
Gallbladder & extrahepatic bile ducts
Cholecystitis
Acute cholecystitis
Authors: Tiffany Sheganoski, D.O., Aaron R. Huber, D.O.
Editorial Board Member: Monika Vyas, M.D.
Deputy Editor-in-Chief: Catherine E. Hagen, M.D.


Last author update: 29 November 2021
Last staff update: 14 September 2023
Copyright: 2003-2024, PathologyOutlines.com, Inc.
PubMed Search: Acute cholecystitis
See also: Acute calculous cholecystitis

Table of Contents
Definition / general | Essential features | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Laboratory | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Clinical images | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Videos | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2 | Board review style question #3 | Board review style answer #3Cite this page: Sheganoski T, Huber AR. Acute cholecystitis. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/gallbladderacutecholecystitis.html. Accessed April 26th, 2024.
Definition / general
- Abrupt destructive process of gallbladder
- Not typical inflammation; neutrophils often absent
- Most often due to stones blocking cystic duct
- ~50% of cases complicated by aerobic bacterial infection
Essential features
- Inflammation of gallbladder induced by choleliths, ischemia or substances
- Gallbladder wall thickening and pericholecystic fluid seen on transabdominal ultrasound
- Complications, such as perforation, seen most often in acalculous cholecystitis
- Cholecystectomy within 72 hours is typically curative
ICD coding
- ICD-9:
- 574.00 - calculus of gallbladder with acute cholecystitis, without mention of obstruction
- 574.01 - calculus of gallbladder with acute cholecystitis with obstruction
- 574.30 - calculus of bile duct with acute cholecystitis, without mention of obstruction
- 574.31 - calculus of bile duct with acute cholecystitis with obstruction
- 574.60 - calculus of gallbladder and bile duct with acute cholecystitis, without mention of obstruction
- 574.61 - calculus of gallbladder and bile duct with acute cholecystitis, with obstruction
- 575.0 - acute cholecystitis
- Reference: Gastroenterol Rep (Oxf) 2017;5:36
Epidemiology
- 10 - 15% of American population
- Native American women have highest rates
- As high as 73% in women > 30 years (Surg Clin North Am 2014;94:455)
Sites
- Gallbladder
Pathophysiology
- Calculous
- Blockage of neck or cystic duct
- Typically by gallstones or biliary sludge
- Continued production of mucus by gallbladder with no outlet
- Increased pressure within gallbladder
- Venous stasis
- Arterial stasis
- Gallbladder ischemia and necrosis (Surg Clin North Am 2014;94:455)
- Blockage of neck or cystic duct
- Acalculous
- Bile stasis and ischemia not provoked by a physical blockade of cystic duct
- Ischemia due to:
- Activated factor XII
- No collateral blood supply; complete reliance on cystic artery (Surg Clin North Am 2014;94:455)
- Ischemia due to:
- Bile stasis and ischemia not provoked by a physical blockade of cystic duct
Etiology
- Calculous
- Due to stones physically blocking cystic duct
- Acalculous
- 2 - 15% of cases (Histopathology 2005;47:485)
- Greater complication risk
- More likely to get gangrenous cholecystitis and subsequent perforation (Infect Dis Clin North Am 2010;24:885)
- AIDS related
- Similar clinical picture
- Due to cytomegalovirus, cryptosporidia or microsporidia
- Cocaine induced (Mills: Sternberg's Diagnostic Surgical Pathology 5th Edition, 2012)
- Seen in young, healthy patients
- Suspect when concurrent vascular thrombosis
Clinical features
- Classic: right upper quadrant pain, nausea, vomiting, anorexia, fever
Diagnosis
- Combination of history, physical, laboratory and imaging findings (Surg Clin North Am 2014;94:455)
Laboratory
- Leukocytosis
- Hyperbilirubinemia and elevated liver function tests
- May indicate choledocholithiasis (Surg Clin North Am 2014;94:455)
Radiology description
- Transabdominal ultrasound
- Gallbladder wall > 4 mm
- Pericholecystic fluid
- Cholescintigraphy
- Hepatic 2,6-dimethyl-iminodiacetic acid (HIDA) injected intravenously
- Gallbladder not visualized (Surg Clin North Am 2014;94:455)
Radiology images
Images hosted on other servers:

Acalculous choleystitis imaging
Prognostic factors
- Complications
- Perforation, pericholecystic abscess, fistula
- Mortality from untreated complications is 20% (BMJ Clin Evid 2008;2008:0411)
Case reports
- 53 and 58 year old women with empyematous cholecystitis and a 75 year old man with perforated cholecystitis, who were treated with robotic cholecystectomy in the emergency setting (Medicine (Baltimore) 2019;98:e16010)
- 59 year old man with COVID-19 pneumonia and ischemic gangrenous cholecystitis (World J Emerg Surg 2020;15:43)
- 66 year old man with COVID-19 pneumonia and acute acalculous cholecystitis (Ann Med Surg (Lond) 2020;58:73)
- 68 year old woman with COVID-19 pneumonia and concurrent acute cholecystitis (BMC Infect Dis 2020;20:437)
Treatment
- Antibiotics
- Cholecystectomy
- Within 72 hours preferred for surgical candidates
- Cholecystostomy drain for critically ill, poor candidates (Infect Dis Clin North Am 2010;24:885)
Clinical images
Images hosted on other servers:

Inflamed gallbladder with exudate
Gross description
- Distention / edema of gallbladder
- Serosa
- Exudate
- Color alteration
- Hemorrhagic
- Wall
- Thickened up to 2 cm
- Edematous
- Hemorrhagic
- Mucosa
- May see ulcers
- Cholelith(s)
- In neck or cystic duct
- Lumen
- May see bile, hemorrhage, fluid mixture of cholesterol and calcium carbonate (J Hepatobiliary Pancreat Surg 2007;14:15)
Gross images
Images hosted on other servers:
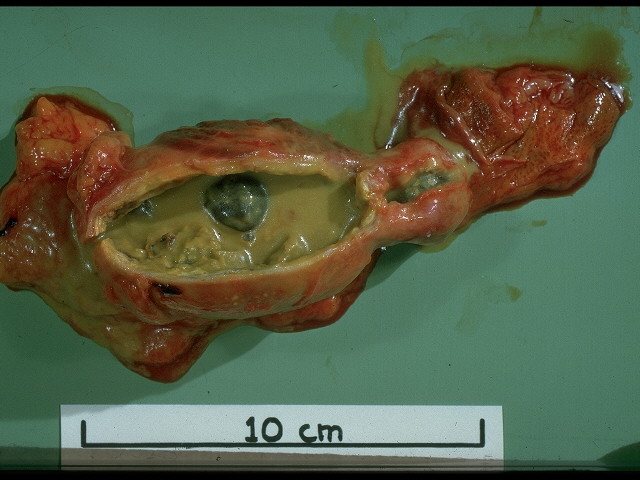
Acute (with
empyema) and
chronic cholecystitis
with gallstone
Microscopic (histologic) description
- May not see acute inflammatory cells unless there is a secondary bacterial infection or choledocholelithiasis
- Erosion of mucosa
- Edema
- Myofibroblasts, lymphocytes, plasma cells, eosinophils and pigment laden macrophages
- Fibrin
- Thrombi in small veins
- Sometimes fibrinoid necrosis (Int J Clin Exp Pathol 2013;6:91)
Microscopic (histologic) images
Contributed by Aaron Huber, D.O.
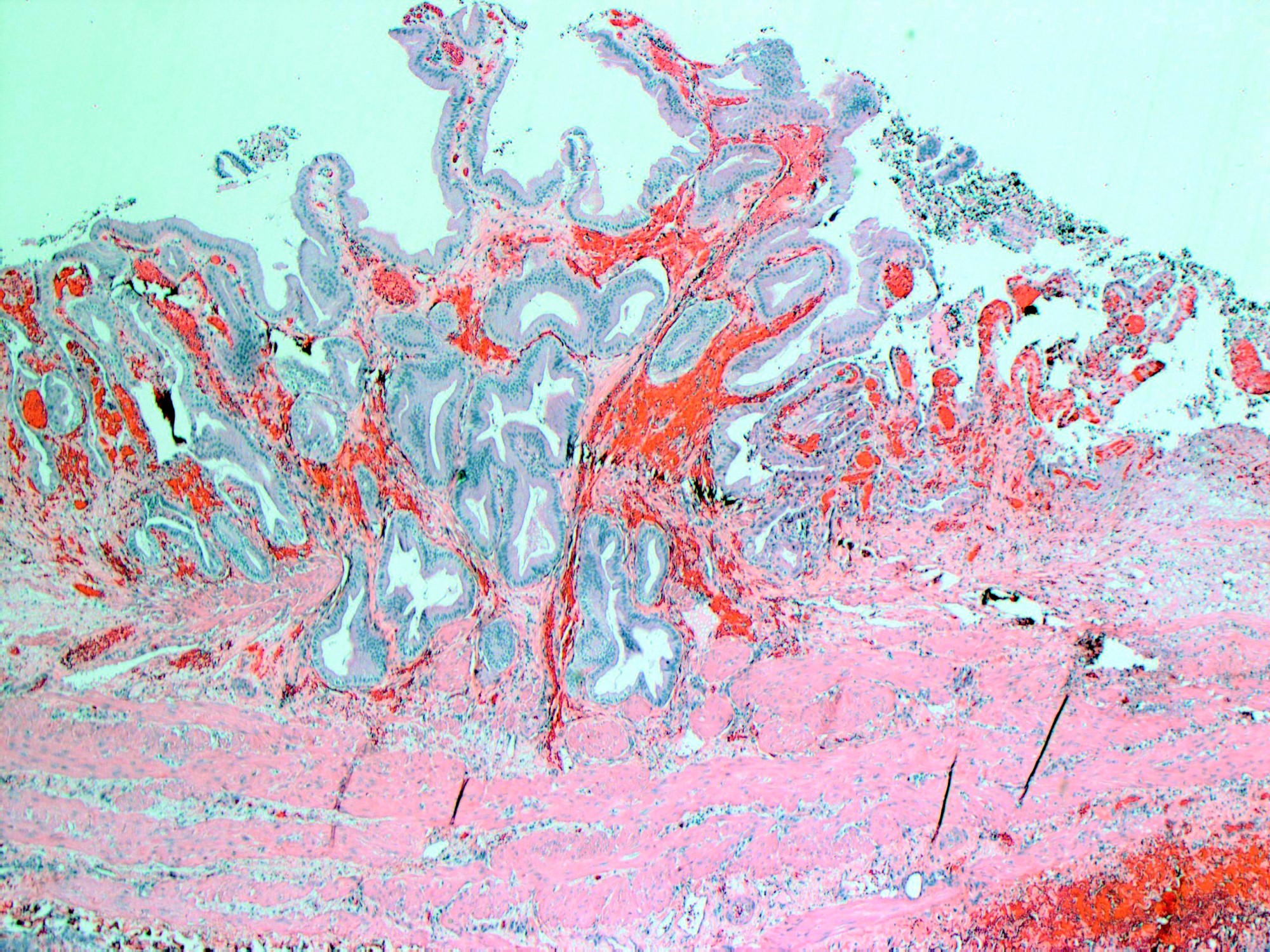
Hemorrhagic mucosa
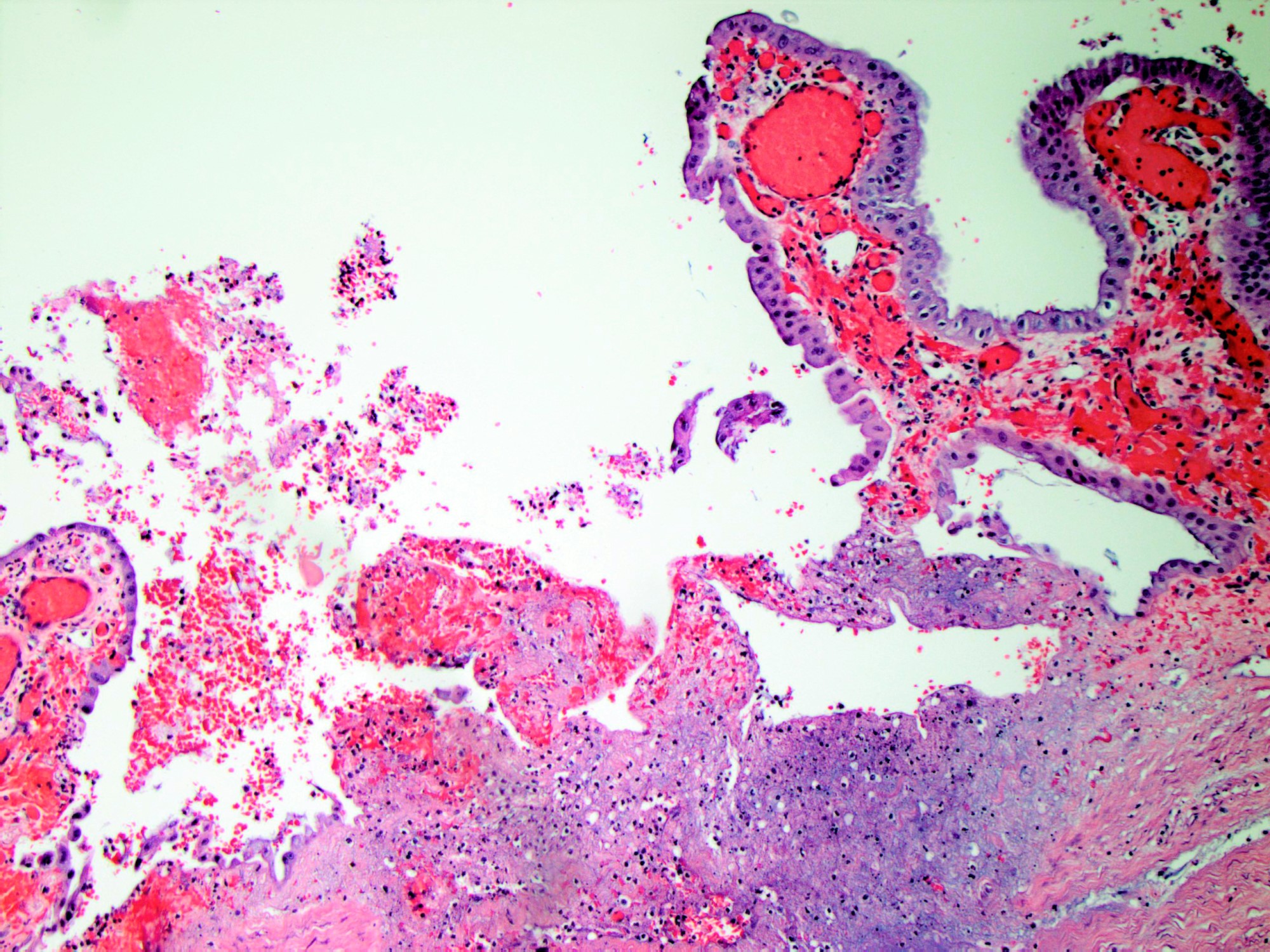
Acute inflammation and erosion
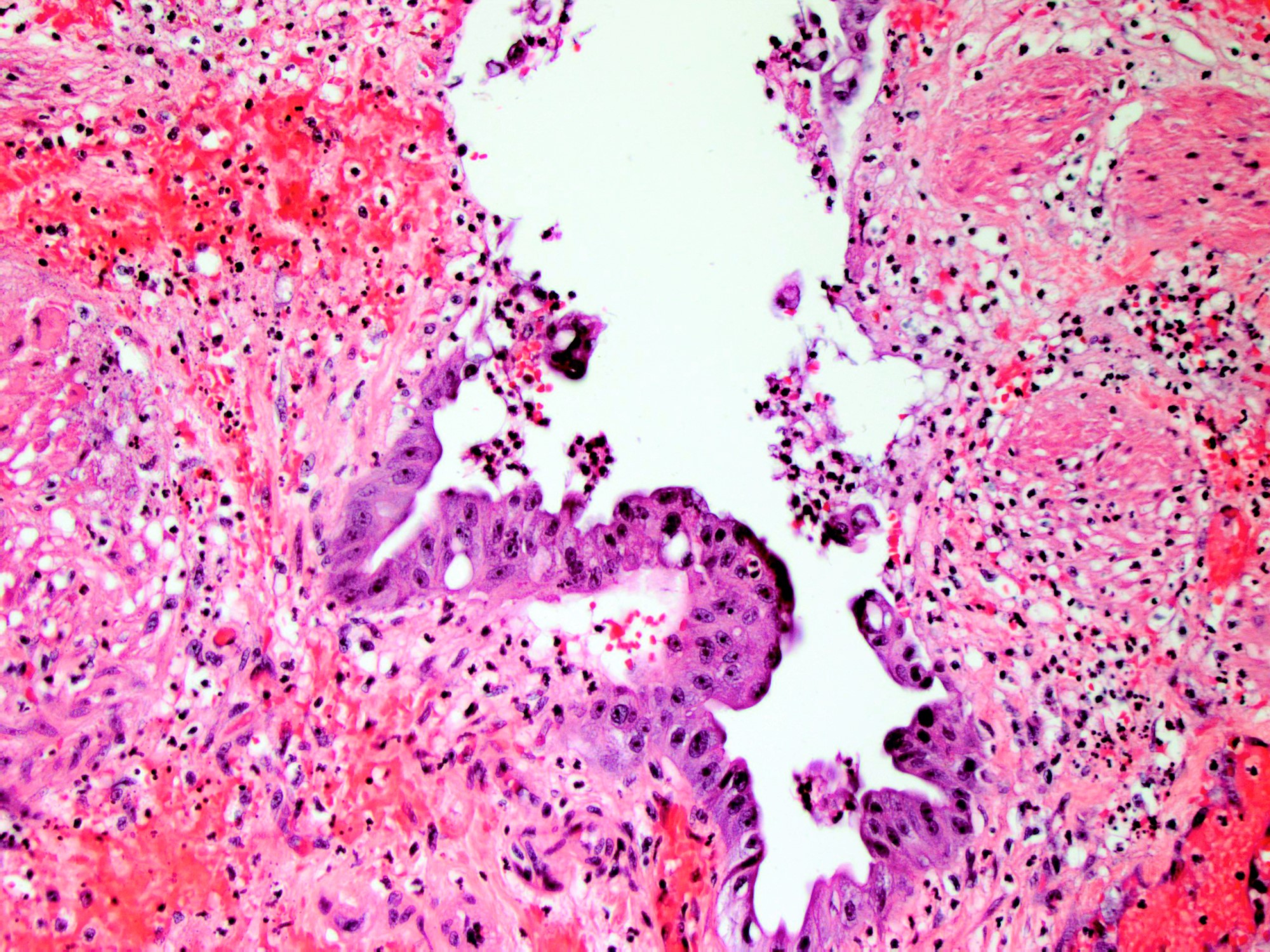
Inflamed and reactive epithelium
Videos
Overview of acute cholecystitis
Imaging findings in cholelithiasis and acute cholecystitis
Sample pathology report
- Gallbladder, cholecystectomy:
- Acute calculous cholecystitis
Differential diagnosis
- Gallbladder cancer:
- Frozen section analysis during cholcystectomy if suspected (Hepatobiliary Pancreat Dis Int 2015;14:300)
Board review style question #1
A patient undergoes removal of the pictured organ. What symptoms or presentation would suggest that the etiology of the condition that leads to removal of this organ is related to cocaine use?
- Amaurosis fugax
- Hematemesis
- Melena
- Vascular thrombosis
Board review style answer #1
D. Cocaine induced cholecystitis is seen in young, otherwise healthy patients and should be suspected when there is vascular thrombosis along with involvement of other parts of the gastrointestinal tract.
Comment Here
Reference: Acute cholecystitis
Comment Here
Reference: Acute cholecystitis
Board review style question #2
What imaging finding would suggest that the pictured organ should be surgically removed in the appropriate clinical context?
- Focal fat stranding
- Gallbladder wall > 4 mm
- Inflamed appendix > 6 mm in diameter
- Round / ovoid collection of barium in the stomach
Board review style answer #2
B. Thickening of the gallbladder wall > 4 mm as well as pericholecystic fluid may be seen on ultrasound imaging in a case of acute cholecystitis.
Comment Here
Reference: Acute cholecystitis
Comment Here
Reference: Acute cholecystitis
Board review style question #3
What factors make the pictured organ susceptible to ischemia necessitating removal, even in the absence of physical blockade of the duct?
- Location in zone 3, furthest from the hepatic artery
- Location within a watershed zone
- No collateral blood supply
- Sensitivity to atherosclerosis of the inferior mesenteric artery
Board review style answer #3
C. Cases of acalculous cholecystitis may occur because the gallbladder is completely reliant on the cystic artery, with no collateral blood supply.
Comment Here
Reference: Acute cholecystitis
Comment Here
Reference: Acute cholecystitis
