

Bone & joints
Chondrosarcoma
Chondrosarcoma (primary, secondary, periosteal)
Authors: Akif K. Guney, M.D., Shadi Qasem, M.D., M.B.A.
Resident / Fellow Advisory Board: Erna Forgó, M.D.
Editorial Board Member: Jose G. Mantilla, M.D.
Last author update: 22 April 2021
Last staff update: 10 May 2023
Copyright: 2003-2024, PathologyOutlines.com, Inc.
PubMed Search: Chondrosarcoma bone
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Etiology | Clinical features | Diagnosis | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Frozen section description | Frozen section images | Microscopic (histologic) description | Microscopic (histologic) images | Virtual slides | Cytology description | Cytology images | Positive stains | Negative stains | Molecular / cytogenetics description | Videos | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Guney AK, Qasem S. Chondrosarcoma (primary, secondary, periosteal). PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/bonechondrosarcoma.html. Accessed April 19th, 2024.
Definition / general
- Locally aggressive or malignant group of tumors characterized by formation of cartilaginous matrix
- Primary: arising without a benign precursor
- Secondary:
- Central: arising in preexisting enchondroma
- Peripheral: arising in preexisting cartilaginous cap of an osteochondroma
- Periosteal chondrosarcoma: occurs on the surface of the bone in association with the periosteum
Essential features
- Locally aggressive or malignant group of tumors characterized by formation of cartilaginous matrix and chondrocytes embedded in lacunae
- Histologic grade, extracompartmental spread and local recurrence are important prognostic factors
- Radiology is essential, especially for low grade lesions
- Change in the size or clinical symptoms might be an indicator of malignant transformation in enchondromas and osteochondromas
- IDH1 and IDH2 mutations in approximately 50% of cases
Terminology
- Atypical cartilaginous tumor = tumors resembling grade 1 chondrosarcoma arising in the appendicular skeleton
- Periosteal chondrosarcoma = juxtacortical chondrosarcoma
- Conventional chondrosarcoma = primary, secondary and periosteal chondrosarcomas
- For low grade tumors, the term low grade cartilaginous neoplasm can be used
Epidemiology
- Accounts for ~20% of all malignant bone tumors
- Second most common primary malignant bone tumor after osteosarcoma (Cancer 1995;75:203)
- Middle aged to older adults (secondary and periosteal chondrosarcoma are seen in younger patients)
- M > F
Sites
- Most common sites are the pelvic bones, femur and humerus (Cancer Imaging 2003;4:36)
- Other sites are the trunk, skull and facial bones
- Involvement of the hands and feet is rare
- Periosteal chondrosarcoma involves the metaphysis of long bones, usually distal femur and humerus
- Conventional type chondrosarcoma is also the most common sarcoma arising in the larynx (Am J Surg Pathol 2002;26:836, Head Neck Pathol 2020;14:707)
Etiology
- Unknown etiology for primary chondrosarcoma
- Malignant transformation from benign precursors in secondary chondrosarcomas (J Am Acad Orthop Surg 2010;18:608)
- Increased risk of secondary chondrosarcoma in patients with Ollier disease and Maffucci syndrome (Oncologist 2011;16:1771)
Clinical features
- Pain, local swelling and enlarging mass are the most common presenting symptoms (Semin Diagn Pathol 2014;31:10)
- Neurological symptoms in skull base tumors (StatPearls: Chondrosarcoma [Accessed 9 March 2021])
- Change in the size and clinical symptoms might be an indicator of malignant transformation in enchondromas and osteochondromas
Diagnosis
- Diagnosis of chondrosarcoma can be made on imaging studies (Xray, CT scan, MRI) in combination with biopsy specimen (Skeletal Radiol 2013;42:611)
- Radiology is essential, especially in low grade lesions
Radiology description
- Xray: popcorn-like calcifications (punctate and ring-like opacities), lytic lesions, endosteal scalloping, thickened cortex, cortical erosion or destruction, soft tissue involvement (Curr Probl Diagn Radiol 2019;48:262)
- Cortical destruction and soft tissue extension of pre-existing enchondromas might be indicators of secondary central chondrosarcoma
- Thick cartilaginous cap > 1.5 - 2 cm in secondary peripheral chondrosarcoma (Radiologe 2016;56:476)
- Multilobular appearance in periosteal chondrosarcoma
- CT scan and MRI: helpful in showing the extent of the tumor
Radiology images
Contributed by Shadi Qasem, M.D.

Soft tissue extension
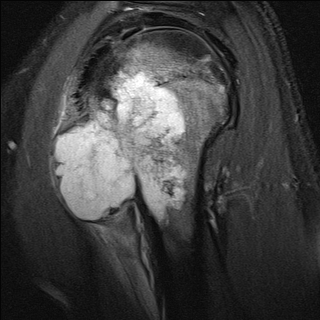
Corresponding MRI for previous image

Finger tumor

Pelvic tumor

Secondary tumor
Prognostic factors
- Histologic grade, extracompartmental spread and local recurrence are important prognostic factors (J Bone Joint Surg Br 2002;84:93)
- Atypical cartilaginous tumor / grade I chondrosarcomas are locally aggressive and have a good prognosis (~85% 5 year survival rate)
- Grade II / III chondrosarcomas have a worse prognosis (~50% 5 year survival rate)
- Local recurrence is related to tumor size and adequacy of surgical margins
Case reports
- 30 year old woman with periosteal chondrosarcoma and bone metastasis (World J Surg Oncol 2015;13:121)
- 35 year old man with postradiation chondrosarcoma (Int J Biol Markers 2014;29:e440)
- 36 year old man presenting with sciatica (J Orthop Case Rep 2020;10:53)
- 43 year old woman presenting with dyspareunia (Rom J Morphol Embryol 2018;59:927)
- 54 year old man with pain and swelling in the left preauricular area (Med Oral Patol Oral Cir Bucal 2009 Jan;14:E39)
Treatment
- Wide surgical resection is the mainstay of treatment
- Low grade chondrosarcomas are often surgically cured
- Chondrosarcomas are in general resistant to chemotherapy and radiotherapy (Curr Opin Oncol 2016;28:314)
- Chondrogenic tumors require a high dose of radiation (Oncologist 2008;13:320)
- Resection with adjuvant radiotherapy yields the best outcome for high grade chondrosarcomas (Neurosurgery 2017;81:520)
Gross description
- Neoplastic hyaline cartilage has a lobular, gray-tan cut surface
- Cystic changes with myxoid or mucoid material
- Mineralization appears as chalky calcium deposits
- Cortical erosion and soft tissue extension can be seen
- Thick cartilage cap (1.5 - 2 cm) with cystic cavities in secondary peripheral chondrosarcoma
- Periosteal chondrosarcoma appears as a large, lobular mass attached to the surface of bone (Am J Surg Pathol 1985;9:666)
Gross images
Contributed by Shadi Qasem, M.D.

Femoral tumor

Pelvic tumor
Frozen section description
- Nodules of hyaline cartilage with variable atypia (Sarcoma 2014;2014:902104)
- For low grade tumors, the term low grade cartilaginous neoplasm can be used
Frozen section images
Contributed by Shadi Qasem, M.D.
Frozen section
Microscopic (histologic) description
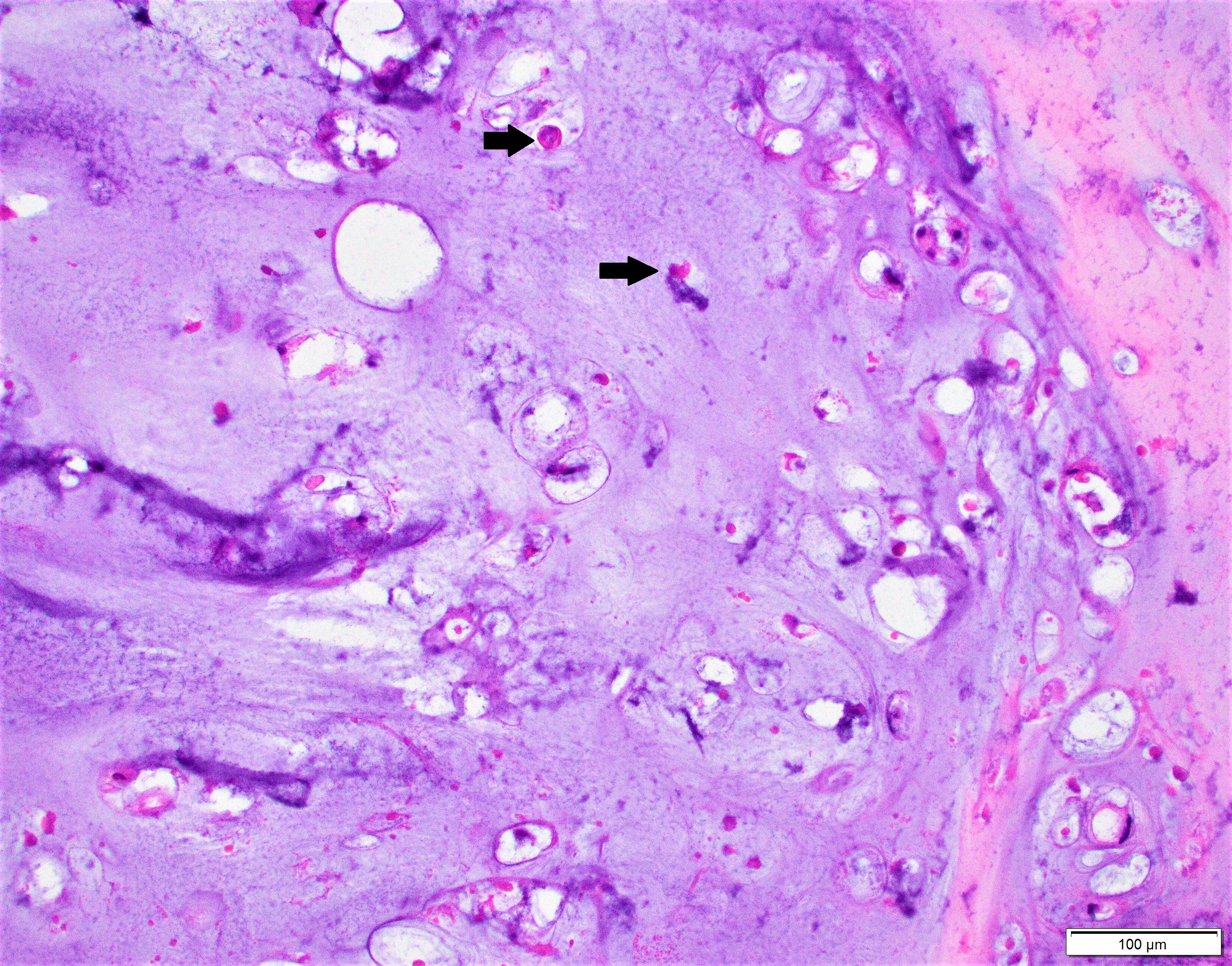
- Abundant cartilaginous matrix with chondrocytes embedded in lacunae
- Lobular or diffuse growth (depending on grade)
- Permeation of intertrabecular spaces
- Varying degrees of increased cellularity, nuclear atypia and mitotic activity
- Grade I: minimally increased cellularity, nodular growth and occasional binucleate nuclei
- Grade II: moderate cellularity and diffuse growth
- Grade III: high cellularity, marked atypical cells, pleomorphic appearance and easily identifiable mitotic figures
- Myxoid changes, chondroid matrix liquefaction and necrosis can be seen
- Formation of nodules and cystic cavities can be seen in secondary peripheral chondrosarcoma (generally low grade tumors)
- Periosteal chondrosarcoma:
- Grade I or II tumors seen on the external surface of the bone
- Cortical invasion, soft tissue extension and size (> 5 cm) can be helpful in distinguishing from periosteal chondroma (AJR Am J Roentgenol 2001;177:1183)
Microscopic (histologic) images
Contributed by Shadi Qasem, M.D.
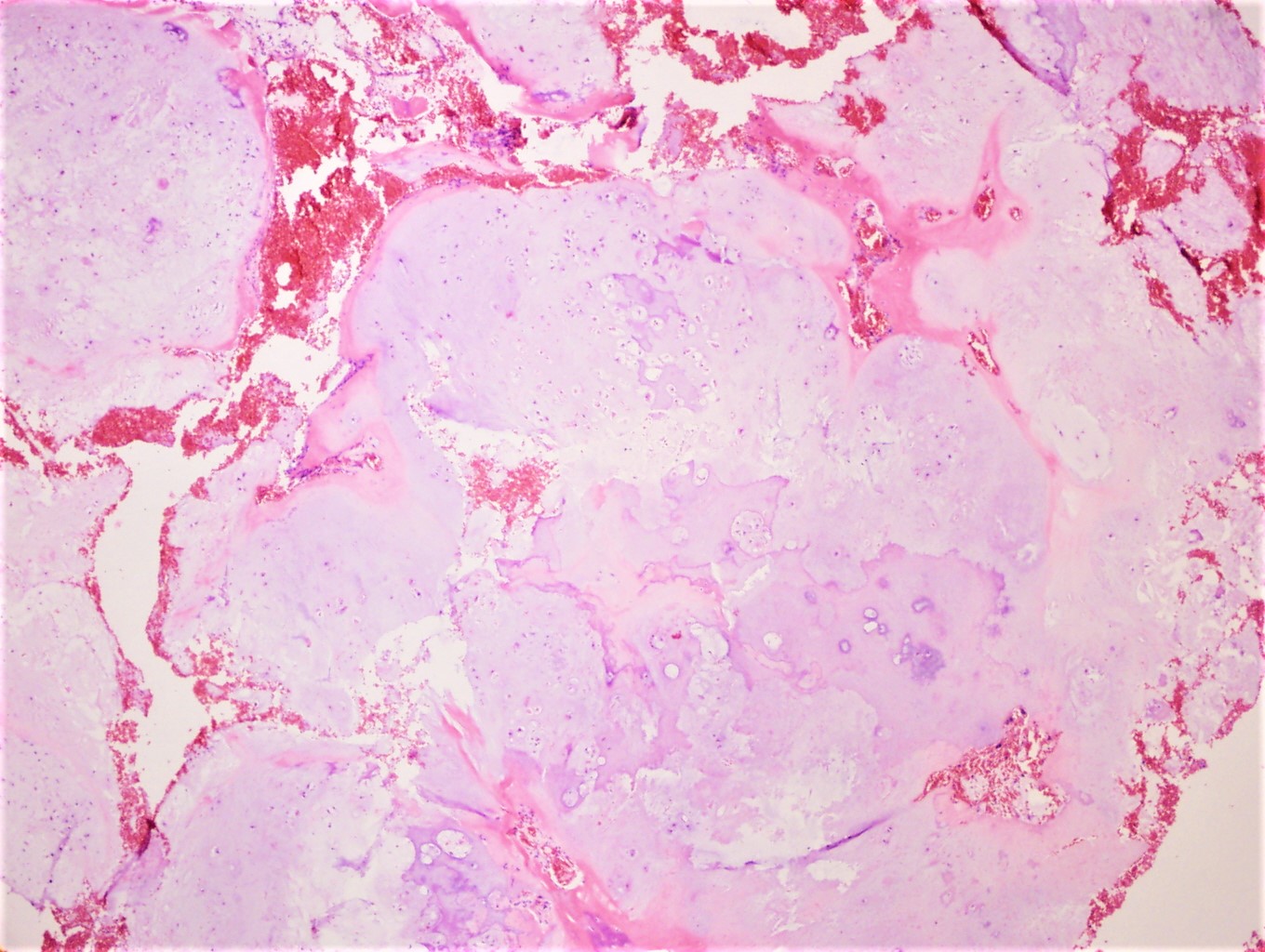
Grade I
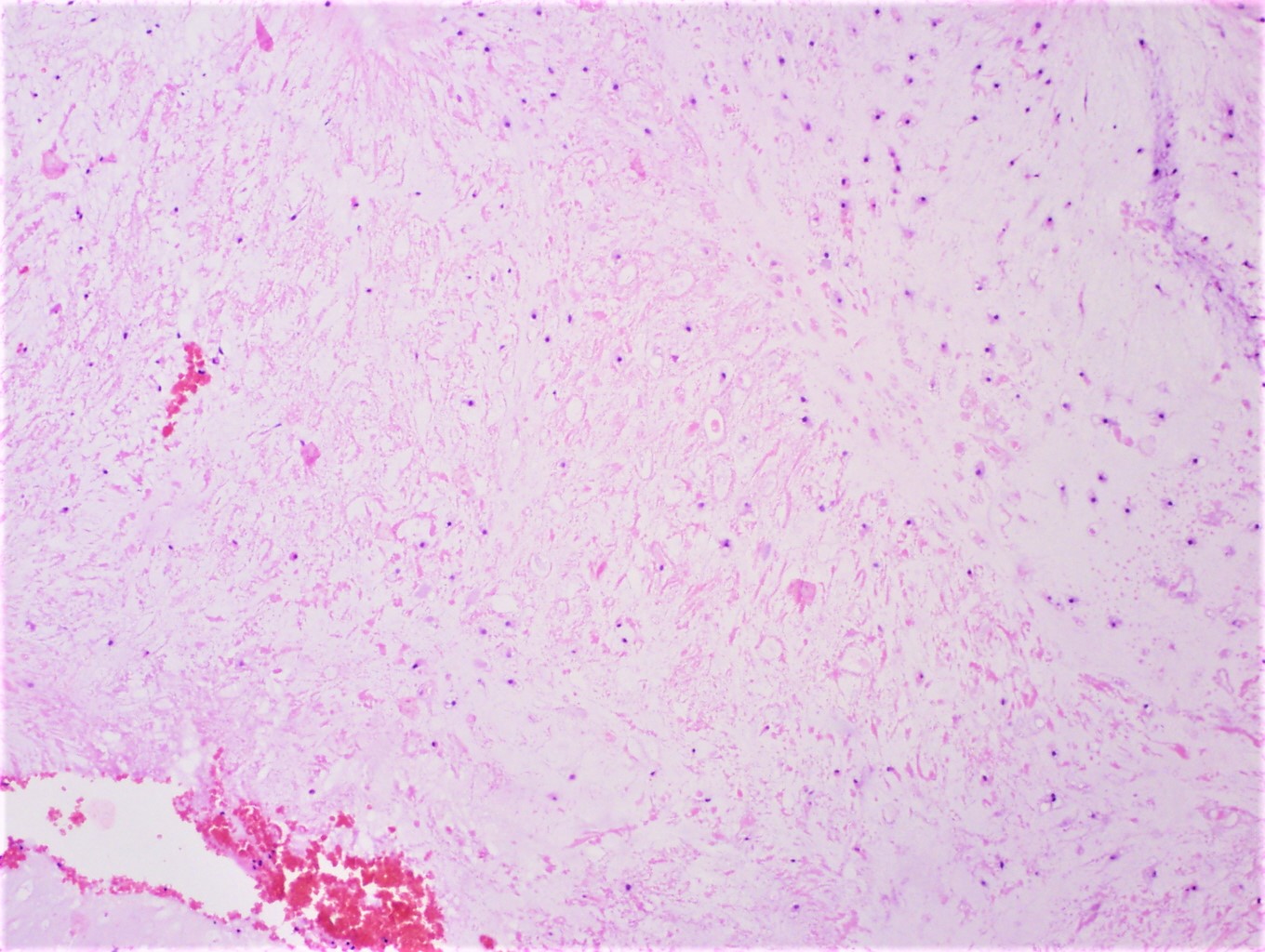
Myxoid degeneration
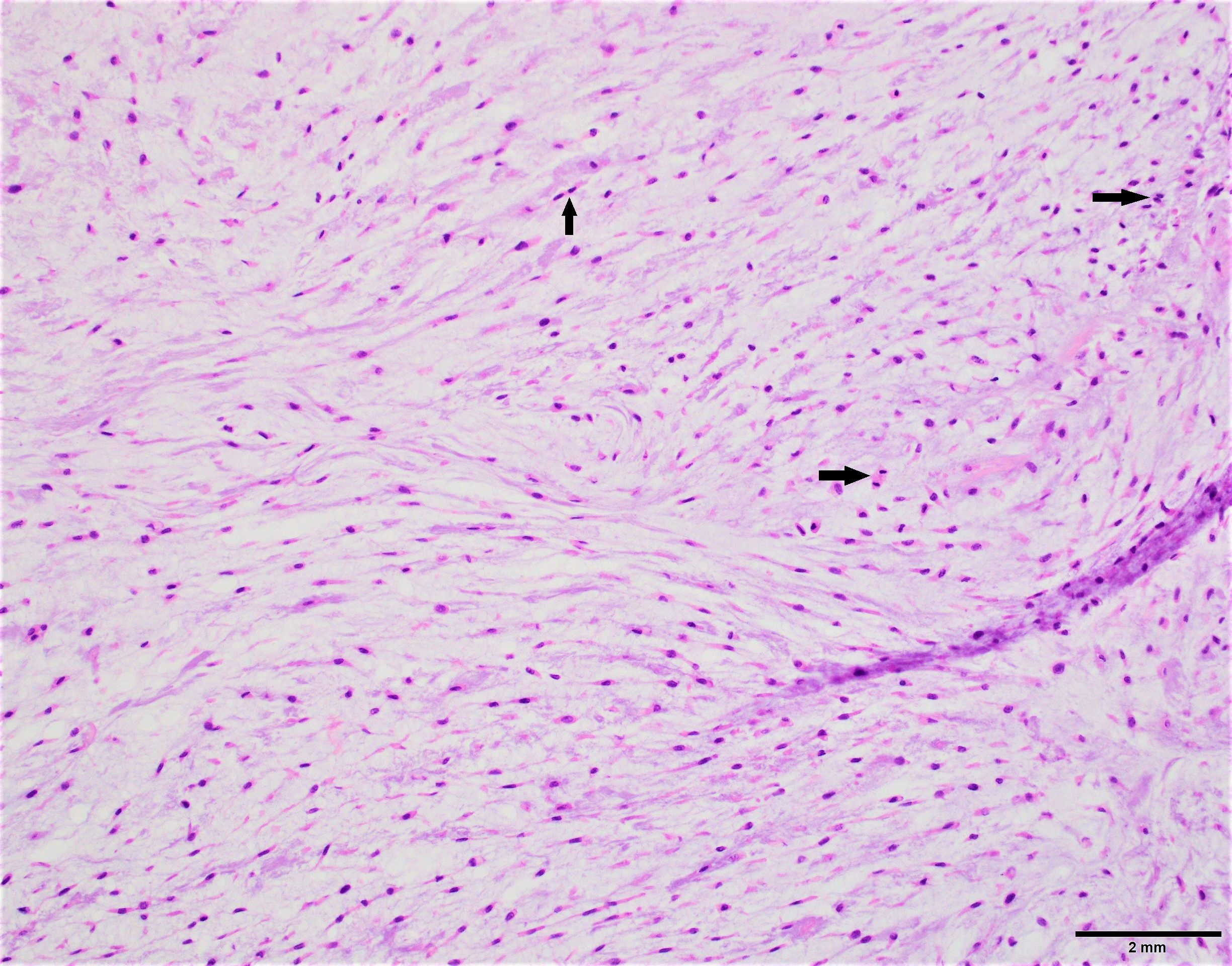
Grade II
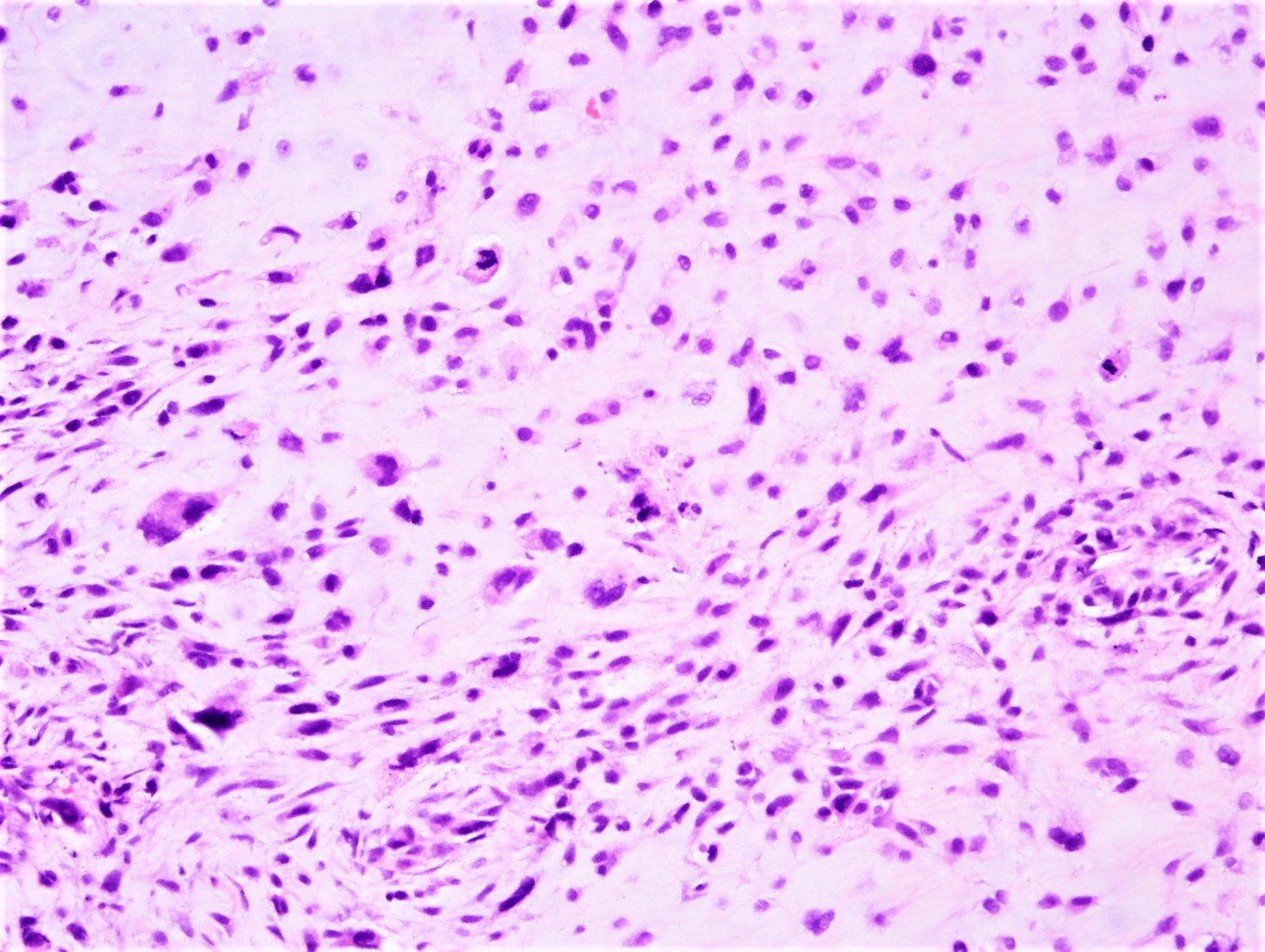
Grade III
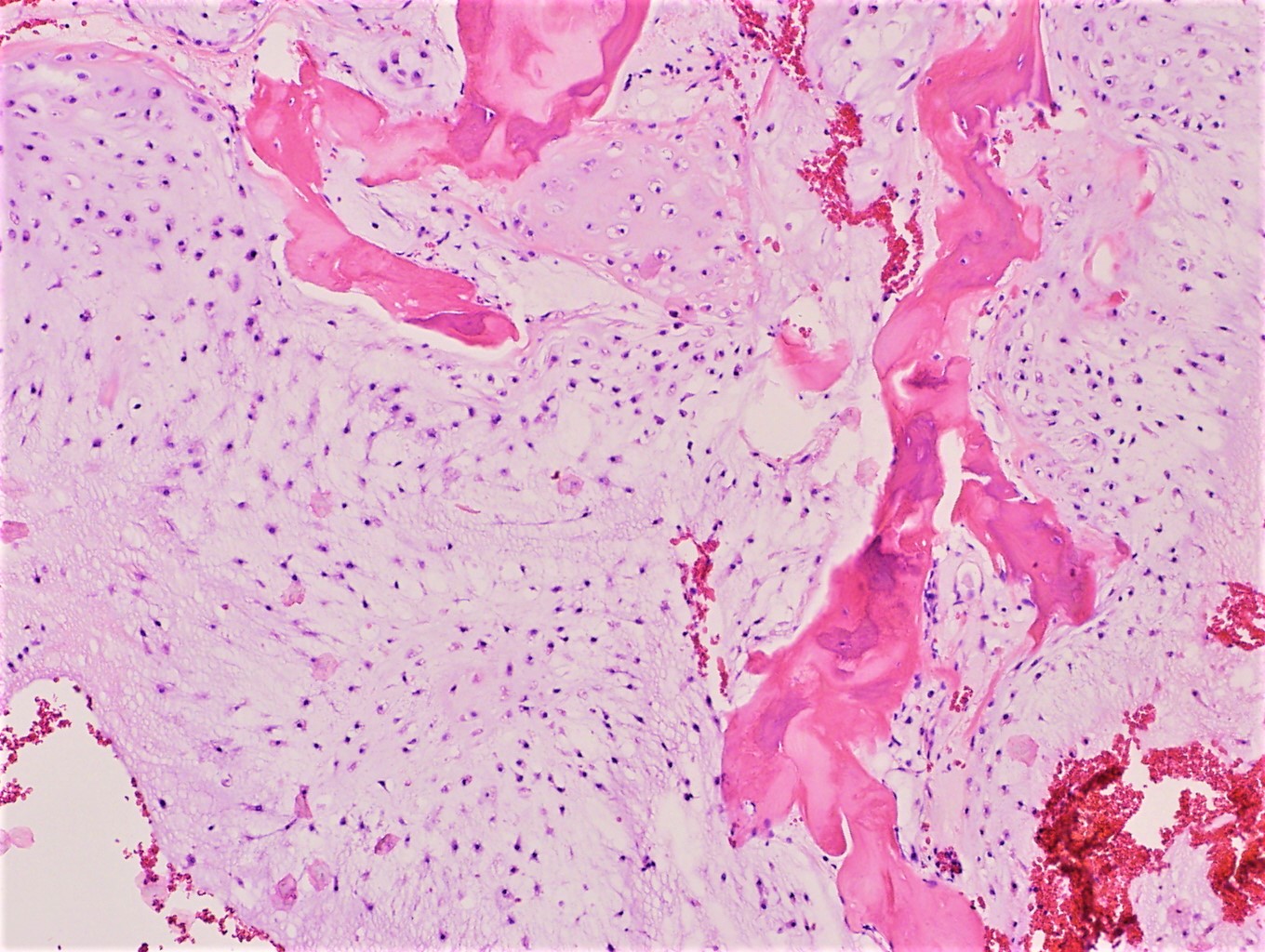
Bone permeation
Virtual slides
Images hosted on other servers:

Grade I


Grade II

Grade III
Cytology description
- Abundance of extracellular matrix material, which is best appreciated on air dried, Giemsa based stained material
- Recognizable lacunae, often containing binucleated or multinucleated chondrocytes
- Atypical cartilaginous tumor / grade I chondrosarcoma is cytomorphologically indistinguishable from an enchondroma
- Grade II / III chondrosarcomas are more cellular, more atypical with more myxoid matrix
- Cytology is more reliable in metastatic than primary tumors (Diagn Cytopathol 2006;34:413)
Cytology images
Contributed by Shadi Qasem, M.D.
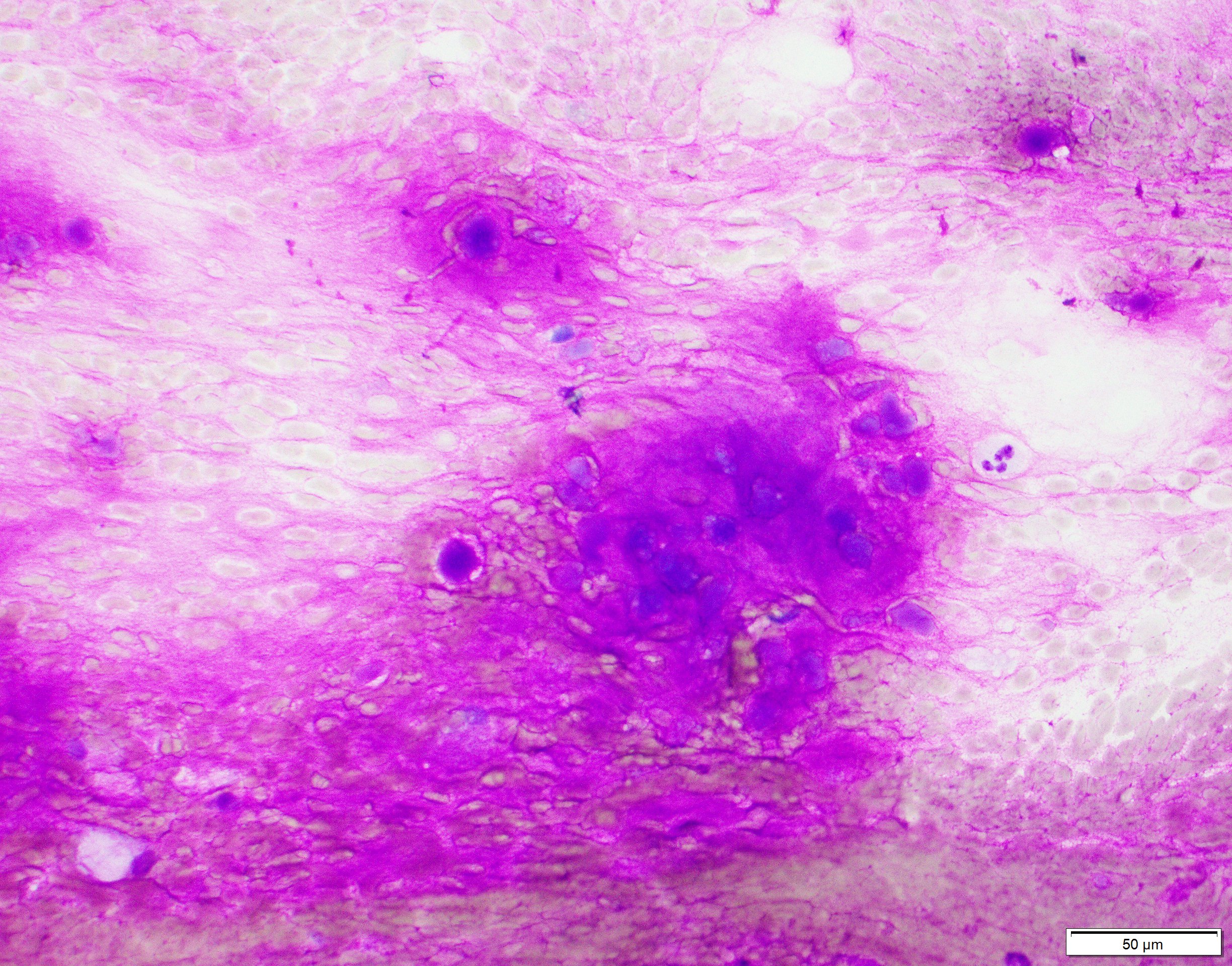
Magenta color matrix
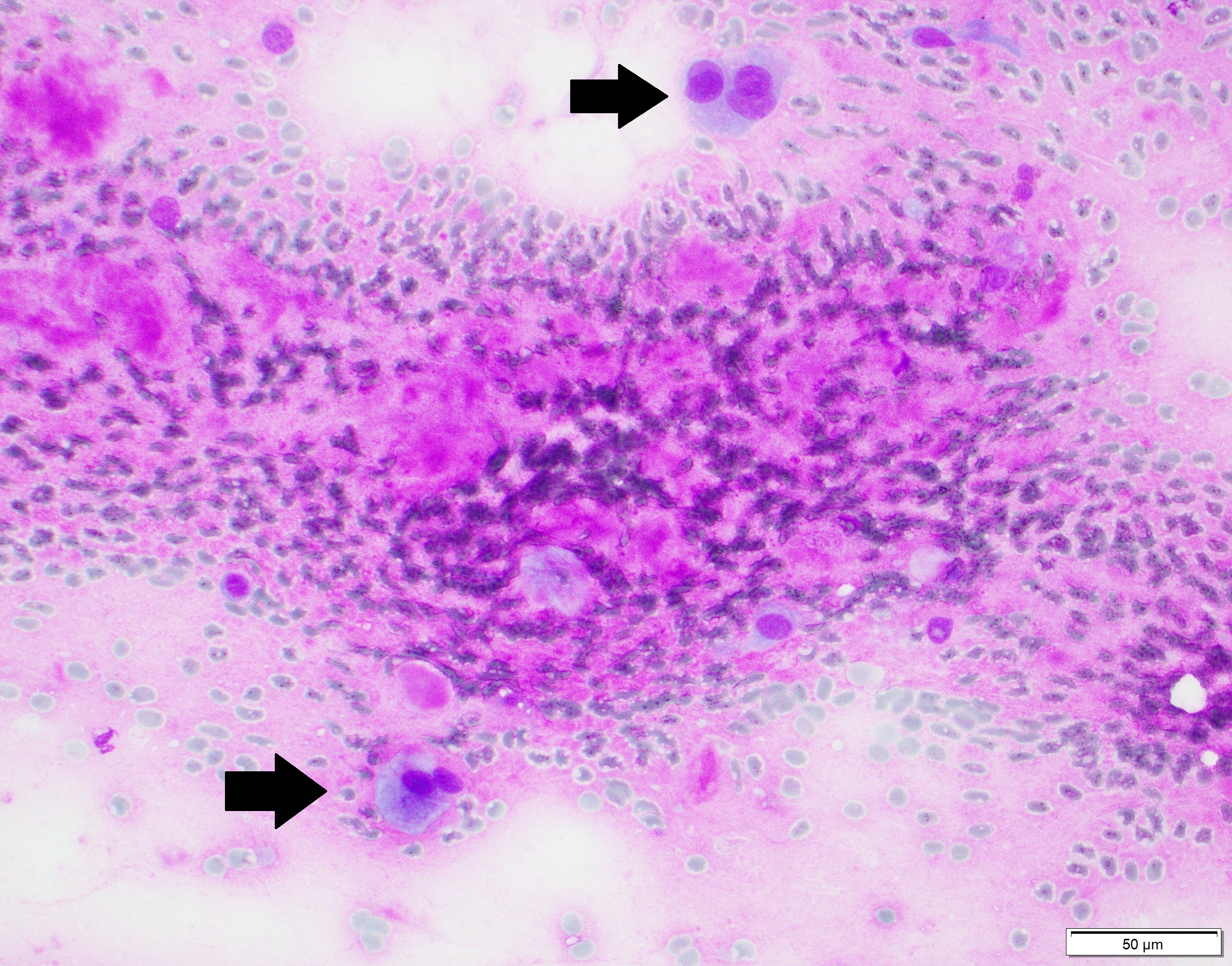
Multinucleation
Contributed by @Elena_PradosMD on Twitter
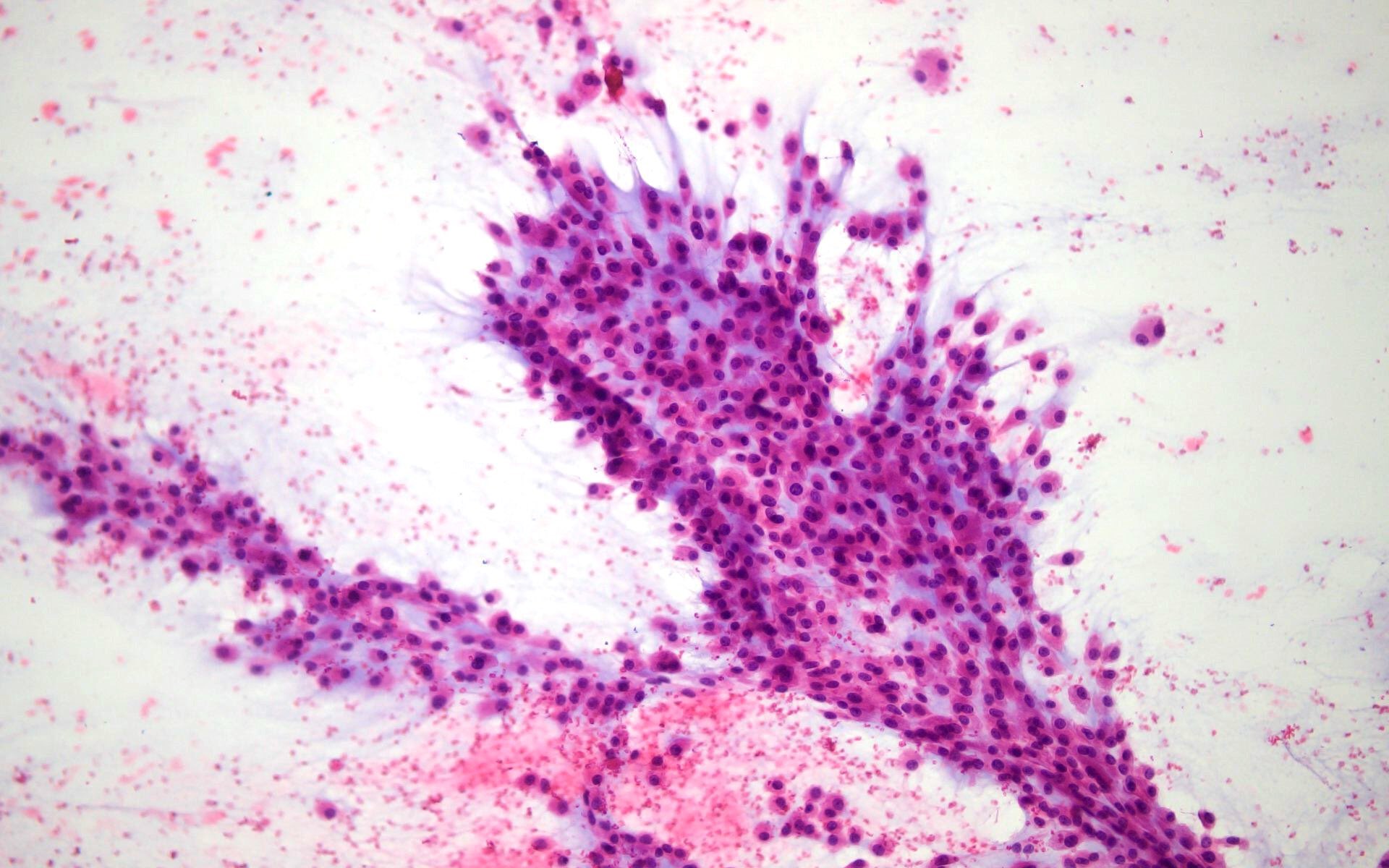
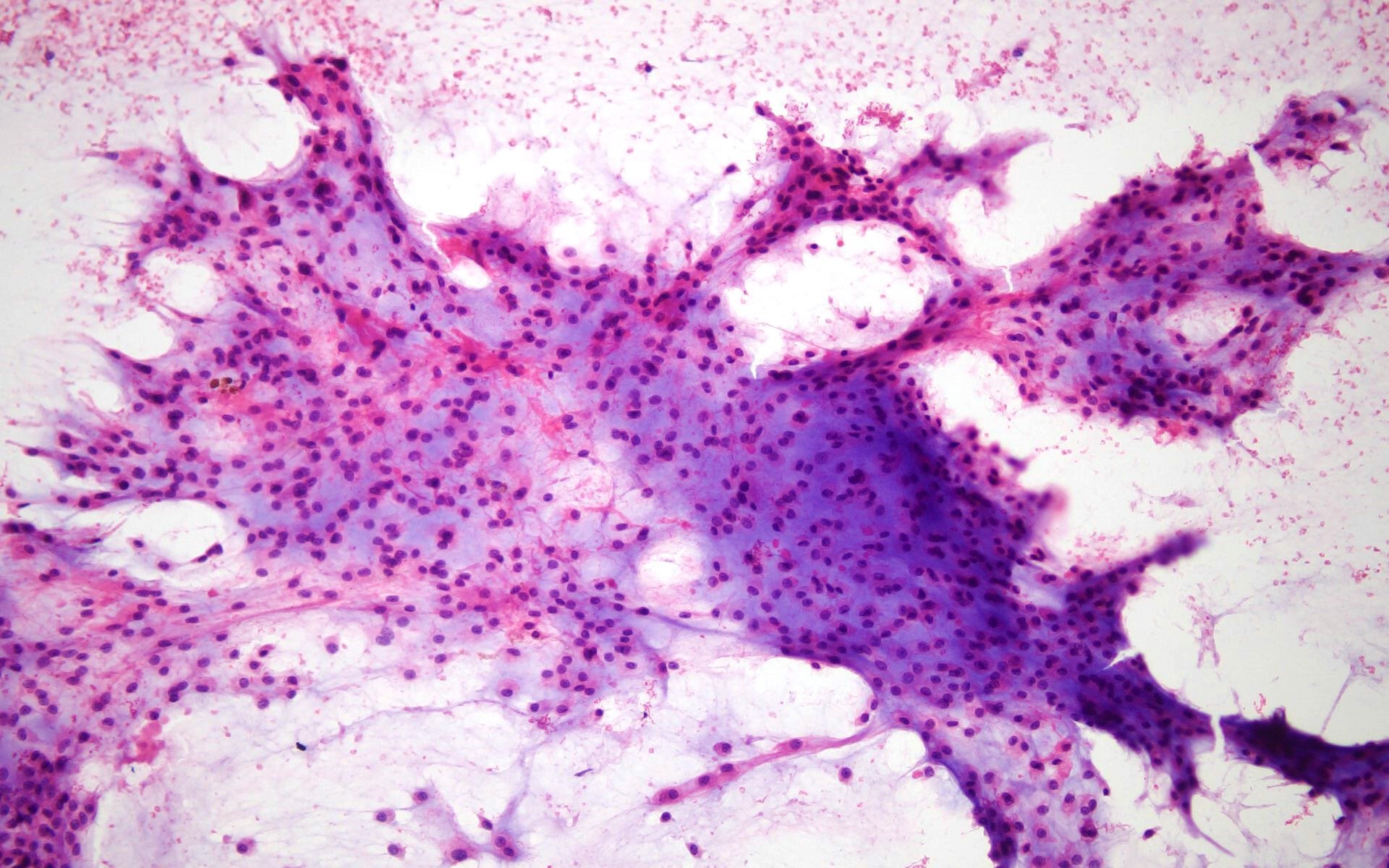
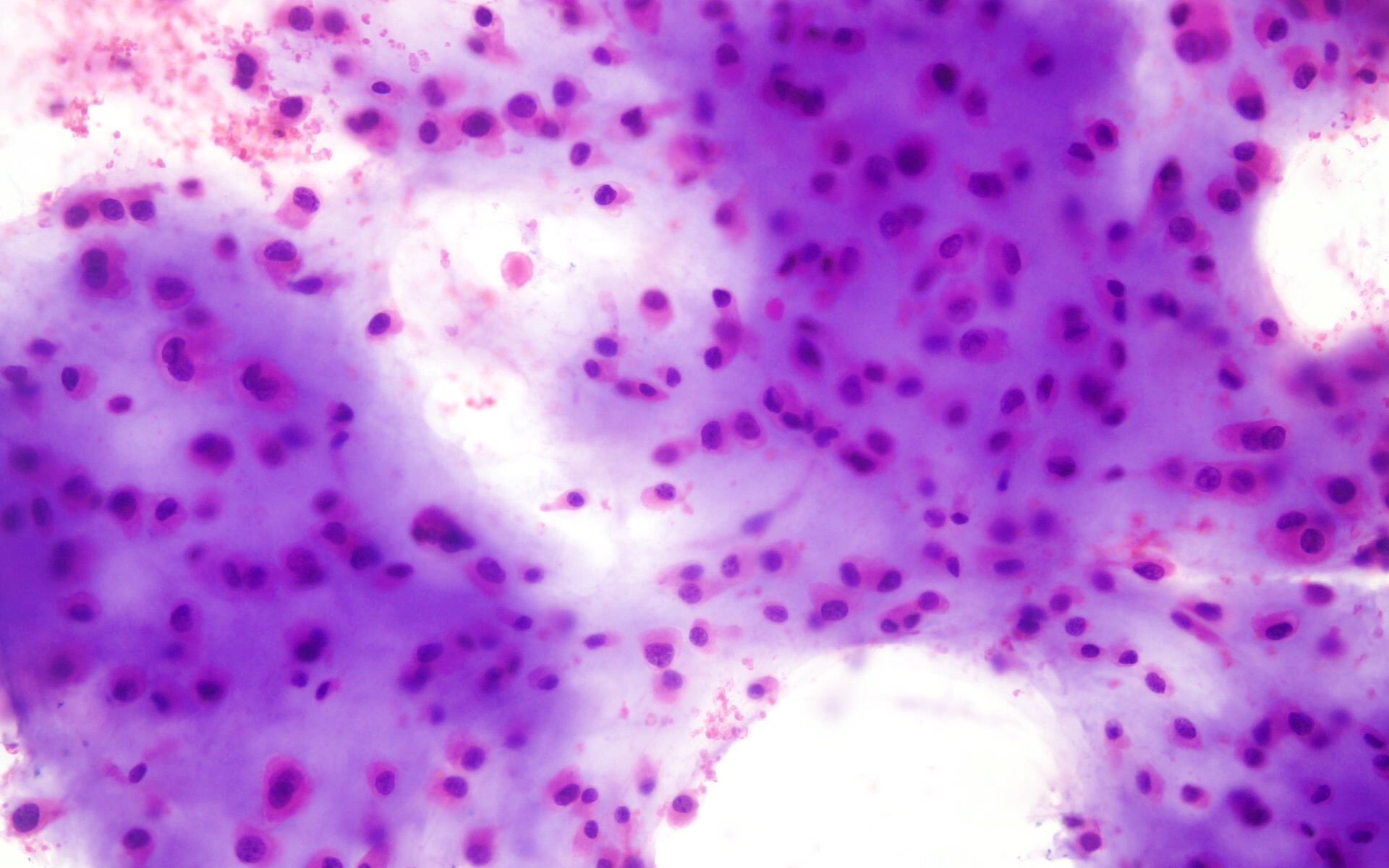
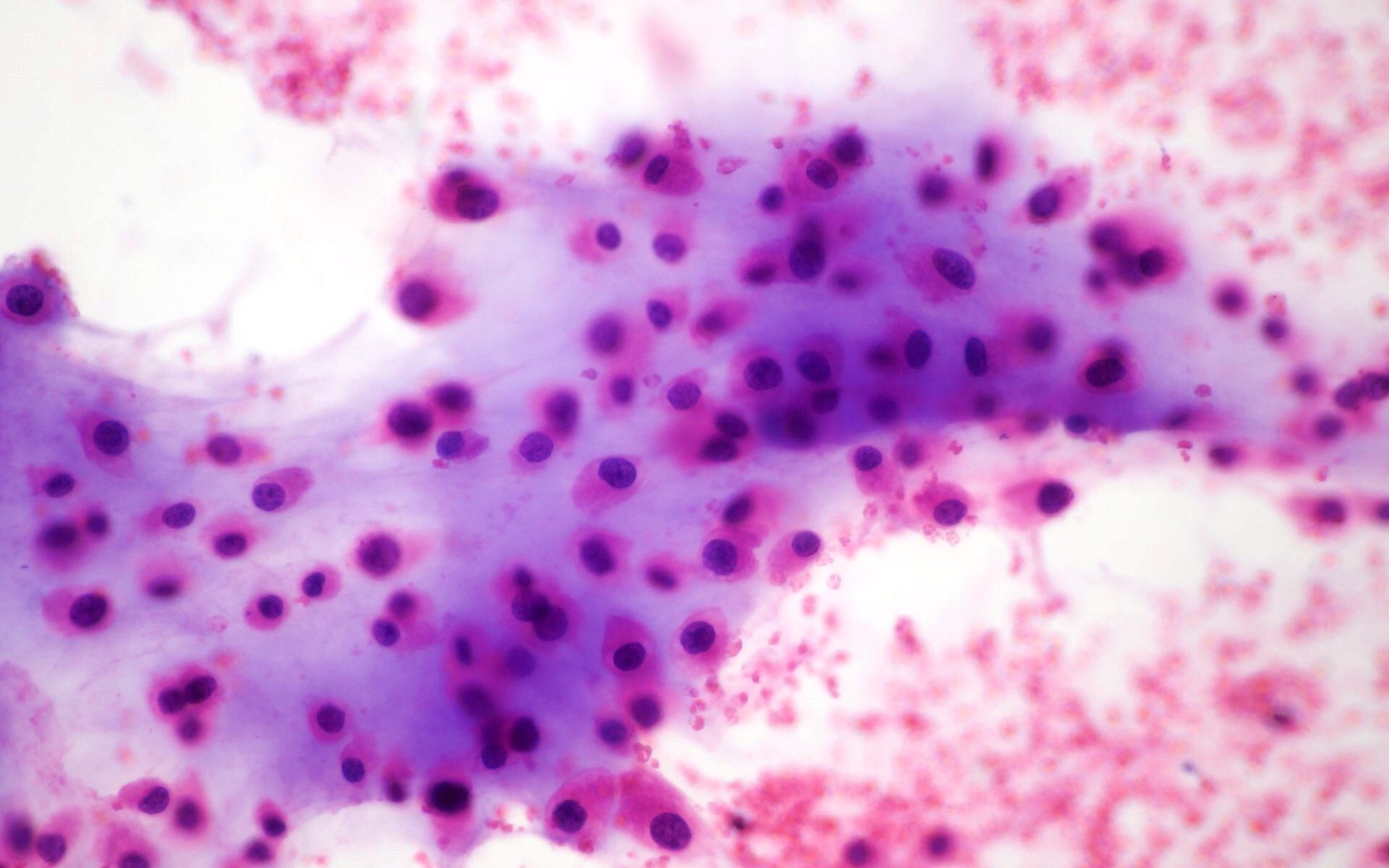
Chondrosarcoma
Positive stains
- Stains are not necessary in the majority of cases
- S100: uniformly strongly positive but in grade III it can be focally negative in less differentiated areas
- D2-40 (Appl Immunohistochem Mol Morphol 2009;17:131)
Negative stains
Molecular / cytogenetics description
- IDH1 and IDH2 mutations in approximately 50% of cases
- Aneuploidy is seen with increasing histologic grade
- TP53 mutations and affected active signaling pathways (RB1, CDKN2A, CDK) are identified particularly in high grade chondrosarcomas (J Cell Mol Med 2009;13:2843)
Videos
Chondrosarcoma versus enchondroma
Sample pathology report
- Tibia, biopsy:
- Low grade cartilaginous neoplasm (see comment)
- Comment: The differential diagnosis includes enchondroma and low grade chondrosarcoma. Clinical and radiologic correlation is recommended.
- Femur, resection:
- Chondrosarcoma, grade II (see comment)
- Surgical margins are negative
- See synoptic report below
- Comment: The diagnosis is made in conjunction with radiologic findings.
Differential diagnosis
- Chondroblastic osteosarcoma:
- If there is significant osteoid formation, then it is osteosarcoma
- Clinical and radiological correlation is helpful (typically younger patients)
- Enchondroma:
- No aggressive features radiologically
- Cytologically almost indistinguishable from low grade chondrosarcoma
- Less cellular, uniform hyaline, abundant matrix calcification
- Small, uniform, round nuclei with homogenous chromatin
- Fracture callus:
- Sometimes can contain abundant proliferating cartilage looking like cartilaginous neoplasia
- Chondroid matrix is less mineralized and dark blue in color
- Clinical and radiological correlation is helpful
- Chondromyxoid fibroma:
- Clinically and radiologically not aggressive
- Stellate cells
- More myxoid and less chondroid background
- SMA positive
Additional references
Board review style question #1
A 54 year old man had an 8 cm mass in the femur, which was resected. Which of the following is the best assessment?
- Radiotherapy is the mainstay of treatment
- Skull is the most common site
- The most likely genetic abnormalities are IDH1 and IDH2 mutations
- The tumor is sensitive to chemotherapy
- There is a female predominance
Board review style answer #1
C. The most likely genetic abnormalities are IDH1 and IDH2 mutations
Comment Here
Reference: Chondrosarcoma (primary, secondary, periosteal)
Comment Here
Reference: Chondrosarcoma (primary, secondary, periosteal)
Board review style question #2
A 45 year old man had a biopsy from a 7 cm mass in the proximal humerus demonstrating a low grade cartilaginous lesion. Which of the following is true?
- Correlation with radiologic findings is essential
- Fingers and toes are common sites for this neoplasm
- Molecular testing is important for diagnosis
- The tumor cells strongly stain with cytokeratin
- This tumor is common in pediatric population
Board review style answer #2
A. Correlation with radiologic findings is essential
Comment Here
Reference: Chondrosarcoma (primary, secondary, periosteal)
Comment Here
Reference: Chondrosarcoma (primary, secondary, periosteal)
