
Appendix
Adenocarcinoma and related tumors
Goblet cell adenocarcinoma
Editorial Board Member: Wei Chen, M.D., Ph.D.
Deputy Editor-in-Chief: Catherine E. Hagen, M.D.


Last author update: 21 January 2022
Last staff update: 21 January 2022
Copyright: 2003-2024, PathologyOutlines.com, Inc.
PubMed Search: Goblet cell adenocarcinoma appendix free full text[SB]
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Laboratory | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Clinical images | Gross description | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Electron microscopy description | Electron microscopy images | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Lollie T, Wang HL. Goblet cell adenocarcinoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/appendixgobletcellcarcinoid.html. Accessed April 20th, 2024.
Definition / general
- Amphicrine neoplasm containing goblet-like mucinous cells with variable numbers of endocrine cells and Paneth-like cells, typically arranged in a tubular or clustered architecture, resembling intestinal crypts
- To be classified as a goblet cell adenocarcinoma, a tumor must demonstrate at least a component of classic low grade goblet cell adenocarcinoma
- Despite previous goblet cell carcinoid terminology, goblet cell adenocarcinoma is considered a variant of adenocarcinoma and is distinct from neuroendocrine neoplasm
Essential features
- Amphicrine tumor containing goblet-like mucinous cells, endocrine cells and Paneth-like cells
- Prognosis dependent on grade and stage of adenocarcinoma
- Important to differentiate from neuroendocrine neoplasm to avoid inappropriate chemotherapeutic regimens and incorrect prognostic indicators
- Mass lesions are typically absent and are often found incidentally or associated with acute appendicitis
- Appendix must be submitted entirely to determine the extent of high grade component, the depth of invasion and the margin status
Terminology
- Acceptable by World Health Organization (WHO) Classification of Tumors (2019):
- Goblet cell carcinoma
- Not recommended by WHO (2019):
- Goblet cell carcinoid
- Adenocarcinoma ex goblet cell carcinoid
- Adenocarcinoid
- Crypt cell carcinoma
- Microglandular carcinoma
- Amphicrine neoplasm
- Mucinous carcinoid
- Mucin producing neuroendocrine tumor or carcinoma
- Mixed goblet cell carcinoid adenocarcinoma
ICD coding
- ICD-O: 8243/3 - goblet cell carcinoid
- ICD-11: 2B81.Y & XH4262 - malignant neoplasms of appendix & goblet cell carcinoid
Epidemiology
- M = F
- Age range of 30 - 85; mean age of 50 - 60 (World J Surg Oncol 2005;3:36)
- ~10 years older than well differentiated neuroendocrine tumor (Neuroendocrinology 2012;95:135)
Sites
- Most often involving distal appendix
- Metastasizes to peritoneum, omentum, abdominal wall and ovaries (Arch Pathol Lab Med 2015;139:782)
Pathophysiology
- Unknown
- Intestinal stem cell theory: arises from pluripotent stem cells capable of dual mucinous and neuroendocrine differentiation (World J Gastrointest Oncol 2010;2:251)
Etiology
- Unknown; large scale sequencing studies have found the following associations:
- Altered Wnt signaling associated genes (USP9X, NOTCH1, CTNNA1, CTNNB1, TRRAP) (Mod Pathol 2018;31:829)
- Mutations in TP53, CDH1 and MLL2 associated with high grade transformation (Mod Pathol 2018;31:989)
- Subset with mutations found in gastric signet ring cell adenocarcinoma (i.e. CDH1, RHOA) (Mod Pathol 2018;31:989, Hum Pathol 2018;77:166)
- Rare to absent mutations in colorectal cancer related genes (i.e. TP53, KRAS, APC) (Mod Pathol 2018;31:829)
Clinical features
- Acute appendicitis
- Perforation / disseminated disease:
- Abdominal pain
- Palpable mass
- Female patients may present with ovarian metastasis (Ann Surg Oncol 2006;13:370)
Diagnosis
- Often found incidentally or associated with acute appendicitis
Laboratory
- Nonspecific; findings associated with acute appendicitis (i.e. leukocytosis with left shift)
- CEA, CA19-9, CA125 may be used to monitor tumor recurrence (Endocr Connect 2018;7:268)
Radiology description
- Nonspecific; findings associated with acute appendicitis (distended edematous appendix) or perforation / disseminated disease
Radiology images
Images hosted on other servers:

CT abdomen: dilated and inflamed appendix

CT / MRI: ovary and appendix
Prognostic factors
- Grade and stage dependent (Arch Pathol Lab Med 2015;139:782):
- Low grade:
- Presents with stage I or II disease
- 33% of patients presented with metastasis in 1 study (Am J Surg Pathol 2008;32:1429)
- 84 - 204 months survival time
- Intermediate grade:
- 60 - 86 months survival time
- High grade / disseminated:
- 29 - 45 months survival time
- Low grade:
Case reports
- 57 year old man with acute appendicitis (Cureus 2021;13:e13511)
- 67 year old woman with metastatic appendiceal goblet cell adenocarcinoma to ovarian mature teratoma, mimicking malignant transformation of a teratoma (Diagn Pathol 2019;14:88)
- 77 year old man with history of adenocarcinoma of the transverse colon status postcolectomy, found to have appendiceal lesion on surveillance colonoscopy (J Med Case Rep 2018;12:275)
Treatment
- Debate on performing appendectomy with clear margins versus right hemicolectomy
- Appendectomy with negative margin and lifelong surveillance
- pT1 / pT2 tumors
- Comorbidities that do not allow further surgical intervention
- Some advocate right hemicolectomy only for:
- pT3 / pT4 tumors
- > 2 cm in size
- High grade tumors
- Involvement of the base of the appendix
- Positive appendectomy margin
- Perforated appendix
- Nodal metastasis
- Appendectomy with negative margin and lifelong surveillance
- Unclear whether cytoreductive surgery and hyperthermic intraperitoneal chemotherapy (HIPEC) improve survival
- Indicated for peritoneal carcinomatosis
- No improvement of survival for patients with high grade goblet cell adenocarcinoma in 1 series (Ann Surg Oncol 2016;23:4338)
- Recent study showed median survival of 30 months, 80% 1 year survival rate and 20% 3 year survival rate (Clin Colorectal Cancer 2011;10:108)
- Unresponsive to anti-EGFR therapies due to absence of KRAS / NRAS mutation
- Prophylactic oophorectomy, particularly for postmenopausal women
- Candidates for right hemicolectomy or chemotherapy
Clinical images
Images hosted on other servers:

Laparoscopic view of an inflamed appendix
Gross description
- Normal to thickened appendiceal wall
- Often overlooked due to absence of gross mass lesion
- Appendix must be entirely submitted with careful attention to the proximal margin
- Reference: Adv Anat Pathol 2019;26:75
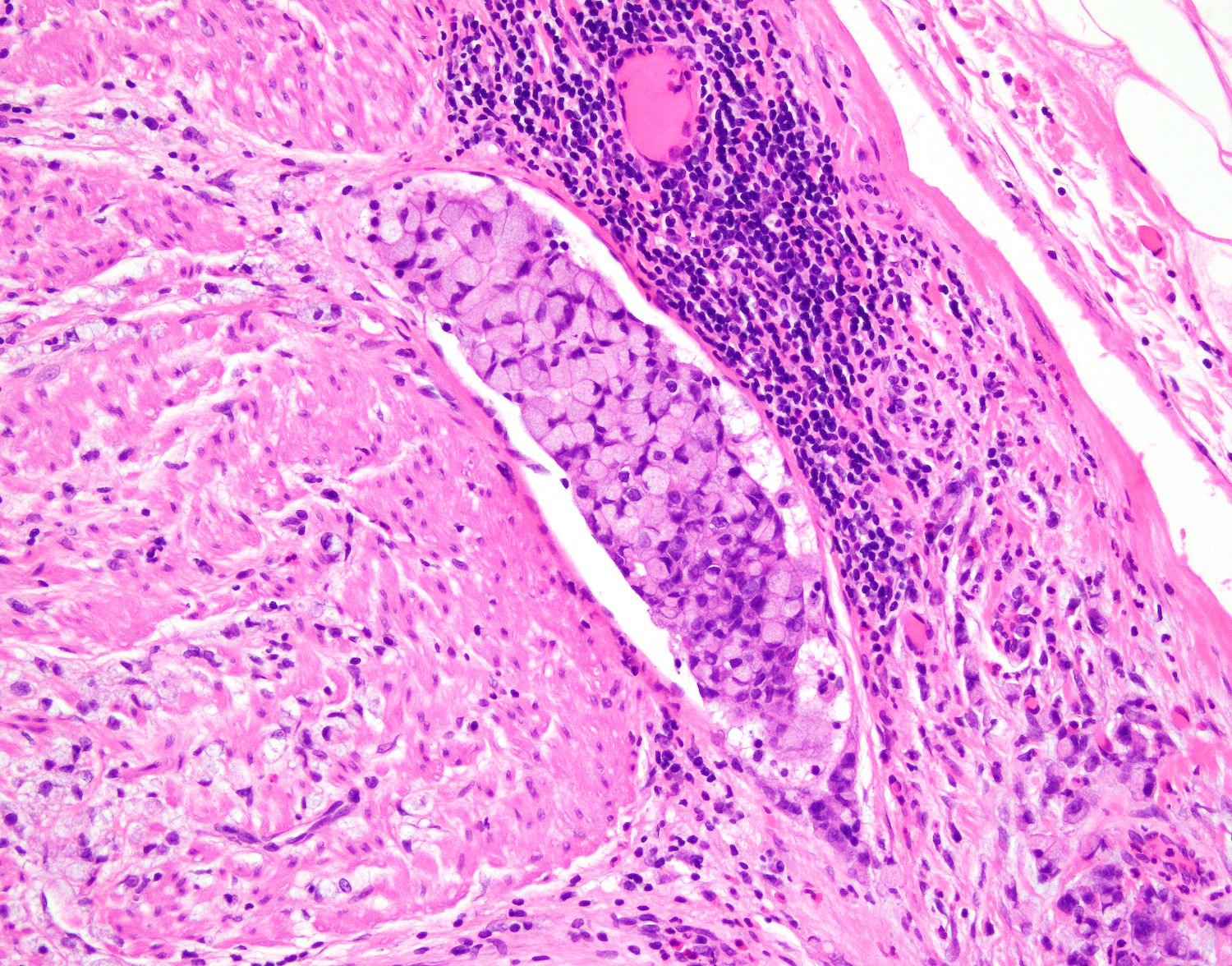
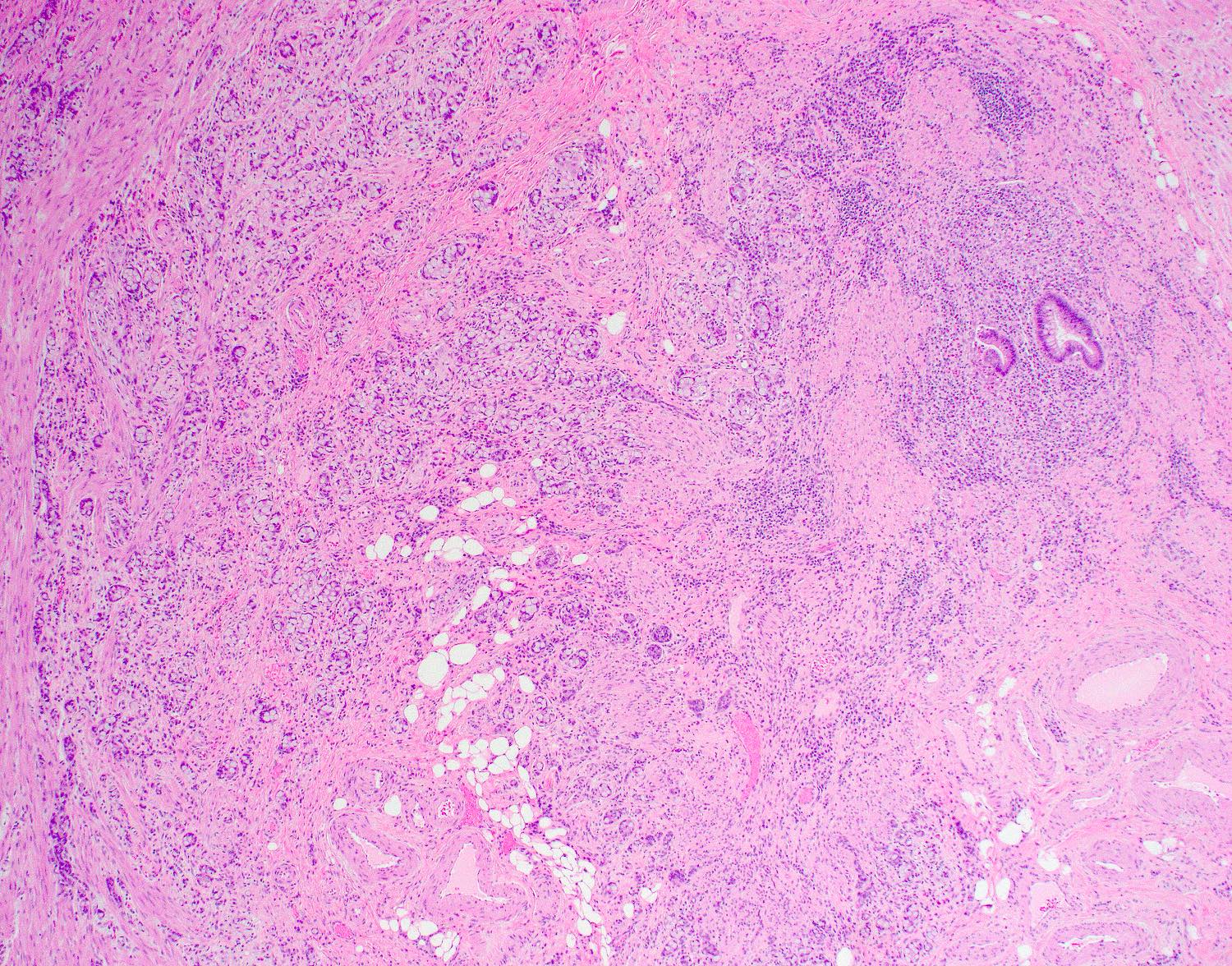
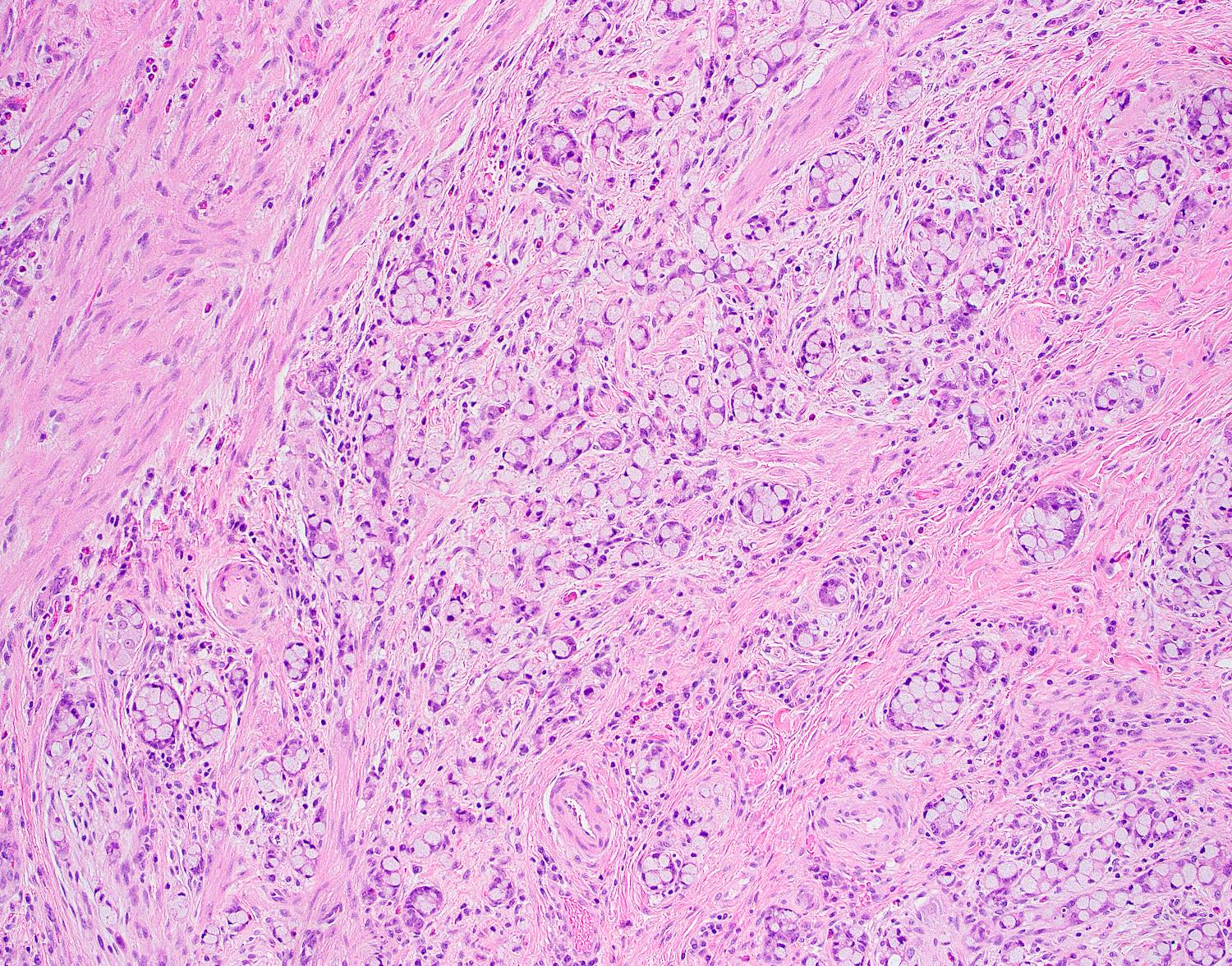
Microscopic (histologic) description
- Concentric / circumferential infiltration of the appendiceal wall by small tubules, nests, clusters or cords of tumor cells with goblet cell morphology (small, compressed nuclei with intracytoplasmic mucin)
- Reference: Adv Anat Pathol 2019;26:75
Low grade versus high grade histological features
Low grade features High grade features - Goblet-like mucinous cells arranged in a tubular pattern
with or without lumens or forming small round to oval
discrete clusters - Variable numbers of endocrine and Paneth-like cells
- Mild nuclear atypia
- Low mitotic rate
- Acceptable:
- Limited tubular fusion or simple trabecular growth
- Occasional single goblet-like cells
- Extracellular mucin, which can be abundant
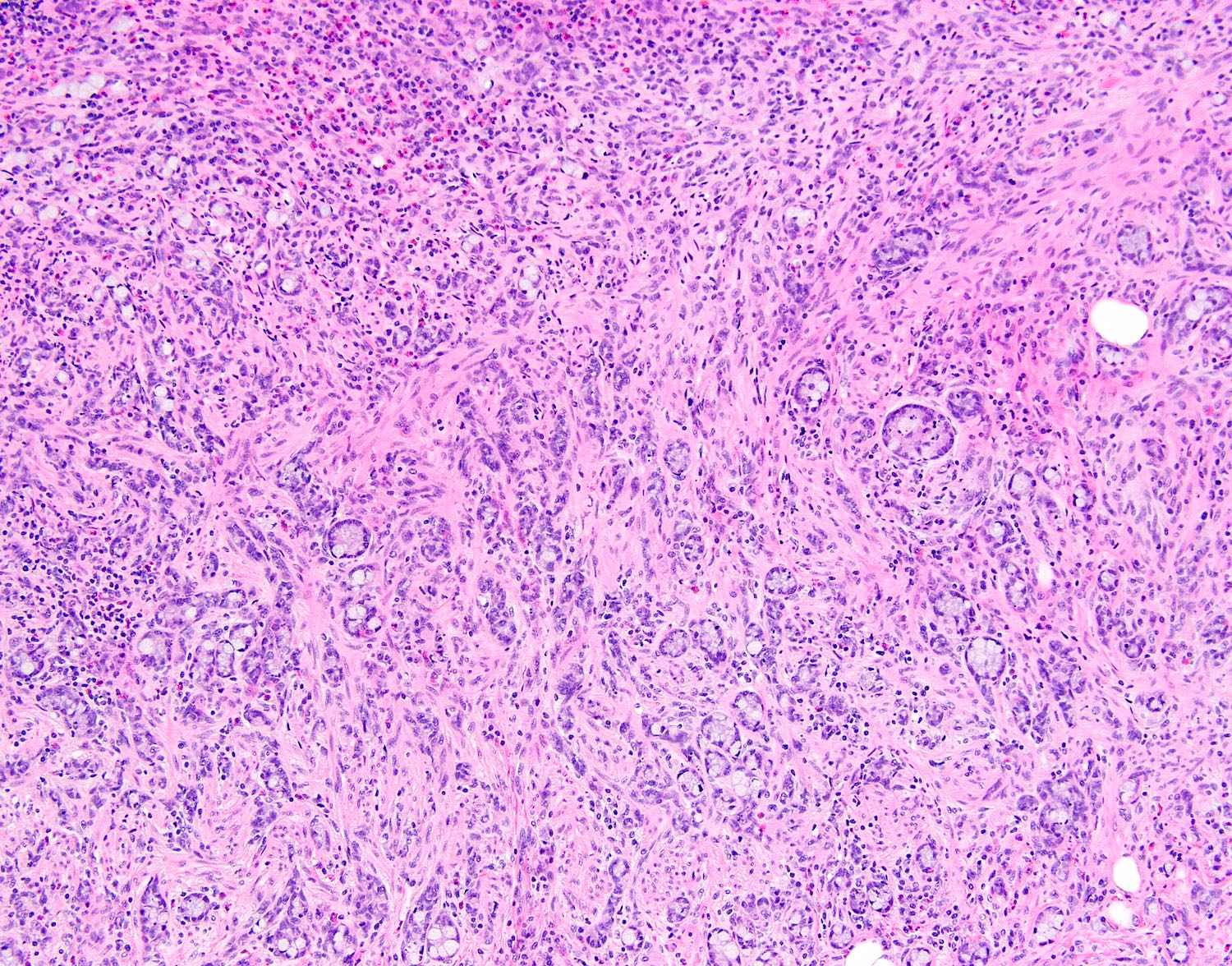
- Complex anastomosing tubules
- Cribriform architecture
- Confluent solid sheets
- Large irregular clusters
- Numerous poorly cohesive goblet-like or nonmucinous cells
- Single file growth pattern
- Single goblet or signet ring-like cells or adenocarcinomatous
glands floating in mucin pools - High grade cytology
- Conventional adenocarcinoma
- Numerous mitoses with atypical mitotic figures
- Necrosis
- Desmoplastic stromal reaction
Yozu 3 tier grading system based on low grade versus high grade patterns
Reference: Am J Surg Pathol 2018;42:898Grade Low grade pattern
(tubular or clustered growth)Any combination of high grade features
(loss of tubular or clustered growth)1 > 75% < 25% 2 50 - 75% 25 - 50% 3 < 50% > 50% - Goblet-like mucinous cells arranged in a tubular pattern
Microscopic (histologic) images
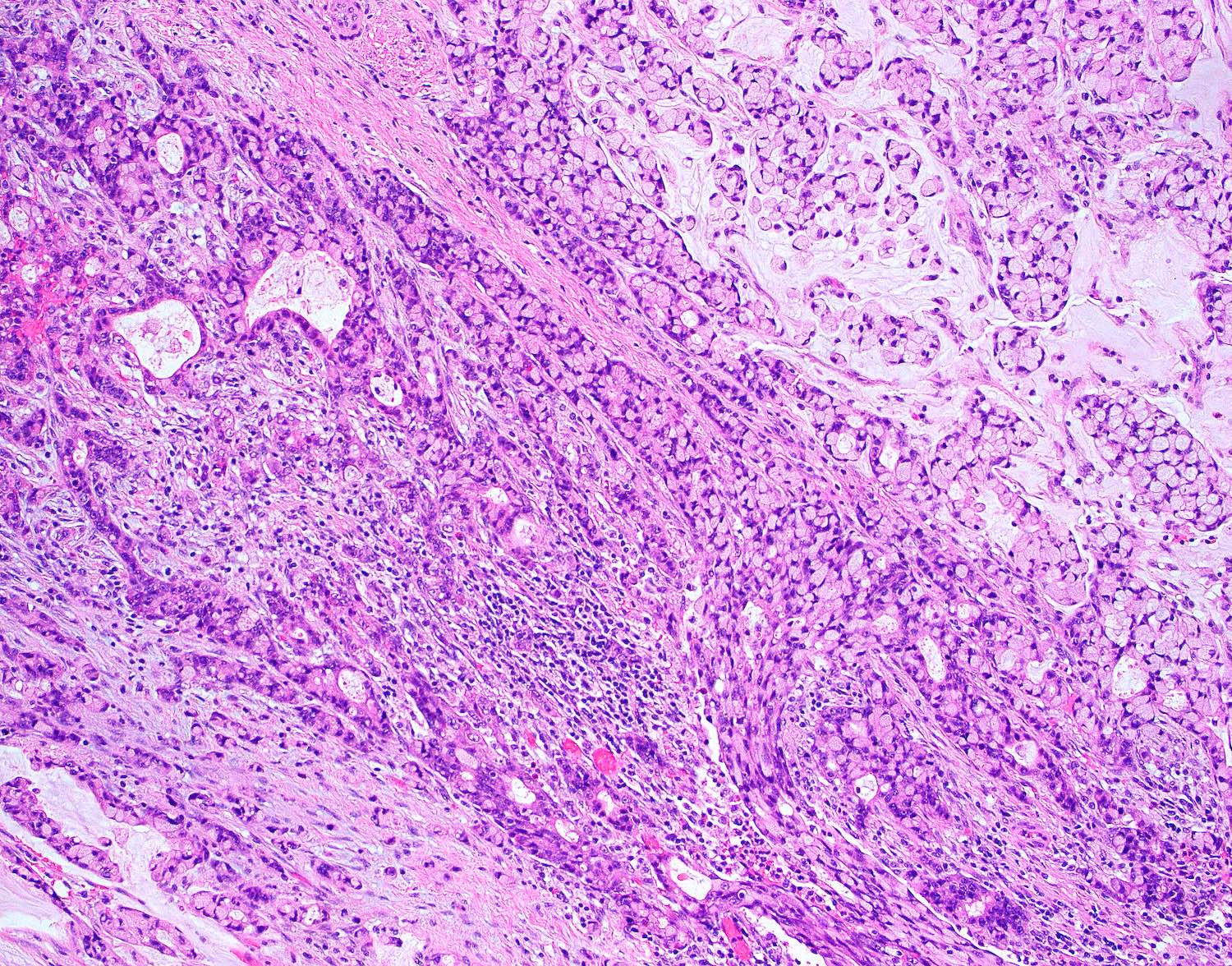
Contributed by Trang Lollie, M.D.
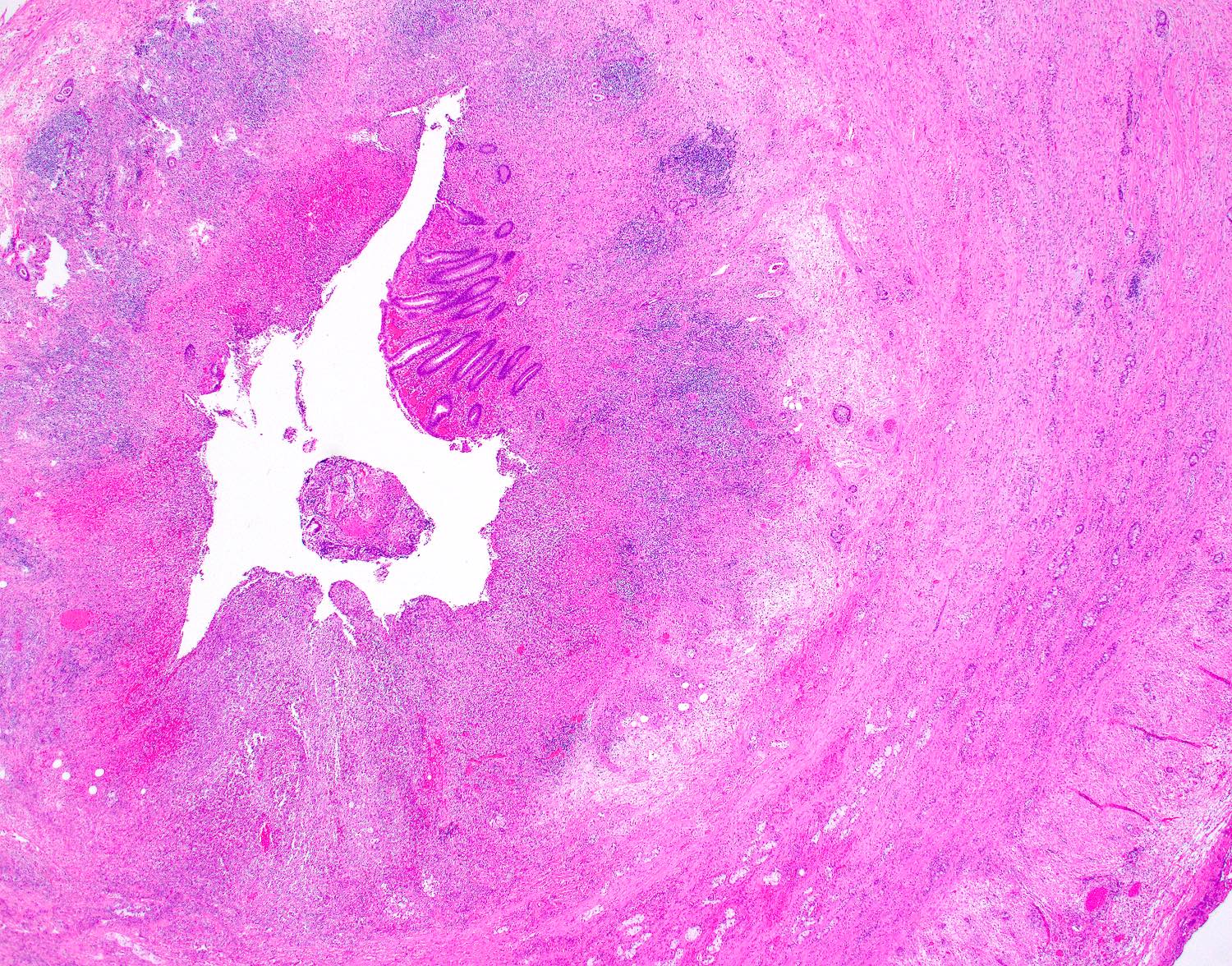
Concentric growth
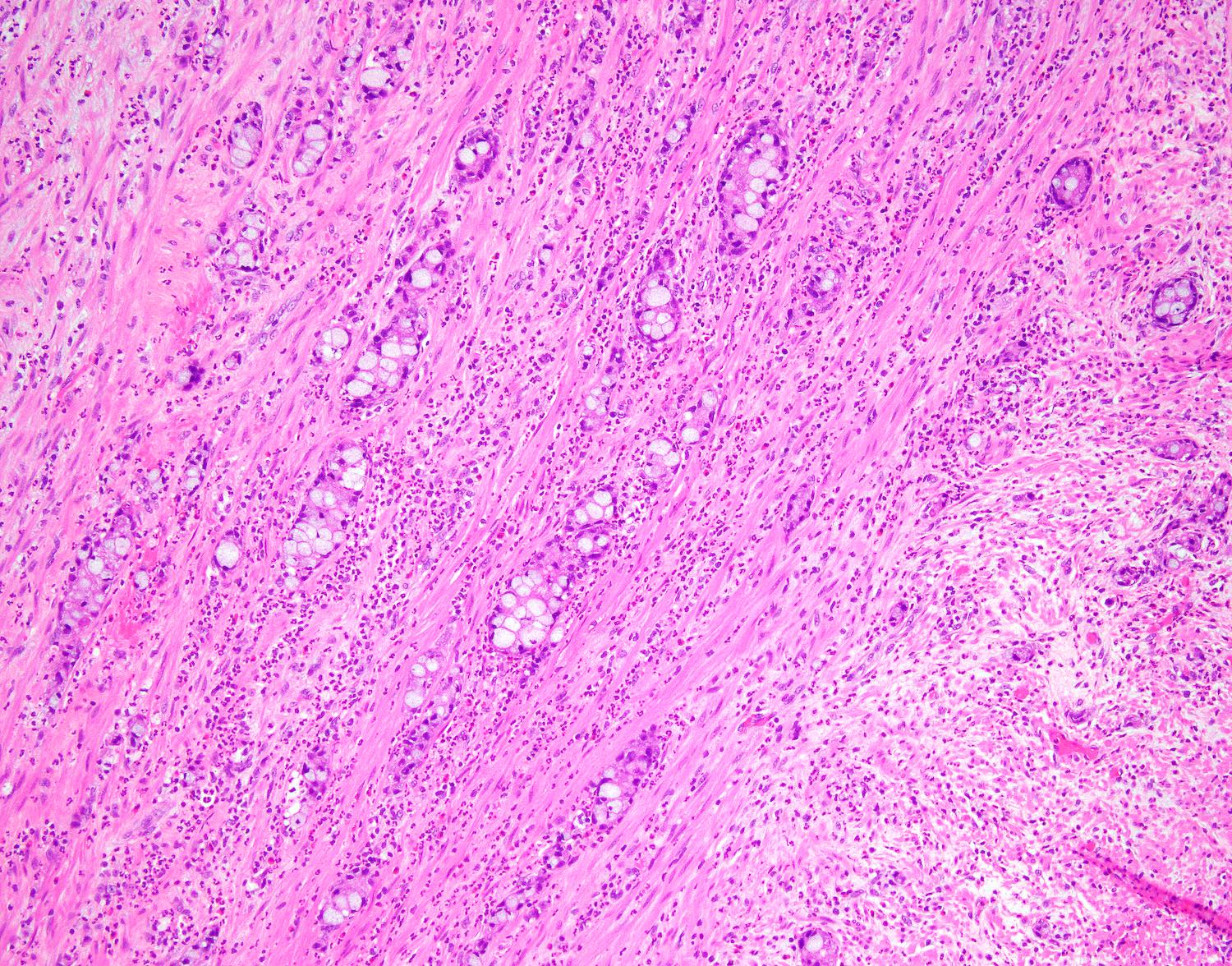
Low grade growth pattern
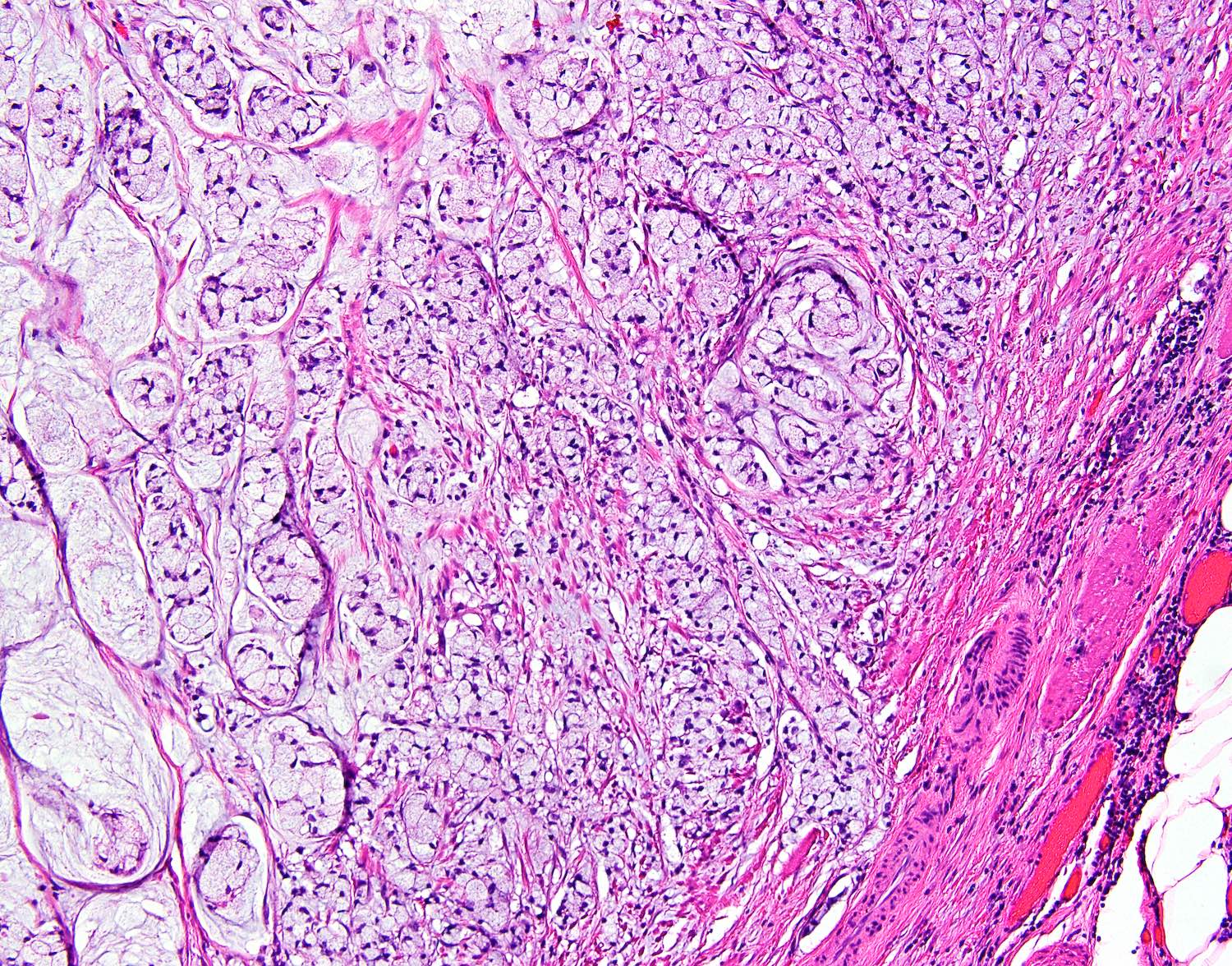

High grade growth pattern
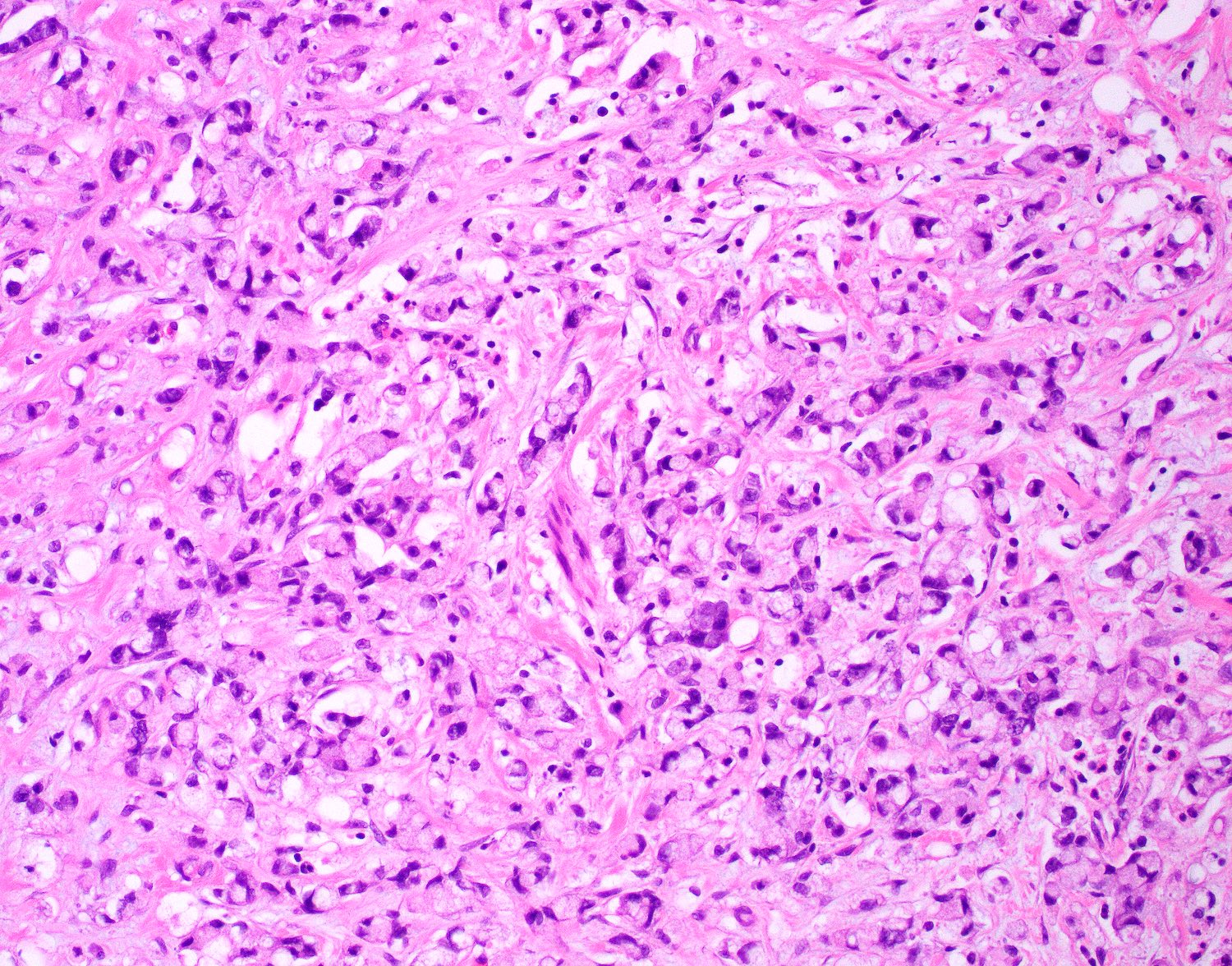
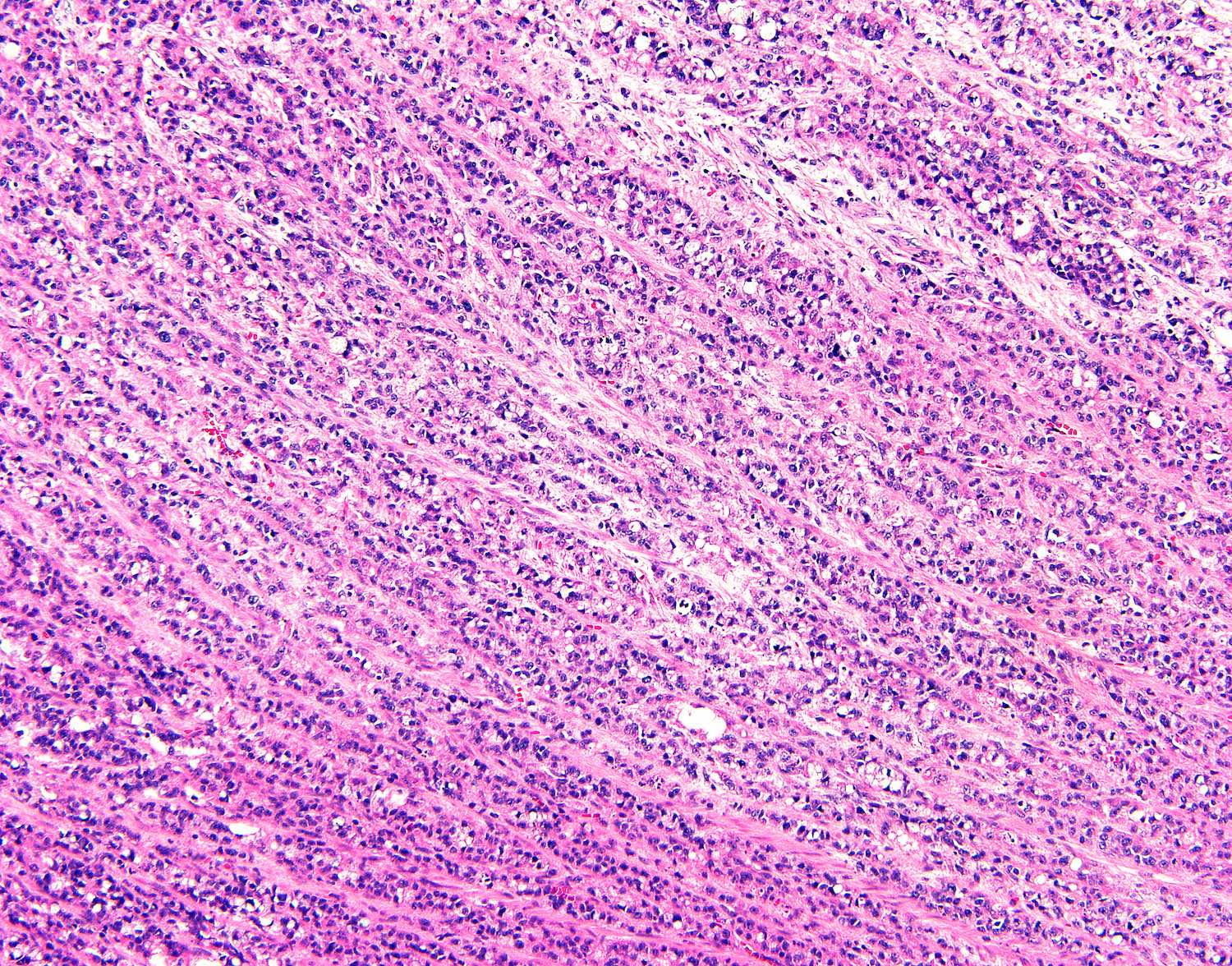
High grade growth pattern
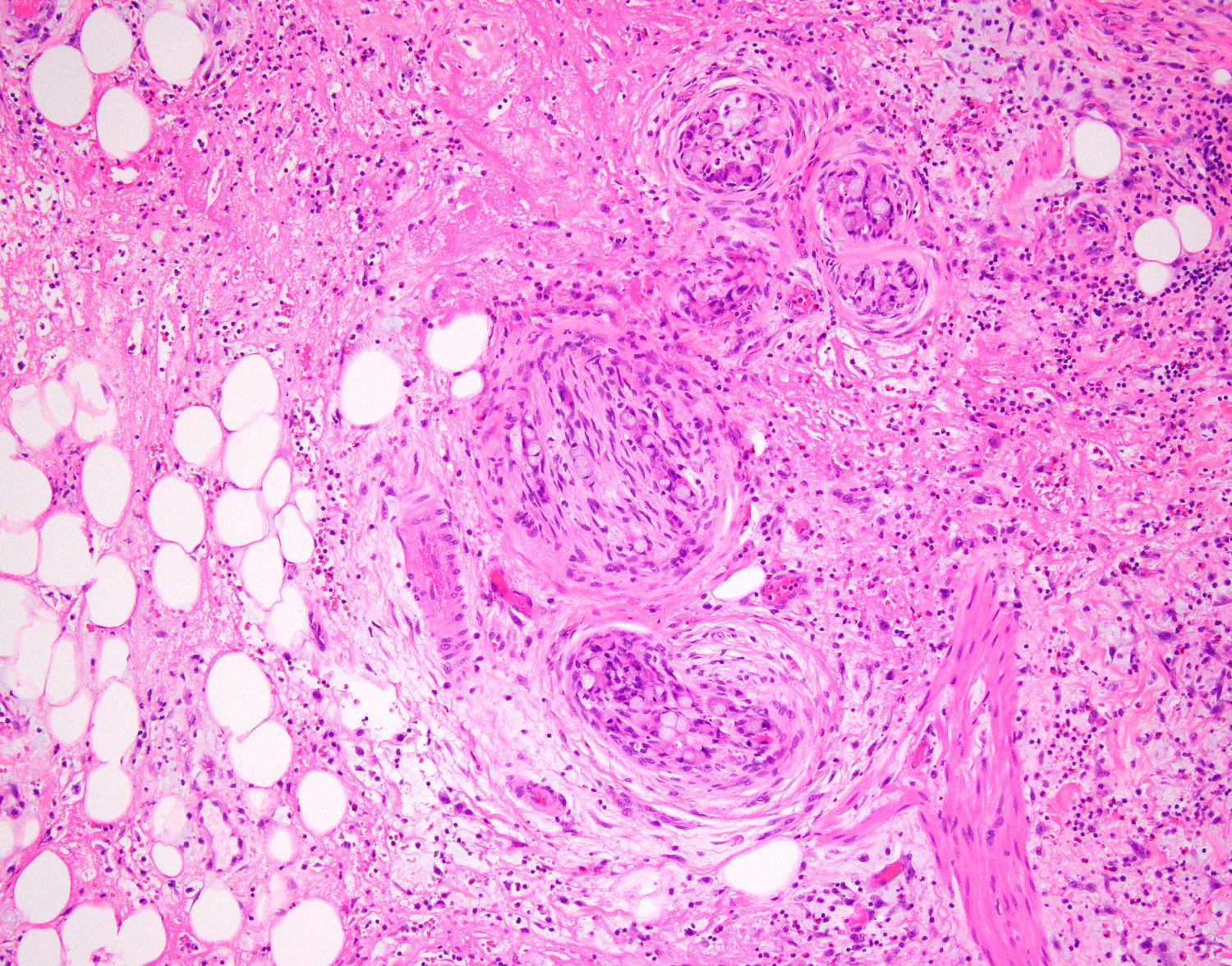
Perineural invasion
Lymphovascular invasion
Positive stains
- Diagnosis and grading are based on morphology; immunohistochemical stains are not required for diagnosis and Ki67 proliferative index is not required for grading
- These stains may be performed:
- Mucicarmine
- CK20: strong and diffuse (Adv Anat Pathol 2019;26:75)
- SATB2 / CDX2 / CEA (Adv Anat Pathol 2019;26:75)
- CK7: strong and diffuse (33 - 75%) (Adv Anat Pathol 2019;26:75)
- Synaptophysin / chromogranin: focal or scattered (85 - 100%) (Adv Anat Pathol 2019;26:75)
- Ki67: variable (0 - 80%)
Electron microscopy description
- Pleomorphic neurosecretory type granules within mucin containing goblet cells (Cancer 1979;44:1700)
- Lysozyme-, secretory component (SC)- and CEA reactive and contained weakly NSE reactive endocrine cells (Pathol Res Pract 1984;178:555)
- In contrast to typical carcinoids: CEA negative and strongly NSE reactive
Electron microscopy images
Images hosted on other servers:

Pleomorphic electron dense granules

Electron dense granules within mucin
Sample pathology report
- Appendix, appendectomy:
- Goblet cell adenocarcinoma, grade 1
- Tumor invades through the muscularis propria into mesoappendix but does not extend to serosal surface
- Proximal appendiceal margin free of tumor
- Mesoappendiceal margin free of tumor
- Perineural invasion present
- No lymphovascular invasion identified
- See synoptic report for additional details
Differential diagnosis
- Well differentiated neuroendocrine tumor:
- Lack of mucin containing goblet-like cells or extracellular mucin
- Usually mass forming with no concentric or circumferential growth pattern
- Signet ring cell adenocarcinoma:
- Poorly cohesive signet ring cells constituting > 50% of tumor volume
- Lack of low grade component of goblet cell adenocarcinoma
- Mucinous adenocarcinoma:
- Mucinous component constituting > 50% of tumor volume
- Lack of low grade component of goblet cell adenocarcinoma
- May harbor KRAS exon 2 mutation (60 - 80%) and GNAS mutations (30 - 70%) (Am J Clin Oncol 2018;41:777)
Additional references
Board review style question #1
Which of the following criteria below should be used to stage the appendiceal tumor in this patient?
- Extent of invasion
- Percentage of gland formation only
- Mitotic activity / Ki67
- Size
Board review style answer #1
A. Extent of invasion. Goblet cell adenocarcinoma behaves (and thus is graded and staged) like adenocarcinoma. Grading should be based on the proportion of low and high grade components. This case would be considered low grade since there is > 75% tubular growth and < 25% high grade component on the representative slide. Purely assessing percentage of glandular formation is used to grade traditional colorectal adenocarcinoma. Mitotic activity and Ki67 proliferative index are used to stage neuroendocrine tumors and should not be used to grade goblet cell adenocarcinomas. Size is used to stage neuroendocrine tumors.
Comment Here
Reference: Goblet cell adenocarcinoma
Comment Here
Reference: Goblet cell adenocarcinoma
Board review style question #2
You are reviewing a case of acute appendicitis and astutely notice the findings in the images provided. What should you do next?
- Immediately alert the surgeon, as the patient requires a right hemicolectomy
- Send the case out for consultation
- Sign it out as goblet cell adenocarcinoma, grade 1 (formerly known as goblet cell carcinoid)
- Submit the remaining appendix
Board review style answer #2
D. Submit the remaining appendix. You are confident with your diagnosis of low grade goblet cell adenocarcinoma and are ready to sign it out; however, the remaining appendix must be submitted to assess the extent of high grade features and the depth of invasion, thus D is the correct answer. There is a controversy over whether patients need a right hemicolectomy. Some features that suggest sufficient surgical management of an appendectomy with negative margins includes pT1 / pT2 tumors, < 2 cm size, confinement to the distal tip, no nodal metastasis and low grade histology.
Comment Here
Reference: Goblet cell adenocarcinoma
Comment Here
Reference: Goblet cell adenocarcinoma
