



















































































































































































































































Primary tumor (pT) and FIGO stages in ( )
- pTX: primary tumor cannot be assessed
- pT0: no evidence of primary tumor
- pT1a (IA): tumor limited to 1 ovary (capsule intact) or fallopian tube; no tumor on ovarian or fallopian tube surface; no malignant cells in ascites or peritoneal washings
- pT1b (IB): tumor limited to both ovaries (capsules intact) or fallopian tubes; no tumor on ovarian or fallopian tube surface; no malignant cells in ascites or peritoneal washings
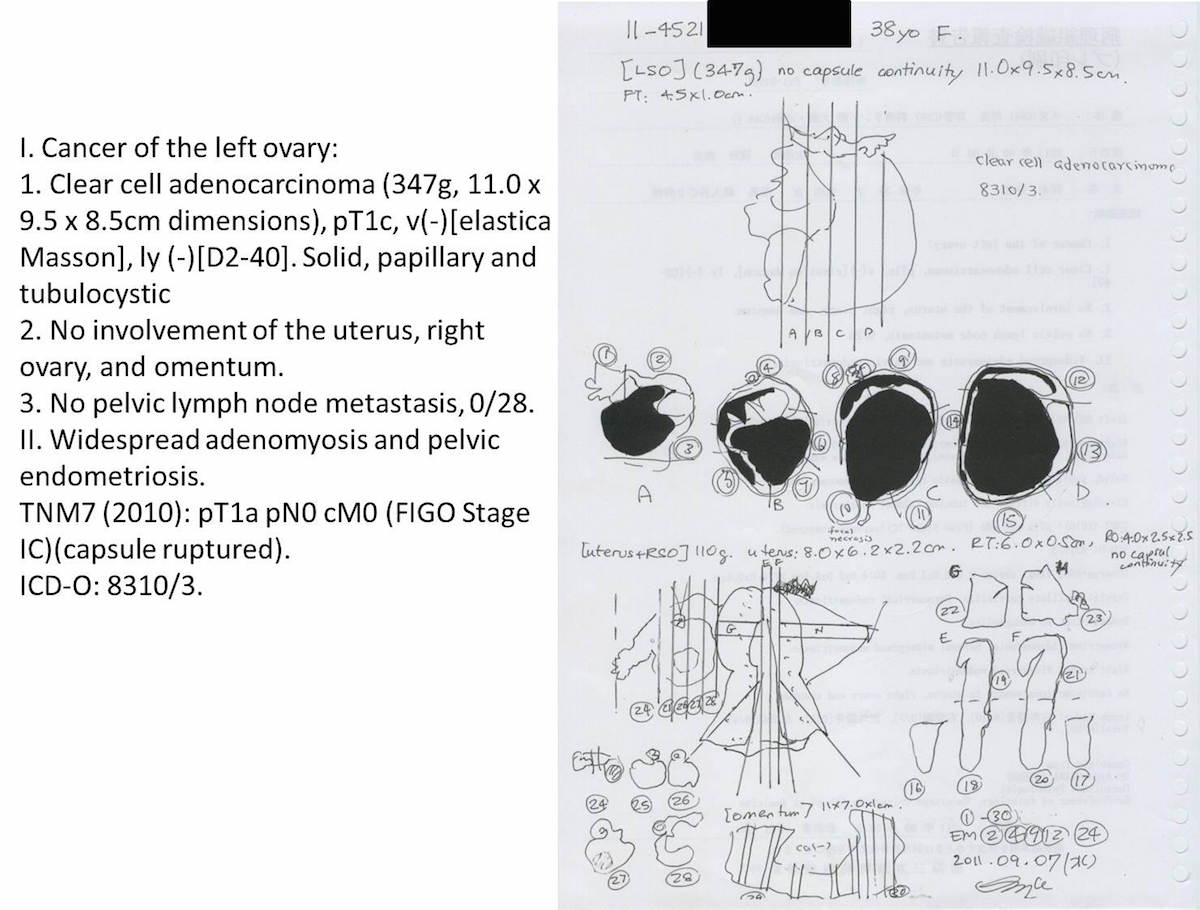
- pT1c (IC): tumor limited to 1 or both ovaries or fallopian tubes, with any of following:
- pT1c1 (IC1): surgical spill
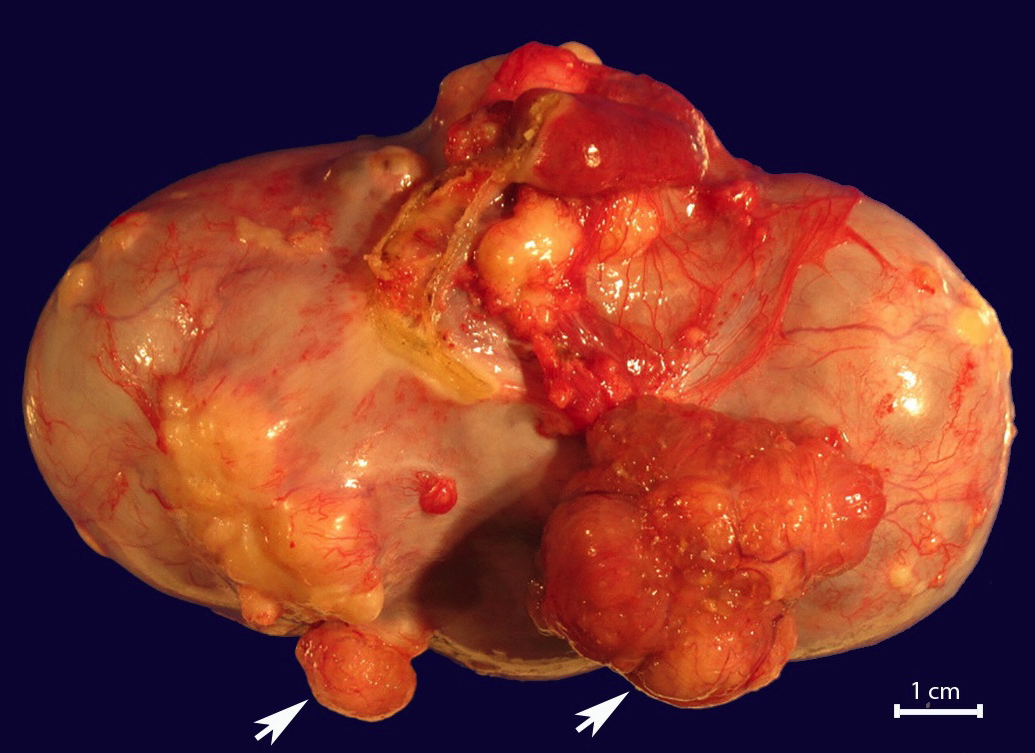
- pT1c2 (IC2): capsule ruptured before surgery or tumor on ovarian or fallopian tube surface
- pT1c3 (IC3): malignant cells in ascites or peritoneal washings
- pT2a (IIA): extension or implants on the uterus or fallopian tube(s) or ovaries
- pT2b (IIB): extension to or implants on other pelvic tissues
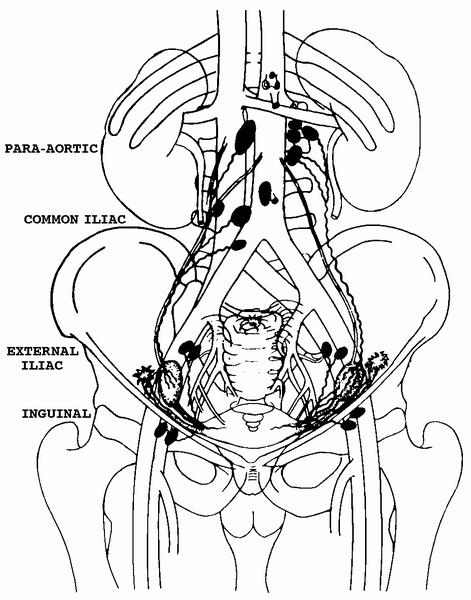
- pT3a (IIIA2): microscopic extrapelvic (above the pelvic brim) peritoneal involvement with or without positive retroperitoneal lymph nodes
- pT3b (IIIB): macroscopic peritoneal metastasis beyond pelvis ≤ 2 cm with or without retroperitoneal lymph node metastasis
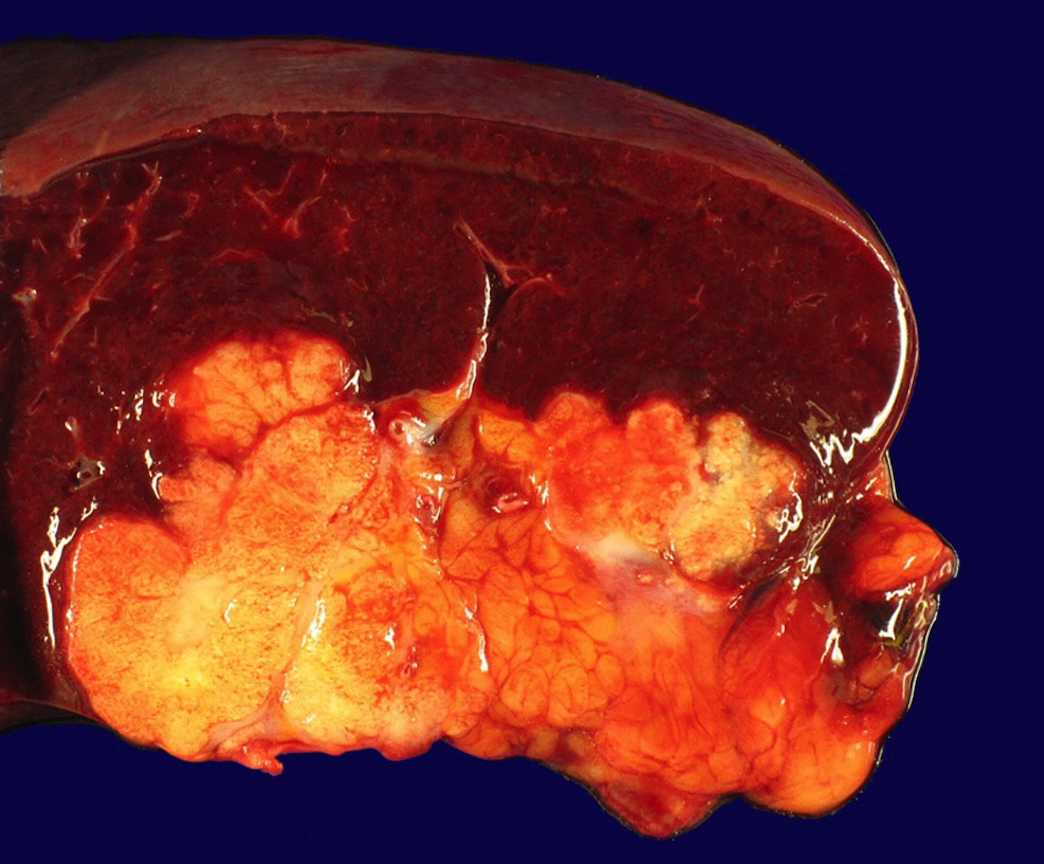
- pT3c (IIIC): macroscopic peritoneal metastasis beyond pelvis > 2 cm with or without retroperitoneal lymph node metastasis (includes extension of tumor to capsule of liver and spleen without parenchymal involvement of either organ)