



- Fallopian tube represents an anatomic bridge between the ovary and the uterus in which fertilization of an egg by sperm may occur followed by delivery of the zygote to the uterus; it also provides the environment needed to sustain the gametes and prevent rejection of the zygote by the body
- Fallopian tube is divided into several anatomic regions (i.e., intramural, isthmus, ampulla and infundibulum) and comprises mucosal, muscular and serosal layers
- Mucosa is composed of 4 cell types that can be readily recognized on H&E staining; however, more cell subtypes can be identified immunohistochemically and molecularly
- Composition of these cell types varies based on location, phase of the menstrual cycle and menopausal status
- A complex immune system moderates tolerance to a fertilized egg, fights infection and plays a role in cancer surveillance
- Other historically used names include tuba uteri, oviduct, uterine tube or tube (J Reprod Fertil 1988;82:843)
- Ciliated cells move egg toward the ampulloisthmic junction
- Ampulloisthmic junction is the site of fertilization
- Growth is encouraged by estradiol
- Deciliation is encouraged by progesterone
- Prolonged exposure to progesterone or removal of estrogen causes epithelial atrophy (Mills: Histology for Pathologists, 5th Edition, 2019)
- Motile cilia beat to provide fluid flow (Int J Gynecol Cancer 2018;28:1535)
- Control gamete and embryo movement (Dev Cell 2022;57:914)
- Secretory cells
- Secrete oviduct fluid
- Complex mixture of materials derived from plasma and proteins specifically formed by the tubal epithelium
- Function of tubal fluid (J Reprod Fertil 1988;82:843)
- Moisturizes surface epithelium
- Bacteriostatic function
- Electrolyte balances may influence the development of embryos into blastocysts, the motility of sperm and the health of the ovum
- Contains nutrients for spermatozoa, oocytes and zygotes and promotes the capacitation of sperm by removing glycoproteins and other molecules from the plasma membrane
- Major constituents are calcium, sodium, chloride, glucose, proteins, bicarbonates, amylase, lactic acid (J Reprod Fertil 1988;82:843)
- Bicarbonates and lactic acid are vital to the sperm's use of oxygen; they also help with postfertilization egg development
- Tubal fluid flows against the action of cilia (i.e., toward the fimbriated end) (J Reprod Fertil 1988;82:843)
- Formation of fallopian tubal fluid (Reproduction 2001;121:339)
- Secrete oviduct fluid
- Intercalated cells are either secretory cells or a form of reserve cells
- After menopause, the lining will contract and the epithelial cells will decrease in number, leading to blunting of the plica
- During pregnancy
- Inactive during gestation
- Mild decidual change in the endosalpingeal stroma during the later half of pregnancy
- Epithelial atrophy
- Birth control pills and tubal ligation can cause changes in morphology (Mills: Histology for Pathologists, 5th Edition, 2019)
- Molecular and transcriptional alterations occur throughout the menstrual cycle and after menopause (medRxiv 2023 Nov 23 [Preprint], Cell Rep 2022;41:111838)
- Immune system (Int J Gynecol Pathol 2014;33:581)
- Prevents infection
- Helps develop tolerance to the zygote
Images hosted on other servers:

Fallopian tube anatomy

Fallopian tube anatomy and ligaments

Fallopian tube blood supply
- Fallopian tubes can be evaluated with hysterosalpingography (Fertil Steril 2022;118:19)
- Dye is injected into the uterus that can be visualized using Xray
- Flow of the dye is visualized to assess the patency of the fallopian tubes
- CA125 can be used to screen for ovarian / fallopian tube cancer (J Ovarian Res 2019;12:28)
- More useful in postmenopausal women
- False positive results are associated with endometriosis, pelvic inflammatory disease and uterine fibroids
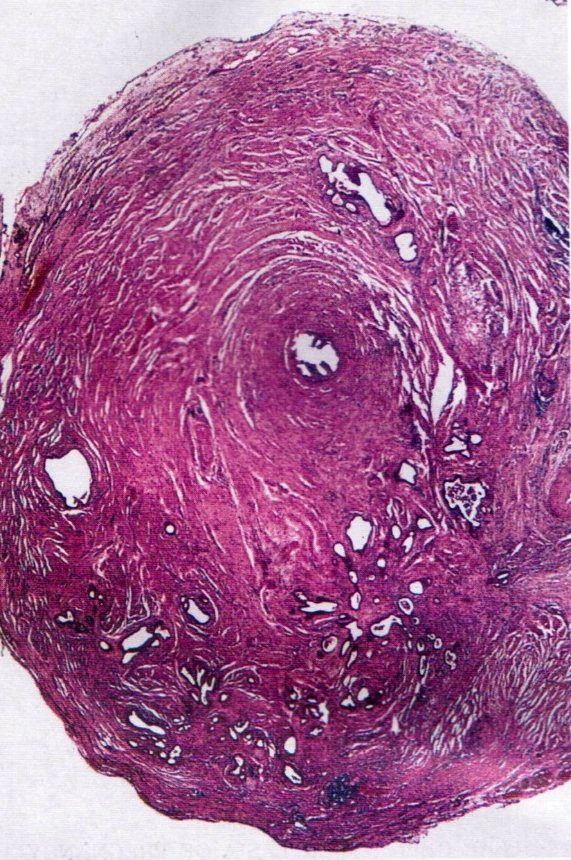
- Bilateral hollow, tubular structures, measuring 8 - 12 cm in length and 0.5 - 1.2 cm in diameter
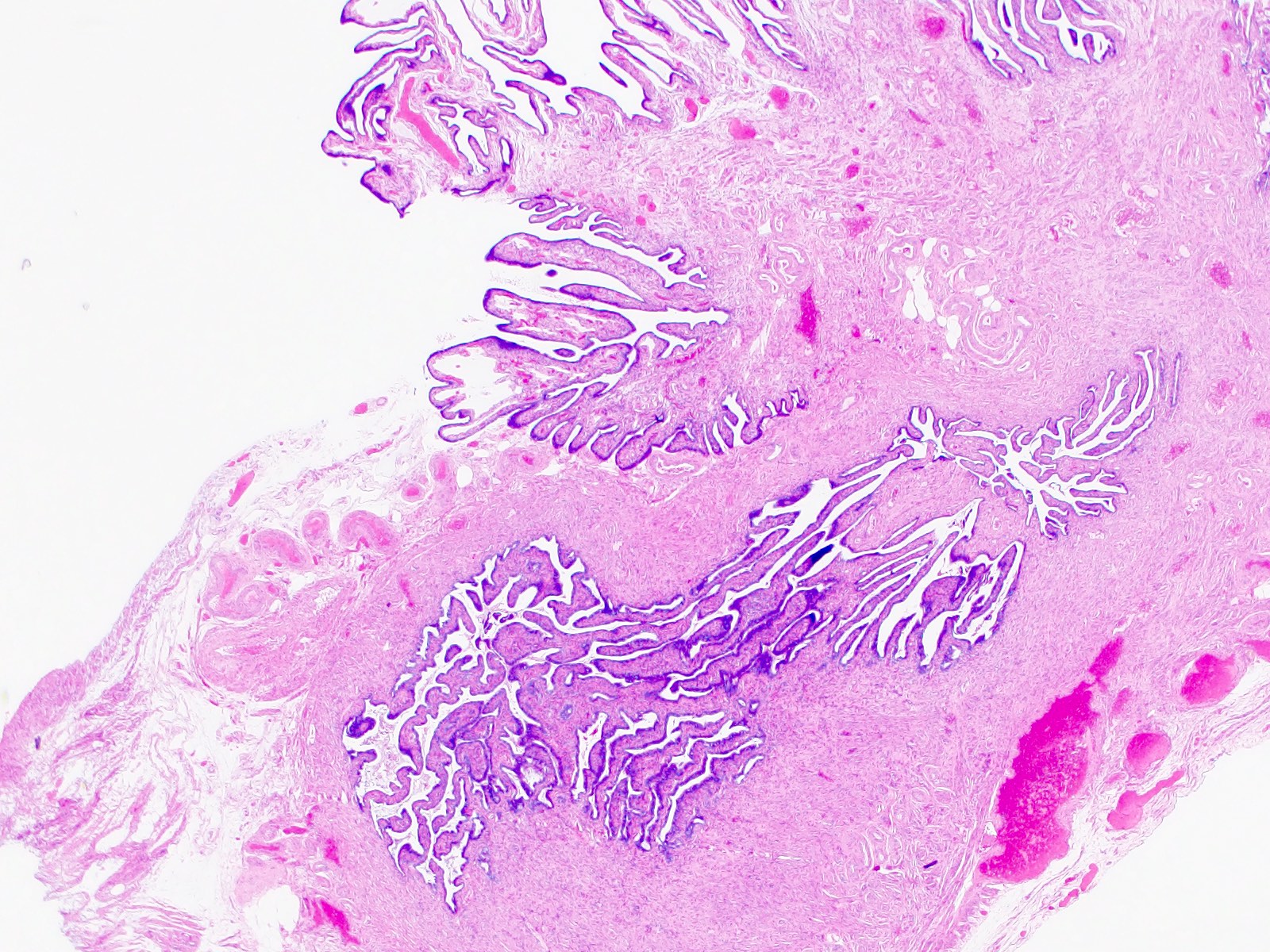
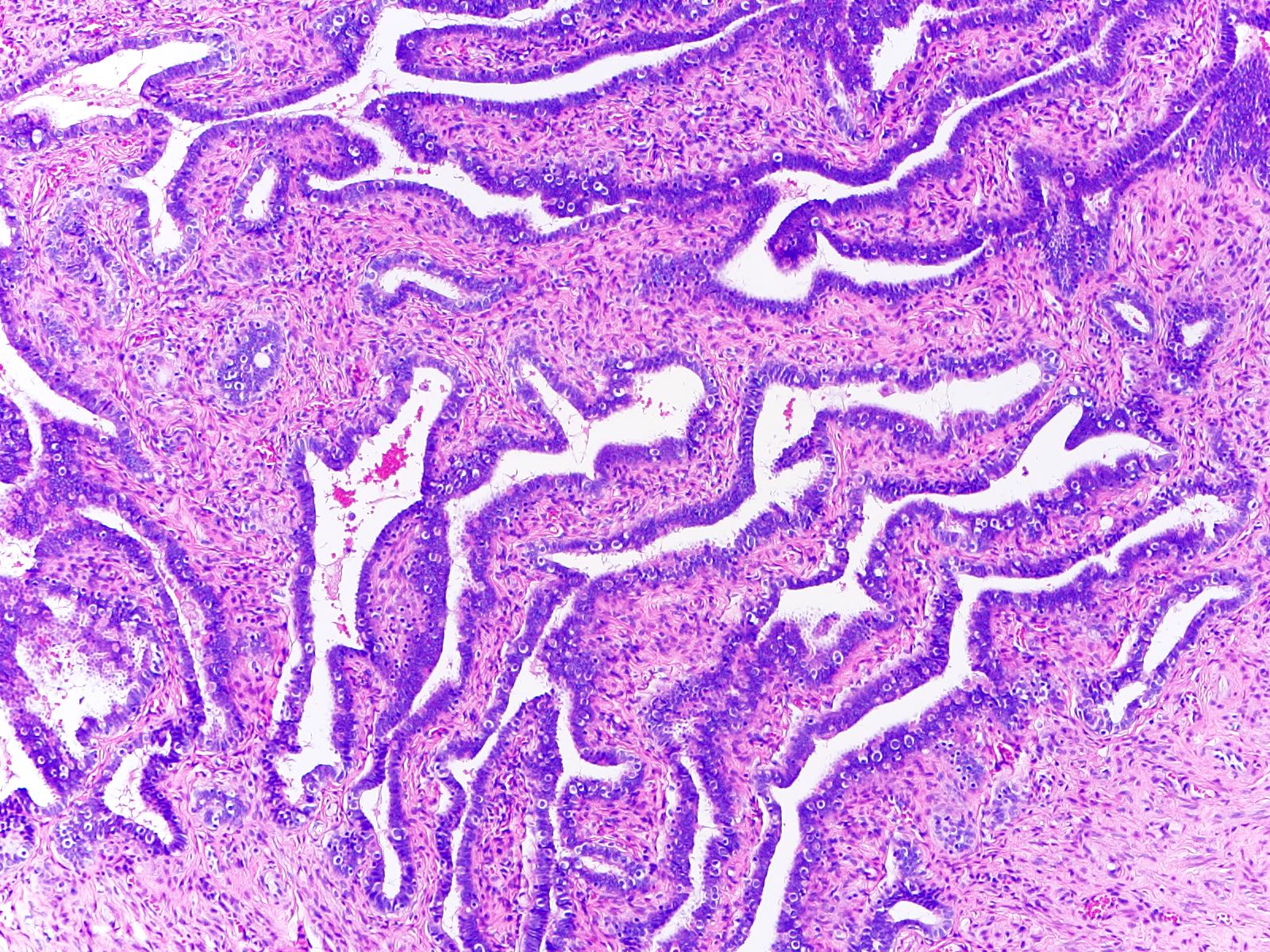
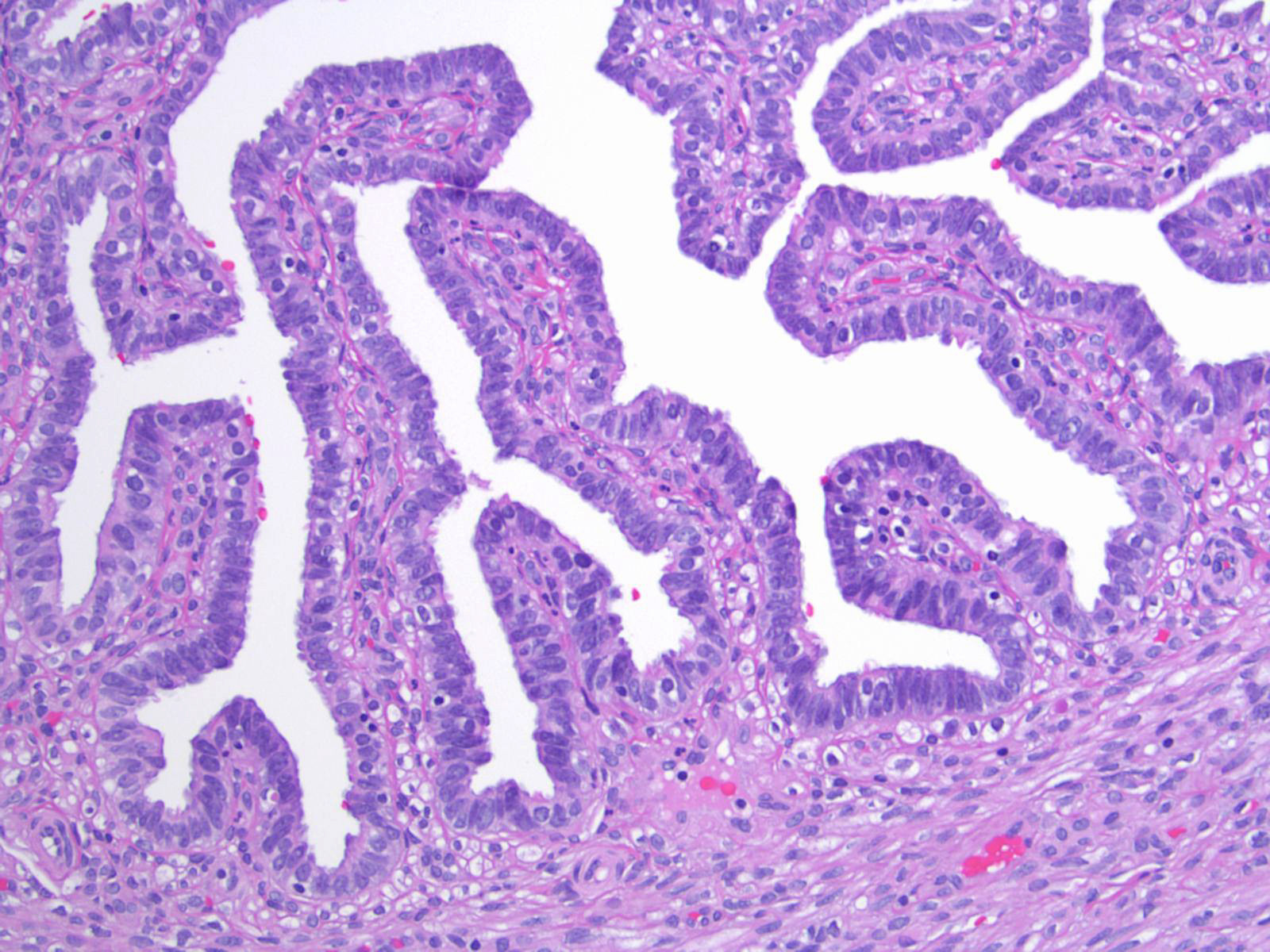
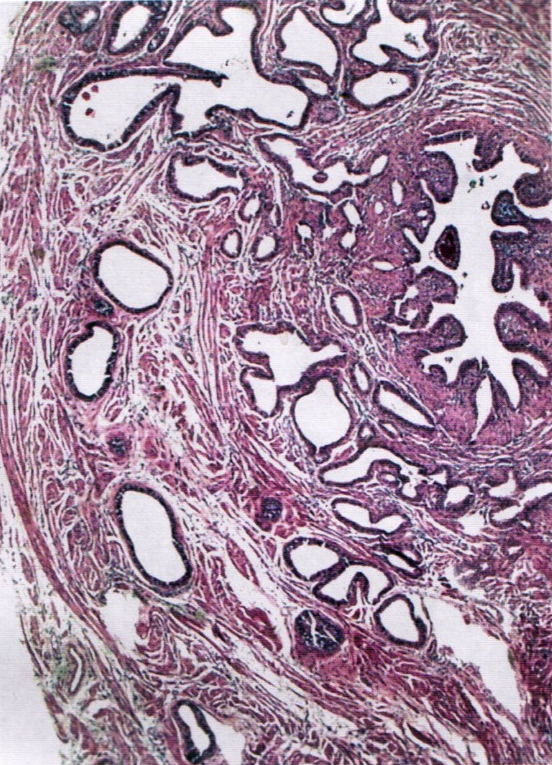
- Lined by a single layer of mucosal epithelium with many folds (plicae), which are most obvious in the ampulla where they subsequently merge with fimbriae
- Extend laterally from the posterior superior uterine fundus and lead to the ovaries
- Connected to broad ligament by mesosalpinx (double fold of peritoneum), to uterine cornu by utero-ovarian ligament and to lateral pelvic sidewall by infundibulopelvic (suspensory) ligament
- Arterial supply is from branches of uterine and ovarian arteries, located within mesosalpinx
- Nerve supply from both sympathetic and parasympathetic fibers
- Sensory fibers run from T11 - T12 and L1
- Lymphatic drainage to para-aortic, internal iliac, external iliac, common iliac and inguinal lymph nodes
- Segments
- Intramural (within wall of uterus)
- Isthmus (thick walled, narrower opening, ~2 cm in length)
- Ampulla (thin walled, major portion, typical site of fertilization)
- Infundibulum (trumpet shaped end lined by fimbriae, attaches to ovary)
- Tubal ostium is an opening to the peritoneal cavity
- Uterotubal junction is an entrance to the uterine cavity
- Reference: StatPearls: Anatomy, Abdomen and Pelvis - Fallopian Tube [Accessed 18 April 2024]
Contributed by Brandon D. Metcalf, M.D.

Salpingectomy specimen
- Fallopian tube specimen is most often received for frozen section as a part of a salpingo-oophorectomy specimen (Hui: Atlas of Intraoperative Frozen Section Diagnosis in Gynecologic Pathology, 1st Edition, 2015)
- Frozen section is not usually performed on grossly identifiable and unremarkable fallopian tubes; however, adherent fallopian tube tissue may occasionally be submitted for intraoperative consultation
- Morphologic features are consistent with normal fallopian tube as described below
- Third week
- Following migration of primordial germ cells from yolk sac, genital ridge forms from intermediate mesoderm and cloaca forms
- Fourth week
- Müllerian (paramesonephric) ducts form from coelomic epithelium invaginating ventrolaterally into Wolffian (mesonephric) duct and genital mesentery
- This site of invagination later becomes the tubal ostium in which the fimbriae develop and septation of the cloaca occurs
- Fifth to eighth weeks
- Unfused cephalic part of Müllerian ducts form fallopian tube
- Fused part forms uterus and upper vagina
- In a female fetus (or male without functioning testes) (Bhatnagar: Essentials of Human Embryology, 3rd Edition, 2000)
- Müllerian structures persist and Wolffian (mesonephric) duct regresses; vestiges may persist as epithelial inclusions
- Development is affected by clomiphene, tamoxifen and to a lesser extent, diethylstilbestrol (DES) (Hum Pathol 1987;18:1132, Hum Pathol 1982;13:190)
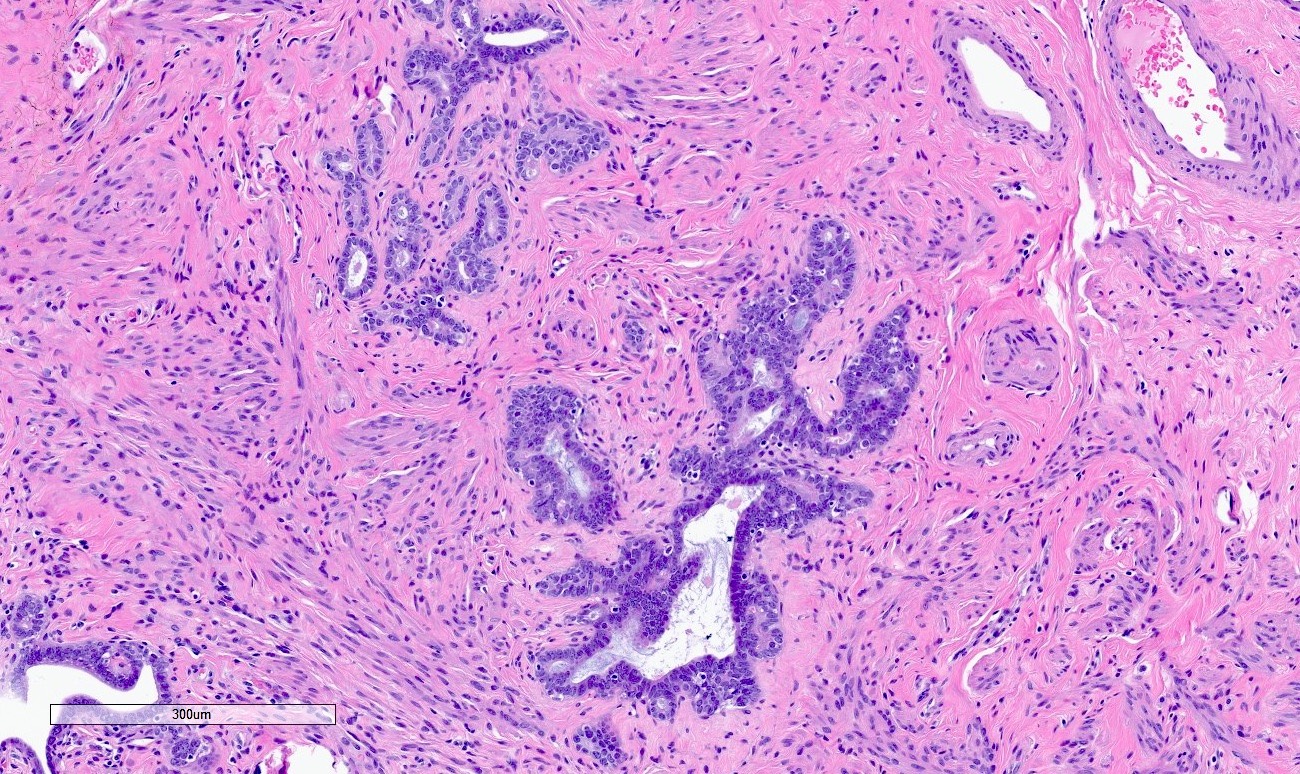
Adult histology
- Fallopian tube wall is composed of mucosal, muscular and serosal layers
- Mucosa comprises luminal epithelium and underlying lamina propria (stroma)
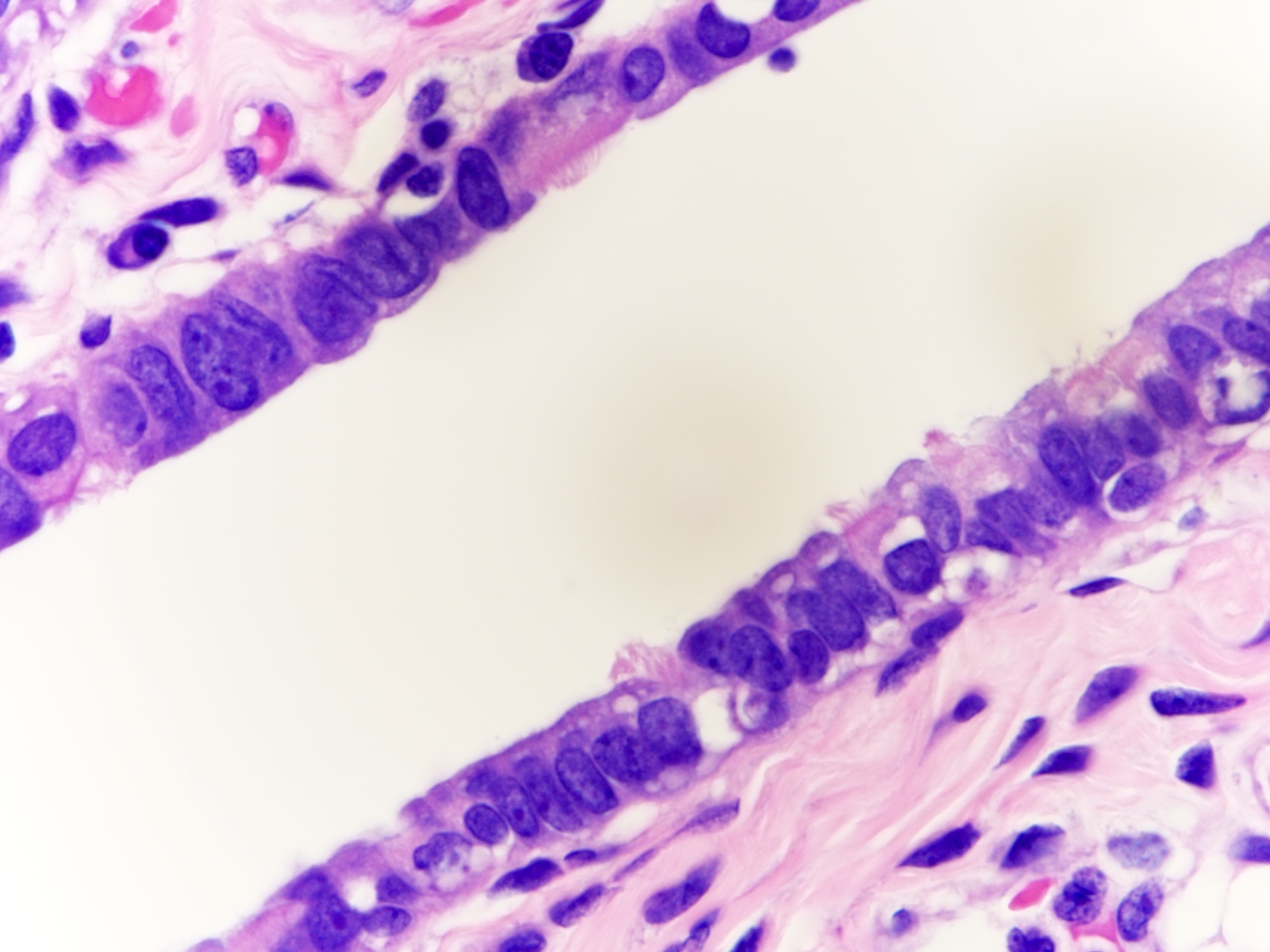
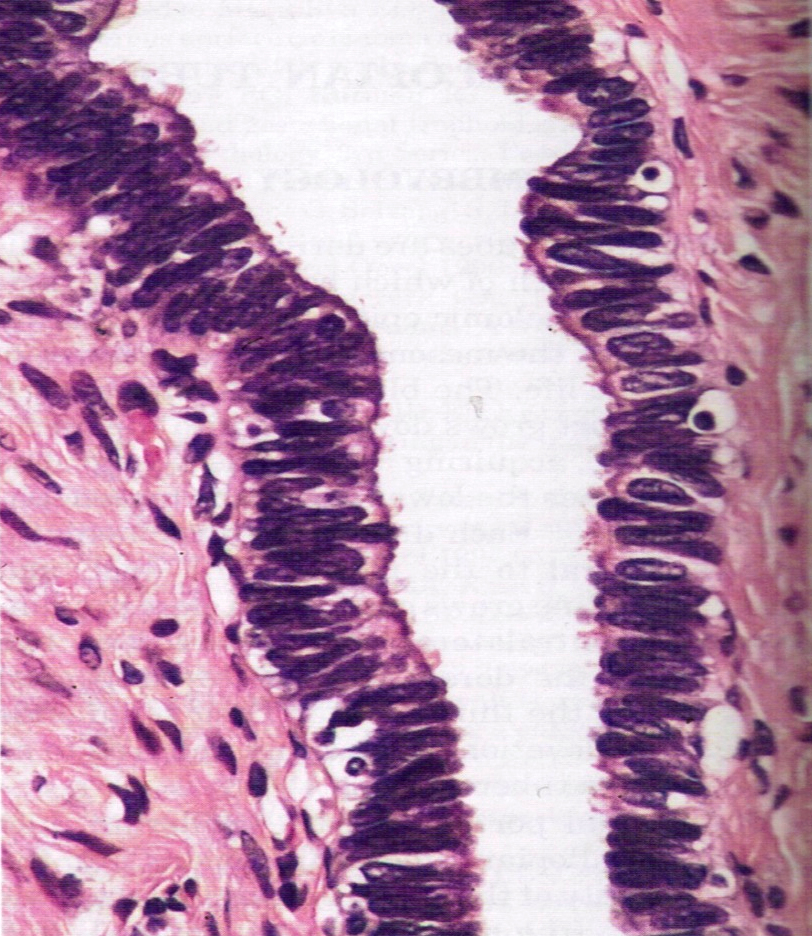
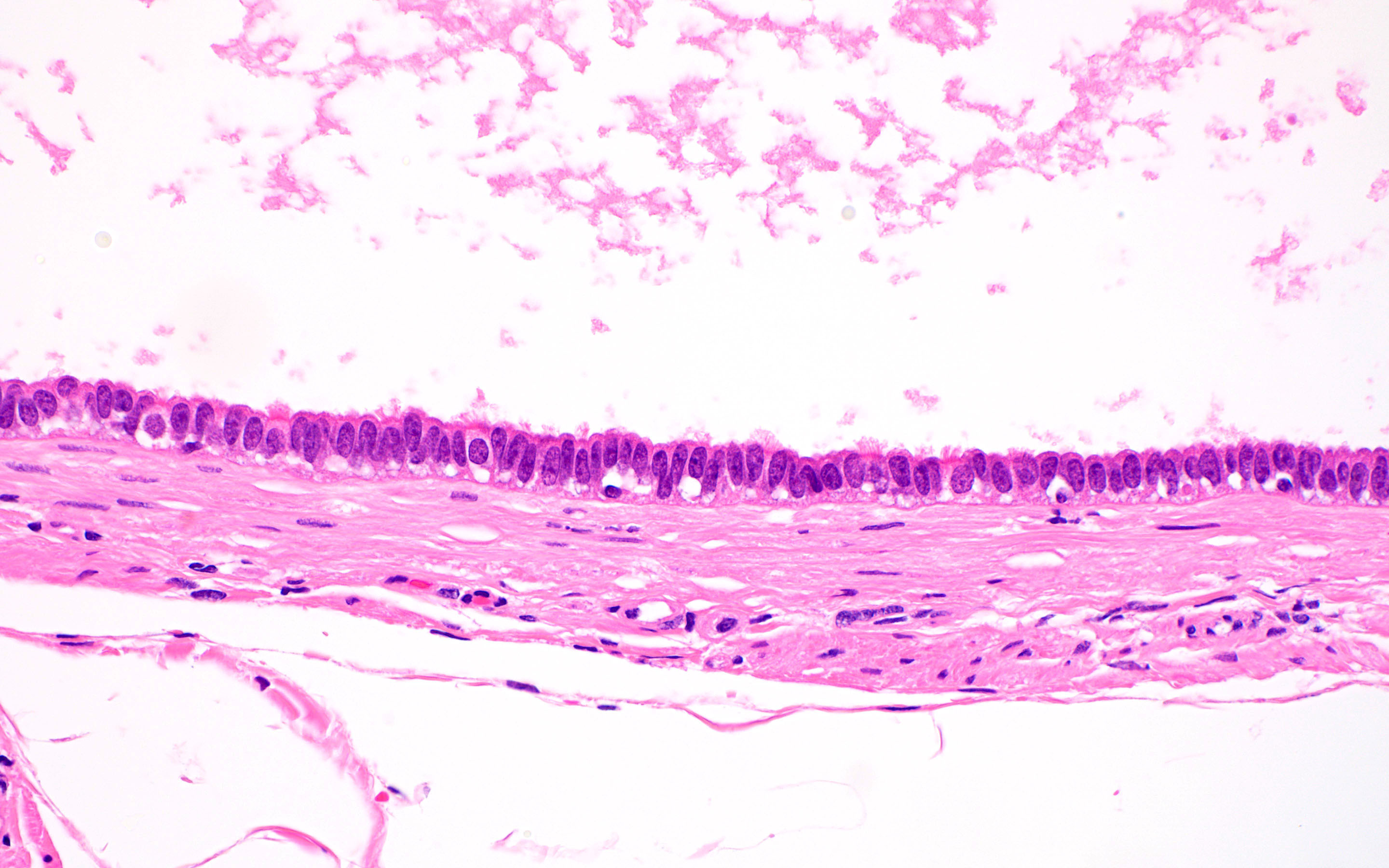
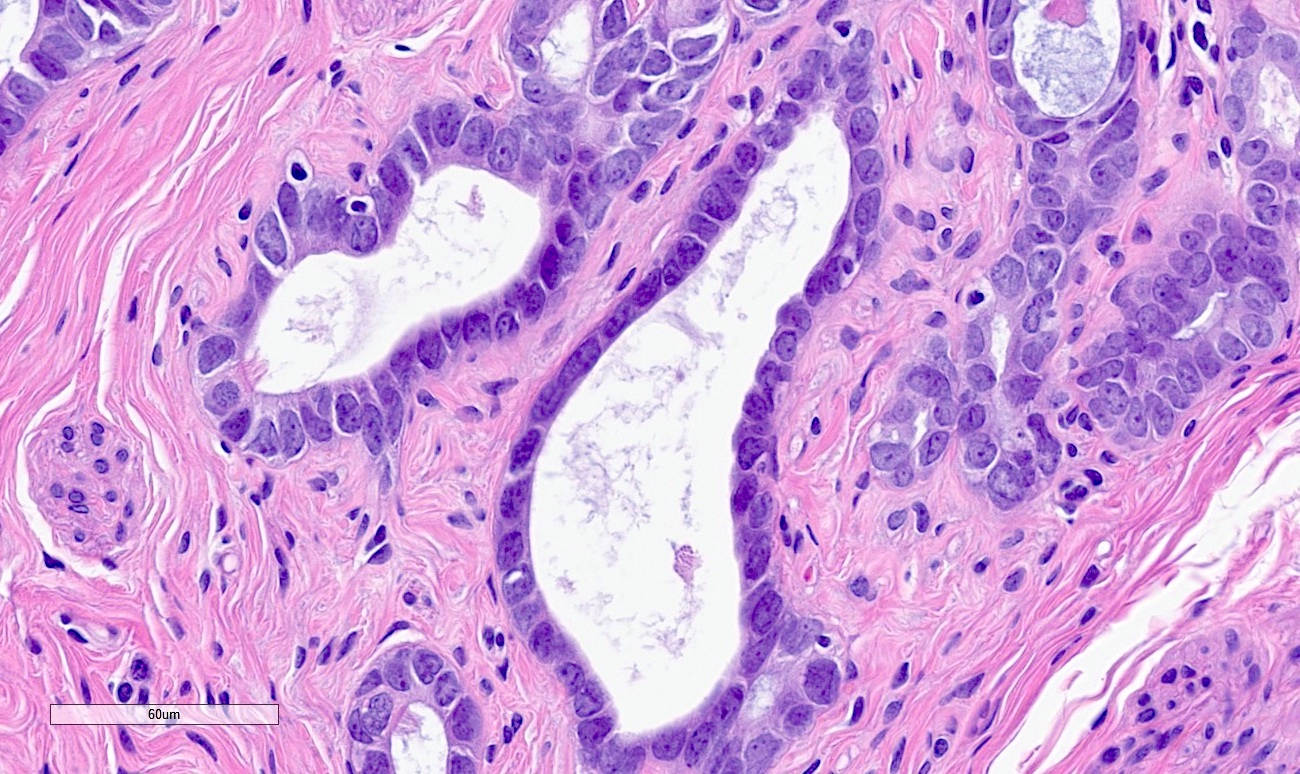
- Luminal epithelium consists of the following cells (Mills: Histology for Pathologists, 5th Edition, 2019)
- Ciliated columnar cells (~25%)
- Most abundant in infundibulum and ampulla
- Estrogen increases production of cilia
- Most often seen at the apex of mucosal folds
- Most common at the ovarian end of the tube, especially in fimbriae
- Most common during midcycle and decrease to the minimum number at menstruation
- Decrease during gestation
- Secretory cells (~60%)
- Nonciliated, containing apical granules and producing tubular fluid
- Exhibit ovoid, dense nuclei
- Most common at the proximal segment of the fallopian tube
- Increase in number in response to progesterone
- Height and secretory activity increase in response to estrogen
- Menstruation cycle changes cell height and appearance
- May exhibit nonmotile primary cilia
- Contain sensory organelles
- React to cilia mediated stimuli and are fully capable of affecting cilia mediated signaling pathways
- Lost in serous tubal intraepithelial carcinoma (Int J Gynecol Cancer 2018;28:1535)
- Peg (intercalated) cells (< 10%)
- Exhibit thin dense nuclei and little cytoplasm
- Hypothesized to be stem / progenitor cells (J Reprod Immunol 2022;152:103646)
- A stage in the cyclic variation during the menstrual cycle of the secretory cells
- Basal cells (Dev Cell 2022;57:914)
- Exhibit round nuclei and a cytoplasmic ring
- Ciliated columnar cells (~25%)
- Lamina propria (stroma) (Dev Cell 2022;57:914)
- Stromal cells resembling fibroblasts, surrounded by dense reticulin network
- Blood vessels
- Possibly Cajal-like cells (Dev Cell 2022;57:914)
- Muscle layer comprising 3 sublayers
- Innermost (obliquely arranged)
- Middle (circular)
- Outermost (longitudinal, extending into fimbriae)
- Serosal layer
- Lined by mesothelium of visceral peritoneum
- Often contains Walthard rests with transitional type epithelium
- Immune cells
- Lymphocytes may be observed in epithelium, lamina propria and muscular wall (Int J Gynecol Pathol 2014;33:581)
- Occasional lymphoid follicles may be seen
- Other immune cells include CD163+ macrophages, CD11c+ dendritic cells, CD8+ T cells and a minor populations CD56+ NK cells, CD4+ T helpers, CD20+ B cells, TCRγδ+ T cells, CD207+ (langerin) Langerhans cells, mast cells (Int J Gynecol Pathol 2014;33:581, Dev Cell 2022;57:914)
- Distribution varies according to menopausal status; T helper and B cells are more common in postmenopausal women, while macrophages are more abundant in premenopausal women (Int J Gynecol Pathol 2014;33:581)
- Play a role in cancer immune surveillance (Int J Gynecol Pathol 2014;33:581)
- Normal histologic variations
- Intramuscular edema in 12.5% of specimens, most frequently postpartum
- Plical fibrosis (35.5%), epithelial vacuolization (6.6%) and epithelial tufting / stratification (3.5%) correlated with increased patient age (Arch Pathol Lab Med 2002;126:951)
- Rare mitotic figures
- Metaplasia, including mucinous, endometrioid or transitional cell (Walthard rests)
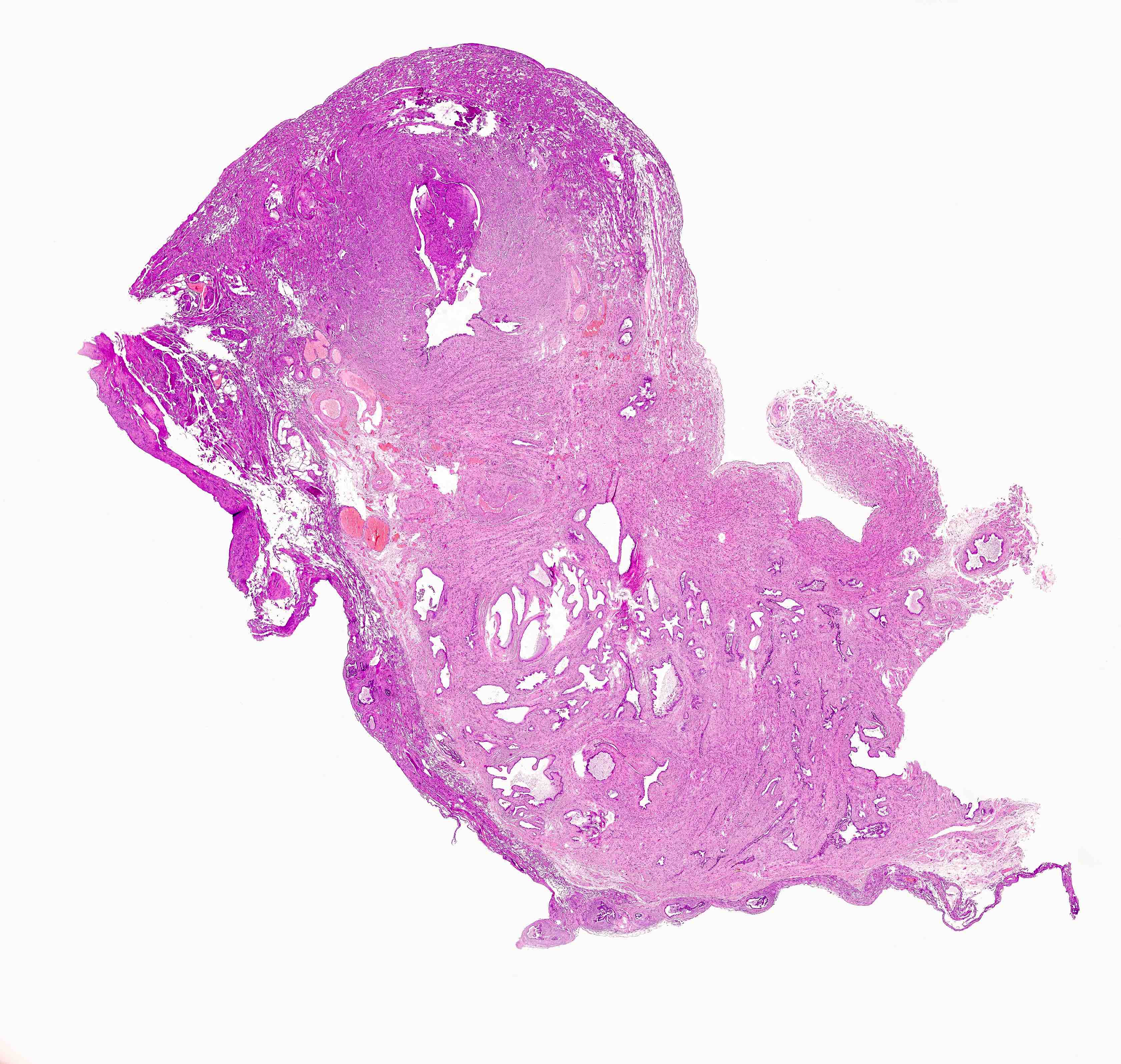
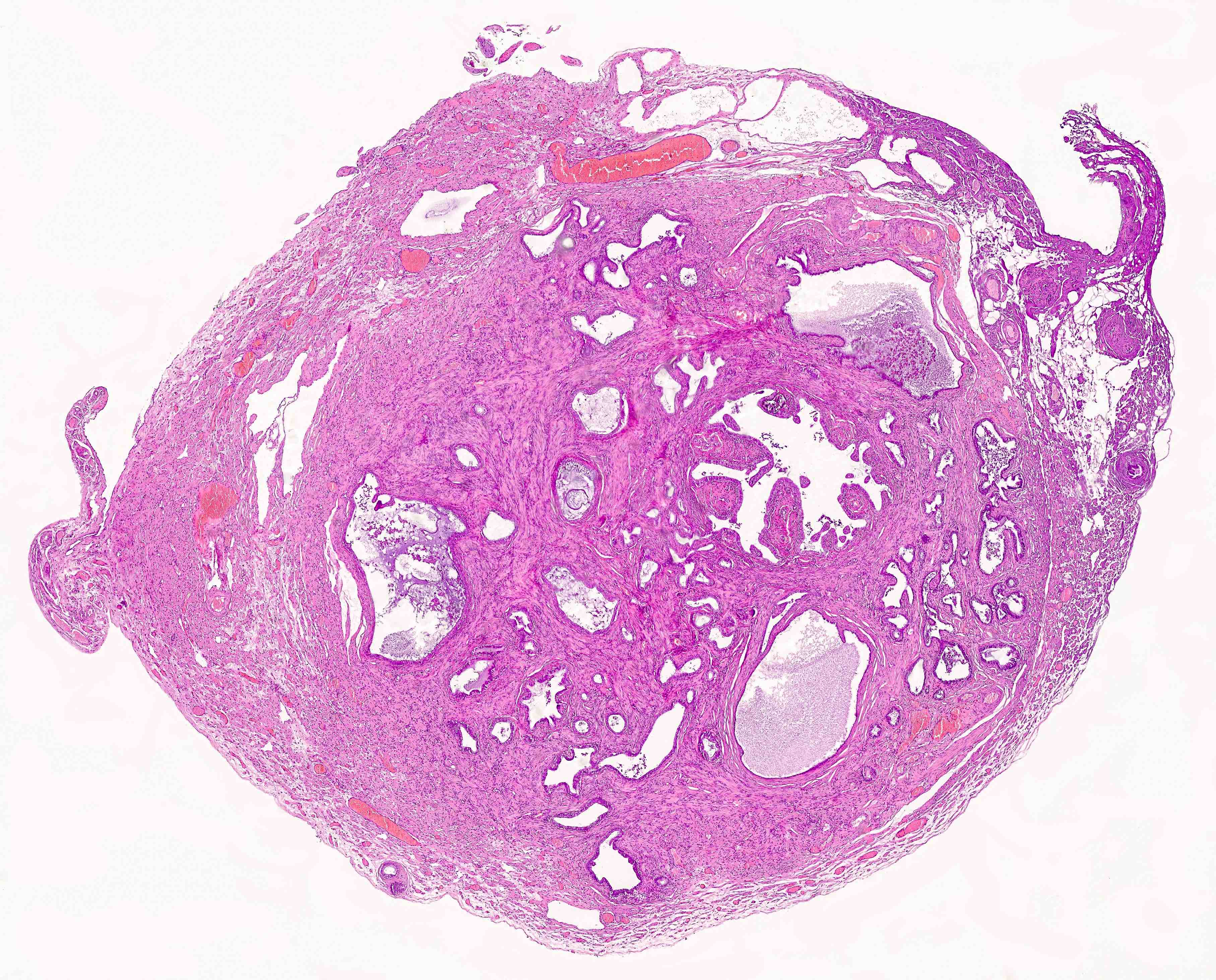
Contributed by Brandon D. Metcalf, M.D. and Nicole D. Riddle, M.D.
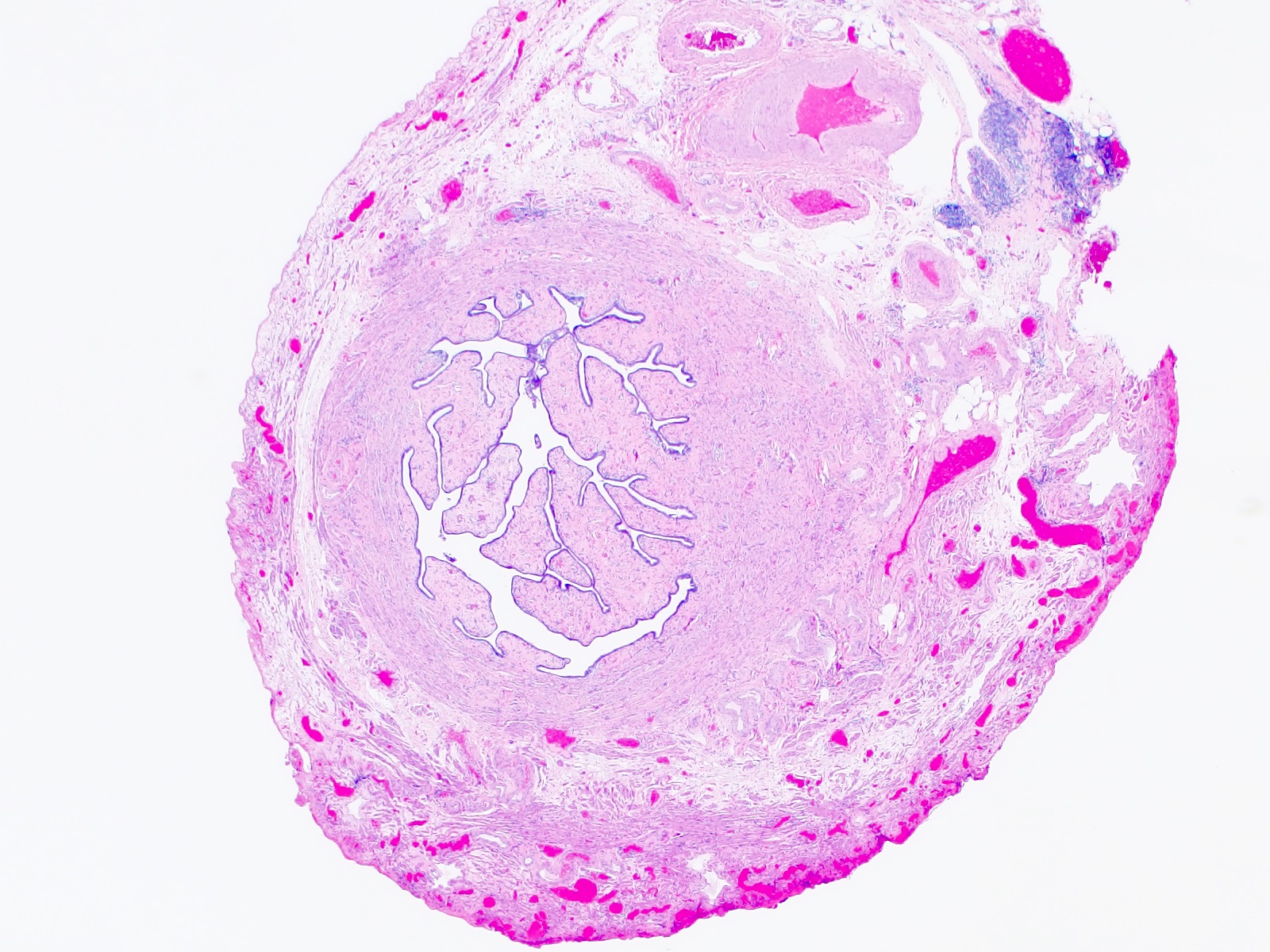
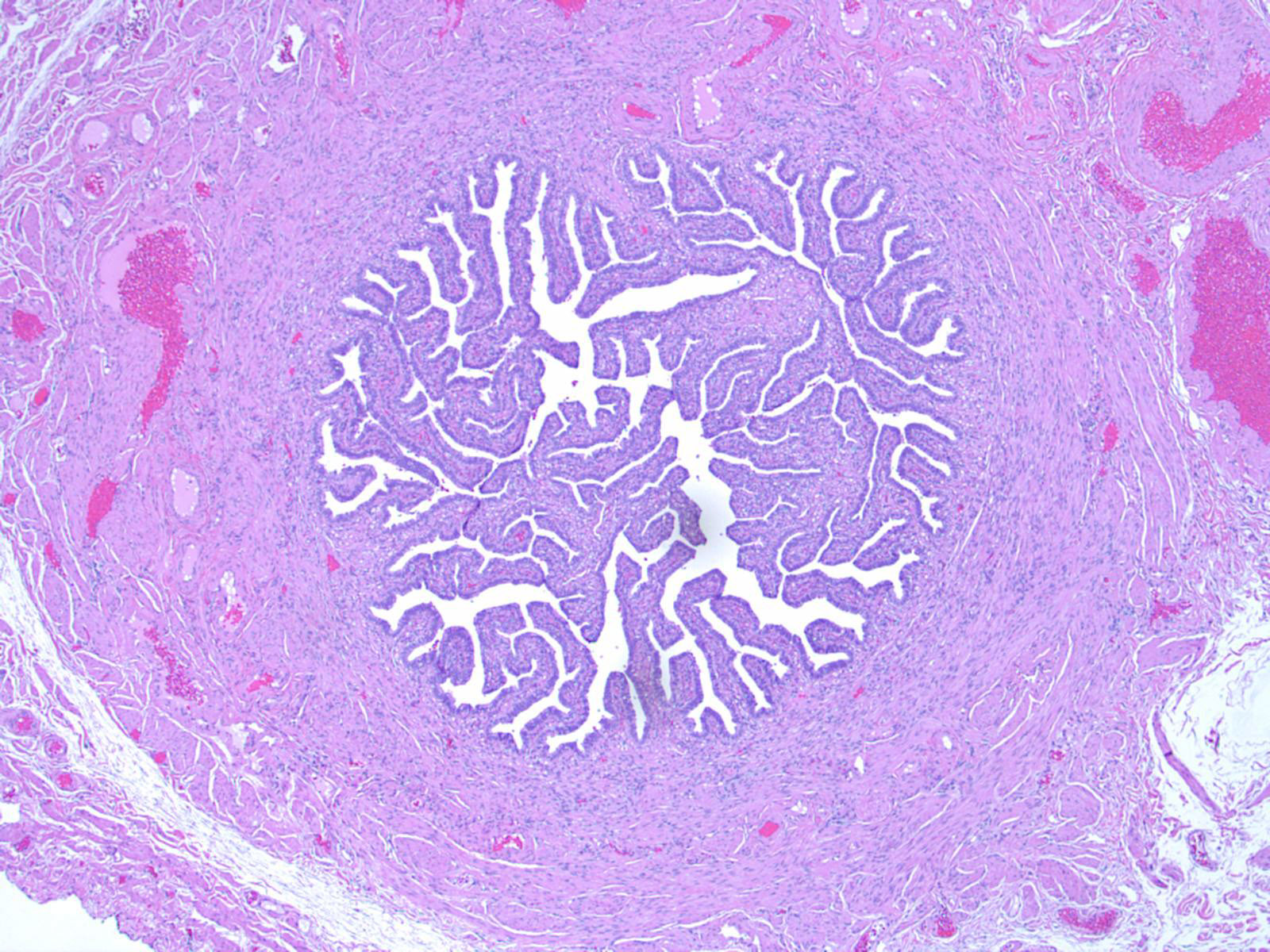
Fallopian tube cross section, postmenopausal
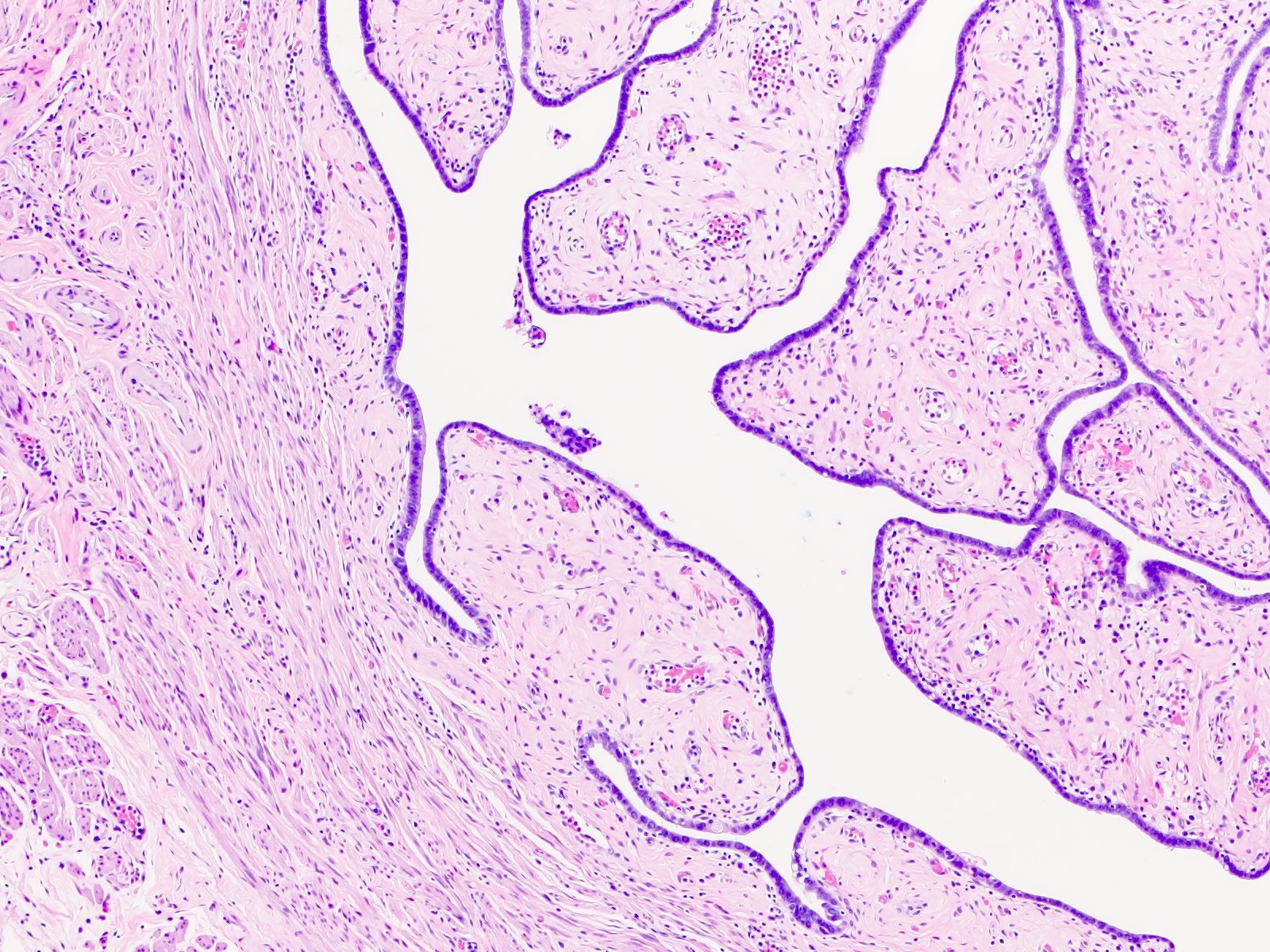
Mucosal plicae
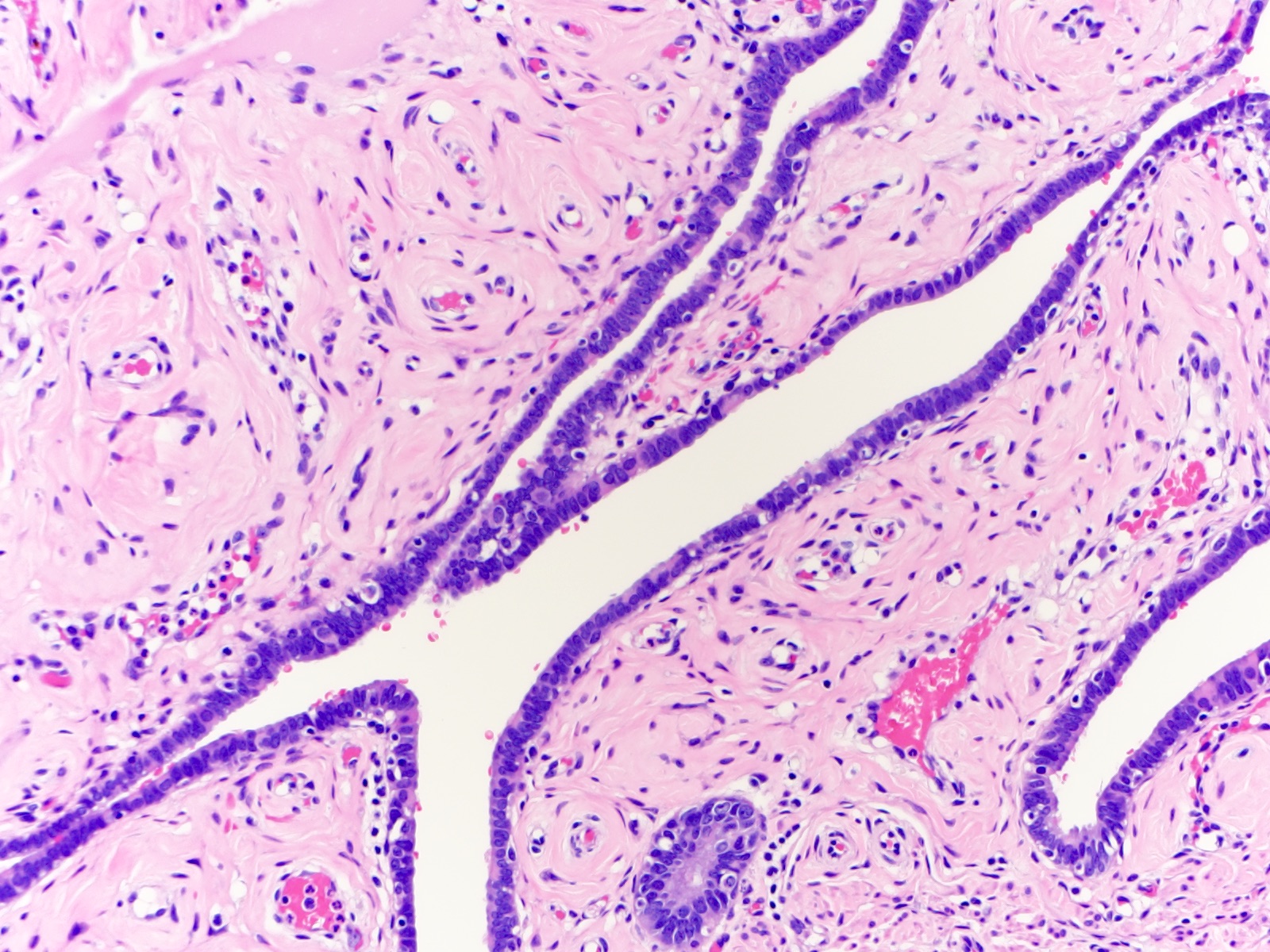
Fallopian tube epithelium
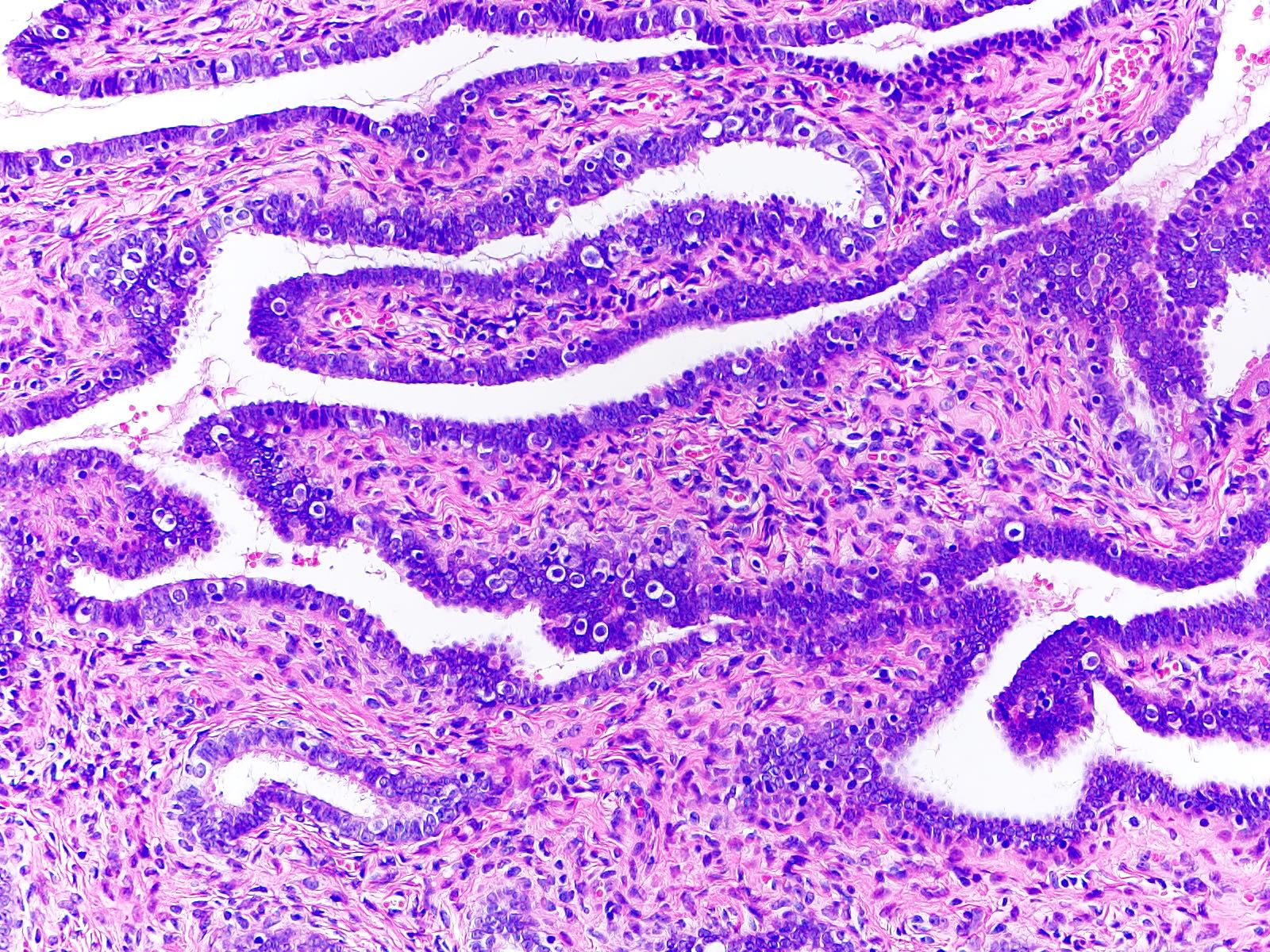
Simple columnar epithelium
Fallopian tube, premenopausal
Mucosal plicae
Fallopian tube epithelium
Simple columnar epithelium
Fimbriae are not thickened
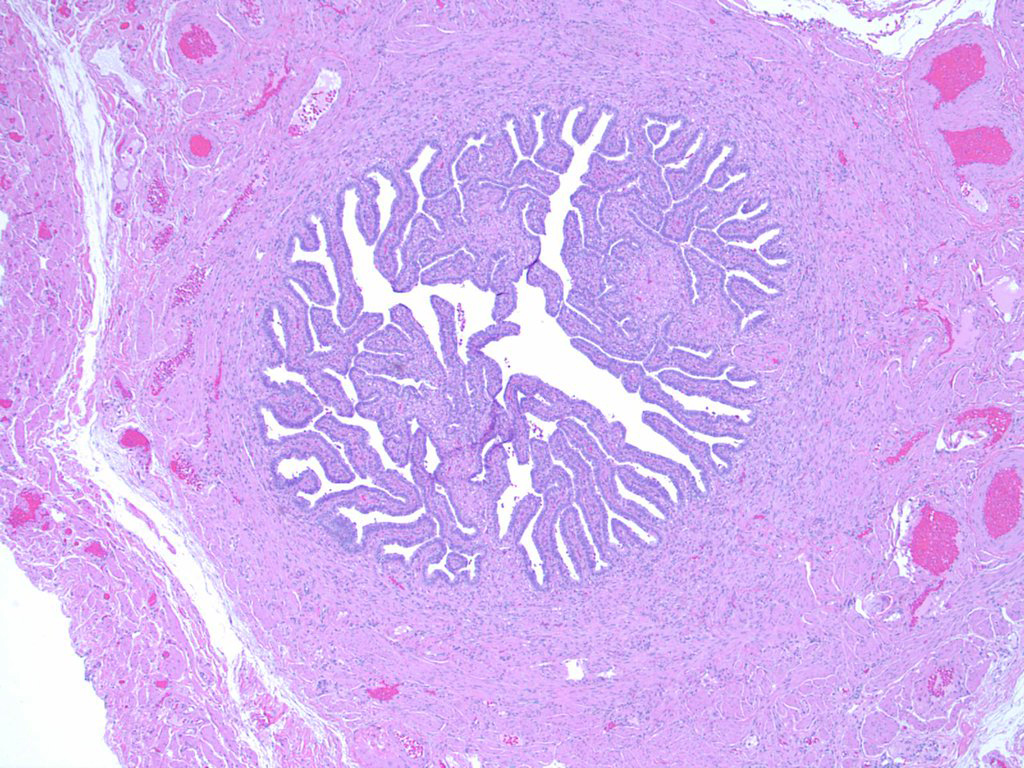
Lumen filled with plicae
Simple columnar epithelium
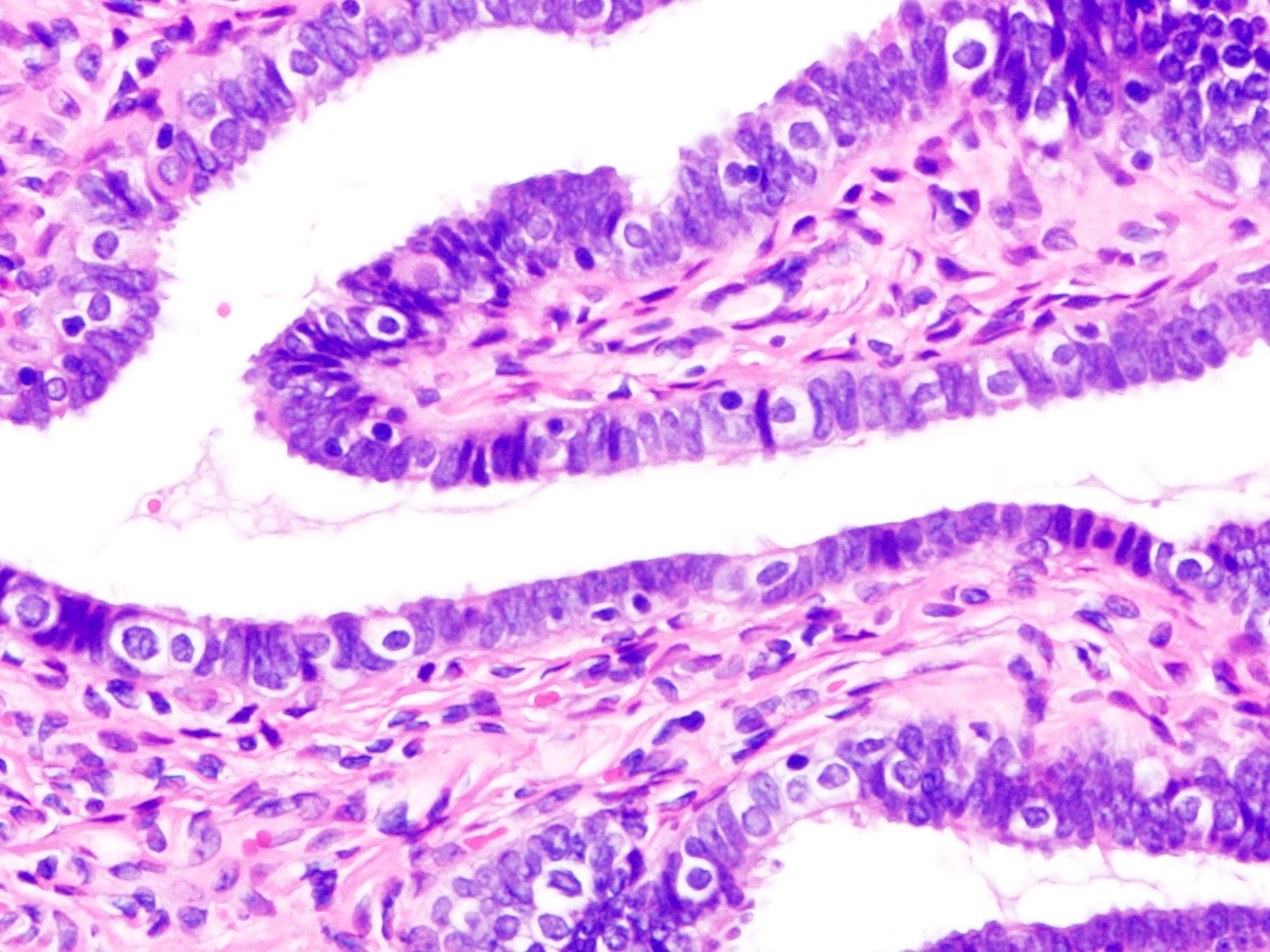
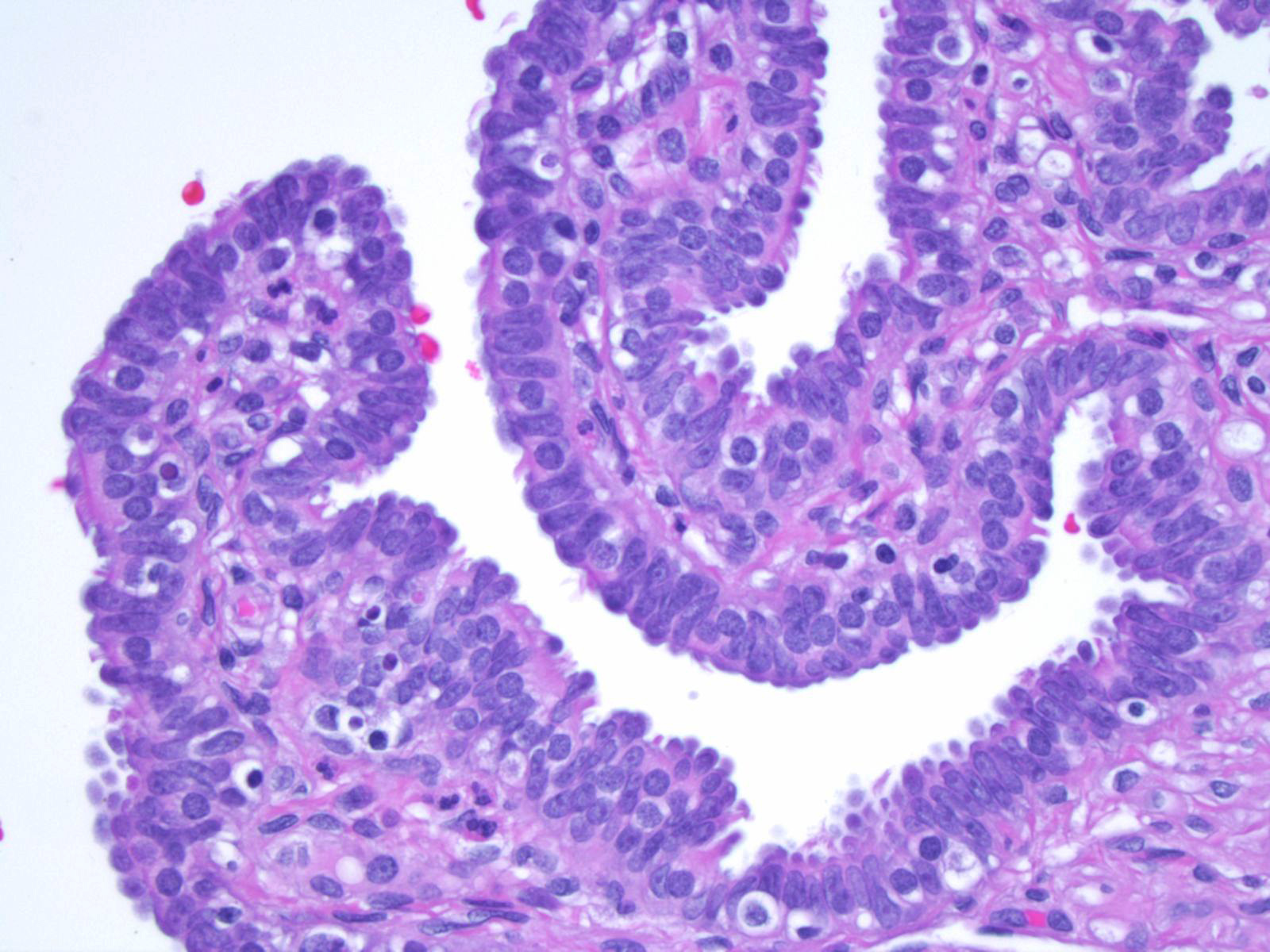
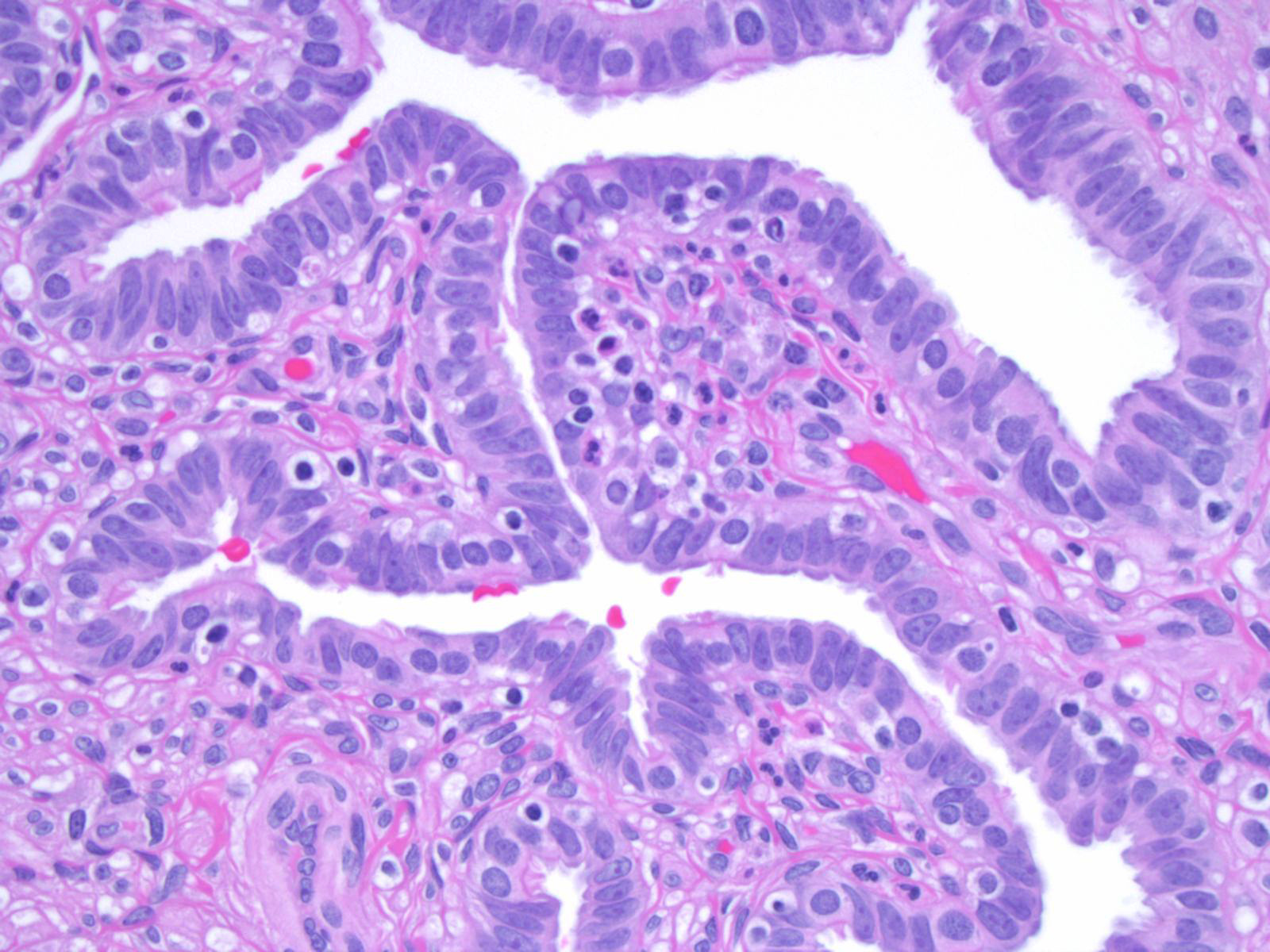
- Ciliated cells in clustered arrangements with round or oval nuclei, hyperchromatic chromatin and mild nuclear membrane irregularity
- Honeycomb / monolayered sheets
- Spindled appearance is not characteristic (Cytojournal 2018;15:28)
- Utility of minimally invasive laparoscopic screening of fallopian tubes in patients at high risk for high grade serous carcinoma is being investigated (J Vis Exp 2017;125:55887, J Am Soc Cytopathol 2023;12:368)
Images hosted on other servers:

Cell clusters

Honeycomb / monolayered sheets
- Ciliated cells (Dev Cell 2022;57:914, Stem Cells 2012;30:2487, Cancer Cell 2020;37:226)
- FOXJ1
- CAPS
- B tubulin
- TUBB4
- CCdC17
- CCDC78
- Secretory cells (Dev Cell 2022;57:914, Stem Cells 2012;30:2487)
- Peg cells (Dev Cell 2022;57:914)
- Basal cells (Dev Cell 2022;57:914)
- Stromal cells
- In postmenopausal fallopian tubes (Cell Rep 2022;41:111838)
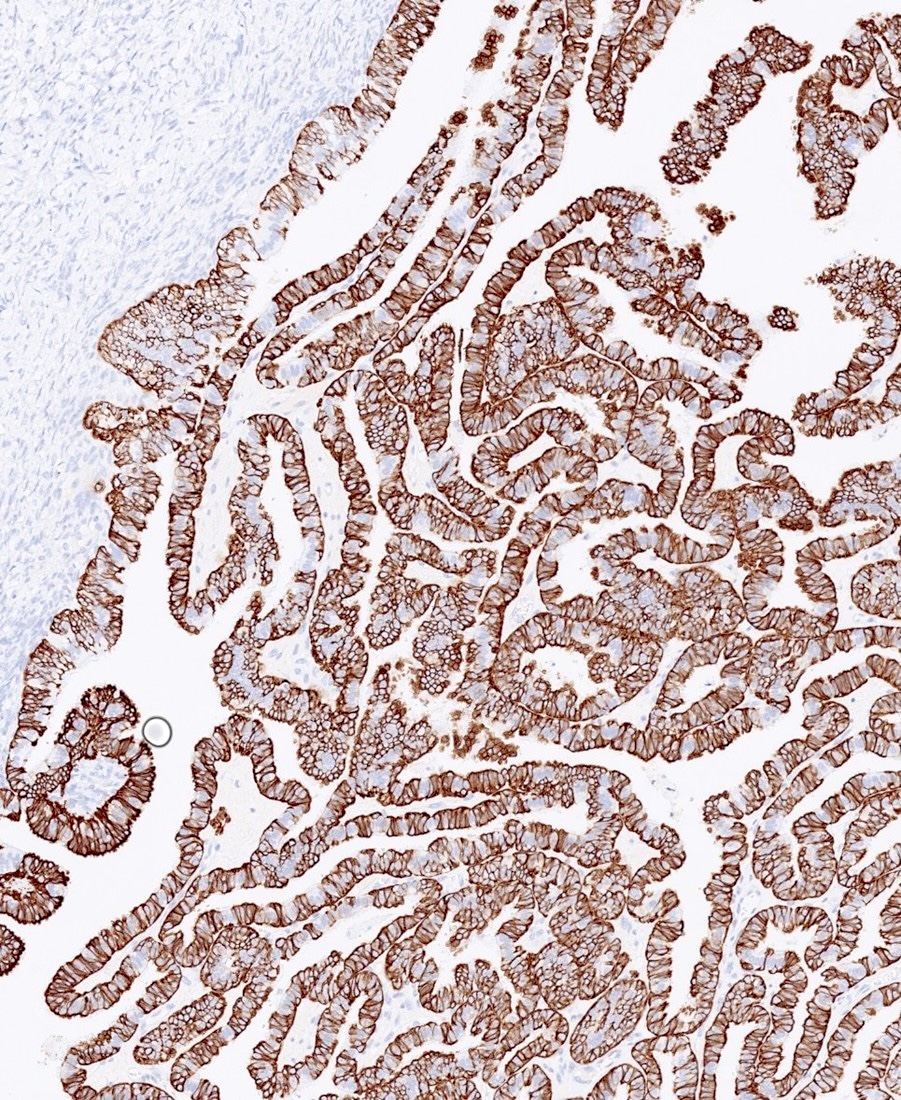
- PAX8 in secretory cells
- FOXJ1, adiponectin, estrogen, insulin and oxytocin in ciliated cells (Cell Rep 2022;41:111838)
- EpCAM mainly in the ampulla and fimbriae (Cell Rep 2022;41:111838)
- AR, ER and PR in stromal cells (Cell Rep 2022;41:111838)
- Dual PolyGlut-tubulin / DNAH5 stain
- Distinguishes motile cilia from primary cilia (Int J Gynecol Cancer 2018;28:1535)
- Variations during menstrual cycle (Physiol Res 2022;71:S137)
- Postmenstrual
- Ciliation is separated by fields of nonciliated flat cells with indistinct cell borders
- Preovulatory epithelium
- Swelling of nonciliated polyhedral cells
- Still maintain overall distribution of ciliated and nonciliated cells.
- Clusters of nonciliated cells bulge up to the height of the cilia tips
- Imparts a more uniform appearance of the surface epithelium
- Ovulatory epithelium
- Nonciliated cells show disrupted membranes after releasing their secretions
- Premenstrual period
- Nonciliated cells
- Regress below the level of the ciliary tips
- Become flattened
- Regain their distinct boundaries
- Clear boundaries: classic feature for differentiating the premenstrual / luteal phase from the postmenstrual phase
- Ciliated cells
- May cluster in elongated fields called tracts
- May form small ciliated clumps
- Nonciliated cells
- Postmenstrual
- Menopausal (Physiol Res 2022;71:S137)
- Surface epithelium is similar to the luteal phase of premenopausal women
- Mucosal folds with tracts of ciliated cells alternate with stretched clumps of ciliated cells
- Postmenopausal (Physiol Res 2022;71:S137)
- More nonciliated cells
- Frequently turn into dome shaped giant cells
- Observe delicate microplicae-like structures (Histol Histopathol 2006;21:219)
- Gradual shortening of microvilli
- More nonciliated cells
Images hosted on other servers:

Primary cilia

Secretory and ciliated cells
Shotgun histology: fallopian tube
UB medical: oviduct histology
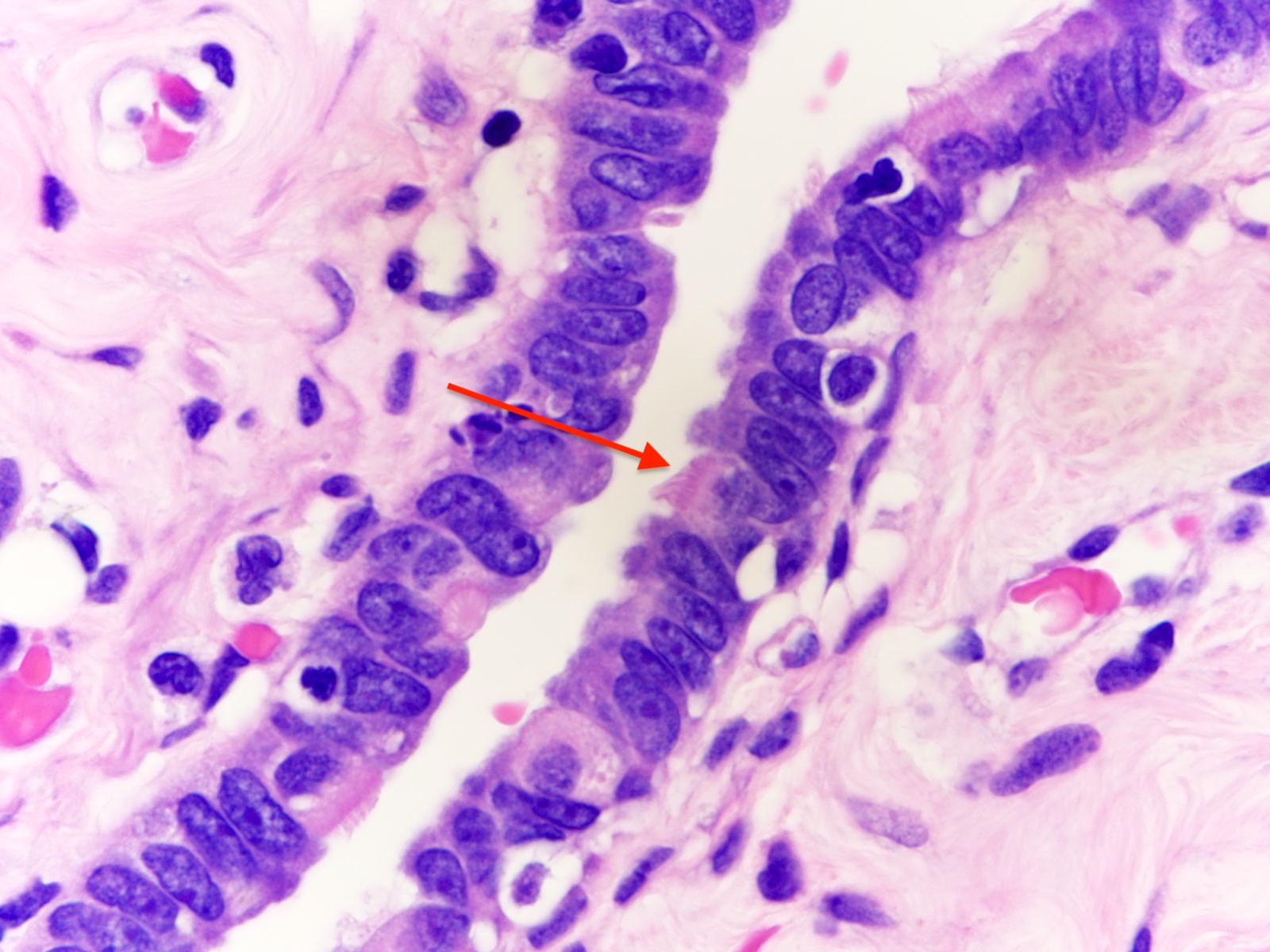
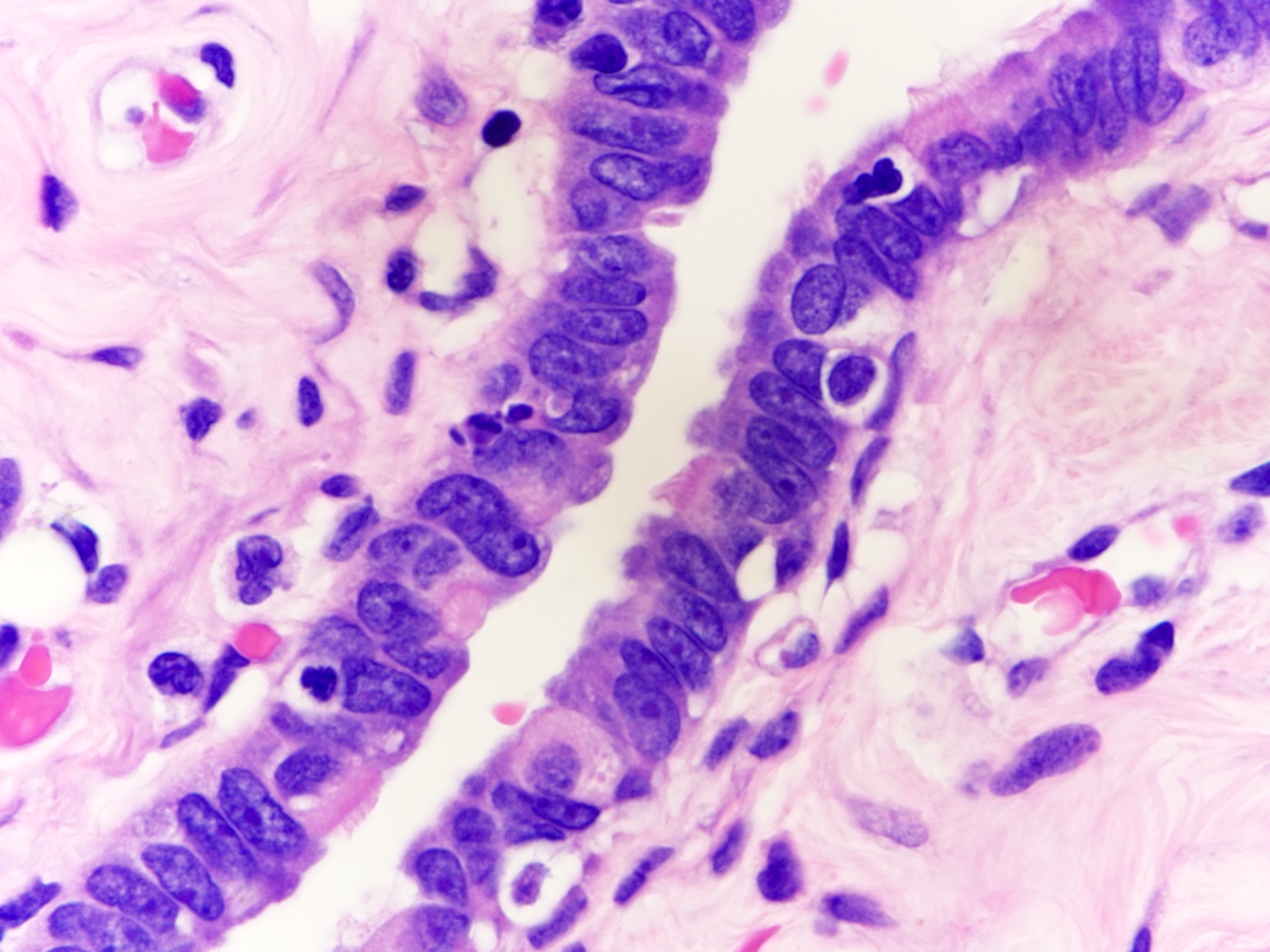
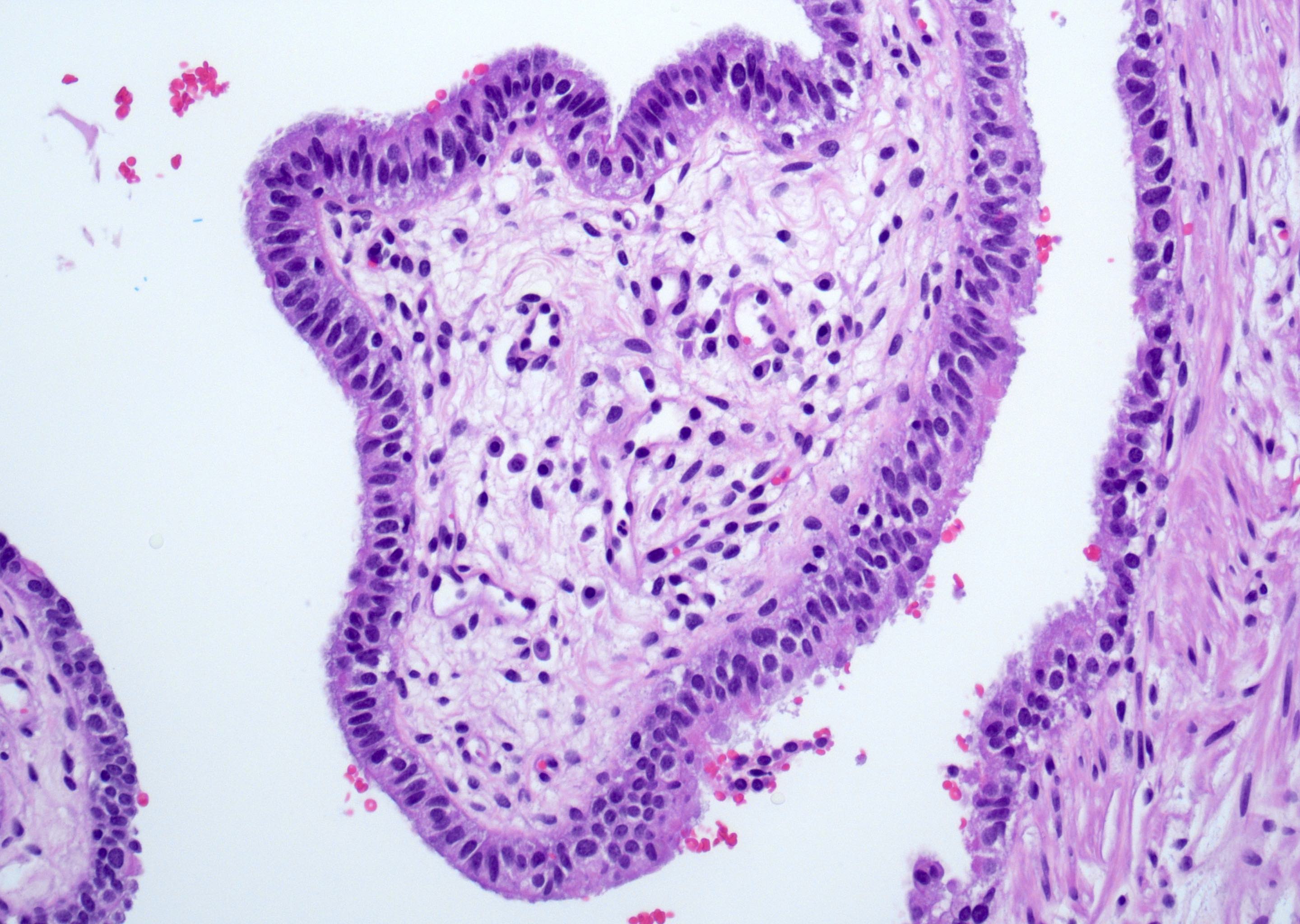
In this photo of fallopian tube epithelium, what cell type is indicated by the arrow and what is its corresponding function?
- Basal cell and production of tubal fluid
- Ciliated cell and movement of the egg
- Ciliated cell and production of tubal fluid
- Secretory cell and movement of the egg
Comment Here
Reference: Fallopian tubes & broad ligament - Anatomy, histology, embryology & features to report
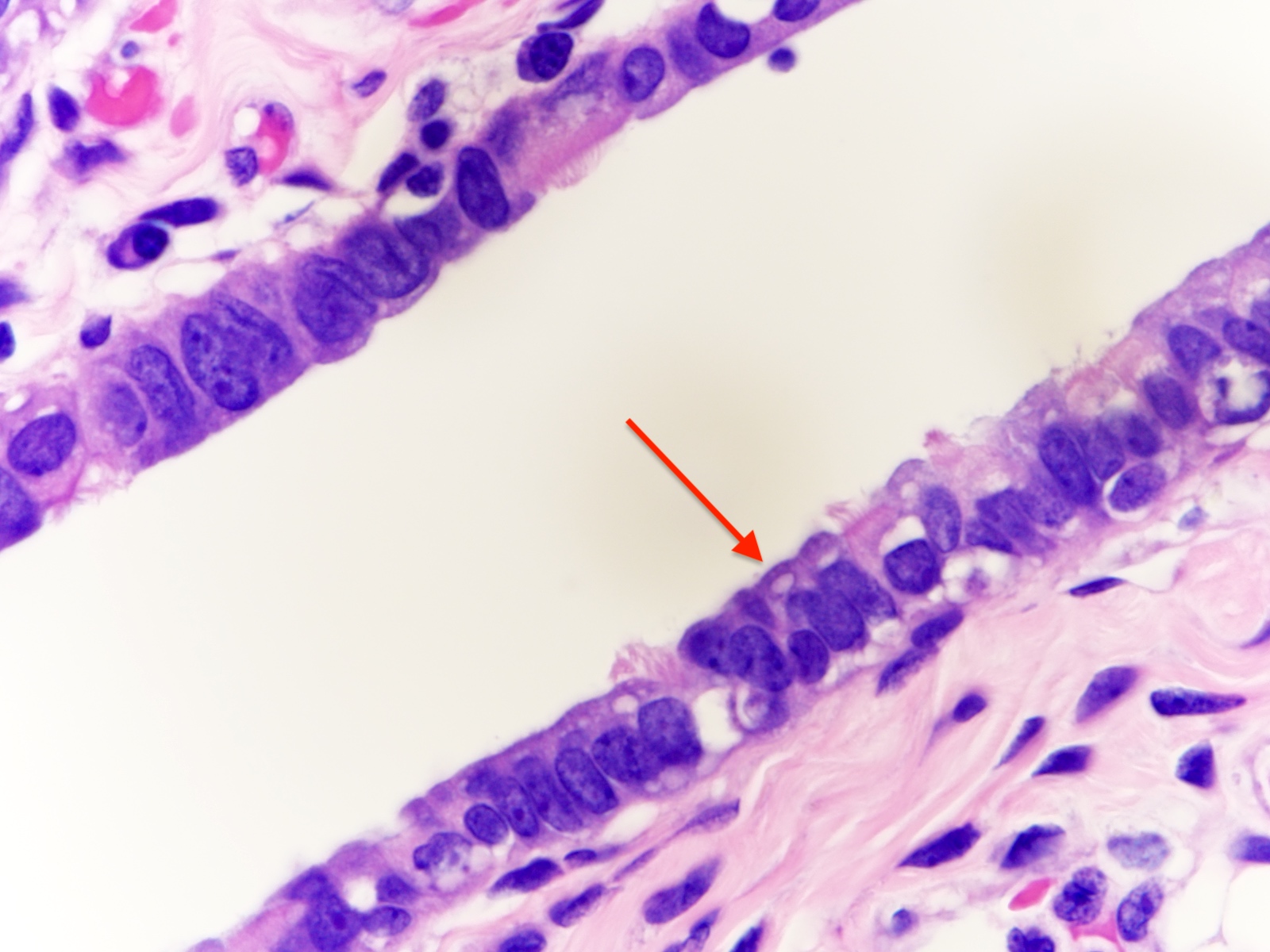
In this section of a fallopian tube, the cell indicated by the arrow stains for which of the following immunohistochemical markers?
- CD44
- EpCAM
- FOXJ1
- PAX8
Comment Here
Reference: Fallopian tubes & broad ligament - Anatomy, histology, embryology & features to report
- Also known as oviducts, uterine tubes, salpinges (singular salpinx means 'trumpet')
- Named after their discoverer, the 16th century Italian anatomist Gabriele Falloppio
- 3rd week:
- Migration of primordial germ cells from yolk sac, genital ridge forms from intermediate mesoderm, cloaca forms
- 4th week:
- Müllerian (paramesonephric) ducts form from coelomic epithelium invaginating venterolaterally into Wolffian (mesonephric) duct and genital mesentery
- This site of invagination later becomes the tubal ostium in which the fimbriae develop; septation of the cloaca occurs
- 5th - 8th weeks:
- Unfused cephalic part of Müllerian ducts form fallopian tube
- Fused part forms uterus and upper vagina
- In a female fetus (or male without functioning testis):
- Müllerian structures persist and Wolffian (mesonephric) duct regresses; vestiges may persist as epithelial inclusions
- Development affected by clomiphene, tamoxifen and to a lesser extent diethylstilbestrol (DES) (Hum Pathol 1987;18:1132, Hum Pathol 1982;13:190)
- In a male fetus:
- Testes produce Müllerian inhibitory substance, which causes regression of Müllerian ducts and persistence of paired Wolffian (mesonephric) ducts, which form epididymis and vas deferens
- The Müllerian remant is the rudimentary appendix testis
- Reference: Bhatnagar: Essentials of Human Embryology, Third Edition, 2000
Images hosted on other servers:
Fallopian tube
- Hollow, tubular structures, bilateral, 8 - 12 cm long and 0.5 - 1.2 cm in diameter, lined by a single layer of mucosal epithelium with many folds (plica)
- Extends from posterior superior uterine fundus laterally and leads to ovaries
- Connected to broad ligament by mesosalpinx (double fold of peritoneum), to uterine cornu by utero ovarian ligament, to lateral pelvic sidewall by infundibulopelvic (suspensory) ligament
- Arterial supply from branches of uterine and ovarian arteries, located within mesosalpinx
- Nerve supply from both sympathetic and parasympathetic fibers
- Sensory fibers run from T11 - T12 and L1
- Lymphatic drainage to para aortic, internal iliac, external iliac, common iliac and inguinal nodes
- Segments: intramural (within wall of uterus), isthmus (thick walled, narrower opening, ~ 2 cm in length), ampulla (thin walled, major portion of lateral tube, typically where fertilization occurs), infundibulum (trumpet shaped end lined by fimbriae, attaches to ovary)
- Tubal ostium: opening to peritoneal cavity
- Uterotubal junction: entrance to uterine cavity
Images hosted on other servers:

Uterine attachment on upper left, fibriae on upper right
- Plica: delicate folds of mucosa on inner aspect of tube, most evident in ampulla, merge with fimbriae
- Mucosa: consists predominately of single layer of cells including:
- Ciliated columnar cells (~25%), most abundant in infundibulum and ampulla, estrogen increases production of cilia
- Secretory cells (~60%), nonciliated, contain apical granules and produce tubular fluid, progesterone increases their number while estrogen increases their height and secretory activity
- Intercalated cells (peg cells, < 10%), which may be inactive secretory cells
- Tubal fluid:
- Contains nutrients for spermatozoa, oocytes and zygotes and promotes the capacitation of sperm by removing glycoproteins and other molecules from the plasma membrane
- Major constituents are calcium, sodium, chloride, glucose, proteins, bicarbonates, amylase, lactic acid
- Bicarbonates and lactic acid are vital to sperm's use of oxygen; also help egg develop postfertilization
- Tubal fluid flows against action of cilia; i.e. toward the fimbriated end
- Formation of fallopian tubal fluid: see Reproduction 2001;121:339
- Muscle layer: 3 smooth muscle layers:
- Innermost - obliquely arranged
- Middle - circular
- Outermost - longitudinal, extends into fimbriae
- Serosal surface: mesothelium of visceral peritoneum
- Stroma:
- Resembles fibroblasts, whorled / storiform pattern, surrounded by dense reticulin network
- Positive for SMA and desmin
- Normal histologic variations:
- Intramuscular edema in 12.5% of specimens, most frequently in postpartum women
- Plical fibrosis (35.5%), epithelial vacuolization (6.6%), and epithelial tufting / stratification (3.5%) correlated with increased patient age
- Inflammatory cells are common; intramuscular mast cells (~70% of cases), plasma cells (~20%), neutrophils (10.5%), and lymphoid follicles (2.1%) (Arch Pathol Lab Med 2002;126:951)
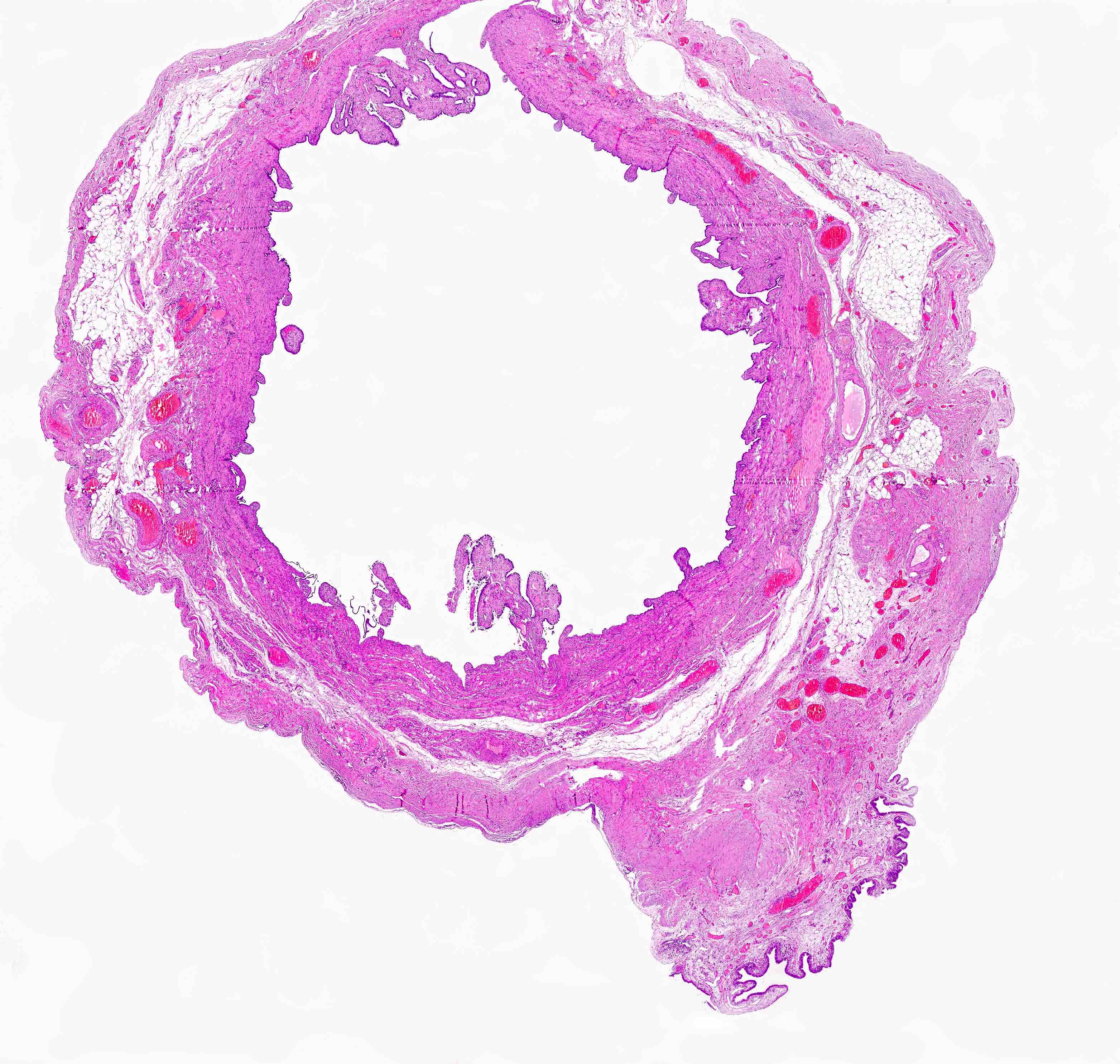
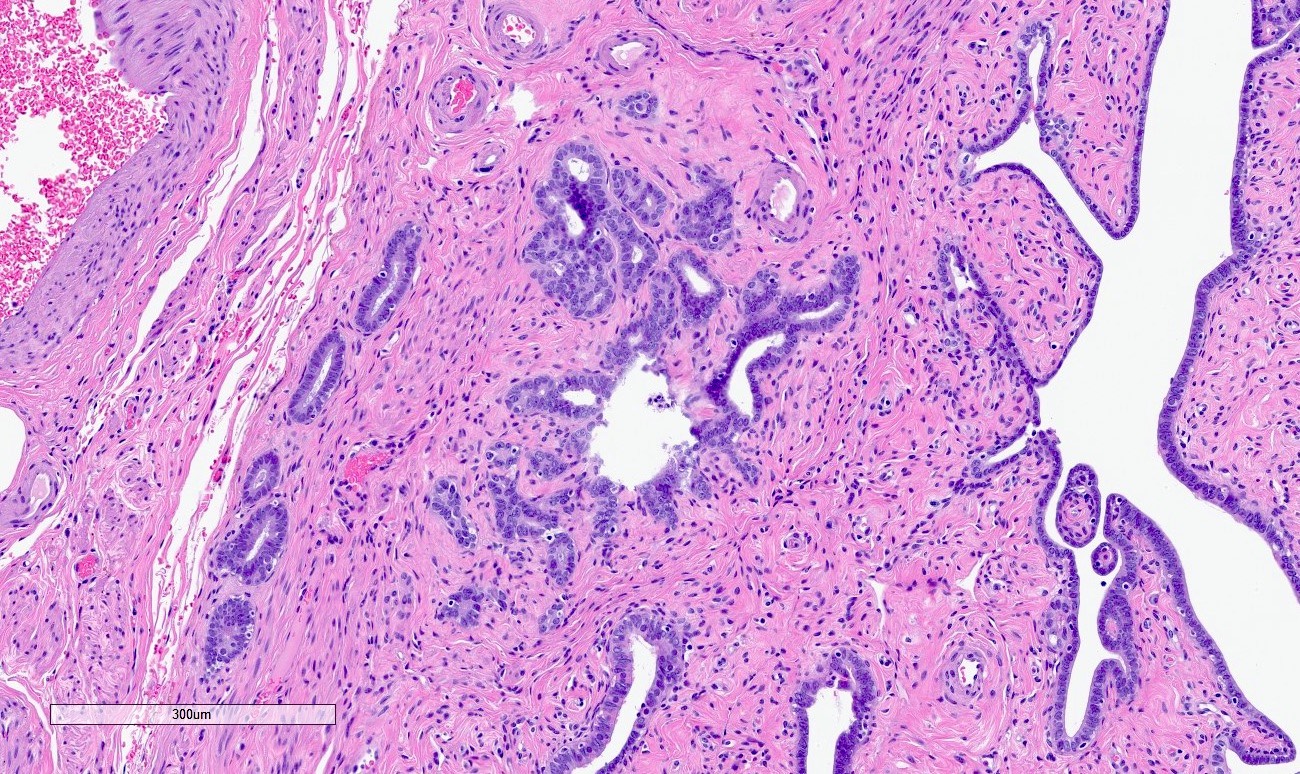
Contributed by Nicole D. Riddle, M.D.
Lumenal center filled with plica
Fimbriae are not thickened
Simple columnar epithelium
AFIP images

Lumen
Tubal epithelium
- Chronic inflammation of fallopian tube with lymphoplasmacytic infiltrate and with or without foamy histiocytes and granulomas
- Presence of plasma cells and lymphocytes in the submucosa
- Plicae are fibrotic, fused, short and thick
- May be associated with epithelial hyperplasia
- Chronic salpingitis, follicular salpingitis, granulomatous salpingitis, ligneous salpingitis, pseudoxanthomatous salpingitis and xanthomatous salpingitis
- Women of reproductive age
- Occurs in up to 50% of ectopic pregnancies
- Fallopian tube, unilateral or bilateral
- May be associated with active or prior history of infection (pelvic inflammatory disease) (Fertil Steril 2000;74:152)
- May be seen in association with endometriosis or tubal ectopic pregnancy
- Other associations include inflammatory bowel disease (with pulse granulomas) or other infectious processes (tuberculosis, sarcoidosis) (Int J Gynecol Pathol 2015;34:275)
- Several bacterial organisms (Neisseria gonorrhoeae, Chlamydia trachomatis, Mycoplasma), foreign body (lubricants, mineral oil, starch), endometriosis
- Usually an incidental finding on microscopic examination
- May be associated with pelvic pain, especially in the setting of pelvic inflammatory disease, endometriosis or tubal ectopic pregnancy
- May show hydrosalpinx, unilateral or bilateral
- 2 year old girl with xanthogranulomatous inflammation (Case Rep Obstet Gynecol 2015;2015:237250)
- 32 year old woman with bilateral tubal gestation (Case Rep Obstet Gynecol 2014;2014:674514)
- 55 year old woman with tuberculous salpingitis (J Clin Diagn Res 2013;7:1186)
- Treating the underlying infection / inflammation if there is concurrent acute salpingitis
- Fused fimbriae, causing blunted end (clubbed tube)
- May form significant tubo-ovarian adhesions and a conglomerated mass
- May show marked tubal dilation (hydrosalpinx)
- May show areas of hemorrhage if associated with endometriosis
AFIP images
Discolored mucosa
- Chronic salpingitis (Fertil Steril 2000;74:152):
- Usually short, thick plicae with fibrous stroma, lymphocytes, plasma cells or both in the mucosa
- Hydrosalpinx may or may not be seen
- Plicae may look normal or fused
- Epithelial hyperplasia may be seen
- Granulomas, either necrotizing or nonnecrotizing, suggest infection (especially tuberculosis), sarcoidosis or other autoimmune disease (e.g., inflammatory bowel disease)
- Pseudoxanthomatous salpingitis (Int J Gynecol Pathol 2015;34:275):
- Abundant hemosiderin laden macrophages within fallopian tube lamina propria with associated lymphoplasmacytic infiltrate
- Endometriosis in the tubal subserosa or ovarian tissue
- Xanthogranulomatous salpingitis:
- Foamy histiocytes, granulomas and chronic inflammation in the fallopian tube submucosa (Int J Gynecol Pathol 2002;21:56)
- May be associated with pelvic inflammatory disease
- Follicular salpingitis (misnomer): later stage of chronic salpingitis with fusing plicae, mimicking a pattern of thyroid follicles
Contributed by Shabnam Zarei, M.D. and Nicole D. Riddle, M.D.
Short thick plicae
Inflammatory cells

Short thick plicae and inflammation
Mucosal inflammation

Stromal fibrosis
Thickened plicae and foamy histiocytes

Foamy histiocytes
Fused and slightly thickened plicae
- Fallopian tube, salpingectomy:
- Chronic salpingitis, xanthogranulomatous salpingitis or pseudoxanthomatous salpingitis
- Fibrotic plica:
- A normal physiologic change in postmenopausal women
- Inflammatory infiltrate is absent
- Physiologic salpingitis during menses:
- Only minimal neutrophilic infiltrate is seen
- Salpingitis isthmica nodosa:
- Nodular thickening of fallopian tube with cystically dilated glands within muscular layer
- No associated inflammation
- Serous tubal intraepithelial carcinoma (STIC):
- Older women
- Cytologic atypia and loss of ciliation
- Abnormal (mutant) pattern of p53 expression by immunohistochemistry
- Endometriosis
- History of prior pelvic surgery
- Inflammatory bowel disease and diverticulosis
- Pelvic tuberculosis
Comment Here
Reference: Chronic salpingitis
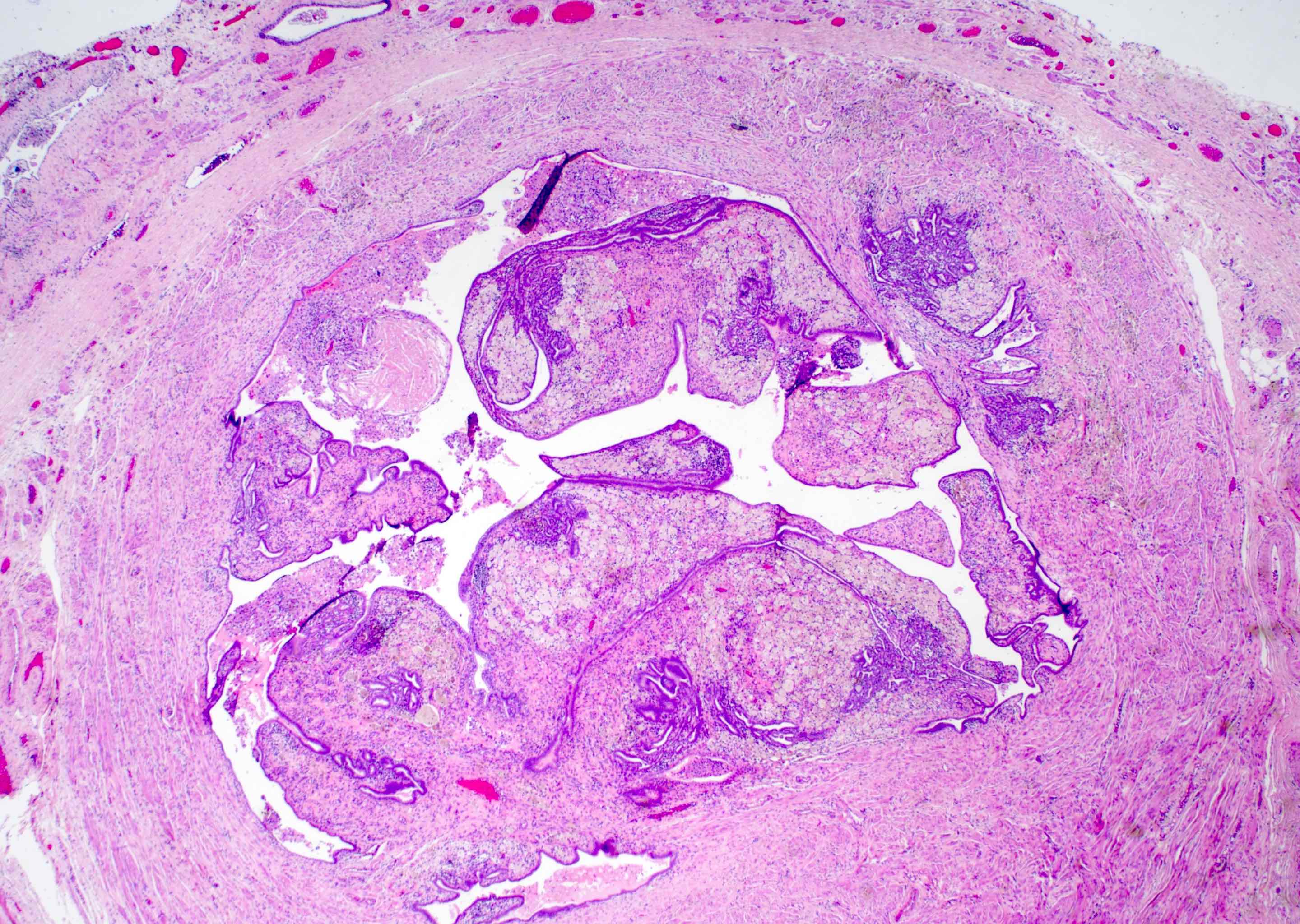
Which of the following statements is true regarding the photomicrograph above?
- Associated hydrosalpinx is uncommon
- Rarely seen in ectopic tubal pregnancy
- The most common inflammatory infiltrates are neutrophils and eosinophils
- When associated with endometriosis, it has distinct gross and microscopic findings
Comment Here
Reference: Chronic salpingitis
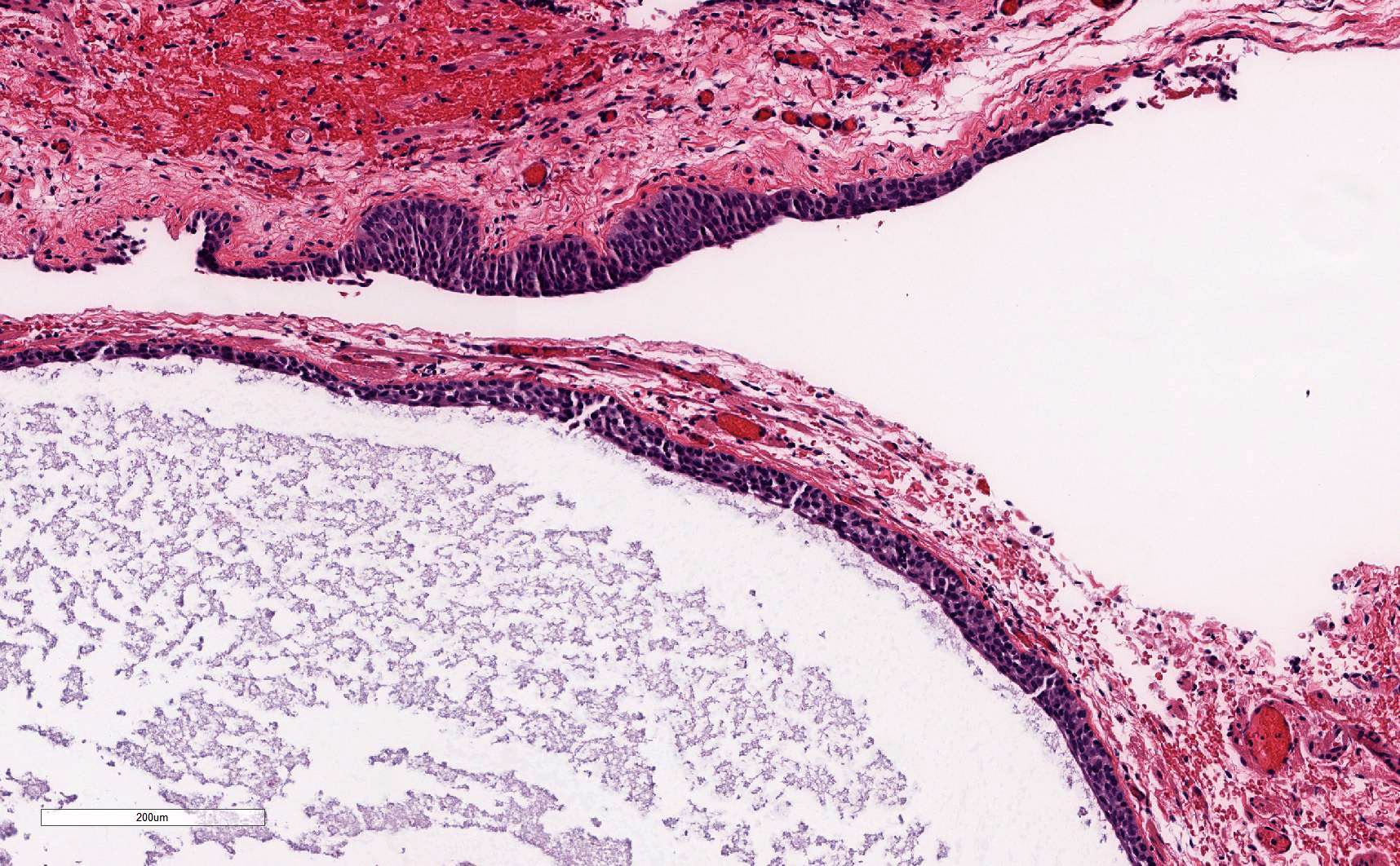
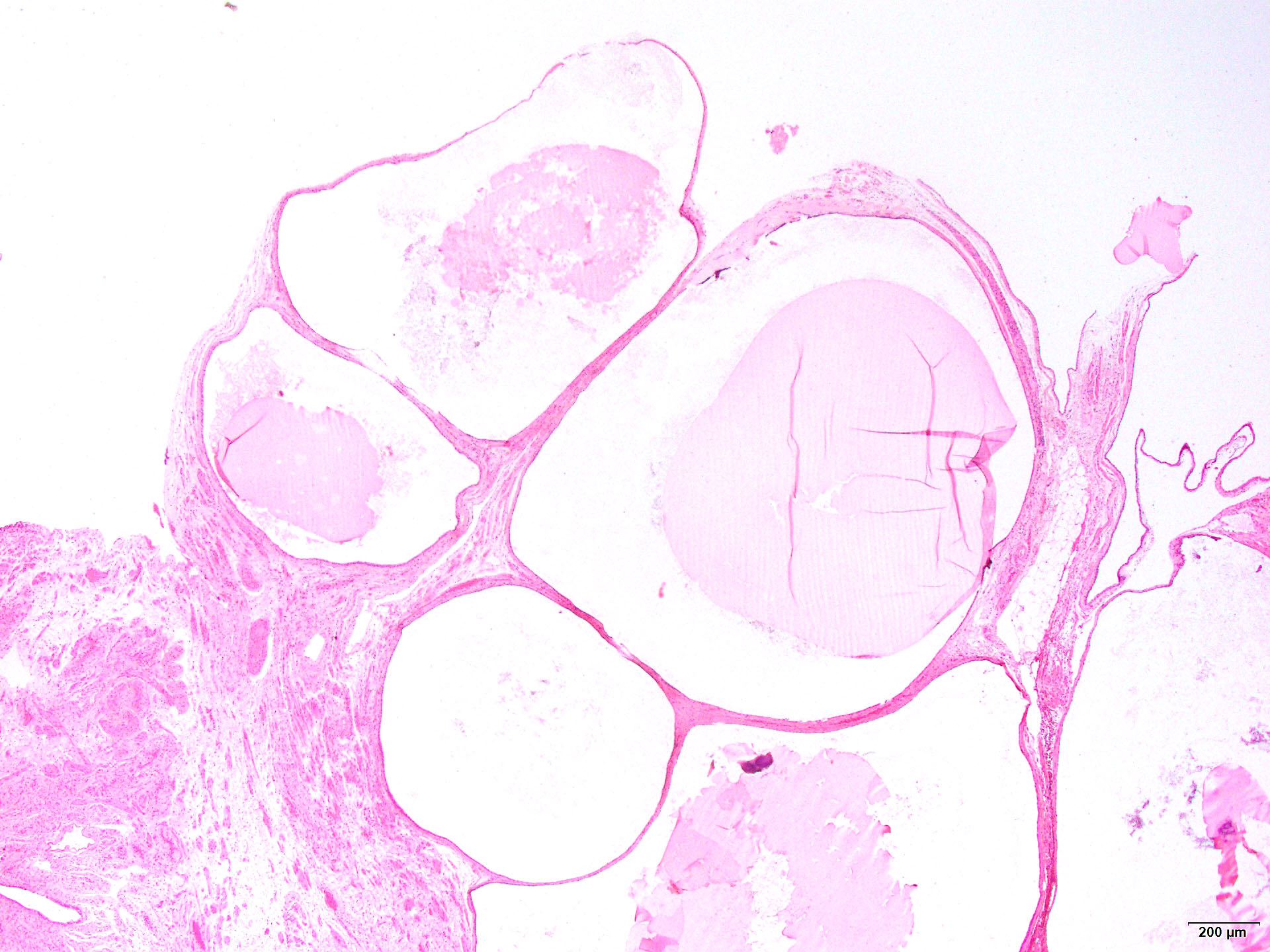
- Benign developmental cysts arising from remnants of Müllerian and Wolffian ducts as well as from mesothelium
- Benign, fluid filled cysts located adjacent to the adnexa (fallopian tube or ovary)
- Cysts are lined by non-stratified epithelium, which can be ciliated (paramesonephric cyst) or flat, cuboidal (mesothelial and mesonephric cysts)
- Usually are incidental findings
- Paratubal cysts, paraovarian cysts, mesothelial (or simple) cyst
- Hydatid cyst of Morgagni (no longer recommended): typically refers to pedunculated cyst located near tubal fimbria (Arch Gynecol Obstet 2012;285:1563)
- ~10% of all adnexal masses (Arch Gynecol Obstet 2012;285:1563)
- Vast majority are Müllerian (paramesonephric) cysts, commonly known as paratubal cysts
- < 2% are Wolffian (mesonephric) cysts (Am J Obstet Gynecol 1977;129:873)
- Adjacent to the adnexa, along broad ligament, between the fallopian tube and the ovary
- Müllerian (paramesonephric) and Wolffian (mesonephric) ducts grow mostly in parallel during development
- Müllerian ducts eventually fuse
- Fusion of Müllerian ducts creates a transverse fold, which becomes the broad ligament
- Broad ligament contains Müllerian and Wolffian duct remnants, which can then become cystic
- Reference: Kurman: Blaustein's Pathology of the Female Genital Tract, 7th Edition, 2019
- Thought to originate from remnants of Müllerian and Wolffian ducts as well as from mesothelium (Am J Obstet Gynecol 1977;129:873, Gynecol Obstet Invest 1981;12:1)
- Usually asymptomatic and incidentally found
- Large cysts can be painful, bleed, rupture or cause ovarian torsion (Arch Gynecol Obstet 2012;285:1563)
- Incidental finding
- If symptomatic, usually diagnosed by ultrasound
- Ultrasound findings: majority are unilocular cysts without papillations (Ultrasound Obstet Gynecol 2006;28:330)
- Presence of papillary projections / solid nodule typically indicates neoplastic cysts
- Benign
- May rarely give rise to serous borderline tumor and carcinoma (Gynecol Oncol Rep 2020;32:100559, Appl Immunohistochem Mol Morphol 2017;25:e21)
- 13 year old girl with bilateral paraovarian cysts (Sultan Qaboos Univ Med J 2021;21:e308)
- 31 year old woman with giant paratubal cyst presented with adnexal torsion (Case Rep Womens Health 2020;27:e00222)
- 85 year old woman with serous borderline tumor arising from a paratubal cyst (Gynecol Oncol Rep 2020;32:100559)
- Surgical excision if large or symptomatic
Images hosted on other servers:

Torsed paraovarian cyst before detorsion

Torsed paraovarian cyst after detorsion

Large paraovarian cyst
- Thin walled, fluid filled cyst(s) located adjacent to fallopian tube or ovary
- Paramesonephric cysts are lined by single layer of bland ciliated tubal epithelium
- Mesonephric cysts are lined by single layer of low cuboidal, nonciliated epithelium with occasional clear cells (rare) (Am J Obstet Gynecol 1977;129:873)
- Mesothelial cysts are lined by single layer of flat or cuboidal, nonciliated cells, which may show transitional cell metaplasia (see Walthard cell nests)
- Distinction between the types of cyst may be difficult but has no clinical implications
Contributed by Lucy Ma, M.D.

Simple cysts adjacent to Walthard nests
Paratubal cysts adjacent to fallopian tube
Ciliated epithelium
- Not essential to include in report, particularly if cysts are small and incidental
- Right fallopian tube, salpingectomy:
- Fallopian tube with paratubal cysts
- Serous cystadenoma:
- Presence of dense collagenized cyst wall
- Absence of rudimentary plicae
- Hydrosalpinx:
- Presence of well developed, smooth muscle wall
- Presence of occasional branching plicae with columnar epithelium containing histologic normal ciliated and secretory cells
- Direct communication with nondilated portion of fallopian tube
A 45 year old patient underwent total hysterectomy and bilateral salpingo-oophorectomy for a myomatous uterus. The left adnexa showed the finding in the image above. What is the next step in management regarding this finding?
- Computed tomography (CT) of the chest
- Germline testing
- No additional therapy
- Serial serum CA-125 levels
- Surgical staging
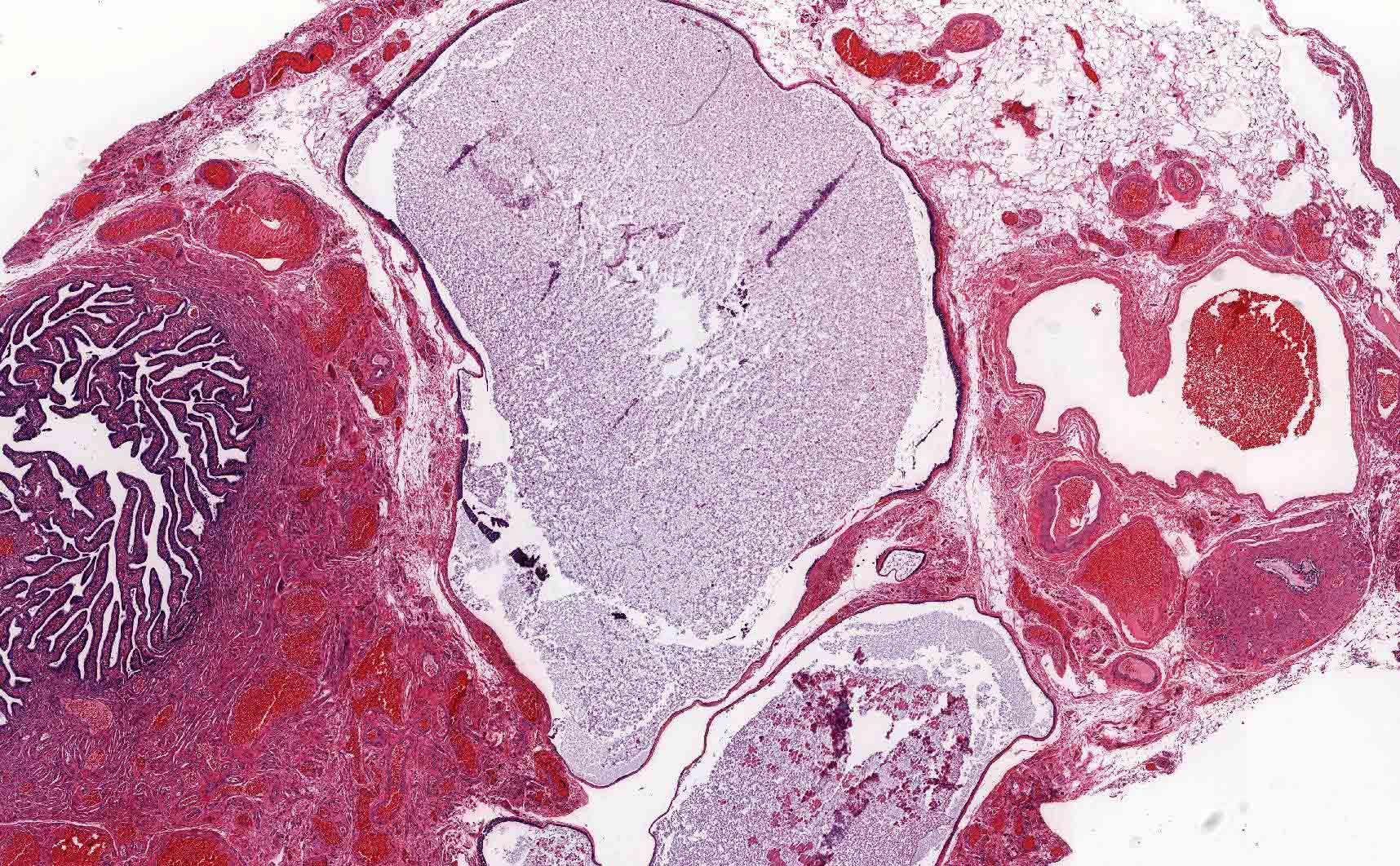
- Extrauterine implantation of a fertilized egg
- Extrauterine implantation of a fertilized egg
- > 95% occur in the fallopian tube
- Diagnosis based on visualization of an extrauterine gestational sac by transvaginal ultrasound (TVUS) or histologic confirmation
- Approximately 2% of all reported pregnancies in the United States are ectopic (MMWR Morb Mortal Wkly Rep 1995;44:46, Fertil Steril 2014;102:1671, Obstet Gynecol 2010;115:495)
- 2.7% of pregnancy related mortalities attributed to ruptured ectopic (Obstet Gynecol 2017;130:366)
- Diagnosis increases with age: 0.29% (15 - 19 years old), ~0.5% (20 - 24 years old), ~0.58% (25 - 29 years old), ~0.7% (30 - 34 years old) and ~0.89% (35 - 44 years old) (South Med J 2017;110:18)
- Fallopian tube accounts for 95.5% of extrauterine implantation sites: 2.4% interstitial, 11.1% fimbrial, 12.0% isthmic and 70% ampullary (Hum Reprod 2002;17:3224)
- 4.5% are extratubal: 3.2% ovarian and 1.3% abdominal (Hum Reprod 2002;17:3224)
- May implant at any place on the abdominal viscera or peritoneal surface (Radiographics 2015;35:946):
- Cervix (J Emerg Med 2019;56:e123)
- Liver (Pathology 2018;50:478)
- Spleen (BMJ Case Rep 2016;2016:bcr2016218291)
- Prior cesarean scars (Clin Imaging 2020;66:26)
- 4 possible mechanisms of ectopic implantation (Sex Transm Infect 2020;96:322):
- Anatomic obstruction preventing passage of the zygote
- Abnormal conceptus
- Tubal motility abnormalities
- Zygote transperitoneal migration
- Pelvic inflammatory disease
- Disruption of tubal anatomy caused by infection is the most likely cause; inflammation of the tube is present in up to 90% of tubal pregnancies, which is 6x more common than in normal tubes
- Cigarette smoking
- Prior fallopian tube pathology
- Infertility
- Intrauterine device
- Previous fallopian tube surgery
- Previous ectopic pregnancy
- Approximately half of ectopic pregnancy patients do not have any identifiable risk factors
- References: Clin Obstet Gynecol 2012;55:376, Fertil Steril 1996;65:1093, Obstet Gynecol 2018;131:e91
- Most common clinical presentationis first trimester vaginal bleeding or abdominal pain
- Symptoms usually appear 6 - 8 weeks after the patient’s last menstrual period but may occur even later, particularly if the pregnancy occurs outside of the fallopian tube
- No confirmed intrauterine pregnancy
- Positive pregnancy test and visualization of an extrauterine gestational sac, with or without an embryo on transvaginal ultrasound
- Visualization at surgery with histologic confirmation
- Positive beta hCG
- Extrauterine gestational sac, with or without an embryo on transvaginal ultrasound
Contributed by Hao Chen, M.D., Ph.D.
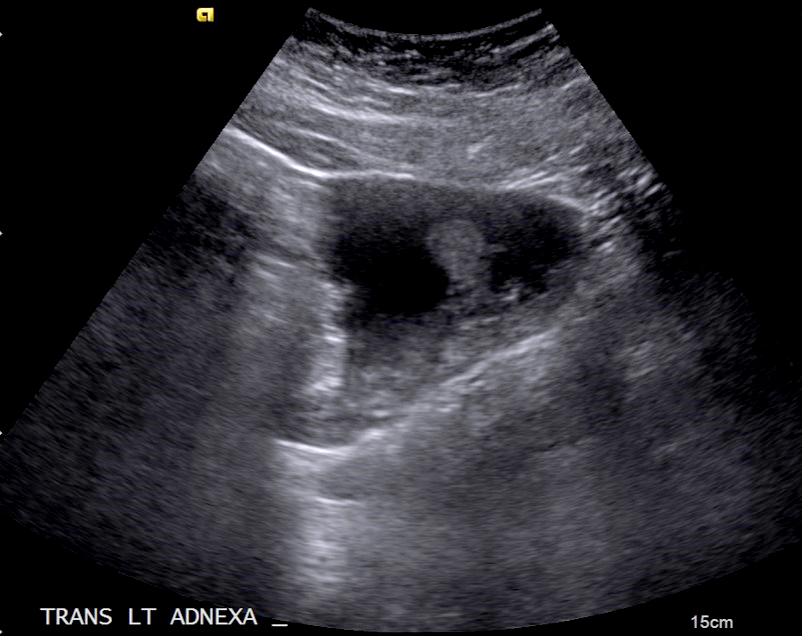
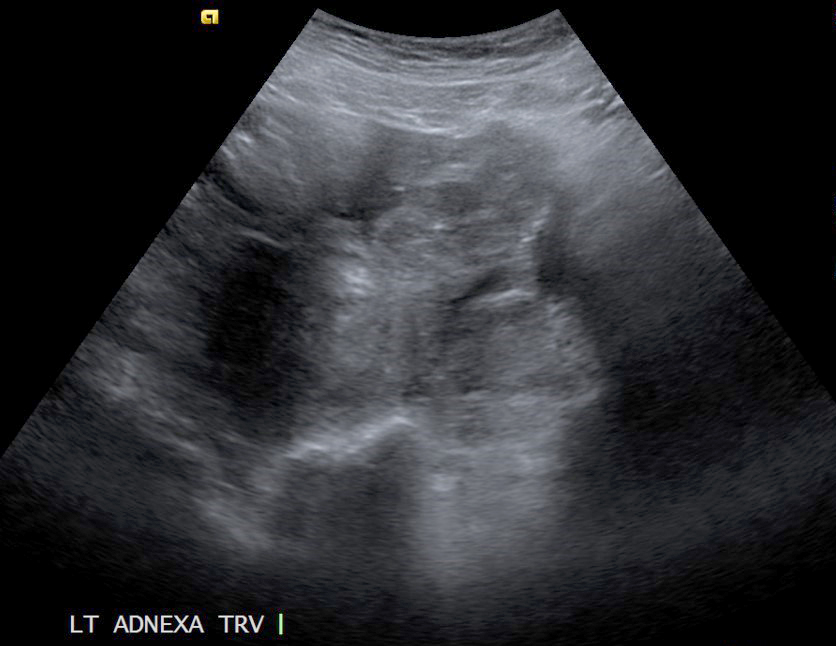
Left adnexal mass
- Significant risk of morbidity and mortality if not promptly recognized and treated
- Patients with earlier ectopic pregnancies and relatively modest beta hCG levels are more likely to have successful treatment with single dose methotrexate therapy (Clin Obstet Gynecol 2012;55:376)
- Following methotrexate therapy, patients not exhibiting at least a 15% decrease in beta hCG from day 4 - 7 are more likely to experience treatment failure (Reprod Biomed Online 2017;34:383)
- 29 year old woman with vaginal bleeding and discharge (Radiol Case Rep 2019;14:354)
- 30 year old woman with abdominal ectopic pregnancy after in vitro fertilization and single embryo transfer (Reprod Biol Endocrinol 2016;14:69)
- 38 year old woman with acute onset of lower abdominal pain associated with a history of amenorrhea (Cureus 2020;12:e10993)
- Surgical management (typically salpingectomy or salpingotomy) for hemodynamically unstable patients
- Methotrexate may be administrated for hemodynamically stable patients (Clin Obstet Gynecol 2012;55:376)
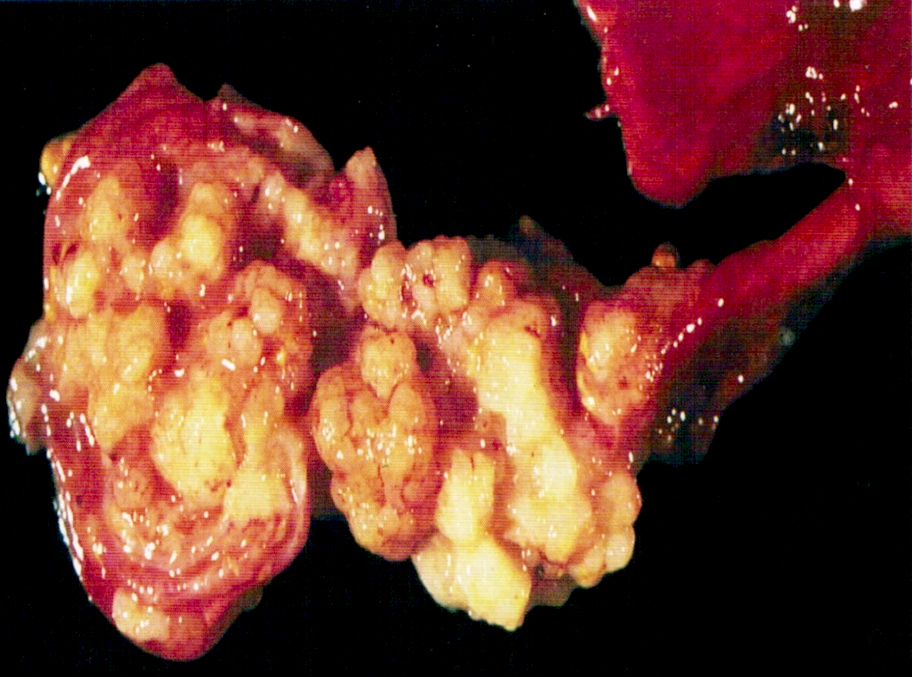
- Dilated tube with distended wall, with or without rupture
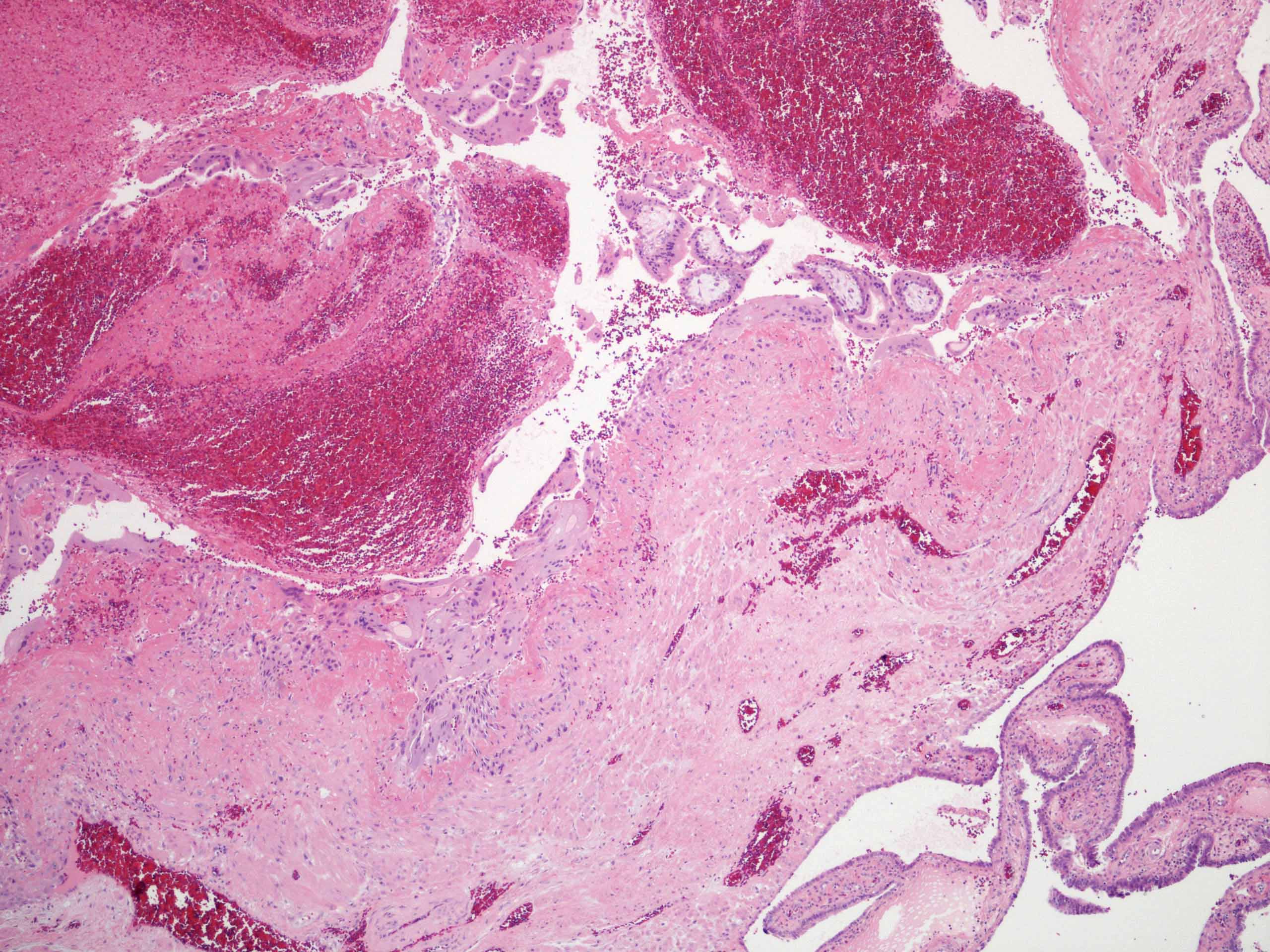
- Lumen contains blood clot, embryo, chorionic villi
Contributed by Hao Chen, M.D., Ph.D. and AFIP

Placenta and fetus
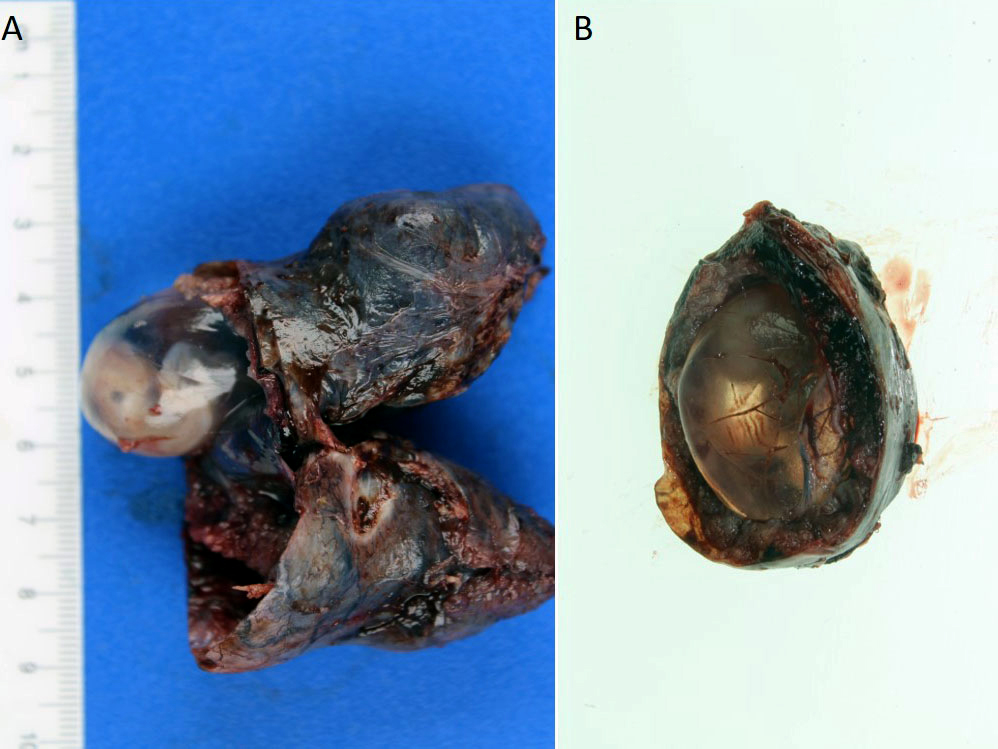
Gestational sac and embryo
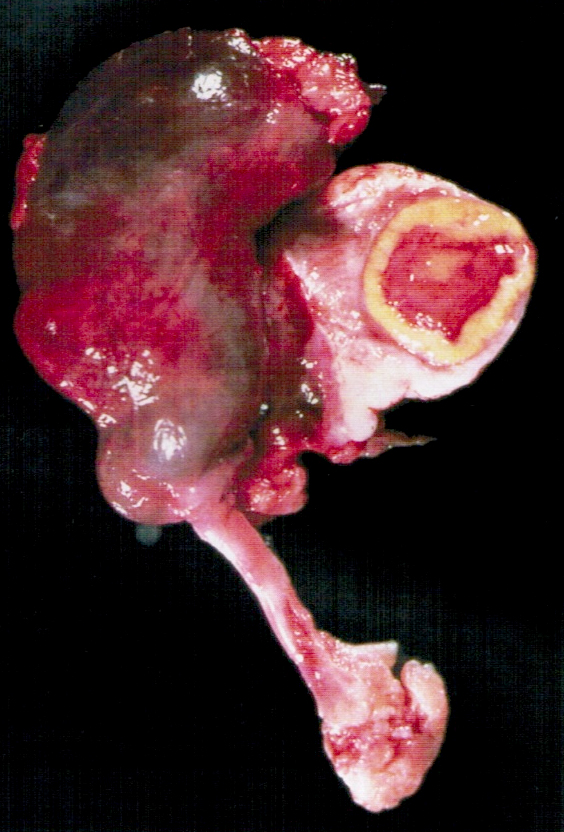

Ectopic pregnancy
Images hosted on other servers

Hemorrhage and placental tissue with fetal part

Rupture and hemoperitoneum
- Presence of extrauterine chorionic villi or extravillous trophoblast is needed for diagnosis
- Fetal tissue may be present
- Endometrial stromal decidualization in isolation is not diagnostic of ectopic pregnancy
- Mesothelial reactive changes, often reactive mesothelial proliferation, may be present (on the surface of the fallopian tube or the closest peritoneum to the site of the ectopic pregnancy); of note, the exaggerated cytological changes and mesothelial proliferation should not be confused with atypical mesothelial proliferation
Contributed by Hao Chen, M.D., Ph.D.
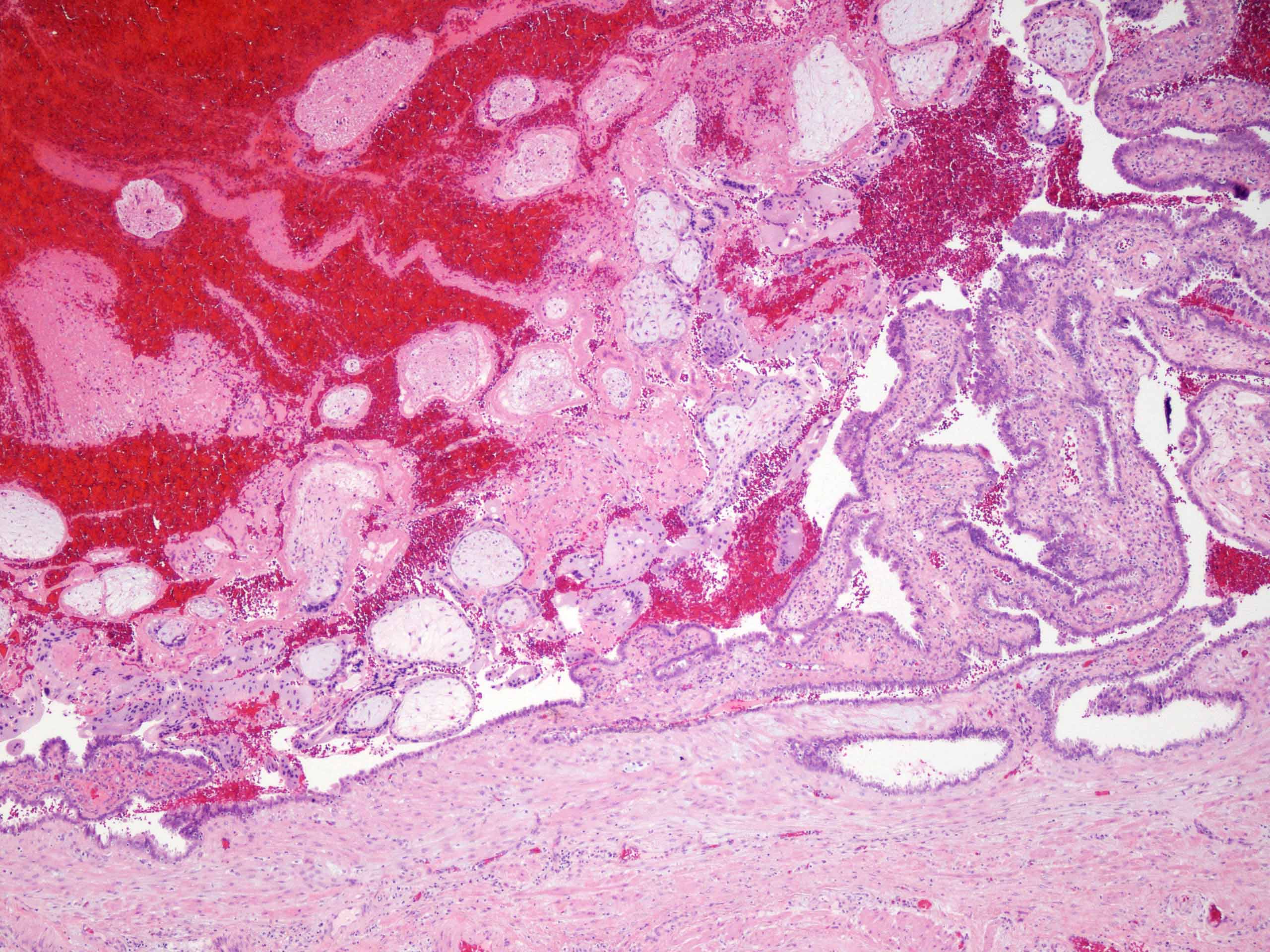
Intraluminal chorionic villi
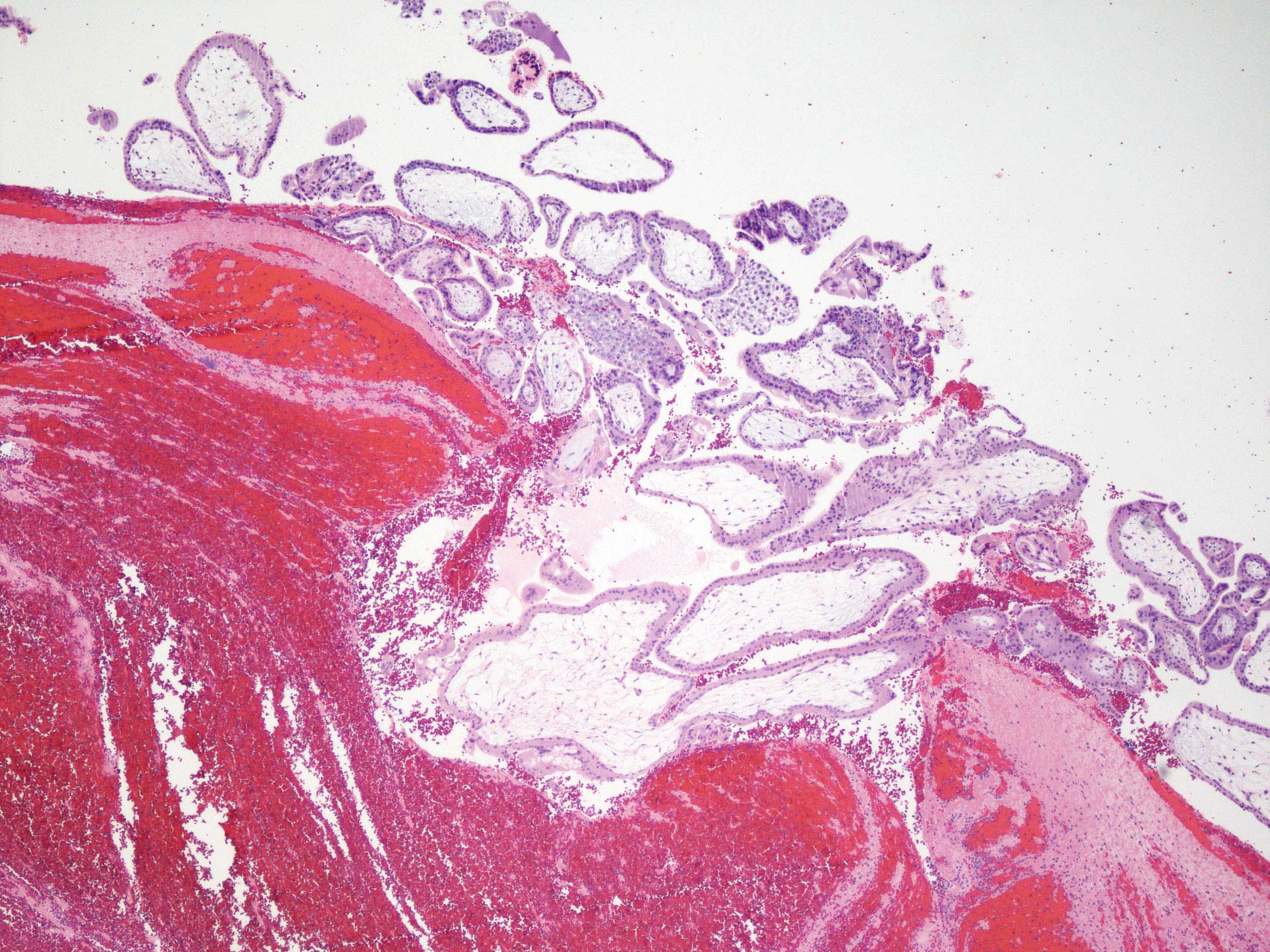
Chorionic villi and blood
- Fallopian tube, salpingectomy:
- Fallopian tube with intraluminal immature chorionic villi, consistent with ectopic (tubal) pregnancy
- Spontaneous abortion:
- Identification of product of conceptions in expelled uterine tissue or endometrial curettage tissue
- Lack of evidence of extrauterine gestational sac / embryo by either transvaginal ultrasound or histological confirmation
- Ampulla
- Fimbria
- Interstitial
- Isthmic
Comment Here
Reference: Ectopic / tubal pregnancy
- Idiopathic
- Infertility
- Intrauterine device
- Pelvic inflammatory disease
Comment Here
Reference: Ectopic / tubal pregnancy
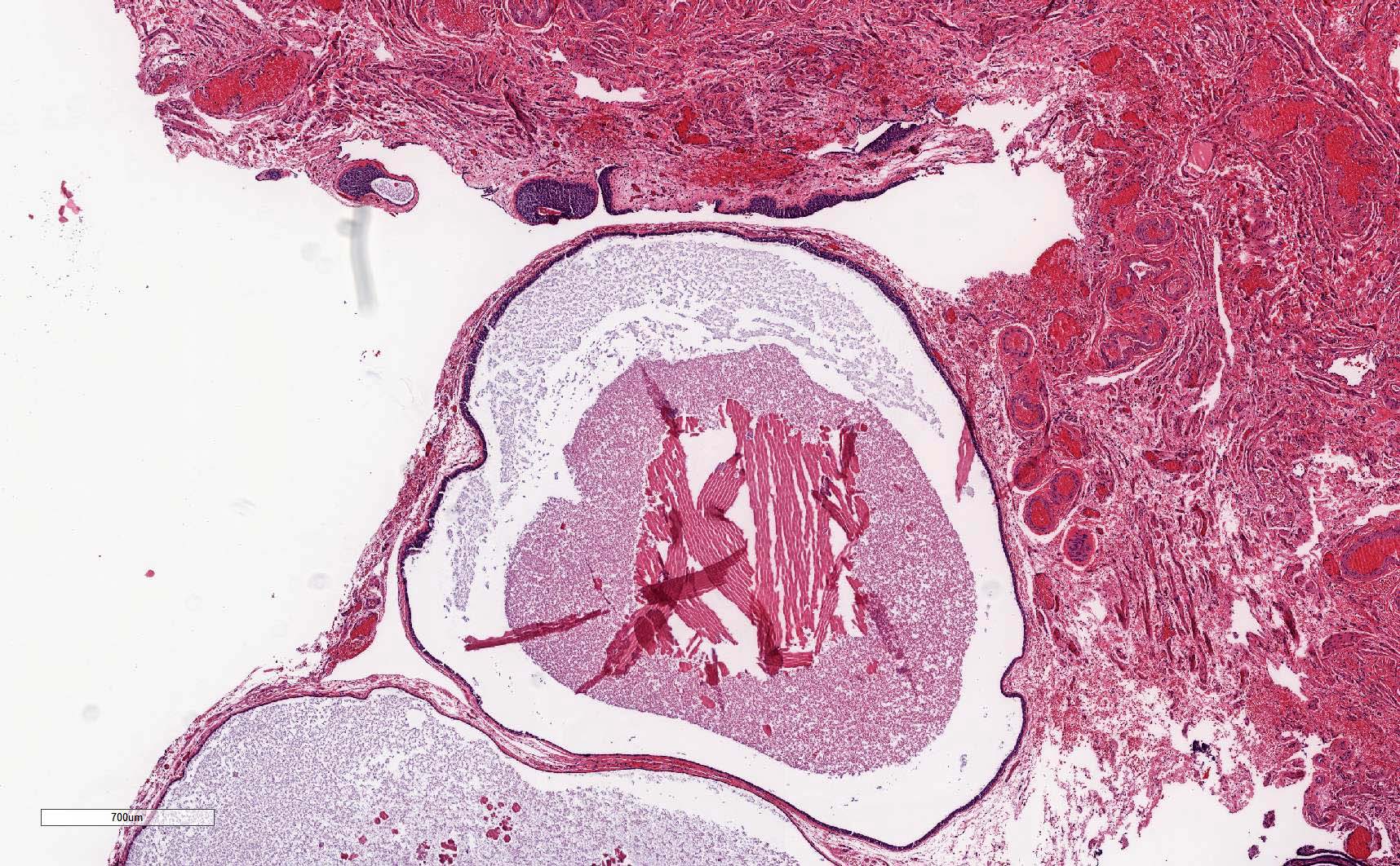
A 28 year old woman presented with acute onset abdominal pain and vaginal bleeding. Pregnancy test was positive. Transvaginal ultrasound showed left adnexal mass. Left salpingectomy was performed. The histological findings were as showed in the above image. The diagnosis is
- Chronic salpingitis
- Ectopic tubal pregnancy
- Tubo-ovarian abscess
- Tubo-ovarian torsion
Comment Here
Reference: Ectopic / tubal pregnancy
- Rare, 0.3 to 1.0% of genital tract malignancies
- Mean age 57 years, rarely teenagers; usually incorrect preoperative diagnosis
- High stage with pelvic extension or positive peritoneal cytology
- To call primary in fallopian tube, should arise from mucosa (endosalpinx), have tubal histologic pattern, involve the lumen, uterus and ovaries must be normal or have foci of malignancy that resemble metastases or independent primaries; if tubal wall is involved, should detect a transition between benign and malignant tubal epithelium
- 5 year survival: stage 1 - 77%, stage 3 - 20%; usually recur intra-abdominally
- Associated with BRCA1 and BRCA2 mutations; for patients with known mutation or family history of breast or ovarian cancer, should submit entire fallopian tube and ovary for microscopic examination (Am J Surg Pathol 2002;26:171, Am J Surg Pathol 2001;25:1283)
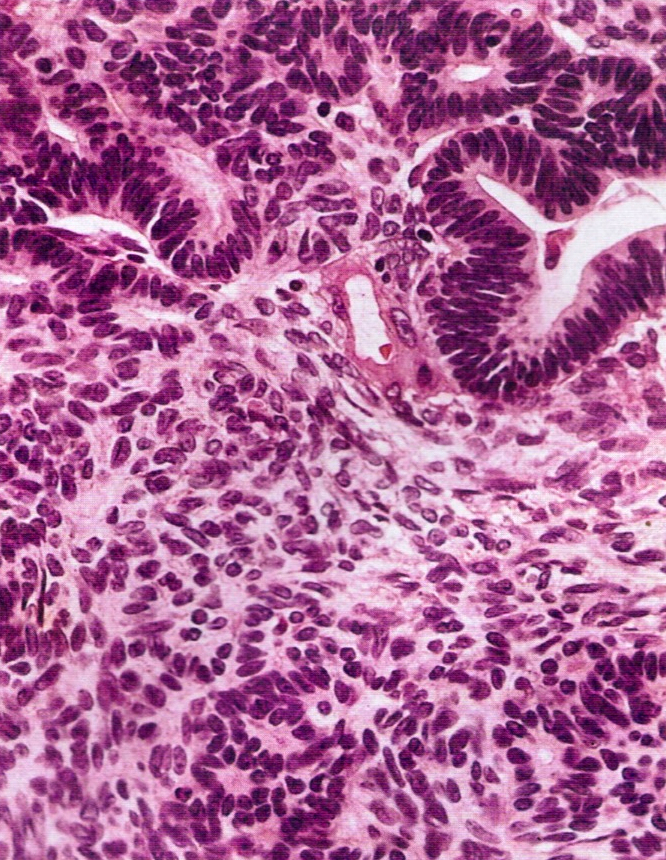
- Carcinomas at this site: 50% serous, 25% endometrioid, 20% transitional or undifferentiated
- Symptoms: vaginal bleeding or discharge (2/3), pain, adnexal mass (triad in 50%); endometrial smear positive in 10%
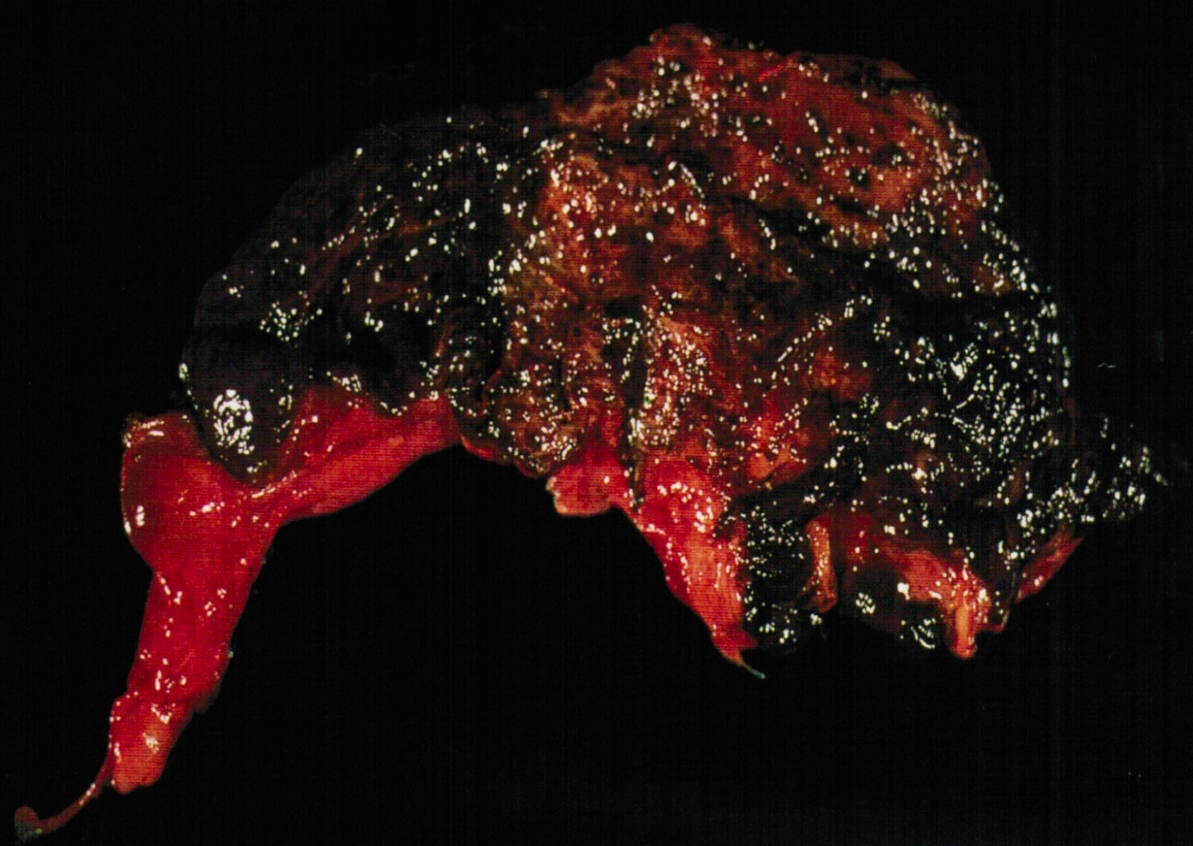
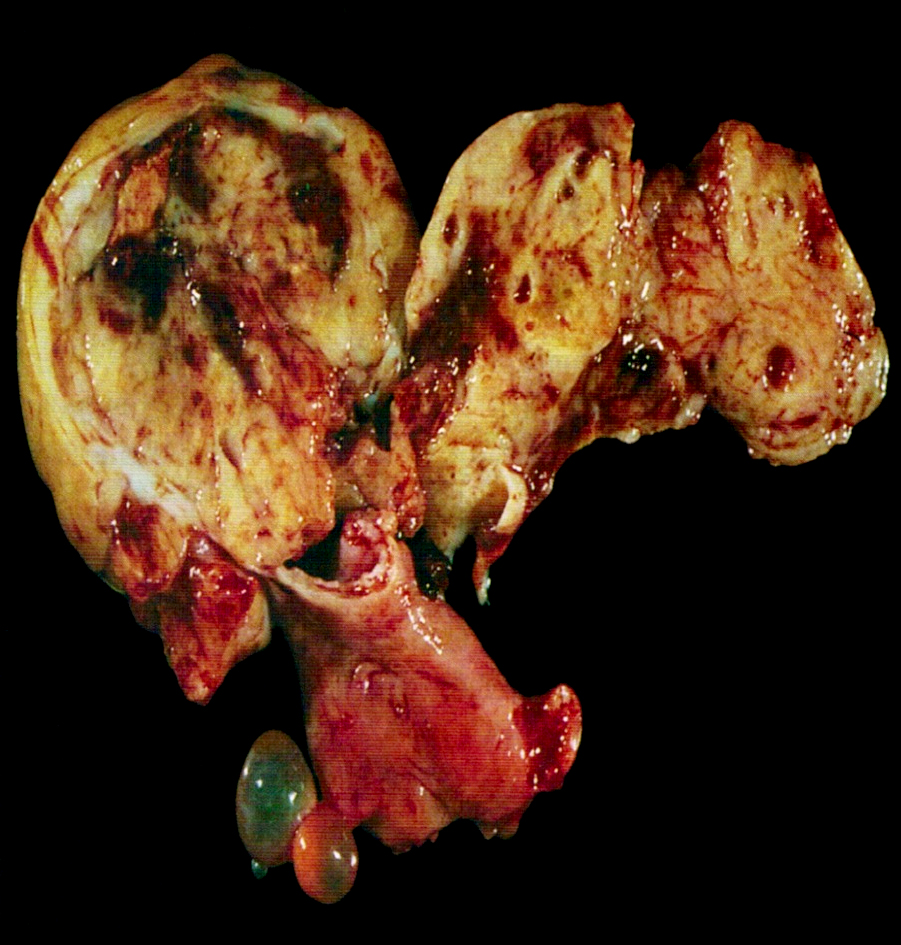
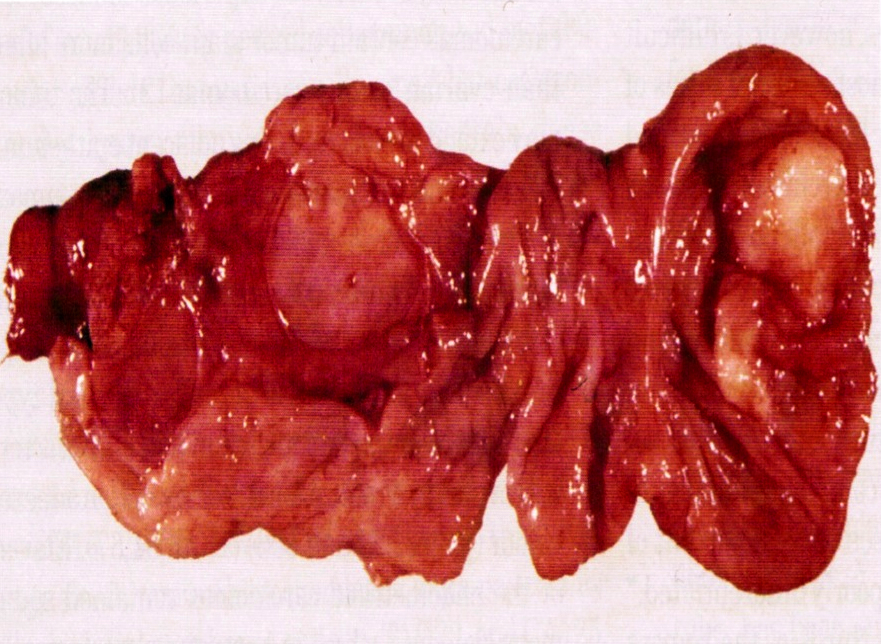
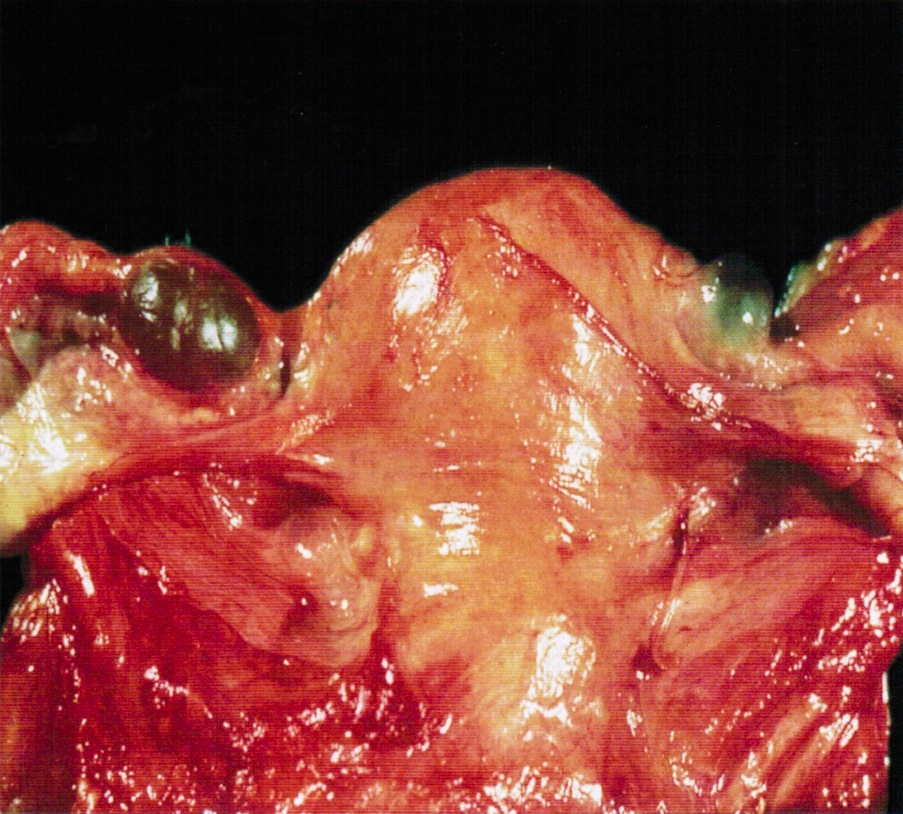
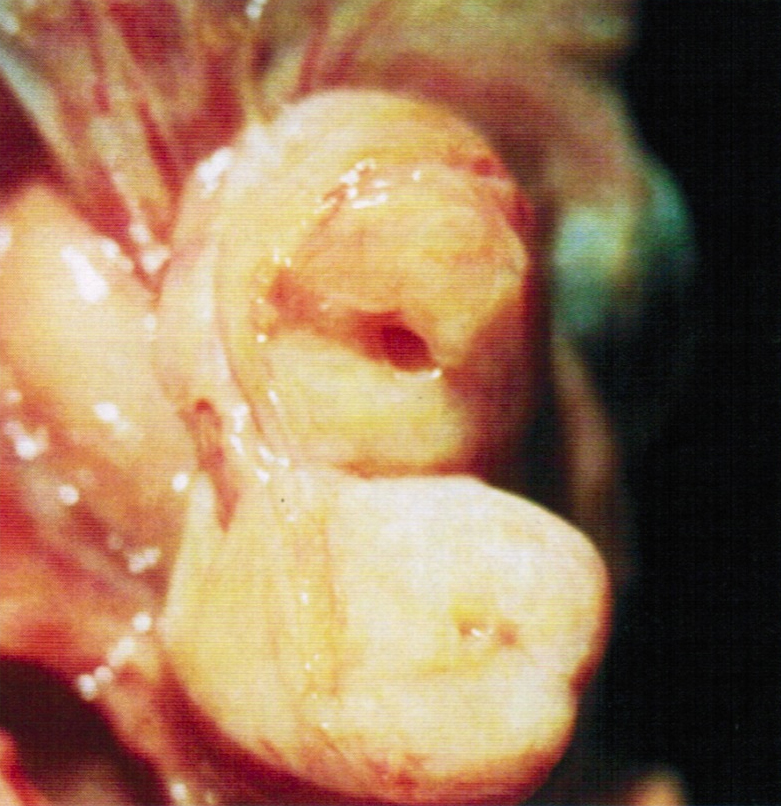
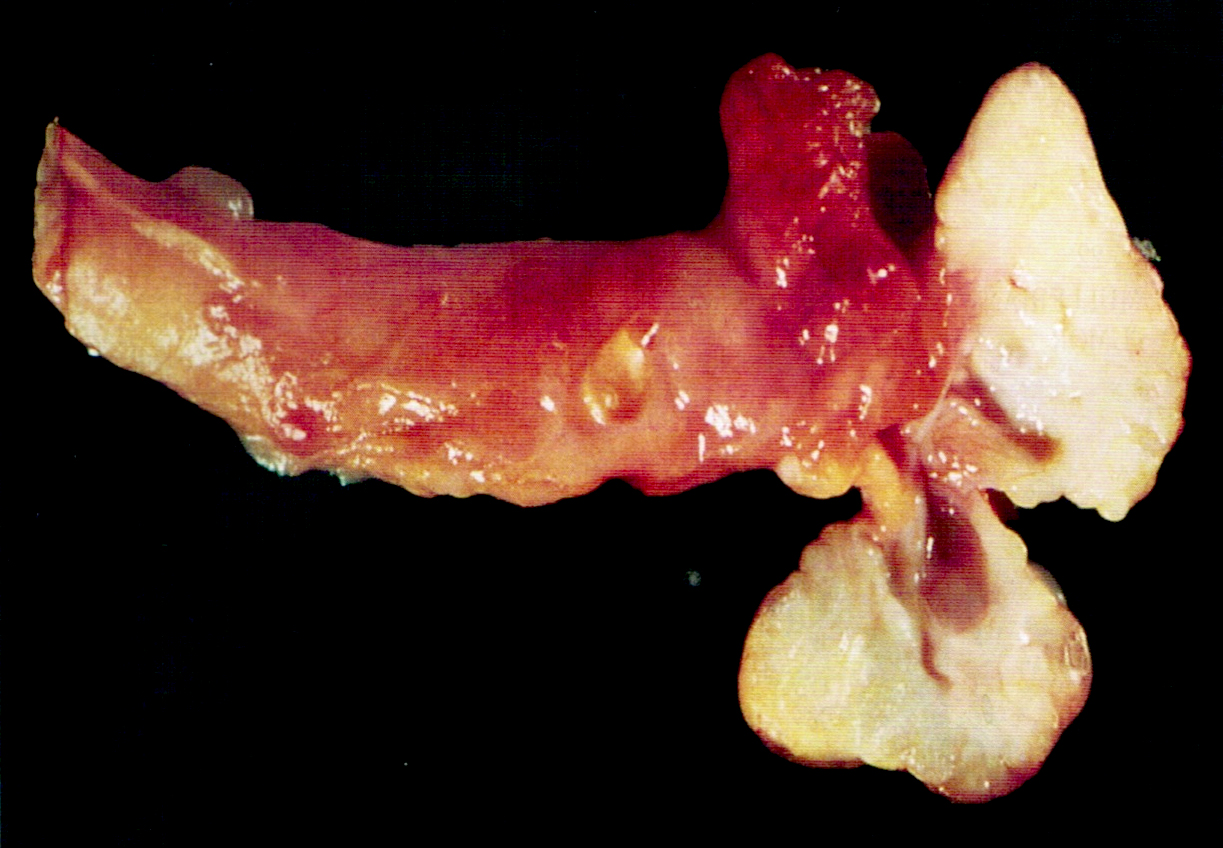
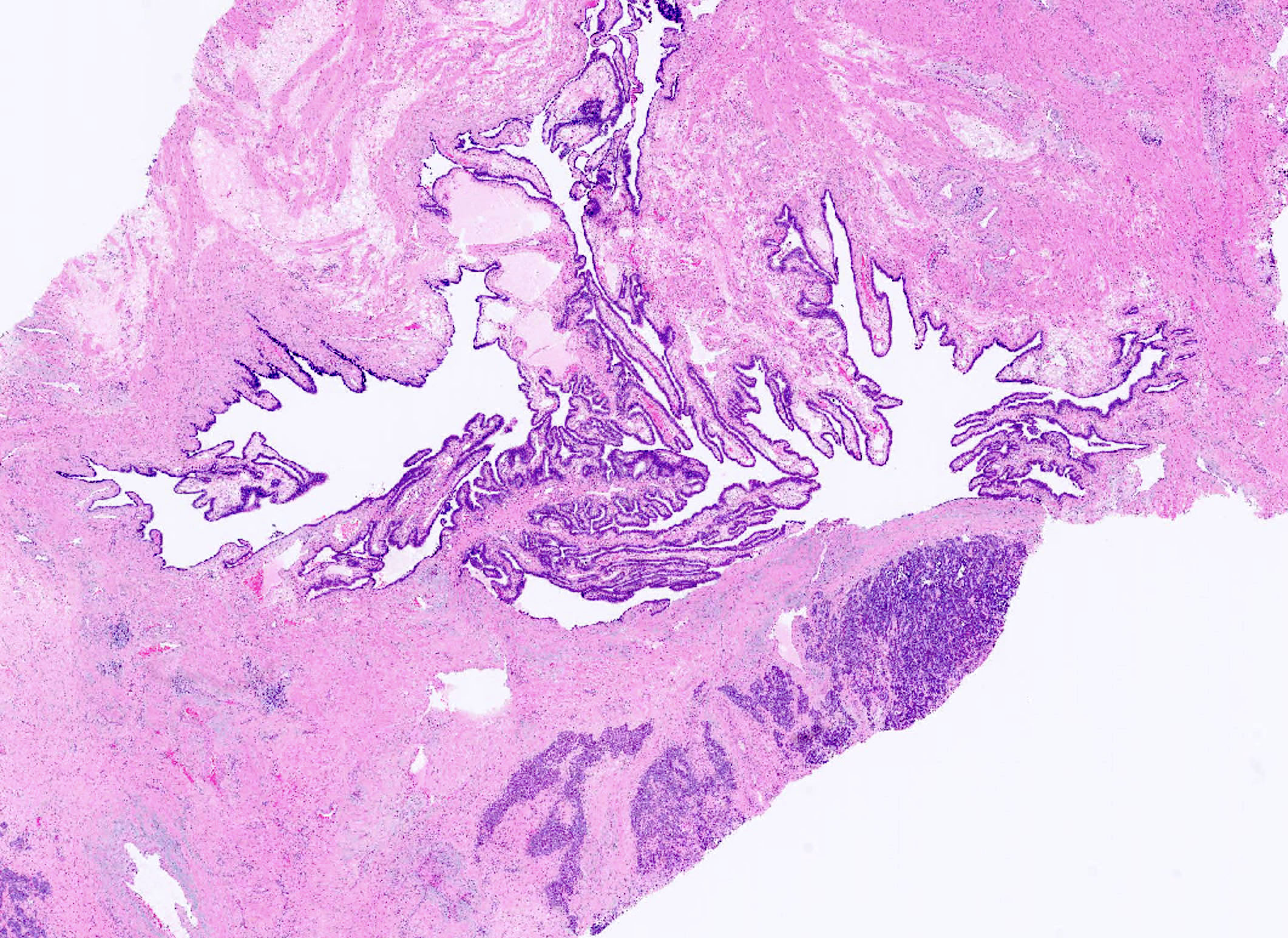
- Enlarged tube, with solid or papillary tumor filling the lumen
- Tumors occasionally are primary in the fimbriae
- 80 - 97% unilateral; hemorrhage, necrosis and cysts common
AFIP images

Diffusely enlarged tube
Papillary tumor attached to mucosa
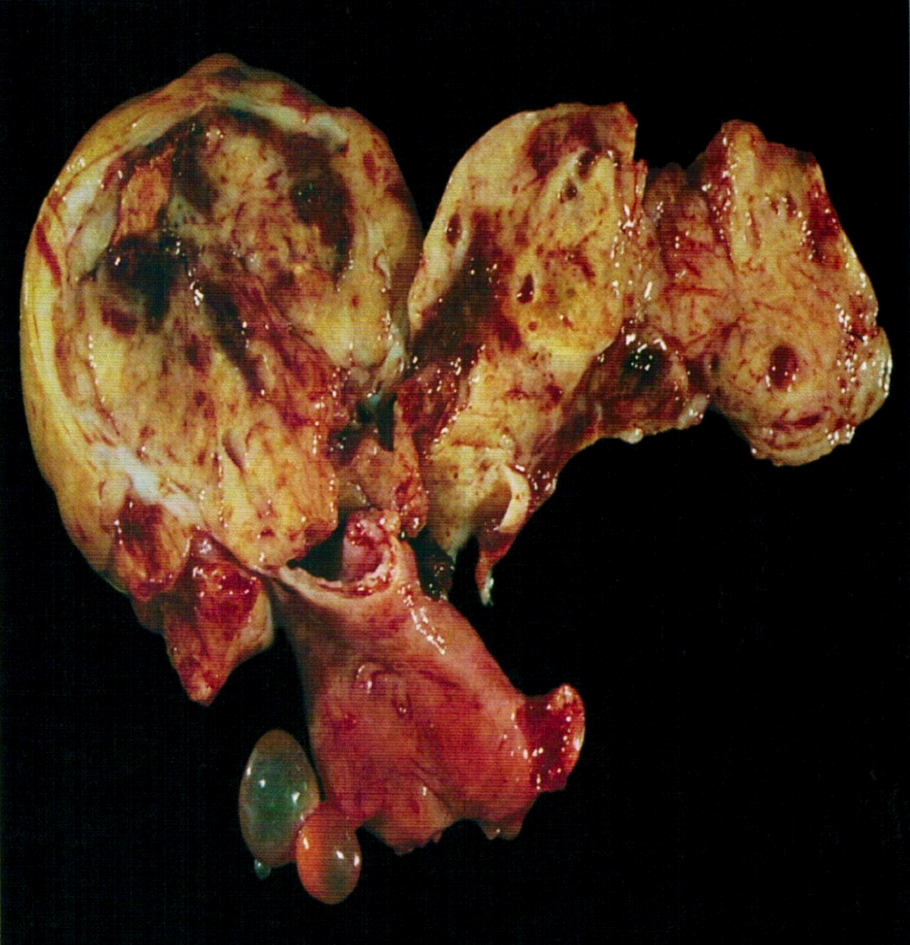
Lumen distended by solid tumor
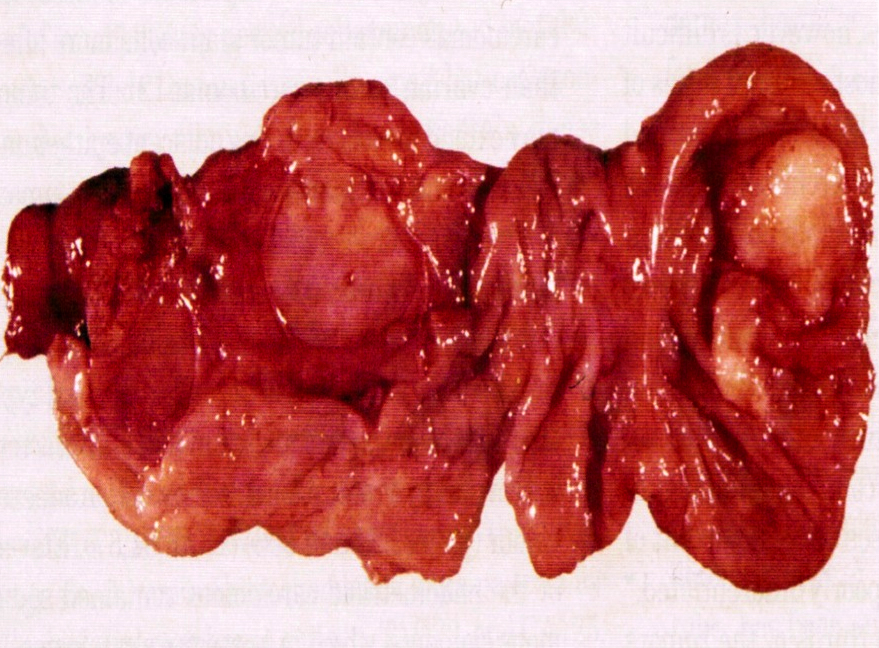
Distended, opened tube
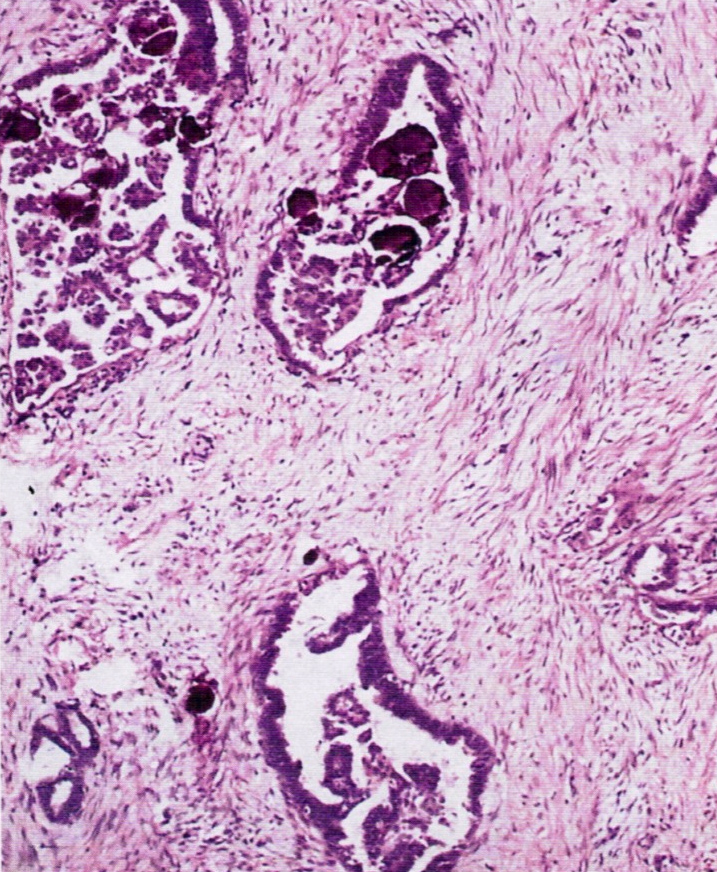
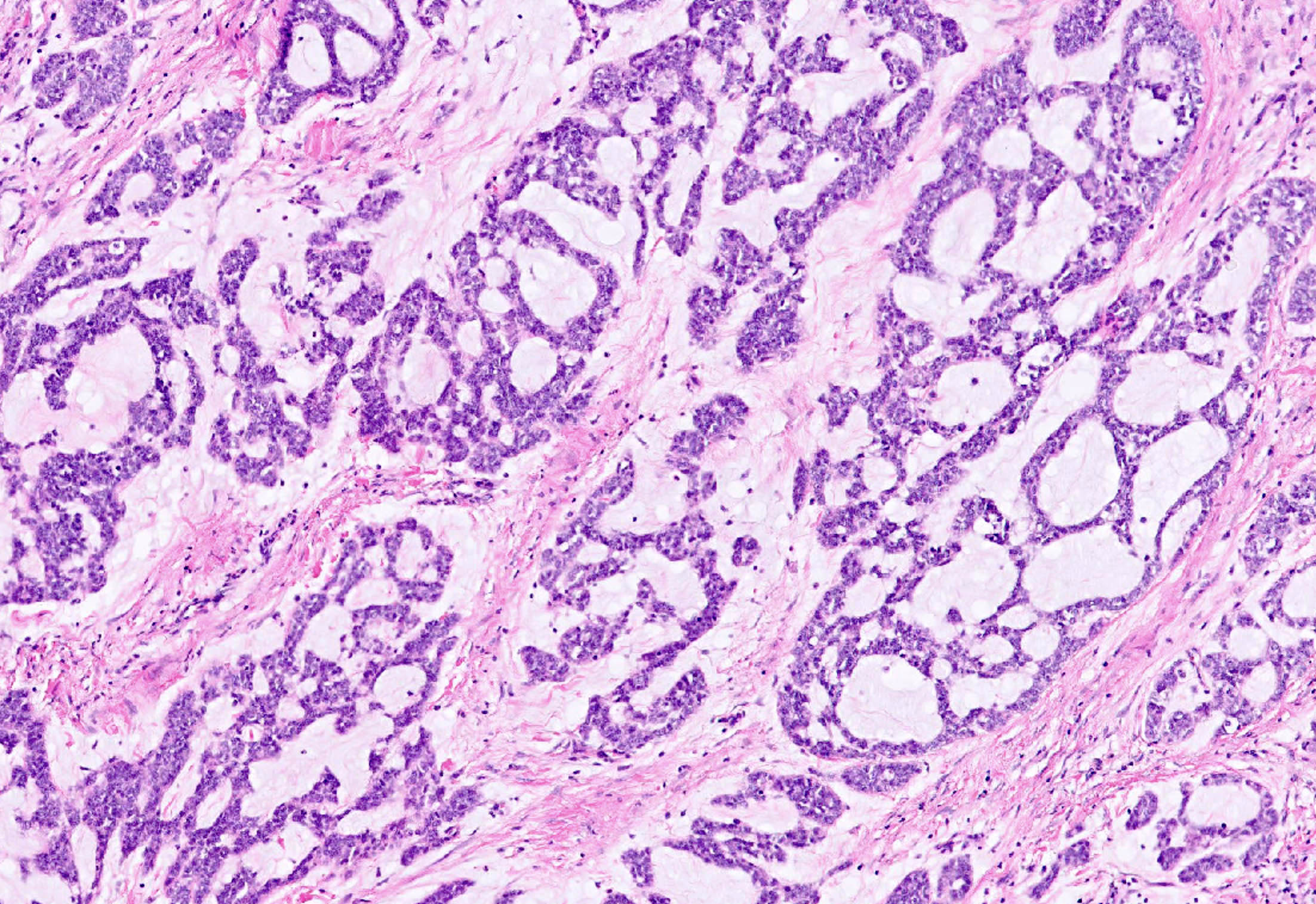
- Endometrioid tumors may be noninvasive, have squamous metaplasia, be associated with endometriosis and contain spindled epithelial cells
- May have small, closely packed cells with numerous glandular spaces of varying sizes, containing PAS+ dense colloid-like secretion, resembling female adnexal tumor of probable Wolffian origin (FATWO), but usually intraluminal, typical endometrioid carcinoma elsewhere, more mitotic activity and atypia, mucin present
AFIP images
Tumor arising in endometriosis
Tumor simulating Wolffian adnexal tumor
- High stage with pelvic extension or positive peritoneal cytology
- To call primary in fallopian tube, should arise from mucosa (endosalpinx), have tubal histologic pattern, involve the lumen, uterus and ovaries must be normal or have foci of malignancy that resemble metastases or independent primaries; if tubal wall is involved, should detect a transition between benign and malignant tubal epithelium
- 5 year survival: stage 1 - 77%, stage 3 - 20%; usually recur intra-abdominally
- Associated with BRCA1 and BRCA2 mutations; for patients with known mutation or family history of breast or ovarian cancer, should submit entire fallopian tube and ovary for microscopic examination (Am J Surg Pathol 2002;26:171, Am J Surg Pathol 2001;25:1283)
- 50% serous, 25% endometrioid, 20% transitional or undifferentiated
- Symptoms: vaginal bleeding or discharge (2/3), pain, adnexal mass (triad in 50%); endometrial smear positive in 10%
- Enlarged tube, with solid or papillary tumor filling the lumen
- Tumors occasionally are primary in the fimbriae
- 80 - 97% unilateral; hemorrhage, necrosis and cysts common
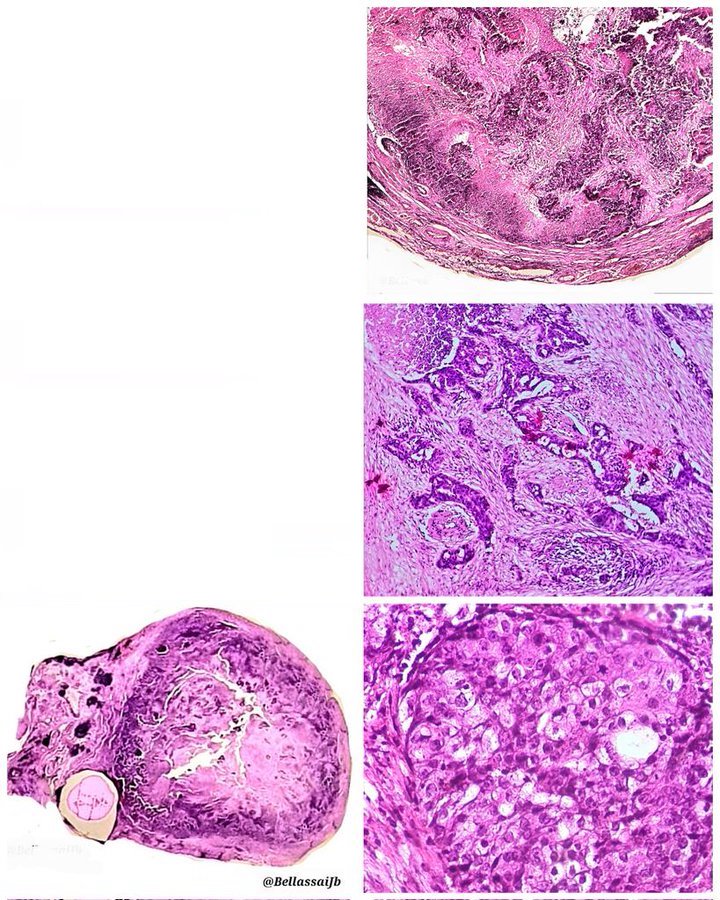
Contributed by AFIP and @BellassaiJb on Twitter
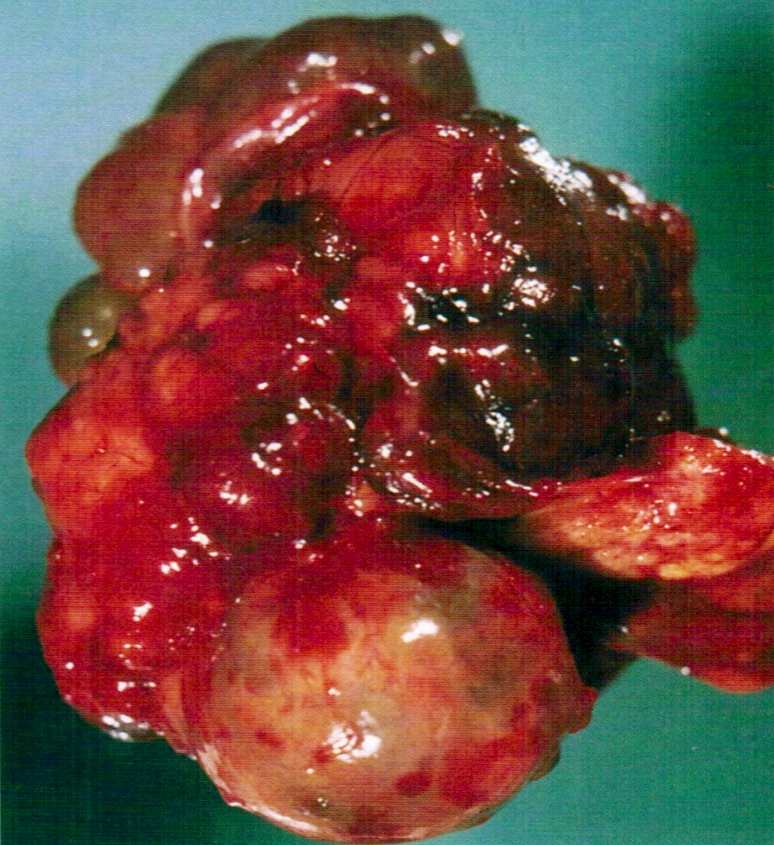
Diffusely enlarged
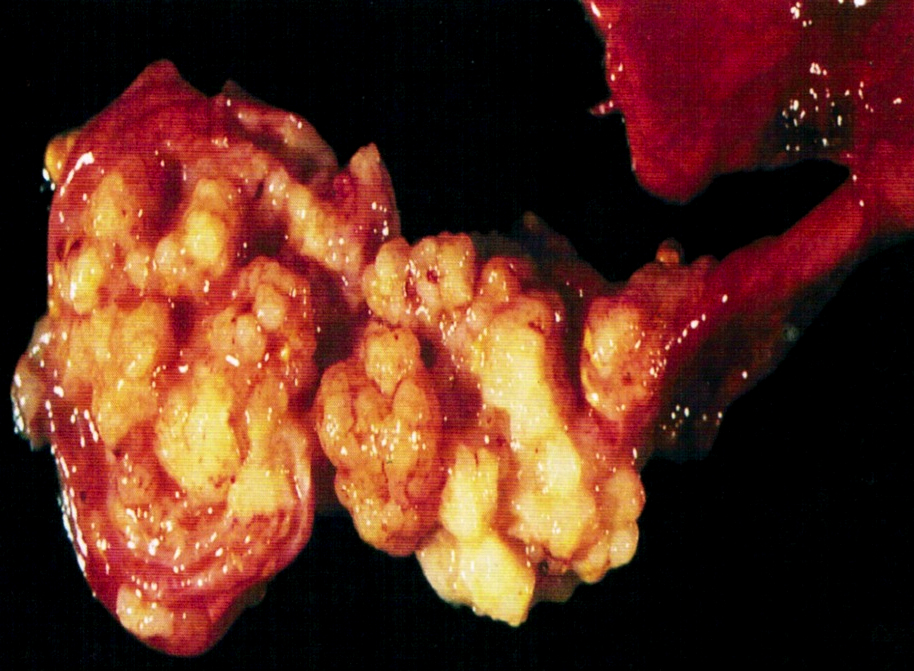
Papillary tumor attached to mucosa
Distended lumen
Solid nodule of tumor

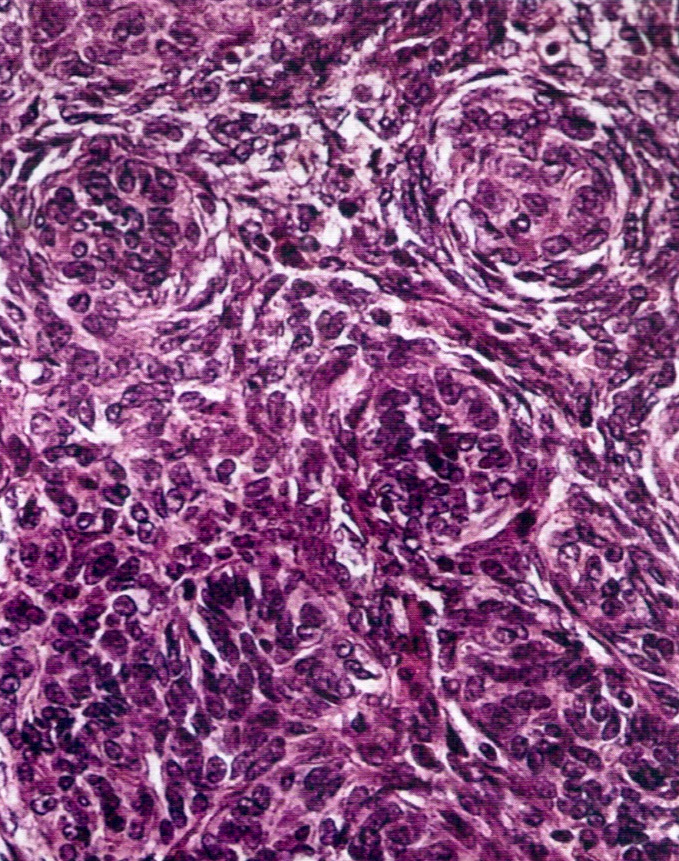
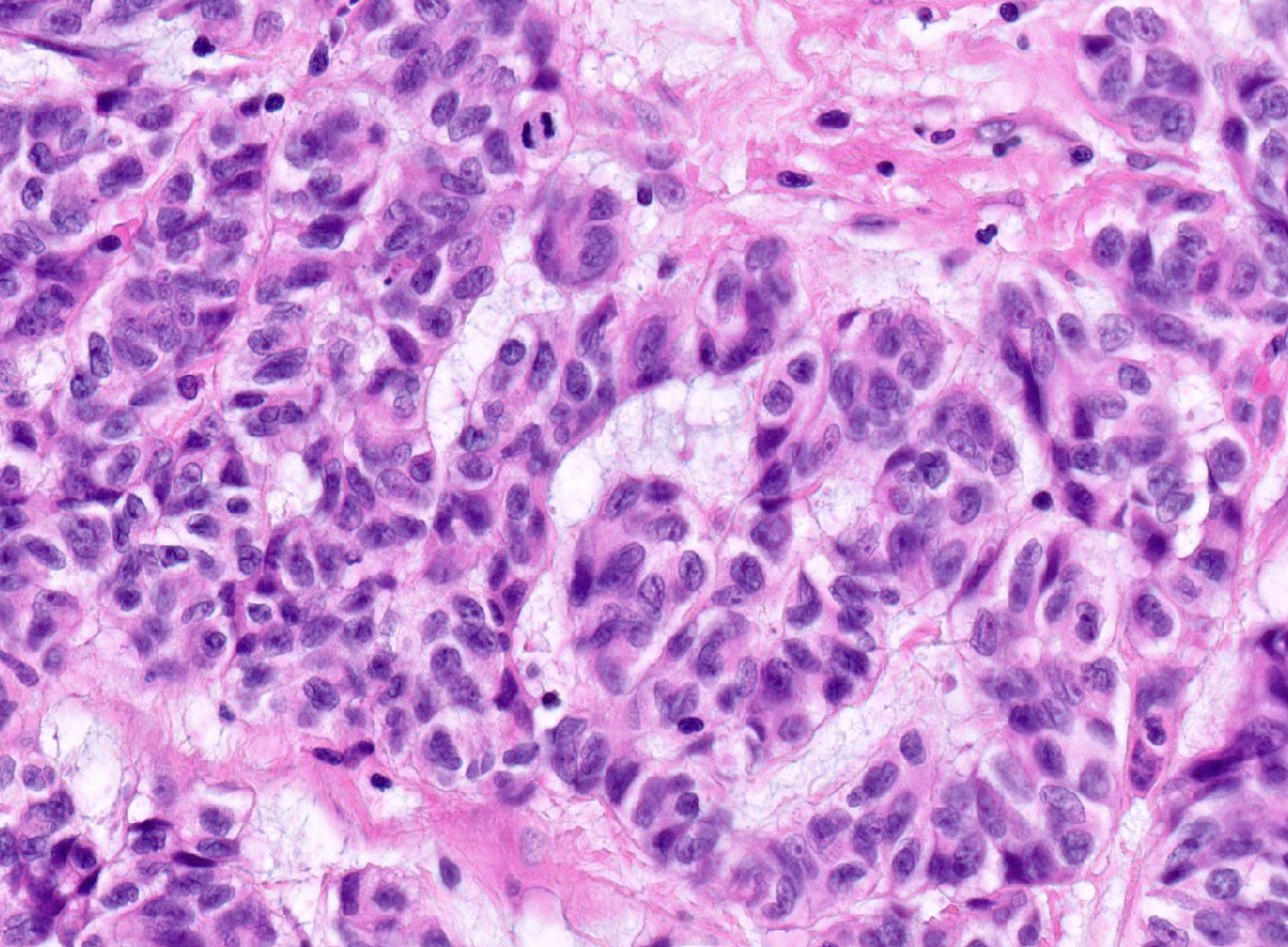
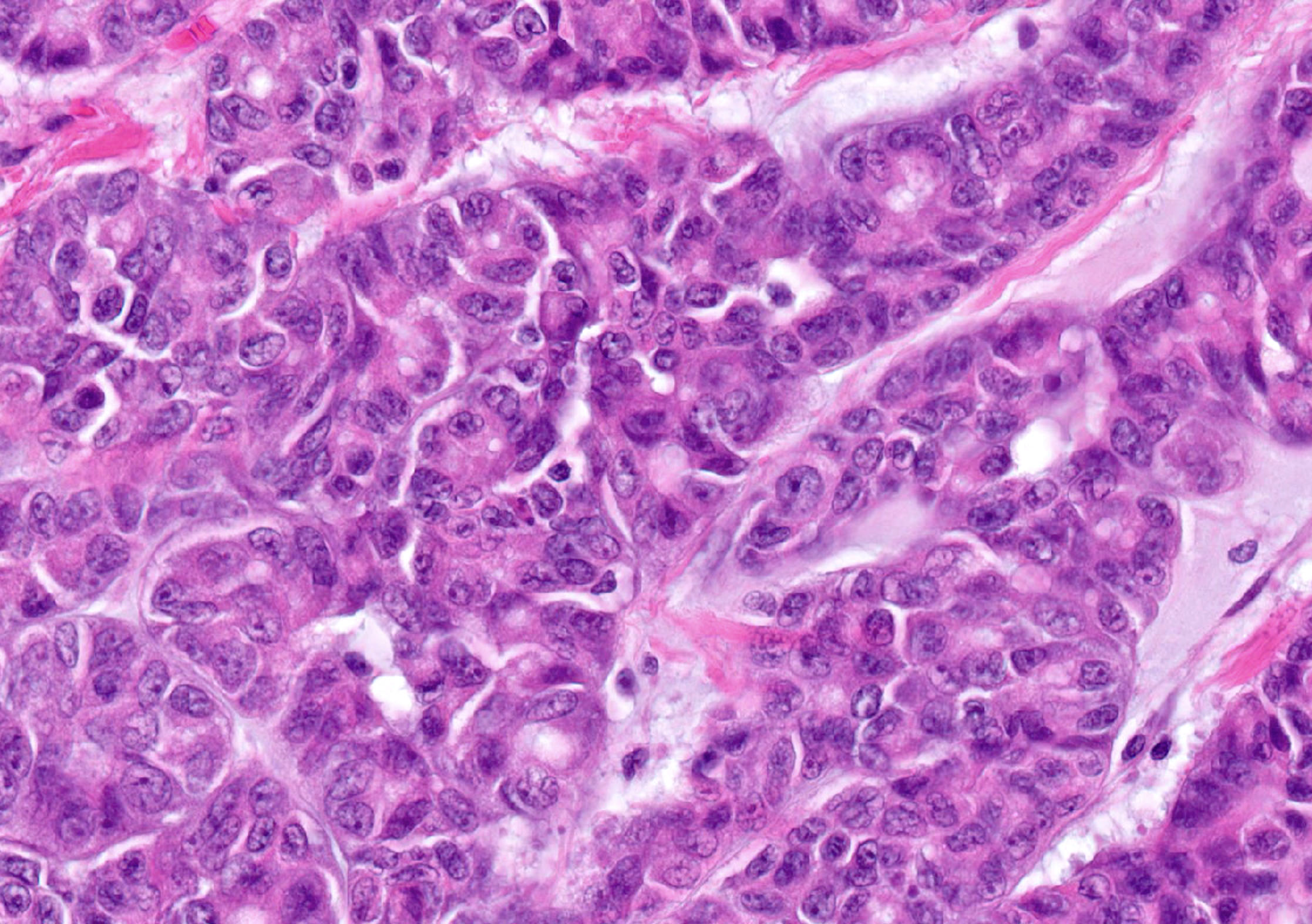
High grade serous carcinoma
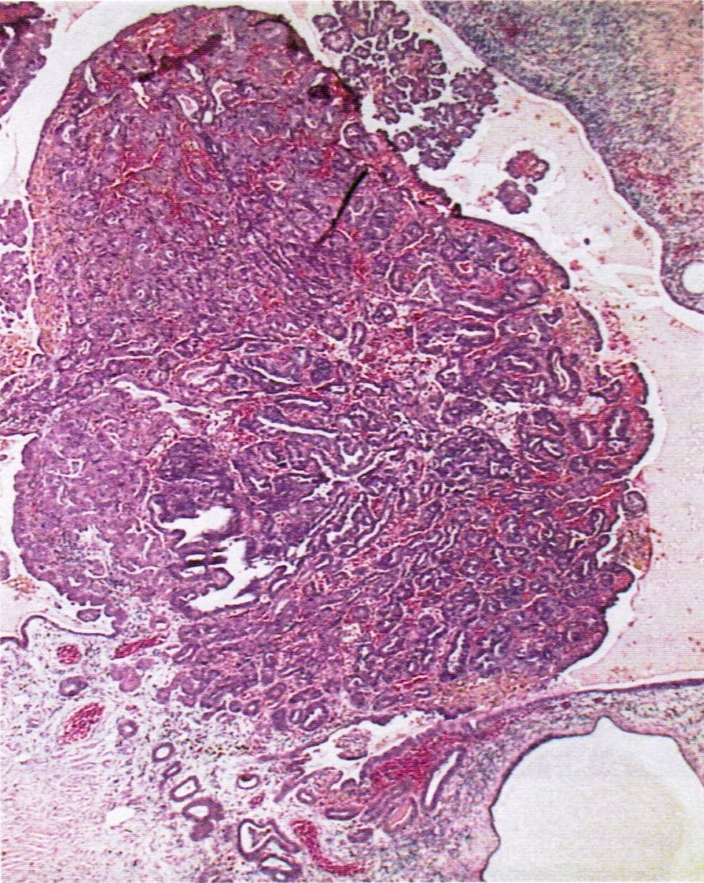
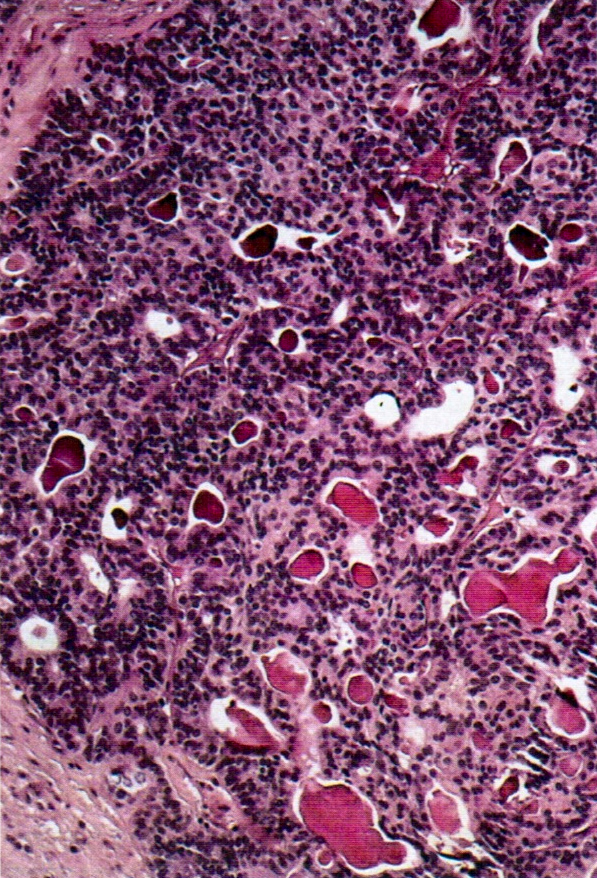
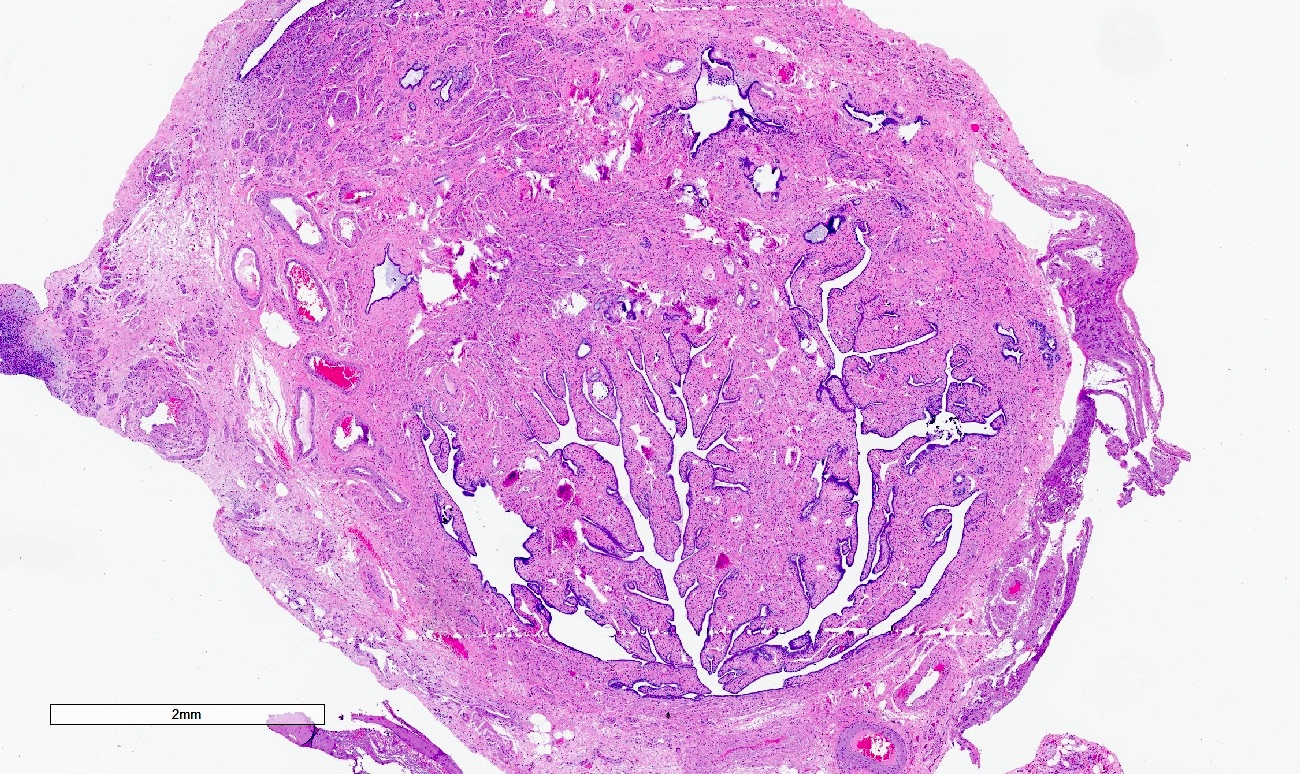
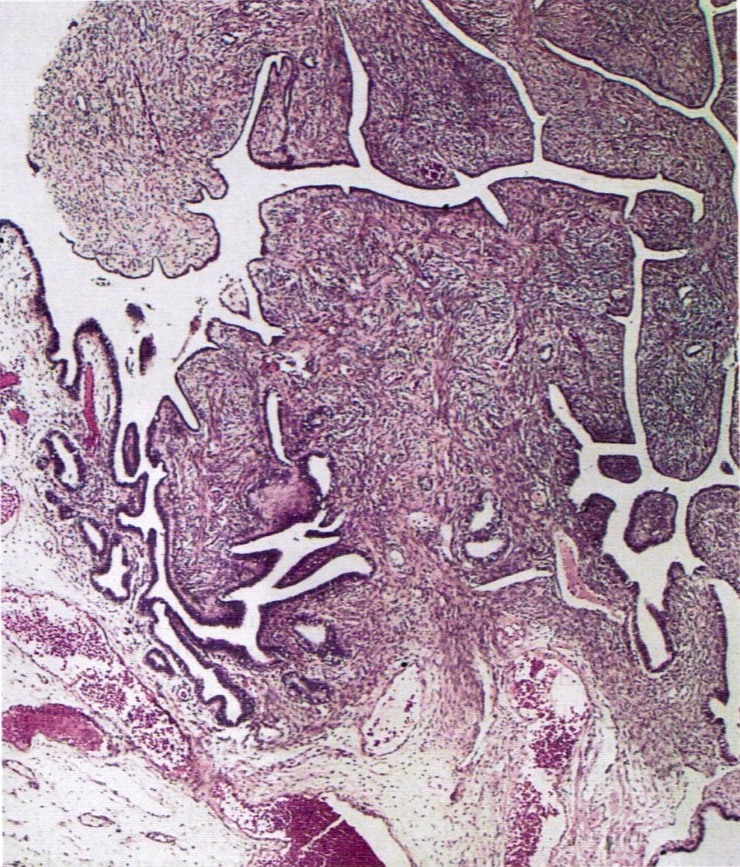
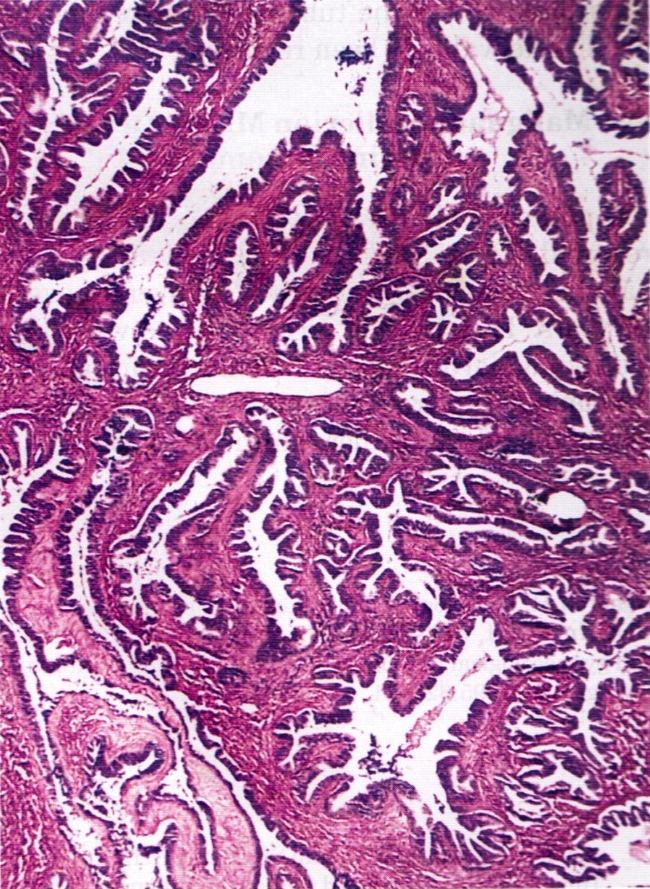
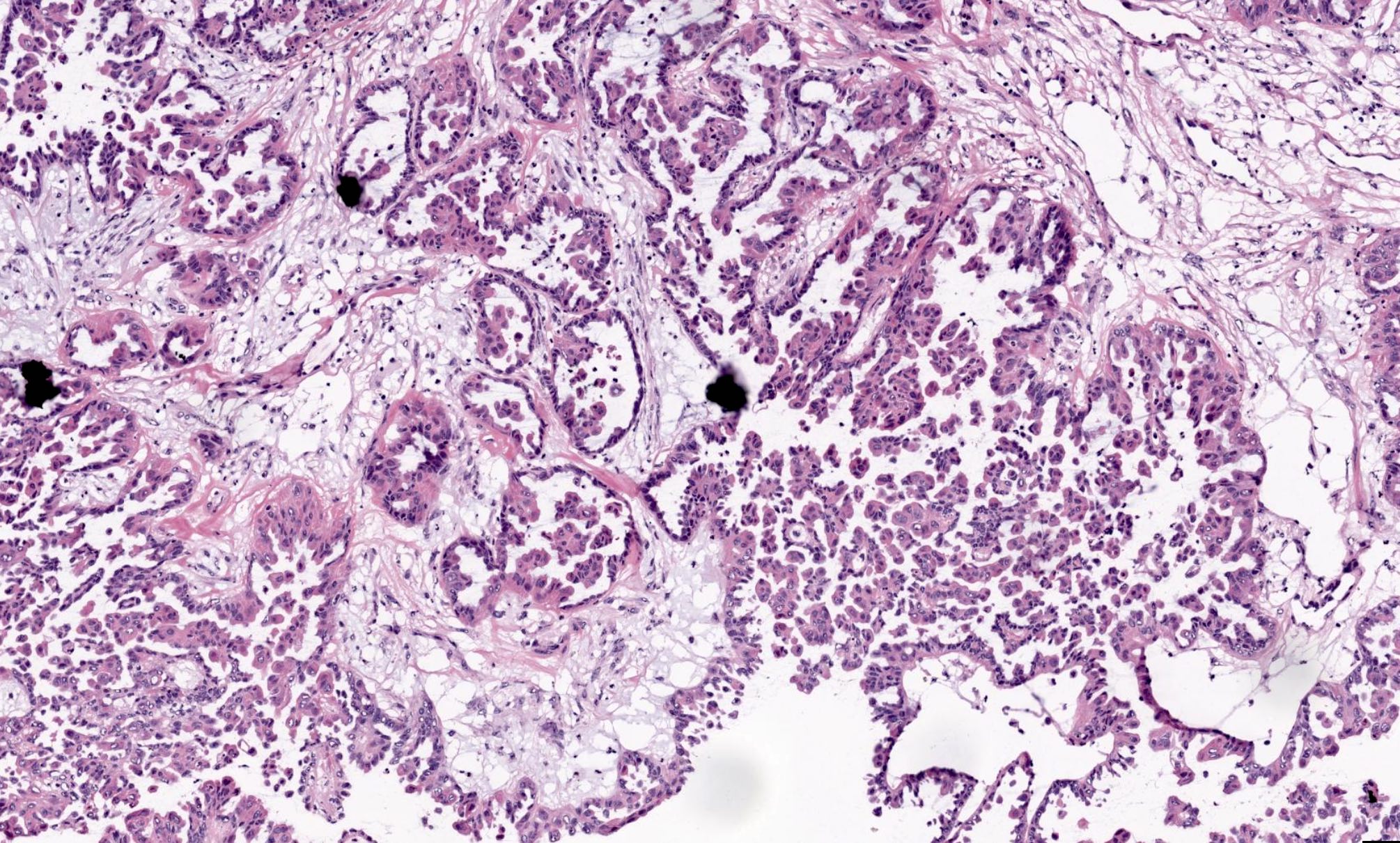
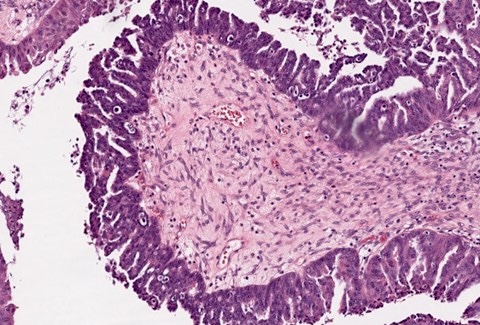
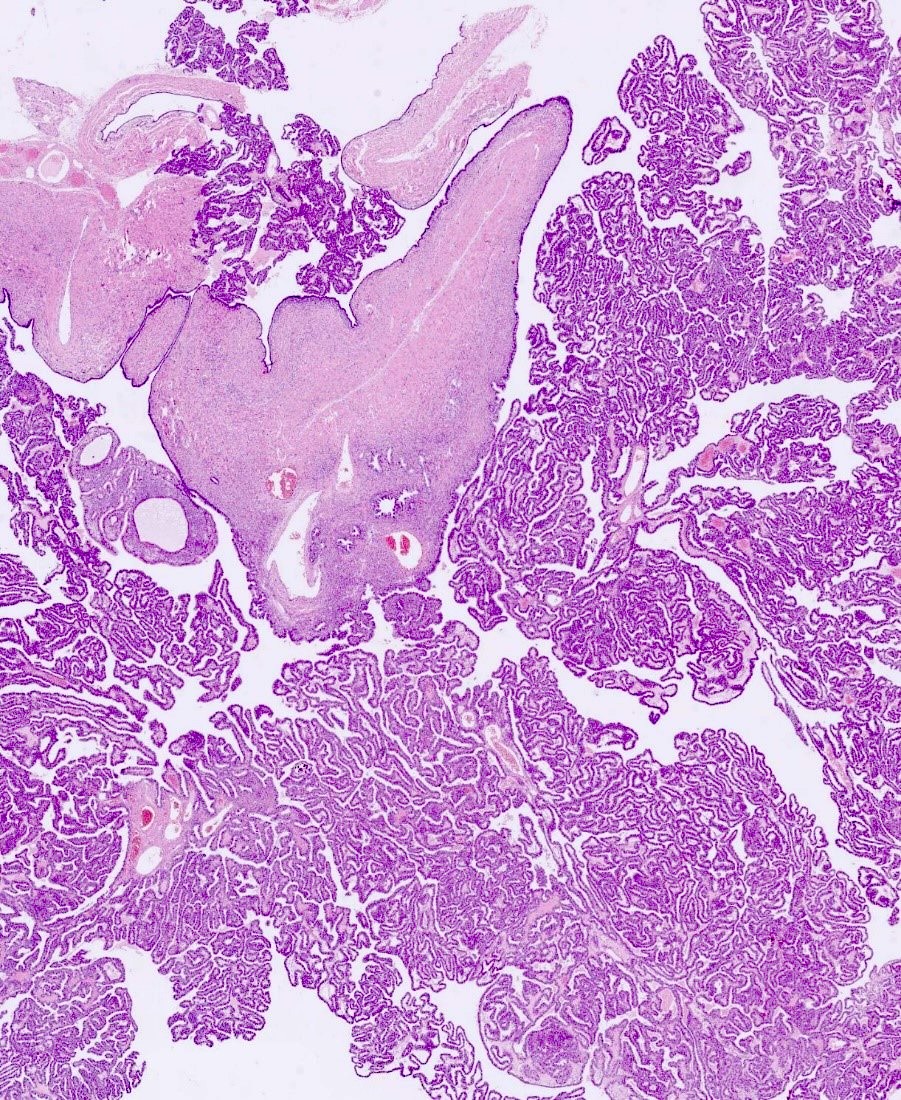
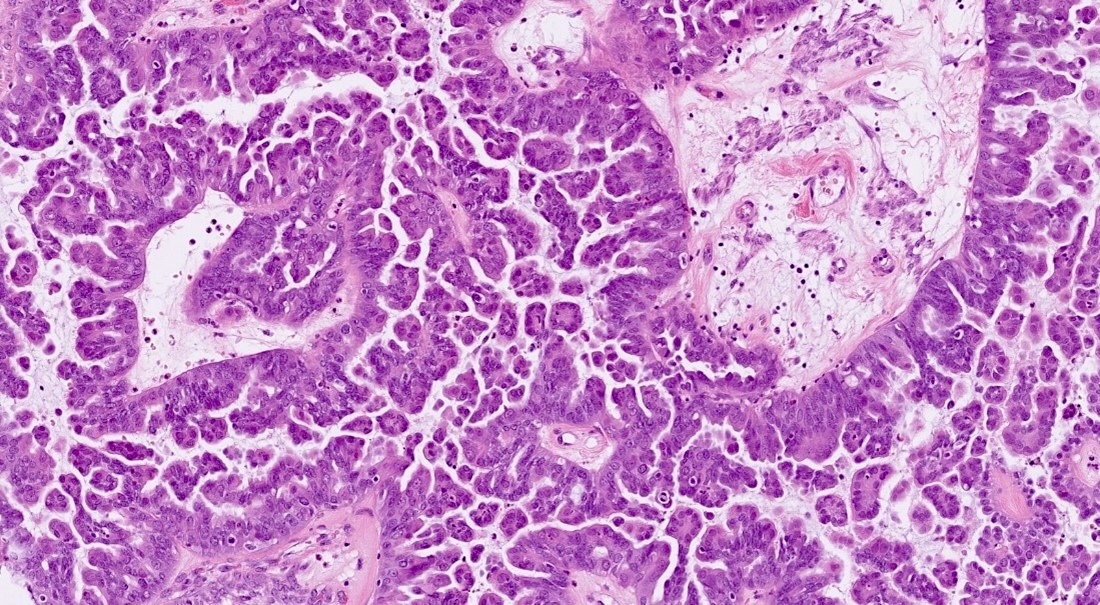
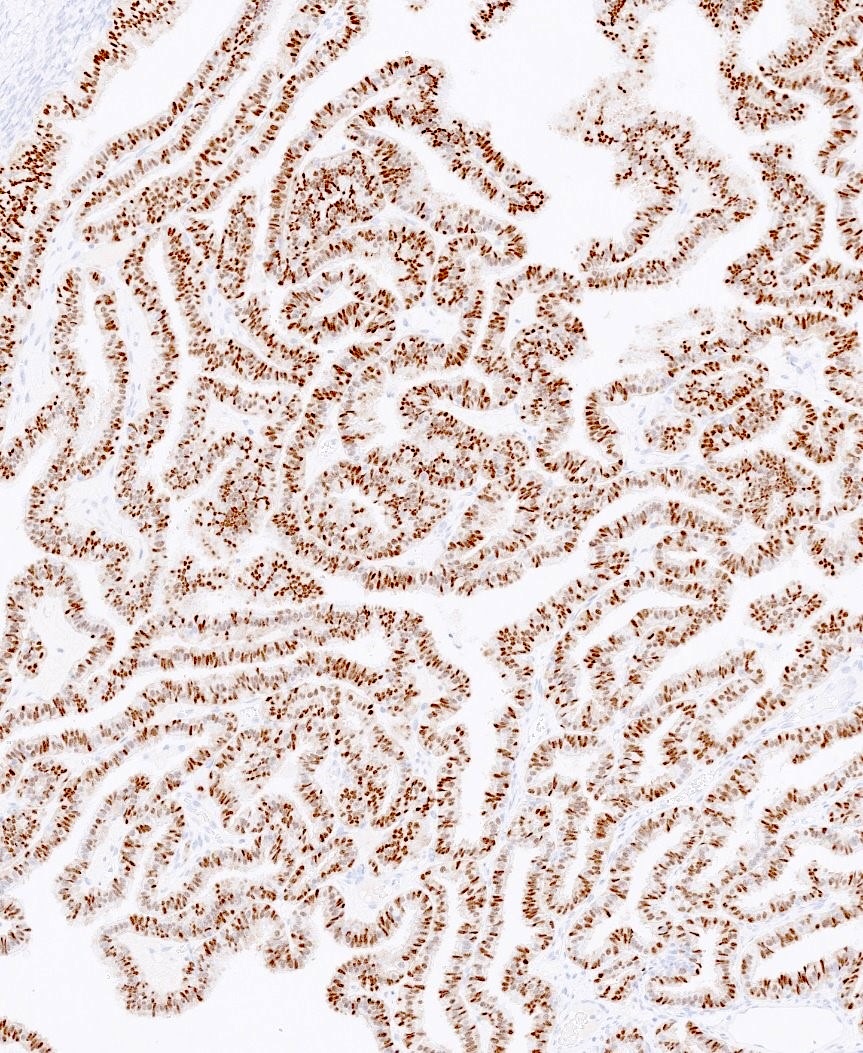
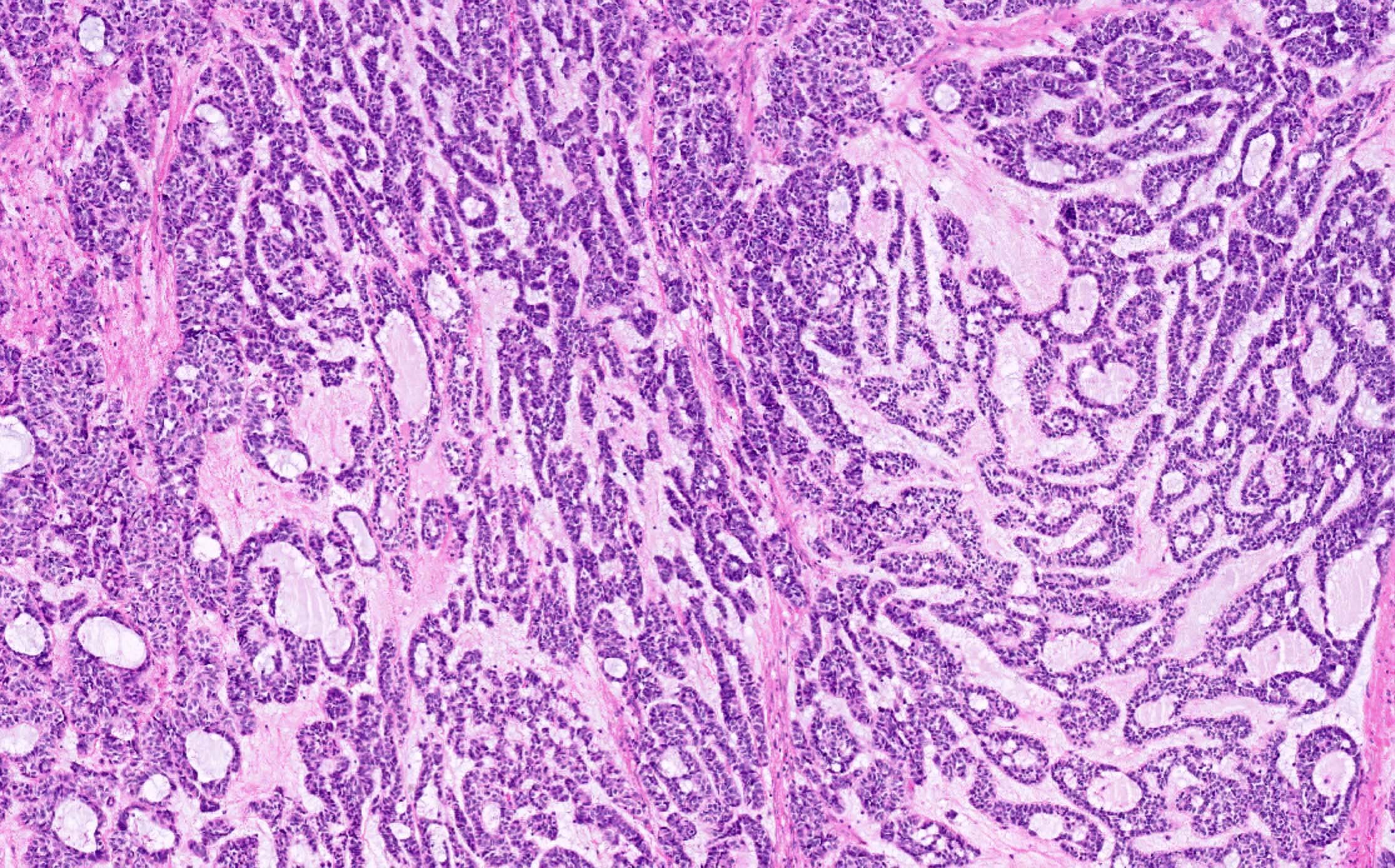
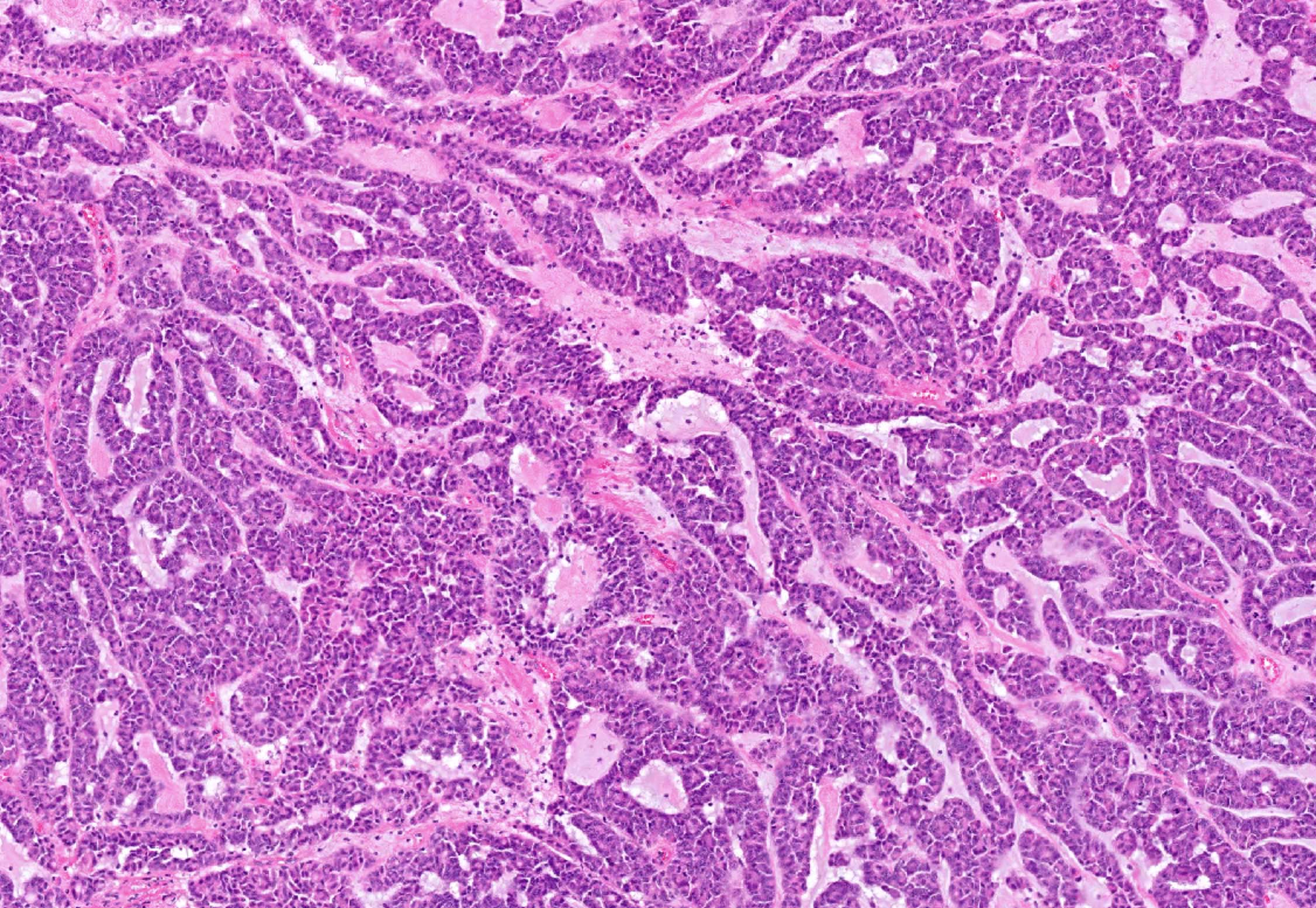
- Invasive papillary adenocarcinoma; may resemble ovarian serous adenocarcinoma with complex papillary architecture
Contributed by AFIP and @BellassaiJb on Twitter
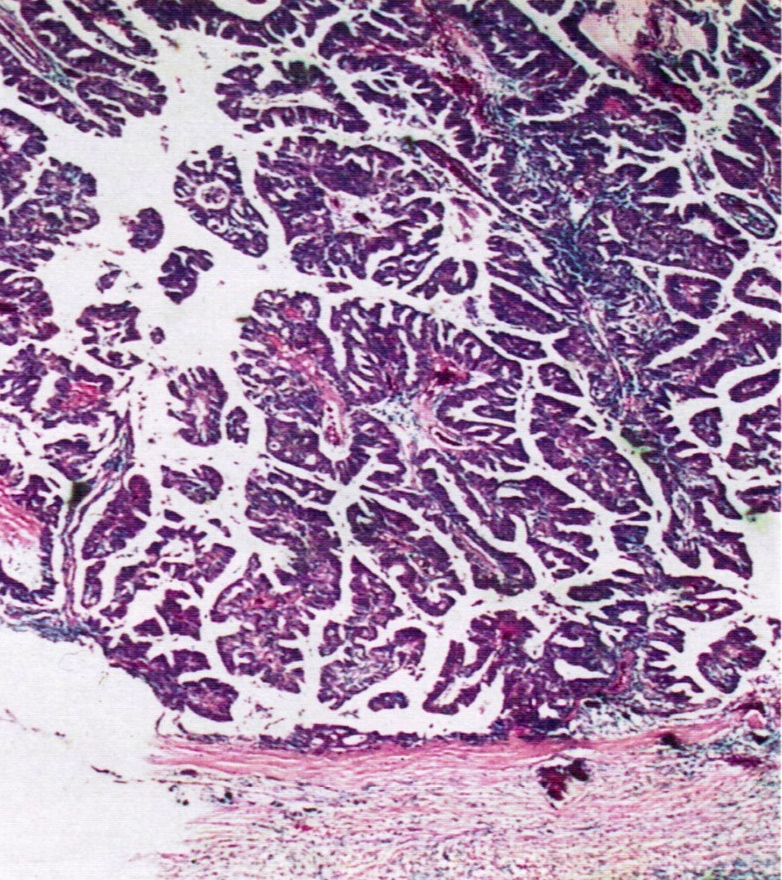
Lumen filled with fine papillae
Desmoplastic stromal response
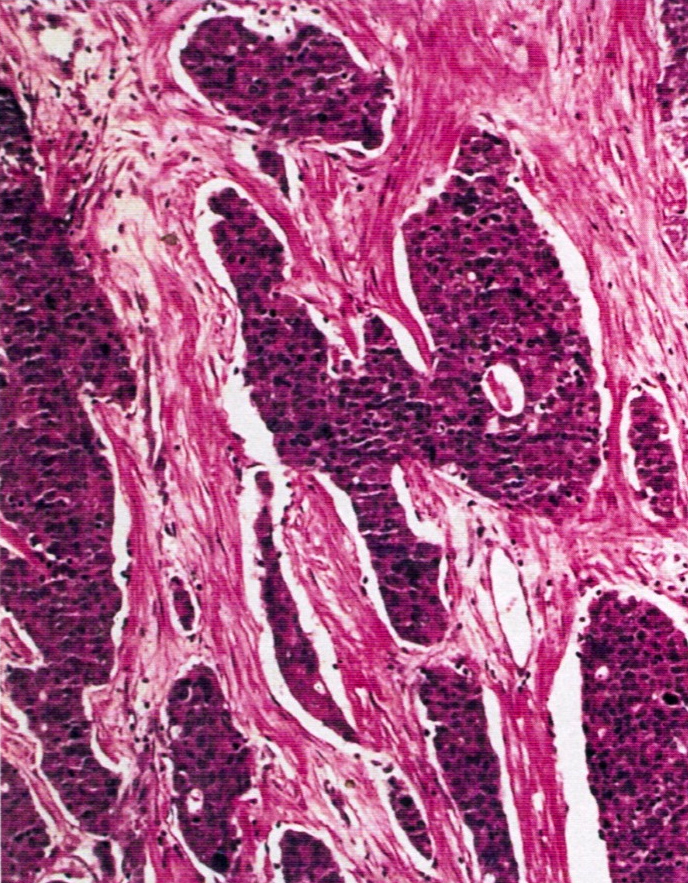
Undifferentiated component in tubal wall
High grade serous carcinoma
- Mesonephric duct is paired organ present during embryogenesis connecting primitive kidney to cloaca, which becomes part of male reproductive organs (Wikipedia: Mesonephric Duct [Accessed 20 December 2018])
- In women, duct regresses but normal remnants remain; however, "abnormal" ductular remnants may remain and cause confusion as they appear as glands "out of place"
- Also known as Wolffian duct, archinephric duct, Leydig duct, nephric duct
- Embryological remnant which occurs in all women of any age
- No known predisposing factors
- Anywhere in pelvic cavity, including broad ligament, cervix (20% of women), fallopian tube, lymph nodes, ovary
- In early development, mesonephric and paramesonephric ducts coexist
- Mesonephric ducts develops in bladder trigone in both sexes
- In men, under influence of testosterone, mesonephric duct develops into epididymis, vas deferens, seminal vesicle
- In women, absence of testosterone causes duct regression; this may be incomplete and inclusions / remnants may persist
- Gartners ducts are paired remnants that may give rise to cysts and are typically located lateral to vaginal wall in broad ligament
- Epoophoron (also known as organ of Rosenmüller or parovarium) is analogous to male epididymis; most cranial portion of remnant, located in lateral broad ligament, between ovary and fallopian tube; may communicate with Gartner ducts
- Paraoophoron is analogous to male paradidymis, usually located in medial broad ligament
- None needed
- Usually no significant gross findings, incidental on microscopy, unless cyst formation
- Small tubules lined by low columnar to cuboidal cells without cilia; surrounded by prominent smooth muscle; may be cystic
- CK903 (may be focal), CD10 (luminal, patchy), vimentin, p16 (Arch Pathol Lab Med 2008;132:402)
- Calretinin (2/3 of mesonephric adenocarcinomas, Histopathology 2003;43:144)
- ER, PR, CEA, p63 (rare focal positivity), PSA in males (Am J Surg Pathol 2011;35:1054)
- Calretinin (benign ducts)
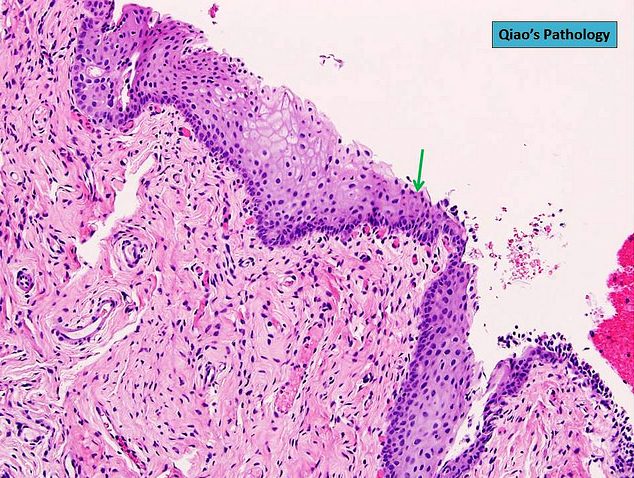
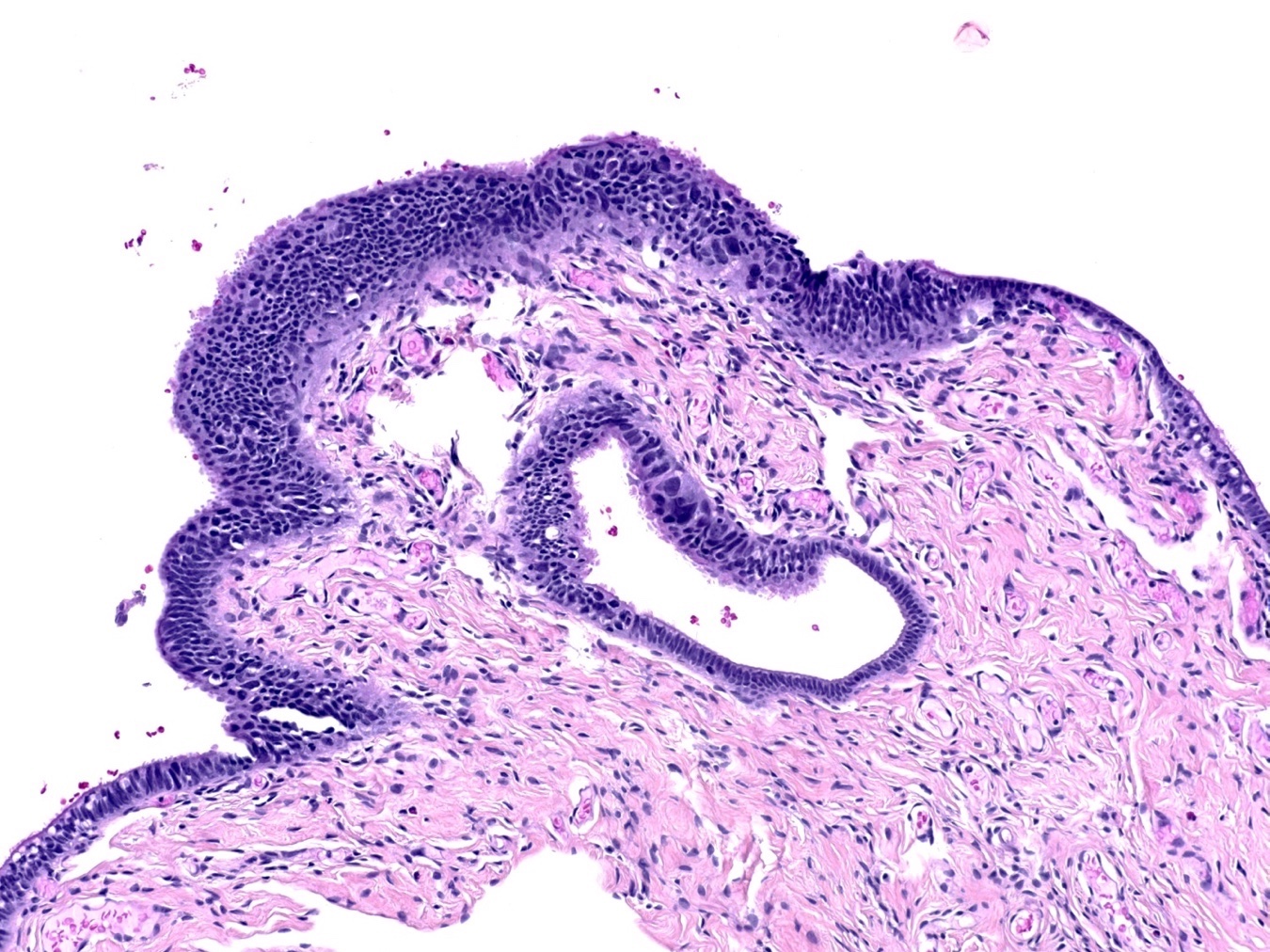
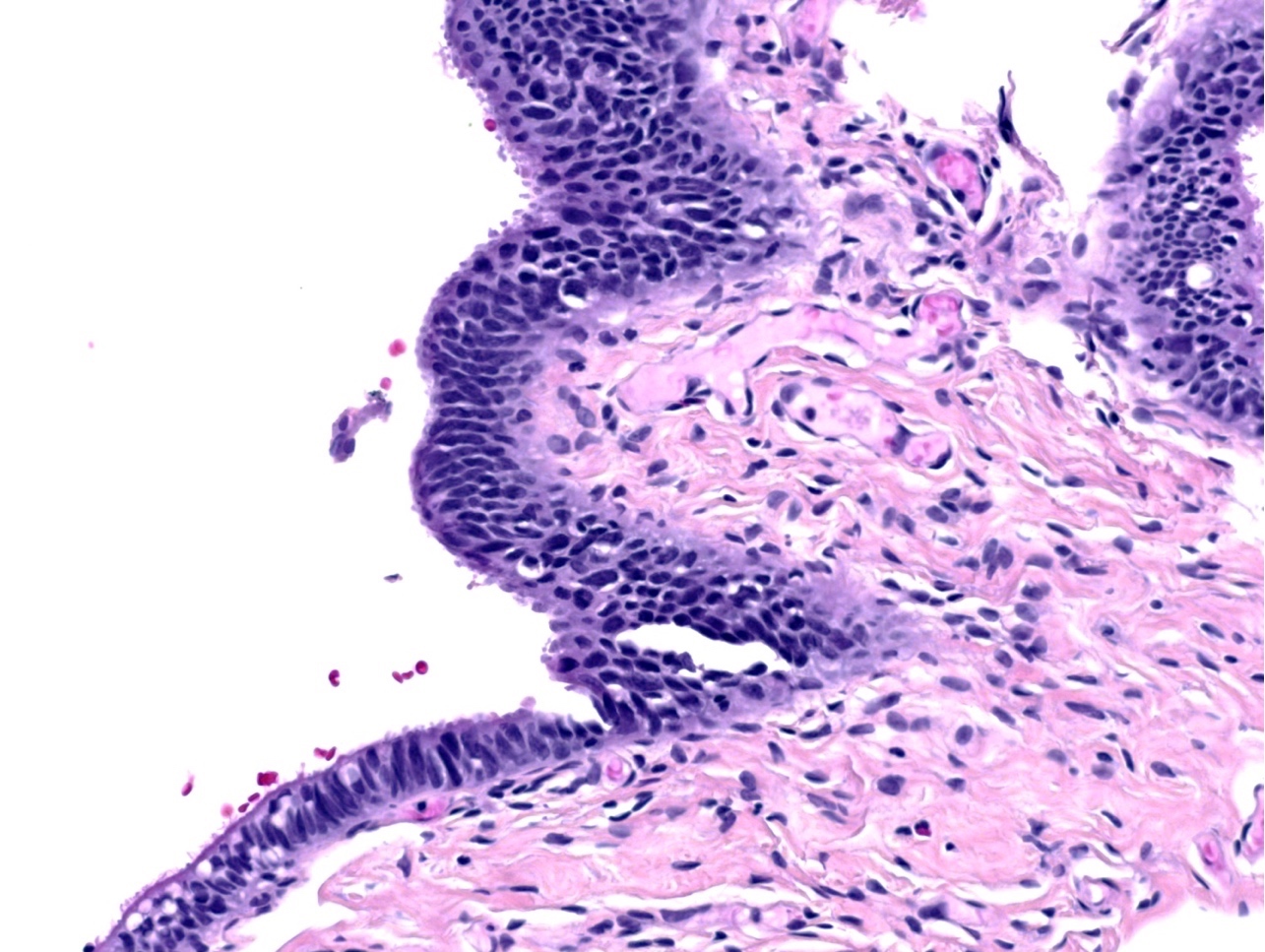
- Defined as alteration in which the normal tubal epithelium is replaced by metaplastic cells resembling benign transitional (urothelial) cells of urinary bladder (Am J Surg Pathol 2009;33:111)
- Transitional cell metaplasia is a benign epithelial alteration but is underrecognized in the tubal fimbriae, where it may mimic serous tubal intraepithelial neoplasm / carcinoma
- It is increasing found because over the past two decades, risk reducing salpingo-oophorectomy (RRSO) for BRCA1 and BRCA2 mutation patients is being performed to identify epithelial atypia and early intraepithelial carcinoma in the distal fallopian tube / fimbriae
- Opportunistic salpingectomy is a viable alternative to salpingo-oophorectomy for BRCA+ women, which reduces the risk of serous carcinoma while preserving ovarian function
- Present in 26% of all RRSO specimens
- Usually multifocal, with involvement of tip, edges or base of the fimbrial plicae
- Average size of a metaplastic focus is 1.3 mm (ranging from 0.1 to 10 mm)
- Also due to fallopian tube prolapse or peritoneal dialysis (squamous) (Int J Gynecol Pathol 2008;27:465)
- Also associated with ovarian mucinous tumors, Peutz-Jeghers syndrome, endometriosis within fallopian tube
- Distal fallopian tube / fimbriae
- Unclear: it is possible that transitional cell metaplasia of the fimbriae is a reaction to mechanical irritation, inflammation or infection
- Findings that only the distal fimbriae are involved and not the isthmus, ampulla or infundibulum supports the notion of a reaction to peritoneal based stimulus
- Prior pregnancy is a potential inciting incident
- Diagnosis of transitional cell metaplasia of fimbriae is only possible after salpingectomy by microscopic examination of distal fallopian tube / fimbriae
- Clinical followup of transitional cell metaplasia of the fimbriae shows no biologic significance
- 45 year old woman with prolapsed fallopian tube with squamous metaplasia (J Postgrad Med 2002;48:241)
- 52 year old woman with papillary syncytial metaplasia of fallopian tube endometriosis (Arch Pathol Lab Med 2013;137:126)
- Generally, such lesions are undetectable grossly and are only identified by careful histologic examination of sections of fallopian tubes; thus, fallopian tubes have to be submitted entirely in serial cross sections whereas fimbriae have to be submitted entirely in longitudinal sections
- Mostly commonly mucinous metaplasia; urethelial and squamous metaplasia less common
- Characteristic features of transitional cell metaplasia are the presence of uniform nuclei with pale chromatin and nuclear grooves and abundant cytoplasm; these features are not seen in serous tubal intraepithelial neoplasia, including serous tubal intraepithelial carcinoma (STIC) and serous tubal epithelial proliferation of uncertain significance
- Careful histologic examination, attention to cytologic details and p53 and Ki67 staining will help prevent the misinterpretation of transitional cell metaplasia as malignancy
Contributed by Jian-Hua Qiao, M.D.
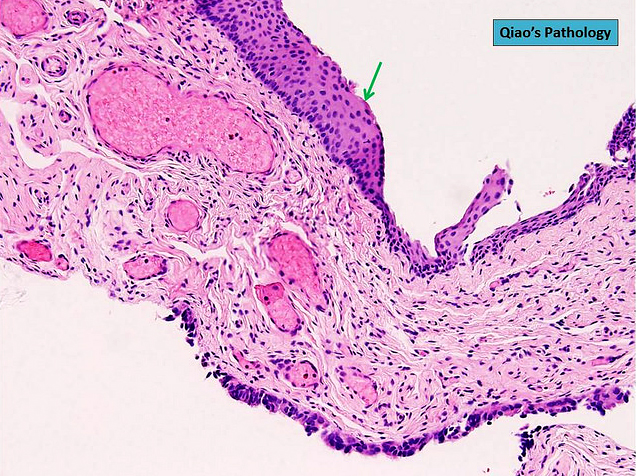
Extensive transitional cell metaplasia
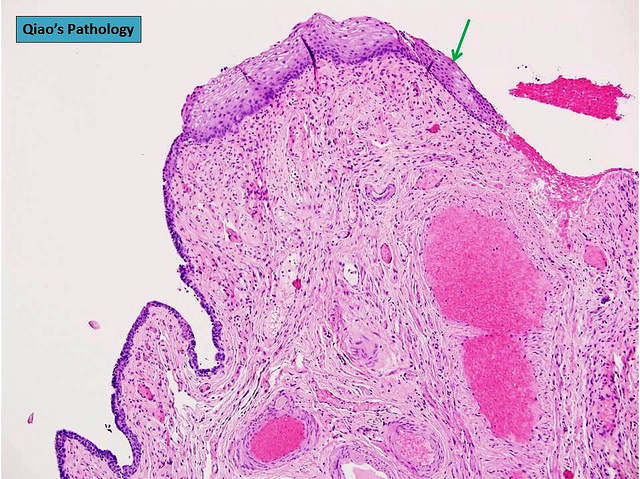
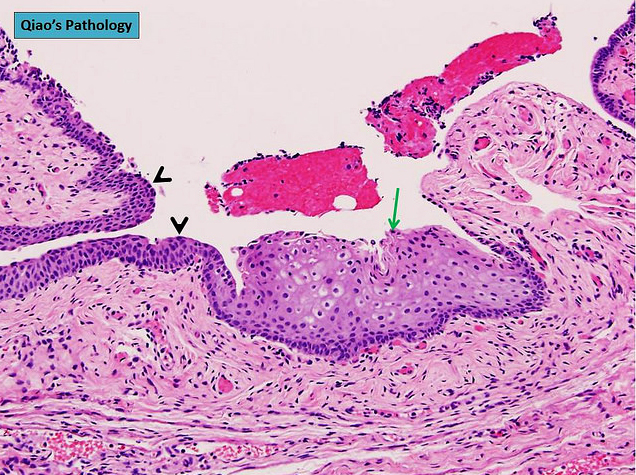
Focal transitional cell metaplasia
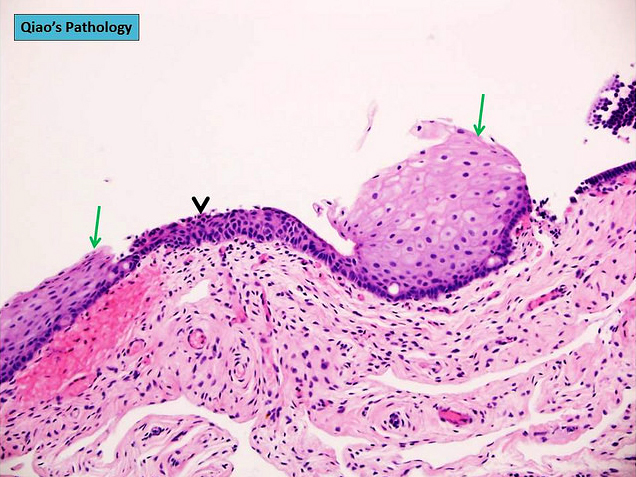
Multifocal transitional cell metaplasia
- Serous tubal epithelial proliferation of uncertain significance: nuclear enlargement, increased N/C ratio and polarity is preserved; evidence of TP53 mutation ("p53 signature") by immunohistochemistry; Ki67 index is variably increased (Mod Pathol 2017;30:710)
- Serous tubal intraepithelial carcinoma (STIC): nuclear enlargement, increased N/C ratio, lost cellular polarity, irregular nuclear stacking, small detached papillary clusters, horizontally oriented surface nuclei and intraepithelial fractures; evidence of TP53 mutation by immunohistochemistry; Ki67 index is variably increased (Mod Pathol 2017;30:710)
- Cells of transitional cell metaplasia show uniform nuclei, pale chromatin and nuclear grooves
- Clinical followup of transitional cell metaplasia of the fimbriae shows no biological significance
- p53 signature and increased Ki67 are usually present in transitional cell metaplasia of the fimbriae
- Transitional cell metaplasia is undetectable by gross examination
- Transitional cell metaplasia shows no evidence of nuclear enlargement, loss of cellular polarity or irregular nuclear stacking
Comment Here
Reference: Metaplastic changes
- A rare, benign, incidental lesion that is usually found during pregnancy or postpartum
- Metaplastic papillary tumor of fallopian tube (Arch Pathol Lab Med 1989;113:545)
- Metaplastic papillary tumor of salpinx (Int J Gynecol Pathol 2011;30:532)
- Not needed
- Usually incidental microscopic finding
- Eosinophilic or mucinous papillae with small cysts
- Large vesicular nuclei with minimal stratification, no crowding or atypia
- Rare mitoses
AFIP images

Metaplastic papillary tumor
- May mimic carcinoma
- Associated with von Hippel-Lindau disease
AFIP images
Simulating serous papillary tumor
Bland, cuboidal epithelial cells
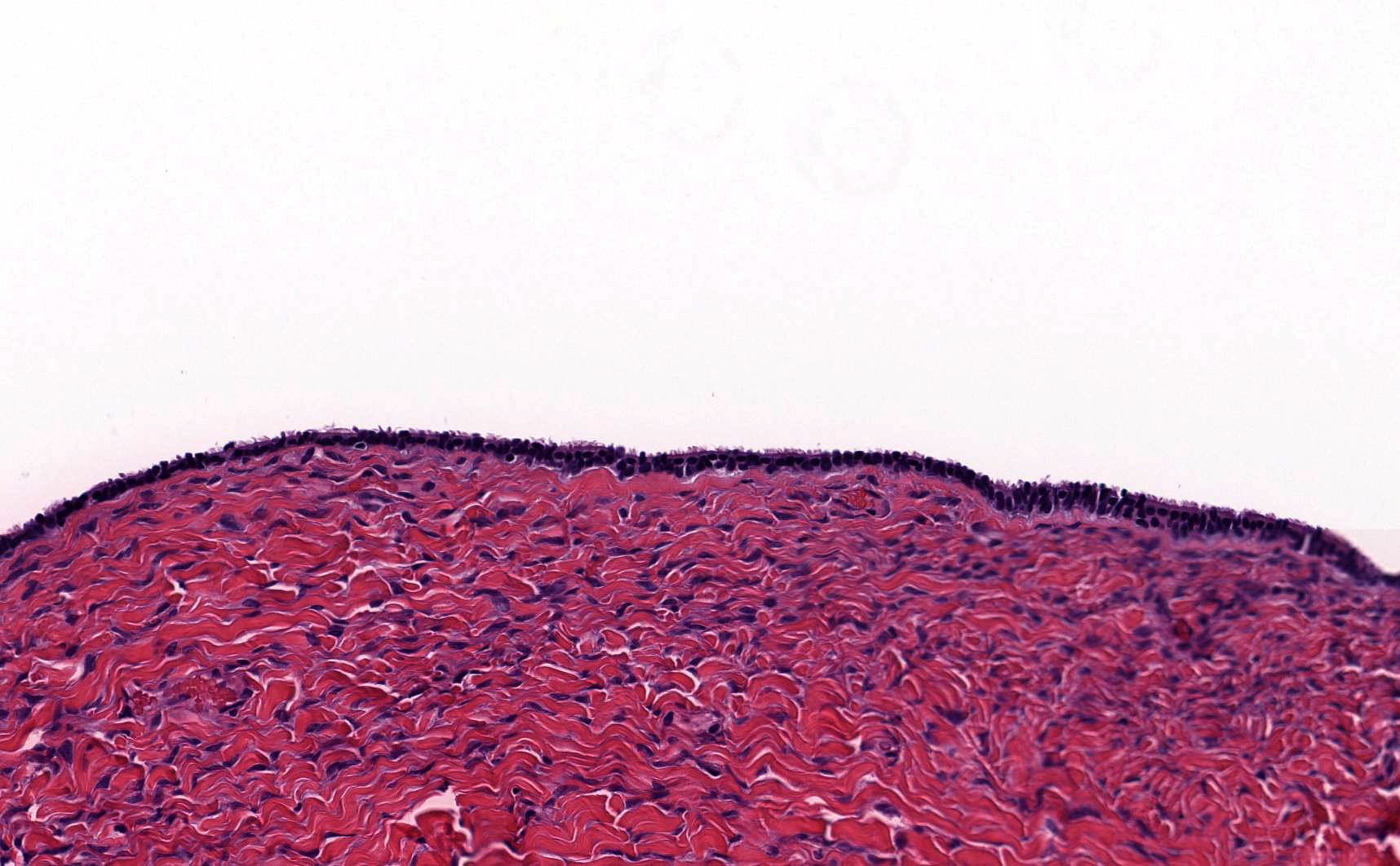
- Fluid filled cyst with ciliated lining adjacent to fallopian tube
- Ciliated cyst adjacent to fallopian tube
- Typically asymptomatic
- Almost always benign, with rare reports of borderline tumor
- Paraovarian cyst
- Hydatid cyst
- Not recommended: hydatid of Morgagni
- ICD-10: N83.8 - other noninflammatory disorders of ovary, fallopian tube and broad ligament
- Common benign incidental finding (~7 - 10% of women) (J Pediatr Surg 2011;46:2161)
- All age groups, most commonly third to fifth decade
- Paratubal (between fallopian tube and ovary)
- Unknown
- Believed to originate from mesothelium or be remnant of Müllerian duct or Wolffian duct
- Most cysts are small and asymptomatic (< 1 to 8 cm; rarely, 20+ cm)
- Size of paratubal cysts may correlate with obesity (J Pediatr Adolesc Gynecol 2017;30:571)
- May be found during surgery or incidentally on radiological study performed for another reason
- Larger lesions may become symptomatic, causing pressure or pain (J Pediatr Surg 2011;46:2161)
- May lead to torsion of adnexa, resulting in acute pain (J Pediatr Surg 2011;46:2161)
- Typically noted incidentally on intraoperative or gross examination
- While not often diagnosed on imaging, paratubal cysts are unilocular and anechoic or hypoechoic on ultrasound (J Clin Endocrinol Metab 2000;85:1021)
- Paratubal cysts are benign
- Rarely gives rise to serous borderline tumor or even more rarely malignancy (Appl Immunohistochem Mol Morphol 2017;25:e21)
- 15 year old girl with giant paratubal serous cystadenoma (J Pediatr Adolesc Gynecol 2020;33:438)
- 17 year old girl with paratubal borderline tumor (J Pediatr Adolesc Gynecol 2016;29:74)
- 34 year old nulligravid woman with paratubal cyst and bilateral hydrosalpinges diagnosed during evaluation of infertility (Taiwan J Obstet Gynecol 2014;53:239)
- Surgical excision of the paratubal cyst represents definitive treatment for symptomatic patients (J Clin Endocrinol Metab 2000;85:1021)
- Benign follow up is expected; treatment is not required for asymptomatic patients
- Simple fluid filled cyst(s) near fallopian tube
Images hosted on other servers:

Benign appearing cyst
- Simple fluid filled cyst lined by ciliated tubal type epithelium
- Focal papillary projections may be seen
Contributed by Stephanie L. Skala, M.D.
Simple cyst near tube
Simple cyst adjacent to fallopian tube
Bland, ciliated, tubal type epithelium
Images hosted on other servers:

Benign fallopian tube with simple paratubal cysts
- Fallopian tubes, bilateral salpingectomy:
- Benign fallopian tubes with paratubal cysts
- Endometriotic cyst:
- Associated with endometrial type stroma with or without hemosiderin laden macrophages
- Serous cystadenoma:
- Histologically identical to paratubal cyst but > 1 cm in size
- Hydrosalpinx:
- Dilation of the fallopian tube lumen with attenuation of the tubal epithelium with or without diminished plicae
- Distinction based largely on location of the cystic space within rather than near the fallopian tube

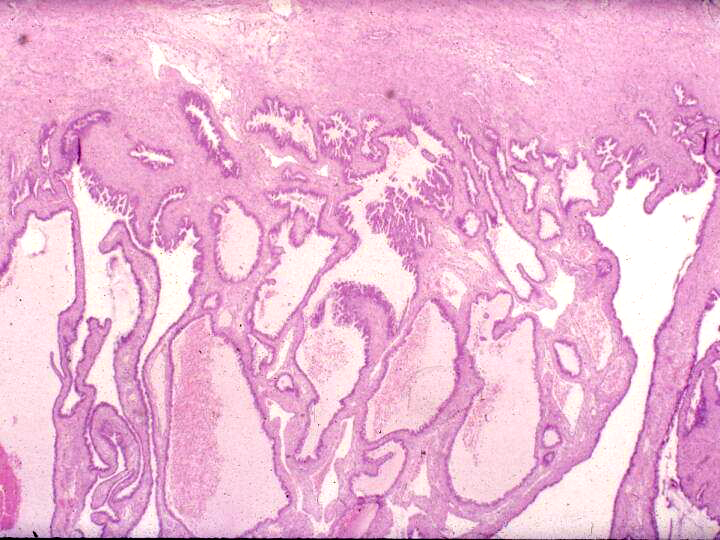
Upon review of a salpingectomy specimen, the lesion shown above is identified next to the fallopian tube. What is the expected outcome?
- Benign follow up
- Local recurrence
- Metastatic disease
- Progression to carcinoma
- Large paratubal cysts may cause torsion
- Large paratubal cysts often progress to borderline tumors
- Paratubal cysts are frequently diagnosed on MRI
- Paratubal cysts are an unusual finding
- Turning of tubes inside out, back into vaginal vault or even more rarely into bladder or uterine cavity
- Rare (less than 100 cases reported), ~80% occur after vaginal hysterectomy (0.5% incidence), presumed due to nonclosure of vaginal vault
- 0.06% incidence after abdominal hystertecomy, less frequent with interposition or colpotomy
- Associated factors include postoperative fever, hematoma formation / failure to maintain adequate hemostasis, poor physical condition, insufficient preoperative vaginal preparation, difficultly with surgical procedure, use of intraperitoneal vaginal drains and packs
- Occurs two months to eight years after surgery
- May present with watery vaginal discharge, lower abdominal pain, dyspareunia
- 27 year old woman with peritoneovaginal fistula (Can J Urol 2010;17:5117)
- 35 year old woman (J Midlife Health 2012;3:40)
- Prolapse of fallopian tube into urinary bladder, resembling carcinoma (Arch Pathol Lab Med 1983;107:613)
- Surgical excision
- Polypoid mass resembling granulation tissue, visible at vaginal apex
- Normal ciliated fallopian tube epithelium with variable surrounding fibrosis, edema, chronic inflammation
Images hosted on other servers:

Fallopian tubal epithelium thrown into papillary folds

Fallopian tube lining
of pseudostratified
ciliated columnar
epithelium
- May be seen on Pap smears
- Columnar cells with cilia and sheets of cells with small granular uniform nuclei in an orderly arrangement; also inflammatory cells and reactive atypia (Diagn Cytopathol 2013;41:146)
- Carcinoma (well differentiated): has glands at odd locations
- Cysts of mesonephric and paramesonephric duct
- Endometriosis
- Vaginal adenosis
- Salpingitis isthmica nodosa (SIN) is an outpouching of the fallopian tube epithelium into the smooth muscle wall (adenomyosis of the tube)
- Multiple discrete lumina are enveloped in smooth muscle and in severe cases, the tubal lumen may be completely obstructed
- SIN can lead to infertility or ectopic pregnancy
- Adenomyosis of the fallopian tube
- Nodular swelling of the isthmic segment of the fallopian tube
- Multiple glands lined by bland tubal epithelium within the tubal wall, separated and surrounded by smooth muscle
- Associated with infertility and ectopic pregnancy
- Diverticulosis of the fallopian tube
- Tubal adenomyosis
- 0.6 - 11% of healthy fertile women (StatPearls: Salpingitis Isthmica Nodosa [Accessed 22 June 2023], Fertil Steril 1993;60:599)
- Incidence is ~1% in the white female population (Fertil Steril 1978;29:164)
- Primarily affects young women of reproductive age (mean: 26 years)
- 10% incidence in cases of ectopic tubular pregnancies (Gynecol Obstet Invest 1992;34:202)
- Fallopian tubes, predominantly the isthmus
- Invasion of the epithelium into the smooth muscle may lead to muscular hypertrophy, generating the nodular appearance of the lesion
- Unclear but early theories include inflammatory or congenital causes (Radiology 1985;154:597)
- Other controversial hypotheses include
- Origination in Wolffian rests or mesonephric rests due to SIN occurring at the location in which these ducts cross during embryologic development (Clin Radiol 1987;38:207)
- Acquired etiology with some studies suggesting diethylstilbestrol exposure; chronic tubal spasm due to increased intramural pressure / weakness in the wall at the site of vasculature (Clin Obstet Gynecol 1987;30:181)
- Infectious etiology due to chronic infection or inflammation
- More common in the background of ectopic pregnancy and infertility
- Associated with infertility in 50% of patients but its presence may not actually affect the number of births (Hum Reprod 1991;6:828)
- Incidence in healthy, fertile women ranges from 0.6 to 11% (Fertil Steril 1993;60:599)
- May be unilateral or bilateral
- Incidental finding during evaluation for pelvic pain or infertility (hysterosalpingogram [HSG], laparotomy, laparoscopy)
- Tubal evaluation for primary infertility may reveal gross lesion
- HSG can demonstrate the nodular swellings (Fertil Steril 1993;60:599)
- No pathognomonic clinical symptomatology
- Hysterosalpingography (HSG)
- Globular 2 mm diameter collections of contrast medium in isthmus
- Tubal occlusion and hydrosalpinx may be observed
Images hosted on other servers:

Nodular swelling of the isthmus

Multiple nodular diveriticula

Small outpouching or diverticula
- Smooth muscle hypertrophy can cause near complete occlusion of the tubal lumen and increase the risk of secondary infection, infertility or ectopic pregnancy
- 29 year old woman with subfertility (Eur J Obstet Gynecol Reprod Biol 2015;184:73)
- 33 year old woman with ruptured salpingitis isthmica nodosum (BMJ Case Rep 2021;14:e237860)
- 42 year old woman with abdominal pain and amenorrhea (J Clin Diagn Res 2013;7:2581)
- Recanalization using interventional radiology (Fertil Steril 1995;63:715)
- Microsurgical tubocornual anastomosis (Fertil Steril 1993;60:599)
- Assisted reproductive technology (ART) for infertility (Eur J Obstet Gynecol Reprod Biol 2015;184:73)
- Firm, nodular swellings of the fallopian tube, ranging in size up to 2 cm in greatest dimension (Br J Radiol 2021;94:20201386)
- May be unilateral or bilateral
- Smooth, intact serosal covering
- Cross section of the nodules reveal gray, yellow or brown tissue punctuated by small cysts that surround the original tubal lumen (StatPearls: Salpingitis Isthmica Nodosa [Accessed 22 June 2023])
- Nodosity of the isthmus may give the uterus a horned appearance
AFIP images
Dark, nodular swelling
Marked thickening
Images hosted on other servers:

Nodules at isthmus
- Regularly spaced glands lined by normal appearing tubal epithelium surrounded by smooth muscle or fibrous tissue
- Tubal lumina are true diverticula that communicate with the central tubal lumen but do not connect with the serosa
- Glands can become cystically dilated (Am J Clin Pathol 1951;21:212)
- No significant atypia, scarring or associated inflammatory / stromal response
- Absence of endometrial stroma differentiates this entity from tubal endometriosis
Contributed by Jessica L. Bentz, M.D., AFIP and @Andrew_Fltv on Twitter
Cystically dilated glands in smooth muscle
Bland nuclear features
Gland-like structures
Numerous gland-like structures
Salpingitis isthmica nodosa
- Right fallopian tube, salpingectomy:
- Salpingitis isthmica nodosa
- Endometriosis:
- Glands are surrounded by endometrial stroma with or without hemosiderin laden macrophages
- Adenocarcinoma:
- Desmoplastic or inflammatory response and prominent cytologic atypia
- Adenomatoid tumor:
- Slit-like glands with thin, tapered septa lined by bland flattened to cuboidal cells
- Ectopic pregnancy
- Endometrioid adenocarcinoma
- Endometriosis
- Fitz-Hugh-Curtis syndrome
- Serous tubal intraepithelial carcinoma (STIC)
Comment Here
Reference: Salpingitis isthmica nodosa
A 48 year old woman with a history of infertility undergoes a hysterectomy with bilateral salpingectomy for abnormal uterine bleeding. What is the most likely diagnosis in her right fallopian tube?
- Endometrioid adenocarcinoma
- Endometriosis
- Endosalpingiosis
- Salpingitis isthmica nodosa (SIN)
- Serous cystadenofibroma
Comment Here
Reference: Salpingitis isthmica nodosa
- Similar to ovarian counterpart
AFIP images
Mostly fibromatous surface
AFIP images
Resembling ovarian fibroma
Endometrioid adenofibroma
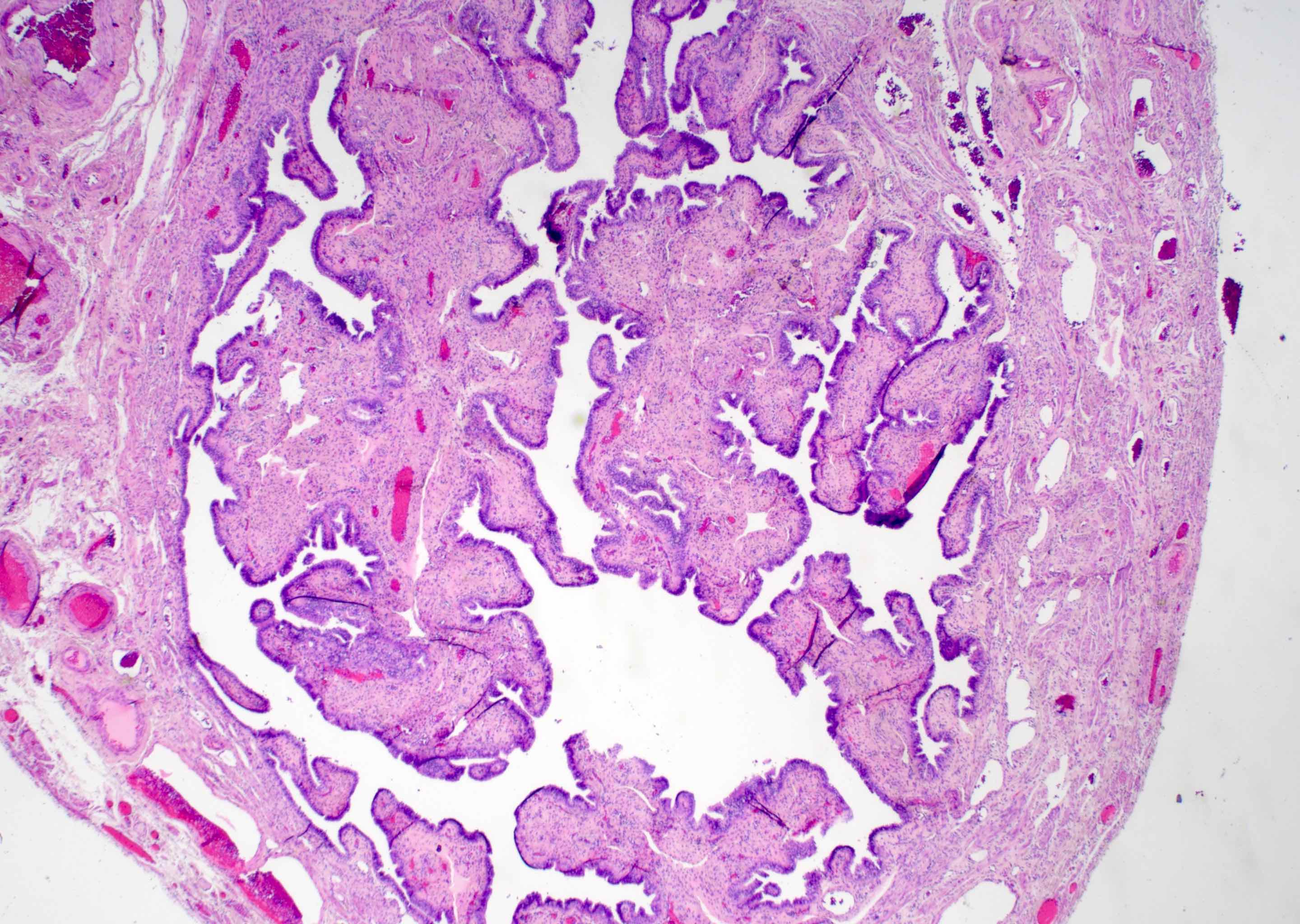
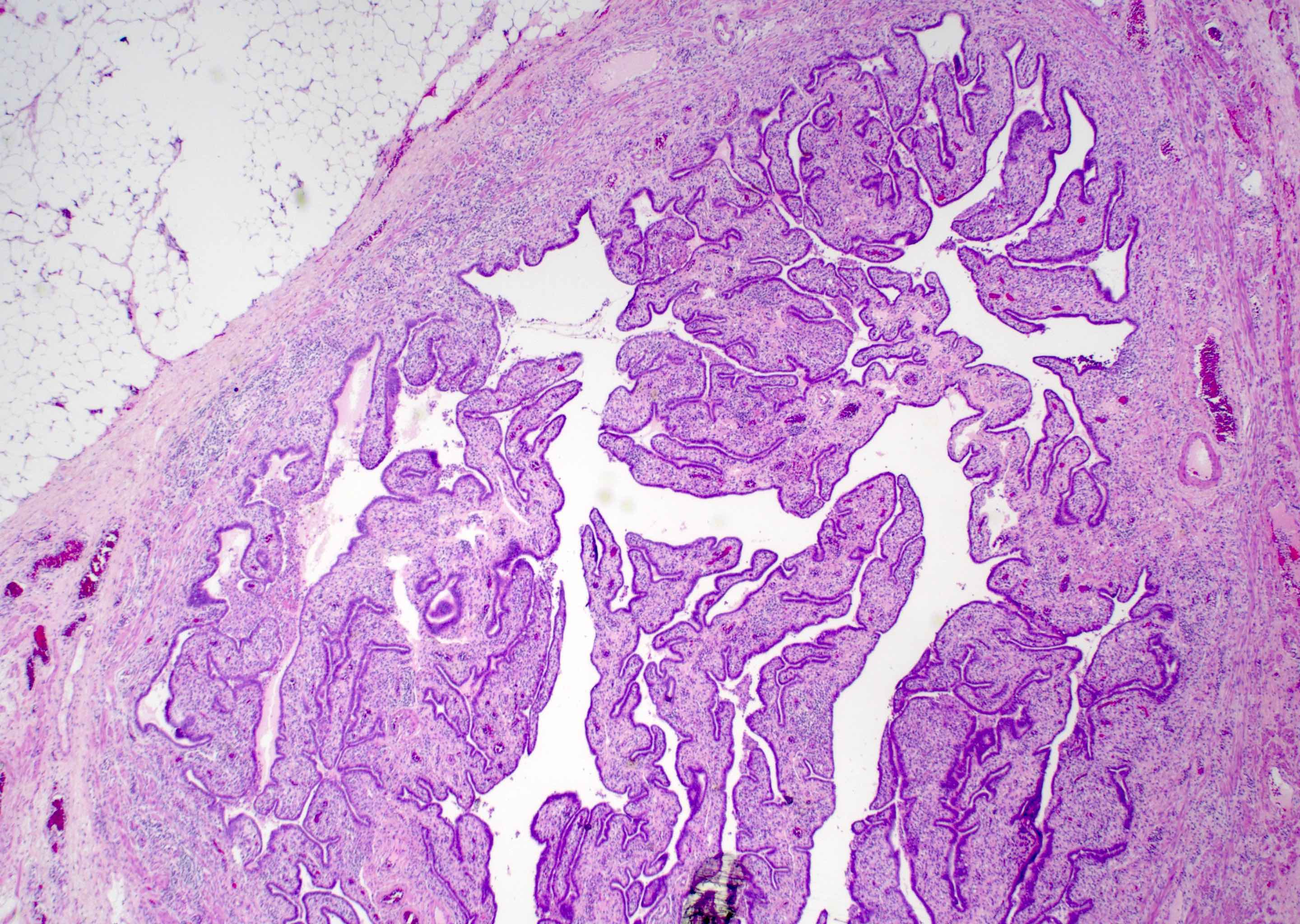
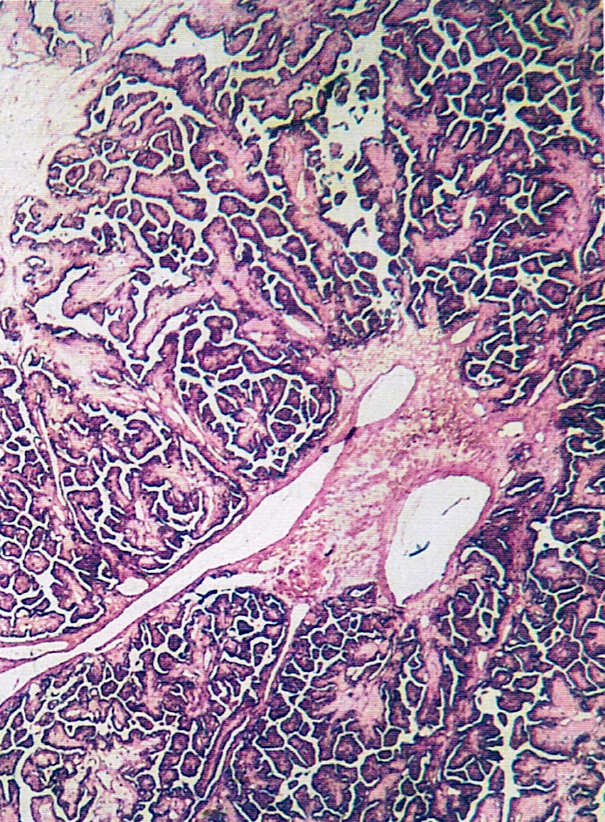
- Serous borderline tumor (SBT) of the fallopian tube is a proliferative epithelial neoplasm that is by definition noninvasive (Pan Afr Med J 2019;32:129)
- Serous borderline tumor arising in the fallopian tube is a rare entity with fewer than 20 cases in the literature
- Microscopically similar to SBT arising in the ovary, with numerous papillae of varying size arborizing down to smaller papillae
- Hobnailing may also be present
- Serous borderline tumor is currently the sole recommended term for primary fallopian tumors
- Not recommended: atypical proliferative serous tumor (Am J Surg Pathol 2011;35:1605)
- ICD-O: 8442/1 - serous borderline tumor, NOS
- ICD-11: 2C74.Y & XH3ZK9 - other specified malignant neoplasms of fallopian tube & serous cystadenoma, borderline malignancy
- Serous borderline tumor of the fallopian tube is a rare neoplasm with fewer than 20 cases reported in the literature (Arch Gynecol Obstet 2011;283:349)
- Age range is broad, from 22 to 83 years (BMC Cancer 2005;5:129)
- Fallopian tube
- Theorized to arise from papillary hyperplasia of the fallopian tube
- May similarly be related to BRAF V600E mutation as in serous borderline tumor of the ovary (J Natl Cancer Inst 2003;95:484)
- Unknown
- Nonspecific, may be asymptomatic or may have abdominal pain (Obstet Gynecol Sci 2014;57:334)
- Adnexal mass may be noted on routine gynecologic exam
- Ultrasound findings may reveal cystic mass near ovary
- On laparoscopy, dilated fallopian tube or hematosalpinx may be noted (BMC Cancer 2005;5:129)
- Generally, CA125 levels are normal (Pan Afr Med J 2019;32:129)
- Hypoechogenic cystic mass on ultrasound, sometimes with intramural papillary projections (Pan Afr Med J 2019;32:129)
Images hosted on other servers:

Ultrasound / CT paratubal mass
- Prognosis is excellent with surgical removal (Clin Case Rep 2023;11:e7140)
- 25 year old woman with lower abdominal pain and abdominal mass (Obstet Gynecol Sci 2014;57:334)
- 30 year old woman with a 1 year history of pelvic pain (Clin Case Rep 2023;11:e7140)
- 61 year old woman with a left fallopian paratubal cyst (Pan Afr Med J 2019;32:129)
- Too few cases to determine optimal treatment, however, most commonly treated through conservative surgical management via salpingectomy or salpingo-oophorectomy for fertility preservation purposes
- At times includes hysterectomy for staging (Obstet Gynecol Sci 2014;57:334)
Images hosted on other servers:

Right fallopian tube cyst
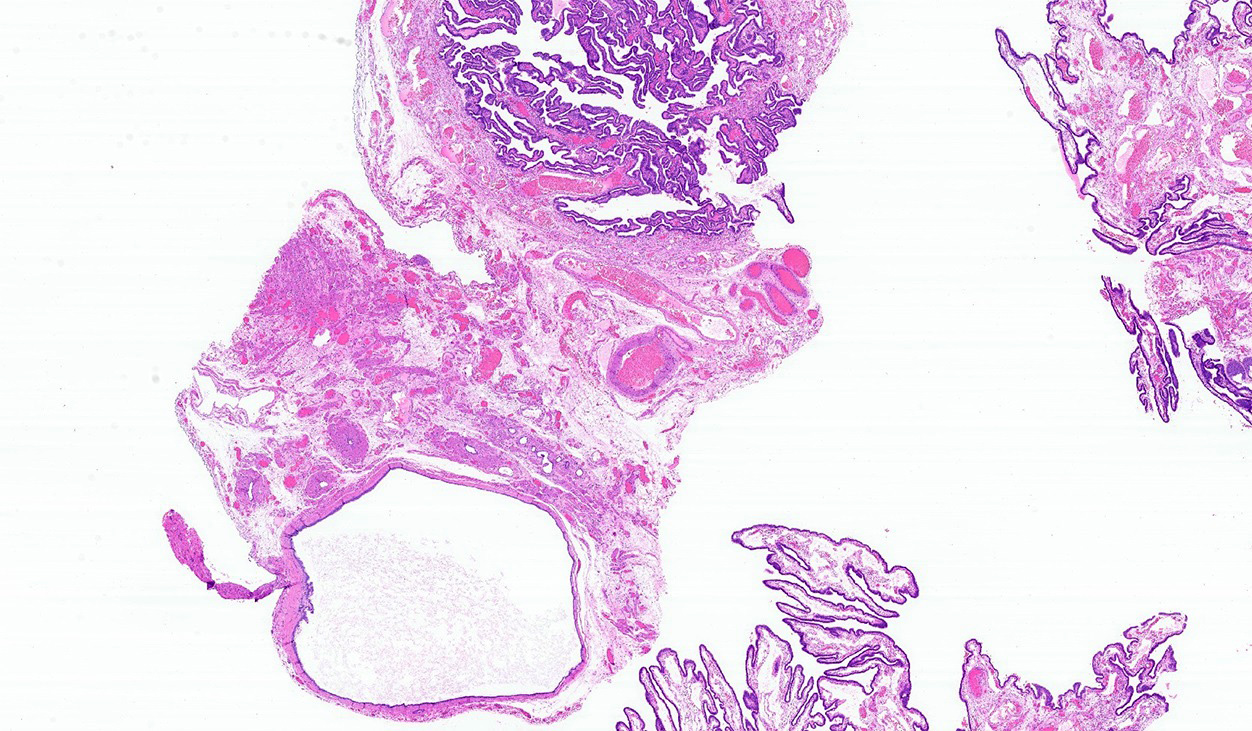
- Received from surgery as cystic mass or distended fallopian tube
- Cut surface
- Multiloculated cystic mass
- Intralocular papillary projections
- Filled with serous fluid
Images hosted on other servers:

Fallopian tube cystic mass
- Gross intraoperative evaluation
- Solid areas and papillary excrescences should be evaluated histologically
- Histologic intraoperative evaluation
- Bulbous papillae branching into smaller papillae on lower power
- Hobnailing or epithelial tufting
- Comparable to serous borderline tumor of the ovary
Contributed by Lewis A. Hassell, M.D. (source: Digital Pathology Association)
SBT of the ovary
- Serous borderline tumors of the fallopian tube closely resemble their ovarian counterparts
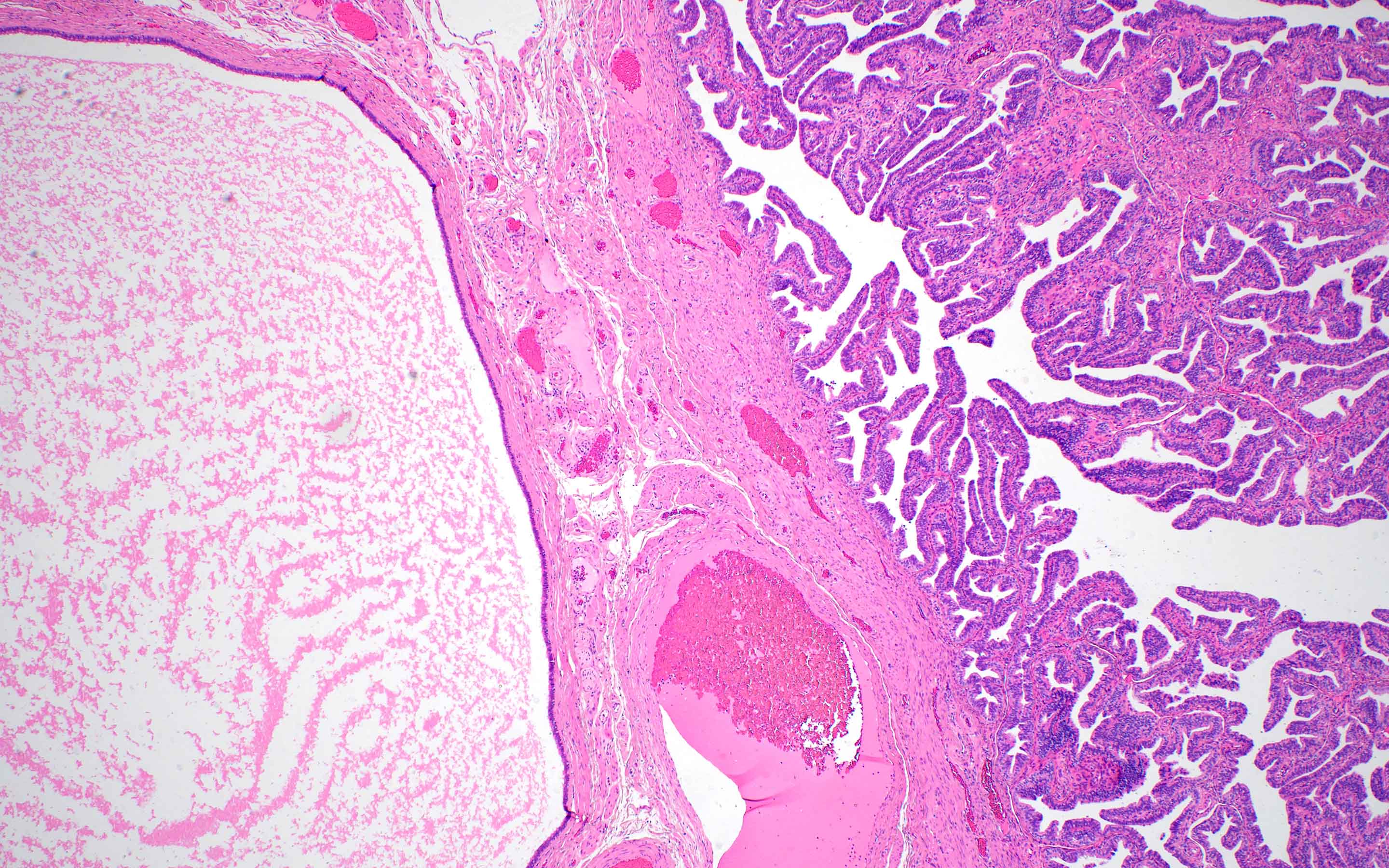
- Architecture
- Numerous papillae of variable size and width (Obstet Gynecol Sci 2014;57:334)
- These papillae occupy a variable extent of a cyst lined by pseudostratified epithelium
- Larger papillae arborize down to smaller papillae which terminate in epithelial clusters or single cells
- Hobnailing or epithelial tufting
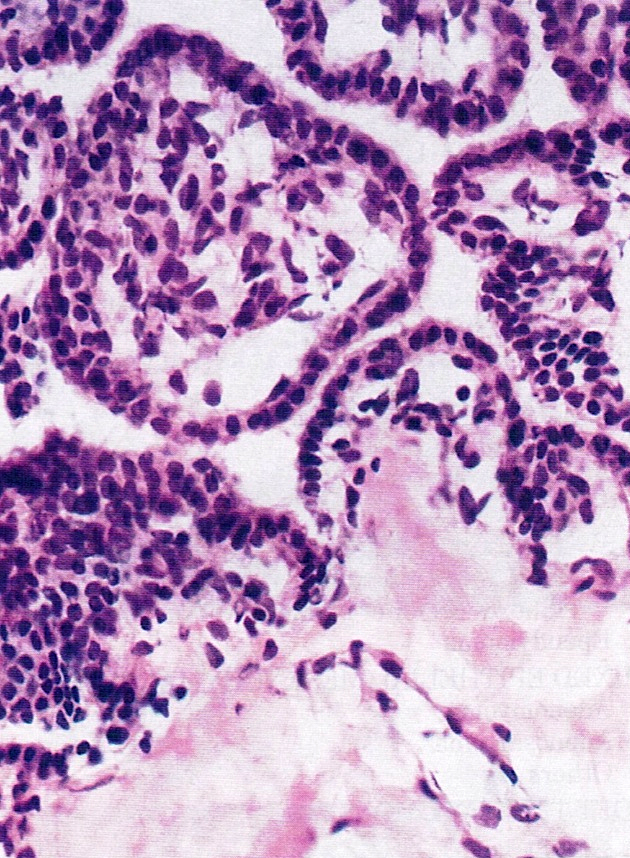
- Cytologic features
- Ciliated cells that are cuboidal to columnar
- Up to moderate atypia - cellular enlargement, coarse chromatin, small nucleoli may be present, minimal mitotic activity
Contributed by Kamaljeet Singh, M.D. and Anna Måsbäck, M.D., Ph.D.

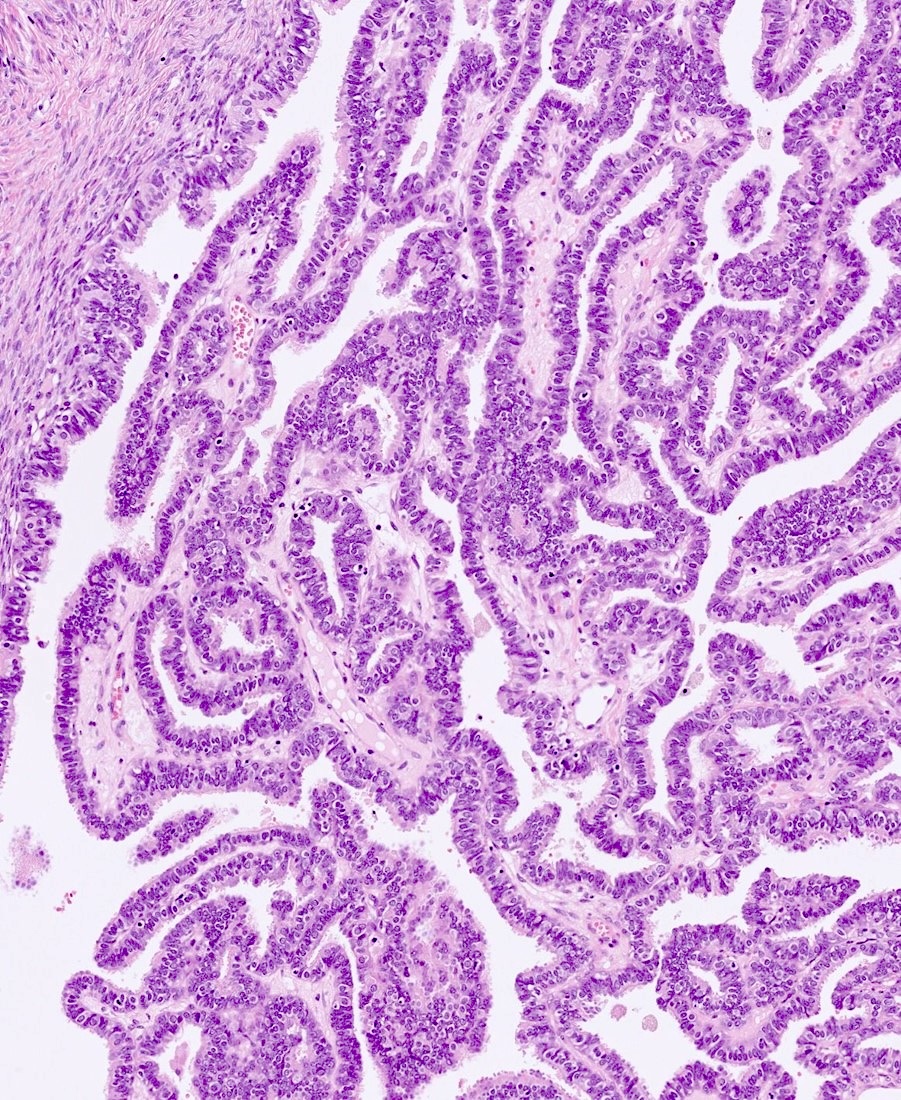
Papillary branching
Epithelial hobnailing
Variably sized papillae

Ciliated cells with hobnailing
Arborizing papillae
PAX8
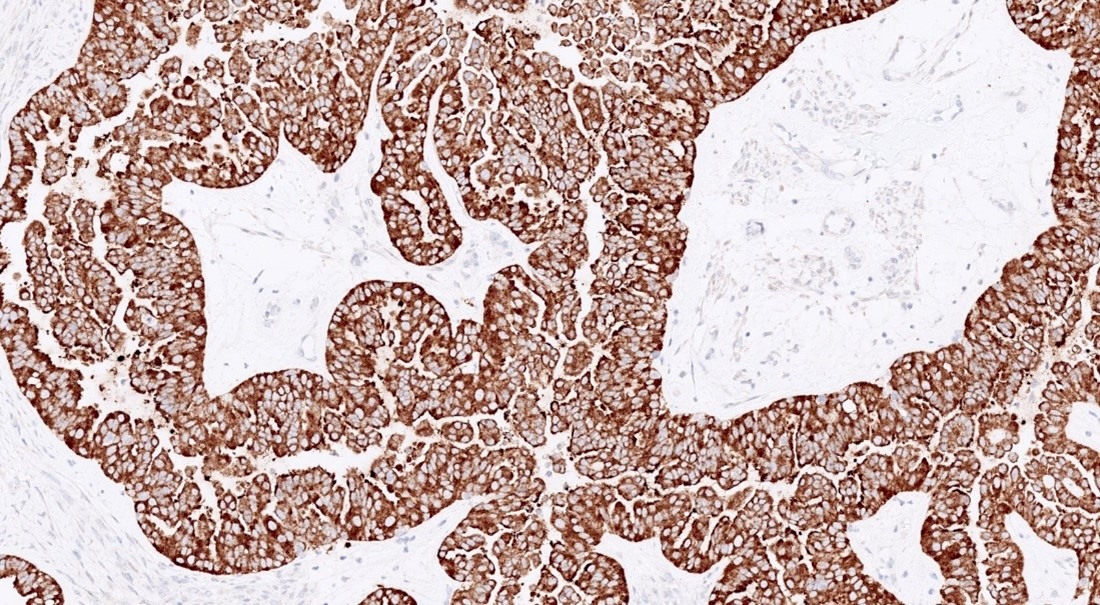
CK7
BRAF
Images hosted on other servers:

SBT with micropapillary features
- Right fallopian tube and ovary, salpingo-oophorectomy:
- Borderline tumor of the fallopian tube (see comment)
- Procedure: unilateral salpingo-oopherectomy, lymphadenectomy
- Specimen integrity: serosa intact
- Surface involvement: absent
- Tumor site: right fallopian tube
- Tumor size: 8.5 cm
- Additional dimensions: 7 x 5 cm
- Histologic type: serous borderline tumor
- Implants: not identified
- Other organ involvement: not identified
- Peritoneal fluid: not submitted
- Regional lymph nodes: all lymph nodes negative for tumor cells
- Number of lymph nodes examined: 4
- Specify sites: right pelvic
- Pathologic stage: pT1, pN0
- FIGO stage: IA
- Comment: Microscopically this lesion shows numerous papillae of varying size and width. These papillae arborize down into smaller papillae. On higher power there is hobnailing, the epithelial cells are cuboidal to columnar and are ciliated. Immunohistochemical stains performed with adequate controls on sections of the right fallopian tube tumor show the tumor cells to be diffusely positive for PAX8, WT1, ER and PR, with focal / weak expression of p53 (wild type expression) and patchy positivity for p16. The combined morphologic and immunohistochemical findings support the above diagnosis (CAP: Protocol for the Examination of Specimens From Patients With Primary Tumors of the Ovary, Fallopian Tube, or Peritoneum [Accessed 19 April 2024]).
- Endosalpingiosis:
- Minimal architectural complexity or cytologic atypia
- Psammomatous calcifications may be present; rarely larger than a few millimeters
- Serous cystadenoma / cystadenofibroma:
- No architectural complexity, e.g., papillae, micropapillae, cribriforming or nesting
- If there is architectural complexity but it constitutes < 10% of overall tumor then it is a serous cystadenoma / cystadenofibroma with focal epithelial proliferation
- Heterogenous population of ciliated and secretory cells but without atypia or mitoses
- Serous borderline tumor with intraepithelial / microinvasive carcinoma:
- Significant cytologic atypia and or evidence of invasion of stroma
- Usually micropapillary
- Clear cell carcinoma:
- Clear cytoplasm
- High grade nuclei
- Napsin A positivity, loss of hormonal markers
The mass shown in the image above was identified in the fallopian tube of a 49 year old woman. What is the most appropriate diagnosis?
- High grade serous carcinoma
- Mesothelioma
- Paratubal cyst
- Serous borderline tumor arising from the fallopian tube
- Well differentiated endometrioid carcinoma
Comment Here
Reference: Serous borderline tumor
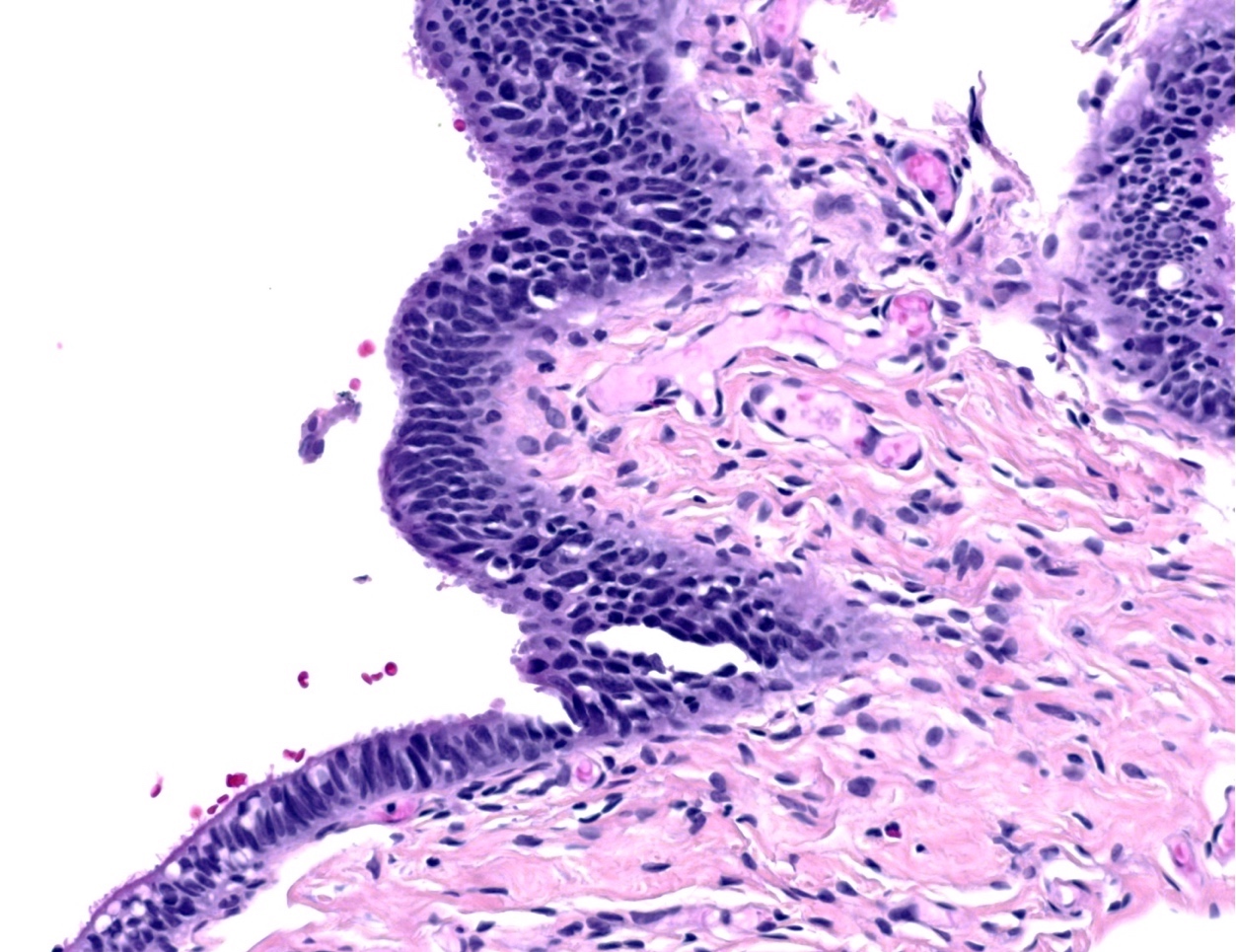
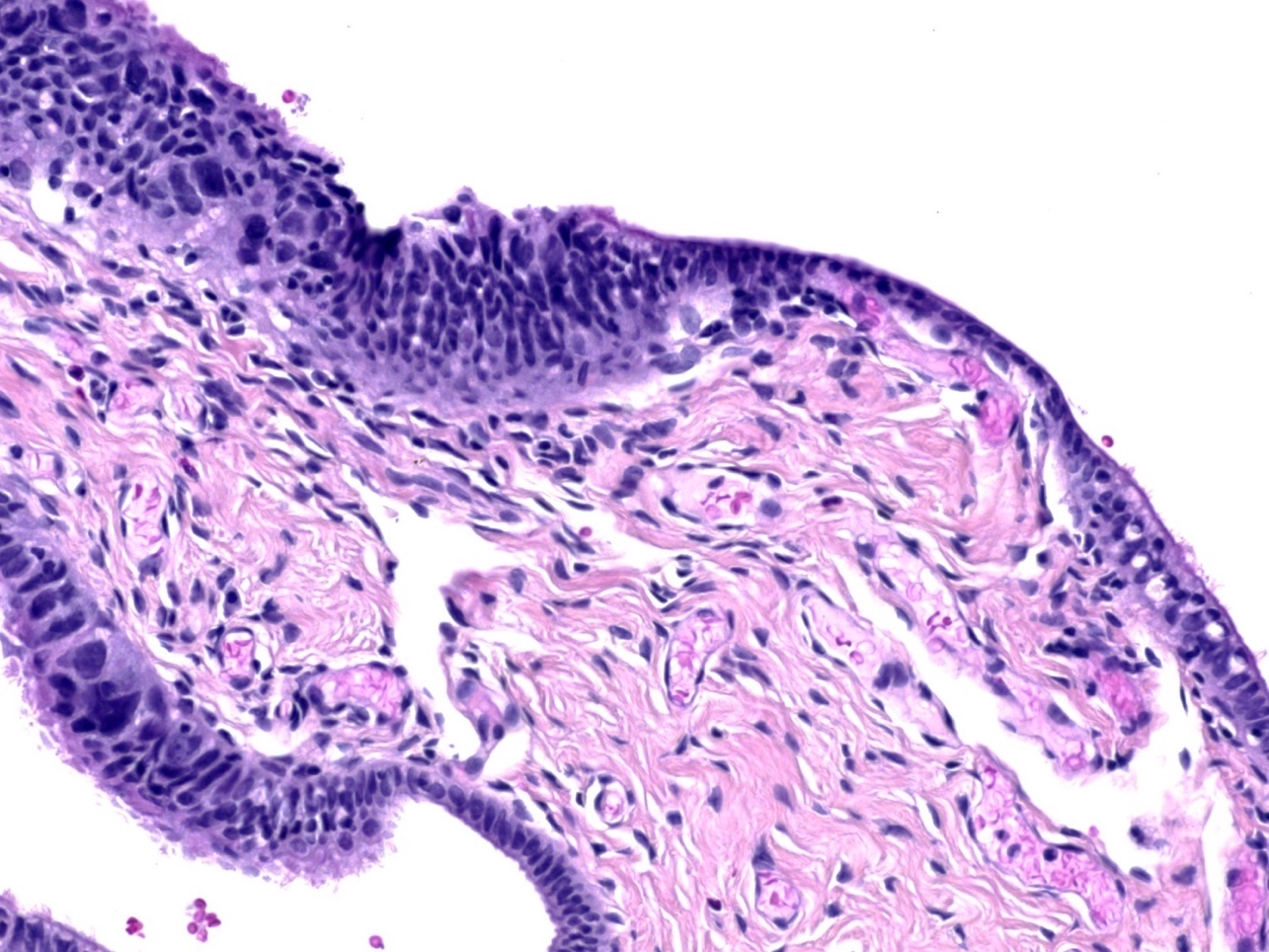
- Lesion that is limited to the fallopian tube epithelium and a precursor to extrauterine (pelvic) high grade serous carcinoma
- Confined to epithelium
- Histologic features: significant atypia, architectural alterations, high proliferative index and mutant pattern of p53 staining
- Important precursor lesion to recognize, as it is a criterion for assigning fallopian tube as primary site of high grade tubo-ovarian serous carcinoma irrespective of presence and size of ovarian and peritoneal disease (Histopathology 2015;67:331)
- Various terms used to describe a spectrum of tubal epithelial alterations:
- Secretory cell outgrowths (SCOUTs): secretory cell expansion with variable ciliation (type 1 / tubal differentiation and type 2 / endometrioid differentiation), wild type p53 staining
- p53 signature: histologically normal epithelium (at least 12 cells) with mutant pattern p53 staining and low proliferation index (MIB1) (typically less than 10%)
- Serous tubal intraepithelial lesion (STIL): abnormal histology (high N/C but preserved polarity), mutant p53 and variable MIB1; STIL is regarded as a lesion of uncertain significance and diagnostic features fall short of STIC
- Serous tubal intraepithelial carcinoma (STIC): abnormal histology (high N/C, loss of polarity, lack of ciliated cells), mutant pattern p53 staining and high proliferation index (MIB1)
- ICD-10: N83.9 - fallopian tube disorder
- Patients with hereditary BRCA mutation have a high risk of high grade serous carcinoma
- Incidence of STIC in risk reducing salpingo-oophorectomies in BRCA+ women is 5 - 8% (Gynecol Oncol 2006;100:58)
- Fallopian tube fimbria is the most common site of origin
- Secretory epithelium of fallopian tube is postulated as the cell of origin (Adv Anat Pathol 2010;17:293)
- Usually discovered incidentally during routine surgery or risk reducing prophylactic salpingo-oophorectomies
- May be seen adjacent to invasive carcinoma
- Reference: Gynecol Oncol 2017;146:69
- Careful morphologic evaluation is key to the diagnosis; immunohistochemistry (p53 and MIB1) is only supportive
- Gross protocol (sectioning and extensively examining the fimbria [SEE-FIM]) influences ability to diagnose (Am J Surg Pathol 2006;30:230):
- Amputation and longitudinal sectioning of the infundibulum and fimbrial segment (distal 2 cm) allows maximal exposure of the tubal plicae; isthmus and ampulla are cut transversely at 2 - 3 mm intervals
- Entire fallopian tube should be submitted for evaluation in women with BRCA mutations or strong family history of ovarian carcinoma
- Extensively examine the fimbriated end
- Controversial role of multiple levels with 1 study finding no impact and another study reporting 25% missed with a single section (Am J Surg Pathol 2009;33:1878, Int J Gynecol Pathol 2013;32:353)
- STIC is staged as pathologic stage pT1
- 48 year old woman with STIC in cervical smears (Diagn Cytopathol 2018;46:945)
- 51 year old postmenopausal woman with STIC and BRCA1 mutation (Jpn J Clin Oncol 2014;44:597)
- 55 year old woman with synchronous papillary serous carcinoma of ovary and endometrium and STIC (Indian J Pathol Microbiol 2017;60:125)
- 56 year old woman with incidental STIC (Case Rep Obstet Gynecol 2015;2015:760429)
- 58 year old woman with retroperitoneal high grade serous carcinoma and STIC (Diagn Pathol 2019;14:17)
- No current consensus among gynecologic oncologists regarding appropriate management of incidental STIC
- Patients have been managed by surgical staging / peritoneal washings / chemotherapy or follow up without additional intervention
- Yield of surgical staging is low and short term clinical outcomes are favorable
- Individualized management is warranted until additional data become available (Int J Gynecol Cancer 2013;23:1603)
- Not evident on gross examination
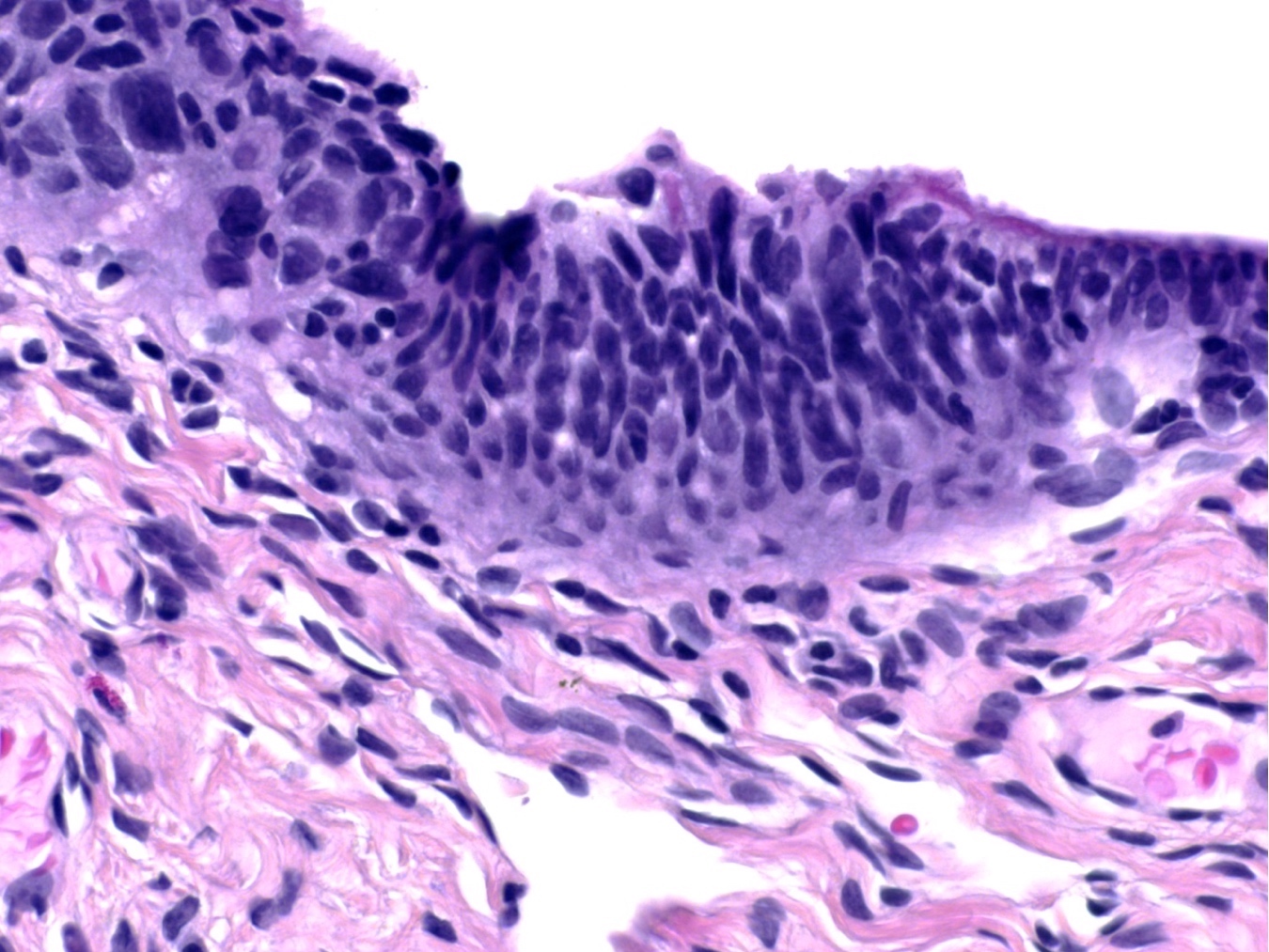
- Epithelial stratification
- Lack of ciliated cells (Mod Pathol 2017;30:710)
- High N/C ratio
- Nuclear pleomorphism, hyperchromasia, prominent nucleoli
- Loss of polarity (may be focal)
- Epithelial fractures (Adv Anat Pathol 2010;17:293)
- Exfoliation of small epithelial clusters
Contributed by Aysha Mubeen, M.D.

Basophilic appearance
Architectural and cytological atypia
STIC in contrast with adjacent normal tubal epithelium
Prominent atypia and multilayering
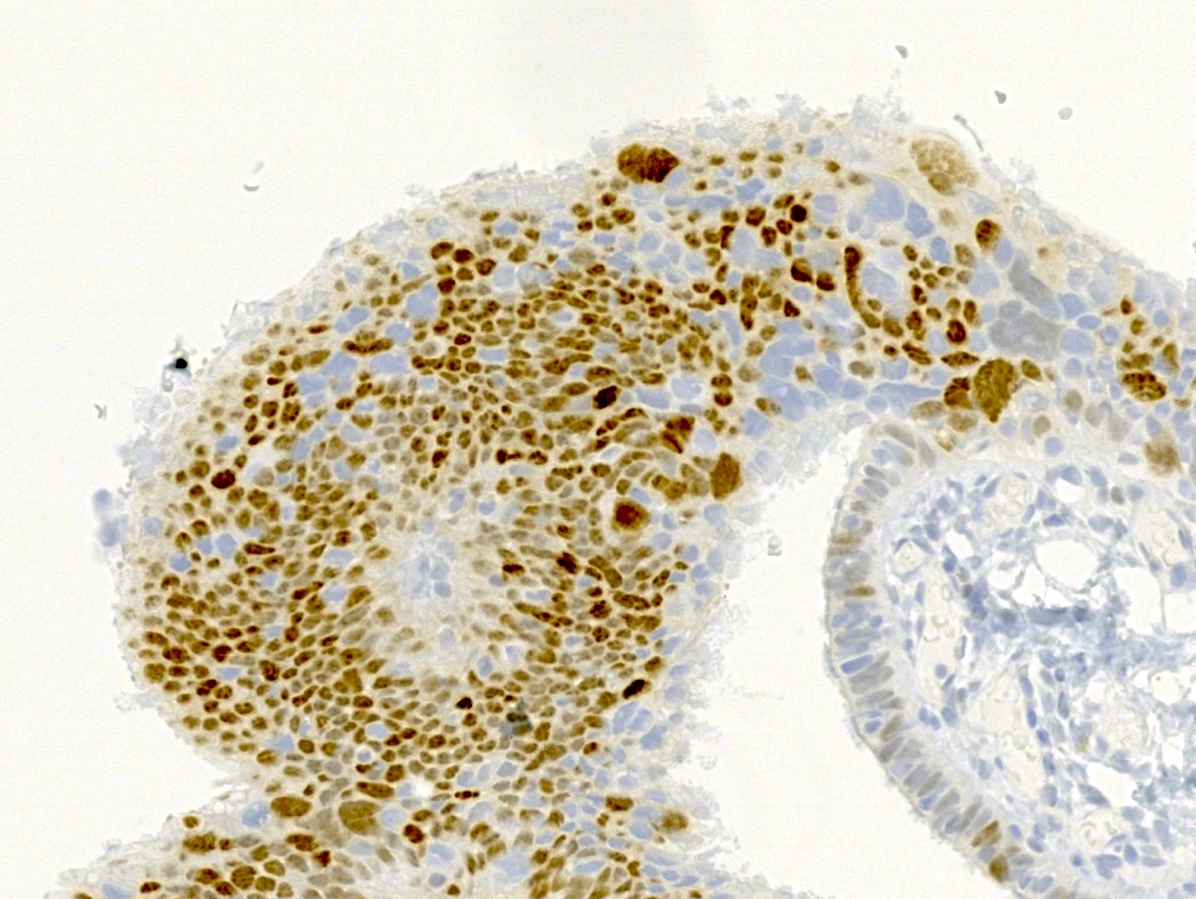
p53
Images hosted on other servers:

Focal epithelial stratification,
loss of polarity,
hyperchromatic and
pleomorphic nuclei
- Brush cytology shows clusters of cells with haphazard pleomorphic nuclei, high N/C ratio and lack of cilia (Cancer Cytopathol 2019;127:192)
- p53: mutant pattern of staining (diffusely positive (nuclear), completely negative (null type) or less commonly, cytoplasmic staining)
- Ki67 / MIB index: high (suggested cutoff of 10%) (Am J Surg Pathol 2011;35:1766, Int J Gynecol Pathol 2012;31:243)
- Bilateral fallopian tubes, salpingectomy:
- Right fallopian tube with serous tubal intraepithelial carcinoma (see comment)
- Left fallopian tube with no pathologic change
- Comment: Immunostain for p53 is diffusely and strongly positive in the lesional cells. Ki67 index is > 10%.
- p53 signature:
- Precursor lesion which shows normal histology with p53 mutant pattern of staining
- Transitional cell metaplasia:
- Uniform cells with nuclear grooves; p53 wild type (Am J Surg Pathol 2009;33:111)
- Florid epithelial hyperplasia and reactive atypia associated with acute salpingitis:
- Has a background of inflammation, retained polarity and presence of ciliated cells; p53 wild type
- Intramucosal fallopian tube metastasis from uterine serous carcinoma:
- May closely mimic STIC; usually WT1 negative (Am J Surg Pathol 2017;41:161)
- Front Biosci (Elite Ed) 2011;3:625, Int J Gynecol Pathol 2010;29:310, Mod Pathol 2009;22:985, Curr Opin Obstet Gynecol 2007;19:3, Adv Anat Pathol 2006;13:1, CAP: Protocol for the Examination of Specimens from Patients with Primary Tumors of the Ovary, Fallopian Tube or Peritoneum [Accessed 5 January 2022]
- p53 signature
- Reactive atypia
- Secretory cell outgrowth (SCOUT)
- Serous tubal intraepithelial carcinoma (STIC)
The grossing protocol for examination of the fallopian tube to identify the diagnosis in the photomicrograph should
- Ensure complete evaluation of the fallopian tube in all cases
- Increase detection of precursor lesions in at risk women
- Require multistep levels in at risk women
- Require tangential sectioning of the infundibulum and fimbrial segment to allow maximal exposure
Comment Here
Reference: Serous tubal intraepithelial carcinoma
- Aggressive tumor that arises in paratubal / paraovarian soft tissues, has variable morphology and immunohistochemistry and harbors pathognomonic alterations in STK11
- Associated with Peutz-Jeghers syndrome in ~50% of cases
- STK11 alterations
- Adnexal or paratubal mass
- ICD-10: C57.4 - malignant neoplasm of uterine adnexa, unspecified
- Age: wide range from middle age to elderly (mean: 40 years old) (Am J Surg Pathol 2021;45:1061)
- Rare pediatric case (16 years old) has been reported (Pediatr Dev Pathol 2023;26:486)
- Paratubal (most common)
- Fallopian tubes
- Ovaries
- Uterine serosa
- Less commonly, the abdomen and pelvis
- Reference: Am J Surg Pathol 2021;45:1061
- Associated with Peutz-Jeghers syndrome in ~50% of cases
- Can be sporadic
- Histogenesis of this tumor (Wolffian versus sex cord stromal versus epithelial or mesothelial origins) remains uncertain (Am J Surg Pathol 2021;45:1061)
- Reference: Pediatr Dev Pathol 2023;26:486
- Abdominal / pelvic pain or mass
- Abdominal distension
- Urinary tract symptoms
- Abnormal uterine bleeding
- Can be incidental finding
- Metastatic tumor at presentation (50%)
- Reference: Am J Surg Pathol 2021;45:1061
- Pelvic ultrasound or MRI and histopathologic diagnosis
- Recurrences at 3 - 79 months (mean: 29) after initial diagnosis, most commonly in the omentum, abdominal wall, peritoneum and pelvis
- Metastasis: most commonly to omentum and uterine serosa; less commonly to bladder peritoneum, anterior abdominal wall, small bowel, liver, paraaortic lymph node and pouch of Douglas
- Reference: Am J Surg Pathol 2021;45:1061
- 16 year old girl with large, bilateral, solid and cystic adnexal masses (Pediatr Dev Pathol 2023;26:486)
- 29 year old woman peritubal neoplastic lesion with STK11 mutation and response to mTOR inhibitor (Gynecol Oncol Rep 2021;37:100838)
- 22 cases of paratubal adnexal tumors that harbored STK11 alterations (Am J Surg Pathol 2021;45:1061)
- Surgery with or without chemotherapy or radiation (Gynecol Oncol Rep 2021;37:100838)
Images hosted on other servers:

Laparoscopic findings
- Adnexal mass that ranges from 4.5 to 25.5 cm in size (mean: 12.4 cm)
- Solid, cystic or both
- Variable in color (tan, white, gray, yellow, pink)
- Hemorrhage and necrosis are often present
- Reference: Am J Surg Pathol 2021;45:1061
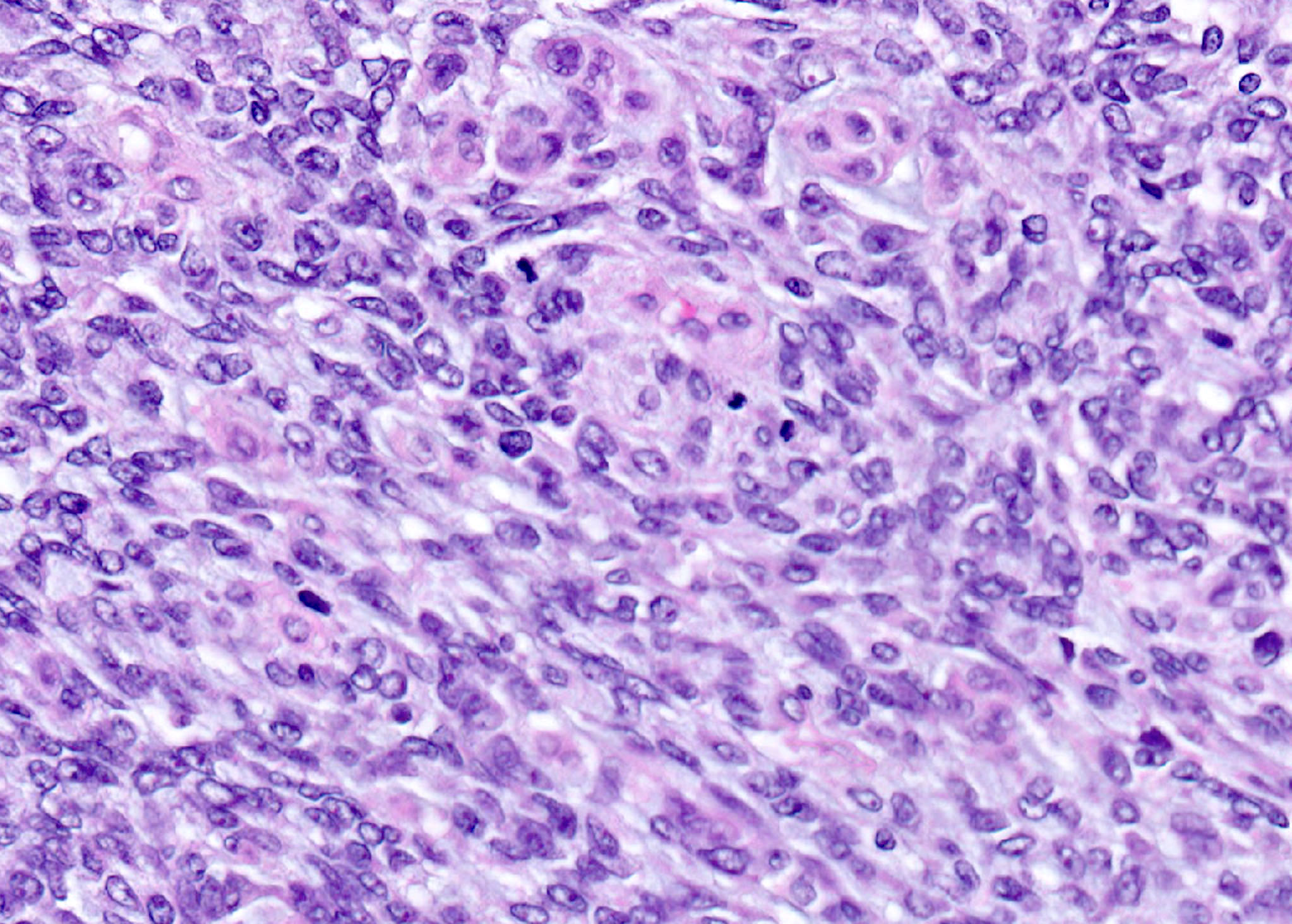
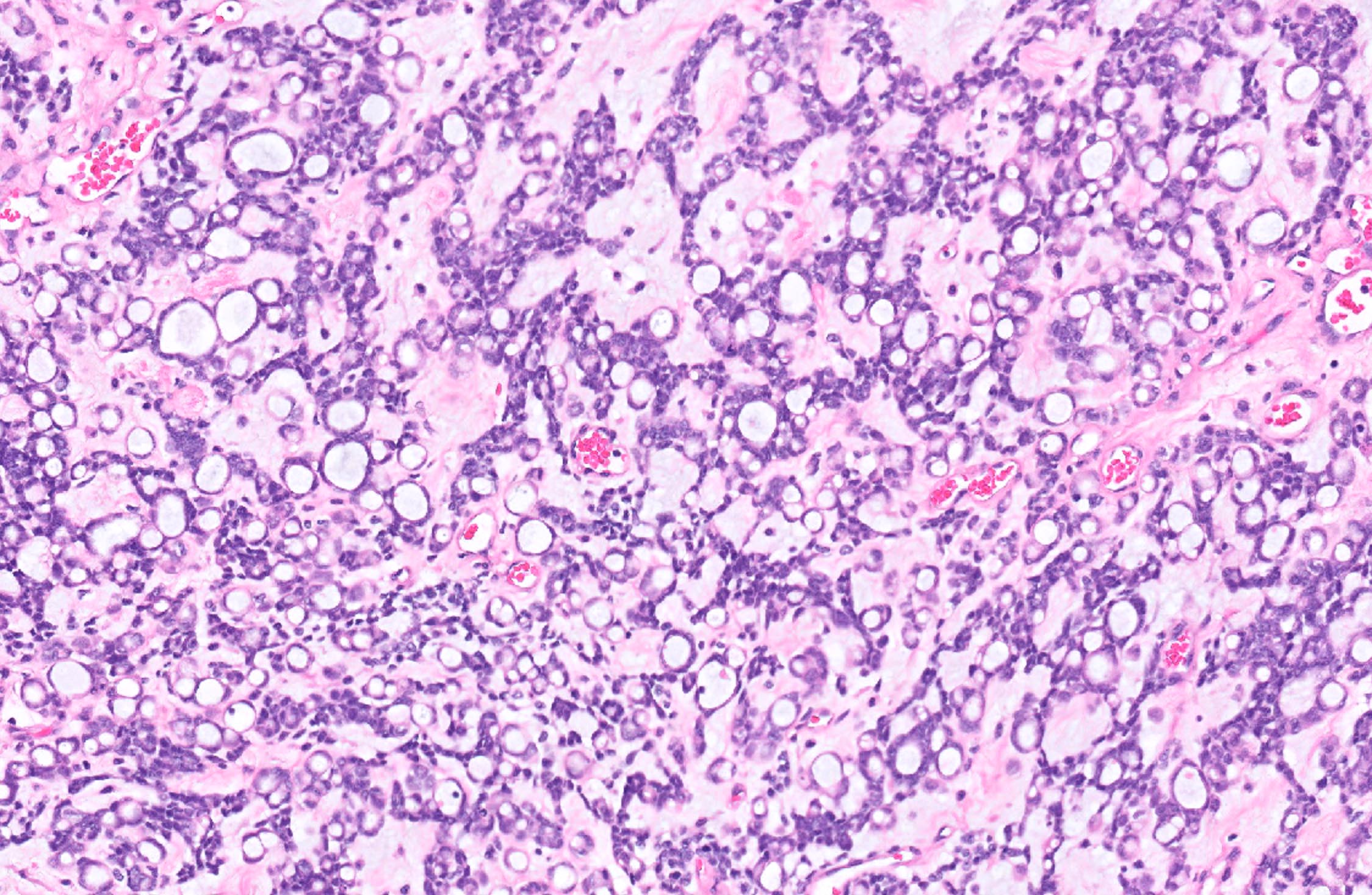
- Mixed architectural patterns are characteristically present within a single tumor and may be key to recognition
- Architecture
- Interanastomosing cords and trabeculae that can form tubular, cystic, cribriform or microacinar architecture
- Solid growth, large nests, broad columns or nodules of varying sizes
- Whorling tumor cells with vaguely glomeruloid appearance
- Focal macrofollicular pattern, pseudofollicular, papillary or pseudopapillary growth
- Villoglandular configuration
- Focally dilated glands or salivary gland type
- Basophilic secretions
- Stroma
- Prominent myxoid stroma (Am J Surg Pathol 2021;45:1061)
- Other ranges from scant to abundant and is either edematous, loosely collagenous or rarely hyalinized
- Cell morphology
- Mostly, columnar to cuboidal cells but a spindled morphology can be seen
- Nuclei are round to ovoid with irregular, often angulated contours and vesicular chromatin
- Prominent nucleoli and inconspicuous nuclear grooves
- Cytoplasm can be eosinophilic, finely vacuolated or clear
- Rarely, squamoid or signet ring-like appearance
- No overt pleomorphism
- Other
- Mitoses range from 2 to 20 (mean: 10) per 10 high power fields
- Incidental findings: sex cord tumor with annular tubules
- References: Pediatr Dev Pathol 2023;26:486, Am J Surg Pathol 2021;45:1061
Contributed by Jennifer A. Bennett, M.D.
Paratubal location
Cord and trabeculae architecture
Cystic architecture
Broad columns
Nuclear features
Mitosis
Signet ring-like cells
Images hosted on other servers:


STK11 adnexal tumor
- Strong CAM5.2 (94%), strong AE1 / AE3 (93%) and focal CK7 (60%)
- Inhibin (90%), calretinin (100%), WT1 (100%)
- AR (93%), ER (80%), PR (76%)
- Variable D2-40 (75%)
- Focal CD10 (81%)
- Reference: Pediatr Dev Pathol 2023;26:486, Am J Surg Pathol 2021;45:1061
- Claudin4
- FOXL2
- TTF1
- Focal SF1 (30% positive) (Am J Surg Pathol 2021;45:1061)
- Focal PAX8 (25% positive) (Am J Surg Pathol 2021;45:1061)
- Weak focal GATA3 (5% positive)
- Weak to moderate EMA staining (Am J Surg Pathol 2021;45:1061)
- Rare p63 (< 1% positive)
- Reference: Pediatr Dev Pathol 2023;26:486
- STK11 alterations
- Pathogenic mutations (most commonly loss of heterozygosity [LOH] event)
- Variants of uncertain significance
- STK11 deletions
- References: Am J Surg Pathol 2021;45:1061, Jpn J Cancer Res 1999;90:629
Pathology of fallopian tube
- Uterus, bilateral fallopian tubes and ovaries:
- Other histologic type: STK11 adnexal tumor (see synoptic summary)
- Clinical history: Peutz-Jehgers syndrome
- Specimen: total hysterectomy with bilateral tubes and ovaries, robotic assisted laparoscopic
- Specimen integrity: not applicable
- Tumor site: right adnexa
- Tumor size: 15 cm; other dimensions: 10 x 9 cm
- Histologic type: other, STK11 adnexal tumor
- Tumor grade: not applicable
- Surface involvement: not identified
- Implants: not identified
- Other tissue involvement: not identified
- Peritoneal fluid involvement: not submitted
- Lymph nodes: none submitted
- Distant metastatic sites: not applicable
- Stage: pT1a pN not assigned; pM not assigned
- FIGO stage: IA
- Note: Tumor can be confidently called stage 1A if the staging biopsies and such are all found to be negative. On the other hand, peritoneal cancers are all classified as stage II. A single adnexal tumor falls conveniently in between these two somewhere but overall, it would still be staged as 1A if all the staging biopsies were negative and if it is a single mass with no surface involvement.
- Female adnexal tumor of probable Wolffian origin (FATWO):
- Sex cord stromal tumor:
- Müllerian adenocarcinoma, endometrioid carcinoma:
- Mesothelioma:
- Diffuse or plaque-like growth
- Rarely, the pleura may harbor STK11 mutations but in association with other alterations (BAP1 mutations or CDKN2A / CDKN2B deletions)
- Loss of BAP1
- Mesonephric adenocarcinoma and mesonephric-like carcinoma:
- Tubular pattern with back to back round tubules with or without eosinophilic secretions
- Uniform nuclei with mild to (at most) moderate cytologic atypia and variable mitotic activity
- AR and inhibin positive in ~33%
- GATA3 and TTF1 positive
- ER / PR, WT1 negative and PAX8 positive
- Positive EMA, claudin4
- KRAS, NRAS mutations
- ARID1A, ARID1B or SMARCA4 mutations ~60%
- Rarely, ovarian adenoid cystic carcinoma:
- Dual population of cells (epithelial / ductal and myoepithelial)
A 45 year old woman presents with a 10 cm adnexal mass demonstrating the pattern of cystic spaces surrounded by cuboidal epithelium shown above. The tumor shows the following immunophenotype: ER / PR positive, CK7 positive, PAX8 positive, GATA3 negative, inhibin positive, TTF1 negative, FOXL2 negative, p53 wild type. Which of the following is the best diagnosis for this tumor?
- Female adnexal tumor of probable Wolffian origin (FATWO)
- High grade serous carcinoma
- Mesonephric adenocarcinoma
- STK11 adnexal neoplasm
- Sex cord stromal tumor, NOS
Comment Here
Reference: STK11 adnexal tumor
- Cutaneous dermatofibromas with hyperpigmentation
- Desmoid type fibromatoses
- Juvenile polyps of the intestinal tract
- Sertoli-Leydig tumors of the ovary or testis
- STK11 adnexal tumors
Comment Here
Reference: STK11 adnexal tumor
- Hyperplasia of tubal epithelium, variable atypia
- Also known as pseudocarcinomatous hyperplasia
- Typically present in women with estrogen producing ovarian tumors (Int J Gynecol Pathol 1989;8:214)
- May also be associated with salpingitis and PID (Am J Surg Pathol 1994;18:1125)
- Often incidental finding
- No specific gross findings
- Papillary, gland-like or cribriform patterns, lined by epithelial cells with mild to moderate nuclear pleomorphism, loss of polarity, stratification, crowding, hyperchromasia and scattered mitotic figures; no invasion
- May be associated with severe inflammation and scarring mimicking adenocarcinoma
AFIP images
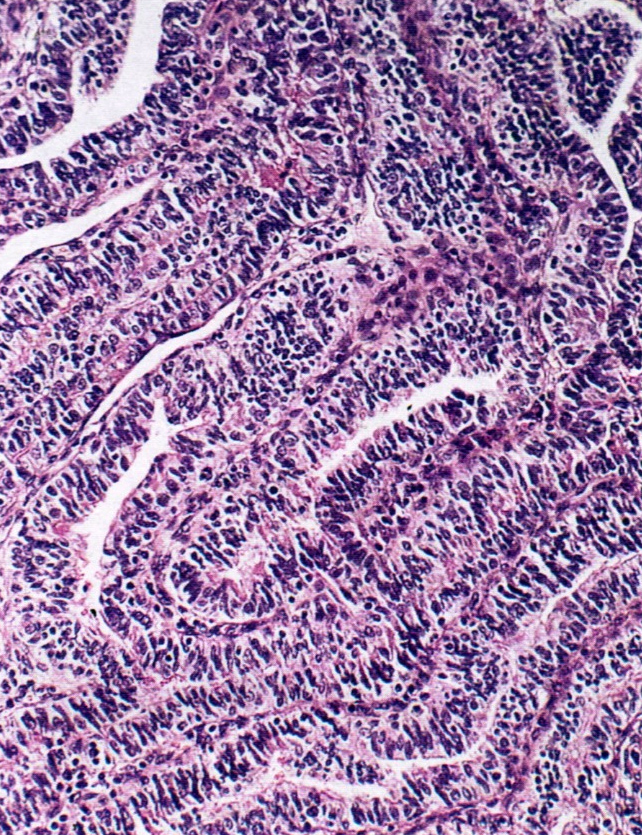
Hyperplasia of tubal epithelium of unknown cause
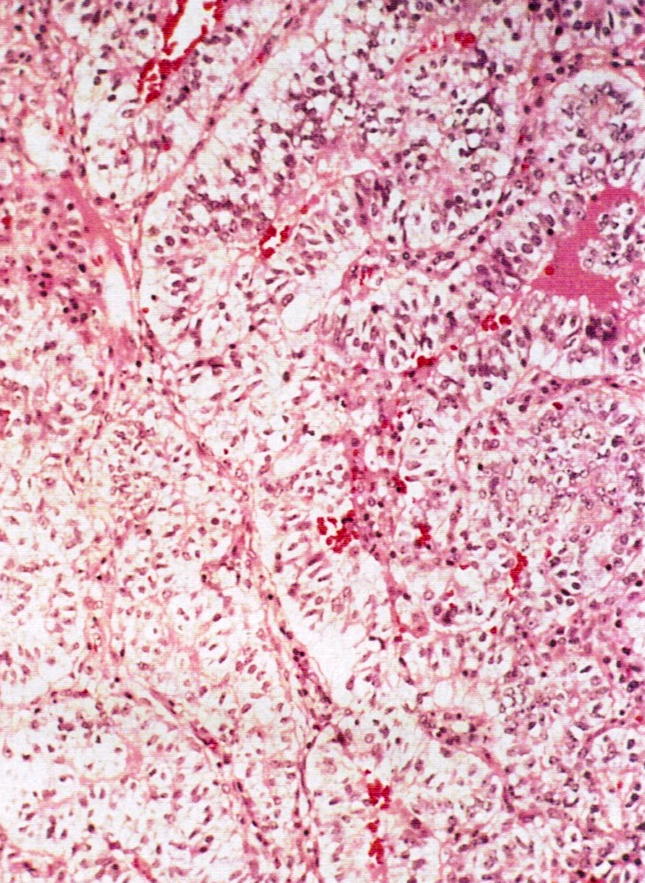
Clear cell hyperplasia of pregnancy
- Carcinoma: typically grossly evident, older age, solid epithelial proliferation, brisk mitotic activity, severe atypia, possible invasion
- Inflammation of fallopian tube, most commonly sexually transmitted due to chlamydia and gonorrhea
- Part of spectrum of pelvic inflammatory disease (PID)
- > 1 million cases of acute salpingitis reported annually in US but actual number probably larger due to incomplete and untimely reporting
- For women 16 - 25 years, salpingitis is most common serious infection; affects 11% of females of reproductive age, 12% of women before age 20
- Salpingitis has higher incidence among lower socioeconomic classes, possibly due to earlier sex debut, multiple partners, poorer health care
- Highest risk for people aged 15 - 24 years, possibly due to multiple partners, less awareness of symptoms, reduced willingness to use protective contraceptives
- Infection also occurs via childbirth, abortion (therapeutic or elective), endometrial biopsy, IUD insertion, miscarriage
- In 2005, World Health Organization (WHO) estimated 448 million new cases of curable STIs occur annually in individuals aged 15 - 49 years
- Bacteria most associated with salpingitis are: actinomyces, Chlamydia trachomatis, enteric gram - negative rods (eg. E. coli), Gardnerella vaginalis, Haemophilus influenza, Mycoplasma, Neisseria gonorrhoeae, rarely other anaerobic and aerobic bacteria, Staphylococcus, Streptococcus, Trichomonos vaginalis, Ureaplasma urealyticum
- Also Herpes and CMV, fungi, parasites
- 30 - 40% are polymicrobial
- In US, chlamydia is #1 most reported sexually transmitted disease associated with PID, N. gonorrhoeae is #2
- 10 - 20% of untreated chlamydial or gonorrheal infections progress to PID
- Symptoms usually appear after a menstrual period; most commonly abdominal pain, abnormal smell and color of vaginal discharge, bloating, fever, lower back pain, nausea, pain during ovulation, pain during periods, pain during sexual intercourse, vomiting
- Tubo-ovarian abscess in 1/3 of women hospitalized for PID
- Often asymptomatic, may be diagnosed clinically by pelvic examination, blood tests, vaginal or cervical swab
- PID has 3 principal complications: chronic pelvic pain (~25%), infertility, ectopic pregnancy (15 - 50%)
- Impaired fertility is major concern; infection and inflammation can lead to scarring and adhesions within tubal lumens
- Of women with tubal factor infertility, 50% have no history of PID but have scarring of fallopian tubes and exhibit antibodies to C. trachomatis
- May lead to tubule ovarian abscess, pelvic peritonitis, Fitz-Hugh-Curtis syndrome (perihepatitis)
- Taiwanese studies of > 60,000 women diagnosed with PID found that PID was independent risk factor for myocardial infarction in women > age 55 (Int J Cardiol 2013;167:416), with increased risk of stroke for 3 years following PID (Stroke 2011;42:2074); also increased risk of ovarian cancer, particularly in women with 5+ episodes of PID (Lancet Oncol 2011;12:900)
- 46 year old woman with S. pneumonia (Hum Pathol 1990;21:1288)
- 50 year old woman with focally calcified cysticercus larva (Hum Pathol 1982;13:665)
- Antibiotics or antifungals
- Pyosalpinx (pus), hematosalpinx
- Enlarged, erythematous, edematous
- May have fibrinous exudate
- Tubo-ovarian abscess common
Images hosted on other servers:

Tubo-ovarian abscess from Neisseria gonorrheae
- Marked neutrophilic infiltrate, congestion and edema
- Mucosal ulceration
- Reactive epithelial changes
- Variable abscess formation, variable presence of microorganisms
Images hosted on other servers:

Neisseria gonorrheae

H&E
- Ectopic pregnancy
- Hydrosalpinx: transudate, follows purulent salpingitis
- Menstruation / pregnancy: neutrophils common but usually don't invade muscularis, no necrosis, no ulceration, no chronic inflammatory infiltrate
- Nests, plaques or cysts (with eosinophilic luminal material) of metaplastic transitional epithelium involving the serosal surface of fallopian tube, mesosalpinx and mesovarium
- Benign common incidental finding
- Benign incidental finding in the subserosa of tubal, paratubal and paraovarian soft tissue
- Bland transitional type epithelium forming small nests / cysts
- CK7+, GATA3+, P63+, PAX8-, CK20- and uroplakin-
- Common incidental finding
- Serosa of fallopian tube, including fimbriated end, fimbrial peritoneal junction, mesosalpinx and meso-ovarium
- Nests or cysts, including mesothelial cells from the tubal and paratubal serosa, that undergo transitional cell metaplasia
- Unknown
- Suggested association between Walthard cell nests and Brenner tumors or mucinous tumors of the ovary (stronger association with the former, though unexplained) (Arch Pathol Lab Med 2008;132:1753)
- Walthard cell nests can be the origin for rare examples of Brenner tumors outside the ovarian parenchyma (Diagn Pathol 2020;15:22)
- Histologically, presence of nests of bland, metaplastic transitional type cells on the serosal surface is diagnostic of Walthard nests
- Pelvic tuberculosis is characterized by granulomatous peritonitis whereas endometriosis will show endometrial type glands and stroma within the serosal surface of adnexal tissue
- Disseminated carcinomatosis shows malignant cells with stromal reaction in the serosal nodules / plaques
- Clinically, Walthard cells are benign asymptomatic and incidental findings, whereas the other differential diagnosis usually presents with abdominal pain, mass, constitutional symptoms or ascites
- Clinically can be mistaken for pelvic tuberculosis (diagnosed based on the presence of granulomas on the tissue along with patient's clinical symptoms) or disseminated tumor (diagnosed based on the presence of malignant tumor cells along with patient's clinical presentation such as abdominal pain / mass, ascites or elevated serum tumor markers)
- 10 year old girl with acute appendicitis and urothelial rests (Fetal Pediatr Pathol 2021 Aug 2 [Epub ahead of print])
- 53 year old postmenopausal woman with extraovarian Brenner tumor of the uterus (Diagn Pathol 2020;15:22)
- Small 1 - 2 mm yellow-white nodules beneath the serosa of the fallopian tube and paratubal soft tissue
AFIP images
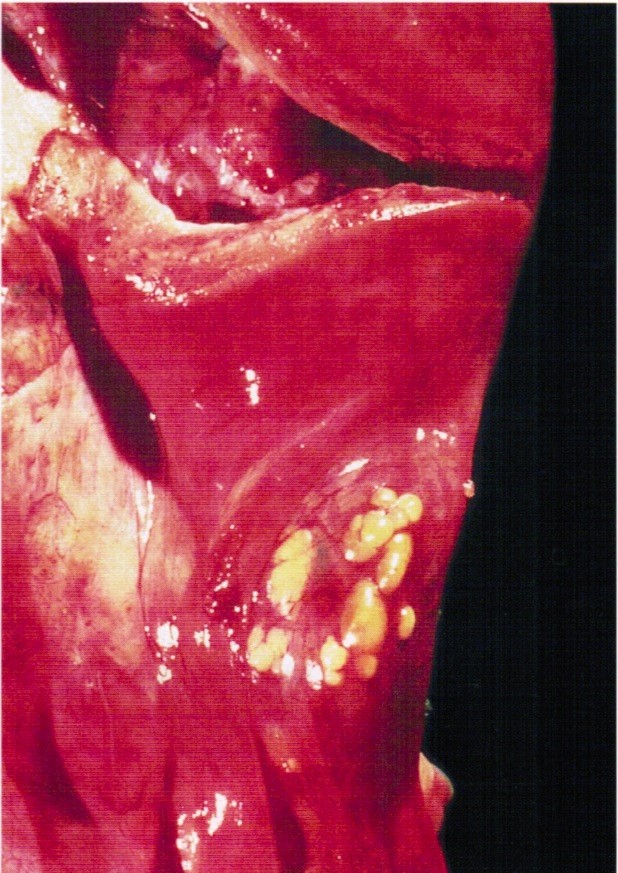
Several small yellow nodules
- Small solid nests or cysts of transitional type epithelium with relatively uniform nuclei with irregular borders and nuclear grooves, located beneath the serosa of tubal / paratubal / paraovarian tissue
- Cystic lesions may have eosinophilic luminal secretions
- Rare or no mitotic figures
Contributed by Shabnam Zarei, M.D. and AFIP images
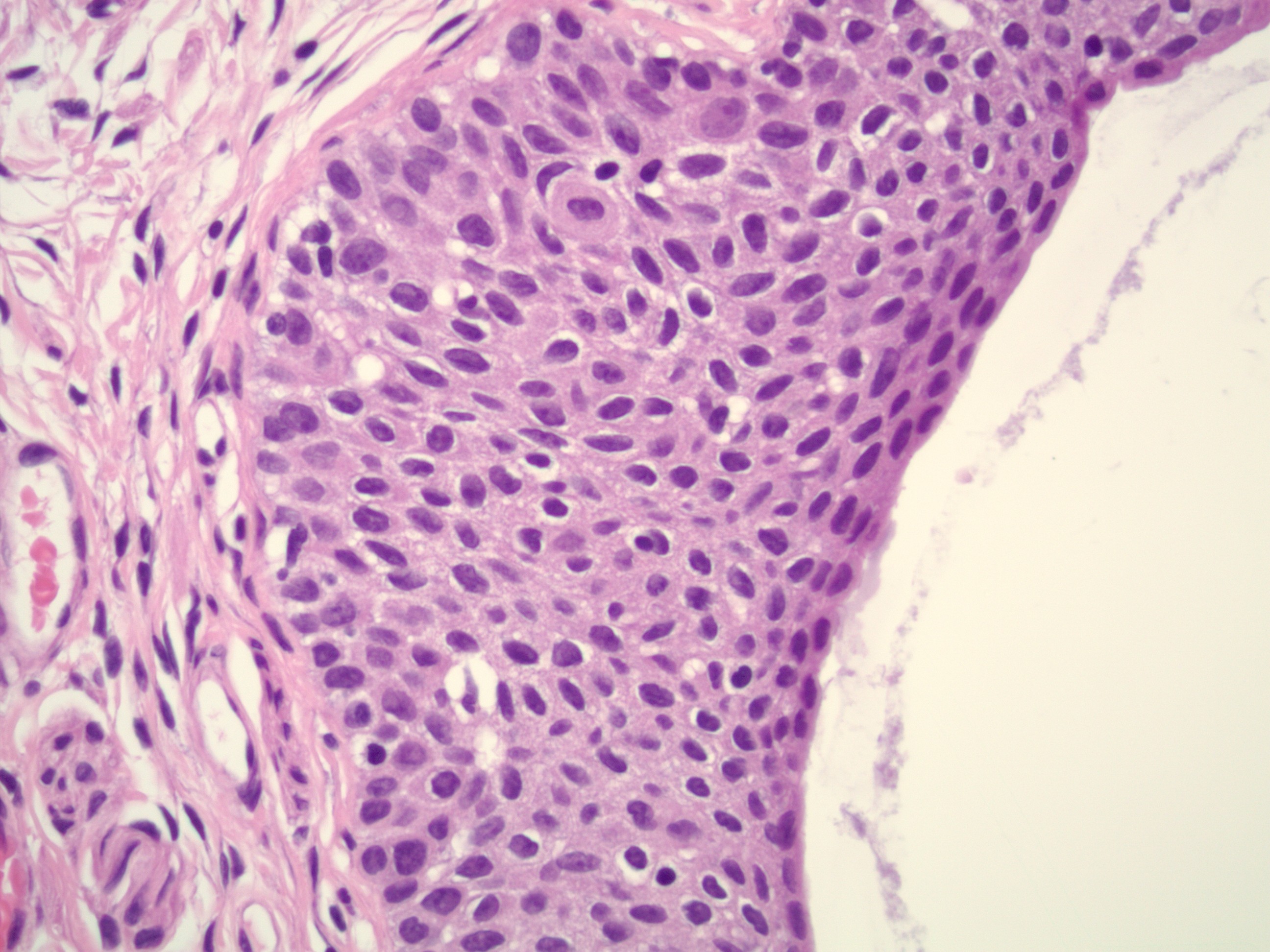
Transitional type epithelium
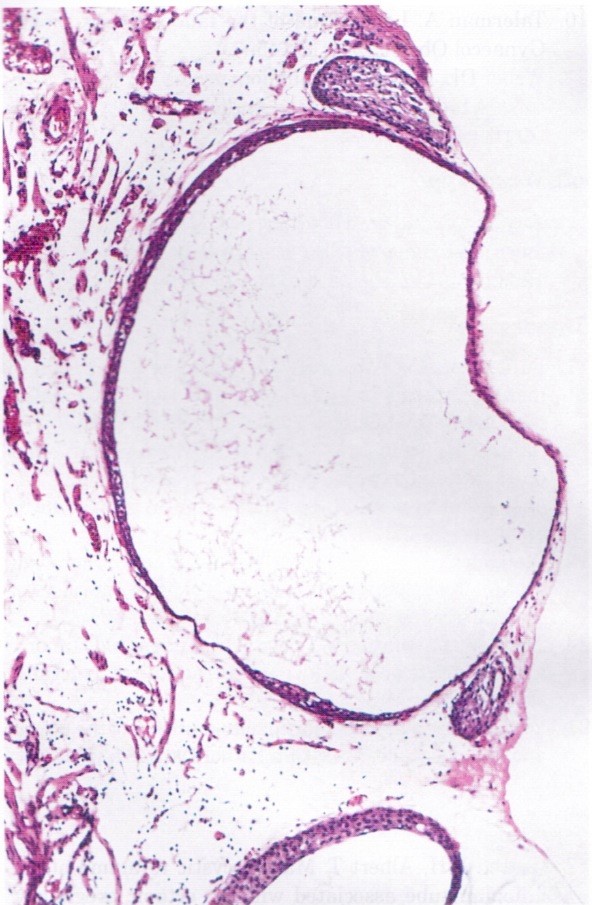
Cystic nests
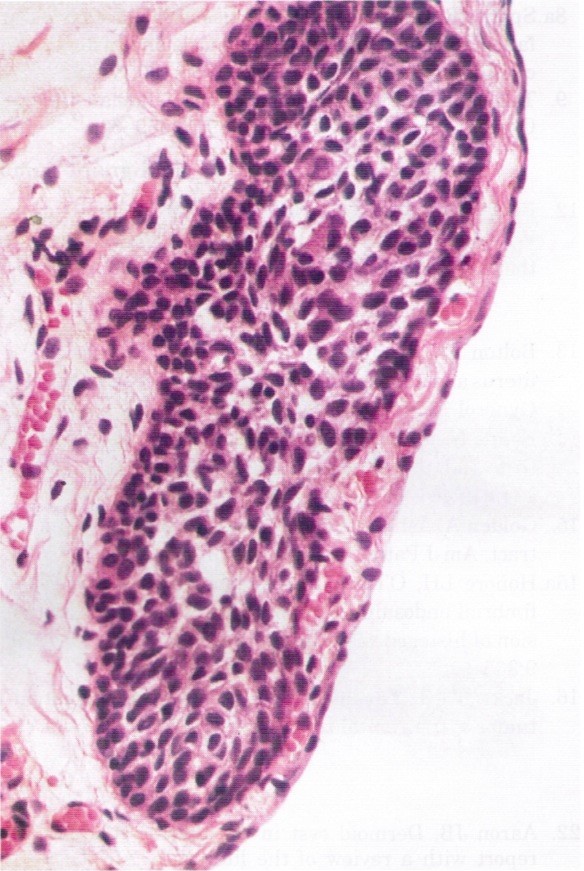
Bland appearing transitional cells
- Dual staining for α tubulin and γ tubulin shows attenuated and patchy distribution of cilia in the metaplastic cells of Walthard cell nests and Brenner tumor, suggesting a common origin from tubal epithelium (Eur J Cancer 2013;49:3839)
- These are benign, incidental findings and are typically not included within the pathology report
- Benign Brenner tumors:
- Endometriosis:
- Presence of endometrial glands, endometrial stroma or hemosiderin laden macrophages
- 2 out of 3 required for the diagnosis
- Paratubal cysts:
- No solid component
- Lined by ciliated tubal type epithelium
- Endosalpingiosis:
- Glands lined by ciliated tubal type epithelium
- Benign Brenner tumors are P63+, GATA3+, uroplakin+, whereas Walthard cell nests are P63+, GATA+ and uroplakin-
- They share the same IHC phenotype
- Walthard cell nests are PAX2 / PAX8- but benign Brenner tumors show diffuse and strong staining with PAX2 / PAX8+
- Walthard cell nests are positive for uroplakin and GATA3; Brenner tumors are positive for GATA3 but negative for uroplakin
Comment Here
Reference: Walthard cell nests
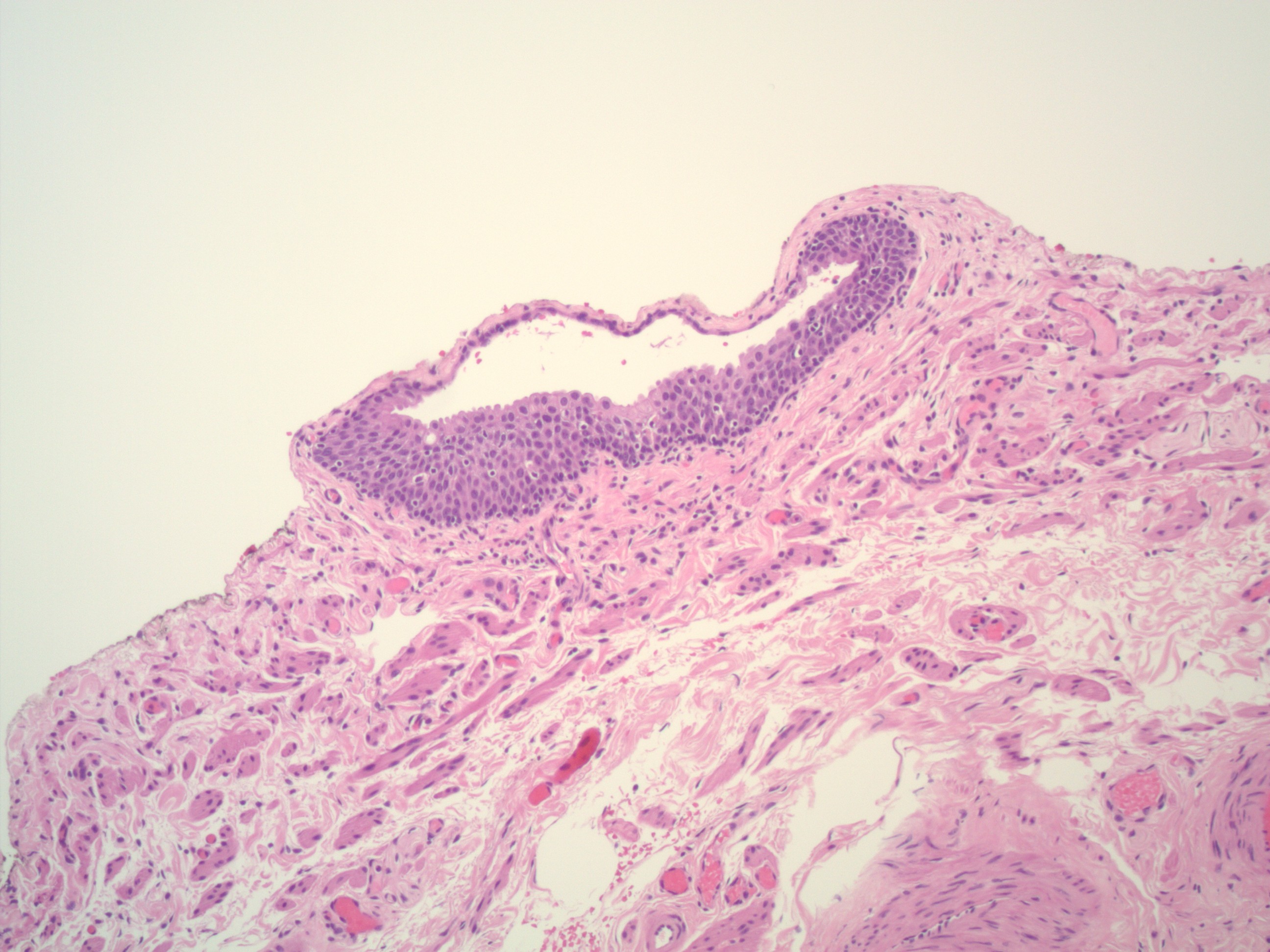
Which of the following is true about the pathologic finding in the image shown above?
- If bilateral, they are associated with higher risk for malignant Brenner tumor
- They are usually GATA3- and PAX8+
- They can mimic peritoneal carcinomatosis by imaging and intraoperatively
- They can only be found on the fallopian tube serosal surface
Comment Here
Reference: Walthard cell nests
- WHO classification of tumors of the female genital tract
- Currently on 5th edition, published in 2020
- No major updates, mostly refined definitions
- Most high grade serous carcinomas of the ovary arise at the fimbriated end of the fallopian tube from a precursor lesion known as serous tubal intraepithelial carcinoma (STIC) (Pathology 2015;47:423, Mod Pathol 2015;28:1101)
- Undifferentiated carcinoma of the fallopian tube is no longer a separate category
-
Epithelial tumors ICD-O
- Serous adenofibroma, NOS9014/0
- Serous borderline tumor, NOS8442/1
- High grade serous carcinoma8461/3
- Endometrioid adenocarcinoma, NOS 8380/3
- Carcinosarcoma, NOS8980/3
-
Tumor-like lesions
- Paratubal cysts
- Tubal hyperplasia
- Tubo-ovarian abscess
- Salpingitis isthmica nodosa
- Metaplastic papillary lesion
- Placental site nodule
- Mucinous metaplasia
- Endosalpingiosis
-
Mixed epithelial and mesenchymal tumors
- Adenosarcoma8933/3
-
Germ cell tumors
- Mature teratoma, NOS9080/0
- Immature teratoma, NOS9080/3
-
Mesenchymal and mixed tumors ICD-O
- Leiomyoma, NOS8890/0
- Adenomyoma, NOS8932/0
- Adenosarcoma8933/3
- Leiomyosarcoma, NOS8890/3
-
Miscellaneous tumors
- Wolffian tumor9110/1
- Papillary cystadenoma, NOS8450/0
- Ependymoma, NOS9391/3
-
Tumor-like lesions
- Adrenocortical remnants
Contributed by Gulisa Turashvili, M.D., Ph.D.
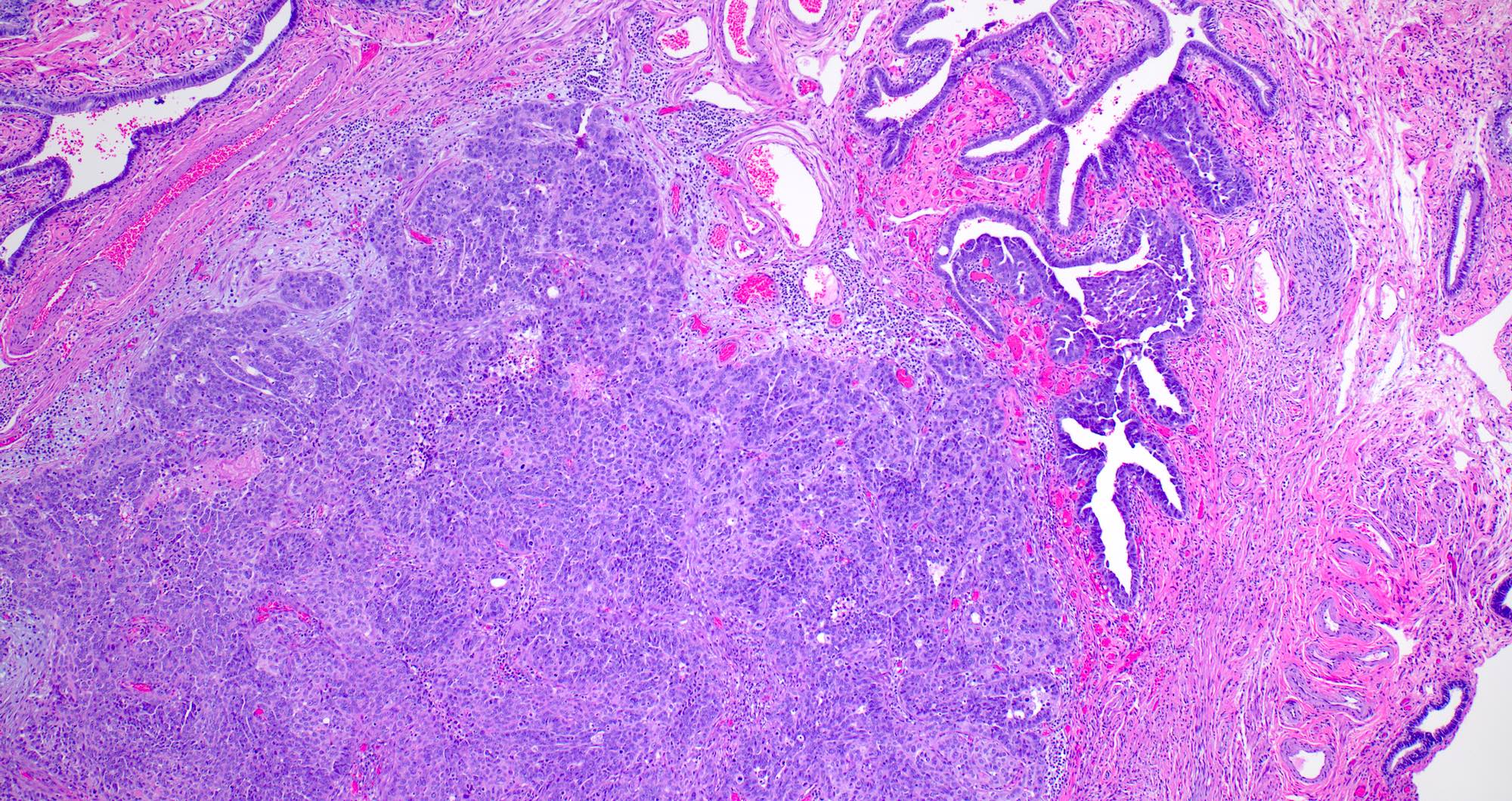
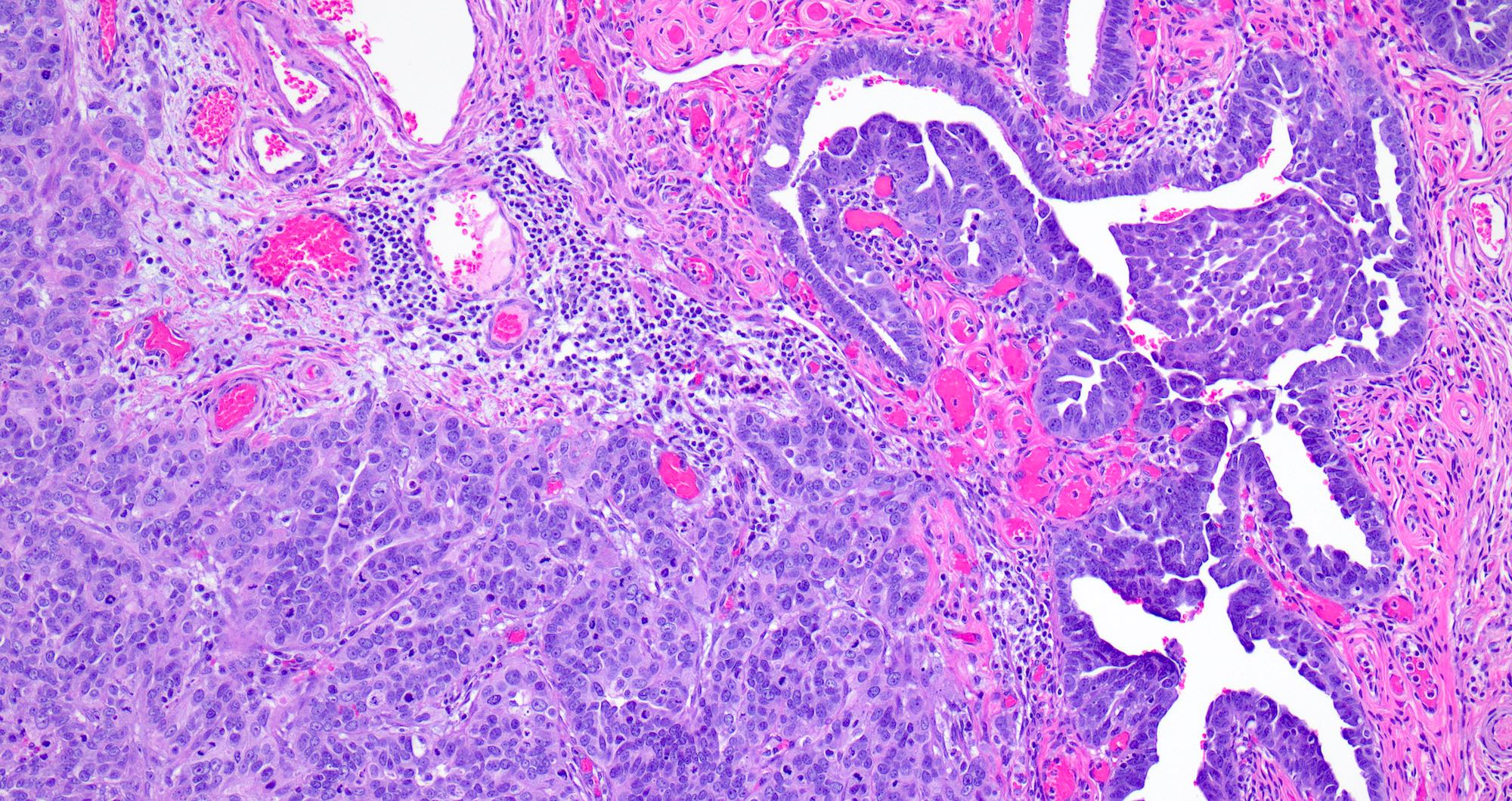
STIC associated with invasion
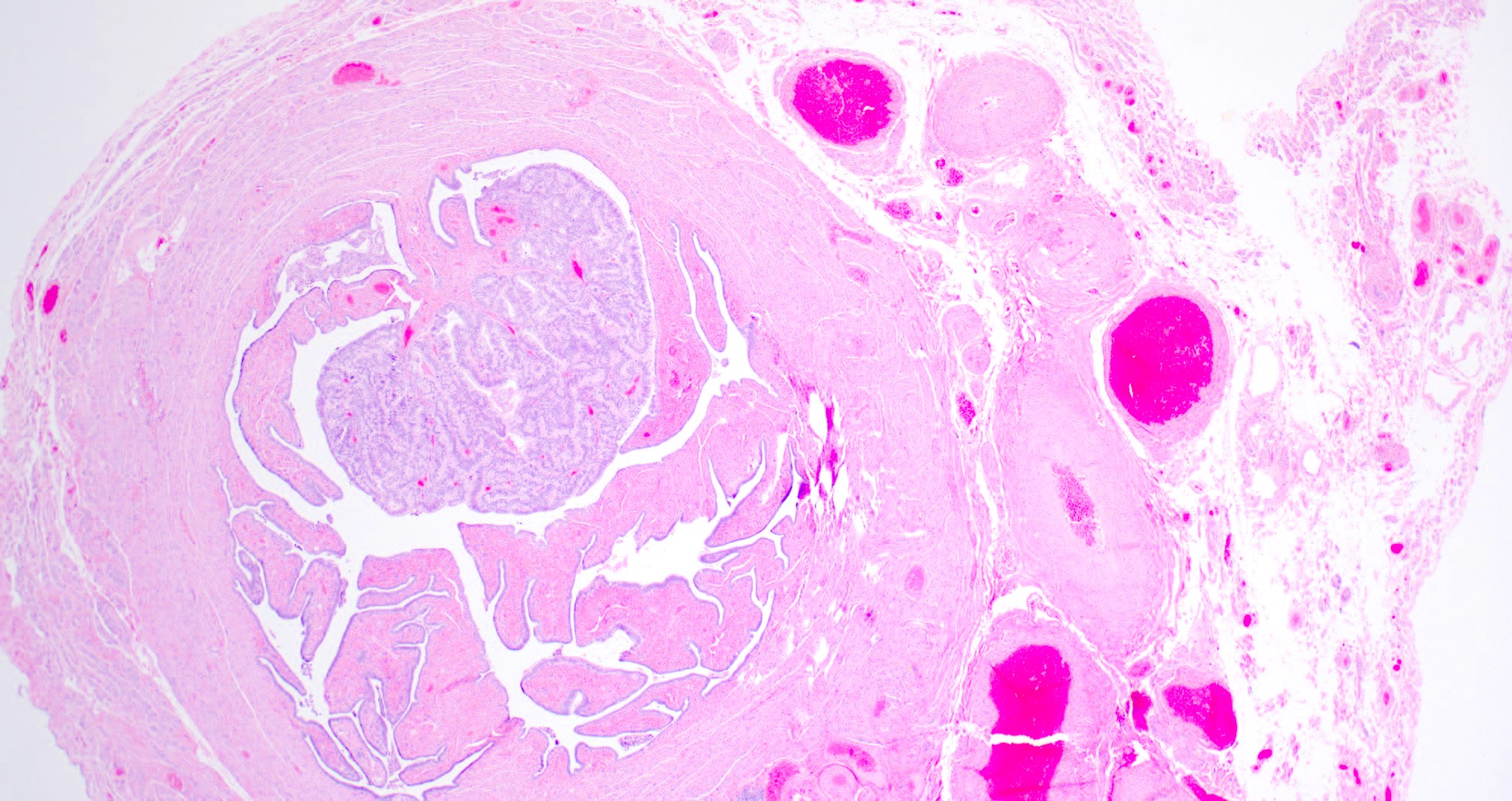
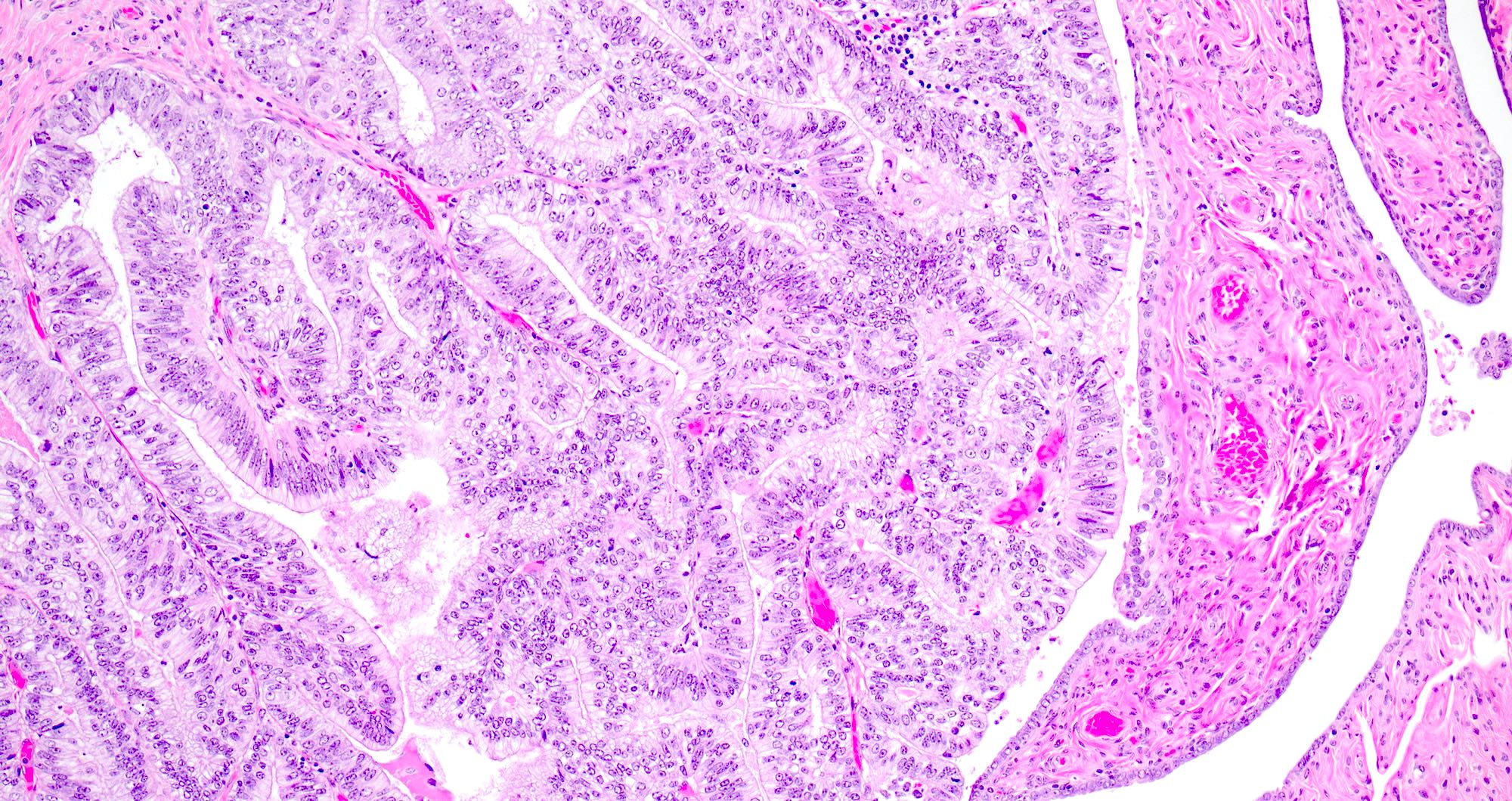
Endometrioid adenocarcinoma

Salpingitis isthmica nodosa
- Low grade serous carcinoma
- Ovarian cortical inclusion cysts
- Paratubal cyst
- Serous borderline tumor
- Serous tubal intraepithelial carcinoma (STIC)
Comment Here
Reference: Fallopian tubes & broad ligament - WHO classification
What is the most likely diagnosis for this salpingectomy specimen?
- Focal tubal hyperplasia
- High grade serous carcinoma
- High grade serous carcinoma and serous tubal intraepithelial carcinoma (STIC)
- Low grade serous carcinoma
- Serous tubal intraepithelial carcinoma (STIC)
Comment Here
Reference: Fallopian tubes & broad ligament - WHO classification
- Adnexal tumor arising from remnants of Wolffian (mesonephric) duct
- Adnexal tumor arising from mesonephric (Wolffian duct) remnants
- Heterogeneous histologic appearance
- Diagnosis based predominantly on the anatomical site and morphology
- Wolffian tumor
- Female adnexal tumor of probable Wolffian origin (FATWO)
- Wolffian adnexal tumor (WAT)
- Wolffian adenoma
- Retiform Wolffian adenoma
- Mesonephric tumor, NOS
- ICD-O: 9110/1 - mesonephric tumor, NOS
- ICD-11: 2F33.Y & XH2WJ5 - benign neoplasm of other or unspecified female genital organs & Wolffian tumor
- Rare, approximately 130 cases reported (Oncol Lett 2017;14:5167)
- Median age 50 years, range 15 - 87 years (Int J Surg Pathol 2008;16:222)
- Broad ligament (most common site) (Hum Pathol 1999;30:856)
- Ovaries (Am J Surg Pathol 1983;7:125)
- Mesosalpinx, fallopian tubes
- Paravaginal (Am J Clin Pathol 1994;101:275)
- Peritoneum
- Believed to originate from mesonephric (Wolffian) duct remnants
- Arises along the trajectory of the Wolffian duct: from the ovarian hilum, along mesosalpinx, broad ligament, lateral aspects of the uterus and cervix, to the outer third of the vagina (Hum Pathol 1999;30:856)
- Unknown
- Adnexal mass with nonspecific symptoms or an incidental finding
- Complaints include lower abdominal pain / distention, pelvic mass, abnormal vaginal bleeding or ascites
- Most tumors are hormonally inert; rare tumors are hormonally active, causing endometrial hyperplasia (Gynecol Oncol 1995;59:304)
- Most tumors are unilateral; rarely bilateral
- Tumor location
- Surgical specimen: gross and microscopic examination
- Well defined, encapsulated, lobulated or ovoid mass, often separate from ovaries, tubes and uterus
- May demonstrate solid and cystic areas
- Low signal intensity rim around the tumor on T2 weighted MRI images; might be a characteristic feature (J Obstet Gynaecol Res 2016;42:1046)
Images hosted on other servers:

CT and MRI: large mass

MRI: mass near ovary
- Low malignant potential; most tumors behave in a benign fashion
- Recurrence or metastases occur in 11 - 20% of cases; median of 48 months to recurrence (range 13 - 96 months) (Gynecol Oncol 2002;86:225)
- Adverse prognostic factors: large size (> 10 cm), capsular invasion and rupture with tumor implants (Histopathology 2005;46:716)
- Aggressive behavior includes intra-abdominal spread, recurrence or distant metastasis, typically to the liver and lungs (Gynecol Oncol 2002;86:225)
- High cellularity, nuclear pleomorphism and high mitotic activity are associated with worse prognosis but tumors with minimal nuclear atypia and low mitotic rate may recur; no single feature is predictive of malignant behavior (Tohoku J Exp Med 1997;181:371)
- 28 year old woman with left paratubal cyst (Gynecol Oncol Rep 2021;36:100726)
- 30 year old woman with an incidental ovarian mass (Gynecol Oncol Rep 2014;10:22)
- 37 year old woman with abdominal pain and adnexal mass (Oncol Lett 2017;13:3403)
- 50 year old woman with bilateral adnexal masses (Int J Gynecol Pathol 2018;37:331)
- 70 year old woman with an abdominal mass (Indian J Pathol Microbiol 2014;57:620)
- Series of 11 cases of FATWO (Arch Pathol Lab Med 2022;146:166)
- Series of 15 tumors of FATWO (Mod Pathol 2020;33:734)
- Hysterectomy and bilateral salpingo-oophorectomy; tumor debulking
- Role of adjuvant chemotherapy or radiation therapy is unknown
- For recurrent / metastatic KIT (CD117) expressing tumors, tyrosine kinase inhibitor Gleevac (STI571) is a treatment option (Int J Gynecol Cancer 2004;14:546)
Images hosted on other servers:

Adnexal mass
- Size from < 1 cm to 30 cm
- Encapsulated mass, often nodular, lobulated appearance
- Often centered within or hanging from broad ligament or fallopian tube by a pedicle
- Solid or partially cystic; may have spongy appearance
- Cut surface is rubbery, variegated, pale yellow, gray-white or tan
- May be hemorrhagic or necrotic
- References: Cancer 1973;31:671, Am J Surg Pathol 1983;7:125, Hum Pathol 1999;30:856
AFIP images
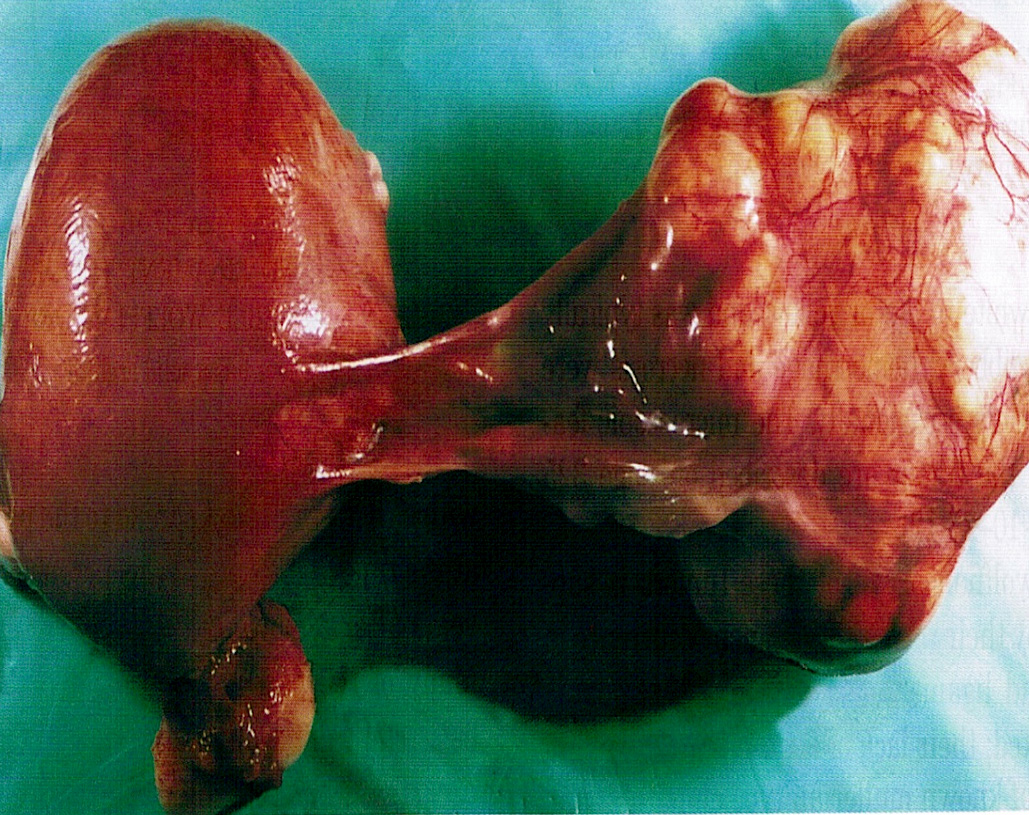
Broad ligament tumor
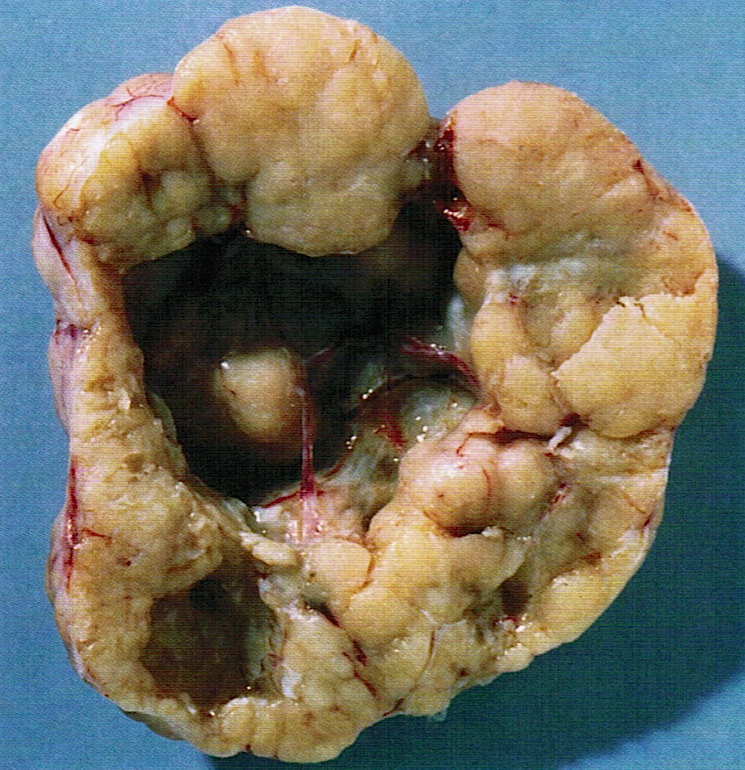
Solid and cystic cut surface

Lobulated cut surface
Images hosted on other servers:

Large peritoneal mass

Mass arising from the fimbriae
- May be mistaken for adenocarcinoma, sex cord stromal tumor or mesonephric carcinoma
- If the tumor is extraovarian, the tumor location (e.g., broad ligament, mesosalpinx) may help to include FATWO in the differential diagnosis during intraoperative consultation
- Variety of patterns may aid with a differential diagnosis, although this may be difficult to appreciate during frozen section due to limited sampling
- Cribriform, tubular, cystic, tubulocystic, sieve-like, solid cords and diffuse growth patterns
- Usually a single pattern predominates but several architectural patterns may coexist (Am J Surg Pathol 1983;7:125)
- Solid sheets of spindle or polygonal cells may be the dominant morphology
- Fibrous stroma varies from scant to large areas of hyalinization
- Intraluminal, bright eosinophilic secretions are often present
- Cells are columnar or cuboidal, may have scant clear cytoplasm, flat or hobnail appearance
- Large cytoplasmic vacuoles and signet ring cell-like forms may be seen (Int J Surg Pathol 2008;16:222)
- Uniform, round or oval nuclei with pale, evenly dispersed chromatin; may have nuclear grooves
- Nuclear atypia is mild to moderate
- Mitotic activity is typically low (up to 1/10 - 3/10 high power fields)
- Malignant tumors have been suggested to present as undifferentiated carcinoma with high cellularity, pleomorphic nuclei or increased mitoses (up to 16/10 high power fields); however, a recent literature review of tumors classified as malignant FATWO indicates that many represent STK11 adnexal tumor or endometrioid carcinoma with unusual features (Am J Surg Pathol 1983;7:125, Histopathology 2022;81:280)
Contributed by Elena Lucas, M.D. and Wenxin Zheng, M.D.
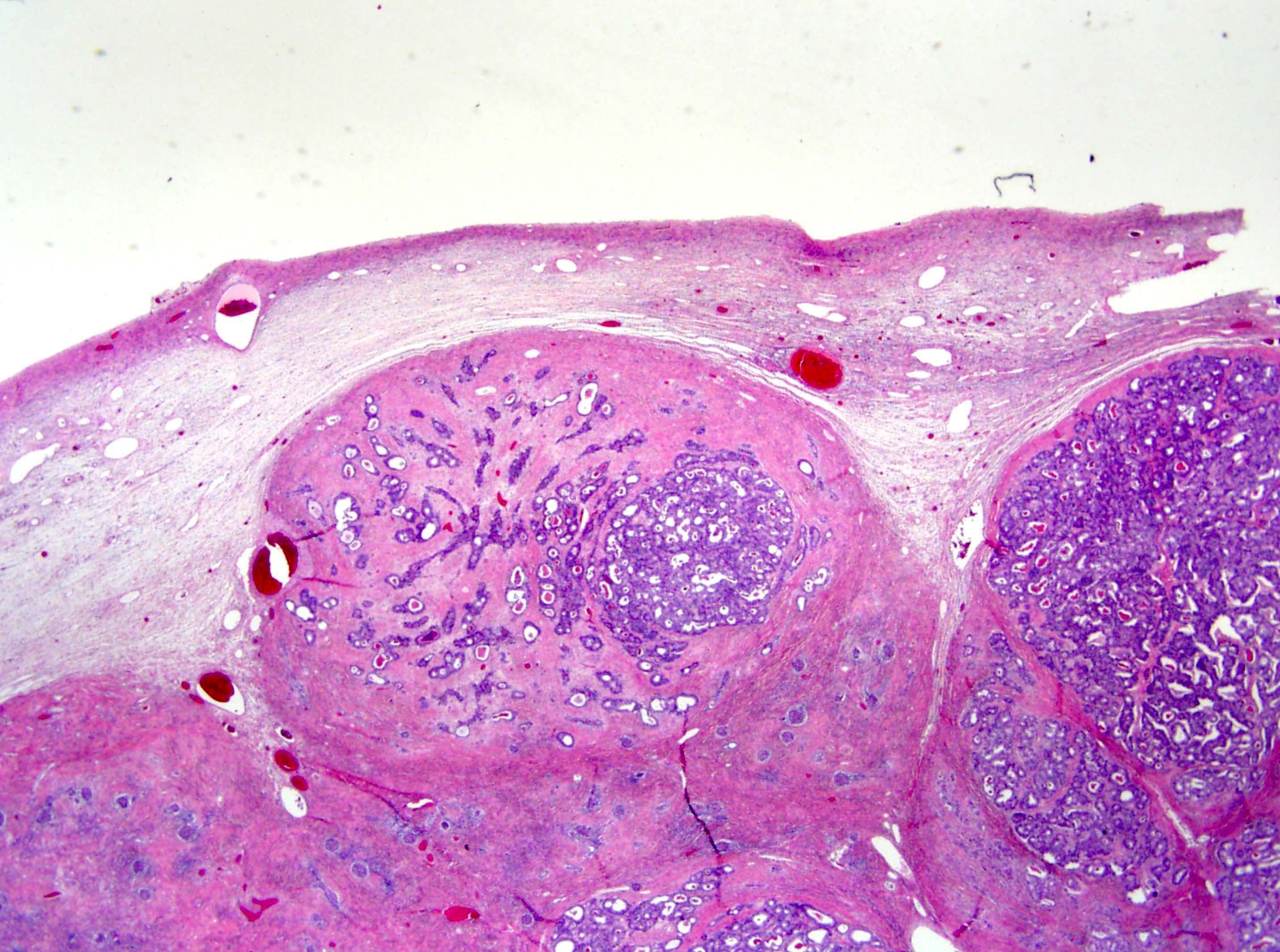
Nodular architecture
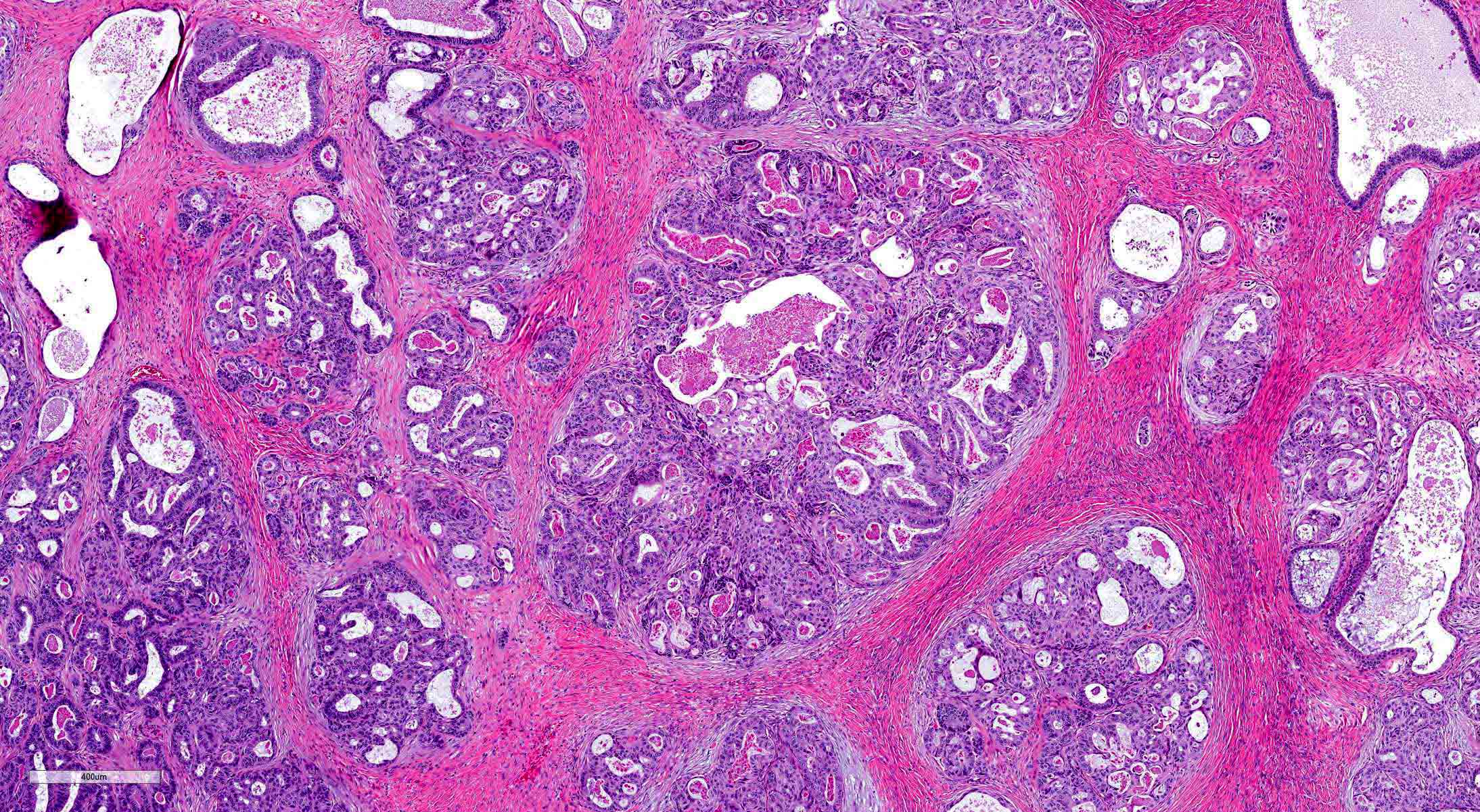
FATWO showing various patterns
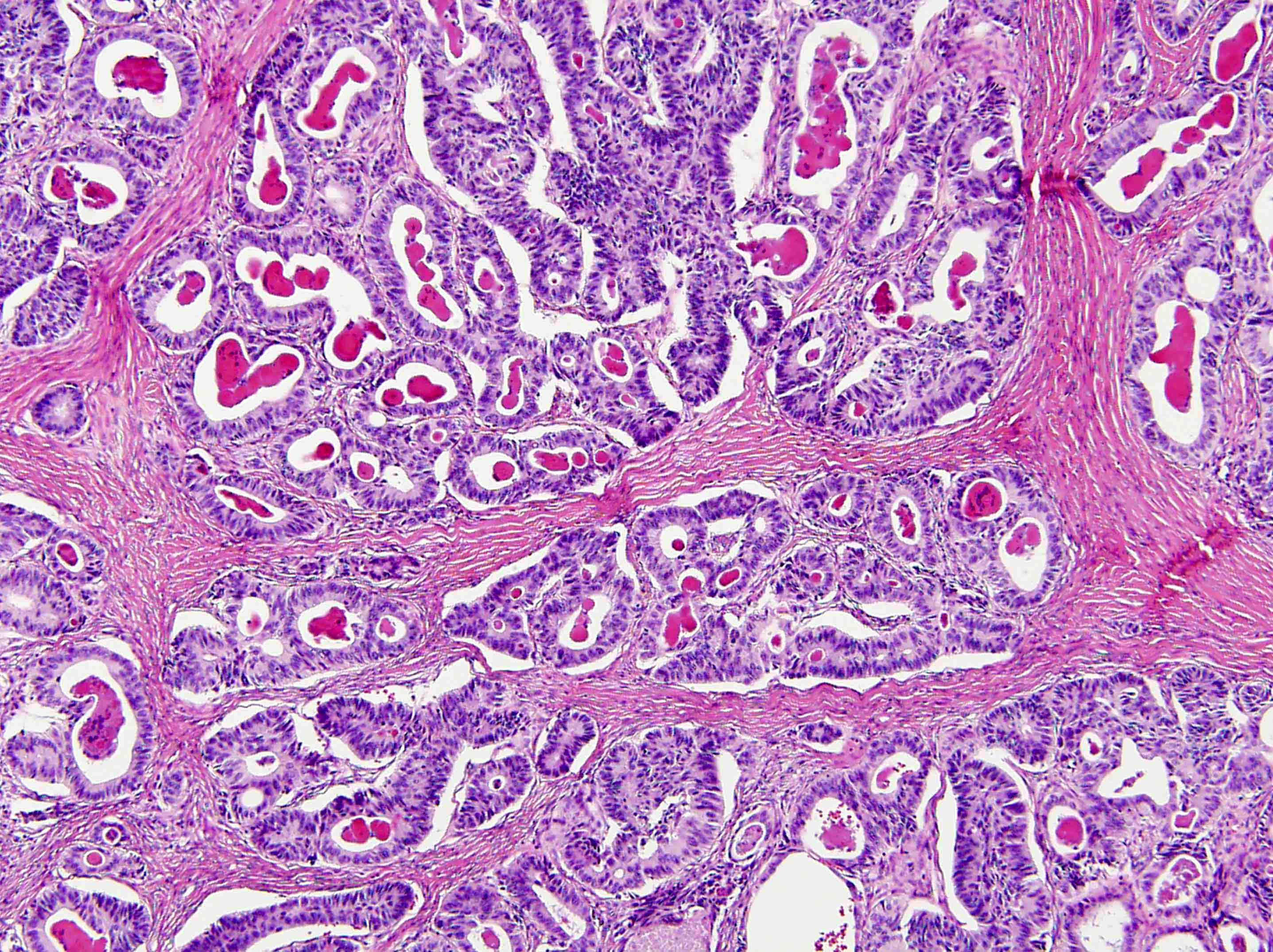
Tubular growth pattern
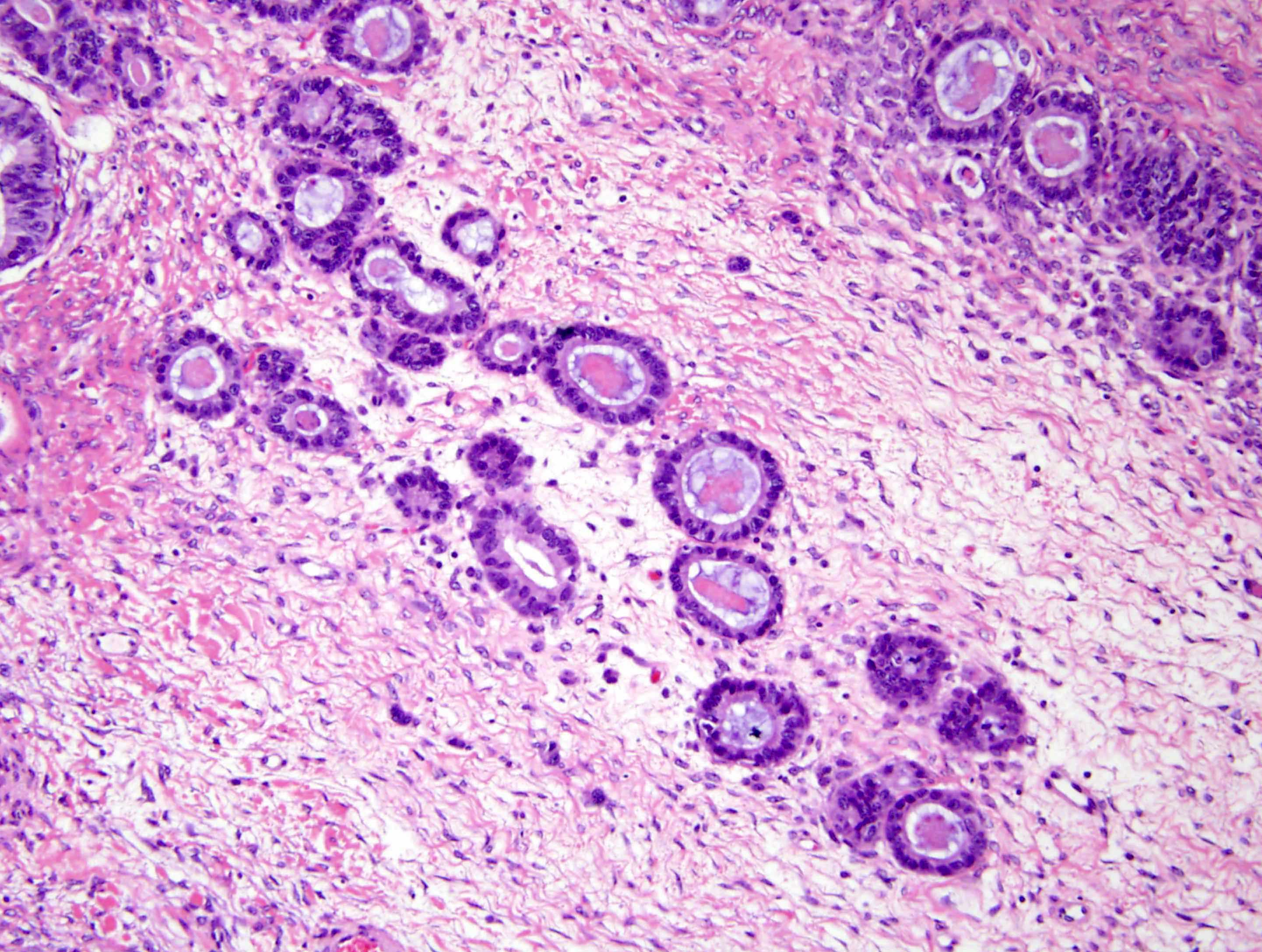
Tubules infiltrating stroma
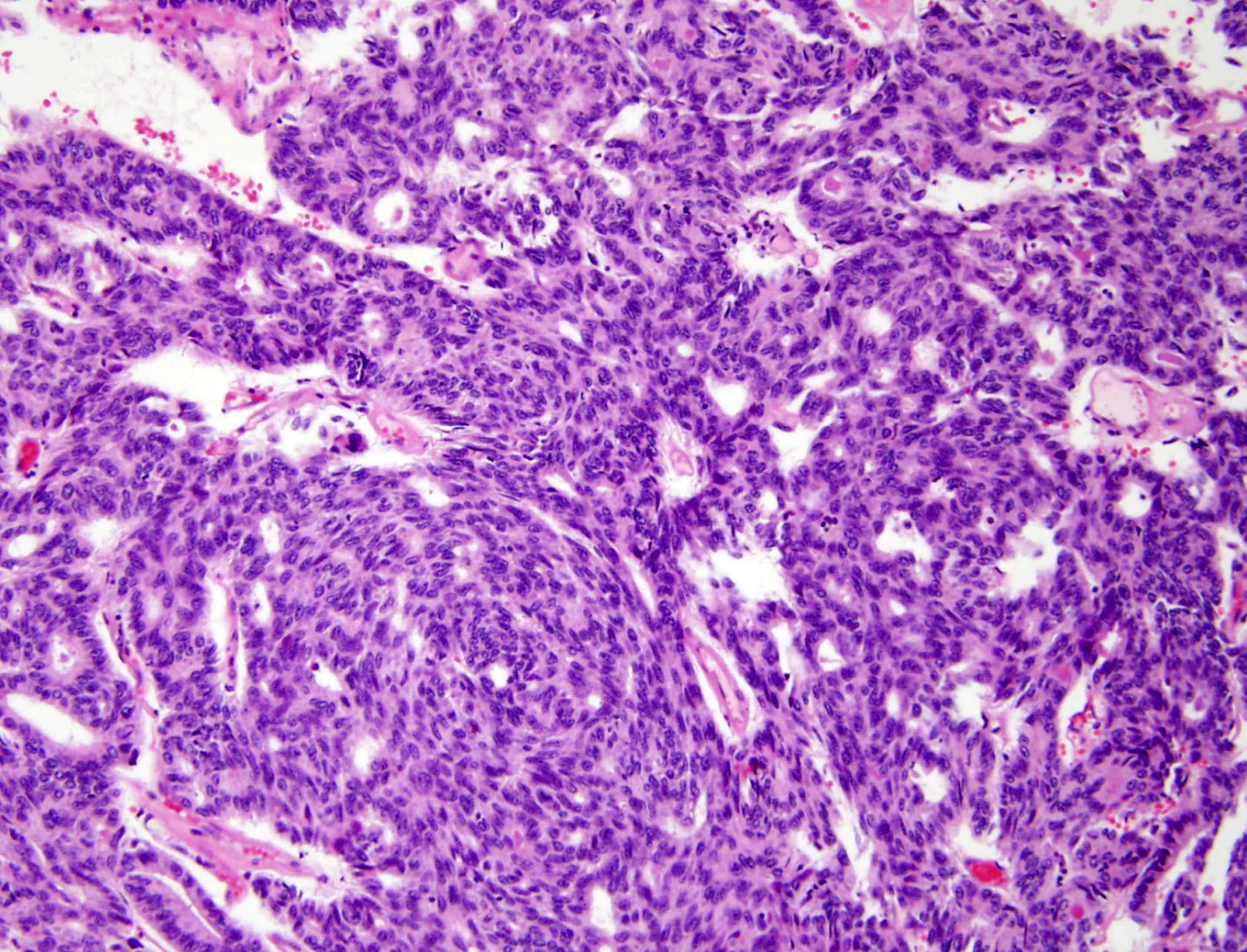
Tubular and solid pattern
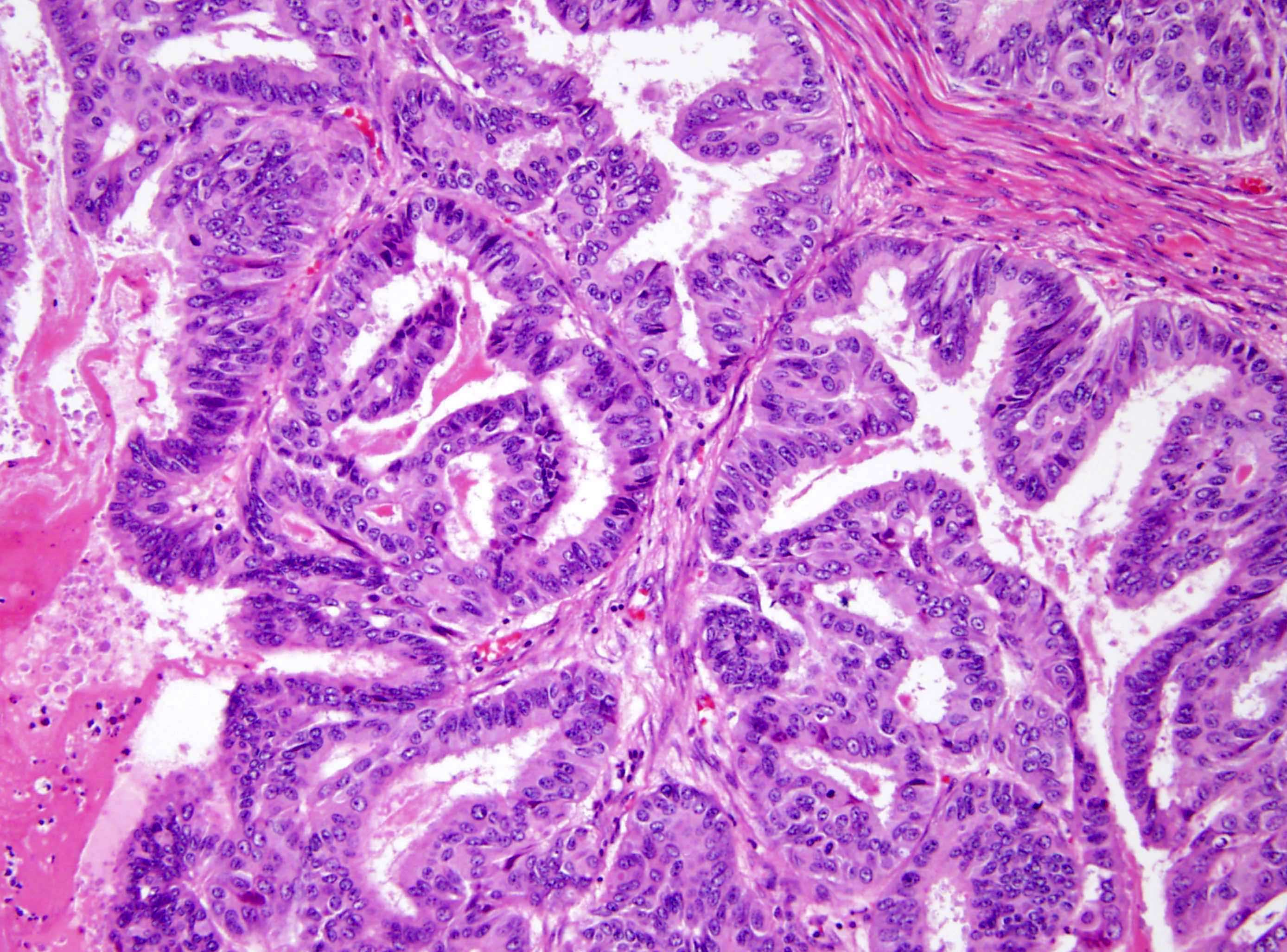
Resembling endometrioid carcinoma
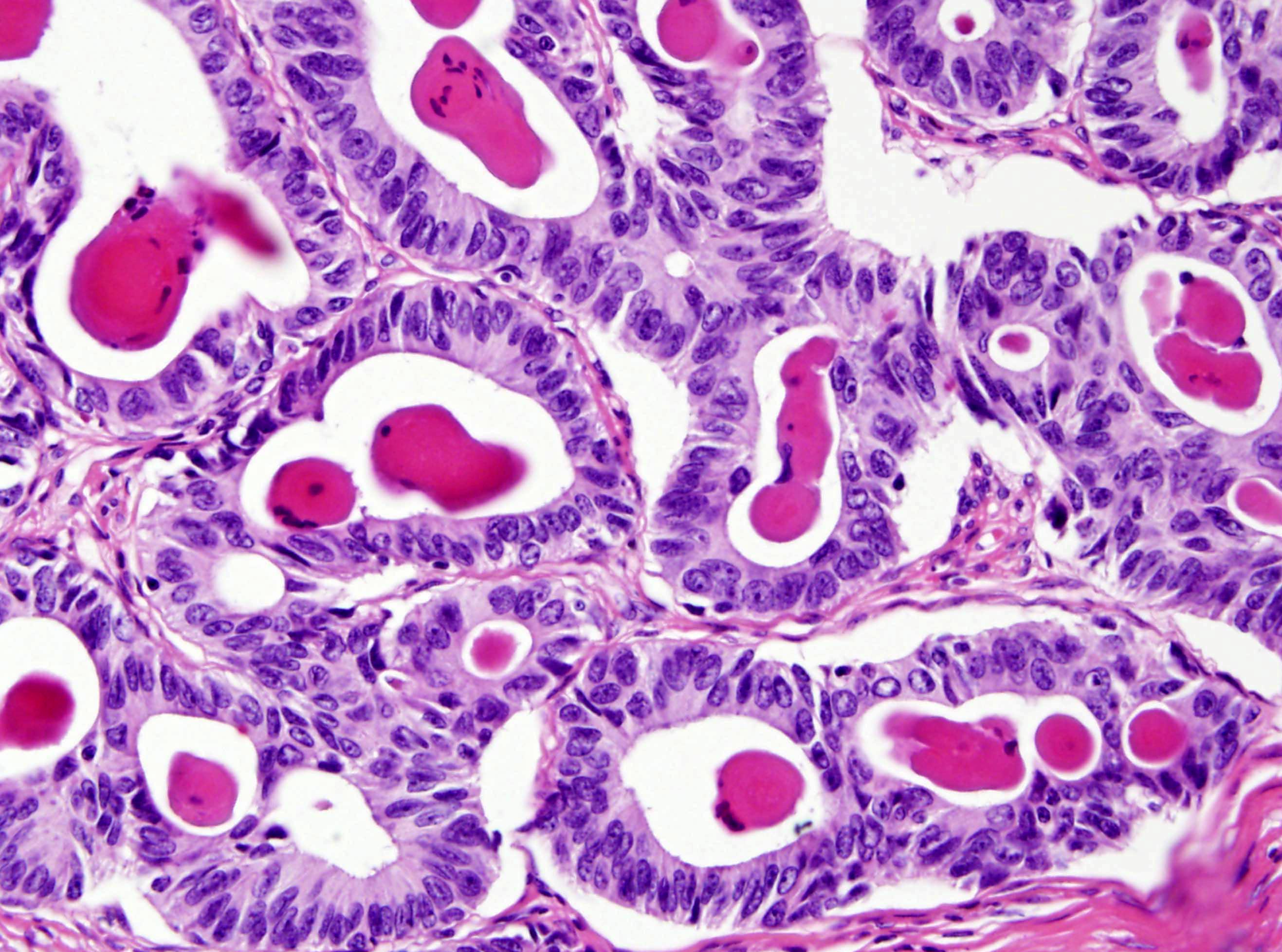
Tubules with eosinophilic secretions
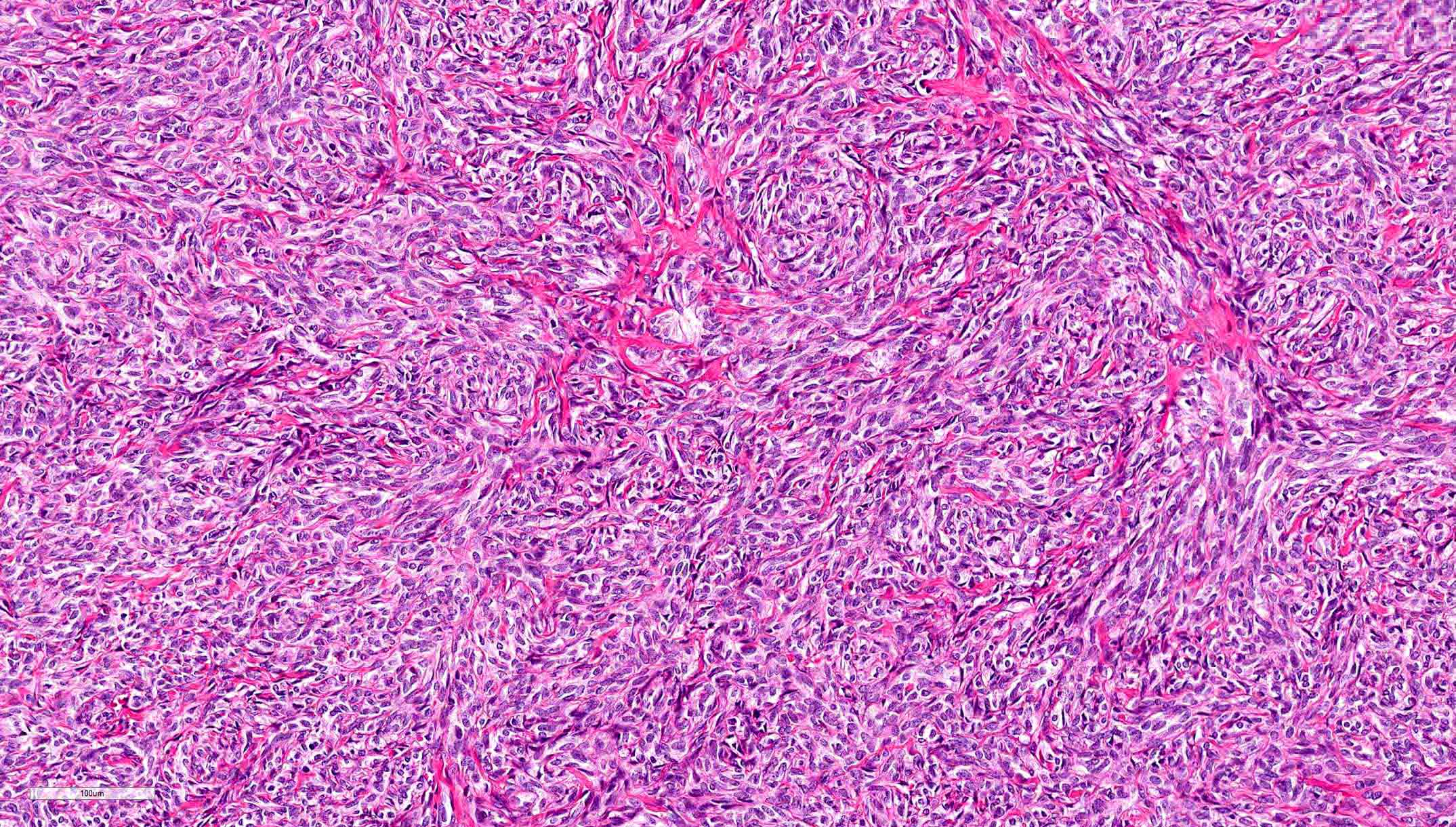
Solid growth pattern
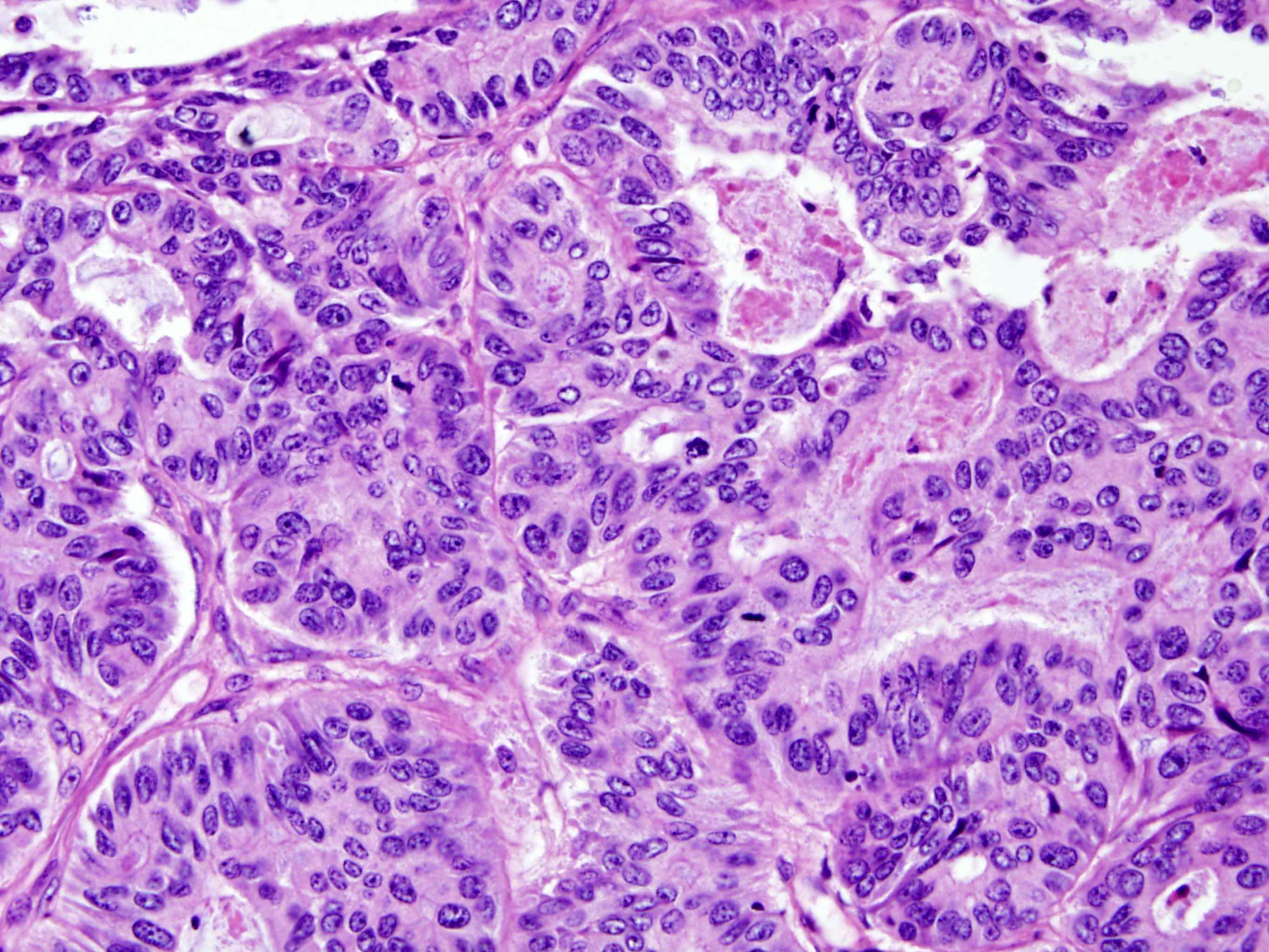
Malignant FATWO
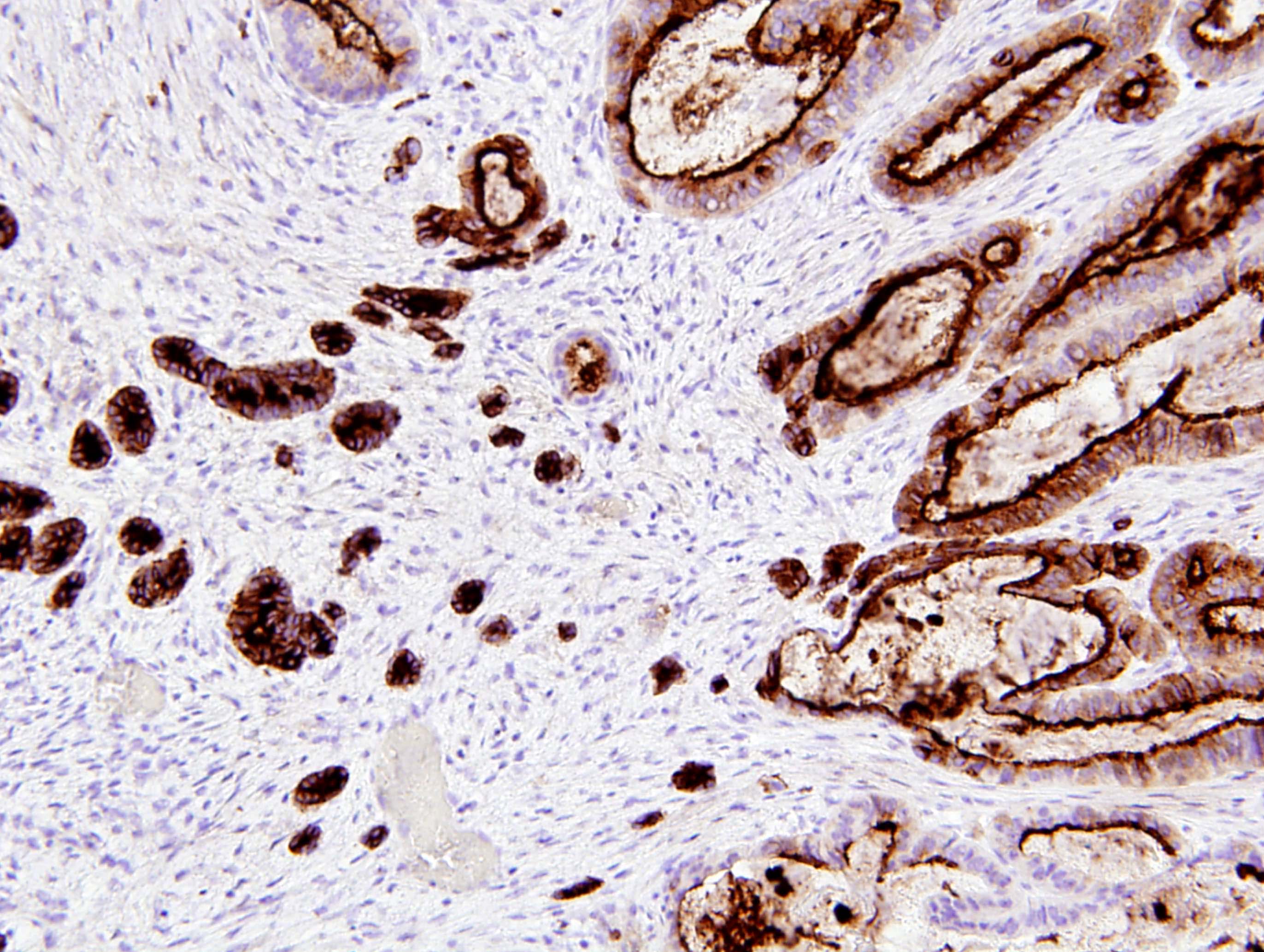
CD10
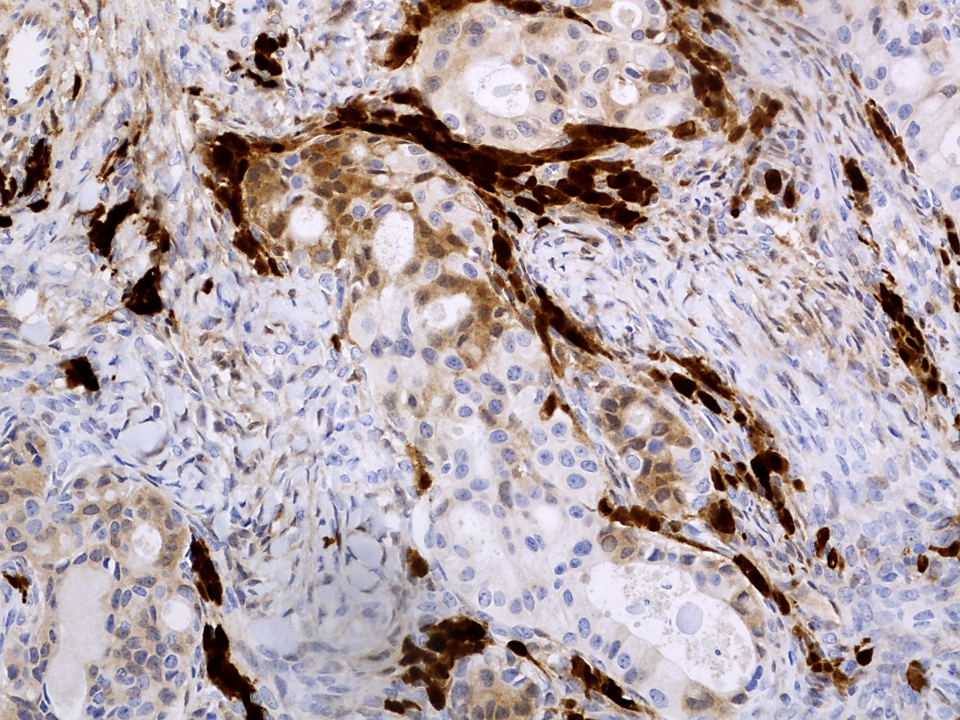
Calretinin
- Pancytokeratin (AE1 / AE3, CAM5.2), CK7, CK19
- Variable: CD10 (50 - 100%), calretinin, inhibin, MelanA, CD99, WT1, ER, PR, androgen receptor, EMA, GATA3, CD117 (KIT), vimentin, SMA (in spindle cell areas)
- References: Hum Pathol 1999;30:856, Int J Gynecol Pathol 2019;38:543, Mod Pathol 2020;33:734, Am J Surg Pathol 2015;39:1411, Arch Pathol Lab Med 2022;146:166
- PAX8 (negative in majority of cases, although focal positivity has been rarely reported) (Mod Pathol 2020;33:734)
- EMA (typically negative; may show focal weak staining)
- CK20, CEA, TTF1, SF1 (Int J Gynecol Pathol 2016;35:167)
- Distinct basal laminae, desmosomal junctions and poorly developed cytoplasmic organelles (Pathol Int 2006;56:95)
- No / minimal cilia, no secretory granules (Pathol Int 2006;56:95)
- No disease defining molecular alterations identified
- Rare tumors harbor APC and MBD4 mutations; KMT2D mutations (Mod Pathol 2020;33:734, Int J Gynecol Pathol 2019;38:543)
- Tumors previously classified as FATWOs with recurring STK11 mutations are now known to represent STK11 adnexal tumors (Histopathology 2022;81:280)
- Despite CD117 positivity in some tumors, no KIT mutations have been detected (Pathol Int 2006;56:95)
- Right adnexal mass, right salpingo-oophorectomy:
- Female adnexal tumor of probable Wolffian origin (FATWO), 6.0 cm (see synoptic report and comment)
- Comment: FATWO (also known as Wolffian tumor) is a rare tumor of low malignant potential. These tumors are thought to arise from mesonephric remnants. Most tumors behave in a benign fashion, although some tumors exhibit aggressive behavior. Although features known to be associated with adverse prognosis (e.g., large size, capsular invasion, rupture, high cellularity, nuclear pleomorphism, high mitotic activity) are absent in this case, cases without these features may also recur. Clinical correlation and follow up are recommended.
- Endometrioid carcinoma:
- Glandular pattern with variable squamous differentiation
- Nuclear atypia
- May show intraluminal mucin
- Positive for PAX8
- High grade serous carcinoma:
- Clear cell carcinoma:
- High grade nuclear features
- Typical architectural patterns (papillary, tubulocystic, solid)
- Positive for PAX8
- Sertoli cell tumor (SCT) and Sertoli-Leydig cell tumors (SLCT):
- Androgenic or estrogenic manifestations; presence of Leydig cells (in SLCT)
- Negative for CD10
- Positive for SF1 and FOXL2
- DICER1 mutation in moderately and poorly differentiated SLCT (Am J Surg Pathol 2017;41:1178)
- Adult granulosa cell tumor:
- Typically solid pattern
- Pale, angulated cells with nuclear grooves
- Hyperestrogenism
- Negative for CD10
- FOXL2 mutation (FOXL2 immunohistochemistry is not specific for mutation status) (N Engl J Med 2009;360:2719)
- STK11 tumors:
- Interanastomosing cords and trabeculae, salivary gland tumor-like growth, tubular, cystic, cribriform, microacinar, nested, nodular, papillary, follicular and solid
- Myxoid, collagenous or hyalinized stroma
- Nuclear atypia with prominent nucleoli, variable mitoses
- Basophilic intraluminal secretions
- Association with Peutz-Jeghers syndrome in ~50%
- Recurrent STK11 alterations (Histopathology 2022;81:280)
- Mesonephric carcinoma:
- Predominantly in the cervix
- May arise in a background of mesonephric hyperplasia
- Mesonephric-like carcinoma:
- Adenomatoid tumor:
- Small, unencapsulated tumor
- Lacks variety of patterns within the same tumor
- Negative for CD10
- Mesothelioma:
- Metastatic carcinoma:
- Higher nuclear grade
- Typically lacks variety of patterns
- Often shows necrosis
- Often positive for CEA
- Final diagnosis is based on ancillary studies
- Minimal nuclear atypia and low mitotic rate are predictive of benign behavior
- Patients often have virilizing symptoms
- Tumor likely originated from mesonephric embryological remnants
- Tumor originated from paramesonephric embryological remnants
Comment Here
Reference: Female adnexal tumor of probable Wolffian origin
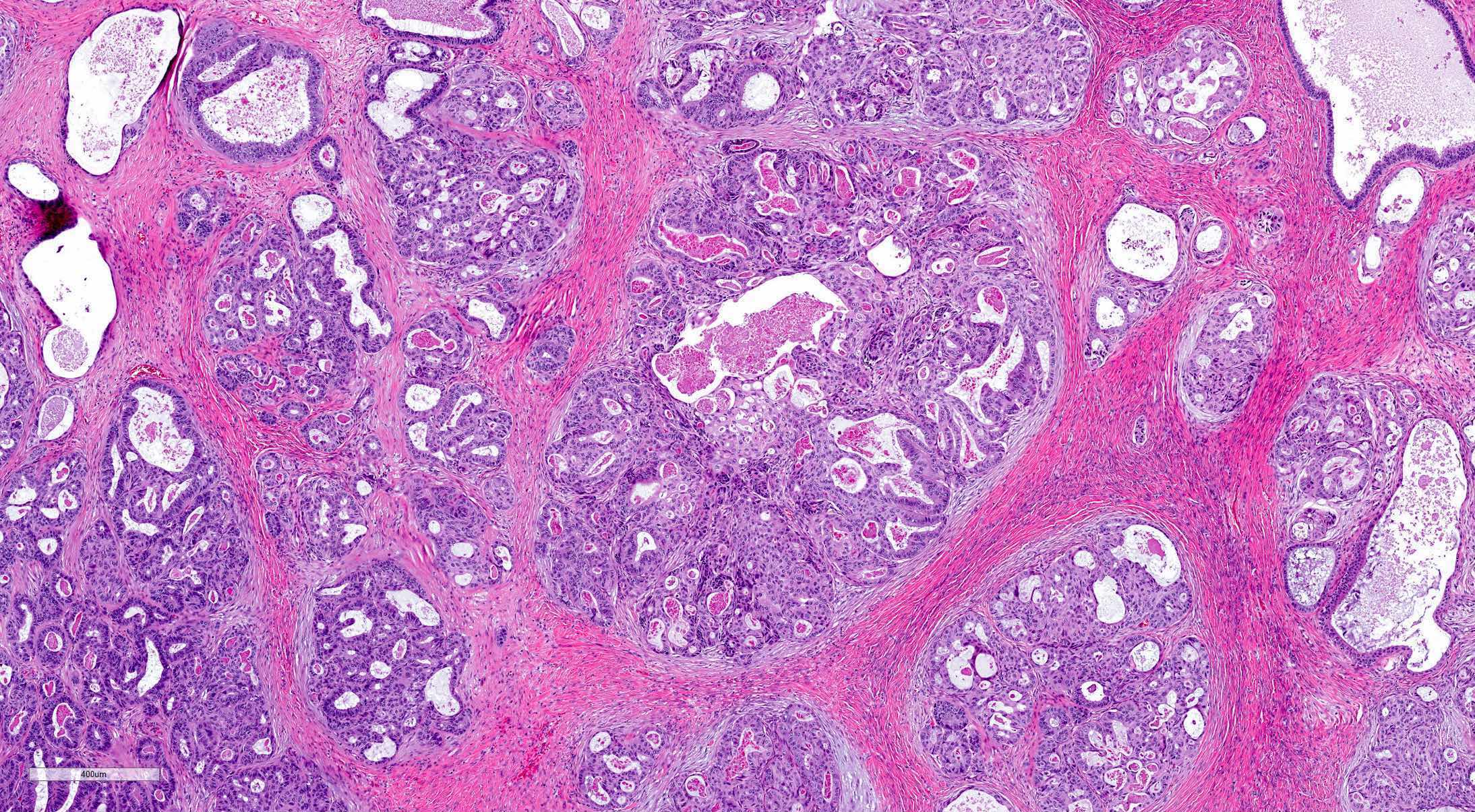
This image is from a 50 year old woman with an encapsulated adnexal mass, found incidentally. Which of the following statements is true?
- Calretinin and inhibin immunostains help to differentiate it from sex cord stromal tumors
- CD117+ tumors harbor KIT mutation
- ER and PR immunostains help to differentiate it from endometrioid carcinoma
- FOXL2 mutation is present in the majority of tumors
- Tumor is typically positive for pancytokeratin and CD10
Comment Here
Reference: Female adnexal tumor of probable Wolffian origin
Carlson: 2023
Clement: 2019
Crum: 2015
Heller: 2015
IARC: 2014
IARC: 2020

Nucci: 2020
Nucci: 2023
Vang: 2017
Find related Pathology books: gynecologic
