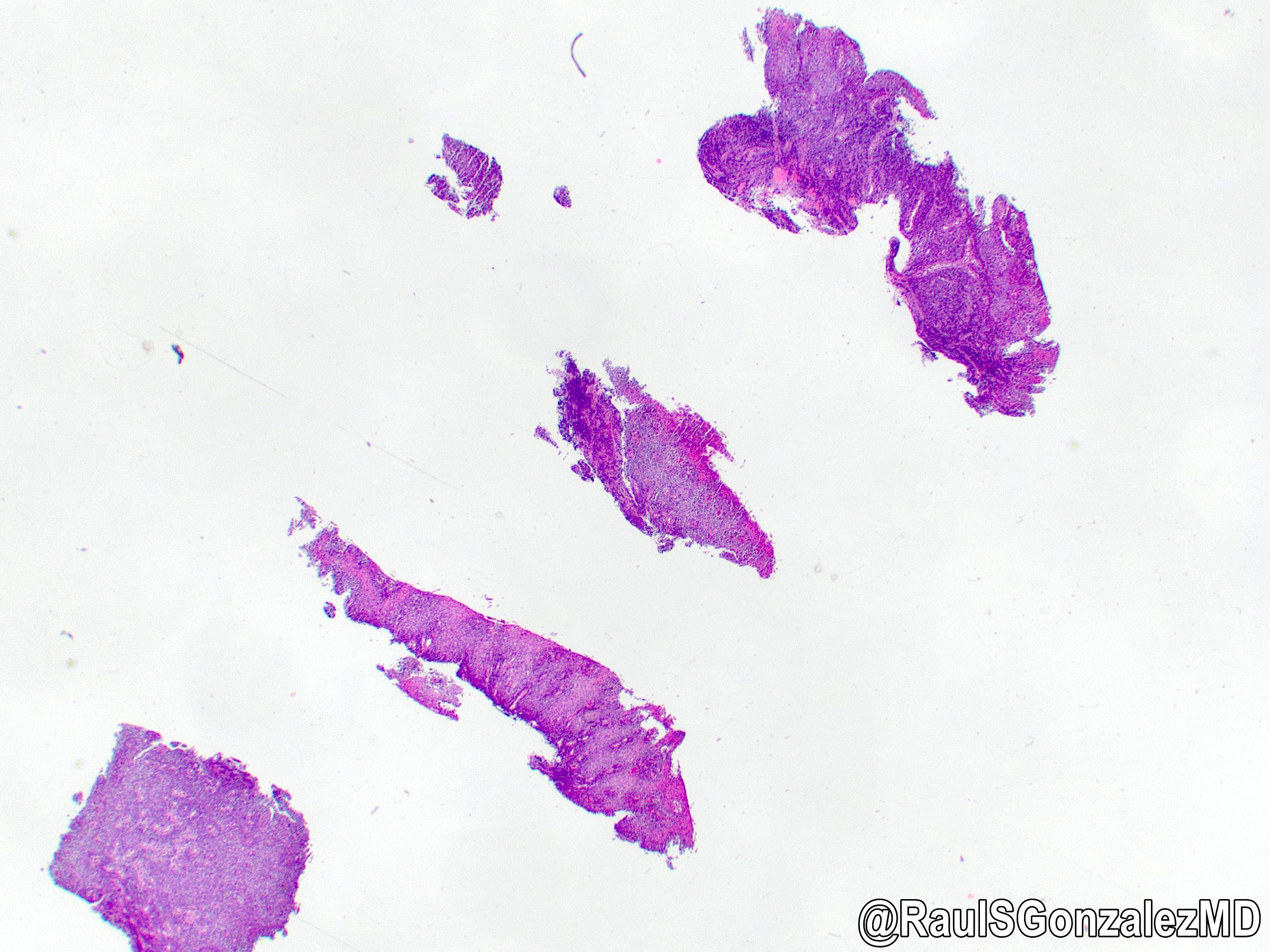
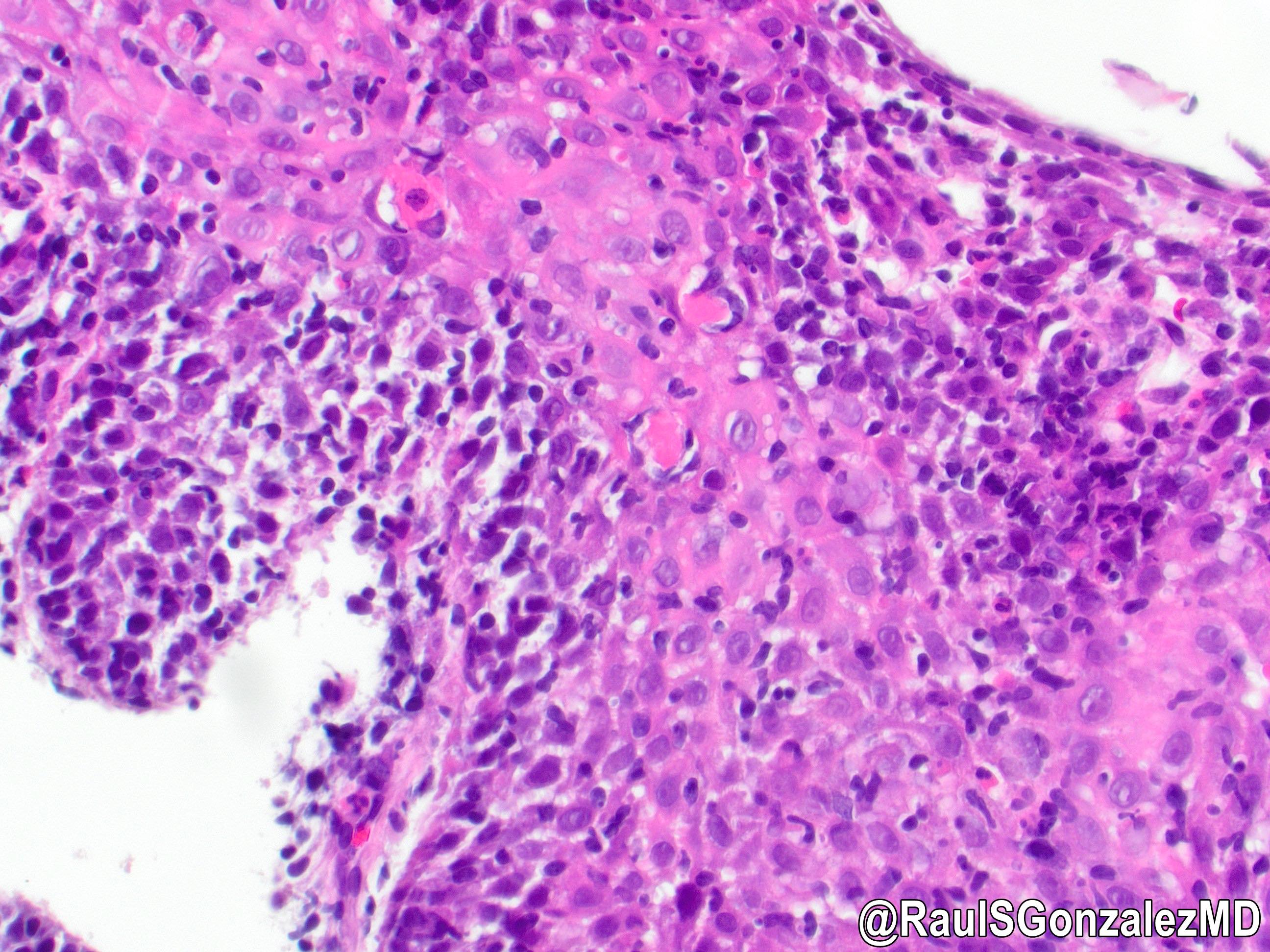
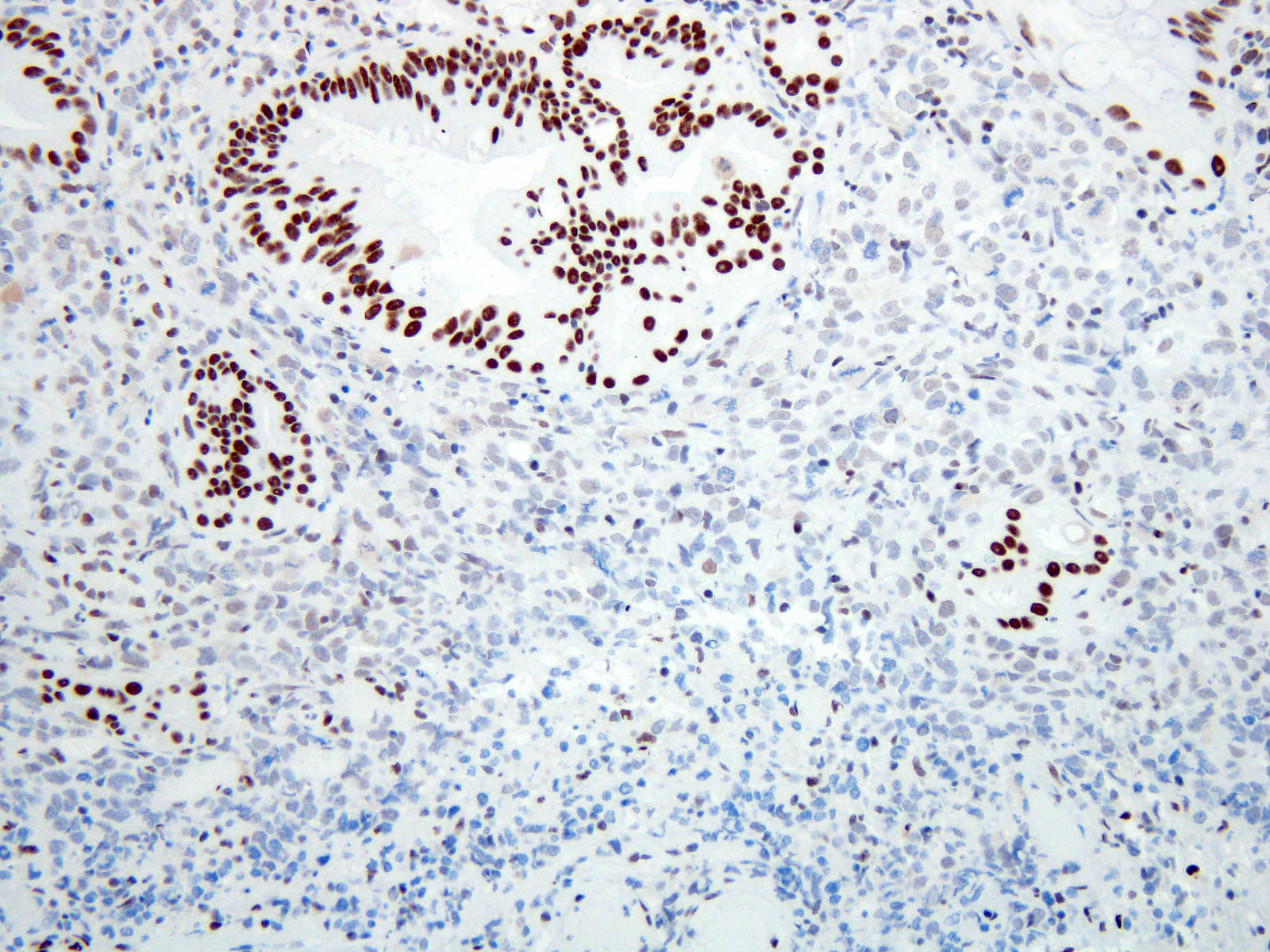
Invasive moderately differentiated adenocarcinoma arising in the background of high grade dysplasia and intestinal metaplasia
Esophagus, distal, endoscopic mucosal resection:
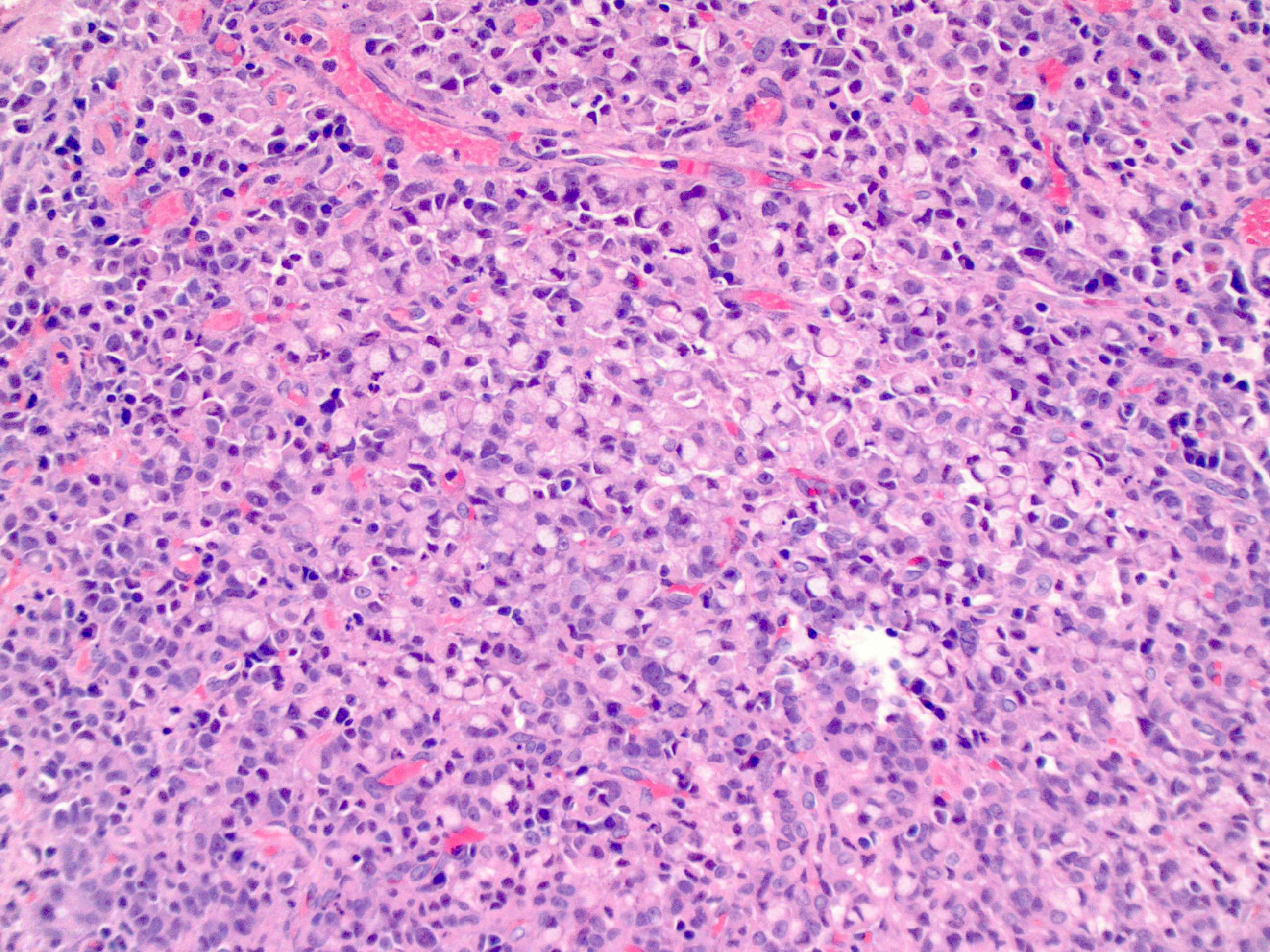
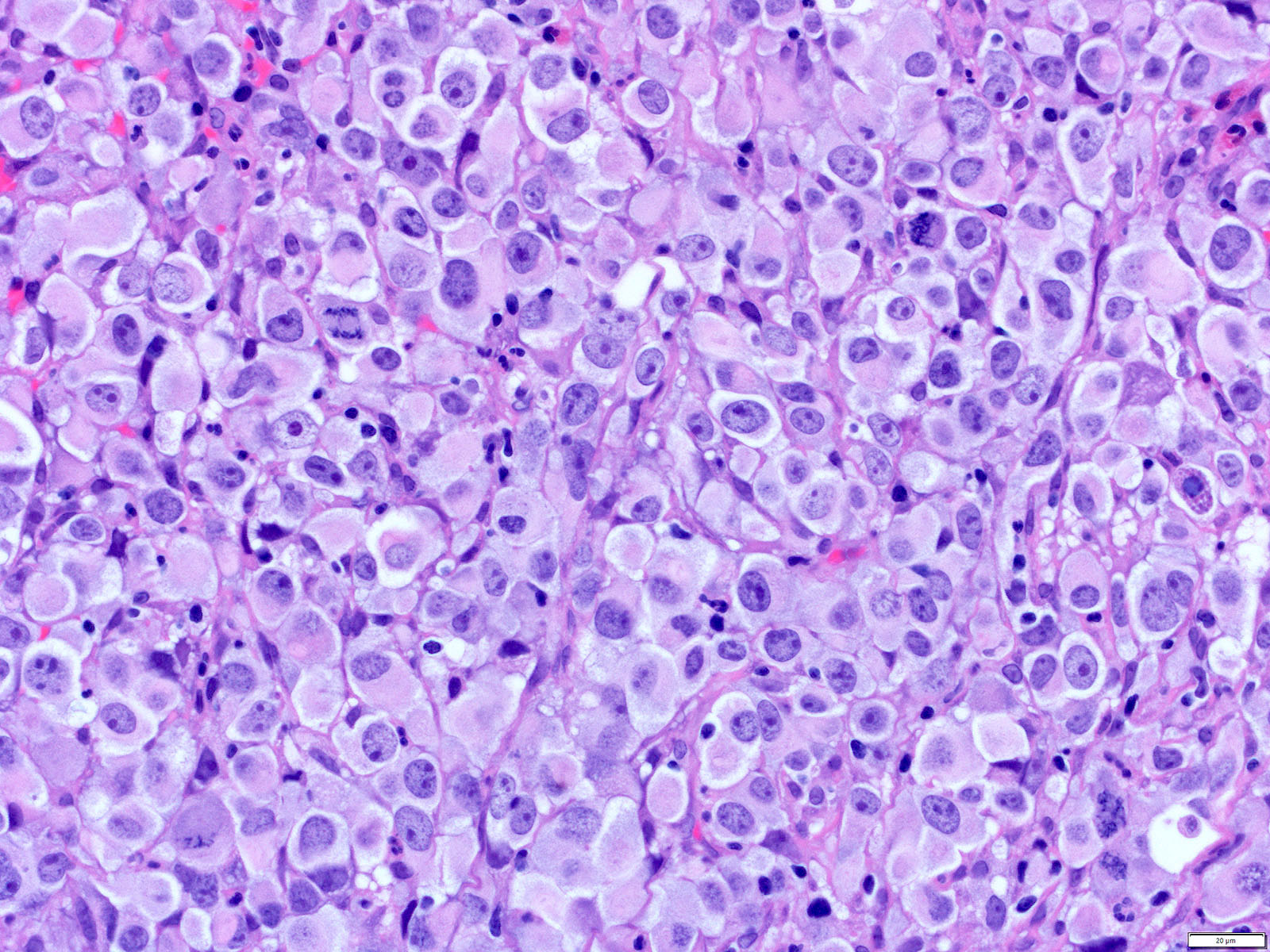
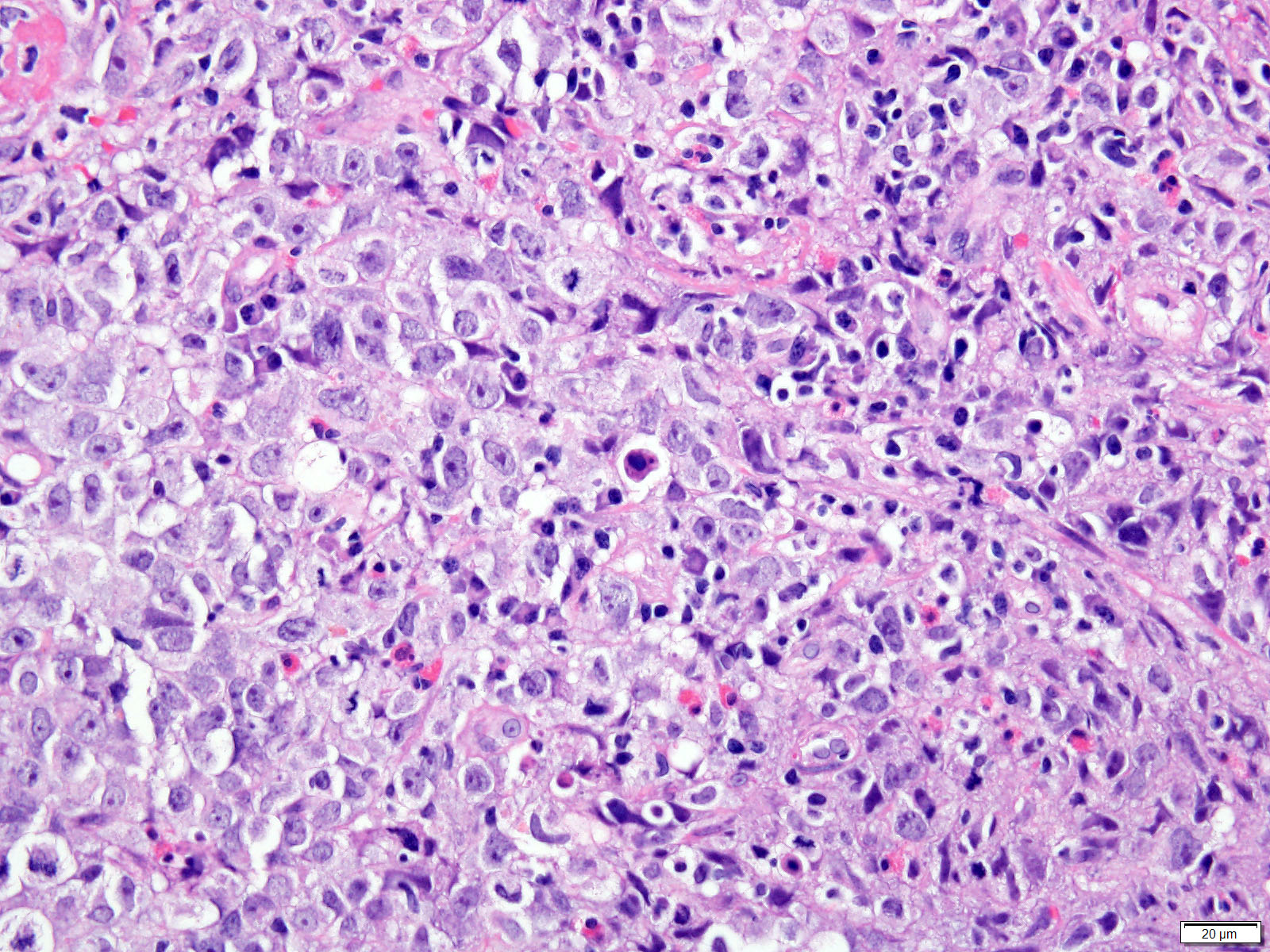
Invasive poorly differentiated adenocarcinoma with signet ring cell differentiation
Tumor is invasive into the submucosa, stage pT1b
Lateral mucosal margin is negative for carcinoma, closest approach is 3 mm
Deep resection margin is focally positive for carcinoma
Negative for lymphovascular and perineural invasion
No lymph nodes are present for evaluation
Esophagogastric junction, distal esophagus and proximal stomach, esophagogastrectomy:
Relationship of tumor to esophagogastric junction: tumor midpoint is located at the esophagogastric junction
Distance of tumor center from eophagogastric junction:
Other (specify): tumor midpoint is the esophagogastric junction
Histologic type: adenocarcinoma
Histologic grade: G2, moderately differentiated
Tumor size: greatest dimension in centimeters is 1.9 cm
Tumor extent: invades muscularis propria
Treatment effect: present, with residual cancer showing evident tumor regression but more than single cells or rare small groups of cancer cells (partial response, score 2)
Lymphovascular invasion: present
Perineural invasion: not identified
Margins: all margins negative for invasive carcinoma
Closest margin to invasive carcinoma: proximal
Distance from invasive carcinoma to closest margin: 1.8 cm
Margin status for dysplasia and intestinal metaplasia: all margins negative for dysplasia and intestinal metaplasia
Regional lymph node status
Tumor present in regional lymph node(s)
Number of lymph node(s) with tumor: 1
Number of lymph node(s) examined: 8
Distant metastasis: not applicable
Pathologic stage classification: ypT2pN1
Additional findings:
Intestinal metaplasia (Barrett esophagus)
Low grade glandular dysplasia
High grade glandular dysplasia
Special studies: HER2 IHC: positive, 3+
Differential diagnosis
Differentiation between high grade glandular dysplasia and invasive adenocarcinoma into the lamina propria may be difficult, especially on small biopsies
Intramucosal adenocarcinoma:
Shows invasion into the lamina propria or into muscularis mucosa but not through the muscularis mucosa
Desmoplasia favors invasive carcinoma when present
A biopsy of a distal esophageal mass shows at least high grade glandular dysplasia. Which lesion is most likely to be present in association with dysplasia?
Barrett esophagus / intestinal metaplasia
Candida esophagitis
Parakeratosis
Proton pump inhibitor therapy
Board review style answer #1
A. Barrett esophagus / intestinal metaplasia. Patients with Barrett esophagus have a 10 - 55 times higher risk of adenocarcinoma. Candida esophagitis (B), parakeratosis (C) and proton pump inhibitor therapy (D) do not increase the risk of glandular dysplasia and adenocarcinoma. Atypical parakeratosis may overlie a focus of squamous dysplasia. Proton pump inhibitor therapy may have some protective effect but this association needs more evidence.
A biopsy of a thoracic lymph node showed a CK7+, CK20- and TTF1+ metastatic adenocarcinoma. Is this immunohistochemistry profile sufficient to distinguish between an esophageal versus a pulmonary primary?
Likely pulmonary primary but esophageal primary needs to be excluded via clinical / endoscopic / radiographic correlation
No, does not support either esophageal or pulmonary primary
Yes, favors esophageal primary
Yes, favors pulmonary primary
Board review style answer #2
A. Likely pulmonary primary but esophageal primary needs to be excluded via clinical / endoscopic / radiographic correlation. A CK7+, CK20- and TTF1+ metastatic adenocarcinoma is likely to be of pulmonary origin; however, since a minority of esophageal adenocarcinomas are TTF1+, it is prudent to rule out that possibility by correlating with clinical findings. Answers B, C and D are incorrect because a CK7+, TTF+ immunohistochemistry profile is seen in both primary lung and esophageal adenocarcinoma.
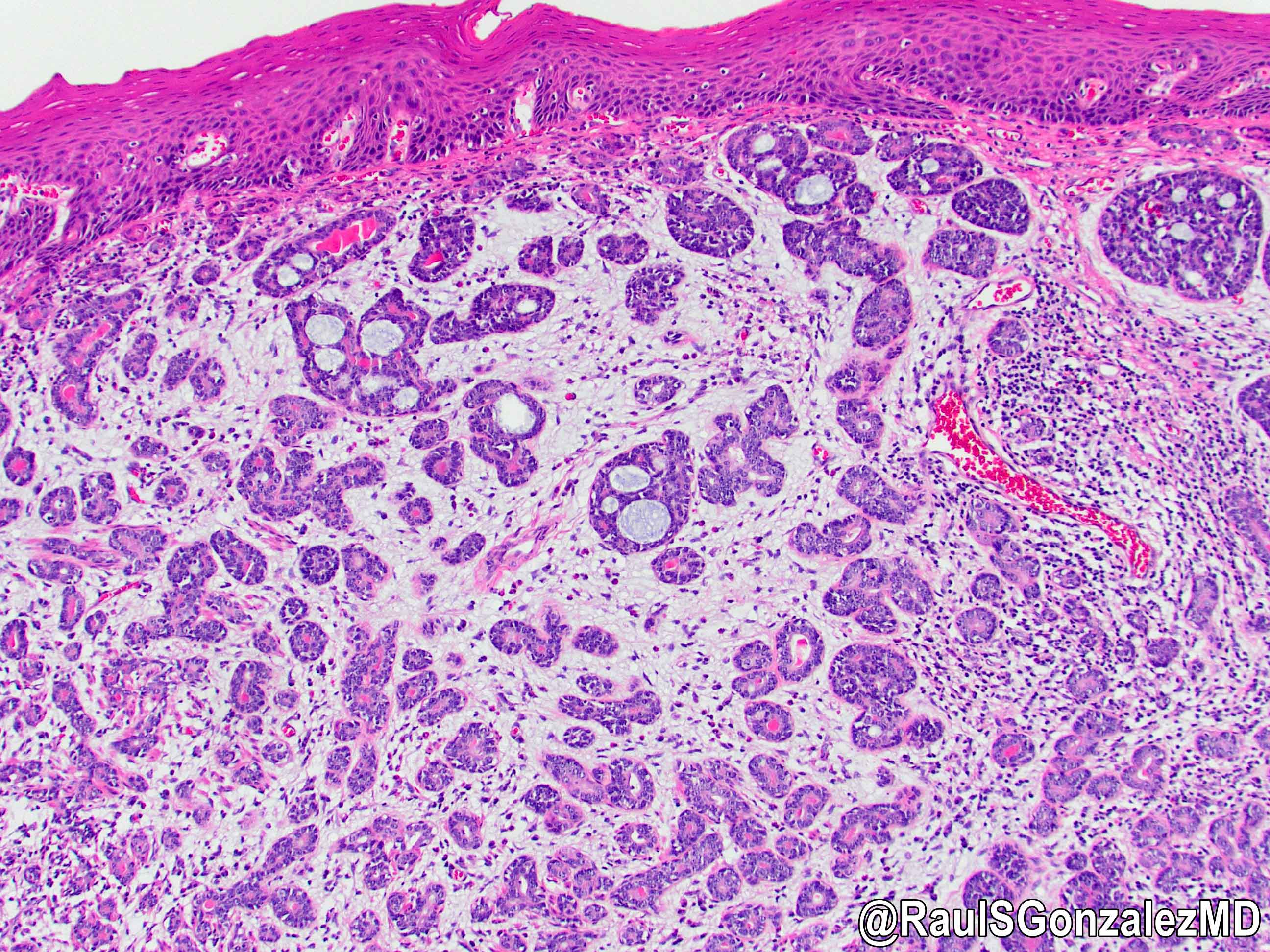
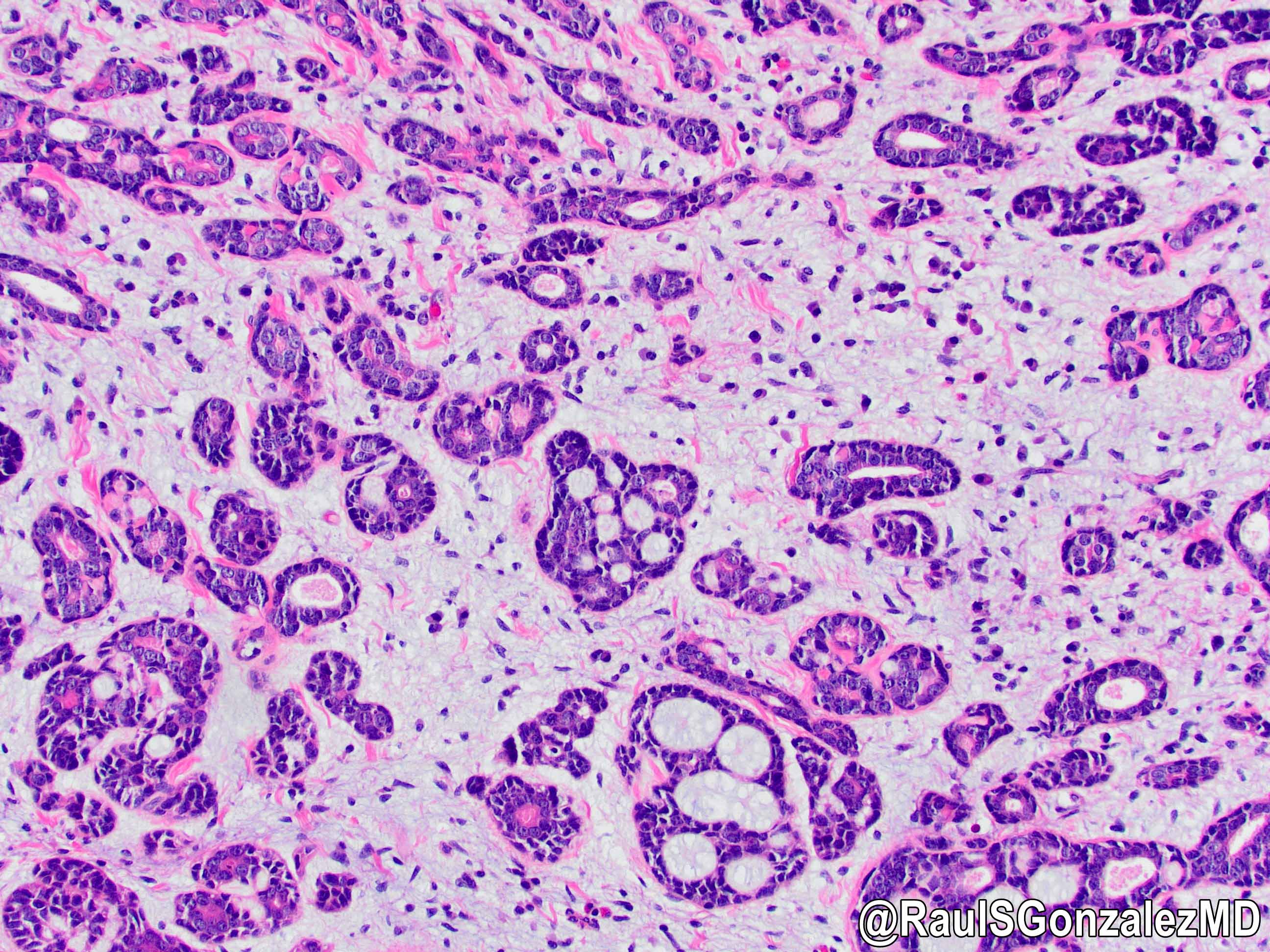
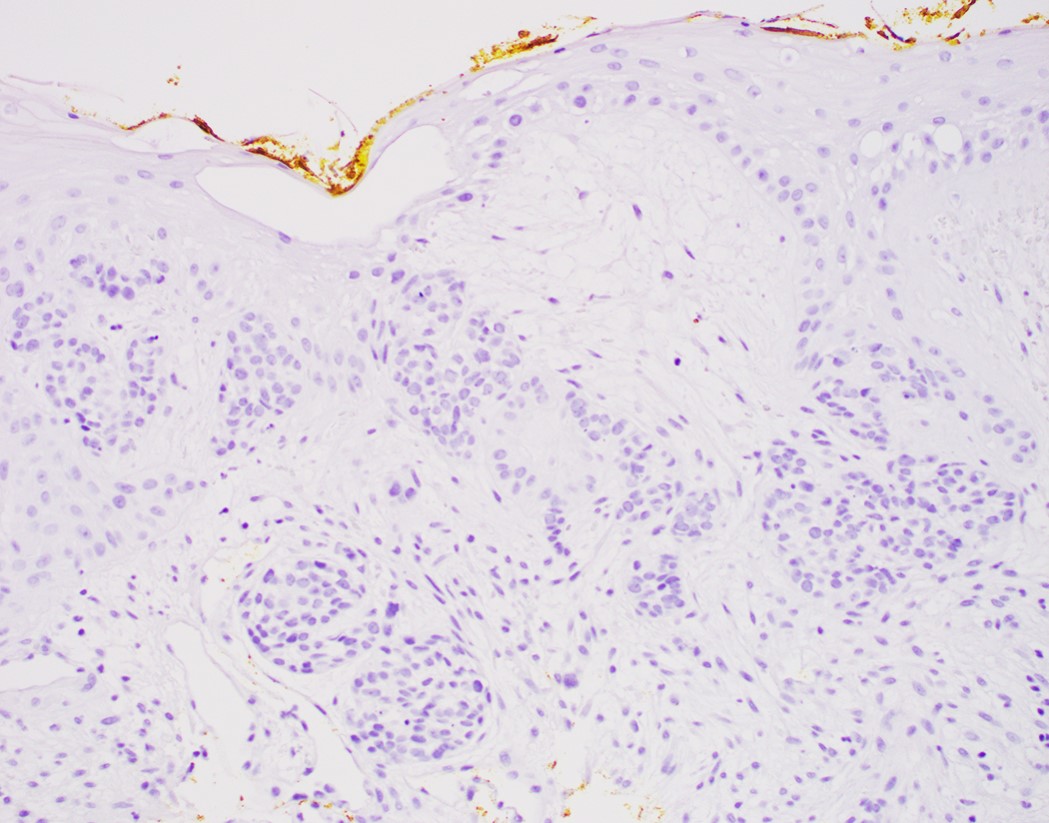
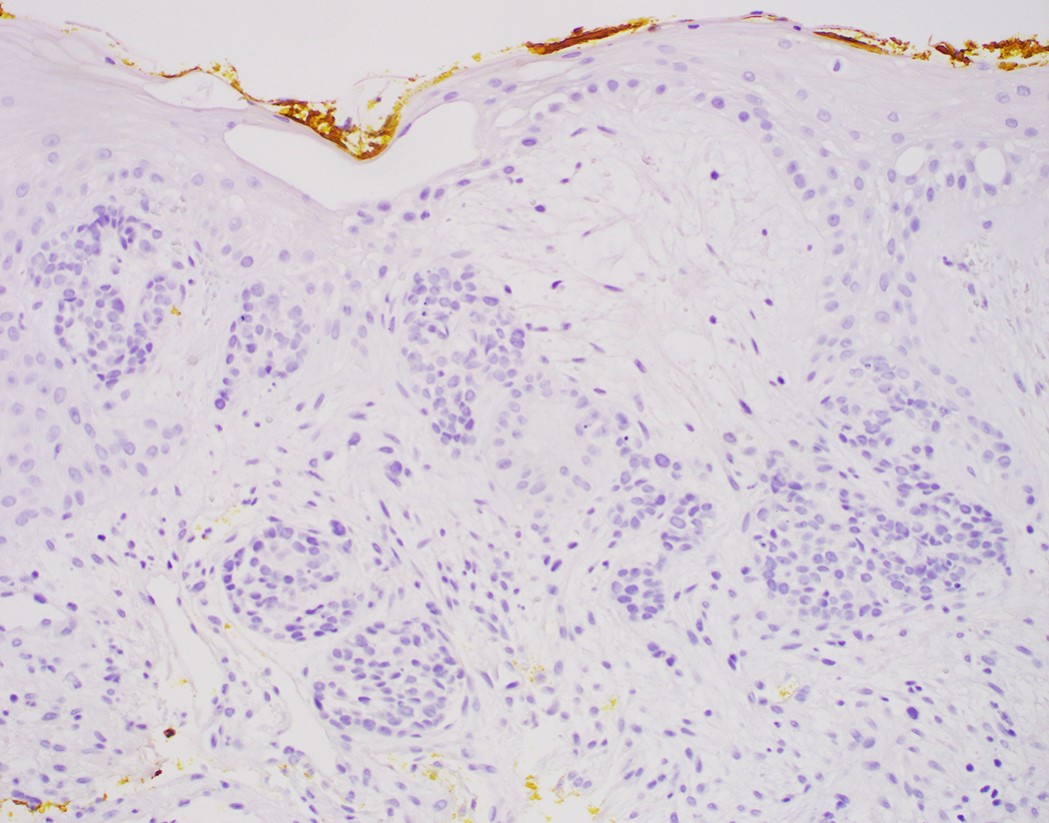
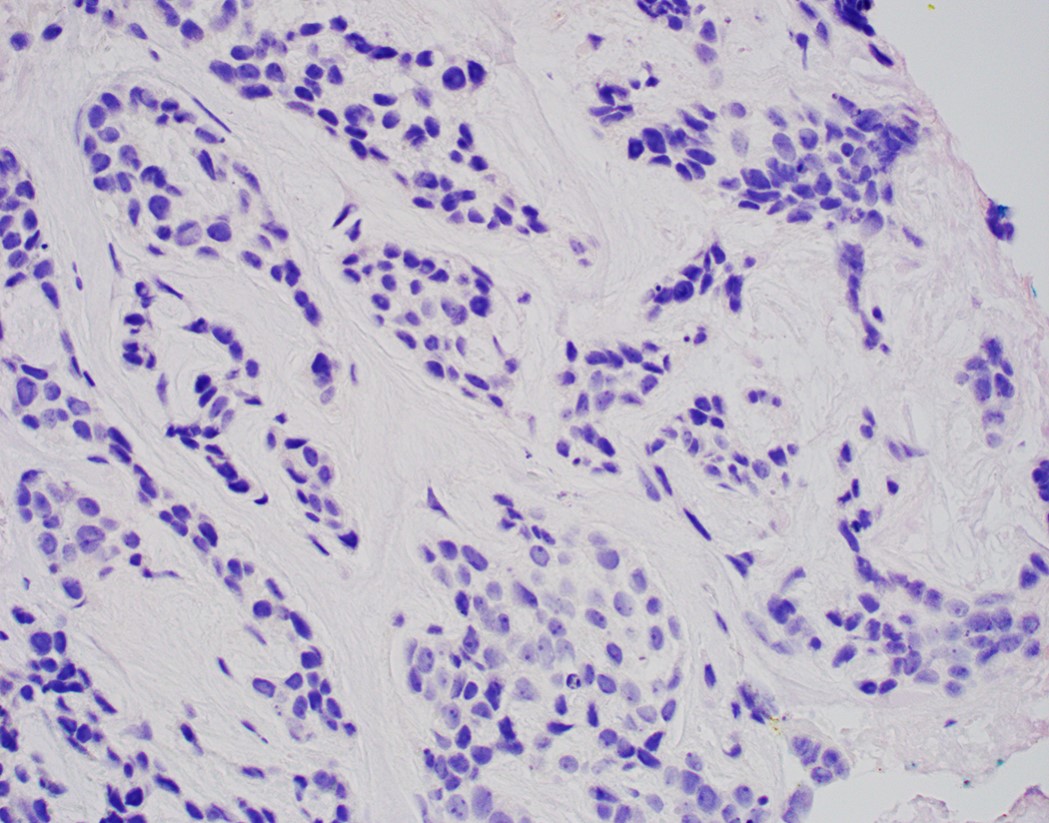
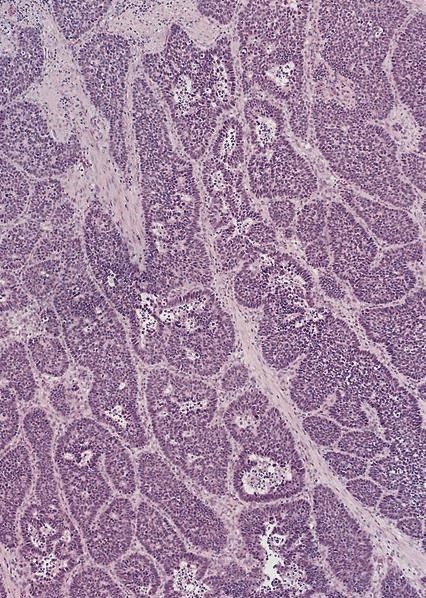
Inner ductal type epithelium and outer modified myoepithlial cells form solid nests or cribriform spaces containing balls of glyocosaminoglycans and basement membrane material
Ductal epithelium is strongly cytokeratin and CEA+, while modified myoepithelial cells are weakly cytokeratin positive with strong S100, actin and vimentin positivity in modified myoepithelial cells
Muscular tubular structure 25 cm long in adults, 10 - 11 cm in newborns; develops from cranial portion of the foregut; connects pharynx and stomach; has cervical, thoracic and abdominal segments
Main purpose is to propel food from pharynx to stomach via peristalsis; secretes mucin for lubrication and to minimize reflux of gastric contents but has no other significant secretory or absorptive functions
Extends from cricopharyngeus muscle in pharynx (level of C6) to lower esophageal sphinchter at gastroesophageal junction (T11 / T12)
Embryology
Notocord induces formation of foregut from endoderm
At day 21 (end of week 3), lateral walls of foregut develop septa that fuse and divide foregut into esophagus and trachea
At week 4, myenteric plexus develops
At weeks 5 - 6, septation of walls ends; initial lining is stratified columnar epithelium, which proliferates and almost occludes the lumen
At weeks 6 - 7, epithelial vacuolization appears, vacuoles coalesce to form a single esophageal lumen
At week 8, ciliated cells appear and extend to almost entire columnar epithelium
At week 9, longitudinal muscle layer develops; interstitial cells of Cajal appear
At week 10, a single layer of columnar cells covers entire esophagus
At month 4, submucosal glands appear due to downward growth of columnar cells, extend distally to cardiac mucosa
At month 5, stratified squamous epithelium initially appears in midesophagus and replaces ciliated epithelium cephalad and caudally; proximal esophagus may retain ciliated epithelium at birth
At month 5, upper esophagus has both striated and smooth muscle
Regions (AJCC)
Cervical (lower border of cricoid cartilage to suprasternal notch / thoracic inlet, 5 cm long, begins 15 cm from incisors); contains striated muscle
Upper thoracic (suprasternal notch to tracheal bifurcation, 5 cm long, begins 20 cm from incisors); has striated and smooth muscle
Midthoracic (tracheal bifurcation to diaphragmatic hiatus, 5 cm long, begins 24 cm from incisors); has striated and smooth muscle
Lower thoracic and abdominal (10 cm long, begins 30 cm from incisors); extends past diaphragm to its junction with stomach; has smooth muscle only
Usual points of narrowing (possible sites of food / pill lodging): cricoid cartilage (due to cricopharyngeus muscle), aortic arch, anterior crossing of left main bronchus and left atrium, where it passes through diaphragm
Gastroesophageal junction: traditionally defined as macroscopic point of flaring of tubular esophagus or proximal limit of gastric rugal folds; endoscopic definition is Z ("zigzag") line at irregular boundary of squamous and columnar mucosa in distal esophagus, which is usually 2 - 3 cm proximal to macroscopic GE junction; histologic definition is proximal limit of gastric oxyntic (fundic) mucosa (Hum Pathol 2006;37:40)
Distal 1 - 2 cm of esophagus is often composed of cardiac or cardiac - oxyntic type of mucosa; there is no consensus if this is normal or due to reflux esophagitis
Esophageal sphincters: two areas of high pressure at rest (physiologic, not anatomic sphincters); upper esophageal sphincter is at cricopharyngeus and inferior pharyngeal constrictor muscles; lower esophageal sphincter is 2 - 4 cm proximal to esophagogastric junction at level of diaphragm (composed of intrinsic esophageal muscles, sling fibers of proximal stomach and crural diaphragm)
Vagotomy does NOT affect tone of lower esophageal sphincter; tone is affected by gastrin, acetylcholine and serotonin
Vessels and nerves
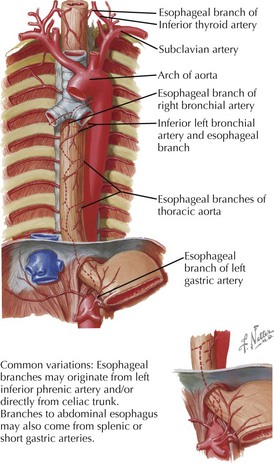
Arterial blood supply: cervical region - inferior thyroid artery; upper thoracic - bronchial and intercostal arteries; lower thoracic - aortic branches; abdominal - left gastric and inferior phrenic arteries; infarction is rare due to numerous anastomoses
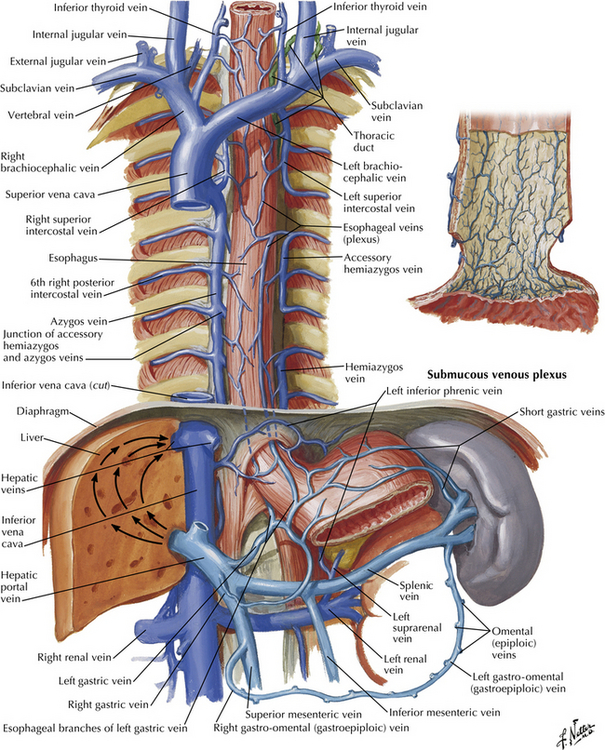
Venous drainage: extensive submucosal venous plexus communicates with periesophageal veins; flows into inferior thyroid (upper 1/3), azygous (middle 1/3) and gastric veins (lower 1/3); azygous vein empties into superior vena cava and gastric veins into portal system; this connection between caval and portal venous systems explains esophageal varices due to portal hypertension
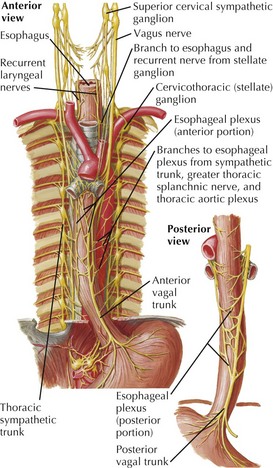
Nerves: left and right vagus nerves run lateral to esophagus, form plexi along anterior and posterior surfaces, then reunite to form anterior and posterior vagal trunks to stomach; have parasympathetic and sympathetic innervation
Lymphatic drainage: freely anastomosing networks in submucosa, muscularis propria and occasionally lamina propria; facilitate lengthwise tumor dissemination; upper third drains into paratracheal and internal jugular nodes, middle third to mediastinal nodes, lower third to nodes around aorta and celiac axis
Adjacent structures: cervical esophagus lies in posterior mediastinum, posterior to trachea and thyroid gland; is bounded by left and right recurrent laryngeal nerves and carotid sheaths; distal esophagus is posterior to left atrium and bounded by azygous veins; passes through opening in diaphragm called the hiatus
Incisura / angle of His: left side of esophagus forms sharp angle where it joins the stomach
Diagrams / tables
Images hosted on other servers:
4 weeks - relation of gut to yolk sac
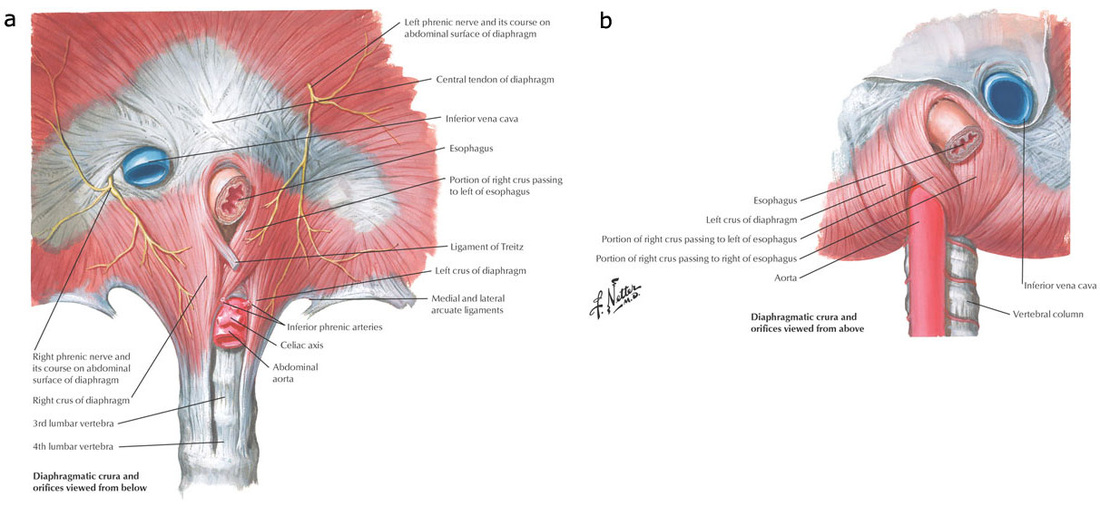
Diaphragmatic crura
Arterial blood supply
Venous drainage
Nerves
Lymphatic drainage
Cervical region
Clinical images
AFIP images
Z line - endoscopic appearance
Gross images
Images hosted on other servers:
Gastroesophageal junction
Microscopic (histologic) images
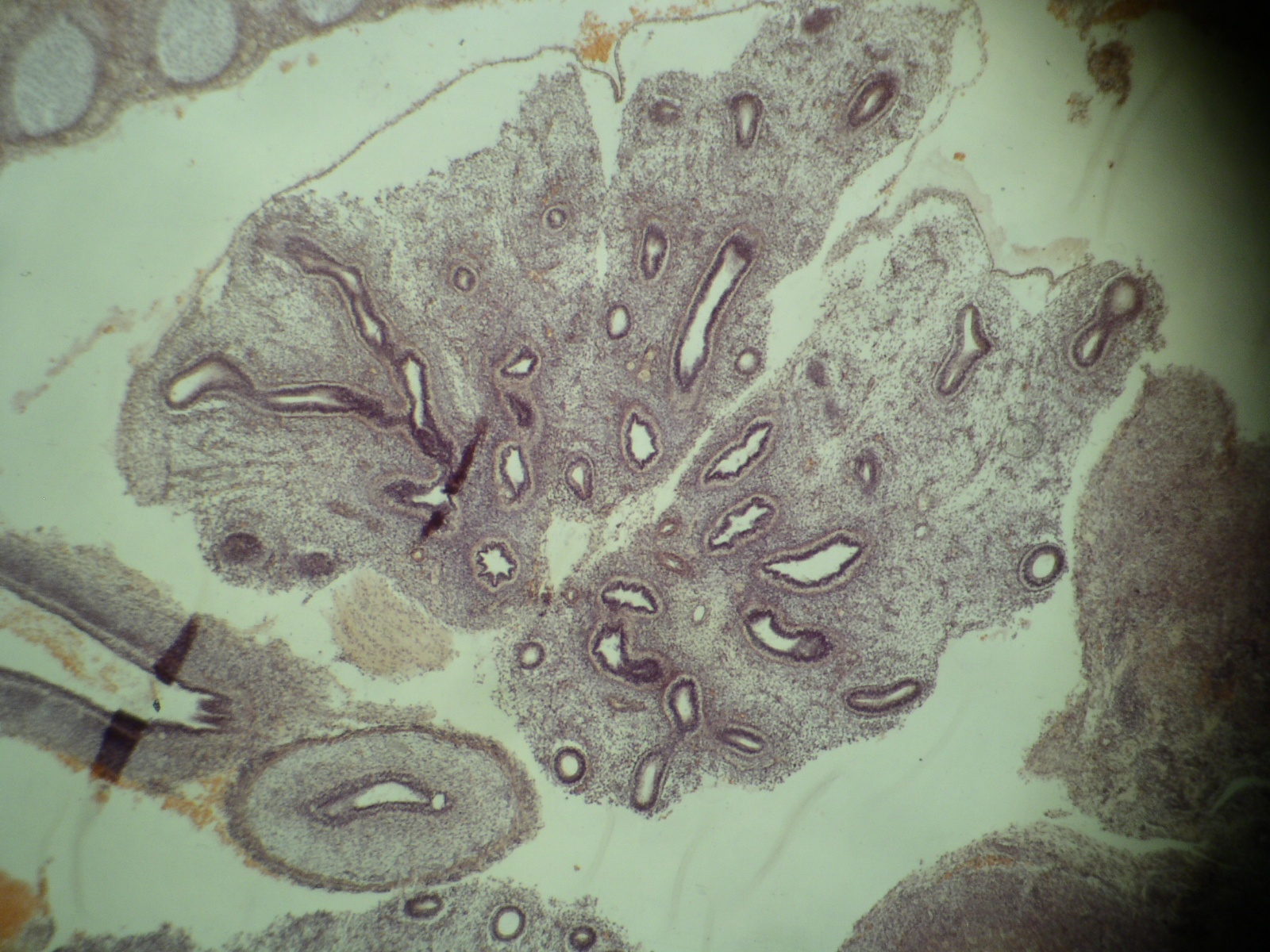
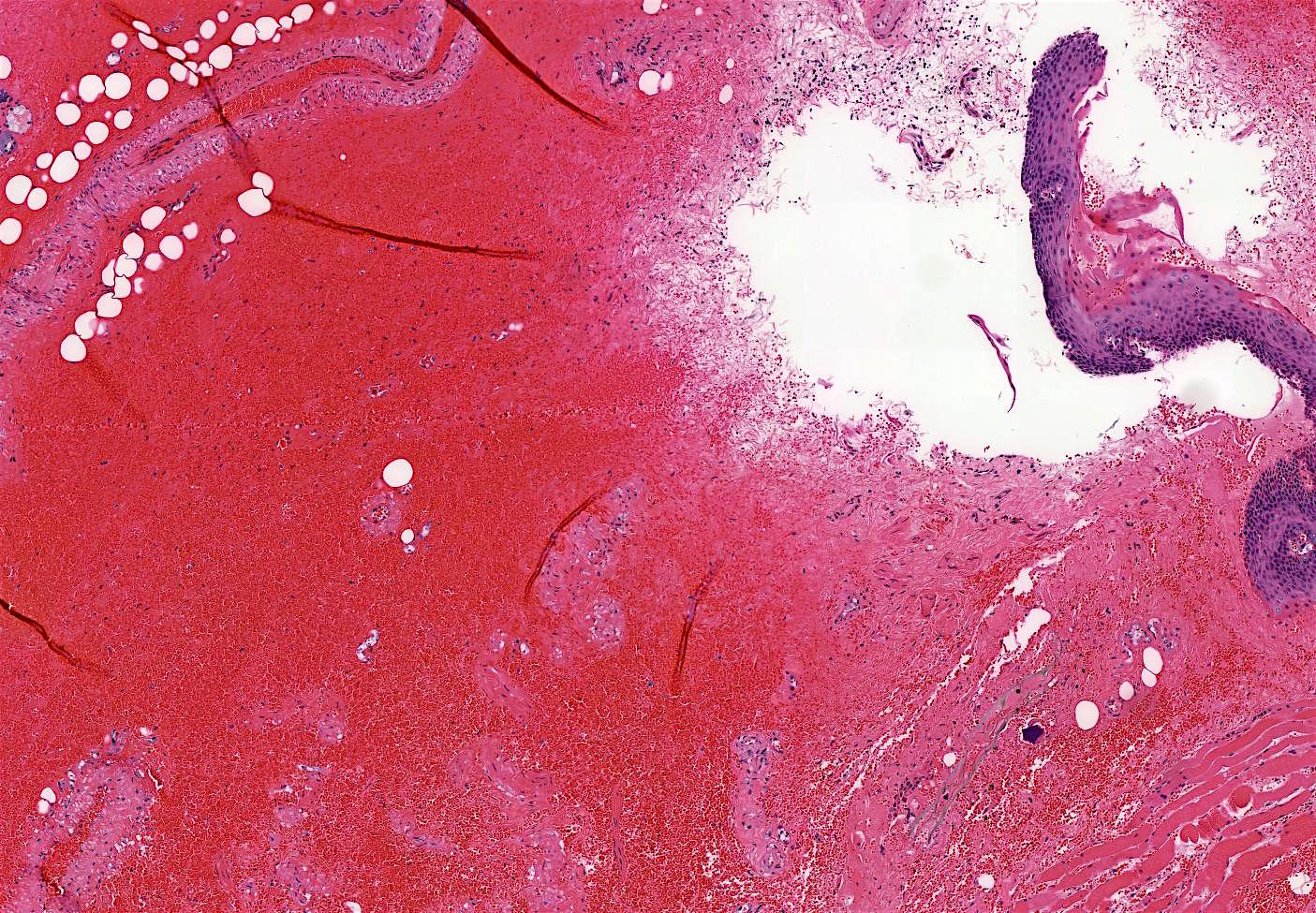
Contributed by Grigory Demyashkin, M.D., Ph.D.
Upper left: small intestine
bottom left: esophagus
center: stomach
top right: pancreas; right: liver
American College of Gastroenterology (ACG) 2016 BE definition: extension of salmon colored mucosa into the tubular esophagus extending ≥ 1 cm proximal to the gastroesophageal (GE) junction with biopsy confirmation of intestinal metaplasia (goblet cells) (Am J Gastroenterol 2016;111:30)
British Society of Gastroenterology 2014 BE definition: columnar epithelium with or without goblet cells extending ≥ 1 cm proximal to the GE junction (Gut 2014;63:7)
Essential features
Secondary to longstanding gastroesophageal reflux disease (GERD)
Necessity of intestinal metaplasia (IM) for diagnosis of BE varies; IM required in United States and part of Europe, IM not necessary in UK and Japan (Am J Gastroenterol 2016;111:30, Gut 2014;63:7)
Screening no longer indicated in women with chronic symptoms of GERD
Screening not recommended for general population (patients without reflux symptoms)
Sites
Distal esophagus, gastroesophageal junction
Pathophysiology
Metaplasia in BE presumably results from cellular reprogramming
GERD induced tissue damage reprograms immature progenitor cells to express columnar development transcription factors
Tissue injury activates signaling pathways such as Hedgehog, BMP4 and NF-KB, and downregulates Notch signaling
Signals lead to increased expression of SOX9 (induces columnar differentiation), FOXA2, CDX1 and CDX2 (induces intestinal differentiation) (J Clin Invest 2014;124:3767)
Transdifferentiation (distinctive type of multilayered epithelium at the squamocolumnar junction with features of both squamous and columnar epithelium) may occur in BE (Am J Gastroenterol 2016;111:30)
Characteristic endoscopic appearance (at least 1 cm segment of abnormal mucosa proximal to GE junction) plus characteristic histologic findings (metaplastic epithelium with intestinal metaplasia in USA)
At least eight random biopsies recommended
When eight biopsies not obtainable (as in short segment BE), at least four biopsies / cm of circumferential BE and one biopsy / cm in tongues of BE recommended
Annual risk of progression with low grade dysplasia (0.7% per year) and high grade dysplasia (7% per year)
Treatment
BE patients should receive once daily proton pump inhibitor therapy
Aspirin, other NSAIDs or antireflux surgery not routinely prescribed or performed
Surveillance should be performed with high definition / high resolution white light endoscopy
For BE without dysplasia, endoscopic surveillance at intervals of three to five years
Endoscopic surveillance should employ four quadrant biopsies at 2 cm intervals in patients without dysplasia and 1 cm intervals in patients with prior dysplasia
For BE dysplasia, refer to BE dysplasia section for surveillance guidelines
Endoscopic mucosal resection or endoscopic ablation therapy: preferred treatment options for patients with dysplasia (refer to BE dysplasia section) (Am J Gastroenterol 2016;111:30)
Clinical images
AFIP images
Normal and BE
Images hosted on other servers:
Salmon colored mucosa
Endoscopy: mucosal erythema of lower esophagus
Gross description
Red / salmon colored mucosa between pale squamous mucosa of lower esophagus and lush pink gastric mucosa; may have tongues extending up from GE junction
Endoscopists utilize the Prague classification to describe disease extent (include circumferential and maximal segment length) in Barrett mucosa (Am J Gastroenterol 2016;111:30)
Microscopic (histologic) description
Esophageal squamous epithelium replaced by columnar epithelium of intestinal type with goblet cells
True goblet cells: rounded shape, clear to bluish cytoplasmic mucin, randomly scattered, mucin usually indents nucleus
Baseline atypia of Barrett mucosa - some basal glands may show nuclear enlargement and stratification but there is complete surface maturation; this is considered negative for dysplasia
Duplication of muscularis mucosae characteristic finding in BE; observed in 92% of BE resections, involving 5% of the Barrett segment (Am J Surg Pathol 2007;31:1719)
Squamous overgrowth over metaplastic epithelium, hybrid glands, presence of esophageal ducts have high specificity for BE (Am J Surg Pathol 2007;31:1733)
Postablation histology: replacement of columnar mucosa to squamous (neosquamous) mucosa; residual metaplastic epithelium may persist beneath the squamous epithelium (known as buried Barrett’s) and progress to dysplasia or carcinoma
Microscopic (histologic) images
Contributed by Dipti M. Karamchandani, M.D.
BE
Goblet cells
Pseudogoblet cells
Four lines
Hybrid glands
Squamous overgrowth
Baseline atypia
Muscularis mucosae duplication
Virtual slides
Images hosted on other servers:
Barrett esophagus
Cytology description
Cytology has good sensitivity (82%) and specificity (88%) for identifying intestinal metaplasia with moderate interobserver agreement (J Am Soc Cytopathol 2015;4:113)
Cytology may be poised to synergize with advances in other techniques for management of patients with Barrett esophagus
H&E remains the gold standard for diagnosis of BE and assessing Barrett dysplasia (Am J Surg Pathol 2016;40:e83)
Alcian blue (at pH 2.5) stain acidic mucin in true goblet cells as bright purple blue; helpful in distinguishing true goblet cells from pseudogoblet cells in challenging cases, reflexive use on biopsies not justified
Use of mucin glycoproteins (MUC2, MUC5AC) to diagnose BE currently not indicated
Use of markers of intestinal phenotype (CDX2, Das-1, villin, HepPar1) to diagnose BE currently not indicated
Use of CK7 and CK20 to distinguish BE from intestinal metaplasia of the gastric cardia not indicated as not adequately specific
Electron microscopy description
Mucin granules in metaplastic cells
Sample pathology report
No endoscopy report provided and there is intestinal metaplasia in the biopsy
Esophagus, distal, biopsy:
Barrett mucosa, negative for dysplasia (see comment)
Comment: Per 2016 ACG guidelines, the diagnosis of Barrett esophagus in this case is made owing to the presence of goblet cells, with the assumption that the biopsy is taken from distal esophagus and the mucosal irregularity extends to at least 1 cm above the top of the gastric folds.
Endoscopy report provided and specifies that mucosal irregularity extends to at least 1 cm proximal to the gastroesophageal junction
Esophagus, distal, biopsy:
Barrett mucosa, negative for dysplasia
No endoscopy report provided, there is intestinal metaplasia in the biopsy and the biopsy is labeled as gastroesophageal junction
Gastroesophageal junction, biopsy:
Gastric cardia type mucosa with intestinal metaplasia, negative for dysplasia (see comment)
Comment: If the biopsy is taken from tubular esophagus and the mucosal irregularity extends to at least 1 cm above the top of gastric folds, then this represents Barrett esophagus. If the biopsy is taken from gastric cardia, then this represents intestinal metaplasia of the gastric cardia.
Below is a picture of endoscopic biopsy from a 60 year old man with a clinical history of reflux symptoms and the biopsy is labeled as gastroesophageal junction. The endoscopy report is not provided. How would you sign out the case?
Barrett esophagus, negative for dysplasia
Gastric mucosa with intestinal metaplasia, consistent with Barrett esophagus
Gastric cardia type mucosa with intestinal metaplasia (see comment)
Barrett esophagus with low grade dysplasia
Board review style answer #1
C. Gastric cardia type mucosa with intestinal metaplasia, with a comment stating that endoscopic evidence of abnormal mucosa for at least 1 cm proximal to the gastroesophageal junction is required for a diagnosis of Barrett esophagus.
Presence of Barrett esophagus related dysplasia remains greatest risk factor for development of esophageal adenocarcinoma (Am J Surg Pathol 2017;41:e8)
Pathologic diagnosis and grading of dysplasia is the gold standard marker for assessing risk of neoplastic progression (Am J Surg Pathol 2016;40:e83)
Diagnosis and grading of Barrett esophagus related dysplasia can be challenging, especially with coexisting inflammation (Hum Pathol 1988;19:166)
Both low grade dysplasia and high grade dysplasia managed by endoscopic therapy, per the latest American
College of Gastroenterology (ACG) guidelines (Am J Gastroenterol 2016;111:30)
Accumulation of multiple genetic and epigenetic alterations causes development and progression of dysplasia (Nat Genet 2014;46:837)
C-myc and cyclins D1, E and B implicated as oncogenes in neoplastic progression in Barrett esophagus (Am J Surg Pathol 2016;40:e45)
Inactivation of tumor suppressor proteins p53, p16, p15, p27 and adenomatous polyposis coli (APC) also implicated in Barrett esophagus carcinogenesis (Am J Surg Pathol 2016;40:e45)
Other mechanisms proposed include increased telomerase expression, increased VEGFA and C, decreased membrane E-cadherin, increased MMP-7 and MMP-9, increased markers of epithelial-mesenchymal transition such as 2EB1/2EB2 and TGF-B1 (Am J Surg Pathol 2016;40:e45)
As Barrett esophagus epithelial cells progress to cancer, they typically manifest aneuploidy, a marker of genomic instability (Am J Surg Pathol 2016;40:e45)
Patients typically have gastroesophageal reflux disease symptoms
No distinct clinical or radiologic manifestations of Barrett esophagus dysplasia
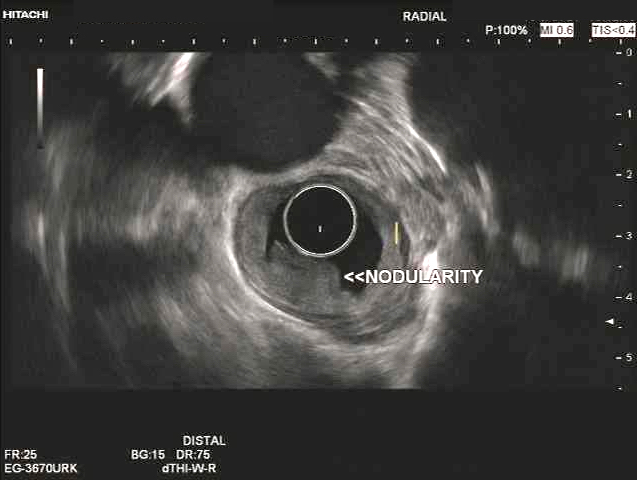
Endoscopically, Barrett esophagus dysplasia may be visible as thickened, flat, irregular or plaque-like area, distinct from adjacent nondysplastic Barrett mucosa (Dig Dis Sci 2003;48:1537, Am J Gastroenterol 2016;111:30)
Mucosal abnormalities (ulceration, stricture, mass, nodules, plaques) associated with increased risk of cancer (Am J Gastroenterol 2016;111:30)
Diagnosis
Recommended for Barrett esophagus with dysplasia to be reviewed by 2 pathologists, at least 1 with specialized expertise in GI pathology (Am J Gastroenterol 2016;111:30)
Barrett esophagus surveillance performed with high definition / high resolution white light endoscopy
Routine use of advanced imaging techniques other than electronic chromoendoscopy not recommended for endoscopic surveillance at this time
Endoscopic surveillance should employ 4 quadrant biopsies at 1 cm intervals in patients with prior dysplasia (Am J Gastroenterol 2016;111:30)
Mucosal abnormalities to be sampled separately, preferably with endoscopic mucosal resection (EMR)
Adjunct use of wide area transepithelial sampling with computer assisted 3 dimensional analysis (WATS) to forceps biopsy markedly improves detection of esophageal dysplasia (United European Gastroenterol J 2018;6:529)
Progression rates of low grade dysplasia to high grade dysplasia and dysplasia to carcinoma directly proportional to number of pathologists who agree on dysplasia diagnosis (Am J Surg Pathol 2016;40:e45, Am J Gastroenterol 2007;102:483)
Treatment
Indefinite for dysplasia:
Repeat endoscopy after acid suppressive medication optimization for 3 - 6 months
In patients with preablation low grade dysplasia, endoscopic surveillance recommended every 6 months in the first year following complete elimination of intestinal metaplasia (CIEM) and annually thereafter (Am J Gastroenterol 2016;111:30)
Endoscopic surveillance following complete elimination of intestinal metaplasia for patients with preablation high grade dysplasia recommended every 3 months for the first year, every 6 months in the second year and annually thereafter (Am J Gastroenterol 2016;111:30)
Clinical images
Images hosted on other servers:
Nodule on endoscopy
Endoscopic mucosal resection
Narrow band imaging
Endoscopic treatment of Barrett high grade dysplasia
Wide area transepithelial sampling
Gross description
Normal appearing or nodule, erosion or polyp
Gross images
Images hosted on other servers:
High grade dysplasia
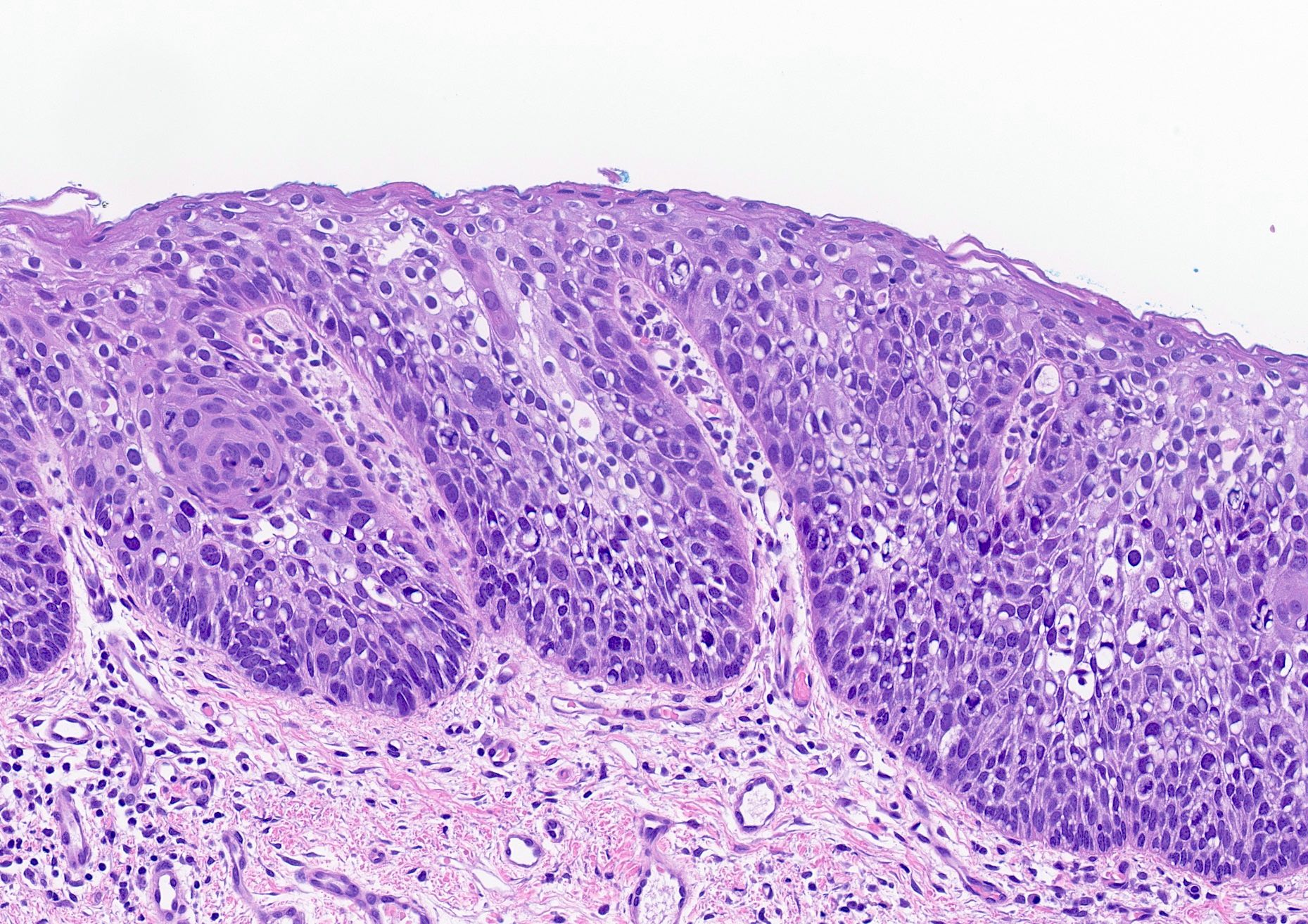
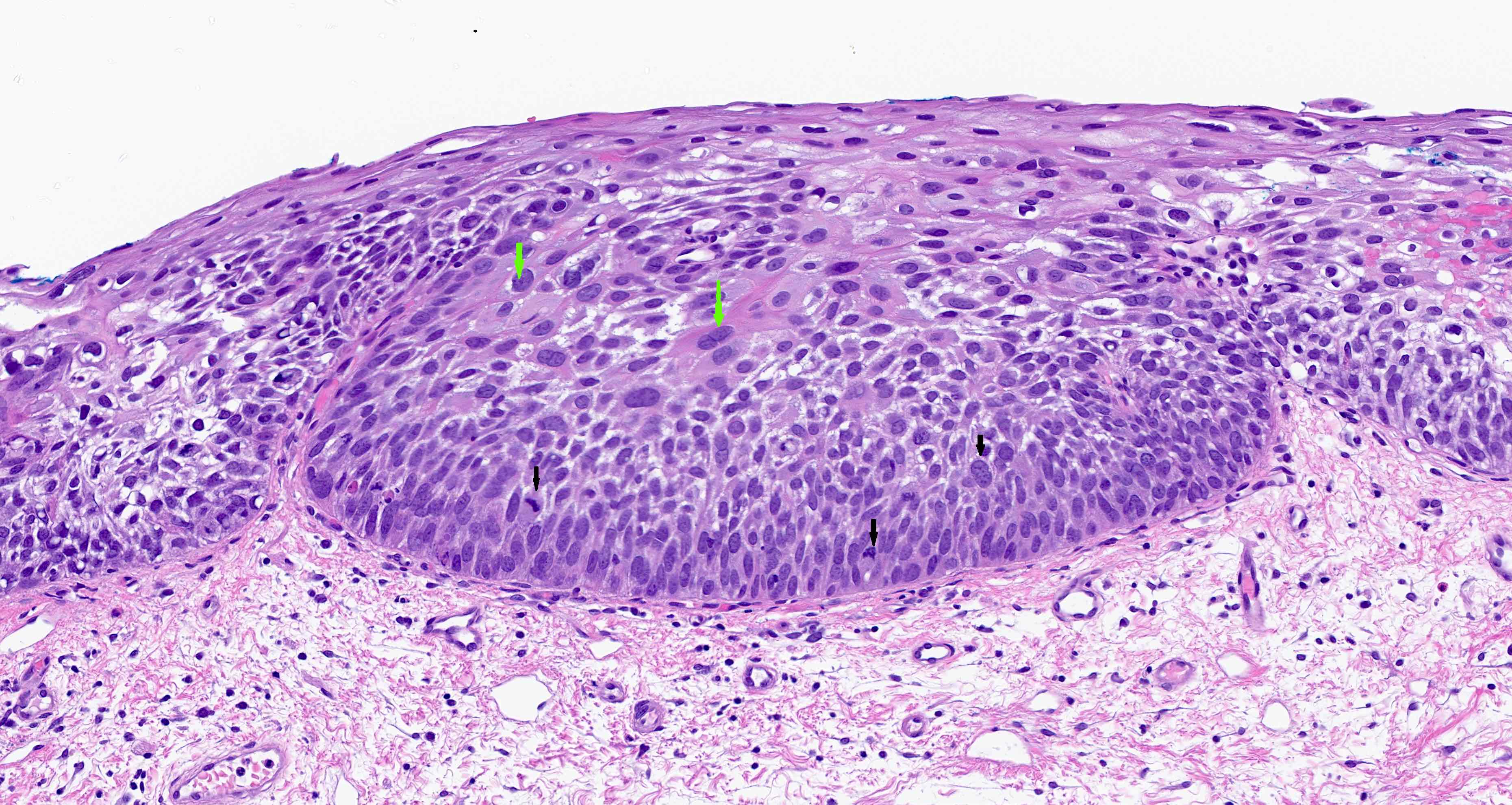
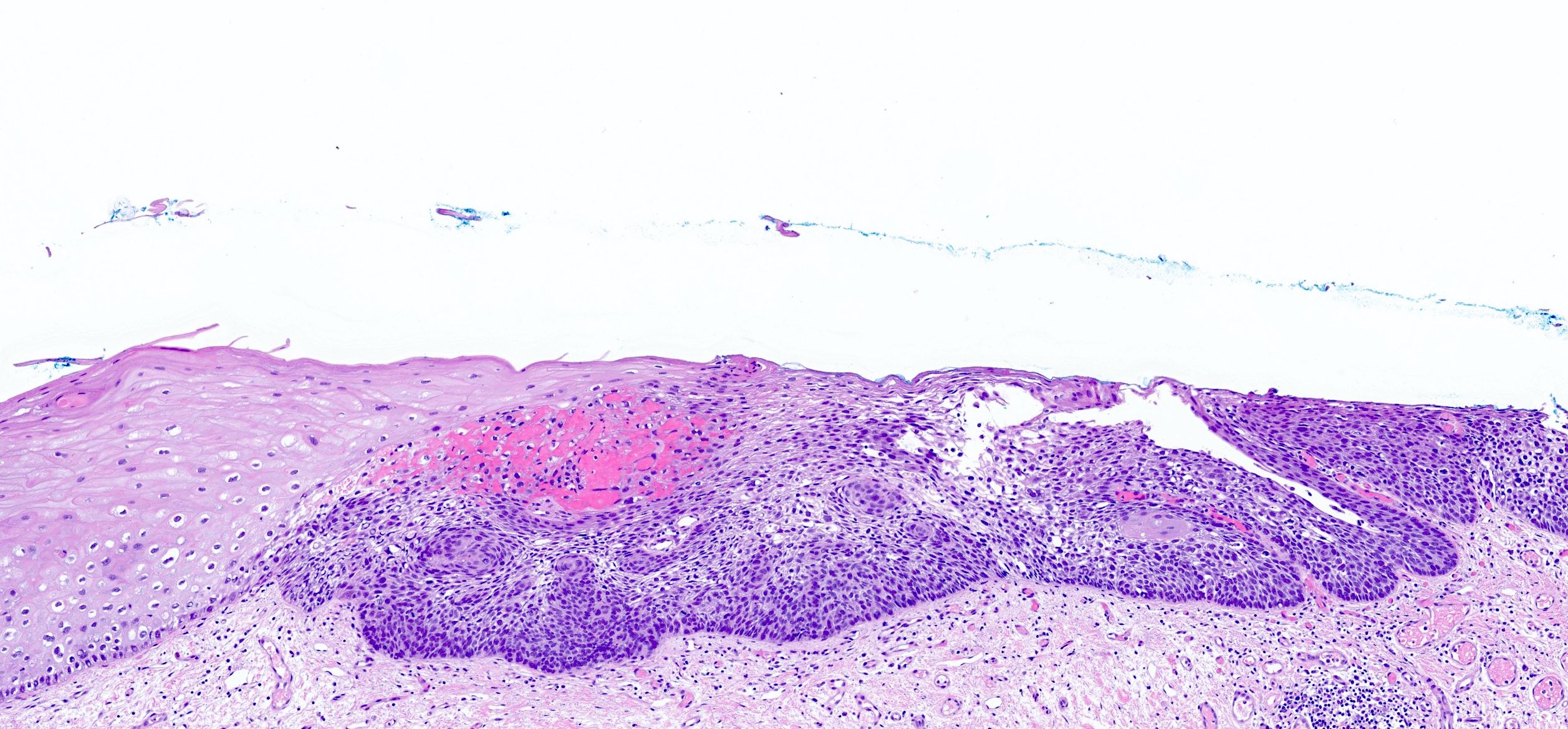
Microscopic (histologic) description
Barrett esophagus dysplasia divided into low grade dysplasia and high grade dysplasia; indefinite for dysplasia also a valid interpretation (but not part of a histologic spectrum of progression) (Hum Pathol 1988;19:166)
Greater degree of cytologic atypia in addition to architectural abnormalities
Architectural abnormalities:
Irregular size and shape of crypts, crowded crypts with little intervening lamina propria, intraluminal budding or cribriforming, rare dilated glands with intraluminal necrotic debris
Cytologic features:
Lack of surface maturation, loss of nuclear polarity, marked nuclear enlargement, pleomorphism and hyperchromasia, irregular nuclear contours
Loss of nuclear polarity considered an important objective criterion to diagnose high grade dysplasia
Used as an adjunct to biopsy in diagnosis of Barrett esophagus and associated neoplasms (Diagn Cytopathol 2003;29:130)
High degree of diagnostic accuracy of cytology for the diagnosis of Barrett associated high grade dysplasia, with reported sensitivity of 82% and specificity of 95% (Diagn Cytopathol 2003;29:130)
Observed sensitivity for low grade dysplasia is low (about 31%)
Gastrointestinal Pathology Society (GIPS) recommendation for p53 in diagnosing Barrett esophagus dysplasia:
Additional studies are needed to develop and validate precise criteria before p53 staining can be fully endorsed and incorporated into the morphologic dysplasia diagnosis algorithm (Am J Surg Pathol 2017;41:e8)
p53 appears promising marker in predicting disease progression but not recommended for routine use at present
Videos
Update on recently developed quality metrics
Sample pathology report
Esophagus, 36 cm, biopsy:
Barrett esophagus with low grade dysplasia
Esophagus, 35 cm, biopsy:
Barrett esophagus with high grade dysplasia
Esophagus, 34 cm, biopsy:
Barrett esophagus with epithelial alterations indefinite for dysplasia
Differential diagnosis
Reactive atypia versus low grade foveolar dysplasia:
Full thickness nuclear atypia with nonstratified nuclei suggests low grade gastric foveolar type dysplasia
Reactive atypia is usually limited to upper mucosa
Histologic features of lamina propria invasion (single cells in more than one focus, never ending glandular pattern, solid sheets of cells, significant cribriforming) is diagnostic of intramucosal adenocarcinoma (Am J Gastroenterol 2008;103:2333)
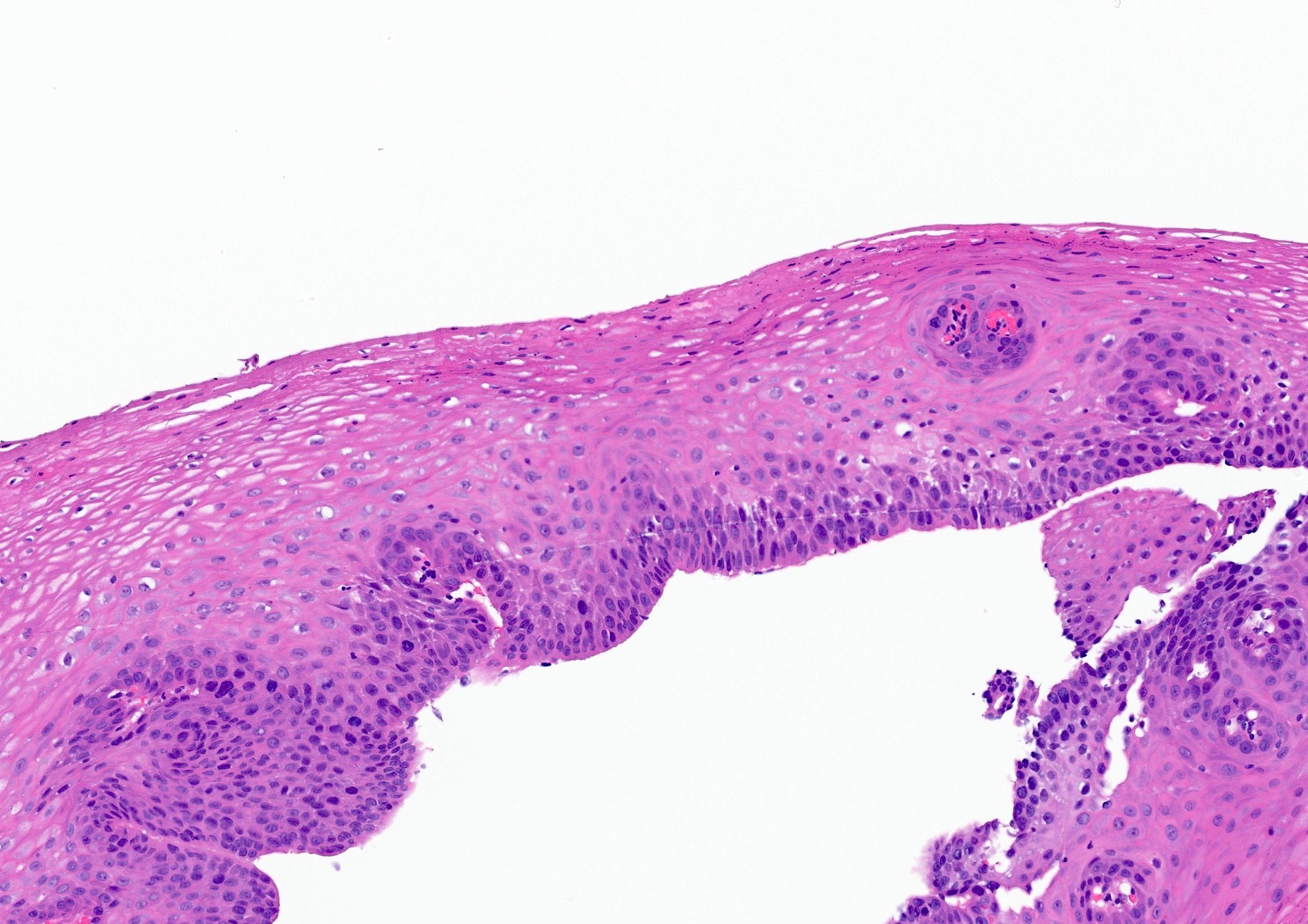
Above is a photomicrograph taken from a biopsy obtained from salmon colored mucosa in the distal esophagus extending to about 2 cm proximal to the gastroesophageal junction. What is your diagnosis?
Barrett esophagus, negative for dysplasia
Barrett esophagus with epithelial alterations indefinite for dysplasia
A nodule is found on surveillance endoscopy of a 60 year old patient with a longstanding history of Barrett esophagus. What should be the next step in patient management?
Endoscopic mucosal resection of the nodule
Esophagectomy
Radiofrequency ablation of the nodule
Use of use of wide area transepithelial sampling with computer assisted 3 dimensional analysis (WATS)
A biopsy diagnosis of low grade dysplasia was made by a pathologist and confirmed by a subspecialized GI pathologist. What is the preferred appropriate management based on the ACG 2016 guidelines?
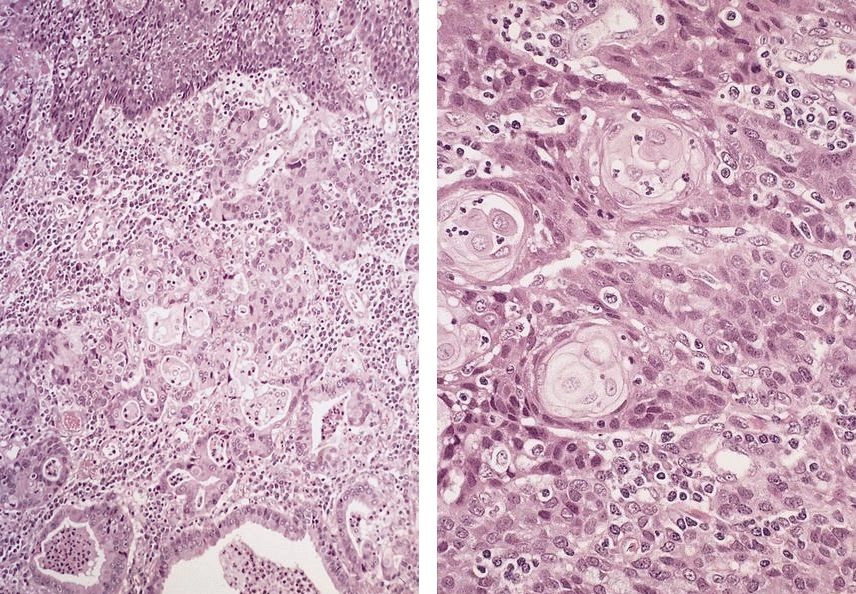
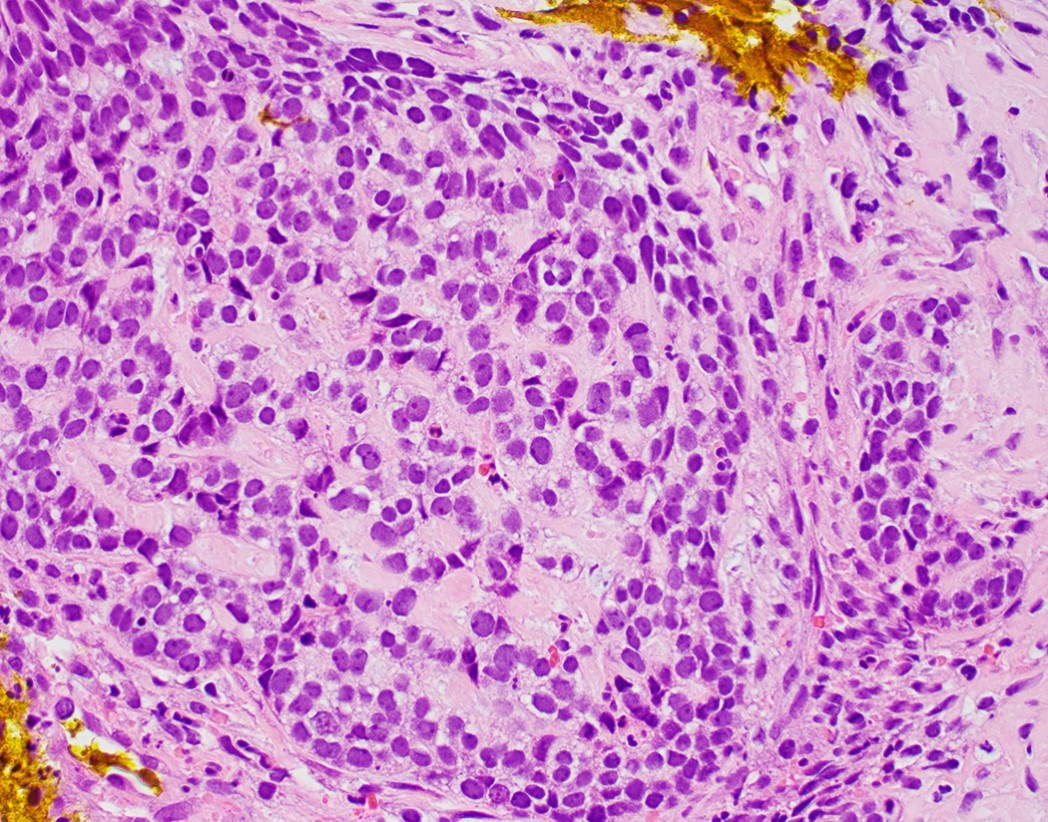
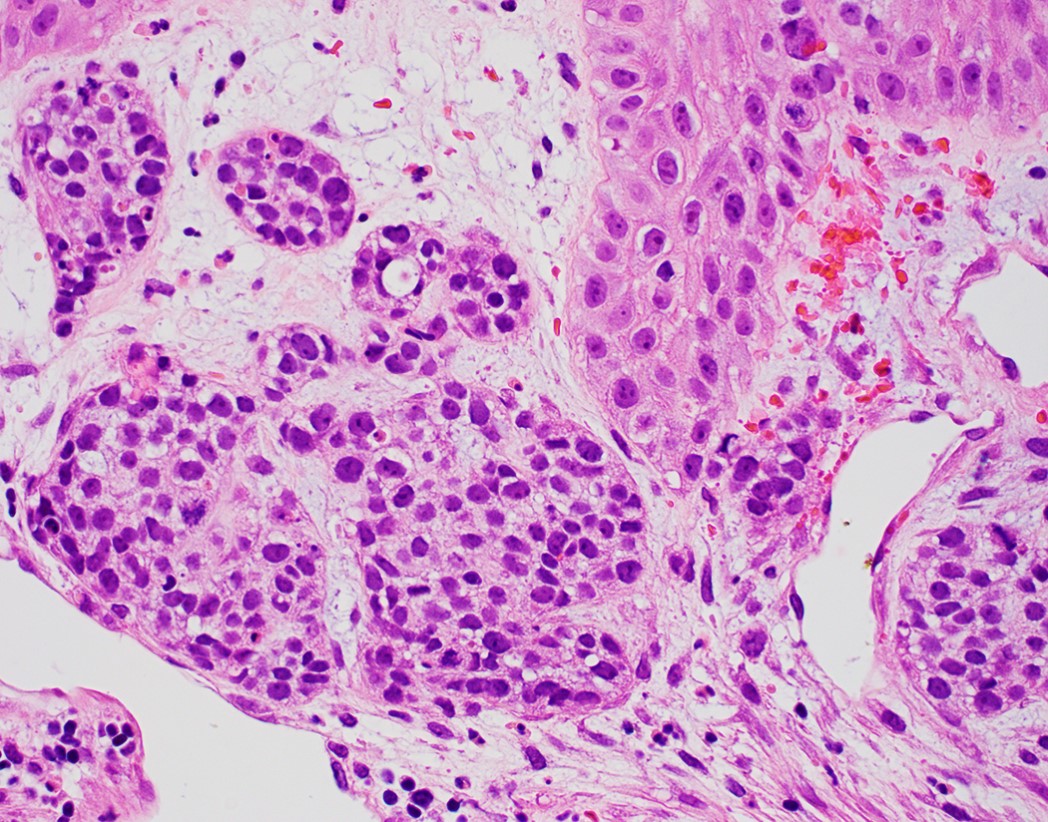
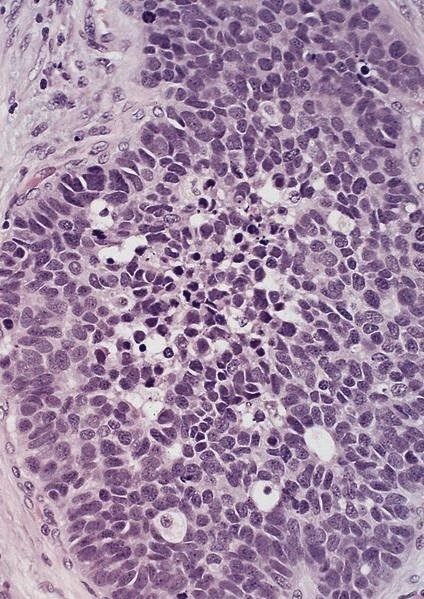
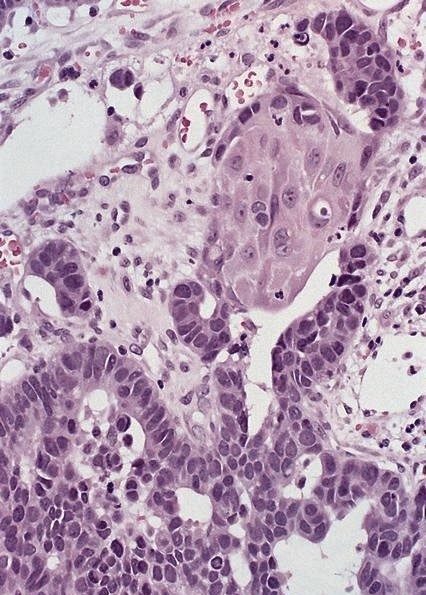
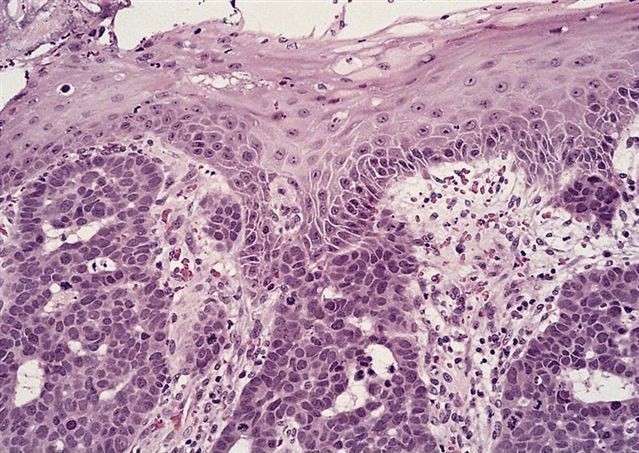
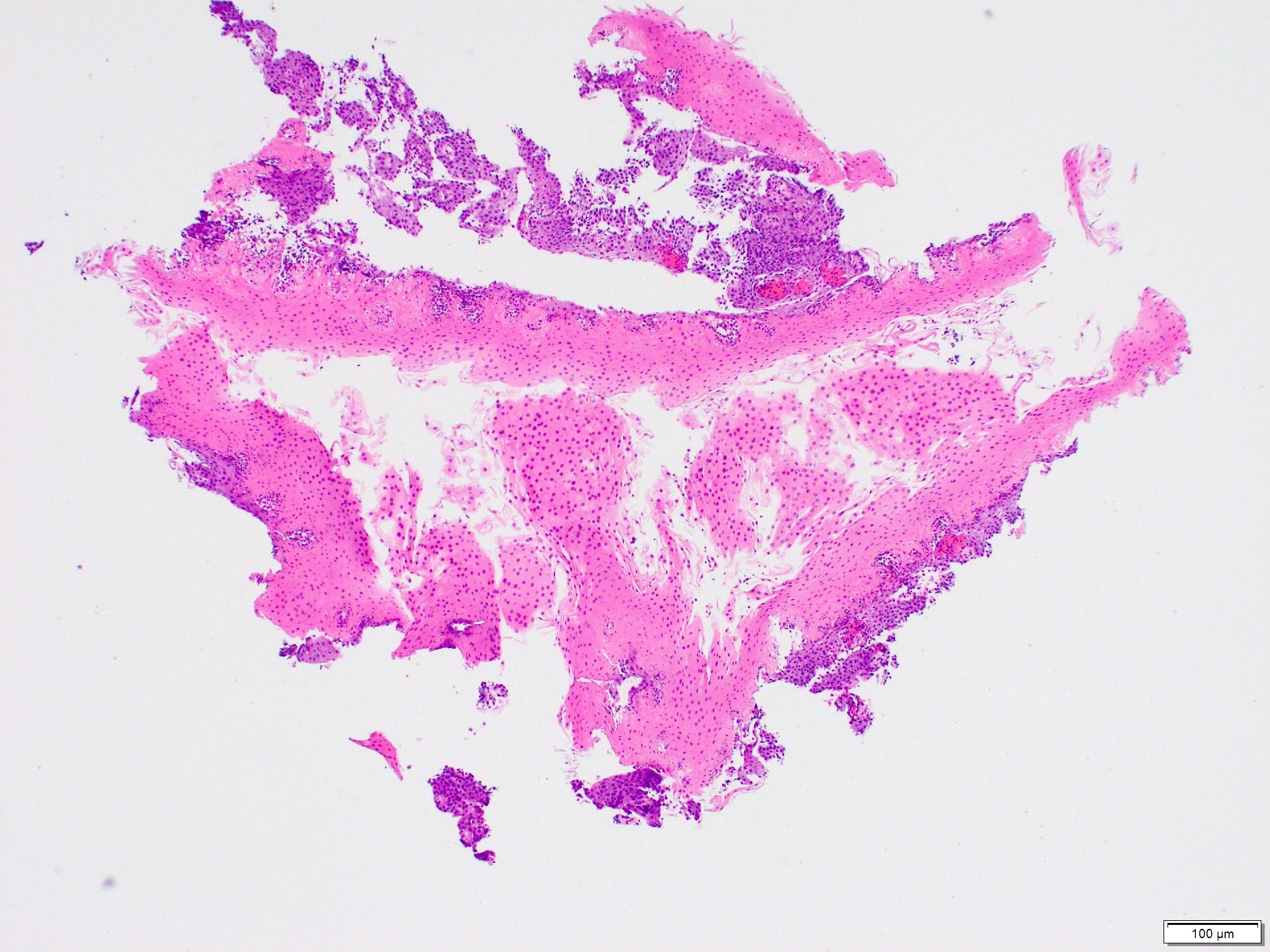
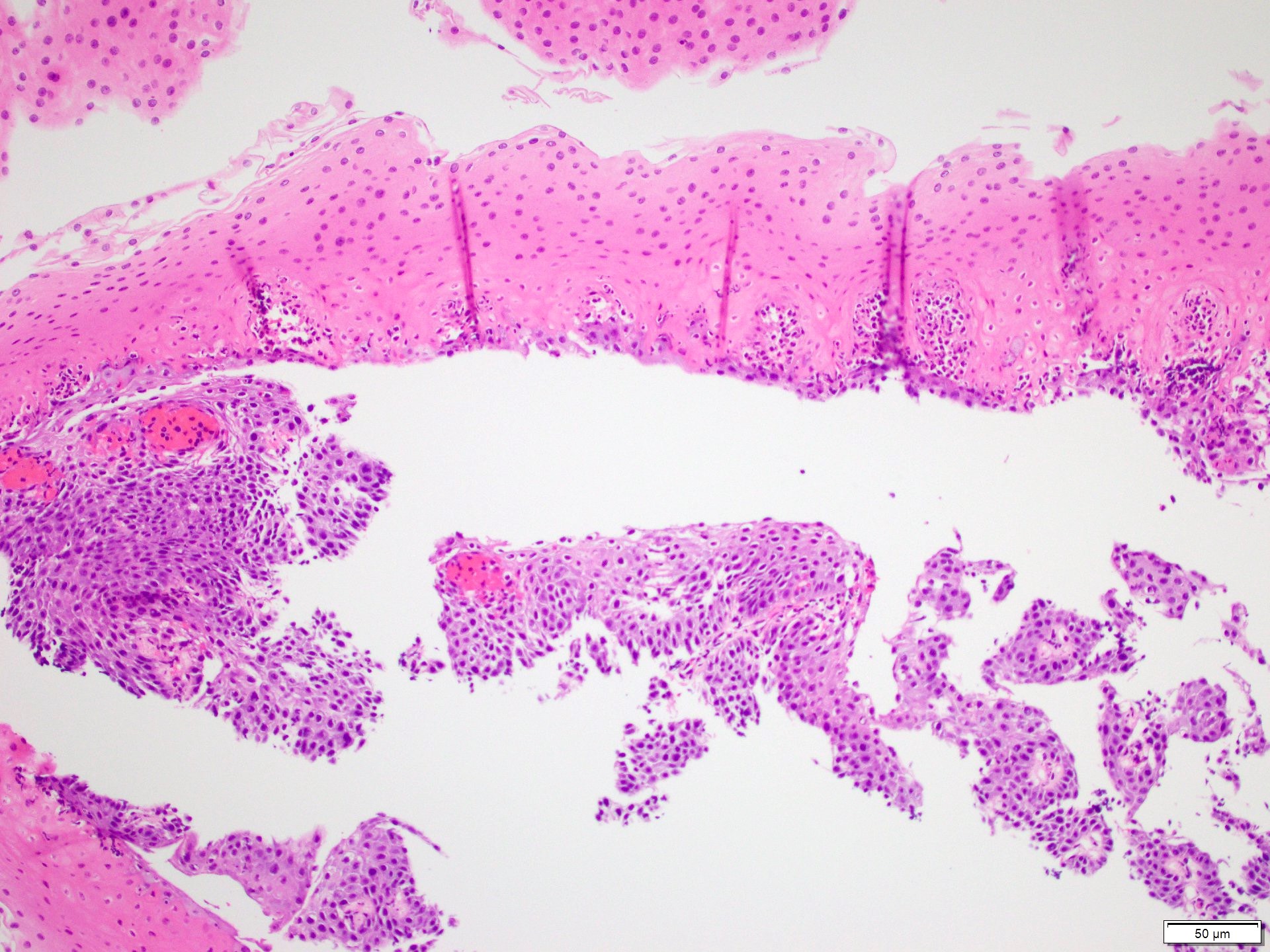
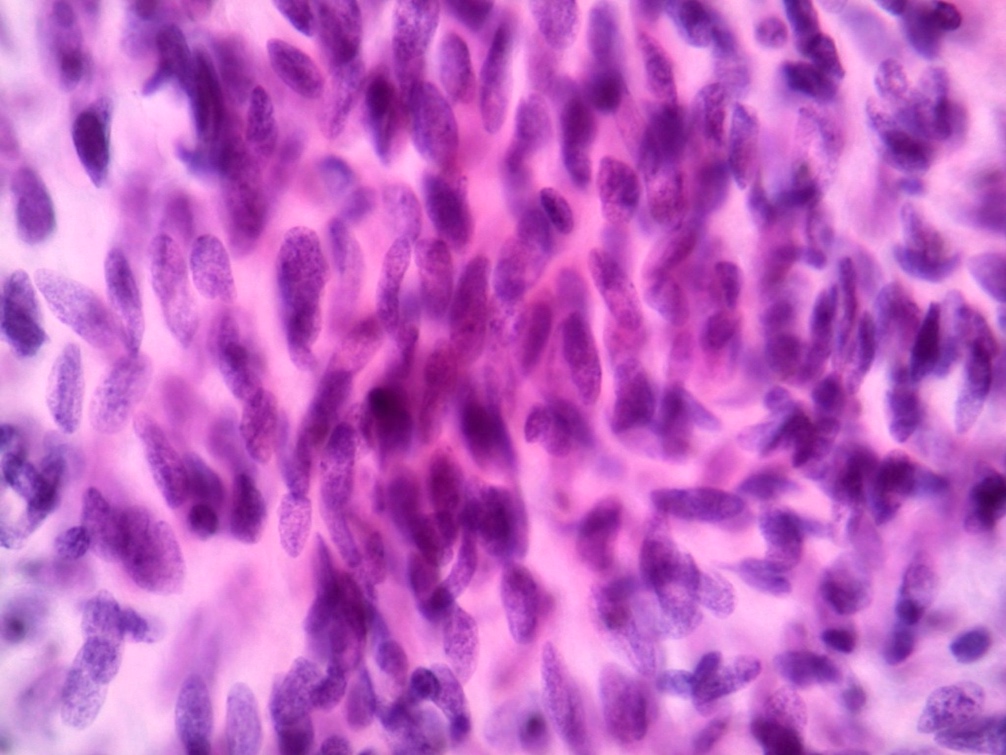
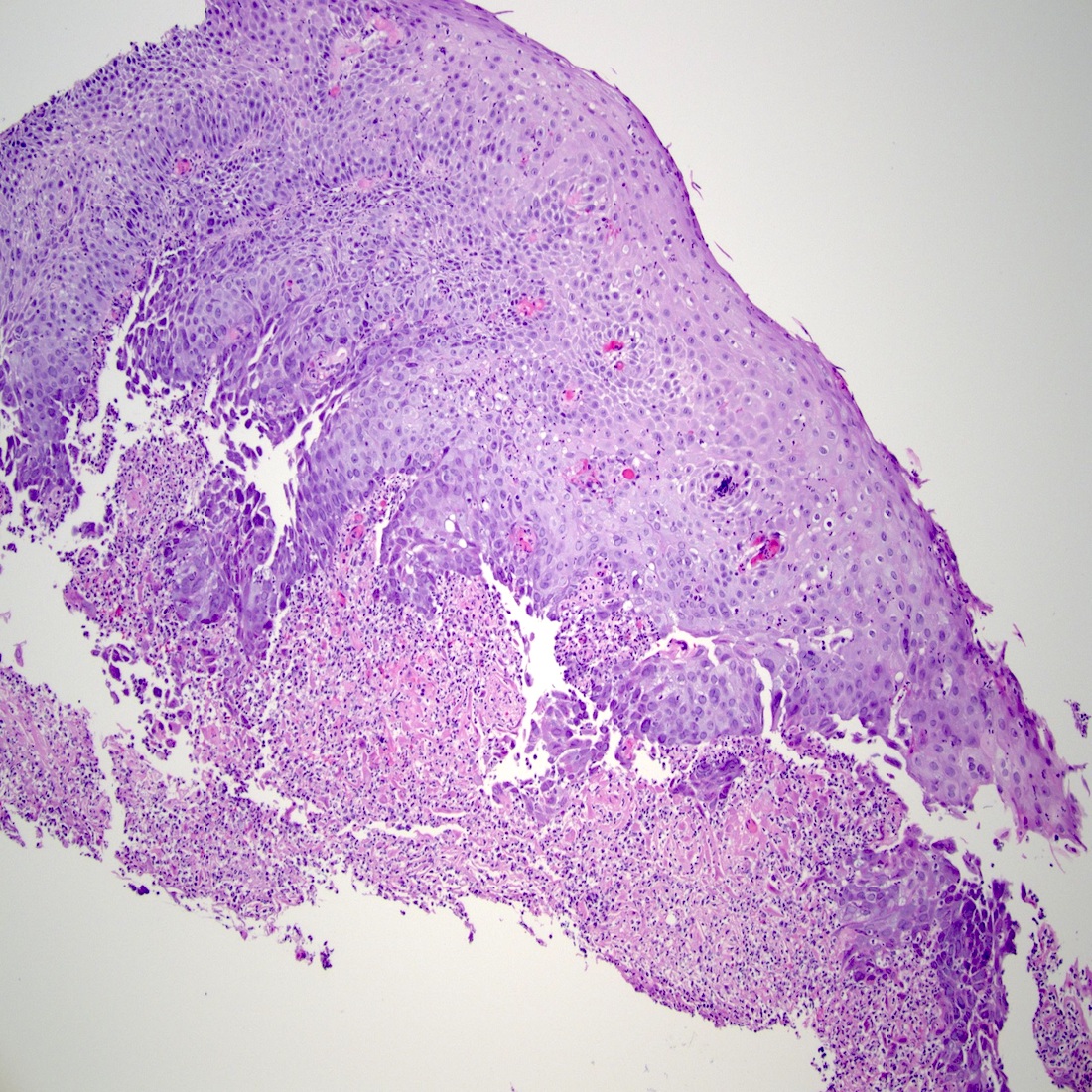
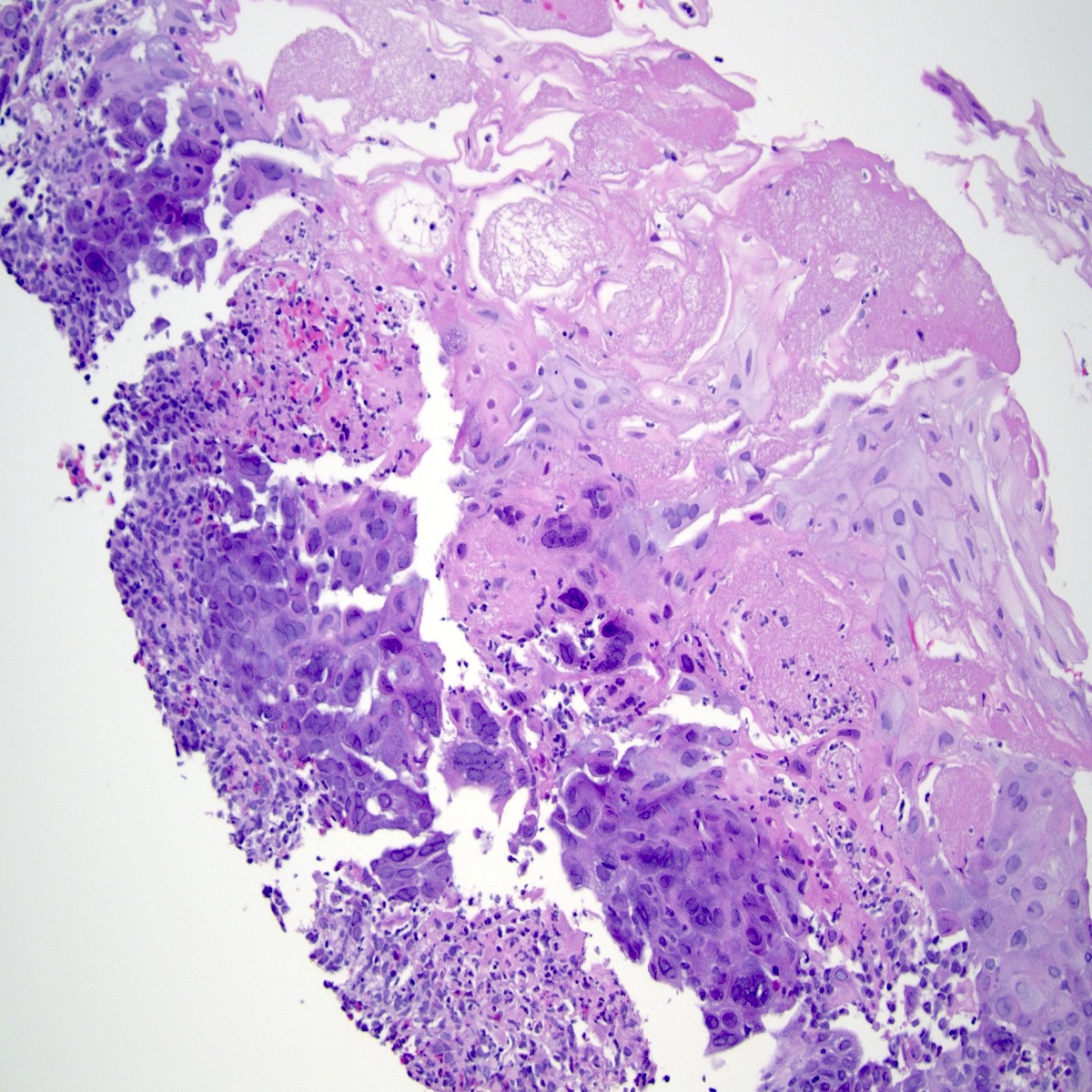
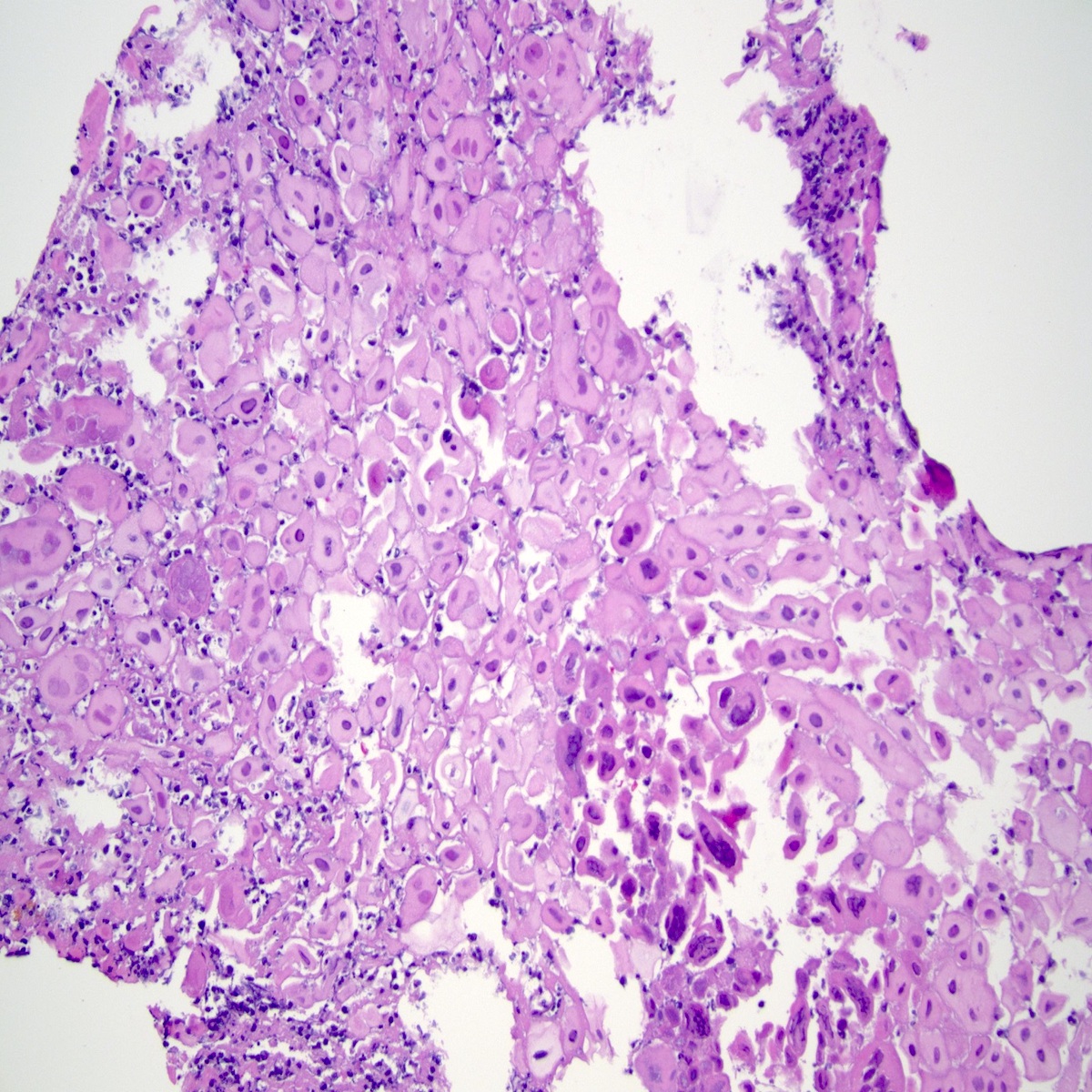
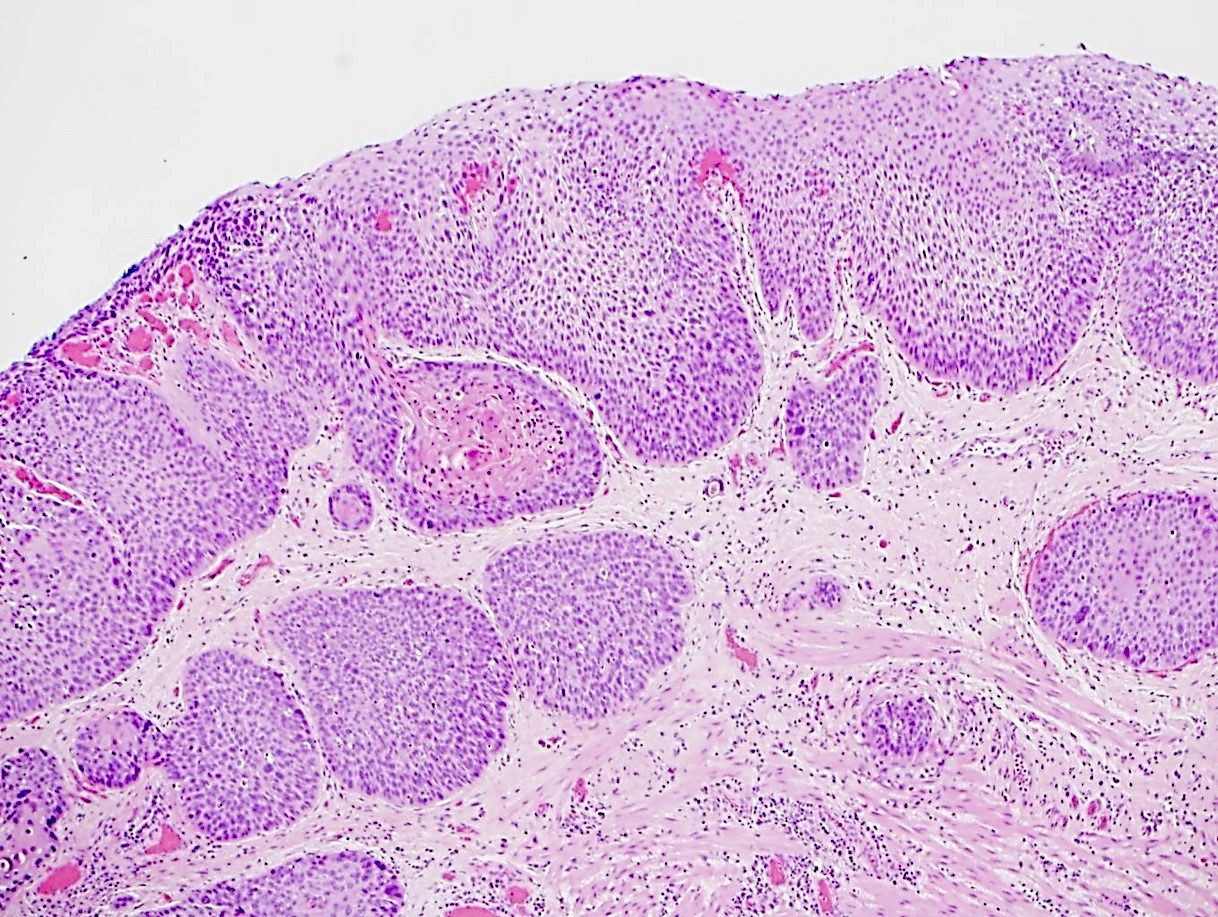
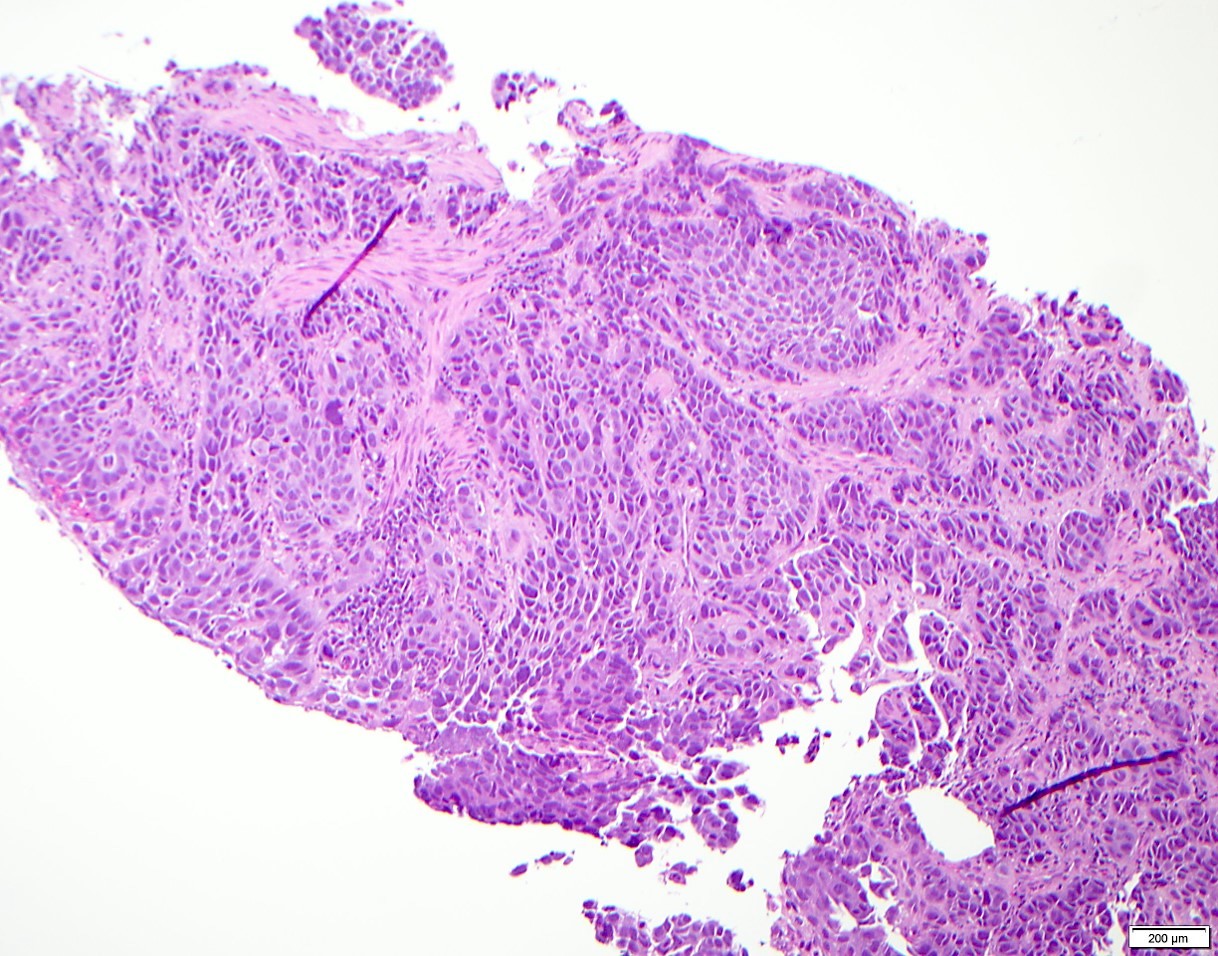
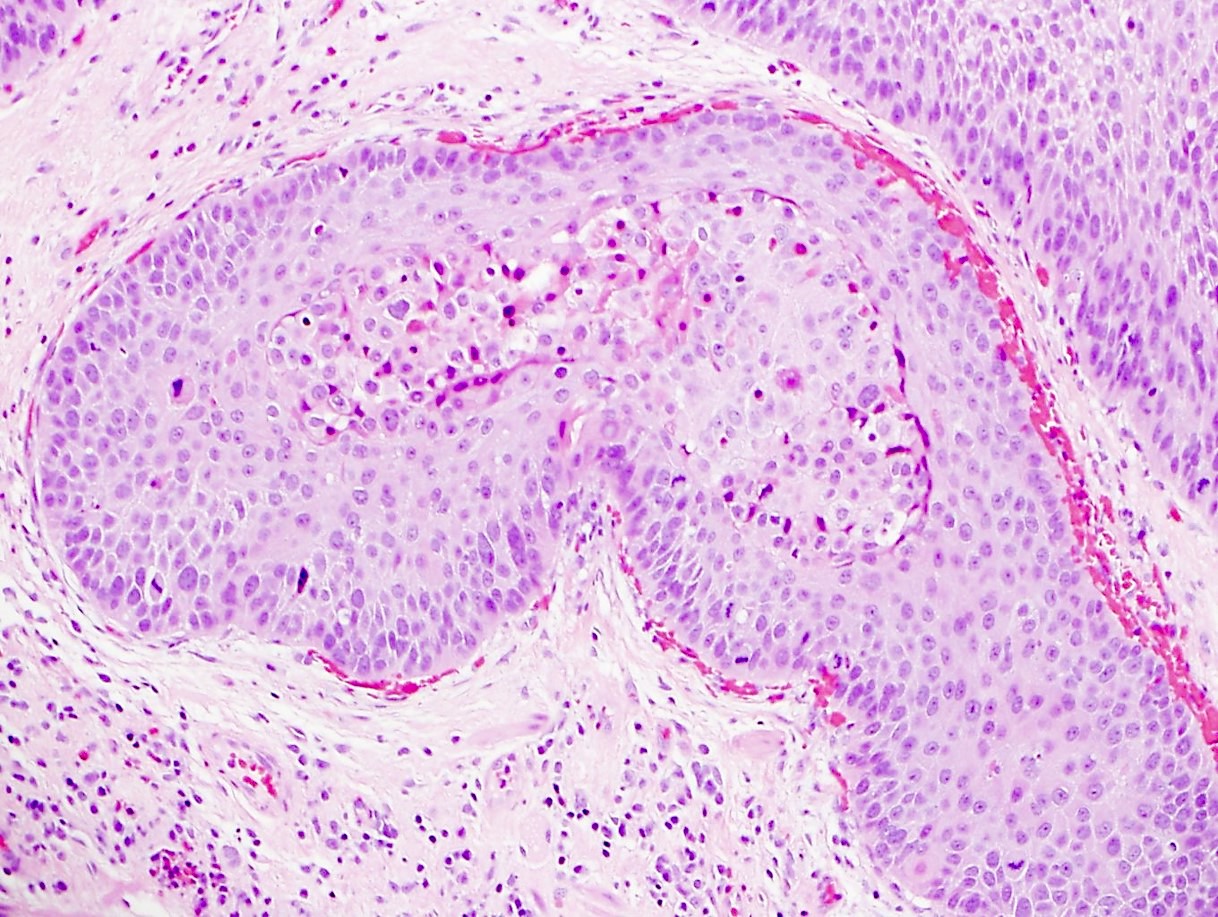
Variant of squamous cell carcinoma with distinct basaloid morphology
Essential features
Esophageal basaloid squamous cell carcinoma (BSCC) is a rare variant of SCC
Morphological differential diagnoses could include adenoid cystic carcinoma, neuroendocrine carcinoma (particularly small cell type), carcinosarcoma and epithelioid sarcoma
BSCC is not human papillomavirus (HPV) related and has a relatively poor prognosis as compared to morphologically similar HPV related SCC
ICD coding
ICD-10: C15.9 - malignant neoplasm of esophagus, unspecified
Even though more likely to be poorly differentiated at presentation, BSCC of the esophagus could have similar clinical features and survival outcomes when compared with SCC (J Am Coll Surg 2018;226:1086, Ann Surg Oncol 2015;22:3659)
Patients with BSCC and SCC should undergo stage specific treatment to achieve optimal outcomes (J Am Coll Surg 2018;226:1086)
Better prognosis that occurs with HPV associated BSCC of upper aerodigestive tract is different from BSCC of esophagus
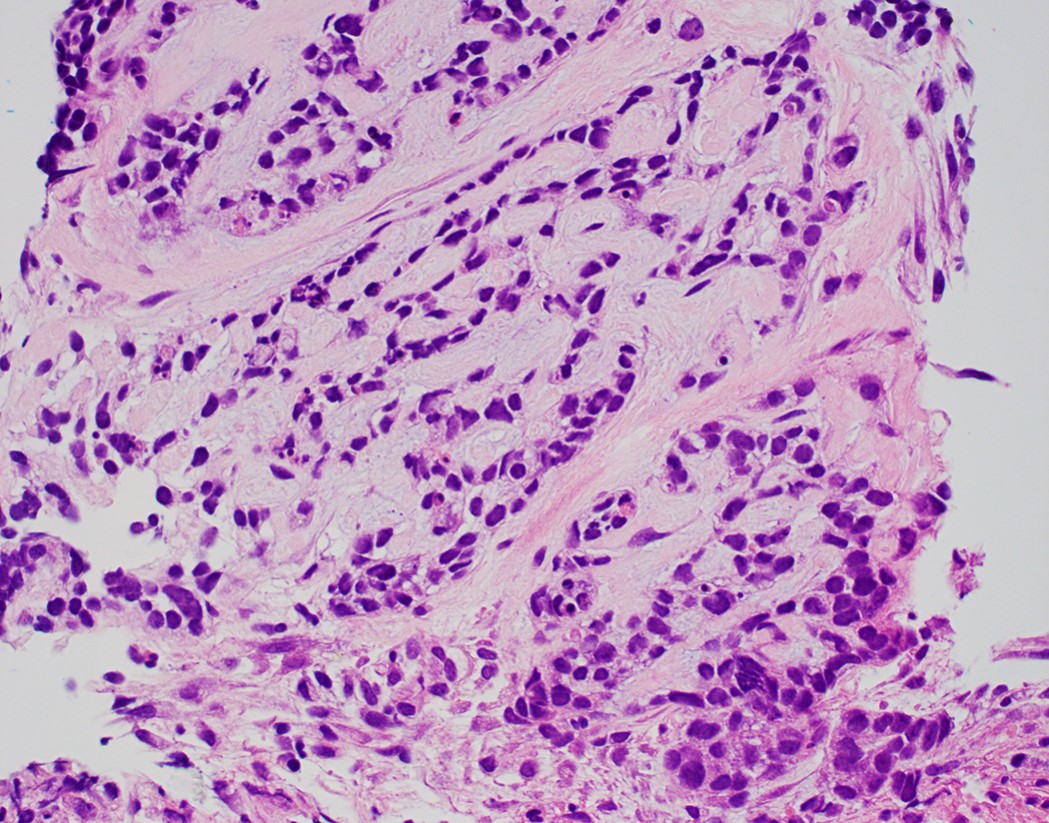
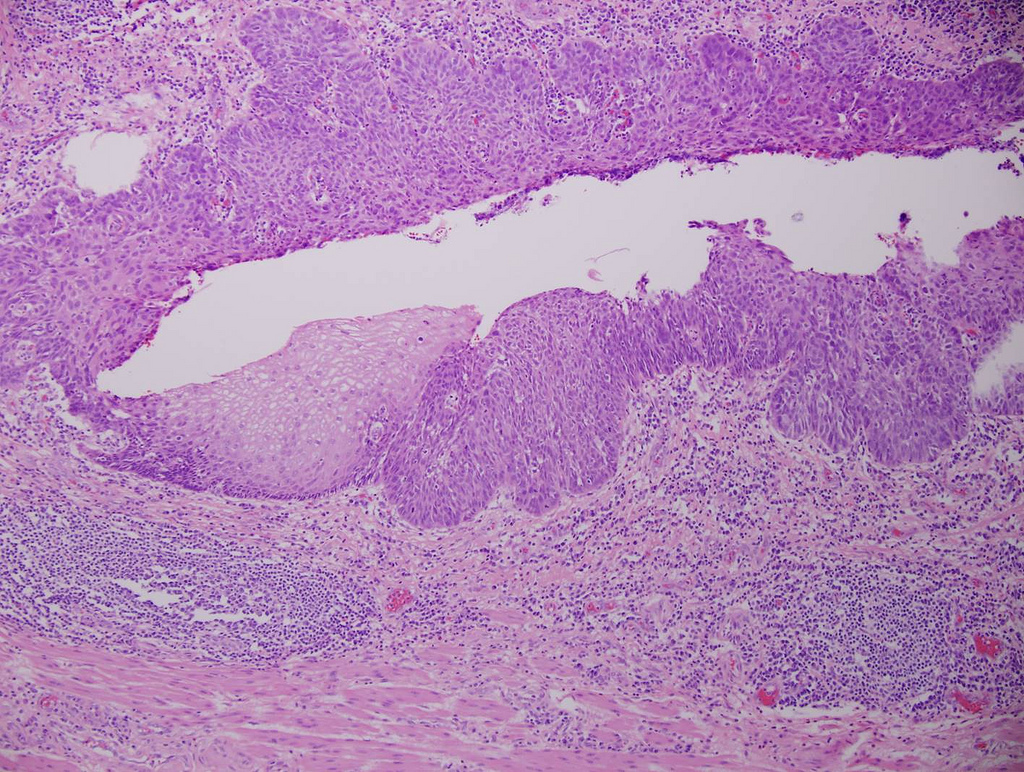
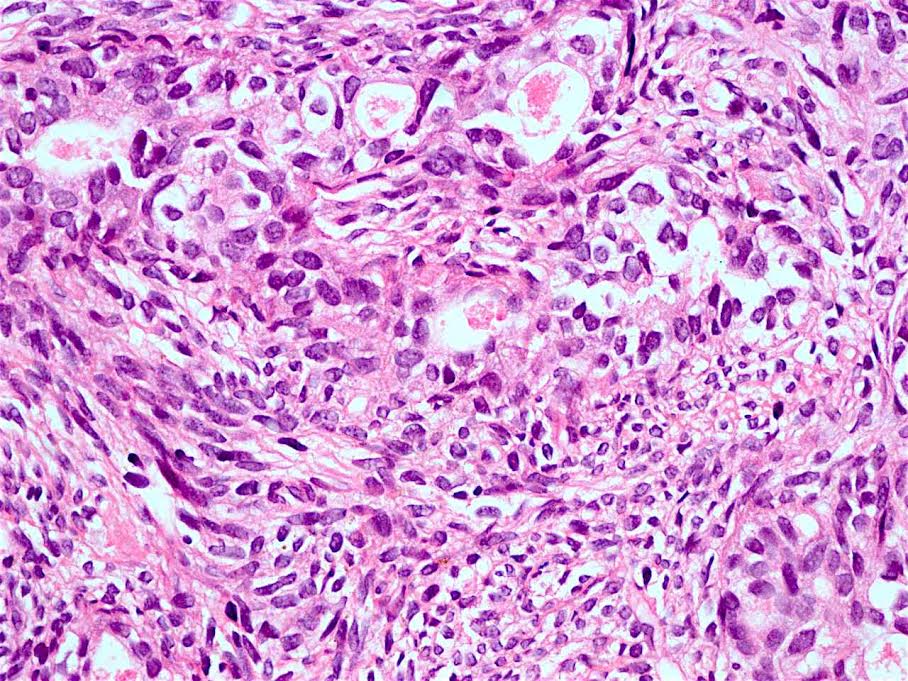
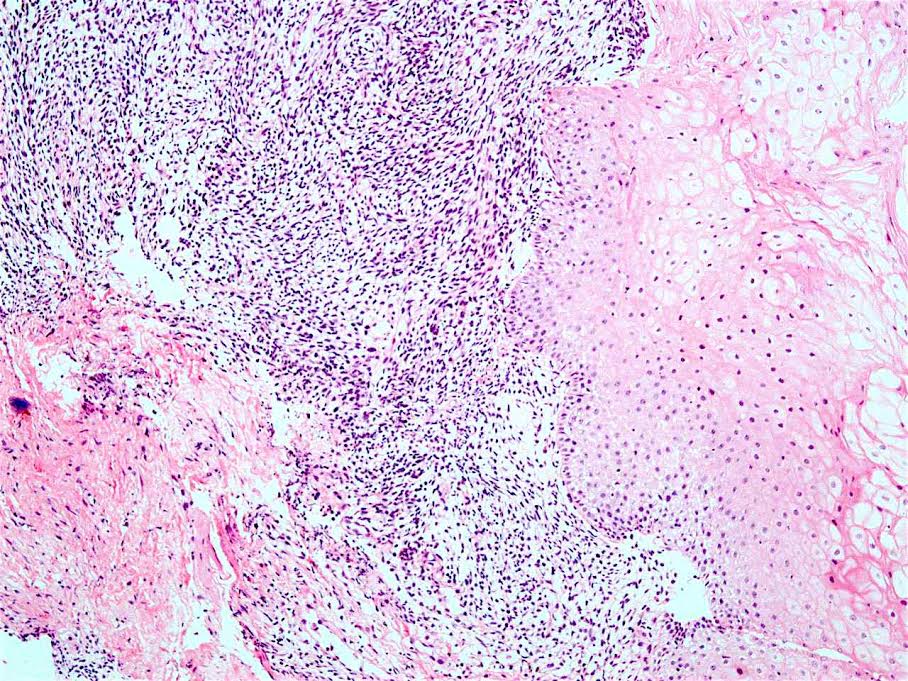
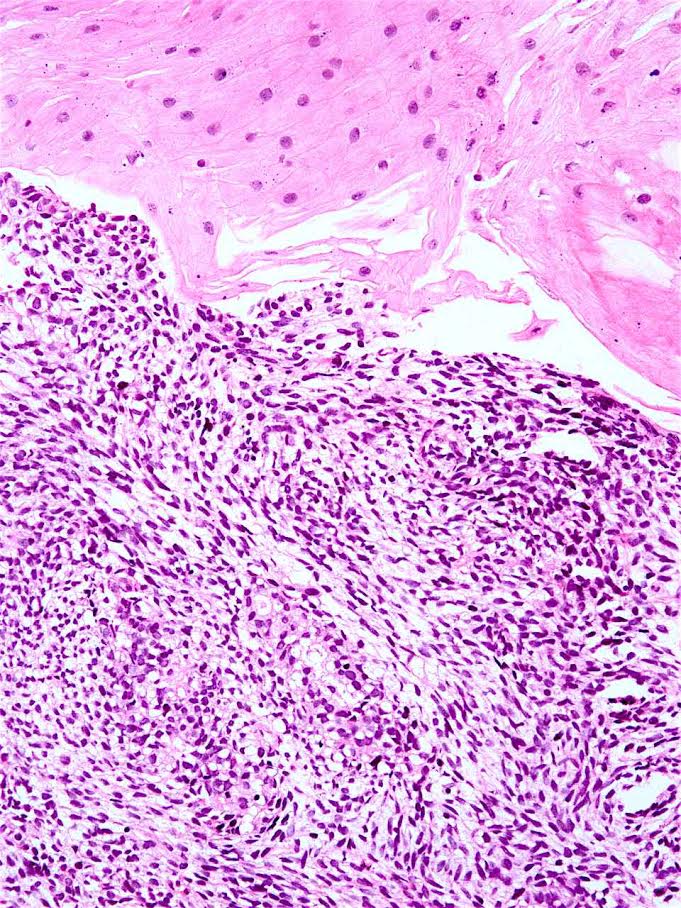
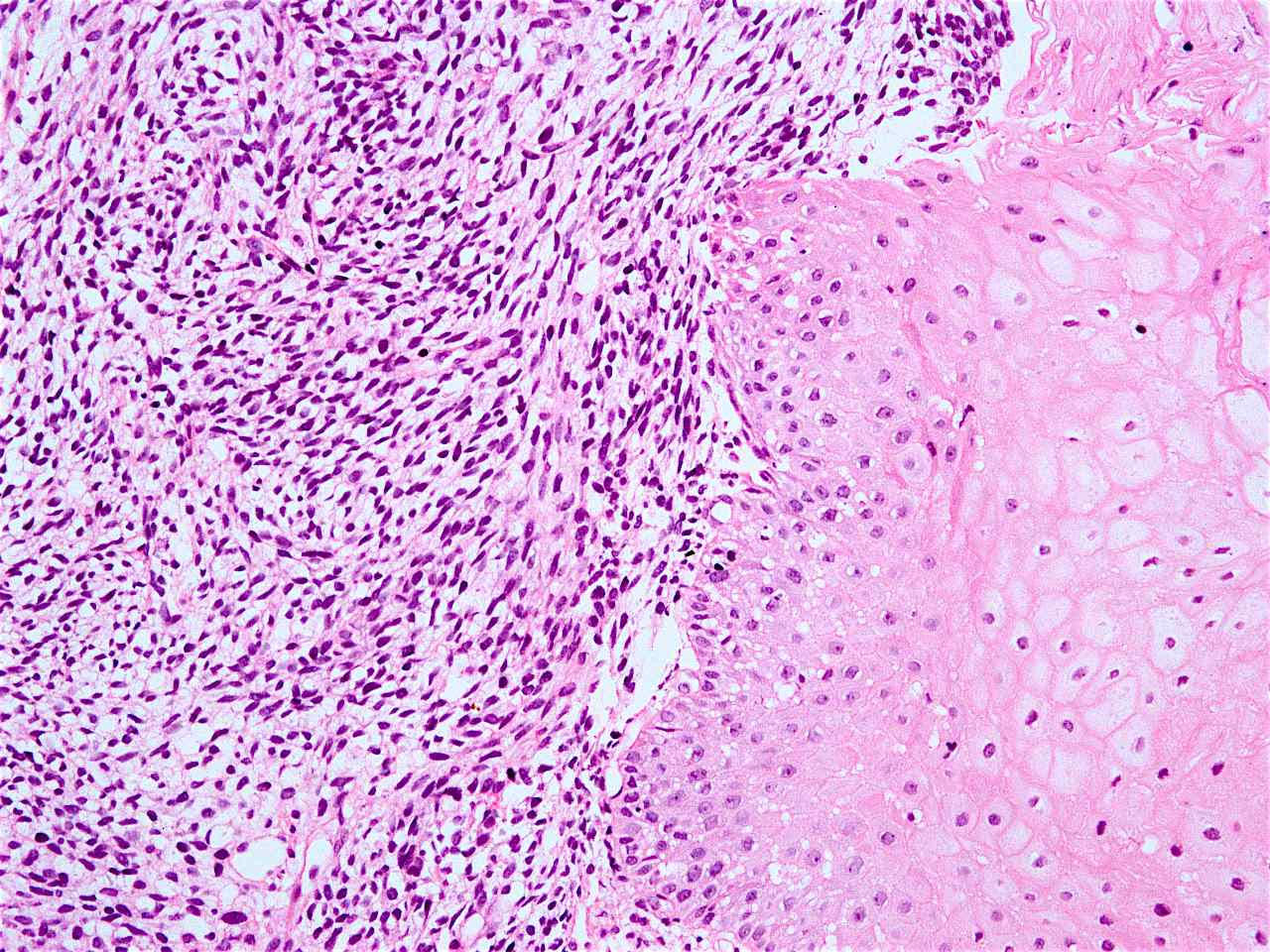
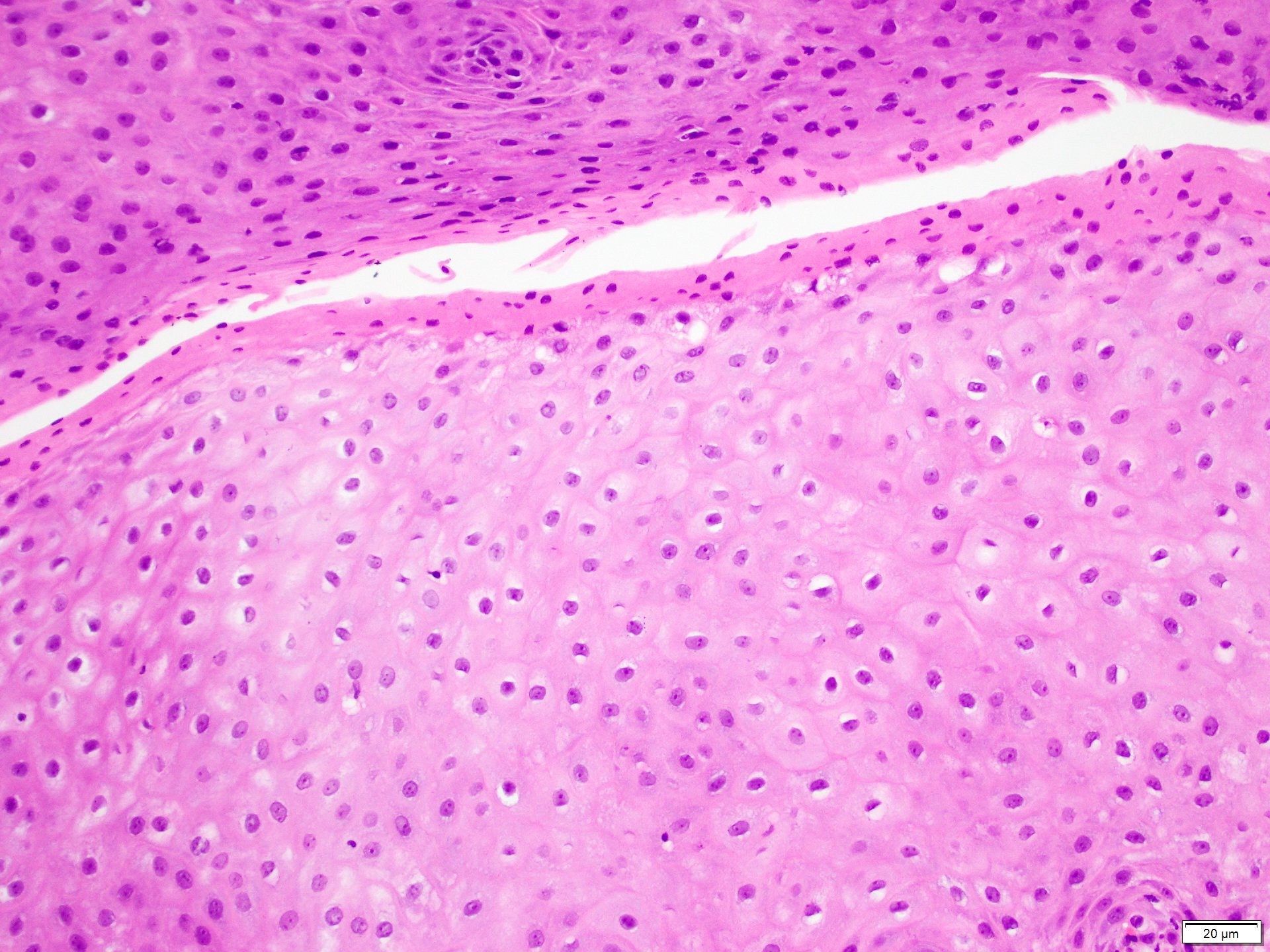
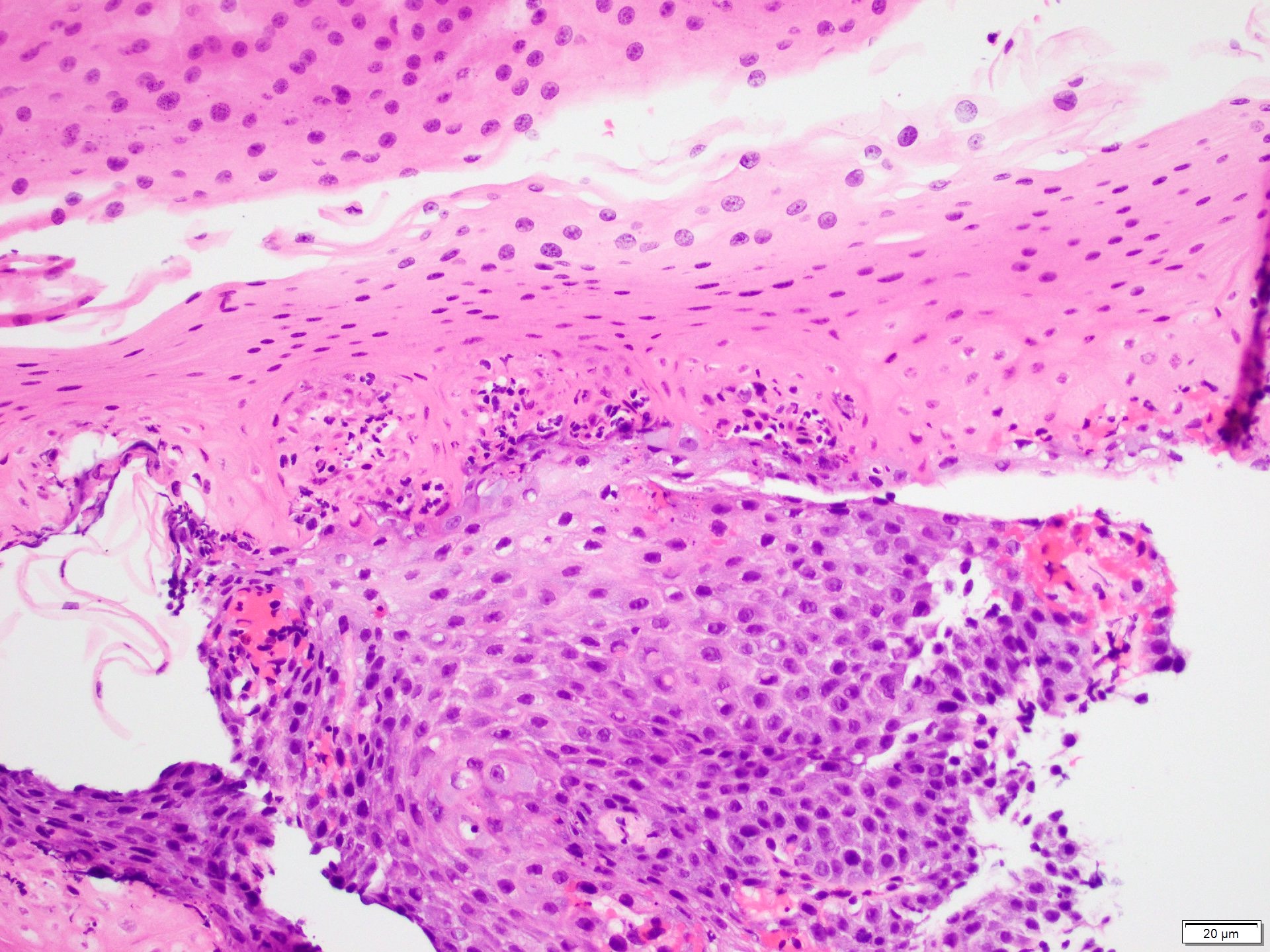
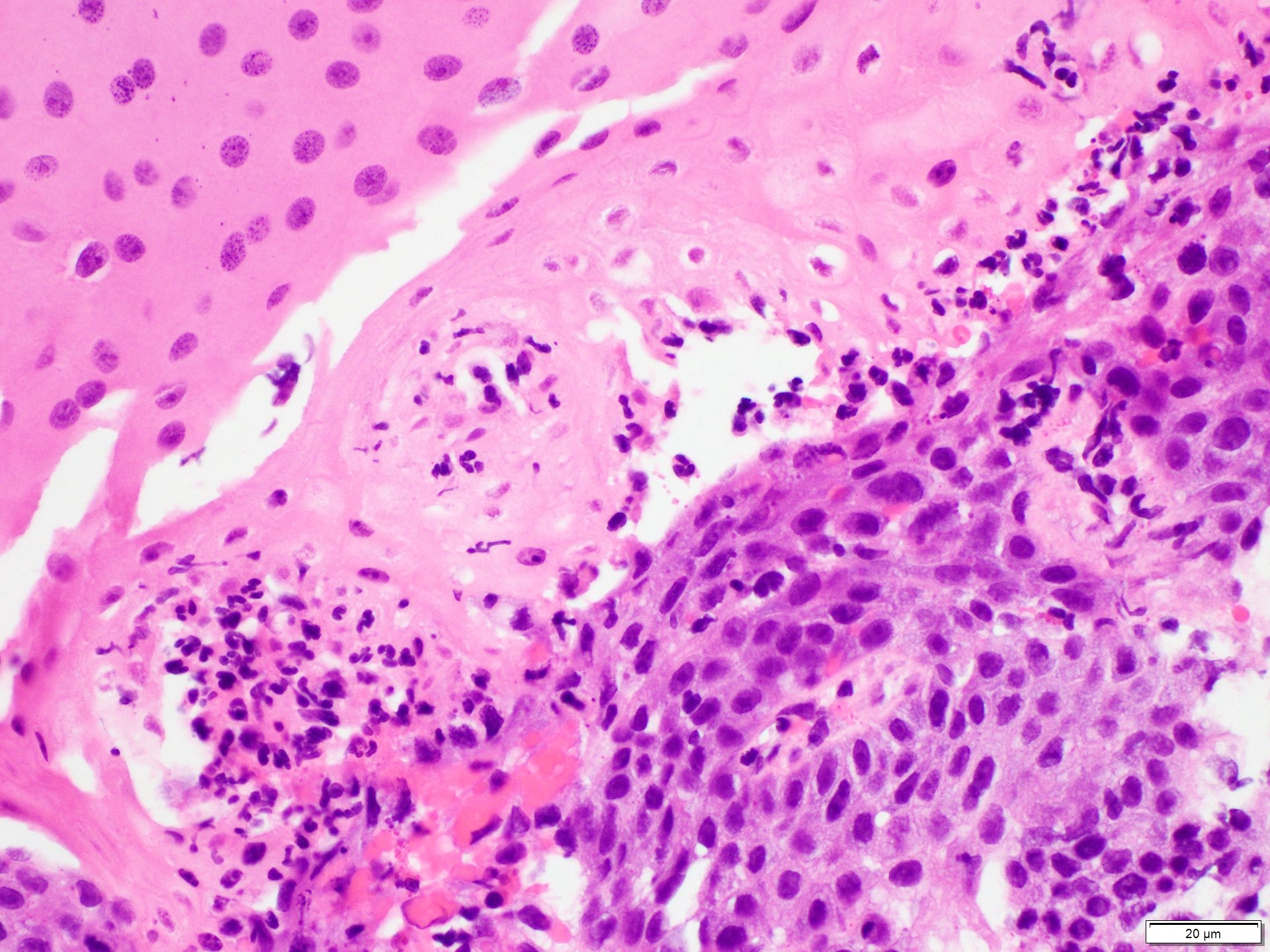
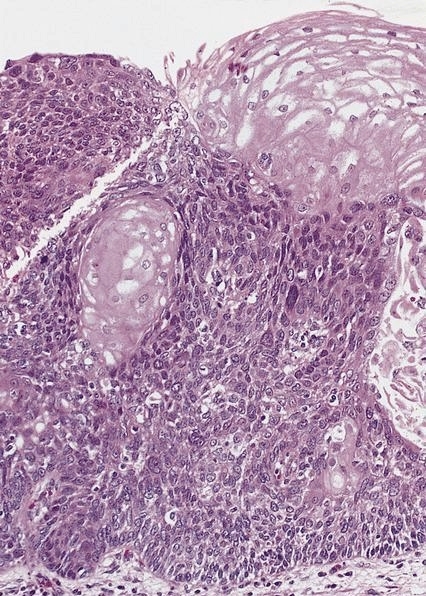
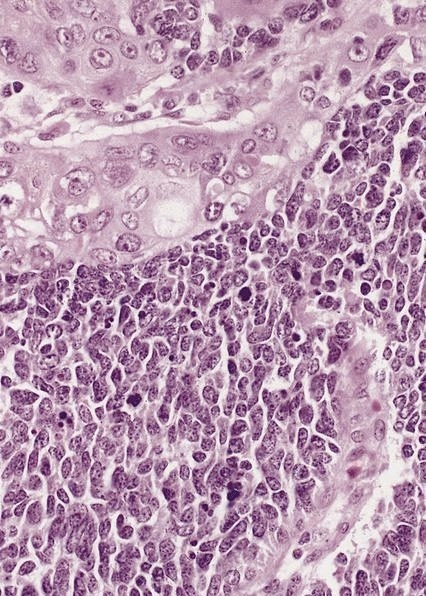
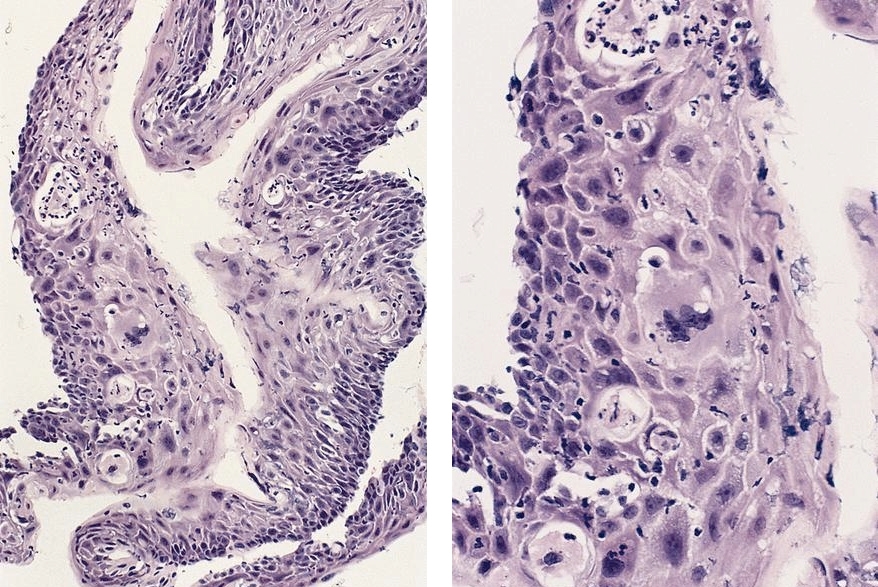
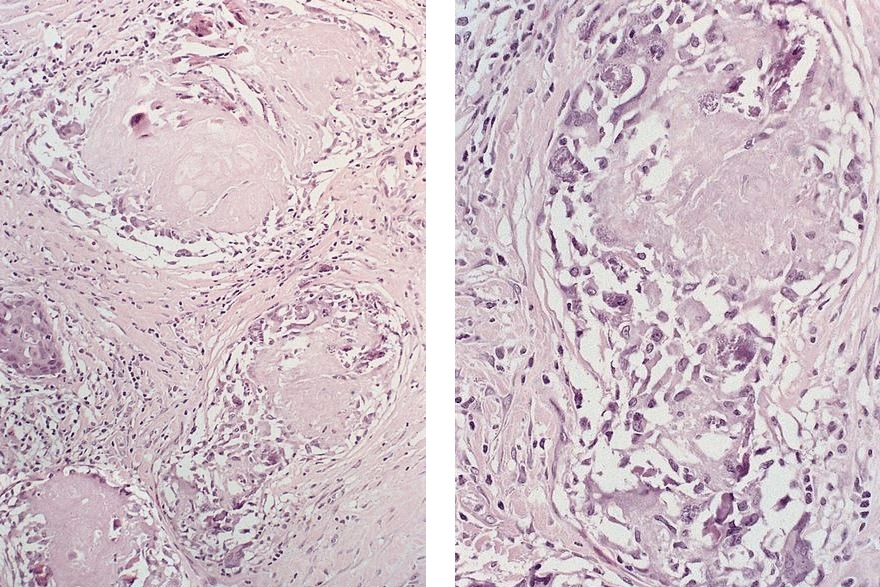
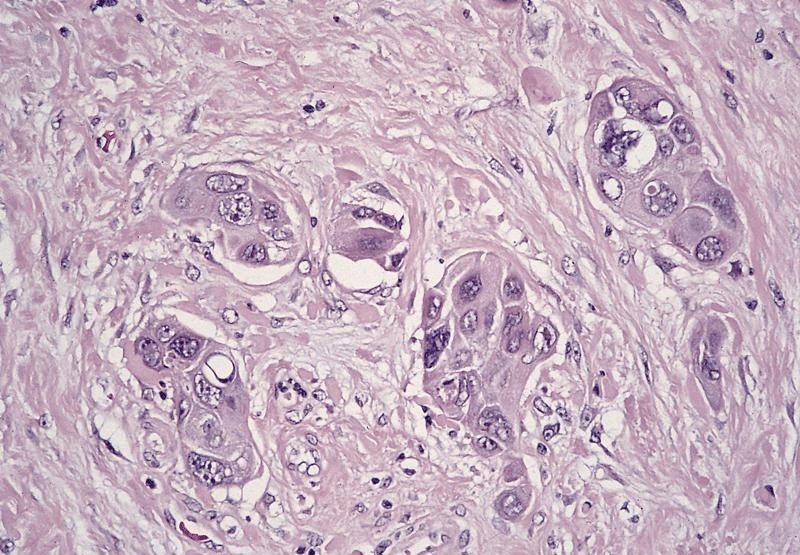
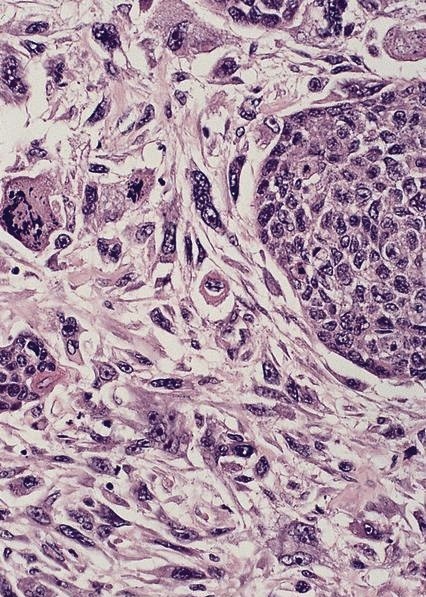
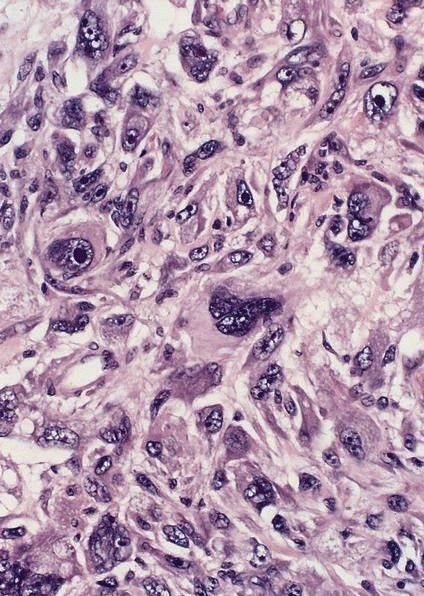
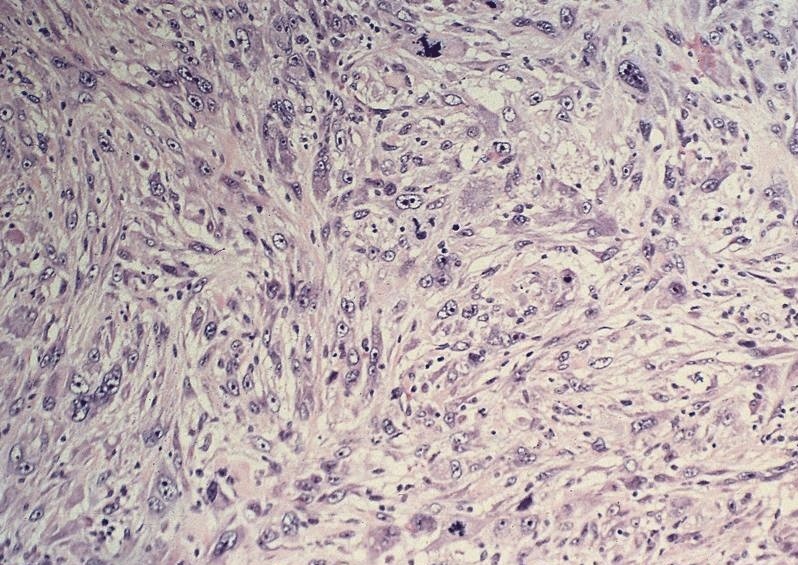
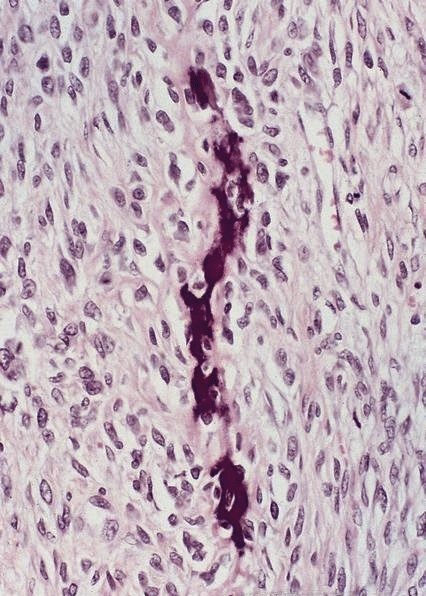
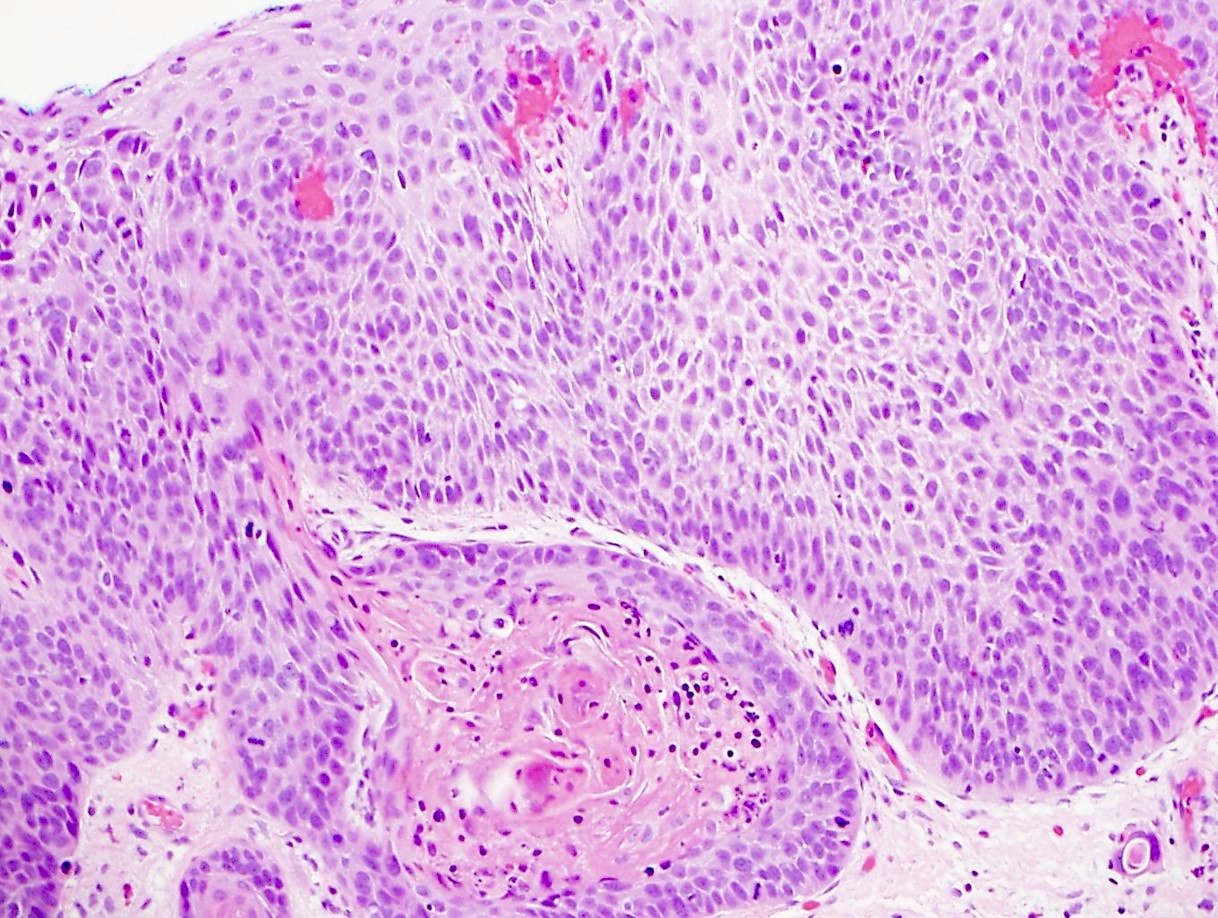
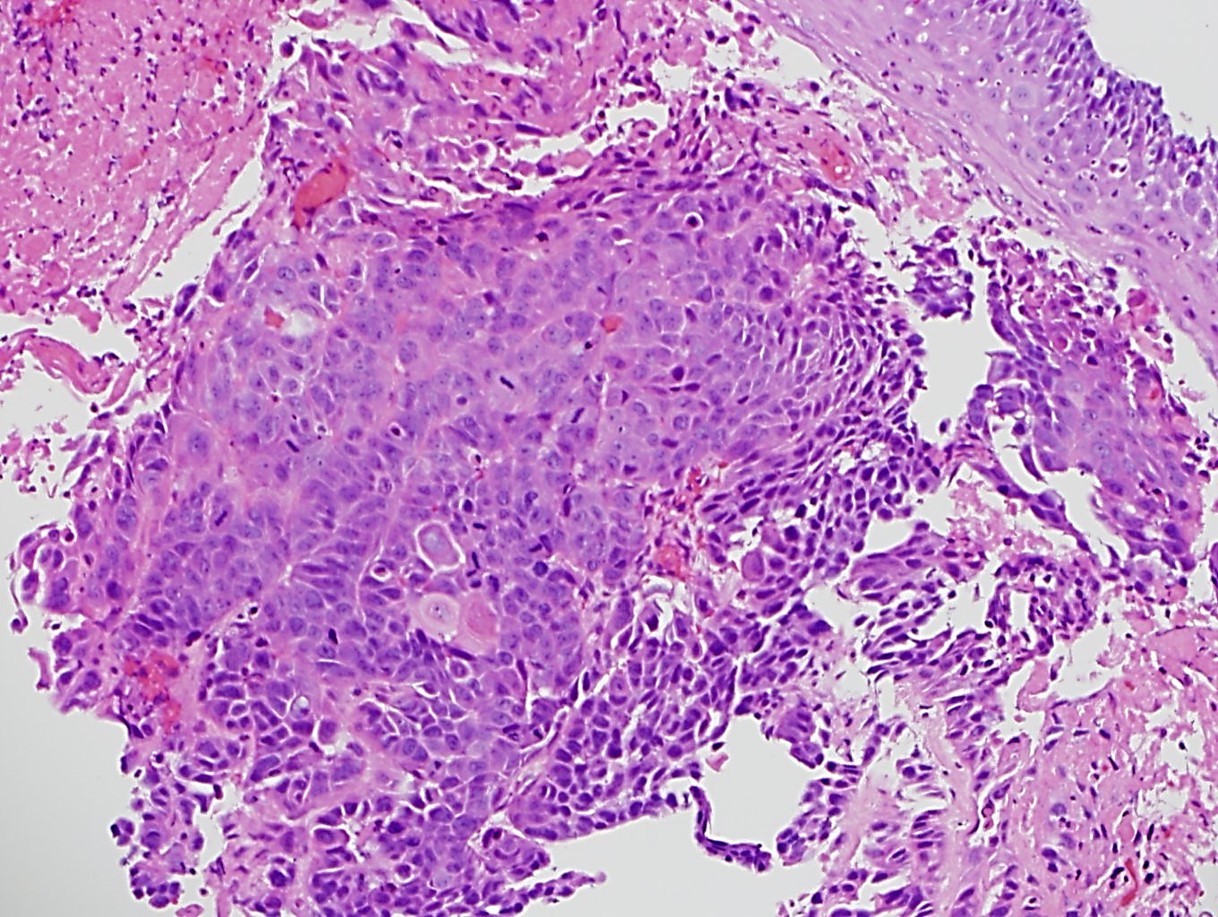
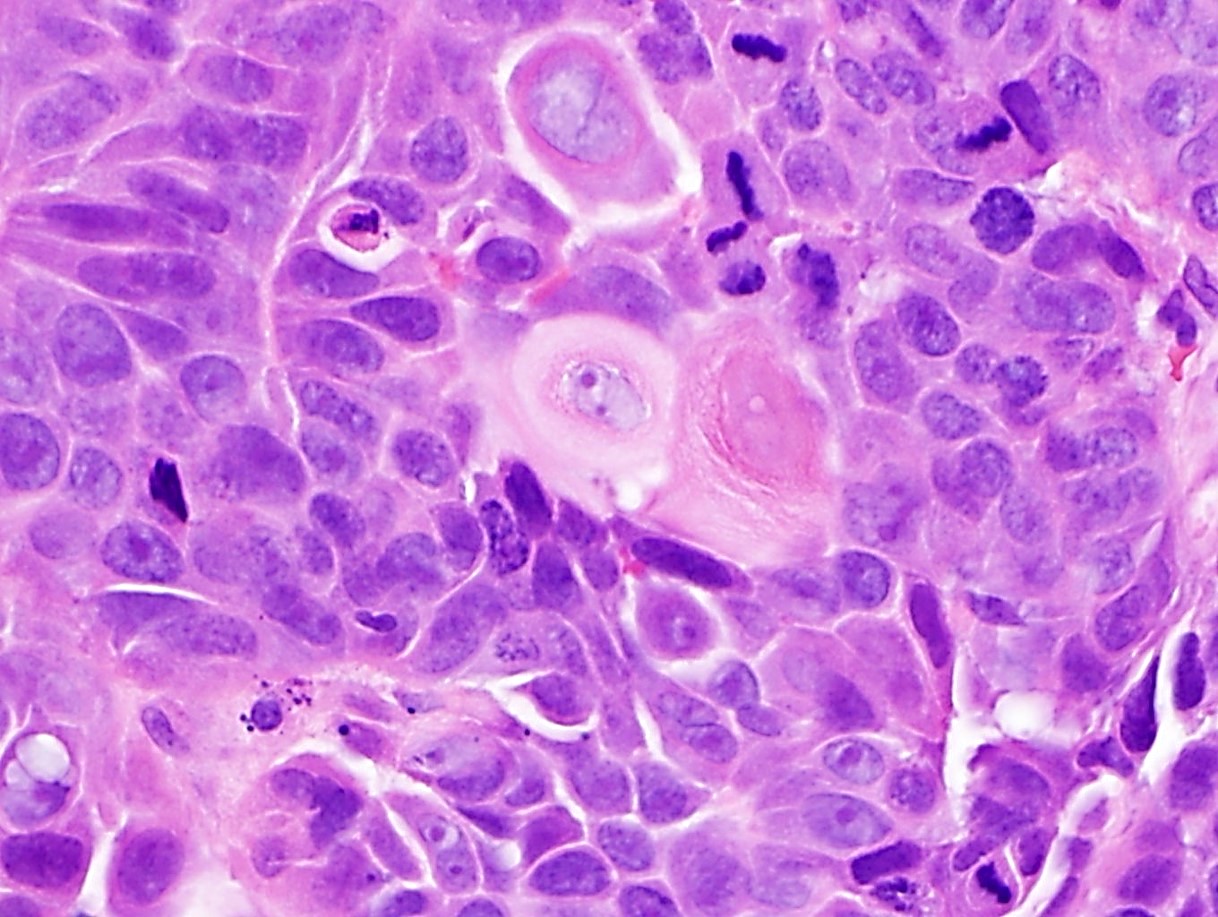
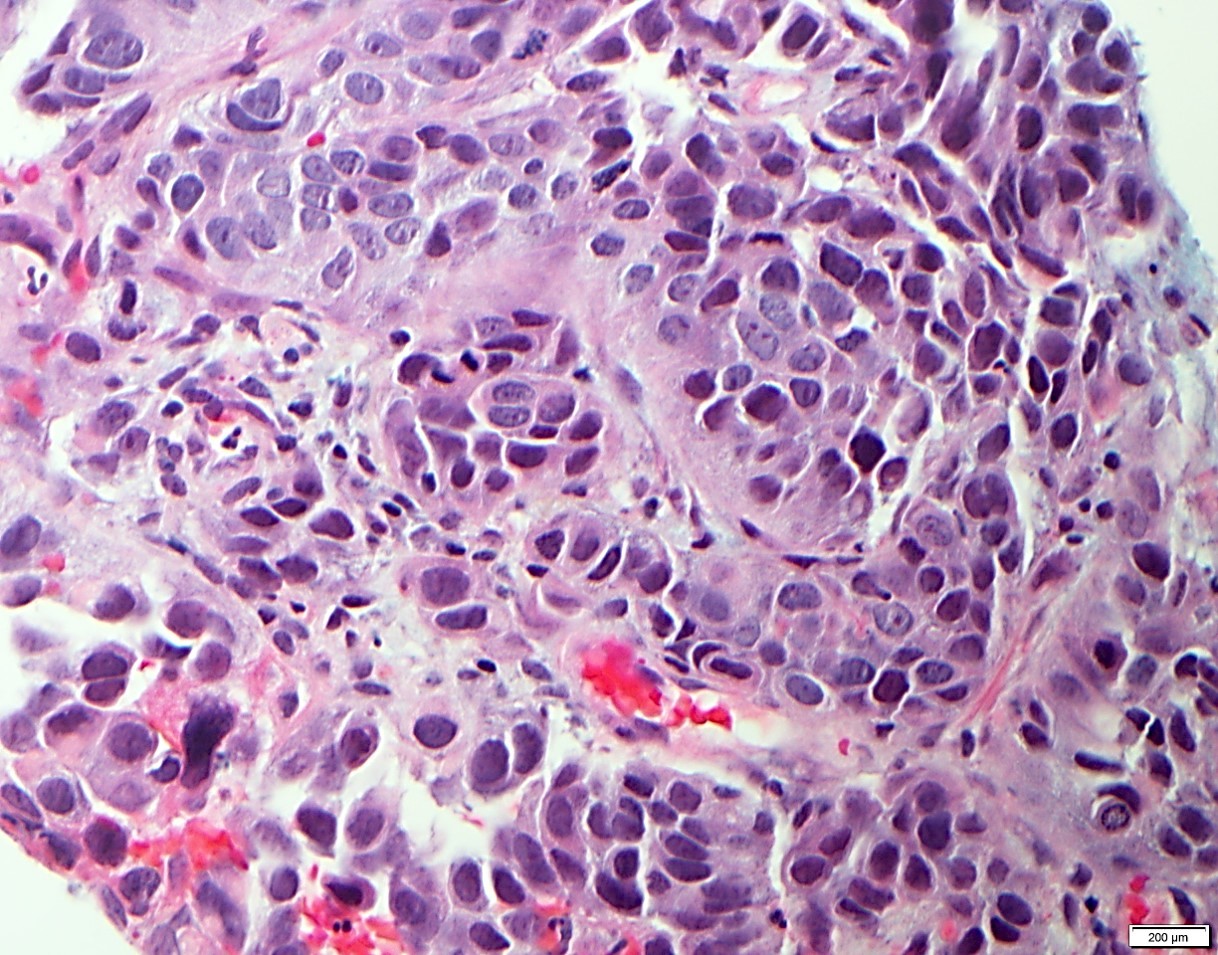
Strands of tumor cells often connected to overlying squamous epithelium
Nuclei are round to oval, hyperchromatic and peripheral palisading, often with central comedo type necrosis
Many mitotic figures
Microcystic pattern contains basophilic material
While microcysts or necrosis may cause a resemblance to lumina, true lumens are lacking
Many have areas of stromal hyalinization
Often admixed with conventional invasive or in situ squamous cell carcinoma and may see admixed adenocarcinoma, small cell carcinoma and spindle cell squamous cell carcinoma
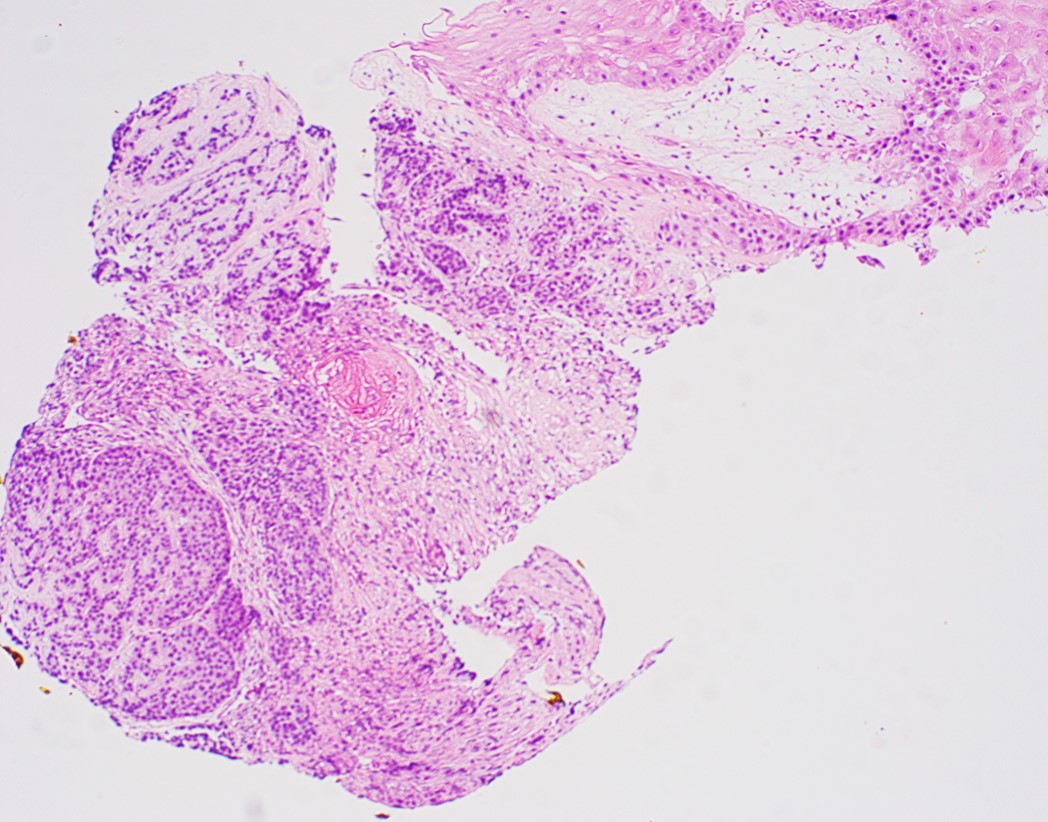
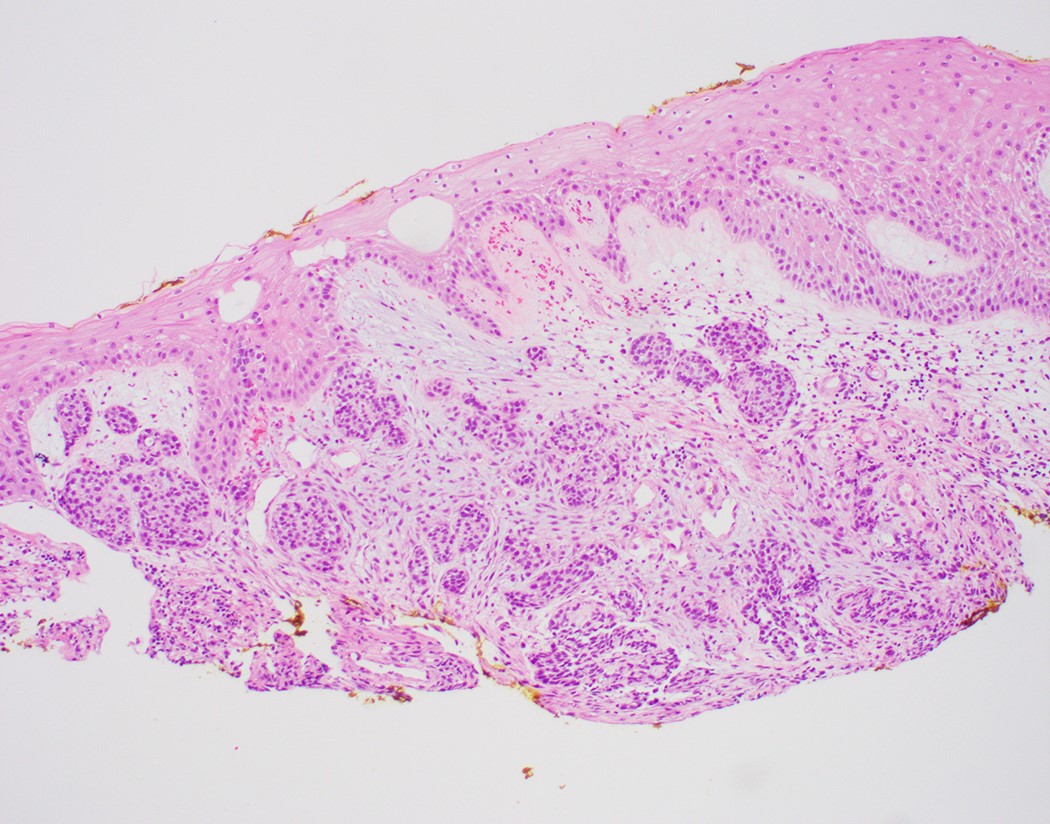
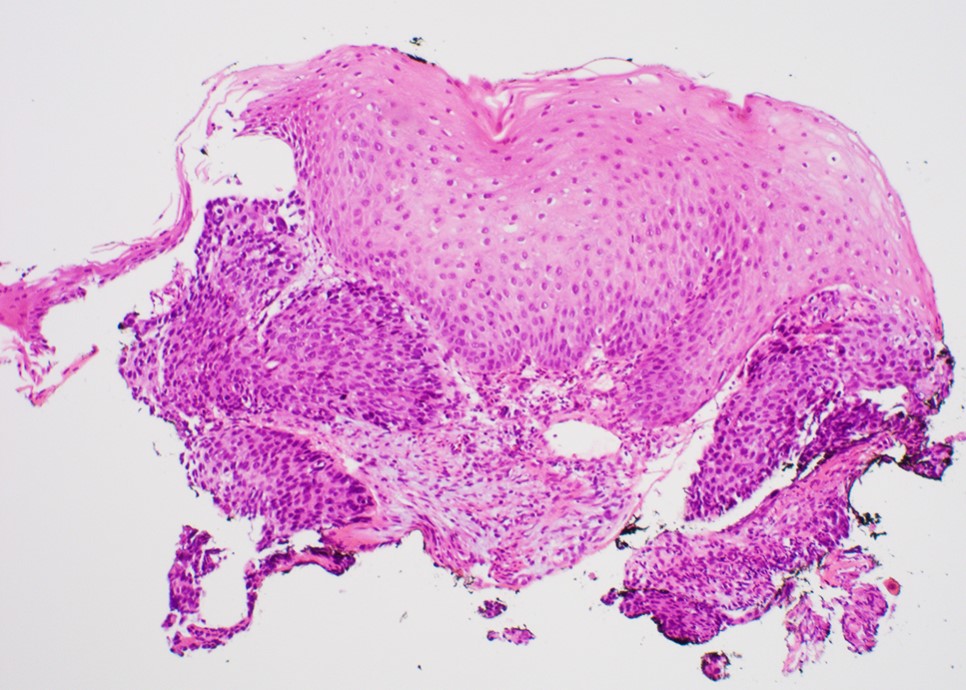
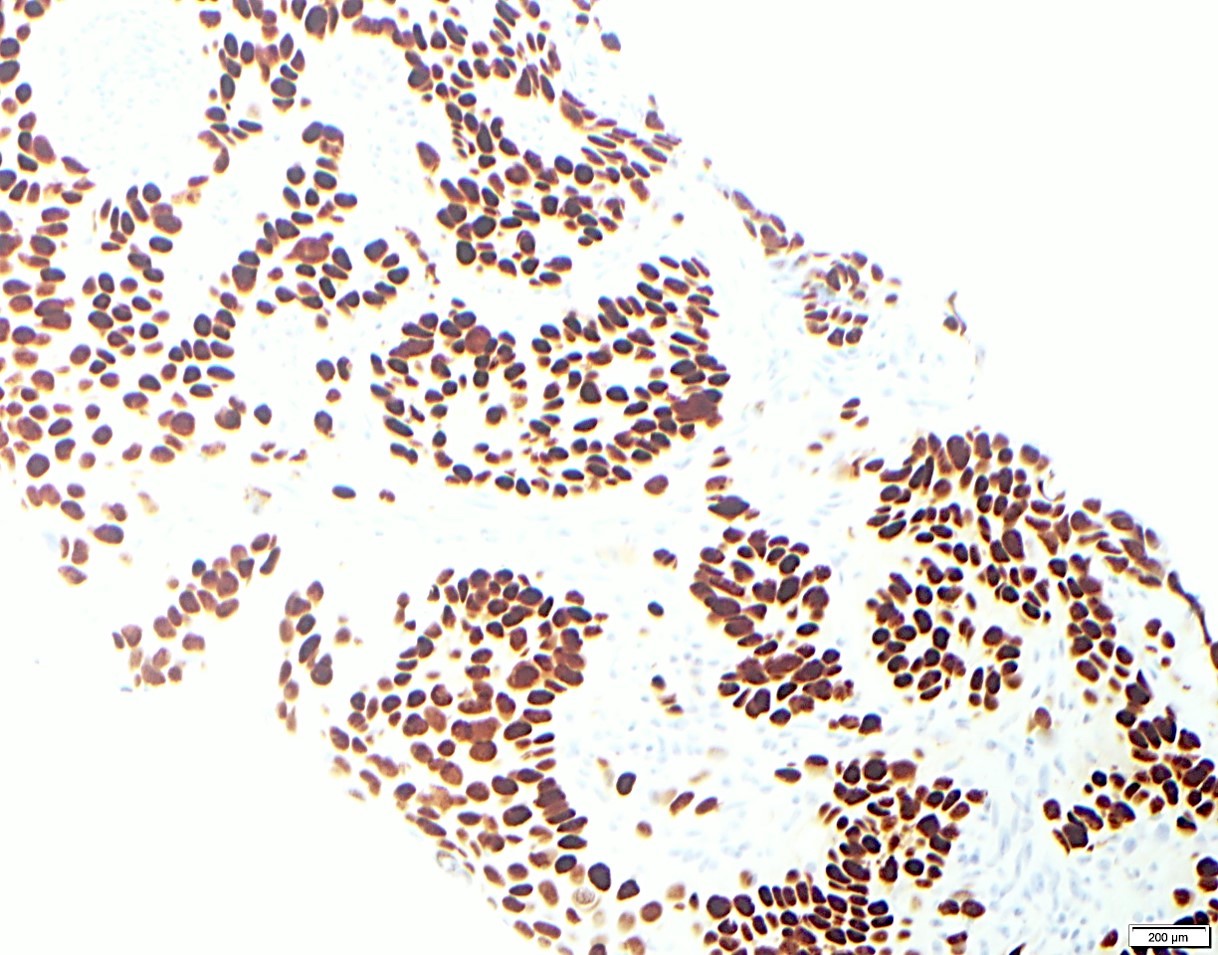
Microscopic (histologic) images
Contributed by Jinping Lai, M.D., Ph.D. and AFIP images
Up to half of esophageal BSCC cases harbor either an EGFR mutation or amplification and partial activation of the Wnt and hedgehog (HH) signaling pathways (Int J Clin Exp Pathol 2015;8:2267)
No KRAS, BRAF or PI3K mutations observed in BSCCs, while 23% of conventional SCC harbored a PIK3CA mutation (Ann Surg Oncol 2015;22:3659)
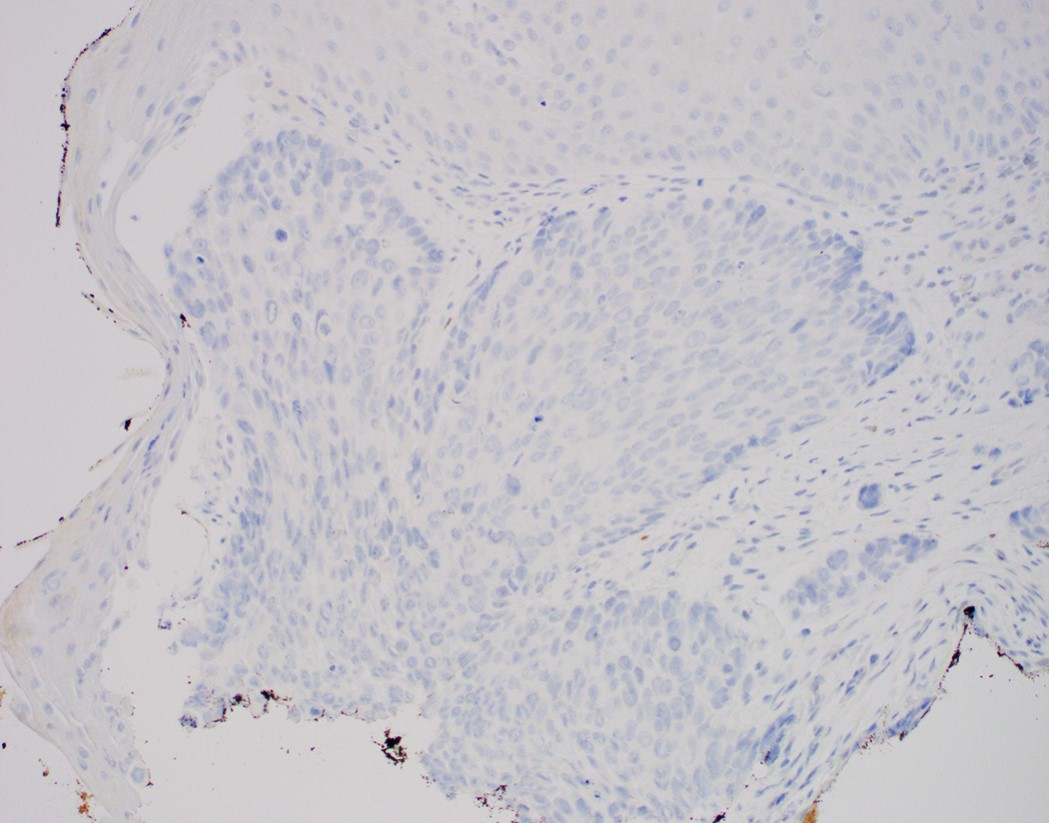
Sample pathology report
Esophagus, mid, mass, biopsy:
Basaloid squamous cell carcinoma (see comment)
Comment: Clinical photos are noted. Sections of the biopsy show subepithelial basaloid neoplasm with microcystic nests, strands, trabeculae of tumor cells infiltrating a myxoid stroma. The tumor cells are positive for p40, p63, p53 and intact INI1, while negative for p16, CK7, CK20, CDX2 and synaptophysin. The histologic features and immunoprofile support the diagnosis.
Compared with conventional squamous cell carcinoma of the esophagus, basaloid squamous cell carcinoma of the esophagus has
Fewer PI3KCA mutations
More p53 mutations
More Rb mutations
More BRAF mutations
More KRAS mutations
Board review style answer #1
A. No PI3KCA mutation has been observed in esophageal basaloid squamous cell carcinoma, while 23% of conventional SCCs of the esophagus harbored a PI3KCA mutation.
56 year old man with a smoking history for 20 years and dysphagia for 6 months. A biopsy is made of a lesion at his mid esophagus, shown in the photo above. The cells are diffusely nuclear positive for p40, p63, p53 and INI1, while negative for p16, CK7, CK20, CDX2 and synaptophysin. What is your diagnosis?
Adenoid cystic carcinoma
Basaloid squamous cell carcinoma
Metastatic oropharyngeal HPV related squamous cell carcinoma
Neuroendocrine carcinoma, small cell type
SMARCB1 deficient carcinoma
Board review style answer #2
B. The most likely diagnosis is basaloid squamous cell carcinoma. The tumor cells only show 1 component and are diffusely positive for p40 and p63, making adenoid cystic carcinoma less likely. The tumor cells show eosinophilic cytoplasm with negative synaptophysin, making small cell carcinoma less likely. The tumor cells have an intact INI1, making SMARCB1 deficient carcinoma less likely. p16 is negative, making HPV related metastatic oropharyngeal squamous cell carcinoma less likely.
Candida albicans, which can be locally invasive, is the most prevalent cause of infectious esophagitis
Other common fungal species relevant to infectious esophagitis are C. tropicalis, C. glabrata, C. krusei and C. parapsilosis
Essential features
Candida esophagitis is one of the most common types of esophagitis in immunosuppressed individuals
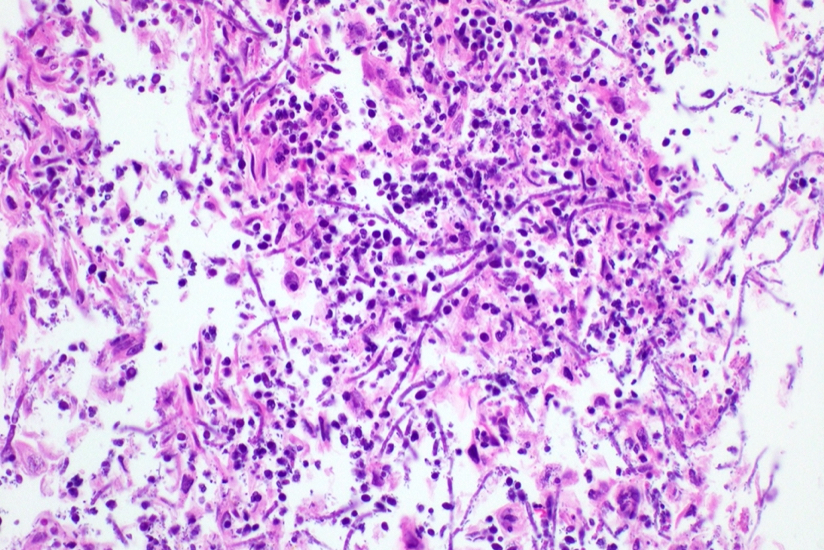
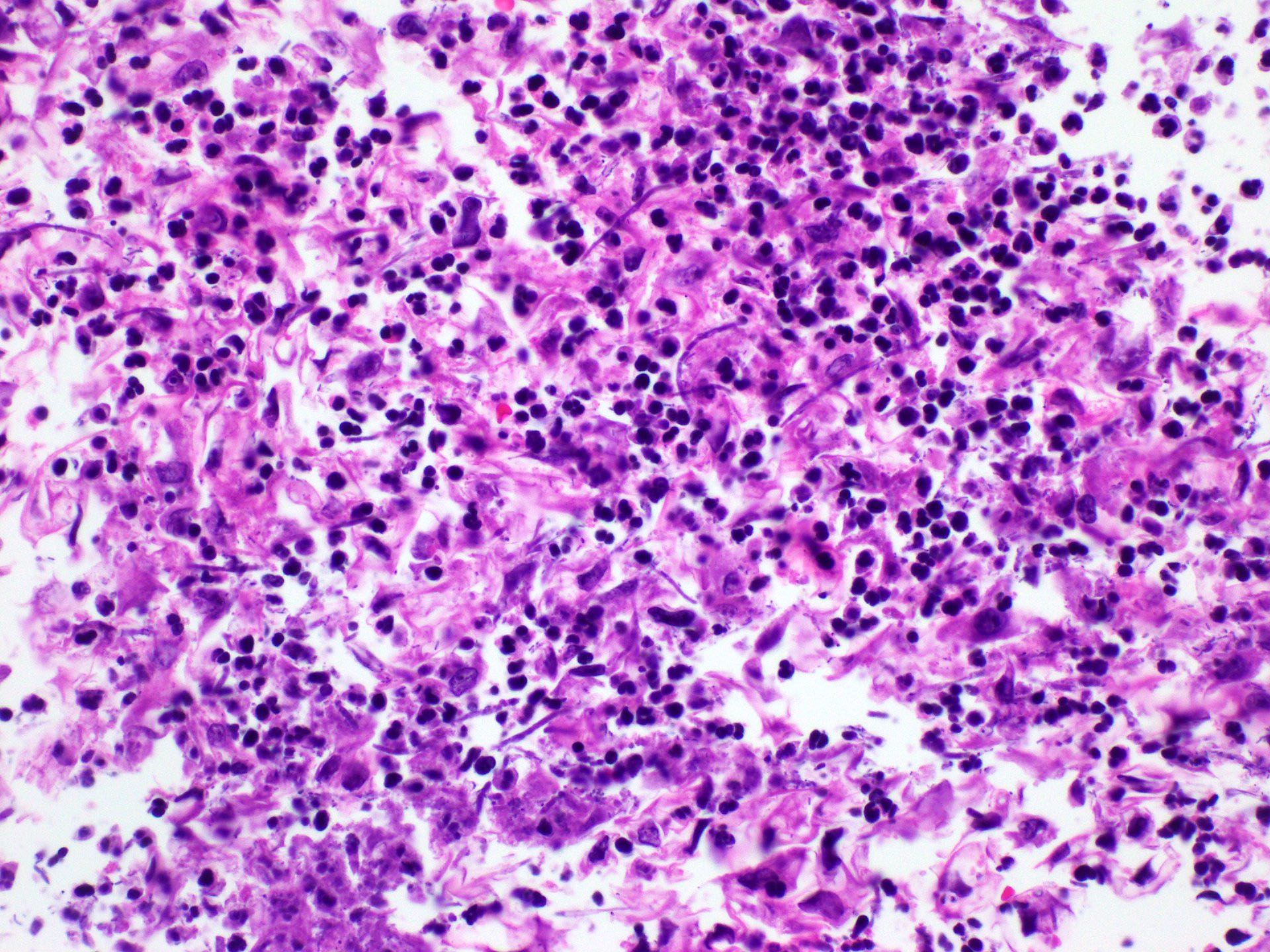
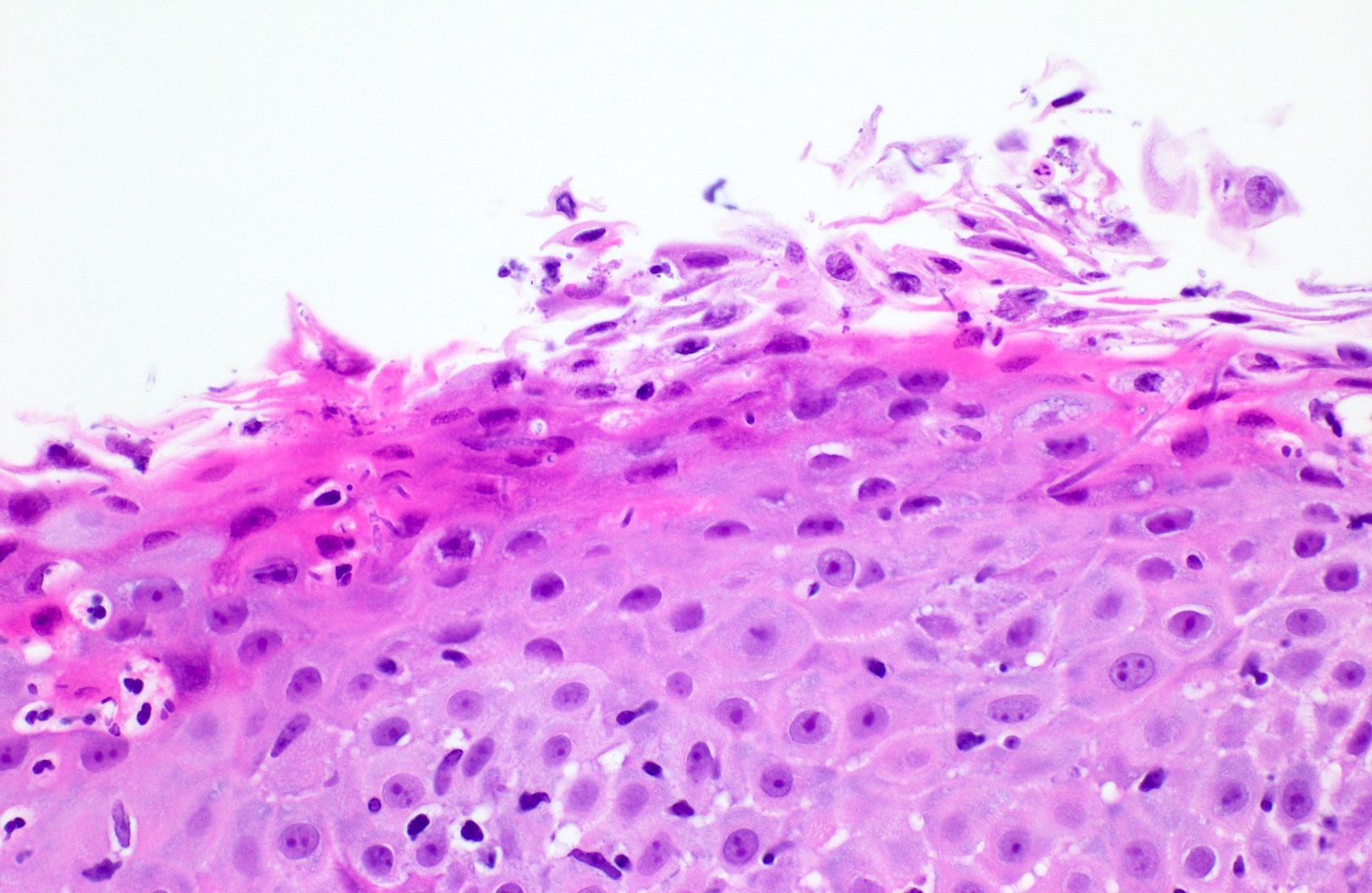
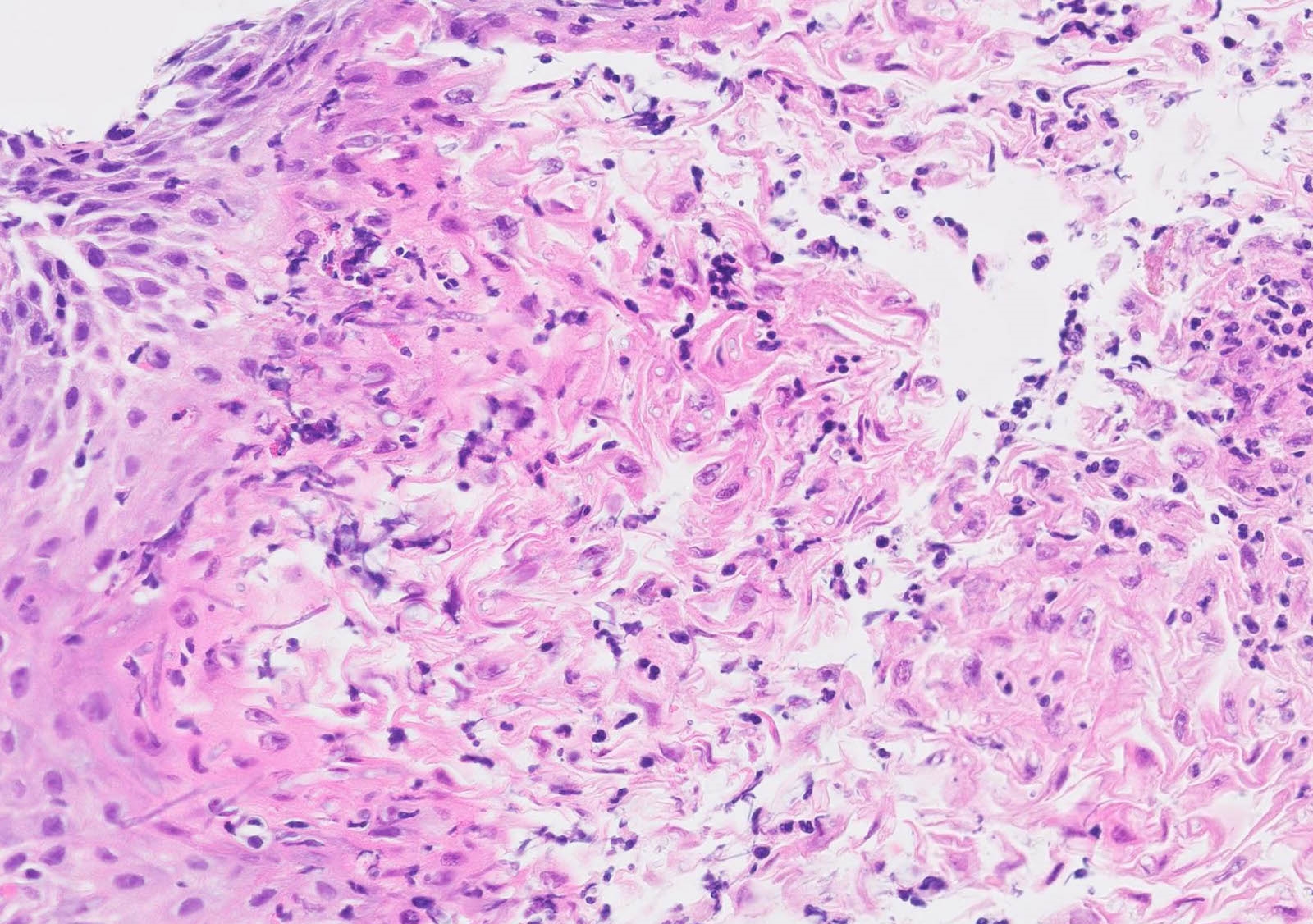
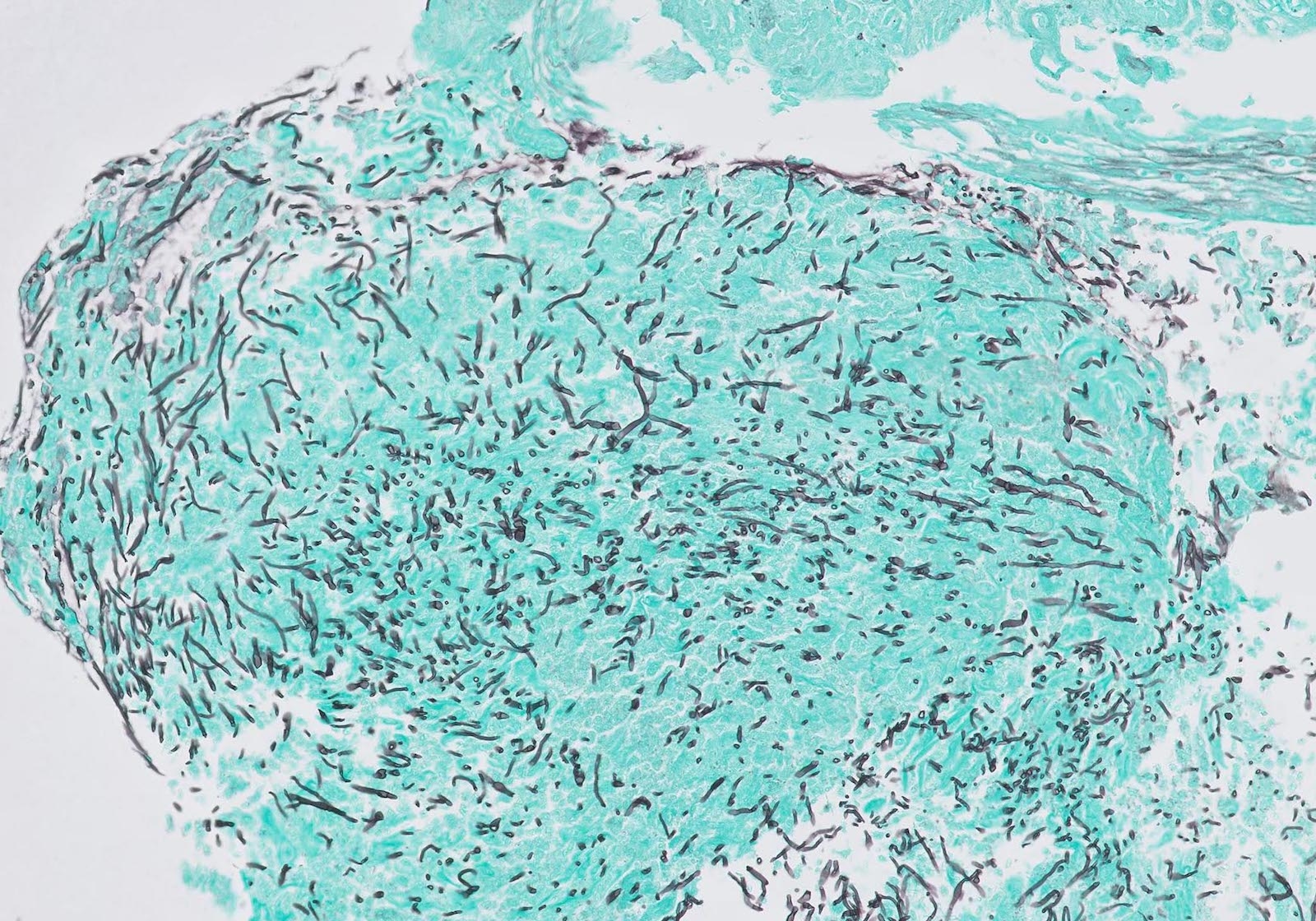
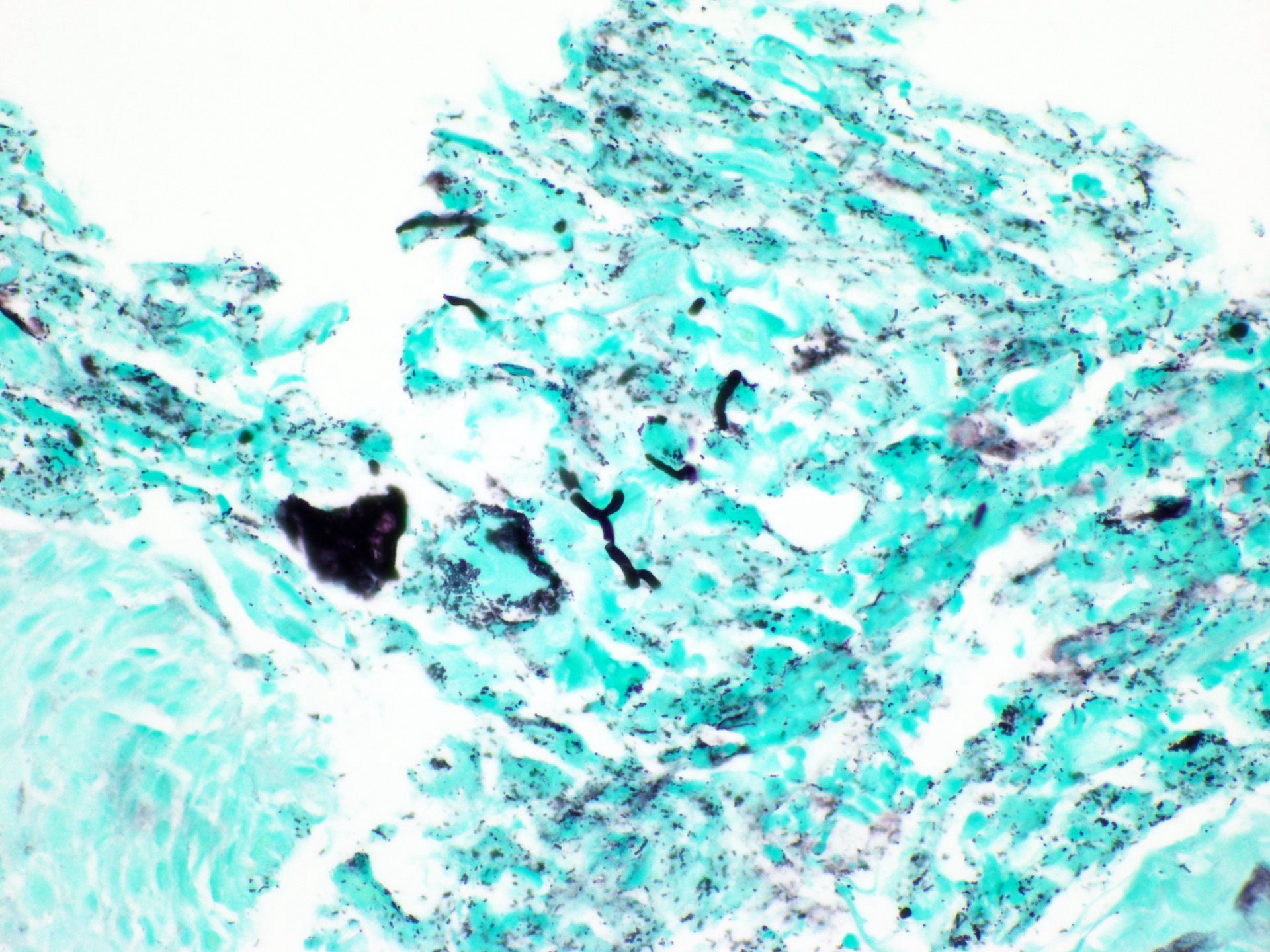
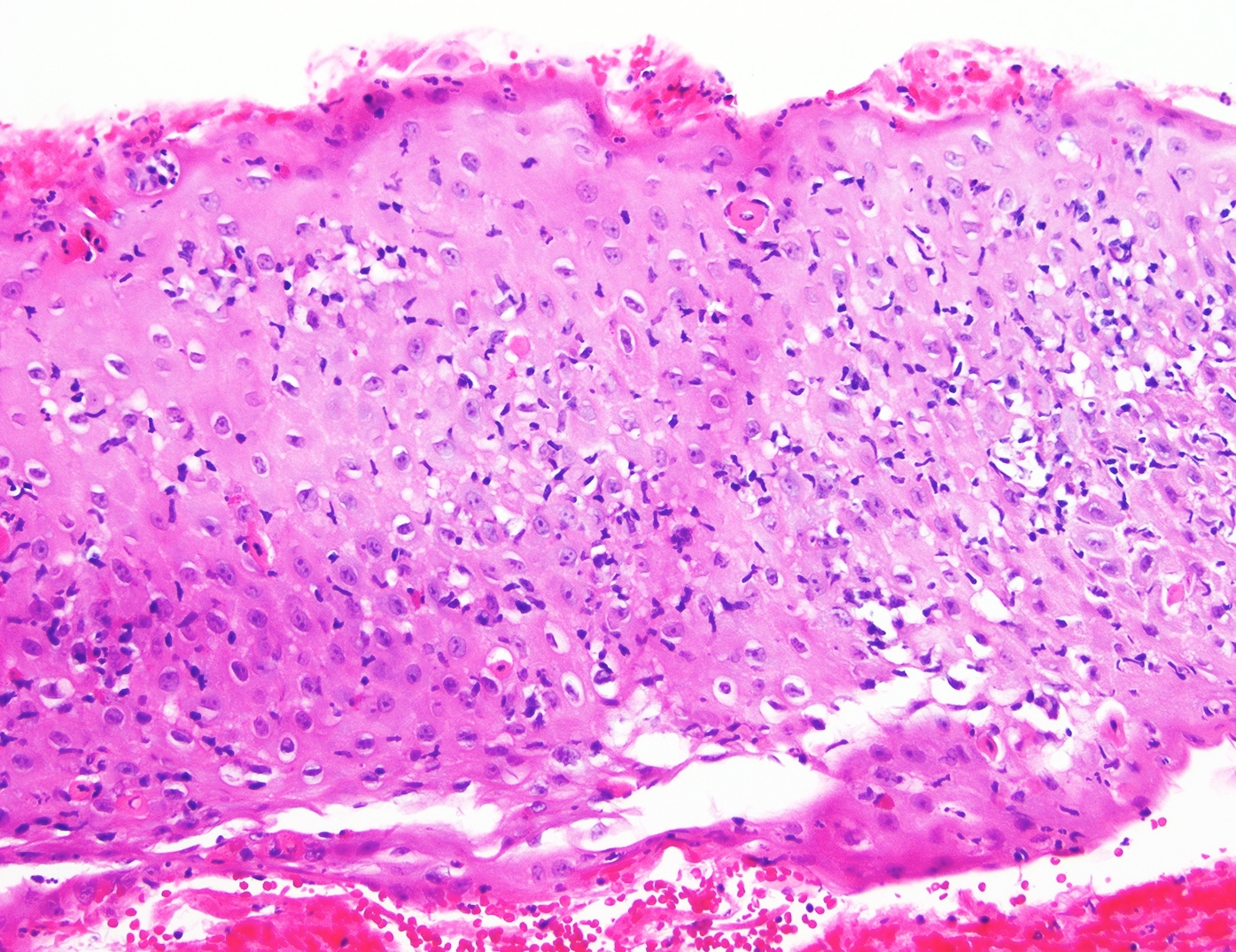
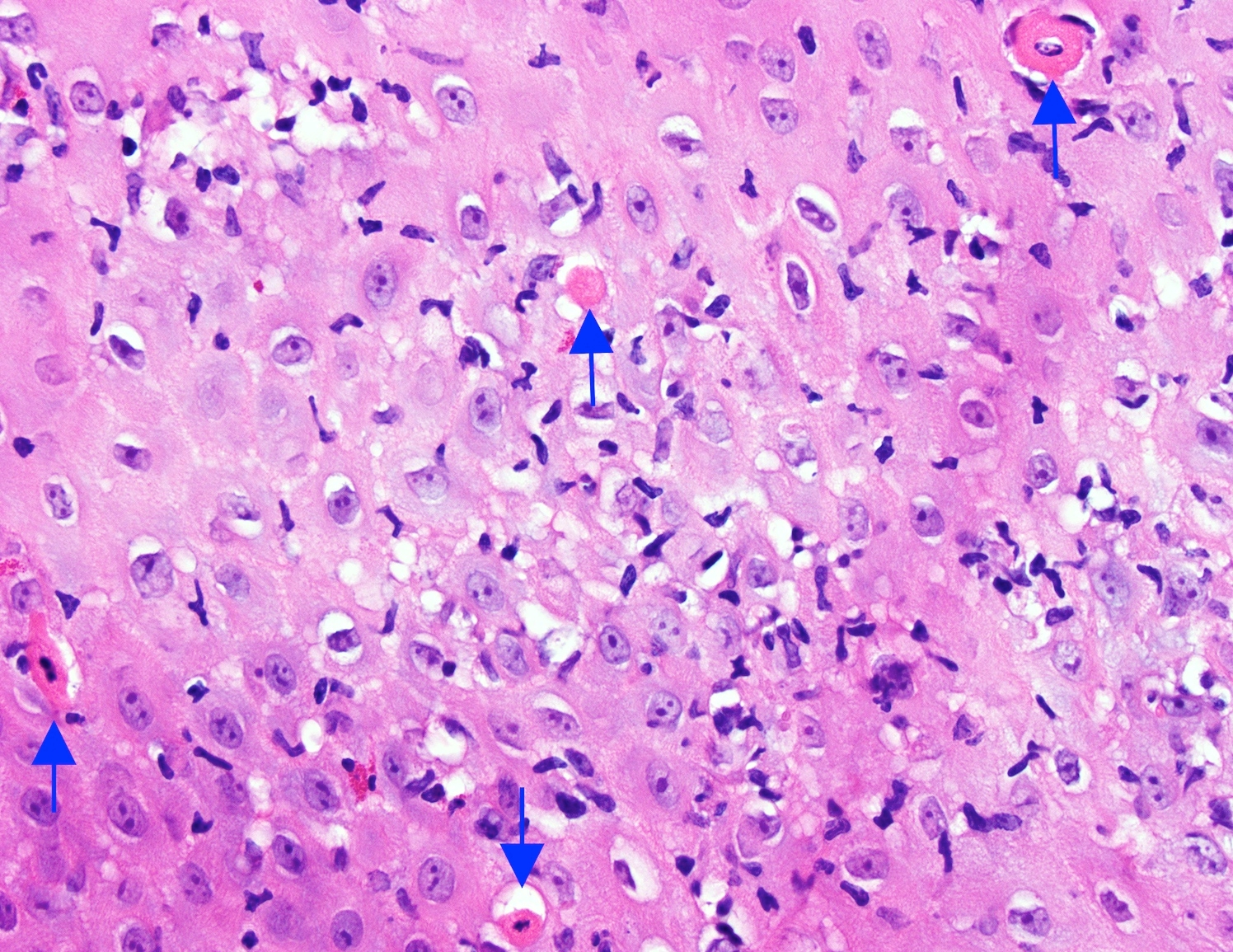
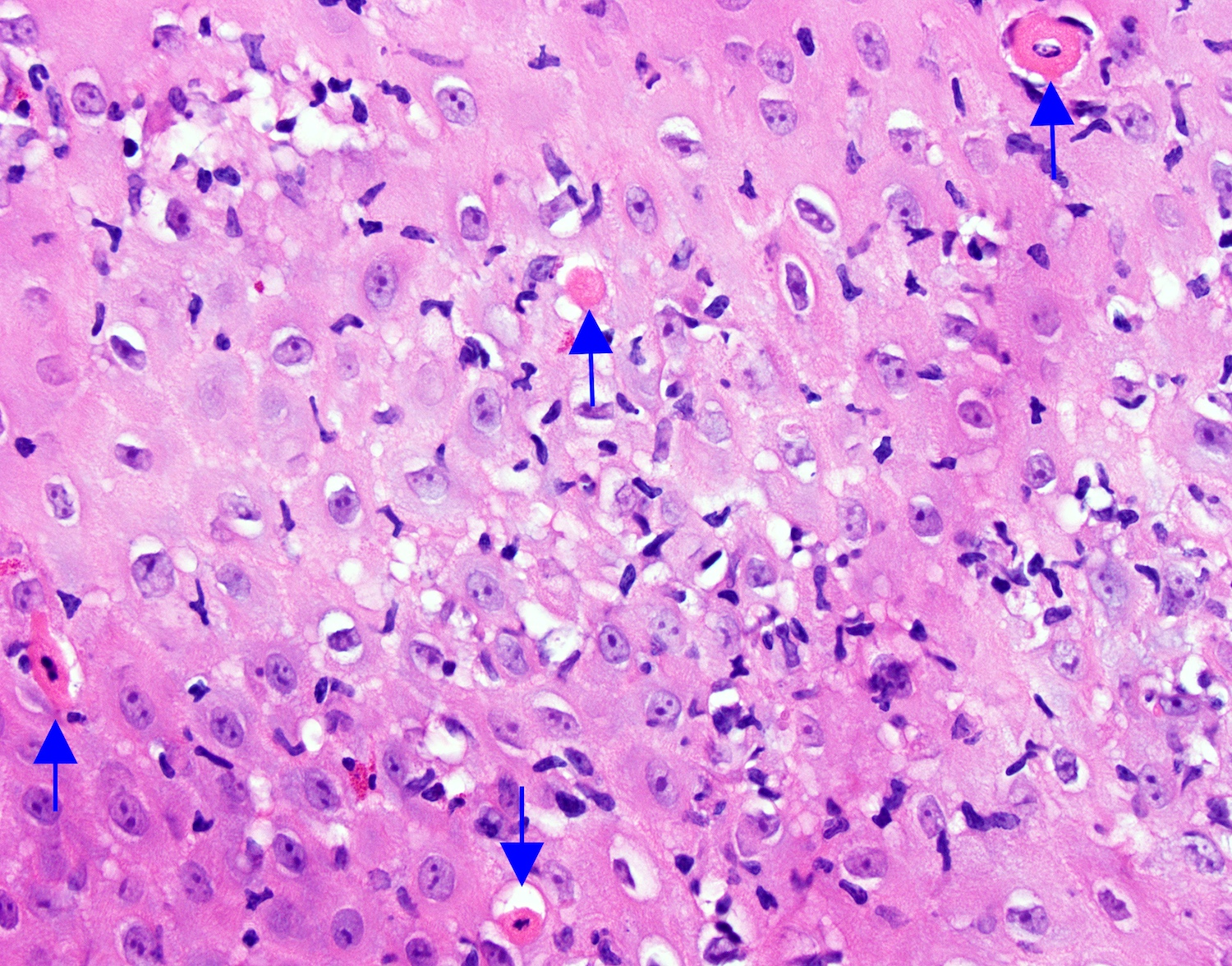
Histological features include acute inflammation, intraepithelial neutrophilic abscesses and epithelial edema; parakeratosis most prominent in the superficial epithelial layers with yeast forms and pseudohyphae
Treated with antifungals, often with good prognosis
Terminology
Esophageal candidiasis, Candida esophagitis or esophageal moniliasis
Typical symptoms include dysphagia, odynophagia and retrosternal pain
Less commonly, abdominal pain, heartburn, diarrhea, nausea, vomiting and weight loss (Am J Clin Pathol 2017;147:33)
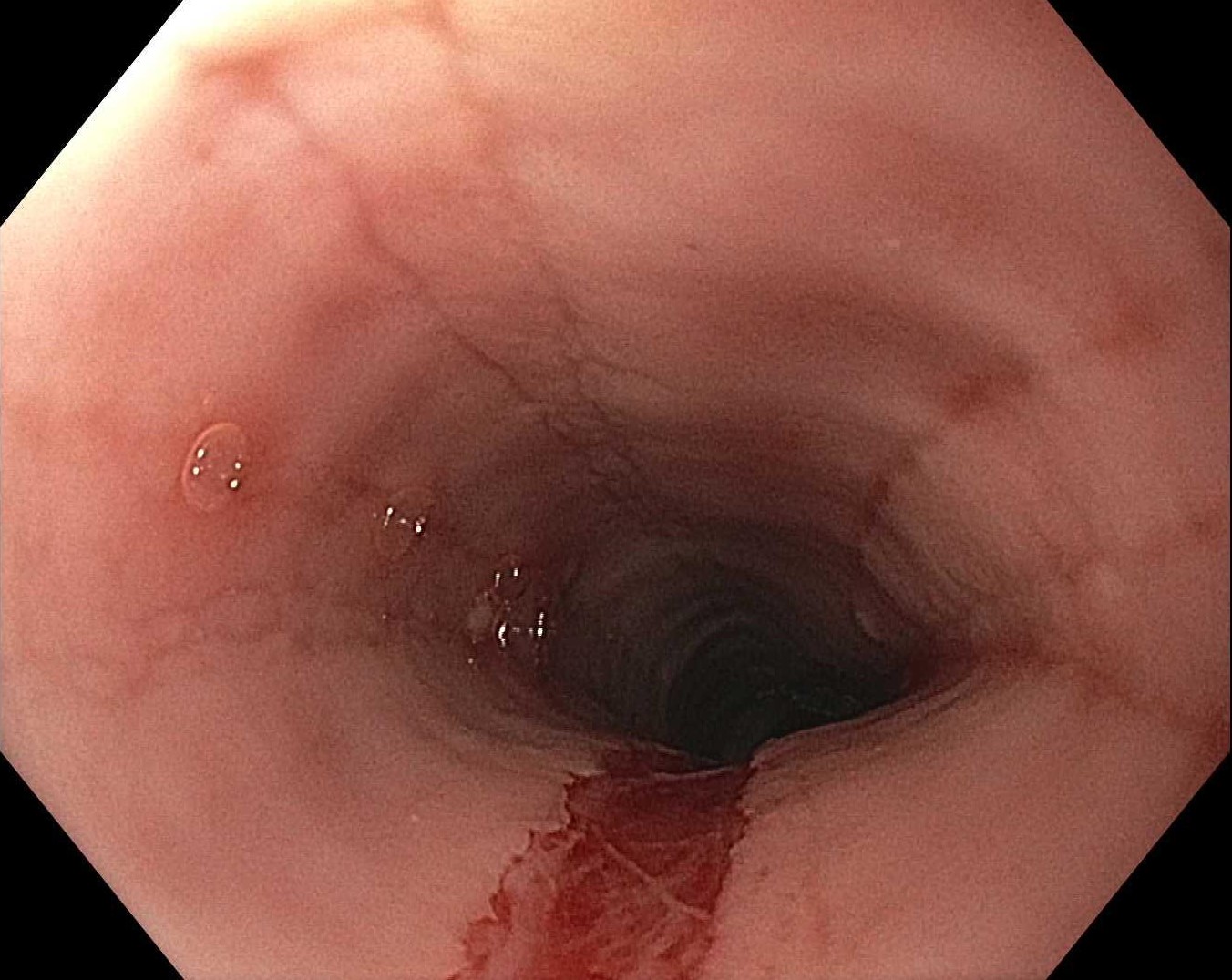
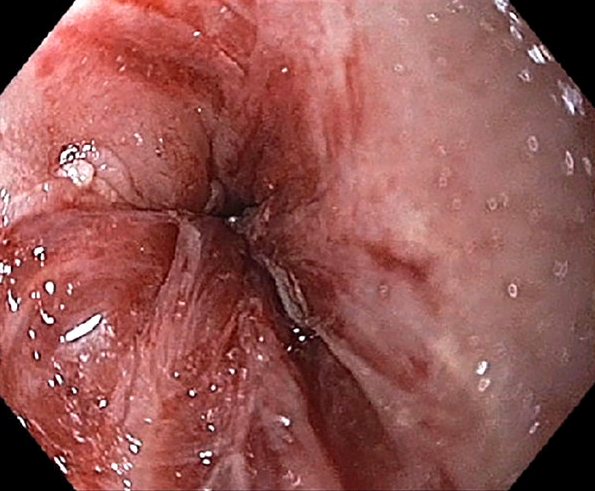
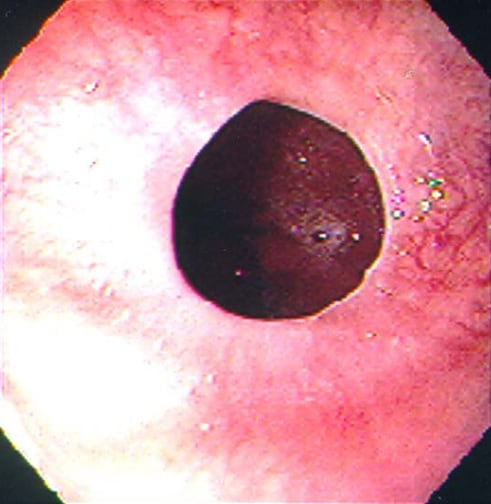
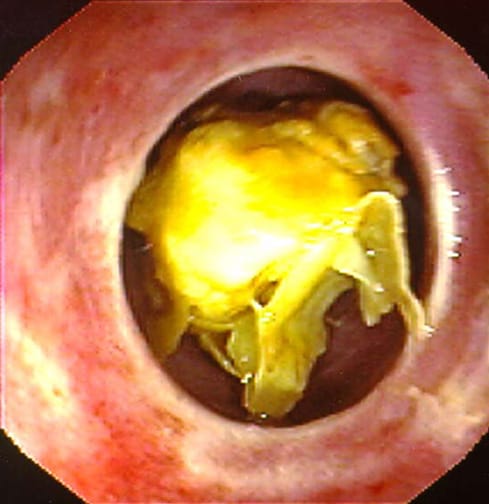
Plaques can be seen on upper endoscopy and do not wash from the mucosa with water irrigation
May coexist with herpes or cytomegalovirus (CMV) esophagitis, oral thrush, esophageal intramural pseudodiverticulosis
Diagnosis
Gold standard for the diagnosis is through histological examination
Biopsy or brushing of the esophageal mucosa is taken during endoscopy
Radiology description
Esophagogram
On double contrast studies, discrete longitudinally oriented linear or irregular plaque-like lesions separated by normal mucosa with small (< 1 cm) punctuate, round or oval ulcers
In advanced cases, the esophagus may have a grossly irregular or shaggy appearance as a result of innumerable plaques and pseudomembranes, with trapping of barium between the lesions
Esophageal obstruction, perforation and tracheoesophageal or aortoesophageal fistula formation are other rare but potentially life threatening complications
Case reports
29 year old Black woman, status post-deceased donor kidney transplant, with difficulty and pain in swallowing (BMJ Case Rep 2019;12:e230410)
Treatment should continue for 1 - 2 weeks after resolution of symptoms
Voriconazole is FDA approved for children at least 12 years of age
Resolution of the radiographic findings sometimes lags behind the clinical recovery, so follow up barium studies may still be abnormal in patients who are asymptomatic
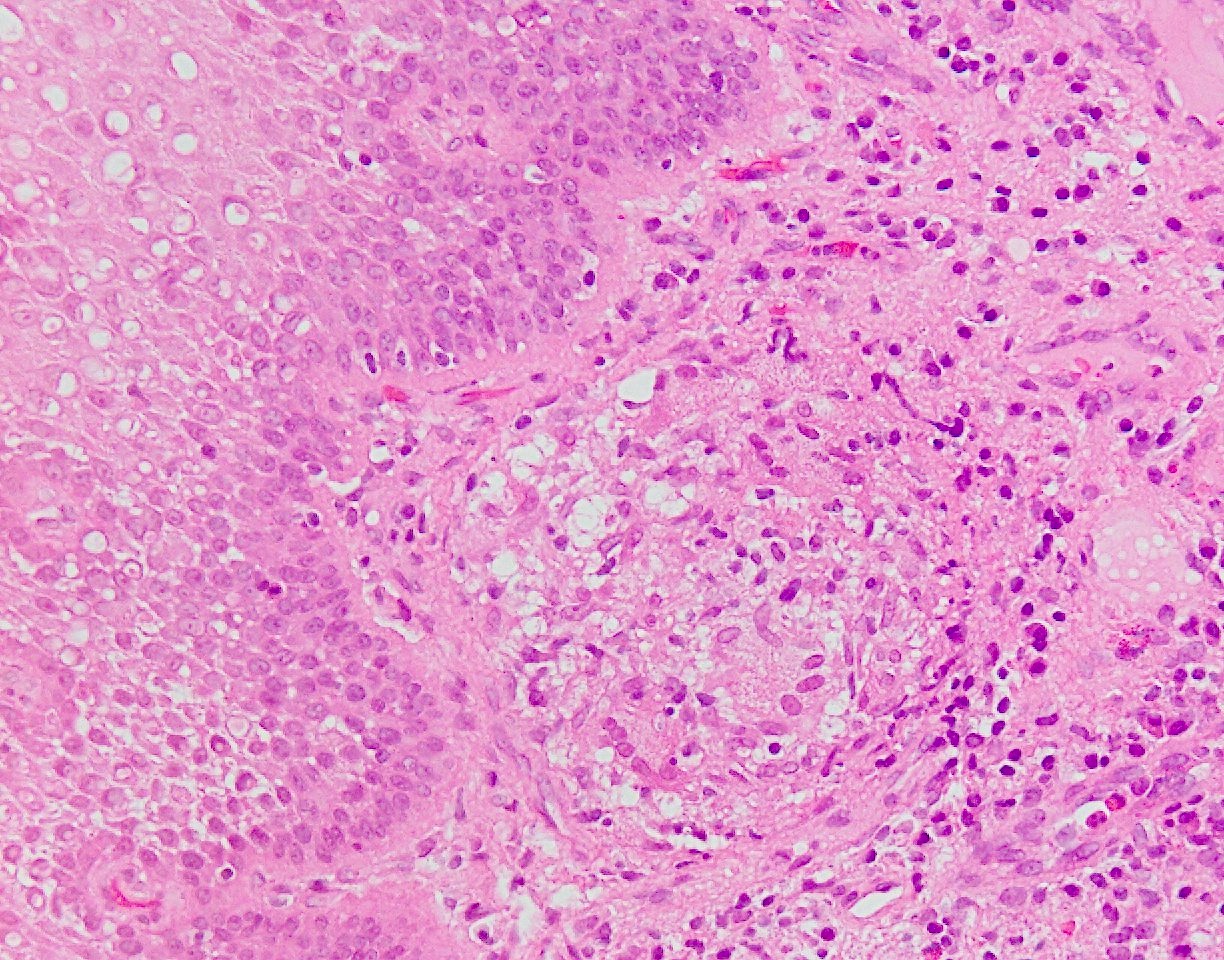
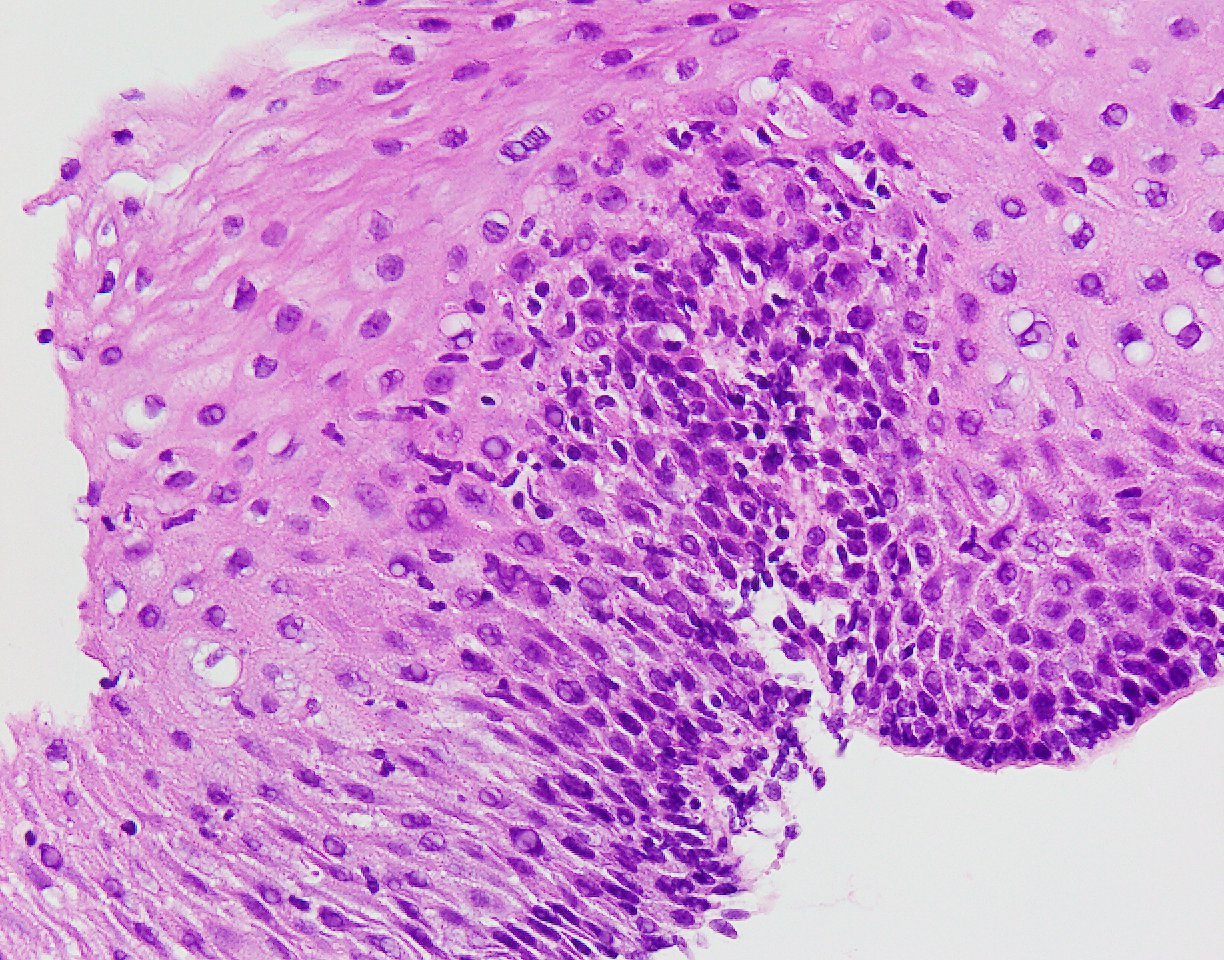
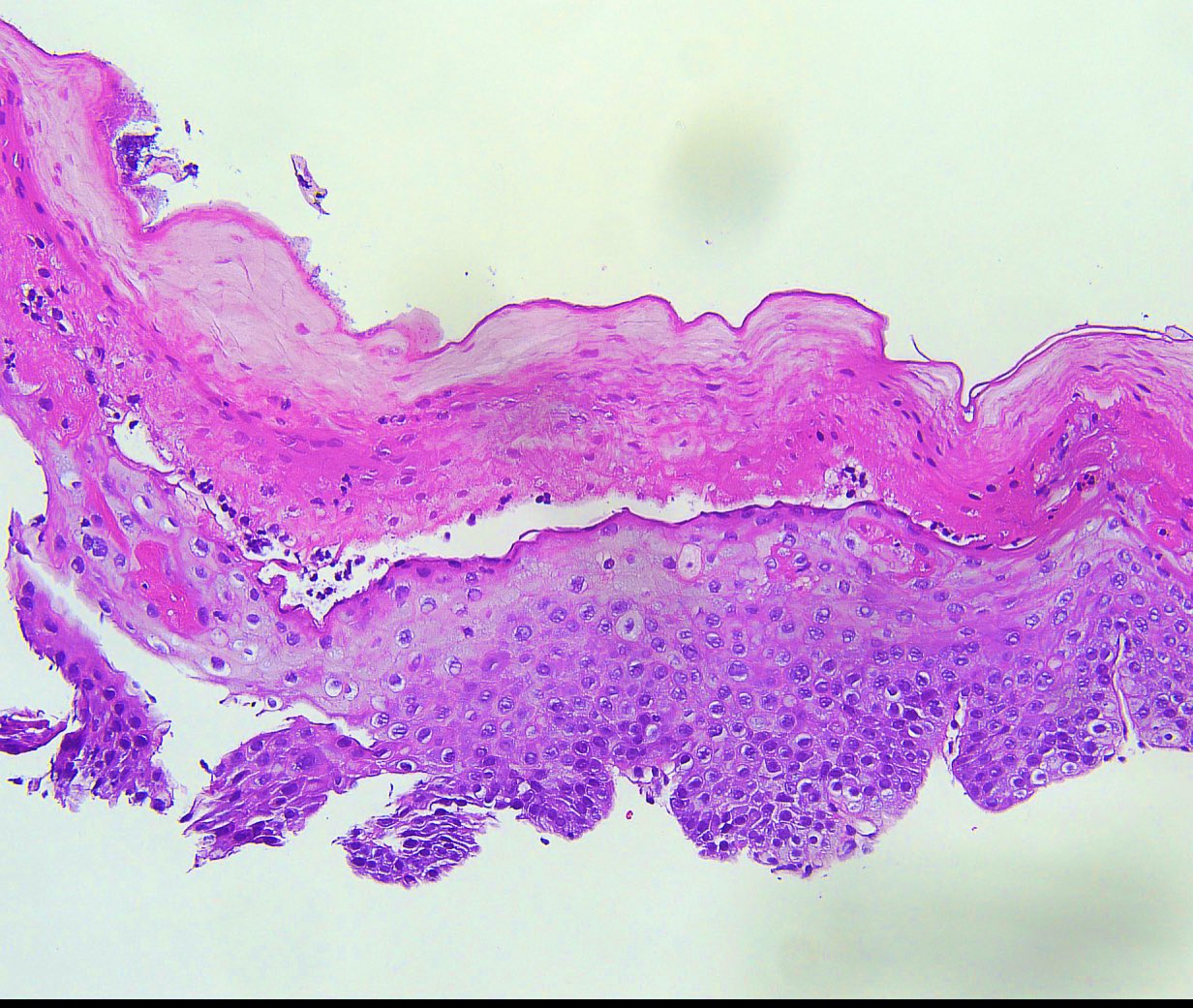
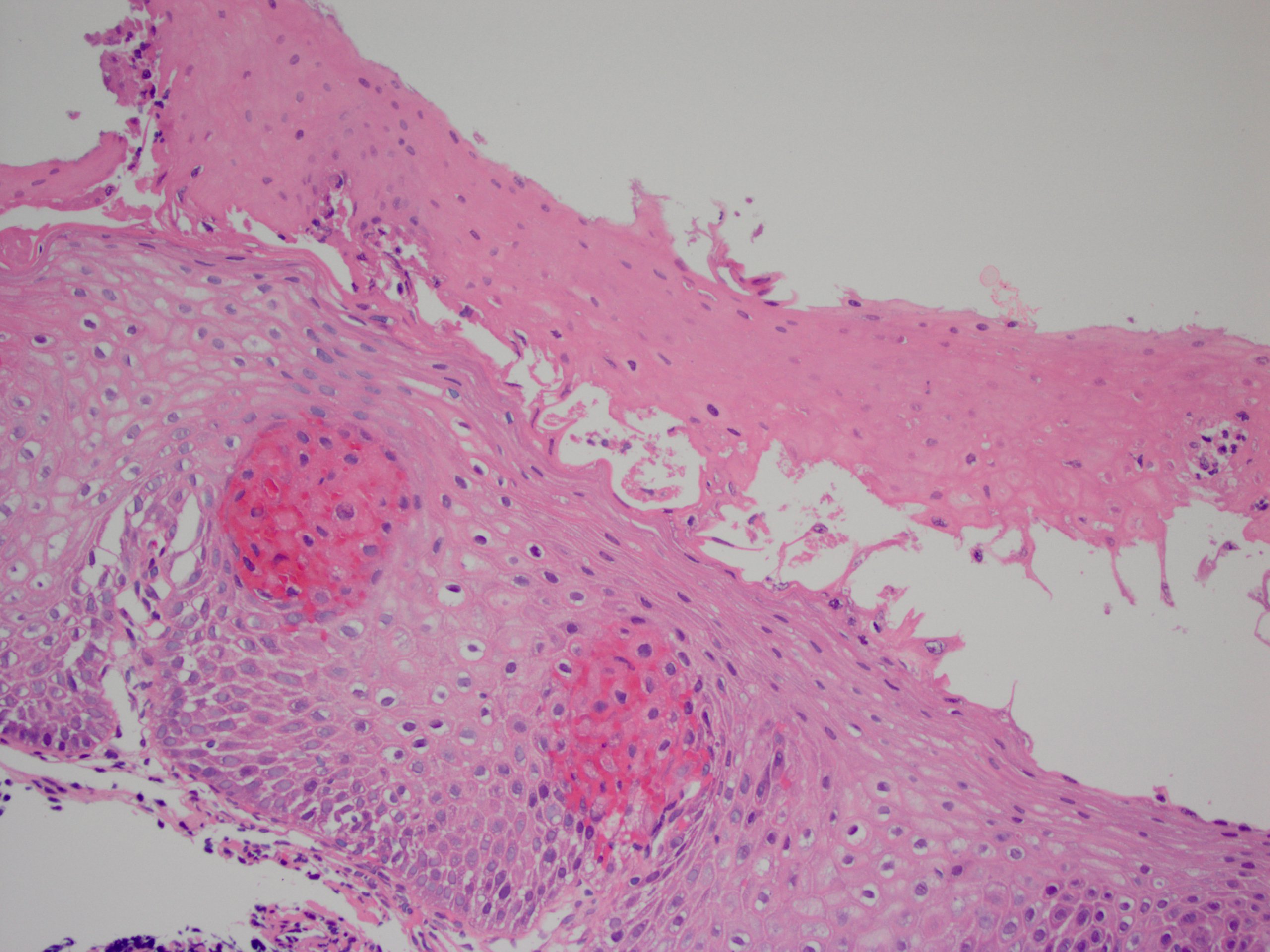
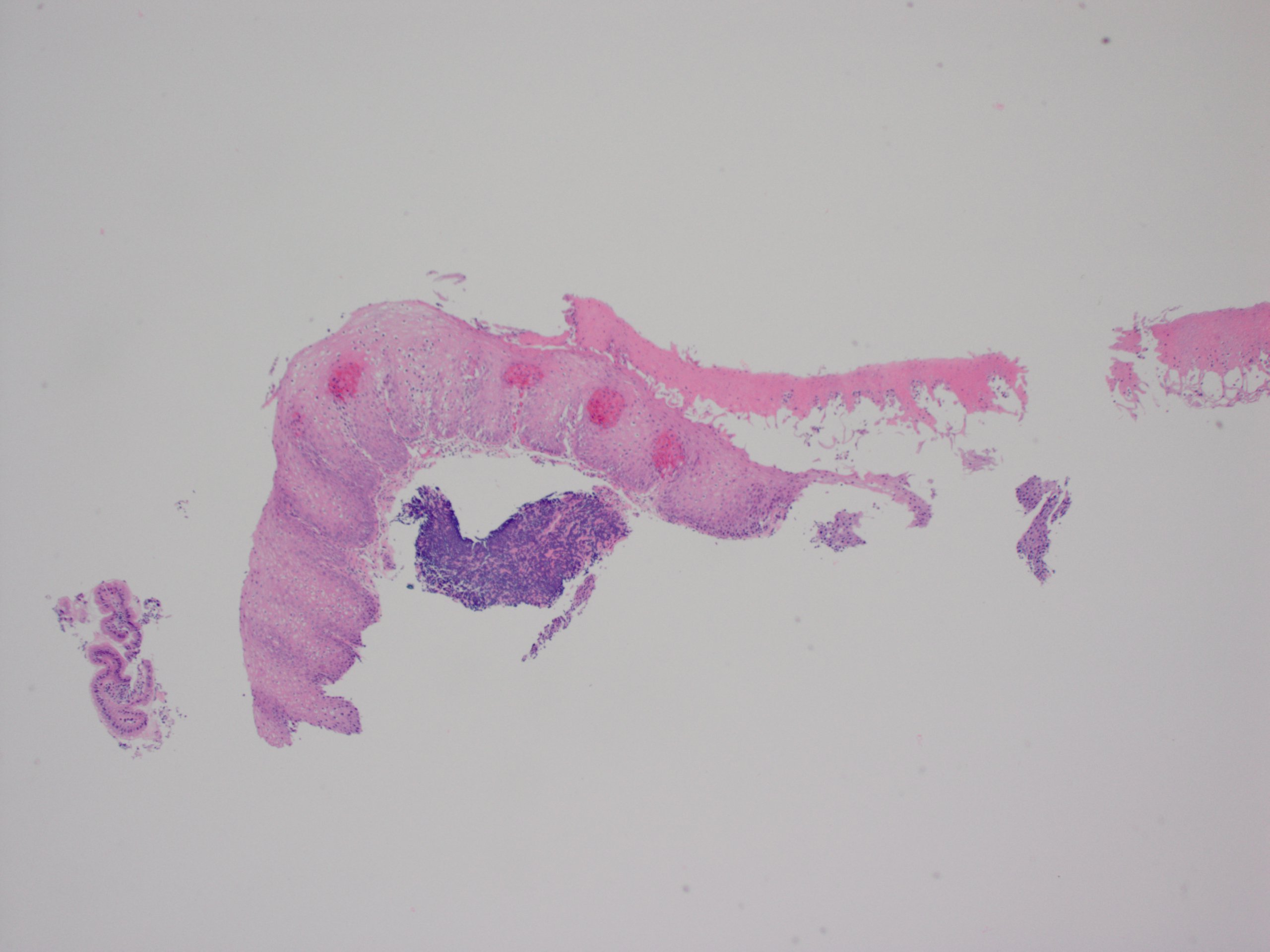
Erosive esophagitis pattern of injury with acute inflammation, intraepithelial neutrophilic abscesses and epithelial edema most prominent in the superficial epithelial layers
Reactive changes including basal zone hyperplasia, parakeratosis and hyperkeratosis are frequently associated
2 forms: yeast cells (often identified on Grocott methenamine silver stain [GMS]) and pseudohyphae
Fungal elements are usually identified within the squamous debris, fibrinopurulent exudate or necrotic debris
HIV patients may have invasion into muscularis propria and adventitia if untreated (Mycoses 1997;40:81)
More commonly presents as a single, isolated and deep, large ulcer rather than multiple small, shallow ulcerations as in herpes simplex virus (HSV) esophagitis
Intranuclear and intracytoplasmic inclusions are more common in mesenchymal and endothelial cells than epithelial cells
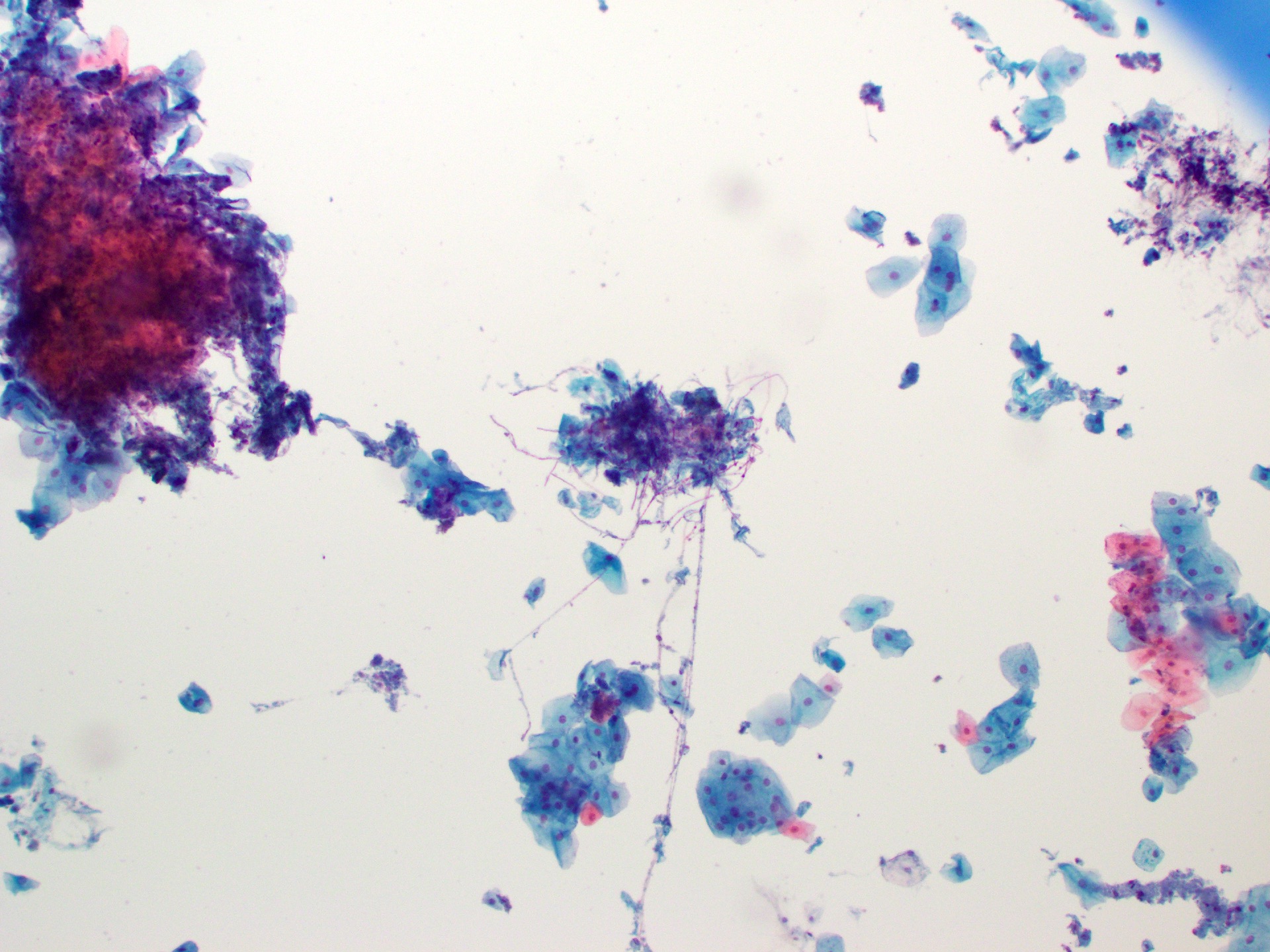
A 46 year old man with a history of human immunodeficiency virus (HIV) presented with odynophagia. Esophagogastroduodenoscopy (EGD) showed white-yellow mucosal plaques in the esophagus. The figure above is from an esophagus biopsy. Which of the following could be the causative agent?
Candida
Cytomegalovirus (CMV)
Herpes simplex virus (HSV)
Iron pills
Board review style answer #1
A.Candida. This patient's history and the EGD findings of the esophagus suggest Candida esophagitis. His history of HIV is an underlying risk factor. The biopsy of the esophagus shows scattered neutrophils with fungal elements including pseudohyphae, supporting the above entity. Answer B is incorrect because pseudohyphae and yeast cells, as shown on the biopsy, are diagnostic for Candida esophagitis. Answer C is incorrect because while HSV esophagitis can affect both immunocompetent and immunocompromised individuals, it is considerably more common in those with compromised immune function. In such cases, these viral infections typically present as ulcerative lesions in the esophagus rather than plaques. To confirm the presence of cytomegalovirus and HSV, it is advisable to perform biopsies of the ulcers. Answer D is incorrect as there was no polarizable crystalline material identified.
Which of the following gross examination findings is consistent with Candida esophagitis?
Bleeding varices
Sloughing of the mucosa
Ulcer in the mid esophagus
Yellow-white mucosal plaques
Board review style answer #2
D. Yellow-white mucosal plaques. Yellow-white plaques, which bleed upon removal, are consistent with Candida esophagitis. Answer C is incorrect as cytomegalovirus (CMV) / herpes simplex virus (HSV) are frequently associated with ulcers. Answer B is incorrect because sloughing of the mucosa can be seen in esophagitis dessecans superficialis. Answer A is incorrect because bleeding varices are associated with portal hypertension.
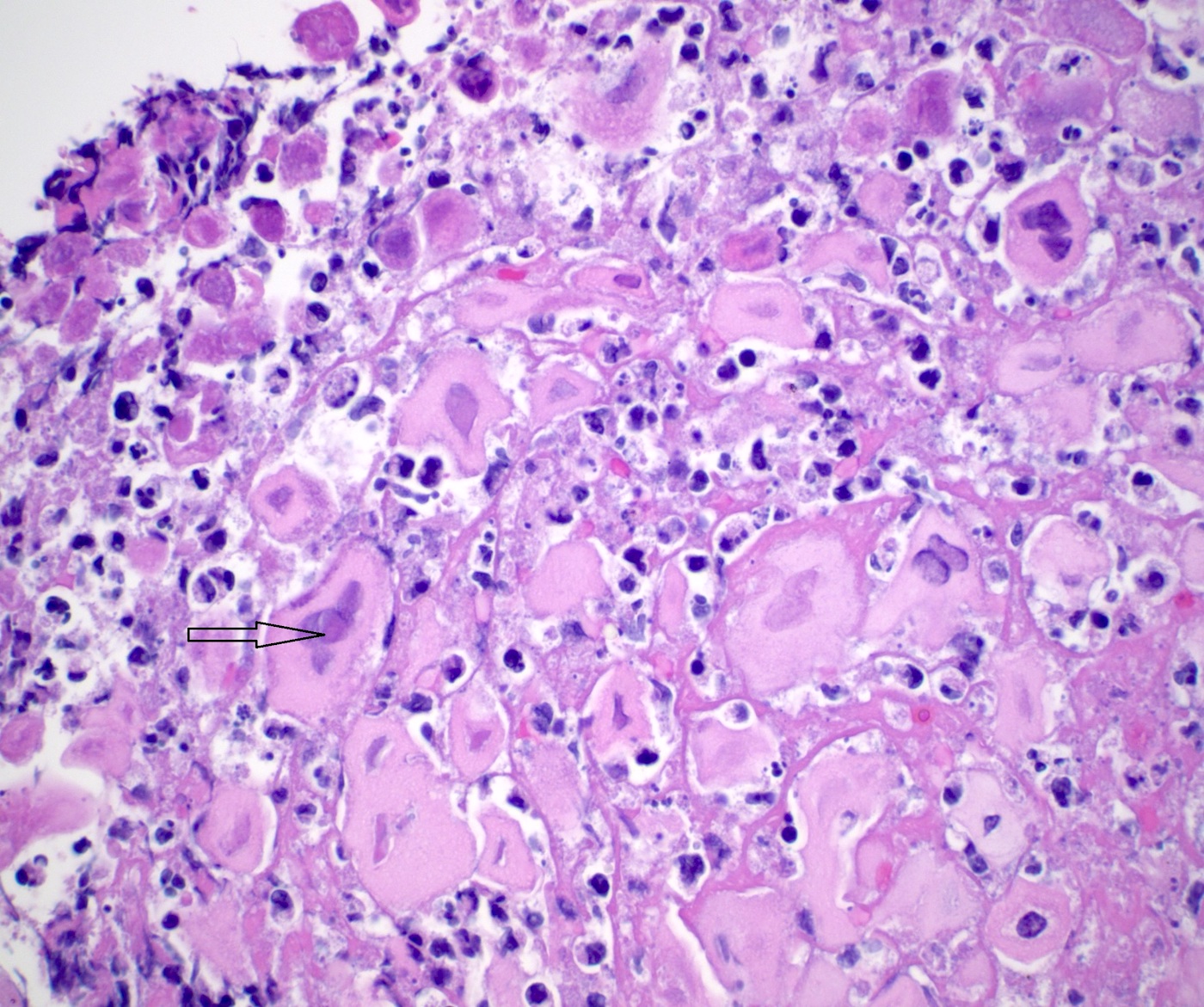
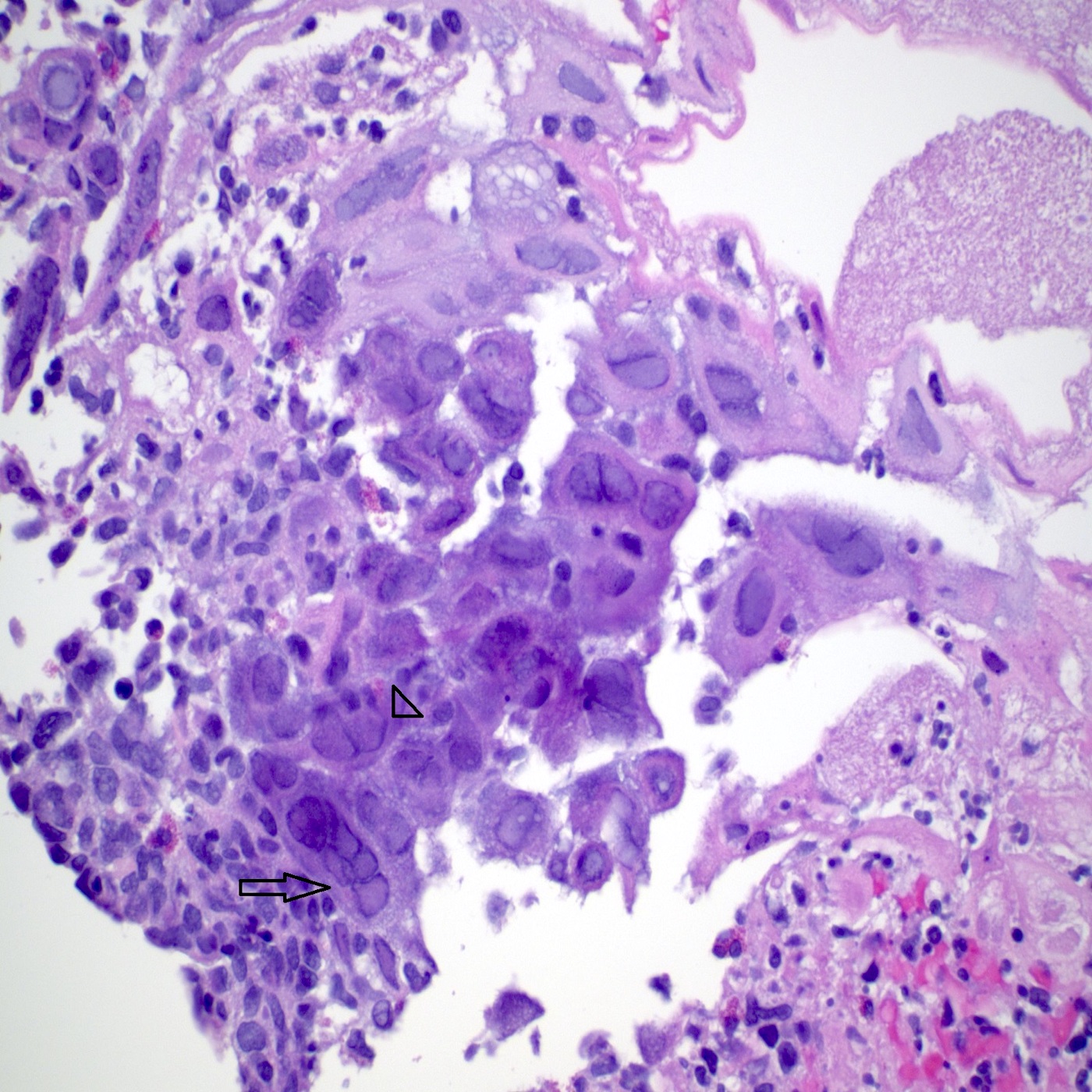
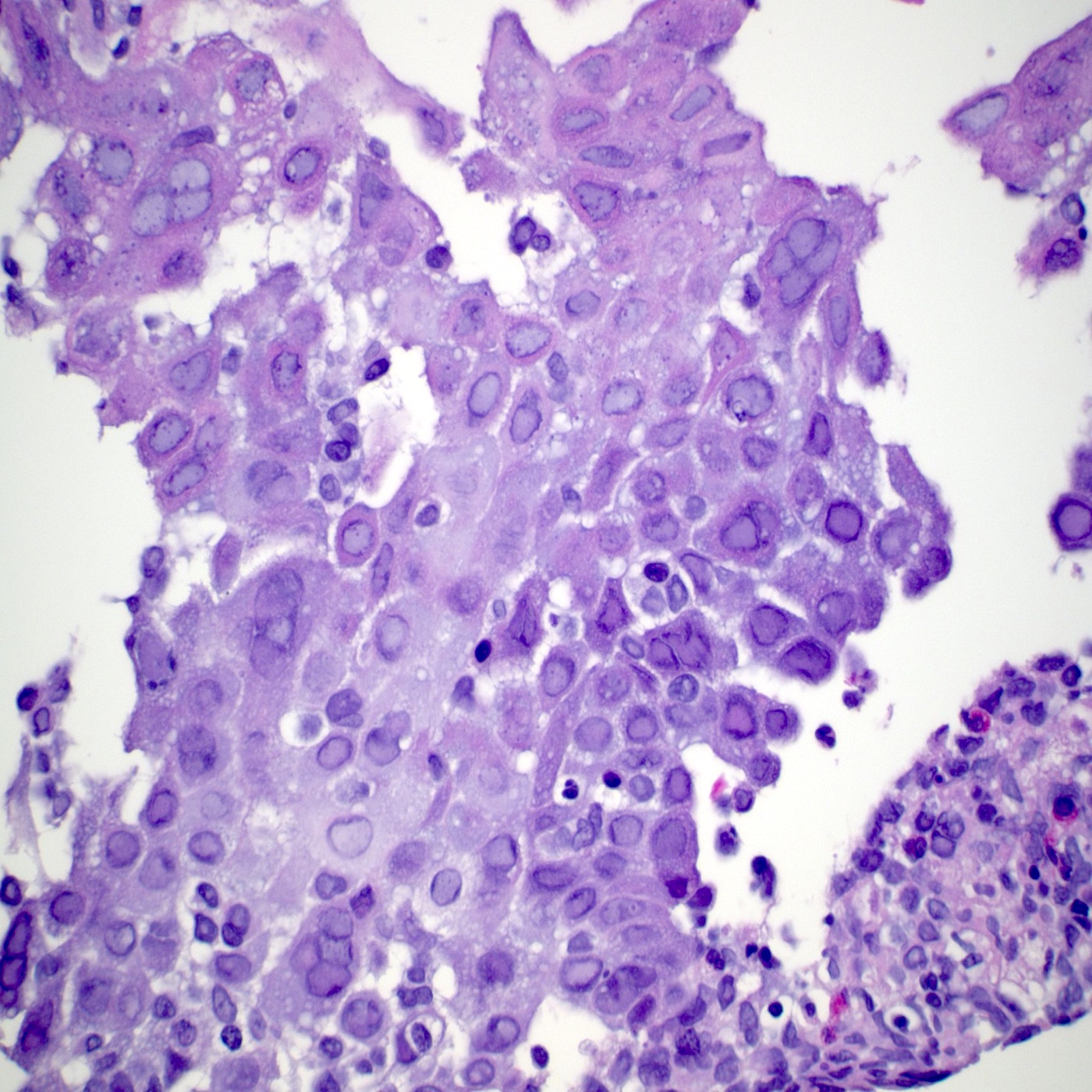
Esophageal infection of adults and children by cytomegalovirus, a double stranded DNA virus of the Herpesviridae family (human herpes virus 5 [HHV5]) spread by blood and other bodily fluids
Rare in immunocompetent patients but causes serious disease in the setting of immunosuppression (e.g., AIDS, solid organ or bone marrow transplant, chemoradiation therapy)
Cytomegalovirus (CMV) is the only herpes virus with both nuclear and cytoplasmic inclusions, identified on routine H&E stain
Essential features
Severe and potentially life threatening esophageal infections occur in immunosuppressed patients (e.g., people living with HIV / AIDS, solid organ or bone marrow transplant recipients, patients undergoing chemoradiation therapy)
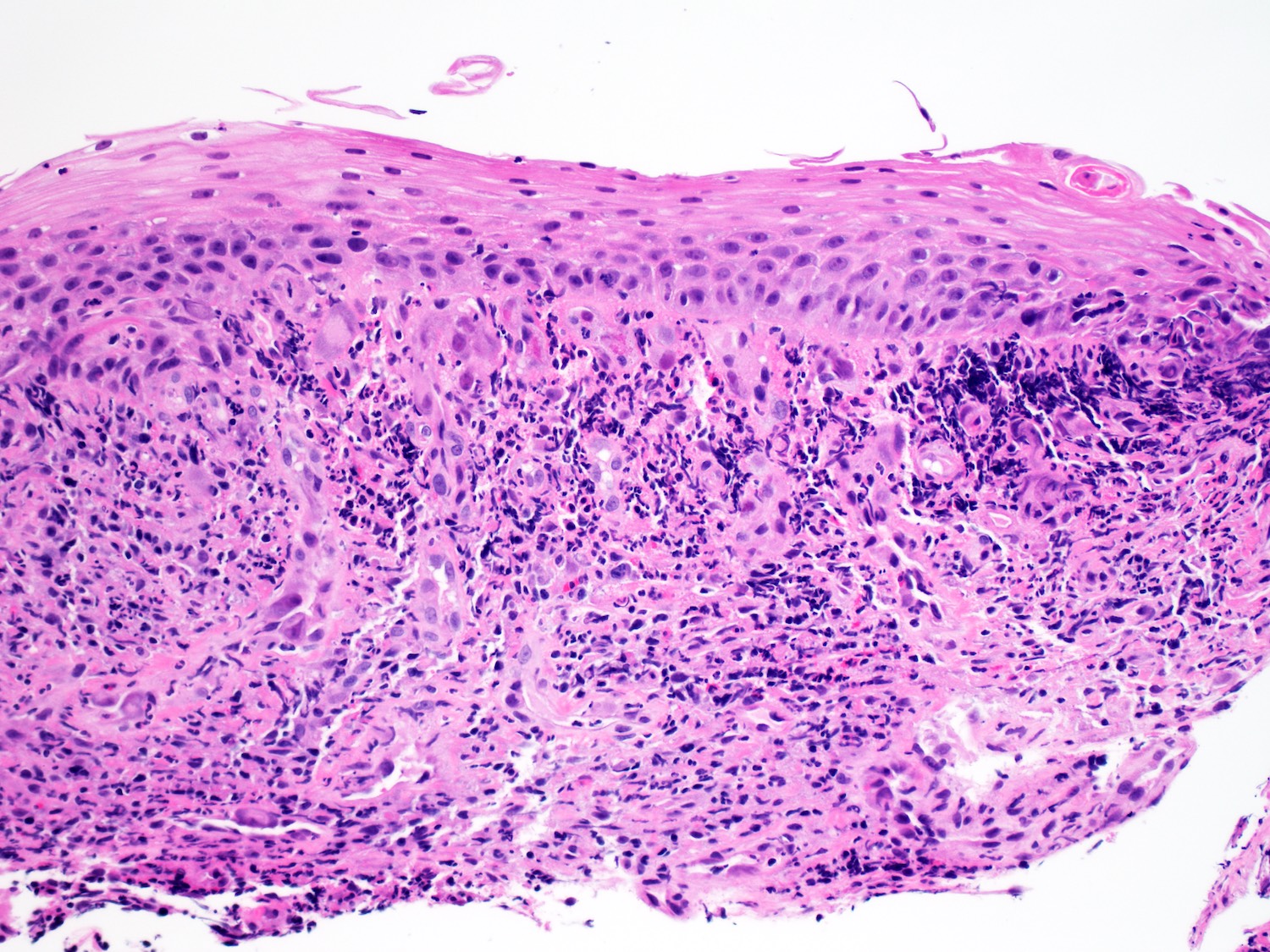
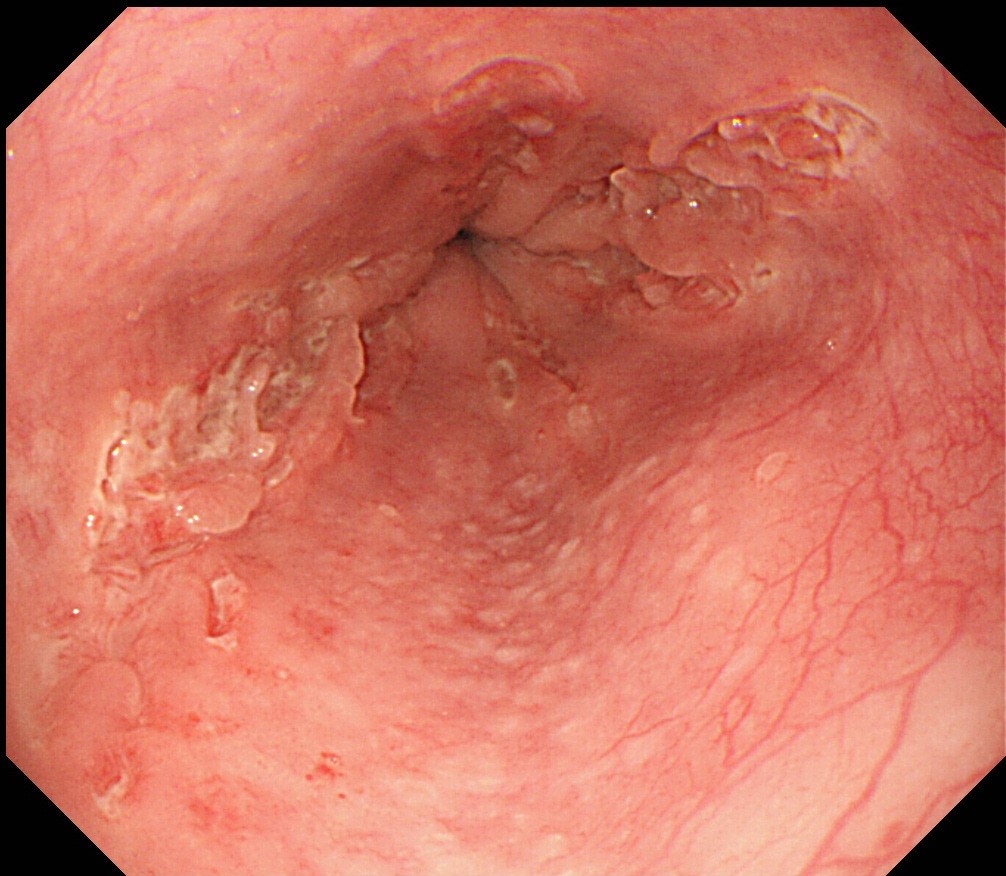
Diagnosis requires endoscopy with tissue biopsy of areas of ulceration or erosion, which typically occur in the mid or distal esophagus
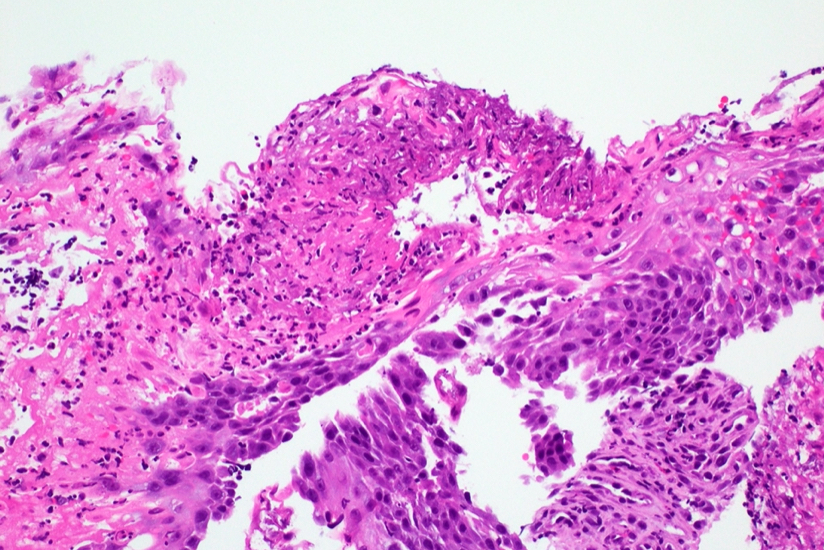
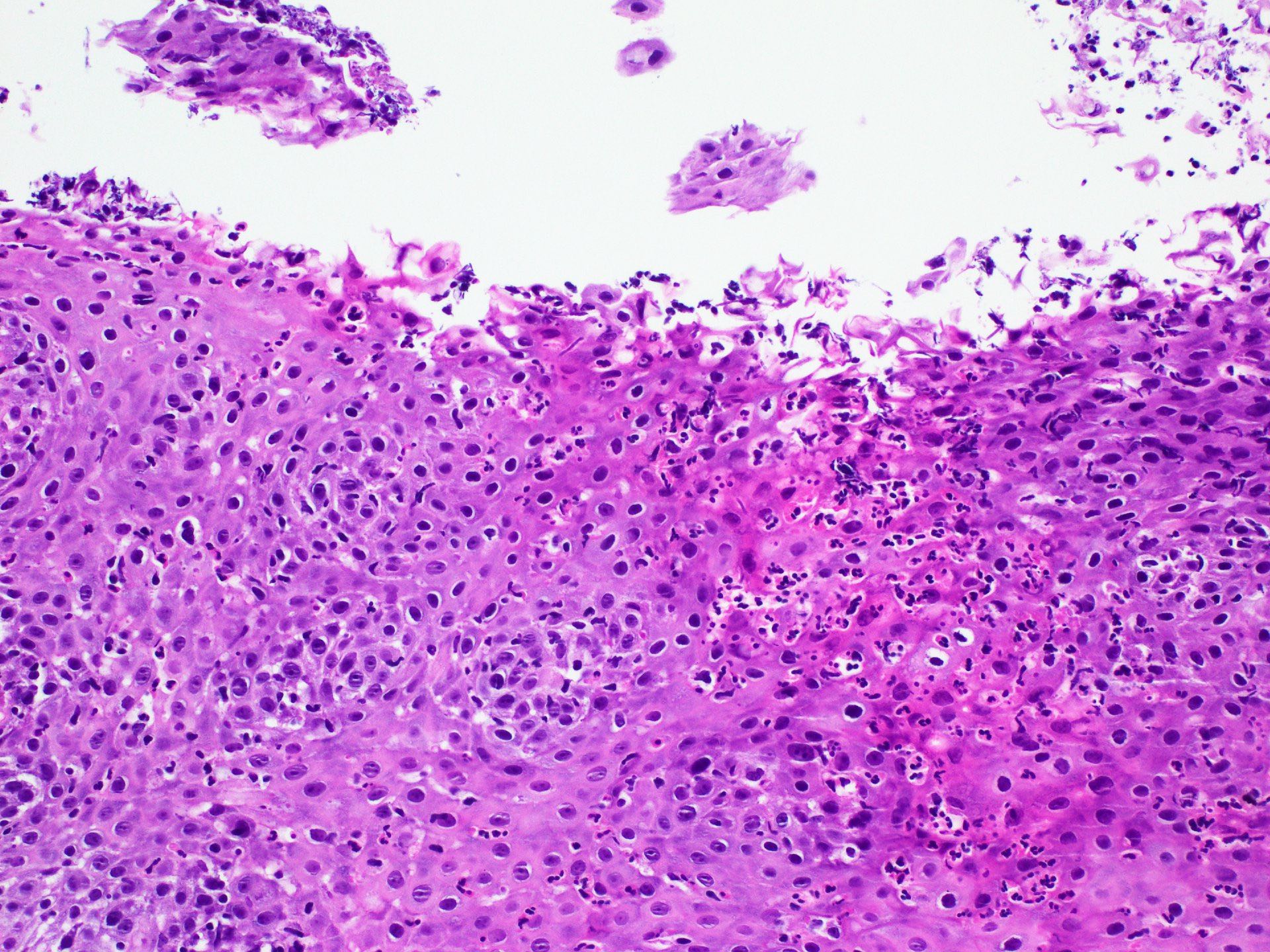
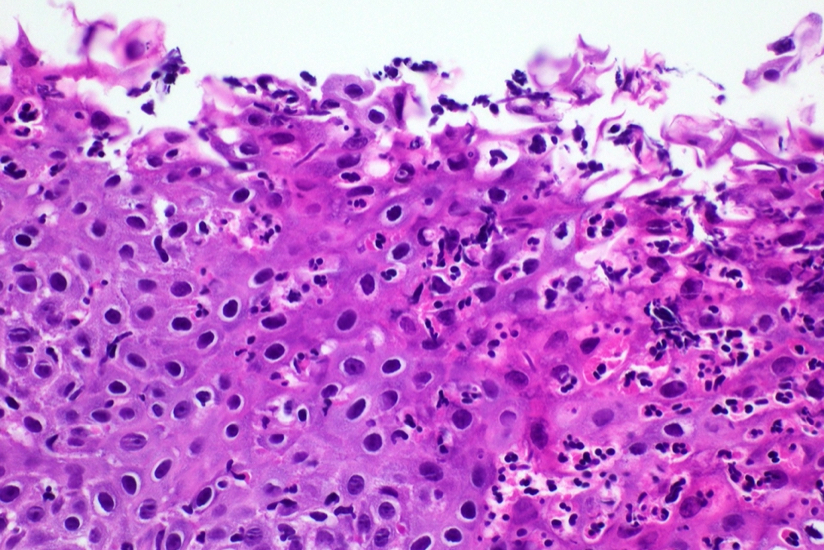
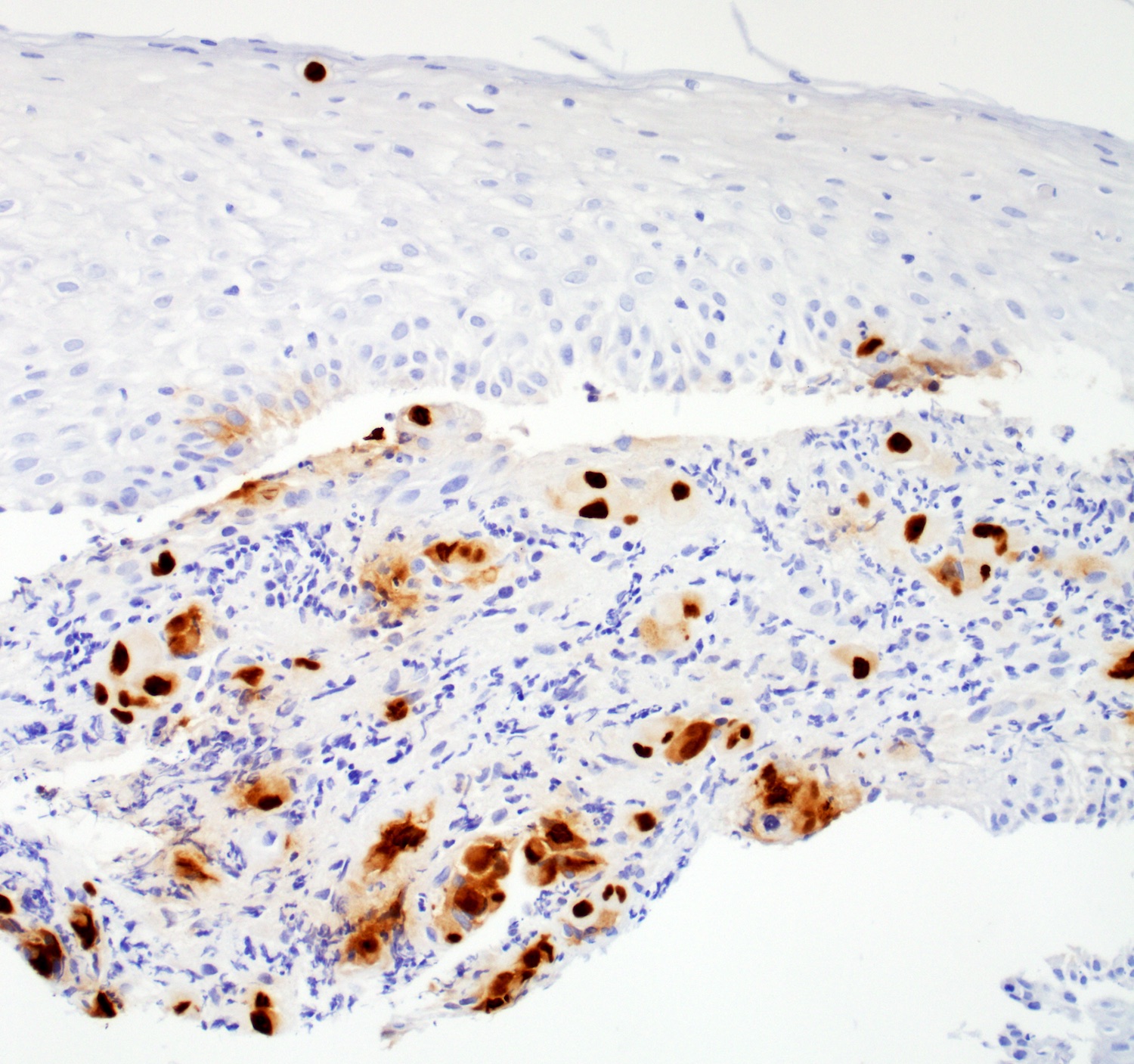
Histopathologic features characterized by ulceration or erosion harboring enlarged cells with intranuclear and cytoplasmic inclusions
Viropathic inclusions can be identified in endothelial cells, stromal fibroblasts or epithelial cells
CMV immunohistochemistry or CMV in situ hybridization aids in the detection of viropathic inclusions
Primary infection usually asymptomatic but can be associated with mononucleosis-like illness (J Infect Chemother 2019;25:431)
CMV establishes latency and persists for life but can be reactivated in the setting of immunosuppression due to the dysfunction of cell mediated immunity (QJM 2012;105:401)
Mucosal infection and replication occur in human epithelial cells, endothelial cells and tissue fibroblasts
Infection leads to an ischemic pattern of tissue erosion or necrosis and inflammation (Ann Intern Med 1993;119:924)
Endoscopic appearance of lesions is variable but most commonly occurs in distal esophagus (65%), followed by mid esophagus (28%) (Clin Gastroenterol Hepatol 2020;18:736)
Requires tissue biopsy and histopathologic diagnosis
Tissue sampling should include granulation tissue or ulcer bed, given predilection for endothelial and stromal cell infection
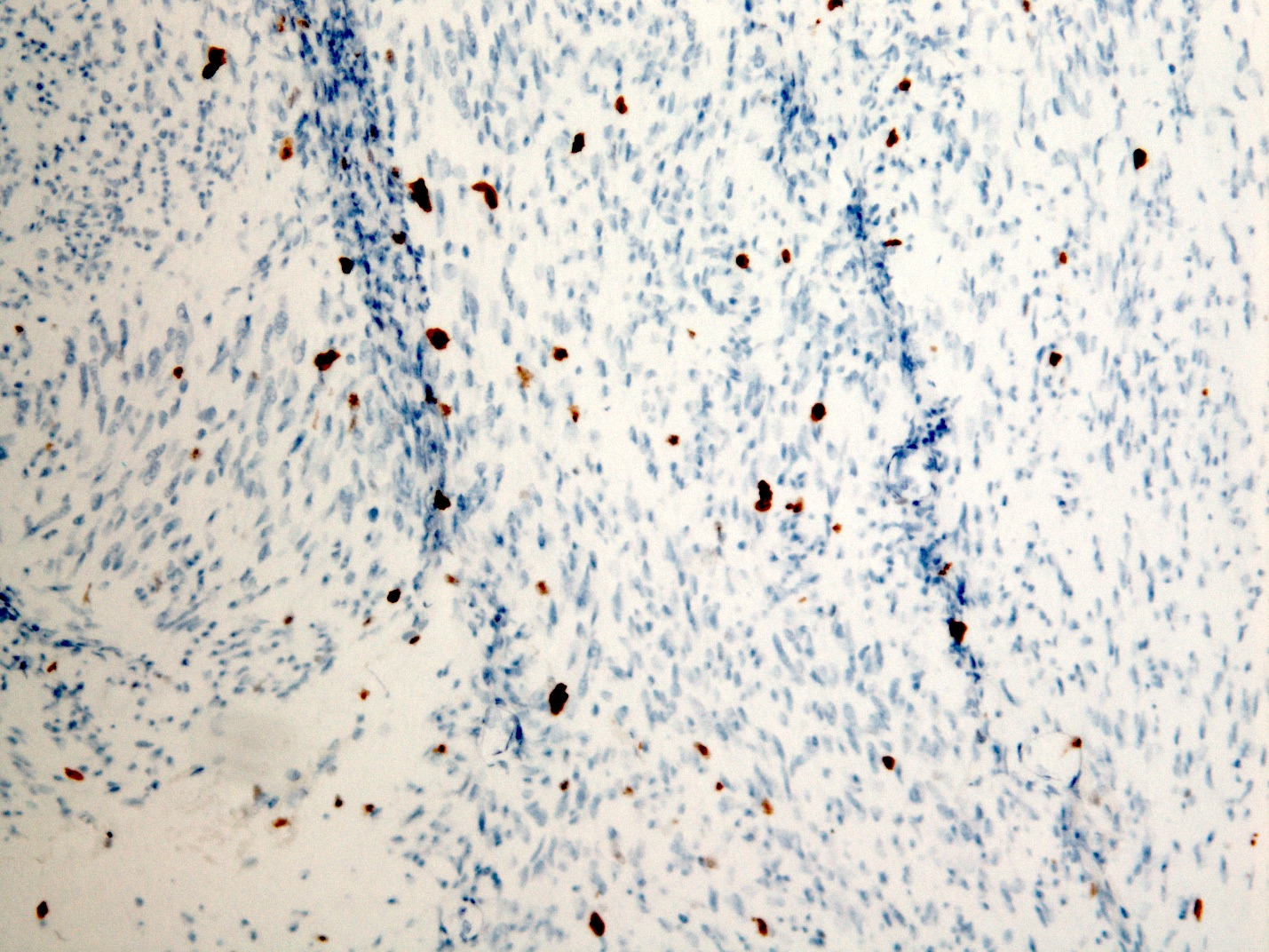
Finding > 2 positive cells by CMV IHC has higher correlation with CMV viremia versus finding rare positive cells (< 2) (Gastroenterology Res 2016;9:92)
Laboratory
CMV antigenemia is a poor predictor of gastrointestinal tract involvement but viral load by real time PCR is more reliable (Bone Marrow Transplant 2004;33:431)
Prognostic factors
ICU requirement and acute kidney injury are risk factors for in hospital mortality
Upper gastrointestinal tract involvement has a 17% mortality rate 1 month after diagnosis and 25% mortality rate 1 year after diagnosis according to a small study of 12 patients (GE Port J Gastroenterol 2017;24:262)
42 year old man who presented to the emergency department (ED) with a 2 week history of abdominal pain and watery diarrhea was found to have a new diagnosis of HIV / AIDS (Cureus 2022;14:e22455)
44 year old man with dermatomyositis on mycophenolate was admitted for acute gastrointestinal bleed (Clin Case Rep 2022;10:e6044)
60 year old woman on immunosuppressive therapy for pemphigus vulgaris presented with odynophagia and was found to have ulcerative CMV and HSV esophagitis (IDCases 2020:22:e00925)
72 year old man with kidney transplant who complained of dysphagia and unintentional weight loss was found to have distal esophageal stricture (ACG Case Rep J 2022;9:e00836)
77 year old immunocompetent man with erosive esophageal lesion was found to have moderately differentiated squamous cell carcinoma and CMV (Gut Pathog 2021;13:24)
Treatment
Intravenous ganciclovir or foscarnet for 3 - 6 weeks; continued maintenance therapy is indicated for patients with concurrent retinitis or recurrent gastrointestinal disease (Am J Gastroenterol 1998;93:317, Arch Intern Med 1998;158:957)
Antiviral prophylaxis is standard of care for high risk solid organ transplant recipients; preemptive therapy preferred for hematopoietic cell transplant recipients (Clin Transplant 2019;33:e13512)
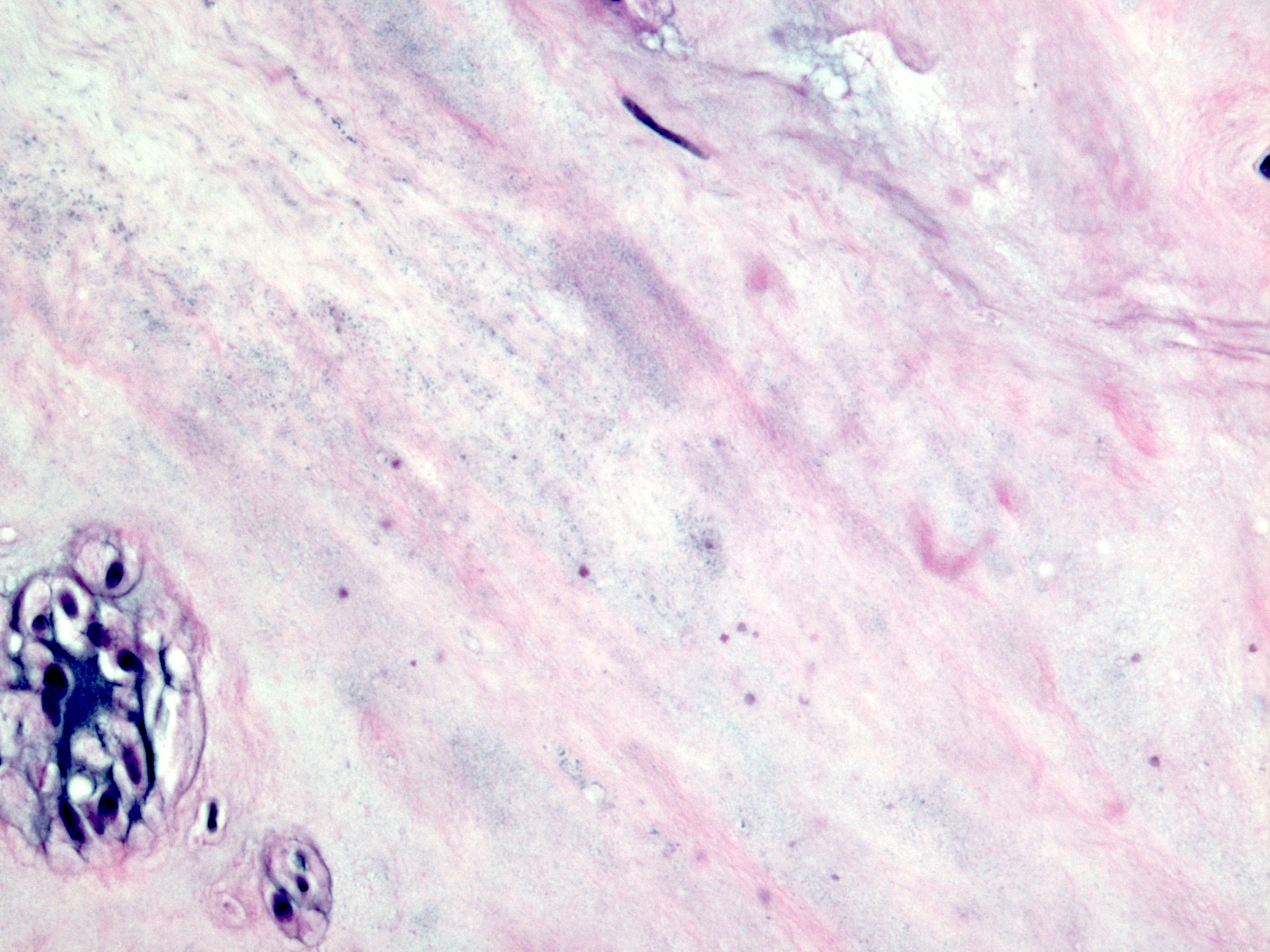
Ulceration and inflamed granulation tissue with necroinflammatory debris
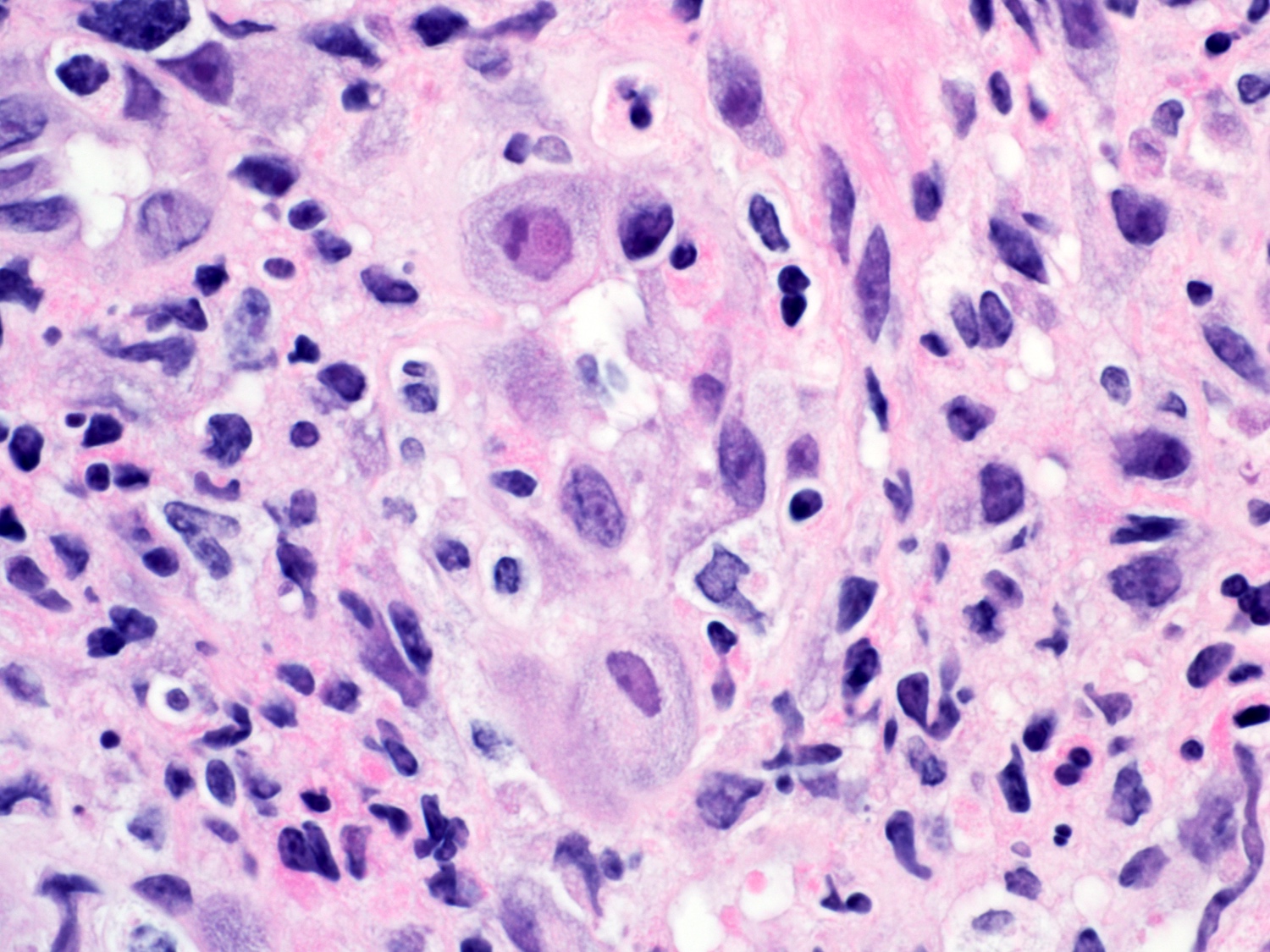
Cytologic enlargement by both intranuclear and intracytoplasmic inclusions
Intranuclear basophilic or amphophilic inclusions; can have owl eye appearance when associated with peripheral clearing (an artifact of fixation) and margination of nuclear chromatin (Cowdry type A body)
Intracytoplasmic basophilic or amphophilic inclusions; can also appear as coarse, eosinophilic inclusions
PAS and GMS stains may weakly highlight intracytoplasmic inclusions, not intranuclear inclusions (Semin Diagn Pathol 2017;34:510)
Viropathic inclusions identified in endothelial cells, stromal cells and epithelial cells
Microscopic (histologic) images
Contributed by Gillian L. Hale, M.D., M.P.H.
Inflammation and CMV inclusions
Numerous viropathic inclusions
Infected endothelial cells
Granular inclusions
CMV IHC
Positive stains
CMV immunohistochemistry or CMV in situ hybridization
Spheroid shaped virions, diameter of 150 - 200 nm, each with dense, protein core comprised of linear, double stranded DNA genome, surrounded by a hyperlucent halo
Electron microscopy images
Images hosted on other servers:
Spheroid virions
Sample pathology report
Esophagus, ulcer, biopsy:
Ulcerated squamous mucosa with intranuclear and basophilic intracytoplasmic inclusions, morphologically consistent with cytomegalovirus (CMV); confirmed by CMV immunohistochemistry
Viropathic inclusions more common in squamous epithelial cells than in stromal and endothelial cells
Intranuclear type A Cowdry inclusion without nuclear enlargement
3 Ms of nuclear changes: molding of nuclear contours, margination of chromatin and multinucleation
No intracytoplasmic inclusions
Varicella zoster virus:
Features similar to HSV 1 / 2 but multinucleation is uncommon
No intracytoplasmic inclusions
Board review style question #1
In the biopsy of the esophagus shown above, what is the most likely clinical presentation of the patient?
2 year old immunocompetent boy with new onset projectile vomiting
21 year old immunocompetent woman presenting with symptoms of gastroesophageal reflux
67 year old female cyclist with new onset shortness of breath and chronic cough
86 year old man undergoing chemoradiation for squamous cell carcinoma
Board review style answer #1
D. 86 year old man undergoing chemoradiation for squamous cell carcinoma. Underlying malignancy and chemoradiation is a risk factor for CMV infection. Answer A is incorrect because the patient is immunocompetent without reported risk factors for CMV infection. Answer B is incorrect because the patient is immunocompetent, which is an unlikely presentation for CMV esophagitis. Answer C is incorrect because the clinical symptoms suggest an acute respiratory infection.
Which herpes virus demonstrates both intranuclear and intracytoplasmic viropathic inclusions?
Cytomegalovirus
Epstein-Barr virus
Herpes simplex virus 1 and 2
Varicella zoster virus
Board review style answer #2
A. Cytomegalovirus. Only CMV virus demonstrates both intranuclear and intracytoplasmic viropathic inclusions. Answer C is incorrect because herpes simplex virus 1 and 2 causes an intranuclear inclusion (Cowdry type A) without an accompanying intracytoplasmic inclusion. Answer D is incorrect because varicella zoster virus also demonstrates an intranuclear Cowdry type A inclusion without an intracytoplasmic inclusion. Answer B is incorrect because Epstein-Barr virus does not cause inclusions in infected cells.
Incidence of esophageal Crohn's disease ranges from 0.3% to 10% in adults with Crohn's disease and from 4.2% to 42% in pediatric patients with Crohn's disease
Aphthous ulcer, longitudinal ulcer, stricture and fistula
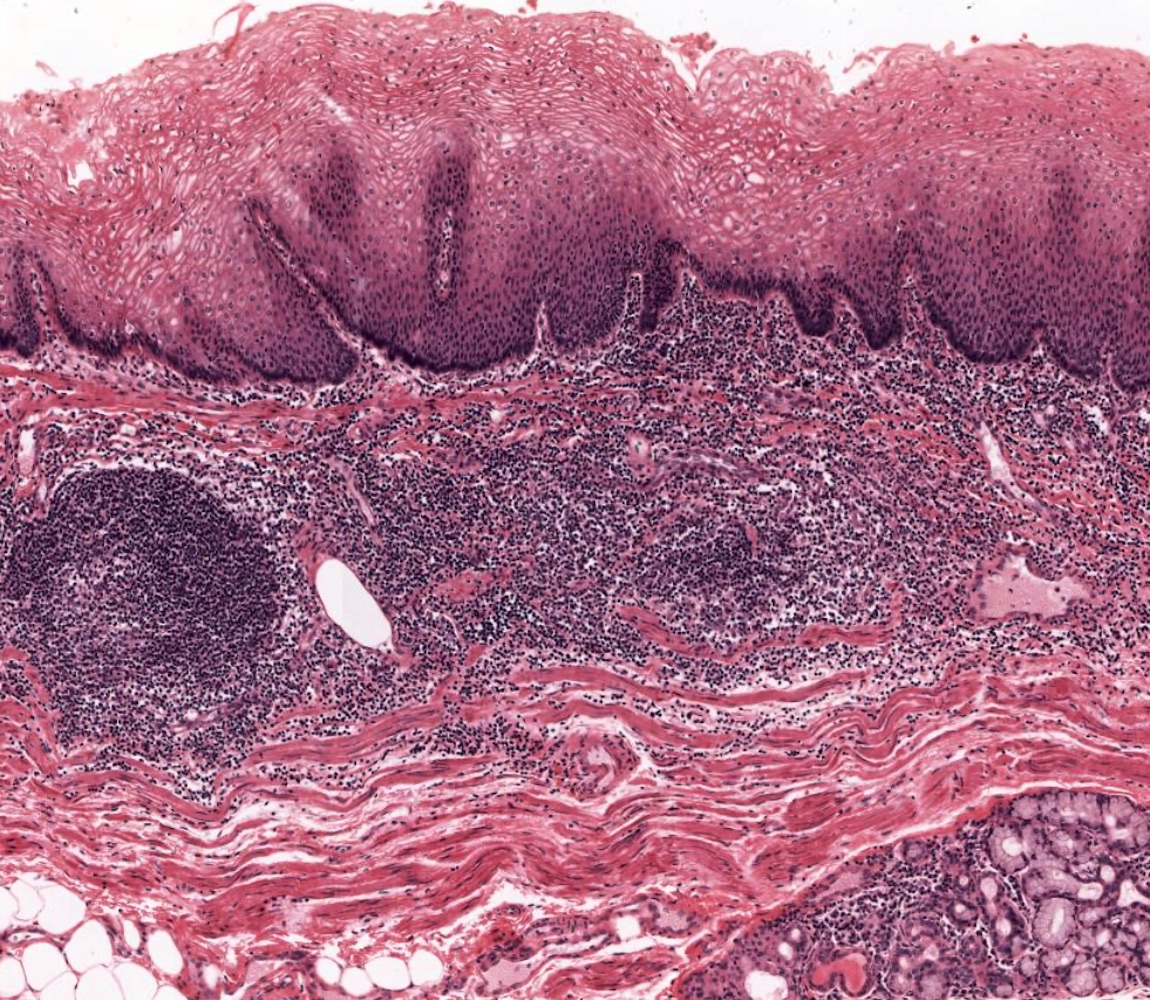
Histologic features of esophageal Crohn's disease are generally nonspecific
Male sex was an independent predictor for upper gastrointestinal tract involvement including the esophagus (J Crohns Colitis 2018;12:1399)
18 of 61 patients (30%) with lymphocyte rich inflammation in the mid or proximal esophagus had Crohn's disease (Am J Surg Pathol 2020;44:198)
Patients in the lymphocytic esophagitis cohort had a higher than normal proportion of patients with Crohn's disease, raising the possibility that lymphocytic esophagitis could be associated with or a manifestation of inflammatory bowel disease (Am J Clin Pathol 2006;125:432, Am J Surg Pathol 2022;46:e55)
Distal esophagus is the most common involved site, either alone or with the involvement of the entire esophagus (J Crohns Colitis 2020;14:624)
Pathophysiology
Crohn's disease is a chronic inflammatory disease mainly affecting the intestine, especially the terminal ileum; Crohn's disease is characterized by the alternating periods of flares and remissions caused by a complex pathogenesis involving a reshaped microenvironment of the intestine (Biol Direct 2020;15:23)
Etiology
Caused by a complex pathogenesis involving the interactions of environmental factors, the immune system, susceptibility genes and the host’s microbiome changes, leading to disruption of the intestinal mucosa; among these, inflammation plays a key role
Etiology of esophageal Crohn’s disease remains unclear, as overall pathogenesis of Crohn’s disease remains poorly understood (Biol Direct 2020;15:23)
Endoscopic findings are nonspecific including erosion, aphthous ulcer, granular and hyperemic mucosa and longitudinal ulcer (J Gastroenterol Hepatol 2018;33:355)
Clinicopathologic diagnosis including the patient's clinical history of Crohn's disease and endoscopic and histologic features, such as aphthous ulcer, longitudinal ulcer and granuloma(s)
30 year old woman with history of severe ileocolonic Crohn's disease presented with odynophagia and progressive dysphagia to liquids and solids (Dig Dis Sci 2017;62:2690)
Transmural chronic inflammation in the esophagectomy specimen, one of the histologic hallmarks of Crohn's disease, has been reported in a patient with uncontrollable stricture due to Crohn's disease (Rev Esp Enferm Dig 2022;114:501)
Squamous mucosa with nonnecrotizing granuloma(s) (see comment)
GMS and PASF stains, negative for fungal infection.
AFB stain, negative for acid fast bacilli.
Comment: Given the patient's clinical history of Crohn's disease and the endoscopic findings of longitudinal and aphthous ulcers, the biopsy findings are compatible with granulomatous inflammation associated with Crohn's disease. Clinical correlation is suggested.
Differential diagnosis
Histologic features of esophageal Crohn's disease are typically nonspecific
In many cases, a definitive diagnosis of esophageal Crohn's disease cannot be established based on histologic features alone and only a diagnosis of compatible with esophageal CD can be achieved
Lymphocytic esophagitis is a term suggested for the finding of intraepithelial lymphocytosis (≥ 20 lymphocytes / high power field) in an esophageal biopsy
Biopsy samples show dense mononuclear cell rich lamina propria inflammation accompanied by band-like chronic inflammation underneath the epithelium
Esophageal tuberculosis:
Caseating granuloma(s) may be found
AFB stain, culture and polymerase chain reaction testing for mycobacterium tuberculosis
Clinical presentation and pathologic features useful for esophageal tuberculosis diagnosis includes fever, night sweaters, transverse ulcer, ileocecal lesion and caseating granuloma(s)
Round deep ulcers with sharp borders in the ileocecal location
Board review style question #1
Which of the following statements regarding the histologic features of esophageal Crohn’s disease is true?
Chronic inflammation with predominantly lymphocytes and plasma cells is the most common finding in biopsy samples
Elderly patients with Crohn's disease tend to show more frequent esophageal involvement
Proximal esophagus is the most common site of involvement
The finding of nonnecrotizing granuloma(s) is diagnostic of Crohn’s disease
Board review style answer #1
A. Chronic inflammation with predominantly lymphocytes and plasma cells is the most common finding in biopsy samples. The biopsy findings of esophageal Crohn's disease are generally nonspecific. Biopsy often shows chronic inflammation only. Epithelioid granuloma(s) may be found up to 50% of cases. Answer C is incorrect because the distal esophagus is the most common site of involvement. Answer D is incorrect because nonnecrotizing granuloma(s) can be seen in various conditions, such as sarcoidosis, tuberculosis and foreign body reaction, among others. Answer B is incorrect because there have been no established evidence / previous reports that elderly patients with Crohn's disease tend to show more frequent esophageal involvement.
Which of the following statements about esophageal Crohn’s disease is true?
Almost all cases have concomitant intestinal Crohn's disease
Granuloma(s) are frequently seen in biopsy samples
Most patients will eventually require esophagectomy
Often shows esophageal stricture
Board review style answer #2
A. Almost all cases have been reported to have concomitant intestinal Crohn's disease. Crohn's disease limited to the esophagus is extremely rare. Answer C is incorrect because esophagectomy is rarely performed for the treatment of esophageal Crohn's disease. Answer B is incorrect because granuloma(s) can be seen in up to (at most) 50% of cases. Answer D is incorrect because esophageal stricture due to Crohn's disease is not frequently seen.
May cause obstruction, aspiration pneumonia, abscess, infection, hemorrhage or be associated with malignancy
Types
Zenker diverticula: also called pharyngoesophageal or pulsion diverticula; most common esophageal diverticula (~70%), more common in elderly; above upper esophageal sphincter, usually posterior wall; due to disordered cricopharyngeal motor dysfunction or weakness in esophageal wall at junction with pharynx; at junction between the pharynx and esophagus (known as the Killian triangle), may accumulate food, cause regurgitation or aspiration pneumonia or simulate a neck mass; malignancy in 0.3%
Mid esophageal / traction diverticula: near mid esophagus at level of tracheal bifurcation; becoming uncommon; previously mostly due to tuberculosis, mediastinal lymphadenitis and scarring; may be due to motor dysfunction, congenital or alkali ingestion (Med Hypotheses 2004;62:931); better prognosis than distal disease (Dysphagia 2006;21:198)
Epiphrenic diverticula: rare; immediately above lower esophageal sphincter (LES); due to lack of coordination of peristalsis and LES relaxation (Am J Surg 2005;190:891); often associated with hiatal hernia, may cause nocturnal regurgitation of massive amounts of fluid, obstruction, aspiration; contains mucosa, submucosa and muscularis mucosae; lined by squamous epithelium, often markedly inflamed
False or pseudodiverticula: mucosa and submucosa only, rare, usually with diffuse esophageal spasm
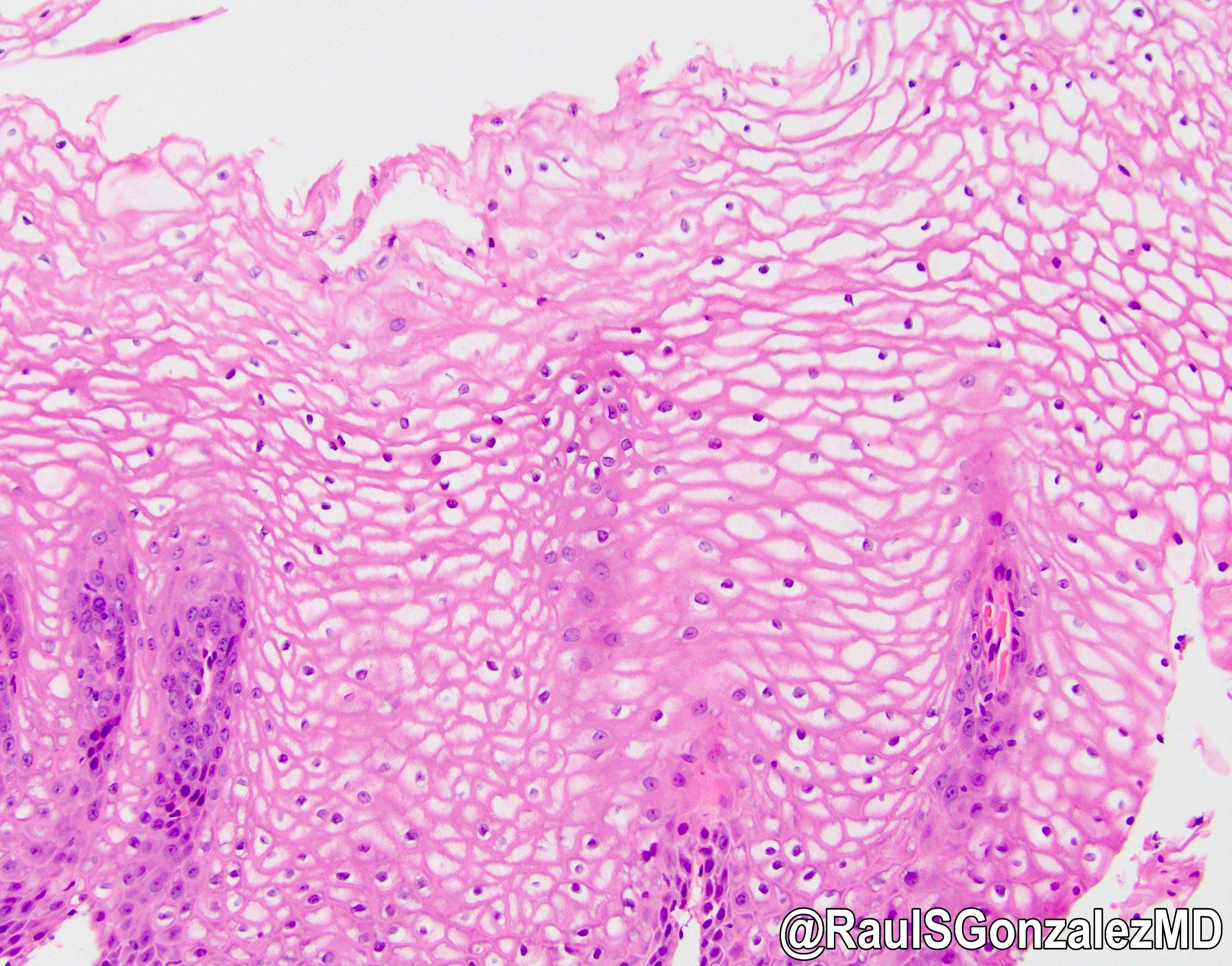
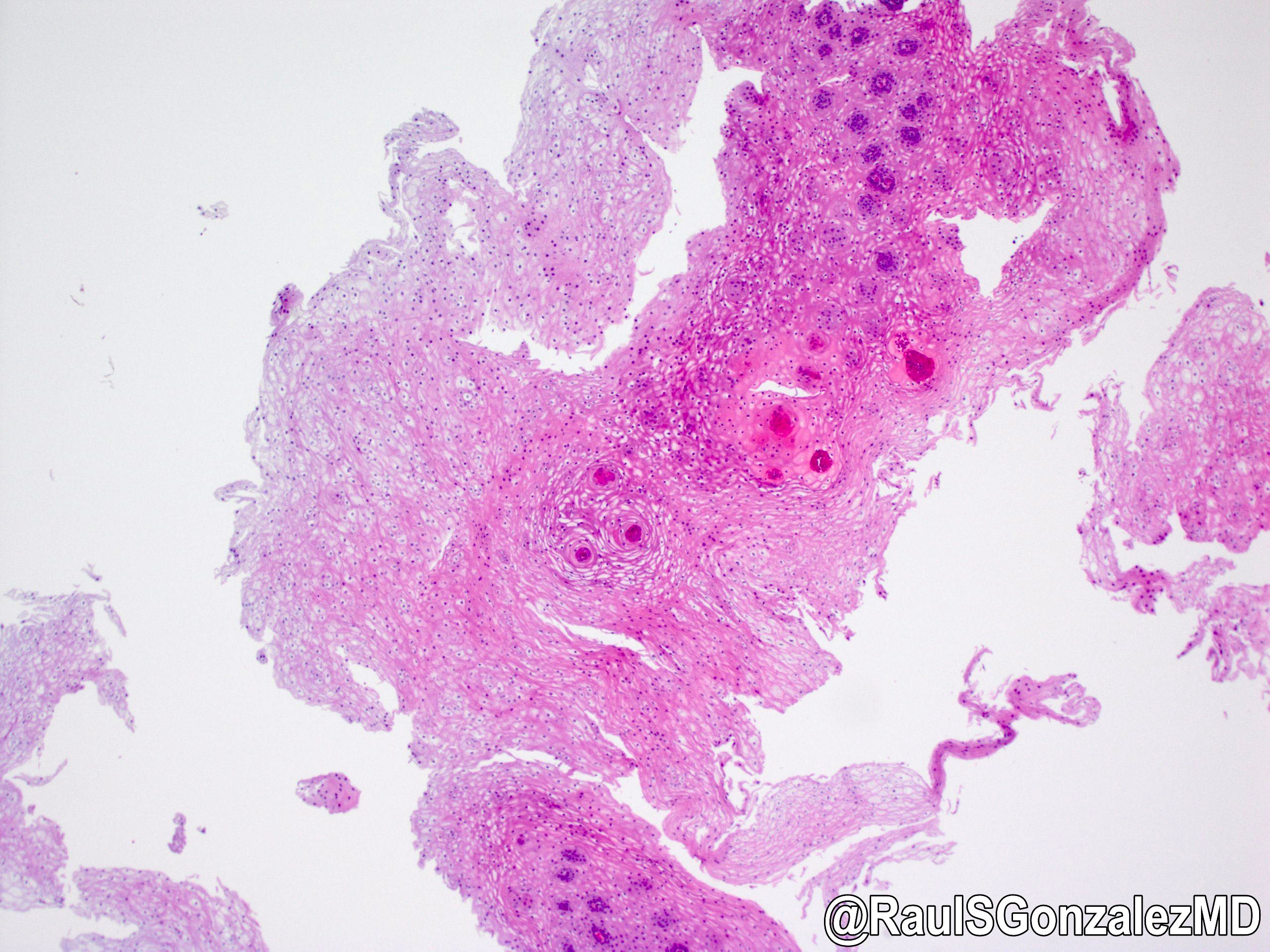
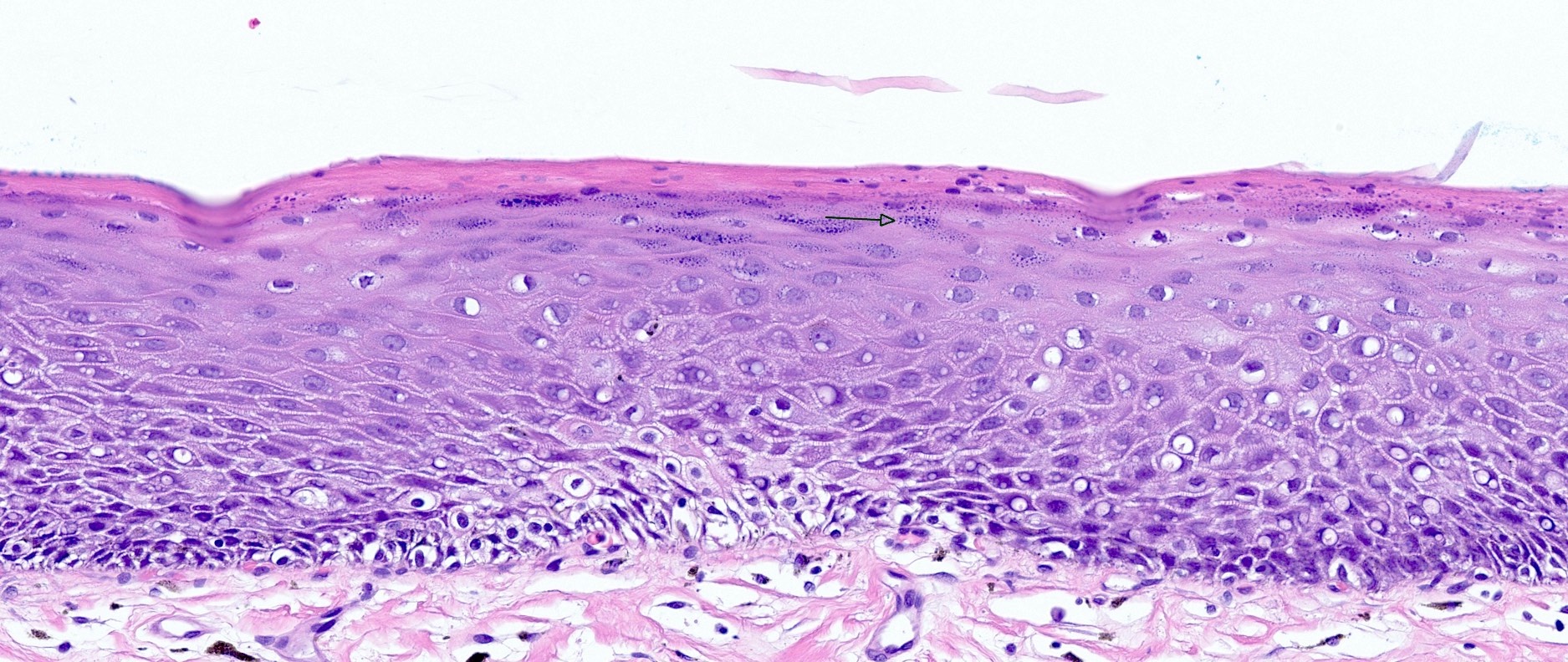
Multifactorial, chronic eosinophilic inflammatory condition affecting the esophagus in both adult and pediatric patients that occurs in the absence of identifiable secondary causes (Med Clin North Am 2019;103:29)
Characterized by a chronic immune reaction to environmental and food allergens leading to a deficient esophageal mucosal barrier (Arch Pediatr 2019;26:182)
Essential features
Major diagnostic criteria of ≥ 15 eosinophils per high power field (40x magnification) in the proper clinical context (Arch Pediatr 2019;26:182)
Terminology
Idiopathic or primary eosinophilic esophagitis
Chronic atopic inflammatory disease of the esophagus
Caucasians have threefold increased prevalence compared with other races
Population based study looking at 7,000 patients diagnosed with eosinophilic esophagitis found 89.3% were Caucasians, 6.1% African American and 5.6% of Asian descent (Gastrointest Endosc Clin N Am 2018;28:27)
Incidence rates vary greatly depending on the geographic location
Pooled incidence rate of 3.7 cases per 100,000 population per year (95% confidence interval, 1.7 - 6.5) from meta analysis (Gastroenterology 2018;154:319)
Included population based studies in North America, Europe and Australia
Pooled incidence rate for adults is 7.0 cases per 100,000 population per year (95% confidence interval, 1 - 18.3) (Aliment Pharmacol Ther 2016;43:3)
Pooled incidence rate for children is 5.1 cases per 100,000 population per year (95% confidence interval, 1.5 - 10.9) (Aliment Pharmacol Ther 2016;43:3)
Prevalence:
Pooled prevalence of 22.7 per 100,000 population (95% confidence interval, 12.4 - 36.0) (Gastroenterology 2018;154:319)
Sites
Can diffusely affect the entire length of the esophagus
Pathophysiology
Intraepithelial eosinophils recruited via chemotaxis act as antigen presenting cells (APCs) recruiting T cells, activating mast cells and activating basophils (Arch Pediatr 2019;26:182)
Eosinophils secrete a cationic protein eosinophilic peroxidase (EPO) and major binding protein (MBP) causing cell damage leading to the symptom of esophageal dysmotility (Arch Pediatr 2019;26:182)
Concentration of eosinophilic peroxidase (EPO) correlates to increased symptomology, not the number of intraepithelial eosinophils (Arch Pediatr 2019;26:182)
Recruited T cells differentiate into Th2 T cells and secrete IL4, IL5 and IL13 (Arch Pediatr 2019;26:182)
Improved hygiene conditions lead to reduced bacterial exposures and alterations in the microbiota, which may alter mucosal permeability (World J Gastroenterol 2019;25:4598)
Gastroesophageal reflux disease (GERD) leads to increased mucosa permeability to food allergens
Genetic variants at multiple loci have been shown to increase the risk of development of atopic diseases, including eosinophilic esophagitis and asthma
Genes found with alterations in patients with eosinophilic esophagitis:
Eosinophilic esophagitis is a clinicopathologic diagnosis and findings should be considered in combination and not independent of each other
Current diagnostic modalities
Esophagogastroduodenoscopy (endoscopy)
Endoscopy may show many characteristic but not pathognomonic changes
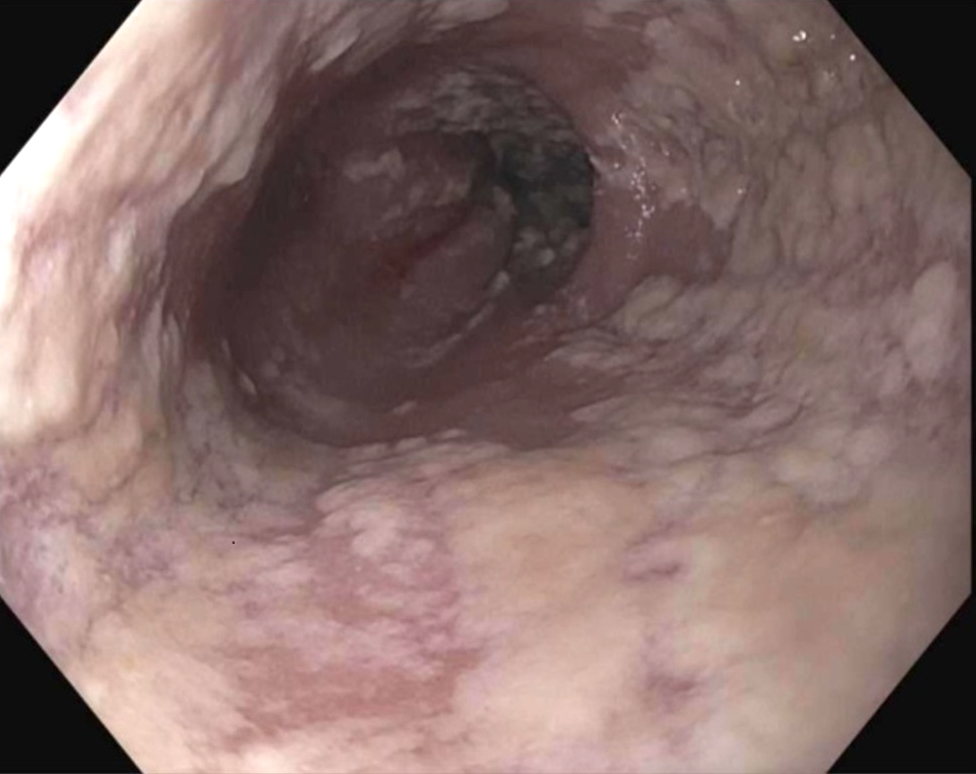
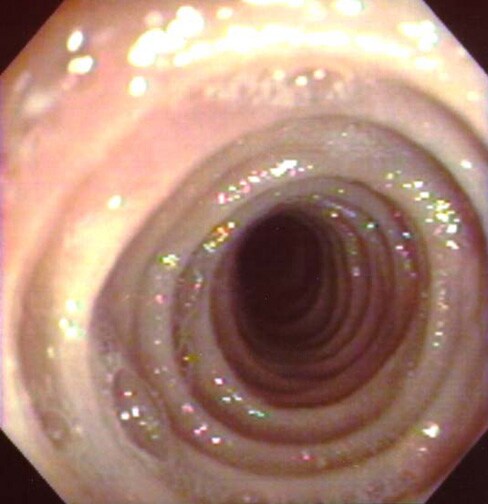
Major criteria: mucosa edema, white exudate, longitudinal furrows, circular esophageal rings (also called pseudotrachea), esophageal stenosis (Gut 2013;62:489)
Minor criteria: feline esophagus (concentric mucosal rings observed with some types of motility that disappear with air insufflation), narrow caliber esophagus, crêpe paper esophagus, mucosal laceration or fragility with passage of instruments before dilation (Gut 2013;62:489)
Major criteria: ≥ 15 eosinophils per high power field (40x magnification) (Arch Pediatr 2019;26:182)
Minor criteria: extreme basal zone hyperplasia with papillary hyperplasia, eosinophils concentrated in the surface epithelium as opposed to the base, eosinophilic microabscesses, eosinophil degranulation, surface desquamation, lamina propria fibrosis (Arch Pediatr 2019;26:182)
Esophageal brushings obtained via endoscopy or via nasogastric tube are analyzed for the presence and quantity of eosinophil derived neurotoxin, which is overexpressed in eosinophilic esophagitis
Barium esophagram is more sensitive than endoscopy for identification of strictures and diffuse small caliber esophagus (Gastrointest Endosc Clin N Am 2018;28:47)
Strictures are classified by the length of fixed narrowing
Concentric mucosal rings observed with some types of motility that disappear with air insufflation
Narrow caliber esophagus
Crêpe paper esophagus
Mucosal laceration or fragility with passage of instruments before dilation
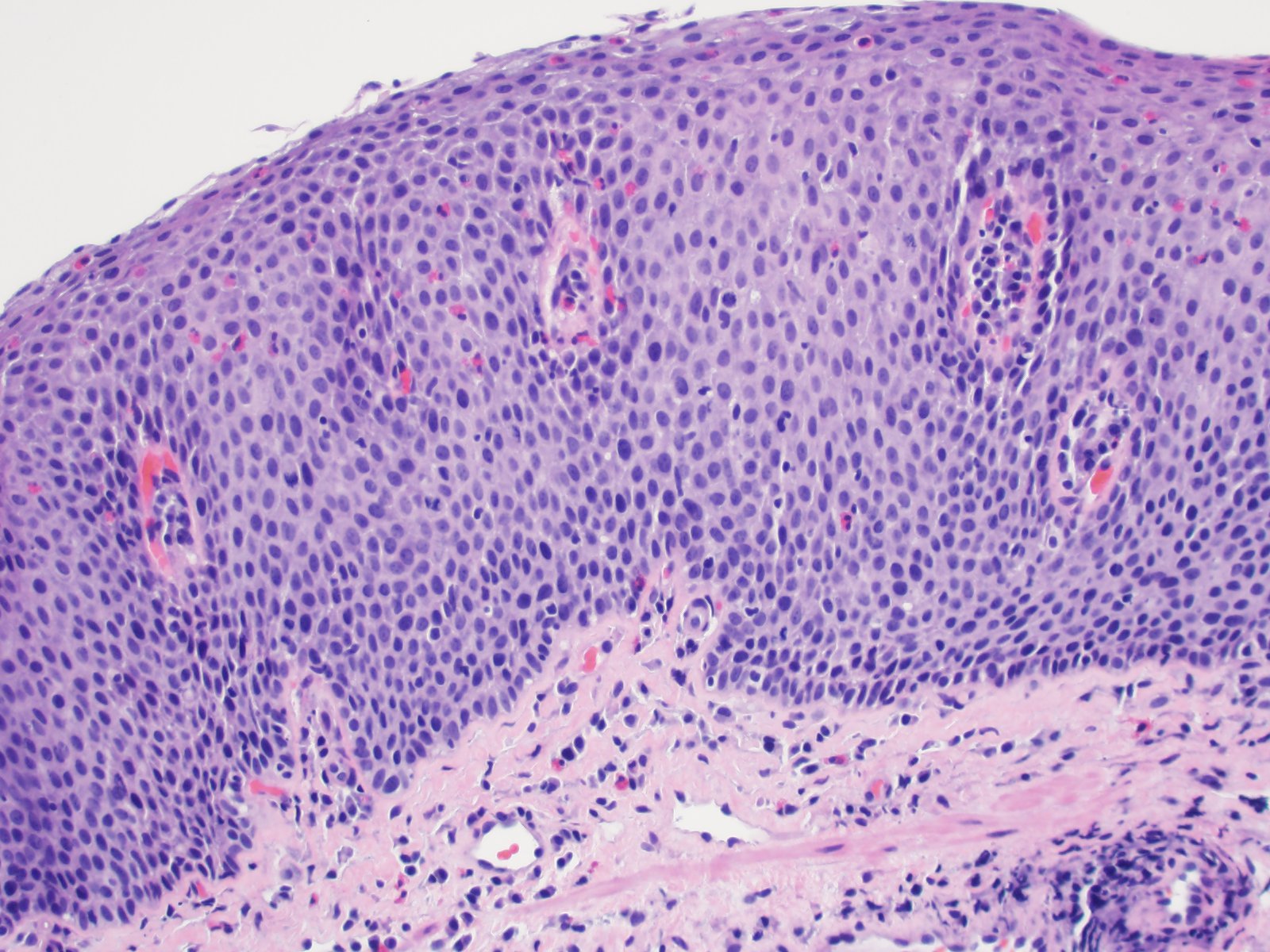
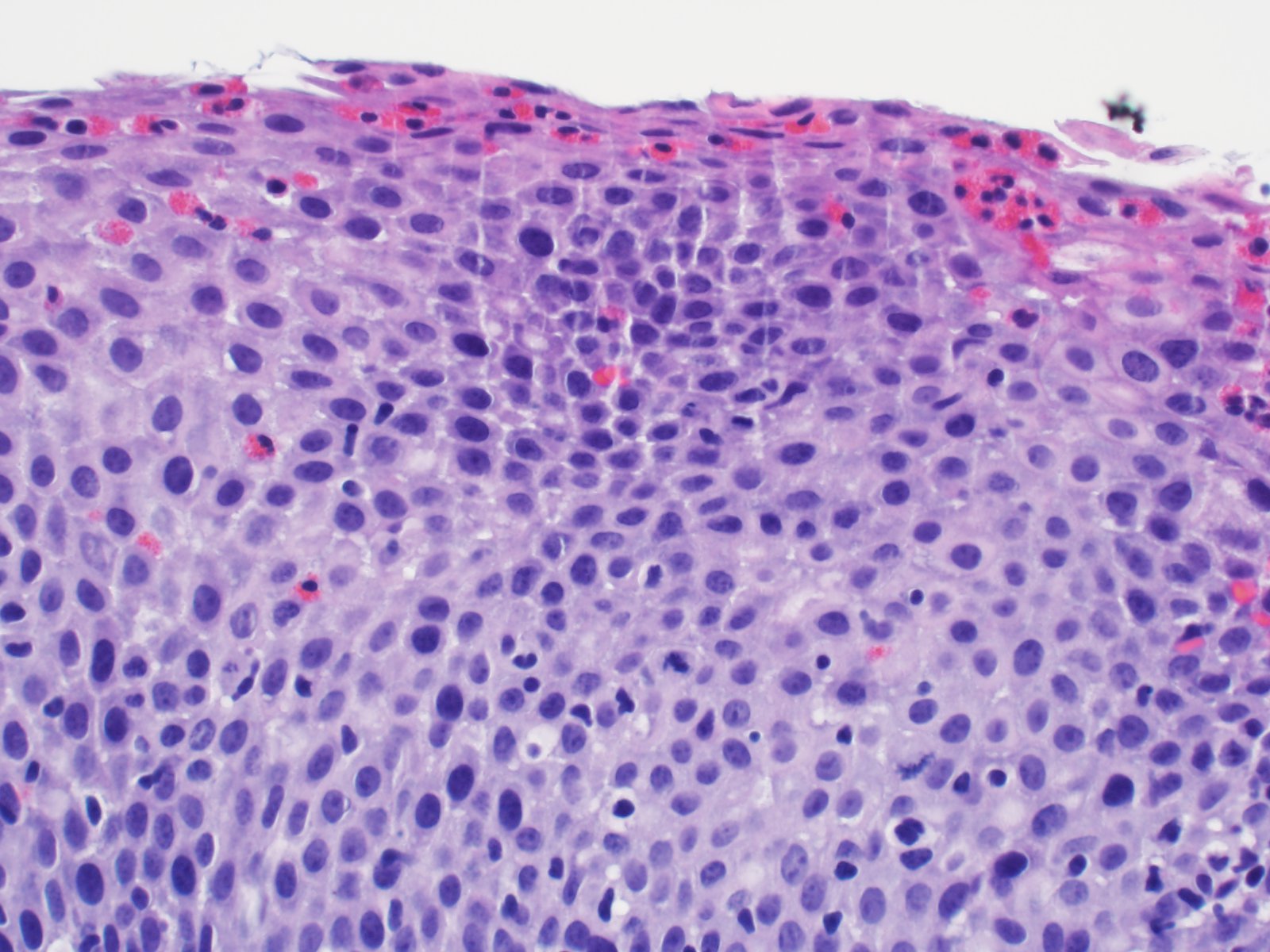
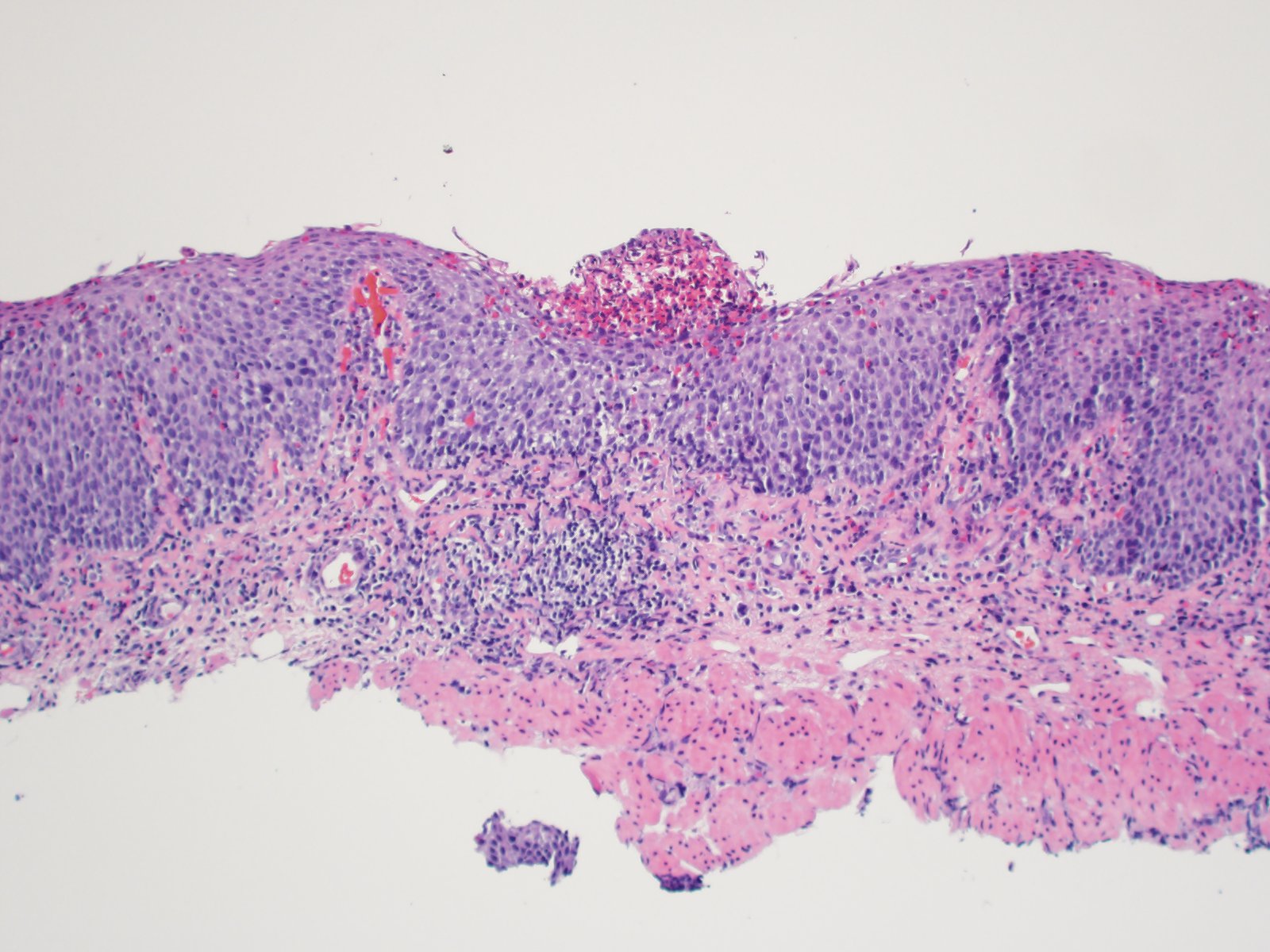
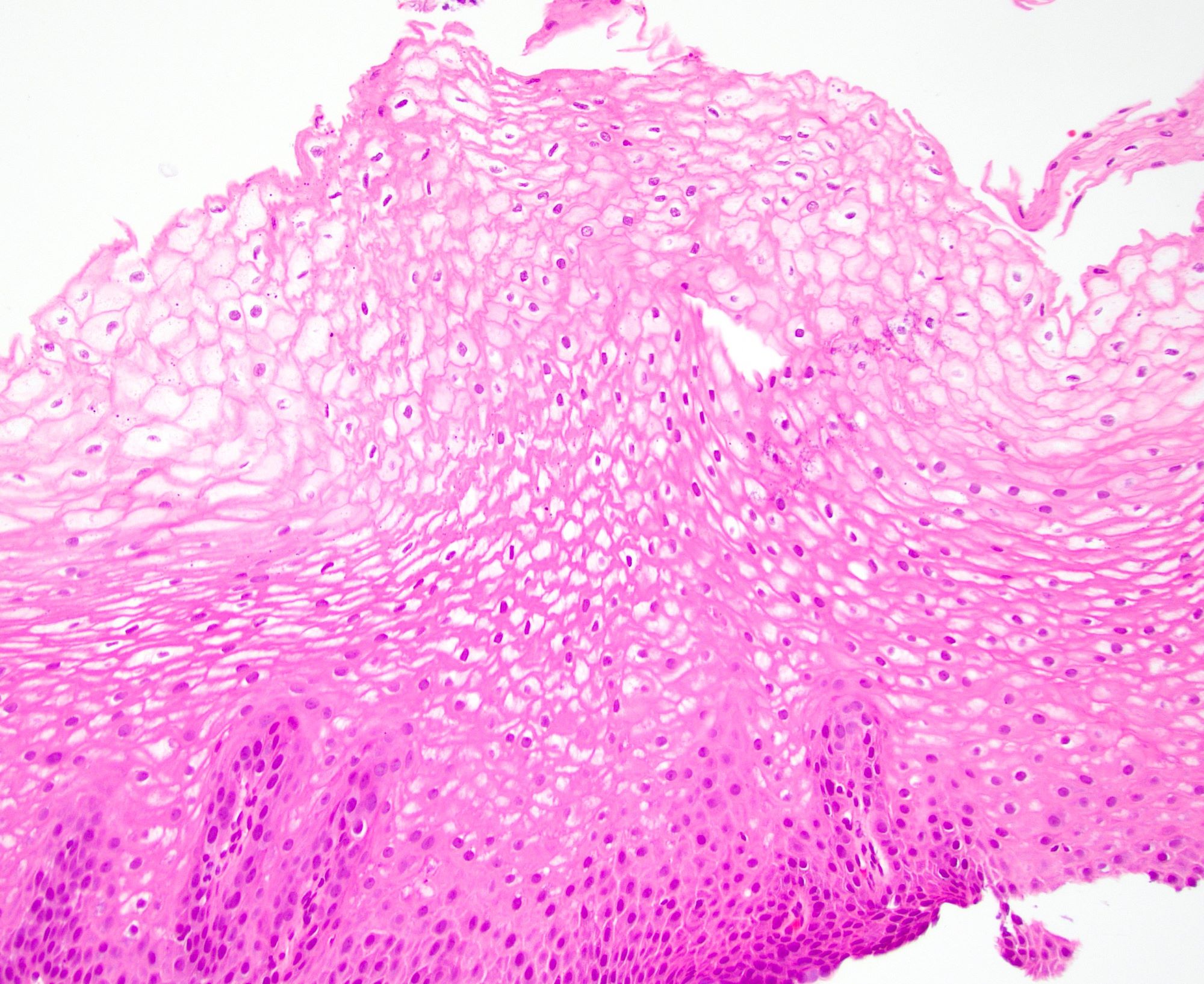
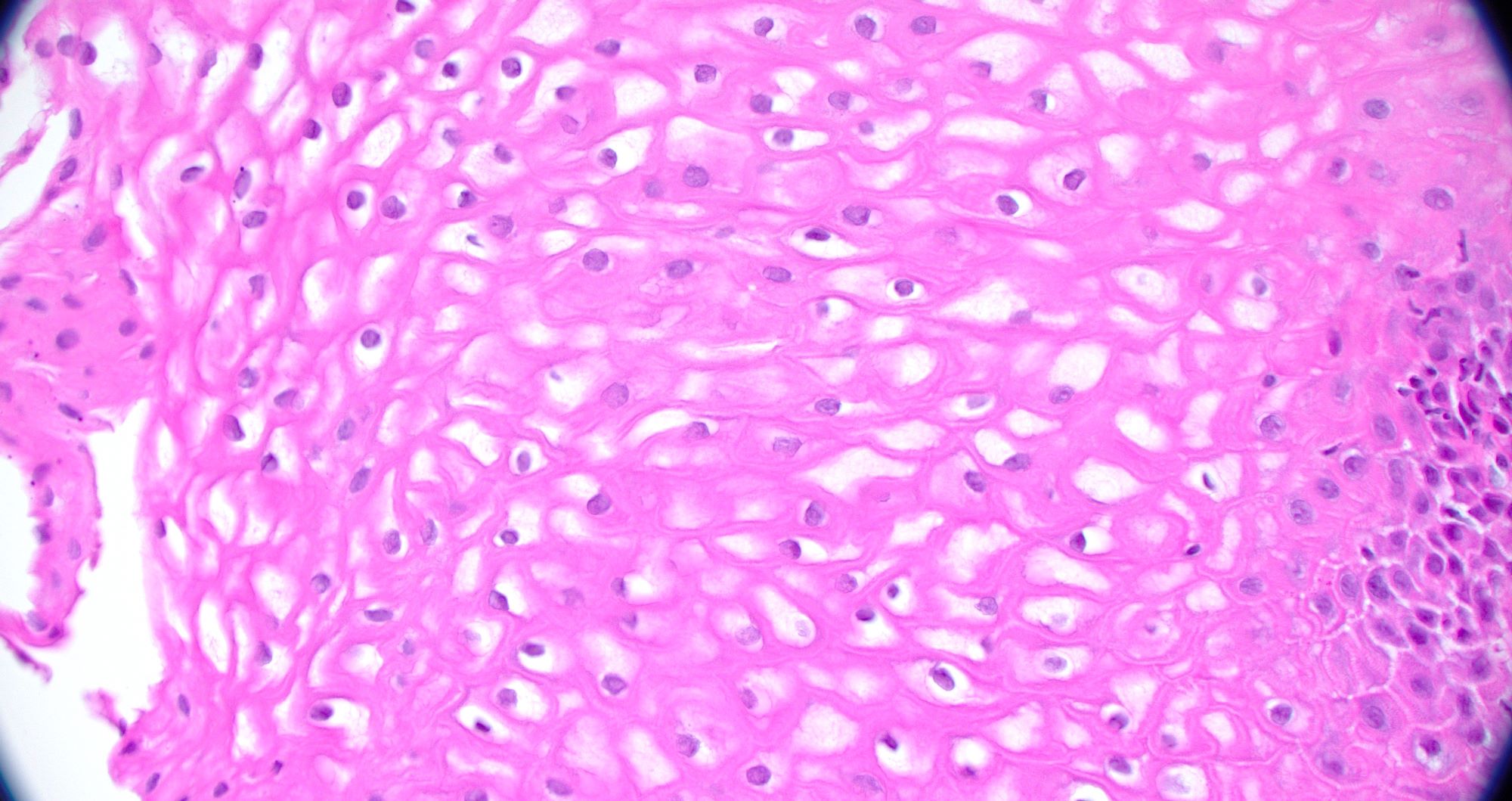
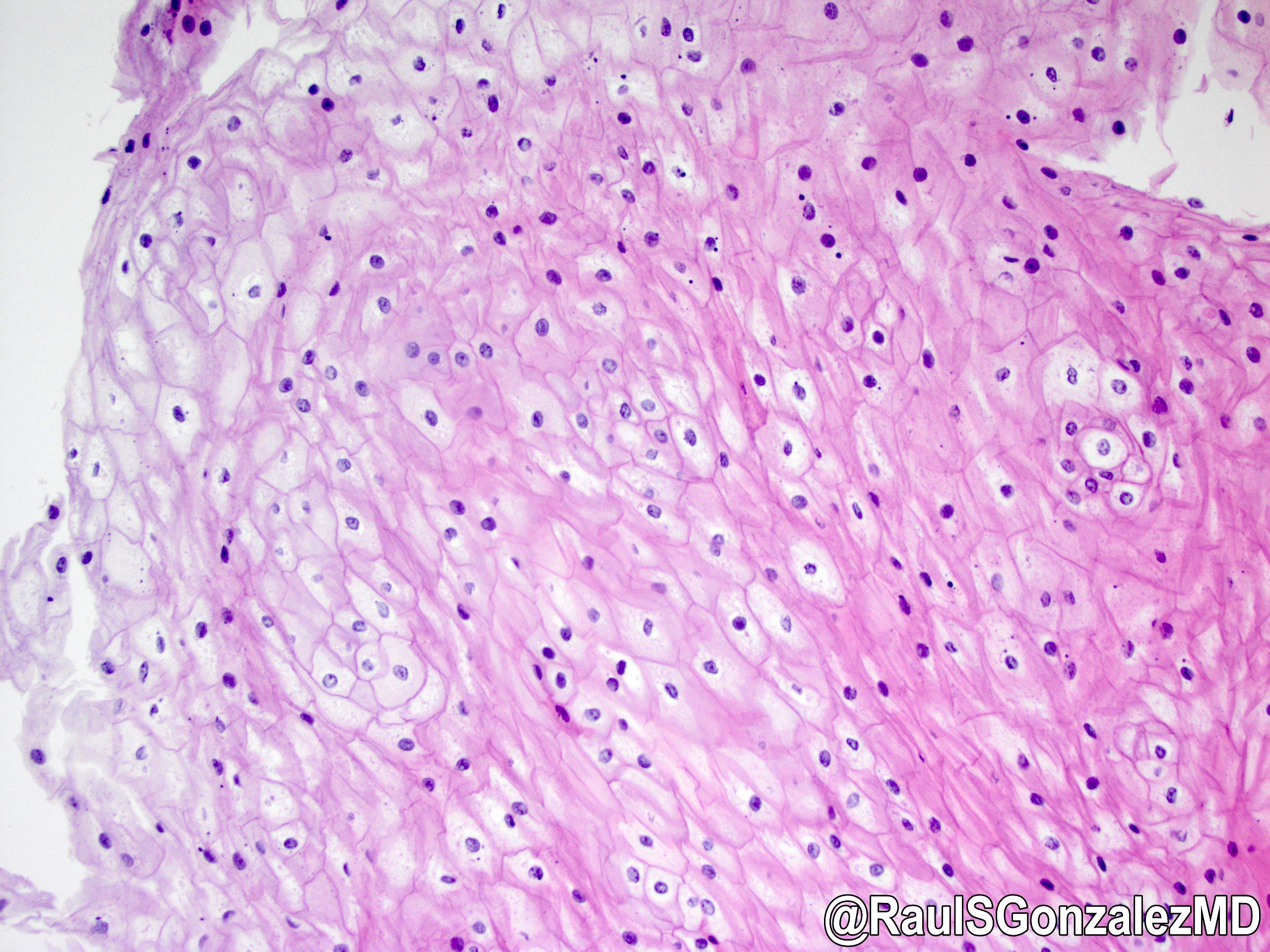
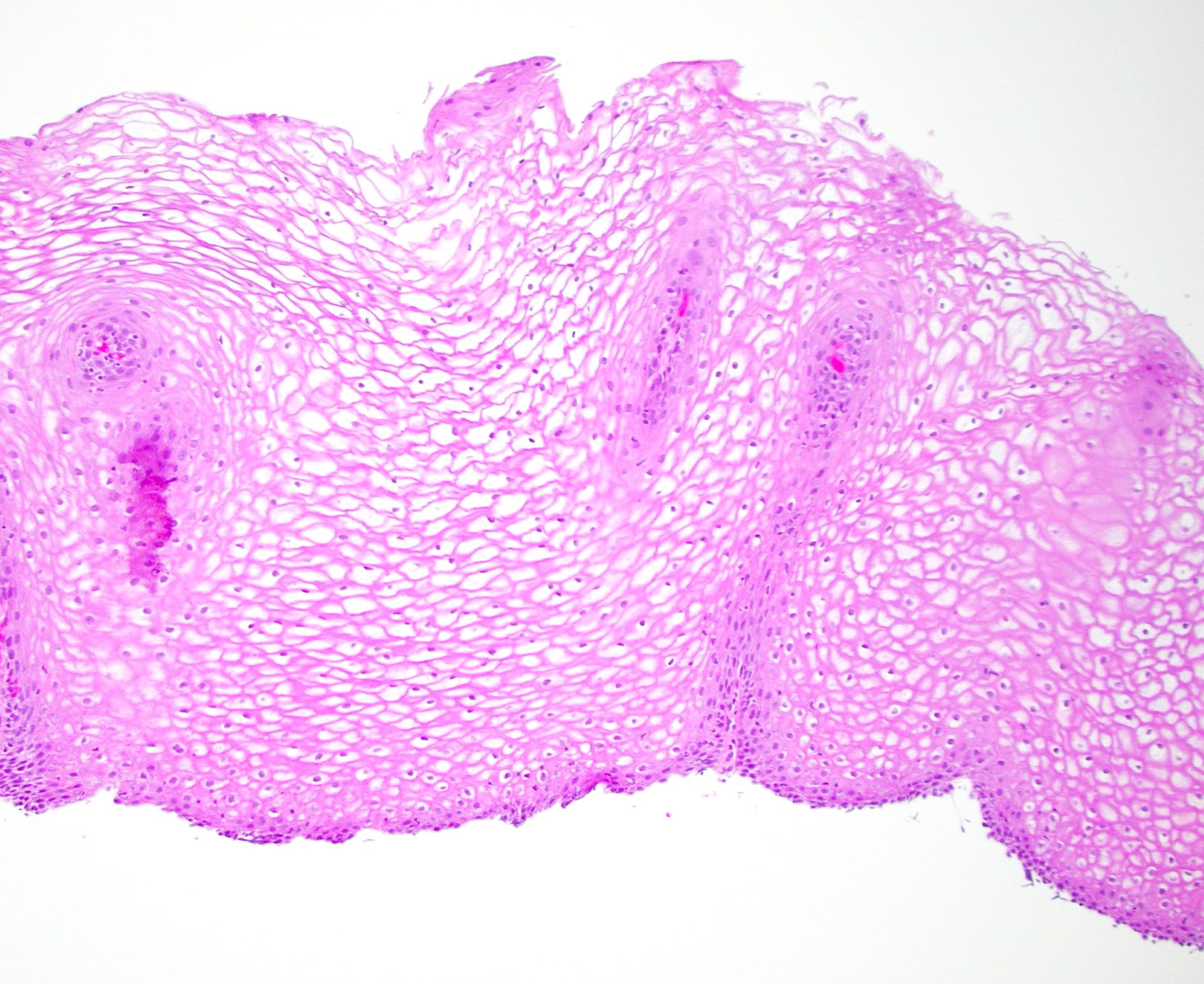
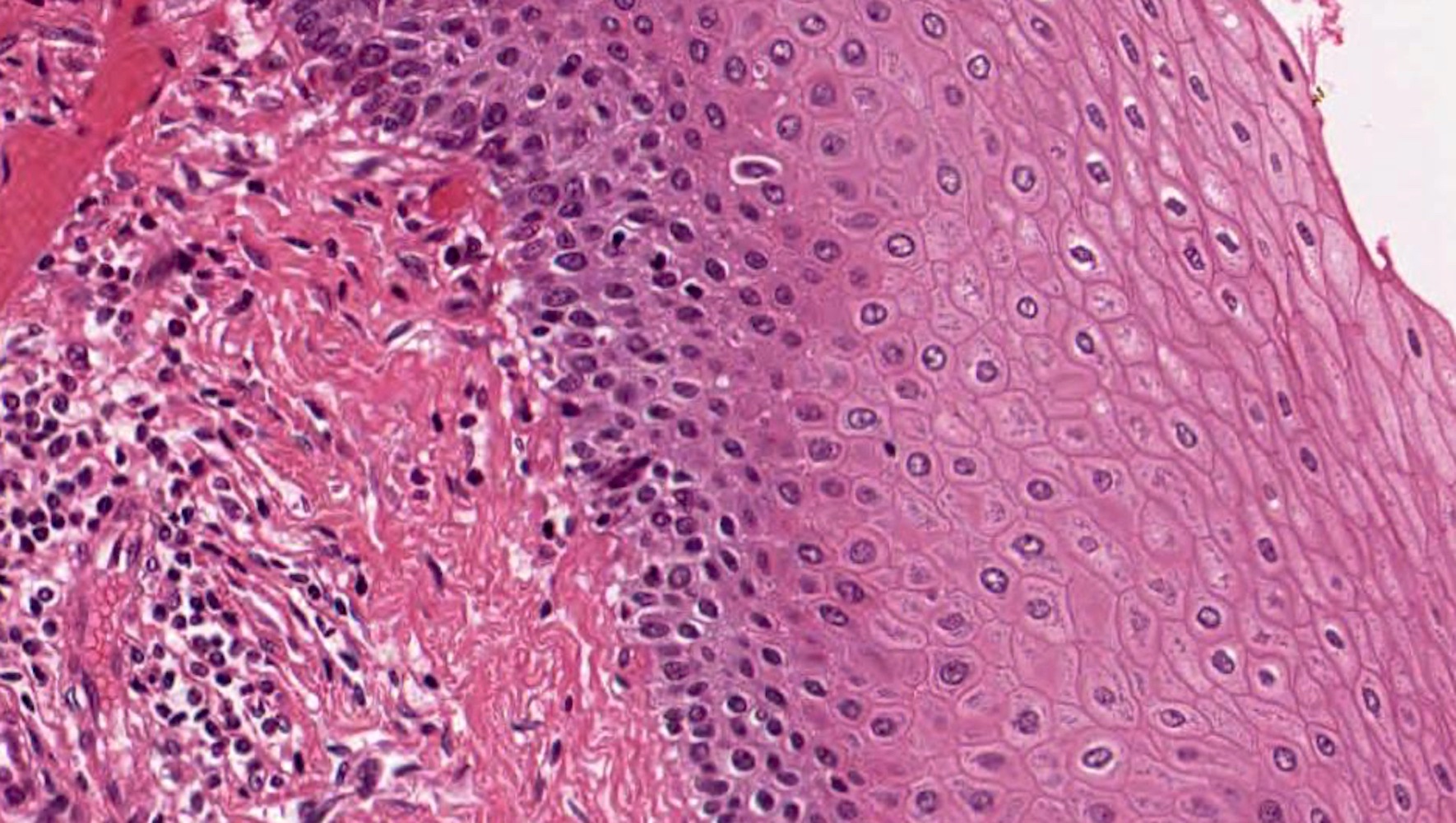
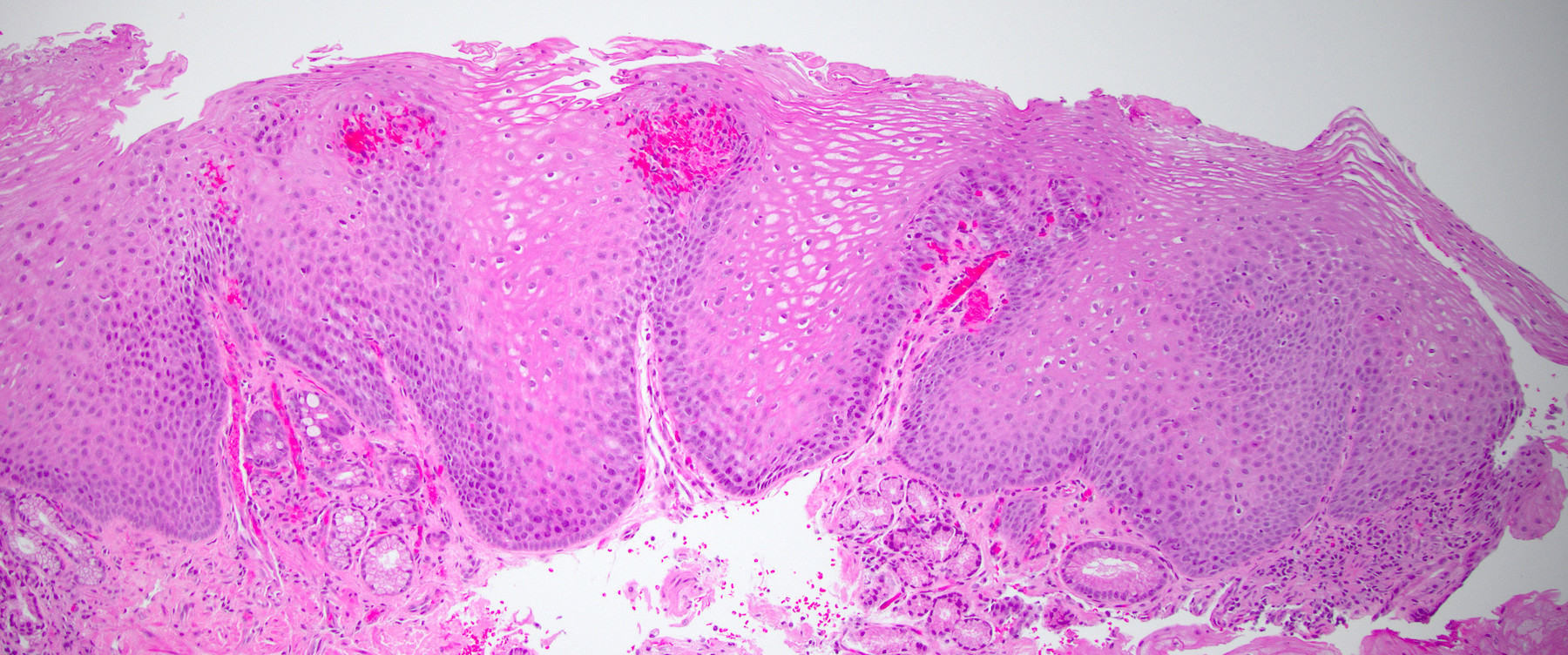
Microscopic (histologic) description
Major criterion: ≥ 15 eosinophils per high power field (40x magnification) present in the squamous mucosa (Arch Pediatr 2019;26:182)
Minor criteria: eosinophils concentrated in the surface epithelium as opposed to the base, extreme basal zone hyperplasia, eosinophilic microabscesses, eosinophil degranulation, surface desquamation, lamina propria fibrosis (Arch Pediatr 2019;26:182)
Microscopic (histologic) images
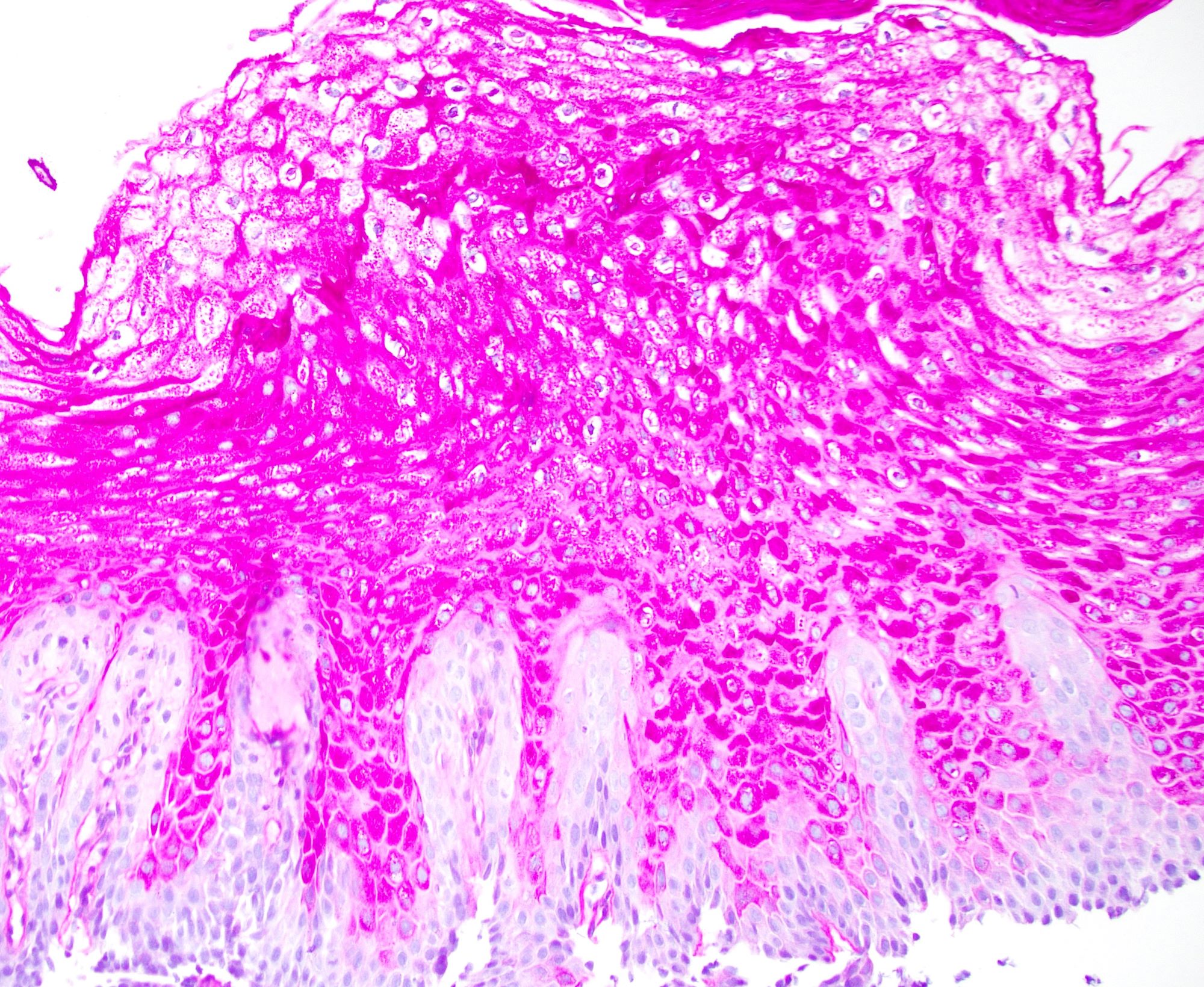
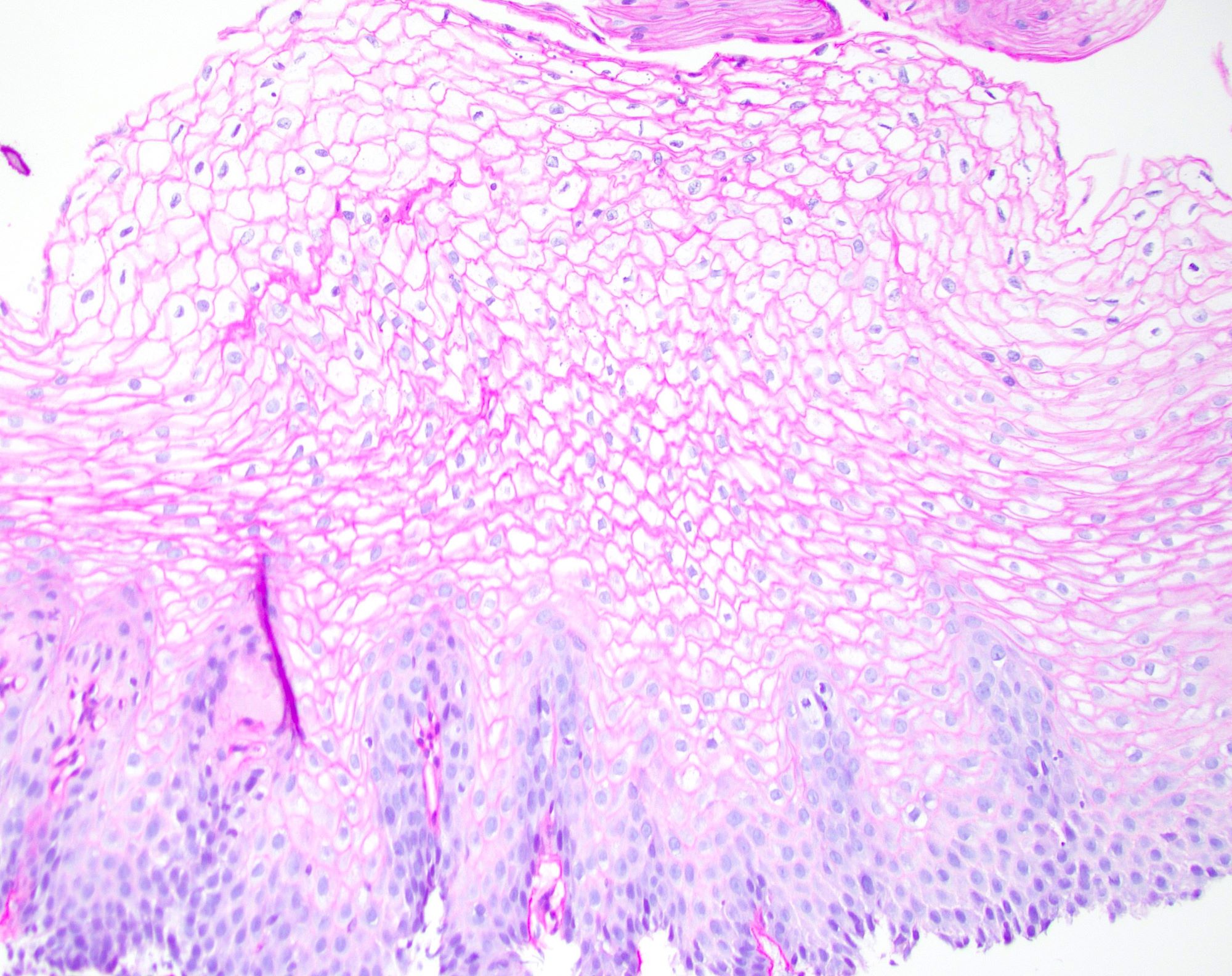
Contributed by Ryan C. Braunberger, M.D. and Joshua A. Hanson, M.D.
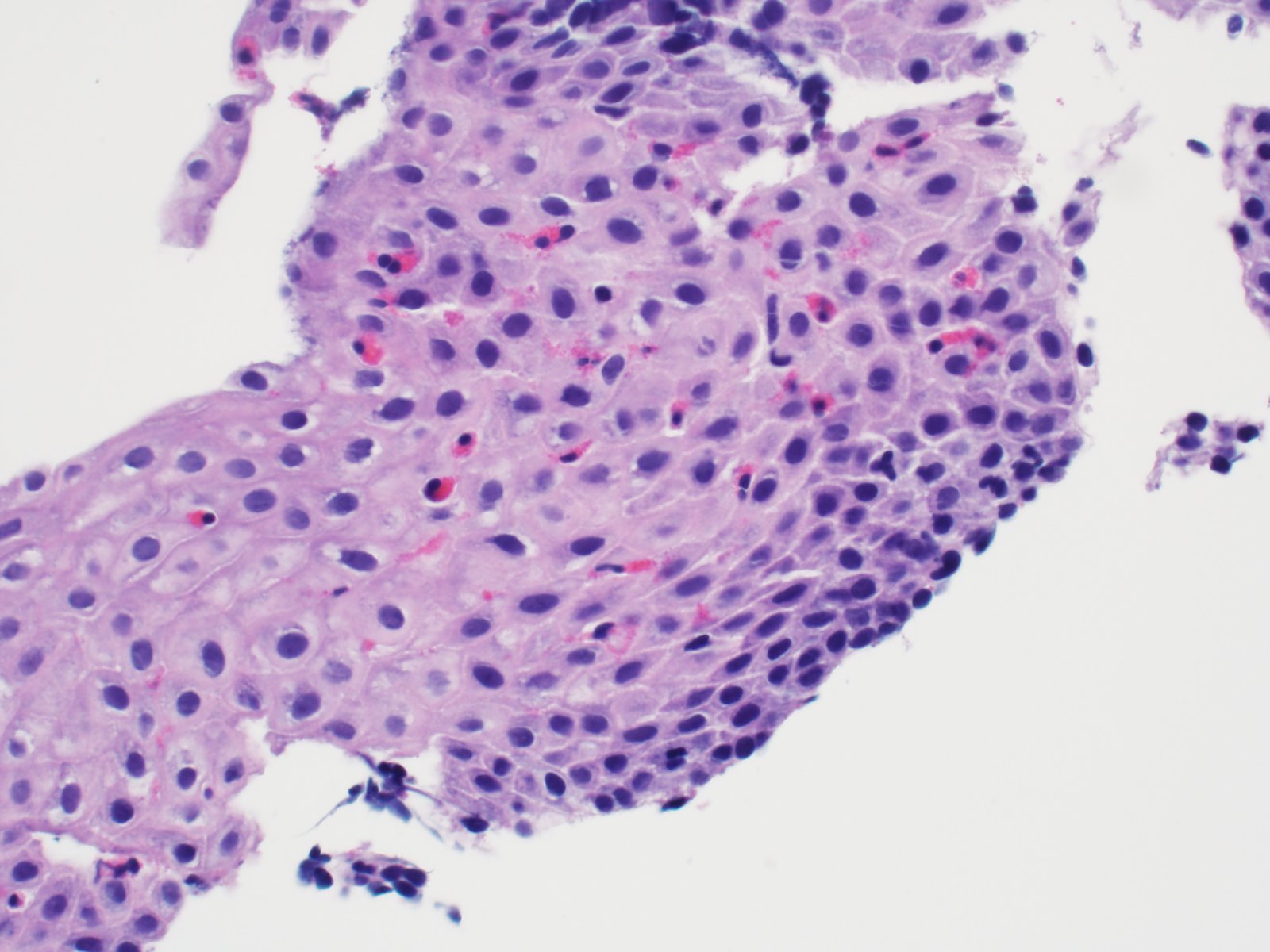
Extreme basal cell hyperplasia
Surface concentration of eosinophils
Eosinophilic microabscess
Eosinophil degranulation
Virtual slides
Images hosted on other servers:
Eosinophilic esophagitis
Perforated esophagus with eosinophilic esophagitis
Videos
Endoscopic features of eosinophilic esophagitis
Sample pathology report
Esophagus, mid, biopsy:
Eosinophil rich esophagitis (> 50 eosinophils per single high power field, maximum count) (see comment)
Comment: The biopsy demonstrates marked reactive basal zone hyperplasia with increased eosinophils. The eosinophils have a top heavy distribution and few eosinophilic microabscesses are identified. These features are consistent with eosinophilic esophagitis in the proper clinical context.
Hyperplasia of lamina propria papillae (greater than two - thirds of the epithelial thickness)
Mild basal zone hyperplasia (approximately 15 - 25% of the epithelial thickness)
Mildly increased intraepithelial eosinophils concentrated at the base of the mucosa as opposed to the surface (usually < 10 per high power field though counts are not pathognomonic for either condition) (Arch Pediatr 2019;26:182)
Eosinophil counts in GERD are generally higher in distal esophageal biopsies compared with more proximal biopsies (this is reversed in eosinophilic esophagitis but is not pathognomonic)
No surface eosinophilic microabscesses
No lamina propria fibrosis
Other intraepithelial inflammatory cells seen in some but not all cases include lymphocytes and neutrophils
Affects any portion of the gastrointestinal tract with the stomach and small bowel being the most common locations (Lancet Gastroenterol Hepatol 2018;3:271)
Symptoms such as diarrhea, intestinal obstruction and ascites are not common in eosinophilic esophagitis
When seen in the esophagus, can be an exact histologic mimic of eosinophilic esophagitis so clinical presentation and correlation with other mucosal biopsies is essential
PPI responsive esophageal eosinophilia:
Same symptomatology and histologic findings as eosinophilic esophagitis but has complete remission with PPI therapy
May actually be the same disease as eosinophilic esophagitis
A 12 year old boy with a history of seasonal allergies and asthma complains of dysphagia and abdominal pain. Endoscopic biopsies reveal increased eosinophils in the esophageal squamous mucosa. What feature shown in the image favors eosinophilic esophagitis over GERD as the most likely diagnosis?
A 36 year old man presents to clinic with the chief complaint of intermittent dysphagia and heartburn that has not responded to over the counter medications. Endoscopy was notable for white plaques in the esophagus, longitudinal furrows and pseudotrachea. Biopsies taken during endoscopy show increased eosinophils in the distal and proximal specimens. Which chemokine producing immune cell plays an essential role in eosinophil infiltration and activation?
2 cases (0.2%) of epidermoid metaplasia out of 1,048 consecutive esophageal biopsies; 50x less common than parakeratosis (11%) (Histopathology 2016;68:988)
37 cases (2%) of epidermoid metaplasia and hyperkeratosis without a prominent granular layer out of 1,845 consecutive esophageal biopsies (Histopathology 2013;63:463)
58 year old Japanese man with epidermization and a concurrent superficial squamous cell carcinoma (Am J Surg Pathol 1997;21:605)
69 year old man with an unusual appearance of epidermoid metaplasia (Endoscopy 2015;47:E100)
69 year old man with epidermoid metaplasia in association with esophageal intramural pseudodiverticulosis and candidiasis (Case Rep Gastroenterol 2021;15:709)
Treatment
Follow up, unless a patient has a concurrent squamous cell carcinoma
Clinical images
Images hosted on other servers:
Scaly white plaque
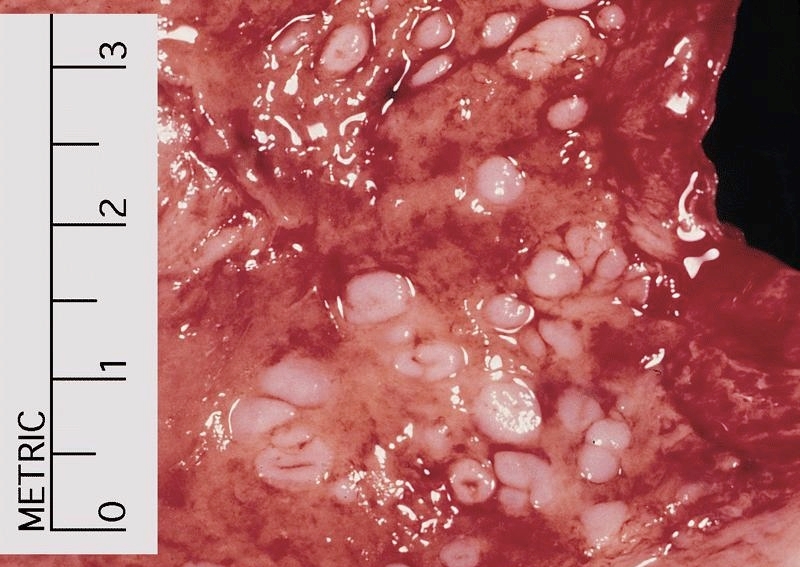
Gross description
Scaly or shaggy white plaque with clear borders (mean size: 2.6 cm) (Mod Pathol 2014;27:38)
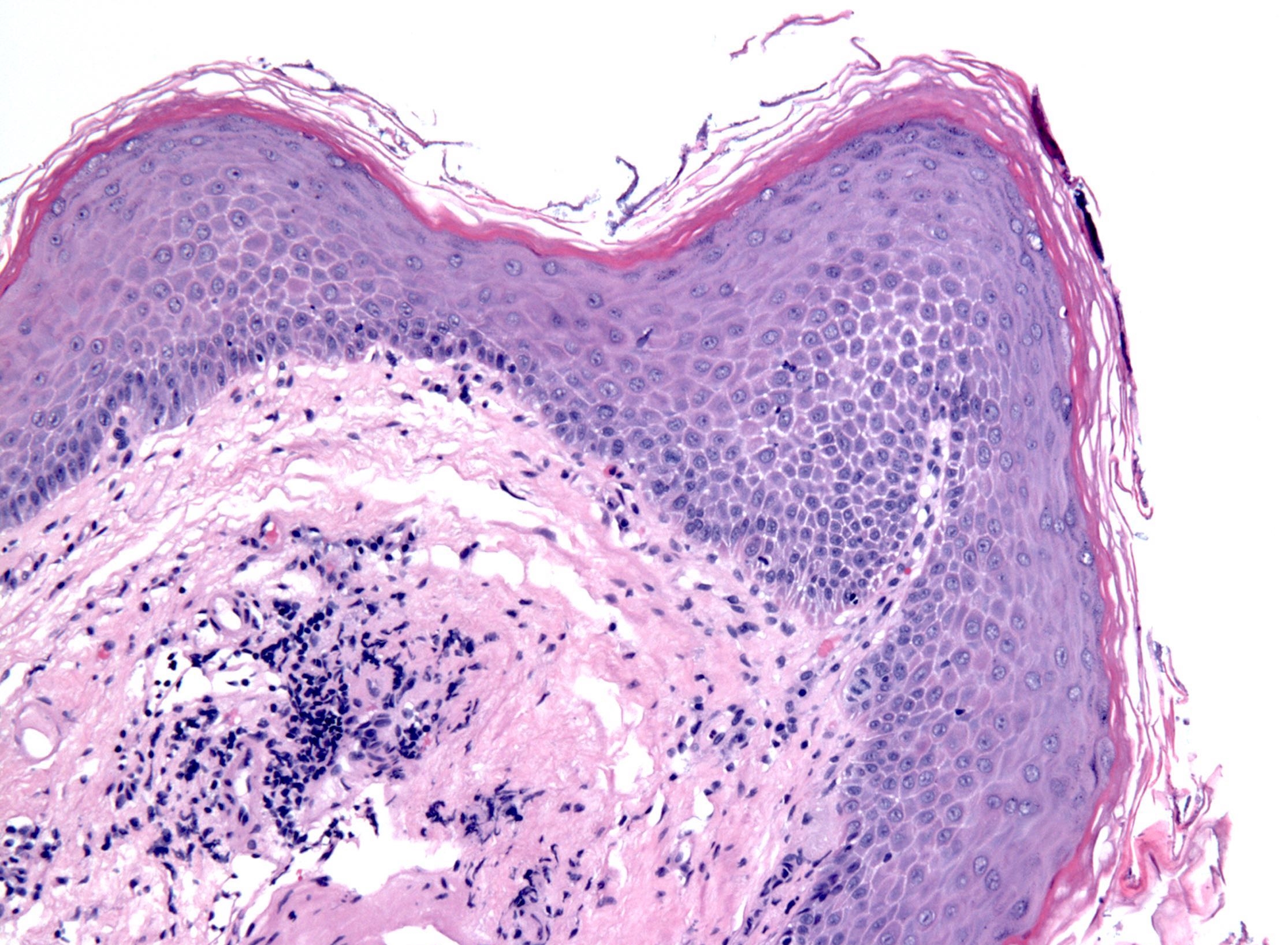
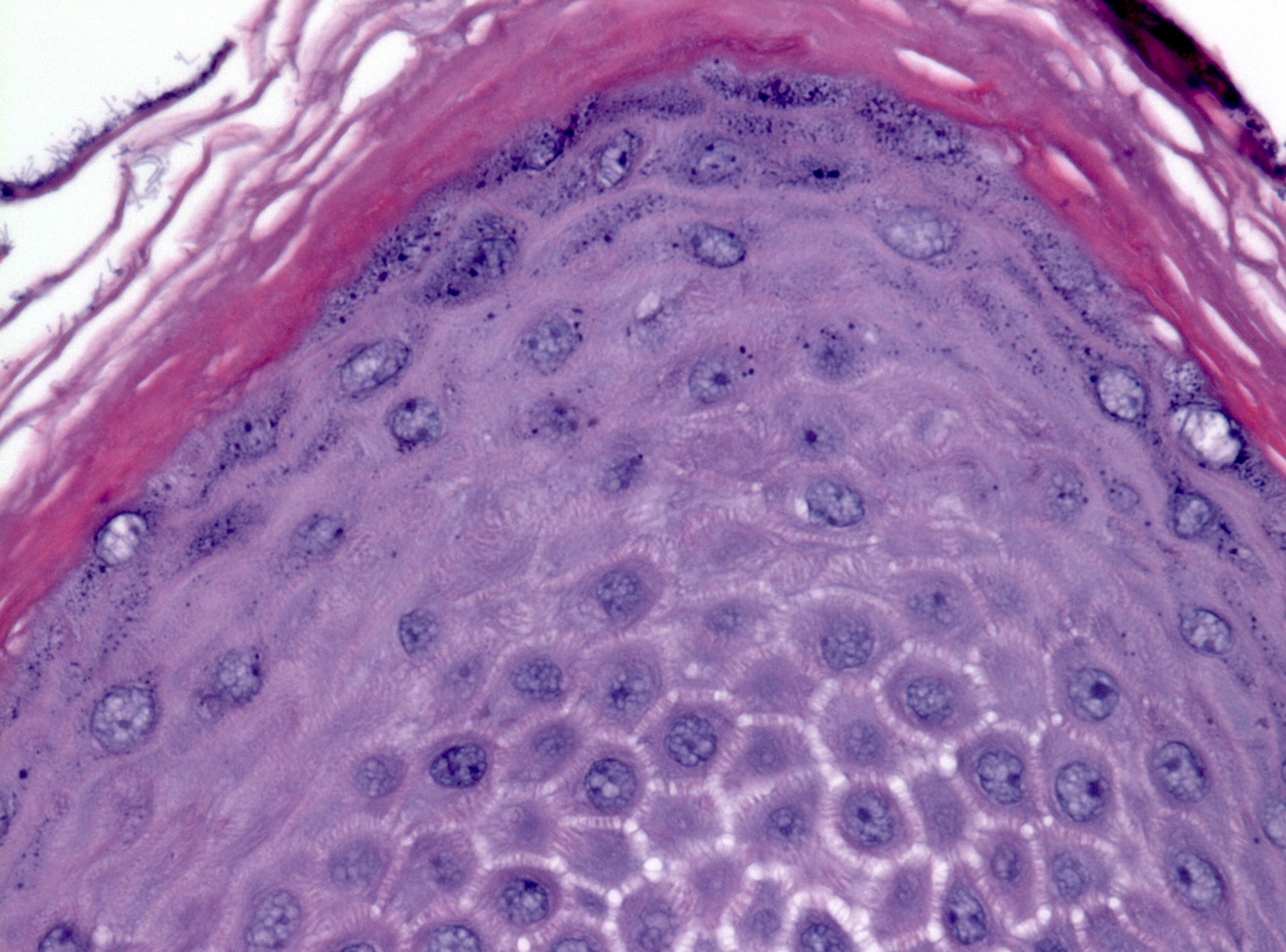
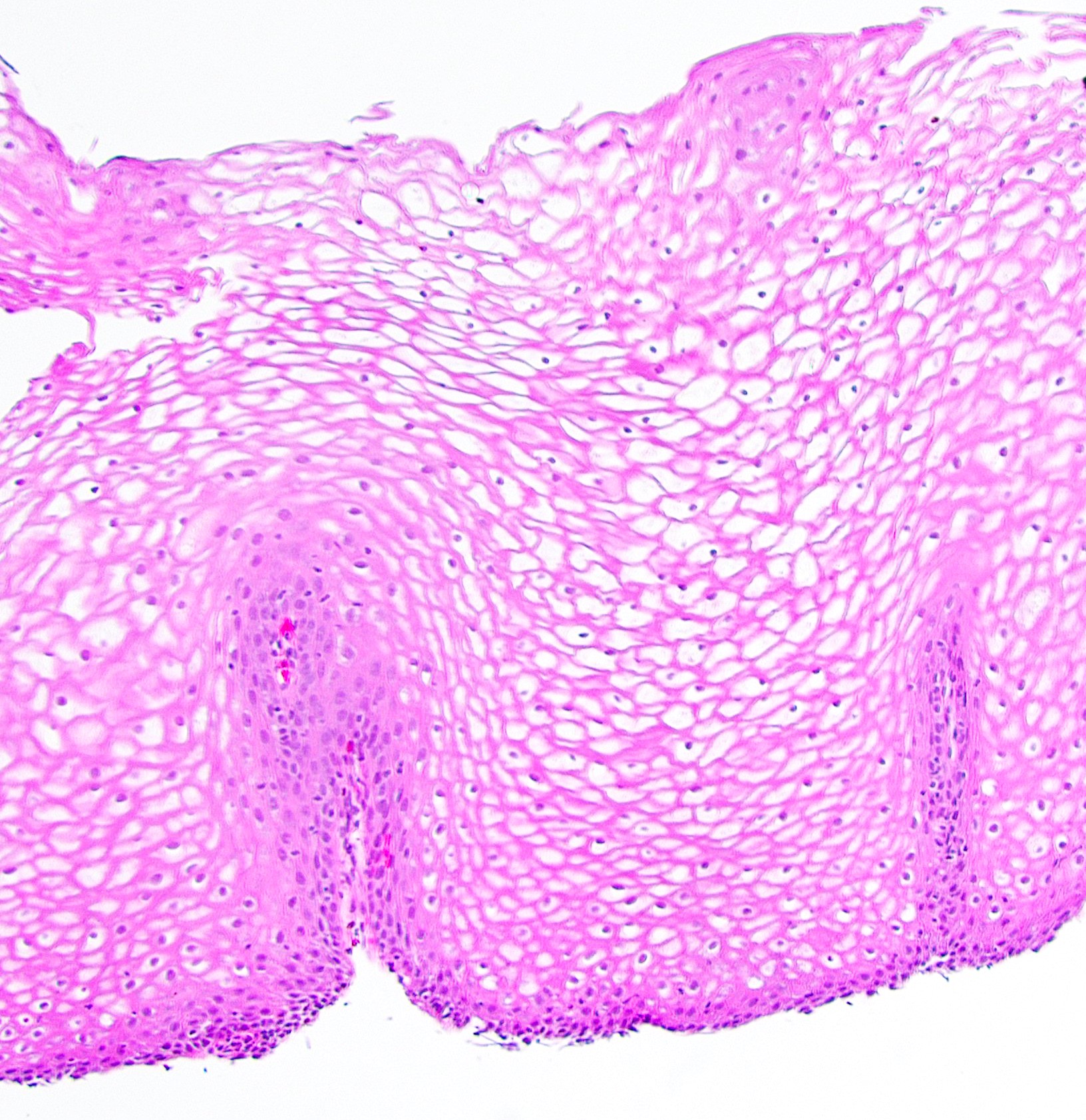
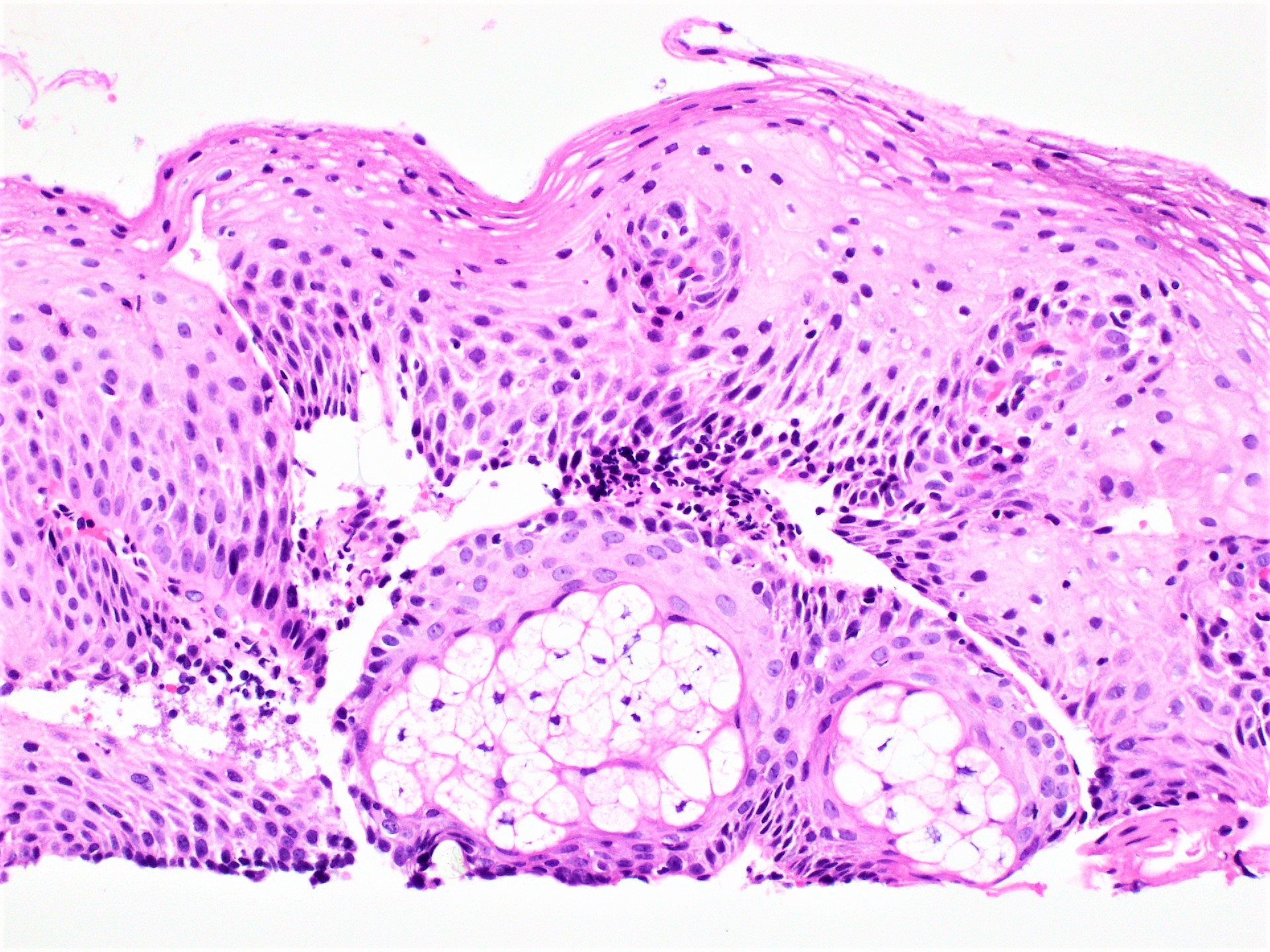
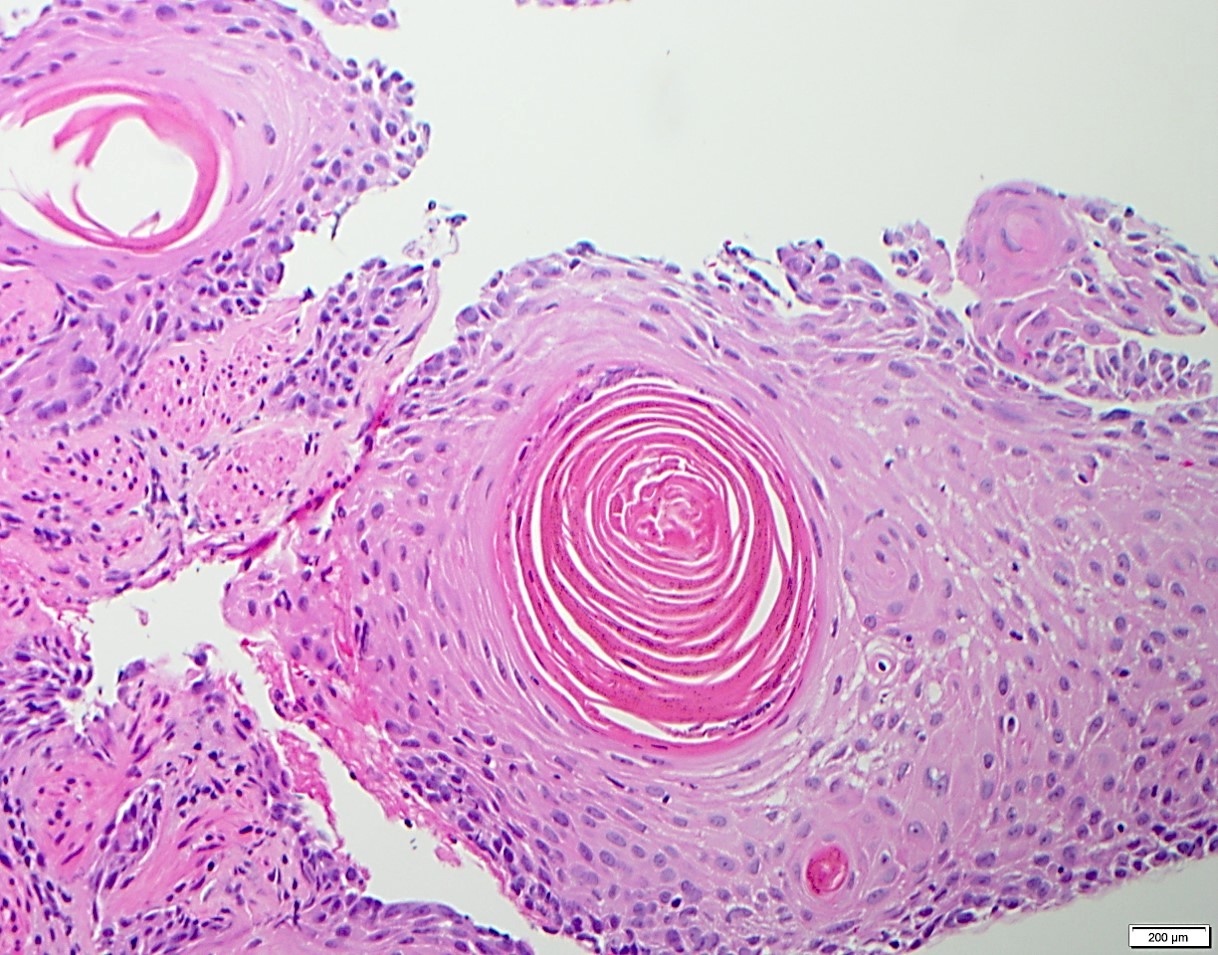
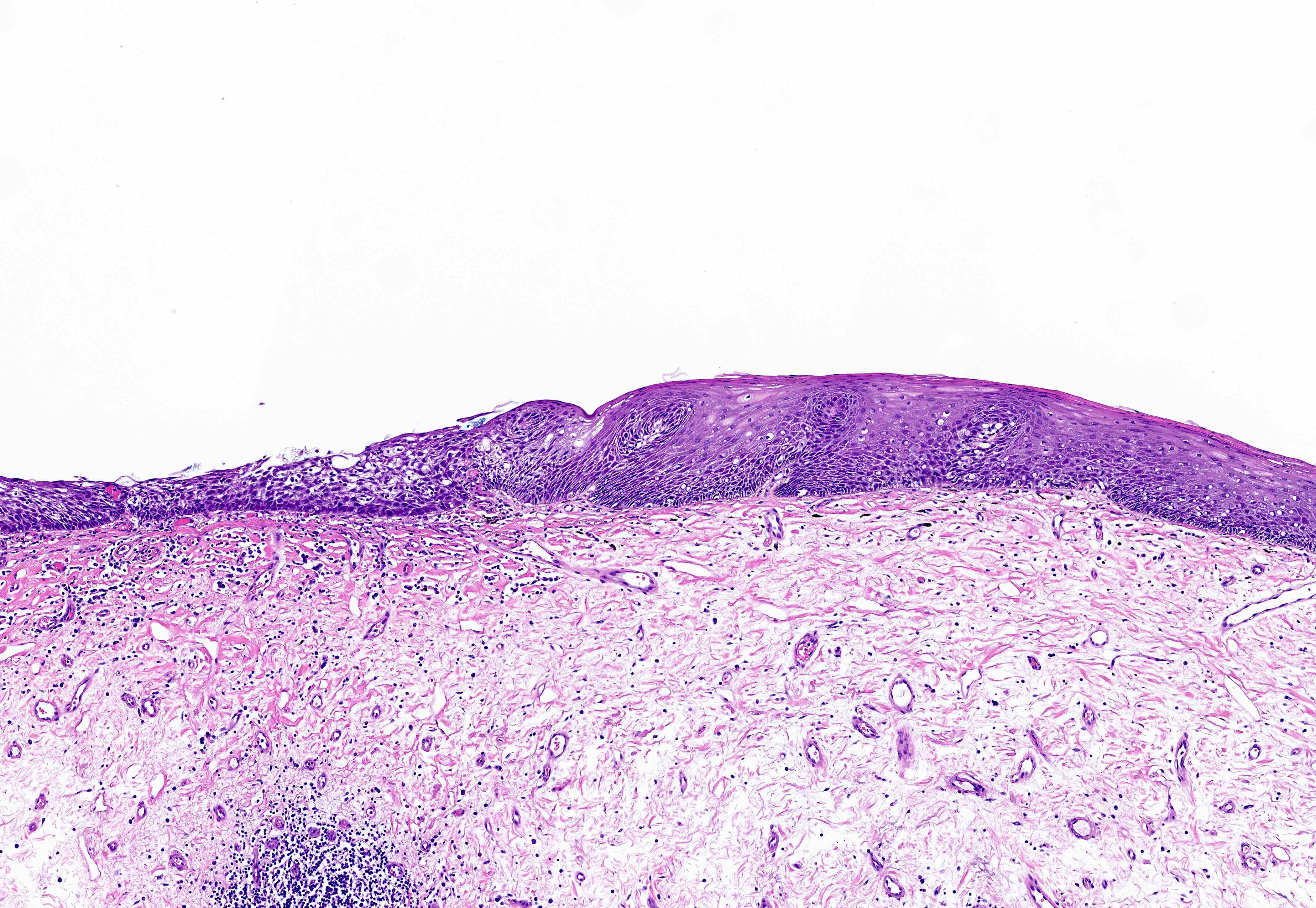
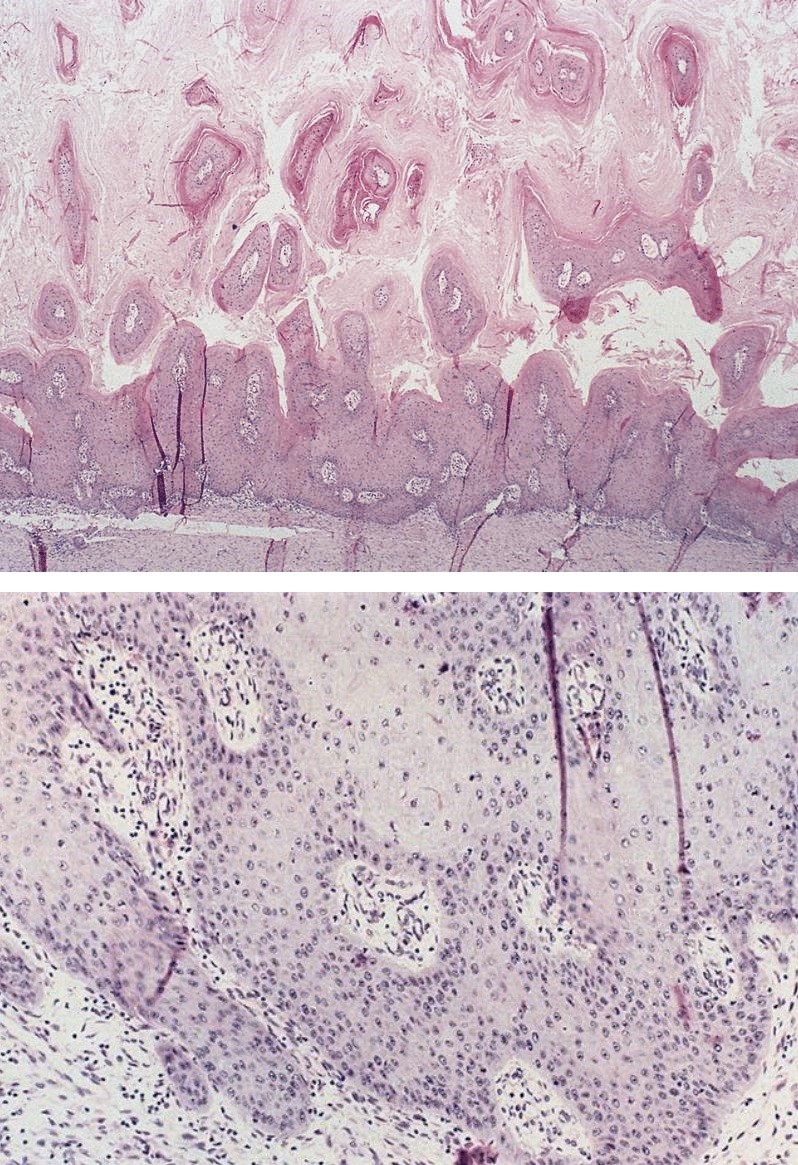
Microscopic (histologic) description
Esophageal squamous epithelium with a compact layer of orthokeratosis / hyperorthokeratosis and a prominent granular layer 1 - 4 cells thick with keratohyalin granules, resembling the epidermis of the skin
Abrupt transition from the adjacent normal squamous epithelium
Which of the following statements about epidermization / epidermoid metaplasia of the esophagus is true?
Characterized by orthokeratosis / hyperorthokeratosis with a prominent granular layer
No association with smoking or excessive alcohol consumption
No association with squamous cell carcinoma and dysplasia
PAS stain highlights epidermoid metaplasia
Board review style answer #1
A. Epidermization / epidermal metaplasia is characterized by orthokeratosis / hyperorthokeratosis with a prominent granular layer, mimicking epidermis.
Which of the following statements about histologic features of epidermization / epidermoid metaplasia of the esophagus is true?
Characterized by the presence of the stratum lucidum beneath the cornified layer
Finding of increased thickness in the cornified layer is called parakeratosis
Granular layer is characterized by the presence of basophilic stained granules known as keratohyalin granules
Orthokeratosis / hyperkeratosis is more frequently seen in the esophagus than parakeratosis
Board review style answer #2
C. Epidermization / epidermoid metaplasia is histopathologically characterized by the presence of the granular layer beneath the cornified layer. The granular layer contains basophilic stained granules known as keratohyalin granules. Parakeratosis is characterized by keratosis with persistence of the cell nuclei. The stratum lucidum is seen only in soles and palms and is not seen in epidermization / epidermoid metaplasia. Parakeratosis is more frequently seen in the esophagus than orthokeratosis / hyperkeratosis.
Adenocarcinoma rarely arises in heterotopic gastric mucosa or submucosal glands
Pathophysiology
Adenocarcinoma: dysplasia - carcinoma sequence occurs in Barrett mucosa with stepwise accumulation of genetic mutations, especially p53, also HER2 / cERB-B2, cyclin D1, cyclin E, RB, p16
Squamous cell carcinoma: genetic alterations include p53, p16INK4a, amplification of cyclin D1, cMYC and EGFR; related to smoking, alcohol, diet, possible nutritional deficiency, genetic factors
Clinical features
Insidious onset, dysphagia to solids, followed by dysphagia to all food
Extreme weight loss due to loss of nutrition and tumor itself
Squamous cell carcinoma may erode through esophagus; invades respiratory tree with fistula formation and pneumonia; aorta with exsanguination; also invades mediastinum or pericardium
Metastasis generally occurs early even in superficial tumors due to extensive lymphatic network in esophagus that allows horizontal and longitudinal spread
Cancers of upper esophagus metastasize to cervical lymph nodes; of mid esophagus to mediastinal, paratracheal and tracheobronchial lymph nodes; of lower esophagus to gastric and celiac lymph nodes
Metastases to liver, lungs and pleura
Recurrences are common
Diagnosis
Endoscopic biopsy
Rarely identified during resection for achalasia or for lesions not amenable to biopsy
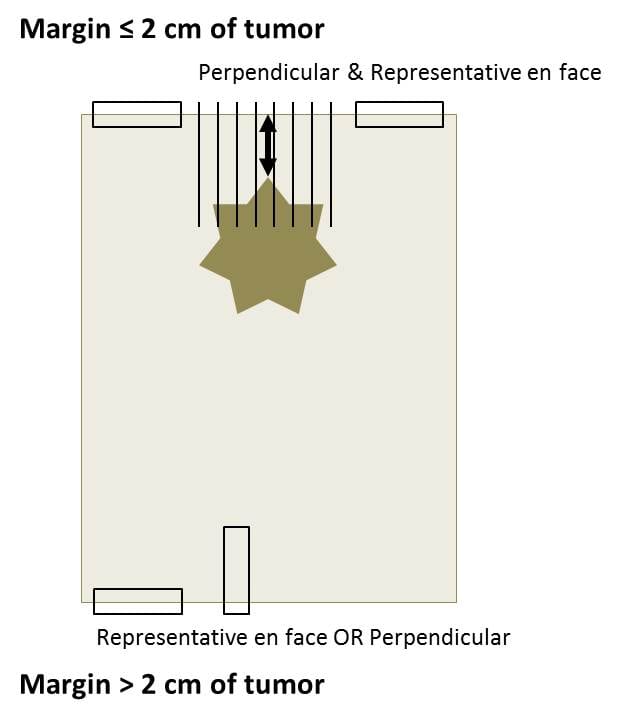
Recommended to submit proximal margins for frozen section to rule out carcinoma underneath a normal appearing mucosa (Arch Pathol Lab Med 2005;129:1558)
Adenocarcinoma is located in distal esophagus and may involve gastric cardia (note: tumors in the proximal 5 cm of the stomach are regarded as esophageal carcinomas in Edge: AJCC Cancer Staging Manual, 7th Edition, 2011)
Flat or raised patches of intact mucosa develop into nodular masses
Squamous cell carcinoma begins as an in situ process
Generally starts as plaque-like lesions which grow to eventually encircle the lumen
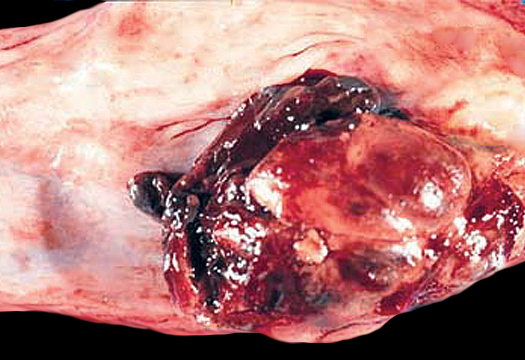
Mostly form protruding cauliflower-like lesions (60%), may be flat (15%) or ulcerated
Gross images
Contributed by Elliot Weisenberg, M.D.
Adenocarcinoma
Squamous cell carcinoma
Microscopic (histologic) description
Overwhelming majority of carcinomas of esophagus are adenocarcinoma and squamous cell carcinoma
Diagnosis usually simple
Generally mucin secreting adenocarcinomas, less often signet ring cell carcinoma
Usually foci of dysplastic mucosa adjacent to cancer
Squamous cells carcinoma tends to be well or moderately differentiated; histologic variants include verrucous, spindle cell or basaloid
Other carcinomas are adenoid cystic carcinoma, adenosquamous carcinoma, mucoepidermoid carcinoma
Special stains only rarely needed for diagnosis
Microscopic (histologic) images
Contributed by Elliot Weisenberg, M.D.
Adenocarcinoma
Adenocarcinoma in lymphatics
Squamous cell carcinoma in situ
Differential diagnosis
Chemoradiationinduced atypia: enlarged hyperchromatic nuclei with prominent mitotic figures but relatively mild pleomorphism in inflammatory background
Reparative processes: atypical cells in granulation tissue but with fine chromatin, few mitotic figures; cells mature at deeper levels, keratin negative
Mucosa, submucosa and muscular layers similar to GI tract; lined by either esophageal squamous, gastric, primitive, ciliated columnar or small intestinal epithelium
Microscopic (histologic) images
Images hosted on other servers:
Cyst wall
Inclusion cysts
Definition / general
Lined by squamocolumnar epithelium, may be ciliated
Retention cysts
Definition / general
Also called mucocele
Derive from obstructed submucosal gland ducts
Small, usually in lower esophagus
May cause intramural pseudodiverticulosis, with multiple flask-like invaginations into esophageal wall (Am J Clin Pathol 1976;65:314)
Associated with chronic esophagitis and fibrosis; also surgically isolated segments of esophagus (Dis Esophagus 2002;15:96)
Microscopic (histologic) description
Saccular or flask shaped dilation of submucosal gland excretory ducts; rarely reaches muscularis propria
In large lesions, muscularis does not accompany the lesion so are not true diverticula
Esophageal manifestation of dermatologic disease (pending)
[Pending]
Esophageal manifestations of collagen vascular disease
No treatment for underlying disease; proton pump inhibitors for reflux esophagitis, dilation for strictures
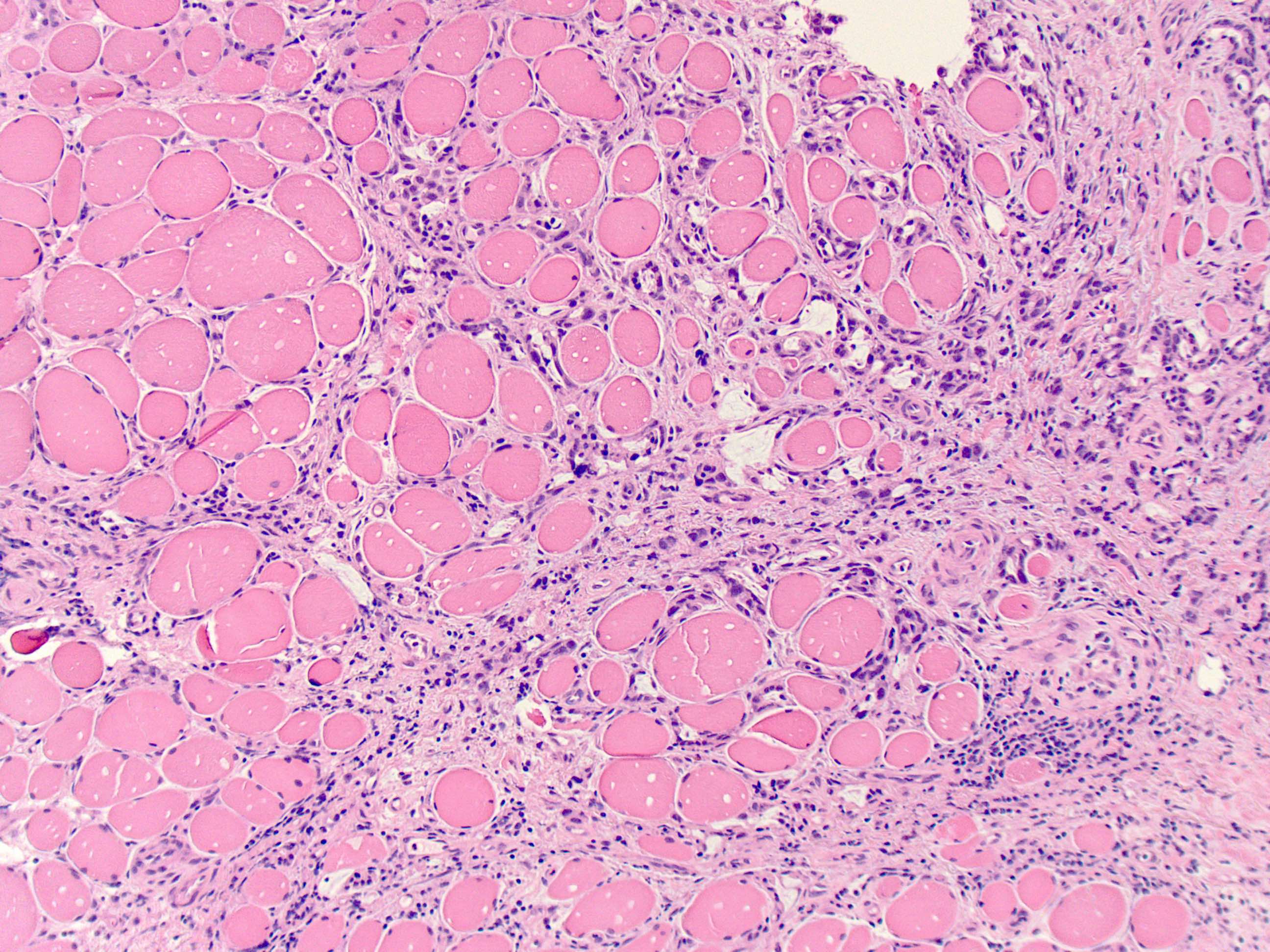
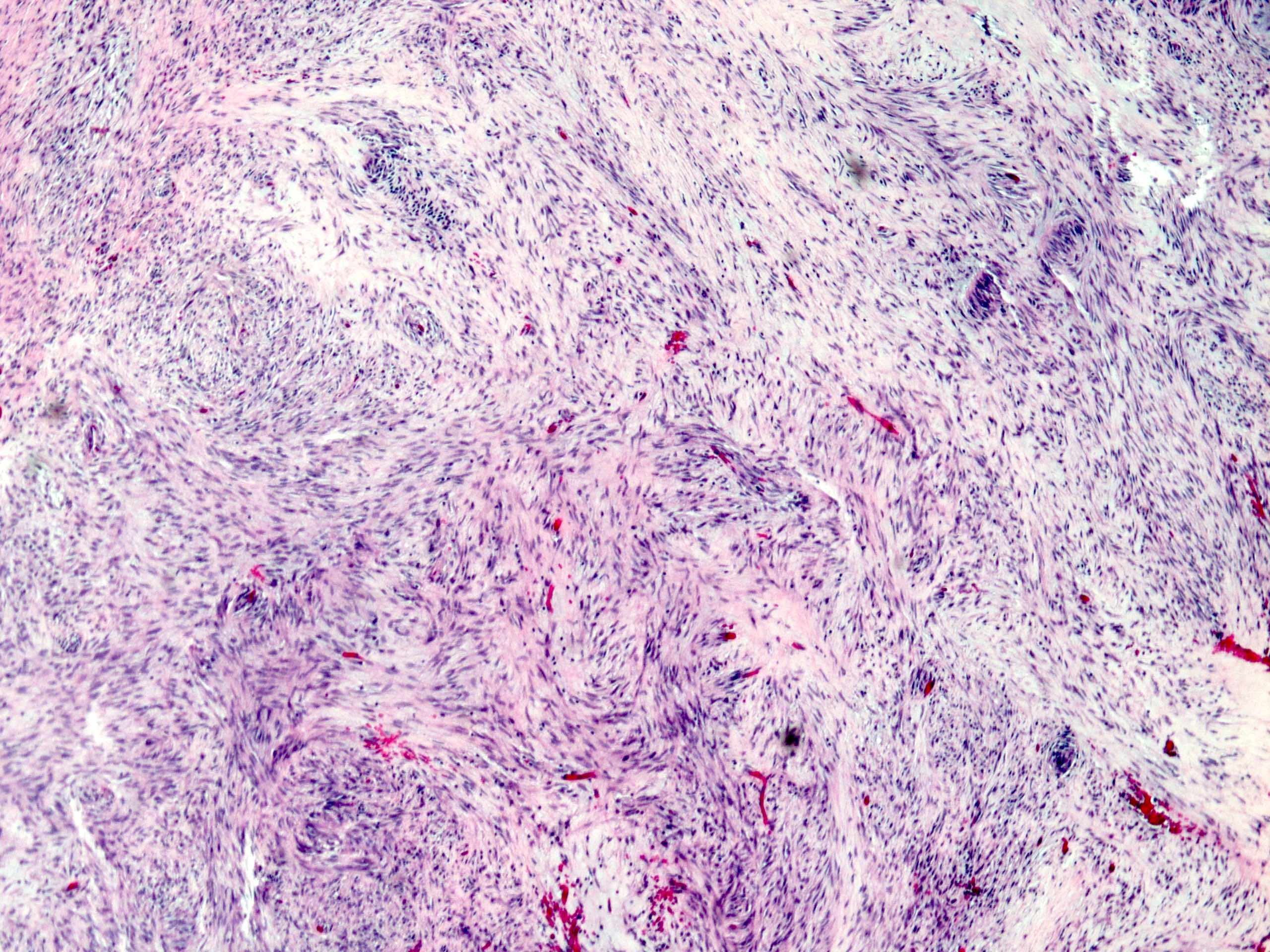
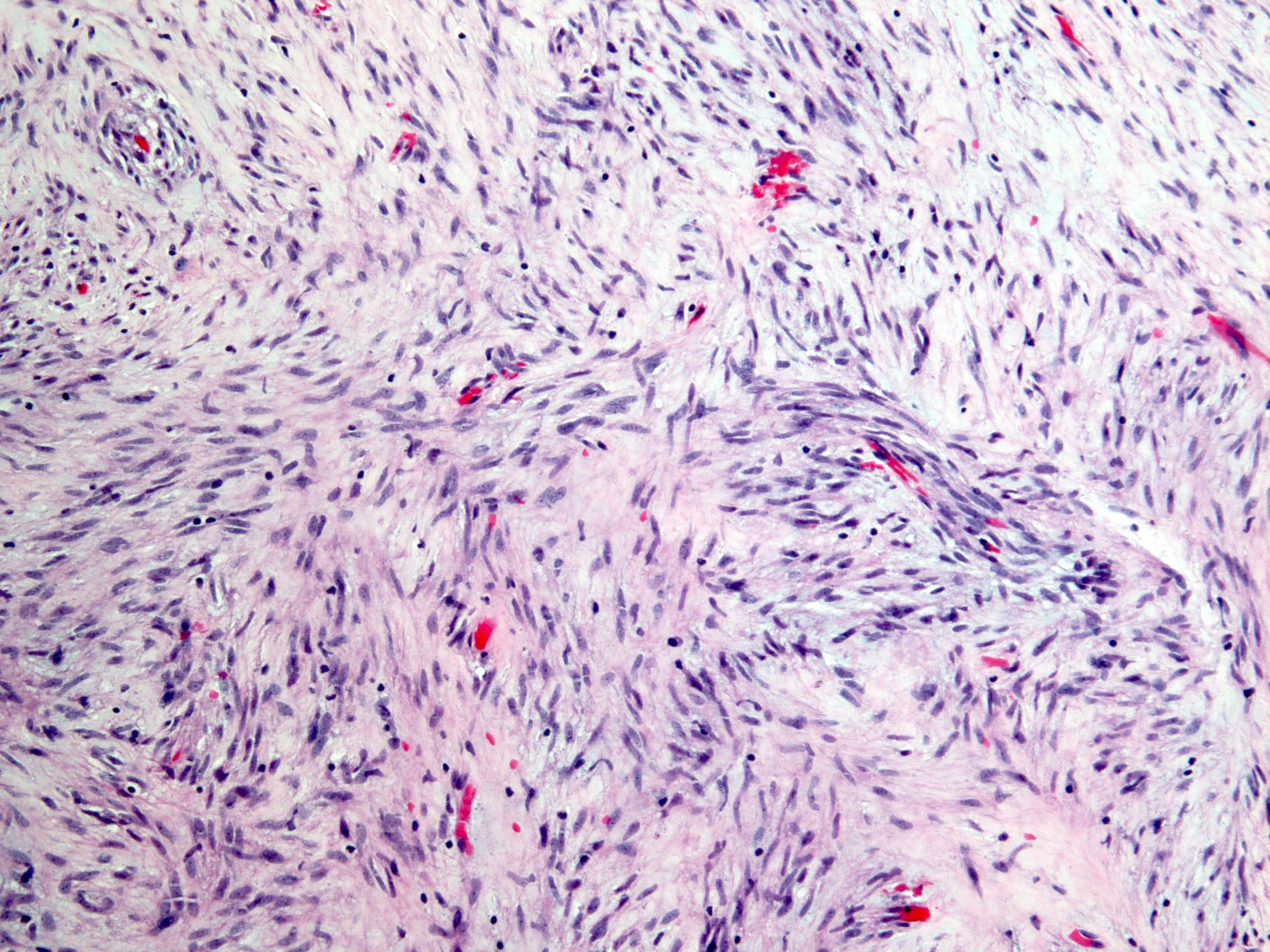
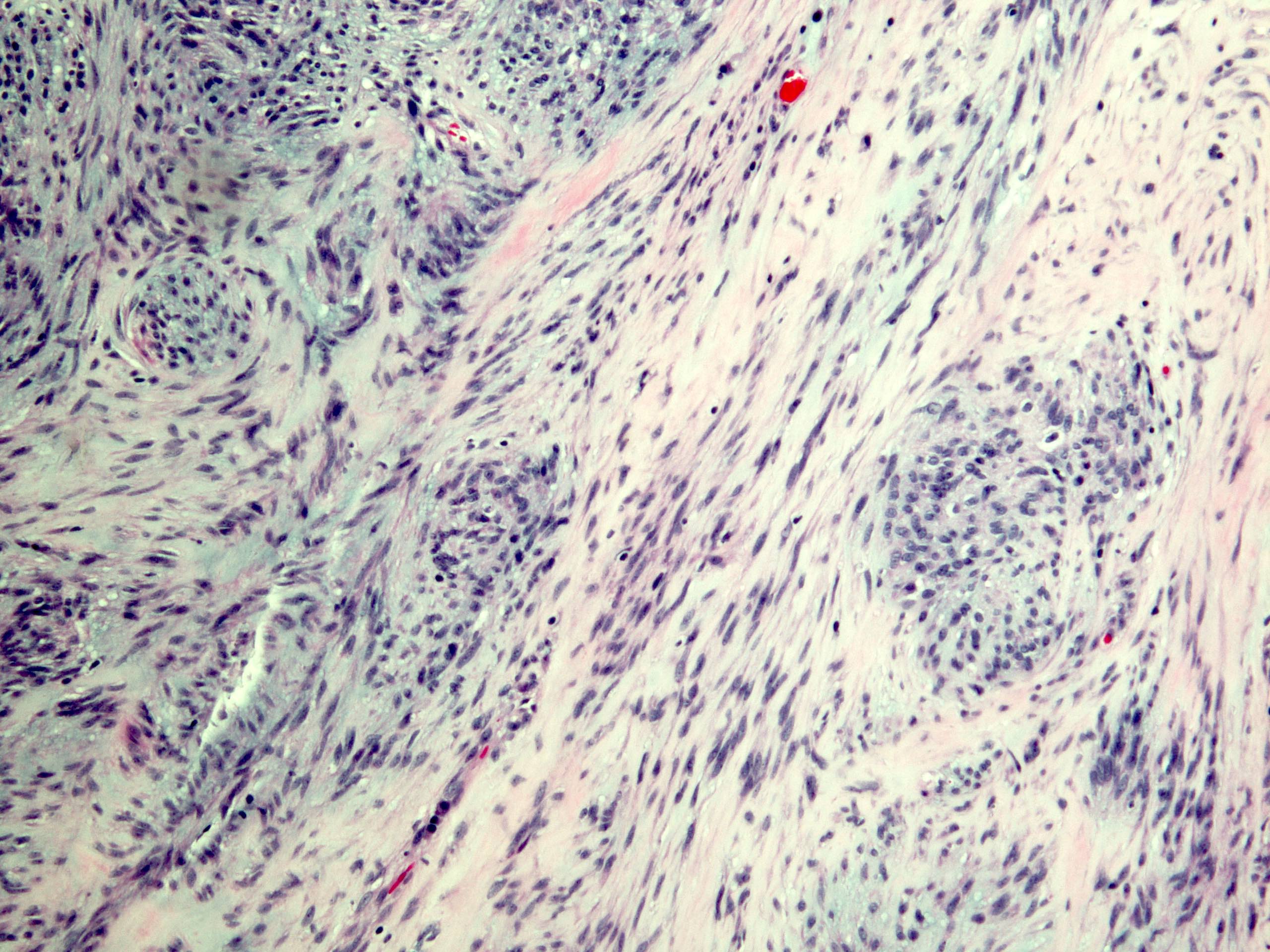
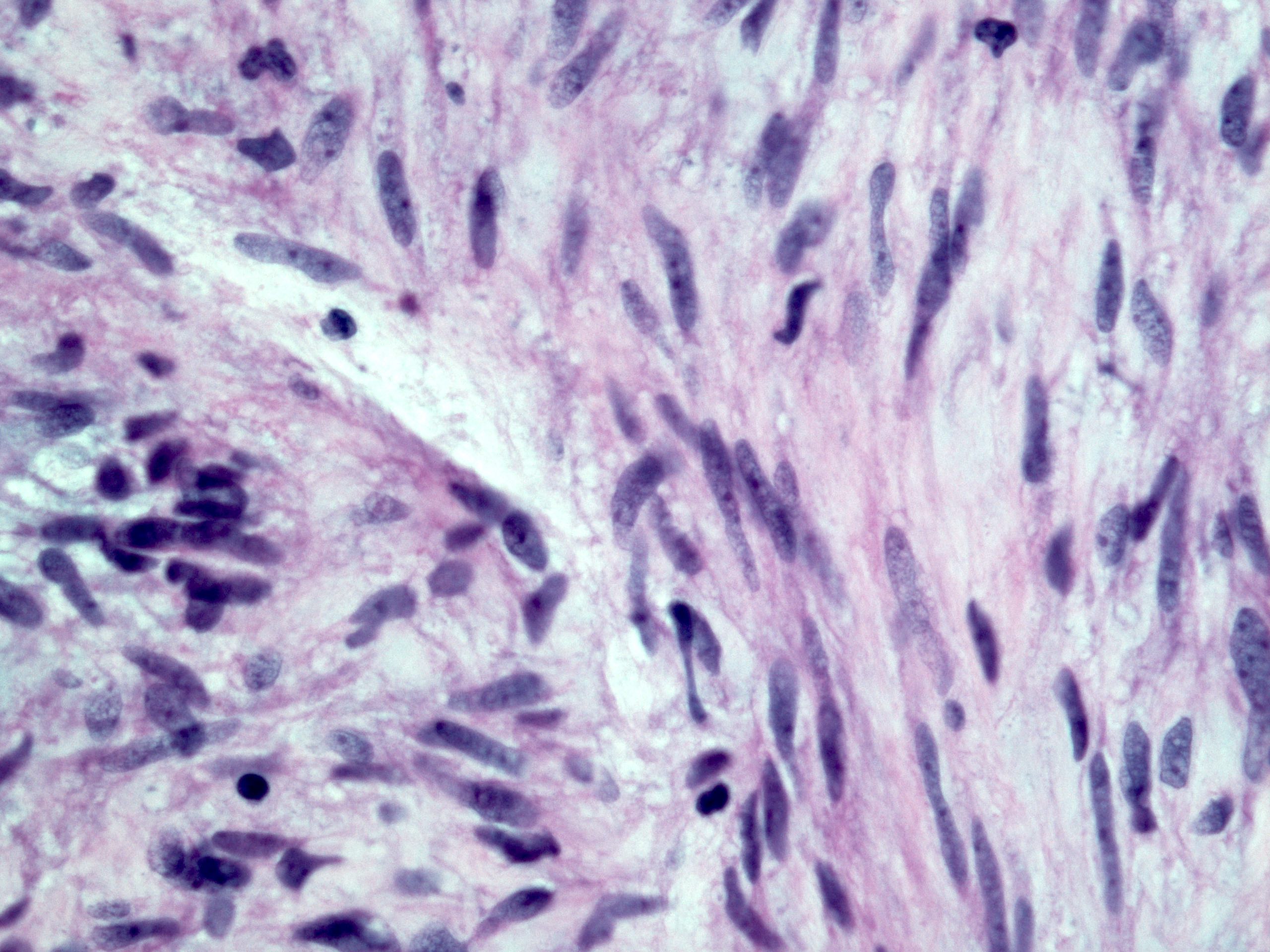
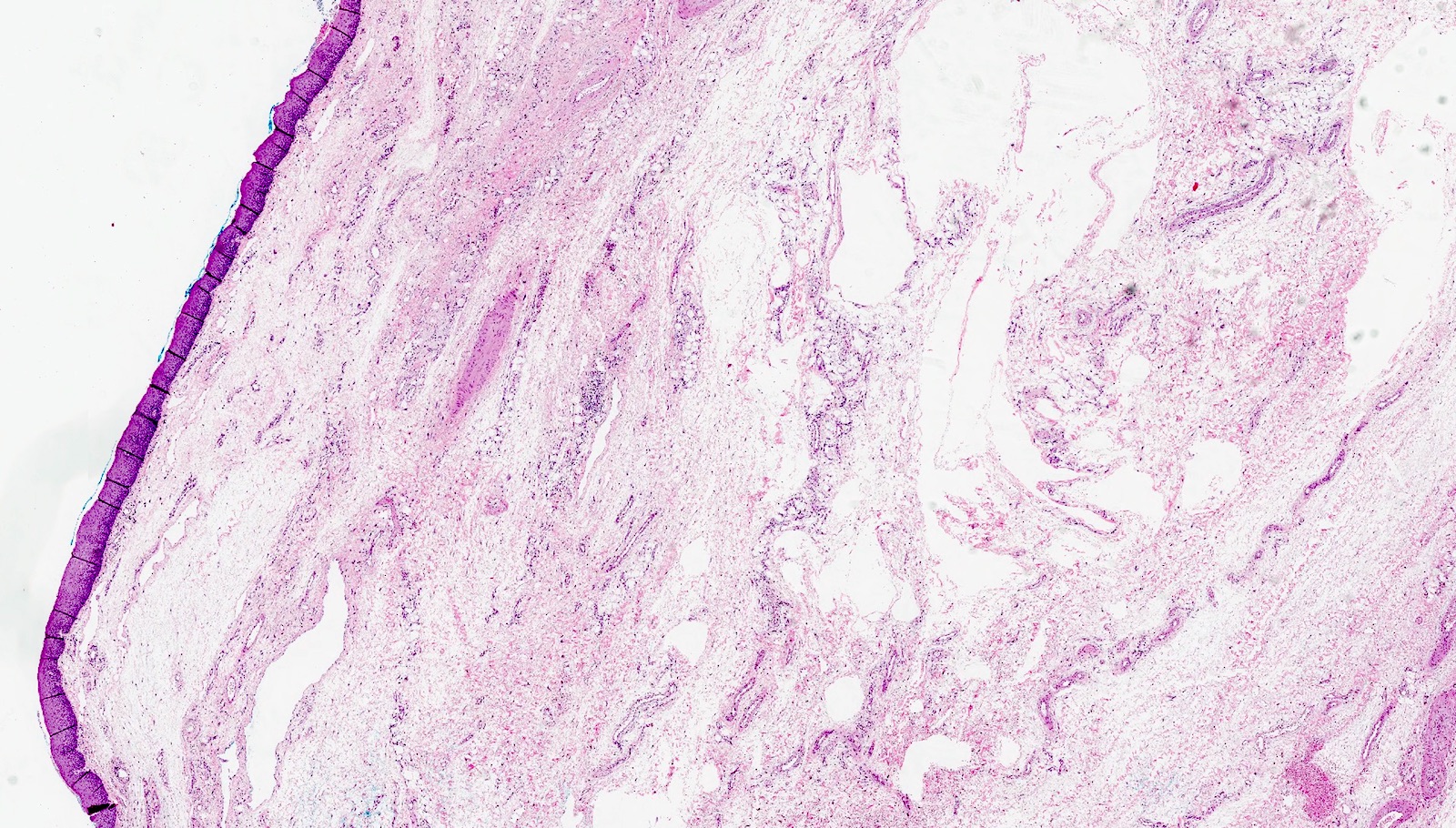
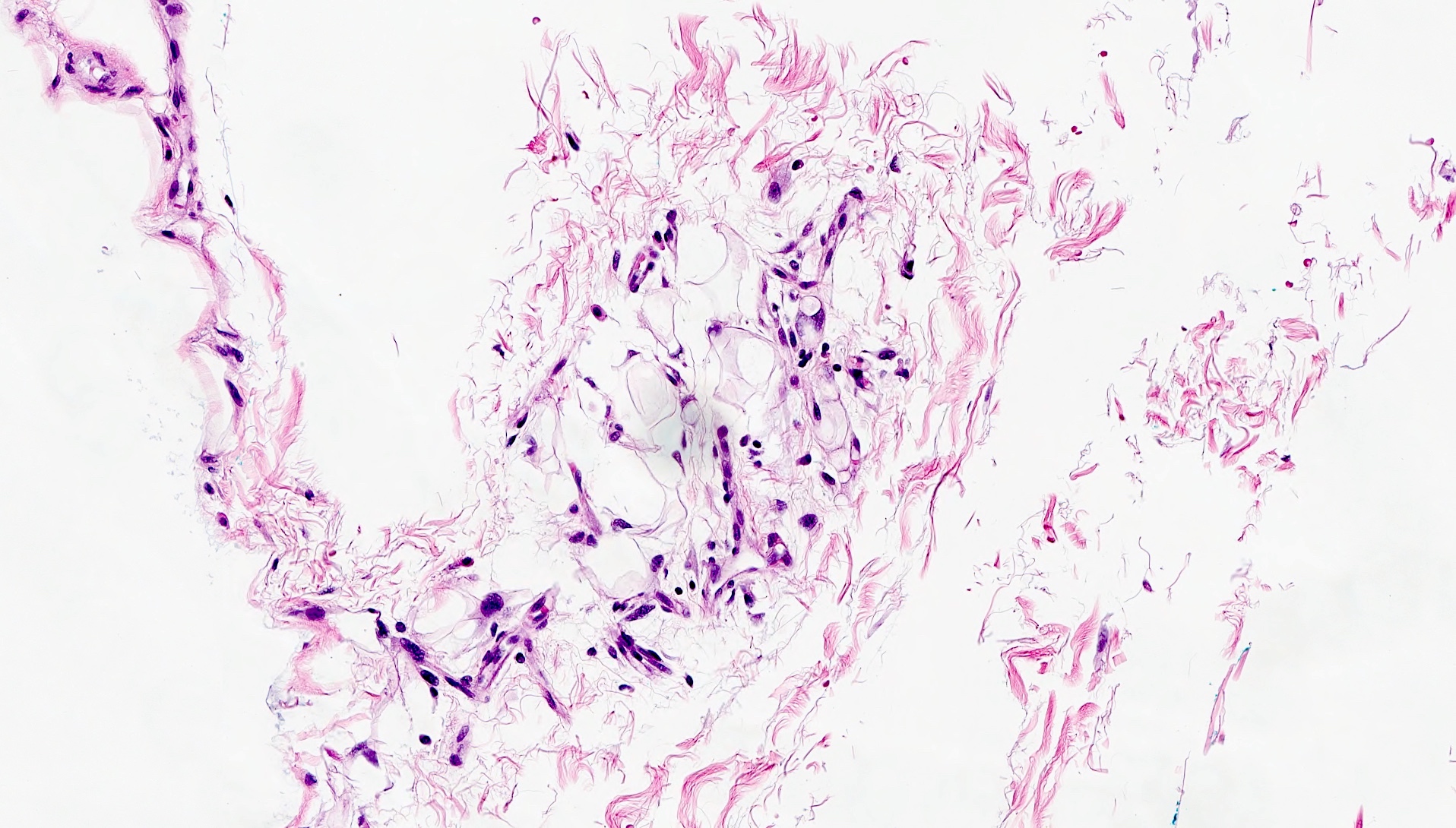
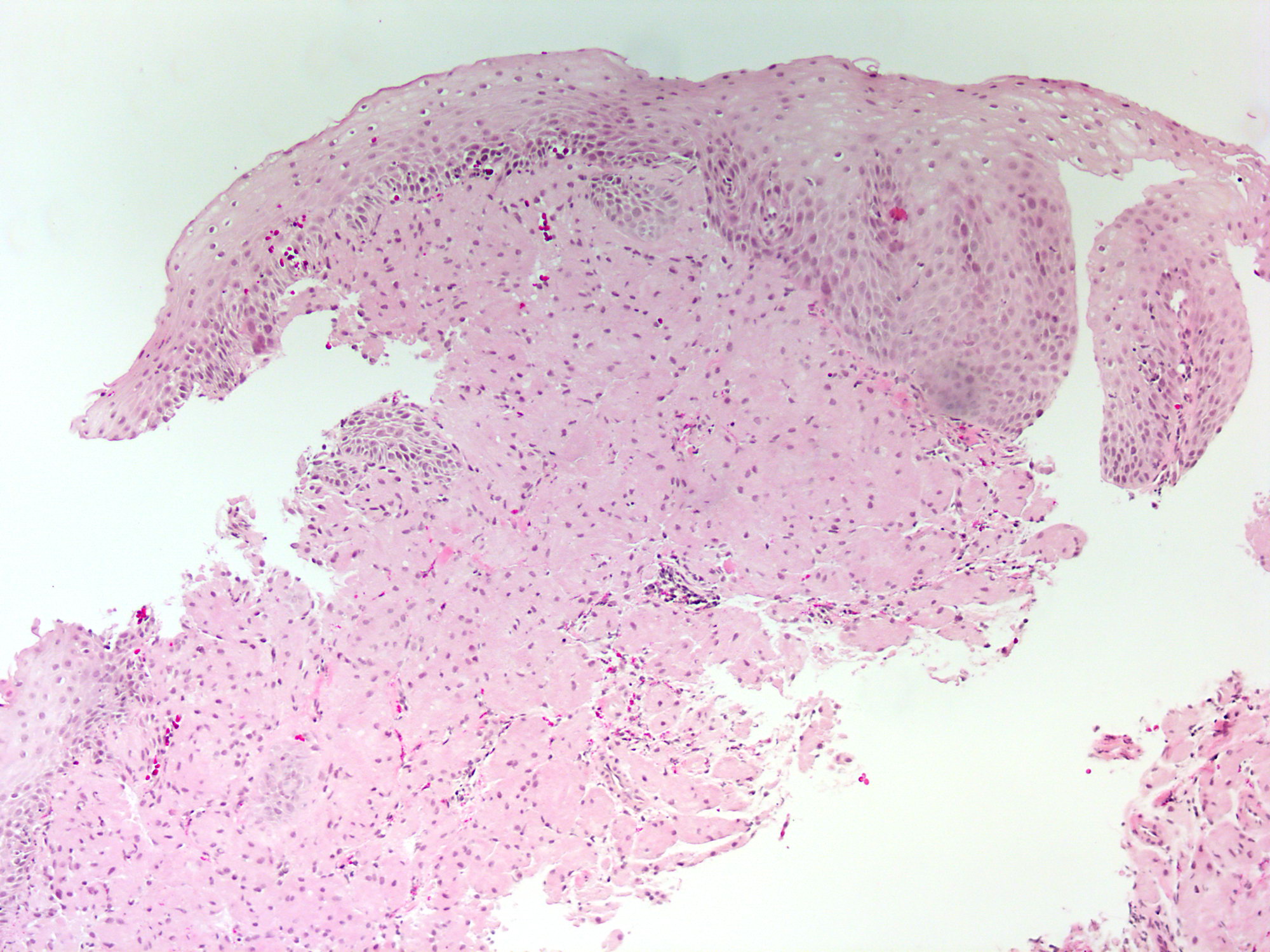
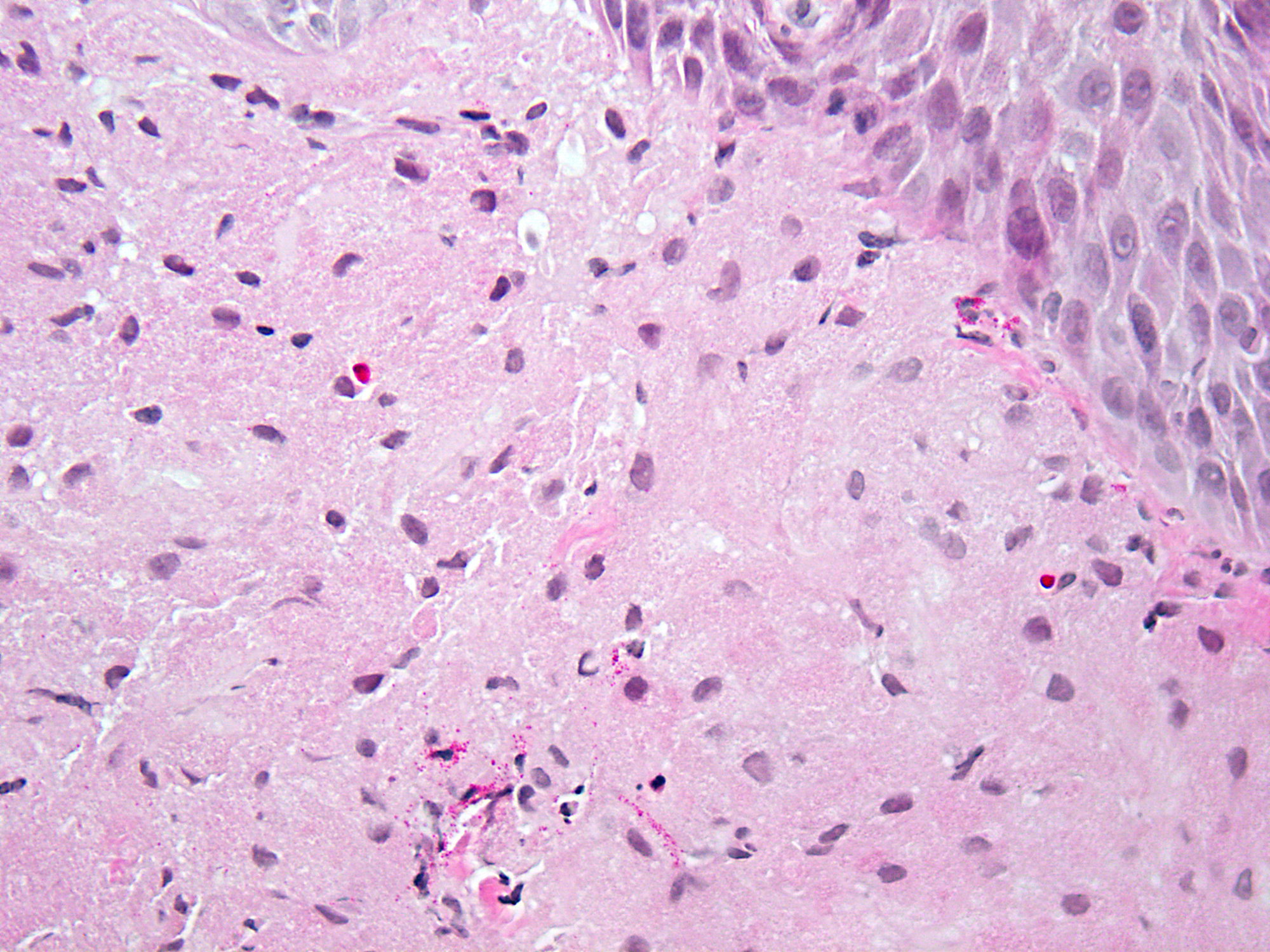
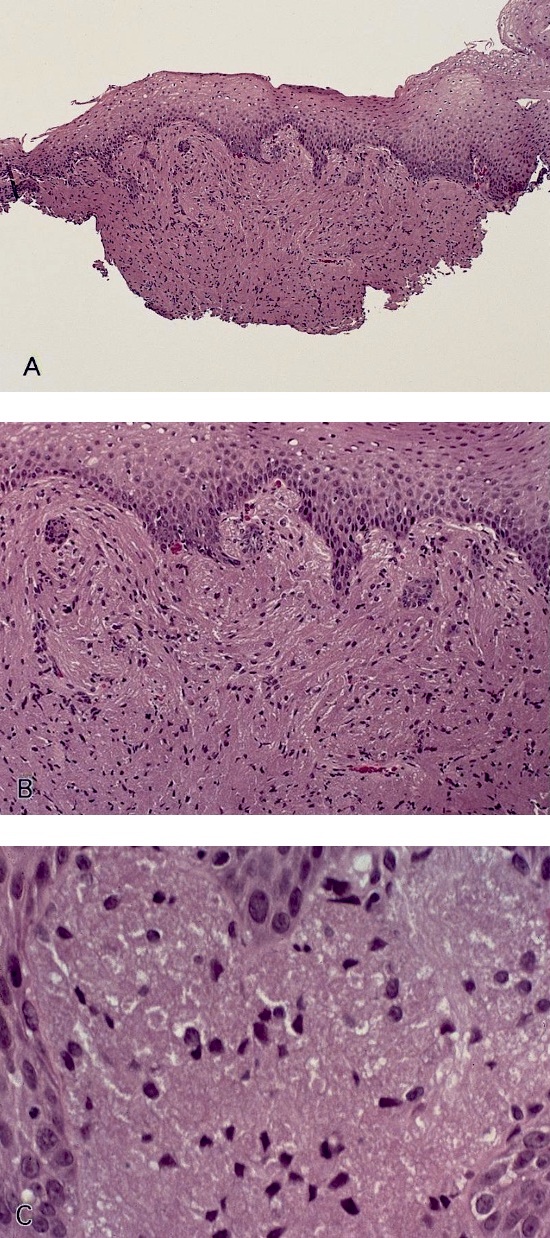
Microscopic (histologic) description
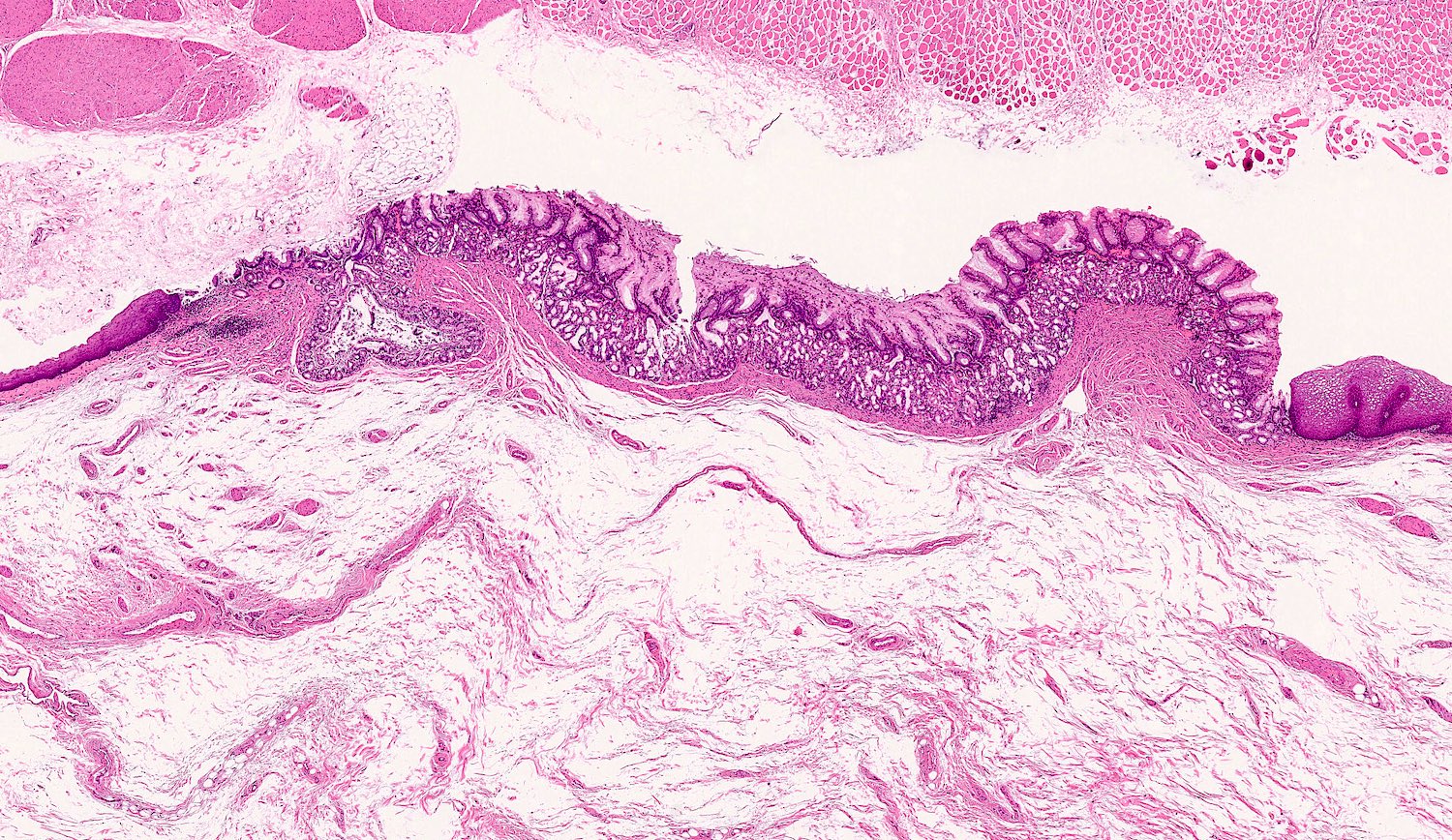
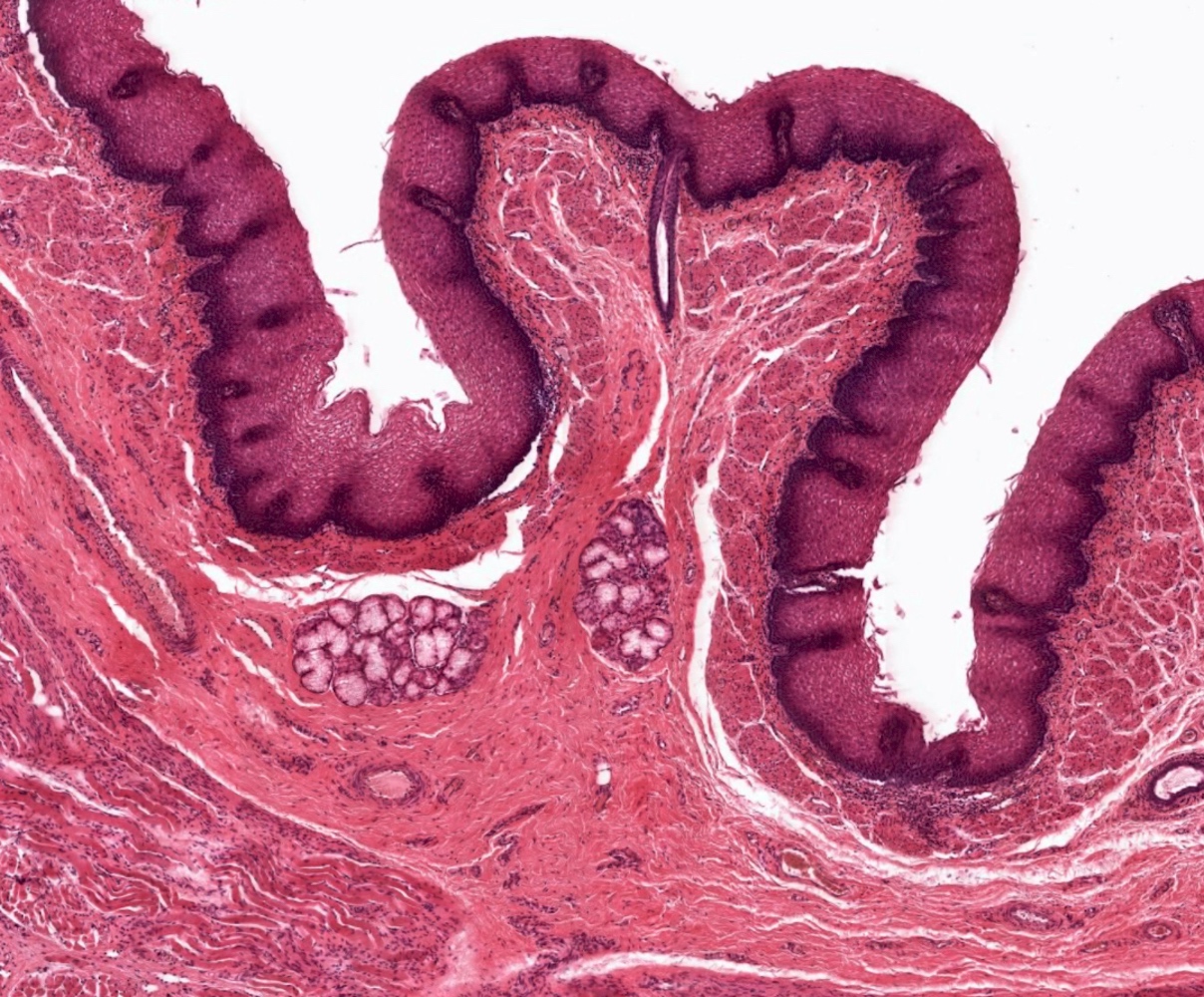
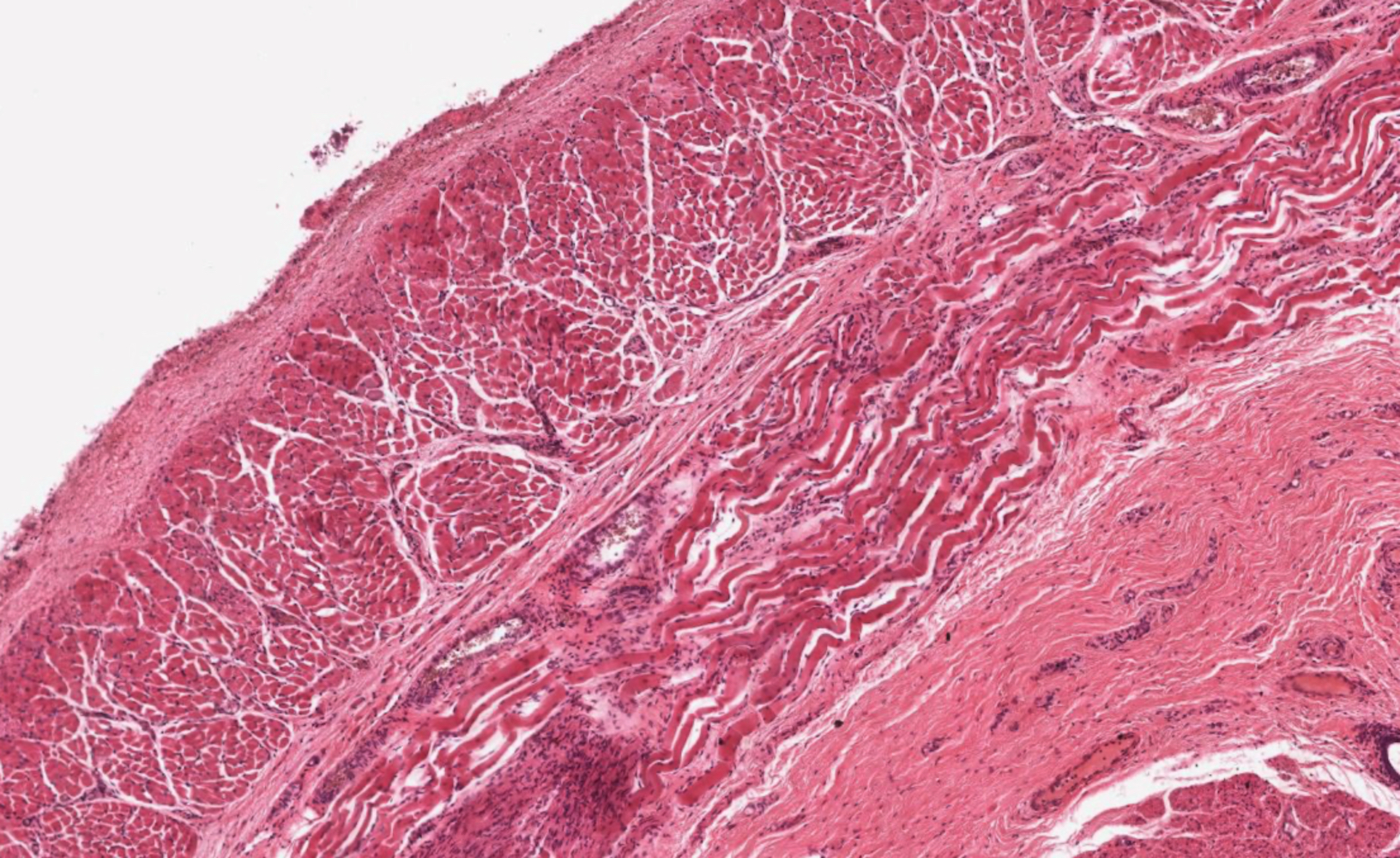
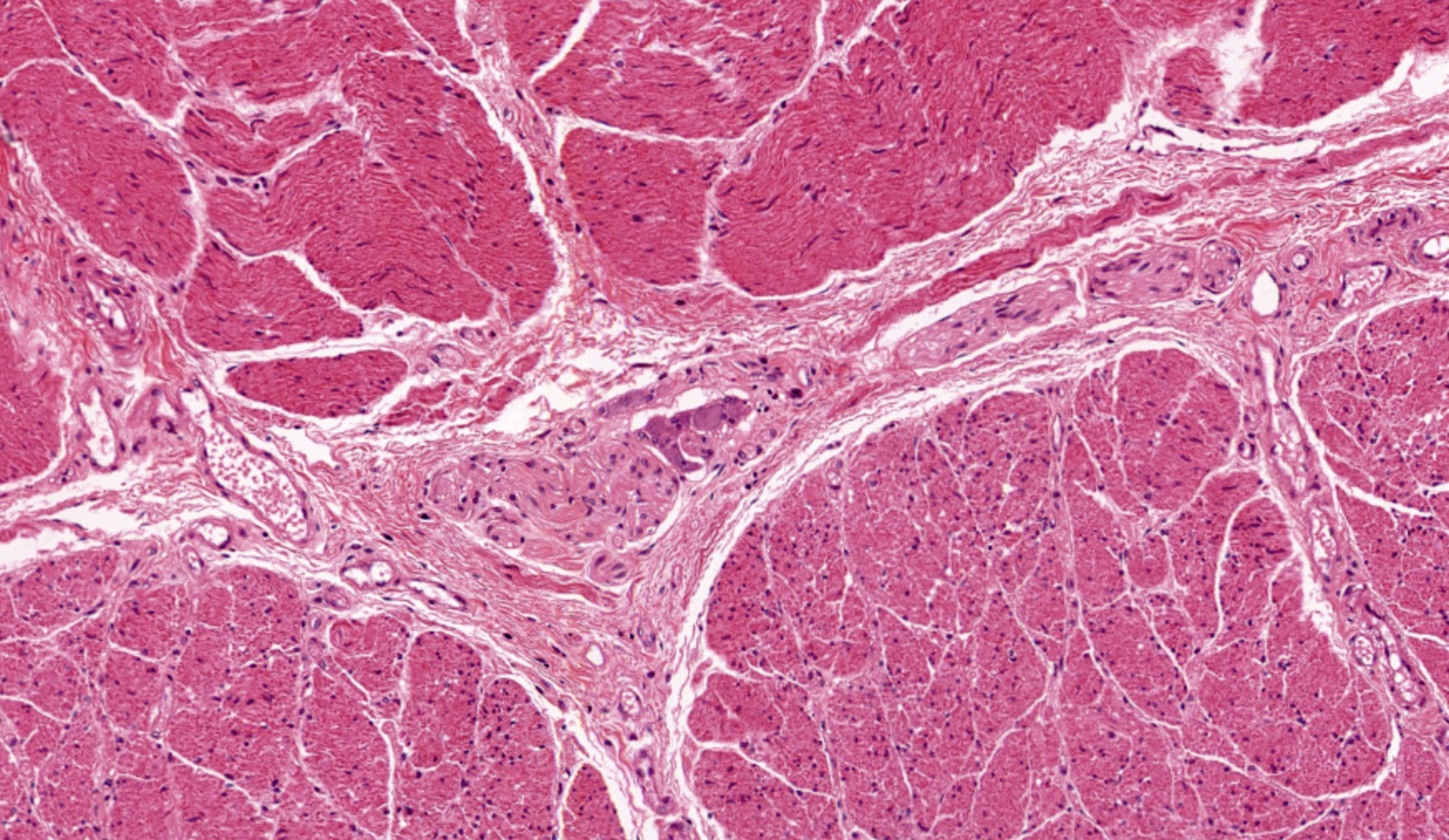
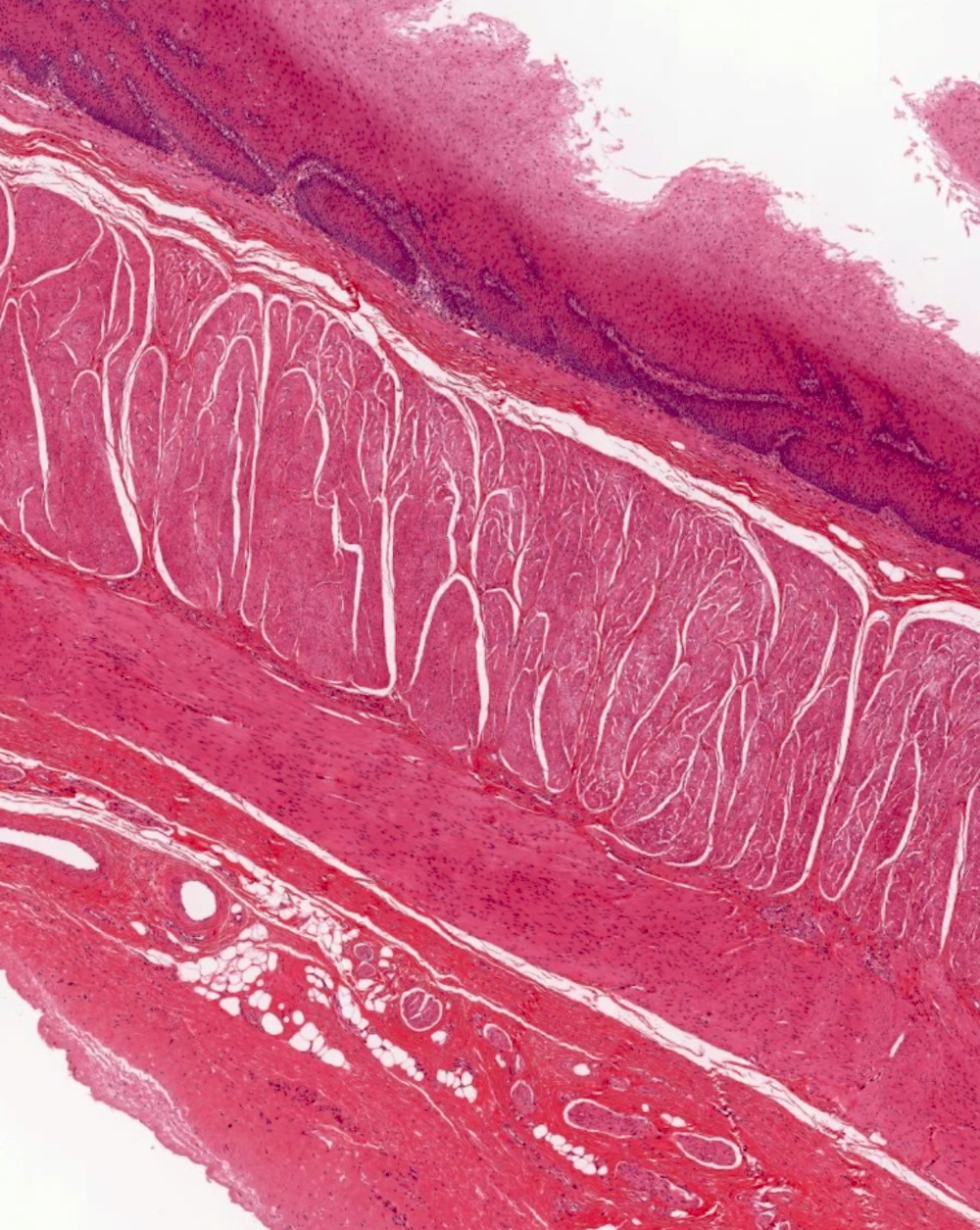
Resection specimens: atrophy and replacement fibrosis of inner circular layer of muscularis propria and resulting stenosis; longitudinal layer is usually involved; also submucosal fibrosis, mild inflammation, intimal proliferation of arterioles (Gut 2006;55:1697)
Biopsies: ulcers or erosions resembling reflux esophagitis, Candida or Barrett
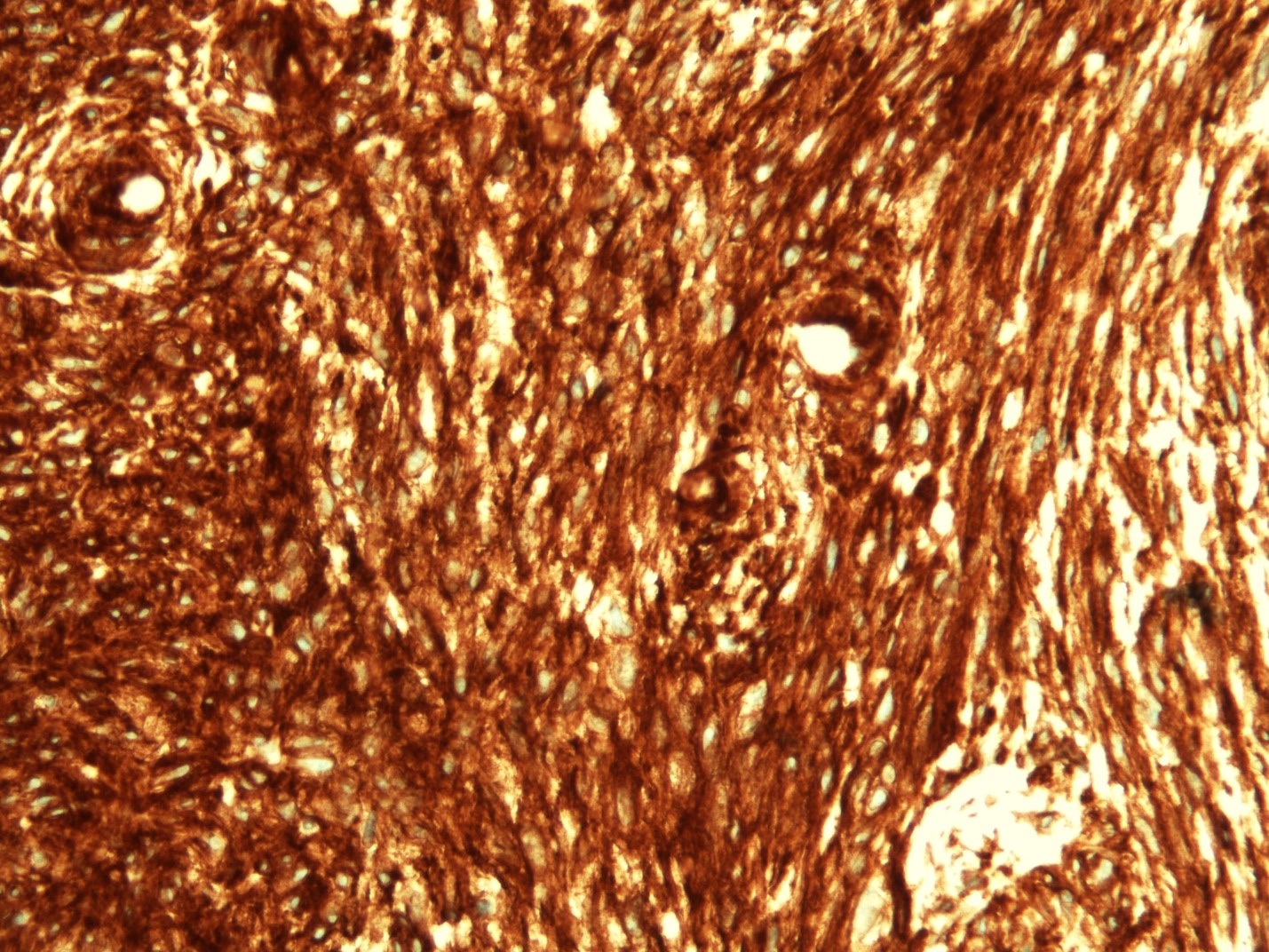
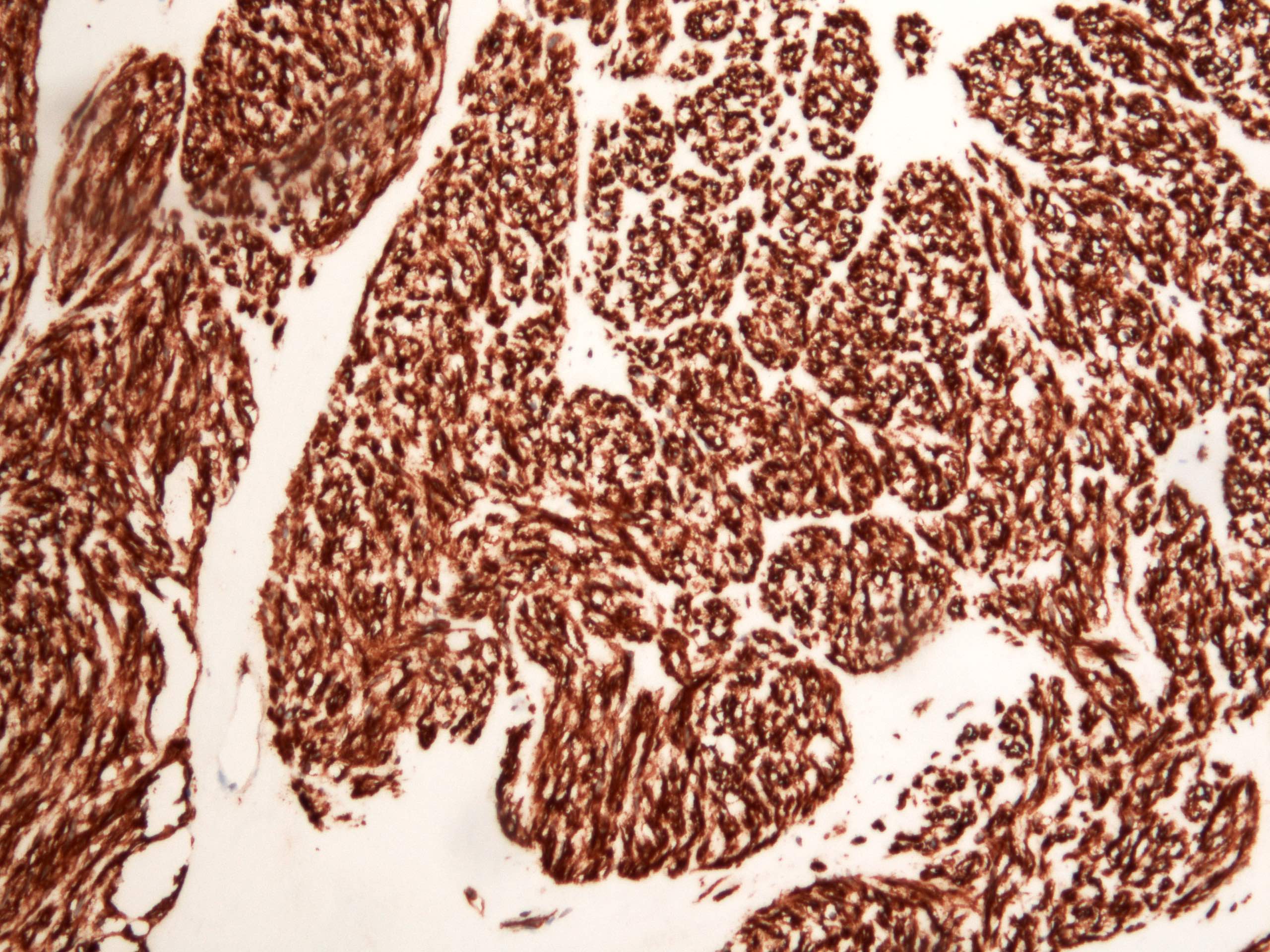
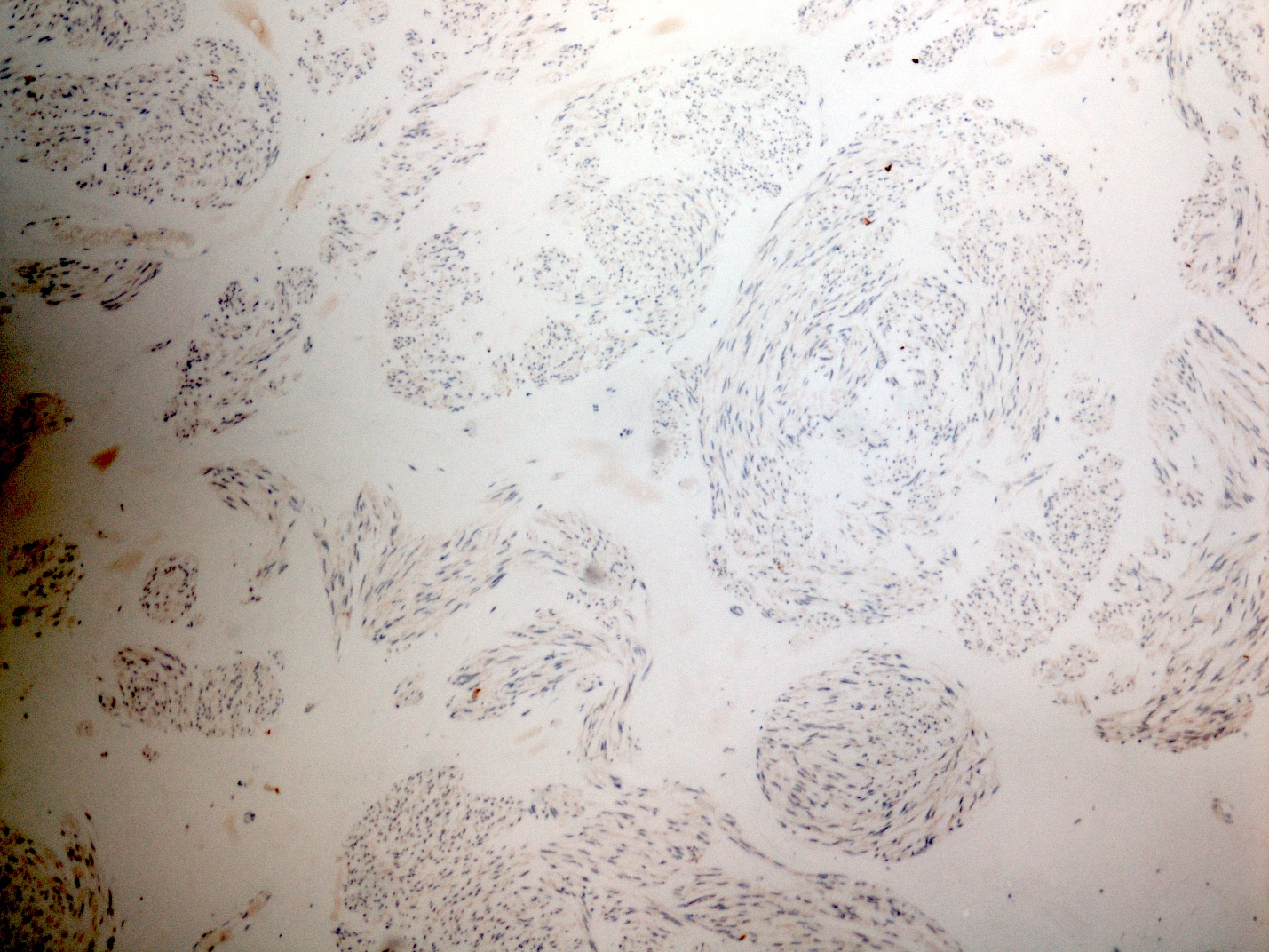
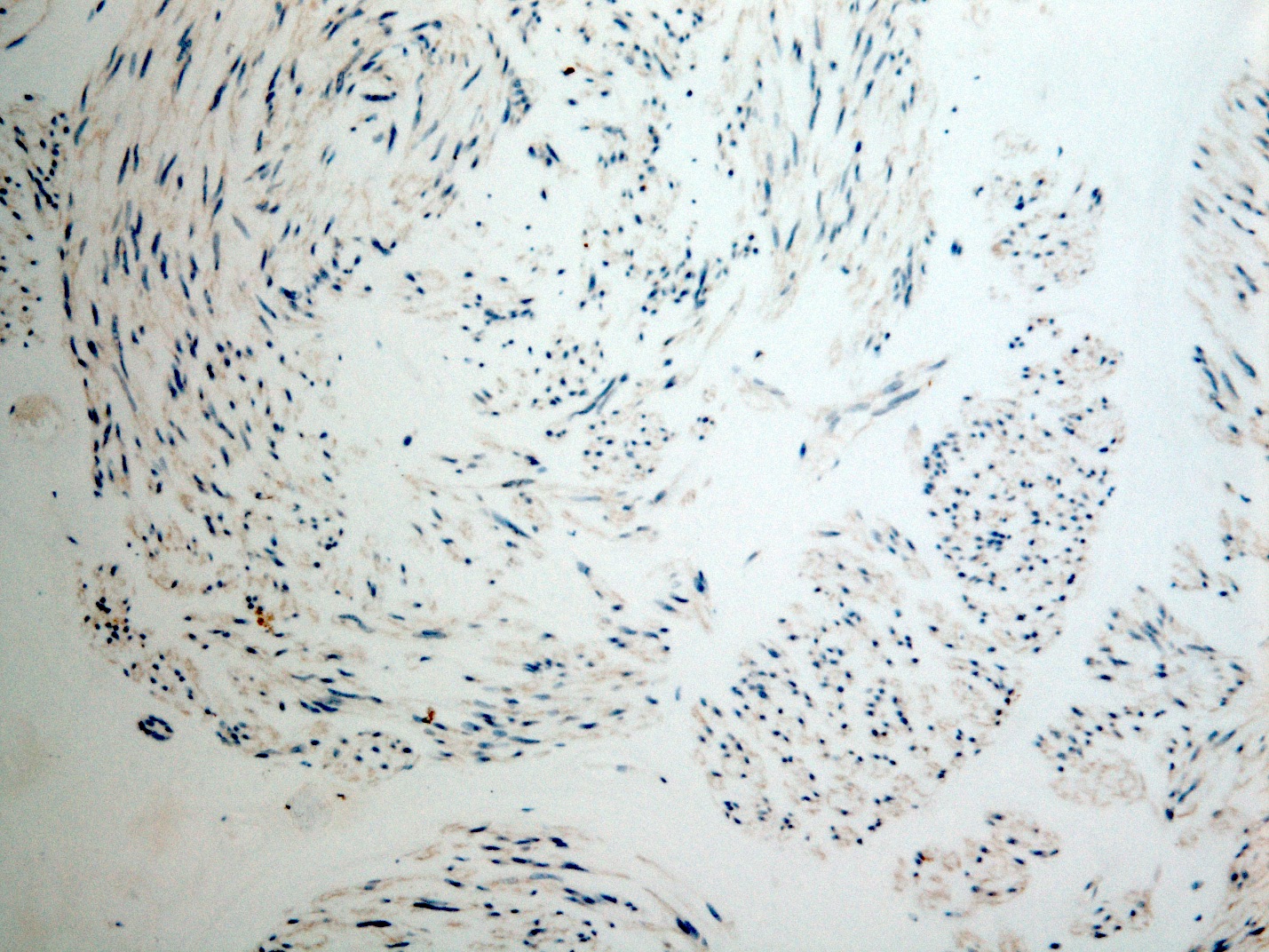
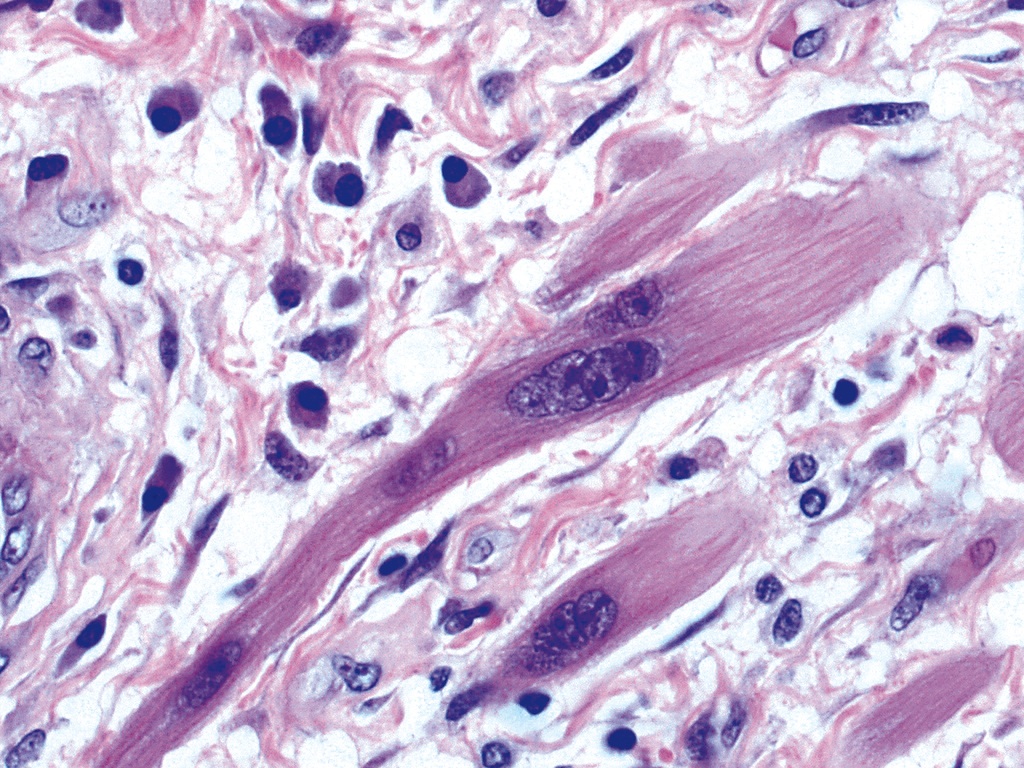
Microscopic (histologic) images
Images hosted on other servers:
Distal and proximal oesophagus
Severe atrophy of circular muscle
Myenteric plexus
Interstitial cells of Cajal
Barrett esophagus
Electron microscopy images
Images hosted on other servers:
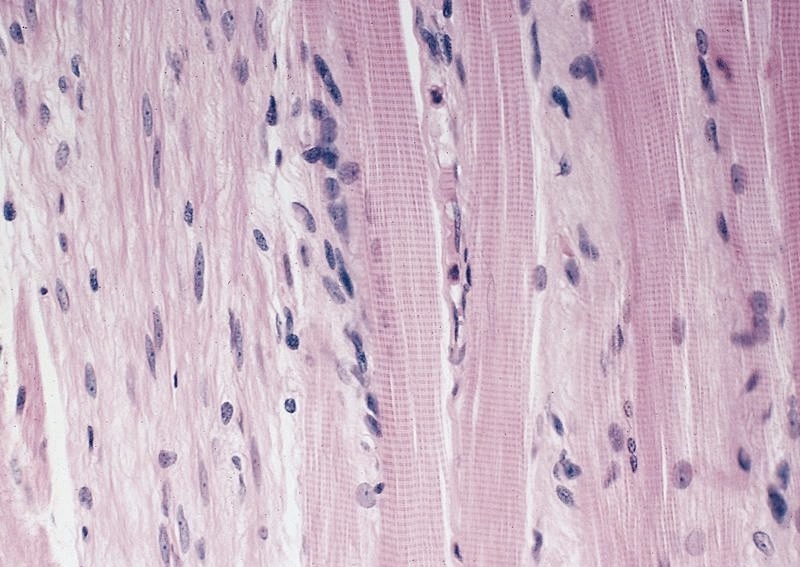
Collagen between
degenerate muscle
fiber (left) and necrotic
muscle fiber (right)
Muscle fibers (M)
separated by collagenous
fibers with widened
intermyofibrillar space
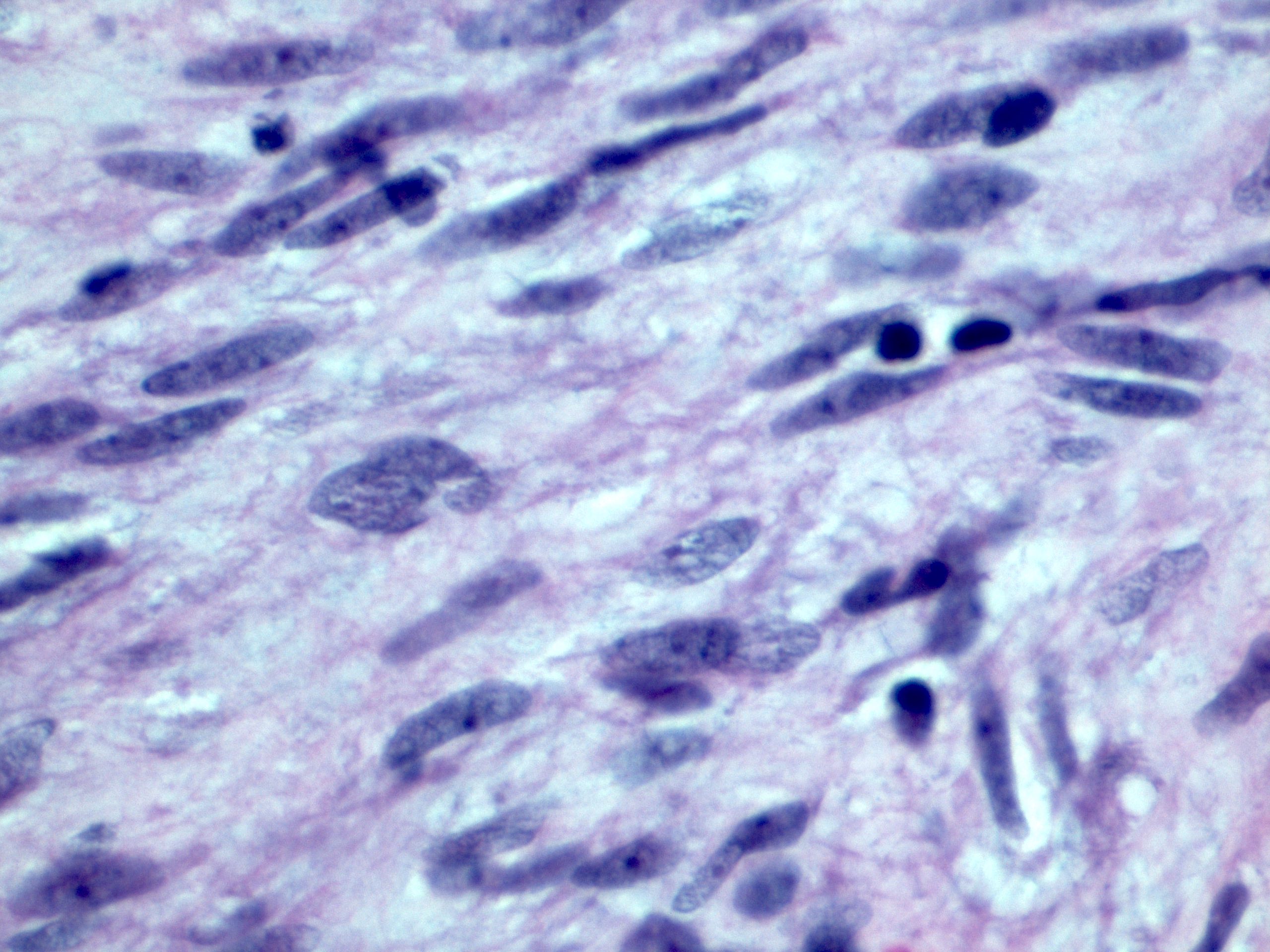
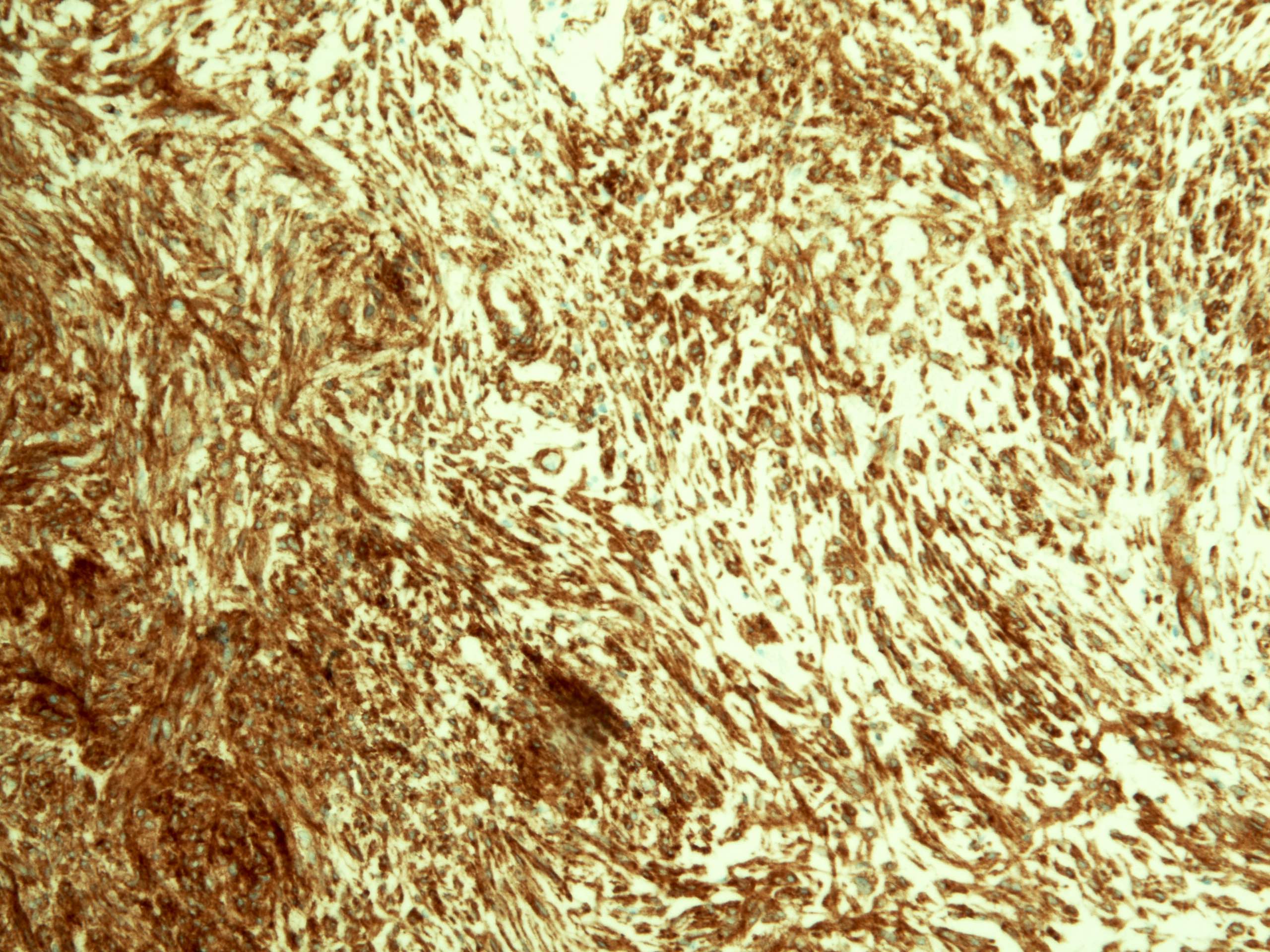
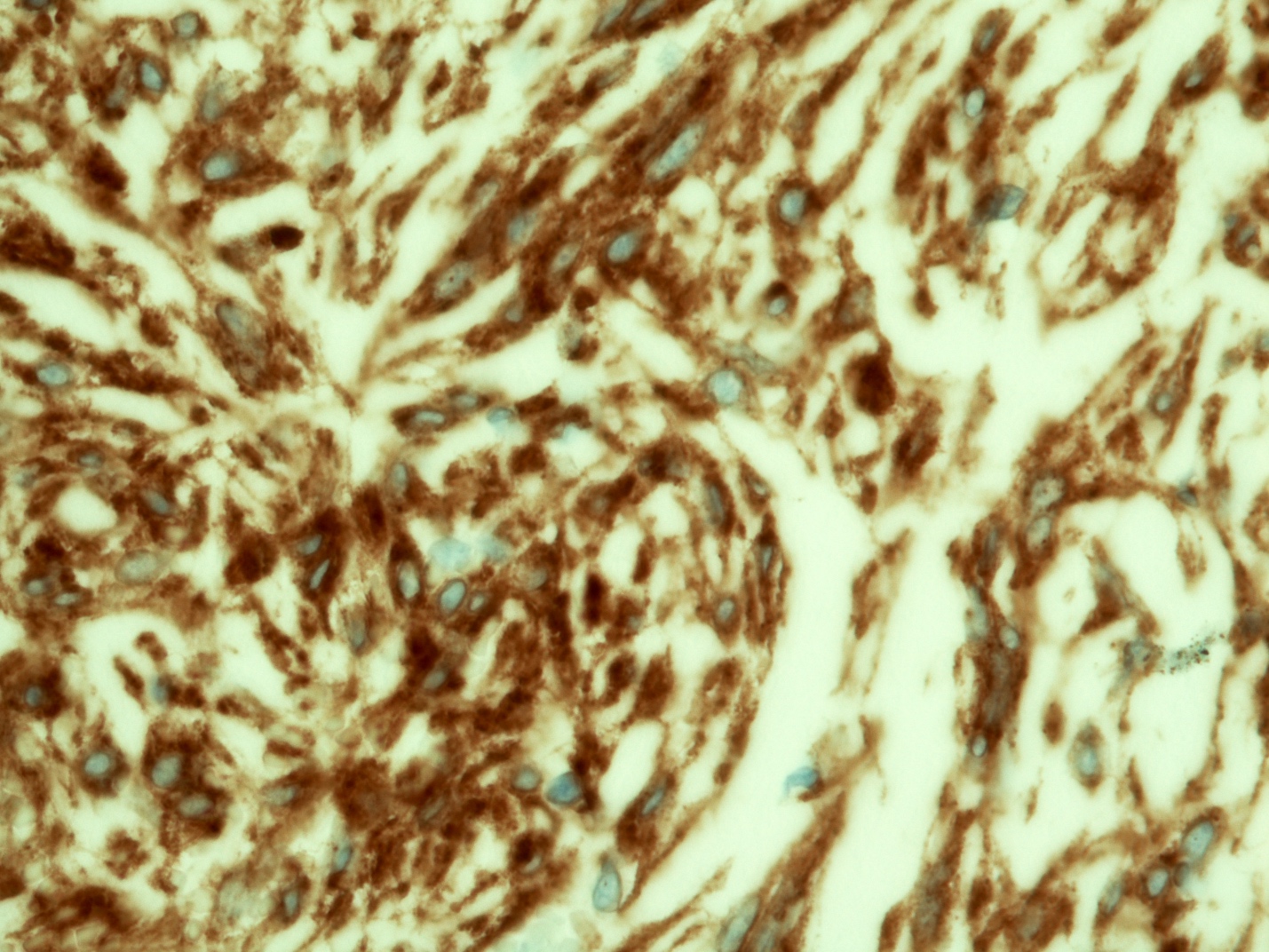
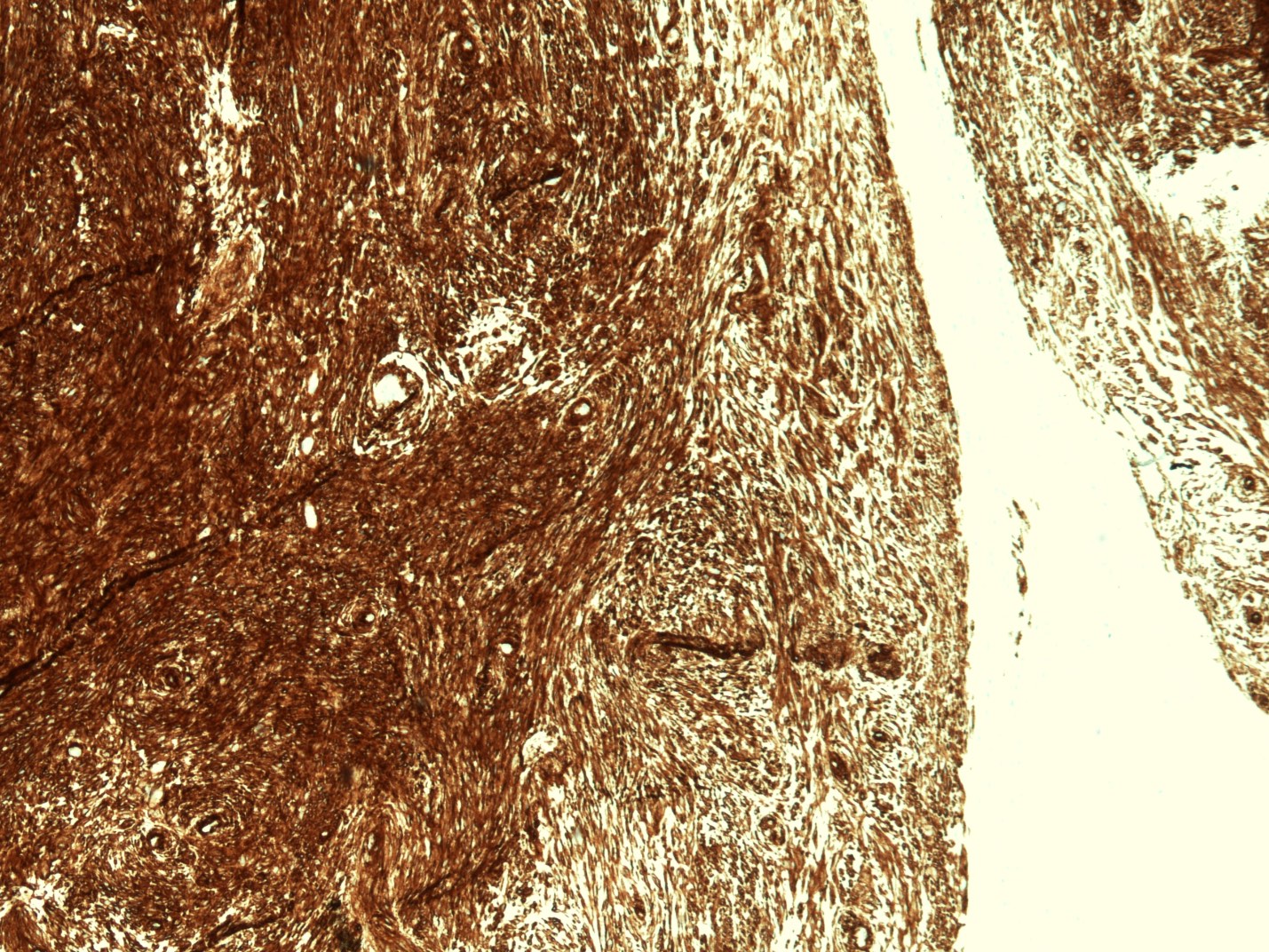
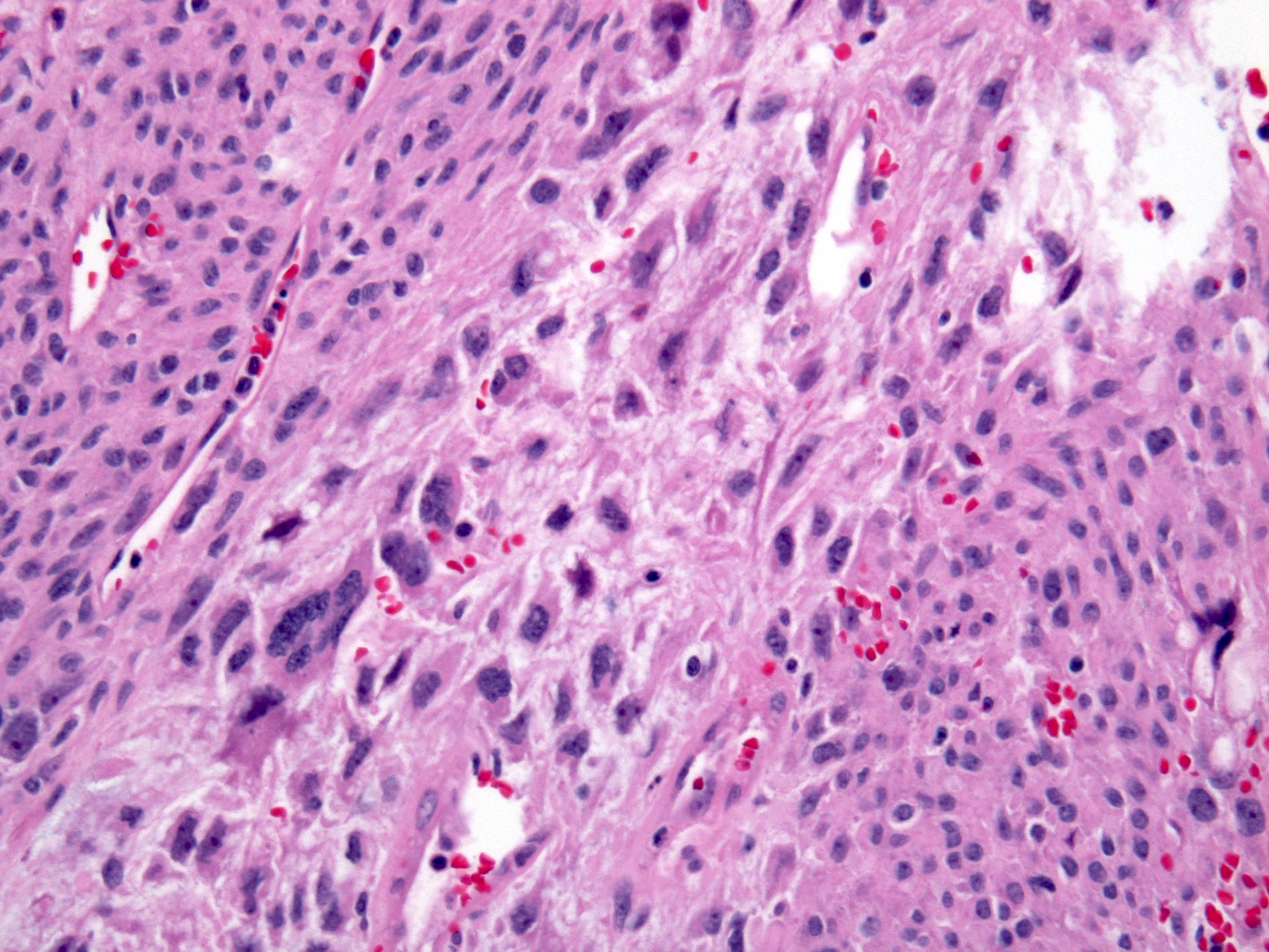
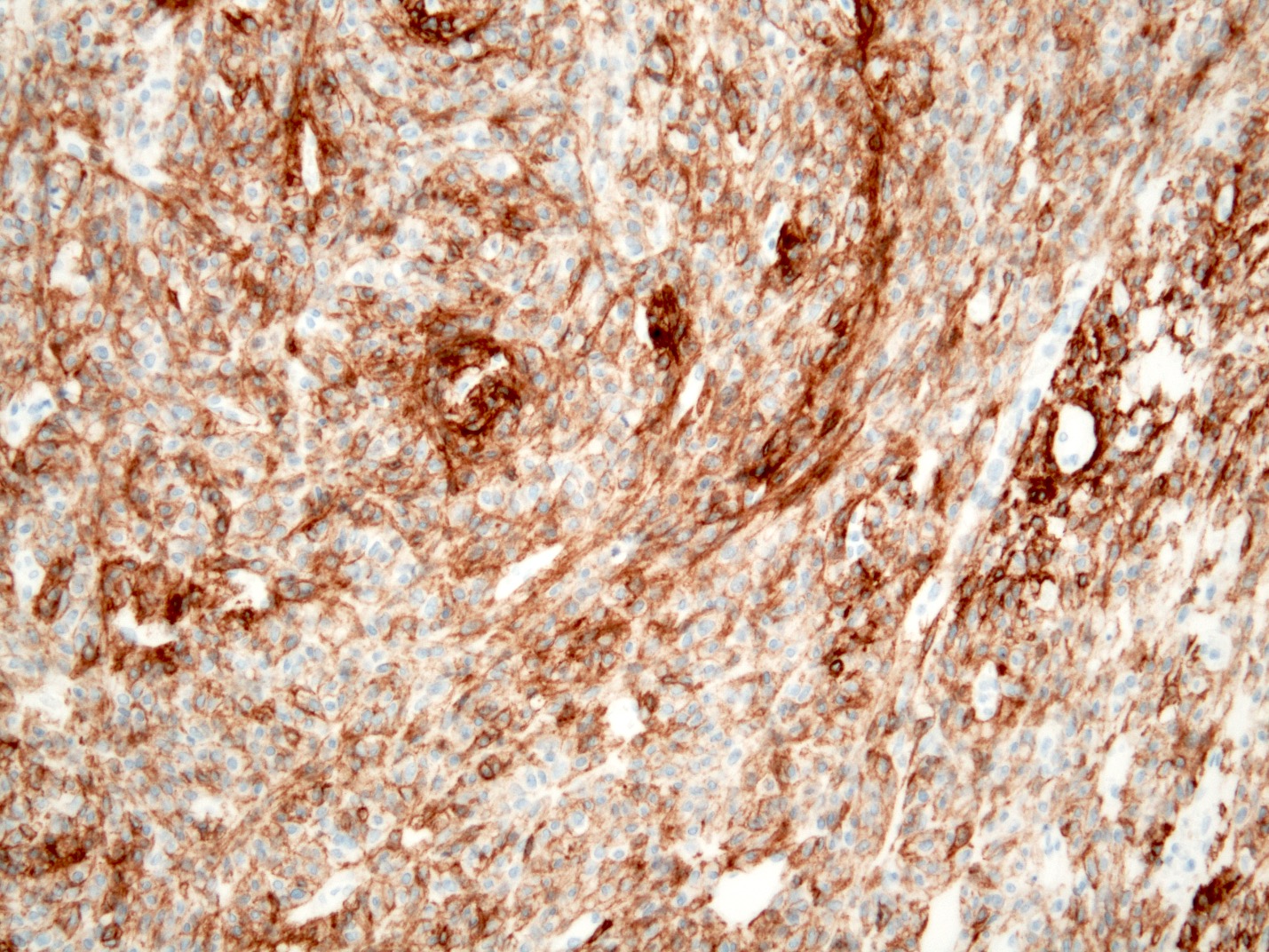
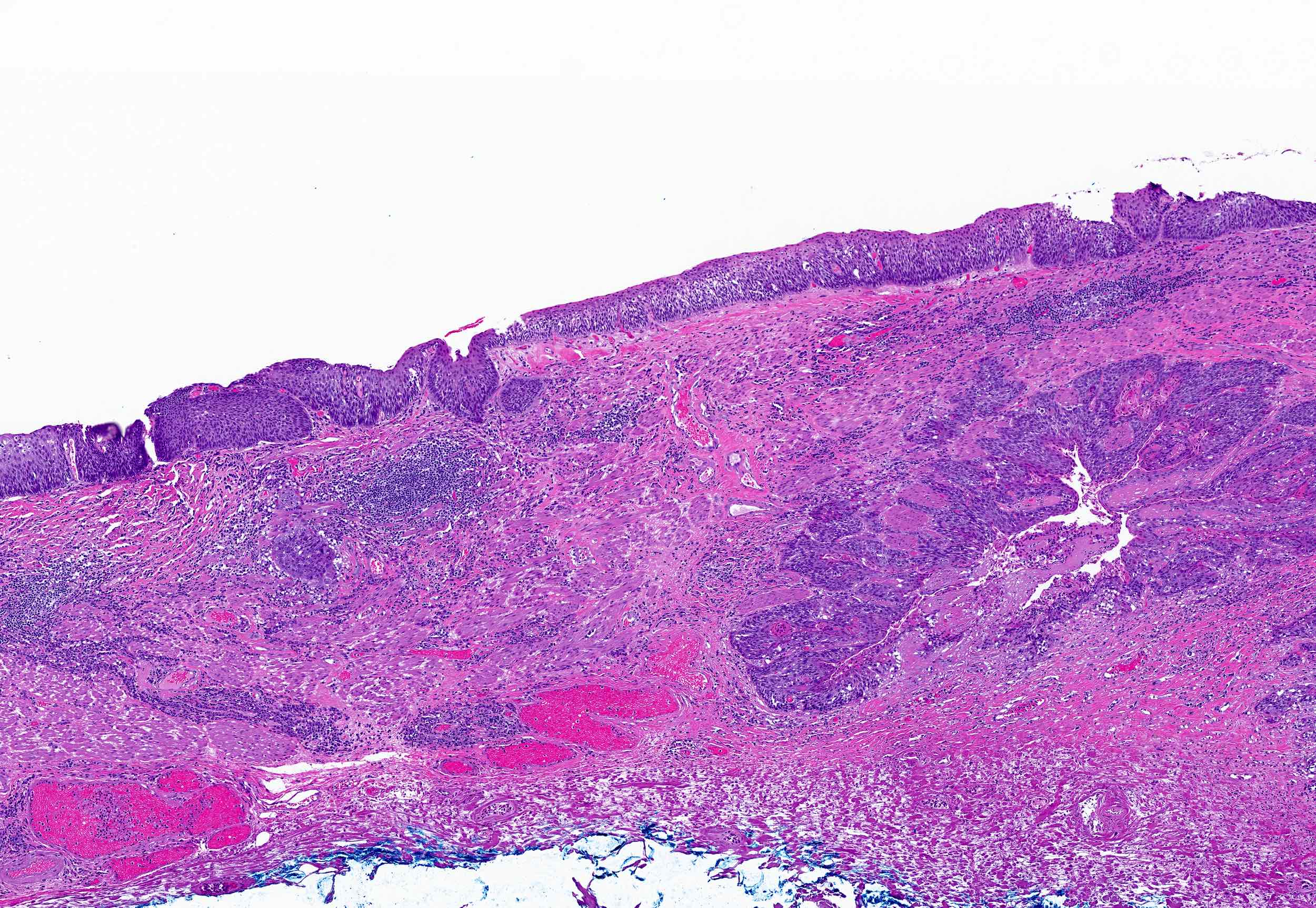
Malignant mesenchymal tumors of the esophagus with variable degrees of differentiation, biologic behavior and prognosis
Examples
Angiosarcoma: high grade malignancy of endothelial cells
Ewing sarcoma: highly malignant small round blue cell tumor characterized by recurrent chromosomal translocations [t(11;22) EWSR1-FLI1 or t(21;22) EWSR1-ERG] and membranous MIC2 / CD99 overexpression
Fibrosarcoma: spindle cell neoplasm of low grade to intermediate grade malignancy
Gastrointestinal stromal tumor (GIST): mesenchymal tumor of digestive tract, likely originating from multipotential progenitors of interstitial cells of Cajal
Hemangiopericytoma (solitary fibrous tumor): ubiquitous mesenchymal tumor showing uncertain line of differentiation (not true microvascular pericytes)
Kaposi sarcoma: uncommon, low grade, vascular malignancy caused by Kaposi sarcoma herpesvirus / human herpesvirus 8 (KSHV / HHV8) infection
GIST: mutually exclusive mutations of activating KIT (95%) or platelet derived growth factor alpha (PDGFRA) receptor tyrosine kinase (5%)
Kaposi sarcoma:HHV8 detected by PCR
Leiomyosarcoma: no consistent genetic events reported
Well differentiated liposarcoma: giant marker or supernumerary ring chromosomes with amplification of 12q12-15 region, including MDM2, CDK4 and other genes
However, it can affect the entire length of the esophagus
Pathophysiology
Unknown
Can result from ischemia or a direct insult to the esophageal mucosa caused by chemical, thermal, physical or immunological mechanisms (Gastroenterology Res 2016;9:108)
Etiology
Mostly idiopathic
Consumption of hot beverages and exposure to chemical irritants
Malignancy
Esophageal trauma
Use of medications such as bisphosphonates, nonsteroidal anti-inflammatory drugs, psychoactive medications (e.g., SSRIs or SNRIs), methotrexate and potassium chloride
Presence of celiac disease, collagen disorders and autoimmune bullous dermatoses (Cureus 2023;15:e43549)
Associated with different autoimmune conditions such as celiac disease, lupus, pemphigus vulgaris, bullous pemphigoid and Stevens-Johnson syndrome (Am J Surg Pathol 2009;33:1789)
Diagnosis
Upper gastrointestinal endoscopy (i.e., EGD) which shows the characteristic appearance of sloughed mucosal fragments, along with a biopsy to confirm the diagnosis and rule out other possible conditions
Meeting 3 of the following endoscopic criteria is consistent with esophagitis dissecans superficialis (EDS) (Ulster Med J 2020;89:39)
Strip(s) of sloughed esophageal mucosa > 2 cm in length
Normal underlying esophageal mucosa
Lack of ulcerations or friability of immediately adjacent esophageal mucosa
Laboratory
Not relevant to this topic
Radiology description
Sloughed out mucosal strips highlighted by barium can be seen on the barium esophagram in few cases (Abdom Radiol (NY) 2021;46:5050)
50 year old man with a past medical history of HIV was hospitalized due to a 3 week course of oropharyngeal dysphagia (Case Rep Infect Dis 2019;2019:4616937)
65 year old woman presented with nausea, vomiting, odynophagia and throat pain after ingesting a colored hair dye (Clin Pract 2021;11:185)
81 year old woman with unintentional weight loss of 8 pounds (Cureus 2023;15:e44372)
Treatment
No standard treatment is available as the condition is self limiting
Treatment is often decided based on the severity of symptoms
Proton pump inhibitors are commonly used, although their primary outcome seems to involve minimizing additional injuries, rather than addressing the root cause (Ann N Y Acad Sci 2016;1380:178)
Morphologic features concerning for esophagitis dissecans superficialis / sloughing esophagitis (see comment)
Negative for intramucosal eosinophilia, dysplasia or malignancy
Comment: The etiology is usually unknown but condition has been associated with some medications, bullous dermatoses, motility disorders, physical / thermal injury and autoimmune diseases.
Erosive esophagitis pattern of injury with acute inflammation, intraepithelial neutrophilic abscesses and epithelial edema most prominent in the superficial epithelial layers on microscopy
Basal zone hyperplasia, parakeratosis and hyperkeratosis are frequently associated
Which histologic feature is commonly seen in esophagitis dissecans superficialis (EDS)?
Dual tone appearance of esophagus
More than 20 eosinophils per high powered field
Prominent granular layer with orthokeratosis
Psuedohyphae and yeast forms
Board review style answer #1
A. Dual tone appearance of esophagus is a common histological finding for EDS. Answer D is incorrect because fungal elements (pseudohyphae and yeast forms) are seen in esophageal candidiasis. Answer B is incorrect because increased eosinophils are usually seen with eosinophilic esophagitis. Answer C is incorrect because a prominent granular layer with orthokeratosis is seen in epidermoid metaplasia.
The image above is from an esophageal biopsy in a 46 year old man with dysphagia. Endoscopy of the esophagus shows strips of sloughed esophageal mucosa. Which of the following would be a possible etiology for these endoscopic findings?
Allergic contact dermatitis
Chemical exposure
Immunosuppression
Use of proton pump inhibitors
Board review style answer #2
B. Chemical exposure can be a causative factor for esophagitis dissecans superficialis (EDS). Answer C is incorrect because immunosuppression can predispose to cause esophageal candidiasis. Answer A is incorrect because allergic dermatitis can be associated with eosinophilic esophagitis. Answer D is incorrect because proton pump inhibitors are commonly used in the treatment of EDS and do not contribute to cause EDS.
Superficial strips of squamous mucosa peel off into the esophageal lumen with normal underlying mucosa
Tends to resolve without sequelae
Essential features
Characteristic endoscopic finding of long, vertical white strips of peeling epithelium with normal underlying mucosa
Constellation of nonspecific histologic findings
Splitting of the squamous epithelium at different levels above the basal layer
Variably sized cysts and bullae
Thick layer of parakeratosis
Basal cell hyperplasia
Focal or minimal inflammation
Terminology
Also called "sloughing esophagitis"
Epidemiology
More common in older individuals (median age in the seventh decade)
Etiology
Unknown
Has been variably associated with certain medications (NSAIDs, bisphosphonates), polypharmacy, prior trauma, underlying motility disorders, heavy smoking, alcohol, hot beverages, immunosuppression, celiac disease, concurrent bullous skin conditions and impaired mobility
Clinical features
Range from asymptomatic to dramatic
Original reports described patients vomiting up casts of esophageal epithelium
Esophageal symptoms such as dysphagia, odynophagia and reflux more common
Can be an incidental finding
Diagnosis
Characteristic endoscopic findings of peeling, white, vertical strips of epithelium > 2 cm long
Normal underlying mucosa
Lack of ulcerations or friability of adjacent mucosa
Biopsy may not be needed unless to rule out other conditions
Case reports
40 year old Hispanic woman with bullous systemic lupus erythematosus associated with esophagitis dissecans superficialis (Case Rep Rheumatol 2015;2015:930683)
67 year old man with unusual appearing esophagus on endoscopy (Case #420)
68 year old man with fungal esophagitis presenting with esophagitis dissecans superficialis (Gastroenterology Res 2016;9:108)
Treatment
Typically proton pump inhibitor therapy and discontinuation of medications that may have triggered the condition
Clinical images
Images hosted on other servers:
Sloughing of large esophageal mucosa fragments
Endoscopy showing EDS
Vertical fissures in
distal esophagus with
sloughing of mucosa
Microscopic (histologic) description
Splitting of the squamous epithelium at different levels above the basal layer
Variably sized cysts and bullae (termed "intraepithelial cystic degeneration" by Hart et al., Dig Dis Sci 2015;60:2049)
Thick layer of parakeratosis that separates off into necrotic fragments
"Two tone" appearance to epithelium
Basal cell hyperplasia
Fungal or bacterial colonies can be associated with the loose fragments
Inflammation is typically minimal or focal (despite "esophagitis" being in the name)
Microscopic (histologic) images
Contributed by Raul S. Gonzalez, M.D. and @Rasamh86 on Twitter
Very rare in esophagus: < 1% of all GIST arise in esophagus (0.7%); they most frequently arise in stomach (60.3%), followed by small intestine (33.2%), rectum (3.1%) and colon (2.9%) (Mod Pathol 2022;35:554)
GISTs arise from interstitial cells of Cajal (ICC)
Driver event involves gain of function mutations in KIT and PDGFRA most frequently
Most of these tumors respond to the tyrosine kinase inhibitor, imatinib
Less frequently, a BRAF V600E mutant is involved as the driving force and these cases are less responsive to imatinib
Etv1, a major transcriptional regulator of ICC - intramuscular and ICC - myenteric, induces BRAF expression in a mouse model
Smooth muscle cells have recently been proposed as an alternative cell of origin for GIST, and these tumors are BRAF V600E driven and resistant to imatinib (J Pathol 2020;252:441)
Etiology
Mostly sporadic
5% of GISTs arise in patients with:
Neurofibromatosis type I syndrome (NF1, multiple small intestinal tumors)
May be an incidental finding during imaging or endoscopic examination for other clinical symptoms
Endoscopy shows as a subepithelial lesion; both leiomyoma and GIST appear similar on CT and EUS (J Thorac Dis 2015;7:E648)
Biopsy with immunohistochemical stains / molecular required for confirmation
Radiology description
Barium studies: smooth intraluminal mass or large ulcerative mass extending intraluminally (see radiology image 1)
Endoscopic ultrasound determines size, shape and intratumoral characteristics of the lesion, its relationship to layers of the bowel wall and enables image guided core needle biopsy or fine needle aspiration (J Gastrointestin Liver Dis 2008;17:131) (see clinical image 1)
CT / MRI: useful for preoperative and metastatic evaluation
Neoadjuvant therapy, small molecule tyrosine kinase inhibitors: imatinib mesylate (STI571, Gleevec), sunitinib maleate may be given preoperatively to reduce the size of tumor
Imatinib is considered in patients with high mitotic rates or larger tumor sizes to obtain negative microscopic margins (R0 resection) and to reduce the risk of intraoperative complications, including tumor rupture (Histopathology 2017;71:805) (see radiology image 4)
Clinical images
Images hosted on other servers:
Endoscopy
Gross description
Lobulated, well circumscribed mass with homogenous fleshy cut surfaces (see gross image 1)
Exophytic or intramural, centered within the muscularis propria
Cystic degeneration, hemorrhage, necrosis (more with high grade)
Overlying esophageal mucosa may be ulcerated (see gross image 2)
Spindle cell type: bland spindle cells with eosinophilic cytoplasm in short fascicles or syncytia, elongated nuclei with inconspicuous nucleoli, indistinct cell borders, paranuclear cytoplasmic vacuoles (more common in gastric), stromal lymphocytes and microcystic stromal degeneration (as in schwannoma), minimal collagen, delicate thin walled vessels, stromal hemorrhage
Subtypes: sclerosing, palisaded, vacuolated, diffuse hypercellular, can have sarcomatoid features with significant nuclear atypia and mitotic activity
Epithelioid type: round cells with vesicular chromatin, eosinophilic or clear cytoplasm in nests or sheets, more pleomorphism than spindle type
Subtypes: sclerosing, discohesive, hypercellular, sarcomatous with significant atypia and mitotic activity
Mixed type: combination of cells with both spindle and epithelioid type, may have abrupt transition between the 2 or complex comingling
SDH deficient: epithelioid or mixed with spindle cell component, multinodular, minimal nuclear pleomorphism, occasional atypical mitosis (gastric location strictly, not seen in esophagus)
Dedifferentiated: anaplastic morphology with unusual phenotype such as loss of KIT expression or aberrant expression of markers such as cytokeratin
Stromal skeinoid fibers (< 20%): hyaline or fibrillary brightly eosinophilic PAS+ structures, representing nodular tangles of collagen fibers; more common in small or large bowel GIST (Case Rep Gastroenterol 2014;8:257)
The image above demonstrates an esophageal mass in a 57 year old man. Of the following, which scenario is associated with best prognosis?
3 cm mass and mitosis < 3/5 mm²
4 cm mass and mitosis > 7/5 mm²
6 cm mass and mitosis < 4/5 mm²
6 cm mass and mitosis > 6/5 mm²
9 cm mass and mitosis < 2/5 mm²
Board review style answer #1
A. 3 cm mass and mitosis < 3/5 mm². Size more than 5 cm, mitosis greater than 5 per 5 mm² and site are associated with disease progression in esophageal GIST. Tumor size > 5 cm and mitotic rate > 5/5 mm² are independent risk factors for progression. Esophageal and colonic GIST are more aggressive than gastric GIST. Of the choices above, A is low risk, D is high risk and others have moderate risk of progression (Mod Pathol 2022;35:554).
Succinate dehydrogenase deficient GIST is seen exclusively in which part of the gastrointestinal system?
Colon
Esophagus
Ileum
Stomach
Board review style answer #2
D. Stomach. Succinate dehydrogenase deficient GIST has a female preponderance and seen almost exclusively in stomach (predilection for distal stomach and antrum) (Am J Surg Pathol 2010;34:636).
Giant fibrovascular polyp used to be considered a nonneoplastic polypoid lesion of the esophagus
The majority of giant fibrovascular polyps of the esophagus now appear to represent well differentiated and dedifferentiated liposarcoma, based on the result of MDM2 FISH (fluorescence in situ hybridization) testing (Mod Pathol 2018;31:337)
Ring or marker chromosomes with regional amplification of chromosome 12q13-21 (Hum Pathol 2012;43:293)
Sample pathology report
Esophagus, mass, endoscopic resection:
Well differentiated liposarcoma / giant fibrovascular polyp (see comment)
Resection margin negative for liposarcoma
Comment: The slightly atypical stromal cells are positive for MDM2 and CDK4 by immunohistochemistry with appropriate controls. The results support the above diagnosis.
Glycogenic acanthosis (GA) is a benign hyperplasia of the esophageal squamous epithelium due to accumulation of intracytoplasmic glycogen of unknown etiology
Endoscopically, affected areas display white plaques or nodular areas (usually 2 - 10 mm in diameter), which may be solitary, multiple or coalesced
First described by Rywlin and Ortega in 1970, glycogenic acanthosis of the esophagus is a common benign lesion seen during upper gastrointestinal endoscopy
Characterized histologically by squamous hyperplasia and intracellular glycogen accumulation
Manifestation of PTEN hamartoma tumor syndrome (Cowden syndrome)
Most common in adults with a mean age of 52 years (range: 45 - 79 years)
Common incidental endoscopic finding seen in up to 3.5% of upper endoscopies
Diffuse involvement of the esophagus is associated with PTEN hamartoma tumor syndrome (Cowden syndrome) and highly predictive of PTEN mutation (80 - 90% of patients)
PTEN hamartoma tumor syndrome (Cowden syndrome) is an autosomal dominant multiple hamartoma syndrome with increased risk of malignant tumors (breast, thyroid and endometrial) due to germline mutations in the tumor suppressor gene PTEN on 10q23
Although the etiology of glycogenic acanthosis is unknown, it is strongly associated with PTEN hamartoma tumor syndrome (Cowden) syndrome
Glycogenic acanthosis has also been associated with tuberous sclerosis, hiatal hernia, reflux esophagitis (GERD) and increased age
Rare reports have noted a possible association with eosinophilic esophagitis or celiac disease
Glycogenic acanthosis has not been found to be associated with disorders of glucose metabolism (diabetes) or skin disorders (psoriasis or acanthosis nigricans)
Given an association with GERD, a postinflammatory hypothesis was raised but has not been proven
Prognosis of glycogenic acanthosis with PTEN hamartoma tumor syndrome (Cowden syndrome) is determined by the risk of various malignant tumors (breast, thyroid, kidney, endometrium or colorectal)
No treatment is required as it is a benign condition
Gross description
Endoscopically and grossly, glycogenic acanthosis is described as raised white plaques or nodular areas (typically 2 - 10 mm in diameter), which may be single, multiple or coalesced (Gastrointest Radiol 1984;9:93)
Gross images
AFIP images
Numerous white islands
Slightly elevated longitudinal plaque
Microscopic (histologic) description
Squamous hyperplasia of the esophageal epithelium with intracellular glycogen accumulation
Glycogen is positive for PAS and sensitive to diastase; a combination of PAS and PASD stains may be helpful to confirm the diagnosis (PAS positive intracellular glycogen is removed with PASD stain, which will be negative)
Comment: Glycogenic acanthosis is a benign esophageal lesion that may be associated with PTEN hamartoma tumor (Cowden) syndrome but is also a common finding in upper endoscopies in nonsyndromic patients. Correlation with clinical and endoscopic findings is recommended.
A 56 year old man underwent an esophagogastroduodenoscopy for reflux symptoms. A biopsy was taken of a small, raised white nodule in the esophagus. The histology is depicted in the H&E image shown above. What is the best diagnosis?
Candidal esophagitis
Epidermoid metaplasia
Glycogenic acanthosis
Mucosal calcinosis
Normal esophageal squamous mucosa
Board review style answer #1
C. Glycogenic acanthosis. The H&E image demonstrates accumulation of intracytoplasmic glycogen in the squamous epithelium and the best diagnosis is glycogenic acanthosis (GA). PAS and PASD stains would be helpful to confirm the diagnosis since glycogen is PAS positive and diastase sensitive. Glycogenic acanthosis can be difficult to distinguish from normal esophageal mucosa, particularly if nonlesional tissue is not present. The endoscopic impression of a nodule is helpful and the diagnosis of glycogenic acanthosis would explain the endoscopic findings. Mucosal calcinosis is rare in the esophagus and would have calcium deposition within the epithelium or mucosa. Epidermoid metaplasia can also appear white on endoscopy but is characterized by a granular cell layer within the squamous epithelium resembling skin, hence the term epidermoid.
A 45 year old woman with a history of hamartomatous gastrointestinal polyps undergoes an esophagogastroduodenoscopy. There are diffuse white plaques and nodules in the esophagus. Biopsies are taken of some of the esophageal lesions and demonstrate hyperplastic squamous epithelium with intracytoplasmic accumulation of glycogen consistent with glycogenic acanthosis. What syndrome does this patient likely have?
Lynch syndrome
Maffucci syndrome
Peutz-Jeghers syndrome
PTEN hamartoma tumor syndrome (Cowden syndrome)
Board review style answer #2
D.PTEN hamartoma tumor syndrome (Cowden syndrome). PTEN hamartoma tumor syndrome (PTHS) is an all encompassing term for Cowden, Bannayan-Riley-Ruvalcaba, PTEN related Proteus and PTEN related Proteus-like syndromes. Cowden syndrome (CS) is an autosomal dominant syndrome caused by a germline mutation in the PTEN tumor suppressor gene on chromosome 10. Esophageal glycogenic acanthosis, particularly if diffuse, is a manifestation of Cowden syndrome and is seen in around 80 - 90% of patients. Maffucci syndrome is characterized by multiple enchondromas and hemangiomas. Peutz-Jeghers syndrome (PJS) is a hamartomatous polyposis syndrome of the gastrointestinal tract with increased risk of certain malignancies. PJS is autosomal dominantly inherited and caused by mutations in the STK11 gene. Lynch syndrome is the most common cause of hereditary colorectal cancer and is due to mutations in mismatch repair genes. Patients with Lynch syndrome are also at risk of other types of cancers. None of these, except Cowden syndrome, have glycogenic acanthosis.
59 year old Japanese man with esophageal tumor 7 years after bronchial tumor (APMIS 2006;114:659)
Treatment
Local excision
Gross description
Intramural nodule(s), poorly circumscribed, up to 2 cm
Microscopic (histologic) description
Identical to granular cell tumors elsewhere; sheets or packets of uniform epithelioid cells with abundant eosinophilic granular cytoplasm and small nuclei that interdigitate with overlying epithelium
Often pseudoepitheliomatous hyperplasia, which may mimic squamous cell carcinoma on small biopsies (J Surg Oncol 1980;13:301)
Often involves superficial lamina propria
May extend into muscularis propria
Microscopic (histologic) images
Contributed by Dr. Oleksandr Grygoruk, AFIP and @RaulSGonzalezMD on Twitter
Received in formalin / unfixed / fresh for intraoperative consultation
Confirm procedure as esophagectomy or other
Orientation: identify anatomic structures, only esophagus or esophagus and portion of stomach or other; look for any sutures to identify the margins
Remove the staple line with scissors, as close to the staples as possible
Locate the lesion by gently palpating the luminal surface
Open the specimen longitudinally
Avoid cutting across any palpable lesions
Measure the length and diameter or circumference and wall thickness of the esophagus and attached proximal stomach, if present
Describe the mucosa, look for any areas of ulceration, glandular mucosa (pink or tan, appears different from pale squamous mucosa) strictures and tumors and the narrowing of the lumen caused by these lesions
Note the dimensions of any lesions and their location, with reference to the proximal / distal / deep margins, the squamocolumnar junction (Z line) and the gastroesophageal (GE) junction
This should be measured on the fresh specimen due to retraction following fixation
Z line is the intersection of squamous and glandular mucosa
GE junction is the junction of the tubular esophagus and saccular stomach, irrespective of the types of mucosa present
Proximal displacement of the Z line above the GE junction suggests Barrett esophagus
Describe the external surface and note areas of retraction, induration, perforation by the tumor or any lymph nodes
Photograph lesions (as appropriate)
Ink the proximal, distal and deep (adventitial) margins underneath the tumor, pin the specimen on a board and fix in 10% formalin; if the tumor is large, make longitudinal cuts to aid in fixation
Depth of invasion: after fixation cut through the tumor or ulcer to assess the depth of invasion into the esophageal wall
Location (including relationship to squamocolumnar junction) (see note)
Note: tumors that have their epicenter at the gastroesophageal junction and extend no more than 2 cm into the proximal stomach are staged as esophageal, while tumors with an epicenter more than 2 cm into the proximal stomach are staged as primary gastric carcinoma even if the tumor involves the gastroesophageal junction
Percent of circumference involved
Luminal diameter at the lesional site
Degree of proximal dilatation
Describe uninvolved mucosa:
Normal squamous esophagus: glistening smooth white mucosa
Normal glandular stomach: velvety pink / red mucosa with rugal folds
Barrett (glandular) mucosa: pale pink / salmon, finely granular, may be discontinuous
Adventitial soft tissue / fat should be thoroughly searched and sectioned for lymph nodes
Nodes may be very small and close to the esophageal or gastric outer surfaces
Should arrive in the laboratory in a fresh state, with margins oriented by the endoscopist
Specimen is usually round or oval
Ink base and lateral mucosal margins with different colors
Stretch the specimen gently and fix overnight in 10% formalin on a rigid board, with mucosal surface up
After fixation the specimens should be serially sectioned at 2 - 3 mm intervals parallel to the long axis (not < 2 mm)
Sections to obtain
Submit tumor: 1 section per centimeter, including maximal depth of invasion and relation to proximal / distal margins
Longitudinal sections preferred
If no gross tumor present (which is often the case after neoadjuvant therapy of the GE junction tumors), then the entire ulcerated / fibrotic area should be blocked off and submitted
Margins: en face sections of proximal / distal margins unless tumor is < 2 cm from the margin then margin can be best demonstrated in perpendicular sections
Esophagus and stomach: representative sections of uninvolved areas
Other gross lesions (including Barrett esophagus): representative sections
If no gross tumor present (which is often the case after neoadjuvant therapy of the GE junction tumors), then the entire ulcerated / fibrotic area should be blocked off and submitted
Examine the specimen for Barrett mucosa, presenting as salmon / pink, granular mucosa (similar to gastric mucosa) above the GE junction, replacing the glistening white squamous mucosa
Tumors that have their epicenter at the gastroesophageal junction and extend no more than 2 cm into the proximal stomach are staged as esophageal, while tumors with an epicenter more than 2 cm into the proximal stomach are staged as primary gastric carcinoma even if the tumor involves the gastroesophageal junction (Amin: AJCC Cancer Staging Manual, 8th Edition, 2017)
15 lymph nodes are recommended for esophageal or GE junction cancer; however, if not found submit entire adventitial tissue for lymph nodes (Ann Surg Oncol 2020;27:1227)
For EMR, immediate pinning and fixing of the specimen helps preserve the size, shape and orientation of the lesion
Portions of esophagus are usually resected to remove neoplasms and less frequently strictures
After checking the history, indication for the procedure and most recent endoscopic findings, proceed as below
Gross images
Images hosted on other servers:
Esophagectomy with proximal portion of stomach
Esophagectomy specimen status posttreatment
Esophageal endoscopic mucosal resection
Sample gross description report
The specimen designated esophagus is received fresh in a container labeled with the patient's name and medical record number and consists of an esophagectomy and partial gastrectomy, including esophagus (20.0 cm length x 3.5 cm circumference) with attached proximal stomach (4.0 cm length x 10.0 cm circumference). There is a tan-pink, firm, fungating mass (2.5 x 2.0 cm), which invades through the muscularis propria into the adjacent soft tissue. The tumor is 15.0 cm from the proximal resection margin, 2.5 cm from the gastroesophageal junction, 6.5 cm from the distal resection margin and 0.2 cm from the deep resection margin (inked in black). The adjacent esophageal mucosa is tan-pink and finely granular from the gastroesophageal junction, up to within 10.0 cm of the proximal margin. The remainder of the mucosal surfaces are unremarkable. The attached soft tissue contains four palpable lymph nodes (range 0.3 - 0.5 cm). Gross photographs are taken. Section code:
Cassette 1: proximal resection margin, en face
Cassette 2: distal resection margin, en face
Cassettes 3 - 4: tumor with deepest extent of invasion and deep margin, longitudinal
Cassette 5: tumor with adjacent esophageal mucosa, longitudinal, representative
Cassette 6: tumor with adjacent gastric mucosa, longitudinal
Other features (esophagitis, Barrett esophagus, dysplasia, specific types of infection)
Board review style question #1
For esophageal or gastroesophageal junction cancers, what is the number of lymph nodes recommended for pathological evaluation?
At least 5
At least 5 - 10
Not less than 15
No number is required but entire adventitia should be submitted
Board review style answer #1
C. The current evidence supports the goal of obtaining at least 15 lymph nodes for pathological evaluation in both primary esophagectomy and postinduction therapy cases. Earlier, no number was required for esophageal or gastroesophageal cancer. If no lymph node is found, the entire adventitia should submitted (Ann Surg Oncol 2020;27:1227).
Heterotopic / ectopic sebaceous glands in the esophagus
Essential features
Incidentally found, small (3 - 4 mm) yellowish plaques with granular or lobulated appearance; the number of lesions varies from single to more than 100
Mature sebaceous gland with excretory duct within the lamina propria of the esophagus
Asymptomatic and benign; no need for treatment
Terminology
Ectopic sebaceous gland
Heterotopic sebaceous gland
ICD coding
ICD-10: K22.8 - other specified diseases of esophagus
Whether heterotopic / ectopic sebaceous glands in the esophagus are the result of congenital anomaly or metaplastic change of squamous epithelium remains unknown (Pathol Int 1999;49:364)
Since the esophagus is of endodermal origin, while sebaceous glands are of ectodermal origin, metaplastic change of squamous epithelium is suspected
Congenital abnormality resulting from an incomplete embryonic esophageal epithelization process (the embryonic esophagus lined by columnar epithelium undergoes gradual replacement of columnar epithelium with squamous epithelium starting from the middle of the esophagus with vertical extension in both directions)
Etiology
No known etiologic factors to cause above mentioned embryonic abnormality
Clinical features
Can be seen in both genders at all ages (no significant difference)
44 year old woman with chronic dysphagia and globus sensation due to multiple inlet patches underwent esophageal dilation and proton pump inhibitor therapy, resulting in a resolution of her symptoms (Cureus 2023;15:e33459)
52 year old man with dysphagia caused by Helicobacter pylori associated inlet patch ulcer (ACG Case Rep J 2020;7:e00405)
65 year old man with alpha fetoprotein (AFP) producing esophageal carcinoma arising from ectopic gastric mucosa in the cervical esophagus (J Gastrointestin Liver Dis 2017;26:193)
Treatment
No treatment for asymptomatic patients
Eradication of H. pylori if positive for H. pylori in heterotopic gastric mucosa
Cytological and structural atypia with invasive growth
Board review style question #1
Which of the following statements regarding the histologic features of heterotopic gastric mucosa of the esophagus is true?
Characterized by the presence of gastric type mucosa with intestinal metaplasia
Double muscularis mucosae is one of the characteristic findings
Most often contains oxyntic type gastric glands
Usually associated with significant inflammation
Board review style answer #1
C. Most often contains oxyntic type gastric glands. Heterotopic gastric mucosa is most often composed of an admixture of oxyntic type gastric glands and mucous glands. Intestinal metaplasia, significant inflammation and double muscularis mucosae are not common findings of heterotopic gastric mucosa.
Which of the following statements about heterotopic gastric mucosa of the esophagus is true?
Often associated with Barrett esophagus
Patients often present with dysphagia
Rare cases of adenocarcinoma arising from heterotopic gastric mucosa have been reported
Surrounding background mucosa should be examined carefully due to possible association with squamous cell carcinoma or squamous dysplasia
Board review style answer #2
C. Rare cases of adenocarcinoma arising from heterotopic gastric mucosa have been reported. Adenocarcinoma arising from heterotopic gastric mucosa is extremely rare but rare cases of adenocarcinoma arising from heterotopic gastric mucosa have been reported. Association with Barrett esophagus is controversial. No association with squamous cell carcinoma or squamous dysplasia. Most patients are asymptomatic.
Esophagus is a muscular tube that extends from the pharynx to the gastroesophageal junction; it has typical gastrointestinal (GI) tract layering (mucosa, submucosa, muscularis propria / externa, adventitia) around a central lumen as well as 2 muscular sphincters (upper and lower)
Essential features
Esophageal tissue is arranged in 4 concentric layers following typical GI layering: mucosa, submucosa, muscularis propria / externa, adventitia
Mucosa lines the lumen of the esophagus and is comprised of epithelium (nonkeratinized stratified squamous), lamina propria, muscularis mucosae
Submucosa lies just deep to the mucosa and is comprised of connective tissue, nerves, Meissner plexus, lymph and blood vessels, and submucosal glands
Muscularis propria / externa is composed 2 concentric layers of muscle cells; these muscle cells are a variable mixture of skeletal and smooth muscle with a greater proportion of skeletal muscle at the proximal end of the esophagus transitioning to solely smooth muscle at the distal end
Esophagus is primarily retroperitoneal and is covered in a connective tissue adventitia and fascia
Physiology
Esophagus is a muscular tube that extends from the oral cavity / pharynx to the stomach; in an adult it is ~25 cm in length (Richter: The Esophagus, 5th Edition, 2012)
Esophagus has cervical, thoracic and abdominal portions; it transitions from the cervical to thoracic region at the suprasternal notch and then passes from the thorax to the abdomen through the diaphragmatic hiatus
In axial cross section, esophagus is located posterior to the trachea and anterior to the vertebral column
Embryologically, esophagus develops from foregut at ~10 weeks; upper esophagus is derived from branchial arches 4 - 6
Arterial blood supply of the esophagus is generally arranged in segments with the inferior thyroid artery supplying the upper esophageal sphincter and cervical esophagus, the aortic esophageal arteries supplying the thoracic esophagus and the left gastric artery and a branch of the left phrenic artery supplying the distal esophagus and lower esophageal sphincter
Esophageal infarction is rare due to the abundant blood supply
Parasympathetic and sympathetic innervation of the esophagus is via the vagus and spinal nerves (sympathetic chain) (J Clin Gastroenterol 2008;42:610)
Auerbach plexus (that lies between the longitudinal and circular layers of the muscularis propria) regulates contraction of the outer muscular layers of the esophagus
Meissner plexus (submucosa) regulates contraction of the muscularis mucosae as well as glandular secretion
Gastroesophageal reflux disease (GERD) can cause chronic esophageal irritation that induces epithelial metaplasia (i.e., Barrett esophagus); this induces an epithelial replacement of cells from the normal stratified squamous to intestinal columnar epithelium with goblet cells (Gastrointest Endosc 2017;85:889)
Laboratory
Biopsy is performed via endoscopy for evaluation of esophageal tissue; diagnostic accuracy is high for identification of malignant versus infectious diseases, as well as in evaluation for dysplasia (Gastrointest Endosc Clin N Am 2000;10:713)
Radiology images
Images hosted on other servers:
Micro CT of human esophagus
Gross description
Esophagus is a muscular tube that extends from the oral cavity / pharynx to the stomach; in an adult, it is ~25 cm in length (Richter: The Esophagus, 5th Edition, 2012)
Esophagus has typical GI layering: mucosa, submucosa, muscularis propria / externa, adventitia
2 muscular sphincters are present: upper and lower esophageal sphincters
Primarily retroperitoneal and is therefore covered in a connective tissue adventitia and fascia
In axial cross section, esophagus is located posterior to trachea and anterior to the vertebral column
Gross images
Images hosted on other servers:
Human cadaveric esophagus
Microscopic (histologic) description
Esophagus is arranged in 4 concentric layers following a typical GI layering scheme; listed from the lumen outward, these layers are mucosa, submucosa, muscularis propria / externa, adventitia
Innermost layer of the esophageal mucosa, lining the lumen
Other cells present: melanocytes, endocrine cells, Langerhans cells, Merkel cells, T cells
Basement membrane separates the epithelium from the underlying lamina propria
Basal layer: < 15% of the mucosal thickness, usually 2 - 3 cells thick, comprised of basophilic proliferative cells with minimal cytoplasm, mitotic figures are found only here (under normal conditions) (Richter: The Esophagus, 5th Edition, 2012)
Intermediate layer: these glycogen rich squamous cells have more cytoplasm than those of the basal layer (i.e., decreased N:C ratio)
Superficial layer: cells appear more flattened as they mature and approach the lumen, many cells are anucleate
Lamina propria: composed of loose fibrovascular connective tissue
Situated between the epithelium and muscularis mucosae
May resemble muscularis propria / externa which is important for accurate American Joint Committee on Cancer (AJCC) staging of adenocarcinoma in this region (J Thorac Dis 2014;6:S289)
Submucosal glands are comprised of mucinous cells surrounding a central lumen that produce acid mucin and empty into the esophagus via squamous lined ducts
Composed of striated skeletal muscle in the proximal third of the esophagus, smooth muscle in the distal third and a mixture of both skeletal and smooth muscle in the middle third
Inner layer is oriented circumferentially while the outer layer is oriented longitudinally; this allows for both segmental contraction and peristalsis
Myenteric plexuses (nerves and ganglia) are found between the inner and outer layer
Adventitia: composed of loose irregular connective tissue
Esophagus is primarily retroperitoneal and the majority is surrounded by fascia
Microscopic (histologic) images
Contributed by Nicole Stringham, Ph.D. (sources: University of Michigan virtual slide box and Duke University virtual slide collection) and AFIP
GI layering, middle third
Epithelium and lamina propria
Mucosal lymph nodule, submucosal gland
Muscularis externa
Myenteric plexus
Lower third
Smooth and skeletal muscle
Virtual slides
Images hosted on other servers:
Esophageal layering, full thickness
Gastroesophageal junction
Cytology description
Esophageal brushing specimens are usually composed of mature superficial type and intermediate type squamous cells with abundant cytoplasm and small round, regular nuclei
Superficial type nuclei are dense and pyknotic; intermediate type contain finely granular chromatin and inconspicuous nucleoli
Cells present as loosely cohesive aggregates, individual cells, large sheets
Cytoarchitecture of the muscularis mucosae and distribution of lymphatic vessels varies between regions of the esophagus (i.e., cervical, thoracic, abdominal); this may affect esophageal cancer infiltration and lymph node metastasis (Esophagus 2019;16:44)
Which of the following cell types comprise the innermost lumen lining layer of a normal esophagus?
Columnar epithelium with goblet cells
Keratinized stratified squamous epithelium
Low columnar epithelium
Nonkeratinized stratified squamous epithelium
Simple columnar epithelium
Board review style answer #1
D. Nonkeratinized stratified squamous epithelium. The innermost layer of the esophageal mucosa, lining the lumen, is made up of nonkeratinized stratified squamous epithelium. Answer A is incorrect because columnar epithelium is normally found in the small intestine but can be found in the esophagus in cases of dysplasia (Barrett esophagus). Answer B is incorrect because keratinized epithelium is generally associated with skin (epithelium on outward facing surfaces of the body). Answer C is incorrect because low columnar epithelium is a type of simple columnar epithelium and is typical of the stomach and intestines, not the esophagus. Answer E is incorrect because simple columnar epithelium is usually found in other areas of the gastrointestinal (GI) tract.
The image shown above is in need of evaluation. Features that are present, both in the image and in subjacent areas include gastrointestinal (GI) layering, Auerbach plexus, submucosal glands and 2 distinct layers of muscularis propria made of smooth and skeletal muscle. What is the anatomical origin of this sample?
Anus
Duodenum
Large intestine
Pylorus
Upper esophagus
Board review style answer #2
E. Upper esophagus. The upper esophagus is the only listed option that has nonkeratinized stratified squamous epithelium (shown in the image) in addition to all of the other listed features. Answer A is incorrect because the anus does not have submucosal glands. Answer B is incorrect because although the duodenum has many of these features, including submucosal glands, it does not have skeletal muscle and is lined by simple columnar (enterocytes) and goblet epithelial cells. Answer C is incorrect because the large intestine is lined by enterocytes with goblet cells and has mucosal rather than submucosal glands. Answer D is incorrect because the pylorus does not have 2 layered muscularized propria with skeletal muscle and the epithelium is simple columnar, not squamous.
Infectious esophagitis is the second most common cause of esophagitis after gastroesophageal reflux disease (GERD) (Gastroenterol Hepatol (N Y) 2013;9:517)
The most common causes of infectious esophagitis are Candida (88%), herpes simplex virus (10%) and cytomegalovirus (2%)
More commonly occurs after reactivation of latent HSV with spread of virus to the esophageal mucosa by way of the vagus nerve or by direct extension of oral - pharyngeal infection into the esophagus (Prz Gastroenterol 2013;8:333)
Can have coexistent herpes labialis, glossitis or oropharyngeal ulcers
May be associated with various opportunistic diseases, such as candidiasis, CMV and Kaposi sarcoma
Endoscopic findings include multiple discrete or coalescent small ulcers, which may be superficial, punched out or volcano-like in appearance (Case Rep Gastrointest Med 2016;2016:7603484)
Viral cytopathic changes are similar to HSV, but it is often pronounced in peripapillary epithelium as compared to superficial epithelium in HSV esophagitis
Esophageal ulcers are more hemorrhagic and less inflammatory as compared to HSV
Clinically, patients often have the cutaneous manifestations of chicken pox or shingles
A patient who underwent liver transplantation had a recent episode of Candida esophagitis treated with fluconazole. Symptoms of pain and dysphagia persisted and repeat endoscopy showed multiple sharply demarcated and superficial ulcers ranging from 2 mm to 2 cm. What is the biopsy diagnosis?
Cytomegalovirus (CMV) esophagitis
Herpes simplex virus (HSV) esophagitis
Nonspecific ulcer
Recurrent or persistent Candida esophagitis
Board review style answer #1
B. HSV esophagitis. The latter image shows the classic histologic findings of herpes esophagitis, including molding of nuclei, margination of nuclear chromatin and multinucleation. CMV infected cells are large and show distinctive intranuclear inclusions in mesenchymal cells. Candida esophagitis shows pseudohyphae or budding spores.
A 63 year old woman presented with dysphagia and esophageal ulcers. The image above shows a section stained with a polyclonal antibody to herpes simplex virus type 1 (HSV1). Which of the following statements about HSV immunohistochemistry is true?
Immunohistochemistry is more sensitive and specific than in situ hybridization for HSV1 and HSV2
The section is likely to react with anti-HSV2 antibody because of cross reactivity
The section is likely to stain positively with an anti-HSV2 antibody because a combined HSV1 and HSV2 infection is common
The section is not likely to stain with an anti-HSV2 antibody because a combined infection with HSV1 and HSV2 is uncommon
Board review style answer #2
B. The section is likely to react with anti-HSV2 antibody because of cross reactivity. Immunohistochemistry of HSV is useful when histology is equivocal. Most antibodies stain both HSV1 and HSV2 precluding reliable identification of the specific HSV. In situ hybridization allows the distinction of HSV1 and HSV2 but is more labor intensive. HSV antibodies may weakly cross react with varicella zoster virus (VZV) but this is usually not a problem.
Circumscribed, mural, solitary mass, 2 - 5 cm (surgical specimens), bulges into lumen, may be polypoid
Pinkish gray white with whorled cut surface; mucosal surface is only rarely ulcerated
Gross images
AFIP images
Bulging, white, whorled cut surface
Images hosted on other servers:
Submucosal tumor
With squamous cell carcinoma
Microscopic (histologic) description
Similar to classic endometrial leiomyoma; circumscribed lesion of circular muscularis propria or muscularis mucosae composed of intersecting fascicles of bland spindle cells with abundant cytoplasm
Variable fibrosis in center of large leiomyomas
Occasional calcification; no / rare mitotic figures; no atypia, no cellular foci
GIST: very rare; solid, myxoid and perivascular patterns; more cellular by H&E and cytology, CD117+, CD34+, variable desmin and actin immunoreactivity (Am J Surg Pathol 2000;24:211)
Predisposing factors for oral lichen planus include medications such as antimalarial drugs, NSAIDs, antihypertensive agents and dental materials such as amalgam
Etiology
Lichen planus
Infections (especially HIV and viral hepatitis)
Upper tract Crohn's disease
Medications: nivolumab and other checkpoint inhibitors, antimalarial drugs, gold, NSAIDs and thiazides (ACG Case Rep J 2017;4:e57)
Mucosa physically damaged by nearby pill esophagitis
Rheumatologic disorders
Clinical features
Rheumatologic diseases more common in patients with lichen planus esophagitis (24%) versus lichenoid esophagitis pattern (11%) (Am J Surg Pathol 2013;37:1889)
Viral hepatitides and human immunodeficiency virus (HIV) infections are associated with lichenoid esophagitis pattern (Am J Surg Pathol 2013;37:1889)
Stricture: risk of stricture formation is higher in patients with lichen planus esophagitis (38%) versus lichenoid esophagitis pattern (9%) (Am J Surg Pathol 2013;37:1889)
Case reports
63 year old woman with dysphagia and areas of friable mucosa and stricture at the upper / mid esophagus (World J Gastroenterol 2013;19:1652)
69 year old woman with dysphagia and odynophagia; endoscopy revealed severe strictures and web-like areas in esophagus (World J Gastroenterol 2013;19:2278)
White plaques or streaks are present, mimicking candidiasis or glycogenic acanthosis
In addition, it may cause ulceration in mid or proximal esophagus
Strictures can also be present
Microscopic (histologic) description
Prominent band-like lymphocytic infiltrate involving the interface of basal epithelium and lamina propria (this feature cannot be evaluated in biopsies lacking lamina propria) (Am J Surg Pathol 2013;37:1889)
Intraepithelial lymphocytosis
Dyskeratotic keratinocytes (Civatte bodies)
Acanthosis
Junctional split seen at the junction of the epithelium and lamina propria (unlike sloughing esophagitis)
Microscopic (histologic) images
Contributed by David Matthew Saulino, D.O. and David Hernandez Gonzalo, M.D.
Lymphocytes and dyskeratosis
Civatte bodies
Immunofluorescence description
Negative in lichenoid esophagitis pattern
In lichen planus esophagitis, globular IgM deposits at the junction of the squamous epithelium and lamina propria as well as complement staining in apoptotic keratinocytes
Positive stains
Predominance of T lymphocytes (CD3) in the epithelium and lamina propria with scattered CD20 positive B lymphocytes
Esophageal squamous mucosa with lichenoid esophagitis pattern of injury (see comment)
Comment: The biopsy demonstrates a prominent band-like lymphocytic infiltrate involving the interface of lamina propria and epithelium, intraepithelial lymphocytes and dyskeratotic keratinocytes. Unfortunately, this pattern of injury is not entirely specific and can be seen as an esophageal manifestation of lichen planus, viral infections (particularly HIV and viral hepatitis), Crohn's disease, medications (NSAIDs, antihypertensive agents, antimalarial drugs) or pill esophagitis. Correlation with the clinical findings (in particular with cutaneous, oral or genital lesions) is suggested. If lichen planus is a consideration, additional biopsies with fresh tissue for immunofluorescence studies are worth performing. No fungal organisms were identified on the GMS stain. There is no dysplasia.
Lymphocytes tend to have a peripapillary distribution while in lichenoid esophagitis pattern prominent band-like lymphocytic infiltrate involves the interface of basal epithelium and lamina propria
In biopsies lacking lamina propria it is a challenge to assess the distribution of lymphocytes
Intraepithelial split while in lichenoid esophagitis pattern split is at the junction of the epithelium and lamina propria
Inflammation not prominent
Isolated esophageal mucous membrane pemphigoid:
Positive immunofluorescence with linear deposits of IgG
Serum anti BP230 or BP180 antibodies
Treatment requires systemic immunosuppression and may be worsened by repeated dilations alone; should be considered in patients with unexplained dysphagia accompanied by mucosal sloughing, strictures and ulcerations (Am J Gastroenterol 2019;114:1695)
A 45 year old woman with dysphagia undergoes an upper endoscopy which demonstrates mucosal breaks involving at least 75% of esophageal circumference in mid esophagus. Tissue submitted for immunofluorescence study is negative and the patient has no skin, oral or genital lesions. An esophageal biopsy demonstrates the findings shown above. Which one of the following has been associated with this pattern of injury?
Cytomegalovirus
Herpes virus I/II
HIV and viral hepatitis
Sarcina ventriculi
Board review style answer #1
C. HIV and viral hepatitis
HIV and viral hepatitis have been associated with lichenoid esophagitis pattern, shown here. Sarcina ventriculi is a Gram positive coccus, recognized in gastric biopsies, particularly of patients with delayed gastric emptying characterized by basophilic staining and tetrad arrangement. Cytomegalovirus causes viral cytopathic effect seen at the base of esophageal ulcers involving endothelial cells. Herpes virus I/II would show multinucleation, margination and molding (3 M’s) within superficial epithelial cells.
Which of the followings is true regarding lichenoid esophagitis pattern of injury?
Dysphagia is not a common symptom in lichenoid esophagitis pattern patients
Stricture formation in mid esophagus can be seen in upper endoscopy
There are no reports of an association with squamous cell neoplasia
White plaques in distal esophagus of young men is the typical clinical scenario
Board review style answer #2
B. Stricture formation in mid esophagus can be seen in upper endoscopy
Lichenoid esophagitis pattern has been rarely reported in association with dysplasia and carcinoma and periodic surveillance should be suggested. White plaques in proximal esophagus of middle aged women is a common endoscopic finding. Endoscopically it may mimic Candida esophagitis or eosinophilic esophagitis. Stricture formation can be seen but is not a common finding in lichenoid esophagitis pattern unlike lichen planus esophagitis. Mid esophagus is more frequently involved in lichenoid esophagitis pattern. Dysphagia is a common symptom at the time of endoscopy.
Controversial diagnosis as a new distinct disease rather than a pattern of injury associated with more prevalent conditions (Am J Surg Pathol 2022;46:e55)
Gastroesophageal reflux disease (GERD), Crohn's disease, dysmotility, achalasia and medication induced esophagitis are some of the underlying conditions associated with lymphocytic esophagitis pattern of injury (Am J Surg Pathol 2022;46:e55)
Several conditions and diseases are associated with this pattern of injury, from autoimmune diseases such as Crohn's, rheumatoid arthritis, dysmotility disorder (achalasia) to medication effect (Dig Dis Sci 2021;66:3976)
28 year old woman with polyvalent sensitization to food and inhalant allergens presented with intermittent dysphagia (Allergy Asthma Clin Immunol 2021;17:56)
66 year old woman complaining of dysphagia for several weeks with the loss of ability to swallow solid foods (Cureus 2022;14:e30300)
71 year old man with a medical history of squamous cell carcinoma of the tongue treated with external beam radiation 17 years ago presented with dysphagia (Cureus 2018;10:e2153)
Treatment
No definitive targeted treatment for lymphocytic esophagitis
Management is pointed towards the underlying condition
1 case report listed empiric therapy with oral steroids, proton pump inhibitor and balloon dilation (Cureus 2022;14:e30300)
Clinical images
Contributed by Omar Aljuboori, M.B.B.S.
Diffuse changes
Microscopic (histologic) description
Characterized by a triad of intraepithelial lymphocytosis, with epithelial damage and no significant granulocytic inflammation
Unequivocal mucosal lymphocytosis; studies have reported various cutoff values for lymphocytes, ranging from 20 - 50/HPF (Am J Surg Pathol 2022;46:e55)
Rare to absent granulocytes (if present abundantly it argues against the diagnosis of lymphocytic esophagitis) (Am J Surg Pathol 2022;46:e55)
Depending on the underlying disease, the T cell population may differ
Crohn's and most GERD patients can have a high CD8:CD4 ratio while dysmotility patients tend to show predominance of CD4 helper T cells with a CD4:CD8 ratio > 1 (neither sensitive nor specific) (Arch Pathol Lab Med 2021;145:1138, Am J Surg Pathol 2015;39:1558)
Microscopic (histologic) images
Contributed by Monica T. Garcia-Buitrago, M.D., Omar Aljuboori, M.B.B.S. and @RaulSGonzalezMD on Twitter
Intraepithelial lymphocytosis
Damaged esophageal epithelium
Lymphocytic esophagitis
Lymphocytic esophagitis
CD3 stain
CD4 stain
CD8 stain
Positive stains
CD3, CD4 and CD8 highlighting T cells (helper and cytotoxic)
On endoscopy, there are visible white plaques that can be scraped off easily from the underlying mucosa
Neutrophilic infiltration is seen in biopsy along with fungal pseudohyphae in sloughed epithelial debris or invading intact squamous epithelium perpendicularly
On endoscopy, mucosal denudation, trachealization and hyperkeratosis are seen; esophageal stenosis may occur
Prominent band-like lymphocytic infiltrate involving the interface of lamina propria and epithelium, intraepithelial lymphocytes and dyskeratotic keratinocytes (Am J Surg Pathol 2013;37:1889)
Direct immunofluorescence shows diagnostic globular IgM deposits and fibrinogen deposits along the basement membrane zone
A 60 year old woman underwent an upper endoscopy for dysphagia. Endoscopy revealed stricture in the mid esophagus. In addition to the findings pictured, no neutrophilic / eosinophilic infiltrate was present. What is the most probable diagnosis?
Candida esophagitis
Gastroesophageal reflux disease (GERD)
Lymphocytic esophagitis
Radiation esophagitis
Board review style answer #1
C. Lymphocytic esophagitis. The presence of increased lymphocytic infiltrates, esophageal swelling and absence of neutrophilic and eosinophilic infiltrate point towards the diagnosis of lymphocytic esophagitis. Answer B is incorrect because eosinophilic and neutrophilic infiltrates associated with basal epithelial changes are characteristic of gastroesophageal reflux disease (GERD). Answer A is incorrect because neutrophilic infiltration along with fungal pseudohyphae in sloughed epithelial debris is a hallmark of Candida esophagitis. Answer D is incorrect because radiation esophagitis is usually associated with mucosal necrosis and marked neutrophilic infiltration.
A 71 year old man with a known history of squamous cell carcinoma of the tongue treated with external beam radiation 17 years prior, presented to the clinic for esophagogastroduodenoscopy (EGD) with dilation for esophageal strictures. His only complaint at this time was dysphagia. A biopsy was taken and showed the findings above. Which of the following are characteristic features of lymphocytic esophagitis?
Basal cell hyperplasia, spongiosis and elongated papillae with intraepithelial lymphocytes can be seen but are accompanied by eosinophils and rare neutrophils
Intraepithelial lymphocytosis, basilar vacuolization, epithelial apoptosis and necrosis with a history of hematopoietic stem cell transplant
Intraepithelial lymphocytosis, epithelial damage and paucity of granulocytes
Prominent band-like lymphocytic infiltrate involving the interface of lamina propria and epithelium, intraepithelial lymphocytes and dyskeratotic keratinocytes
Board review style answer #2
C. Intraepithelial lymphocytosis, epithelial damage and paucity of granulocytes. The presence of lymphocytic infiltrate, esophageal swelling and absence of neutrophilic and eosinophilic infiltrate are the clinical features of lymphocytic esophagitis. Answer D is incorrect because these are the features of esophageal lichenoid planus. Answer B is incorrect because these are the features of graft versus host disease (GVHD). Answer A is incorrect because these are the features of gastroesophageal reflux disease (GERD).
Which of the following stains highlights most of the cells in lymphocytic esophagitis?
CD3
CD20
CD68
CD138
Board review style answer #3
A. CD3. CD3 stain identifies T cells, increased in lymphocytic esophagitis cases. Answer B is incorrect because CD20 stain shows rare B cells in lymphocytic esophagitis. Answer C is incorrect because CD68 stain is expressed in histiocytic and monocytic cells. Answer D is incorrect because CD138 stain is expressed in plasma cells.
Classic Hodgkin lymphoma: Reed-Sternberg cells and variants in a reactive background
R-S cells: CD30+, CD15±, PAX5+, ALK-, CD45-, CD3-
Nodular lymphocyte predominant Hodgkin lymphoma: vague nodules of small B cells and interspersed large tumor cells (LP cells) with thin nuclear membranes, fine chromatin and variable nucleoli
LP cells: CD45+, CD20+, CD15-, CD30-
Microscopic (histologic) images
Images hosted on other servers:
Diffuse large B cell lymphoma
Mantle cell lymphoma
Mantle cell lymphoma
Mycosis fungoides
MALT lymphoma:
Dense submucosal lymphocytic infiltrate
Vaguely nodular growth pattern
Monocytoid appearance
Germinal centers
CD20+
CD20+
BCL6+ in germinal centers
BCL6+
CD10
Ki67
Kappa / lambda
Cytology description
Discohesive, single abnormal lymphoid cells
Cytology images
Images hosted on other servers:
DLBCL
Burkitt lymphoma
MALT lymphoma
Peripheral smear description
Peripheral blasts if leukemic spread
Positive stains
CD45 (leucocyte common antigen): most hematopoietic neoplasms
Melanocytic proliferation in basal layer of esophageal squamous epithelium with increased quantity of melanin; overlying epithelium may demonstrate hyperplasia, acanthosis or hyperkeratosis; variable inflammation, melanophages, fibrosis and telangiectasia; no atypia
Long dendritic cytoplasmic processes that extend between keratinocytes, melanosomes; mildly hyperchromatic nuclei with uniform chromatin and indented nuclei; no desmosomes or tonofilaments (Virchows Arch A Pathol Anat Histopathol 1991;418:515)
Mostly epithelioid tumor cells with at least focal melanin pigment (Mod Pathol 2019;32:957)
Associated melanoma in situ component (junctional melanocytic activity / junctional melanocytic component / tumor nests at the epithelium - lamina propria junction / horizontal tumor spread in the basal layer of the epithelium) and melanocytosis / melanosis (Mod Pathol 2019;32:957, Ann Thorac Surg 2013;96:1002)
Microscopic (histologic) images
Contributed by Yukihiro Nakanishi, M.D., Ph.D. and @RaulSGonzalezMD on Twitter
Neuroendocrine markers (chromogranin and synaptophysin); neuroendocrine markers can be expressed in malignant melanomas / malignant melanomas with neuroendocrine differentiation have been reported (Histopathology 2005;47:402)
NGS analysis revealed NF1 (30%), SF3B1 (20%), KRAS (10%), BRCA2 (10%), KIT (10%) and TP53 (10%) mutations; no BRAF mutations were detected (Histopathology 2021;78:240)
Sample pathology report
Esophagus, mass, biopsy:
Malignant melanoma (see comment)
Comment: The infiltrating epithelioid tumor cells are positive for S100, HMB45, MelanA and negative for AE1 / AE3, CAM5.2, synaptophysin and chromogranin. The morphology and immunoprofile are consistent with malignant melanoma.
Rare high grade epithelial tumor with neuroendocrine differentiation divided into small cell or large cell types by morphology; follows an aggressive clinical course and has a poor prognosis
Essential features
Rare malignant tumor of the esophagus with poor prognosis and frequent locoregional or distant metastasis at the time of diagnosis
Usually involves mid or distal third of the esophagus
Positive for either synaptophysin or chromogranin
Divided into either small cell or large cell type by morphology, using the same criteria as for other sites in the gastrointestinal tract
Small cell: minimal cytoplasm, nuclei with fine chromatin and nuclear molding, inconspicuous nucleoli, frequent mitoses, necrosis
Large cell: moderately abundant cytoplasm, nuclei with clumped chromatin and prominent nucleoli, frequent mitoses, necrosis
Terminology
Poorly differentiated endocrine carcinoma, small cell carcinoma, large cell carcinoma
63 year old woman with esophageal small cell carcinoma coexisting with paraneoplastic neurological syndrome (Jpn J Clin Oncol 2006;36:109)
66 year old man with rare collision tumor of squamous carcinoma and small cell carcinoma in esophagus with separate lymph node involvement (J Thorac Dis 2013;5:E203)
Multimodal therapy (surgery, platinum based chemotherapy or radiation) improves survival in patients with locoregional and metastatic disease (Dis Esophagus 2014;27:152)
Folinic acid, fluorouracil and irinotecan (FOLFIRI) can be considered for second line therapy after platinum etoposide first line chemotherapy (Lancet Oncol 2023;24:297)
Associated with a high rate of inactivating mutations in 5 well known genes: TP53, RB1, NOTCH1, FAT1, FBXW7 and 3 genes not previously associated with esophageal carcinogenesis: PDE3A, PTPRM and CBLN2 (Cell Res 2018;28:771)
Molecular / cytogenetics images
Not available
Videos
Not available
Sample pathology report
Esophagus, mass, biopsy:
Poorly differentiated neuroendocrine carcinoma, small cell type (see comment)
Comment: Sections show sheets of crowded tumor cells with round to oval nuclei, inconspicuous nucleoli, prominent nuclear molding and numerous mitoses. There are broad zones of necrosis and necroinflammatory debris within the tumor. The tumor cells are highlighted by stains for pankeratin (strong, diffuse), synaptophysin (strong, diffuse) and chromogranin A (weak, patchy). Ki67 highlights a proliferative index of > 80%. The morphologic features and immunophenotype are those of a poorly differentiated neuroendocrine carcinoma, small cell type.
There are no reliable means of differentiating a primary esophageal neuroendocrine carcinoma from a metastatic pulmonary neuroendocrine carcinoma (Hum Pathol 2020:96:8)
For the lower esophageal tumor depicted in the image above, which of the following statements is true?
Synaptophysin immunohistochemistry has greater sensitivity than chromogranin in detection
There are established consensus guidelines on the treatment of this large cell carcinoma
This tumor has a favorable prognosis with a median survival of 10 years
Tumors with a concomitant adenocarcinoma or squamous cell carcinoma component have a worse prognosis
Board review style answer #1
A. Synaptophysin immunohistochemistry has greater sensitivity than chromogranin in detection. This is an esophageal small cell carcinoma, which expresses synaptophysin or chromogranin, although synaptophysin has greater sensitivity than chromogranin. Answer C is incorrect because this tumor has a poor prognosis. Answer D is incorrect because tumors with an adenocarcinoma or squamous cell carcinoma component tend to have a better prognosis than pure small cell carcinoma. Answer B is incorrect because the image depicts a small cell carcinoma (not large cell carcinoma) and there is no consensus approach to the treatment of neuroendocrine carcinomas given the rarity of the tumor and lack of randomized controlled trials; however, treatment often includes a combination of approaches including surgery, platinum based chemotherapy and radiation.
Epithelial neoplasm with prominent neuroendocrine differentiation
Pathologic spectrum from low grade neuroendocrine tumors (carcinoid, atypical carcinoid) to high grade neuroendocrine carcinoma (small cell or large cell neuroendocrine carcinoma)
Malignant epithelial tumor consisting or small cells with scant cytoplasm, ill defined cell borders, finely granular nuclear chromatin and absent or inconspicuous nucleoi
Cells are round, oval and spindle shaped
Nuclear molding is prominent
Necrosis is typically extensive and the mitotic count is high
66 year old man with rare collision tumor of squamous carcinoma and small cell carcinoma in esophagus in separate lymph nodes (J Thorac Dis 2013;5:E203)
Small cell carcinoma (upper), squamous cell carcinoma (lower)
Microscopic (histologic) description
Well differentiated (low grade) tumors
Uniform, small, bland tumor cells in solid, trabecular, gyriform or glandular patterns
May have Paneth cell differentiation
Poorly differentiated (high grade) carcinomas
Large cell type: nests of pleomorphic, large cells with prominent nucleoli and a moderate amount of cytoplasm
Small cell type: sheets and nests of small cells with hyperchromatic nuclei and a minimal to moderate amount of cytoplasm; prominent crush artifact and Azzopardi phenomenon, as in small cell carcinomas at other sites
Necrosis
Increased mitotic activity
Angiolymphatic invasion common
Solid to cribriform growth
Usually in lamina propria
May be associated with heterotopic oxyntic mucosa or Barrett esophagus (large cell carcinoma)
Neuroendocrine carcinoma may have small component(s) of adenocarcinoma or squamous cell carcinoma differentiation
Microscopic (histologic) images
Contributed by Mark R. Wick, M.D. and AFIP images
Small cell carcinoma of esophagus
In muscularis
Small cell neuroendocrine carcinoma:
Diffusely infiltrating sheets of small cells
In situ component
Squamous cell differentiation
Cytology description
Low grade tumors
Flat sheets or loosely cohesive groups / cords of monotonously uniform plasmacytoid cells
Endoscopy: erosions, kissing ulcers, multiple small ulcerations with bleeding, mainly in mid esophagus
Kayexalate damage
Kayexalate (sodium polystyrene sulfonate) in sorbitol is used to treat hyperkalemia
Symptoms are from sorbitol, given orally though NG tube or as an enema, may crystallize in esophagus, stomach or duodenum and produce endoscopic ulcers and erosions resembling carcinoma or Candida (Am J Surg Pathol 2001;25:637)
Colonic infarction and erosions reported
Crystals are lightly basophilic with a faint crystalline mosaic pattern, better seen with PAS / Alcian blue
Crystals are refractile but not polarizable, luminal and adherent to intact surface epithelium or mixed with inflammatory exudate in patients with ulcer or erosion
Chronic injury: due to fractionated doses of 60 gray or more; submucosal fibrosis, capillary telangiectasia, thick walled arterial vessels, mucus glandular atrophy, atypical fibroblasts; grossly are ulcers, strictures or fistulas
Gross images
AFIP images
Esophageal squamous cell carcinoma
Radiation has destroyed tumor
Deep ulcer with necrotic base
Microscopic (histologic) description
Variably sized cells in all layers, often increased cytoplasm but usually normal nuclear to cytoplasmic ratio
Nuclei enlarged with bizarre shapes, may be hyperchromatic or smudged
May have large eosinophilic nucleoli; usually no mitotic figures
Microscopic (histologic) images
AFIP images
Normally oriented epithelium is thinner than normal
Reflux esophagitis (RE) / gastroesophageal reflux disease (GERD) is the reflux of gastric contents into the esophagus that results in symptoms or complications; reflux esophagitis / gastroesophageal reflux disease is objectively defined as mucosal injury seen at endoscopy or abnormal esophageal acid exposure on a reflux monitoring study
Remains one of the most common diseases seen by gastroenterologists, surgeons and primary care physicians (Am J Gastroenterol 2022;117:27)
Essential features
One of the most common diseases in everyday pathology practice
May affect all ages and is more common in men
Caused by reflux of gastric contents into the distal esophagus
Minimum criteria for histologic diagnosis have not been established
3 main histologic features are basal cell hyperplasia, elongation of the lamina propria papillae and inflammatory infiltrates
Mainstay of therapy is proton pump inhibitors
ICD coding
ICD-10:
K21.0 - gastroesophageal reflux disease with esophagitis
K21.9 - gastroesophageal reflux disease without esophagitis
Epidemiology
Affects an estimated 20% of the United States population
Prevalence is increasing worldwide
Males affected more commonly than females
All ages, including infants and children
One of the most costly gastrointestinal diseases in the United States, exceeding $14 billion dollars annually
Lower esophageal sphincter (LES) is a circular muscle layer at the distal esophagus that creates a higher pressure than the intra-abdominal pressure
Physiologic reflux does occur and is termed transient lower esophageal sphincter relaxations (TLESRs)
TLESRs are a normal mechanism for the stomach to vent and may be activated by things such as gastric distension
TLESRs are increased in those with reflux esophagitis / gastroesophageal reflux disease
Inappropriate relaxation of the LES allows gastric acid to enter the distal esophagus
Chemoreceptors are stimulated and irritation occurs, causing symptoms
Symptoms result from mucosal injury and are directly related to frequency of the reflux, duration of reflux and the injurious potential of the refluxate
Certain drugs may relax the tone of the LES and worsen reflux
Hiatal hernias are associated with reflux esophagitis / gastroesophageal reflux disease
Caused by reflux of gastric contents into the lower esophagus
Clinical features
May be asymptomatic
Typical symptoms are heartburn and regurgitation
May have so called extraesophageal symptoms, including hoarseness, cough, odynophagia, reflux induced asthma, laryngitis and aspiration pneumonia
Atypical or severe symptoms (hematemesis, weight loss, dysphagia) may indicate a stricture or malignancy, endoscopic evaluation is recommended as the first test
54 year old woman with idiopathic pulmonary fibrosis and gastroesophageal reflux disease (Respir Med Case Rep 2016;17:40)
Treatment
Diet and lifestyle modifications: weight loss for obese patients, elevating the head of the bed, tobacco and alcohol cessation, avoiding late night meals and bedtime snacks, staying upright after eating and not ingesting foods known to make reflux worse (coffee, chocolate, carbonated beverages, spicy foods, acidic foods and fatty foods)
Proton pump inhibitors (PPIs) are the mainstay of therapy
Histamine 2 receptor antagonists may be added to PPIs for persistent nocturnal symptoms
Surgical treatment (e.g., fundoplication) is an option for those with chronic gastroesophageal reflux disease whose symptoms do not respond to medical management or have a defective lower esophageal sphincter (LES) (Goldblum: Rosai and Ackerman’s Surgical Pathology, 11th Edition, 2017)
The 3 major features of reflux esophagitis / gastroesophageal reflux disease are:
Inflammatory cells in the squamous epithelium
Elongation of the lamina propria papillae
Basal cell hyperplasia
Inflammatory infiltrate may be composed of neutrophils, eosinophils and lymphocytes
Numerous neutrophils suggest severe injury; eosinophils are seen in 50% of cases
Lymphocytes are present as squiggle cells, in between the squamous epithelial cells
Normal basal cell layer is only 1 - 4 cells in thickness and makes up only the bottom 10 - 15% of the epithelial thickness; basal cell hyperplasia is defined as more than 15% of the thickness of the epithelium
Lamina propria papillae elongation, to a height > two - thirds of the epithelial thickness, is commonly seen in reflux esophagitis / gastroesophageal reflux disease
Capillaries within the lamina propria papillae may show congestion and red blood cell extravasation
Distended squamous epithelial cells are nonspecific and termed balloon cells
Spongiosis is common and may be a marker of early injury without endoscopic findings; this is seen in up to 80% of NERD cases
Notably, none of these features are specific for reflux esophagitis / gastroesophageal reflux disease
Minimum criteria for a diagnosis of reflux esophagitis / gastroesophageal reflux disease remain undefined
A 43 year old man complains of several months of reflux and regurgitation that is worse after eating and while lying down. Upper endoscopy shows mucosal erythema and erosions of the distal esophagus. After esophageal pH monitoring, the patient is diagnosed with gastroesophageal reflux disease. A histologic image of the esophageal biopsy is shown above. What are the 3 main histologic features of reflux esophagitis / gastroesophageal reflux disease?
Basal cell hyperplasia, elongation of the lamina propria papillae, inflammatory infiltrates
Basal cell hyperplasia, loss of polarity, > 15 - 20 eosinophils per high power field
Elongation of the lamina propria papillae, necrosis, increased apoptotic bodies
Full thickness atypia, inflammatory infiltrates, > 15 - 20 eosinophils per high power field
Board review style answer #1
A. Basal cell hyperplasia, elongation of the lamina propria papillae, inflammatory infiltrates
Initially described as a constant, symmetrical and diaphragm-like narrowing at the GE junction, associated with a small sliding hiatus hernia (Am J Roentgenol Radium Ther Nucl Med 1953;70:911)
May be congenital or a scar from drinking caustic liquids
Type A: lower muscular ring; rare; thickened circular smooth muscle with overlying squamous mucosa; usually 1.5 cm proximal to squamocolumnar junction, usually asymptomatic (Am J Gastroenterol 2000;95:43)
Type B: lower mucosal ring / Schatzki ring; 5% of normal esophagi; upper surface is lined by stratified squamous epithelium, undersurface is lined by columnar type epithelium; ring contains connective tissue and fibers of muscularis mucosae; located at squamocolumnar junction at proximal margin of hiatal hernia; associated with meat impaction ("steakhouse syndrome," Surg Endosc 1989;3:195), "swallow syncope" (Dysphagia 2005;20:273) and a reduced incidence of Barrett esophagus (Dig Dis Sci 2004;49:770)
Type C: rare; refers to indentation on radiographic studies caused by diaphragmatic crura; usually asymptomatic
Squamous cell carcinoma with a variable spindle cell component (WHO definition)
Terminology
WHO uses the term "spindle cell (squamous) carcinoma"
Spindle cell carcinoma (Odze) and sarcomatoid carcinoma (Rosai) are also commonly used
Synonyms include carcinosarcoma, pseudosarcomatous squamous cell carcinoma, polypoid carcinoma, metaplastic carcinoma, squamous cell carcinoma with a spindle cell component, Lane tumor, carcinoma with mesenchymal stroma and pseudosarcoma
Epidemiology
Uncommon, usually middle aged to elderly men
Sites
Typically in mid esophagus
Pathophysiology
In the vast majority of cases the epithelial component is squamous and the lesion is generally regarded as a variant of squamous cell carcinoma
Very rare examples of spindle cell carcinoma associated with adenocarcinoma are known
Spindle cell component dominates, has growth advantage over epithelial component, although both evolve from same clone
Clinical features
Patients generally present with short history of dysphagia, weight loss and pain
Diagnosis
Endoscopic biopsy or resection
Radiology description
Large polypoid lesion, typically with narrow pedicle leads to characteristic "cupola" sign
Prognostic factors
Better survival than typical squamous cell carcinoma, overall survival about 50%
Tends to present at low stage with intraluminal instead of intramural growth
30% have nodal metastases at presentation (usually epithelial or both components)
Sarcomatous component thought to represent sarcomatous metaplasia of malignant epithelial cells; has malignant potential
64 year old man with esophageal carcinosarcoma with basaloid squamous carcinoma and rhabdomyosarcoma components with p53 mutation (Pathol Int 2004;54:803)
Dilated cisternae of rough endoplasmic reticulum, peripheral cytoplasmic intermediate filaments
Also some intermediate type junctions and subplasmalemmal linear densities
Sarcomatous cells may retain epithelial features including tonofibril bundles or desmosomes or lack epithelial elements and have fibrohistiocytic differentiation (Hum Pathol 1987;18:692)
WHO definition: a malignant epithelial tumor displaying squamous cell differentiation characterized by keratinocyte type cells with intercellular bridges or keratinization
Essential features
Esophageal squamous cell carcinoma (ESCC) is the most common esophageal cancer worldwide
Distinct from esophageal adenocarcinoma in terms of cell origin, epidemiology, etiology, pathogenesis and location in the esophagus
Rich lymphovascular network facilitates early tumor spread
Early diagnosis is critical to improve survival and endoscopic surveillance with biopsy evaluation is the standard of care in high risk groups
ICD-11: 2B70.1 - squamous cell carcinoma of esophagus
Epidemiology
Incidence worldwide, the most common esophageal cancer
Great regional and ethnic variation
Highest incidence regions (> 50 cases/100,000 person years) stretching from Eastern to Central Asia
Intermediate rates (10 - 50 cases/100,000 person years) observed along the Indian coast of Africa, in southern Brazil and Uruguay and in parts of the Caribbean
Trending down and less common in the U.S., Europe, Australia and many other Western countries than esophageal adenocarcinoma
Ratio varies with the M:F ratio reaching 4:1 in low risk areas (such as U.S.) and the ratio being lower or even exceeding 1:1 in high incidence areas of China and Iran (Gastroenterology 2018;154:360)
Most commonly in middle third of esophagus, followed by lower third and upper third, respectively
Pathophysiology
Develops by stepwise progression, with accumulating genetic abnormalities driving progression from histologically normal squamous mucosa to low grade intraepithelial neoplasia (dysplasia) to high grade intraepithelial neoplasia and finally to invasive squamous cell carcinoma
TP53 mutation is a key early driver mutation developing at the stage of intraepithelial neoplasia
Other key genetic abnormalities, including cell cycle regulators (e.g., CDKN2A [p16], RB1, NFE2L2, CHECK1, CHECK2, CCND1, CKD4, CDK6 and MDM2), EGFR signaling pathway, PI3Kinase signaling pathway, histone modification, NOTCH and WNT pathway, Hedgehog signaling and other genetic changes, including aneuploidy, copy number alterations (Ann N Y Acad Sci 2018;1434:342)
Specific mutations required for the invasion beyond the basement membrane are still unknown
Acquisition of invasive and migratory capability via epithelial mesenchymal transition is important; EIF5A2 amplification has been shown to be a factor in inducing this phenotype
Etiology
Multifactorial and strongly population dependent
Low socioeconomic status is one of the most consistent factors, even after adjusting other confounding factors (e.g., tobacco use and alcohol consumption)
Tobacco use
Remains a key risk factor in developed countries but a weaker effect in developing countries
Dependent on both exposure duration and intensity, with duration outweighing intensity
Tobacco specific nitrosamines (TSNA) and polycyclic aromatic hydrocarbons (PAH) are thought to be the major carcinogenic substances in tobacco
Alcohol beverage
Alcoholic beverage consumption has been causally linked to ESCC by International Agency for Research on Cancer (IARC)
Consumption of > 3 drinks per day is associated with a risk almost 5 times that in individuals who consume 1 drink per day
Acetaldehyde, a metabolite of ethanol, is linked to the increase in risk of ESCC, particularly in Eastern Asian population, which was found to exclusively have ALDH2 and ALDH1A1 mutations leading to accumulation of acetaldehyde following alcohol consumption
Other risk factors: betel quid, diets low in fruit and vegetables, pickled vegetables, deficiency of selenium or riboflavin, hot foods and beverages, PAH, increased BMI, poor oral health
Associated medical conditions: Plummer-Vinson syndrome, achalasia, caustic ingestion injury, radiotherapy to the chest area and Fanconi anemia
Esophageal leukoplakia or epidermoid metaplasia has been associated with esophageal squamous cell carcinoma and dysplasia (Mod Pathol 2014;27:38)
Genetic factors: tylosis, a keratosis disorder caused by an autosomal dominant mutation in RHBDF2al, 17q25.3, is highly associated with ESCC (> 90% of patients develop ESCC by the age of 65 years)
HPV infection is unlikely to be a substantial risk factor in the current consensus
Most common symptom is progressive dysphagia and weight loss
Insidious onset with dysphagia to solids, followed by dysphagia to all food
Chest pain, painful swallowing and weight loss can also present
Usually advanced at presentation
Chronic gastrointestinal blood loss from ESCC is common and may result in iron deficiency anemia
Hoarseness or cough may occur if the recurrent laryngeal nerve is invaded
May erode the esophageal wall, causing fistulas; the adjacent respiratory tree, causing pneumonia; the aorta, causing exsanguination or the mediastinum and pericardium
Horizontal and longitudinal spread are facilitated by rich lymphovascular network
Lymph node metastases vary by region:
Upper third: cervical nodes
Middle third: mediastinal, paratracheal and tracheobronchial node
Lower third: gastric and celiac nodes
Most common sites for distant metastasis are the lungs, liver, bones, adrenal glands, kidneys
Contributed by Xiaoqin Liu, M.D., Ph.D. and Aaron R. Huber, D.O.
Obstructing lesion of esophagus
Eccentric esophageal wall thickening
Prognostic factors
Stage is most important; American Joint Committee on Cancer / Union for International Cancer Control (AJCC / UICC) TNM the 8th edition (2017) is the current staging system to predict prognosis (Ann Cardiothorac Surg
2017;6:119)
Tumor length is an independent predictor of mortality when controlled for depth of invasion in patients with localized disease (Thorac Cancer 2014;5:204, Cancer 2002;95:1434)
TP53 hotspot mutation p.R213* and TENM3 mutation are reported as independent prognostic factors (Ann Oncol 2018;29:938)
64 year old man with esophageal squamous cell carcinoma with neuroendocrine, basaloid and ciliated glandular differentiation (Clin J Gastroenterol 2021;14:32)
67 year old man with esophageal squamous cell carcinoma arising from esophageal squamous papillomatosis (Int J Surg Case Rep 2020;71:335)
Treatment
Early lesion (T1) can be managed by endoscopic submucosal dissection or esophagectomy
Neoadjuvant chemoradiation followed by esophagectomy is widely accepted for advanced lesion (Surg Clin North Am 2019;99:479)
Definitive chemoradiation is an acceptable alternative in patients who are not surgical candidates or patients who wish to avoid surgery (Surg Clin North Am 2019;99:479)
Although salvage therapy is a viable option, longterm outcomes are unclear but it can be considered in select patients (Surg Clin North Am 2019;99:479)
By integrating molecular profiling as part of the management of patients with esophageal cancer, future treatment guidelines will provide a more personalized and effective approach to this disease
Clinical images
Contributed by Xiaoqin Liu, M.D., Ph.D. and Aaron R. Huber, D.O.
Mucosal tearing and ulceration
Gross description
Fungating / exophytic / polypoid lesions
Ulcerative or infiltrative (intramural causing thick, rigid esophageal wall with luminal narrowing, linitis plastica pattern and only minor mucosal defect, associated with stricture)
Contributed by Xiaoqin Liu, M.D., Ph.D. and Aaron R. Huber, D.O.
Fungating / exophytic lesion
Polypoid lesion
Ulcerated lesion
Cavitary lesion
Microscopic (histologic) description
Essential diagnostic criteria: histological evidence of vertical and horizontal growth of neoplastic squamous epithelium, with definite evidence of invasion
Should be staged using the 8th editions (2017) of the UICC / AJCC cancer staging manual
Depth of invasion provides a clinically relevant division of esophageal squamous cell carcinoma into superficial (or early) disease versus advanced (or late) disease
Superficial disease is invasion restricted to the mucosa and submucosa; it has a low risk of regional lymph node metastasis
Advanced disease is invasion beyond the muscularis propria, with a high risk of regional or systemic metastasis
Grading is based on the degree of cytological atypia, mitotic activity and presence of keratinization
Grade 1 (well differentiated):
Contains enlarged cells with abundant eosinophilic cytoplasm and keratinization
Cytological atypia is minimal and the mitotic rate is low
Invasive margin is pushing and the cells remain well ordered
Grade 2 (moderately differentiated):
Has evident cytological atypia and the cells are less ordered
Mitotic figures are easily identified
Grade 3 (poorly differentiated):
Consists predominantly of basal-like cells forming nests with or without central necrosis
Treatment effect often involved in both tumor cells and the peritumor stroma
Cellular changes include nuclear enlargement or shrinkage, nuclear vacuolation, apoptosis and necrosis
Neutrophilic or chronic inflammatory cell response may be seen
There is fibrosis and sometimes stromal elastosis
Subtypes:
Verrucous squamous cell carcinoma: usually at the gastroesophageal junction, associated with reflux; shows a very well differentiated histology with a pushing border and surface papillary projection and metastases are uncommon
Spindle cell squamous cell carcinoma: biphasic morphology with conventional squamous cell carcinoma and a high grade spindle cell component with heterogeneous differentiation
Basaloid squamous cell carcinoma: shows a solid or nested growth pattern of basaloid cells, sometimes with central comedonecrosis and occasionally with pseudoglandular cribriform formations
Microscopic (histologic) images
Contributed by Xiaoqin Liu, M.D., Ph.D. and Aaron R. Huber, D.O.
Well differentiated carcinoma
Moderately differentiated carcinoma
Poorly differentiated carcinoma
Carcinoma with pagetoid cells
Keratinizing well differentiated carcinoma
Desmoplastic changes
Lymphovascular invasion
p40 stain
Kreyberg stain
Cytology description
Nuclear membrane alterations, nuclear hyperchromasia and enlargement, loss of nuclear polarity, prominent nucleoli
Positive stains
Immunohistochemistry is useful in confirming poorly differentiated and spindle cell squamous cell carcinoma
NOTCH1 and NOTCH3 mutations detected in up to 28% of cases
EGFR overexpression reported in 59.6 - 76% of cases
Mutations or amplification in RAS and AKT family seen in at least 75% of cases
Genetic alterations involved in cell cycle regulation, epigenetic factors, copy number alterations, chromosome aneuploidy (in particular, gains in chromosome 3, 10, 12 and 20) were reported
Associated with tylosis and Fanconi anemia
Sample pathology report
Esophagus, at 35 to 28 cm, biopsy:
Invasive moderately differentiated squamous cell carcinoma (see comment)
Comment: Immunohistochemical / special stains were performed and show the tumor is positive for p40 and negative for Kreyberg for intracellular mucin. The morphology and immunoprofile are consistent with squamous cell carcinoma.
A 65 year old man presented with progressive dysphagia and weight loss. Esophageal biopsy confirmed squamous cell carcinoma and esophagectomy was performed. What is the T staging according to the H&E section above?
Neoplastic alteration of squamous esophageal mucosa without invasion
Precursor lesion to squamous cell carcinoma (SCC)
Low grade dysplasia is characterized by atypia limited to the lower half of the epithelium while high grade dysplasia is characterized by atypia involving greater than half of the epithelium
Essential features
Precursor lesion to squamous cell carcinoma
Occurs predominantly in the middle third of the esophagus
Often encountered at the periphery of invasive squamous cell carcinoma
Comprises both architectural and cytologic abnormalities
Terminology
Squamous intraepithelial neoplasia, squamous carcinoma in situ
Environmental exposures, predisposing conditions and genetic factors interplay in the pathogenesis of squamous dysplasia; risk factors are similar to those of SCC (Gastroenterology 2018;154:360)
Substantial alcohol use and smoking
Chronic esophageal irritation associated with conditions such as achalasia, esophageal diverticula, gastroesophageal reflux disease (GERD), Plummer-Vinson syndrome and chronic strictures
Low socioeconomic status
Dietary factors and drinking very hot beverages
Increased body mass index
Male sex
Genetic conditions
Nonepidermolytic palmoplantar keratoderma (tylosis), a rare autosomal dominant disorder with hyperkeratosis of palms and soles, confers a > 90% risk of development of SCC (Orphanet J Rare Dis 2015;10:126)
Epidermoid metaplasia, also termed esophageal leukoplakia, is thought to represent a precursor lesion to squamous dysplasia
Magnitude of risk is not known, although targeted next generation sequencing supports that epidermoid metaplasia shares molecular signatures with squamous dysplasia and squamous cell carcinoma (Mod Pathol 2017;30:1613)
Current consensus is that human papillomavirus (HPV) is unlikely to be a substantial risk factor (Gastroenterology 2018;154:360)
Clinical features
Patients may present with dysphagia or be asymptomatic
Endoscopically, dysplasia is usually flat and requires enhancing techniques such as methylene blue or Lugol iodine with chromoendoscopy or narrow band imaging (Ann Gastroenterol 2015;28:41)
Diagnosis
Endoscopic biopsy with histologic examination
Prognostic factors
Patients with high grade dysplasia have a greater risk of progressing to SCC
In a study of Chinese patients over a period of 3.5 years, 5% of patients with mild dysplasia progressed to SCC versus 65% with severe dysplasia (Cancer 1994;74:1686)
Endoscopic mucosal resection (EMR) or endoscopic submucosal dissection (ESD) is the definitive treatment with endoscopic surveillance for recurrence or progression
Which of the following is thought to represent a precursor lesion to squamous dysplasia of the esophagus?
Epidermoid metaplasia
Intestinal metaplasia
Pancreatic acinar metaplasia
Pyloric gland metaplasia
Board review style answer #1
A. Epidermoid metaplasia. Epidermoid metaplasia (leukoplakia) is thought to represent a precursor lesion to esophageal squamous dysplasia, although the magnitude of risk is unknown. Answer B is incorrect because intestinal metaplasia (i.e., Barrett esophagus) is a precursor for glandular dysplasia in the esophagus. Answer C is incorrect because pancreatic acinar metaplasia is usually an incidental finding seen at the gastroesophageal (GE) junction with no known neoplastic risk. Answer D is incorrect pyloric gland metaplasia is usually seen in the intestine and not in the esophagus.
The image above shows an endoscopic biopsy of a lesion noted as a white plaque that did not stain with Lugol iodine in the middle third of the esophagus. What is your diagnosis?
Barrett esophagus with dysplasia
High grade squamous dysplasia
Low grade squamous dysplasia
Reactive atypia, negative for dysplasia
Board review style answer #2
B. High grade squamous dysplasia. A full thickness high grade squamous esophageal dysplasia with cytologic atypia is seen on the right side of the image with sharp demarcation from the normal nondysplastic squamous epithelium on the left. Answer C is incorrect because low grade dysplasia encompasses less than half of the mucosa. Answer A is incorrect because Barrett esophagus or intestinal metaplasia, which by definition is columnar epithelium with or without goblet cells that extends ≥ 1 cm proximal to the gastroesophageal junction, is commonly seen in distal esophagus and gastroesophageal (GE) junction. Answer D is incorrect because the full thickness atypia present exceeds what would be expected for reactive atypia.
Benign esophageal epithelial polyp composed of squamous epithelium with a papillary growth pattern
Essential features
Papillary proliferation of nondysplastic squamous epithelium with fibrovascular cores of lamina propria
Etiologic factors include irritation (alcohol consumption, smoking and reflux esophagitis, metal stent and chronic food impaction), infection (HPV infection) and genetic syndromes (Goltz-Gorlin syndrome and angioma serpiginosum)
Human papilloma virus infection rate: 10.5 - 57%
Often seen in the distal esophagus in the U.S. (58.3 - 70%) and the middle esophagus in Asian countries (52.6 [Japan] - 57.5% [Taiwan])
Pathologic TNM staging of carcinomas of the esophagus, AJCC 8th edition
Definition / general
All carcinomas of the esophagus, including poorly differentiated neuroendocrine carcinomas, are covered by this staging system
Esophagus cancers are defined as having an epicenter within the esophagus, within the gastroesophageal junction or no more than 2 cm into the proximal stomach
Well differentiated neuroendocrine tumors of the true esophagus are extremely rare and do not have a separate staging system, unlike other gastrointestinal organs
Well differentiated neuroendocrine tumors of the gastroesophageal junction and cardia are staged using the stomach neuroendocrine system
A patient undergoes esophagogastrectomy for a tumor of the distal esophagus. A representative hematoxylin and eosin photomicrograph of the lesion is shown. The tumor lacks any immunohistochemical signs of differentiation, including negativity for pancytokeratin, MelanA, synaptophysin, chromogranin and CD34. An esophageal carcinoma of this subtype is characterized by what immunophenotype?
Keratin 7 expression
Wild type p53
Loss of SMARCA4 or SMARCA2
Expression of Rb
Board review style answer #1
C. Loss of SMARCA4 or SMARCA2. This is an undifferentiated carcinoma of the esophagus.
Collaterals in lower esophagus divert flow from portal vein, through coronary veins of stomach, into esophageal veins, then azygous veins, then into vena cava
Clinical features
Present in 90% of cirrhotic patients, usually due to alcoholism; acute alcohol intake may cause death, often outside the hospital (Arch Pathol Lab Med 2002;126:1197)
May rupture and cause massive hemorrhage (cause of death in 50% with advanced cirrhosis)
40% die in first episode of bleeding varices; rebleeding occurs in 50% of survivors within 1 year with 40% mortality
Blood stains at death scene and unusual body positions of deceased are clues to fatal esophageal variceal hemorrhage
#2 cause of bleeding varices worldwide is hepatic schistosomiasis
Highly differentiated variant of squamous cell carcinoma that is locally invasive with a pushing, as opposed to an infiltrative border, that is identical to lesions of the same name in the upper aerodigestive tract
Metastases are uncommon
Epidemiology
Extremely rare
Male predominance
Ages 36 - 76 years
Pathophysiology / etiology
Cases related to chronic mucosal irritation, lye ingestion, diverticular disease, reflux esophagitis (Gastroenterology 1996;110:904)
Superficial biopsies may be diagnosed as squamous papillomas or other benign lesions
Papillomas are generally under 3 cm in dimension, generally do not demonstrate circumferential growth, lack ulceration, do not cause stricture and do not invade submucosa or muscularis, which are common findings in verrucous carcinoma (Can J Gastroenterol 2004;18:459, Am J Gastroenterol 1996;91:1031)
Well differentiated epithelial neoplasm with prominent neuroendocrine differentiation
Pathologic spectrum from low grade neuroendocrine tumor (carcinoid, atypical carcinoid) to high grade neuroendocrine carcinoma (small or large cell carcinoma)