
Chemistry, toxicology & urinalysis
Organ specific
Adrenal
Hypercortisolism
Author: Renu Virk, M.D.

Last author update: 1 January 2010
Last staff update: 2 April 2020
Copyright: 2002-2024, PathologyOutlines.com, Inc.
PubMed Search: Hypercortisolism [title]
Table of Contents
Definition / general | Terminology | Epidemiology | Clinical features | Diagnosis | Laboratory | Clinical images | Gross images | Additional referencesCite this page: Virk R. Hypercortisolism. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/chemistryadrenalhypercortisolism.html. Accessed April 25th, 2024.
Definition / general
- Disorder of chronic exposure to high levels of cortisol in the blood, either endogenous or exogenous
Terminology
- Also called Cushing syndrome in Adrenal Chapter
- Cushing disease refers to a pituitary adenoma that produces excess ACTH
- Subclinical hypercortisolism:
- Due to incidental adrenal masses that may secrete cortisol autonomously, with no signs or symptoms of hypercortisolism (Eur J Endocrinol 2009;160:87)
- Associated with high prevalence of hypertension, diabetes mellitus (Eur J Endocrinol 2005;153:837), obesity, dyslipidemia and osteoporosis
Epidemiology
- Adrenal adenoma (eMedicine - Adrenal Incidentaloma) or hyperplasia
- Adrenal carcinoma
- ACTH secreting pituitary adenoma (Cushing disease)
- Other tumors with ectopic ACTH production
- Exogenous glucocorticoids
Clinical features
- Obesity (buffalo hump is characteristic), hypertension, glucose intolerance, moon facies, easy bruisability, striae, proximal muscle weakness, bone loss, osteonecrosis of femur head, menstrual irregularities
- With androgen excess, females show virilization
- Some patients may present with neuropsychological changes
Diagnosis
- A single test cannot be used to diagnose hypercortisolism
- Primary hypercortisolism: high serum cortisol, low plasma ACTH
- Secondary hypercortisolism: high serum cortisol, high plasma ACTH
Laboratory
- Increase in daily urinary cortisol excretion
- High midnight salivary cortisol levels
- Increase in late evening serum cortisol levels
Low dose dexamethasone suppression test:
- Absence of suppression supports a diagnosis of Cushing syndrome (J Clin Endocrinol Metab 2006;91:2582), but suppression also occurs in some patients with Cushing syndrome (J Clin Endocrinol Metab 2004;89:1222)
- This test is not very helpful in patients with abnormal levels of cortisol binding globulin
High dose dexamethasone suppression test:
- This test is useful in differentiating primary hypercortisolism from ACTH secreting pituitary adenoma
- No suppression is noted in patients with ectopic ACTH secretion or adrenal adenoma
CRH after dexamethasone test:
- Makes the dexamethasone test more sensitive
- Urinary and salivary cortisol should be measured twice (N Engl J Med 1986;314:1329)
CRH stimulation test:
- Usually done with equivocal plasma ACTH levels
- Indicated to differentiate Cushing disease from Cushing syndrome
- Pituitary tumor will show increase in ACTH and cortisol levels
- Adrenal tumor and ectopic ACTH production will not show any increase
Clinical images
Images hosted on other servers:
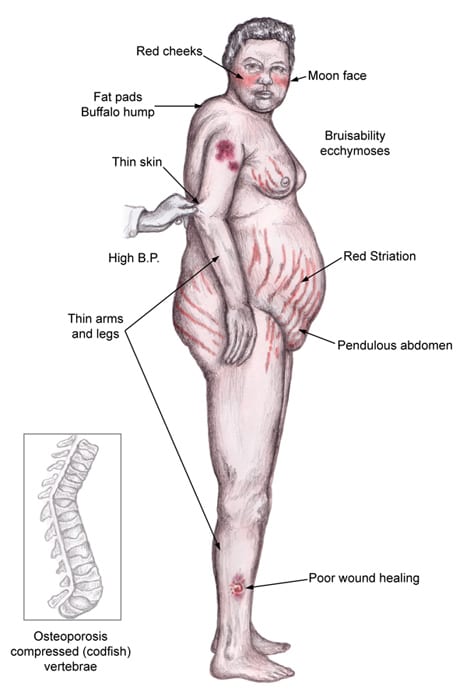
Physical features

Patient description
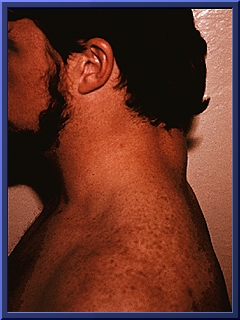
Buffalo hump
Gross images
Images hosted on other servers:

Adrenal adenoma
Additional references
