Risk factors include poor contact lens hygiene (e.g., wearing lenses overnight or during swimming / showering) and orthokeratology (specially fitted lenses) (J Clin Med 2021;10:942)
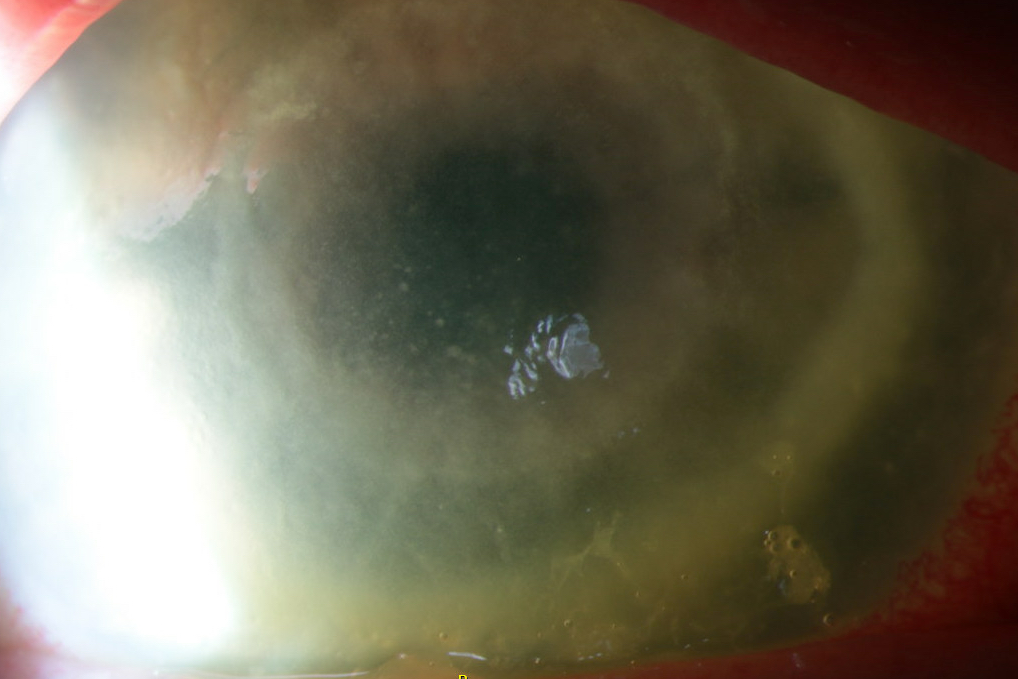
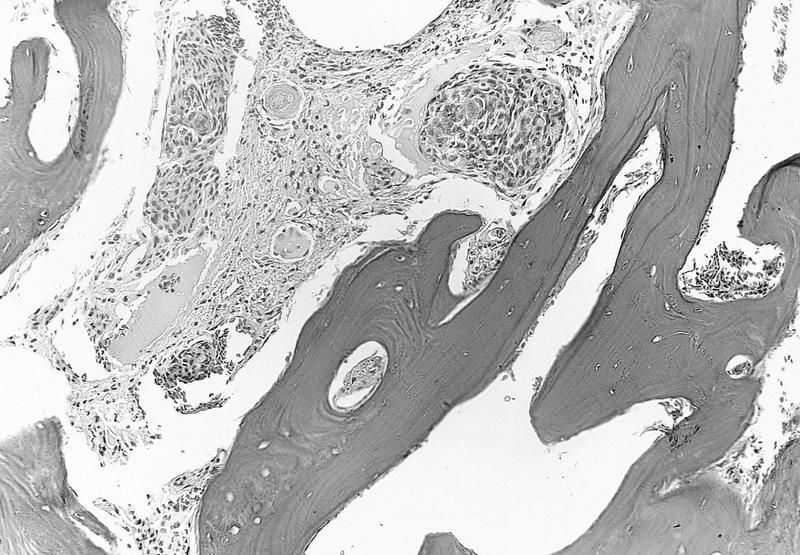
20 year old man with orthokeratology contact lenses, right eye pain and redness for 2 days and dendrite-like anterior stromal keratitis coinfected with Acanthamoeba and Pseudomonas (Taiwan J Ophthalmol 2019;9:131)
26 year old woman with history of immunocompetence and contact lens use presented with severe pain, photophobia, tearing and decreased visual acuity of her left eye for 2 months (Parasitol Res 2021;120:1121)
53 year old woman with contact lens use and a 2 month history of a persistent left corneal ulcer (Hum Pathol 2013;44:918)
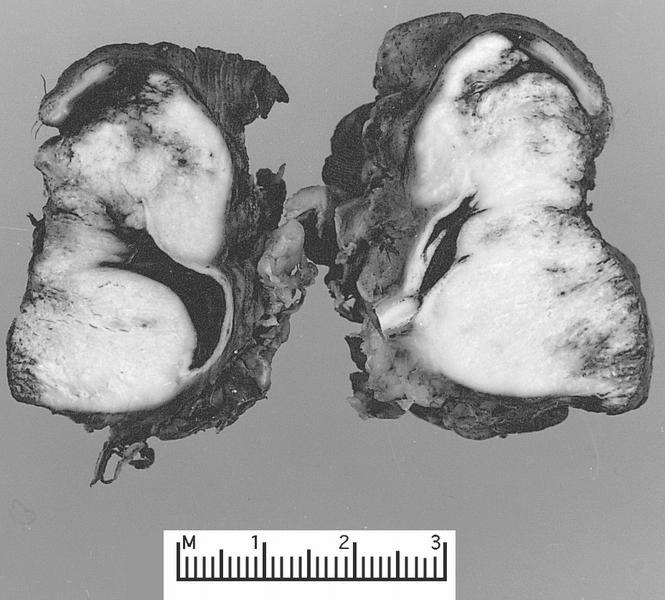
65 year old man presented with a 10 year history of bilateral uveitis, scleritis and eventual complete loss of vision and severe pain in both eyes (bilateral enucleation) (Am J Ophthalmol Case Rep 2020:20:100970)
74 year old woman with history of extended soft contact lens use and intense painful ring corneal ulcer refractory to conventional antibiotics (Pathogens 2021;10:323)
76 year old man with rigid gas permeable lens use in the setting of keratoconus presented after a 4 month history of corneal ulcer of the left eye (BMJ Case Rep 2021;14:e241864)
Treatment
Acanthamoeba trophozoite form is susceptible but the cystic form is highly drug resistant and may persist for months
Principal initial treatment is topical biguanide, such as polyhexamethylene biguanide (PHMB) 0.02 - 0.08% or chlorhexidine 0.02 - 0.06% (J Clin Med 2021;10:942)
Immunohistochemical stains for Acanthamoeba spp. exist but are not readily available in most clinical settings (Mod Pathol 2007;20:1230)
Negative stains
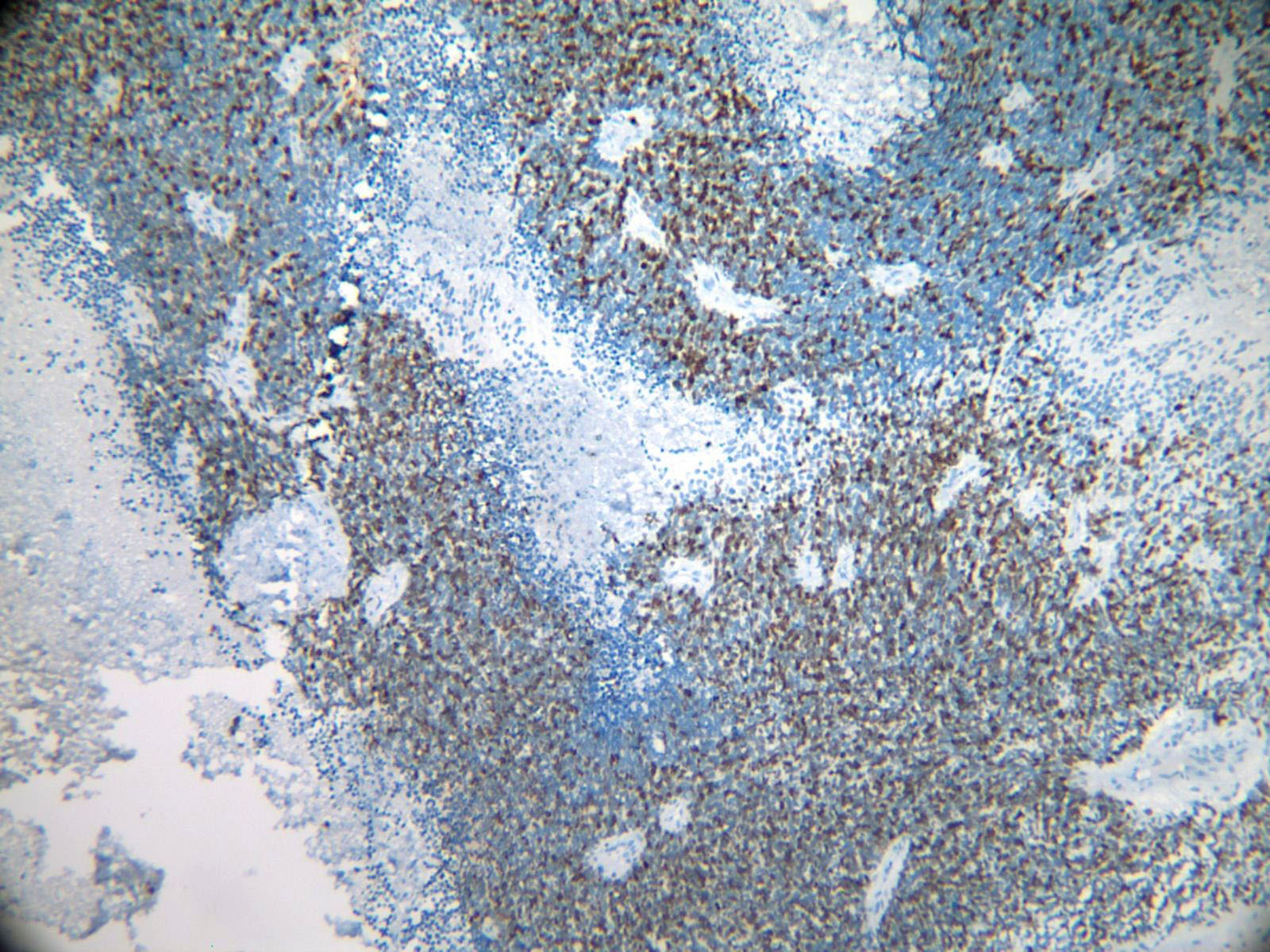
CD68 or CD163 highlight macrophages in background; stain is negative in amoebic organisms
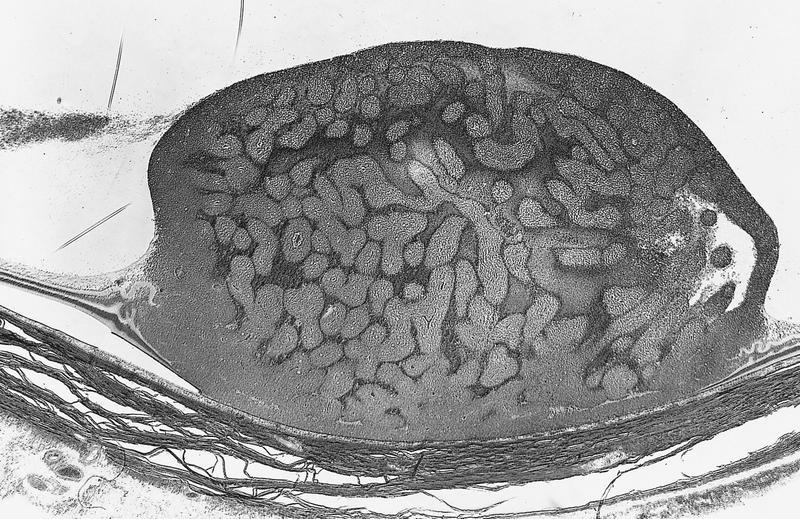
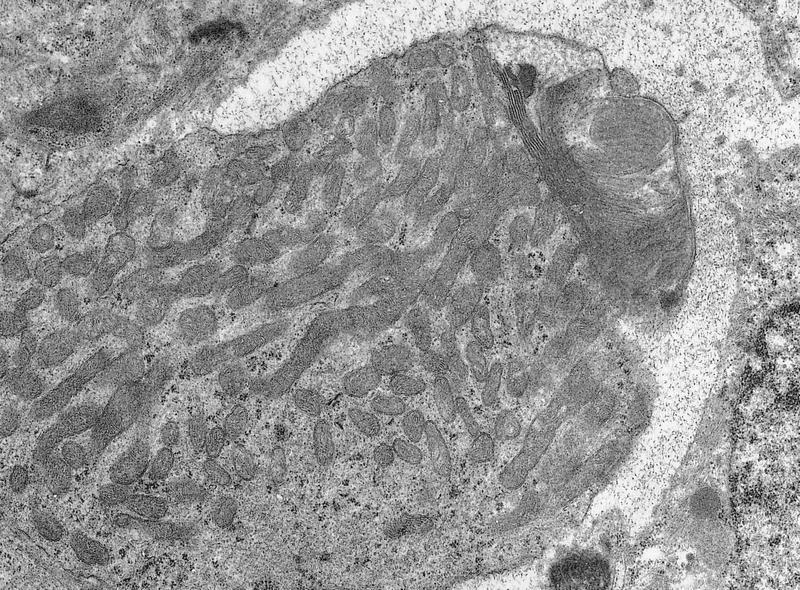
Electron microscopy description
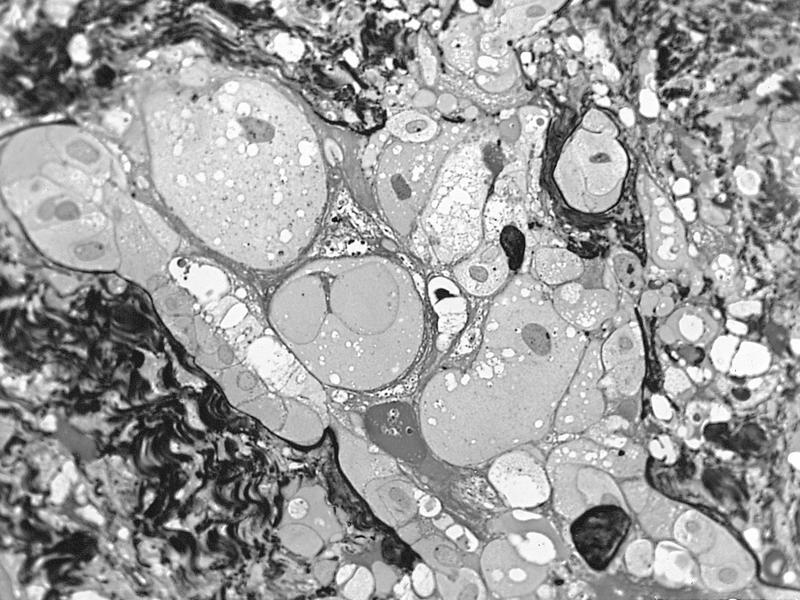
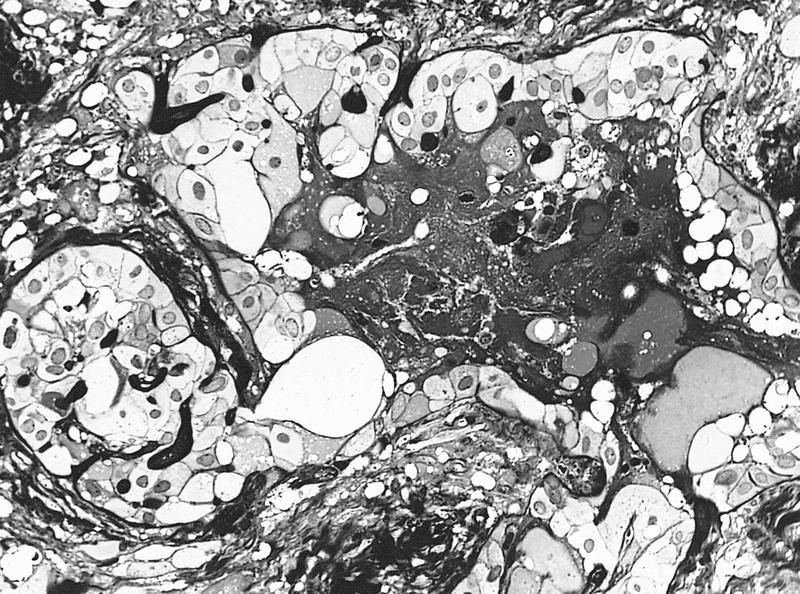
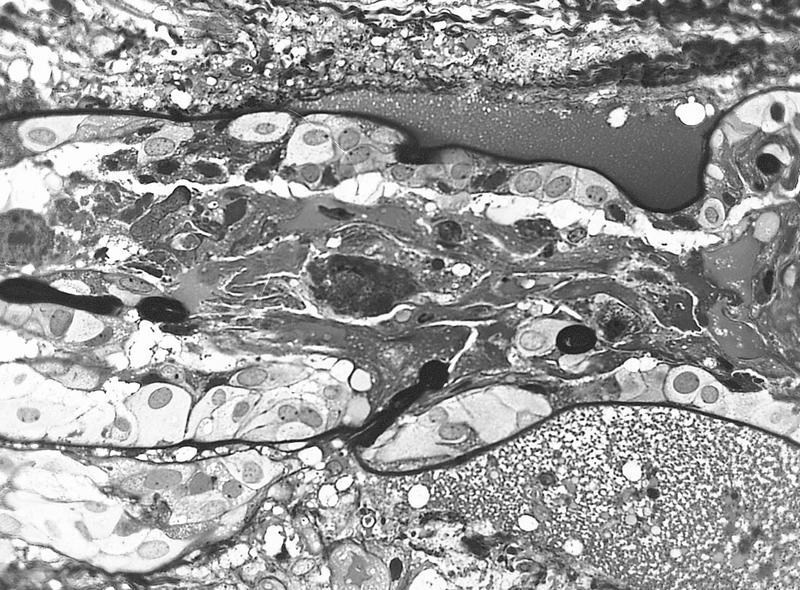
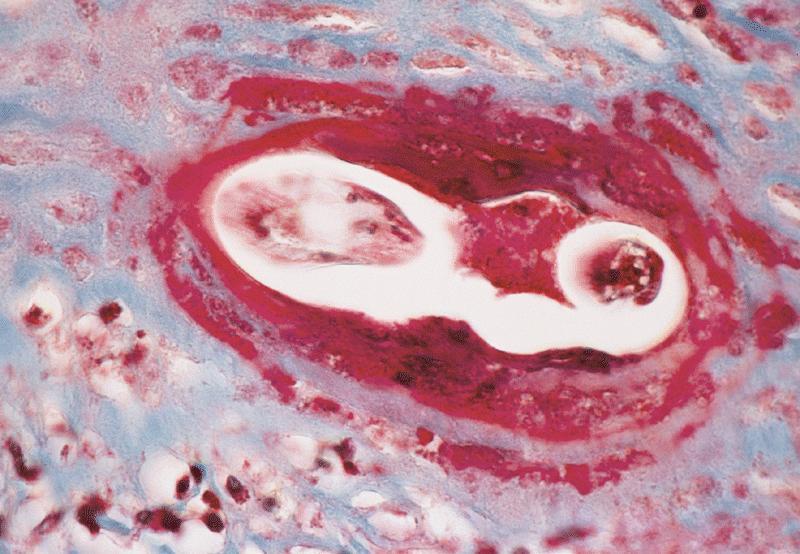
Typically for education / research rather than diagnosis: transmission electron micrograph showing an encysted Acanthamoeba organism with outer ectocyst layer, mitochondria, lipid vacuoles and lysosomes; adjacent neutrophils (Am J Ophthalmol 1987;103:626)
Videos
Clinical presentation of Acanthamoeba keratitis
Sample pathology report
Eye, (side) cornea, biopsy or keratoplasty:
Acanthamoeba keratitis (see comment)
Comment: The cornea is ulcerated with necrosis and neutrophils. PAS and GMS stains highlight amoebic forms. PAS also highlights the Descemet membrane.
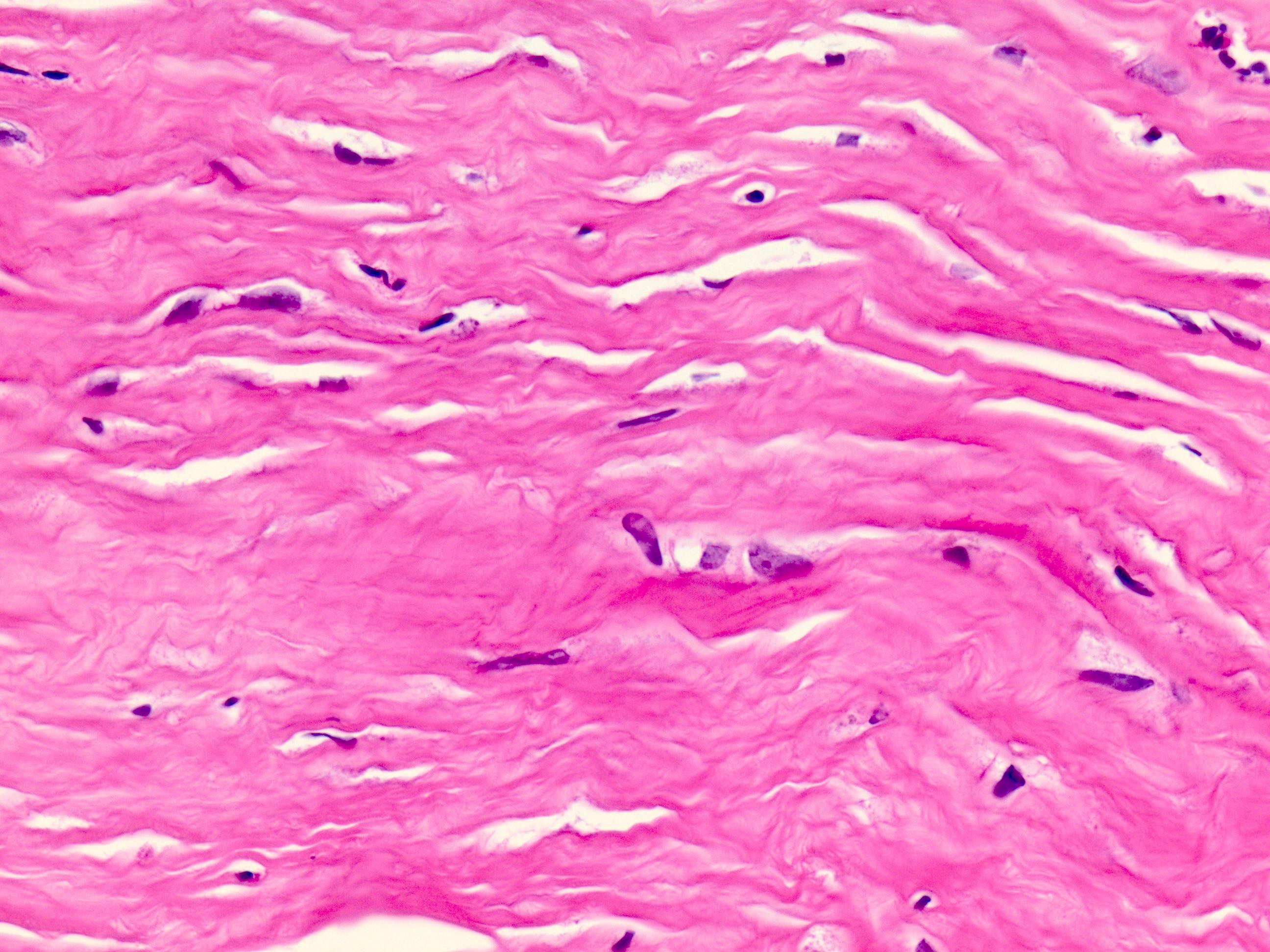
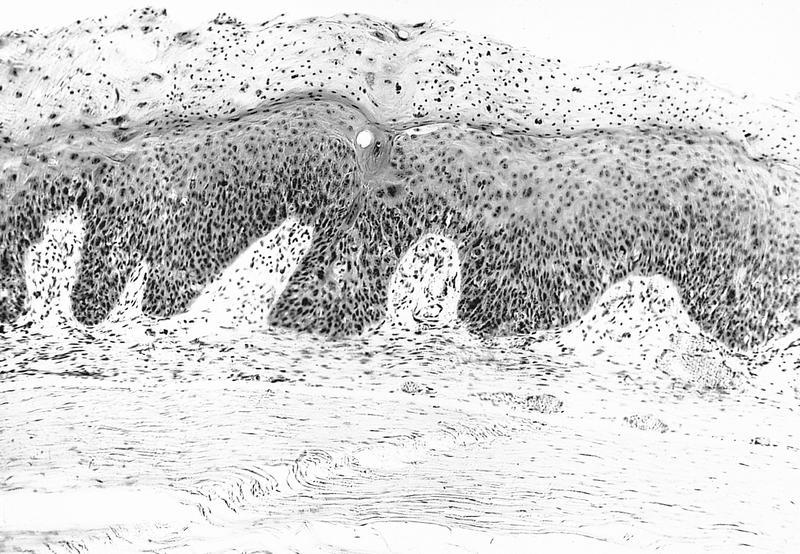
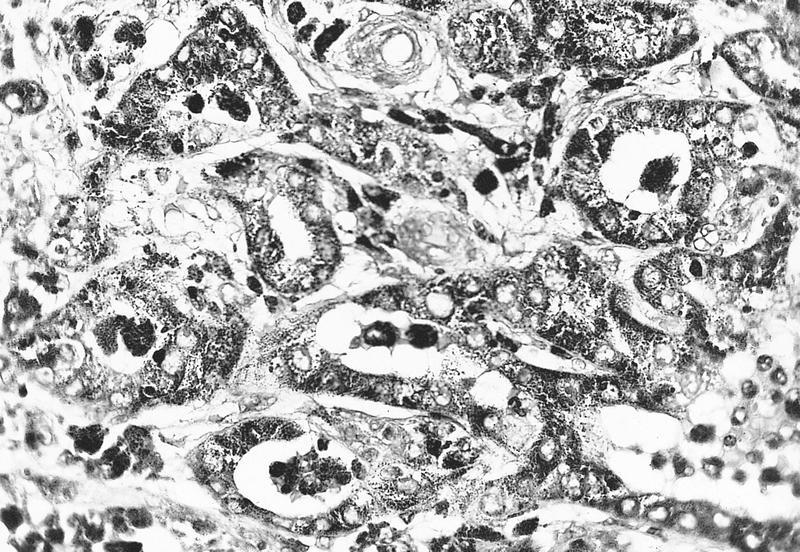
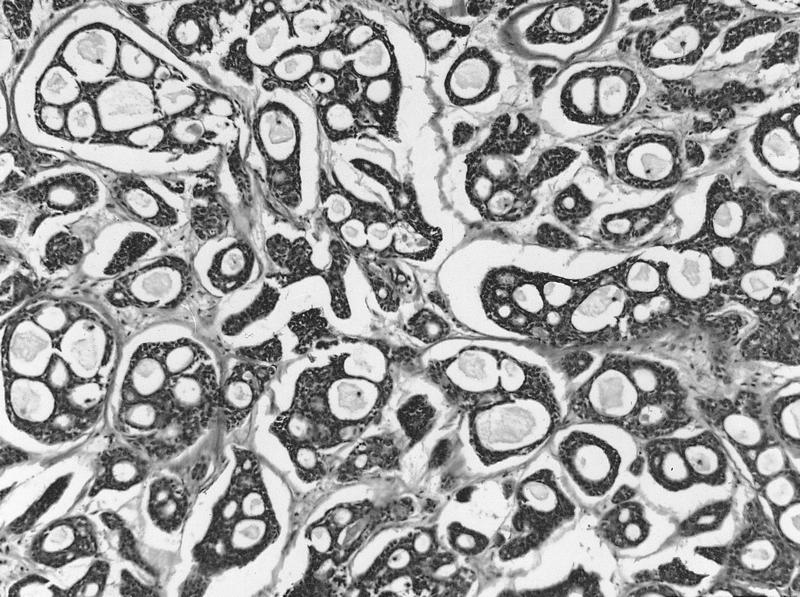
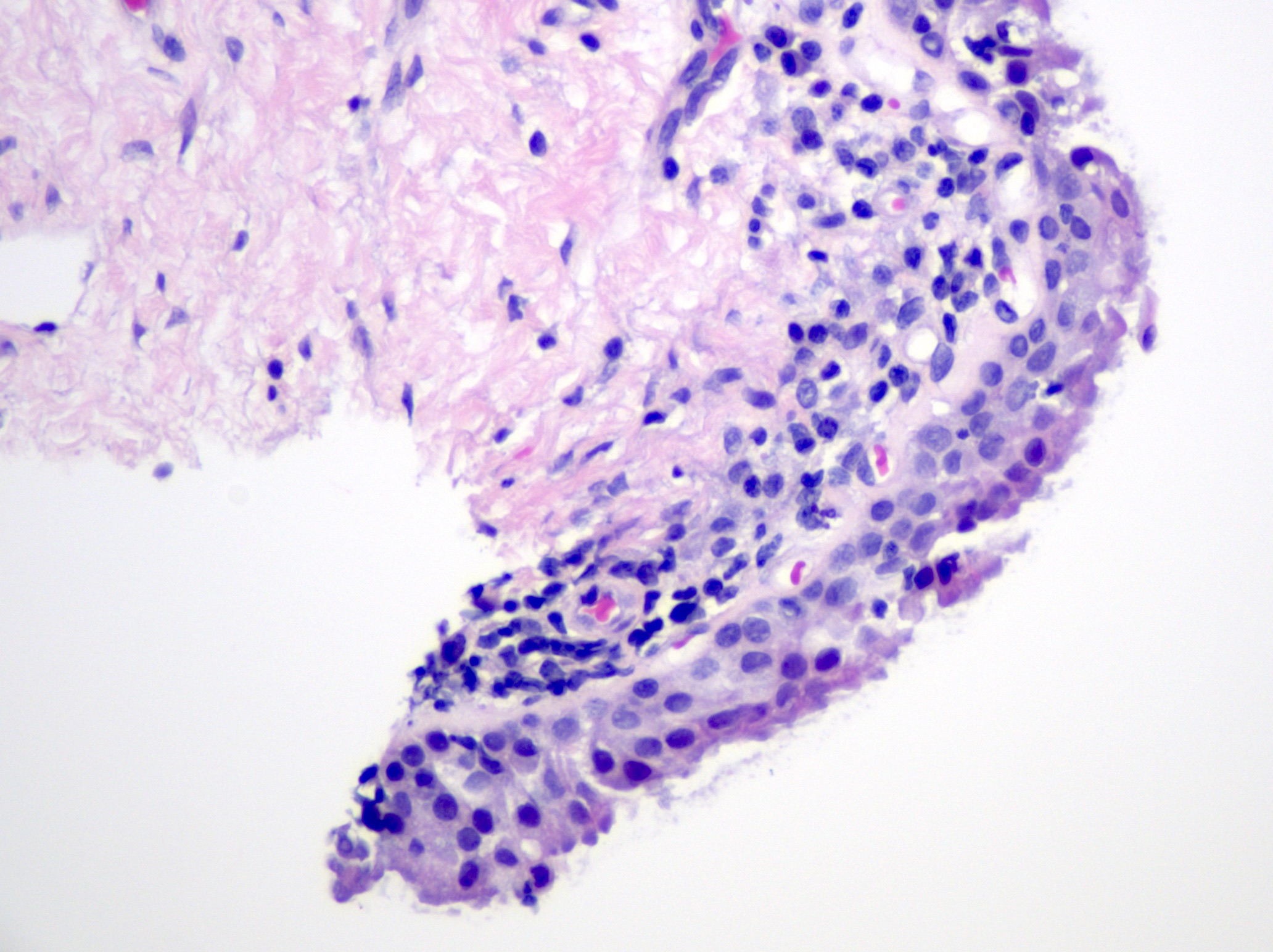
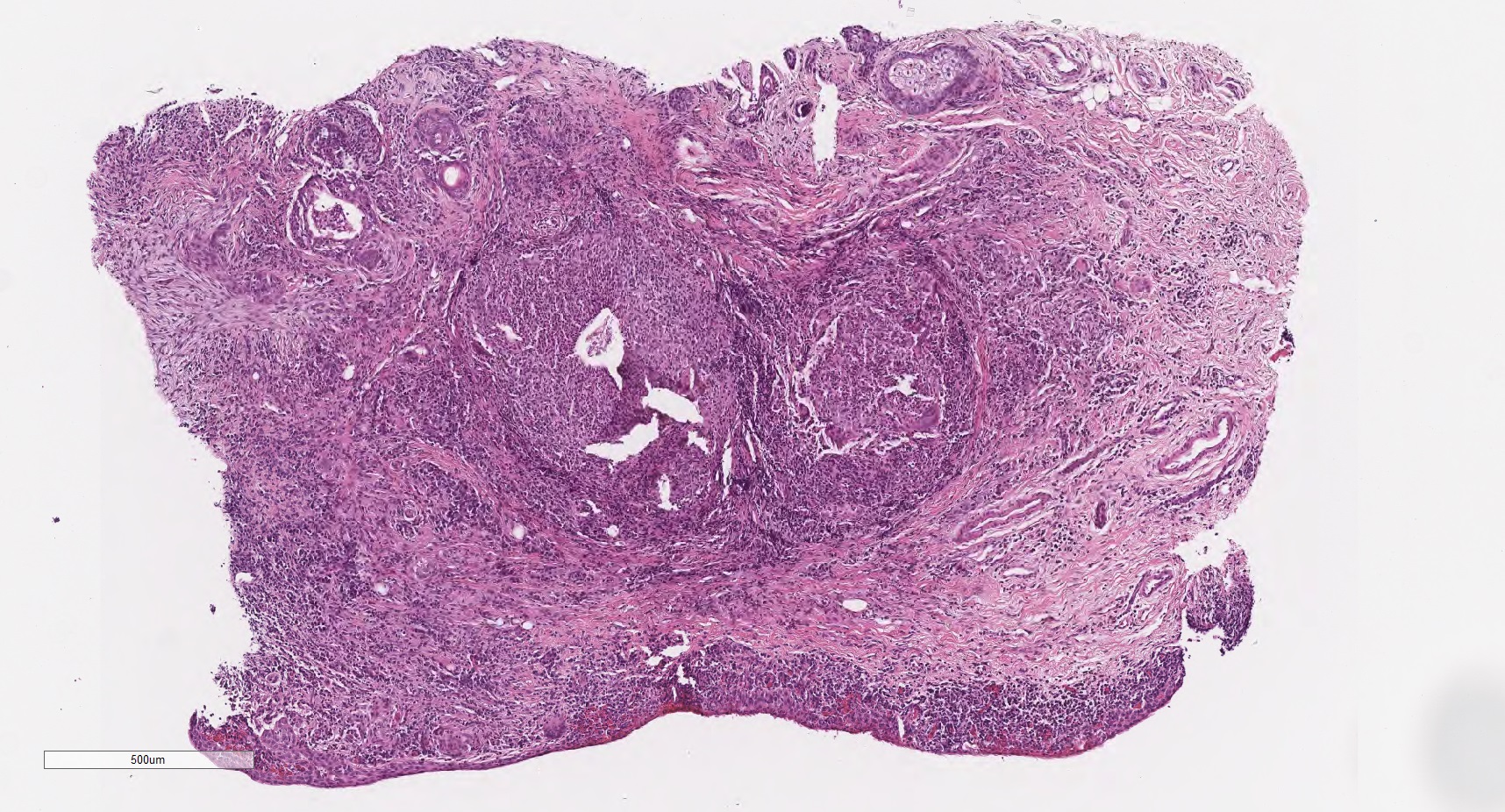
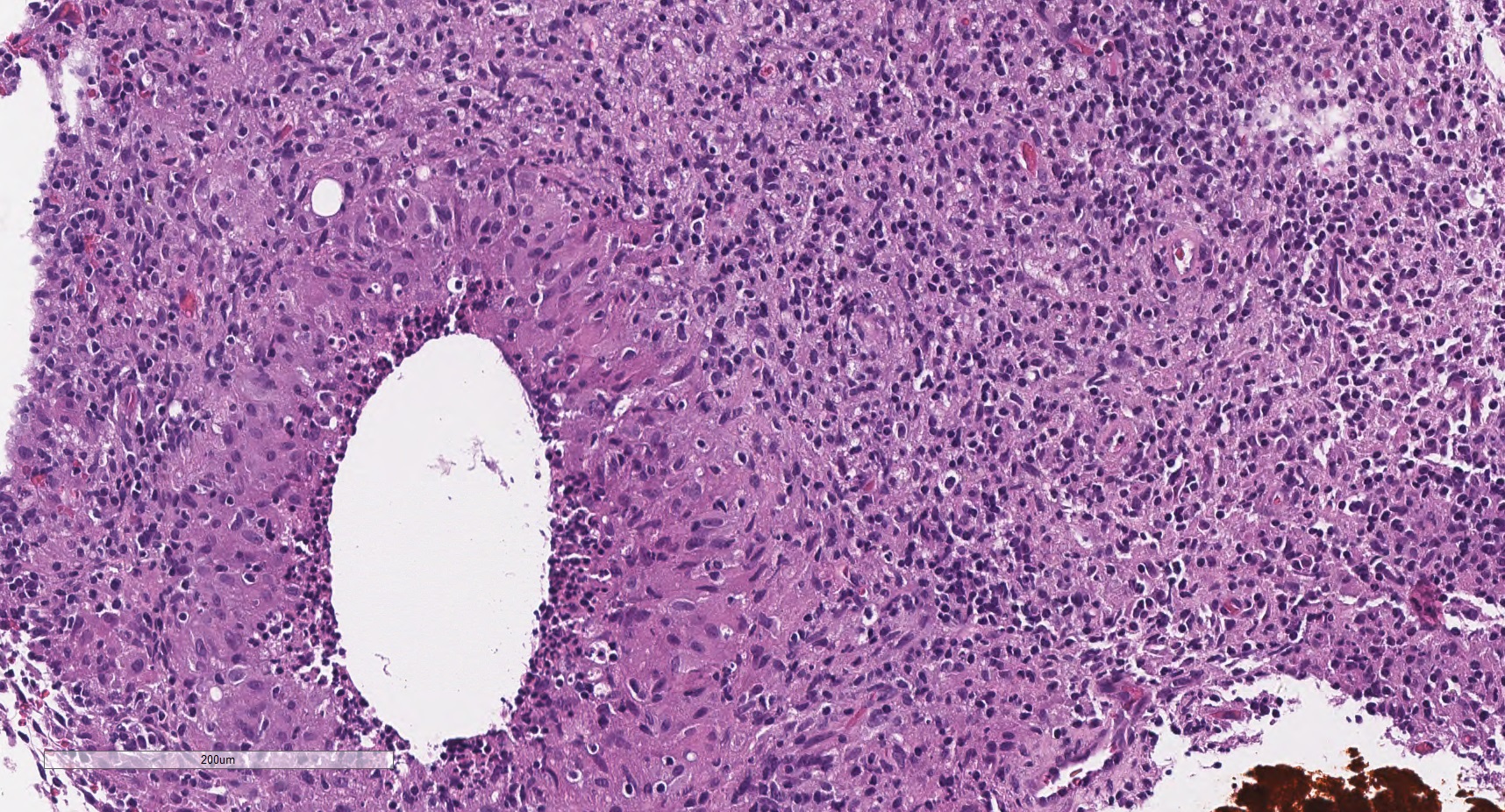
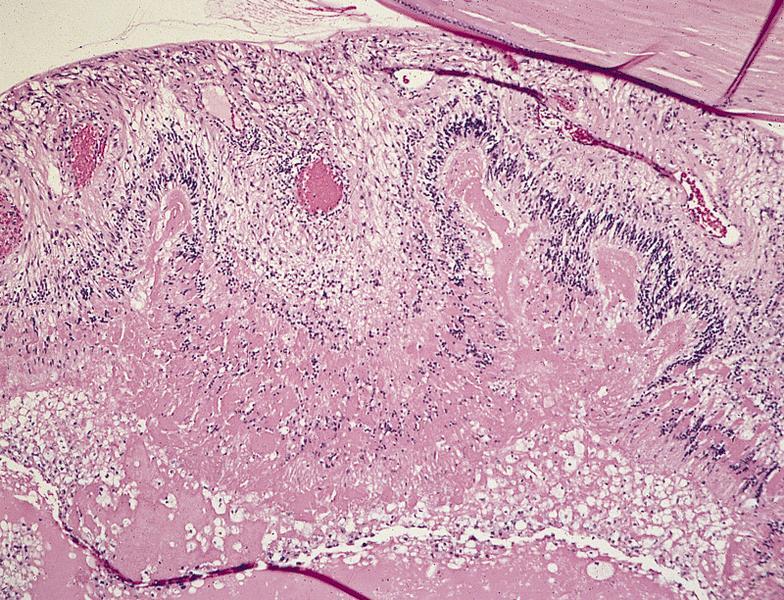
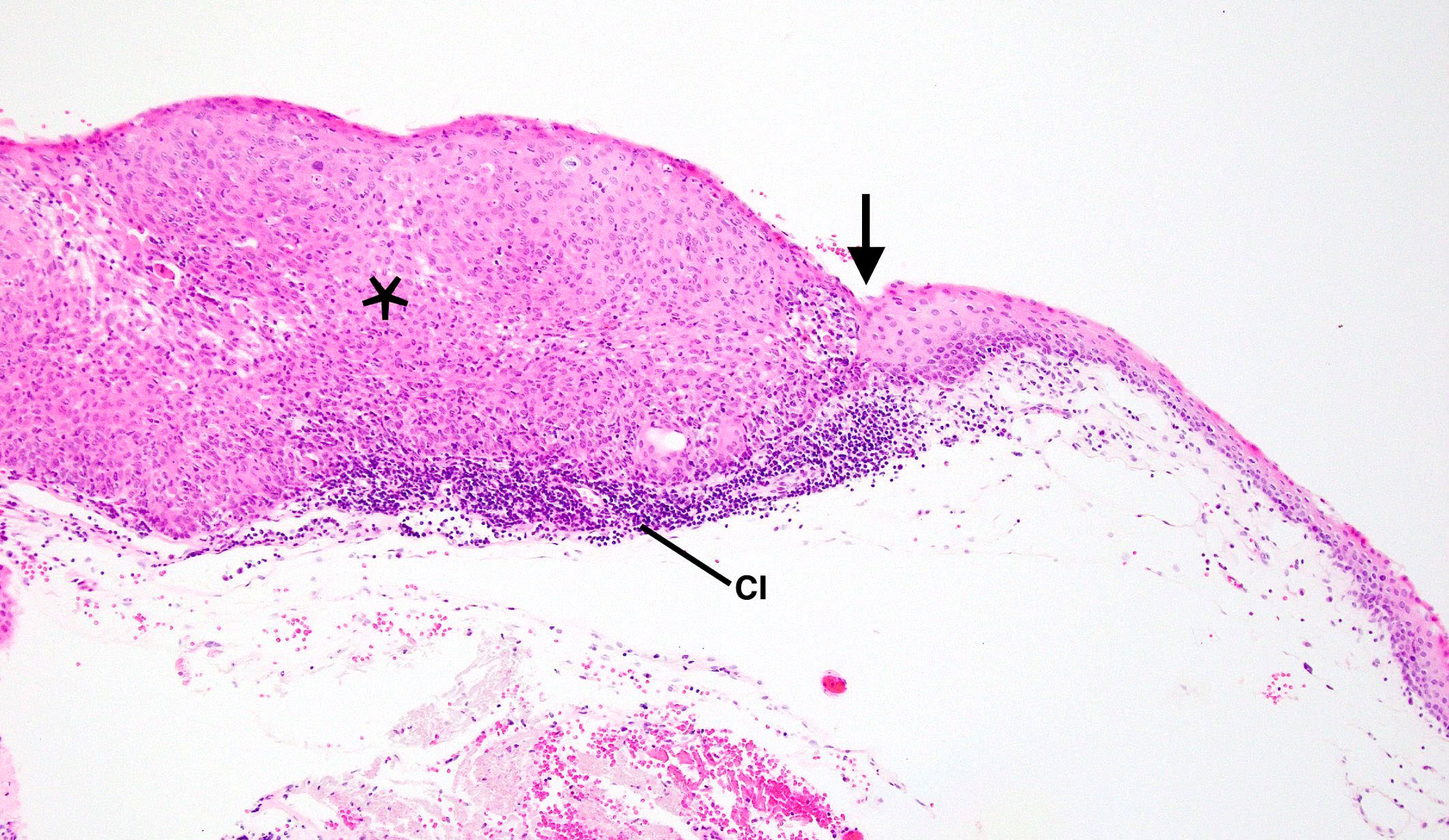
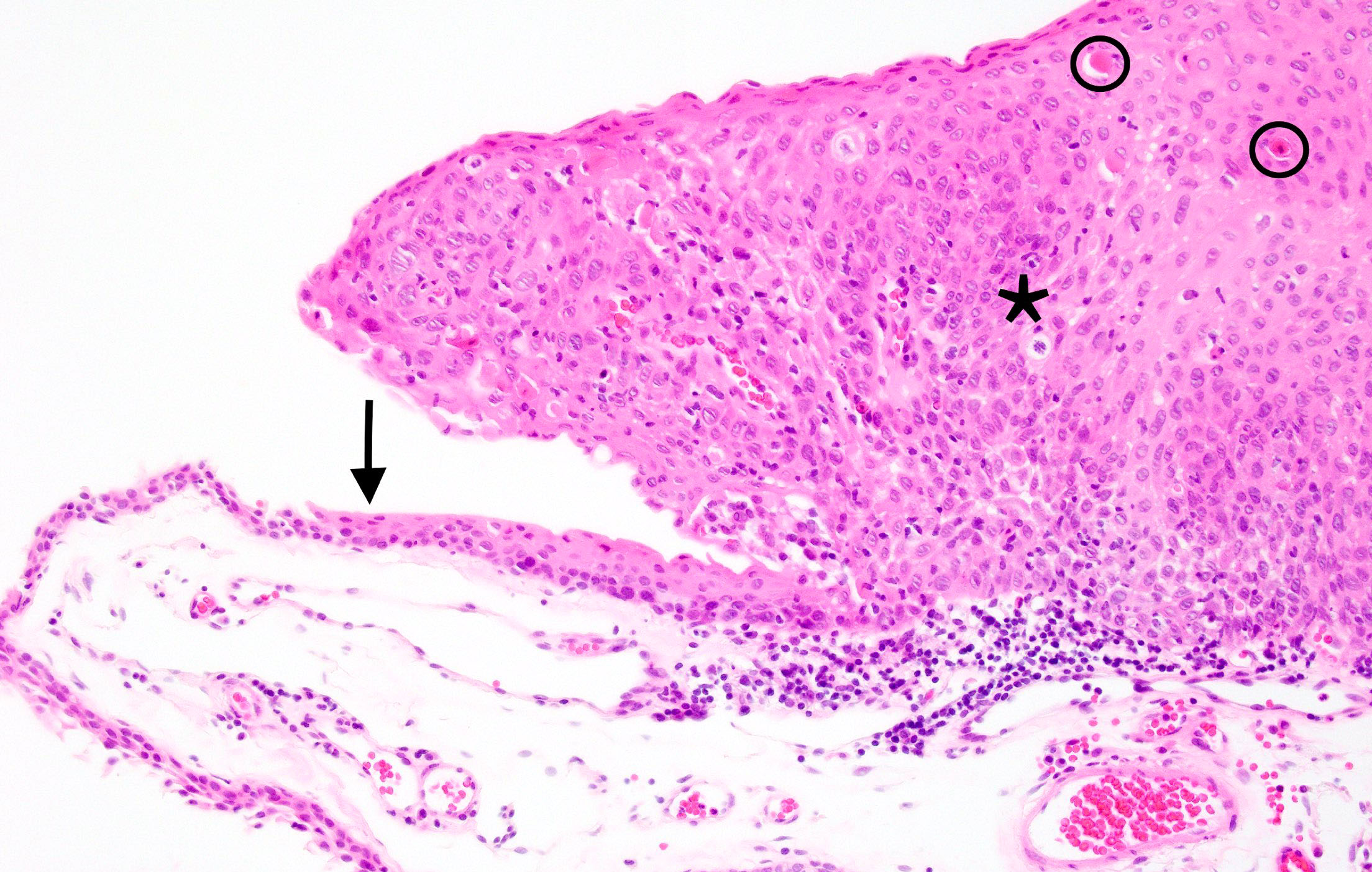
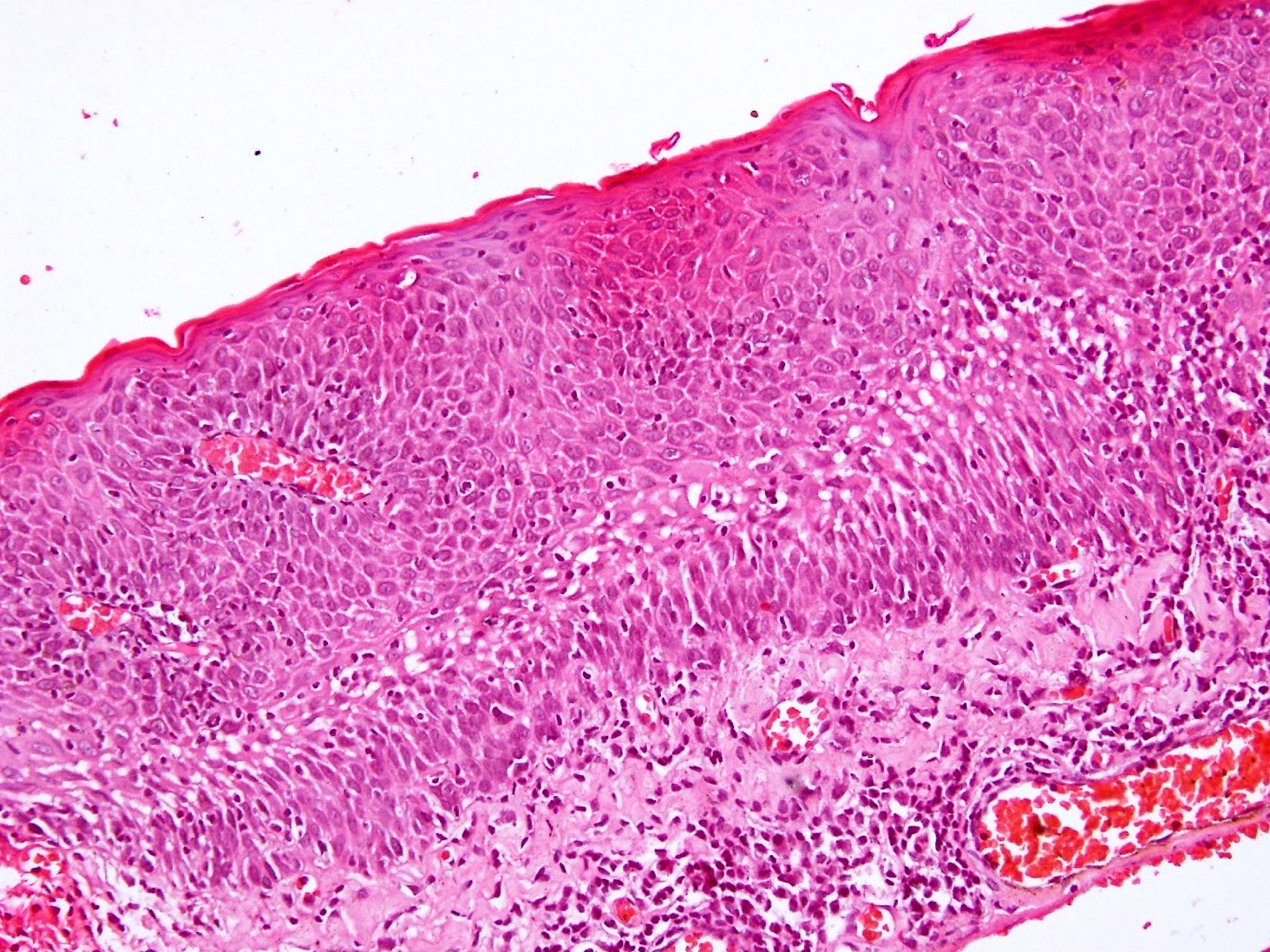
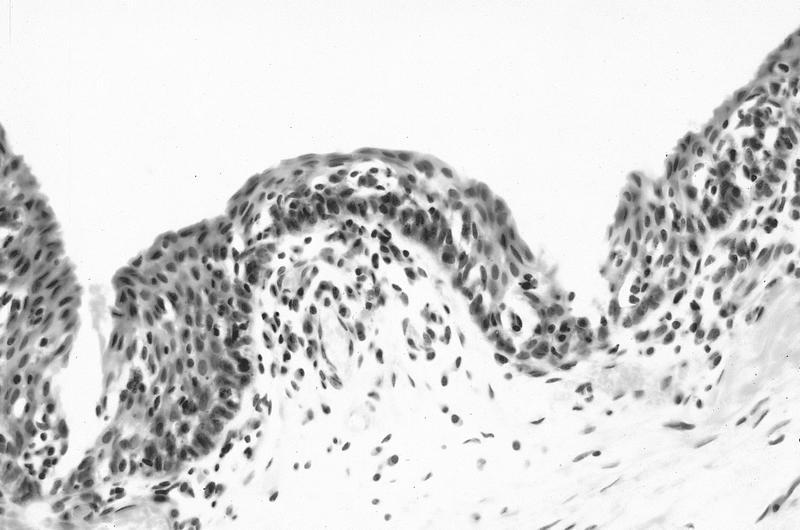
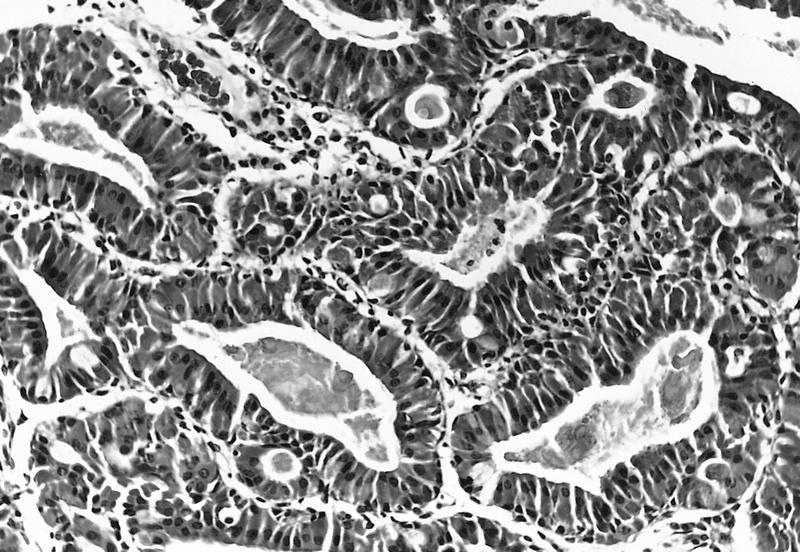
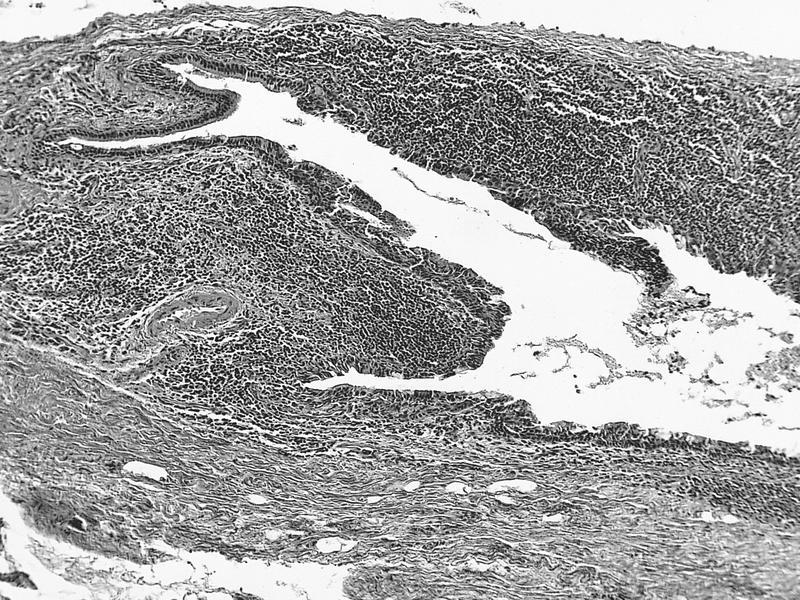
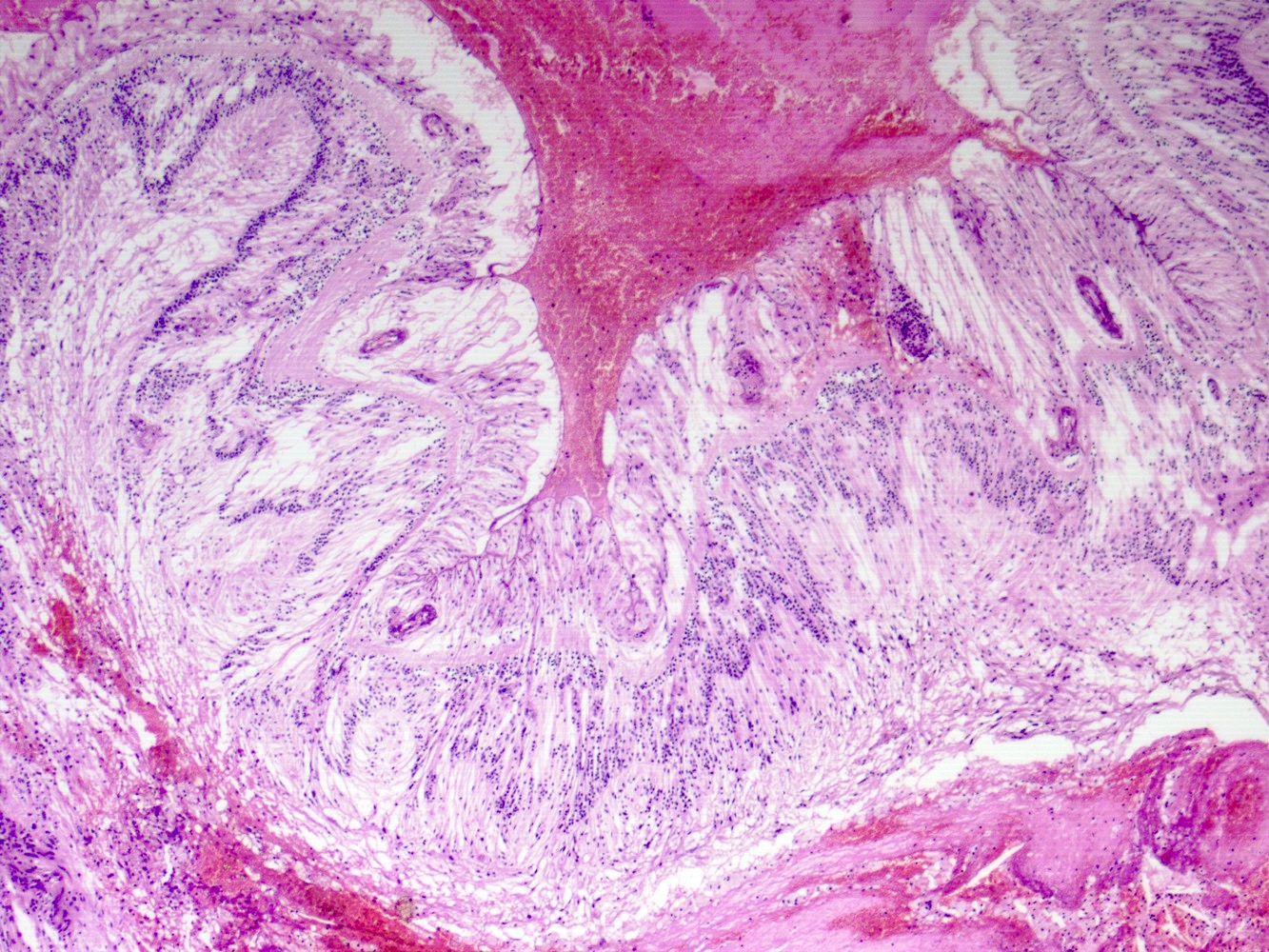
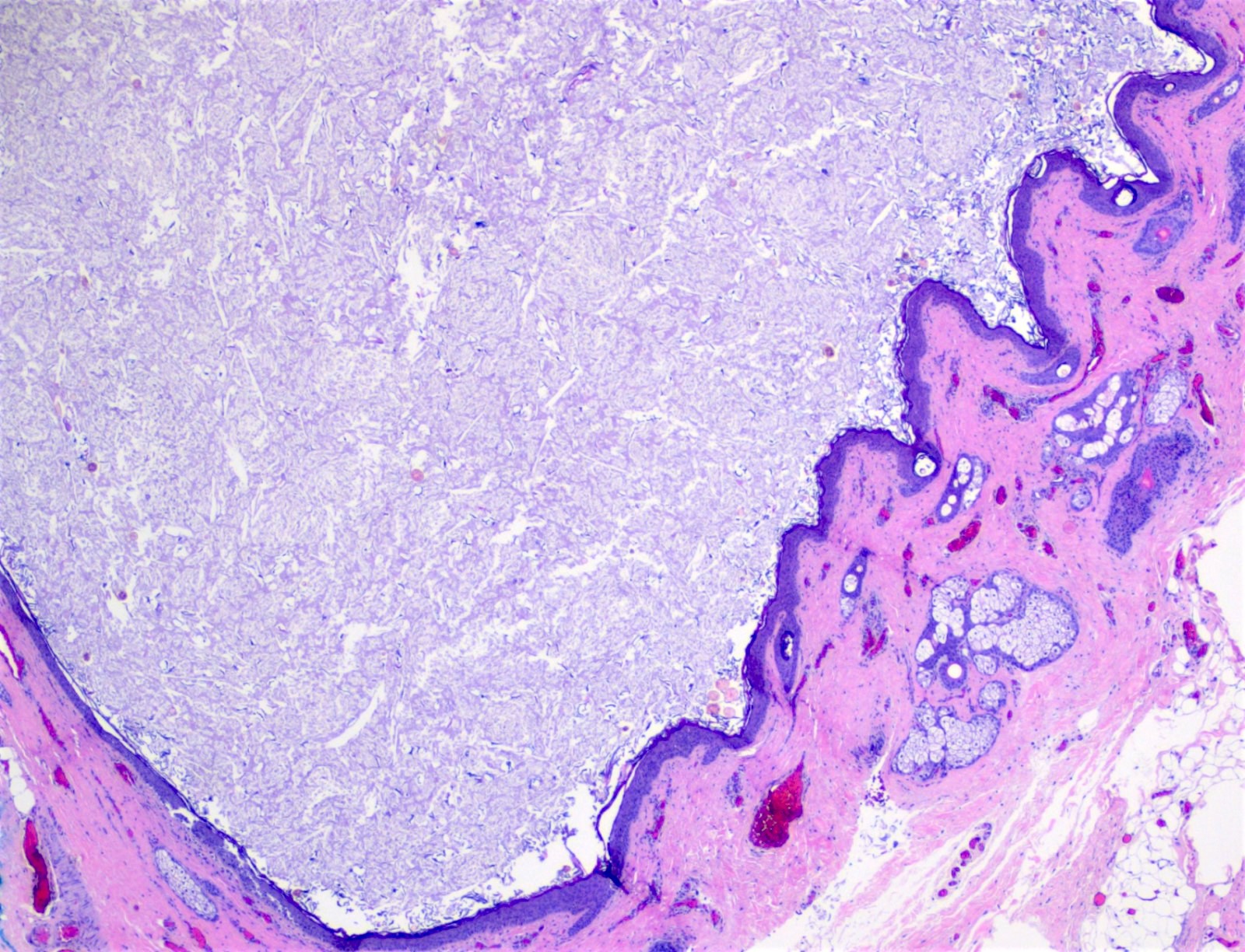
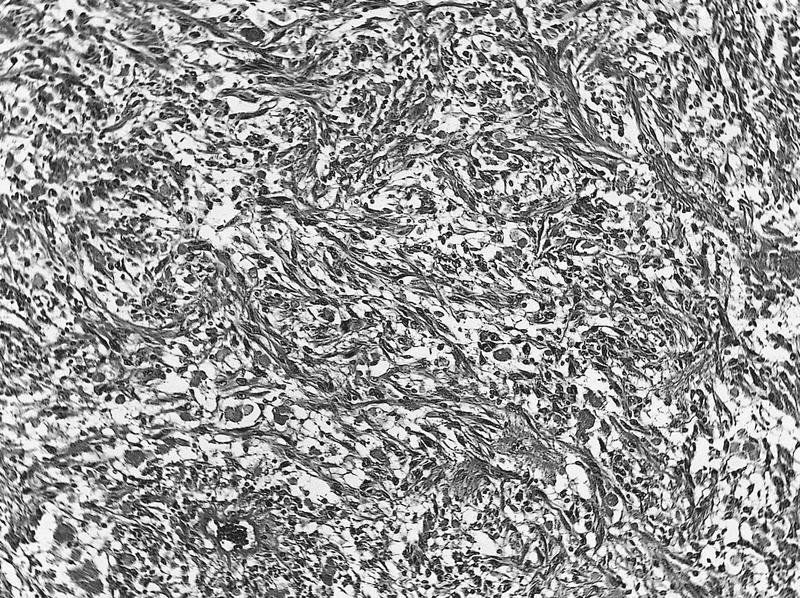
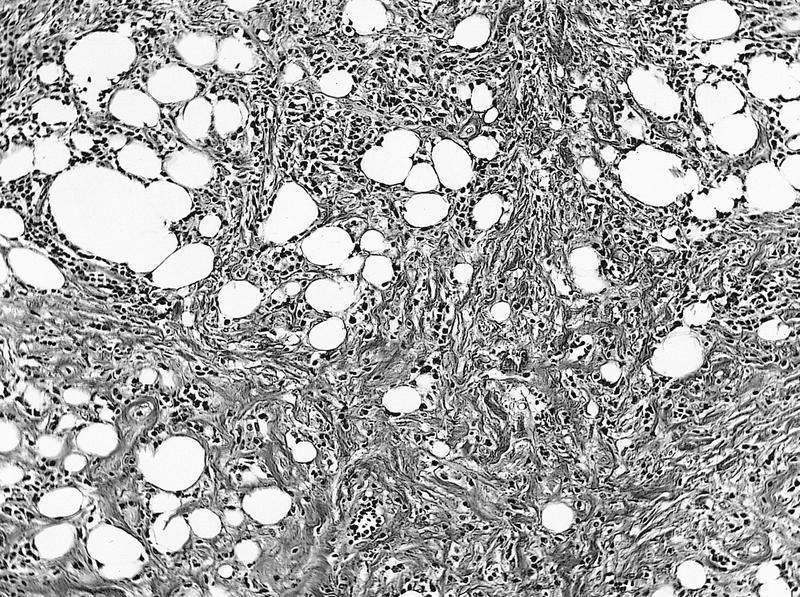
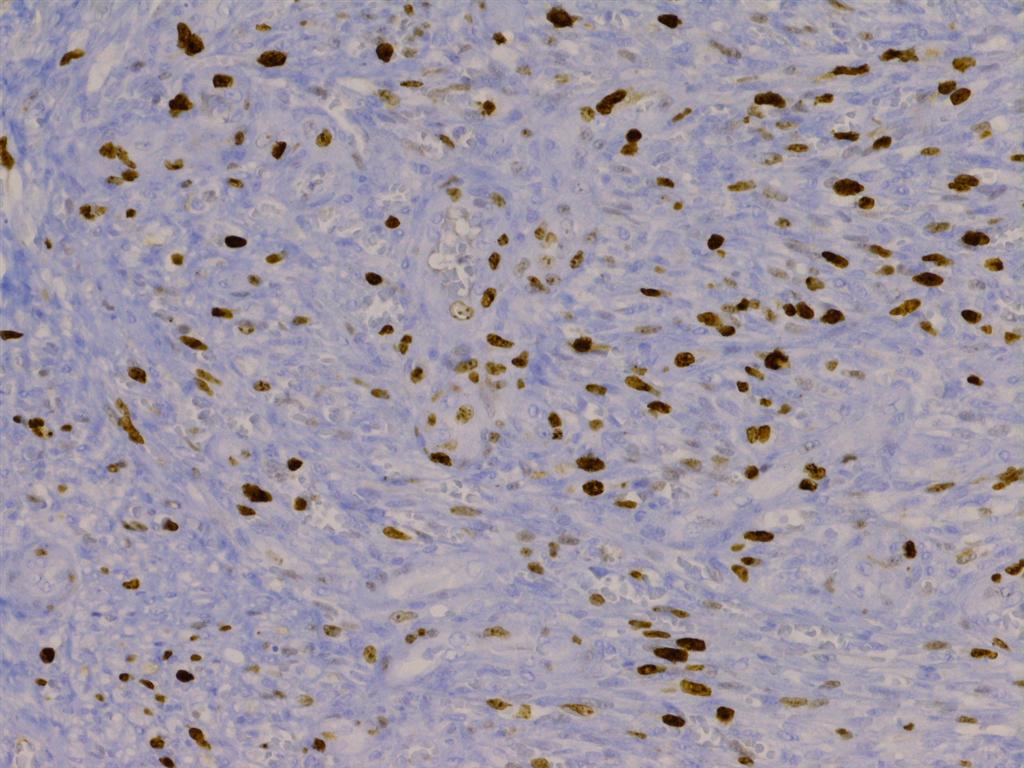
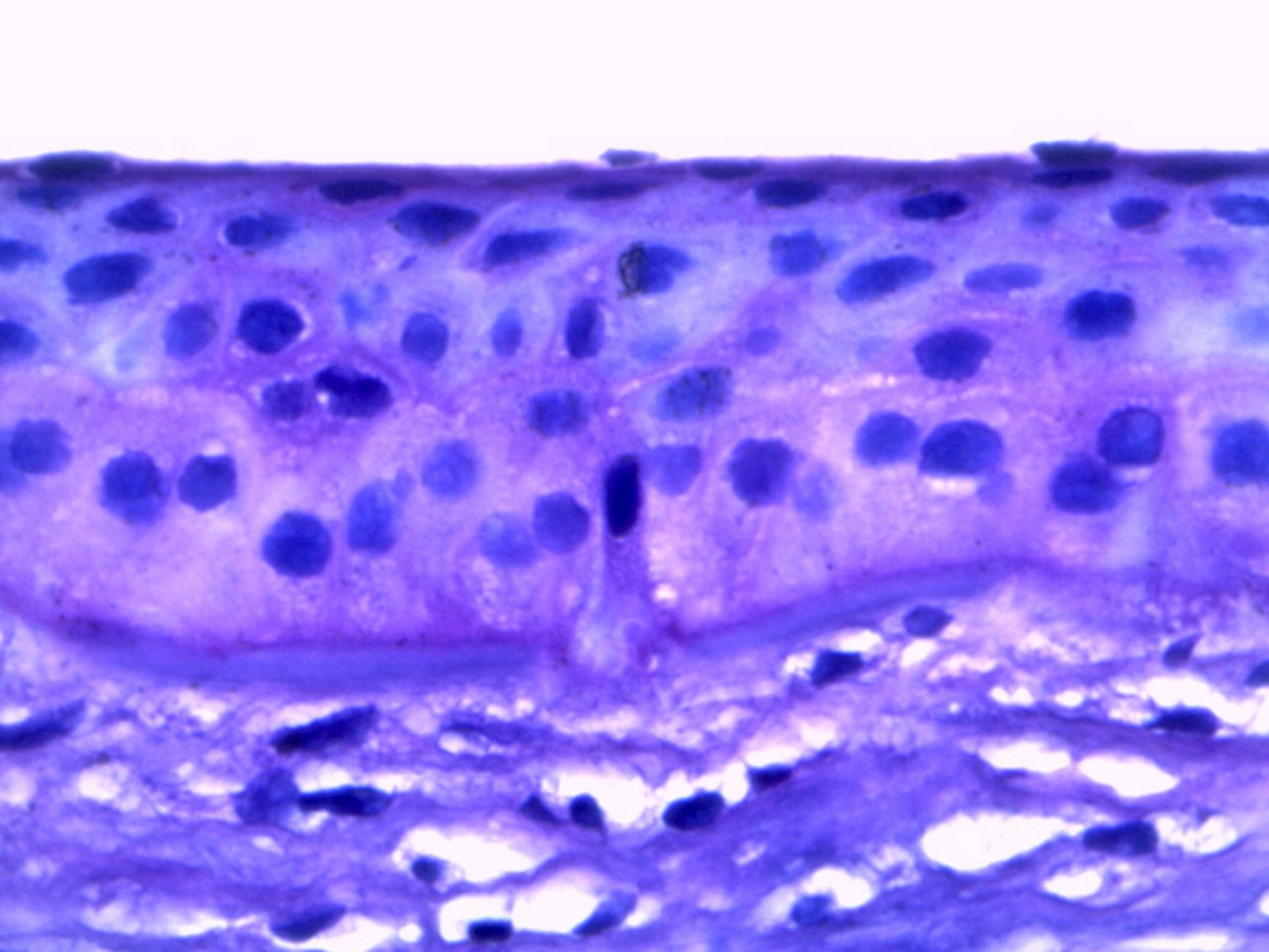
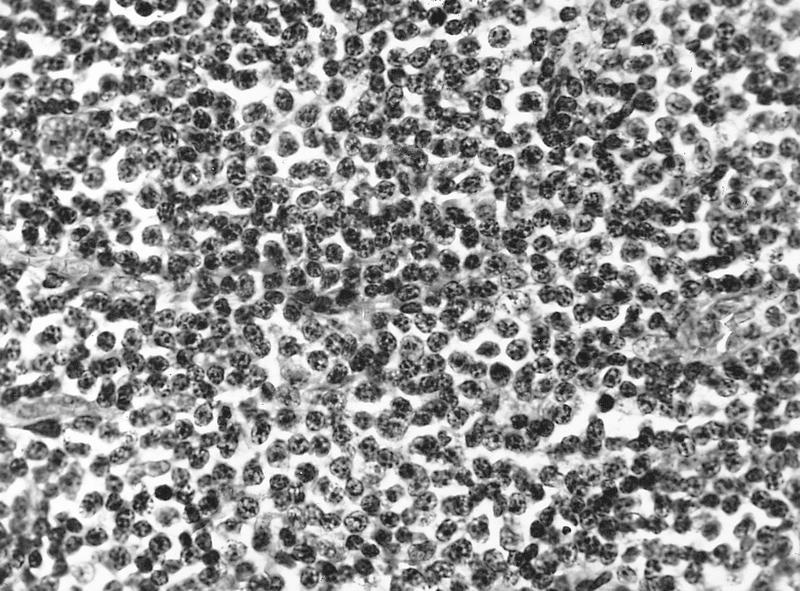
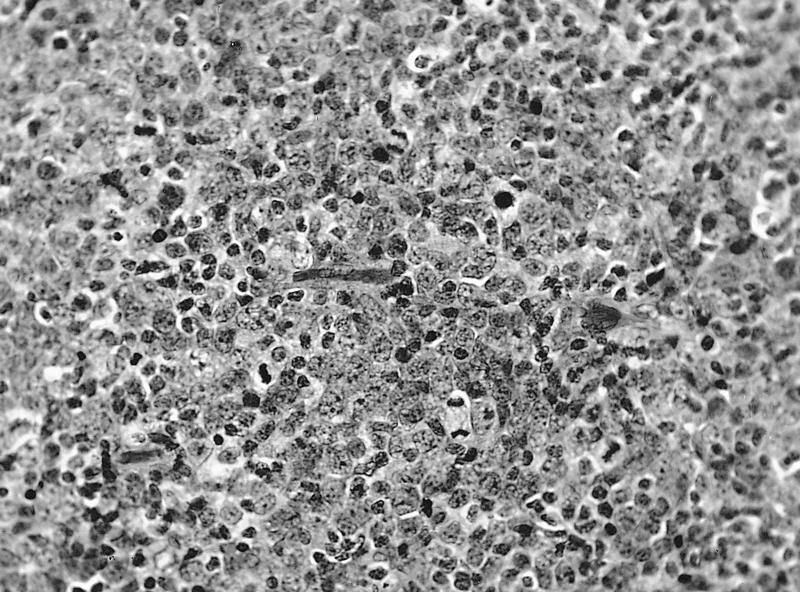
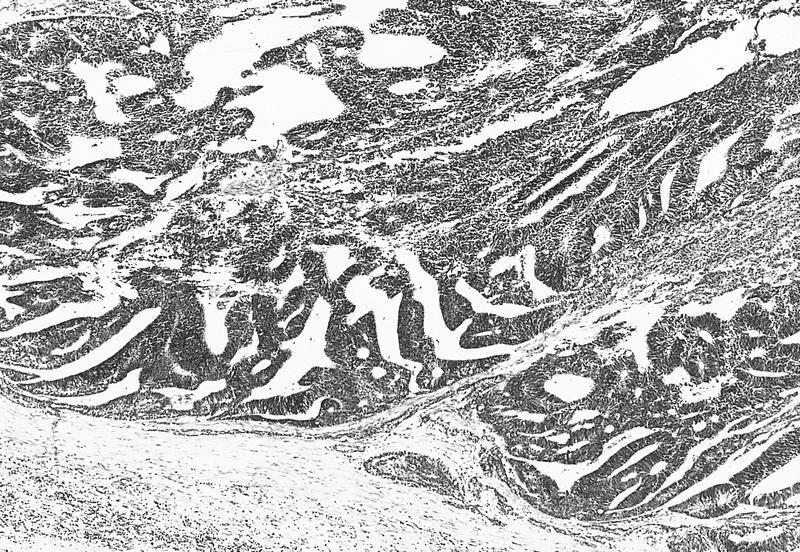
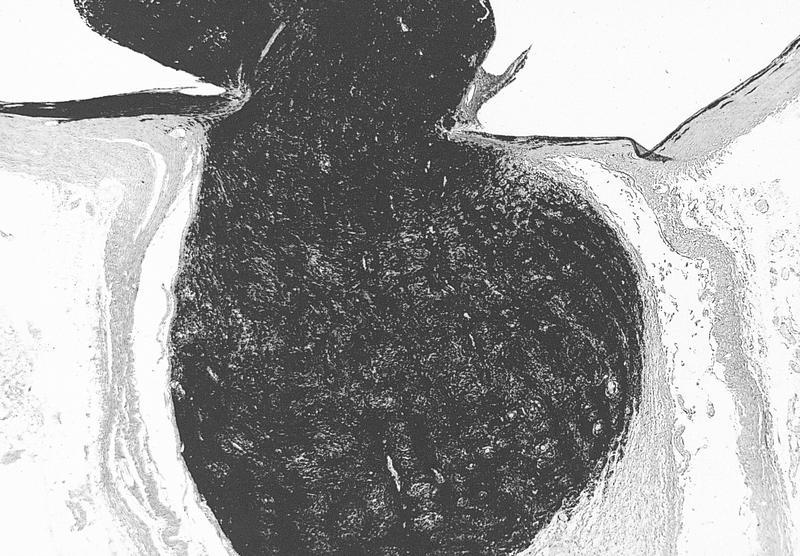
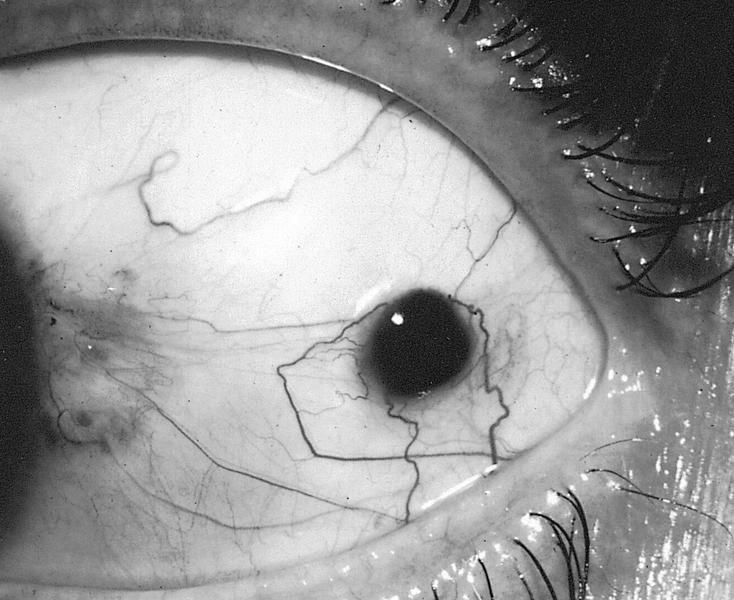
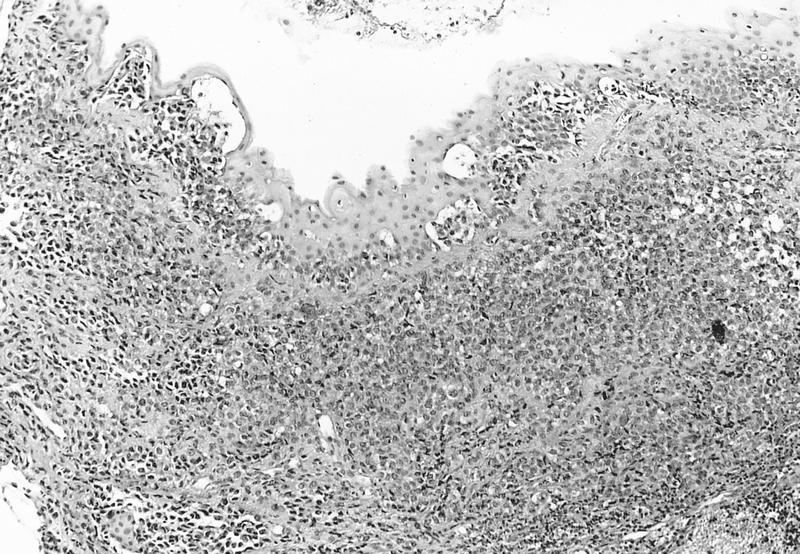
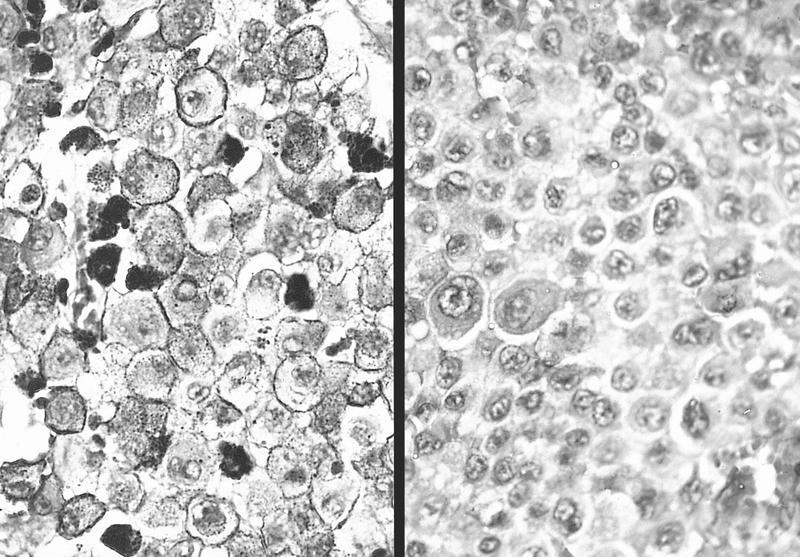
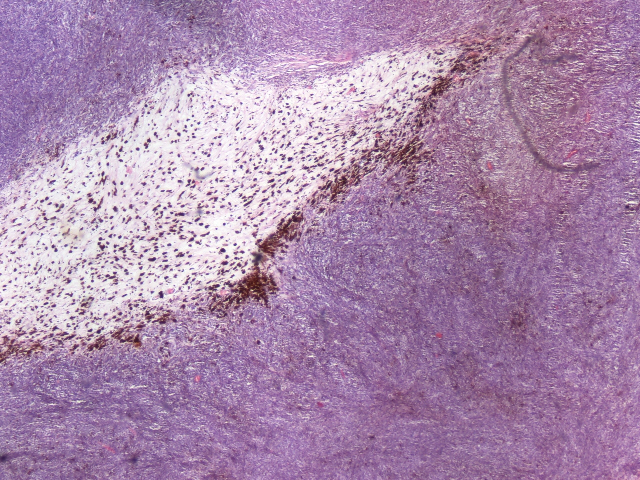
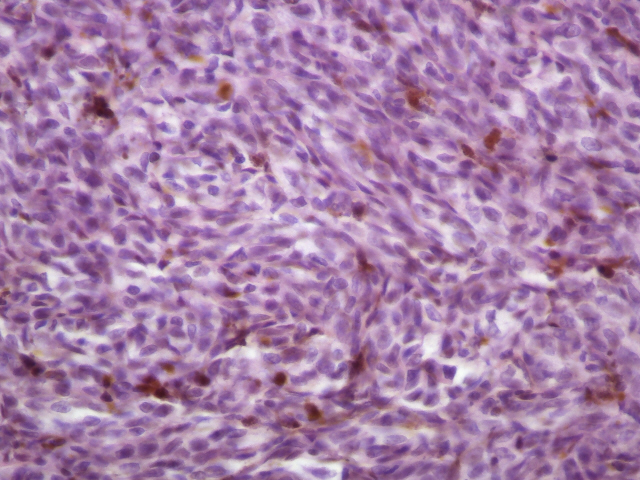
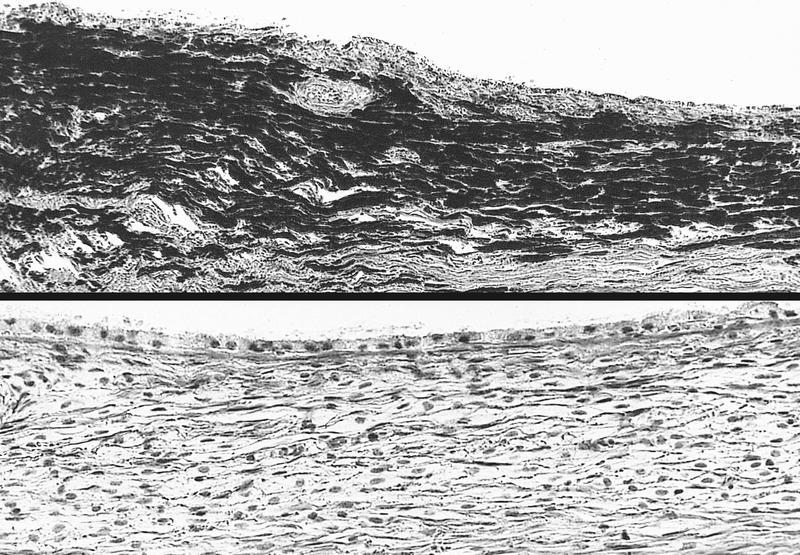
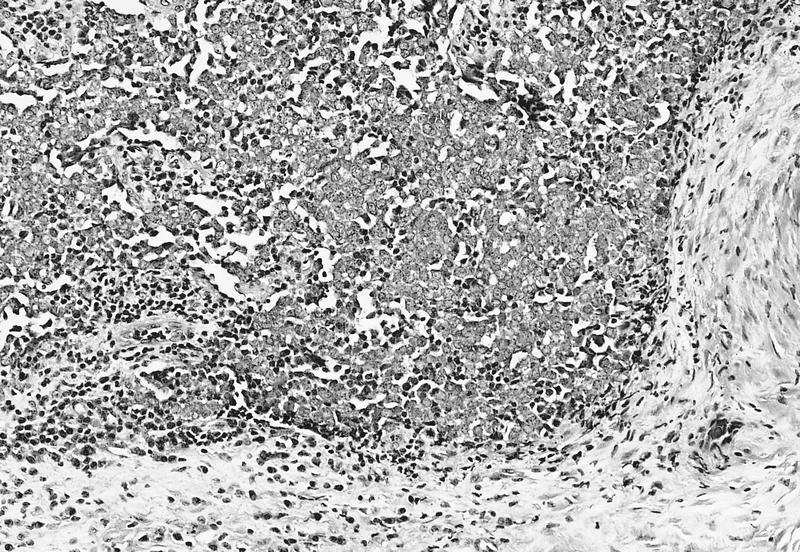
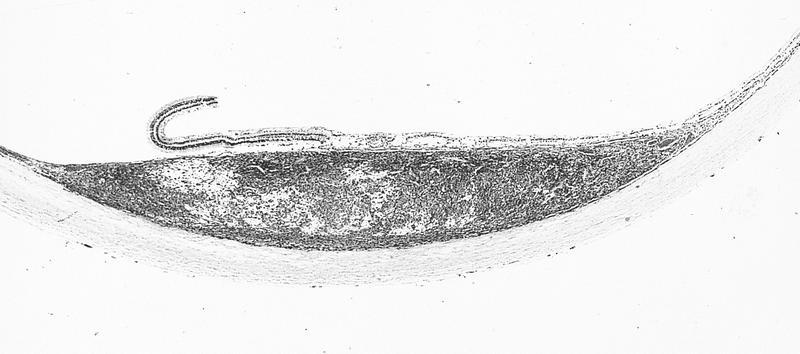
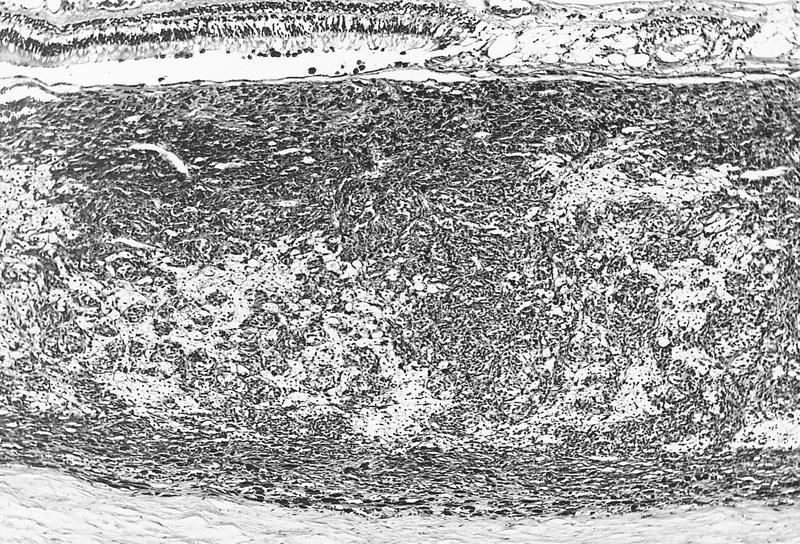
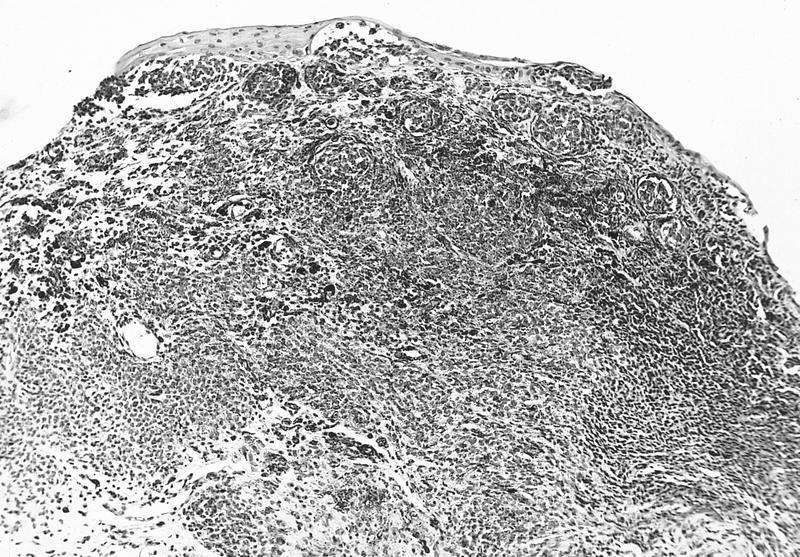
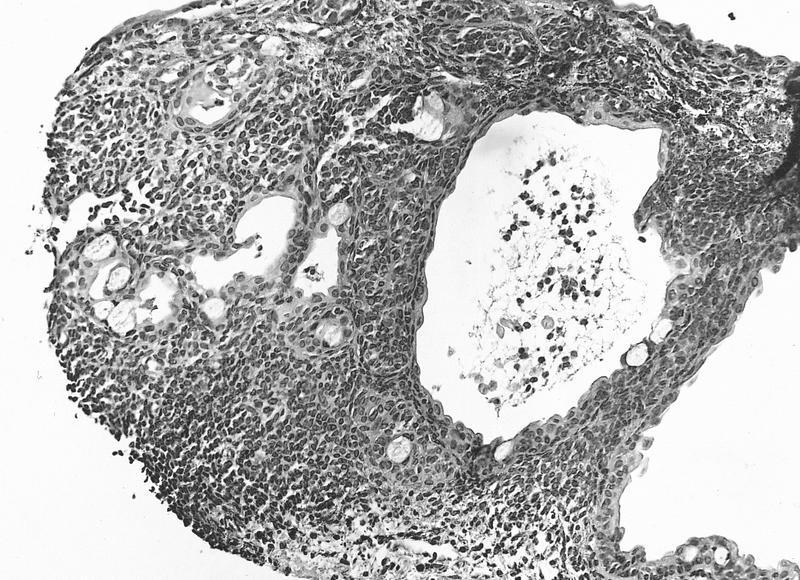
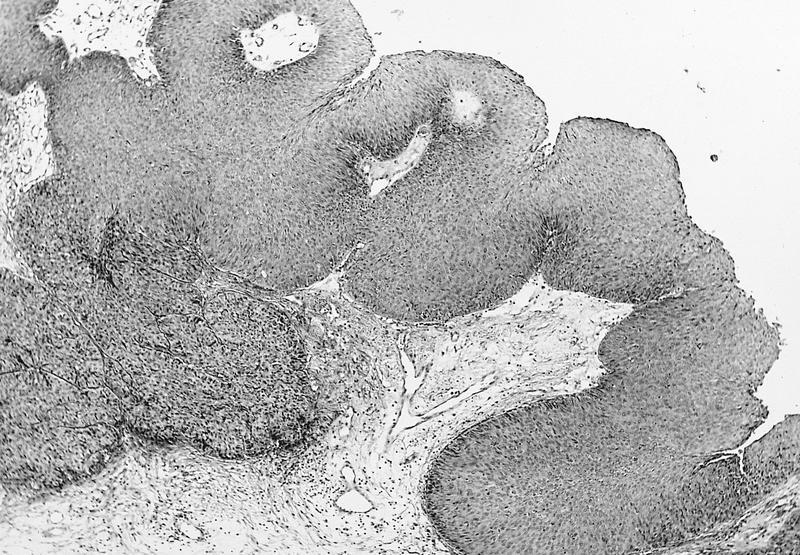
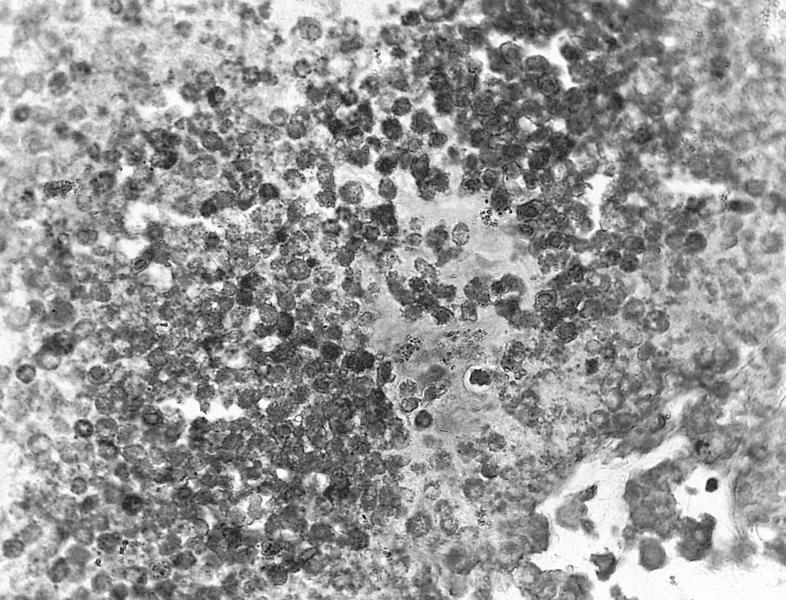
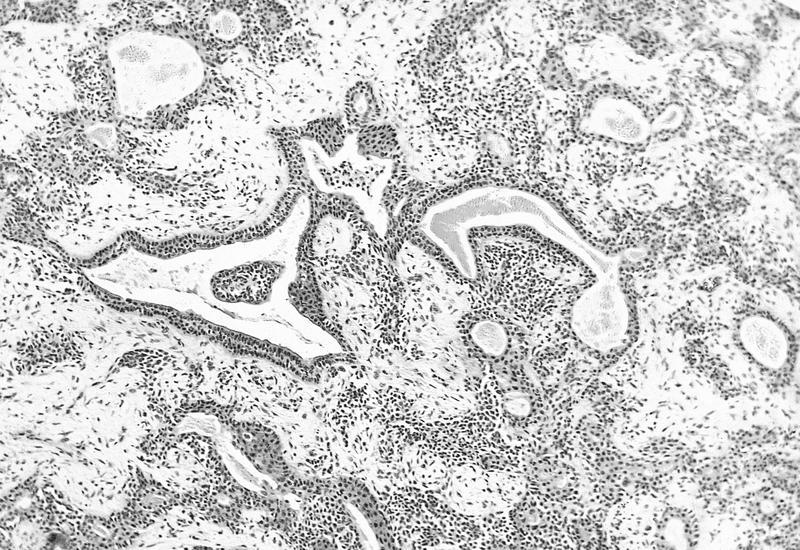
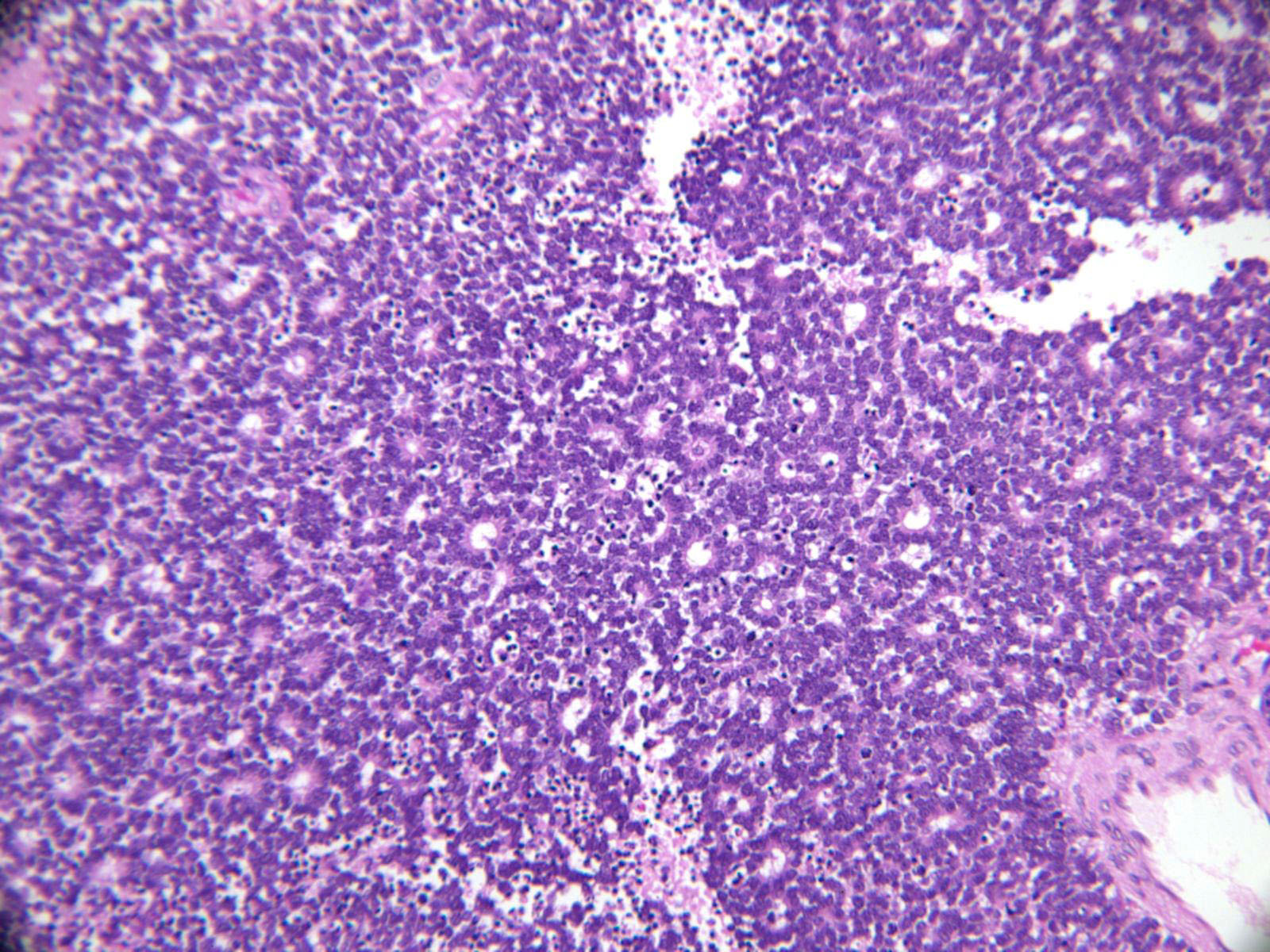
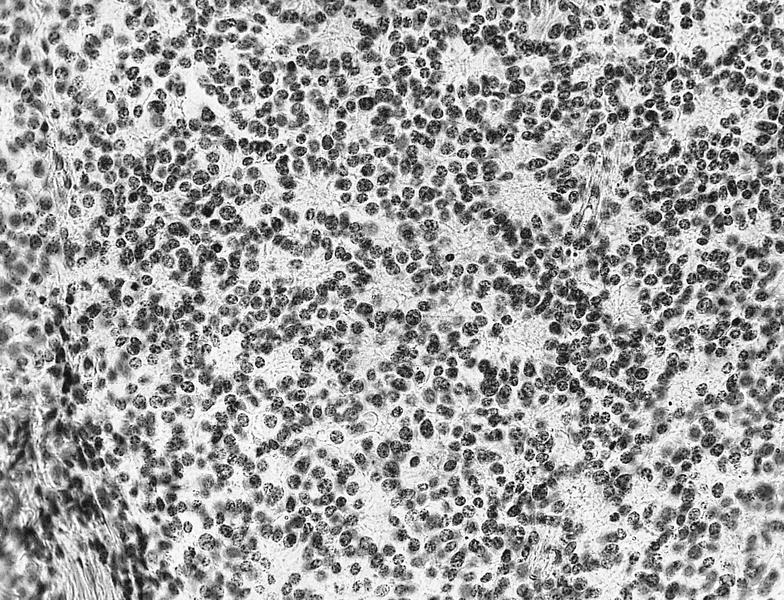
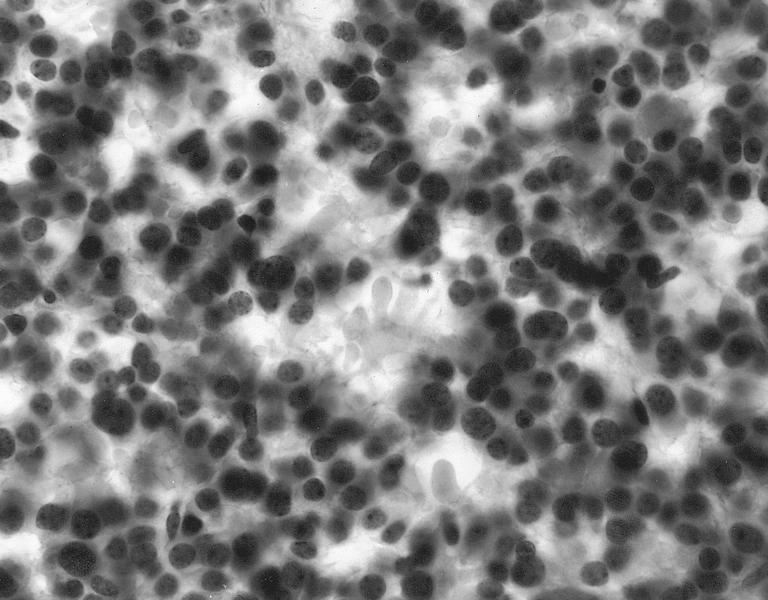
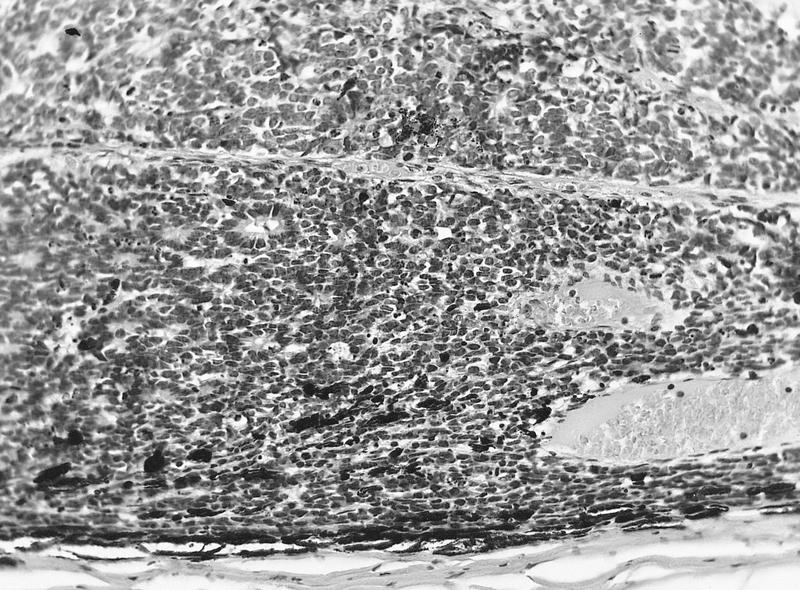
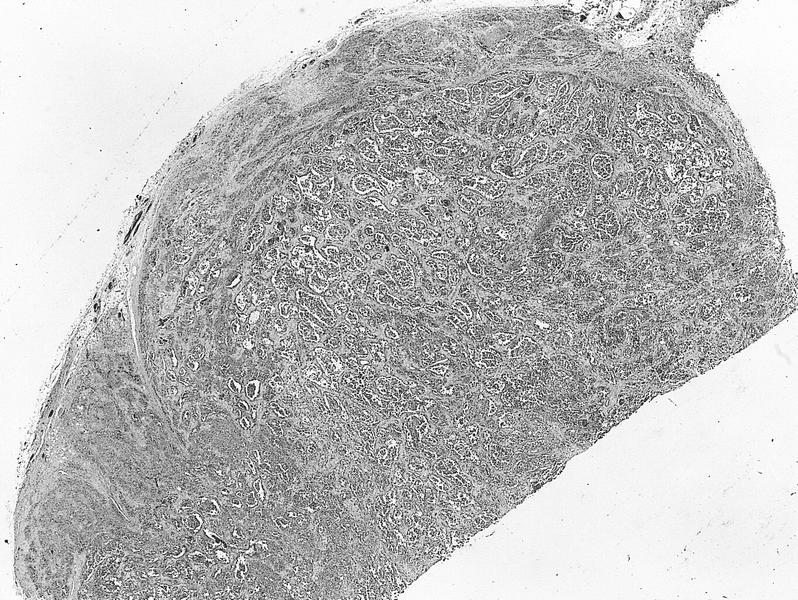
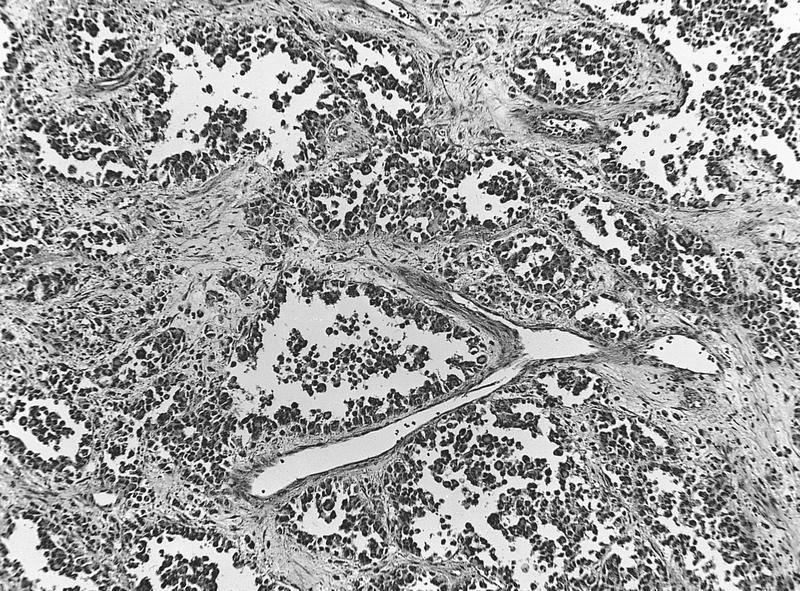
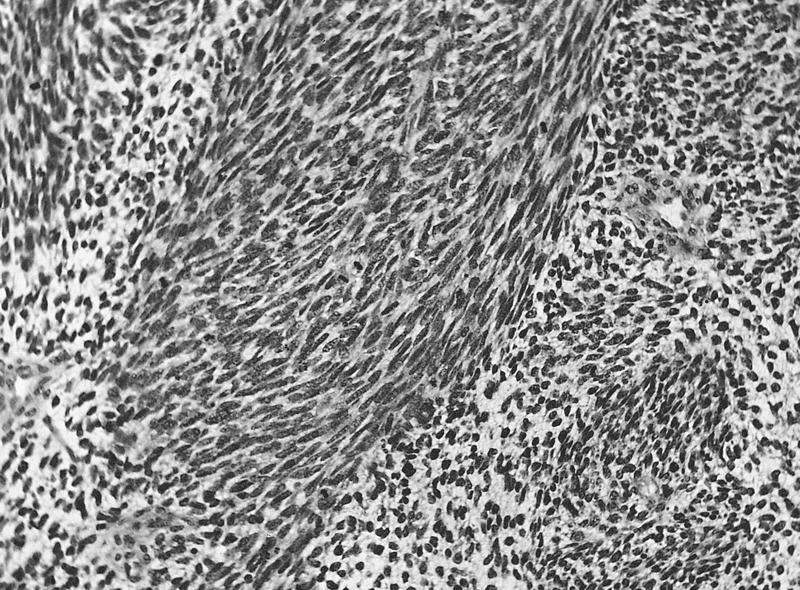
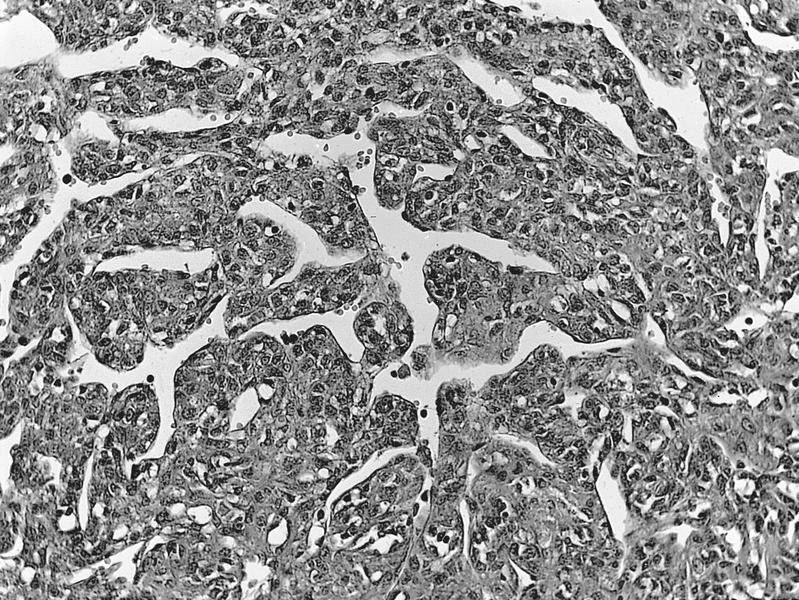
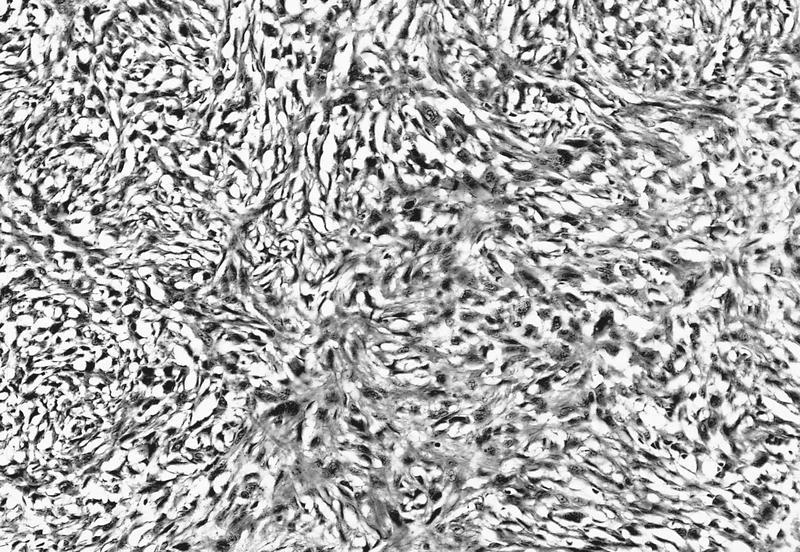
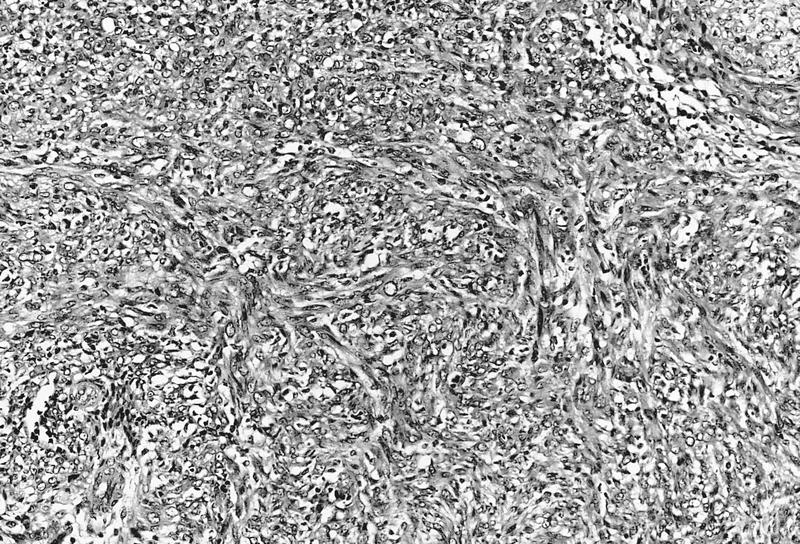
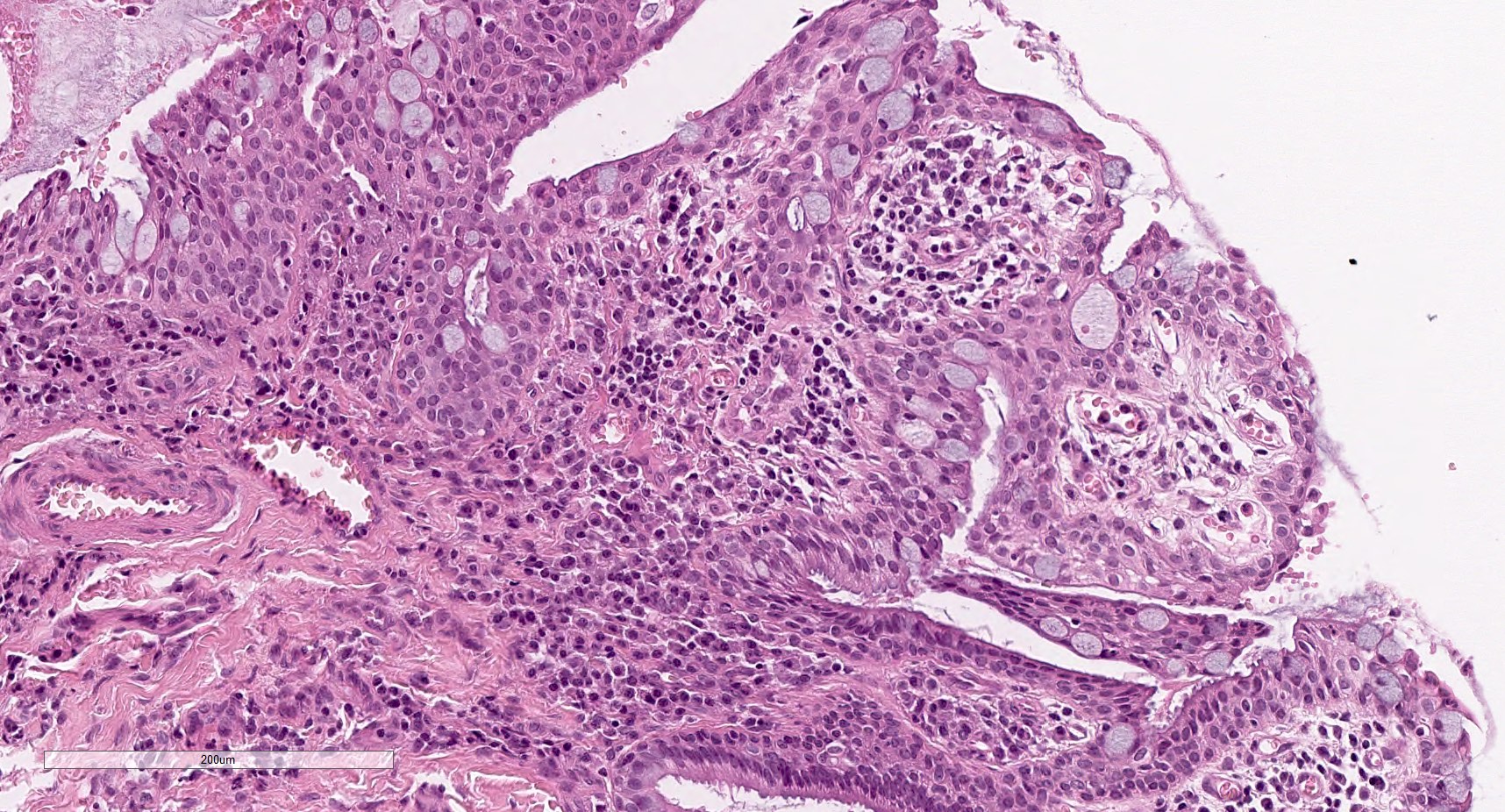
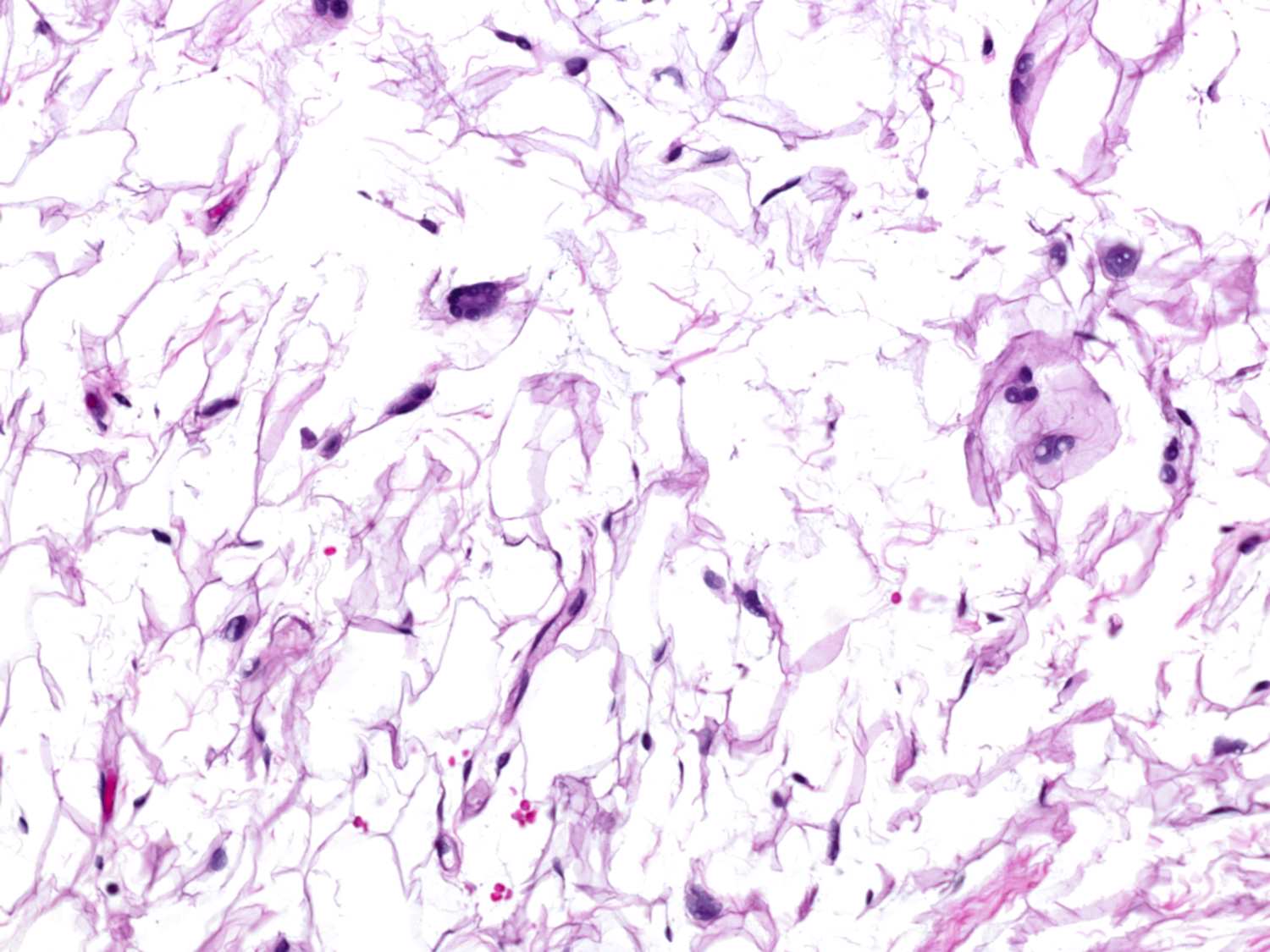
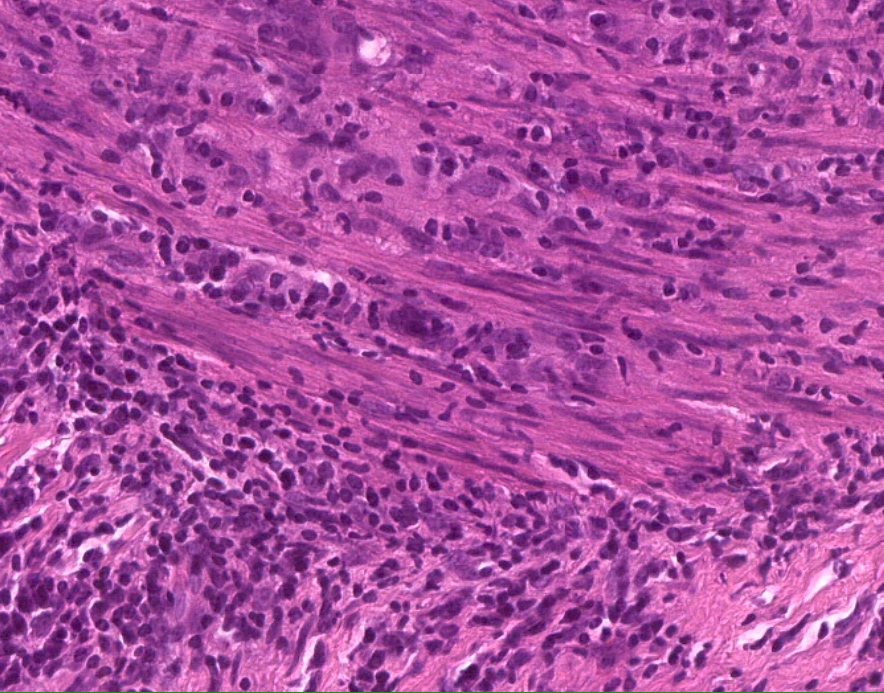
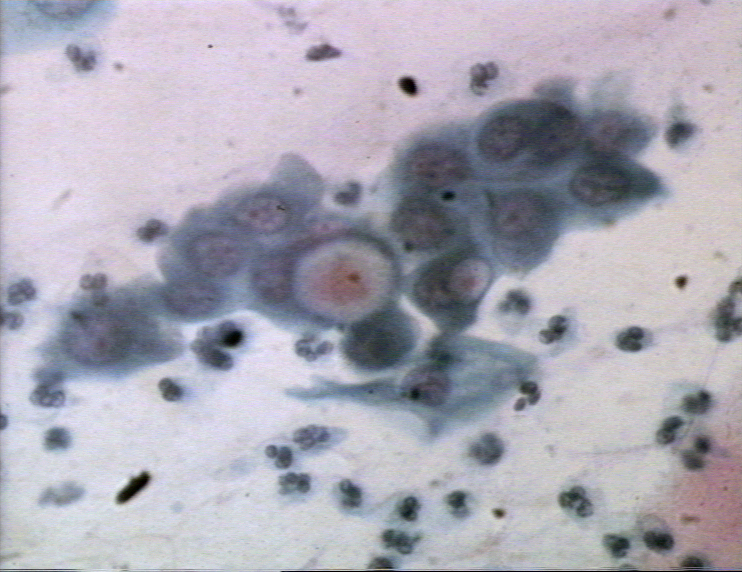
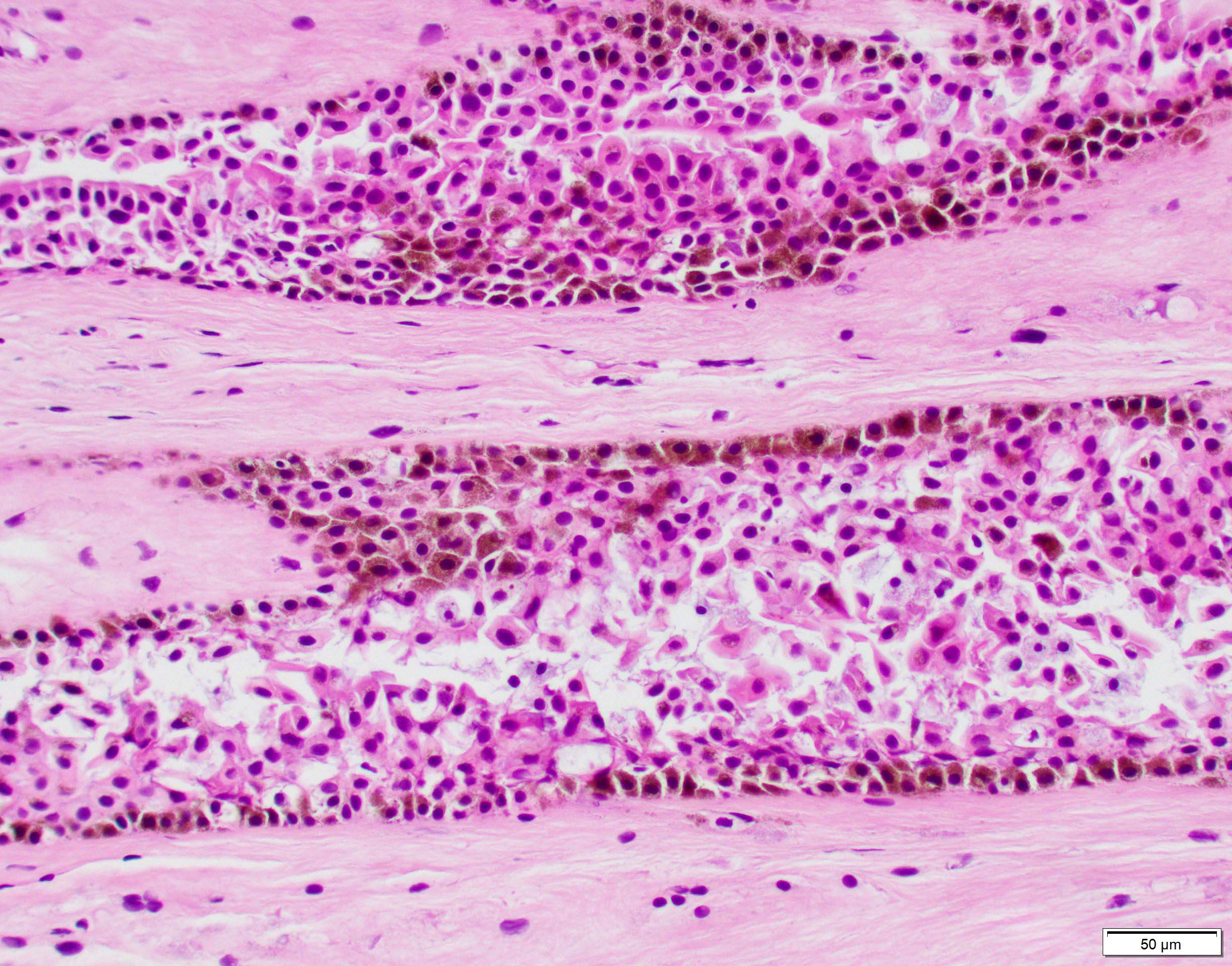
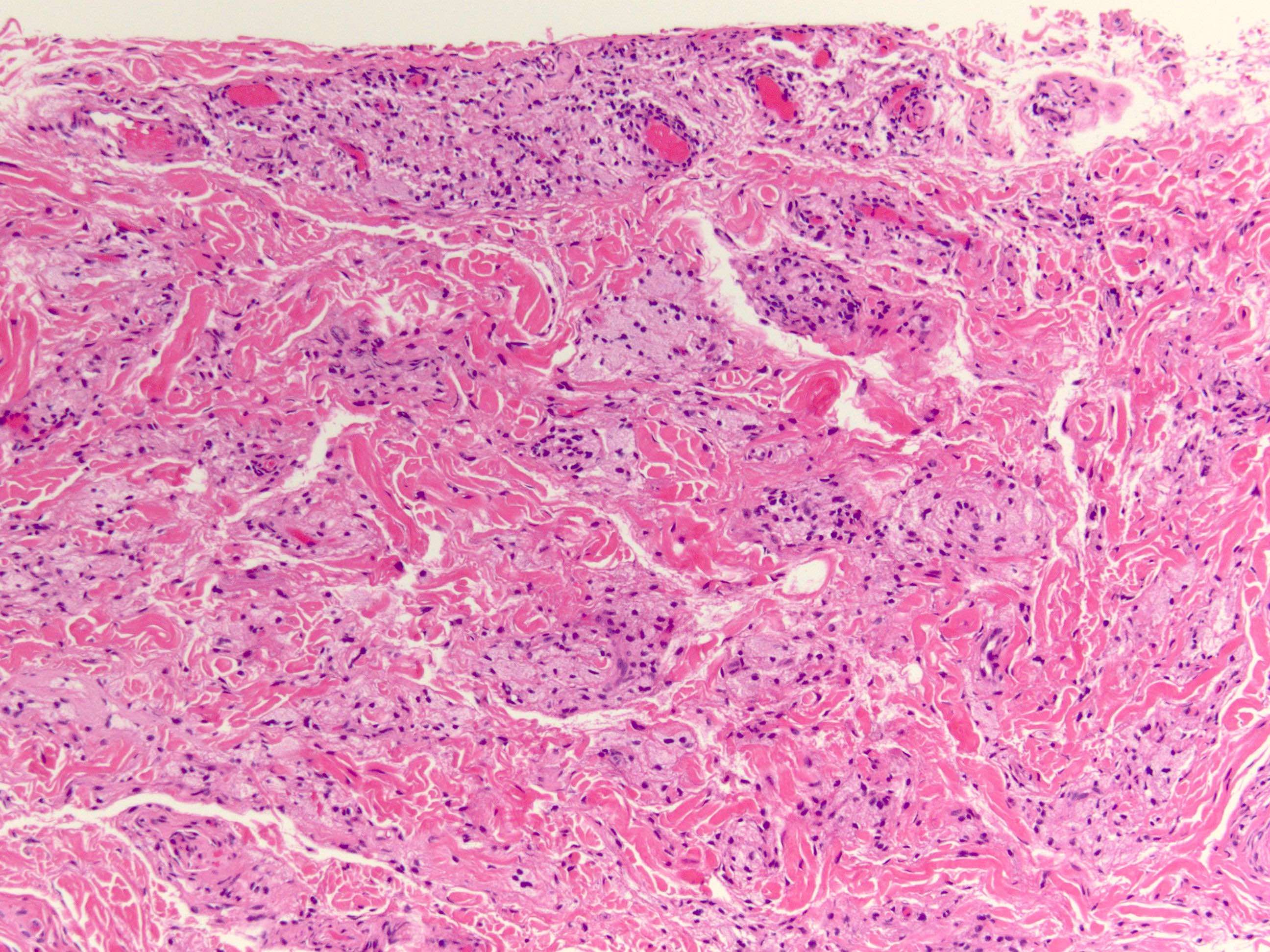
A 25 year old man with orthokeratology (specially fitted lenses) presents with severe pain in his left eye. The slit lamp examination shows a pattern of radial perineural and ring infiltrate in cornea. Corneal biopsy following negative direct smear examination on corneal scrapes shows focal ulceration of the surface with loss of epithelium; infiltrate of inflammatory cells, mainly polymorphonuclear cells and macrophages, are shown in the image above. What is the most likely diagnosis?
Acanthamoeba keratitis
Bacterial keratitis
Herpetic keratitis
Mycotic (fungal) keratitis
Board review style answer #1
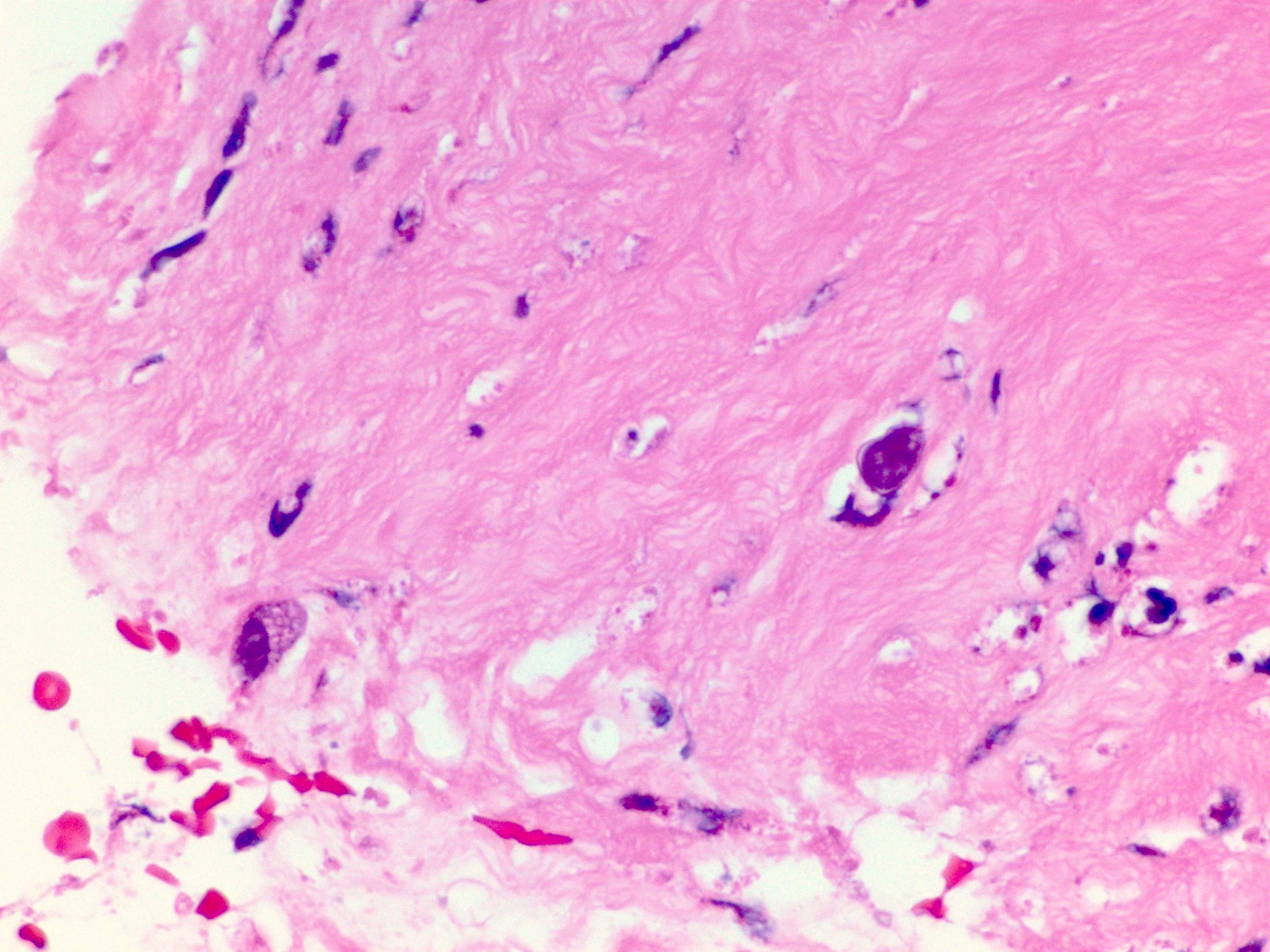
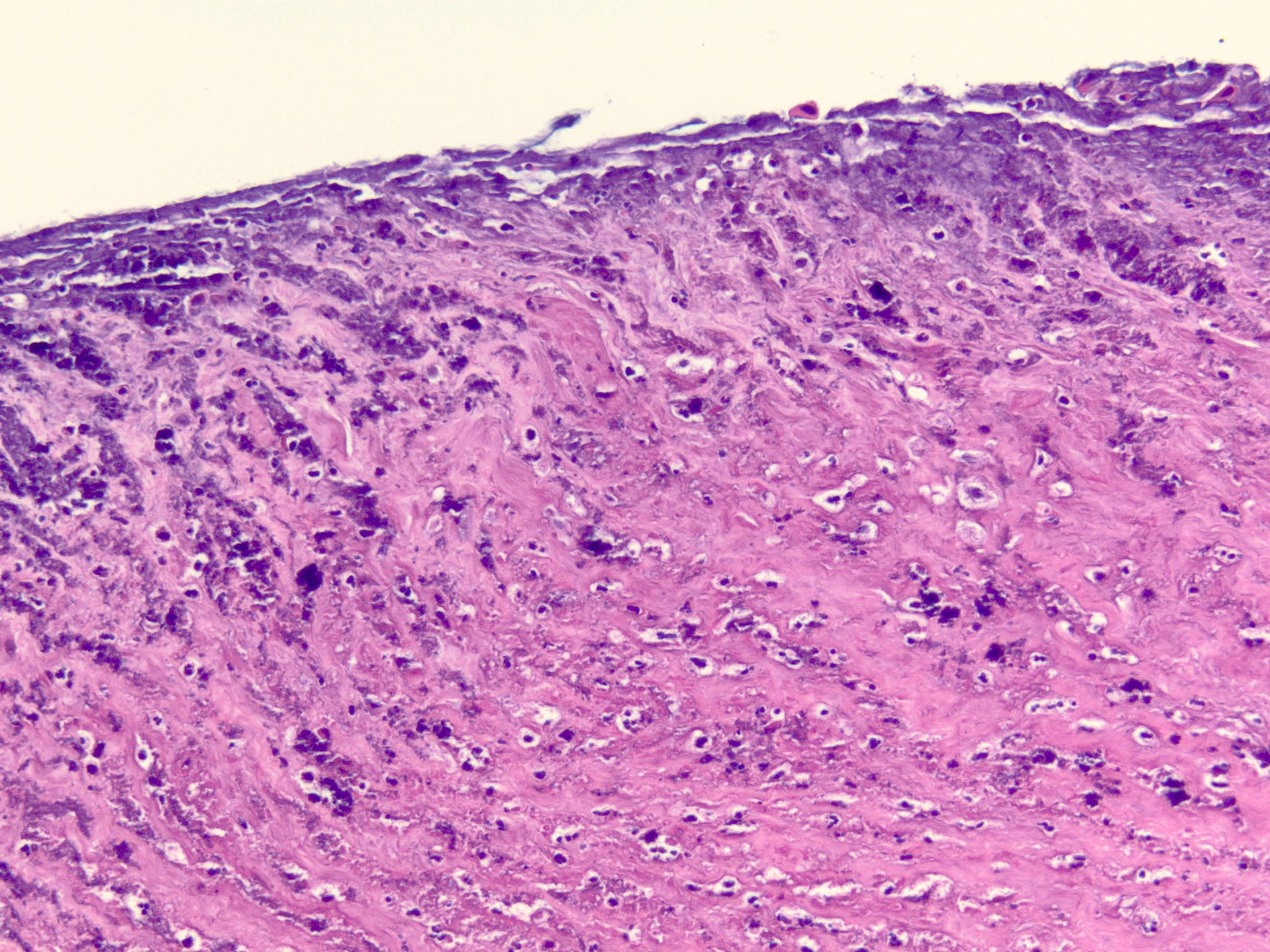
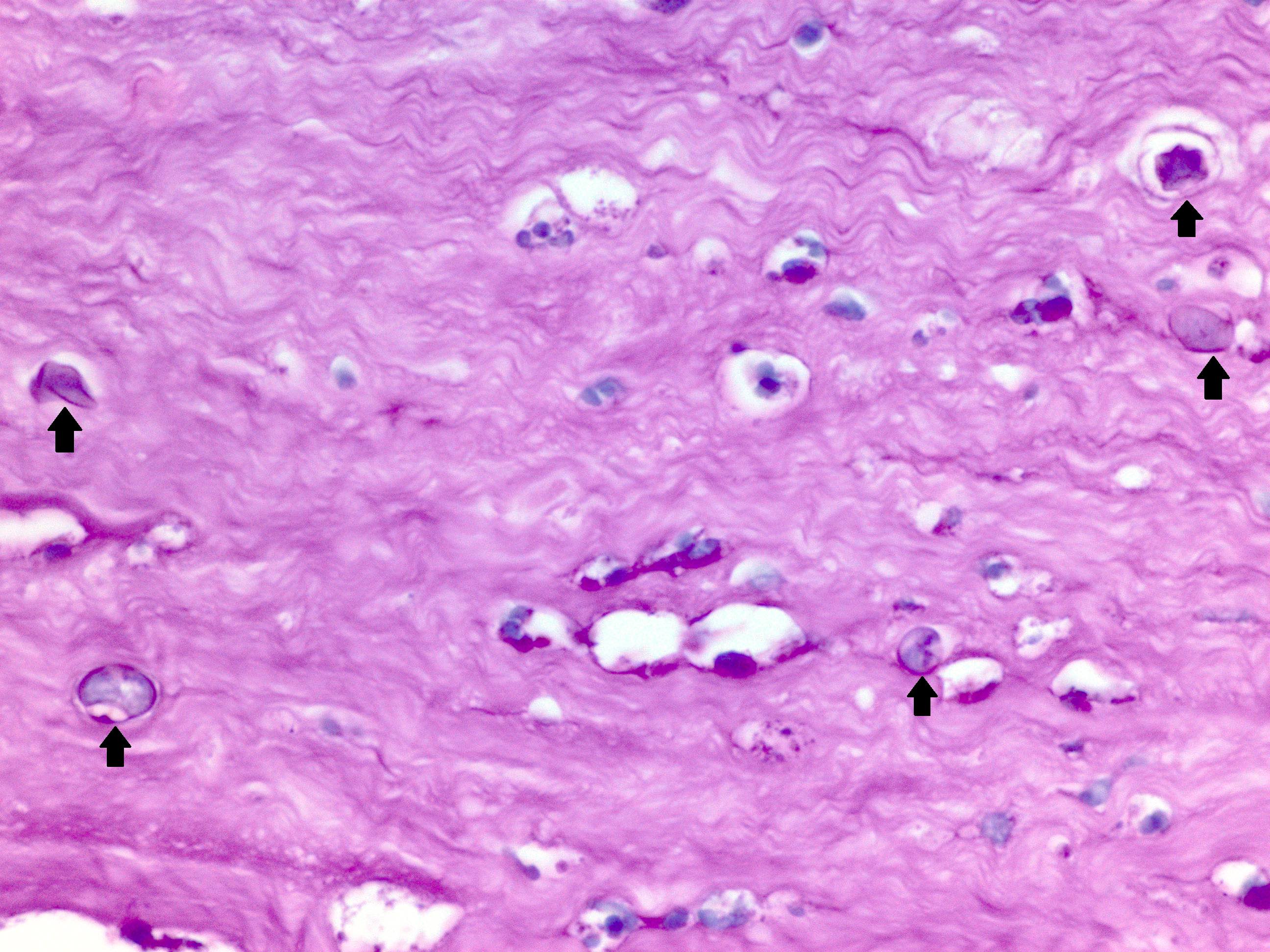
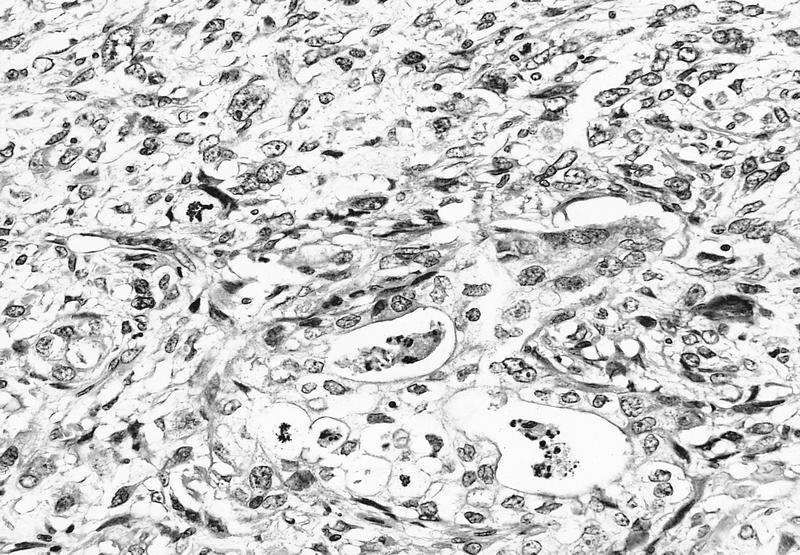
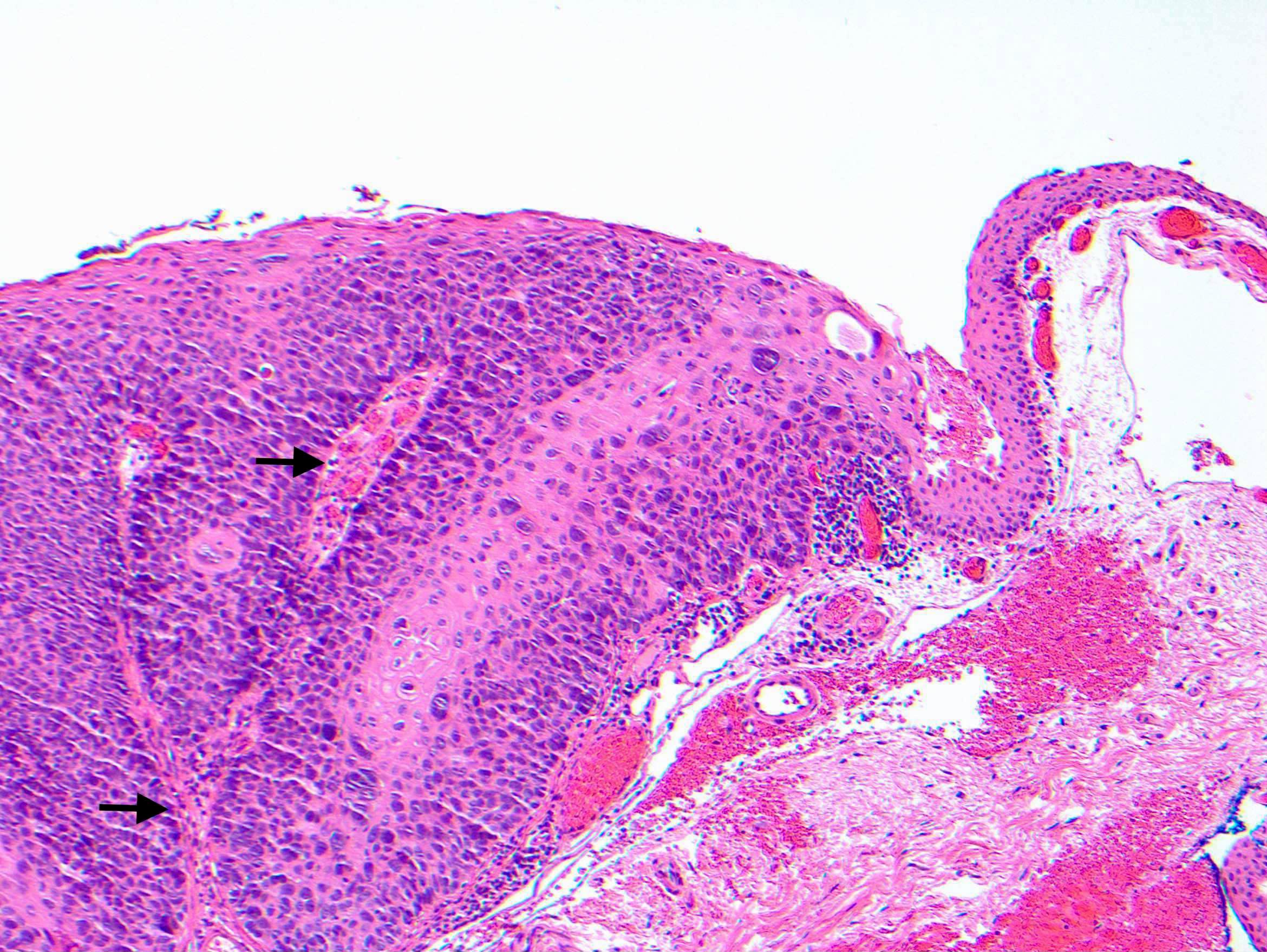
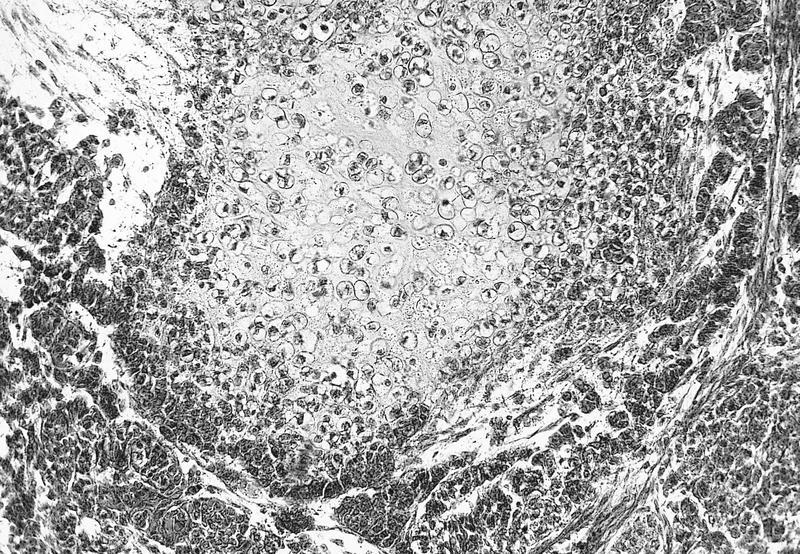
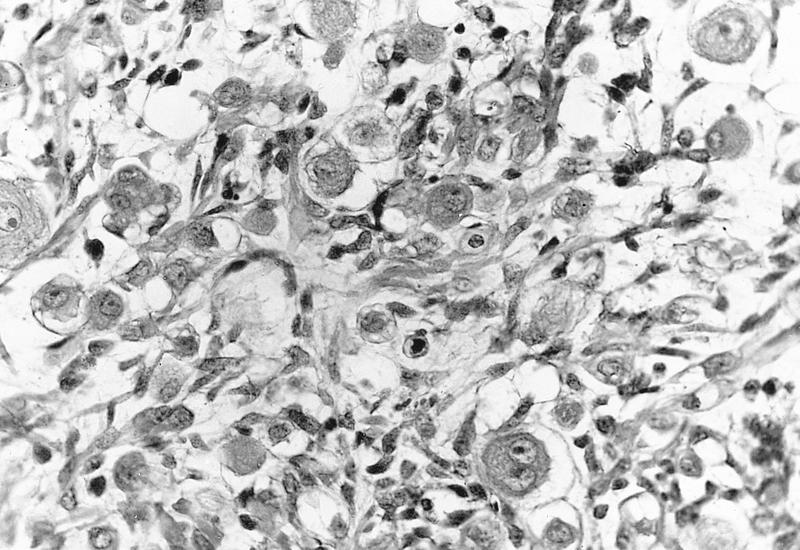
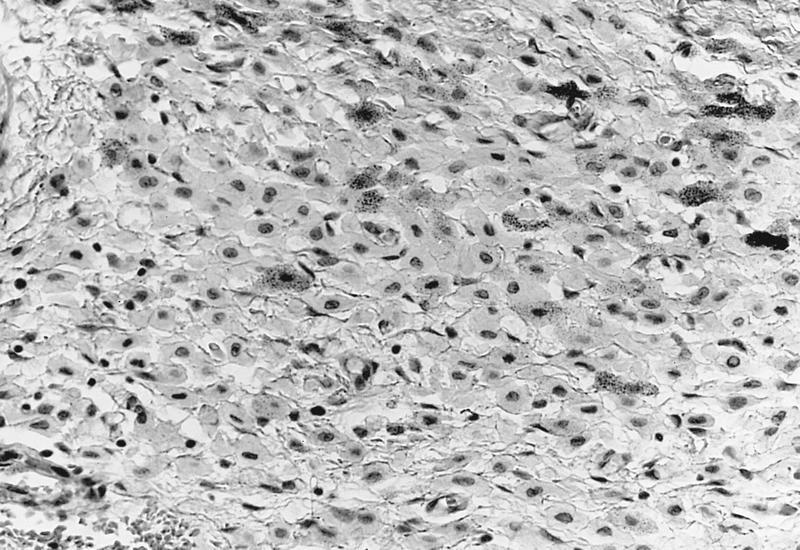
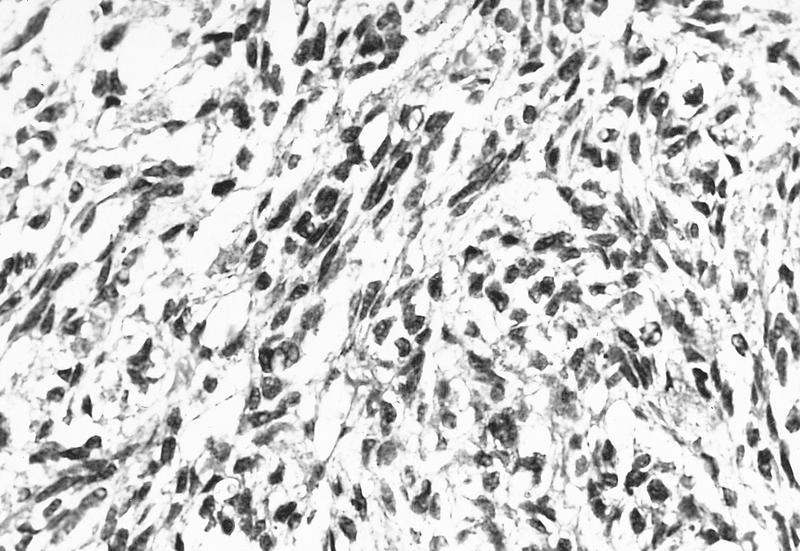
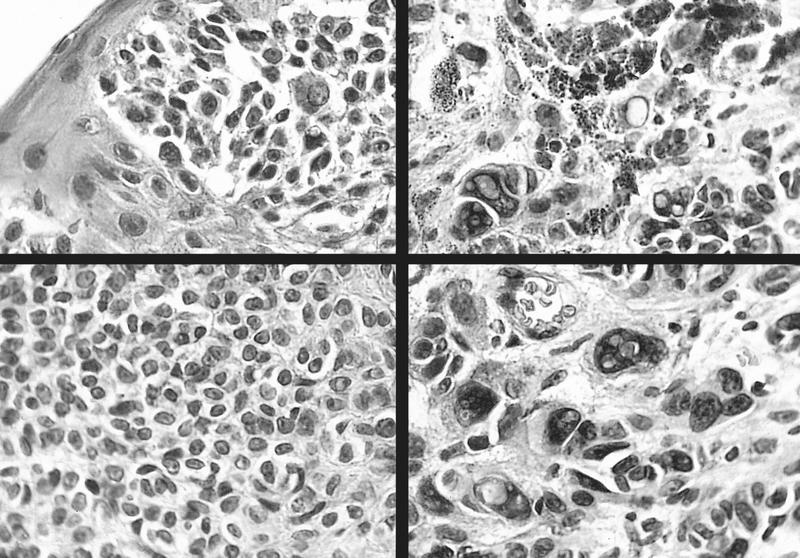
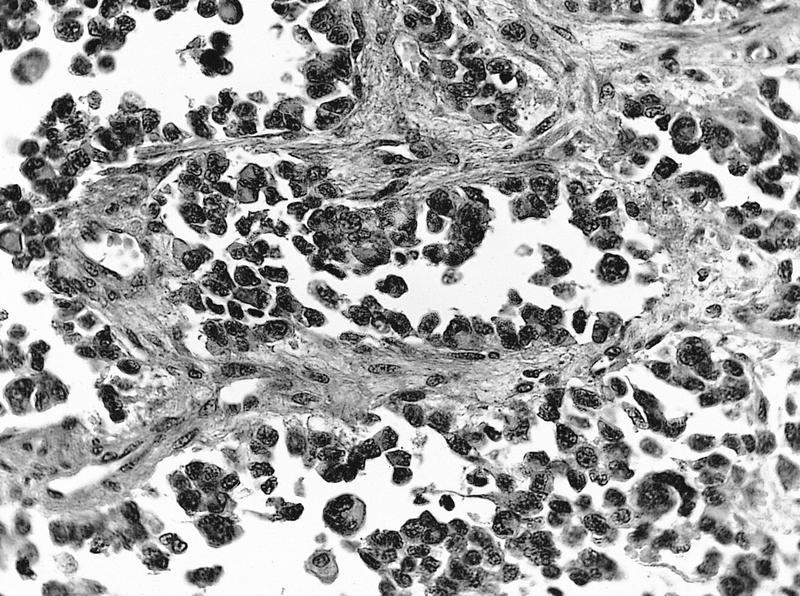
A. Acanthamoeba keratitis. H&E sections at high power show several Acanthamoeba infiltrating corneal stroma in varying states of degeneration. Microscopic features on corneal biopsy also include ulceration, necrosis, neutrophilic and macrophage infiltrates; may show nonnecrotizing granulomatous inflammation. Encysted forms may be highlighted with PAS or GMS stains. Answer C is incorrect because a corneal biopsy for herpetic keratitis shows inflammatory infiltrates of mainly lymphocytes, plasma cells with stromal vascularization on H&E sections. Multinucleated giant cells around Descemet membrane are also identified. Answer D is incorrect because a corneal biopsy for mycotic (fungal) keratitis shows granulomatous, chronic nongranulomatous or rarely purulent inflammation on H&E sections; PAS or GMS positive for yeast or hyphal forms. Answer B is incorrect because microscopic findings of infiltration of the stroma by polymorphonuclear leukocytes occur in acute bacterial keratitis. The endothelium is often damaged and may have associated hypopyon and corneal perforation. Gram stain often shows bacteria in the stroma bordering the inflammatory infiltrate.
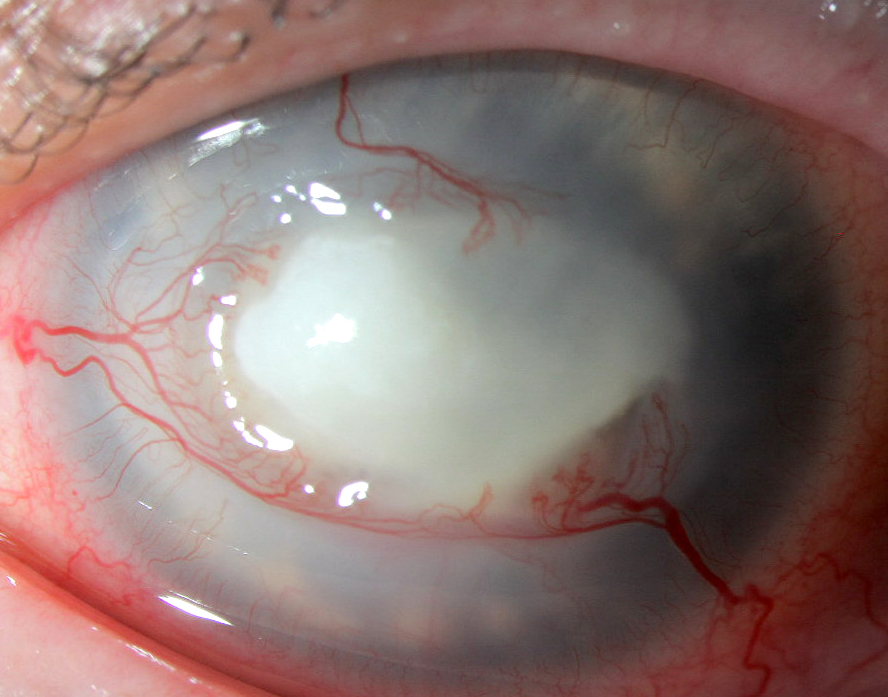
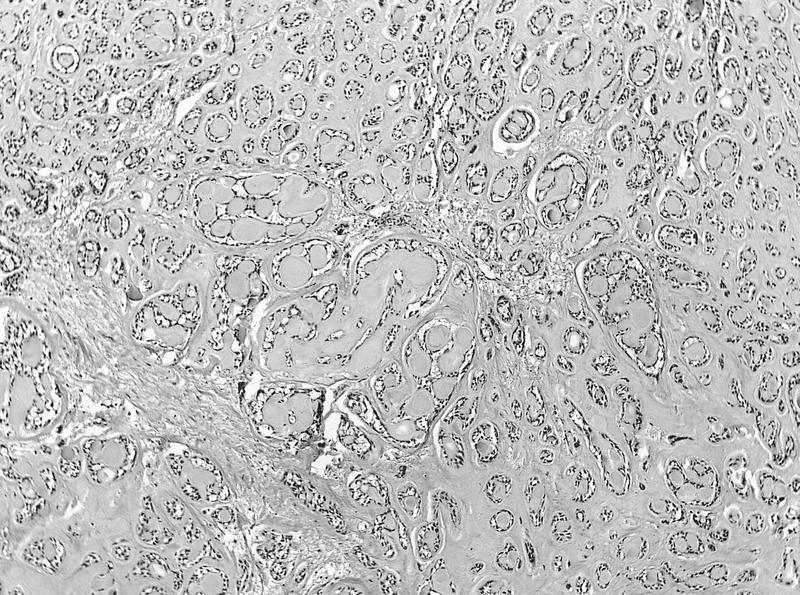
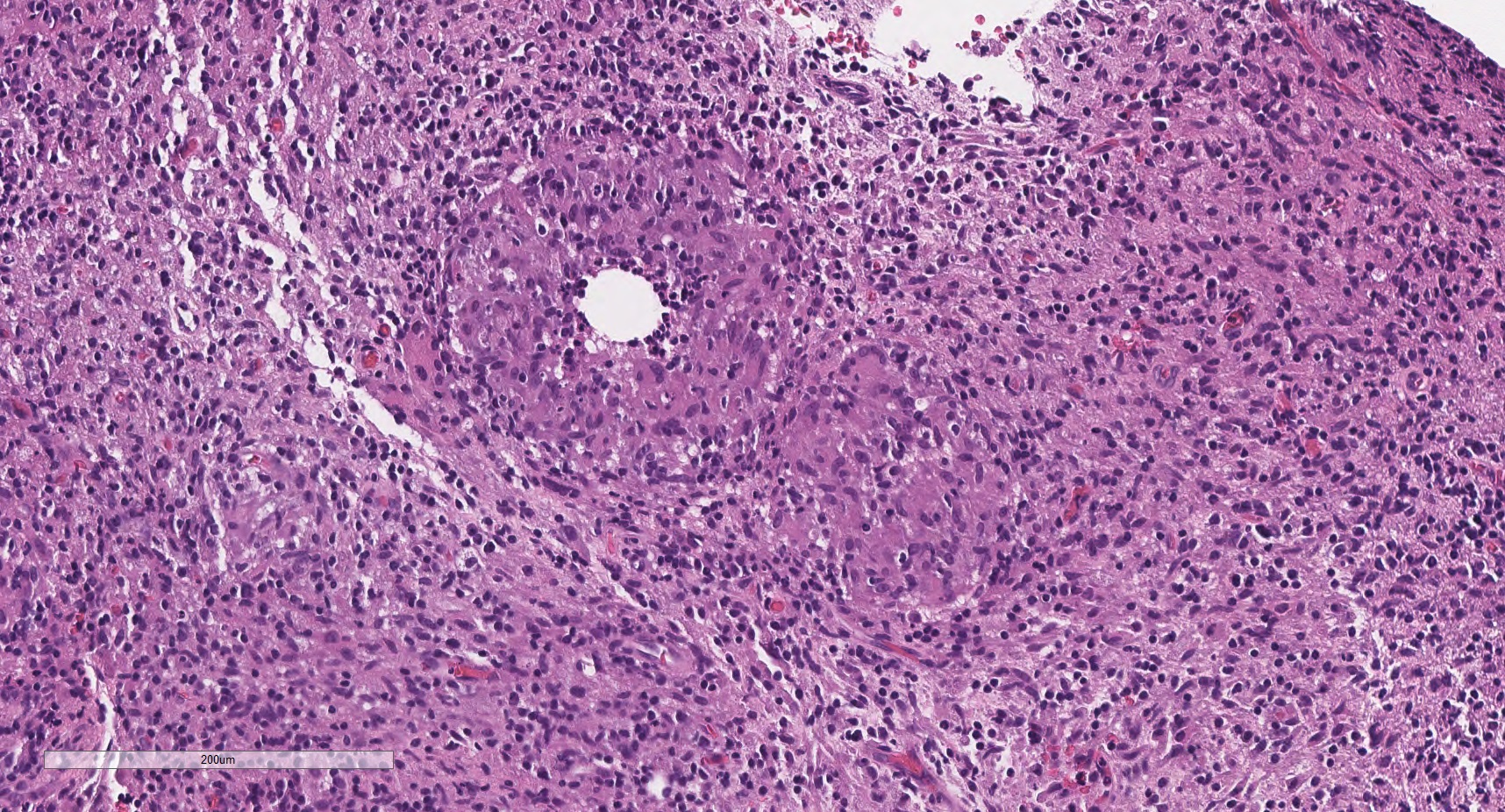
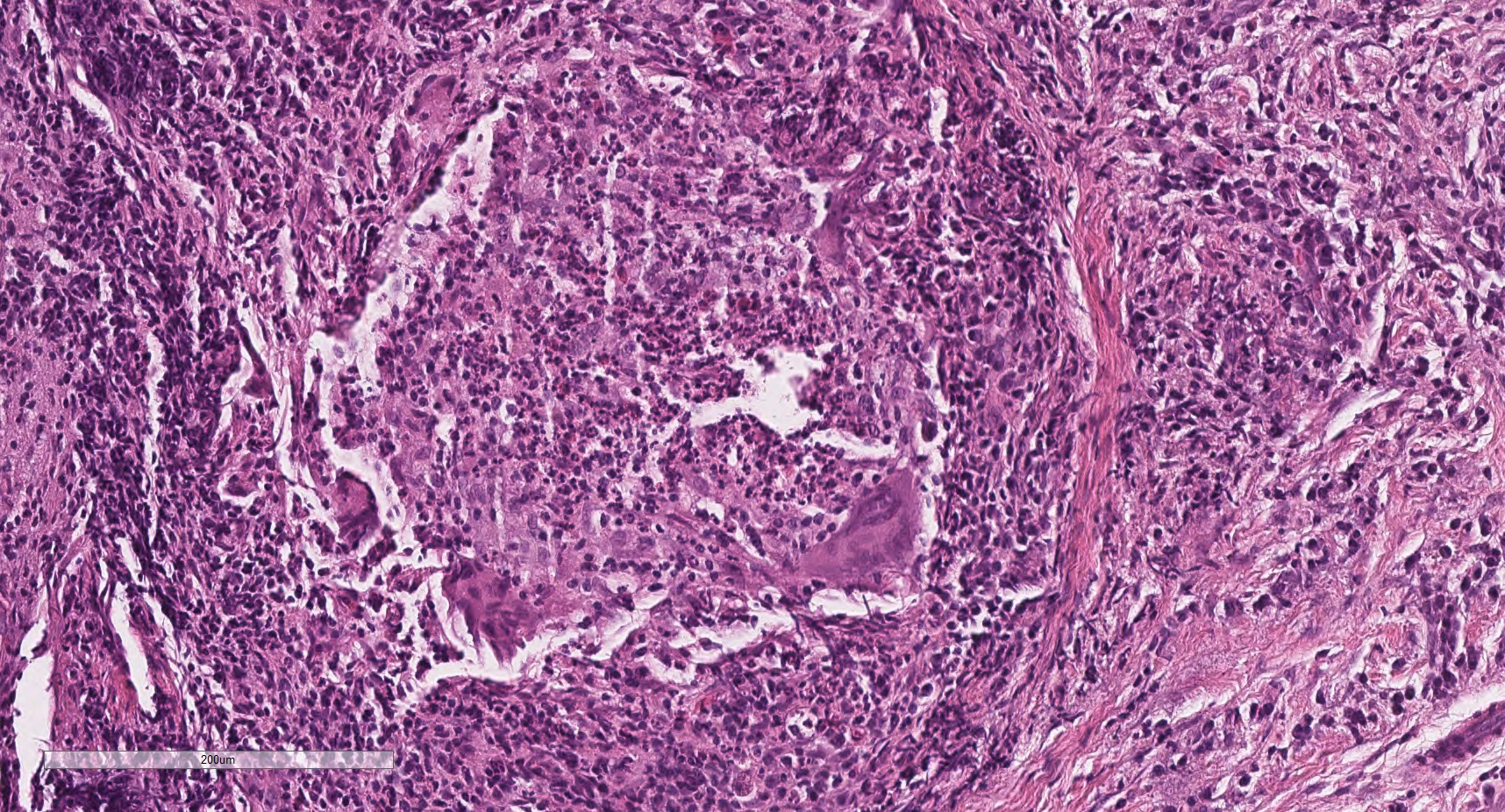
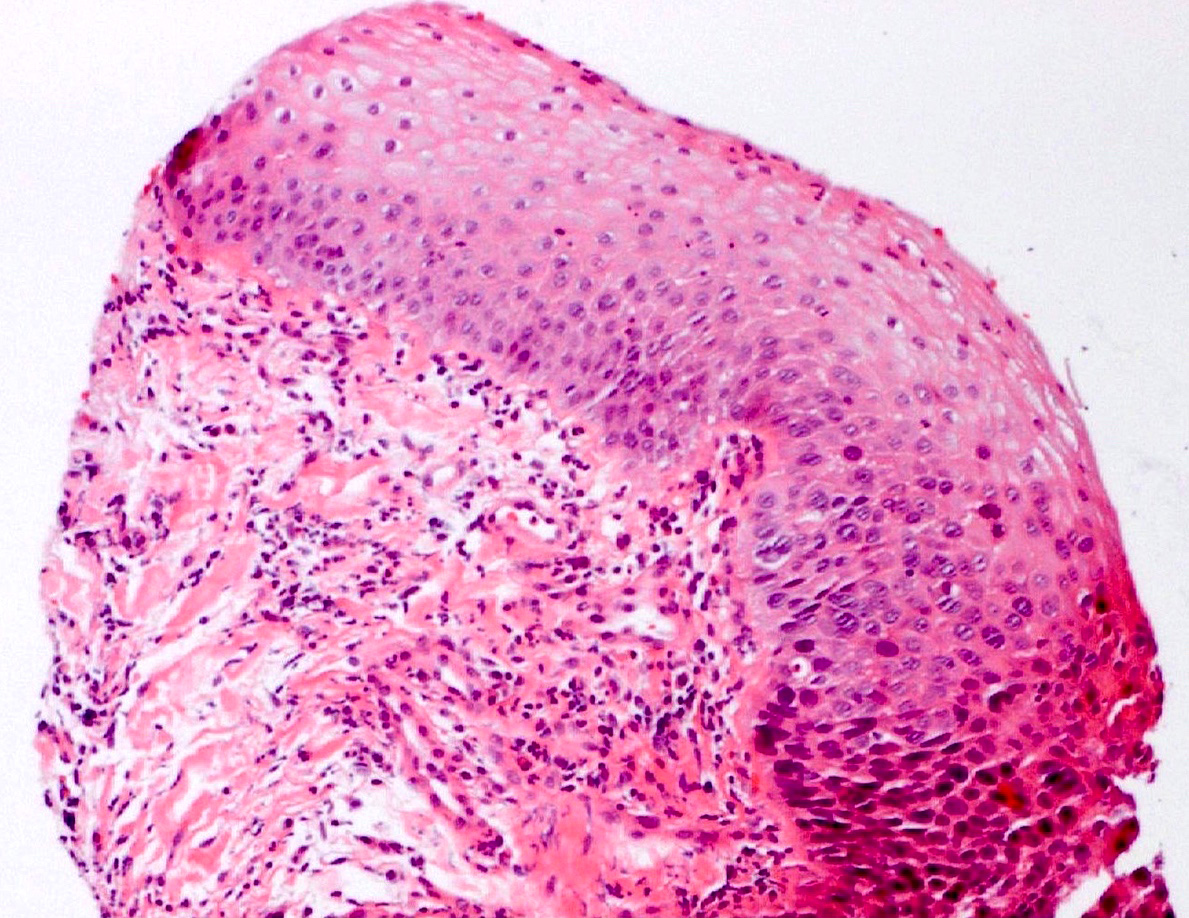
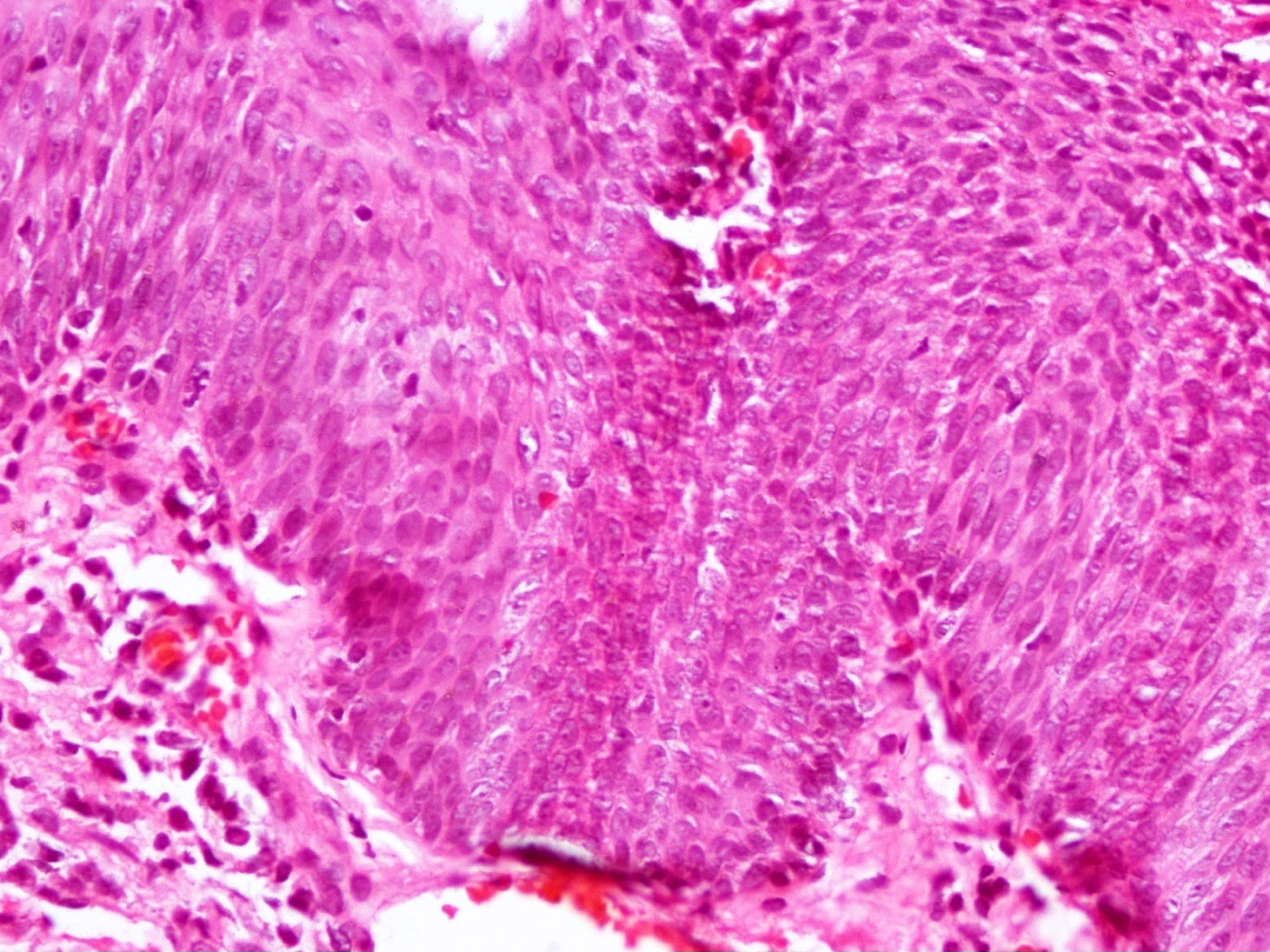
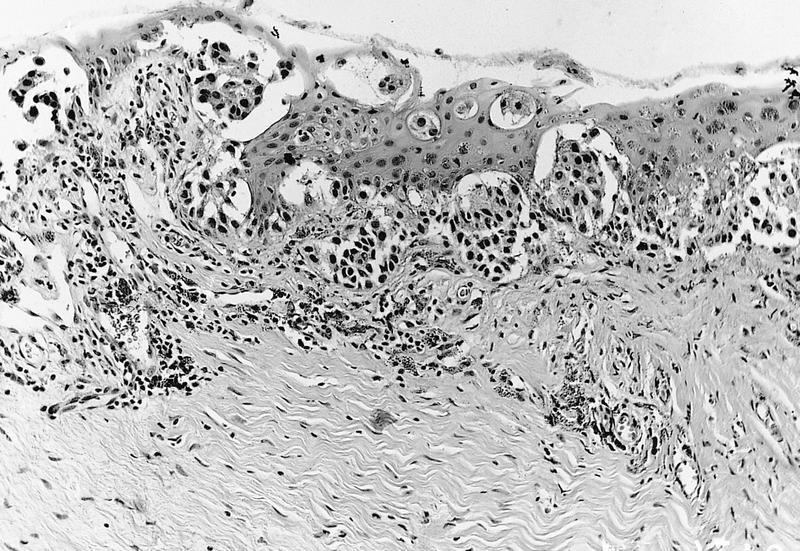
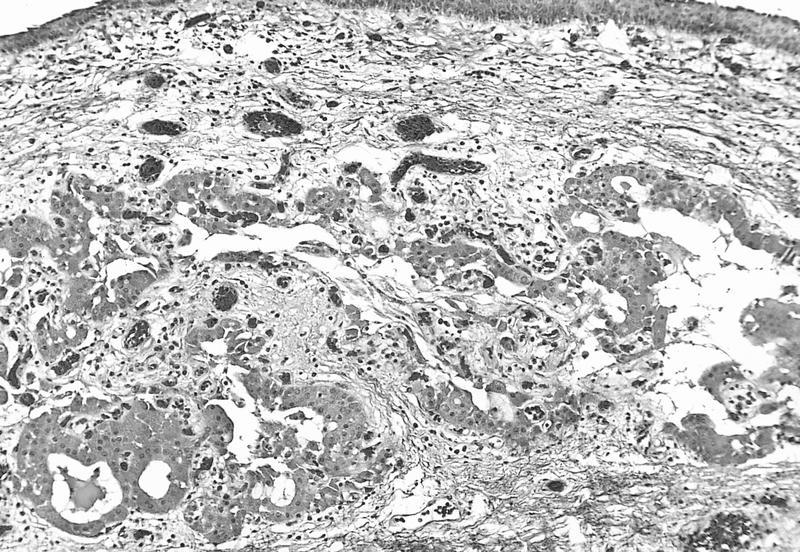
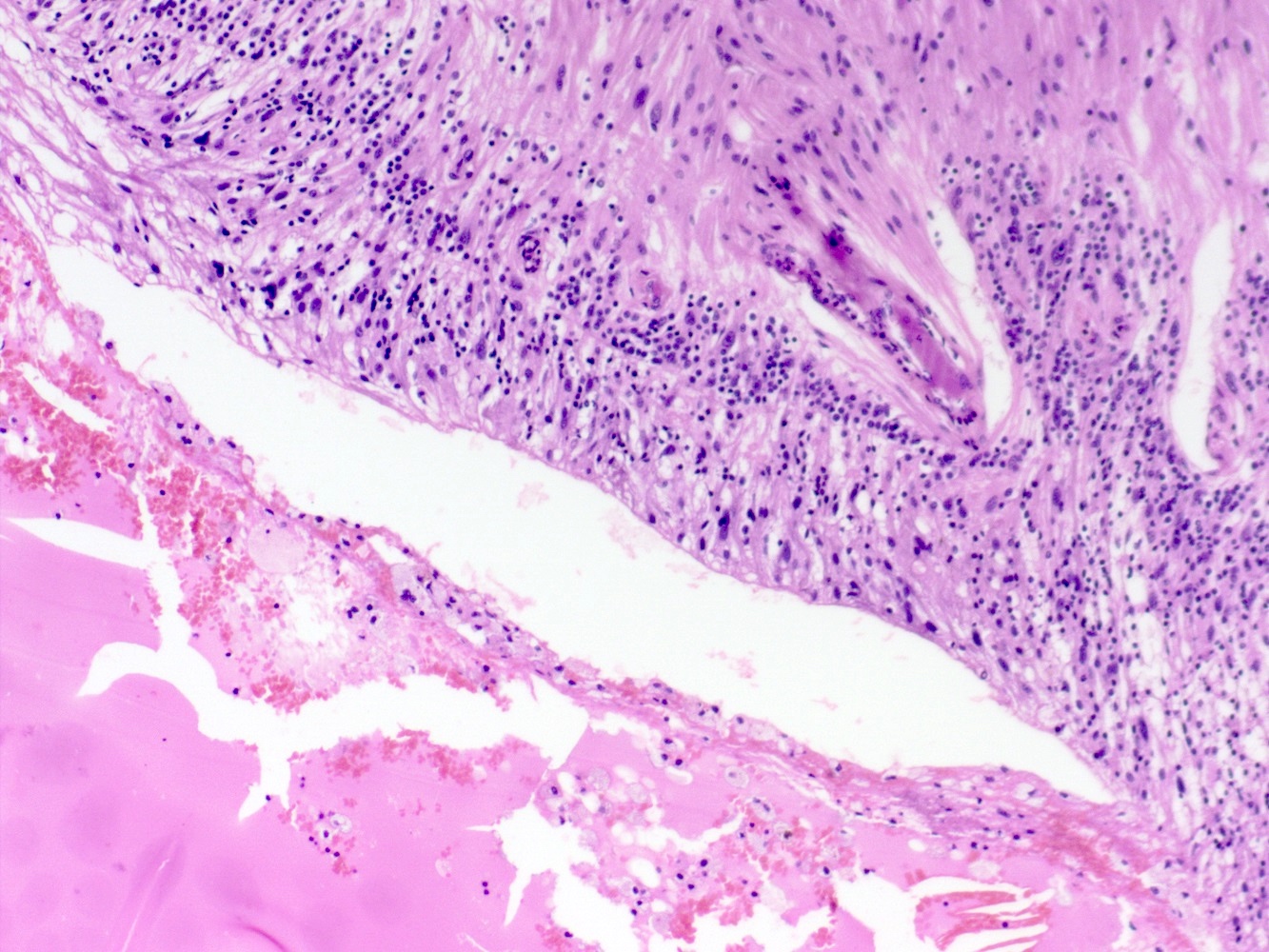
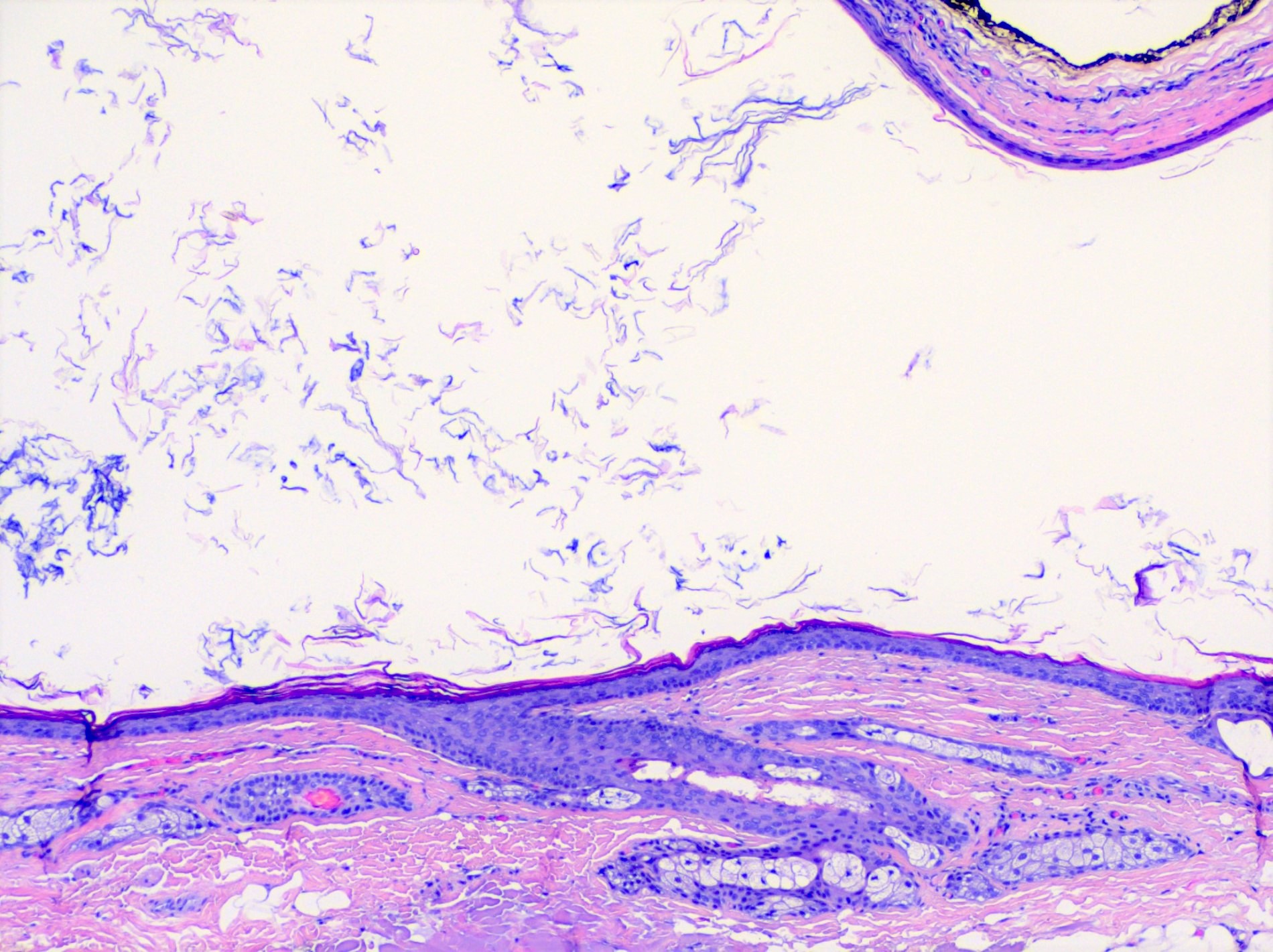
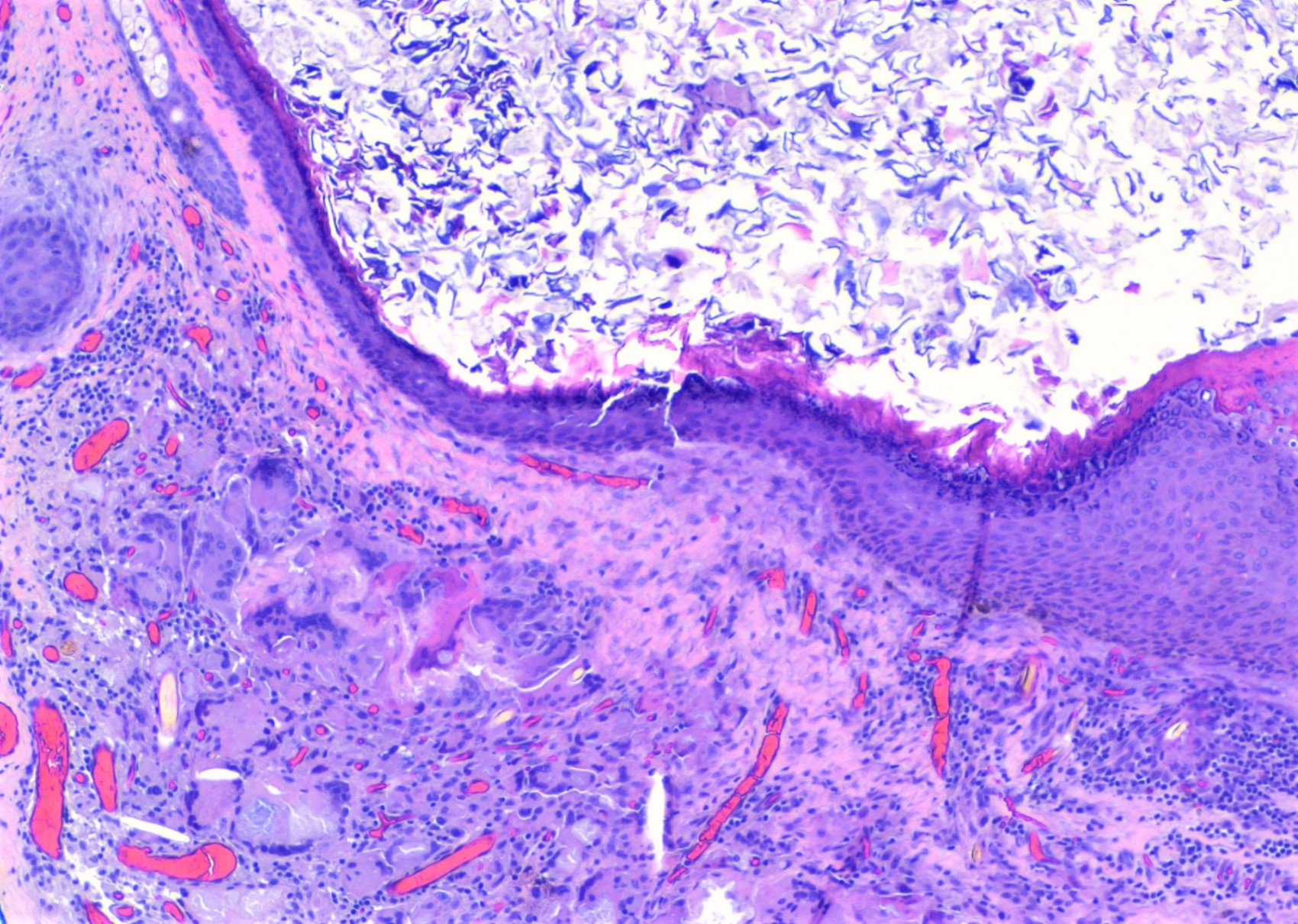
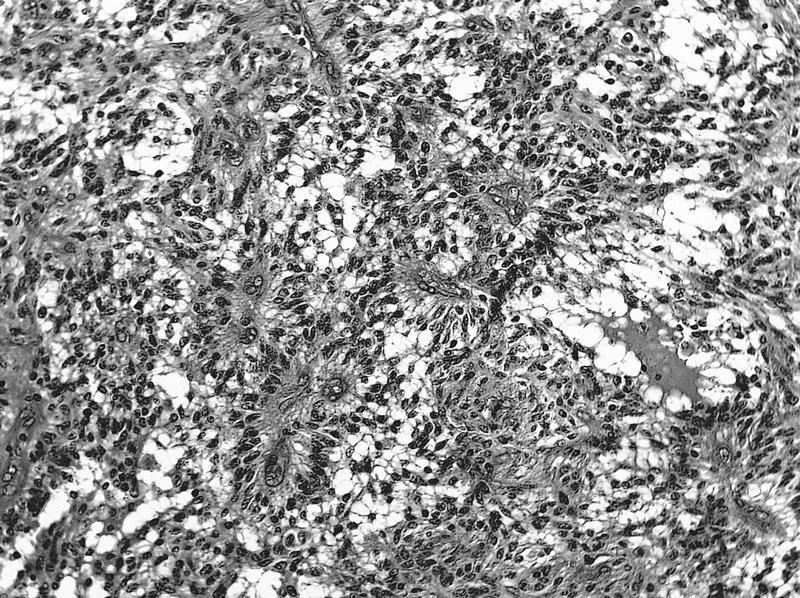
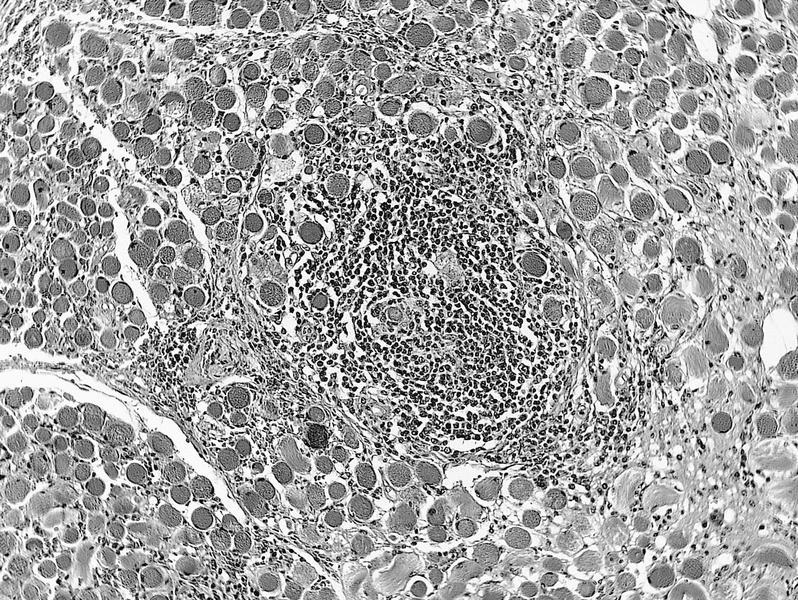
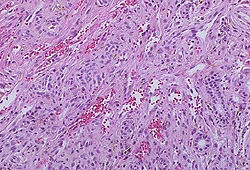
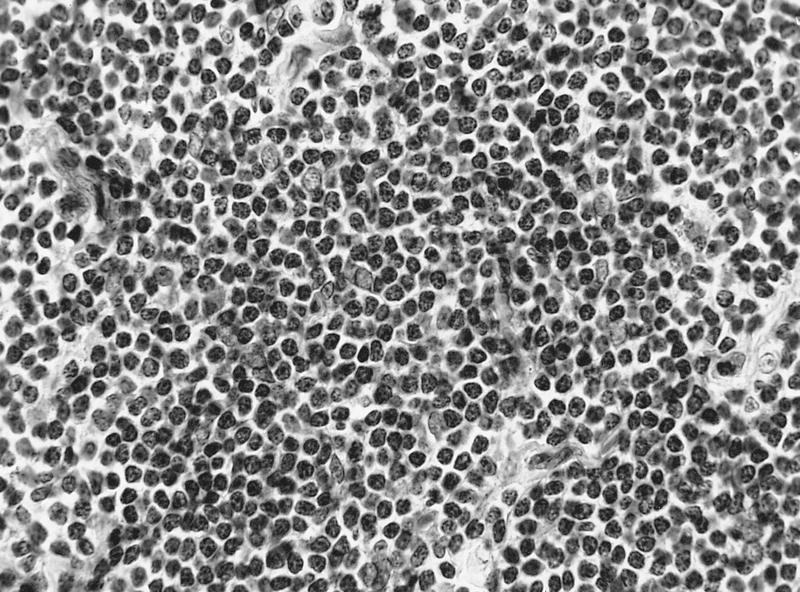
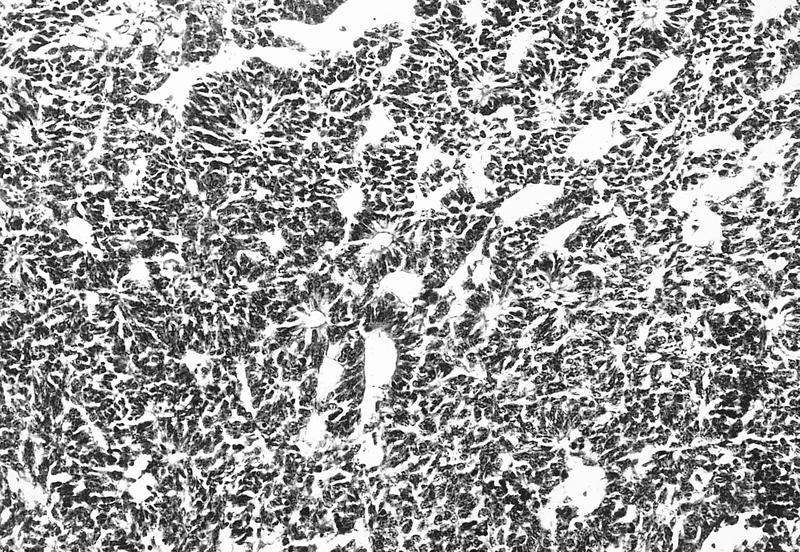
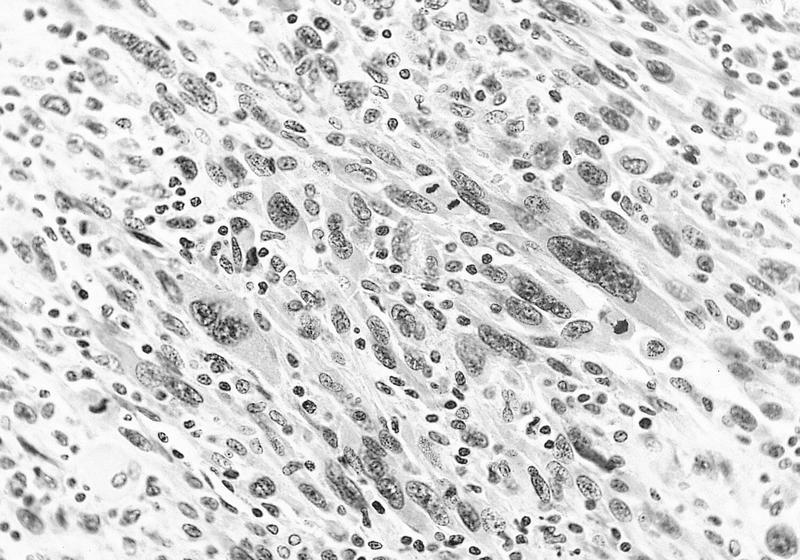
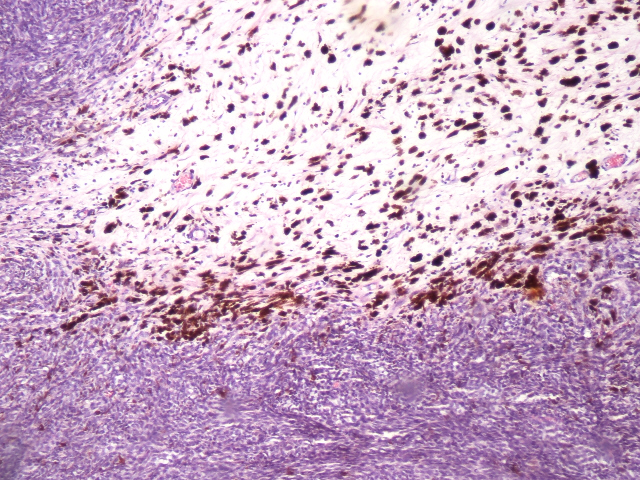
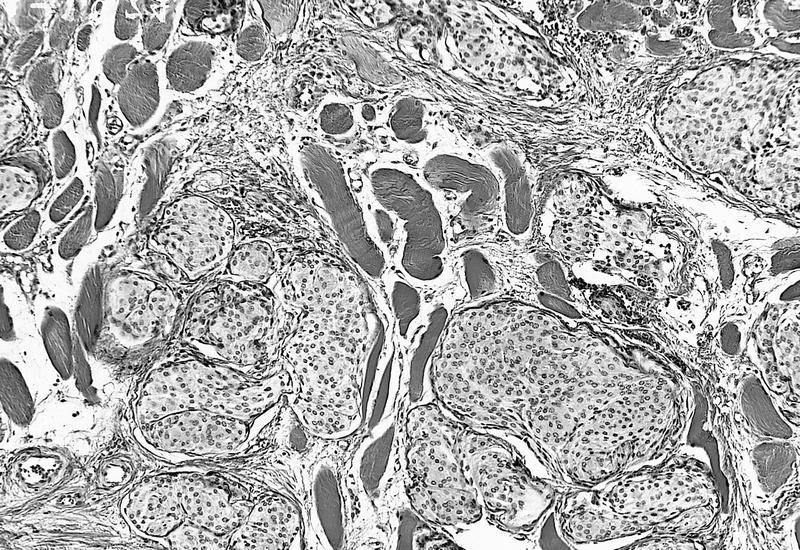
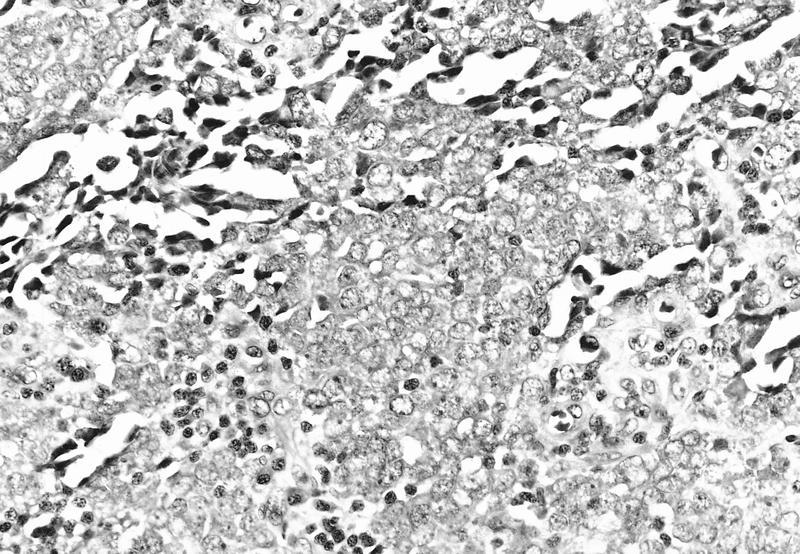
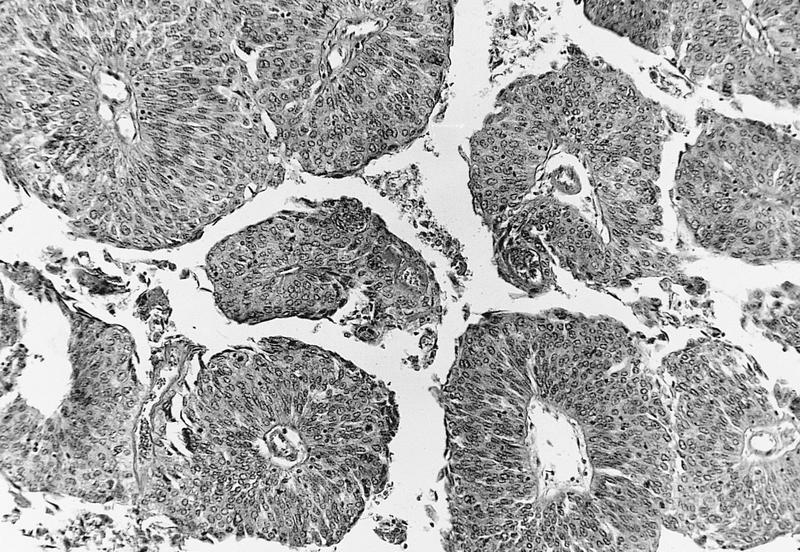
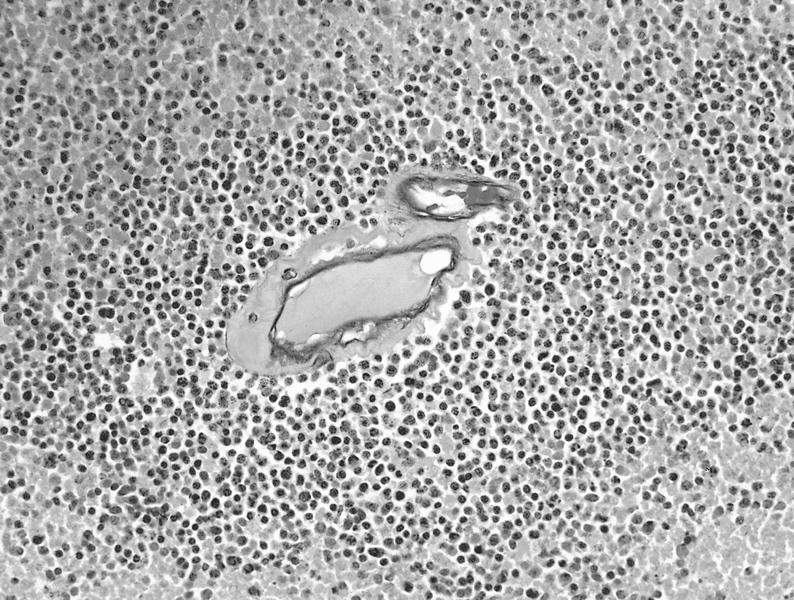
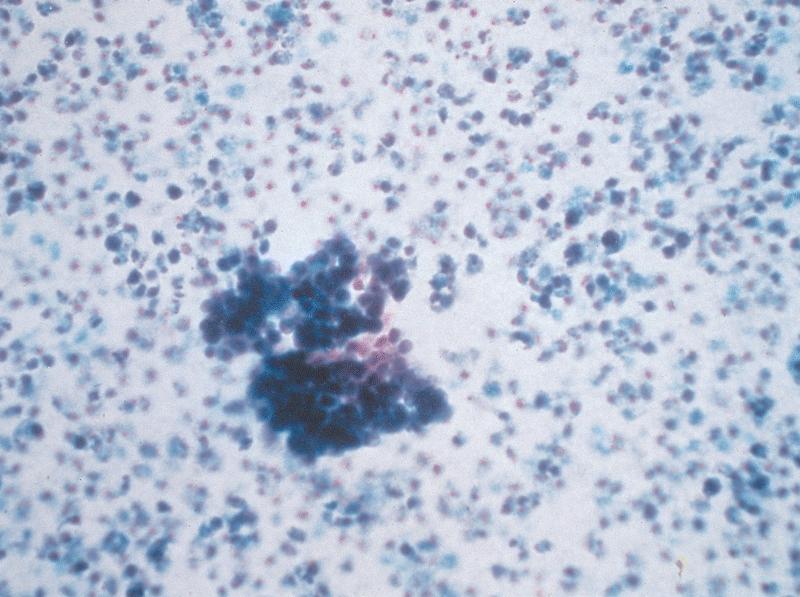
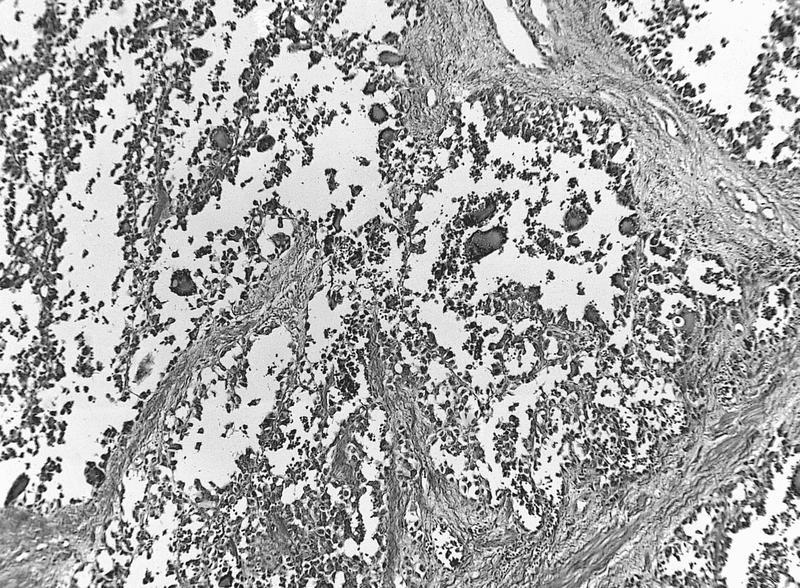
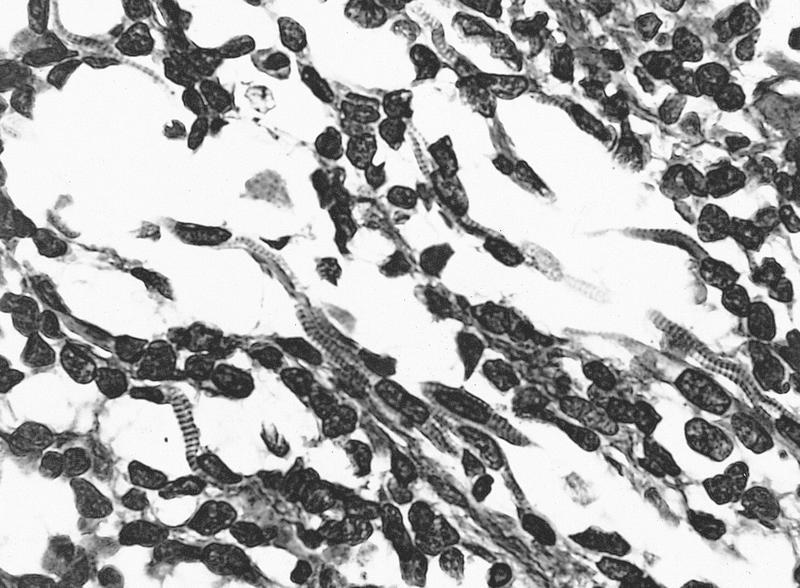
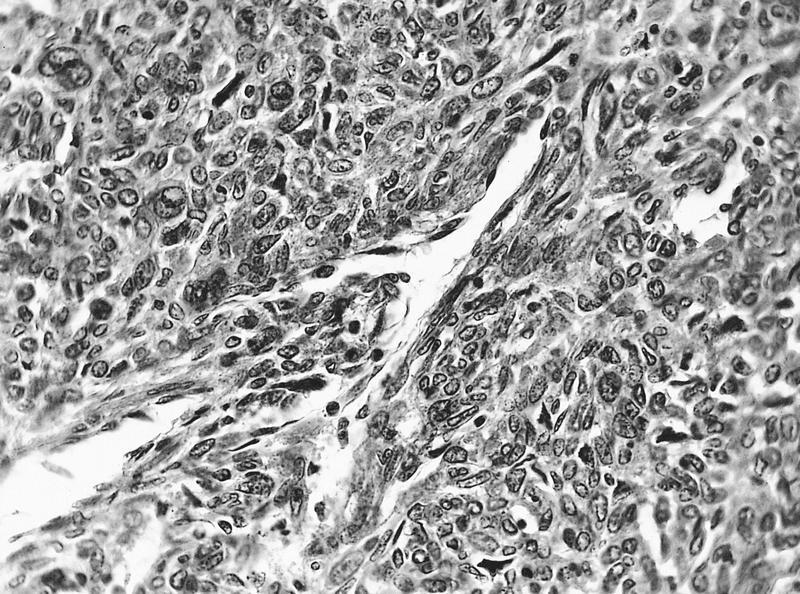
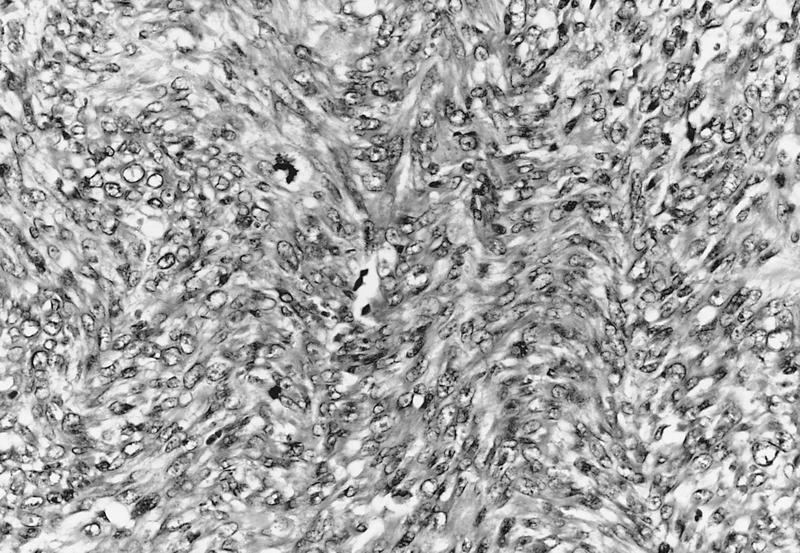
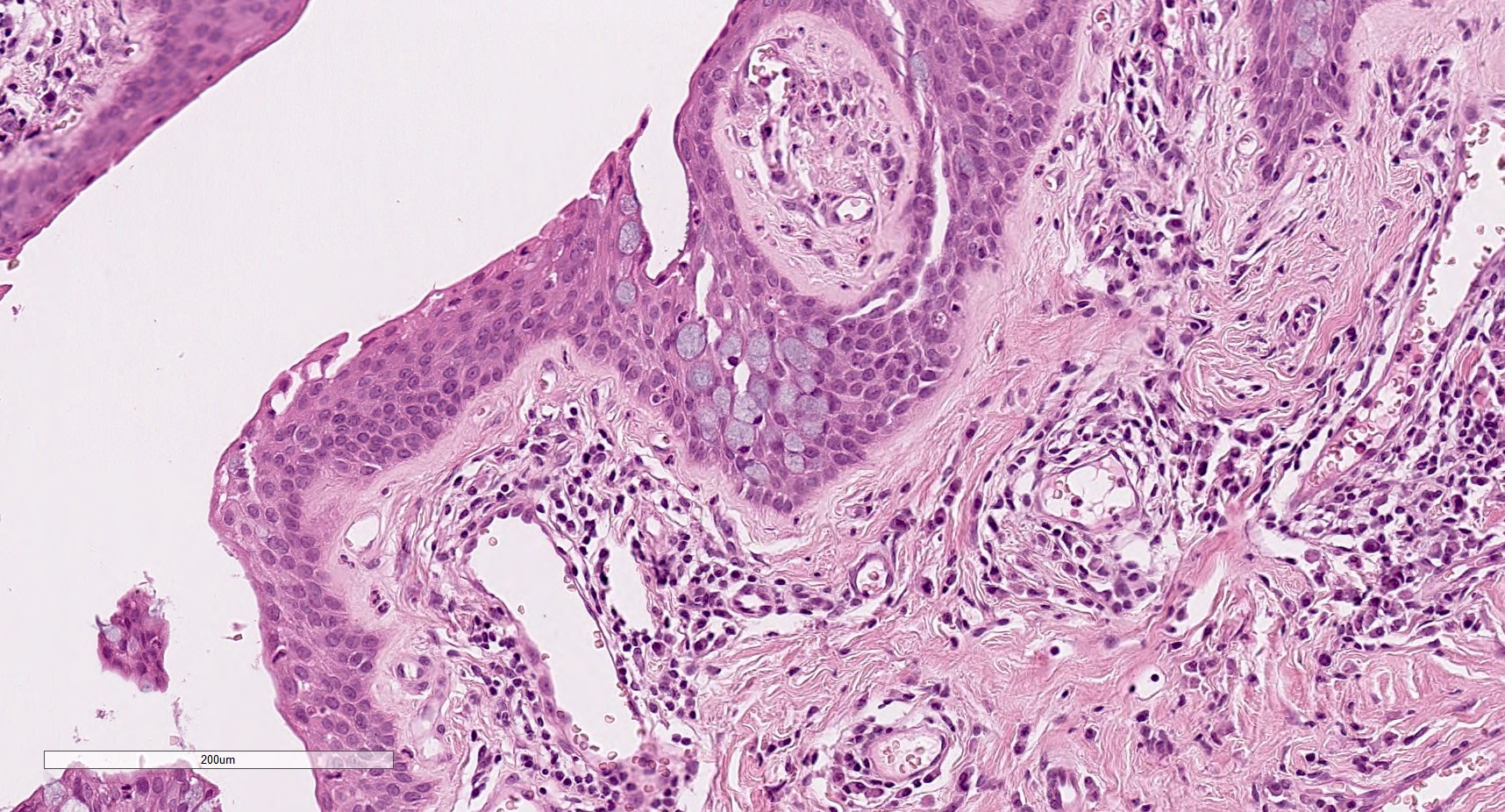
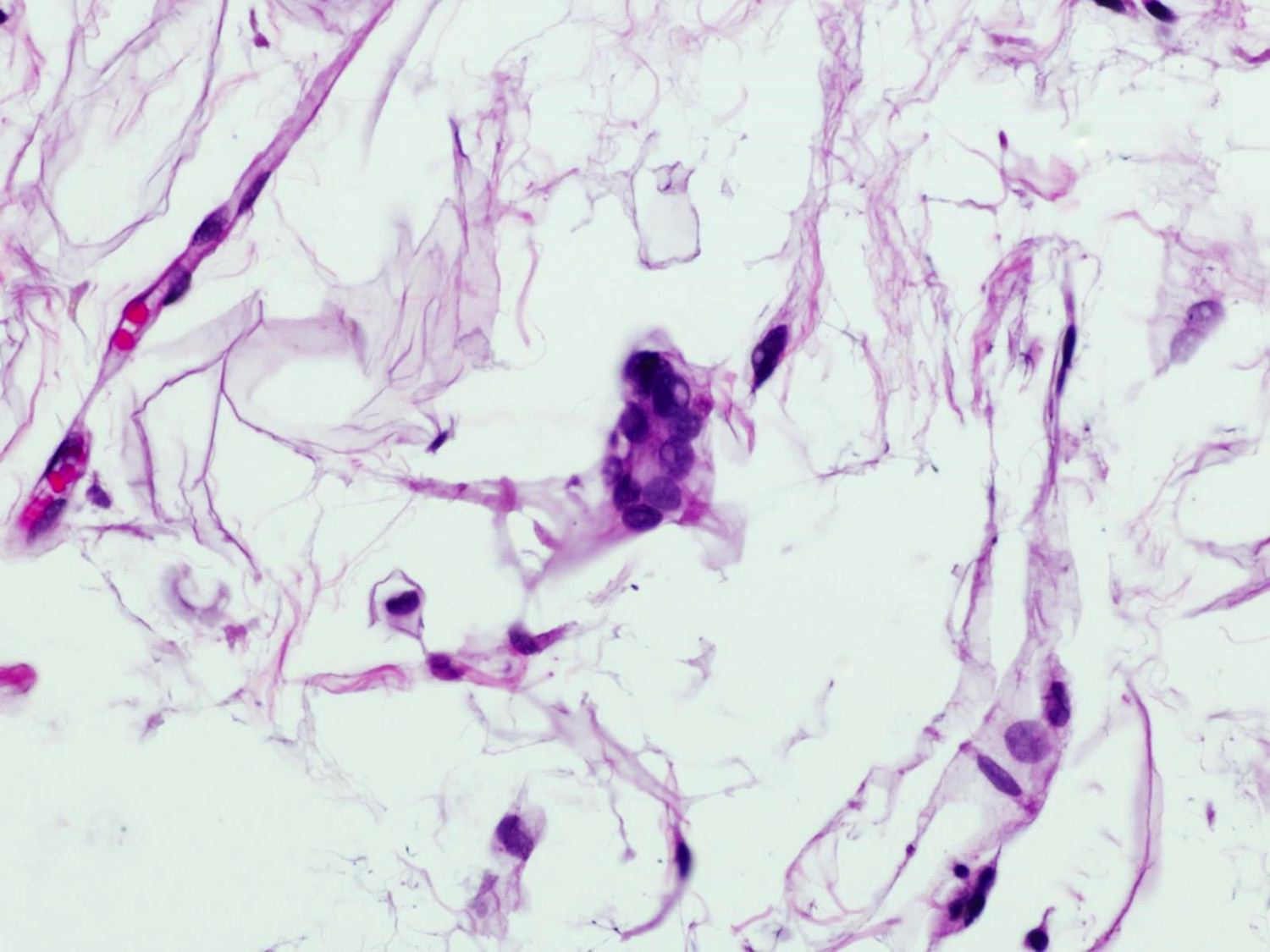
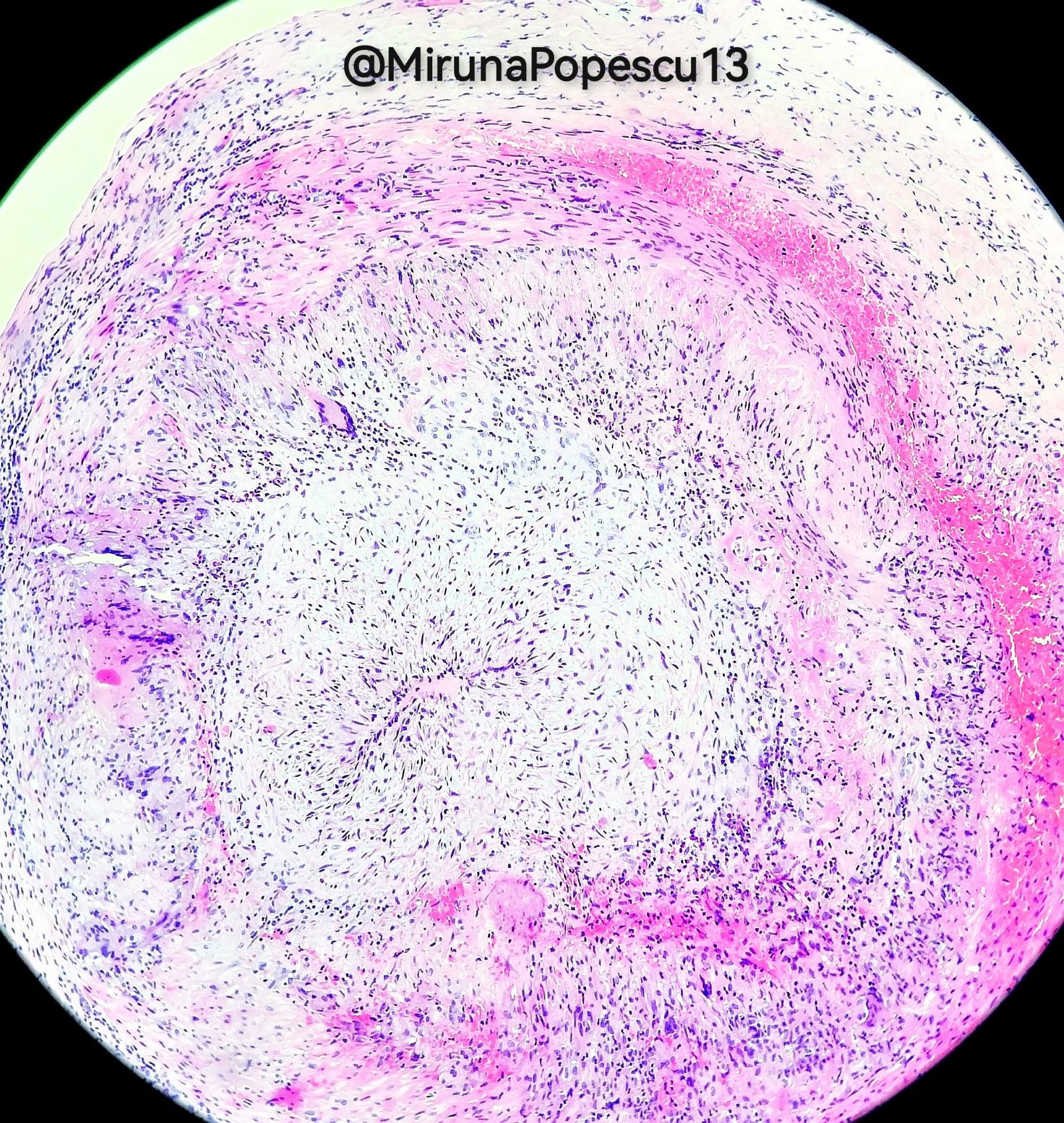
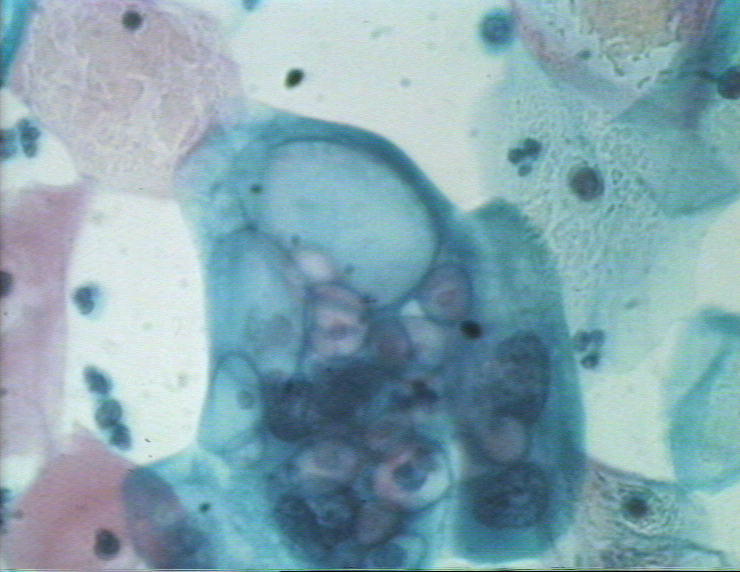
A 52 year old man who is a soft contact lens wearer presents with left eye pain and vision changes. Ophthalmic exam shows a ring shaped corneal stromal defect. Corneal biopsy reveals necrosis, neutrophilic infiltrates as shown in the image above. Which of the following is the best choice of stain to confirm the diagnosis?
AFB Fite
AFB Ziehl-Neelsen
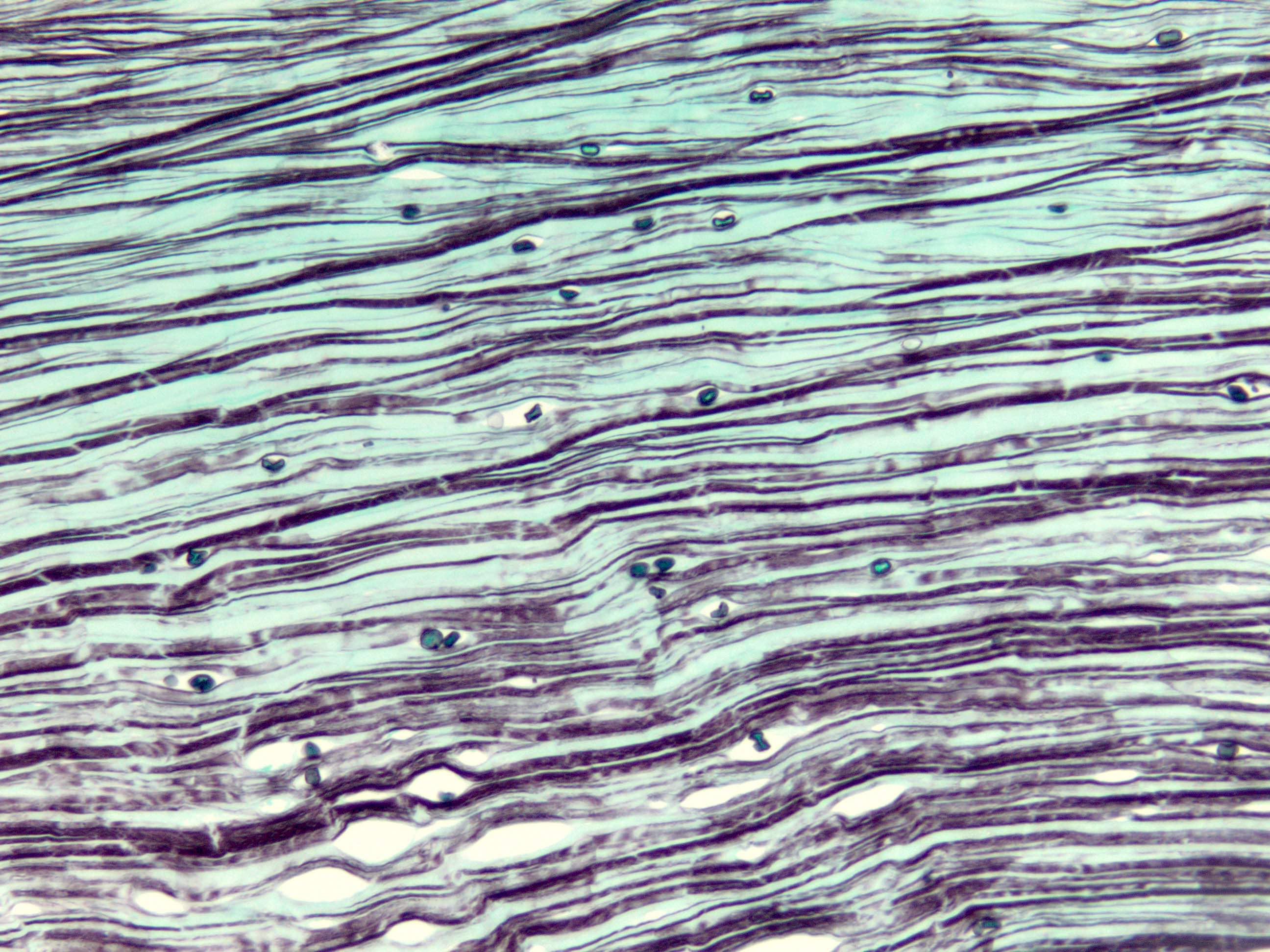
GMS
Gram
Mucicarmine
Board review style answer #2
C. GMS. GMS staining will highlight the encysted forms of amoeba in this description of Acanthamoeba keratitis. Answer A is incorrect because AFB Fite is used for Nocardia and would not stain amoebic forms. Answer B is incorrect because AFB Ziehl-Neelsen identifies acid fast organisms such as tuberculosis but would not stain amoebic forms. Answer D is incorrect because Gram stain is typically for bacterial organisms and would not be helpful in amoebic keratitis. Answer E is incorrect because mucicarmine is a stain for mucin and highlights cryptococcal forms, for example but is not helpful in this case of Acanthamoeba keratitis.
Middle segment of uveal tract, between iris and choroid
Composed of pars plicata and pars plana
Holds lens in place
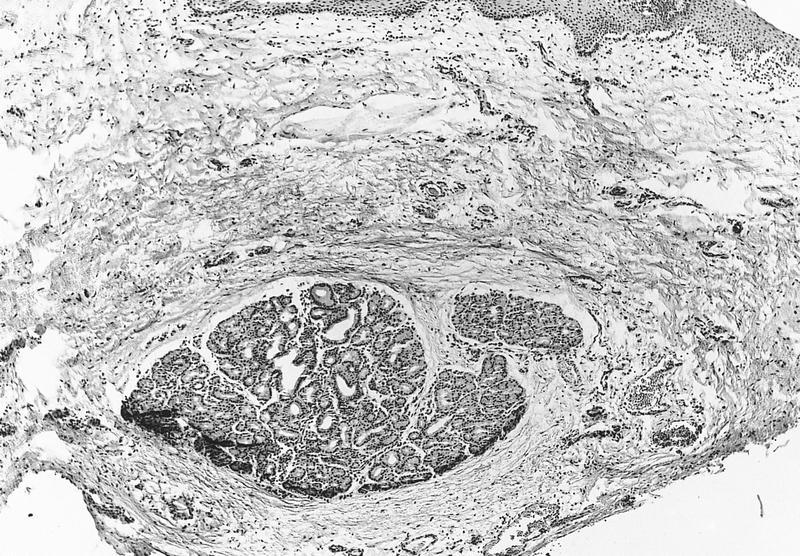
Cyclectomy: resecting portion of ciliary body containing tumor; may also include other surrounding structures
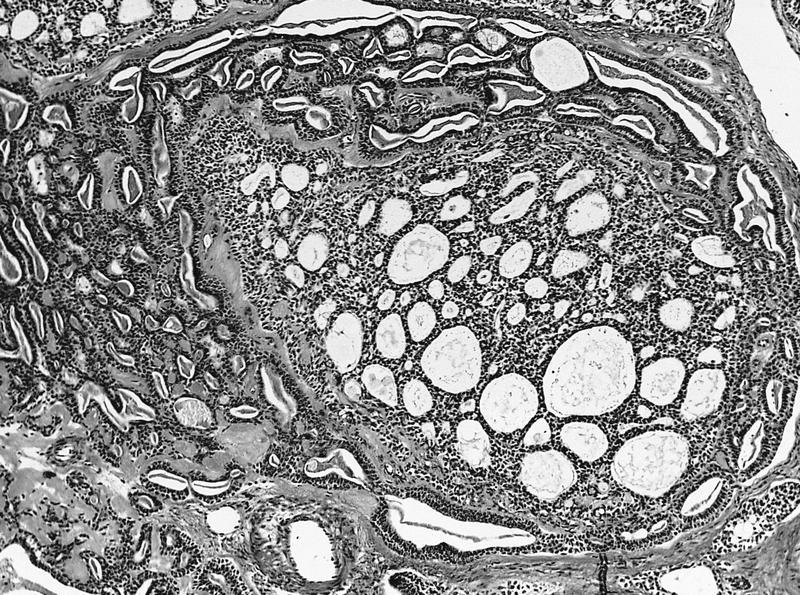
Pars plicata: 70 sagitally oriented folds or ciliary processes that gradually merge with posterior flat pars plana, which merges posteriorly with serrated, anterior border of retina (ora serrata)
Ciliary epithelium composed of inner epithelial layer (nonpigmented, contiguous with aqueous of posterior chamber) and outer epithelial layer (pigmented, unites with retinal pigment epithelium at ora serrata)
Outer epithelial layer overlies PAS+ basal lamina that thickens in diabetes mellitus
Zonules: acellular fibers that attach crests of nonpigmented ciliary epithelium in pars plicata to capsule of crystalline lens
Ciliary body has 3 distinct bundles of smooth muscle which assist in accommodation; as muscle contacts, ciliary body extends forward, reducing pressure on zonules, enabling lens to become less concave, thereby increasing its refractive power
Mucous membrane that covers, protects and lubricates the posterior surface of the eyelids (palpebral, also known as tarsal, conjunctiva) and anterior surface of the globe (bulbar conjunctiva) as well as provides redundant folds (forniceal conjunctiva) to aid eye movement
Essential features
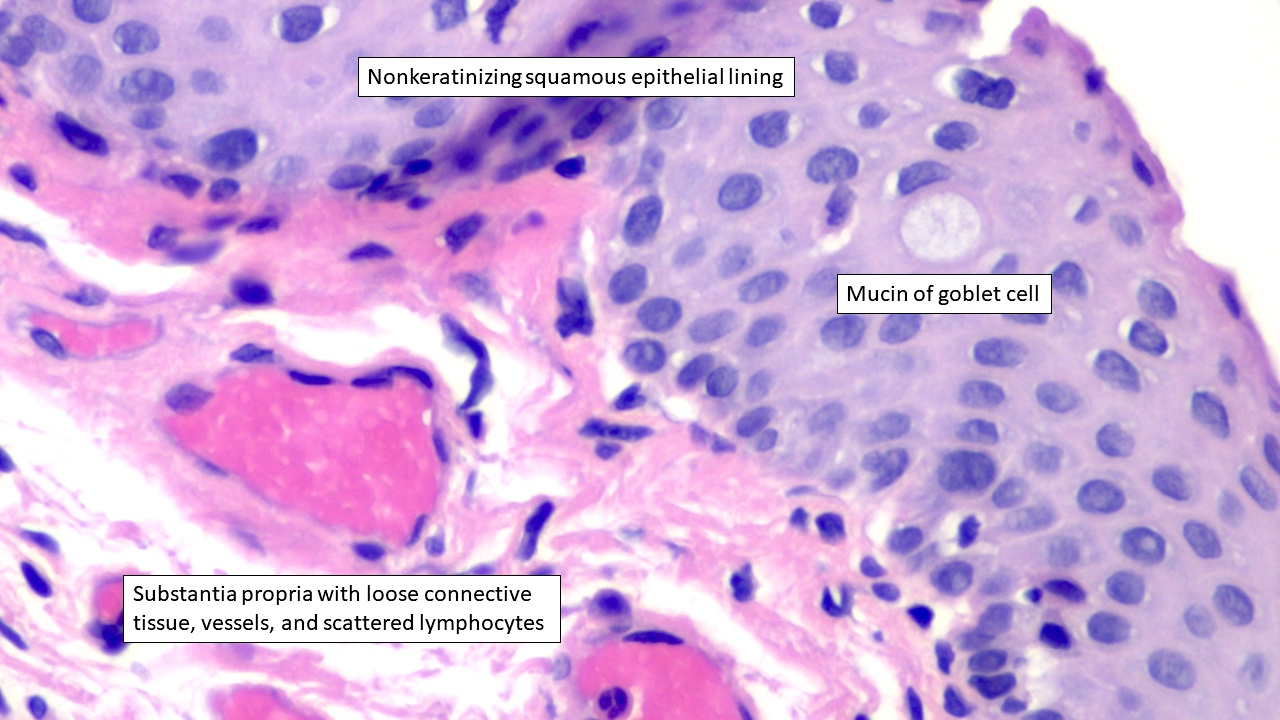
Nonkeratinizing squamous epithelium with goblet cells overlying loose connective tissue
Aids in protecting and lubricating the eye
Bulbar conjunctiva covers the anterior globe
Palpebral conjunctiva covers the posterior surface of the eyelids
Forniceal conjunctiva forms redundant folds to aid eye movement
Terminology
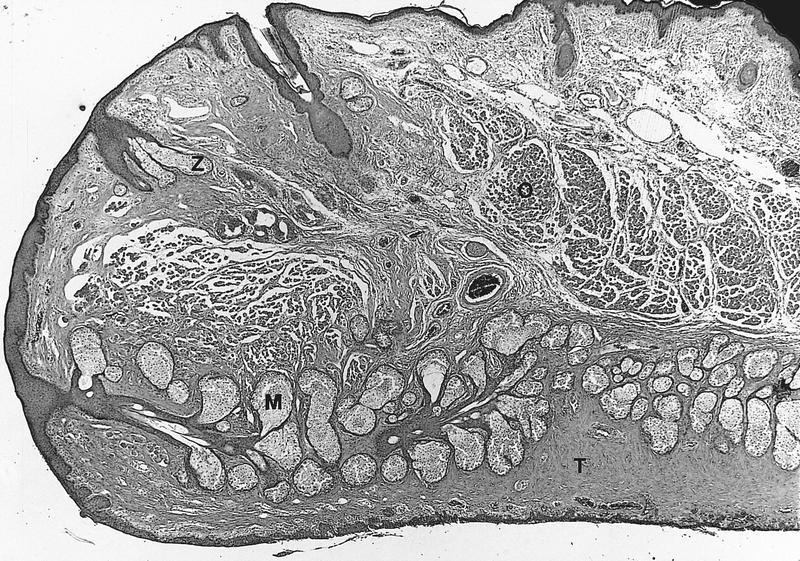
Palpebral (tarsal) conjunctiva covers the posterior surface of the eyelid and is associated with the tarsal plate and sebaceous (Meibomian) glands
Tarsal plate is the thick fibroconnective tissue that provides structural support to the eyelid and houses sebaceous (Meibomian) glands (J Anat 2005;206:37)
Meibomian glands are sebaceous glands of the tarsal plate that secrete meibum through holocrine secretion (Ophthalmology 2017;124:S20)
Bulbar conjunctiva covers the anterior globe (excluding the cornea) and can be further divided into scleral conjunctiva, limbal conjunctiva and plica semilunaris
Scleral conjunctiva covers the sclera, the dense, fibrous connective tissue of the eye
Limbal conjunctiva forms an annular rim around the cornea
Plica semilunaris is a fold of conjunctiva lateral to the caruncle
Limbus includes the border between the corneal and conjunctival epithelium and is an important location for multipotent stem cells (Eye (Lond) 1989;3:101)
Characterized by fibrovascular ridges that exist in a radial orientation, known as the palisades of Vogt, which are interspaced by limbal epithelial crypts that house stem cells that mediate corneal epithelial regeneration and superficial wound healing (Trans Am Ophthalmol Soc 1982;80:155, Br J Ophthalmol 2005;89:529)
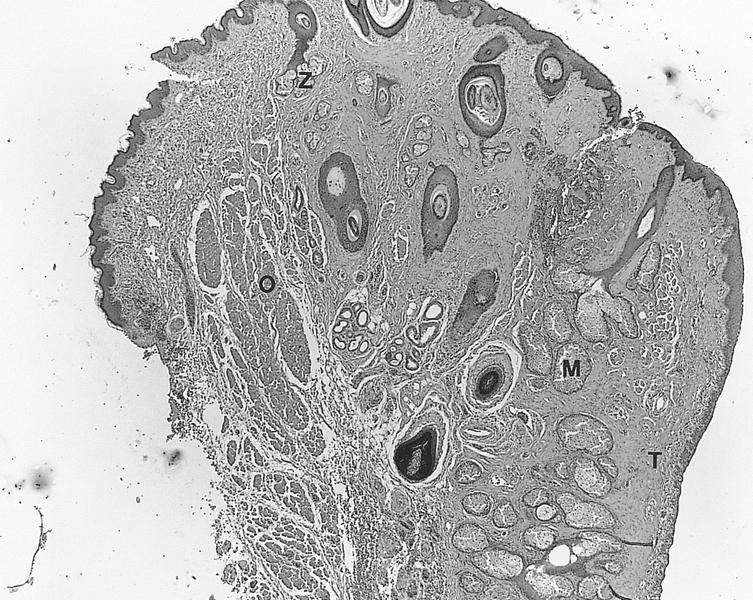
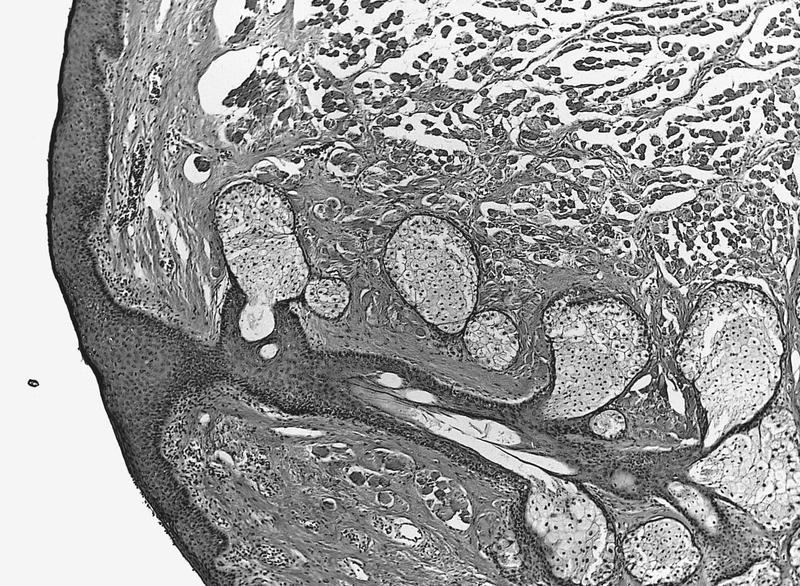
Caruncle is the fleshy pink prominence at the medial aspect of the eye; it contains conjunctiva, skin, hair follicles and other adnexal structures (Eye (Lond) 2009;23:1004)
Forniceal conjunctiva forms redundant folds in the cul de sac of the upper and lower fornices (the areas where the bulbar and palpebral conjunctivas meet) and allows for movement of the globe and eyelids (StatPearls: Mucous Membrane Graft [Accessed 28 June 2023])
Pseudoglands of Henle are infoldings, invaginations or tangentially sectioned conjunctival epithelium that resemble glands, often in the context of chronic inflammation (Ophthalmology 2001;108:135)
Conjunctival vascular supply
Conjunctival blood supply is primarily derived from the ophthalmic artery and its branches, such as the anterior ciliary arteries (Eye (Lond) 1988;2:533)
Routine surgical specimens of benign conjunctiva are typically small, unoriented fragments of tan-pink tissue
Microscopic (histologic) description
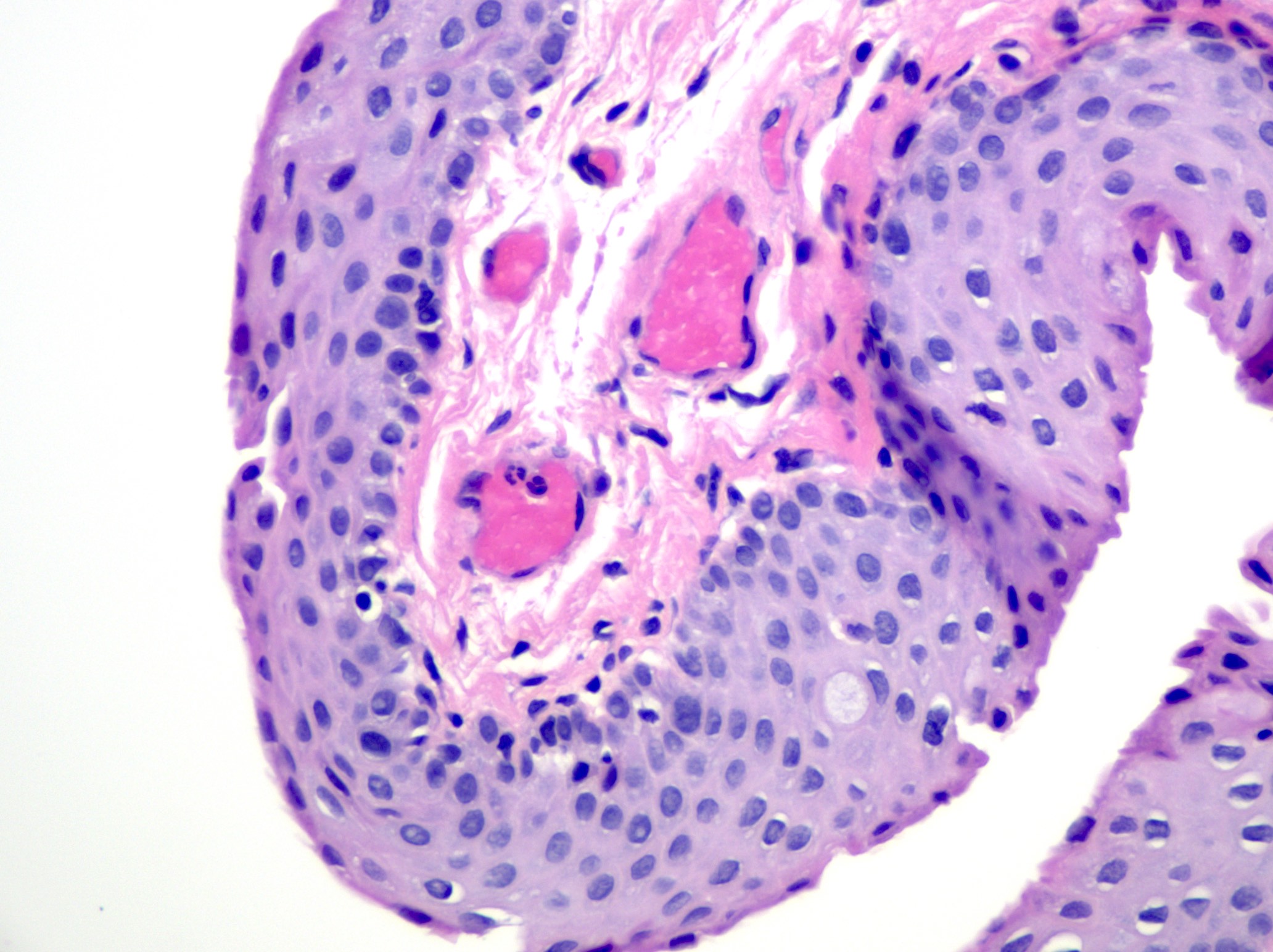
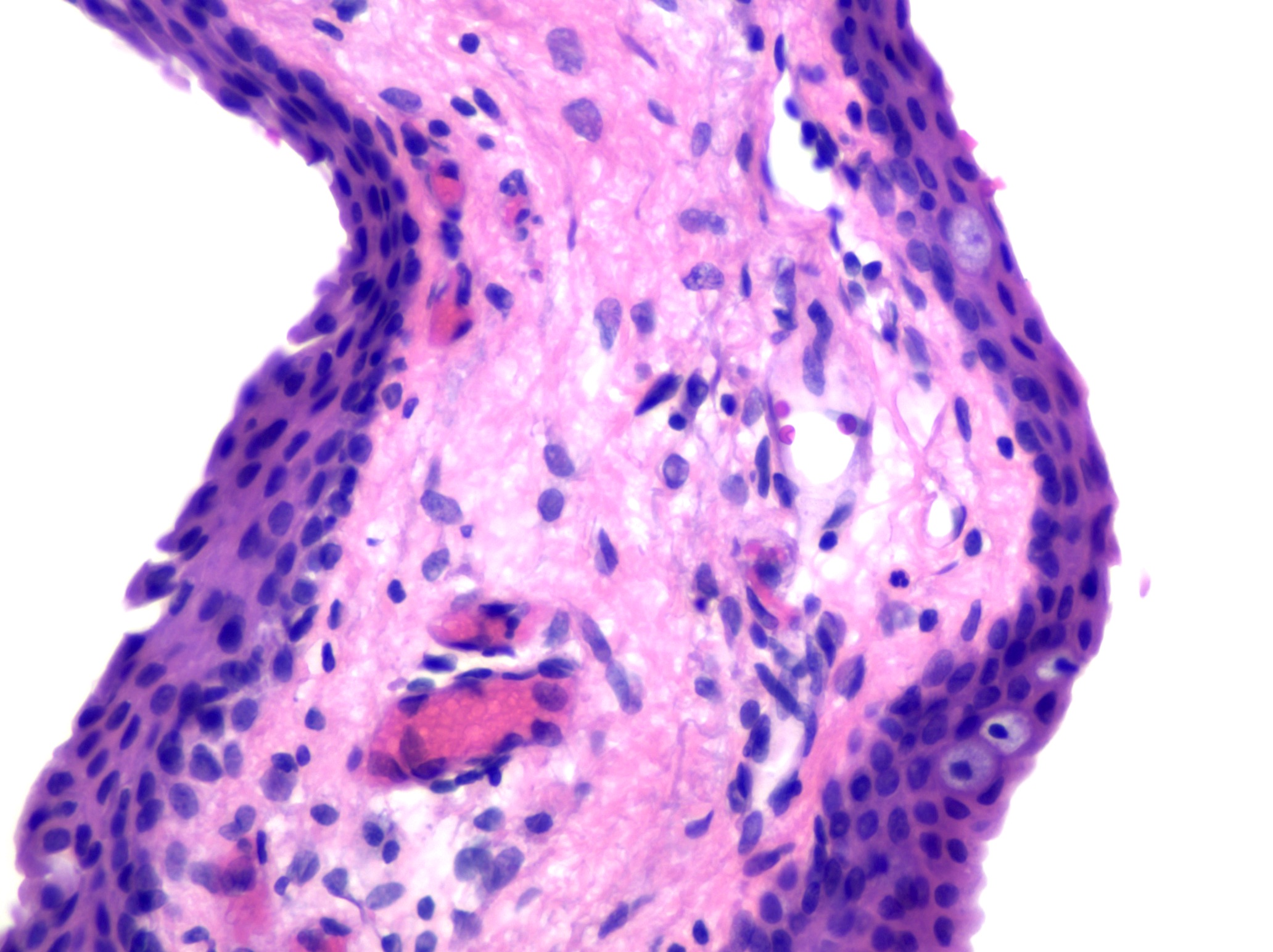
Nonkeratinizing squamous epithelium with scattered goblet cells overlying loose connective tissue of the substantia propria with limited chronic inflammation (including lymphocytes and plasma cells) and subepithelial glands, such as sebaceous (Meibomian) glands in the vicinity of the tarsal plate (Exp Eye Res 2014;129:172, Invest Ophthalmol Vis Sci 2011;52:1938)
Tarsal plate is identified by dense fibroconnective tissue in association with sebaceous (Meibomian) glands (J Anat 2005;206:37)
Infoldings of conjunctival epithelium, particularly in the context of chronic conjunctivitis, may mimic glandular tissue, a histologic appearance known as pseudoglands of Henle (Ophthalmology 2001;108:135)
Caruncle is identified by the presence of adnexal structures in addition to conjunctiva
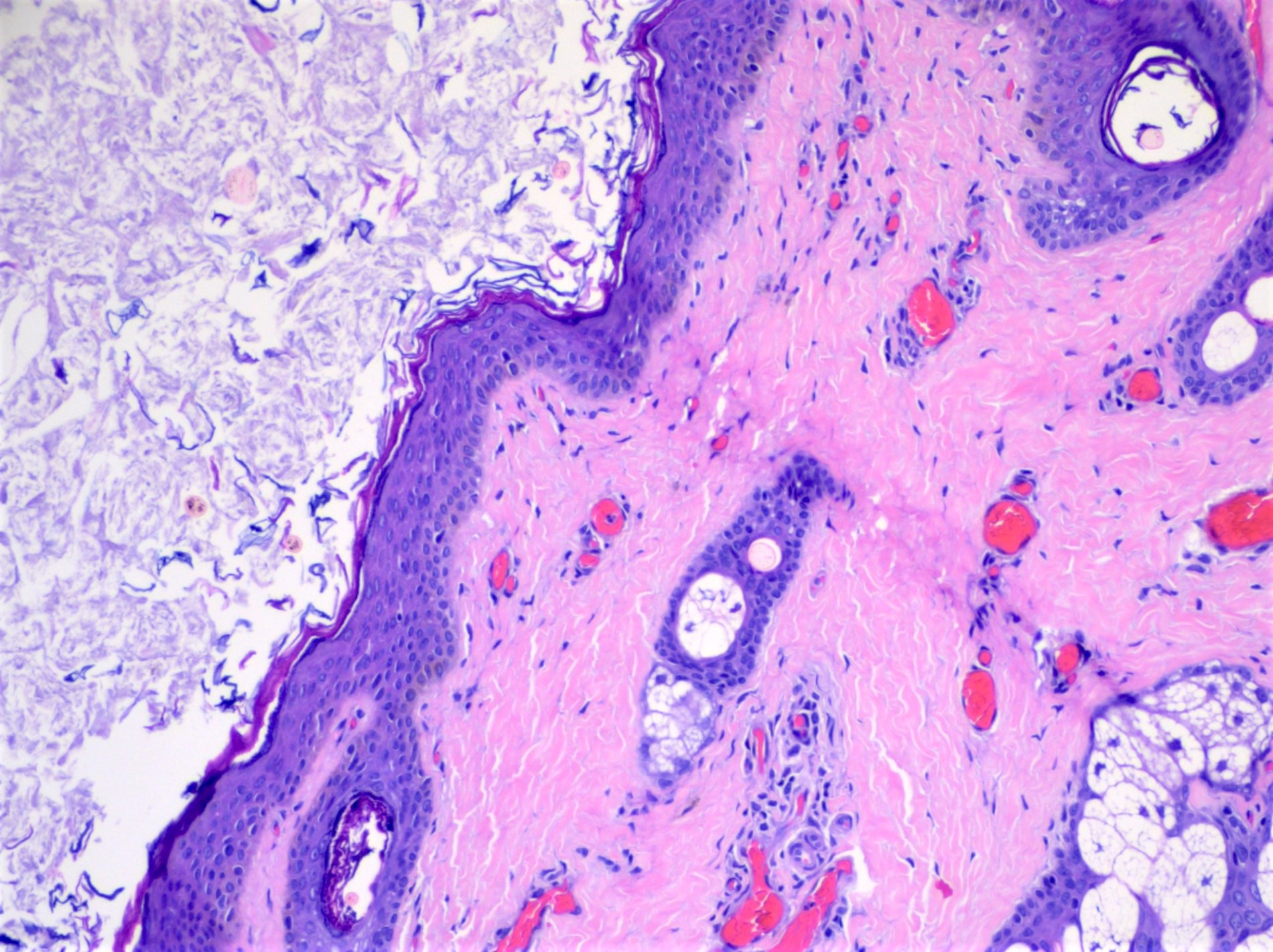
Degenerative changes related to the conjunctiva include pterygium and pinguecula; both are caused by ultraviolet light damage
Pterygium histologically appears as benign conjunctival epithelium with corneal Bowman membrane, underlying elastotic (solar) degeneration and neovascularization (see Pterygium) (Am J Pathol 2011;178:817)
Follicular conjunctivitis is comprised of lymphocytic nodules in the substantia propria and causes a bulge of the overlying epithelium; etiologies include infections, drug reaction, manifestations of systemic diseases and idiopathic causes
Papillary conjunctivitis is a polygonal distortion of the epithelium, often affecting tarsal conjunctiva and may be caused by chronic mechanical irritation, allergy, topical drugs and as a complication of contact lenses (Ocul Surf 2020;18:396)
Granulomatous conjunctivitis may be caused by foreign material, infection, systemic diseases or sarcoidosis (see Granulomatous conjunctivitis)
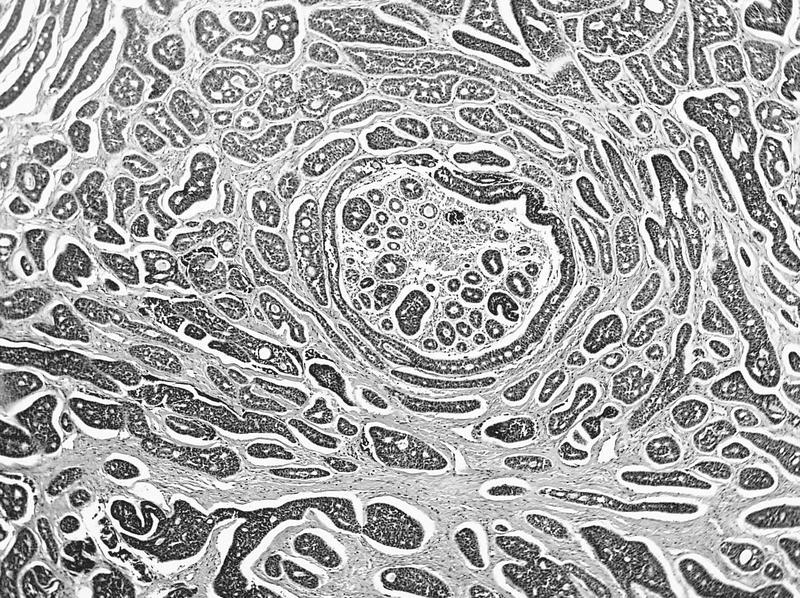
Based on the histologic features shown above, from what location is the biopsy taken?
Bulbar conjunctiva
Caruncle
Cornea
Forniceal conjunctiva
Palpebral conjunctiva
Board review style answer #1
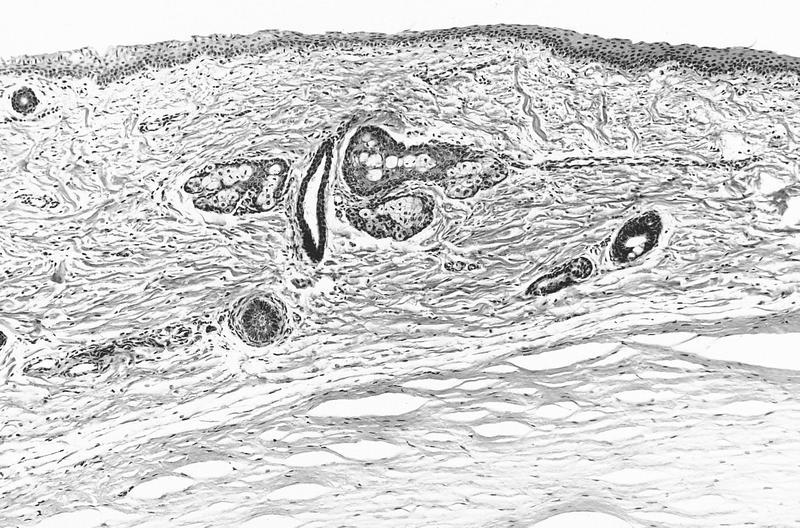
E. Palpebral conjunctiva. The presence of dense fibroconnective tissue constituting the tarsal plate and sebaceous (Meibomian) glands is helpful for identifying the palpebral (tarsal) conjunctiva. Answer B is incorrect because the caruncle is identified by the presence of adnexal structures, such as pilosebaceous units. Answer C is incorrect because the cornea features corneal epithelium, Bowman membrane, corneal stroma, Descemet membrane and endothelium. Answers A and D are incorrect because the bulbar and forniceal conjunctivas are not seen in association with the tarsal plate.
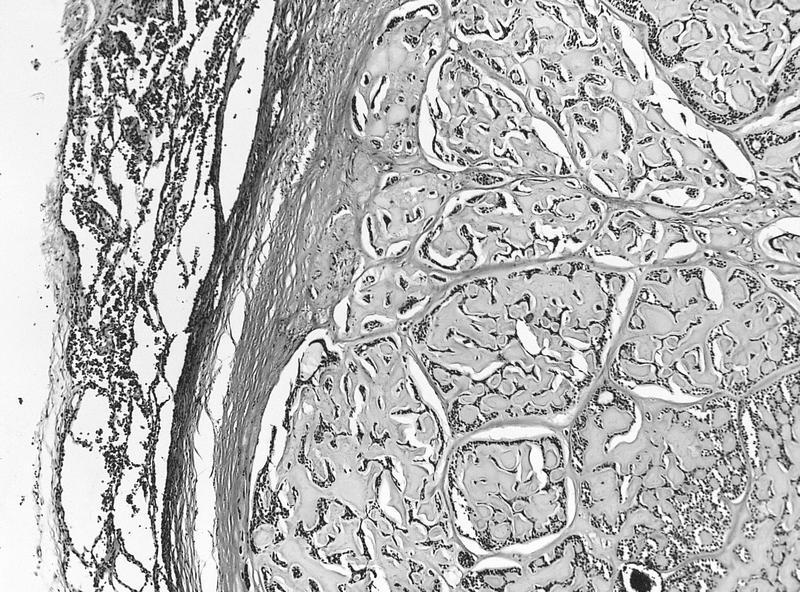
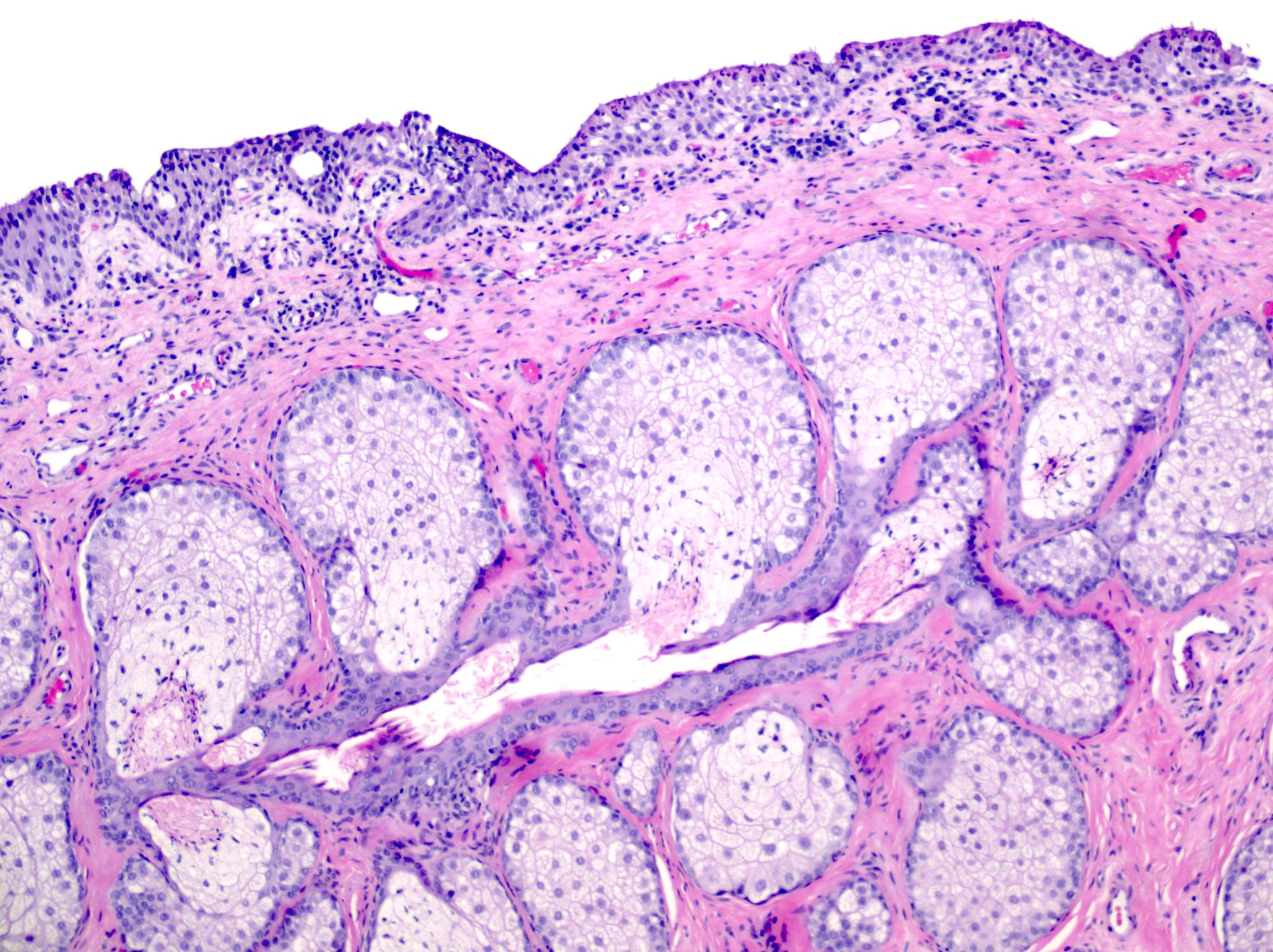
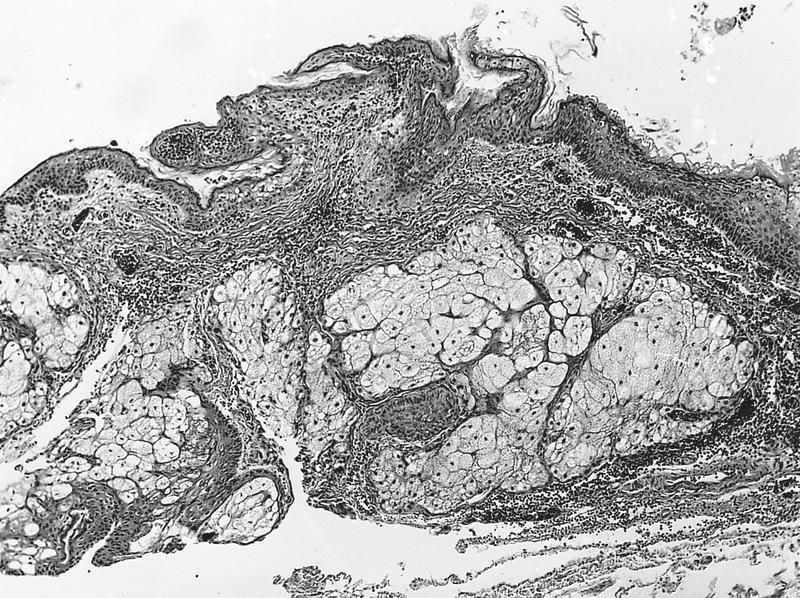
Based on the histologic features shown, from what location is the following biopsy with increased chronic inflammation and reactive changes taken?
Bulbar conjunctiva
Caruncle
Cornea
Forniceal conjunctiva
Palpebral conjunctiva
Board review style answer #2
B. Caruncle. The caruncle is identified by the presence of adnexal structures, such as the pilosebaceous unit seen in this histologic image. Answer E is incorrect because thick fibroconnective tissue of the tarsal plate and sebaceous (Meibomian) glands would be helpful for identifying the palpebral conjunctiva. Answer C is incorrect because the cornea features corneal epithelium, Bowman membrane, corneal stroma, Descemet membrane and endothelium. Answers A and D are incorrect because the bulbar and forniceal conjunctivas would not feature an associated pilosebaceous unit.
Wider than tall (11.7 mm horizontally vs. 10.6 mm vertically)
Thickness varies from 0.5 mm (central) to 0.67 mm (peripheral)
Cornea and overlying tear film are major refractive surface of eye, not the lens
6 distinct layers (outside to inside):
Outer epithelium: stratified squamous, nonkeratinized, 5 layers thick centrally, thicker peripherally, polygonal at basal layer but flatten as they approach surface; basal cells may have mitotic figures; Langerhans cells are CD1a+; note: layers often rubbed off while grossing specimen
Epithelial basal lamina (basement membrane): highlighted with PAS stain
Bowman layer: most anterior stroma, acellular, 8 - 14 microns thick, not a true basement membrane, composed of randomly oriented delicate collagen fibers, does not regenerate
Stroma: also called substantia propria, no blood vessels or lymphatics, 90% of cornea's thickness, contains regularly spaced collagen fibrils; normally separated by glycoprotein and mucoprotein which makes cornea transparent; normally see stromal lamellae separated by clefts, a processing artifact, absence of clefts is caused by stroma edema (causes corneal clouding), due to damage of endothelium
Descemet [pronounced DEZMET] membrane: a true basal lamina produced by underlying corneal endothelial cells; 3 - 4 microns at birth, 10 - 12 microns in adults; does not regenerate; site of copper deposition in Kayser-Fleisher ring of Wilson disease
"Endothelium": single layer of very flat cells, does not regenerate, functions as pump to keeps cornea dehydrated and transparent
Neural crest origin (S100+); does not line blood vessels or lymphatic spaces; directly contacts aqueous humor of anterior chamber, often rubbed off while grossing specimen
Hasall-Henle bodies (warts)
Focal excrescences that form on peripheral Descemet membrane with normal aging
Not seen in surgically excised corneal buttons because are too peripheral in location
Hyperopia
Eye too short for its refractive power
Laser assisted in situ keratomileusis (LASIK)
Sculpt cornea and change its refractive properties to eliminate need for glasses
Limbus
Junction of peripheral cornea and anterior sclera, 1.5 to 2.0 mm wide
Not a distinct anatomic site but a significant clinical landmark
Composed of conjunctiva (epithelium and stroma), cornea and scleral stroma, episclera, Tenon capsule (fibrous tissue that covers the globe)
Descemet membrane terminates at limbus and gives rise to Schwalbe ring
15% have prominent area of thickening at this site
Contains trabecular meshwork and Schlemm canal
Site of incisions for surgery on anterior eye
Restricts deeper extension of superficial tumors
Myopia
Eye too long for its refractive power
Schlemm canal and trabecular meshwork
Schlemm canal
Anterior and superficial to trabecular meshwork
Endothelial lined venous canal that completely encircles limbus
Separated from trabecular meshwork by thin connective tissue and separate endothelial linings
Trabecular meshwork
With Schlemm canal, are apparatus for removal of aqueous from eye
Collection of finely branching and delicately pigmented connective tissue bands
Lining cells are continuous with corneal endothelium
Posteriorly, trabecular meshwork extends to scleral connective tissue called scleral spur
Vasculature
No blood vessels or lymphatics within cornea
Arterial plexus is present at junction of cornea and sclera
Is also nourished by aqueous humor of anterior chamber
Palpebral (tarsal) conjunctiva lines interior of eyelid
Very thin
Continuous with bulbar conjunctiva that covers the sclera
Becomes papillary with allergic or bacterial conjunctivitis
Contains eccrine and apocrine glands (glands of Moll) and sebaceous glands
Sebaceous glands (Meibomian glands within eyelid fibrous tarsus and glands of Zeis associated with eyelashes) create lipid layer of tear film which retards evaporation of tears
The orifices of Meibomian glands open just in front of the posterior edge of the lid margin and are separated from the more anteriorly placed eyelashes by a gray line
Muscular layer is composed primary of orbicularis oculi muscle
Pathophysiology
Specimens received are often from cosmetic blepharoplasty or other reparative surgery with no abnormalities
Other lesions are similar to those in skin
Creates tear film via accessory lacrimal glands embedded above fibrous tarsus of eyelid
Helps to protect and lubricate the globe
Tumors may prevent complete closure of eyelid, leading to exposure and ulceration of cornea
Gray line
Divides the eyelid into anterior and posterior parts
It corresponds with the position of the pretarsal orbicularis muscle
Defined as eyeball itself plus intraocular tissues, or eye proper without its appendages
Dimensions: anterior-posterior 24 mm, vertical and horizontal dimensions are both 23 to 23.5 mm
Six extraocular muscles:
4 rectus and 2 oblique muscles
Arise in posterior orbit from fibrous ring called annulus of Zinn, and insert into sclera
Muscles are surrounded by fascia
Inferior oblique inserts on sclera, other muscles insert on tendons
Equator: midway between anterior and posterior poles
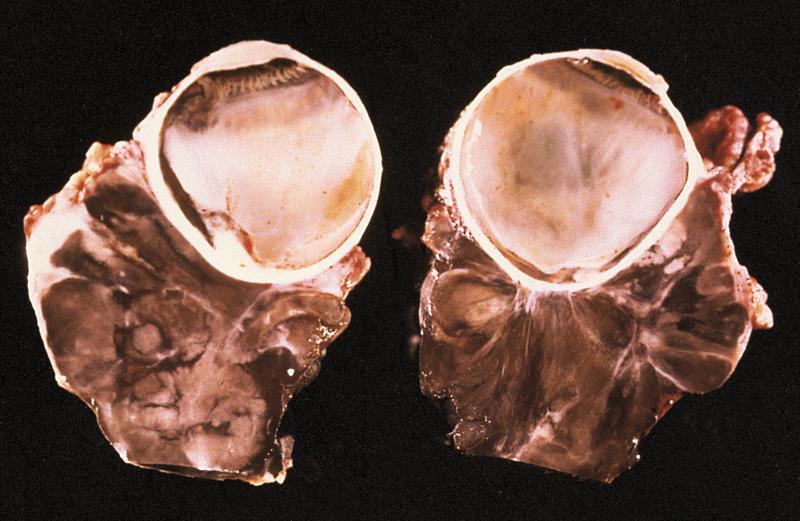
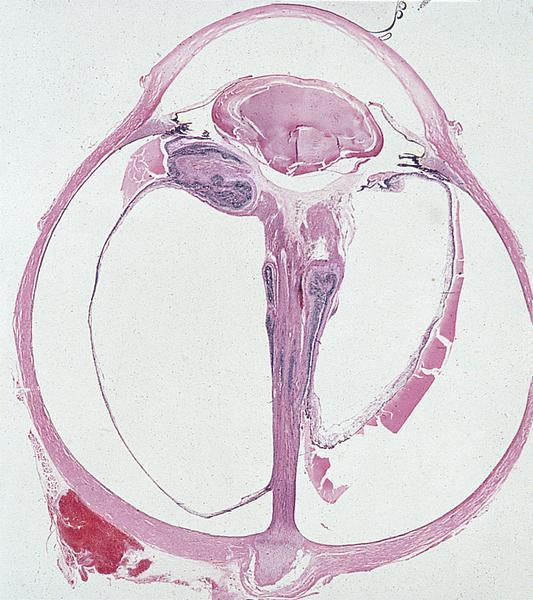
Specimen is the result of enucleation, performed because eye is nonfunctional, painful, unsightly, infectious, contains neoplasm, post-trauma (may be removed to prevent sympathetic uveitis) or has chronic glaucoma
Globe usually intact but free of extraocular muscles and orbital fat
Globe may be eviscerated, with only fragments available for microscopic study
Initial pathologic processes may be obscured by subsequent pathologic processes
Enucleation: due to tumor (48%, usually melanoma), glaucoma (13%), phthisis bulbi (12%), recent trauma (11%)
Specimens also received after evisceration (10%) or exenteration (9%) to manage malignant orbital tumors (Am J Clin Pathol 2003;119:594)
During 1990 to 2000, decrease in percentages due to neoplasms, increase due to glaucoma and phthisis bulbi
Lacrimal duct & gland
Lacrimal gland located in superiotemporal aspect of orbit, not palpable
Contributes secretions to tear film including IgA
Accessory lacrimal glands are embedded above fibrous tarsus of eyelid and in conjunctival fornix
Serous with minor mucinous component
Larger ducts have myoepithelial layer
Normally may have lymphocytes and plasma cells
Drainage apparatus is composed of puncta, canaliculi, lacrimal sac and nasolacrimal duct
Tears drain toward medial canthus, then through lacrimal punctum into lacrimal canaliculi, then nasolacrimal sac, then nasolacrimal duct, then nose
Puncta:
Opening in medial aspect of eyelid where tear fluid drains
Canaliculi (lacrimal duct):
Tubular structures 0.5 mm in diameter where puncta drains
Nonkeratinizing squamous epithelium surrounded by fibrous tissue
Lacrimal sac:
Merging of canaliculi, encased by bones of orbit
Stratified columnar epithelium with goblet cells
Nasolacrimal duct:
Drains lacrimal sac, 1 cm long, connects to inferior meatus of nose
Stratified columnar epithelium with goblet cells
Lacrimal duct disorders often cause epiphora (tears flow over lid margin onto cheek), induration, inflammation of lower eyelid
Tumors tend to displace eye downward because adjacent orbit restricts growth
Tumors are difficult to resect completely leading to high recurrence rate
Lacrimal gland is considered a minor salivary gland for tumor reporting
Regional lymph nodes are preauricular (parotid), submandibular and cervical
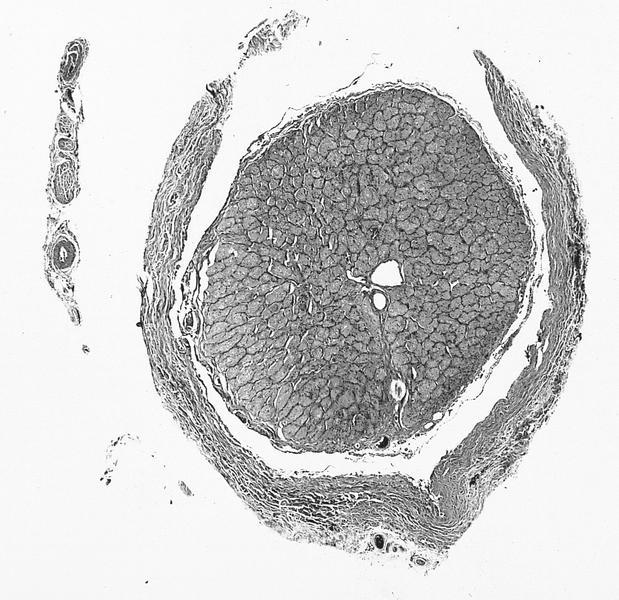
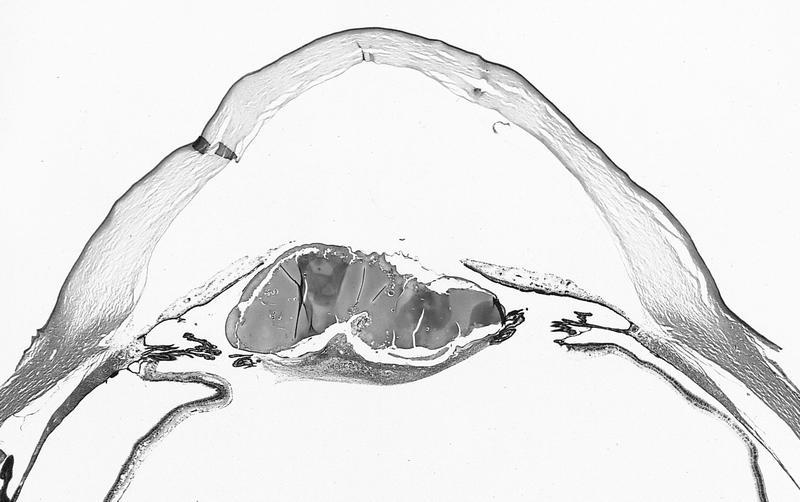
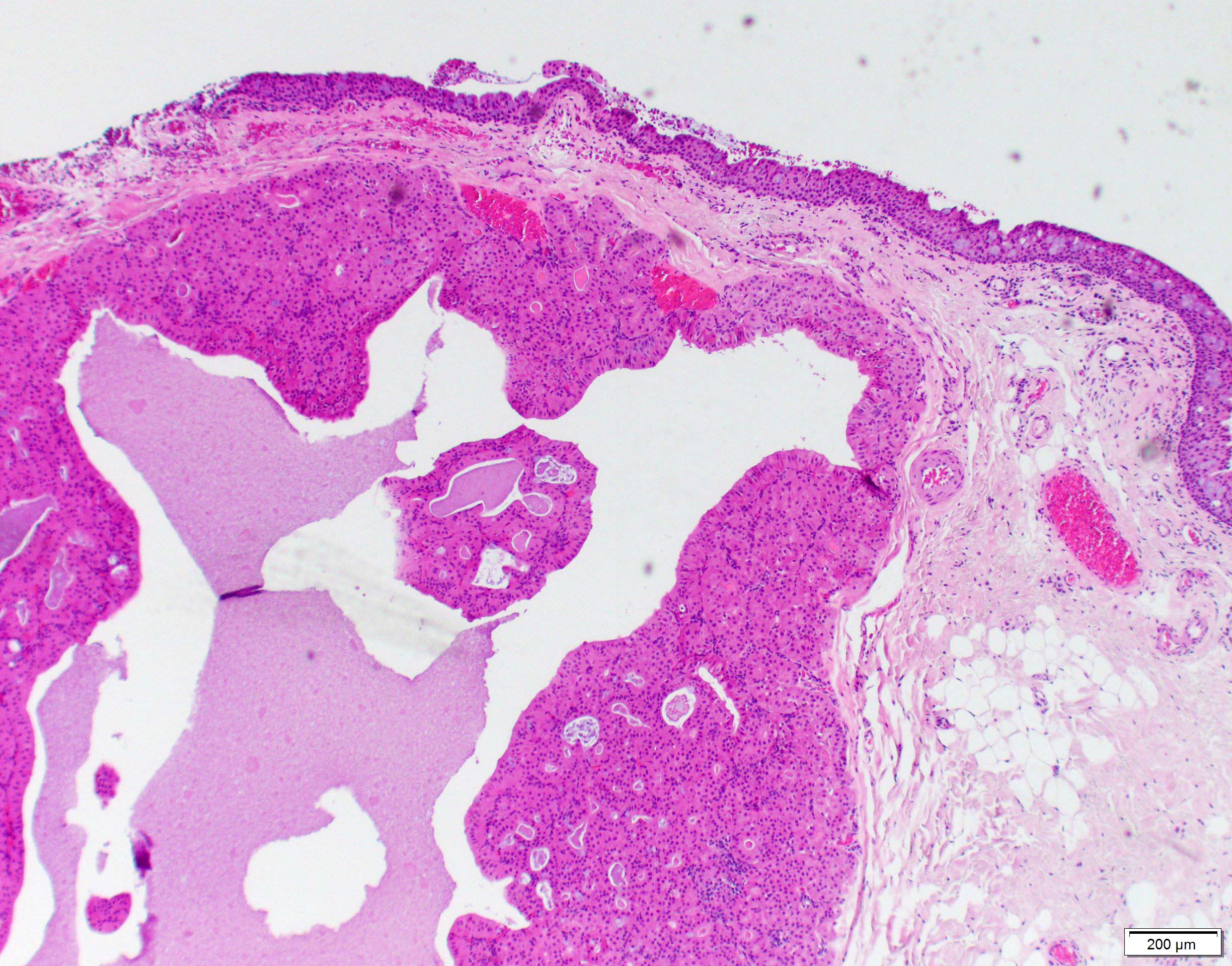
Lens
Most surgical specimens are cataracts or prosthetic intraocular lens
Normal lens is biconvex, behind pupil / iris, in front of vitreous, in posterior chamber
10 mm in diameter by 4 - 5 mm in width
Usually Gross Examination Only (report as transparent - Yes or No), don't section
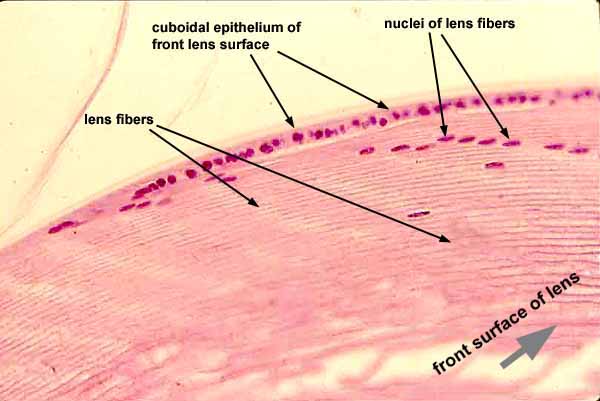
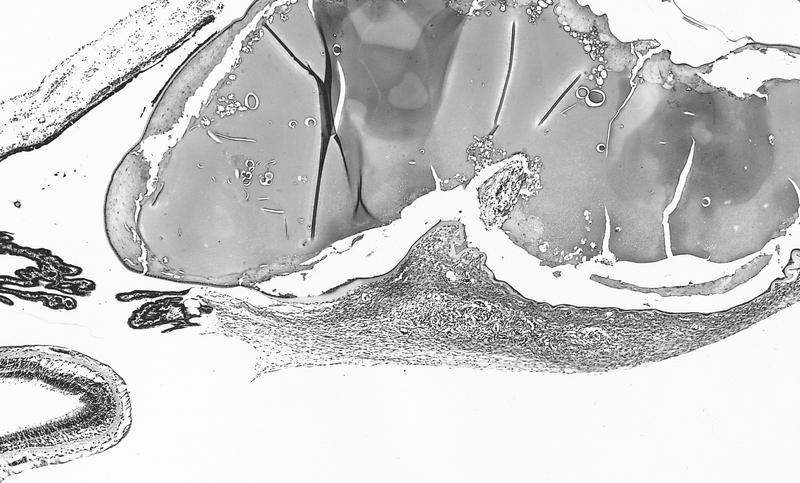
Anterior lens capsule is eosinophilic acellular band overlying single layer of epithelial cells
Lens capsule is strongly PAS+, holds lens in place
Lens has thinner capsule posteriorly, without epithelial cells
Lens in held in place by zonules that connect to pars plicata of ciliary body
Lens normally opacifies with age due to globules of degenerate lens fibers
Is a closed epithelial system with lens capsule (epithelium) that totally envelops the lens
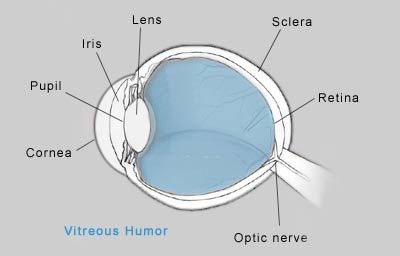
Vitreous humor:
Avascular
Extends from lens to sensory retina
Contains gel-like material composed of water, protein, hyaluronic acid and "hyalocytes"
Gel consistency is due to randomly oriented collagen fibrils
May appear as amorphous material on H&E
Orbit & optic nerve
Orbit contains globe and its fibrous covering (Tenon capsule), lacrimal gland, optic nerve and its meningeal covering, extraocular muscles, cartilaginous trochlea, blood vessels and delicate fibroadipose connective tissue
Floor of orbit is roof of maxillary sinus
Medial wall of orbit (lamina papyracea) separates orbit from ethmoidal sinuses
Proptosis: forward displacement of eyeball (or other organs), due to any disease that increases orbital contents, since orbit is closed medially, laterally and posteriorly
Exophthalmos: abnormal protrusion of eyeball
Common symptom of orbital disease, although often due to thyroid disease and not biopsied
Other common causes of exophthalmos are mucocele from paranasal sinus, hemangioma, inflammatory pseudotumor
Optic nerve:
Surrounded by meninges; part of central nervous system
Not usually biopsied
Often has psammoma bodies or drusen (calcified acellular globular concretions of nerve fibers)
Site of convergence of one million axons from retinal nerve fiber layer
Nerve head accounts for physiologic blind spot in normal visual field
Receives blood supply from branches of ophthalmic artery
Surrounded on both sides by short posterior ciliary arteries
Lamina cribrosa:
Site of myelination of optic nerve axons
Highlighted with Luxol fast blue or other myelin stains
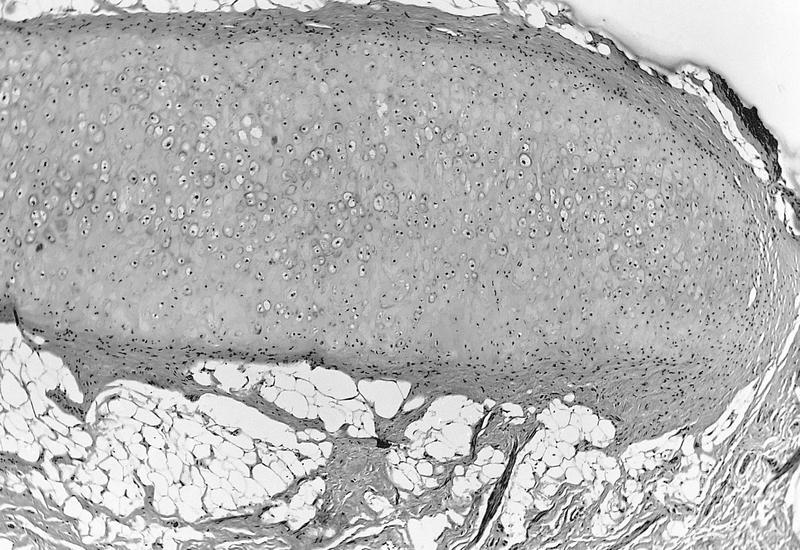
Trochlea:
Arc shaped structure through which tendon of superior oblique muscle passes before insertion upon eyeball
The only cartilaginous structure in normal orbit
Tumors should be reported using formats published for their counterparts elsewhere in body
Drainage through submandibular, parotid and cervical lymph nodes through vascular anastomosis
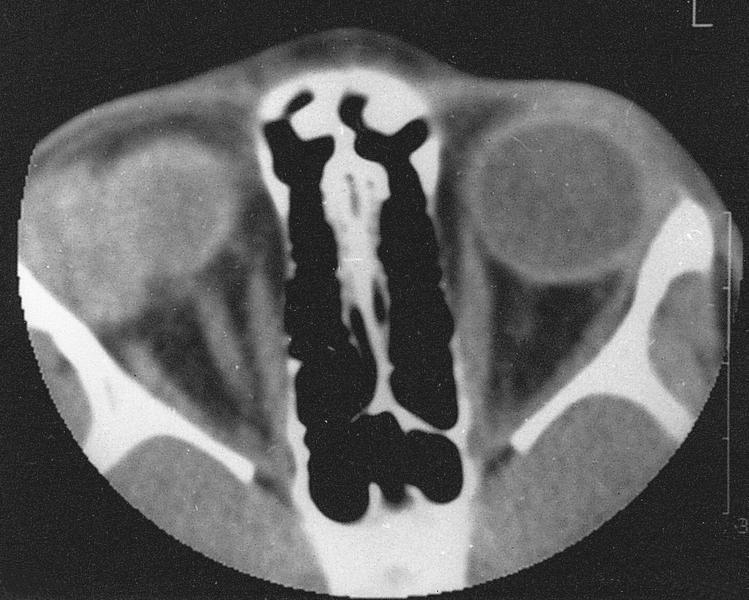
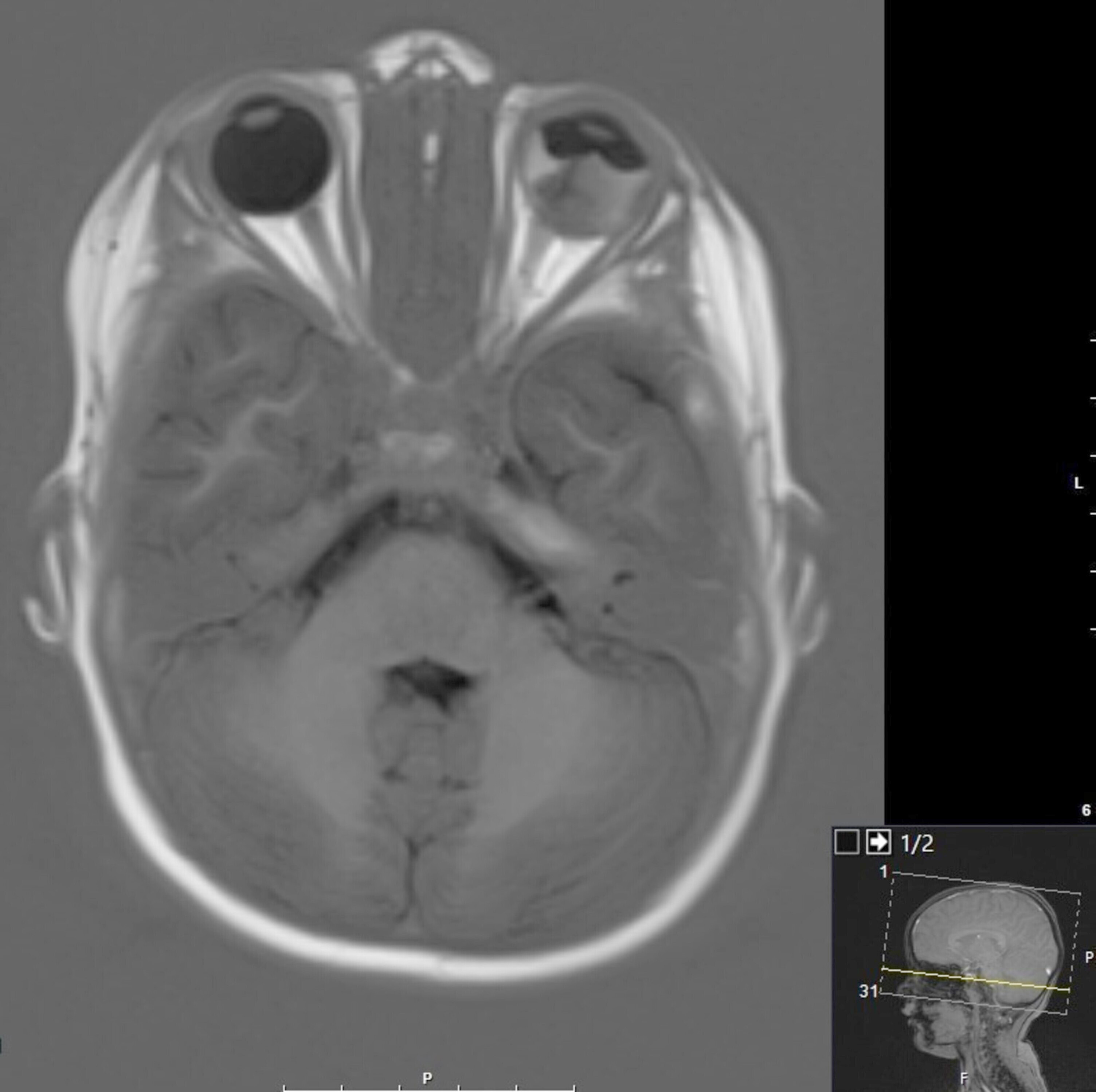
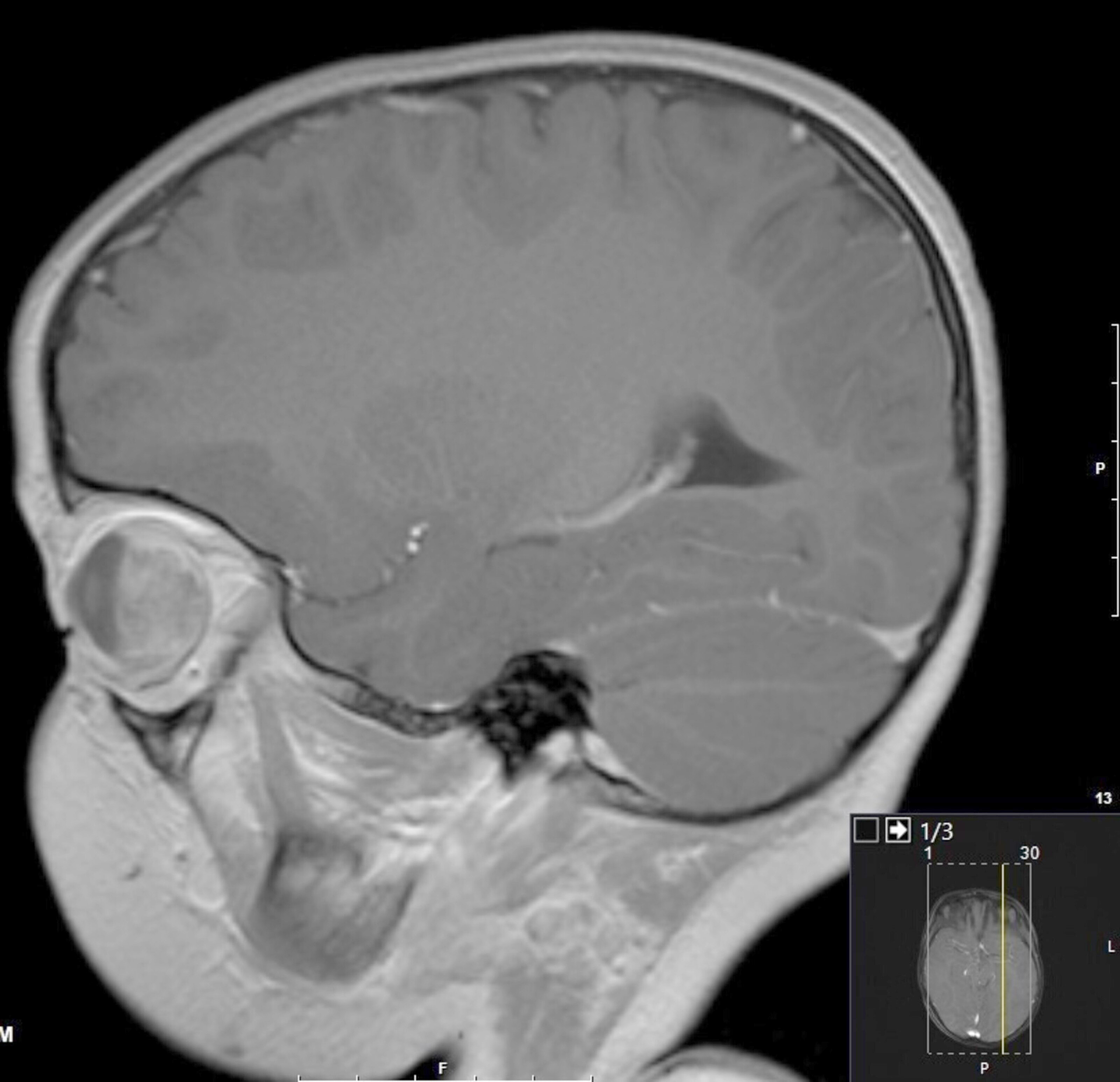
Radiology images
AFIP images
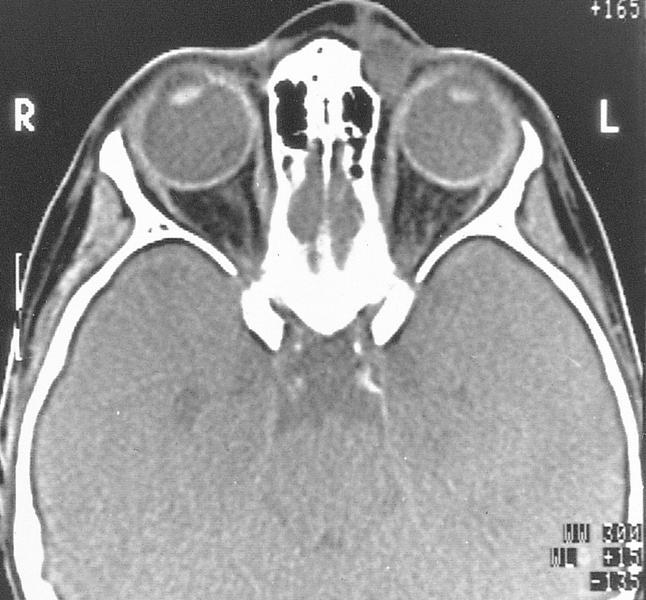
Normal eye and orbital contents
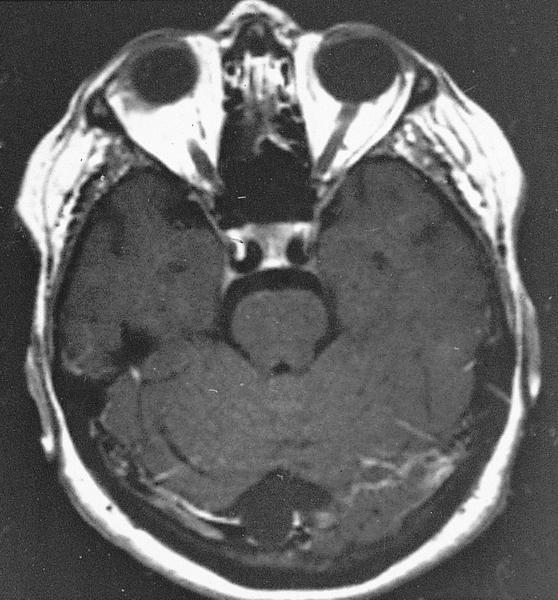
MR #1 (T1 weighted)
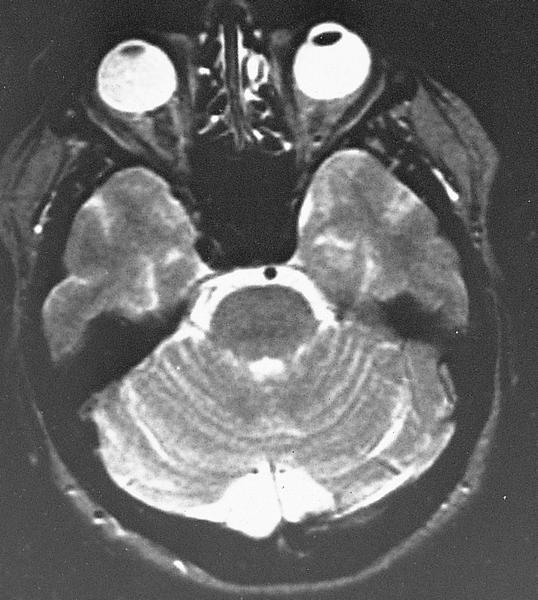
MR #2 (T2 weighted)
MR #3 (T1 weighted) shows coronal section of orbital contents posterior to globe
Drawings
Images hosted on other servers:
Lacrimal apparatus
Lens
Optic nerve
Orbit
Extraocular muscles in orbit
Cross section
Globe
Microscopic (histologic) description
Anterior but not posterior lens has single epithelial layer
Microscopic (histologic) images
AFIP images
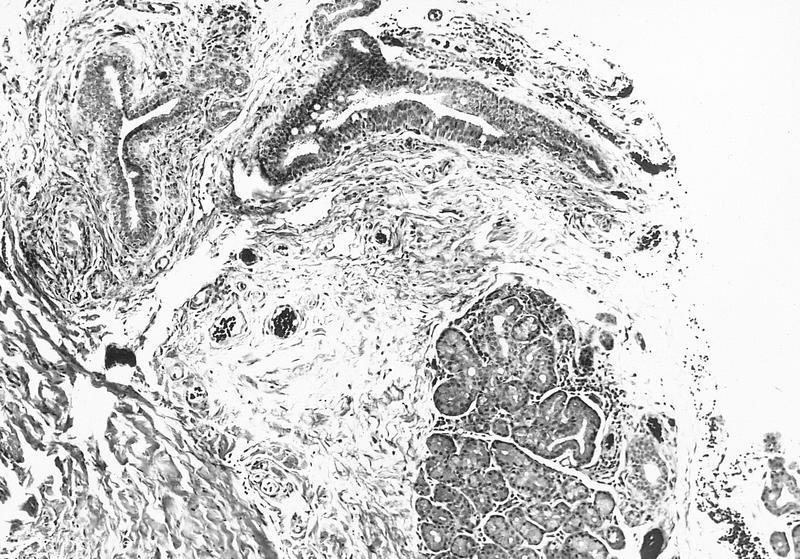
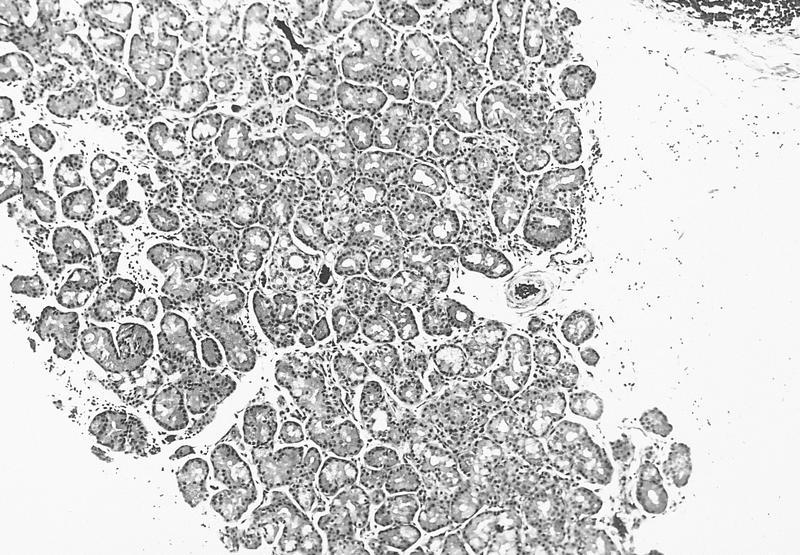
Glandular lobule next to ducts
Lobule of acinic and mucinous cells
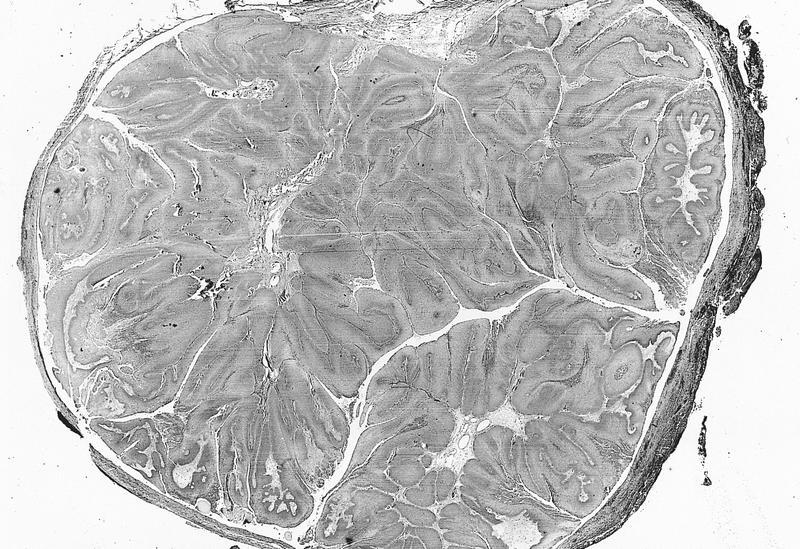
Intraocular and orbital portions of optic nerve
Cross section of optic nerve parenchyma and meninges
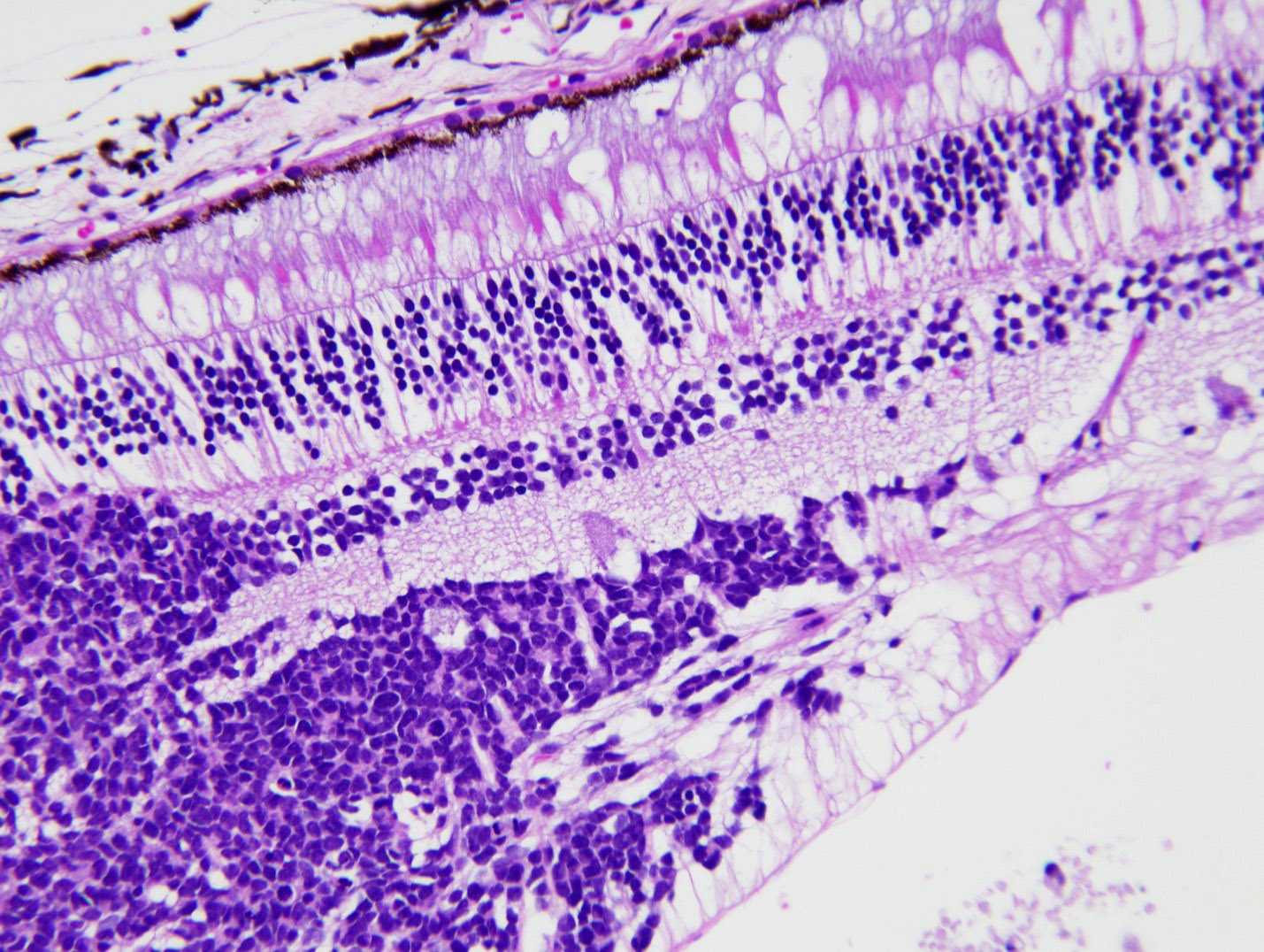
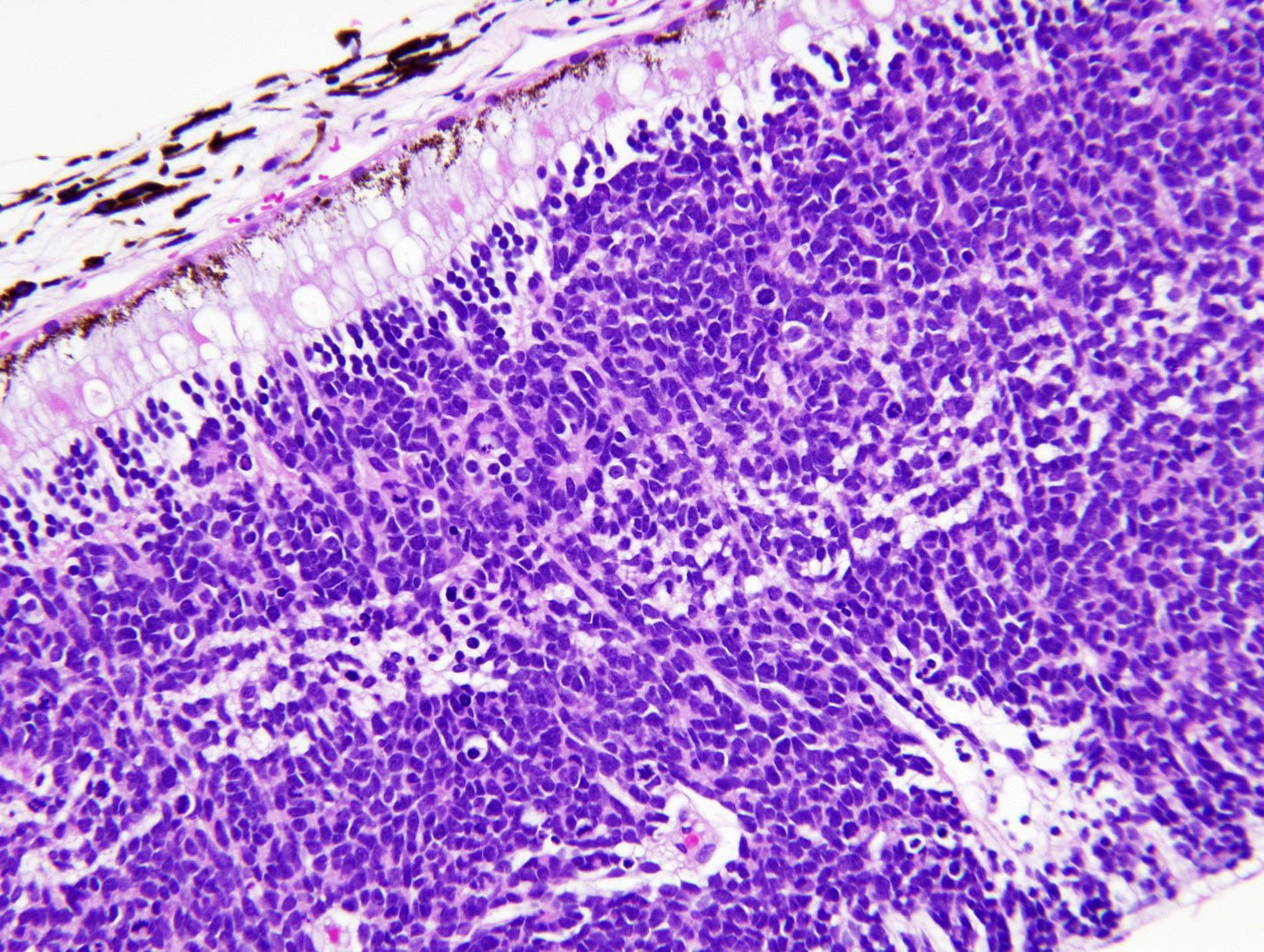
Specialized nervous tissue of the posterior eye that is responsible for the detection of light
Essential features
Embryologic derivative of the optic vesicle, which arises from the diencephalon and enables detection of light (Dev Biol 2007;305:1)
Composed of photoreceptors, first order neurons, second order neurons and glia (including Müller cells), the latter of which account for gliotic reaction
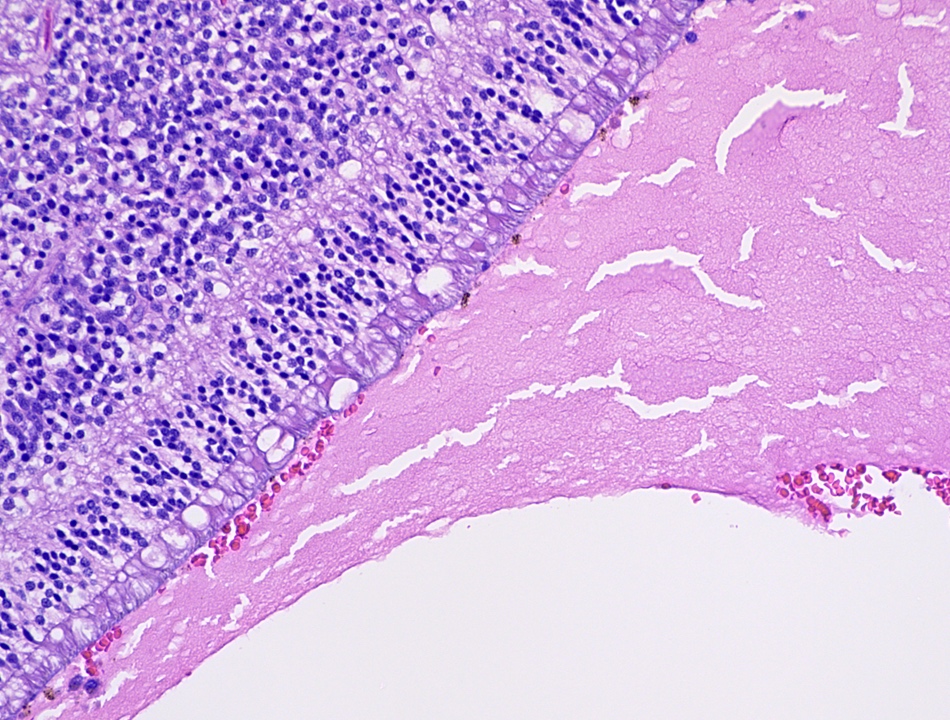
Lines the innermost layer (or coat) of the eye, extending posteriorly from the ora serrata and situated between the vitreous body and choroid
Terminology
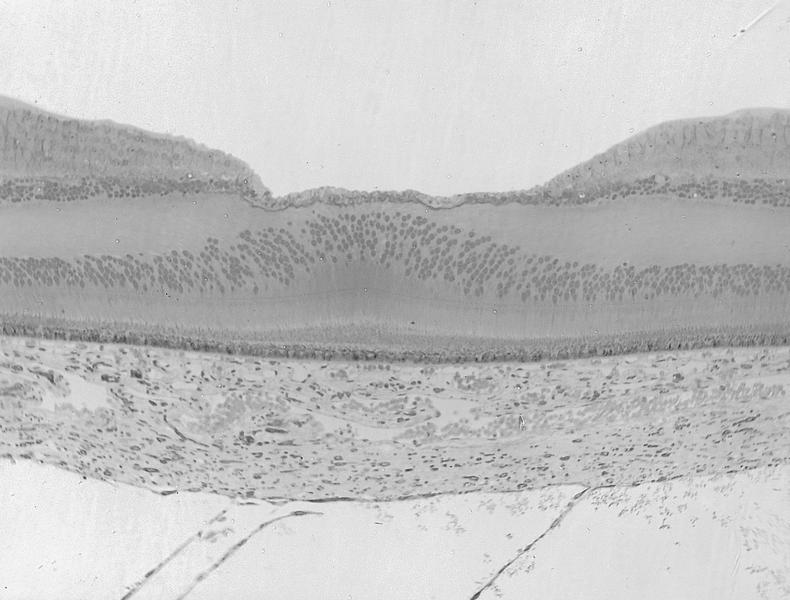
Macula: highest density of photoreceptors and ganglion cells, responsible for high acuity vision and identified histologically by an increased number of ganglion cells and increased layer thickness
Ora serrata: point of transition between anterior ciliary body and posterior retina
Bruch membrane (not part of retina): separates choroid from overlying retinal pigment epithelium and features a 5 layer structure (basement membrane of retinal pigment epithelium, inner collagenous layer, elastin layer, outer collagenous layer and basement membrane of choriocapillaris); thickens with age and acquires focal extracellular deposits known as drusen (Prog Retin Eye Res 2010;29:1)
Anatomy and physiology
Light is detected by the rods and cones of the photoreceptor layer and signals are transmitted through the layered retina to the optic nerve
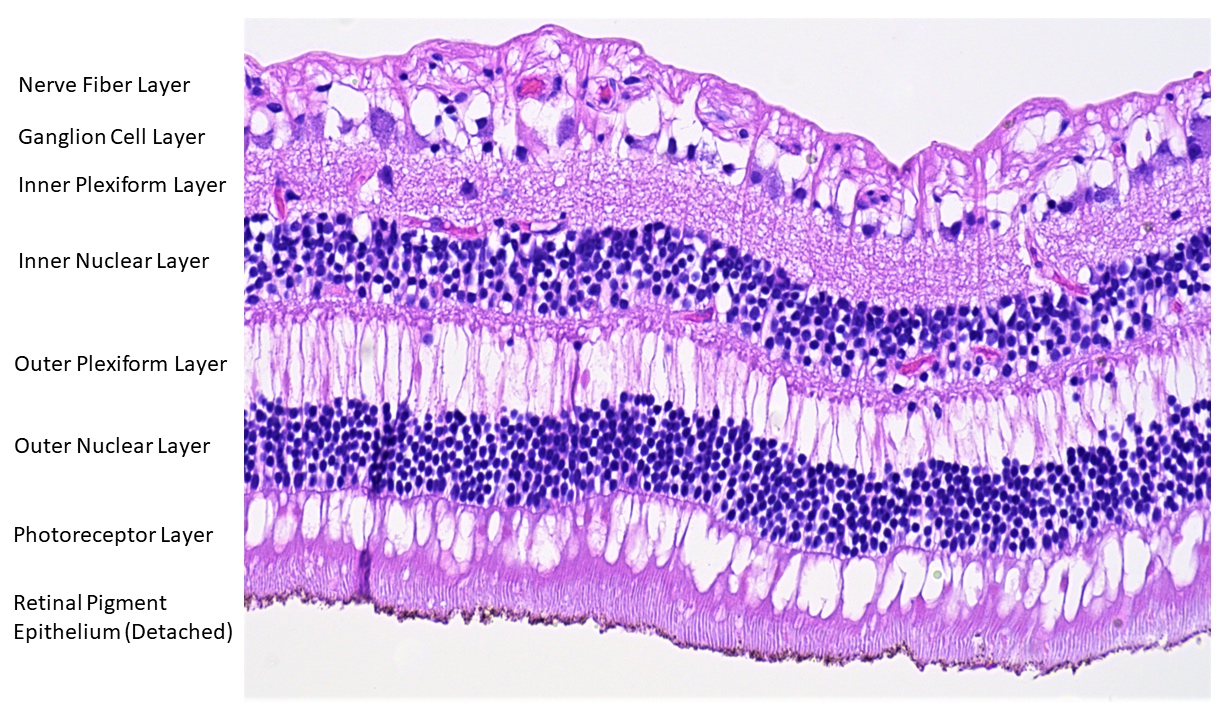
Anatomical structure of retina and surrounding structures (outer to inner):
Orientation
Outer: nearest the limits of the globe (sclera)
Inner: nearest the center of the globe (vitreous body)
Retinal pigment epithelium: single layer of microvillous, cuboidal cells containing melanosomes that aid in light absorption by melanin, nutrient and fluid transport and phagocytosis that assists in photoreceptor turnover; forms the outer limit of the retina adjacent to Bruch membrane (Curr Mol Med 2010;10:802)
Photoreceptor (rods and cones) layer: composed of the outer segments of the rods and cones (the photoreceptors that convert light into signal impulses) (J Cell Sci 2015;128:4039)
External (outer) limiting membrane: permeable adherent junctions between photoreceptors and Müller cells (J Comp Neurol 1990;295:155)
Outer nuclear layer: contains the photoreceptor nuclei
Outer plexiform layer: located between the outer nuclear and inner nuclear layers and contains axons and dendrites of photoreceptors and bipolar cells (first order neurons), including Henle fibers (photoreceptor axons) that are prominent in the perifoveolar region and features a line of synapses known as the middle limiting membrane (Dev Ophthalmol 2016;55:7)
Inner plexiform layer: network of neuronal processes between the inner nuclear layer and the ganglion cell layer
Ganglion cell layer: accommodates the ganglion cells, varying in thickness and density up to 5 - 8 layers in the macula; it is responsible for various functions in the relaying of received visual information out of the retina (Front Neurol 2021;12:661938)
Nerve fiber layer: comprised of the axons of ganglion cells
Internal limiting membrane: the only true basement membrane of the retina; it is located adjacent to the vitreous body where it serves as an anchor point for collagen fibers of the vitreous cortex (Exp Eye Res 2021;206:108545)
Relevant vasculature to the retina:
Central retinal artery: a branch of the ophthalmic artery that supplies the inner retina, including the nerve fiber layer, ganglion cell layer, inner plexiform layer and a portion of the inner nuclear layer
Choriocapillaris: supplies the outer retina, including the photoreceptor layer and the innermost portion of the choroid adjacent to Bruch membrane (Prog Retin Eye Res 2022;87:100997)
Central retinal vein and branches: drain the inner retina
Retina lacks lymphatics
Diagrams / tables
Contributed by J. Stephen Nix, M.D.
Retina anatomy
Clinical features
Central retinal artery occlusion: often presents with sudden, painless vision loss and damage to the inner aspect of the retina (Eye (Lond) 2013;27:688)
Hemorrhages of the nerve fiber layer appear streaked or flame shaped, while hemorrhages of deeper layers appear dot-like or blot-like on ophthalmoscopic examination (Pediatr Emerg Care 2018;34:665)
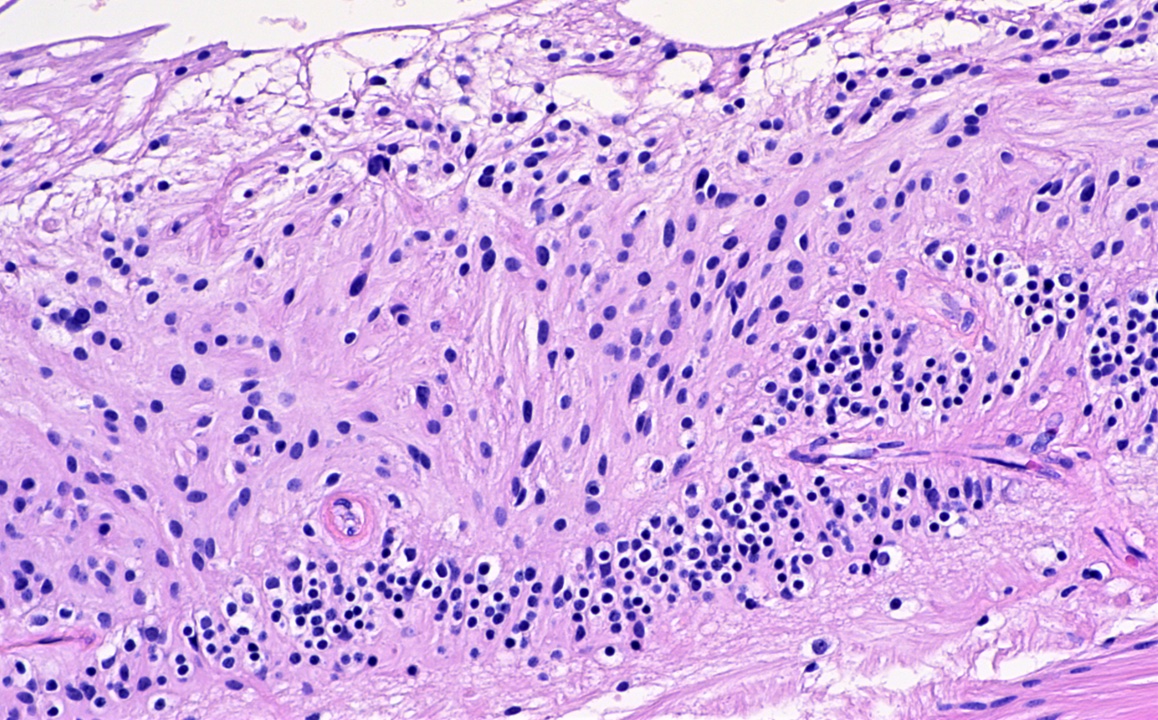
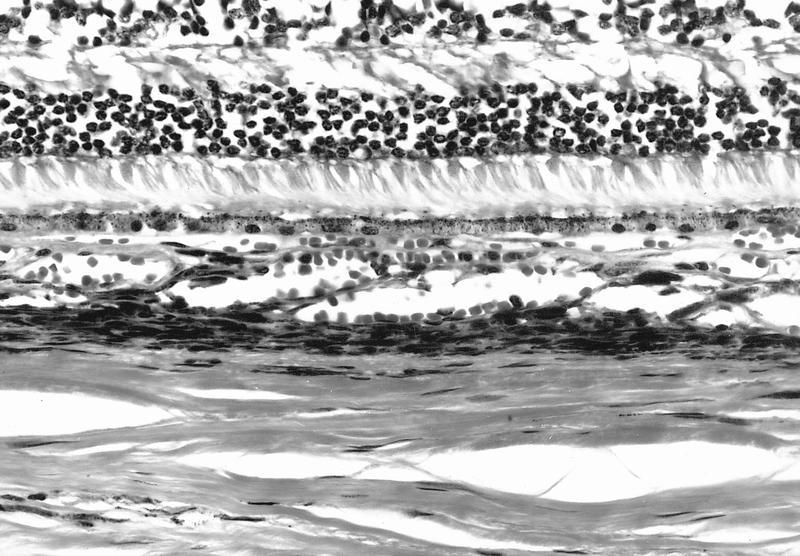
Microscopic (histologic) description
Gliotic reaction due to the presence of glia (including Müller cells) are seen as a hypercellularity of variably spindled cells with oblong nuclei
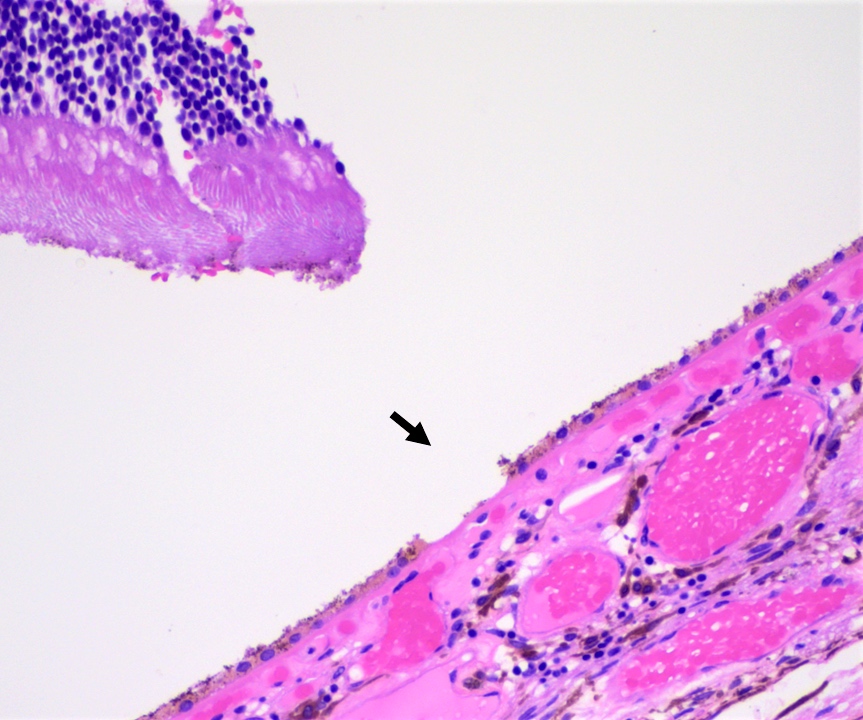
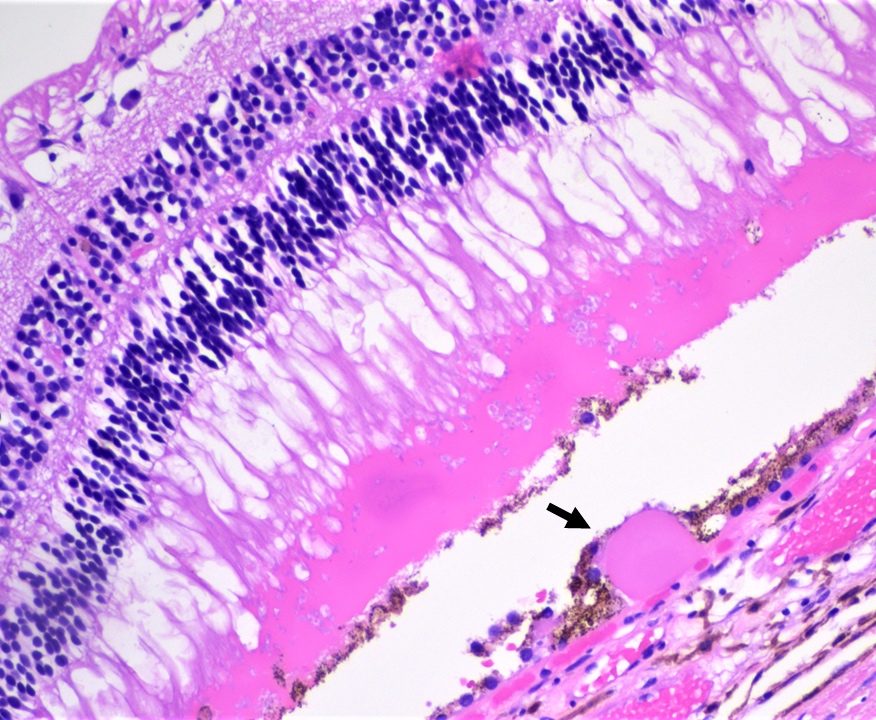
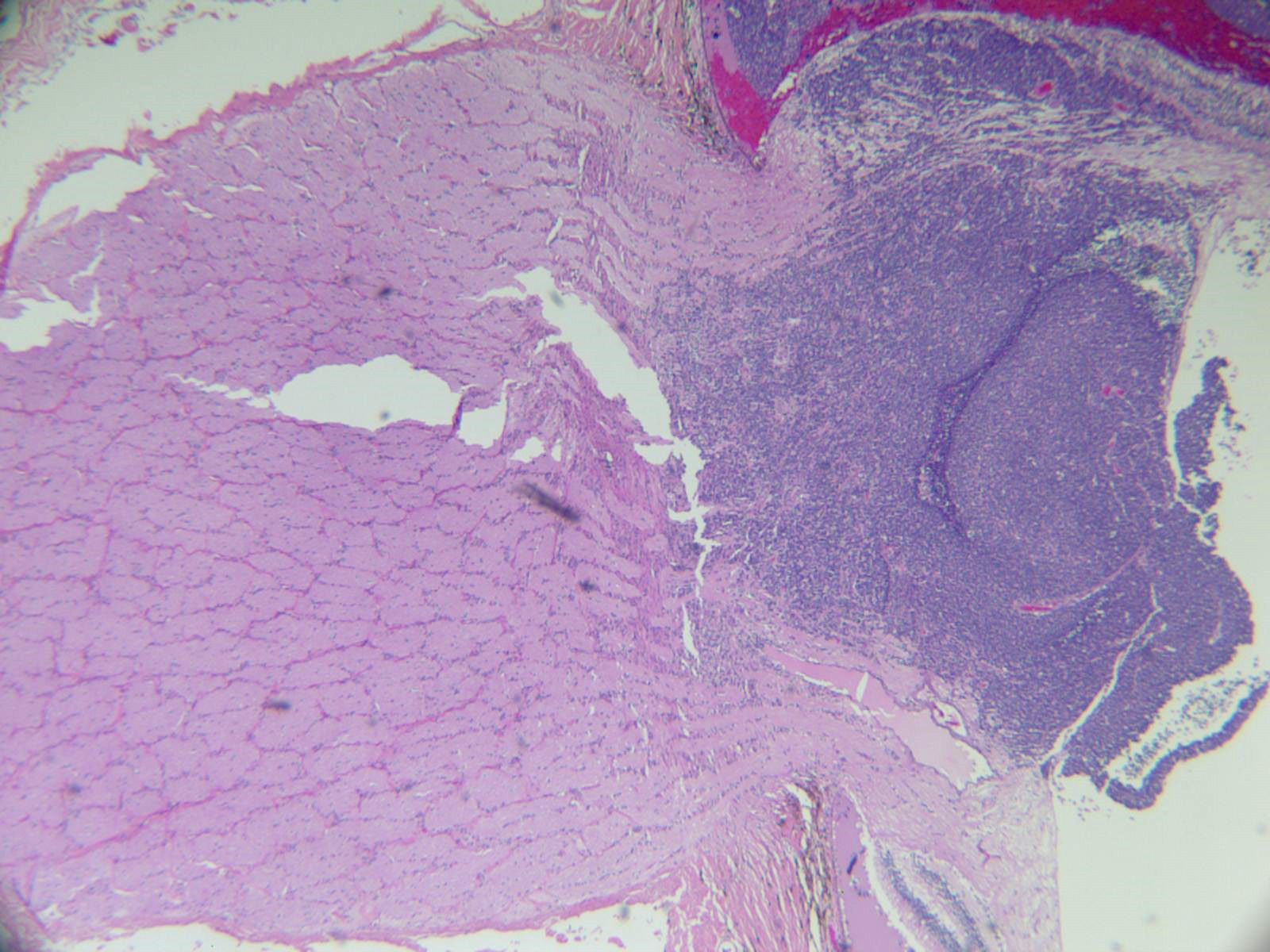
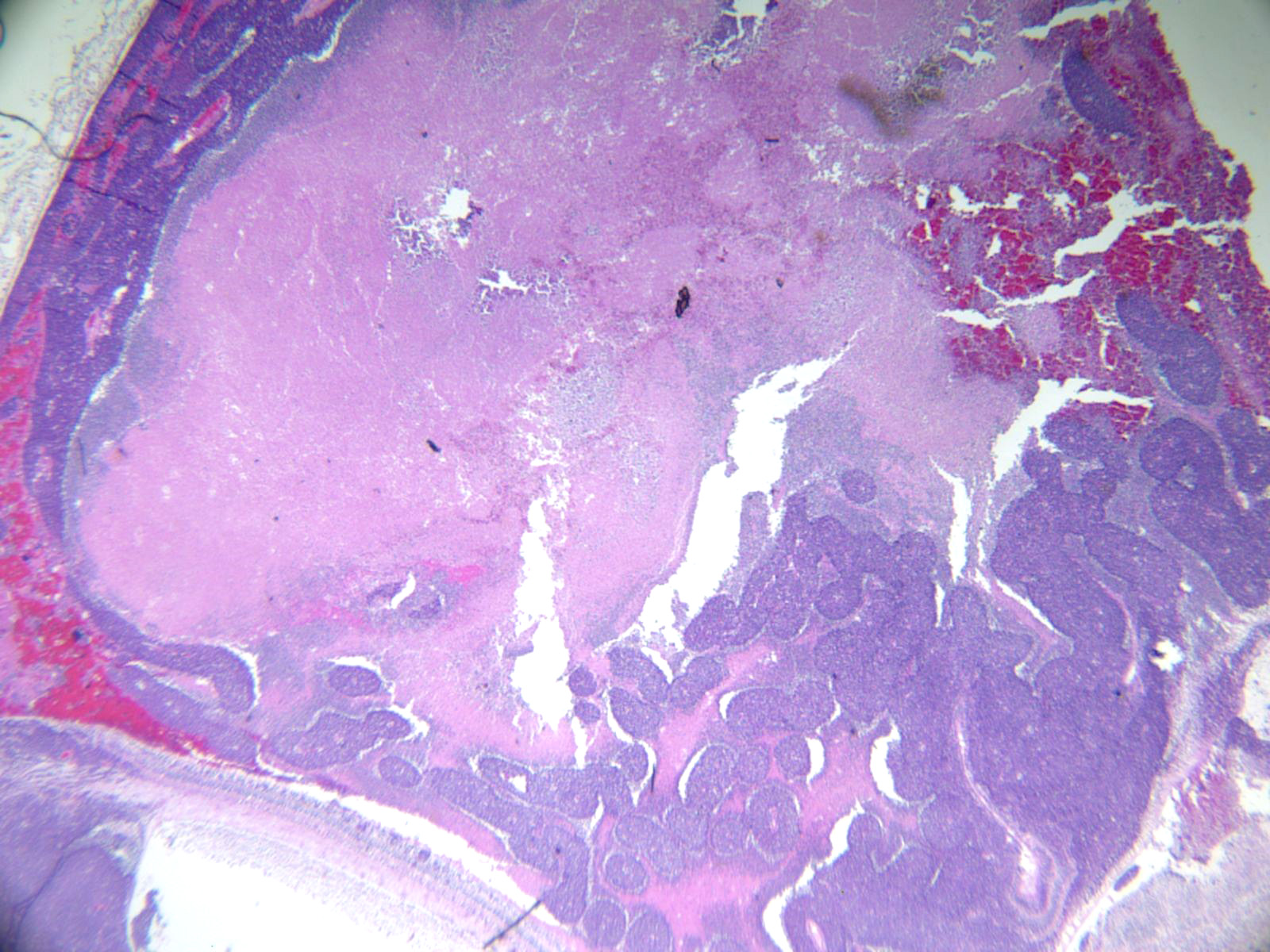
Retinal detachment: separation of neurosensory retina (rods and cones) from retinal pigment epithelium
Peripheral microcystoid degeneration: commonly encountered cystoid spaces of the outer plexiform layer near the ora serrata in adults > 20 years of age
Hard drusen are eosinophilic nodules that are observed between the retinal pigment epithelium and Bruch membrane and are encountered in aging
Microscopic (histologic) images
Contributed by J. Stephen Nix, M.D. and AFIP images
A patient with sudden, painless vision loss is diagnosed with central retinal artery occlusion. What layer of the retina would be expected to be affected?
Ganglion cell layer
Outer nuclear layer
Outer plexiform layer
Photoreceptor layer
Board review style answer #2
A. Ganglion cell layer. The central retinal artery supplies the inner layers of the retina, including much of the inner nuclear layer, the inner plexiform layer, the ganglion cell layer and the nerve fiber layer.
Associated with tuberous sclerosis (57%), neurofibromatosis (14%), or no syndrome (29%)
Tuberous sclerosis patients usually have multiple, peripheral retinal tumors with giant astrocytes vs. disc based tumors in non tuberous sclerosis patients
Pigmented thickening of conjunctival epithelium, may be normal finding in dark skinned individuals - bilateral, continues throughout life
(Surv Ophthalmol 2004;49:3)
Present in 92% of blacks, 36% of Asians, 28% of Hispanics, 5% of whites
Defined as progressive opacity of crystalline lens that decreases visual acuity
Usually develops in older individuals, rarely in infancy or childhood
Associated with systemic diseases (galactosemia, diabetes mellitus, Wilson disease, atopic dermatitis), corticosteroids, radiation (ultraviolet light or radiation therapy), trauma, glaucoma, uveitis, retinitis pigmentosa, steroids
Age related cataract is due to opacification of lens nucleus, which becomes brown and distorts perception of blue color
Changes occur in lens nucleus, cortex and subcapsular regions
Nuclear changes due to progressive crosslinking and insolubility of crystalline proteins
Cortical changes begin as small peripheral water clefts and diffuse degenerative changes that coalesce into dense bands of opaque cortical material
Anterior lens epithelial cells may undergo fibrous metaplasia, creating a thick fibrous plaque between the anterior lens capsule and the anterior epithelial cells
Congenital cataract:
Becomes apparent within first 6 months of life
Posterior subcapsular cataract:
Migration of lens epithelium posterior to lens equator
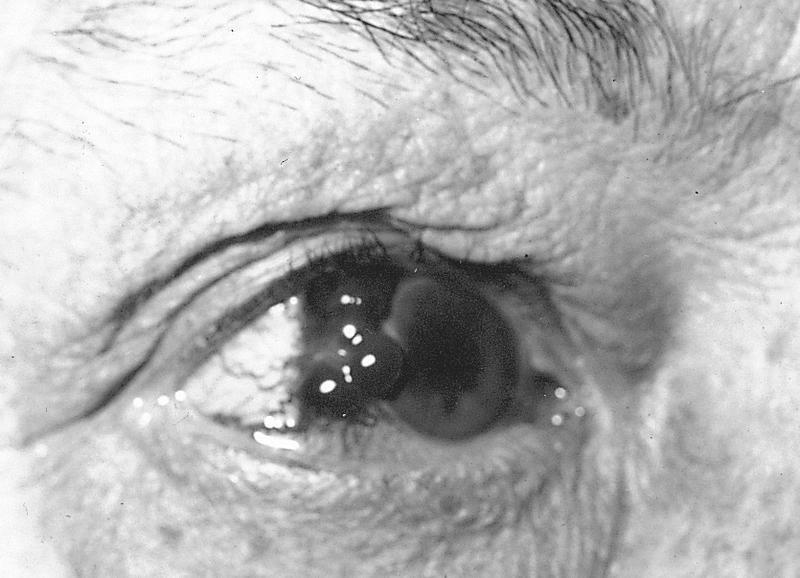
Morgagnian cataract:
Long standing cataract that undergoes liquefaction of lens cortex with sinking of nucleus into fluid filled sac and clinical brown nucleus
Soemmering ring cataract:
Peripheral donut or ring shape due to loss of lens nucleus and much of anterior and posterior cortex
Also proliferating lens epithelial cells in periphery and equatorial region of lens
Treatment
Often high frequency sound waves are used to disintegrate the lens (phacoemulsification), then lens contents aspirated and disposed of (not submitted for examination)
Lens capsule is intact
Then placement of prosthetic intraocular lens
Gross description
Senile cataracts are yellow-brown
Microscopic (histologic) description
Homogenous eosinophilic lens fibers, vacuolization of superficial cortical fibers, extracellular clefts and eosinophilic globules of variable size (morgagnian globules) between lens fibers
Very common, inflammatory eyelid lesion, characterized by granulomatous inflammation with lipogranulomas
All specimens with tissue should be submitted to rule out malignant neoplasms and other masquerading conditions; most of the time they are not submitted
Essential features
Very frequent inflammatory eyelid lesion
More frequent in the upper eyelid
Broad histopathological spectrum from acute to more chronic findings
Lipogranulomas, suppurated granulomas, granulation tissue and fibrosing inflammation
More common in younger adults than in children, uncommon in late life
Sites
Eyelid
Pathophysiology
Probably due to obstruction or nonspecific inflammation (blepharitis) surrounding sebaceous gland ducts, leading to discharge of sebaceous material into surrounding tissue and resulting in intense foreign body granulomatous inflammatory reaction
Superficial chalazion from Zeis gland
Deep chalazion from Meibomian gland
May erupt through conjunctival surface of eyelid (internal chalazion)
Etiology
More significant: history of chalazion and blepharitis
Less significant: rosacea, gastritis, anxiety and smoking (Cornea 2011;30:1376)
There is no evidence that cosmetics in the eyelid causes, aggravates or protects from this condition
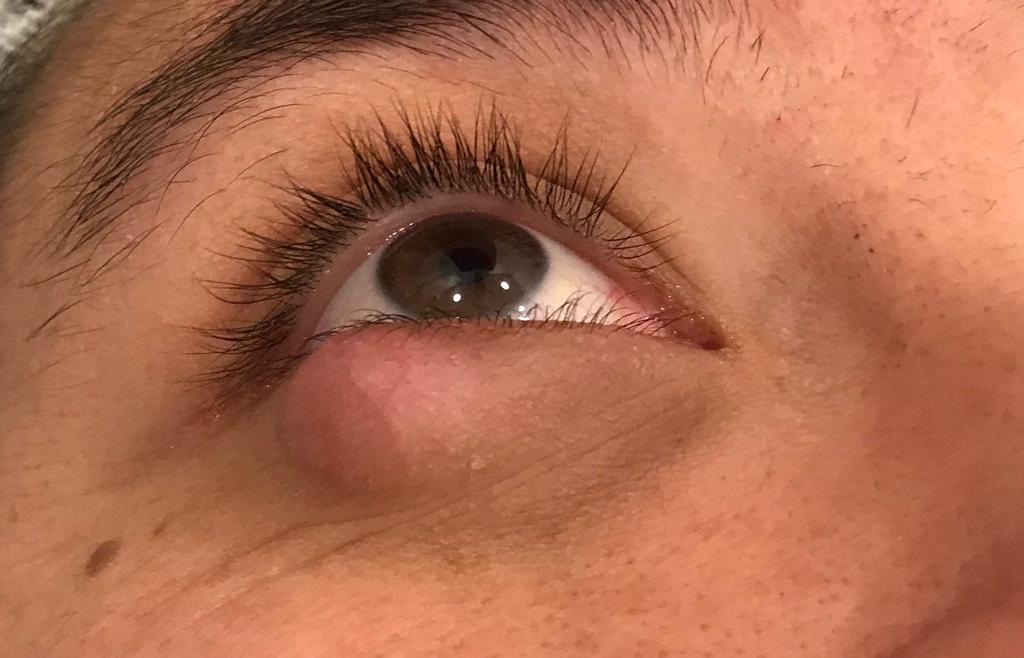
Clinical features
Upper eyelid > lower eyelid
Slowly growing mass with variability in size on a day to day basis
Solitary, nontender nodule; eversion helps to identify the lesion
Clinically may masquerade as sebaceous carcinoma and other neoplasms (Eye (Lond) 2004;18:135)
Diagnosis
Typically suspected upon clinical examination
Histologic examination of resected tissue can confirm the diagnosis
Treatment
Medical treatment includes applying of heat and massage at least twice a day
No benefit with antibacterial topical preparations except when infected (hordoleum) (BMJ 2010; 341 :c4044)
Surgical management using incision and curettage is a second line of treatment
Clinical images
Contributed by Eugenia Abusleme, M.D.
Chalazion
Microscopic (histologic) description
Lipogranuloma (empty spaces surrounded by epithelioid and foamy histiocytes with multinucleated foreign body and or Touton type giant cells)
Some lesions have granulation tissue, fibrosis or suppurative inflammation
Early lesions can have necrotizing (neutrophilic) granulomas
Conchoidal bodies and asteroid bodies can be observed
Microscopic (histologic) images
Contributed by Pablo Zoroquiain, M.D.
Chronic conjunctival inflammation
Large lipogranuloma
Small lipogranuloma
Neutrophilic granuloma
Positive stains
Oil Red O: positive in the lipid droplets (central clearings)
Lymphoplasmacytic infiltrate with storiform fibrosis
Lymphoid aggregates
Obliterative phlebitis
IgG4/IgGt ratio higher than 60%
Board review style question #1
What is the key finding for chalazion seen in this photo?
Exuberant granulation tissue
Fibrosing chronic inflammation
Lipogranulomas
Lymphoplasmacytic chronic inflammation of the tarsal plate
Board review style answer #1
C. Lipogranulomas. This is the key morphological finding in chalazion. The granulomas are usually nonnecrotizing. All the other changes such as lymphoplasmacytic chronic inflammation of the tarsal plate, exuberant granulation tissue and fibrosing chronic inflammation could be present but are nonspecific.
Middle layer of globe between outer sclera and inner retina
Highly vascular but no lymphatics
Extends from ciliary body to optic nerve
Inner aspect is adherent to retinal pigment epithelium; outer surface is loosely attached to overlying sclera
Stroma contains abundant pigmented melanocytes
Bruch membrane: separates choroid from overlying retinal pigment epithelium, is 2 - 4 microns thick, has 5 distinct layers (basal lamina of overlying retinal pigment epithelium, collagenous layer, elastic fiber rich layer, collagenous layer and basal lamina of endothelial cells of choriocapillaris), thickens with age, has focal excrescences known as drusen
Choriocapillaris: in innermost choroidal stroma adjacent to Bruch membrane, connects with arterial and venous channels from vessels in outer choroidal stroma to nourish outer retinal layers
Considered to be a premalignant lesion that can progress to invasive squamous cell carcinoma
Essential features
Dysplastic changes of conjunctiva
Precursor to squamous cell carcinoma
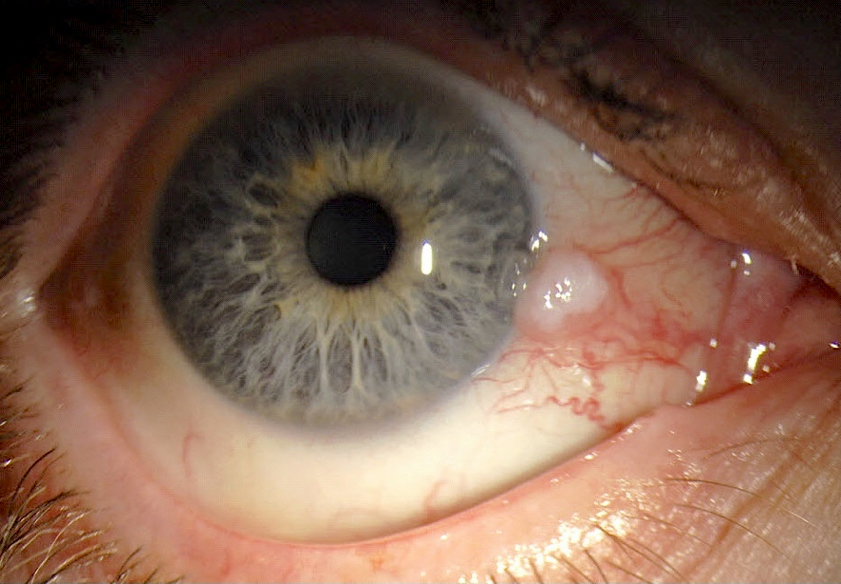
Typical clinical presentation is a lesion at the limbus within the interpalpebral fissure
Terminology
Conjunctival intraepithelial neoplasia (1, 2 or 3)
Also called conjunctival dysplasia (mild, moderate or severe), conjunctival epithelial dyskeratosis, Bowen disease
Falls within the broad spectrum of ocular surface squamous neoplasia (OSSN), which encompasses neoplastic squamous abnormalities of the conjunctival, limbal and corneal epithelium, including squamous cell carcinoma
ICD coding
ICD-O: 8077/2 - conjunctival squamous intraepithelial neoplasia (conjunctival intraepithelial neoplasia and carcinoma in situ)
ICD-10: C69.00 - malignant neoplasm of unspecified conjunctiva
Incidence rate varies worldwide; highest rates in Africa (3.4 cases per 100,000 per year in Zimbabwe) (Trop Med Int Health 2013;18:1424)
Reported incidence of OSSN was 0.53 cases/million/year (conjunctival intraepithelial neoplasia: 0.43 cases/million/year; squamous cell carcinoma: 0.08 cases/million/year) in the United Kingdom (Eye (Lond) 2019;33:283)
Third most common conjunctival lesion in adults (after pterygium and nevus) (Cornea 1987;6:78)
2 disease patterns:
In northern high latitude areas, mostly affects elderly males
Close to the equator, males and females are equally affected at a younger age; also associated with HIV
HIV testing should be considered in patients < 40 years old with no other risk factors
Risk factors include exposure to UV light, especially in light skinned individuals, human papillomavirus infection (HPV 16 / 18), immunosuppression, tobacco use, vitamin A deficiency, ocular surface injury and exposure to petroleum products (Ophthalmology 1994;101:360, Ophthalmology 2002;109:542, Cornea 2003;22:687)
Sites
Typically occurs in the bulbar conjunctiva in the interpalpebral fissure (sun exposed area) arising at the limbus (where stem cells reside)
Can spread onto the cornea
Occasionally occurs in the forniceal or palpebral conjunctiva
Arises from conjunctival epithelial cells that originate from the ocular surface ectoderm
Preferred limbal location suggests that most cases arise from limbal stem cells; limbal stem cells are sensitive to oncogenic factors and are susceptible to DNA alterations secondary to UV light
Actinic keratosis growth pattern has a good prognosis while diffuse growth pattern has poorer prognosis with more recurrences because tumoral margin is not well defined
Case reports
41 year old HIV positive man with low CD4 counts presented with conjunctival epithelial dysplasia and viral retinitis (Indian J Ophthalmol 2019;67:116)
48 year old white man with a leukoplakic conjunctival growth 3 months after total body phototherapy for mycosis fungoides (MF) (Am J Ophthalmol Case Rep 2019;14:98)
56 year old woman with conjunctival intraepithelial neoplasia presented as a pigmented conjunctival lesion (Case Rep Ophthalmol 2021;12:77)
Surgical excision using a no touch technique with 2 - 4 mm margins, alcohol application and supplemental surgical margin cryotherapy (Arch Ophthalmol 1997;115:808)
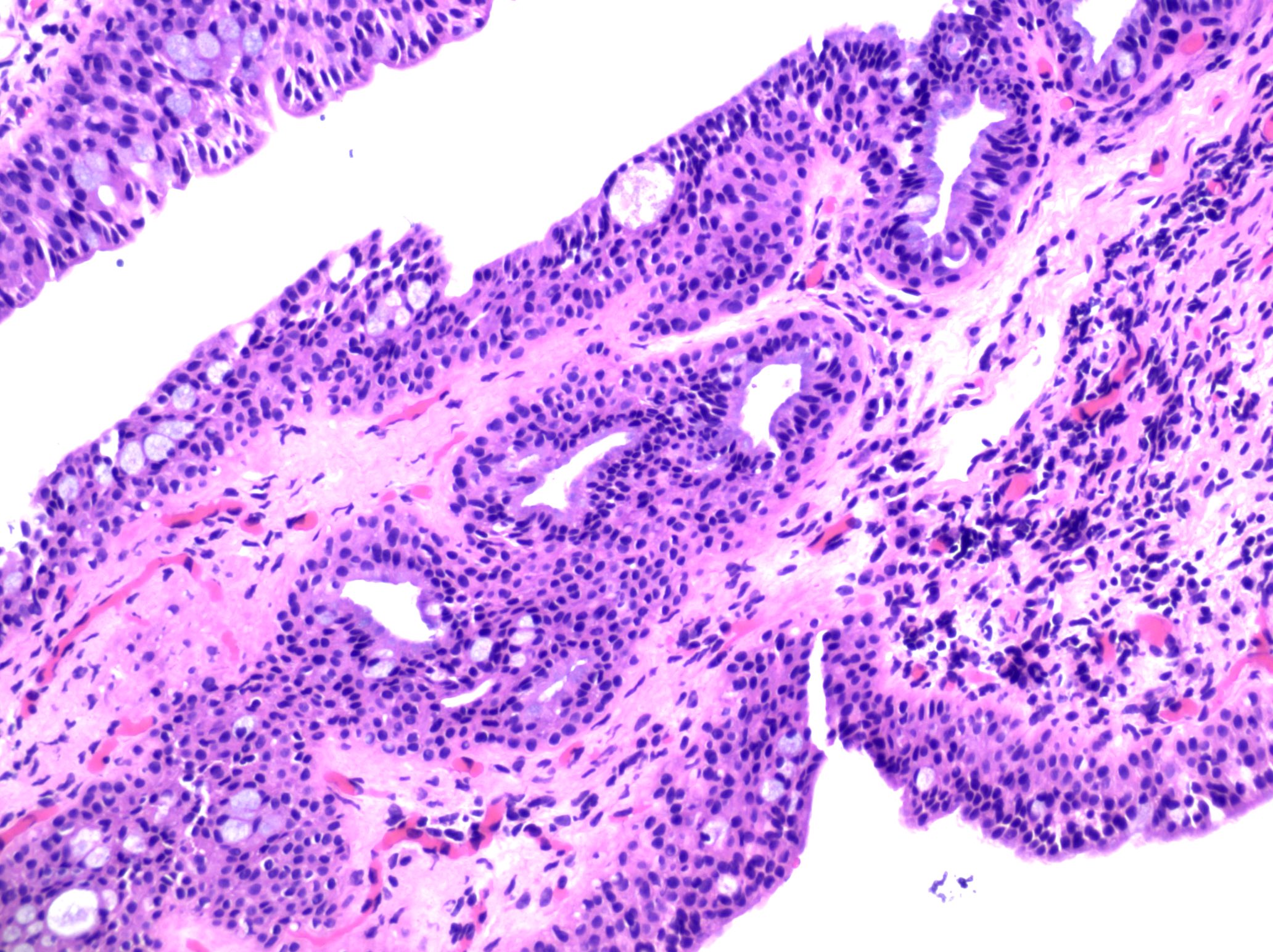
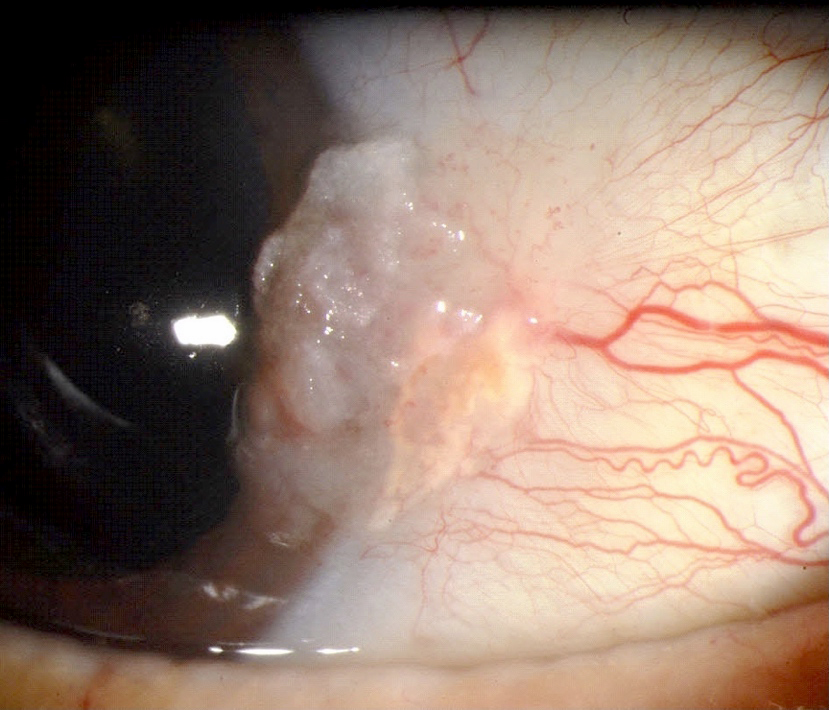
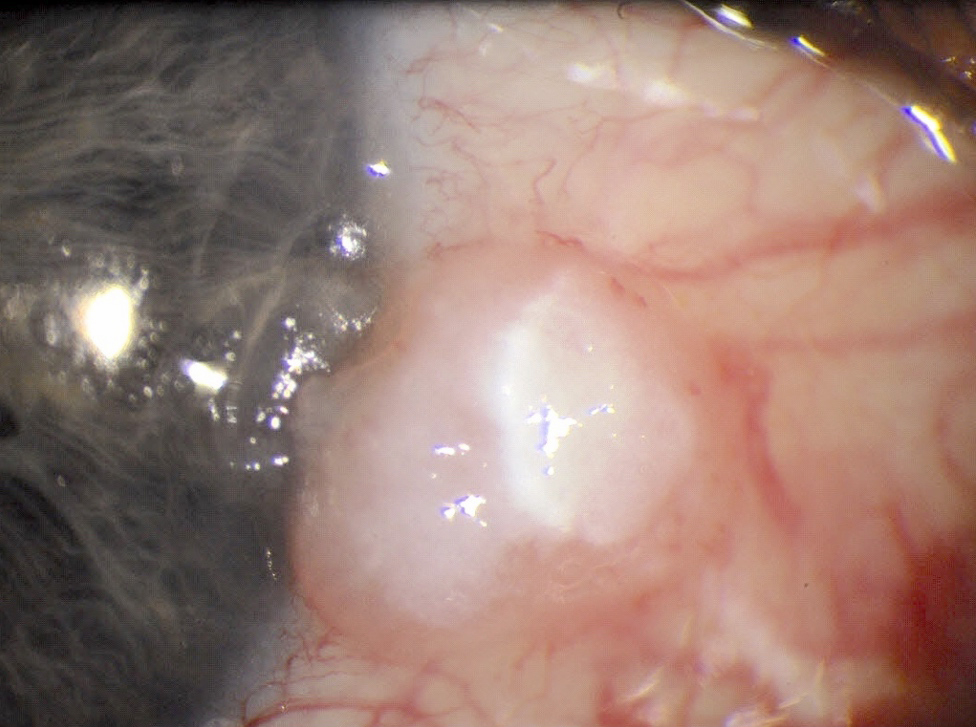
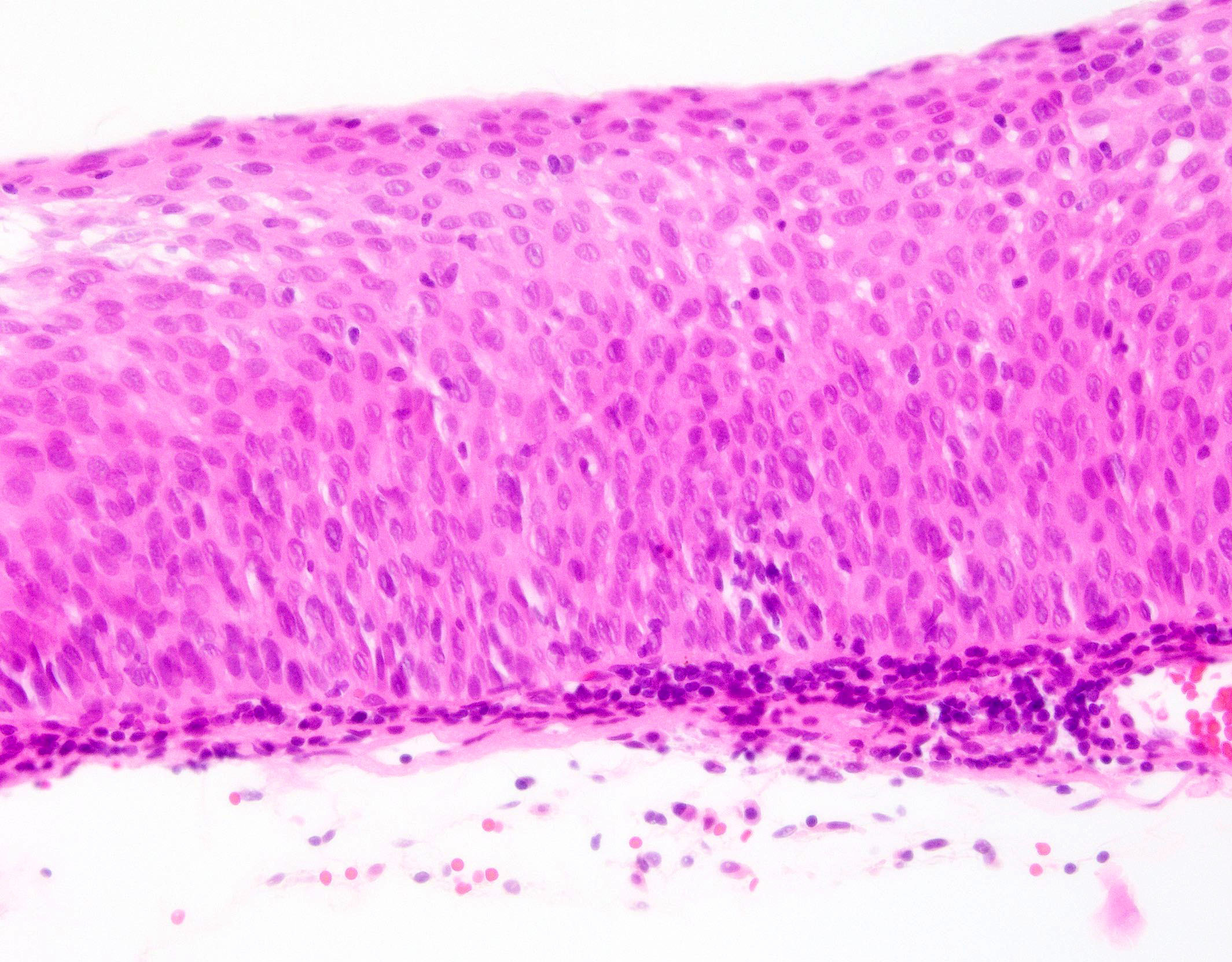
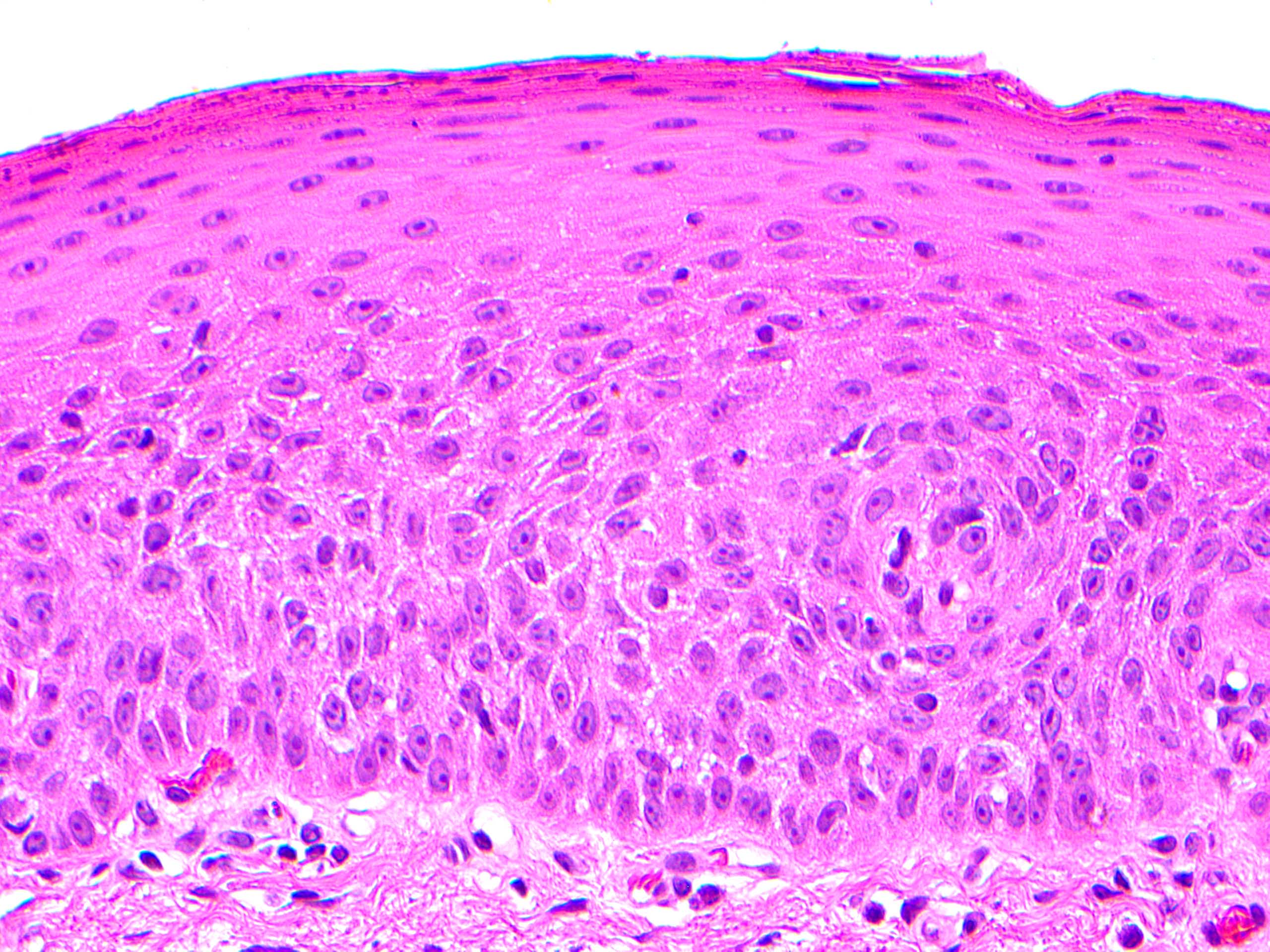
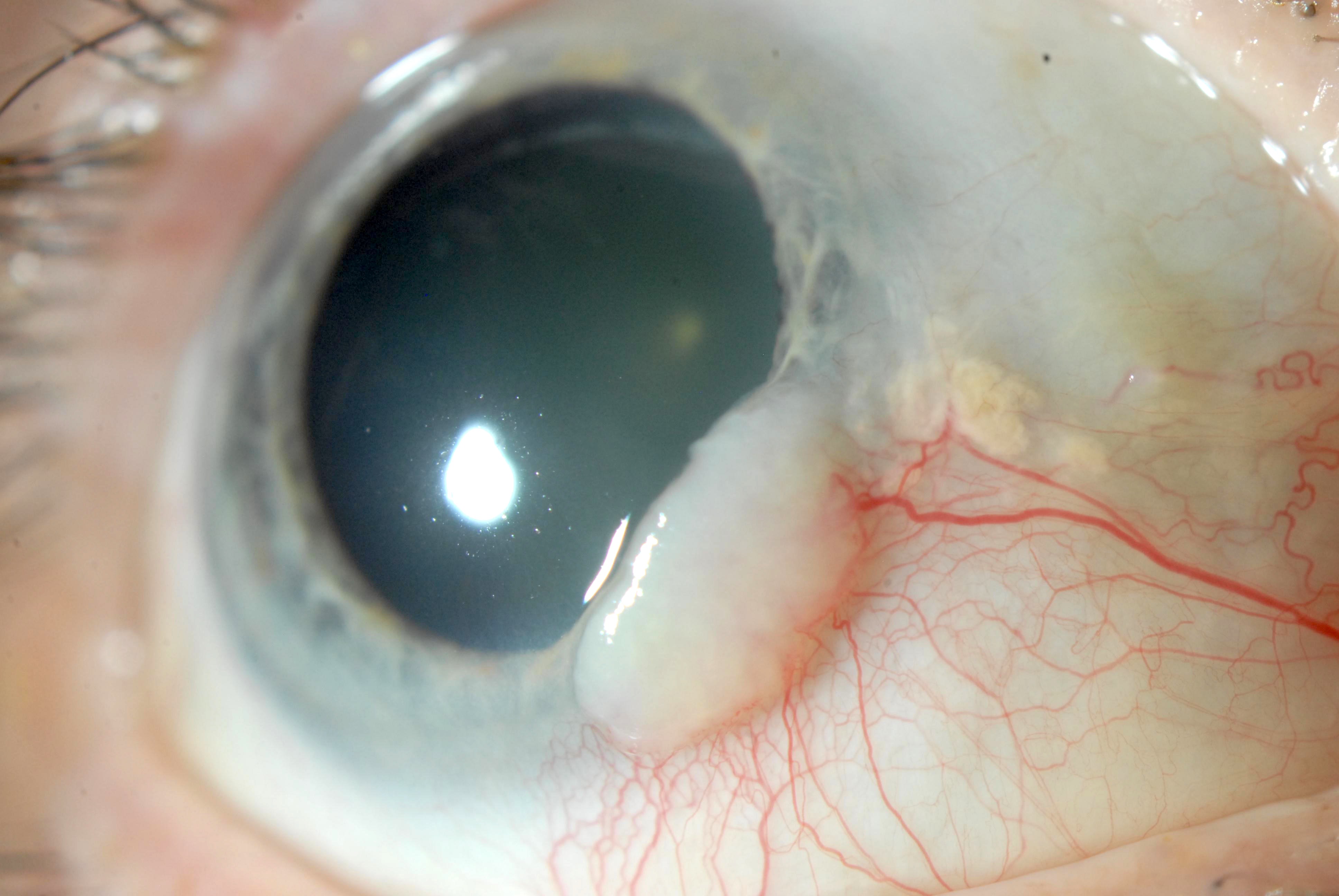
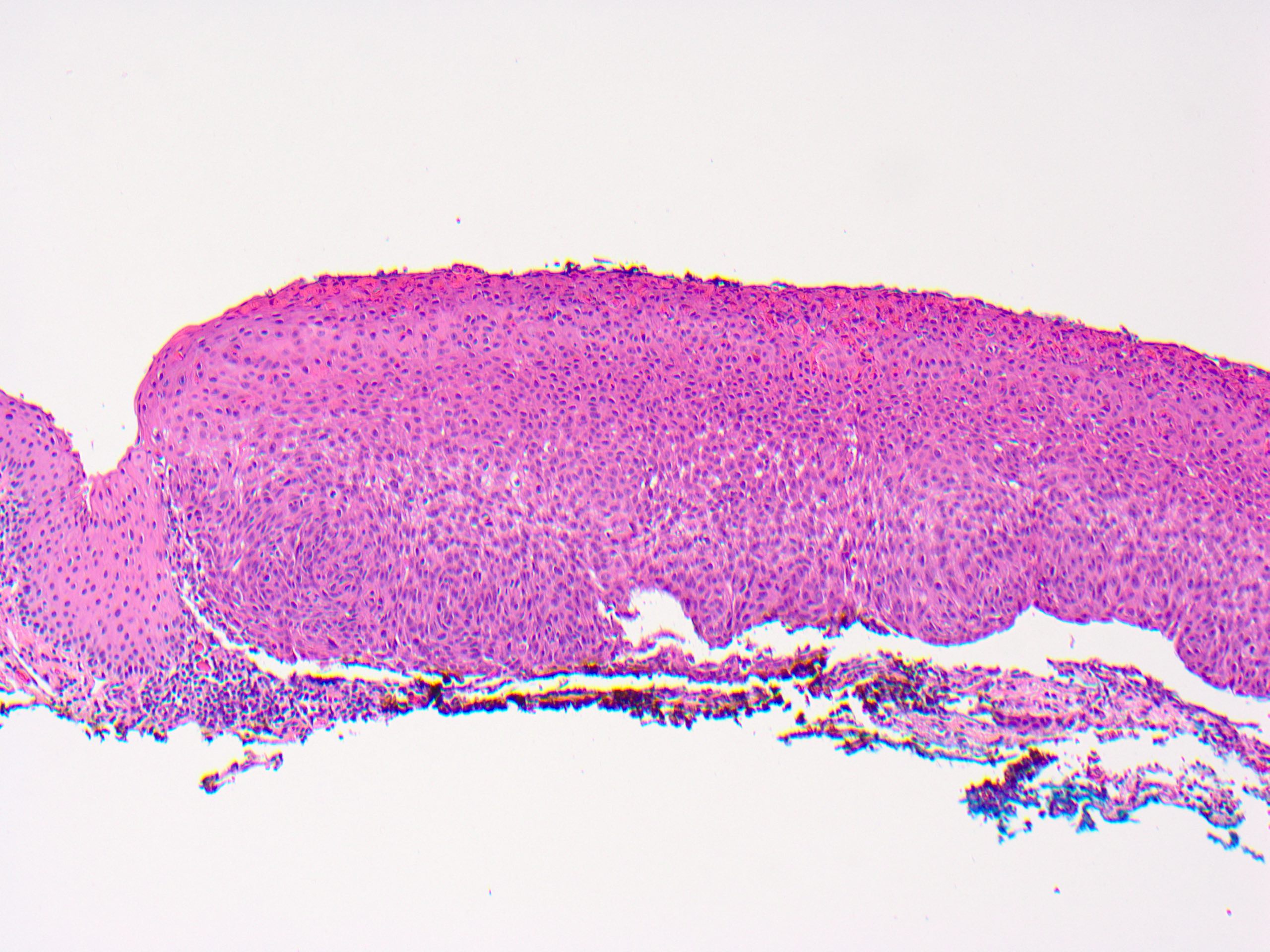
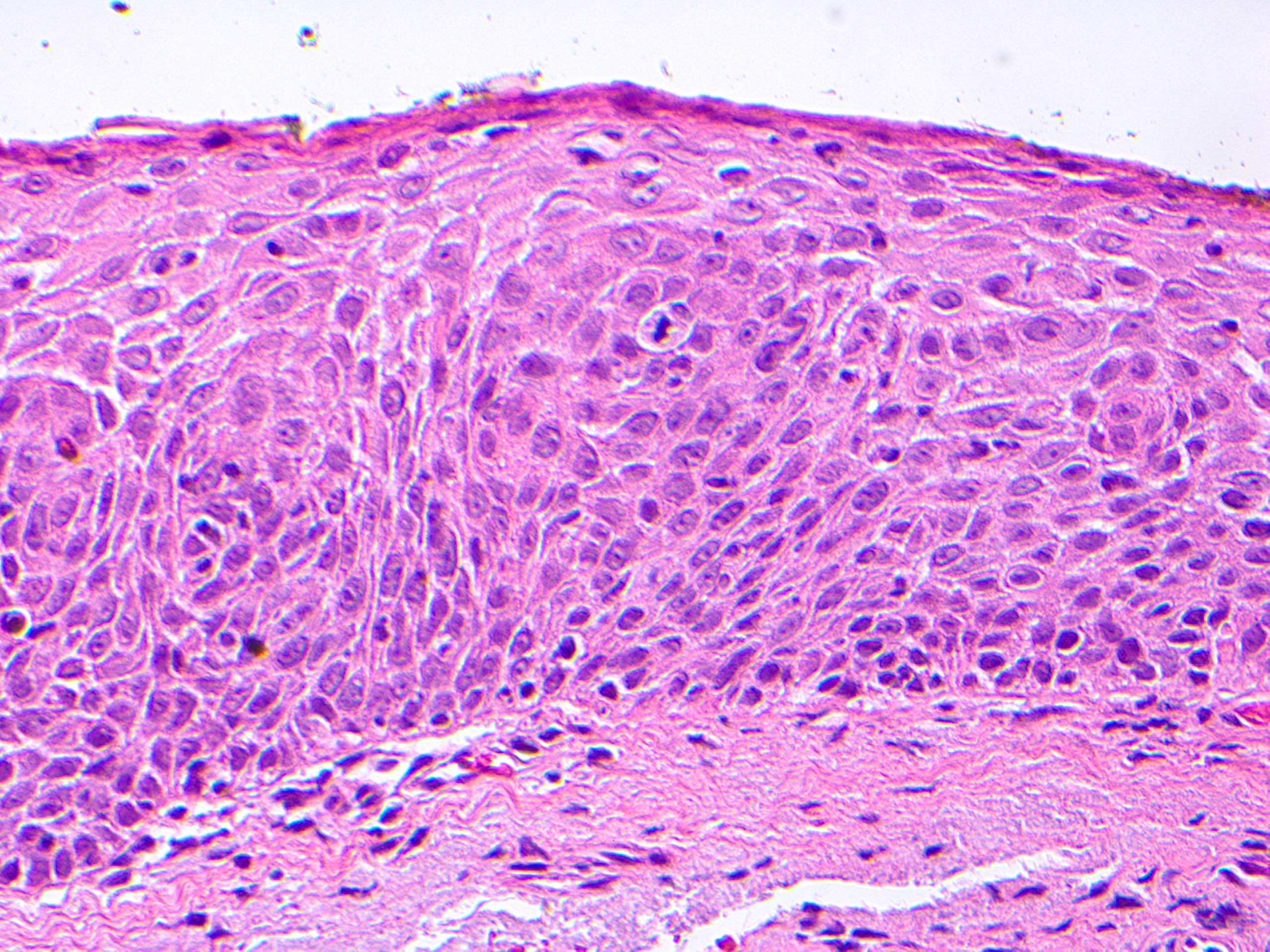
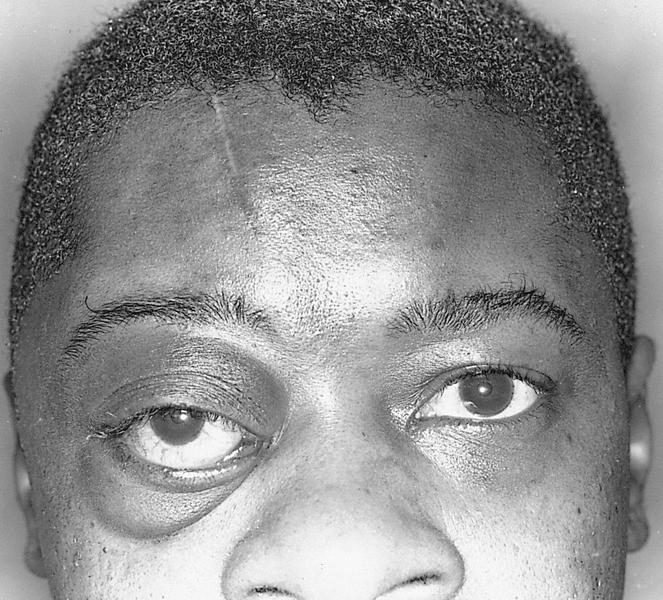
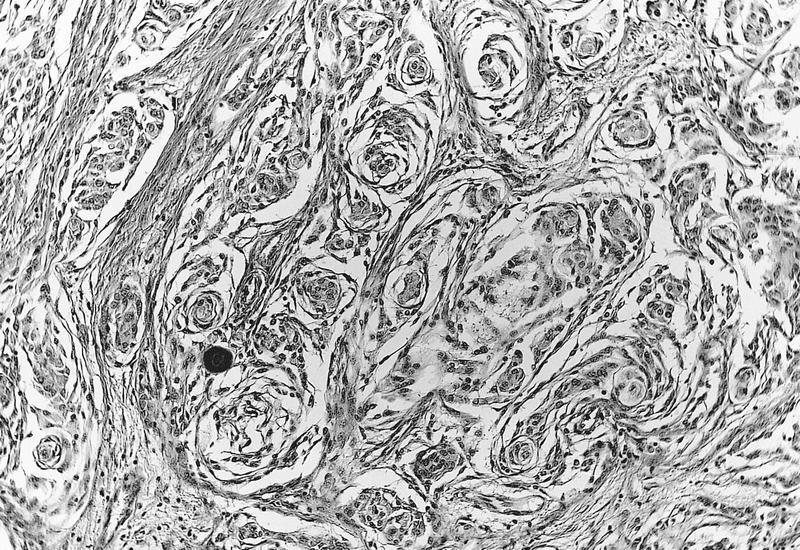
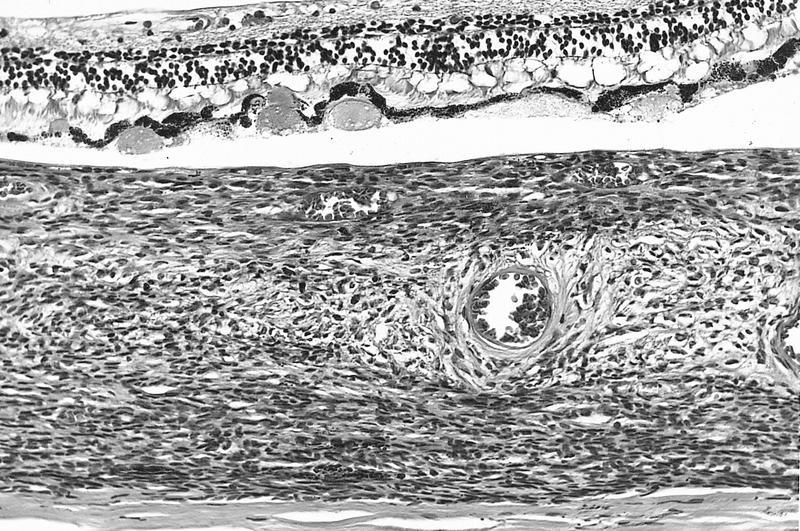
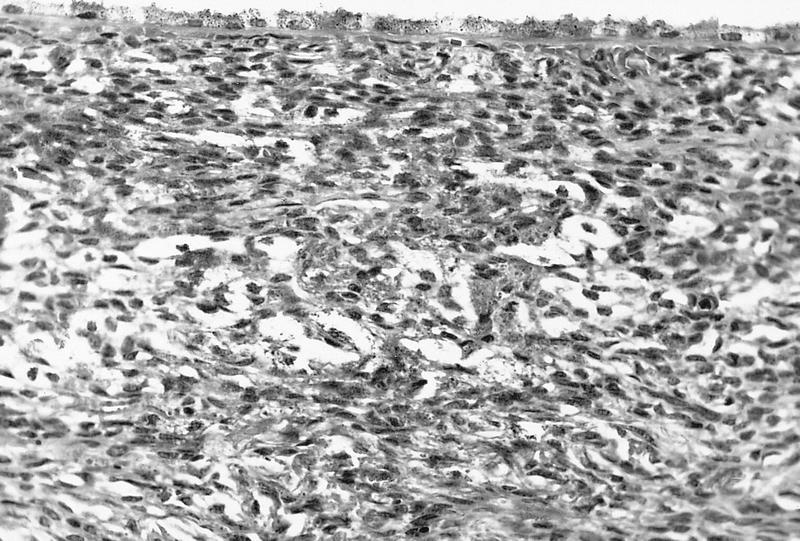
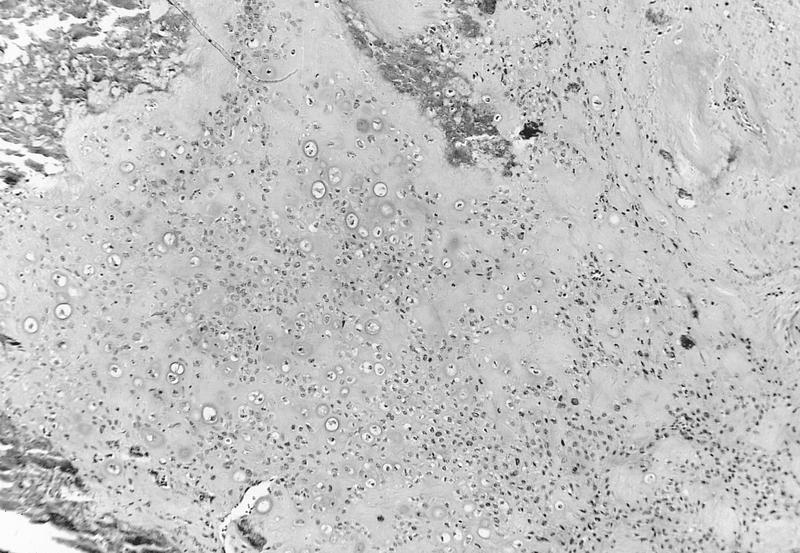
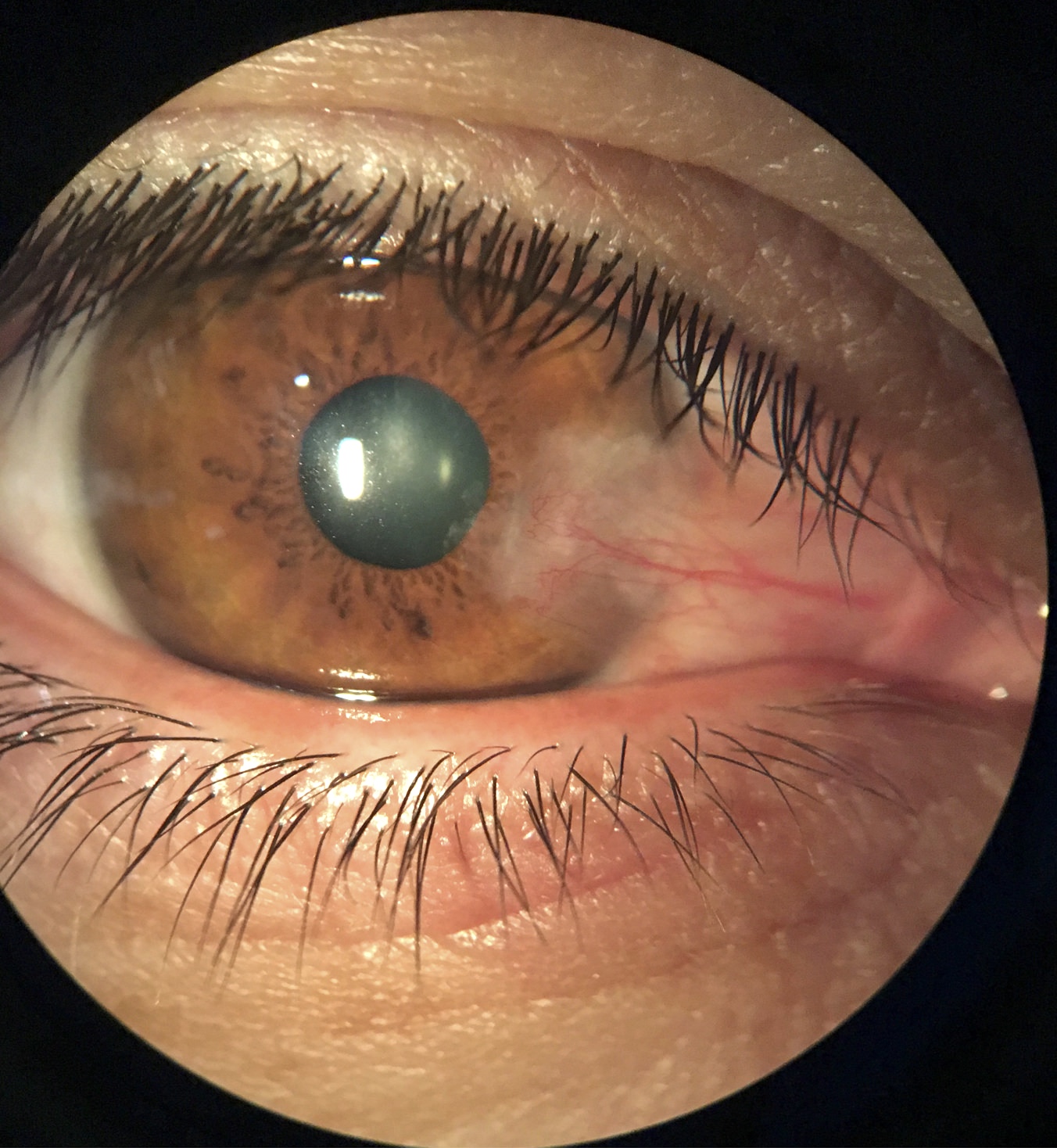
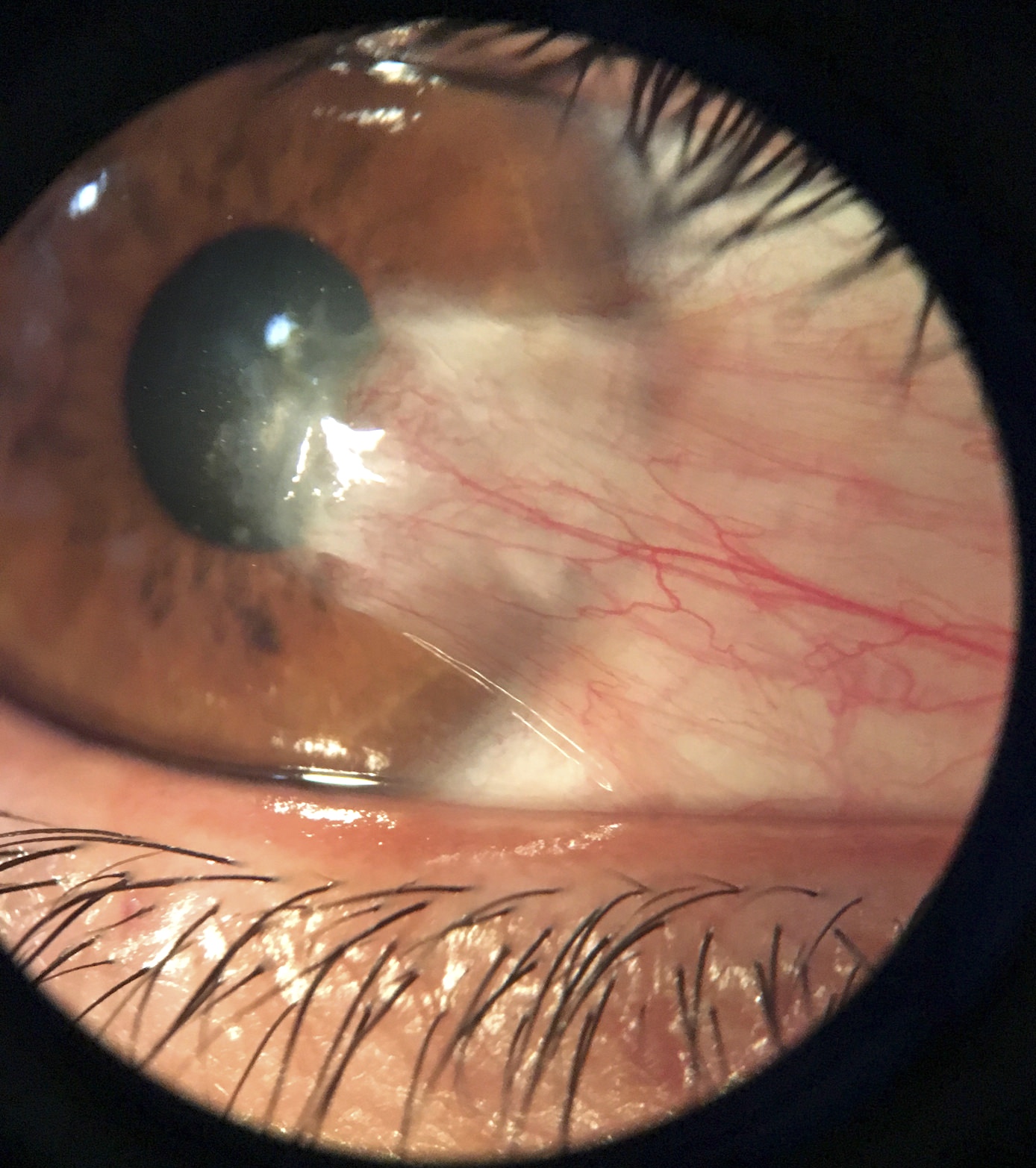
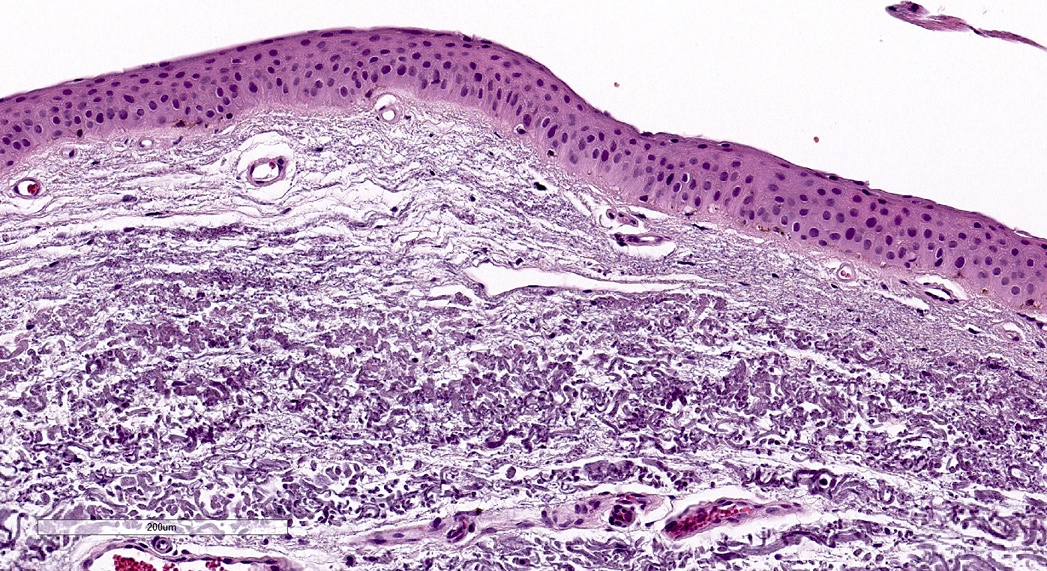
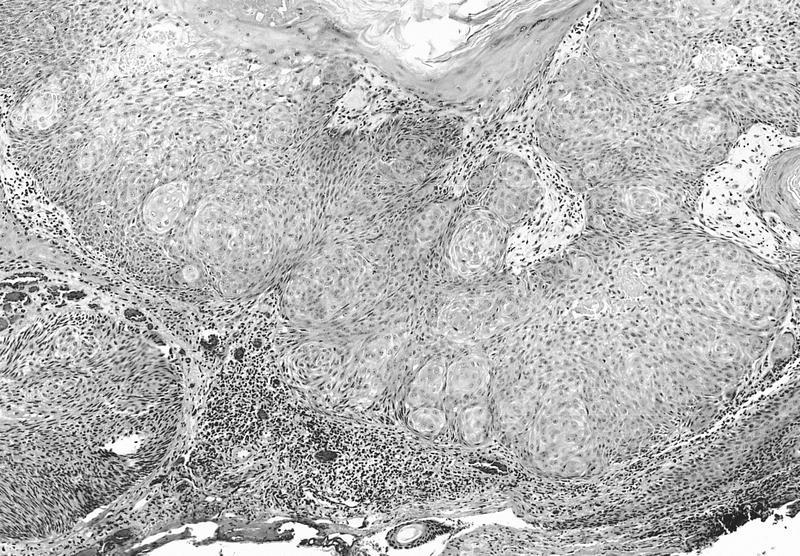
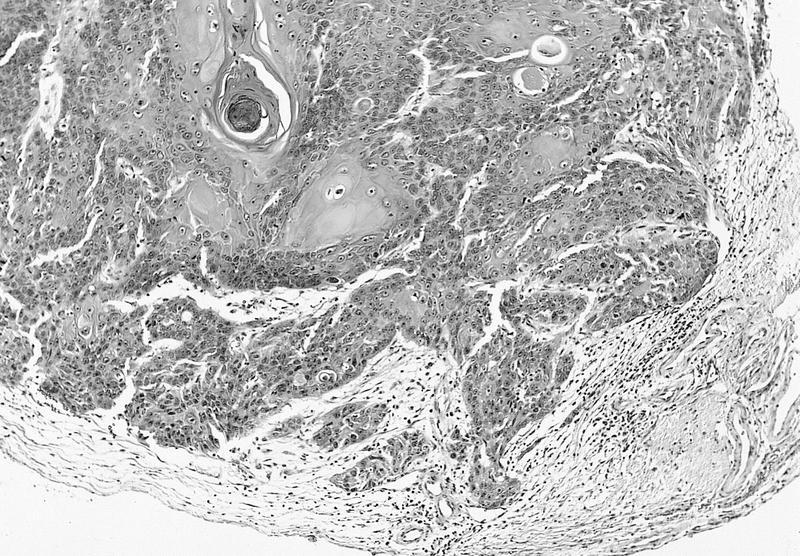
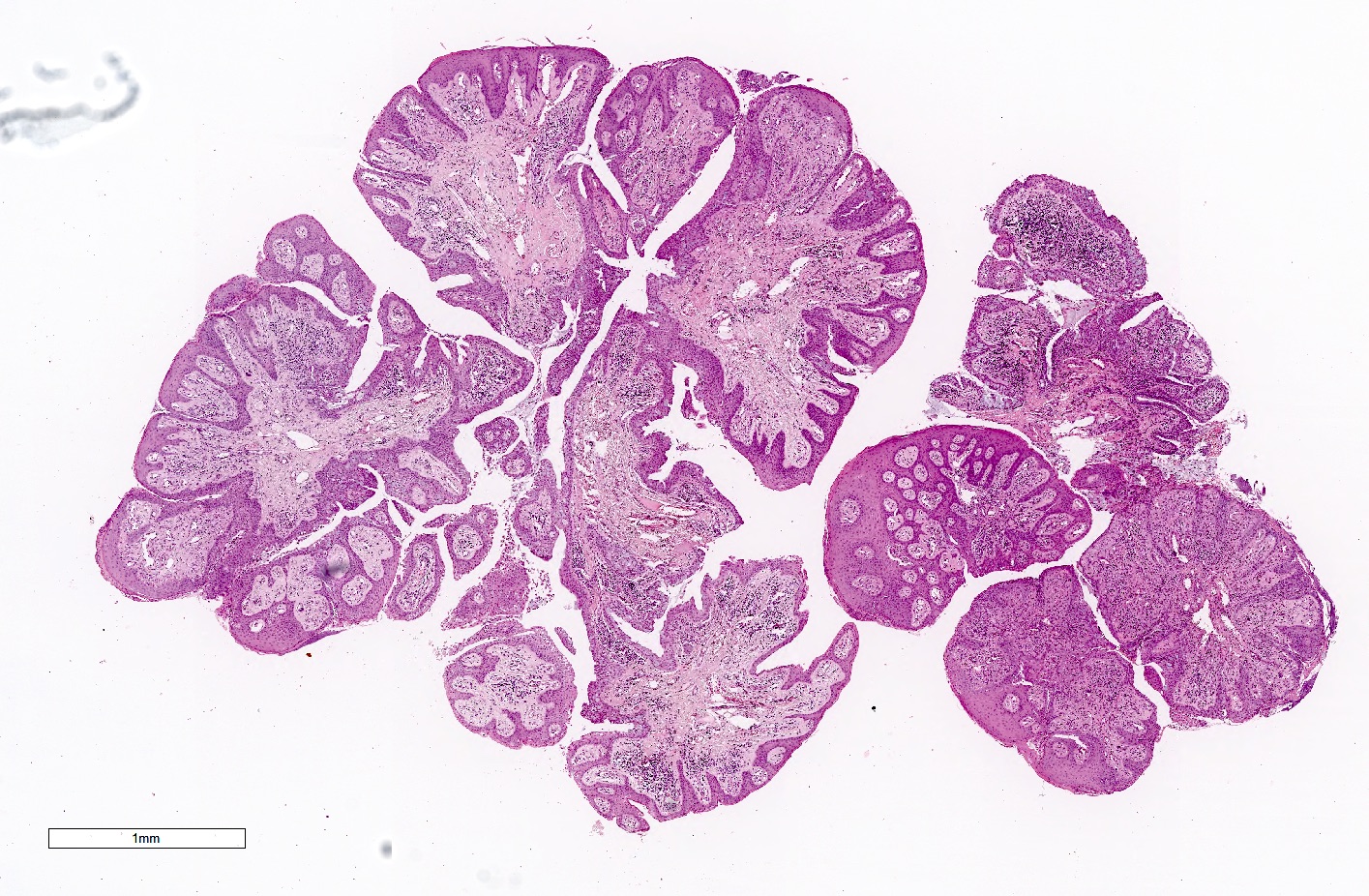
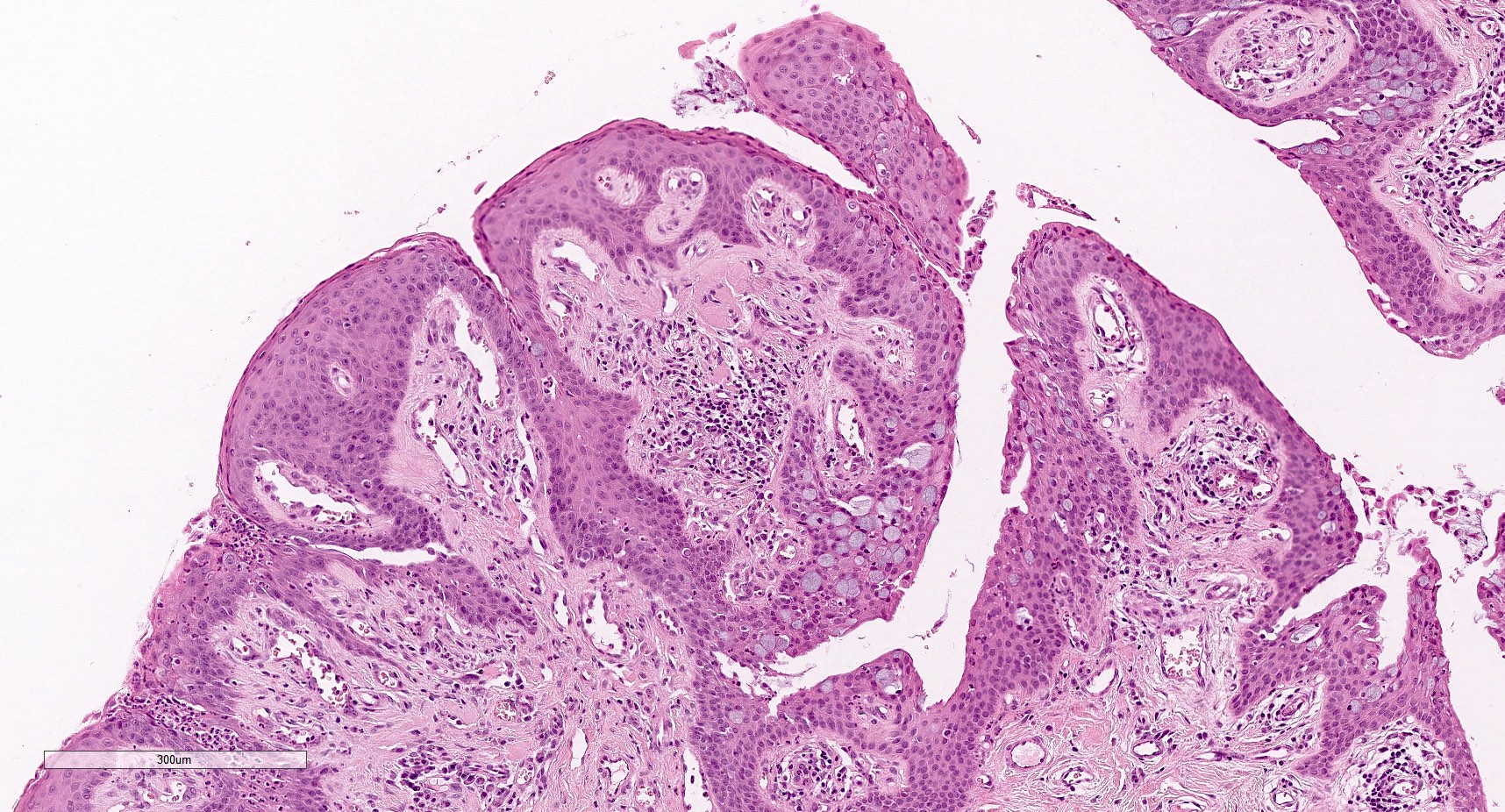
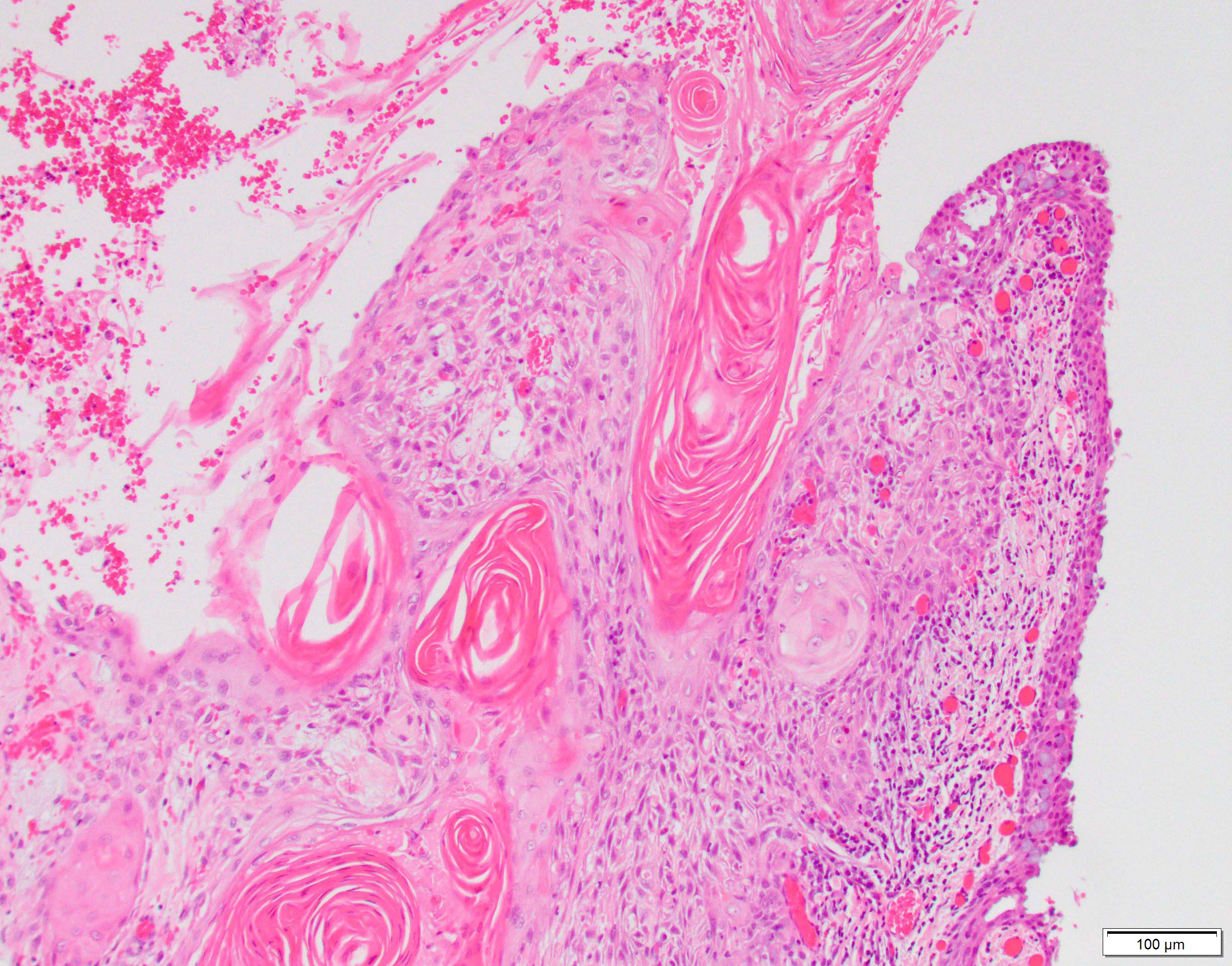
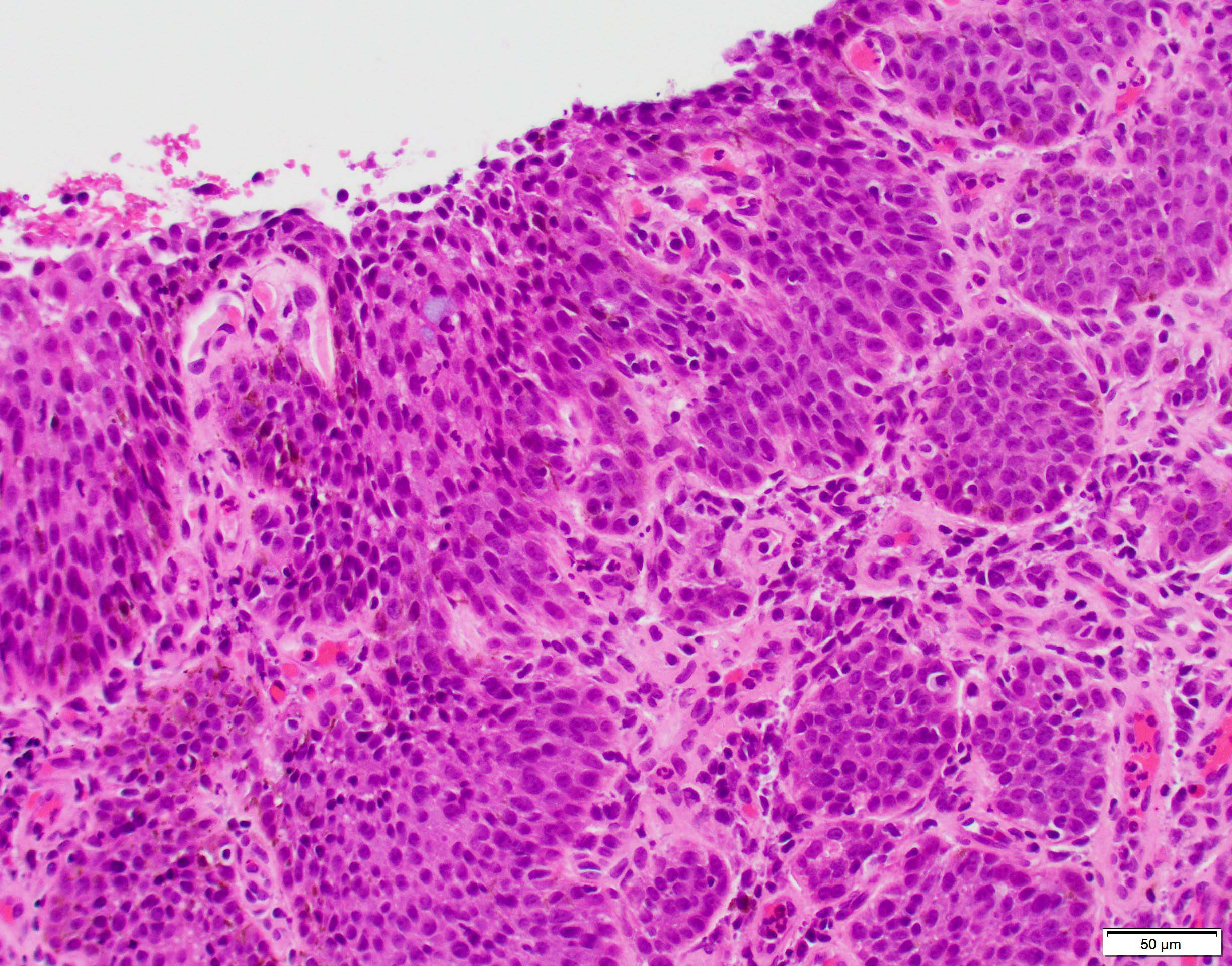
A 66 year old Caucasian male construction worker presents with the lesion shown above. Biopsy reveals the following histopathology. What is the likely diagnosis?
Conjunctival intraepithelial neoplasia grade 3
Primary acquired melanosis
Pterygium
Squamous cell carcinoma
Board review style answer #1
A. Conjunctival intraepithelial neoplasia grade 3.
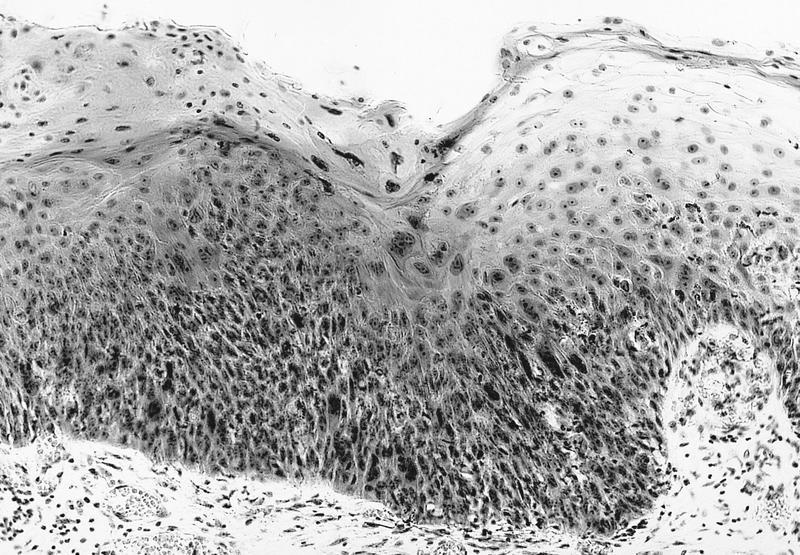
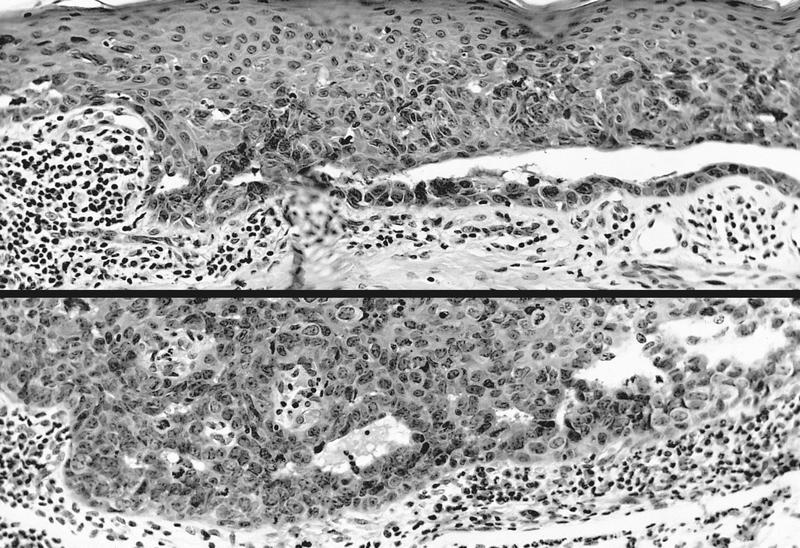
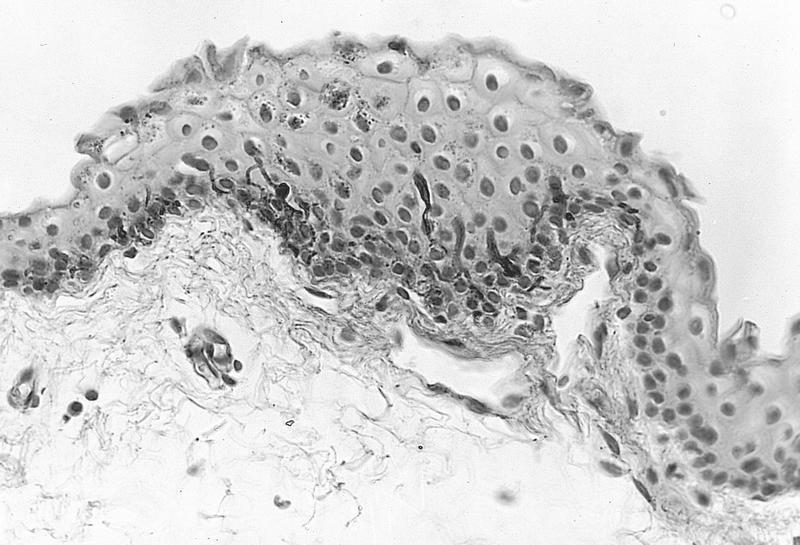
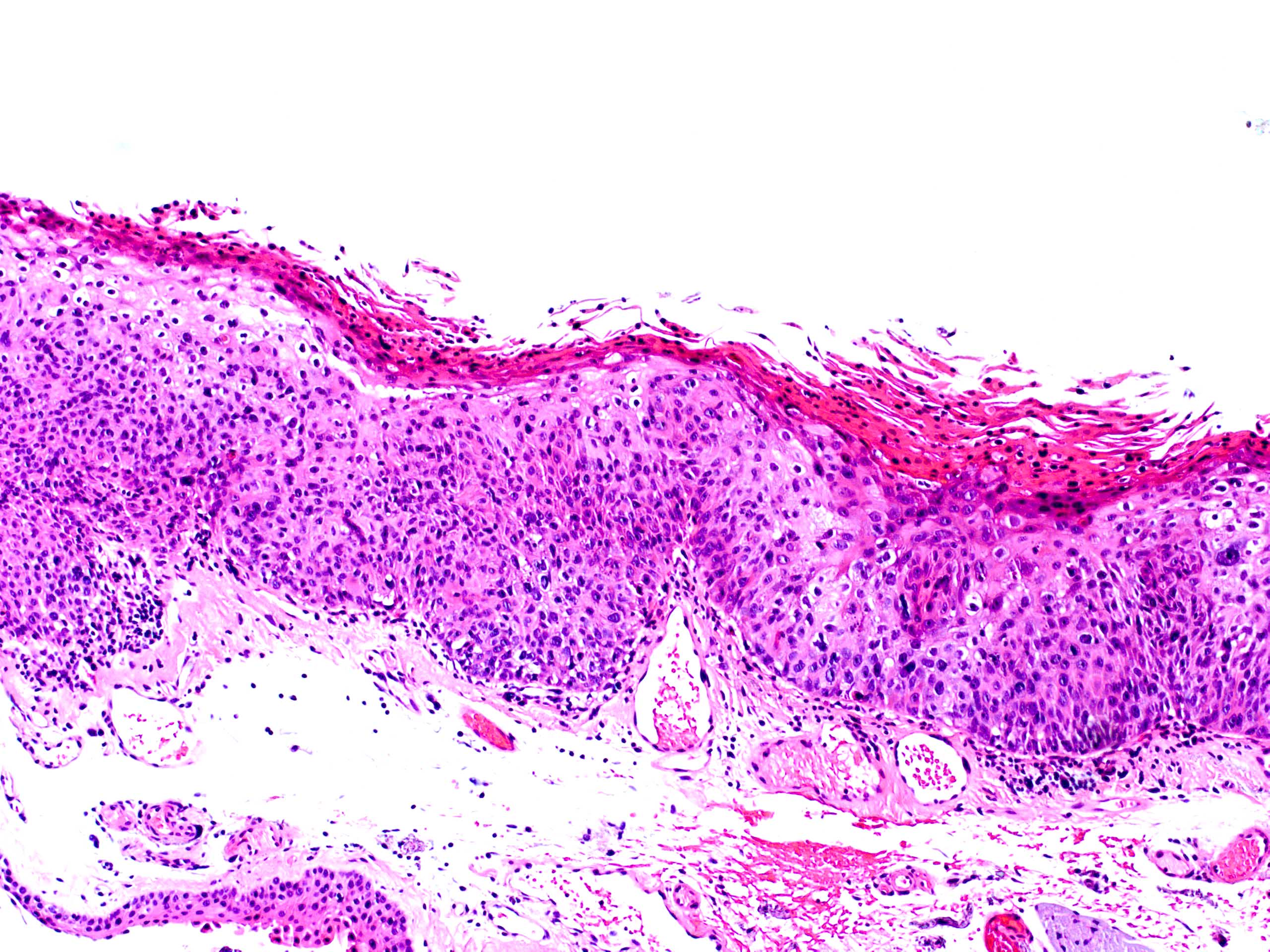
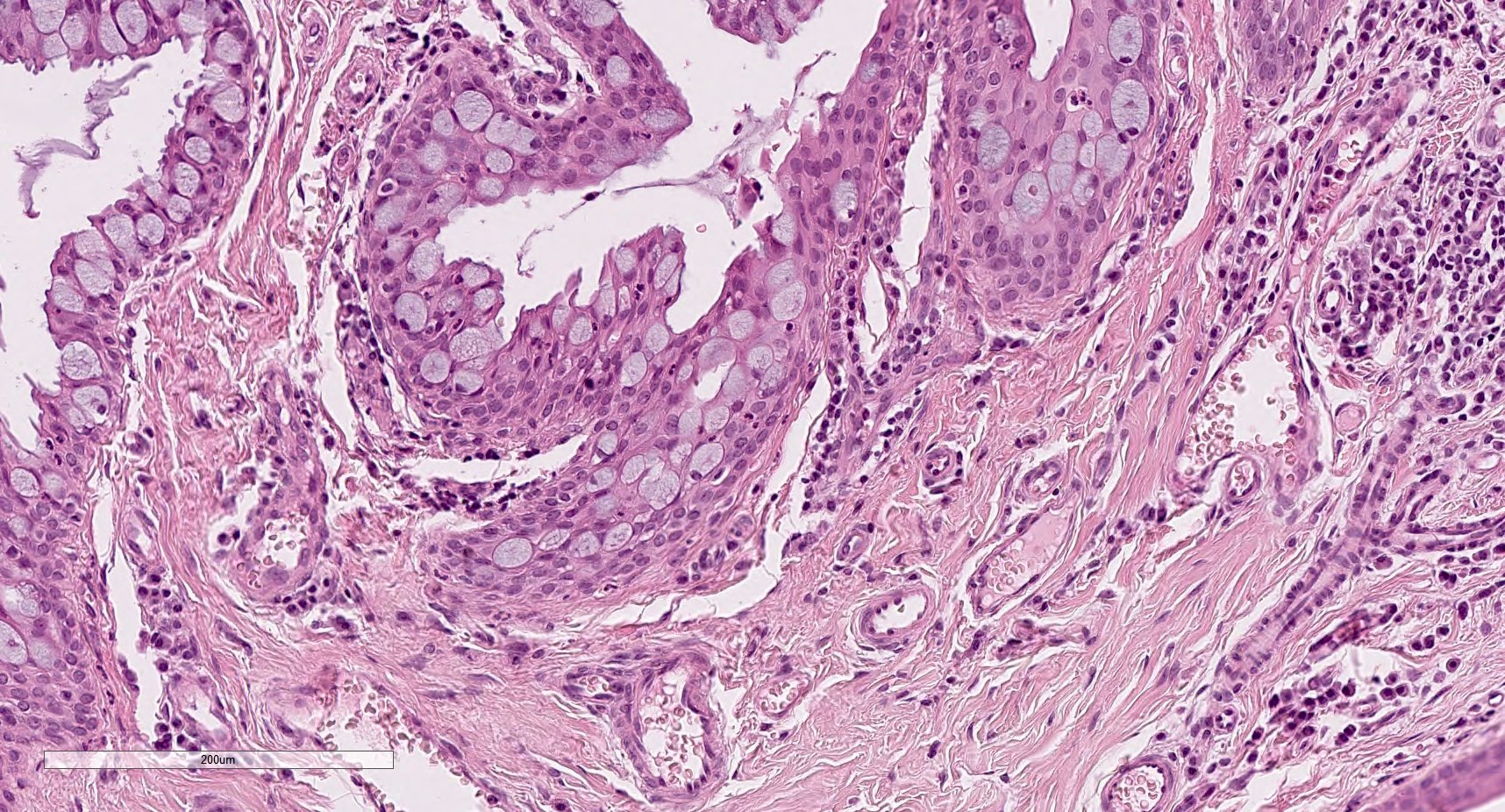
The patient is an older, light skinned man, likely with significant UV exposure, putting him at higher risk for the conditions listed in the choices. The clinical image shows a gelatinous conjunctival lesion with feeder vessels at the limbus in the interpalpebral zone. The biopsy shows thickened conjunctival epithelium with loss of the normal maturation sequence. There is a proliferation of dysplastic squamous cells with high N/C ratios, mitotic activity, hyperchromatic and pleomorphic nuclei involving > two - thirds of the epithelial thickness (conjunctival intraepithelial neoplasia 3 / severe dysplasia). The basement membrane is intact.
Primary acquired melanosis (choice B) is a proliferation of intraepithelial melanocytes that typically grow in a nested pattern.
Pterygium (choice C) would present clinically as a wing-like, fleshy conjunctival lesion. Histopathology would show thin epithelium without dysplasia and underlying stromal fibrovascular tissue with solar elastosis.
Conjunctival intraepithelial neoplasia is a precursor of squamous cell carcinoma (choice D). In squamous cell carcinoma, dysplastic cells invade beyond the basement membrane.
Which of the following is a feature of conjunctival intraepithelial neoplasia?
Association with HPV 6 and 11
Goblet cell containing epithelium without dysplasia
Positivity for CK7 and periodic acid Schiff (PAS)
Proliferation of atypical squamous cells, which may be a precursor to squamous cell carcinoma
Board review style answer #2
D. Proliferation of atypical squamous cells, which may be a precursor to squamous cell carcinoma.
Conjunctival intraepithelial neoplasia is characterized by a proliferation of neoplastic squamous cells showing cellular atypia. It is considered a premalignant lesion that may progress to invasive squamous cell carcinoma.
HPV 6 and 11 (choice A) are associated with squamous papilloma. HPV 16 and 18 are associated with conjunctival intraepithelial neoplasia.
Goblet cell containing epithelium without dysplasia (choice B) is seen in other entities that may mimic conjunctival intraepithelial neoplasia, such as pterygium, pingueculae and squamous papilloma.
CK7 (choice C) is expressed in normal conjunctiva and squamous papillomas but usually negative in dysplasia. PAS is positive in normal conjunctiva and squamous papillomas due to presence of goblet cells; however, goblet cells are usually lacking in conjunctival intraepithelial neoplasia.
Cases with atypia usually recur or develop new foci
Clinical images
AFIP images
Flat diffuse pigmentation
Gross description
Diffuse granular conjunctival pigmentation, usually in bulbar conjunctiva, also cornea, palpebral conjunctiva, eyelid skin
Microscopic (histologic) description
See C-MIN scoring system above
Intraepithelial proliferation of abnormal melanocytes with variable atypia
Early: pigmentation of basilar epithelium only
Later:
Basilar melanocytic hyperplasia with nests, resembling Paget disease
Cells have retracted cytoplasm, larger nuclei than neighboring cells, clumped chromatin and prominent basophilic nucleoli
Cells may be small with scant cytoplasm and small round nuclei
Classification: with or without atypia
High risk of progression: atypia plus epithelioid features including abundant cytoplasm, vesicular nuclei, prominent nucleoli, may be mixed with low risk areas (almost all are associated with invasion,
Am J Surg Pathol 2007;31:185)
Low risk of progression: atypia plus primarily single cell lentinginous growth, small / medium size, high N/C ratio, small / medium hyperchromatic nuclei, no nucleoli, 15% risk of invasion
Pitfalls: don't interpret melanophages as invasive tumor cells
Grade 1: melanocytes with dendritic processes and transferred melanin in epithelial cells
Grade 2: melanocytes have short dendritic processes, incomplete melanin transfer and immature melanosomes, irregular nuclei with clumped chromatin and large nucleoli
Grade 3: epithelioid cells, no cytoplasmic processes, large irregular nuclei with large prominent nucleoli and abnormal melanin transfer
Solid nests and cords of polyhedral cells with abundant, finely granular acidophilic cytoplasm and round / oval paracentral nuclei, usually with one prominent nucleolus
May have microcystic areas with occasional goblet cells
(Am J Dermatopathol 2007;29:279),
may have malignant histology and behavior
Most frequent allergens are tree and grass pollens
More severe forms
Chronic vernal keratoconjunctivitis: more common in spring (vernal); conjunctival scarring, eyelid thickening, ptosis, corneal neovascularization, ulceration, thinning, infection, keratoconus, and vision loss
Atopic keratoconjunctivitis: eyelid tightening, loss of eyelashes, cataracts
Lymphocyte and eosinophil predominant, versus predominance of mast cells and eosinophils in allergic cases
Vernal keratoconjunctivitis
Chronic conjunctivitis
Pathophysiology
Conjunctivitis that persists for 4+ weeks
Etiology
Unilateral:
Due to keratitis, nasolacrimal duct obstruction, occult foreign body, neoplasm, tuberculosis, phthiriasis palpebrarum (due to lice, Int Ophthalmol 2012;32:467)
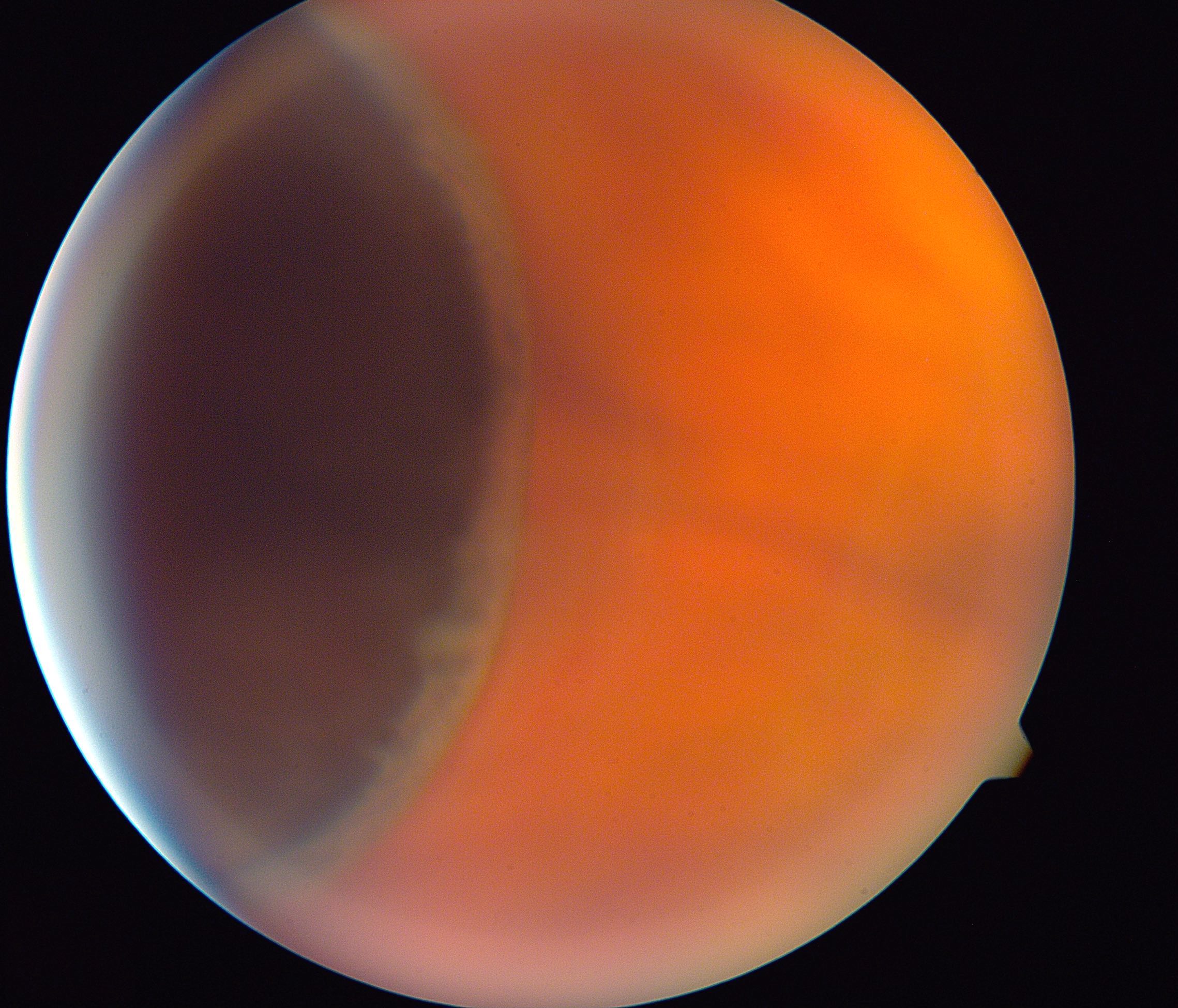
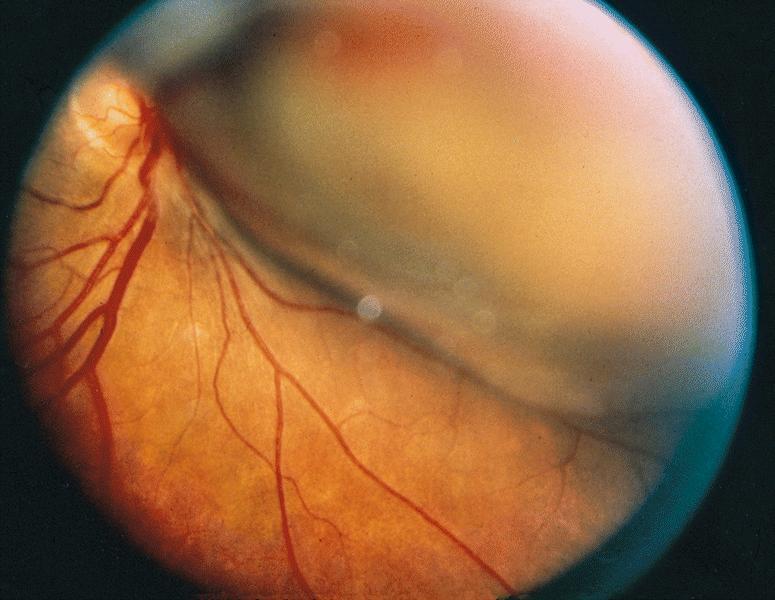
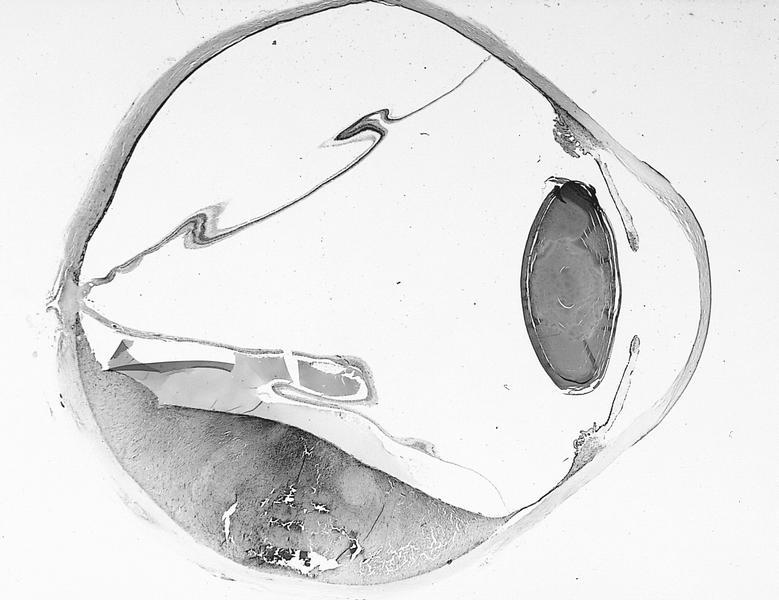
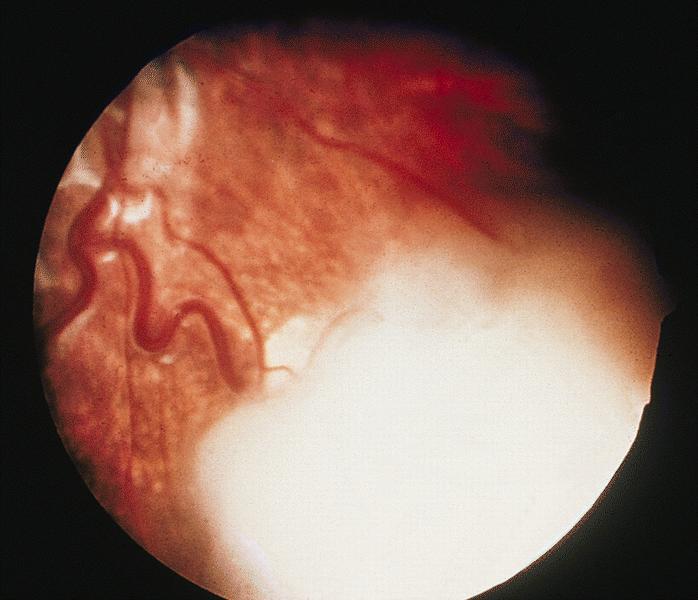
Separation of neurosensory retina (rods and cone and more superficial layers) from retinal pigment epithelium
Rhegmatogenous ("due to a rupture or fracture") detachment: associated with full thickness retinal defect, such as collapse of vitreous, causing traction on retinal internal limiting membrane, causing tears and seepage of vitreous between neurosensory layer and retinal pigment epithelium; treated by relieving vitreous traction
Nonrhegmatogenous detachment: no retinal break; due to significant exudates or conditions causing leakage of fluid from choroidal circulation beneath the retina, such as choroidal tumors and malignant hypertension
Chronic retinal detachment may cause loss of photoreceptor outer segments, gliosis and development of microcystic spaces in detached retina
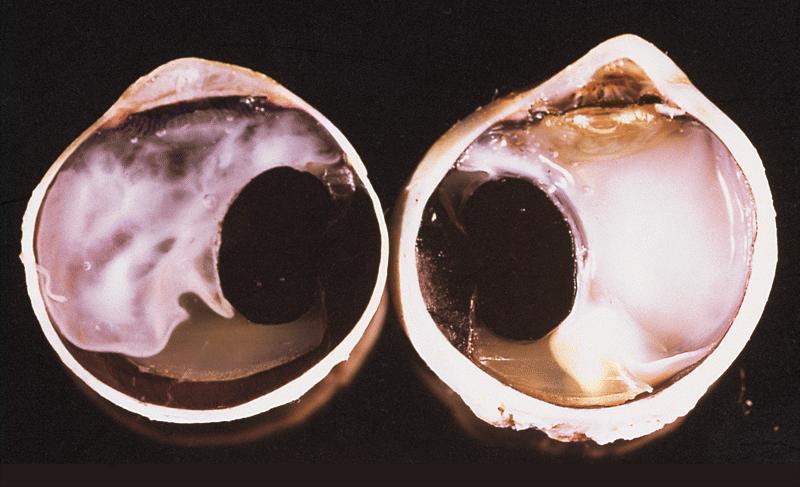
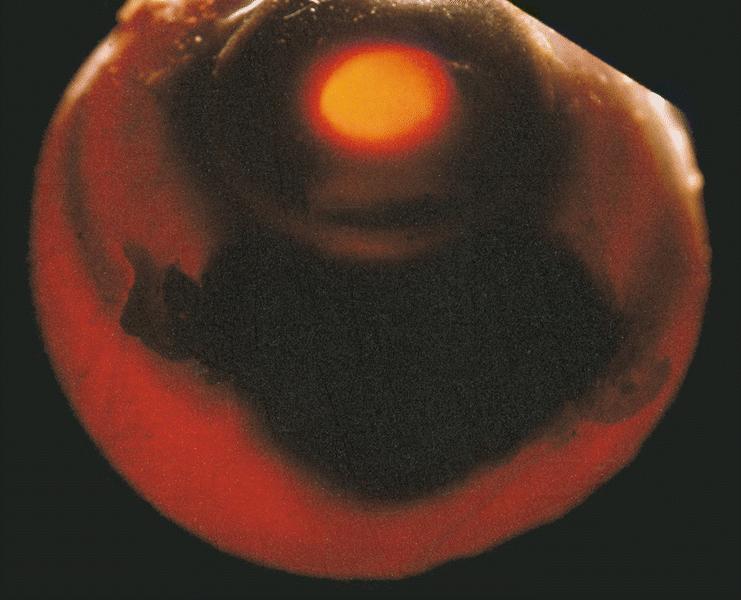
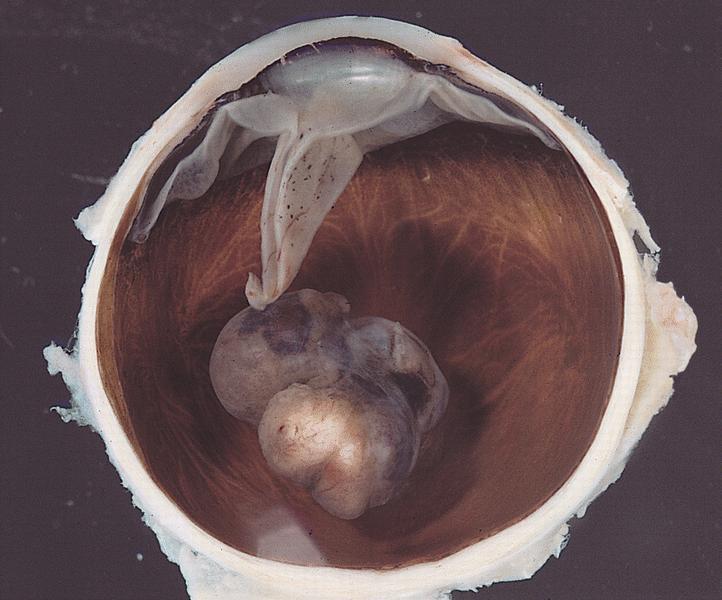
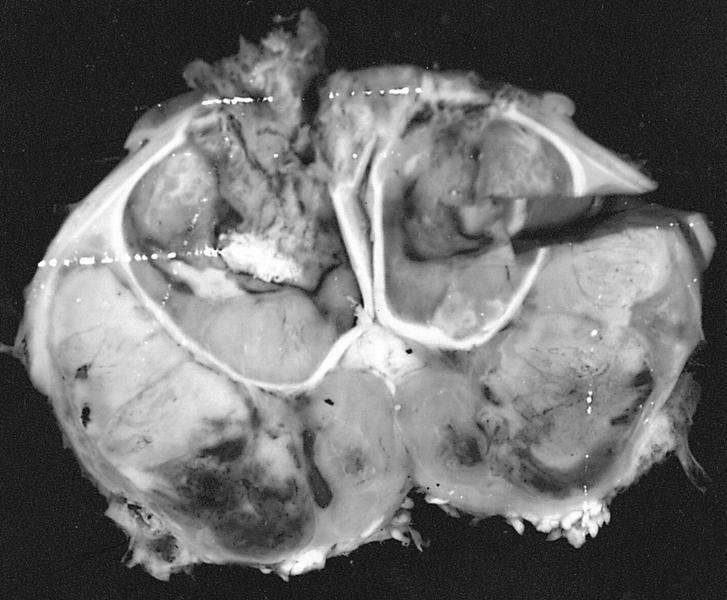
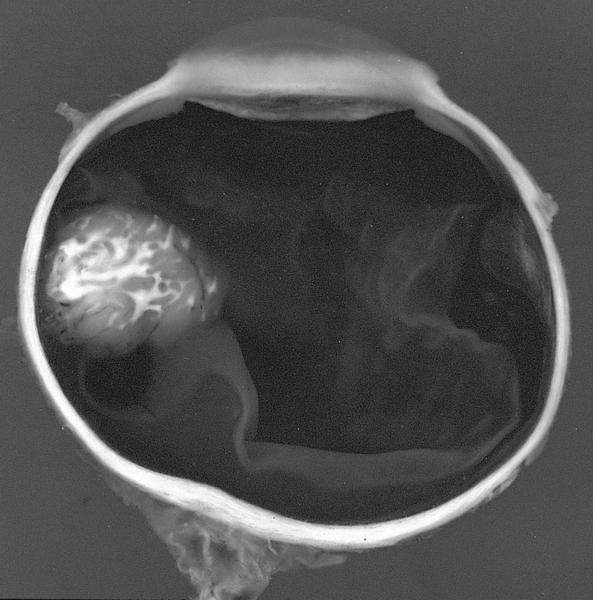
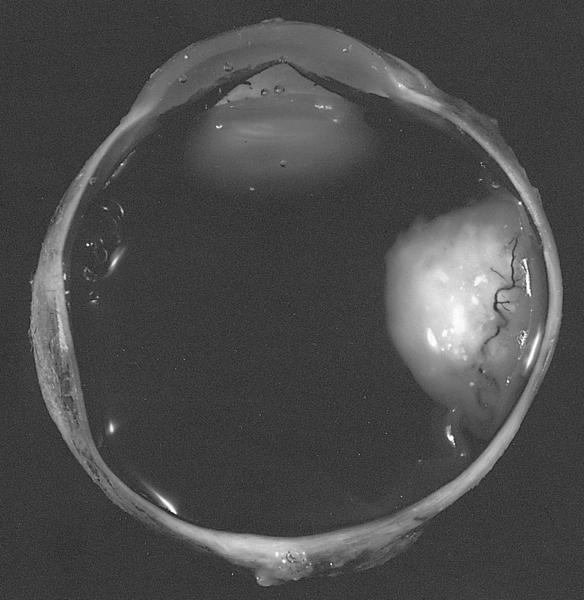
Gross images
Contributed by Anita Kumari, M.D.
Retinal detachment
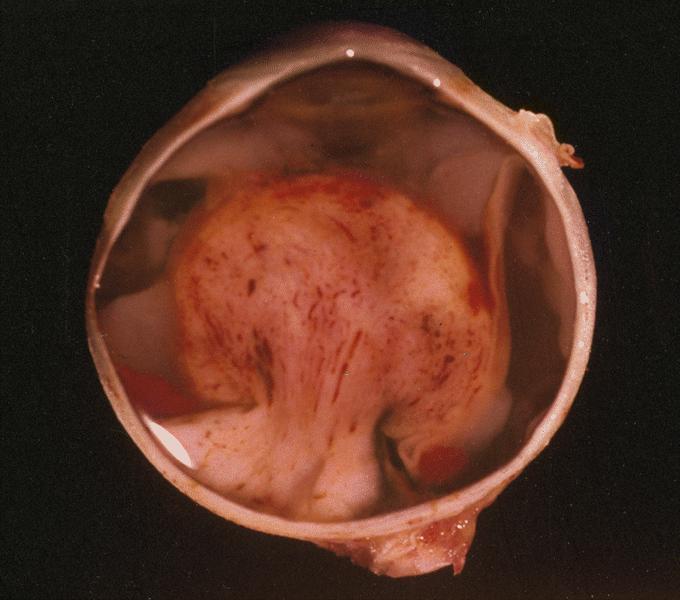
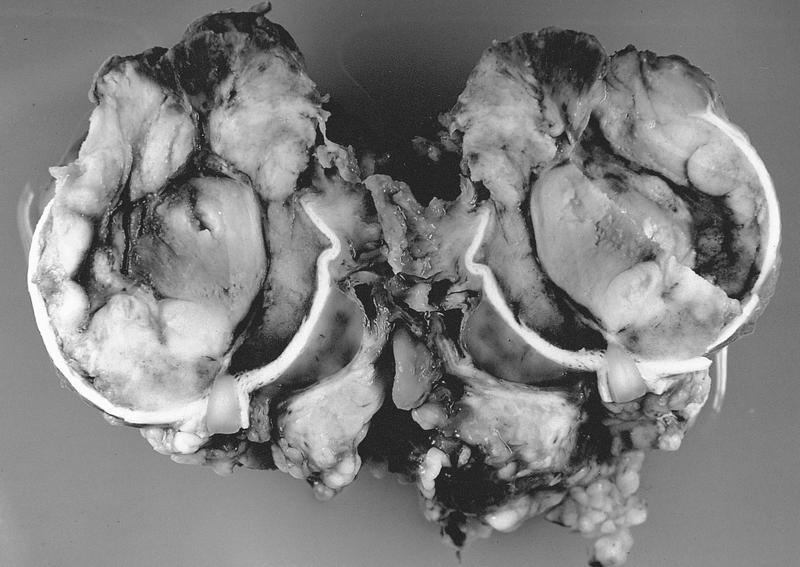
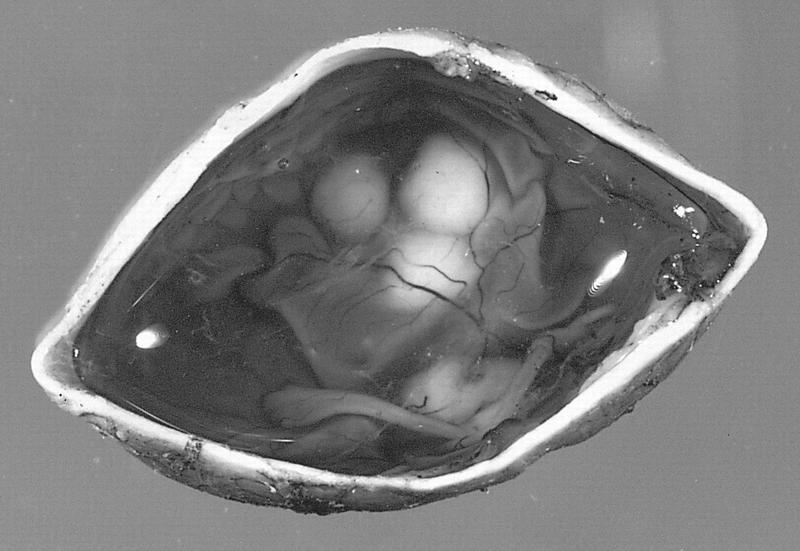
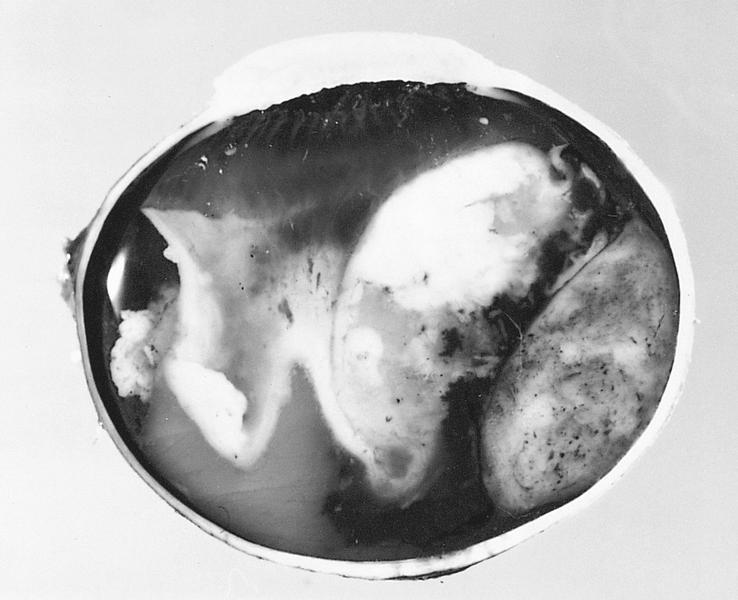
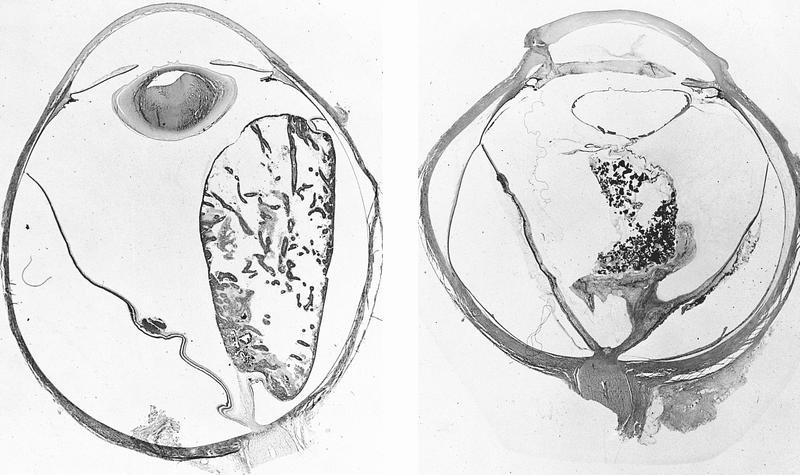
Whole mount images
Contributed by Anita Kumari, M.D.
Retinal detachment
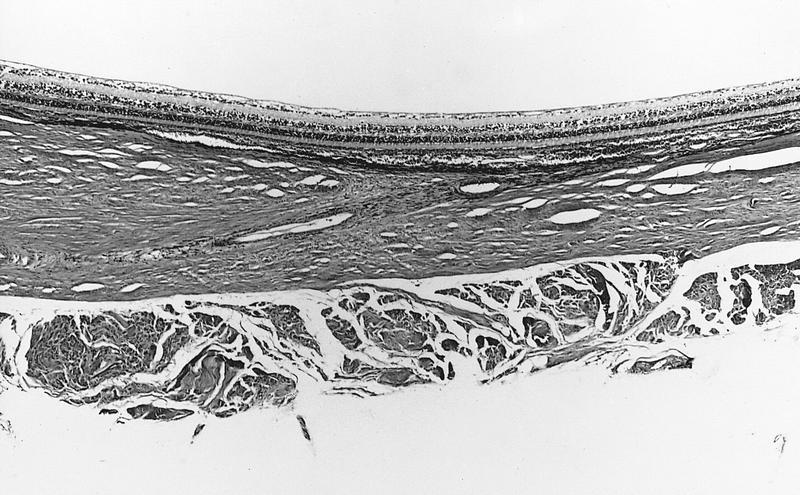
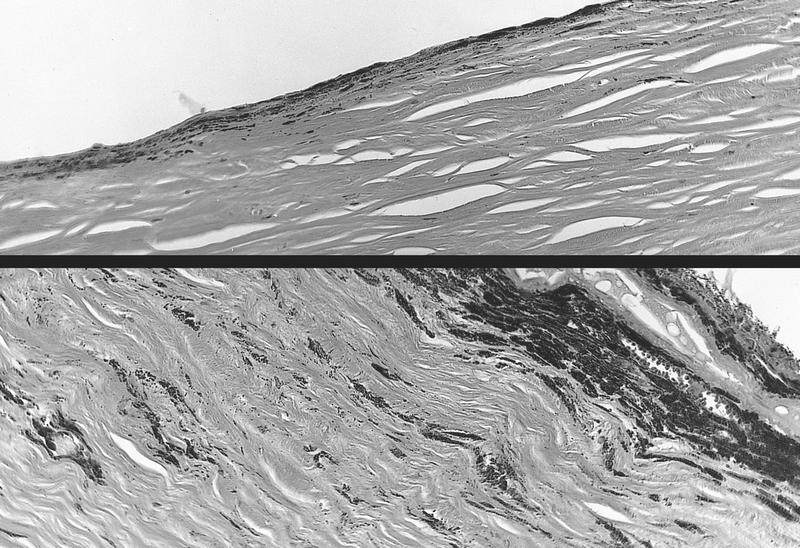
Microscopic (histologic) description
Early changes are degeneration of outer retinal layers and photoreceptors with subretinal exudates
Late changes are disruption and atrophy of retinal architecture with marked gliosis and proliferative vitreoretinopathy
Microscopic (histologic) images
Contributed by Anita Kumari, M.D.
Microscopic images of a case of retinal detachment
Classified as background, preproliferative or proliferative retinopathy
Background retinopathy: initial lesion is capillary microangiopathy
Preproliferative retinopathy: changes of background diabetic retinopathy plus significant venous dilation / beading, cotton wool spots (due to focal infarcts in nerve fiber layer), extensive formation of intraretinal microvascular abnormalities (due to vascular shunts) and extensive ischemia
Proliferative retinopathy: growth of neovascular tissue from inner surface of retina into vitreous; causes retinal detachment, treat with laser photocoagulation; may occur without clinically visible background diabetic retinopathy
Retinopathy is associated with duration of diabetes - 60% at 15 years
May cause rubeosis iridis (neovascularization of iris) and secondary glaucoma
Also causes thickening of basement membrane of pars plicata of ciliary body
Also causes vacuolization of iris pigment epithelium with glycogen containing vacuoles related to blood glucose level at time of enucleation
Microscopic (histologic) description
Background retinopathy: retinal capillary microaneurysms and cotton wool spots (due to hypoxia from microvascular obstructions and nonperfusion) with PAS+ deposits on endothelium, basement membrane thickening, loss of pericytes; also venous anomalies, hemorrhage (flame shaped between fibers of nerve fiber layer), exudates (hard, yellow, waxy protein and lipid of outer plexiform layer appears eosinophilic) and edema
Proliferative retinopathy: new vessels that sprout from existing vessels on surface of optic nerve head or retina and penetrate the internal limiting membrane of the retina; thickened basement membrane, reduction in number of pericytes (causes microaneurysms and arteriovenous shunts)
A type of choristoma (congenital, nonneoplastic lesion composed of cytologically normal tissue not normally found at that location), often at limbus
Mainly children
No malignant potential
May be associated with colobomas of iris and ciliary body, Goldenhar syndrome (ocular dermoid tumors, extra-auricular appendages, vertebral anomalies,
East Afr Med J 2002;79:502),
organoid nevus syndrome (also called linear nevus sebaceus of Jadassohn,
Br J Ophthalmol 1987;71:268)
Diagrams / tables
Images hosted on other servers:
Complex choristoma (figure 1b)
Clinical images
Images hosted on other servers:
Lipodermoid
Gross description
Bulbar tumors are firm, localized, elevated, opaque, yellow-white masses at limbus
Microscopic (histologic) description
Dermoid:
Solid (not cystic) choristoma mass with surface epithelium resembling epidermis and dermis and containing a few hairs, overlying thick bundles of collagen, which make up bulk of mass
(eMedicine: Limbal Dermoid [Accessed 17 April 2018])
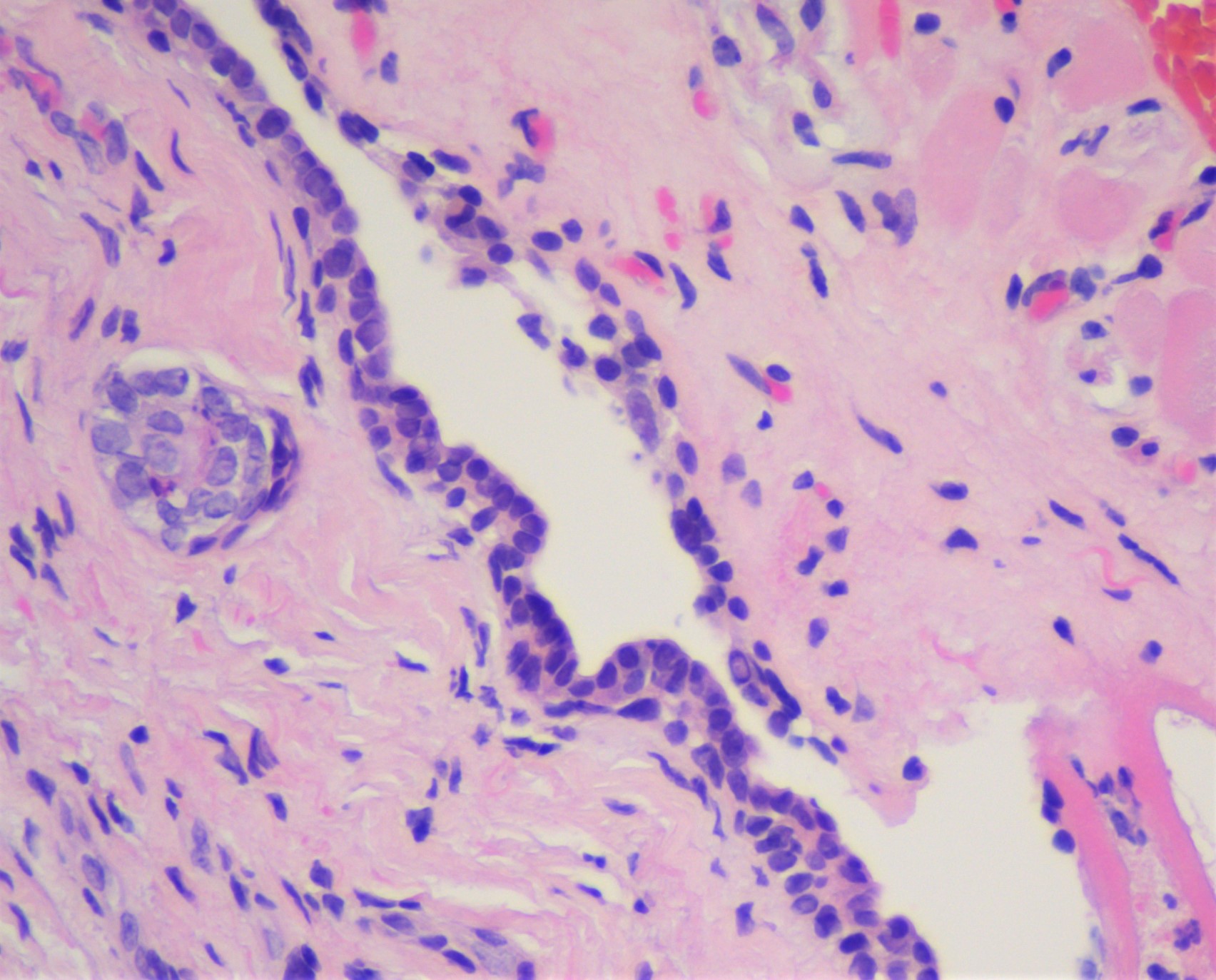
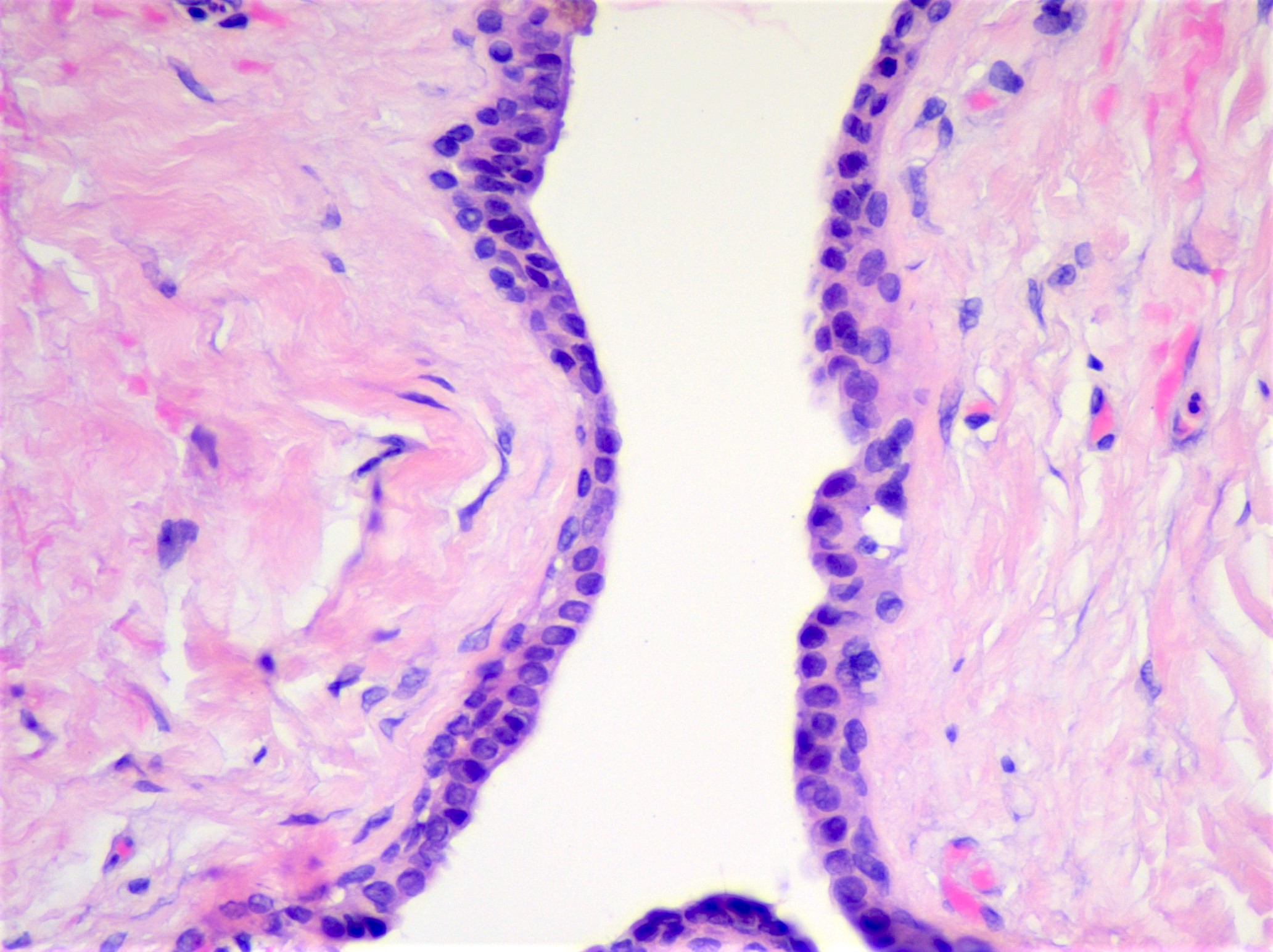
Benign cystic lesions of the eyelid, most of which are caused by blockages of ducts (hidrocystomas) or hair follicles (epidermal cyst) or are consequence of entrapped benign, embryologic tissue (dermoid cyst)
Includes epidermal cyst, dermoid cyst, eccrine hidrocystoma and apocrine hidrocytoma, all of which are generally cured by excision
Essential features
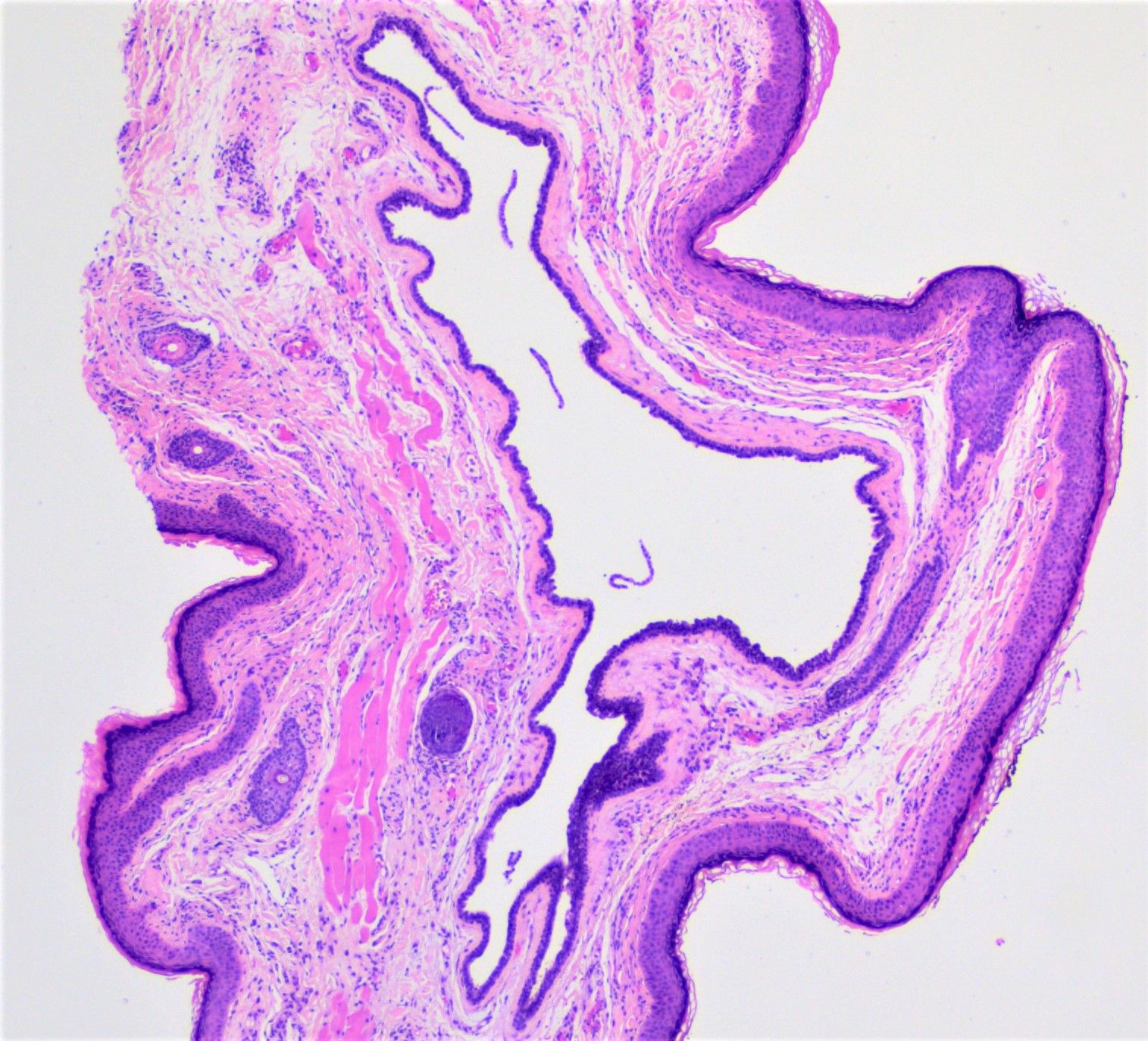
Epidermal cysts feature a lining of benign keratinizing stratified squamous epithelium with a granular layer (in the absence of adnexal structures) and contain keratinaceous debris
Dermoid cysts are embryologically derived lesions histologically identified by the presence of adnexal structures in conjunction with benign, stratified squamous epithelial cyst lining
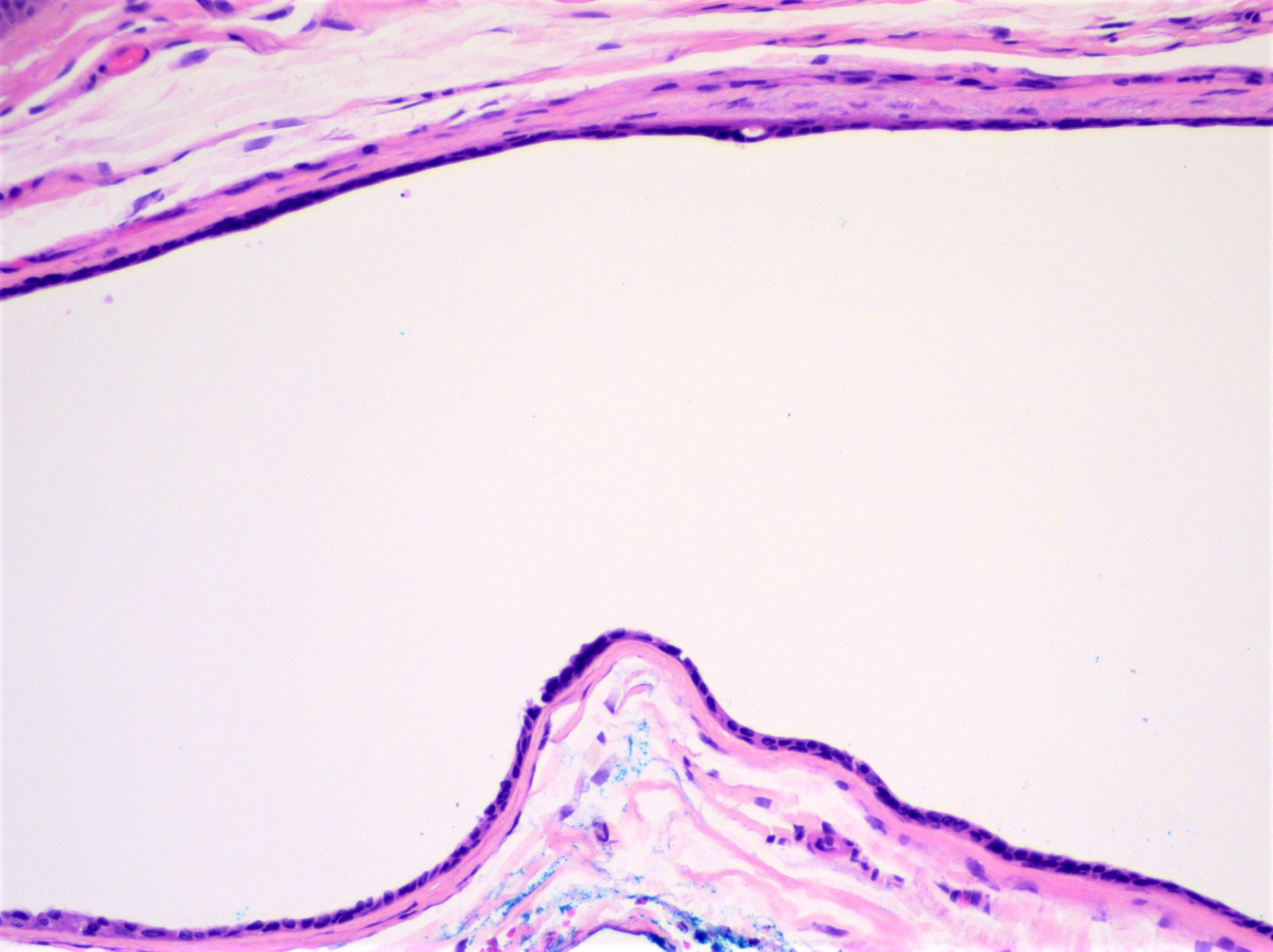
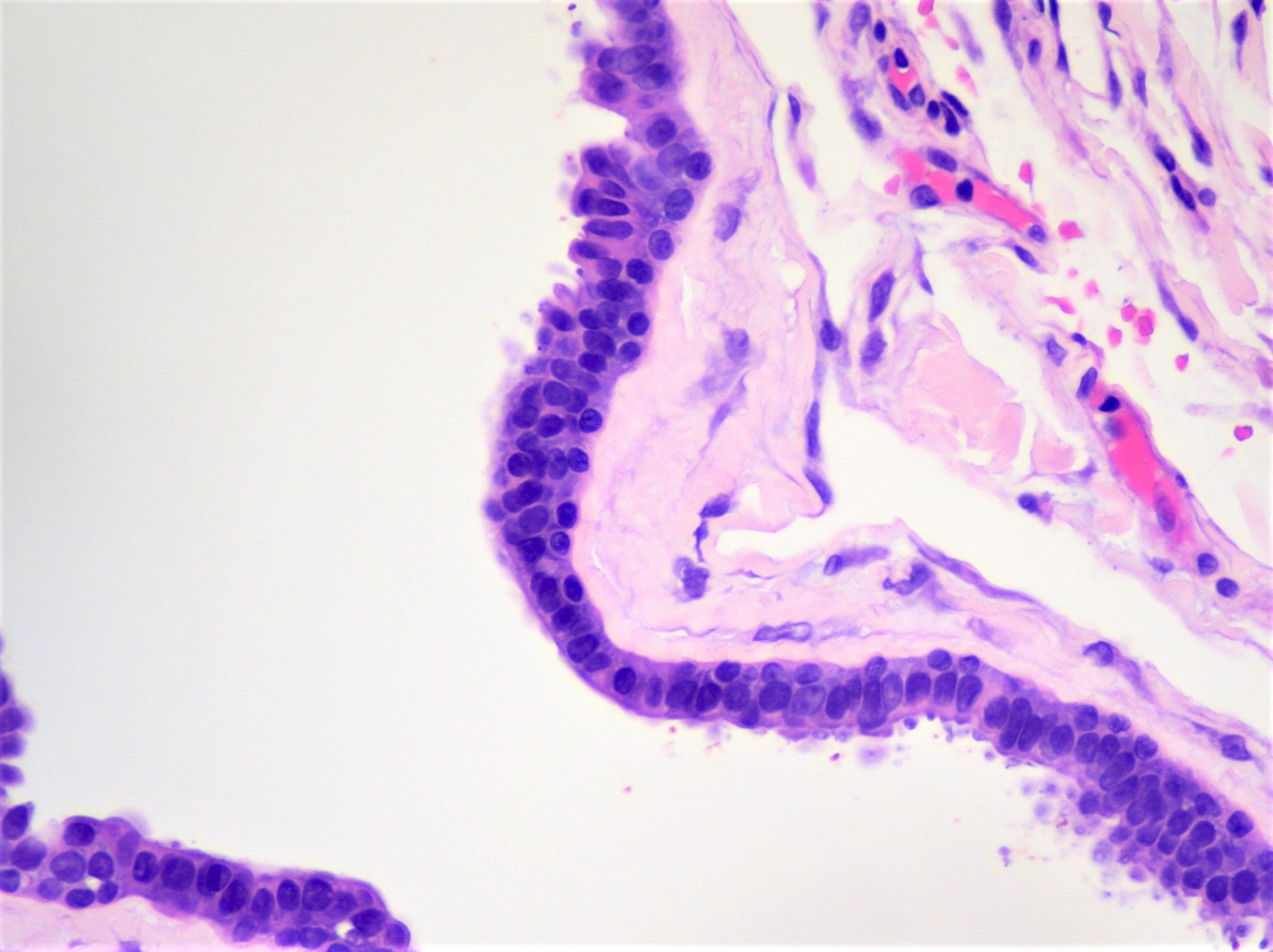
Eccrine hidrocystomas are caused by obstruction of eccrine sweat glands and are histologically identified by a dual layer of bland, cuboidal epithelial cells
Apocrine hidrocystomas are caused by obstruction of apocrine sweat glands and are histologically identified by the presence of an inner layer of elongated, epithelial cells with apical snouts and decapitation secretions
Periocular dermoid cysts are most often encountered in pediatric patients, with many cases arising in the superotemporal region within the first year of life (Ophthalmic Epidemiol 2019;26:117)
Eccrine hidrocytomas generally arise along the medial or lateral eyelid in middle aged to older adults (Eye (Lond) 2005;19:77)
Apocrine hidrocystomas often occur near the canthus in middle aged and older adults but may rarely be seen in the pediatric population (MedGenMed 2006;8:57)
Etiology
Most epidermal cysts are thought to arise secondary to occlusion of hair follicles (Arch Ophthalmol 1988;106:270)
Dermoid cysts present as subcutaneous nodules, often superotemporally in the vicinity of the zygomaticofrontal suture (Int Ophthalmol 2011;31:93)
Most hidrocystomas appear as single, dome shaped lesions with varying tints (including transparent, skin colored, brown, blue and blue-black hues) though examples of multiple hidrocystomas do occur (MedGenMed 2006;8:57)
Subepithelial cyst with an inner epithelial lining of elongated (columnar), eosinophilic cells with apical snouts and decapitation secretions
Unilocular or multilocular
Like eccrine hidrocystomas, the cyst cavity may appear clear / empty or contain eosinophilic, proteinaceous material
Microscopic (histologic) images
Contributed by J. Stephen Nix, M.D.
Epidermal cyst, keratinaceous contents
Epidermal cyst, granular layer
Dermoid cyst, keratinaceous contents
Dermoid cyst, adnexal structures
Dermoid cyst with rupture
Eccrine hidrocystoma
Eccrine hidrocystoma, cuboidal bilayer
Eccrine hidrocystoma, attenuated lining
Apocrine hidrocystoma
Apocrine hidrocystoma, inner cyst lining
Virtual slides
Images hosted on other servers:
Apocrine hidrocystoma of skin
Videos
Hidrocystoma: 5 minute pathology pearls by Dr. Jared Gardner
Dermoid cyst: 5 minute pathology pearls by Dr. Jared Gardner
Sample pathology report
Eyelid, left upper, excision:
Epidermal cyst (see comment)
Comment: Histologic examination shows a cyst with a bland keratinizing squamous epithelial lining with a granular layer and keratinaceous cyst contents in the absence of adnexal structures.
Periocular nodule, excision:
Dermoid cyst (see comment)
Comment: Histologic examination shows a cyst with a bland keratinizing squamous epithelial lining and adjoining adnexal structures.
Eyelid, right upper, excision:
Apocrine hidrocystoma (see comment)
Comment: Histologic examination shows a subepithelial cyst that features an inner layer of elongated, eosinophilic cells with apical snouts and decapitation secretions.
Eyelid, left lower, excision:
Eccrine hidrocystoma (see comment)
Comment: Histologic examination shows a subepithelial cyst with an epithelial lining composed of a dual layer of flattened, cuboidal cells.
Eyelid, left upper, excision:
Epidermal cyst (see comment)
Comment: Histologic examination shows a cyst with a bland keratinizing squamous epithelial lining with a granular layer and keratinaceous cyst contents in the absence of adnexal structures.
Periocular nodule, excision:
Dermoid cyst (see comment)
Comment: Histologic examination shows a cyst with a bland keratinizing squamous epithelial lining and adjoining adnexal structures.
Eyelid, right upper, excision:
Apocrine hidrocystoma (see comment)
Comment: Histologic examination shows a subepithelial cyst that features an inner layer of elongated, eosinophilic cells with apical snouts and decapitation secretions.
Eyelid, left lower, excision:
Eccrine hidrocystoma (see comment)
Comment: Histologic examination shows a subepithelial cyst with an epithelial lining composed of a dual layer of flattened, cuboidal cells.
A 68 year old man presents with a skin colored nodule of the lateral left lower eyelid. Based on the histologic image, what is the most likely etiology of the lesion?
Blockage of an apocrine sweat gland
Blockage of an eccrine sweat gland
Entrapped embryologic tissue
Obstruction of a pilosebaceous unit
Board review style answer #1
B. Blockage of an eccrine sweat gland. The histologic image shows an epithelial lining composed of a dual layer of cuboidal cells, consistent with the diagnosis of eccrine hidrocystoma. Eccrine hidrocystomas are caused by blockages of eccrine sweat glands. Apocrine hidrocystomas result from blockages of apocrine sweat glands (A). Entrapped embryonal tissue is encountered in a dermoid cyst (C) and obstruction of a pilosebaceous unit may result in an epidermal cyst (D).
A 1 year old girl undergoes excision of a superotemporal periocular nodule and the histologic findings are provided in the associated image. What is the diagnosis?
Apocrine hidrocystoma
Dermoid cyst
Eccrine hidrocystoma
Epidermal cyst
Board review style answer #2
B. Dermoid cyst. Periocular dermoid cysts most often occur in pediatric patients and are diagnosed histologically by the presence of adnexal structures in association with a bland stratified squamous epithelial cyst lining. Apocrine hidrocystomas demonstrate a cyst lining with an inner layer of elongated, eosinophilic cells with apical snouts and decapitation secretions (A). Eccrine hidrocystomas feature a cyst lining composed of a dual layer of cuboidal cells (C). Epidermal cysts have a cyst lining of bland keratinizing stratified squamous epithelium with a granular layer in the absence of adnexal structures (D).
Diverse etiologies, causes widespread degeneration of ocular tissue
Defined as optic neuropathy with distinct excavation of optic nerve head and incremental loss of visual field sensitivity
Almost always due to increased intraocular pressure (due to impaired outflow of aqueous humor) which causes optic nerve damage and degenerative changes below
Normal circulation of aqueous humor
Aqueous humor is produced by pars plicata of ciliary body, discharged into posterior chamber, flows between lens and iris, through pupil, into anterior chamber, then through trabecular meshwork (in deep layers of peripheral cornea just in front of angle of anterior chamber), into Schlemm canal, leaves eye via plexus of intrascleral and episcleral veins along limbus
Drawings
Images hosted on other servers:
Anterior chamber
Microscopic (histologic) images
AFIP images
Iris and ciliary body with open anterior chamber angle
Slow growing tumor within orbital segment of optic nerve
Usually ages 0 - 9 years with symptoms of minimal exophthalmos, optic nerve atrophy or papilledema
Associated with neurofibromatosis type 1
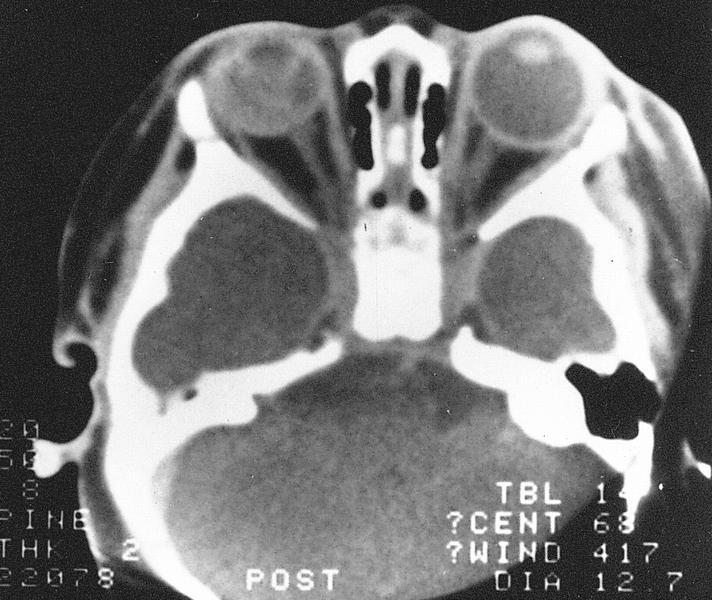
Radiology description
Thickening of nerve on CT scan
May enlarge optic canal
Radiology images
AFIP images
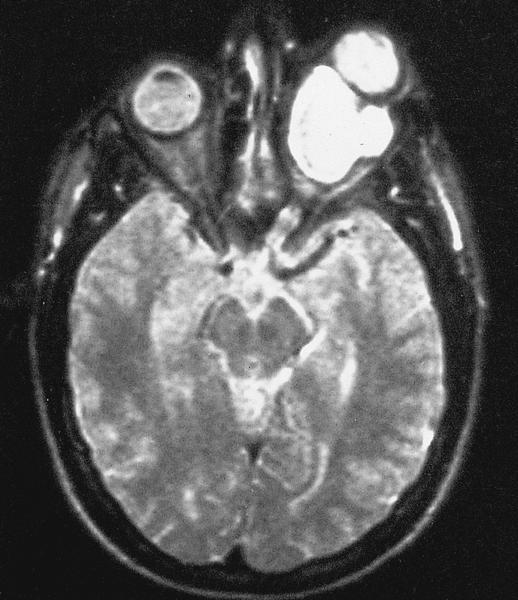
MR of large retrobulbar optic nerve tumor
Treatment
Resection for tumors limited to optic nerve
Also radiation therapy for more extensive lesions
Gross description
Small tumors are limited to optic nerve
Larger tumors form bulbous enlargement of nerve, often infiltrate pia causing arachnoid thickening
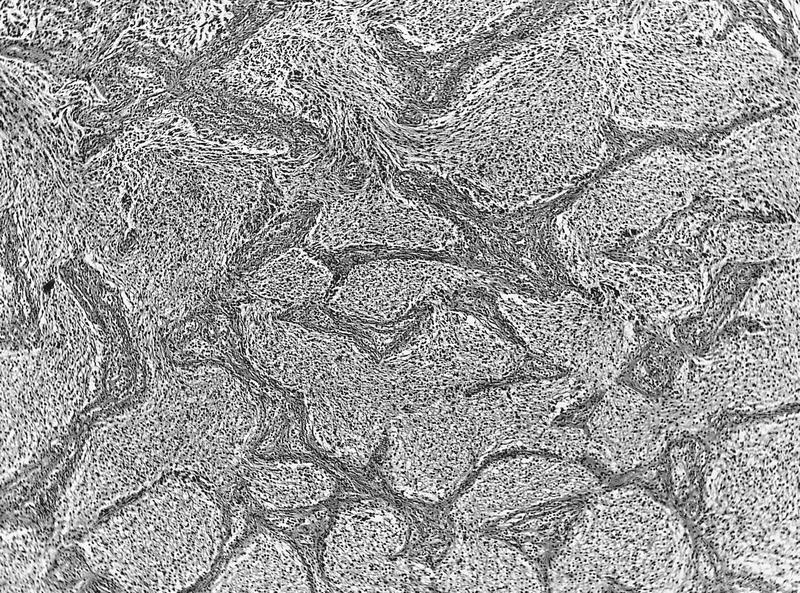
Microscopic (histologic) description
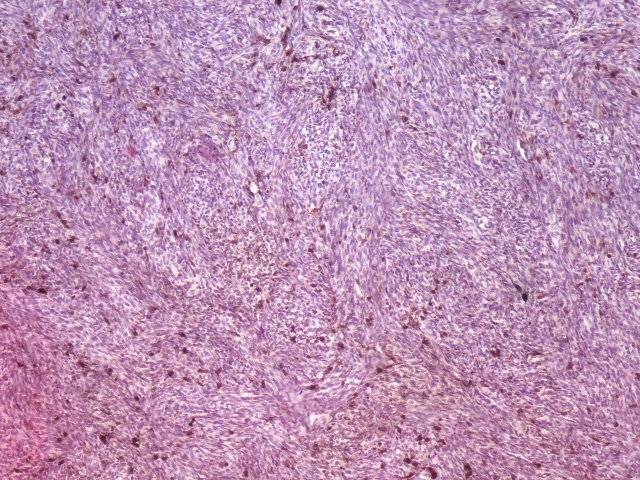
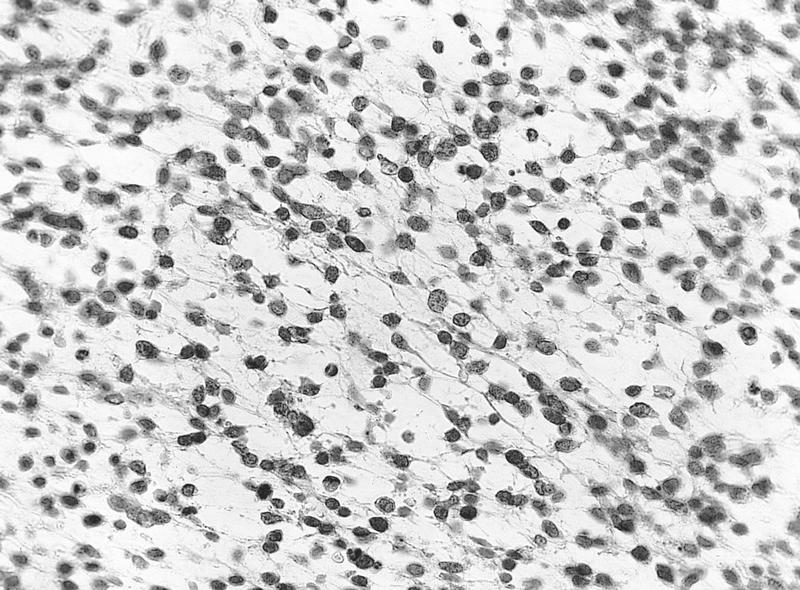
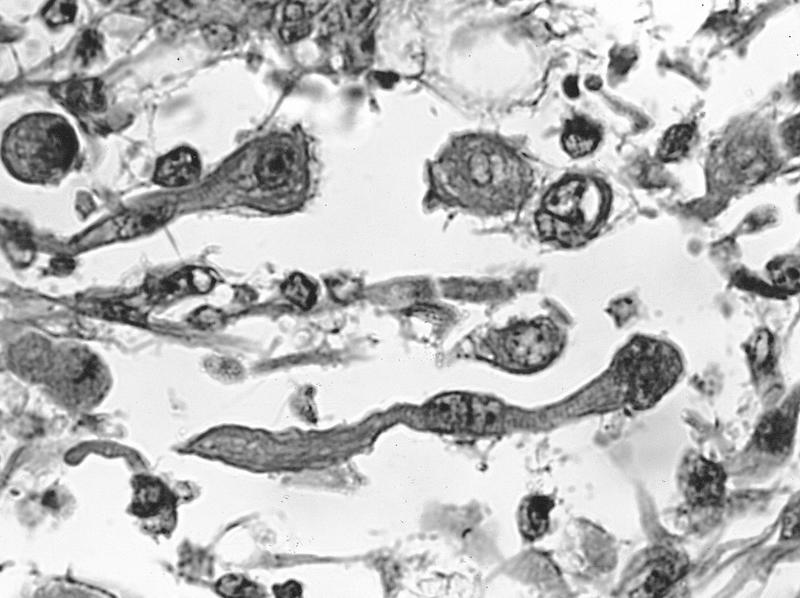
Variable cytology and cellularity, even within same tumor, but usually are low grade pilocytic astrocytomas similar to cerebellar and third ventricle tumors with round to spindled nuclei and dendrite-like cytoplasmic processes
Often Rosenthal fibers (fusiform, cigar shaped eosinophilic structures within astrocyte cytoplasmic processes, are a nonspecific degenerative change)
Rarely are hypercellular with brisk mitotic activity, marked pleomorphism, necrosis and vascular proliferation
Difficult to differentiate reactive vs. neoplastic resection margins
Typically has intense mucinous degeneration with tumor cells in pools of mucin
Infiltrating tumor may cause reactive proliferation of arachnoid cells resembling meningioma
Specimens are thin and tend to fold when placed in fixative
Surgeon should spread lesion onto filter paper, allow to dry for a few seconds, then place in specimen container
Relevant landmarks should be labeled
For lesions that extend to limbus, cut so sections are perpendicular to limbus
Don't use methylene blue or toluidine blue ink for margins as they bleed into sample
Don't place specimens on sponges which expand in fixative and distort specimen
Conjunctiva tumors - features to report
Histologic type
Degree of differentiation
Precise anatomic location: bulbar by quadrant, palpebral (superior or inferior), fornix (superior or inferior), caruncle, plica semilunaris, limbus, cornea
Tumor size
Involvement of corneal stroma, episclera, orbital fat
Involvement (noninvolvement) of other tissues present
Margins (deep and lateral, minimum clearance)
Presence of angiolymphatic, perineural, intraocular or intraorbital invasion
Presence of ulceration
For melanomas, also indicate thickness (from top of epithelium to deepest tumor cell in substantia propria using ocular micrometer) and mitotic activity
Presence of foreign bodies (in traumatic specimens)
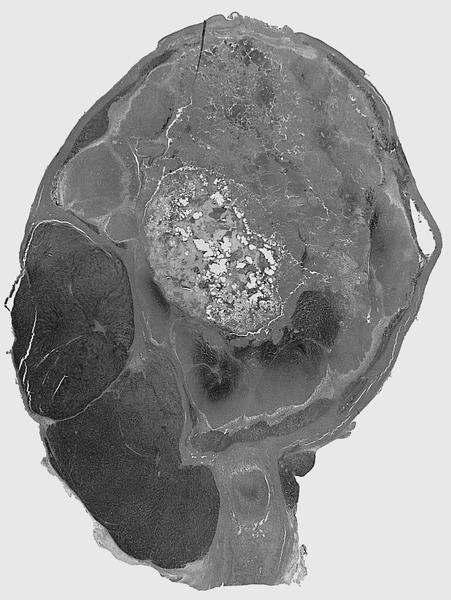
For tumors, describe location, dimensions, shape, ulceration, color, consistency, hemorrhage, necrosis, calcification, ocular structures involved, extension into optic nerve, tumor distance to optic nerve and limbus, rupture of Bruch membrane
Transillumination findings
Globe - sectioning
Grossing
Enucleation: globe and part of optic nerve are removed from orbit
For retinoblastoma, may need fresh tissue for genetic studies:
Identify tumor location by transillumination
Submit optic nerve margin separately before cut into globe
Cut small window in sclera overlying tumor and obtain small tumor sample
Try to avoid seeding of tumor cells onto optic nerve or elsewhere
Fix in formalin (300 ml of 10% neutral buffered formalin) for 24 - 48 hours before sectioning
Do not open or puncture the eye
Wash in running tap water for 5 - 15 minutes
Optionally place in 60 - 70% ethyl alcohol for 1 - 2 hours (firms up eye and restores color of vessels)
Review clinical history and results of ophthalmologic examination prior to sectioning
"Temporal" is same as lateral; "nasal" is same as medial
Orient globe based on:
Cornea is wider than tall by 1 mm
Optic nerve distance to limbus (junction of cornea and sclera) is less medially than laterally (i.e. optic nerve is medial (nasal) to posterior pole)
Superior oblique muscle tendon inserts in upper outer quadrant of posterior globe behind superior rectus muscle insertion and insertion points towards anterior nasal eye
Inferior oblique muscle has muscular insertion in lower outer (temporal) quadrant of sclera and fibers run posteriorly and medially
Long posterior ciliary arteries are in horizontal plane
Four vortex veins exit posterior sclera
Transilluminate globe to find tumor and cut accordingly
Can use a substage microscope lamp in a dark room
Rotate globe over light, mark abnormal shadows on sclera with indelible pencil
Take Xray before opening globe if foreign body or retinoblastoma is suspected
If choroidal melanoma is suspected, sample at least one vortex vein from each of four quadrants and submit separately
Central section is called "pupil-optic nerve" section; other fragments are called calottes
Try to include optic nerve, pupil, cornea, lens and large cut surface of tumor in same section, about 8 mm thick
Use sharp razor to cut, holding globe with nondominant hand, cornea down against cutting block using blade between thumb and middle finger of dominant hand
Open eye with sawing motion from back (adjacent to optic nerve) to front (1 mm inside limbus through peripheral cornea)
If no tumor, cut globe at superior and inferior edges of iris in horizontal plane from back to front (5 mm above and below the optic nerve, missing the lens)
Quick freeze first in liquid nitrogen to minimize artifacts
Excision, but lesions commonly recur; no malignant transformation
Gross description
Gray-white, inflamed, horseshoe shaped elevated lesions of conjunctiva and oral mucosa; bilateral corneal involvement
(Cornea 2011;30:1481)
Microscopic (histologic) description
Acanthotic and dyskeratotic epithelium of conjunctiva and oral mucosa
Overlying multilayered parakeratotic mantle with pyknotic nuclei and epithelial ghosts, middle and superficial layers have large squamous cells and dyskeratotic cells but no atypia
May not be a specific disease process, but due to various causes (paranasal sinus tumors, Rosai-Dorfman disease, inflammatory fibrosclerosis, dysthyroid ophthalmopathy, cholesterol or keratin granulomas, traumatic fat necrosis, prior hemorrhage or abscess)
More common than infectious granulomas
Usually ages 20 - 49 years with good health and sudden onset of exophthalmos with variable lid or conjunctival edema
Case reports
50 year old man with intraocular inflammatory myofibroblastic tumor with ALK overexpression (Arch Pathol Lab Med 2004;128:e5)
Treatment
Steroids (alleviate signs and symptoms)
Excision
Gross description
Indurated orbital mass, often surrounding optic nerve and enveloping extraocular muscles
Gross images
AFIP images
Fibrotic mass surrounds the eye
Microscopic (histologic) description
General:
Edematous tissue with excessive production of ground substance, chronic inflammatory cells, vascular proliferation and hyperplastic connective tissue
May have periphlebitis with tissue eosinophilia
Inflammatory myofibroblastic tumor:
Combinations of fibroblasts and myofibroblasts in background of plasma cells and other inflammatory cells
Rosai-Dorfman related:
Large histiocytes, some with lymphocytophagocytosis, lymphocytes and plasma cells, often with prominent fibrosis
Contact lens wearers are susceptible to Pseudomonas and Acanthamoeba
Keratitis caused by microfilaria of Onchocerca volvulus is the leading cause of blindness worldwide, outside US
Granulomatous keratitis
Due to HSV1, juvenile xanthogranuloma, leprosy, sarcoidosis
Herpes keratitis
Most common cause of corneal ulcers
Usually unilateral, may recur
Usually HSV1
Diagnosis difficult in recurrent cases; may need EM, PCR, ISH or immunohistochemistry since cultures are usually negative and inclusions are rarely identified
Microscopic (histologic) description
Similar histologic findings for all organisms
Destruction of corneal epithelium, Bowman layer and stroma
Necrosis and prominent neutrophils
Discontinuities of Descemet membrane with corneal perforation
Crystal-like stromal opacities with Streptococcus viridans
May need special stains to detect organisms
Herpes keratitis:
Diffuse epithelial edema causing bullae between epithelium and Bowman layer
Also patchy loss of Bowman layer
Irregular epithelium
Infiltration of anterior stroma by lymphocytes and plasma cells with stromal fibrosis and neovascularization
Severe cases have granulomatous reaction surrounding Descemet membrane
Thin diaphragm of tissue with central opening (pupil)
Forms boundary of anterior and posterior chamber
Highly textured with folds and crypts
Part of middle layer of eye (also ciliary body and choroid)
Normally rests gently upon lens and bulges slightly forward
Consists of stroma and posterior epithelial lining (two closely apposed epithelial layers, with numerous melanosomes); contains sphincter muscle within stroma that controls pupil
Anterior iris lacks a cellular lining
Color is due to number of stromal melanocytes; blue irises have few stromal melanocytes; brown irises have numerous melanocytes
Blood vessels are usually surrounded by a thick collar of collagen fibers, resembling arteriolosclerosis
Fewer melanosomes and melanocytes in patients with ocular and oculocutaneous albinism
Regulates amount of light reaching pupil; muscles of iris dilate or constrict pupil in response to parasympathetic or sympathetic nerve impulses; normal diameter of pupil is 1 - 8 mm
Iridectomy: excision of small segment of iris; place on filter paper to avoid folding
Ectropion uveae: fibrovascular tissue on anterior surface of iris everts the papillary margin and pulls pigmented epithelia onto anterior surface of iris
Drawings
Images hosted on other servers:
Iris: front view
Choroid and iris
Microscopic (histologic) images
AFIP images
Iris and ciliary body with open anterior chamber angle
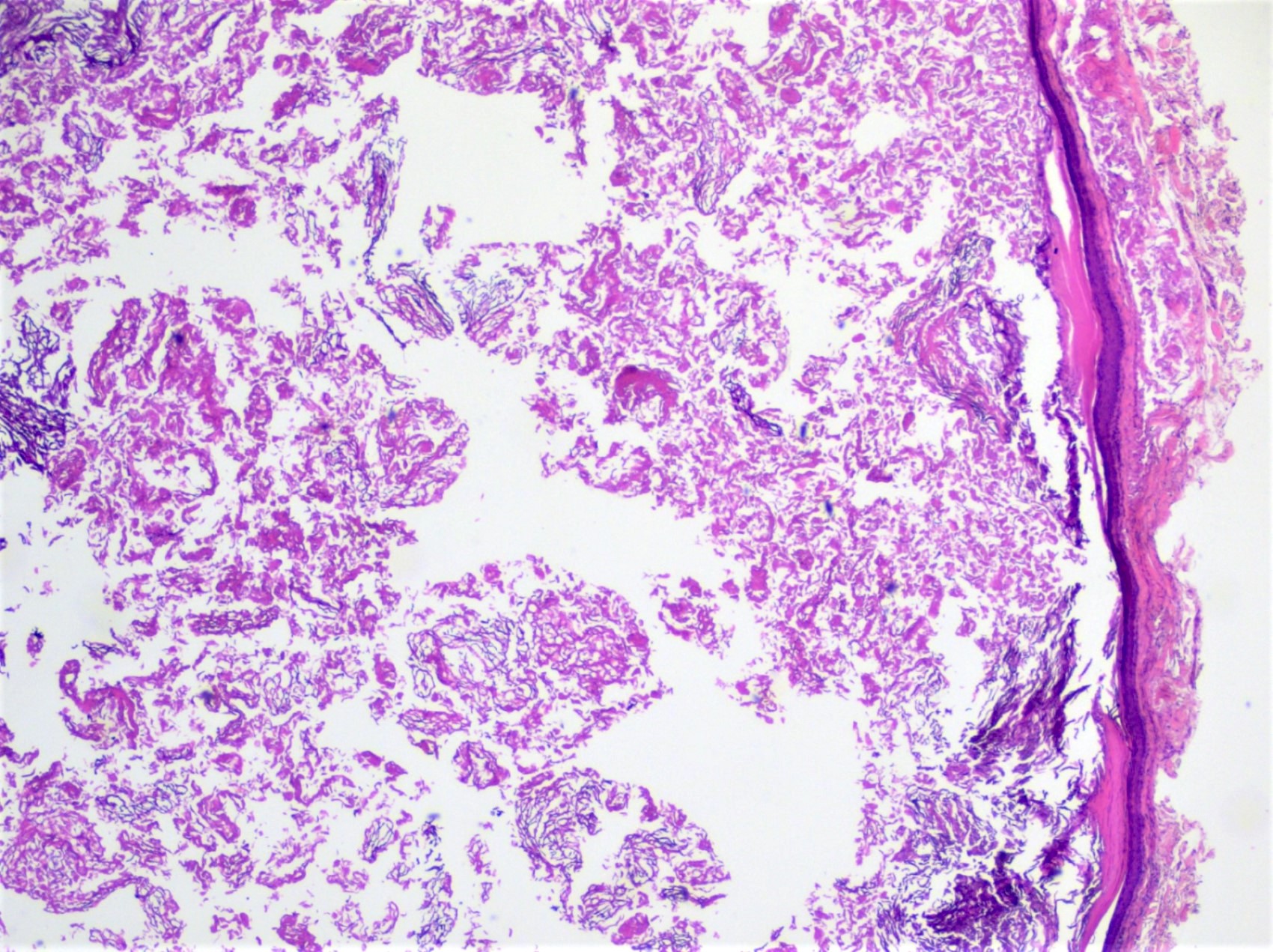
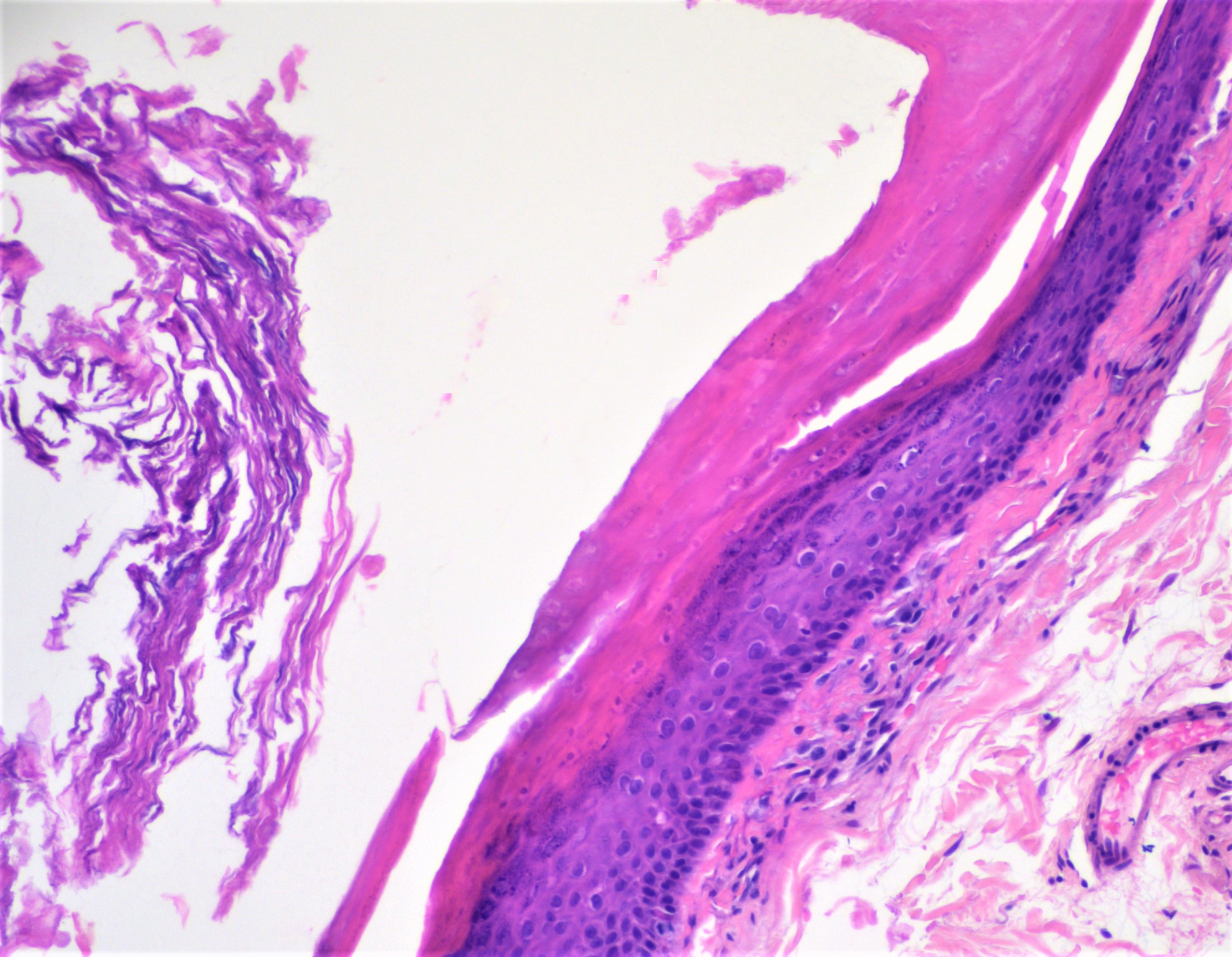
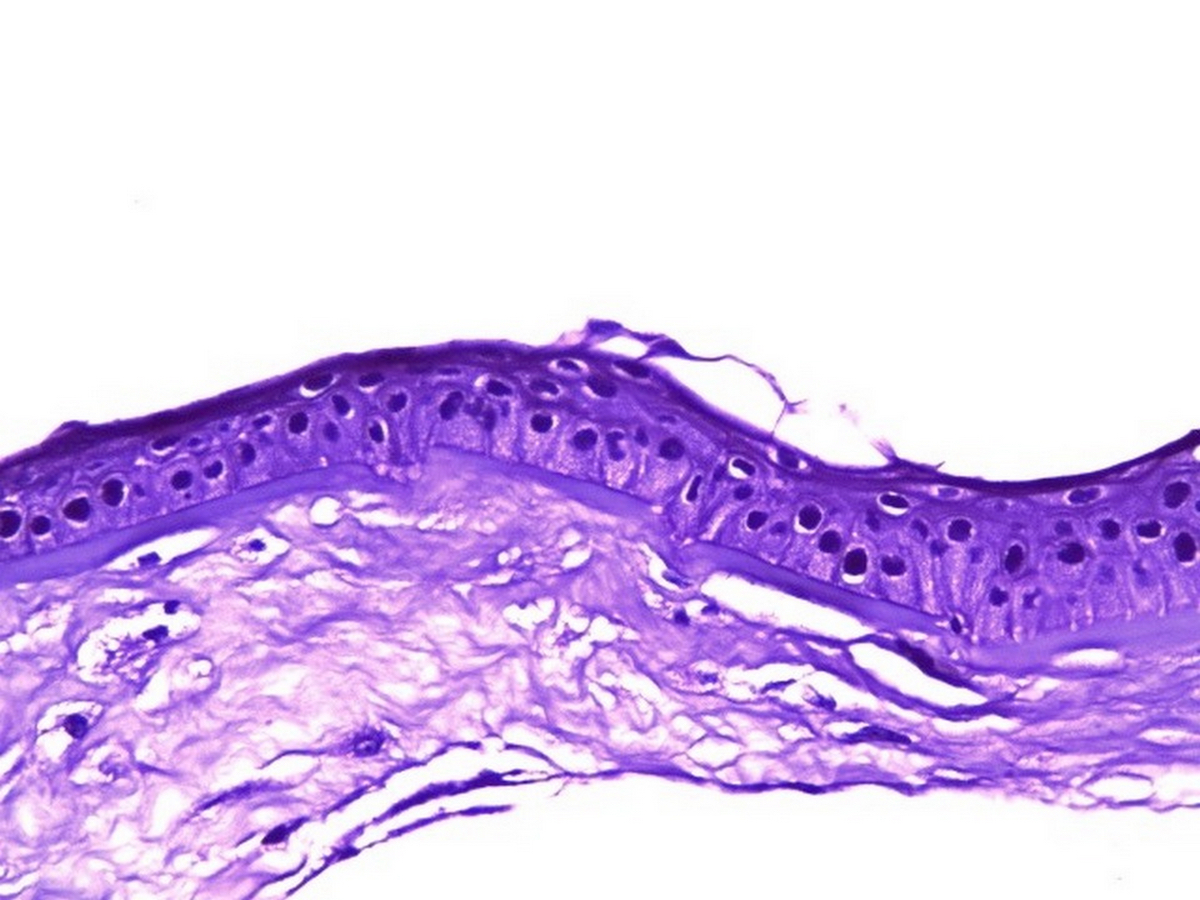
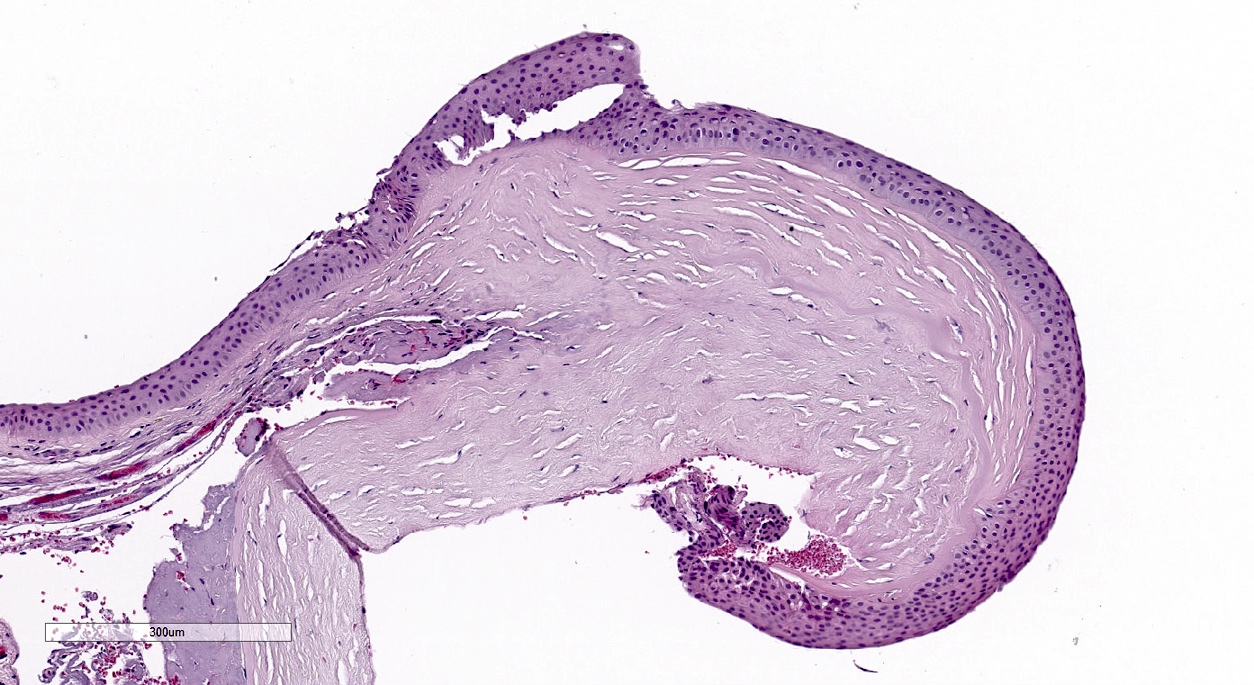
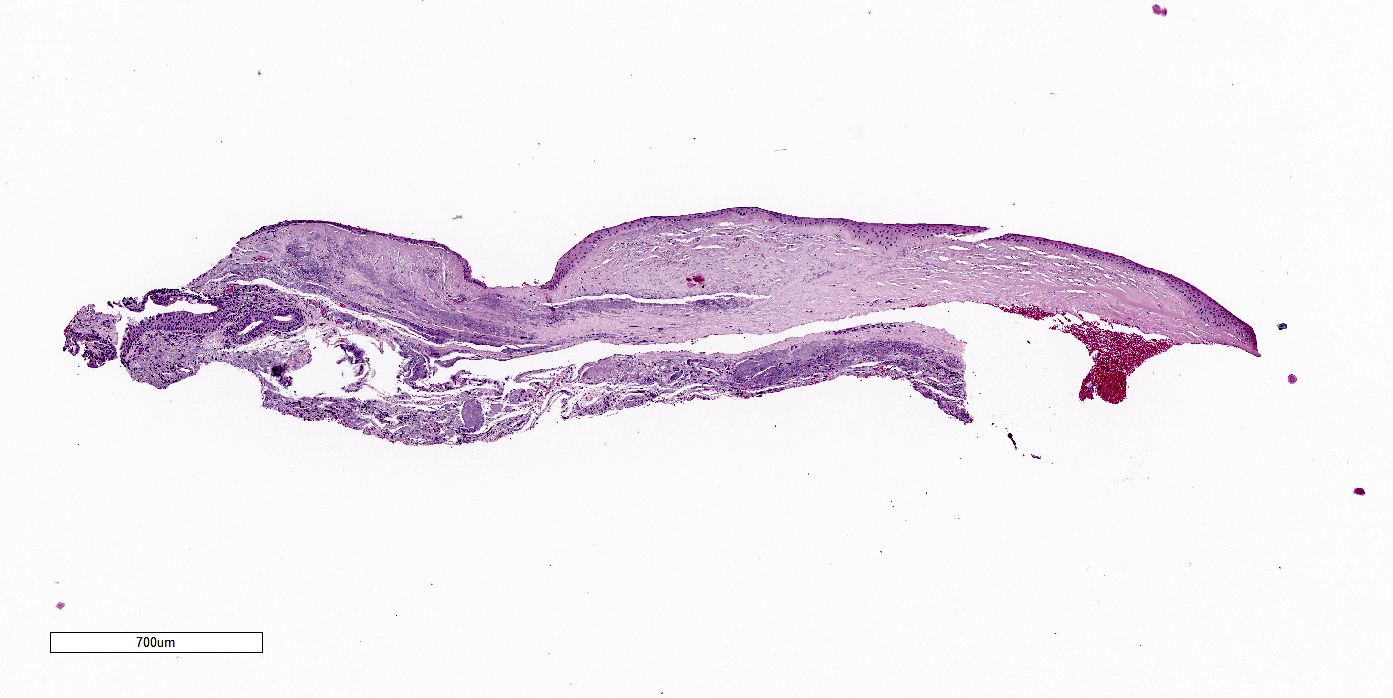
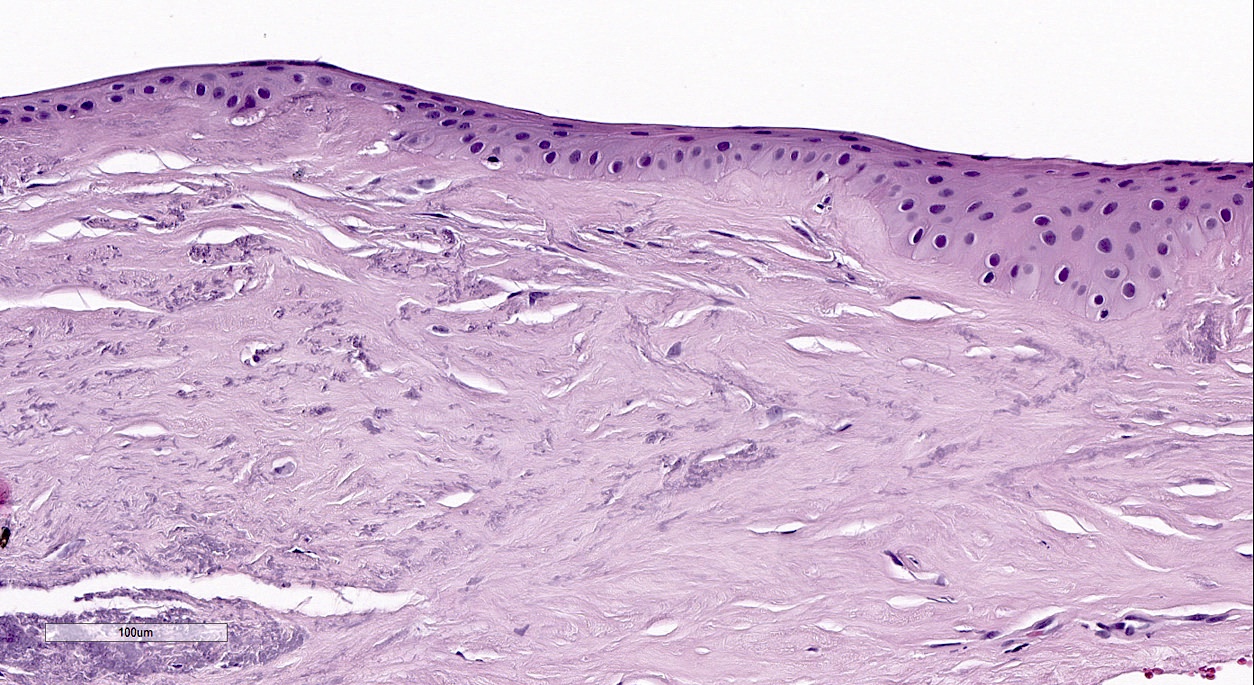
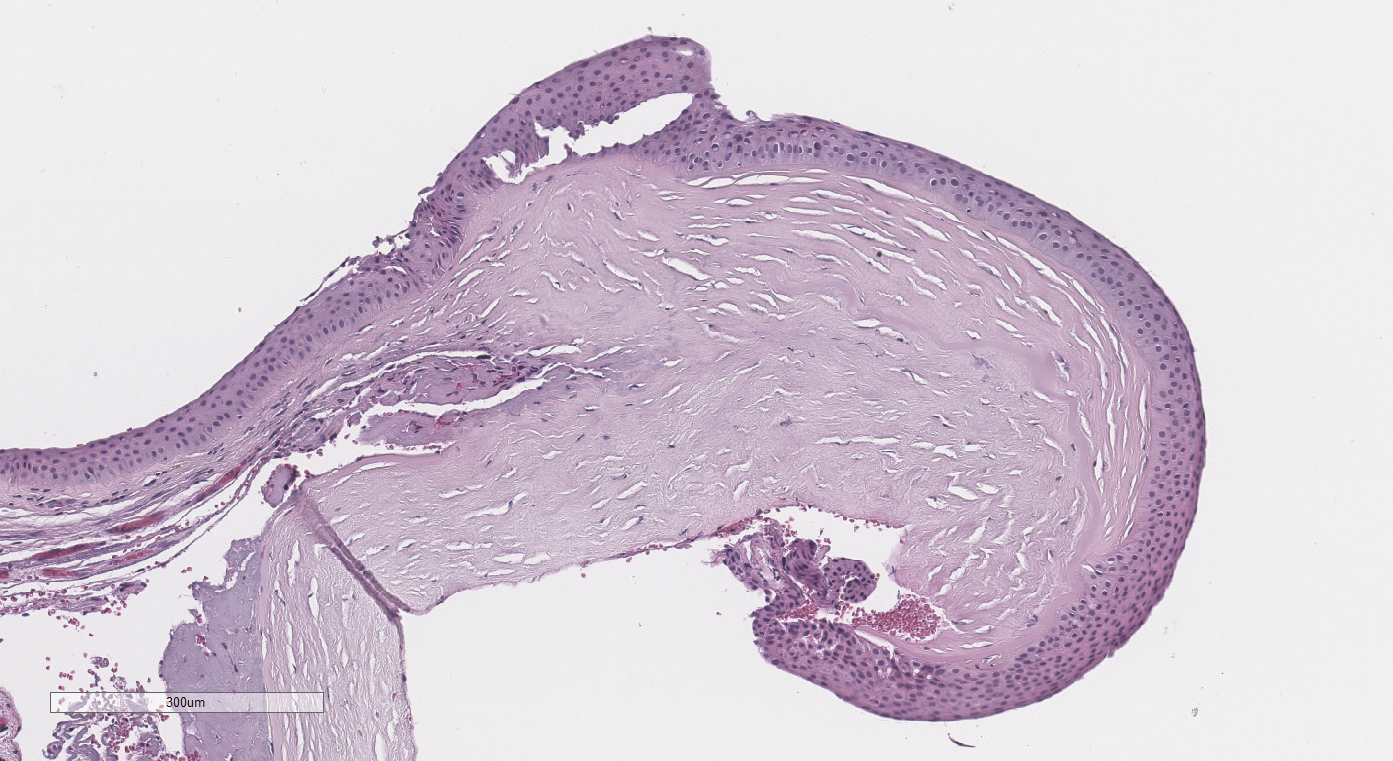
All layers of the cornea are believed to be affected
Characteristic structural changes include:
Epithelial basement membrane fragmentation and scarring
Breaks in the anterior limiting lamina (i.e. Bowman membrane)
Axial stromal thinning and scarring
Deposition of iron in the basal epithelial cells forms Fleischer rings
Breaks and folds close to the Descemet membrane form commonly seen striae and rarely, acute hydrops when aqueous humor enters corneal stroma
Keratoconic corneas have been shown to have:
Altered antioxidant enzymes, accumulations of cytotoxic reactive oxygen / nitrogen species, activated caspase pathways and mitochondrial DNA damage
Abnormal oxidative stress related properties that can induce activation of degradative enzymes and degradation of tissue inhibitors of metalloproteinases
Genomic deletion in the superoxide dismutase 1 (SOD1) gene has also been associated with the disease
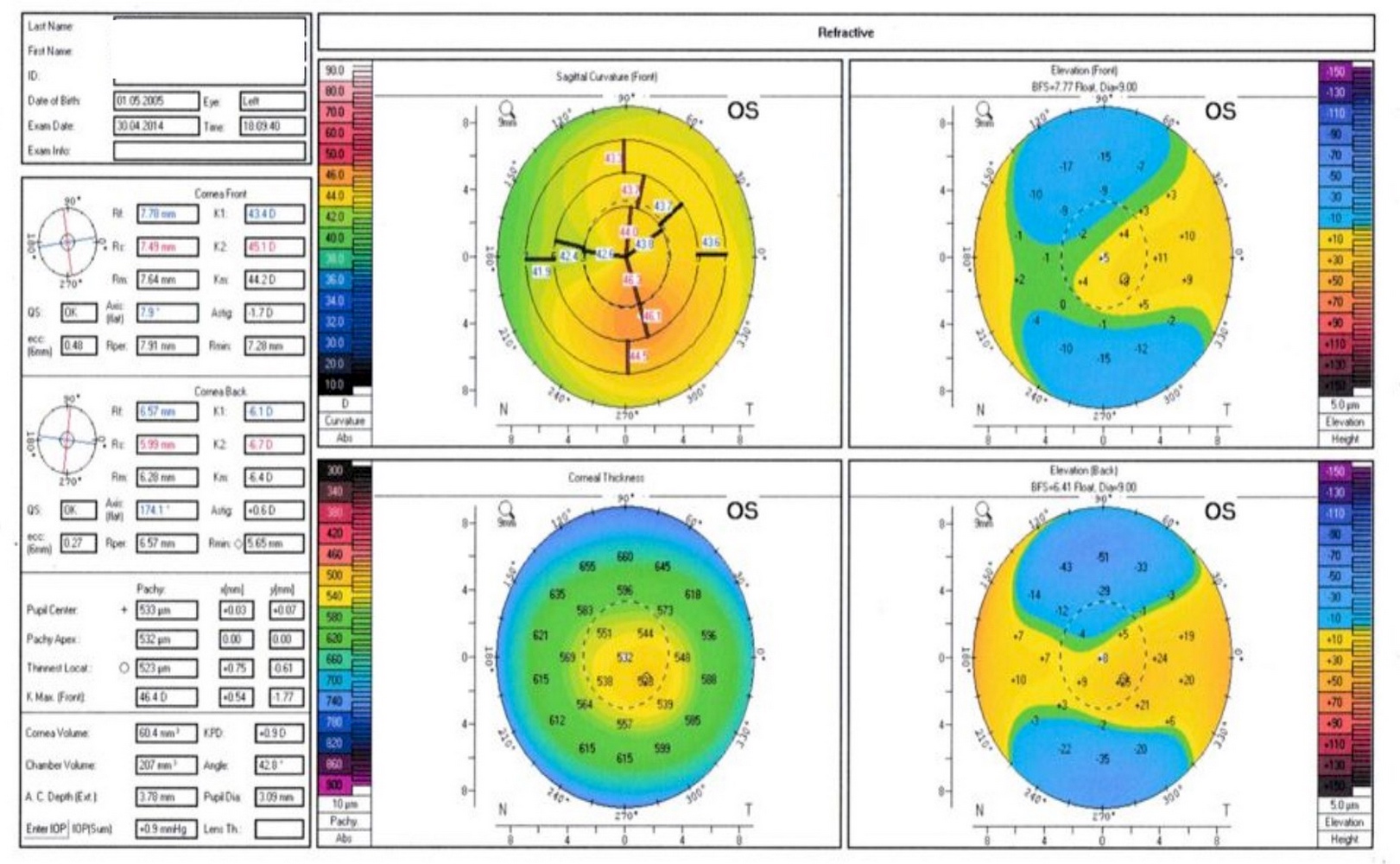
Eye examination with measuring corneal curvature using a manual keratometer
Slit lamp examination:
Fleischer ring: a ring of yellow-brown to olive-green pigmentation
Vogt striae: fine stress lines within the cornea caused by stretching and thinning
Munson sign: V shaped indentation in the lower eyelid when the person's gaze is directed downwards is highly pronounced
Handheld keratoscope: for noninvasive visualization of the surface of the cornea by projecting series of concentric rings of light onto the cornea
Corneal topography provides map indicating any distortions or scarring in the cornea, including steepening of curvature that is usually below the centerline of the eye; helps in detection at early stages
Severe vision threatening disorder that commonly indicates corneal transplantation
Case reports
17 year old girl, 21 year old man and 22 year old man with rare complications of stromal thinning up to Descemet membrane 3 - 6 years post corneal collagen crosslinking (CXL) (Indian J Ophthalmol 2020;68:224)
In vitro study of fixed, processed corneas with light microscopy shows 2 microscopic patterns:
Typical pattern (identified in > 80%): both stromal and central epithelial thinning with multiple Bowman layer breaks
Atypical pattern: lacks breaks in Bowman layer and has less thinning of the central epithelium
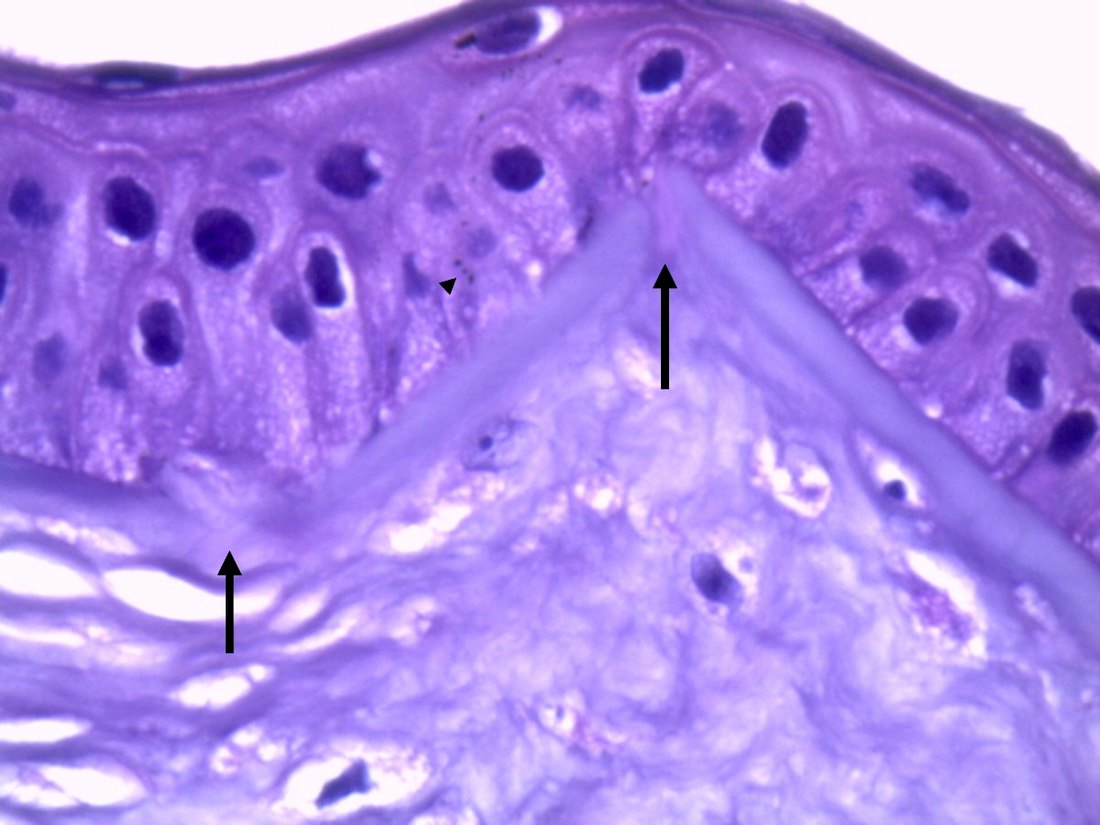
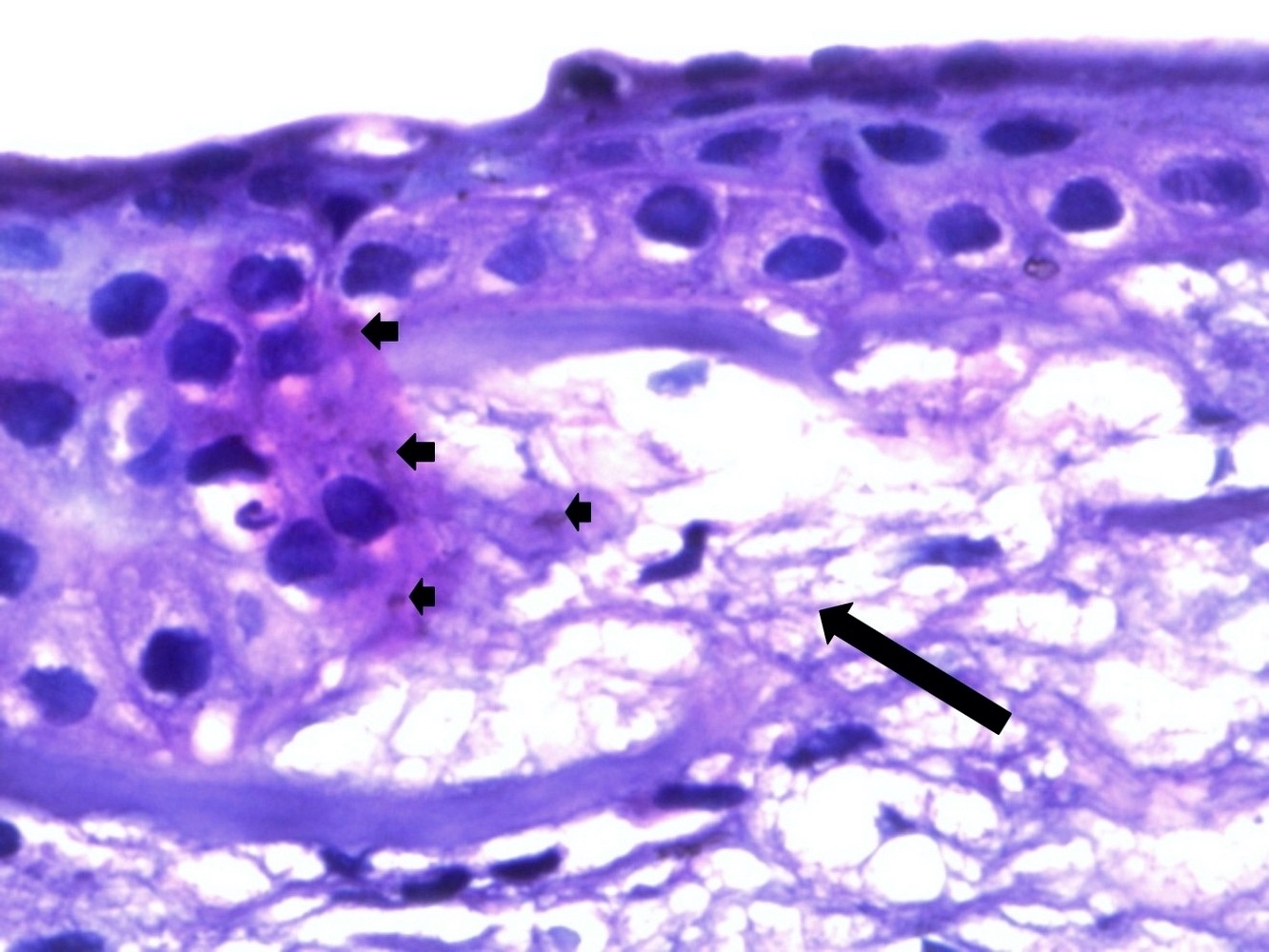
Alterations in different layers of cornea are:
Epithelium: cellular enlargement with irregular arrangement and apoptosis
Stroma: loss in collagenous lamella, reduction in keratocyte density with appearance of nonkeratocyte cells
Descemet membrane: morphological folds and irregularities; its rupture with entering of aqueous humor into corneal epithelium and stroma is a serious complication for keratoconus known as acute corneal hydrops
Endothelium: does not exhibit any changes during keratoconus progression
Using optical coherence tomography (OCT) for in vivo examining cornea, Sandali et al. proposed a classification system for keratoconus with 5 distinct stages (Ophthalmology 2013;120:2403):
Stage 1: thinner corneal epithelium and stroma at the conus than control
Stage 2: hyperreflective anomalies in Bowman layer are noticed with thickening epithelium and opaque stroma
Stage 3: increased epithelial thickening and stromal thinning with disruptions in Bowman layer
Stage 4: shows panstromal scarring
Stage 5: considered as the acute form of keratoconus (hydrops) with Descemet membrane rupture and total corneal scar
Comment: Sections in keratoconus cornea show stromal and central epithelial thinning with multiple Bowman layer breaks. Brown iron deposits are seen within basal layer of corneal epithelium.
Differential diagnosis
Pellucid marginal degeneration:
Often considered a variant of keratoconus
Corneal thinning occurs about 1 mm above the inferior limbus, resulting in advanced against the rule corneal astigmatism that may be observed on corneal topography or tomography
Terrien marginal corneal degeneration:
Slowly progressive noninflammatory, unilateral or asymmetrically bilateral peripheral corneal thinning
Associated with corneal neovascularization, opacification and lipid deposition
Keratoglobus:
Extremely rare corneal disease in which the entire cornea thins from limbus to limbus, sometimes to the point where spontaneous perforation becomes possible
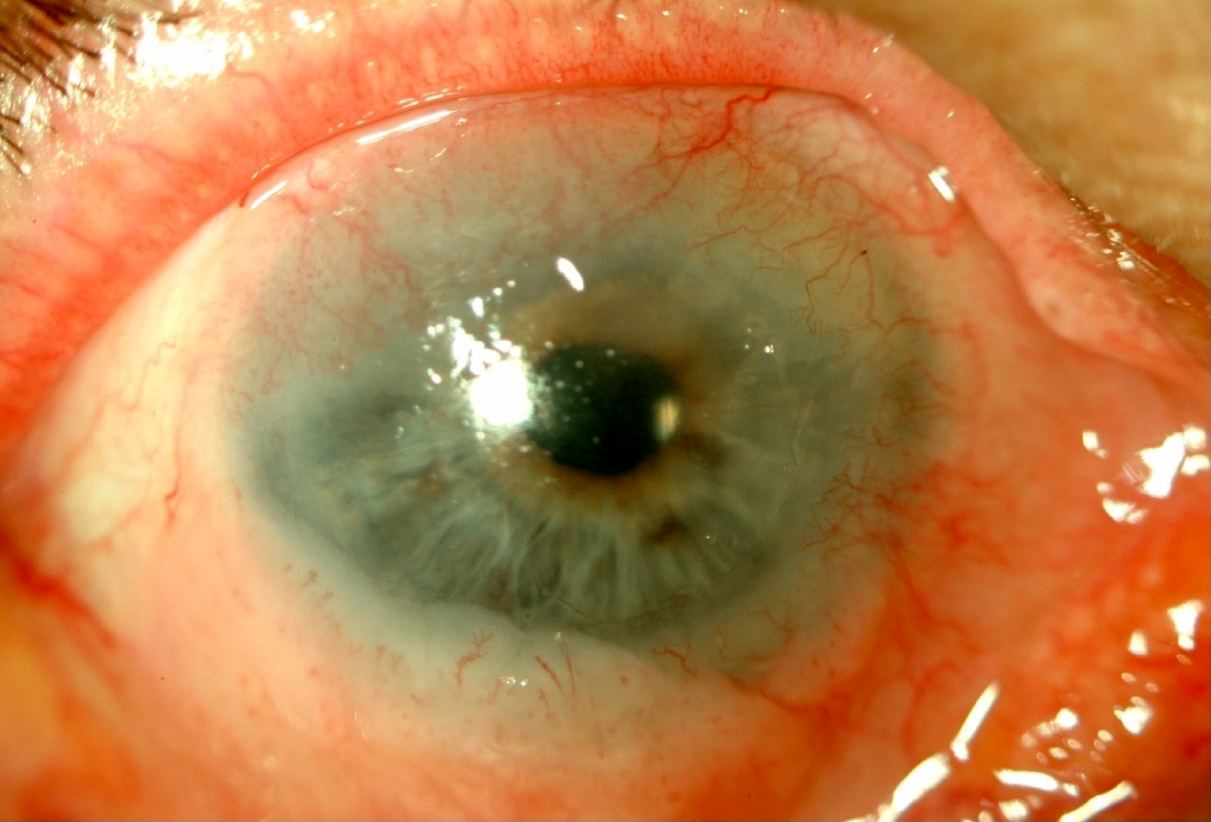
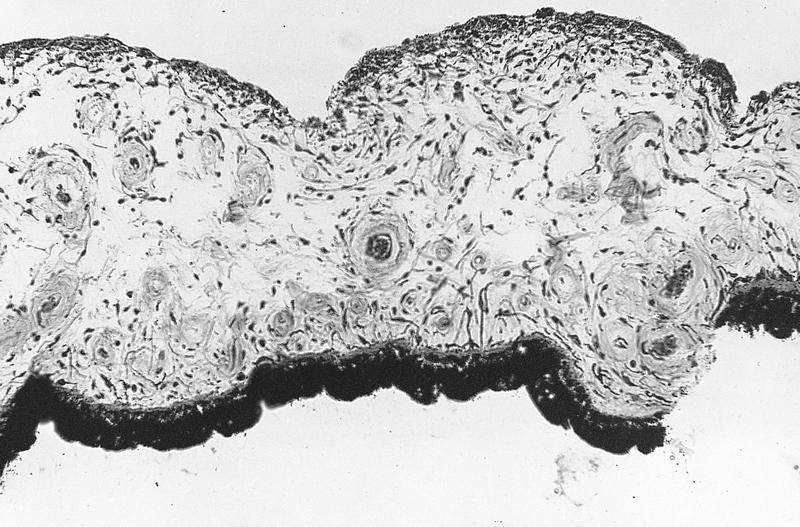
A 25 year old woman complaining of blurred vision and polyopia comes to the ophthalmology department. On examination, a bilateral V shaped indentation in the lower eyelids is apparent when she looks downwards and corneal topography shows steeping of corneal curvature. She undergoes keratoplasty and the removed cornea is sent for pathological examination. What is the most likely diagnosis?
Severe form of Vitamin A deficiency with diffuse, severe keratinization of mucous membrane epithelia, including corneal and conjunctiva epithelia (xerophthalmia)
Leading cause of blindness in developing world
Associated with secondary bacterial infection, corneal ulceration / necrosis, which causes corneal perforation and panophthalmitis
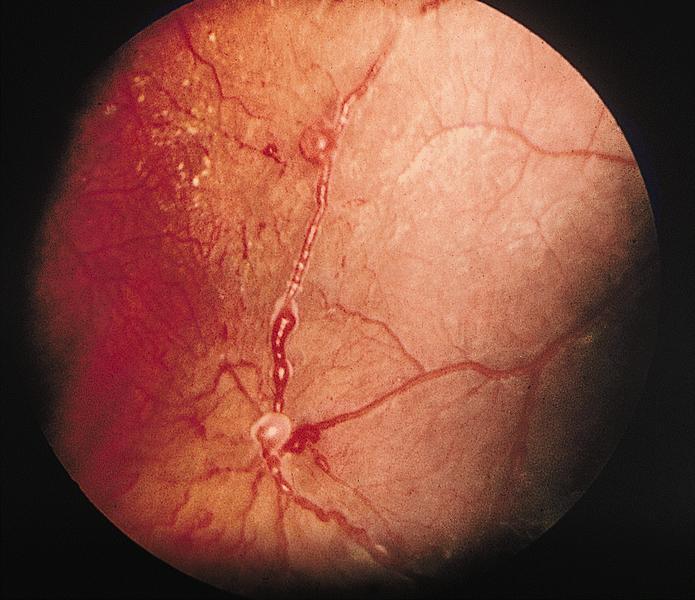
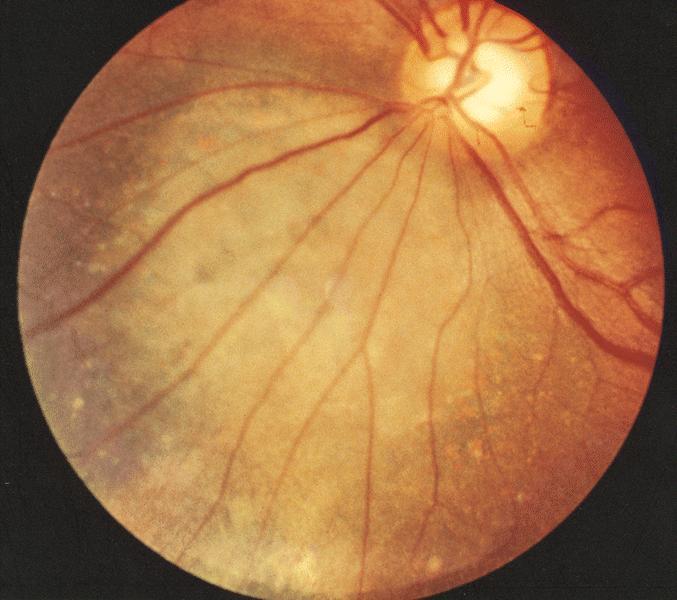
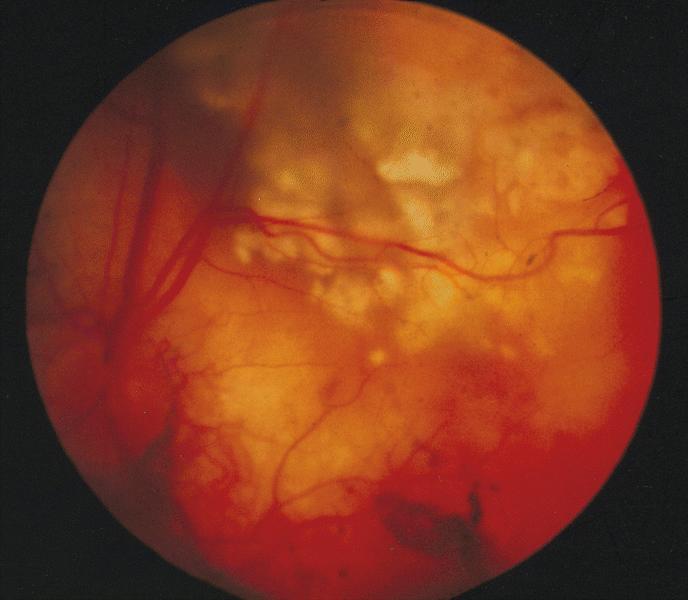
Bilateral condition that involves retina peripherally between ora serrata and equator
Associated with hyperpigmentation, condensed overlying vitreous forming adhesions to margins of lattice degeneration that may cause subsequent retinal detachment
Fundoscopy: circumferential area of involvement with small criss-crossing white lattice lines (thickened hyalinized blood vessels)
Microscopic (histologic) description
Atrophic and thinned retina with superficial gliosis
Thickened and hyalinized retinal vessels
Overlying liquefaction of vitreous with vitroretinal adhesions at edge of lattice lesion
Chronic relapsing pseudomembranous conjunctivitis with woody induration of eyelid and tarsal conjunctiva and pseudomembrane on tarsal conjunctiva
Also affects other mucosa
Terminology
"Ligneous" means resembling wood
Liesegang rings:
Rings of precipitated iron and calcium (a phenomenon of chemical systems) seen in conjunctiva and eyelid, associated with inflammation, necrosis, fibrosis or cysts
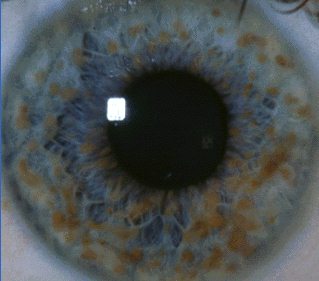
Associated with neurofibromatosis type 1, also familial angiolipomatosis, a benign condition with no malignant potential (Arch Pathol Lab Med 1999;123:946)
Clinical images
Images hosted on other servers:
Lisch nodules
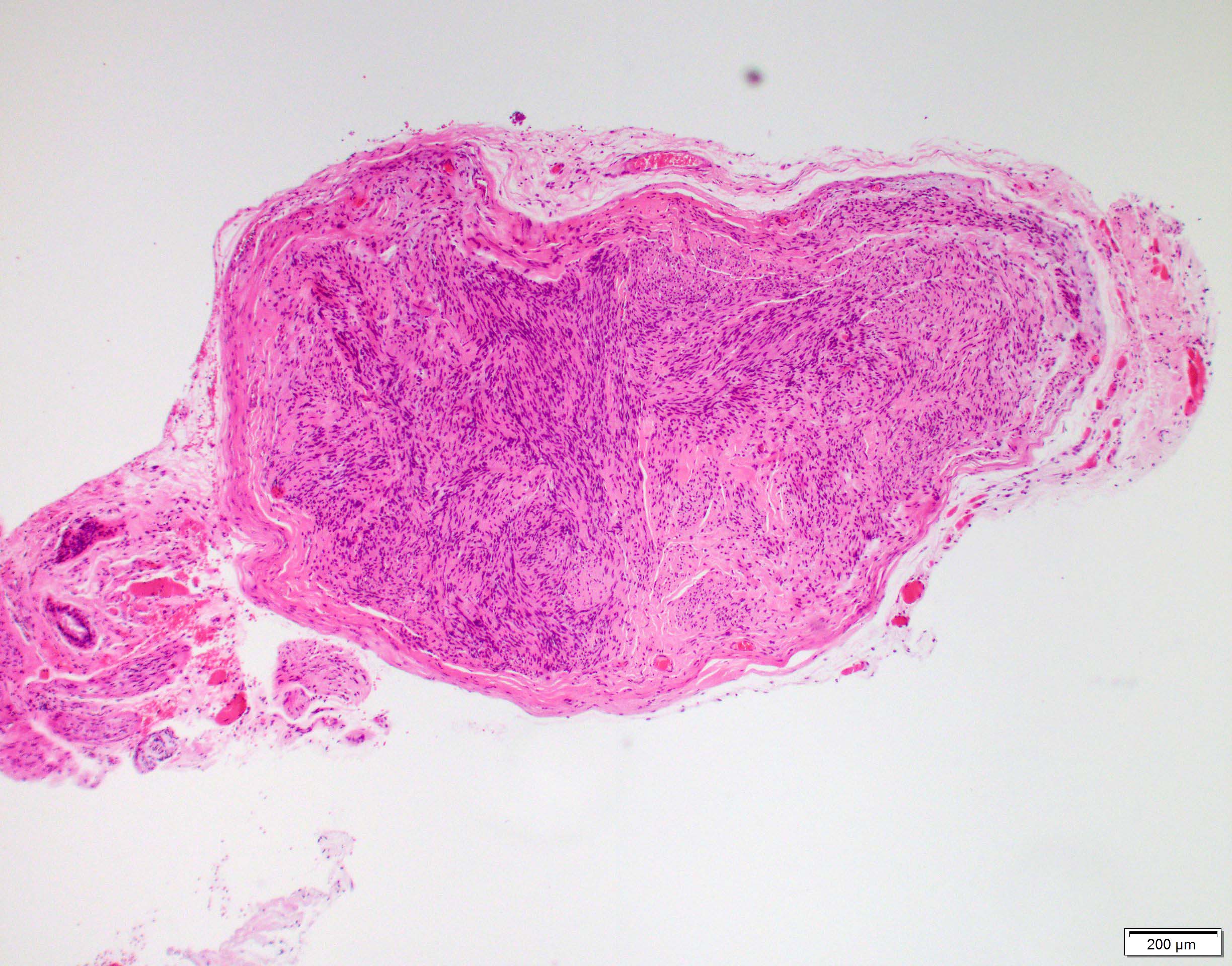
Microscopic (histologic) description
Dome shaped papules on anterior surface of iris consisting of aggregates of ovoid to round cells
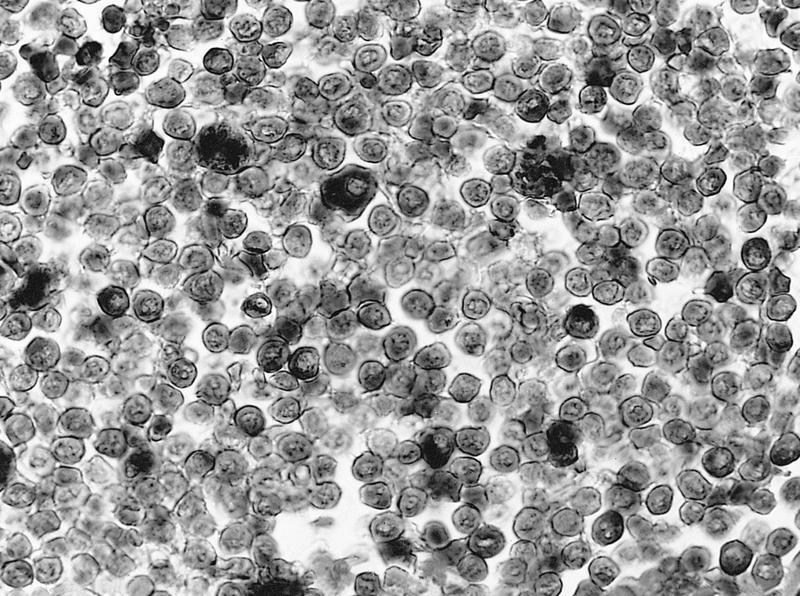
MALT: well differentiated, monoclonal small B lymphocytes, occasionally exhibits overt monocytoid cytology, prominent plasmacytic features or lymphoepithelial lesions (Am J Surg Pathol 2007;31:792)
Molecular / cytogenetics description
MALT may have t(14;18)(q32;q21) involving IgH and MALT1 genes
B cell clonality in 55% of MALT and 60% of diffuse large B cell lymphomas (Mod Pathol 2001;14:641)
Tumors composed of small lymphocytic proliferations confined to orbit are usually indolent and associated with long survival, even with minimal treatment
MALT lymphoma:
Uniform and monotonous proliferation of small lymphocytes infiltrating into orbital fat, blood vessels and nerves
May have plasmacytoid features with Dutcher bodies (intranuclear inclusions) and serum paraproteinemia
Light chain restriction
Radiology images
AFIP images
Homogeneous tumor
Case reports
5 year old girl with an angiocentric orbital lesion with an immature natural killer cell immunophenotype (Hum Pathol 2001;32:339)
Nasal-type NK/T cell lymphoma of the orbit with distant metastases (Hum Pathol 2003;34:290)
Clinical images
AFIP images
Burkitt lymphoma: bilateral
Lymphoplasmacytic lymphoma: bilateral
Microscopic (histologic) images
AFIP images
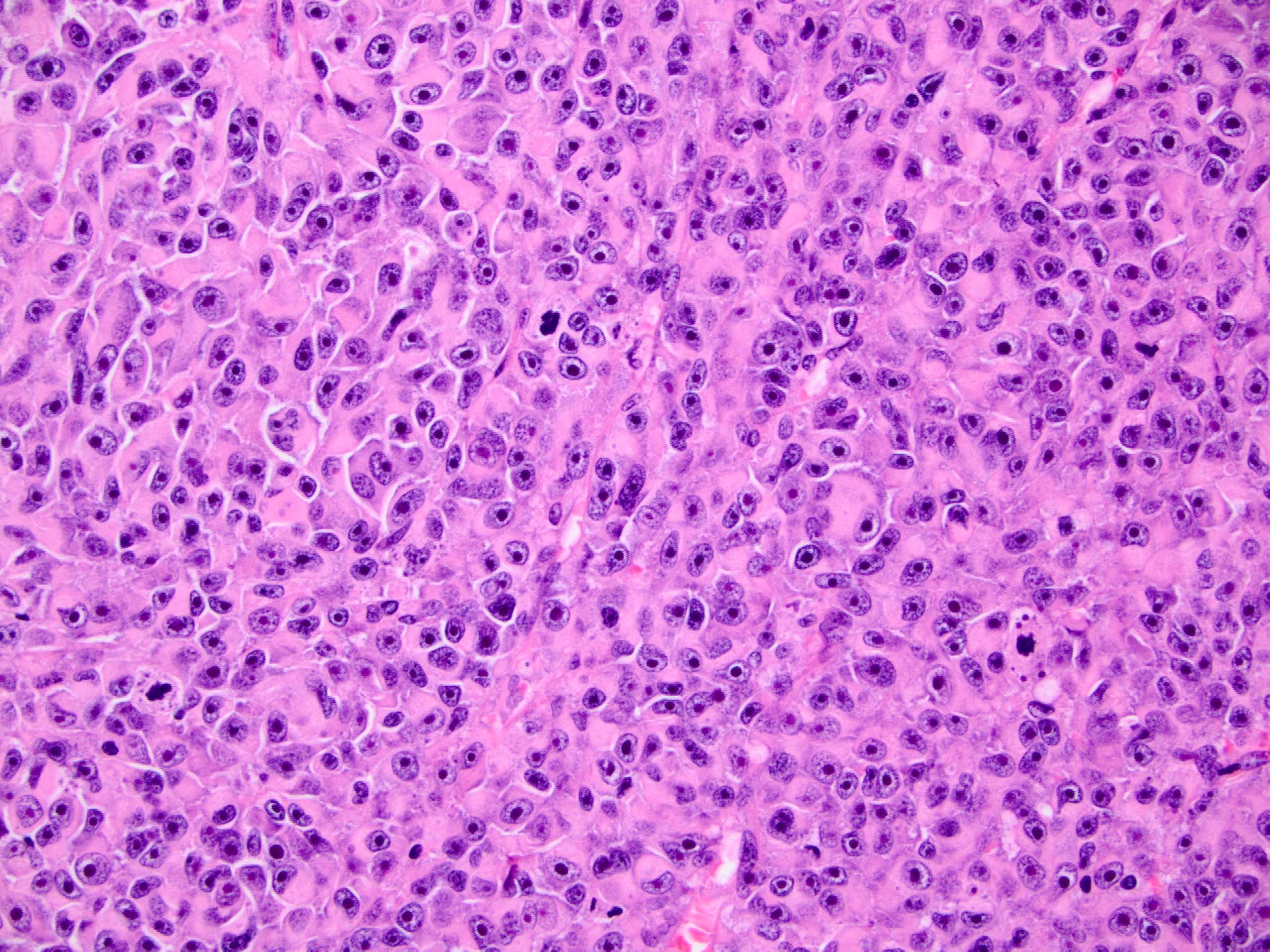
Low grade tumor
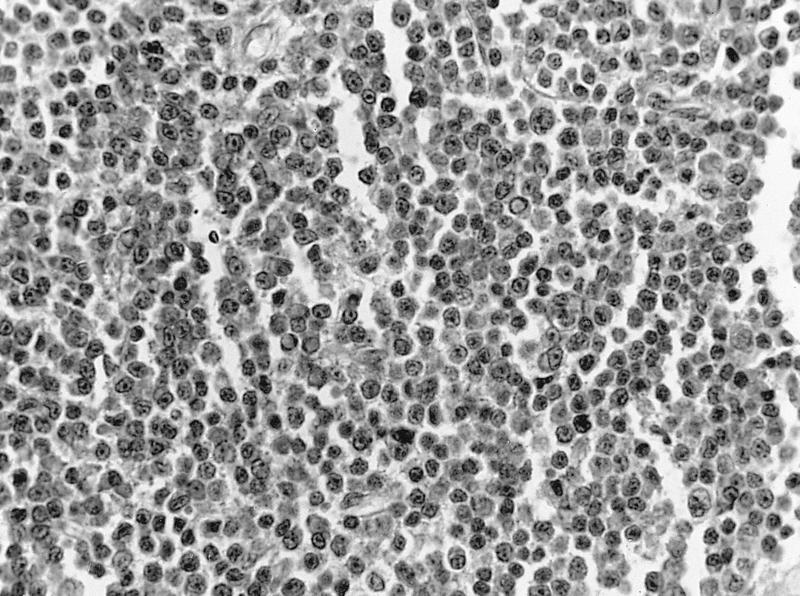
Well differentiated lymphoma
Irregularly shaped mass
Uniform population of well differentiated lymphocytes
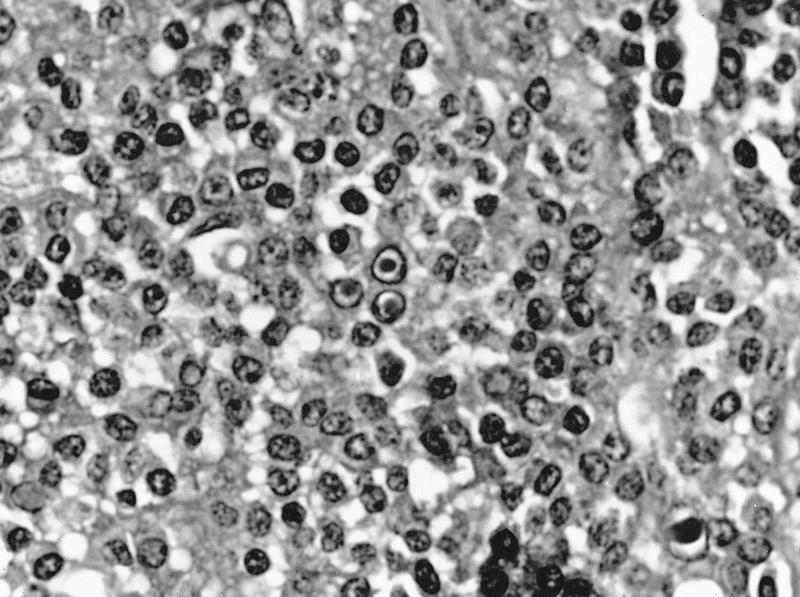
Small cleaved cells
Small population of T cells
Numerous CD20+ B cells
Burkitt lymphoma
Granulocytic leukemia - Leder stain positive
Lymphoplasmacytic lymphoma - lymphoid cells, some with plasmacytic differentiation
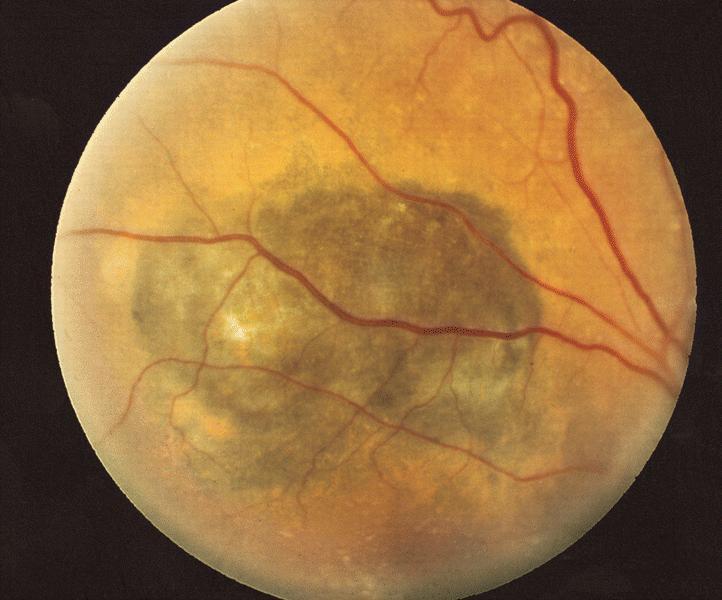
Age related (senile) macular degeneration is the most common cause of irreversible visual loss in US
Causes loss of central portion of vision
May be due to vascular disease in choriocapillaris and retinal pigment epithelium
Non-disciform (atrophic, dry type) causes slow, bilateral visual loss in elderly with atrophy and degeneration of retinal pigment epithelium and choriocapillaris; also drusen
Disciform (wet, exudative type) is associated with more severe and acute vision loss; often after non-disciform degenerative changes and due to hemorrhagic retinal detachment secondary to neovascularization, as vessels from choriocapillaris penetrate through Bruch membrane beneath the retinal pigment epithelium and leak fluid / blood which organizes into macular scars
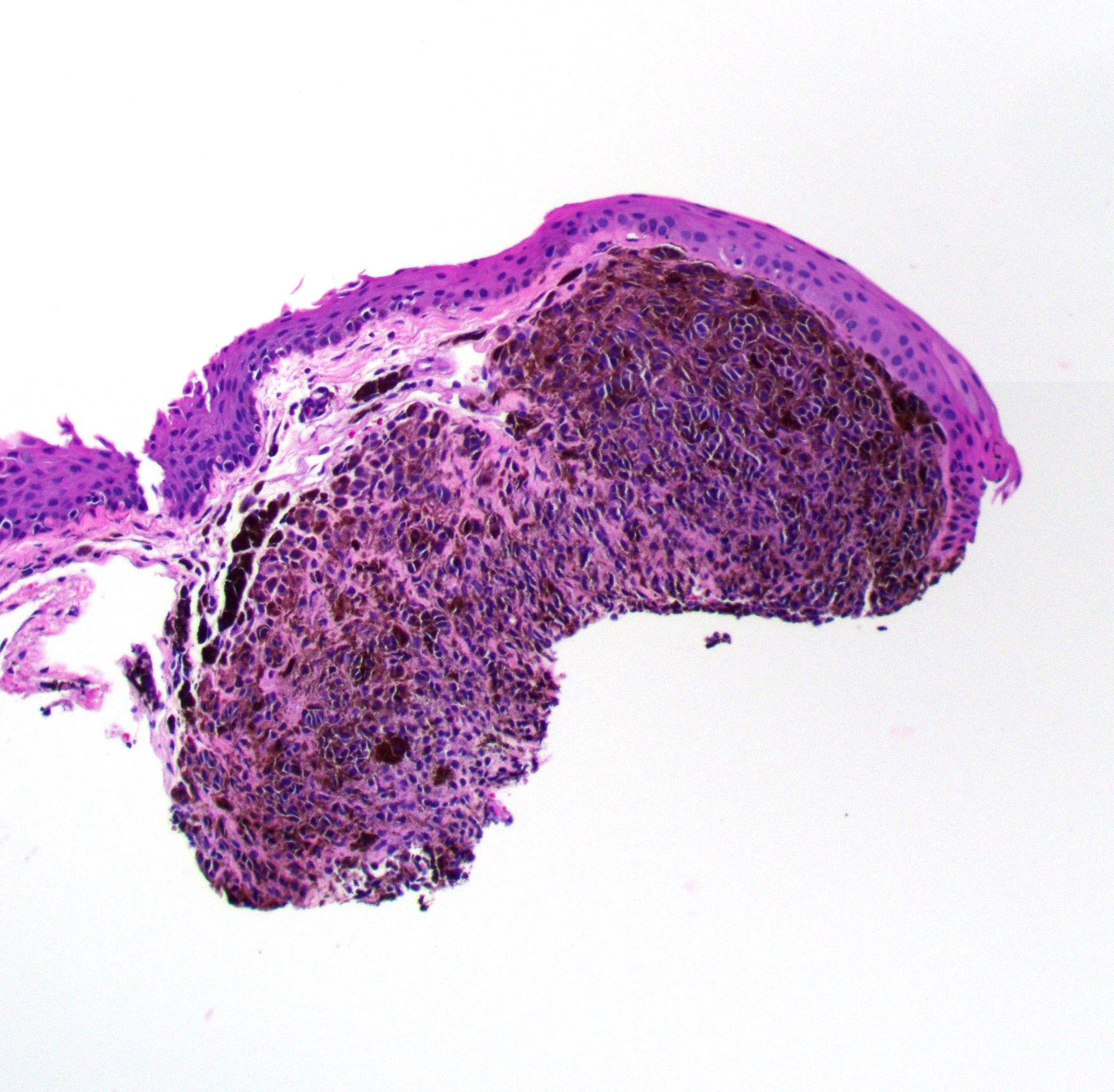
Pigmented lesion adjacent to primary acquired melanosis
Elevated melanotic nodule
Large neglected melanoma
Gross description
Vascular, pigmented, nodular
Gross images
AFIP images
Large heavily pigmented nodule covers cornea
Whole mount images
AFIP images
Exophytic tumor covers conjunctiva and cornea
Microscopic (histologic) description
Invasion of atypical melanocytes into epithelial connective tissue
Usually thin surface epithelium
Bizarre polygonal epithelioid cells with eosinophilic cytoplasm, large atypical nuclei, prominent eosinophilic nuclei
Also spindle cells, smaller cells, balloon cells containing lipid
Often lymphocytes at base or tumor margins
Report: presence of primary acquired melanosis or nevi, presence of pagetoid spread at edge of excision, atypical intraepithelial melanocytes, nevus cells; also tumor thickness from surface of lesion to deepest margin using calibrated micrometer
Microscopic (histologic) images
AFIP images
Nodular tumor at limbus
Anaplastic melanocytes within epithelial nests
Pigmented epithelioid cells with prominent nucleoli
Tumor size, location and cell type are the most important histopathologic prognostic factors but molecular testing plays an increasing clinical role in prognostication
Half of cases are asymptomatic and discovered on exam; half present with visual disturbance
Melanoma of iris: presents as elevated mass with variable pigmentation, often with distortion of pupil and prominent vessels
Melanoma of choroid: irregular, slate gray, solid, choroidal tumor that may extend through Bruch membrane into retina and vitreous producing retinal detachment, macular edema, choroidal hemorrhage; occasionally spreads along scleral canals into orbit, rarely invades optic nerve
Melanoma of ciliary body: may interfere with accommodation or cause localized cataract
Contributed by Lynn R. Schoenfield, M.D. and AFIP images
Fundoscopy
Ciliary body tumor
Orange pigment
Vessels over tumor are out of focus
Gross description
Small uveal melanomas may be difficult to distinguish from a nevus clinically; size criteria are used
Gross findings suspicious for melanoma include:
Orange pigment
Subretinal fluid
Tumor thickness > 2 mm
Low internal reflectivity on ultrasound examination
Gross images
Contributed by Lynn R. Schoenfield, M.D. and AFIP images
Uveal melanoma
Heavily pigmented choroidal tumor
Large transillumination defect
Ruptured Bruch membrane
Subretinal hemorrhage and total retinal detachment
Partially organized hemorrhage
Amelanotic tumor with retinal detachment
Extraocular extension
Iridocyclectomy
Tumor of ciliary body
Subluxation of lens
Extraocular extension
Vortex vein invasion
Whole mount images
AFIP images
Tightly packed melanoma cells
Tumor with exudative retinal detachment
Uveal tract diffuse tumor
Choroidal tumor with extraocular extension
Microscopic (histologic) description
There are 2 distinct cell types and most tumors contain a combination of the 2:
Spindle B cells: spindle shaped cells with large oval nuclei and distinct nucleoli
Epithelioid cells: large polygonal cells with atypical nuclei, 1 or more prominent nucleoli and sometimes intranuclear pseudoinclusions
Note that spindle A cells also exist, which are spindle shaped cells with slender nuclei that lack visible nucleoli; these are typically benign and are the melanocytes of uveal nevi
Excision if on eyelid margin to prevent infection of ocular surface
Gross description
Multiple raised skin nodules with umbilicated centers
Microscopic (histologic) description
Lobules of acanthotic epithelium that surround intracytoplasmic eosinophilic inclusion bodies (molluscum bodies) which become larger as they reach superficial epithelium
Excision or watchful waiting, only rarely transforms (1 per 150K)
Excise if newly acquired in adults, clinical growth, change in pigmentation, cosmetic reasons
Clinical images
Images hosted on other servers:
Balloon cell nevus
Variations in pigmentation
Variations in size
Variations in location
Variations in associated clinical features
Variations in clinical appearance
Change in nevus appearance over time
Gross description
Discrete, flat or slightly elevated; circumscribed, pink, yellow-tan, brown or nonpigmented, in interpalpebral zone near limbus; 1/3 are amelanotic
Microscopic (histologic) description
Nevomelanocytes organized into intraepithelial nests of oval cells (type A), sheets of oval to cuboidal cells (type B), and spindled cells in subepithelium (type C)
Often (50%) with solid and prominent cystic inclusions of conjunctival epithelium and chronic inflammatory infiltrate
May have atypical features and mitotic figures during growth periods
Compound (70 - 78%):
Most common, nevi cells in epithelium and subepithelial connective tissue
Cells have cysts lined by cuboidal and goblet cells and intranuclear inclusions
May have large pigmented cells with prominent basophilic nucleoli
Usually mixed inflammatory cells
Junctional (5%):
Contiguous nests of round / spindle melanocytes near basal cell region with oval nuclei, small nucleoli
Nucleoli may be basophilic and prominent but no atypia
Uncommon except in young children
Resembles primary acquired melanosis with atypia
Subepithelial (9%):
Nevus cells only in subepithelial connective tissue, no pigment, bland nuclei
May have clear cytoplasm due to lipid and central round nucleus (balloon cell nevus)
Microscopic (histologic) images
AFIP images
Compound nevus: variability in cytology
Atypical compound nevus melanocytes in junctional area
Cystic compound nevus:
Multiple large cysts
Nevoid cells
Sheets of melanocytes
Diffuse proliferation of melanocytes
Images hosted on other servers:
Benign nevus (B), amelanotic nevus (C)
Conjunctival nevi
Epithelioid cell (clonal or inverted) nevi
Granular cell nevus
Balloon cell:
Various images
Balloon cell compound nevus composed of large clear cells
Microscopic (histologic) description: proliferation of fibrovascular tissue under epithelium in anterior cornea
Ulceration
Due to any process that causes uneven distribution of the tear film across cornea
Bacterial ulcers often destroy epithelium and Bowman layer with variable stromal destruction; due to Staphylococcus aureus, Streptococcus pneumoniae, E. coli, Klebsiella, Pseudomonas
Complications include corneal perforation and scarring
Fungal ulcers occur 8 - 15 days after trauma, usually involving vegetative matter; due to Candida, Aspergillus, Cephalosporium, Fusarium
50% of cases involve conjunctiva, usually 10 years or more after onset of cutaneous or other mucosal disease; may occasionally demonstrate purely ocular disease
(Ophthalmology 1999;106:355)
Divide sample in two - one for formalin, one in transport media for immunofluorescent studies
Diagnosis
Compatible clinical picture plus linear deposition of IgA and IgG along conjunctival basal lamina or circulating anti-basement membrane antibodies
(Ophthalmology 2004;111:45)
Loss of function of optic nerve with gliosis, loss of capillaries and loss of axonal tissue
Due to damage from within the eye (optic neuritis, papilledema, glaucoma, retina-choroid lesions), to optic nerve or brain (trauma, tumor, demyelinating disorders, hydrocephalus) or congenital (Leber optic atrophy)
Gross description
White, pale disc
Microscopic (histologic) description
Loss of substance of optic nerve due to degeneration of myelin sheaths and axons
Rarely due to spontaneous rupture of swollen lens with a cataract
Granulomatous reaction may be due to acquired hypersensitivity to lens proteins
May coexist with sympathetic uveitis
Microscopic (histologic) description
Granulomatous inflammation surrounding area of lens perforation, with zonal pattern of central neutrophils around disintegrating lens fibers and peripheral macrophages, epithelioid cells and giant cells
Degenerative change of globe involving all tissues
Usually takes several years to develop
Often due to accidental or post-surgical trauma
Also found in eyes removed for blindness, pain, glaucoma, inflammation
Due to reduced production of aqueous humor causing reduced intraocular pressure (hypotony) and shrinkage of globe
Also due to organization of inflammatory exudate
Degenerative changes and degree of shrinkage are variable in different tissues
May be calcification and ossification with bone marrow
Note: must decalcify globe
Microscopic (histologic) description
Typically disorganization of intraocular contents, opaque media, corneal scars, exudate in anterior and posterior chambers, advanced cataracts, destruction of vitreous, scleral thickening, cyclitic membrane extends from one ciliary body behind the lens to the other ciliary body, complete detachment of retina; also ossification or bone formation
Usually histology does not disclose initial condition leading to phthisis bulbi
Occasionally occult melanoma or lymphoma is found
Microscopic (histologic) images
AFIP images
Regressed retinoblastoma
Disorganized intraocular contents with ossification and calcification
May cause uneven distribution of tear film, leading to focal dehydration and saucer like depression in corneal tissue ("dellen"); associated with conjunctivochalasis (Acta Ophthalmol 2012;90:773) and contact lens induced subconjunctial hemorrhage (Am J Ophthalmol 2010;150:656)
Treatment
Excision for cosmetic reasons or to remove mild irritation; otherwise no treatment
Gross description
Elevated yellow lesion (due to solar elastosis) in bulbar conjunctiva in interpalpebral region near nasal limbus; conjunctiva is atrophic or thickened
Microscopic (histologic) description
Band of subepithelial actinic elastosis with variable hyalinization and calcification
May have acanthosis or dyskeratosis resembling carcinoma
May have foreign body giant cell reaction around elastotic material (actinic granuloma)
Microscopic (histologic) images
Images hosted on other servers:
Lamina propria shows
basophilic elastosis
and hyalinization
Type of primary endothelial dystrophy or endothelial decompensation
Most common endothelial dystrophy and common indication for corneal transplantation in US
Damage (decompensation) to endothelium, which normally pumps out fluid from corneal stroma, leads to chronic edema of stroma and epithelium, pain from rupture of epithelial bullae, eventually diffuse scarring and reduced vision
Women ages 50+
Some cases are autosomal dominant
Some cases are due to mutation in COL8A2 at 1p34.3-p32.3
Gross description
Bilateral
Often asymmetric
Microscopic (histologic) description
Corneal edema and cysts due to endothelial damage with paucity of endothelial cells and thickening of Descemet membrane
Epithelium is separated from Bowman layer
Papillary excrescences (guttae) in middle of cornea (must bisect cornea at equator and embed at equator to see)
If severe, may see edema of basal cells, bullae formation and pannus formation (fibrovascular ingrowth between Bowman layer and epithelium)
Differential diagnosis
Interstitial keratitis: inconspicuous ghost vessels in most posterior corneal stroma
Primary choroidal lymphoma (pending)
[Pending]
Primary vitreoretinal large B cell lymphoma (pending)
Frequent, degenerative ocular surface lesion, characterized by invasion of the cornea by a fibrovascular tissue originating from the bulbar conjunctiva (Surv Ophthalmol 2018;63:719)
Most frequent in the interpalpebral area, nasal side
Thought to be UV light associated; not associated with human papillomavirus (HPV) (Br J Ophthalmol 200;91:1016)
Develops from limbal epithelial progenitors; may be a stem cell disorder with possible premalignant features (Am J Pathol 2011;178:817)
Essential features
Frequent, degenerative ocular surface lesion
Similar to pinguecula but with corneal infiltration
UV related
Can masquerade as a neoplastic process
Fibrovascular connective tissue that migrates to cornea
Prevalence of 12%, with a geographic variation of 53% in China and 0.07% in Saudi Arabia (Surv Ophthalmol 2018;63:719)
Sites
Corneoconjunctival limbus and cornea
Pathophysiology
There are many hypotheses but its pathogenesis is still unknown
Environmental factors have been suggested, due to high prevalence in hot and dry climates
UV radiation has been proposed, due to the similarity with the histopathology of solar elastosis
Other proposed hypotheses are corneal stem cell deficiency, inflammation, angiogenic disregulation, ultraviolet albedo (reflected, scattered light) in the anterior eye (Br J Ophthalmol 1993;77:734)
Etiology
Older age, M > F, rurality, outdoor activities, prolonged exposure to UV light and alcohol consumption are known risk factors (Surv Ophthalmol 2018;63:719)
Clinical features
Causes significant changes in corneal refractive status that increases with grade of pterygia (Indian J Ophthalmol 2007;55:383)
High prevalence (18%) in those older than 40 living at high altitude in Mongolia (Eye (Lond) 2009;23:421)
Clinically, may resemble ocular surface squamous neoplasia or melanoma
65 year old man with recurrent lesion treated with small incision lenticule extraction (J Int Med Res 2018;46:2474)
Treatment
Treatment for cosmetic reasons, visual impairment, recurrent inflammation, mild irritation
Medical therapy:
Symptoms can be alleviated using over the counter vasoconstrictor drops and lubricating agents such as ointments or drops
Corneal extension should be followed to determine the growth ratio to the visual axis
Surgery:
Excision with adjunctive therapies (radiotherapy, mitomycin C or fluorouracil [5FU]): low recurrence and fast but can have complication secondary to the use of the adjunctive
agents
Conjunctival flap or graft: considered the gold standard with recurrence as low as 1/1,000 with autografts; it is a lengthier procedure and technically more difficult
Epithelial dysplasia; can coexist and be overlooked
Board review style question #1
Which finding in the sample seen above is characteristic of pterygium?
Bowman layer fragmentation
Elastosis of the lamina propria with corneal invasion
Epithelial atrophy with goblet cell loss
Neovascularization of the stroma
Board review style answer #1
B. Elastosis of the lamina propria with corneal invasion. Elastosis is the key morphological finding in pterygia. The infiltration of the corneal stroma is important to be able to differentiate it from a pinguecula when there is no clinical information. Epithelial atrophy with goblet cell loss is nonspecific and can be seen in dry eye syndrome or superior limbic
keratoconjunctivitis. Neovascularization is present in most of pterygia but is also seen in many other
conjunctival inflammatory processes. Fragmentation of the Bowman layer may be present but is
also seen in keratoconus and other chronic keratitis.
Which of the following is the most important risk factor of pterygium?
Chlamydia psittaci infection
Human papillomavirus
Sun exposure
Tobacco and alcohol consumption
Board review style answer #2
C. Sun exposure is the most important risk factor. Human papillomavirus is not strongly associated with either pterygium or conjunctival intraepithelial neoplasia. Chlamydia psittaci has been associated with some MALT lymphomas but has not been associated with pterygium. Alcohol and tobacco have been listed as possible predisposing factors but are not as prevalent as sun exposure.
Retinoblastoma is the most common intraocular malignancy in children characterized by hyperchromatic small round blue cells with scant cytoplasm arranged in sheets, nests and trabeculae
Prognosis dependent on many factors; histopathological evaluation determines metastatic risk, including tumor invasion into anterior chamber, significant invasion into choroid (at least 3 mm) and postlaminar optic nerve invasion
Retinoma / retinocytoma is the benign form of retinoblastoma
Can be trilateral (pineoblastoma) or very rarely quadrilateral (pineoblastoma and suprasellar primitive neuroectodermal tumor) (Pediatr Blood Cancer 2010;55:570)
Pathophysiology
Loss or inactivation of both alleles of the retinoblastoma 1 gene (RB1)
Tumor suppressor gene located at 13q14.2 locus
Encodes RB1 protein
Knudson 2 hit hypothesis
Results from 2 separate mutations:
First mutation is somatic or germline
Second mutation is somatic
Germline mutations in RB1 lead to inherited / familial retinoblastoma
An 8 year old girl had an enucleation that showed a white, chalky intraocular tumor. A histologic image is shown above. Which of the following statements is true regarding this entity?
Enucleation remains the best initial treatment
Involvement of the optic nerve is not considered a significant prognostic factor
Majority of these tumors have MYCN mutations
Recommended initial treatment paradigm is chemoreduction
Strabismus is never seen in patients with this tumor
Board review style answer #1
D. Recommended initial treatment paradigm is chemoreduction
Retinoblastomas can occur both in sporadic and familial forms. Which of the following features is more indicative of a sporadic tumor?
Bilateral retinoblastomas
Development of subsequent melanoma or osteosarcoma
Early age of onset
Germline mutation of Rb gene
Late age of onset
Board review style answer #2
E. Late age of onset. Familial tumors result from germline mutations in the Rb gene and are more likely to be bilateral or trilateral. They have an early age of onset and are prone to the development of other malignancies, including osteosarcoma, melanoma, sarcoma and breast cancer.
Occurs in premature infants given oxygen therapy; related to level and duration of oxygen, degree of prematurity at birth and status as carrier for defect in Norrie disease gene
Immature vessels of premature infants are damaged by high or even physiologic oxygen; rarely occurs in term infants
Pathophysiology
Oxygen therapy causes vasoconstriction and obliteration of immature retinal vessels in lateral (temporal) retina which causes ischemia and failure of retina to vascularize
Then vasoproliferative phase and angiogenesis
Vessels grow into vitreous or leak serum or fluid, 25% have associated scarring which causes retinal detachment
Defined as formation of cavernous spaces in retrolaminar portion of proximal optic nerve due to focal loss of myelin and axons and accumulation of hyaluronic acid
Present in < 0.1% of eyes at autopsy; 80% are women, mean age 88 years (range 54 - 103 years)
Associated with severe vascular anomalies (75%), glaucoma (24%)
Grading of cavernous degeneration: I - clearly present but < 10% of diameter of optic nerve at point of most severe involvement; II - 10 - 25%; III - 50 - 75%; IV - > 75%
Begins at periphery of cornea, extends posteriorly to optic nerve
Relatively rigid; protects eye from trauma and maintains intraocular pressure
Visible anteriorly under transparent conjunctiva; white in adults
Thickness varies; 0.3 mm at insertion of rectus muscles, 0.8 mm at limbus and 1.0 mm at insertion of optic nerve
Weakly attached to underlying choroid by thin collagen fibers
Heals poorly due to few blood vessels or fibroblasts
Aging related changes include calcification between collagen fibers, senile scleral plaques
Composed of episclera, stroma and lamina fusca
Episclera: most superficial part of sclera, located between fibrous structure that envelopes the globe (Tenon capsule) and scleral stroma; composed of loose collagen fibers and fibroblasts with numerous vessels, occasional melanocytes and mononuclear white blood cells
Stroma: largest component of sclera, randomly arranged bands of collagen with occasional elastic fibers and fibroblasts; minimal blood vessels except in perforating emissiary canals, accompanied by nerves and scattered melanocytes; rarely contains a prominent nerve (nerve loop of Axenfeld) in an emissiarial canal near limbus, which may mimic a neurofibroma; anterior ciliary arteries perforate sclera near insertion of rectus muscles, posterior ciliary arteries pass through sclera near optic nerve; vortex veins exit sclera posterior to equator of eye
Lamina fusca: innermost layer of sclera with loose collagen fibers, fibroblasts and scattered melanocytes
Rarely metastasize to lymph nodes (more common if large or multiple recurrences)
Clinical images
Images hosted on other servers:
Nodular tumor with prominent vascularity at limbus
Gross description
Papillary or exophytic gray-white mass, often at limbus
Occasionally jet black resembling melanoma (in heavily pigmented individuals)
Surrounded by inflamed conjunctiva
Gross images
AFIP images
Large limbal tumor invades anterior chamber
Tumor has destroyed eye and invaded orbit
Microscopic (histologic) description
Atypia throughout full thickness of epithelium (conjunctival intraepithelial neoplasia) with individual tumor cells or nests extending into underlying stroma
Dense sclera usually limits deepest margins
Epithelium may be keratinized
Cells have eosinophilic or clear cytoplasm, intercellular bridges, dyskeratosis, coarse chromatin, prominent nucleoli
Dense lymphoplasmacytic infiltrate is present with germinal center formation
Epithelium is thin
Board review style question #1
What do the intraepithelial clear spaces in this image represent?
Atypical nonpigmented melanocytes
Goblet cells
Procesing artifact classically in this lesions
Sebaceous cells in pagetoid spread
Board review style answer #1
B. Goblet cells are classically observed in these cases. Sometimes they are very numerous and they are characteristically slightly basophilic. Pagetoid spread of sebaceous cells is represented by malignant cells with atypical nuclei and optically empty vacuolated cytoplasm. Amelanotic spread of melanoma cells must show malignant features of the nuclei and is usually centrally located. An artifact will not be structured as observed in the cells here.
Squamous papilloma is more frequently associated with
Herpex simplex virus
Human papillomavirus 6 and 11
Human papillomavirus 16 and 18
Sun exposure
Board review style answer #2
B. The most frequent associations are with HPV 6 and 11. Sun exposure is an important association in limbal papillomas but is less frequent than HPV. Herpes virus is not associated with squamous papilloma. HPV 16 and 18 are associated with ocular surface squamous neoplasia.
Not applicable to uveal melanomas with secondary involvement of conjunctiva
Essential features
AJCC 7th edition staging was sunset on December 31, 2017; as of January 1, 2018, use of the 8th edition is mandatory
Terminology
Bulbar conjunctiva is the mucosal epithelium lining the surface of the eye
Palpebral conjunctiva is the mucosal epithelium lining the inner surface of the eyelid
Caruncle is the fleshy protuberance in the inner corner (canthus) of the eye
Fornix (plural fornices) is the loose fold of conjunctiva at the reflection from the bulbar to the palpebral conjunctiva, present superiorly and inferiorly
pT1a: tumor of the bulbar conjunctiva with ≤ 2 mm of invasion of substantia propria
pT1b: tumor of the bulbar conjunctiva with > 2 mm of invasion of substantia propria
pT2: tumor of nonbulbar conjunctiva (i.e. palpebral, forniceal or caruncle)
pT2a: tumor of the nonbulbar conjunctiva with ≤ 2 mm of invasion of substantia propria
pT2b: tumor of the nonbulbar conjunctiva with > 2 mm of invasion of substantia propria
pT3: tumor of any size with local invasion
pT3a: invasion of the globe
pT3b: invasion of the eyelid
pT3c: invasion of the orbit
pT3d: invasion of the nasolacrimal duct, lacrimal sac or paranasal sinuses
pT4: tumor of any size with invasion of the central nervous system
Regional lymph nodes (pN)
pNX: regional lymph nodes cannot be assessed
pN0: no regional lymph node metastasis
pN1: regional lymph node metastasis
Notes:
Regional lymph nodes are the preauricular, parotid, postauricular, submandibular and cervical
Distant metastasis (pM)
pM0: no distant metastasis
pM1: distant metastasis
Prefixes
y: preoperative radiotherapy or chemotherapy
r: recurrent tumor stage
AJCC prognostic stage groups
There are currently no proposed prognostic groups
Registry data collection variables
Tumor thickness: depth of invasion measure in millimeters into substantia propria from the surface of the conjunctiva
Presence or absence of epithelioid cytology
Mitotic count: number of mitoses per square millimeter
Margin status
Presence or absence of
Ulceration
Epithelioid cytology
Growth regression
Lymphatic invasion
Angioinvasion
Perineural invasion
Conjunctival melanoma in situ
Conjunctival nevus
Microsatellites / in transit metastases
Histologic grade (G)
Grading is not performed
Histopathologic type
Spindle cell
Epithelioid
Anaplastic
Board review style question #1
The AJCC 8th edition staging for the conjunctiva should be used for which of these tumors
Caruncle melanoma
Eyelid melanoma
Uveal melanomas with secondary involvement of conjunctiva
Metastatic melanoma
Board review style answer #1
A. Caruncle melanoma
This staging should be used for melanomas arising from bulbar and palpebral conjunctiva, the caruncle and the fornices but not for primary eyelid skin melanomas or uveal melanomas with secondary involvement of conjunctiva. Although not specifically described in this topic, primary staging systems in general should not be used for metastases.
Pathologic TNM staging of carcinoma of the eyelid, AJCC 7th edition
Definition / general
Applies to clinical and pathologic staging
Note: excludes melanoma and malignancies other than carcinoma
Primary tumor (T)
TX: Primary tumor cannot be assessed
T0: No evidence of primary tumor
Tis: Carcinoma in situ
T1: Tumor 5 mm or less in greatest dimension, not invading the tarsal plate or eyelid margin
T2a: Tumor more than 5 mm, but not more than 10 mm in greatest dimension, or any tumor that invades the tarsal plate or eyelid margin
T2b: Tumor more than 10 mm, but not more than 20 mm in greatest dimension, or involving the full thickness eyelid
T3a: Tumor more than 20 mm in greatest dimension, or any tumor that invades adjacent ocular or orbital structures, or any T with perineural tumor invasion
T3b: Complete tumor resection requires enucleation, exenteration or bone resection
T4: Tumor is not resectable due to extensive invasion of ocular, orbital, craniofacial structures or brain
Regional lymph nodes (N)
NX: Regional lymph nodes cannot be assessed
cN0: No regional lymph node metastasis, based on clinical evaluation or imaging
pN0: No regional lymph node metastasis, based on lymph node biopsy
T2: lymphoma with orbital involvement +/- any conjunctival involvement
T2a: anterior orbital involvement (+/- any conjunctival involvement)
T2b: anterior orbital involvement (+/- any conjunctival involvement but with lacrimal involvement)
T2c: posterior orbital involvement (+/- any conjunctival involvement, +/- anterior involvement, +/- any extraocular muscle involvement)
T2d: nasolacrimal drainage system involvement (+/- conjunctival involvement but not including nasopharynx)
T3: lymphoma with preseptal eyelid involvement (infiltrates preseptal tissues such as dermis or orbicularis muscle of anterior eyelid skin) +/- orbital involvement, +/- any conjunctival involvement
T4: orbital adnexal lymphoma extending beyond orbit to adjacent structures such as bone and brain
T4a: involvement of nasopharynx
T4b: osseous involvement (including periosteum)
T4c: involvement of maxillofacial, ethmoidal or frontal sinuses
T4d: intracranial spread
Regional lymph nodes (N)
NX: involvement of lymph nodes not assessed
N0: no evidence of lymph node involvement
N1: involvement of ipsilateral regional lymph nodes
N2: involvement of contralateral or bilateral regional lymph nodes
N3: involvement of peripheral lymph nodes not draining ocular adnexal region
N4: involvement of central lymph nodes
Notes: regional lymph nodes include preauricular (parotid), submandibular and cervical
Distant metastasis (M)
M0: no evidence of involvement of other extranodal sites
M1a: noncontiguous involvement of tissues or organs external to the ocular adnexa (e.g. parotid glands, submandibular gland, lung, liver, spleen, kidney, breast, etc.)
M1b: lymphomatous involvement of the bone marrow
M1c: both M1a and M1b involvement
Stage grouping
No stage grouping is presently recommended by AJCC 7th edition
Uveal tract is the middle layer of the eye, between sclera and retina
Uveal tract consists of the iris, ciliary body and the choroid
Essential features
AJCC 7th edition staging was sunset on December 31, 2017; as of January 1, 2018, use of the 8th edition is mandatory
There are 2 separate pT classification systems for uveal melanomas: one for the iris and one for the ciliary body and choroid melanomas
Tumors with < 50% of their volume located in the iris should be categorized using the ciliary body and the choroid pT classification
Clinical and pathological T categories are the same
Some patients with iris melanoma experience a secondary open angle glaucoma caused by the tumor cells and tumor pigment laden macrophages becoming trapped in and obstructing the trabecular meshwork
pT1a: tumor limited to the iris, not more than 3 clock hours in size
pT1b: tumor limited to the iris, more than 3 clock hours in size
pT1c: tumor limited to the iris, with secondary glaucoma
pT2: tumor extending into the ciliary body, choroid or both
pT2a: tumor extending into the ciliary body, without secondary glaucoma
pT2b: tumor extending into the ciliary body and choroid, without secondary glaucoma
pT2c: tumor extending into the ciliary body, choroid or both, with secondary glaucoma
pT3: tumor extending into the ciliary body, choroid or both, with scleral extension (but without extrascleral extension)
pT4: tumor with extrascleral extension
pT4a: tumor with extrascleral extension ≤ 5 mm in largest diameter
pT4b: tumor with extrascleral extension > 5 mm in largest diameter
Ciliary body and choroid:
pT1: tumor size category 1
pT1a: tumor size category 1 without ciliary body involvement or extraocular extension
pT1b: tumor size category 1 with ciliary body involvement
pT1c: tumor size category 1 without ciliary body involvement but with extraocular extension ≤ 5 mm in largest diameter
pT1d: tumor size category 1 with ciliary body involvement and extraocular extension ≤ 5 mm in largest diameter
pT2: tumor size category 2
pT2a: tumor size category 2 without ciliary body involvement or extraocular extension
pT2b: tumor size category 2 with ciliary body involvement
pT2c: tumor size category 2 without ciliary body involvement but with extraocular extension ≤ 5 mm in largest diameter
pT2d: tumor size category 2 with ciliary body involvement and extraocular extension ≤ 5 mm in largest diameter
pT3: tumor size category 3
pT3a: tumor size category 3 without ciliary body involvement or extraocular extension
pT3b: tumor size category 3 with ciliary body involvement
pT3c: tumor size category 3 without ciliary body involvement but with extraocular extension ≤ 5 mm in largest diameter
pT3d: tumor size category 3 with ciliary body involvement and extraocular extension ≤ 5 mm in largest diameter
pT4: tumor size category 4 or any tumor with extraocular extension > 5 mm
pT4a: tumor size category 4 without ciliary body involvement or extraocular extension
pT4b: tumor size category 4 with ciliary body involvement
pT4c: tumor size category 4 without ciliary body involvement but with extraocular extension ≤ 5 mm in largest diameter
pT4d: tumor size category 4 with ciliary body involvement and extraocular extension ≤ 5 mm in diameter
pT4e: any tumor size category with extraocular extension > 5 mm in largest diameter
Notes:
Largest basal diameter and tumor thickness are used to determine size category (see table above), required to assign pT category to melanomas of the ciliary body and choroid
Proper grossing technique is required to obtain largest basal diameter and tumor thickness in enucleation specimens
Globe should be transilluminated with strong light source to map out the tumor shadow on the sclera in order to determine the best orientation of pupil-optic nerve section
Pupil-optic nerve section should capture the largest basal diameter based on the shadow
In clinical practice, largest basal diameter may be estimated in optic disc diameters (dd) (average 1 dd = 1.5 mm) and tumor thickness may be estimated in diopters (average 3 diopters = 1 mm)
Regional lymph nodes (pN)
pNX: regional lymph nodes cannot be assessed
pN0: no regional lymph node metastasis
pN1: regional lymph node metastasis or discrete orbital tumor deposits
pN1a: metastasis in one or more regional lymph nodes
pN1b: discrete orbital tumor deposits discontinuous with the globe without regional lymph node metastases
Notes:
Regional lymph nodes include preauricular, submandibular and cervical
Distant metastasis (pM)
pM0: no distant metastasis
pM1: distant metastasis
pM1a: largest diameter of the largest metastasis is ≤ 3 cm
pM1b: largest diameter of the largest metastasis is 3.1 - 8.0 cm
pM1c: largest diameter of the largest metastasis is > 8 cm
There is a lack of agreement on the proportions needed for the diagnosis of spindle cell and epithelioid types; 10% and 90% are provided for guidance only
Gross images
AFIP images
Gross extraocular extension
Whole mount images
AFIP images
Choroidal melanoma with extraocular extension
Microscopic (histologic) images
Contributed by Martin Hyrcza, M.D., Ph.D., M.Sc.
Scleral invasion
Extrascleral extension
Board review style question #1
Uveal melanoma involving 2 mm of iris, all of ciliary body and 9 mm of the choroid has a thickness of 12 mm and largest basal diameter of 16 mm. There is no extraocular extension present and no glaucoma. The pT category is
57 year old man and 85 year old man with intratarsal keratinous cysts of the meibomian gland (Am J Dermatopathol 2011;33:624)
Treatment
Simple excision with removal of cyst wall intact
Clinical images
Images hosted on other servers:
Pale yellow lesion
Gross description
Flesh colored or yellowish, well circumscribed, soft, mobile, and non-tender
On incision contains oily sebum
Microscopic (histologic) description
Cystic space lined by nonkeratinizing squamous epithelium with an eosinophilic cuticle and sebaceous lobules within the cyst wall, but no granular layer
Microscopic (histologic) images
Images hosted on other servers:
Cyst lined by squamous epithelium with sebaceous glands in cyst wall
Prolapsed intraconal fat due to dehiscence of tenon capsule precipitated by age, disease, trauma or surgery
Typically occurs in elderly obese men
Presents as small (up to 2.5 cm), raised, convex, yellow, compressible mass in the superotemporal quadrant of the eye (Optom Vis Sci 2015;92:1021, Figure 1 & 2)
Unilateral or bilateral
Low recurrence rate after simple excision
Essential features
Rare entity, caused by forward movement of intraconal fat due to dehiscence of tenon capsule precipitated by age, disease, trauma or surgery
Typically presents in elderly obese men as a small, raised, yellow, compressible mass in the superotemporal quadrant of the eye
Composed of an admixture of mature adipocytes, delicate fibrovascular septae, Lochkern cells and floret-like giant cells
Principal differential diagnosis includes pleomorphic lipoma and atypical lipomatous tumor
Composed of uniformly shaped mature adipocytes separated by a delicate fibrovascular septae
Scattered Lochkern cells (adipocytes with enlarged nuclei containing intranuclear vacuoles) and floret-like giant cells (multinucleated giant cells with a wreath like arrangement of bland, uniform, often vacuolated nuclei)
Varying numbers of inflammatory cells, including lymphocytes, plasma cells, histiocytes and mast cells
Regarding subconjunctival herniated orbital fat, which of the following statements is true?
Associated with MDM2 amplification
Floret-like giant cells with nuclear hyperchromasia and pleomorphism are typically seen in SHOF
Nuclei of Lochkern cells and floret-like giant cells are highlighted by CD34 immunohistochemistry
Has an aggressive course and the management includes radiation therapy
Board review style answer #1
C. The nuclei of Lochkern cells and floret-like giant cells in SHOF are highlighted by CD34 immunohistochemistry (although not necessary for diagnosis)
Temporal (or giant cell) arteritis is a systemic and discontinuous nonnecrotizing, granulomatous vasculitis of elastic and muscular arteries
Essential features
Presents in patients in the sixth decade of life or older with new onset headache
Risk of permanent vision loss if left untreated
Diagnosis requires morphologic confirmation (biopsy is the preferred modality)
Classic findings include lymphocytes and macrophages arranged in concentric rings surrounding the external and internal elastic lamina as well as an association with intimal hyperplasia and loss / fragmentation of elastic fibers
Useful stains: elastic stain, CD3 and CD68
Terminology
Temporal arteritis
Giant cell arteritis
Horton disease
Horton giant cell arteritis
Cranial arteritis
ICD coding
ICD-10
M31.5 - giant cell arteritis with polymyalgia rheumatica
EULAR 2018: diagnostic confirmation can be performed by imaging or histology (Ann Rheum Dis 2020;79:19)
ACR / Vasculitis Foundation 2021: temporal artery biopsy is the preferred modality for diagnostic confirmation (Arthritis Rheumatol 2021;73:1349)
Ultrasonography: offers good sensitivity and specificity in treatment naive patients (up to 4 days of treatment)
Temporal artery biopsy (TAB): offers good sensitivity and specificity within 2 - 4 weeks of glucocorticoid treatment (BMC Musculoskelet Disord 2016;17:363)
Optimal length of biopsy: > 1 cm with at least 1.5 cm preferred by some groups (ANZ J Surg 2018;88:191)
Unilateral temporal artery biopsy is the preferred modality as an initial approach over bilateral biopsies, though bilateral biopsies are recommended by some groups due to possible discordant findings (J Vasc Surg 2022;76:1704, Can J Ophthalmol 2014;49:157)
Segment of muscular artery with thickened, nodular and rubbery wall
Grossing and processing differ between institutions but should be thorough and account for the possibility of skip lesions or the uneven distribution of pathologic changes
Serially section vessel at 3 mm intervals
Embed in cross section (ink may be used to indicate which surface should be embedded to ensure uniform examination along the entire length of the artery)
Some prefer cutting 30 levels with 1 H&E slide performed every third level, leaving intervening unstained slides for additional stains as needed
Transmural inflammation pattern with lymphocytes and macrophages arranged in concentric rings, surrounding the external and internal elastic lamina and associated with intimal hyperplasia and loss of elastic fibers
50 - 70% of cases exhibit giant cells but giant cells are not required for the diagnosis
Neutrophils are uncommon (1.8%)
Unusual findings include necrosis, well formed granulomas and thrombosis
Borderline arteritis - lymphocytic and histiocytic infiltrate restricted to the following localizations
Vasa vasorum vasculitis (6.5% of cases): inflammation of vasa vasorum in the absence of medial inflammation
Inflammation limited to the adventitia (7% of cases): crescent shaped configuration limited to the adventitia and external elastic lamina, with sparing of the media
Small vessel vasculitis (9% of cases): inflammatory lymphocytic infiltrate surrounding (cuffing) small periadventitial vessels
Healed arteritis - fibrotic changes without inflammatory lymphocytic infiltrate
Marked intimal thickening
Intimal, medial and adventitial fibrosis and scarring, with neovascularization
Loss of elastic fibers
Microscopic (histologic) images
Contributed by José Tomás Peña, M.D., Pablo Zoroquiain, M.D. and @MirunaPopescu13 on Twitter
Vasculitis Foundation giant cell arteritis webinar
Giant cell arteritis by Nicholas J. Volpe, European Society of Ophthalmology
Temporal artery biopsy technique
Giant cell arteritis (temporal arteritis) pathology by Jerad Gardner, M.D.
Sample pathology report
Right temporal artery, biopsy:
Morphological findings consistent with temporal arteritis (see comment)
Comment: There is lymphocytic and macrophagic infiltration within the vascular wall. Multinucleated giant cell phagocytizing elastic fibers (elastic stain) are observed, supporting the diagnosis.
Gross description: Specimen A is received in formalin in a container and labeled with the patient’s name and specimen number and designated right temporal artery. The specimen consists of a tan, tubular structure, consistent with a muscular artery, that measures 1.5 cm in length and is notable for nodularity and thickening. The specimen is serially cross sectioned at 3 mm intervals, placed between sponges and submitted entirely in a cassette.
Differential diagnosis
Age related changes:
Intimal hyperplasia, duplication of the elastic inner lamina, adventitial fibrosis
Absence of mononuclear infiltration of the arterial wall
Another vasculitis (up to 5% of cases):
Neutrophil infiltration, abundant fibrinoid necrosis, microthrombi and leukocytoclasis
In addition to special staining to evaluate elastic fibers, which of the following antibody panels is most useful for evaluating temporal arteritis?
CD3 / CD68
CD4 / CD8
CD20 / CD138
CD34 / CD68
Board review style answer #1
A. CD3 / CD68. The hallmark of temporal arteritis is a transmural lymphocytic (T cells) and macrophagic infiltrate, which can be demonstrated with antibodies against CD3 and CD68, respectively. Answer C is incorrect because B cells (CD20+) and plasma cells (CD138+) are not diagnostic findings. Answer D is incorrect because the combination of CD34 and CD68 highlights histiocytes, myofibroblasts and small blood vessels but excludes T cells. Answer B is incorrect because although CD4+ and CD8+ are T cell markers, this panel does not stain macrophages.
A patient is diagnosed with temporal arteritis. What key finding is demonstrated with the special stain used in the image above?
Intimal hyperplasia
Loss of elastic fibers
Myxoid degeneration
Tunica media fibrosis
Board review style answer #2
B. Loss of elastic fibers. The Verhoeff-Van Gieson stain is a special stain used to demonstrate elastic fibers. In the setting of temporal arteritis, it can be used to evaluate areas of loss and disorganization of elastic fibers. Answer A is incorrect because intimal hyperplasia is visible with H&E and does not require special stains. Answer D is incorrect because tunica media fibrosis is a nonspecific finding and can be observed in the scenario of healed arteritis. Answer C is incorrect because myxoid degeneration is not a characteristic finding of temporal arteritis.
Conjunctival inflammatory infiltrates (lymphoid follicles and diffuse infiltrates)
Followed by pannus formation (fibrovascular tissue in conjunctival and corneal stroma) with Chlamydia elementary bodies and larger basophilic initial bodies seen
Also lymphocytes, plasma cells, neutrophils
Stage II:
Florid inflammation, more follicles, epithelial thickening, severe pannus
Macrophages with ingested debris (Leber cells) in conjunctiva
Stage III:
Scarring
No follicles
Cicatricial entropion (inversion of upper lid)
Misdirected lashes (trichiasis)
Stage IV:
Arrest of disease due to entropion and trichiasis but with continuing corneal damage and infection
Consist of epithelial tumors originating in skin and conjunctival surfaces (squamous cell and basal cell carcinoma), glandular tumors originating from sebaceous, sweat and apocrine glands and hair follicles
Also lymphoid and melanocytic tumors
Occasionally Kaposi sarcoma, fibrous histiocytoma and other sarcomas
Regional lymph nodes are pretarsal and posttarsal plexuses, which are anastamosed
Lateral 2/3 of upper eyelid and lateral 1/3 of lower eyelid drain into preauricular nodes
Remaining lymphatics drain into submandibular nodes
Local extension includes soft tissue of orbit, lacrimal gland and globe
Frozen section (Mohs technique) useful to minimize size of excised tissue
Metastases to cervical, axillary and mediastinal lymph nodes, lung, liver and other viscera
Diffuse infiltration by plasma cells, occasionally nodular lymphocytic infiltrates
Associated with obliteration of anterior chamber and adherence of iris to cornea
May be seen in juvenile rheumatoid arthritis
Posterior uveitis (choroiditis, chorioretinitis):
Diffuse, focal or scattered chronic inflammatory infiltrate, often involving retina
May form cyclitic membrane that contracts, leading to detachment of retina and ciliary body
Not painful, so enucleation often not necessary
Enucleation if recurrence leads to adhesions between iris and cornea (anterior synechiae) or iris and anterior surface of lens (posterior synechiae) causing secondary glaucoma
Cause usually cannot be determined; known causes are herpes zoster, Behcet's disease (obliterative vasculitis of retinal vessels), Pneumocystis carinii
Granulomatous uveitis:
May be due to sarcoidosis
Also tuberculosis, leprosy, syphilis, tularemia, CMV, varicella zoster virus, fungi and parasites
Usually produced by Toxocara canis in children ages 3 - 14 years without systemic disease
Single migrating larva enters eye hematogenously and rests in vitreous or inner surface of retina with accompanying acute and chronic inflammatory cells and intense eosinophilia
Late changes are scarring, retinal detachment and leukokoria, simulating retinoblastoma
Dead larvae may cause minute granulomas, found with serial sectioning
WHO classification of tumors of conjunctiva and caruncle
Currently on 5th edition (to be published in 2023; beta version now available online)
Major updates
5th edition is now available online in beta form
This edition contains updated information on molecular pathology, expression profiling and molecular classification of tumors; however, the focus remains on morphologic classification
Additional classification and incorporation of tumor lineage (e.g., epithelial, adnexal, melanocytic) has been emphasized.
Selected entities reclassified in this edition
Phakomatous choristoma has been removed (now classified under eyelid)
Sebaceous carcinoma has been removed (now classified under eyelid)
Spitz nevus has been removed (now classified under eyelid)
Keratoacanthoma of the conjunctiva is no longer listed as a separate tumor type
Spindle squamous cell carcinoma and squamous cell carcinoma with mucinous differentiation are included within the broader group of squamous cell carcinoma
WNT activated deep penetrating / plexiform melanocytoma has been included as a new entity in the WHO 5th edition
Includes an update on pathogenesis and molecular genetics of melanocytic conjunctival lesions
Within the melanocytic lesions, nomenclature for premalignant and malignant lesions has been updated.
Nonneoplastic pterygium and pinguecula were added as tumor-like lesions to delineate them from conjunctival squamous intraepithelial neoplasia
Soft tissue tumors, hematolymphoid neoplasms and secondary tumors of the conjunctiva are discussed in separate chapters
WHO (2023)
Tumor-like lesions and choristomas of the conjunctiva
Among melanocytic lesions of the conjunctiva, which of the following statements is true about the lesion shown in the above image?
It has a high risk for transformation into malignant melanoma
It is best treated by enucleation
It is commonly found as a poorly defined, pigmented mass
It is most commonly found in ages 70 - 90 years
It is the most common melanocytic lesion of the conjunctiva
Board review style answer #1
E. It is the most common melanocytic lesion of the conjunctiva. This is a conjunctival melanocytic nevus, which accounts for up to 53% of all conjunctival neoplasms. Differentials include primary acquired melanosis, racial melanosis, ocular melanocytosis and malignant melanoma. Answer A is incorrect because conjunctival nevi have a low rate of conversion to conjunctival melanoma (less than 1%). Answer B is incorrect because treatment is usually for cosmetic reasons; conjunctival melanocytic nevus is typically managed by periodic observation and serial photographic comparison. Answer C is incorrect because the morphology is usually a well defined, slightly elevated mass. The classic location is the interpalpebral bulbar conjunctiva, caruncle or plica semilunaris. Answer D is incorrect because most often these lesions are apparent within the first or second decade of life as a discrete, pigmented lesion.
46 year old Japanese woman with a 1 year history of asymptomatic yellowish papules on the neck and elbow (J Dermatol 2019;46:e362)
66 year old man presented with longstanding lesions on the 4 eyelids for several years, recently becoming larger and heavily pigmented (Am J Dermatopathol 2023;45:646)
A 56 year old woman presents with bilateral eyelid lesions. Histopathology is shown. Which of the following is the most likely diagnosis?
Chalazion
Erdheim-Chester disease
Langerhans cell histiocytosis
Ruptured epidermal inclusion cyst
Xanthelasma
Board review style answer #1
E. Xanthelasma is correct because there are abundant foamy histiocytes in the superficial dermis. Answer A is incorrect because chalazion typically shows mixed acute and chronic inflammation with extracellular lipid deposits; it is sometimes granulomatous. Answer B is incorrect because Erdheim-Chester is a non-Langerhans histiocytosis with intermixed lymphocytes, which may involve the orbit but also has involvement of other organ systems: bone, CNS, pituitary. Answer C is incorrect because there is not an abundant mixed inflammatory infiltrate with histiocytes showing grooved nuclei. Answer D is incorrect because ruptured epidermal inclusion cyst would show portions of epithelial lines cyst with a surrounding mixed inflammatory infiltrate, often with keratin debris and foreign body giant cells, many of which may contain keratin fragments.
A 50 year old woman presents with bilateral medial upper eyelid yellow plaques. Which systemic medical condition is most likely associated with this pathology?
Acromegaly
Atherosclerosis
Breast cancer
Colon cancer
Board review style answer #2
B. Atherosclerosis. Xanthelasma characteristically presents with symmetric medial upper eyelid yellow plaques. It may be associated with cirrhosis, atherosclerosis, thyroid disorders, nephrotic syndrome, primary hyperlipidemias (especially type 2a) and diabetes mellitus. Answer A is incorrect because acromegaly is growth hormone overproduction and is not associated with xanthelasma. Answer C is incorrect because breast cancer is not associated with xanthelasma. Metastatic breast cancer can cause enophthalmos but not yellow plaques. Answer D is incorrect because colon cancer is not associated with xanthelasma.