

Kidney nontumor / medical renal
Glomerular disease
Other primary glomerular disease
Crescentic glomerulonephritis overview
Editorial Board Member: Nicole K. Andeen, M.D.
Editor-in-Chief: Debra L. Zynger, M.D.


Last author update: 25 March 2021
Last staff update: 20 January 2023
Copyright: 2002-2024, PathologyOutlines.com, Inc.
PubMed Search: Rapidly progressive crescentic glomerulonephritis
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Laboratory | Prognostic factors | Case reports | Treatment | Microscopic (histologic) description | Microscopic (histologic) images | Immunofluorescence description | Immunofluorescence images | Positive stains | Electron microscopy description | Electron microscopy images | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Murshed KA, Taha NM, Akhtar M. Crescentic glomerulonephritis overview. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/kidneyrpgn.html. Accessed April 16th, 2024.
Definition / general
- Rapidly progressive glomerulonephritis (RPGN) is a clinical syndrome, not a pathologic diagnosis
- Often presents with a rapid decline in kidney function, hematuria, proteinuria, oliguria or hypertenison
- Often crescentic glomerulonephritis (CGN) is characterized by glomerular crescents in > 50% of glomeruli
Essential features
- Often crescent formation in > 50% of the glomeruli
- Immunofluorescence and serologic findings distinguish etiology:
- Antiglomerular basement membrane (GBM) disease is characterized by circulating anti-GBM antibody, linear staining for immunoglobulin (Ig) G on immunofluorescence microscopy and absent electron dense deposits on electron microscopy
- Immune complex mediated glomerulonephritis (GN) occurs in various glomerulonephritis (lupus, IgAN) and is characterized by granular staining for Ig and complements immunofluorescence with electron dense deposits on electron microscopy
- Pauci-immune complex mediated / vasculitic type glomerulonephritis is frequently associated with circulating antineutrophil cytoplasmic antibody (ANCA) and is characterized by negative or scanty Ig deposits on immunofluorescence (pauci-immune complex pattern) and electron microscopy
Terminology
- Rapidly progressive nephritic syndrome
- Rapidly progressive nephritic syndrome, diffuse crescentic glomerulonephritis
- Rapidly progressive nephritic syndrome with extracapillary glomerulonephritis
ICD coding
Epidemiology
- CGN accounts for < 10% of all patients presenting with primary glomerulopathy
- M:F = 1:1, more common in white population, rare in Africans
- Bimodal age distribution: first peak around age 30 and second after 60
- Pauci-immune complex glomerulonephritis is the most common subtype of CGN in adults (Kidney Int 2003;63:1164)
- Anti-GBM disease is the most aggressive form of CGN (Kidney Int 2003;63:1164)
Sites
- Kidney
- Kidney and lung (pulmonary renal syndrome, Goodpasture’s syndrome)
- Systemic, including various organs such as skin, lung, gastrointestinal and nervous system, if associated with vasculitis and connective tissue disease
Pathophysiology
- For pathophysiology of crescents, endothelial injury is a key driver, which leads to breaks and rupture of GBM (J Pathol 2012;228:482)
- This triggers coagulation cascade within Bowman space, ultimately leading to fibrin deposition
- Fibrin stimulates parietal epithelial cells to proliferate, resulting in formation of cellular crescents
- Cellular crescents lead to increase in counter pressure, collapse of glomerular tuft and tubular outflow obstruction
- This will result in decline in the single nephron glomerular filtration rate
- Multilevel growth of parietal epithelial cells may lead to epithelial - mesenchymal transition in cell phenotype, which leads to the formation of fibrocellular and fibrous crescents (Curr Opin Nephrol Hypertens 2020;29:302)
Etiology
- Anti-GBM disease: circulating antibodies directed against the noncollagenous domain of alpha 3 chain of type IV collagen
- Immune complex mediated crescentic GN: secondary to immune complex deposition in conditions such as postinfectious GN, lupus nephritis, membranoproliferative GN, IgA nephropathy and cryoglobulinemia
- Pauci-immune complex crescentic GN: 80 - 90% are associated with ANCA
- ANCA associated vasculitis includes granulomatosis with polyangiitis, microscopic polyangiitis, eosinophilic granulomatosis with polyangiitis or renal limited vasculitis (J Am Soc Nephrol 2010;21:1628)
- Variety of drugs may also cause the disease (hydralazine, penicillamine, rifampicin)
- Mixed antibody patterns may also occur (anti-GBM + ANCA, antidouble stranded DNA + ANCA, antidouble stranded DNA + anti-GBM)
Clinical features
- Rapid deterioration of renal function over short period (days to weeks)
- Acute nephritic syndrome: (Clin Exp Nephrol 2016;20:322)
- Oliguria
- Hypertension
- Hematuria, macroscopic and less frequently microscopic
- Proteinuria
Diagnosis
- Clinicopathological diagnosis, mainly achieved on renal biopsy
Laboratory
- Elevated serum creatinine and blood urea nitrogen (BUN) (Clin Exp Nephrol 2016;20:322)
- Elevated C reactive protein (CRP) and erythrocyte sedimentation rate (ESR)
- Hematuria
- Red blood cell casts
- Proteinuria (usually nonnephrotic range)
- Complement levels
- Autoantibodies (J Am Soc Nephrol 2016;27:1278)
- Anti-GBM antibody
- ANCA, antimyeloperoxidase (pANCA) and antiproteinase 3 (cANCA)
- Antidouble stranded DNA antibody
Prognostic factors
- Best predictor of outcome for all types of crescentic glomerulonephritis is the severity of renal failure at time of initiation of therapy (Kidney Int 2003;63:1164)
- Dialysis dependency at presentation is considered a poor prognostic sign
- Cellular crescents are usually reversible with prompt and aggressive treatment or may resolve spontaneously in postinfectious GN
- Fibrocellular and fibrous crescents are irreversible in terms of potential recovery of single nephron glomerular filtration rate (Curr Opin Nephrol Hypertens 2020;29:302)
Case reports
- 26 year old woman with necrotizing CGN related to sarcoidosis (J Med Case Rep 2015;9:282)
- 59 year old man presented with membranous nephropathy with crescents (J Am Soc Nephrol 2011;22:1804)
- 68 year old woman with CGN due to coexistent anti-GBM disease and fibrillary glomerulonephritis (Clin Kidney J 2016;9:97)
- 74 year old woman with systemic lupus erythematosus presented with RPGN secondary to IgA nephropathy (Case Rep Nephrol 2019;2019:8354823)
Treatment
- Anti-GBM disease: plasmapheresis and immunosuppressive agents (glucocorticoids and cyclophosphamide)
- Immune complex mediated crescentic GN: depends on the underlying etiology
- Pauci-immune complex crescentic GN: immunosuppressive agents, rituximab (Clin J Am Soc Nephrol 2017;12:1162)
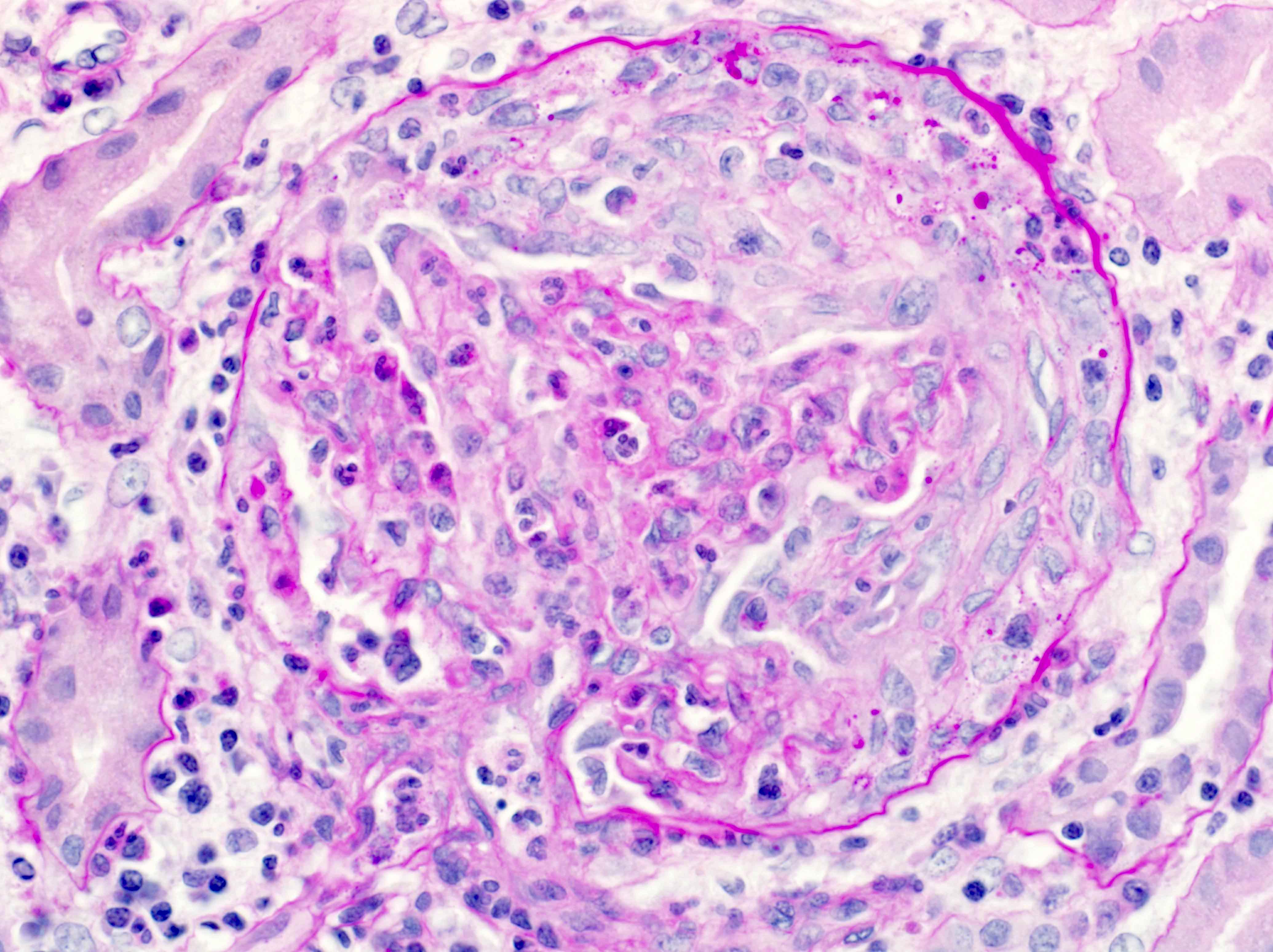
Microscopic (histologic) description
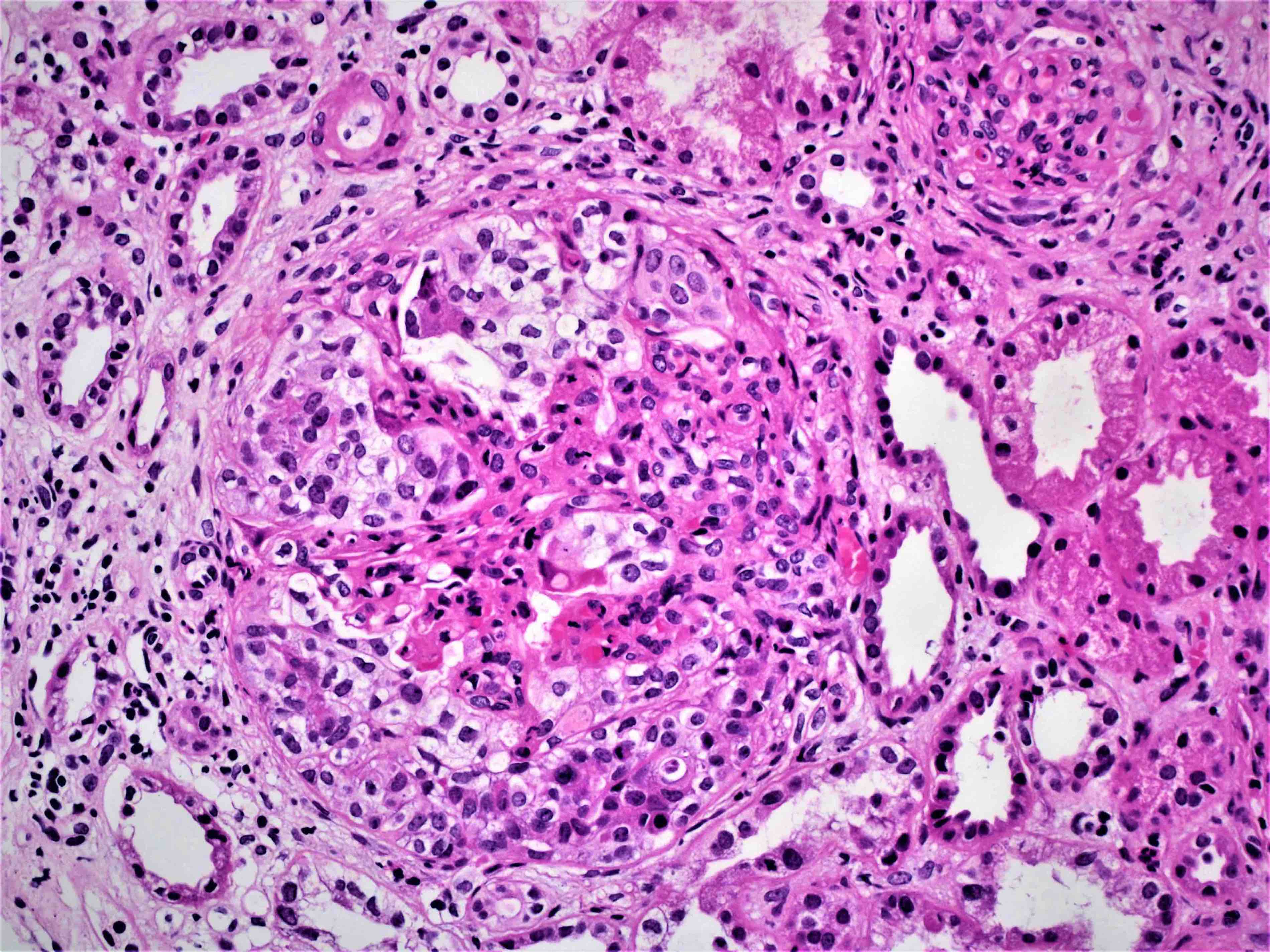
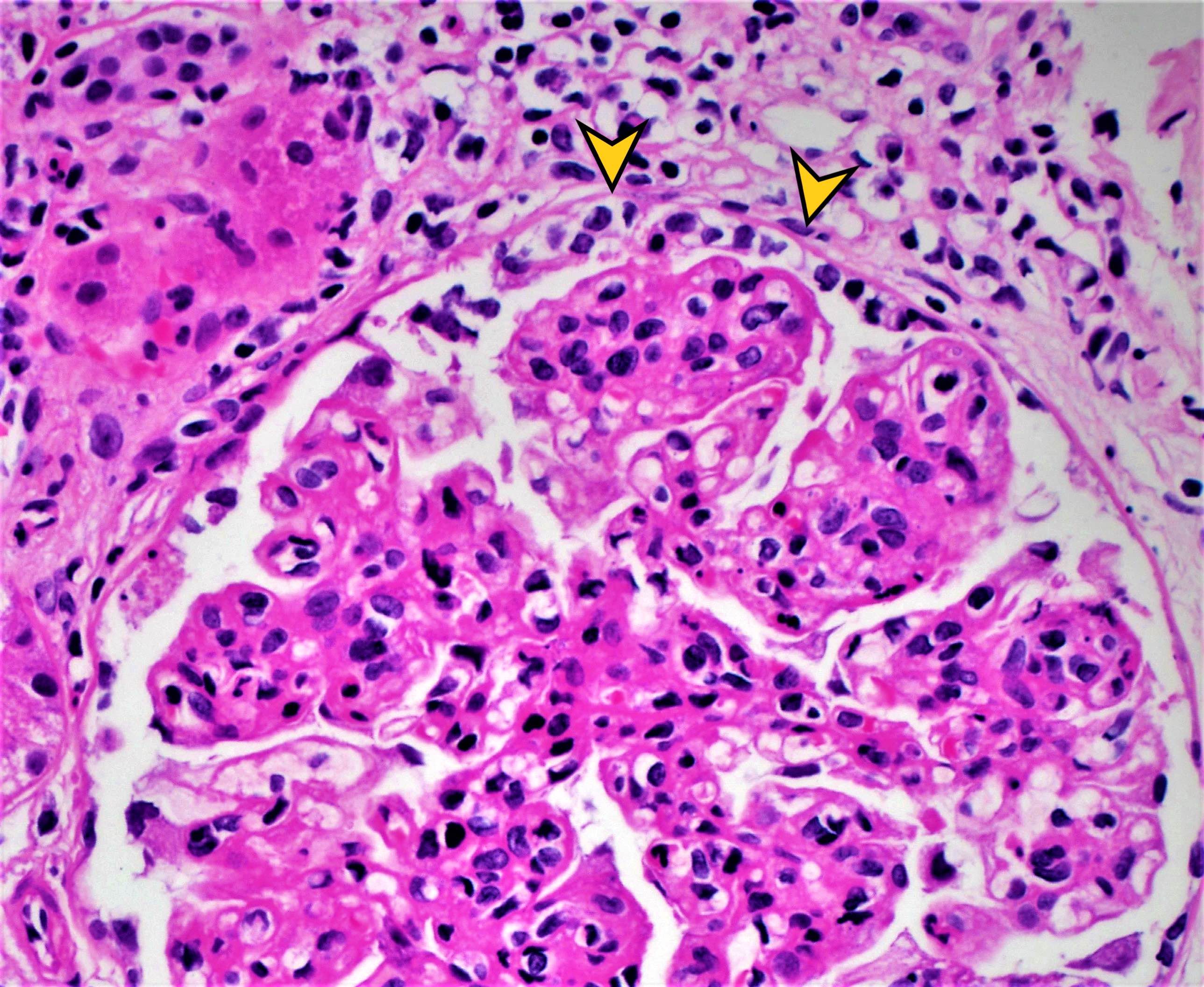
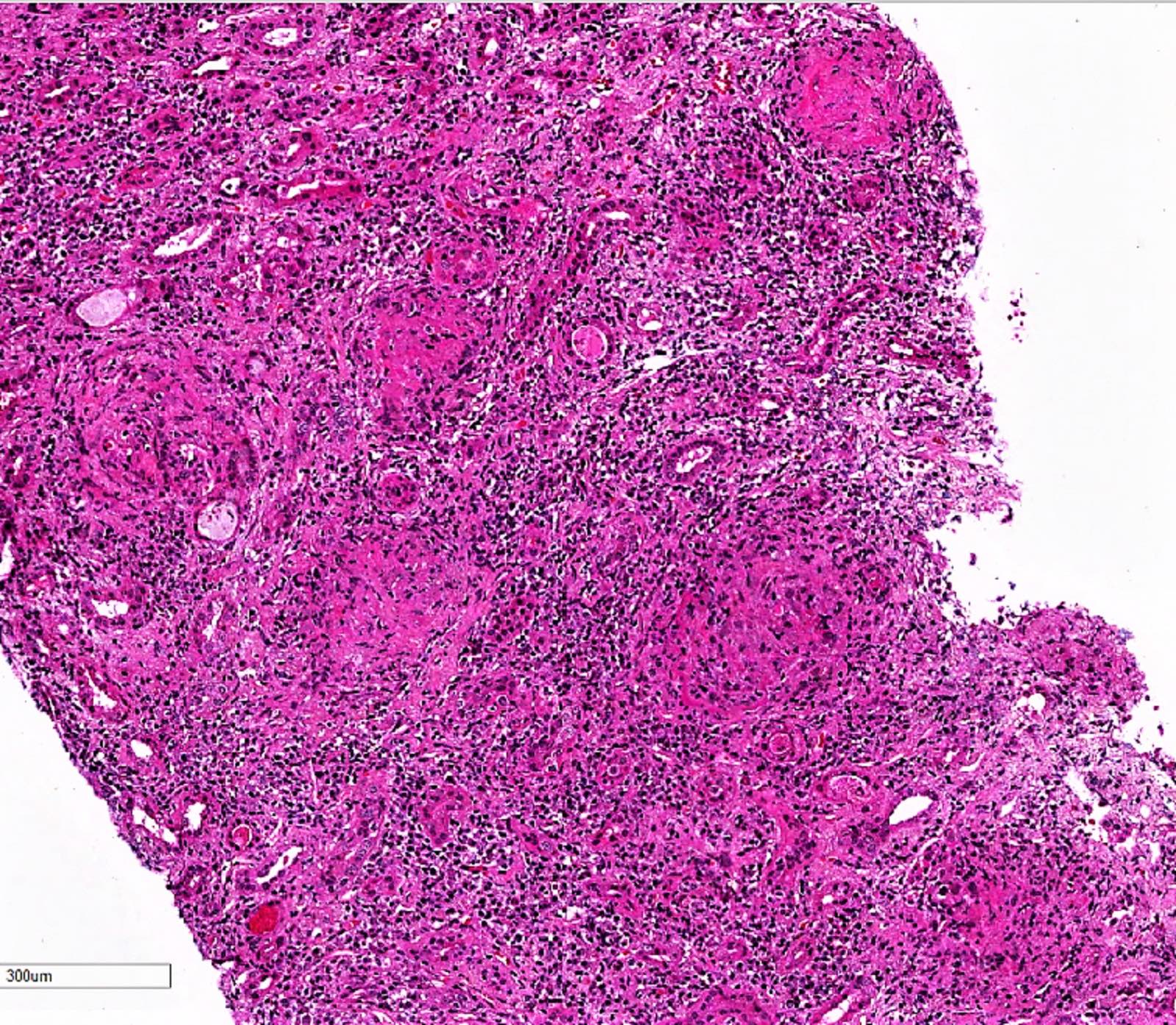
- Extracapillary cellular proliferation (crescents) composed of parietal epithelial cells, macrophages and fibrin
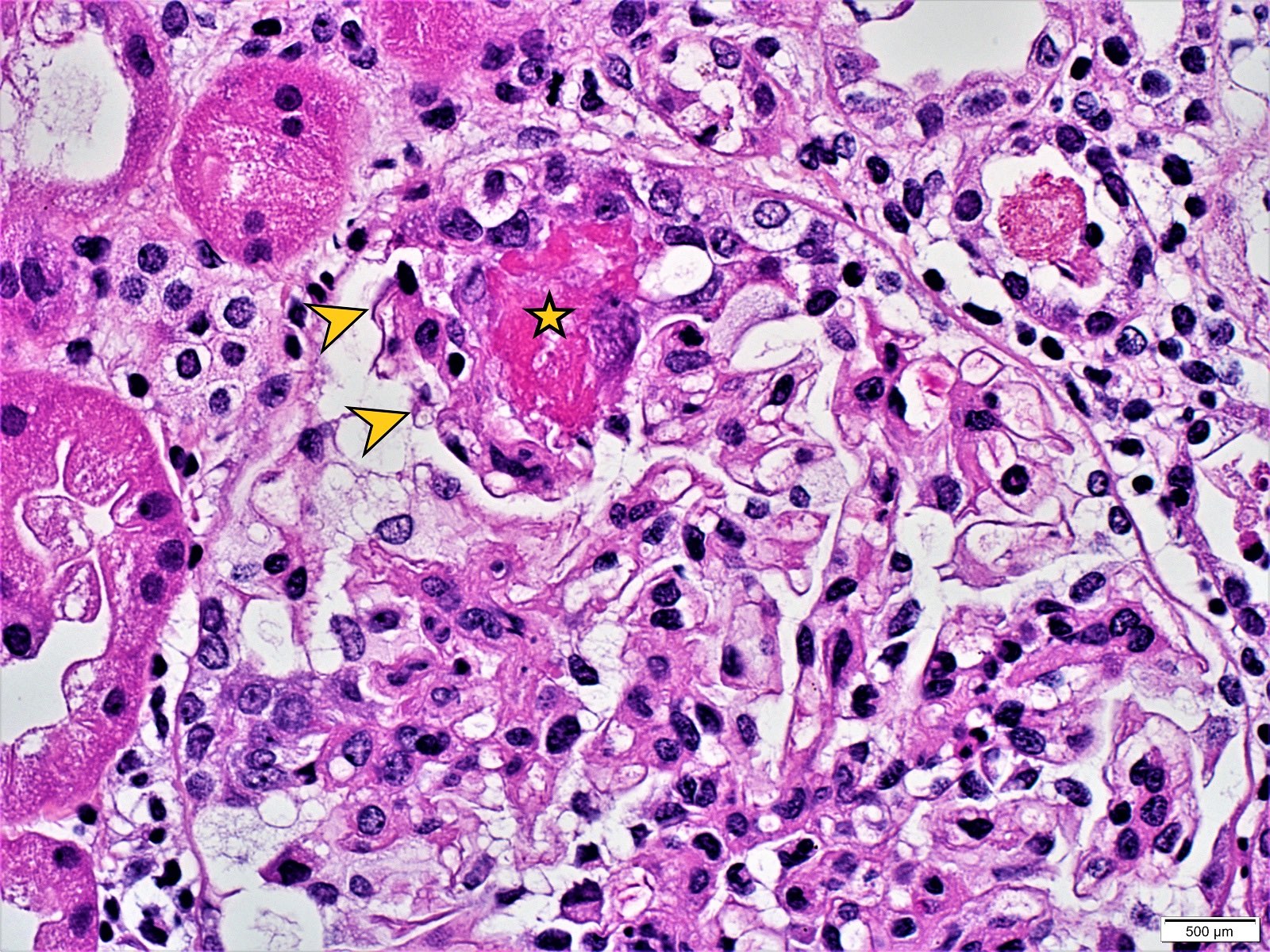
- Segmental fibrinoid necrosis of the glomerular tufts
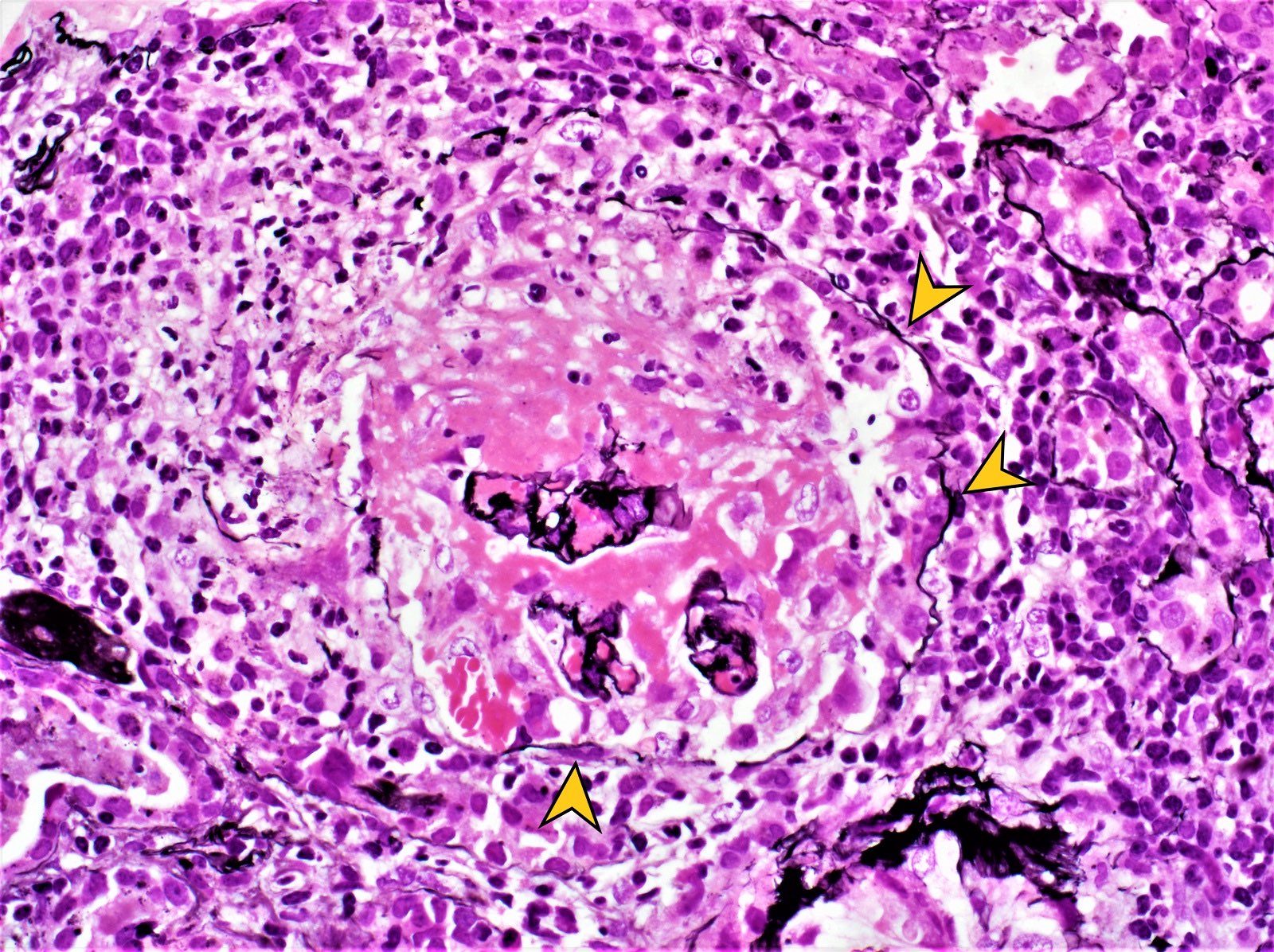
- Active periglomerular inflammation in cases with rupture of Bowman capsule
- In anti-GBM disease, crescents are uniform and temporally homogeneous, showing the same stage of activity and chronicity (Adv Anat Pathol 2021;28:59)
- In pauci-immune complex crescentic GN, crescents are heterogeneous at variable ages with mixture of cellular, fibrocellular and fibrous crescents; the underlying glomerular architecture is generally normal (Adv Anat Pathol 2021;28:59)
- In immune complex mediated crescentic GN, there are often underlying glomerular architectural changes including esangial or endocapillary proliferation (systemic lupus erythematosus, IgAN)
- Small vessel vasculitis is a feature for pauci-immune complex crescentic glomerulonephritis CGN
- Crescents are classified based on their composition and age into: (J Am Soc Nephrol 2016;27:1278)
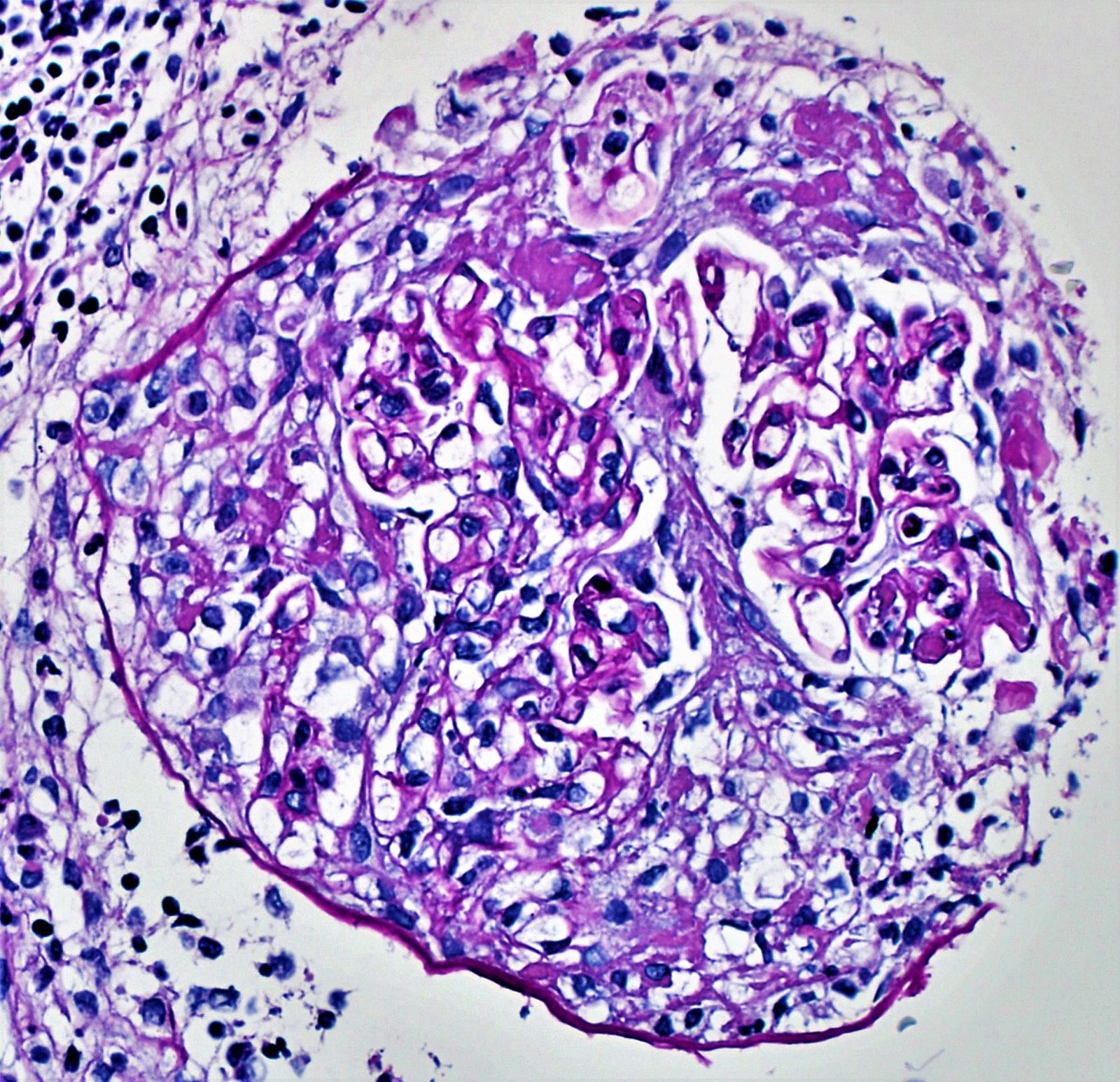
- Cellular crescent: extracapillary cell proliferation of more than 2 cell layers, involving at least 10% of glomerular circumference with > 50% of the lesion occupied by cells
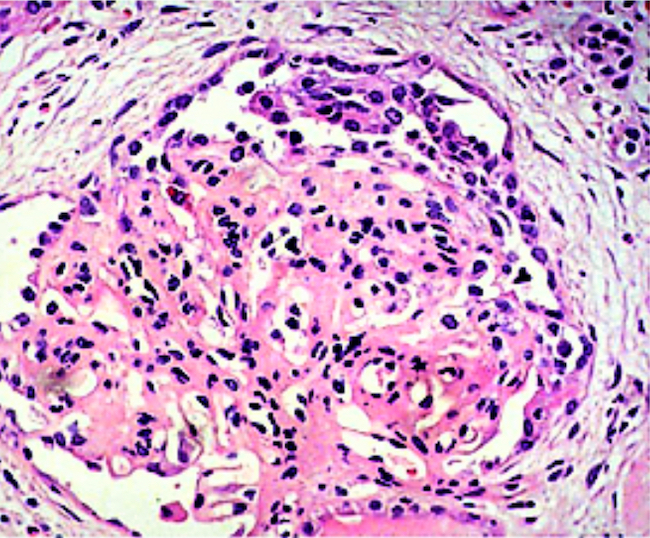
- Fibrocellular crescent: extracapillary lesion comprising cells and extracellular matrix with < 50% cells and < 90% matrix
- Fibrous crescent: extracapillary crescents with > 90% matrix
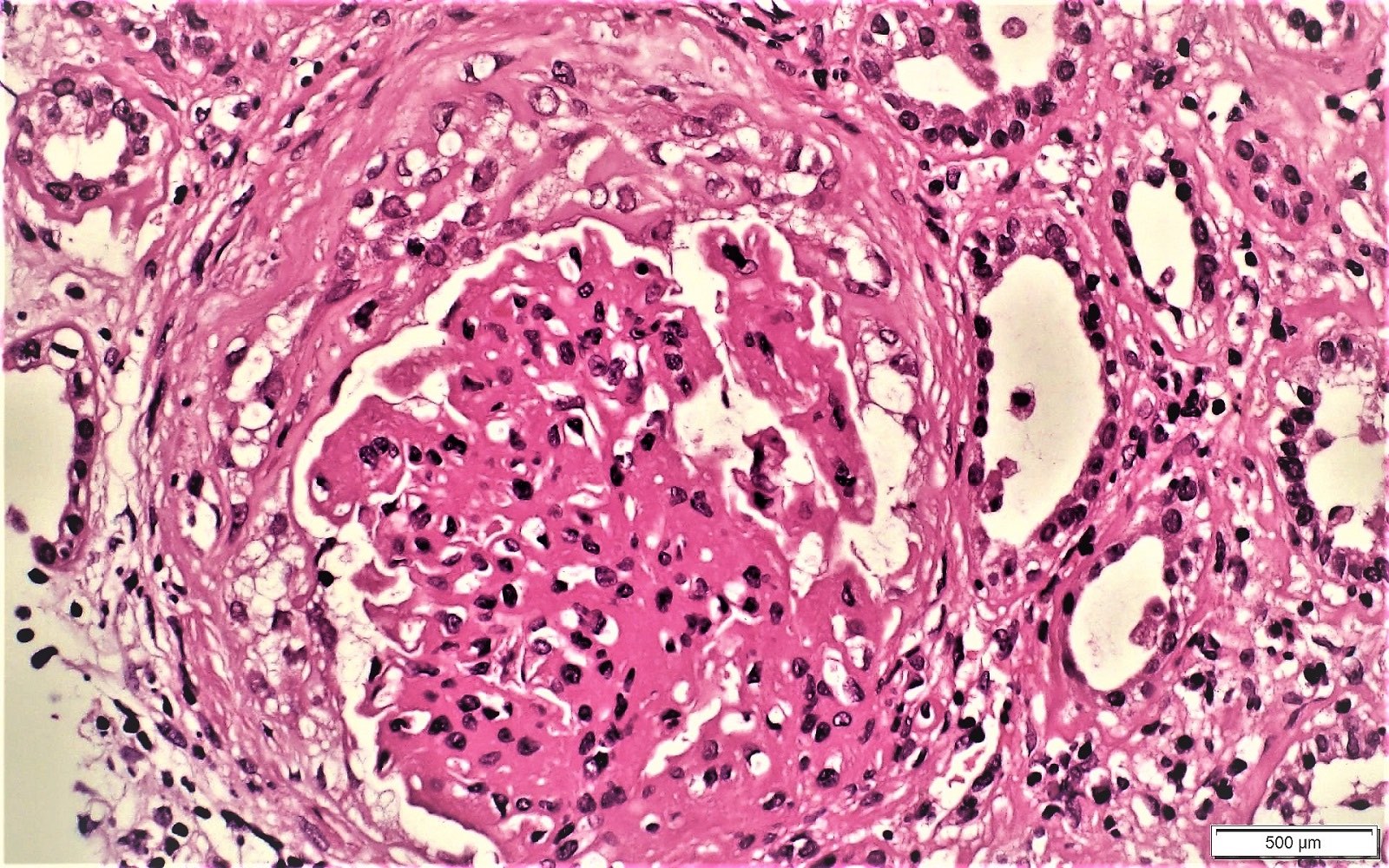
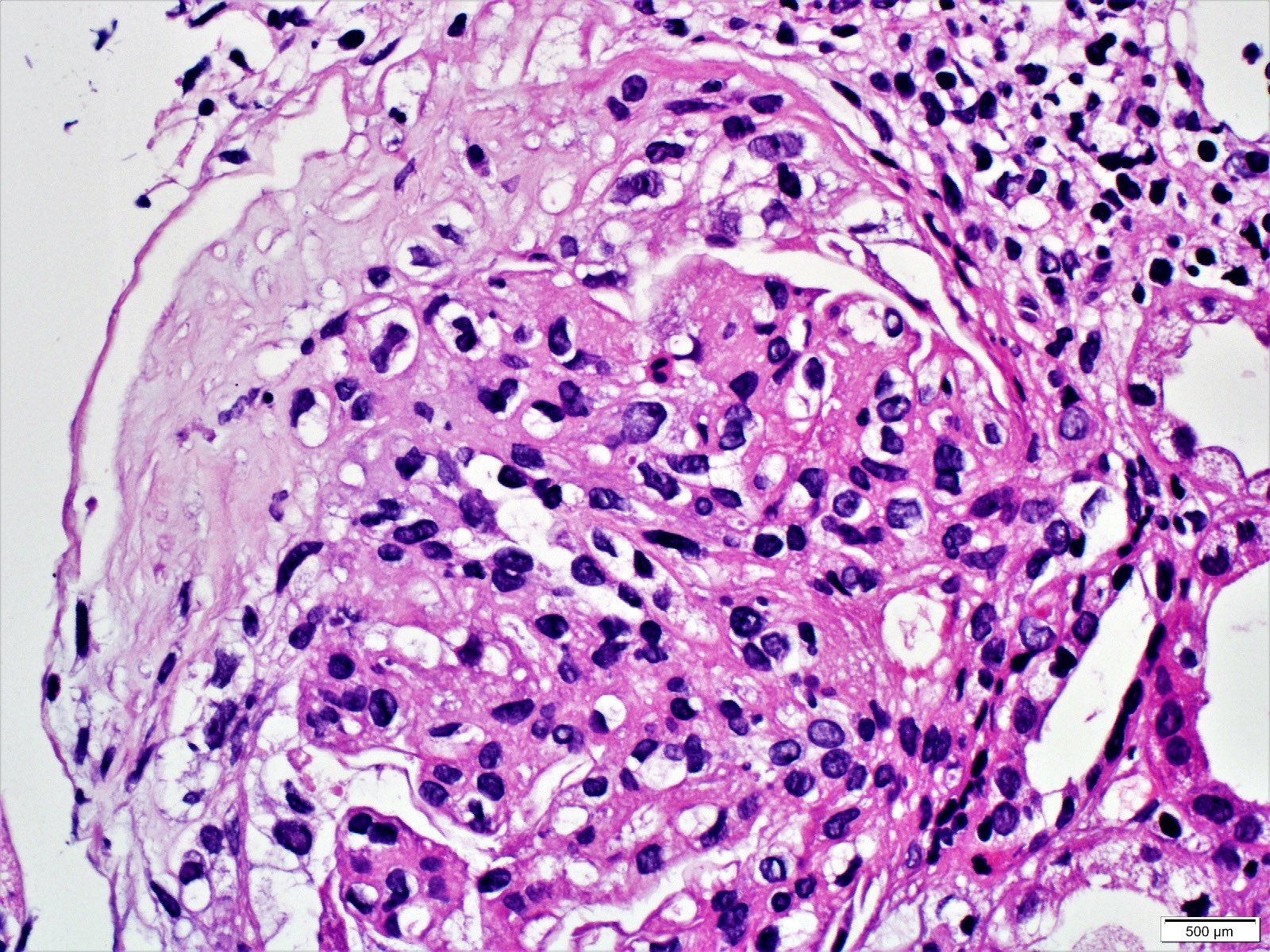
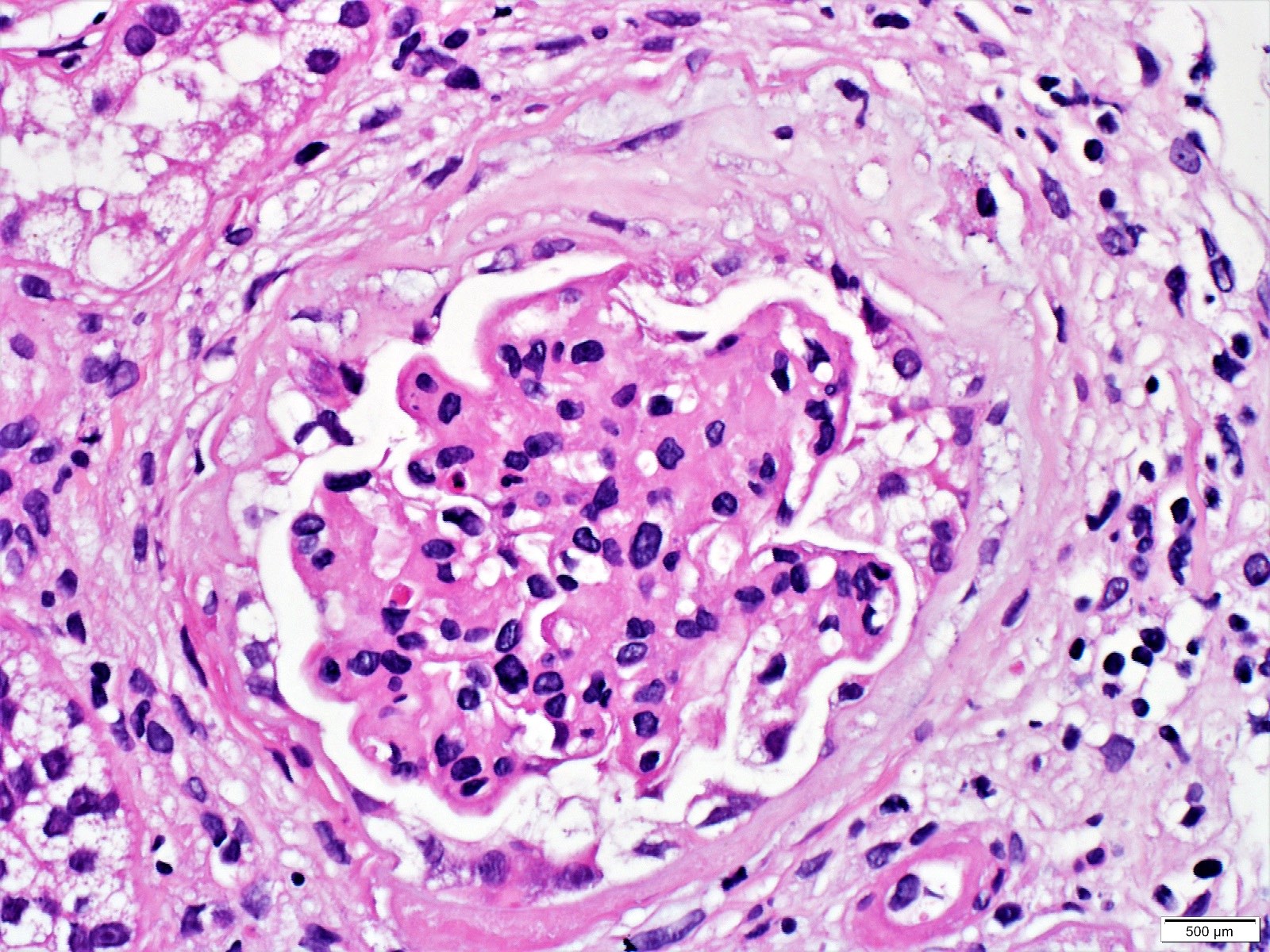
Microscopic (histologic) images
Contributed by Khaled A. Murshed, M.D., Noheir M. Taha, M.B.B.Ch., M.D. and Mohammed Akhtar, M.D.
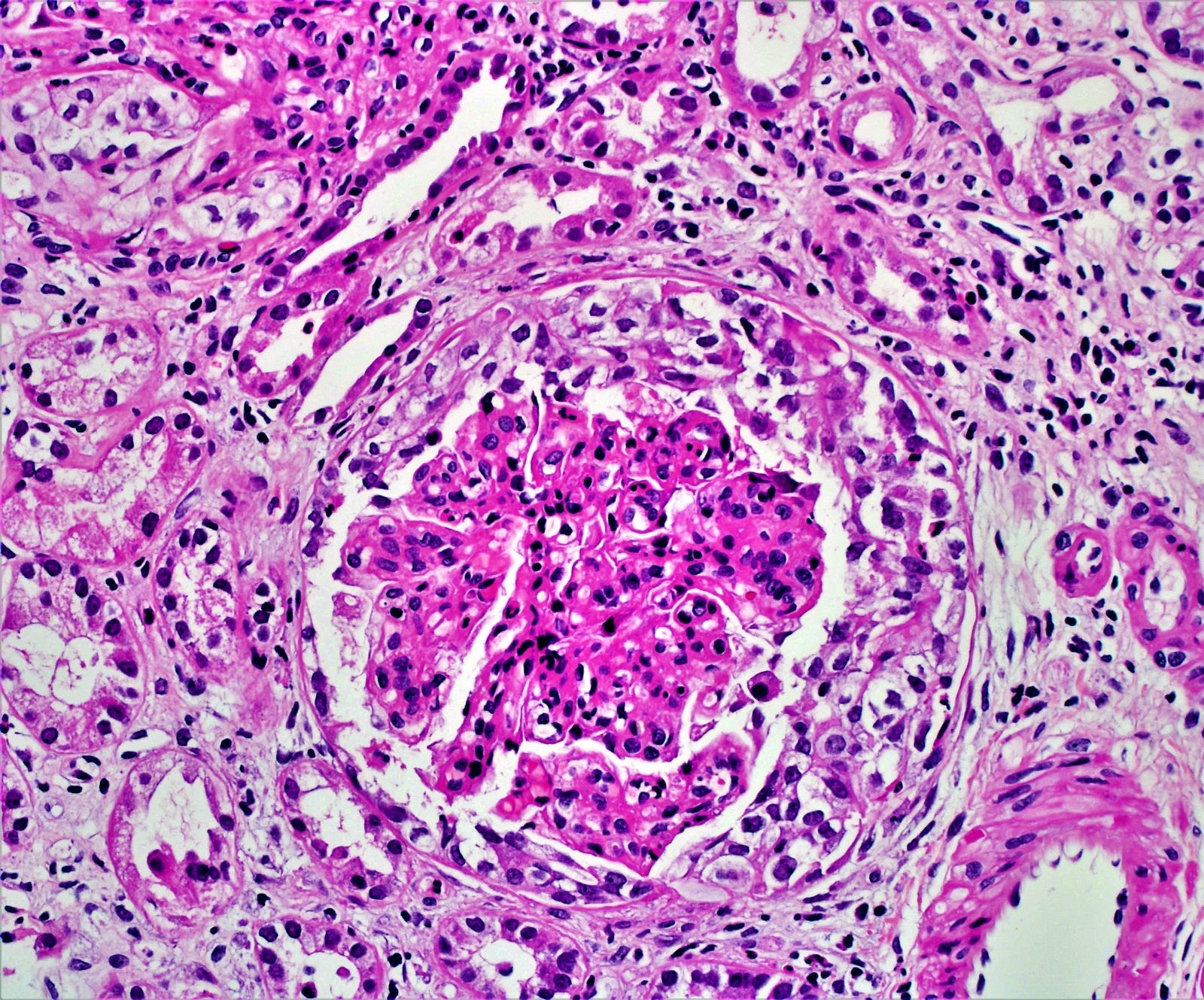
Cellular crescent
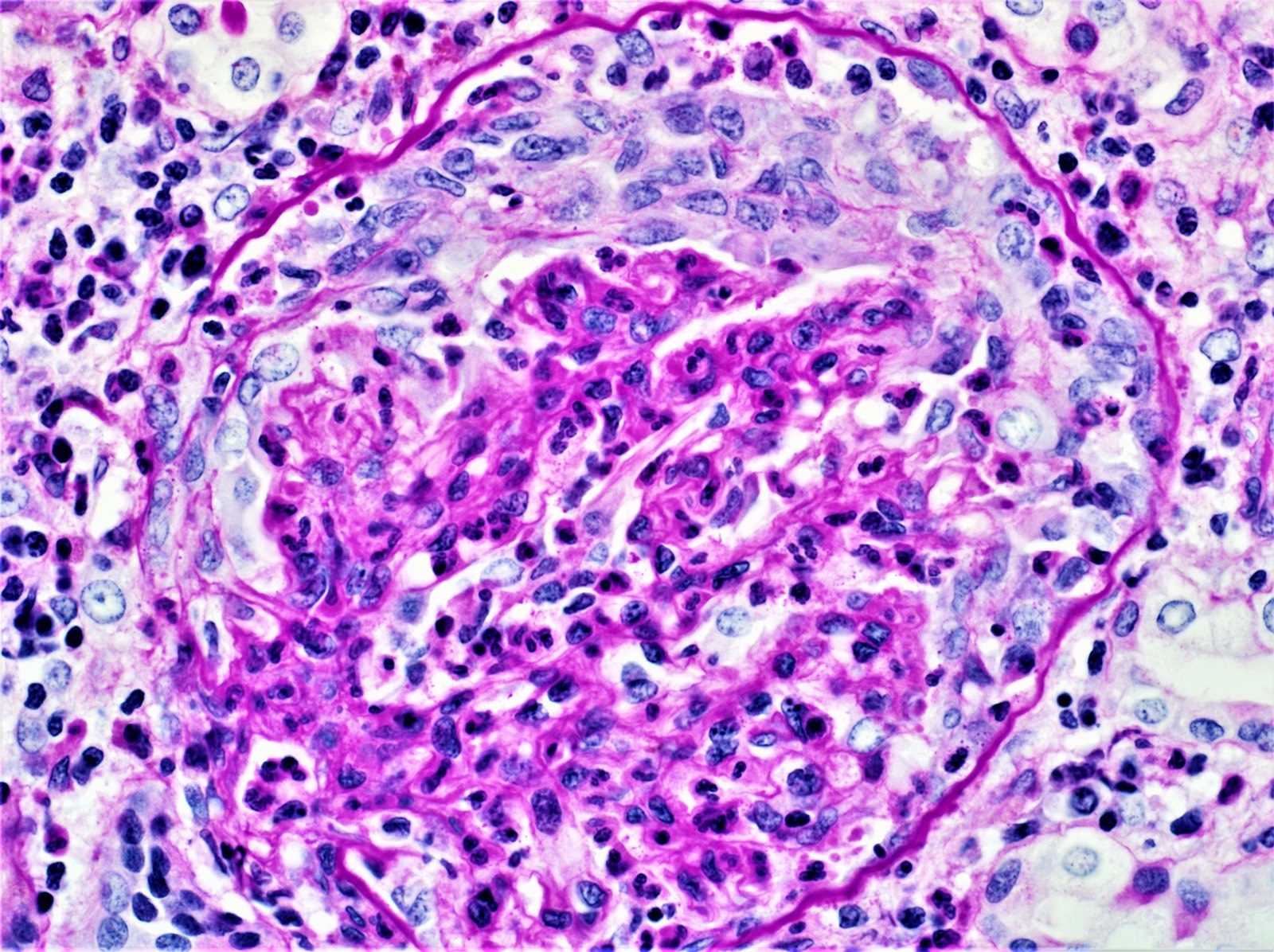
Cellular crescent high magnification
Fibrin and PEC proliferation
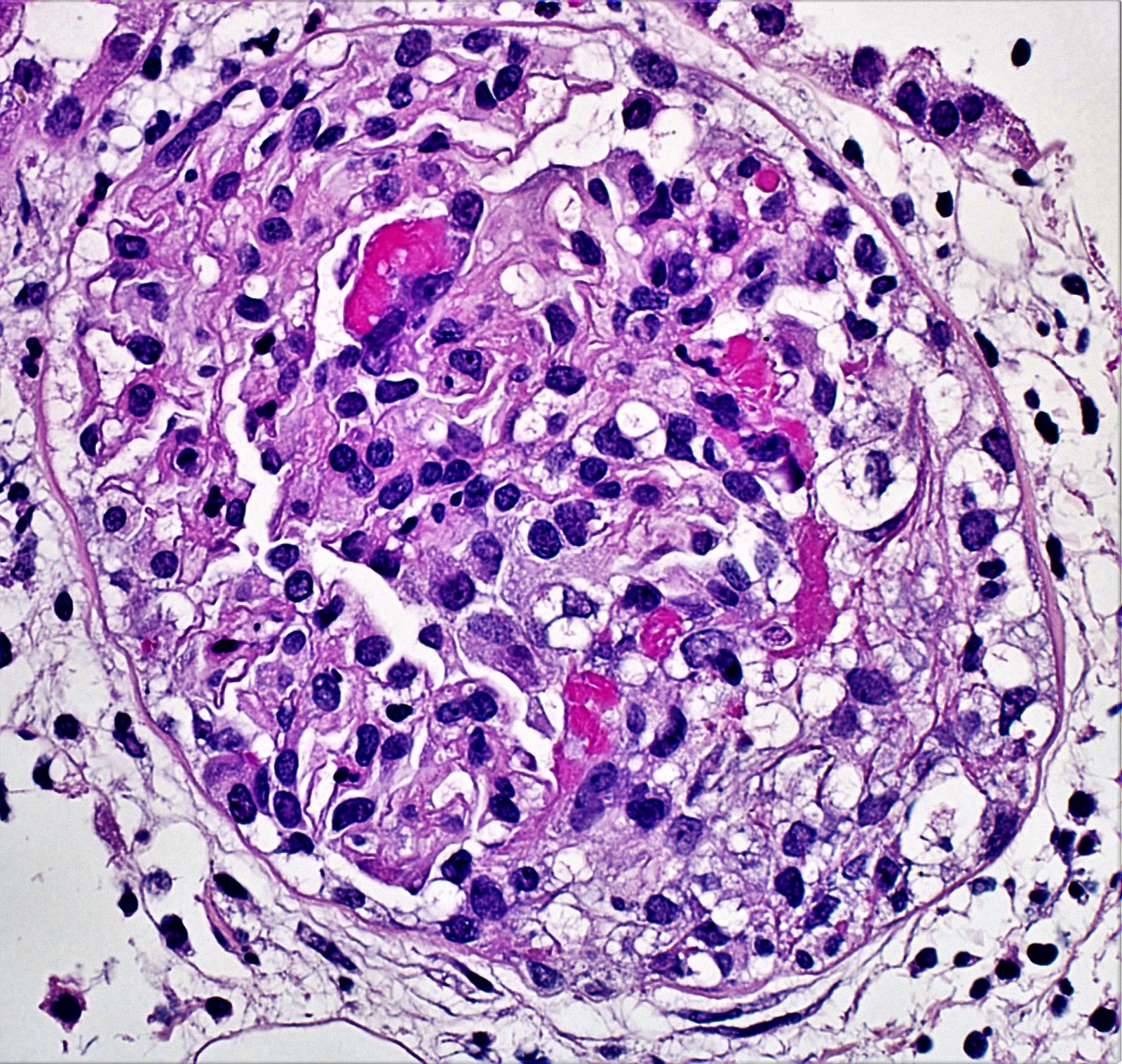
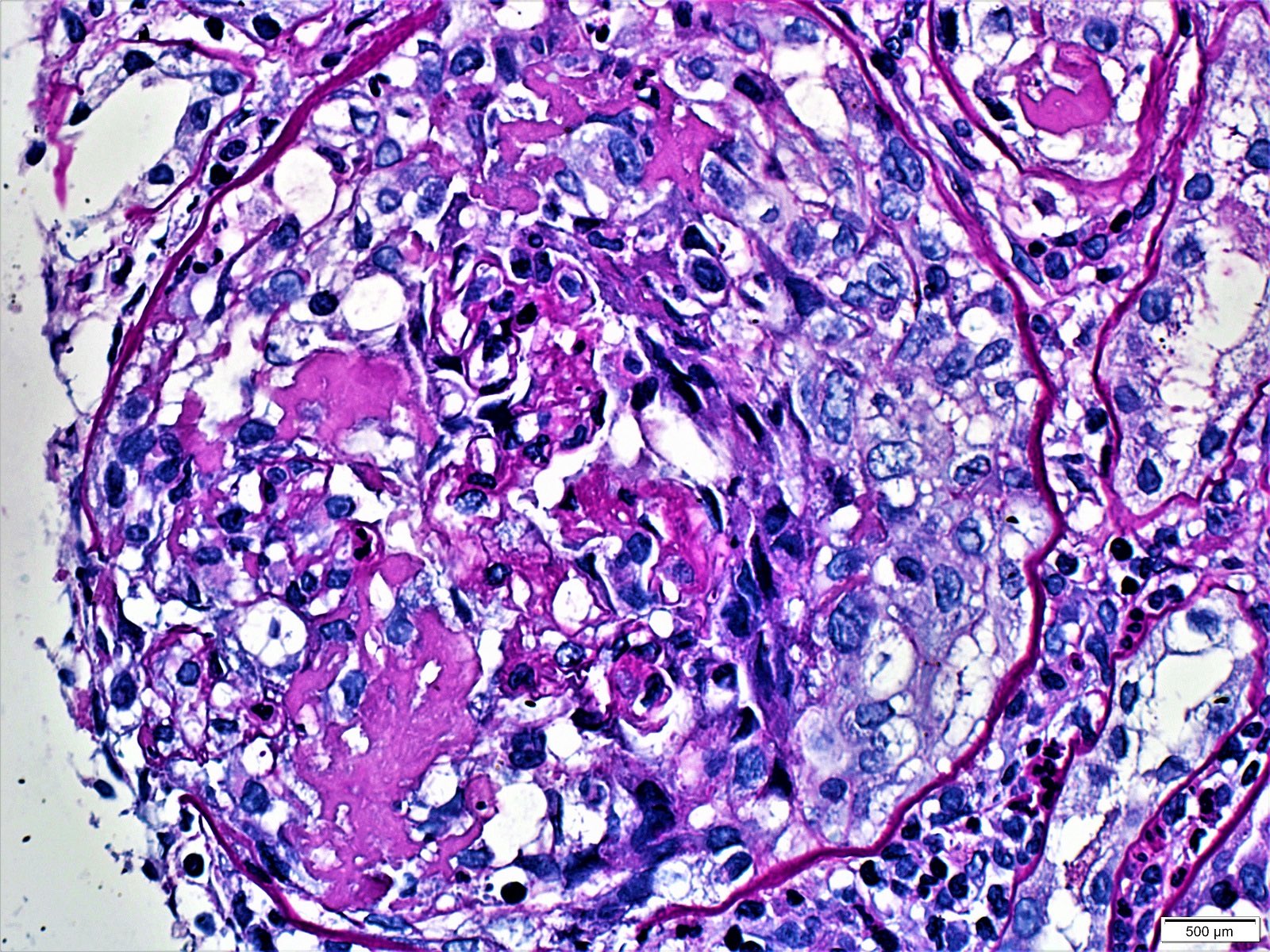
Cellular crescent with fibrin
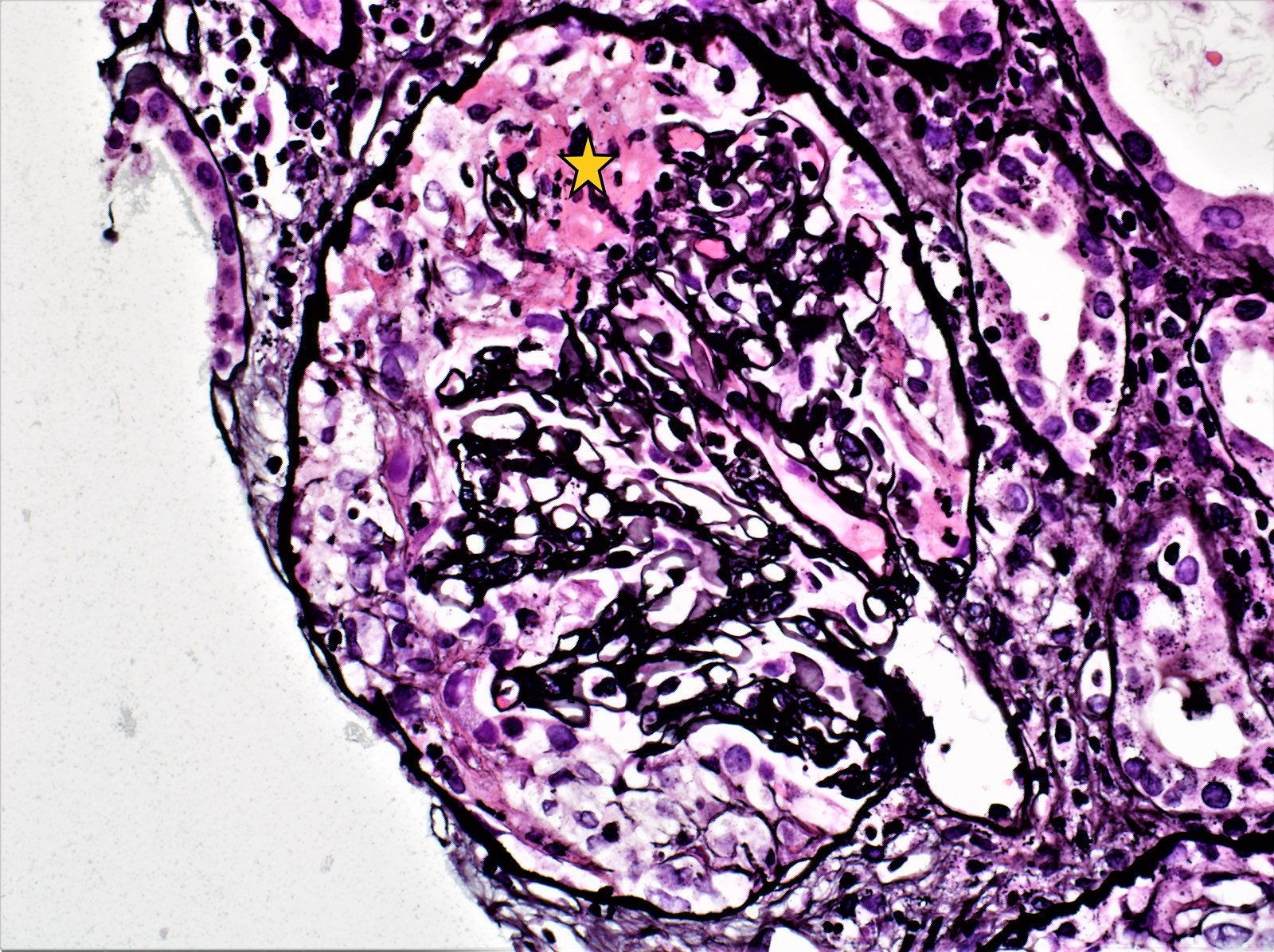
Fibrinoid necrosis
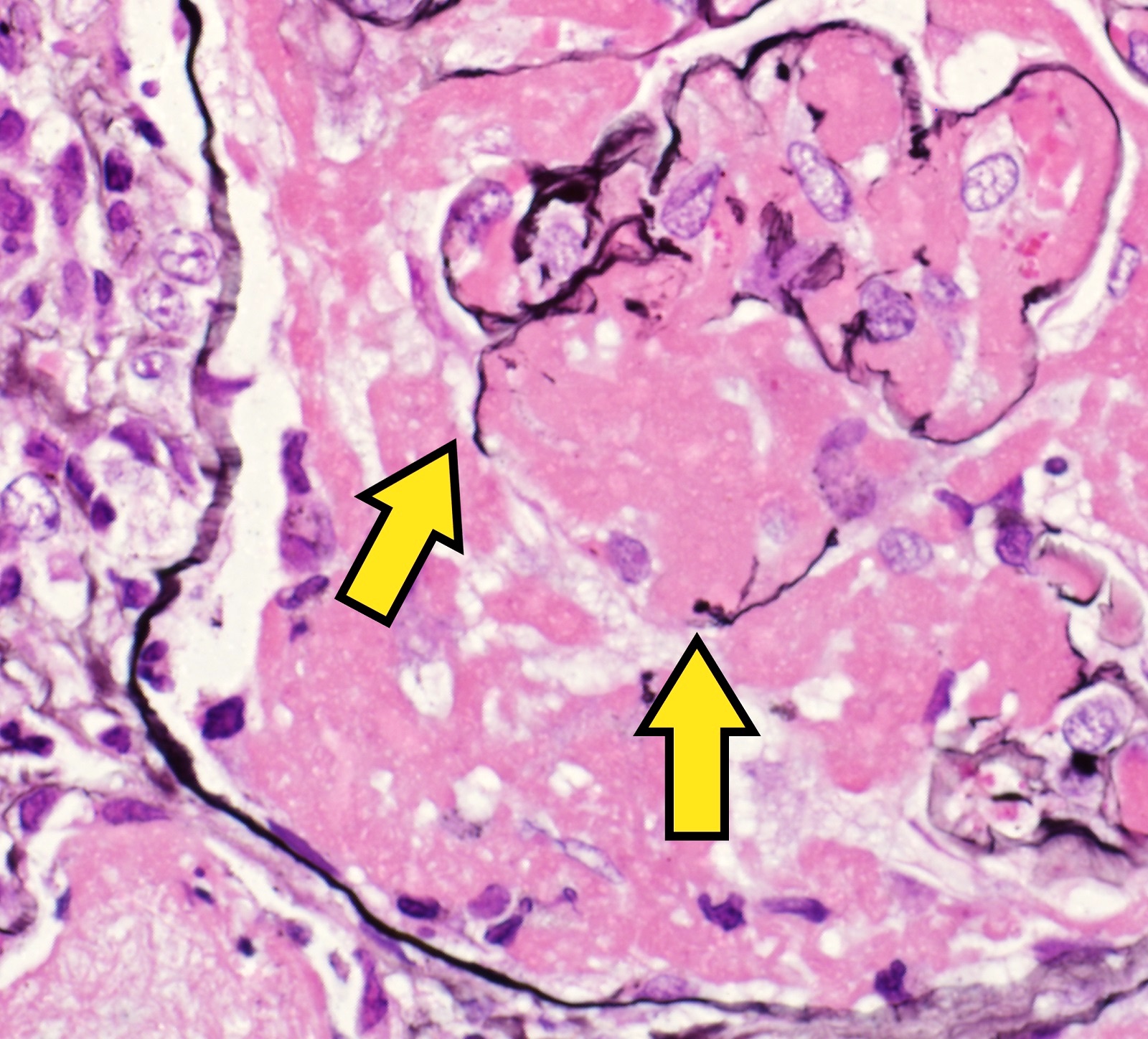
Capillary wall defect high magnification
Bowman capsule defect
Circular crescent
Monolayer PEC proliferation
Early crescent
Fibrocellular crescent
Fibrocellular fibrous crescent
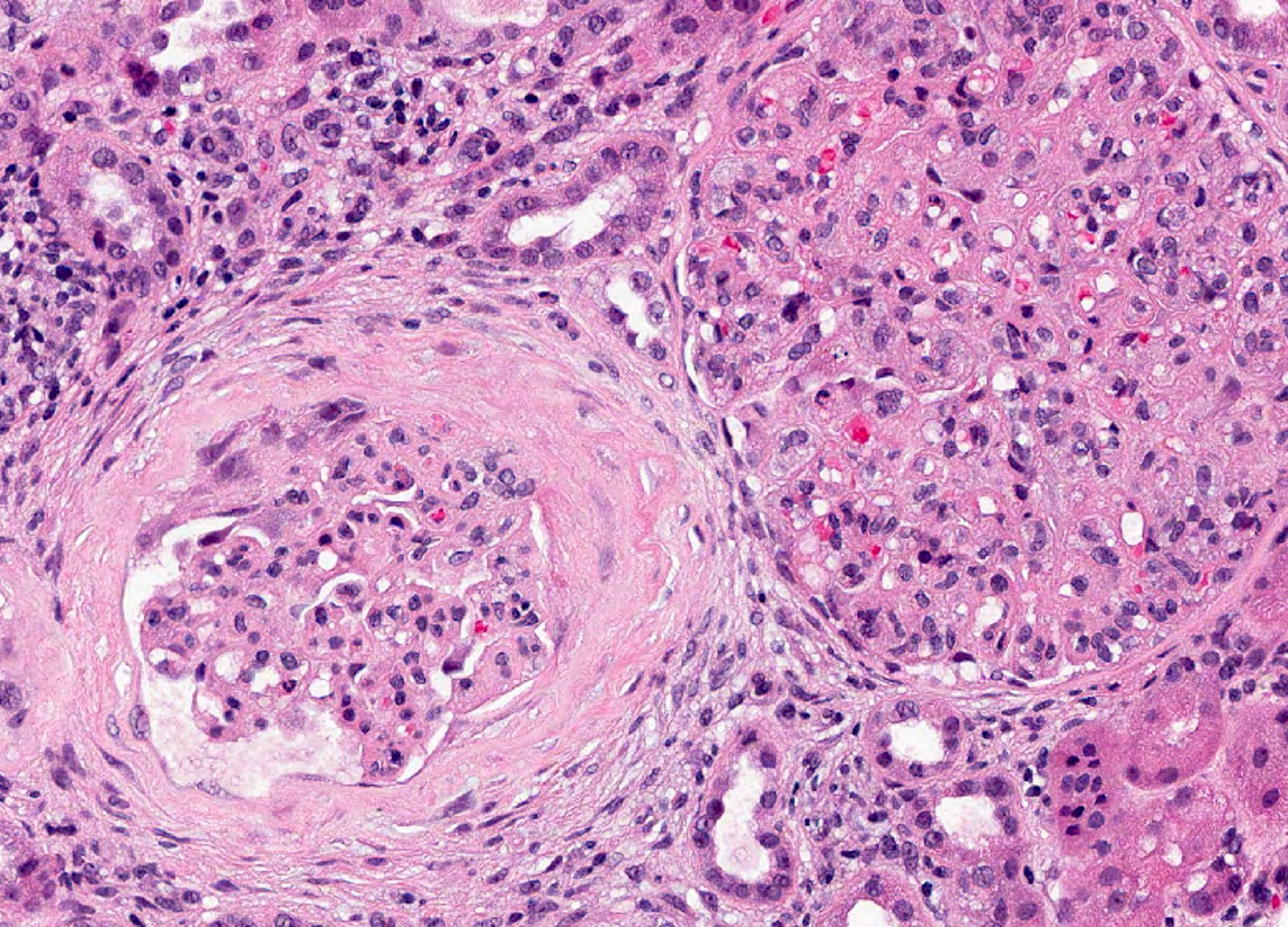
Fibrous crescent
Anti-GBM disease

ANCA associated GN
Immunofluorescence description
- Anti-GBM disease: strong linear staining of IgG and frequently C3 along GBM (Adv Anat Pathol 2021;28:59)
- Similar pattern along tubular basement membranes in some cases
- Immune complex mediated crescentic GN: granular deposits of Ig and complement; their type and location (subepithelial, subendothelial, mesangial) depend on the underlying etiology
- Pauci-immune complex crescentic GN: negative or weak (≤ 1+) staining of Ig and complement (pauci-immune pattern)
- Fibrin deposition in cellular crescents and foci of fibrinoid necrosis
Immunofluorescence images
Contributed by Khaled A. Murshed, M.D., Noheir M. Taha, M.B.B.Ch., M.D. and Mohammed Akhtar, M.D.
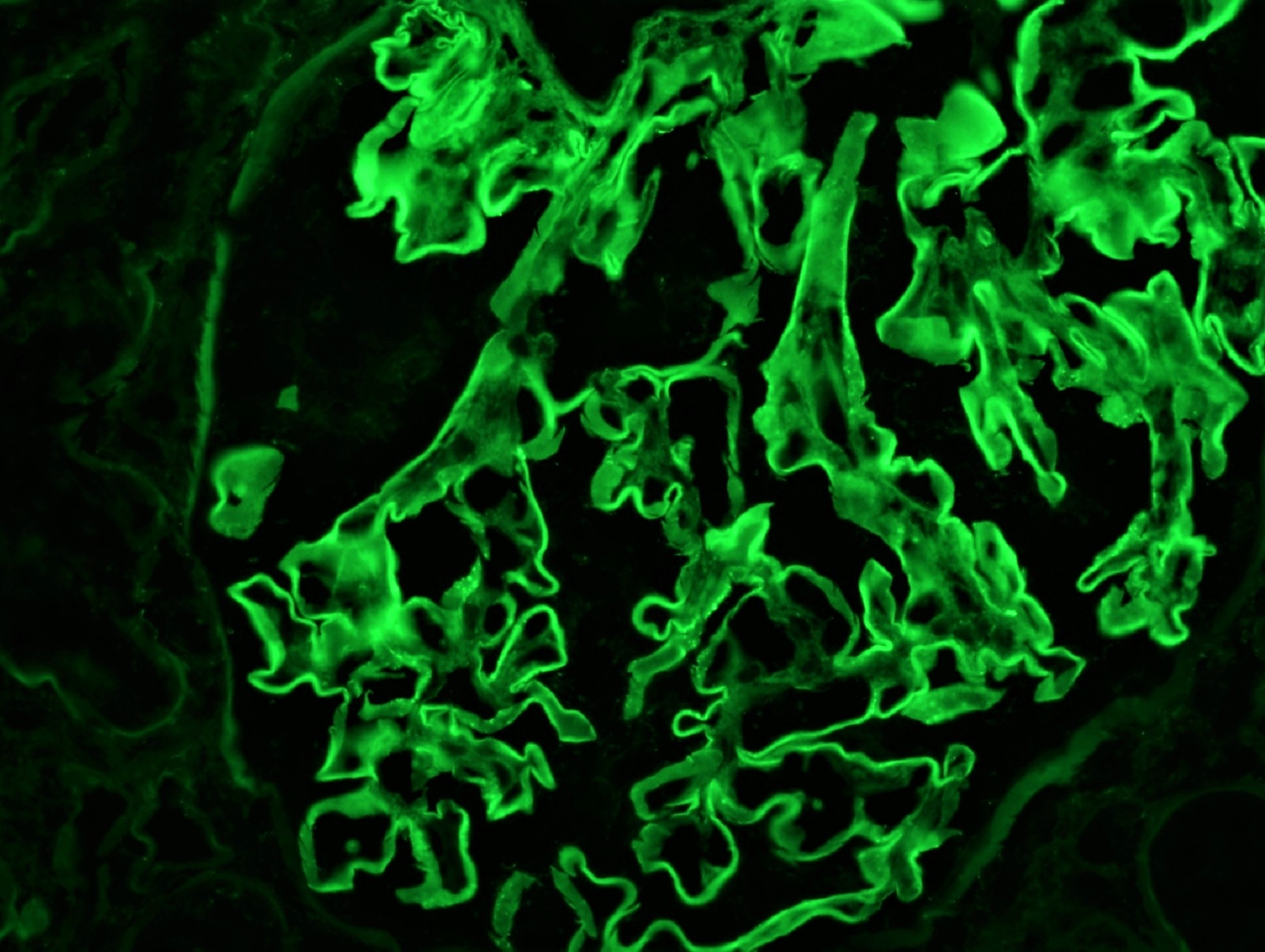
Anti-GBM disease
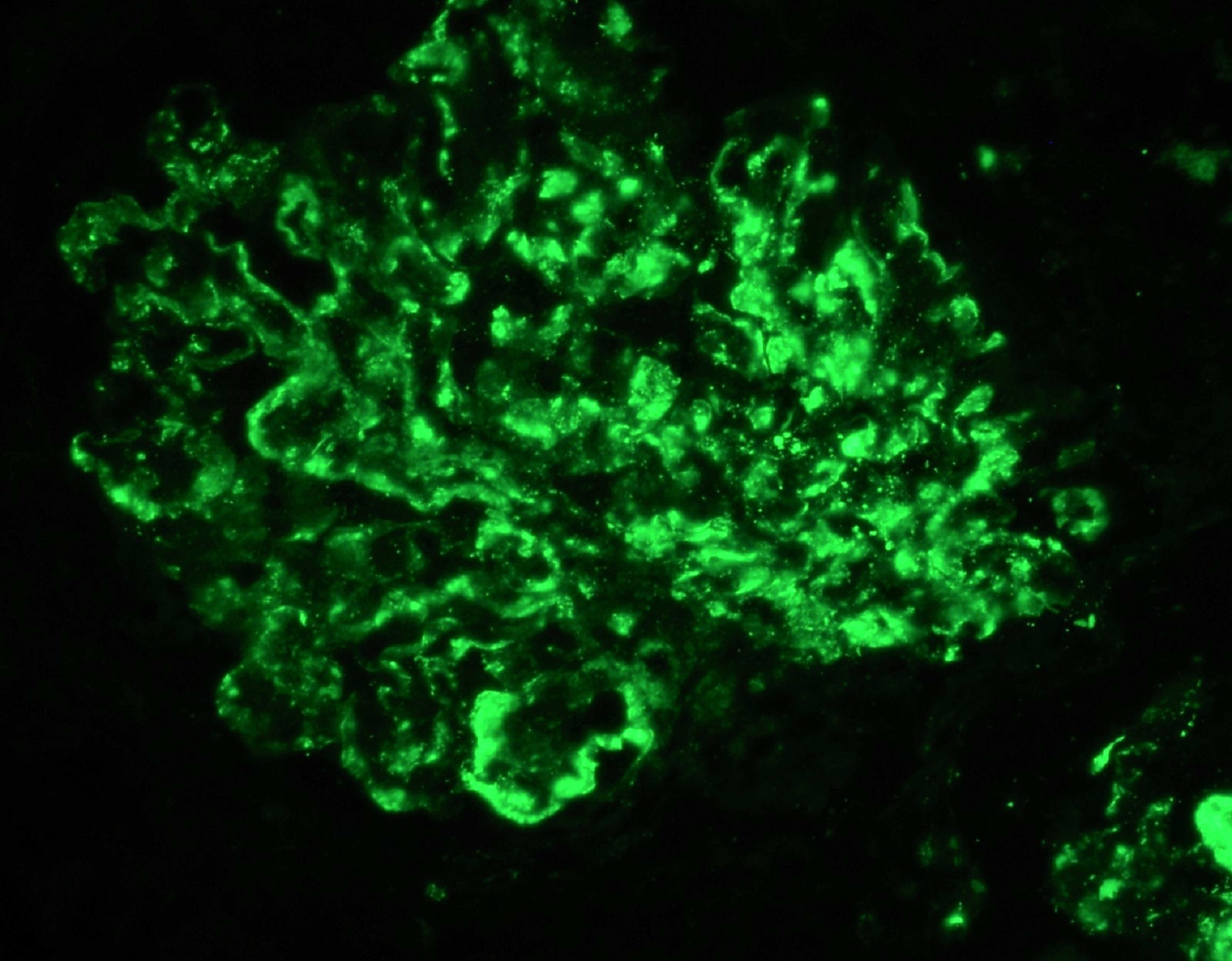
Immune complex GN
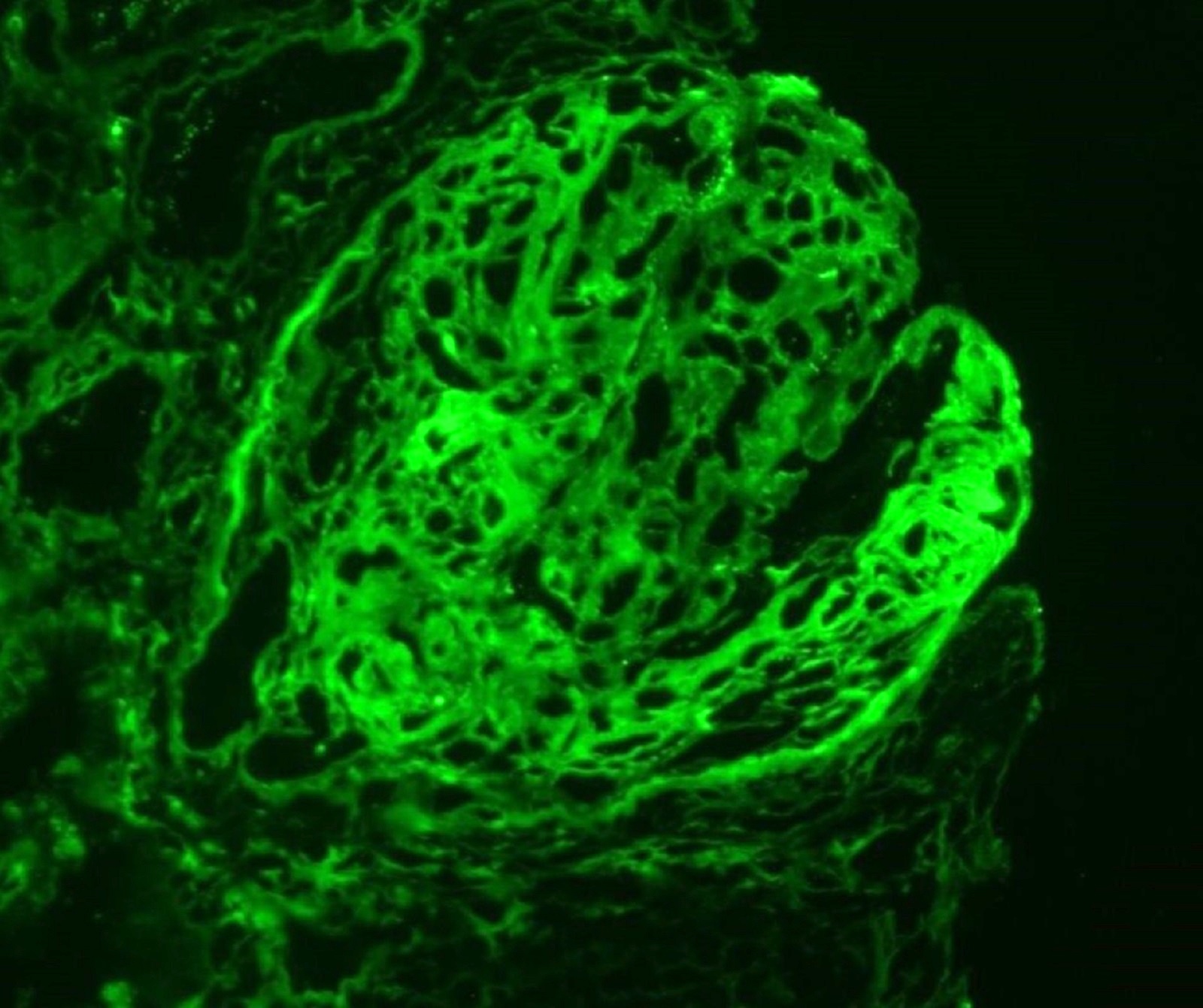
Fibrinogen staining in crescent
Positive stains
- PAS, Jones methenamine silver and trichrome are used to evaluate the morphology
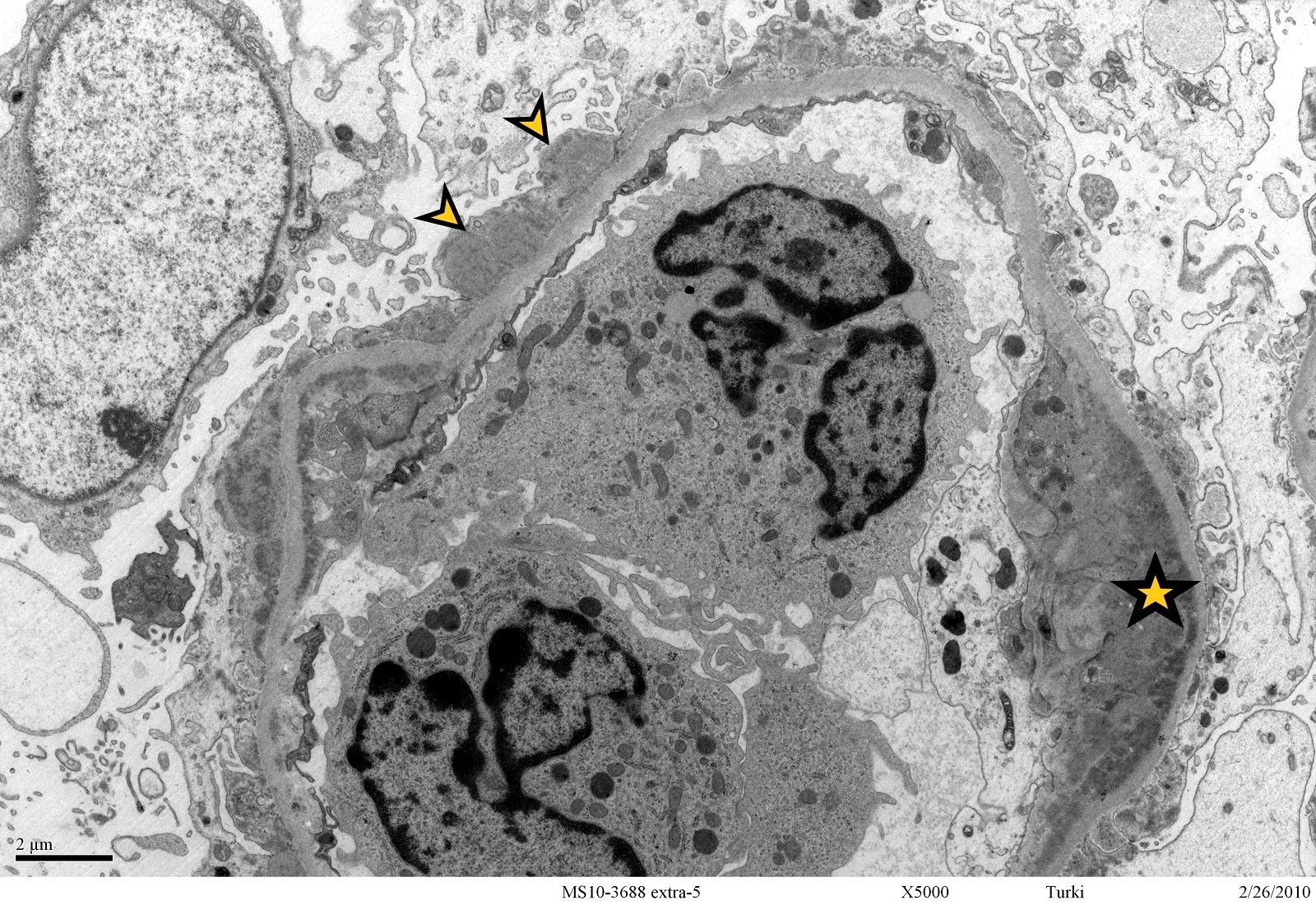
Electron microscopy description
- Anti-GBM disease: no electron dense deposits
- Immune complex mediated crescentic GN: electron dense deposits are present within glomeruli; their location depends on the underlying etiology (J Am Soc Nephrol 2016;27:1278)
- Pauci-immune complex crescentic GN: no electron dense deposits
- Breaks and rupture of GBM
Electron microscopy images
Contributed by Khaled A. Murshed, M.D., Noheir M. Taha, M.B.B.Ch., M.D. and Mohammed Akhtar, M.D.
Electron dense deposits

Pauci-immune
Sample pathology report
- Left kidney, needle core biopsy:
- Crescentic glomerulonephritis secondary to anti-GBM disease (see comment)
- Cellular crescent (9/13), fibrocellular / fibrous crescents (0/13)
- Global glomerulosclerosis (0/13), segmental glomerulosclerosis (0/13)
- Interstitial inflammation, moderate
- Tubular atrophy and interstitial fibrosis, mild
- Arteriosclerosis, moderate
- Comment: Indirect immunofluorescence studies show diffuse linear staining of IgG (2+) and C3 (2+) along the GBM and tubular basement membrane with negative staining for IgA, IgM and C1q. The findings are consistent with anti-GBM disease.
Differential diagnosis
- RPGN is a clinical diagnosis, not a pathology diagnosis so the differential is most important to nephrologists, not pathologists; the usual pathology correlate is a crescentic glomerulonephritis due to different etiologies
Board review style question #1
Which of the following is true about the glomerular disease depicted in the image?
- It presents clinically as a slowly progressive disease
- Immune complex mediated crescentic glomerulonephritis (type 2) is associated with linear staining of IgG along glomerular basement membrane
- Anti-GBM disease (type 1) is associated with granular staining of IgG along glomerular basement membrane
- In pauci-immune complex crescentic GN (type 3), electron dense deposits are commonly present
- Pauci-immune complex crescentic GN (type 3) is the most common subtype of crescentic glomerulonephritis
Board review style answer #1
E. Pauci-immune complex crescentic GN (type 3) is the most common subtype of crescentic glomerulonephritis
Comment Here
Reference: Crescentic glomerulonephritis overview
Comment Here
Reference: Crescentic glomerulonephritis overview
Board review style question #2
Regarding the pathogenesis of crescentic glomerulonephritis, which of the following is the first and most crucial event that leads to crescent formation?
- Podocyte injury
- Epithelial mesenchymal transition
- Podocyte effacement
- Endothelial cell injury
- Parietal cell damage
Board review style answer #2
