

Kidney tumor
Benign / borderline adult tumors
Angiomyolipoma
Author: Tatjana Antic, M.D.
Editorial Board Member: Debra L. Zynger, M.D.
Deputy Editor-in-Chief: Maria Tretiakova, M.D., Ph.D.
Last author update: 4 April 2023
Last staff update: 4 April 2023
Copyright: 2019-2024, PathologyOutlines.com, Inc.
PubMed Search: Renal angiomyolipoma
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Clinical features | Diagnosis | Laboratory | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Positive stains | Negative stains | Electron microscopy description | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Antic T. Angiomyolipoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/kidneytumorangiomyolipoma.html. Accessed April 24th, 2024.
Definition / general
- Member of perivascular epithelioid cell (PEC) tumor family
Essential features
- Angiomyolipoma, classic variant, is a benign mesenchymal neoplasm composed of admixture of thick dysmorphic blood vessels, smooth muscle and adipose tissue
- Amount of each component is variable
- Some cases show significant sclerosis
- Epithelioid variant has potential to metastasize
- Angiomyolipoma can occur in extrarenal sites
Terminology
- PEComa: perivascular epithelioid cell (PEC) tumor family
ICD coding
- ICD-O: 8860/0 - angiomyolipoma
Epidemiology
- Reported in 0.13 - 2.2% of asymptomatic adults who underwent imaging studies (Eur Urol 1995;27:124, Am J Kidney Dis 2012;59:611)
- Occurs sporadically or in patients with tuberous sclerosis
- Majority are sporadic cases (80%) and usually diagnosed in middle aged adults (F > M) (Yonsei Med J 2010;51:728)
- Tuberous sclerosis cases occur in young patients and have no sex predilection (J Urol 2017;197:500)
- Constitutes ~1% of all resected renal tumors
- A large autopsy study demonstrated that 9% of an unselected population had angiomyolipomas (Hum Pathol 2016;58:41)
Sites
- Kidney; can occur in extrarenal sites such as liver and lymph nodes
- Rarely occurs in the ovary (Int J Gynecol Pathol 2002;21:69, Internet Journal of Pathology 2006;6:1)
Pathophysiology
- Presumably arises from perivascular epithelioid cells, which have no known body counterpart
Clinical features
- Usually asymptomatic in screened tuberous sclerosis patients due to smaller size when discovered
- May coexist with renal cell carcinoma in nontuberous sclerosis patients, particularly clear cell carcinoma (Mod Pathol 2001;14:157)
- Tumors can be quite large, multifocal and can extend into the renal vein or vena cava
- Classic variant is benign but may be complicated by hemorrhage if the tumor is large
Diagnosis
- Imaging is often sufficient to render the diagnosis for classic angiomyolipoma (Radiology 2011;260:158, Int J Urol 2011;18:727, AJR Am J Roentgenol 2012;198:377, Radiology 2012;263:160)
- Definitive diagnosis by light microscopic examination of tissue
- So called fat poor and epithelioid variants may additionally require immunohistochemistry
Laboratory
- Routine laboratory within normal limits
Radiology description
- Characteristic radiologic appearance with fat content in the classic variant
- Radiologic findings depend on the amount of fat within the tumor (AJR Am J Roentgenol 2017;209:826)
Radiology images
Images hosted on other servers:

CT with renal mass
Prognostic factors
- Benign course in angiomyolipoma, classic variant
- Tumors with epithelioid and pleomorphic features can have a more aggressive course (Mod Pathol 2013;26:1355, Ann Diagn Pathol 2020;47:151538, Urol Oncol 2022;40:18)
- Sarcomatous transformation with distant metastasis is extremely rare
- Retroperitoneal hemorrhage is an important complication (Urology 2008;72:1077)
- Patients with bilateral disease can have renal failure
- Death can occur due to involvement of contiguous organs particularly blood vessels
Case reports
- 33 year old woman with retroperitoneal hemorrhage, tuberous sclerosis and bilateral tumors (Am J Case Rep 2017;18:1309)
- 34 year old woman with a giant angiomyolipoma (Mol Clin Oncol 2017;7:298)
- 41 year old man with extension into vena cava and pulmonary arteries (J Thorac Dis 2018;10:E166)
- 48 year old woman and 62 year old man with malignant epithelioid variant (Medicine (Baltimore) 2018;97:e11805)
- 64 year old woman with angiosarcoma arising in angiomyolipoma (Diagn Pathol 2018;13:53)
Treatment
- Tumors may be embolized or undergo surgical excision (Eur Urol 2009;55:1155)
- mTOR inhibitors such as everolimus can be used if large or extending into the vena cava (Urol Case Rep 2017;11:11)
Gross description
- Tumor ranges from 0.5 to 25 cm with a mean of 6 cm
- Circumscribed, not encapsulated with pushing border
- Cut surface can have red (vascular component), gray-white (smooth muscle component) or yellow (adipose component) appearance
- May involve the intrarenal venous system, the renal vein or the vena cava despite being benign (Arch Pathol Lab Med 1990;114:65)
- Tumors rarely have a cystic component (Mod Pathol 2006;19:669)
- Tumors are usually unilateral and unifocal
- Multiple (~33%) or bilateral (15%) tumors suggest underlying tuberous sclerosis
Gross images
Contributed by Tatjana Antic, M.D.

Classic variant

Predominant adipose tissue
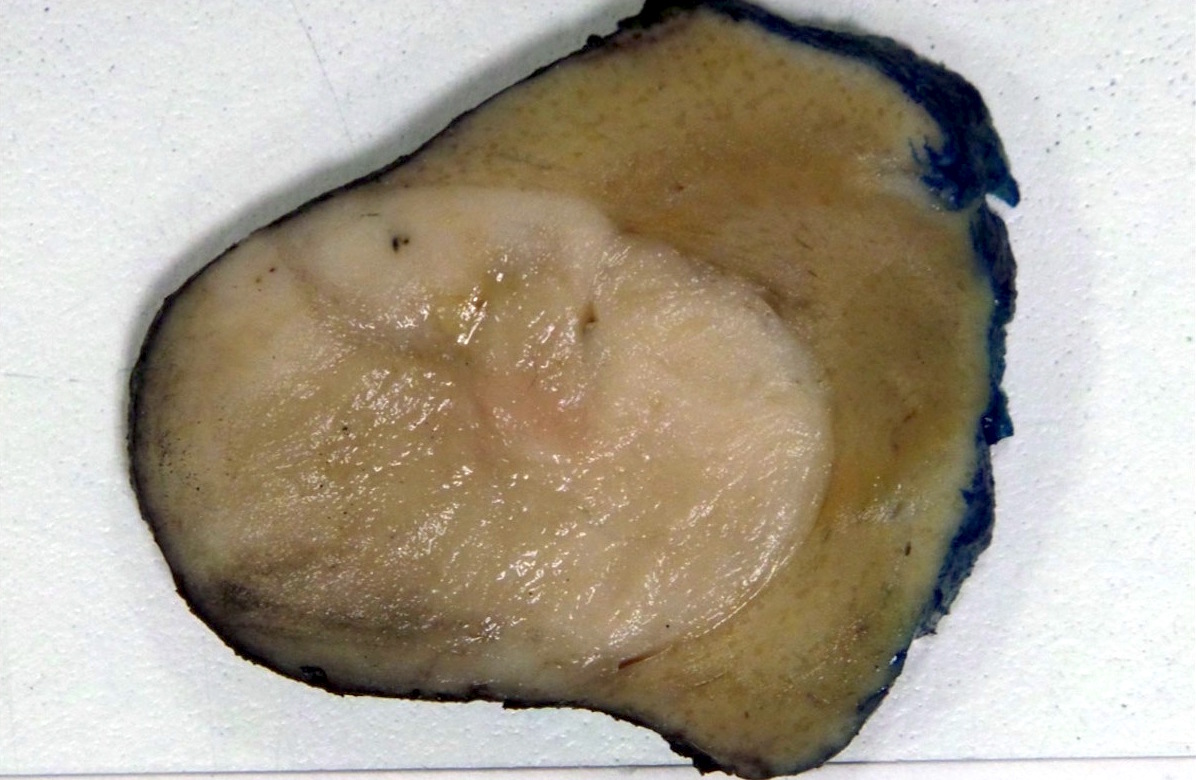
Fat poor
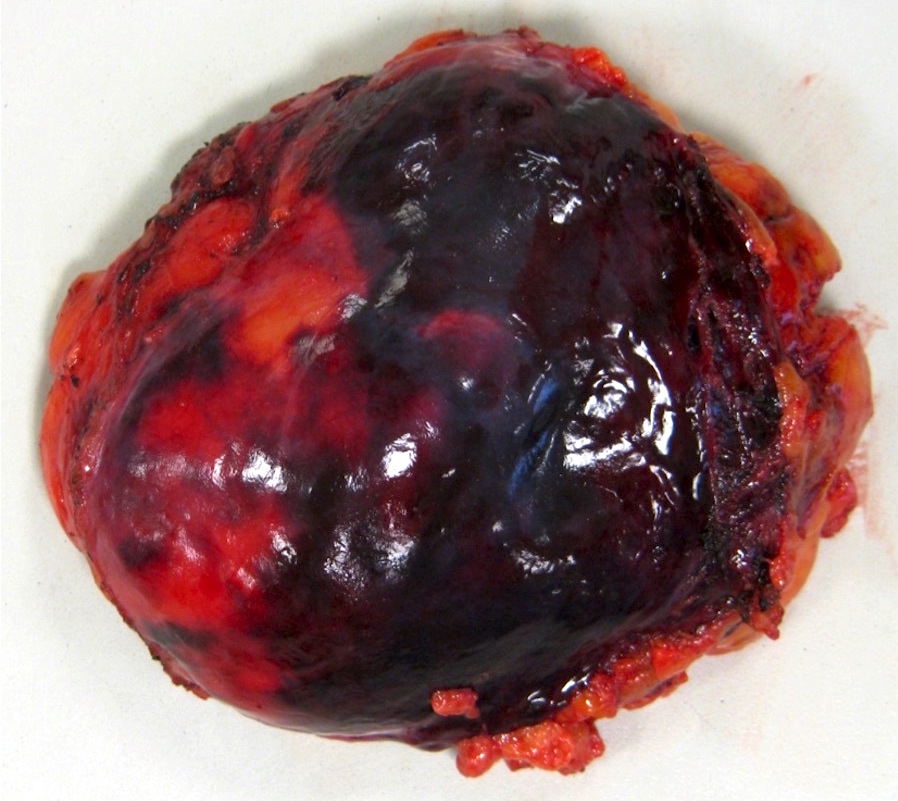
Hemorrhagic angiomyolipoma
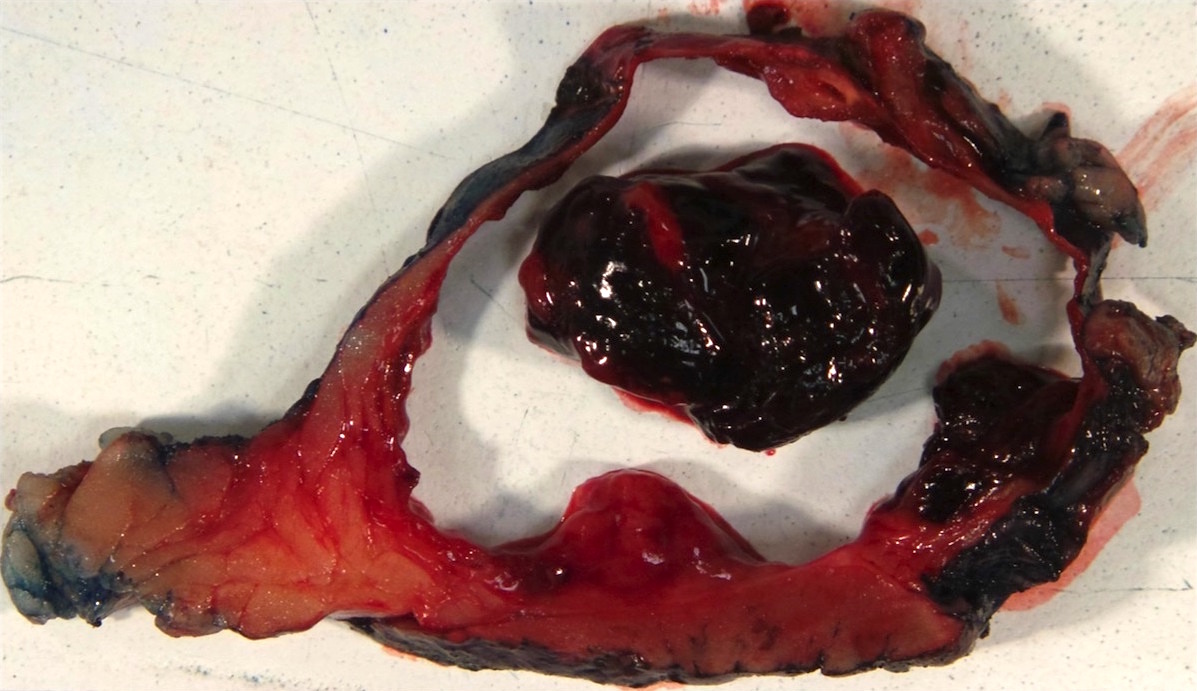
Cystic epithelioid angiomyolipoma with hemorrhage
Microscopic (histologic) description
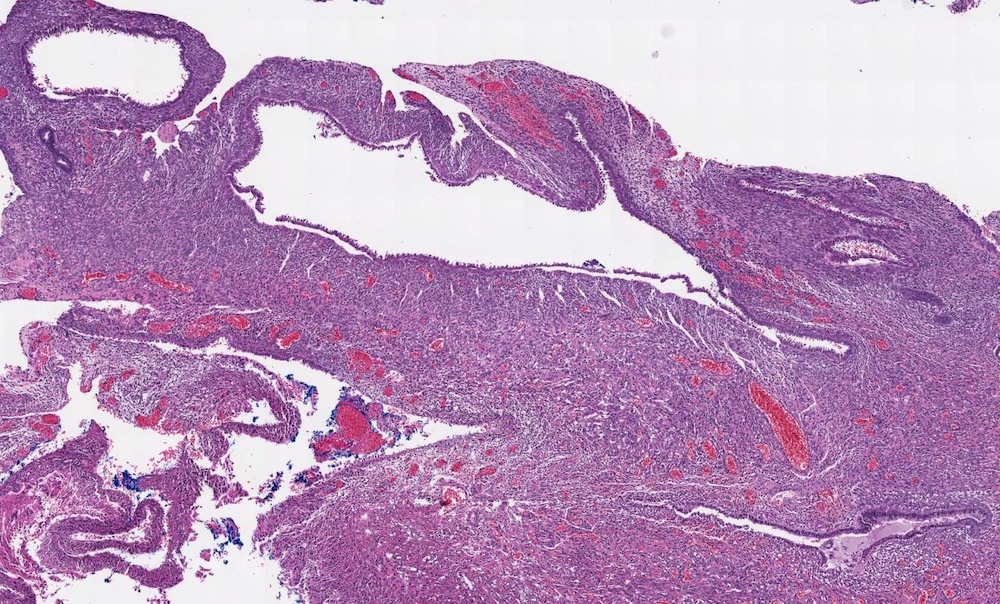
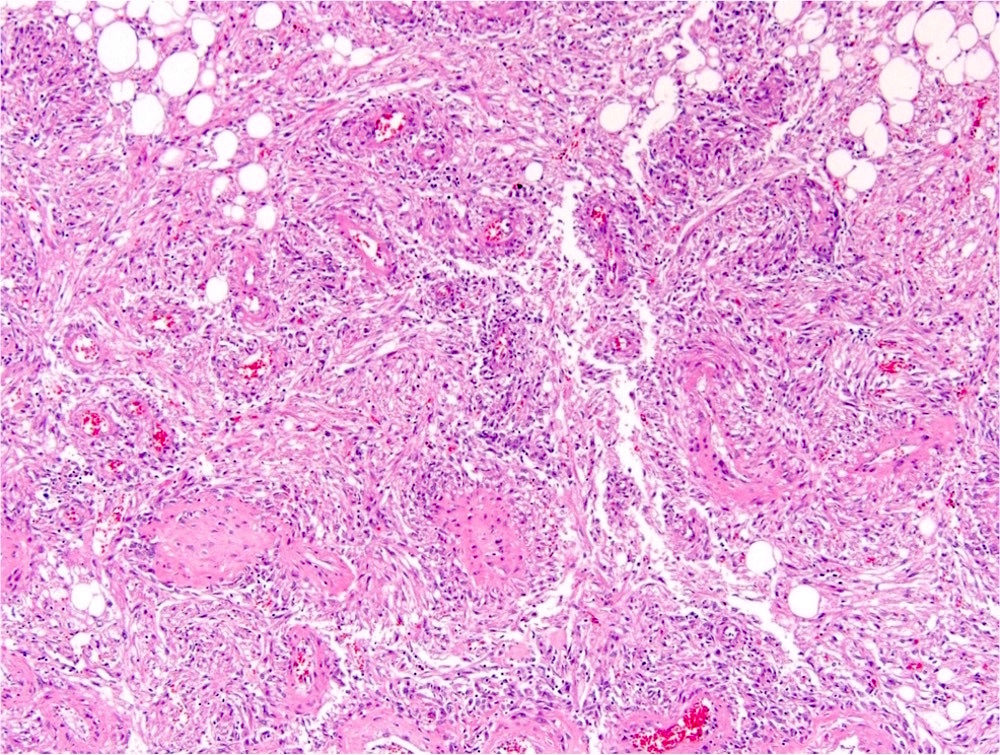
- Classic triphasic with myoid spindle cells, mature adipose tissue and dysmorphic thick walled blood vessels without elastic lamina
- Smooth muscle component appears to originate from vessel walls and may be hypercellular, atypical, pleomorphic or epithelioid
- Vascular component is in the form of thick walled hyalinized vessels
- Fat component is in the form of mature adipose tissue and is seen in > 90% of tumors
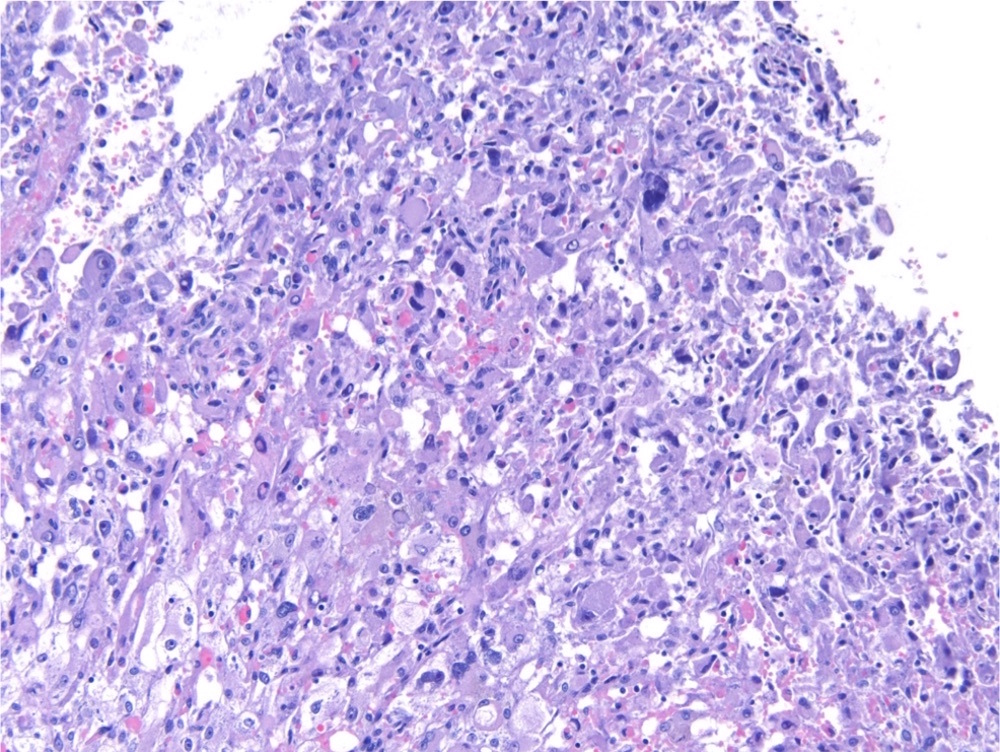
- Epithelioid variant (Mod Pathol 2013;26:1355):
- Pure or predominant population of polygonal cells with clear or densely eosinophilic cytoplasm, large hyperchromatic bizarre nuclei
- Multilobated nuclei and multinucleation is common
- Hemorrhage, mitotic figures and necrosis are common
- Angiomyolipoma with epithelial cysts (AMLEC) represents a morphologic spectrum of the tumors that is characterized by cysts lined by cuboidal or hobnail epithelial cells reminiscent of renal tubular epithelium
Microscopic (histologic) images
Contributed by Tatjana Antic, M.D. and Ankur R. Sangoi, M.D. (Case #359)
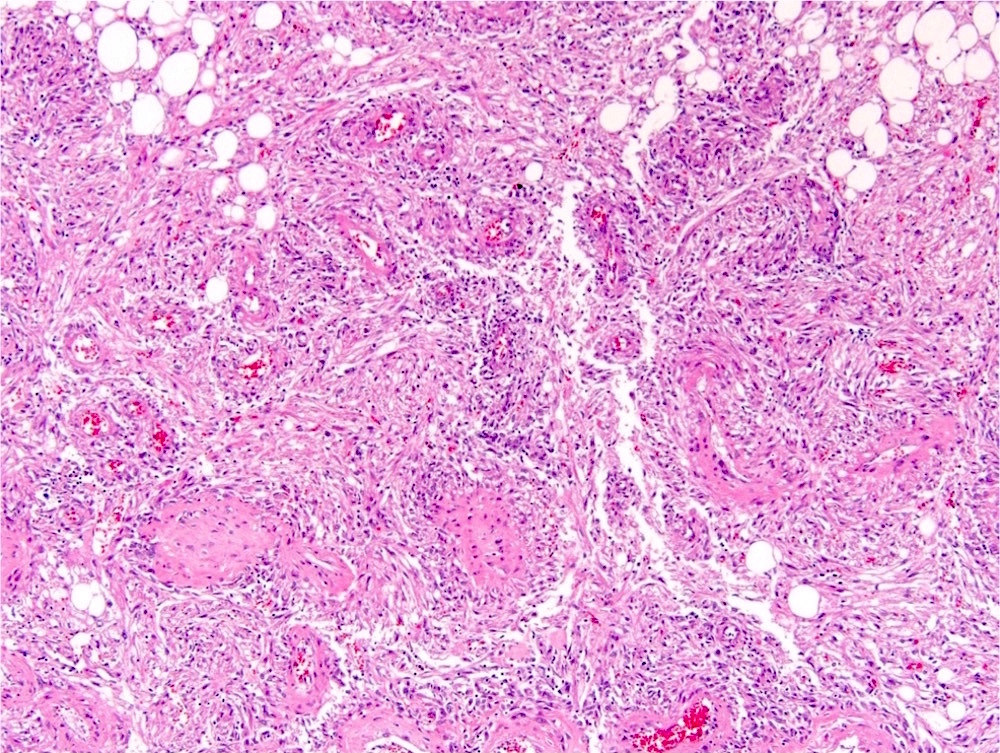
Classic
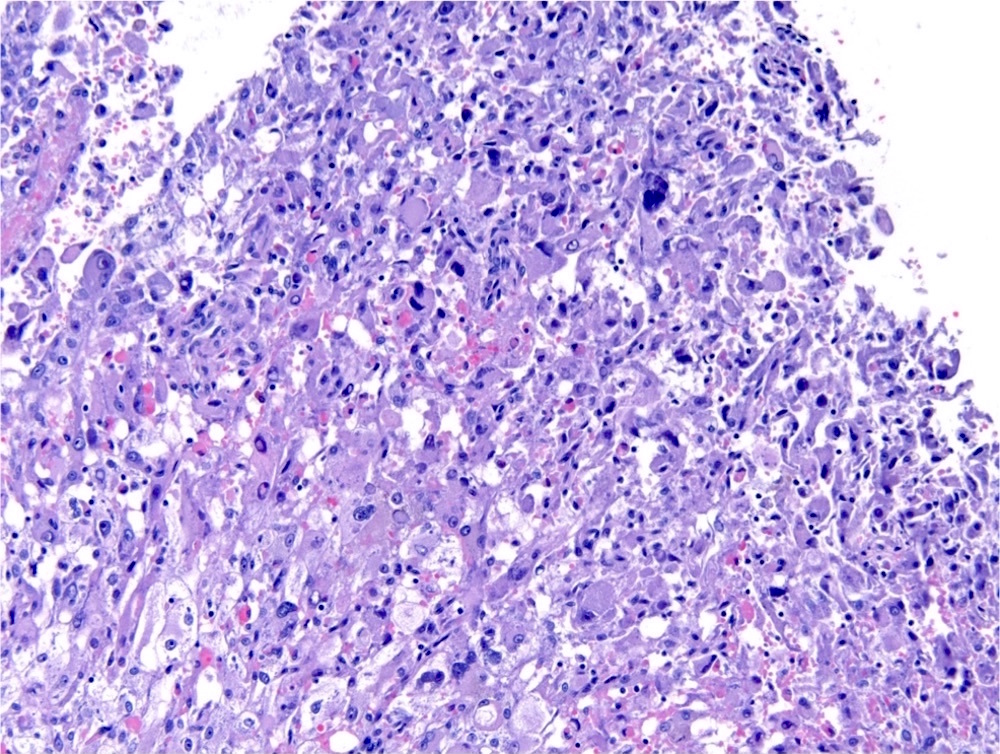
Epithelioid
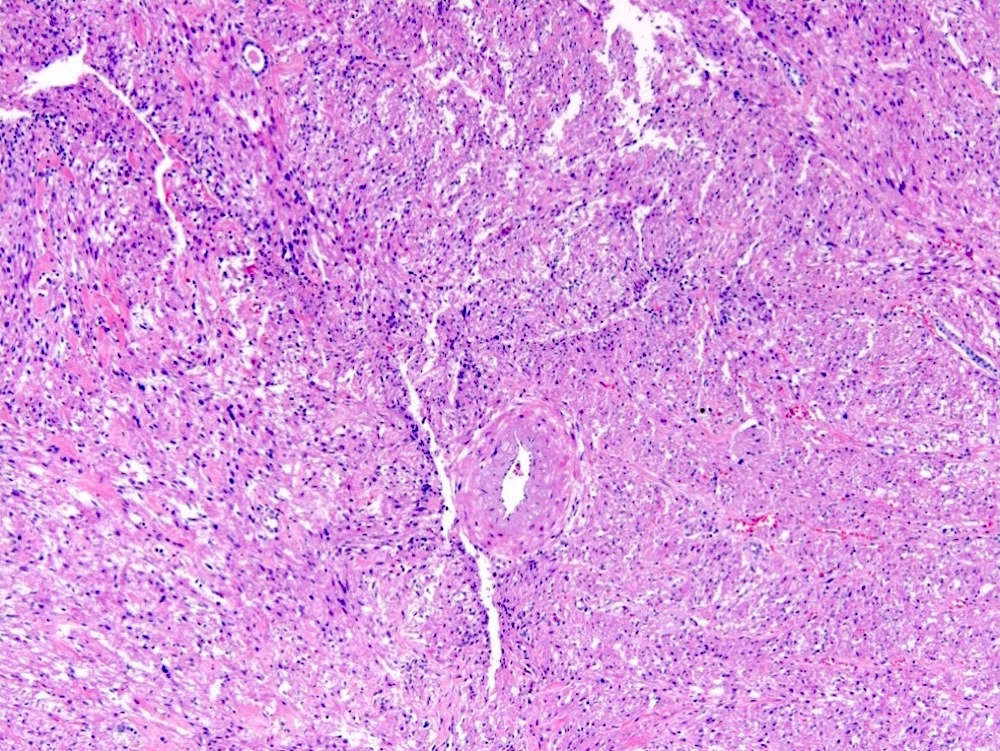
Fat poor

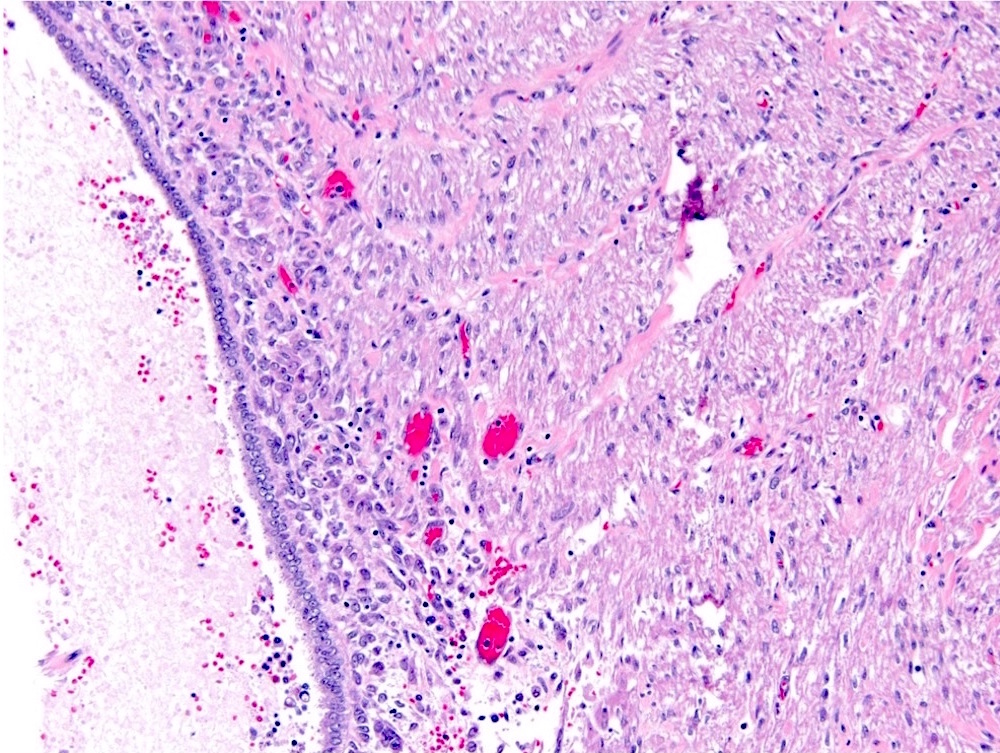
Epithelial cysts (AMLEC)
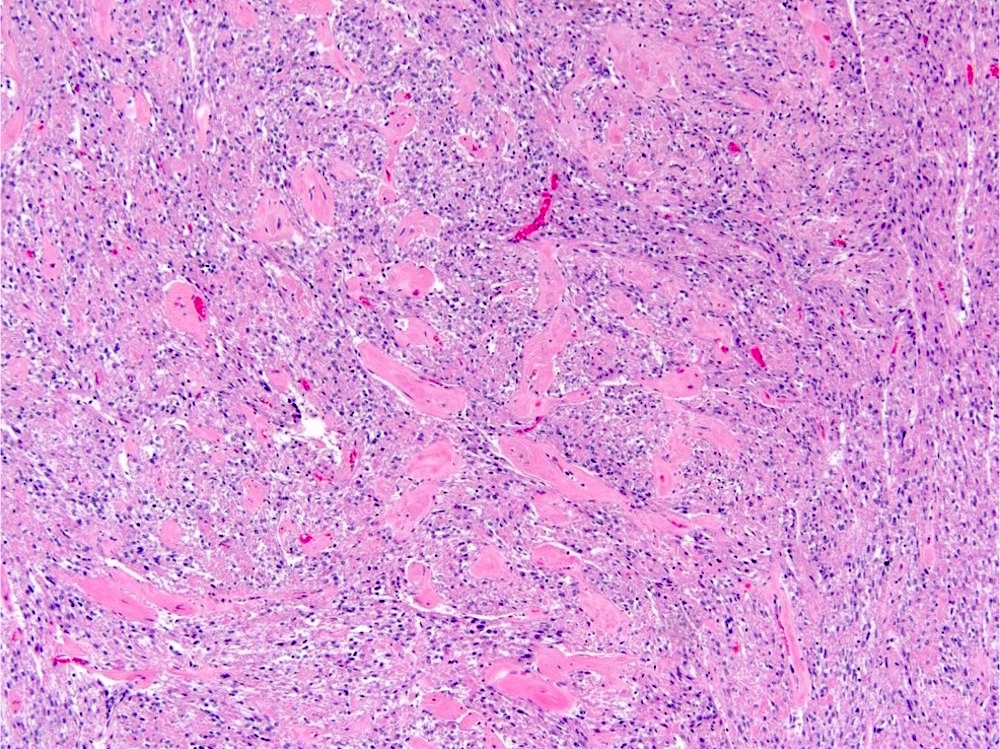
Sclerosis
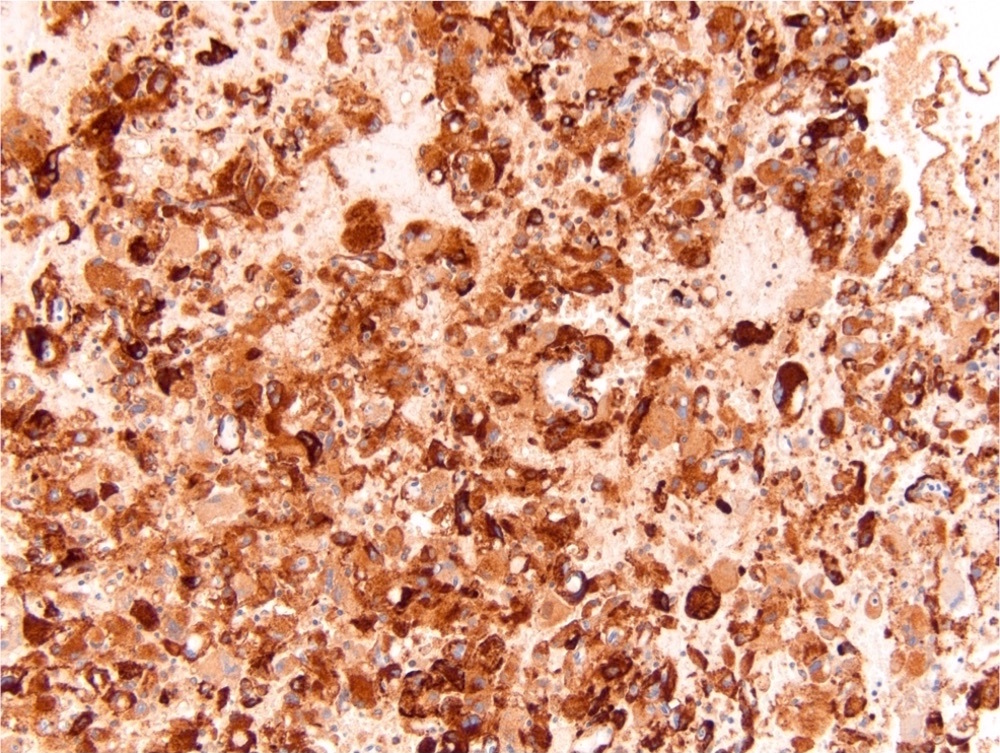
SMA
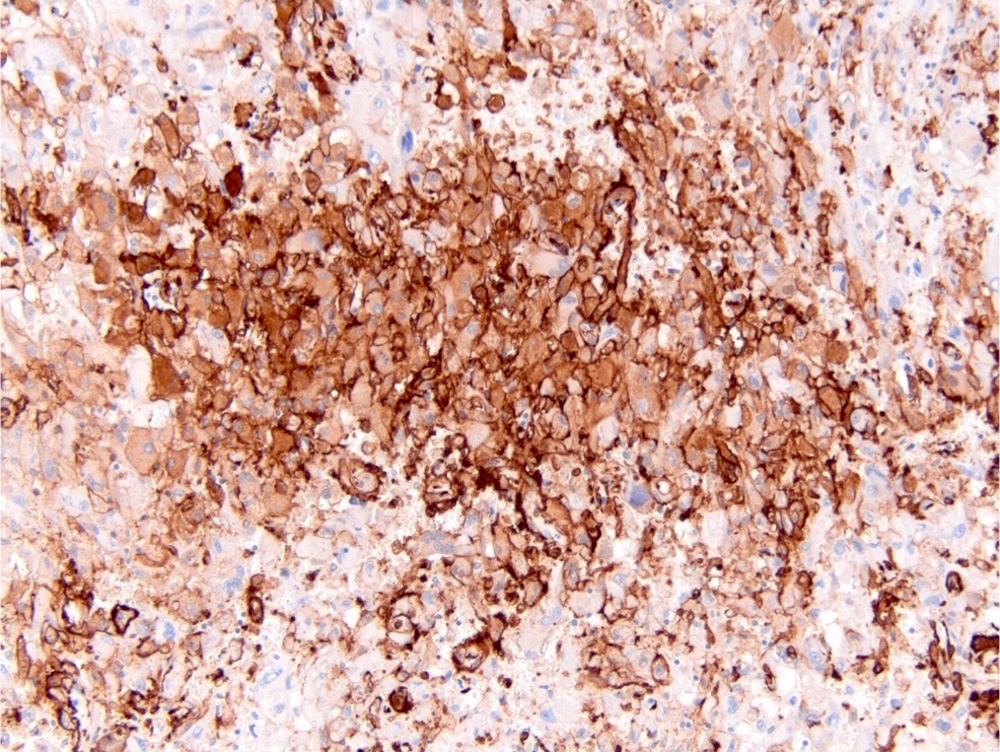
HMB45
Cytology description
- Oval to spindled cells and cohesive stromal fragments, adipose tissue and branching blood vessels in a hemorrhagic background (Diagn Cytopathol 2019;47:1190)
- No mitotic figures (Cytopathology 2007;18:250)
Positive stains
- Coexpression of melanocytic and smooth muscle markers in myoid and lipoid components can be seen with stronger expression of melanocytic markers in epithelioid areas and stronger expression of muscle markers in spindled areas
- HMB45 (adipose 90%, smooth muscle 85%, vessel 80%) (Arch Pathol Lab Med 2007;131:122)
- MART1 / MelanA (adipose 70%, smooth muscle 60%, vessel 40%) (Arch Pathol Lab Med 2007;131:122)
- Cathepsin K, SMA, MSA, calponin, caldesmon (Mod Pathol 2012;25:100, Arch Pathol Lab Med 2001;125:751, Am J Surg Pathol 2009;33:289, Am J Surg Pathol 2015;39:349)
Negative stains
- Cytokeratin
- PAX8
- CAIX
- GATA3
- Inhibin
- CD117 (adipose 20%, smooth muscle 40%) (Arch Pathol Lab Med 2007;131:122)
Electron microscopy description
- Premelanosomes
Molecular / cytogenetics description
- TSC2 (most commonly) or TSC1 mutations in sporadic angiomyolipomas (PLoS One 2011;6:e24919)
- Copy neutral LOH on chromosome 16p (PLoS Genet 2016;12:e1006242)
- 5q (Hum Pathol 1999;30:295)
- P53 mutation in epithelioid angiomyolipomas (Urol Oncol 2022;40:18)
- Rare cases of MDM2 amplification by fluorescence in situ hybridization in fat predominant angiomyolipomas (Virchows Arch 2020;477:661)
Sample pathology report
- Right kidney, mass, partial nephrectomy:
- Angiomyolipoma, classic variant, measuring 3.5 cm in greatest dimension (see comment)
- Surgical margins, negative for tumor
- Comment: The sections show well circumscribed tumor composed of adipose tissue, thick walled blood vessels and smooth muscle. There are vessel walls with prominent sclerosis. Immunohistochemical stain SMA is diffusely positive in the vessel walls and the smooth muscle component. HMB45 is focally staining adipose tissue and smooth muscle.
Differential diagnosis
- Renal cell carcinoma, clear cell type:
- Well differentiated liposarcoma:
- No vascular component
- Negative for melanocytic markers and SMA
- Leiomyoma:
- No vascular or adipose component
- Negative for melanocytic markers
- Leiomyosarcoma:
- Prominent atypia, infiltrative, usually no vascular or adipose component
- Negative for melanocytic markers
- Pleomorphic rhabdomyosarcoma:
- Smooth muscle component is markedly atypical, tumor is infiltrative, no vascular or adipose component
- Negative for melanocytic markers
- Melanoma:
- Marked atypia, no adipose or vascular component
- Negative for SMA
- Adrenal cortical carcinoma:
- Oncocytoma:
- Cytologically bland oncocytes
- No adipose or vascular component
- Negative for melanocytic markers and SMA
- Mixed epithelial and stromal tumor of the kidney (MEST):
- Solid component of MEST can resemble a spindle cell component of so called fat poor angiomyolipoma
- Ovarian stroma-like spindle cells of the solid MEST component are positive for SMA, desmin, ER, PR and FOXL2 and negative for melanocytic markers
- Epithelial component of MEST is similar to AMLEC and is positive for PAX8
Board review style question #1
- A 16 year old girl with history of seizures was found to have bilateral renal masses containing a fat component on the CT imaging study. Histology is shown in the image above. Which hereditary disease is this patient likely to have?
- Birt-Hogg-Dubé
- Familiar papillary renal cell carcinoma
- Hereditary leiomyomatosis
- Tuberous sclerosis
- von Hippel-Lindau
Board review style answer #1
D. Tuberous sclerosis. This H&E image of an angiomyolipoma, together with the clinical history of seizures in a young female, is consistent with tuberous sclerosis.
Comment Here
Reference: Angiomyolipoma
Comment Here
Reference: Angiomyolipoma
Board review style question #2
- A renal tumor from a 43 year old woman shows proliferation of epithelioid cells with abundant eosinophilic cytoplasm and prominent nuclear atypia. What is the best initial immunohistochemical panel for this case?
- Cytokeratin, PAX8, CAIX, CD10, vimentin
- Cytokeratin, PAX8, CK7, CK20, p53
- Cytokeratin, PAX8, MDM2, MyoD1, desmin
- Cytokeratin, PAX8, MITF, S100, tyrosinase
- Cytokeratin, PAX8, SMA, HMB45, inhibin
Board review style answer #2
E. Cytokeratin, PAX8, SMA, HMB45, inhibin. Differential diagnosis includes high grade renal cell carcinoma, epithelioid angiomyolipoma and metastatic tumors such as melanoma and adrenal cortical carcinoma. Although the panel including cytokeratin and PAX8 could provide a diagnosis of renal cell carcinoma and any panel including HMB45 should be helpful in diagnosing melanoma, the only panel that can help with a diagnosis of epithelioid angiomyolipoma is one that includes SMA.
Comment Here
Reference: Angiomyolipoma
Comment Here
Reference: Angiomyolipoma
