

Kidney nontumor / medical renal
Vascular disease
Other vascular disorders
Arterionephrosclerosis
Authors: Husam Jum'ah, M.D., Santhi Ganesan, M.D.
Editorial Board Members: Nicole K. Andeen, M.D., Jonathan E. Zuckerman, M.D., Ph.D.


Last author update: 12 June 2023
Last staff update: 12 June 2023
Copyright: 2002-2024, PathologyOutlines.com, Inc.
PubMed Search: Arterionephrosclerosis
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Laboratory | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Immunofluorescence description | Positive stains | Electron microscopy description | Genetics | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2 | Board review style question #3 | Board review style answer #3Cite this page: Jum'ah H, Ganesan S. Arterionephrosclerosis. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/kidneyarterionephrosclerosis.html. Accessed April 19th, 2024.
Definition / general
- Sclerosis of renal arterioles and small arteries, strongly associated with nonmalignant hypertension
- Hypertension can be both a cause and consequence of nephrosclerosis
- Hypertension associated nephrosclerosis is an important cause of chronic kidney disease (CKD) that affects African Americans disproportionately (Kidney Int Rep 2016;1:10)
Essential features
- Arterionephrosclerosis is a chronic kidney disease attributed to nonmalignant hypertension
- Histopathological features include hyaline changes involving terminal branches of interlobular arteries, global glomerulosclerosis and proportional tubulointerstitial changes
- Individuals of African descent have strong predisposition to chronic kidney disease (CKD) and end stage renal disease (ESRD)
- APOL1 associated arterionephrosclerosis with risk alleles G1 and G2 tend to progress towards more advanced levels of CKD (Curr Opin Nephrol Hypertens 2013;22:266)
Terminology
- Also called hypertension associated kidney disease
- The term hypertensive nephrosclerosis is becoming obsolete
ICD coding
Epidemiology
- Advanced age
- More common in the African American population, especially at a younger age (as young as 20s) (Kidney Int 2002;62:172)
- M > F
- Strongly associated with hypertension
Sites
- Renal arterioles and small arteries
- Glomerulus
- Tubulointerstitium
Pathophysiology
- Medial and intimal thickening of small arteries and arterioles as a response to hemodynamic changes, aging, genetics or combination of factors
- Hypertension can be associated with vasoregulatory dysfunction at the level of the glomerular microcirculation (Curr Opin Nephrol Hypertens 2013;22:266)
- Arteriolar hyalinosis due to extravasation of plasma proteins through injured endothelium and increased deposition of basement membrane matrix
- Subsequent vascular narrowing and ischemia leading to glomerulosclerosis, chronic tubulointerstitial injury and reduced functional renal mass
Etiology
- Hypertension
- Aging
- Genetics (G1 and G2 risk allele variants of apolipoprotein L1 [APOL1]) (Curr Opin Nephrol Hypertens 2013;22:266)
- Oxidative stress, chronic inflammation and smoking
Clinical features
- Progressive proteinuria, nephrotic range at times
- Low estimated glomerular filtration rate (eGFR) (Kidney Int Rep 2019;5:339)
- Renal insufficiency when associated with African descent, concomitant diabetes and poorly controlled blood pressure
- End stage kidney disease in 25 - 30% of patients (Am J Kidney Dis 2016;67:e21)
Diagnosis
- Arterionephrosclerosis is a diagnosis of exclusion as it can be the cause and consequence of hypertension
- Arterionephrosclerosis is often misdiagnosed and likely includes cases of both focal segmental glomerulosclerosis (FSGS) and non-FSGS glomerular diseases (J Am Soc Nephrol 2008;19:2047)
- Hyperechogenic kidneys on ultrasound
Laboratory
- Deteriorating kidney function in a patient with high blood pressure
- Progressive proteinuria
Prognostic factors
- Individuals with APOL1 risk variants tend to progress to more advanced levels of CKD (Curr Opin Nephrol Hypertens 2013;22:266)
- Individuals of African descent have strong predisposition to CKD and end stage kidney disease
- Concomitant causes of microvascular pathology such as smoking, obesity, diabetes, aging and oxidative stress
Case reports
- 31 year old woman with retinitis pigmentosa who had been diagnosed with renal failure due to nephrosclerosis related to hypertensive disorders of pregnancy (BMJ Case Rep 2020;13:e236137)
- 44 year old Hispanic woman, smoker, with hypertension and peripheral arterial disease who presented with nephrotic syndrome for 2 weeks (J Bras Nefrol 2020;42:484)
- 74 year old man, with hypertension and heavy smoking history, who presented with nephrotic proteinuria and chronic kidney disease (Clin Nephrol Case Stud 2022;10:82)
Treatment
- Strict blood pressure control
- Fluid and salt restriction to manage chronic kidney disease
Gross description
- Kidneys can be either normal or smaller with fine cortical granularity resembling grain leather; smaller size is due to cortical scarring and shrinkage
Gross images
Contributed by Husam Jum’ah, M.D.

Renal cortical surface with granularity
Images hosted on other servers:

Characteristic granular appearance
Microscopic (histologic) description
- 3 glomerular morphological patterns
- Obsolescent glomerulus, which may be a partially or wholly collapsed glomerular tuft, with accumulation of extracellular material in Bowman space
- Solidified global glomerulosclerosis, in which the glomerular tuft remains expanded but replaced by collagen and possibly other matrix material
- Segmental glomerulosclerosis, possibly due to glomerular hyperfiltration (Curr Opin Nephrol Hypertens 2013;22:266)
- Hyaline arteriolosclerosis predominantly involving the afferent arteriole; this is characterized by thickening of the arteriolar wall due to the accumulation of homogeneous material that stains pink on H&E stained slides
- Arterial medial thickening and subintimal fibrosis
- Proportional tubulointerstitial fibrosis
- Solidified and disappearing glomerulosclerosis, thyroidization type tubular atrophy and microcystic tubular dilatation may be seen more in African Americans with arterionephrosclerosis, with APOL1 risk variants (Mod Pathol 2015;28:95)
Microscopic (histologic) images
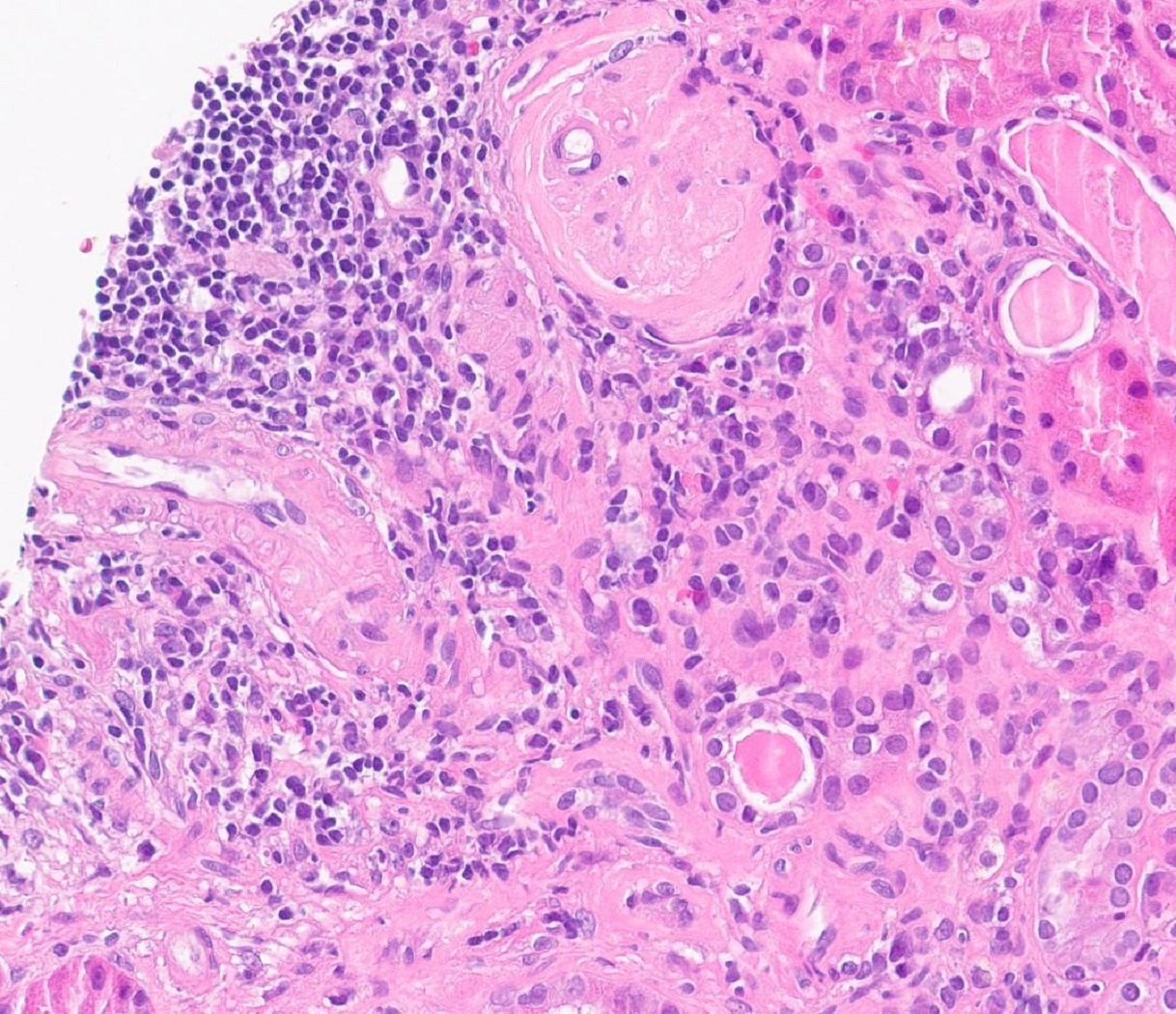
Contributed by Santhi Ganesan, M.D.
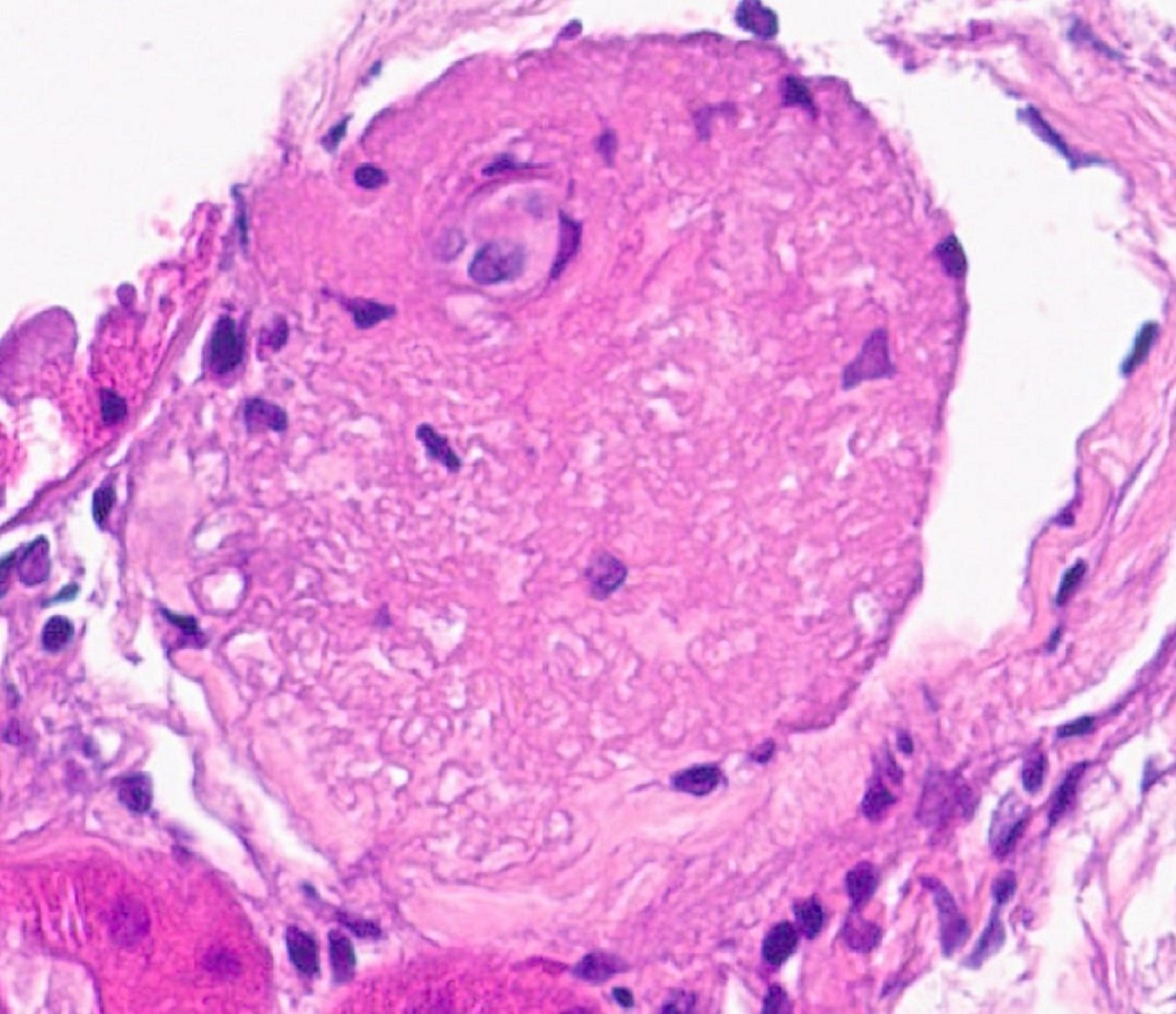
Global
glomerulosclerosis
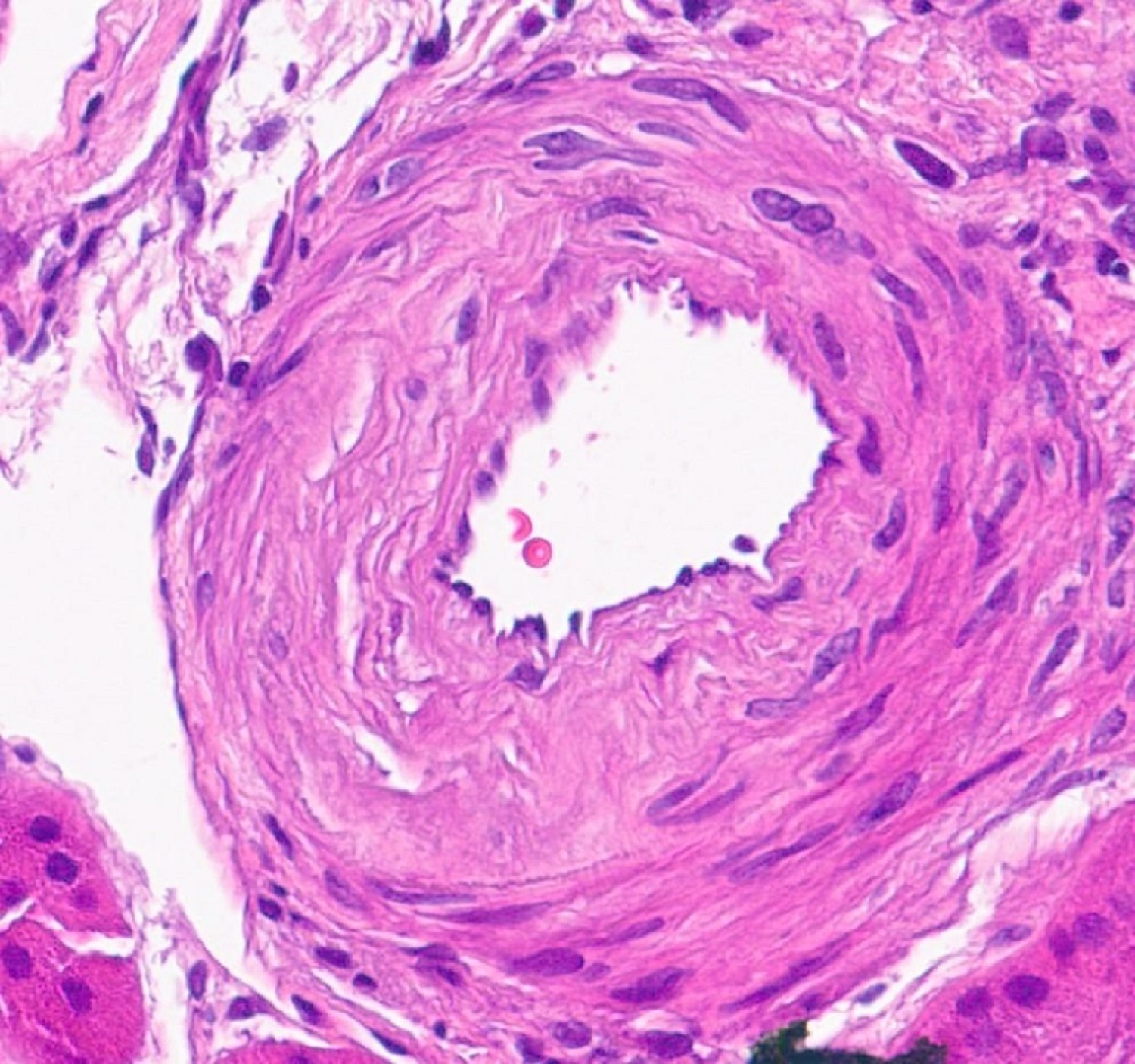
Arterial medial thickening
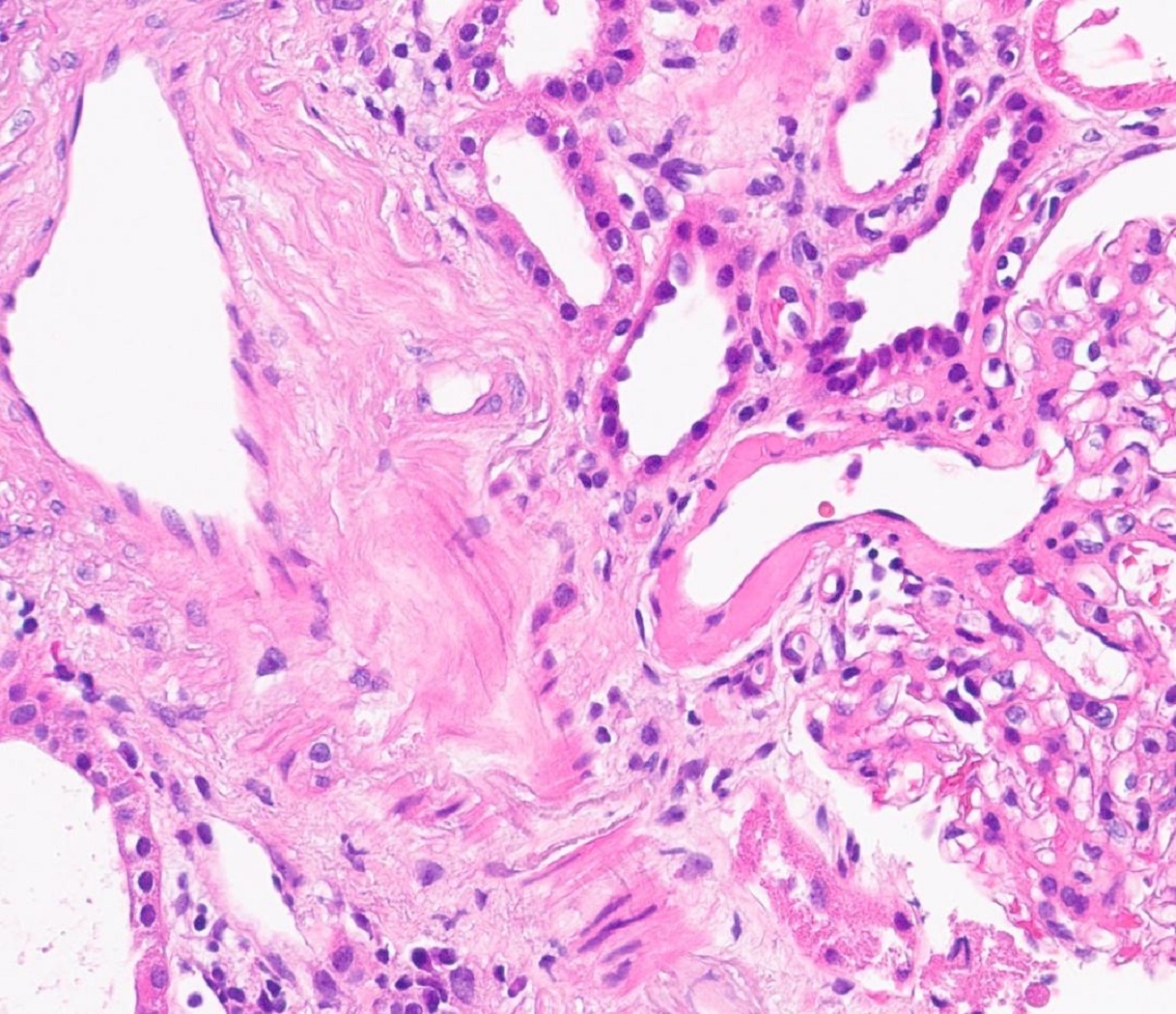
Hyaline vascular changes
Obsolescent glomerulus
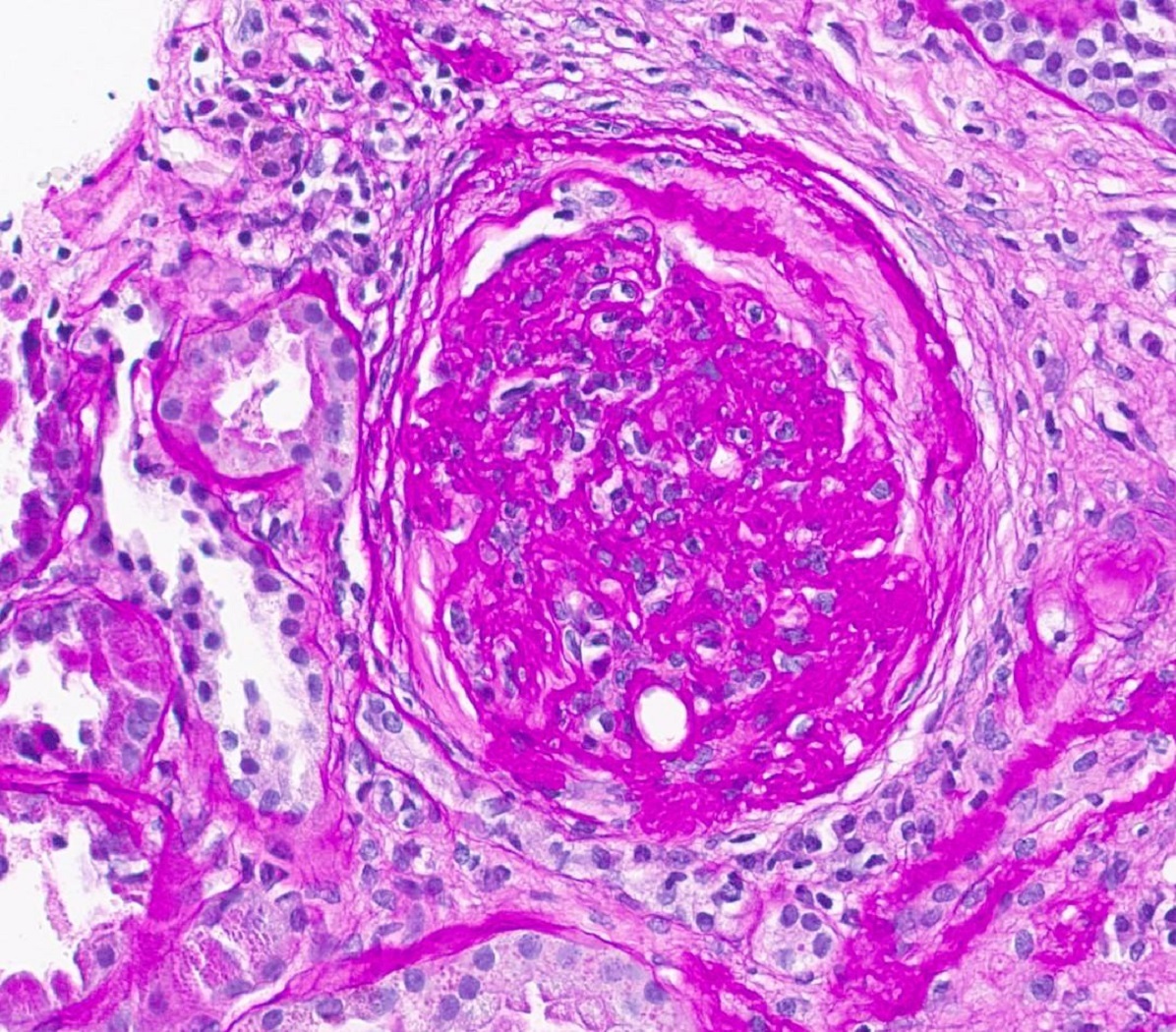
Global
glomerulosclerosis
PAS
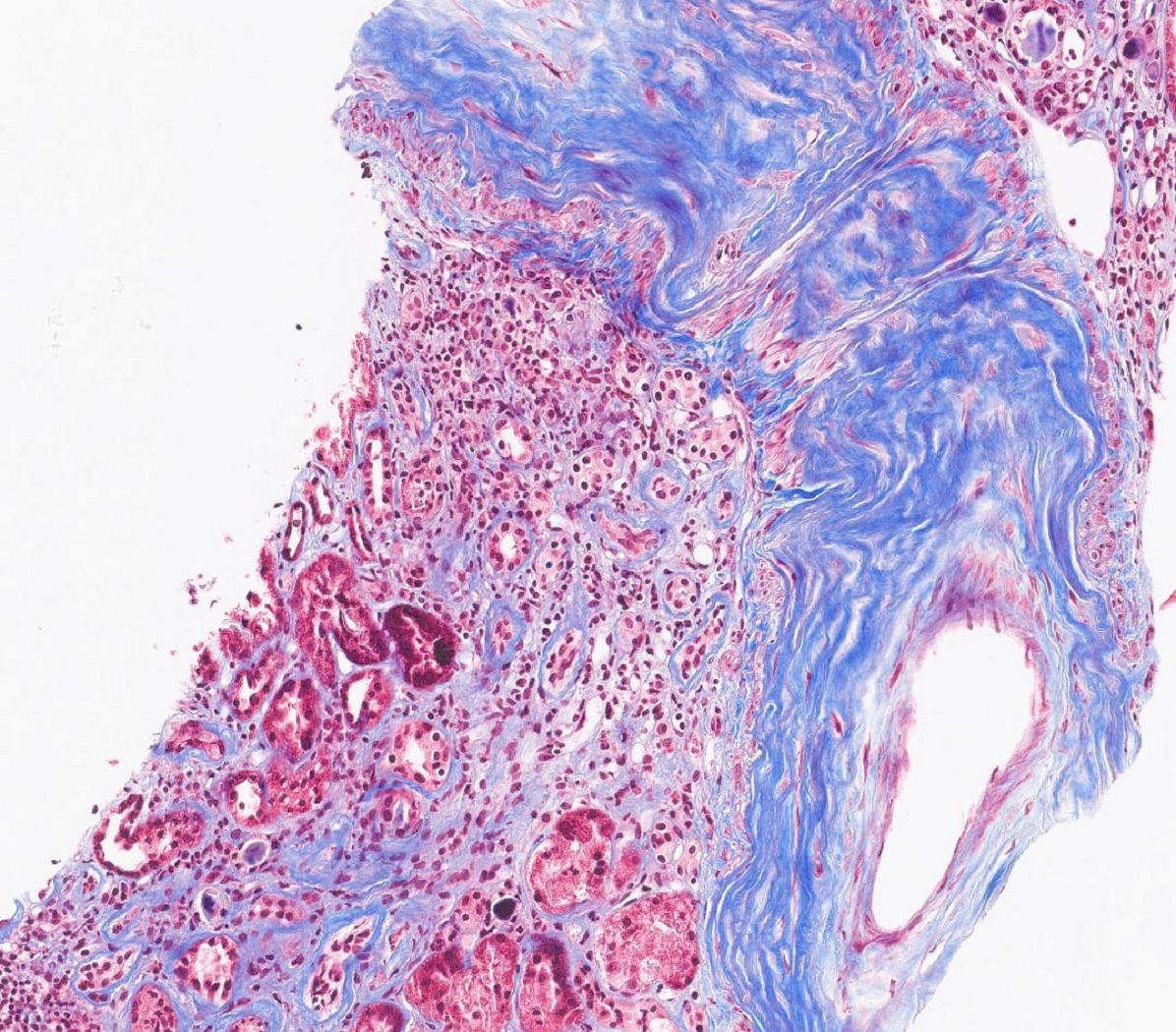
Subintimal fibrosis trichrome
Immunofluorescence description
- Low intensity staining for IgM, C3 and C1q in areas of hyalinosis
Positive stains
- PAS: highlights hyaline arteriolosclerosis and glomerulosclerosis
- Jones silver: highlights wrinkled glomerular basement membrane, global and segmental glomerulosclerosis (Kidney Int 2002;62:172)
- Trichrome: highlights tubulointerstitial fibrosis (Semin Diagn Pathol 2018;35:360)
Electron microscopy description
- Corrugated and thickened glomerular basement membrane
- Expansion of lamina rara interna
Genetics
- G1 and G2 risk allele variants of apolipoprotein L1 (APOL1)
Sample pathology report
- Kidney, biopsy:
- Arterionephrosclerosis (see comment)
- Comment: Marked global glomerulosclerosis is seen in a background of hyaline arteriolosclerosis, medial smooth muscle hyperplasia, subintimal fibrosis and proportional tubulointerstitial fibrosis. Immunofluorescence study results show low intensity mesangial staining for IgM. Electron microscopic evaluation does not show significant podocytopathy. Overall findings are reflective of chronic benign hypertensive related changes.
Differential diagnosis
- Primary (idiopathic) focal segmental glomerulosclerosis:
- Prominent foot process changes (Am J Kidney Dis 2016;67:e21)
- Fewer hyaline vascular arteriosclerotic changes
- Diabetic glomerulosclerosis:
- Diffusely thickened glomerular basement membrane and nodular mesangial expansion
- Hyaline arteriolosclerosis involving both afferent and efferent arterioles
Board review style question #1
Which of the following vasculature is affected by hyalinosis in arterionephrosclerosis?
- Afferent arteriole
- Both afferent and efferent arterioles
- Efferent arteriole
- Interlobar artery
Board review style answer #1
A. Afferent arteriole. Arterionephrosclerosis (hypertension associated kidney disease) affects terminal branches of interlobular arteries, especially afferent arterioles as a response to hemodynamic changes and insudation of plasma proteins and subsequent afferent arteriolar hyalinosis.
Answers B and C are incorrect because efferent arterioles are not affected. Diabetic nephropathy involves afferent and efferent arteriolar hyalinosis. Answer D is incorrect because interlobar artery shows medial thickening and subintimal fibrosis but no hyalinosis.
Comment Here
Reference: Arterionephrosclerosis
Comment Here
Reference: Arterionephrosclerosis
Board review style question #2
Hypertension associated chronic kidney disease (CKD) can be associated with
- Apolipoprotein E (APOE) genotype
- COL4A5 mutations
- G1 and G2 risk allele variants of apolipoprotein L1 (APOL1)
- Phospholipase A2 receptor (PLA2R) antibodies
Board review style answer #2
C. G1 and G2 risk allele variants of apolipoprotein L1 (APOL1). The presence of 2 APOL1 risk alleles (G1 and G2) can be associated with more proteinuria, more severe kidney disease and progression to end stage renal disease (ESRD) on follow up. Answer D is incorrect because PLA2R antibodies are associated with membranous glomerulopathy. Answer B is incorrect because COL4A5 mutations can be seen in association with focal segmental glomerulosclerosis. Answer A is incorrect because apolipoprotein E (APOE) genotype is implicated in Alzheimer disease.
Comment Here
Reference: Arterionephrosclerosis
Comment Here
Reference: Arterionephrosclerosis
Board review style question #3
The vascular changes depicted in the image above represent which of the following processes or outcomes?
- Atherosclerosis
- Extravasation of plasma proteins through injured endothelium and increased deposition of basement membrane matrix in hypertension associated kidney disease
- Fibrinoid necrosis of small vessel vasculitis
- Misfolded proteinaceous material with a characteristic beta pleated sheet on electron microscopic examination
Board review style answer #3
B. Extravasation of plasma proteins through injured endothelium and increased deposition of basement membrane matrix in hypertension associated kidney disease. Hypertension can be associated with vasoregulatory dysfunction at the level of the glomerular microcirculation. This image represents afferent arteriolar hyalinosis due to extravasation of plasma proteins through injured endothelium and increased deposition of basement membrane matrix in arterionephrosclerosis (hypertension associated kidney disease). This results in accumulation of homogeneous material that stains pink on H&E stained slides. Answer C is incorrect because fibrinoid necrosis of vasculitis is amorphous and stains bright pink in H&E stained slides. Answer D is incorrect because misfolded protein with beta pleated sheet of amyloid appears glassy and homogeneous and stains lighter pink in H&E stained slides. Answer A is incorrect because atherosclerosis is associated with atheromatous plaque and involves arterial walls characterized by accumulation of lipid, matrix material and calcium.
Comment Here
Reference: Arterionephrosclerosis
Comment Here
Reference: Arterionephrosclerosis
