
Colon
Polyps
Inflammatory polyp
Authors: Andrew L.J. Dunn, M.D., Raul S. Gonzalez, M.D.
Deputy Editor-in-Chief: Catherine E. Hagen, M.D.


Last author update: 21 April 2021
Last staff update: 7 December 2023
Copyright: 2002-2024, PathologyOutlines.com, Inc.
PubMed Search: "Inflammatory polyp" colon

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Clinical features | Case reports | Treatment | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Negative stains | Molecular / cytogenetics description | Videos | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1Cite this page: Dunn ALJ, Gonzalez RS. Inflammatory polyp. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/colontumorinflammatory.html. Accessed April 19th, 2024.
Definition / general
- Generic term for nonneoplastic mixture of epithelial and stromal components admixed with inflammatory cells
- Often related to inflammatory bowel disease (Crohn's disease or ulcerative colitis), anastomosis, ischemic colitis or infection
Essential features
- Nonneoplastic colon polyp composed of inflamed mucosa
- Typically shows surface erosion with surrounding granulation tissue and epithelial distortion
Terminology
- Inflammatory polyp as a diagnosis is generally used to describe small foci of nonspecifically inflamed colonic mucosa or inflammatory pseudopolyps
- Inflammatory polyp as a category includes several subtypes, including:
- Inflammatory cap polyp
- Inflammatory fibroid polyp
- Inflammatory myoglandular polyp
- Prolapse associated polyps
ICD coding
- ICD-10: K51.4 - inflammatory polyps of colon
Epidemiology
- Typically second and third decades for inflammatory bowel disease; incidence range of 10 - 20% in ulcerative colitis patients (World J Gastroenterol 2017;23:1541)
- May occur in older patients with peripheral vascular disease
Sites
- Can arise anywhere in the colon, especially at the ileocecal region in Crohn’s disease
- May form at anastomotic sites
Pathophysiology
- Believed to be secondary to repeated bouts of intense inflammation
- Formation of inflammatory polyps may be related to increases in C reactive protein, C4 and procollagen III peptide (World J Gastroenterol 2003;9:619)
Clinical features
- Sporadic inflammatory polyps are usually incidental at colonoscopy
- May present with intussusception or obstructive symptoms
- Presence of pseudopolyps in inflammatory bowel disease may represent recent flare, although lesions are found in active or dormant disease (World J Gastroenterol 2017;23:1541)
- Also may be related to arthropathy or other extracolonic symptoms (Lancet 1969;2:555)
Case reports
- 28 year old woman with pseudosarcomatous changes in inflammatory polyp (Korean J Gastrointest Endosc 2007;35:51)
- 47 year old man with intussusception due to 3 cm inflammatory polyp (Asian J Surg 2005;28:58)
- 62 year old man with inflammatory polyp due to Kirschner wire (Intern Med 2014;53:699)
- 74 year old man with inflammatory polyp with osseous metaplasia (Gastroenterology Res 2012;5:74)
- Patient with inflammatory polyp containing schistosomiasis (bilharzial polyp) (J Clin Gastroenterol 1983;5:169)
Treatment
- Typically treated endoscopically via polypectomy
- Examples related to inflammatory bowel disease may improve with infliximab (J Crohns Colitis 2010;4:707)
- Argon plasma coagulation or ablation for bleeding control
- Surgical resection if profuse bleeding, obstruction or intussusception
Gross description
- Usually sessile and less than 3 cm
- May be pedunculated or filiform
Gross images
Images hosted on other servers:

Inflammatory pseudopolyps in ulcerative colitis
Microscopic (histologic) description
- Often consists of normal colonic mucosa in a polypoid configuration, with increased inflammation (expanded lamina propria and crypt abscesses or cryptitis)
- Epithelium can show various degrees of surface erosion, crypt distortion / dilation or hyperplasia, along with reactive nuclear features within the mucosal epithelial cells
- May consist entirely of granulation tissue (abundant thin walled and dilated vessels surrounded by mixed neutrophilic and lymphoplasmacytic inflammation)
- Reactive stromal cells may be markedly pleomorphic and mimic sarcoma
- Cases associated with inflammatory bowel disease may rarely show epithelial dysplasia
Microscopic (histologic) images
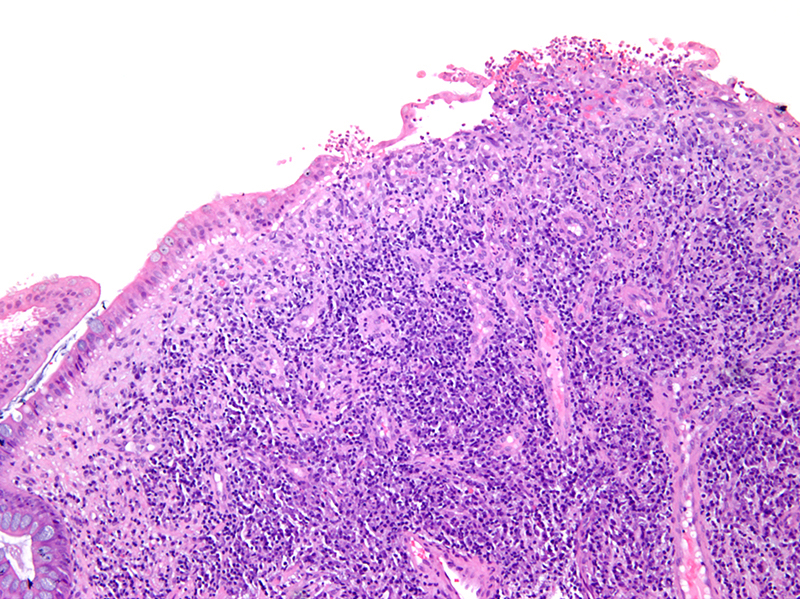
Contributed by Andrew L.J. Dunn, M.D.
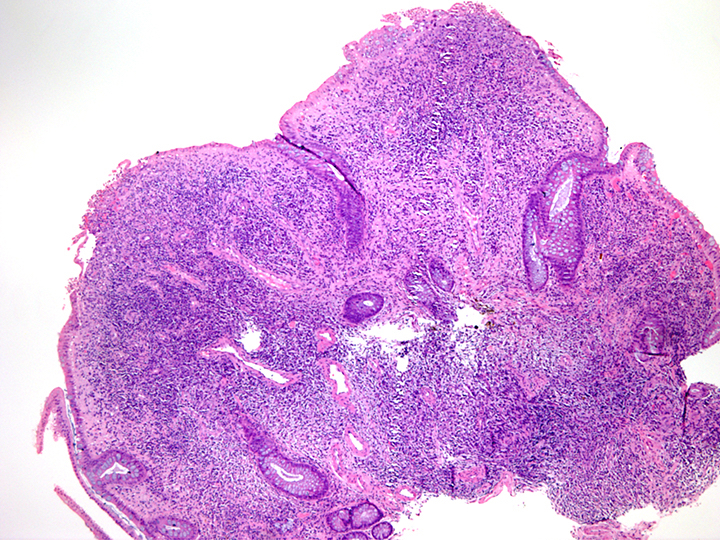
Dense inflammation in lamina propria
Surface mucosal ulceration
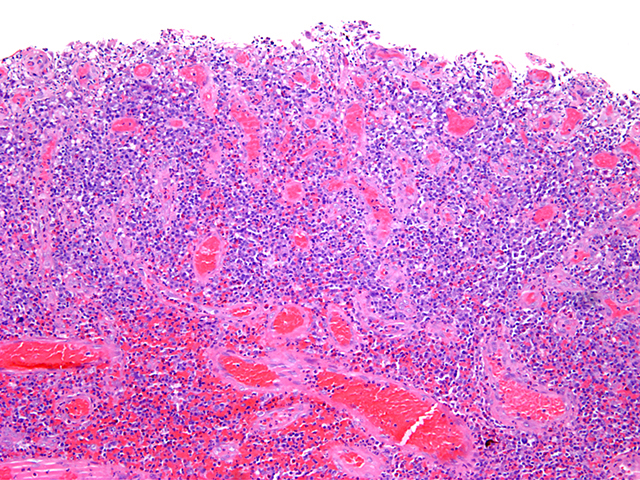
Surface erosion with granulation tissue
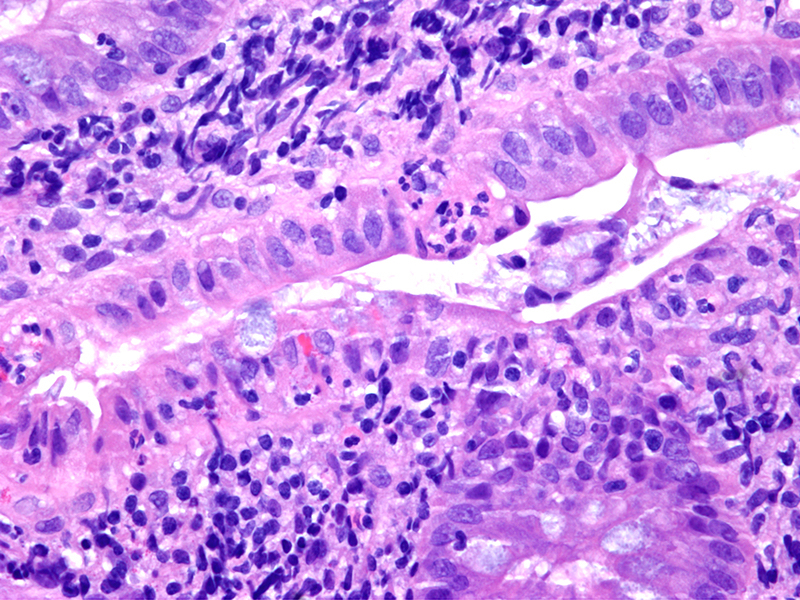
Cryptitis
Negative stains
- S100, cytokeratin (reactive stromal cells), CMV
Molecular / cytogenetics description
- Usually no abnormalities
Videos
Inflammatory polyp on colonoscopy
Sample pathology report
- Sigmoid colon, polypectomy:
- Inflammatory polyp
Differential diagnosis
- Juvenile polyp:
- Large cystically dilated glands; wide histologic overlap and the distinction is of little importance in adult patients
- Pyogenic granuloma:
- Lobular arrangement of capillaries within edematous stroma (Ann Diagn Pathol 2005;9:106)
Board review style question #1
Which of the following is not a typical feature of colonic inflammatory polyps?
- Crypt distortion / branching
- Granulation tissue changes
- Microsatellite instability
- Surface mucosal erosion
Board review style answer #1
C. Microsatellite instability. Inflammatory polyps are a benign process with various degrees of mucosal erosion, increased vascular density similar to granulation tissue and architectural changes.
Comment here
Reference: Inflammatory polyp
Comment here
Reference: Inflammatory polyp
