

Heart & vascular pathology
Benign tumors / other nonneoplastic
Cardiac fibroma
Editorial Board Members: David B. Chapel, M.D., Jefree J. Schulte, M.D.


Last author update: 5 January 2023
Last staff update: 5 January 2023
Copyright: 2007-2024, PathologyOutlines.com, Inc.
PubMed Search: Cardiac fibroma
Table of Contents
Definition / general | Essential features | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Laboratory | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Frozen section description | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Negative stains | Electron microscopy description | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Toba S, Carreon CK. Cardiac fibroma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/hearttumorfibroma.html. Accessed April 19th, 2024.
Definition / general
- Cardiac fibroma is rare but is also the second most common cardiac tumor in children and may occur in association with basal cell nevus syndrome (BCNS), also known as Gorlin syndrome (Eur J Cardiothorac Surg 1997;12:730, JACC Clin Electrophysiol 2019;5:563, J Thorac Cardiovasc Surg 1994;108:862, Am J Cardiol 2022;182:95)
- Usually arises within the ventricle or ventricular septum and can cause heart failure due to obstruction of blood flow or sudden death from ventricular arrhythmia (JACC Clin Electrophysiol 2019;5:563)
Essential features
- Second most common primary cardiac tumor in children (34%) but also occurs in adolescents and adults (~40%) (J Thorac Cardiovasc Surg 1994;108:862)
- Solid, unencapsulated tumor arising predominantly from the ventricles
- Microscopically consists of bland fibroblasts, varying amounts of collagen and immature mesenchymal cells with little or no atypia and interdigitating / entrapped myocardium (particularly toward the tumor - normal myocardium interface) (JACC Clin Electrophysiol 2019;5:563)
- Known association with BCNS (Gorlin syndrome)
- Complete surgical resection may cure ventricular arrhythmias but incomplete removal may result in persistence of arrhythmias (JACC Clin Electrophysiol 2019;5:563)
ICD coding
Epidemiology
- Second most common primary cardiac tumor in children (34%) (J Am Coll Cardiol 2011;58:1903)
- Majority of patients are < 10 years old but a substantial proportion (~40%) are older
- Age range: newborn to 62 years old (J Am Coll Cardiol 2011;58:1903, Cardiovasc Pathol 2022;56:107381, Eur J Med Res 2012;17:5)
- No sex or race predilection reported (J Am Coll Cardiol 2011;58:1903, Cardiovasc Pathol 2022;56:107381)
Sites
- Predominantly affects the ventricles (JACC Clin Electrophysiol 2019;5:563):
- Left ventricle: up to 90%
- Right ventricle: 7%
- Interventricular septum: 3%
- Could also involve the right atrium, left and right ventricular outflow tracts and main pulmonary artery: 1 - 7% (Cardiovasc Pathol 2022;56:107381)
- Size range: 0.5 - 17 cm (Cardiovasc Pathol 2022;56:107381, JACC Clin Electrophysiol 2019;5:563)
Pathophysiology
- Multinodular architecture of cardiac fibromas suggests a multifocal origin of the tumor arising from proliferation of scattered resident stromal fibroblasts / myofibroblasts interspersed between cardiomyocytes from multiple foci, with progressive nodular growth and subsequent formation of a larger and more compact solid tumor mass (JACC Clin Electrophysiol 2019;5:563)
- Prominent multilobulation observed in some of these tumors is also consistent with this hypothesis
Etiology
- Poorly understood; often congenital (Eur J Med Res 2012;17:5)
- Isolated deletions and translocations involving chromosome 9 suggests potential role of a critical region in chromosome 9 regardless of syndromic association (JACC Clin Electrophysiol 2019;5:563)
- PTCH1 gene, which is involved in Gorlin syndrome, has been localized to chromosome 9q22.3 (Lancet 1992;339:581, Cell 1996;87:553)
Clinical features
- Children present with arrhythmia (32%), murmur (20%) and abnormal chest Xray (20%) (J Am Coll Cardiol 2011;58:1903)
- Heart failure, arrhythmias, sudden death and chest pain (J Thorac Cardiovasc Surg 1994;108:862)
- Ventricular tachycardia occurs in 64% of children with fibroma (J Am Coll Cardiol 2011;58:1903, JACC Clin Electrophysiol 2019;5:563)
- Possibly asymptomatic
Diagnosis
- Patient work up often follows clinical presentation
- Echocardiography (echogenic or complex echogenicity) (J Thorac Cardiovasc Surg 1994;108:862)
- MRI (see Radiology description)
- ECG may reveal ventricular tachycardia (J Am Coll Cardiol 2011;58:1903)
Laboratory
- No laboratory findings specific to cardiac fibromas have been reported
Radiology description
- Cardiomegaly, calcifications on chest Xray (J Thorac Cardiovasc Surg 1994;108:862)
- Homogenous or heterogenous enhancement on CT (J Thorac Cardiovasc Surg 1994;108:862)
- MRI (J Am Coll Cardiol 2011;58:1044):
- Intramyocardial location involving the ventricular septum or free wall
- Well defined borders with a thin rim of myocardium
- Strong hyperenhancement on myocardial delayed enhancement (MDE) imaging, with or without hypoenhancing core
- Hypointense on first pass perfusion (FPP) or magnetic resonance angiogram
- Heterogeneous appearance on T1 and T2 weighted turbo spin echo (TSE) sequences with variable areas of slightly hypointense or hyperintense areas
Radiology images
Contributed by Stephen P. Sanders, M.D.
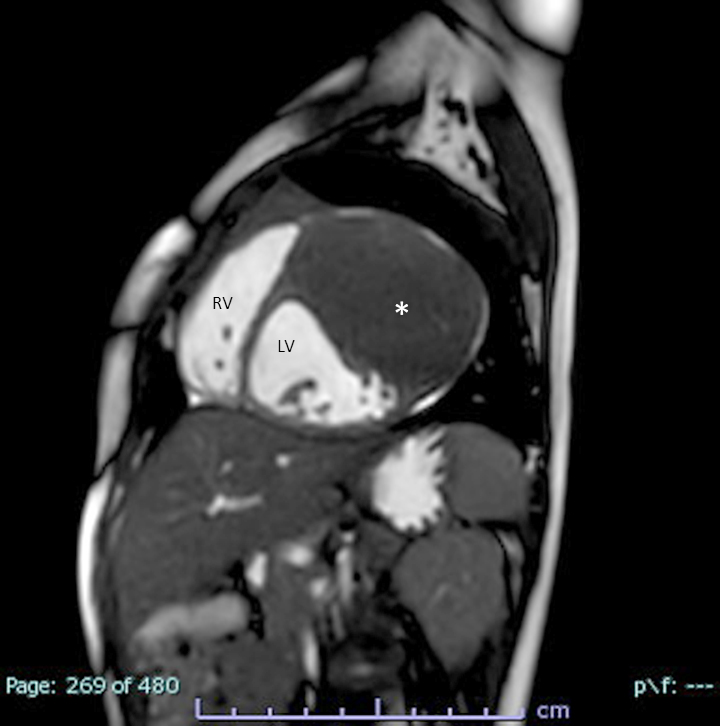
MRI (cine SSFP)
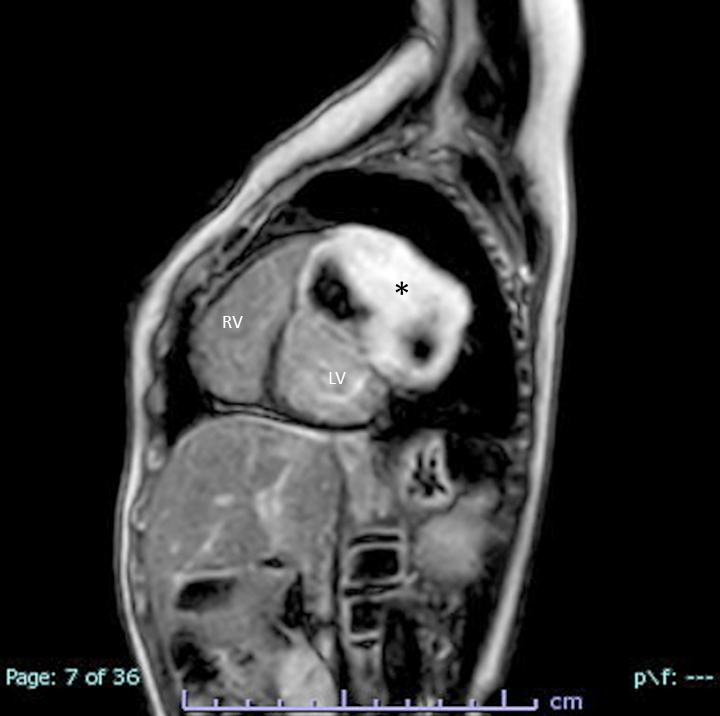
MRI (LGE technique)
Prognostic factors
- Unfavorable prognostic factors:
- Younger age at diagnosis: worse survival; higher incidence of fatal arrhythmias in children < 3 years old, suggesting a period of vulnerability with increased sudden death events in this age group (Eur J Med Res 2012;17:5, JACC Clin Electrophysiol 2019;5:563)
- Involvement of interventricular septum: worse survival (Eur J Med Res 2012;17:5)
- Larger tumor volume index: postoperative regional wall motion abnormality (Circ Cardiovasc Imaging 2021;14:e011748)
- Diffuse myocyte interdigitation: sustained arrhythmia (JACC Clin Electrophysiol 2019;5:563)
- Postoperative mitral regurgitation (Circ Cardiovasc Imaging 2021;14:e011748)
Case reports
- 3 month old girl with a fibroma in the right ventricle (Cardiol Young 2020;30:129)
- 5 month old girl with a fibroma in the right ventricle (J Cardiothorac Surg 2017;12:49)
- 14 year old man with a fibroma in the left ventricle (Innovations (Phila) 2020;15:283)
- 40 year old man with a fibroma in the right atrium (Ann Card Anaesth 2018;21:65)
- 46 year old woman with a fibroma in the left ventricle (Eur Heart J Case Rep 2020;4:1)
Treatment
- Surgical resection / excision has been shown to cure arrhythmias (J Am Coll Cardiol 2011;58:1903, JACC Clin Electrophysiol 2019;5:563)
- Heart transplants are sometimes considered and performed, particularly for large tumors that are not amenable to surgical removal (J Thorac Cardiovasc Surg 1993;106:1208, J Heart Lung Transplant 1995;14:382)
Gross description
- Tumors are often large and multinodular and may include attenuated epicardial tissue on the surface
- May be singular or multilobulated (Cardiovasc Pathol 2022;56:107381)
- Depending on the surgical approach, the tumor may be received intact or in multiple pieces
- Cut surfaces are grayish white to light beige, whorled to trabeculated, with rubbery to firm consistency (J Thorac Cardiovasc Surg 1994;108:862, Eur J Med Res 2012;17:5, Circ Cardiovasc Imaging 2021;14:e011748, JACC Clin Electrophysiol 2019;5:563)
- Tumor is almost always unencapsulated and adherent to surrounding myocardium (JACC Clin Electrophysiol 2019;5:563)
- Entrapped or interdigitating strands of myocardium are sometimes visible on closer examination (JACC Clin Electrophysiol 2019;5:563)
Gross images
Contributed by Chrystalle Katte Carreon, M.D. and AFIP
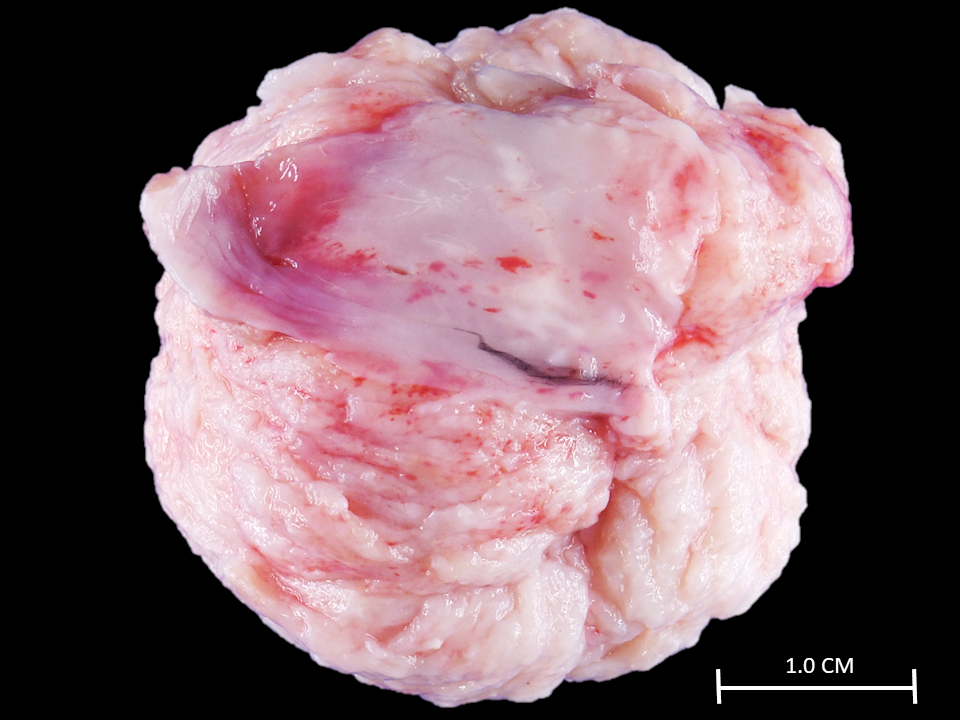
Macroscopic features
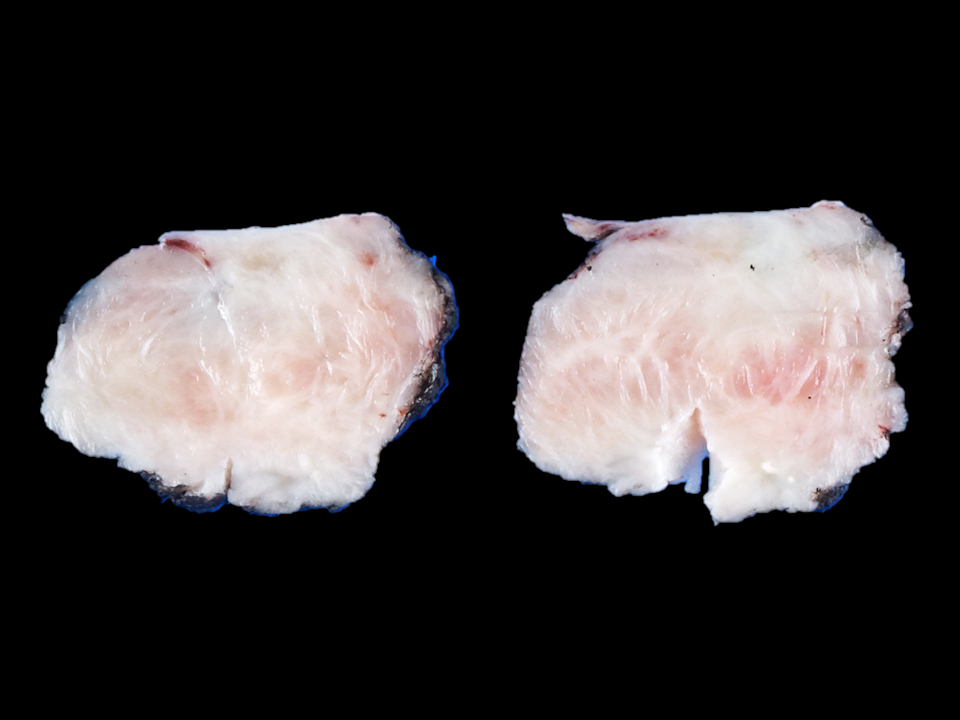
Cut surface features

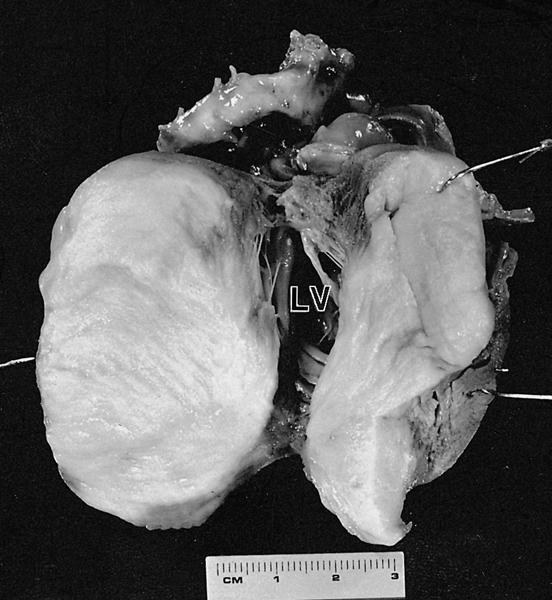
Large septal mass

Homogeneous mass
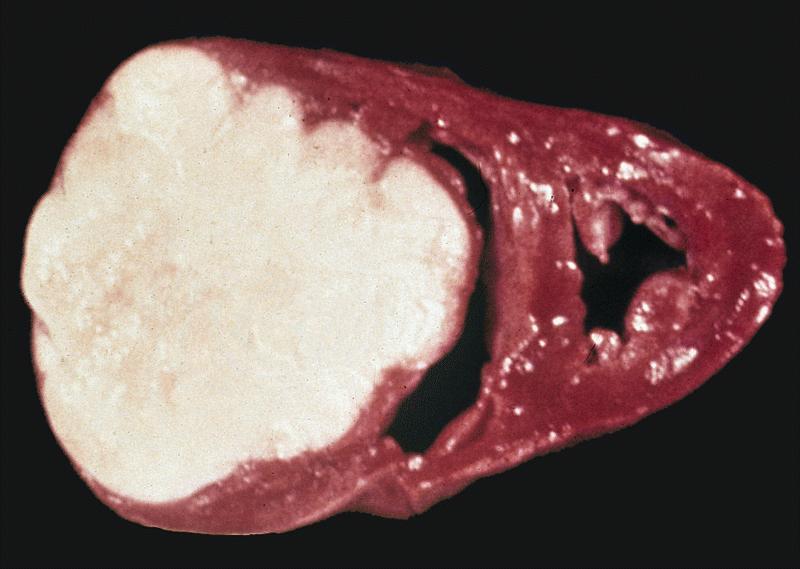
Large circumscribed mass
Frozen section description
- Intraoperative frozen sections are usually not performed on cardiac fibromas unless there are concerns for malignancy on imaging
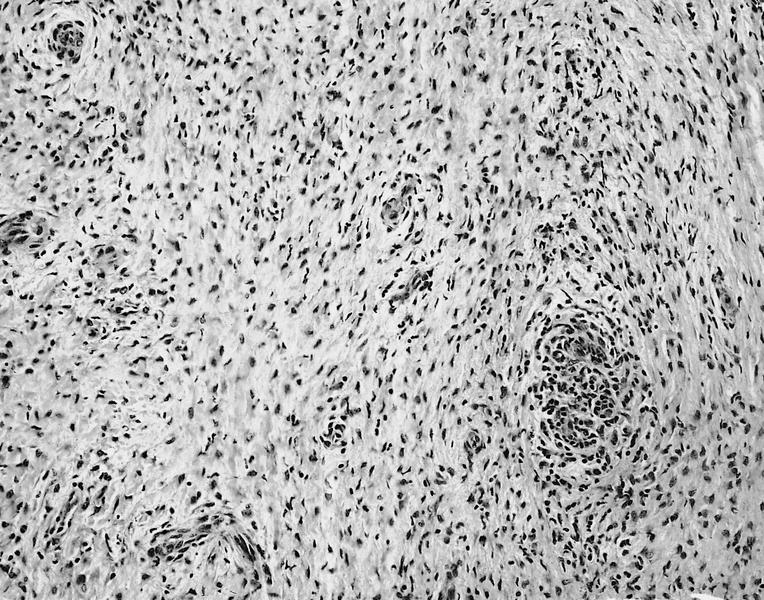
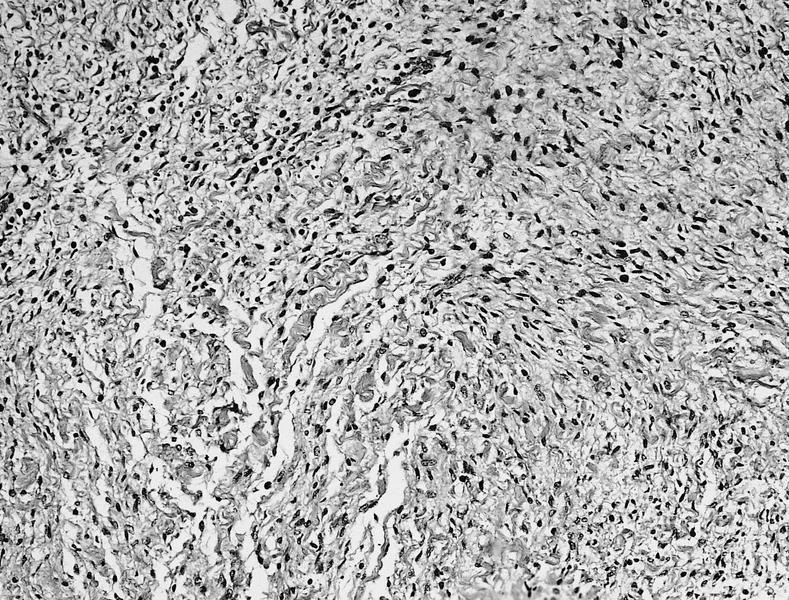
Microscopic (histologic) description
- Bland spindle cell / fibroblastic proliferation with abundant collagen, sometimes immature mesenchymal cells, with little or no atypia (Eur J Med Res 2012;17:5)
- Cellularity tends to decrease while collagen increases with age (JACC Clin Electrophysiol 2019;5:563)
- Occasional findings within the tumor include calcification, aggregates of lymphocytes and histiocytes, prominent elastic fibers, extramedullary hematopoiesis, necrosis and ossification (J Thorac Cardiovasc Surg 1994;108:862, JACC Clin Electrophysiol 2019;5:563)
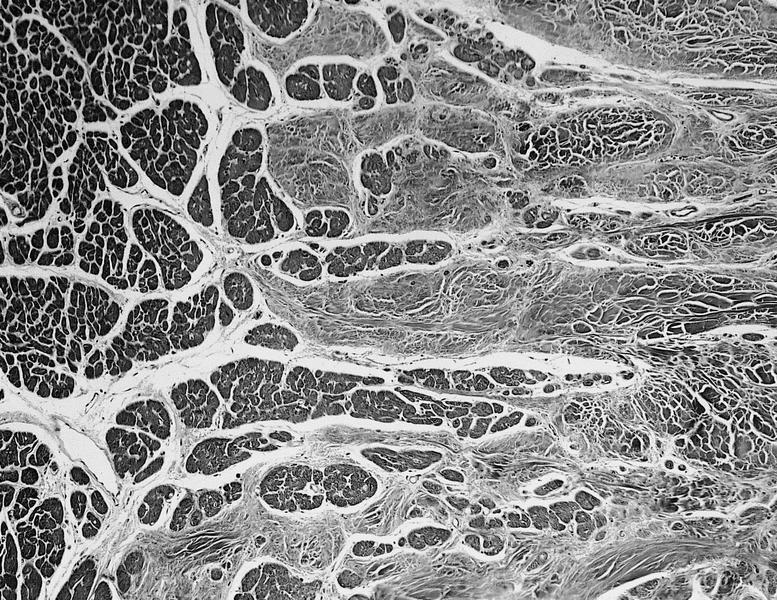
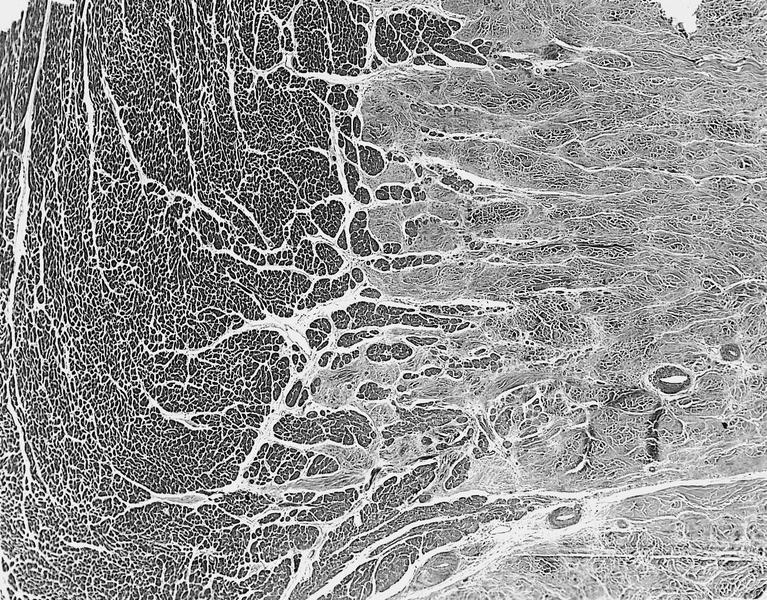
- Tumor may infiltrate into surrounding myocardium; isolated islands of entrapped myocardium may also be seen
- Increased mitotic activity or atypia is usually not observed
Microscopic (histologic) images
Contributed by Chrystalle Katte Carreon, M.D.
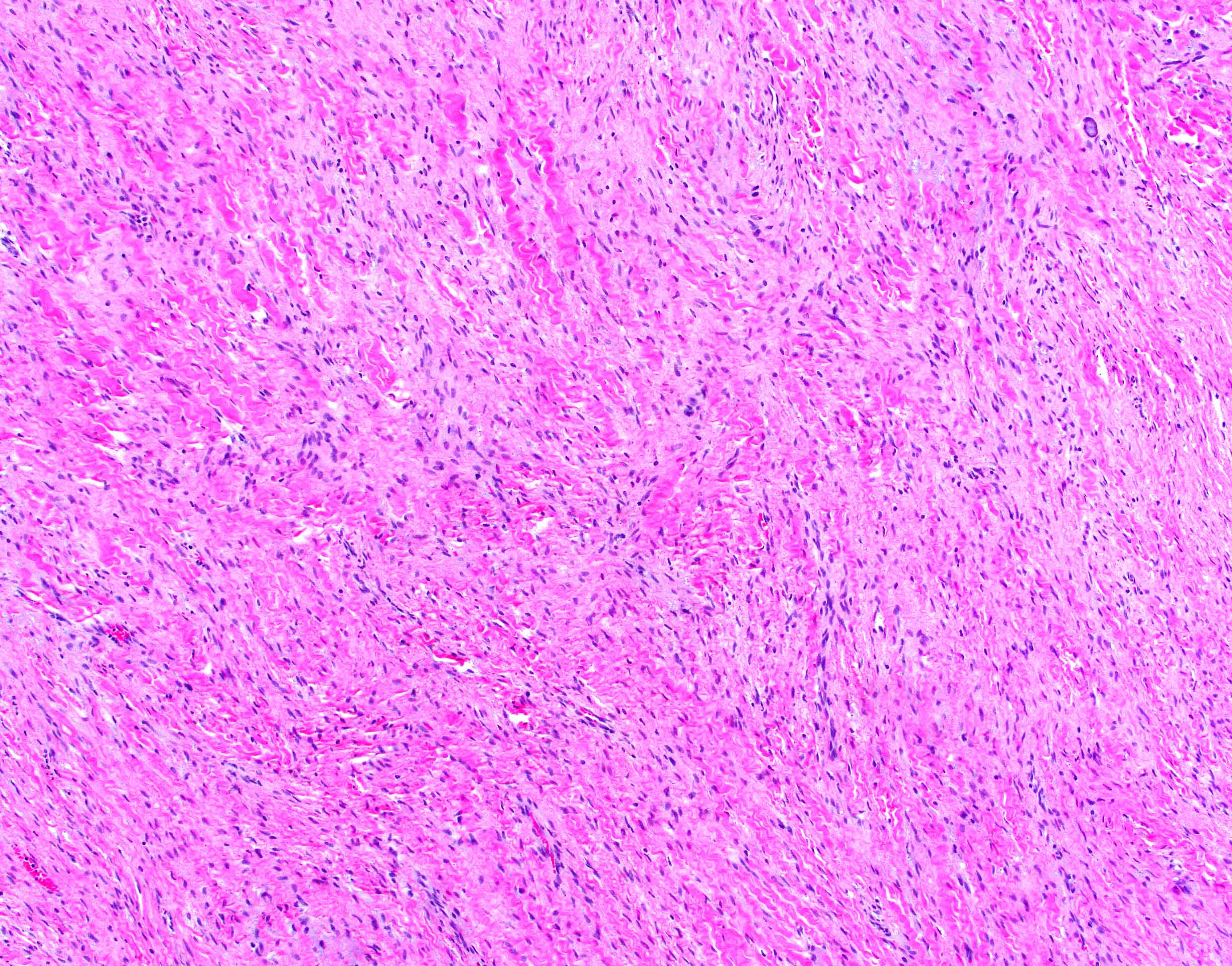
Abundant collagen
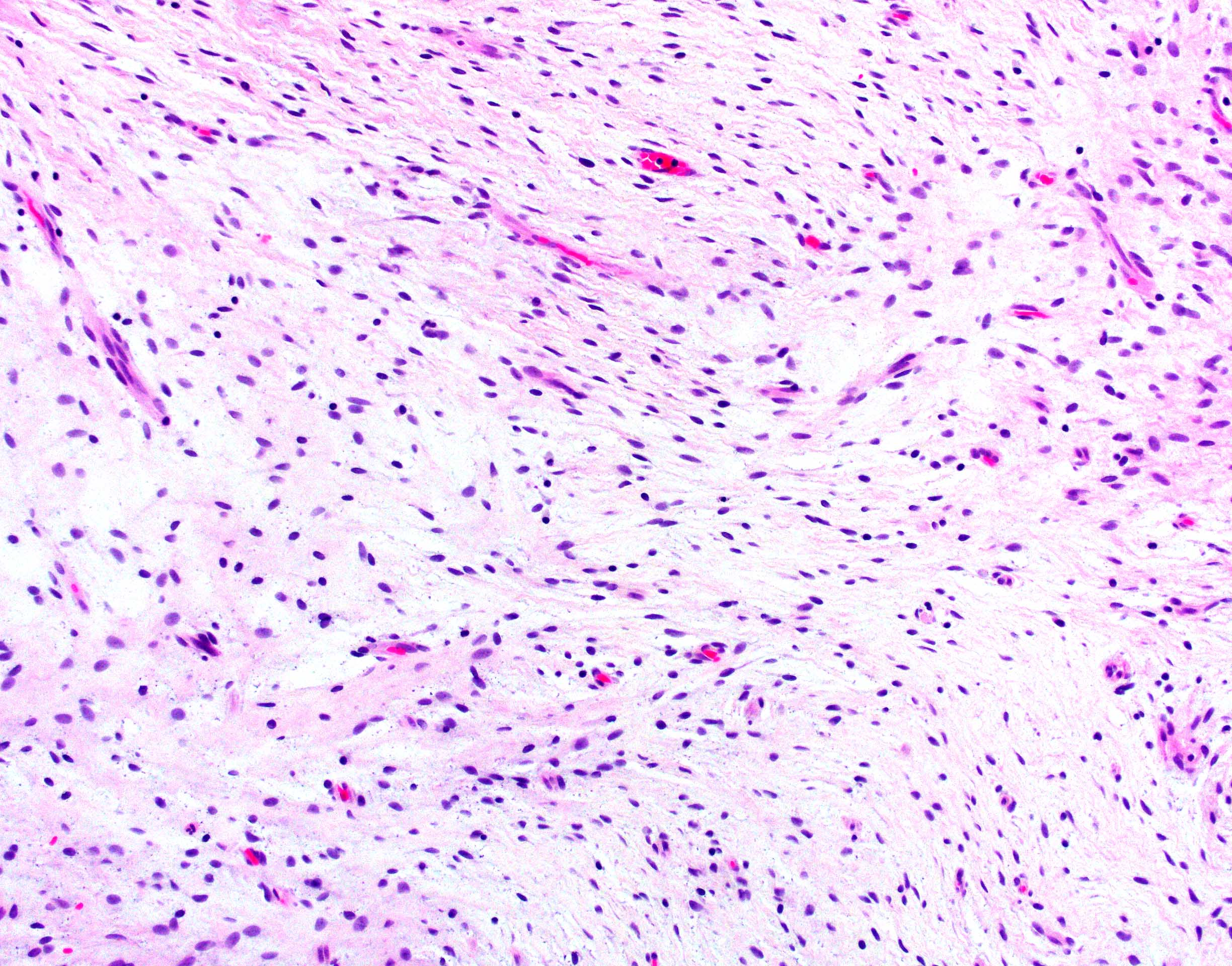
Immature appearance
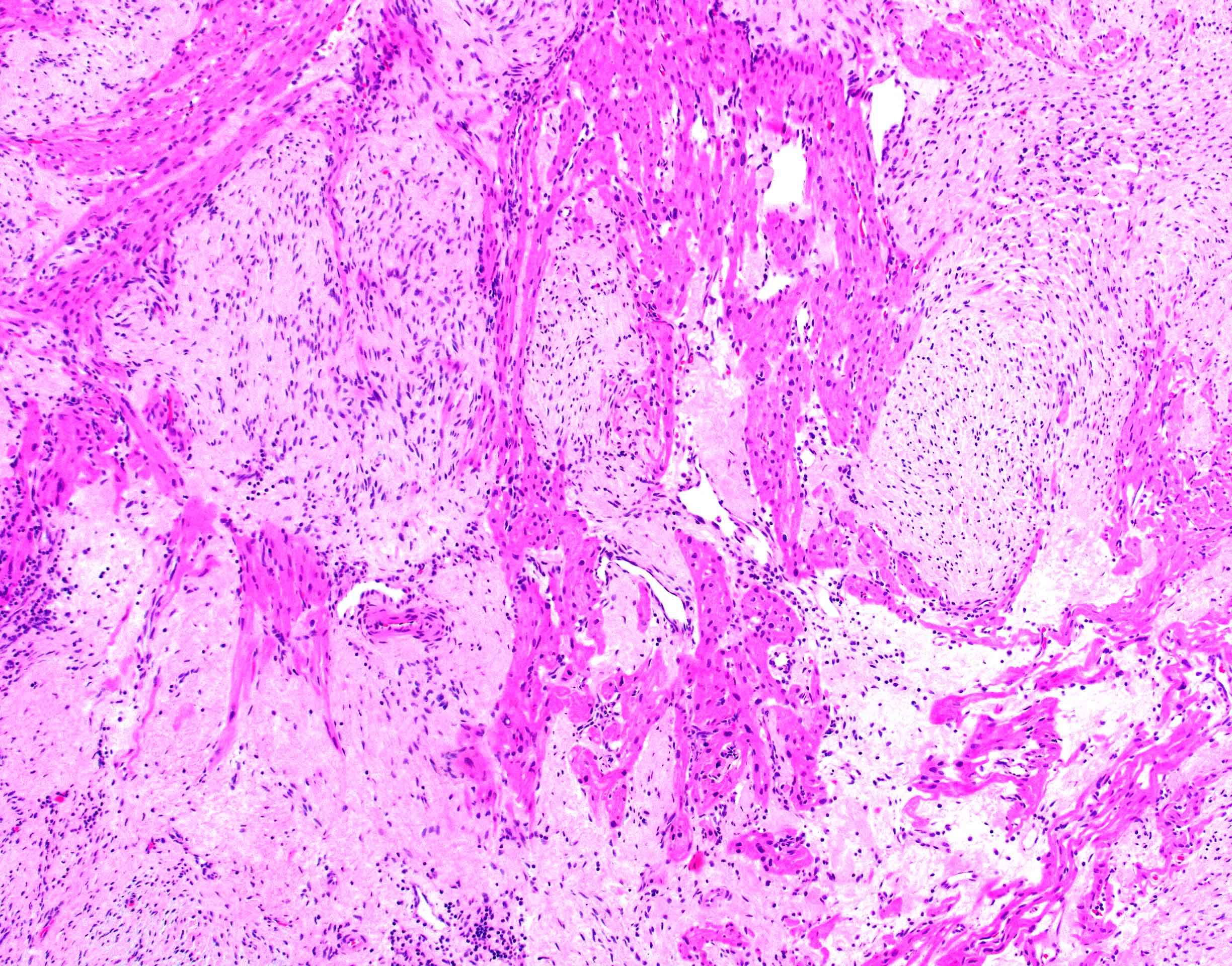
Entrapped myocardium
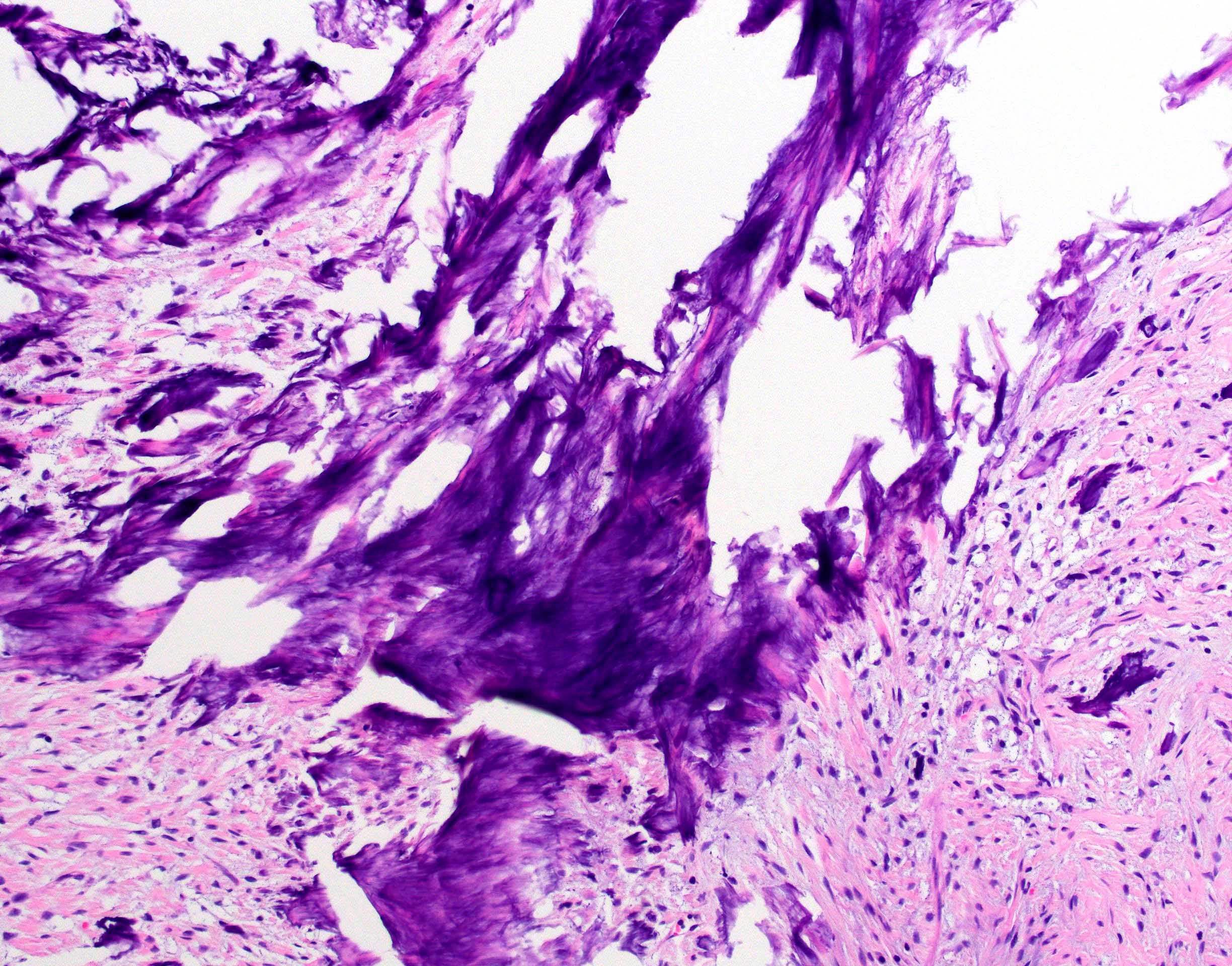
Dystrophic calcifications
Lack of tumor capsule

Entrapped myocardium (desmin)
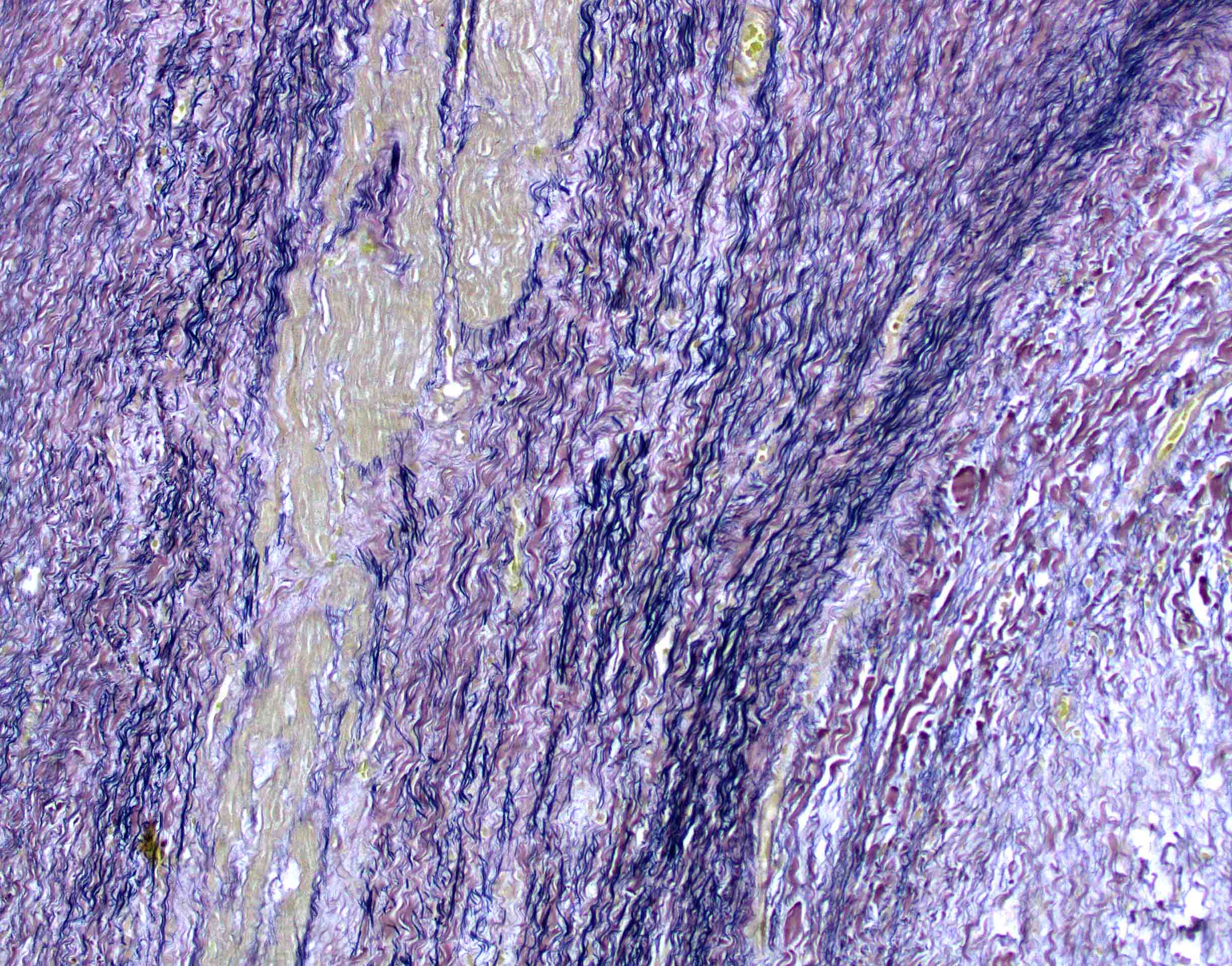
Abundant elastic fibers
AFIP images
Cellular lesion in infant
Collagen deposition

Central fibroma cells

Calcification
Infiltrative margin
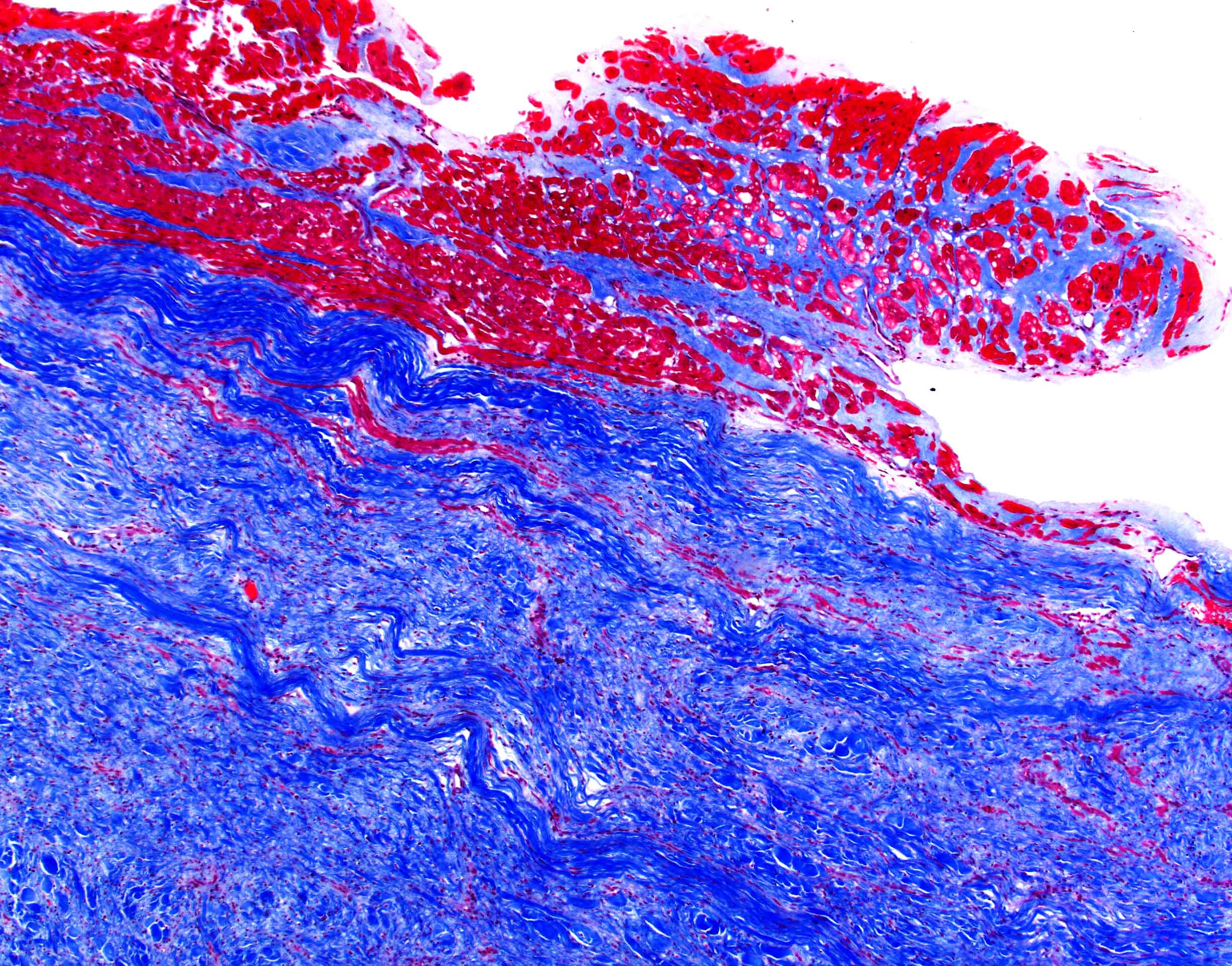
Trichrome
Von Gieson elastin
Positive stains
- Smooth muscle actin and vimentin (Cardiovasc Pathol 2022;56:107381)
- CD31 and CD34 highlights scattered vascular channels (Cardiovasc Pathol 2022;56:107381)
- Trichrome stain highlights collagen bundles (JACC Clin Electrophysiol 2019;5:563)
- Elastic stain highlights abundant elastic fibers (Case Rep Cardiol 2015;2015:713702)
Negative stains
- AE1 / AE3, desmin, myoglobin, ALK, S100, calretinin or STAT6 (J Am Coll Cardiol 2011;58:1903)
- In contrast to the tumor, entrapped myocardium is positive for desmin (JACC Clin Electrophysiol 2019;5:563)
Electron microscopy description
- Fibroblasts with abundant, rough endoplasmic reticulum
- Intercellular space contains collagen fibers that are regularly banded and arranged in whorls, clustered elastic fibers and ground substance (J Thorac Cardiovasc Surg 1993;106:1208)
Molecular / cytogenetics description
- Cytogenetics: deletions in chromosomes 9 and 3 (Cancer Genet Cytogenet 1996;87:34, Cardiol Young 2003;13:101, Cardiovasc Pathol 2008;17:93, JACC Clin Electrophysiol 2019;5:563)
- Isolated translocations, t(4;13), t(5:11) and t(1;9), are reported (JACC Clin Electrophysiol 2019;5:563)
- FISH: homozygous and heterozygous loss of the PTCH1 locus (Cardiovasc Pathol 2008;17:93)
- High resolution microarray analysis showed losses of somatic copy numbers on chromosome 9q21.33 to q22.33, encompassing the PTCH1 locus as well (Cancer Genet 2015;208:615)
Sample pathology report
- Heart, left ventricular mass, resection:
- Cardiac fibroma (4.5 cm) (see comment)
- Comment: Immunohistochemical stain for desmin shows entrapment of cardiomyocytes within the tumor.
Differential diagnosis
- Inflammatory myofibroblastic tumor:
- Denser proliferation of myofibroblastic cells within an inflammatory background, mostly consisting of plasma cells and lymphocytes
- Cytoplasmic staining for ALK correlates with ALK gene rearrangement, seen in up to 60% of cases
- Variable staining for SMA and desmin
- Focal cytokeratin staining may be observed; immunostain positive (Cardiovasc Pathol 2022;56:107381)
- Fibrosarcoma:
- Mitotically active, with prominent cellular atypia
- Solitary fibrous tumor:
- Scar:
- Lacks a mass-like growth
- Often associated with chronic ischemic change in surrounding myocardium
Board review style question #1
Which microscopic feature may be observed in cardiac fibroma?
- Extensive necrosis
- High mitotic count
- Marked atypia
- Prominent calcifications
Board review style answer #1
D. Prominent calcifications. Other microscopic features that may be observed in cardiac fibromas include dystrophic calcifications, lymphocytic infiltrate and extramedullary hematopoiesis, among others. High grade features are absent.
Comment Here
Reference: Cardiac fibroma
Comment Here
Reference: Cardiac fibroma
Board review style question #2
Cardiac fibromas may be a manifestation of which of the following syndromes?
- Carney complex
- Gorlin syndrome
- Holt-Oram syndrome
- Tuberous sclerosis
Board review style answer #2
B. Gorlin syndrome, also known as basal cell nevus syndrome (BCNS), is caused by mutations in a tumor suppressor gene called PTCH1. This gene is located on chromosome 9. Mutations in this gene may increase the risk for other tumors, including keratocystic odontogenic tumors, medulloblastomas and ovarian fibromas.
Comment Here
Reference: Cardiac fibroma
Comment Here
Reference: Cardiac fibroma
