

Kidney tumor
General
WHO classification
Resident / Fellow Advisory Board: Alcino Pires Gama, M.D.
Editorial Board Member: Debra L. Zynger, M.D.


Last author update: 4 October 2023
Last staff update: 11 April 2024
Copyright: 2003-2024, PathologyOutlines.com, Inc.
PubMed Search: Kidney / renal tumor WHO classification
Table of Contents
Definition / general | Major updates | WHO (2022) | Microscopic (histologic) images | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Rizkalla C, Tretiakova M. WHO classification. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/kidneytumorWHOclass.html. Accessed April 25th, 2024.
Definition / general
- The new World Health Organization (WHO) 2022 classification of urinary and male genital tumors (5th edition) replaces the previous WHO 2016 classification
- Diagnostic criteria, molecular correlates and nomenclature have been updated
Major updates
- Grouping of renal tumors into broader categories
- Clear cell renal tumors
- Papillary renal tumors
- Papillary renal cell carcinoma (PRCC)
- Subclassification into type 1 and type 2 PRCC is no longer recommended
- Previously known type 1 PRCC is regarded as classic PRCC
- Previously known type 2 PRCC has now been recognized to be other entities (e.g., sporadic fumarate hydratase deficient renal cell carcinoma [FH deficient RCC], acquired cystic disease associated RCC, TFE3 altered RCC, etc.) (Mod Pathol 2021;34:1167, Pathologica 2022;115:8)
- Morphologic spectrum is expanded to include biphasic PRCC and Warthin-like PRCC; papillary renal neoplasm with reverse polarity recognized as separate provisional entity (Pathologica 2022;115:8)
- Subclassification into type 1 and type 2 PRCC is no longer recommended
- Renal papillary adenoma
- Papillary renal cell carcinoma (PRCC)
- Oncocytic and chromophobe renal tumors
- New category: other oncocytic tumors of the kidney
- Includes emerging entities such as low grade oncocytic tumor (LOT) and eosinophilic vacuolated tumor (EVT)
- Includes the entity oncocytic renal neoplasms of low malignant potential not otherwise specified (NOS) for tumors with features in between an oncocytoma and chromophobe RCC (Mod Pathol 2021;34:1167)
- Includes the entity hybrid oncocytic tumors (HOT) for oncocytic tumors with borderline features that occur in a hereditary setting (Mod Pathol 2021;34:1392)
- New category: other oncocytic tumors of the kidney
- Collecting duct tumors
- Other renal tumors
- Includes a diverse set of renal tumors that do not fit in any of the other categories
- Clear cell papillary renal cell tumor replaces previously named clear cell papillary renal cell carcinoma due to benign behavior (Pathologica 2022;115:8)
- Molecularly defined renal carcinomas
- Reflects recent discoveries in renal tumor genomics (Mod Pathol 2021;34:1167)
- TFE3 rearranged RCC and TFEB altered RCC are now separated into separate diagnostic entities, rather than both being considered as microphthalmia transcription factor (MiT) family of RCC (Pathologica 2022;115:8)
- New entities (Mod Pathol 2021;34:1167)
- Eosinophilic solid and cystic renal cell carcinoma (ESC RCC)
- ELOC (formerly TCEB1) mutated renal cell carcinoma
- Anaplastic lymphoma kinase (ALK) rearranged RCC
- Grading of renal carcinomas is based on the single high power field showing the greatest degree of pleomorphism, rather than the predominant grade (Histopathology 2019;74:4)
- World Health Organization / International Society of Urological Pathology (WHO / ISUP) grading is not equally significant for all RCC subtypes; the WHO divides them into several categories based on grading value
WHO (2022)
| Renal cell tumors | ICD-O | ICD-11 |
| ||
| 8310/3 | 2C90.0 & XH46F1 | |
| 8316/1 | 2F35 & XH7PR9 | |
| ||
| 8260/0 | 2F35 & XH09B0 | |
| ||
| 8290/0 | 2F35 & XH9Z86 | |
| 8317/3 | 2C90.0 & XH6153 | |
| 2F98 | ||
| ||
| 8319/3 | 2C90.0 & XH4SQ4 | |
| ||
| 8323/1 | 2C90.0 & XH9T60 | |
| 8480/3 | 2C90.0 & XH5EQ2 | |
| 8316/3 | 2C90.0 & XH7K79 | |
| 8316/3 | 2C90.0 & XH0RU3 | |
| 8311/3 | 2C90.0 | |
| 8312/3 | 2C90.0 & XH05V6 | |
| ||
| 8311/3 | 2C90.0 | |
| 8311/3 | 2C90.0 | |
| 8311/3 | 2C90.0 | |
| 8311/3 | 2C90.0 | |
| 8311/3 | 2C90.0 & XH8EN1 | |
| 8311/3 | 2C90.0 | |
| 8510/3 | 2C90.Y & XH2YP5 | |
| Metanephric tumors | ICD-O | ICD-11 |
| 8325/0 | 2F35 & XH0JC7 | |
| 9013/0 | 2F35 & XH7ZU2 | |
| 8935/1 | 2F35 & XH4N88 | |
| Mixed epithelial and stromal renal tumors | ICD-O | ICD-11 |
| 8959/0 | 2C90.Y & XH0533 | |
| 8959/0 | 2F35 & XH7TJ0 | |
| Renal mesenchymal tumors | ICD-O | ICD-11 |
| ||
| 8860/0 | 2F35 & XH4CC6, 2C90.Y & XH4CC6 | |
| 8860/1 | 2F35 & XH0QR3, 2B5F.2 & XH0QR3 | |
| 9161/1 | 2F98 & XH6810 | |
| 8361/0 | 2F35 & XH6M13 | |
| 8966/0 | 2F35 & XH3470 | |
| ||
| 8967/0 | 2F35 & XH3SR2 | |
| 8960/1 | 2C90.Y & XH10F1 | |
| 8963/3 | 2C90.Y & XH3RF3 | |
| 8964/3 | 2C90.Y & XH0765 | |
| Embryonal neoplasms of the kidney | ICD-O | ICD-11 |
| ||
| 8959/1 | 2C90.Y & XH1JB4 | |
| 8960/3 | 2C90.Y & XH5QN3 | |
| Miscellaneous renal tumors | ICD-O | ICD-11 |
| 9084/0, 9084/3, 9071/3, 9085/3 | 2C90.Y & XH83G5, 2C90.Y & XH09W7 |
Microscopic (histologic) images
Contributed by Maria Tretiakova, M.D., Ph.D.
ALK rearranged renal cell carcinoma
Eosinophilic solid and cystic renal cell carcinoma
ELOC (formerly TCEB1) mutated renal cell carcinoma
Fumarate hydratase deficient renal cell carcinoma
Macronucleoli
Low grade oncocytic tumor
Board review style question #1
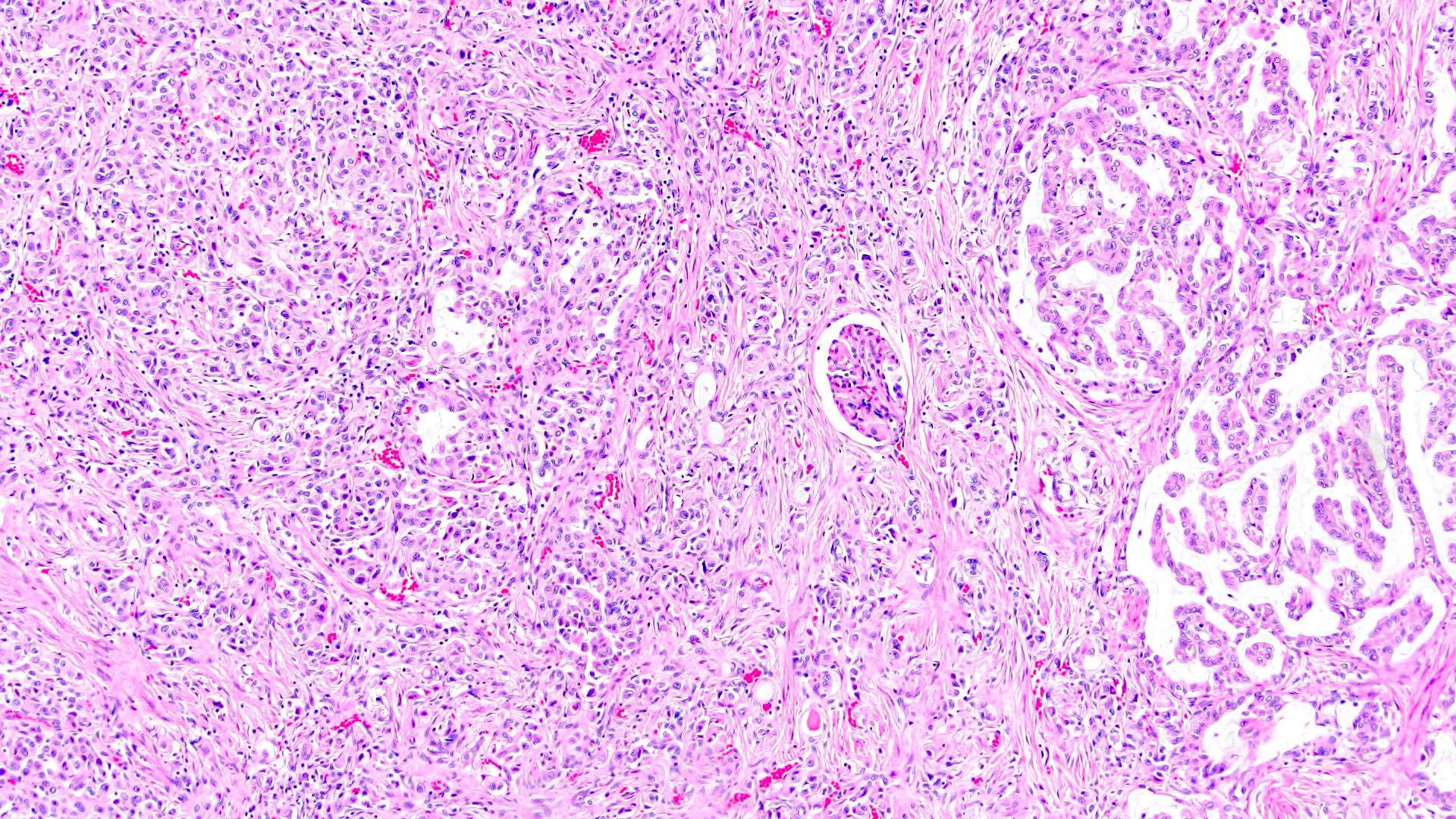
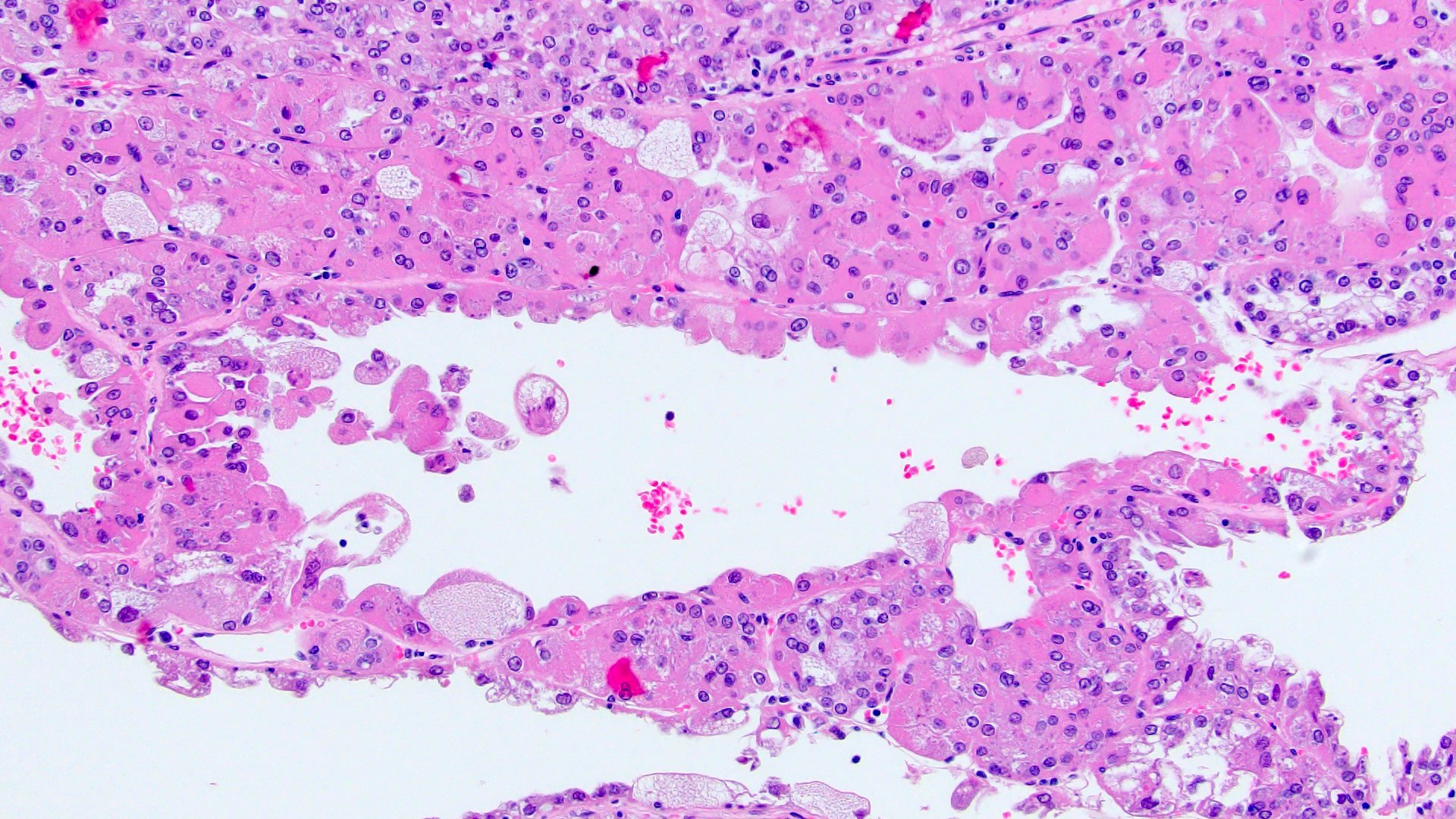
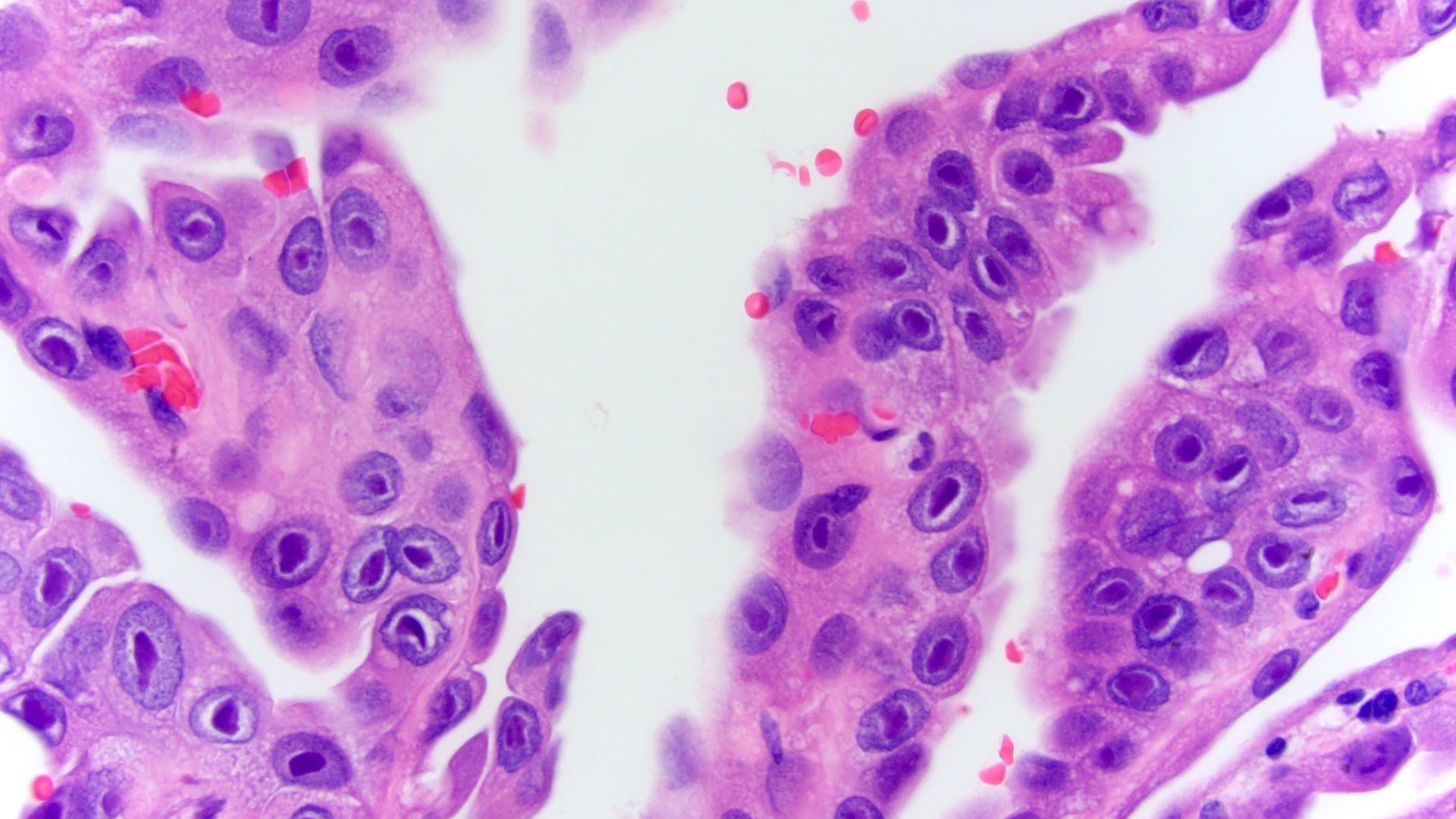
Based on the microscopic images of a renal tumor, what is the most likely diagnosis?
- Clear cell renal cell carcinoma
- Fumarate hydratase deficient renal cell carcinoma
- Papillary renal cell carcinoma type 1
- Papillary renal cell carcinoma type 2
Board review style answer #1
B. Fumarate hydratase deficient renal cell carcinoma. A key feature of this diagnostic entity is prominent eosinophilic inclusion-like nucleoli with perinucleolar clearing. Answer A is incorrect because these RCCs were previously misdiagnosed as papillary RCC grade 2 due to their tubulopapillary architecture and higher grade cytology. Answers C and D are incorrect because the diagnostic entities papillary RCC grade 1 and 2 no longer exist; papillary RCC grade 1 is now considered classic type PRCC and type 2 PRCC is now recognized to be one of several other entities (e.g., FH deficient RCC, acquired cystic disease associated RCC and more).
Comment Here
Reference: Kidney tumor - WHO classification
Comment Here
Reference: Kidney tumor - WHO classification
Board review style question #2
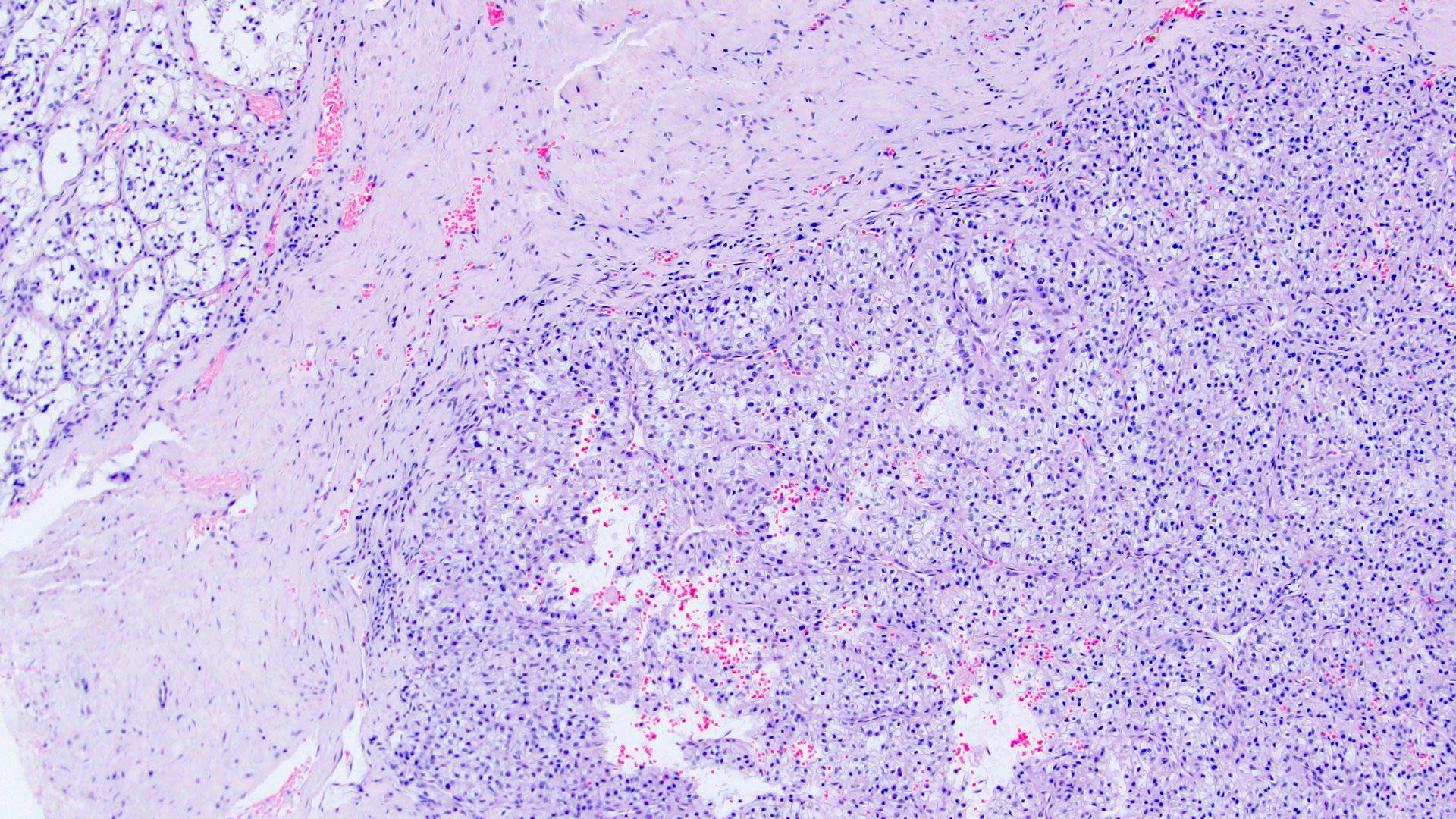
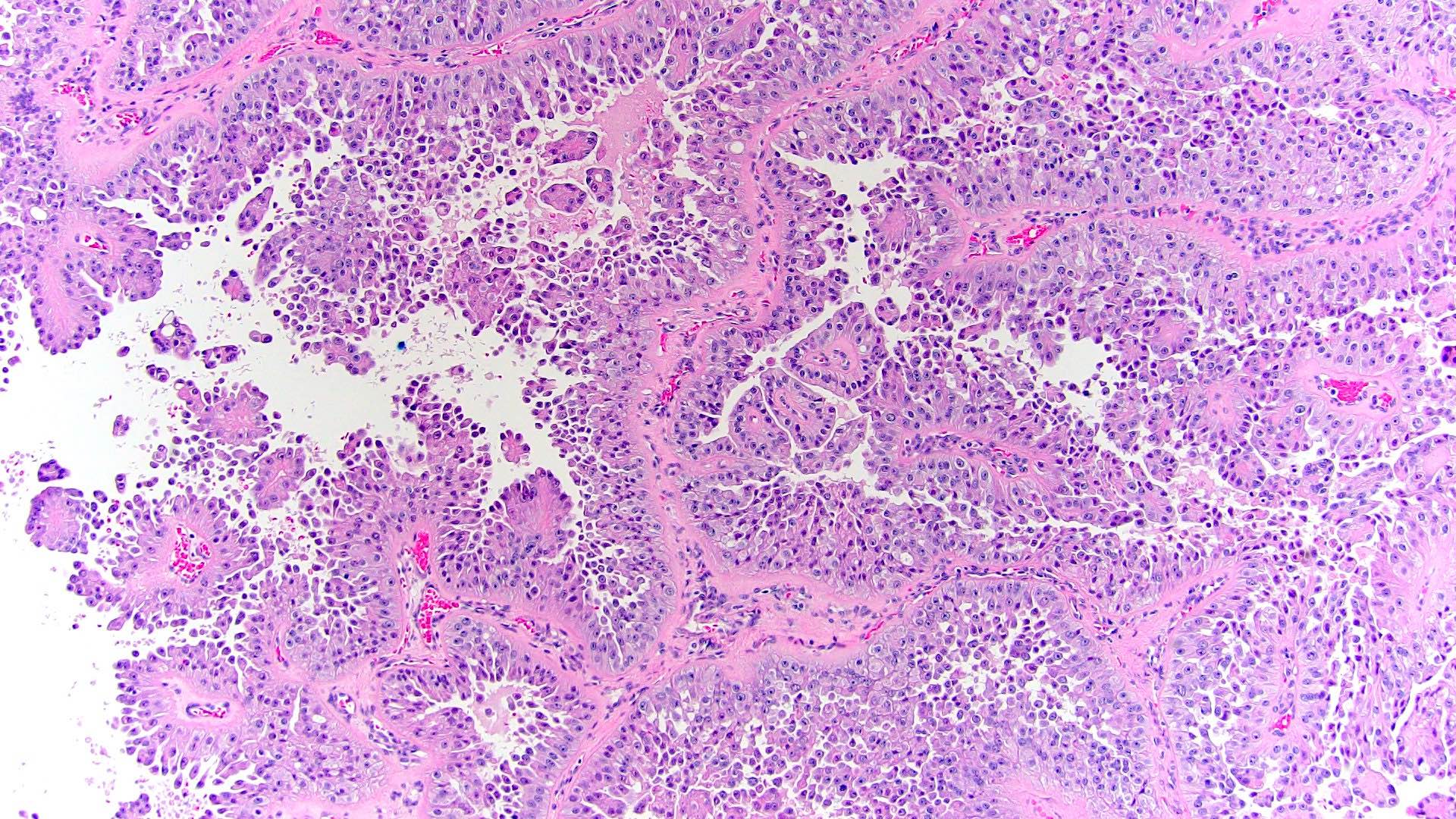
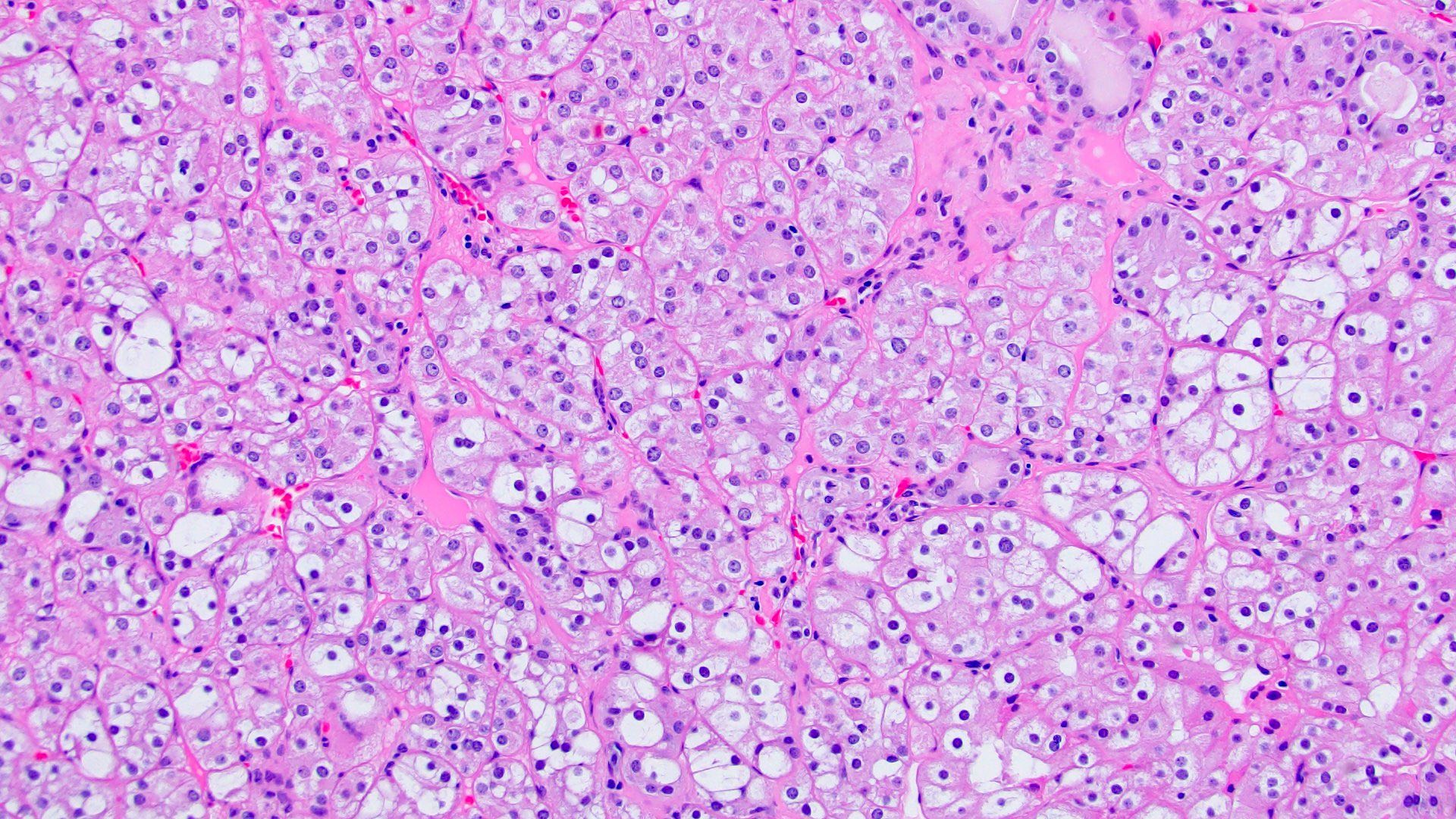
The microscopic image above shows a needle core biopsy from a patient with multiple bilateral renal masses. Immunohistochemical stains were performed and are positive for CK7, KIT and succinate dehydrogenase B (SDHB). Which syndrome does this patient likely have?
- Birt-Hogg-Dubé syndrome
- Cowden syndrome
- Fumarate hydratase deficiency / hereditary leiomyomatosis
- Succinate dehydrogenase deficient tumor syndrome
Board review style answer #2
A. Birt-Hogg-Dubé syndrome. The microscopic image shows an oncocytic neoplasm with a solid alveolar pattern with a predominantly oncocytoma type morphology (round regular nuclei, small inconspicuous nucleoli, occasional binucleation) mixed with nests of cytoplasmic clearing and perinuclear halos, mimicking chromophobe renal cell carcinoma. Birt-Hogg-Dubé syndrome is characterized by a diagnostic triad including: skin manifestations (e.g., fibrofolliculomas, acrochordons), lung manifestations (e.g., pneumothorax) and renal cell carcinomas. These patients tend to have an increased incidence of oncocytic tumors (oncocytoma, chromophobe RCC, hybrid oncocytic tumors), which can affect bilateral kidneys as multiple lesions.
Answer B is incorrect because Cowden syndrome is associated with a PTEN mutation. Patients can present with a wide clinical spectrum: breast cancer, endometrial cancer, hamartomas, trichilemmomas. Renal cell carcinomas have not been described as part of this syndrome. Answer C is incorrect because hereditary leiomyomatosis is a syndrome defined by multiple cutaneous or uterine leiomyomata and a renal cell carcinoma with a characteristic loss of fumarate dehydrogenase. These tumors were previously misclassified under PRCC type 2 due to their high grade cytology and papillary architecture, however, now they are recognized as a separate entity. A key diagnostic feature is prominent eosinophilic inclusion-like nucleoli with perinucleolar clearing, which is not present in these images. Answer D is incorrect because succinate dehydrogenase deficient tumor syndrome is characterized by a loss of succinate dehydrogenase B (SDHB); patients can present with SDH deficient RCC, paraganglioma or GISTs. Although these tumors are eosinophilic, the question stem indicated positive SDHB staining.
Comment Here
Reference: Kidney tumor - WHO classification
Answer B is incorrect because Cowden syndrome is associated with a PTEN mutation. Patients can present with a wide clinical spectrum: breast cancer, endometrial cancer, hamartomas, trichilemmomas. Renal cell carcinomas have not been described as part of this syndrome. Answer C is incorrect because hereditary leiomyomatosis is a syndrome defined by multiple cutaneous or uterine leiomyomata and a renal cell carcinoma with a characteristic loss of fumarate dehydrogenase. These tumors were previously misclassified under PRCC type 2 due to their high grade cytology and papillary architecture, however, now they are recognized as a separate entity. A key diagnostic feature is prominent eosinophilic inclusion-like nucleoli with perinucleolar clearing, which is not present in these images. Answer D is incorrect because succinate dehydrogenase deficient tumor syndrome is characterized by a loss of succinate dehydrogenase B (SDHB); patients can present with SDH deficient RCC, paraganglioma or GISTs. Although these tumors are eosinophilic, the question stem indicated positive SDHB staining.
Comment Here
Reference: Kidney tumor - WHO classification
