
































































































































































































































Primary tumor (pT)
- pTX: cannot be assessed
- pT0: no evidence of primary tumor
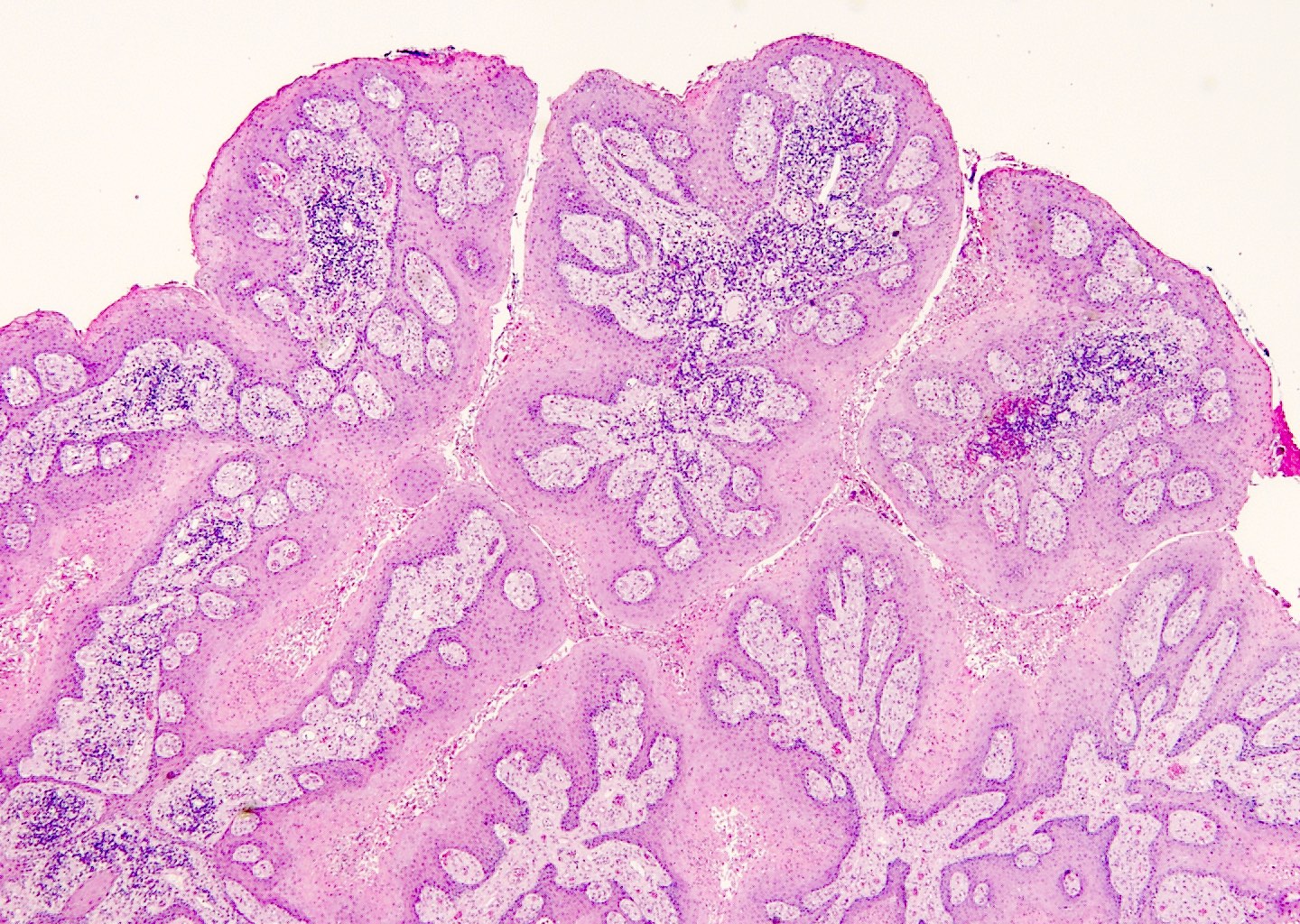
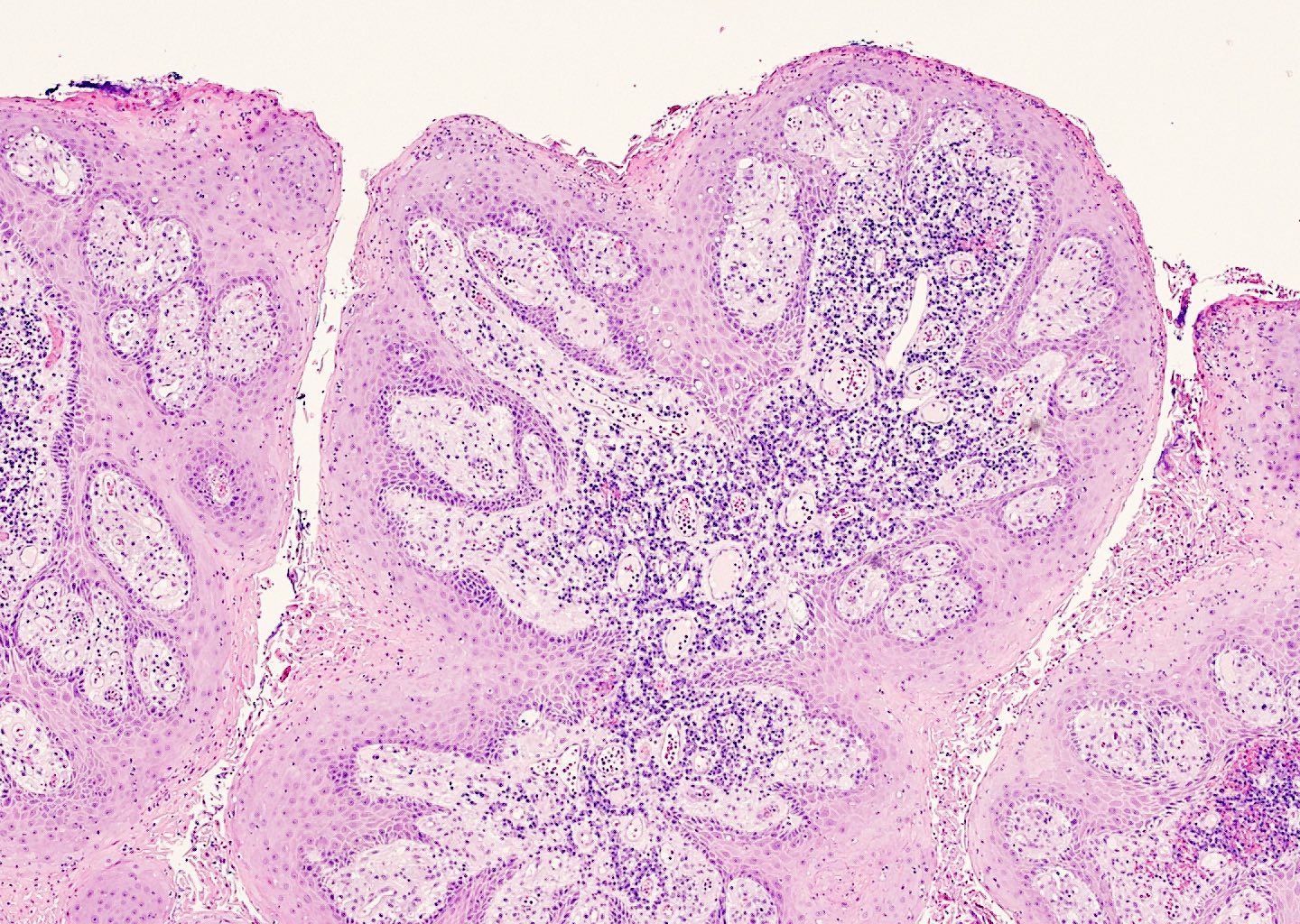
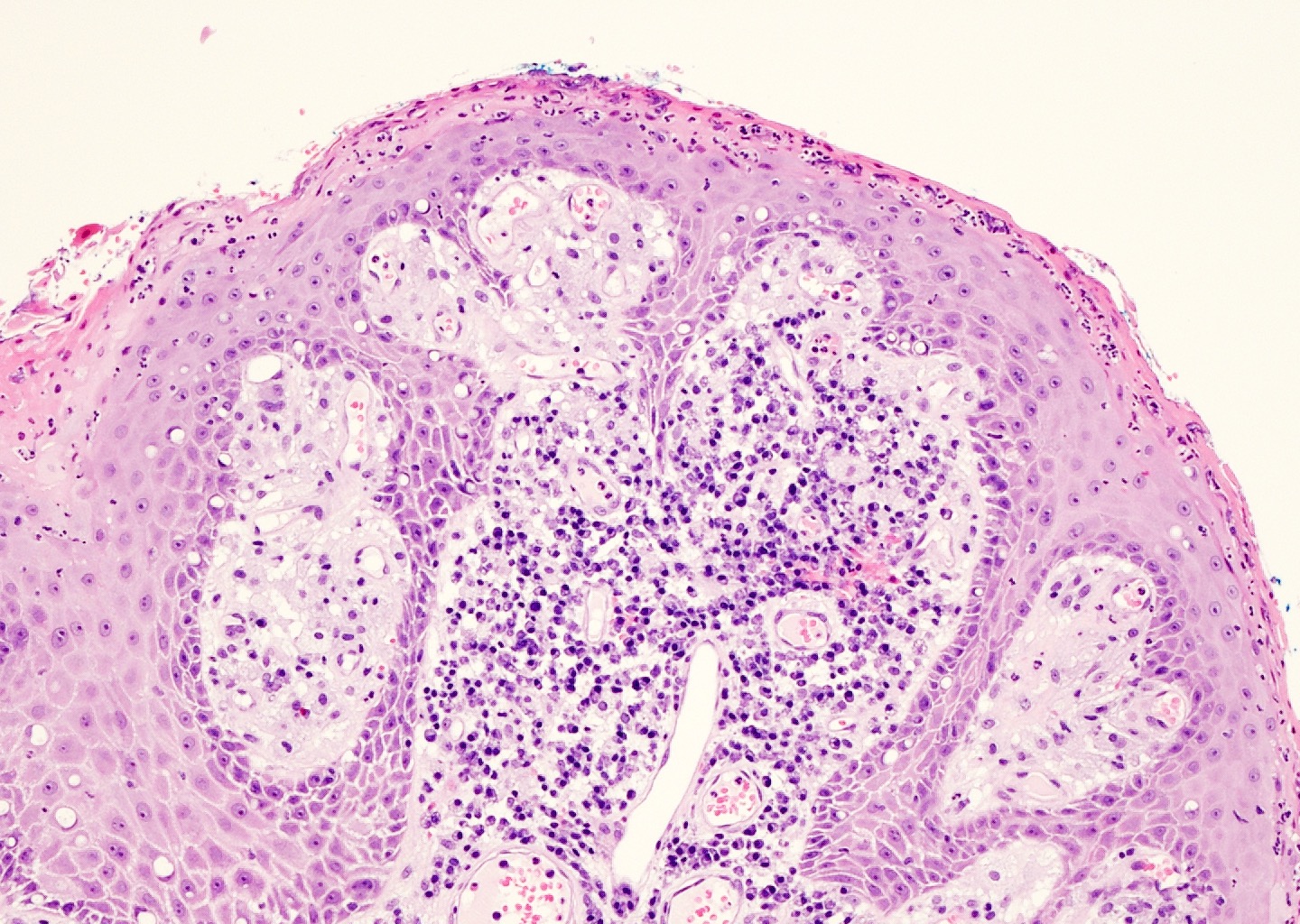
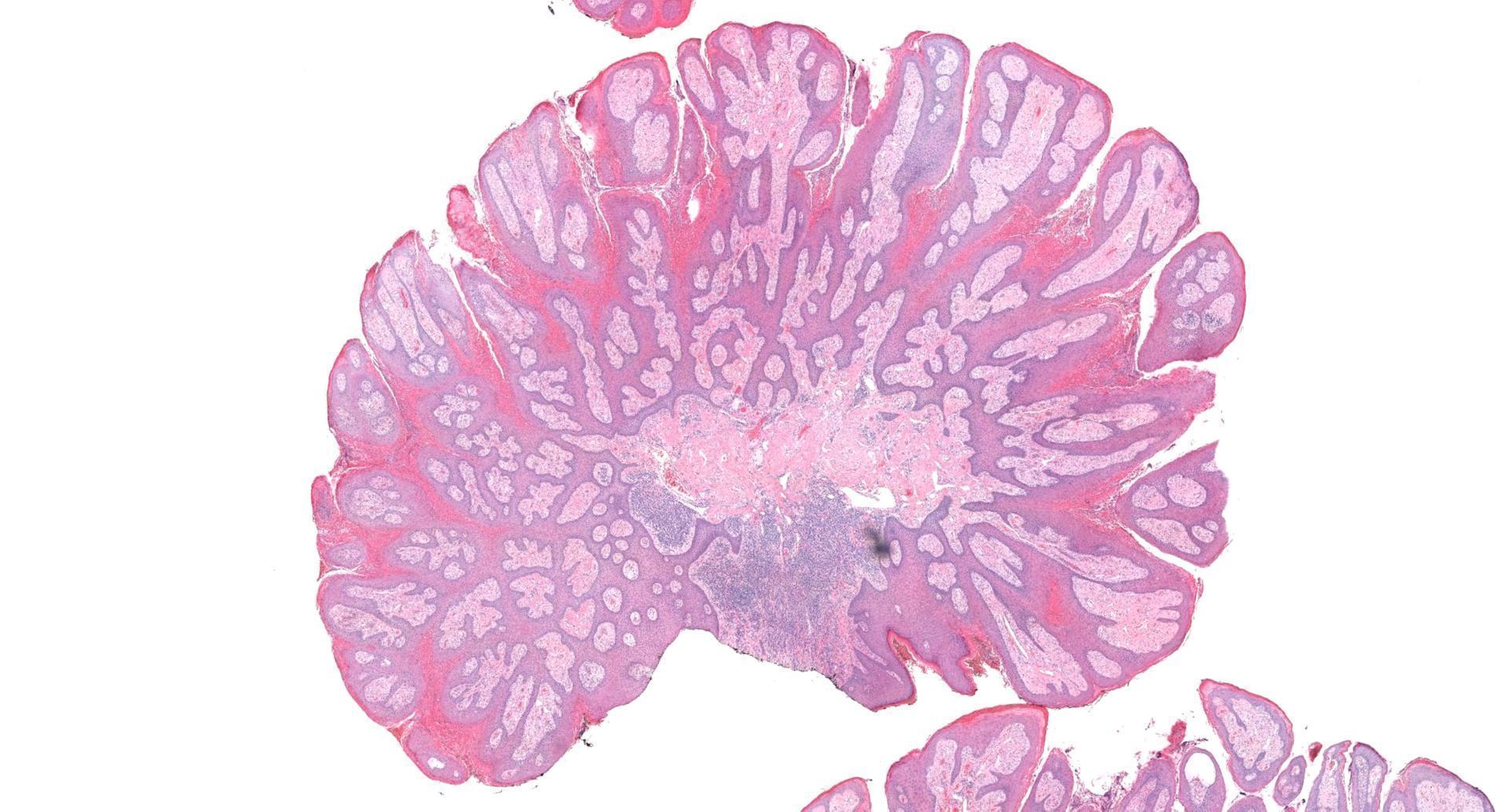
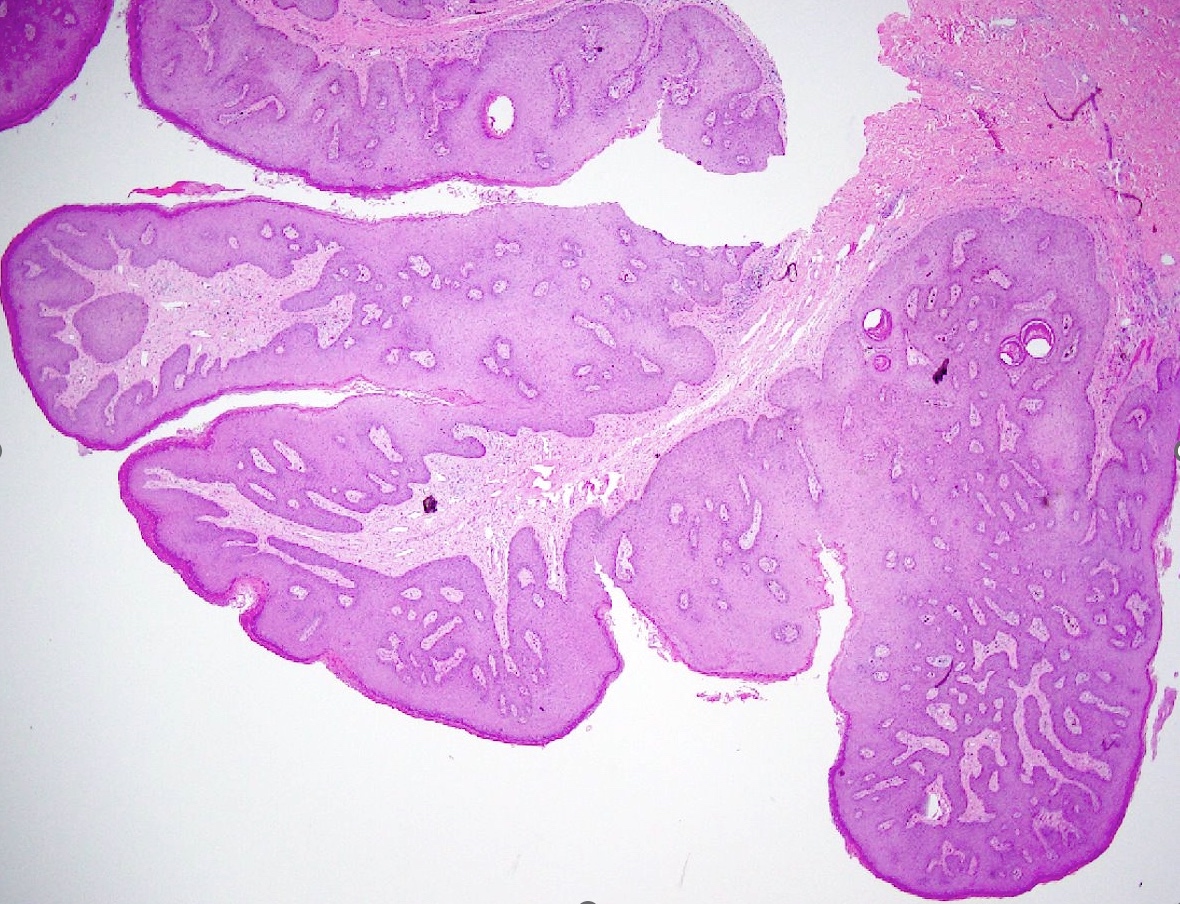
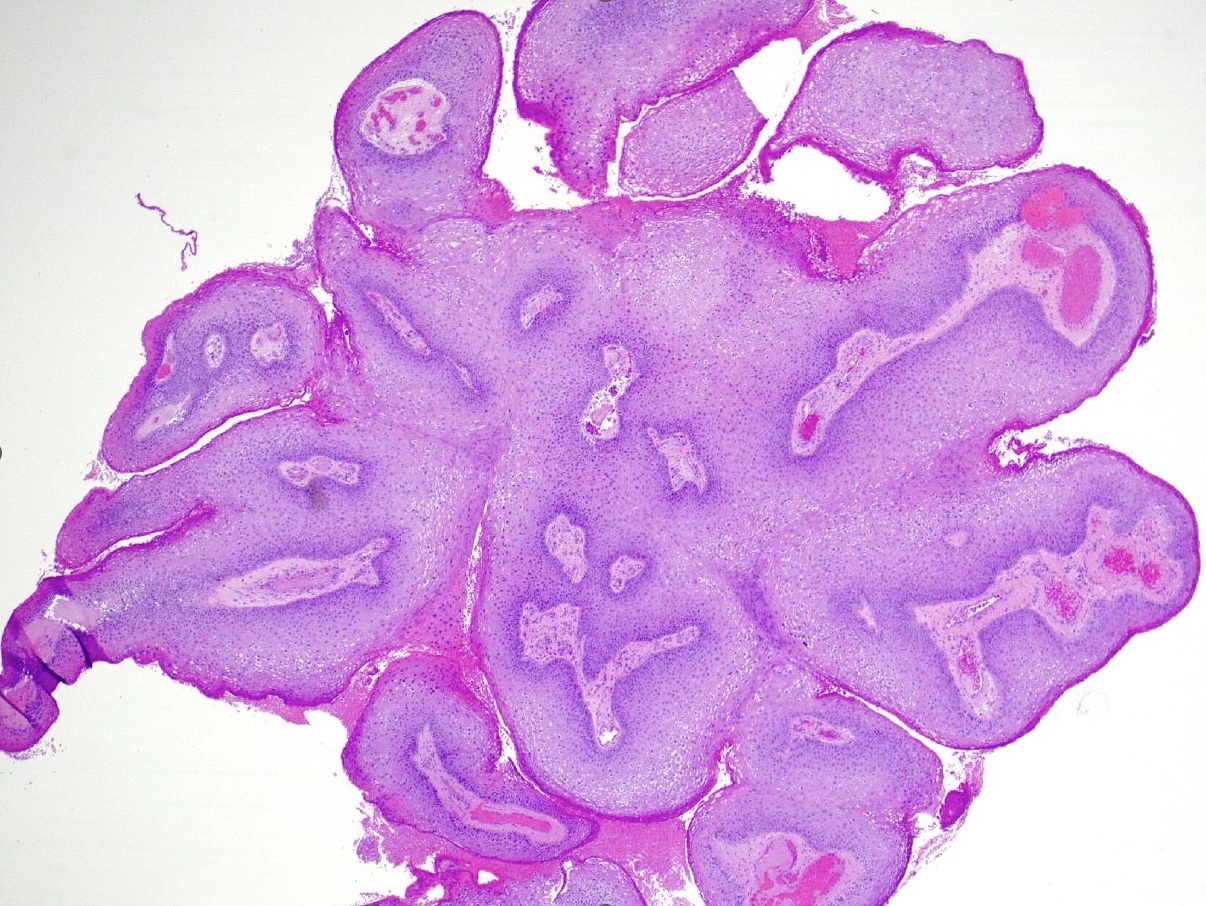
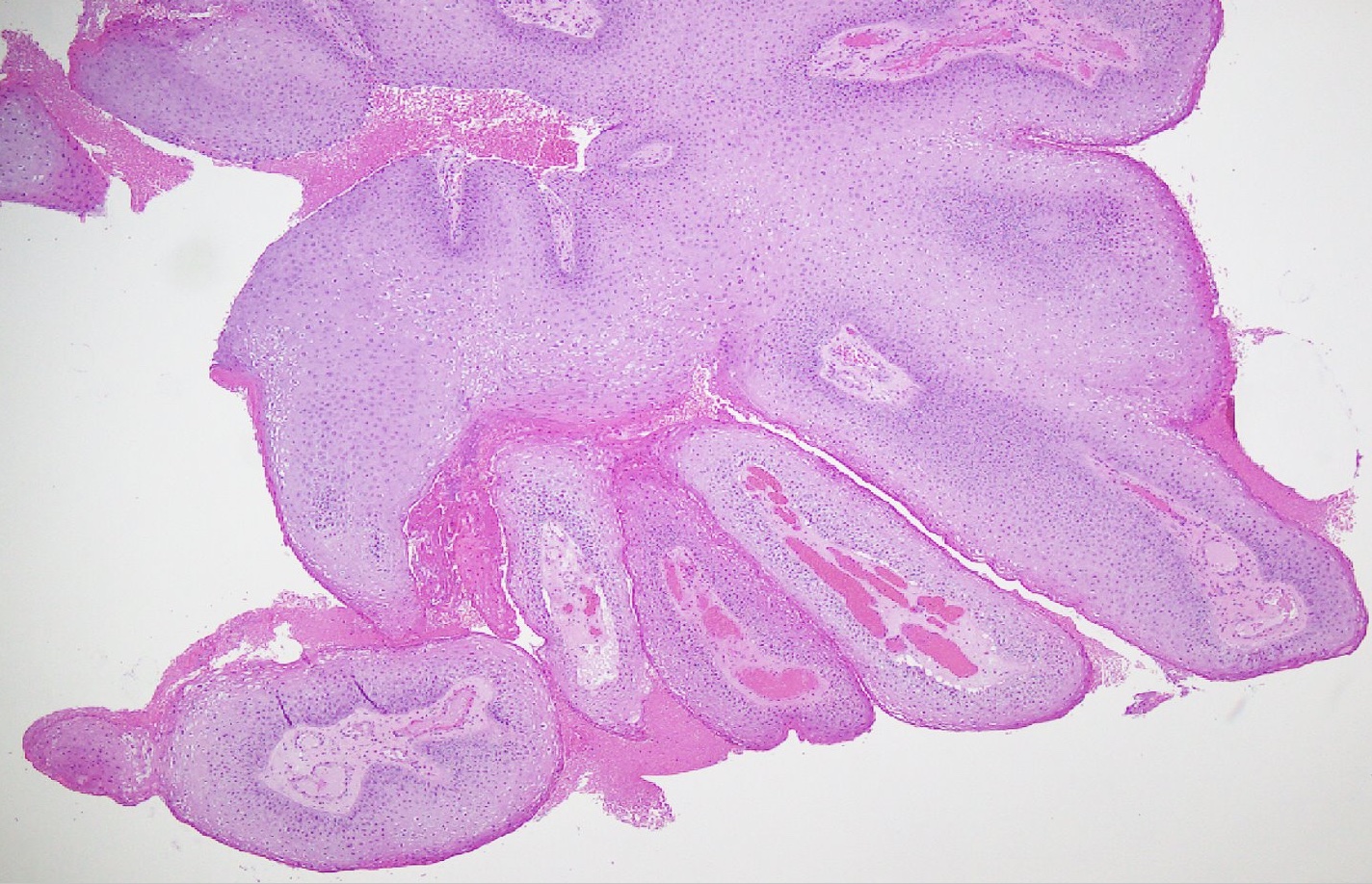
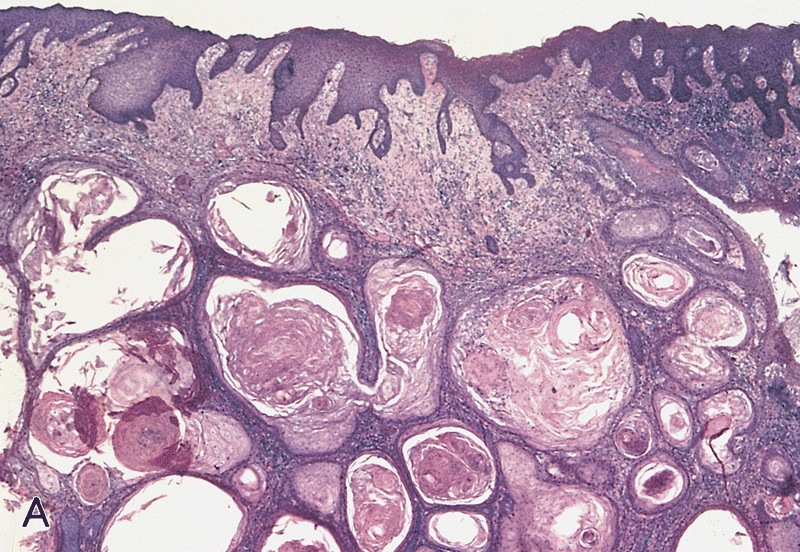
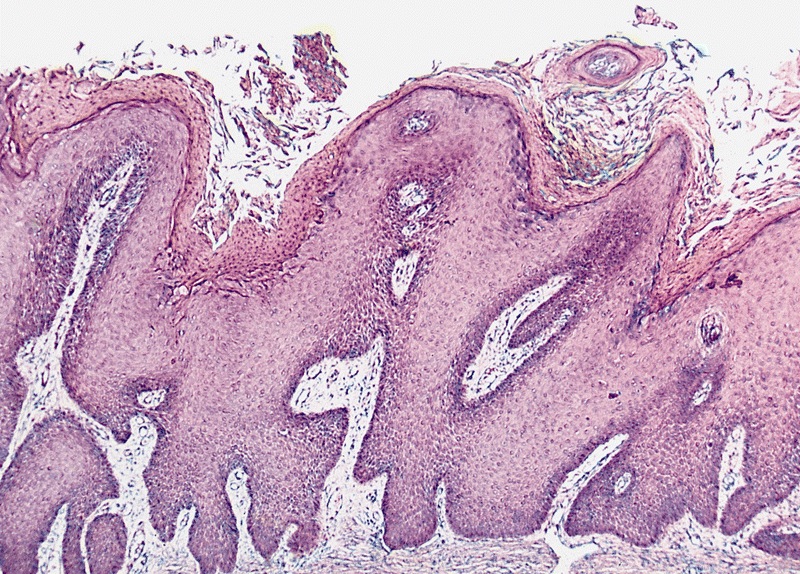
- pTa: noninvasive carcinoma (broad pushing penetration is permitted)
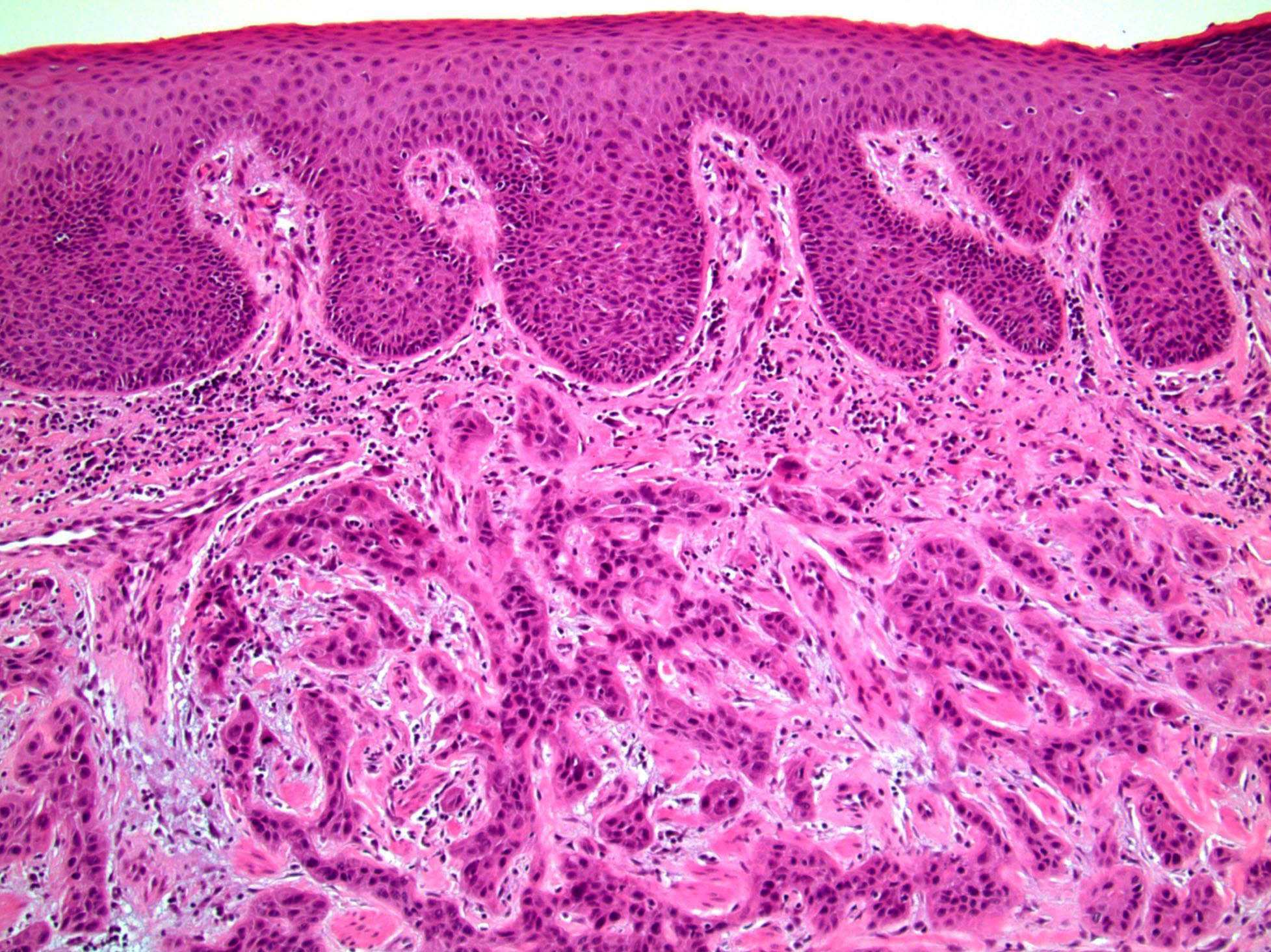
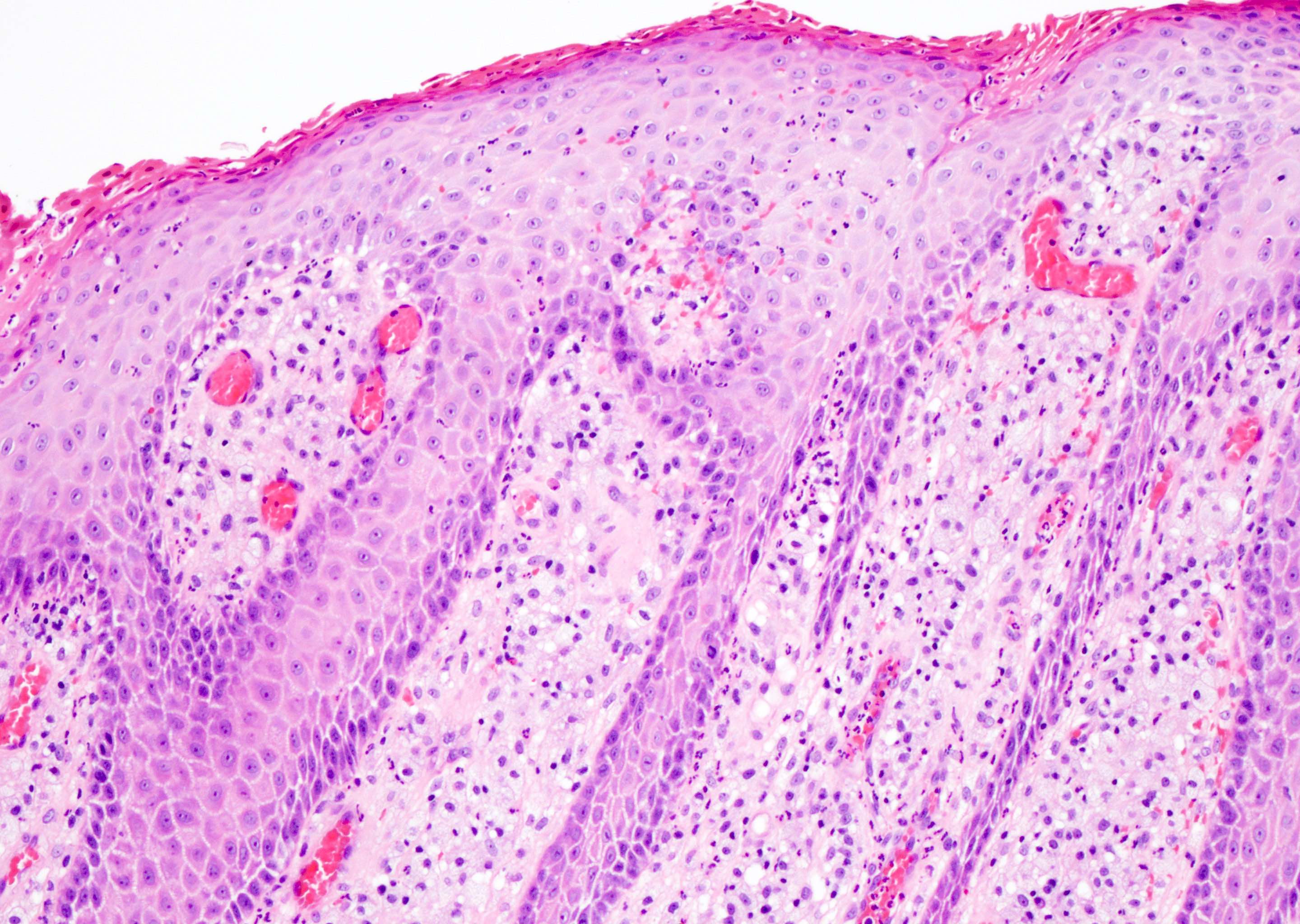
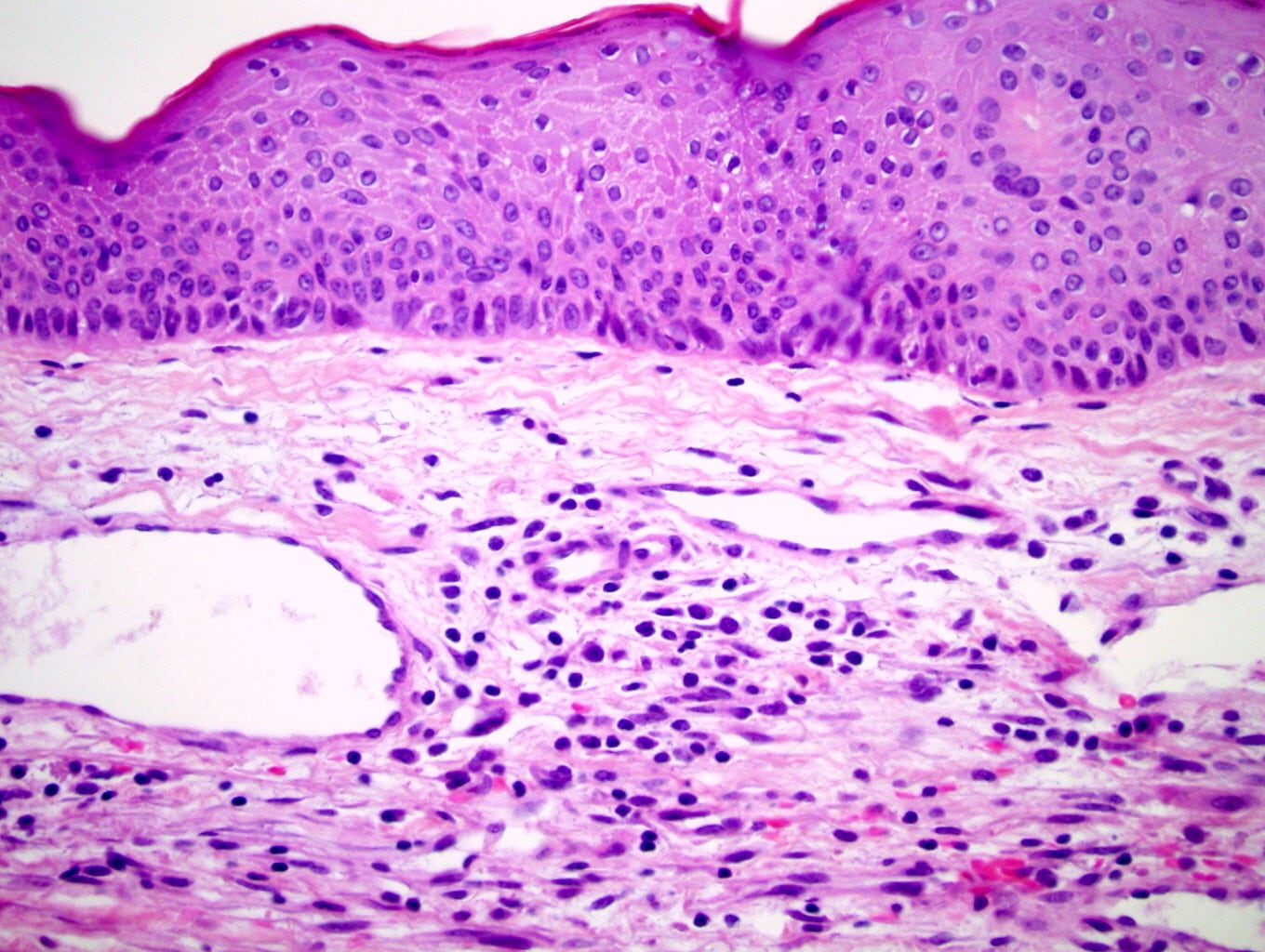
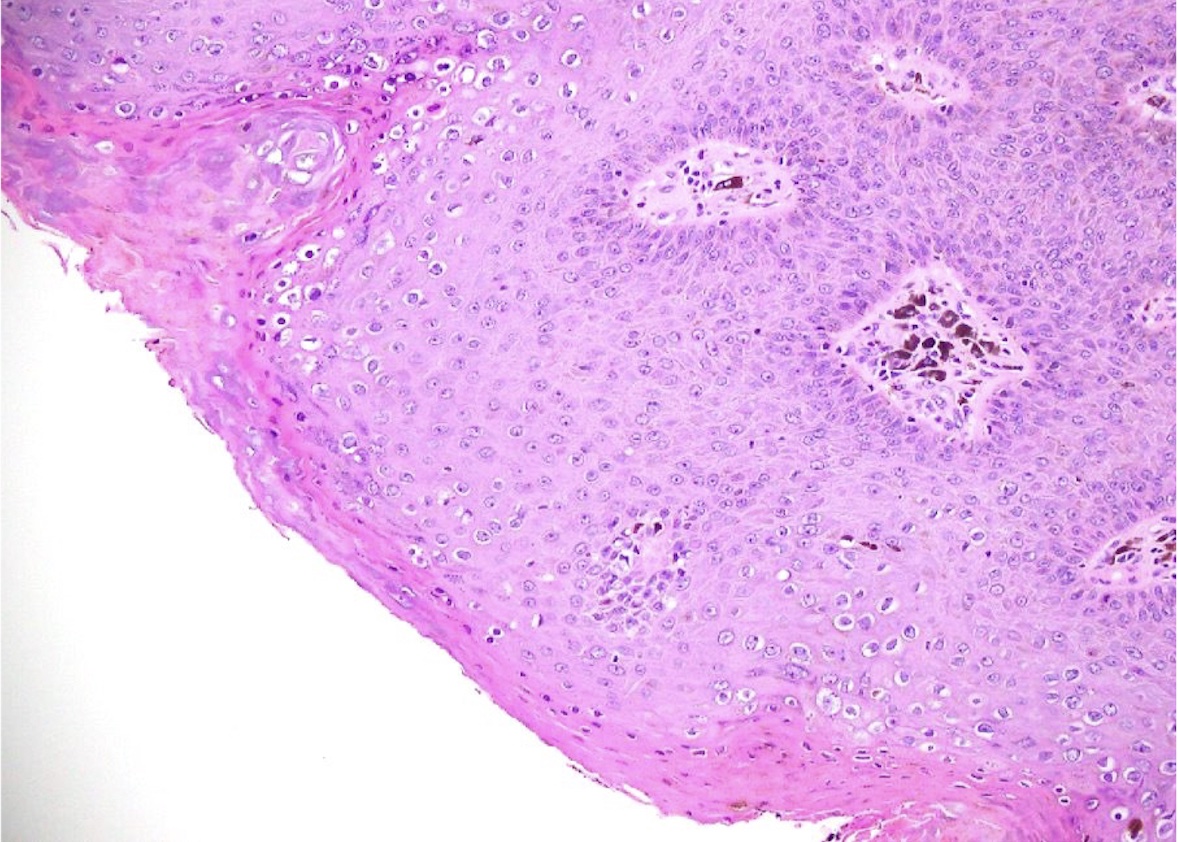
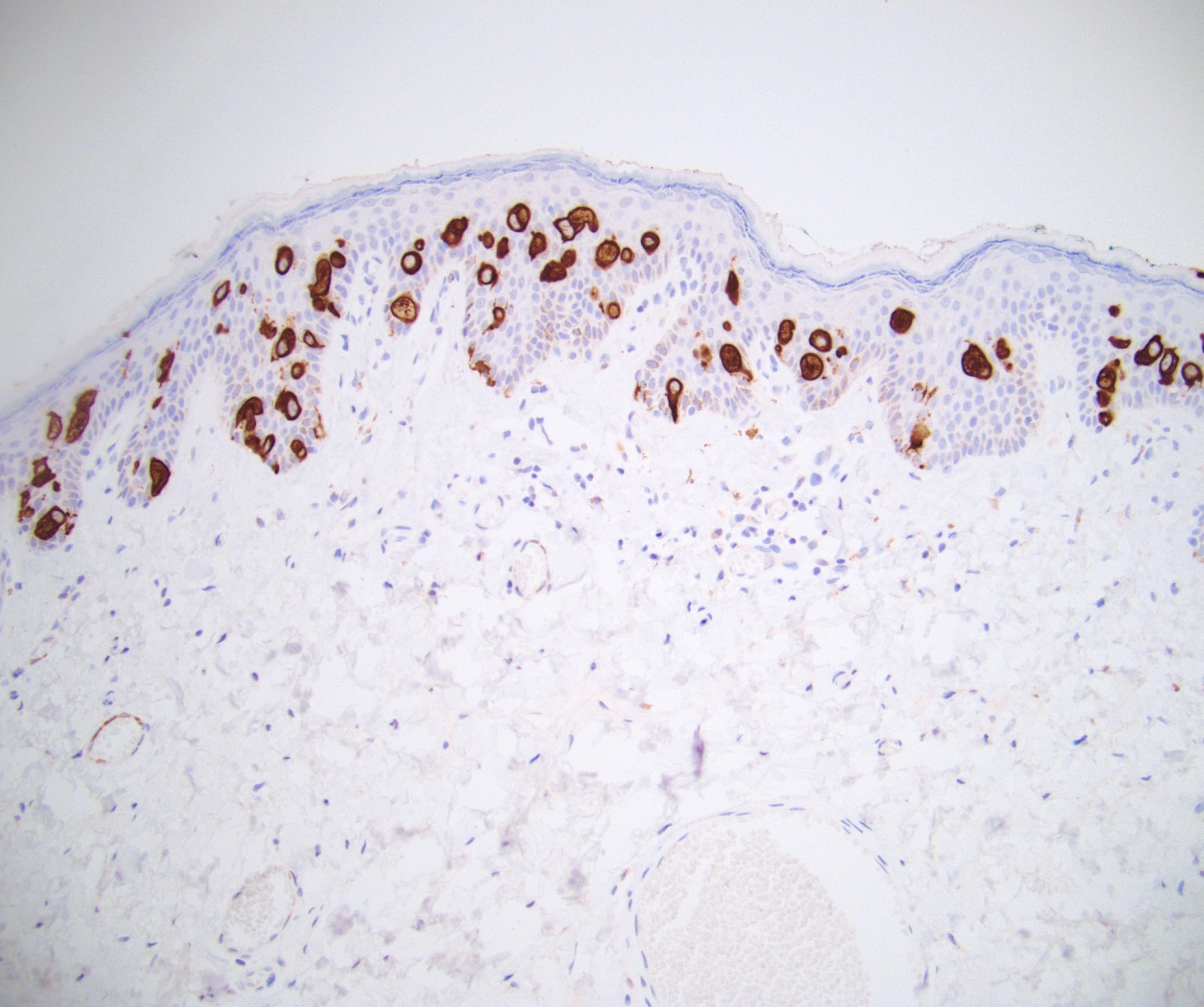
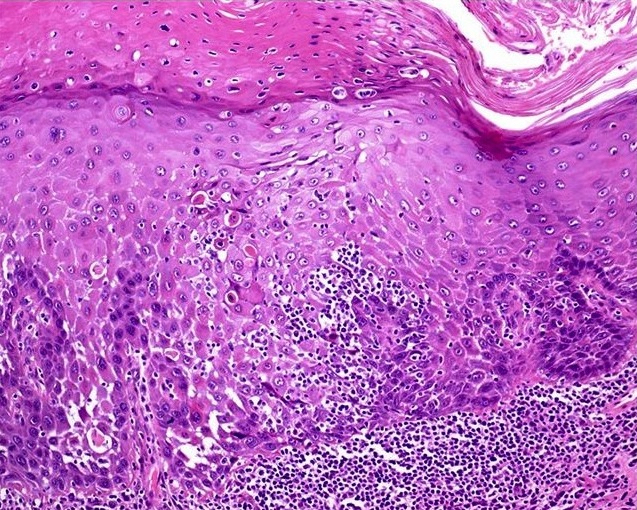
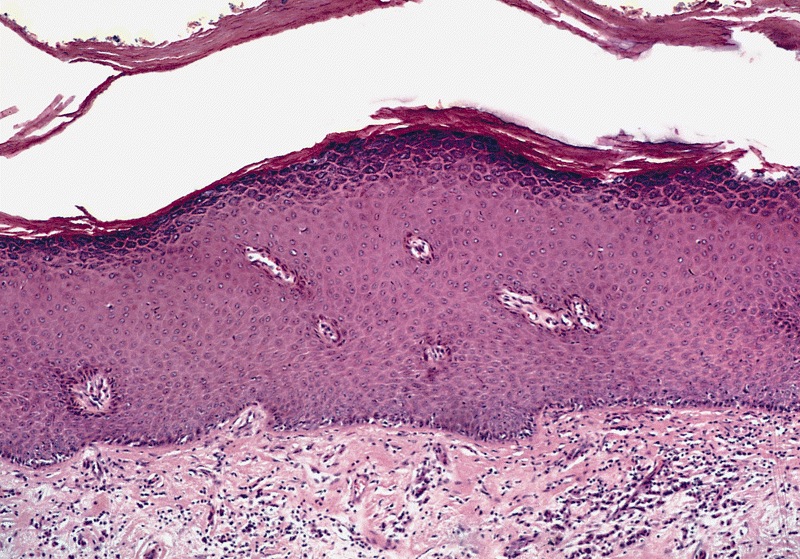
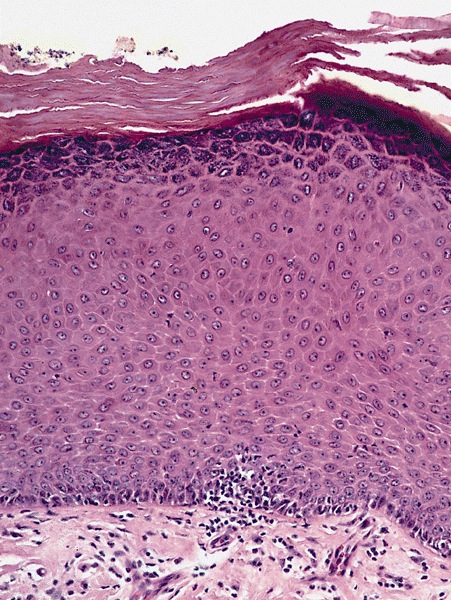
- pTis: carcinoma in situ
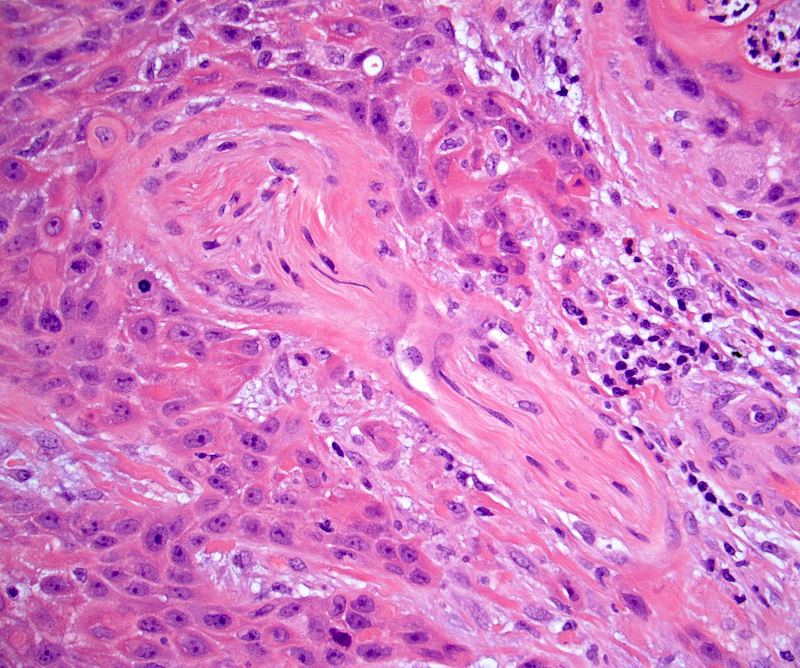
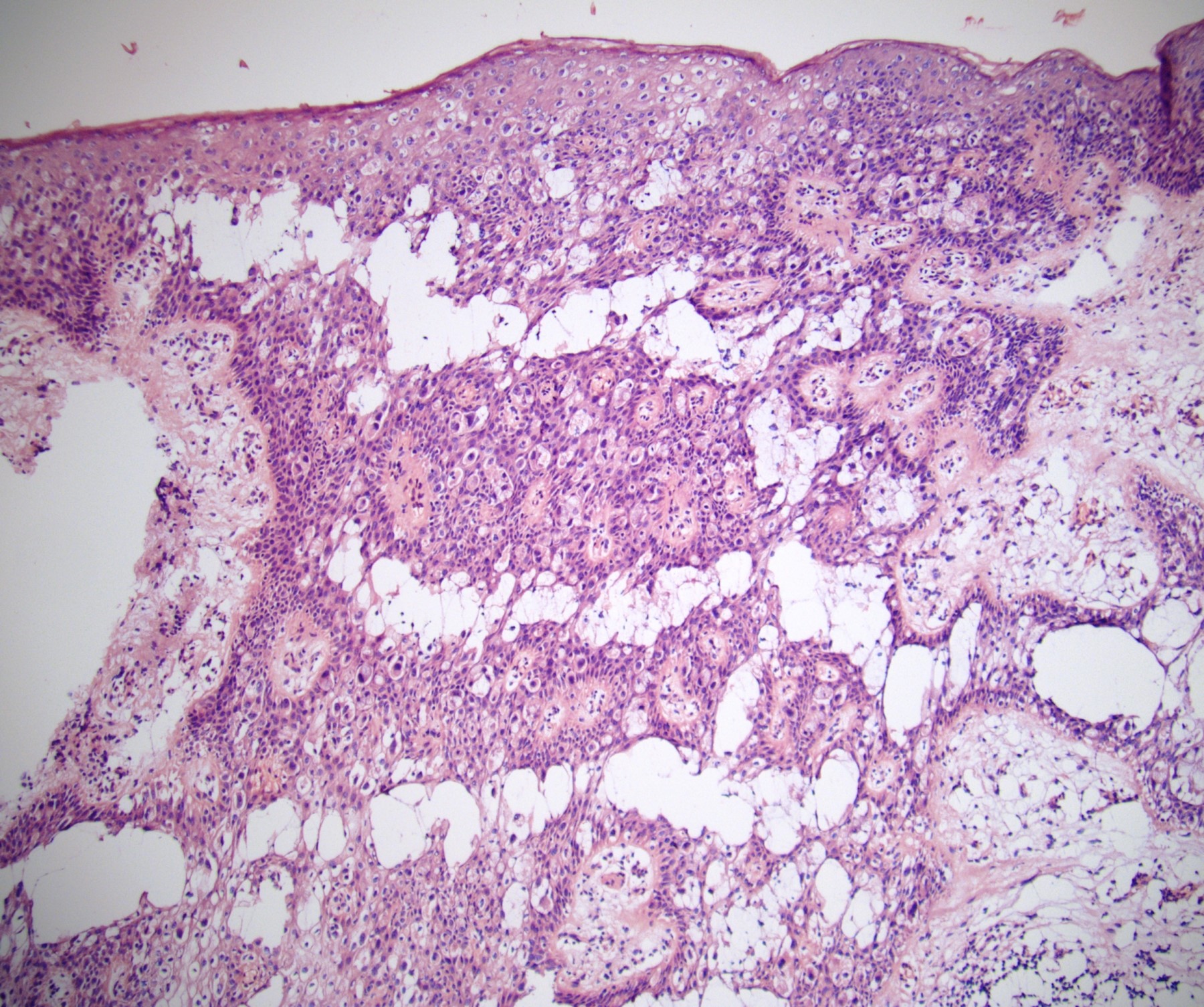
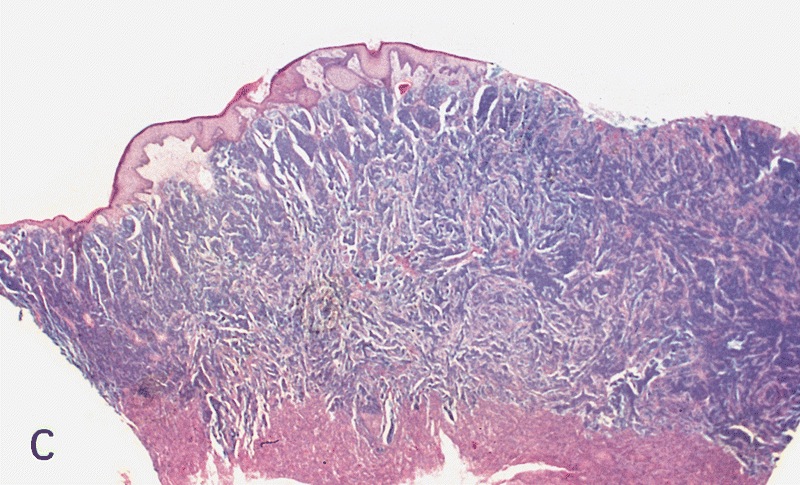
- pT1a: subepithelial invasion without lymphovascular invasion, perineural invasion or grade 3
- pT1b: subepithelial invasion with lymphovascular invasion, perineural invasion or grade 3
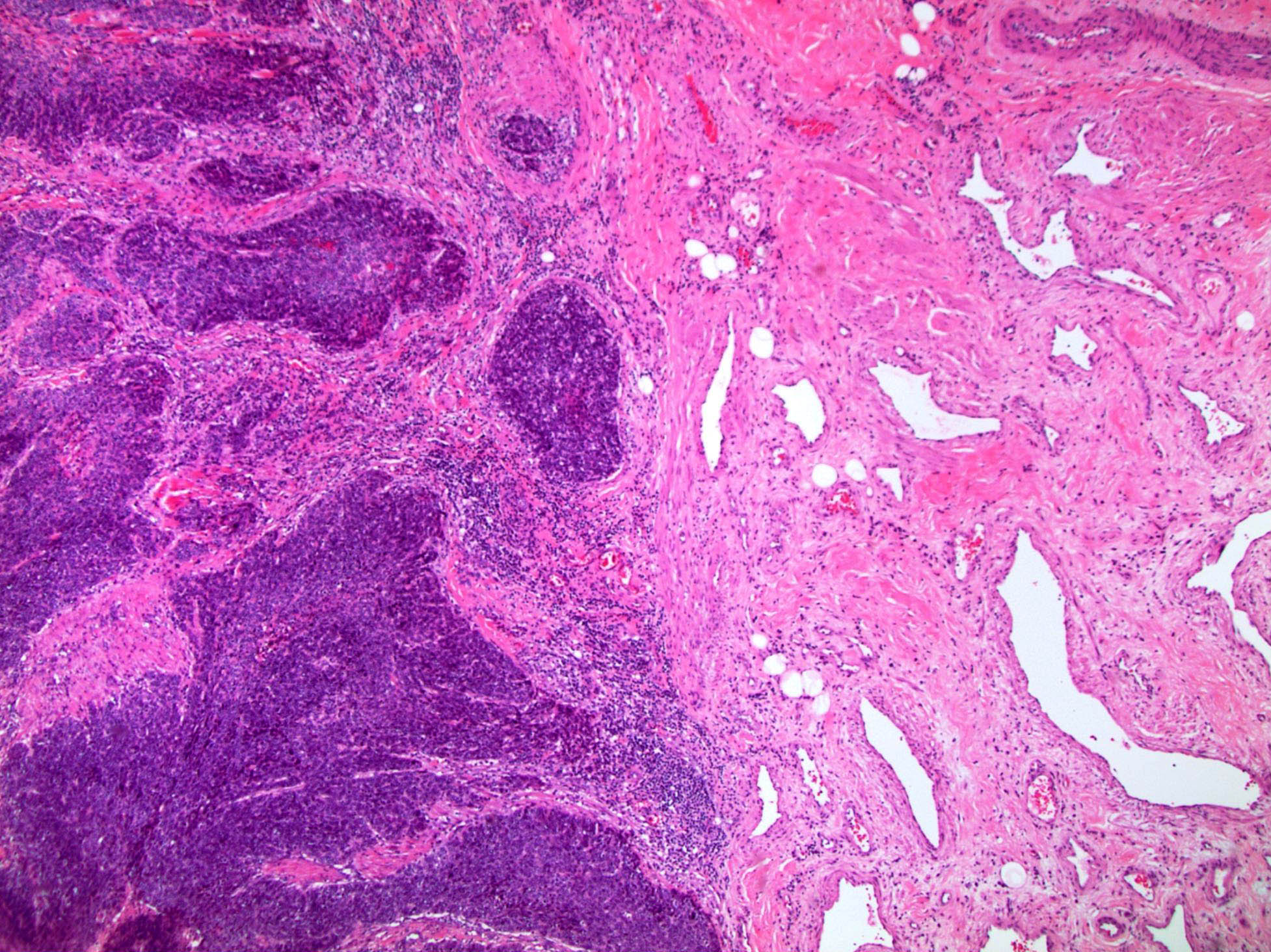
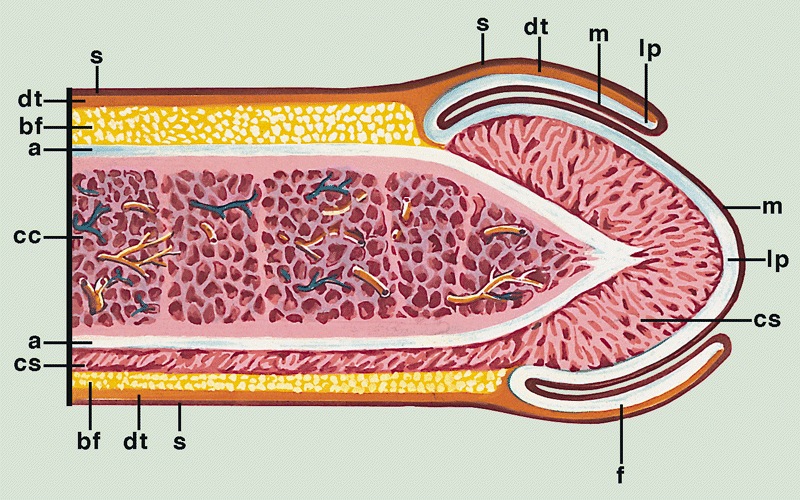
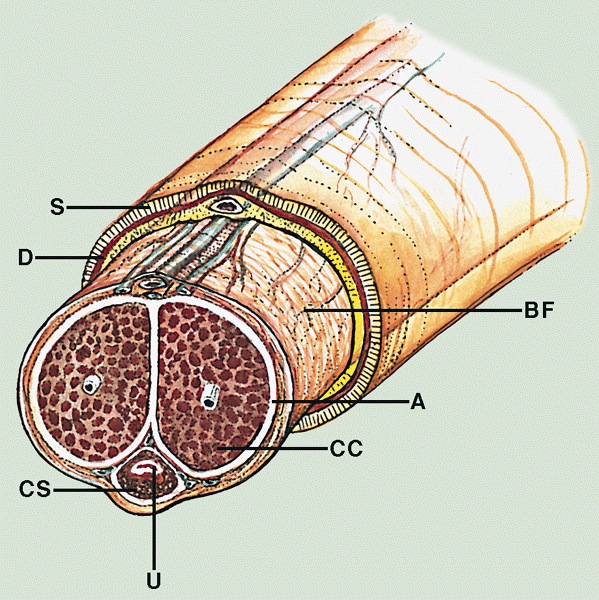
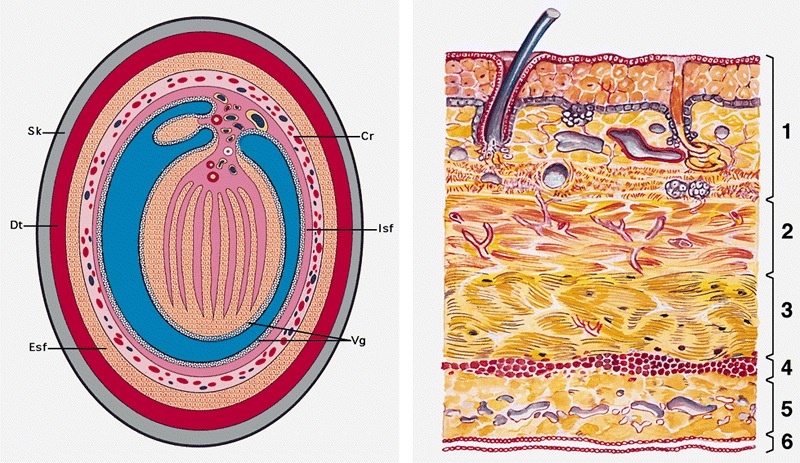
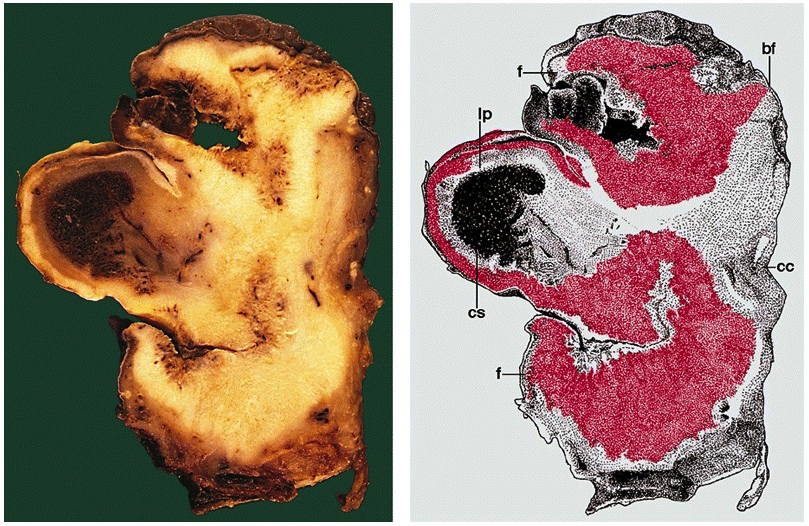
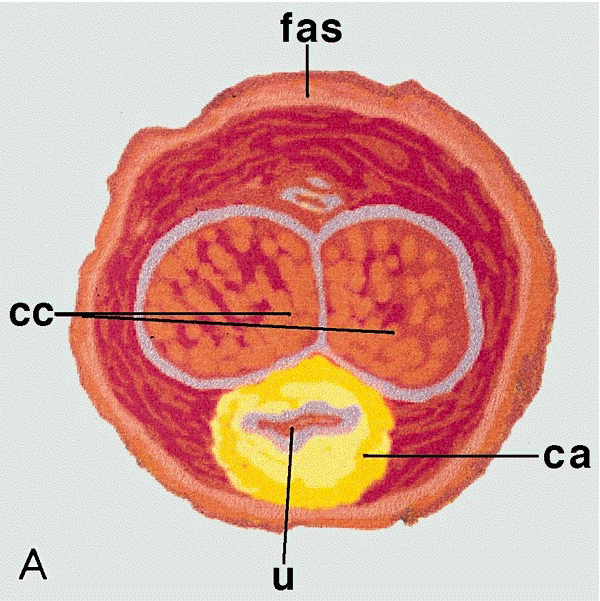
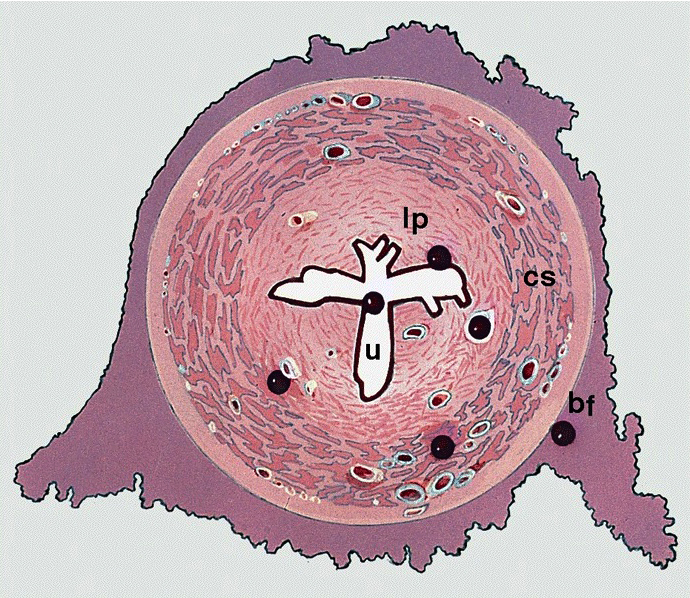
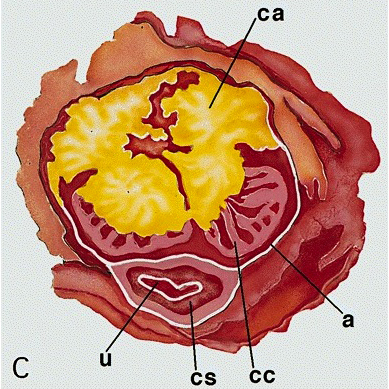
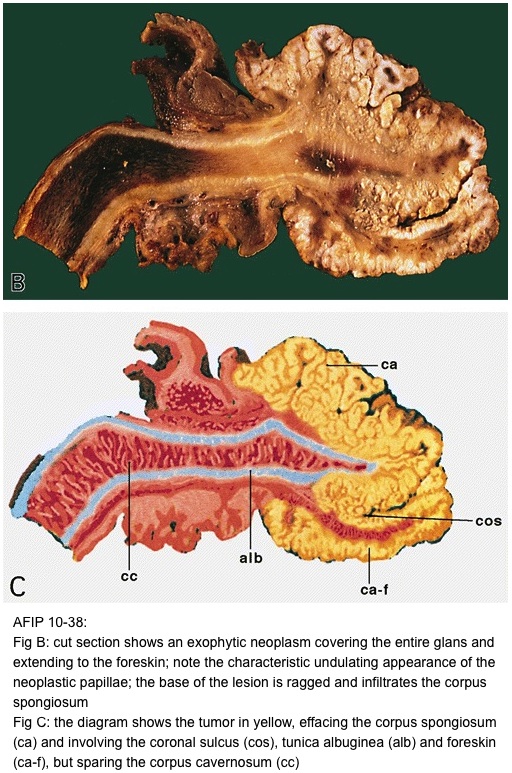
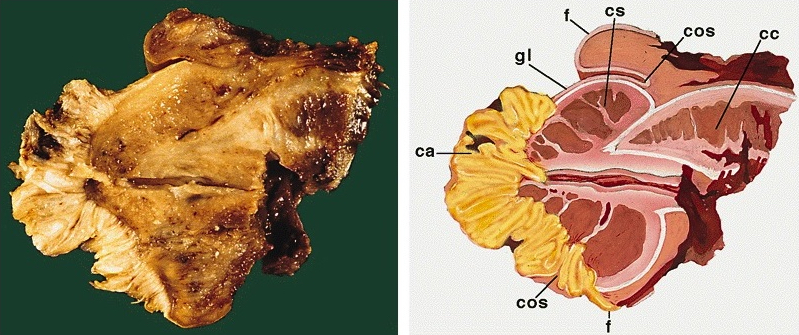
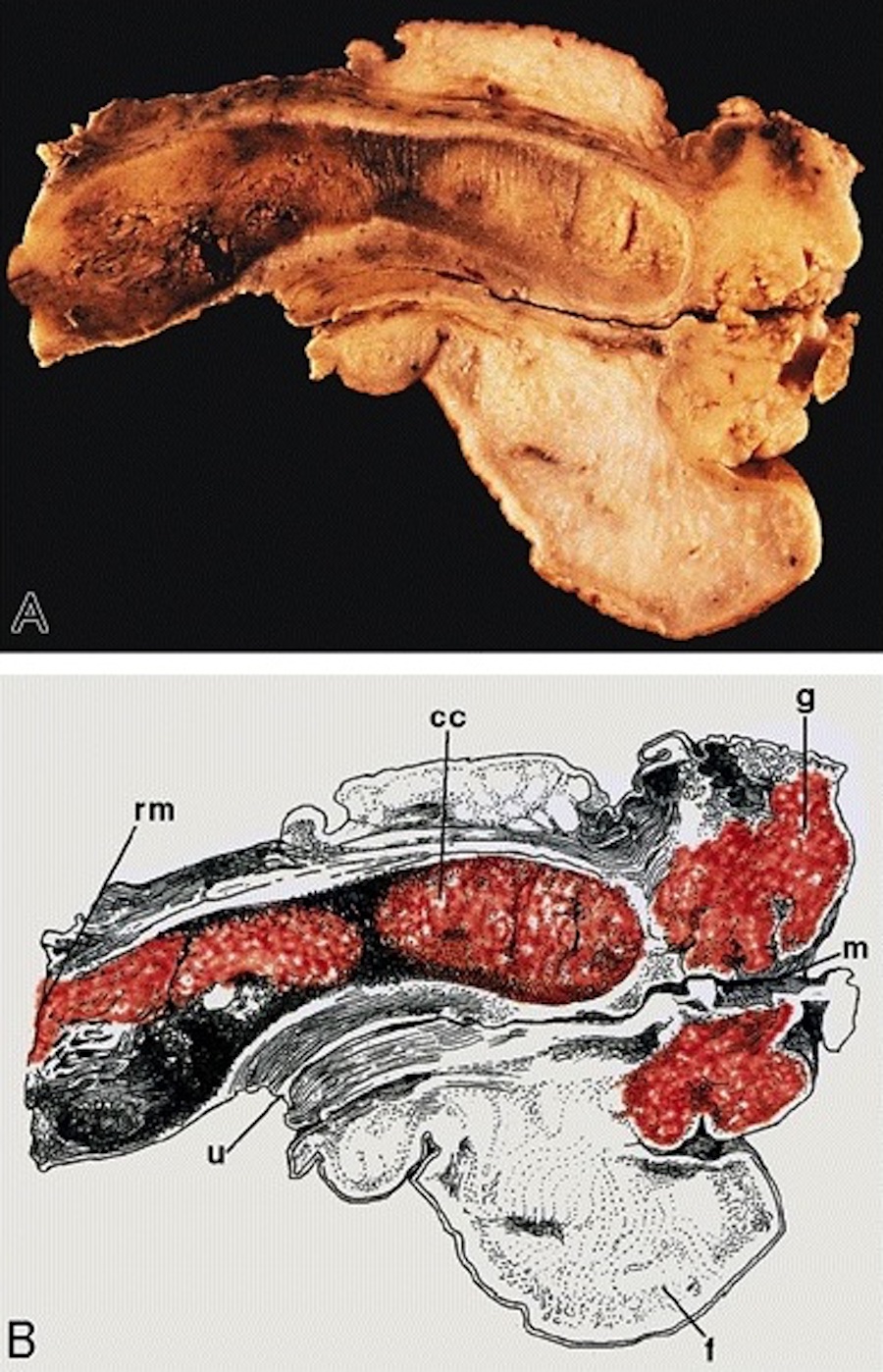
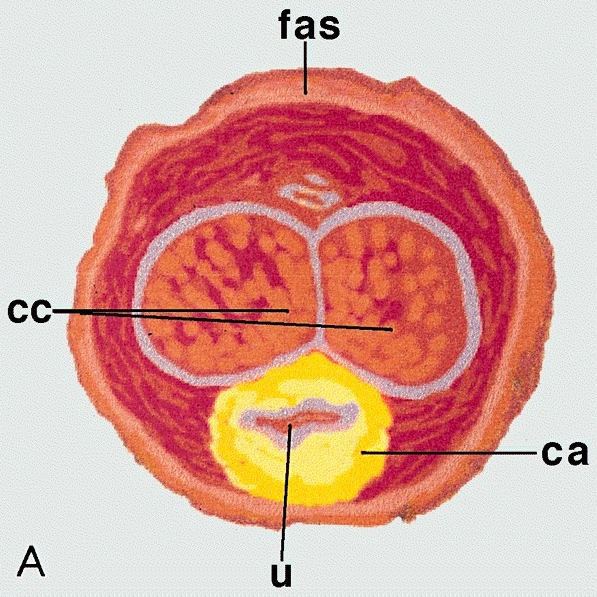
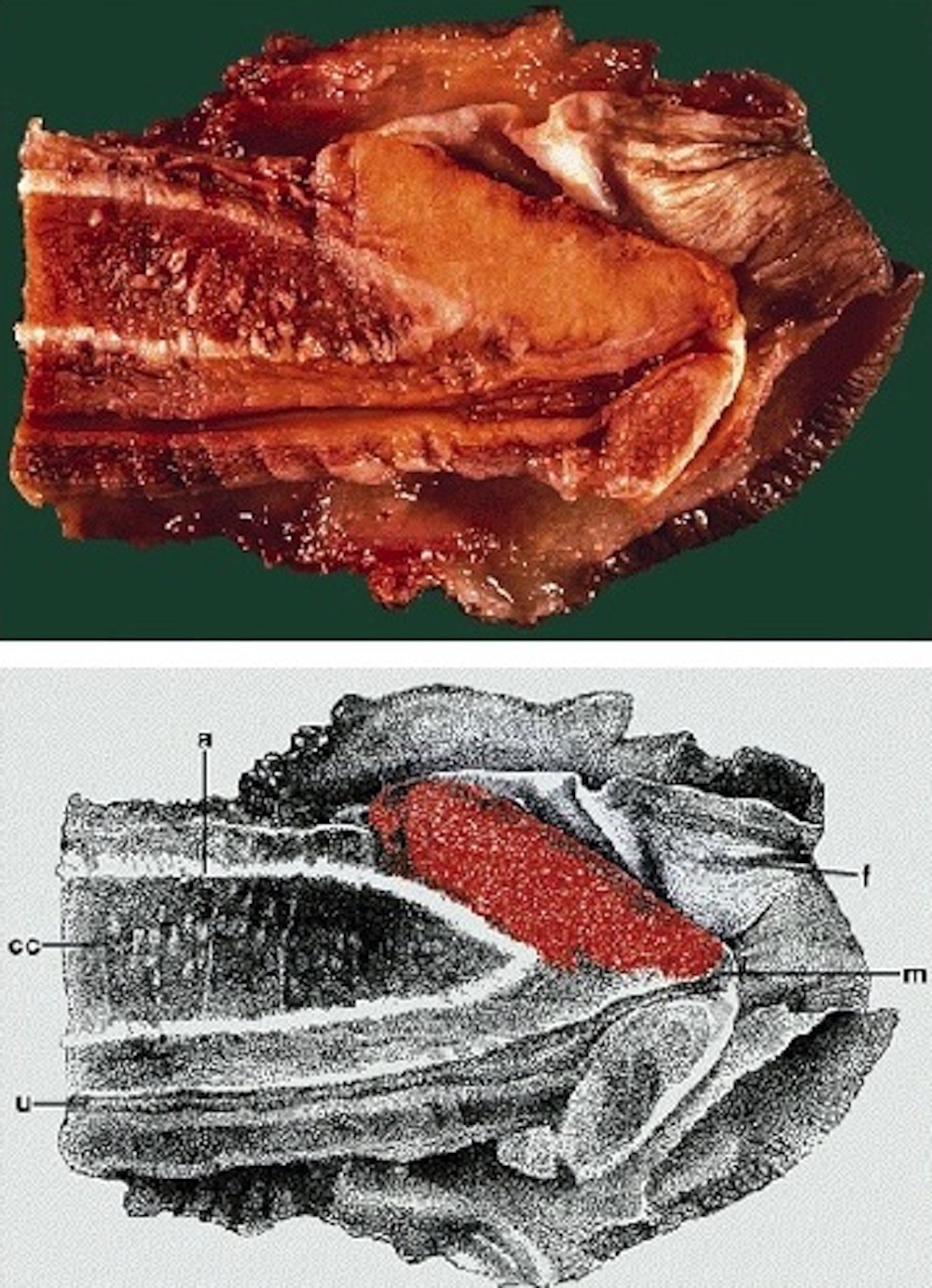
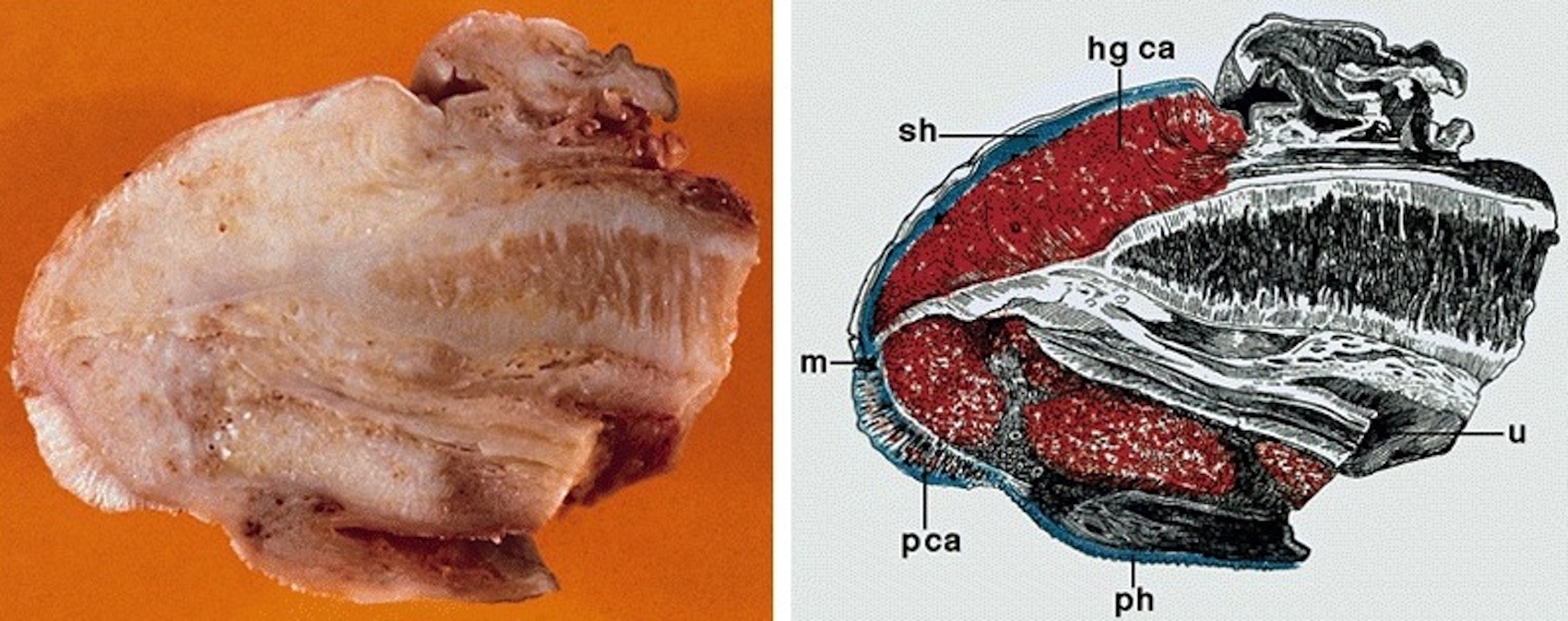
- pT2: invasion of corpus spongiosum
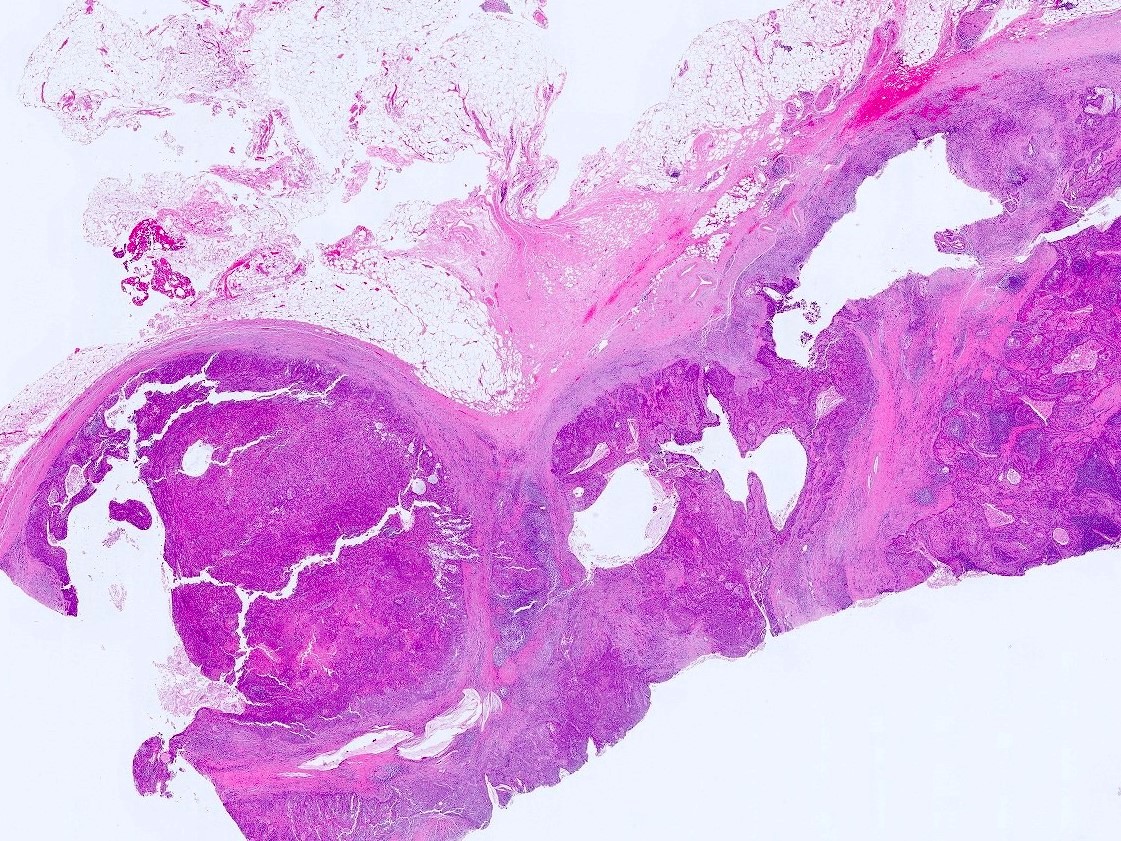
- pT3: invasion of corpus cavernosum
- pT4: invasion of adjacent structures including scrotum, prostate and pubic bone