
Colon
Diverticular disease
Diverticulosis
Authors: Bindu Challa, M.D., Martha M. Yearsley, M.D.
Editorial Board Member: Naziheh Assarzadegan, M.D.
Deputy Editor-in-Chief: Catherine E. Hagen, M.D.


Last author update: 7 June 2022
Last staff update: 7 June 2022
Copyright: 2003-2024, PathologyOutlines.com, Inc.
PubMed Search: Diverticulosis

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Diagrams / tables | Clinical features | Diagnosis | Laboratory | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Clinical images | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Virtual slides | Videos | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Challa B, Yearsley MM. Diverticulosis. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/colondiverticulosis.html. Accessed April 19th, 2024.
Definition / general
- Anatomic change in the colon characterized by outpouchings of mucosa and submucosa through the muscularis (Clin Geriatr Med 2021;37:141)
- Diverticulosis: presence of diverticula, regardless of symptoms
- Diverticular disease: clinically relevant symptomatic diverticulosis
Essential features
- Anatomic change in the colon characterized by outpouchings of mucosa and submucosa through the muscularis
- Diverticulosis can be asymptomatic or symptomatic
- Sigmoid colon / left colon, most common site (90%)
- Mucosa normal to markedly abnormal
- Expansion of lamina propria by lymphoplasmacytic infiltrate, lymphoglandular complexes, mucin depletion and focal Paneth cell metaplasia may be seen
- No rationale for treatment of asymptomatic colonic diverticulosis
Terminology
- Most colonic diverticula are false diverticula
- Mucosa and submucosa herniate through defect or weakness in muscularis layer and is covered by serosa
- True diverticula are uncommon
- Involves the outpouching of all layers of the intestinal wall (e.g., Meckel diverticulum) (Expert Rev Gastroenterol Hepatol 2018;12:683)
- Diverticulosis can be asymptomatic or symptomatic
- Symptomatic diverticulosis:
- Symptomatic uncomplicated diverticular disease (SUDD)
- Diverticulitis (acute, chronic or recurrent)
- Diverticular hemorrhage
- Segmental colitis associated with diverticulosis (SCAD)
- Diverticulitis: uncomplicated or complicated
- Complicated diverticulitis includes abscess, fistula, perforation, obstruction (Clin Geriatr Med 2021;37:141)
ICD coding
- ICD-10: K57.90 - diverticulosis of intestine, part unspecified, without perforation or abscess without bleeding
Epidemiology
- Highest incidence in Western world
- Prevalence increases with age
- > 75% people above 75 years of age
- < 50 years of age: more common in males
- 50 - 70 years of age: slightly more common in females
- > 70 years of age: significantly increased incidence in females (Expert Rev Gastroenterol Hepatol 2018;12:683)
- Left sided diverticula: more common in Western world
- Right sided diverticula: more common in Asia
- Diverticular bleeding 5 - 15%
- Usual source is right sided diverticula
- Possibly due to thinner wall on right side of colon, widened necks and domes of right sided diverticula
- Diverticulitis: in 4 - 15% of patients with diverticula
Sites
- Sigmoid colon / left colon, most common site (90%)
- Right sided colon (5 - 15%)
- Pancolonic involvement (2%) (Int J Colorectal Dis 2018;33:1299)
Pathophysiology
- Occurs in weaker portions of the colonic wall where vasa recta infiltrate the circular muscle layer
- Abnormal colonic motility → exaggerated segmental contractions → increased intraluminal pressure and separation of colonic lumen into chambers (Expert Rev Gastroenterol Hepatol 2018;12:683)
- Sigmoid colon, segment with smallest diameter and largest intraluminal pressure
- In diverticula, vasa recta are separated from intestinal lumen by a layer of mucosa alone
- Exposed to greater amount of injury and can lead to bleeding
Etiology
- Host of complex factors are implicated
- Altered colonic motility
- Visceral hypersensitivity
- Inflammation
- Genetic susceptibility
- Diet, tobacco use
- Medication
- Gut microbiome imbalances (Clin Geriatr Med 2021;37:141)
- Connective tissue disease, Marfan syndrome, Ehlers-Danlos and autosomal dominant polycystic kidney disease
- Can cause structural changes in intestinal walls
Diagrams / tables
Images hosted on other servers:

Physiological activity
Clinical features
- Usually asymptomatic
- Abdominal pain, cramping, altered bowel functions, painless bleeding
- Resembles irritable bowel syndrome (IBS) (Dig Dis 2012;30:64, Curr Opin Gastroenterol 2019;35:27)
Diagnosis
- Frequently is an incidental finding during colonoscopy
- Symptomatic patients, classic presenting symptoms and confirmation with radiology or via colonoscopy (Mayo Clin Proc 2016;91:1094)
- Colonoscopy or Xray following barium enema (StatPearls: Diverticulosis [Accessed 21 April 2022])
- Colonoscopy should be avoided in acute diverticulitis (Mayo Clin Proc 2016;91:1094)
Laboratory
- Fecal calprotectin measurement
- Calprotectin is a calcium and zinc binding protein; can be considered neutrophil specific
- Marker of gastrointestinal inflammation
- Can help in distinguishing IBS from diverticular disease (Expert Rev Gastroenterol Hepatol 2018;12:791)
- Increased white blood cell (WBC), erythrocyte sedimentation rate (ESR), C reactive protein (CRP) in diverticulitis
Radiology description
- Barium enema: barium filled outpouchings; can look similar to polyps
- Ultrasound: gas filled outpouchings
- CT: diverticula outlined by gas
- Intramural diverticula seen as a tiny focus of gas or contrast within the colonic wall (J Clin Gastroenterol 2004;38:S11)
- CT allows grading of severity and detection of complications (Br J Radiol 2020;93:20200670)
Radiology images
Contributed by Bindu Challa, M.D. and Martha M. Yearsley, M.D.

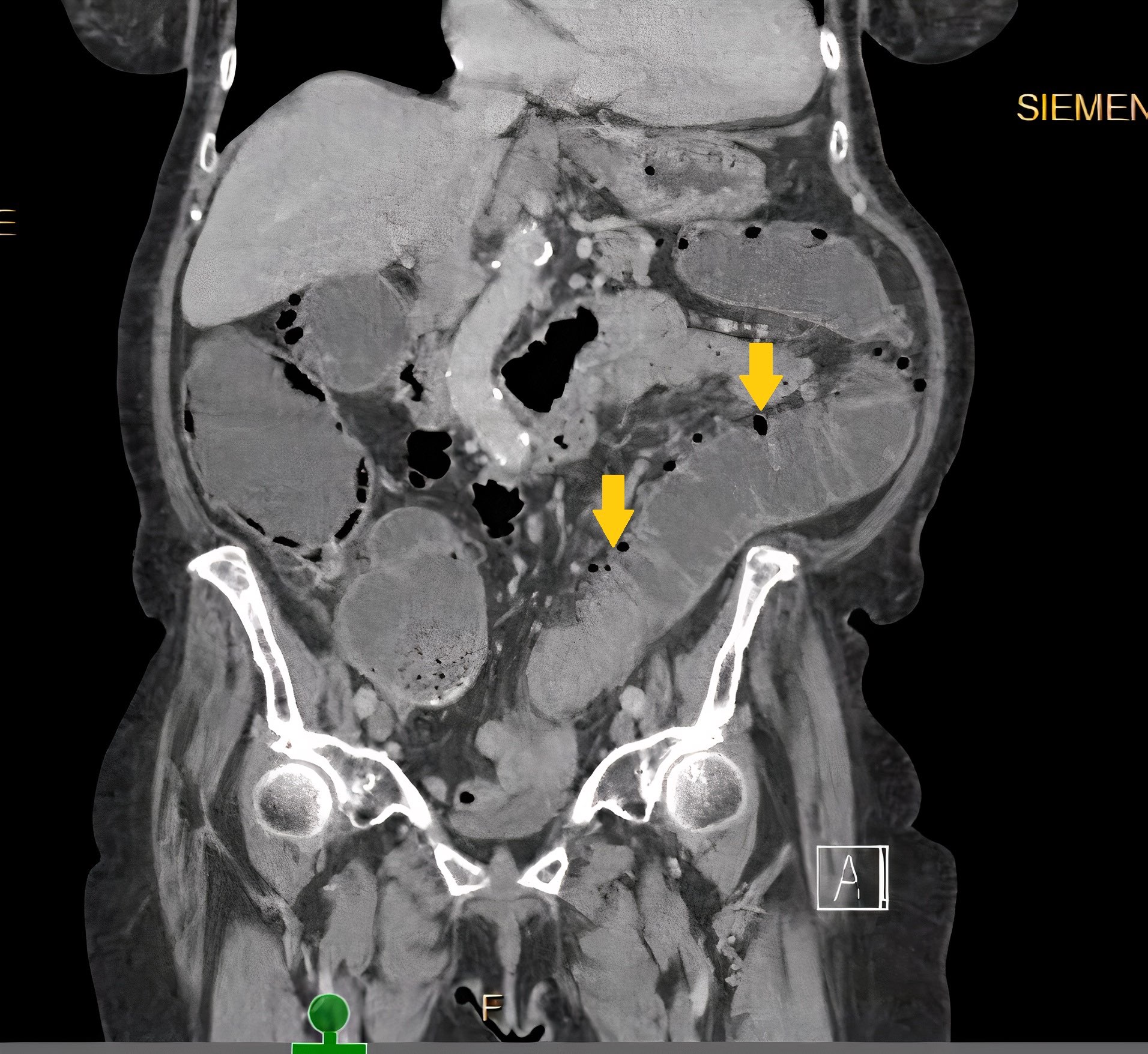
CT of abdomen and pelvis
Prognostic factors
- Mortality rate in uncomplicated diverticulitis is negligible (StatPearls: Acute Diverticulitis [Accessed 21 April 2022])
- Complicated diverticulitis requiring surgery may lead to death in ~5% of patients
- Perforation of the bowel with resulting peritonitis, risk of death increases to 20%
Case reports
- 15 year old boy with dysmorphic features and learning disabilities presents with acute onset abdominal pain, nausea and vomiting (ACG Case Rep J 2019;6:1)
- 50 year old man with longstanding history of ulcerative colitis and severe diverticulosis on colonoscopy (Rev Esp Enferm Dig 2021;113:550)
- 68 year old man with lower gastrointestinal bleeding and arteriovenous malformations within jejunal diverticulosis (BMC Surg 2019;19:70)
- 83 year old woman with history of chronic abdominal pain is found to have partial midgut volvulus (Am J Case Rep 2021;22:e933180)
- 88 year old man presents with hematochezia and perianal pain (Cureus 2021;13:e14900)
Treatment
- No rationale for treatment of asymptomatic colonic diverticulosis (Pol Przegl Chir 2015;87:203, United European Gastroenterol J 2014;2:413)
- Symptomatic uncomplicated diverticular disease (SUDD)
- Dietary modifications to increase fiber, use of probiotics has been proposed (Neurogastroenterol Motil 2015;27:305)
- Antibiotics in acute complicated diverticulitis (Gastroenterology 2015;149:1944)
Clinical images
Contributed by Bindu Challa, M.D. and Martha M. Yearsley, M.D.
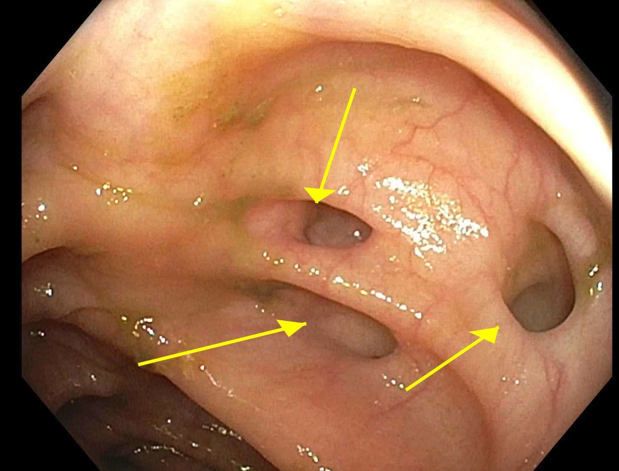
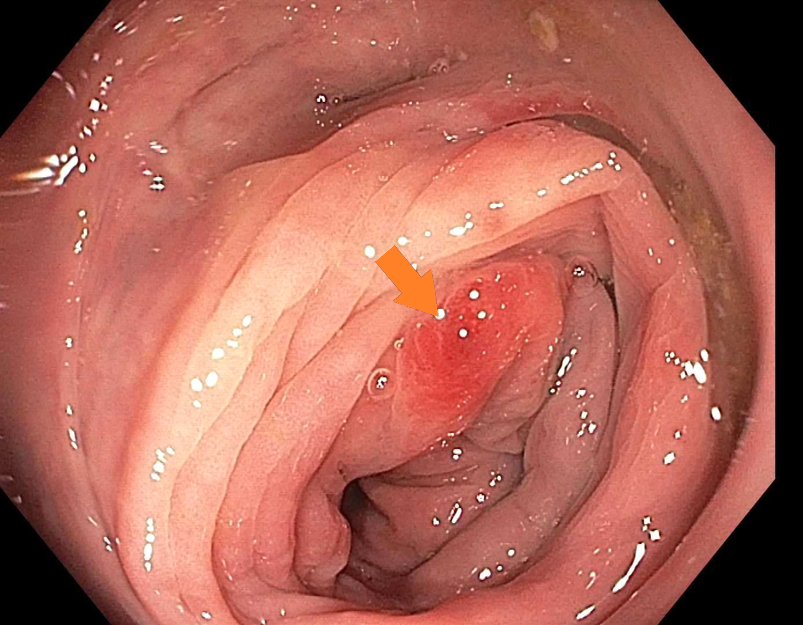
Colonoscopy
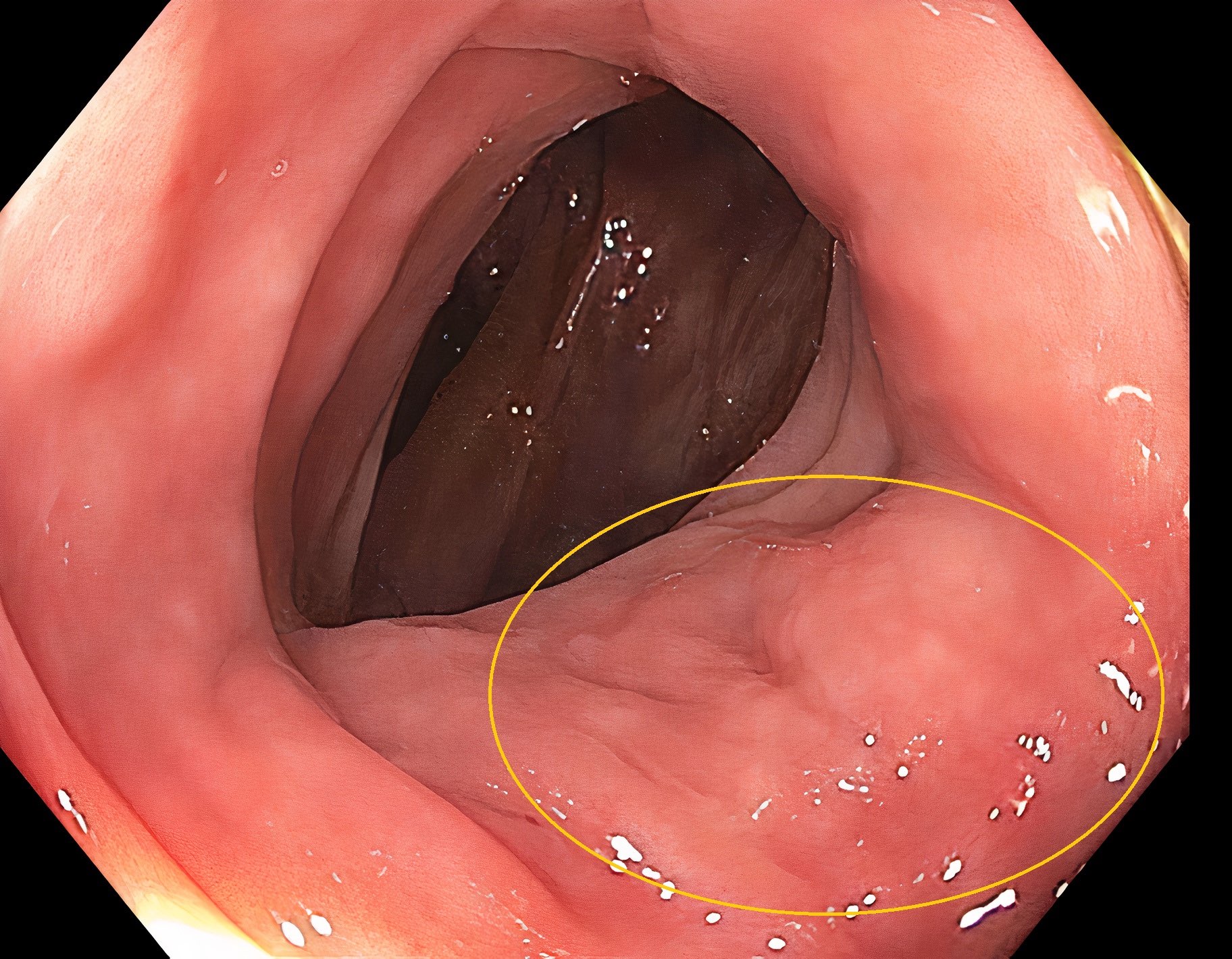
Colonoscopy
Gross description
- Specimen should be fixed and opened longitudinally for easy sampling of diverticula
- Usually, multiple flask shaped invaginations of colonic wall
- Wall thickening may be present (Surg Endosc 2011;25:2586)
- Narrowing of lumen, shortening of tenia and marked thickening of circular muscle layer may be present (J Clin Gastroenterol 2006;40:S108)
- If it extends deeply, perforation and serosal adhesions may be seen
Gross images
Images hosted on other servers:


Multiple diverticula

Multiple diverticula


Multiple diverticula

With bowel wall stenosis

Blue-gray diverticula

Perforated single true diverticulum

False diverticulum
Microscopic (histologic) description
- Mucosa may be normal to markedly abnormal
- Expansion of lamina propria by lymphoplasmacytic infiltrate (more prominent in basal half)
- Lymphoglandular complexes, mucin depletion, focal Paneth cell metaplasia (in chronic cases) may be seen (J Clin Gastroenterol 2004;38:S11)
- Muscularis mucosa extends towards surface between elongated crypts
- Shortening of the affected bowel and hypertrophy of circular muscle layer (myochosis) leads to exaggerated mucosal folds (Am J Surg Pathol 1991;15:871)
- Some cases can show lamina propria fibrosis, crypt elongation on the tips of prominent mucosal folds, like mucosal prolapse syndrome in rectum and anus (J Clin Gastroenterol 2008;42:1137)
- Hemosiderin deposition in submucosa may be seen (StatPearls: Diverticulosis [Accessed 21 April 2022])
- Can mimic inflammatory bowel disease
- Hyperplasia of lymphoid aggregates is one of the earliest signs of diverticulitis
- Cryptitis, crypt abscesses, peridiverticular abscess and fistulas may be superimposed on this background in acute diverticulitis
- Tracking abscesses can spread longitudinally or circumferentially and can cause diverticular colitis
- Persistent localized inflammation can lead to phlegmon which is a thickened, firm segment of bowel wall that can lead to strictures and acute or subacute large bowel obstruction (Best Pract Res Clin Gastroenterol 2002;16:543)
Microscopic (histologic) images
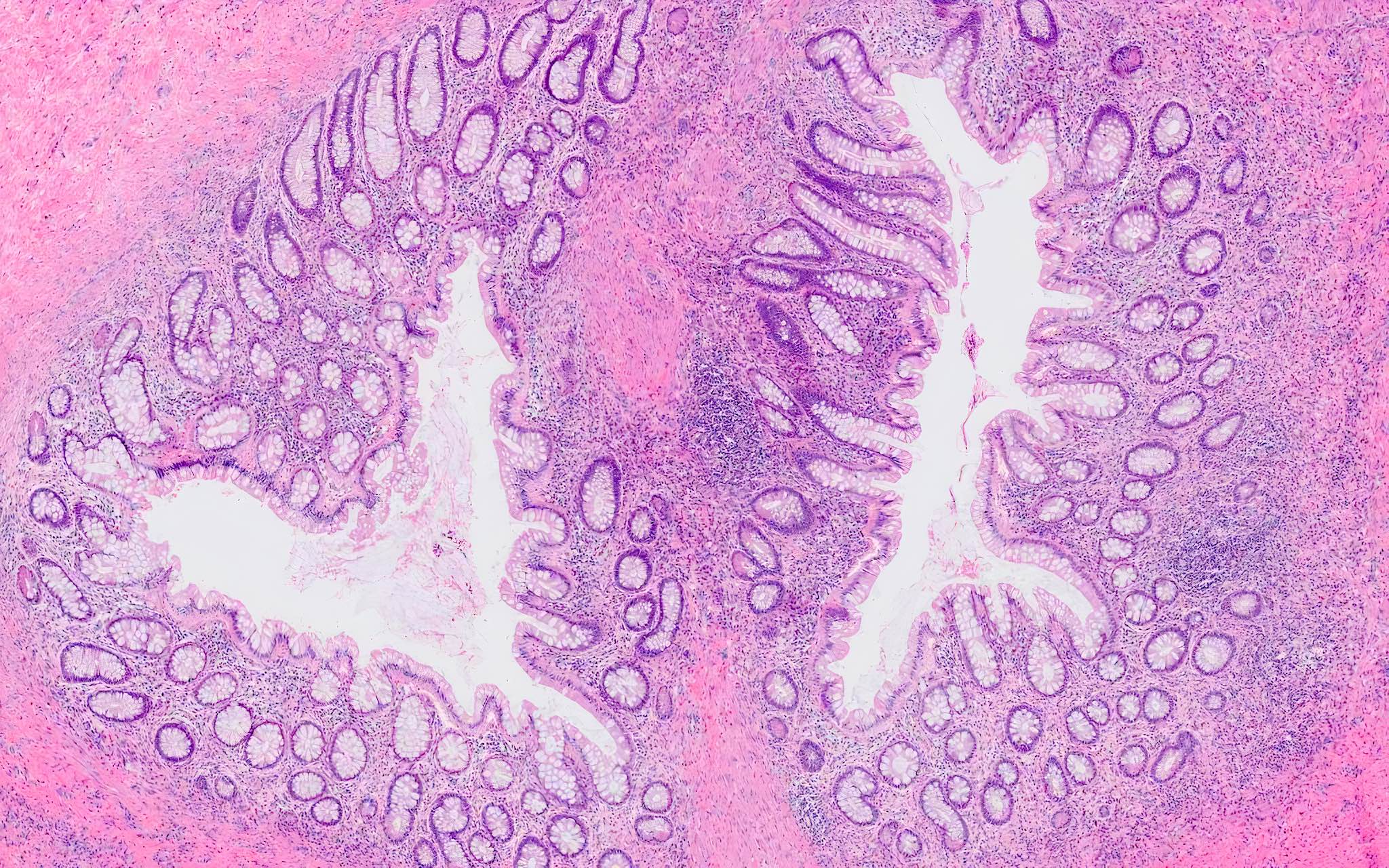
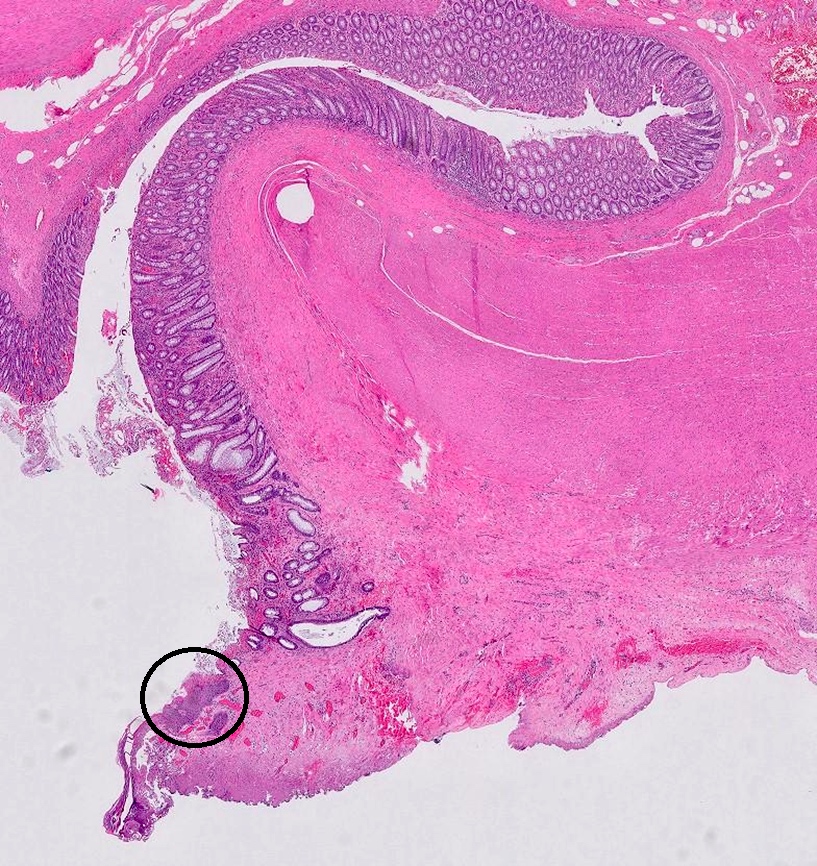
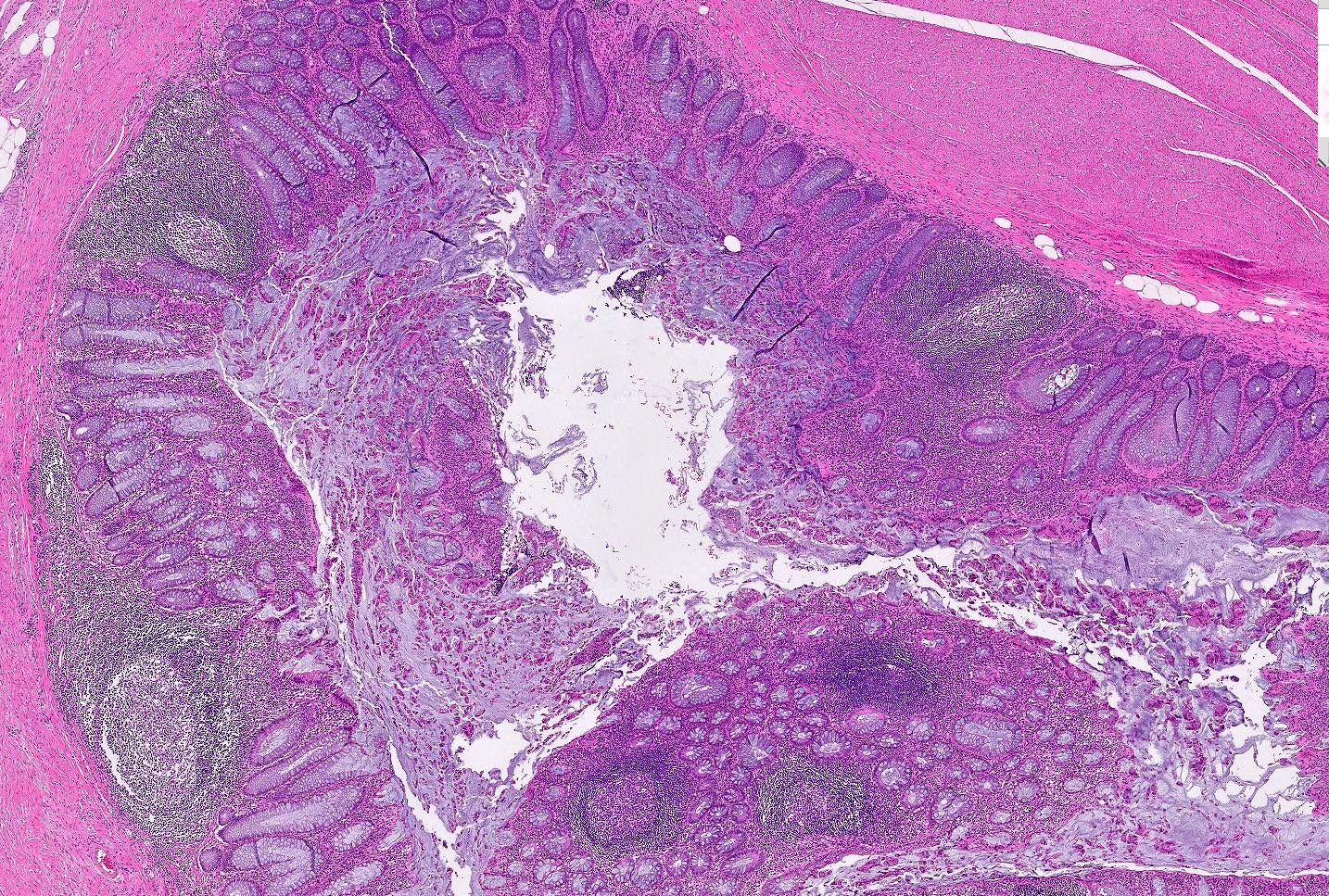
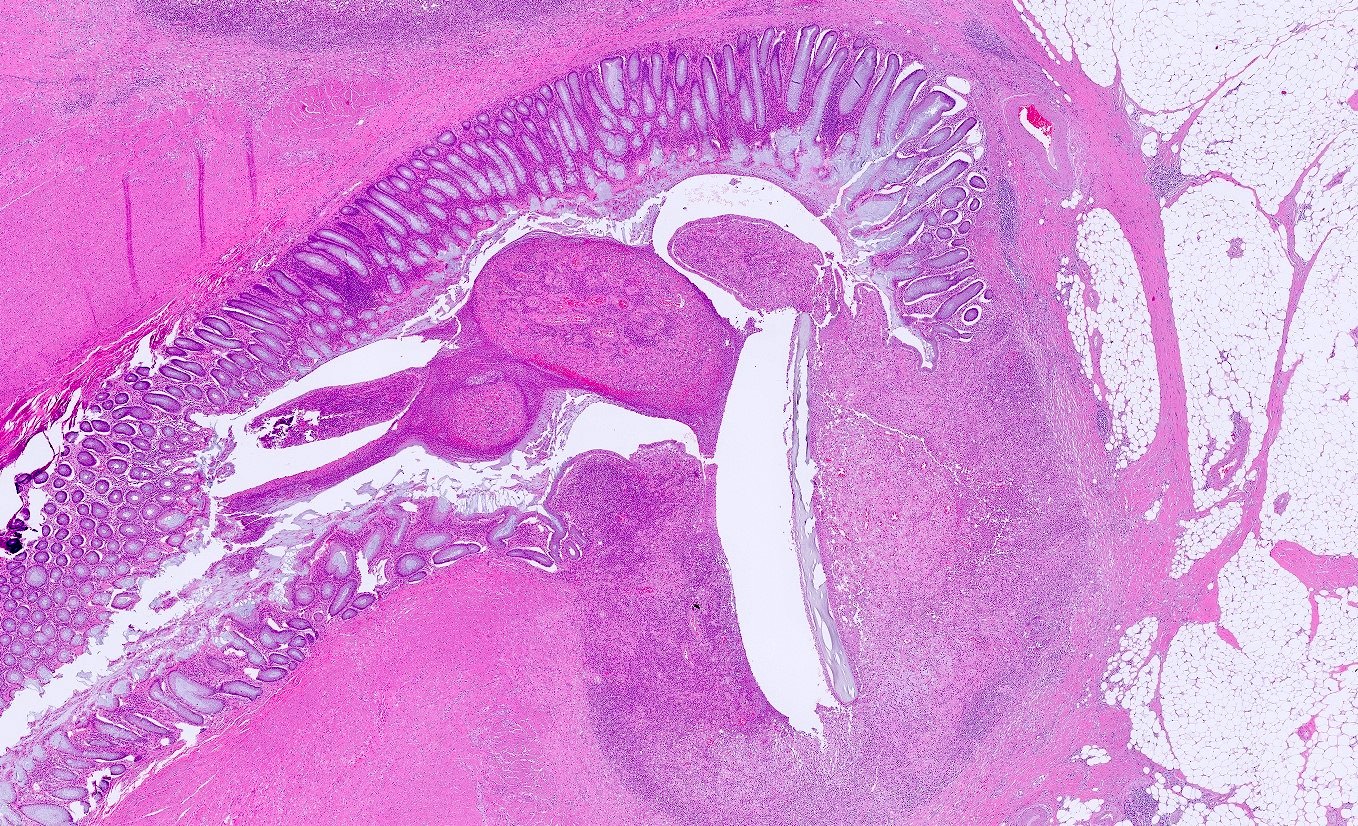
Contributed by Bindu Challa, M.D. and Martha M. Yearsley, M.D.
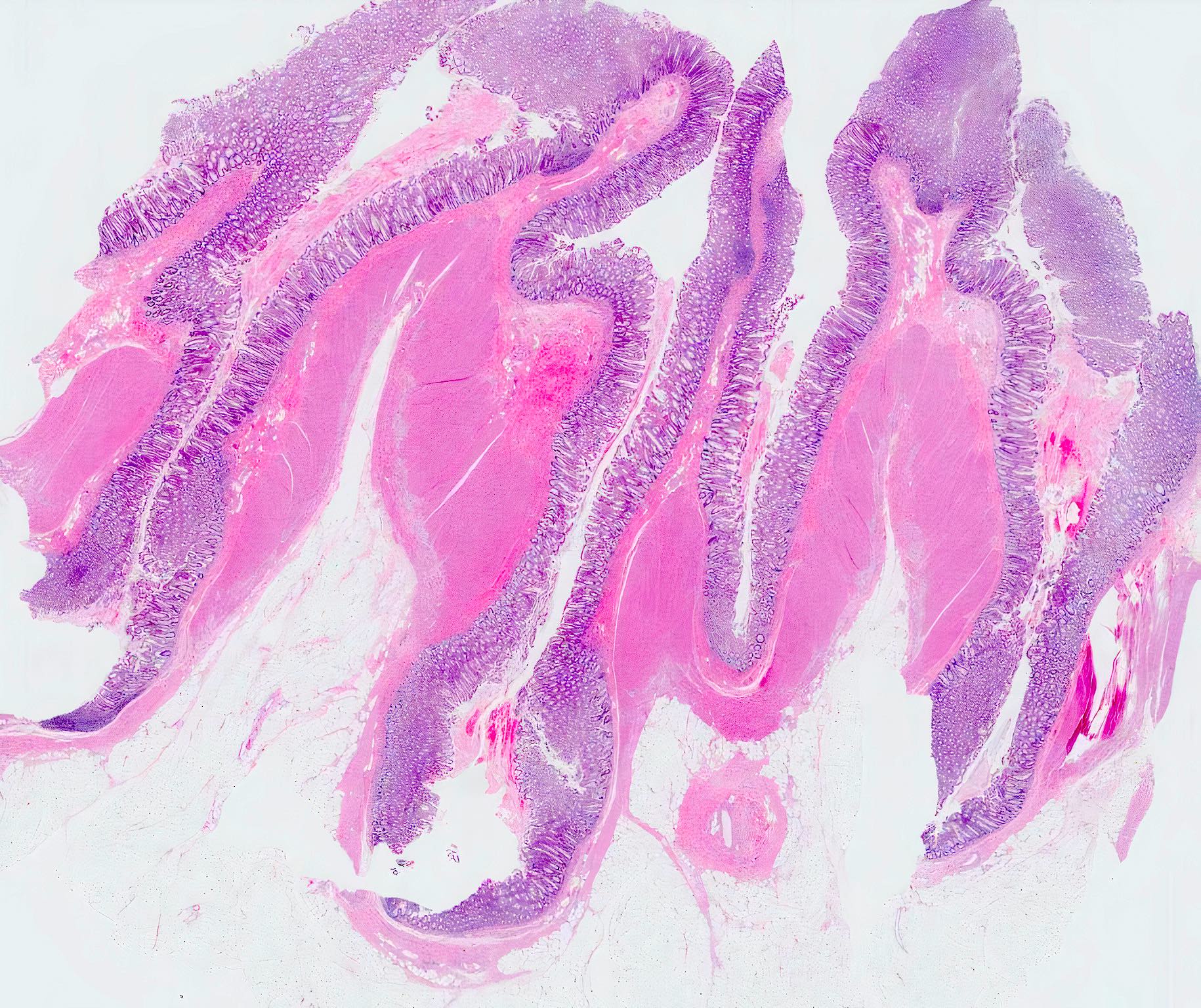
Diverticula
Multiple diverticula
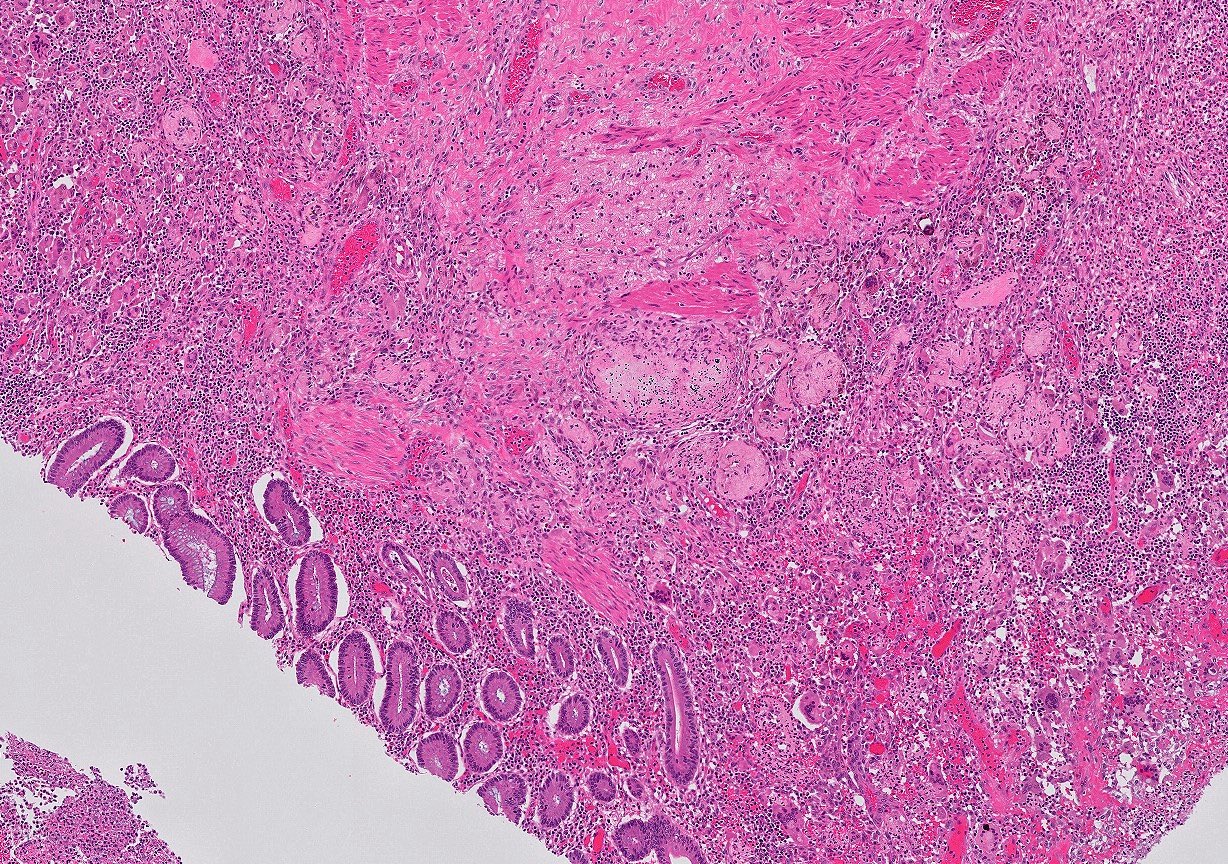
Diverticular abscess
Enterocutaneous fistula
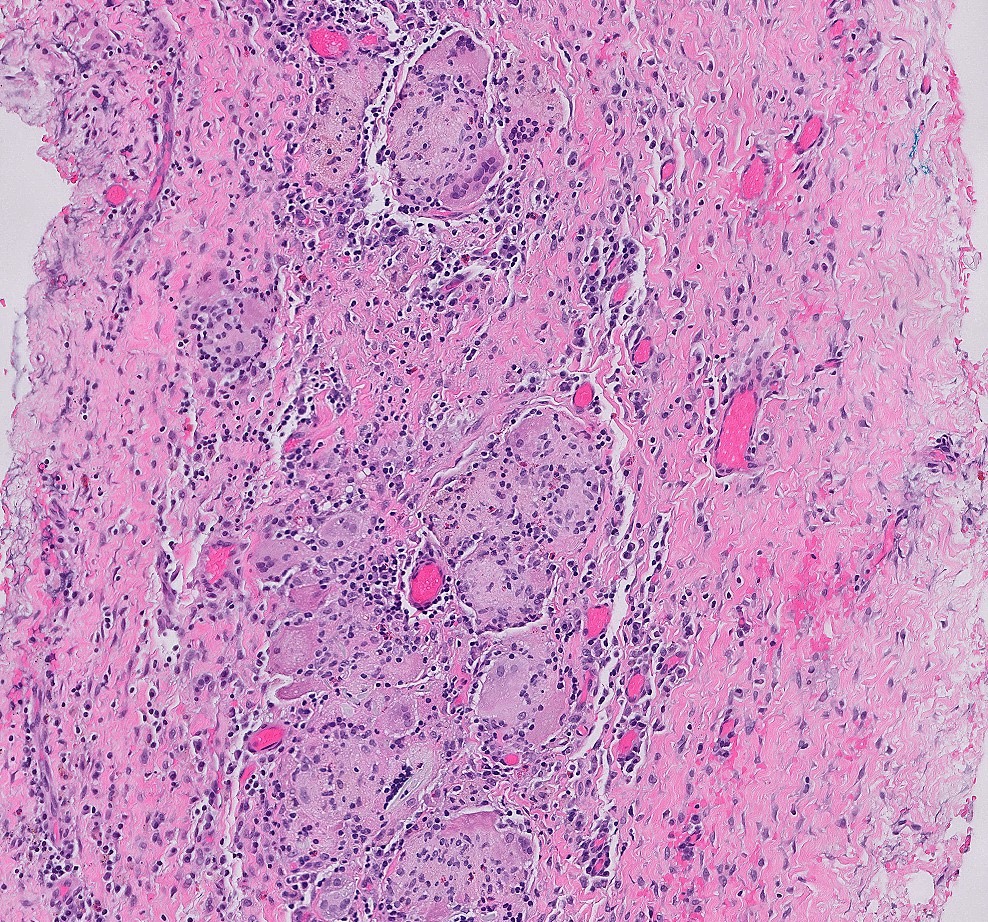
Chronic inflammation in diverticular wall
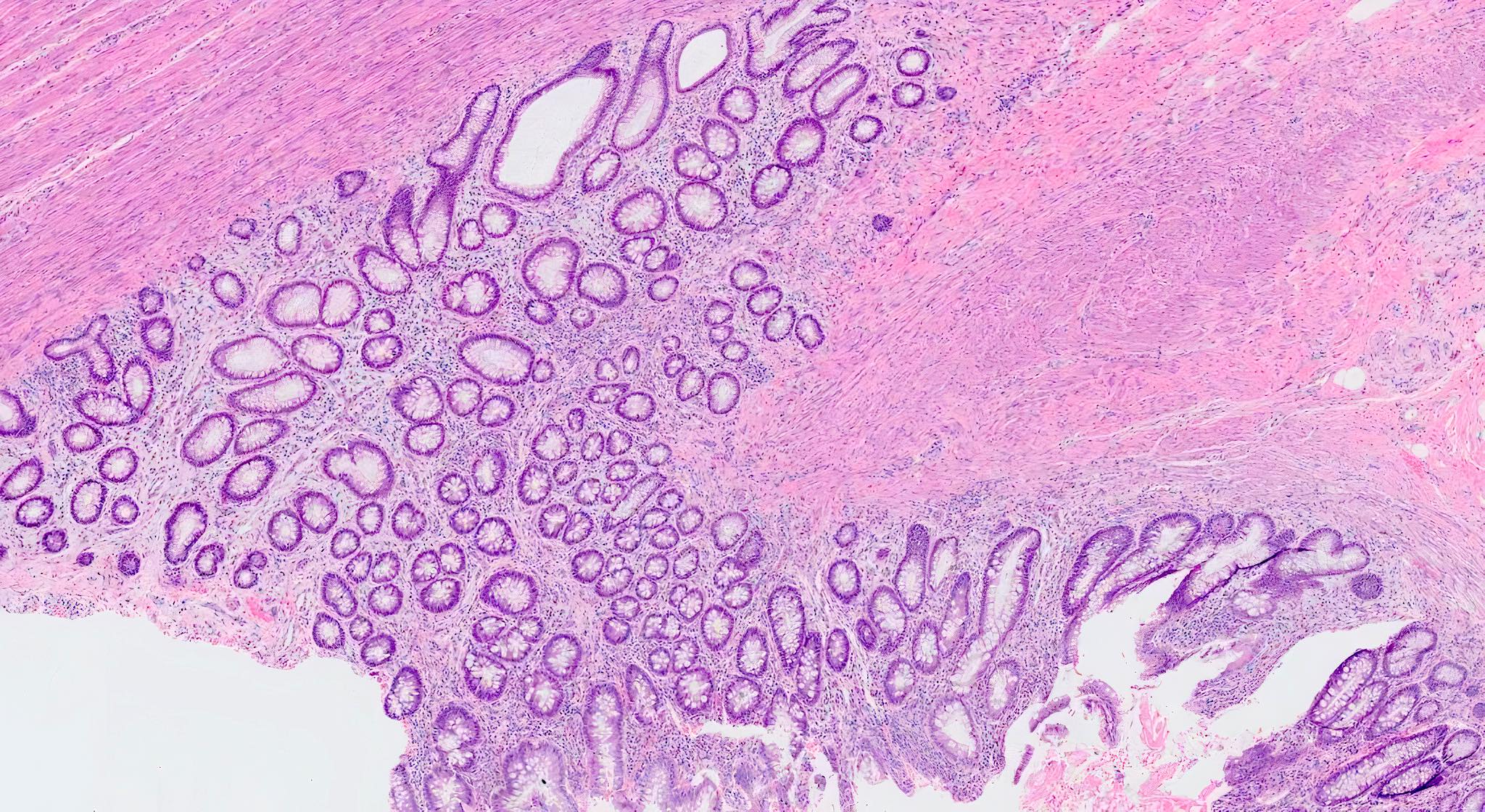
Diverticular disease associated chronic colitis
Lymphoid aggregates in diverticular wall
Diverticulitis with complications
Virtual slides
Images hosted on other servers:

Diverticulosis with diverticulitis
Videos
Histopathology of diverticular disease
Whole slide image of case of diverticulosis with diverticulitis
Sample pathology report
- Colon, sigmoid, segmental resection:
- Diverticulosis
- Two lymph nodes, negative for tumor
- Colon, sigmoid, partial colectomy:
- Segment of colon with diverticulosis, diverticulitis and abscess formation
- Colon, total colectomy:
- Colonic diverticular disease with perforated diverticulum
Differential diagnosis
- Inflammatory bowel disease:
- Diverticular disease associated chronic active colitis can resemble ulcerative colitis
- Wall thickening, transmural lymphoid aggregates and granulomas can mimic Crohn's disease
- Solitary rectal ulcer syndrome and inflammatory cloacogenic polyp:
- Prominent mucosal folds / prolapsed folds adjacent to diverticula can mimic these conditions
- Angiodysplasia:
- Abnormal, tortuous, thin walled blood vessels in mucosa and submucosa
Additional references
Board review style question #1
What is the most common site of occurrence for the condition shown in the image?
- Appendix
- Jejunum
- Rectum
- Sigmoid colon
Board review style answer #1
D. Sigmoid colon. Diverticulosis occurs most commonly in sigmoid colon in 90% of cases.
Comment Here
Reference: Diverticulosis
Comment Here
Reference: Diverticulosis
Board review style question #2
What is the laboratory test that can help distinguish irritable bowel syndrome from diverticular disease?
- Aspartate transaminase
- Fecal calprotectin
- Fecal lactoferrin
- Gamma glutamyl transferase
Board review style answer #2
B. Fecal calprotectin is a marker of gastrointestinal inflammation. Elevated fecal calprotectin favors diverticular disease and helps in distinguishing it from functional gastrointestinal disorders like irritable bowel syndrome.
Comment Here
Reference: Diverticulosis
Comment Here
Reference: Diverticulosis
