
Autopsy & forensics
Types of injuries
Sharp force injuries
Authors: Lorenzo Gitto, M.D., Ponni Arunkumar, M.D.
Deputy Editor-in-Chief: Patricia Tsang, M.D., M.B.A.


Last author update: 25 August 2021
Last staff update: 20 May 2022
Copyright: 2012-2024, PathologyOutlines.com, Inc.
PubMed search: Sharp force [title] injuries forensic
Table of Contents
Definition / general | Essential features | Incised wounds | Stab wounds | Chop wounds | Atypical weapons | External examination and autopsy | Postmortem radiology | Radiology images | Manner of death | Determination of force required to produce stab wounds | Case reports | Clinical images | Gross images | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Gitto L, Arunkumar P. Sharp force injuries. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/autopsysharpforce.html. Accessed April 24th, 2024.
Definition / general
- Sharp force injuries: injuries produced by sharp objects
- Sharp object: an object that has a sharp edge or pointed extremity
- Numerous objects can produce sharp force injuries; knives are the most commonly used weapons (Int J Legal Med 2000;113:259, J Forensic Sci 2020;65:833)
- Typical knife contains:
- Handle: the portion that can be gripped; it can be used as a blunt force weapon, producing patterned injuries
- Guard (or finger guard): a metal bar at right angles between the blade and the hilt; the guard may include the quillon, protuberances extending perpendicularly to the long axis of the knife that stop the fingers from sliding forward onto the knife blade and cutting edge; the quillon may produce patterned skin injuries (Italian Journal of Legal Medicine 2012;1:4)
- Blade: can have a plain edge or serrated edge with rounded or pointed extremity and a single or double edge
- Atypical sharp and pointed objects that can be used to produce sharp force injuries include but are not limited to scissors, screwdrivers, fragments of glass (e.g. broken bottleneck or glasses), forks, ice picks, etc. (Forensic Sci Int 2001;123:135)
- Typical knife contains:
- Numerous objects can produce sharp force injuries; knives are the most commonly used weapons (Int J Legal Med 2000;113:259, J Forensic Sci 2020;65:833)
- Sharp force wounds typically show cleanly divided edges and may involve different types of tissue with the same contact
- Depth of the wound track relative to the length of the cutaneous wound distinguishes a stab from an incision
- Sharp force injuries can be subcategorized as follows:
- Incised wounds
- Stab wounds
- Chop wounds
- Atypical wounds (atypical weapons, combined incised and stab wounds)
Essential features
- Incised wounds are typically superficial and longer than they are deep
- Incised wounds must be distinguished from laceration: tissue bridges are the hallmark of laceration
- Stab wounds generally are deeper than their cutaneous length
- Chop wounds are produced by heavy, relatively blunt objects with at least 1 sharp edge
- Number and location of the wounds can give clues regarding the manner of death
- Multiple deep stab wounds are generally seen in homicides
- Progressively deeper wounds with a single fatal stab wound are typically seen in suicides
- Accidental fatal sharp force deaths are rarely described
Incised wounds
- Also called cuts or slashes
- Surgical incision is a typical example of an incised wound
- Wounds caused by sharp objects that contain a blade with at least 1 sharp edge (knives, razors, swords, etc.)
- Produced by a tangential movement of the blade to the skin
- Typically, wounds are superficial and longer than they are deep
- In most cases, incised wounds tend to be deeper at the point of the first contact with the skin (entrance) and become progressively more superficial as the wound approaches the distal end (exit)
- Wounds show clear separation of the injured and uninjured tissues
- Tissue bridges absent in the center of the wound (BMC Med Imaging 2012;12:32)
- Tissue bridging is caused by incomplete separation of stronger tissue elements, such as blood vessels and nerves
- Critical feature to differentiate incised wounds from laceration (tear in tissue caused by blunt trauma, e.g. tearing or crushing)
- Based on the depth of penetration and the energy applied to the blade, there may be different wounds:
- Abrasions: though typically produced by blunt objects, when the blade affects the superficial layer of the skin involving just the epidermis, it may leave superficial linear scratches (abrasions)
- Cuts: the blade penetrates deeper, resulting in skin and soft tissue splitting
- Mutilations: the blade is used vigorously on protruding body areas, resulting in their complete detachment
- Wound tails: tails are superficial, linear scratches localized at the level of the wound's extremities that are due to the blade movement on the skin; as a general rule, the tail is shorter and deeper at the entrance point (entrance tail) where there is higher pressure applied to the blade; it is longer and more superficial at the exit point (exit tail) as the blade progressively rises from the skin, decreasing the pressure toward the end
- Tails may give information about the direction in which an incised wound was inflicted; associated skin and soft tissue injuries or clothing defects need to be considered to evaluate the direction
- Tails can be absent
- Entrance tail can be absent if the applied pressure is too vigorous, causing skin separation without scratching
- Exit tail may be absent or shorter than the entrance tail when the affected body area is convex: the involved surface escapes the sliding action of the cutting edge
- If the skin surface is not flat but folded (hands, knuckles, breast, etc.), a single cut can determine more than 1 wound (wrinkle wounds); the sharp edge of the object moves from crest to crest, leaving intact skin between the incised wounds
- Incised wounds are rarely fatal but can be life threatening if they affect body areas with superficial major blood vessels, such as the neck and the wrist
Stab wounds
- Also called puncture wounds
- Wounds caused by a sharp pointed object that enters the body during a more or less perpendicular movement
- Penetration mechanism is the critical feature of stab wounds
- Penetration is related to pressure (P), which is the force (F) applied perpendicular to a surface per unit area (A)
- P = F/A
- Penetration is related to pressure (P), which is the force (F) applied perpendicular to a surface per unit area (A)
- Stab wounds are typically deeper than their cutaneous length (Med Sci Law 1994;34:67)
- Sharp pointed objects penetrate the body producing:
- Entrance wound: may show additional injuries due to the blunt mechanism of the knife's handle or guard (patterned injuries, abrasions, bruises, etc.)
- Wound track, usually with a dead end
- Rarely, an exit wound; for example, stab wounds to the upper extremities or high energy stab wounds (e.g. arrows)
- No tissue bridges are present in the center of the wound
- Critical feature to differentiate stab wounds from laceration
- When the knife is twisted into the body before withdrawal, there may be peculiar wound shapes: V, L, Y or irregular
- Imprint abrasions from the handle can be present (handle's mark) (Italian Journal of Legal Medicine 2012;1:4)
- Indicates that the entire blade penetrated the body
- Requires vigorous pressure
Chop wounds
- Mixed injuries showing both patterns of sharp and blunt force injuries (J Clin Forensic Med 1999;6:24)
- Produced by various objects that are generally heavy, relatively blunt and with at least 1 sharp edge
- Chop wound appearance:
- Clean center due to the action of the sharp edge of the object on the tissues
- Margins are less clean and regular than classic sharp force injuries due to:
- Increased weight and thickness of the blade
- Decreased sharpness of the blade
- Bruising, abrasions and crushing are usually present surrounding the center of the wound
- Significant weight of the weapon allows for a high energy pressure mechanism that results in a cut of the tissues together with evidence of bruising, abrasion and crushing
- Wound depth is usually variable due to the irregular penetration of the blade
- No wound tails are typically observed due to the primary pressure mechanism
- Chop wound mechanism involves high energy forces:
- Skin and soft tissues are usually lacerated
- Fractures may be observed
- When the head is involved, a typical linear dent is observed on the external surface of the cranium due to the action of the heavy blade
- If the force exceeds the elastic threshold of the cranium, then fractures develop
- When the extremities are involved, partial or full amputations may occur
- Typical chop wounds (J Forensic Sci 2001;46:228):
- Axes: crushing, fragmenting wounds with fractures
- Cleavers: clean, narrow wounds without fractures at the entry site
- Machetes: wider, less clean wounds with small fragments of bone at the entry site and fractures in the bed of the cut
- Atypical chop wounds:
- Boat propellers: typically observed in bodies found in water
- Characteristic large, parallel wounds, variable in depth, usually set a few centimeters apart and showing a sliced nature (J Forensic Sci 2000;45:917)
- Evidence of hemorrhage within the soft tissues surrounding the wound is highly indicative of an antemortem injury
- Absence of hemorrhage within the soft tissues surrounding the wound does not exclude an antemortem injury
- Prolonged immersion in water washes away the blood from the soft tissues
- Tangential cuts may result in partial or complete skin and soft tissue flap wounds
- Boat propellers: typically observed in bodies found in water
Atypical weapons
- Scissors (J Am Acad Dermatol 2020 Sep 15 [Epub ahead of print]):
- Closed pair of scissors usually produce a singular skin wound with a triangular, rhomboid or Z shape
- Open scissors usually produce 2 separate stabs wounds separated by a bridge of intact skin
- Broken glass (Med Leg J 2019;87:196, Med Sci Law 2005;45:81):
- Broken bottleneck or glass injuries may resemble the shape and diameter of the object; 1 or more glass spikes can produce multiple stab wounds connected by a circular or superficial semicircular cut
- Screwdrivers (J Forensic Sci 2007;52:1243):
- Cross shaped tip screwdrivers generally result in wounds showing 4 equally spaced cuts, resembling the cross shape of the tip
- Flathead screwdrivers generally result in wounds showing a rectangular morphology, resembling the flat end of the tip
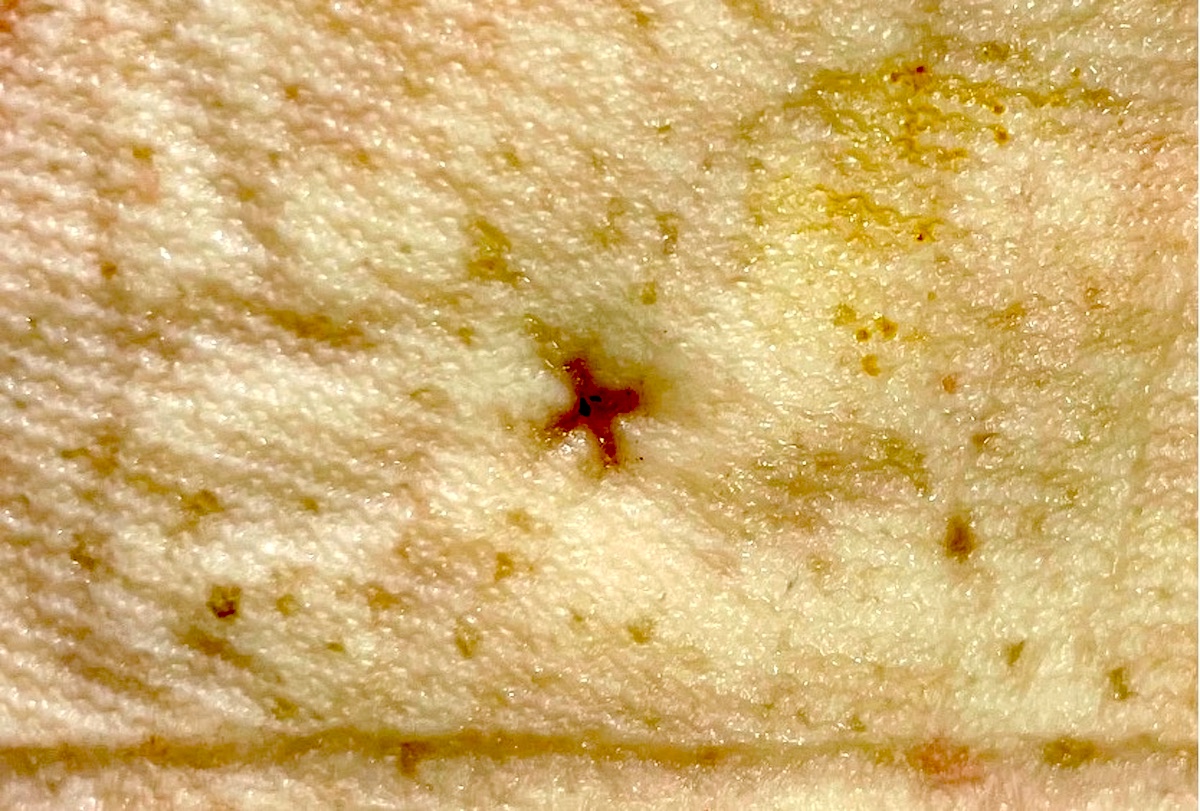
- Ice pick (J Forensic Leg Med 2013;20:803):
- Purely pointed with no or very limited sharp surface
- Mechanism of injury is related to its high penetration ability
- Resulting wounds are usually small, round or slit-like; their diameter may vary based on the depth of penetration of the object
- May grossly resemble a mole
- Forks (Int J Image Graph Signal Process 2018;10:1):
- Kitchen forks generally cause 4 circular defects separated by a short distance, corresponding to the fork prongs
- Barbecue forks with 2 or 3 prongs generally cause groups of 2 or 3 wounds, with regular or irregular unremarkable skin between the wounds based on the angle of penetration
External examination and autopsy
- Before manipulating the body, it is critical to take photographs of the body as it is received
- Medical interventions may alter the shape and size of the wound
- Clothing must be examined thoroughly to compare the number, size and location of tissue defects to the wounds observed on the body
- Anatomical location of the wounds must be described
- Location can give clues regarding the manner of death
- Number of wounds:
- Wounds can be described singularly or in clusters, depending on the case
- Each wound or cluster should be sequentially numbered
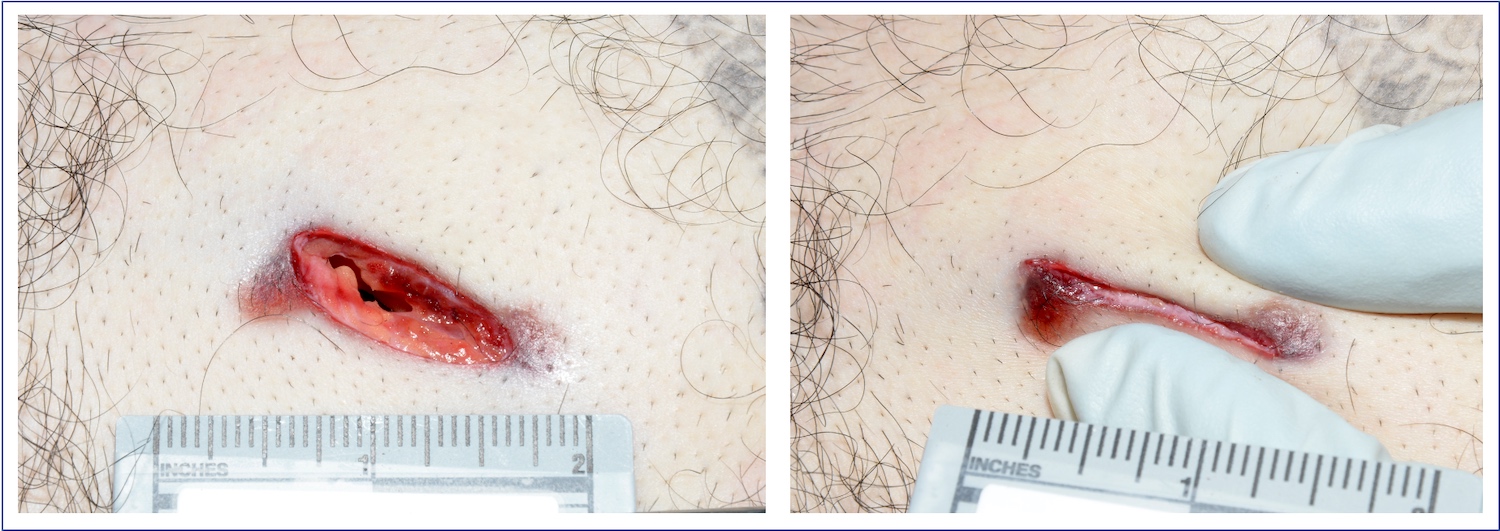
- Size and shape of wounds:
- Wound margins can be more or less apposed, resulting in size and shape artifacts
- Due to the skin and soft tissue elasticity and the direction of fibroelastic fibers (Langer lines or Langer lines of skin tension)
- Wound edges should always be gently apposed to evaluate the length and the shape of the lesion better
- Wound margins can be more or less apposed, resulting in size and shape artifacts
- Wound's path and direction:
- Always remember that stabbing deaths are dynamic rather than static situations
- Direction of the thrust is based both on the skin wound feature and the wound track
- Must be determined during the internal examination
- Involved organs must be included in the report
- Always remember that stabbing deaths are dynamic rather than static situations
- Depth of the wounds:
- Due to the soft tissue elasticity, the wound depth does not necessarily represent the length of the blade
- Vigorous stab can indent the body surface (i.e. abdomen) and compress the soft tissues allowing the blade to reach deep tissues and organs at a greater distance than the blade length
- Suggested to describe the maximal depth, as recorded during the autopsy (e.g. "The wound depth is not less than…” or “The wound depth is approximately...”)
- Due to the soft tissue elasticity, the wound depth does not necessarily represent the length of the blade
- Internal organs:
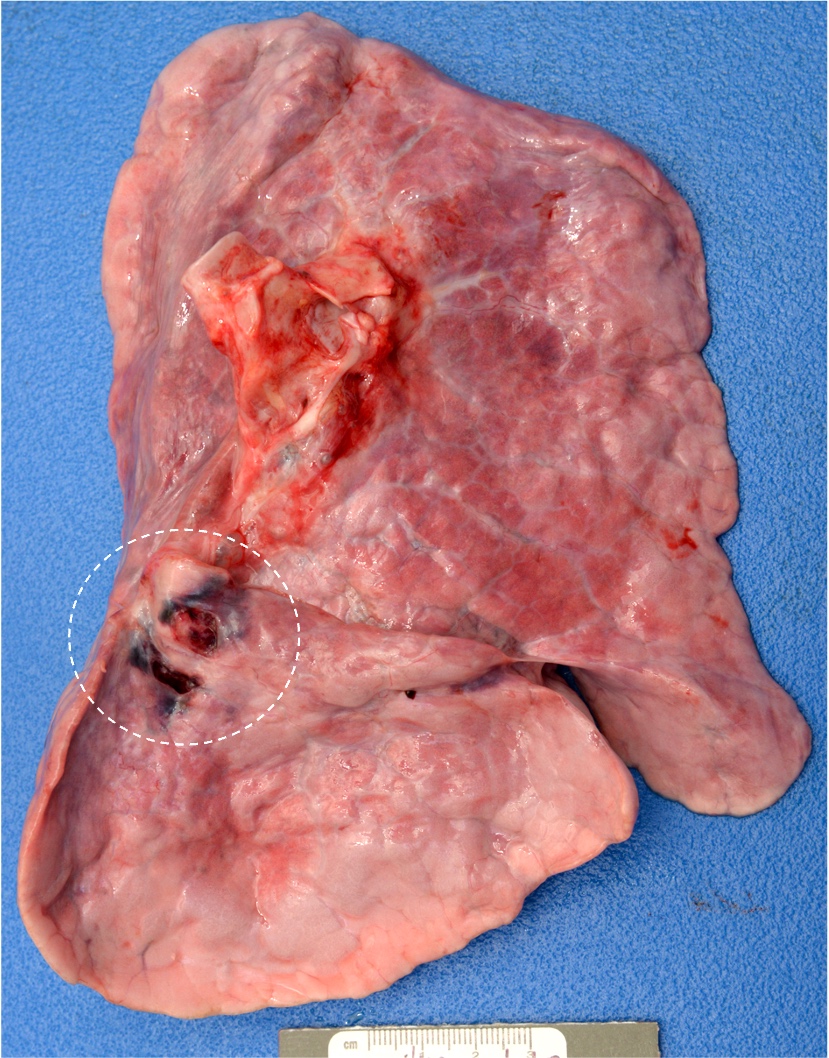
- Direct evidence of stab wounds can be observed in the involved organs (e.g. heart, lungs, liver)
- Due to the respiratory phases, the lung can show injuries that are longer or shorter than the actual blade length
- During inspiration, the lung expands and comes close to the chest wall, thus becoming easier to be involved by the stab wound
- During the exhalation, the contraction of lung brings it away from the chest wall, making it harder to be reached by the blade
- Direct evidence of stab wounds can be observed in the involved organs (e.g. heart, lungs, liver)
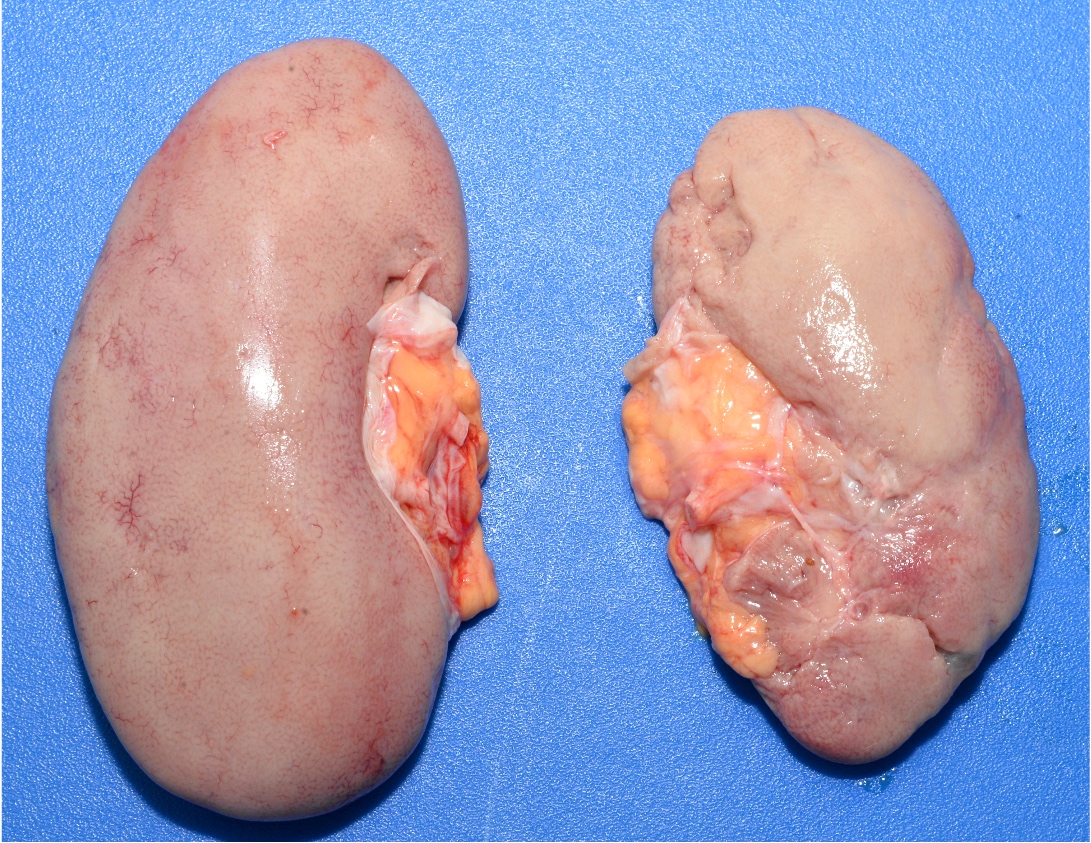
- Evaluation of blood loss following sharp force trauma is suggested (Int J Legal Med 2020;134:1123)
- Signs of severe blood loss include extreme paleness of the internal organs, even if they are not directly involved (e.g. kidneys)
- Sometimes bleeding is not extensive and death is due to vascular injury complications (e.g. air embolism to the heart)
Postmortem radiology
- Radiology studies can be helpful in sharp force traumas (Acta Radiol 2010;51:92)
- Postmortem Xrays or computed tomography may show (Leg Med (Tokyo) 2009;11:4):
- Retained weapons or their fragments
- Allow for collection as evidence
- Help in preventing autopsy operators from accidental injuries
- Pneumothorax
- Air embolism
- Additional autopsy techniques are required to confirm
- Retained weapons or their fragments
Radiology images
Contributed by Lorenzo Gitto, M.D., Ponni Arunkumar, M.D., Luigi Bonaccorso, M.D. and the Cook County Medical Examiner's Office

Postmortem radiology
Manner of death
- Homicidal sharp force injuries:
- No specific anatomical location (random)
- Usually, numerous deep wounds
- Mostly stab wounds (Forensic Sci Med Pathol 2018;14:295)
- Additional injuries are often present:
- Defense injuries (J Forensic Leg Med 2012;19:207)
- Active: on the palms of the hand in the attempt of the victim to grab the blade
- Passive: on the dorsal or anterior aspects of the forearm or hands in the attempt of the victims to protect themselves from the blade
- Clothes are typically involved
- Suicidal sharp force injuries:
- Typical location
- Wrist
- Neck
- Thorax
- Only accessible areas of the body are involved
- Posterior aspects are virtually never involved
- Mostly incised wounds
- If present, usually 1 deep stab wound
- Rarely a few stab wounds can be present
- Hesitation marks are typically observed (J Forensic Sci 2016;61:1515)
- Typically, linear, parallel, superficial incised wounds involving the upper extremities
- Hesitation stab wound can also be observed, especially on the chest; typically, there are progressively deeper stab wounds and a single stab wound penetrating into the chest wall, hitting an internal organ
- Remote hesitation marks are usually in the form of linear, parallel scars
- No additional injuries are present
- No defense injuries
- Clothes generally are not involved
- Victims tend to remove clothes to be sure that they will cut / stab the right anatomical location
- Typical location
- Accidental sharp force injuries:
- Rarely described (Am J Forensic Med Pathol 2001;22:358)
- Rarely reported in the literature (Arch Kriminol 2011;228:108)
- Hard to demonstrate
- Only a comprehensive medicolegal death investigation helps determine the manner of death
- Fixation of the blade, meaning that the knife is securely gripped and held firmly, seems the primary factor in determining accidental stabbing fatalities
- Common defense theory in court is about the possibility of the victim running or falling onto a knife and sustaining a stab wound
- Rarely described (Am J Forensic Med Pathol 2001;22:358)
Determination of force required to produce stab wounds
- Frequently asked question to the forensic pathologist in stab wound deaths
- Knight found that the velocity and sharpness of the blade are critical factors in consideration of the amount of force needed to cause any given stab wound (Forensic Sci 1975;6:249)
- Green found that the skin was the most resistant tissue to penetration (J Forensic Sci Soc 1978;18:161)
- Clothing increased the force required to produce a stab wound
- O'Callaghan confirmed that the skin was the most resistant tissue to penetration (Forensic Sci Int 1999;104:173)
- Gitto et al. performed a study on cadaveric chest tissues (skin and soft tissue, cartilage and bone) using 3 different types of blades (Am J For Med Path 2021 May 4 [Epub Ahead of Print])
- Skin is the most resistant tissue encountered by the blade
- Maximum peak force of 261 N has been recorded to penetrate the chest tissues
- Serrated edge blades showed difficulties in penetrating chest bones and cartilage compared with the plain edge blades
Case reports
- 21 year old man who died due to accidental femoral vessels injuries by a broken glass (Med Leg J 2019;87:196)
- 24 year old man who committed suicide by a transcranial stab wound (Am J Forensic Med Pathol 2008;29:268)
- 42 year old man who committed suicide by more than 90 stab wounds (Int J Legal Med 2001;115:167)
- 45 year old man who committed suicide by an atypical cut throat injury (J Forensic Leg Med 2009;16:492)
- 45 year old man killed with a dessert spoon (For Sci Int Rep 2020;100094)
- 59 year old woman died due to accidental impalement by a broken rose bush (Am J Forensic Med Pathol 2018;39:341)
Clinical images
Contributed by Lorenzo Gitto, M.D., Ponni Arunkumar, M.D., Luigi Bonaccorso, M.D. and the Cook County Medical Examiner's Office

Incised wounds

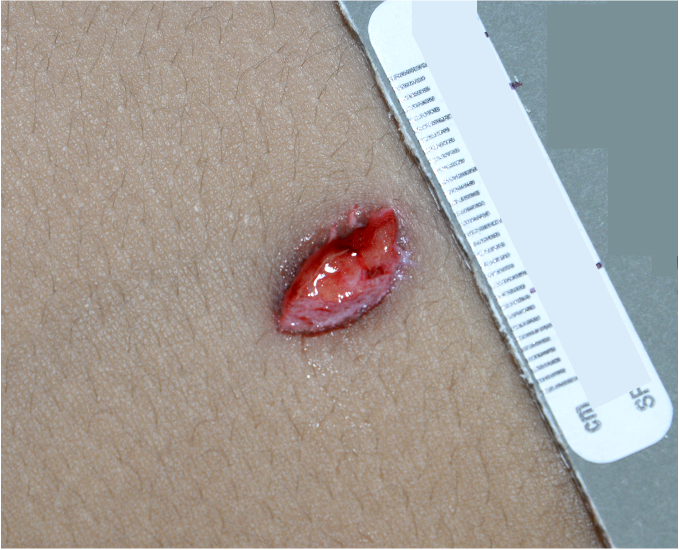
Stab wound

Chop wounds to the head
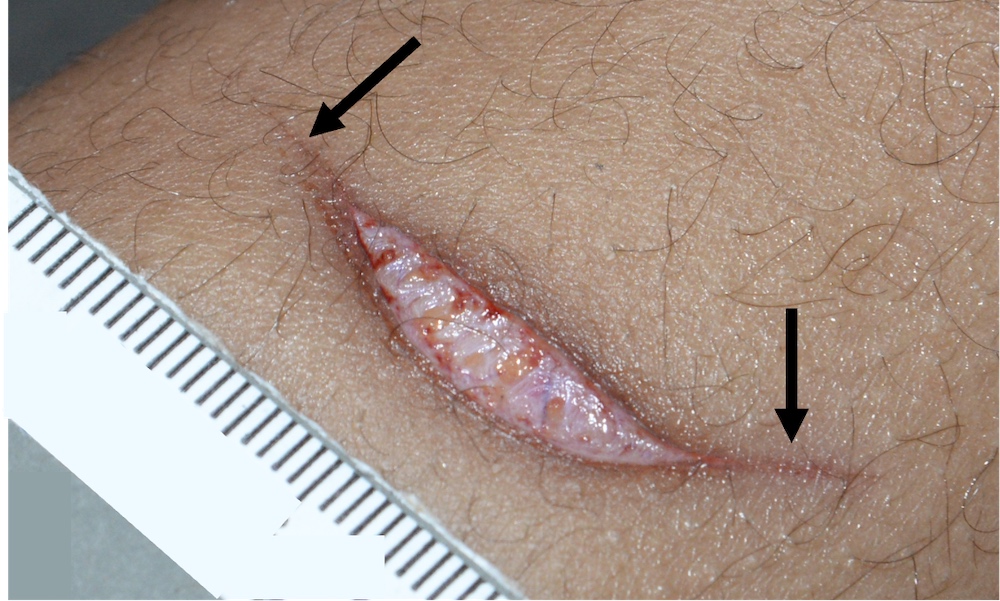
Wound tailing
Wound margin approximation

Hesitation marks - recent

Hesitation marks - remote

Medical intervention

V shaped stab wound

Vascular injury
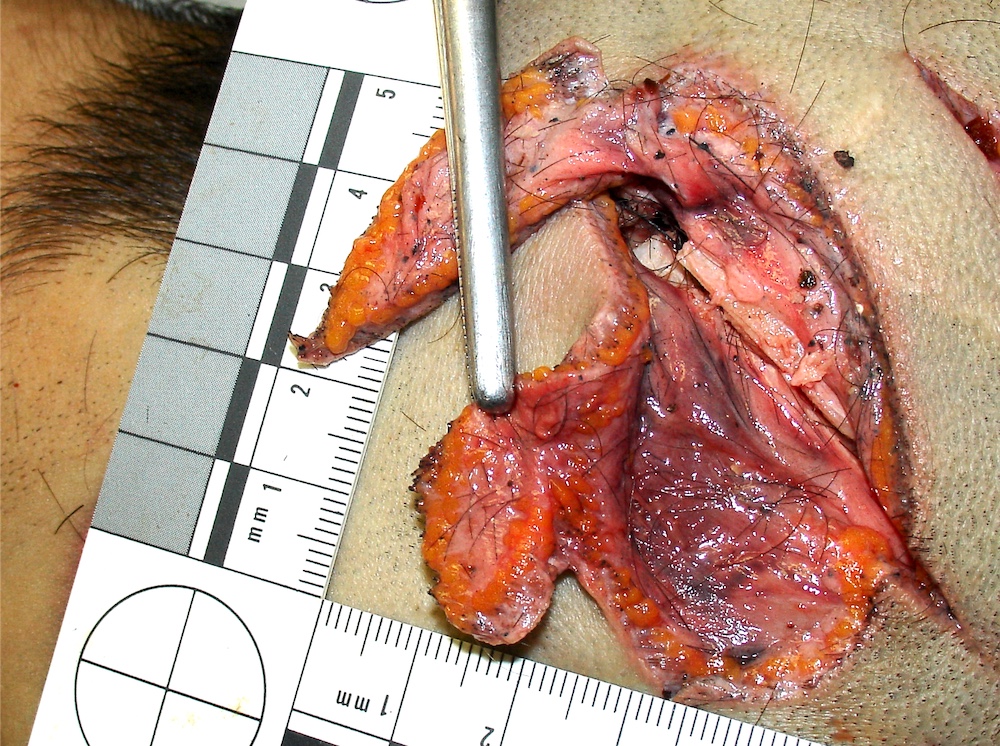
Partial skin flap

Active defense wounds

Passive defensive wounds

Broken glass

Broken glass - causative object
Scissors
Cross tip screwdriver

Flathead screwdriver
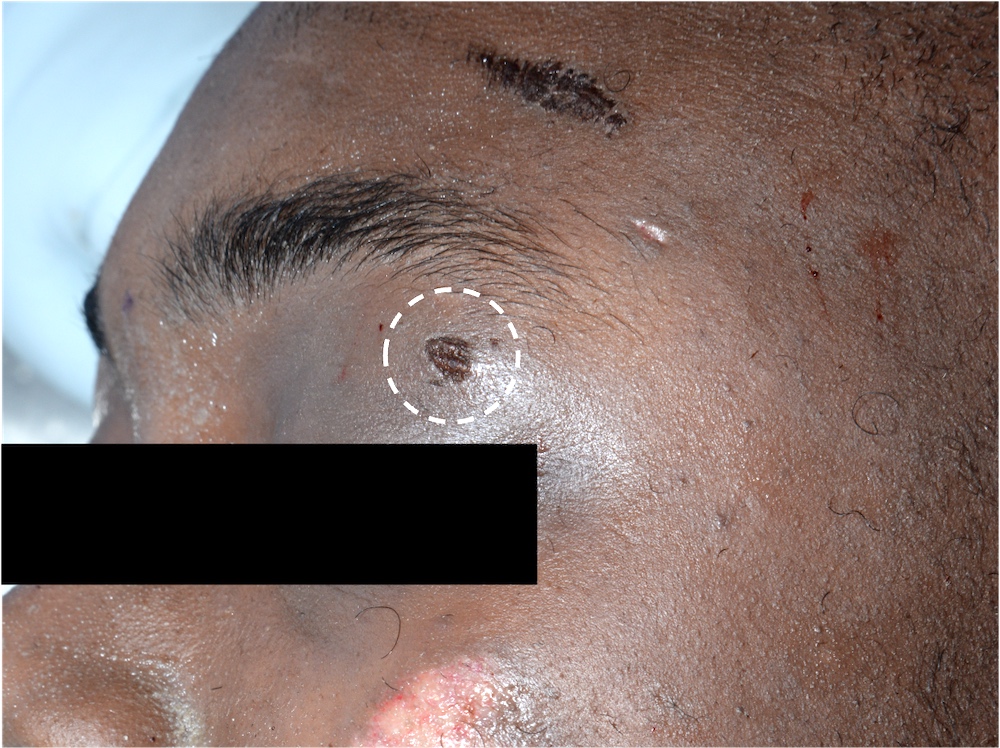
Ice pick - cutaneous lesion
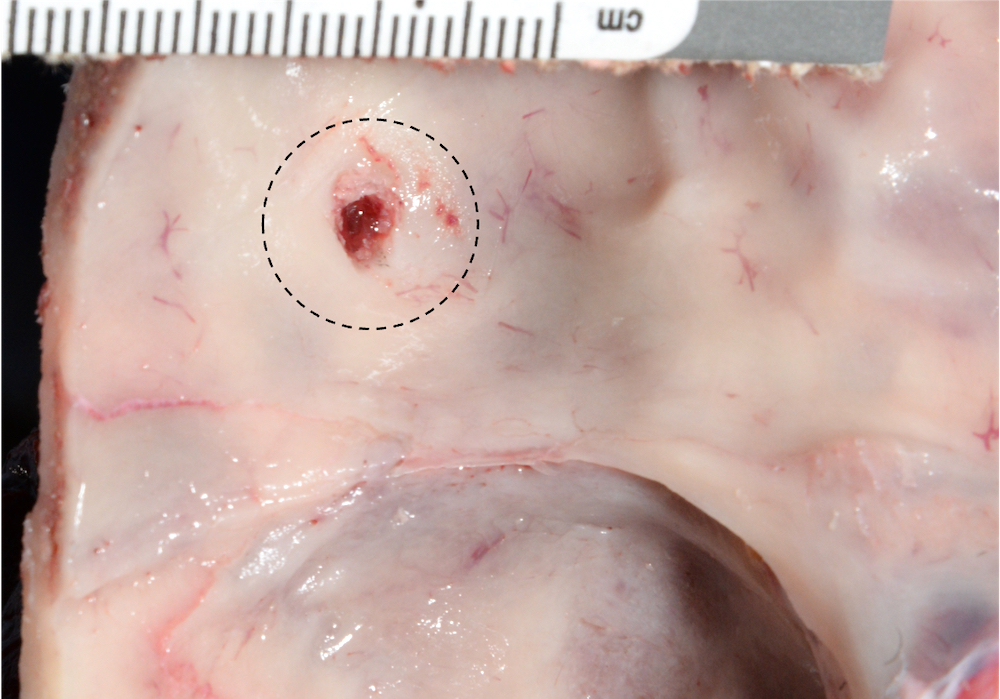
Ice pick - skull lesion

Barbecue fork
Gross images
Contributed by Lorenzo Gitto, M.D., Ponni Arunkumar, M.D., Luigi Bonaccorso, M.D. and the Cook County Medical Examiner's Office
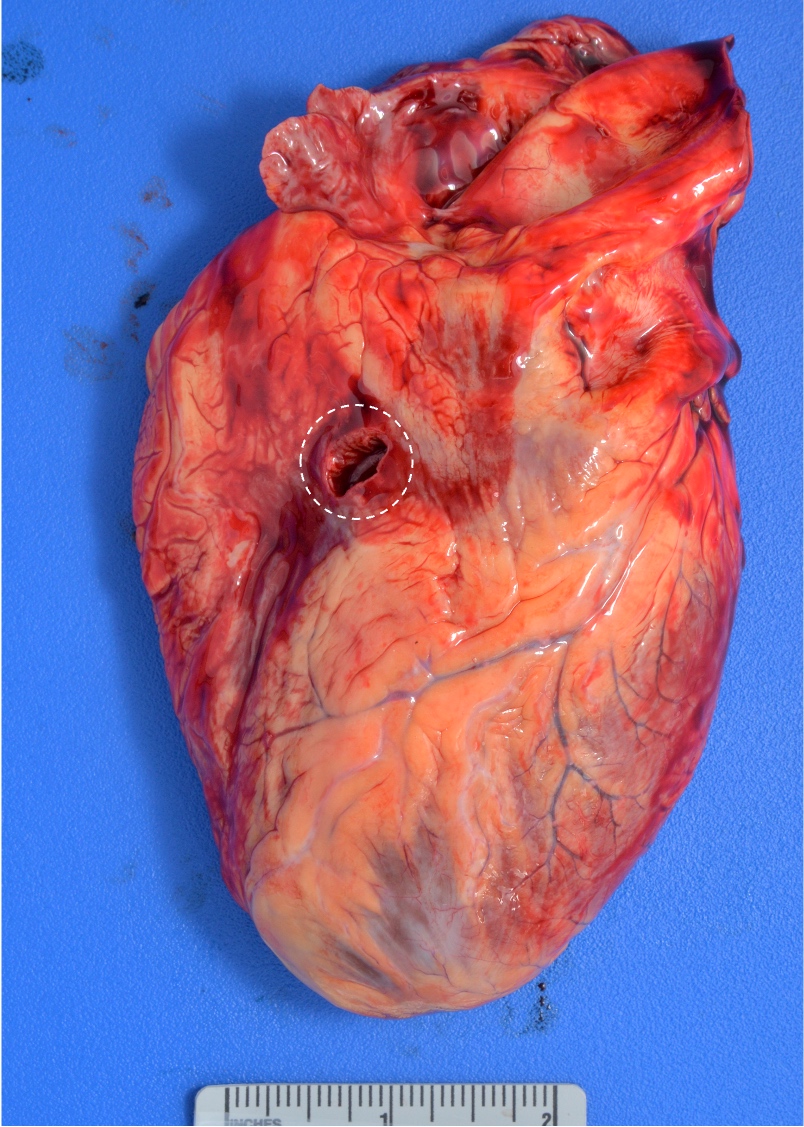
Heart stab wound
Lung stab wound
Pale organs
Board review style question #1
What is the injury shown in the picture?
- Chop wound
- Incised wound
- Laceration
- Scissor wound
- Stab wound
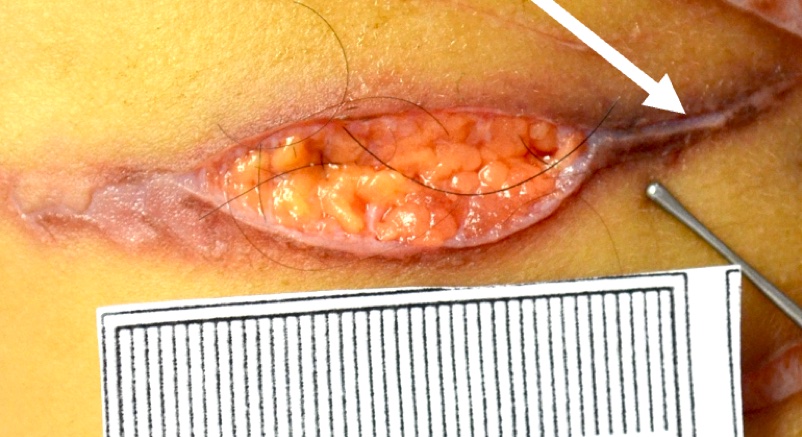
Board review style answer #1
B. Incised wound. The wound shown in the picture is a typical example of an incised wound. The white arrow indicates the wound tail that is commonly observed in incised wounds. These wounds are superficial and longer than they are deep. It is mandatory to distinguish them from lacerations (answer C) that are produced by blunt objects. The presence of tissue bridges in the center of the wound is the hallmark of lacerations. A stab wound (answer E) is typically deeper than its cutaneous length. A wound track can be frequently observed in the center of the lesion. Chop wounds (answer A) are produced by objects that are generally heavy, relatively blunt and with at least 1 sharp edge. The center of the wound is usually cleaner and deeper than incised wounds. Scissors (answer D) produce different stab wounds based on their action (open or closed).
Comment Here
Reference: Sharp force injuries
Comment Here
Reference: Sharp force injuries
Board review style question #2

Based on the findings shown in the picture, what is the most probable manner of death?
- Accident
- Homicide
- Natural
- Suicide
- Undetermined
Board review style answer #2
B. Homicide. The picture shows a typical example of an active defense wound. These wounds are generally produced by the attempt of the victims to grab the blade. Suicidal sharp force injuries (answer D) are generally multiple and located to the wrist, neck or chest. Accidental sharp force injuries (answer A) are rarely described in the literature and they generally involve random body areas. A natural death (answer C) can be excluded by the evidence of a sharp force injury. An undetermined manner of death (answer E) could be an option if there is no clear evidence of an assault. In this case, this typical active defense wound is most consistent with homicide.
Comment Here
Reference: Sharp force injuries
Comment Here
Reference: Sharp force injuries
