

Kidney nontumor / medical renal
Glomerular disease
Obesity related glomerulopathy
Obesity related glomerulopathy
Editorial Board Member: Nicole K. Andeen, M.D.
Editor-in-Chief: Debra L. Zynger, M.D.

Last author update: 9 November 2020
Last staff update: 11 March 2021
Copyright: 2020-2024, PathologyOutlines.com, Inc.
PubMed Search: Obesity related glomerulopathy "free full text"[SB]
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Laboratory | Prognostic factors | Case reports | Treatment | Microscopic (histologic) description | Microscopic (histologic) images | Immunofluorescence description | Immunofluorescence images | Electron microscopy description | Electron microscopy images | Genetics | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Samiei A, Zuckerman JE. Obesity related glomerulopathy. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/kidneyobesity.html. Accessed April 24th, 2024.
Definition / general
- Glomerulomegaly with or without accompanying focal segmental glomerulosclerosis occurring in the setting of obesity with or without the metabolic syndrome
Essential features
- Glomerulomegaly is the pathological hallmark (Kidney Int 2001;59:1498)
- Hypertrophied glomeruli that fill the microscopic visual field at 40x objective lens
- Often secondary / maladaptive focal segmental glomerulosclerosis present (Nephron 2017;136:273)
- Segmental patchy podocyte foot process effacement (Nephron 2017;136:273)
- Proteinuric presentation, most often subnephrotic
Terminology
- Obesity related glomerulopathy
- Metabolic syndrome related glomerulopathy
ICD coding
- ICD-10: N08 - glomerular disorders in diseases classified elsewhere
Epidemiology
- Associated with obesity and preterm birth (Nat Rev Nephrol 2016;12:453)
- 46% of patients have class 1 or class 2 obesity and 54% have class 3 obesity (Kidney Int 2001;59:1498)
Sites
- Kidney
Pathophysiology
- Congenital or functional low nephron endowment (Kidney Int 2000;58:770)
- Glomerular filtration rate (GFR) is increased in order to maintain adequate natriuresis in obesity
- Leads to adaptive hemodynamic modulations and glomerular hypertension
- Chronic glomerular hypertension causes nephron injury, which manifests as glomerular hypertrophy, basement membrane thickening and podocyte damage
- Subsequent podocyte loss from continued mechanical injury eventually leads to podocyte loss and segmental sclerosis (Kidney Int 1992;42:148, Am J Hypertens 1988;1:335)
- May also be contributions from endocrinopathies of metabolic syndrome
- Obstructive sleep apnea may also be a contributing factor
Etiology
- Obesity (Nat Rev Nephrol 2016;12:453)
- Metabolic syndrome
- Possibly congenital reduced nephron mass (e.g. preterm birth) (Nephrology (Carlton) 2013;18:180)
Clinical features
- Middle aged adults (35 - 45 years) (Am J Kidney Dis 2008;52:58)
- Slowly progressive proteinuria (Kidney Int 2001;59:1498)
- Proteinuria often subnephrotic but may reach nephrotic range
- Nephrotic syndrome is rare
- Slow decline in renal function
- Sometimes present without overt clinical disease
Diagnosis
- Diagnosis is made on renal biopsy (Kidney Int 2008;73:947)
- Can be suspected clinically in obese patients with proteinuria
Laboratory
- Patients commonly present with proteinuria, sometimes in nephrotic range
- Median estimated glomerular filtration rate (eGFR) of 30 ml/min/1.73 m² (Kidney Int 2019;95:647)
Prognostic factors
- Body mass index (BMI) is directly proportional to risk of end stage renal disease
Case reports
- 37 year old Caucasian man with a BMI of 38 kg/m² presented to general nephrology clinic with a 3+ proteinuria on urinalysis (Oxf Med Case Reports 2020;2020:omz148)
- 49 year old morbidly obese Caucasian man was found to have obstructive sleep apnea, proteinuria and renal insufficiency (Am J Kidney Dis 1987;10:470)
- 69 year old Caucasian man, with previous normal renal function, suffering from diabetes mellitus, obesity (BMI = 38 kg/m²), hypercholesterolemia, hypertension and coronary artery disease started hemodialysis because of severe acute renal failure (Bioimpacts 2015;5:155)
Treatment
- Weight loss
- Renin angiotensin system blockade
- Bariatric surgery
Microscopic (histologic) description
- Glomerular hypertrophy in 100% of cases (Kidney Int 2001;59:1498)
- Cross sectional glomerular diameter of > ½ 40x high power field
- Often perihilar segmental sclerosis (Nephron 2017;136:273)
- Reduced glomerular density (Clin J Am Soc Nephrol 2012;7:735)
- Focal global glomerulosclerosis
- Mild thickening of glomerular basement membrane (Kidney Int 2001;59:1498)
- Mild mesangial sclerosis may be present
- Variable interstitial fibrosis and tubular atrophy
- Variable arteriosclerosis and arteriolosclerosis
- Focal afferent arteriole dilation (Am J Physiol Renal Physiol 2000;278:F817)
- Tubular hypertrophy may also be present
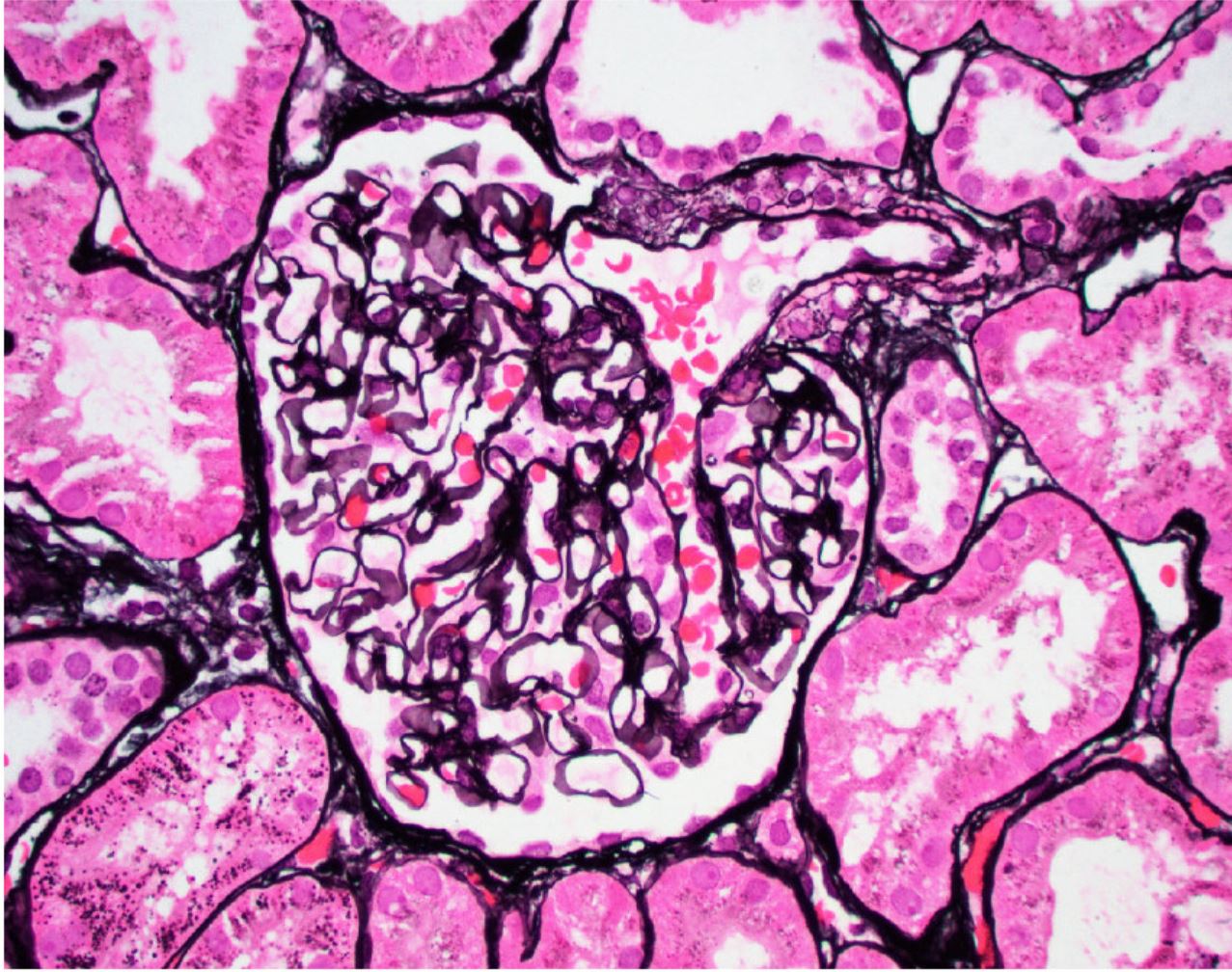
Microscopic (histologic) images
Contributed by Jonathan E. Zuckerman, M.D., Ph.D.
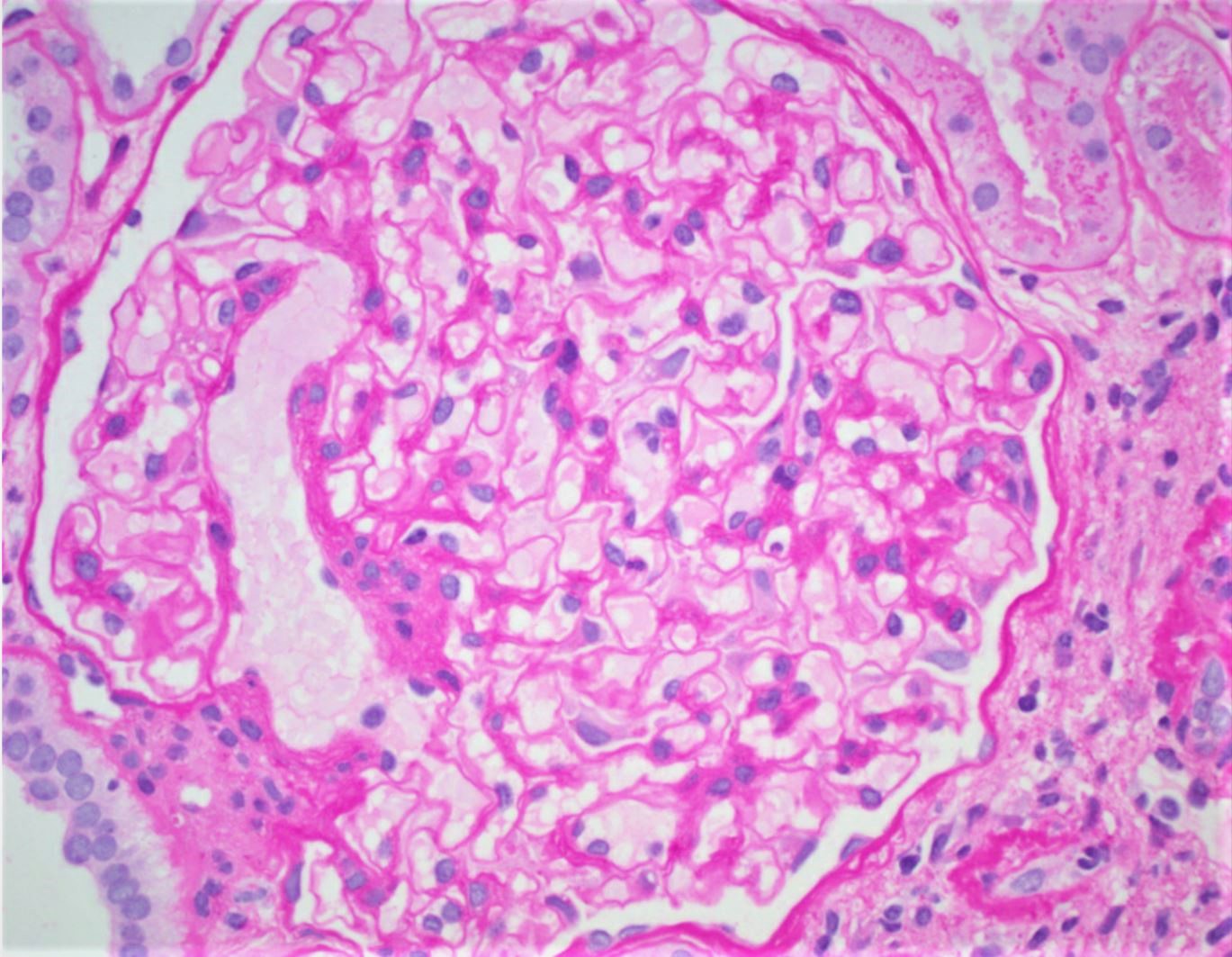
Glomerulomegaly

Perihilar focal segmental glomerulosclerosis
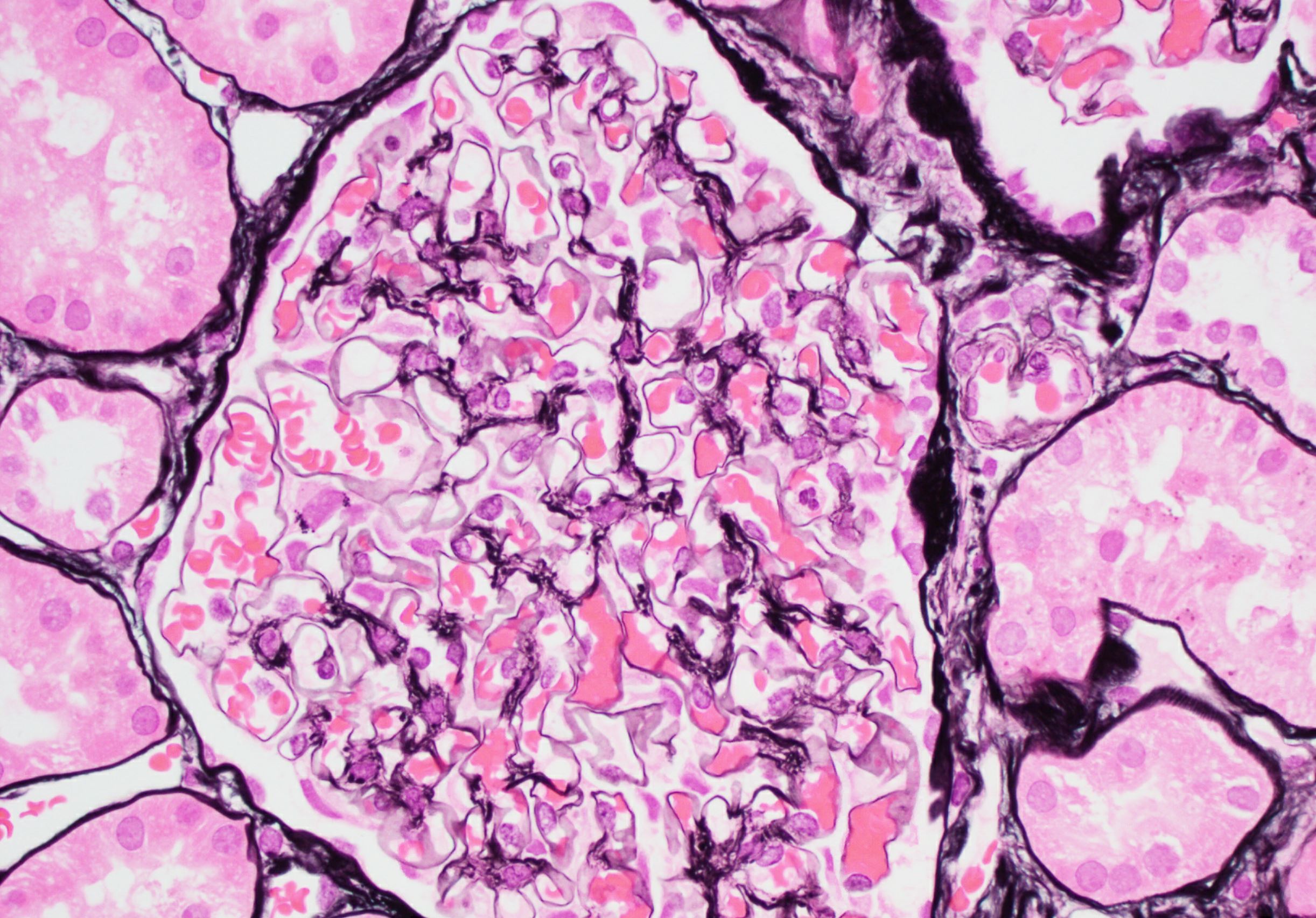
Glomerulomegaly
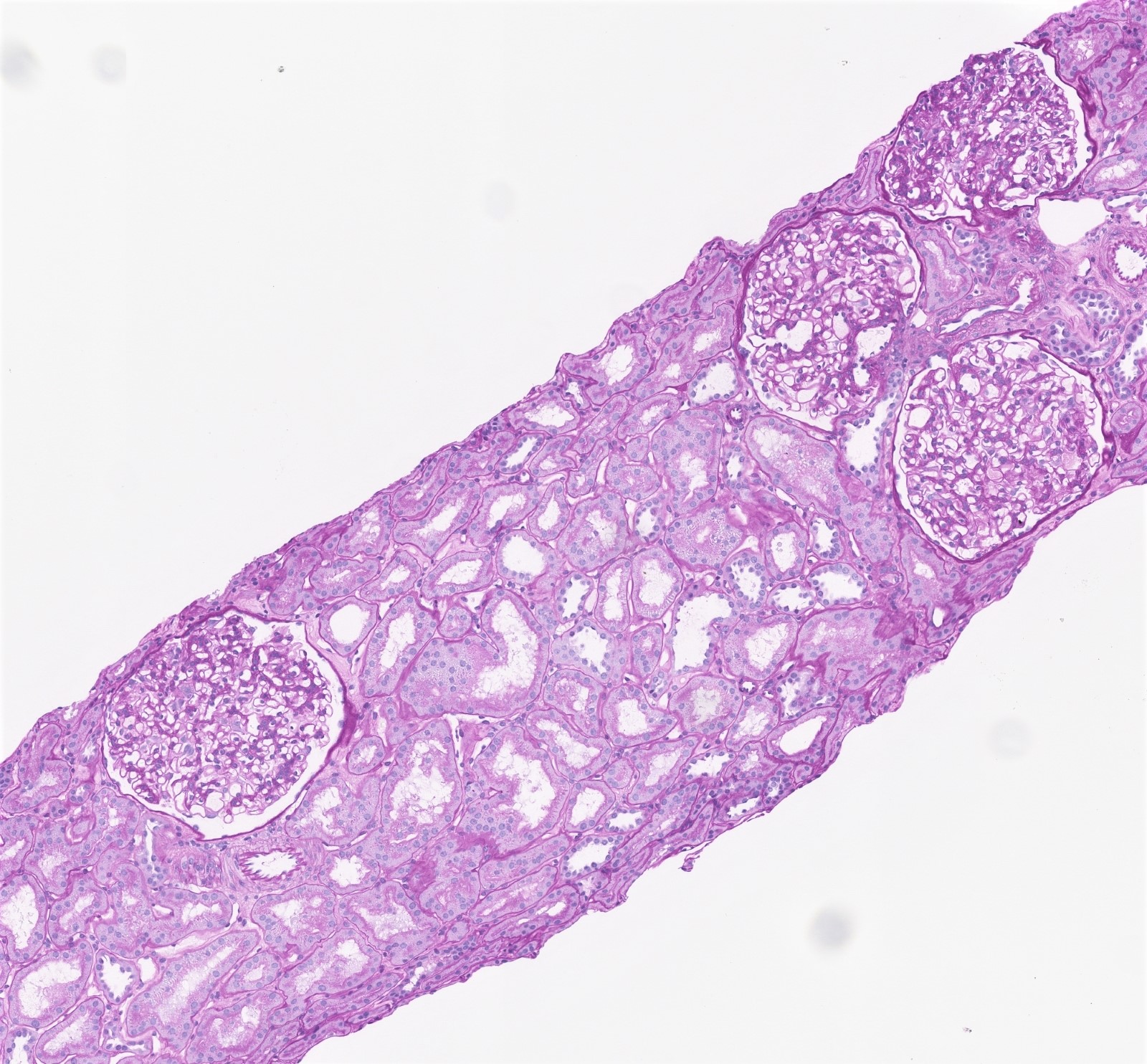
Glomerulomegaly, tubular hypertrophy
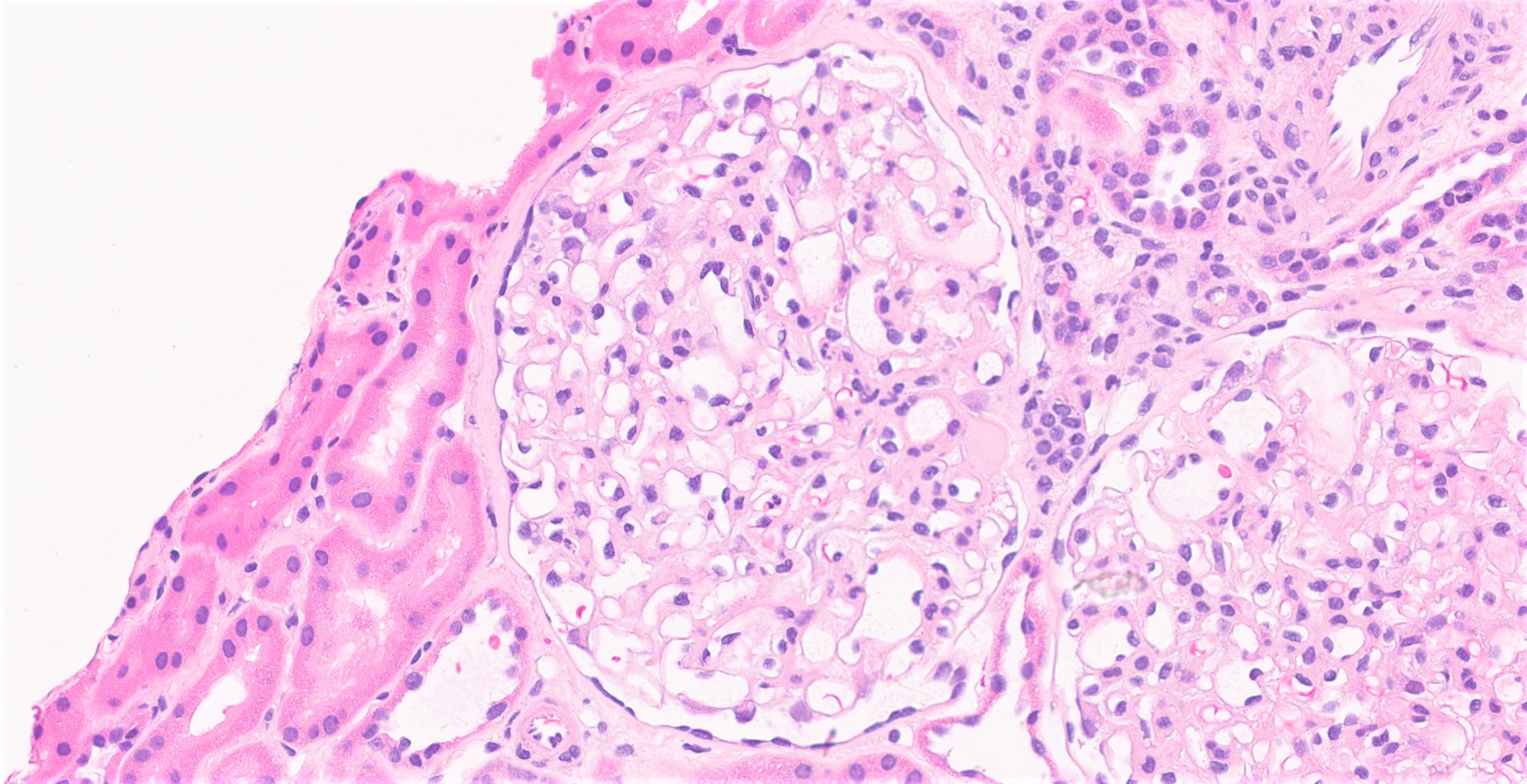
Perihilar focal segmental glomerulosclerosis
Normal glomerulus
Immunofluorescence description
- Glomeruli negative for immune complex deposits
- Nonspecific accumulation of IgM and complement C3 in sclerotic and hyalinized lesion (Kidney Int 2001;59:1498)
- Podocytes may contain intracytoplasmic protein resorption droplets that stain for IgG, IgA and albumin
Immunofluorescence images
Contributed by Jonathan E. Zuckerman, M.D., Ph.D.
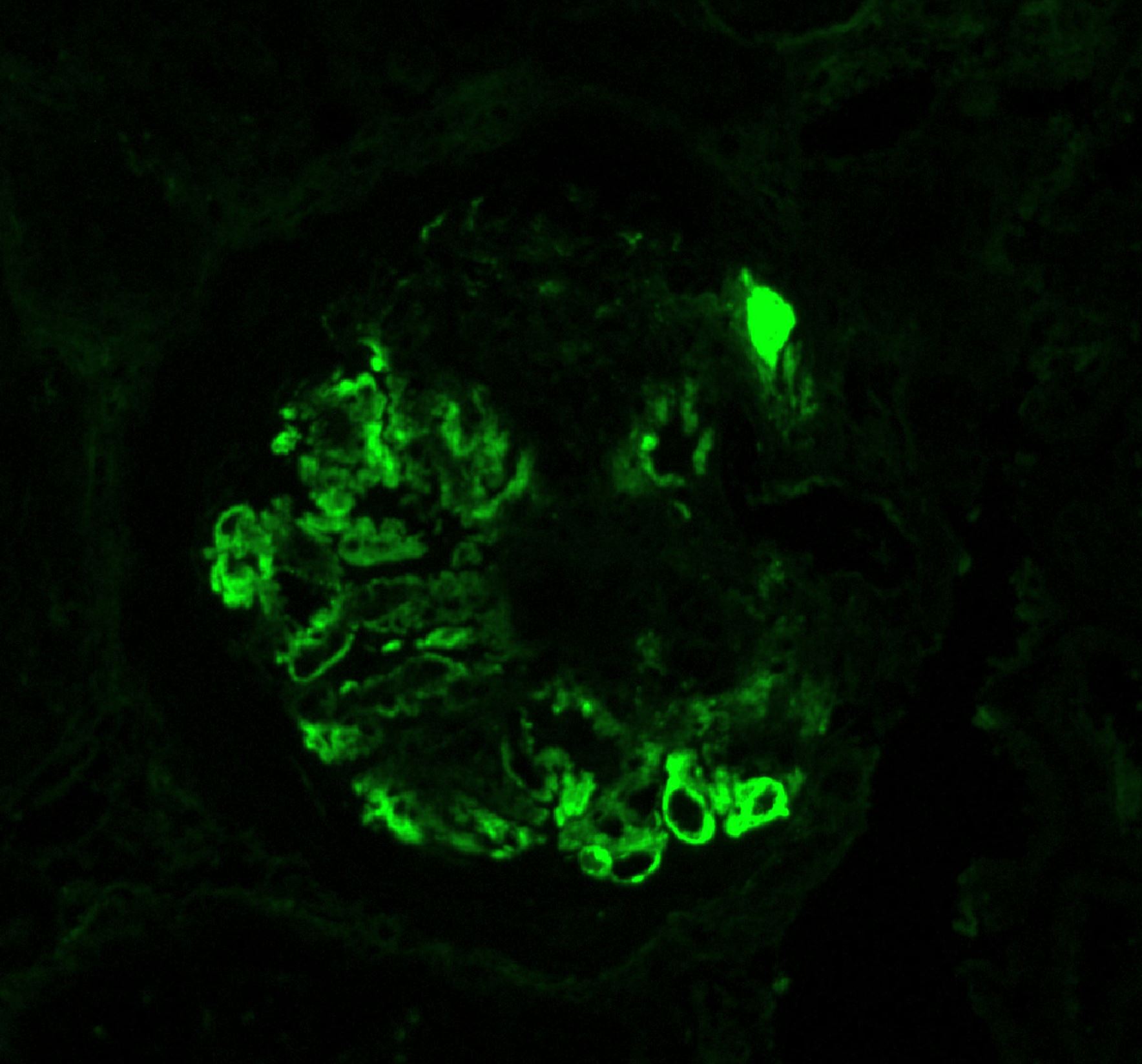
Focal segmental glomerulosclerosis
Electron microscopy description
- Podocytes exhibit segmental foot process effacement (25 - 40%)
- Mild thickening of glomerular basement membrane
- Mild mesangial sclerosis
- Podocytes and mesangial cells will contain lipid droplets (Lancet Diabetes Endocrinol 2014;2:417)
- Lipid vacuoles can be seen in the tubular epithelial cells of the proximal tubule
- No immune complex deposits
Electron microscopy images
Contributed by Jonathan E. Zuckerman, M.D., Ph.D.
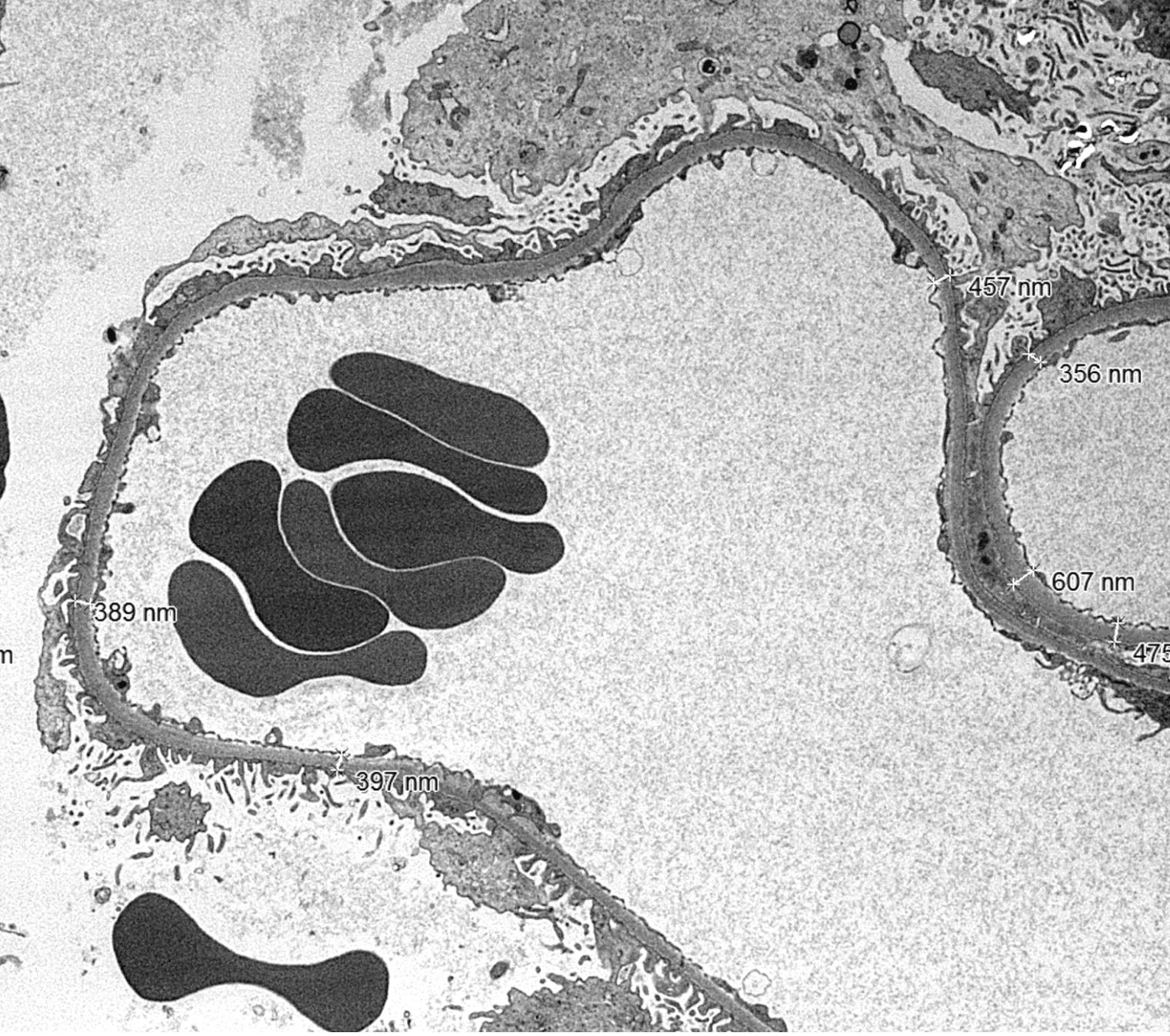
Mild GBM thickening
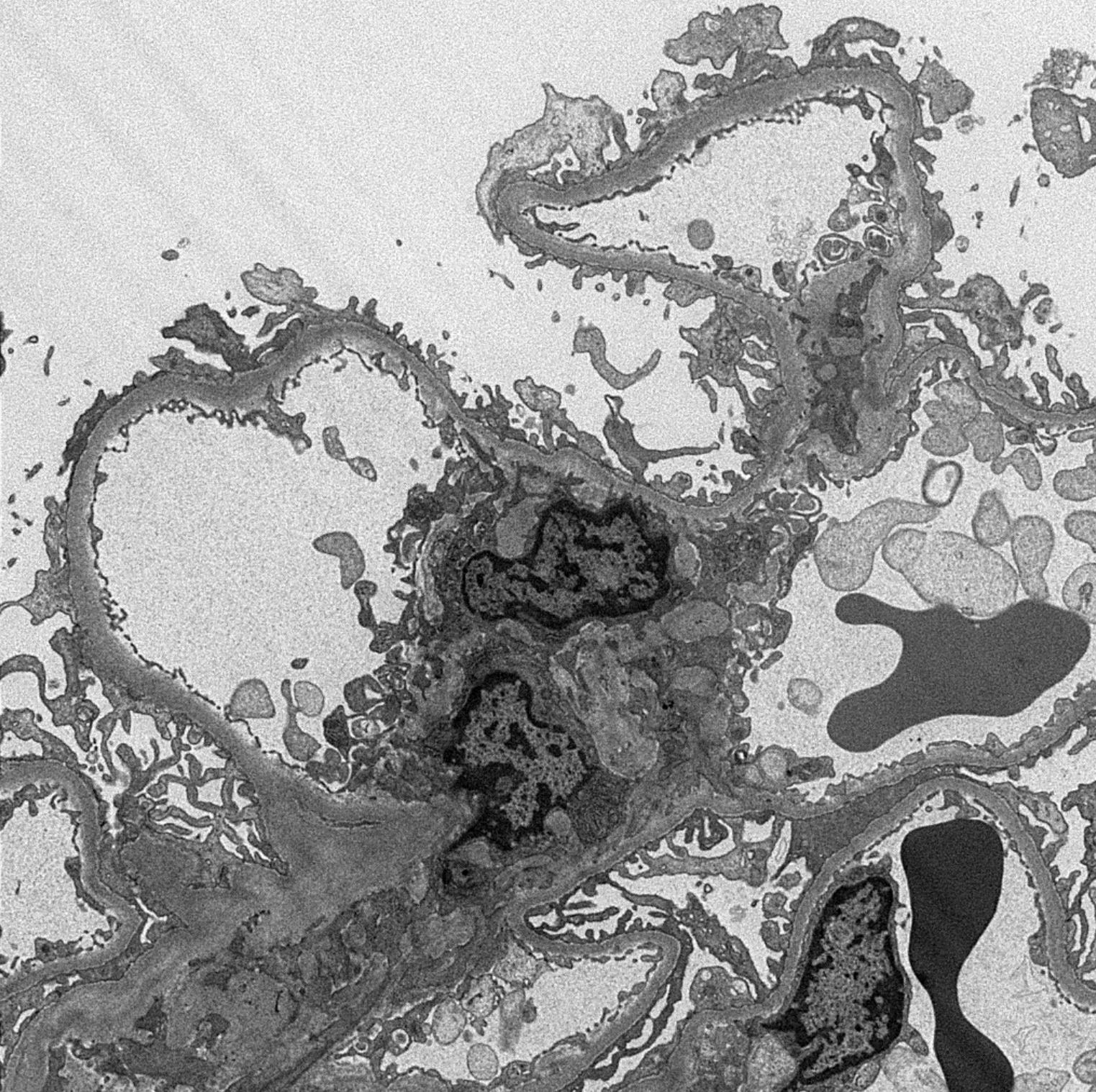
Segmental foot process effacement
Genetics
- Unknown at this time
Sample pathology report
- Left kidney, native, needle core biopsy:
- Glomerulomegaly with secondary focal segmental glomerulosclerosis (FSGS), perihilar variant consistent with obesity related glomerulopathy (see comment)
- Comment: In addition to obesity, other clinical risk factors for these biopsy findings may include obstructive sleep apnea, chronic hypertension and diabetes. These findings may also reflect situations of congenital or acquired states of low nephron number (e.g. low birth weight) or congenital susceptibility to maladaptive glomerular injury.
Differential diagnosis
- Primary focal segmental glomerulosclerosis (FSGS) (Kidney Int 2001;59:1498):
- Sudden onset of proteinuria
- Hypoalbuminemia and edema
- > 75% podocyte foot process effacement
- Diabetic nephropathy:
- Glomerulomegaly in early diabetic nephropathy
- Hyperglycemia and elevated A1C
- Hyalinization of afferent and efferent arterioles
- Difficult to distinguish on morphologic grounds alone
- Sickle cell anemia (N Engl J Med 1992;326:910):
- Glomerulomegaly may be present
- Sickled red blood cells may be present in capillaries
- Requires clinical correlation
- Congenital cyanotic heart disease (Nephrol Dial Transplant 2002;17:144):
- Glomerulomegaly may be present
- Requires clinical correlation
- Congenital renal hypoplasia / oligomeganephronia (Nephrol Dial Transplant 2011;26:2202):
- Glomerulomegaly may be present
- Tubular hypertrophy may also be present
- Kidneys may be small
- Absence of obesity
- Difficult to exclude in obese patients
- Other etiologies of secondary forms of FSGS:
- Due to arteriosclerosis / ischemia / chronic glomerulonephritis
- Perihilar segmental sclerosis
- Glomerulomegaly may not be present
- Often more severe interstitial fibrosis / tubular atrophy and vascular sclerosis than obesity related glomerulopathy
- Some genetic forms of FSGS:
- ACTN4 mutations associated FSGS often exhibit perihilar FSGS (J Am Soc Nephrol 2009;20:961)
- Irregularly aggregated electron dense material in the podocyte cytoplasm
- Autosomal dominant, correlation with family history and genetic testing may be required
- Other etiologies of glomerular hypertrophy:
- Preterm birth
- Sickle cell disease (N Engl J Med 1992;326:910, Kidney Int 1985;27:711)
- Congenital cyanotic heart disease (Nephrol Dial Transplant 2002;17:144)
Additional references
Board review style question #1
A morbidly obese patient has a renal biopsy for subnephrotic range proteinuria that has been gradually worsening. Her serologic workup is negative. A renal biopsy is performed and is significant for the histologic finding shown above. Immunofluorescence is negative and there are no electron dense deposits or glomerular basement membrane abnormalities by light microscopy. What is the most likely diagnosis?
- IgA nephropathy
- Lupus nephritis
- Minimal change disease
- Obesity related glomerulopathy
Board review style answer #1
Board review style question #2
A 50 year old Caucasian woman is found to have mild proteinuria during routine urinary screening. Her serologic workup is negative. A renal biopsy is performed and is significant for the finding shown above. Immunofluorescence is negative and there are no electron dense deposits or glomerular basement membrane abnormalities by light microscopy. In which clinical settings is this biopsy finding typically seen?
- Advanced diabetic disease
- Elevated BMI
- Lupus
- Mild essential hypertension
Board review style answer #2
