
Coagulation
Acquired bleeding disorders
Disseminated intravascular coagulation (DIC)
Author: Dong Chen, M.D., Ph.D.
Editorial Board Member: Kyle Annen, D.O.
Deputy Editor-in-Chief: Patricia Tsang, M.D., M.B.A.

Last author update: 4 January 2022
Last staff update: 4 January 2022
Copyright: 2002-2024, PathologyOutlines.com, Inc.
PubMed Search: Disseminated intravascular coagulation [title] "last 5 years"[DP] Review[ptyp]
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Pathophysiology | Diagrams / tables | Clinical features | Diagnosis | Laboratory | Prognostic factors | Case reports | Treatment | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2 | Board review style question #3 | Board review style answer #3 | Board review style question #4 | Board review style answer #4Cite this page: Chen D. Disseminated intravascular coagulation (DIC). PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/coagulationDIC.html. Accessed April 18th, 2024.
Definition / general
- First descriptions of DIC appeared in the 19th century (Semin Thromb Hemost 2014;40:874)
- DIC is a systemic activation of the coagulation system, which results in microvascular thrombosis and simultaneously potentially life threatening hemorrhage attributed to consumption of platelets and coagulation factors
- DIC is a complication to various underlying clinical conditions, including infection, malignancies, obstetrical complications, trauma (especially head trauma) and vascular disorders (e.g. Kasaback-Merritt syndrome, aortic aneurysms, etc.); of these conditions, infection related DIC is most common
- Based on the severity and stage, DIC can be categorized as nonovert (early) and overt (decompensated); DIC can present either acutely or chronically and can be subclinical
- In general, DIC patients can suffer from both bleeding and thrombosis, although thrombosis may not be readily apparent
Essential features
- Essential features of DIC can be classified as clinical and laboratory features
Terminology
- Most widely used definition of DIC was issued by a subcommittee of the Scientific and Standardization Committee (SSC) of the International Society on Thrombosis and Hemostasis in 2001 (Thromb Haemost 2001;86:1327)
ICD coding
- ICD-10: D65 - Disseminated intravascular coagulation (defibrination syndrome)
Epidemiology
- Prevalence of DIC in patients with various medical conditions:
- 1% of hospitalized patients are estimated to develop DIC
- 10 - 30% of patients in the intensive care unit (ICU)
- 20% of patients with acute respiratory distress syndrome (ARDS)
- 30 - 40% of patients with severe head trauma
- 30 - 60% of patients with severe sepsis
- See Table 1 for secondary causes
- Reference: Br J Haematol 2021;192:803
Pathophysiology
- Increased tissue factor activity and thrombin generation
- Tissue factor is expressed on circulating activated monocytes in sepsis related DIC and on the surface of the malignant cells or circulating tumor derived microparticles in cancer related DIC
- In obstetric DIC, placental abruption and amniotic fluid embolism expose the circulating blood to tissue factor
- Through activation of coagulation factor (F) VII and FX, increased tissue factor activity leads to thrombin generation
- Increased platelet activation in DIC occurs through interaction with activated endothelium and the direct action of thrombin on platelets; in sepsis related DIC, inflammatory cells, cytokines and pathogens interact directly with platelets and contribute to their activation
- Levels of antithrombin, protein C and protein S decrease due to consumption, decreased synthesis in the liver and degradation by neutrophil elastase
- Fibrinolysis can be either impaired (hypofibrinolysis) or enhanced (hyperfibrinolysis) according to the pathophysiology of the underlying disease
- Both tissue plasminogen activator (tPA) and plasminogen activator inhibitor 1 (PAI1) are released from the activated endothelium, such as in patients with vascular malformations (see Table 1)
- In sepsis, the net effect is impaired fibrinolysis in most cases; in contrast, cancer is often associated with increased fibrinolytic activity
- Primary hyperfibrinolysis is a common feature of acute promyelocytic leukemia; these patients often present with severe hyperfibrinolysis and bleeding due to increased plasminogen activation on the malignant cell surface
- Reference: Br J Haematol 2021;192:803
Diagrams / tables
Images hosted on other servers:

Clinical diagnosis / management of patients with DIC
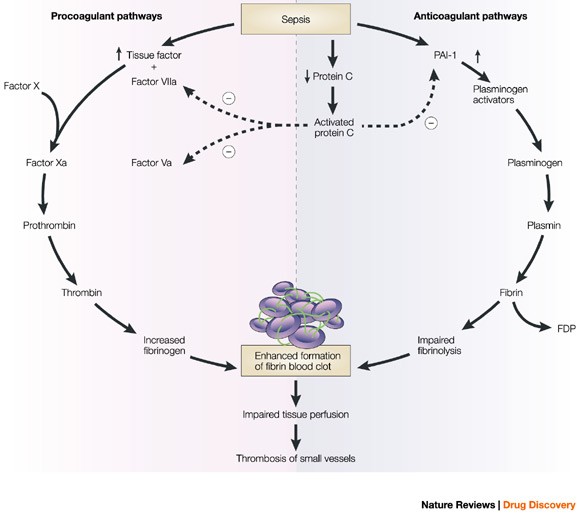
Key events in DIC
Table 1: secondary causes
| Severe infectious diseases | Gram positive or negative organisms, malaria, hemorrhagic fevers |
| Malignancy | Solid tumors (e.g. adenocarcinomas), acute promyelocytic leukemia or monocytic leukemia |
| Trauma | Multitrauma, brain injury, burns |
| Obstetrical complications | Abruptio placentae, amniotic fluid embolism |
| Vascular malformations | Kasabach-Merrit syndrome, giant hemangiomas Other vascular malformations, large aortic aneurysms |
| Severe immunologic reactions | Transfusion reaction |
| Heat stroke | |
| Postcardiopulmonary resuscitation |
Table 2: DIC scoring systems by the JAAM and the ISTH (AMIA Annu Symp Proc 2015;2015:804)
| SIRS* criteria | |
| ≥ 3 | +1 |
| 0 to 2 | 0 |
| Platelet count | |
| < 80 × 109/L or > 50% decrease within 24 hours | +3 |
| ≥ 80 < 120 × 109/L or > 30% decrease within 24 hours | +1 |
| ≥ 120 × 109/L | 0 |
| Prothrombin time (value of patient / normal value) | |
| ≥ 1.2 | +1 |
| < 1.2 | 0 |
| Fibrin / fibrinogen degradation products | |
| ≥ 25 mg/L | +3 |
| ≥ 10 < 25 mg/L | +1 |
| < 10 mg/L | 0 |
| Diagnosis: if ≥ 4, there is positive diagnosis of DIC | |
| *Systemic inflammatory response syndrome | |
| Platelet count | |
| < 50 × 109/L | +2 |
| ≥ 50 < 100 × 109/L | +1 |
| ≥ 100 × 109/L | 0 |
| Elevated fibrin related marker | |
| Strong increase | +3 |
| Moderate increase | +2 |
| No increase | 0 |
| Prolonged prothrombin time | |
| ≥ 6 seconds | +2 |
| ≥ 3 < 6 seconds | +1 |
| < 3 seconds | 0 |
| Fibrinogen level | |
| < 100 g/mL | +1 |
| ≥ 100 g/mL | 0 |
| Diagnosis: if > 5, there is positive diagnosis of overt DIC; if < 5, suggestive (not affirmative) of nonovert DIC | |
Clinical features
- Without adequate treatment, DIC can eventually lead to multiorgan dysfunction / failure
- Patients can present with bleeding, thrombosis or both
- Septic patients are more likely to have thrombosis than bleeding
- Bleeding can present as surgical site, venipuncture site or mucocutaneous bleeding (most common)
- Gastrointestinal bleeding, CNS bleeding, hematuria or ecchymoses
- Thrombosis can present as purpura fulminans (manifestation of subdermal microthrombi with skin necrosis)
- Cold, pulseless limb
- Sudden loss of vision
- Oliguria
- Mental status changes, seizures, behavioral changes or adrenal insufficiency
- Causes of DIC can be acute (meningococcemia), chronic (retained dead fetus), localized (abdominal aortic aneurysm) or systemic (acute promyelocytic leukemia)
- Chronic causes of DIC are typically malignancy, liver disease, retained dead fetus syndrome, abdominal aortic aneurysm, giant hemangioma and head trauma
- Without adequate treatment, DIC can eventually lead to multiorgan dysfunction / failure
- Reference: Br J Haematol 2021;192:803
Diagnosis
- Most widely used DIC diagnostic scoring systems are the JAAM and ISTH (Crit Care 2016;20:287, Thromb Haemost 2001;86:1327)
- See Table 2 for a comparison of both scoring systems
Laboratory
- Prolonged prothrombin time (PT), activated partial thromboplastin time (APTT) and thrombin time (TT)
- Elevated D dimers and other fibrin degradation products (but D dimer may be falsely positive in HIV+ Castleman disease due to interference from monoclonal gammopathy (Am J Clin Pathol 2004;122:178, Arch Pathol Lab Med 2004;128:328)
- Fall in platelet count (usually not lower than 30,000 - 40,000 x 109/L)
- Consumptive deficiency of fibrinogen, antithrombin, alpha 2 antiplasmin and plasminogen
- Presence of schistocytes and microspherocytes on peripheral blood smear
- With chronic causes, fibrinogen and platelets may actually be elevated as acute phase reactants
- All coagulation factors may be variably decreased due to factor activation and consumption
- Multiorgan dysfunction may manifest as elevated cardiac enzymes or elevated BUN / creatinine
- Baseline coagulation studies and serial follow up are needed to follow the trends
Prognostic factors
- DIC is a devastating condition with a poor prognosis; the clinical course is primarily determined by the age of the patient, presence of comorbidities, identification and treatment of underlying etiologies, initial treatment response and severity of organ dysfunction, including the degree of hemostatic abnormalities
- A multicenter study of critically ill patients with DIC found that the 28 day mortality was 21.9%, which was significantly higher than non-DIC patients (11.2%) (Crit Care Med 2008;36:145)
- Another study found the mortality rate was significantly higher in sepsis patients than trauma patients (Thromb Haemost 2008;100:1099)
Case reports
- 30 year old woman with DIC due to amniotic fluid embolism (Arch Pathol Lab Med 2002;126:869)
- 48 year old woman, 63 year old man and 68 year old man with DIC (Blood 2018;131:845)
- 66 year old woman with DIC due to underlying lymphoma (Chest 2017;151:e41)
Treatment
- Treat underlying disease
- Keep fibrinogen levels above 100 mg/dL with cryoprecipitate or fresh frozen plasma
- Monitor PT, PTT, platelet count, fibrinogen and possibly antithrombin levels
- If bleeding predominates, replace coagulation factors and fibrinogen with fresh frozen plasma (FFP) and cryoprecipitate
- Consider plasmapheresis (ASFA Category III indication), platelet transfusions and immunoabsorption
- Because prothrombin concentrates (PCC) may increase the risk for thromboembolism, they are not recommended for patients with DIC, with an only rare exception in patients with potentially life threatening coagulation factor deficiency when no other alternative treatment is available
- If platelet count is lower than 50,000 x 109/L with active bleeding or lower than 10,000 x 109/L, give platelet transfusion
- If thrombosis predominates (chronic DIC), heparinization should be considered
- See Diagram 1 for diagnosis and treatment strategies
- Reference: Br J Haematol 2021;192:803
Board review style question #1
Tissue factor can be released from which of the following blood cells during infection?
- Eosinophils
- Lymphocytes
- Monocytes
- Neutrophils
- Red cells
Board review style answer #1
Board review style question #2
Which of the following laboratory findings is typical in a patient with DIC?
- Decreased fibrinogen
- Elevated plasminogen
- Elevated protein S and C
- Normal clotting times (PT, APTT and TT)
- Thrombocytosis
Board review style answer #2
Board review style question #3
Which of the following is true of disseminated intravascular coagulation?
- Clotting times are usually shortened
- DIC rarely happens in patients with cancer or a hematologic malignancy
- Patient’s fibrinogen activity is usually elevated
- Patients with promyelocytic leukemia may have markedly elevated D dimer levels
- Treatment strategy should focus on stopping bleeding for virtually all cases of DIC
Board review style answer #3
D. Patients with promyelocytic leukemia have an increased risk of DIC and may show marked elevated D dimer levels
Comment Here
Reference: Disseminated intravascular coagulation (DIC)
Comment Here
Reference: Disseminated intravascular coagulation (DIC)
Board review style question #4
Which of the following is the most common underlying condition or mechanism that leads to DIC?
- Patient with breast cancer
- Pregnant woman (30 weeks) with severe hypertension
- Patient with end stage liver disease due to hepatitis C
- Patient was involved in an automobile accident with fractures of his lower extremities
- Leukemic patient who received chemotherapy and developed a high fever and hypotension
Board review style answer #4
E. Leukemic patient who received chemotherapy and developed a high fever and hypotension
Comment Here
Reference: Disseminated intravascular coagulation (DIC)
Comment Here
Reference: Disseminated intravascular coagulation (DIC)
