50% of those with jaundice have coexisting choledocholithiasis
Due to stone impaction, versus biliary colic, which is due to intermittent obstruction
50% have bacterial infection (E. coli, Enterobacter, Enterococcus, Klebsiella, Clostridium, Peptostreptococcus, Bacteroides)
1% mortality
Perforation unlikely if early operation
Pathophysiology
Chronic obstruction causes increased intraluminal pressure, vascular compromise, stasis and concentration of bile within lumen, mucosal damage, release of cellular enzymes, release of inflammatory mediators such as lysolecithin and prostagladins
Gall bladder volume increases as acute cholecystitis progresses to gangrene or empyema
Gallstone formation is associated with poorer contractility and larger volume in gallbladders that contain stones
(World J Gastroenterol 2010;16:4341)
As the weight, volume and size of the stone increases, gall bladder mucosa changes from cholecystitis, hyperplasia, metaplasia, dysplasia, to carcinoma (Trop Gastroenterol 2012;33:39)
53 and 58 year old women with empyematous cholecystitis and a 75 year old man with perforated cholecystitis, who were treated with robotic cholecystectomy in the emergency setting (Medicine (Baltimore) 2019;98:e16010)
A patient undergoes removal of the pictured organ. What symptoms or presentation would suggest that the etiology of the condition that leads to removal of this organ is related to cocaine use?
Amaurosis fugax
Hematemesis
Melena
Vascular thrombosis
Board review style answer #1
D. Cocaine induced cholecystitis is seen in young, otherwise healthy patients and should be suspected when there is vascular thrombosis along with involvement of other parts of the gastrointestinal tract.
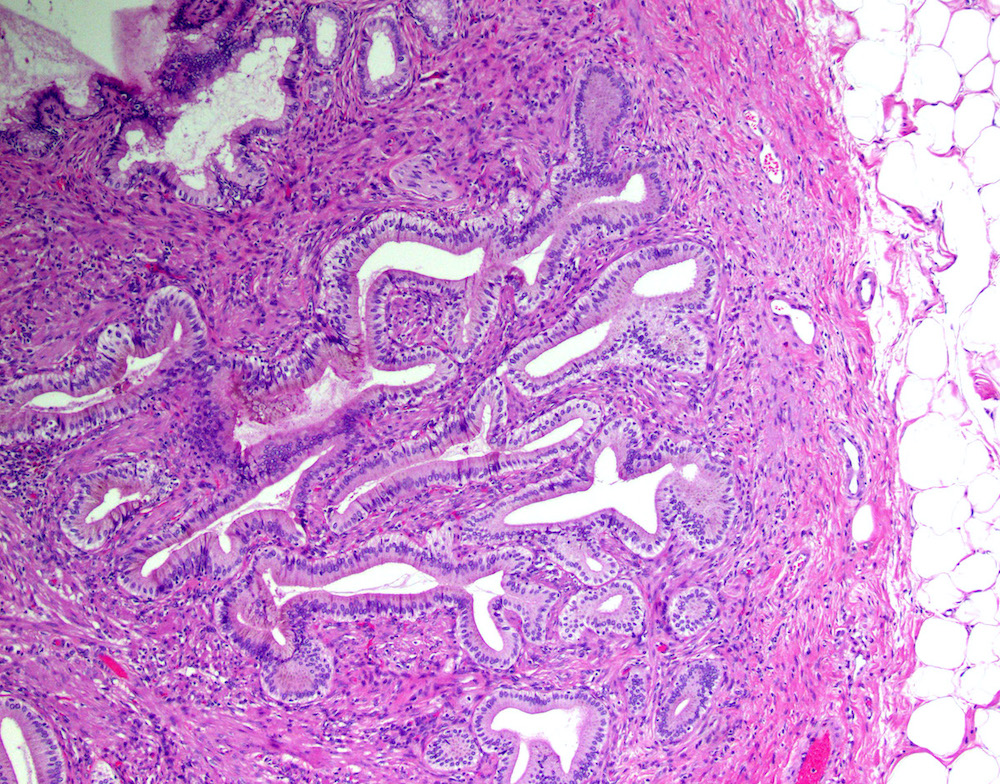
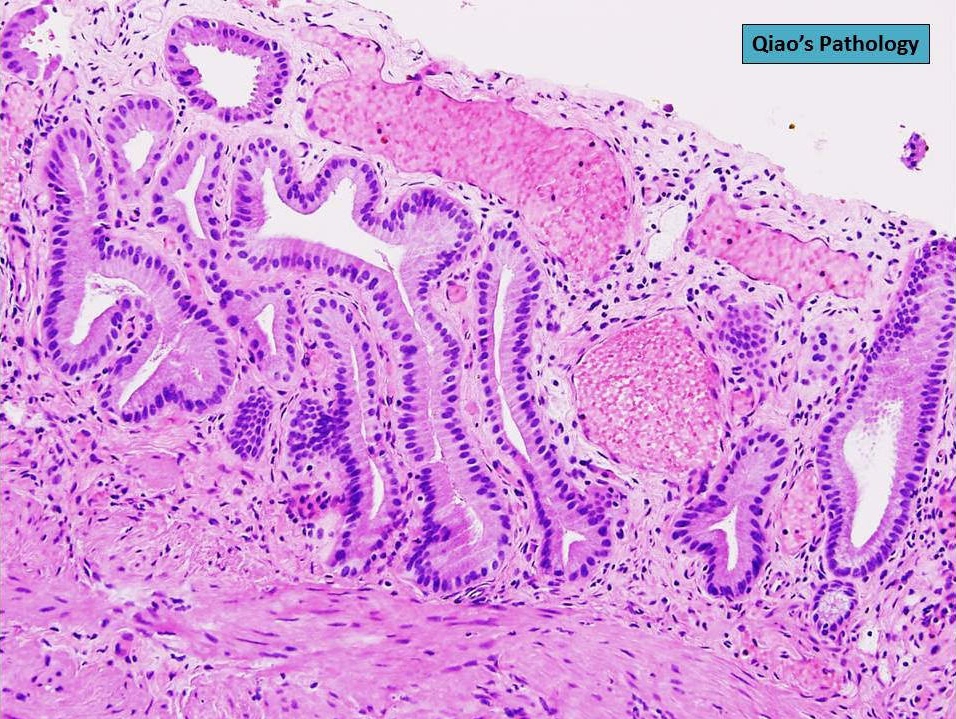
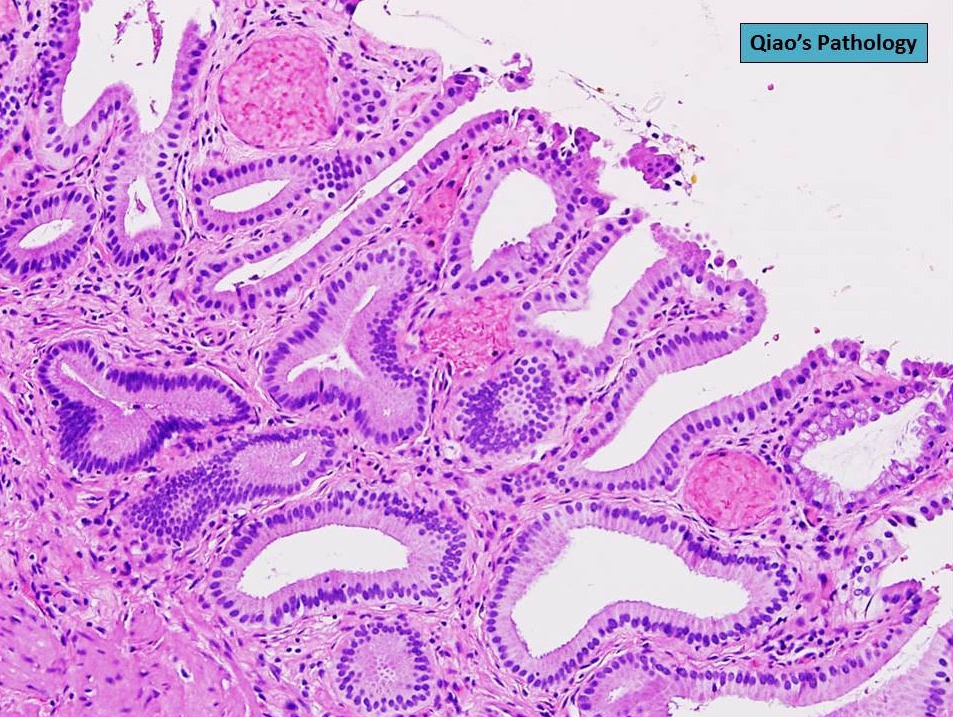
Glands are distinct from the Rokitansky-Aschoff sinuses, which are epithelial diverticula, usually multifocal and occur throughout gallbladder secondary to injury, versus adenomyomatous nodule (distinct localized lesion of the gallbladder wall, 1 - 1.5 cm mural nodule in the fundus) (Am J Surg Pathol 2020;44:1649)
Rarely, benign glands are seen in proximity to nerves, appearing as perineural and intraneural invasion only in the subserosal layer (benign gland-like structures may migrate into nerves due to chemotactic factors or signaling substances with activation of cell receptors) (Am J Surg Pathol 2007;31:1598)
Adenomyomatous nodules may rarely show dysplastic / carcinomatous transformation, whereas dysplasia in Rokitansky-Aschoff sinuses appears to be more common; however, the true association between adenomyomatous nodules and neoplasia has not yet been determined (Am J Surg Pathol 2020;44:1649)
Recently, papillary dysplastic lesions of adenomyomas have been identified (intracholecystic neoplasms of adenomyomas), demonstrating cystic and solid areas with papillary projections that show biliary, gastric and intestinal phenotypes, with low or high grade dysplasia (Am J Surg Pathol 2020;44:1649)
In general, biliary dysplasia (biliary intraepithelial neoplasia [BilIN]) can be either low grade or high grade and is recognized by the abrupt transition from normal mucosa with nuclear hyperchromasia, overlapping and enlargement in low grade, with the inclusion of those features as well as loss of nuclear polarity/nuclear stratification seen in high grade dysplasia
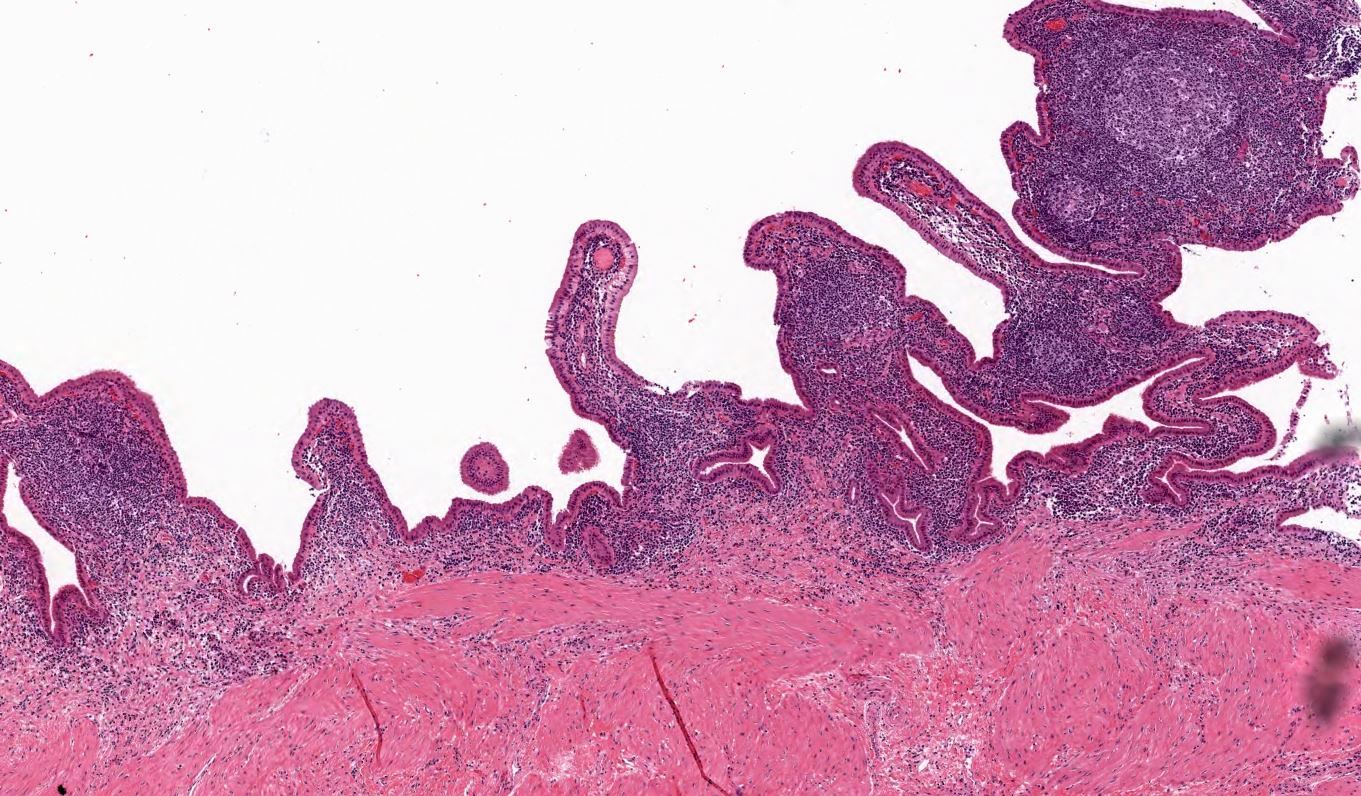
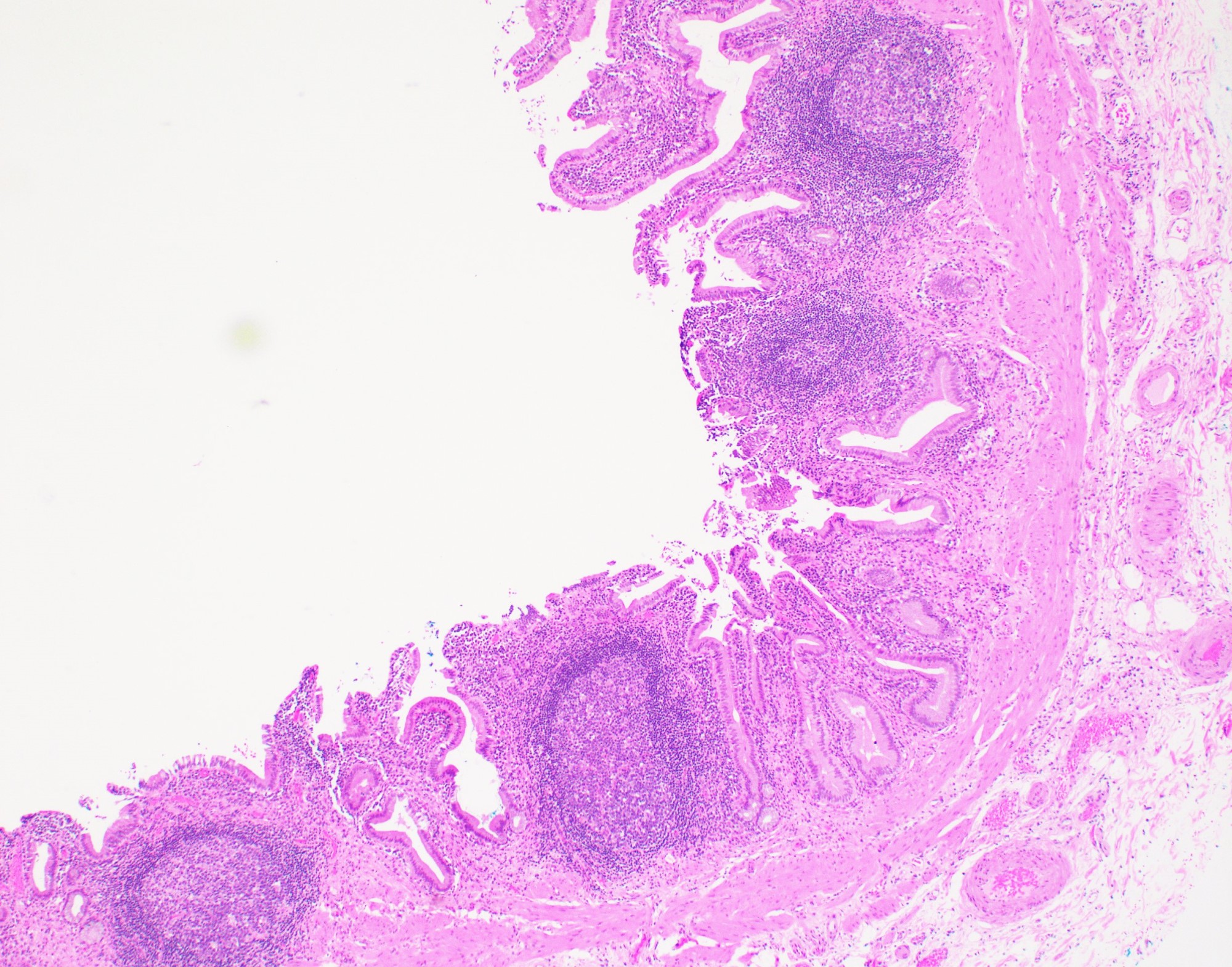
Lymphoplasmacytic infiltrates in lamina propria, may extend deeper, occasionally form lymphoid aggregates / follicles, occasionally may contain eosinophils
May contain Rokitansky-Aschoff sinuses: epithelial diverticula that can occur throughout gallbladder secondary to injury
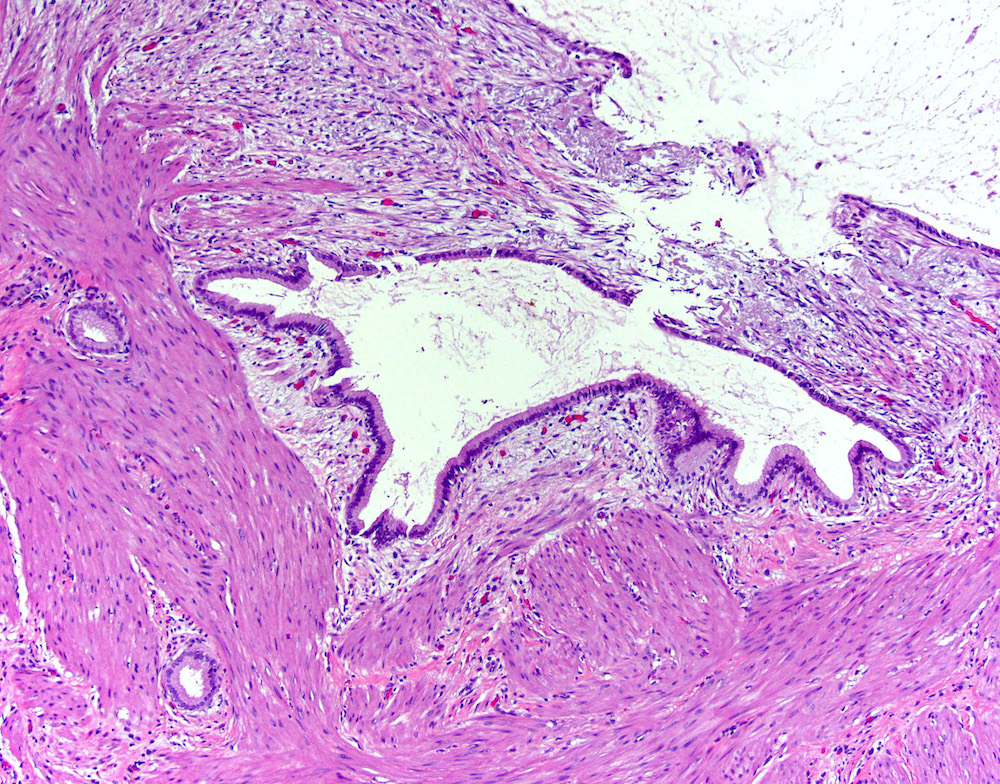
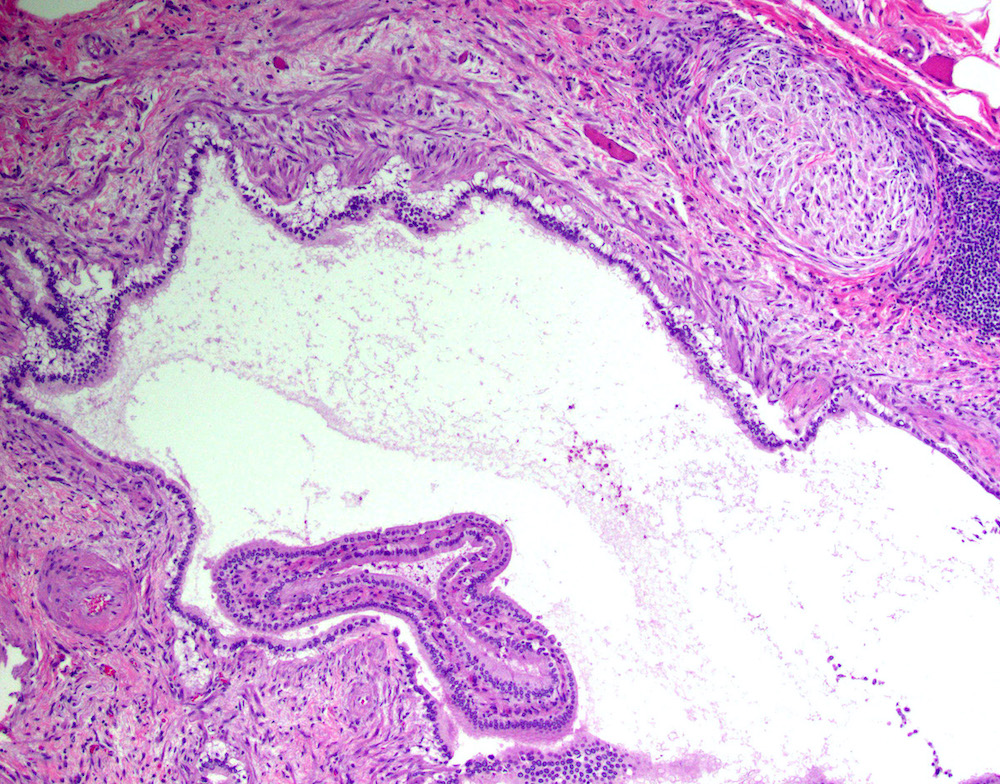
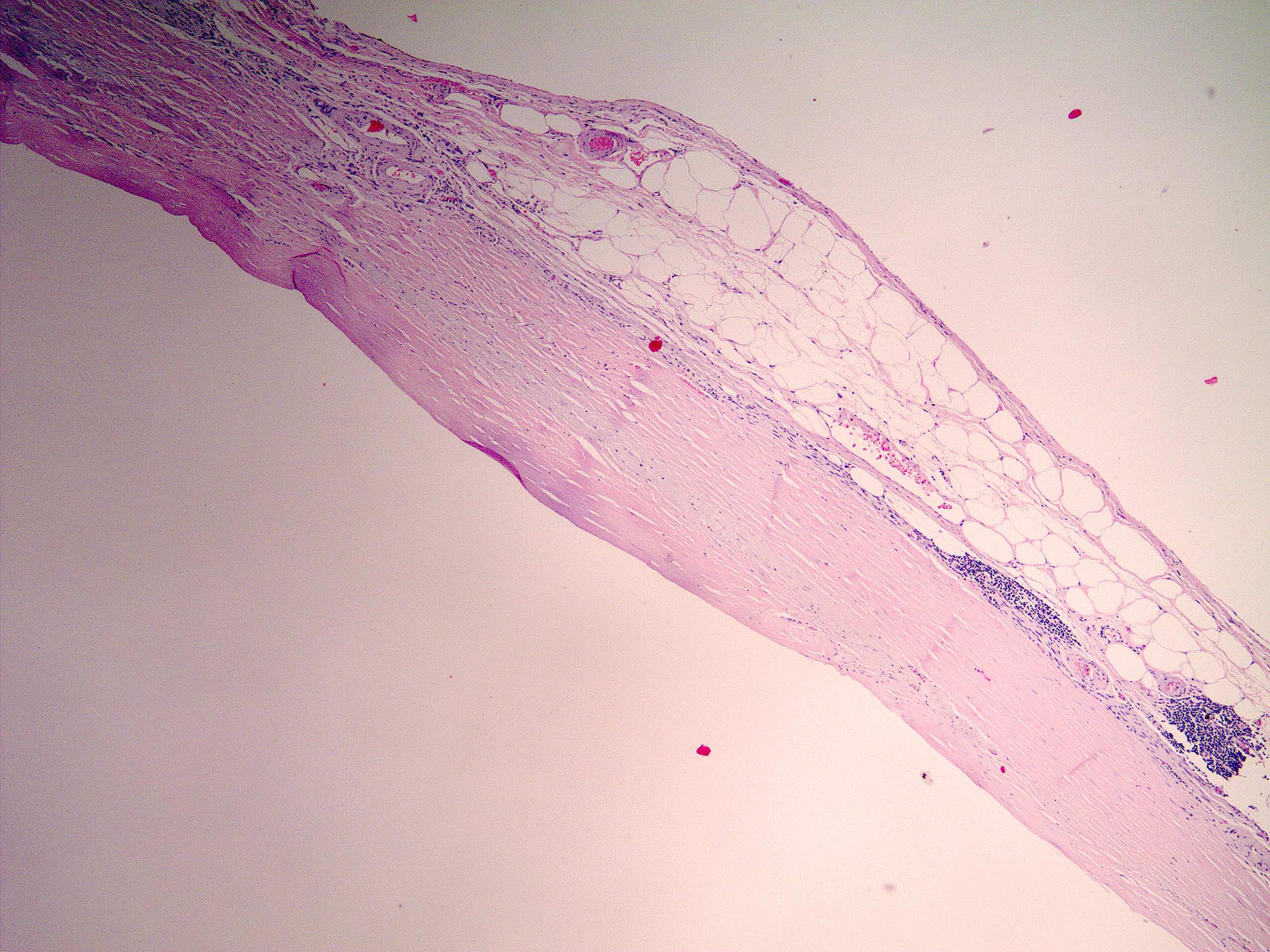
The gallbladder is a pear shaped saccular organ connected to the extrahepatic biliary system via the cystic duct
Essential features
Gallbladder wall is 1 - 2 mm thick and composed of mucosa, muscularis propria and serosa
No muscularis mucosae or submucosa is present
With the exception of the common bile duct and the cystic duct at the junction with the gallbladder, the extrahepatic bile ducts do not have a muscle layer
Physiology
Gallbladder:
Pear shaped saccular structure located on the inferior surface of the right hepatic lobe
Wall thickness: 1 - 2 mm
Composed of fundus, body and neck
Distal fundus: extends beyond the anterior liver margin
Central body: most of the gallbladder
Neck: narrows as it joins the cystic duct
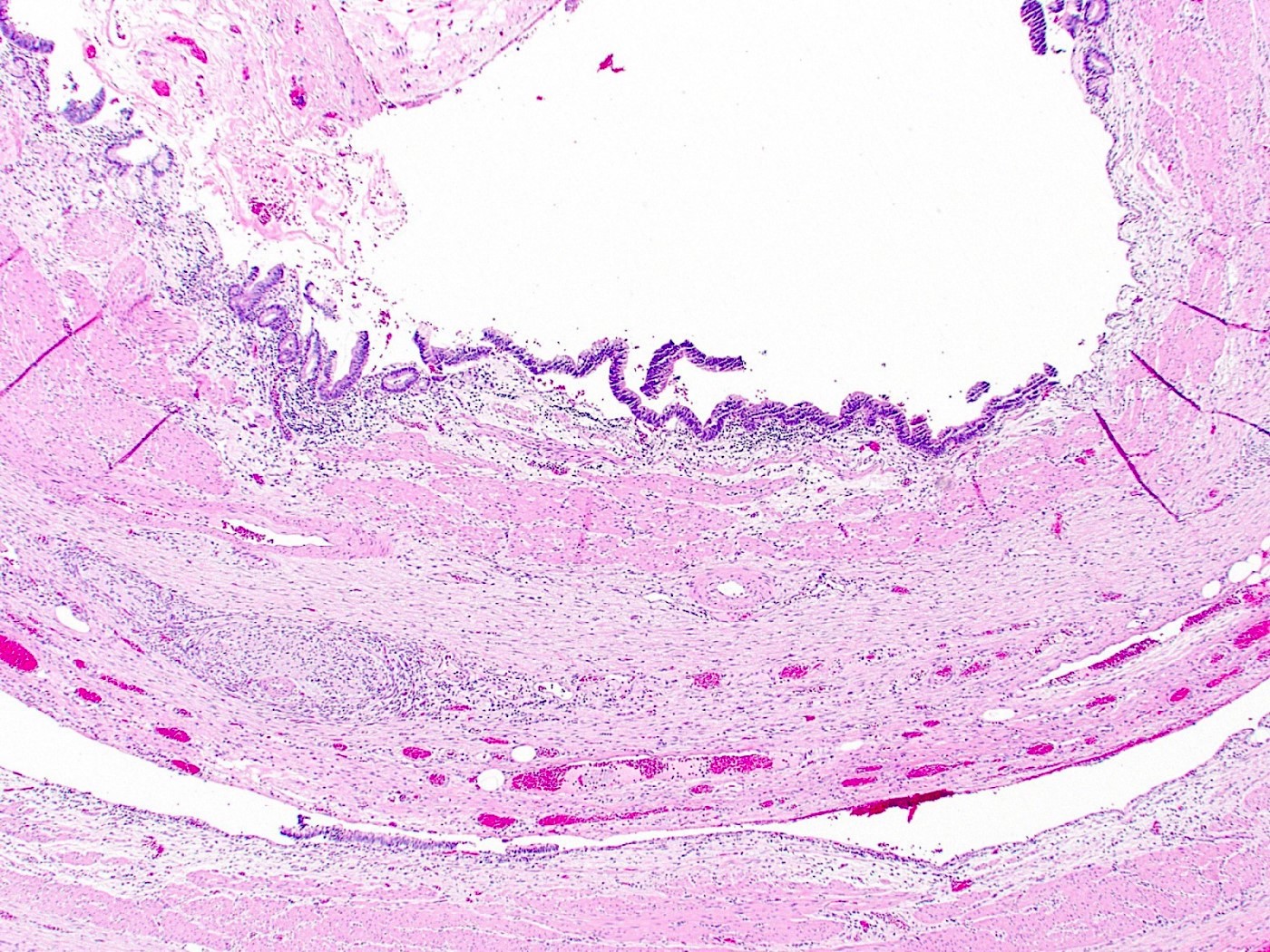
Extrahepatic biliary tree:
Right and left hepatic ducts:
Join to form common hepatic duct (CHD) in the porta hepatis (hilum of liver)
Common hepatic duct:
Joins cystic duct to form common bile duct
Cystic duct:
Connects gallbladder to common hepatic duct (CHD)
Has spiral valve of Heister (mucosal folds that avoid collapse)
Common bile duct:
Results from the fusion of CHD and cystic duct
2 - 9 cm long; passes posterior to the first portion of duodenum, traverses the head of pancreas, enters the second part of duodenum through the ampulla of Vater and discharges gallbladder contents into the duodenal lumen
60% of the population have common channel for pancreatic duct and common bile duct
Remainder of the population have 2 ducts in parallel
Gallbladder stores and releases bile
Gallbladder empties into cystic duct, which connects it to the extrahepatic biliary tree
Extrahepatic biliary tree serves as conduit for bile flow
Bile excretion is normally 500 - 1000 mL/day
Bile is concentrated 5 - 10x via active absorption of electrolytes accompanied by passive movement of water
Cholecystokinin causes gallbladder contraction and release of stored bile into the gut
Bile is critical for intestinal absorption of dietary fat but the gallbladder is not
Bile is 66% bile salts, is bicarbonate rich and has 3% organic solutes
95% of secreted bile salts are reabsorbed in the ileum and are subsequently returned to the liver via portal blood (called enterohepatic circulation of bile salts)
Cholesterol is eliminated via loss of 0.5 g of bile salts per day
Family of water soluble sterols with carboxylated side chains
Highly effective detergents, solubilize water insoluble lipids secreted by the liver (usually lecithin) into the biliary tree and promote dietary lipid absorption within the gut
Lecithin (phosphatidylcholine):
Hydrophobic, nonaqueous
Has minimal solubility in water
Diagrams / tables
Images hosted on other servers:
Inferior surface of the liver
Posterior and inferior surfaces of the liver
Gallbladder and bile ducts laid open
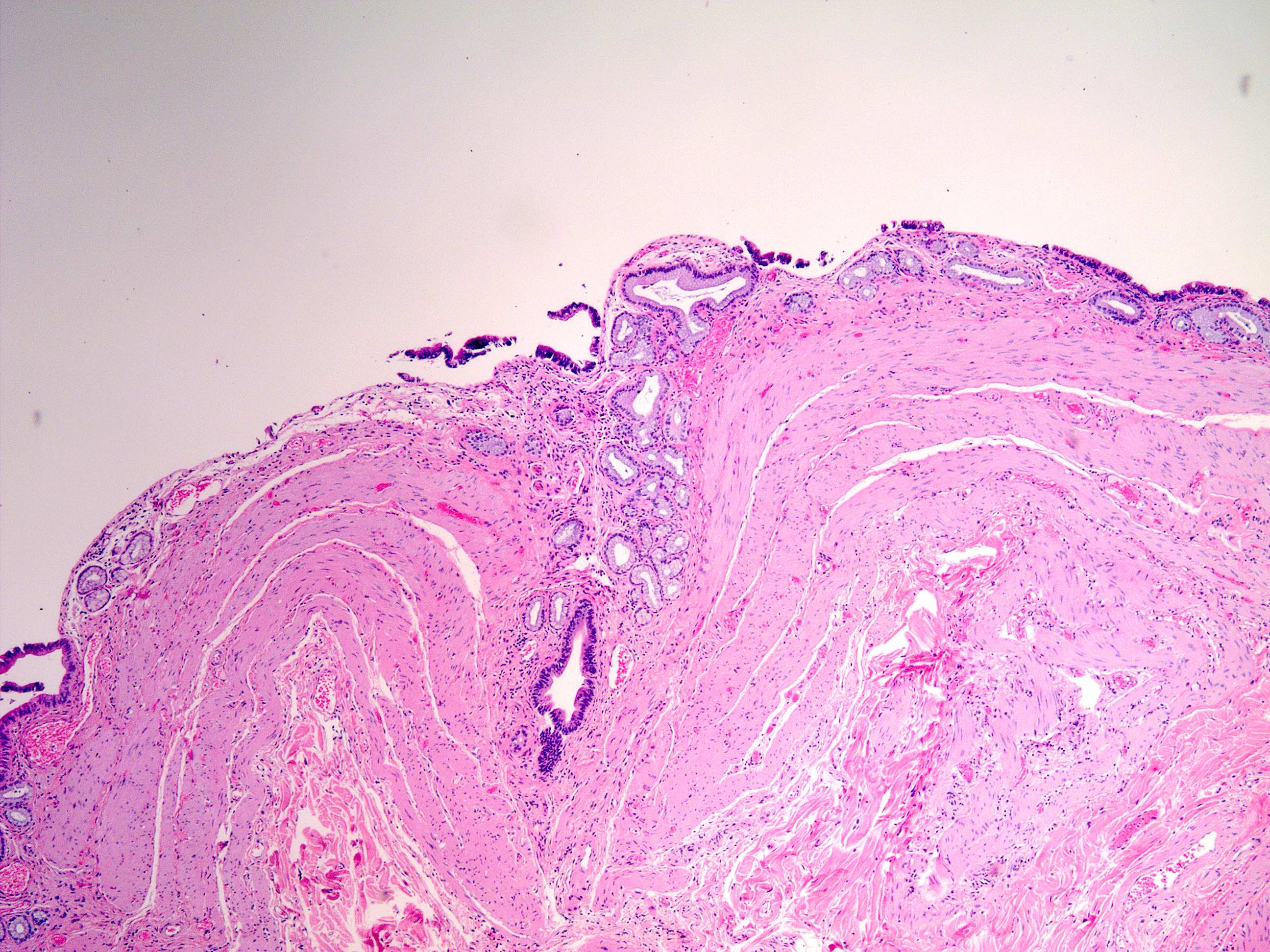
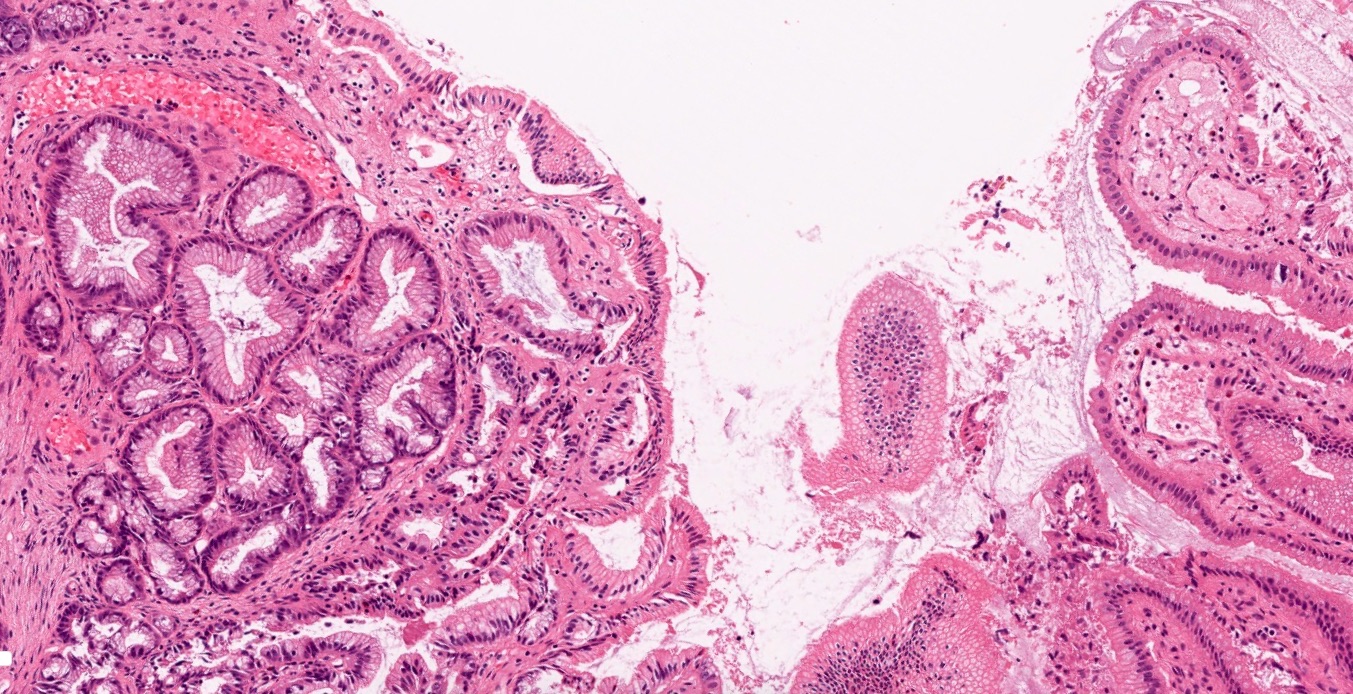
Microscopic (histologic) description
Gallbladder:
Microscopic layers: mucosa, muscular wall, perimuscular subserosal connective tissue and serosa; muscularis mucosae and submucosa are not present
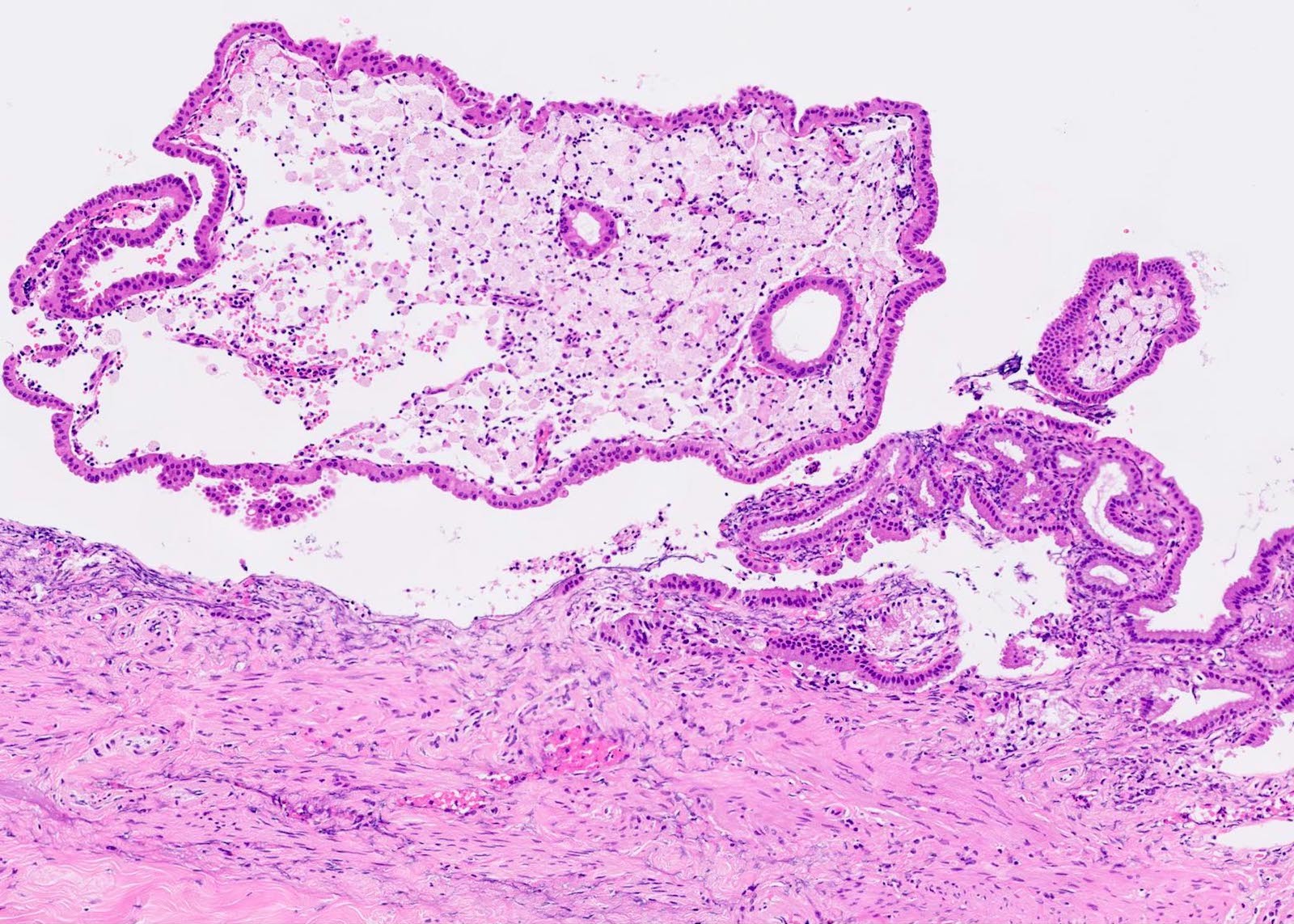
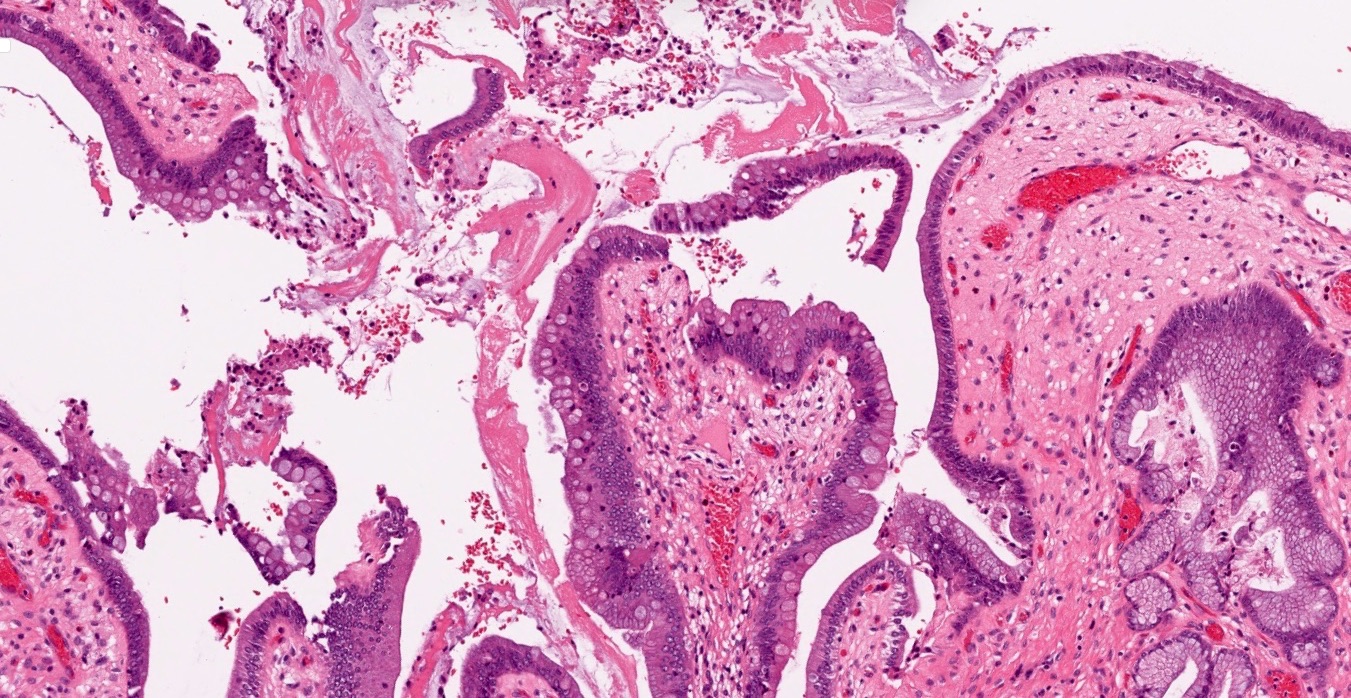
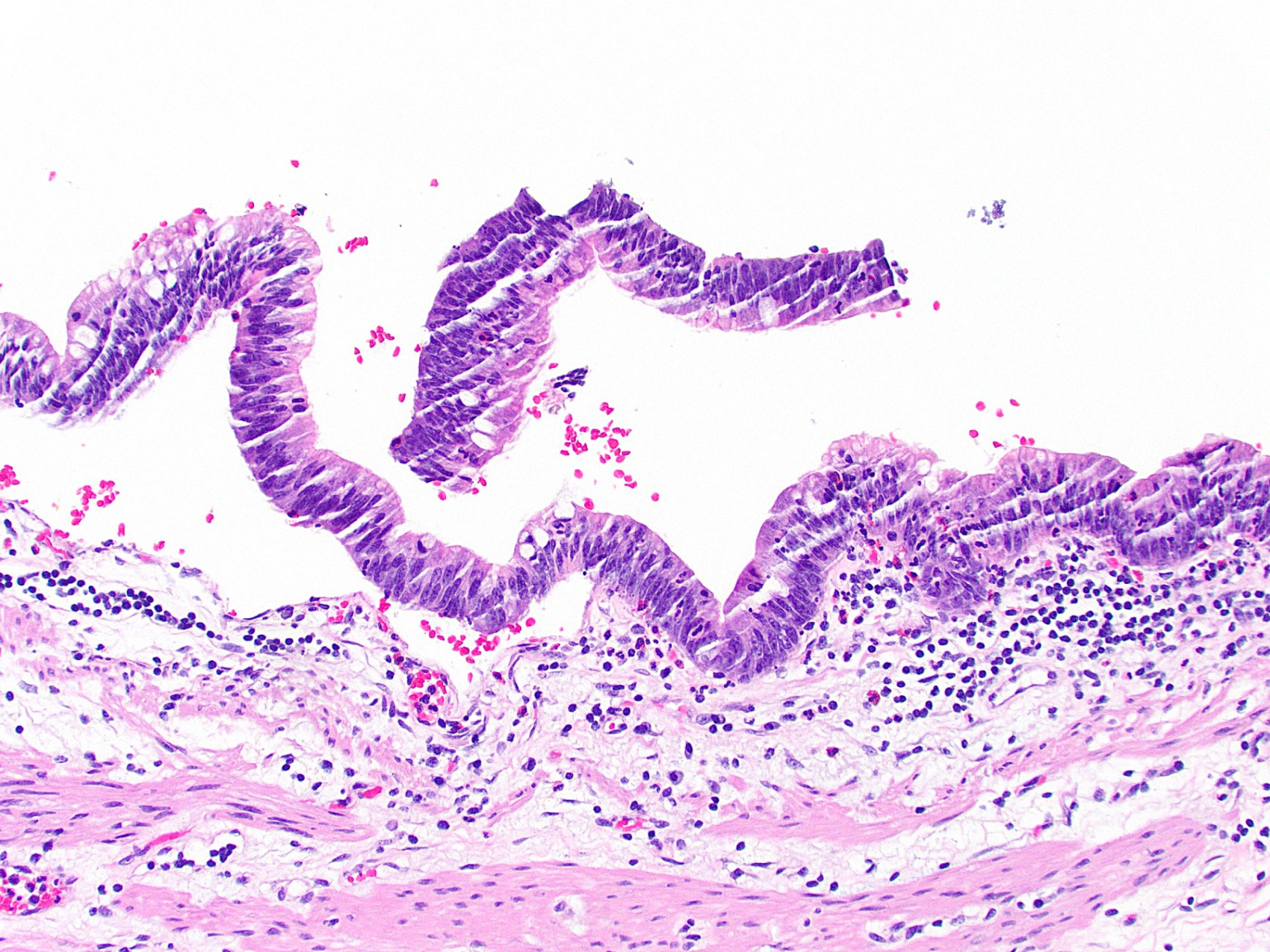
Mucosa:
Branching folds composed of surface epithelium and lamina propria
Cores of lamina propria are lined by a single layer of columnar epithelial cells
Epithelial cells have eosinophilic cytoplasm with variably present apical vacuoles; nuclei are basally oriented, oval and uniform, with inconspicuous nucleoli
There are also inconspicuous scattered basal epithelial cells located above the basement membrane
Tubuloalveolar mucus glands are present only in the neck region; true glands are not present outside the neck in normal gallbladder
Goblet cells are not present in normal gallbladder epithelium
Lamina propria is composed of loose connective tissue, blood vessels and lymphatics; few lymphocytes, plasma cells, mast cells and histiocytes are usually present (Mills: Histology for Pathologists, 3rd Edition, 2007)
Muscular wall:
Loose bundles of smooth muscle fibers without well formed distinct layers
Resembles muscularis mucosae
Adjacent to lamina propria without an intervening submucosa
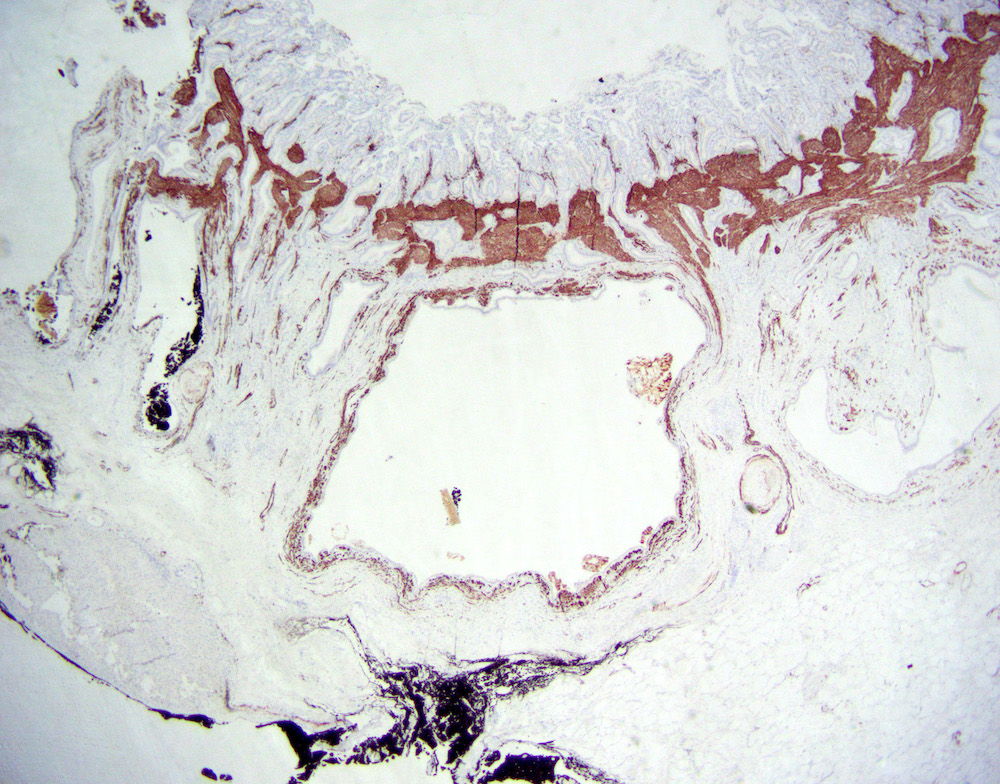
Perimuscular connective tissue composed of collagen, elastic tissue, fat, vessels, lymphatics and nerves
May contain lymph nodes and paraganglia
Serosa:
Peritoneum covers the portion of gallbladder that is not connected to the liver
Aberrant bile ducts (ducts of Luschka):
Present in 10% of cholecystectomy specimens, often buried in gallbladder wall adjacent to liver, may contain a collar of fibrous tissue, may communicate with intrahepatic bile ducts
Histologically composed of lobular aggregates of small ductules lined by bland cuboidal to columnar biliary type epithelium (Am J Surg Pathol 2011;35:883)
Rokitansky-Aschoff sinuses:
Outpouchings of gallbladder mucosa that penetrate the muscle wall
Which of the following is true about normal gallbladder and extrahepatic tree histology?
Gallbladder lacks muscularis mucosae and submucosa
Goblet cells are present in normal gallbladder epithelium
Muscle layer is not present along the common bile duct and at the junction of the cystic duct and gallbladder
Tubuloalveolar mucus glands are present throughout the entire gallbladder
Board review style answer #1
A. Gallbladder lacks muscularis mucosae and submucosa, unlike any other luminal GI structure. Tubuloalveolar mucus glands are present only in the neck region. True glands are not present outside the neck in normal gallbladder. Muscle layer is present along the common bile duct and at the junction of the cystic duct and gallbladder. Goblet cells are not present in normal gallbladder epithelium.
Persistent chronic inflammation and cytokine stimulation to biliary epithelium induces neoplastic changes, with involvement of different molecular pathways (Histopathology 2011;59:867)
KRAS mutations are an early event in biliary carcinogenesis and are present in almost 33% of BilINs, while TP53 mutations occur as a late molecular event (Cancer 2013;119:1669)
Contributed by Satyapal Chahar, M.D. and Monica T. Garcia-Buitrago, M.D.
Low grade dysplasia
Acute inflammation
Rokitansky-Aschoff sinus involvement
High grade dysplasia
High grade dysplasia
High grade dysplasia
High grade dysplasia
Cytology description
BilINs are microscopic, non mass forming lesions; not amenable to sampling via fine needle aspiration
Bile duct brushing cytology: increased nuclear to cytoplasmic ratio, nucleomegaly, anisonucleosis, nuclear border irregularity, hyperchromasia, visible or prominent nucleoli are associated with next generation sequencing (NGS) positivity (clonal somatic mutations) (J Am Soc Cytopatol 2020;9:520)
Approximately 33% of BilIN lesions show KRAS mutations, which occur as an early molecular event during the progression of BilIN; p53 overexpression occurs as a late molecular event (Surg Oncol Clin N Am 2009;18:215)
Multifocal high grade biliary intraepithelial lesion (BilIN3), extending to Rokitansky-Aschoff sinuses (see comment)
Comment: The specimen is entirely submitted for microscopic examination. No invasive carcinoma is identified. Cystic duct margin is negative for dysplasia.
Gallbladder, cholecystectomy:
Chronic cholecystitis with cholelithiasis and focal low grade biliary intraepithelial lesion (BilIN) (see comment)
Comment: The specimen is entirely submitted for microscopic examination. No invasive carcinoma is identified. Cystic duct margin is negative for dysplasia.
Differential diagnosis
Reactive changes:
Background acute and chronic inflammation present
Gradual transition between benign epithelium and reactive epithelium
Biliary intraepithelial neoplasia is a preneoplastic lesion and is most commonly cured by cholecystectomy. Which feature is most suggestive of possible recurrence?
Advanced age
Extensive lesion with Rokitansky-Aschoff sinus involvement
Female gender
Granular velvety mucosa
Radiologically identifiable mass
Board review style answer #2
B. Extensive lesion with Rokitansky-Aschoff sinus involvement
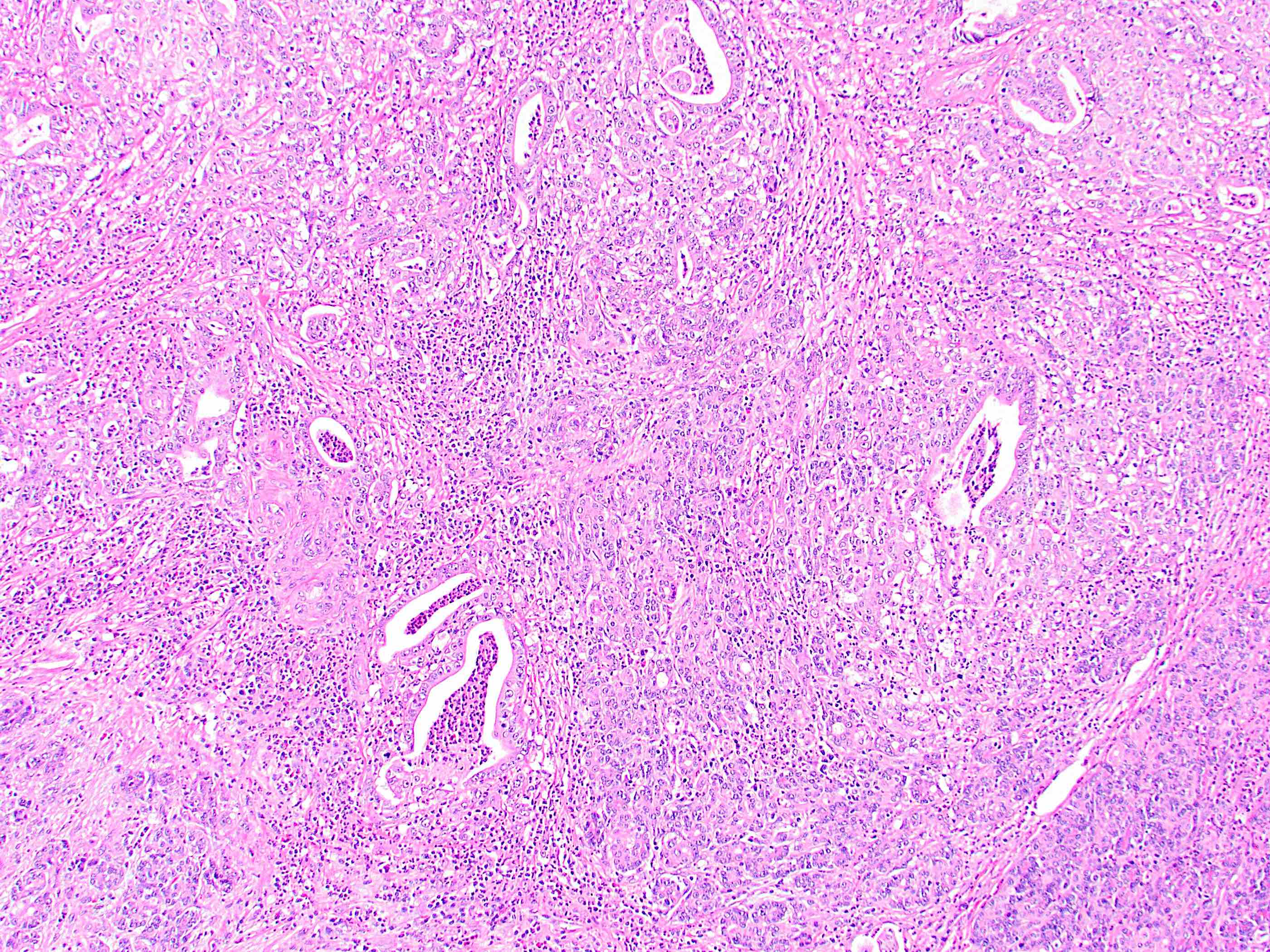
Rare malignant adenocarcinoma arising from extrahepatic bile ducts
Biliary adenocarcinomas (cholangiocarcinomas) typically divided into intrahepatic bile duct origin, gallbladder origin, perihilar bile origin (this topic) and distal extrahepatic bile duct origin (this topic), including right and left hepatic ducts, common hepatic duct and common bile duct
Essential features
Adenocarcinoma arising from the biliary system outside the liver, with several risk factors
Histology is similar to intrahepatic cholangiocarcinoma, particularly large duct type
Poor prognosis
Terminology
Some prefer to restrict the term cholangiocarcinoma to intrahepatic adenocarcinomas only but others use the term for any adenocarcinoma of the biliary system
Klatskin tumor refers to a hilar cholangiocarcinoma arising at the bifurcation of the right and left hepatic ducts
ICD coding
ICD-11
2C15.0 - adenocarcinoma of biliary tract, distal bile duct
May arise de novo, without risk factors being present
Diagrams / tables
Images hosted on other servers:
Bismuth-Corlette classification
Clinical features
Signs of biliary obstruction may occur, including jaundice (most characteristic and common symptom), pruritis, acholic stools and dark urine (Liver Int 2019;39:98)
Patients can present with nonspecific symptoms, including abdominal pain, nausea / vomiting, anorexia, weight loss and malaise (Liver Int 2019;39:98)
Many patients present with unresectable disease
Diagnosis
Early diagnosis is challenging and is often delayed due to asymptomatic early stage disease (World J Hepatol 2021;13:166)
Lack of a standardized screening protocol
MRI and magnetic resonance cholangiopancreatography (MRCP) can assess size and extent of tumor
Endoscopic ultrasound (EUS) and EUS guided FNA can be utilized in the diagnosis and staging of cholangiocarcinoma
Intraductal ultrasound is suggested for patients with obstructive jaundice for local tumor staging and bile duct stricture assessment
Intrapancreatic cases have a better prognosis than pancreatic ductal adenocarcinoma but a worse prognosis than ampullary adenocarcinoma (Mod Pathol 2016;29:1358)
Preoperative C reactive protein to albumin ratio (CAR) is an accurate prognostic biomarker, predicting overall survival and disease free survival (J Surg Oncol 2020;122:1516)
CAR is the most valuable prognostic biomarker in patients with resected extrahepatic cholangiocarcinoma (Dig Surg 2022;39:65)
Requires careful gross examination and correlation with clinical and imaging findings
May be impossible to definitively determine for advanced lesions
Reactive change:
Can involve biliary surface epithelium or peribiliary glands
On cytology specimens, features of malignancy include 3 dimensional clusters, pleomorphism, 2 cell population and chromatin pattern changes (Mod Pathol 2017;30:1273)
Board review style question #1
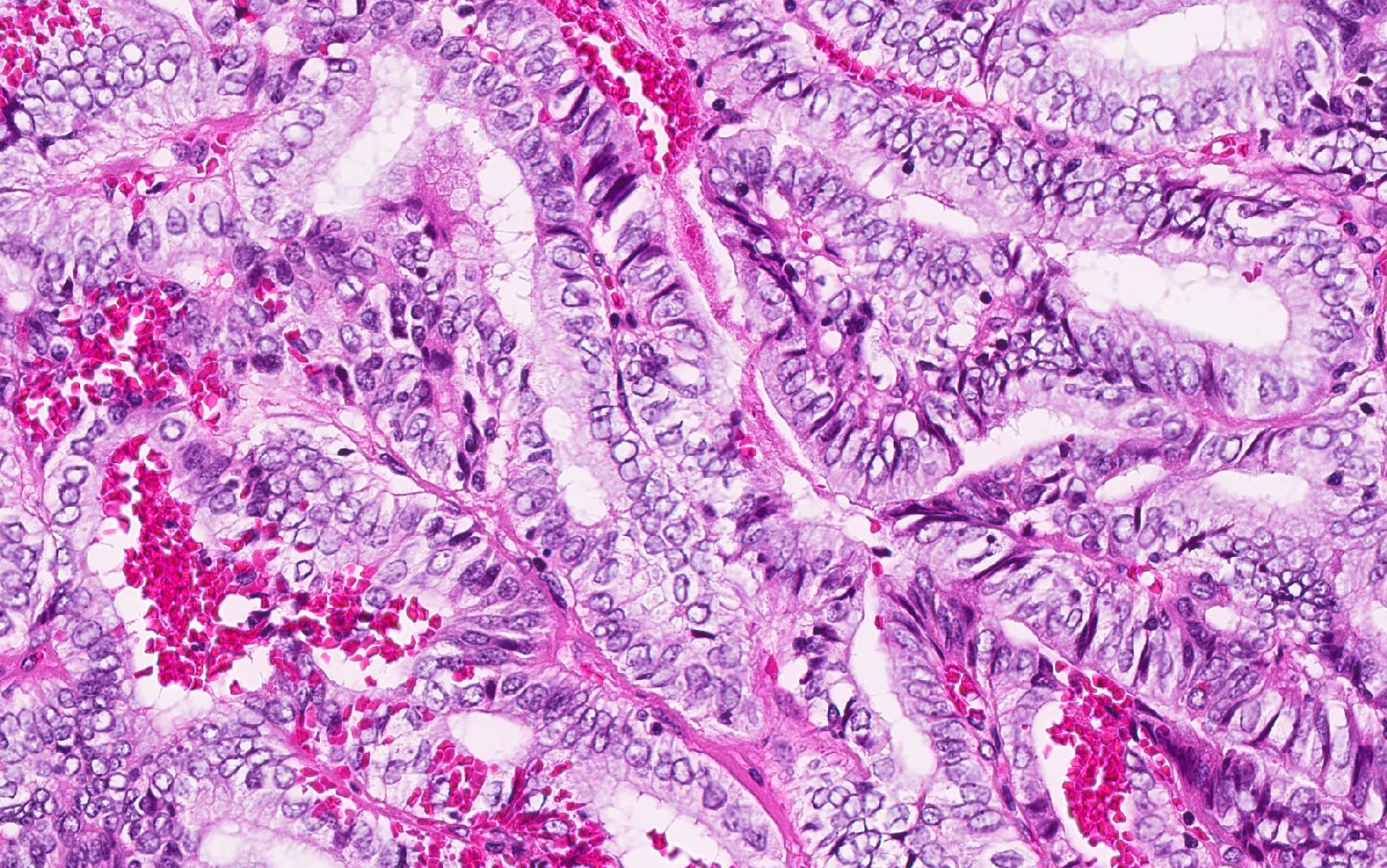
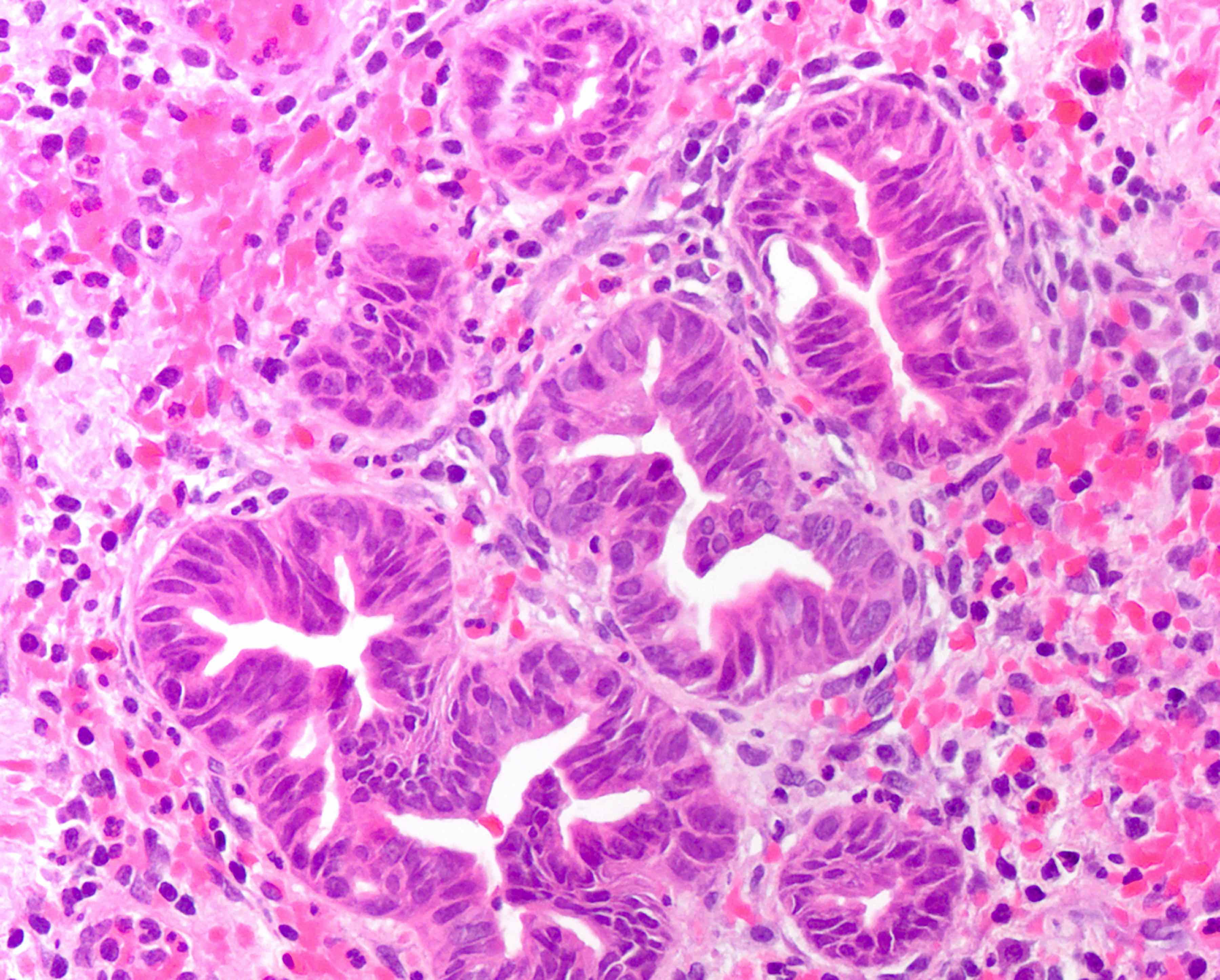
This image shows a cholangiocarcinoma arising within the pancreas. Which of the following is true regarding extrahepatic cholangiocarcinoma?
It has a good prognosis
It often shows a prominent neutrophilic infiltrate
It resembles the small duct type of intrahepatic cholangiocarcinoma
Peak onset is in the third decade of life
Primary biliary cholangitis is a risk factor
Board review style answer #1
B. It often shows a prominent neutrophilic infiltrate. This finding is often seen in pancreatobiliary adenocarcinomas in general, including extrahepatic cholangiocarcinoma. Answer A is incorrect because this disease has a poor prognosis. Answer D is incorrect because peak onset is in the sixth and seventh decades of life. Answer E is incorrect because primary sclerosing cholangitis is a risk factor, not primary biliary cholangitis. Answer C is incorrect because histologically, it most resembles the large duct type of intrahepatic cholangiocarcinoma.
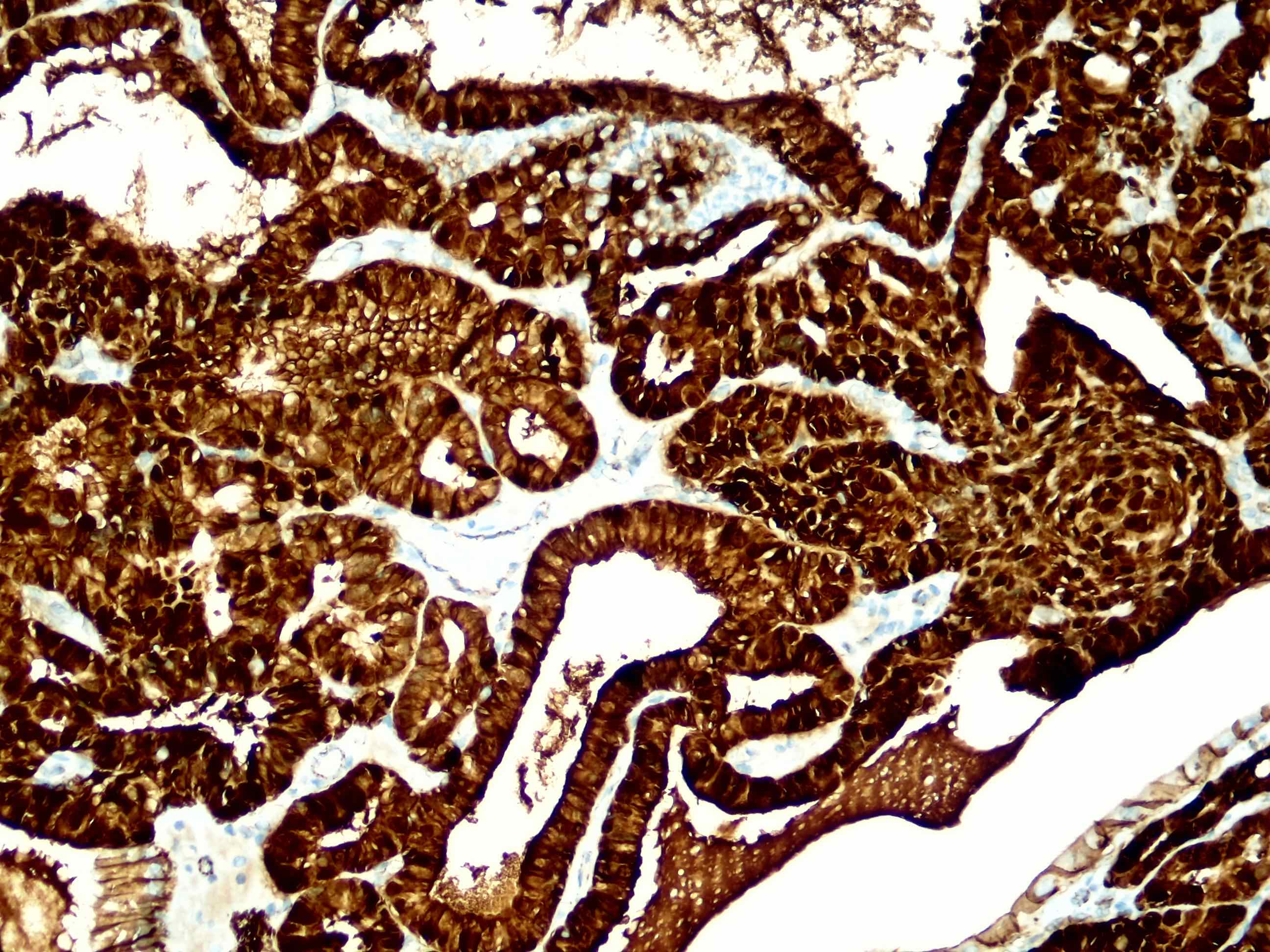
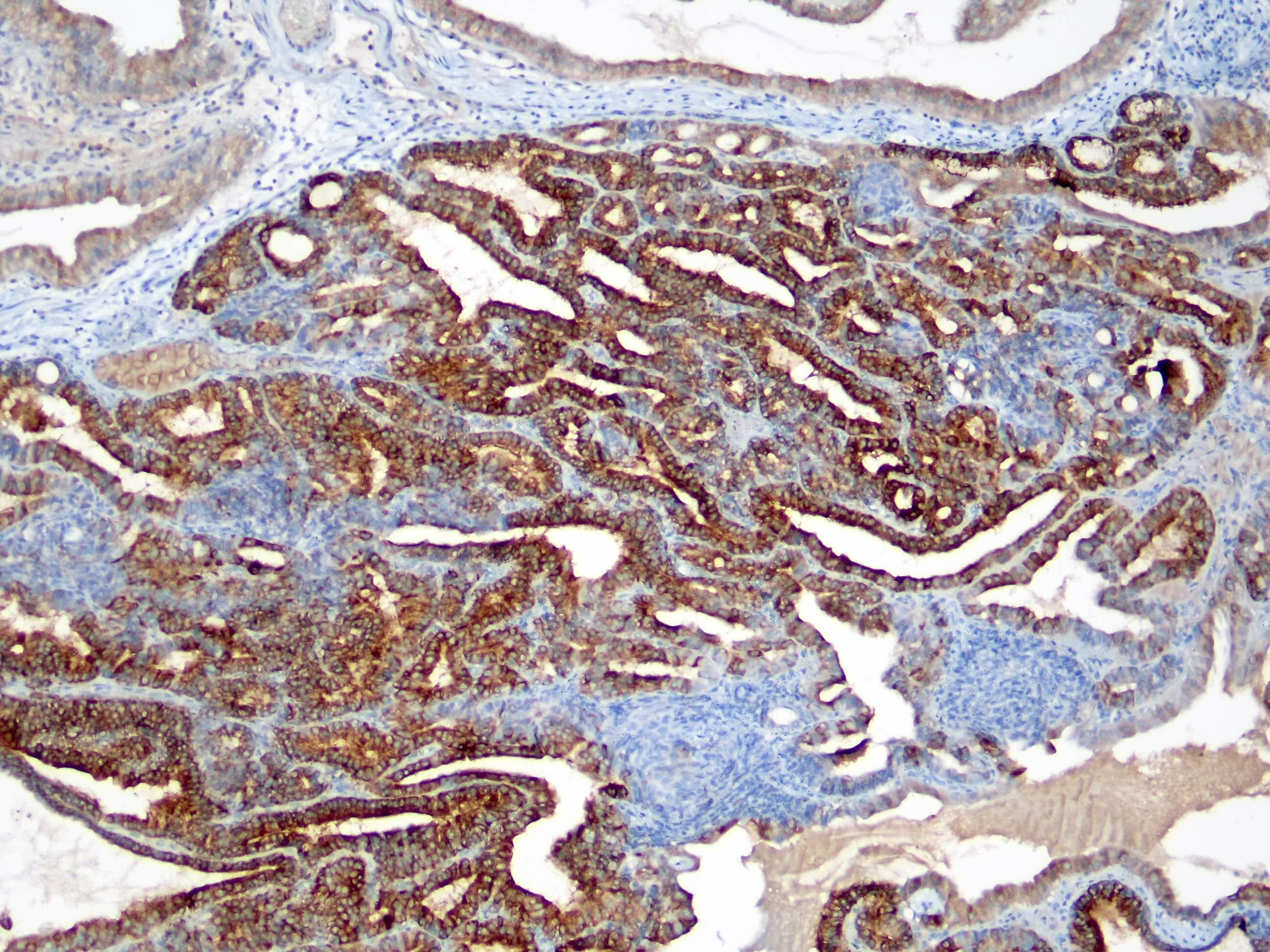
Which of the following immunohistochemical stains is typically positive in extrahepatic cholangiocarcinoma?
CDX2
CK7
CK20
PAX8
TTF1
Board review style answer #2
B. CK7. As with most pancreatobiliary adenocarcinomas, extrahepatic cholangiocarcinoma is positive for CK7. Answers A and C are incorrect because CDX2 and CK20 are variable but more often negative than positive. Answer E is incorrect because TTF1 positivity would suggest lung origin. Answer D is incorrect because PAX8 positivity would suggest renal or gynecologic origin.
Associated with other hepatobiliary tract abnormalities
May rupture spontaneously, be associated with reflux of pancreatic enzymes into bile duct
Associated with stones in 1 - 30% of cases
Not actually a cyst but a dilation of common bile duct which may secondarily obstruct other biliary ducts or the duodenum
2 - 8% develop biliary tract carcinoma (20x normal risk) at mean age 34 years, lower risk if surgery earlier in life (age 10 years or less), carcinoma may develop within wall of cyst, within gallbladder or bile ducts
Affects 10% of adults in developed countries (80% are silent) vs. < 1% of children
80% of gallstones in West are cholesterol stones with 50% or more crystalline cholesterol monohydrate
20% of gallstones in West are pigment stones composed of bilirubin calcium salts
Gallstones impact at neck just proximal to cystic duct
Typically within lumen but may be intramural
Risk factors:
Pima, Hopi or Navajo (75% of stones are pure cholesterol vs. 25% in industrialized vs. minimal in developing countries), also Scandinavians, Chileans, Mexican Americans, increasing age (> 50% risk by age 80)
Fat, fertile [multiple pregnancies], forty, female, obesity (Korean J Gastroenterol 2012;59:27), rapid weight loss, gallbladder stasis, genetic disorders that impair bile salt synthesis / secretion or increase cholesterol levels (serum or biliary), low HDL levels
Estrogens from birth control pills or pregnancy increase expression of hepatic LDL receptors, which increase cholesterol uptake, which stimulate HMG CoA reductase, which synthesizes cholesterol
Pigment stone risk factors are increased unconjugated bilirubin (from hemolytic syndromes, ileal dysfunction / bypass, bacterial contamination of biliary tree)
Clofibrate:
Anticholesterol drug that increases HMG CoA reductase activity and decreases conversion of cholesterol to bile acids by reducing cholesterol 7 alpha hydroxylase activity, causes excess biliary secretion of cholesterol
Symptoms:
Usually none but may have biliary colic (severe, right upper quadrant pain)
Complications:
1 - 2% have acute or chronic cholecystitis, choledocholithiasis, cholangitis, empyema, gallstone ileus, acute pancreatitis
Mirizzi syndrome:
Rare
Stone impacting in cystic duct or gallbladder neck causes extrinsic compression or obstruction of common bile duct, causing jaundice
Report:
Presence of biliary sludge, number, size and type of gallstones
Clinical features
Gallstones are composed of insoluble bile components: cholesterol, calcium bilirubinate, calcium salts (organic and inorganic), bile salts, mucin glycoproteins
In U.S., 75 - 85% are cholesterol stones, 15 - 25% are pigment stones
Calcium stones are gray white and amorphous; very uncommon
Calcium carbonate may fill lumen as thick, inspissated, cream gray to yellow green putty-like material
Choledocholithiasis: stones in common bile duct
40% of common bile duct stones are brown stones, usually associated with recurrent pyogenic cholangitis and older age (J Int Med Res 2009;37:1220)
Primary: originate in common bile duct
Secondary: originate in gallbladder
ERCP (95% sensitive and specific), ultrasound is only 50% sensitive
Cholesterol stones
75 - 85% of all gallstones
Only 10% are pure (at least 90% cholesterol), the remainder are mixtures with at least 60% cholesterol by weight
Cholesterol monohydrate precipitates when no longer soluble in bile
Initially bile supersaturation with cholesterol occurs
Then nucleation (initial crystallization), then stone growth facilitated by bile stasis and mucin hypersecretion
Pure and mixed occur predominantly in women
Also associated with increasing age, obesity, rapid weight loss, diabetes, ileal disease, multiple pregnancies, total parenteral nutrition, various drugs, specific ethnic groups
Adenomatous hyperplasia and Rokitansky-Aschoff sinuses:associated with mixed and cholesterol stones; not associated with pigment stones (Trop Gastroenterol 2002;23:25)
Pigment stones
15 - 25% of all gallstones
Associated with increasing age
Less than 25 - 35% cholesterol
Composed of calcium bilirubinate, calcium salts, mucin glycoprotein
Brown (not black) stones associated with infected bile (usually E. coli) due to acute cholecystitis or choledocholithiasis with cholangitis
Black stones associated with older age, chronic hemolysis, cirrhosis, sclerosing cholangitis (increased unconjugated bilirubin in bile)
Diagnosis
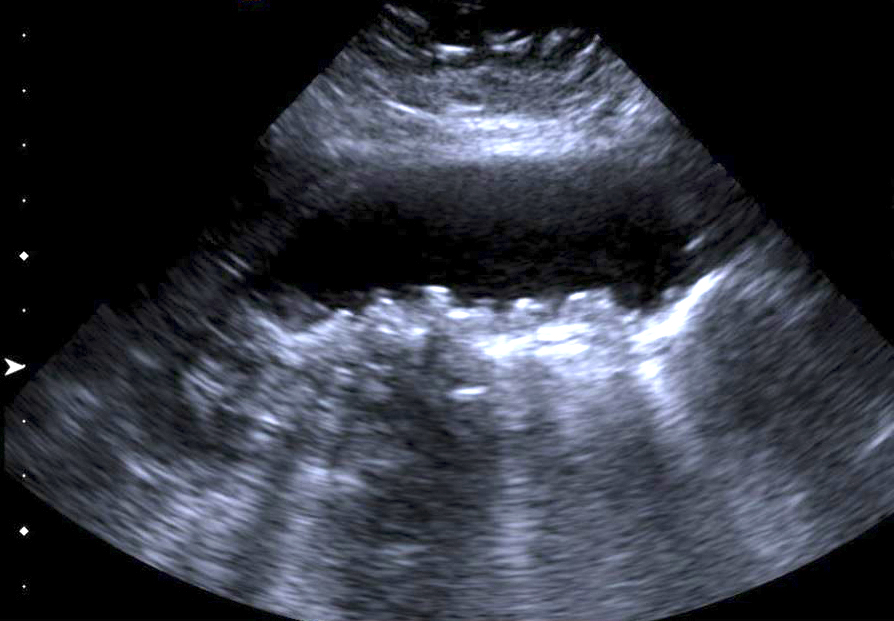
Ultrasound (95% sensitive and specific for gallstones 2 mm or larger or gallbladder sludge), Xrays detect 10 - 25% of gallstones that are radiopaque due to calcium
Treatment
Laparoscopic cholecystectomy if symptomatic or in children, Native Americans, patients with sickle cell disease or porcelain gallbladder, stones 3 cm or larger
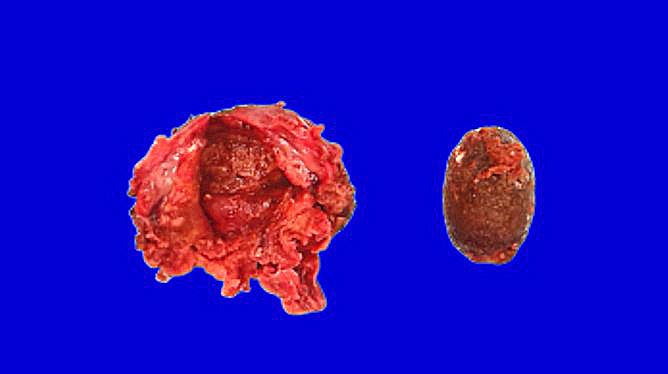
Gross description
85% are 2 cm or less
Cholesterol stones: < 1 cm to 4 cm; single or multiple; white yellow, round / oval with crystalline cut surface
Pigmen stones: multiple shiny black stones, 0.2 to 5 cm, rarely brown in U.S. (more commonly brown in Japan)
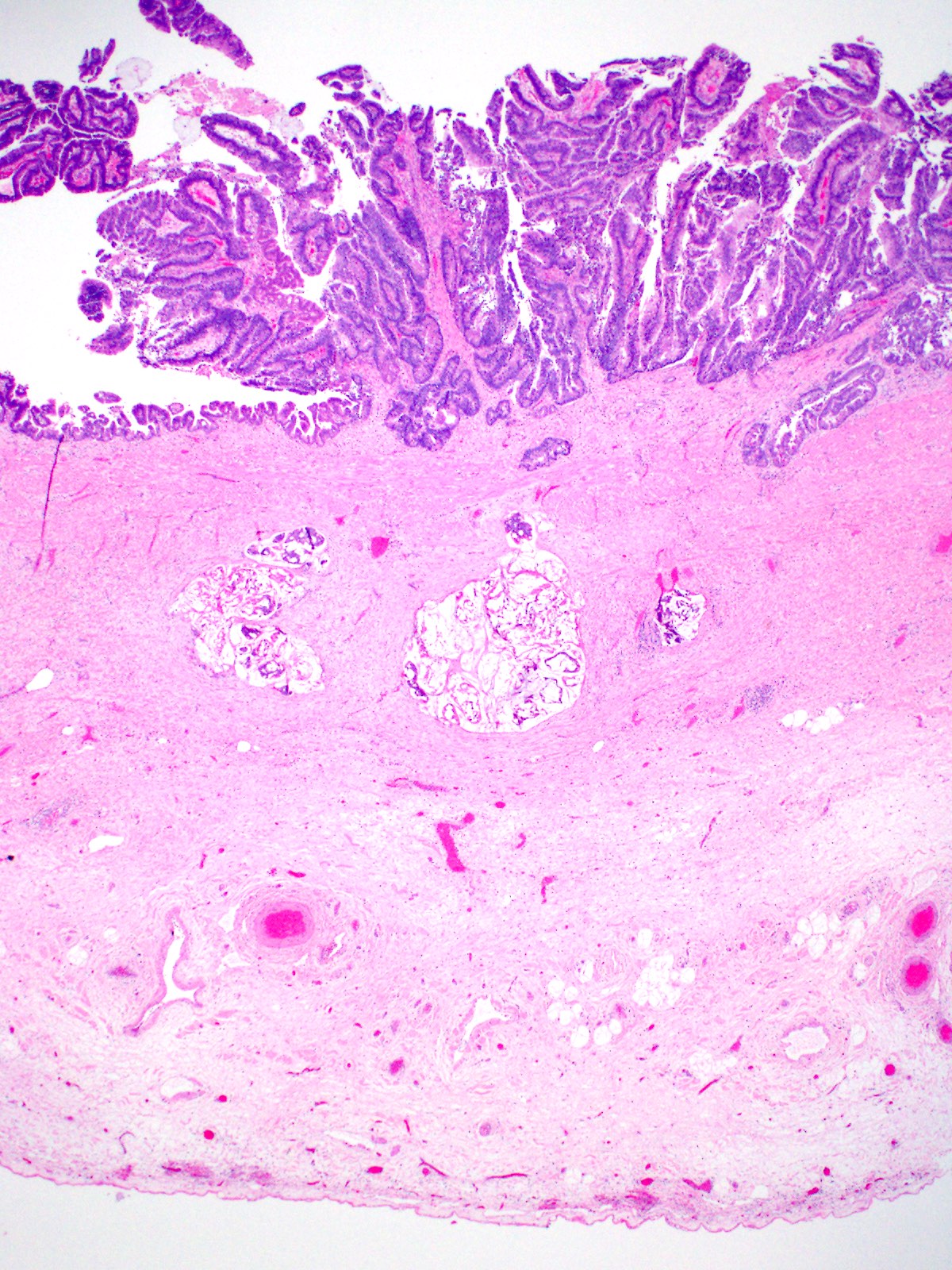
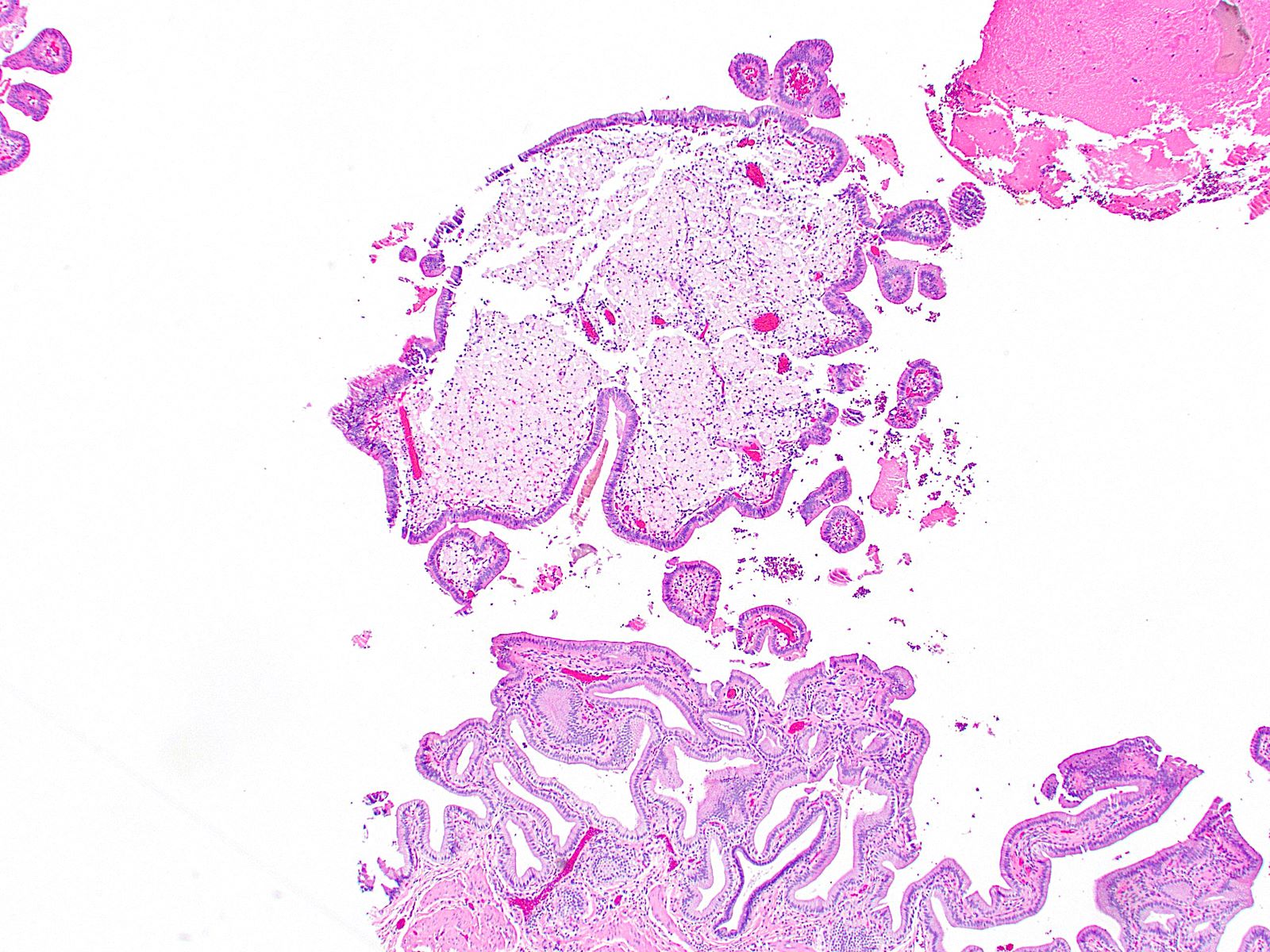
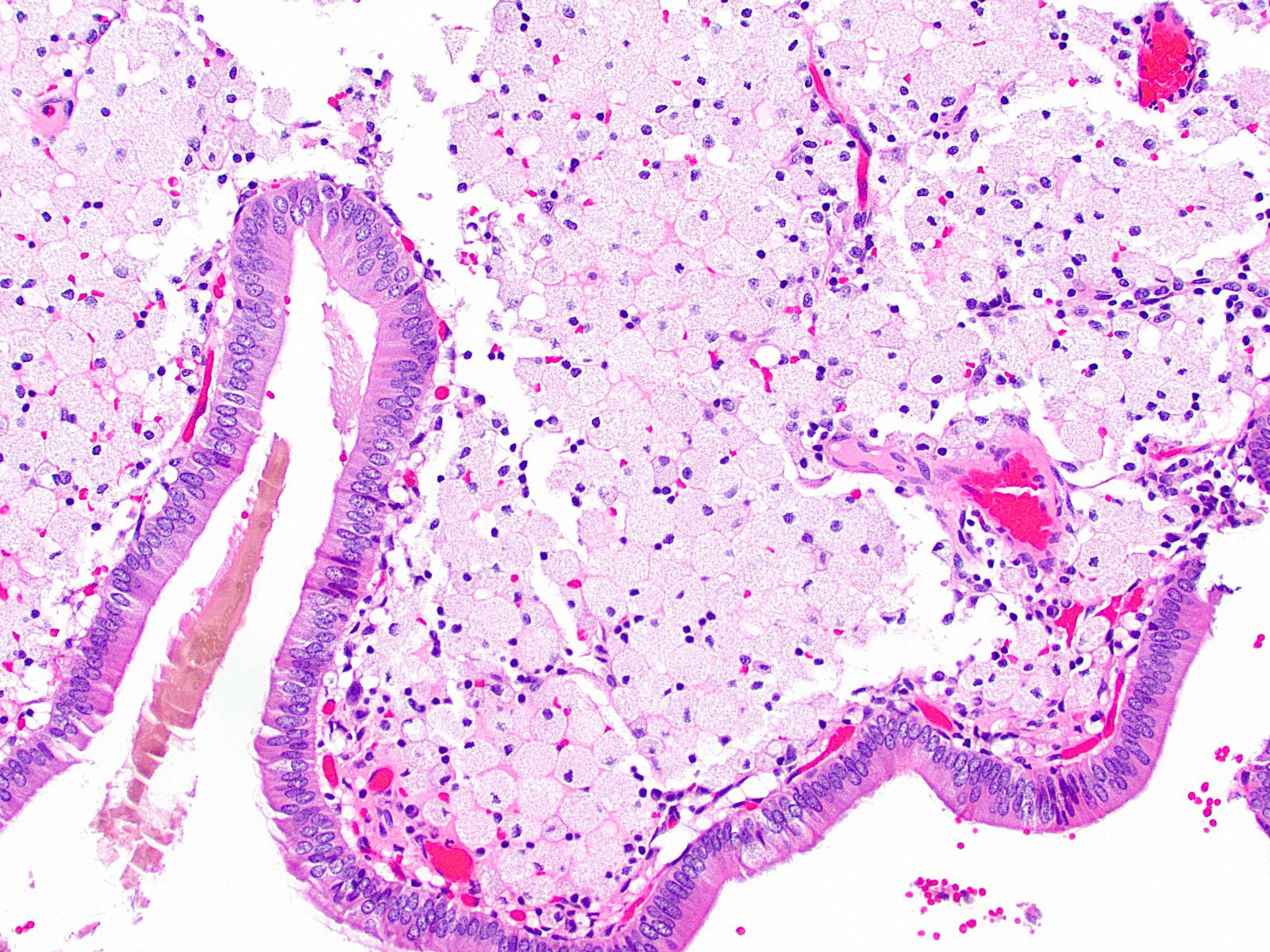
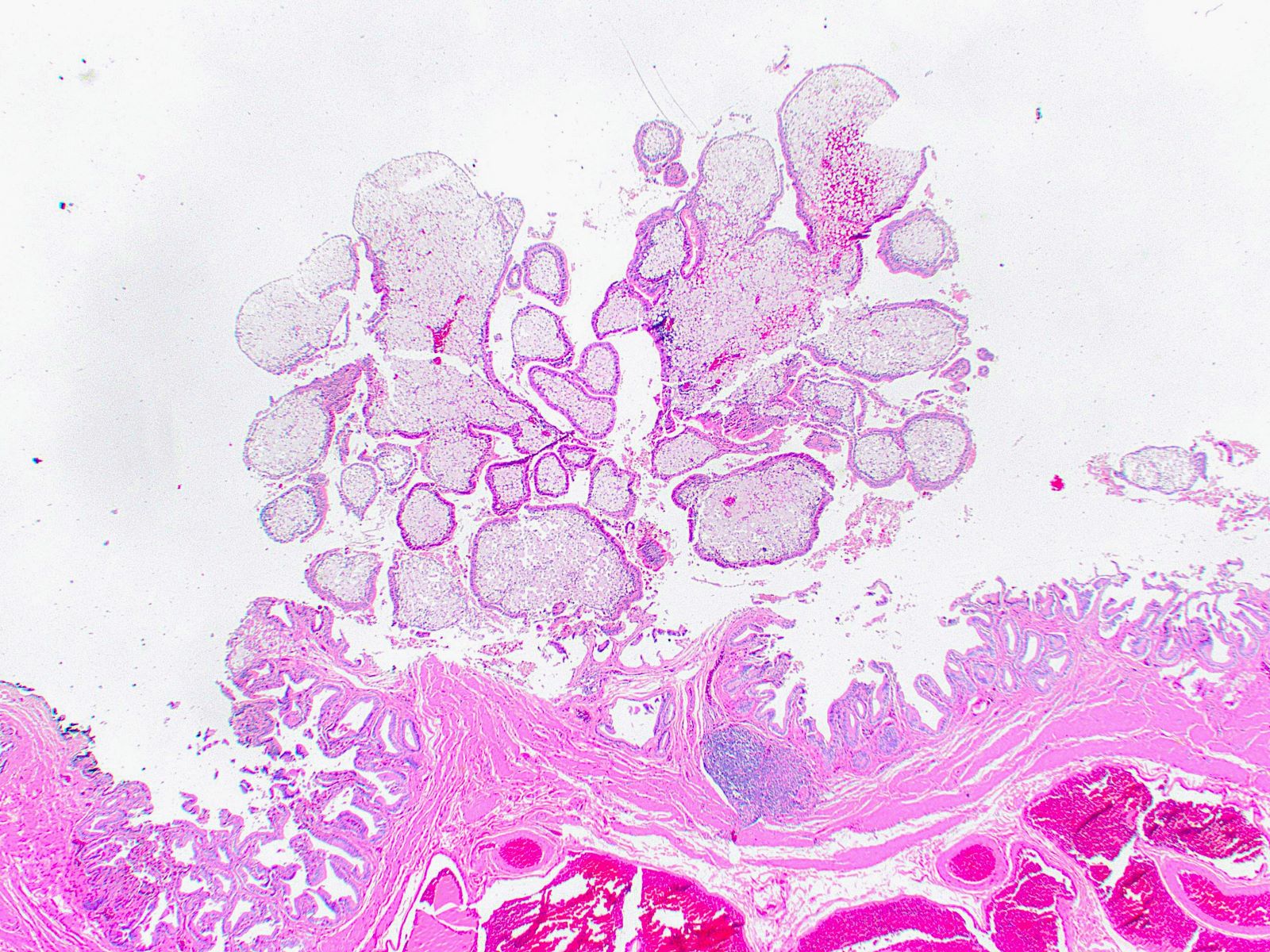
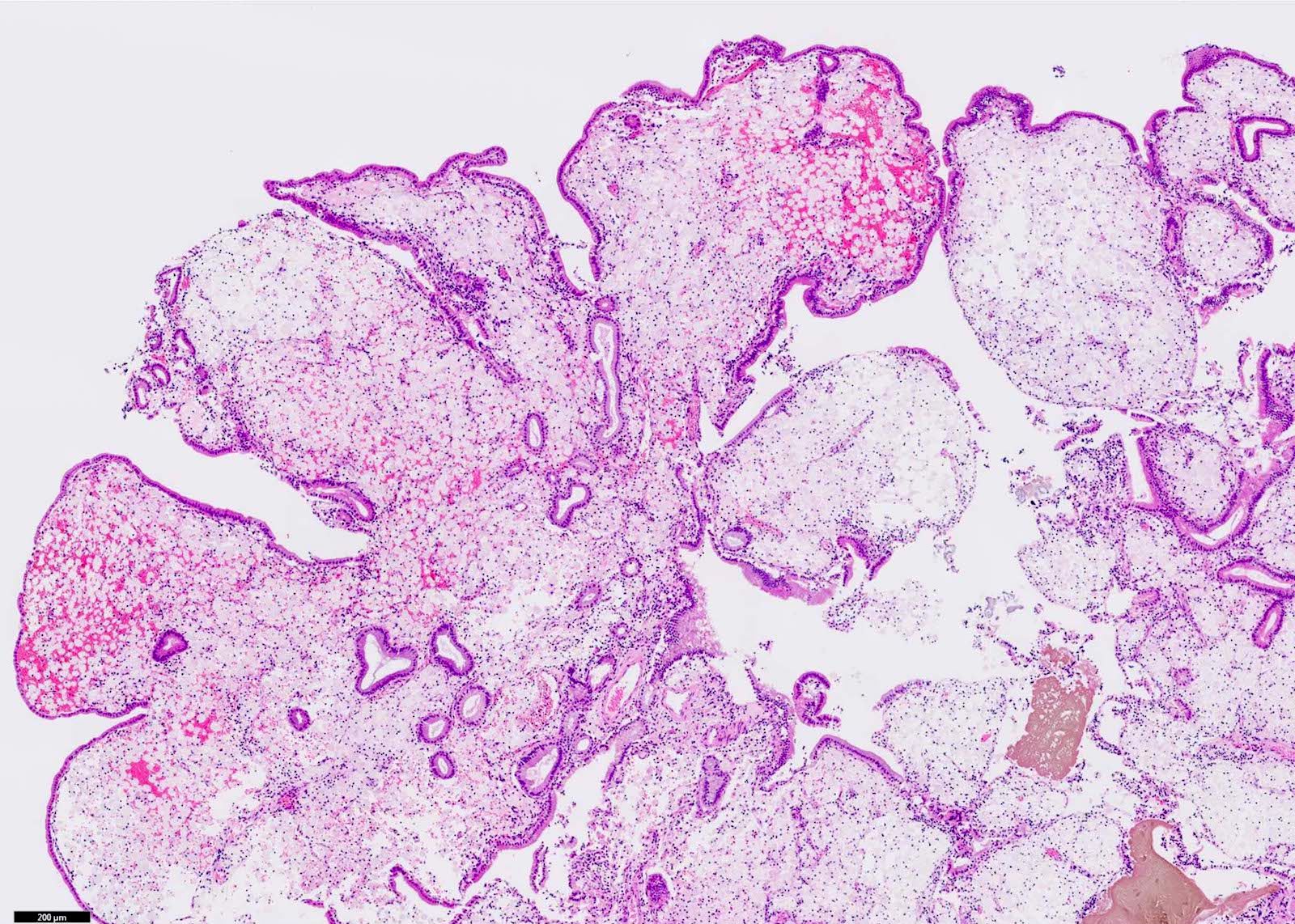
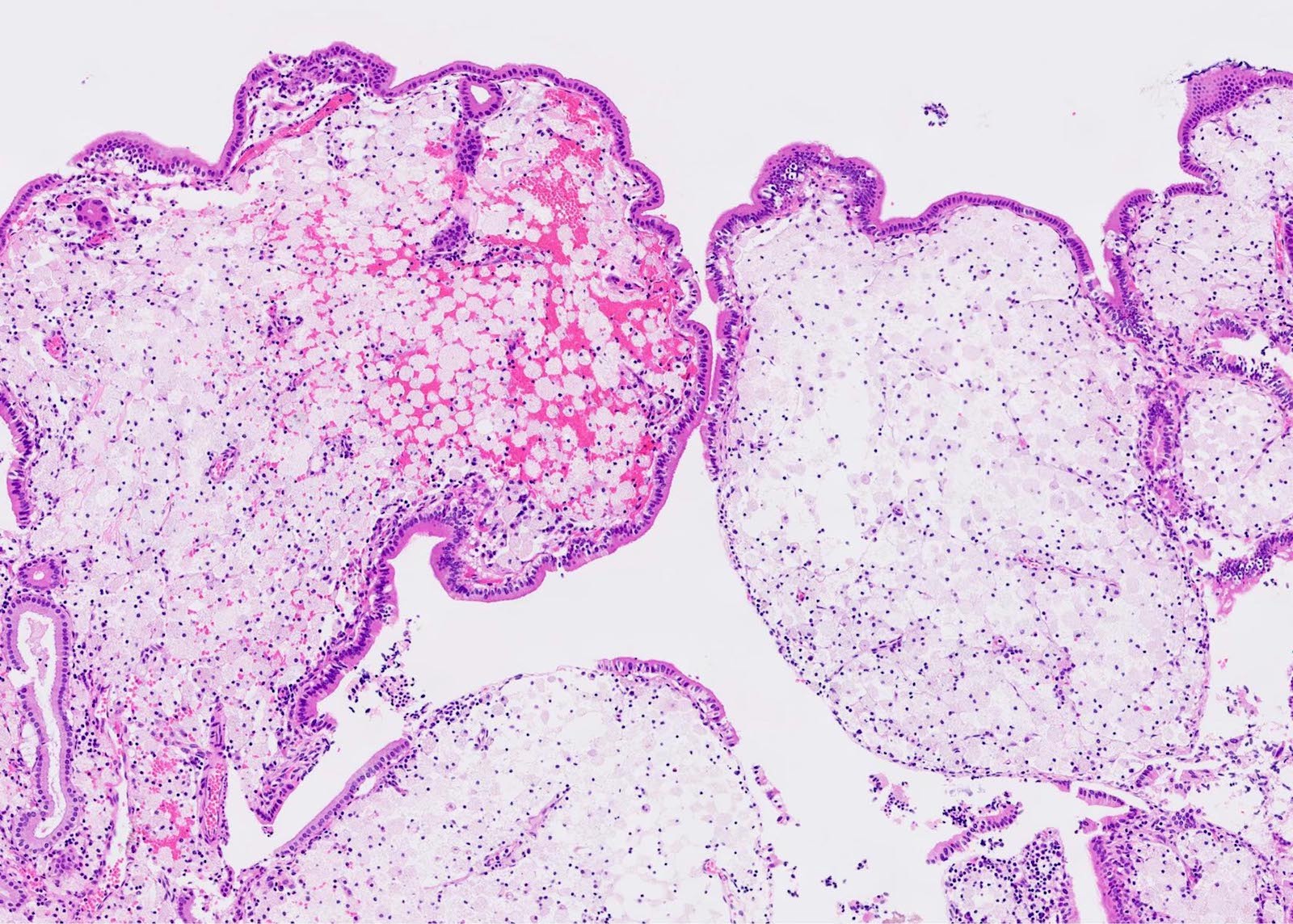
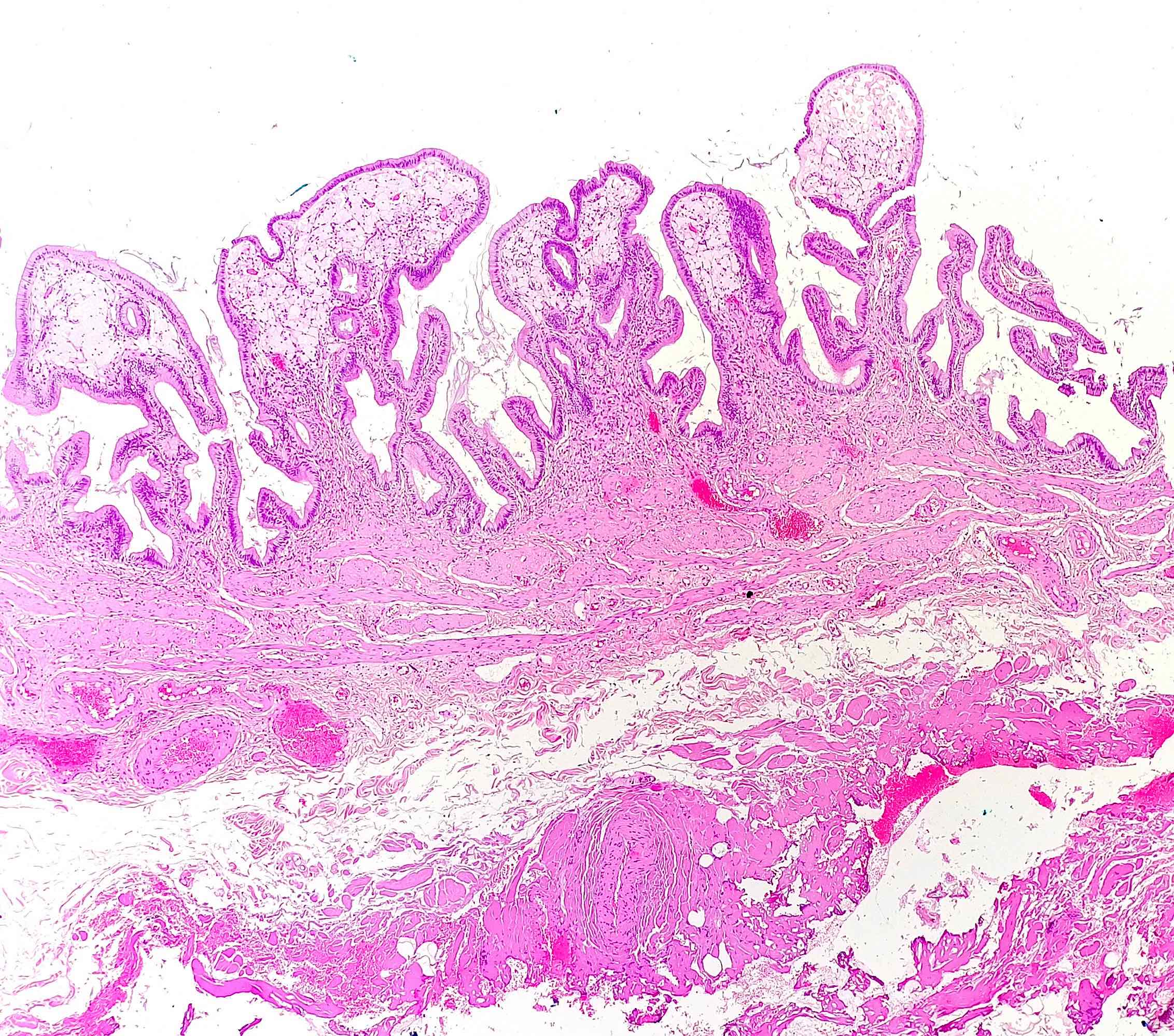
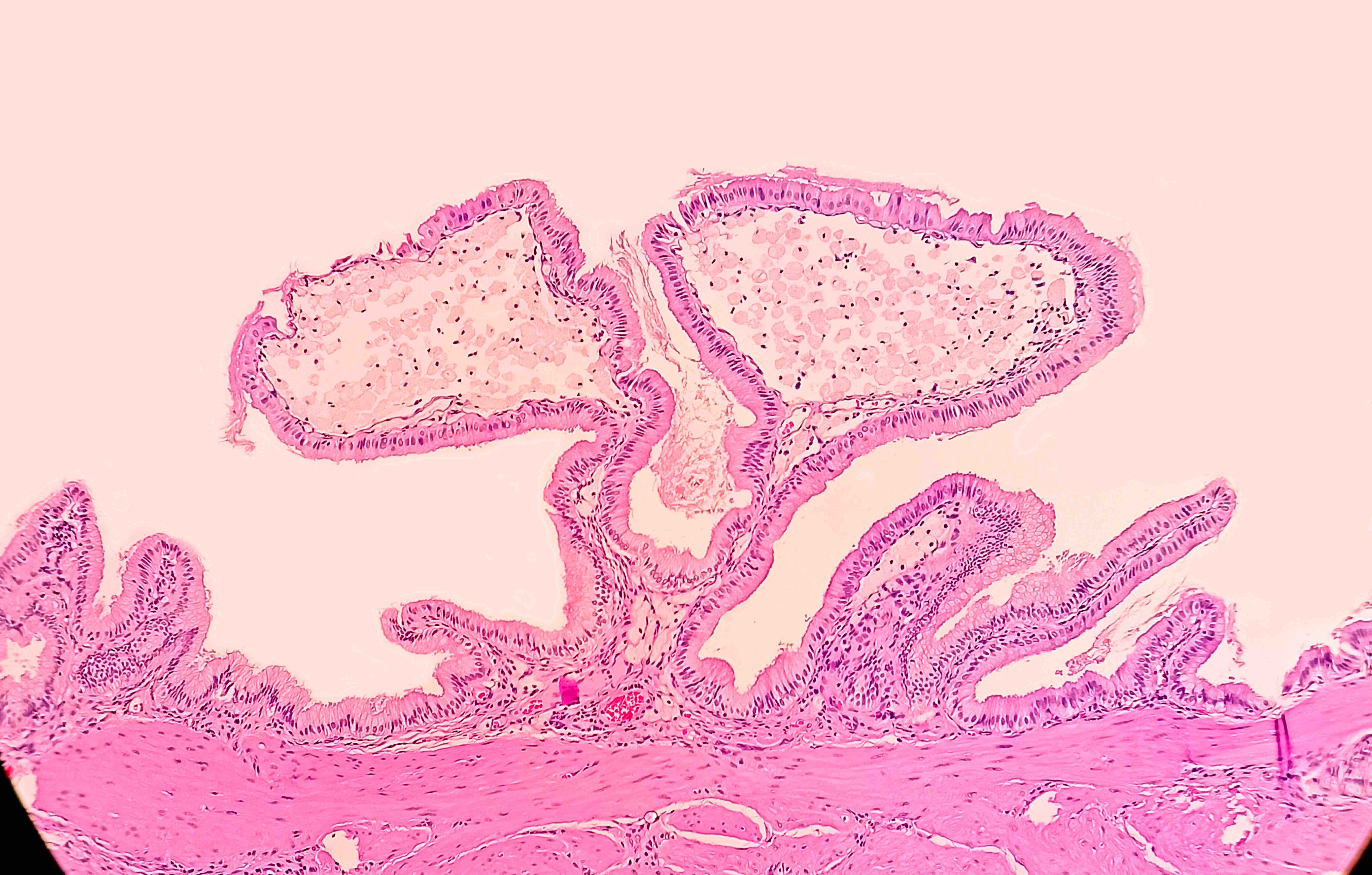
Resorption of the macrophages in a cholesterol polyp leaves behind edematous acellular stroma that might mimic neoplastic polyps (Am J Surg Pathol 2020;44:467)
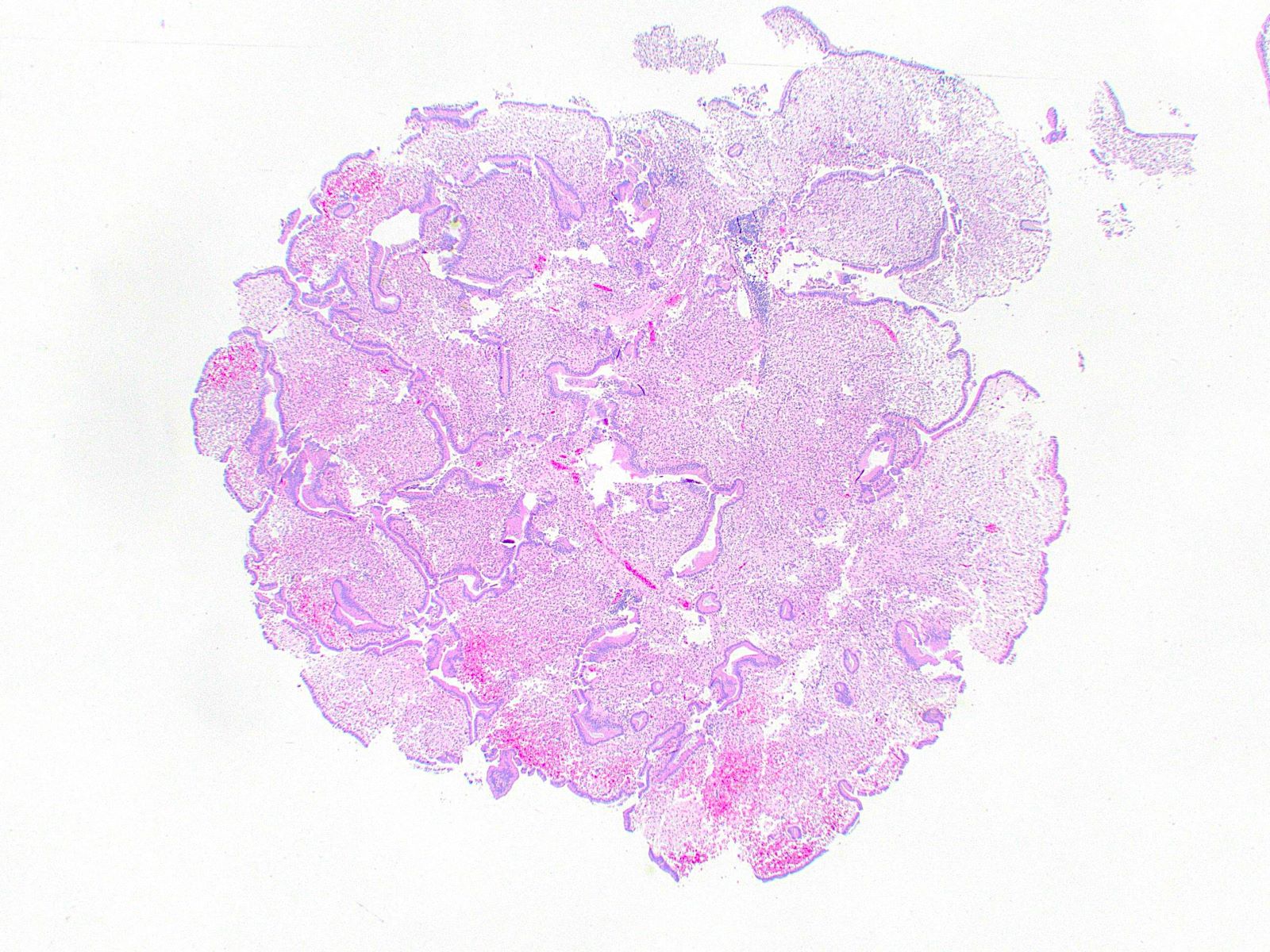
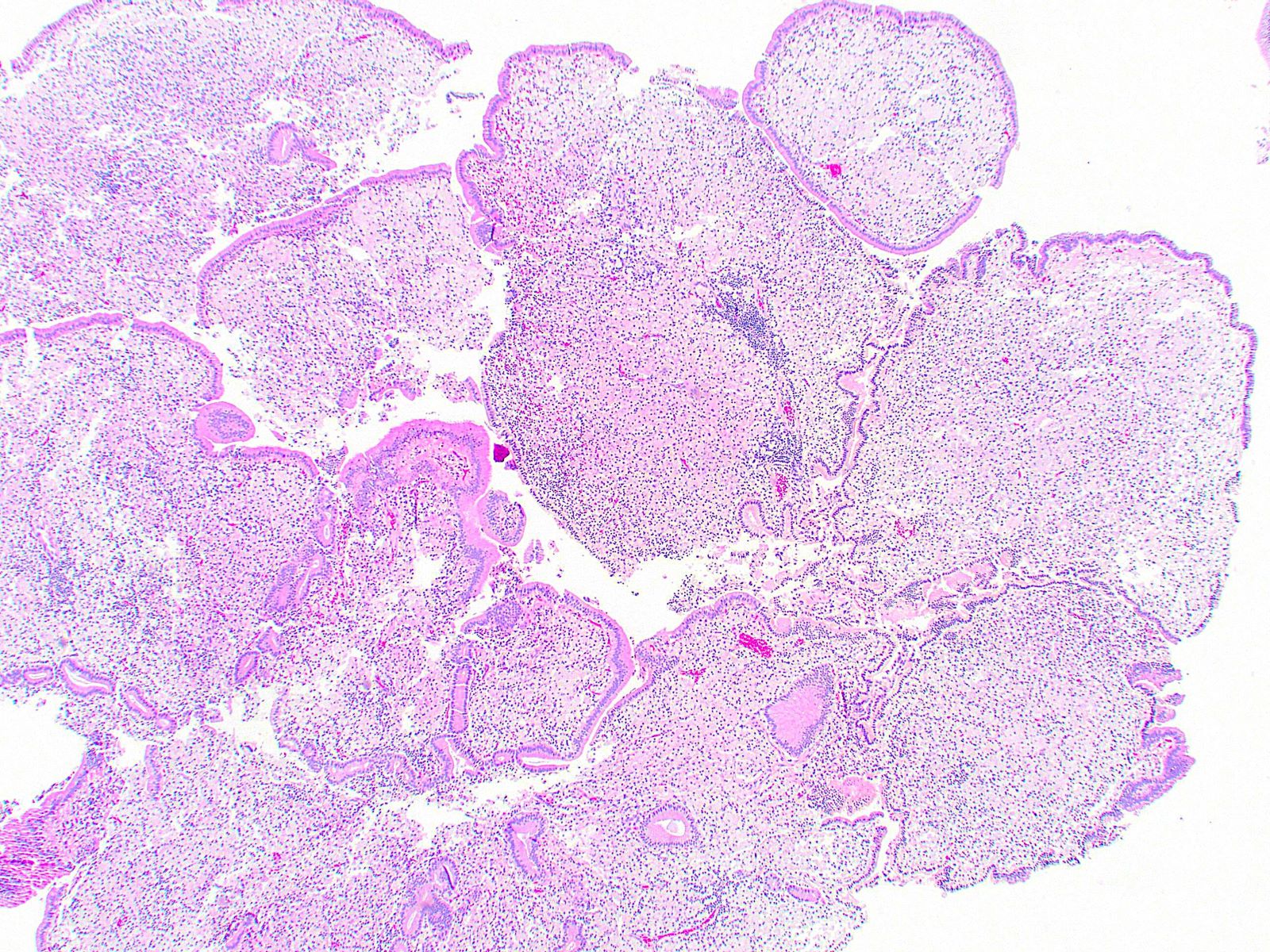
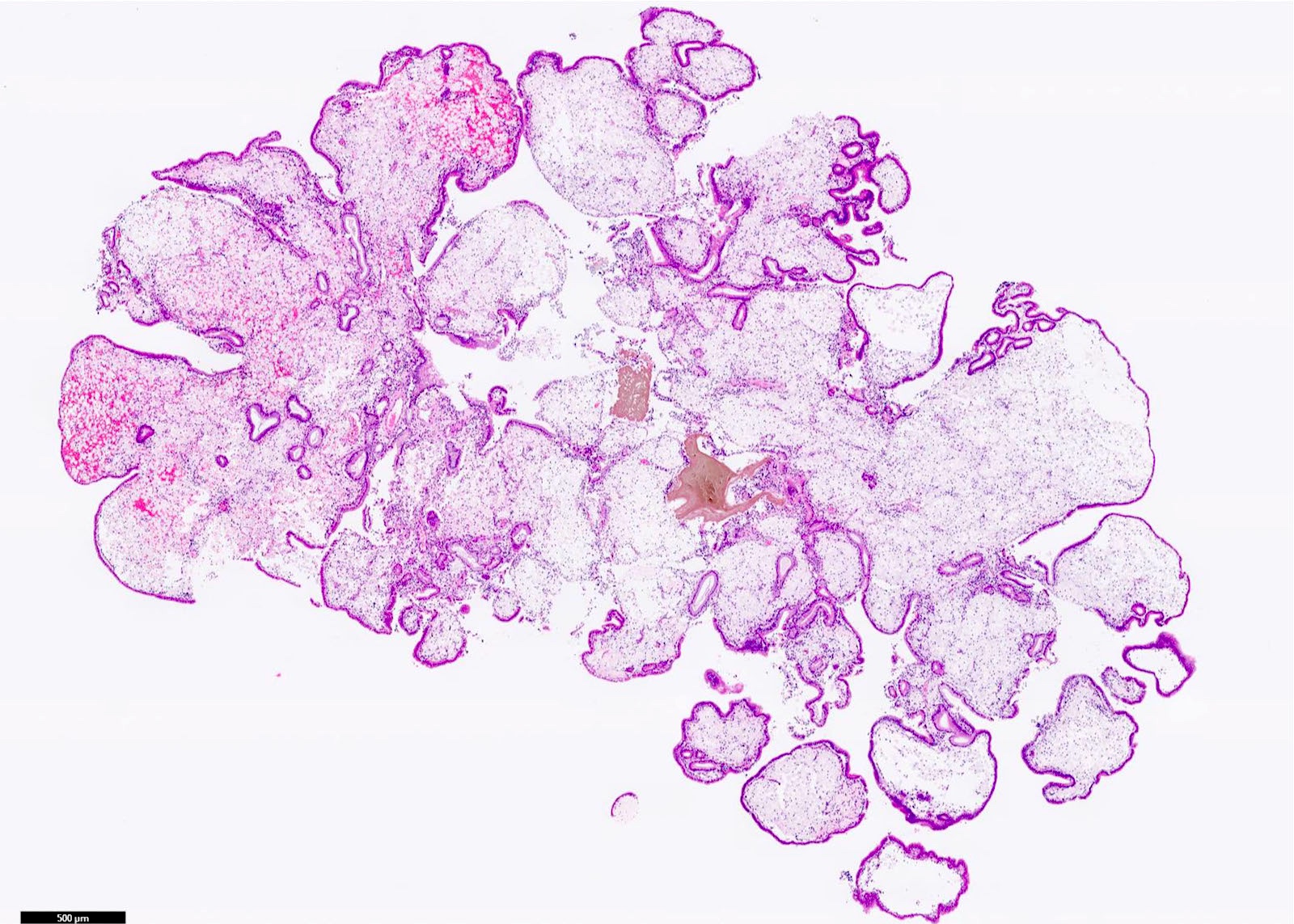
A gallbladder resection specimen is found to contain a polyp with the histologic appearance shown above. What is the diagnosis?
Adenomyomatosis
Cholesterol polyp
Hyperplastic polyp
Inflammatory polyp
Intracholecystic papillary neoplasm
Board review style answer #1
B. Cholesterol polyp. Cholesterol polyps have cauliflower-like architecture and are made of foamy lipid laden macrophages (both features seen in the image provided above). Answer E is incorrect because the polyp lining epithelium is normal biliary epithelium unlike in intracholecystic papillary neoplasms. Answer D is incorrect because the body of the polyp does not show inflammatory cells as in inflammatory polyps. Answer A is incorrect because the body of the polyp does not show hyperplastic smooth muscle as in adenomyomatosis. Answer C is incorrect because the polyp does not show hyperplastic gallbladder epithelium with elongated villi as in hyperplastic polyps.
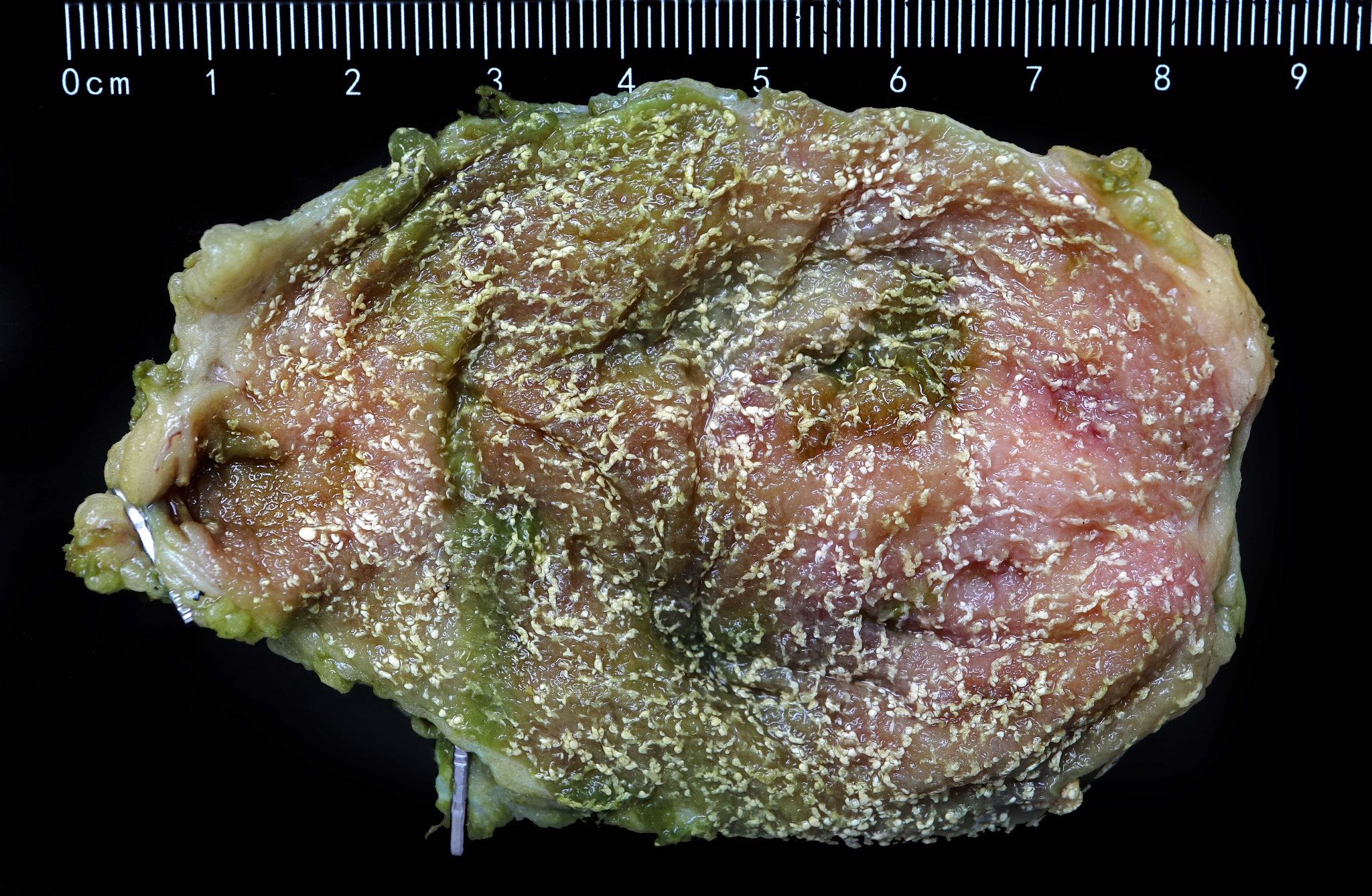
Which of the following is a gross feature of cholesterol polyps of the gallbladder?
Most are > 1 cm
Most are sessile
The surface exhibits a gritty texture
They are usually solitary
They exhibit a yellowish color
Board review style answer #2
E. They exhibit a yellowish color. Answer C is incorrect because cholesterol polyps have a smooth yellowish surface. Answer B is incorrect because most are pedunculated. Answer A is incorrect because most are < 1 cm. Answer D is incorrect because multiple / multifocal cholesterol polyps often coexist.
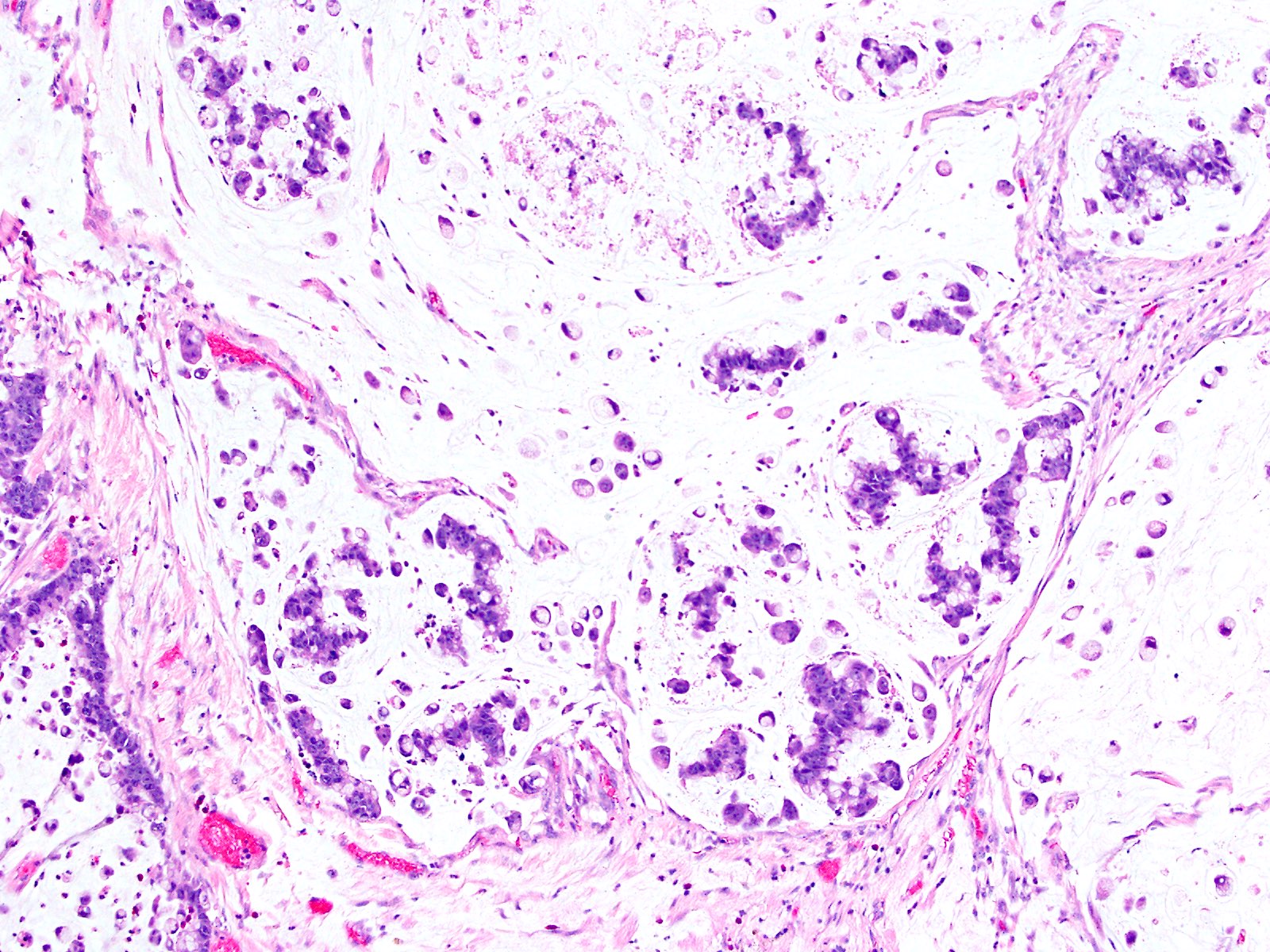
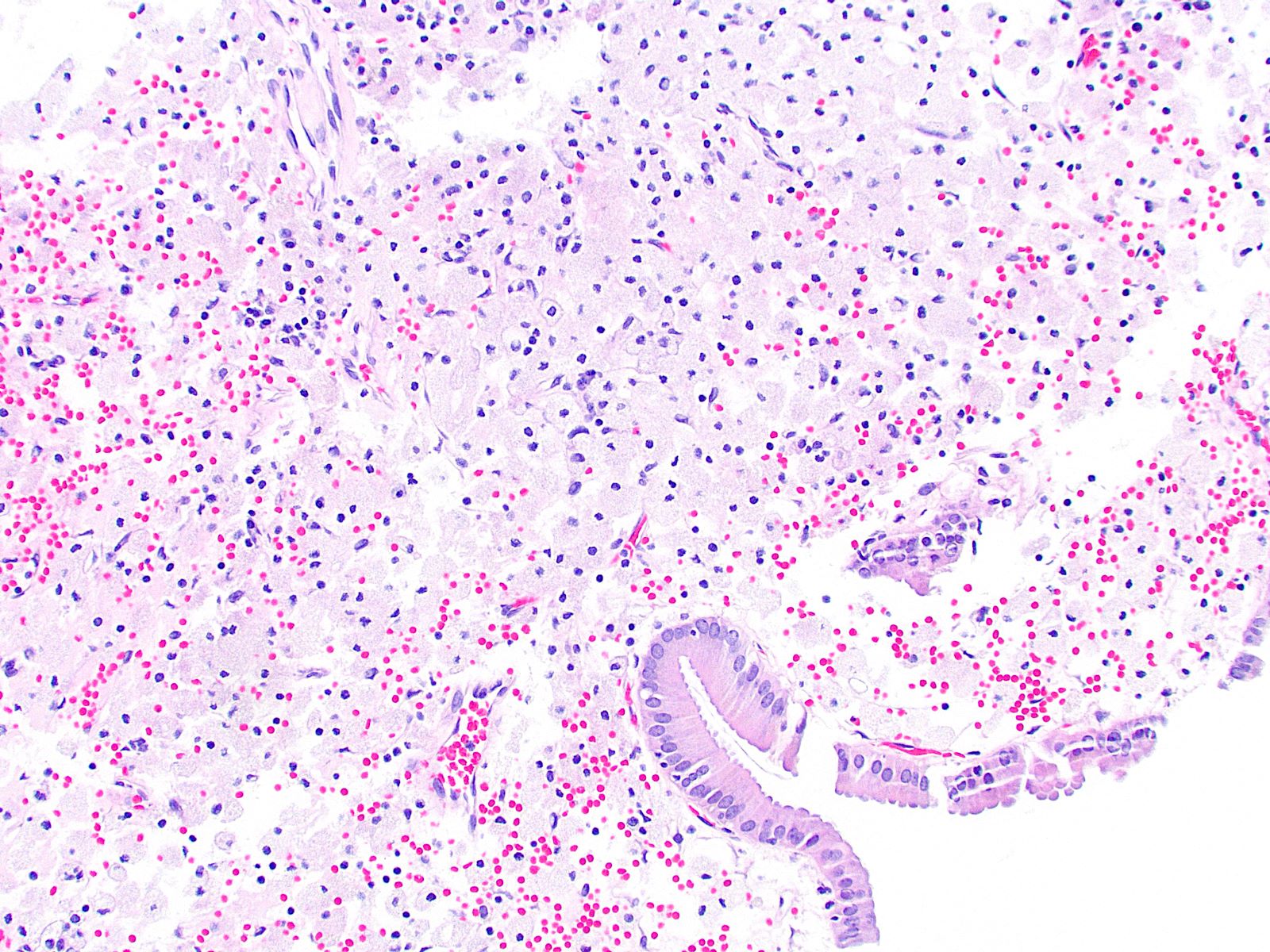
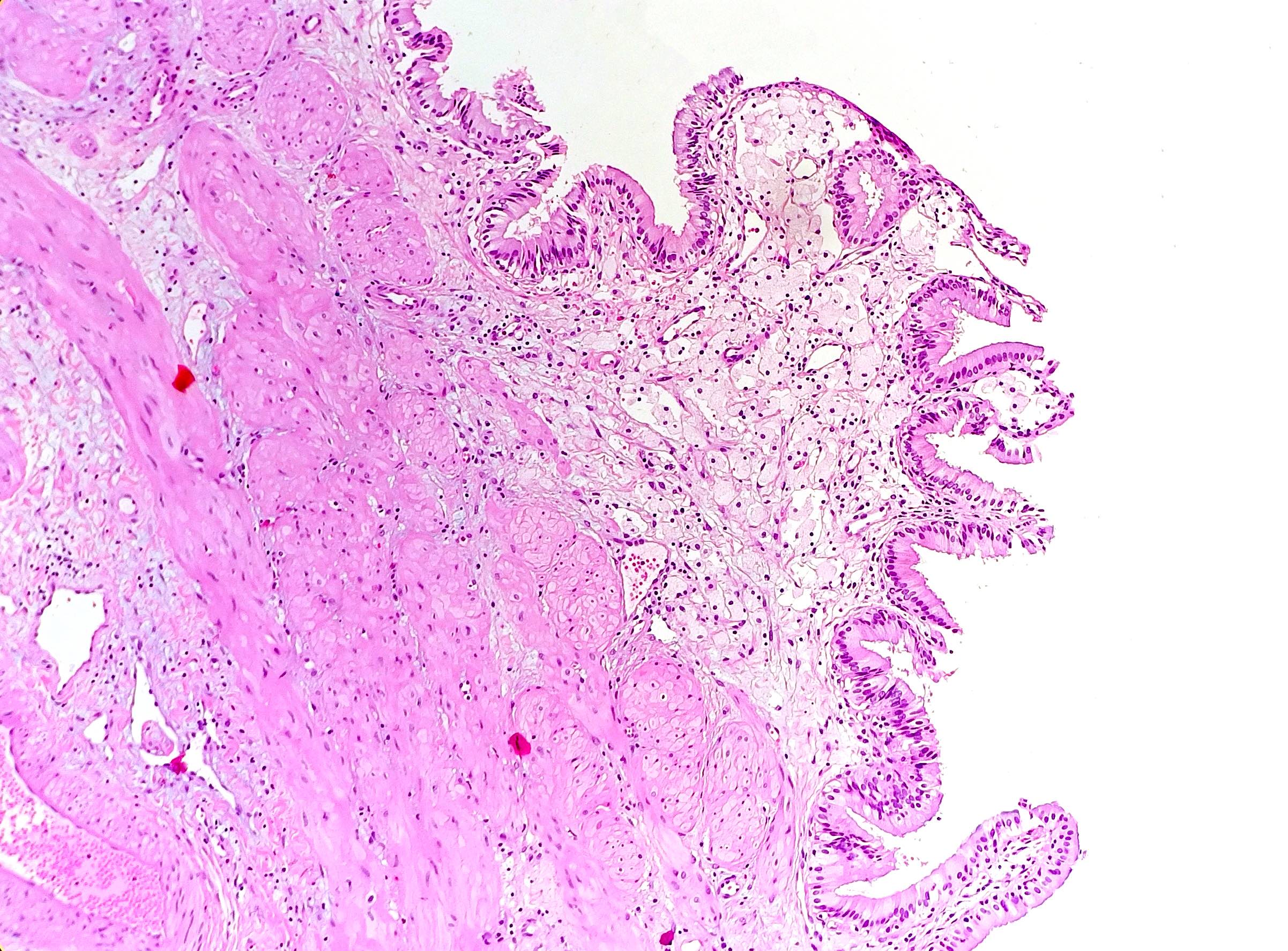
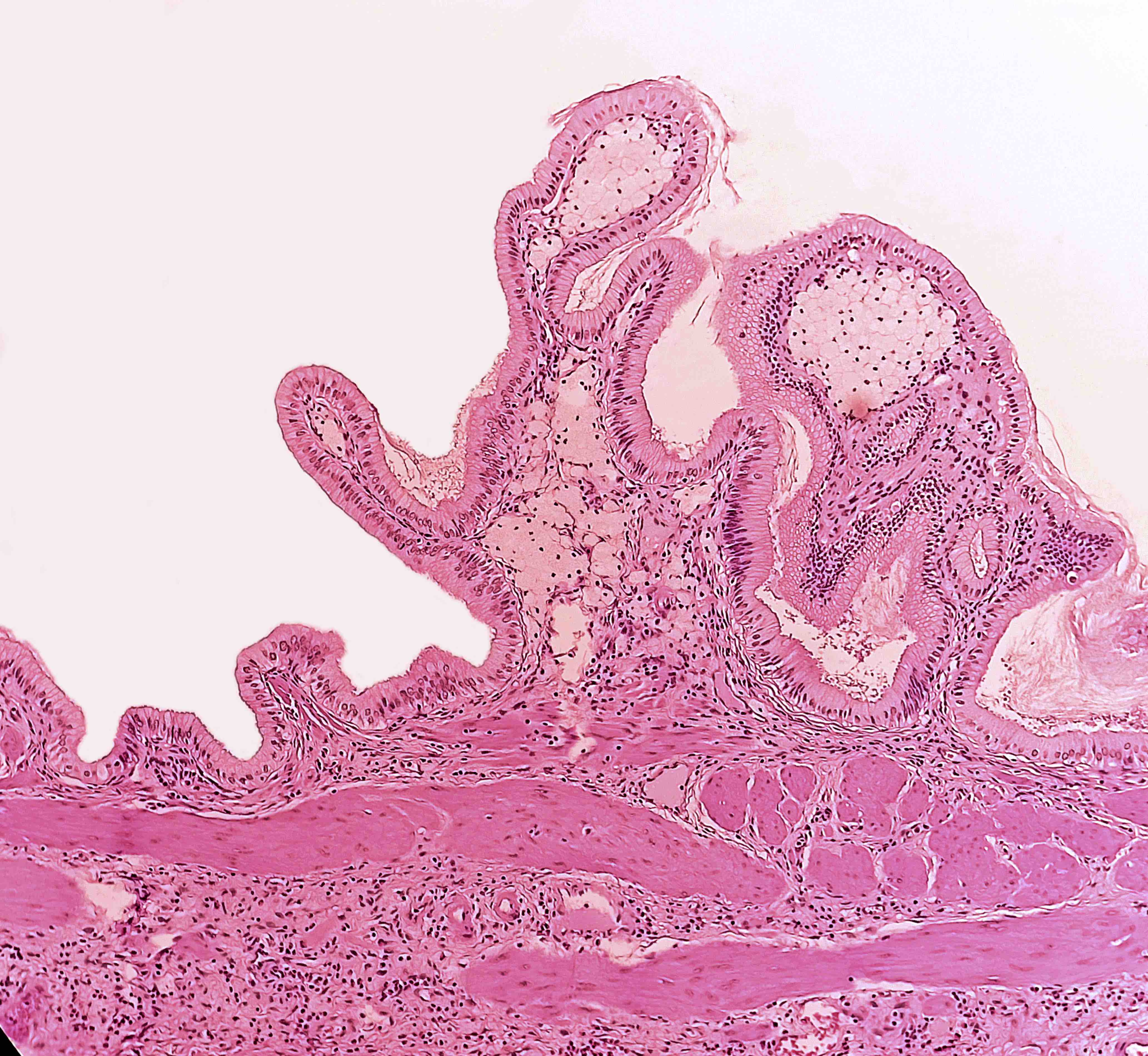
Accumulation of lipids (triglycerides, cholesterol precursors and cholesterol esters) within subepithelial macrophages in the lamina propria of the gallbladder (J Ultrasound 2021;24:131)
Bile is supersaturated with cholesterol in both cholesterolosis and gallstone disease, perhaps due to excess bile production
Patients who are unable to fully solubilize cholesterol will form cholesterol gallstones
Patients who are able to keep cholesterol fully solubilized may have increased mucosal cholesterol uptake and develop cholesterolosis (J Clin Pathol 1987;40:524)
This likely occurs in patients with increased acyl-CoA cholesterol ester acyltransferase activity in gallbladder mucosa (Am J Gastroenterol 1998;93:1518)
The enzyme causes increased synthesis of cholesterol esters, which accumulate in mucosal macrophages (Am J Gastroenterol 1998;93:1518)
Incidentally found during abdominal sonography (appears as a pseudopolyp; see Radiology description for details) or diagnosed on histopathology of surgical specimens (J Ultrasound 2021;24:131)
Microscopic examination provides the definitive diagnosis
Cholesterolosis may form pseudopolyps that appear as single or multiple hyperechoic parietal foci generating comet tail artifacts (J Ultrasound 2021;24:131)
A variant of chronic cholecystitis, with lipid laden macrophages and acute and chronic inflammatory cells in the wall of the gallbladder (World J Radiol 2016;8:183)
Poorly defined benign entity characterized by mucosal hyperplasia including elongated villi, sometimes with metaplastic changes but never with dysplasia; macrophages are not part of this process
Board review style question #1
The lesion shown above is observed during microscopic examination of a cholecystectomy specimen. Which of the following is most likely true?
The lesion caused severe clinical symptoms
The lesion has a high risk of progression to malignancy
The patient is female
The patient is very thin
Board review style answer #1
C. The patient is female. Cholesterolosis tends to occur in overweight female patients. It is generally asymptomatic and has no risk of progression to malignancy.
Which of the following is the most likely pathophysiologic cause of gallbladder cholesterolosis?
Increased synthesis and deposition of cholesterol esters
Infiltration of macrophages due to subclinical infection
Mucosal irritation due to longstanding inflammation
Slow degradation and absorption of gallstones
Board review style answer #2
A. Increased synthesis and deposition of cholesterol esters. Cholesterolosis appears to occur when excess bile is converted to cholesterol esters via acyl-CoA cholesterol ester acyltransferase. The esters are then stored in mucosal macrophages. Choleliths, inflammation and infection do not play a role in the development of cholesterolosis.
Chronic inflammation of the gallbladder, typically secondary to gallstones
Essential features
The most common disease of the gallbladder, typically secondary to cholelithiasis
Variety of histologic findings, including variable amounts of mononuclear cell predominant inflammation, mucosal changes including metaplasia, muscular hypertrophy and transmural fibrosis
Rokitansky-Aschoff sinuses and ducts of Luschka should not be mistaken for invasive adenocarcinoma
Typically related to cholelithiasis, either through direct mucosal irritation or via intermittent mechanical obstruction with associated alteration of bile chemistry
Altered mechanics of gallbladder emptying plays crucial role
Risk factors correspond to those that increase risk of cholelithiasis: female sex, obesity, rapid weight loss, pregnancy, advanced age (Gastroenterol Nurs 2016;39:297)
44 year old man with gallstones and chronic cholecystitis revealing metachronous gallbladder metastasis from renal clear cell carcinoma (ANZ J Surg 2019 Jun 23 [Epub ahead of print])
45 year old woman with porcelain gallbladder secondary to chronic cholecystitis, without adenocarcinoma (Mymensingh Med J 2019;28:694)
53 year old man with history of colorectal adenocarcinoma with progressively elevating CEA secondary to chronic cholecystitis (J Surg Case Rep 2019;2019:rjz138)
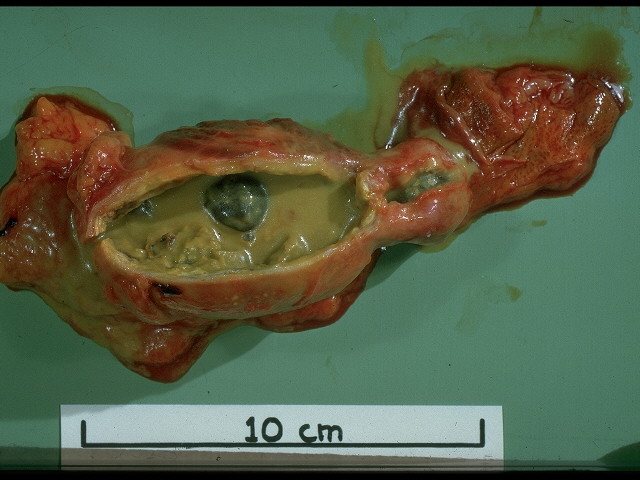
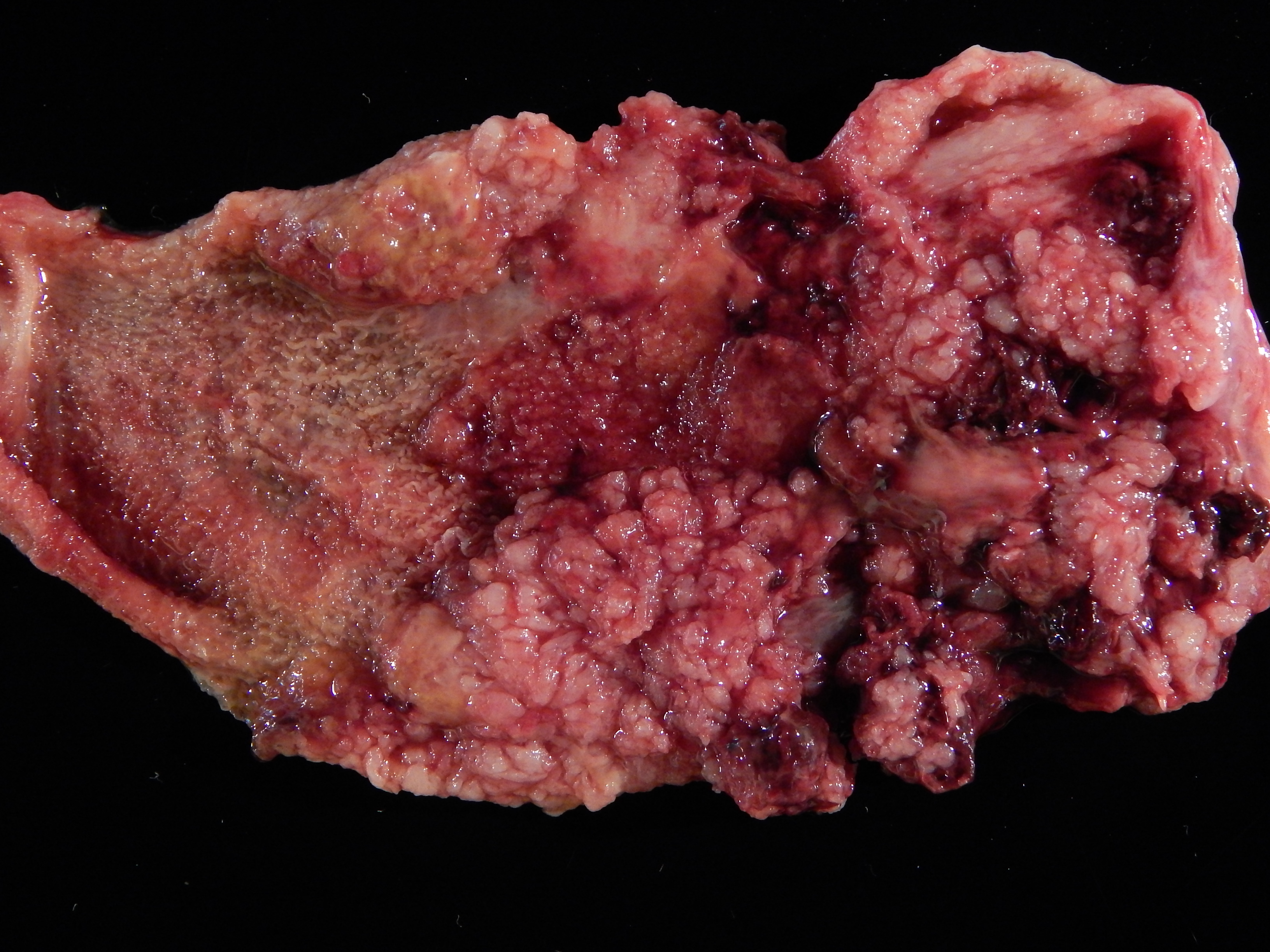
Gallbladder may appear shrunken due to marked fibrosis
Severe cases show adhesions to adjacent organs
Variable mucosal appearance: can be granular, ulcerated, polypoid
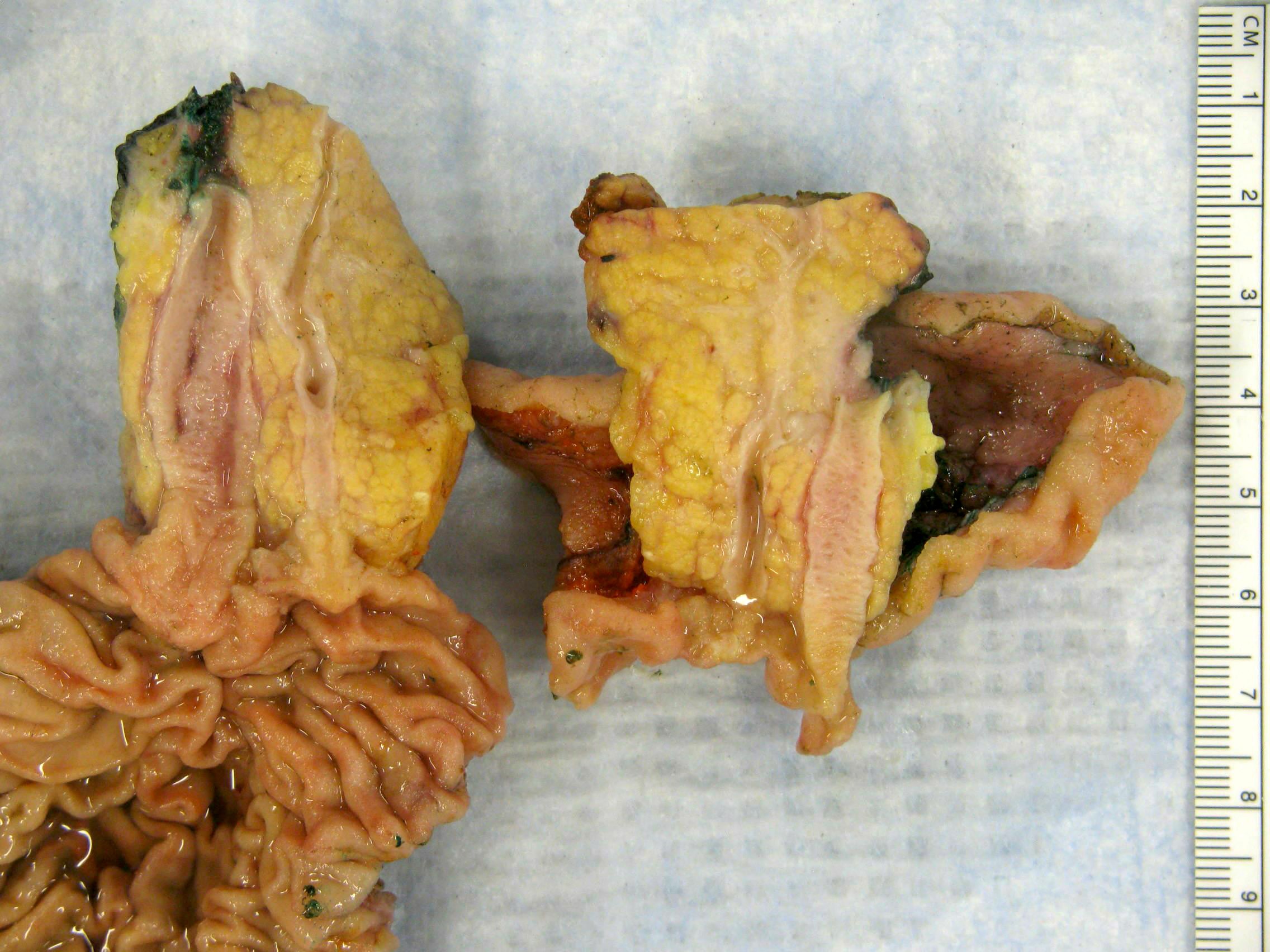
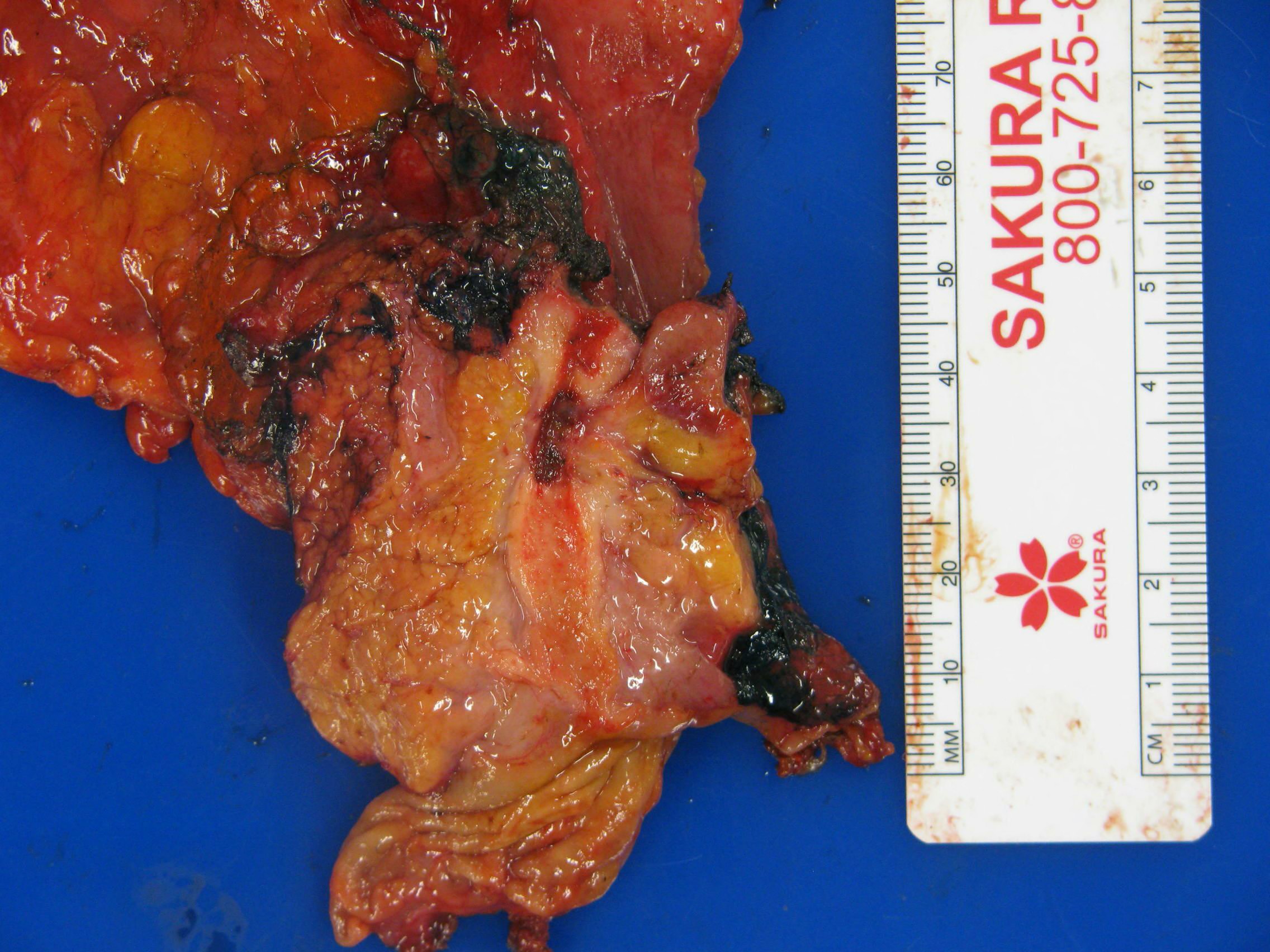
Gross images
Contributed by Kelsey E. McHugh, M.D.
Contracted gallbladder with stones
Distended gallbladder with stones
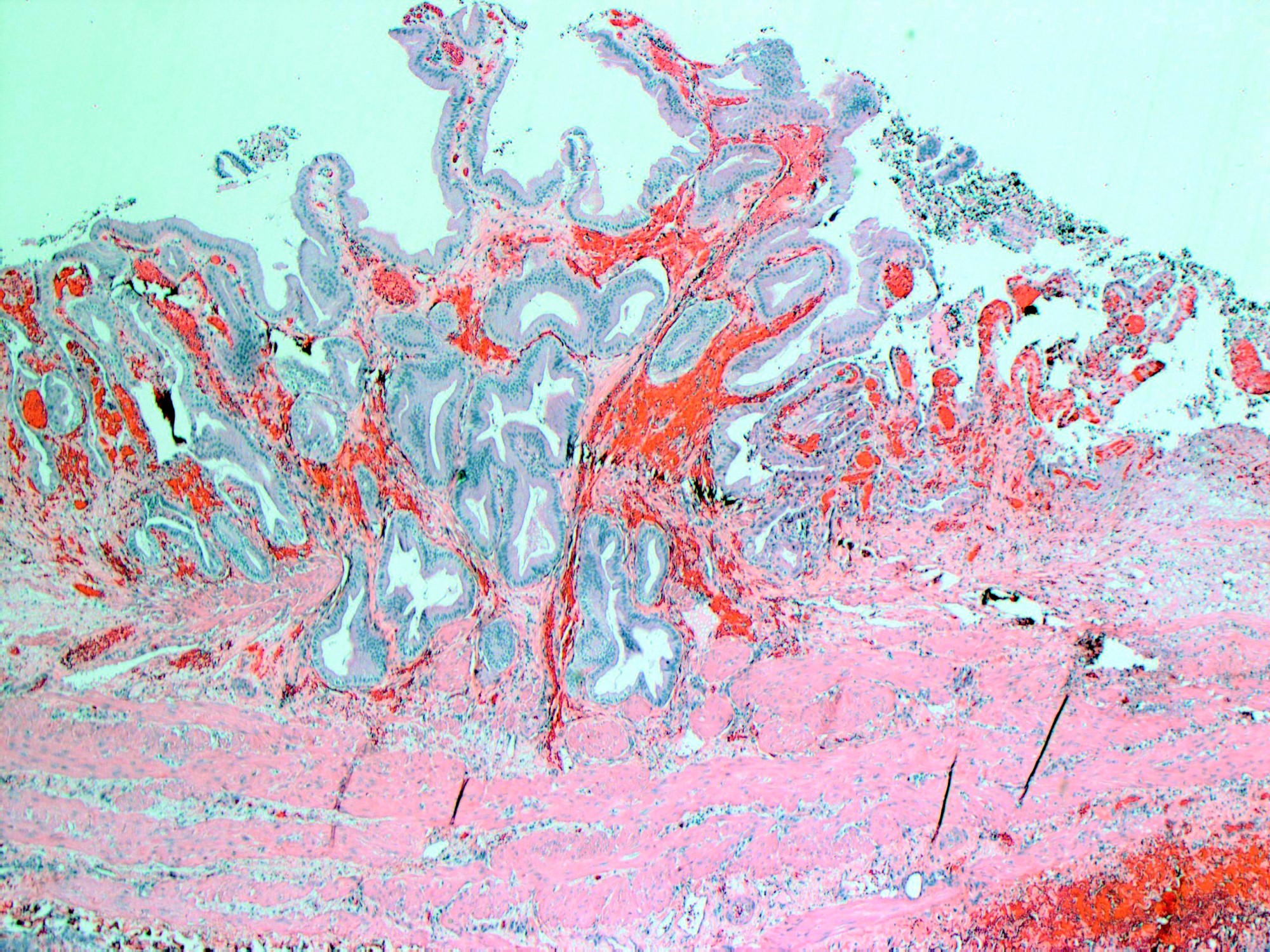
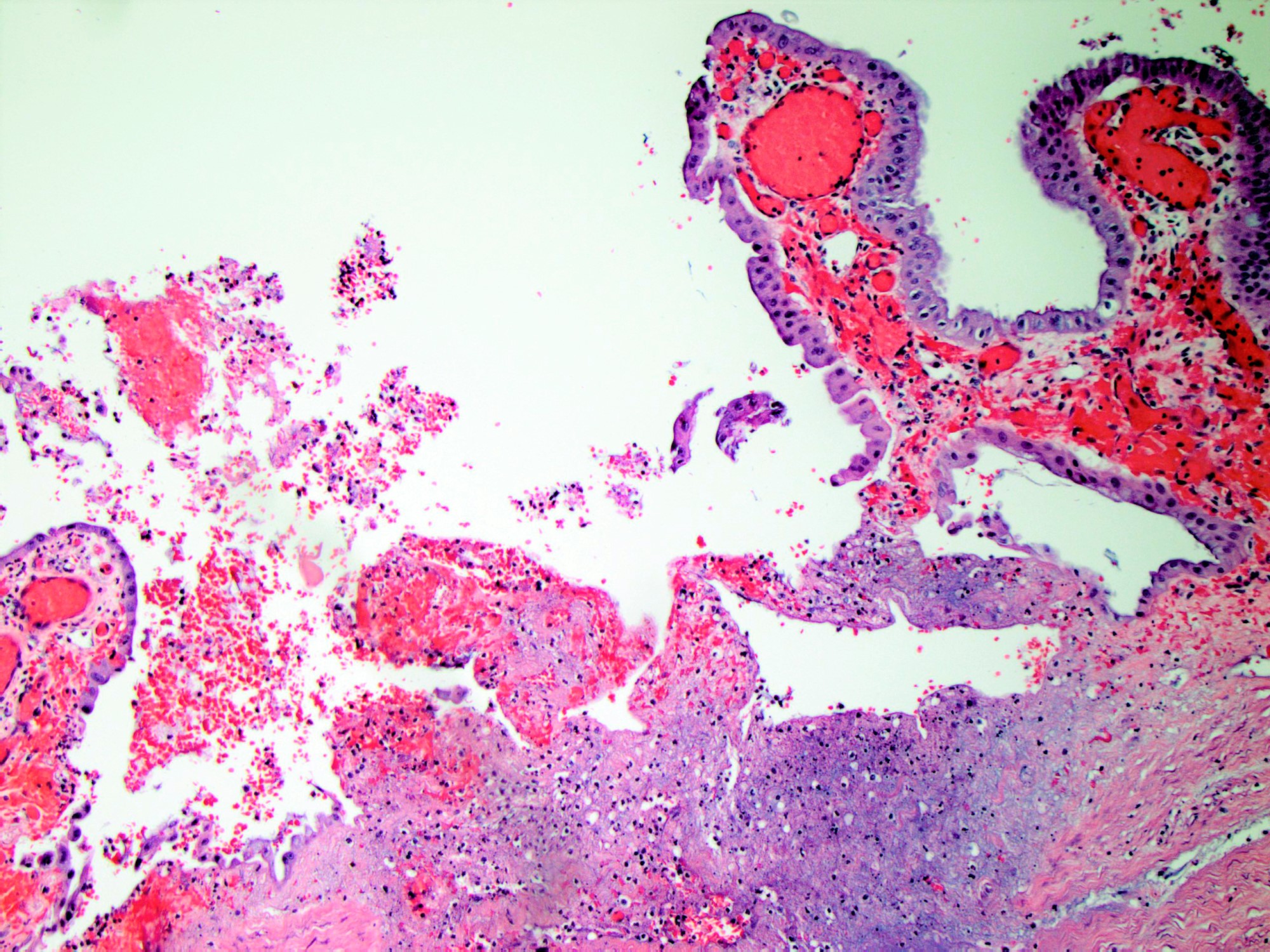
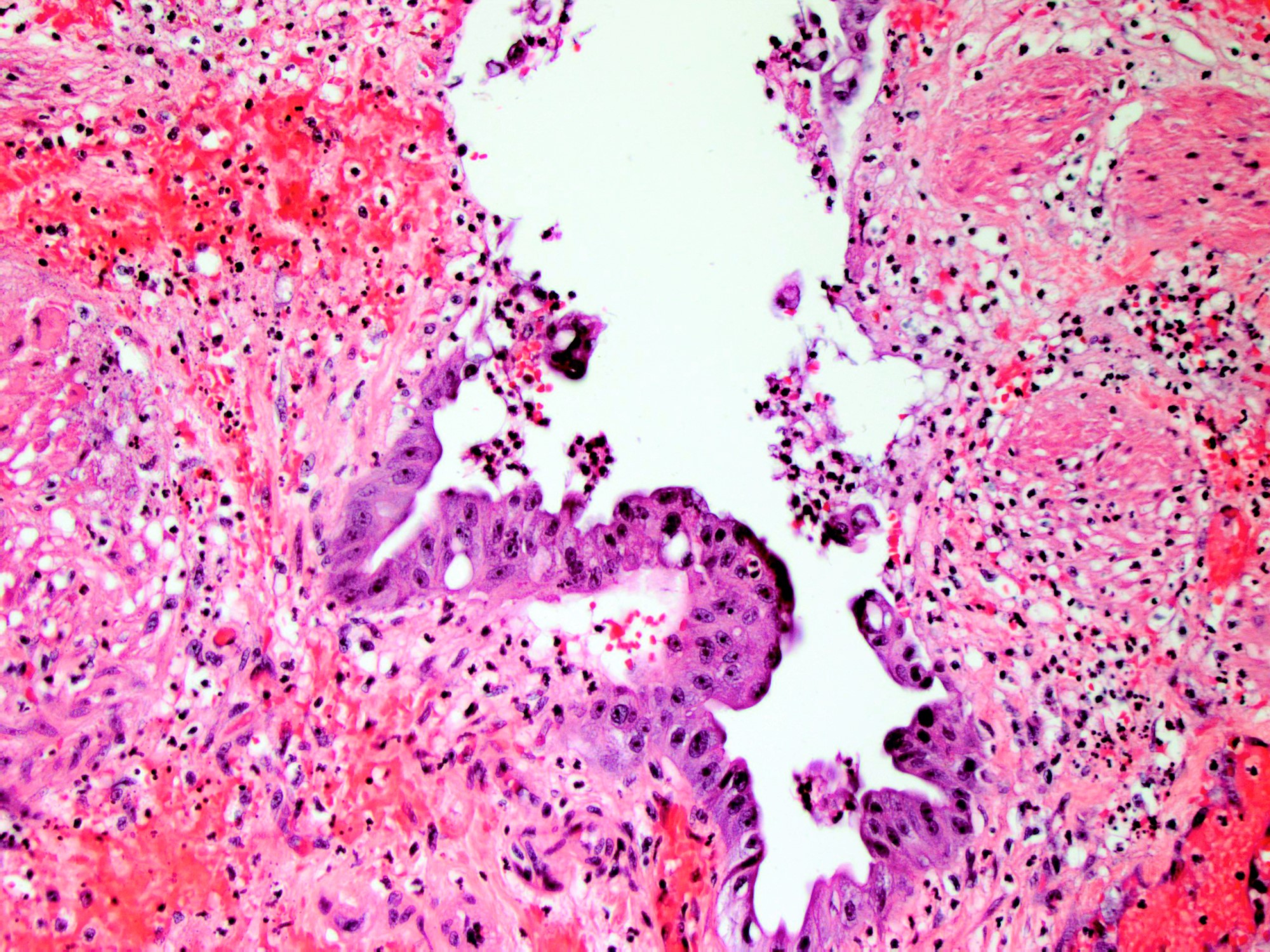
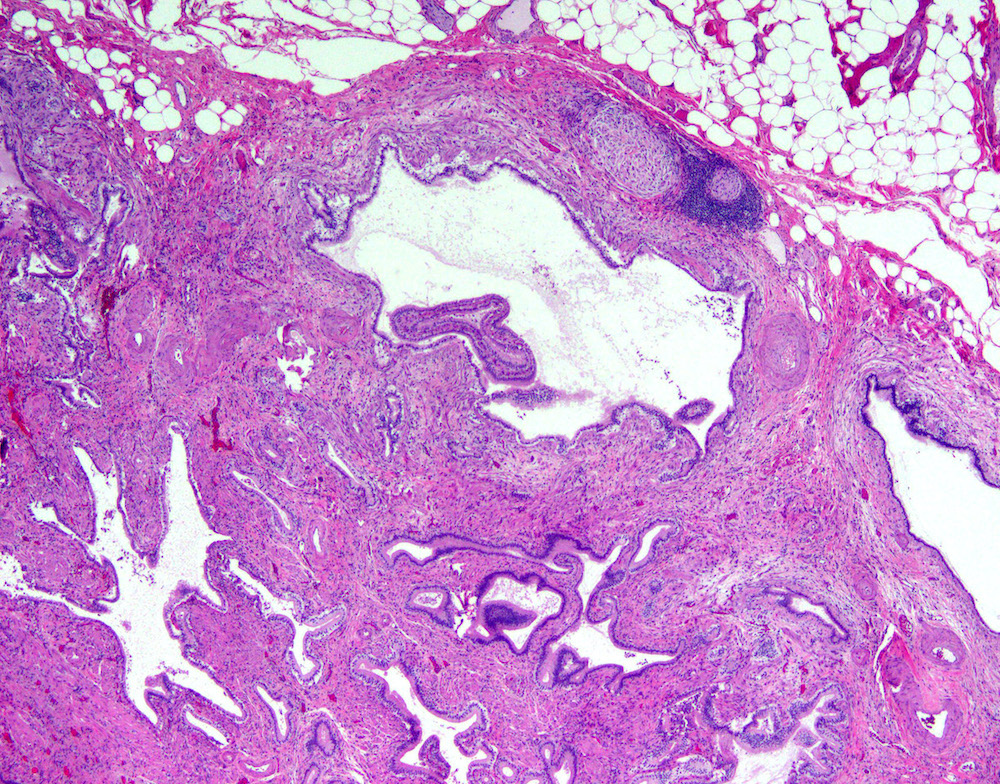
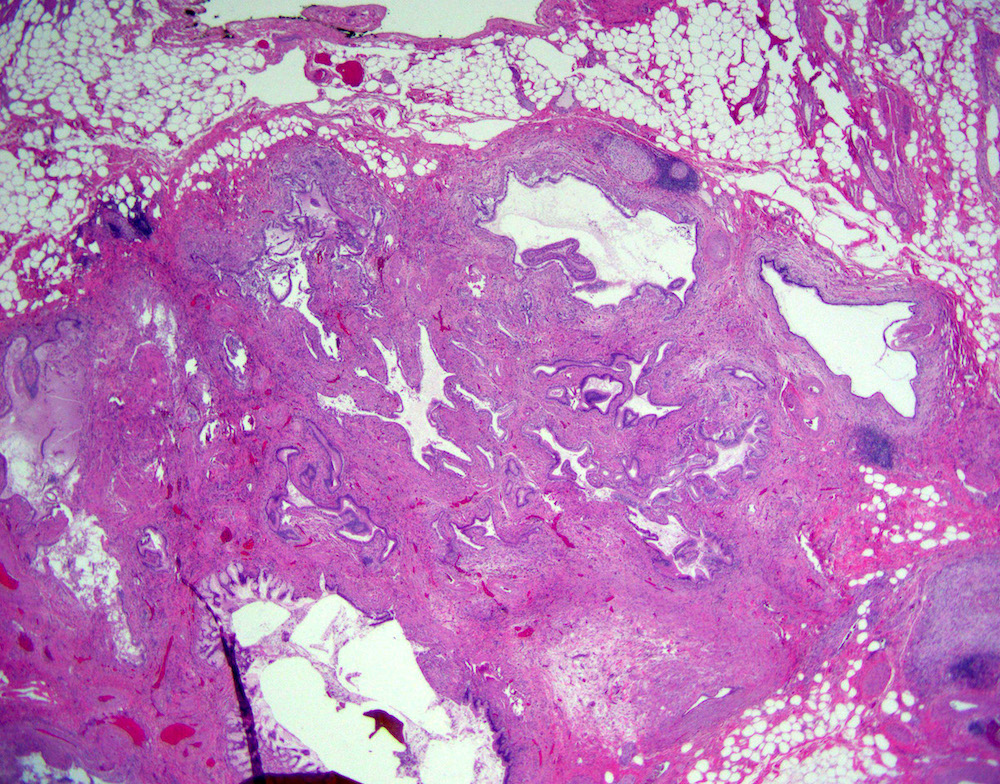
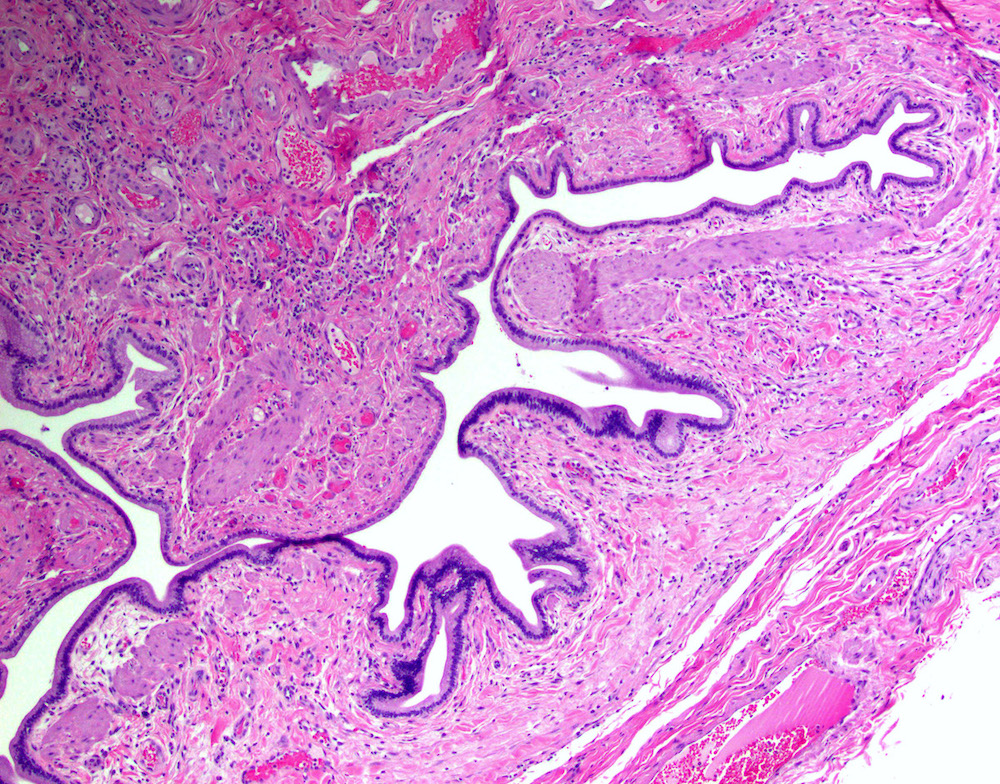
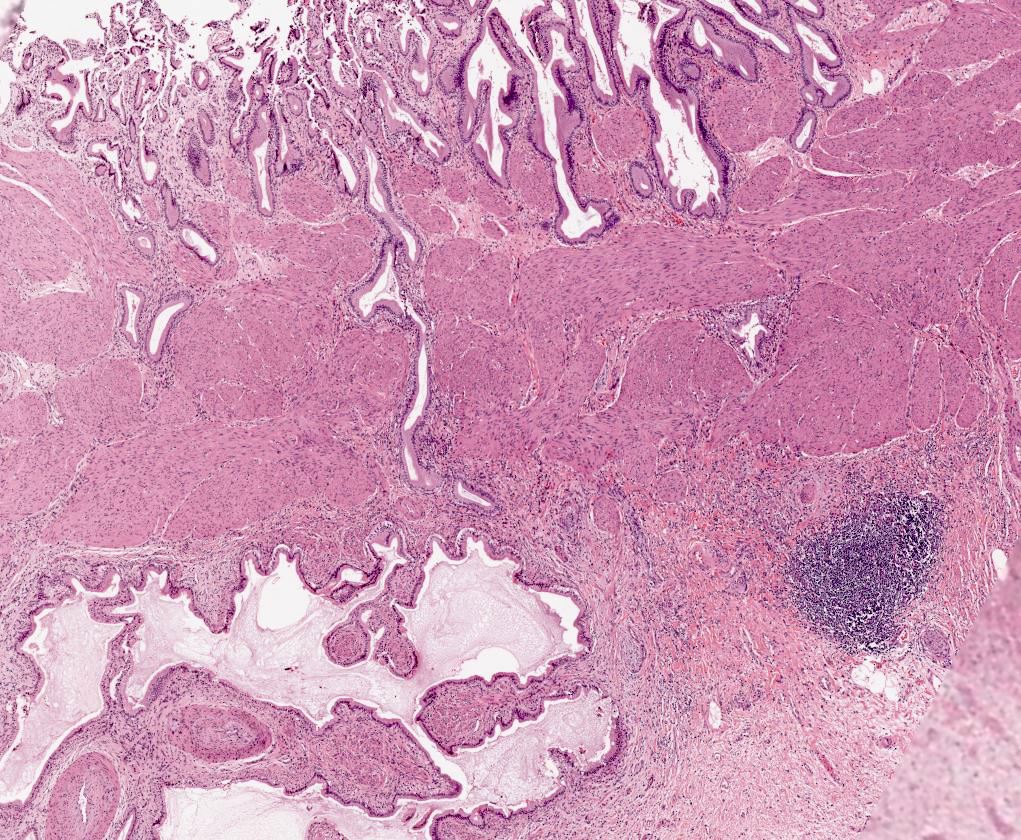
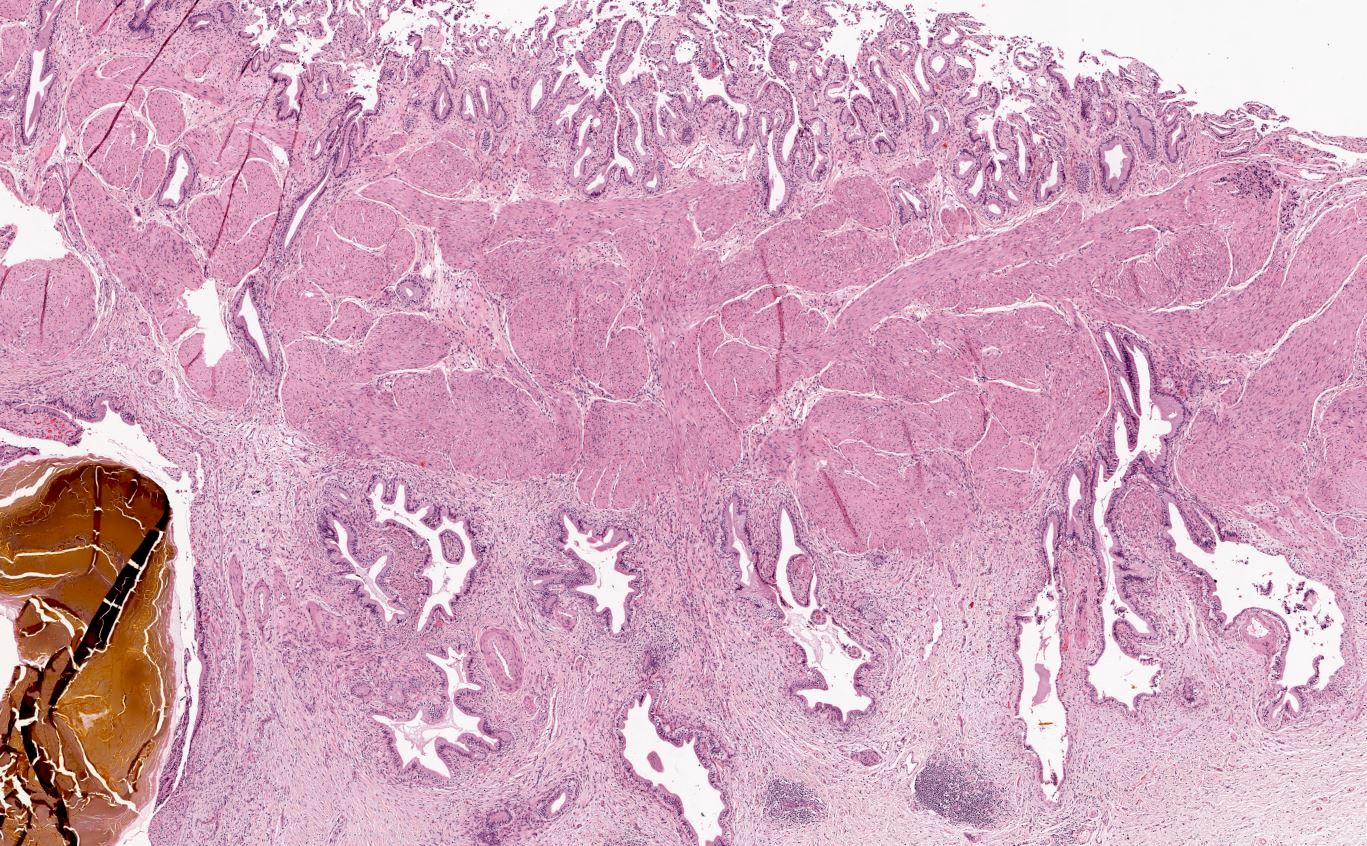
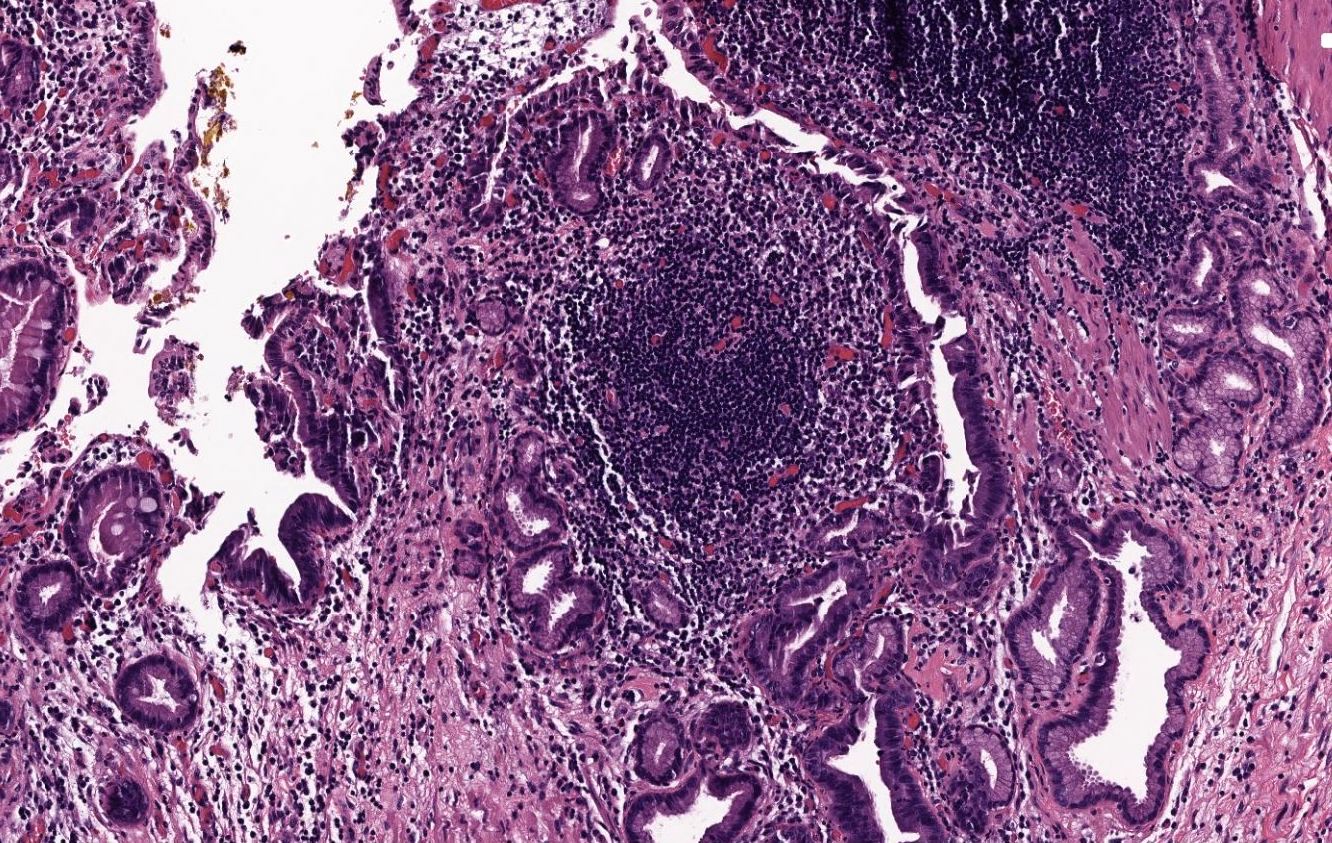
Microscopic (histologic) description
Variable amounts of predominantly mononuclear inflammatory infiltrate in lamina propria, which may extend into the muscularis and pericholecystic tissues
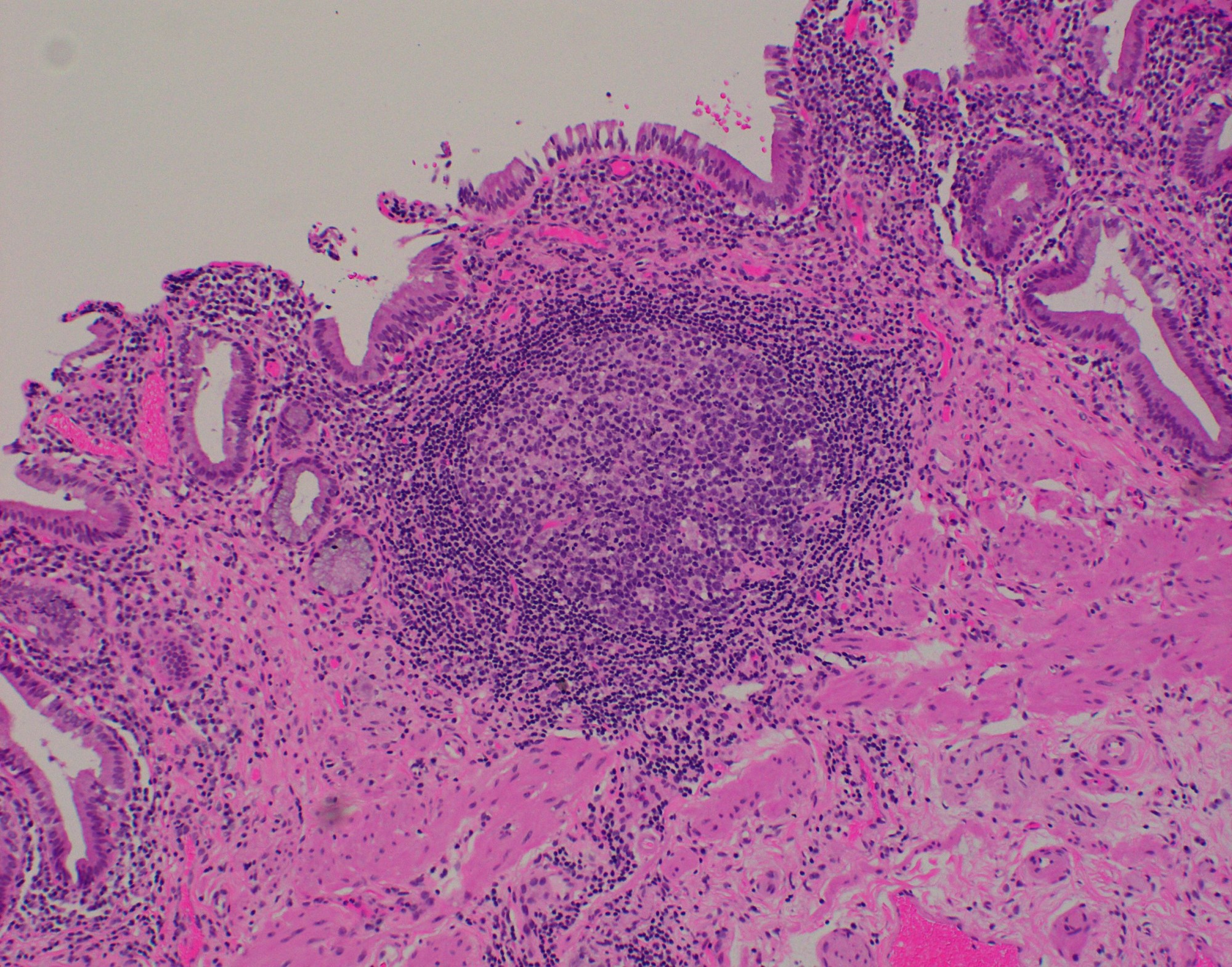
Inflammatory infiltrate predominantly consists of T lymphocytes, with some plasma cells, histiocytes and occasional eosinophils (Ann Diagn Pathol 2003;7:147)
Inflammation typically rather minimal; occasional lymphoid follicles may be seen in lamina propria
Hypertrophy of muscularis and variable degrees of mural fibrosis, elastosis, neural hyperplasia
Accentuation of Rokitansky-Aschoff sinuses (pseudodiverticula)
Hyalinizing variant: dense paucicellular hyalinizing fibrosis effacing ≥ 80% of normal histologic structures, resulting in a thinned gallbladder wall with (porcelain gallbladder) or without dystrophic calcification
Primary MALT lymphoma of gallbladder is typically identified on presurgical imaging as gallbladder wall thickening or a polypoid lesion
Lymphoplasmacytic cholecystitis:
Plasma cell rich inflammatory infiltrate that diffusely involves the mucosa and is primarily confined to the lamina propria (Am J Surg Pathol 2003;27:1313)
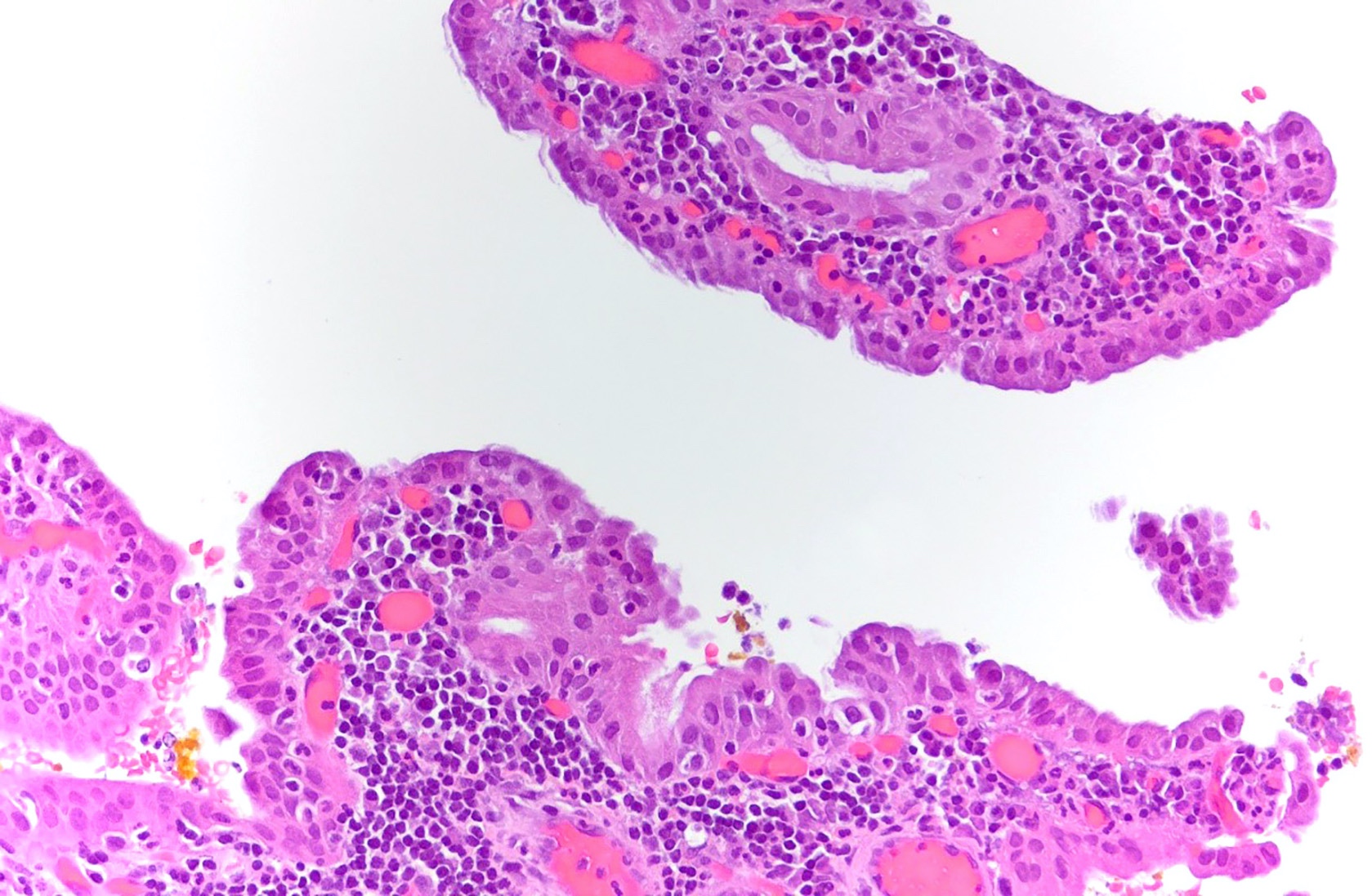
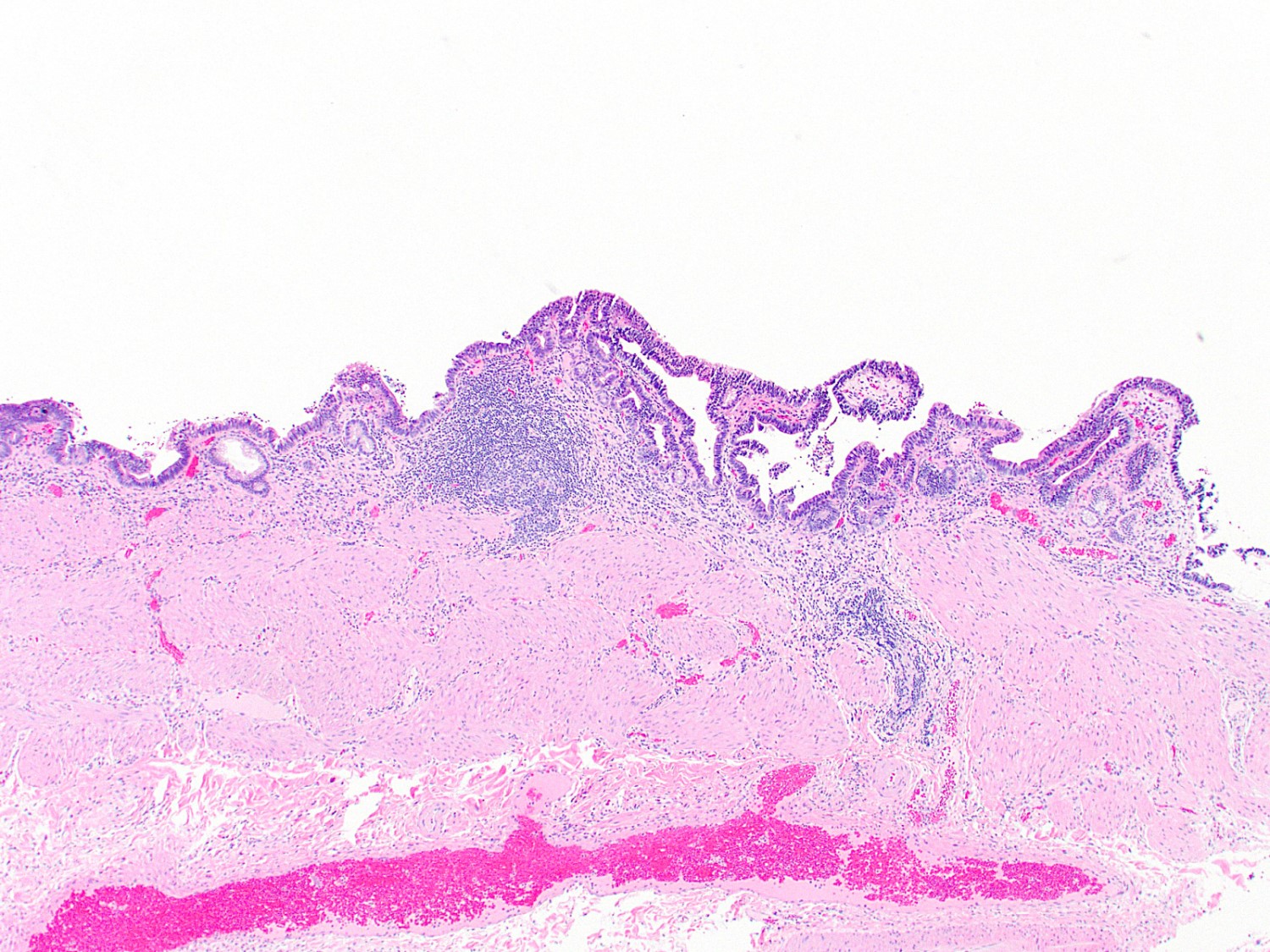
A 40 year old woman with a BMI of 36 undergoes cholecystectomy for intermittent, dull right upper quadrant abdominal pain, reproducible on physical examination with deep palpation. Sections of gallbladder wall show the following
What is the best interpretation of these findings?
Dysplasia is unlikely to cover > 20% of the gallbladder in patients without carcinoma (Hum Pathol 2018;82:87)
Pathophysiology
Chronic inflammation leads to epithelial metaplasia (most commonly intestinal metaplasia), then low grade dysplasia, then high grade dysplasia and finally invasive carcinoma (Arch Pathol Lab Med 2005;129:386, Hum Pathol 2018;82:87)
Diagrams / tables
Images hosted on other servers:
Low grade dysplasia distribution in gallbladder
Clinical features
Ranges from asymptomatic to vague, nonspecific signs and symptoms
Clinical presentation can overlap with cholelithiasis / cholecystitis (Histopathology 2021;79:2)
Low grade dysplasia: 4 additional sections (consider more in high risk patients or populations)
High grade dysplasia: at least 4 additional sections but strongly consider submitting entire remaining gallbladder (high risk of malignancy elsewhere in gallbladder)
Radiology description
Usually no findings
US, CT or MRI can show nonspecific focal or diffuse gallbladder wall thickening or a space occupying lesion (Ann Diagn Pathol 2018;37:7)
Prognostic factors
Increases risk for carcinoma of the gallbladder and elsewhere in the pancreatobiliary tract (J Gastrointest Surg 2019;23:686)
Contributed by Raul S. Gonzalez, M.D. and Monica T. Garcia-Buitrago, M.D.
Cancer and dysplasia
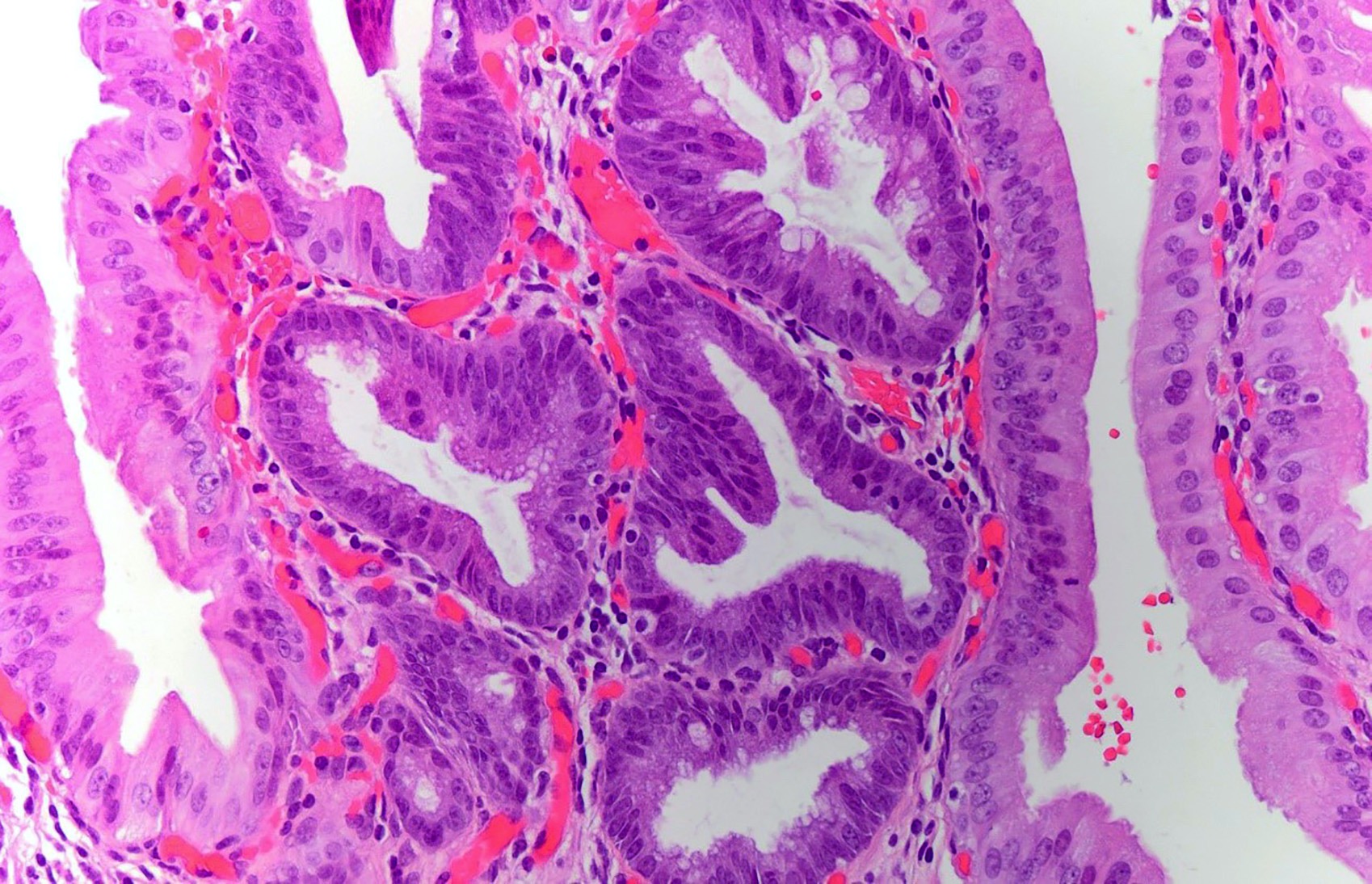
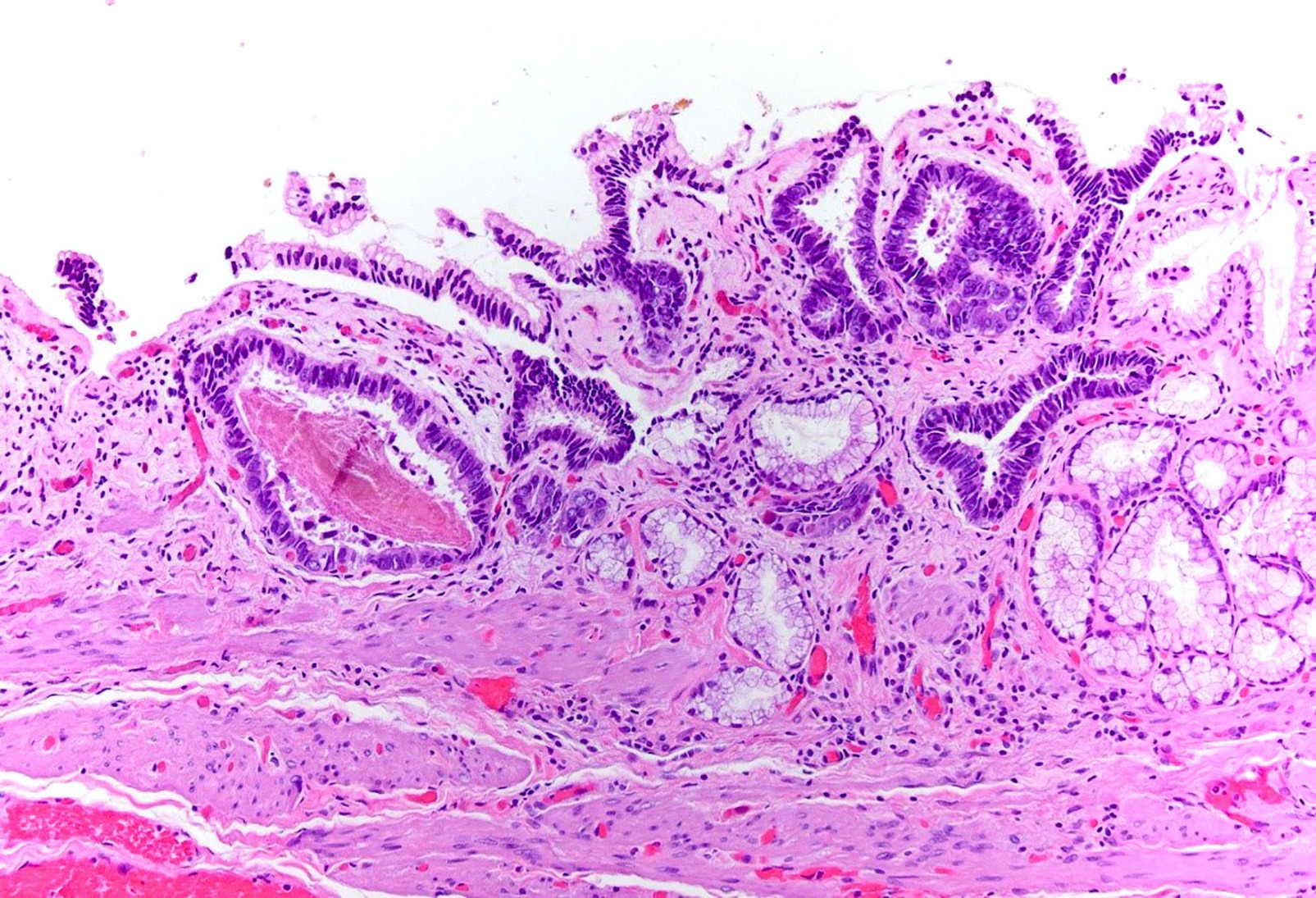
High grade BilIN
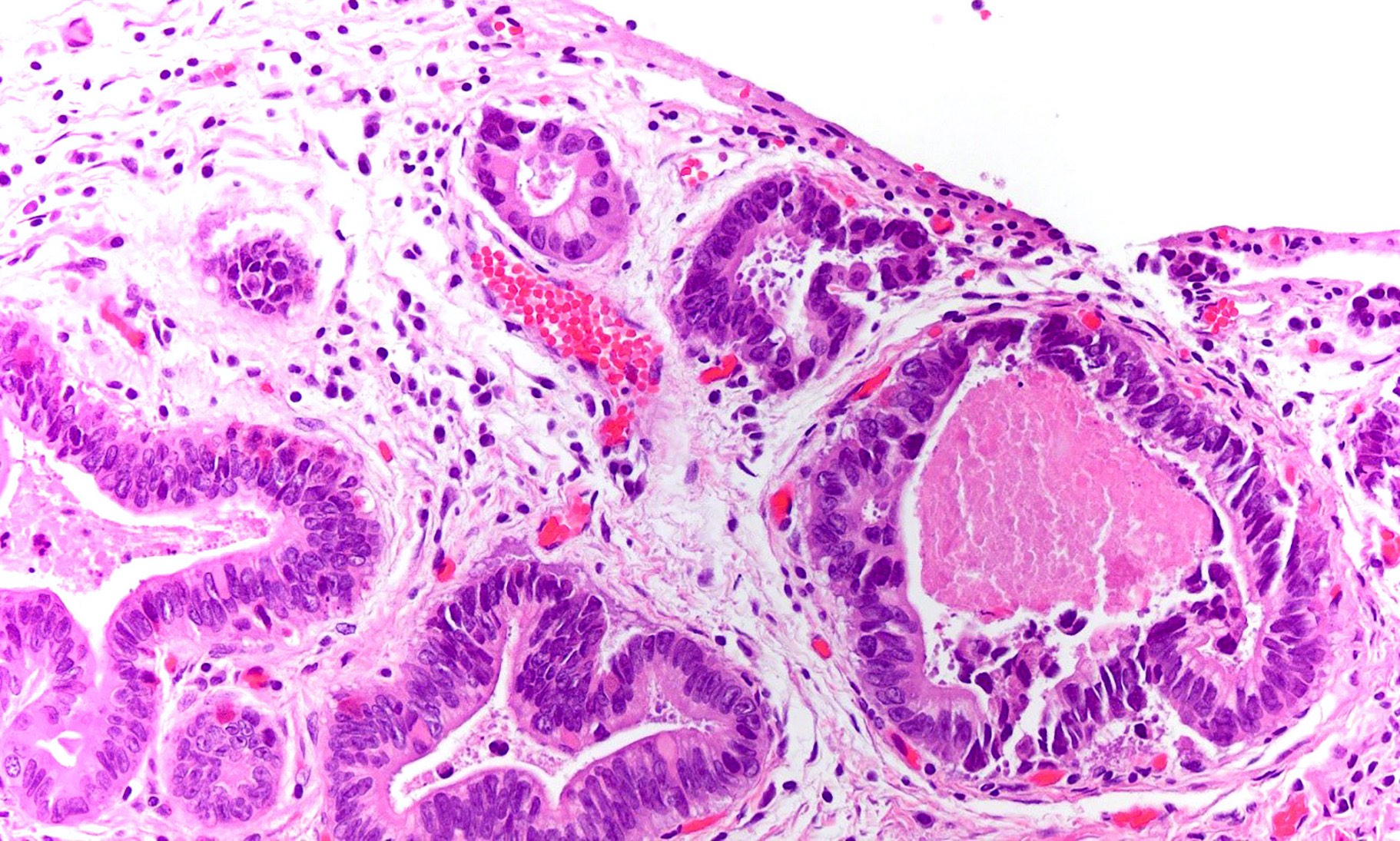
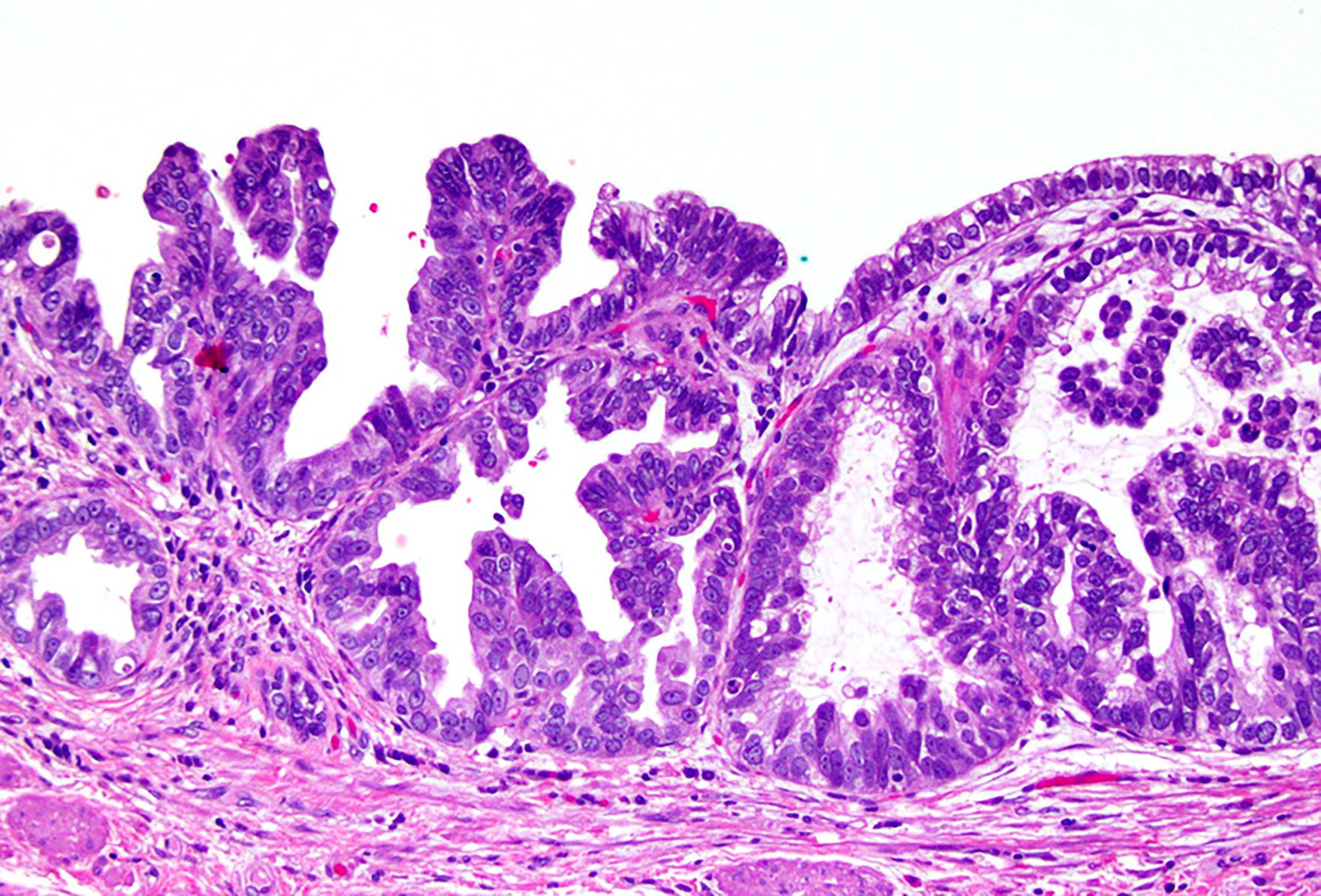
Microscopic (histologic) description
Gallbladder dysplasia can be difficult to reproducibly define, in particular low grade dysplasia (Histopathology 2021;79:2)
Low grade dysplasia
Elongated (pencillate) hyperchromatic nuclei that may show pseudostratification but still maintain basal polarity, with moderate N:C ratios
Mucosal surface often remains flat
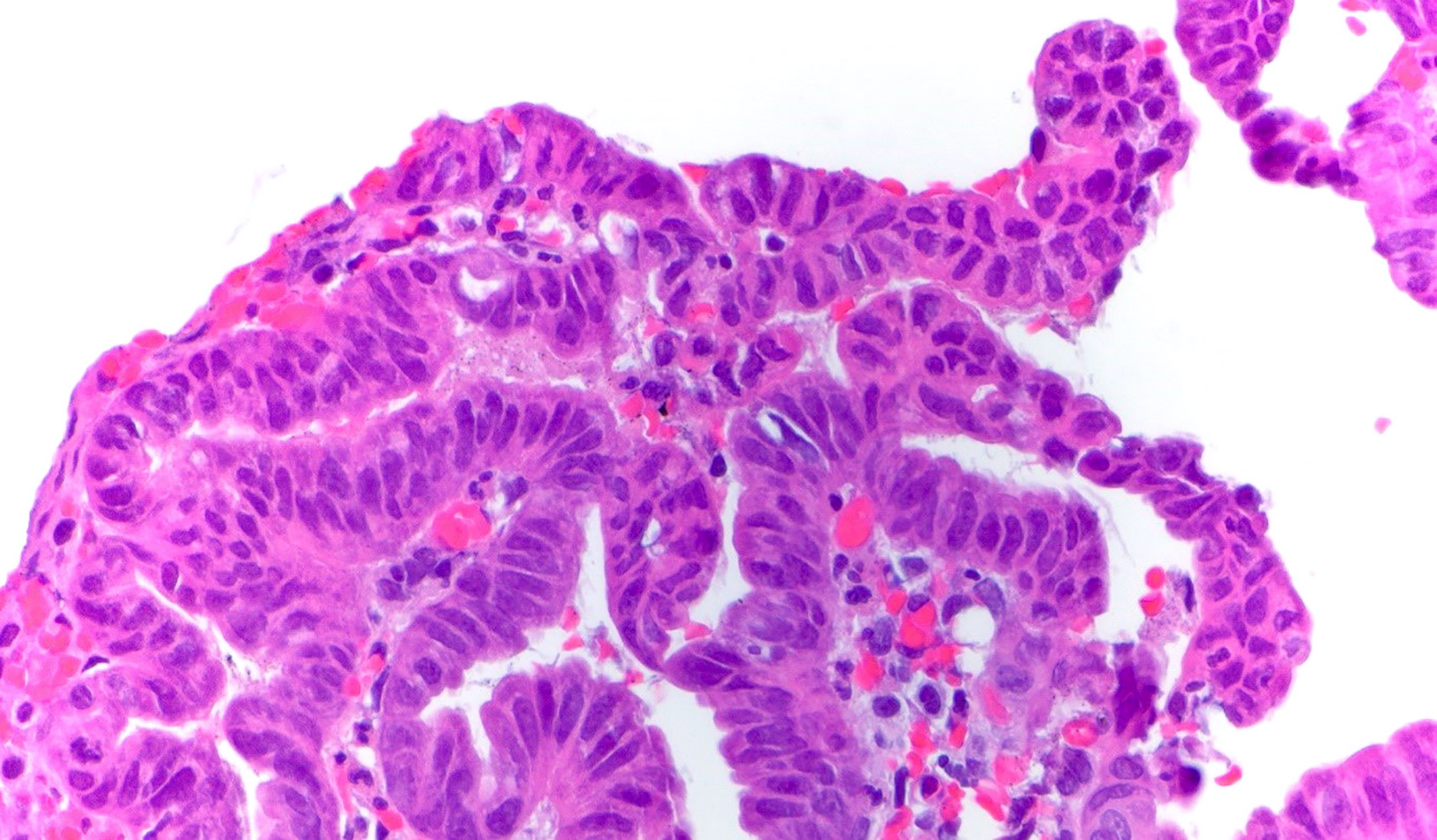
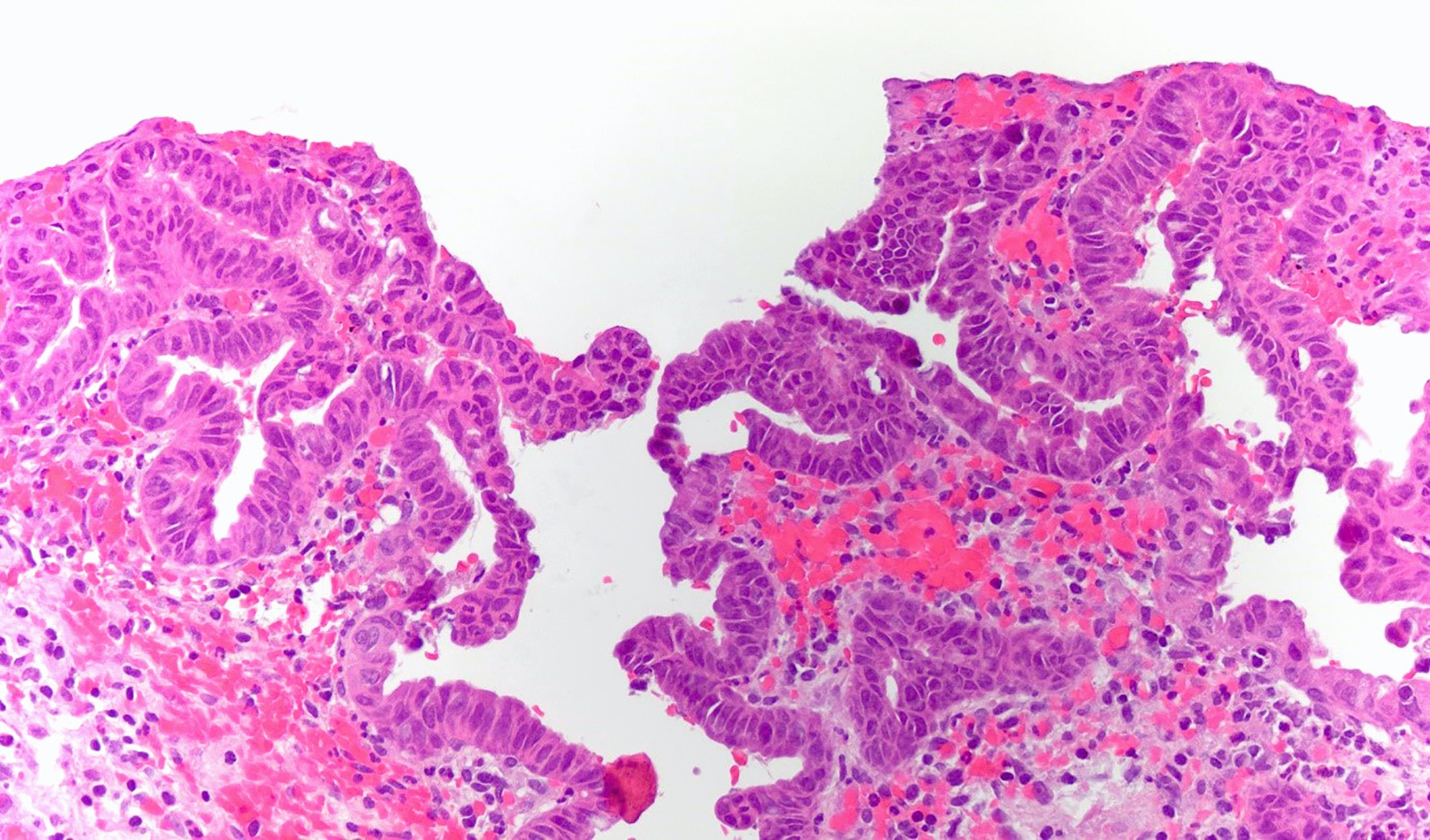
High grade dysplasia
Markedly atypical nuclei with rounding, nucleoli and loss of polarity, with high N:C ratios and more complex surface architecture
Low grade dysplasia often accompanies high grade dysplasia
Intestinal metaplasia is often present in the background
Neutrophils (acute inflammation) may be present in dysplastic epithelium, raising consideration for reactive atypia but erosion or ulceration is uncommon
Interobserver variability exists for these diagnoses; strict diagnostic criteria have been proposed to address this (Mod Pathol 2007;20:701)
Dysplastic process that forms a discrete polypoid lesion, rather than remaining relatively flat
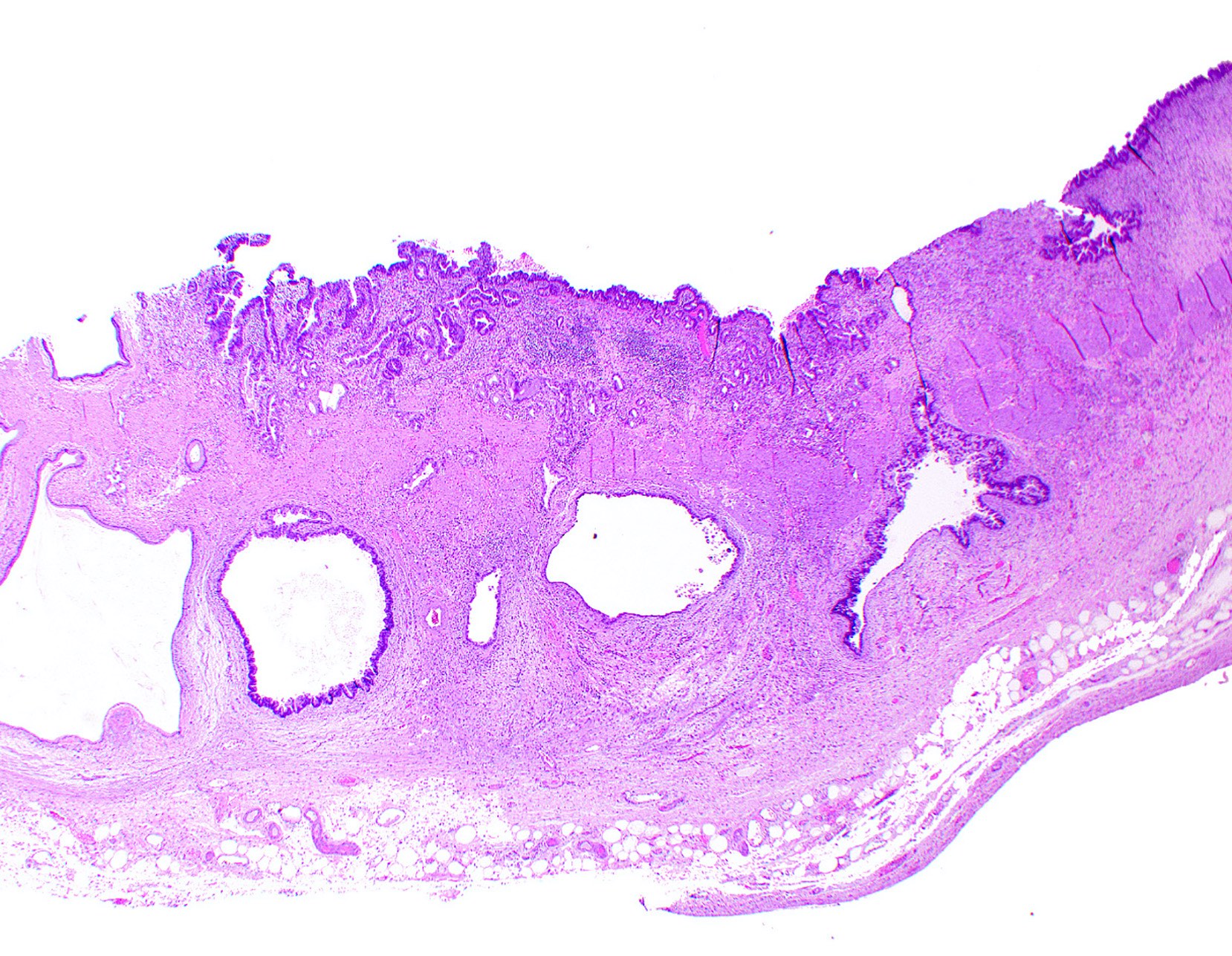
Board review style question #1
A 72 year old woman presented to the emergency department with symptoms of cholecystitis and underwent laparoscopic cholecystectomy. The gallbladder grossly looked normal but the one routine section submitted for histology showed the changes seen in the image above. What is the most appropriate next step in the workup of this case?
Sign out the pathology report
Submit 1 - 2 additional cassettes
Submit the entire gallbladder
Tell the surgeon the patient needs urgent hepatectomy
Board review style answer #1
C. Submit the entire gallbladder. The image shows high grade dysplasia, which can be found incidentally in gallbladder specimens. It would be inappropriate to sign out the case without going back to the specimen. While recommendations vary, some experts suggest that discovery of high grade dysplasia means the entire gallbladder should be submitted for thorough histologic inspection to rule out invasive gallbladder carcinoma.
Answer A is incorrect because high grade dysplasia warrants further investigation so as to not miss a cancer diagnosis.
Answer B is incorrect because submitting 1 - 2 more sections errs on the insufficient side.
Answer D is incorrect because the patient does not necessarily need more surgery, though if carcinoma is found, definitive treatment may require additional surgery.
Which of the following countries has the lowest incidence of gallbladder dysplasia and carcinoma?
Chile
India
Japan
United States
Board review style answer #2
D. United States. Answer A - C are incorrect because Chile, India and Japan are all known to have a high incidence of gallbladder dysplasia and carcinoma, unlike the United States, which has a more standard incidence. In those countries, it may be prudent to submit additional sections from gallbladder specimens to rule out incidental dysplasia.
Aggressive cancer, with an overall 5 year survival rate of < 10%
Cholelithiasis is a major risk factor
Up to 50% are detected incidentally in routine cholecystectomy specimens due to absence of gross abnormalities; systematic sampling of these specimens is therefore crucial to detect incidental gallbladder adenocarcinomas (Am J Surg Pathol 2019;43:1668)
Terminology
Carcinoma of gallbladder; adenocarcinoma of gallbladder; malignant epithelial neoplasm of gallbladder
Primarily affects the fundus (60%), body (30%) or neck (10%) of gallbladder
Advanced tumors involve the liver and extrahepatic biliary tree
Pathophysiology
Longstanding cholelithiasis and cholecystitis give rise to metaplastic changes (intestinal or pseudopyloric types) in the gallbladder mucosa (Cancer 1993;72:1878)
Prognosis of adenocarcinoma, NOS depends on tumor stage:
Superficially invasive cancers limited to the lamina propria (pT1a) have excellent prognosis as they are completely cured by cholecystectomy (Ann Surg 2017;266:625)
High histologic grade (poor differentiation) and vascular invasion have adverse outcomes (Cancer 1992;70:1493)
Rokitansky-Aschoff sinus involvement by carcinoma and cystic duct margin status are suspected predictors of progression (Am J Clin Pathol 2014;141:675)
Case reports
22 year old man with primary signet ring cell carcinoma of gallbladder in the absence of choleliths (Int J Surg Pathol 2010;18:358)
Cholecystectomy with a negative cystic duct margin is curative in pT1a tumors (Ann Surg 2017;266:625)
Hilar / portal lymphadenectomy, plus resection of hepatic bed and the common bile duct to achieve negative margins, is necessary for tumors that extend into a muscle or beyond (pT1b - pT3) (HPB (Oxford) 2015;17:681)
Chemotherapy or radiation for metastatic tumors
Gross description
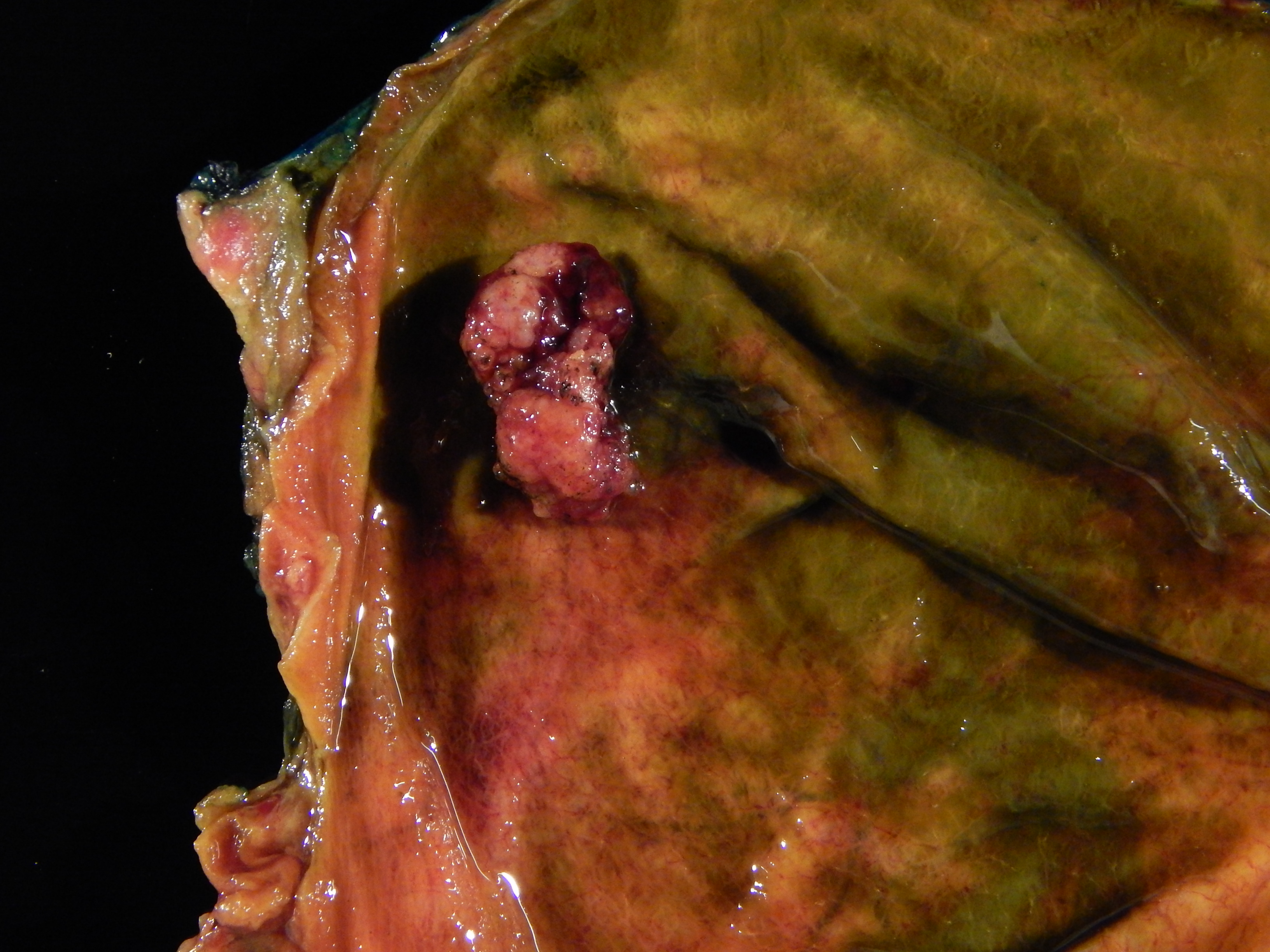
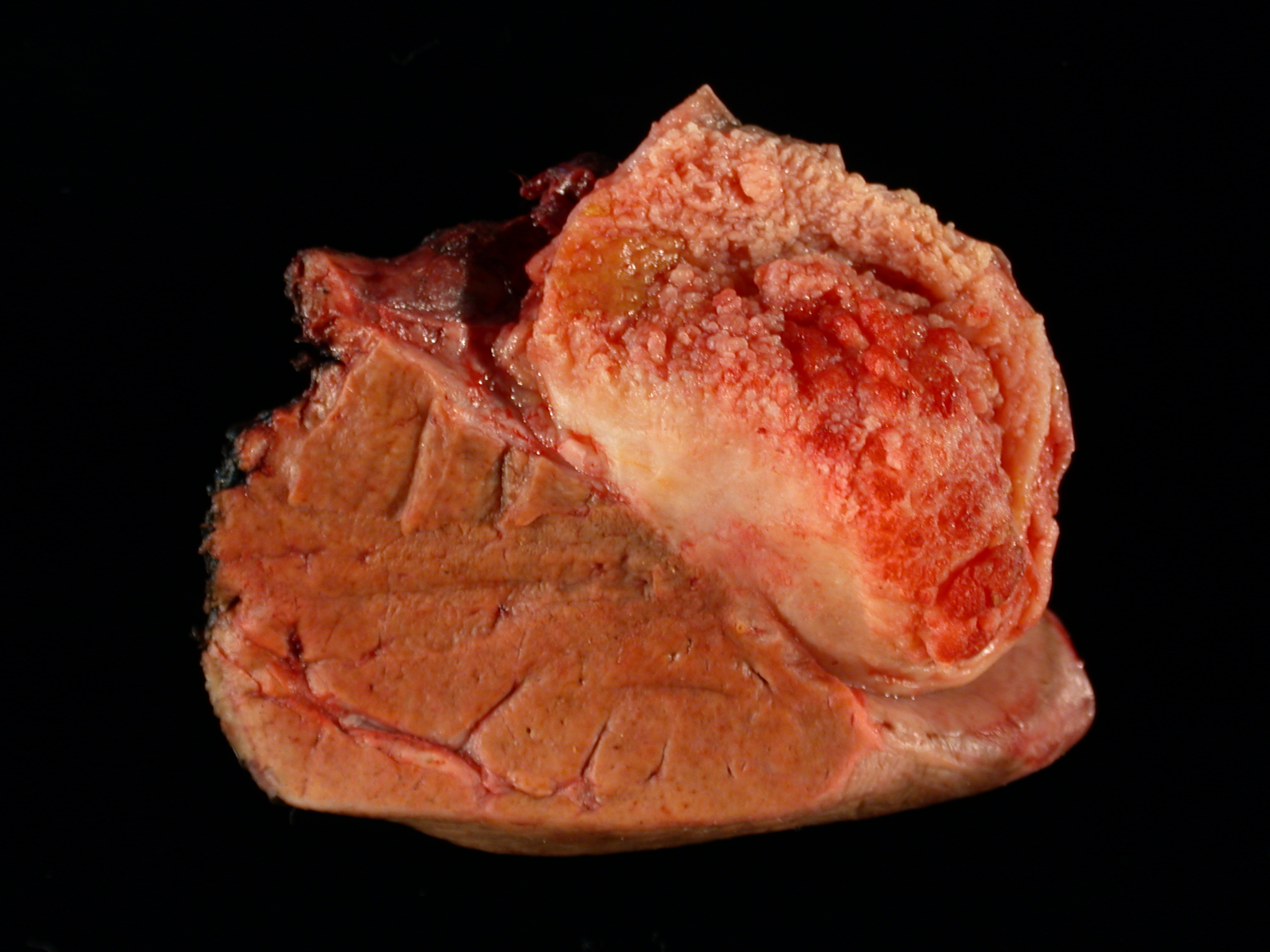
Incidental gallbladder cancer in routine cholecystectomy specimens can be grossly subtle, with areas of mucosal granularity / irregularity, minimally raised / polypoid mucosal lesions or focally thickened fundus / body (Am J Surg Pathol 2019;43:1668)
Frank tumors may have one or more of the following features:
Thickened and indurated gallbladder wall
Exophytic or polypoid friable mucosal lesions (especially those arising from intracholecystic papillary neoplasm)
Firm, gritty, tan-white to yellow-gray cut surface
Gross images
Contributed by Ashwin S. Akki, M.D., Ph.D.
Papillary proliferation
Carcinoma in a polyp
Gallbladder cancer invading liver
Diffusely thickened gallbladder wall
Microscopic (histologic) description
Histologic variants recognized by WHO include:
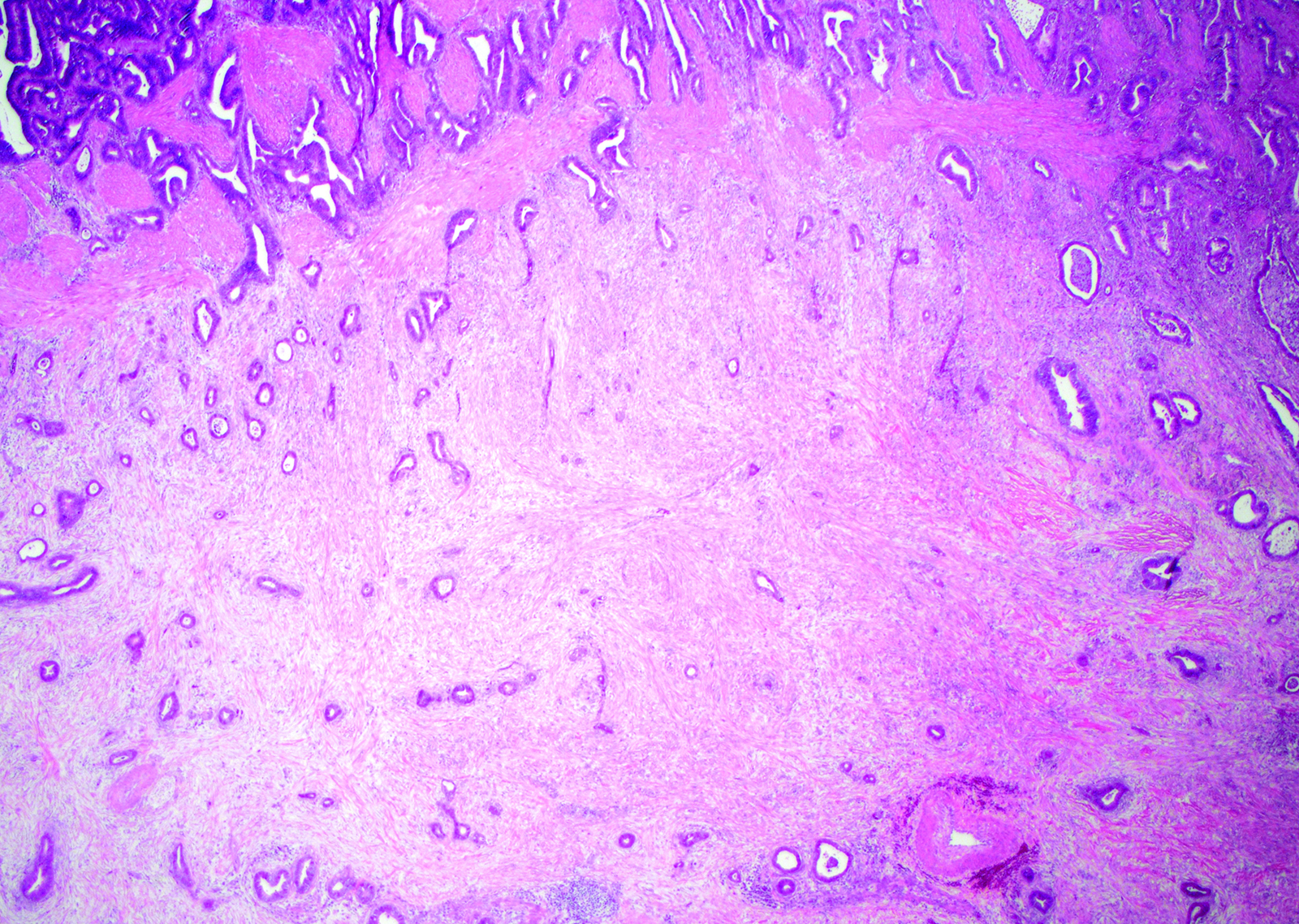
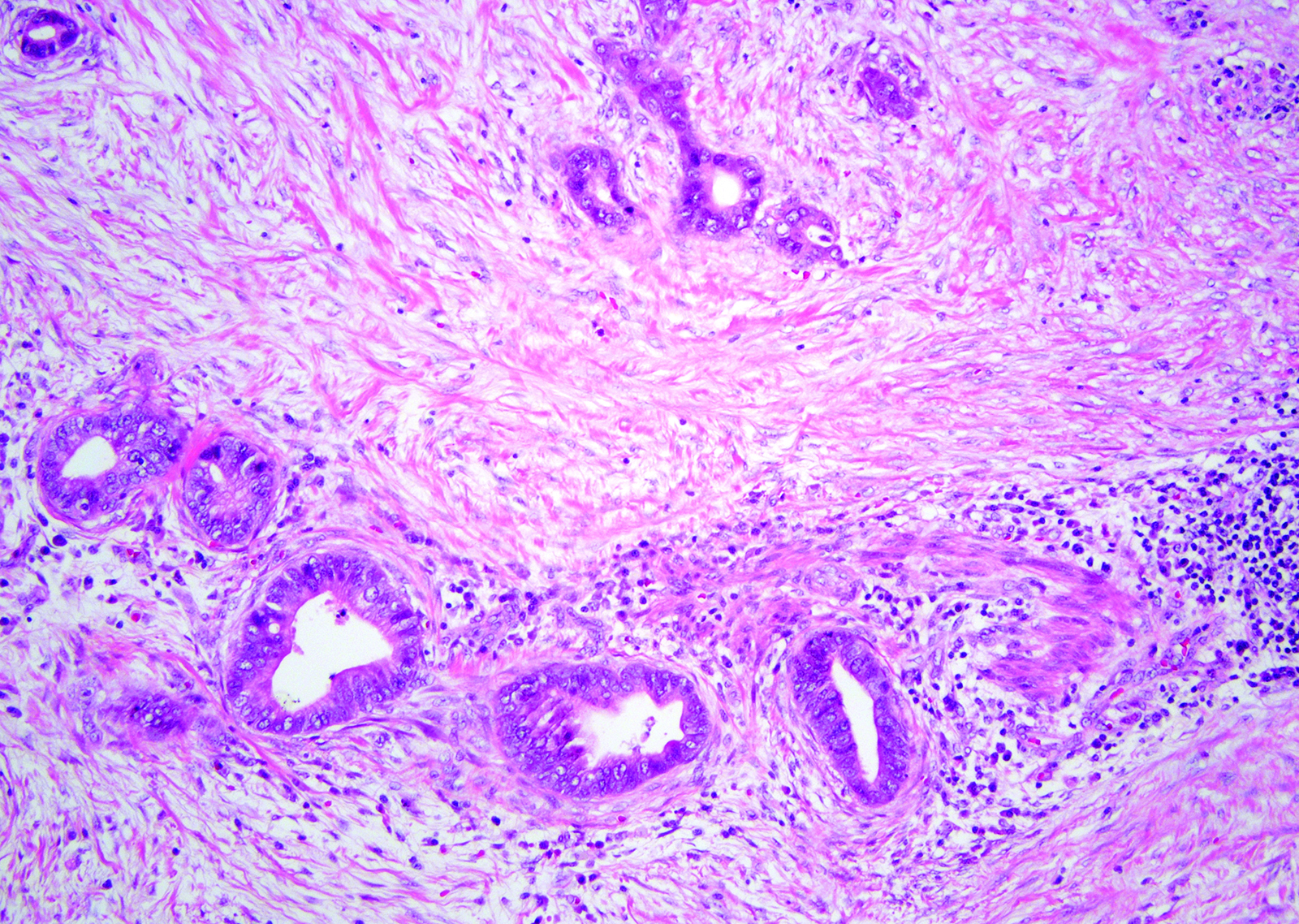
Biliary type adenocarcinoma (~75%):
Similar to pancreatic ductal adenocarcinoma
Includes adenocarcinoma, NOS (most common), papillary, micropapillary
Composed of tubules (lined by cuboidal to columnar cells) embedded in a desmoplastic stroma
Moderately differentiated is more common but has a wide histologic spectrum, from deceptively bland to poorly differentiated
Intestinal type adenocarcinoma:
Tubules lined by columnar cells with elongated hyperchromatic nuclei, very similar to colonic adenocarcinomas
Mucinous carcinoma:
Comprised of > 50% extracellular mucin
Clear cell carcinoma:
Sheets of clear cells in an alveolar arrangement separated by blood vessels, similar in appearance to metastatic clear cell renal carcinoma
Signet ring cell carcinoma:
Signet ring cells are the predominant or exclusive component
Hepatoid carcinoma:
> 50% with abundant eosinophilic cytoplasm, enlarged nuclei and prominent nucleoli arranged in a trabecular pattern
Sarcomatoid carcinoma (carcinosarcoma):
Predominant spindle cell morphology with or without heterologous differentiation (e.g. skeletal muscle, bone and cartilage)
Differentiation
Well differentiated:
Well formed glands lined by columnar cells with minimal cytologic abnormality
Glands in perimuscular connective tissue, nuclear irregularities and mitoses may be the only clues
Desmoplasia may be subtle
Moderately differentiated:
Irregular / angulated glands lined by polygonal tumor cells with enlarged nuclei showing vesicular chromatin, prominent nucleoli and increased mitoses
Desmoplasia is usually prominent
Poorly differentiated:
Incomplete or poorly formed tubules / glands, single cells or sheets of pleomorphic tumor cells with bizarre nuclei
Amplifications of ERBB2 (HER2) have been reported in 16% of cases and microsatellite instability (MSI) in 10% of cancers, both of which have therapeutic implications (Cancer 2016;122:3838, Histopathology 2009;55:218)
A higher KRAS mutation rate is noted in lesions related to pancreatobiliary maljunction (Hum Pathol 1999;30:21)
Videos
Extended cholecystectomy
Sample pathology report
Gallbladder; cholecystectomy:
Invasive adenocarcinoma, moderately differentiated, biliary type (2.7 cm in largest dimension), arising in a background of extensive high grade biliary intraepithelial neoplasia (BilIN).
Adenocarcinoma invades perimuscular connective tissue on the peritoneal side, without involvement of the serosa (visceral peritoneum).
Cystic duct margin is free from biliary intraepithelial neoplasia (BilIN) or carcinoma.
Epicenter in the colon, intestinal phenotype, CK20 strong and diffuse
Board review style question #1
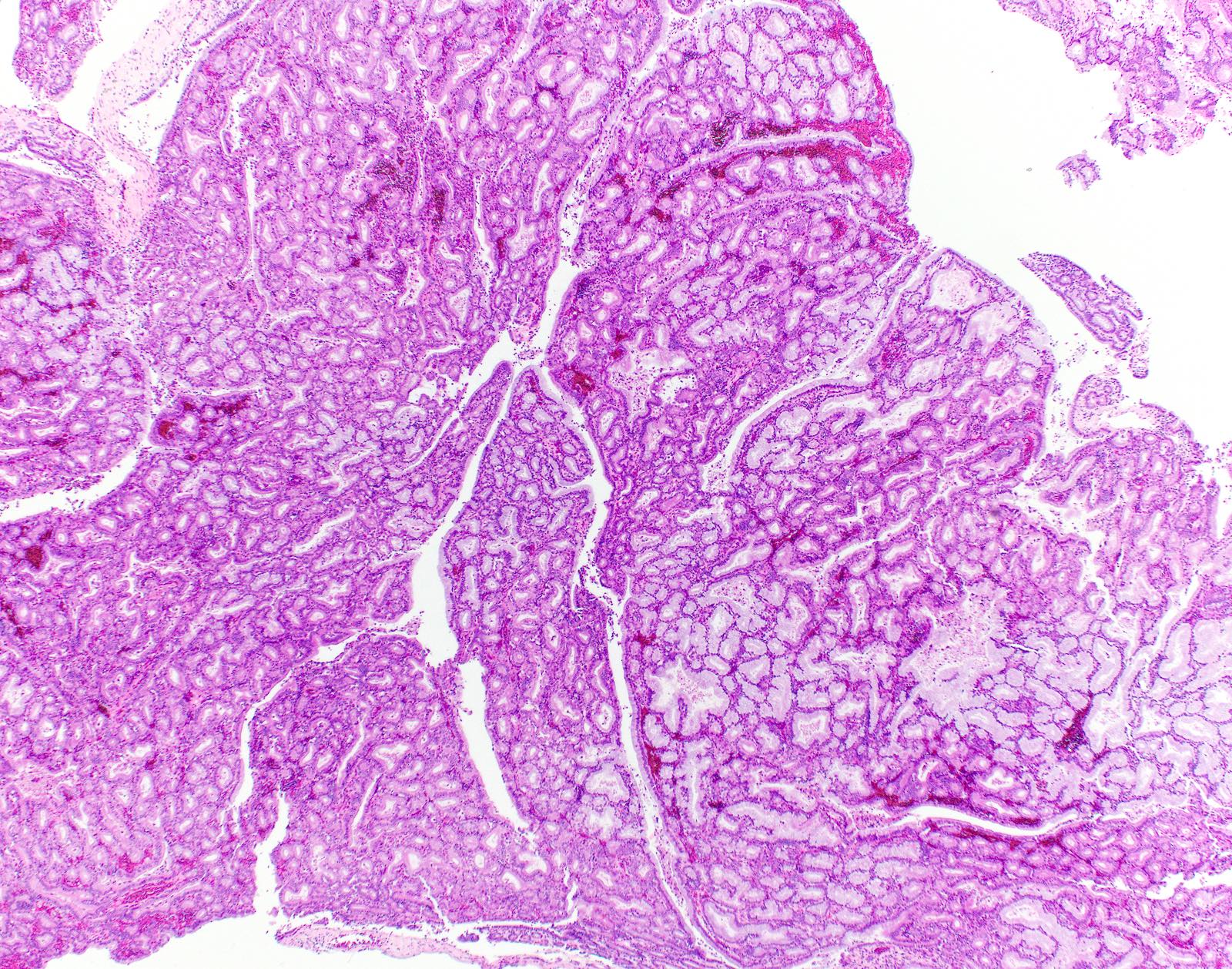
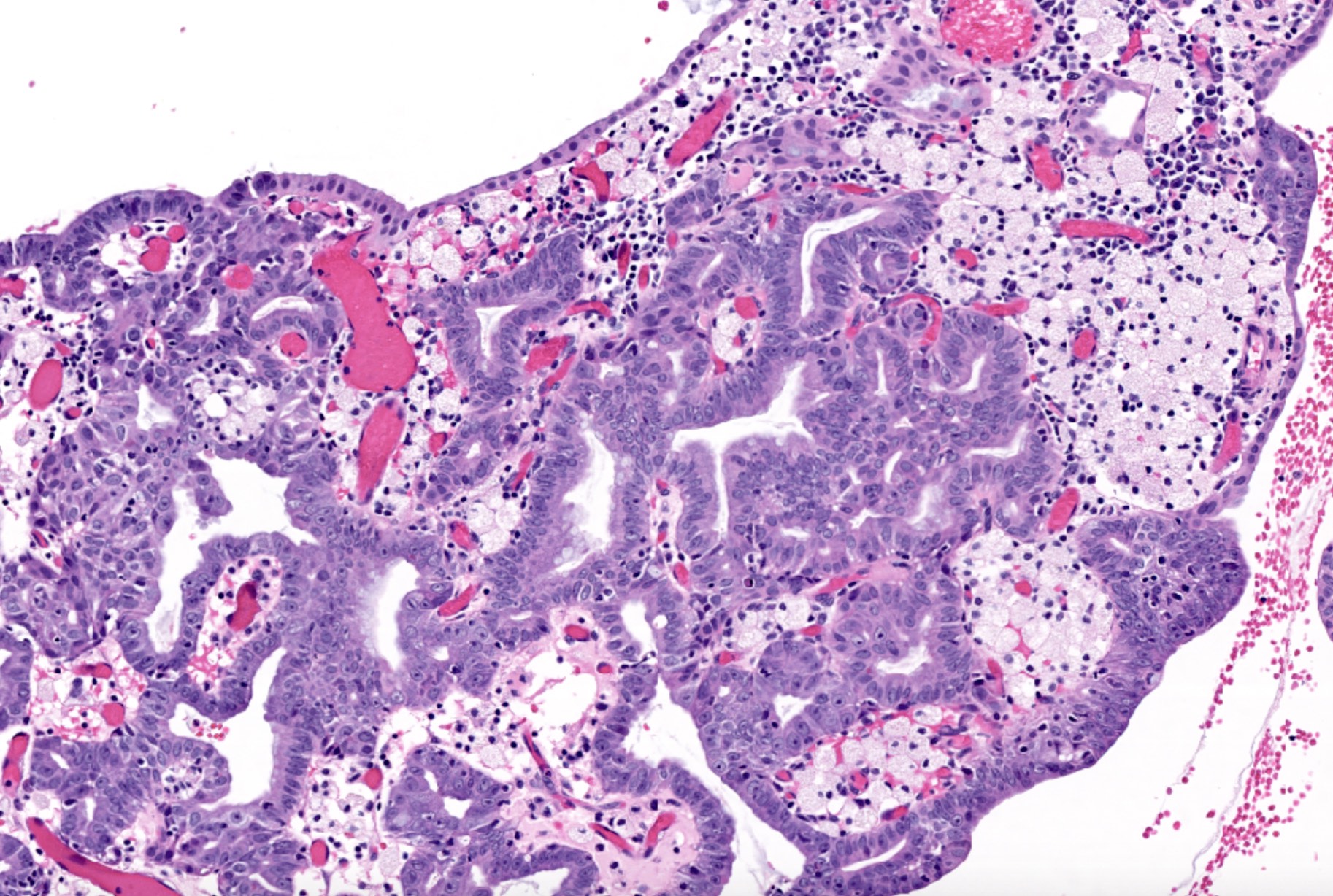
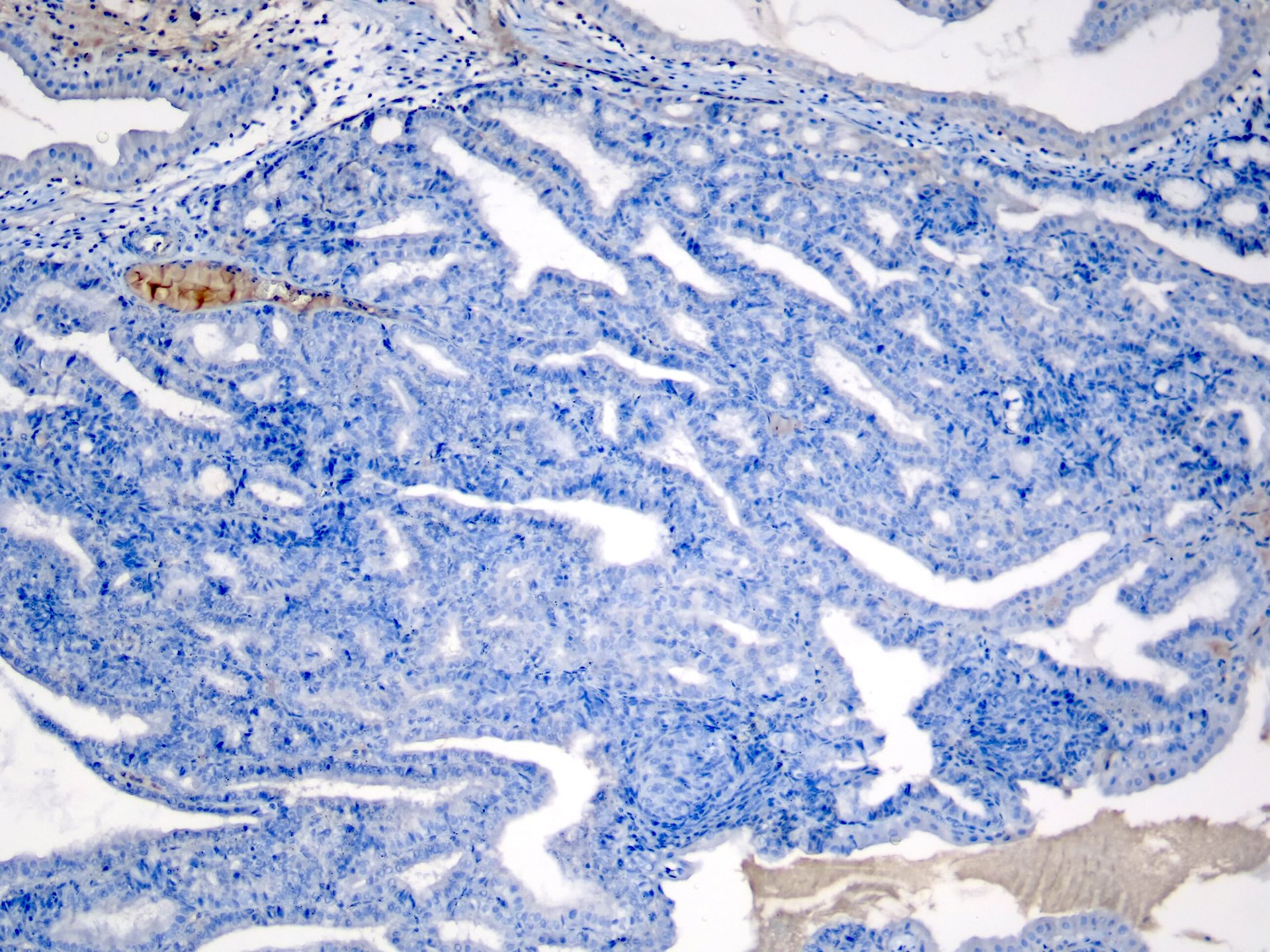
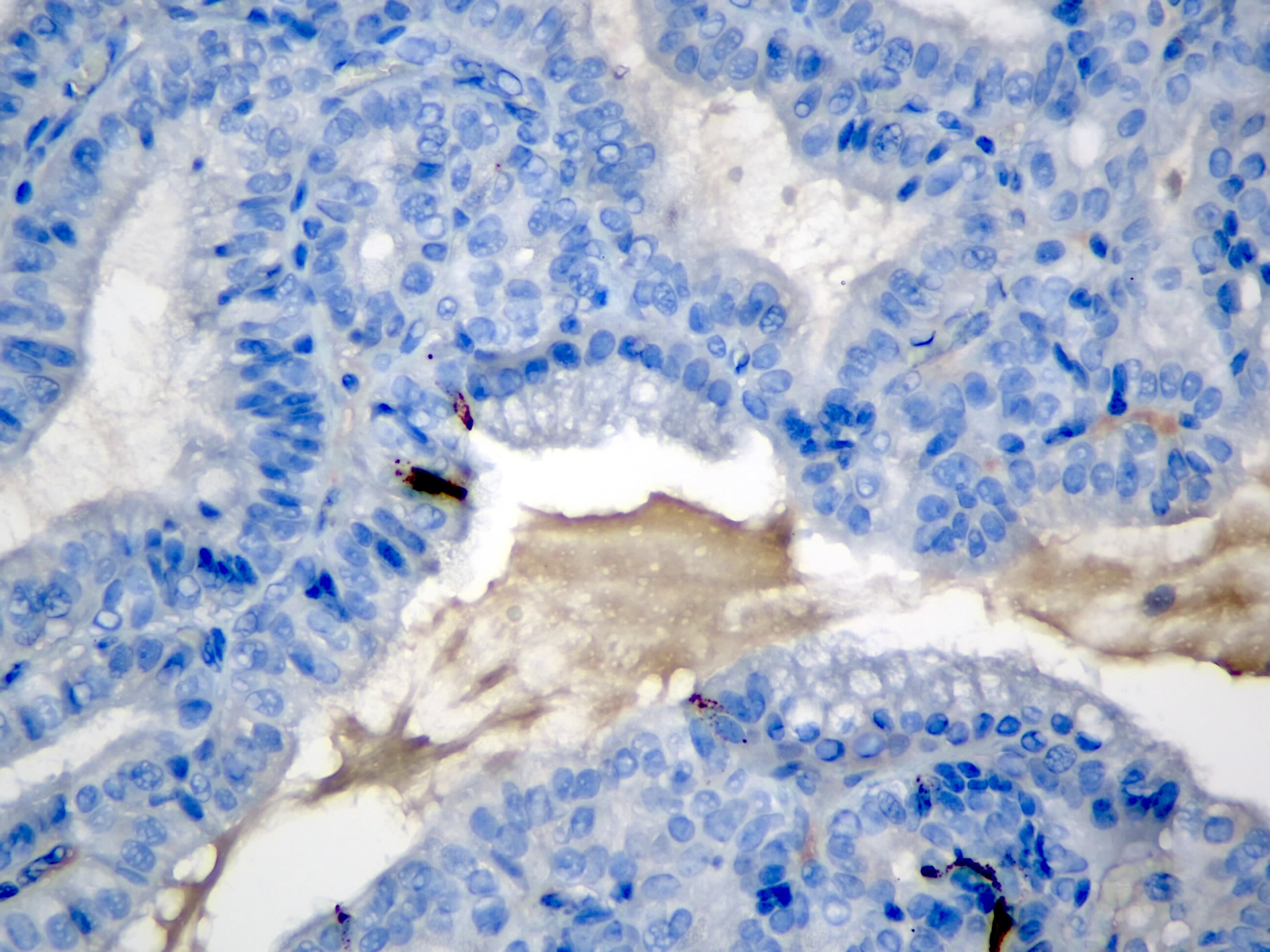
A 58 year old woman presents with right upper quadrant pain. Imaging reveals a polypoid lesion in the gallbladder. Patient undergoes cholecystectomy. Pathology shows the finding seen in the image above. Which of the following is true about this entity?
Has aggressive dissemination potential
Has a more favorable prognosis than conventional nonpapillary gallbladder adenocarcinomas
Immunoreactive to hepatocellular markers
Is not detected early on imaging
Board review style answer #1
B. Invasive papillary carcinomas have the most favorable prognosis than conventional nonpapillary gallbladder adenocarcinomas because they have an exophytic growth pattern, exhibit delayed invasion into the gallbladder wall, and are detected early due to obstructive symptoms (Arch Pathol Lab Med 2005;129:905).
Optimally should have clinical data and serum AFP levels available
Should know if specimen is from a mass
Indication: presence of a polypoid mucosal lesion or a suspicious thickening of the gallbladder wall (Arch Pathol Lab Med 2005;129:1610)
Features to report - Gallbladder
Tumor size and location
Tumor histologic type and pattern
Depth of invasion
Number and size of tumor nodules
Tumor extension to adjacent structures
Status of resection margins (cystic duct, liver bed, other)
Cystic duct involvement
Liver bed involvement
Regional lymph nodes: number identified, number with tumor
Angiolymphatic invasion
Perineural invasion
Presence of carcinoma in situ or dysplasia
Additional pathologic findings to report:
Chronic cholecystitis, metaplasia (squamous, pyloric gland, intestinal metaplasia), inflammatory bowel disease, porcelain gall bladder, presence or absence of stones (gallbladder cancer occurring without stones may be caused by anomalous choledochopancreatic junction or associated with chronic inflammatory bowel disease, Arch Pathol Lab Med 2000;124:37)
Features to report - Extrahepatic bile ducts
Bile duct wall thickness, external surface, obstruction, stones
Tumor size and location
Tumor histologic type, pattern and grade
Depth of invasion
Number and size of tumor nodules
Tumor extension to adjacent structures
Status of resection margins
Regional lymph nodes: number identified, number with tumor
3 - 15 mm, red gray brown, usually sessile and single
Gross images
Images hosted on other servers:
Smooth surfaced polyp
Microscopic (histologic) description
Sessile mucosal projections with a surface of columnar epithelial cells covering a fibrous stroma with chronic inflammatory cells and lipid laden macrophages in granulation type tissue
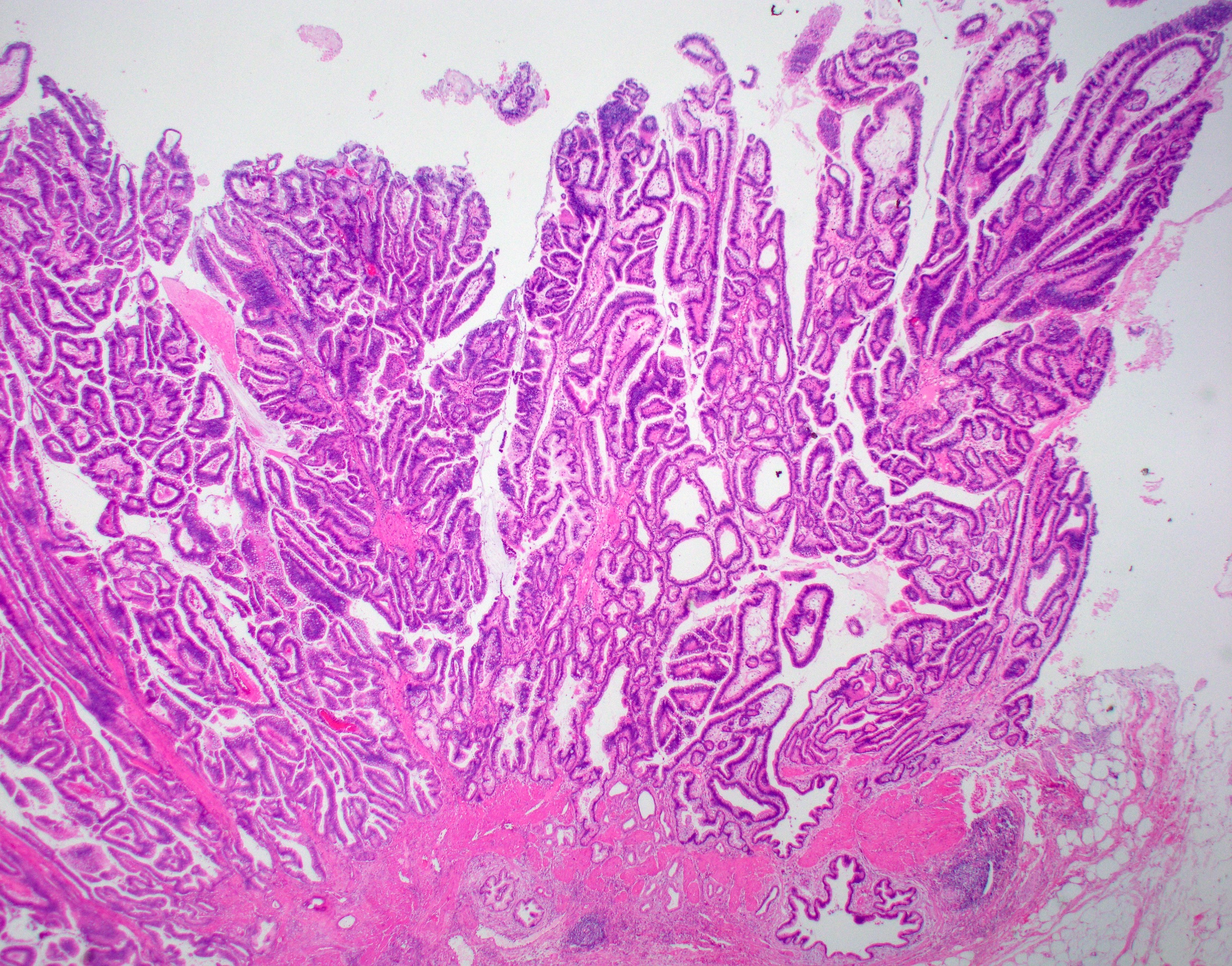
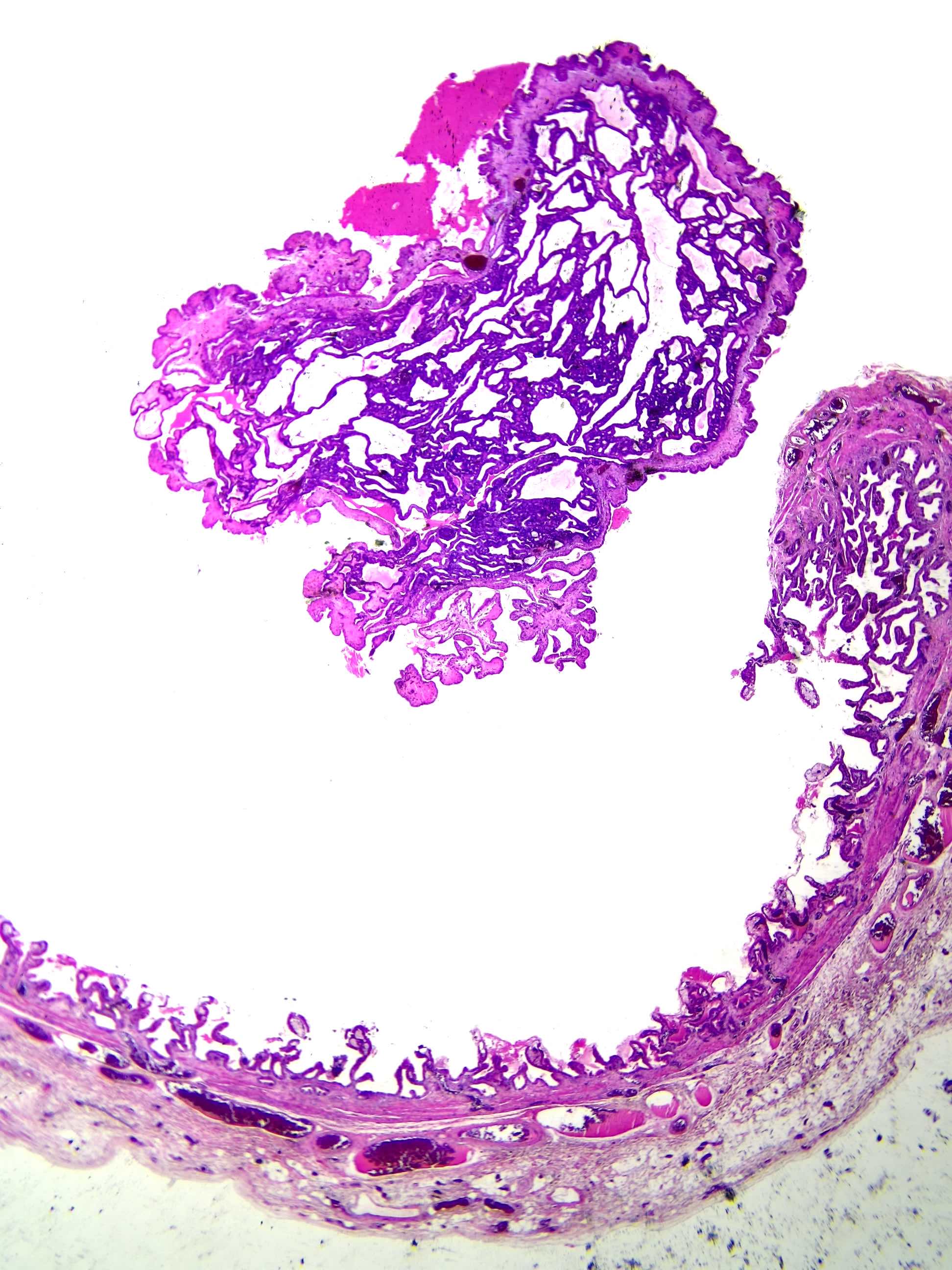
2019 WHO recognizes as a distinct type of preinvasive neoplasm of gallbladder under the name of intracholecystic papillary neoplasm (ICPN)
Exhibits many similarities to pancreatic intraductal papillary mucosal neoplasms as they demonstrate a spectrum of variable configurations, different cell lineages (often in a mixture) and dysplastic changes as well
Characteristic imaging findings include contrast enhanced tumor on CT image and on MR cholangiopancreatography examination a tumor-like defect within the gallbladder with dilatation of the upstream bile duct (Clin J Gastroenterol 2019;12:197)
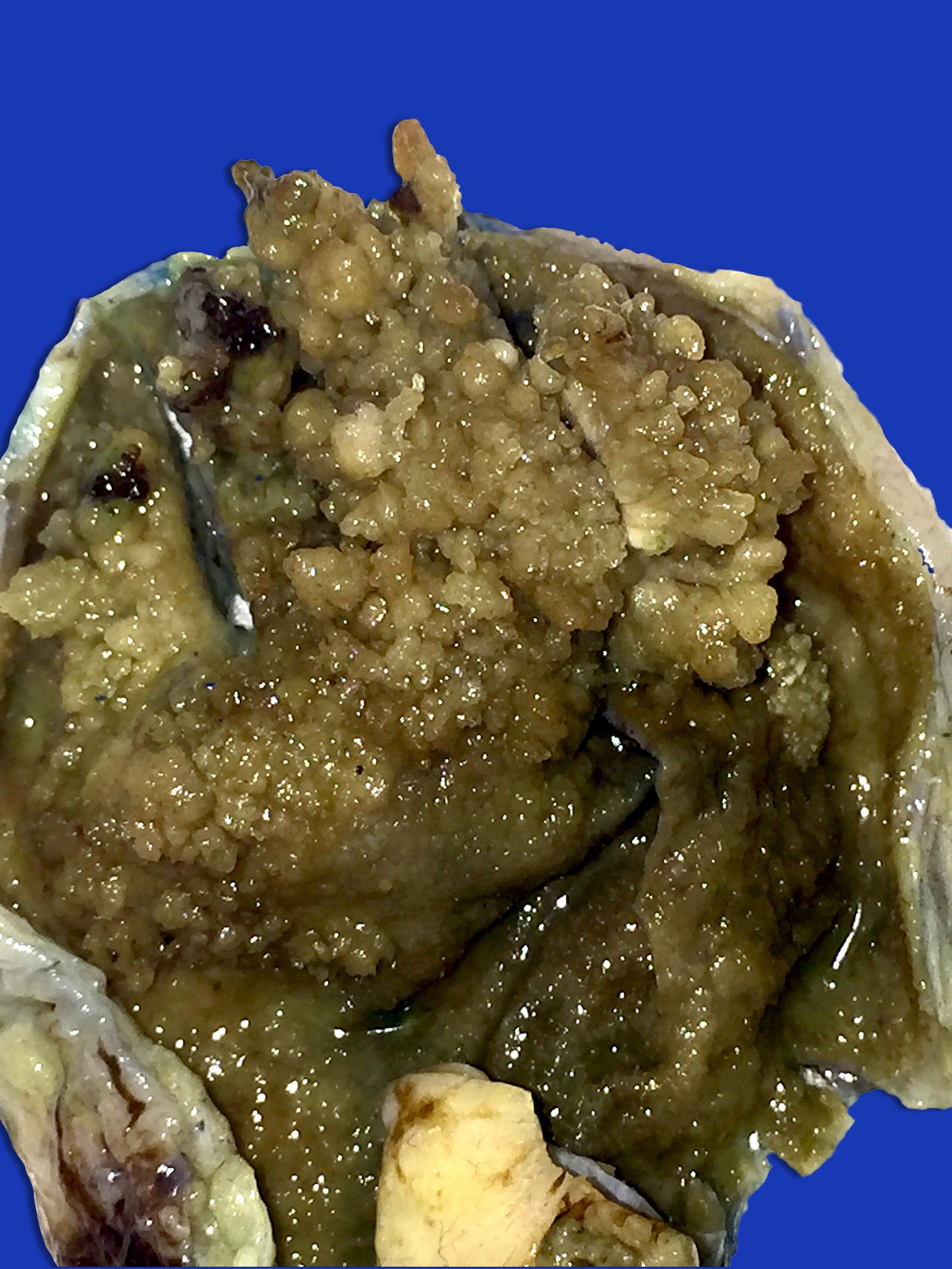
Prominent exophytic growth within the gallbladder or granular, friable soft tan excrescences
Friable excrescences loosely attached to the lumen may be mistaken as sludge or debris in the lumen and not adequately sampled during initial macroscopic examination
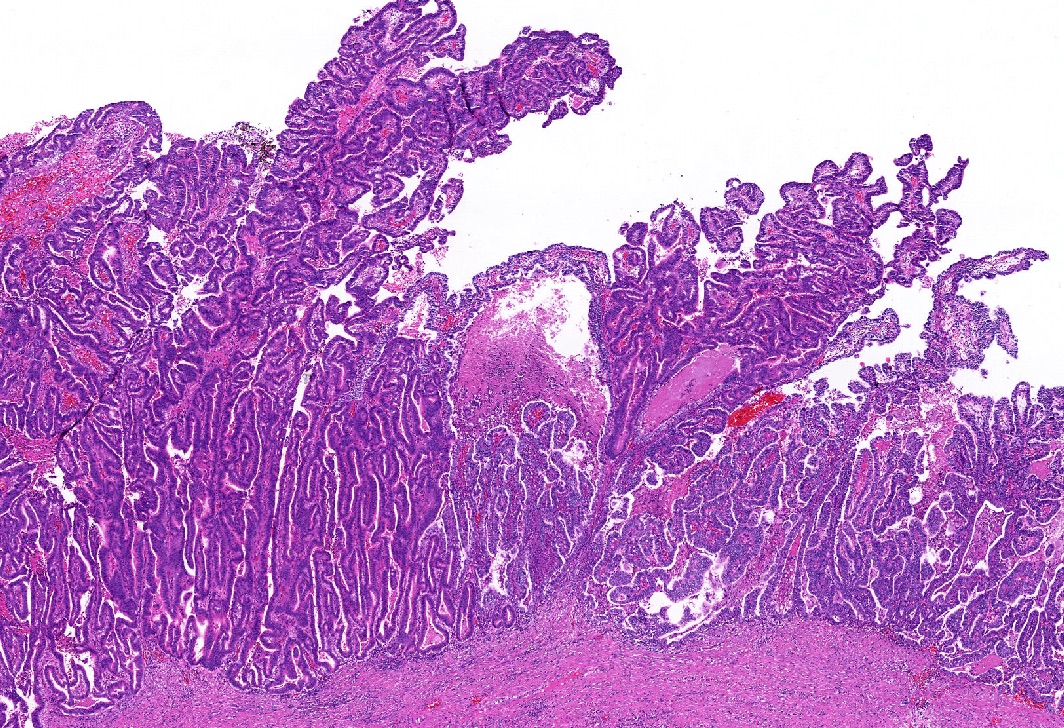
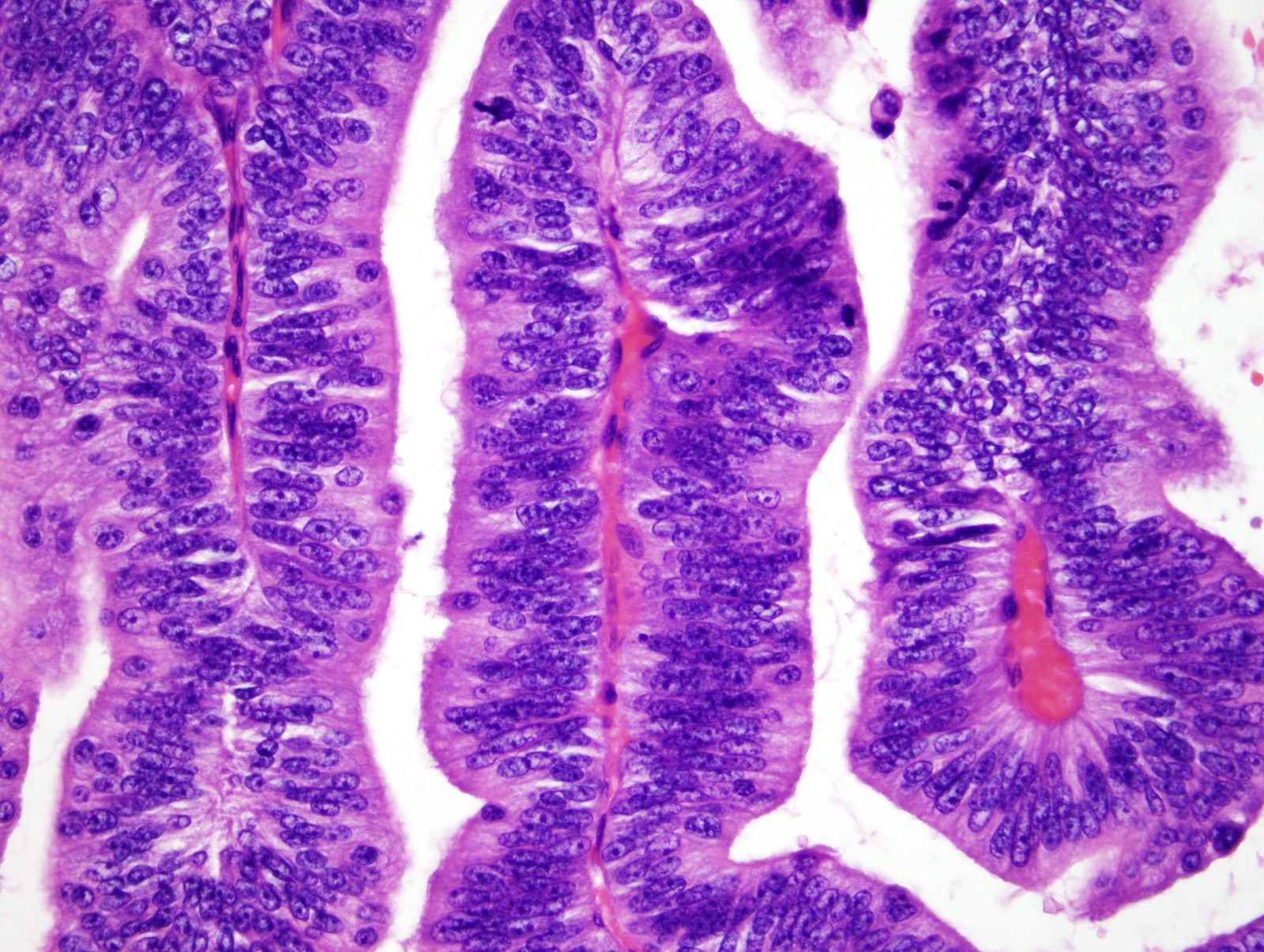
Biliary phenotype: most common phenotype characterized by papillae lined by cuboidal cells with clear to eosinophilic cytoplasm and enlarged nuclei with distinct nucleoli; carries the highest risk for associated invasive carcinoma
Gastric phenotype:
Pyloric type:
Intracholecystic neoplasms characterized by back to back mucinous glands with features characteristic of gastric pyloric glands were originally described as one of the subtypes of ICPN
However, current (2019) WHO classifies these neoplasms as a distinct entity (i.e. pyloric gland adenoma)
These carry the lowest risk for associated invasive carcinoma
Foveolar type: large elongated glands lined by tall columnar mucinous epithelium with pale cytoplasm
Intestinal phenotype: morphologically similar to colonic adenoma showing pseudostratified cigar shaped nuclei and overall basophilia
Oncocytic phenotype: least common subtype characterized by arborizing papillae that are lined by oncocytic cells (large, granular cytoplasm and prominent, large, eccentric nucleoli) with atypia
Mixed phenotypes are common
Lesions histologically characterized by abundant cytoplasm, small and uniform nuclei and distinct nucleoli are classified as low grade dysplasia; those with architectural complexity as well as nuclear atypia have high grade dysplasia (Am J Surg Pathol 2012;36:1279)
For the noninvasive cases, it is important to assess the presence and amount of high grade dysplasia
Associated invasive carcinoma is detected in more than half of the cases at the time of diagnosis, mostly in lesions with biliary phenotype and high grade dysplasia (Am J Surg Pathol 2012;36:1279, Ann Diagn Pathol 2019;40:88)
Associated invasive carcinoma is mostly pancreatobiliary type adenocarcinoma but other types of carcinomas, such as colloid or poorly differentiated neuroendocrine carcinoma, may also be seen (GE Port J Gastroenterol 2019;26:356, Surg Case Rep 2016;2:62)
Invasive carcinoma may be grossly inapparent and may even occur away from the ICPN, therefore thorough sampling and careful microscopic evaluation are extremely important (Semin Diagn Pathol 2012;29:127)
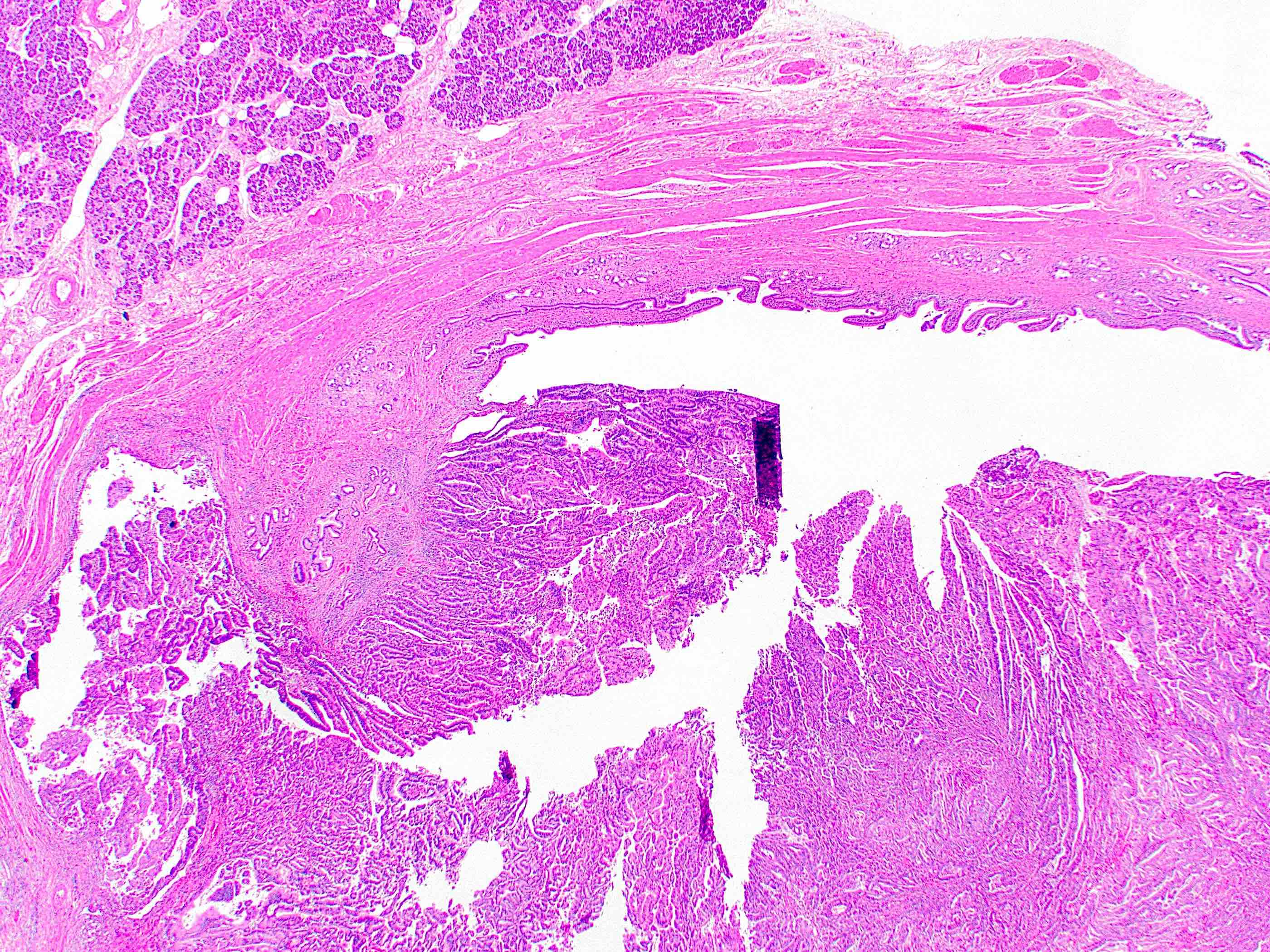
Microscopic (histologic) images
Contributed by Gokce Askan, M.D. and Olca Basturk, M.D.
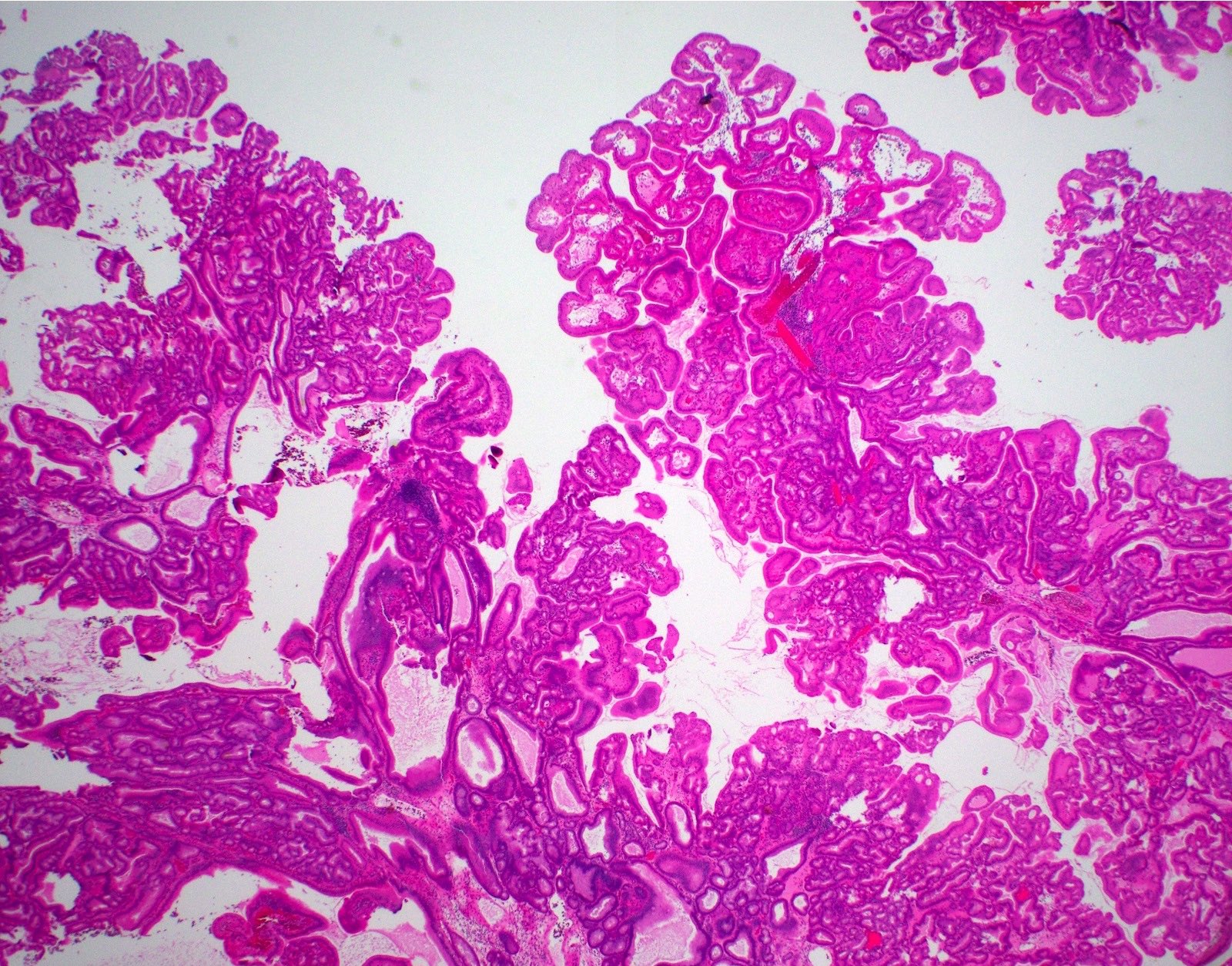
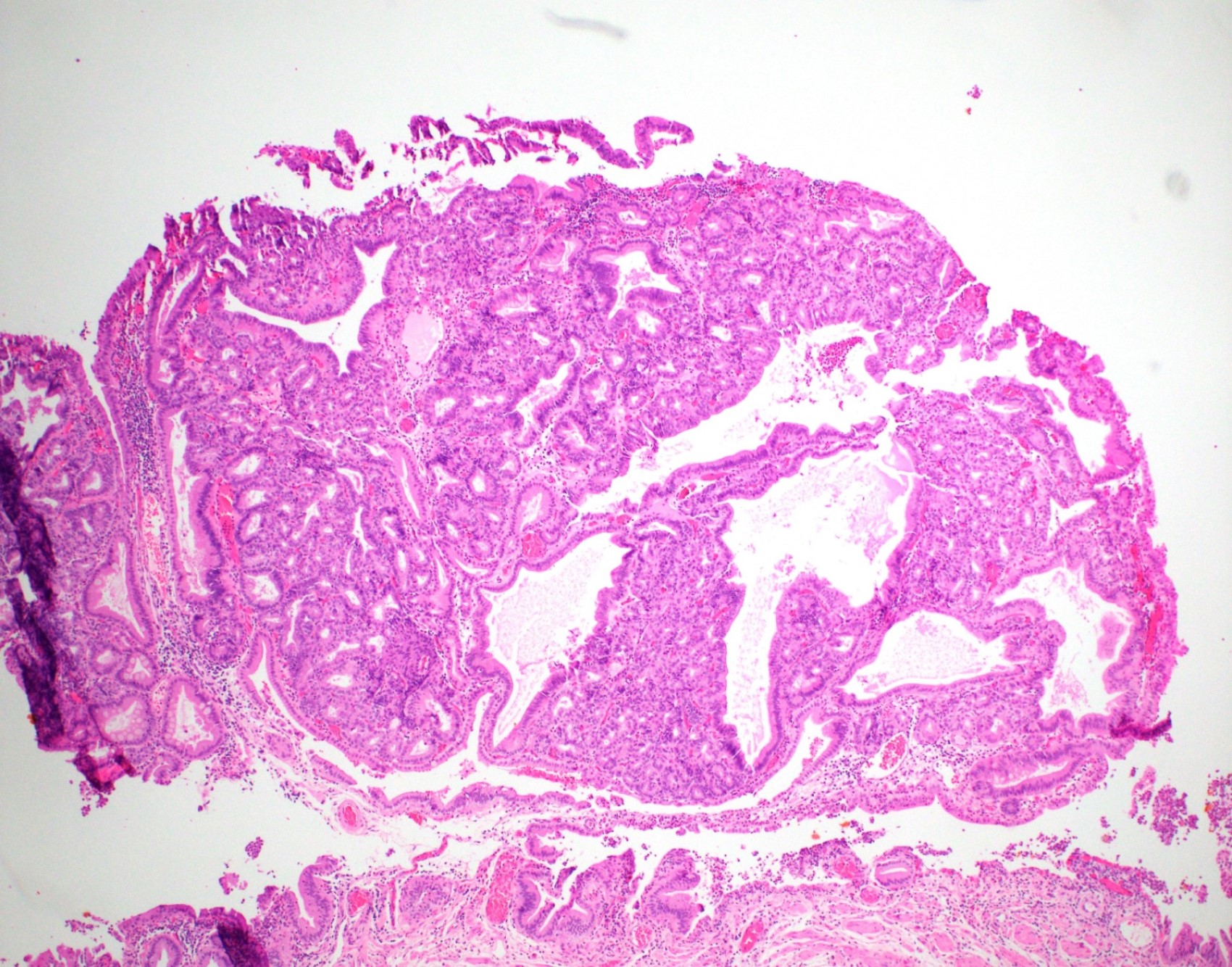
Intracholecystic papillary neoplasm of gallbladder (ICPN), biliary type, with extensive high grade dysplasia (> 75% of the tumor) (see comment)
Comment: The gallbladder was submitted entirely for microscopic evaluation and no invasive carcinoma is identified. The ICPN measures 3.5 cm in greatest dimension. Cystic duct margin is free of ICPN.
Gallbladder, cholecystectomy:
Invasive adenocarcinoma, moderately differentiated, colloid type, arising in an intracholecystic papillary neoplasm (ICPN), intestinal type, with high grade dysplasia (see comment)
Comment: The entire tumor is 5.3 cm in greatest dimension; the invasive carcinoma component is 1.5 cm in greatest dimension. The carcinoma invades through the muscularis layer (pT2). Cystic duct margin is free of invasive carcinoma but reveals high grade dysplasia.
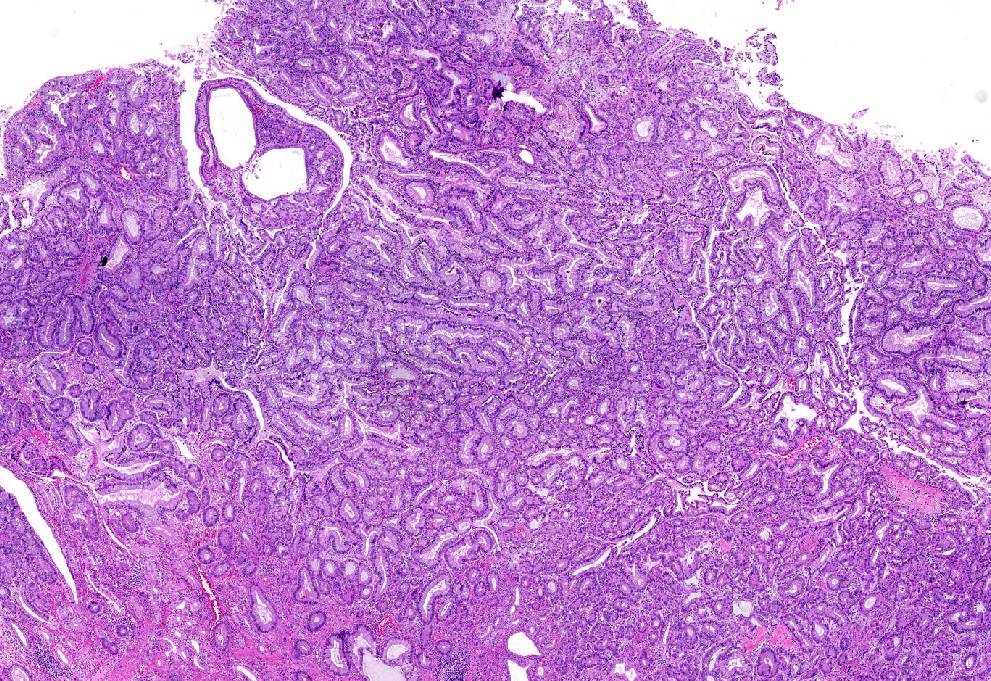
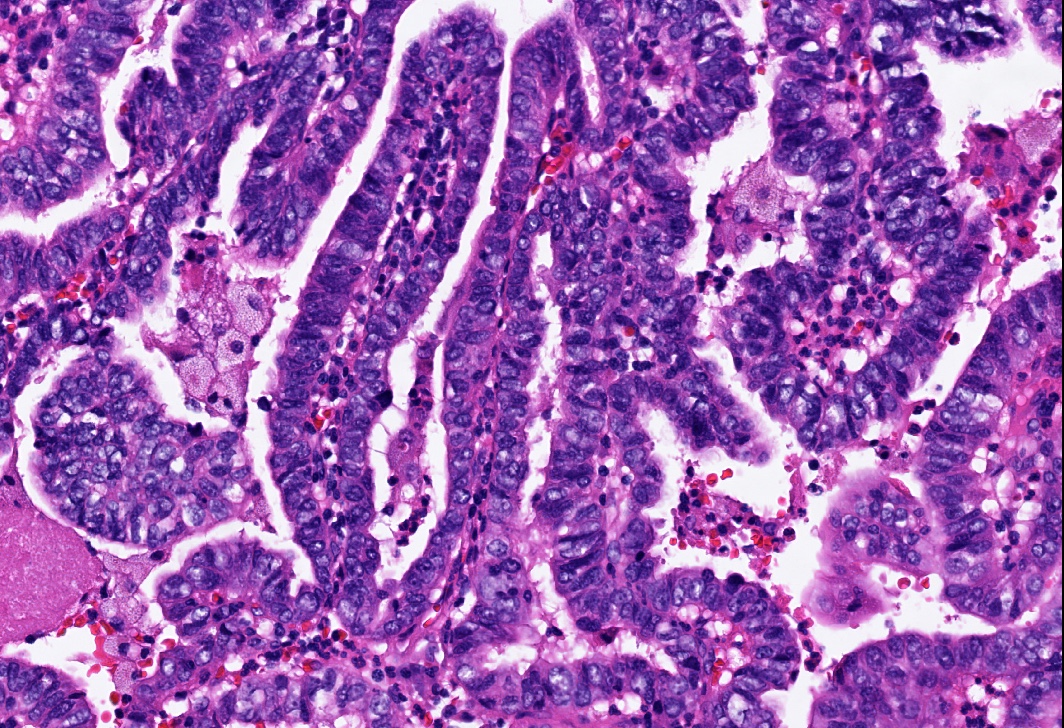
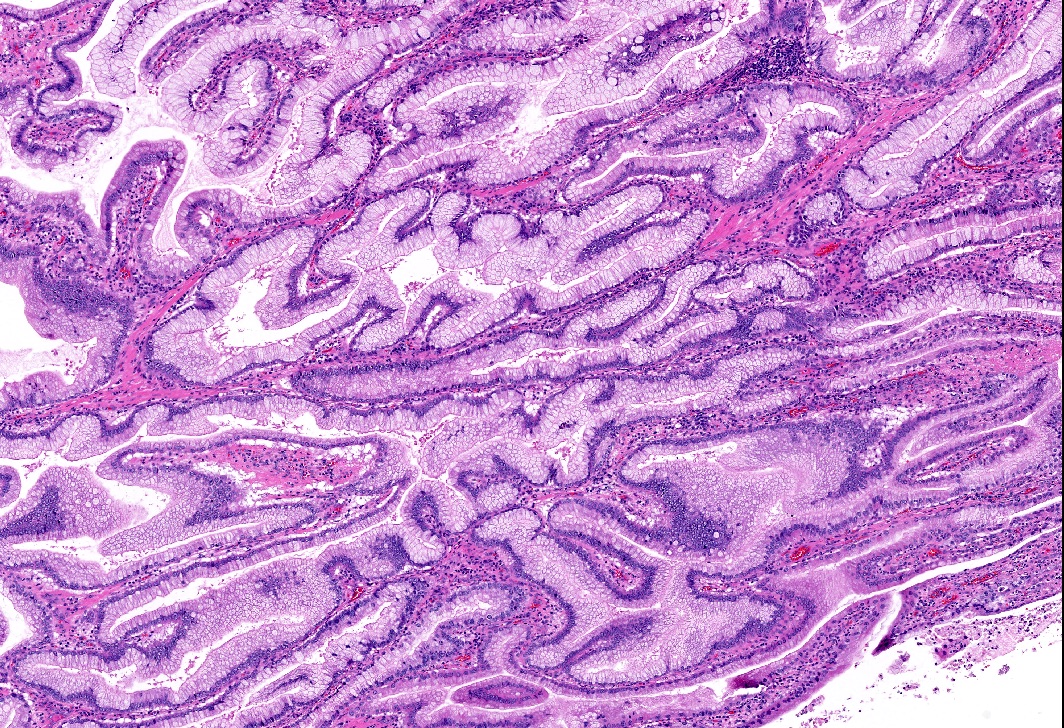
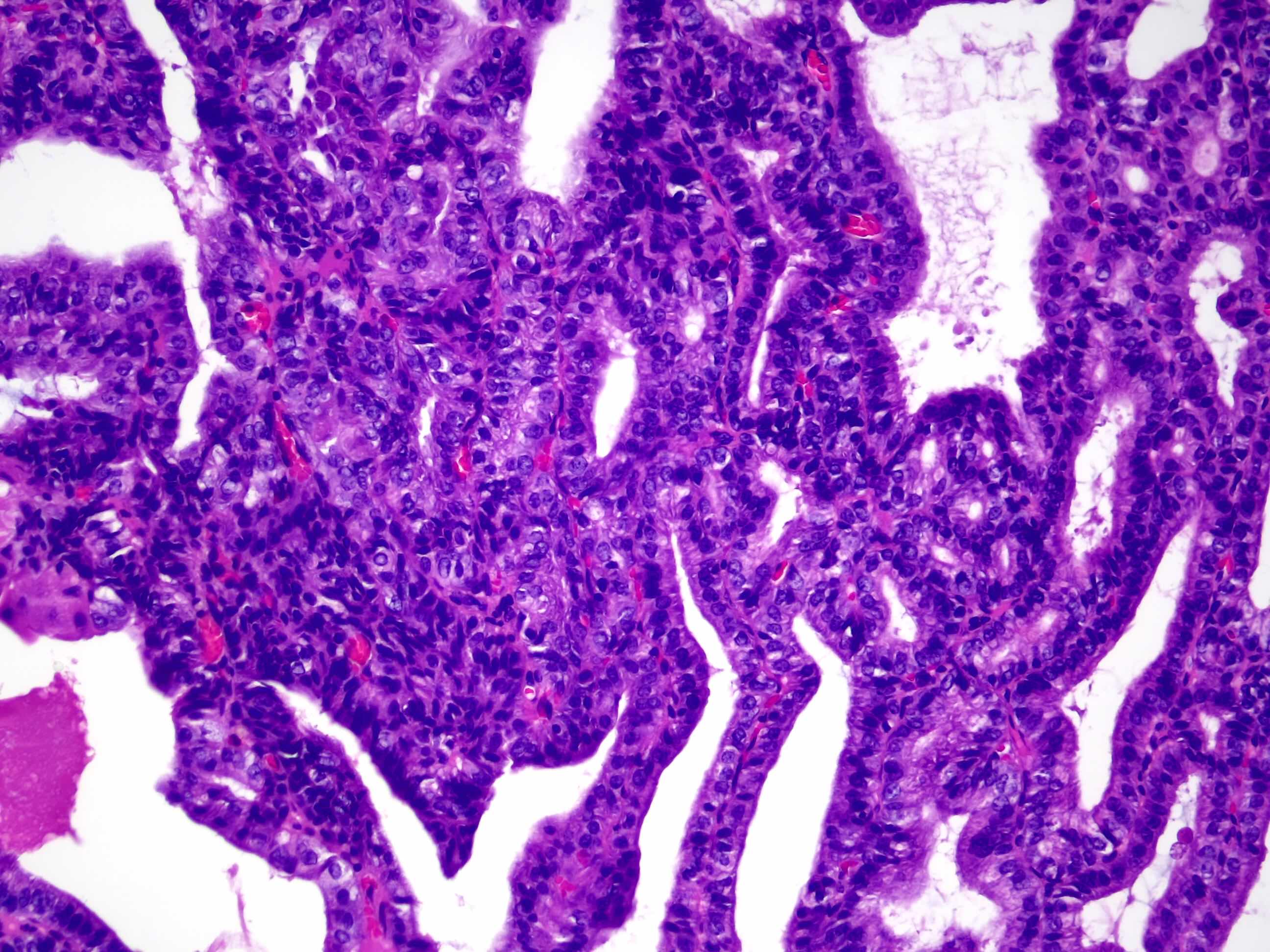
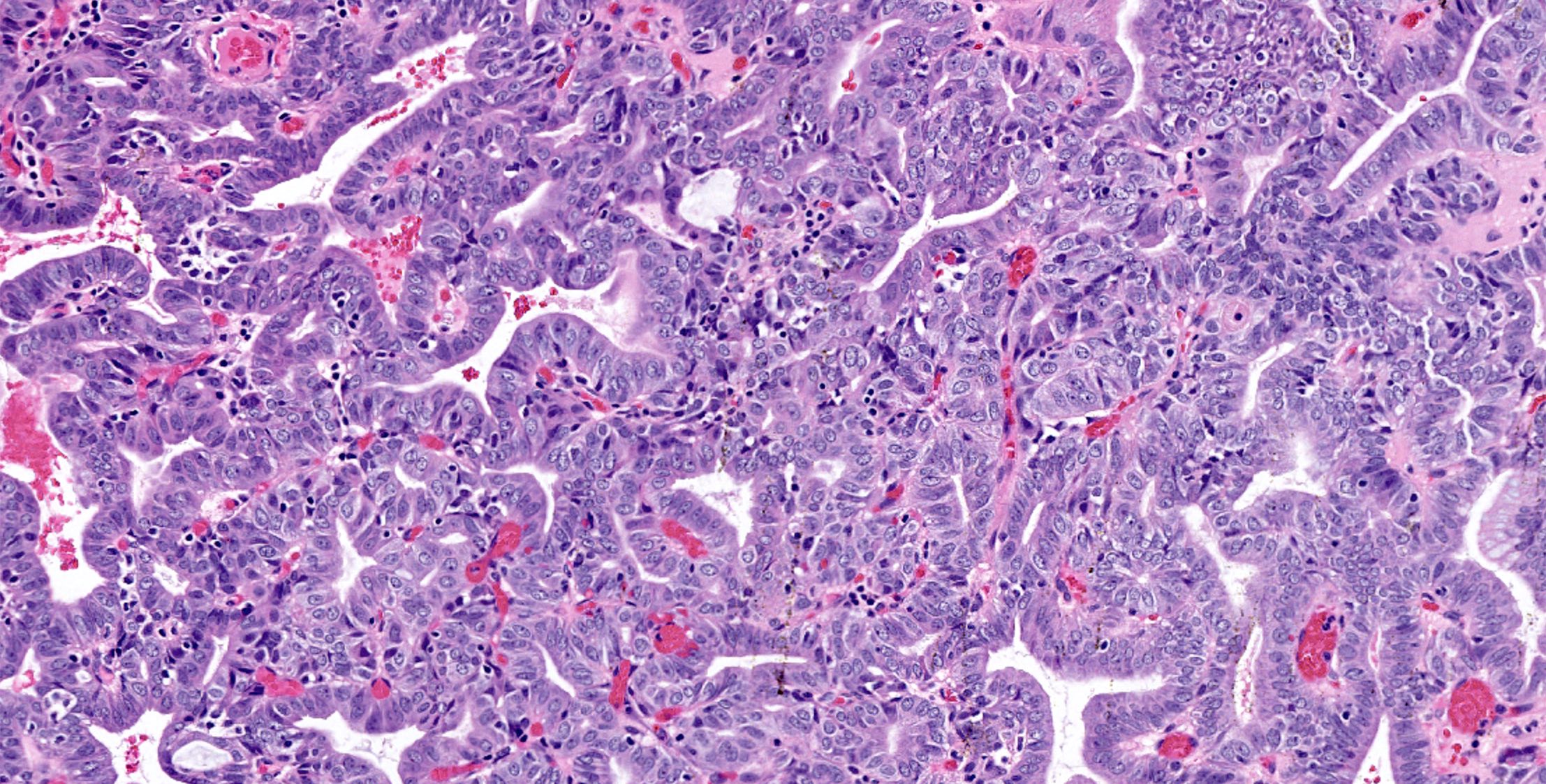
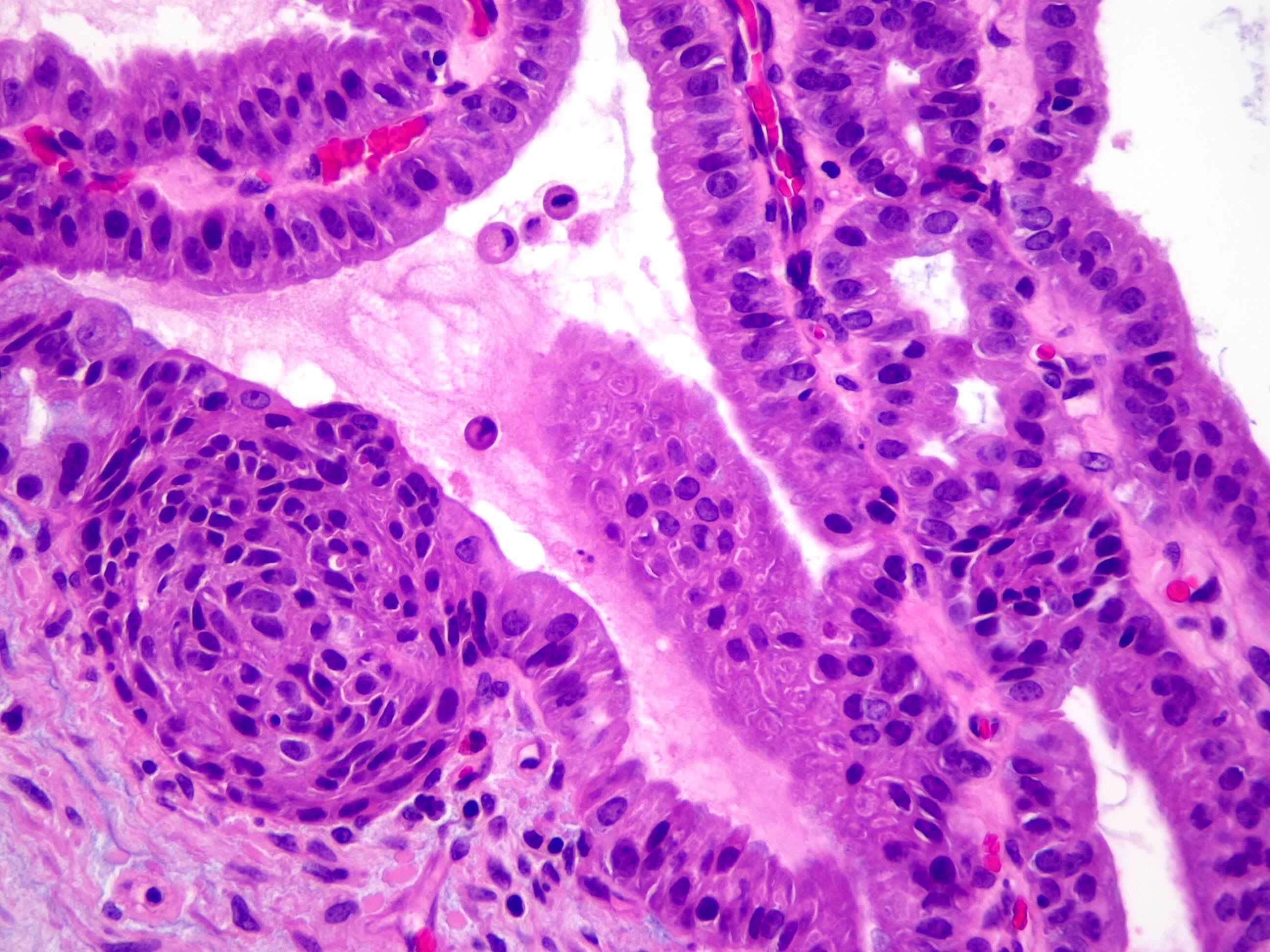
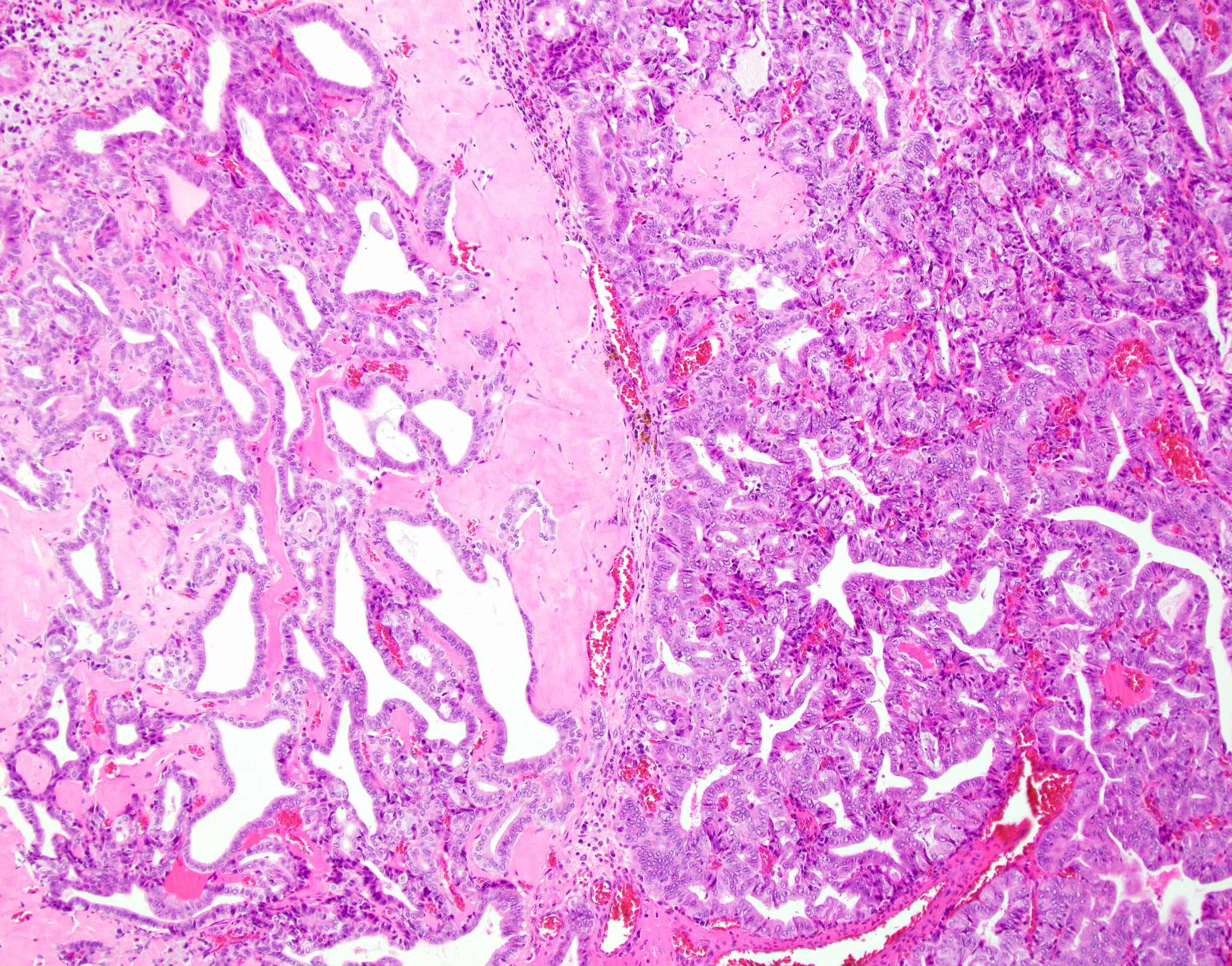
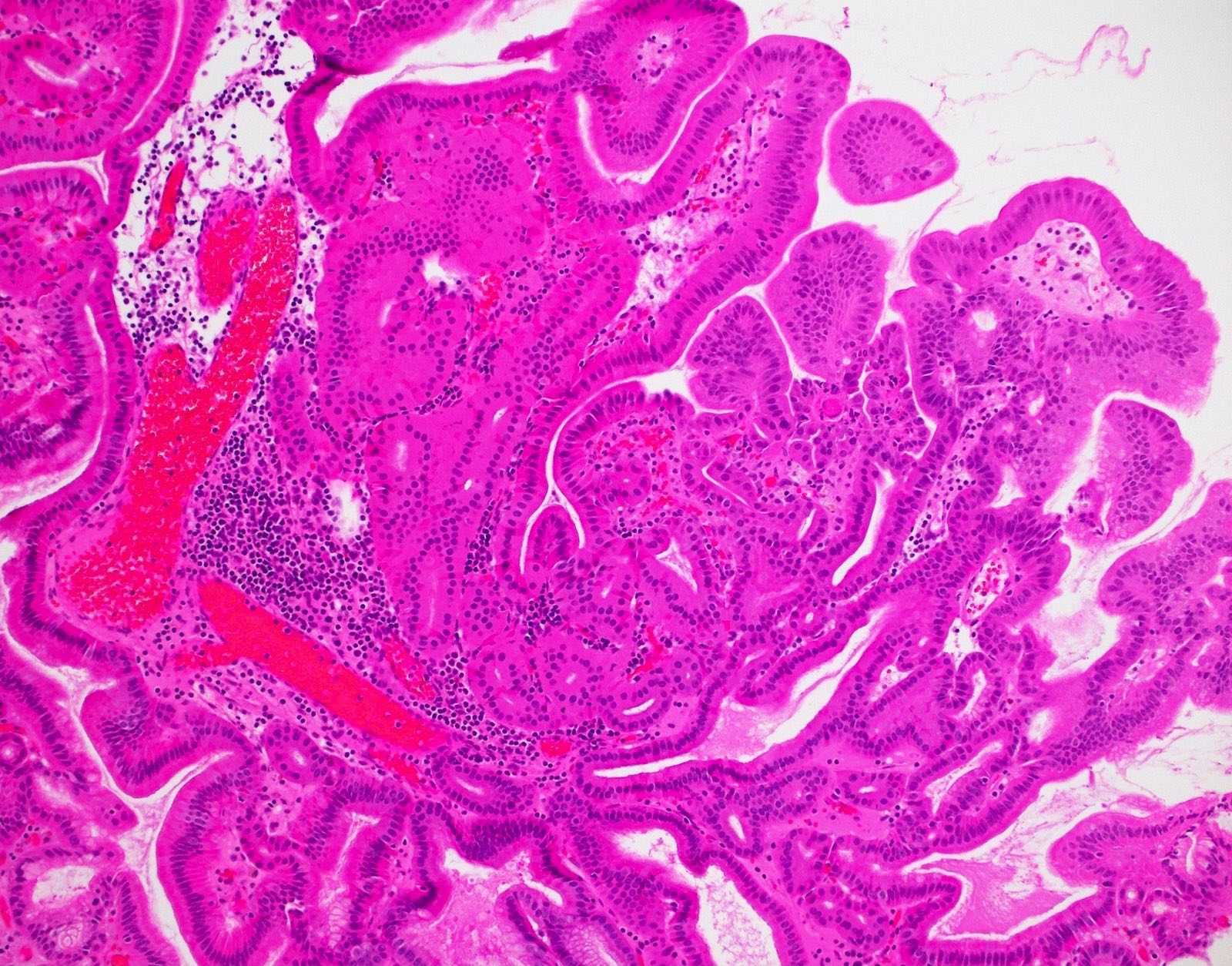
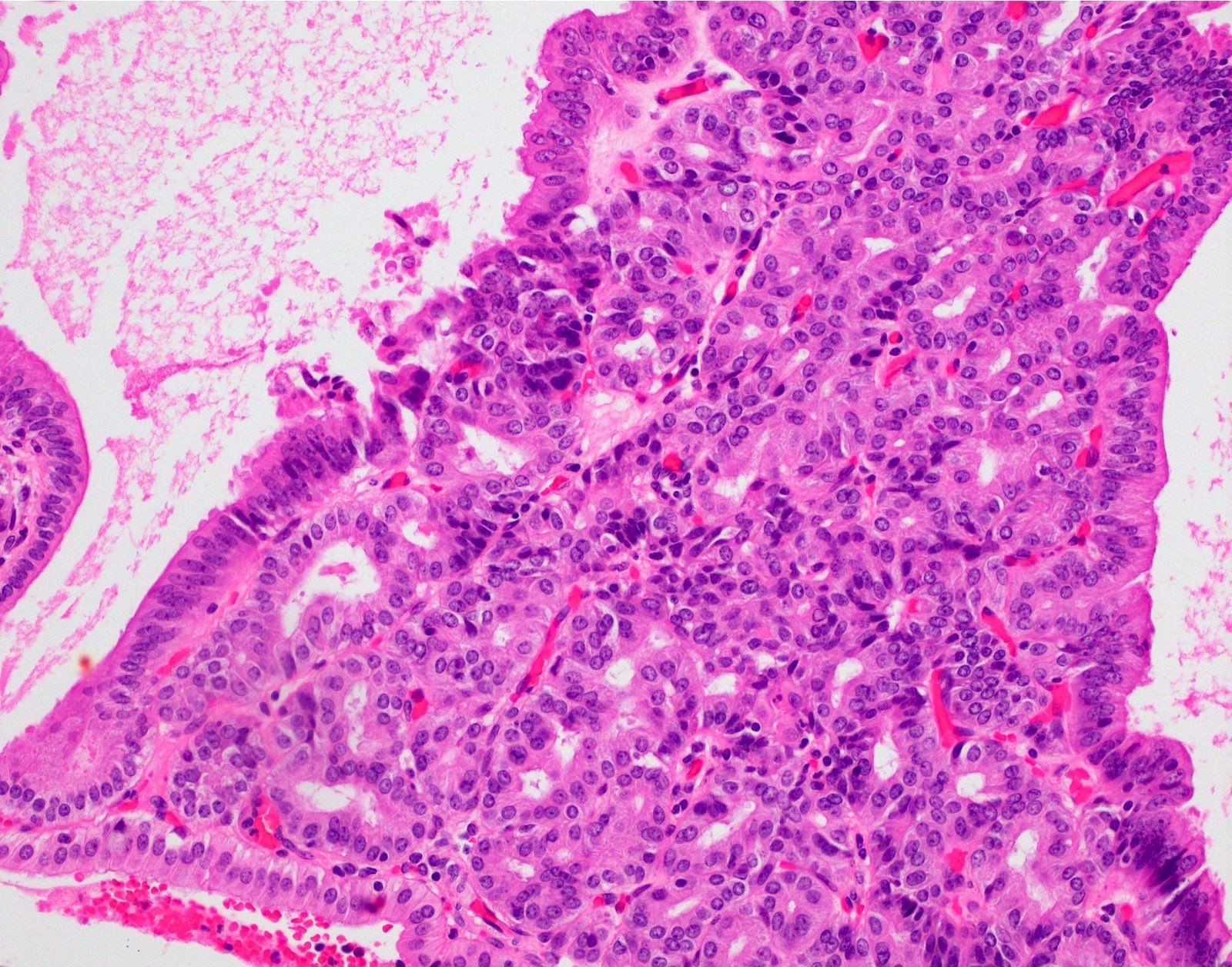
Presents as a mass forming gallbladder neoplasm characterized by cauliflower-like architecture and is comprised of compact, back to back, small tubular units showing variable complexity
Tubules are lined by low cuboidal, nonmucinous epithelium
Nuclei are either round and have visible nucleoli or are more ovoid, overlapping and have optically clear chromatin, creating a picture highly reminiscent of papillary thyroid carcinoma
Squamoid / meningothelial-like morules and neuroendocrine cell clusters are frequent
Despite their cytoarchitectural complexity, they are not associated with invasive carcinoma
Noninvasive epithelial neoplasm of the gallbladder that forms pedunculated polyps composed exclusively of small, nonmucinous tubules, often with squamoid morules (Virchows Arch 2021;478:435)
Despite the cytoarchitectural complexity that warrants high grade dysplasia diagnosis, almost never associated with invasion (Virchows Arch 2021;478:435)
Essential features
Pedunculated, typically solitary polyps with cauliflower architecture composed of lobules of back to back small acinar-like tubular units; possible association with cholesterol polyps
Morules are common but can be subtle; they can be highlighted by beta catenin nuclear labeling
Usually no dysplasia in the background gallbladder, uninvolved gallbladder is typically devoid of inflammation or chronic changes
Virtually no association with invasive carcinoma (unlike other preinvasive neoplasia of the gallbladder) (Virchows Arch 2021;478:435)
Does not appear to have field effect risk for biliary tract
Not defined as a distinct entity in WHO 2019; mentioned as intracholecystic papillary neoplasm showing gastric pyloric, nonmucinous morphology or presumably included in pyloric gland adenoma category
Use of older terms, such as biliary adenoma, tubulopapillary adenoma or papillary carcinoma is not recommended
ICD coding
No specific ICD code present; can be regarded under adenoma or intracholecystic papillary neoplasms
ICD-O: 8503/2 - intracystic papillary neoplasm with high grade intraepithelial neoplasia
Considering the WNT / beta catenin alterations along with the common presence of morules, may be regarded as a part of the so called BROCN family tumors (morule forming with biotin rich optically clear nuclei, namely fetal type pulmonary adenocarcinoma, pancreatoblastoma, cribriform morular thyroid carcinomas and some endometrial adenocarcinomas) (Mod Pathol 2003;16:1124, Mod Pathol 2002;15:617, J Pathol 2001;194:59, Am J Pathol 2001;159:1619)
Intracholecystic tubular nonmucinous neoplasm (ICTN) (see comment)
No dysplasia identified in the remainder of the gallbladder
No invasive carcinoma is identified
Cholesterolosis (if present)
Comment: Although there is high grade dysplasia within the lesion, intracholecystic tubular nonmucinous neoplasm (ICTN) typically has an innocuous behavior and does not seem to bear any risk for invasive carcinoma in the gallbladder or biliary tract.
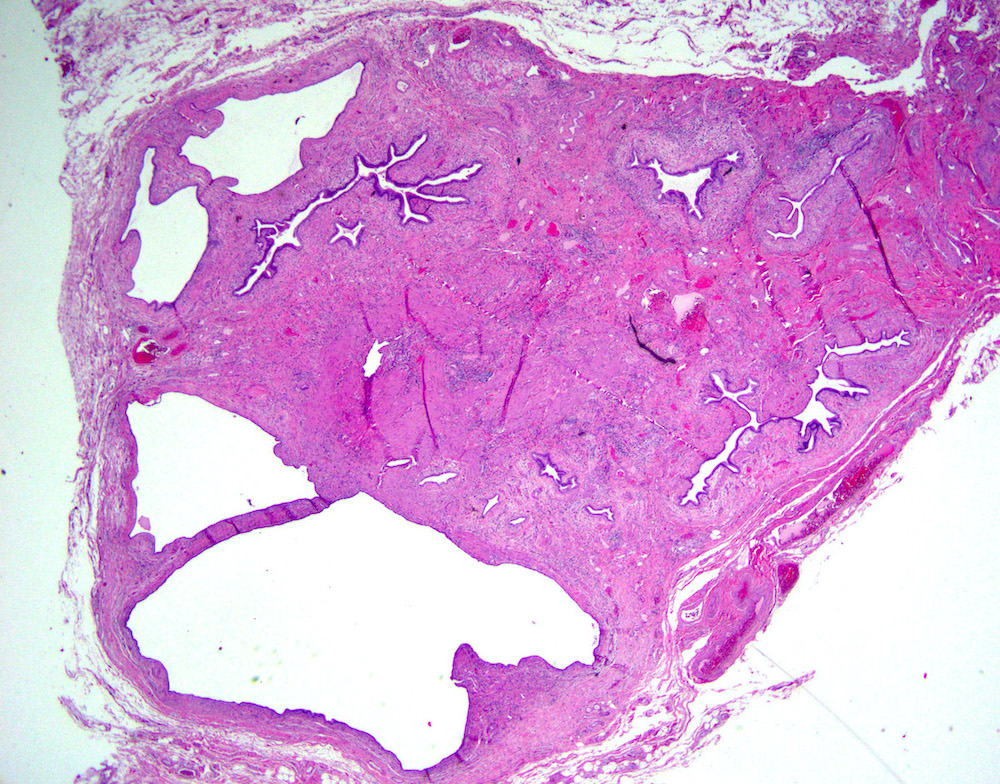
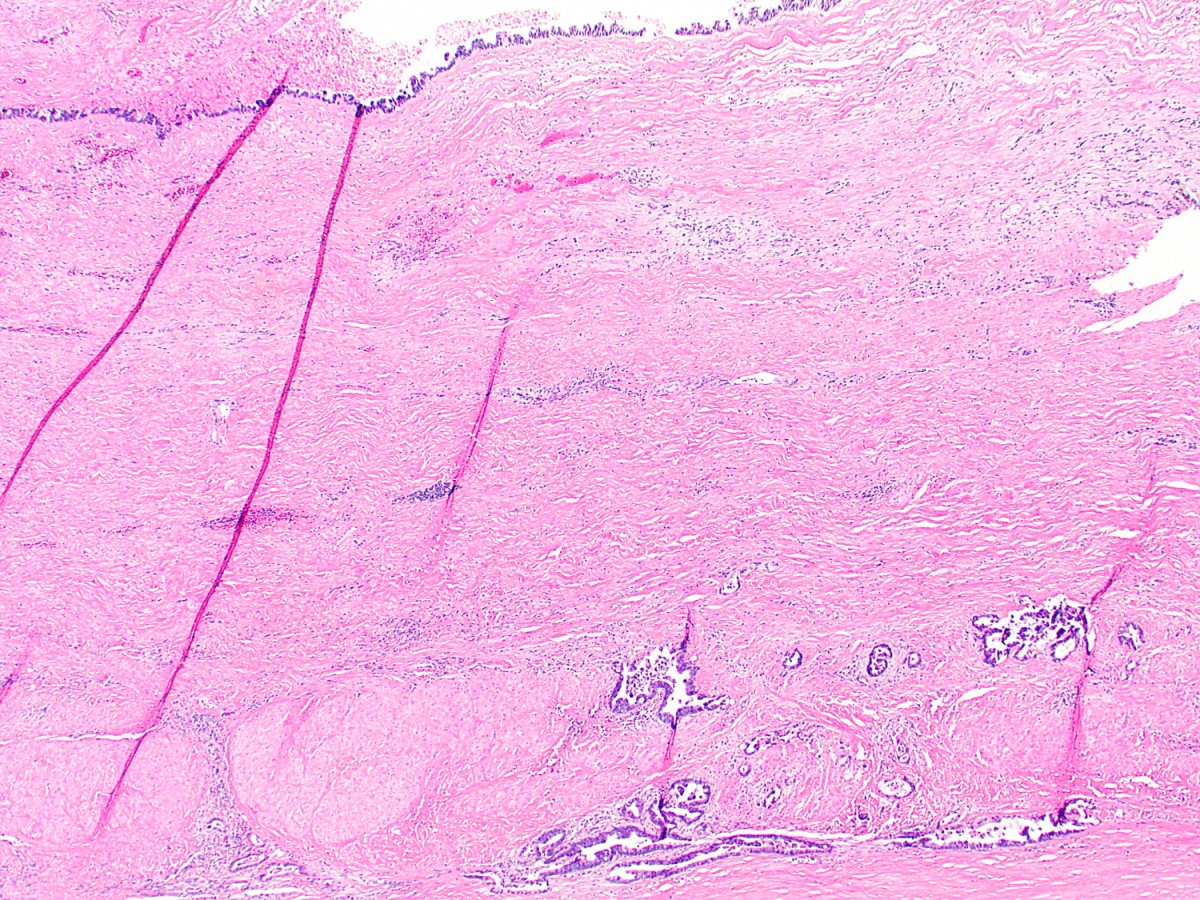
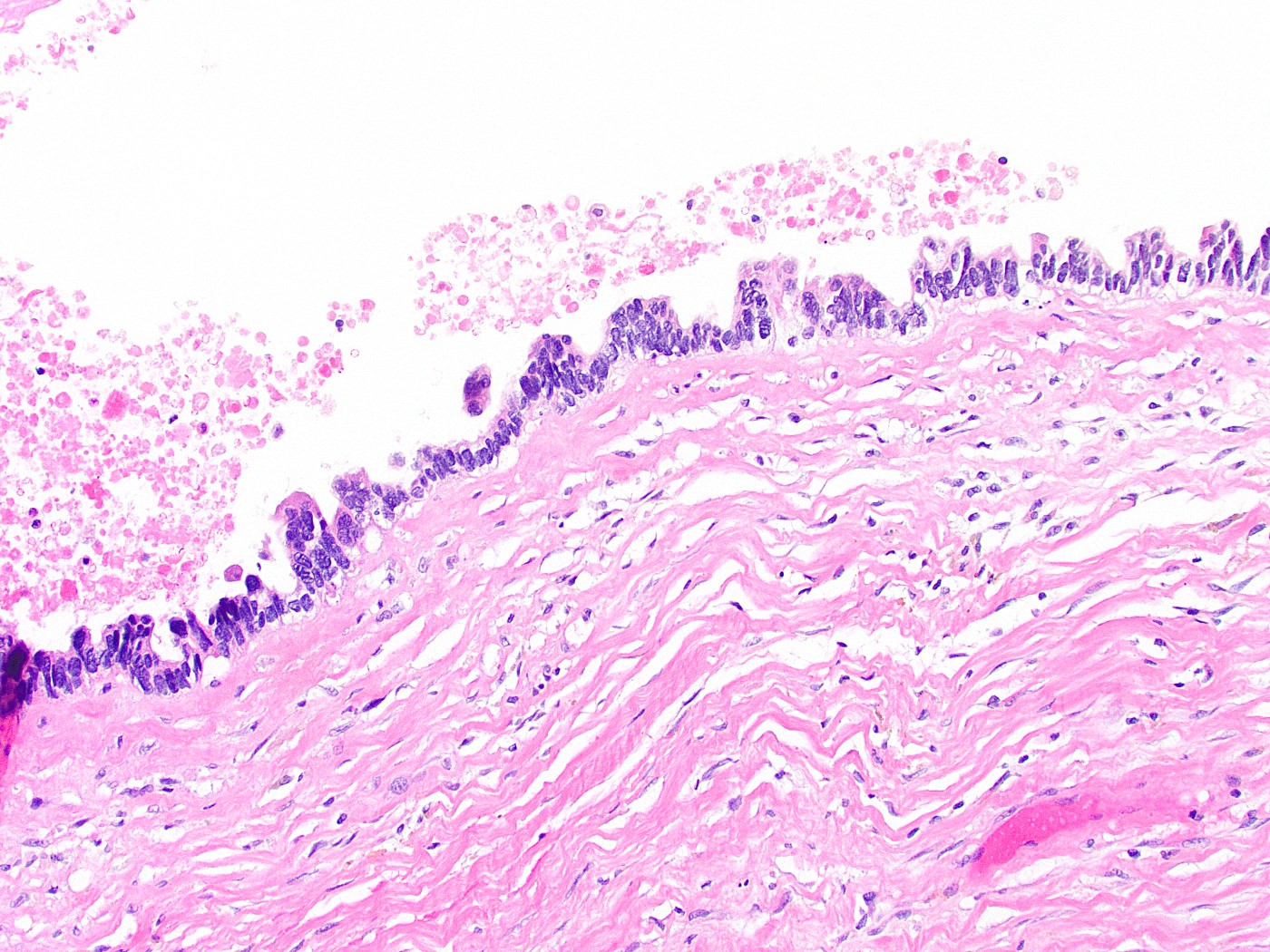
Dense, paucicellular hyaline fibrosis transforming gallbladder wall into relatively thin and uniform band
Diffusely effaces most of normal structure, some cases show calcifications
Also called hyalinizing cholecystitis
0.5% of cholecystectomies - 20% of cases associated with gallbladder carcinoma
Gross description
Pearly white appearance due to dystrophic calcification
Gross images
Images hosted on other servers:
Porcelain gallbladder
Microscopic (histologic) description
Widely scattered and bland appearing glands embedded in thin band of hyaline stroma, commonly showing a disappearing lining, leaving behind granular, necrotic intraluminal debris (regression) with or without calcification (Am J Surg Pathol 2011;35:1104)
Surface epithelium, if preserved, typically shows carcinoma in situ of either denuding or micropapillary types
Glandular elements in wall should raise suspicion of carcinoma, since benign glands are usually sparse
Glands have longitudinal axis parallel to the surface, irregular contours, clear cytoplasm with distinct borders, nuclear irregularities, washed out chromatin
Chronic cholestatic disorder of unknown origin (possibly autoimmune) involving entire biliary tract from ampulla of Vater to small intrahepatic bile ducts or gallbladder
Much less common than secondary sclerosing cholangitis
Clinical features
Rule of 70s: 70% men, 70% have chronic inflammatory bowel disease (particularly ulcerative colitis which is usually detected first; only 4% with ulcerative colitis have primary sclerosing cholangitis, which is unaffected by colectomy), 70% younger than age 45
Also associated with chronic pancreatitis (15 - 25%), Riedel thyroiditis, retroperitoneal and mediastinal fibrosis, orbital pseudotumor, Sjögren syndrome, angioimmunoblastic lymphadenopathy
End stage disease is associated with hyperplasia of glands of extrahepatic bile ducts, with low incidence of dysplasia and adenocarcinoma
(Am J Surg Pathol 2003;27:349)
Bile ducts in PSC show two distinct pathways of dysplasia-carcinoma, based on differences in cell morphology, growth patterns, immunophenotypes and grade of malignancy (Histopathology 2011;59:1100)
Symptoms: fatigue, jaundice, pruritis
Complications:
Biliary cirrhosis and liver failure in all cases with median survival 9 - 12 years
Cholangiocarcinoma (10 - 43%), colon carcinoma
Staging:
Inflammation without expansion of portal tracts or piecemeal necrosis
Piecemeal necrosis or fibrosis without bridging
Bridging necrosis or fibrosis
Cirrhosis
Laboratory
Elevated serum alkaline phosphatase, IgM, IgG
Variable bilirubin
May be pANCA positive
Radiology description
Xray: beading of barium column in cholangiogram due to irregular strictures and dilations of affected bile ducts
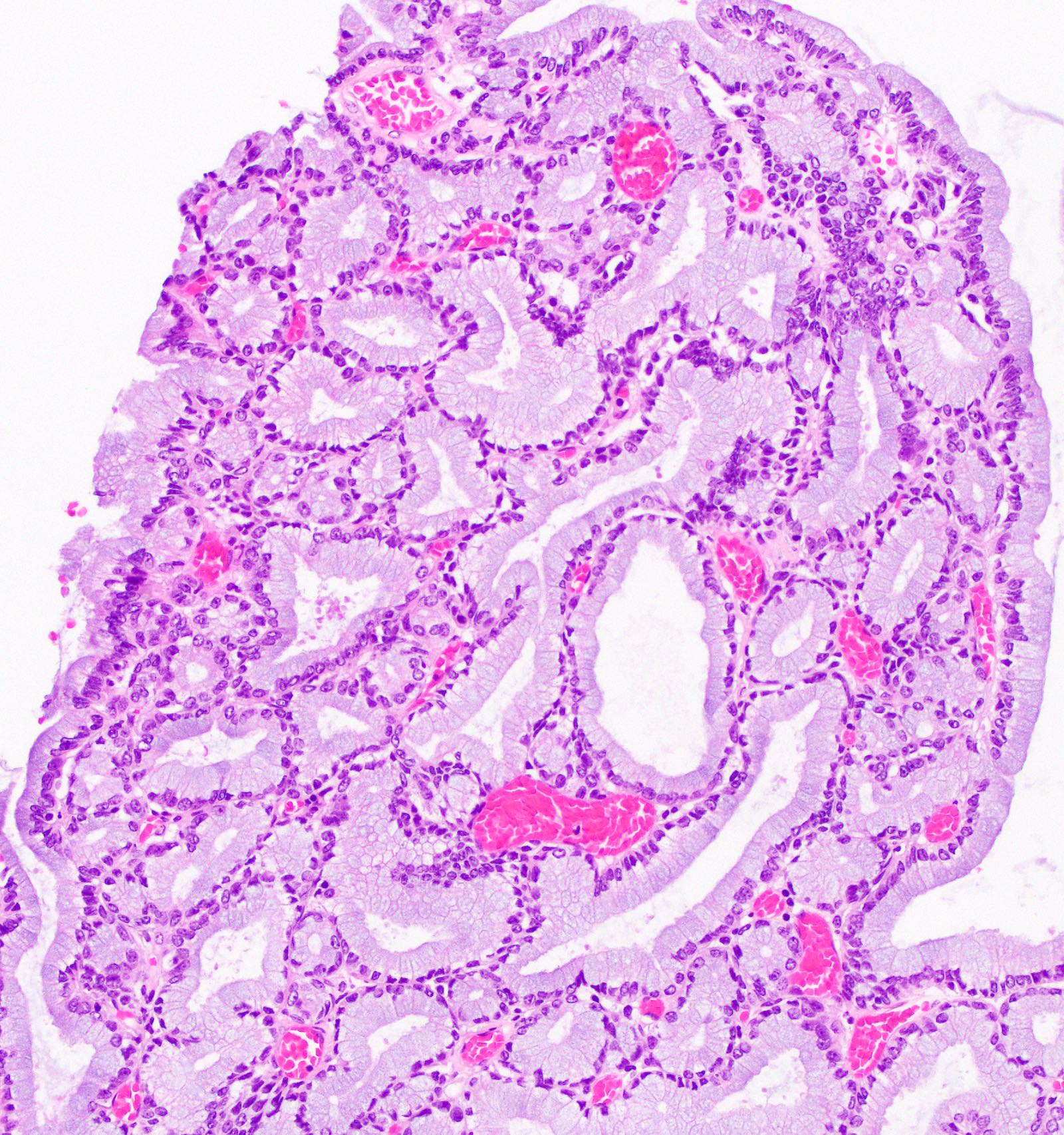
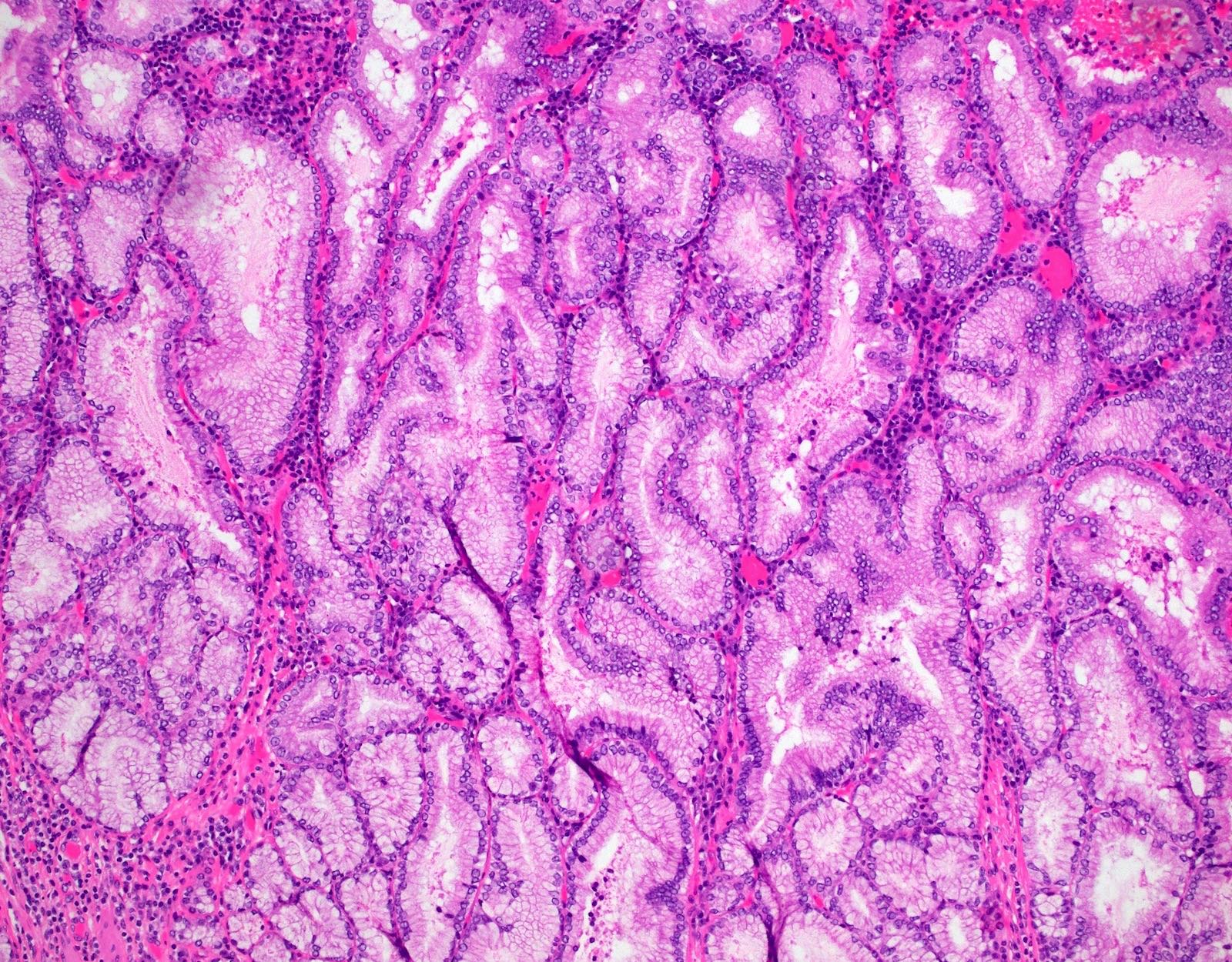
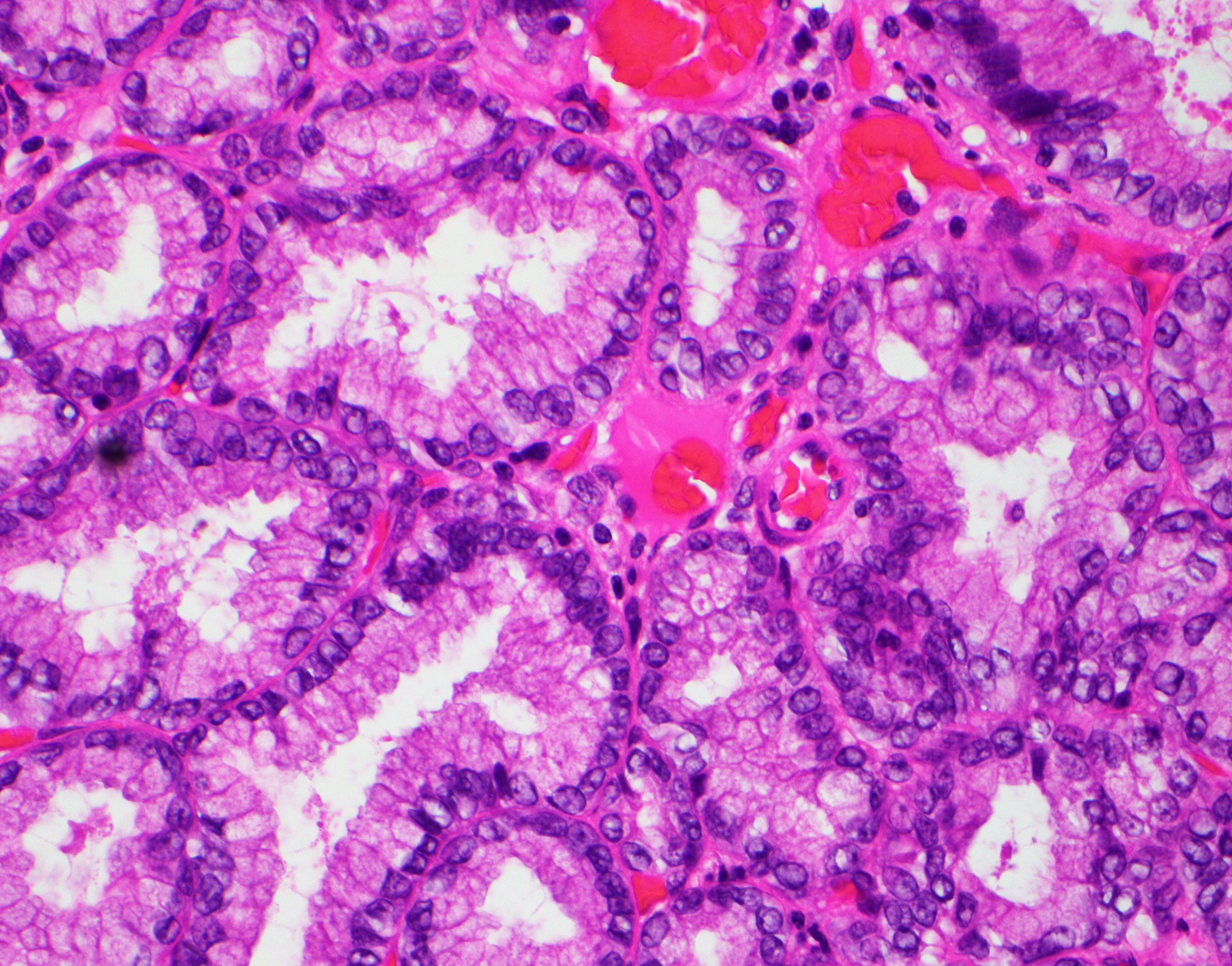
Grossly visible, noninvasive neoplasm of the gallbladder composed of uniform back to back mucinous glands arranged in a tubular configuration
WHO classification
Architecture is often complex
Glands are bland looking pyloric type or Brunner gland-like
There is minimal cytological atypia in most of the lesions
By definition, the cytologic atypia is sufficient for low grade dysplasia
Foci of high grade dysplasia can be seen in larger lesions
If lesion is > 1 cm with dysplasia present, classification as intracholecystic papillary (tubular) neoplasm is recommended by some authors (Am J Surg Pathol 2012;36:1279)
Essential features
Grossly visible, complex, back to back, uniform mucinous glands of pyloric type or Brunner gland-like
Usually > 0.5 cm and < 2 cm
< 0.5 cm should be distinguished from nodular pyloric gland metaplasia, which by definition bears no cytologic atypia or dysplasia
> 1 cm with dysplasia may be classified as intracholecystic papillary (tubular) neoplasm
Terminology
Intracholecystic papillary tubular neoplasm, gastric pyloric, simple mucinous type
62 year old man with a 2 cm tumor with transition into well differentiated adenocarcinoma and high grade biliary intraepithelial neoplasia (BMC Cancer 2012;12:570)
Treatment
Surgery (cholecystectomy) is indicated for any polypoid lesions ≥ 1 cm
Considered an umbrella term for any neoplastic polyps, adenomas and papillary neoplasms that are ≥ 1 cm
Can be further divided into several categories by morphology
Biliary, gastric, intestinal and oncocytic
Pyloric gland adenoma is currently not included under this umbrella
However, terms may be interchangeable between intracholecystic papillary (tubular) neoplasm and pyloric gland adenomas that are ≥ 1 cm with invasive carcinoma
A polypoid lesion of the gallbladder is identified by ultrasound and is resected. Based on the photomicrograph above, which of the following statements is true?
Aberrant expression of CDX2 is a frequent feature
Frequently shows MUC5AC positivity
It is a precursor lesion for most of the gallbladder adenocarcinomas
Occurs predominantly in males
Usually CK7 positive
Board review style answer #1
E. Usually CK7 positive, as this is a pyloric gland adenoma. Answer A is incorrect because they do not often express CDX2. Answer B is incorrect because they frequently show MUC6 positivity. Answer C is incorrect because it is a precursor lesion to some but not most of the gallbladder adenocarcinomas. Answer D is incorrect because they occur predominantly in female patients.
Regarding pyloric gland adenoma of the gallbladder, which of the following is correct?
Frequently shows p53 aberrant expression
Lesions > 1 cm can be reclassified as intracholecystic papillary neoplasm
They are not associated with chronic cholecystitis
Those are benign lesions and never progress to cancer
Board review style answer #2
B. Lesions > 1 cm can be reclassified as intracholecystic papillary neoplasm. If the lesion is > 1 cm with dysplasia present, classification as intracholecystic papillary (tubular) neoplasm is recommended by some authors. Answer C is incorrect because pyloric gland adenoma is often associated with background chronic cholecystitis. Answer A is incorrect because p53 usually shows normal wild type expression in those lesions. Answer D is incorrect because they can progress to cancer.
All carcinomas of the distal common bile duct (with an epicenter between the cystic duct / common hepatic duct confluence and the ampulla of Vater), including poorly differentiated neuroendocrine carcinomas, are covered by this staging system
Cystic duct lesions are staged using the gallbladder template and common hepatic duct lesions are staged using the perihilar template
Essential features
AJCC, 7th Edition staging was sunset on December 31, 2017; as of January 1, 2018, use of the
AJCC, 8th Edition, 2018 is mandatory
Terminology
These lesions are generally referred to as adenocarcinoma, rather than cholangiocarcinoma
ICD coding
C24.0: malignant neoplasm of extrahepatic bile duct
Primary tumor (pT)
TX: primary tumor cannot be assessed
T0: no evidence of primary tumor
Tis: carcinoma in situ / high grade dysplasia
T1: tumor invades the bile duct wall with a depth less than 5 mm
T2: tumor invades the bile duct wall with a depth of 5 - 12 mm
T3: tumor invades the bile duct wall with a depth greater than 12 mm
T4: tumor invades the celiac axis, superior mesenteric artery or common hepatic artery
Notes: careful perpendicular or longitudinal sections of the bile duct wall must be taken in order for accurate measurements of invasion to be made
Regional lymph nodes (pN)
NX: regional lymph nodes cannot be assessed
N0: no regional lymph node metastasis
N1: metastasis in one to three regional lymph nodes
N2: metastasis in four or more regional lymph nodes
Notes: regional lymph nodes include the common bile duct, hepatic artery, anterior and posterior pancreaticoduodenal and right lateral superior mesenteric artery nodes
Distant metastasis (pM)
M0: no distant metastasis
M1: distant metastasis
Stage grouping
Stage 0:TisN0M0
Stage I:T1N0M0
Stage IIA:T1N1M0
T2N0M0
Stage IIB:T2N1M0
T3N0 - 1M0
Stage IIIA:T1 - 3N2M0
Stage IIIB:T4N0 - 2M0
Stage IVB:any Tany NM1
Registry data collection variables
Tumor location: cystic duct, perihilar bile ducts or distal bile duct
CEA
CA19-9
Histologic grade
GX: grade cannot be assessed
G1: well differentiated
G2: moderately differentiated
G3: poorly differentiated
Histopathologic type
Adenocarcinoma, biliary type
Adenocarcinoma, intestinal type
Adenocarcinoma, gastric foveolar type
Mucinous adenocarcinoma
Clear cell adenocarcinoma
Signet ring cell carcinoma
Squamous cell carcinoma
Adenosquamous carcinoma
Undifferentiated carcinoma
Neuroendocrine carcinoma
Small cell neuroendocrine carcinoma
Large cell neuroendocrine carcinoma
Mixed adenoneuroendocrine carcinoma
Intraductal papillary neoplasm with an associated invasive component
Mucinous cystic neoplasm with an associated invasive component
Residual tumor
R0: complete resection with grossly and microscopically negative margins of resection
R1: grossly negative but microscopically positive margins of resection
R2: grossly and microscopically positive margins of resection
Board review style question #1
Bile duct adenocarcinoma arising in the pancreas and invading 10 mm into the bile duct wall, focally involving the pancreas but no other local structures, would be staged as which of the following using AJCC 8th edition criteria?
T1: tumor invades lamina propria or muscular layer
T1a: tumor invades lamina propria
T1b: tumor invades muscular layer
T2: tumor invades the perimuscular connective tissue on the peritoneal side, without involvement of the serosa (visceral peritoneum) or tumor invades the perimuscular connective tissue on the hepatic side, with no extension into the liver
T2a: tumor invades the perimuscular connective tissue on the peritoneal side, without involvement of the serosa (visceral peritoneum)
T2b: tumor invades the perimuscular connective tissue on the hepatic side, with no extension into the liver
T3: tumor perforates the serosa (visceral peritoneum) or directly invades the liver or one other adjacent organ or structure, such as the stomach, duodenum, colon, pancreas, omentum or extrahepatic bile ducts
T4: tumor invades the main portal vein or hepatic artery or invades two or more extrahepatic organs or structures
Regional lymph nodes include the common bile duct, hepatic artery, portal vein and cystic duct nodes
Distant metastasis (pM)
M0: no distant metastasis
M1: distant metastasis
Stage grouping
Stage 0:
Tis
N0
M0
Stage I:
T1
N0
M0
Stage IIA:
T2a
N0
M0
Stage IIB:
T2b
N0
M0
Stage IIIA:
T3
N0
M0
Stage IIIB:
T1-3
N1
M0
Stage IVA:
T4
N0-1
M0
Stage IVB:
any T
N2
M0
any T
any N
M1
Registry data collection variables
Specimen type
Extent of liver resection
Free peritoneal side versus hepatic side for T2 tumors
Histologic grade
GX: grade cannot be assessed
G1: well differentiated
G2: moderately differentiated
G3: poorly differentiated
Histopathologic type
Adenocarcinoma, biliary type
Adenocarcinoma, intestinal type
Adenocarcinoma, gastric foveolar type
Mucinous adenocarcinoma
Clear cell adenocarcinoma
Signet ring cell carcinoma
Squamous cell carcinoma
Adenosquamous carcinoma
Undifferentiated carcinoma
Neuroendocrine carcinoma
Small cell neuroendocrine carcinoma
Large cell neuroendocrine carcinoma
Mixed adenoneuroendocrine carcinoma
Intraductal papillary neoplasm with an associated invasive component
Mucinous cystic neoplasm with an associated invasive component
Residual tumor
R0: complete resection with grossly and microscopically negative margins of resection
R1: grossly negative but microscopically positive margins of resection
R2: grossly and microscopically positive margins of resection
Board review style question #1
Which of the following AJCC T-category staging options for gallbladder carcinoma is substaged depending on whether the tumor arises from the peritoneum facing or liver facing side of the gallbladder?
All carcinomas of the perihilar bile ducts (arising predominantly in the main lobar extrahepatic bile ducts, distal to segmental bile ducts and proximal to the cystic duct), including poorly differentiated neuroendocrine carcinomas, are covered by this staging system
Cystic duct lesions are staged using the gallbladder template and common bile duct lesions are staged using the distal bile duct template
Essential features
AJCC, 7th Edition staging was sunset on December 31, 2017; as of January 1, 2018, use of the
AJCC, 8th Edition, 2018 is mandatory
Terminology
AJCC advocates the term cholangiocarcinoma for adenocarcinomas of this region
ICD coding
C24.0: malignant neoplasm of extrahepatic bile duct
T1: tumor confined to the bile duct, with extension up to the muscle layer or fibrous tissue
T2: tumor invades beyond the wall of the bile duct to surrounding adipose tissue or tumor invades adjacent hepatic parenchyma
T2a: tumor invades beyond the wall of the bile duct to surrounding adipose tissue
T2b: tumor invades adjacent hepatic parenchyma
T3: tumor invades unilateral branches of the portal vein or hepatic artery
T4: tumor invades the main portal vein or its branches bilaterally or the common hepatic artery; or unilateral second order biliary radicles with contralateral portal vein or hepatic artery involvement
Regional lymph nodes (pN)
NX: regional lymph nodes cannot be assessed
N0: no regional lymph node metastasis
N1: one to three positive lymph nodes typically involving the hilar, cystic duct, common bile duct (choledochal), hepatic artery, posterior pancreatoduodenal and portal vein lymph nodes
N2: four or more positive lymph nodes from the sites described for N1
Notes: regional lymph nodes are listed above, in the N1 criteria
Distant metastasis (pM)
M0: no distant metastasis
M1: distant metastasis
Stage grouping
Stage 0:TisN0M0
Stage I:T1N0M0
Stage II:T2a - bN0M0
Stage IIIA:T3N0M0
Stage IIIB:T4N0M0
Stage IIIC:any TN1M0
Stage IVA:any TN2M0
Stage IVB:any Tany NM1
Registry data collection variables
Tumor location and extent according to Bismuth-Corlette classification:
I: tumor is limited to the common hepatic duct, below the level of the confluence of the right and left hepatic ducts
II: tumor involves the confluence of the right and left hepatic ducts
IIIa: tumor with type II involvement plus extension to the right second order ducts
IIIb: tumor with type II involvement plus extension to the left second order ducts
IV: tumor extends into both right and left second order ducts
Mucinous cystic neoplasm with an associated invasive component
Residual tumor
R0: complete resection with grossly and microscopically negative margins of resection
R1: grossly negative but microscopically positive margins of resection
R2: grossly and microscopically positive margins of resection
Board review style question #1
Which of the following histologic patterns portends a good prognosis for perihiliar bile duct cholangiocarcinoma and therefore is considered a registry data collection variable?
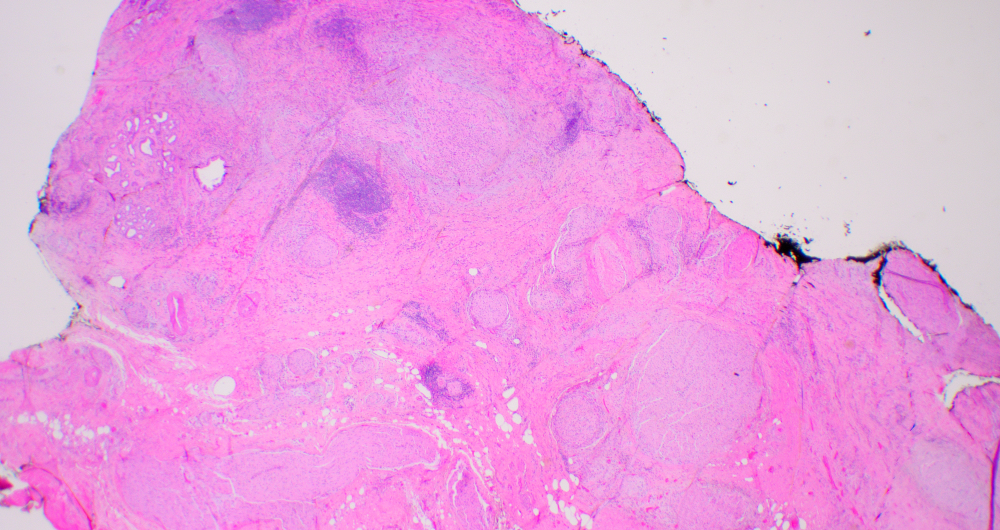
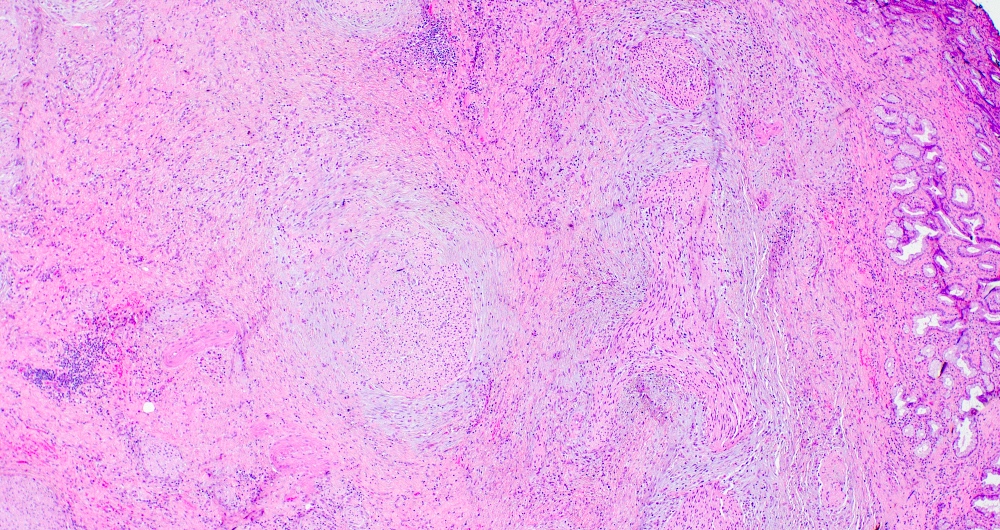
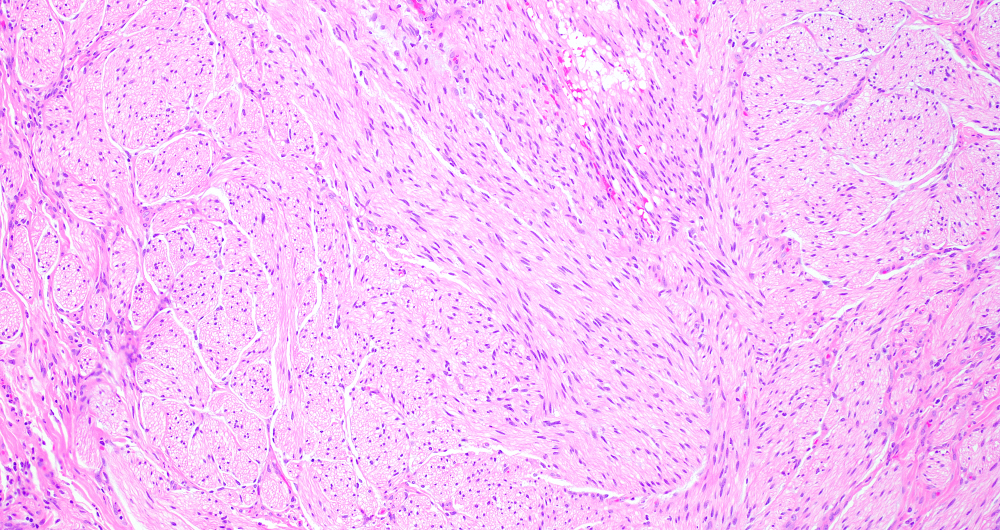
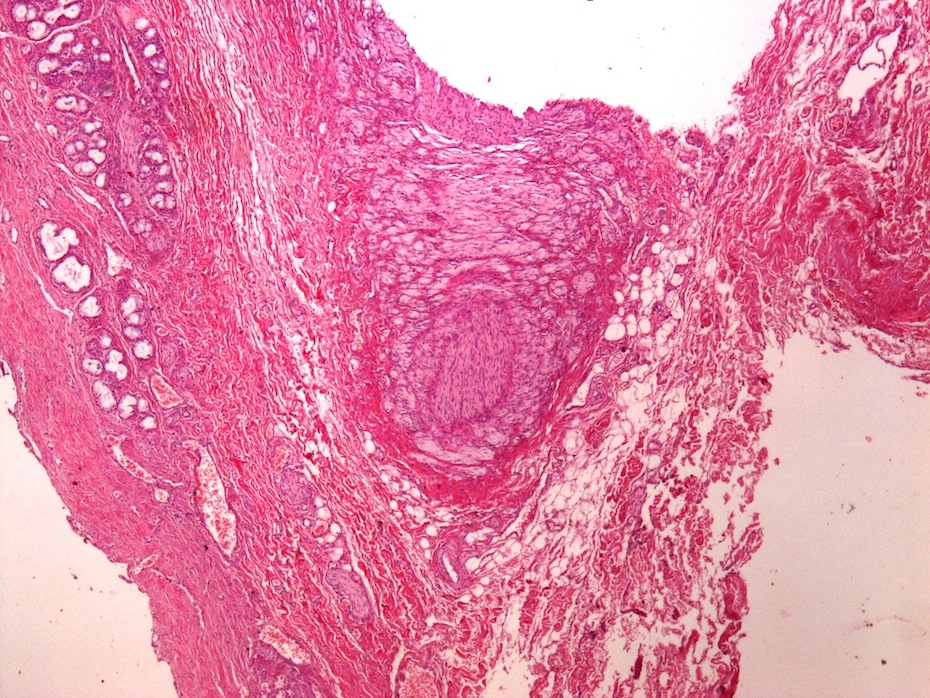
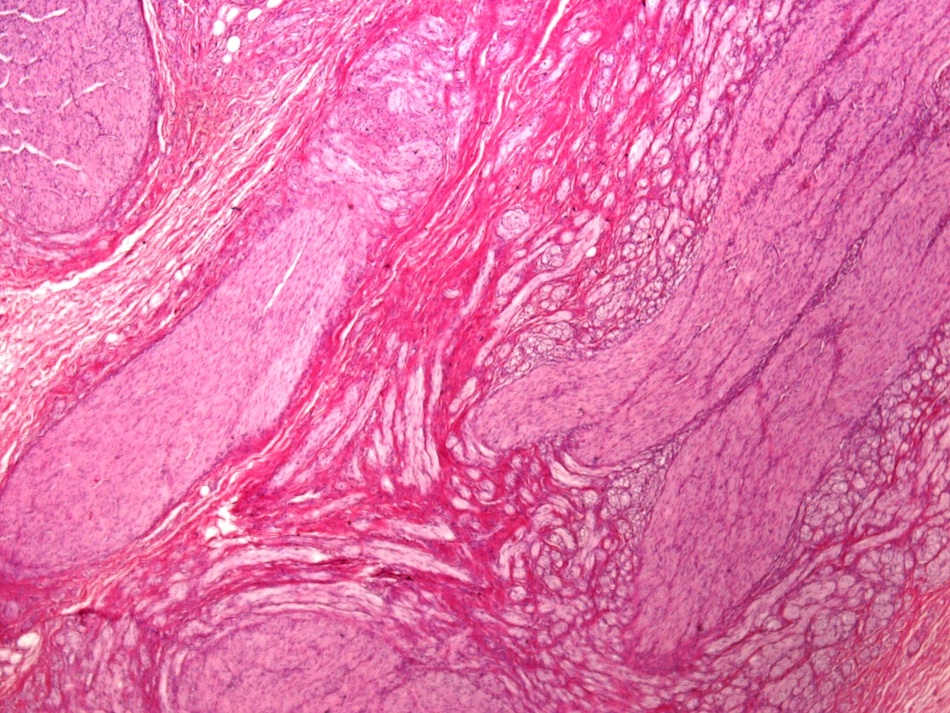
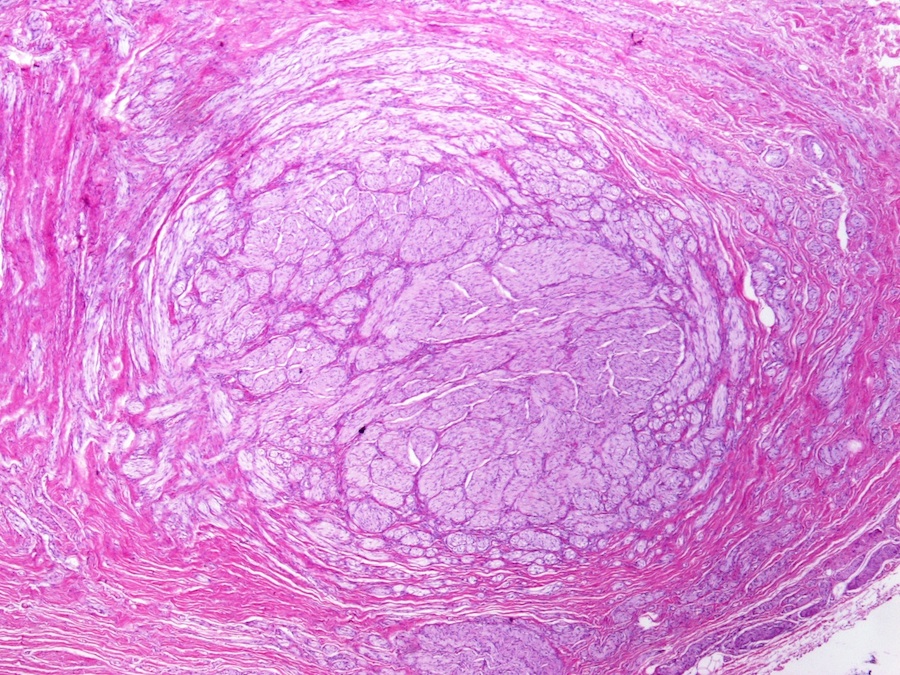
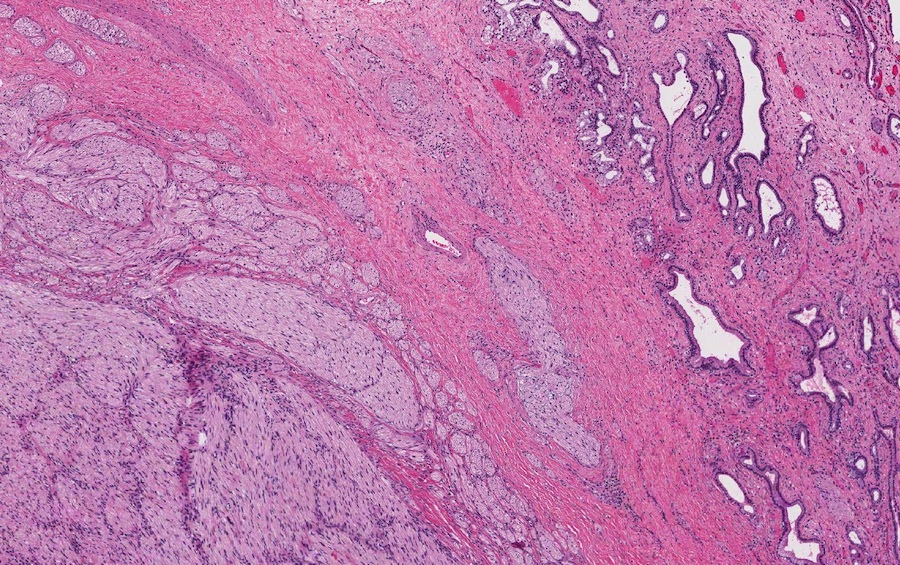
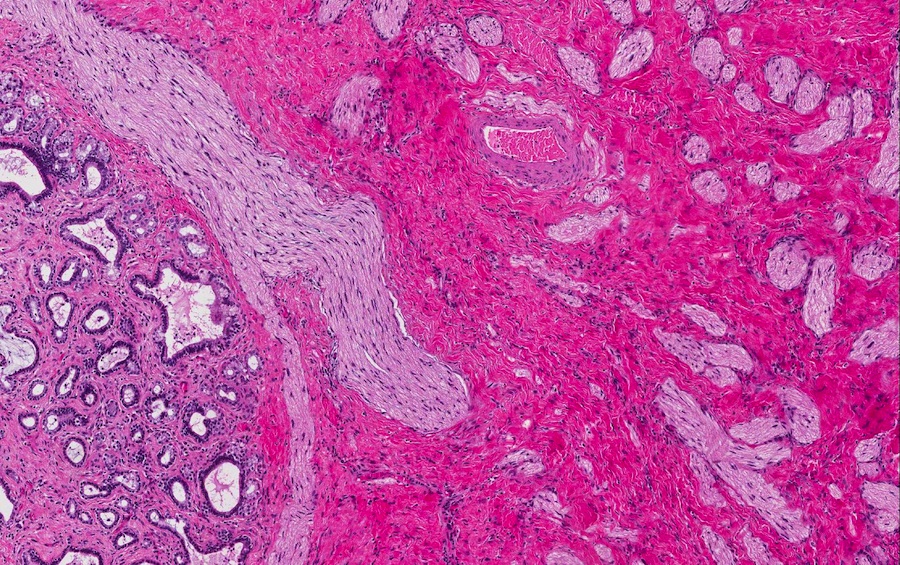
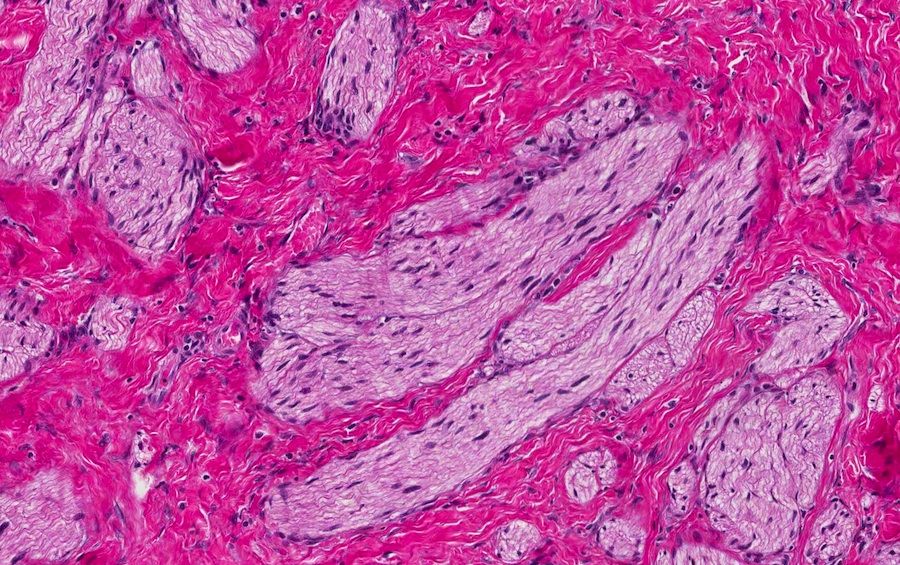
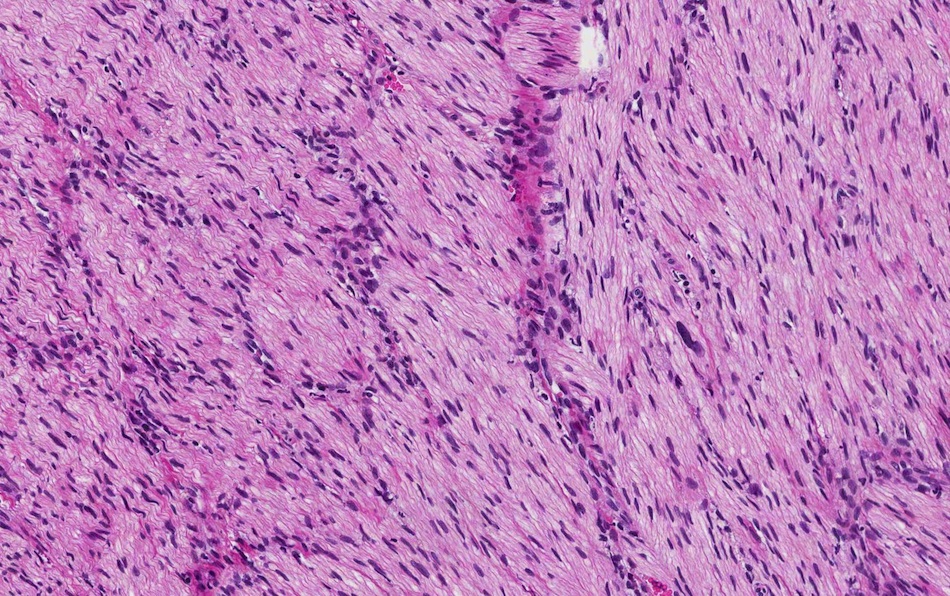
Proximal nerve stump attempts to regenerate resulting in disorganized proliferation of normal nerve components, including nerve fibers, Schwann cells and perineural cells arranged in fascicles
Etiology
Presents after surgery or procedure (i.e., laparoscopic or open cholecystectomy, biliary surgery for cholangiocarcinoma, liver transplantation, gallbladder biopsy)
Most are asymptomatic without any specific physical examination findings
Can present with right upper quadrant pain, obstructive jaundice, ascending biliary cholangitis (upper abdominal pain, fever, jaundice) and mass (Ann Hepatobiliary Pancreat Surg 2019;23:282)
Symptoms can present decades after the initial injury
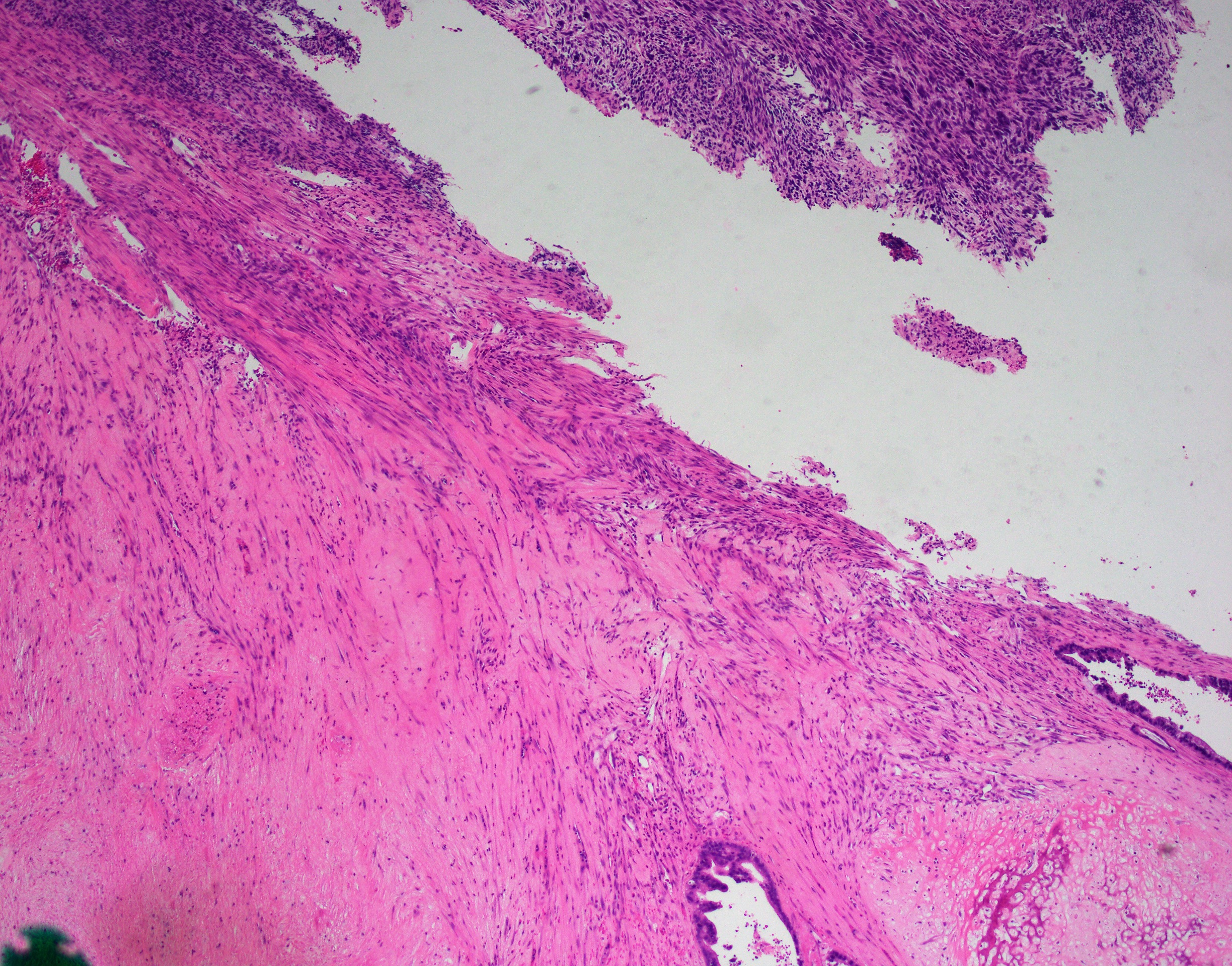
Portion of bile duct with benign traumatic neuroma; no malignancy seen (see comment)
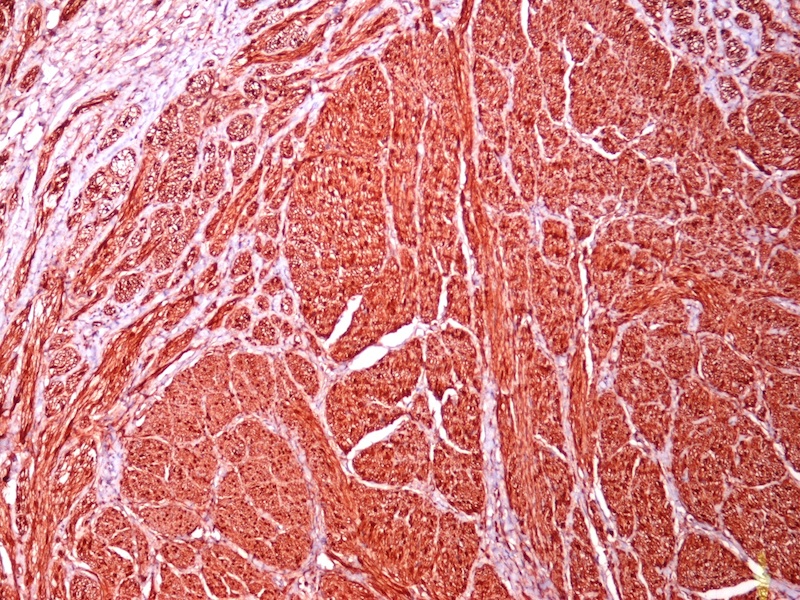
Comment: The patient's history of obstructive jaundice, biliary stricture, perihilar mass and previous cholecystectomy is noted. Histological examination reveals a benign haphazard proliferation of nerve fascicles in the fibromuscular layer of the bile duct, features consistent with a postcholecystectomy traumatic neuroma. The lesion focally displays areas of nuclear palisading and we considered the possibility of a benign nerve sheath tumor such as plexiform schwannoma. However, the lesion lacks encapsulation and has interspersed, normal appearing nerves. Immunostains show that the lesional cells are immunoreactive with S100 protein and SOX10. Ki67 proliferation index is not increased. EMA highlights the perineurium. CD34 highlights the myofibroblasts. Traumatic neuromas are a rare, nonneoplastic cause of long distance bile duct stenosis and progressive jaundice; in particular, in patients with a history of cholecystectomy or surgical history in this abdominal region.
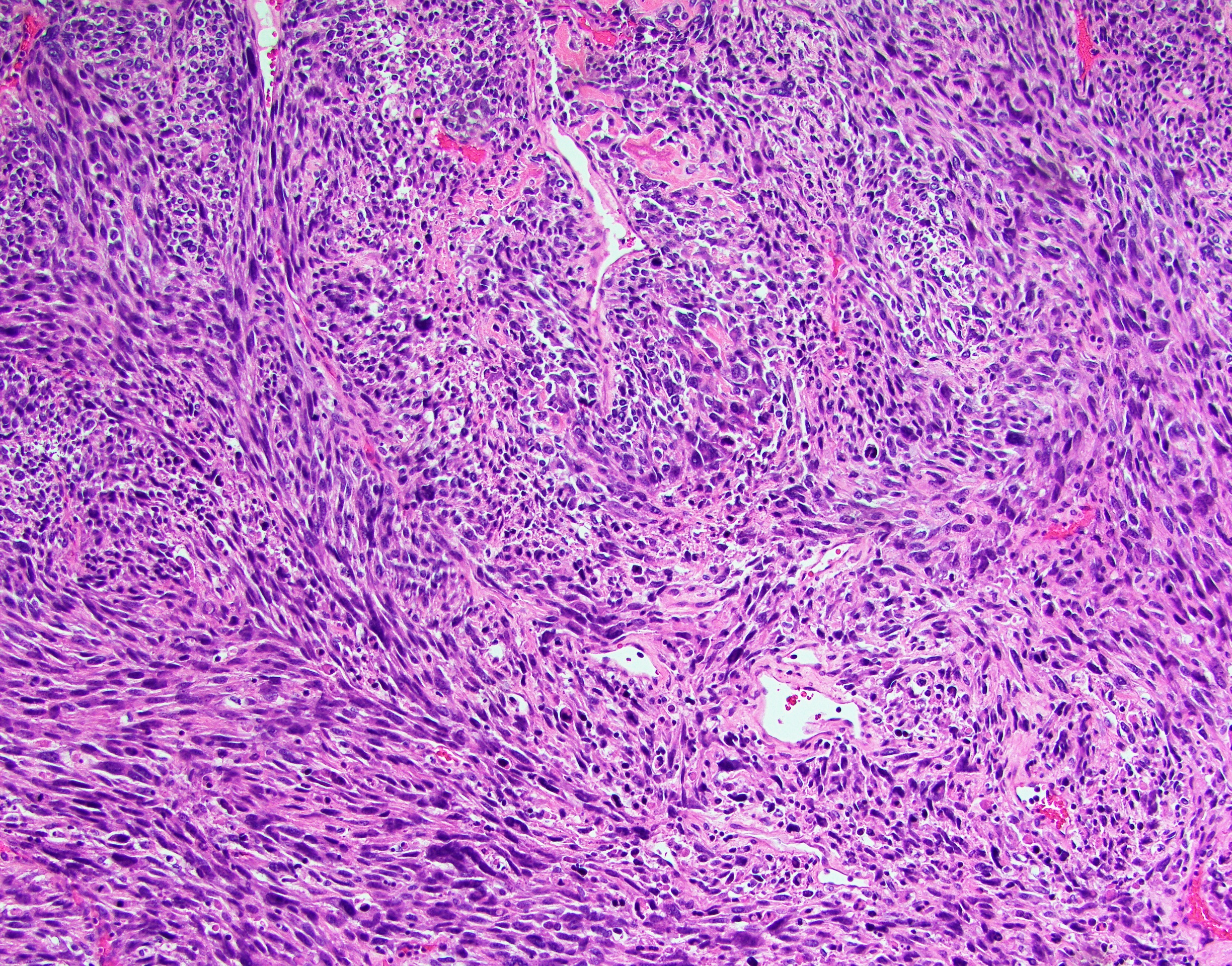
A woman with a history of cholecystectomy presents with obstructive jaundice. A contrast enhanced CT shows a 3 cm mass compressing the cystic duct stump. The histologic appearance of the tumor is shown above. What is the diagnosis?
Cholangiocarcinoma
Neurofibroma
Schwannoma
Traumatic neuroma
Board review style answer #1
D. Traumatic neuroma. The lesion is composed of disorganized proliferation of nerve fascicles in a collagenous stroma and in the clinical context of cholecystectomy is in keeping with traumatic neuroma.
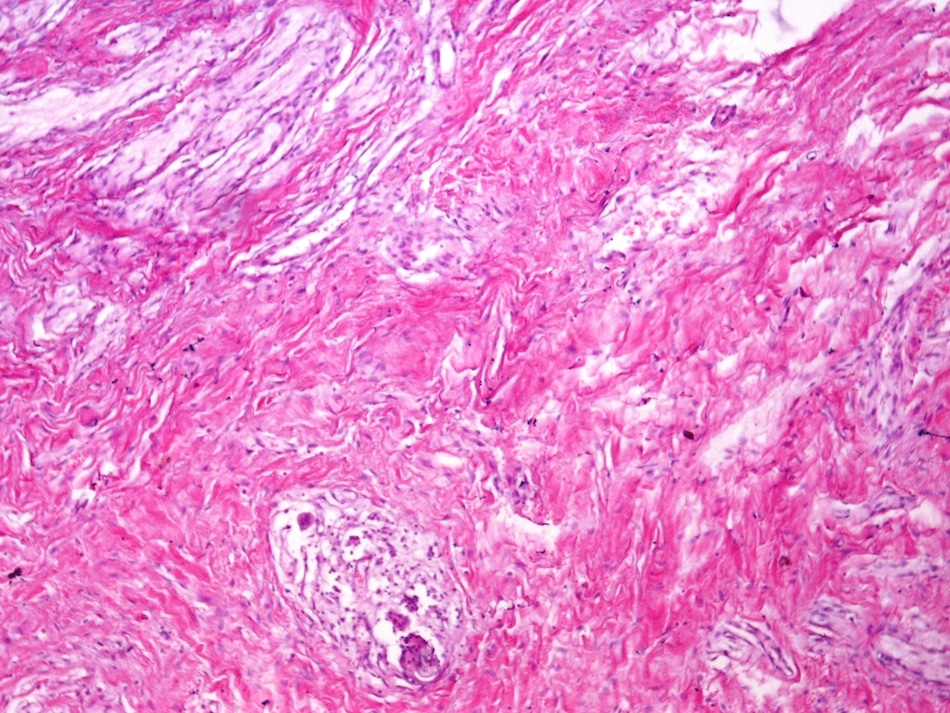
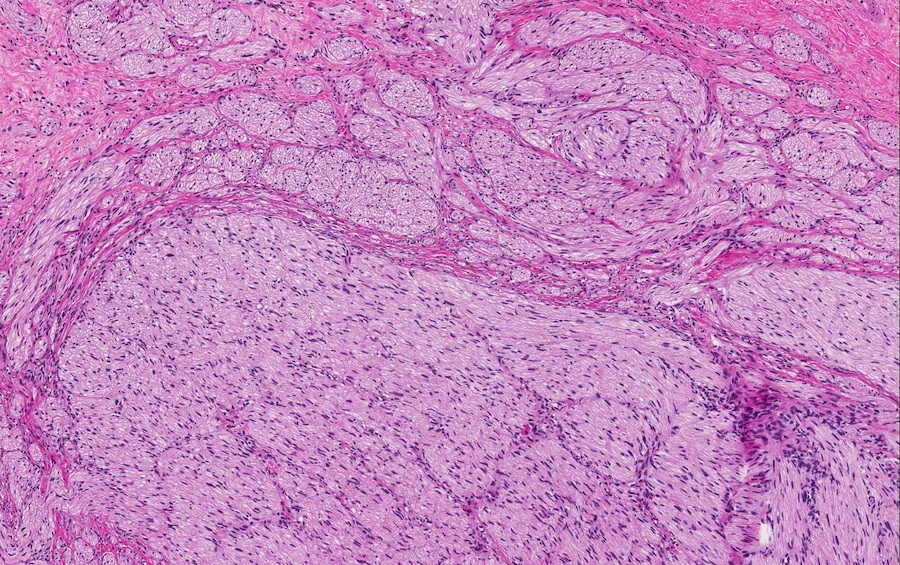
A patient with a history of cholecystectomy presents with a mass near the cystic duct stump. Histologic examination is consistent with a traumatic neuroma. Which of the following best describes the gross and microscopic findings in traumatic neuroma?
Large, heterogeneous mass with fascicles of uniform spindle cells with frequent mitoses and areas of coagulative necrosis in vascularized, myxoid to collagenous stroma
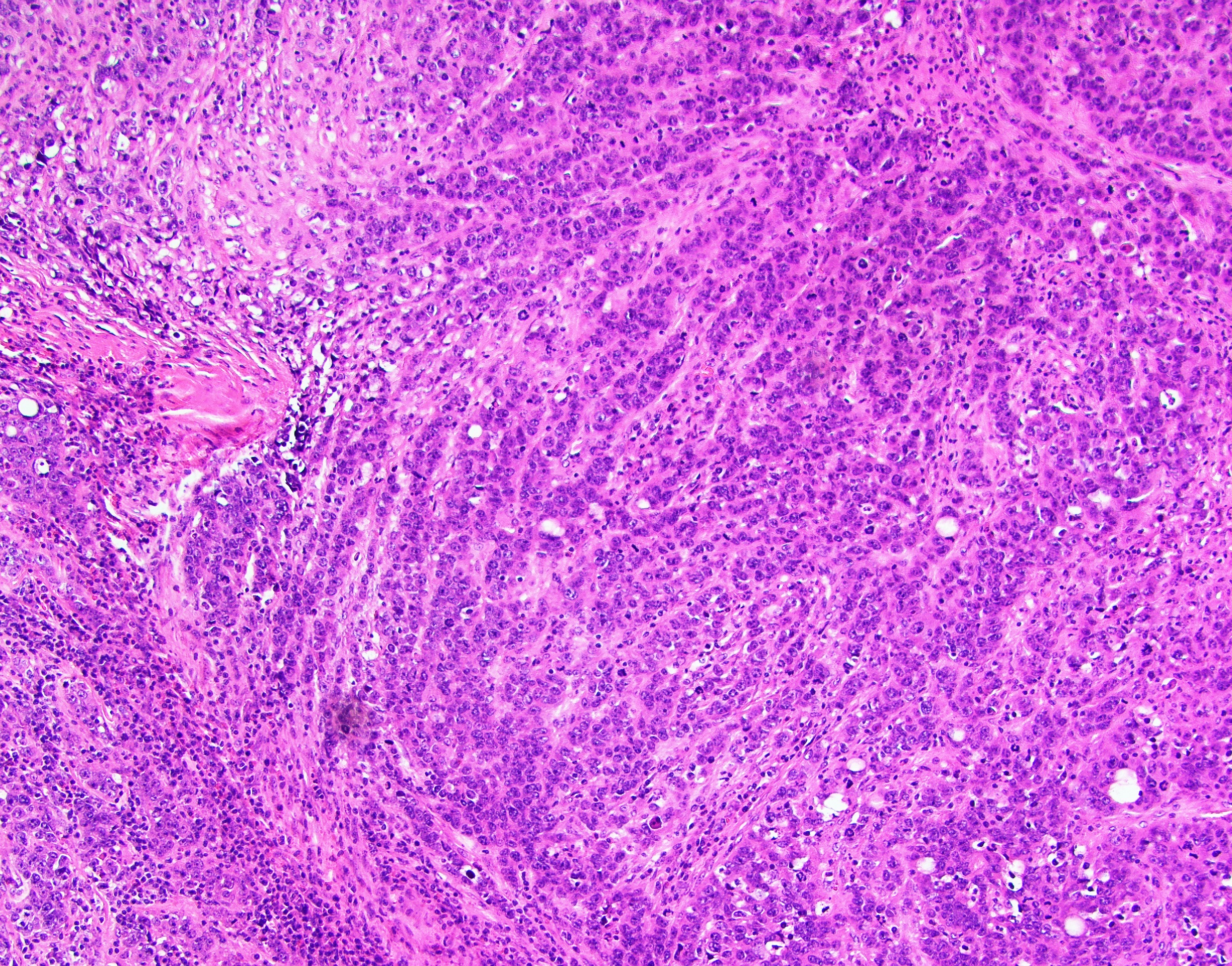
Well circumscribed, encapsulated, tan-gray mass with spindle cells arranged in biphasic hypercellular and hypocellular areas with diffuse staining of S100 and SOX10
Well circumscribed, gray-white mass with haphazard proliferation of benign nerve fascicles
Well circumscribed, nonencapsulated, tan-gray mass with haphazard spindle cells, mast cells, rare axons in shredded carrot collagenous stroma with hypocellular and myxoid areas
Board review style answer #2
C. Well circumscribed, gray-white mass with haphazard proliferation of benign nerve fascicles. Traumatic neuromas are benign lesions with haphazard proliferation of benign nerve fascicles. They usually occur after damage to peripheral nerves from surgery, trauma or inflammation. Choice A describes findings in malignant peripheral nerve sheath tumors. Choice B describes the findings in schwannoma. Choice D describes findings in neurofibromas.
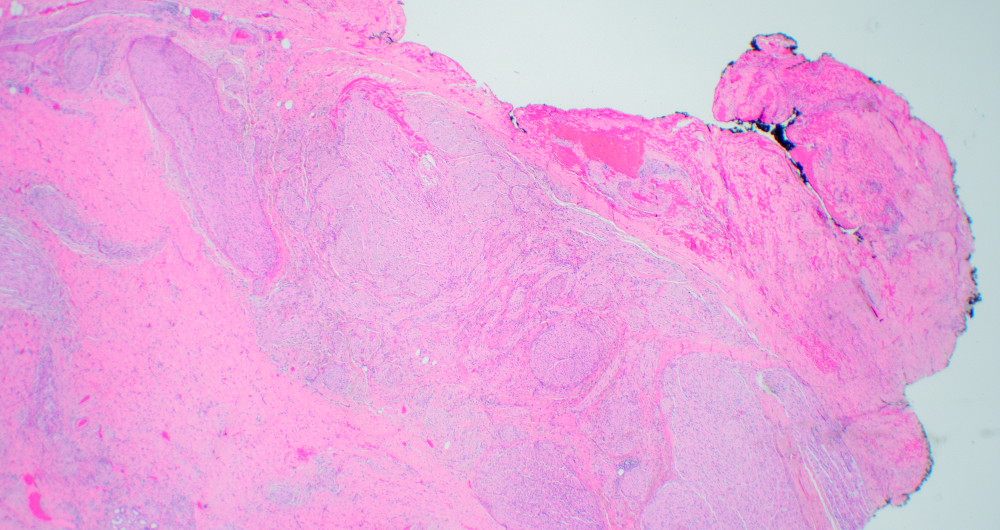
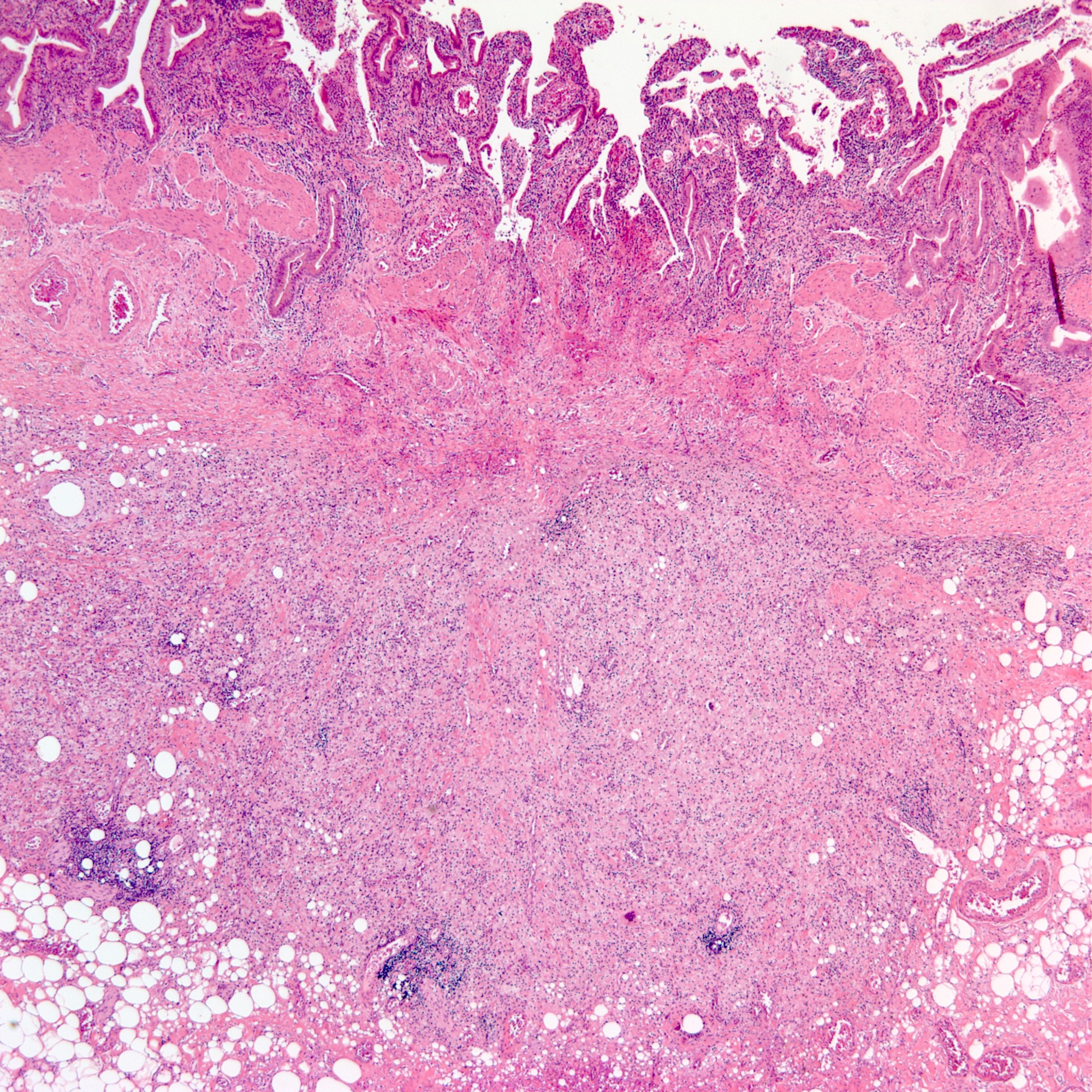
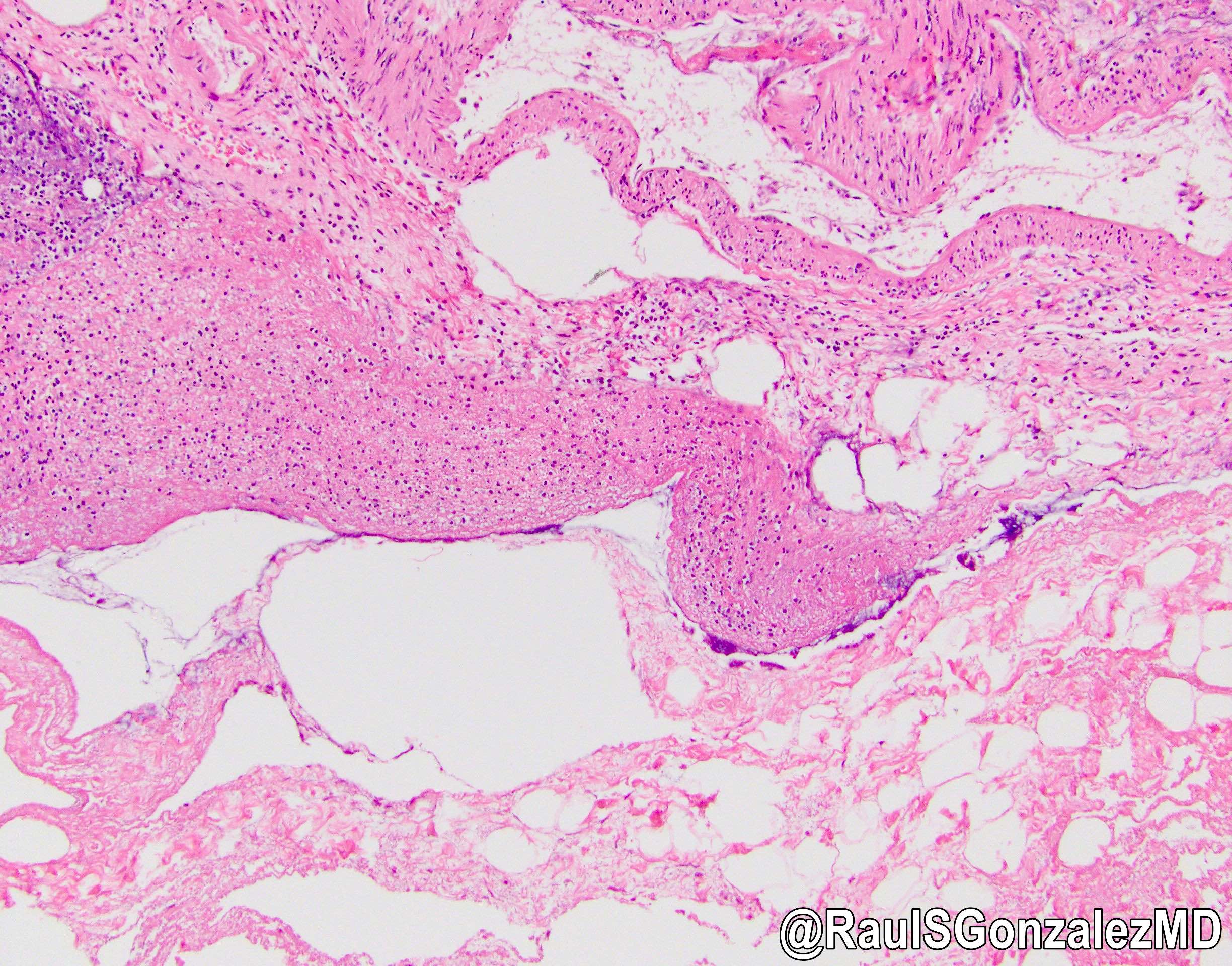
Unusual histologic variant of chronic cholecystitis
Infiltration of foamy histiocytes and fibrosis in the background of chronic active inflammation
Essential features
Xanthogranulomatous cholecystitis (XGC), in clinical and radiologic findings, can frequently mimic gallbladder cancer
Pathologic findings are quite characteristic with foamy histiocytes, fibrosis and chronic active inflammation; when XGC is confused with gallbladder cancer, frozen examination can be useful in excluding malignancy
Increased intraluminal pressure due to obstruction of bile flow (various etiologies: gallstone, cancer, etc.) ⇢ rupture of Rokinstanky-Aschoff sinuses ⇢ bile spillage ⇢ inflammatory reaction (Gastroenterol Res Pract 2014;2014:253645, World J Radiol 2016;8:183)
Etiology
Gallstones
Clinical features
Patients' symptoms manifest as acute cholecystitis
Diagnosis
XGC is usually diagnosed with histopathologic examination
Radiologic imaging, including computed tomography, ultrasonography and magnetic resonance imaging, can be helpful but are limited for diagnosis
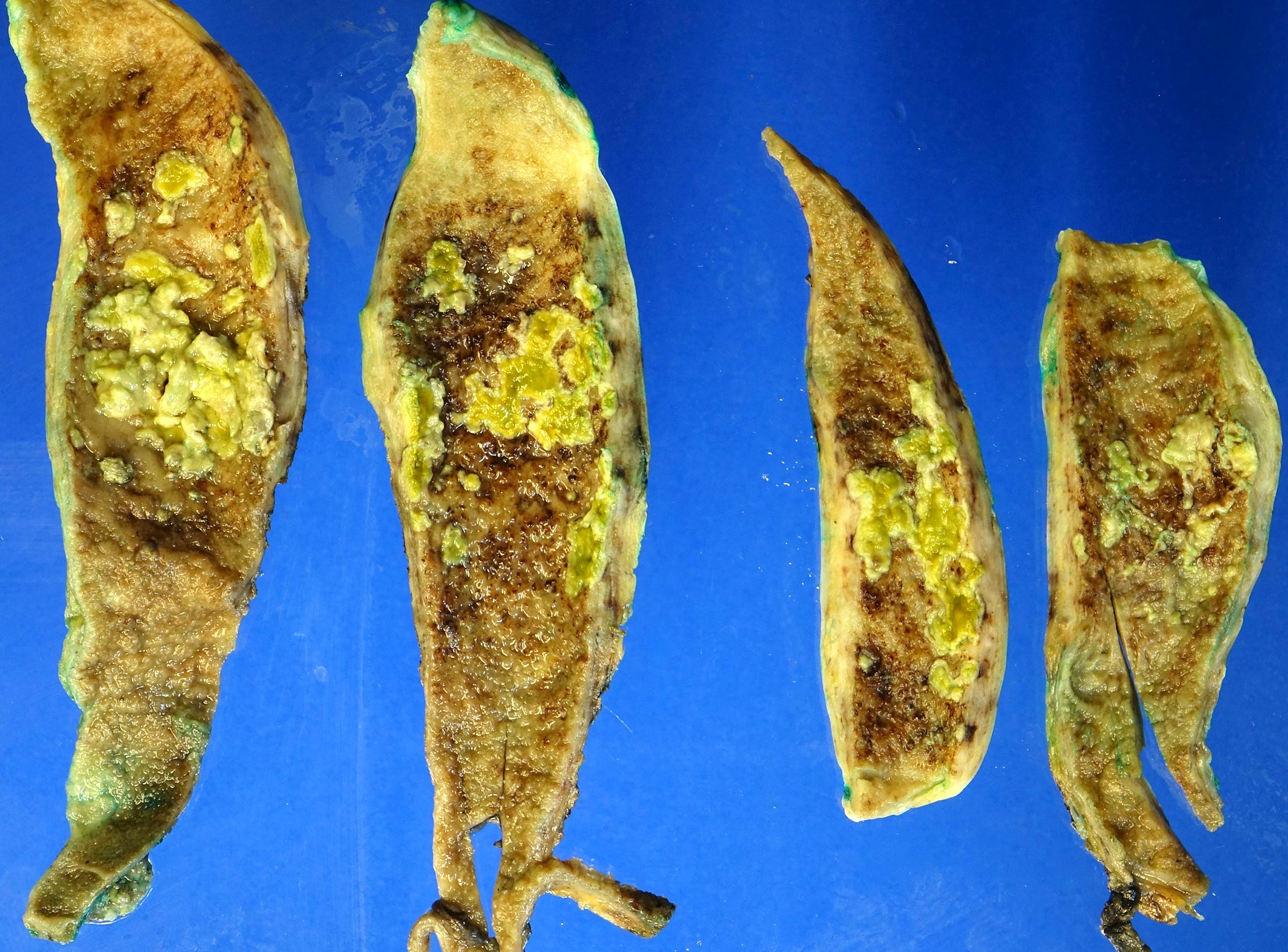
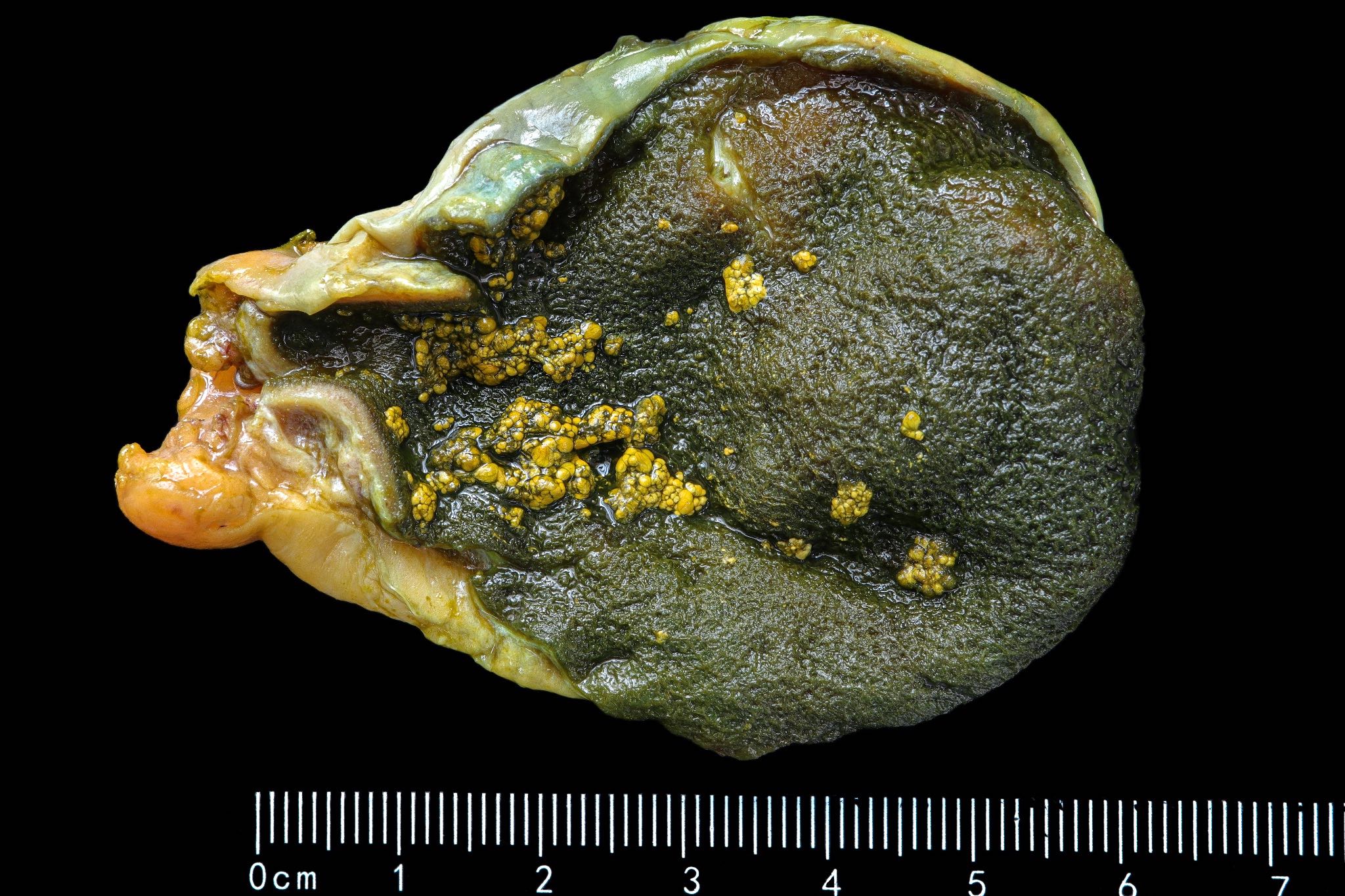
Irregular thickening of the gallbladder wall with multiple yellow nodules
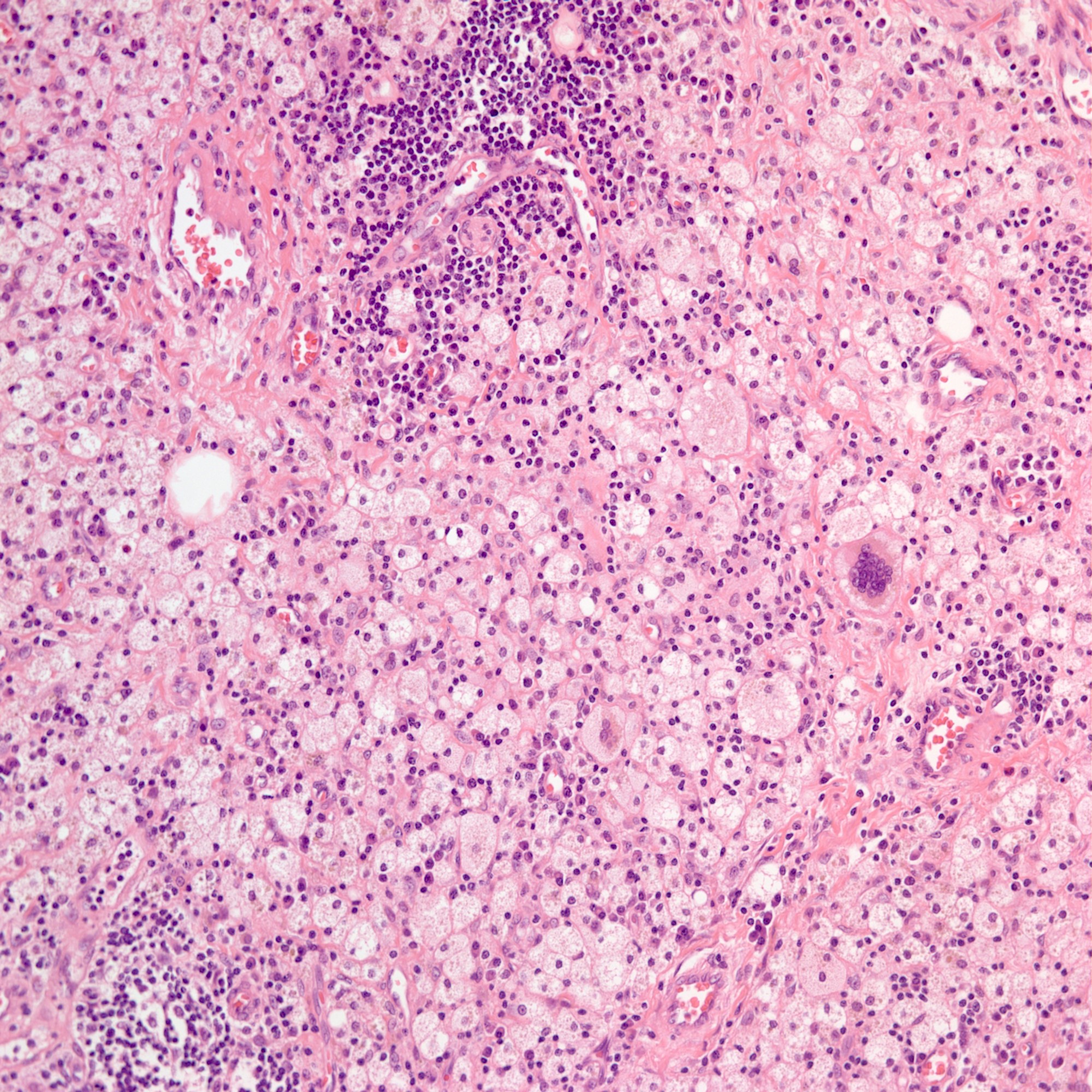
Microscopic (histologic) description
Round to spindled shaped, lipid laden macrophages, giant cells and proliferative fibrosis in the background of chronic active inflammation (lymphocytes, plasma cells, neutrophils and eosinophils)
Transmural inflammation, mural and extramural inflammatory nodule
Small foci of xanthomatous inflammation associated with chronic cholecystitis cannot be qualified as XGC
In a resected gallbladder, histopathologic examination showed sheets of histiocytes in the gallbladder. PAS staining demonstrated intracytoplasmic granules in histiocytes. What is the best diagnosis?
Hemophagocytosis
Malakoplakia
Rosai-Dorfmann disease
Signet ring cell carcinoma
Xathogranulomatous cholecystitis
Board review style answer #1
B. Malakoplakia. Malakoplakia is rare but can occur in the gallbladder. The histologic findings are very similar to those of xanthogranulomatous cholecystitis; however, histiocytes in malakoplakia are typically positive for PAS, while those in xanthogranulomoatus cholecystitis are negative.
A 63 year old patient visited the hospital with upper quadrant abdominal pain. Gallbladder cancer was strongly suspected in preoperative computed tomography. After the operation, histologic examination showed the findings in the image above. What is the best diagnosis?
Acute emphysematous cholecystitis
IgG4 related cholecystitis
Mycobacterial infection
Signet ring cell carcinoma
Xanthogranulomatous cholecystitis
Board review style answer #2
E. Xanthogranulomatous cholecystitis. Xanthogranulomatous cholecystitis is a rare variant of cholecystitis. It frequently mimics gallbladder malignancy according to radiologic examination. Histopathologic examination shows round to spindled shaped, lipid laden macrophages, giant cells and proliferative fibrosis in the background of chronic active inflammation (lymphocytes, plasma cells, neutrophils and eosinophils).













































_histopathology.jpg)