
Breast
Fibrocystic changes
Usual ductal hyperplasia
Authors: Sofia Lérias, M.D., Melinda Lerwill, M.D.
Editorial Board Member: Gary Tozbikian, M.D.
Editor-in-Chief: Debra L. Zynger, M.D.


Last author update: 11 February 2021
Last staff update: 25 April 2022
Copyright: 2002-2024, PathologyOutlines.com, Inc.
PubMed Search: Usual ductal hyperplasia[TIAB] free full text[SB]
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Radiology description | Prognostic factors | Case reports | Treatment | Gross description | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Cytology images | Positive stains | Molecular / cytogenetics description | Videos | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2 | Board review style question #3 | Board review style answer #3Cite this page: Lérias S, Lerwill M. Usual ductal hyperplasia. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/breastepithelialductalhyperplasia.html. Accessed April 23rd, 2024.
Definition / general
- Benign intraductal proliferation of progenitor epithelial cells with varying degrees of solid or fenestrated growth
Essential features
- Component of fibrocystic changes
- Mild cytologic variability
- Streaming growth pattern with fenestrated spaces and lack of cellular polarity
- Immunoreactive for high molecular weight cytokeratins
- Associated with slight increase in subsequent breast cancer risk (1.5 - 2 times)
Terminology
- Also called epithelial hyperplasia, intraductal hyperplasia, hyperplasia of usual type, ductal hyperplasia without atypia, epitheliosis
ICD coding
Epidemiology
- Mean age is 54 (N Engl J Med 2005;353:229)
- Most significant finding in 20% of benign breast biopsies (Cancer 2006;106:732)
Sites
- Terminal duct lobular units
- Occasionally, extralobular ducts
Pathophysiology
- Proliferation of CK5+ progenitor cells that can differentiate along glandular or myoepithelial lineages; glandular progenitor cells appear to predominate and show intermediate levels of differentiation (J Pathol 2002;198:458)
Etiology
- No specific etiologic factors
Clinical features
- No specific clinical findings
Diagnosis
- Diagnosis by histologic examination of tissue removed via biopsy or surgical excision
Radiology description
- No specific mammographic findings; occasional examples are associated with microcalcifications
- Can involve an underlying lesion (e.g. radial scar or papilloma) that is identified on imaging
- May show enhancement on magnetic resonance imaging (Arch Pathol Lab Med 2017;141:1513)
Prognostic factors
- Associated with 1.5 - 2 times increased risk for subsequent breast cancer (N Engl J Med 2005;353:229, Cancer 2006;107:1240)
- Risk may be slightly higher for patients with a positive family history of breast cancer (Cancer 2006;107:1240)
- Indicator of general breast cancer risk rather than direct precursor lesion
Case reports
- 30 year old woman with immature-like usual ductal hyperplasia in a fibroadenoma (Breast Dis 2016;36:157)
- 75 year old woman with malignant phyllodes tumor with liposarcomatous differentiation and intraductal hyperplasia (Breast Dis 2015;35:59)
- Usual ductal hyperplasia within gynecomastia-like changes of the female breast (Arch Pathol Lab Med 2001;125:506)
Treatment
- No treatment necessary
Gross description
- No macroscopic findings
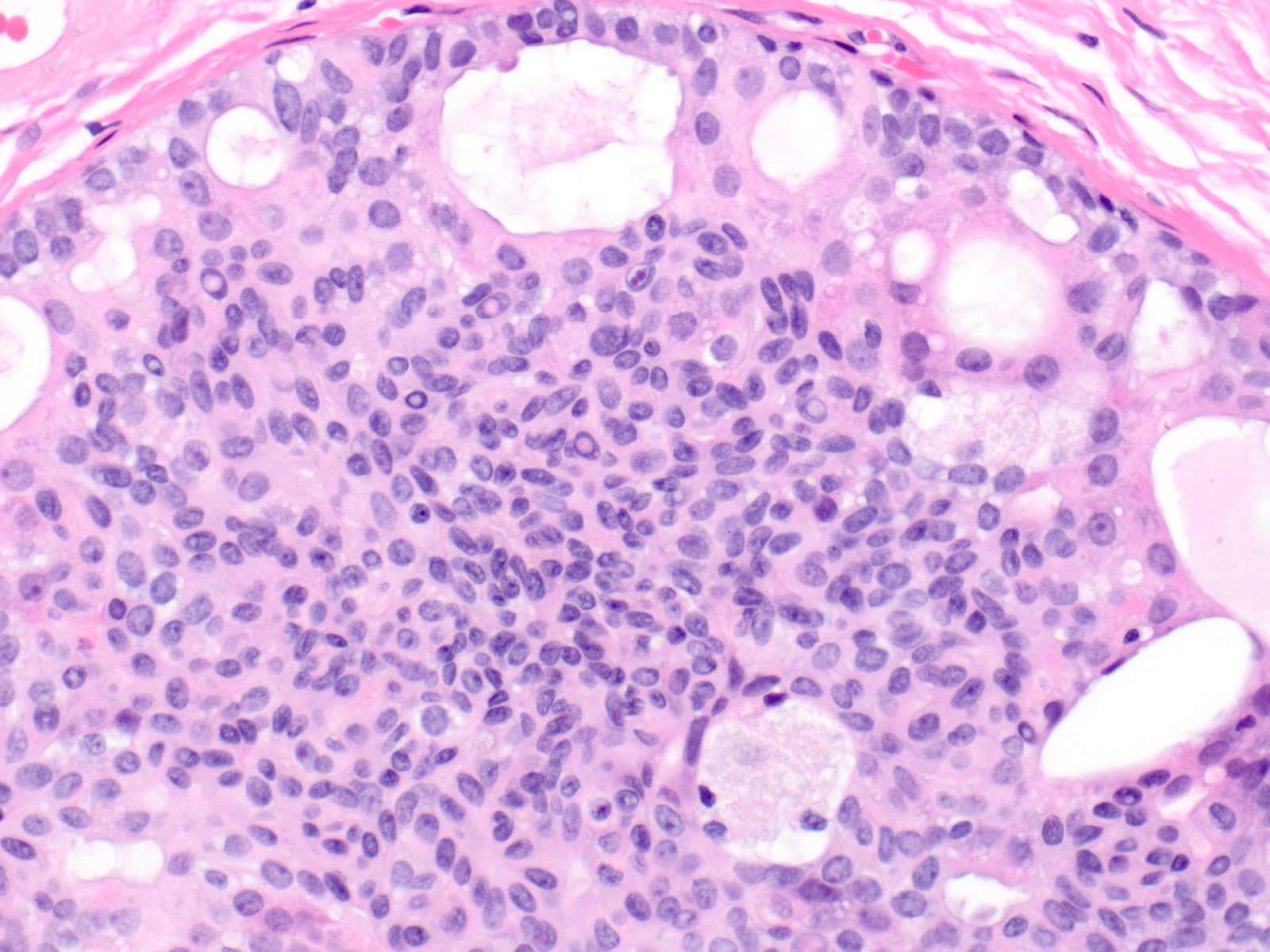
Microscopic (histologic) description
- Proliferation of cells of luminal and myoepithelial lineages, occasionally with intermixed apocrine cells
- Cytologic features (Semin Diagn Pathol 2004;21:10)
- Mild variation in cellular and nuclear size and shape
- Relatively small ovoid nuclei with frequent elongated or asymmetrically tapered (pear shaped) forms
- Lightly granular euchromatic chromatin and small nucleoli
- Frequent longitudinal nuclear grooves (coffee bean-like) and occasional nuclear pseudoinclusions
- Many examples demonstrate cellular maturation, where the cells shrink as they progress from a basal location to the center of the proliferation, becoming small and nearly pyknotic
- Eosinophilic, nonabundant cytoplasm with indistinct cell borders
- Architectural features (Semin Diagn Pathol 2004;21:10)
- Cohesive proliferation with haphazard, jumbled cell arrangement or streaming growth pattern
- Fenestrated, solid and occasional micropapillary patterns
- Irregular slit-like fenestrations are common, especially along periphery
- Cells run parallel to the edges of secondary spaces and do not exhibit a polarized orientation (this contrasts with the cells of atypical ductal hyperplasia and ductal carcinoma in situ, which have apical-basal polarity and radially orient their apical poles toward the spaces)
- Variant patterns and features
- Micropapillary
- Typically focal in a background of conventional pattern usual ductal hyperplasia
- Mild duct dilation
- Short stubby papillae of roughly uniform height
- Cytologic features of usual ductal hyperplasia
- Cellular maturation present, with tips of papillae formed by tight knots of mature cells
- Lack of polarization
- Immature
- Uncommon variant
- Larger immature basal hyperplastic cells predominate or are increased beyond their usual 1 - 2 cell layers and are instead several cell layers thick
- Cellular maturation is still present
- Most often encountered in fibroepithelial lesions with cellular stroma
- Necrosis
- Florid usual ductal hyperplasia can rarely demonstrate central necrosis
- Typically occurs within a radial scar / complex sclerosing lesion, nipple adenoma or juvenile papillomatosis
- Mild nuclear enlargement in radial scars
- Florid usual ductal hyperplasia within radial scars / complex sclerosing lesions can occasionally have more active appearing nuclei with mild nuclear enlargement
- Other cytologic and architectural features of usual ductal hyperplasia remain intact
- Micropapillary
Microscopic (histologic) images
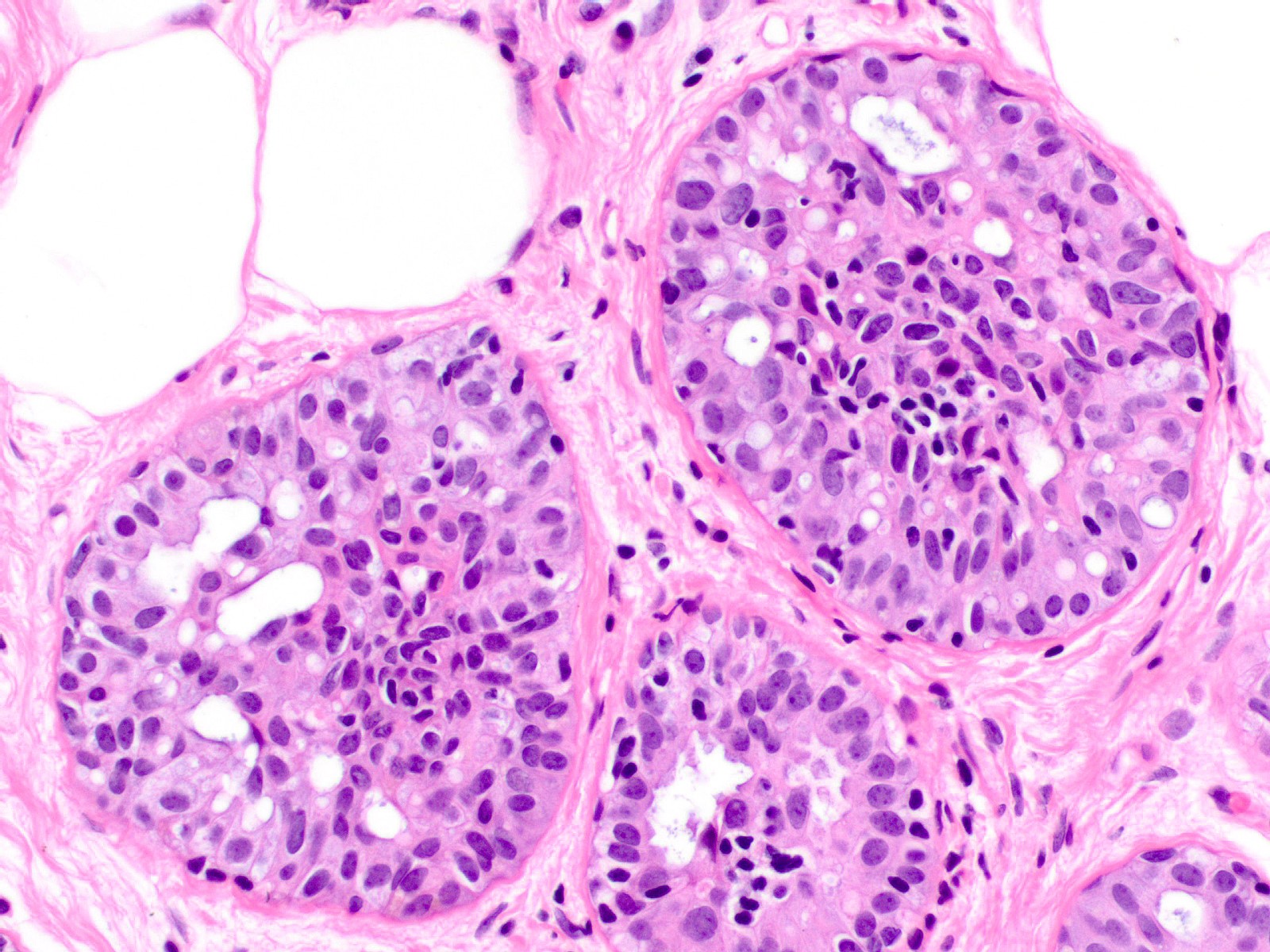
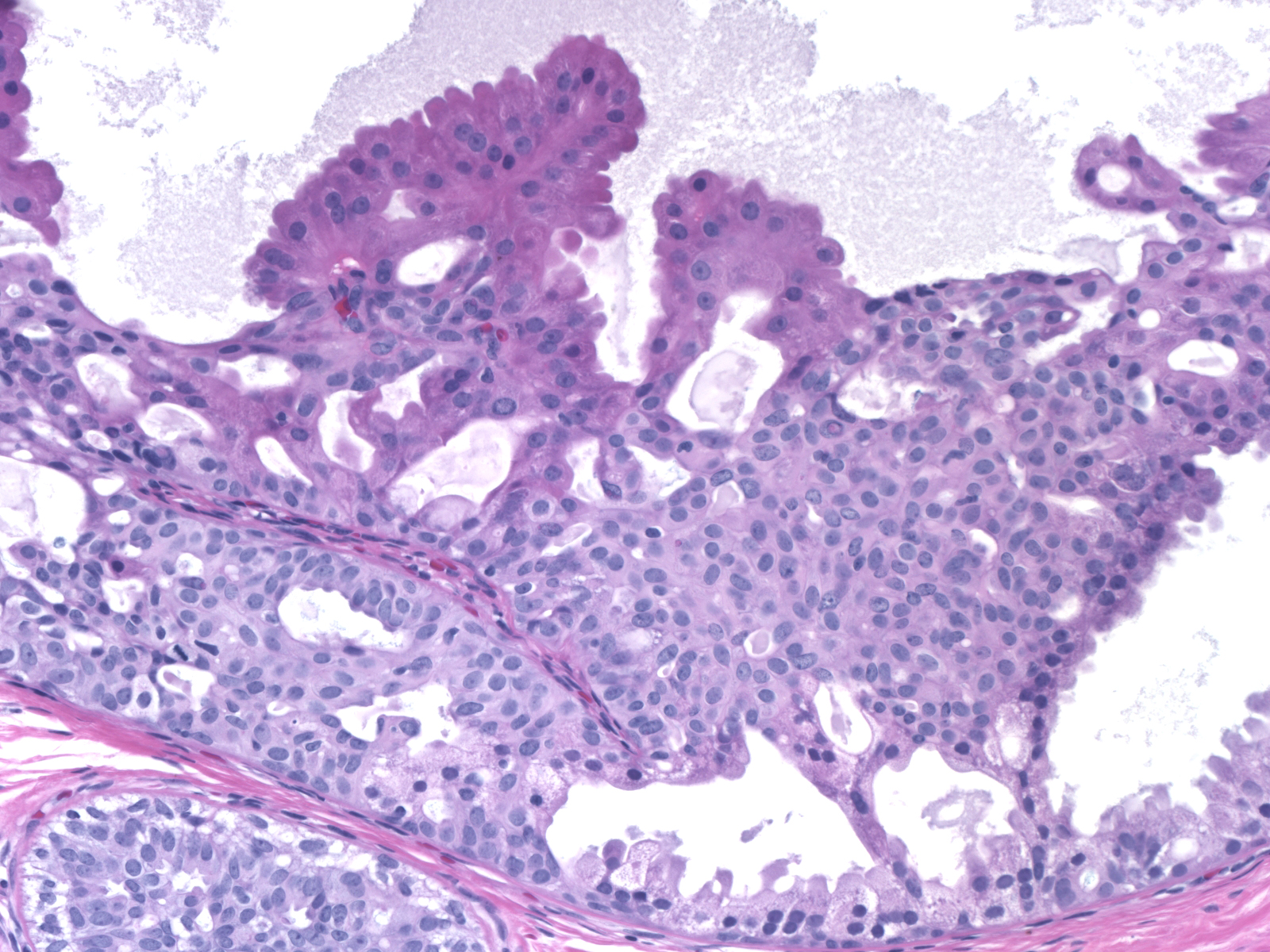
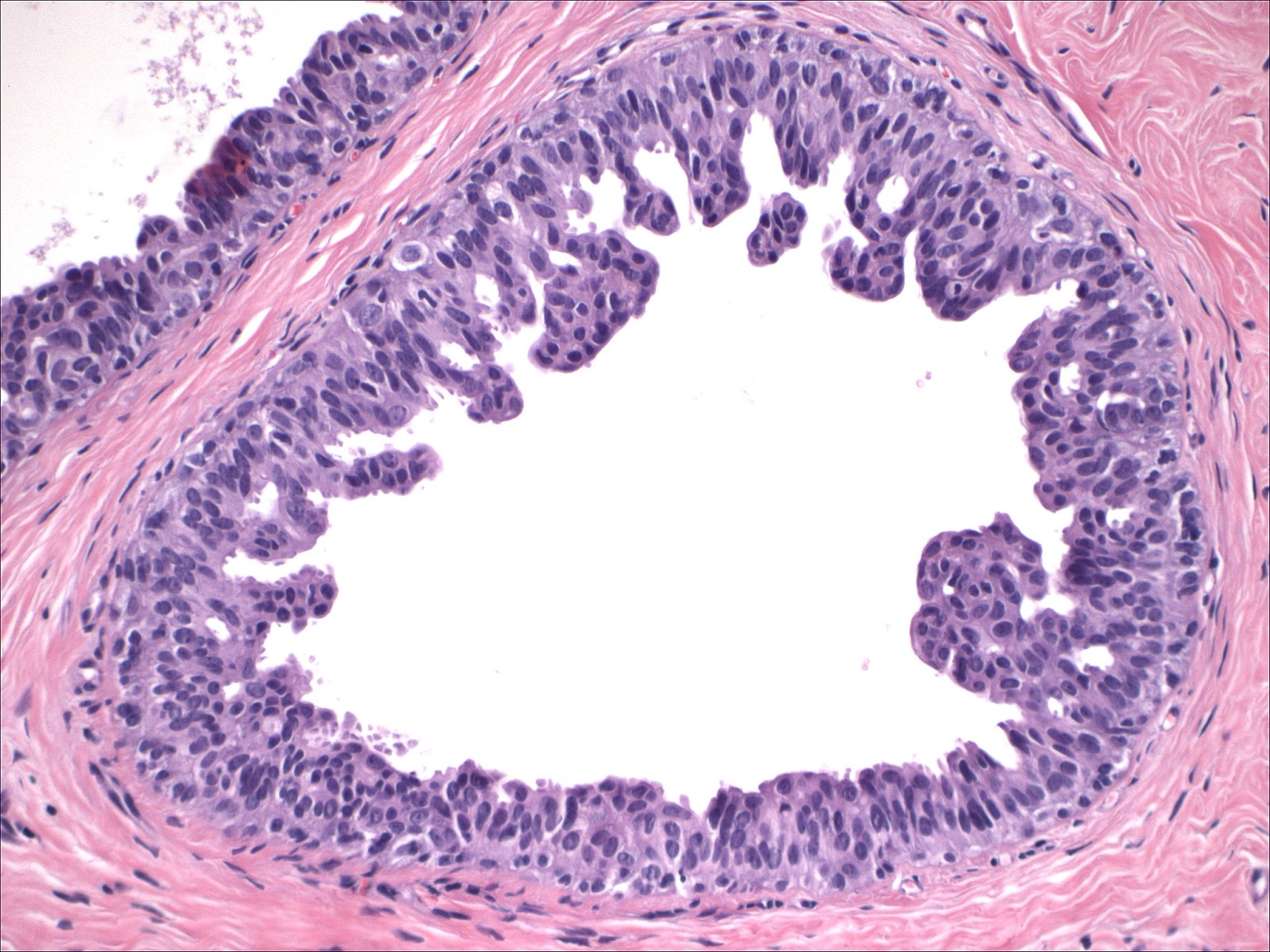
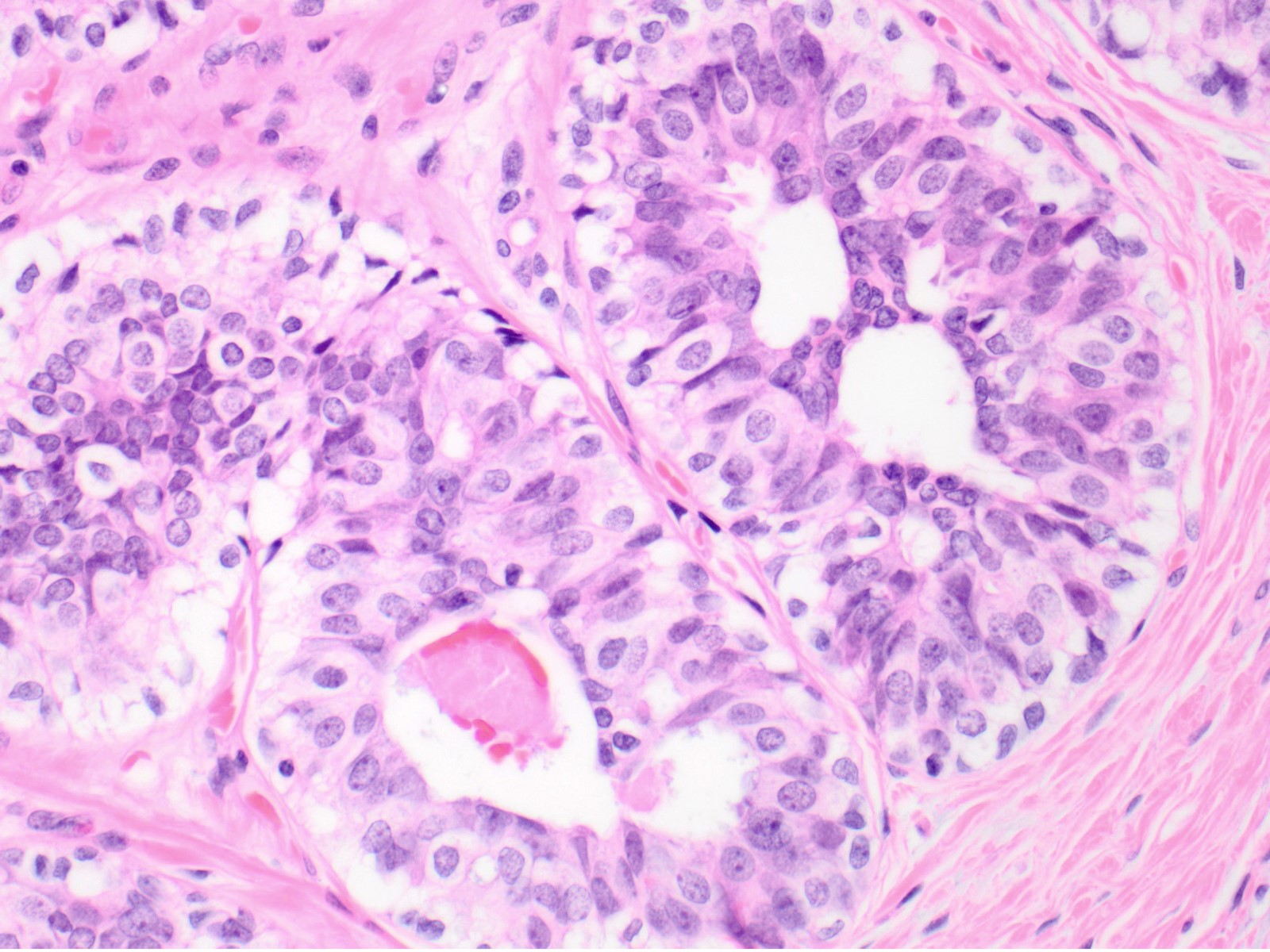
Contributed by Melinda Lerwill, M.D.
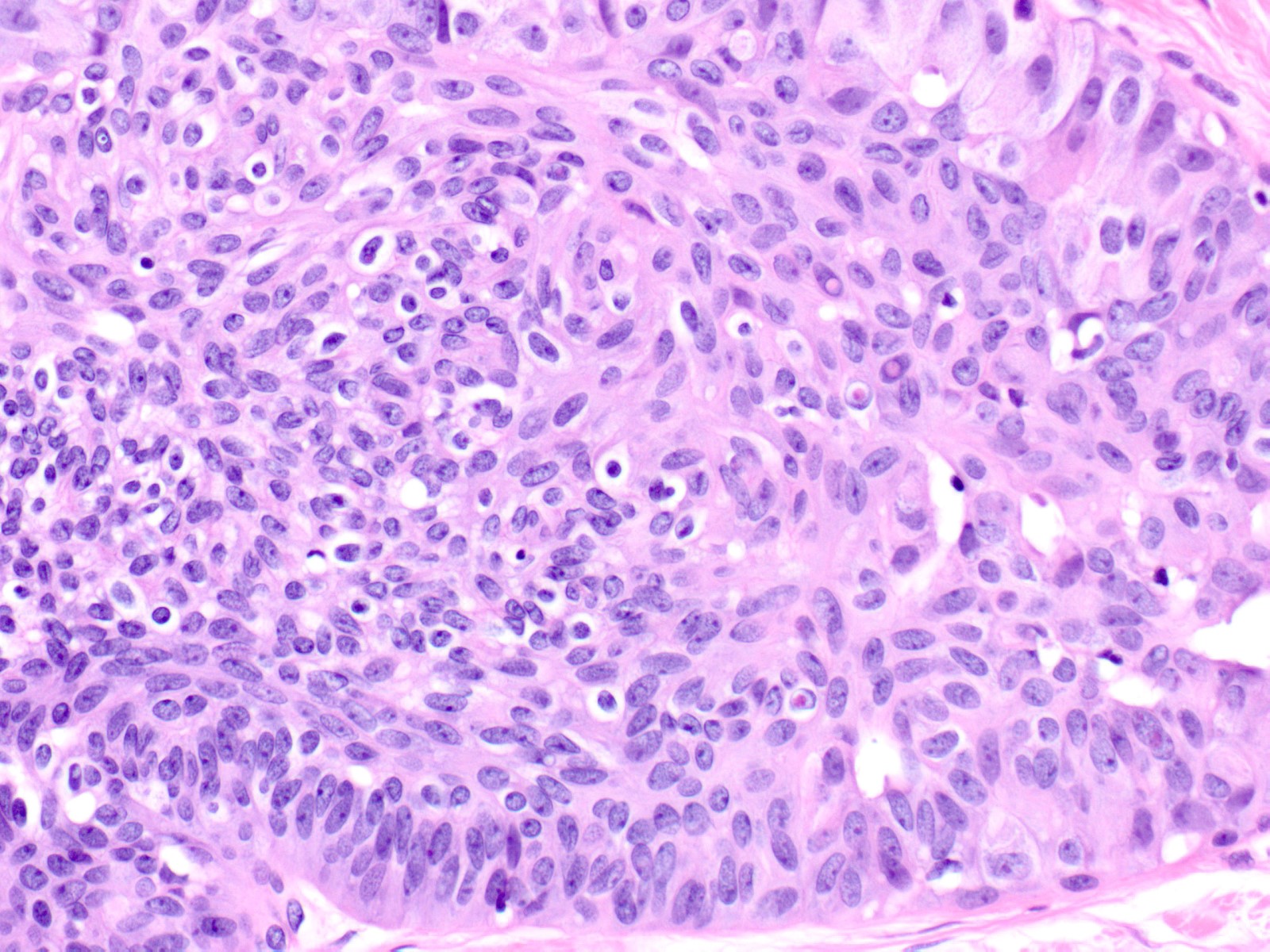
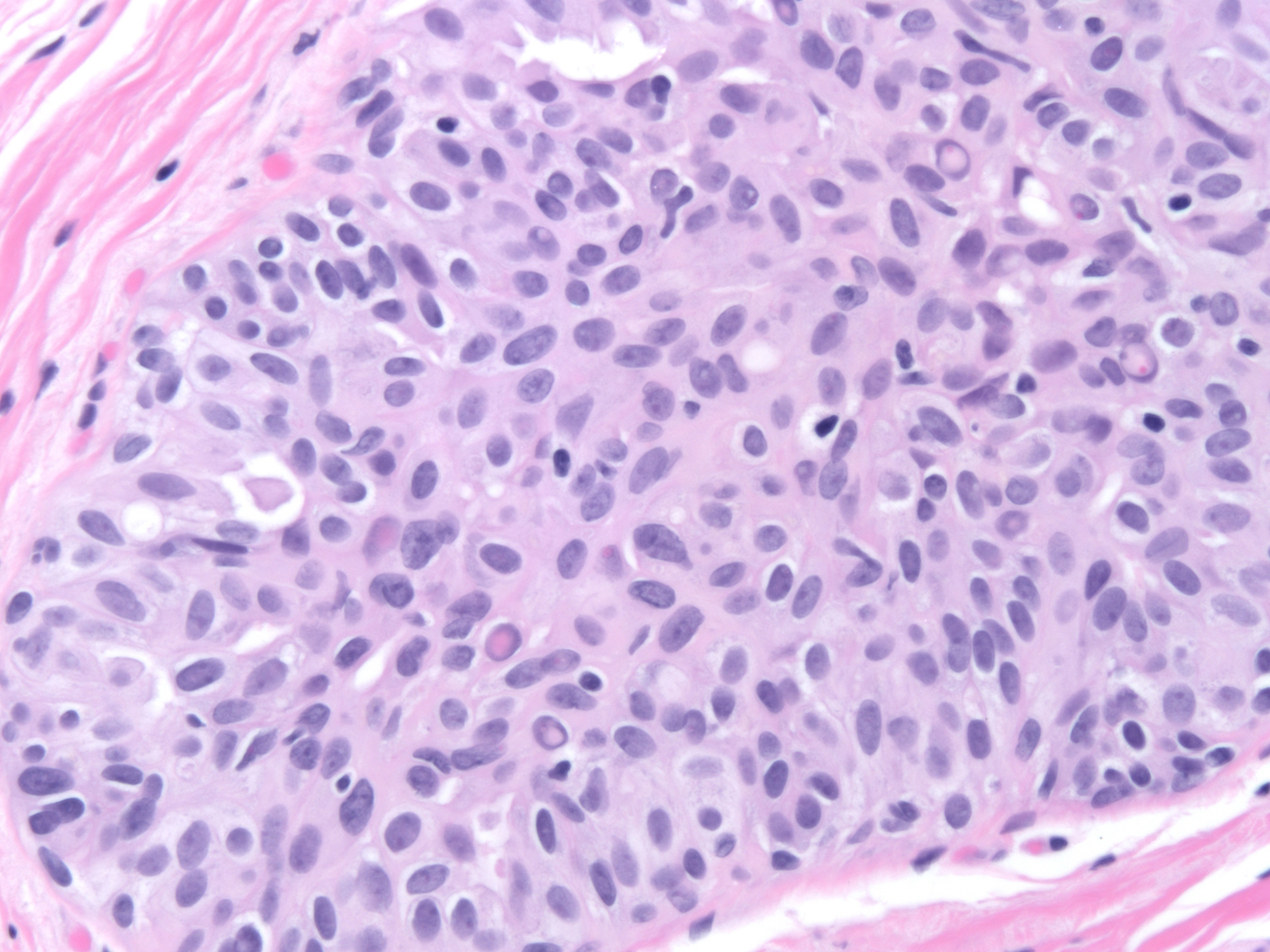
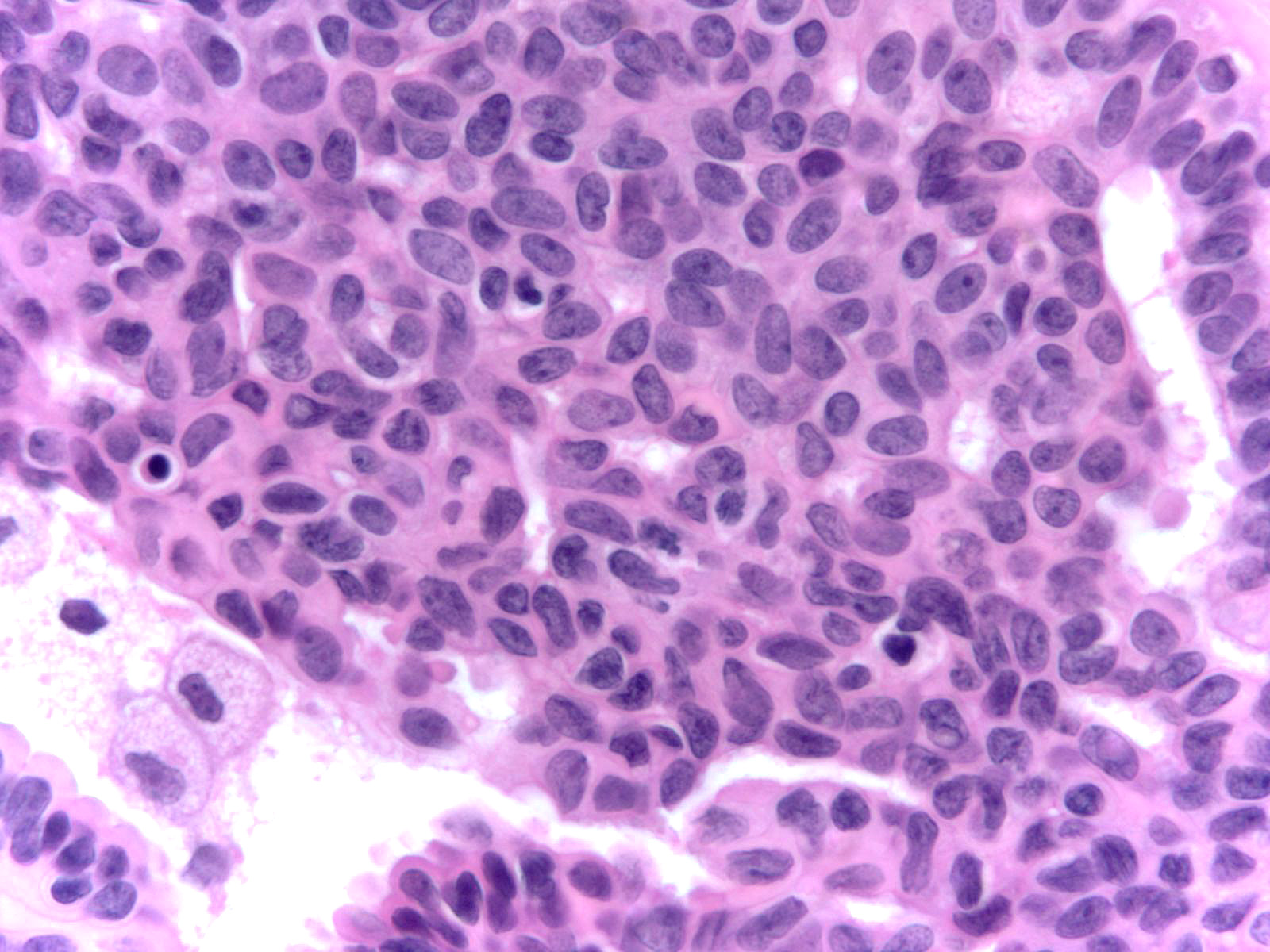
Cytologic features
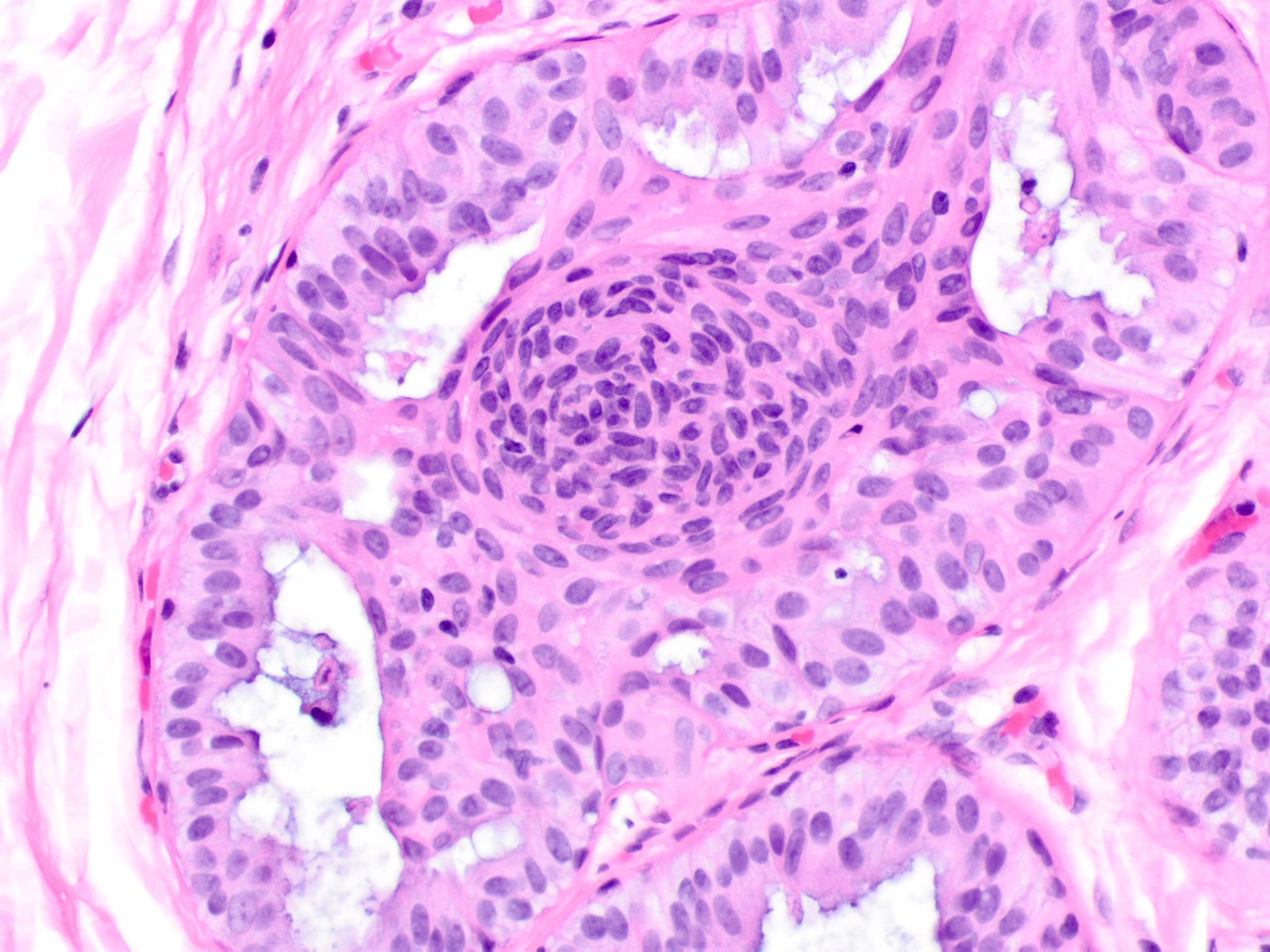
Cellular maturation
Merging with apocrine metaplasia
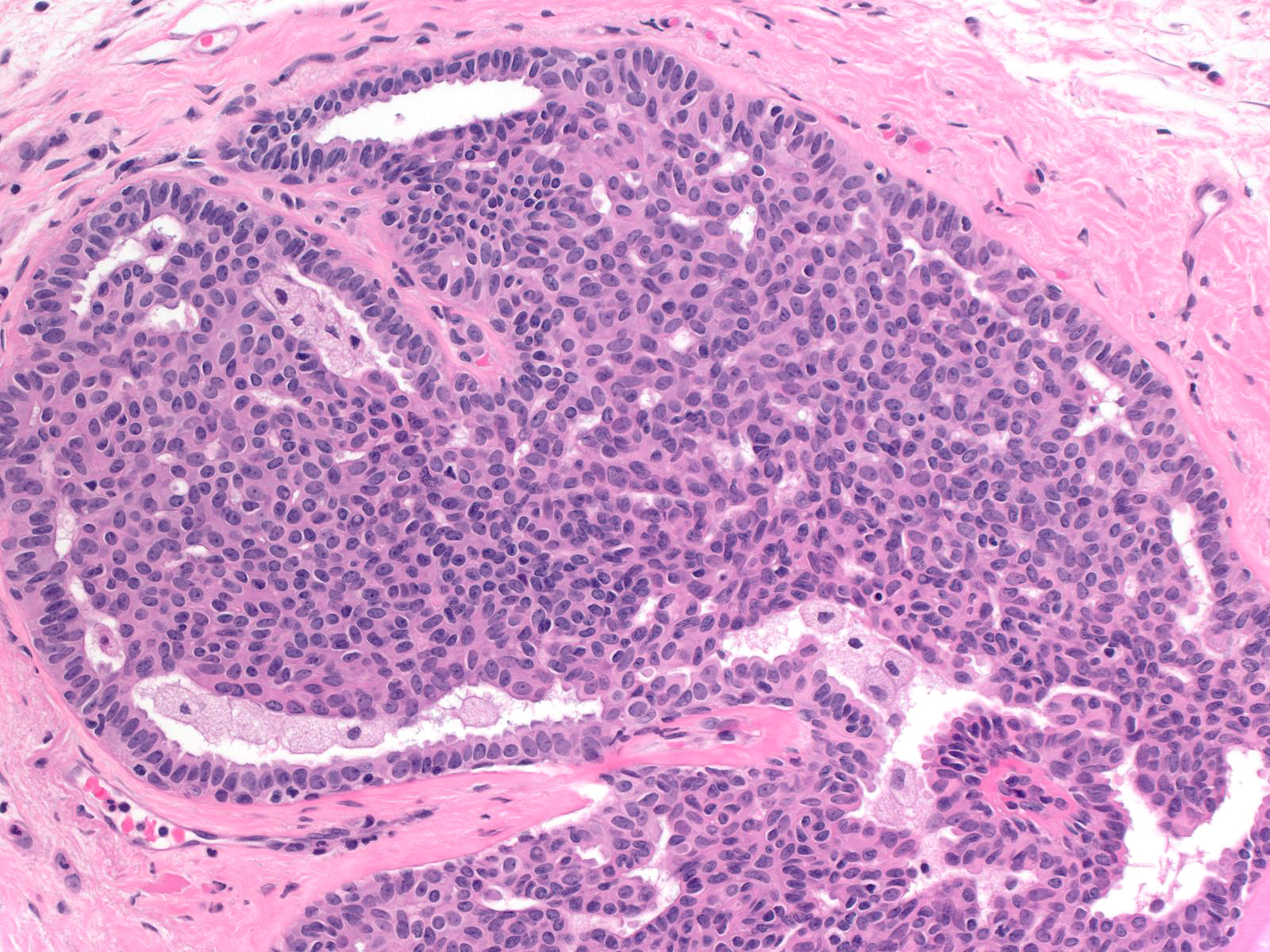
Fenestrated spaces
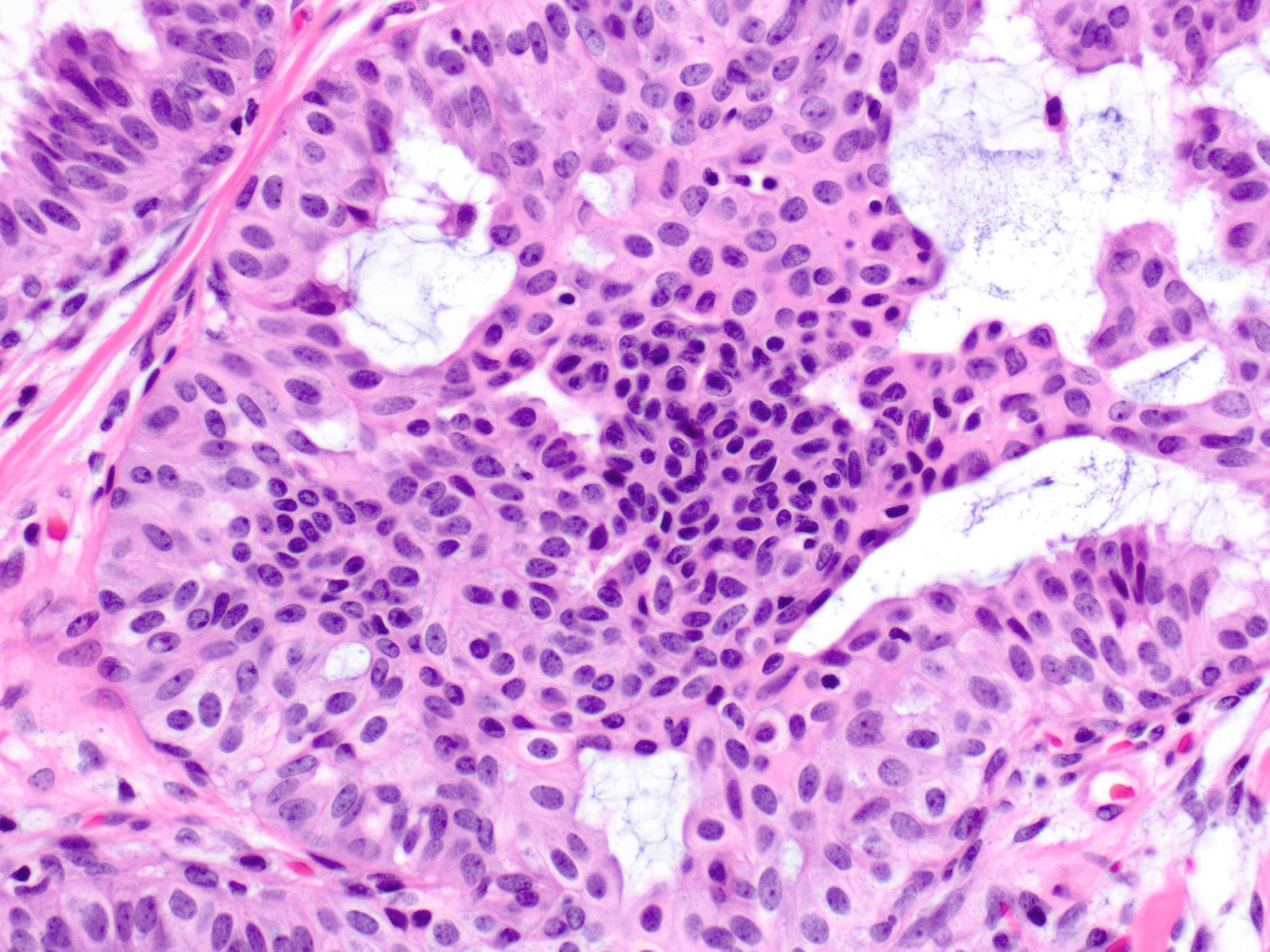
Lack of cellular polarity
Micropapillary usual ductal hyperplasia
Immature usual ductal hyperplasia

Florid usual ductal hyperplasia in radial scar
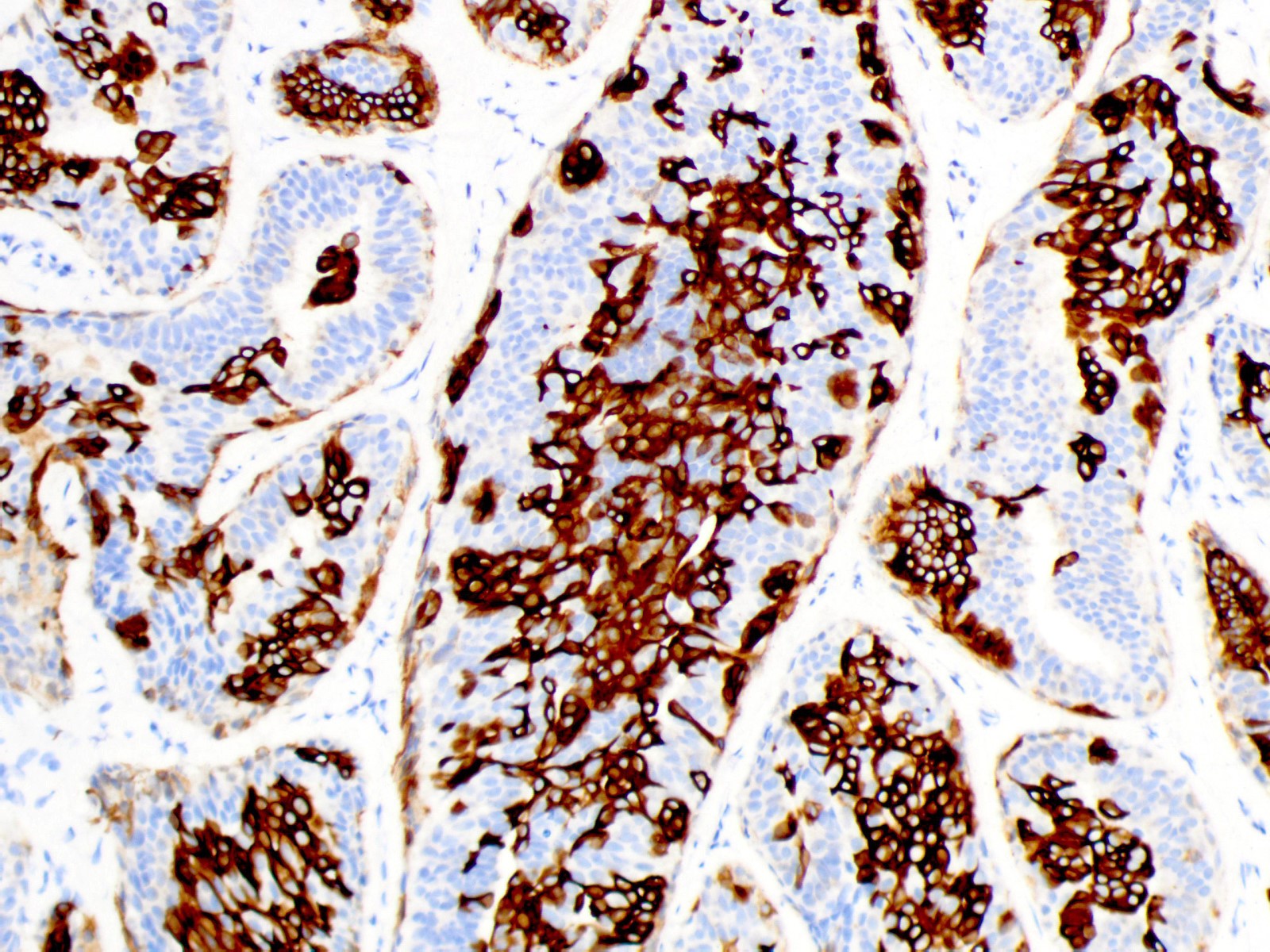
Cytokeratin 5/6
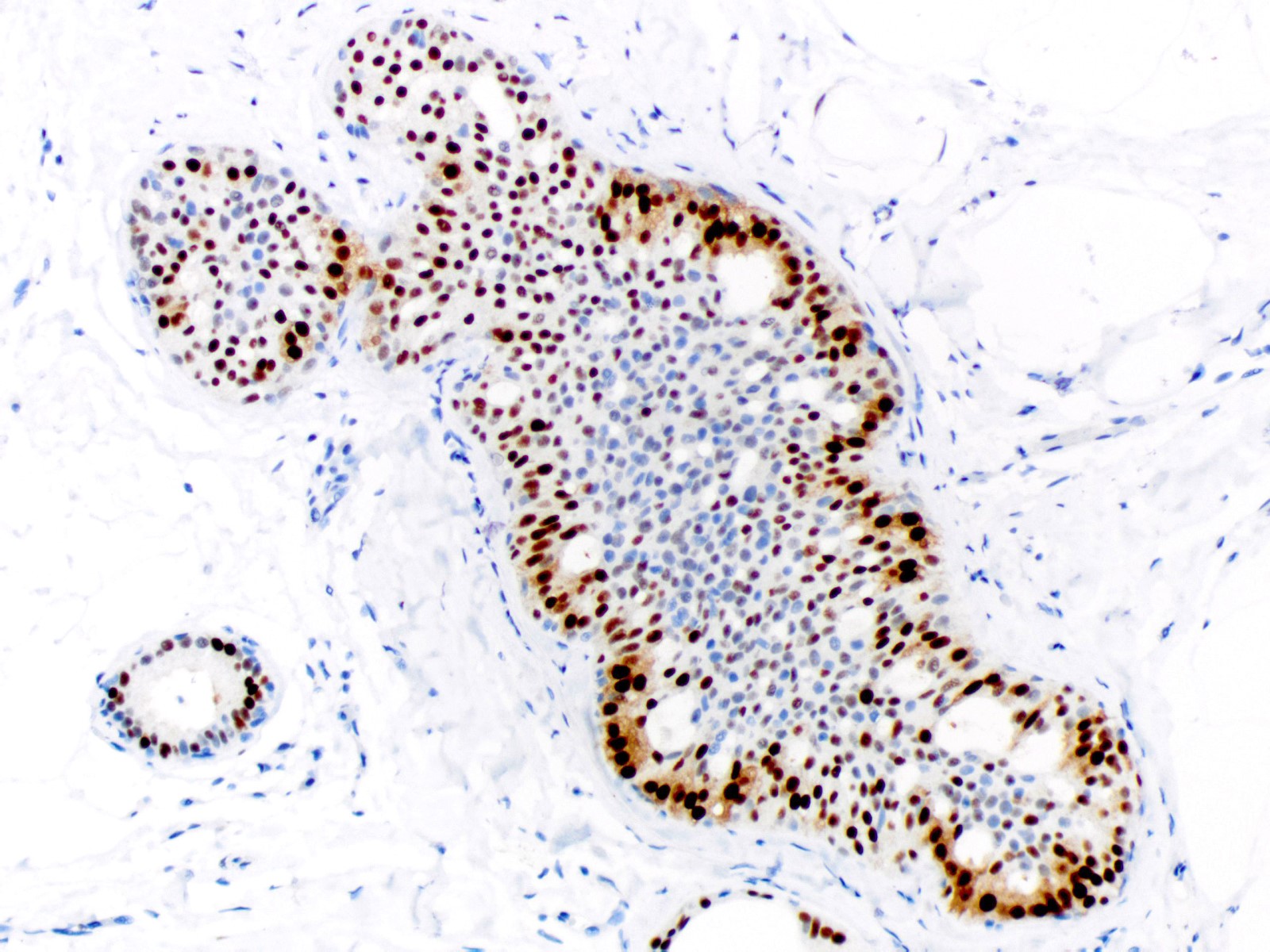
Estrogen receptor
Cytology description
- Sample may be moderately to highly cellular
- Sheets and cohesive clusters of bland ductal cells with regular spacing and associated myoepithelial cells (Am J Clin Pathol 1995;103:438)
- Lack of significant nuclear overlap / crowding
- Ductal cell nuclei with finely granular chromatin and inconspicuous small nucleoli
- Lack of ductal cell discohesion
- Naked myoepithelial cell nuclei in the background may be present
Cytology images
Contributed by Amy Ly, M.D.
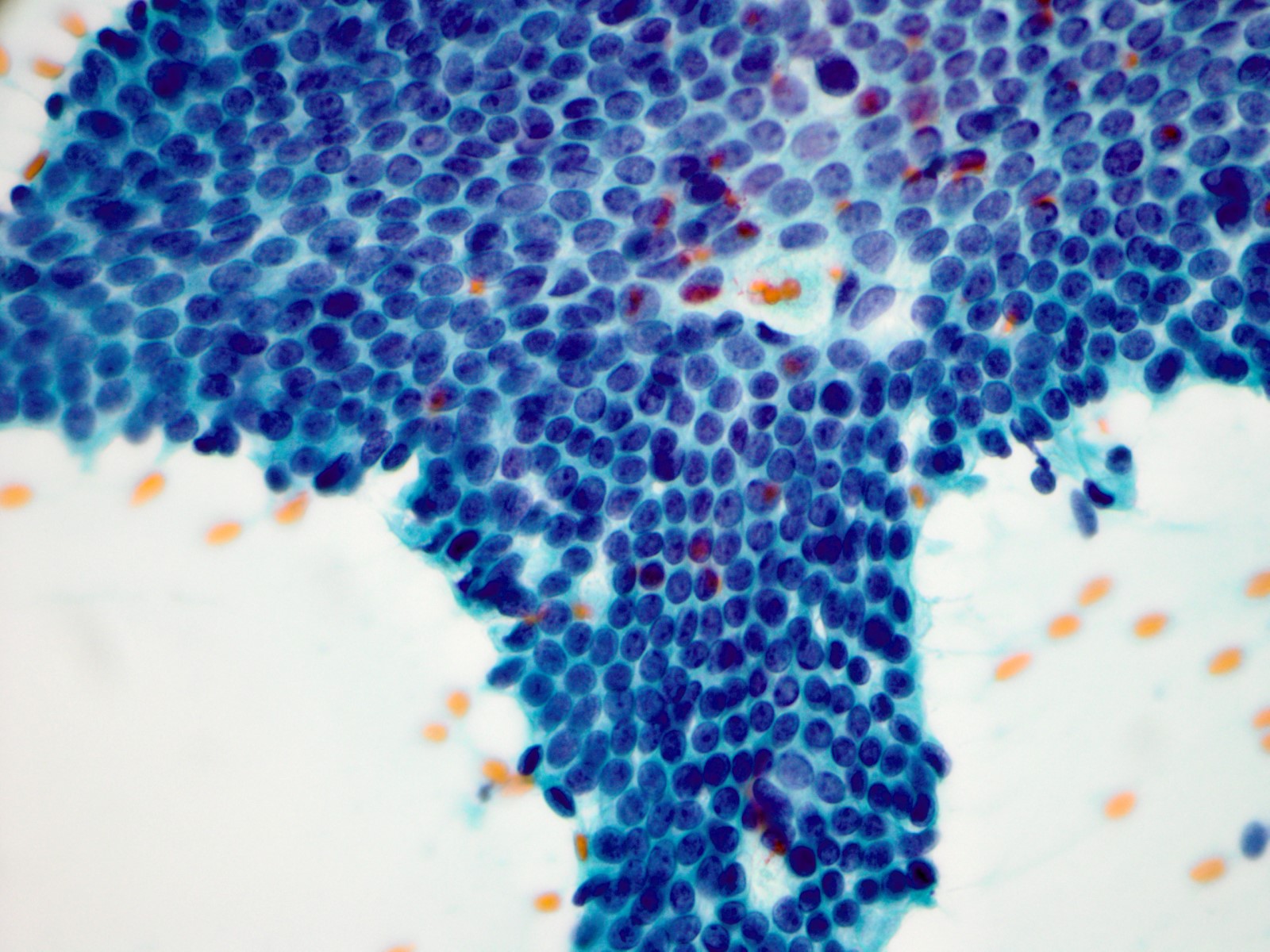
Fine needle aspiration
Positive stains
- High molecular weight cytokeratins (e.g. CK5, CK14, 34 beta E12): mosaic to occasionally diffuse pattern of positivity (Histopathology 2000;37:232)
- Estrogen receptor: heterogeneous positivity with variation in staining intensity
- E-cadherin
- Low molecular weight cytokeratins (e.g. CK7, CK8, CK18)
Molecular / cytogenetics description
- Activating mutations in the PI3K / AKT / mTOR pathway may play a role in pathogenesis (Am J Pathol 2016;186:15)
Videos
High yield breast pathology cases
Sample pathology report
- Left breast, needle core biopsy:
- Usual ductal hyperplasia
Differential diagnosis
- Atypical ductal hyperplasia / low grade ductal carcinoma in situ:
- Monomorphic cell population
- Round to oval nuclei with homogeneous, fine and hyperchromatic chromatin; inconspicuous nucleoli; and smooth nuclear contours
- Increased amounts of pale eosinophilic to amphophilic cytoplasm with conspicuous cell borders
- Cellular maturation absent
- Cellular polarization around luminal and secondary spaces
- Atypical architectural patterns formed by polarized growth (cribriform spaces, Roman arches, trabecular bars, micropapillae)
- High molecular weight cytokeratin / CK5 negative and estrogen receptor diffusely positive (Arch Pathol Lab Med 2016;140:686)
- Micropapillary ductal carcinoma in situ:
- Often extensive (Mod Pathol 2010;23:260)
- Moderate to marked duct dilation
- Variation in papillae size and shape
- Elongated, bulbous or complex papillae
- Cellular polarization
- Cytologic atypia
- Lack of maturation
- Frequent luminal cellular debris
- High molecular weight cytokeratin / CK5 negative and estrogen receptor diffusely positive in low and intermediate grade cases
- Intermediate grade ductal carcinoma in situ:
- Populational uniformity (one cell type)
- Moderate nuclear enlargement throughout the proliferation
- Abnormal chromatin, which may be hyperchromatic, cleared and clumped or coarsely granular
- May show marked nuclear irregularity
- Can have red nucleoli
- Polarized architectural atypia
- Necrosis may be present
- Usually high molecular weight cytokeratin / CK5 negative
- Estrogen receptor often positive but more variability in degree of staining than in low grade ductal carcinoma in situ
- Uncommon basal-like examples may have a high molecular weight cytokeratin / CK5 positive and estrogen receptor negative phenotype (Breast Cancer Res 2008;10:R67)
- Solid papillary carcinoma:
- Solid epithelial proliferation showing marked expansion of multiple circumscribed duct spaces (Arch Pathol Lab Med 2012;136:1308)
- Thin fibrovascular cores punctuate the proliferation, with cellular palisading around the cores
- Myoepithelial cells often sparse or absent along fibrovascular cores
- Nuclei may superficially resemble those in usual ductal hyperplasia but demonstrate greater populational uniformity, are slightly larger and have abnormal chromatin
- Granular cytoplasm may be present
- Intra or extracellular mucin common
- High molecular weight cytokeratin / CK5 negative and estrogen receptor diffusely positive
- Often positive for neuroendocrine markers (synaptophysin or chromogranin)
Board review style question #1
- What is the risk for subsequent breast cancer associated with the illustrated lesion?
- 1.5 - 2 times increased risk
- 2 - 3 times decreased risk
- 4 - 5 times increased risk
- 8 - 11 times increased risk
- No change in risk compared to control populations
Board review style answer #1
A. 1.5 - 2 times increased risk
This is usual ductal hyperplasia. Usual ductal hyperplasia is associated with a slight increase in risk (1.5 - 2 times) for subsequent breast cancer. Risk appears to be slightly higher in those patients with a positive family history of breast cancer.
Comment Here
Reference: Usual ductal hyperplasia
This is usual ductal hyperplasia. Usual ductal hyperplasia is associated with a slight increase in risk (1.5 - 2 times) for subsequent breast cancer. Risk appears to be slightly higher in those patients with a positive family history of breast cancer.
Comment Here
Reference: Usual ductal hyperplasia
Board review style question #2
- What is the typical high molecular weight cytokeratin / estrogen receptor (HWMCK / ER) immunoprofile for usual ductal hyperplasia of the breast?
- HMWCK negative / ER diffusely positive
- HMWCK negative / ER negative
- HMWCK mosaic positive / ER diffusely positive
- HMWCK mosaic positive / ER heterogeneously positive
- HMWCK mosaic positive / ER negative
Board review style answer #2
D. HMWCK mosaic positive / ER heterogeneously positive
Usual ductal hyperplasia is positive for HMWCK in a mosaic to occasionally diffuse pattern and demonstrates heterogeneous positivity for ER.
Comment Here
Reference: Usual ductal hyperplasia
Usual ductal hyperplasia is positive for HMWCK in a mosaic to occasionally diffuse pattern and demonstrates heterogeneous positivity for ER.
Comment Here
Reference: Usual ductal hyperplasia
Board review style question #3
- Which of the following is a feature of usual ductal hyperplasia that aids in distinguishing it from low grade ductal carcinoma in situ?
- Cellular maturation
- Monomorphic hyperchromatic nuclei
- Palisading around fibrovascular cores
- Polarization around secondary spaces
- Red macronucleoli
Board review style answer #3
A. Cellular maturation
Many examples of usual ductal hyperplasia demonstrate cellular maturation, where the cells shrink as they progress from a basal location to the center of the proliferation, becoming small and nearly pyknotic. Cellular maturation is not a feature of low grade ductal carcinoma in situ or atypical ductal hyperplasia.
Comment Here
Reference: Usual ductal hyperplasia
Many examples of usual ductal hyperplasia demonstrate cellular maturation, where the cells shrink as they progress from a basal location to the center of the proliferation, becoming small and nearly pyknotic. Cellular maturation is not a feature of low grade ductal carcinoma in situ or atypical ductal hyperplasia.
Comment Here
Reference: Usual ductal hyperplasia
