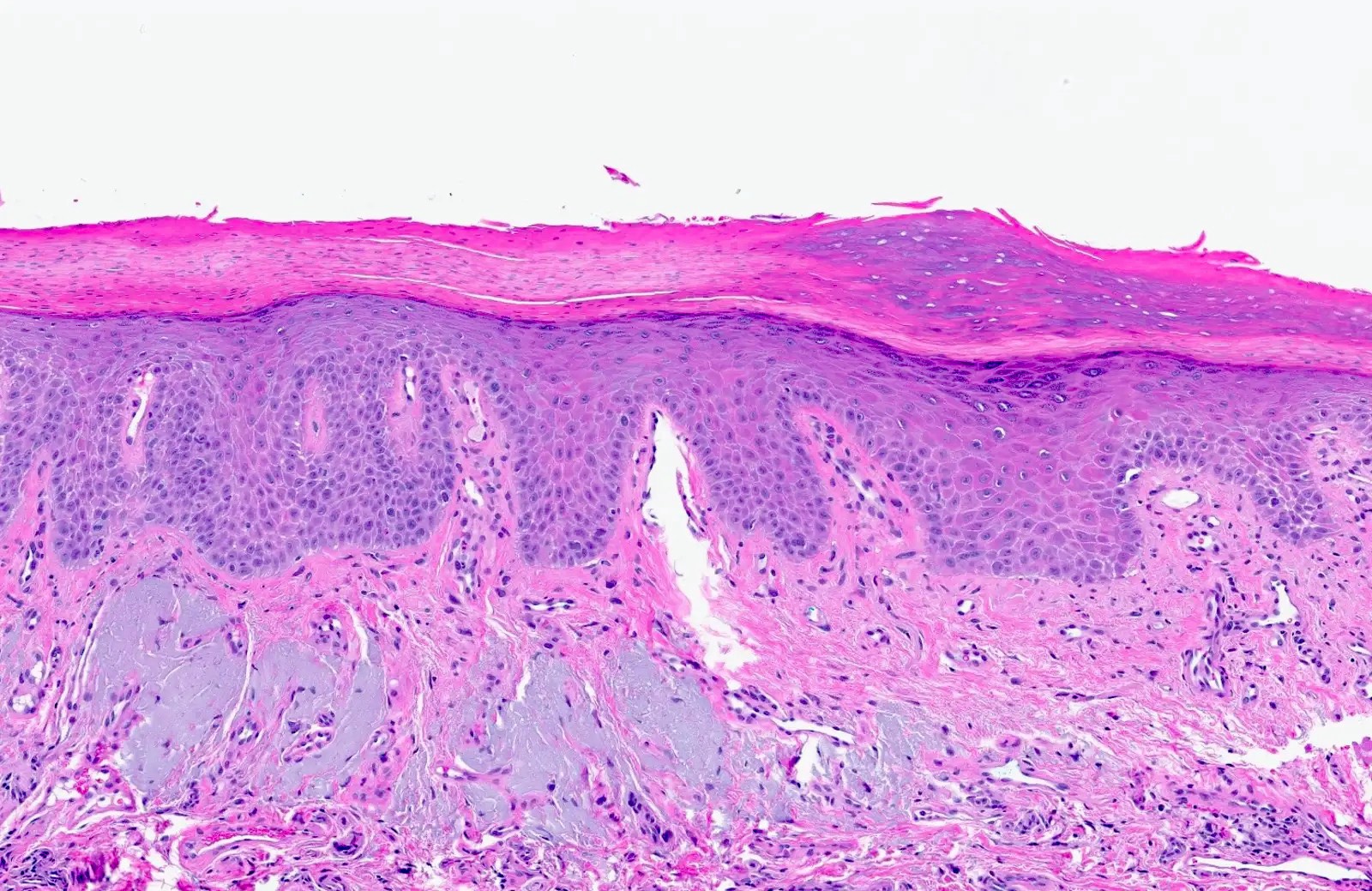
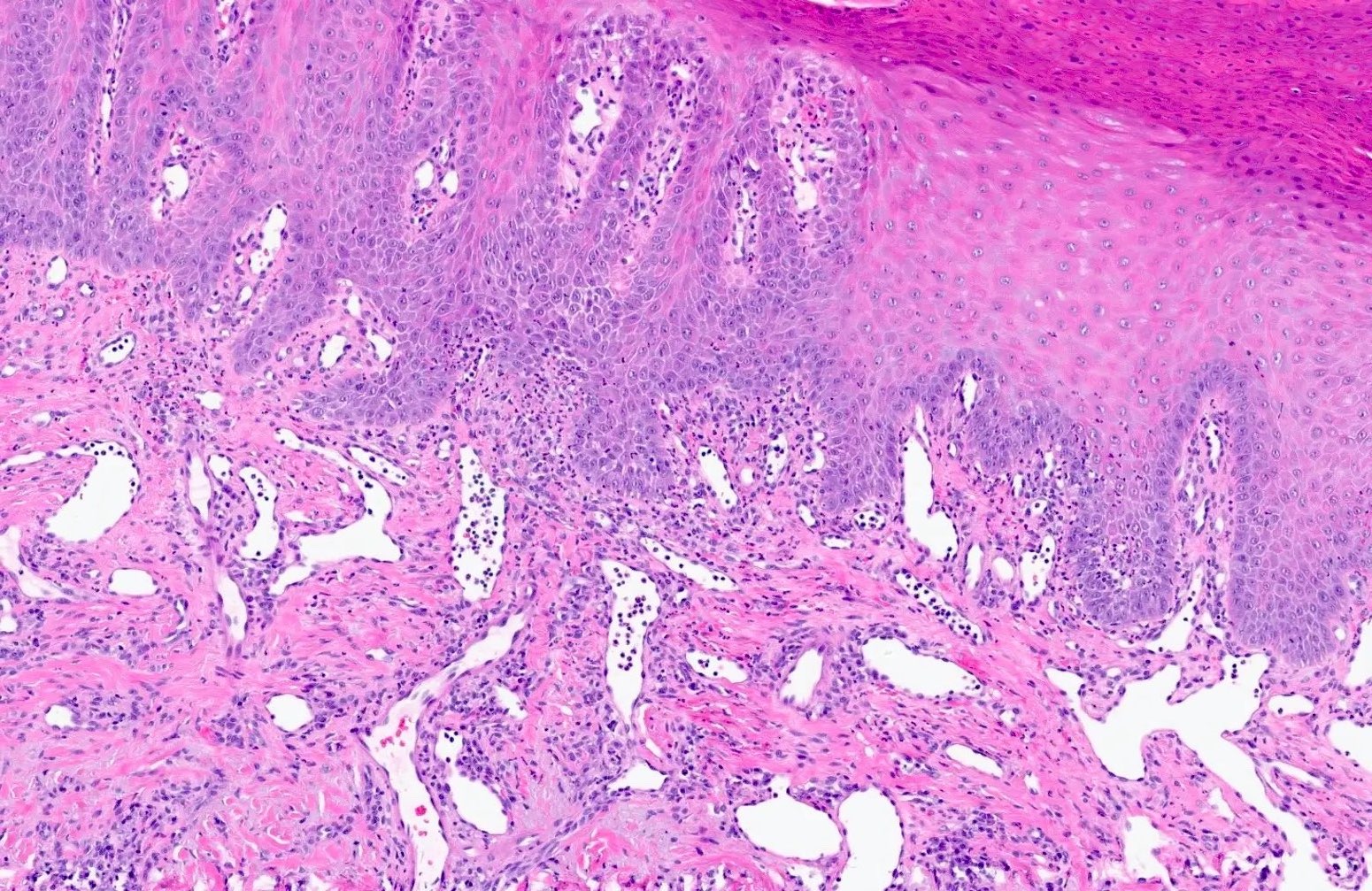
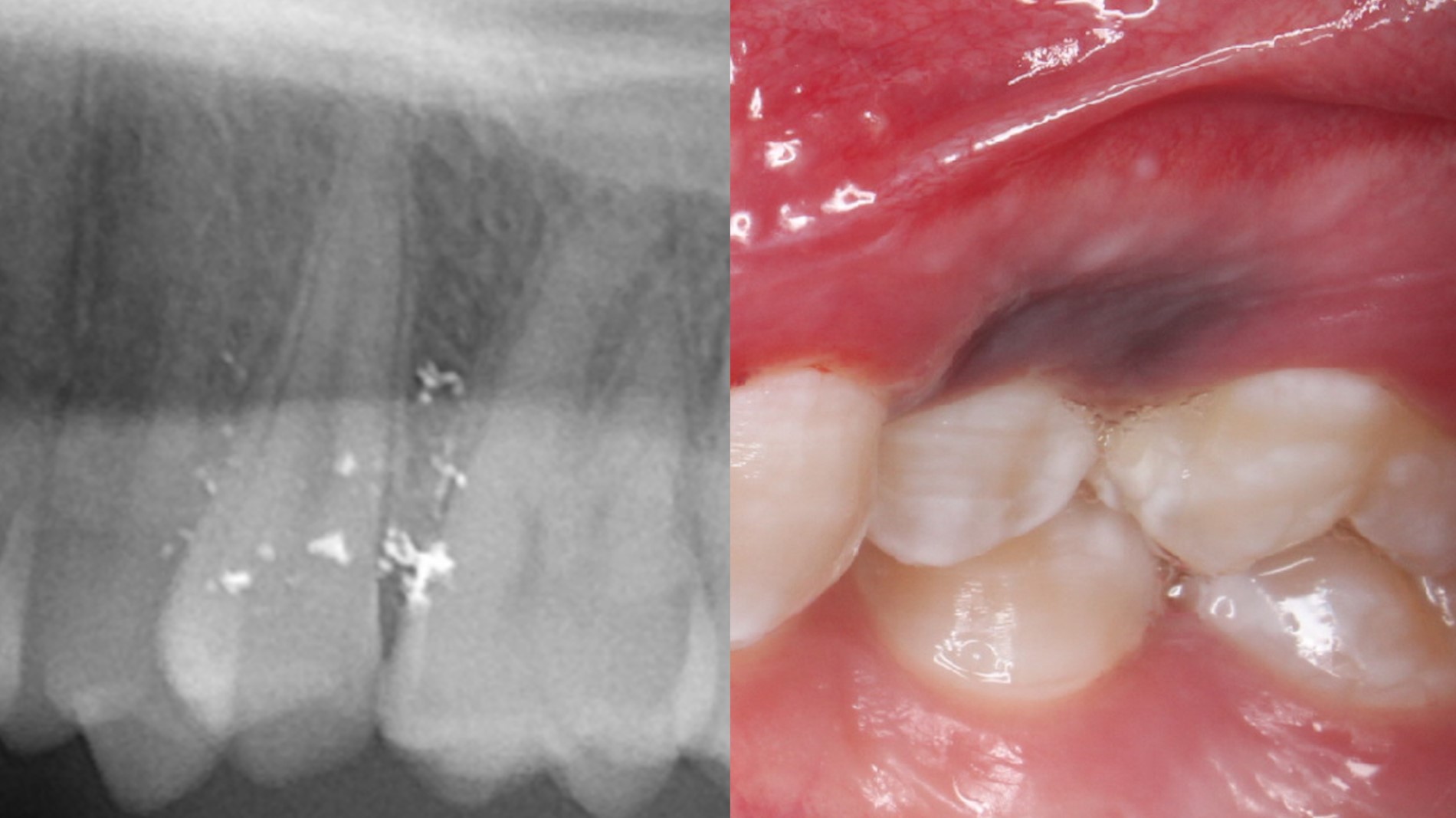
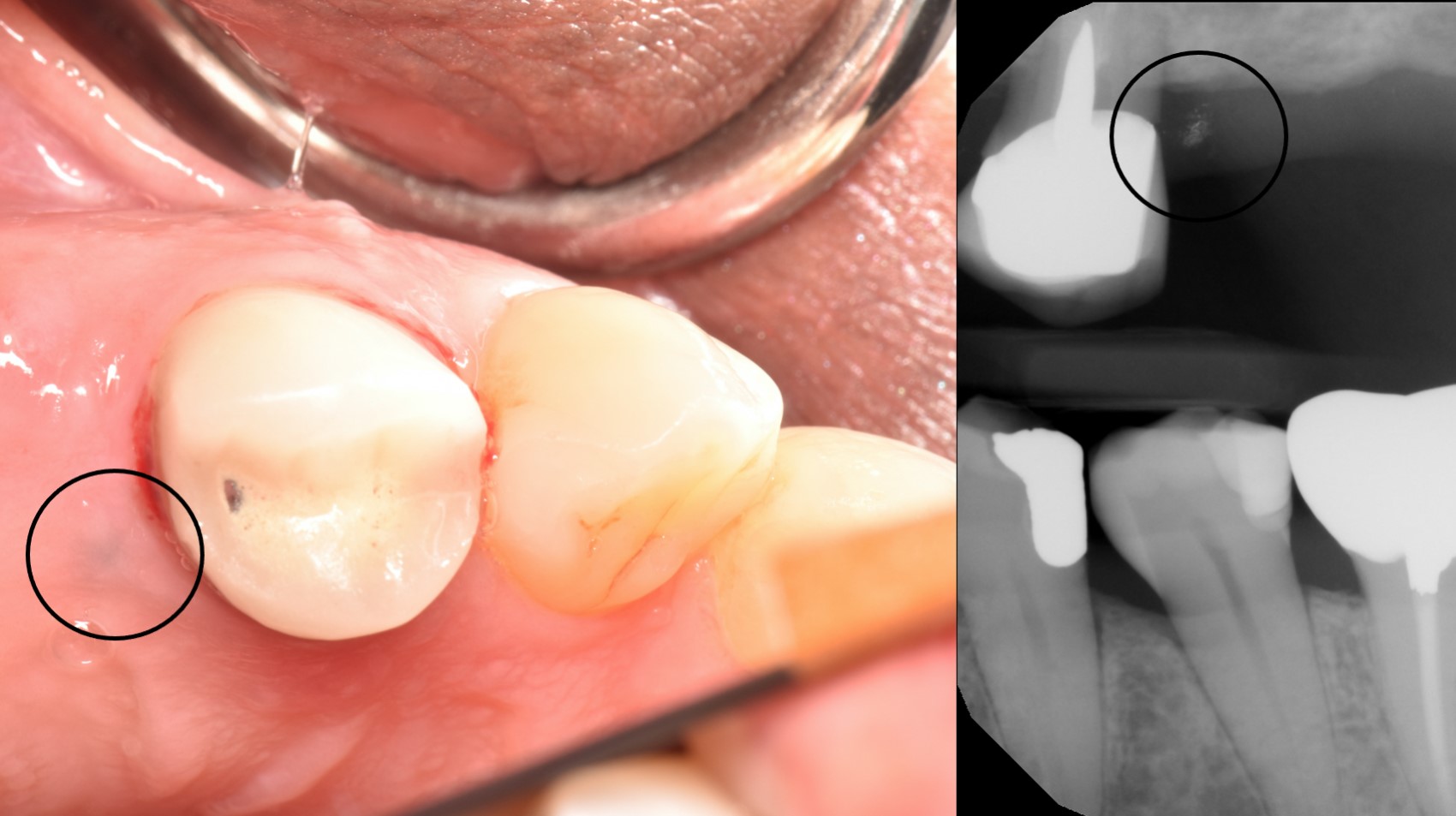
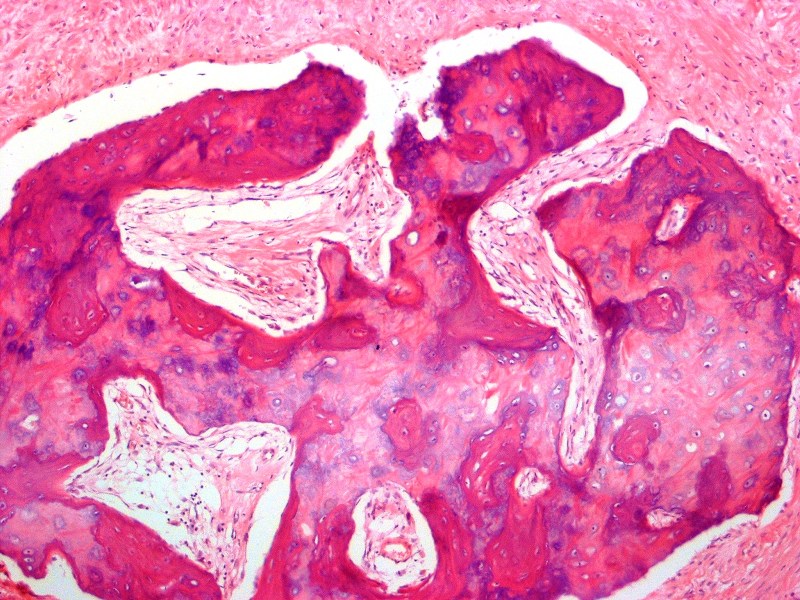
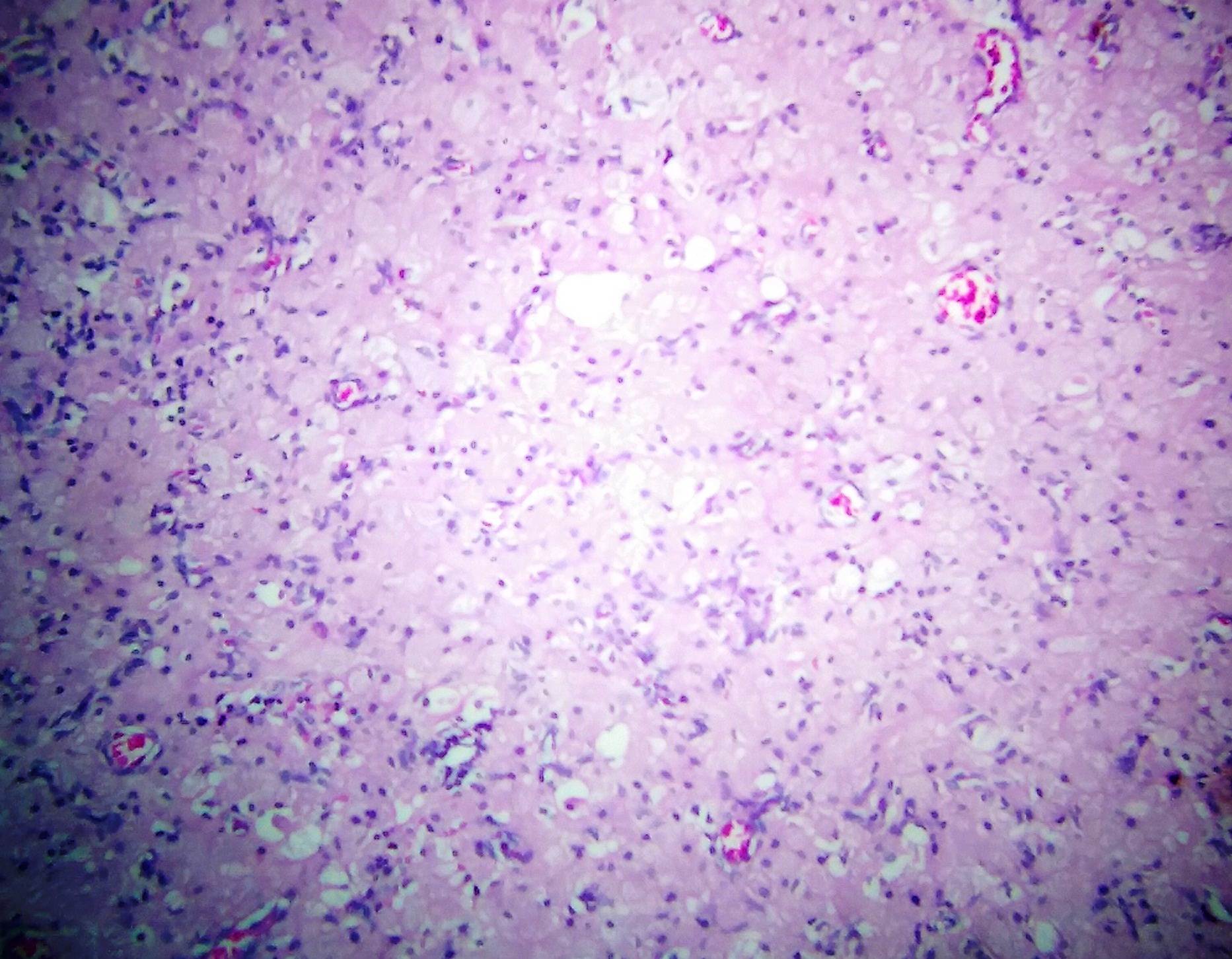
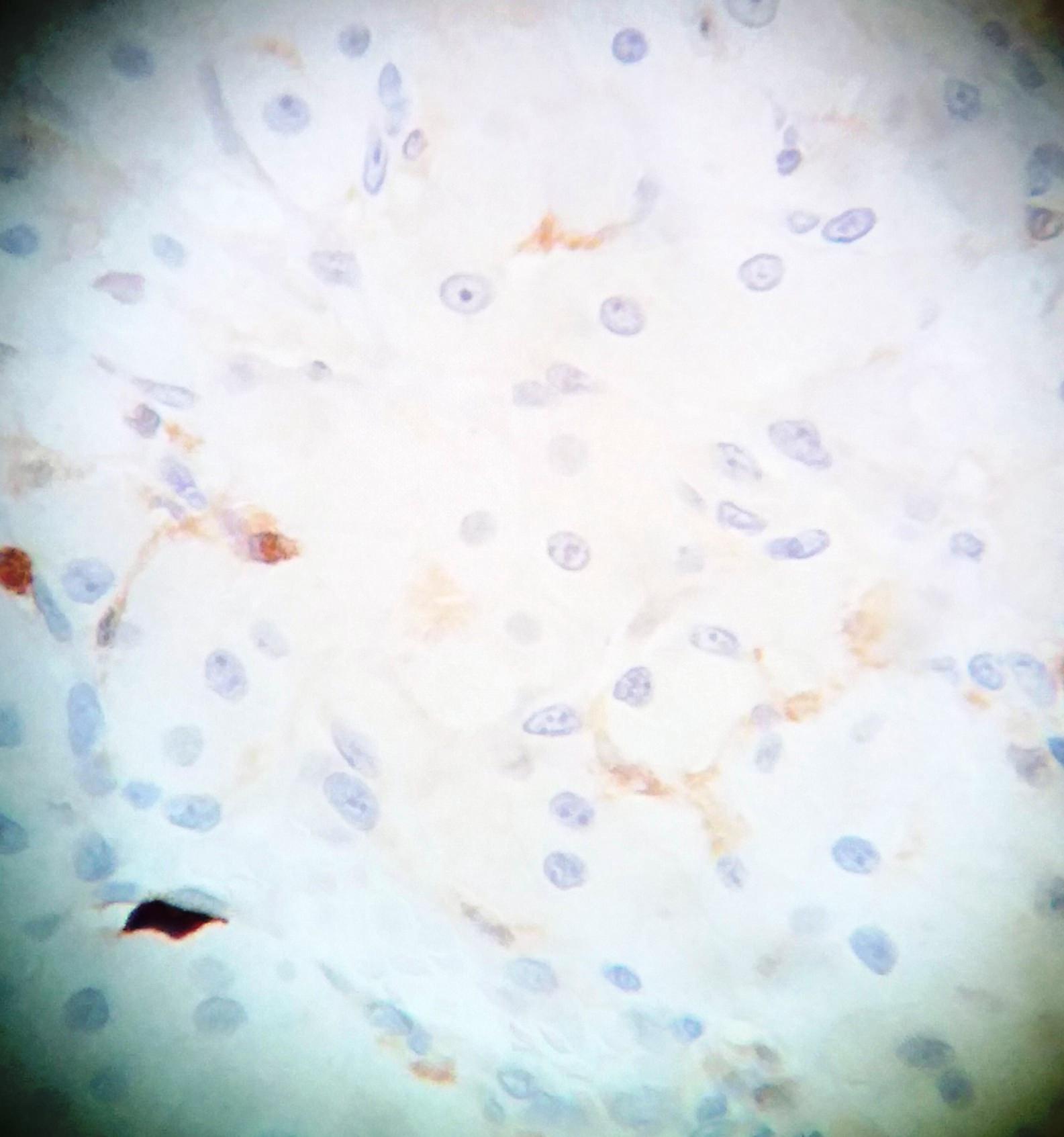
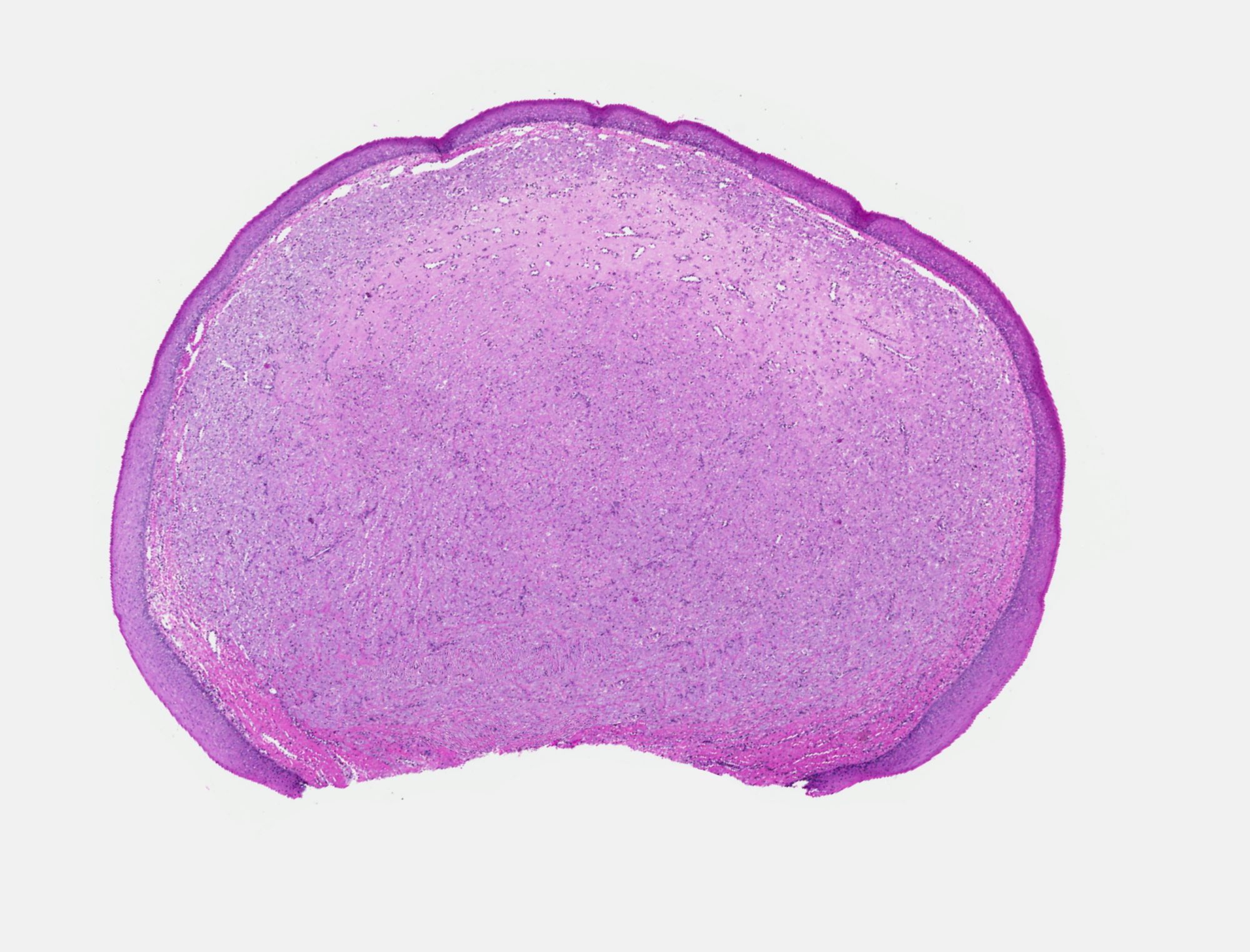
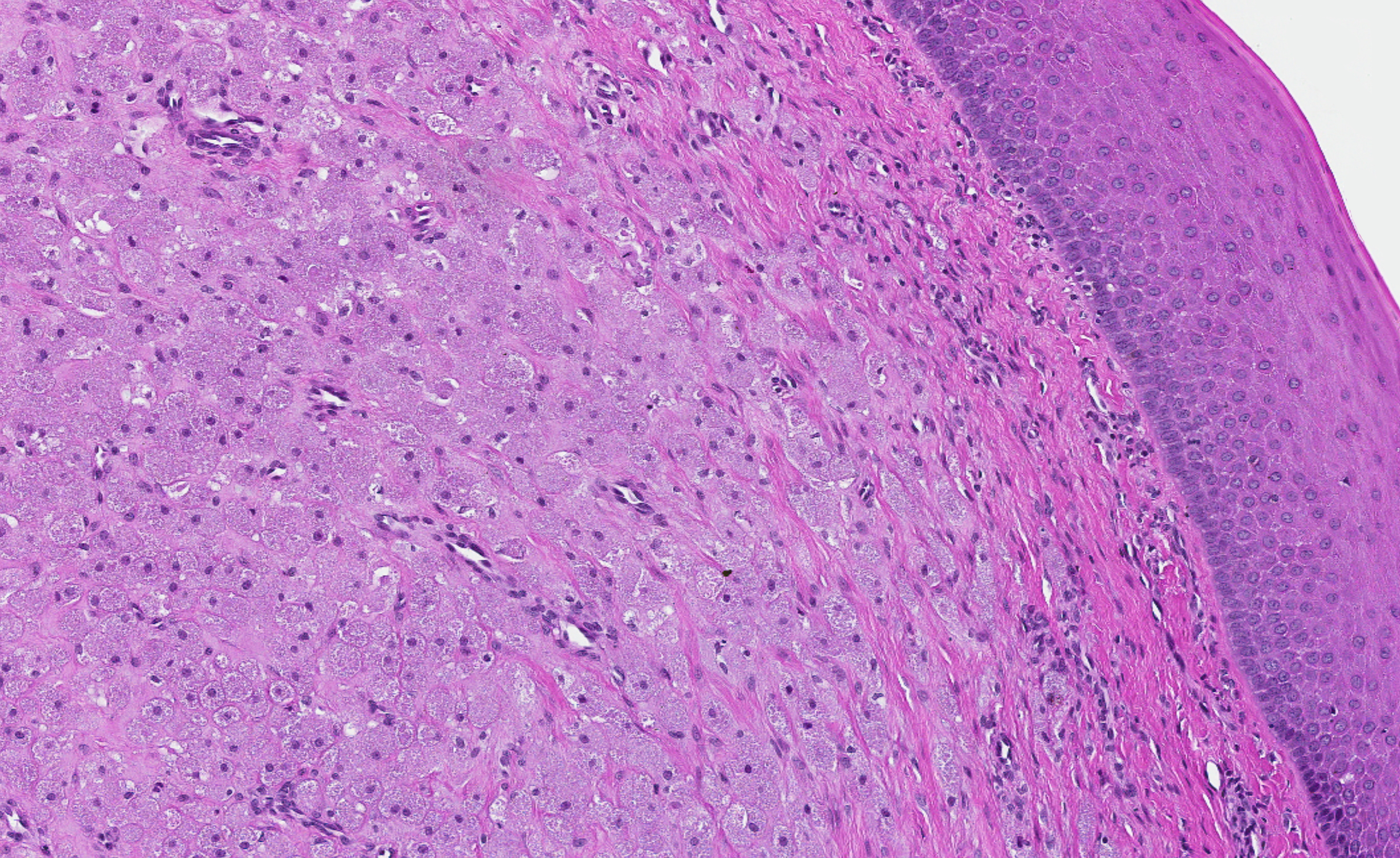
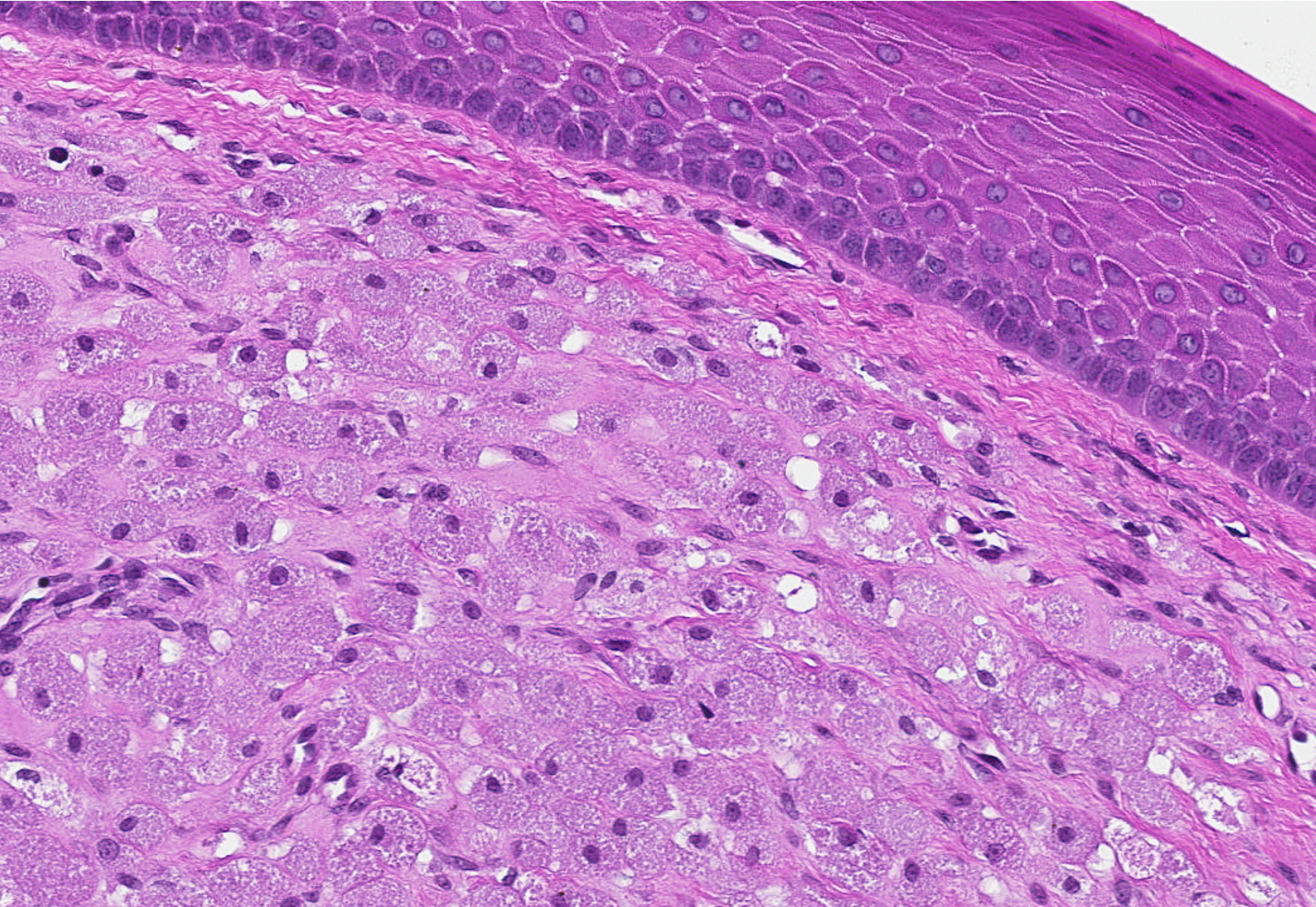
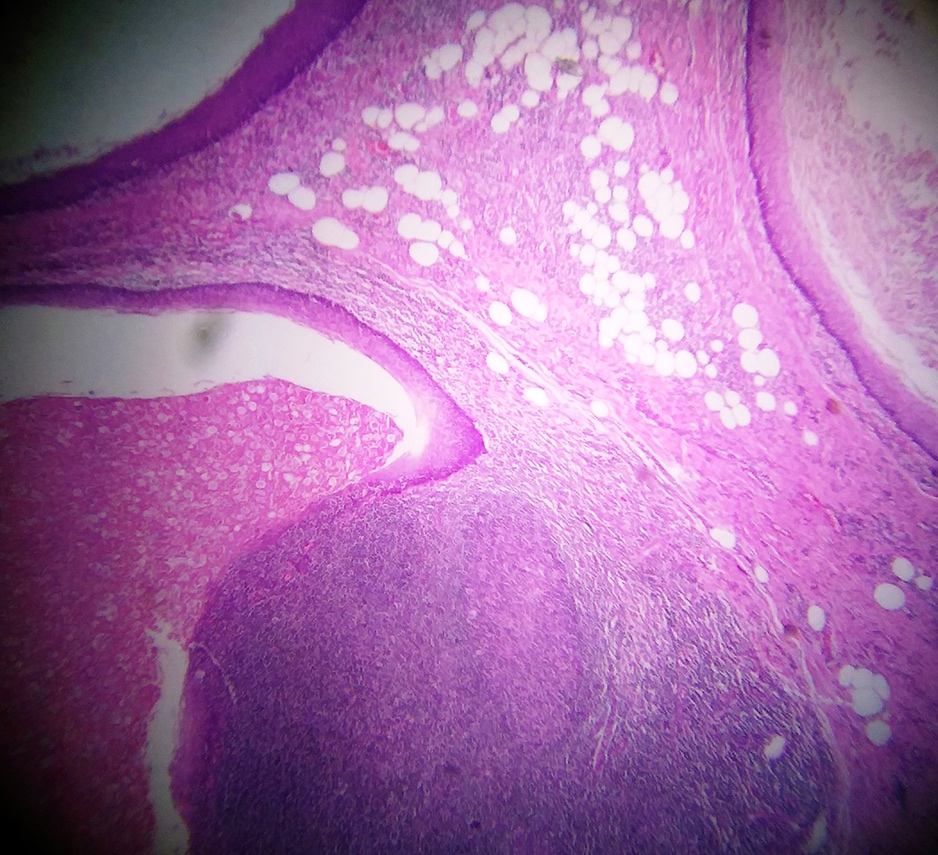
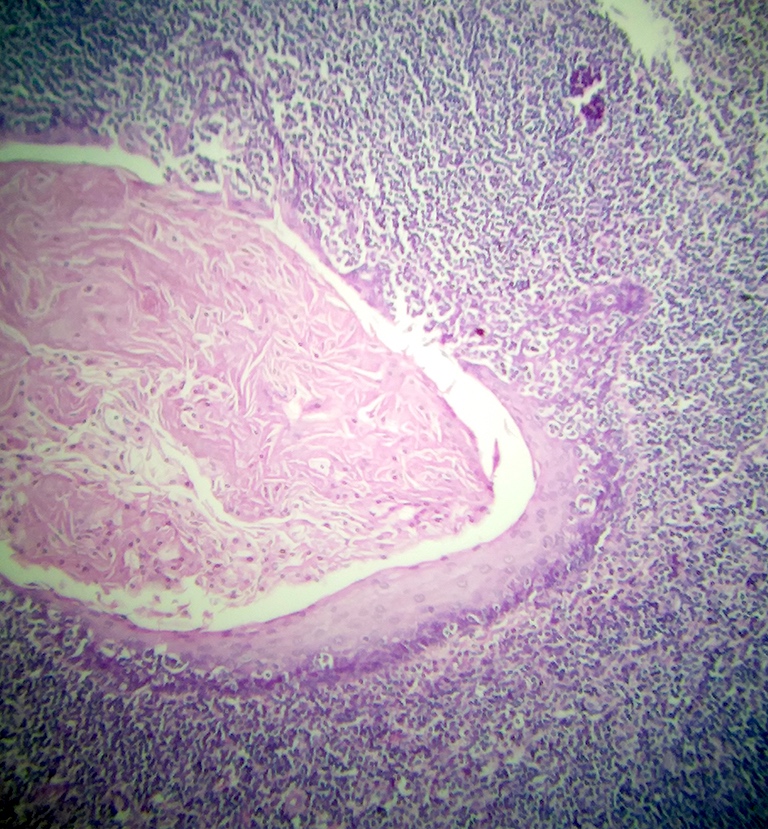
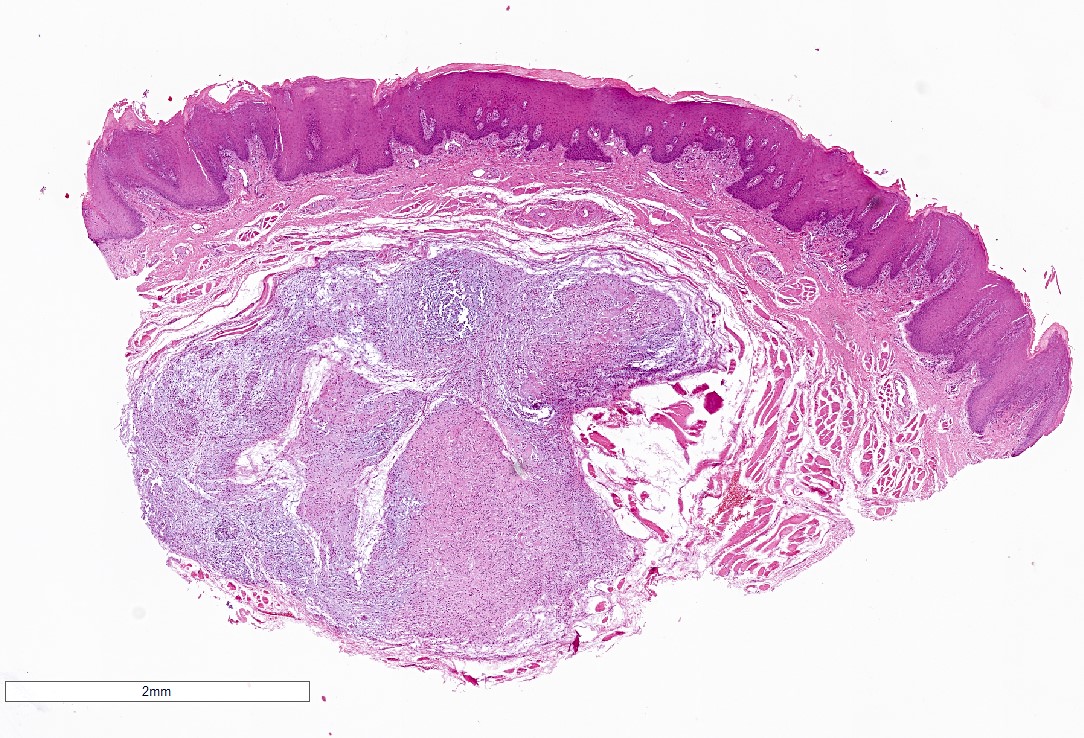
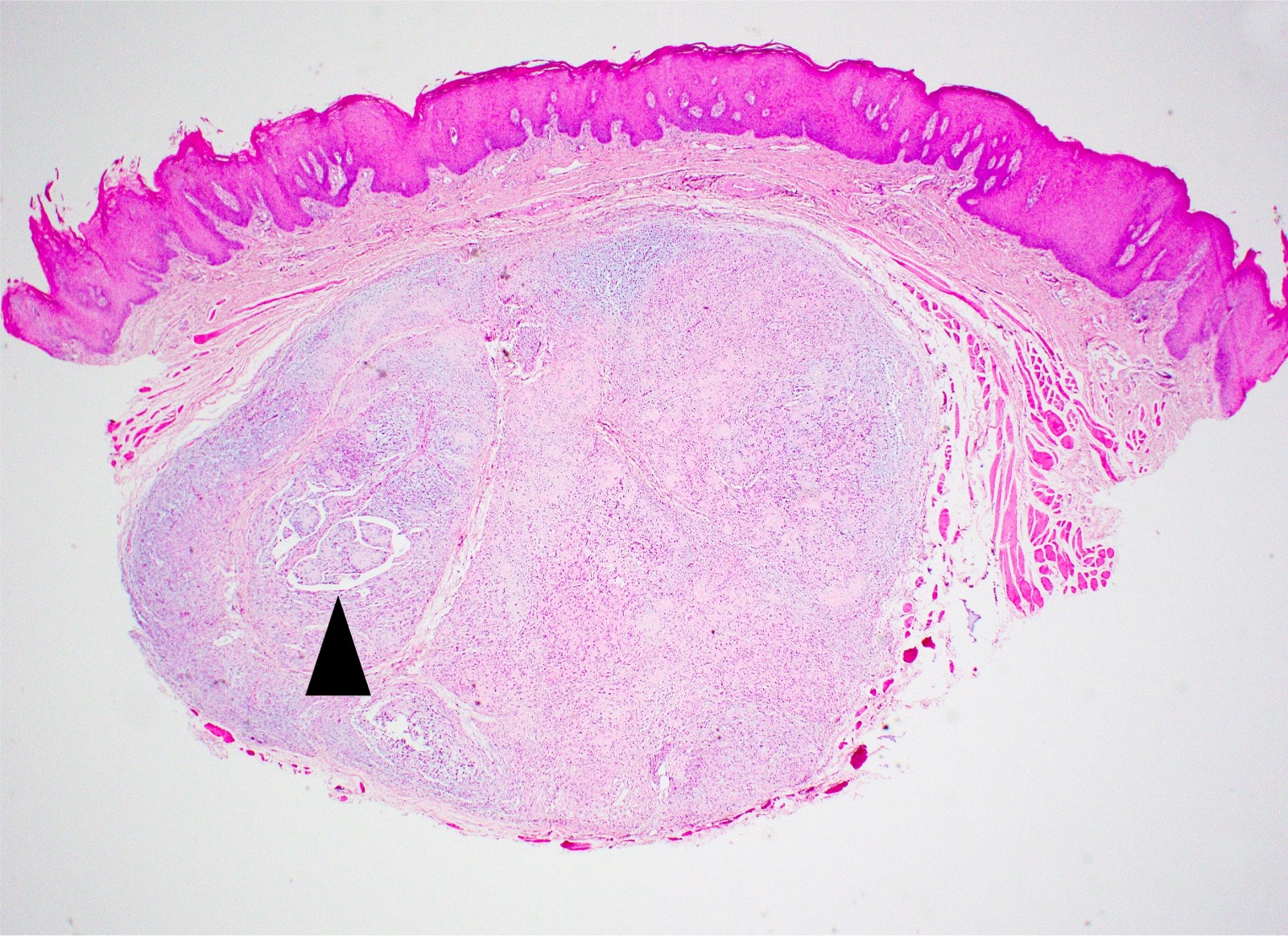
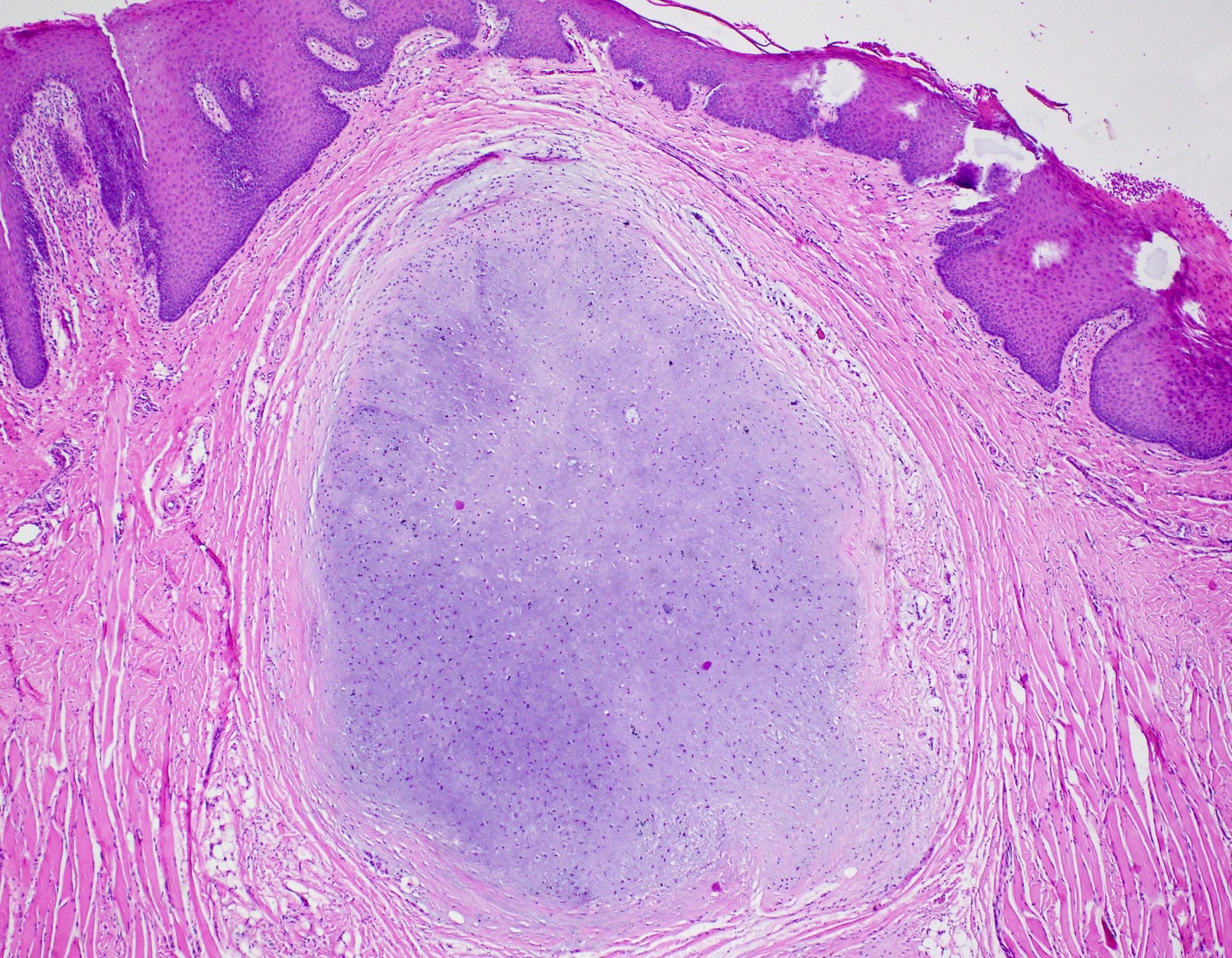
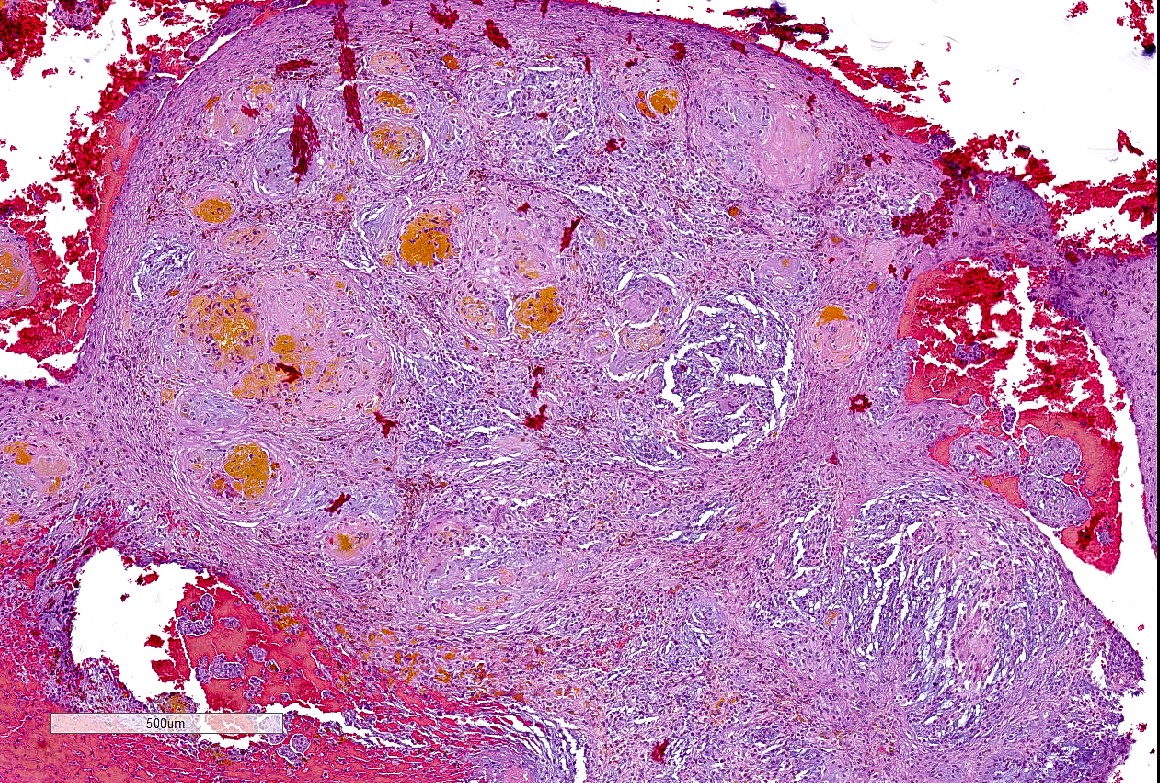
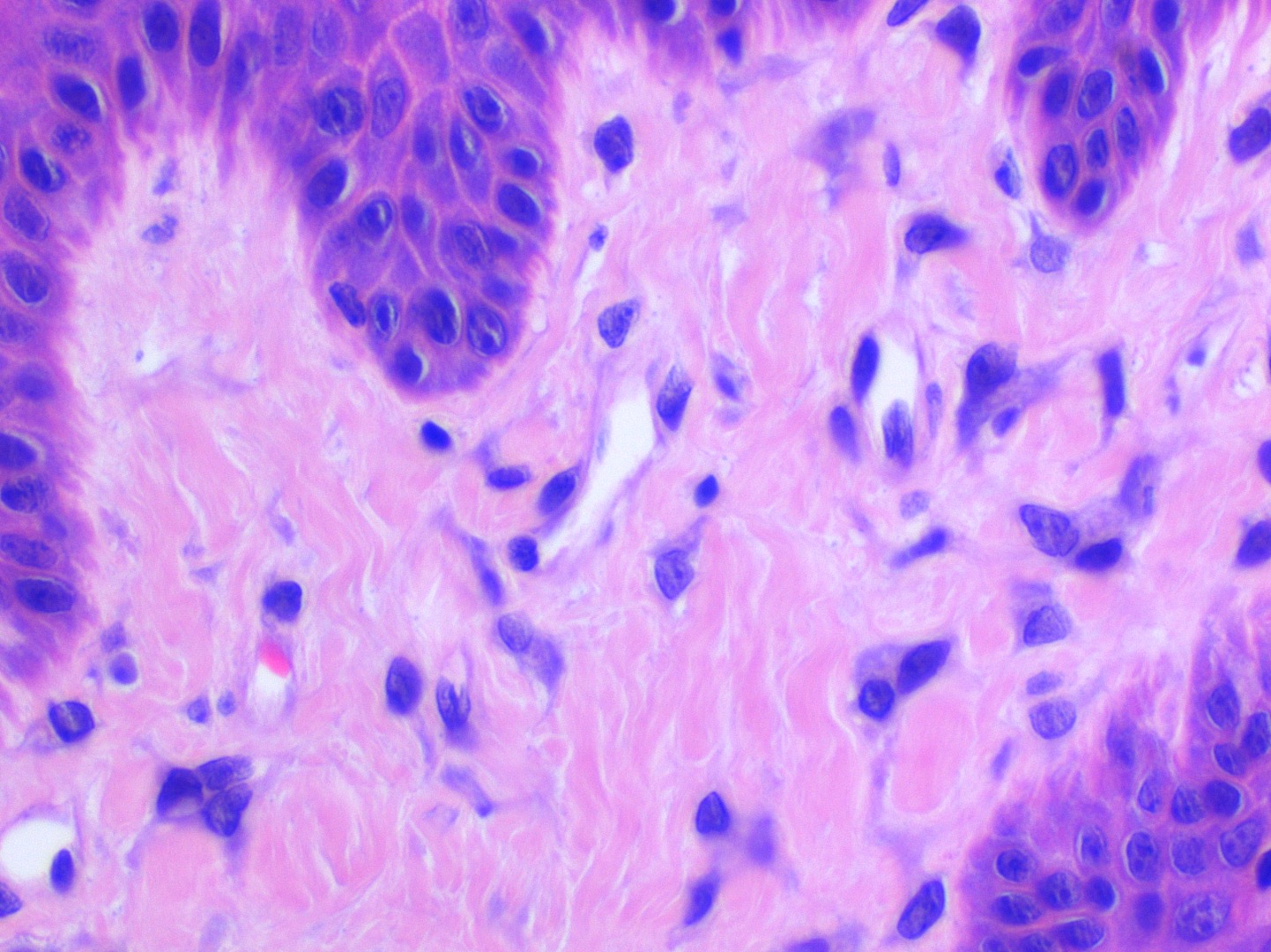
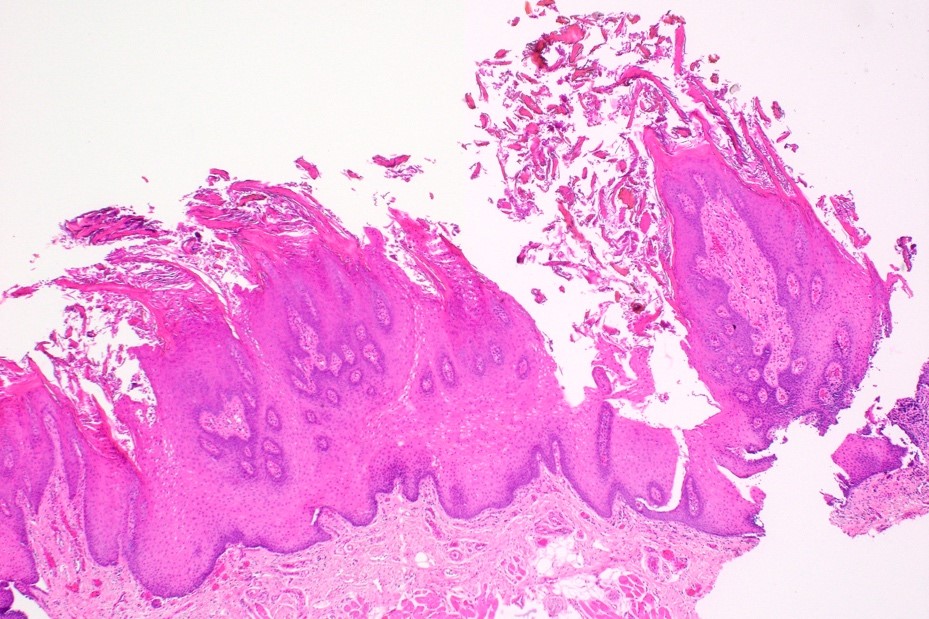
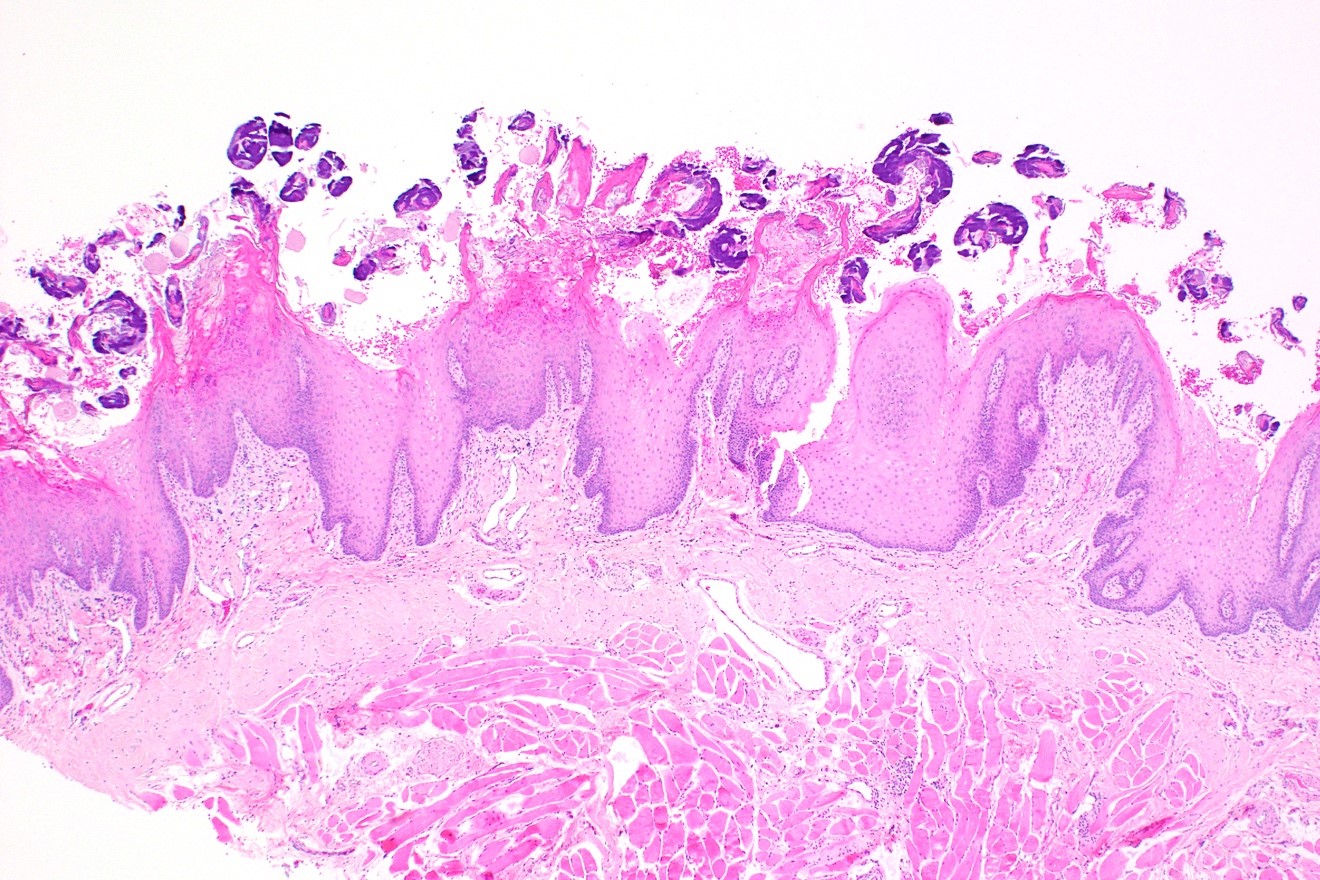
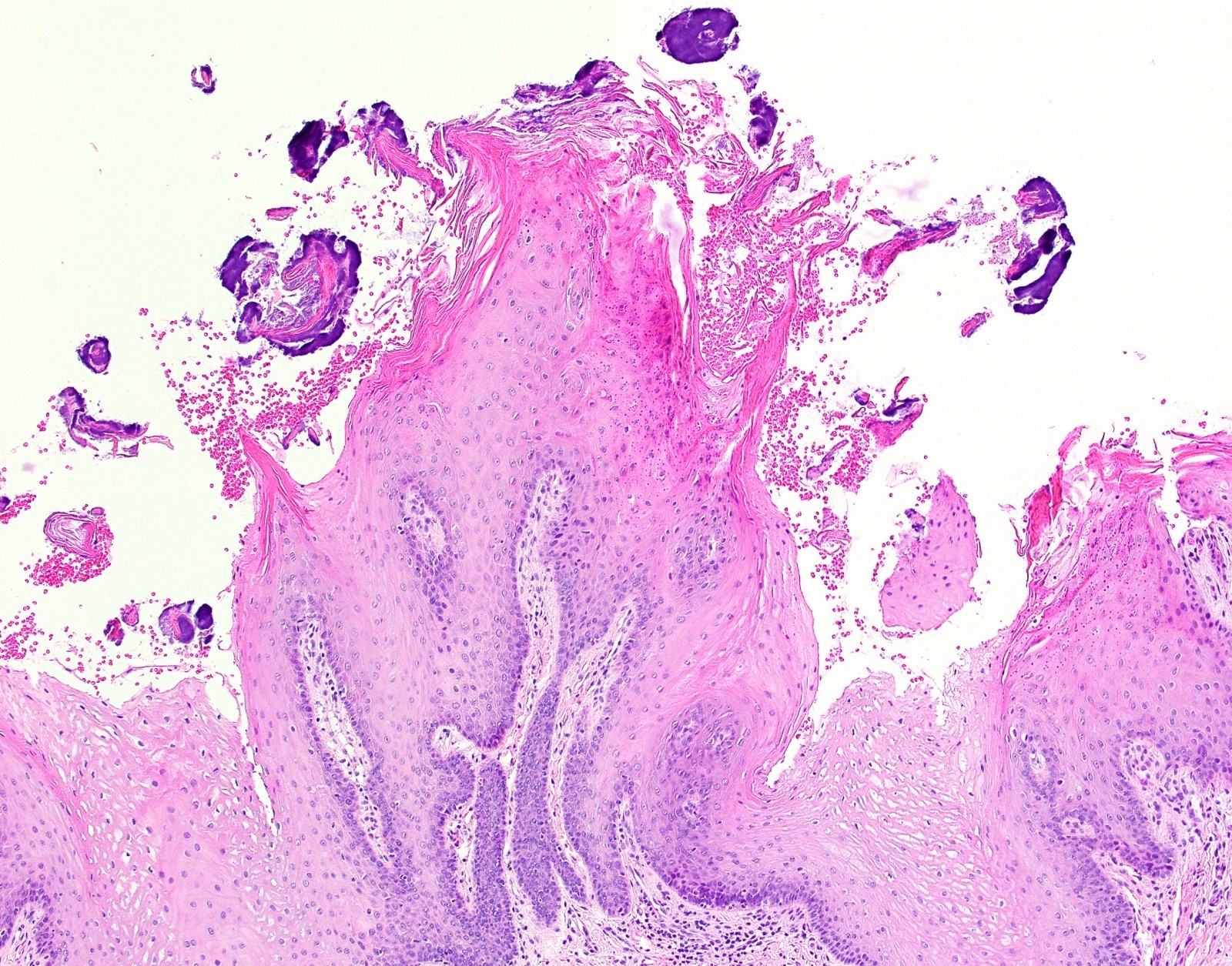
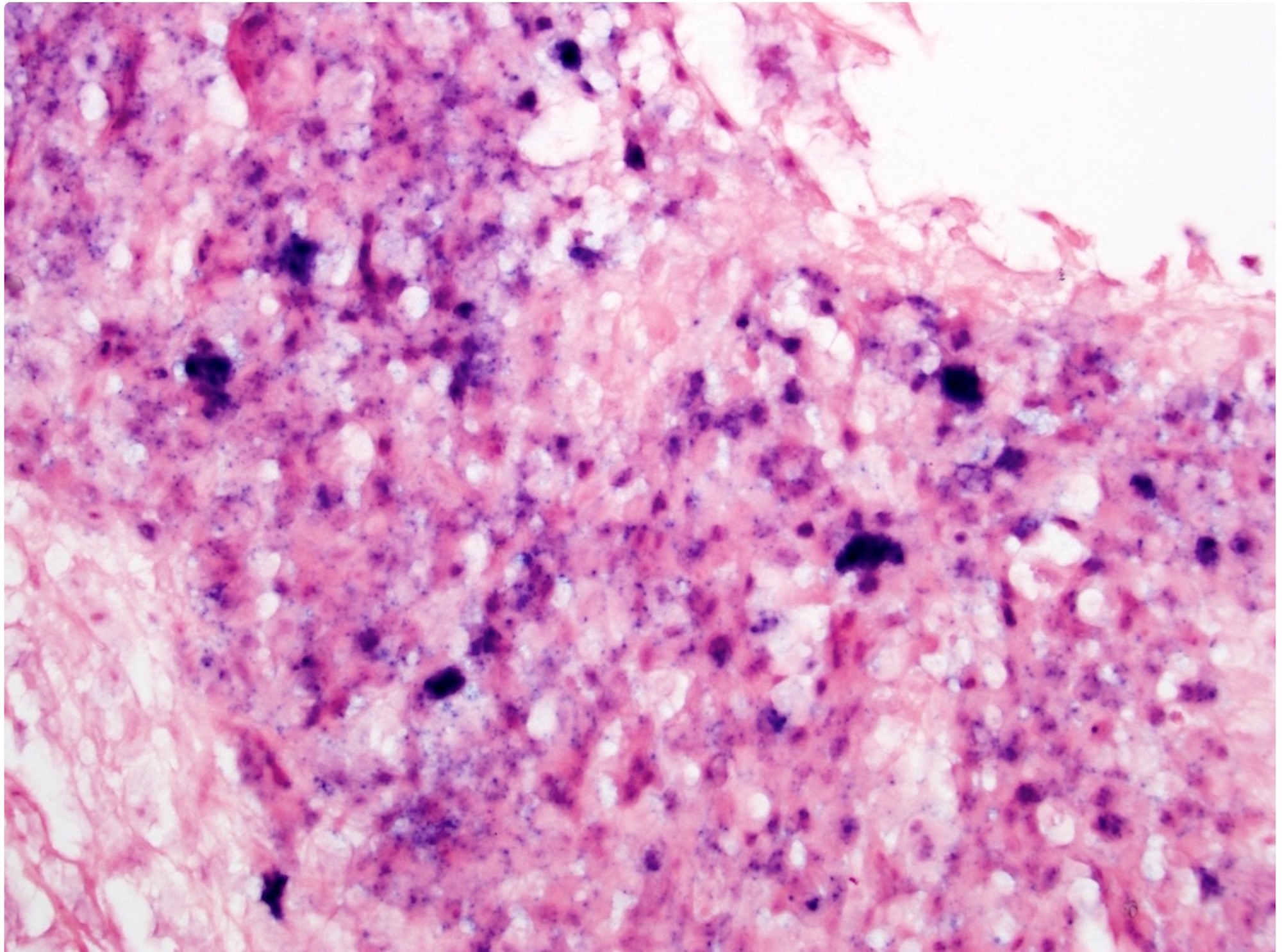
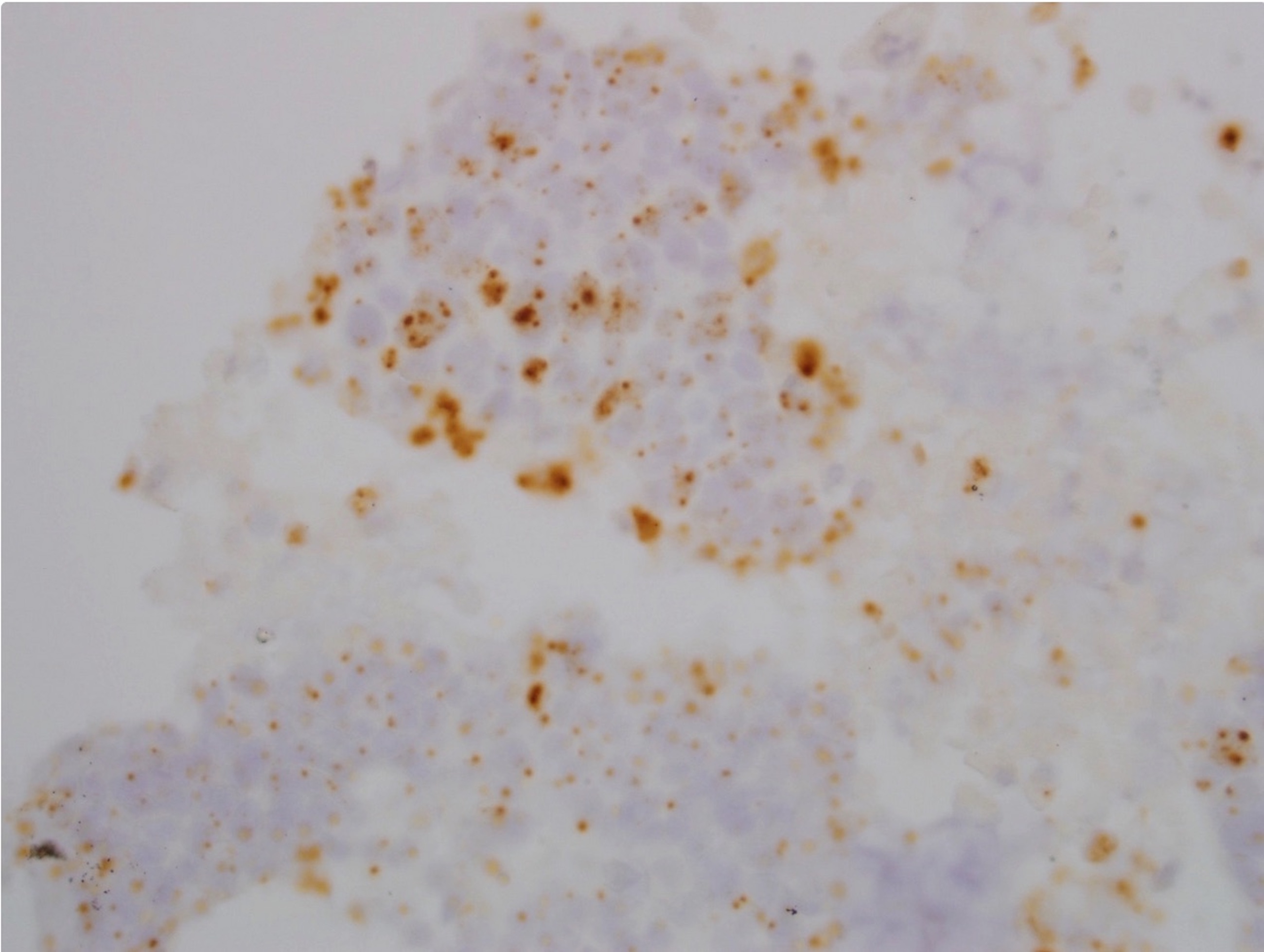
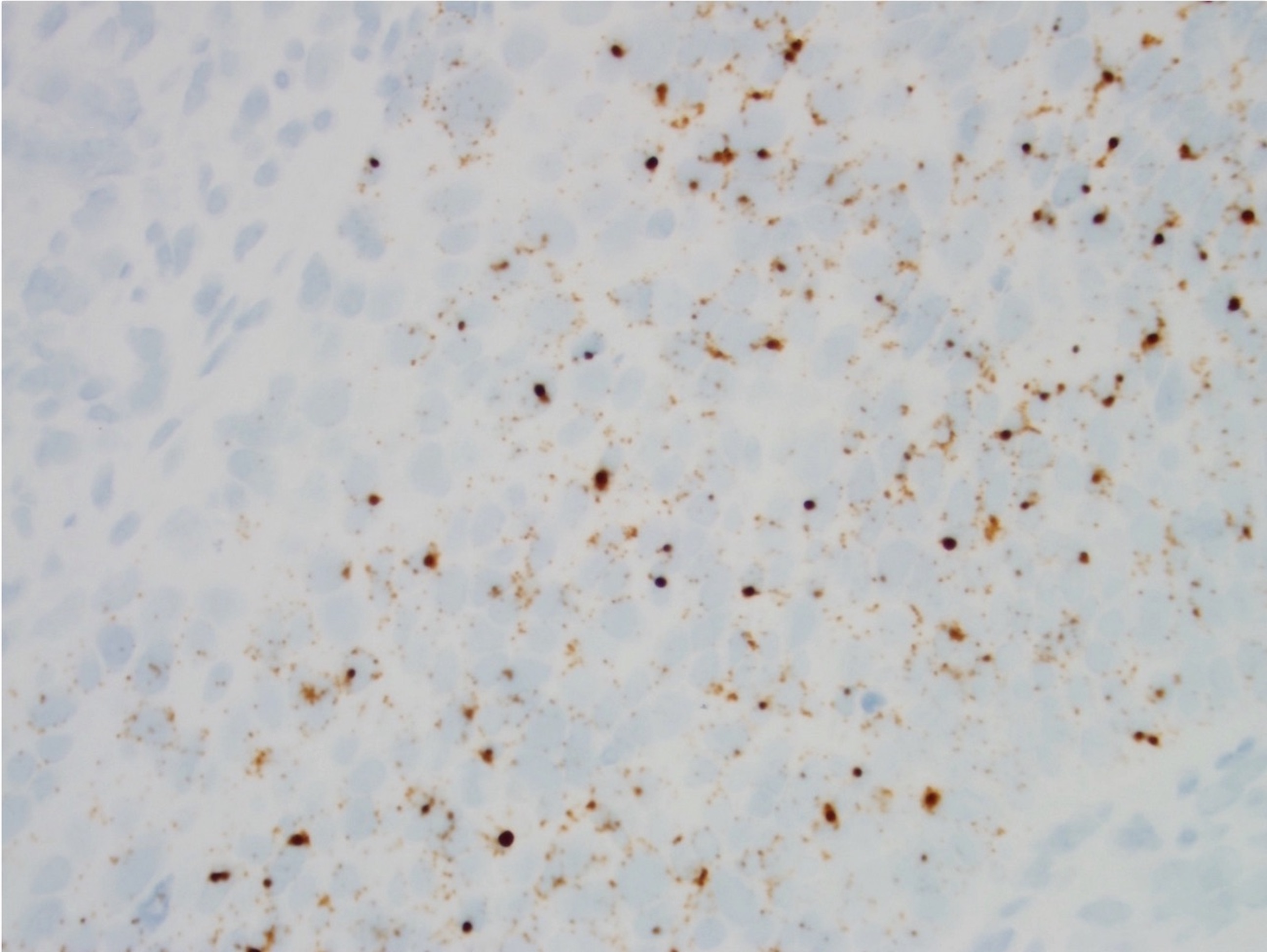
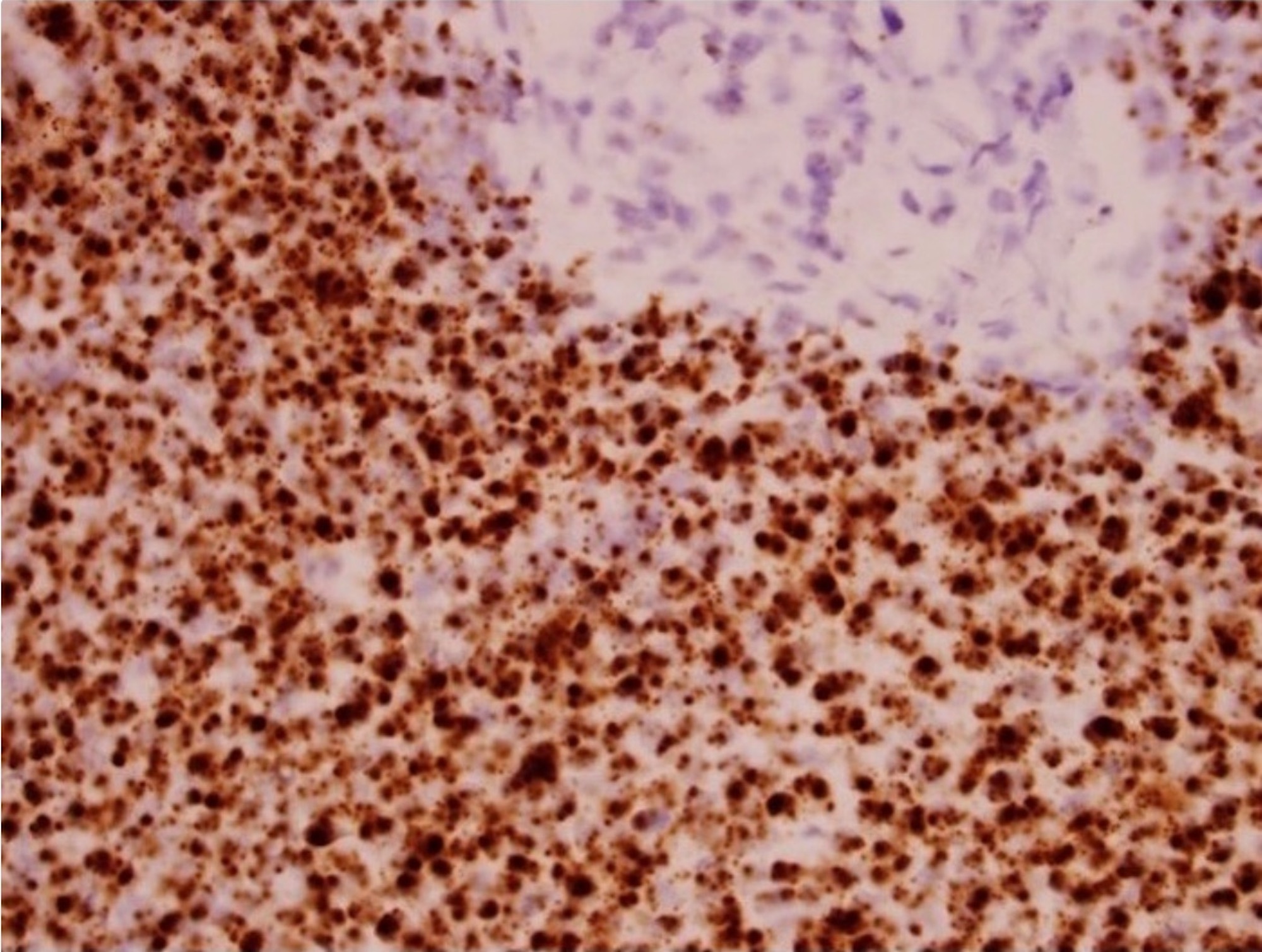
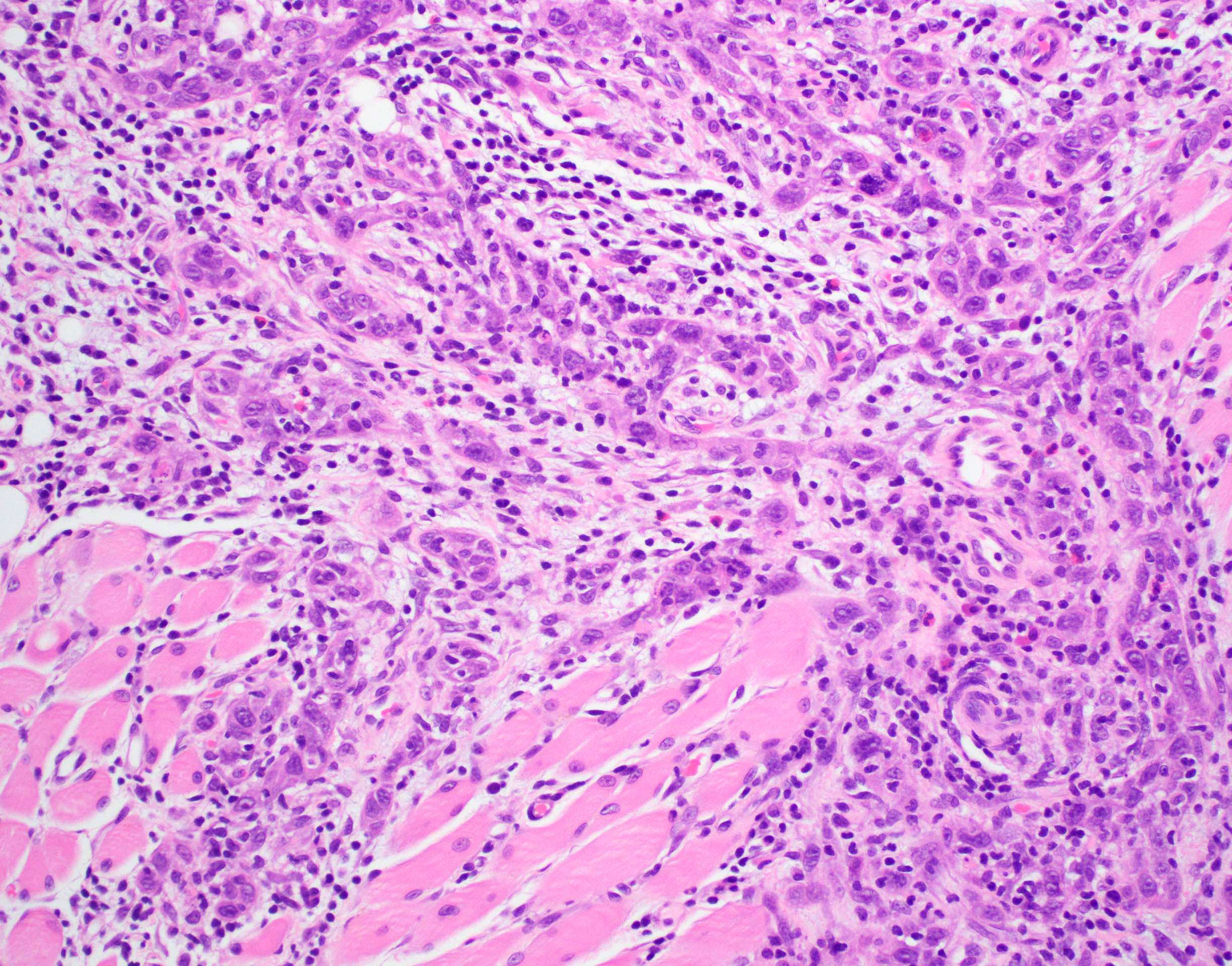
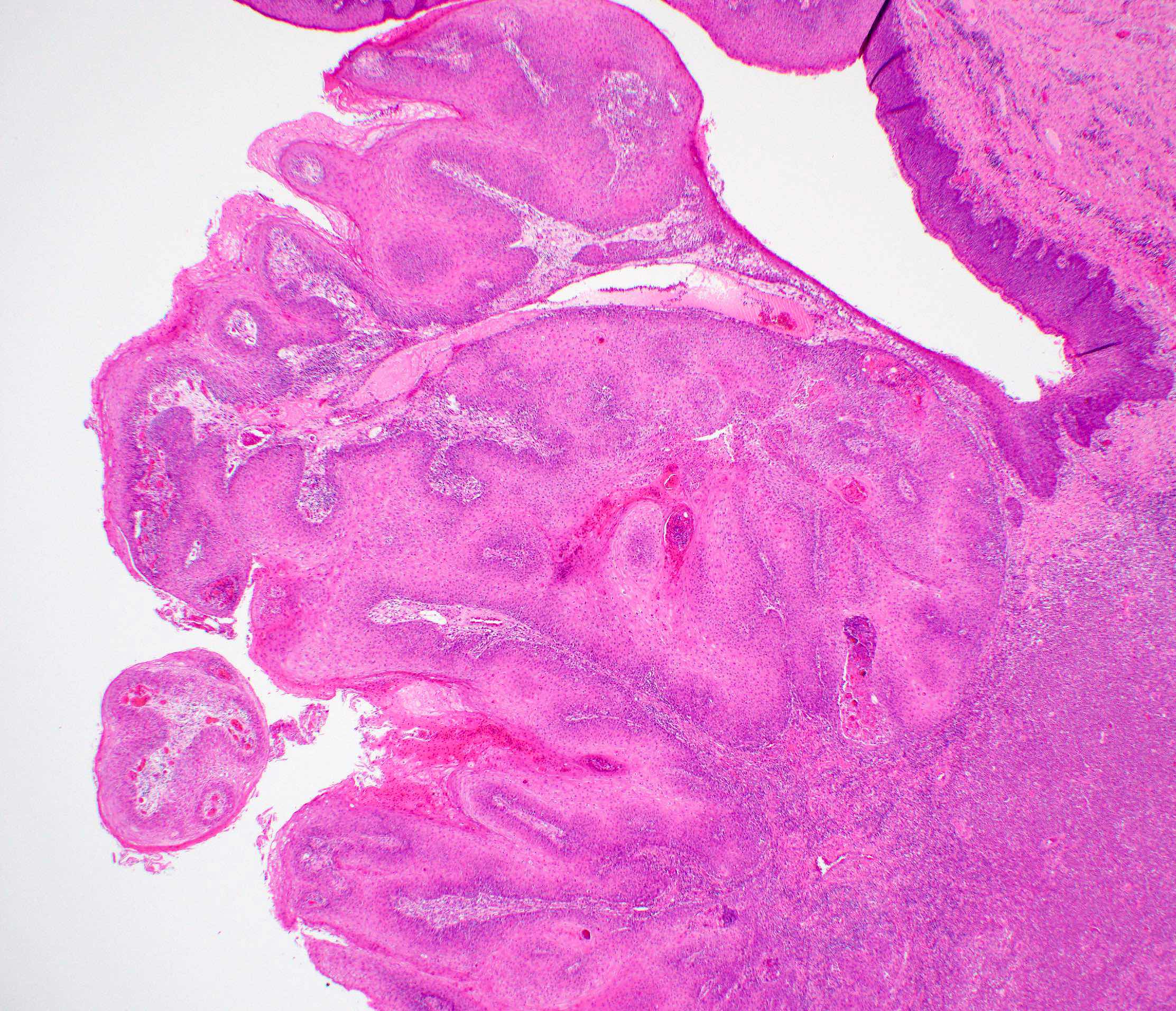
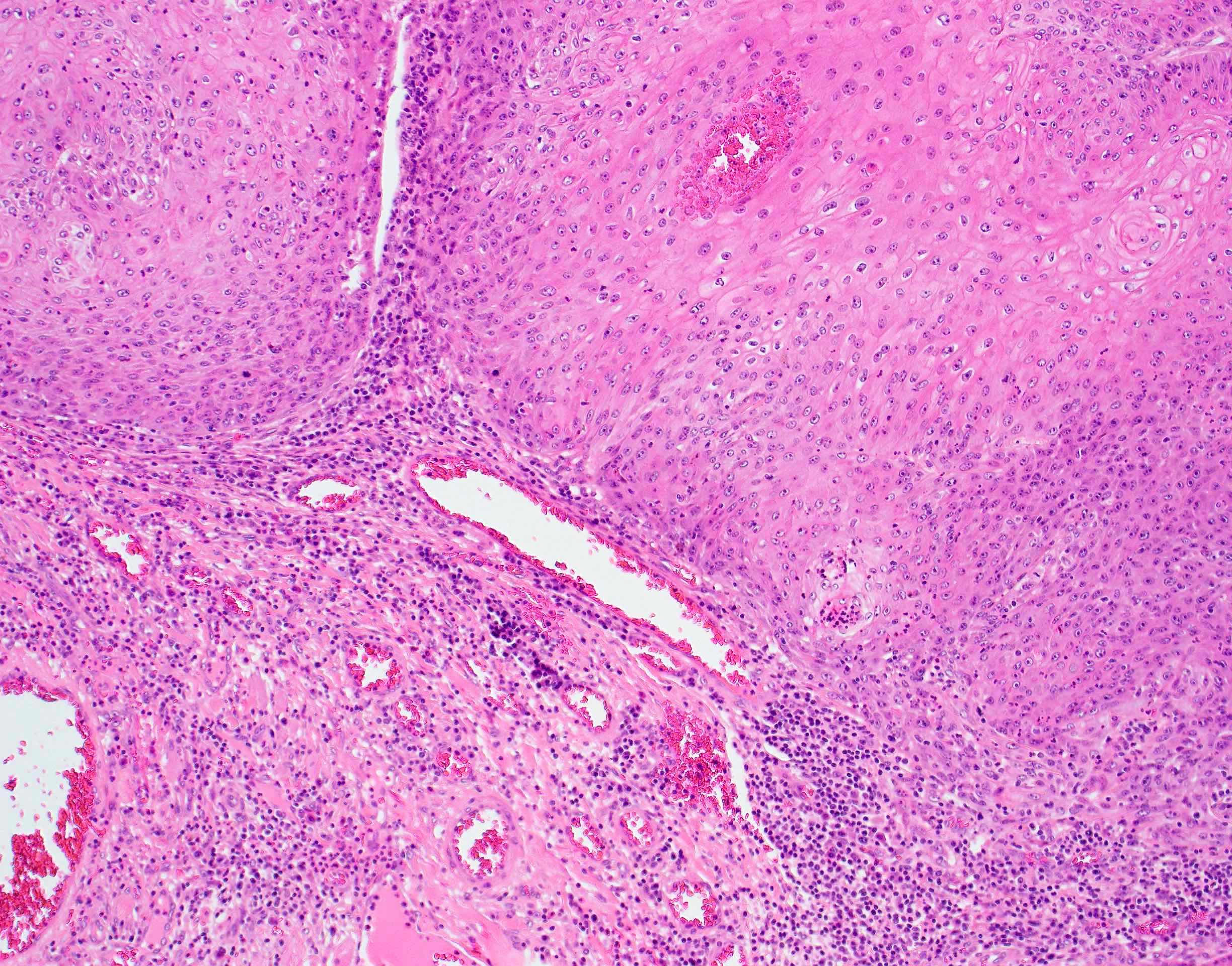
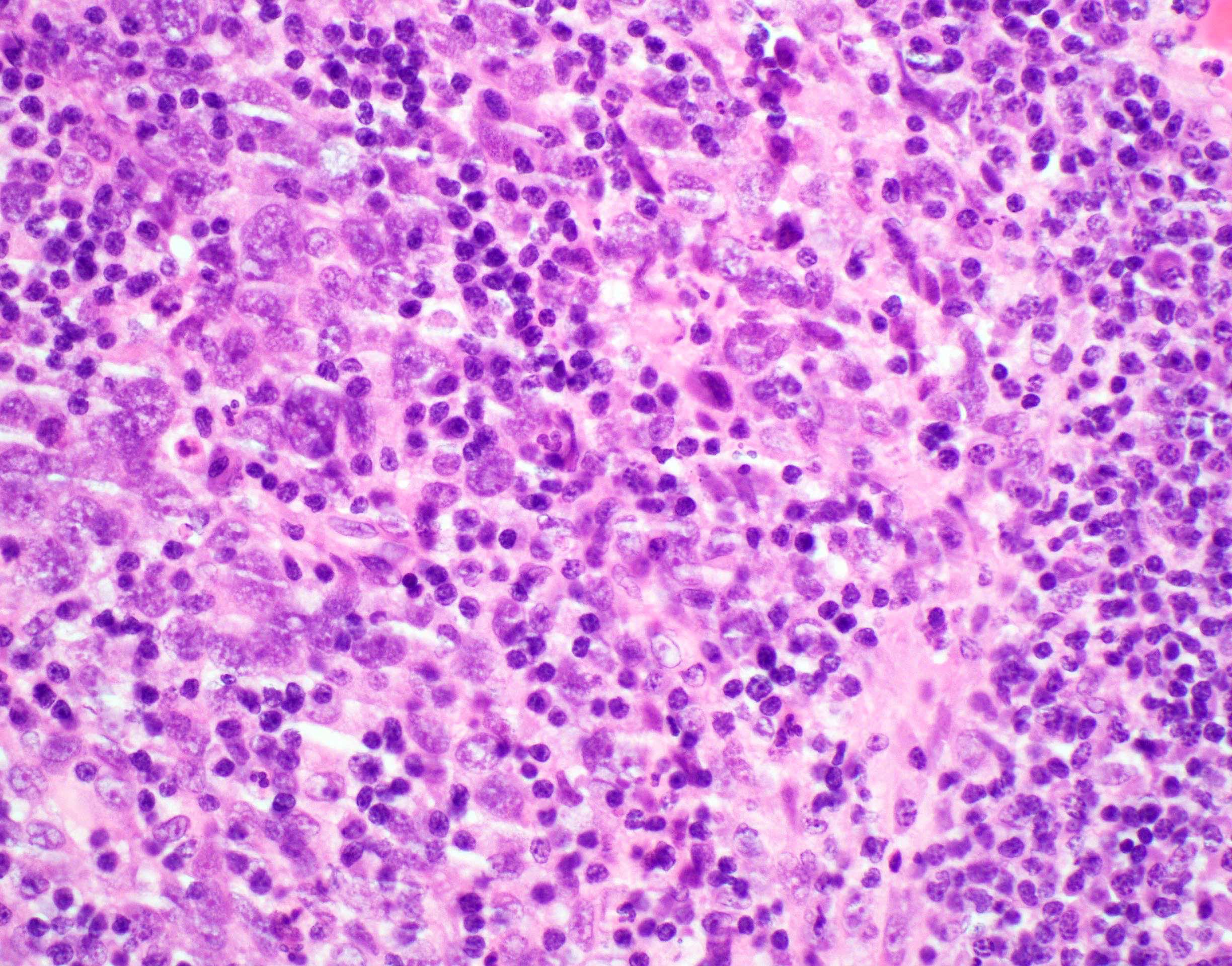
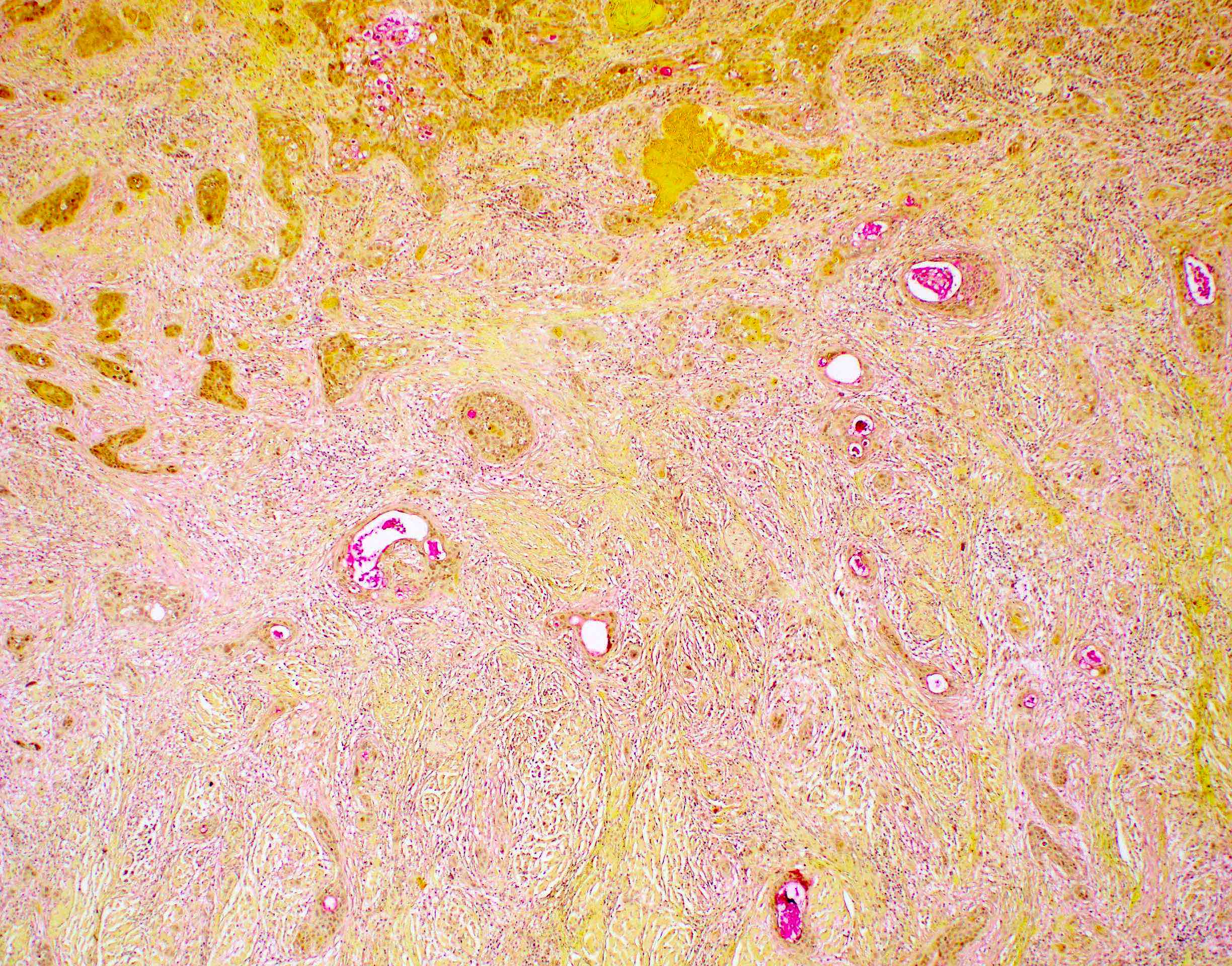
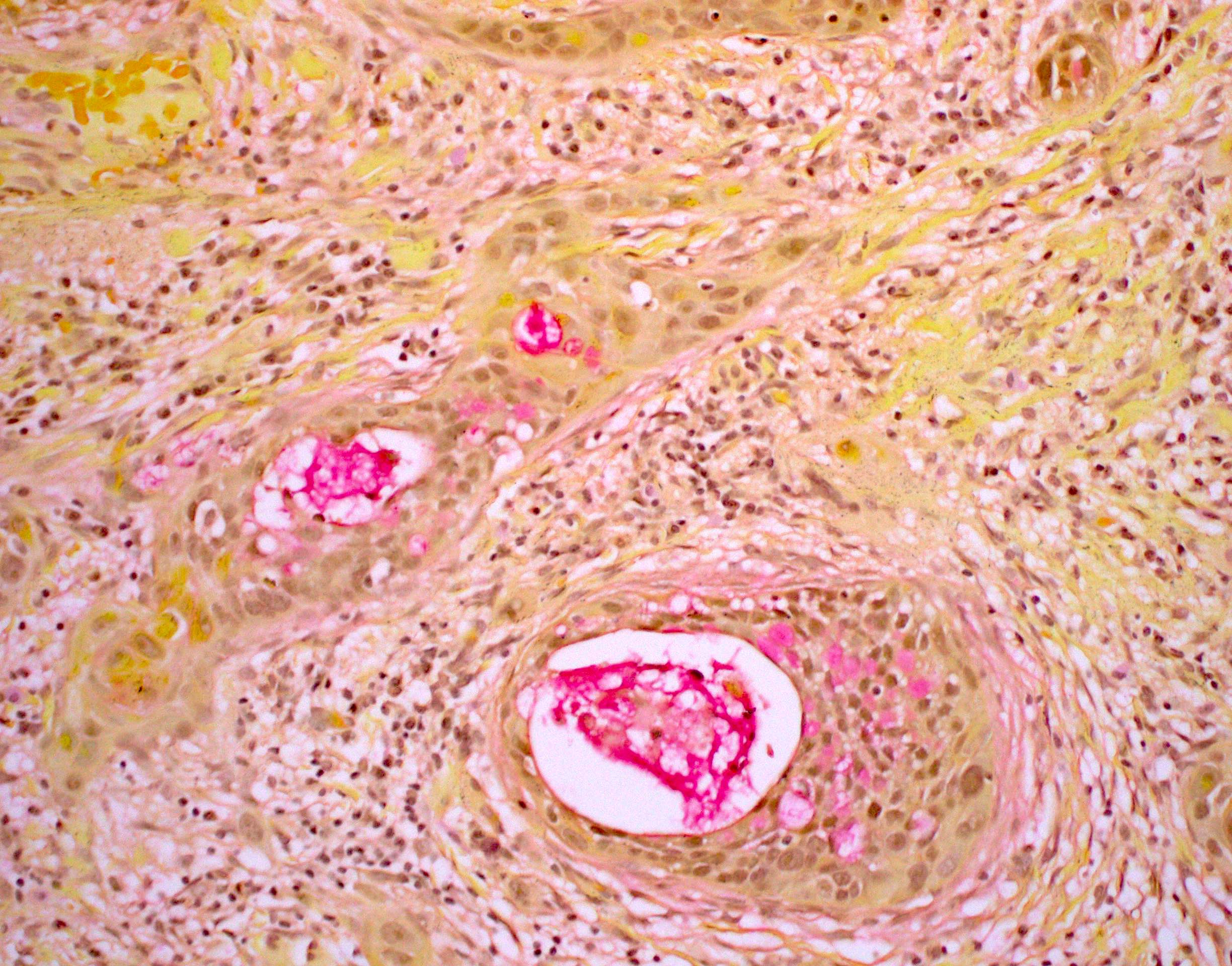
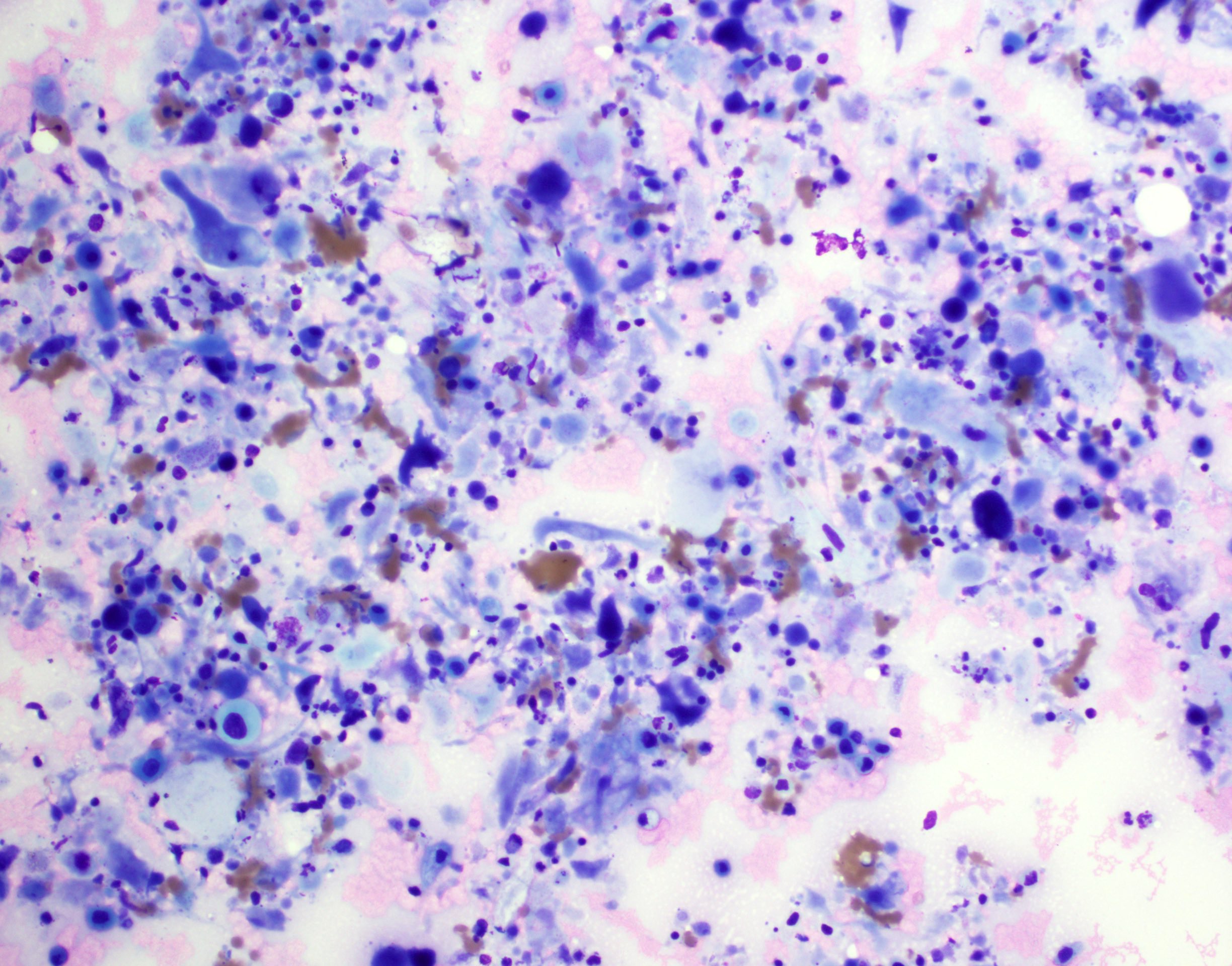
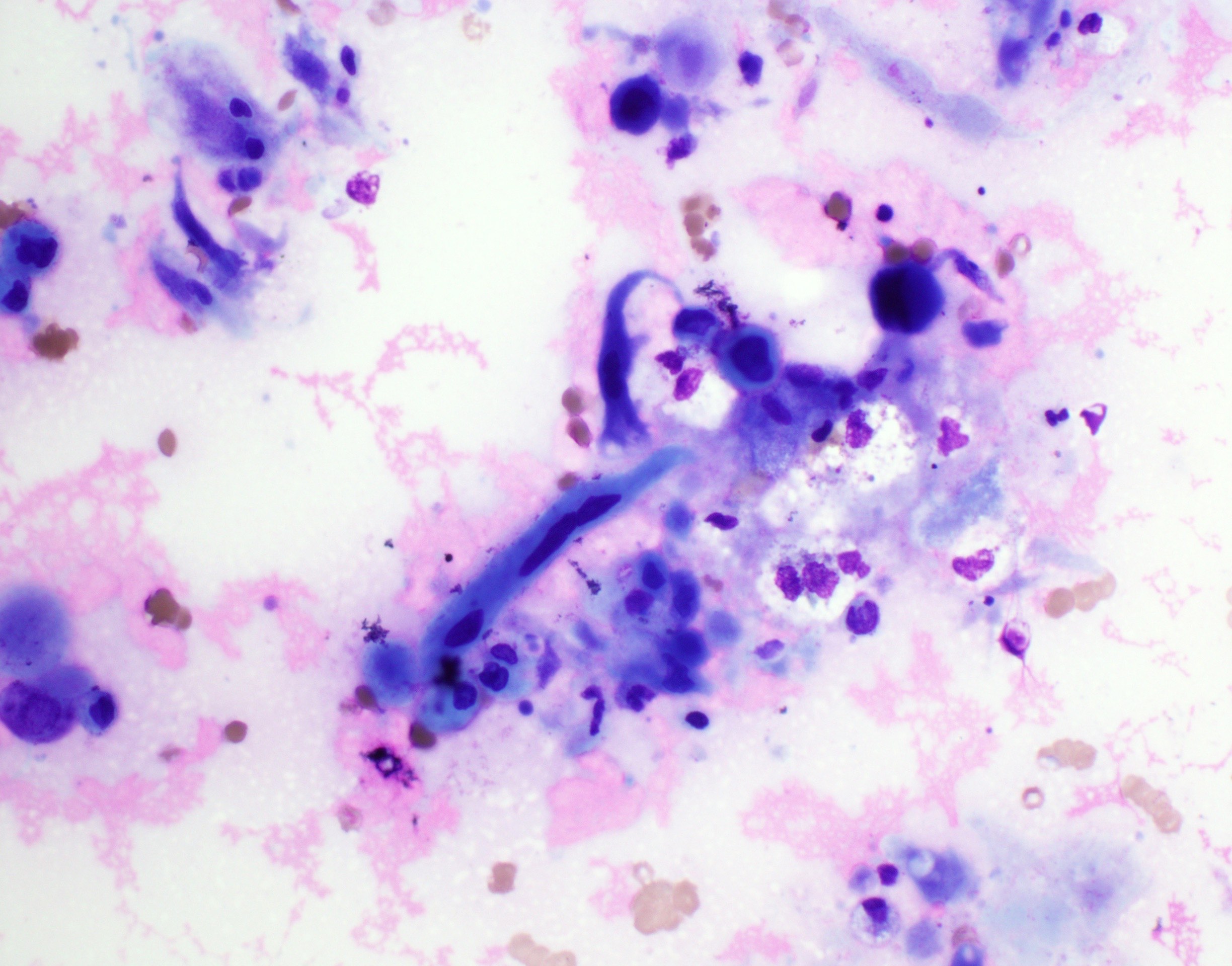
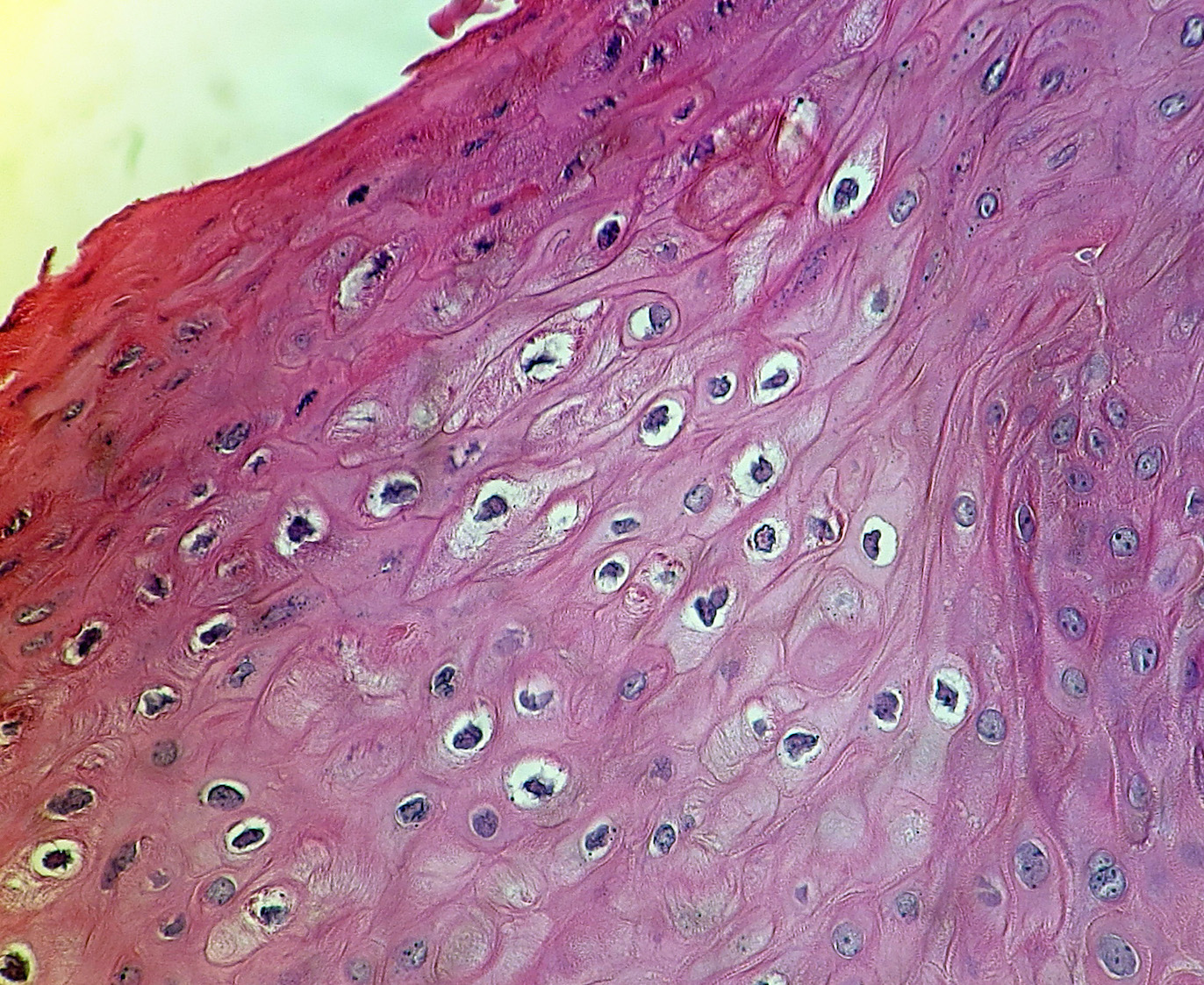
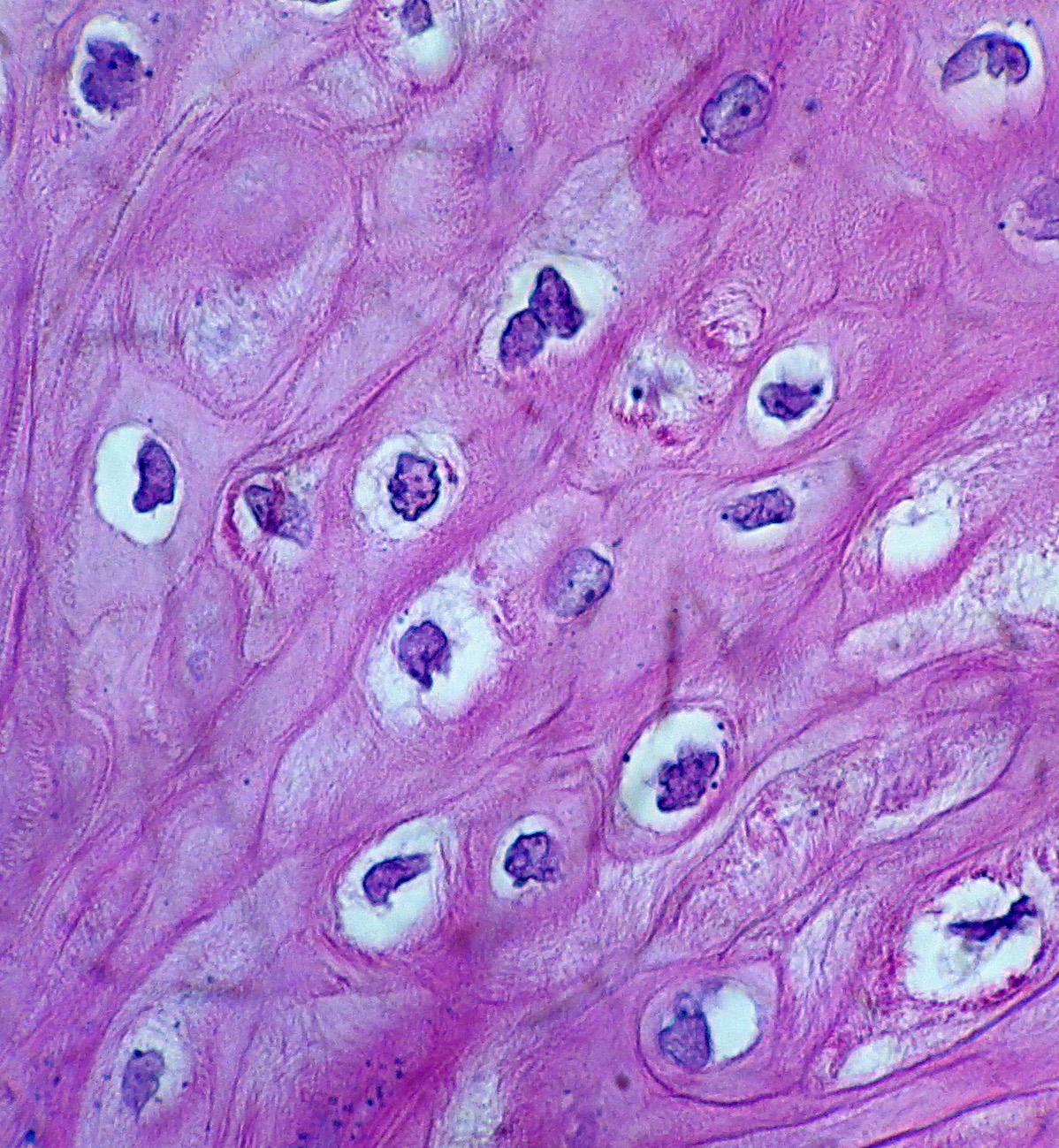
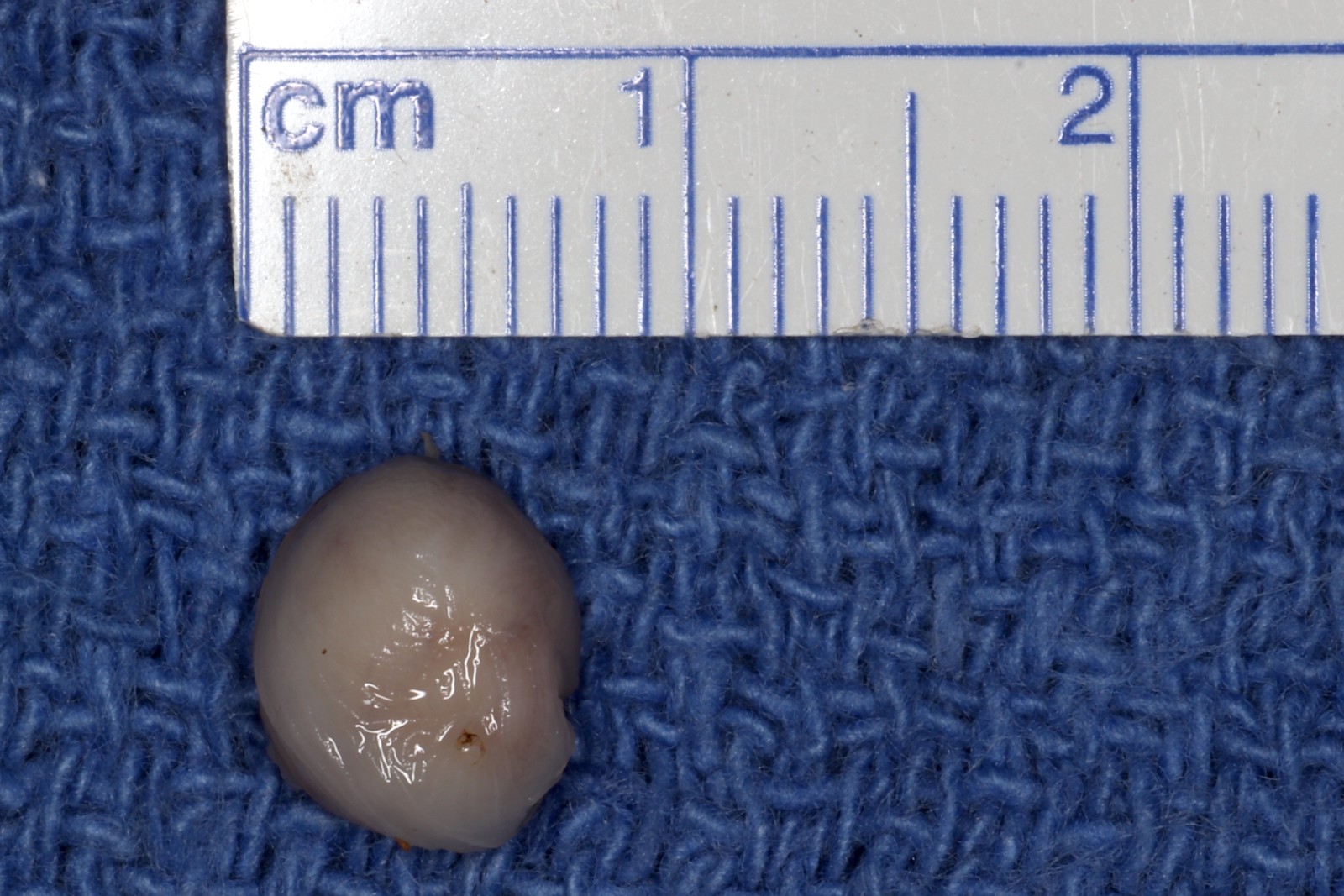
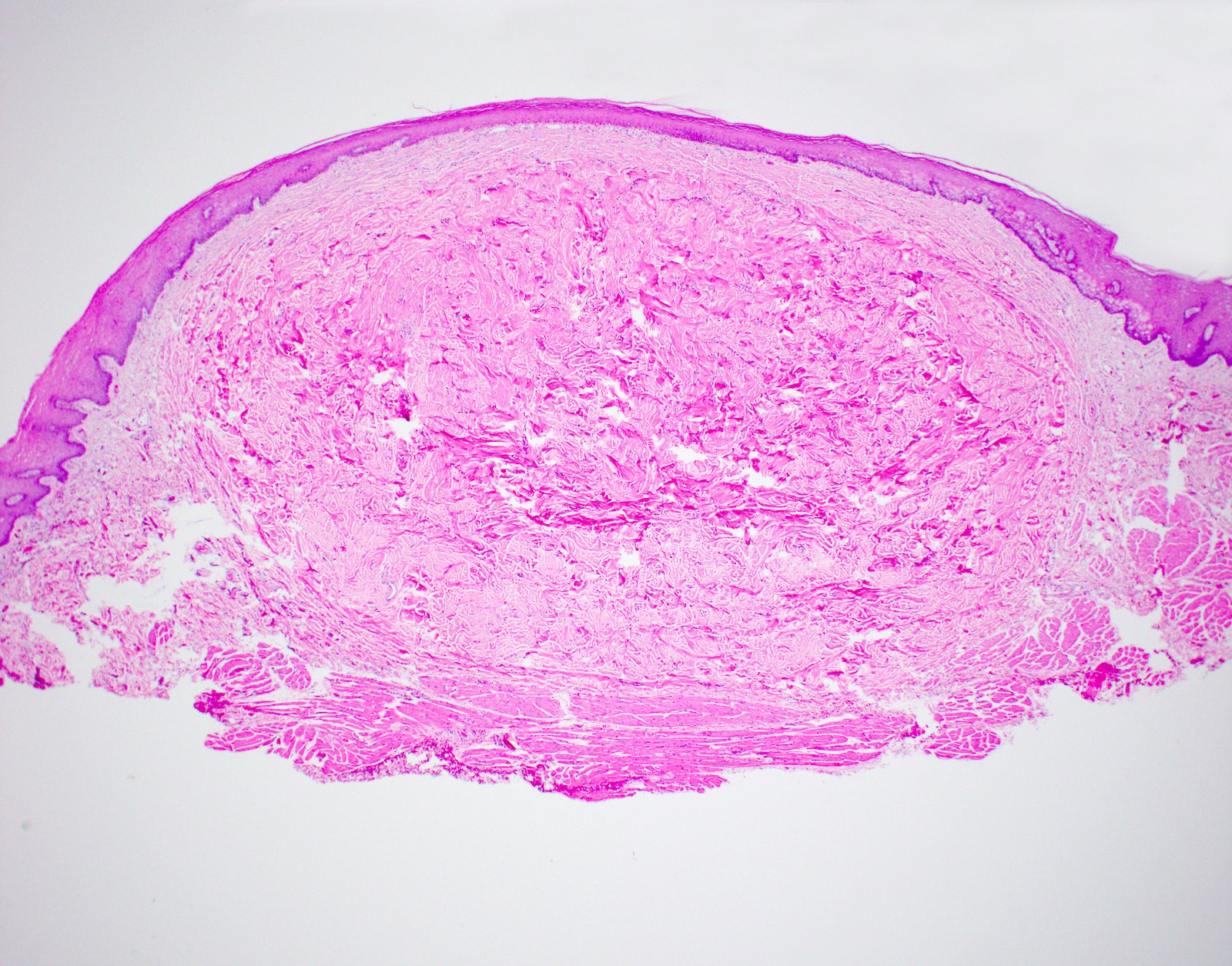
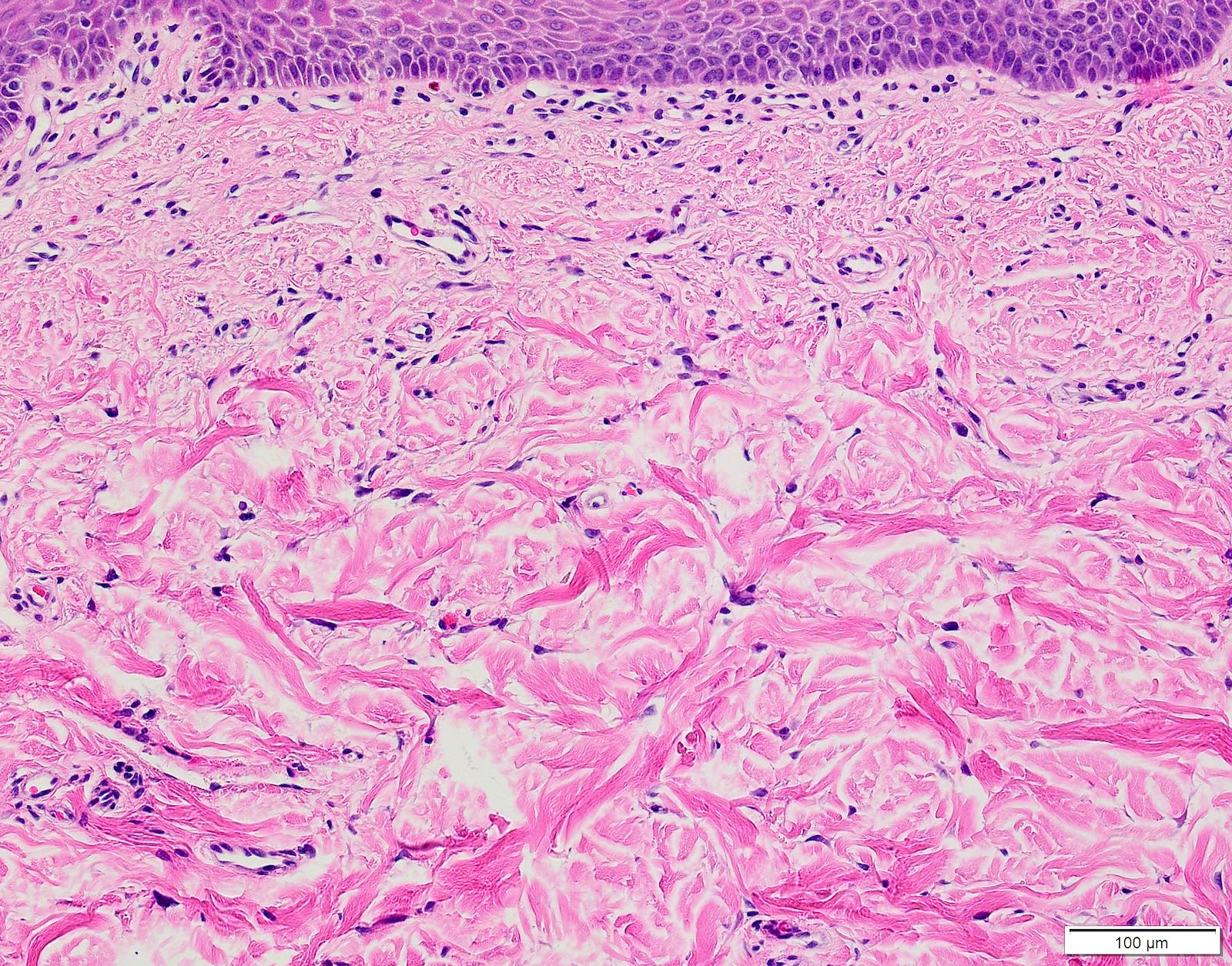
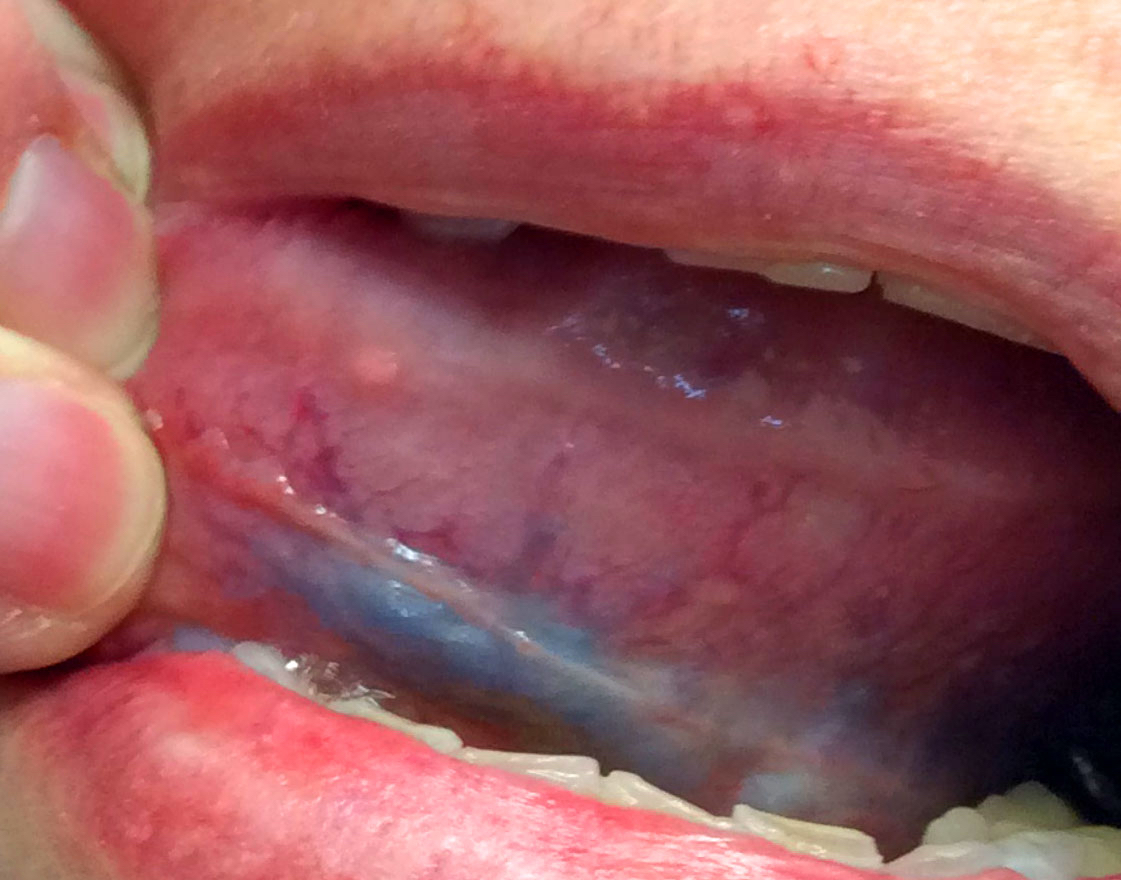
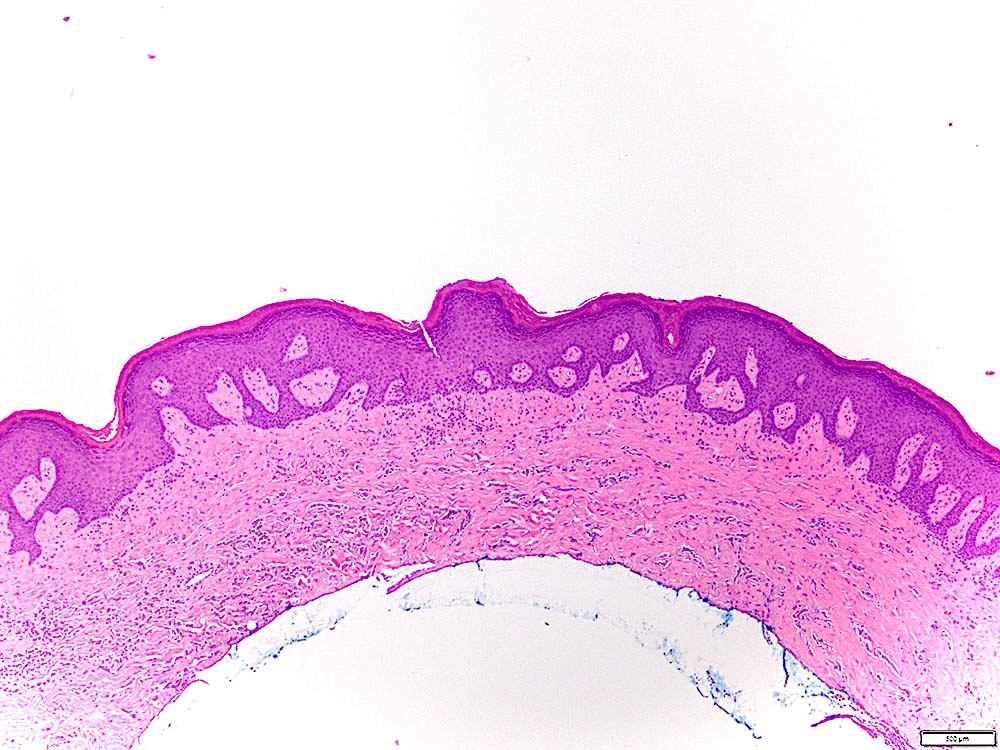
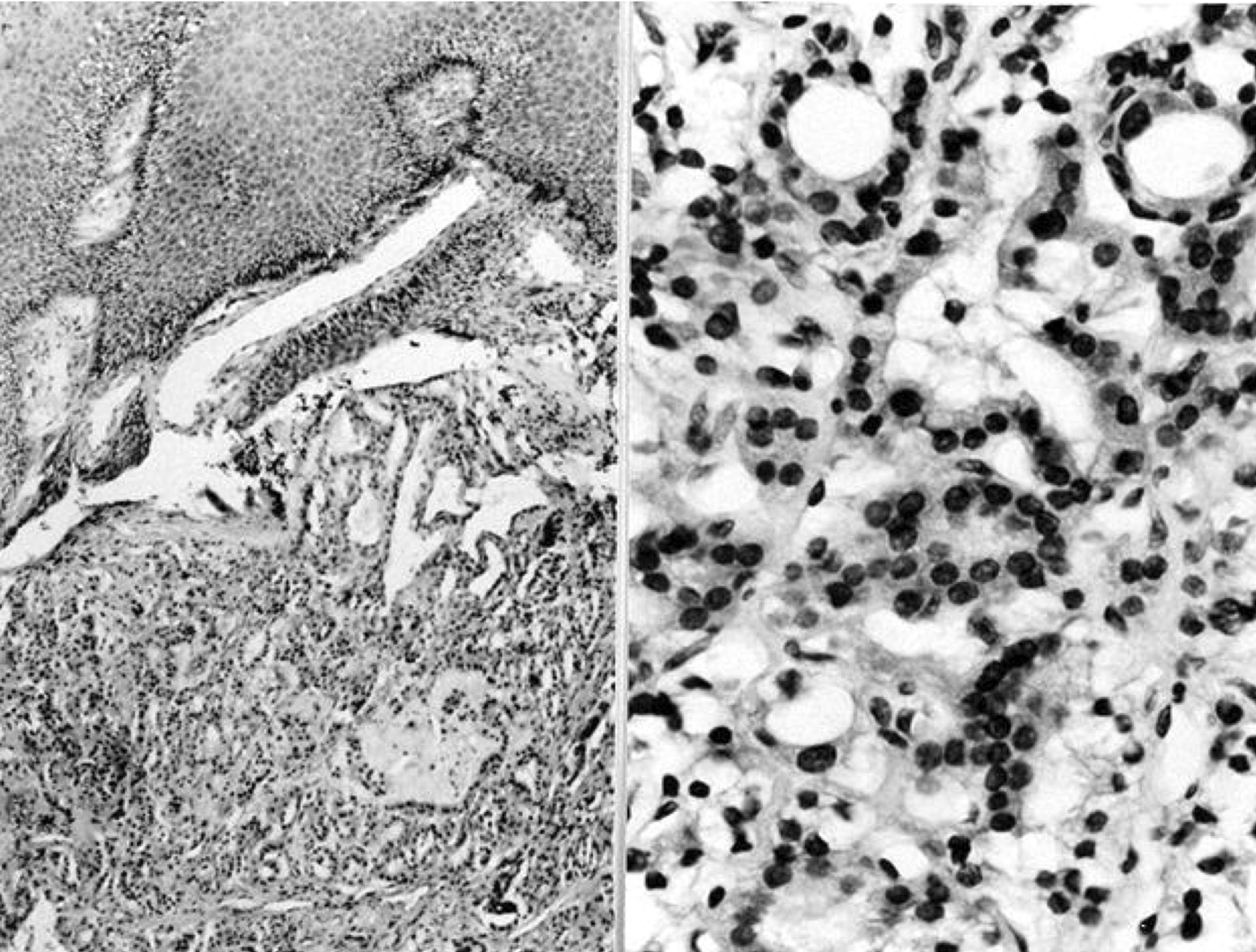
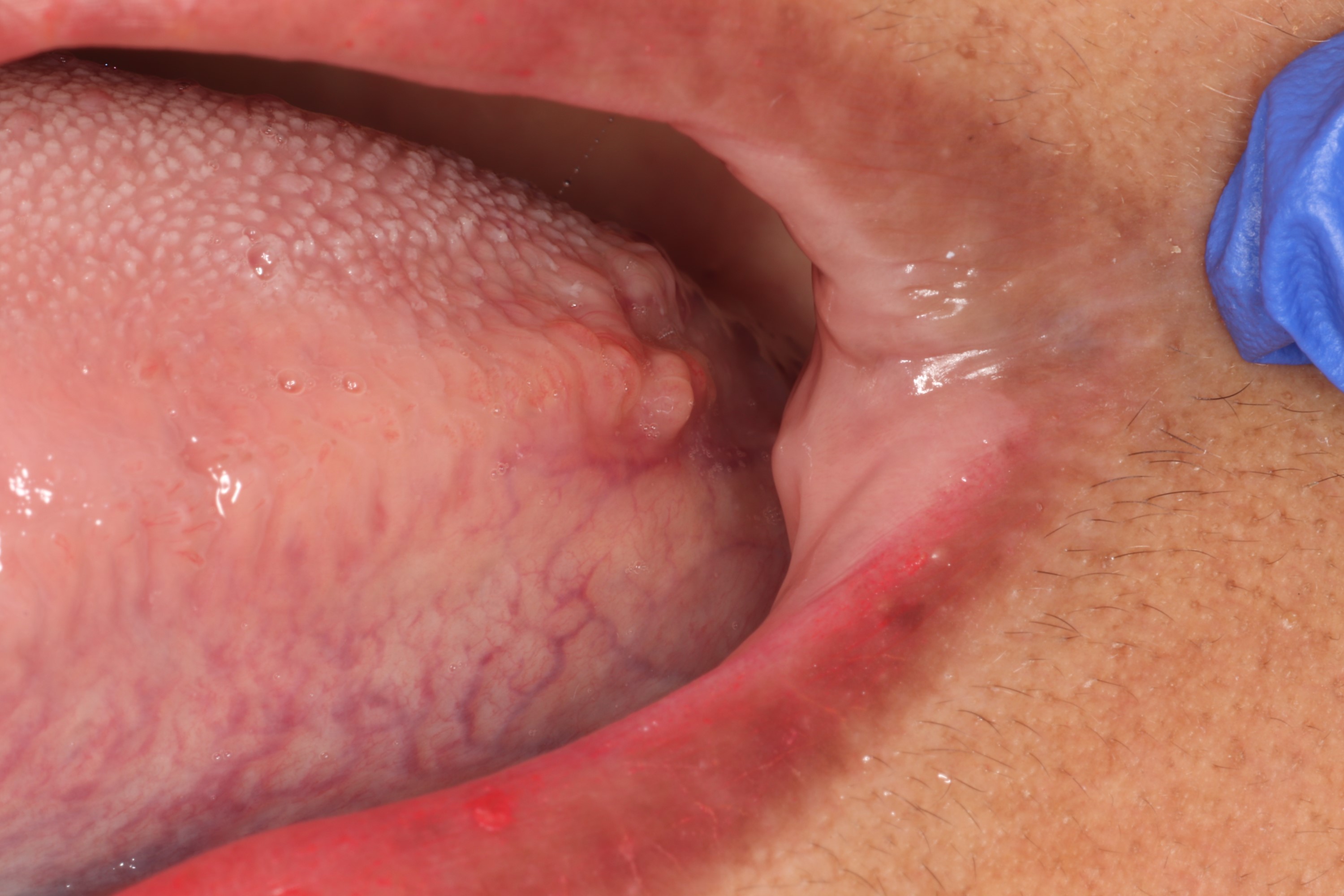
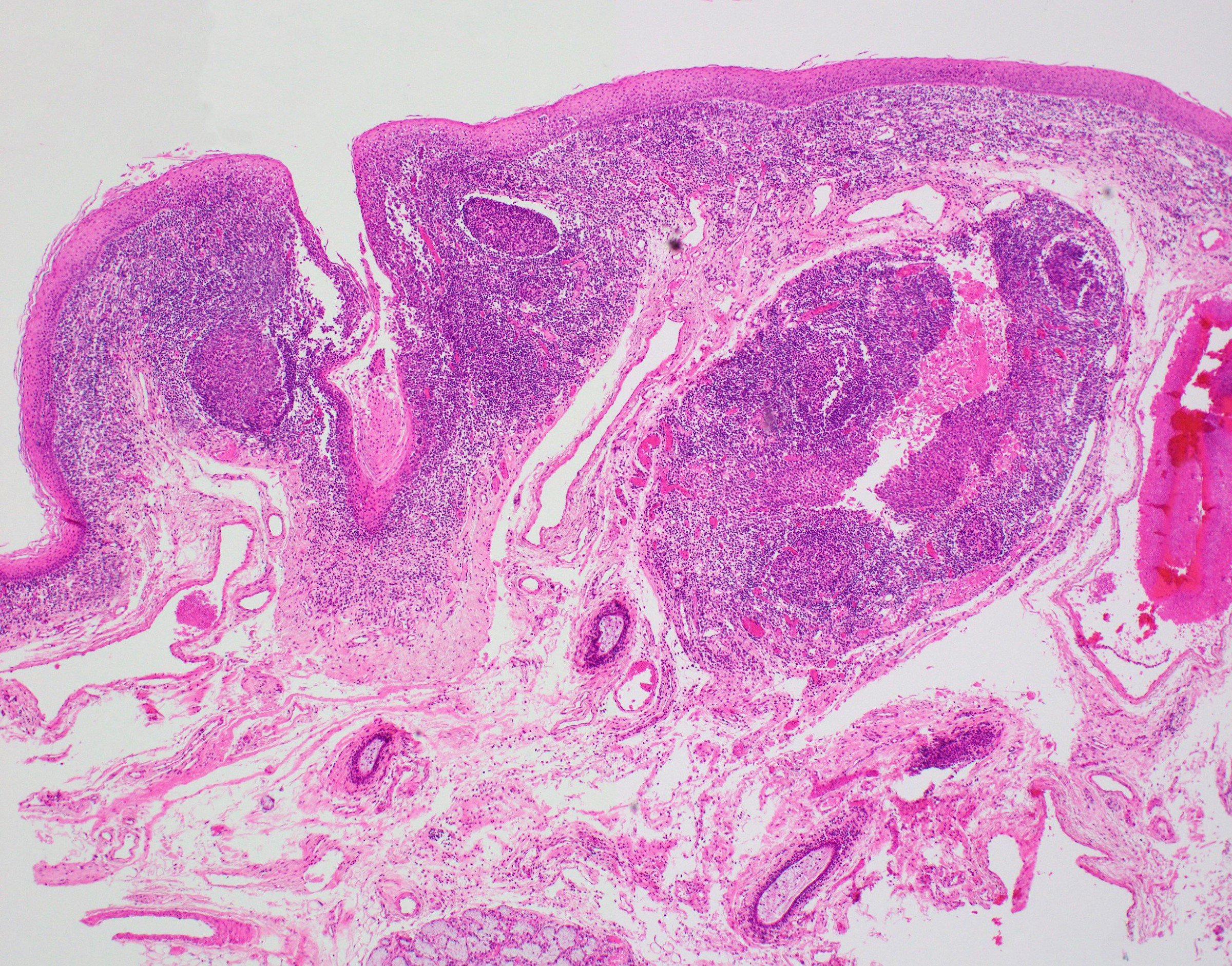
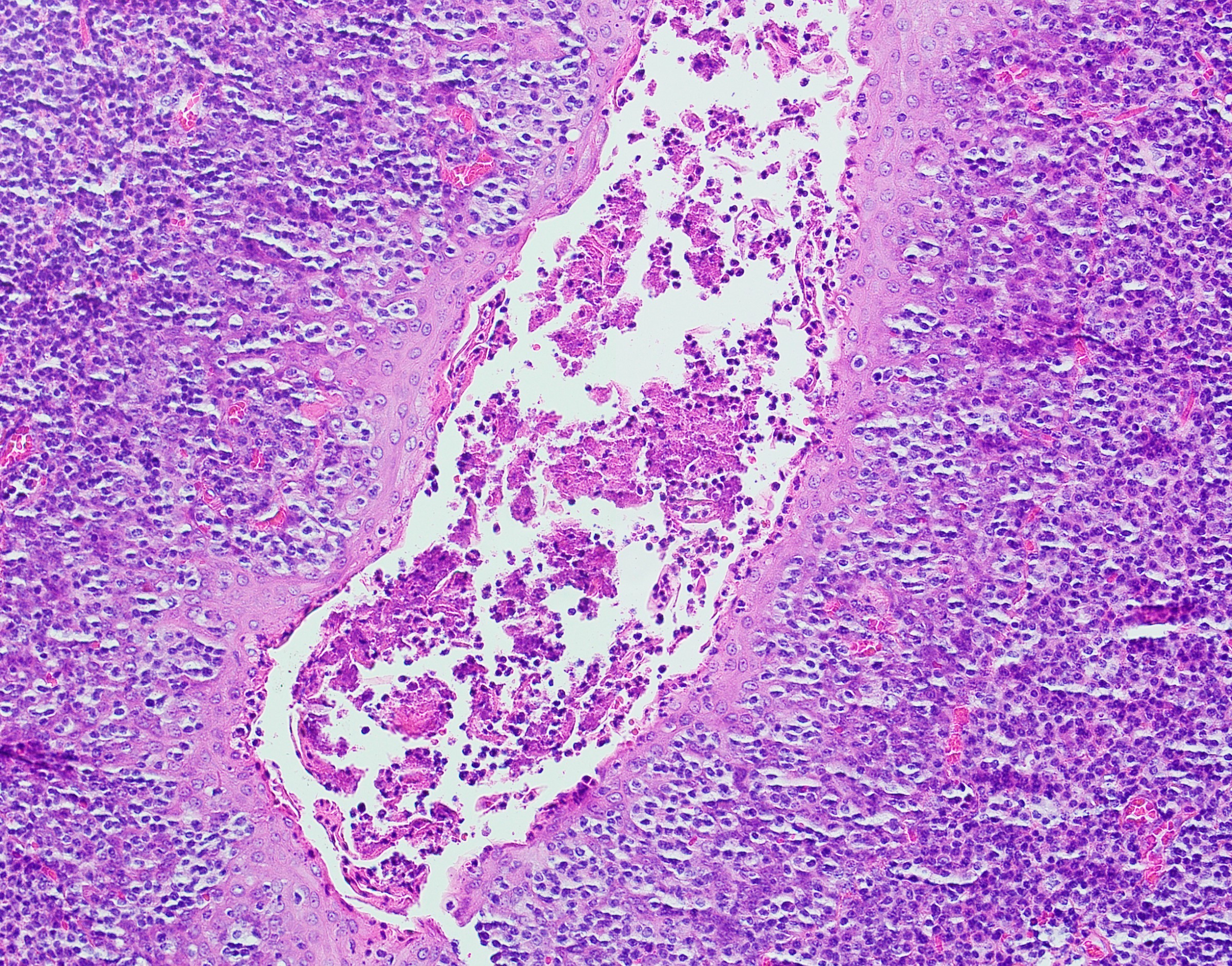
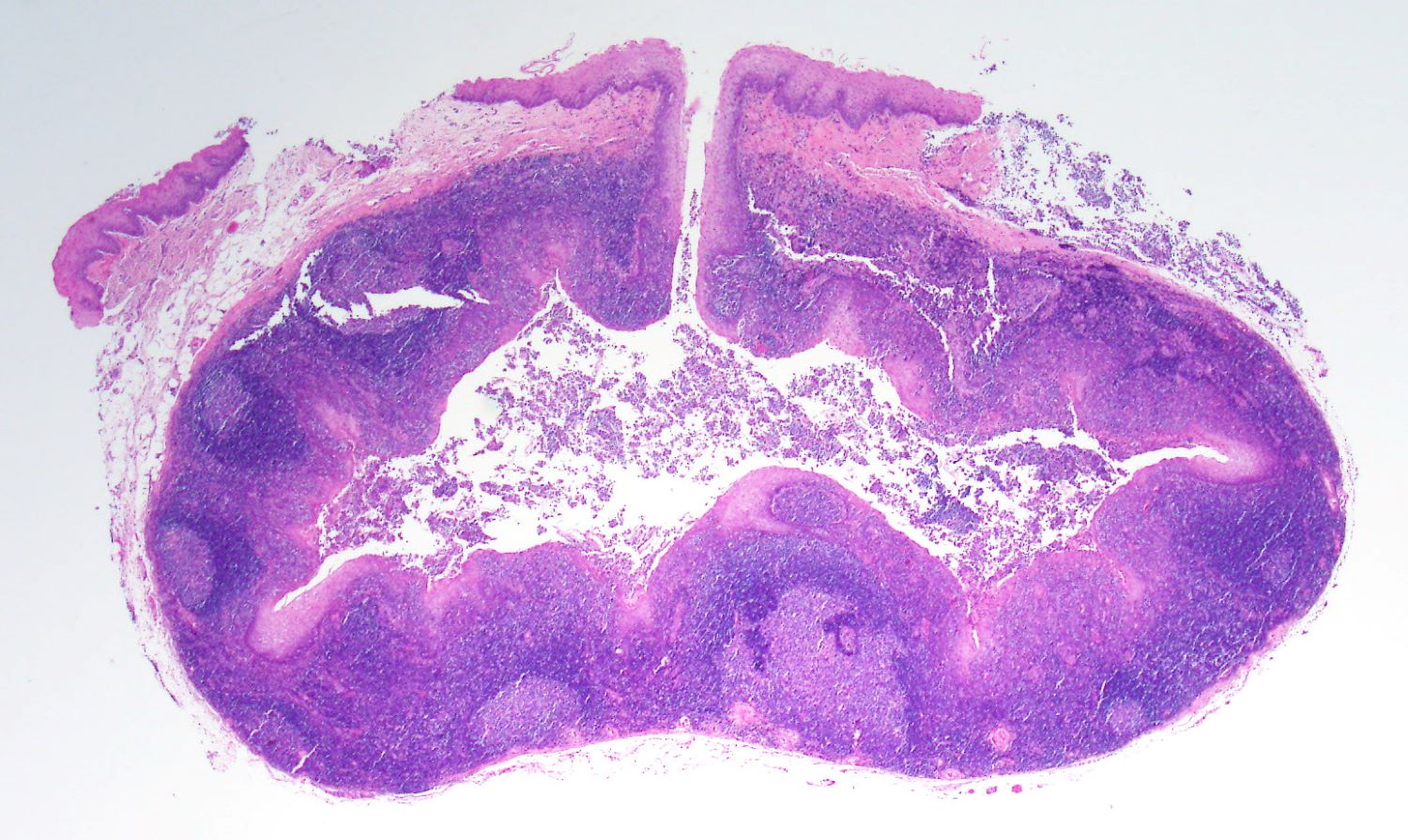
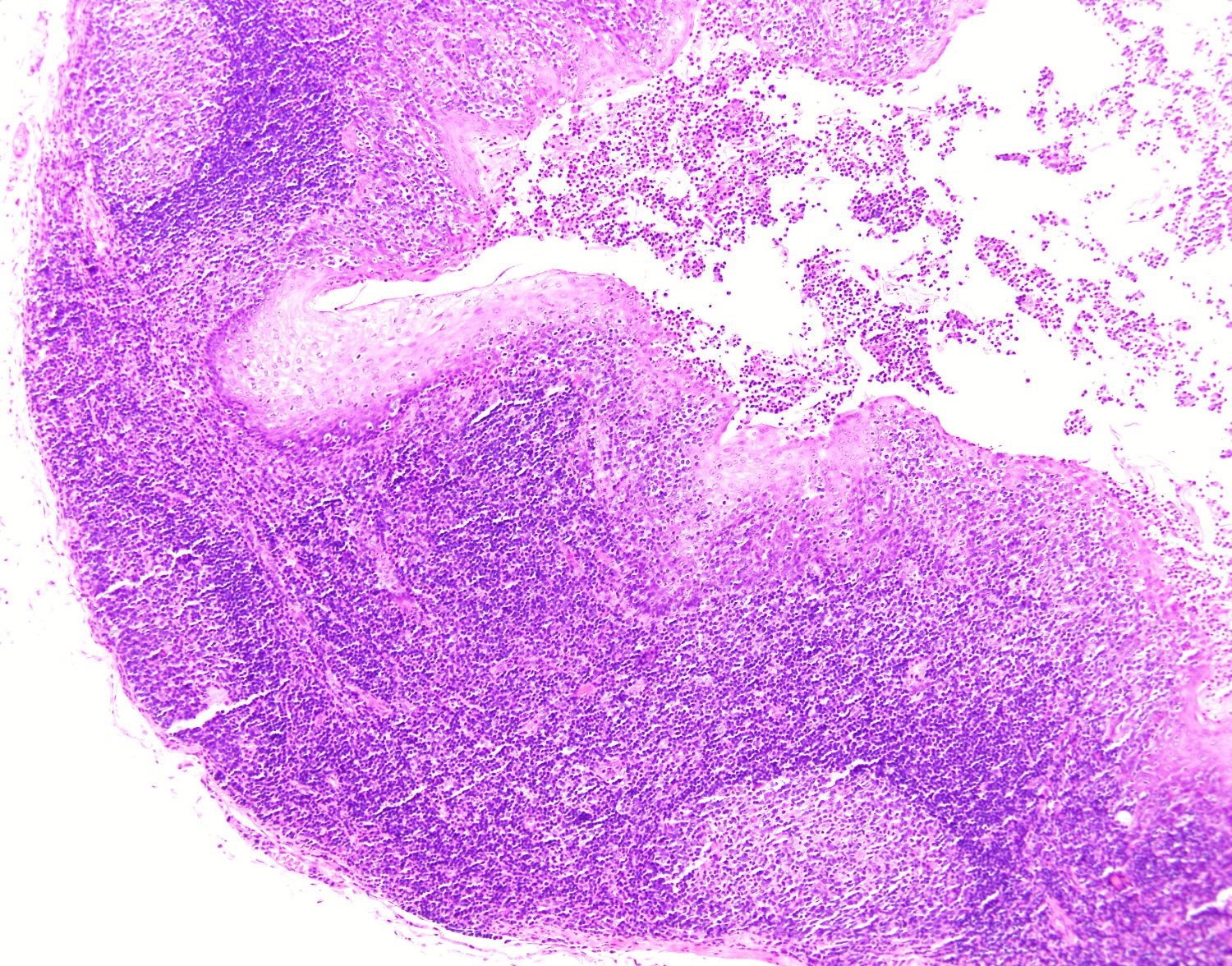
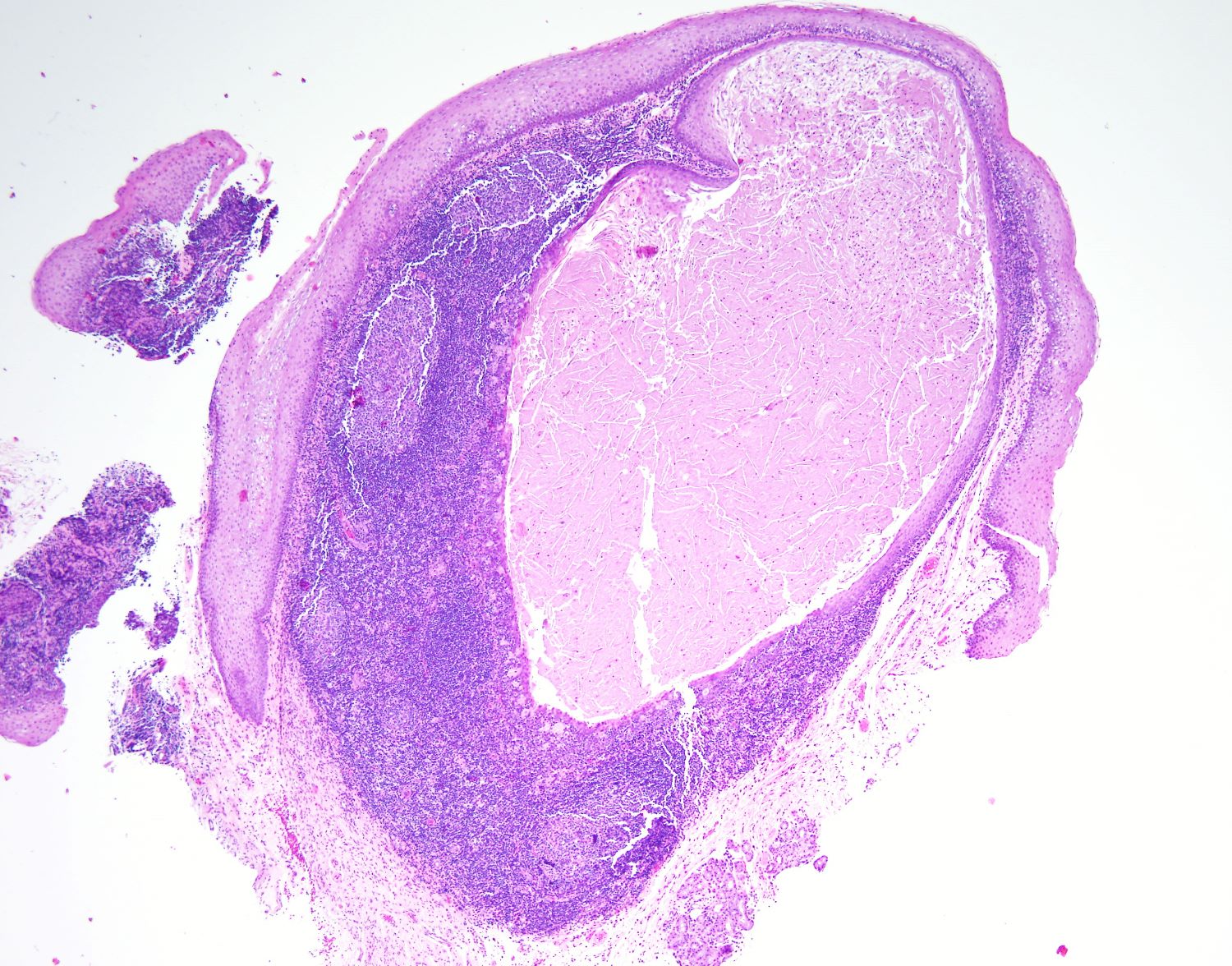
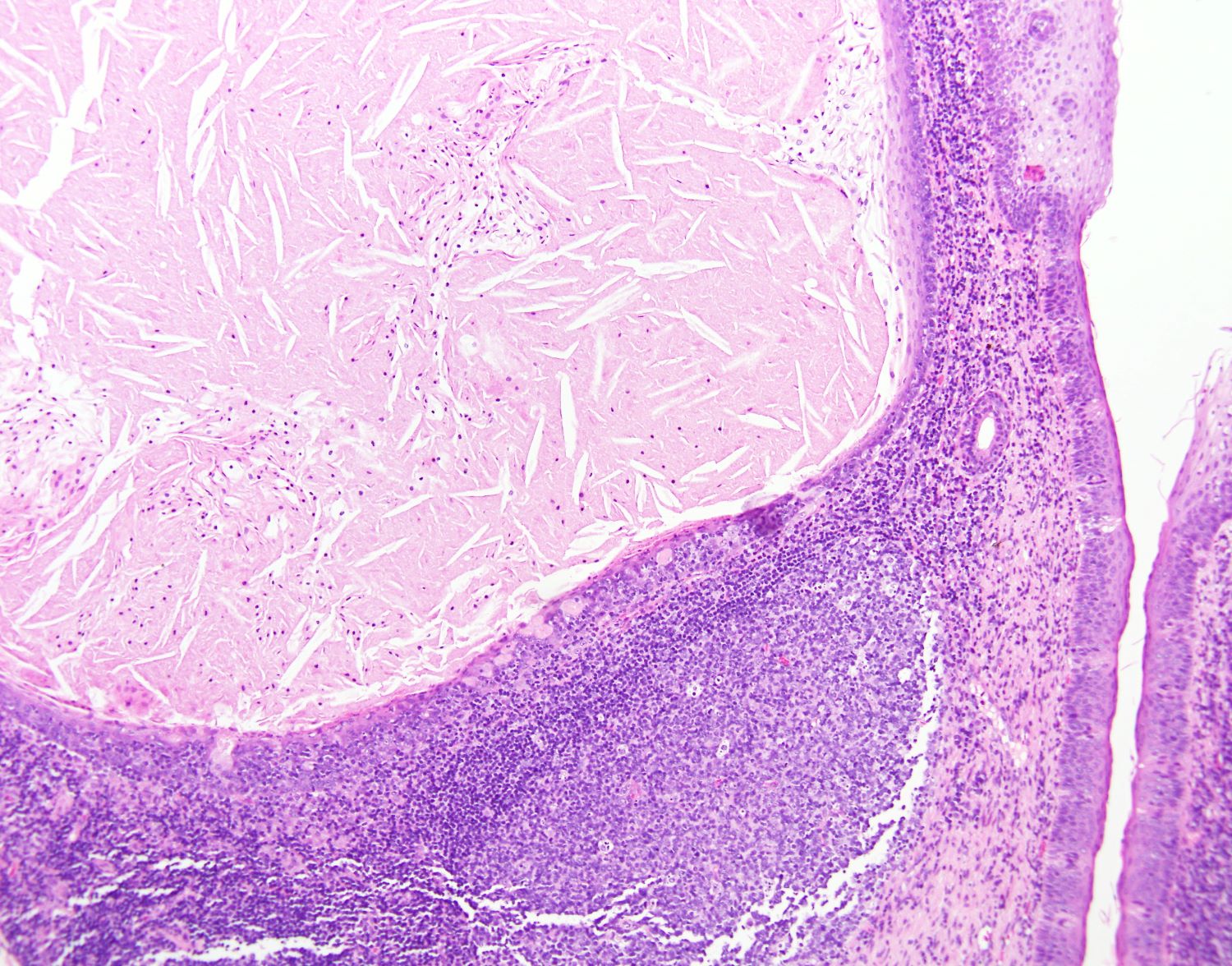
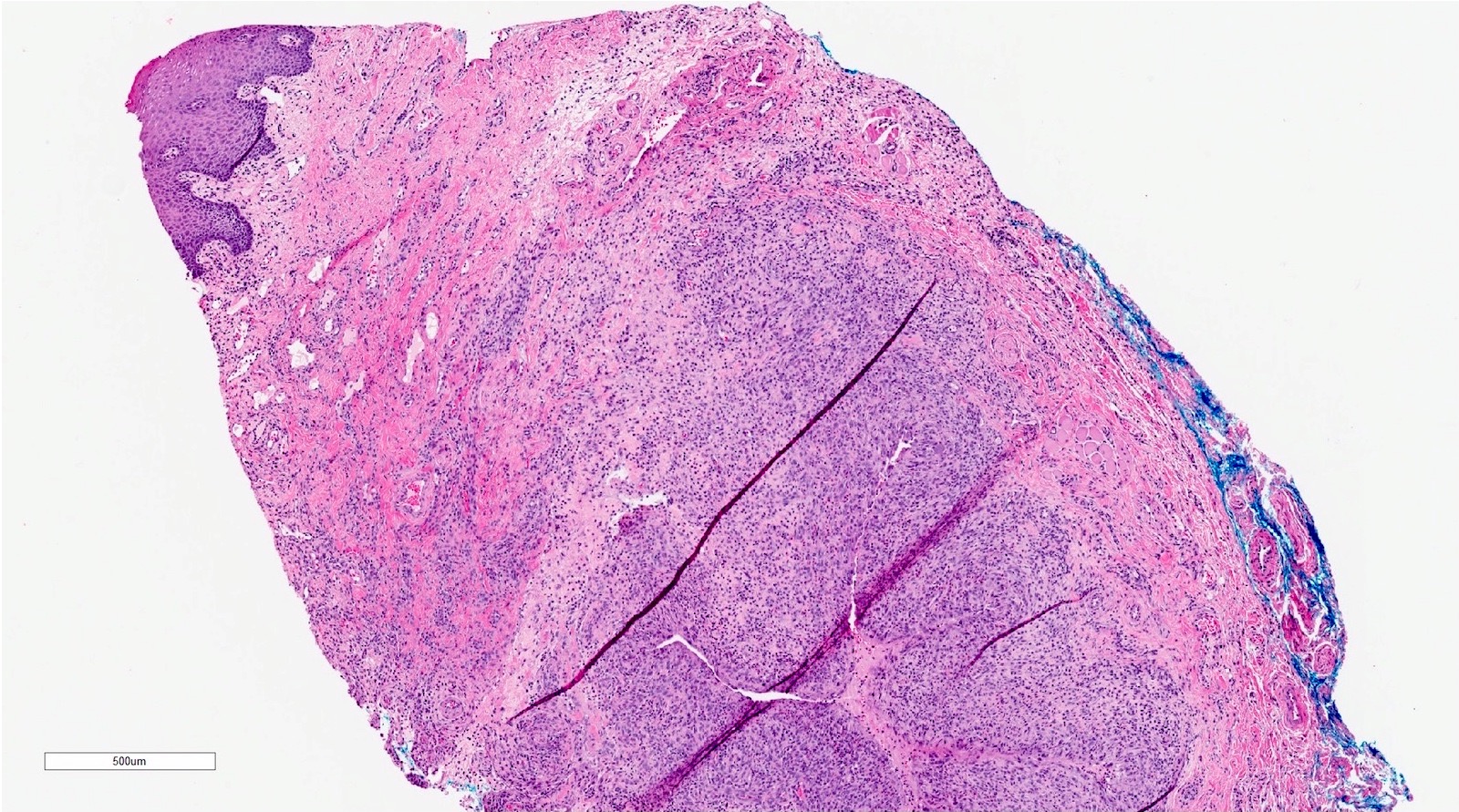
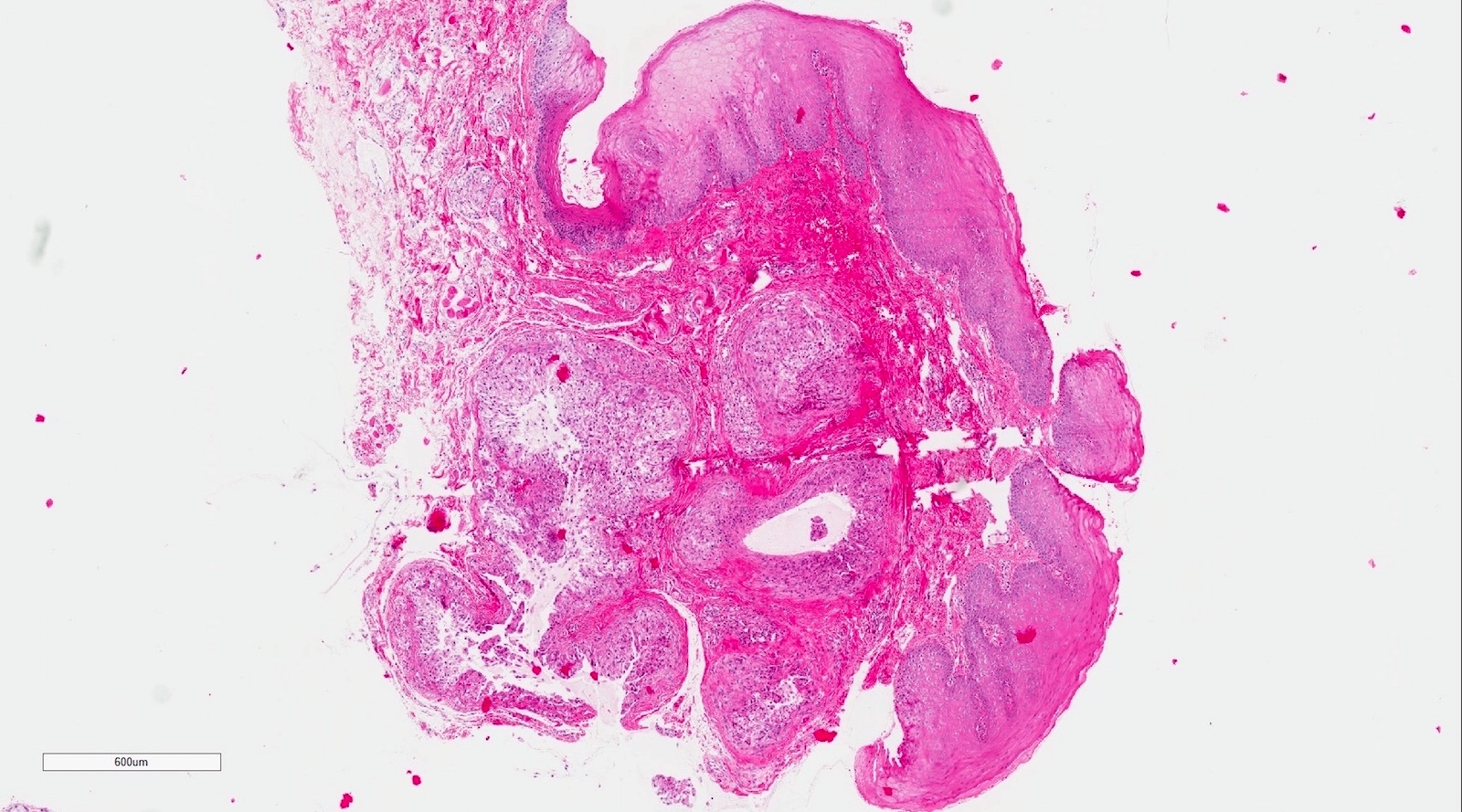
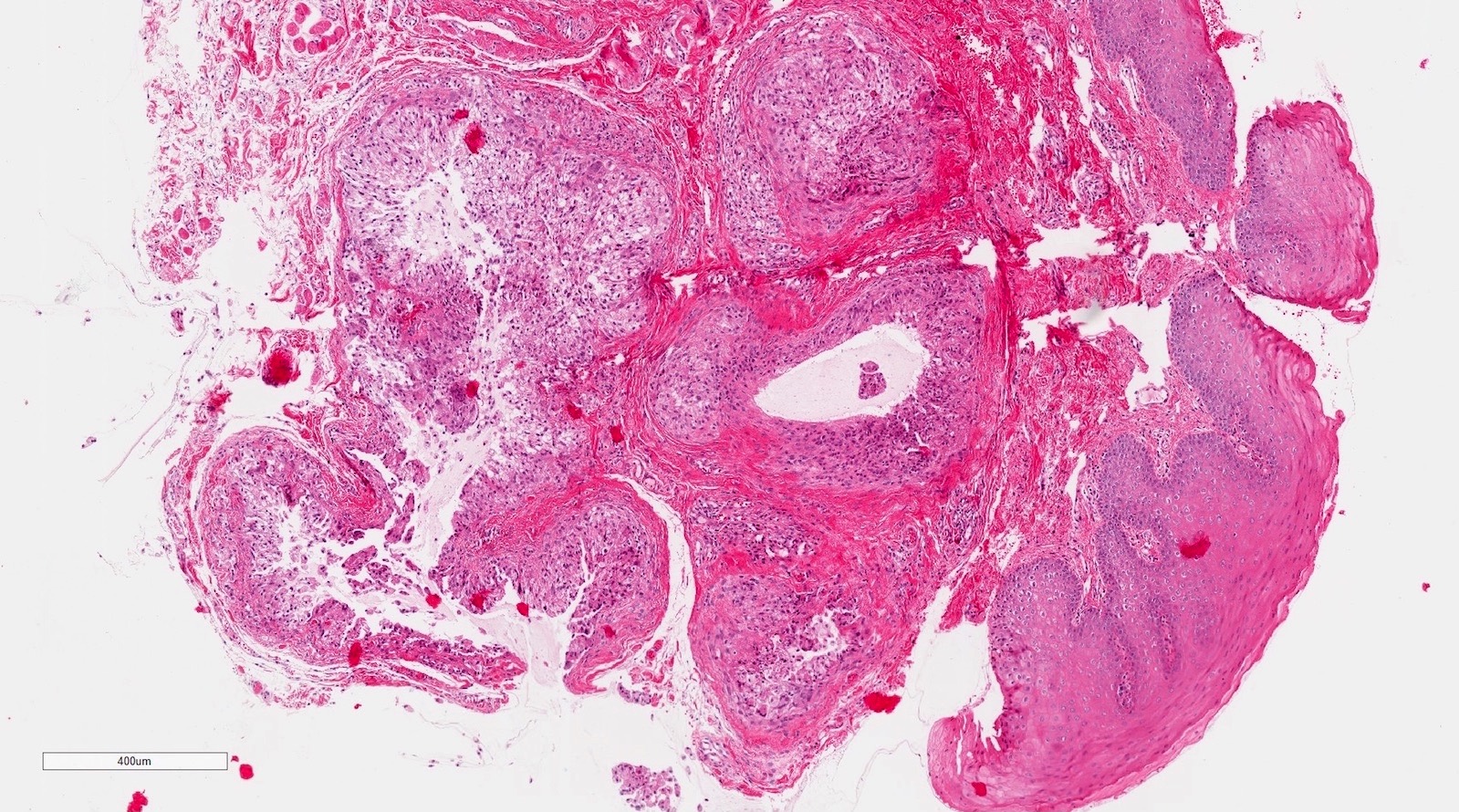
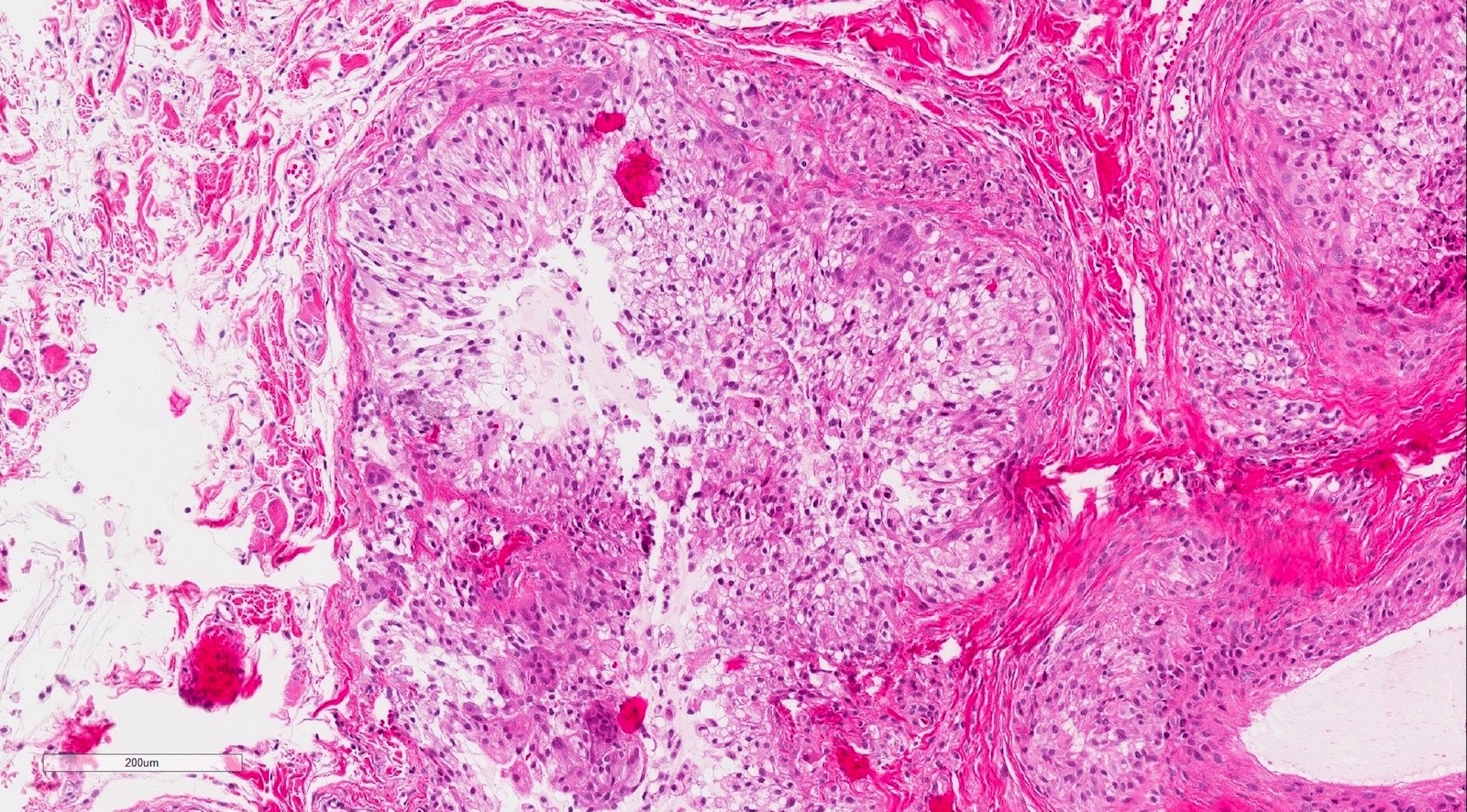
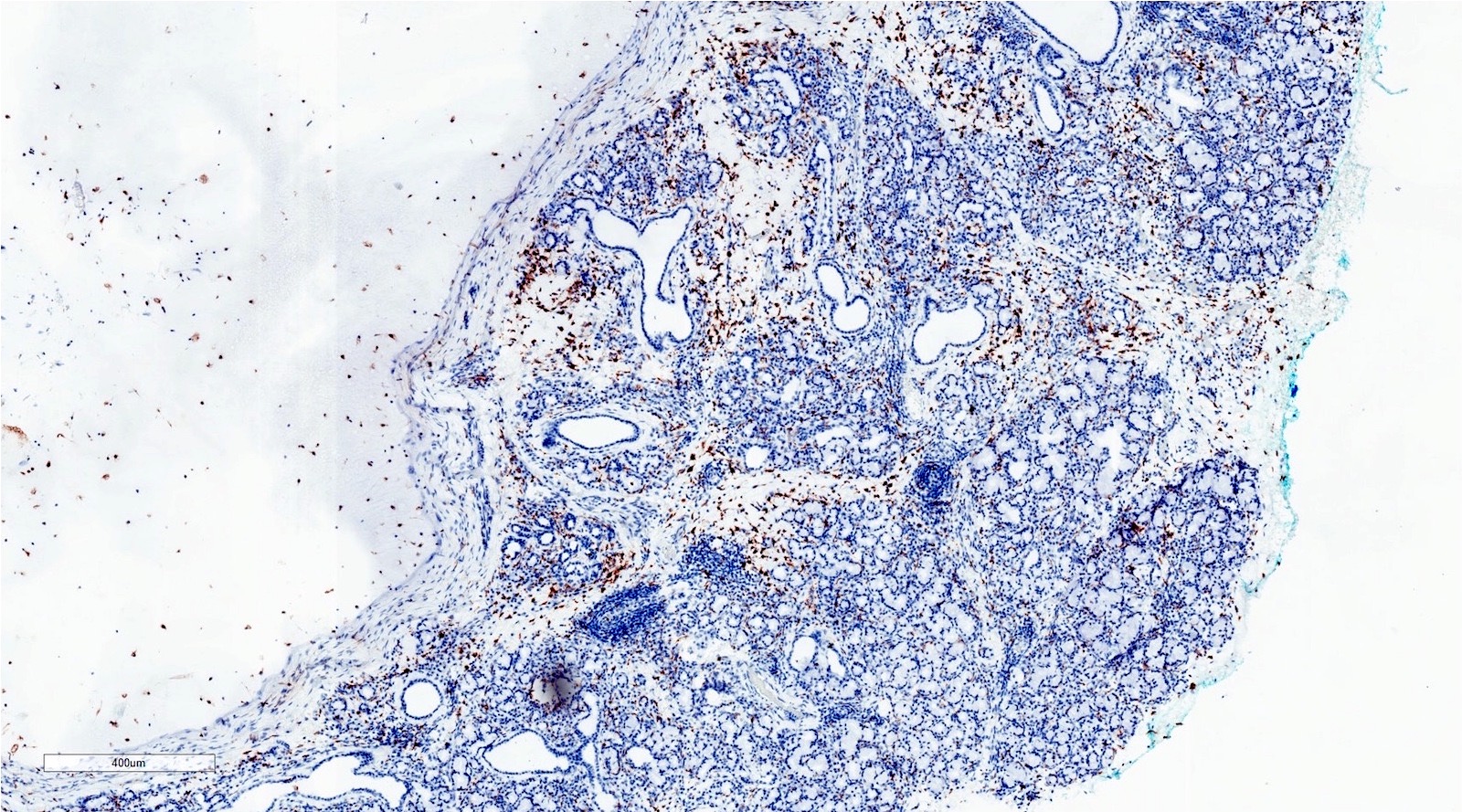
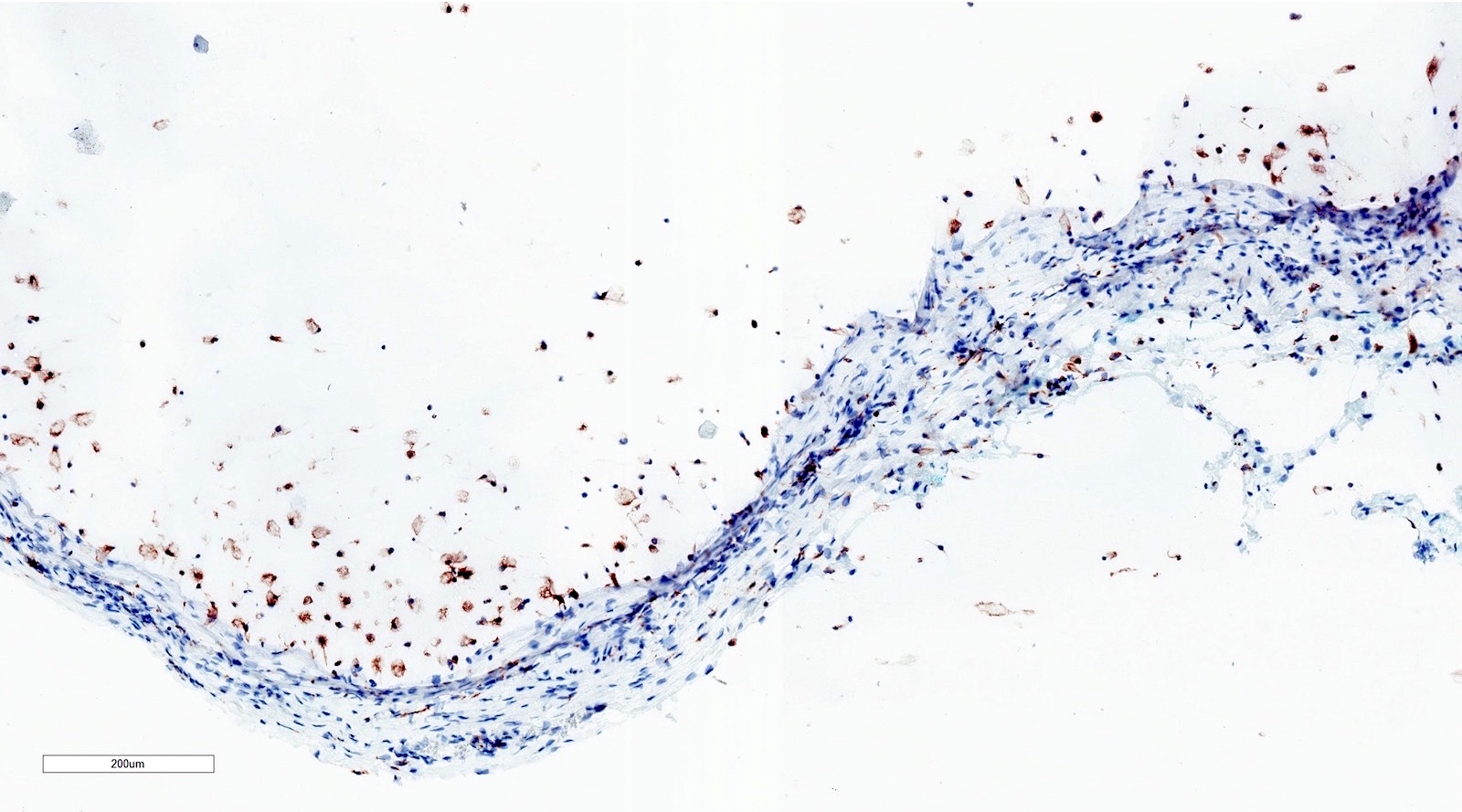
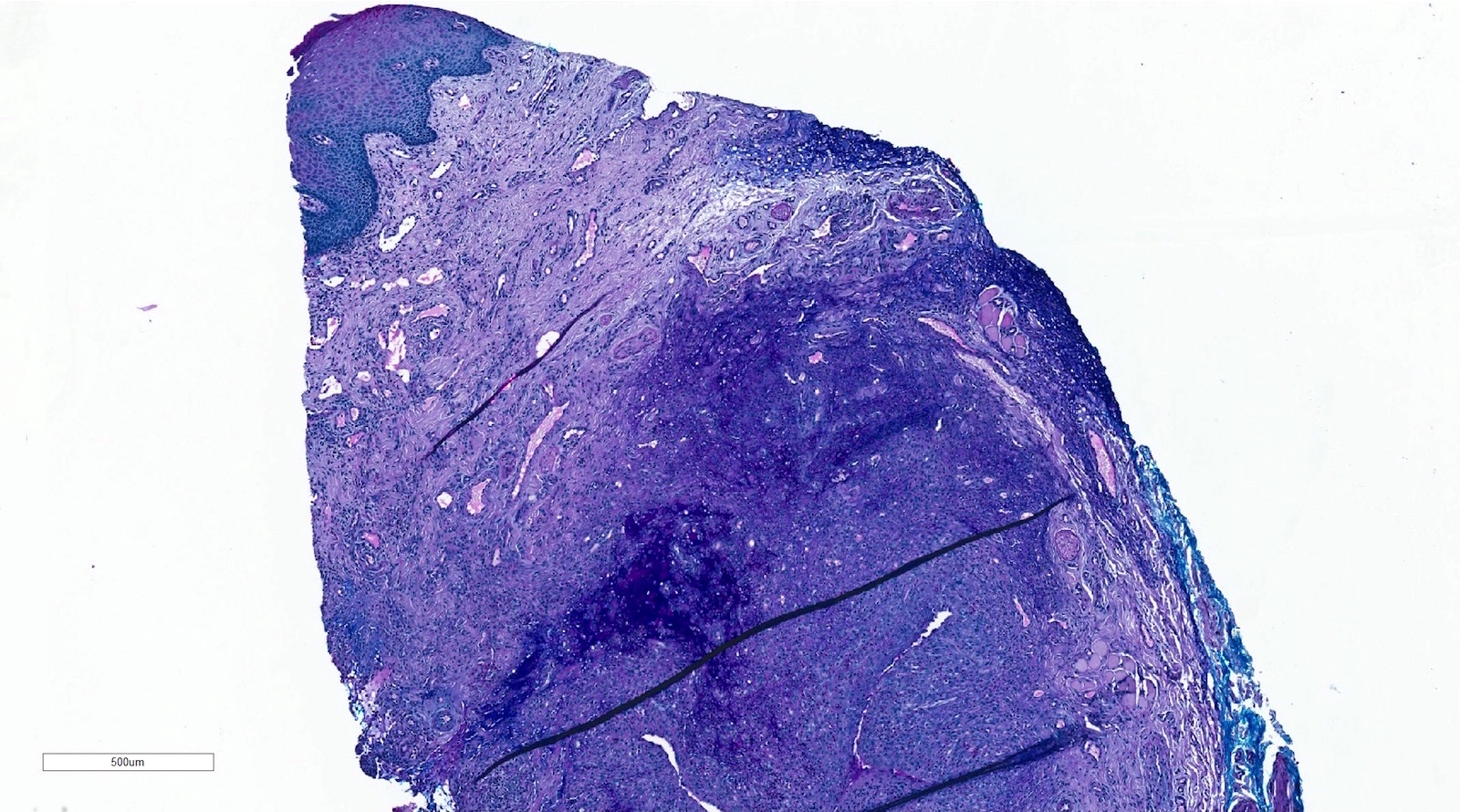
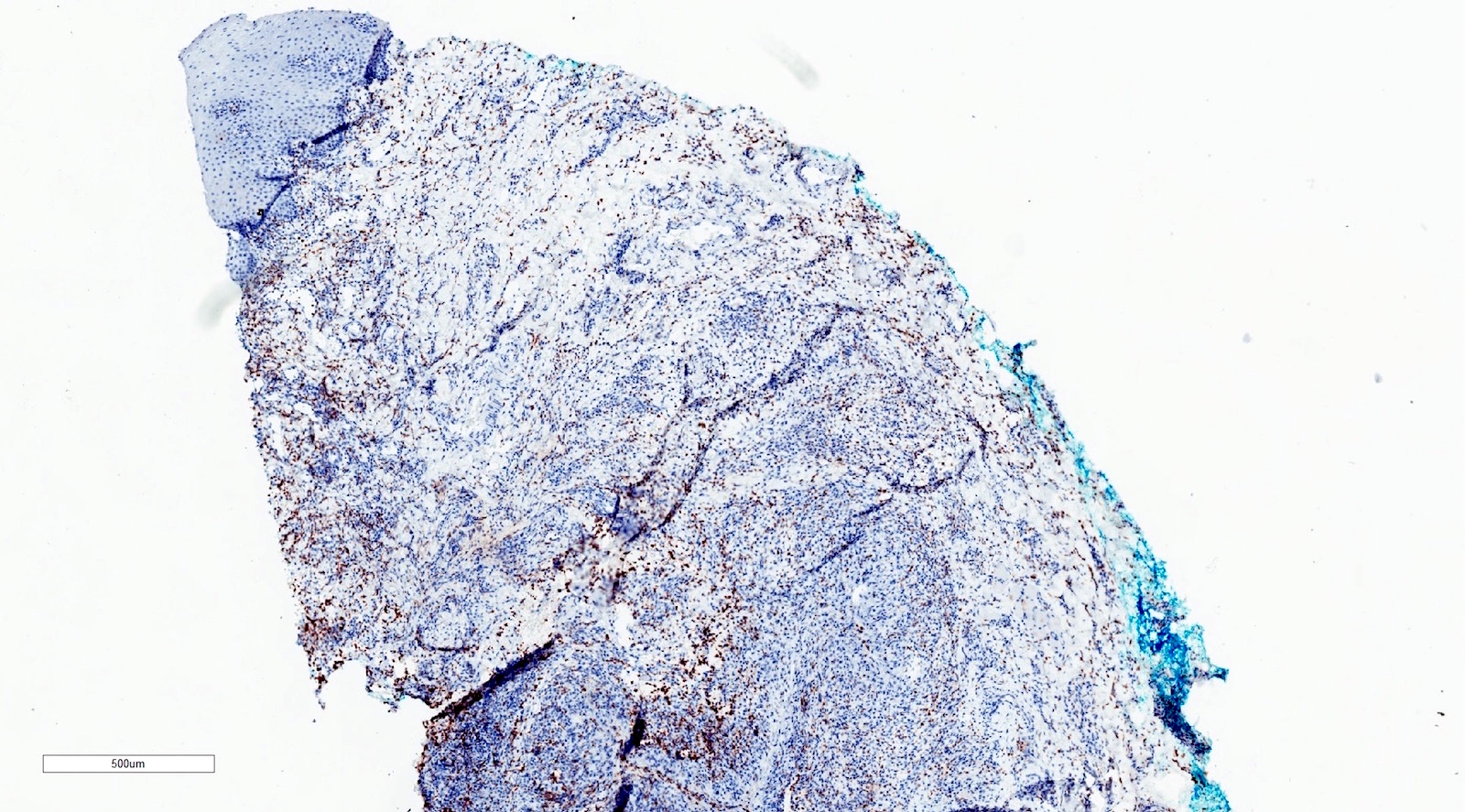
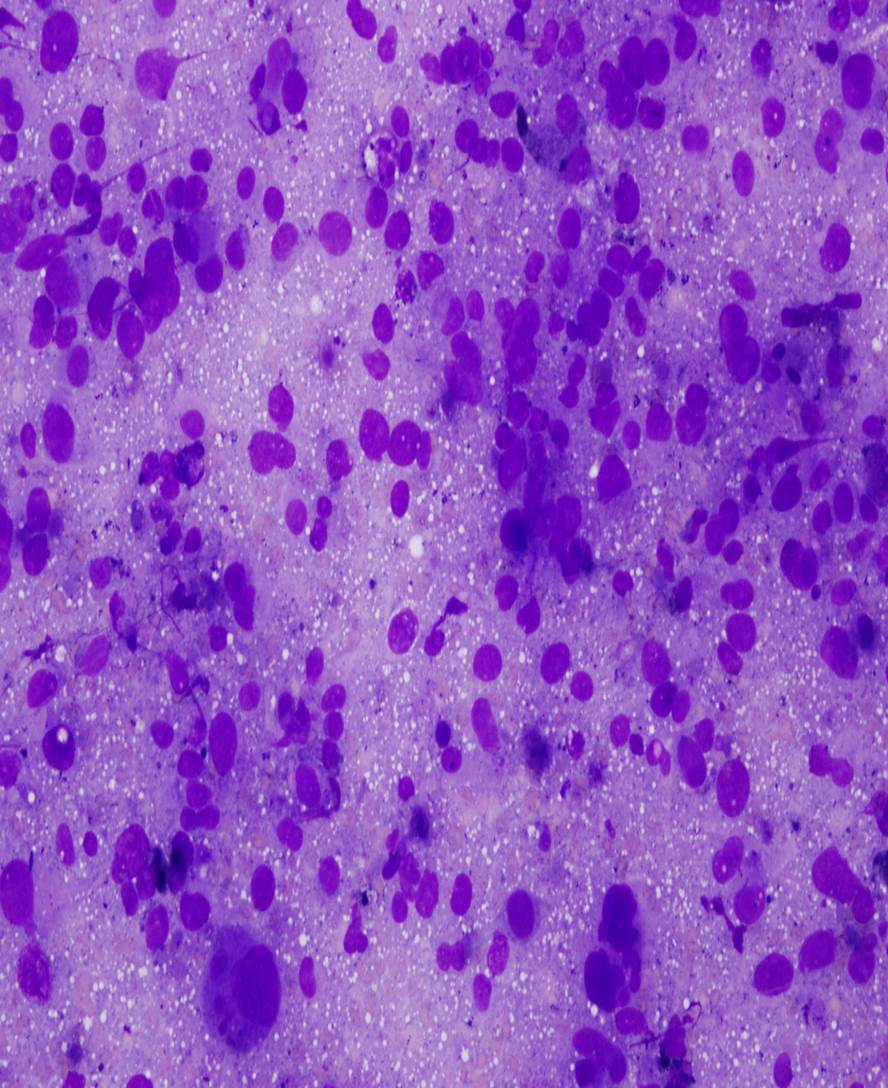
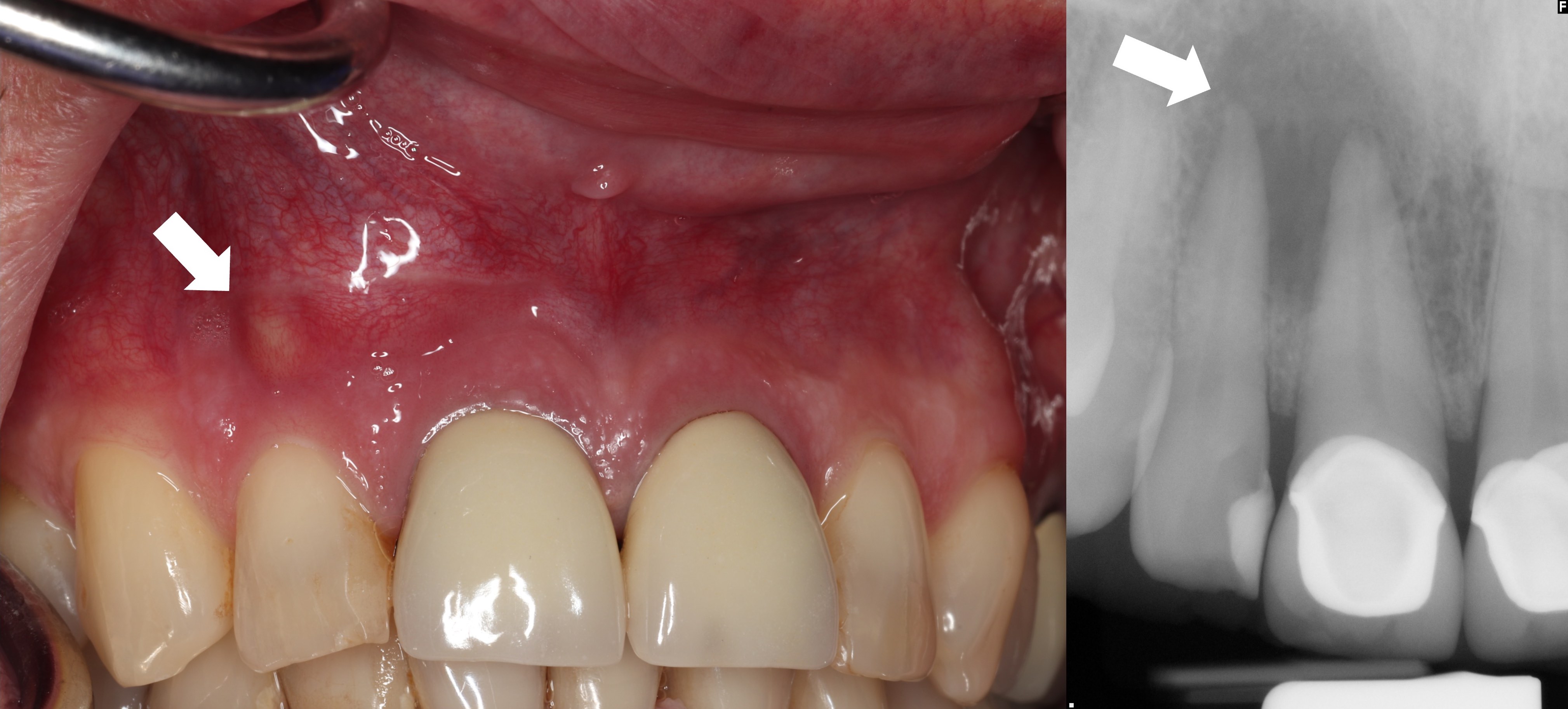
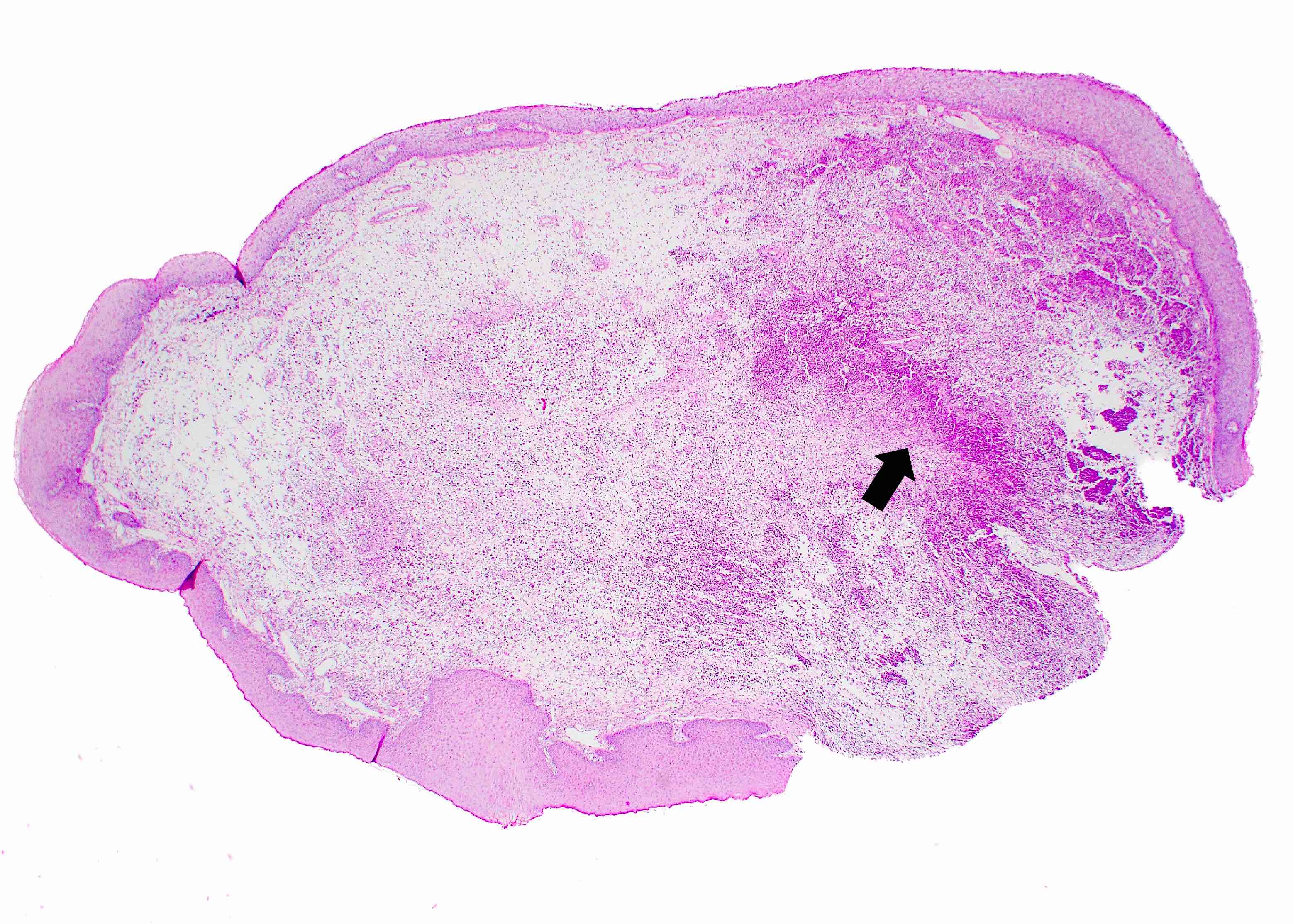
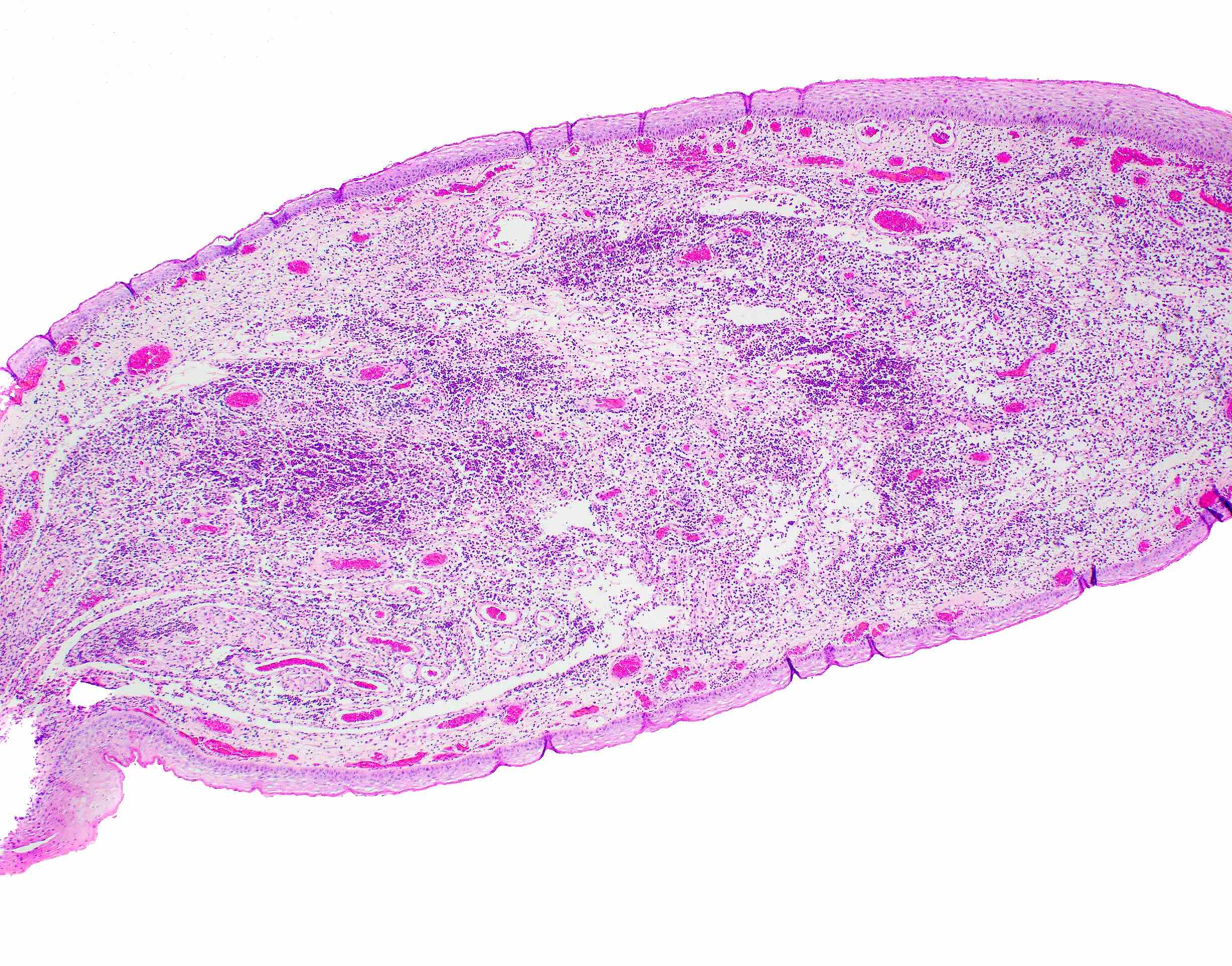
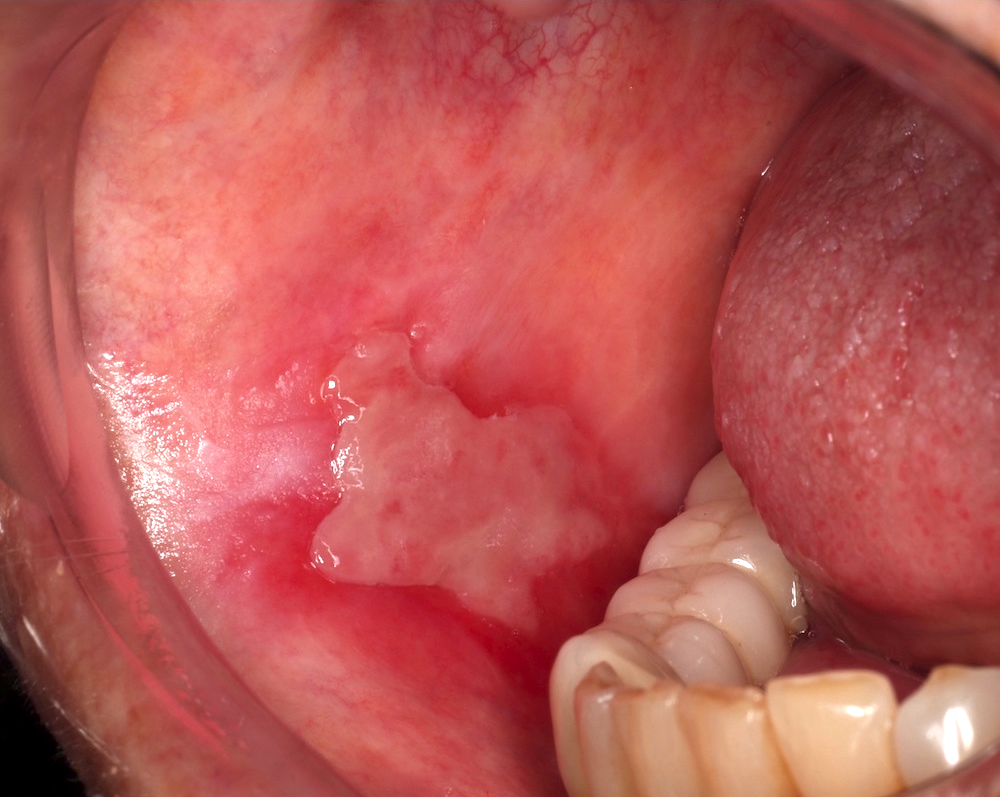
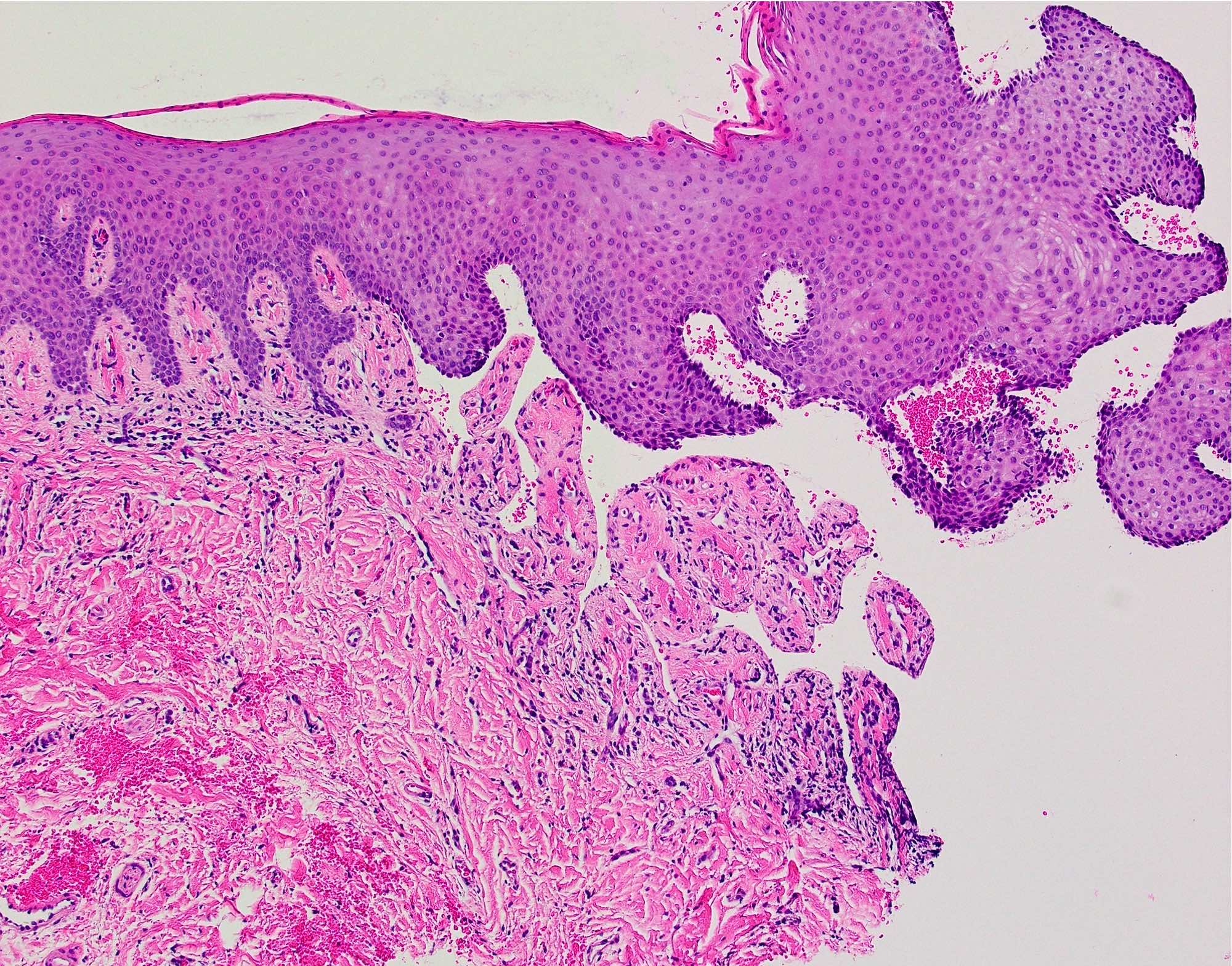
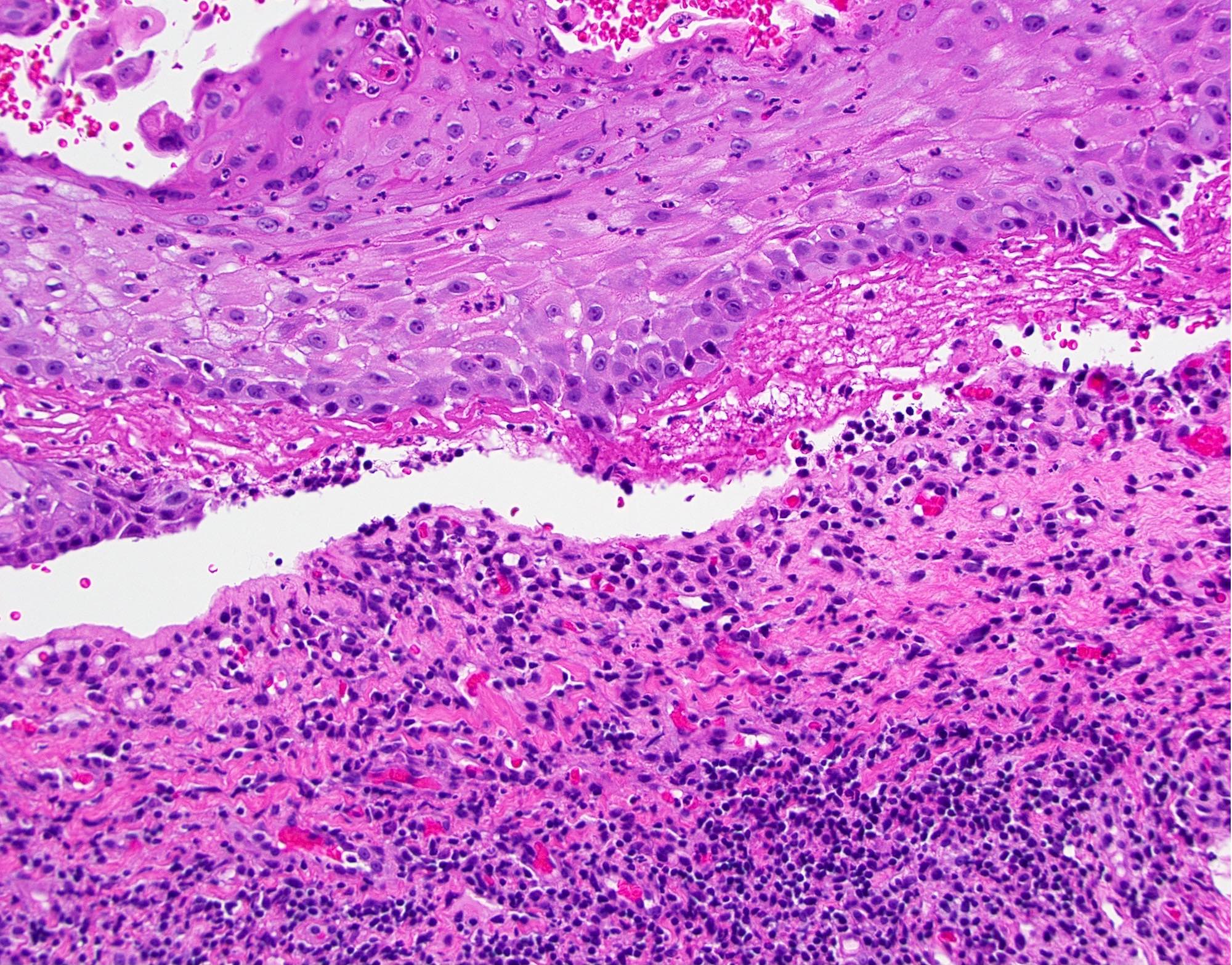
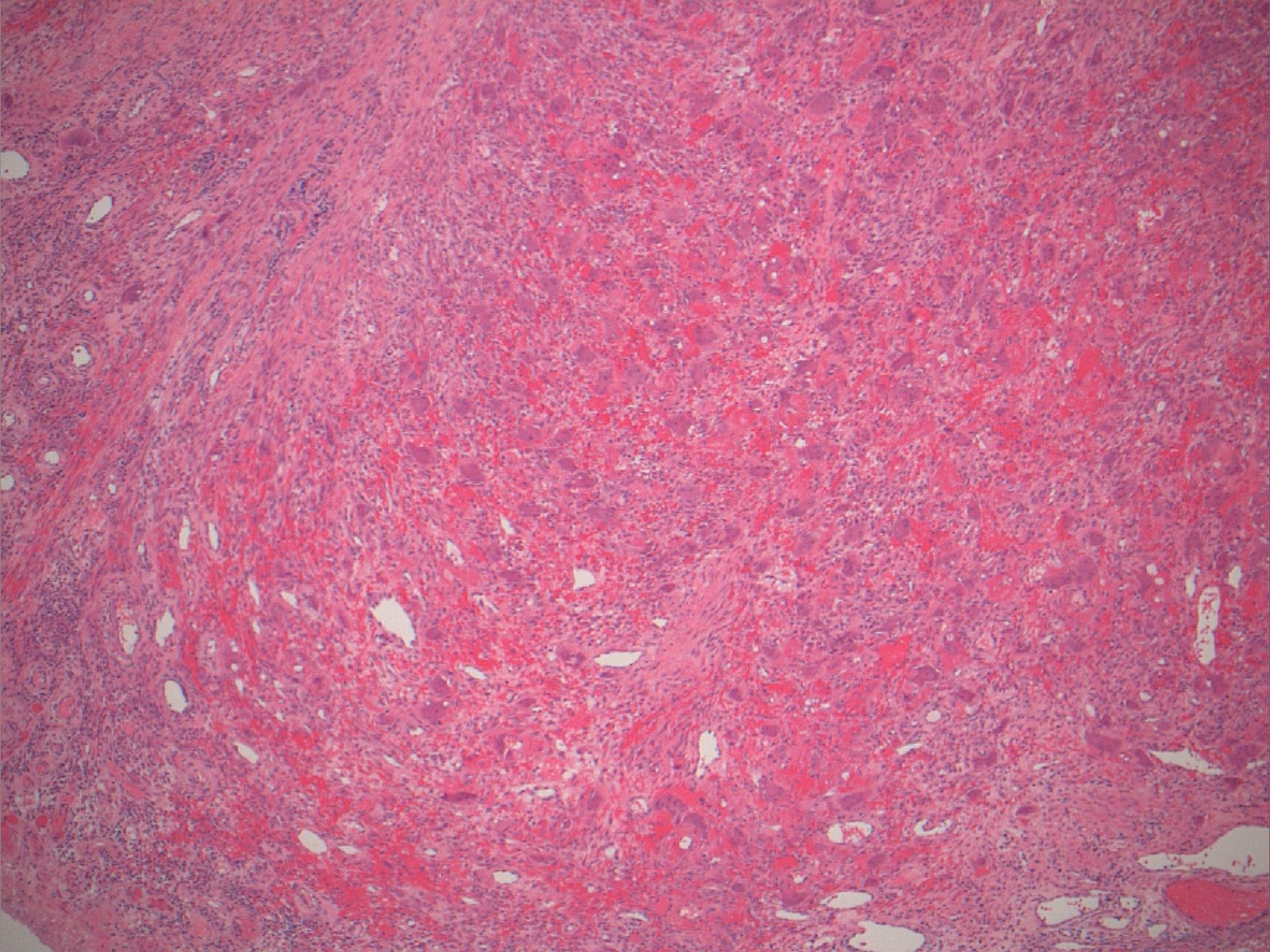
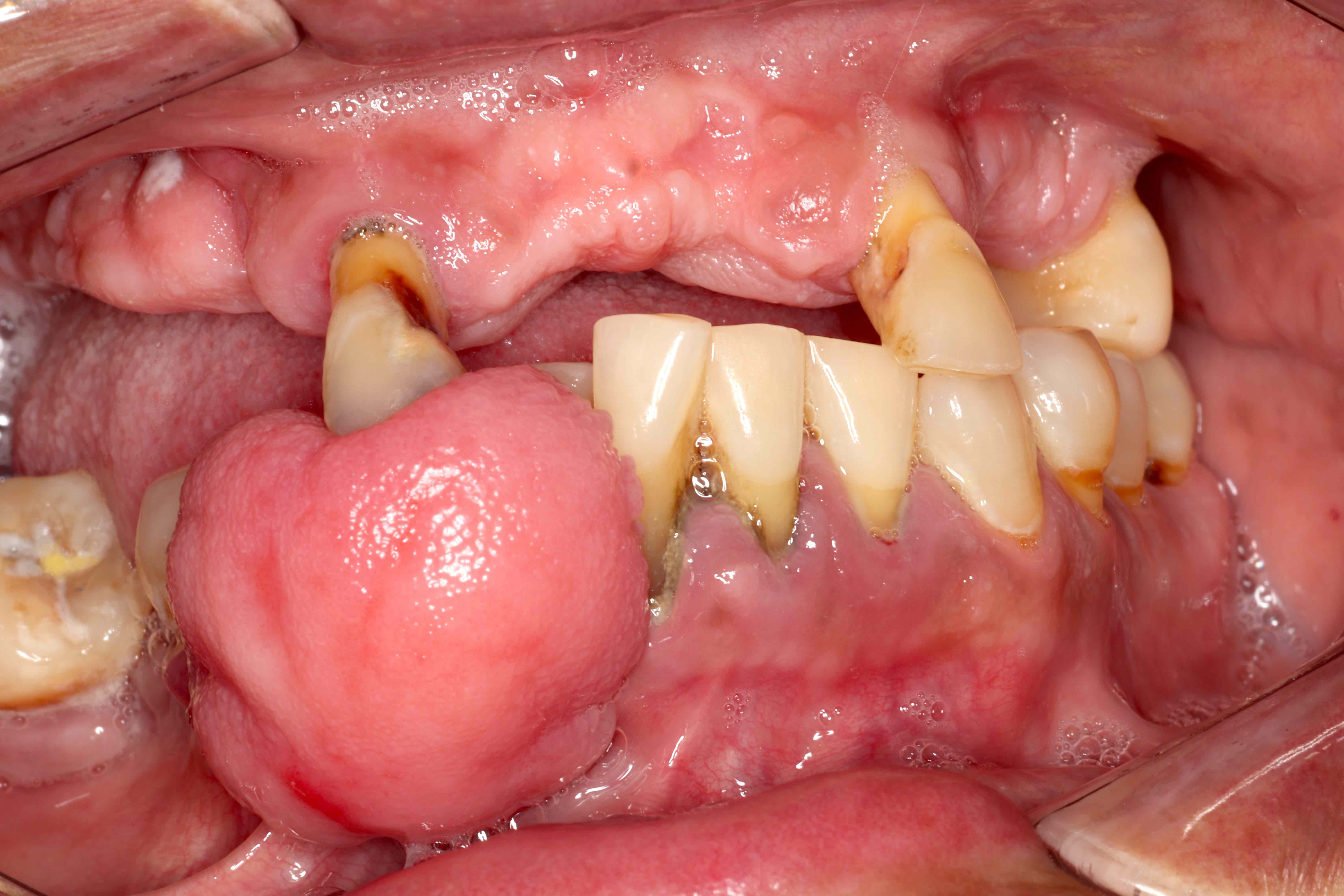
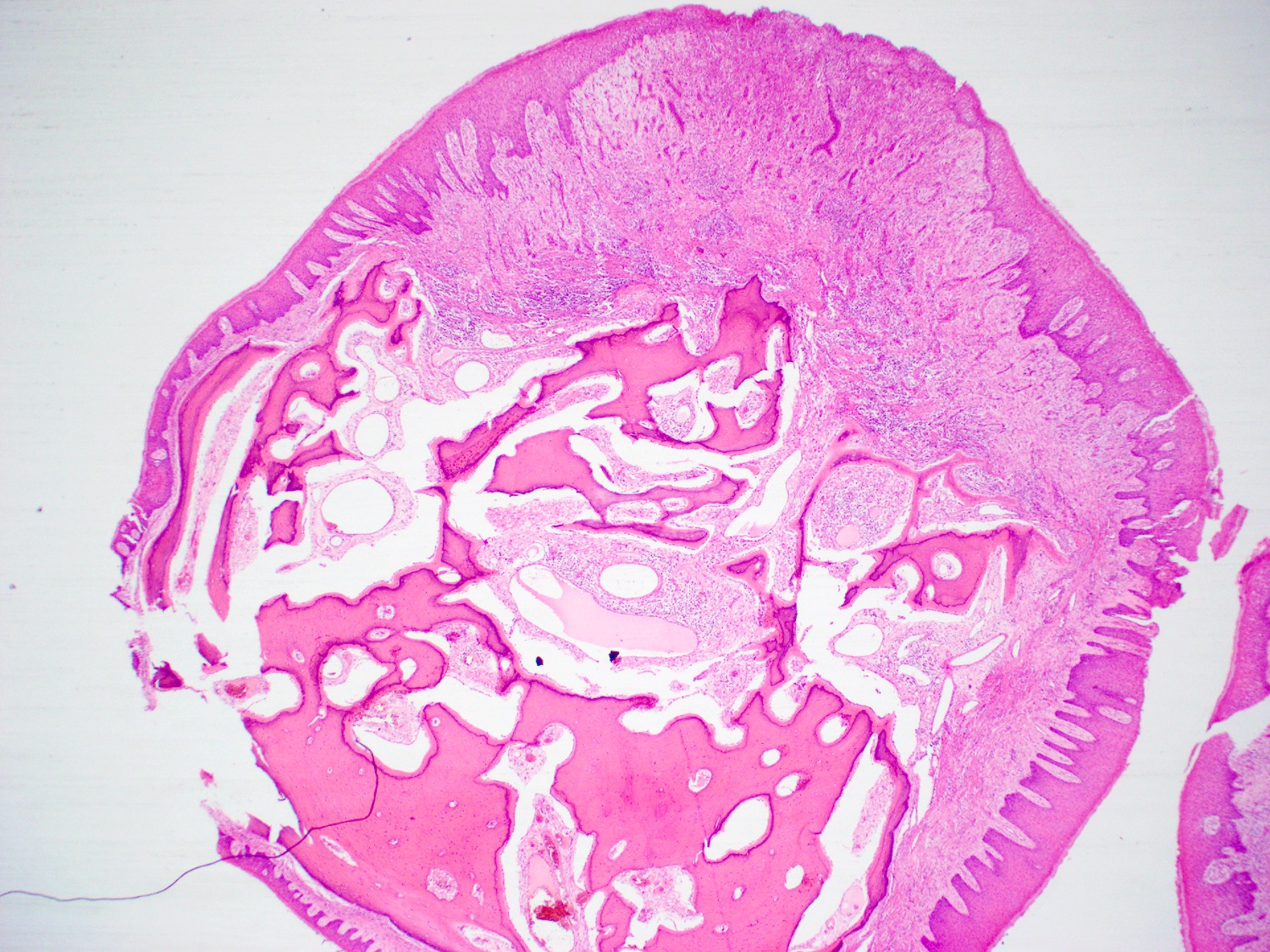
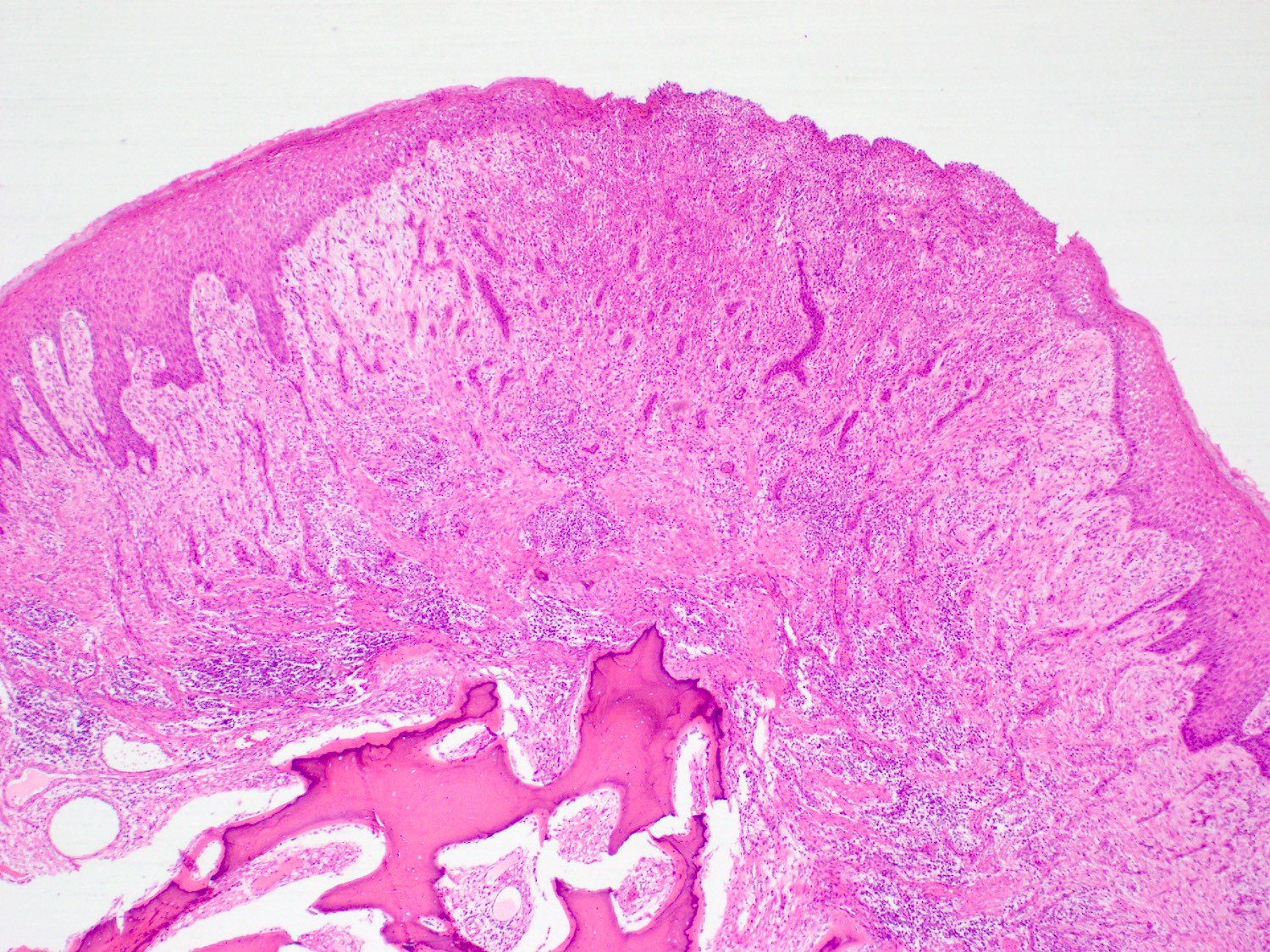
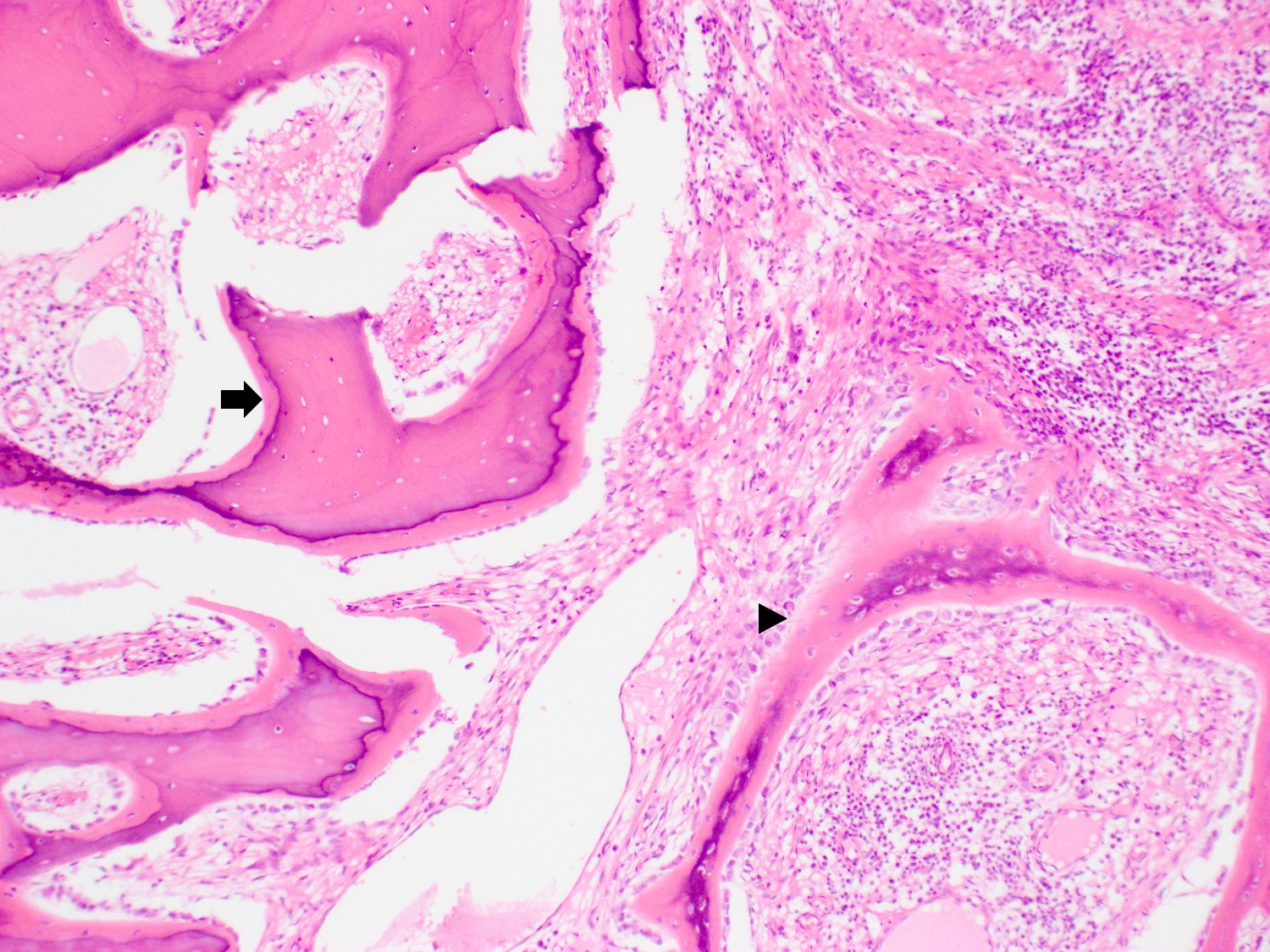
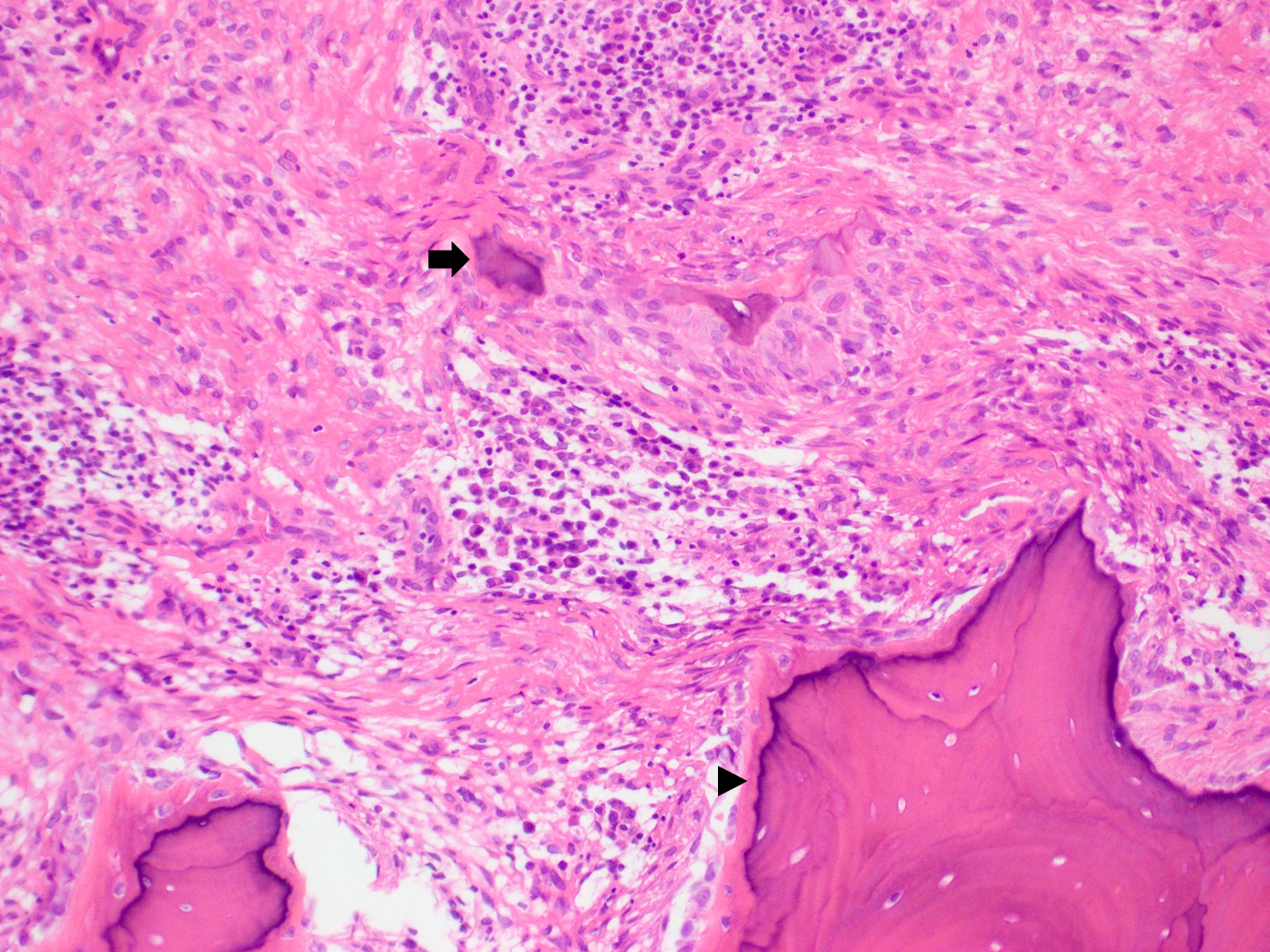
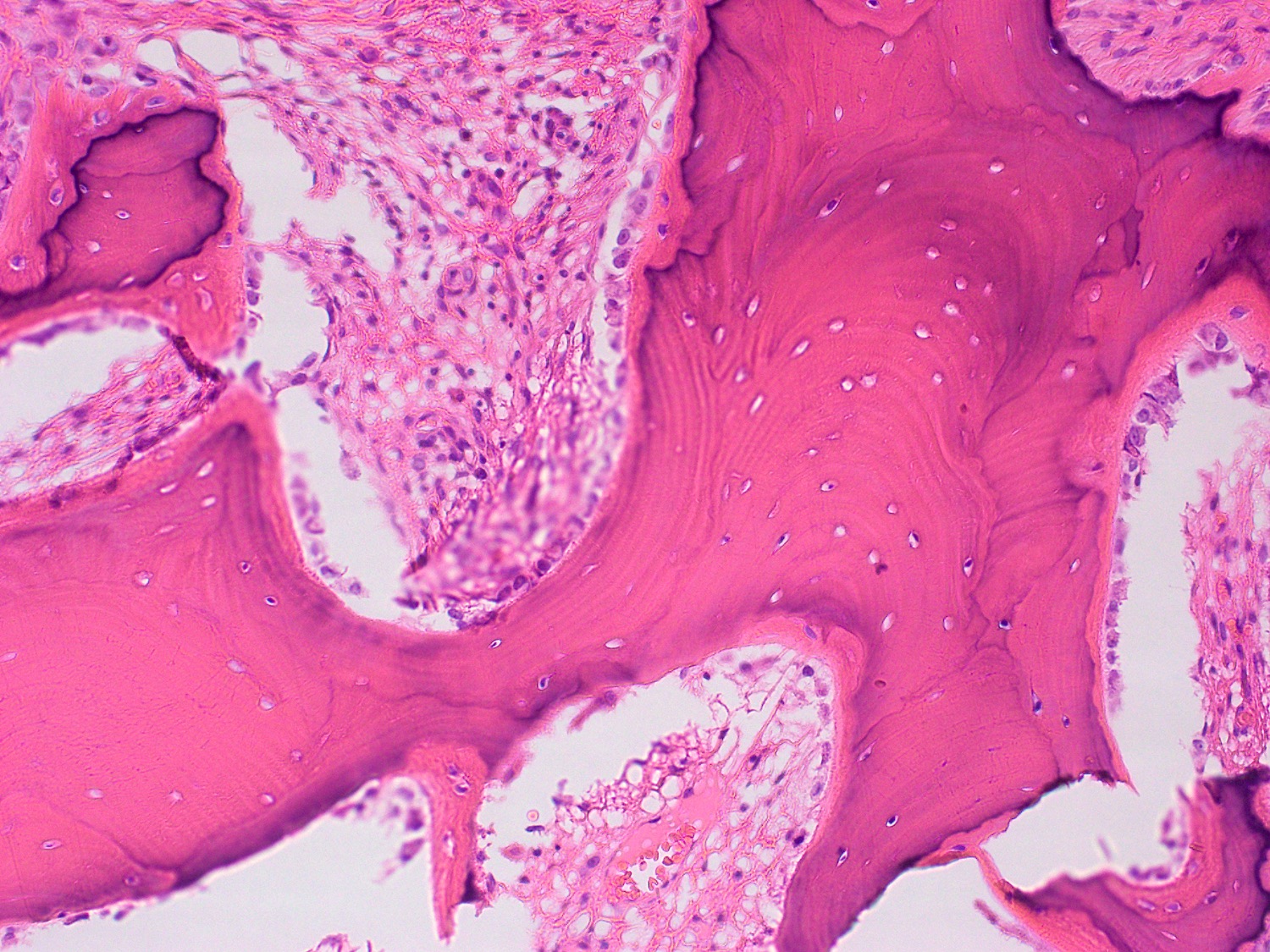
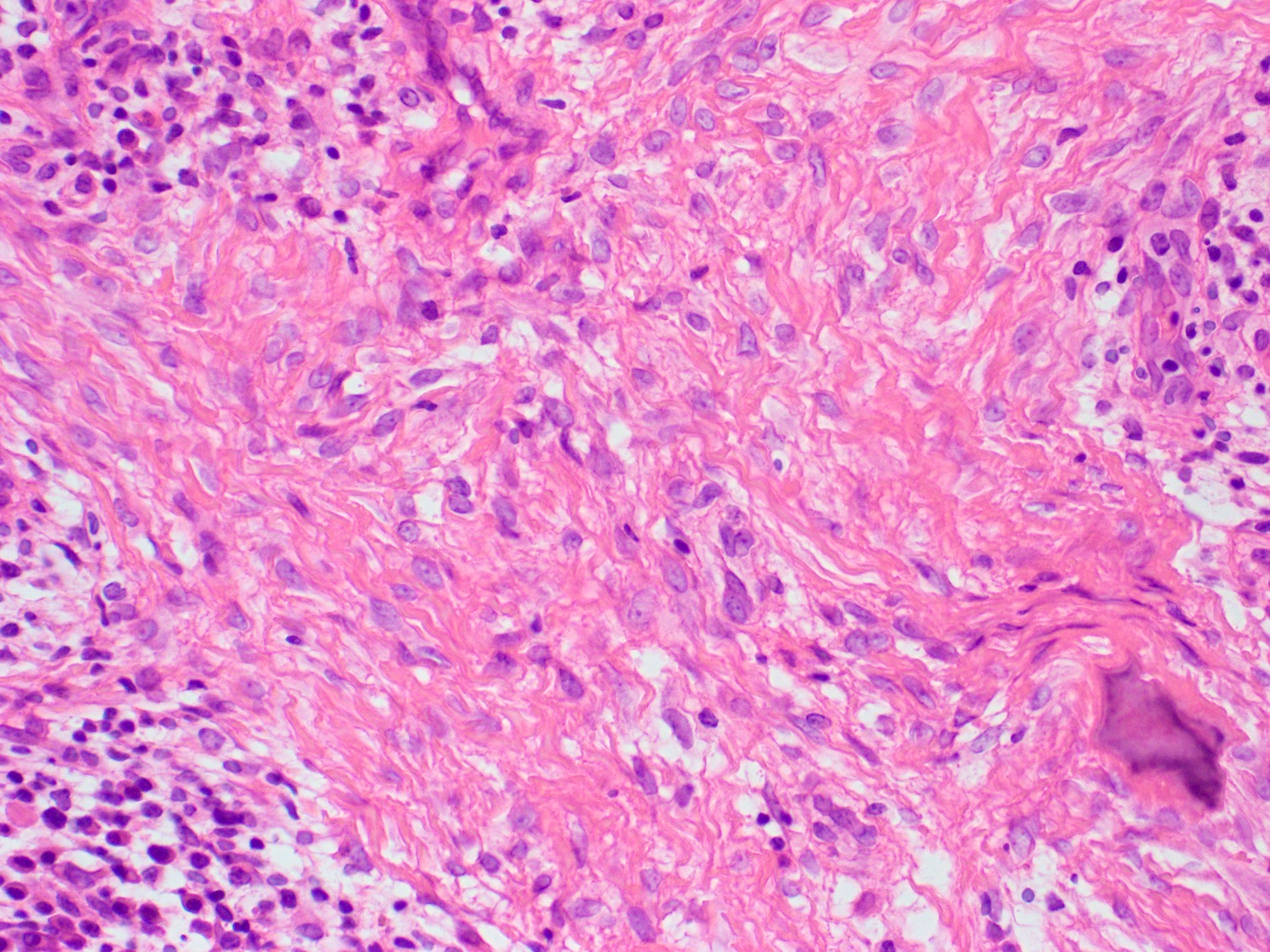
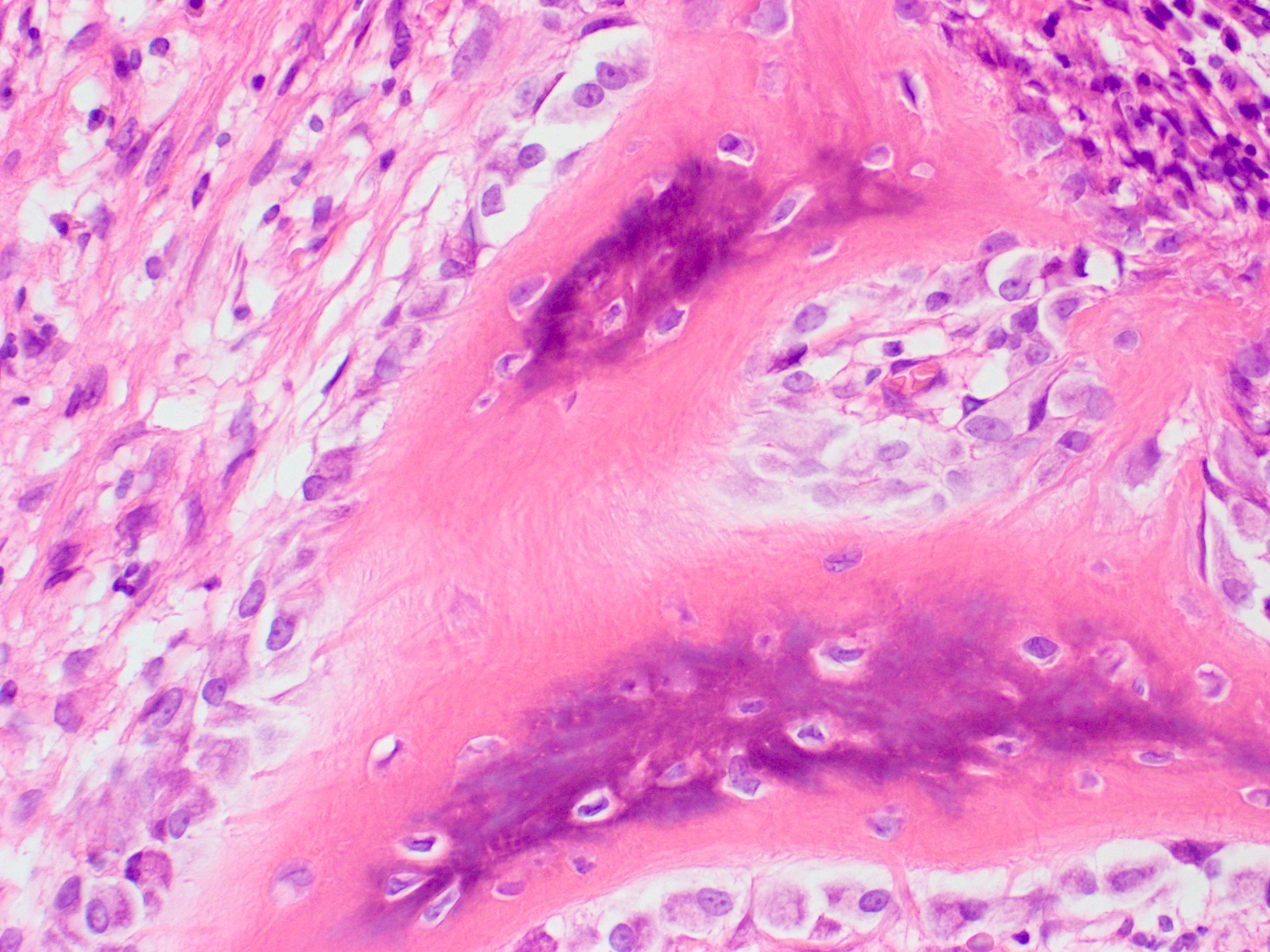
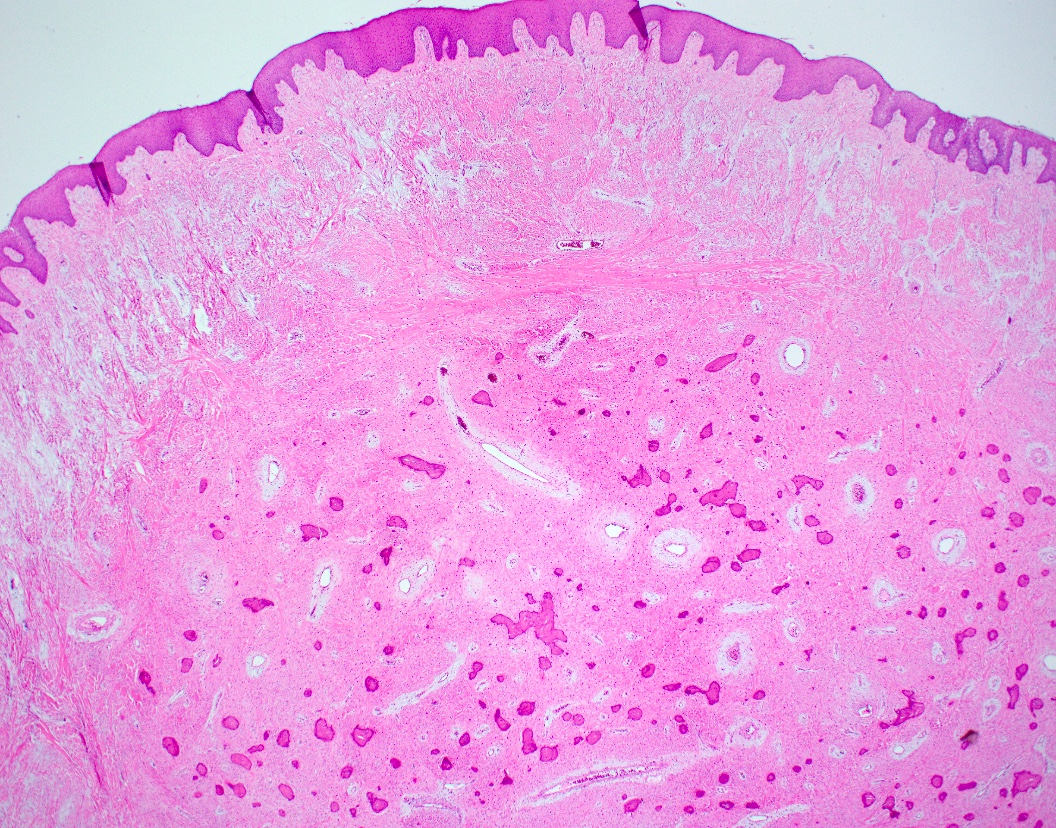
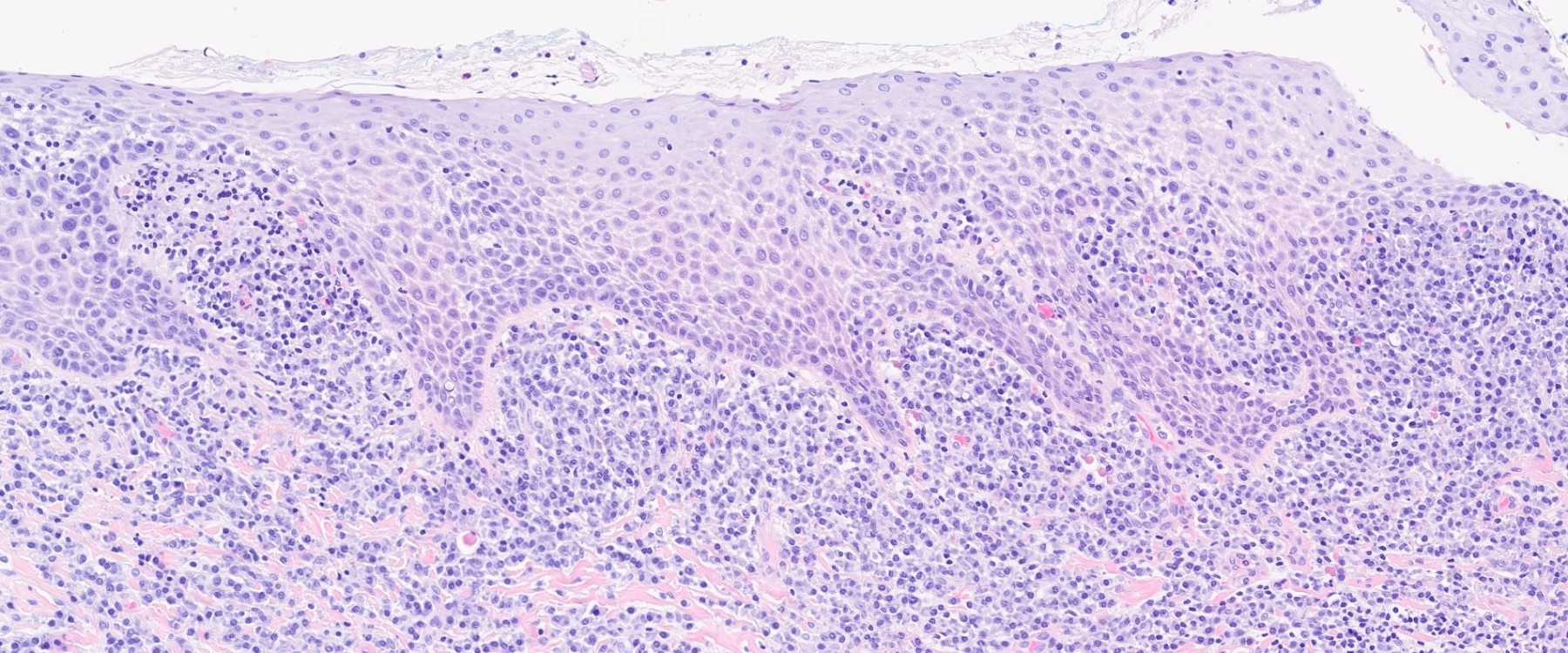
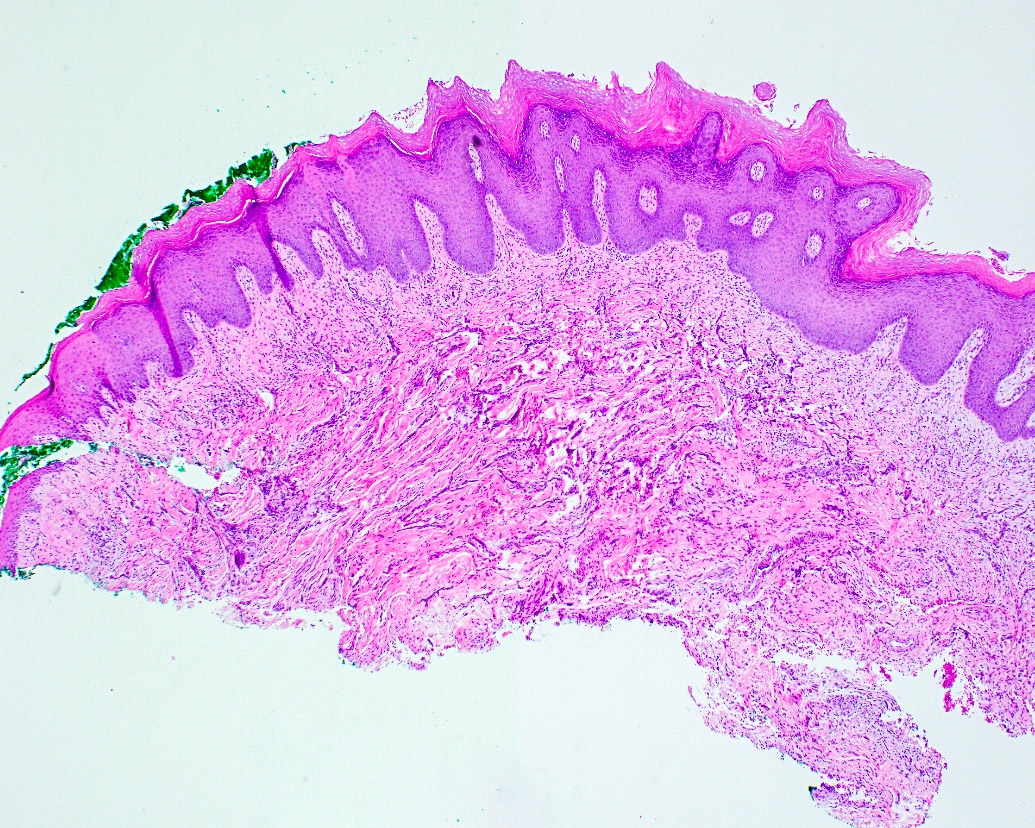
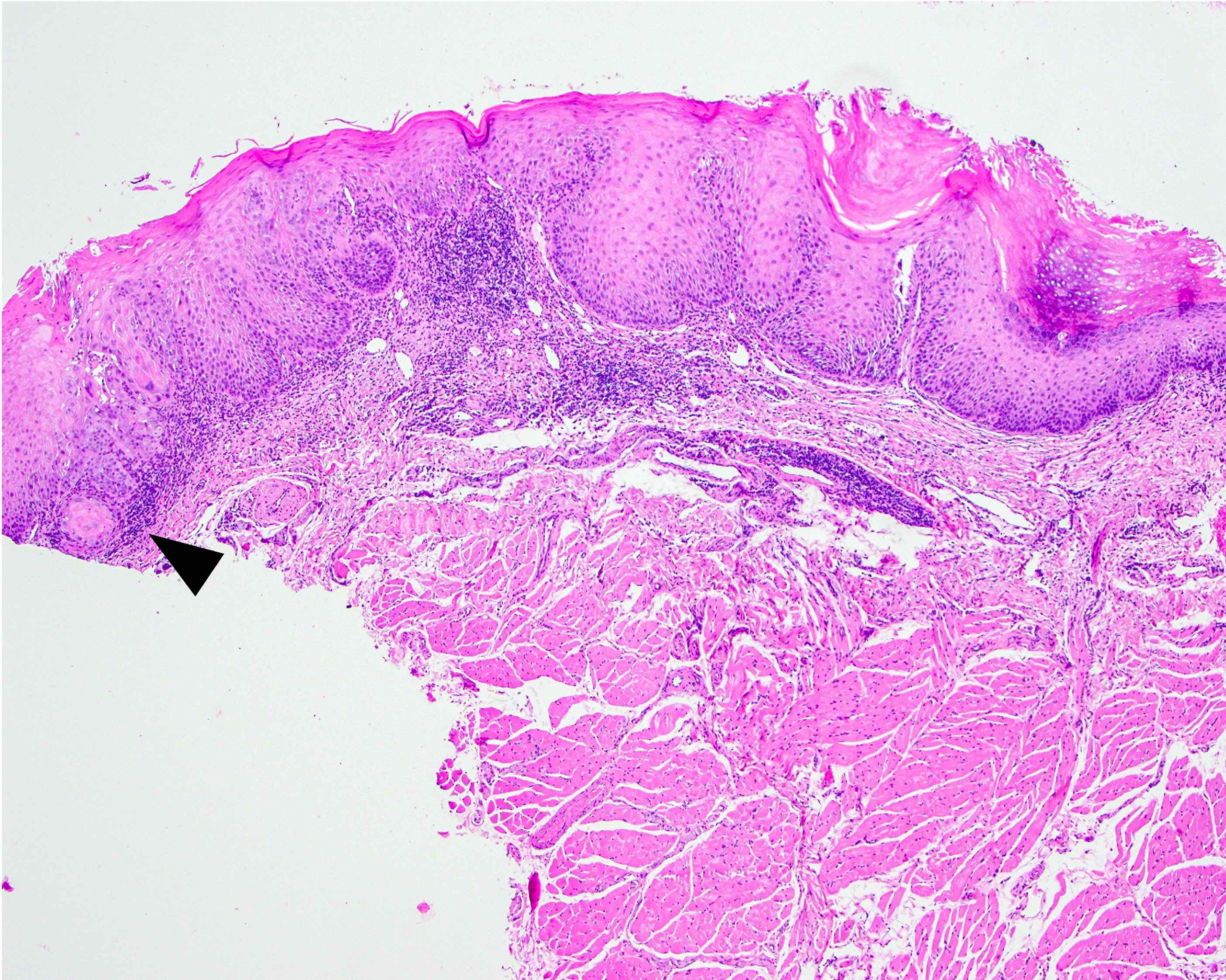
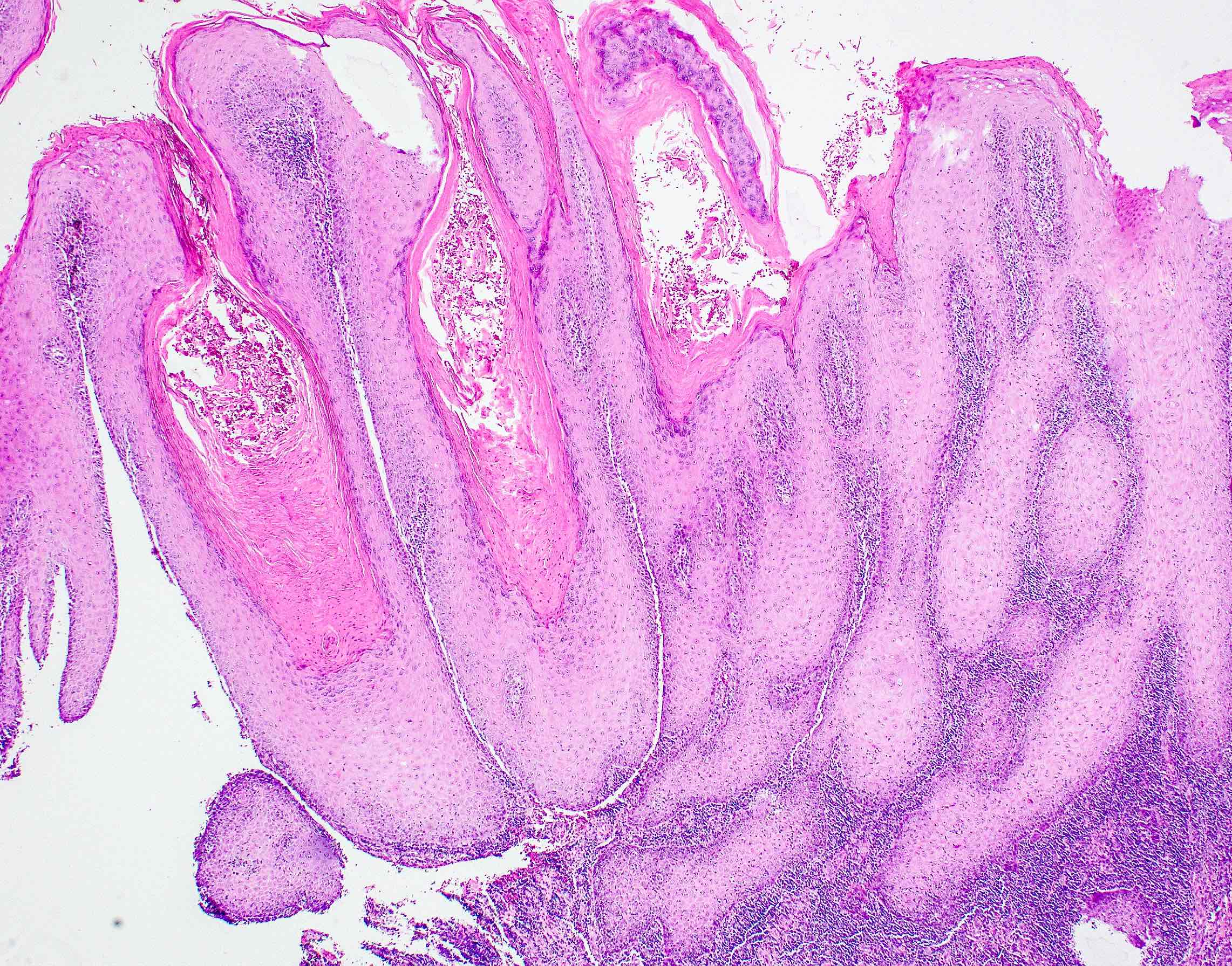
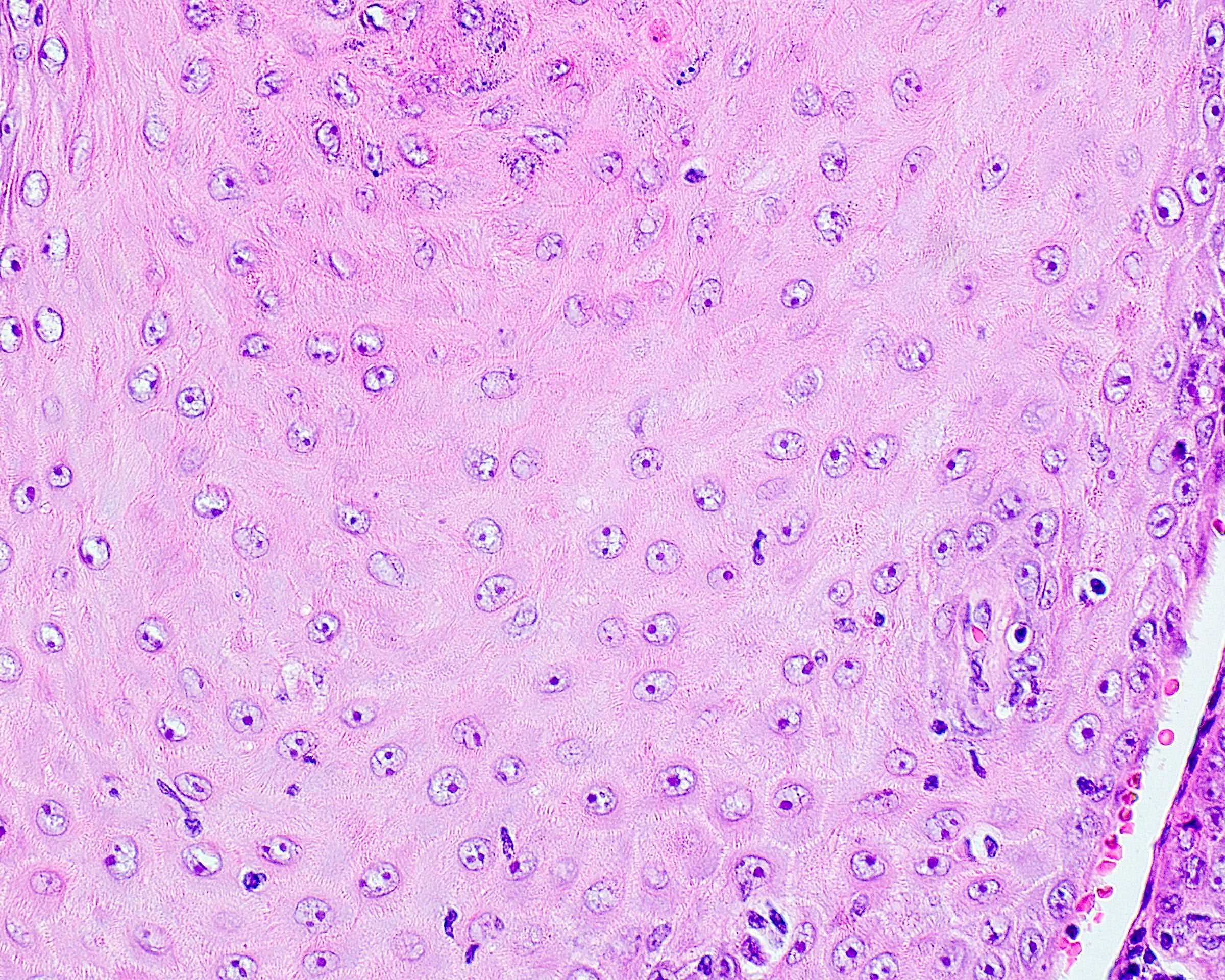
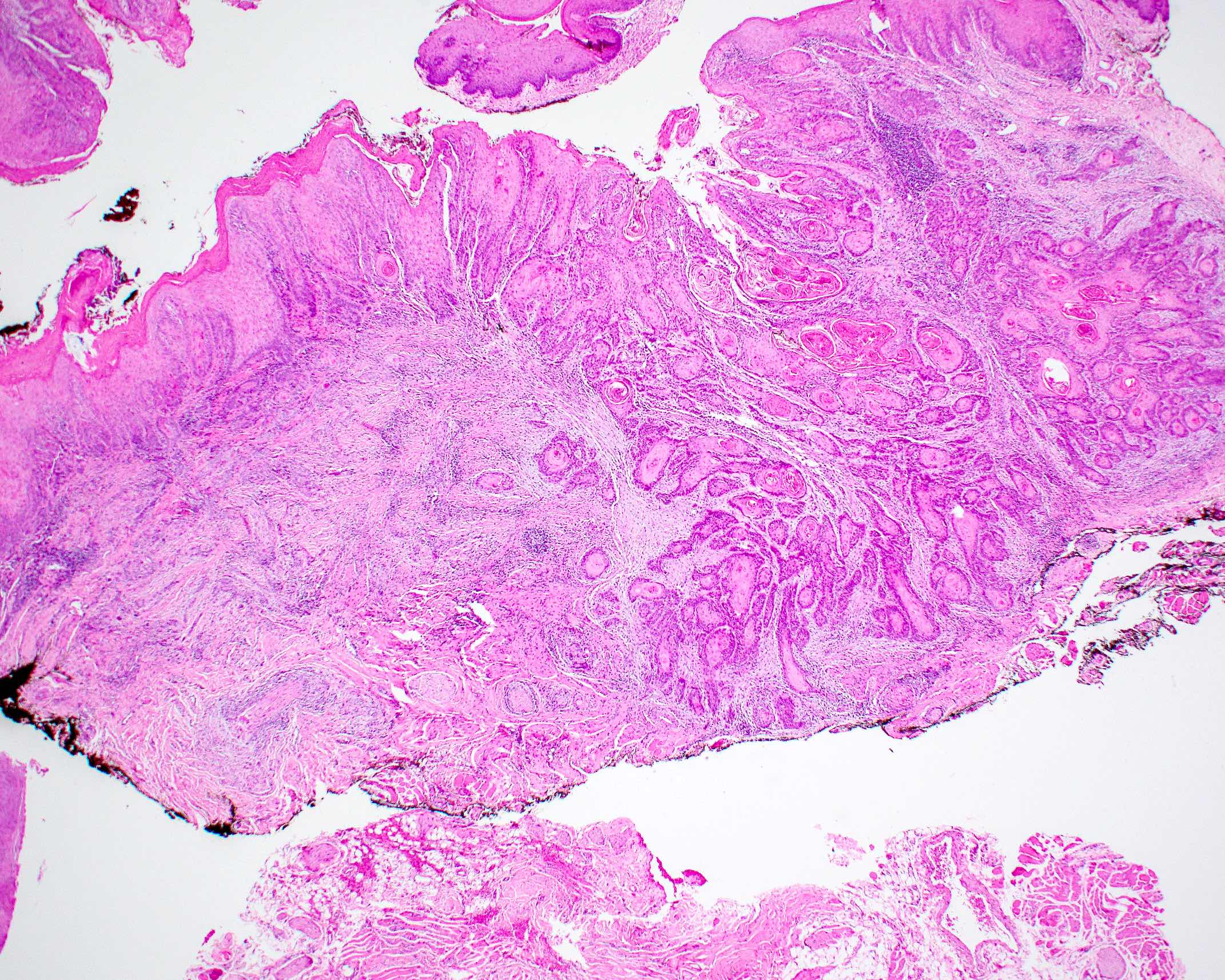
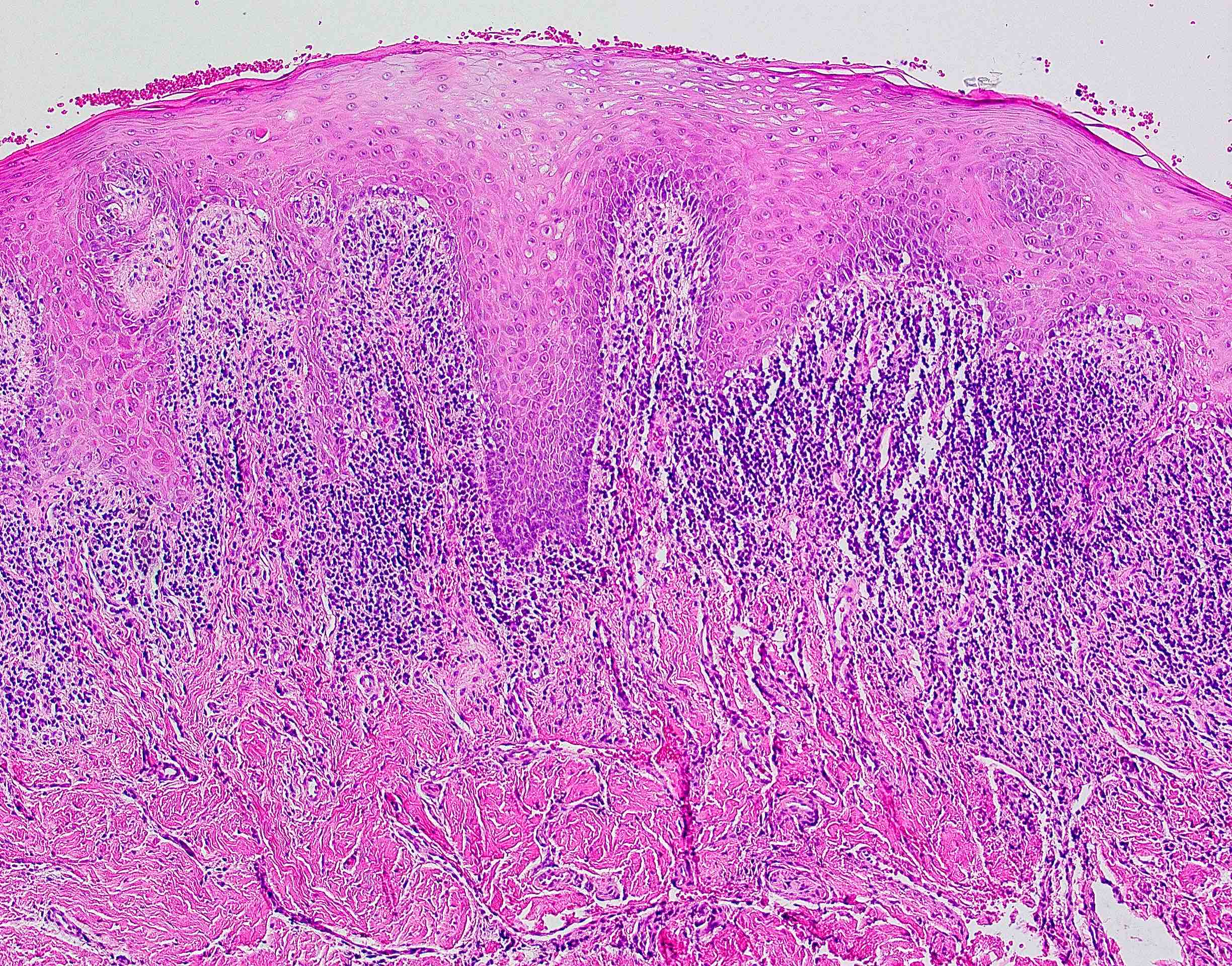
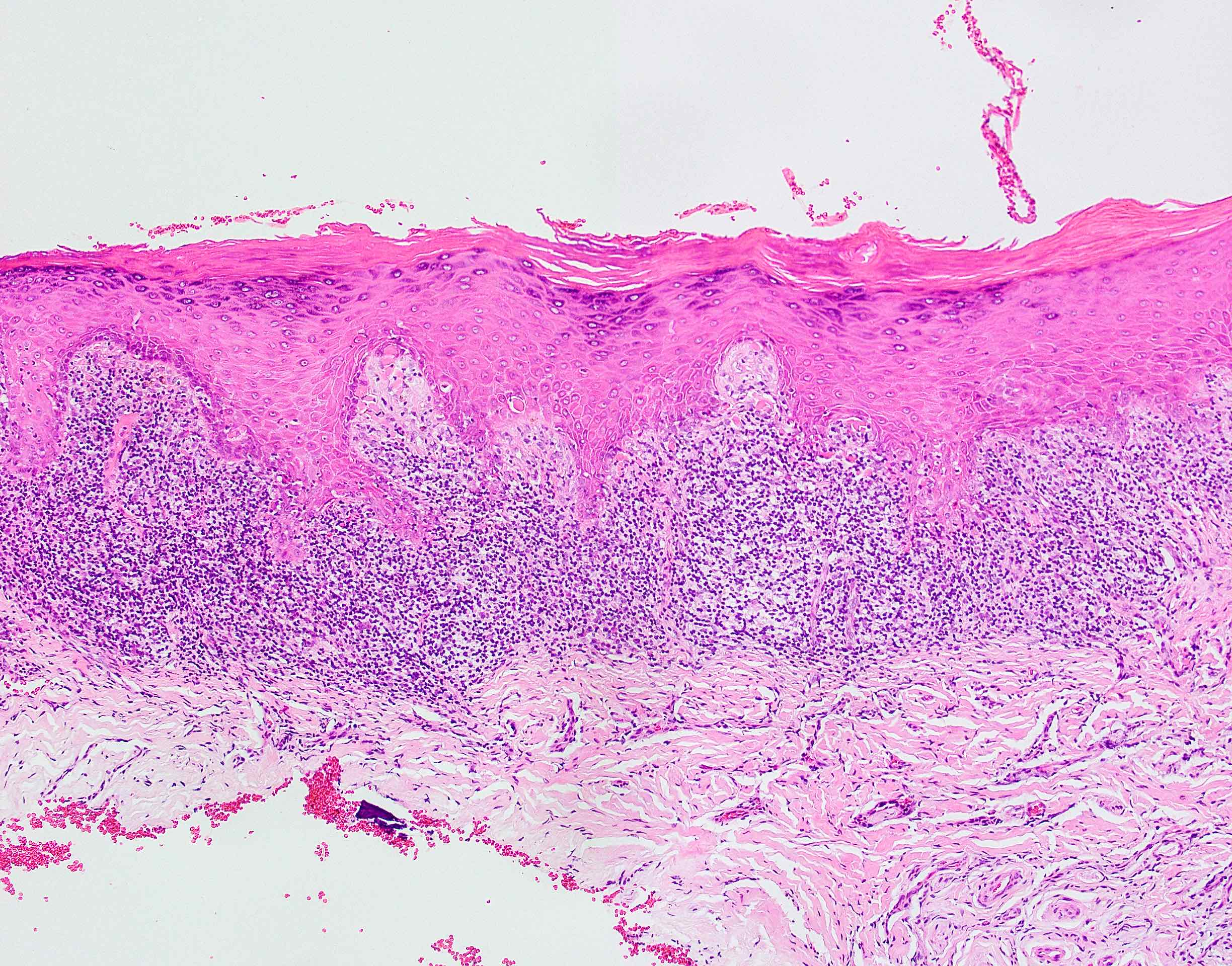
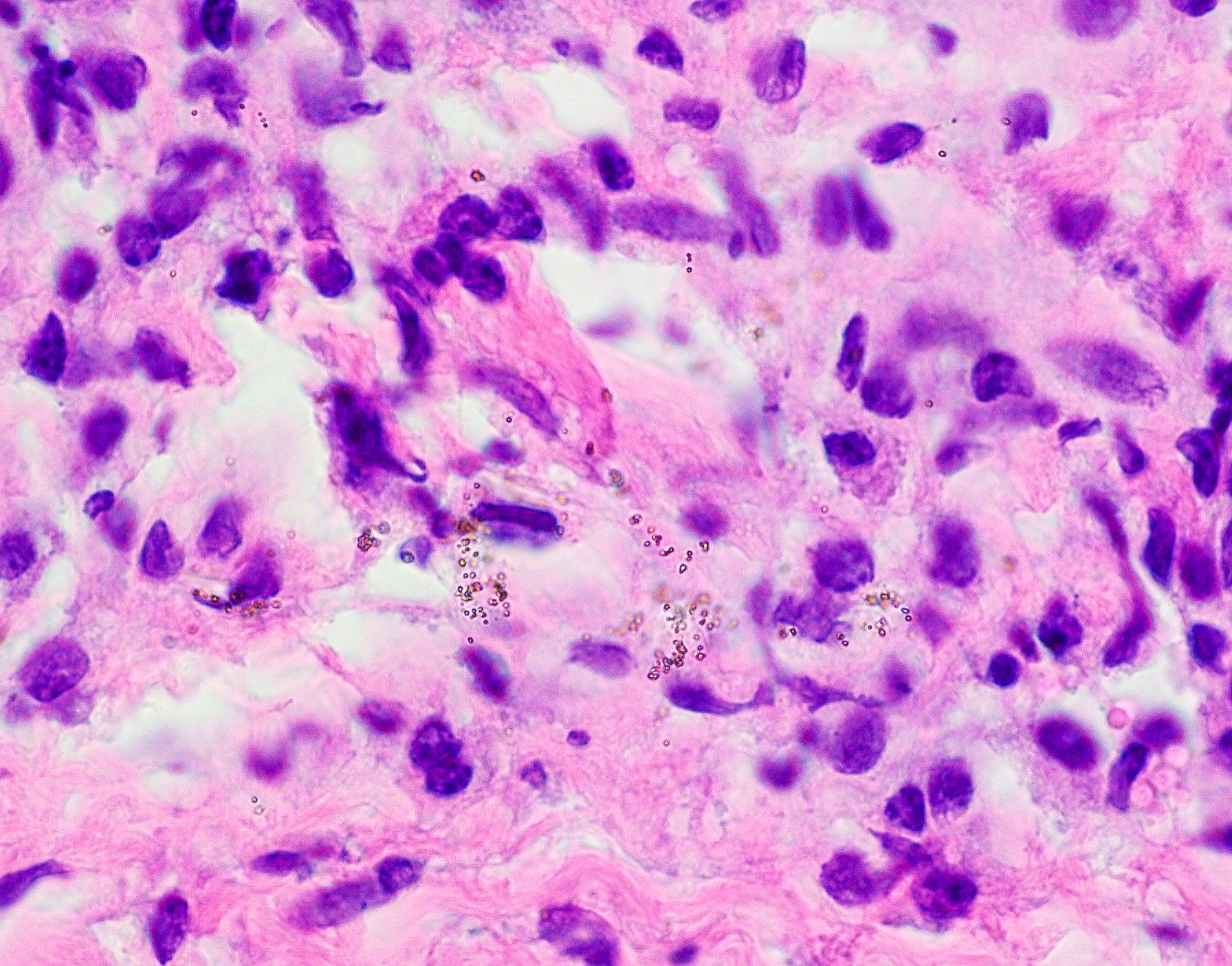
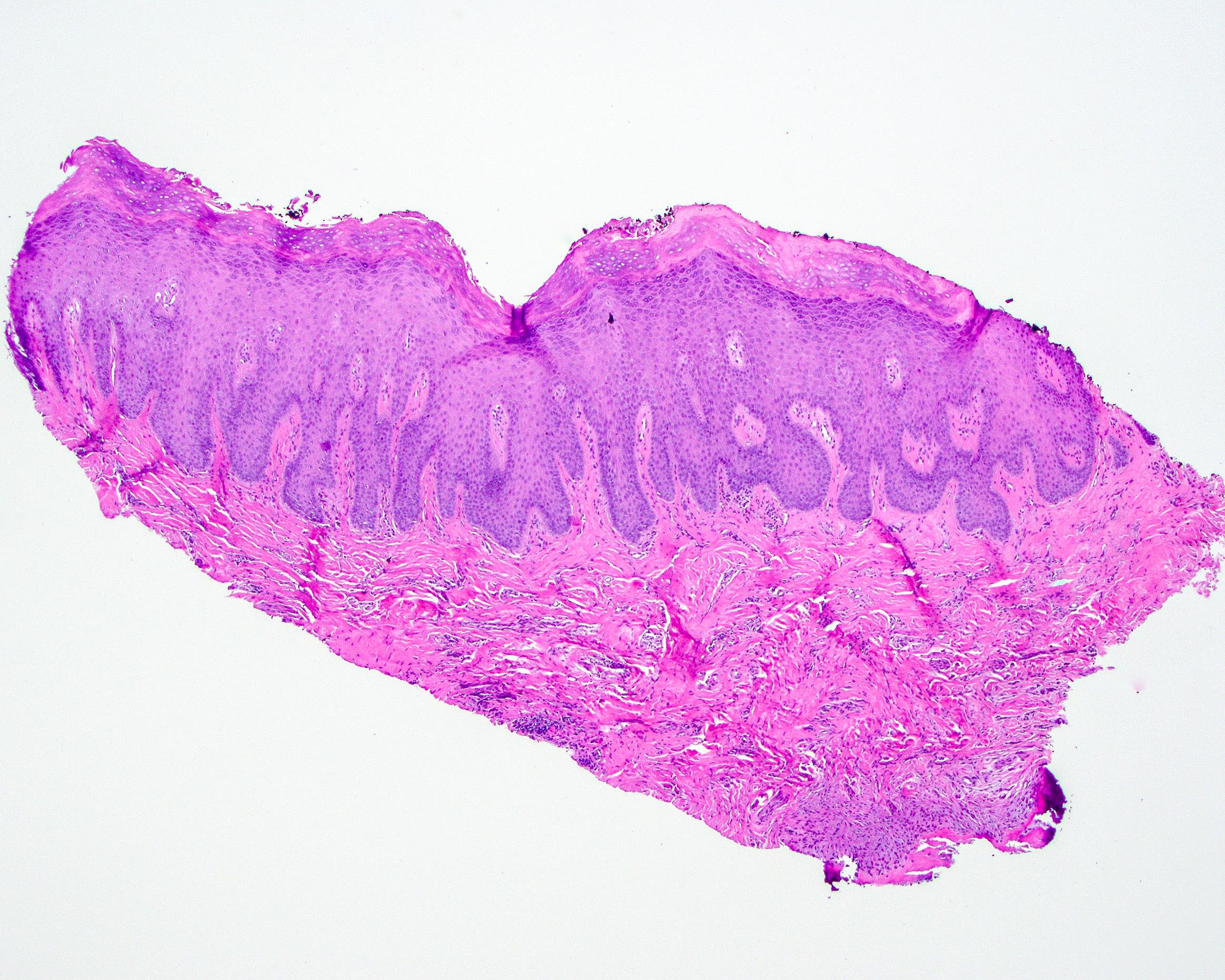
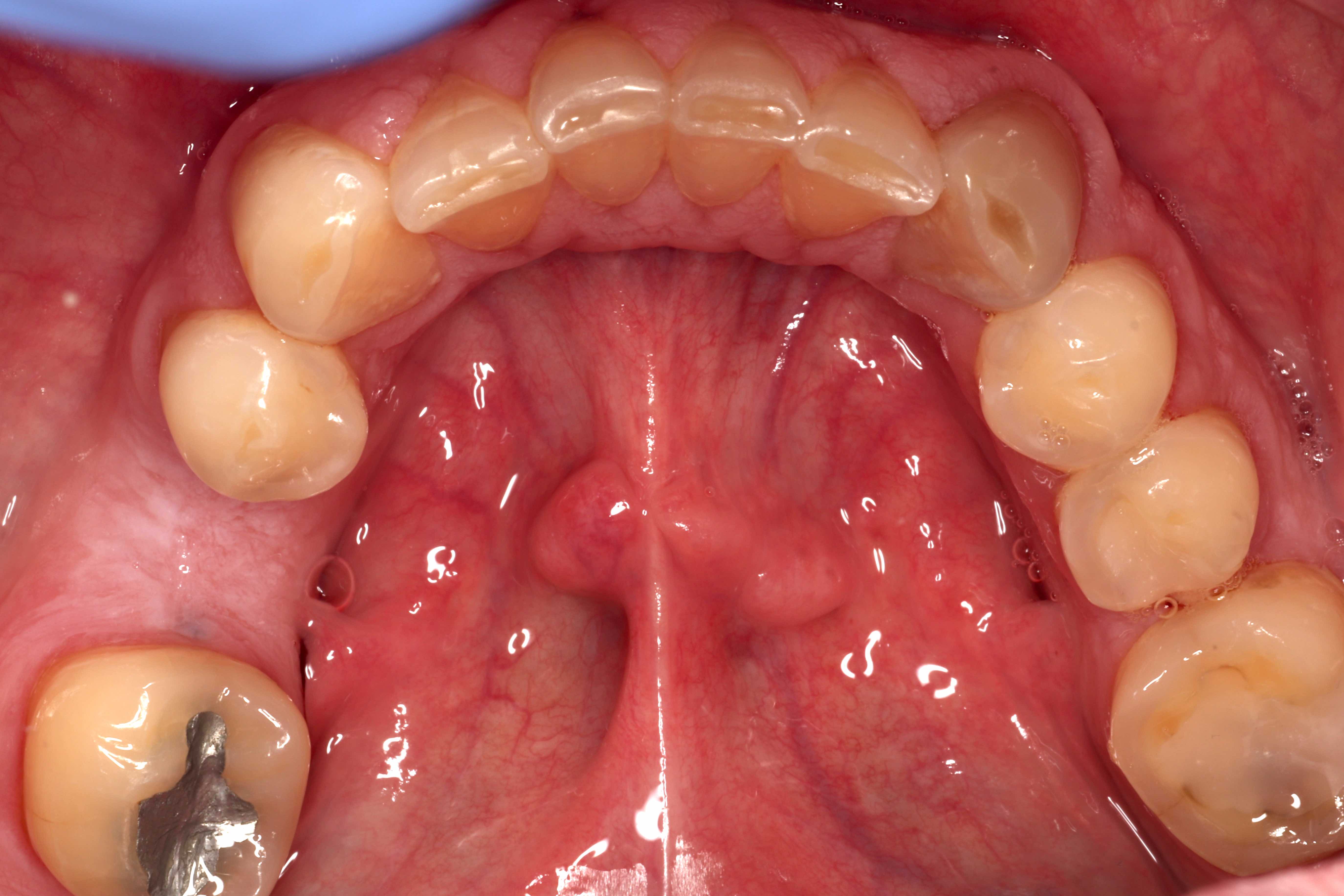
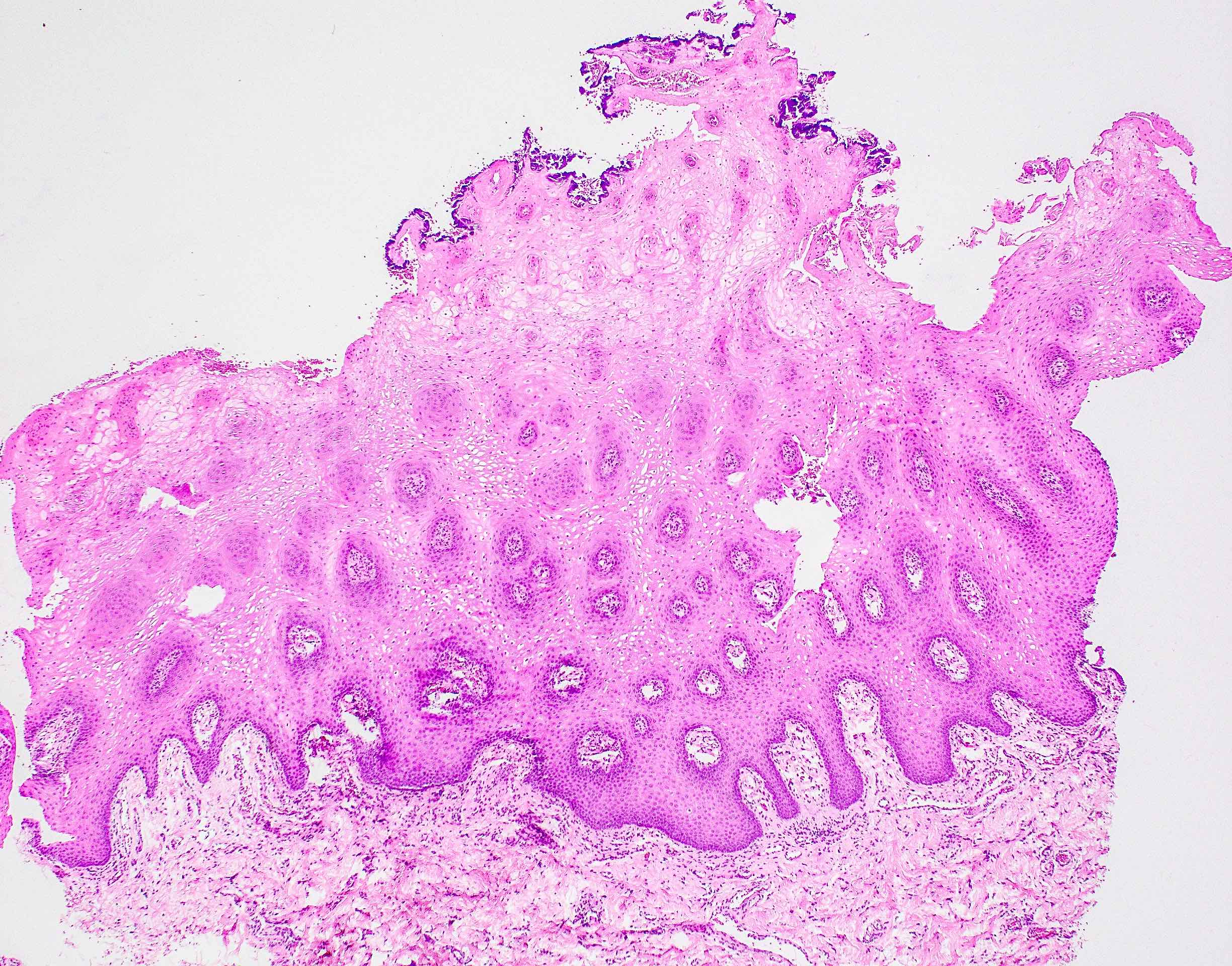
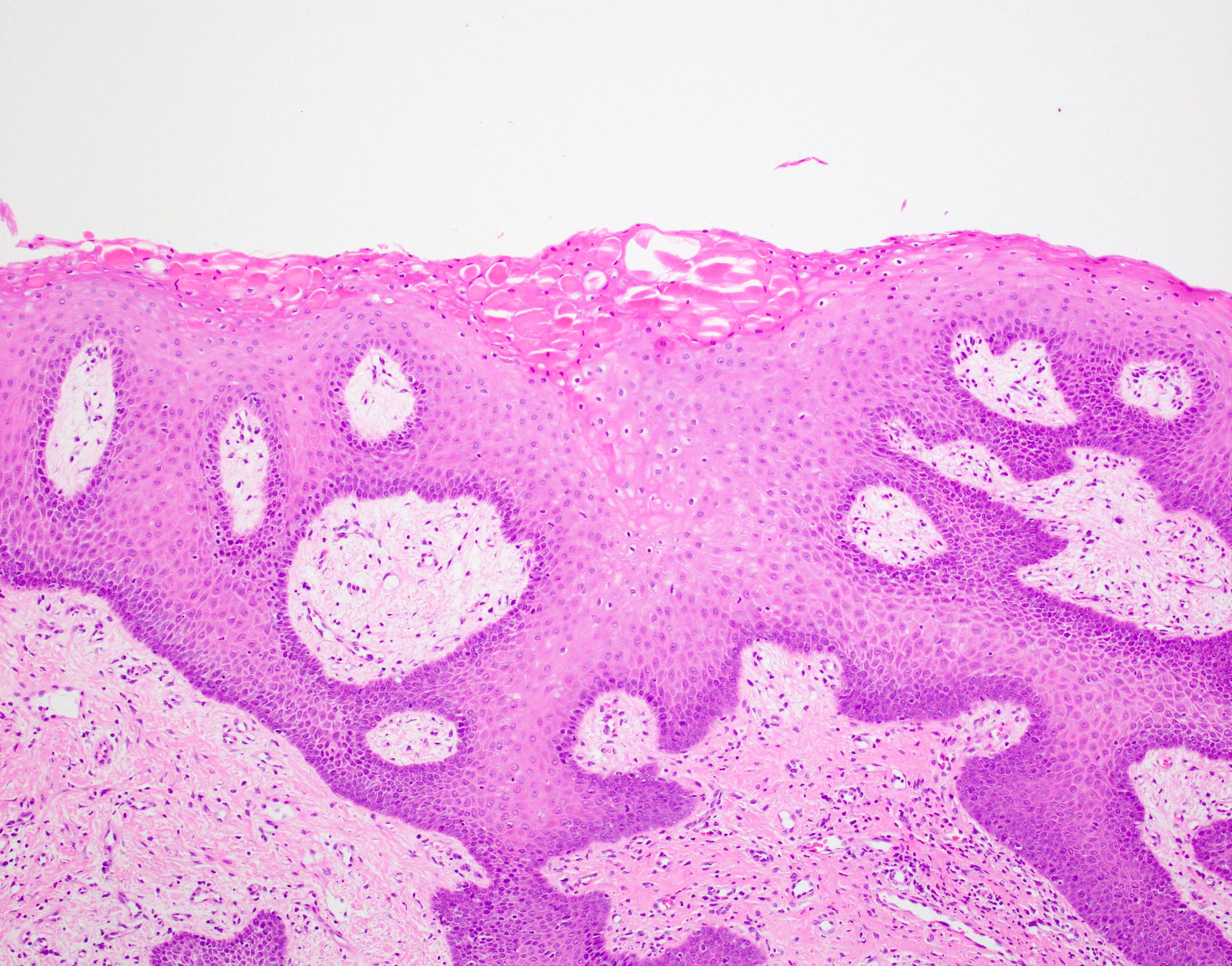
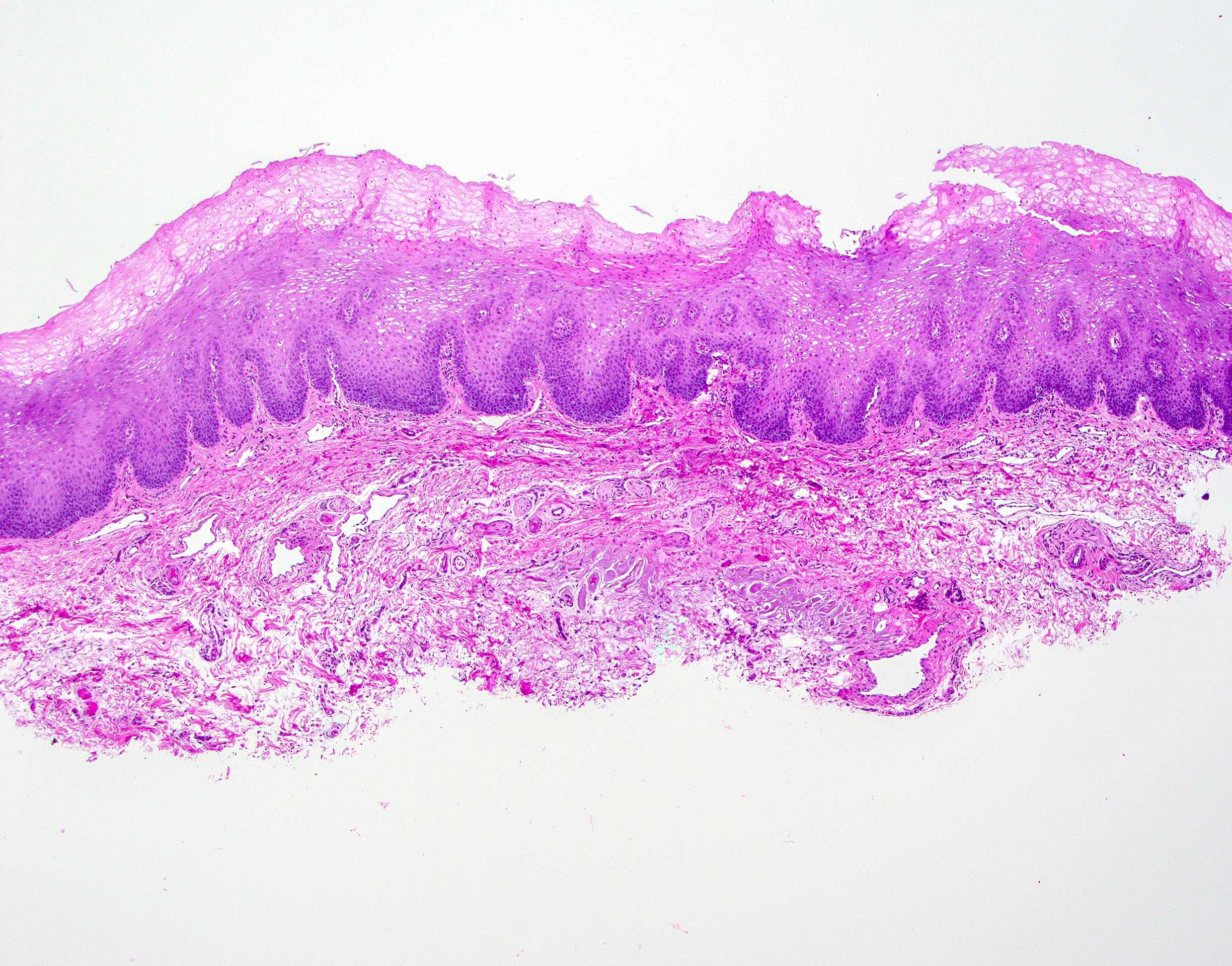
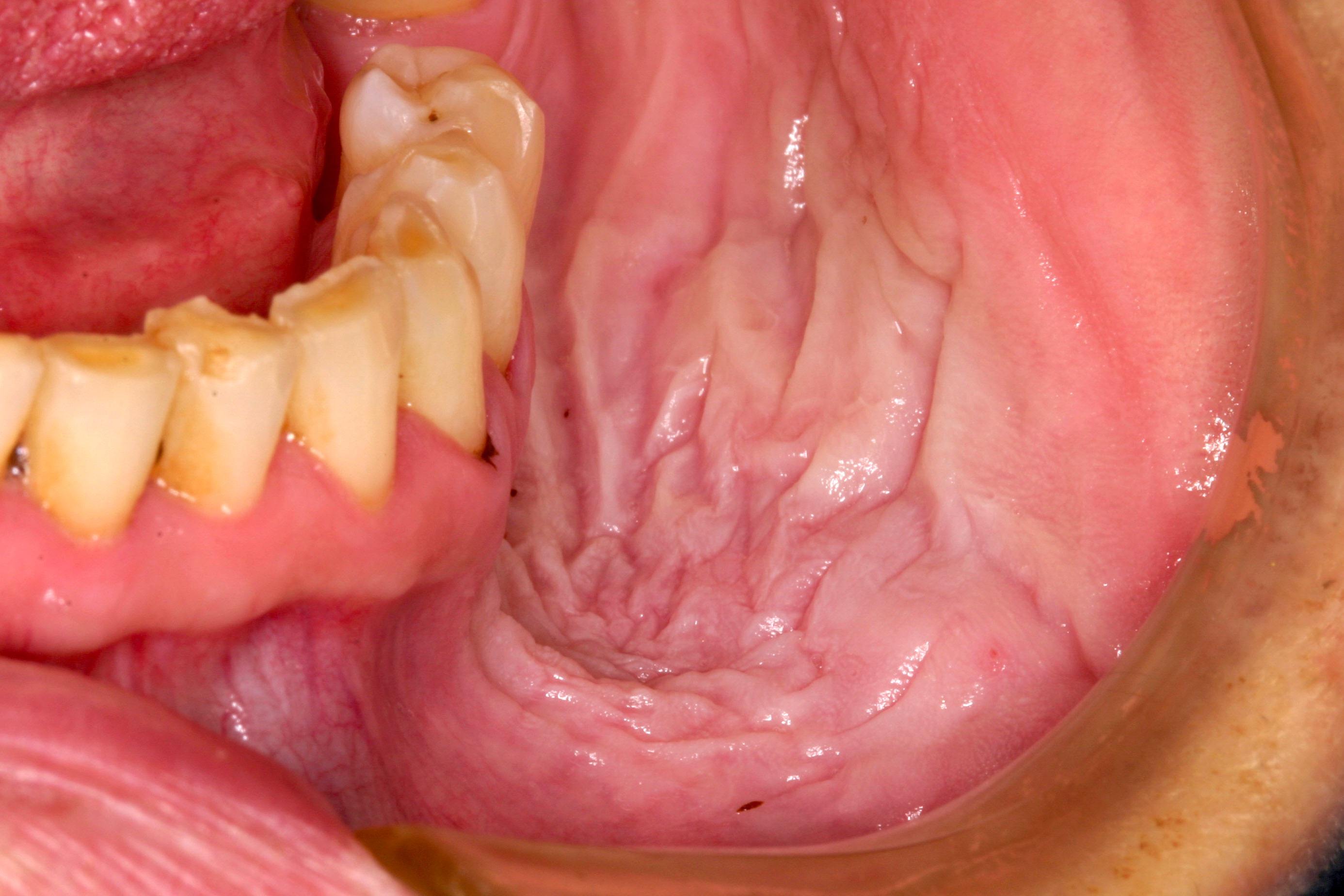
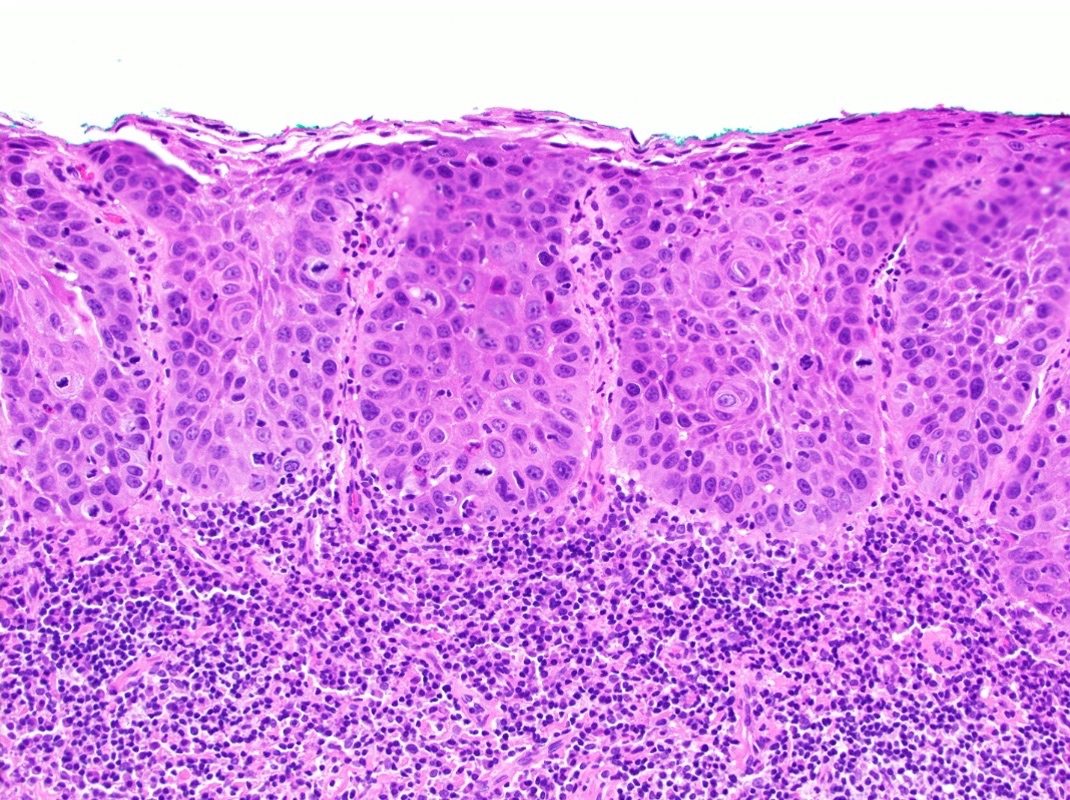
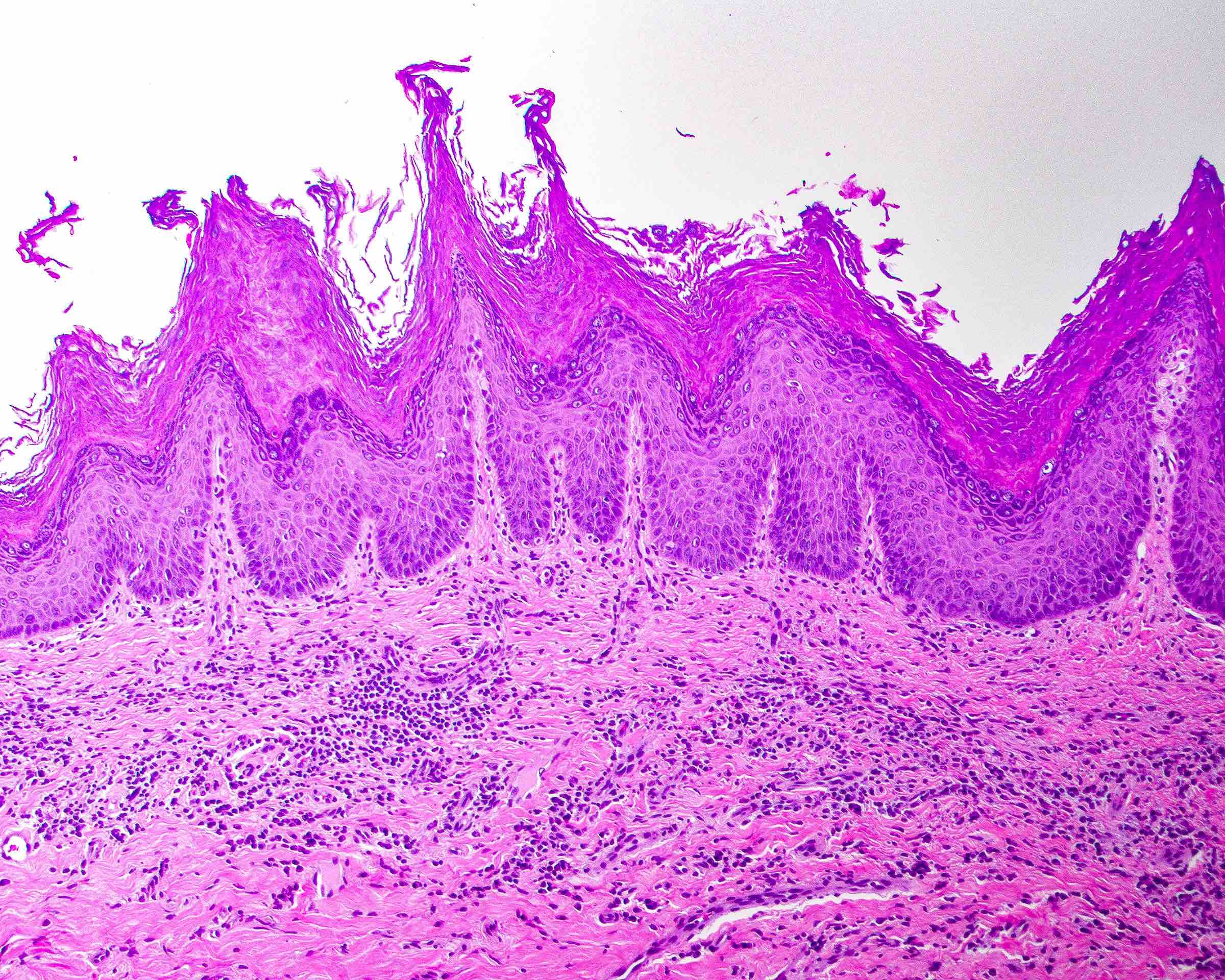
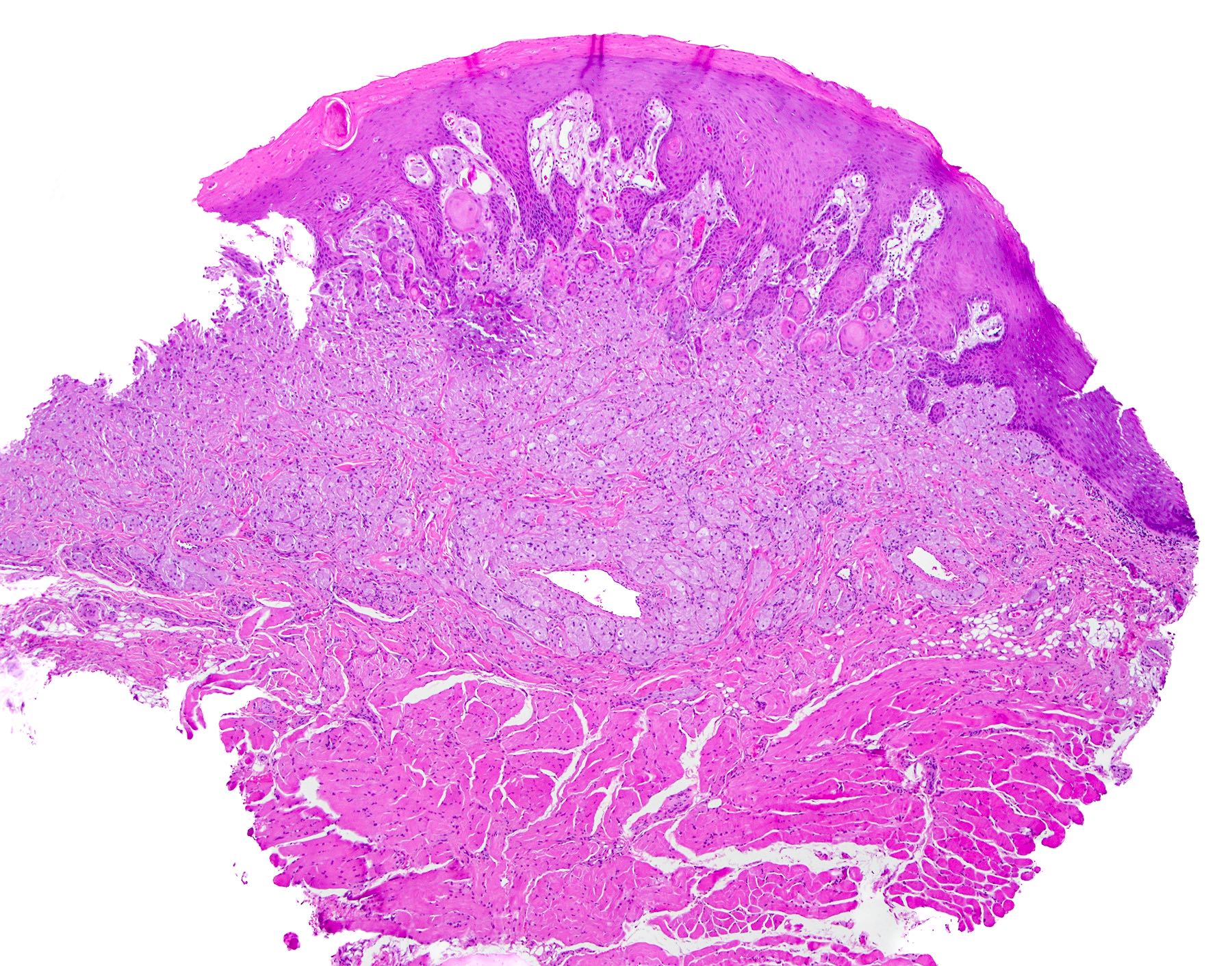
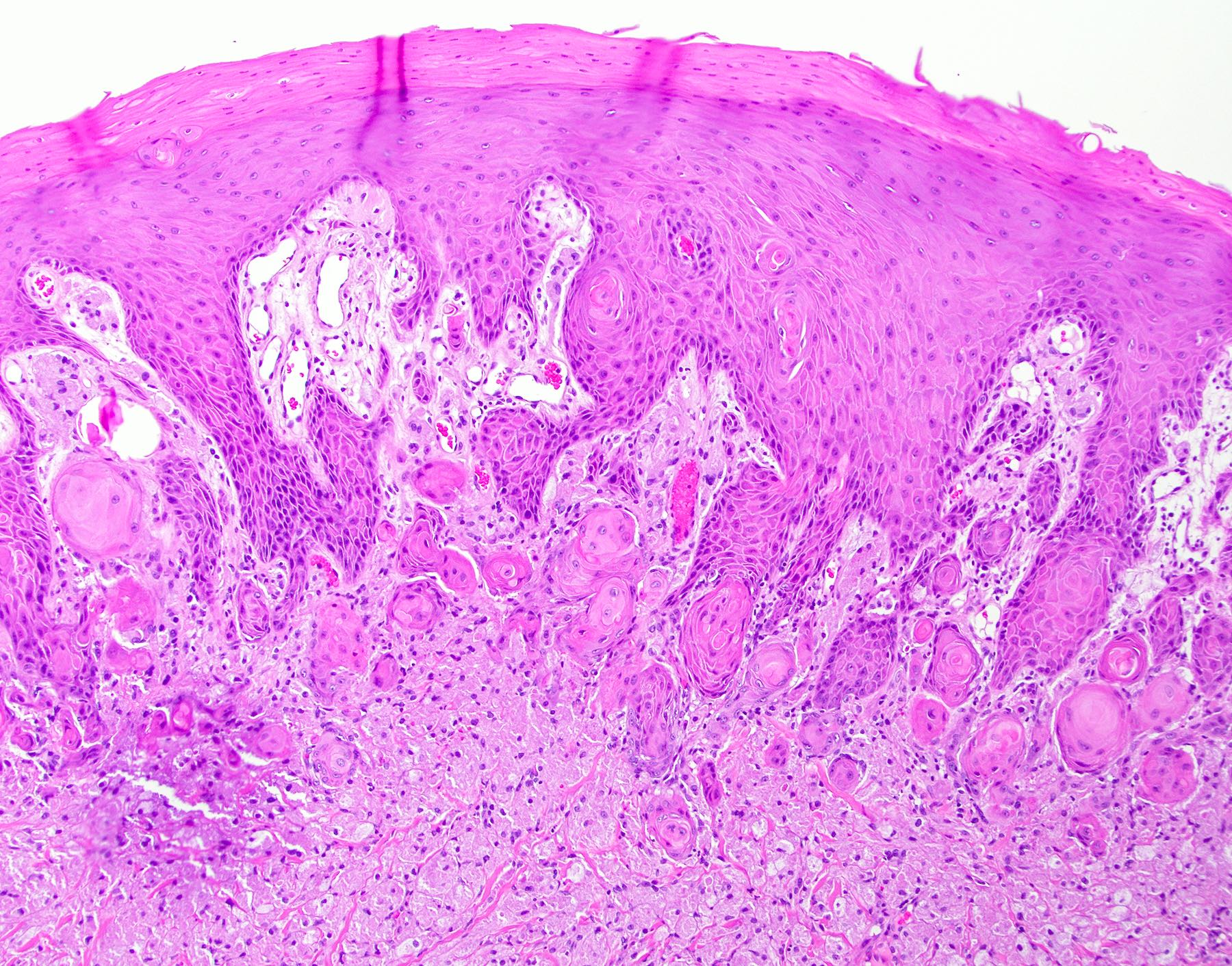
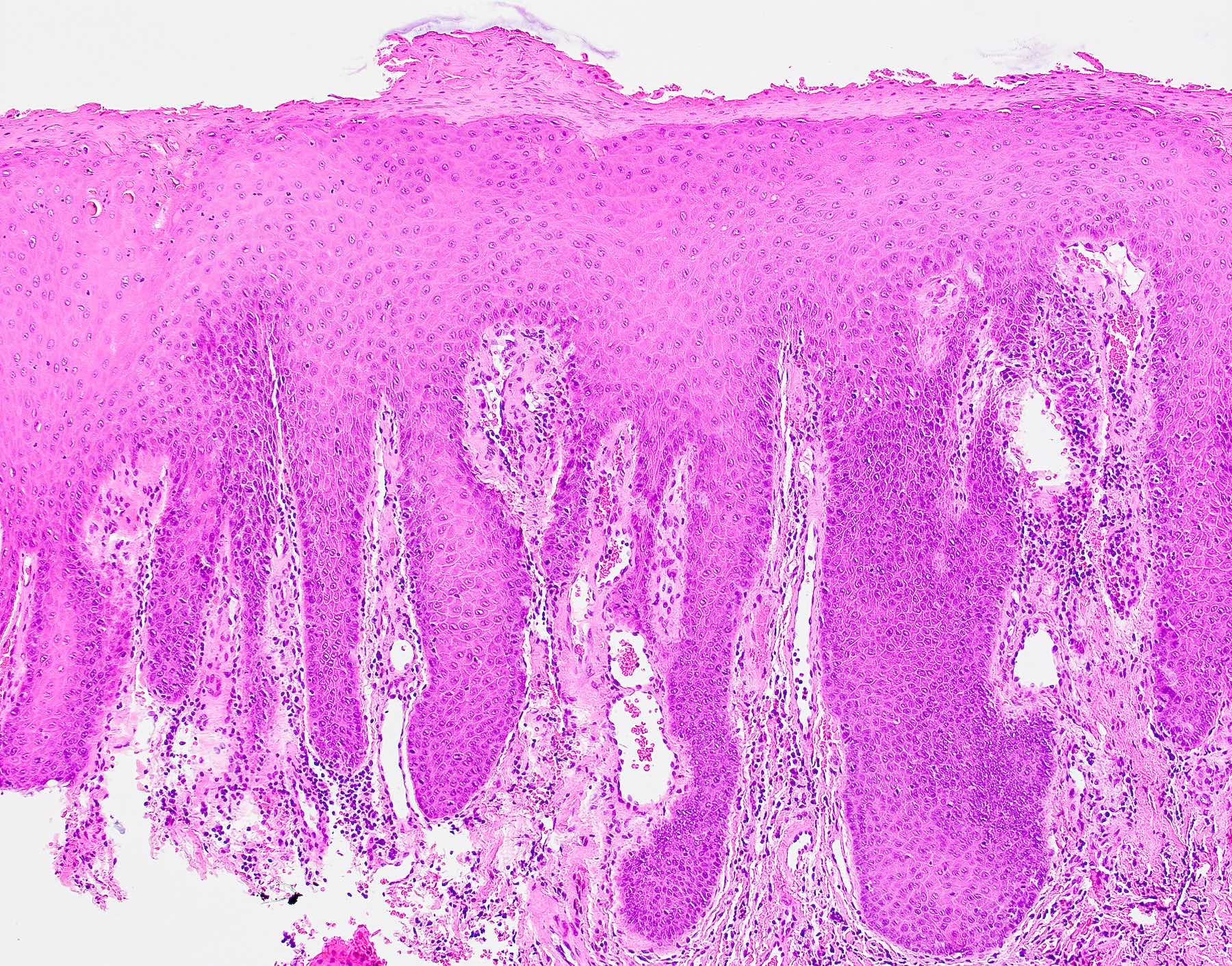
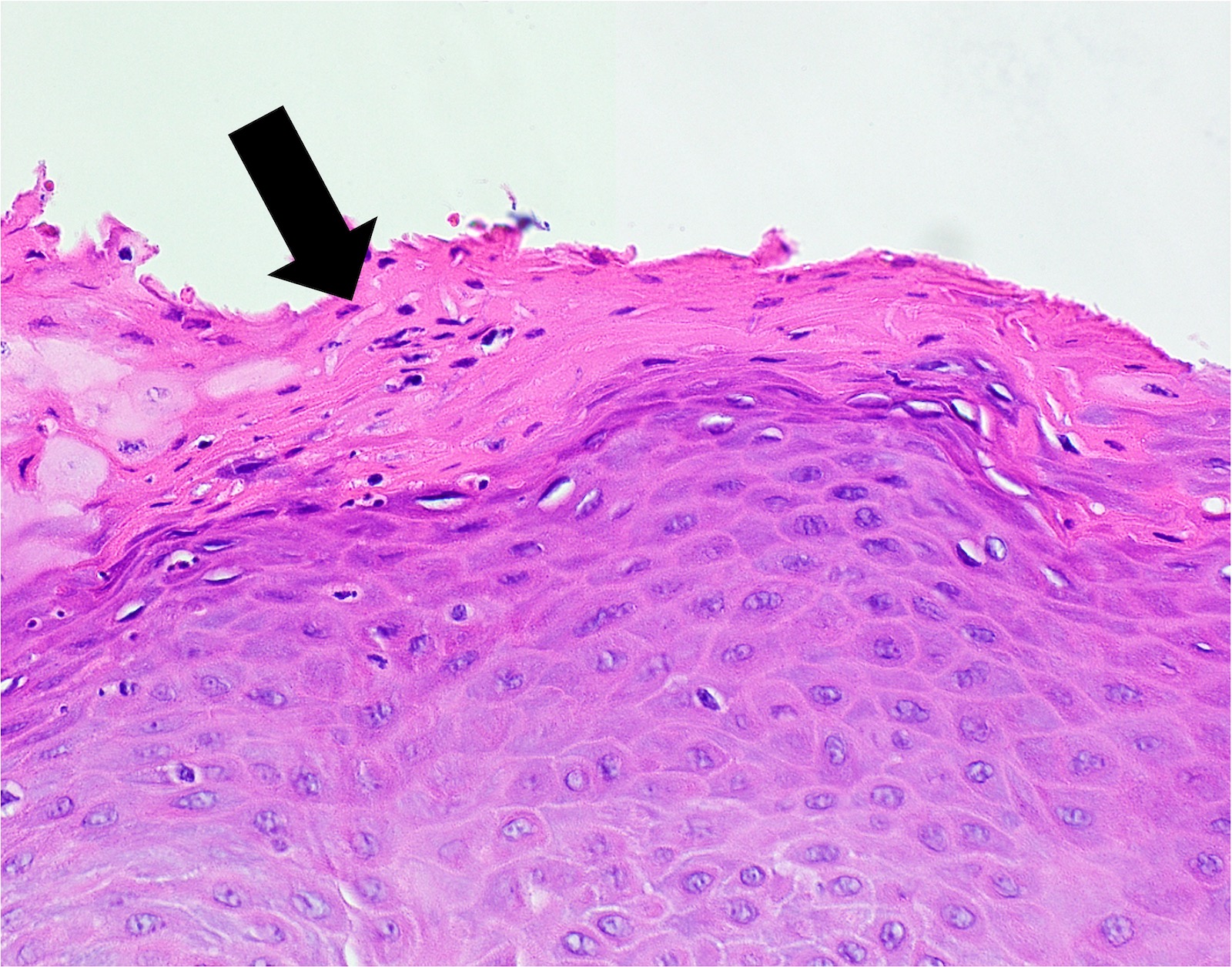
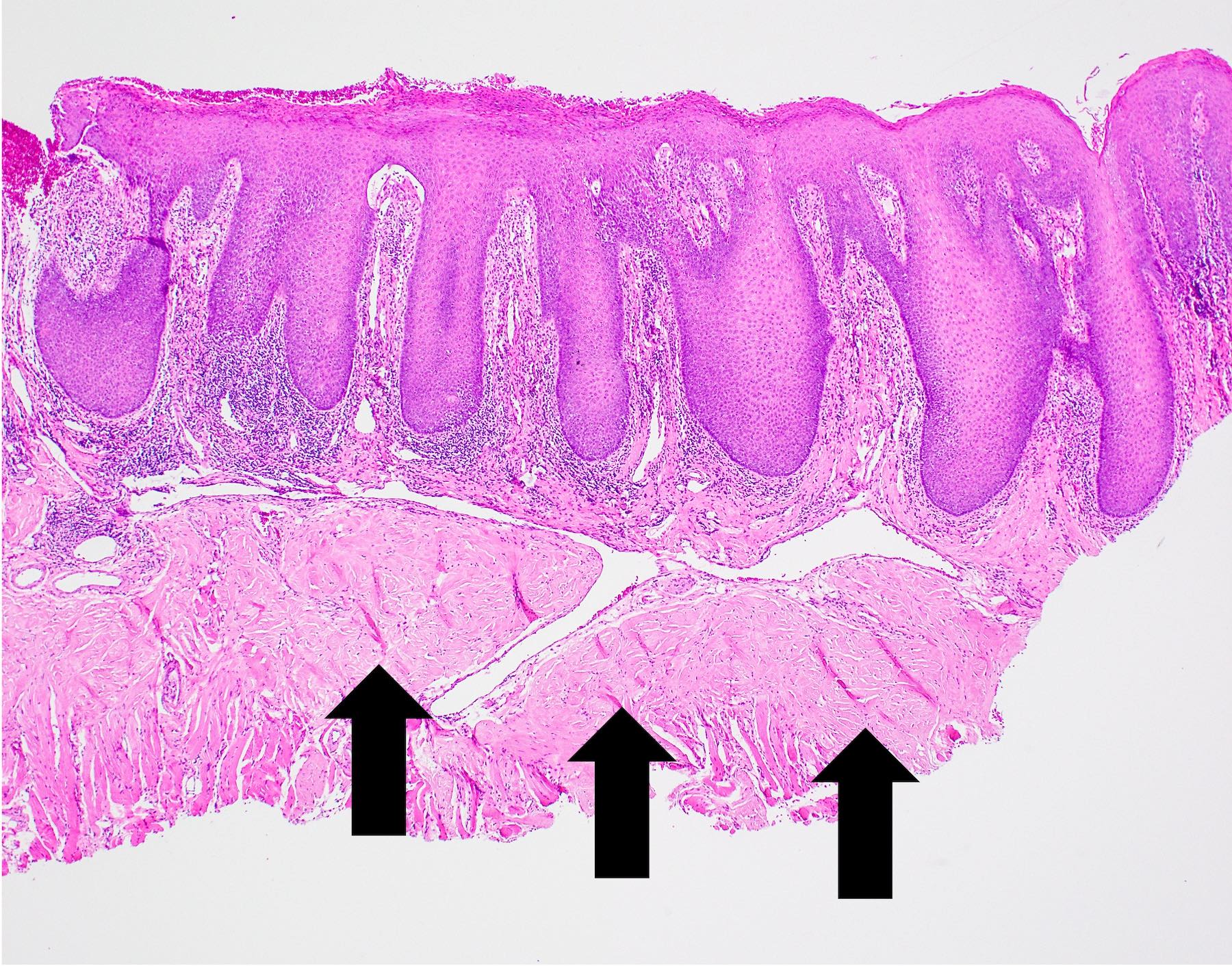
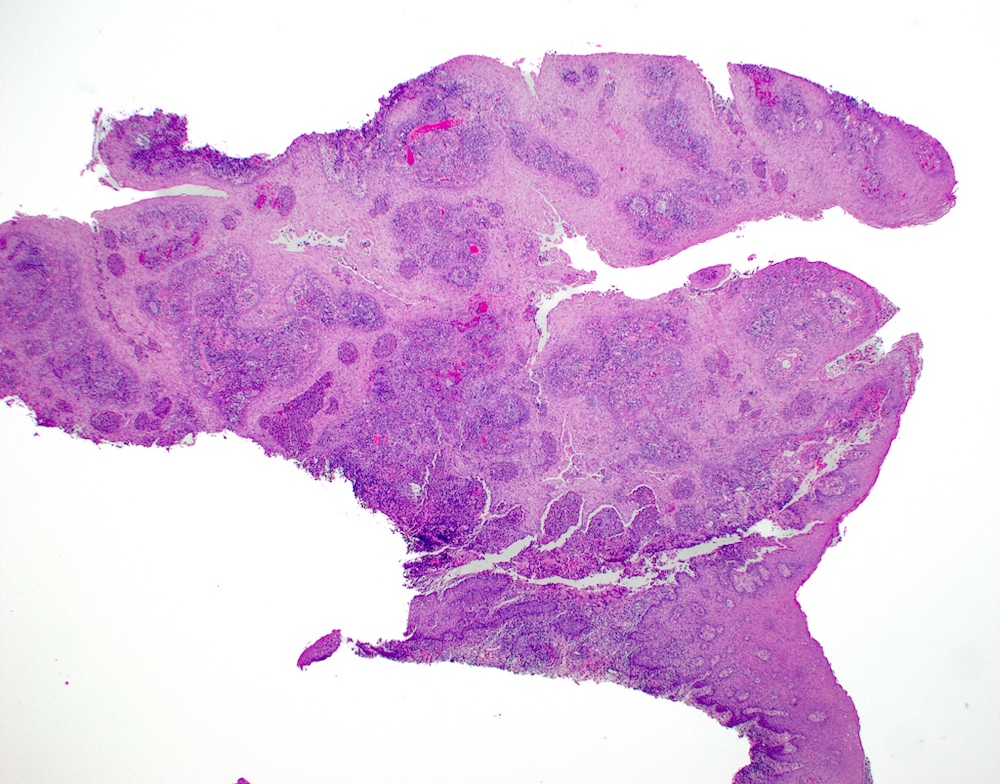
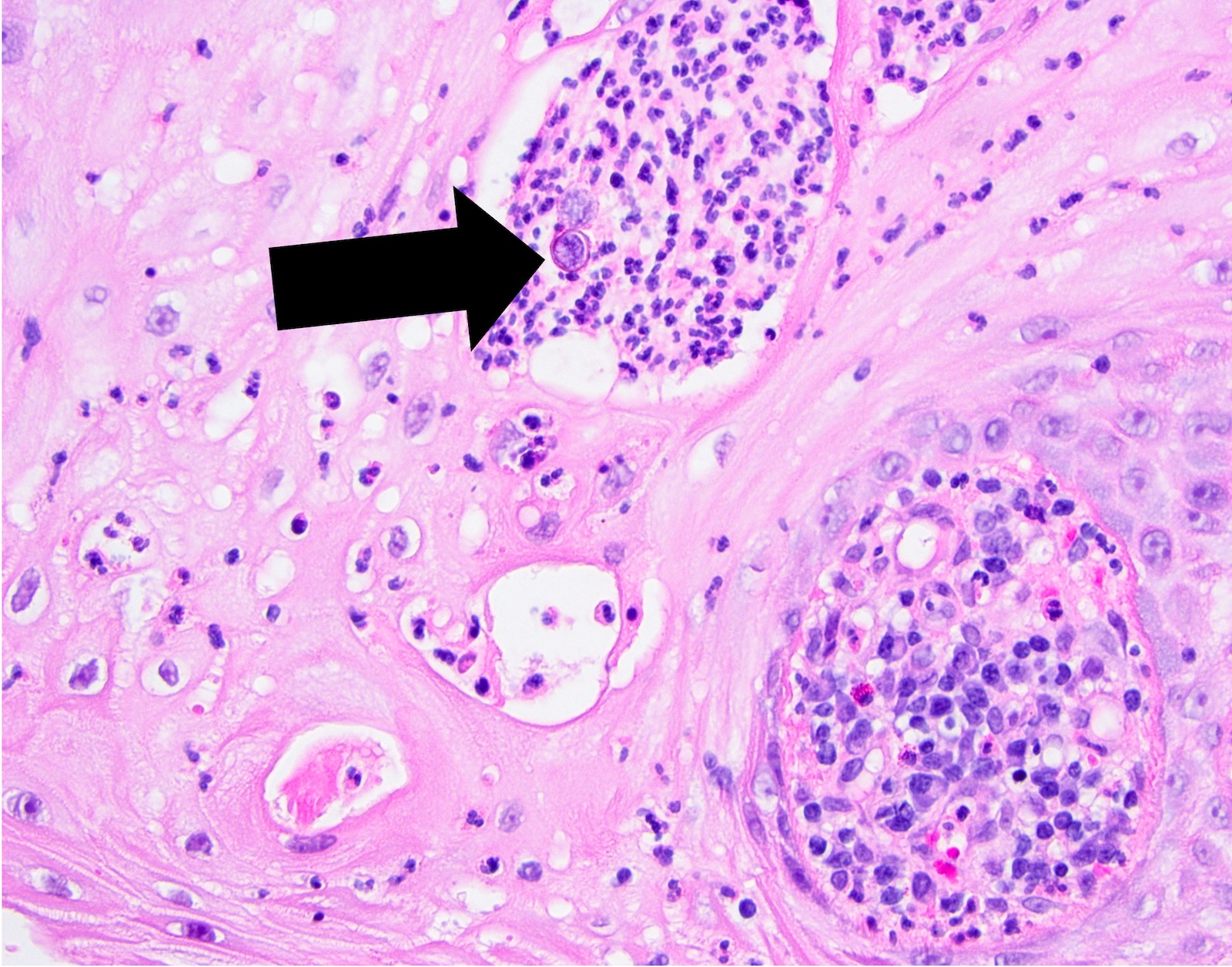
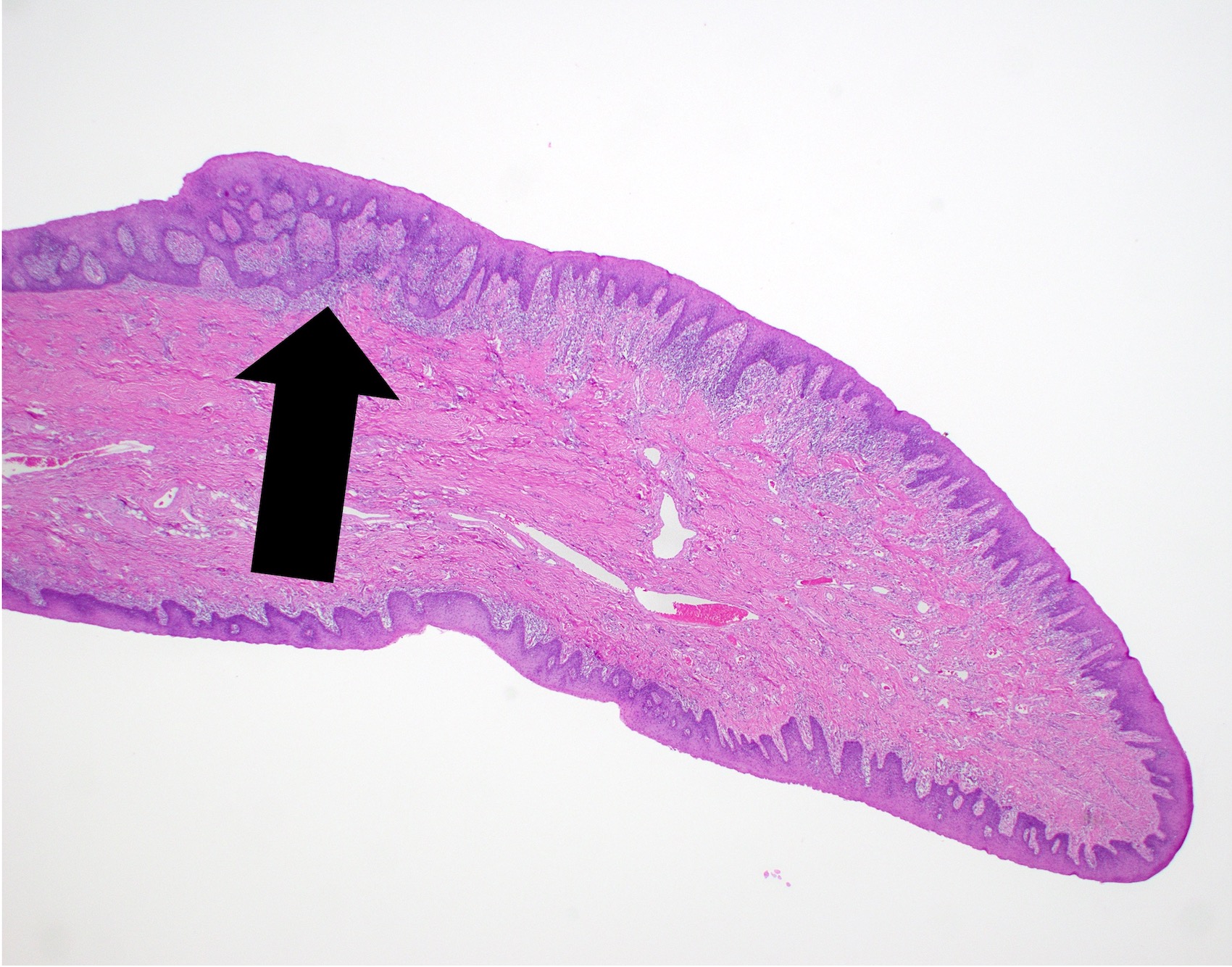
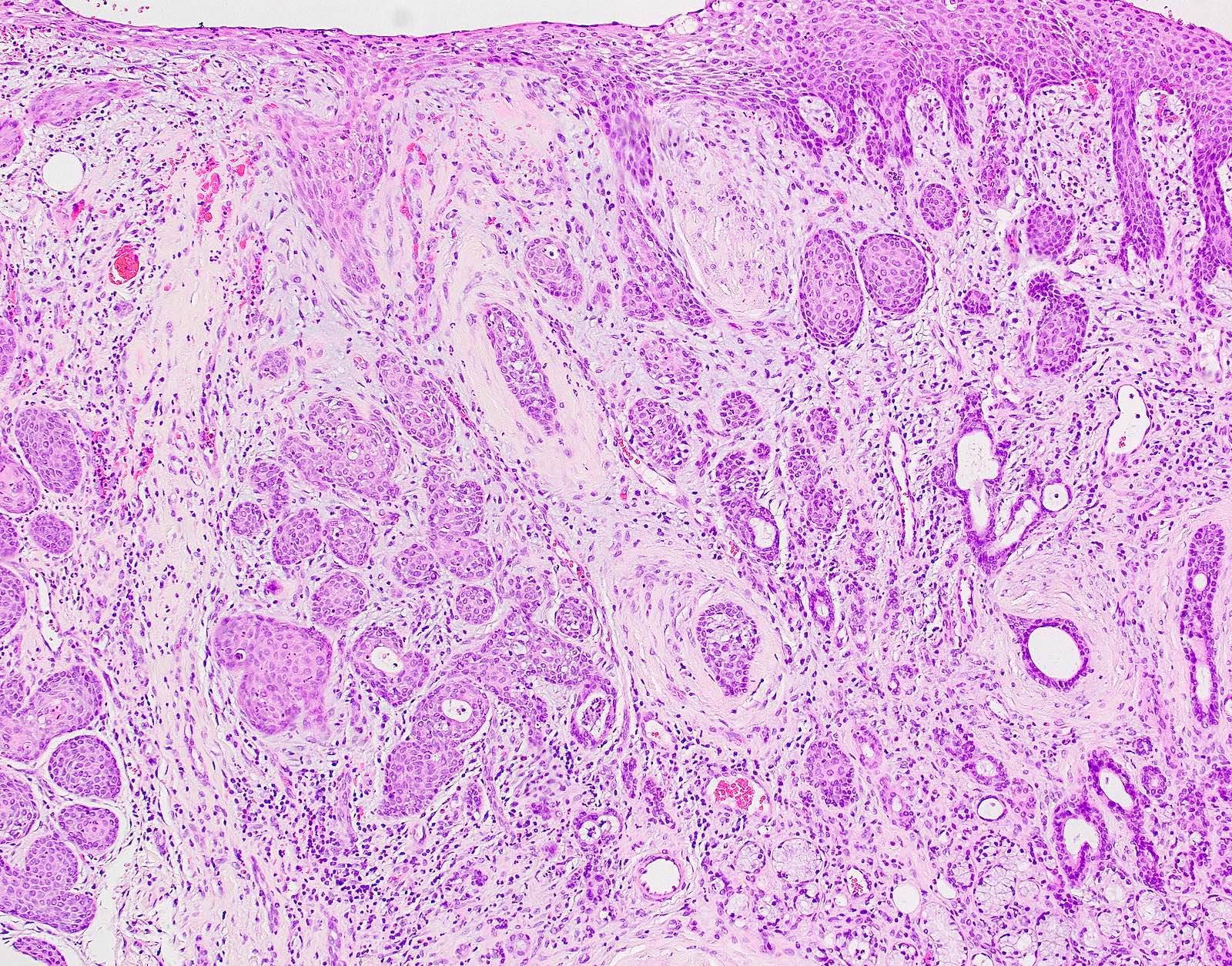
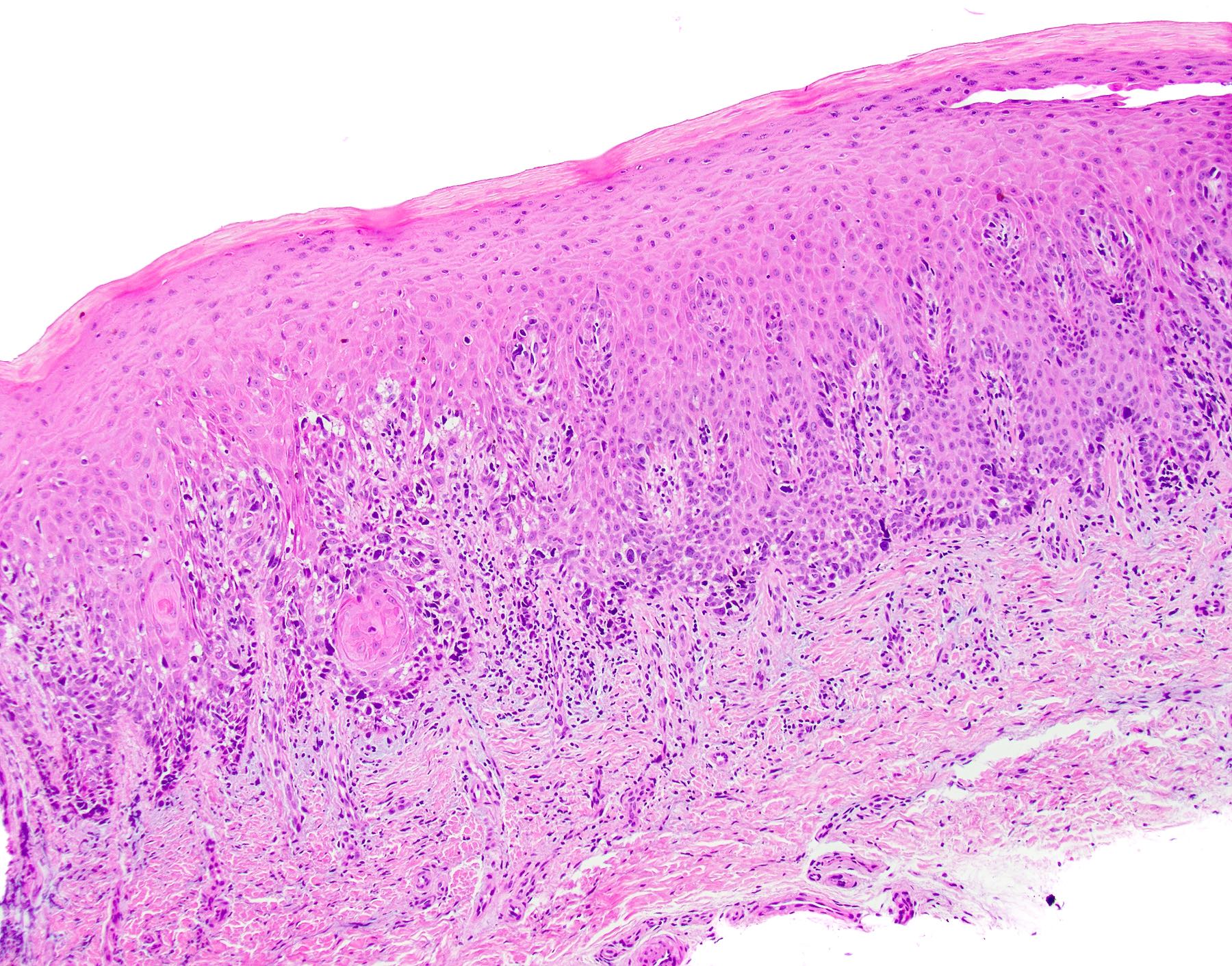
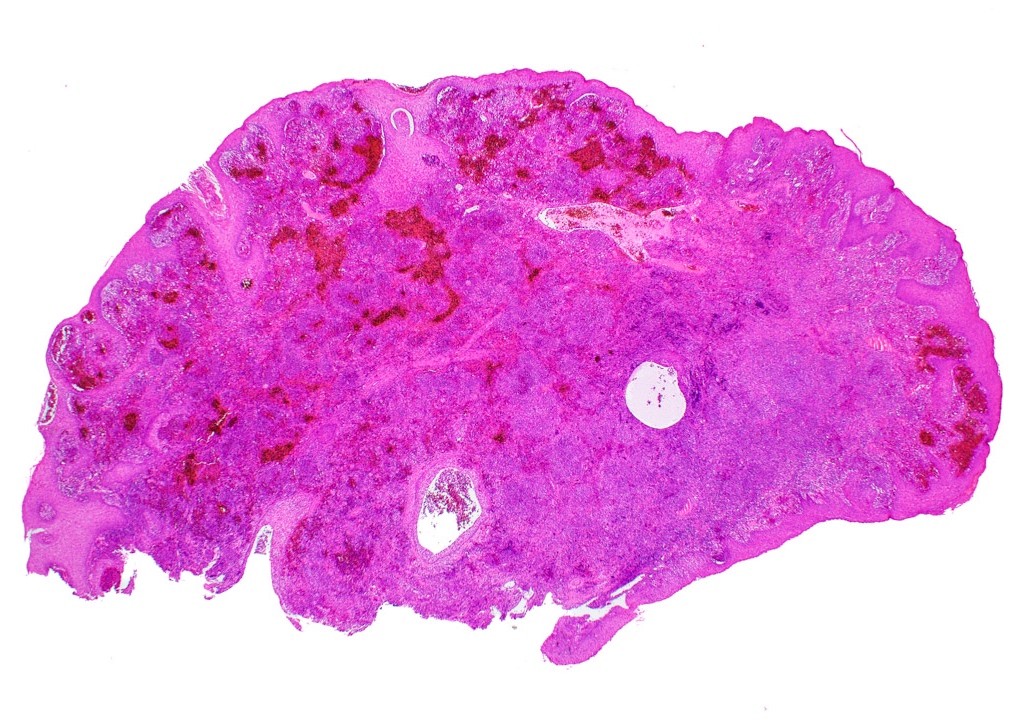
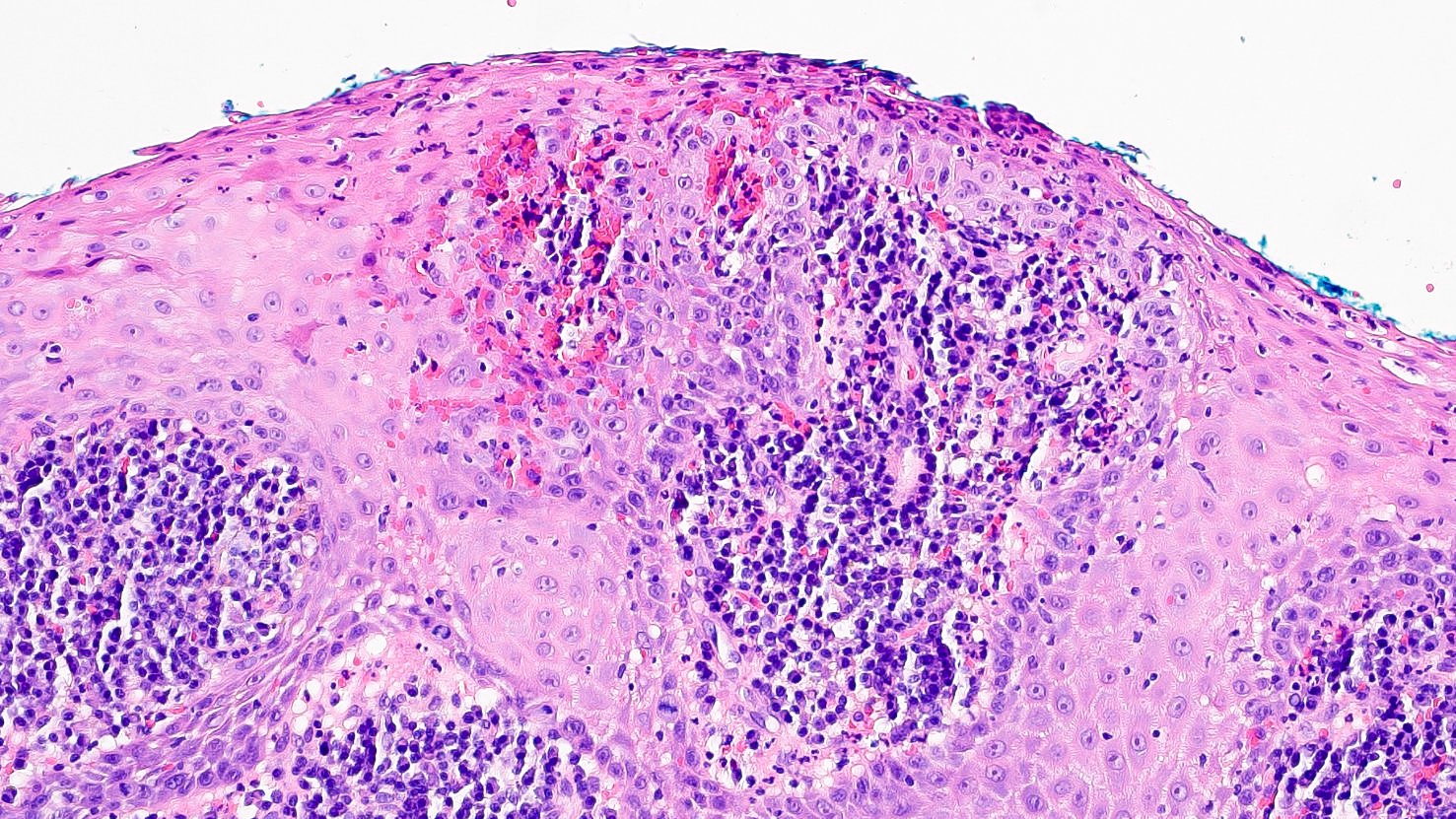
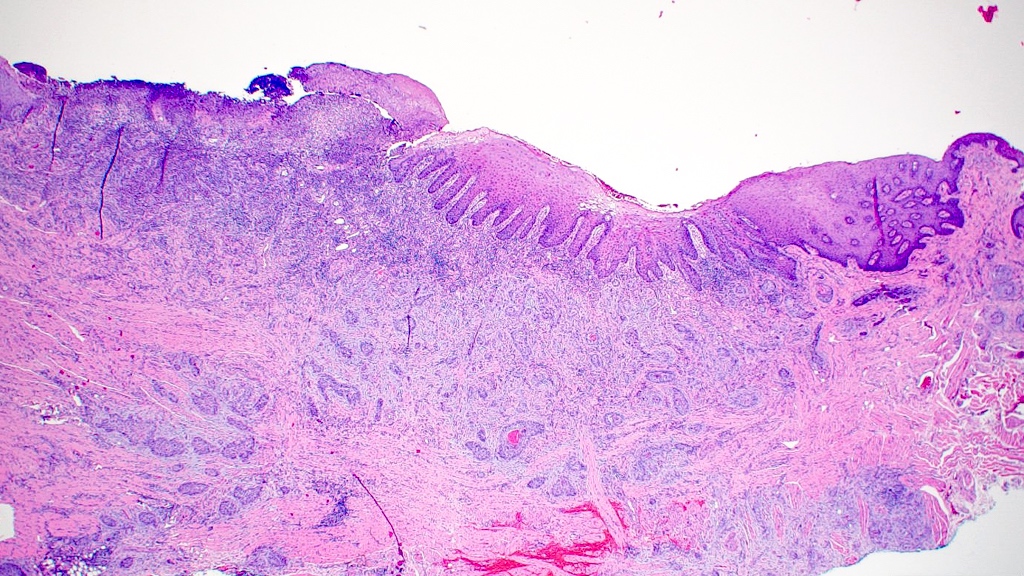
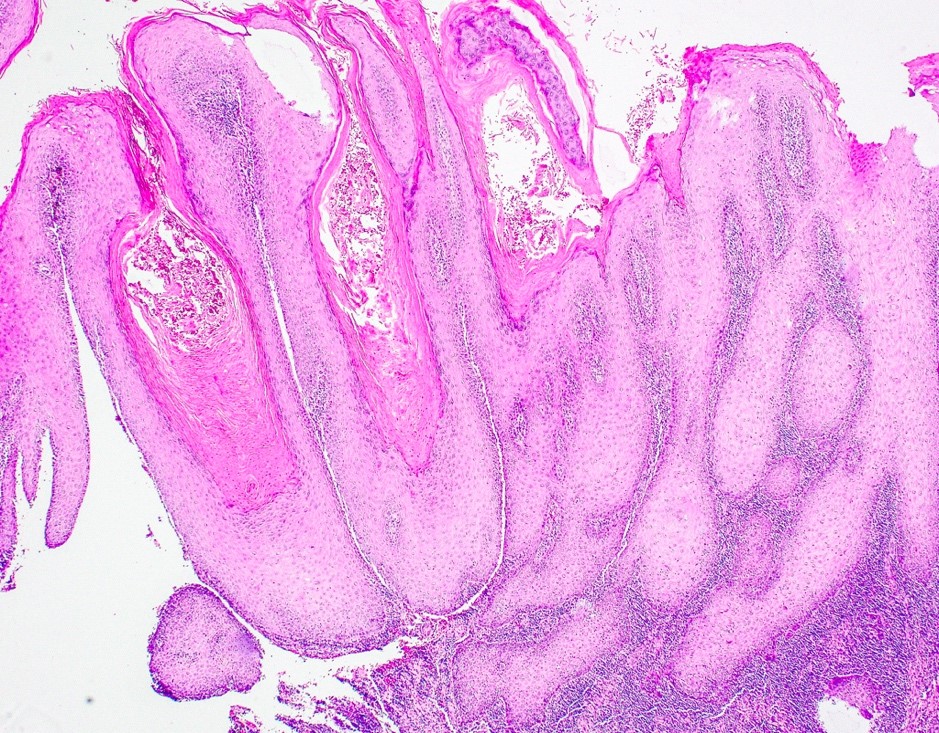
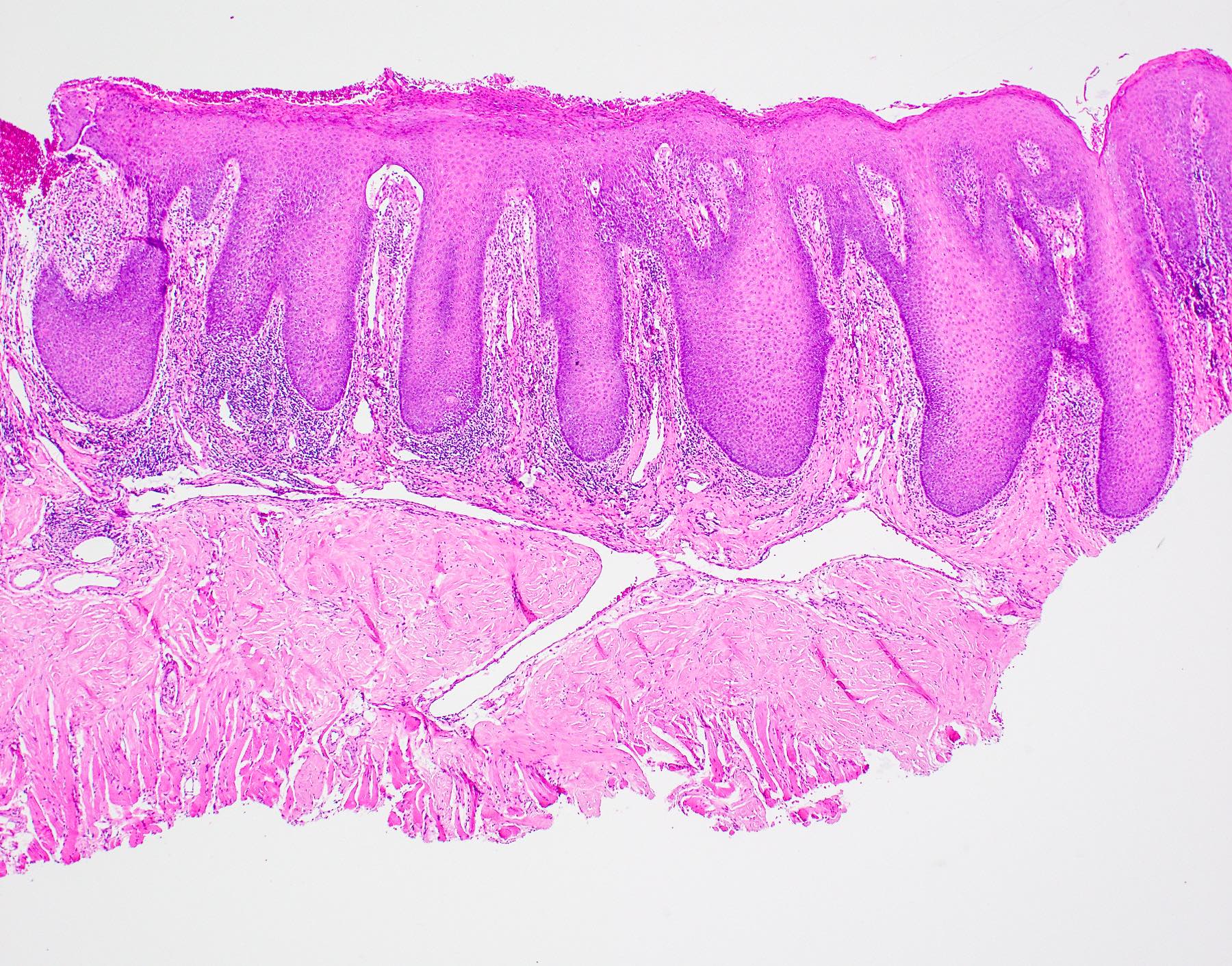
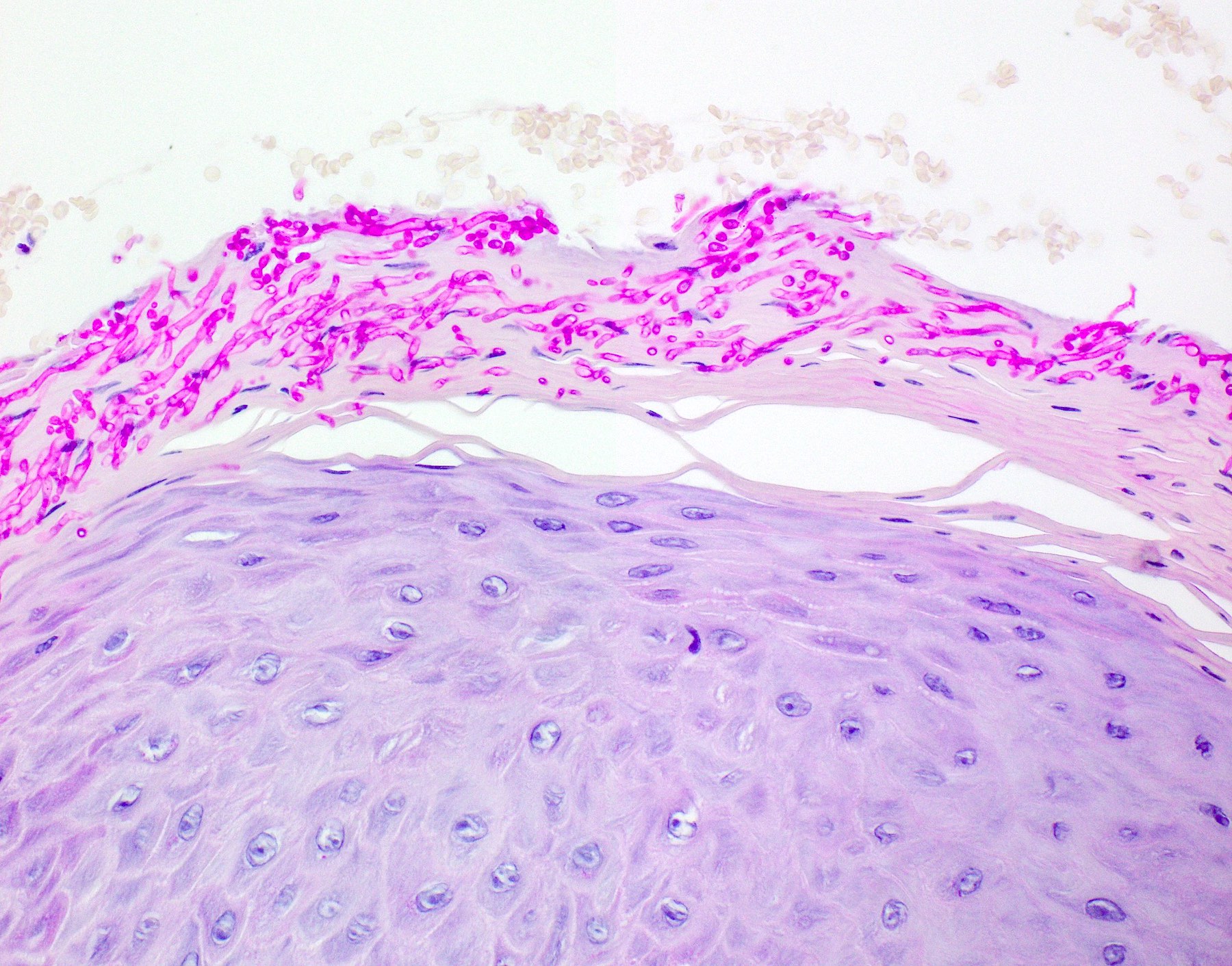
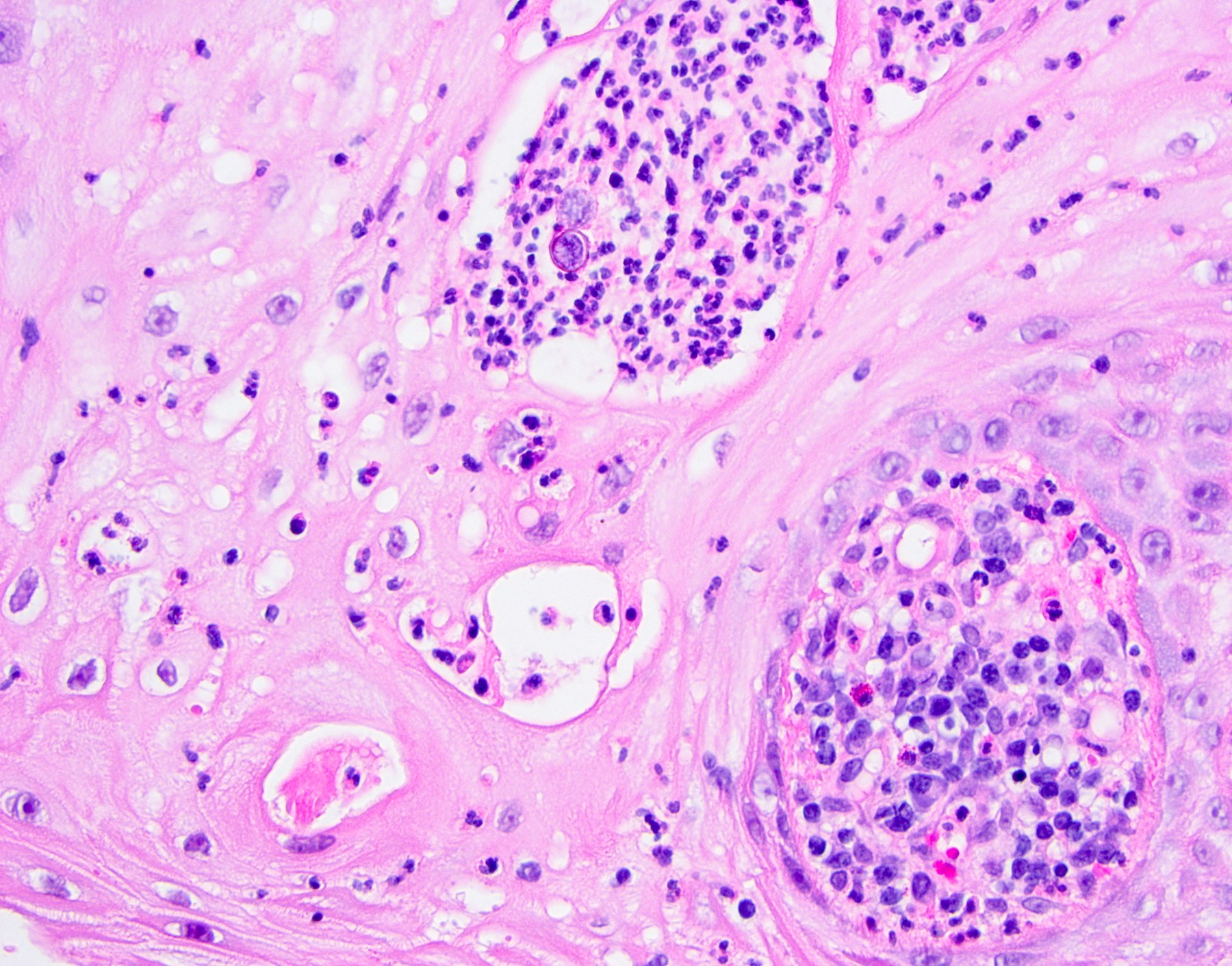
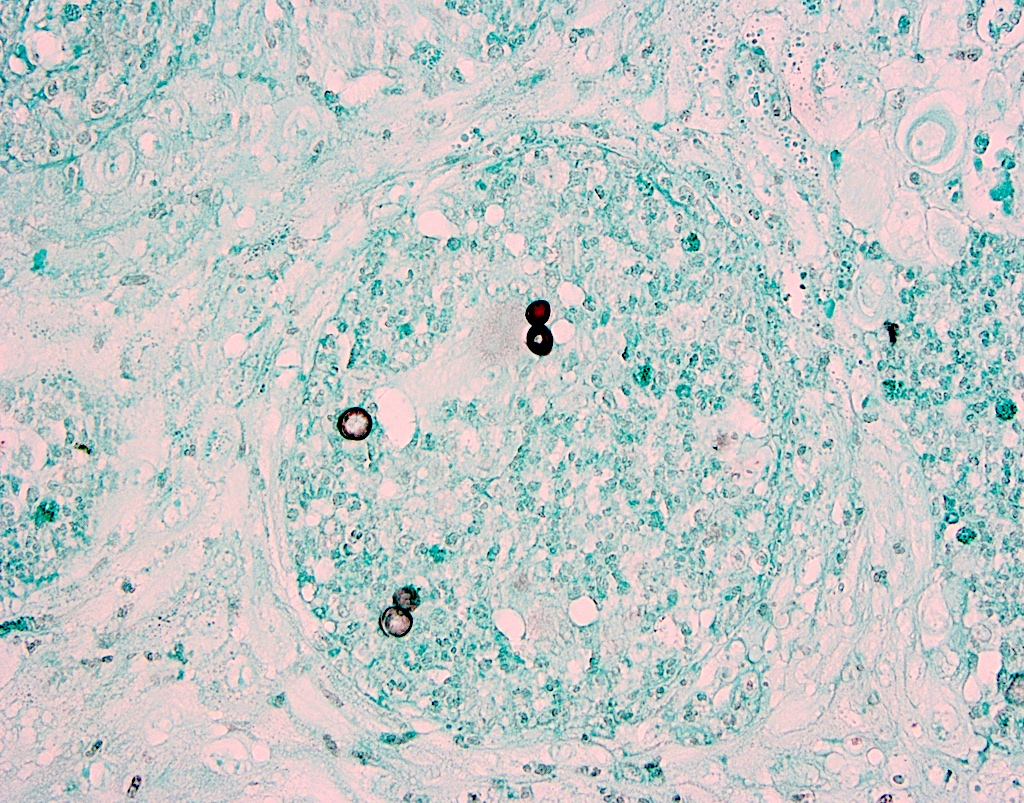
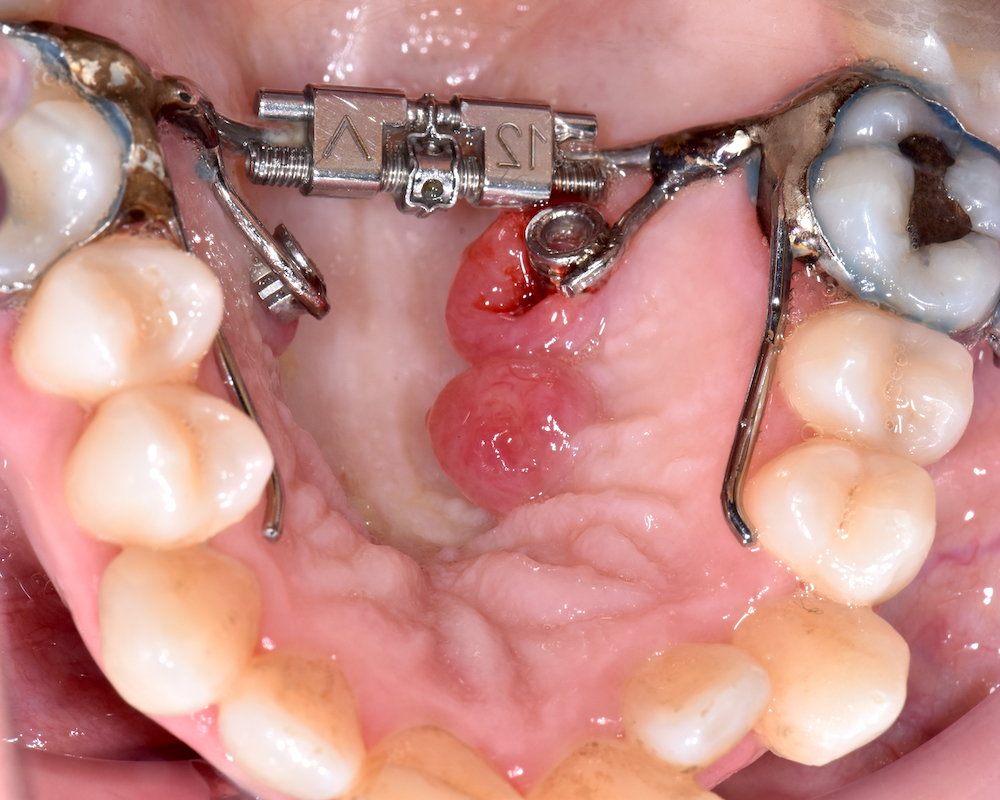
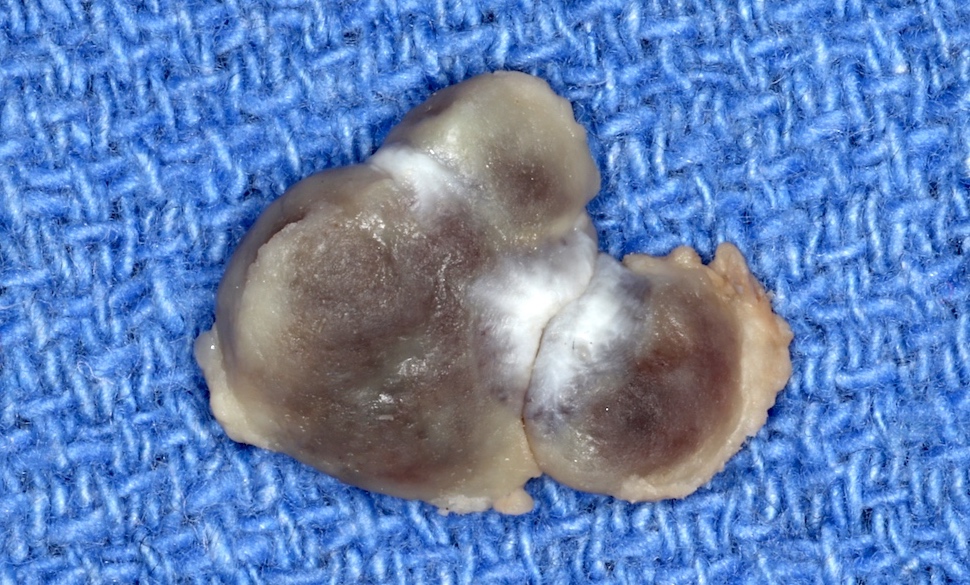
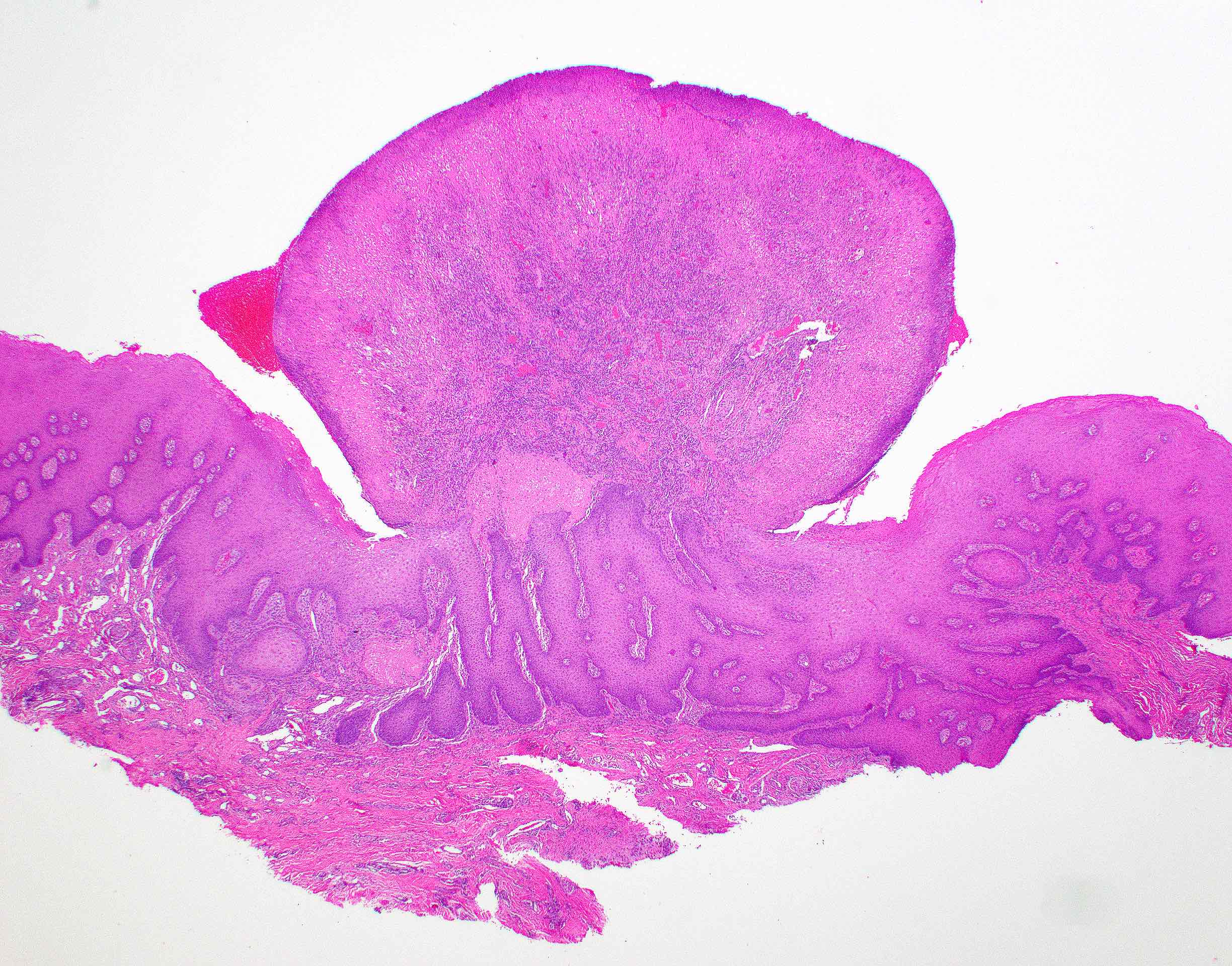
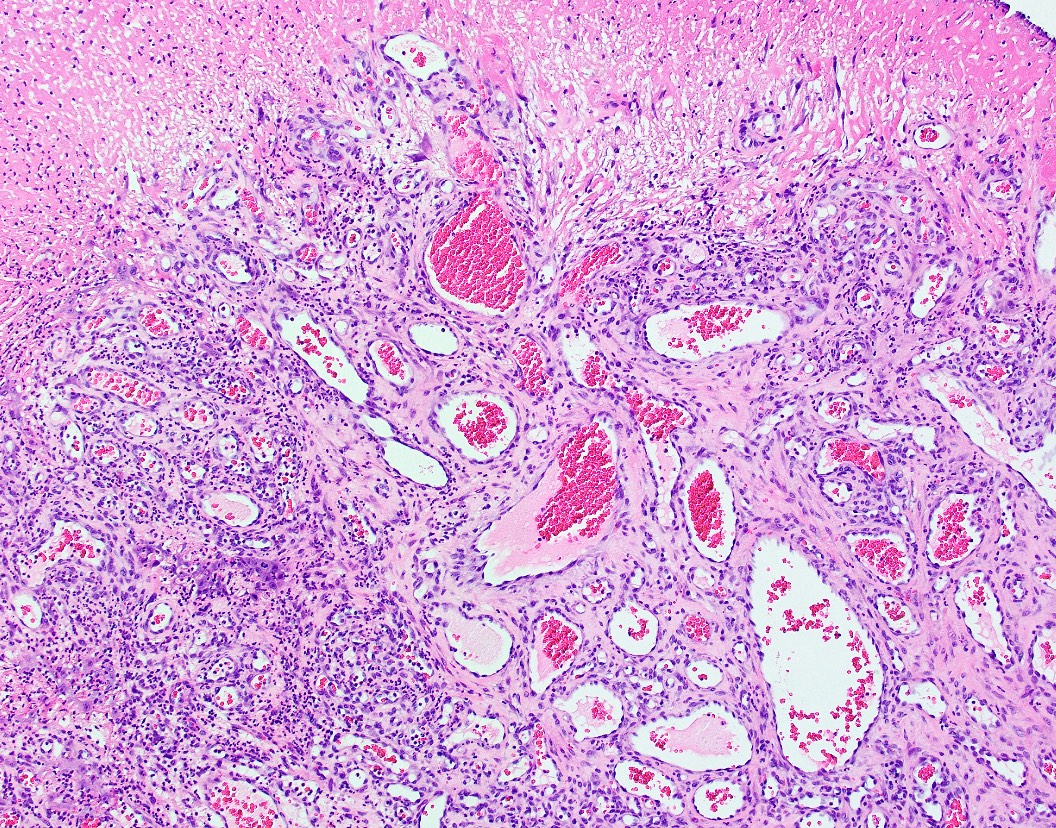
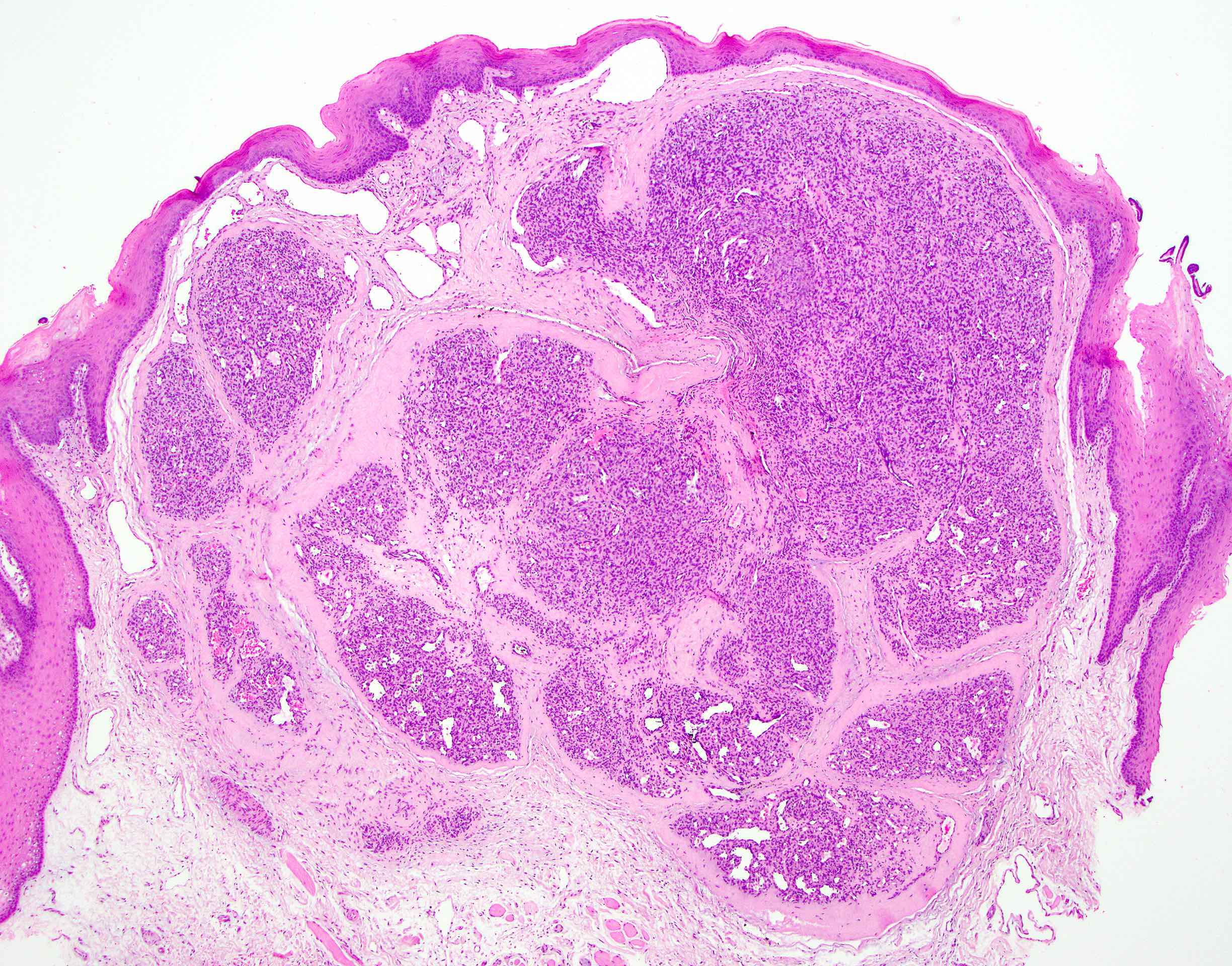
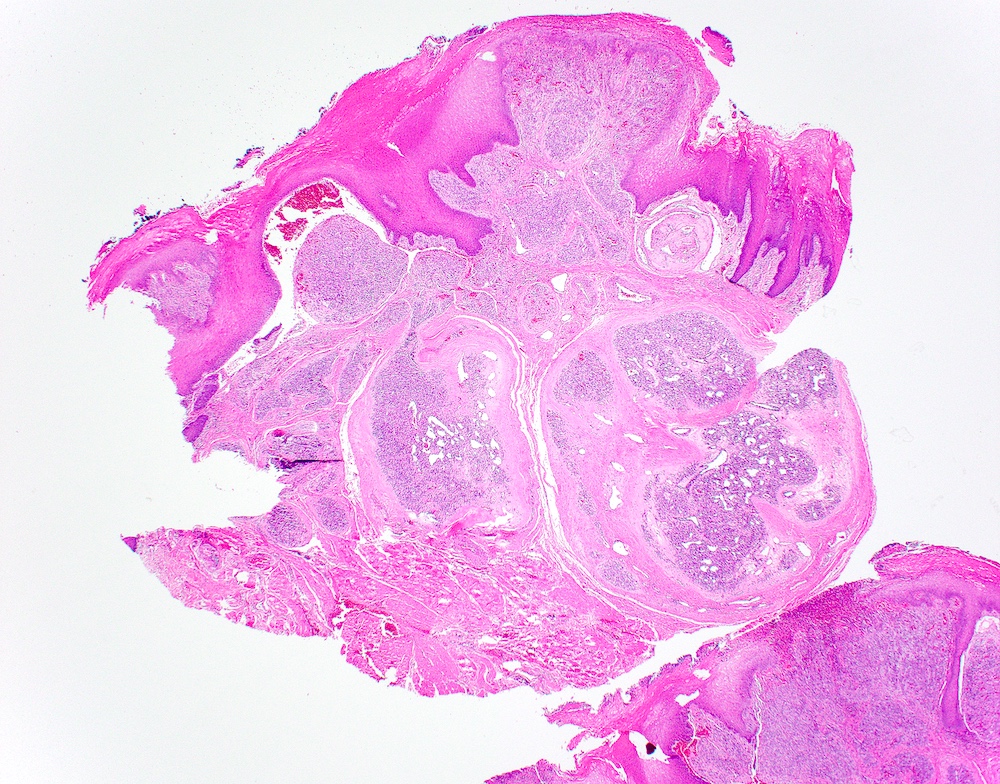
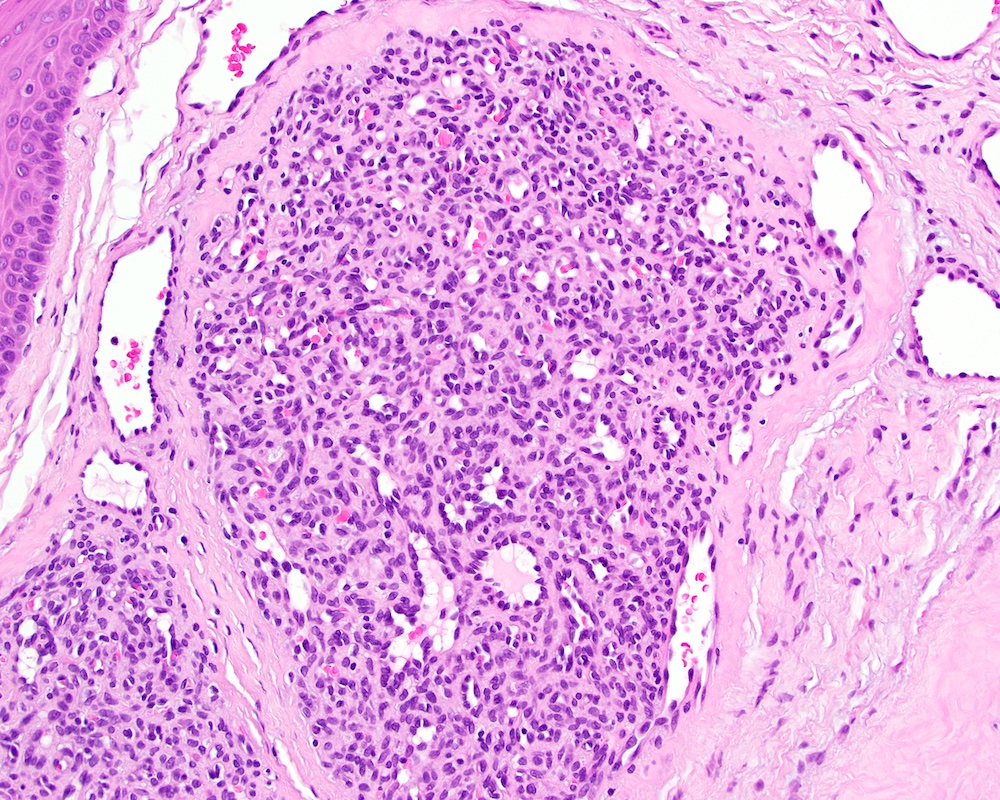
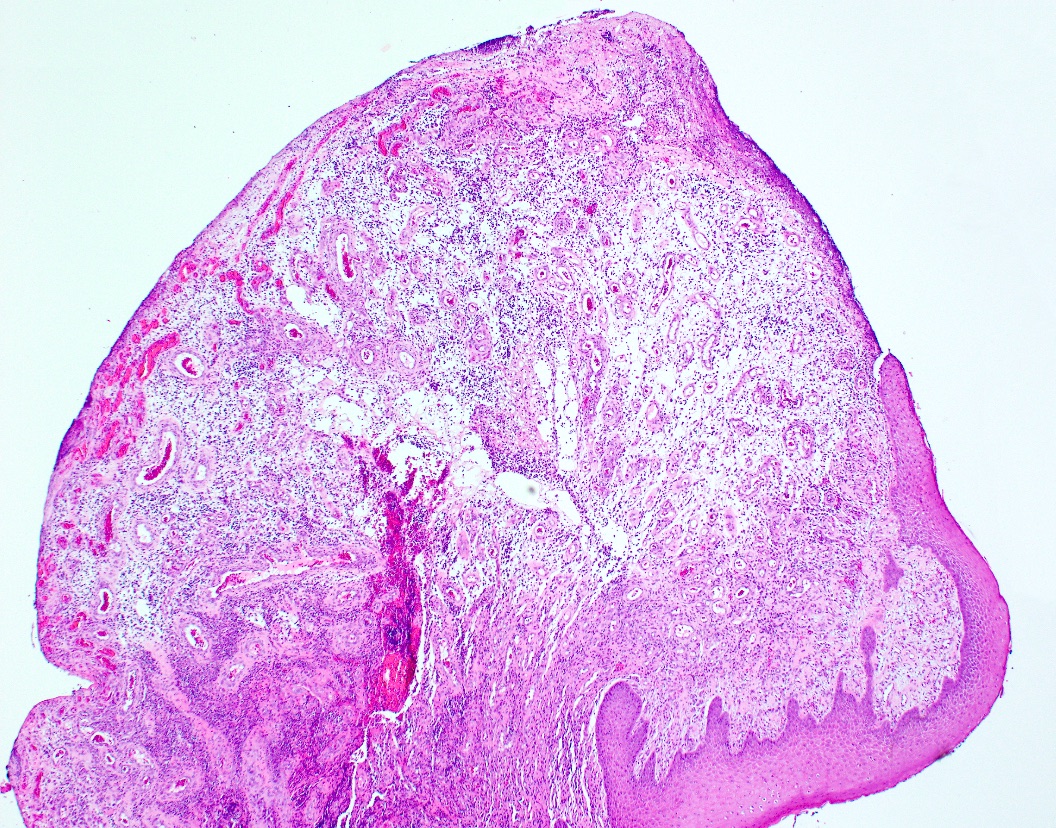
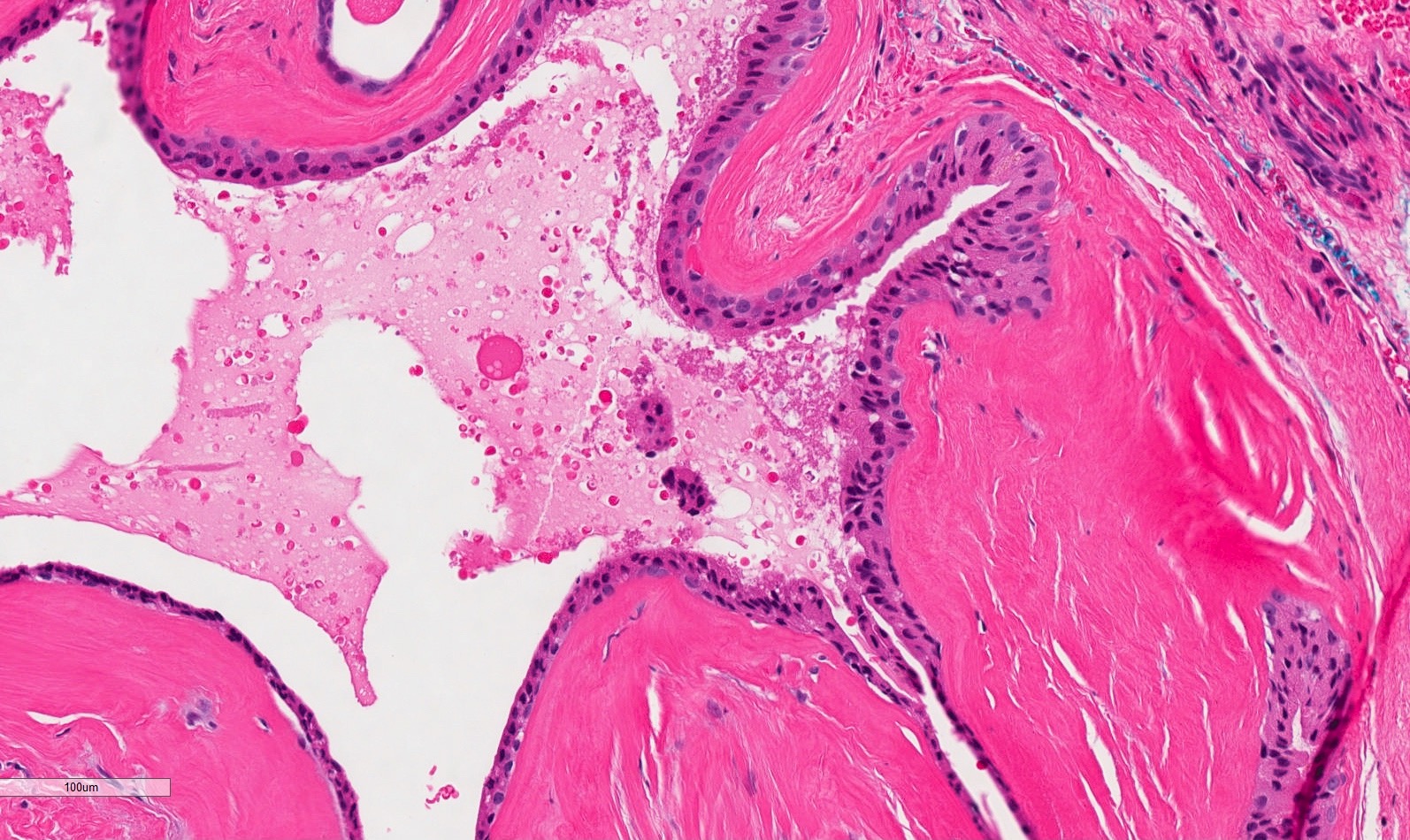
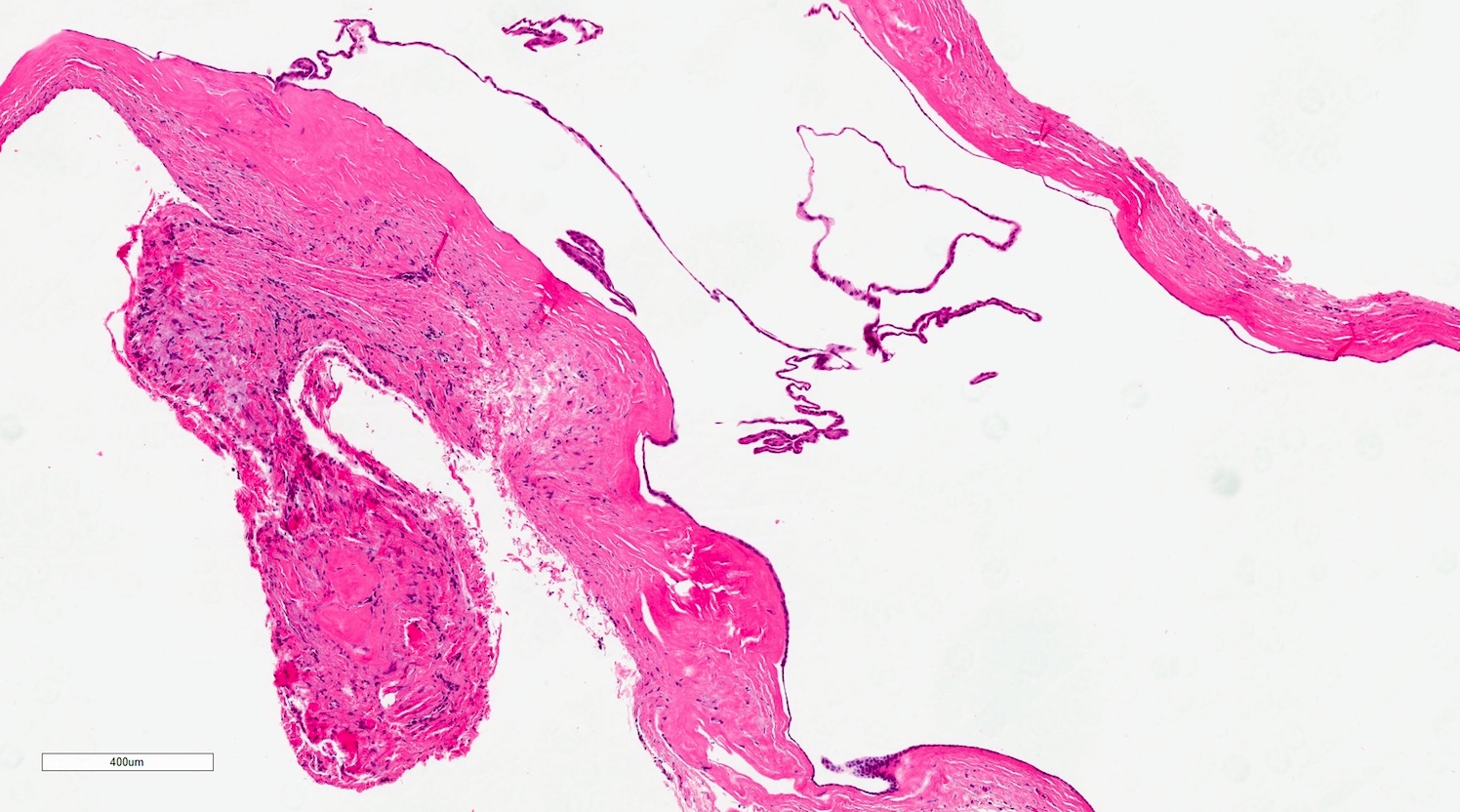
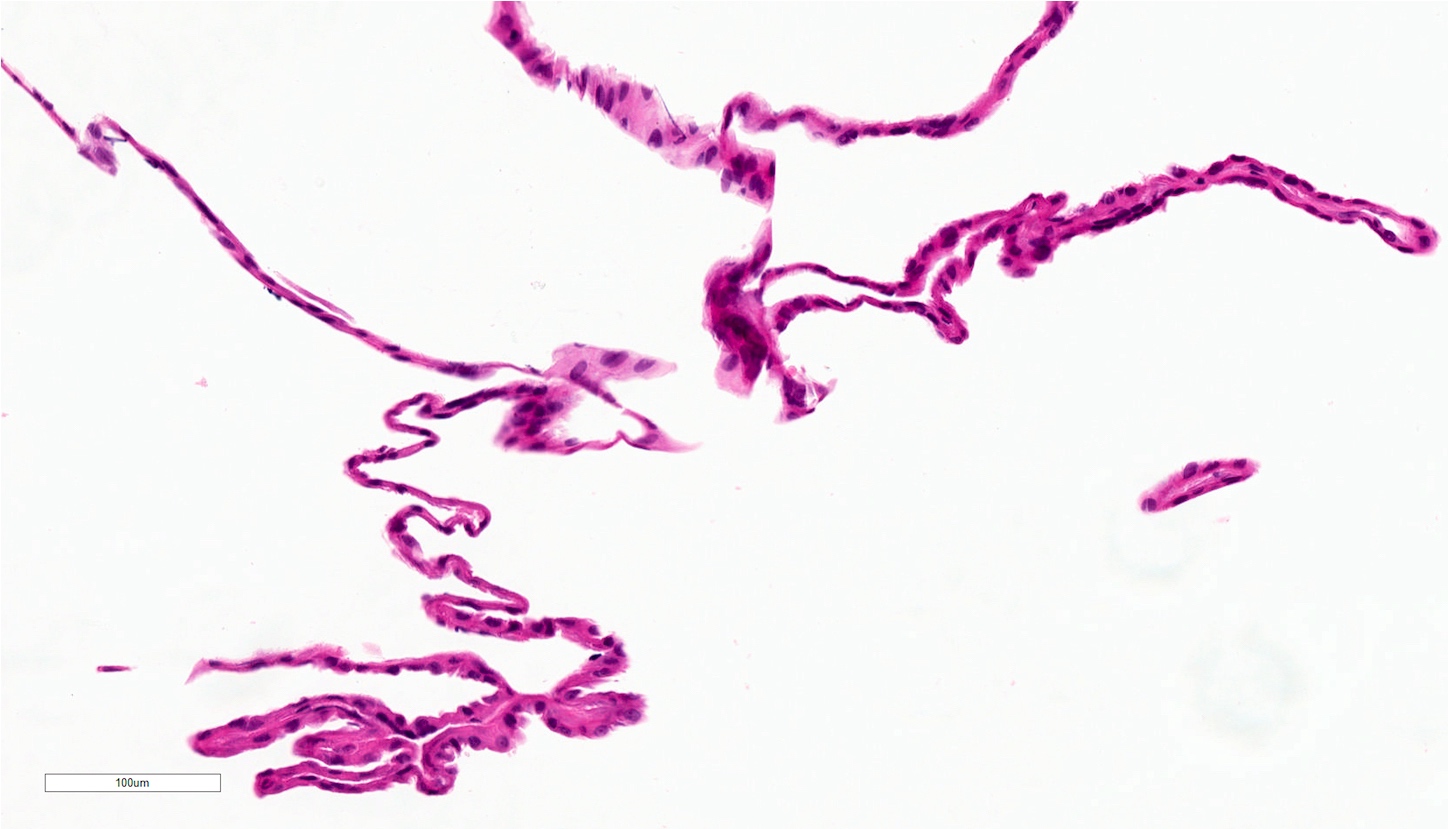
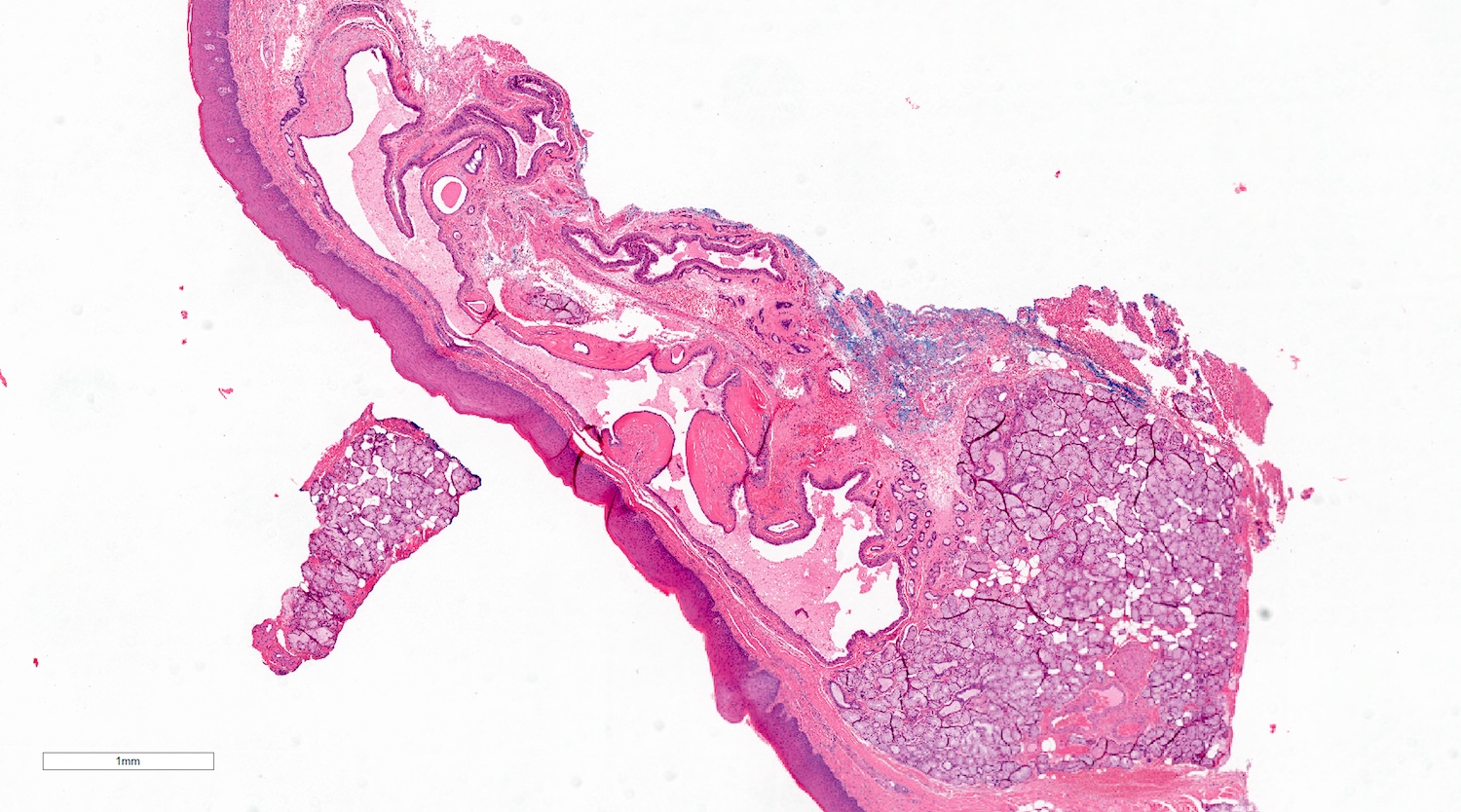
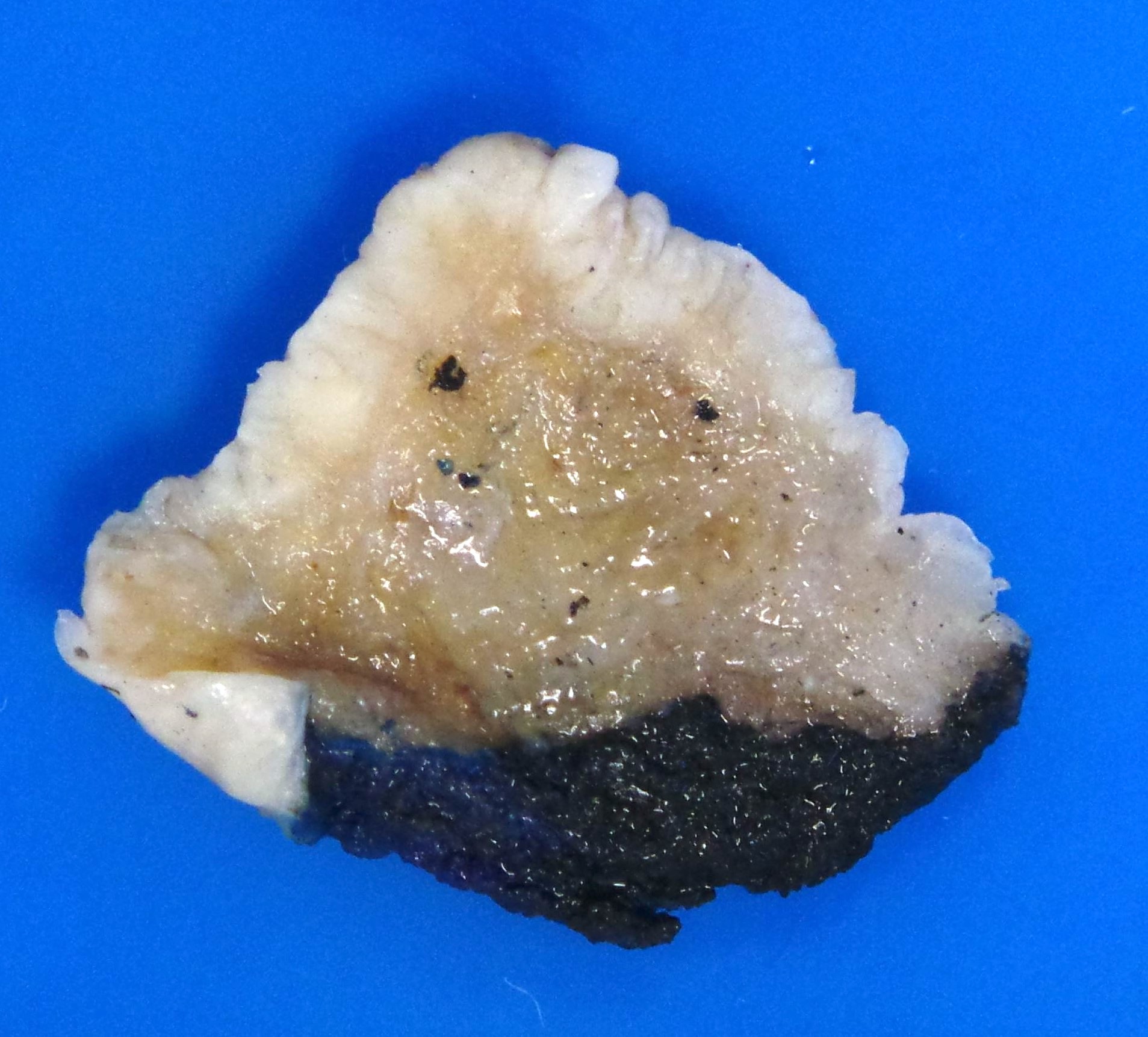
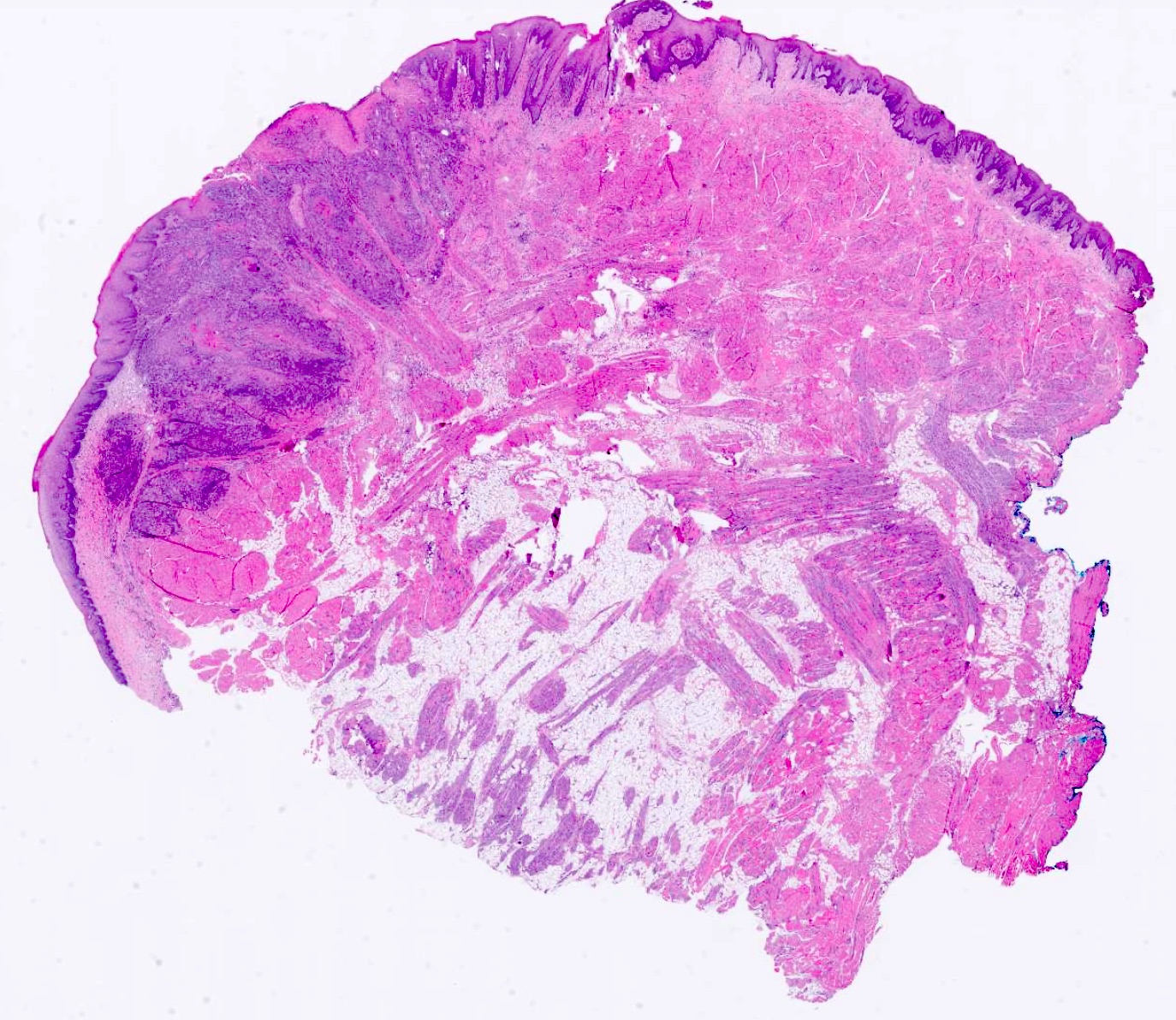
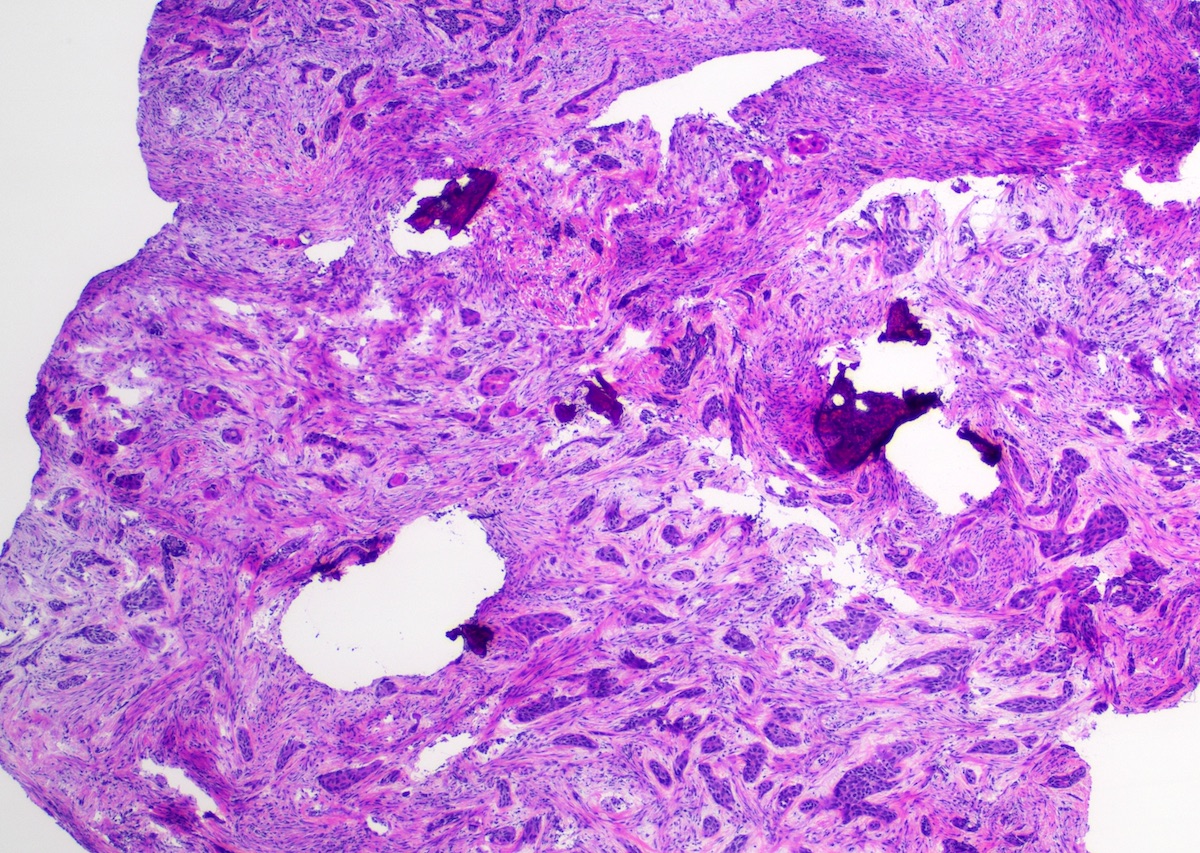
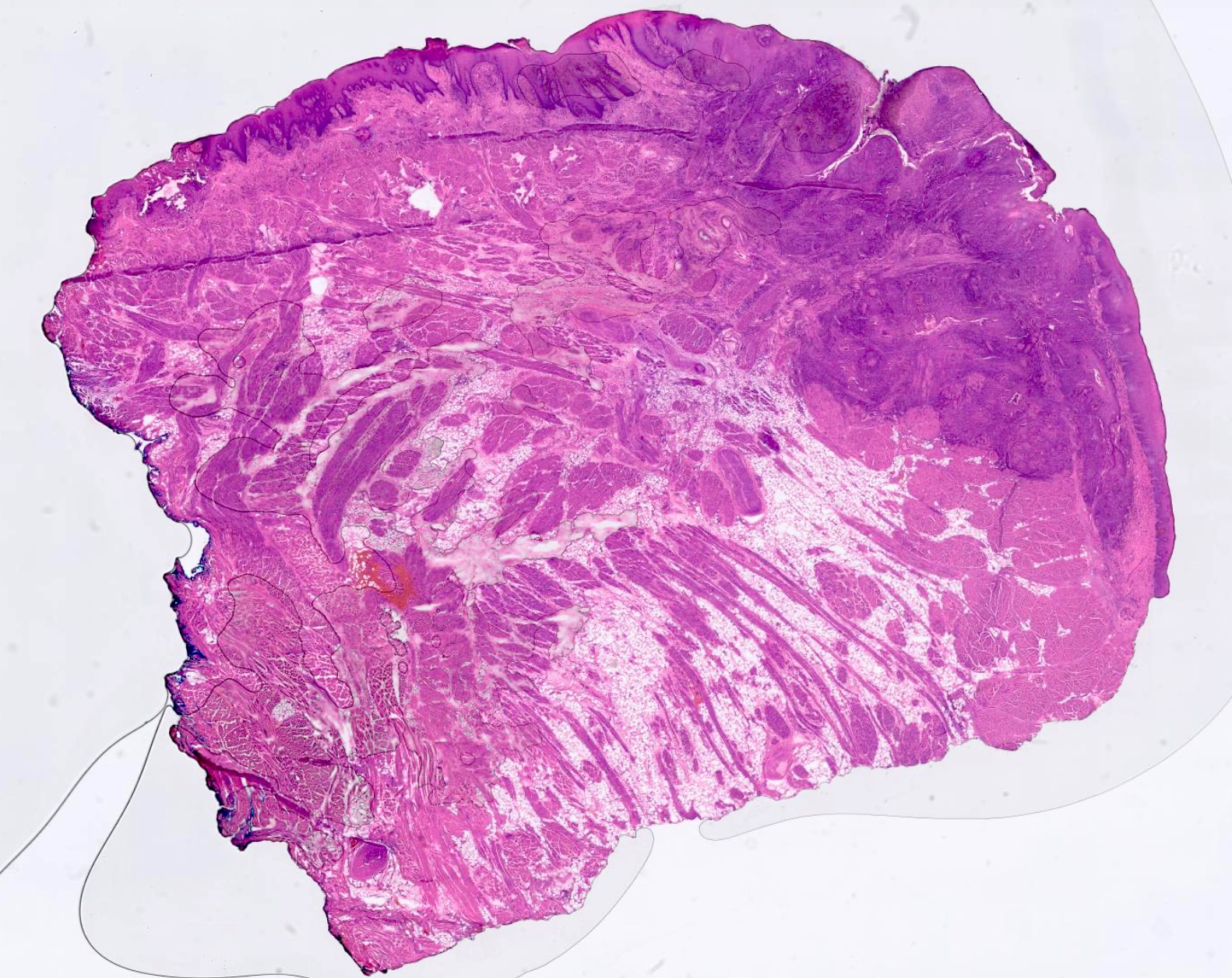
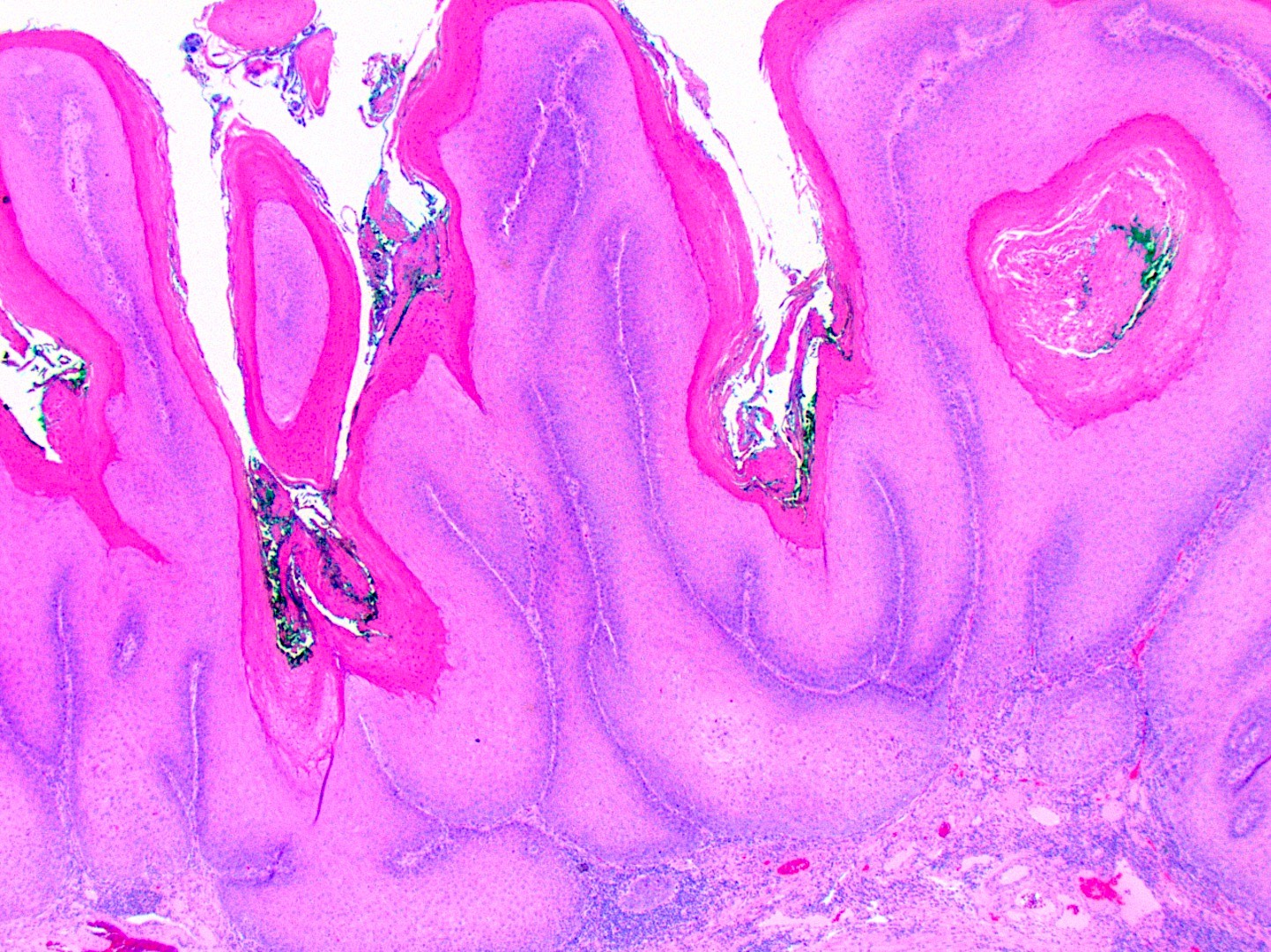
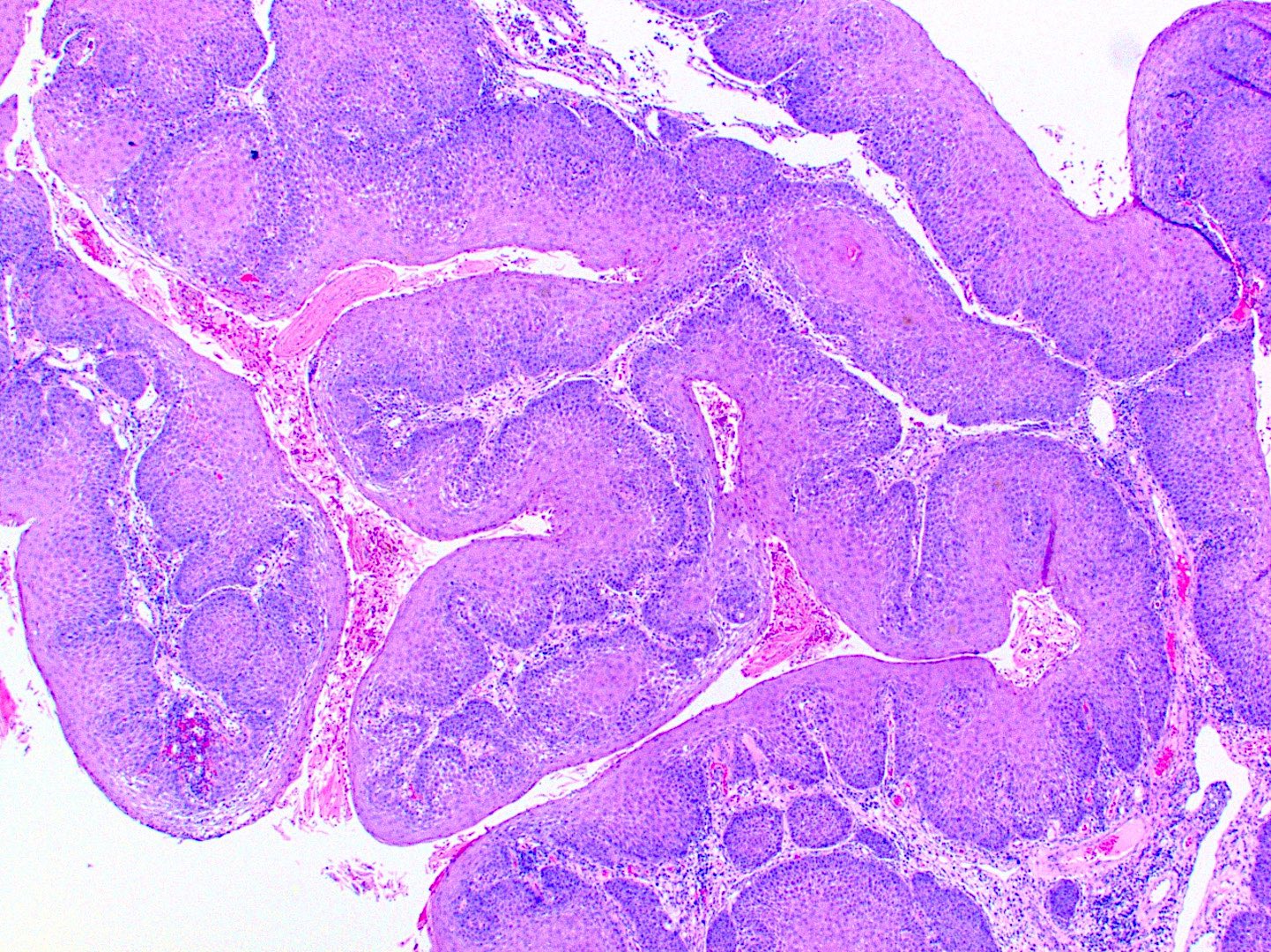
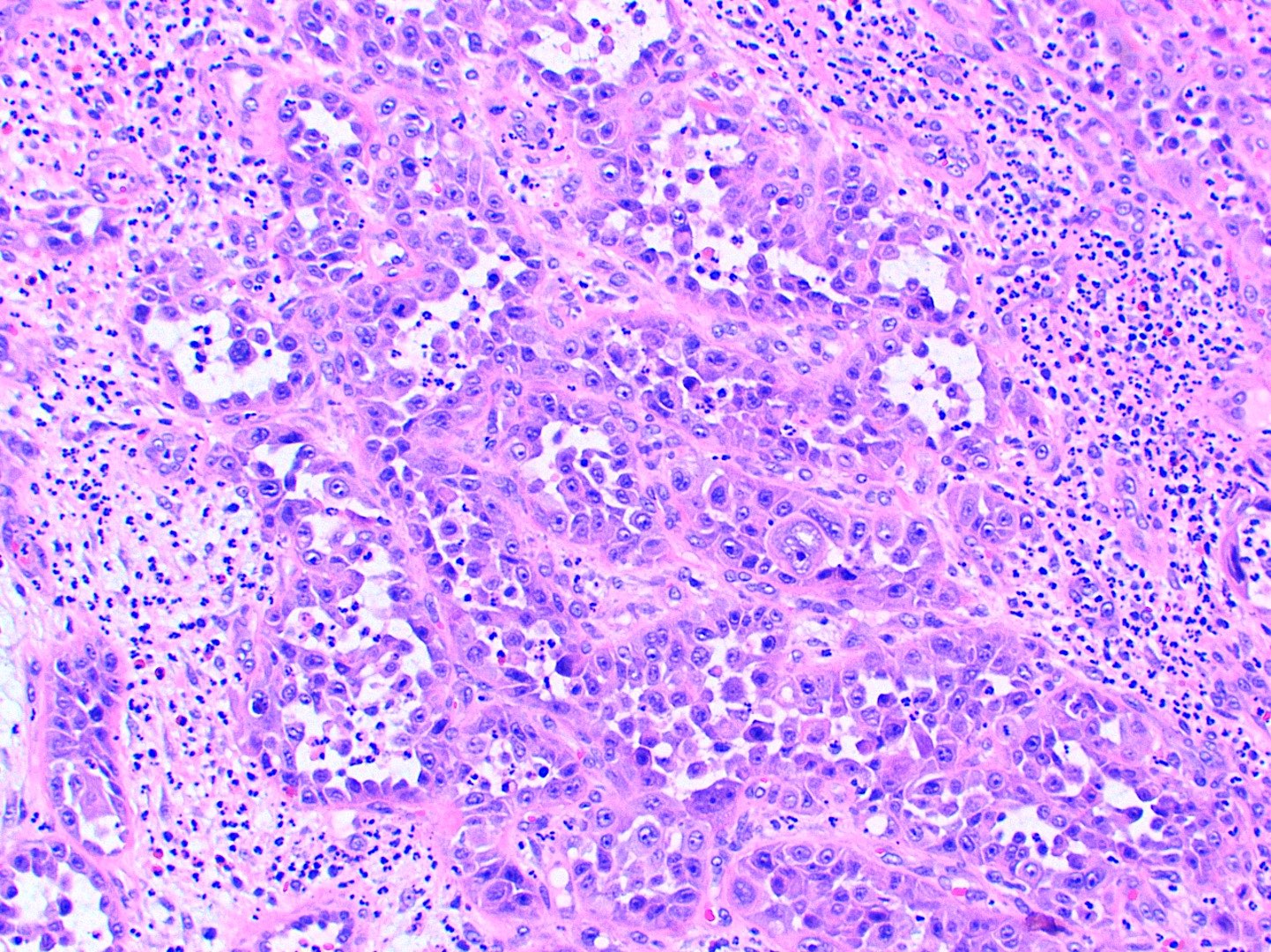
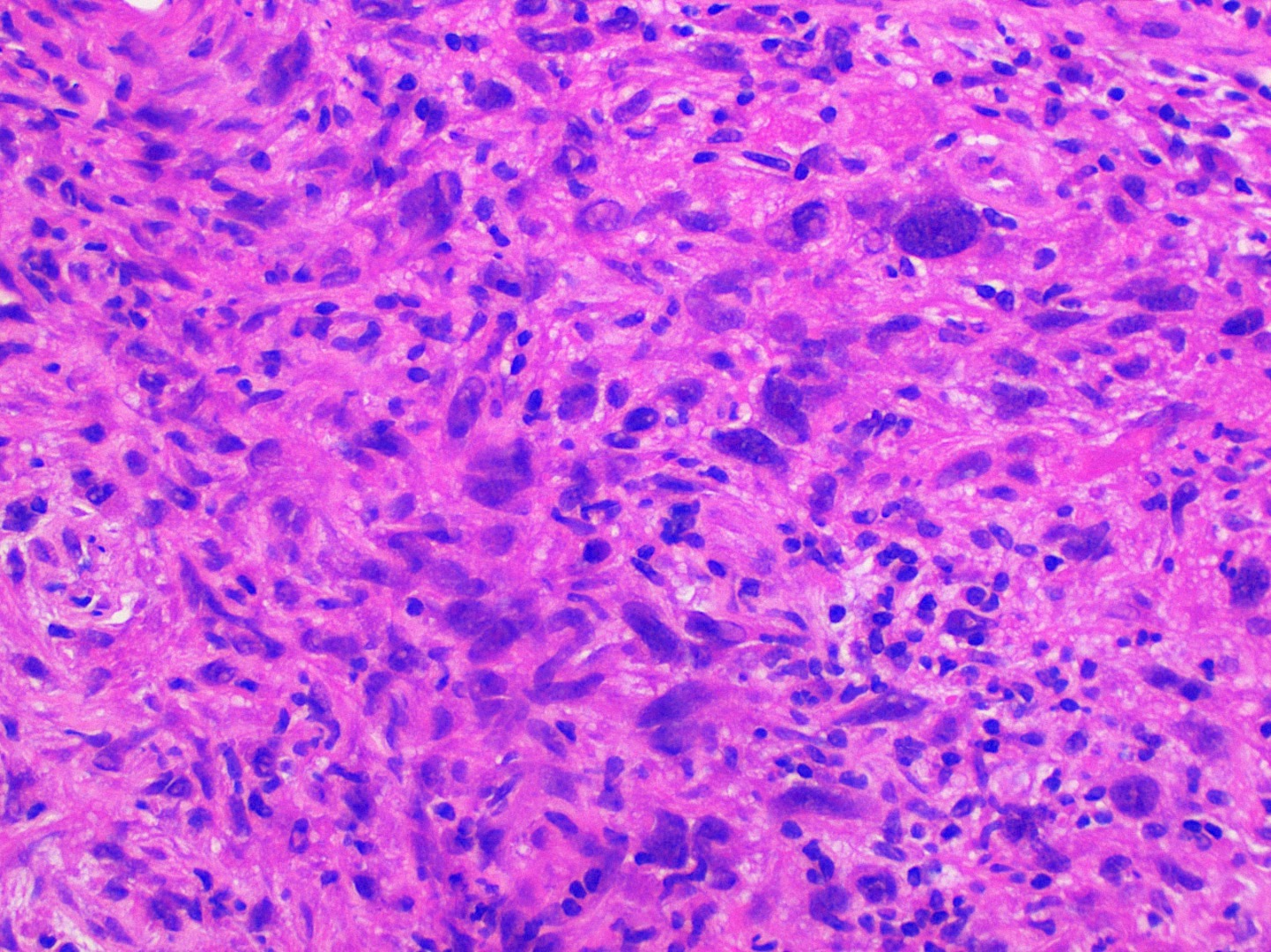
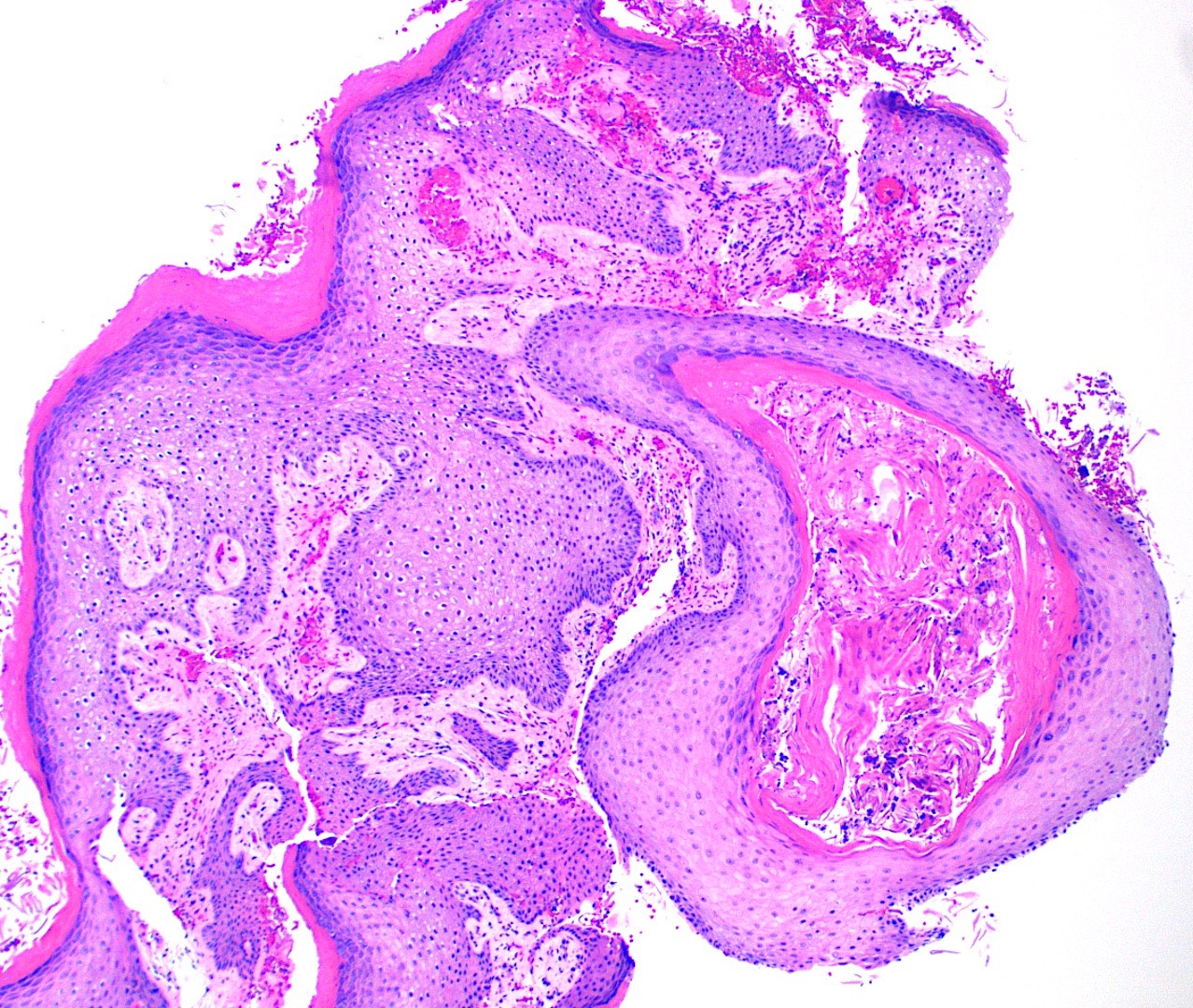
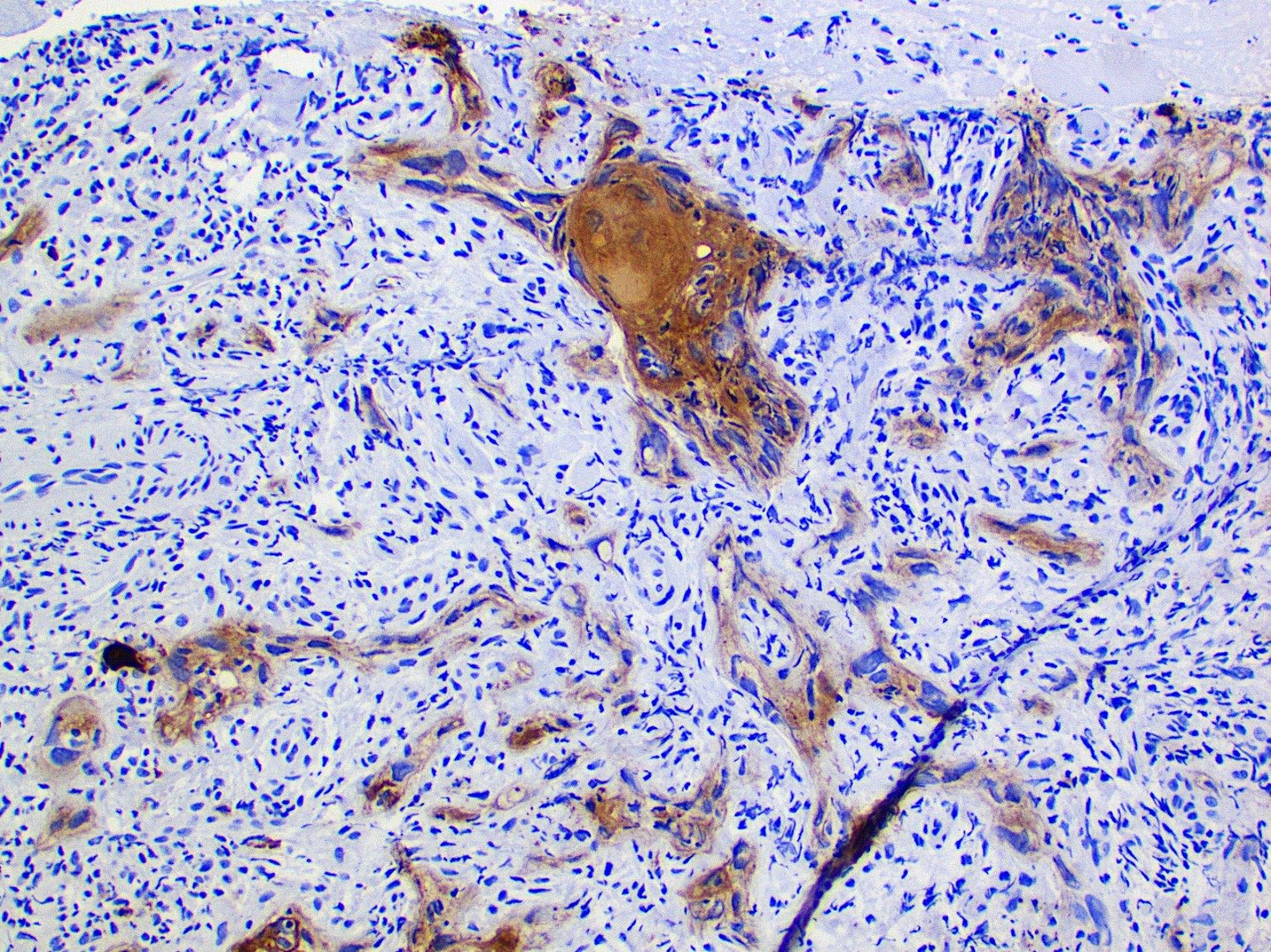
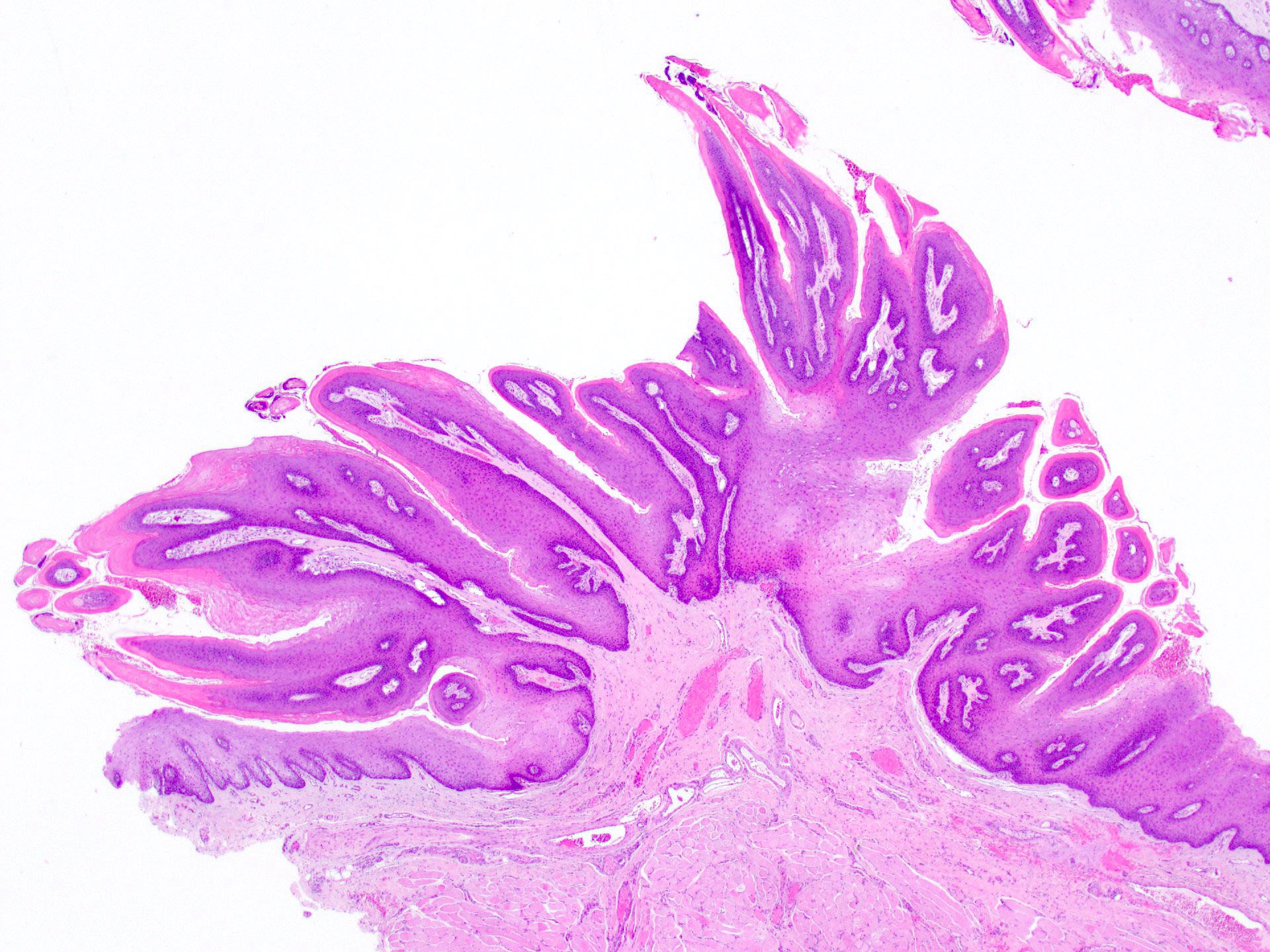
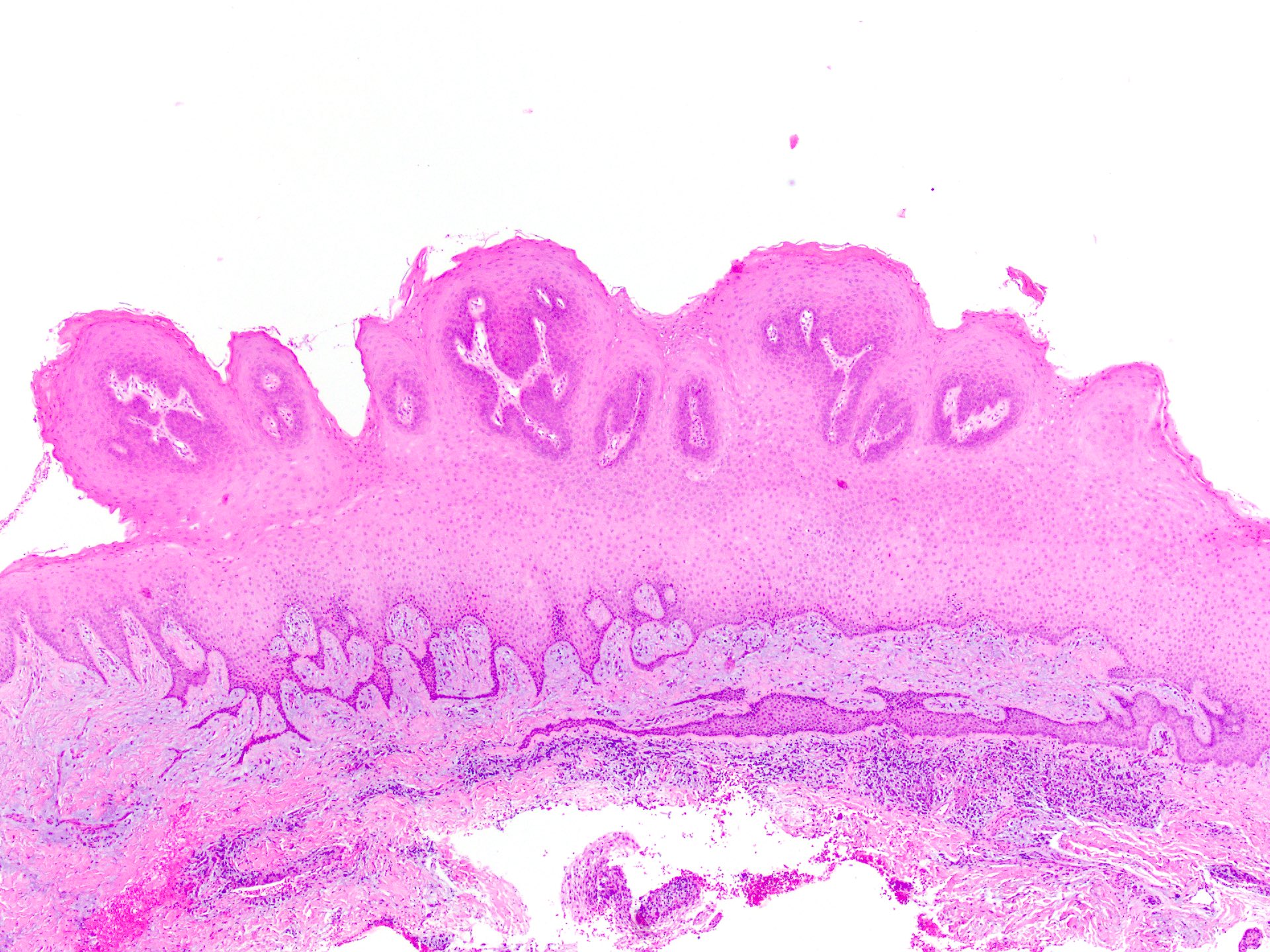
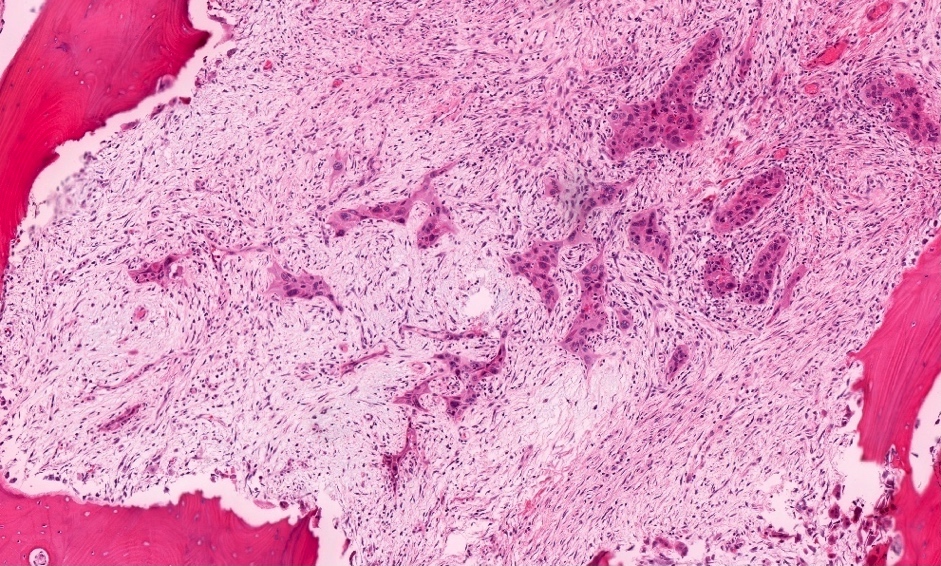
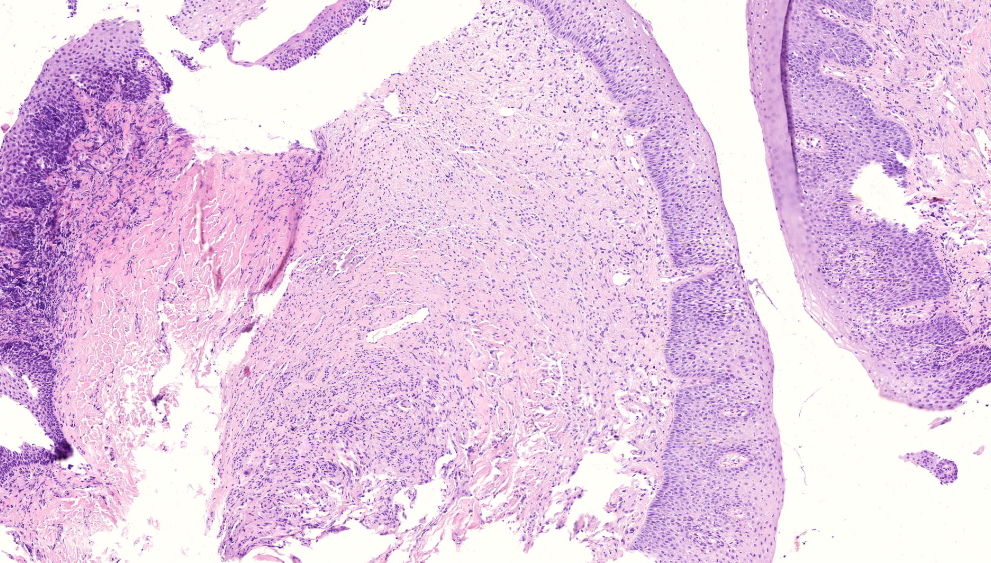
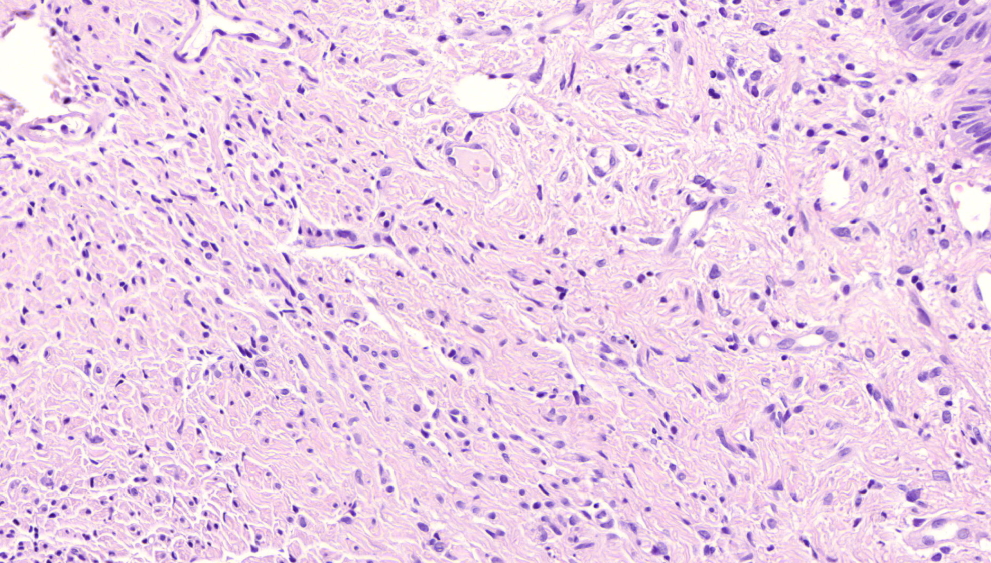
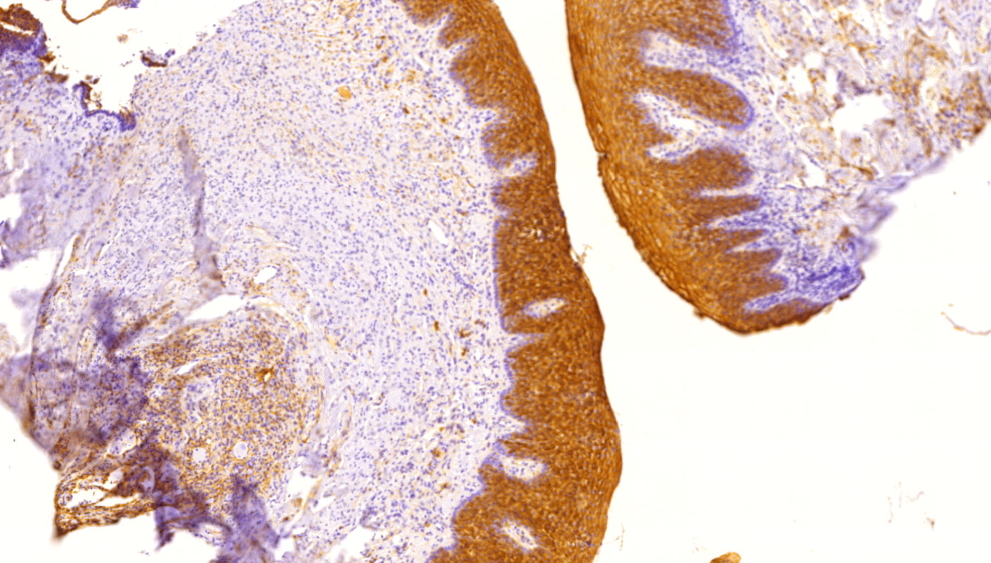
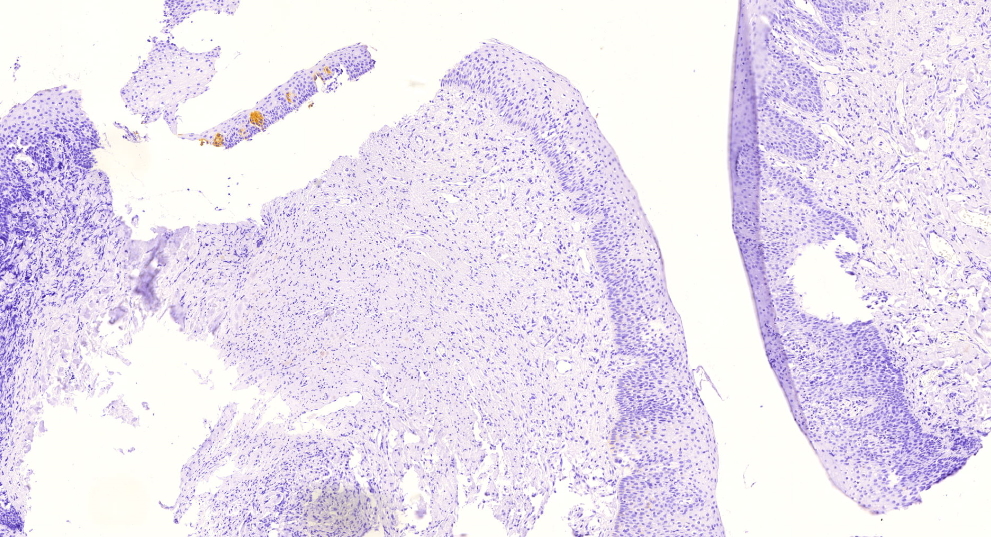
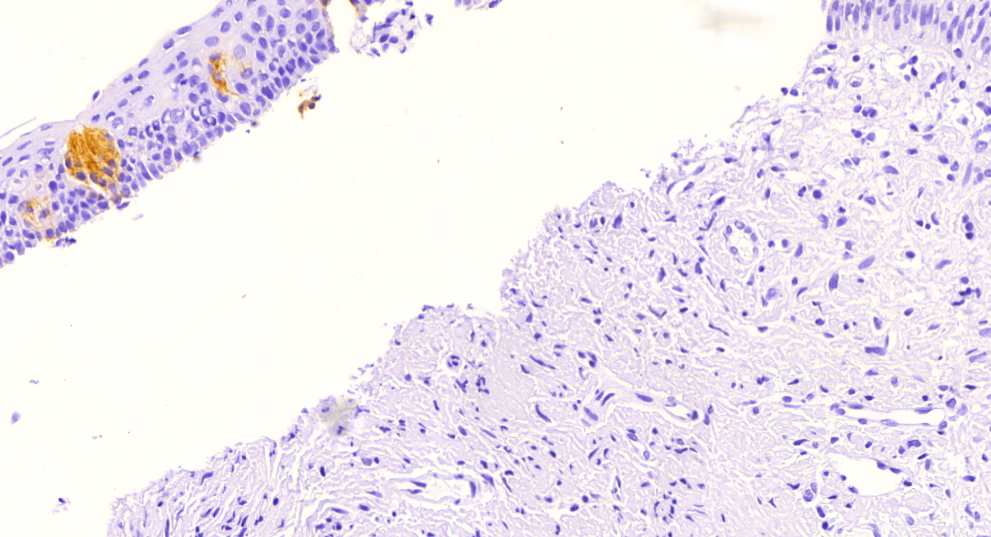
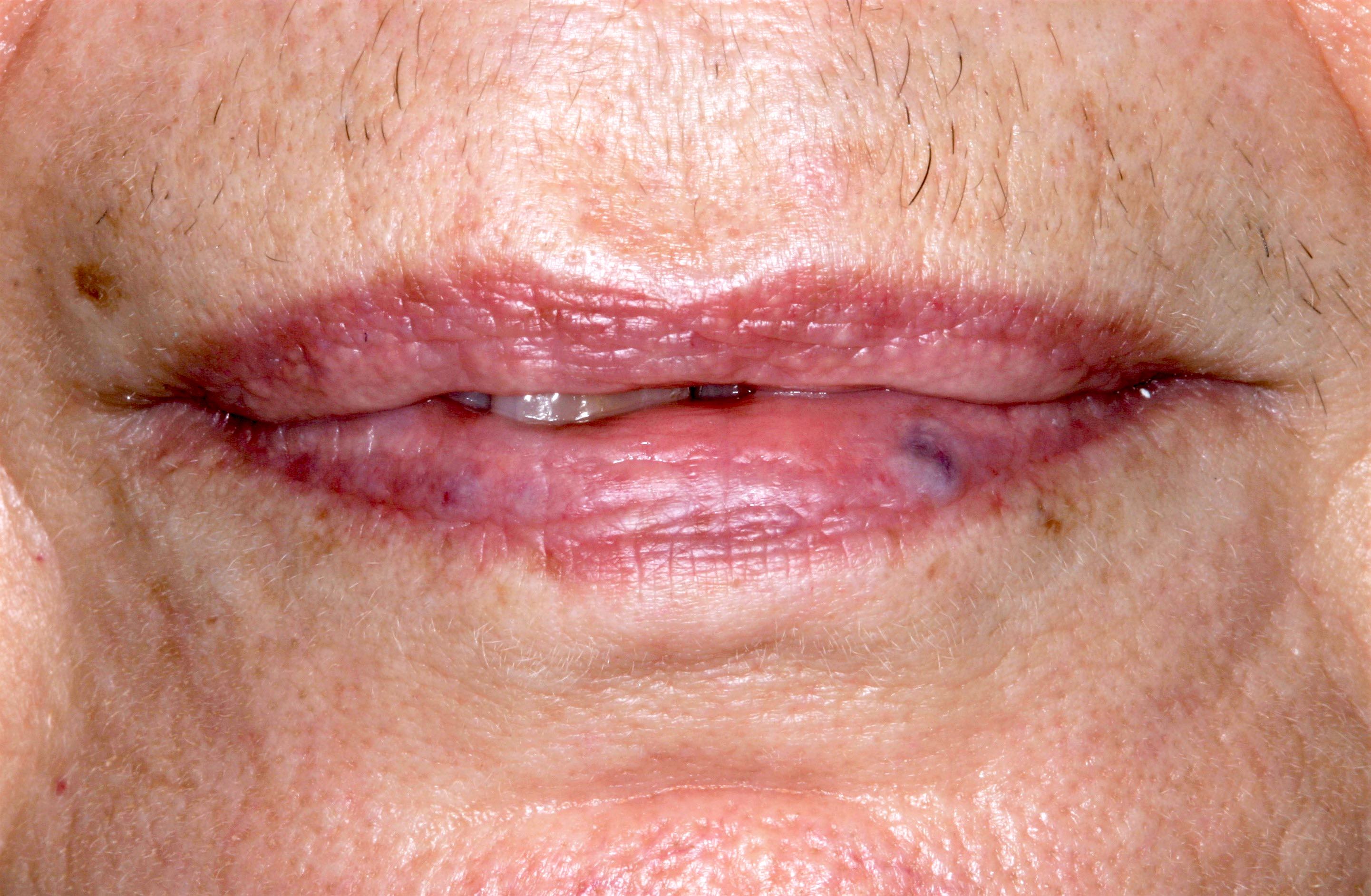
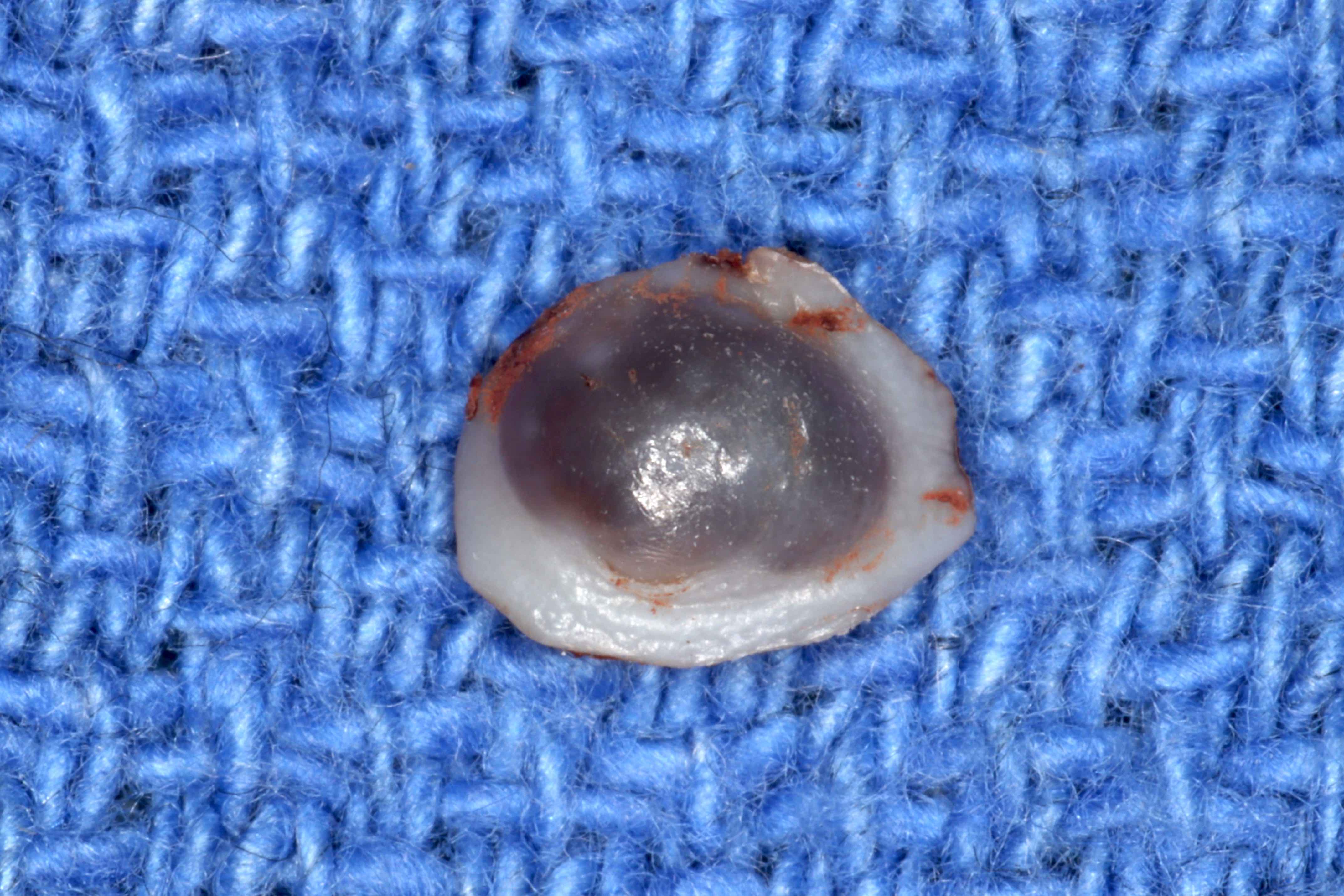
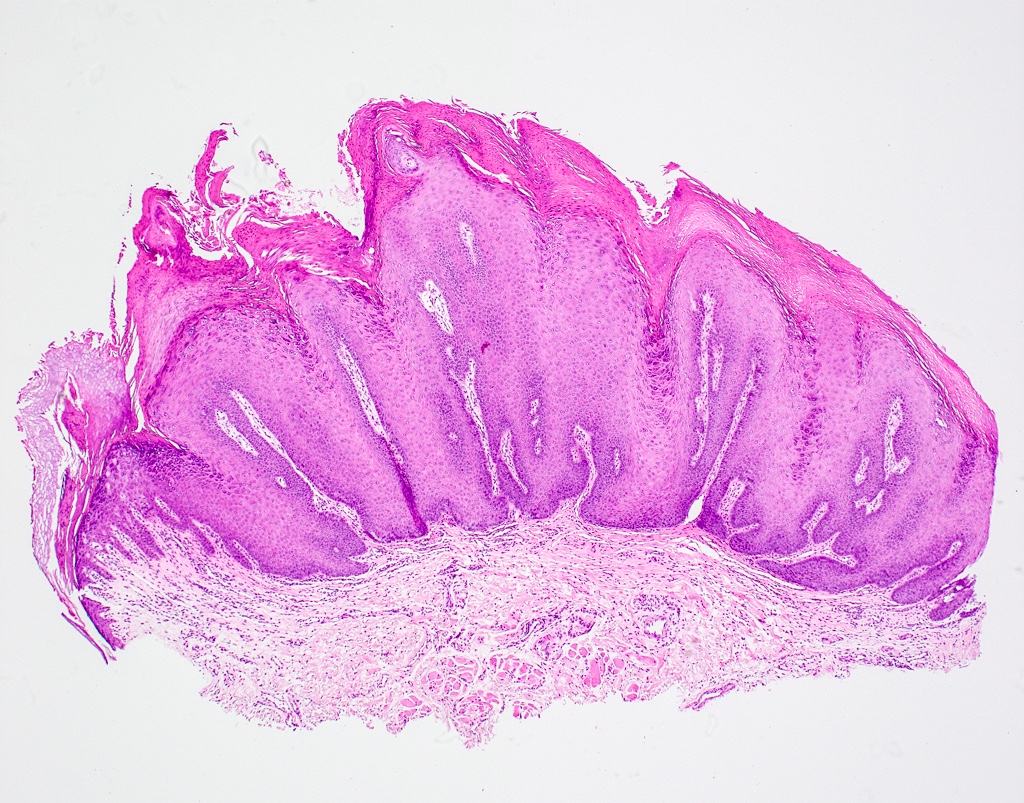
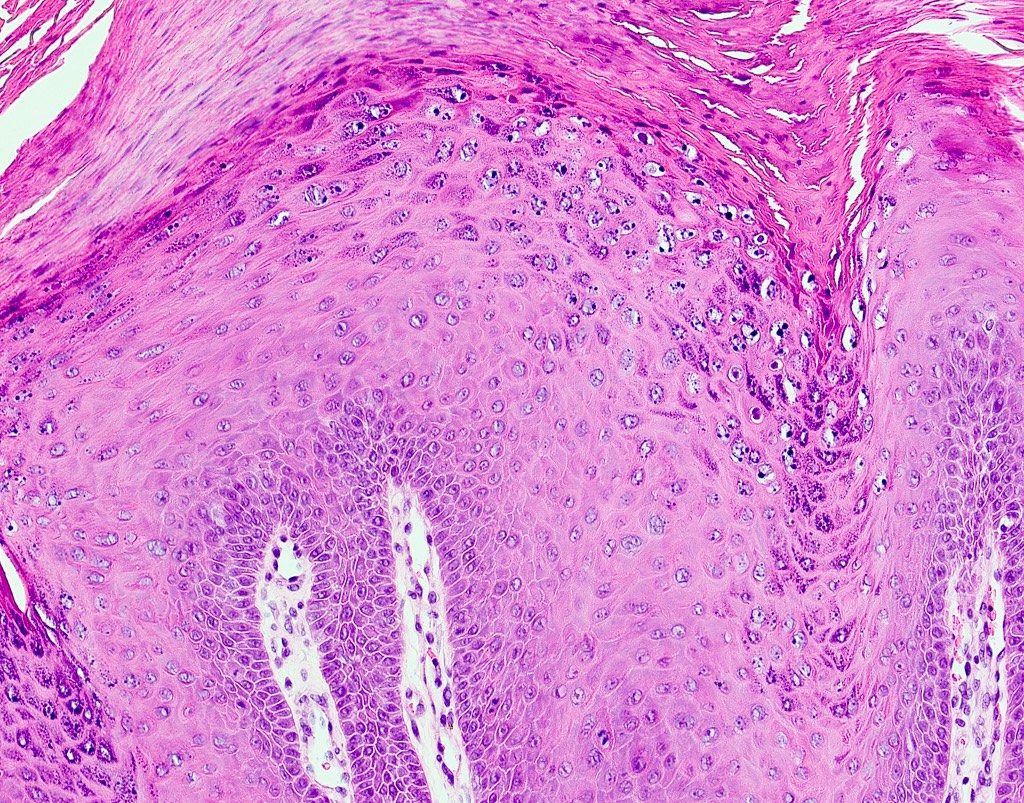
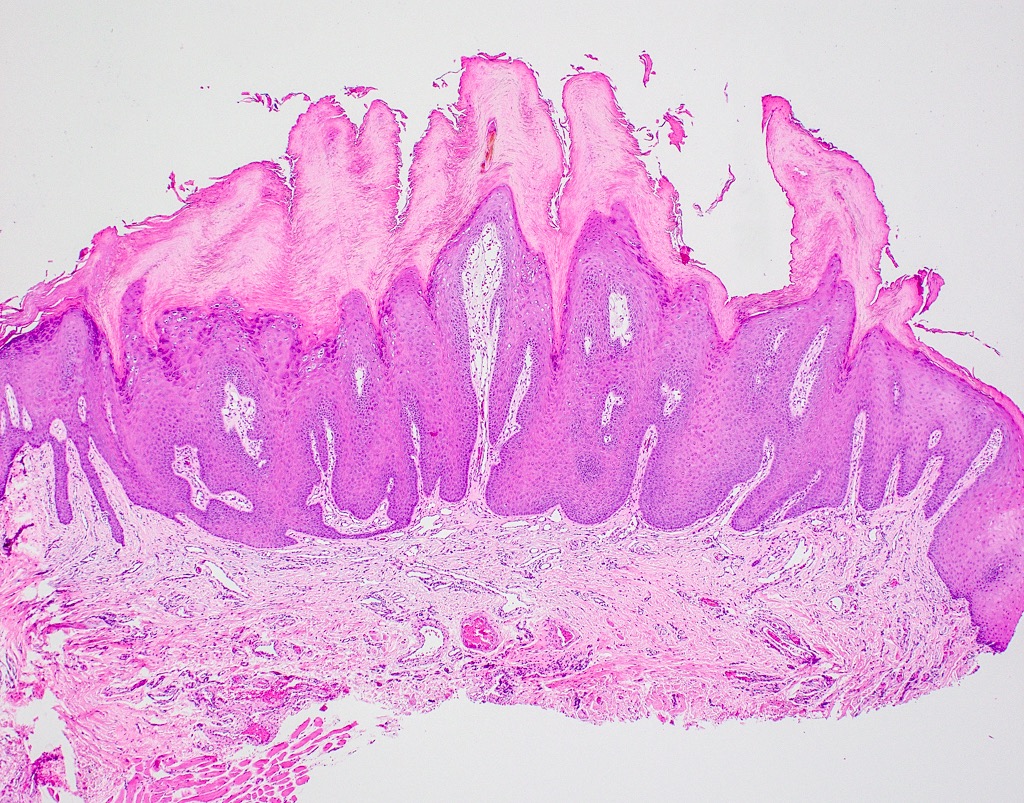
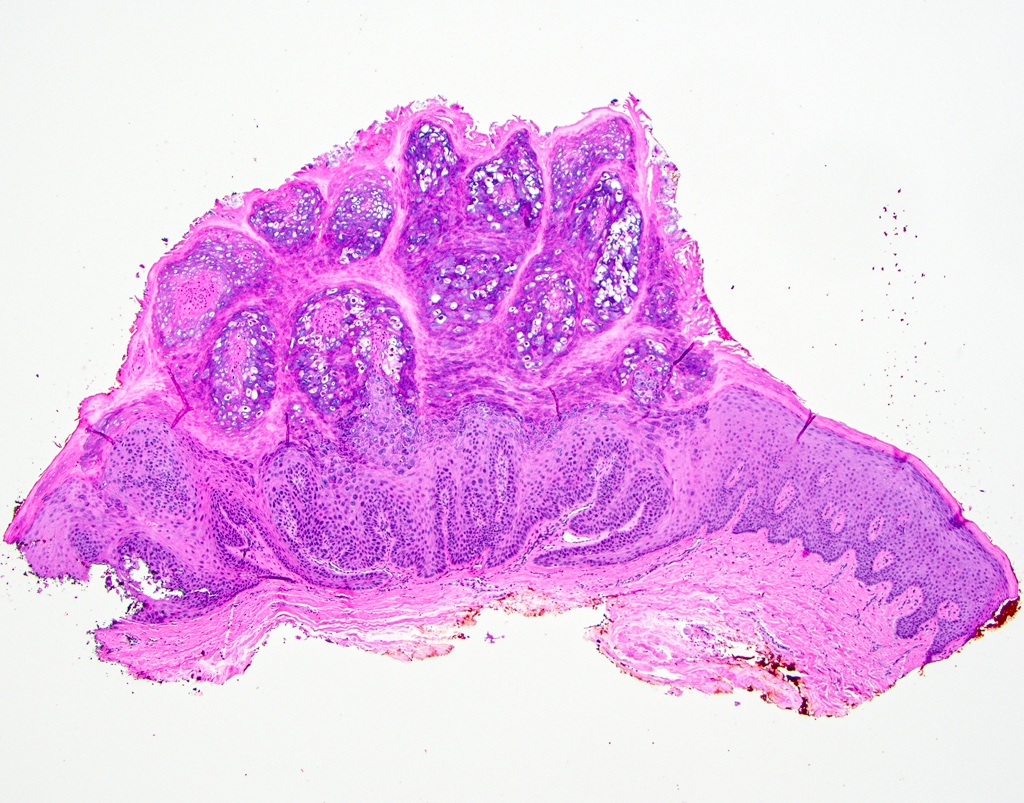
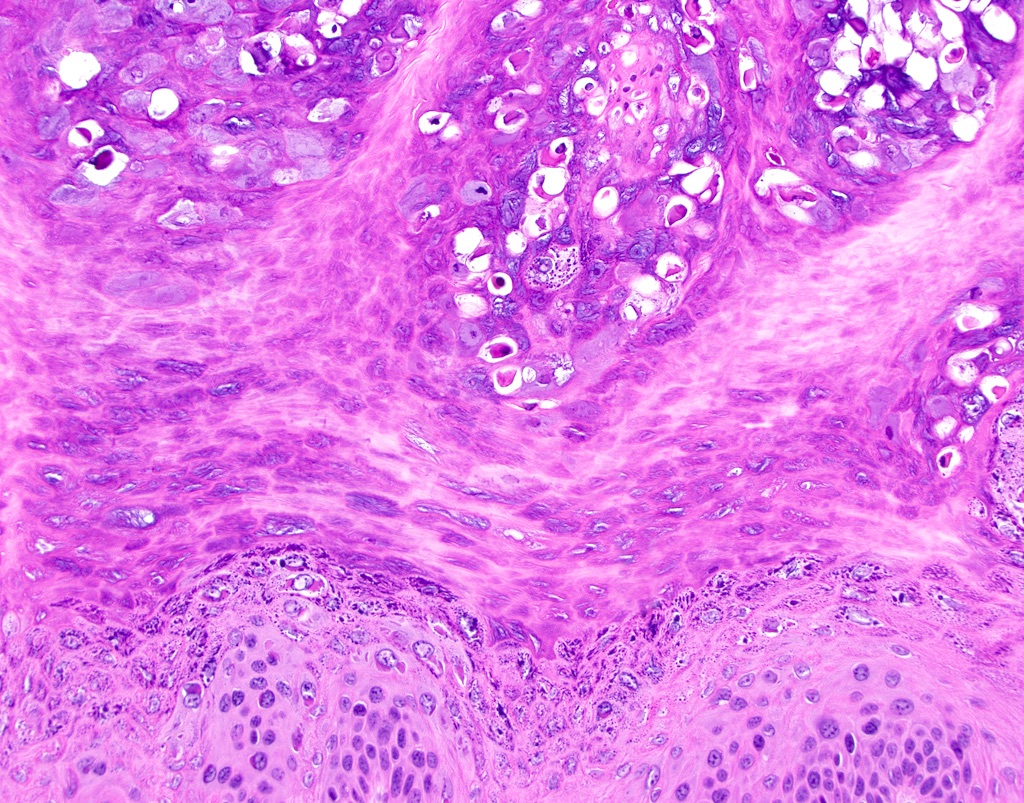
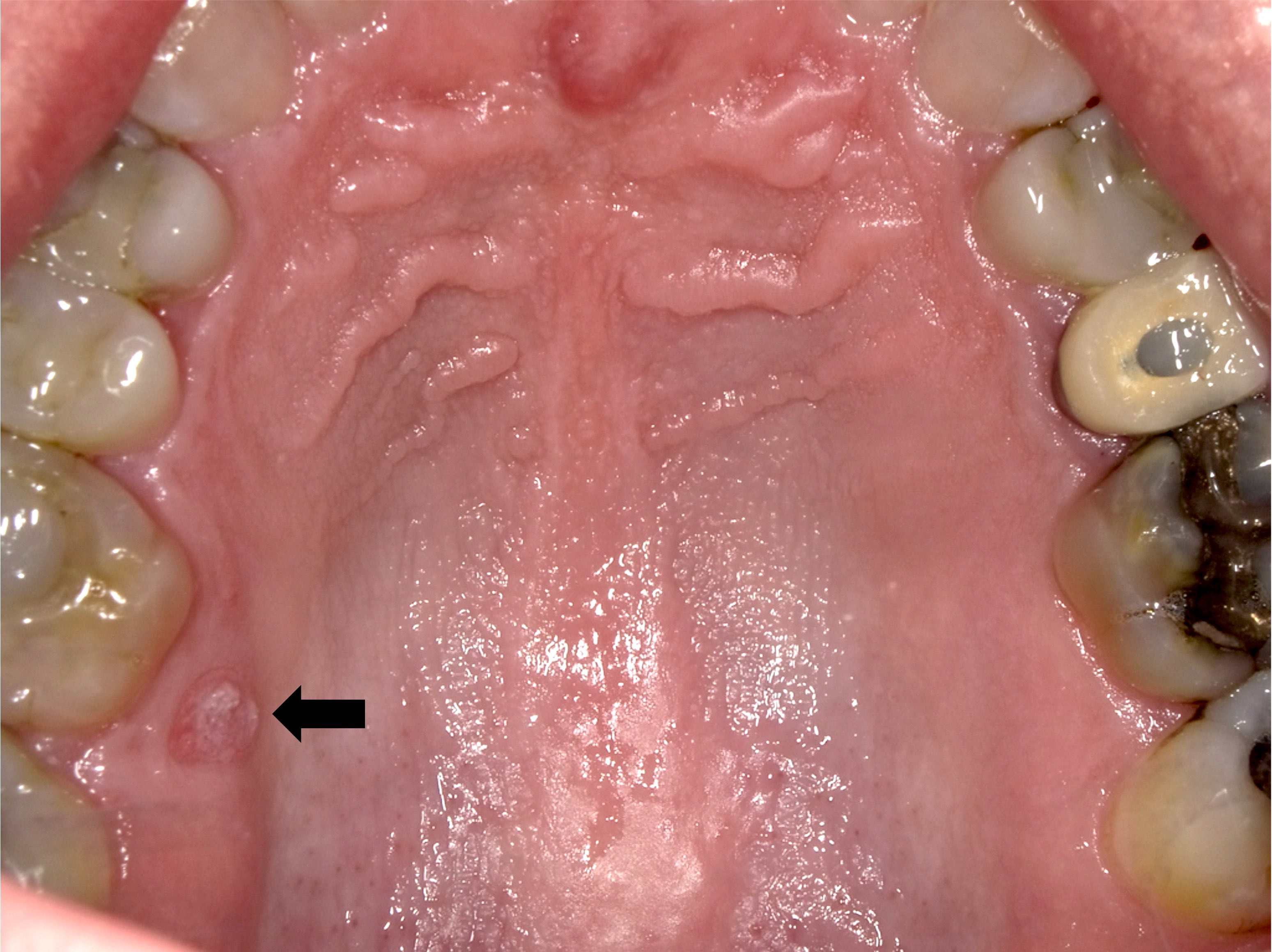
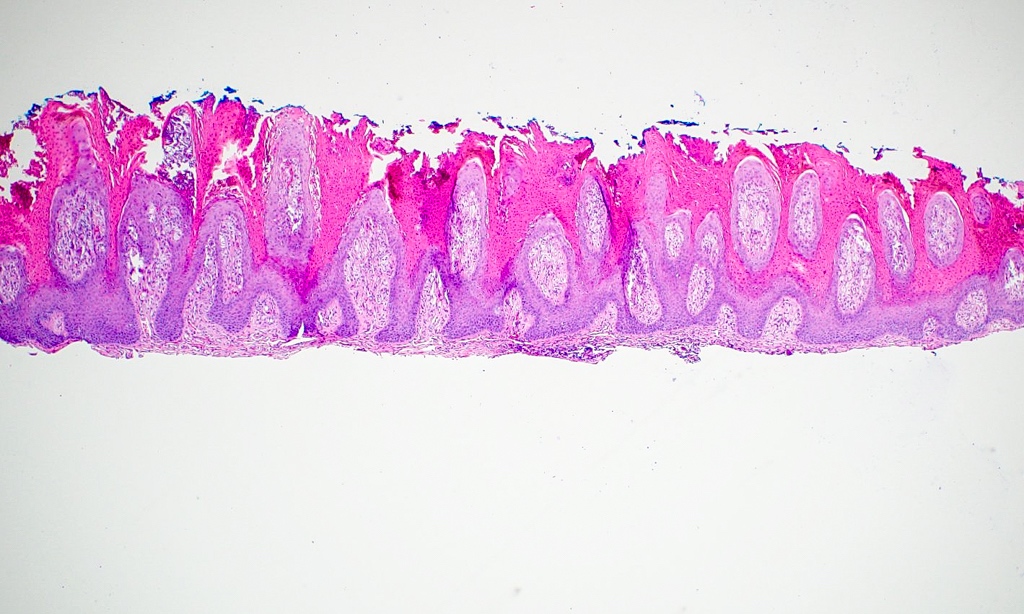
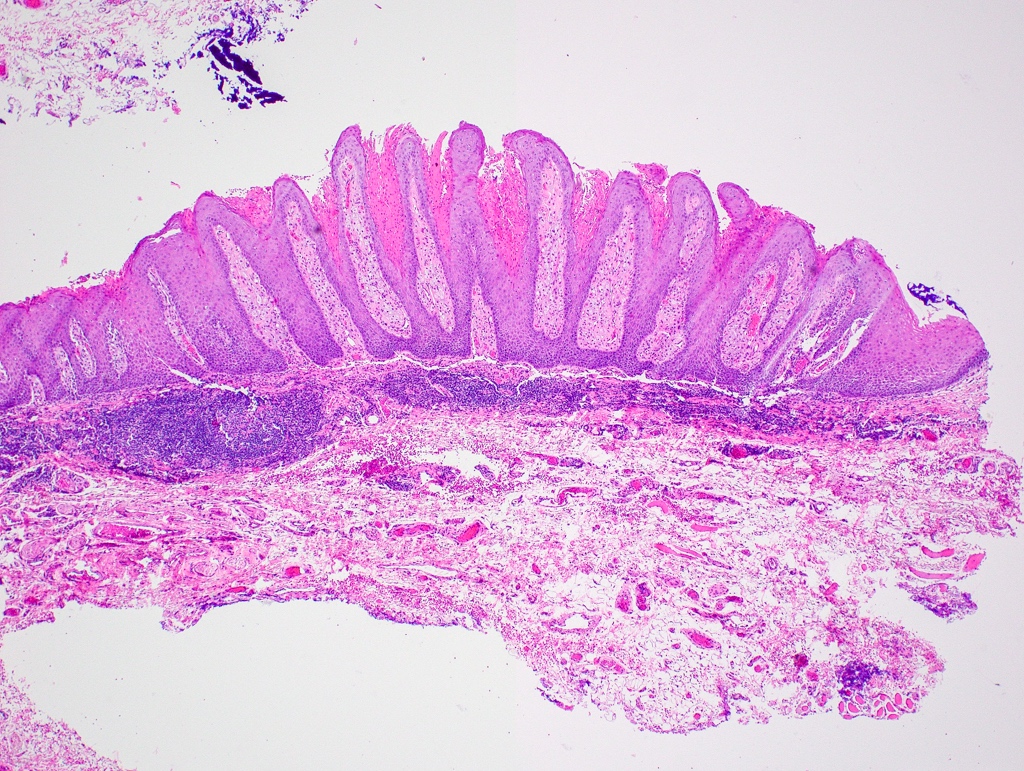
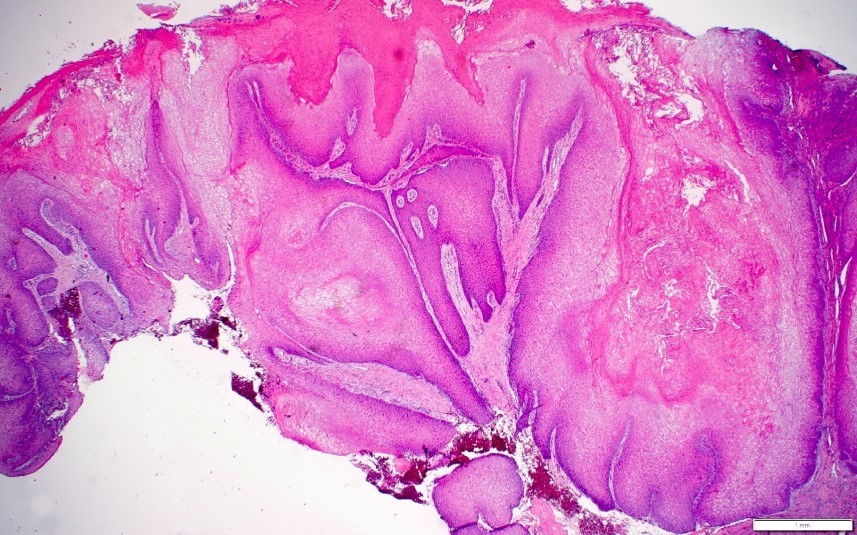
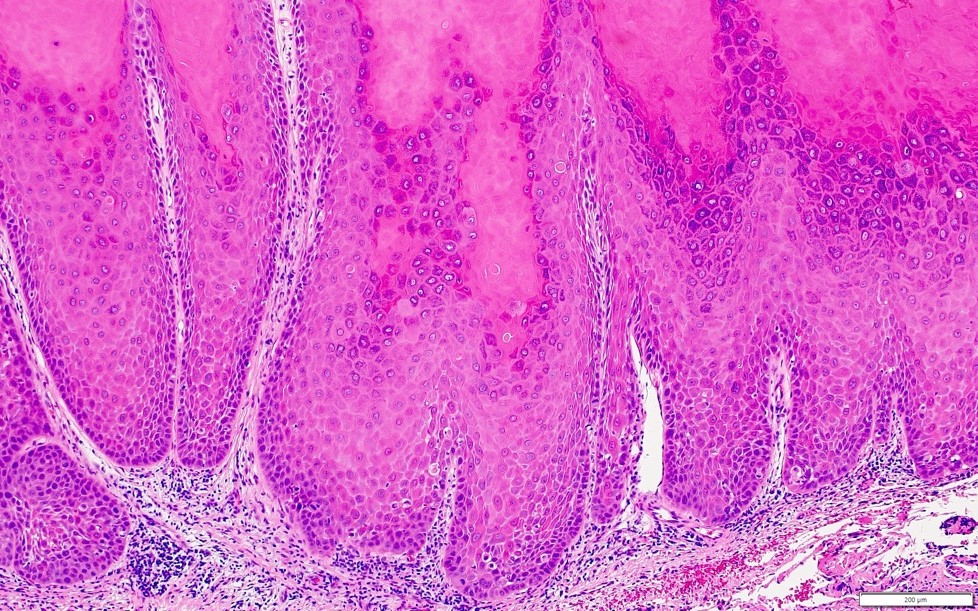
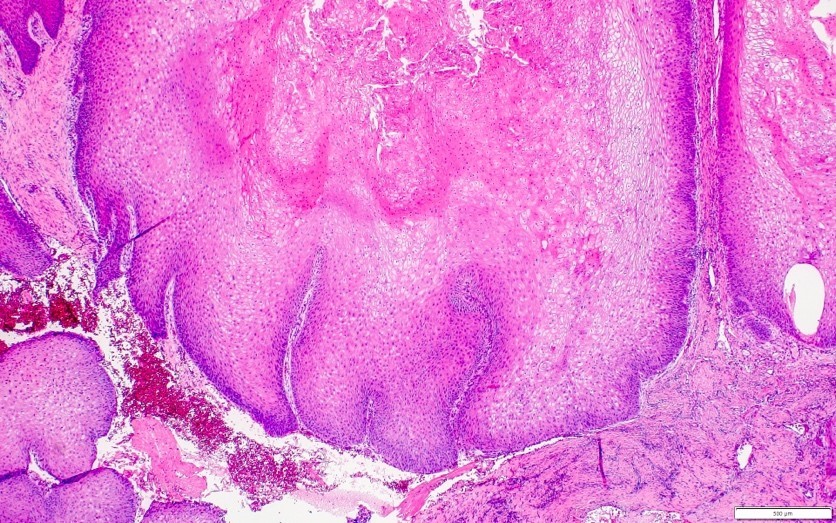
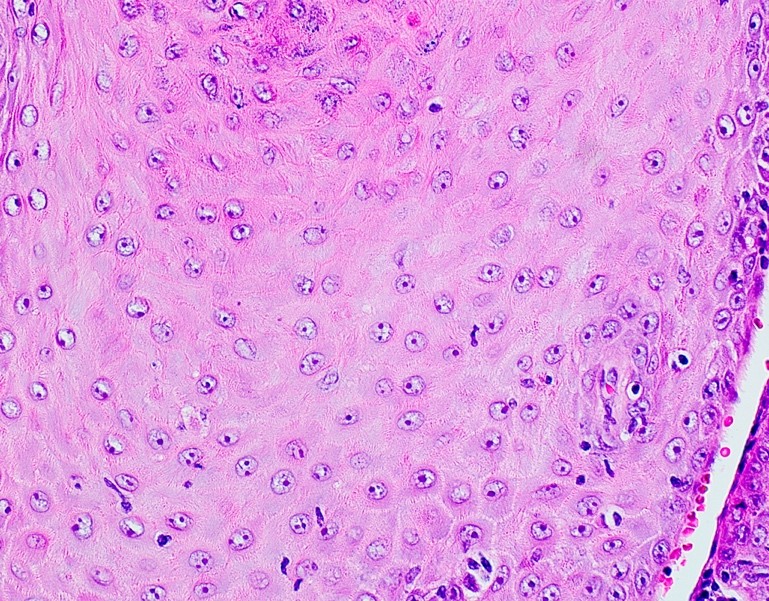
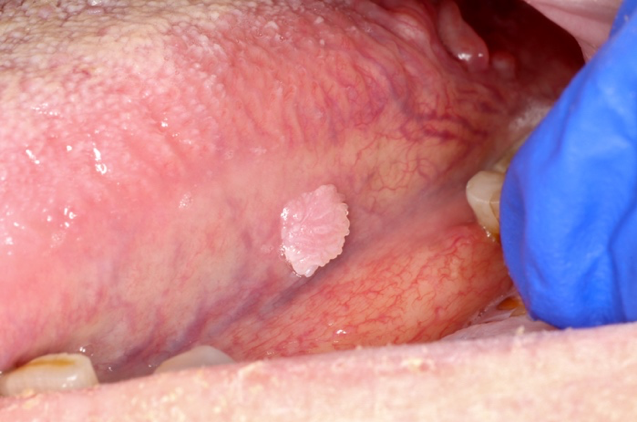
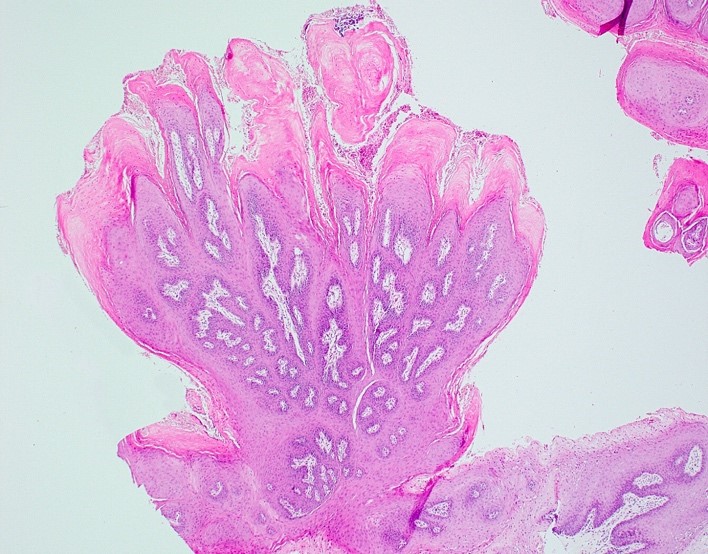
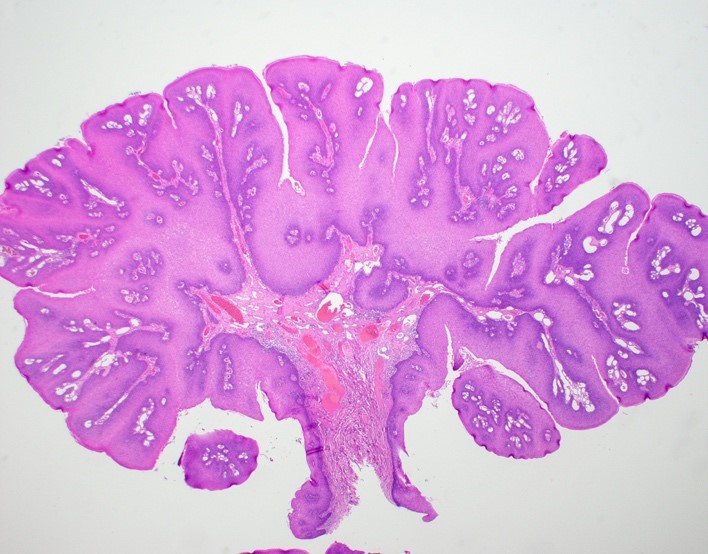
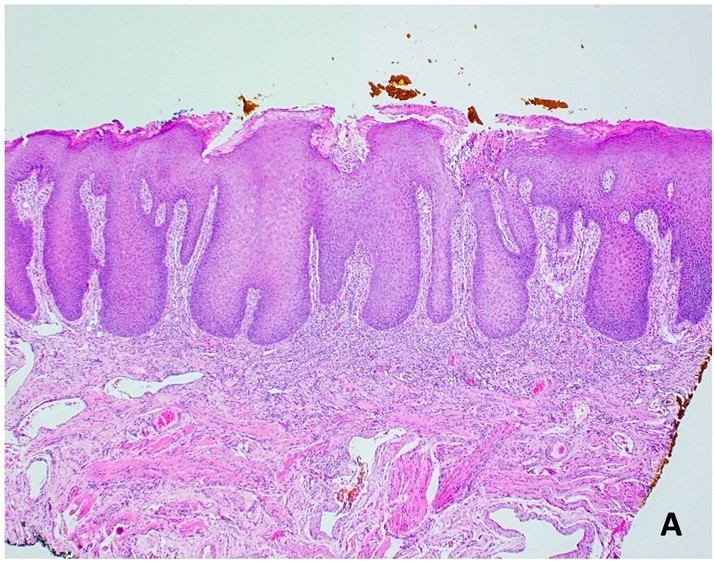
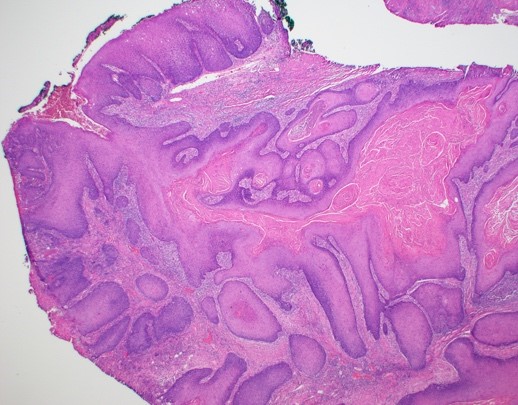
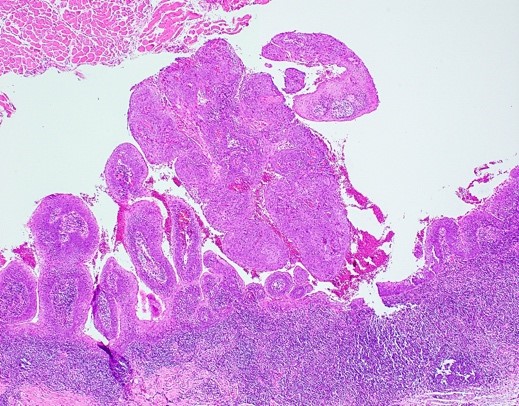
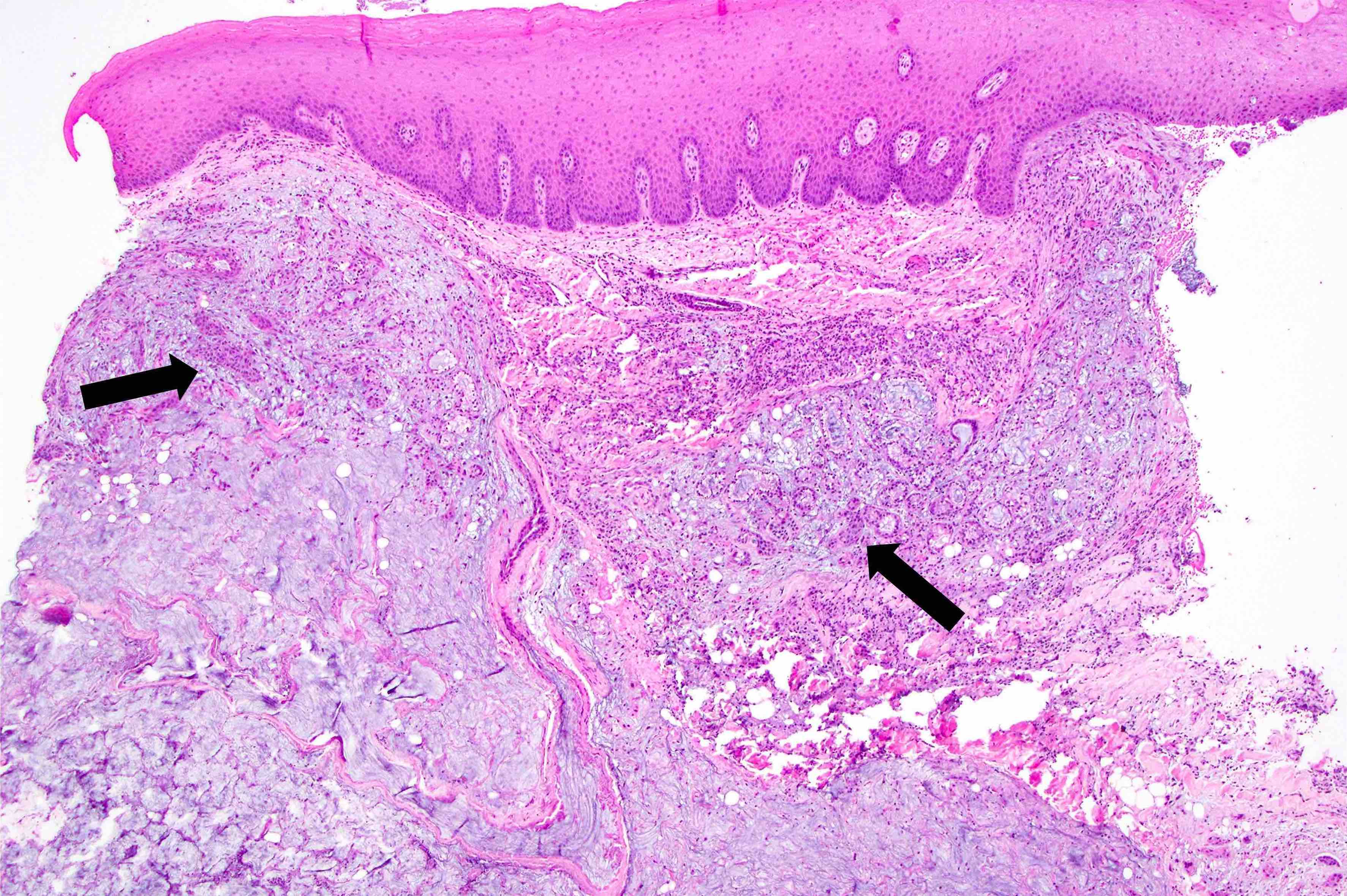
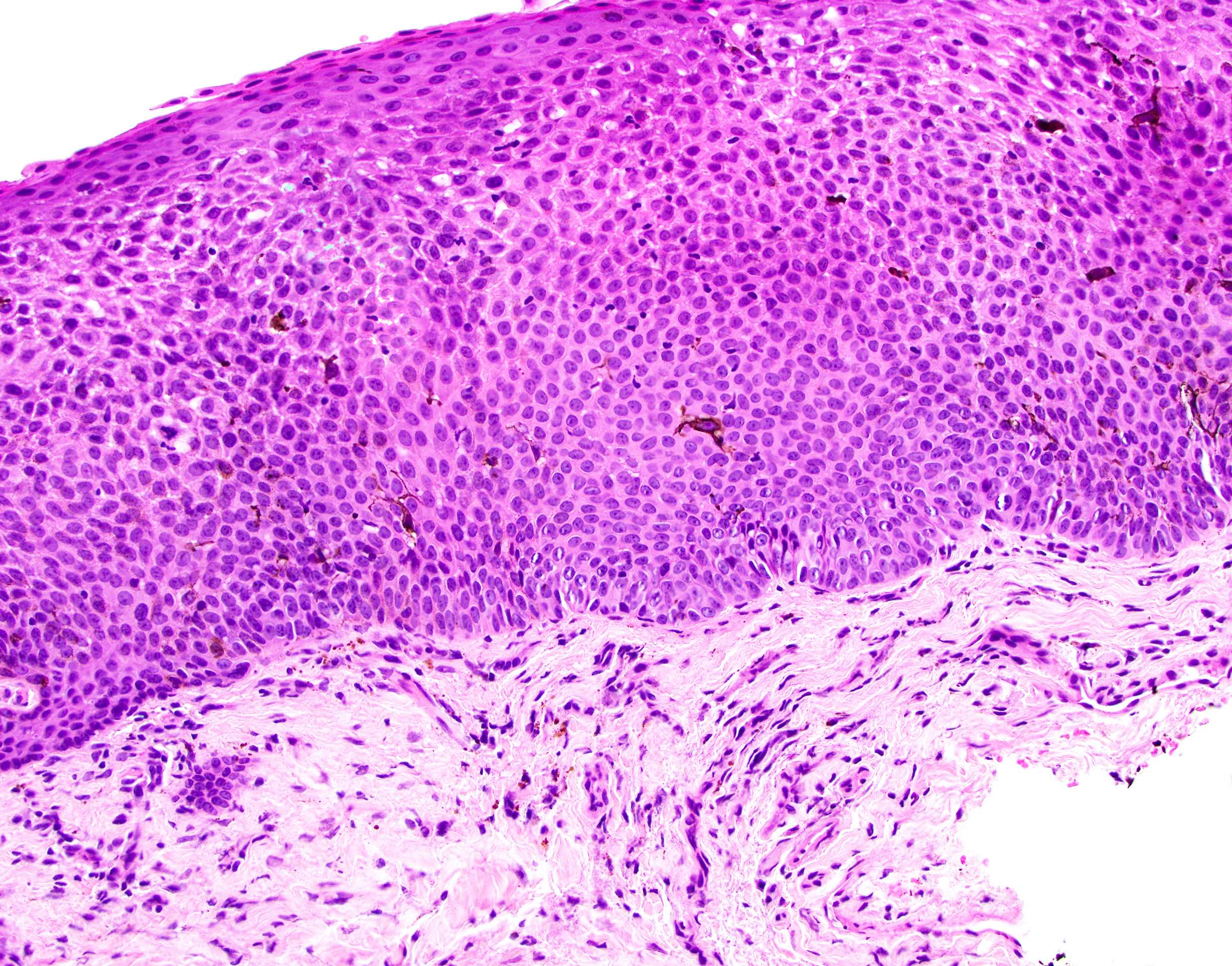
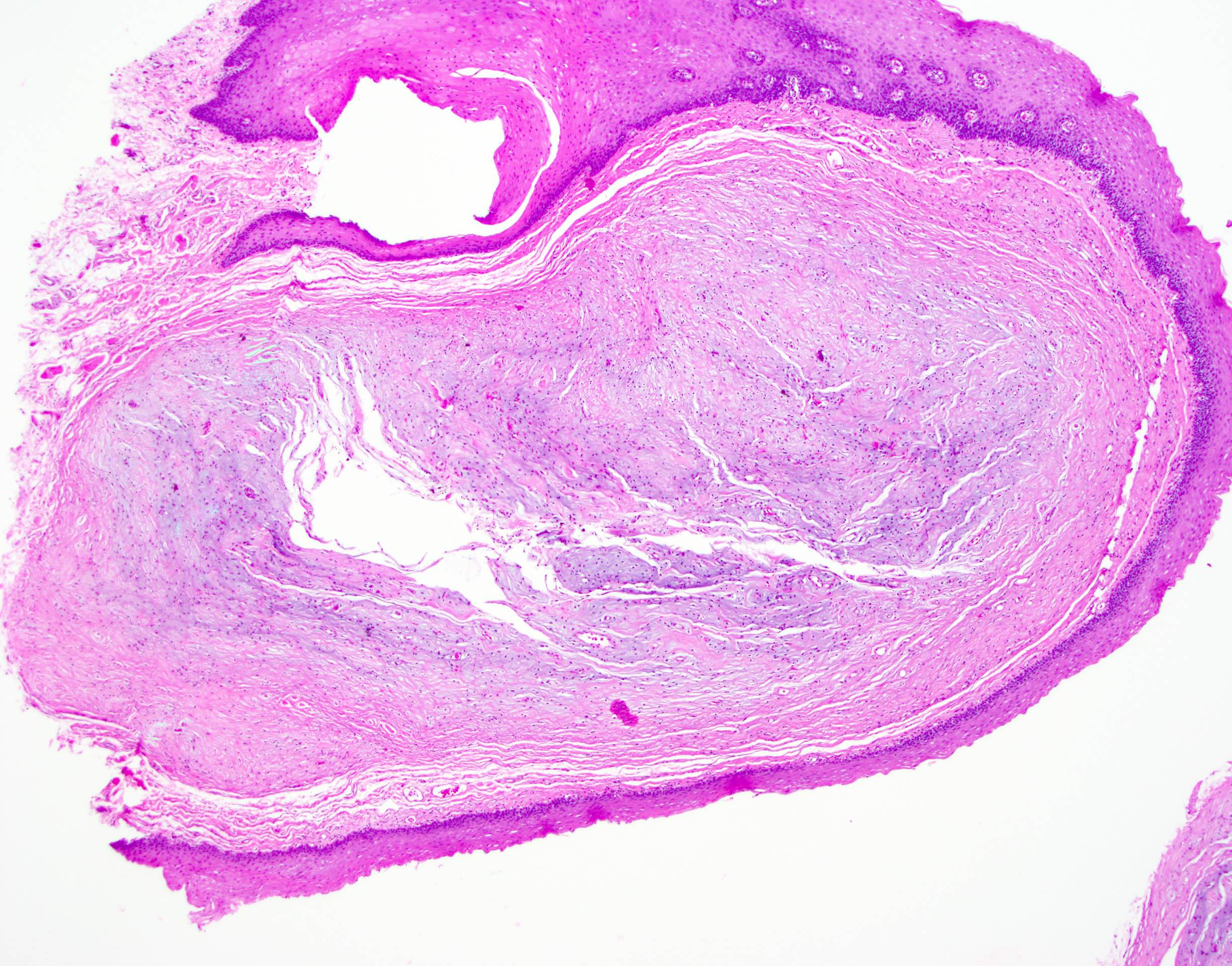
C. Parulis. The main distractor for this gingival nodule comprised of inflamed granulation tissue is a pyogenic granuloma; however, the description of dense accumulations of neutrophils at the base of the specimen favors a parulis, a soft tissue mass representing the intraoral opening of a draining odontogenic (dental) infection. Although both entities are benign, differentiating the two entities is important, as treatment modalities are different.
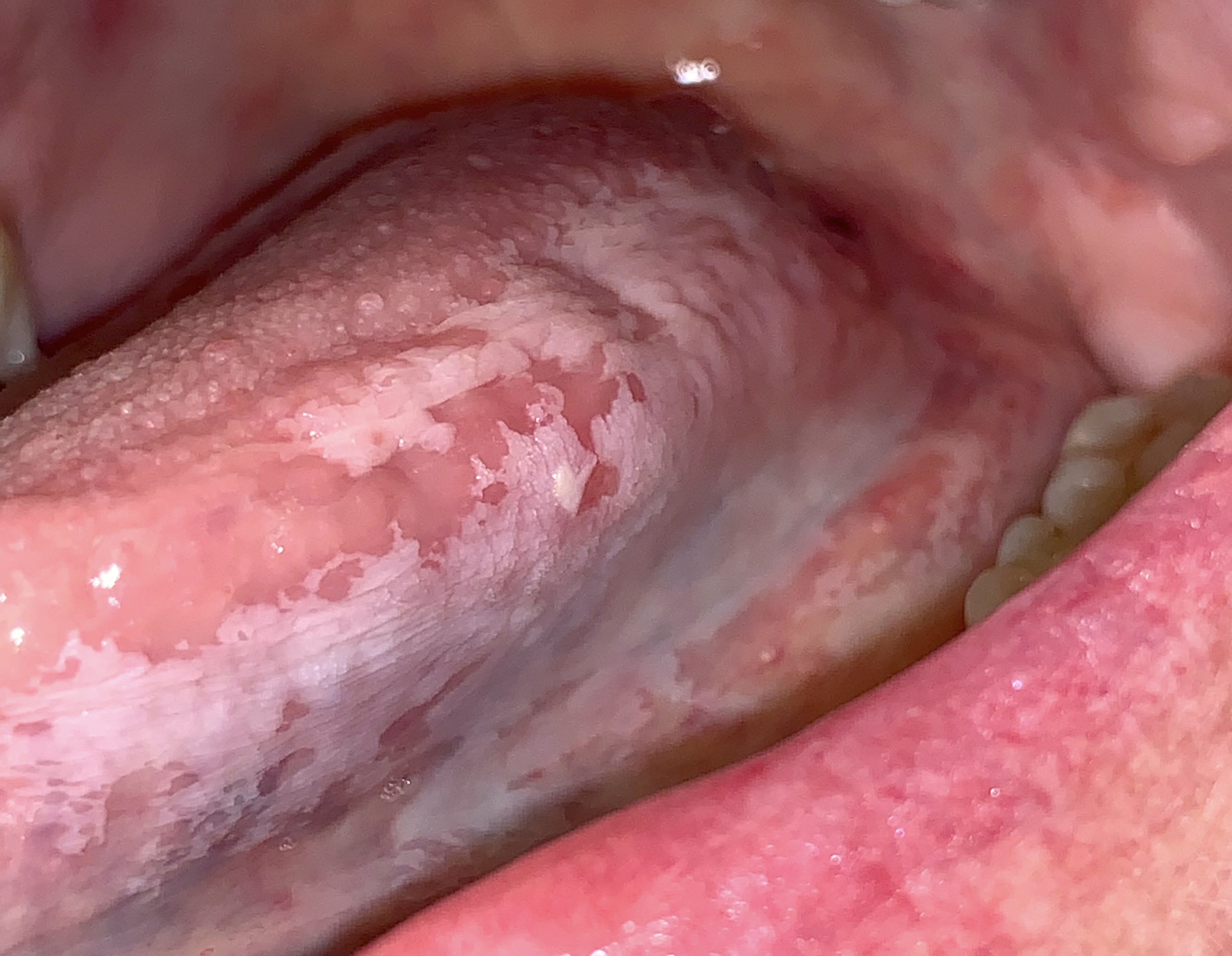
Although accumulations of dermal filler may present as a yellow nodule in the oral cavity, dermal filler accumulates under unattached mucosa rather than attached gingiva. Past medical history regarding previous cosmetic injections may also aid in excluding this entity from the differential diagnosis.
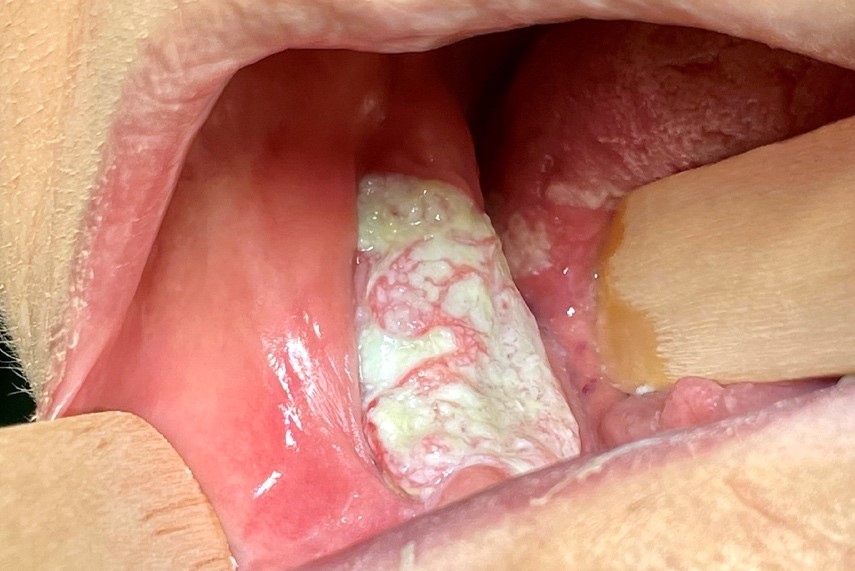
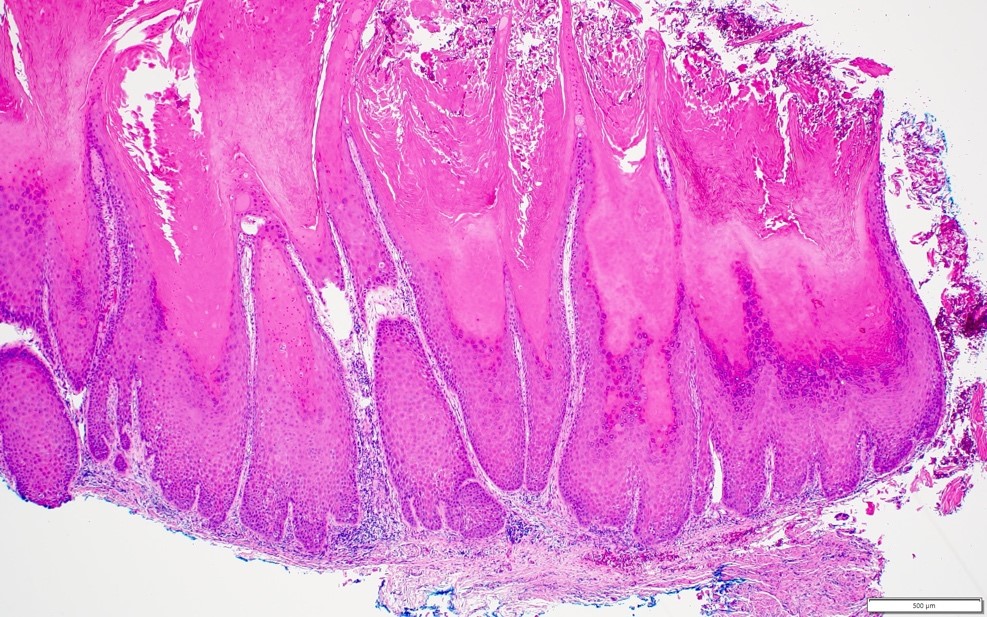
Leukoplakia is a flat, white patch of the oral cavity and does not clinically present as a nodule or histopathologically as granulation tissue.
Comment Here
Reference:
Parulis