| Primary tumor (T)
|
| TX
|
| Primary tumor thickness cannot be assessed (i.e., diagnosis by curettage)
|
| T0
|
| No evidence of primary tumor (i.e., axillary metastases without known primary tumor)
|
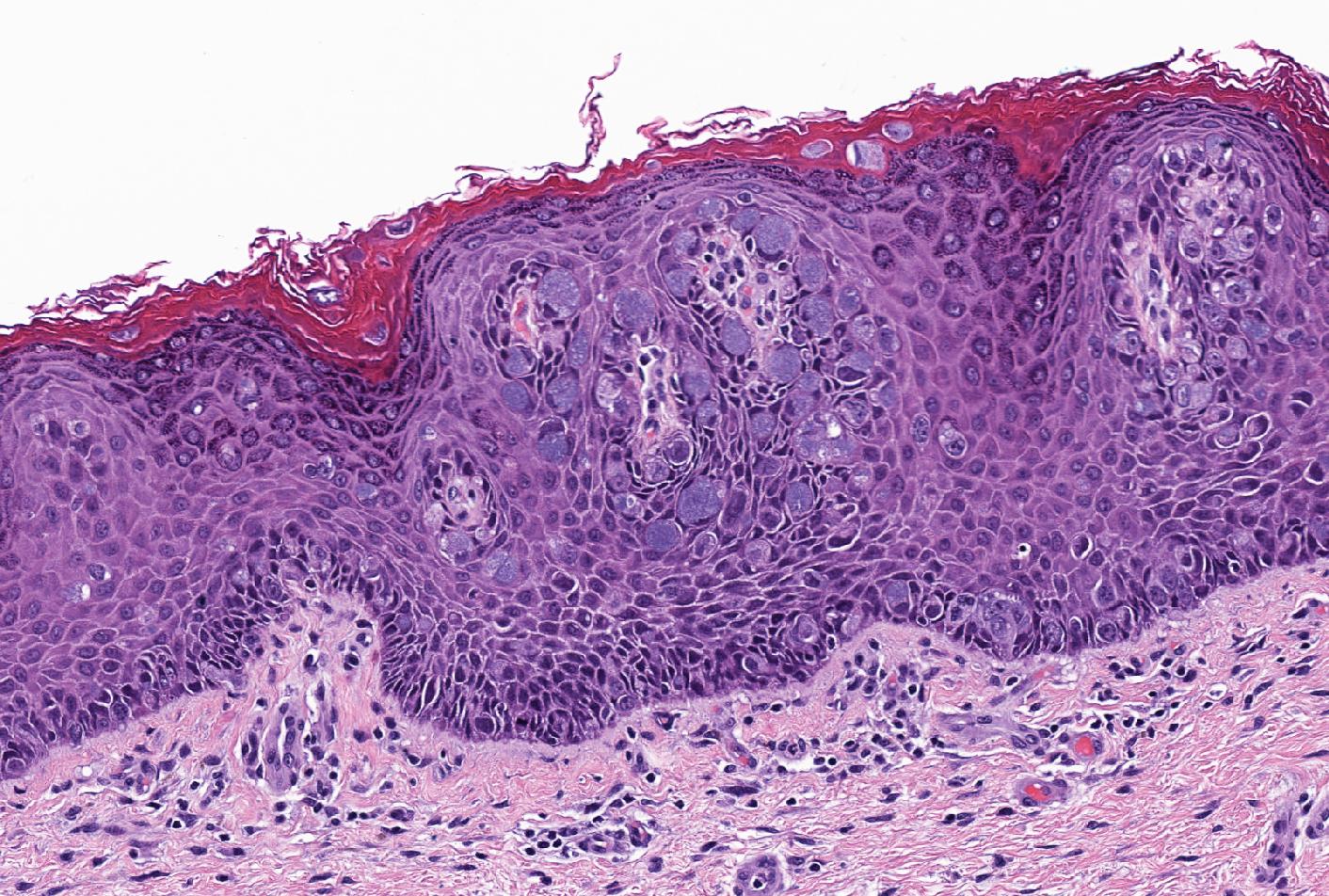
| Tis
|
| Intraepithelial (i.e., melanoma in situ)
|
| T1
|
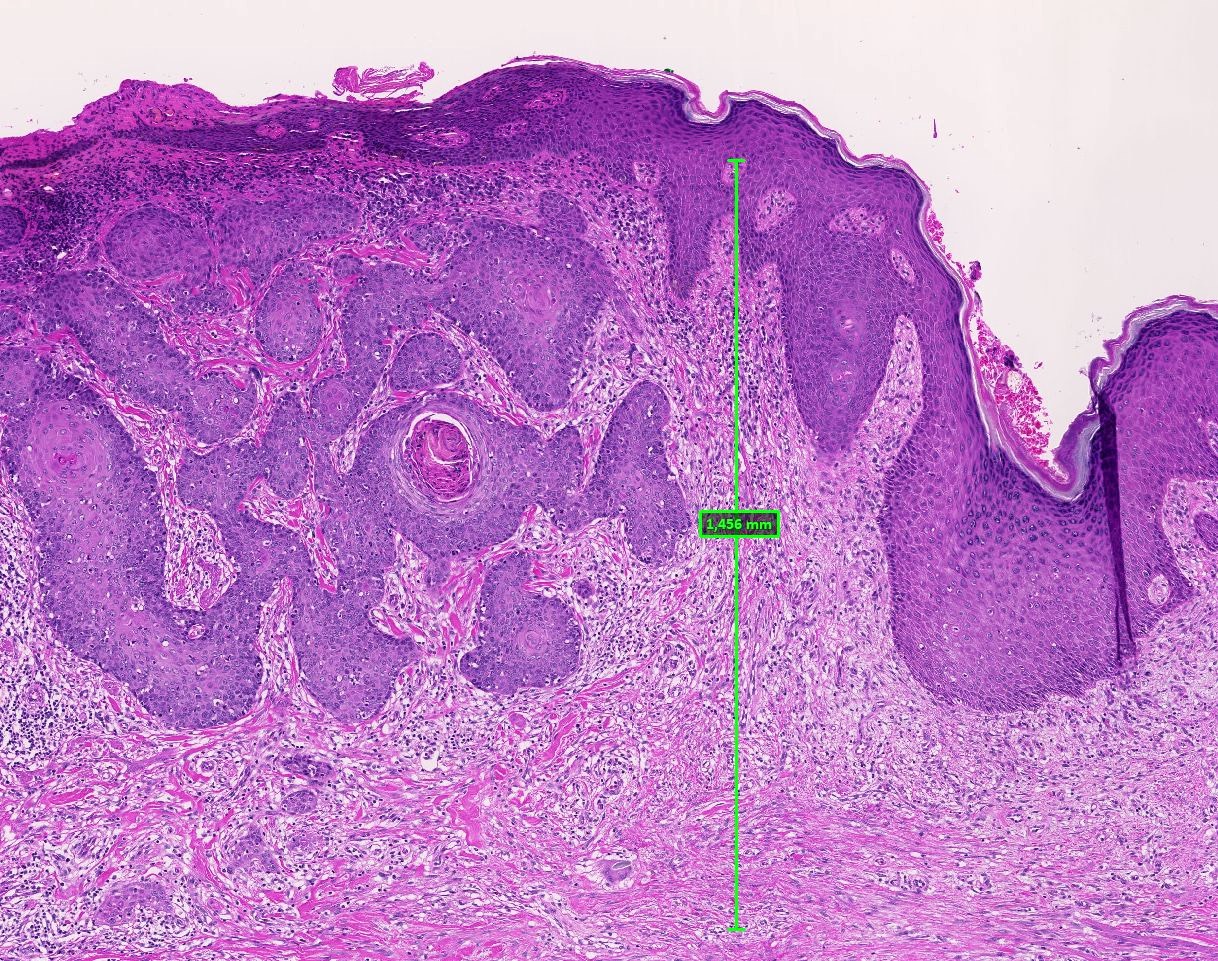
| Tumor ≤ 1.0 mm thick, without or with ulceration
|
| T1a
| ≤ 0.8 mm thick and Clark level II or III, without ulceration
|
| T1b
| < 0.8 mm thick and Clark level IV or V or with ulceration
0.8 - 1.0 mm thick and Clark level IV or V, with or without ulceration
|
| T2
|
| Tumor 1.01 - 2.0 mm thick, without (T2a) or with ulceration (T2b)
|
| T3
|
| Tumor 2.01 - 4.0 mm thick, without (T3a) or with ulceration (T3b)
|
| T4
|
| Tumor > 4.0 mm thick without (T4a) or with (T4b) ulceration
|
| Regional lymph node (N)
|
| Nx
|
| Regional lymph nodes cannot be assessed
|
| N0
|
| No regional lymph node metastasis
|
| N1
|
| Metastasis to 1 lymph node or in transit, satellite or microsatellite metastases with no tumor involved nodes
|
| N1a
| Clinically occult (i.e., detected by SLNB)
|
| N1b
| Clinically apparent (i.e., macroscopic)
|
| N1c
| In transit, satellite or microsatellite metastases with no tumor involved nodes
|
| N2
|
| Metastasis to 2 or 3 regional lymph nodes or in transit, satellite or microsatellite metastases with no tumor involved nodes
|
| N2a
| Clinically occult (i.e., detected by SLNB)
|
| N2b
| Clinically apparent (i.e., macroscopic)
|
| N2c
| In transit, satellite or microsatellite metastases combine with 1 clinically occult or apparent
|
| N3
|
| Metastasis to 4 or more regional lymph nodes, matted lymph nodes or combination of in transit metastasis or satellite(s) and metastatic regional lymph node(s)
|
| N3a
| Clinically occult (i.e., detected by SLNB)
|
| N3b
| Clinically apparent (i.e., macroscopic) or presence of matted nodes
|
| N3c
| In transit, satellite or microsatellite metastases combine with 2 or more clinically occult or clinically detected or presence of matted nodes
|
| Distant metastasis (M)
|
| Mx
|
| Distant metastasis cannot be assessed
|
| M0
|
| No distant metastasis
|
| M1
|
| Distant metastasis, LDH status (designated as 0 for not elevated and I for elevated level; no suffix is used if LDH is not recorded or is unspecified)
|
| M1a
| Distant skin, subcutaneous or lymph node
|
| M1b
| Lung
|
| M1c
| All other non-central nervous system (CNS) visceral sites
|
| M1d
| CNS
|























































































































































































































{kind=link}