
Gallbladder & extrahepatic bile ducts
Gallbladder dysplasia and malignancy
Gallbladder carcinoma
Author: Ashwin S. Akki, M.D, Ph.D.
Deputy Editor-in-Chief: Raul S. Gonzalez, M.D.
Last author update: 21 April 2020
Last staff update: 1 June 2021
Copyright: 2003-2024, PathologyOutlines.com, Inc.
PubMed Search: Gallbladder carcinoma[TI] bile ducts
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Laboratory | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Virtual slides | Positive stains | Negative stains | Molecular / cytogenetics description | Videos | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2 | Board review style question #3 | Board review style answer #3Cite this page: Akki A. Gallbladder carcinoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/gallbladdercarcinoma.html. Accessed April 19th, 2024.
Definition / general
- Carcinoma arising from the gallbladder epithelium (WHO Classification of Tumours Editorial Board: Digestive System Tumours (Medicine), 5th Edition, 2019)
Essential features
- Aggressive cancer, with an overall 5 year survival rate of < 10%
- Cholelithiasis is a major risk factor
- Up to 50% are detected incidentally in routine cholecystectomy specimens due to absence of gross abnormalities; systematic sampling of these specimens is therefore crucial to detect incidental gallbladder adenocarcinomas (Am J Surg Pathol 2019;43:1668)
Terminology
- Carcinoma of gallbladder; adenocarcinoma of gallbladder; malignant epithelial neoplasm of gallbladder
ICD coding
Epidemiology
- Commonly occurs in the sixth and seventh decades
- F:M = 3:1
- Highest incidence in women from Chile (27.3/100 000), India (21.5/100 000), Pakistan (13.8/100 000) and Ecuador (12.9/100 000) (Int J Cancer 2010;127:2446, Histopathology 2009;55:218)
- Incidence 1.1 per 100,000 in the United States (Cancer Epidemiol Biomarkers Prev 2015;24:1319)
- Overall 5 year survival rate of < 10%
Sites
- Primarily affects the fundus (60%), body (30%) or neck (10%) of gallbladder
- Advanced tumors involve the liver and extrahepatic biliary tree
Pathophysiology
- Longstanding cholelithiasis and cholecystitis give rise to metaplastic changes (intestinal or pseudopyloric types) in the gallbladder mucosa (Cancer 1993;72:1878)
- Metaplasia (especially intestinal type) gives rise to epithelial dysplasia and carcinoma in situ (J Hepatobiliary Pancreat Surg 2000;7:556)
- Progression from dysplasia to advanced gallbladder carcinoma takes around 15 years (Gastroenterology 1996;111:232)
Etiology
- Risk factors include:
- Cholelithiasis (major risk factor)
- Chronic cholecystitis, especially hyalinizing cholecystitis
- Obesity
- Infections (esp. Salmonella and Opisthorchis viverrini)
- Porcelain gallbladder
- Primary sclerosing cholangitis
- Pancreaticobiliary maljunction (supra-Oddi union of common bile duct with the main pancreatic duct)
- Occasionally occurs in patients with Lynch syndrome or familial adenomatous polyposis (FAP)
Clinical features
- Asymptomatic in a large majority of patients
- Symptoms when present are vague
- Right upper quadrant pain (most common)
- Weight loss
- Fever
- Disease is usually advanced by the time patient develops symptoms
Diagnosis
- 50% are diagnosed incidentally on routine cholecystectomy specimens
- Finding a thickened gallbladder wall or polypoid lesions in the gallbladder on imaging done for other reasons should prompt surgical resection
Laboratory
- Elevated alkaline phosphatase in advanced cancers (HPB (Oxford) 2008;10:446)
- CEA only has 50% sensitivity (Int J Cancer 1990;45:821)
Radiology description
- Imaging findings are variable from subtle (in early disease) to obvious (in late disease)
- Thickening of the gallbladder wall
- Raised / polypoid lesion in the gallbladder wall / lumen
- Mass occupying or replacing the gallbladder lumen
- Gallbladder mass invading the liver (in advanced disease)
- Ultrasound is the primary imaging modality for screening purposes in suspected cases
- Abnormal findings on ultrasound are further investigated by CT and MRI that provide detailed information, including staging parameters
Radiology images
Images hosted on other servers:

Heterogeneous mass
Prognostic factors
- Noninvasive papillary carcinomas, regardless of size and differentiation, do not metastasize
- Invasive papillary carcinomas have the most favorable prognosis (Arch Pathol Lab Med 2005;129:905)
- Prognosis of adenocarcinoma, NOS depends on tumor stage:
- Superficially invasive cancers limited to the lamina propria (pT1a) have excellent prognosis as they are completely cured by cholecystectomy (Ann Surg 2017;266:625)
- Advanced cancers (i.e. muscle invasive and beyond; pT1b - pT4) have a higher chance of recurrence and have poorer outcomes (J Gastrointest Surg 2007;11:631, Ann Surg 2011;254:320)
- High histologic grade (poor differentiation) and vascular invasion have adverse outcomes (Cancer 1992;70:1493)
- Rokitansky-Aschoff sinus involvement by carcinoma and cystic duct margin status are suspected predictors of progression (Am J Clin Pathol 2014;141:675)
Case reports
- 22 year old man with primary signet ring cell carcinoma of gallbladder in the absence of choleliths (Int J Surg Pathol 2010;18:358)
- 56 year old woman with clear cell carcinoma of the gallbladder (Int J Surg Case Rep 2017;32:36)
- 59 year old woman with hepatoid carcinoma of the gallbladder (World J Surg Oncol 2011;9:103)
- 62 year old man with carcinosarcoma of the gallbladder with chondroid differentiation (Int J Clin Exp Pathol 2015;8:7464)
Treatment
- Cholecystectomy with a negative cystic duct margin is curative in pT1a tumors (Ann Surg 2017;266:625)
- Hilar / portal lymphadenectomy, plus resection of hepatic bed and the common bile duct to achieve negative margins, is necessary for tumors that extend into a muscle or beyond (pT1b - pT3) (HPB (Oxford) 2015;17:681)
- Chemotherapy or radiation for metastatic tumors
Gross description
- Incidental gallbladder cancer in routine cholecystectomy specimens can be grossly subtle, with areas of mucosal granularity / irregularity, minimally raised / polypoid mucosal lesions or focally thickened fundus / body (Am J Surg Pathol 2019;43:1668)
- Frank tumors may have one or more of the following features:
- Thickened and indurated gallbladder wall
- Exophytic or polypoid friable mucosal lesions (especially those arising from intracholecystic papillary neoplasm)
- Firm, gritty, tan-white to yellow-gray cut surface
Gross images
Contributed by Ashwin S. Akki, M.D., Ph.D.
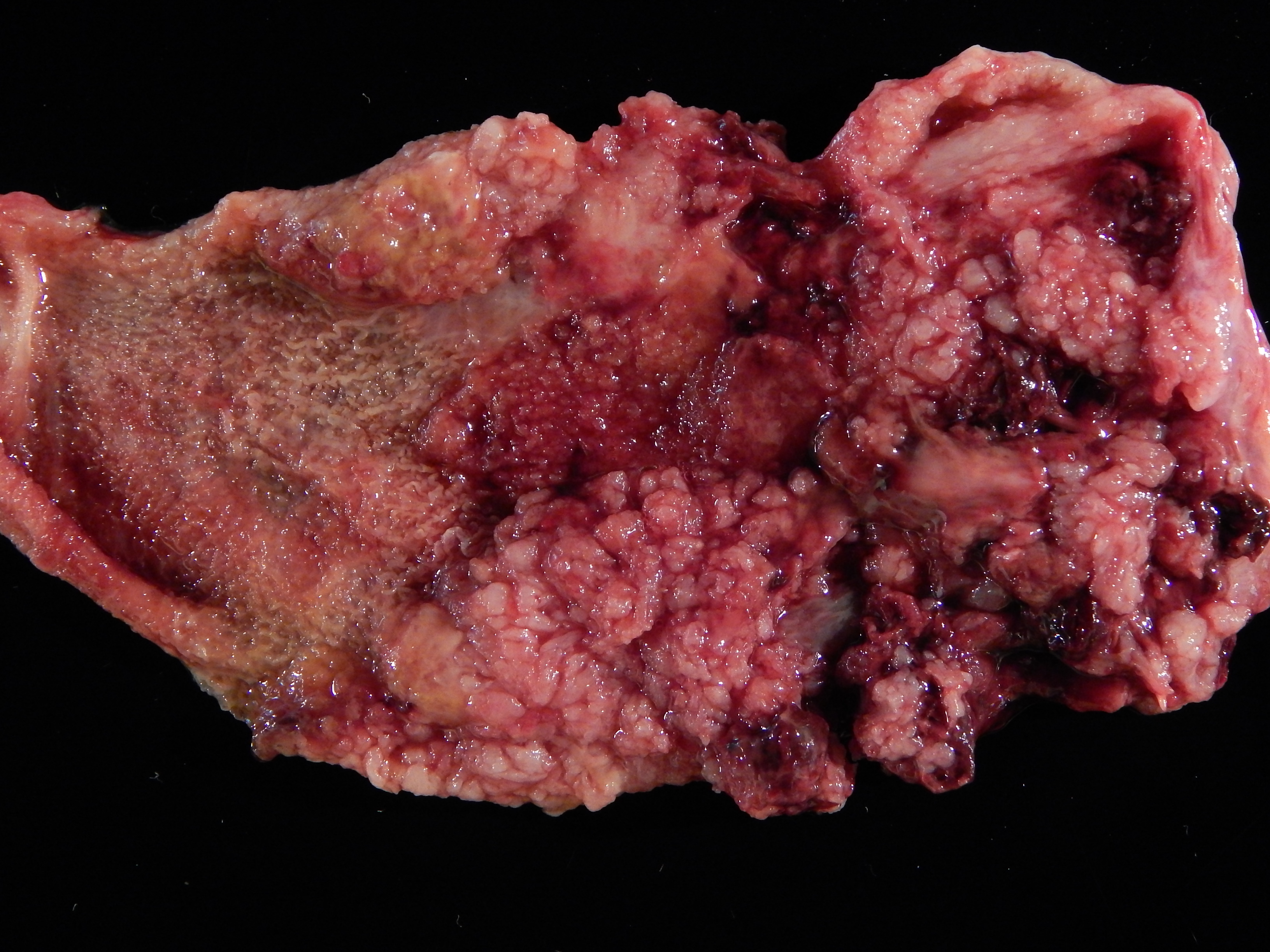
Papillary proliferation
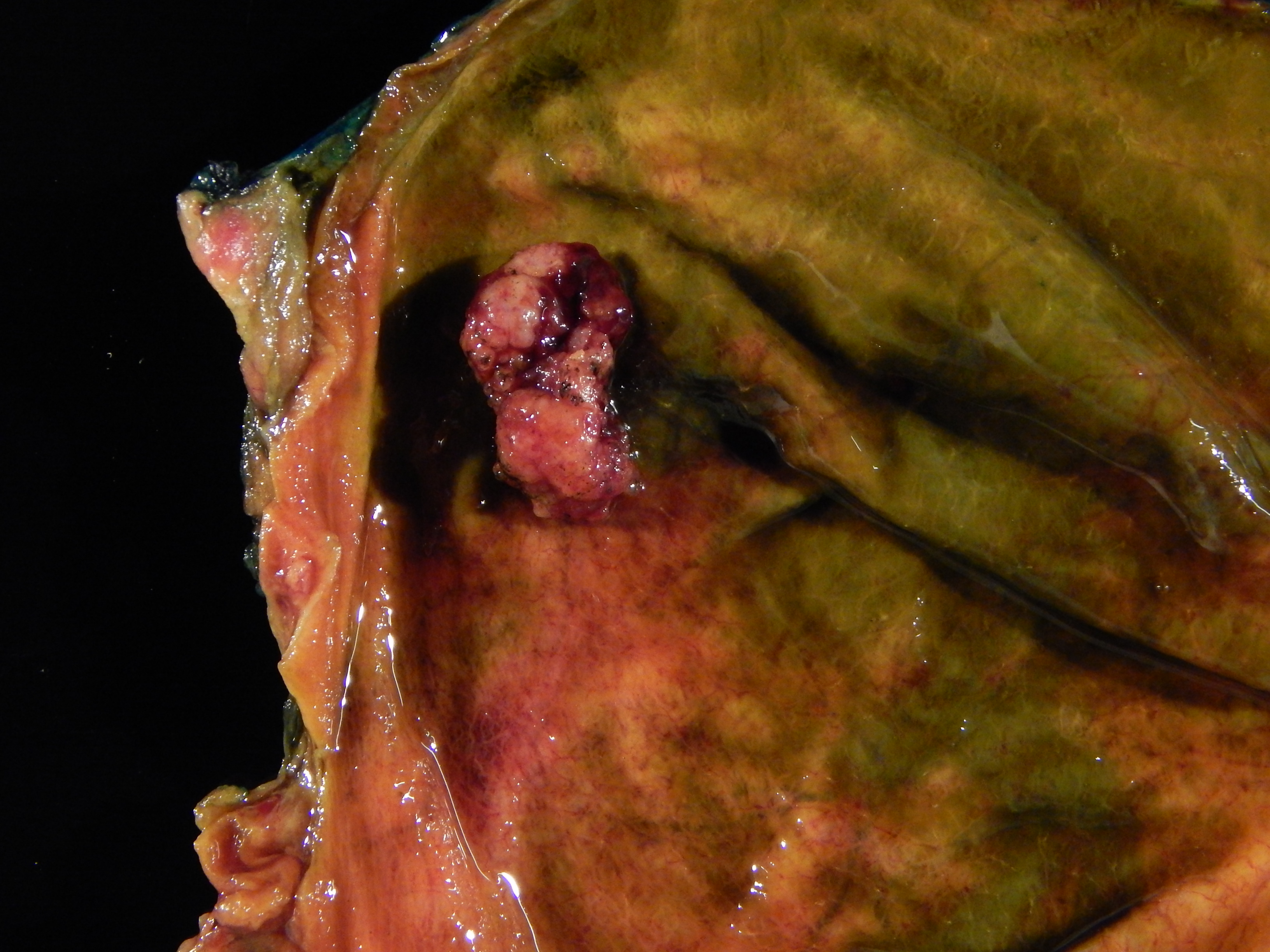
Carcinoma in a polyp
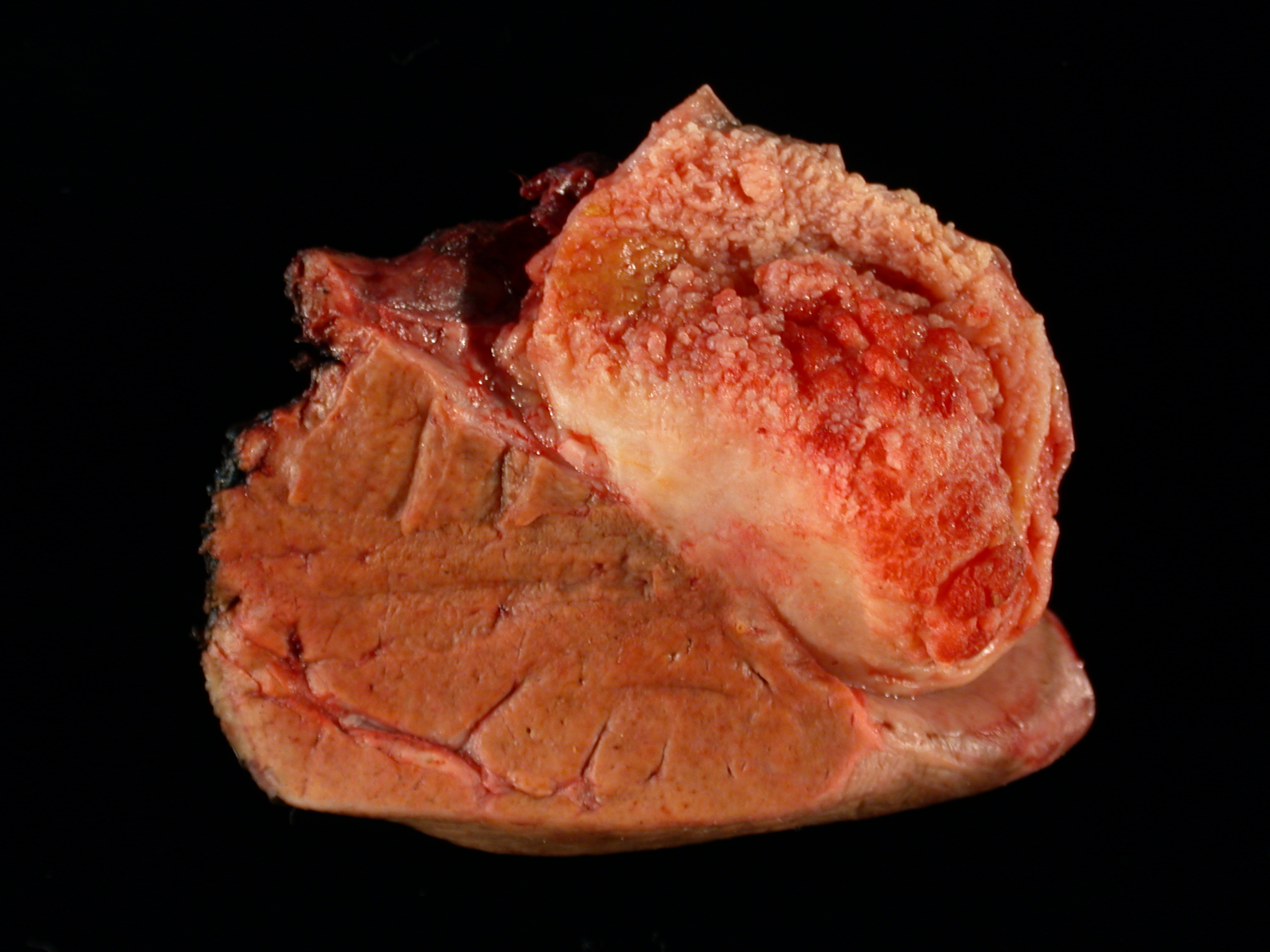
Gallbladder cancer invading liver

Diffusely thickened gallbladder wall
Microscopic (histologic) description
- Histologic variants recognized by WHO include:
- Biliary type adenocarcinoma (~75%):
- Similar to pancreatic ductal adenocarcinoma
- Includes adenocarcinoma, NOS (most common), papillary, micropapillary
- Composed of tubules (lined by cuboidal to columnar cells) embedded in a desmoplastic stroma
- Moderately differentiated is more common but has a wide histologic spectrum, from deceptively bland to poorly differentiated
- Intestinal type adenocarcinoma:
- Tubules lined by columnar cells with elongated hyperchromatic nuclei, very similar to colonic adenocarcinomas
- Mucinous carcinoma:
- Comprised of > 50% extracellular mucin
- Clear cell carcinoma:
- Sheets of clear cells in an alveolar arrangement separated by blood vessels, similar in appearance to metastatic clear cell renal carcinoma
- Signet ring cell carcinoma:
- Signet ring cells are the predominant or exclusive component
- Hepatoid carcinoma:
- > 50% with abundant eosinophilic cytoplasm, enlarged nuclei and prominent nucleoli arranged in a trabecular pattern
- Sarcomatoid carcinoma (carcinosarcoma):
- Predominant spindle cell morphology with or without heterologous differentiation (e.g. skeletal muscle, bone and cartilage)
- Biliary type adenocarcinoma (~75%):
- Differentiation
- Well differentiated:
- Well formed glands lined by columnar cells with minimal cytologic abnormality
- Glands in perimuscular connective tissue, nuclear irregularities and mitoses may be the only clues
- Desmoplasia may be subtle
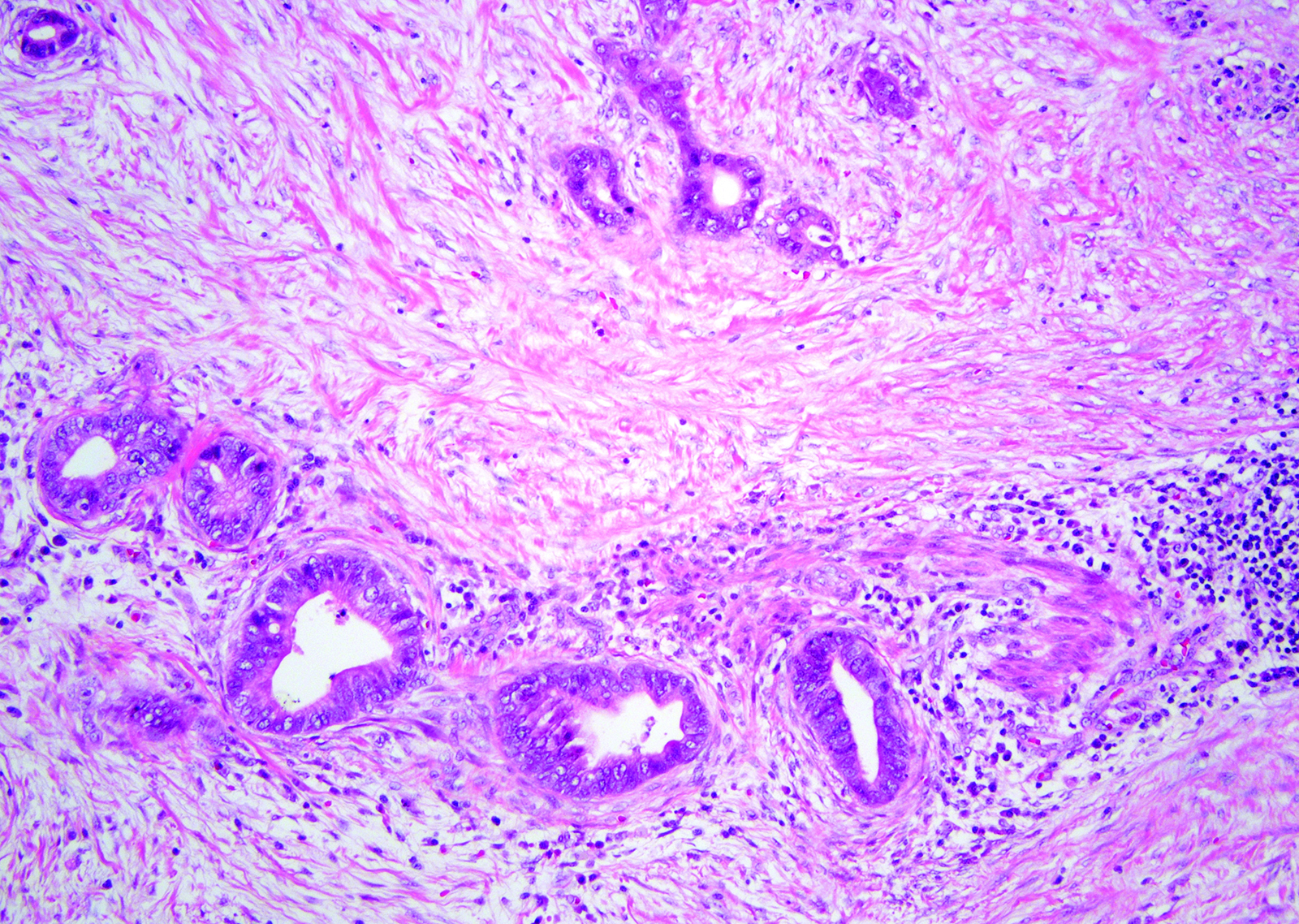
- Moderately differentiated:
- Irregular / angulated glands lined by polygonal tumor cells with enlarged nuclei showing vesicular chromatin, prominent nucleoli and increased mitoses
- Desmoplasia is usually prominent
- Poorly differentiated:
- Incomplete or poorly formed tubules / glands, single cells or sheets of pleomorphic tumor cells with bizarre nuclei
- Well differentiated:
Microscopic (histologic) images
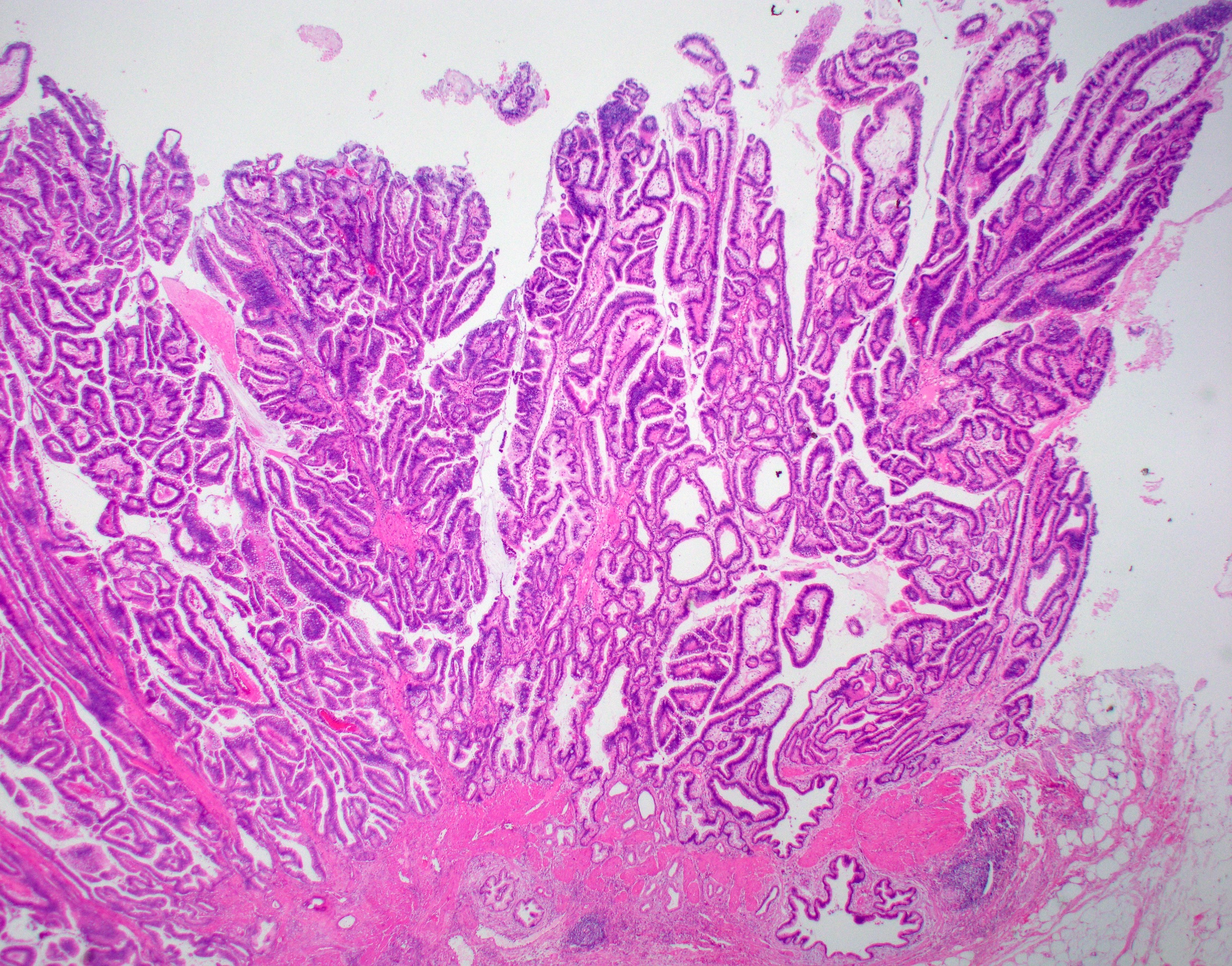
Contributed by Ashwin S. Akki, M.D., Ph.D.
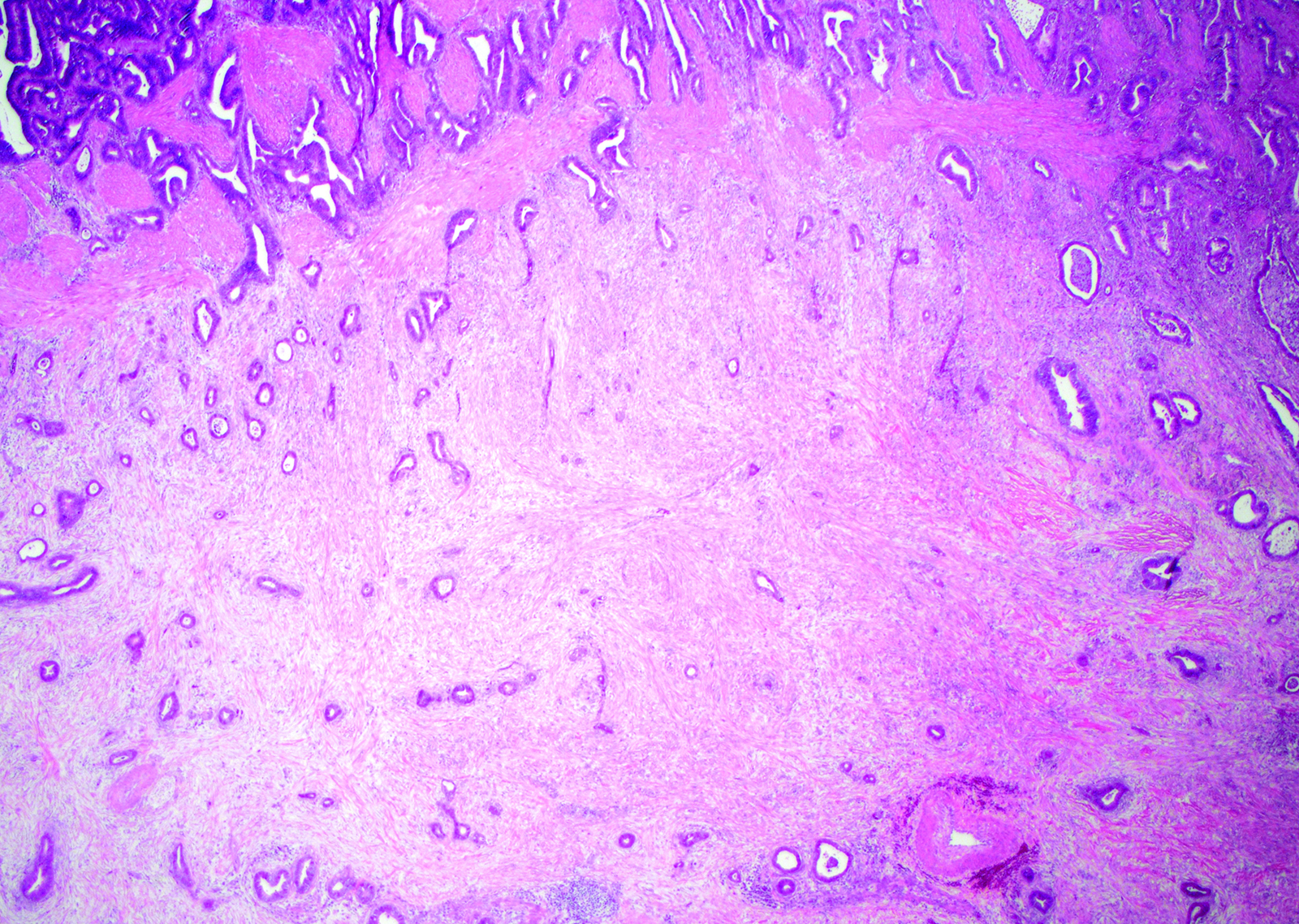
Desmoplasia
Well formed glands

Intermediate gland formation
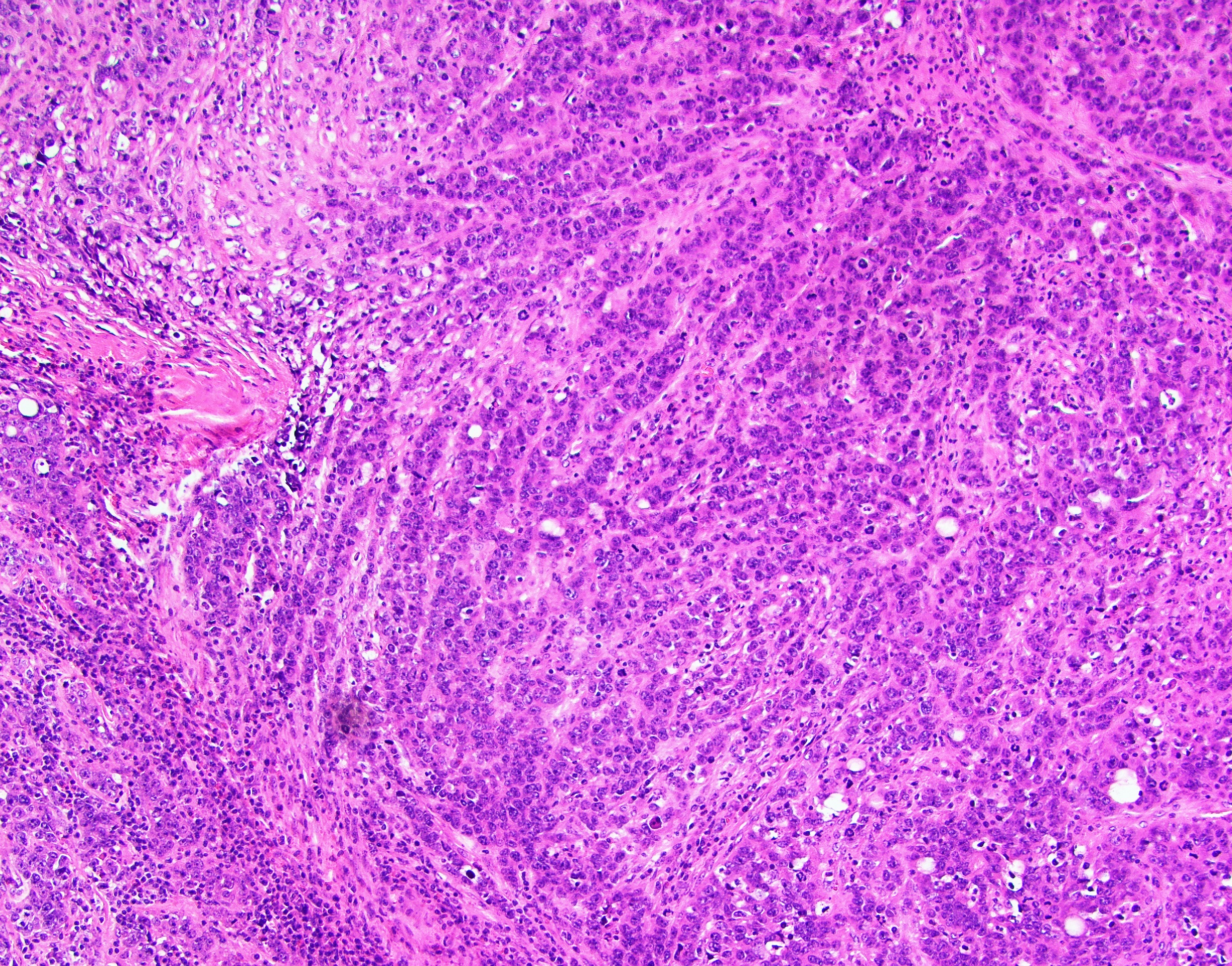
Poor gland formation
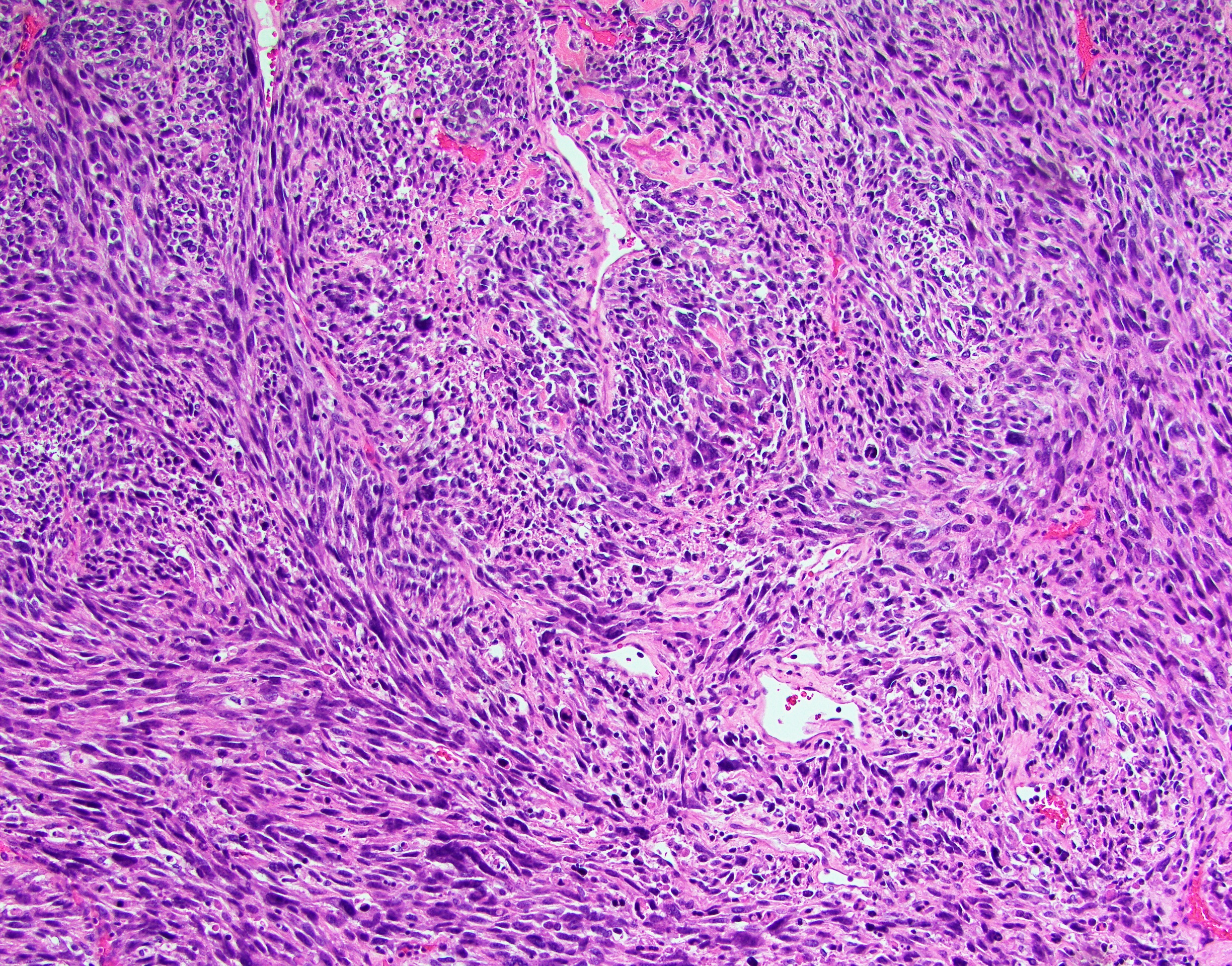
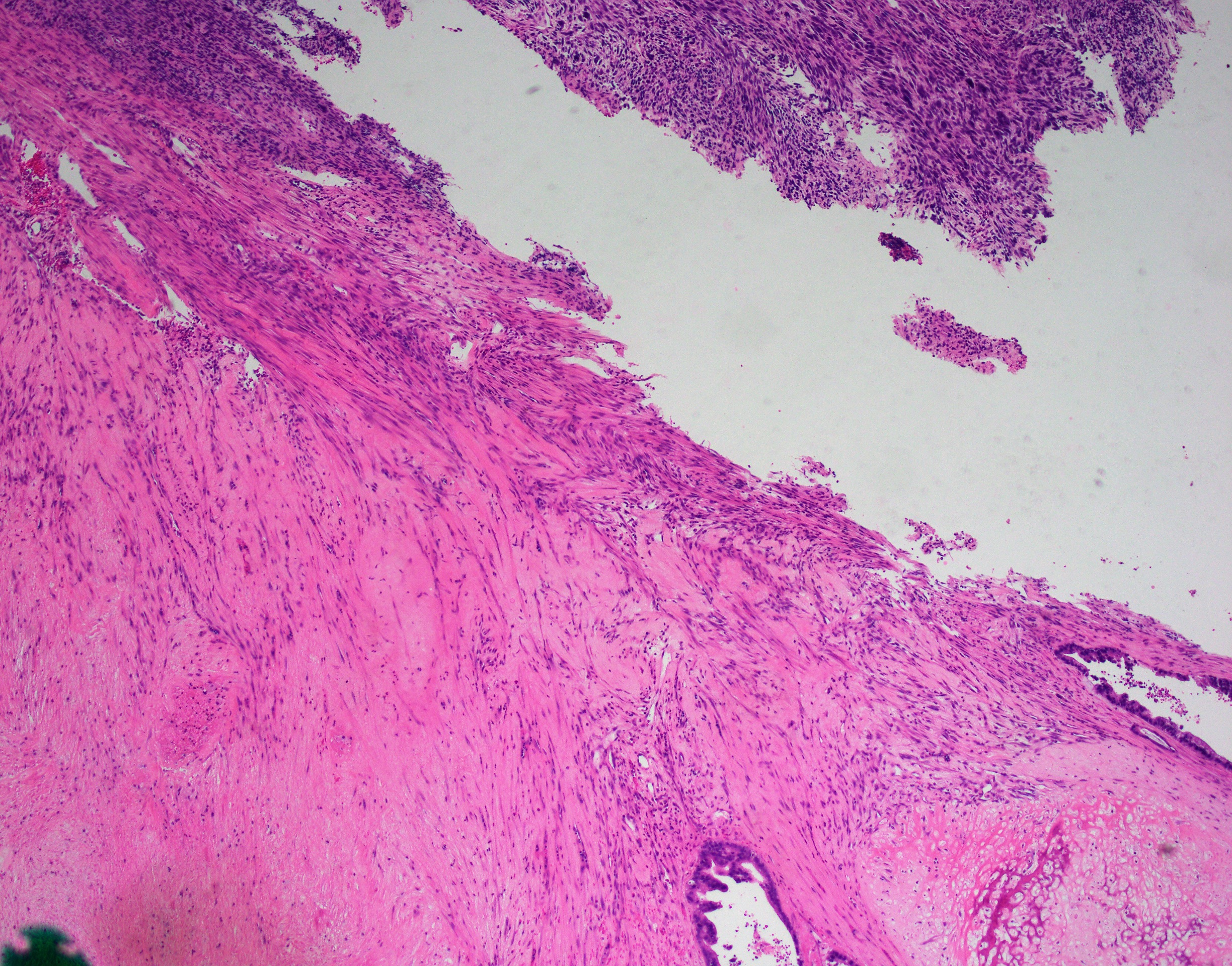
Sarcomatoid differentiation
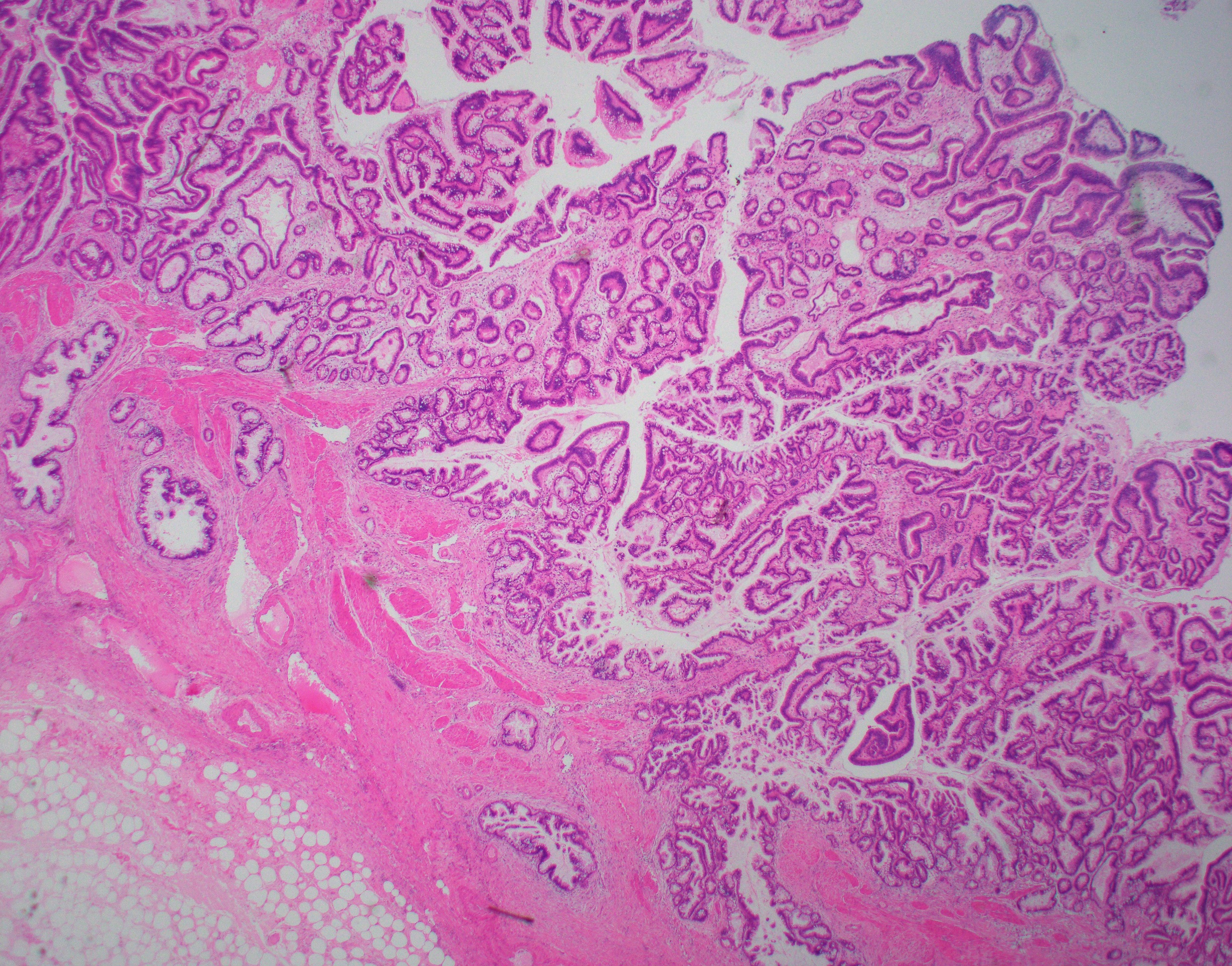
Papillary proliferation with invasion
Virtual slides
Images hosted on other servers:
_histopathology.jpg)
Invasive adenocarcinoma
Positive stains
- CK7 (strong and diffuse) (Arch Pathol Lab Med 2000;124:1196), p53 (majority), CEA and CA19-9 (70 - 90%), IMP3 (80%) (Arch Pathol Lab Med 2017;141:1155), Maspin (60 - 100%), S100P and MUC1 (75%), HER2 (> 60%), CK20 and CDX2 (focal)
- Hep par1 and alpha-fetoprotein (AFP) (Positive in hepatoid variant)
Negative stains
- p16 (not expressed in a majority of cases akin to normal gallbladder) (Hepatogastroenterology 2010;57:18)
- PAX8, CD10 and CAIX
Molecular / cytogenetics description
- Common genetic alterations include TP53 (seen in > 50% of cases), CDKN2A (20%), ARID1A (13%), PIK3CA (10%) and CTNNB1 (10%) (WHO Classification of Tumours Editorial Board: Digestive System Tumours (Medicine), 5th Edition, 2019)
- Amplifications of ERBB2 (HER2) have been reported in 16% of cases and microsatellite instability (MSI) in 10% of cancers, both of which have therapeutic implications (Cancer 2016;122:3838, Histopathology 2009;55:218)
- A higher KRAS mutation rate is noted in lesions related to pancreatobiliary maljunction (Hum Pathol 1999;30:21)
Videos
Extended cholecystectomy
Sample pathology report
- Gallbladder; cholecystectomy:
- Invasive adenocarcinoma, moderately differentiated, biliary type (2.7 cm in largest dimension), arising in a background of extensive high grade biliary intraepithelial neoplasia (BilIN).
- Adenocarcinoma invades perimuscular connective tissue on the peritoneal side, without involvement of the serosa (visceral peritoneum).
- Cystic duct margin is free from biliary intraepithelial neoplasia (BilIN) or carcinoma.
- One lymph node, negative for carcinoma (0/1).
- Lymphovascular invasion is not identified.
- pT2a, N0, M-not applicable (AJCC 8th edition). Please see synoptic report
- Background gallbladder with chronic cholecystitis.
- Cholelithiasis.
Differential diagnosis
- Pancreatic ductal adenocarcinoma:
- Cholangiocarcinoma (both intrahepatic and extrahepatic):
- Epicenter in the bile ducts; CK19+
- Colonic adenocarcinoma:
- Epicenter in the colon, intestinal phenotype, CK20 strong and diffuse
Board review style question #1
- A 58 year old woman presents with right upper quadrant pain. Imaging reveals a polypoid lesion in the gallbladder. Patient undergoes cholecystectomy. Pathology shows the finding seen in the image above. Which of the following is true about this entity?
- Has aggressive dissemination potential
- Has a more favorable prognosis than conventional nonpapillary gallbladder adenocarcinomas
- Immunoreactive to hepatocellular markers
- Is not detected early on imaging
Board review style answer #1
B. Invasive papillary carcinomas have the most favorable prognosis than conventional nonpapillary gallbladder adenocarcinomas because they have an exophytic growth pattern, exhibit delayed invasion into the gallbladder wall, and are detected early due to obstructive symptoms (Arch Pathol Lab Med 2005;129:905).
Comment Here
Reference: Gallbladder carcinoma
Comment Here
Reference: Gallbladder carcinoma
Board review style question #2
- What is the amount of extracellular mucin needed to diagnose a mucinous adenocarcinoma of the gallbladder?
- > 25%
- > 30%
- > 50%
- > 90%
Board review style answer #2
Board review style question #3
- What are actionable molecular targets in the treatment of advanced GBCs?
- HER2 and MSI
- KRAS and ARID1A
- TP53 and CDKN2A
- PIK3CA and CTNNB1 (beta-catenin)
- p16
Board review style answer #3
