

Fallopian tubes & broad ligament
Broad ligament tumor-like lesions
Developmental cysts
Author: Lucy Ma, M.D.
Editorial Board Member: Gulisa Turashvili, M.D., Ph.D.
Deputy Editor-in-Chief: Jennifer A. Bennett, M.D.

Last author update: 1 November 2022
Last staff update: 1 November 2022
Copyright: 2003-2024, PathologyOutlines.com, Inc.
PubMed Search: Paraovarian cyst


Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Radiology description | Prognostic factors | Case reports | Treatment | Clinical images | Gross description | Microscopic (histologic) description | Microscopic (histologic) images | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1Cite this page: Ma L. Developmental cysts. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/fallopiantubesdevelopmentalcysts.html. Accessed April 25th, 2024.
Definition / general
- Benign developmental cysts arising from remnants of Müllerian and Wolffian ducts as well as from mesothelium
Essential features
- Benign, fluid filled cysts located adjacent to the adnexa (fallopian tube or ovary)
- Cysts are lined by non-stratified epithelium, which can be ciliated (paramesonephric cyst) or flat, cuboidal (mesothelial and mesonephric cysts)
- Usually are incidental findings
Terminology
- Paratubal cysts, paraovarian cysts, mesothelial (or simple) cyst
- Hydatid cyst of Morgagni (no longer recommended): typically refers to pedunculated cyst located near tubal fimbria (Arch Gynecol Obstet 2012;285:1563)
ICD coding
Epidemiology
- ~10% of all adnexal masses (Arch Gynecol Obstet 2012;285:1563)
- Vast majority are Müllerian (paramesonephric) cysts, commonly known as paratubal cysts
- < 2% are Wolffian (mesonephric) cysts (Am J Obstet Gynecol 1977;129:873)
Sites
- Adjacent to the adnexa, along broad ligament, between the fallopian tube and the ovary
Pathophysiology
- Müllerian (paramesonephric) and Wolffian (mesonephric) ducts grow mostly in parallel during development
- Müllerian ducts eventually fuse
- Fusion of Müllerian ducts creates a transverse fold, which becomes the broad ligament
- Broad ligament contains Müllerian and Wolffian duct remnants, which can then become cystic
- Reference: Kurman: Blaustein's Pathology of the Female Genital Tract, 7th Edition, 2019
Etiology
- Thought to originate from remnants of Müllerian and Wolffian ducts as well as from mesothelium (Am J Obstet Gynecol 1977;129:873, Gynecol Obstet Invest 1981;12:1)
Clinical features
- Usually asymptomatic and incidentally found
- Large cysts can be painful, bleed, rupture or cause ovarian torsion (Arch Gynecol Obstet 2012;285:1563)
Diagnosis
- Incidental finding
- If symptomatic, usually diagnosed by ultrasound
Radiology description
- Ultrasound findings: majority are unilocular cysts without papillations (Ultrasound Obstet Gynecol 2006;28:330)
- Presence of papillary projections / solid nodule typically indicates neoplastic cysts
Prognostic factors
- Benign
- May rarely give rise to serous borderline tumor and carcinoma (Gynecol Oncol Rep 2020;32:100559, Appl Immunohistochem Mol Morphol 2017;25:e21)
Case reports
- 13 year old girl with bilateral paraovarian cysts (Sultan Qaboos Univ Med J 2021;21:e308)
- 31 year old woman with giant paratubal cyst presented with adnexal torsion (Case Rep Womens Health 2020;27:e00222)
- 85 year old woman with serous borderline tumor arising from a paratubal cyst (Gynecol Oncol Rep 2020;32:100559)
Treatment
- Surgical excision if large or symptomatic
Clinical images
Images hosted on other servers:

Torsed paraovarian cyst before detorsion

Torsed paraovarian cyst after detorsion

Large paraovarian cyst
Gross description
- Thin walled, fluid filled cyst(s) located adjacent to fallopian tube or ovary
Microscopic (histologic) description
- Paramesonephric cysts are lined by single layer of bland ciliated tubal epithelium
- Mesonephric cysts are lined by single layer of low cuboidal, nonciliated epithelium with occasional clear cells (rare) (Am J Obstet Gynecol 1977;129:873)
- Mesothelial cysts are lined by single layer of flat or cuboidal, nonciliated cells, which may show transitional cell metaplasia (see Walthard cell nests)
- Distinction between the types of cyst may be difficult but has no clinical implications
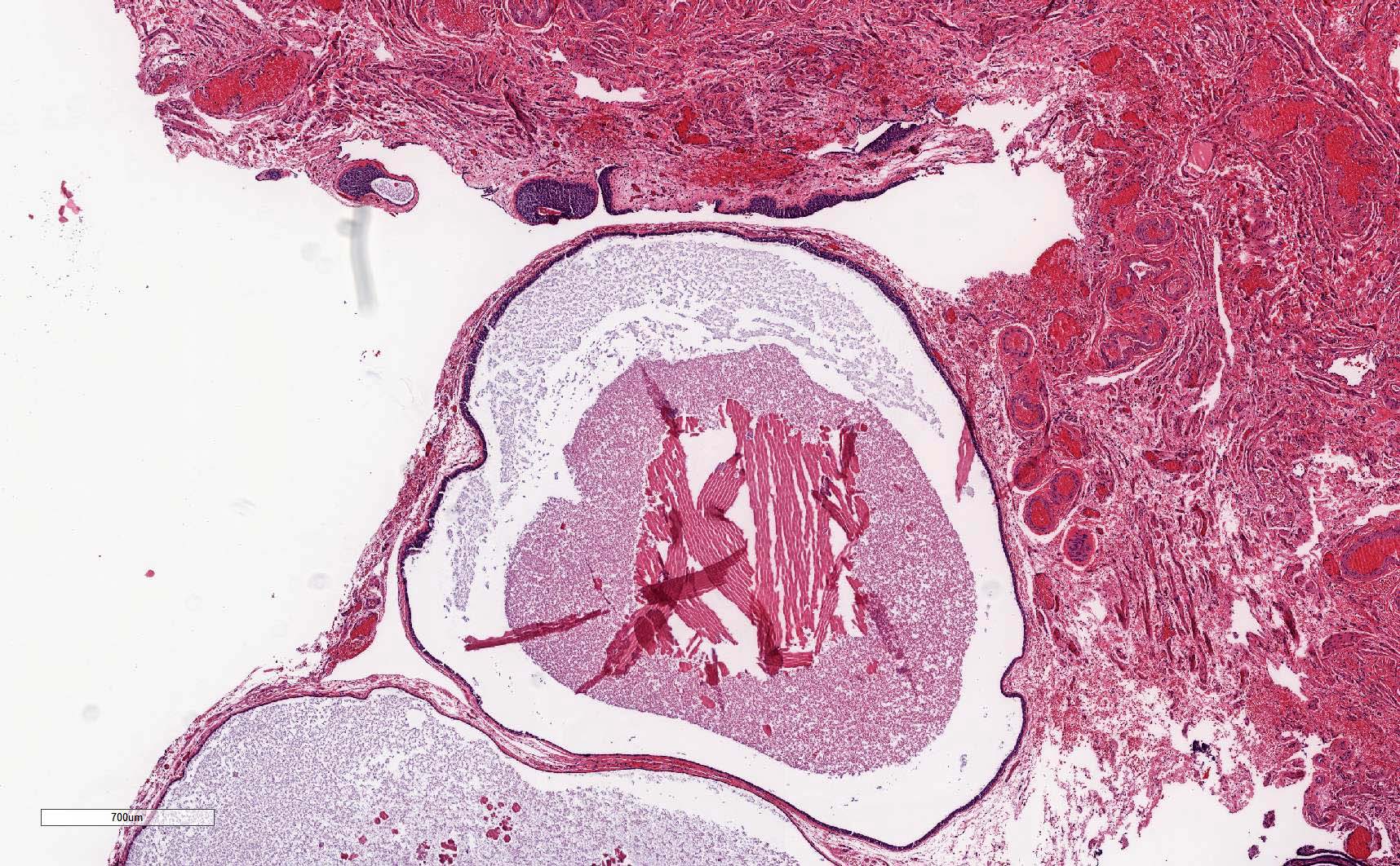
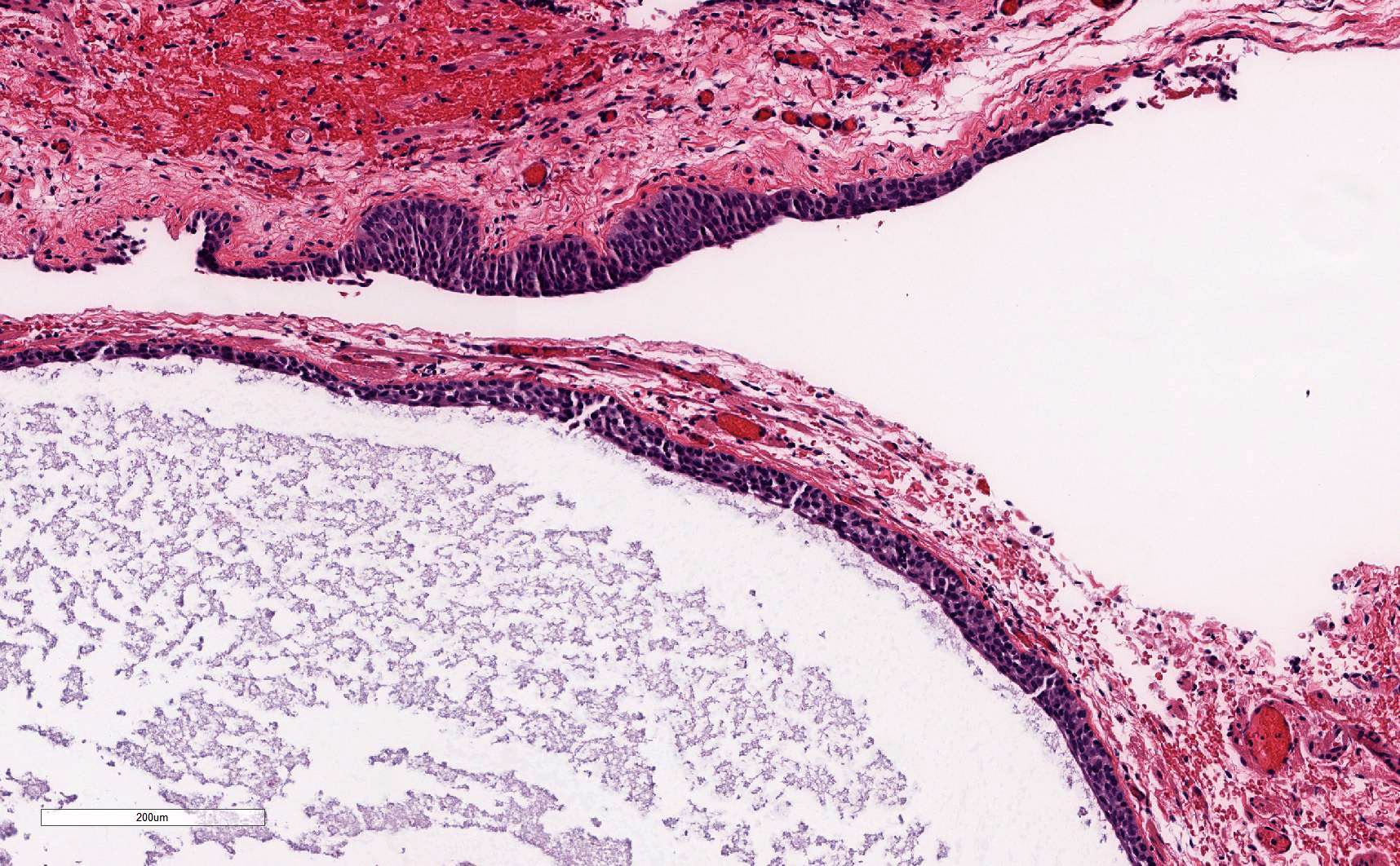
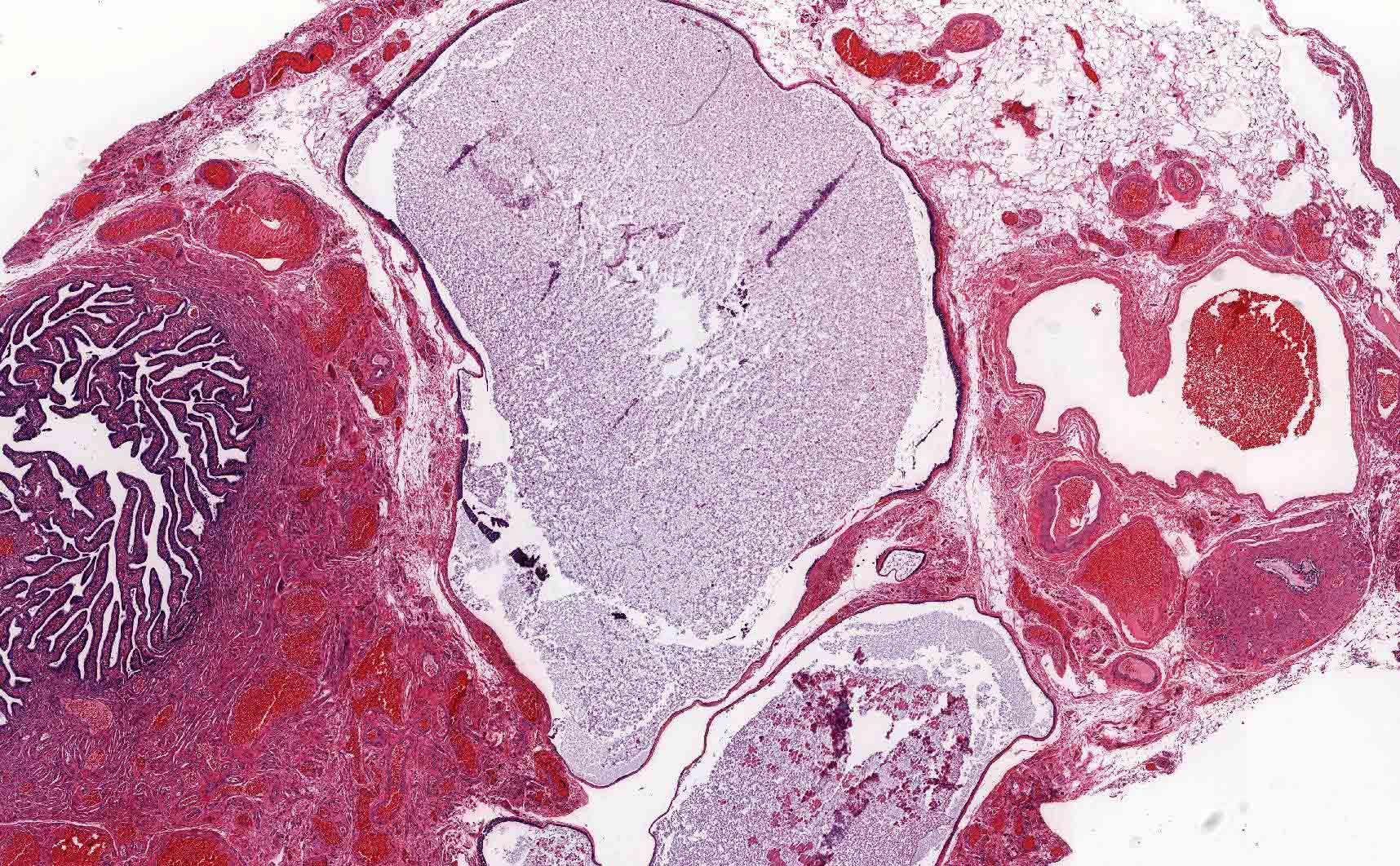
Microscopic (histologic) images
Contributed by Lucy Ma, M.D.

Simple cysts adjacent to Walthard nests
Paratubal cysts adjacent to fallopian tube
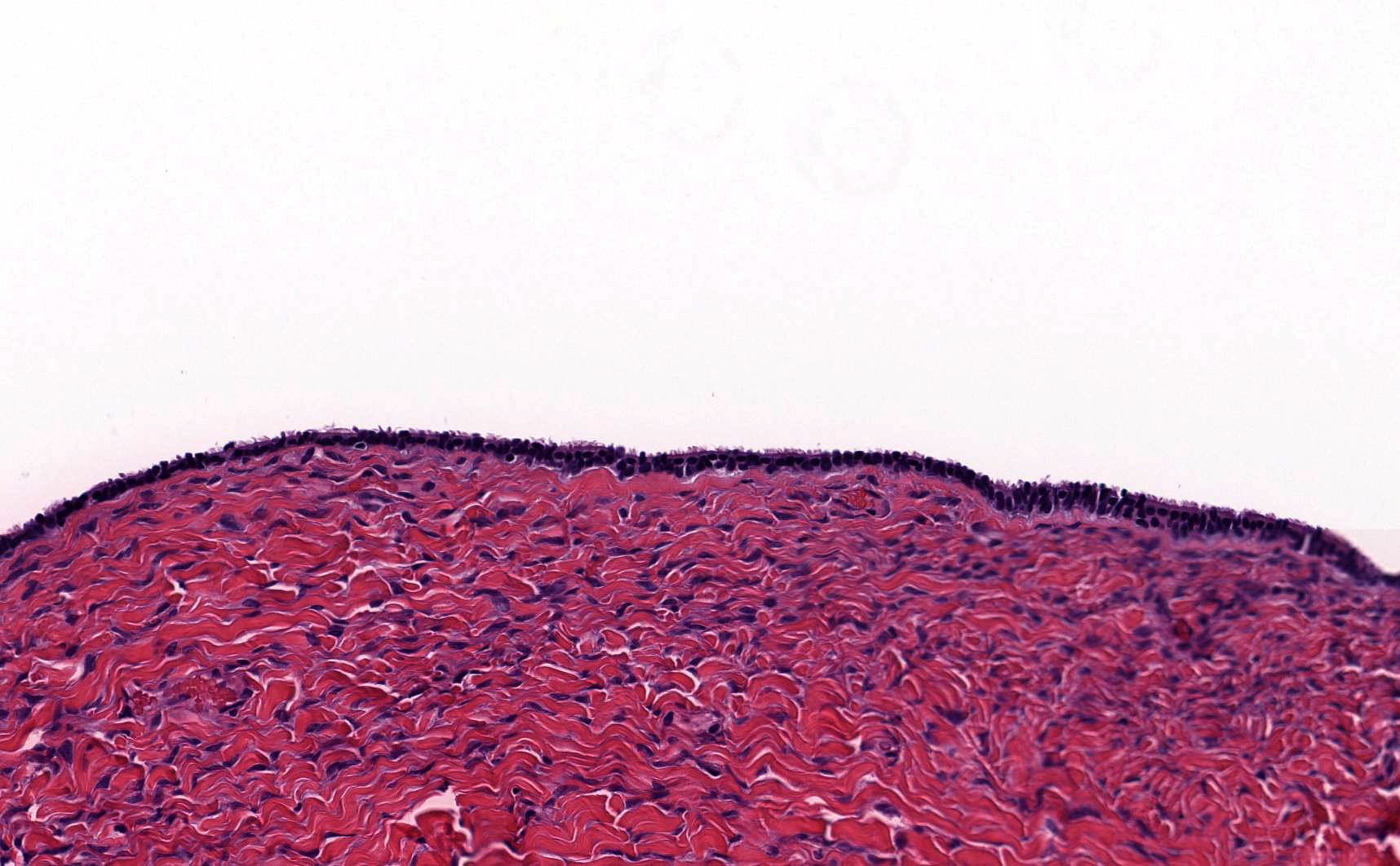
Ciliated epithelium
Sample pathology report
- Not essential to include in report, particularly if cysts are small and incidental
- Right fallopian tube, salpingectomy:
- Fallopian tube with paratubal cysts
Differential diagnosis
- Serous cystadenoma:
- Presence of dense collagenized cyst wall
- Absence of rudimentary plicae
- Hydrosalpinx:
- Presence of well developed, smooth muscle wall
- Presence of occasional branching plicae with columnar epithelium containing histologic normal ciliated and secretory cells
- Direct communication with nondilated portion of fallopian tube
Additional references
Board review style question #1
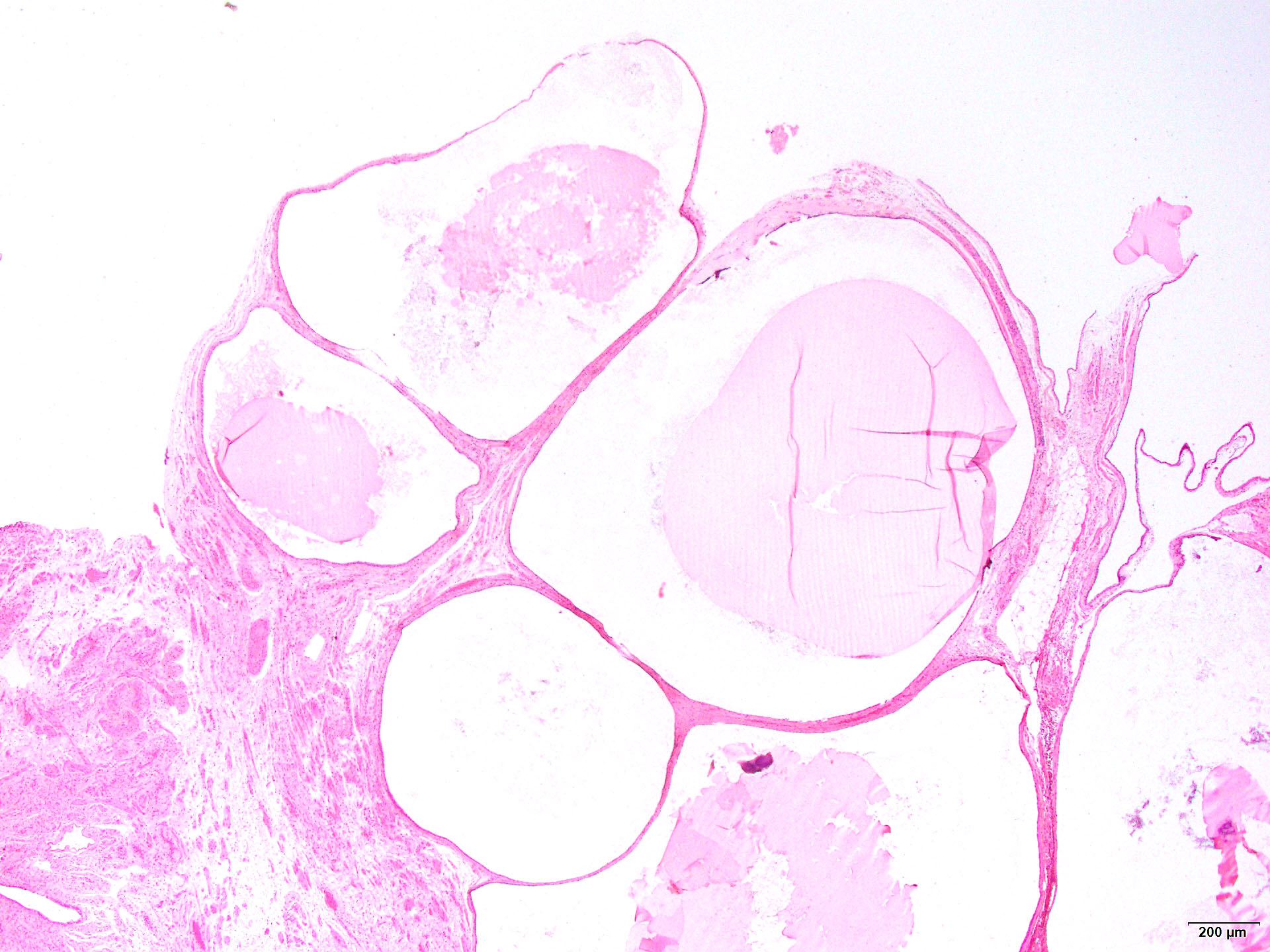
A 45 year old patient underwent total hysterectomy and bilateral salpingo-oophorectomy for a myomatous uterus. The left adnexa showed the finding in the image above. What is the next step in management regarding this finding?
- Computed tomography (CT) of the chest
- Germline testing
- No additional therapy
- Serial serum CA-125 levels
- Surgical staging
Board review style answer #1
