
































































































































































































































Primary tumor (pT)
- TX: primary tumor cannot be assessed
- T0: no evidence of primary tumor
- Tis: carcinoma in situ
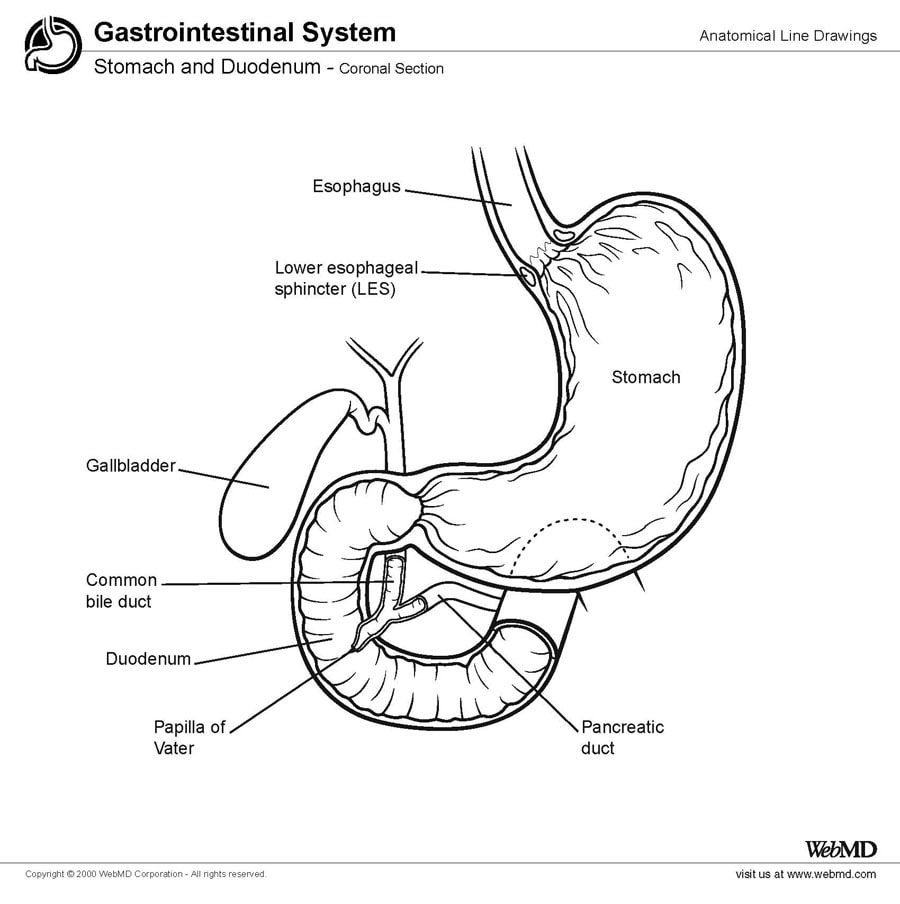
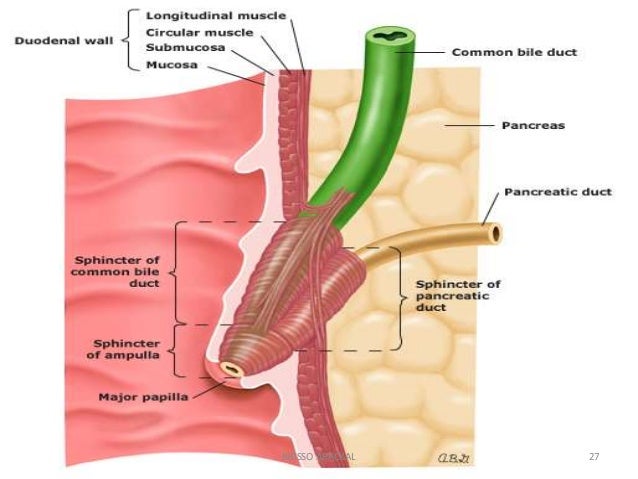
- T1: tumor limited to Ampulla of Vater of sphincter of Oddi or tumor invades beyond the sphincter of Oddi (perisphincteric invasion) or into the duodenal submucosa
- T1a: tumor limited to Ampulla of Vater of sphincter of Oddi
- T1b: tumor invades beyond the sphincter of Oddi (perisphincteric invasion) or into the duodenal submucosa
- T2: tumor invades into the muscularis propria of the duodenum
- T3: tumor directly invades into the pancreas (up to 0.5 cm) or tumor extends more than 0.5 cm into the pancreas or extends into peripancreatic or periduodenal tissue or duodenal serosa without involvement of the celiac axis or superior mesenteric artery
- T3a: tumor directly invades the pancreas (up to 0.5 cm)
- T3b: tumor extends more than 0.5 cm into the pancreas or extends into peripancreatic tissue or periduodenal tissue or duodenal serosa without involvement of the celiac axis or superior mesenteric artery
- T4: tumor involves the celiac axis, superior mesenteric artery or common hepatic artery, irrespective of size