
















































































Primary tumor (pT)
- pTX: cannot be assessed
- pT0: no evidence of primary tumor
- pT1: tumor limited to the ipsilateral parietal surface with or without involvement of visceral pleura, mediastinal pleura or diaphragmatic pleura
- pT2: tumor involves each of the ipsilateral pleural surfaces (parietal, mediastinal, diaphragmatic and visceral pleura) and has at least one of the following
- Diaphragmatic muscle involvement
- Extension from visceral pleura into the underlying pulmonary parenchyma
- pT3: tumor is locally advanced but potentially resectable; tumor involves all the ipsilateral pleural surfaces (parietal, mediastinal, diaphragmatic and visceral pleura) and has at least one of the following
- Endothoracic fascia involvement
- Mediastinal fat involvement
- Solitary completely resectable focus of tumor extending into soft tissue of chest wall
- Nontransmural involvement of the pericardium
- pT4: tumor is locally advanced and technically unresectable; tumor involves all the ipsilateral pleural surfaces (parietal, mediastinal, diaphragmatic and visceral pleura) and has at least one of the following
- Diffuse extension or multifocal masses in chest wall
- Direct transdiaphragmatic extension to peritoneum
- Direct extension to the contralateral pleura
- Direct extension to mediastinal organs
- Direct extension into spine
- Extension to internal surface of the pericardium
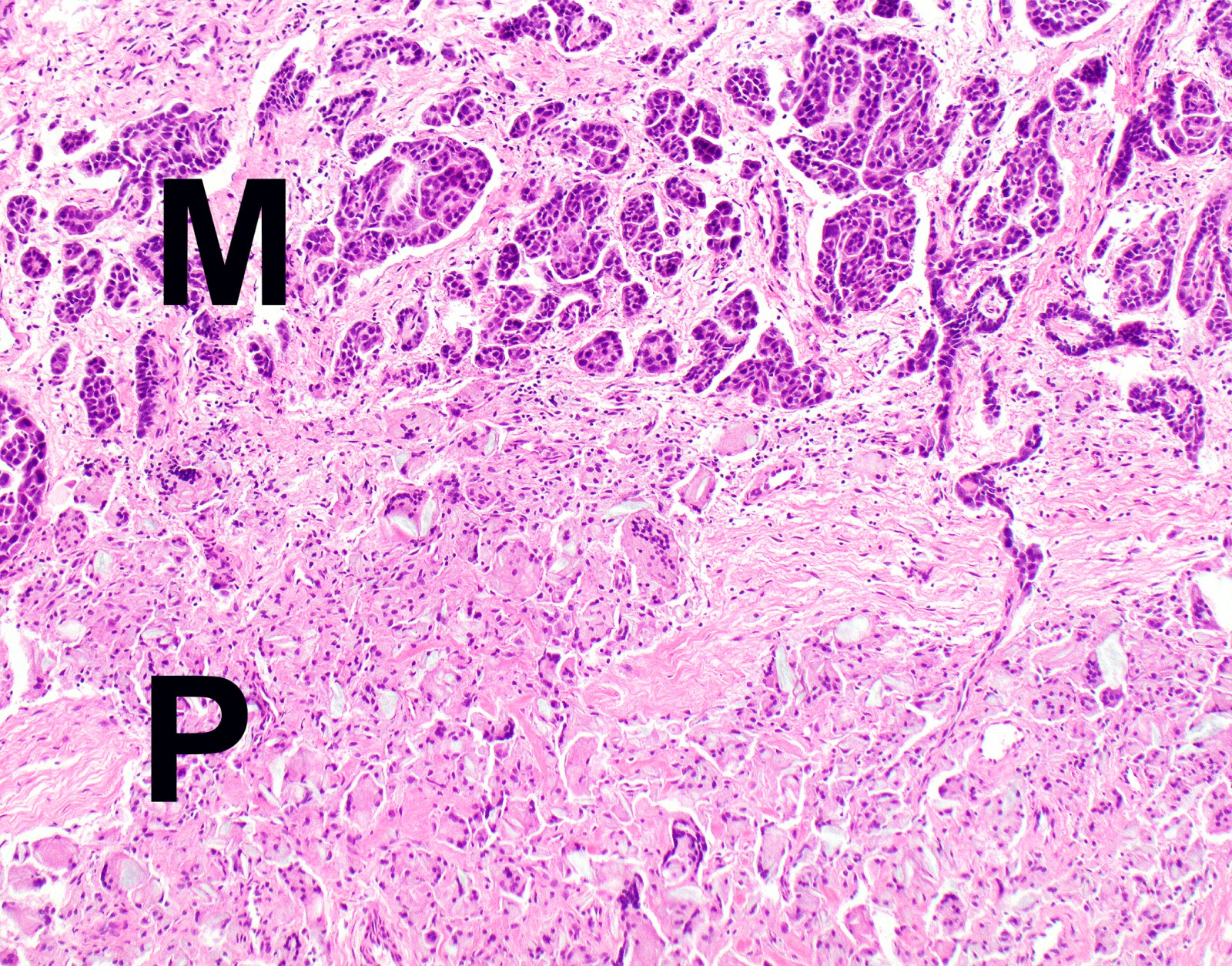
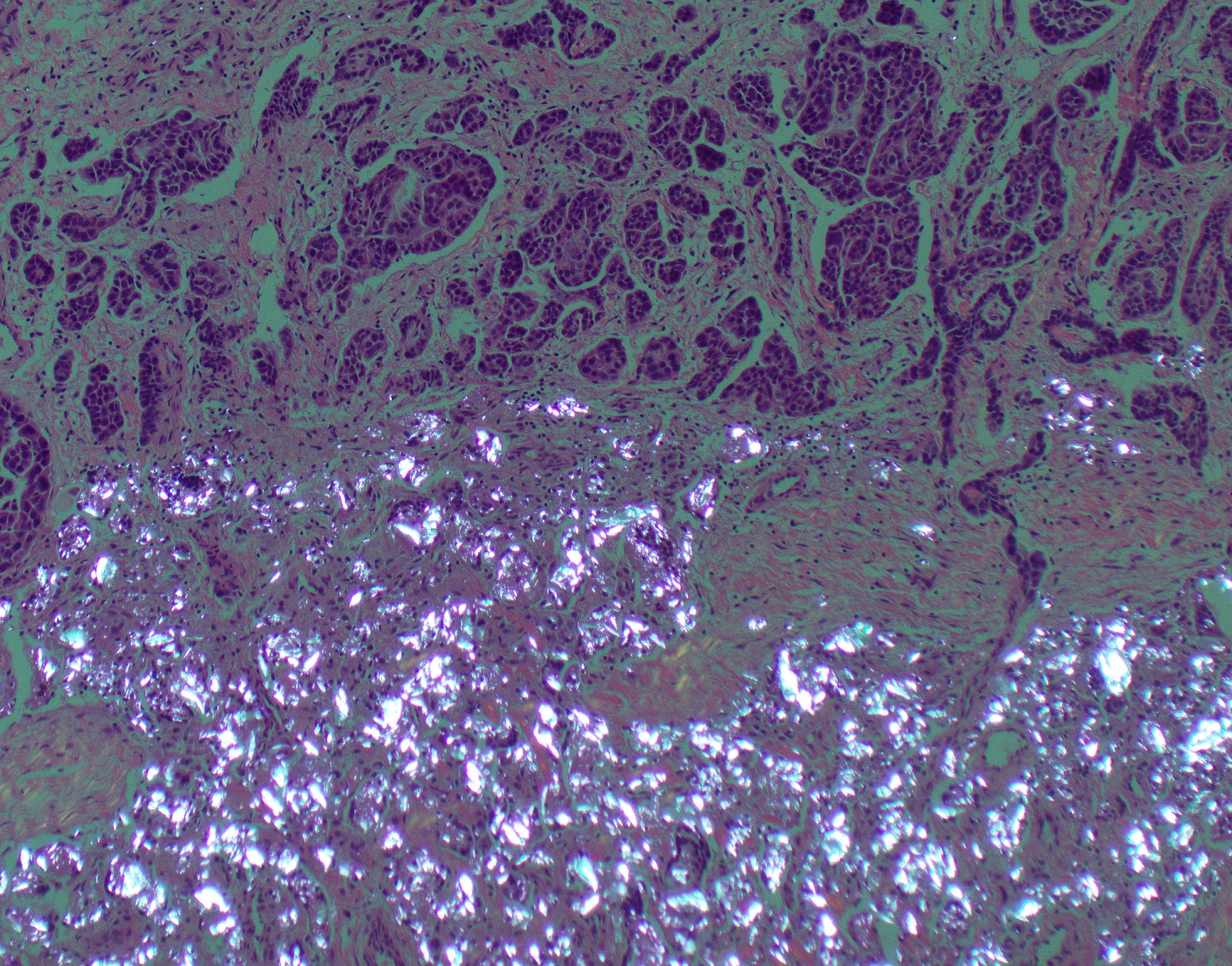
- Myocardium involvement