
Breast
General
Histology
Authors: Indu Agarwal, M.D., Luis Blanco, Jr., M.D.
Editorial Board Members: Gary Tozbikian, M.D., Julie M. Jorns, M.D.


Last author update: 2 August 2021
Last staff update: 9 May 2022
Copyright: 2002-2024, PathologyOutlines.com, Inc.
PubMed Search: Breast histology
Table of Contents
Definition / general | Essential features | Embryology | Histology | Menstrual cycle related changes | Pregnancy / lactation | Menopause | Neonatal breast | Male breast | Transsexual breast | Clinical features | Gross description | Gross images | Microscopic (histologic) images | Positive stains | Negative stains | Electron microscopy images | Videos | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Agarwal I, Blanco L. Histology. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/breastnormal.html. Accessed April 24th, 2024.
Definition / general
- Mammary glands located on the upper anterior thorax that produce and secrete milk in females
Essential features
- Adult female breast consists of branching ducts and acini; the acini group together to form lobules
- Ductal - lobular system: composed of ducts and acini lined by a dual inner (luminal) epithelial cell layer and outer (basal) myoepithelial cell layer, resting on a basement membrane, enveloped by stroma
- Exhibits physiologic histomorphologic changes during menstrual cycle, pregnancy / lactation, menopause, exogenous hormone therapy
Embryology
- Considered an epidermal gland, as it develops as diverticula of epidermis into dermis
- Mammary gland development begins at week 5
- Week 5:
- Ectodermal thickenings called mammary ridges develop along ventral embryo, extending from axilla to medial thigh
- Ridges eventually disappear, except at fourth intercostal space where mammary gland develops
- Week 15 - 20:
- Mesenchyme condenses around epithelial stalk under testosterone influence
- Solid epithelial columns develop within mesenchyme
- Week 20 - 32:
- Differentiation of mesenchyme into fat within collagenous stroma
- Stroma of reticular dermis forms suspensory ligaments of Cooper, attaching breast to skin and subdividing breast into lobes
- Areola formed by ectoderm
- Week 32 - 40:
- Epithelial cords canalize and branch, forming lobuloalveolar structures
- Depression in epidermis forms at the convergence of lactiferous ducts: mammary pit
- Near term birth: nipple formed by evagination of mammary pit
- Reference: Mills: Histology for Pathologists, 4th Edition, 2012
Histology
- Ductal - lobular system:
- Consists of large lactiferous ducts that open to the surface of the nipple via lactiferous sinuses, which branch into ducts and terminal ductules which terminate in acini
- Acini are grouped together in clusters to form lobules (terminal duct lobular unit)
- Ductal - lobular system is arranged in series of segments (5 - 10)
- Cellular lining of the ductal - lobular system is bilayered and consists of:
- Inner (luminal) epithelial cells: cuboidal to columnar epithelium with pale eosinophilic cytoplasm
- Outer (basal) myoepithelium: variably distinctive, varies in appearance from flattened cells with compressed nuclei to prominent epithelioid cells with abundant clear cytoplasm, can sometimes have myoid appearance
- Both epithelial and myoepithelial cells thought to arise from a bipotent progenitor cell (Oncotarget 2017;8:10675)
- Basement membrane surrounds mammary ducts, ductules and acini (Virchows Arch A Pathol Anat Histopathol 1992;421:323)
- Basement membrane contains type IV collagen and laminin, demarcates ductal - lobular system from the surrounding stroma
- Transgression of the myoepithelial layer and basement membrane by tumor cells defines invasion
- Stroma:
- Consists of varying amounts of fibrous tissue and adipose tissue and can be divided into:
- Interlobular stroma:
- Surrounds large ducts and terminal duct lobular units (TDLUs), denser, more collagenous than intralobular connective tissue
- Multinucleated giant cells of unknown significance are sometimes present (Virchows Arch 2001;439:768)
- Intralobular stroma: surrounds acini within TDLUs, loose, contains fibroblasts, scattered inflammatory cells and histiocytes
- Interlobular stroma:
- Consists of varying amounts of fibrous tissue and adipose tissue and can be divided into:
- Nipple - areolar complex: skin variably pigmented, contains numerous sebaceous glands
- Independent of hair follicles, except at periphery of areola; contains dense fibrous stroma with bundles of smooth muscle
- Montgomery tubercles: sebaceous glands sharing ostium with a lactiferous duct, more prominent during pregnancy and lactation
- Epidermis may contain occasional clear cells, either clear keratinocytes or Toker cells (epidermally located mammary duct epithelium)
- Toker cells found in 10% of normal nipple (Histol Histopathol 2009;24:367)
- Stratified squamous epithelium extends into duct lumens for 1 - 2 mm (Clin Radiol 2012;67:e42)
Pregnancy / lactation
- Dramatic increase in the number of lobules, as well as acinar units
- Increased epithelial cell proliferation and lobuloalveolar differentiation
- Decrease in intralobular and interlobular stroma
- Second and third trimester:
- Increase in size of epithelial cells and cytoplasmic vacuolization, myoepithelial cells difficult to discern
- Lactation:
- Abundant secretory material and prominent cytoplasmic vacuoles, epithelial cells may have bulbous or hobnail appearance
- Myoepithelial cells remain inconspicuous
- Rarely areas of infarction (Exp Ther Med 2015;10:1888)
Menopause
- Reduction of estrogen and progesterone causes involution and atrophy of TDLUs
- Reduction in size and complexity of acini, loss of specialized intralobular stroma
- Hyalinized stroma with relative increase in fat
- Reference: Mills: Histology for Pathologists, 4th Edition, 2012
Neonatal breast
- Identical in males and females at birth
- Breast enlargement due to neonatal prolactin production, caused by falling maternal estrogen
- Associated with production of colostrum
- Extramedullary hematopoiesis may be seen (J Pediatr Hematol Oncol 2012;34:229)
Male breast
- Composed of ductal structures only within collagenized stroma, with no / rare acini
Transsexual breast
- Female to male conversion results from prolonged androgen administration, starting prior to mastectomy
- Reduction in glandular tissue and prominence of stroma (J Histochem Cytochem 2006;54:905)
- Calcifications more frequent (J Pathol 1993;170:37)
- Male to female conversion involves prolonged estrogen therapy and chemical castration with progestational agents
- Changes include well developed lobular structures and pregnancy related changes
Clinical features
- Gross anatomy:
- Lies on the anterior chest wall over the pectoralis major muscle, extends from second to sixth rib vertically and from sternal edge to midaxillary line horizontally
- Also projects into the axilla as the tail of Spence
- Microscopic foci of glandular tissue may extend through the pectoral fascia
- Clinical relevance: total mastectomy does not remove all glandular breast tissue
- Arterial supply, lymphatic flow:
- Principal arterial supply by the internal mammary and lateral thoracic arteries
- Lymphatic drainage: > 90% to axillary lymph nodes, remaining to internal mammary and posterior intercostal nodes
- Relevance to staging, as metastasis to internal mammary node is higher nodal stage
- Breast tissue is typically less nodular, late follicular phase is the optimal time for mammography (Radiol Phys Technol 2018;11:20)
- Loss of myoepithelium is usually considered evidence of invasion, with the exception of microglandular adenosis, encapsulated papillary carcinoma and solid papillary carcinoma
- Transsexual breast may develop any benign or malignant process seen in nontranssexual breast (Hoda: Rosen's Breast Pathology, 4th Edition, 2014)
Gross description
- Mastectomy attempts to remove all breast tissue
- Different types of mastectomies: simple, modified radical, prophylactic, skin sparing, nipple sparing and radical
- Axillary dissections performed for the staging of invasive carcinoma
- Number of lymph nodes with metastases is the most important prognostic factor for breast carcinoma
- Reference: Lester: Manual of Surgical Pathology, 3rd Edition, 2010
Gross images
Images hosted on other servers:

Mastectomy specimen, anterior view
Microscopic (histologic) images
Contributed by Indu Agarwal, M.D.
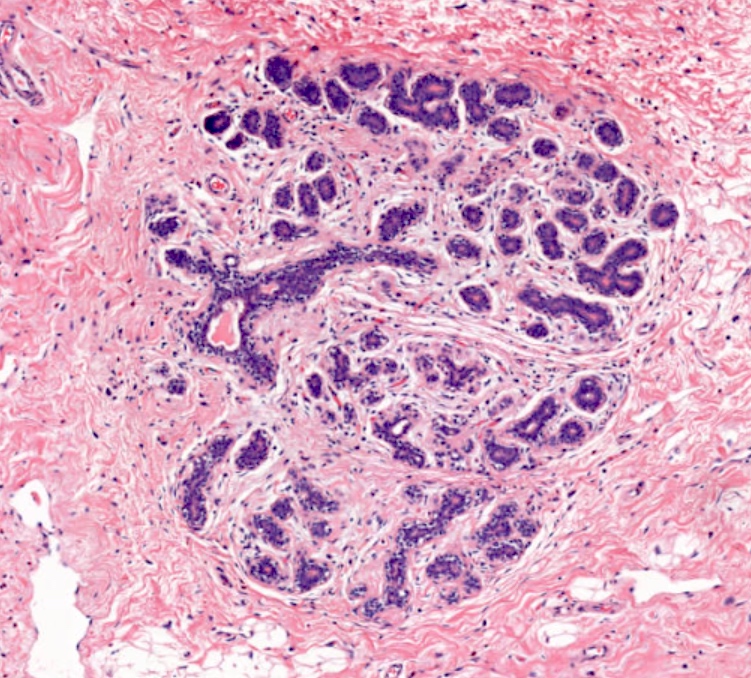
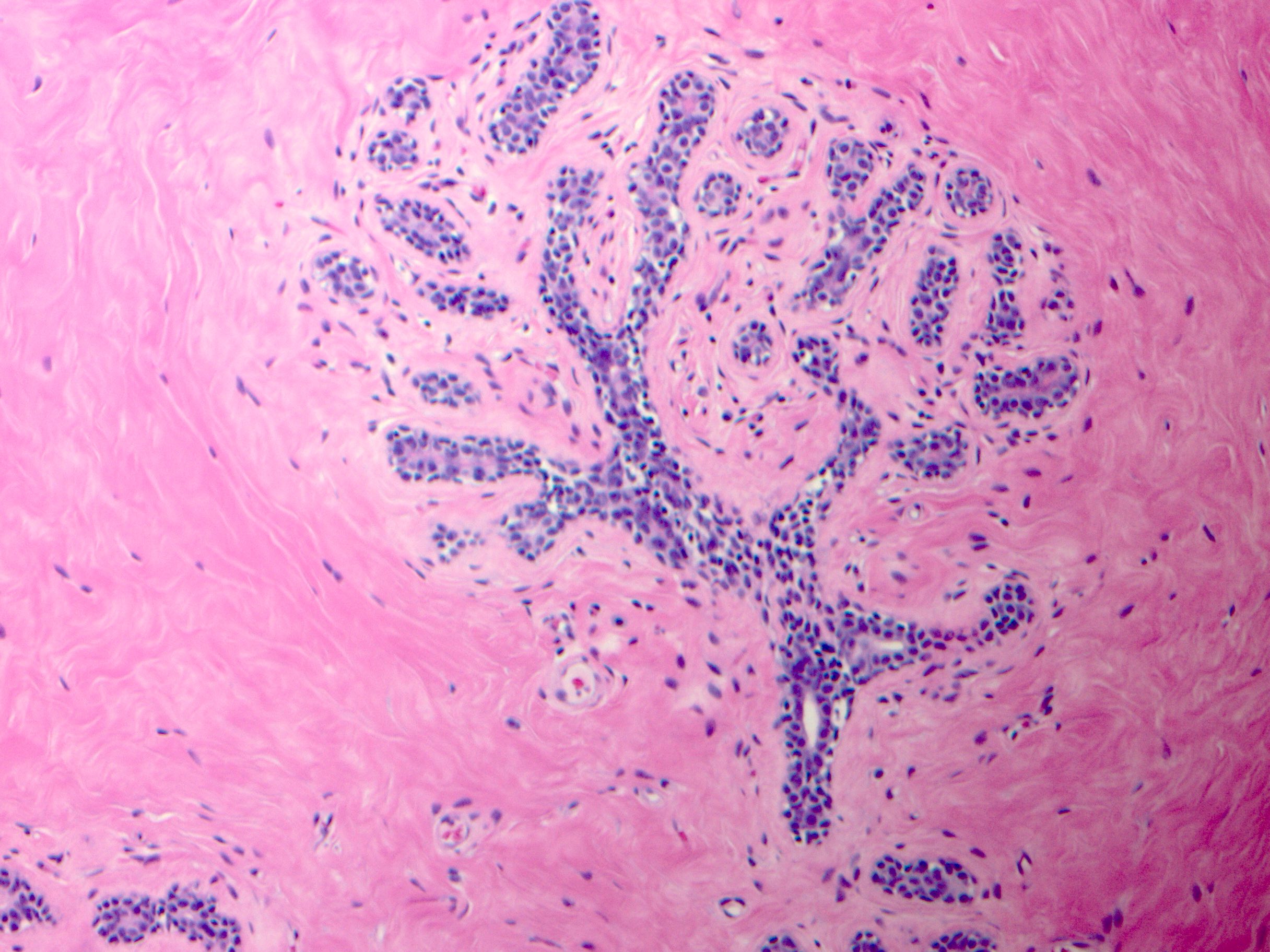
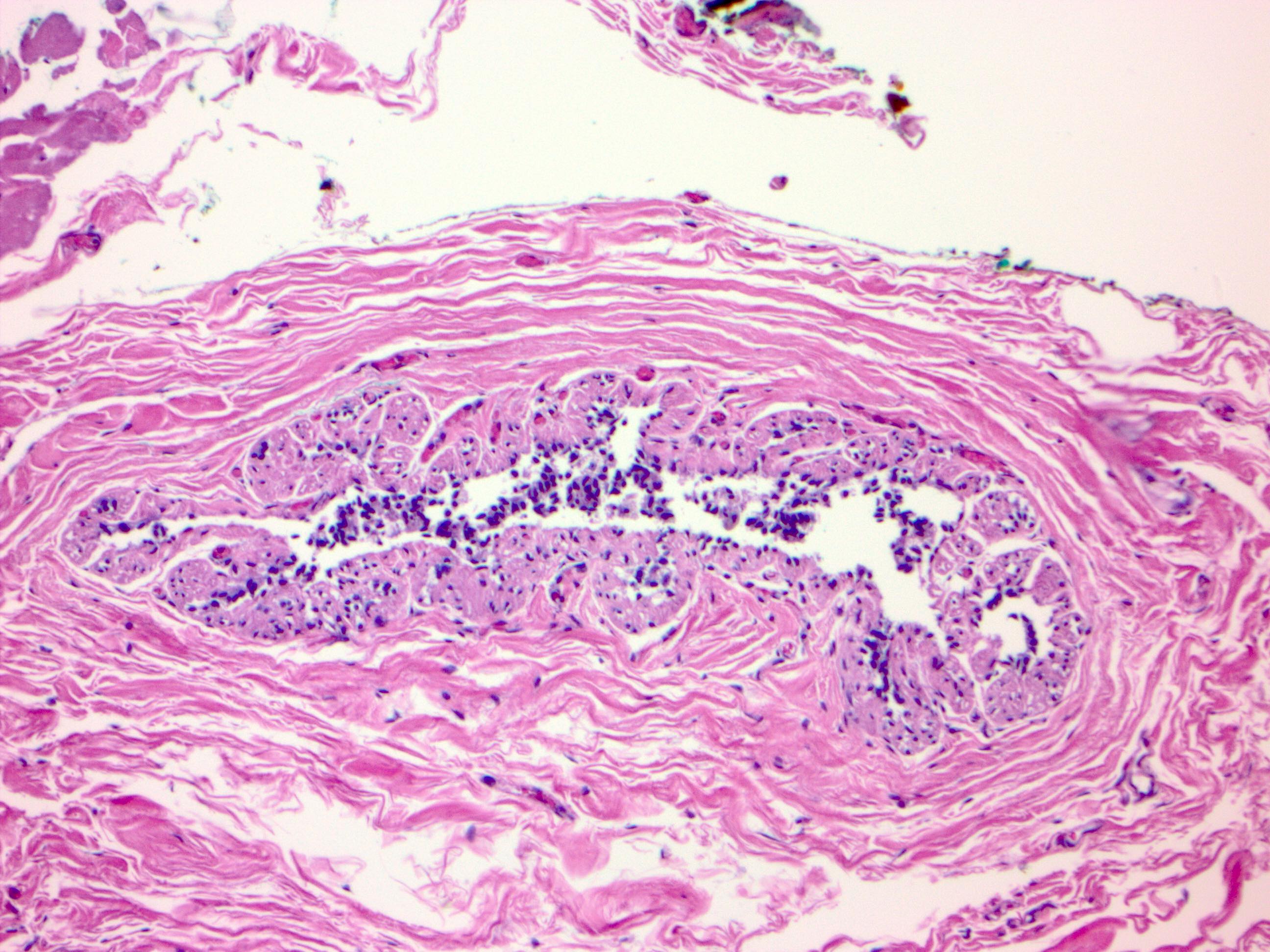
Terminal duct lobular unit (TDLU)
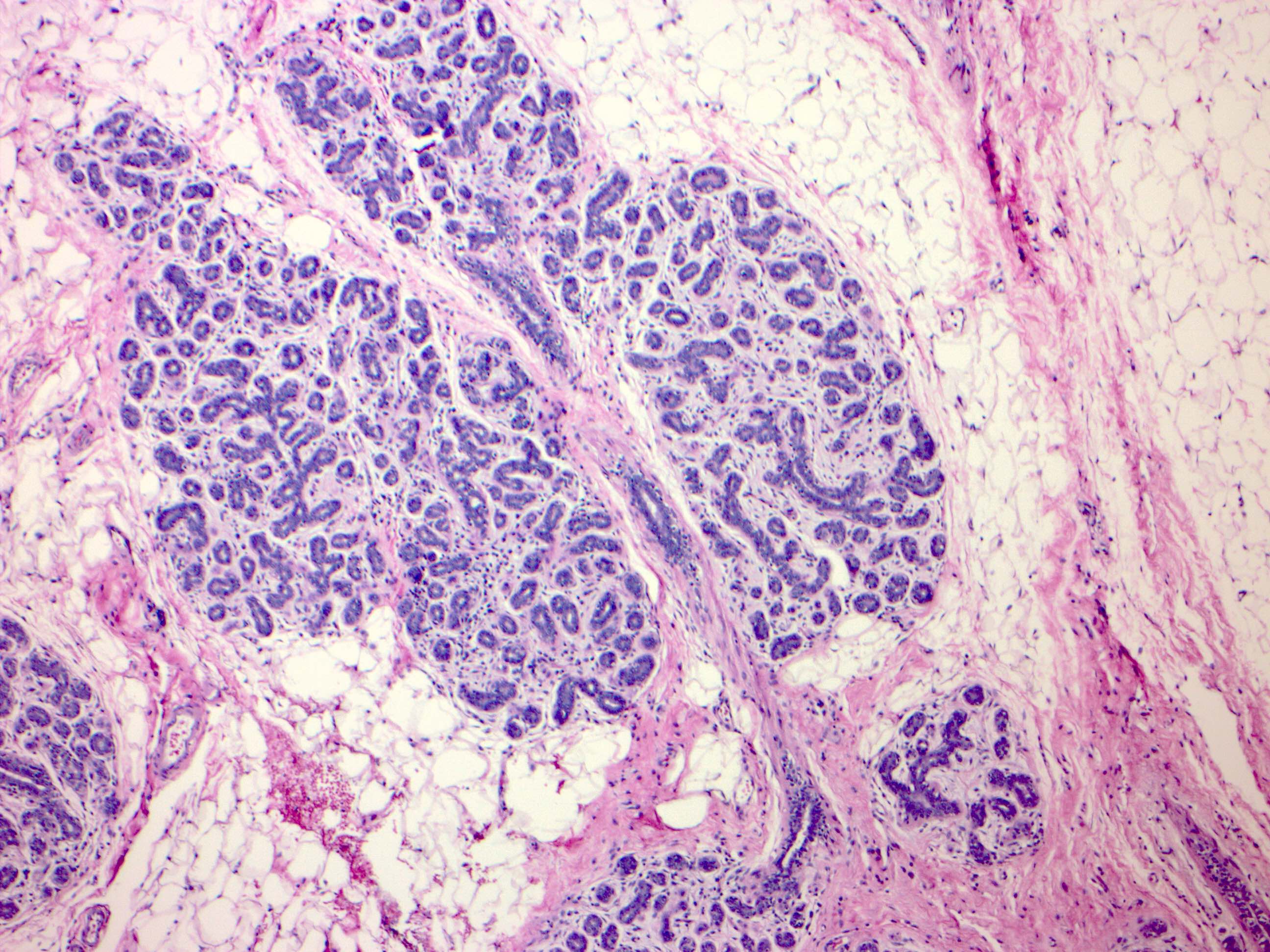
Extralobular and TDLU
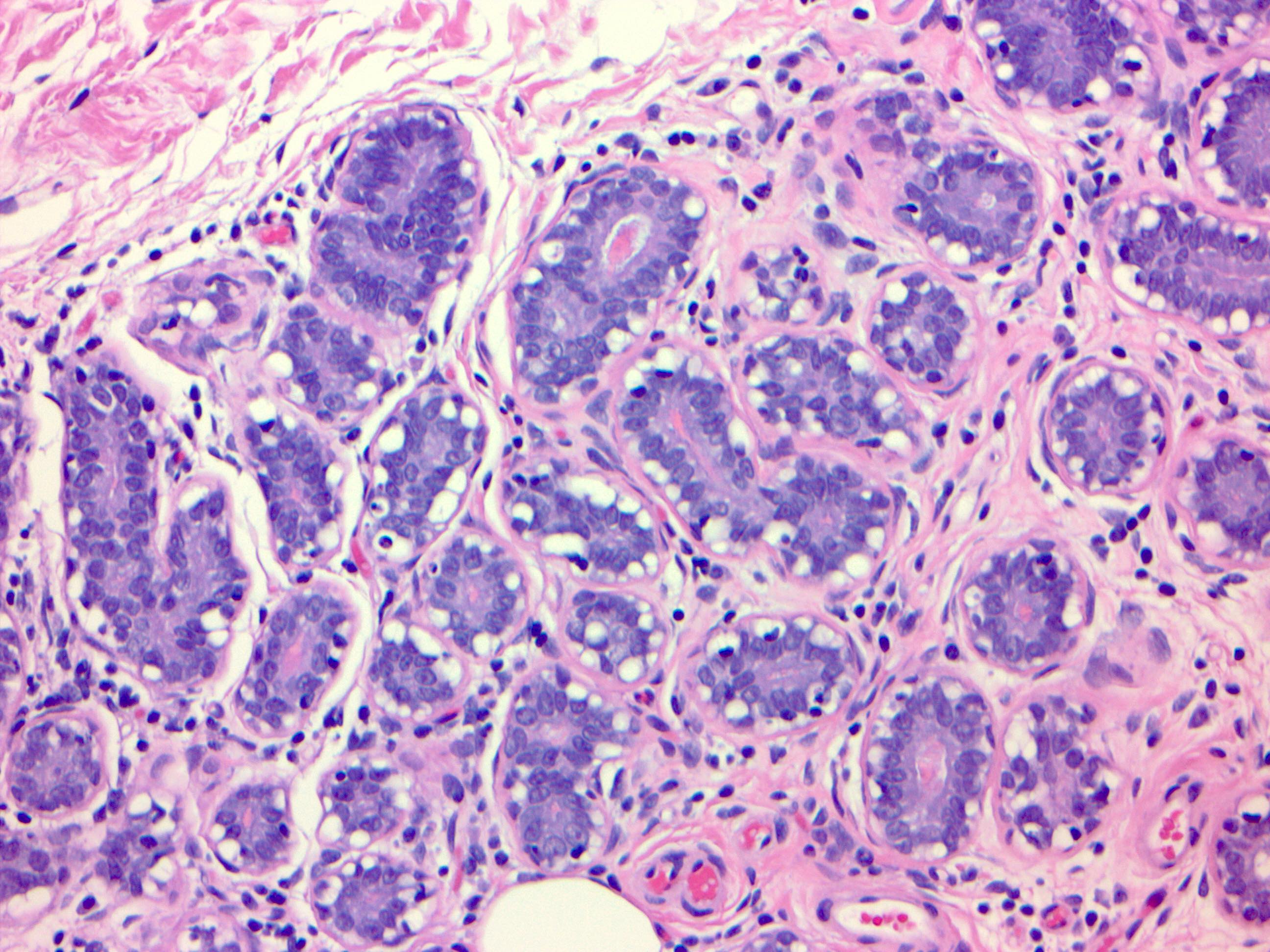
Myoepithelial cells
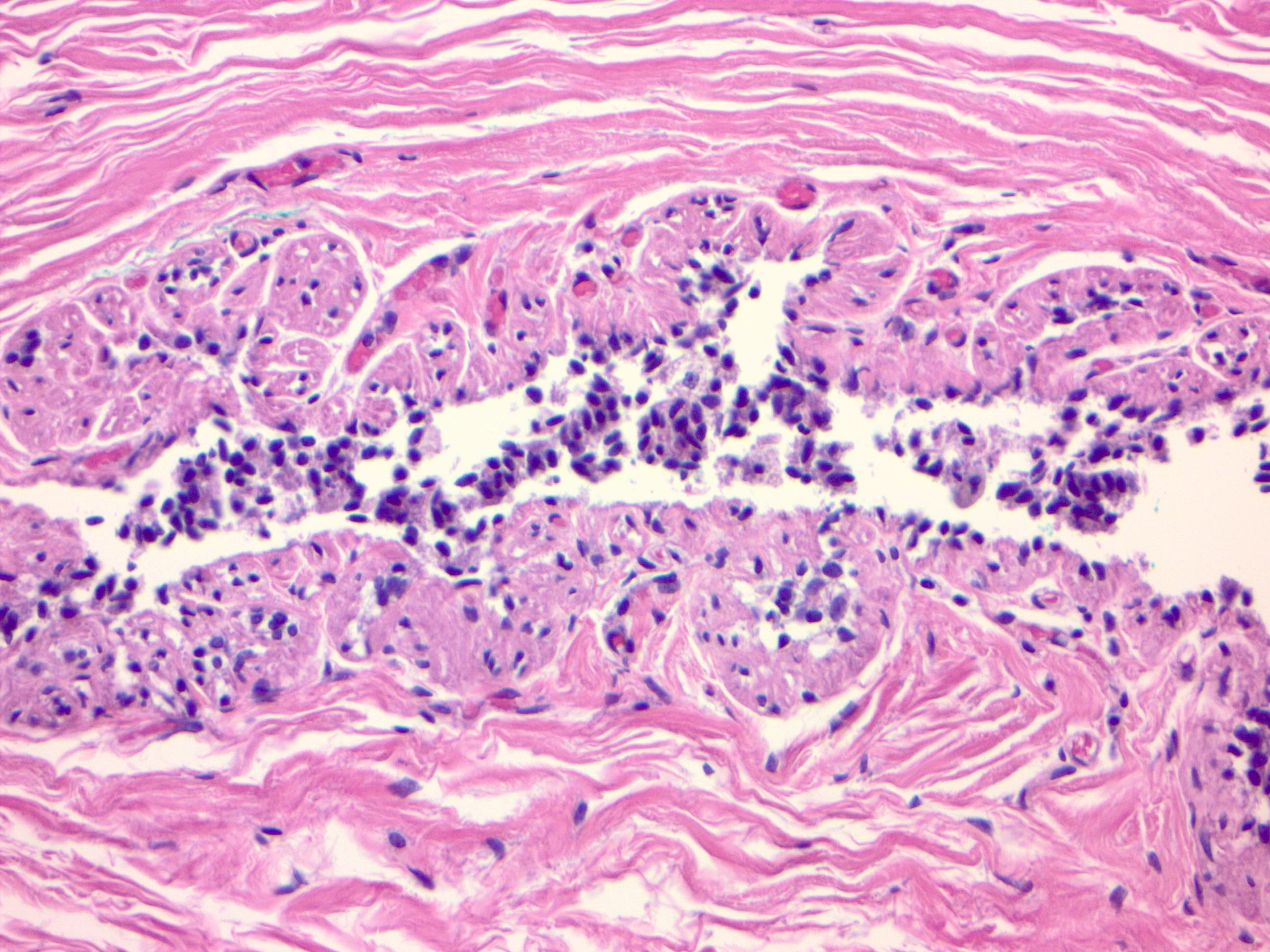
Myoid appearance

Clear cell change
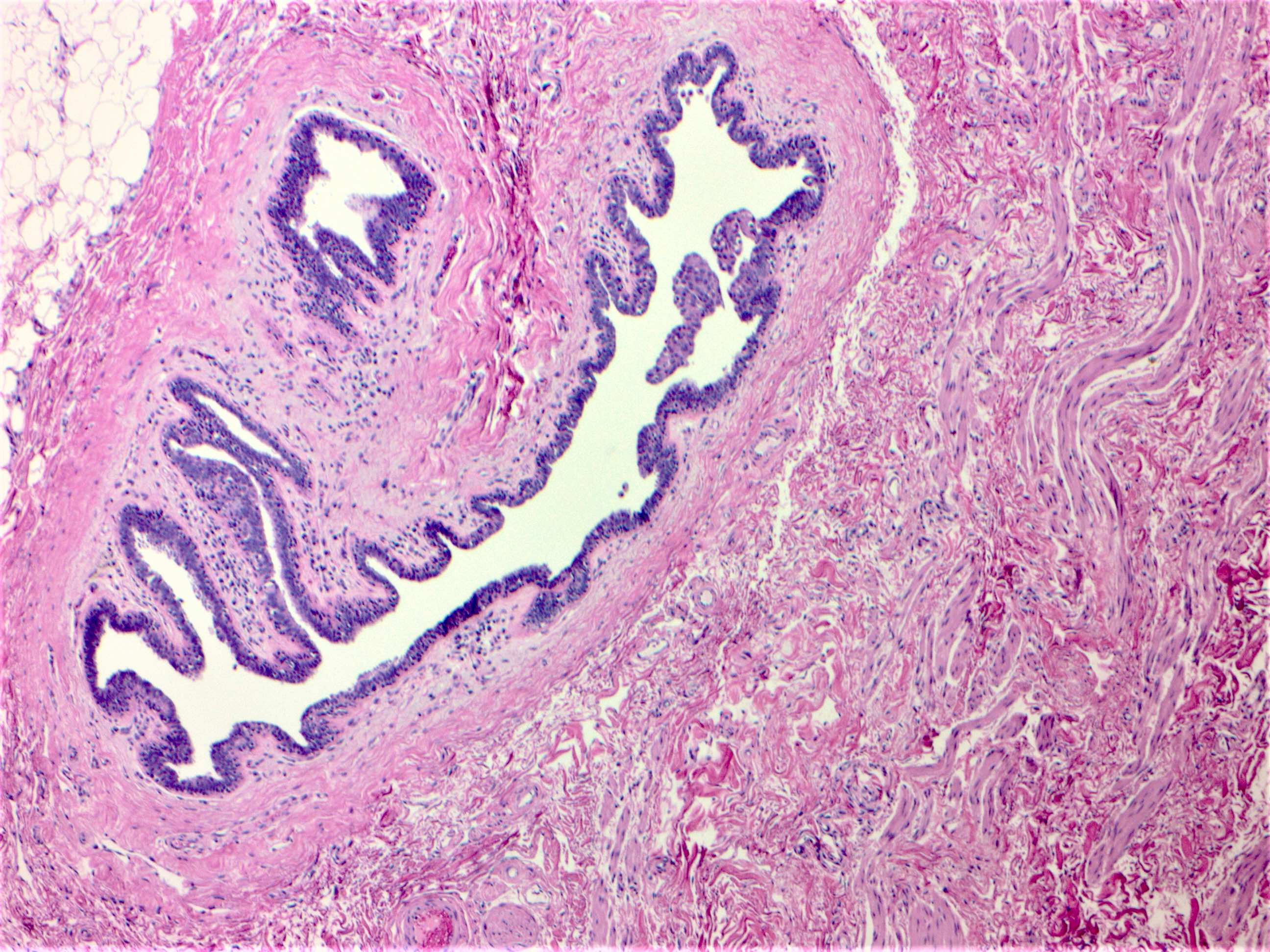
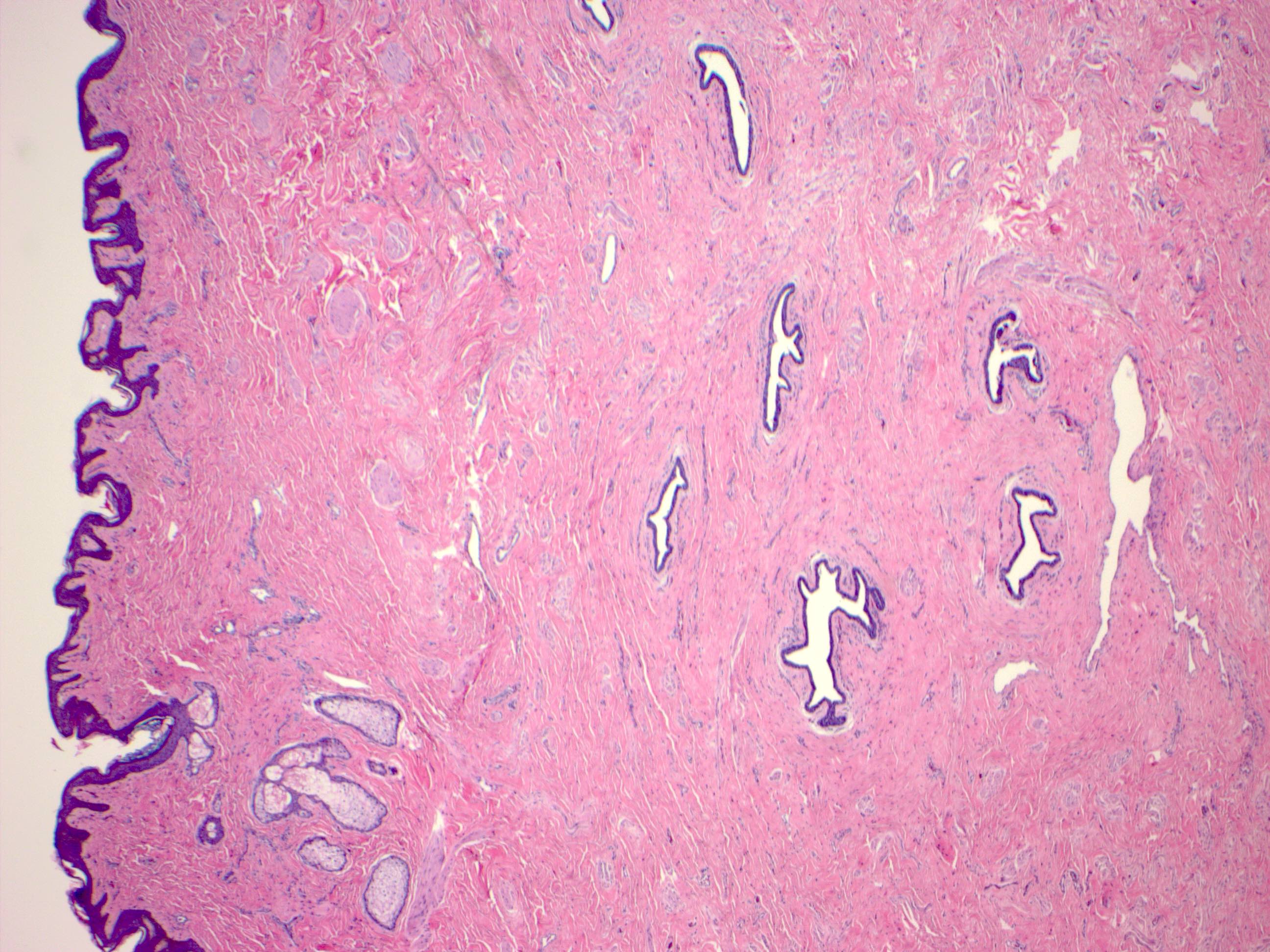
Cross section of nipple
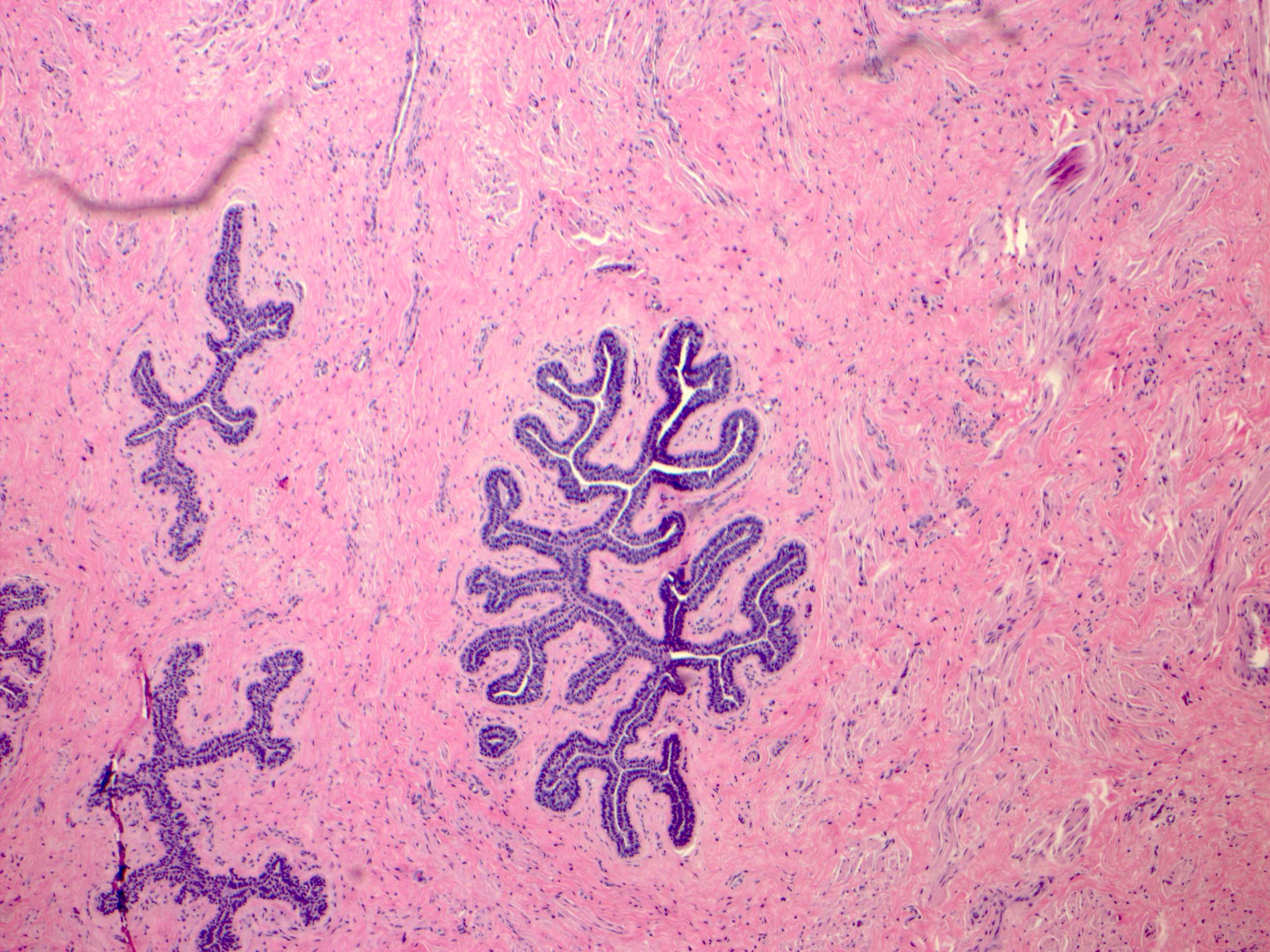
Lactiferous duct
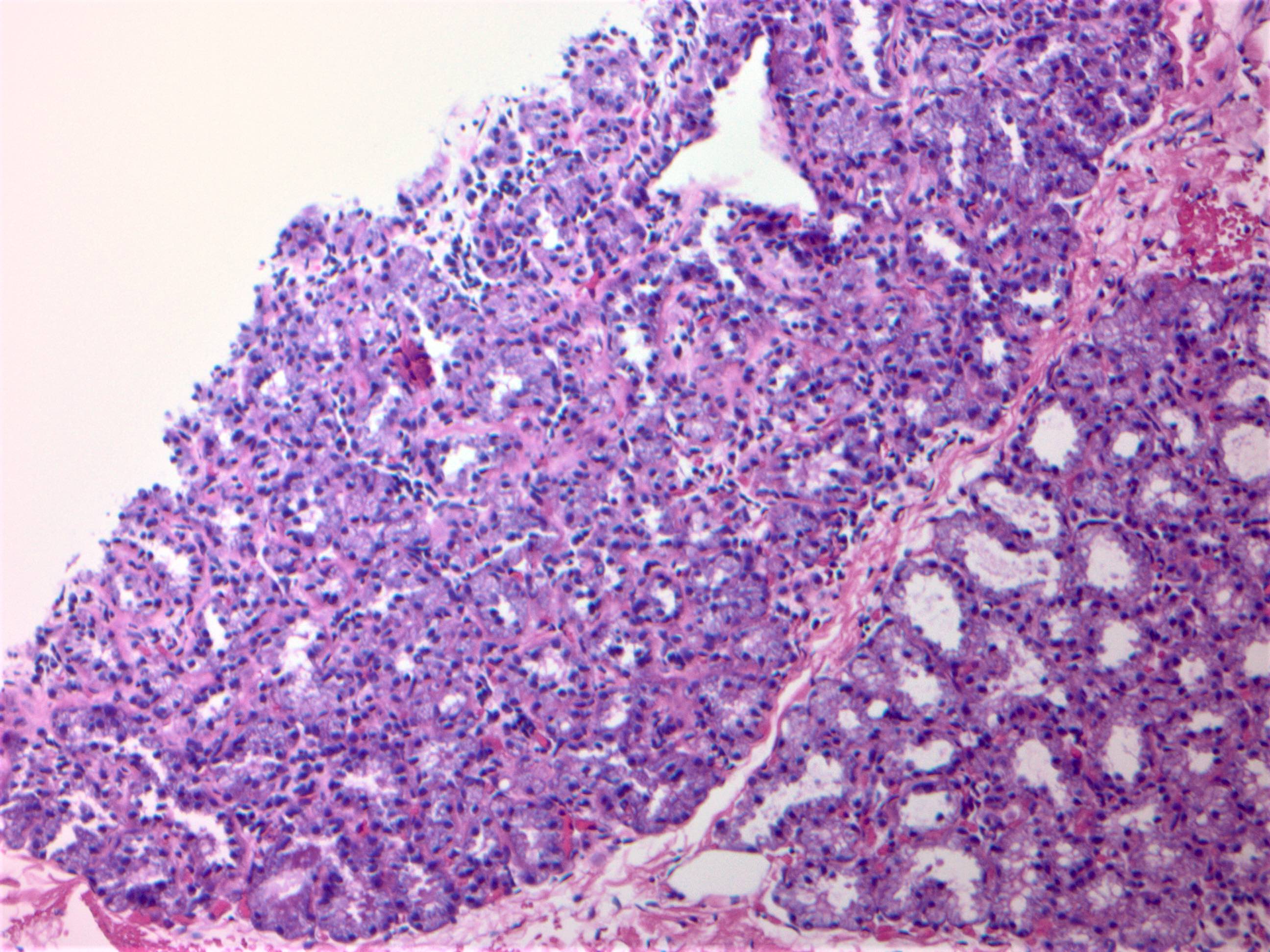
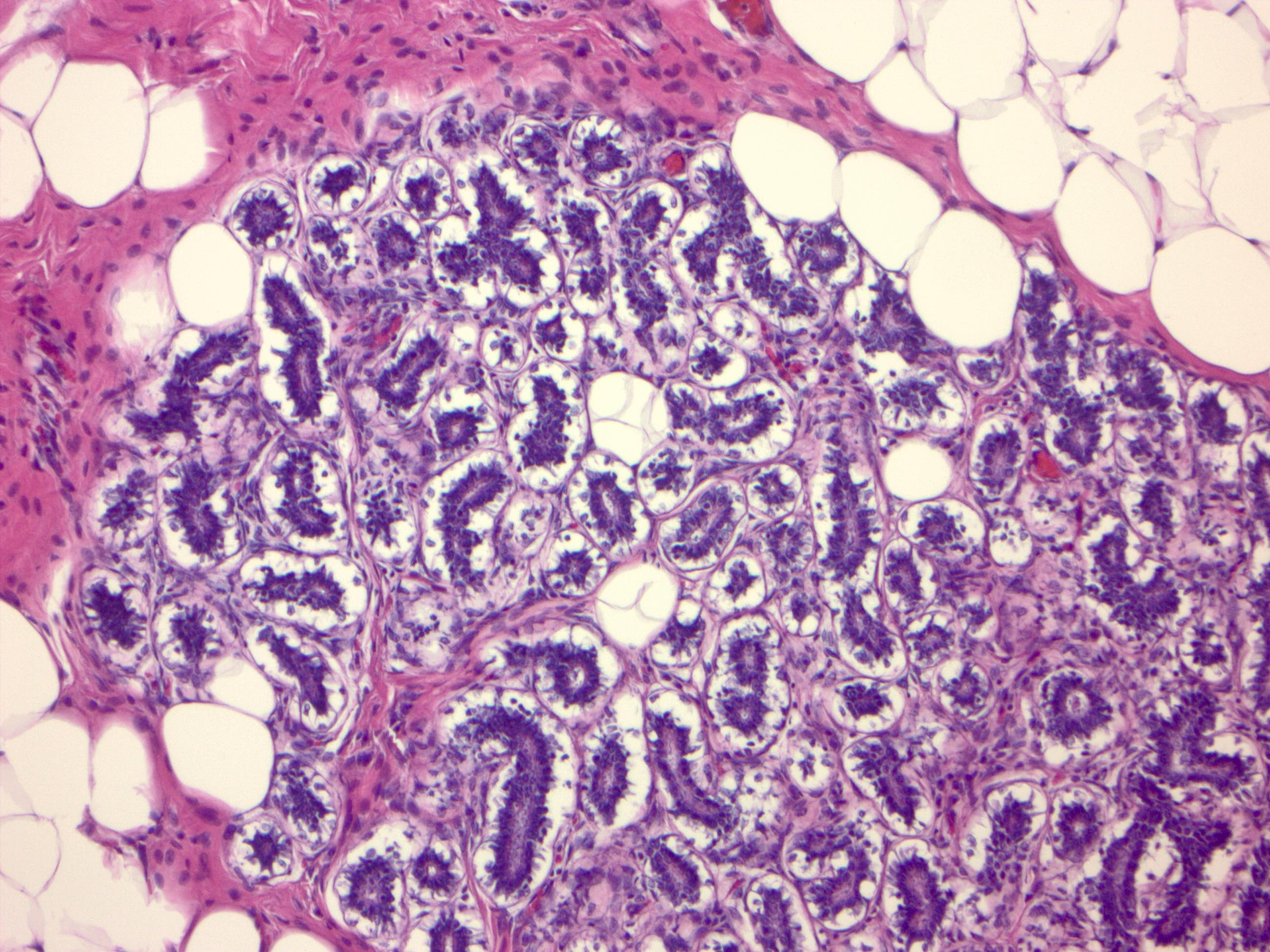
Lactational changes
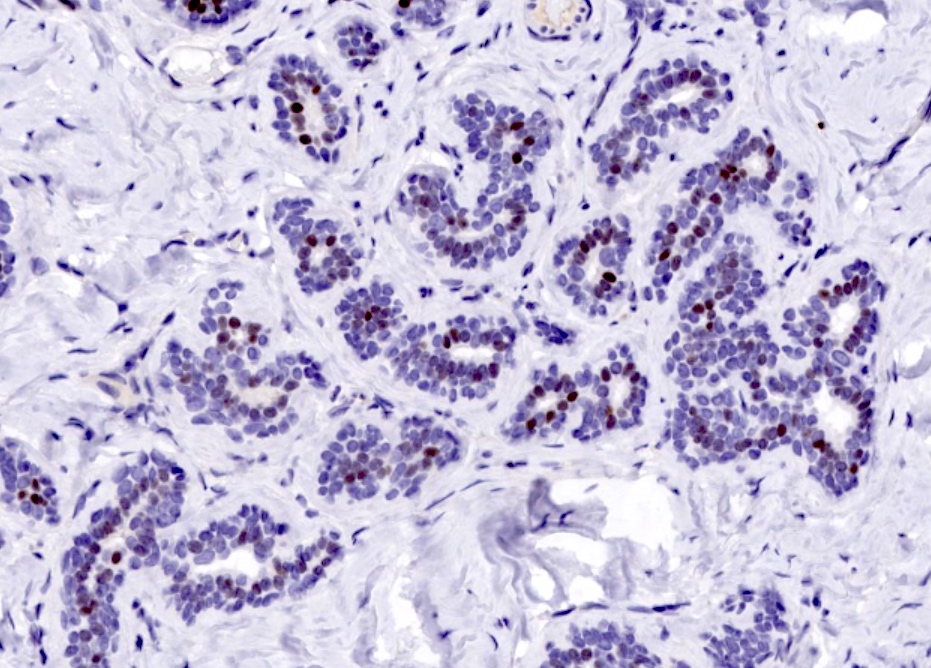
Immunostain ER
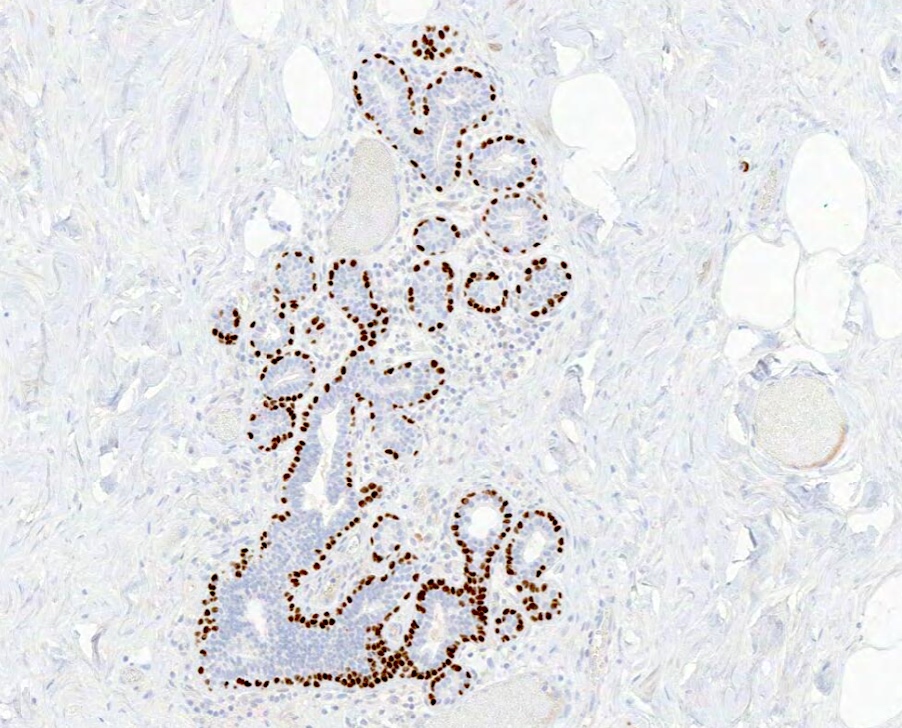
Immunostain p63
Positive stains
- Basement membrane: laminin, type IV collagen and reticulin
- Epithelium / luminal cells:
- Usually express luminal cytokeratins: LMWCK, CK7, CK8, CK18, CK19 (J Pathol 2004;203:661)
- Also express mammaglobin, gross cystic disease fluid protein (GCDFP)
- Most express ER alpha or PR in a heterogeneous pattern
- E-cadherin, p120, beta catenin in membranous pattern
- Myoepithelial cells:
- Basal cytokeratins: HMWCK, CK5/6, CK14 (Front Biosci (Landmark Ed) 2010;15:226)
- P-cadherin, calponin, smooth muscle myosin heavy chain (SMMHC), smooth muscle actin, CD10, S100 (Arch Pathol Lab Med 2008;132:349)
- At least 2 markers, 1 with a nuclear staining pattern (e.g. p63) and 1 with cytoplasmic staining (e.g. SMMHC) recommended
- Toker cells: CK7, EMA and usually positive for ER and PR
Negative stains
- HER2 / neu overexpression or amplification not seen in normal breast, restricted to carcinomas (J Clin Oncol 2000;18:267)
Electron microscopy images
Images hosted on other servers:

Acini

Glandular and myoepithelial cells
Videos
Shotgun histology inactive breast
Additional references
Board review style question #1

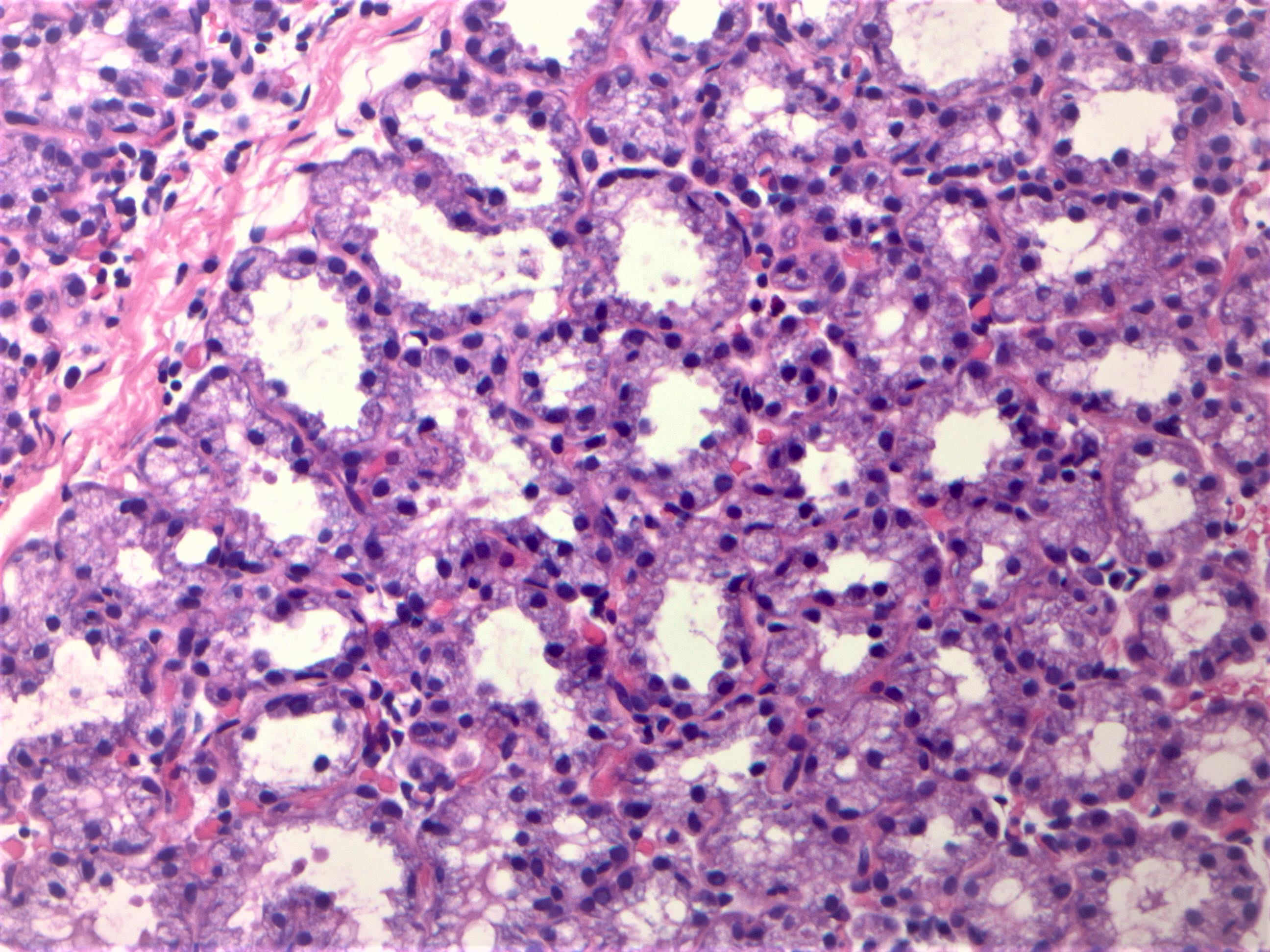
From the image above, what is the most likely diagnosis?
- Atypical apocrine adenosis
- Lactational changes
- Microglandular adenosis
- Secretory carcinoma
Board review style answer #1
B. Lactational changes. During lactation, epithelial cells are enlarged and have a bulbous or hobnail appearance with attenuated myoepithelial cells. These florid changes seen can be alarming and can be mistaken for atypia or malignancy.
Comment Here
Reference: Breast - Histology
Comment Here
Reference: Breast - Histology
Board review style question #2
Myoepithelial cells are always retained in which of the following?
- Atypical ductal hyperplasia
- Encapsulated papillary carcinoma
- Invasive tubular carcinoma
- Microglandular adenosis
Board review style answer #2
A. Atypical ductal hyperplasia. Myoepithelium is retained in atypical ductal hyperplasia and most benign and in situ lesions, with the exception of microglandular adenosis and a few in situ lesions, e.g. encapsulated papillary carcinoma.
Comment Here
Reference: Breast - Histology
Comment Here
Reference: Breast - Histology
