

Kidney tumor
Benign / borderline adult tumors
Hemangioma
Editorial Board Members: Debra L. Zynger, M.D., Bonnie Choy, M.D.


Last author update: 3 January 2022
Last staff update: 6 January 2022
Copyright: 2003-2024, PathologyOutlines.com, Inc.
PubMed Search: Hemangioma kidney [TIAB] "last 5 years"[dp]
Table of Contents
Definition / general | Essential features | Terminology | Epidemiology | Sites | Etiology | Clinical features | Diagnosis | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Gross description | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Negative stains | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Wondimu B, Tretiakova M. Hemangioma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/kidneytumorhemangiomas.html. Accessed April 19th, 2024.
Definition / general
- Benign vascular proliferation, rarely diagnosed in kidney (more common in skin or superficial soft tissue)
- Subtypes: capillary, cavernous, mixed, anastomosing
Essential features
- Benign, circumscribed, unencapsulated proliferation of capillaries with endothelial lining in kidney
- Can appear radiologically similar to renal cell carcinomas, angiosarcomas or other malignancies (Arch Pathol Lab Med 2020;144:240)
- Anastomosing hemangioma: sinusoidal vessels with anastomotic arrangement, hobnail endothelial cells, with or without extramedullary hematopoiesis (Histopathology 2014;65:309)
Terminology
- Benign, neoplastic vascular proliferation
Epidemiology
- M:F = 1.8:1 (Am J Surg Pathol 2010;34:942)
Sites
- Pelvis or medullary pyramid, rarely in renal cortex or capsule
- Hemangiomas more commonly found in skin or soft tissues
Etiology
- Often associated with end stage renal disease (Histopathology 2014;65:309)
- Can be associated with acquired cystic kidney disease, polycythemia or renal cell carcinoma
Clinical features
- Typically asymptomatic but can present with hematuria or flank / abdominal pain
- Often incidentally found on imaging
- May be associated with vascular malformation syndromes, including Klippel-Trenaunay and Sturge-Weber (Virchows Arch 2012;461:669)
Diagnosis
- May be diagnosed radiologically but can be difficult to distinguish from renal cell carcinoma or other tumors on imaging
- Diagnosis often made on biopsy or nephrectomy (Radiol Case Rep 2019;14:750)
Radiology description
- Nonspecific echogenicity on ultrasound
- CT: hypoattenuation, arterial enhancement, can be concerning for malignancy
- Difficult to distinguish radiographically from malignant lesions; biopsy or excision often needed for definitive diagnosis (Radiol Case Rep 2019;14:750)
Radiology images
Images hosted on other servers:

Kidney ultrasound

Noncontrast CT

Contrast CT
Prognostic factors
- Excellent prognosis with excision
Case reports
- 23 year old man with end stage renal disease with isoechoic left kidney mass (Radiol Case Rep 2019;14:750)
- 35 year old woman with end stage renal disease and a renal mass (BMC Nephrol 2021;22:262)
- 40 year old woman with abdominal pain and left kidney mass (Indian J Pathol Microbiol 2020;63:292)
- 47 year old man with end stage renal disease and left kidney mass (Diagn Pathol 2017;12:14)
- 64 year old woman with back pain (Diagn Pathol 2017;12:14)
Treatment
- May regress spontaneously (J Urol 2002;167:488)
- Variable; can include no treatment, endoscopic ablation or nephrectomy (Am J Case Rep 2017;18:255)
- In healthy patients with minimal symptoms and confirmed diagnosis, observation favored
- Nephrectomy often occurs when difficult to distinguish from carcinoma
Gross description
- Unilateral, solitary, well circumscribed, red to brown mass
- Most commonly present in papillary tips; can also be found in submucosa, medulla (Am J Surg Pathol 2010;34:942)
Microscopic (histologic) description
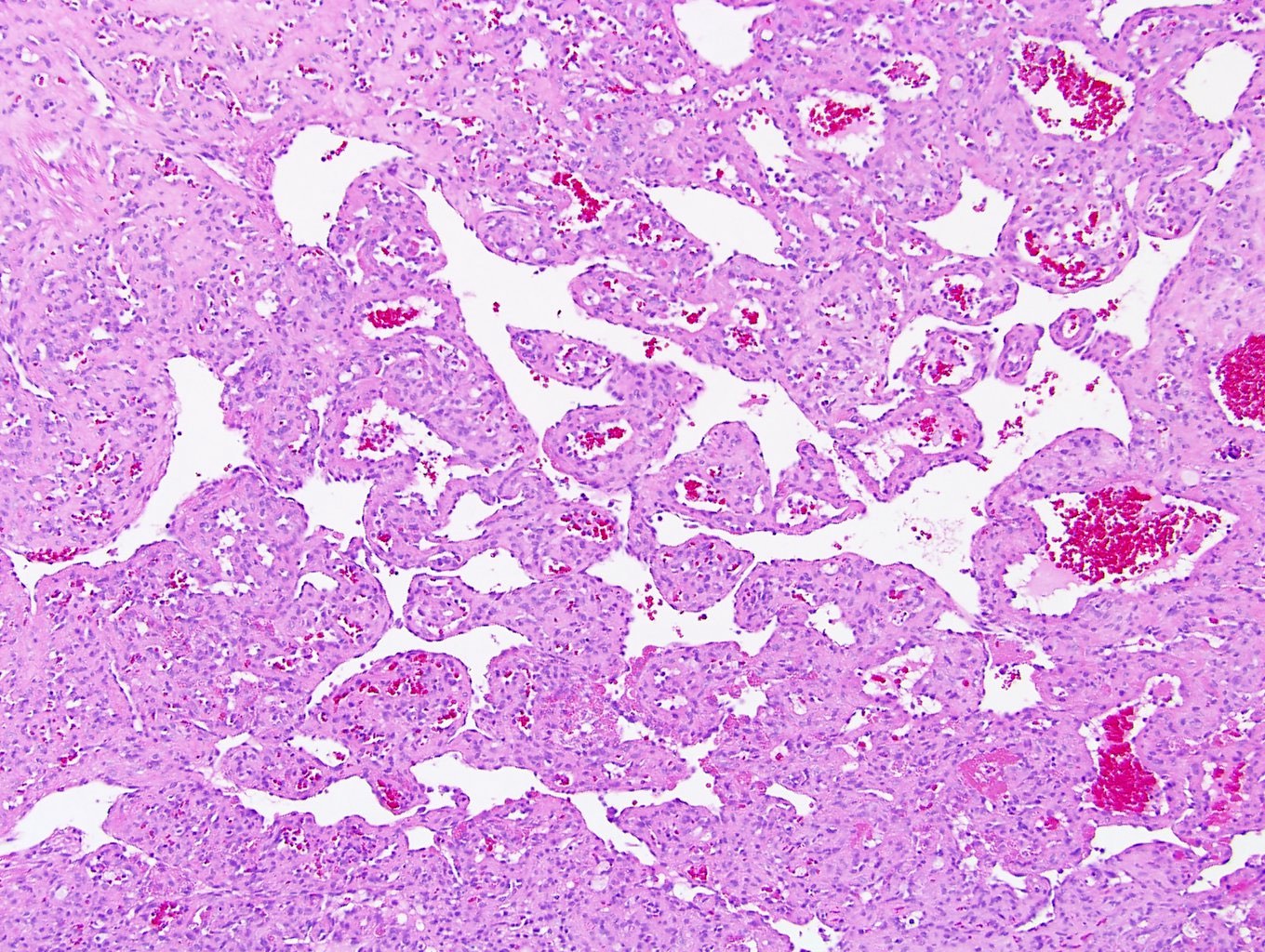
- Circumscribed, unencapsulated proliferation of irregular, blood filled vascular spaces lined by a single layer of endothelial cells
- May or may not show lobular growth pattern with large feeding vessels at periphery (Virchows Arch 2012;461:669)
- Multiple subtypes:
- Capillary: more common, characterized by slit-like vascular spaces
- Cavernous: characterized by dilated vessels
- Mixed: features of both capillary and cavernous
- Anastomosing hemangioma (variant of capillary)
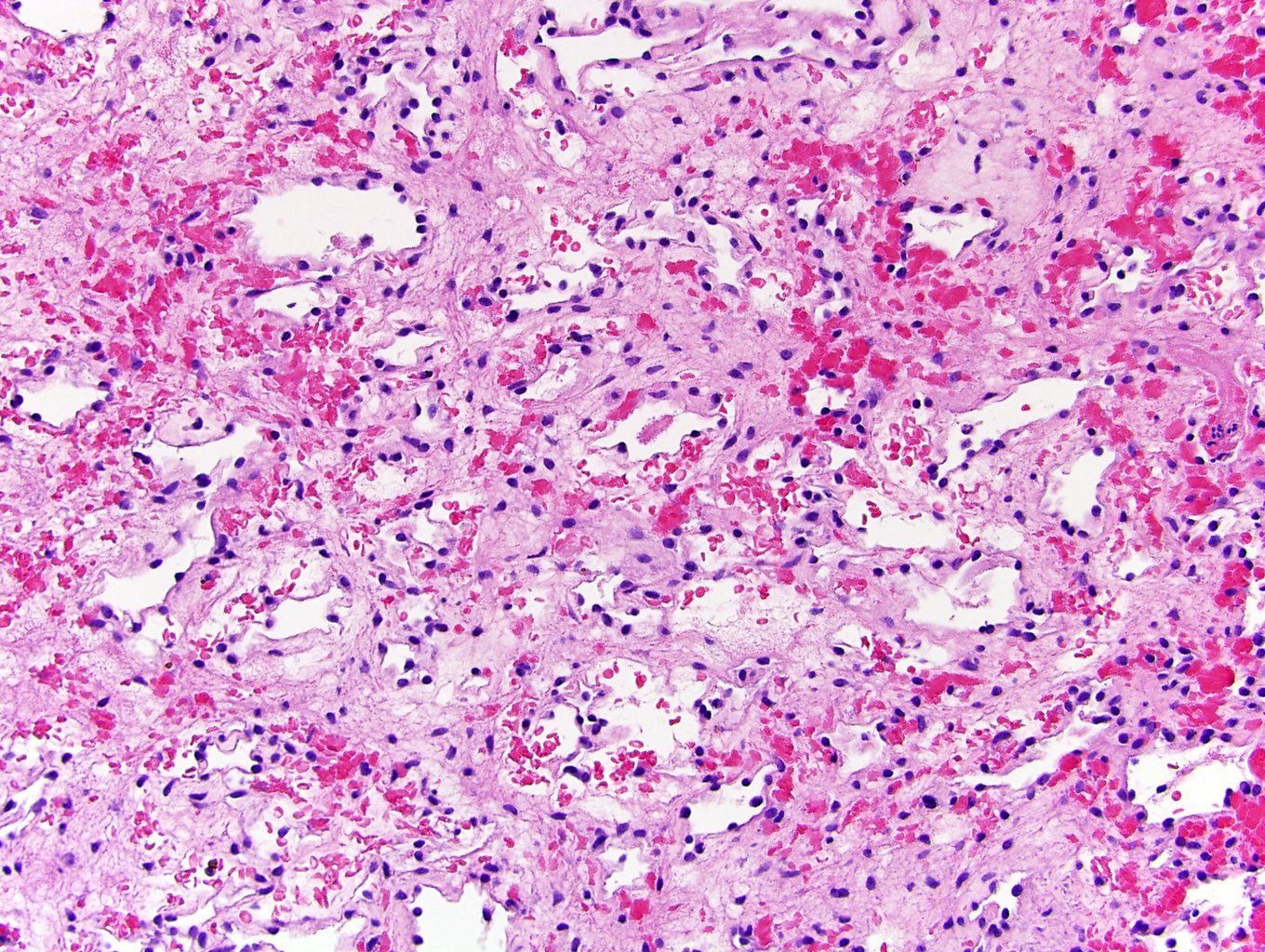
- Anastomosing hemangioma (AH):
- Capillary sized sinusoidal vessels with anastomotic arrangement
- Scattered hobnail endothelial cells
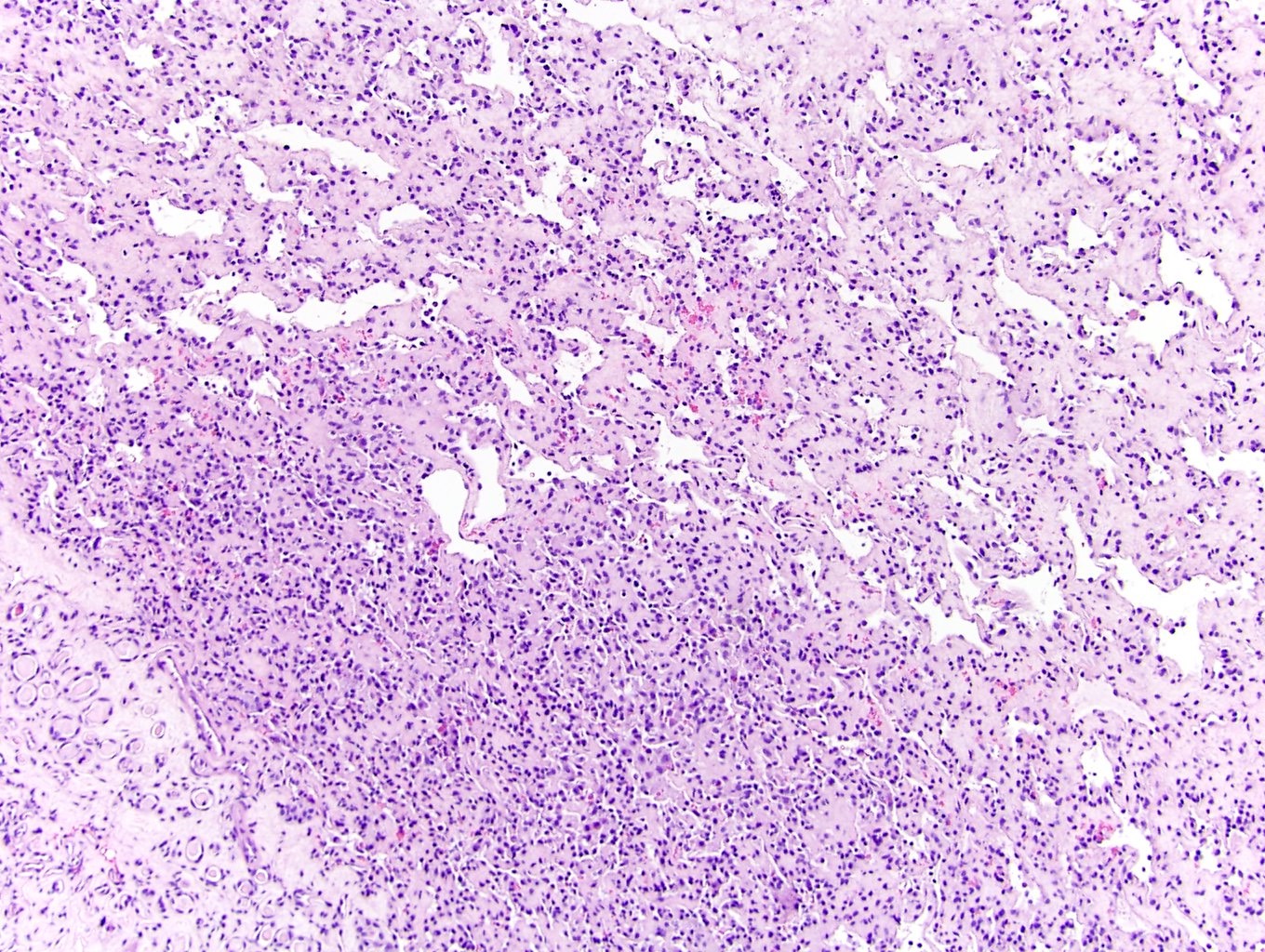
- Extramedullary hematopoiesis, fibrin thrombi, extensive perirenal fat entrapment, intravascular growth and mast cells may be seen (Histopathology 2014;65:309)
- Cytologic atypia and mitotic activity rare
- Regressive changes, including hyalinization, cystic changes and fatty overgrowth (Histopathology 2014;65:309)
Microscopic (histologic) images
Contributed by Maria Tretiakova, M.D., Ph.D. and AFIP images
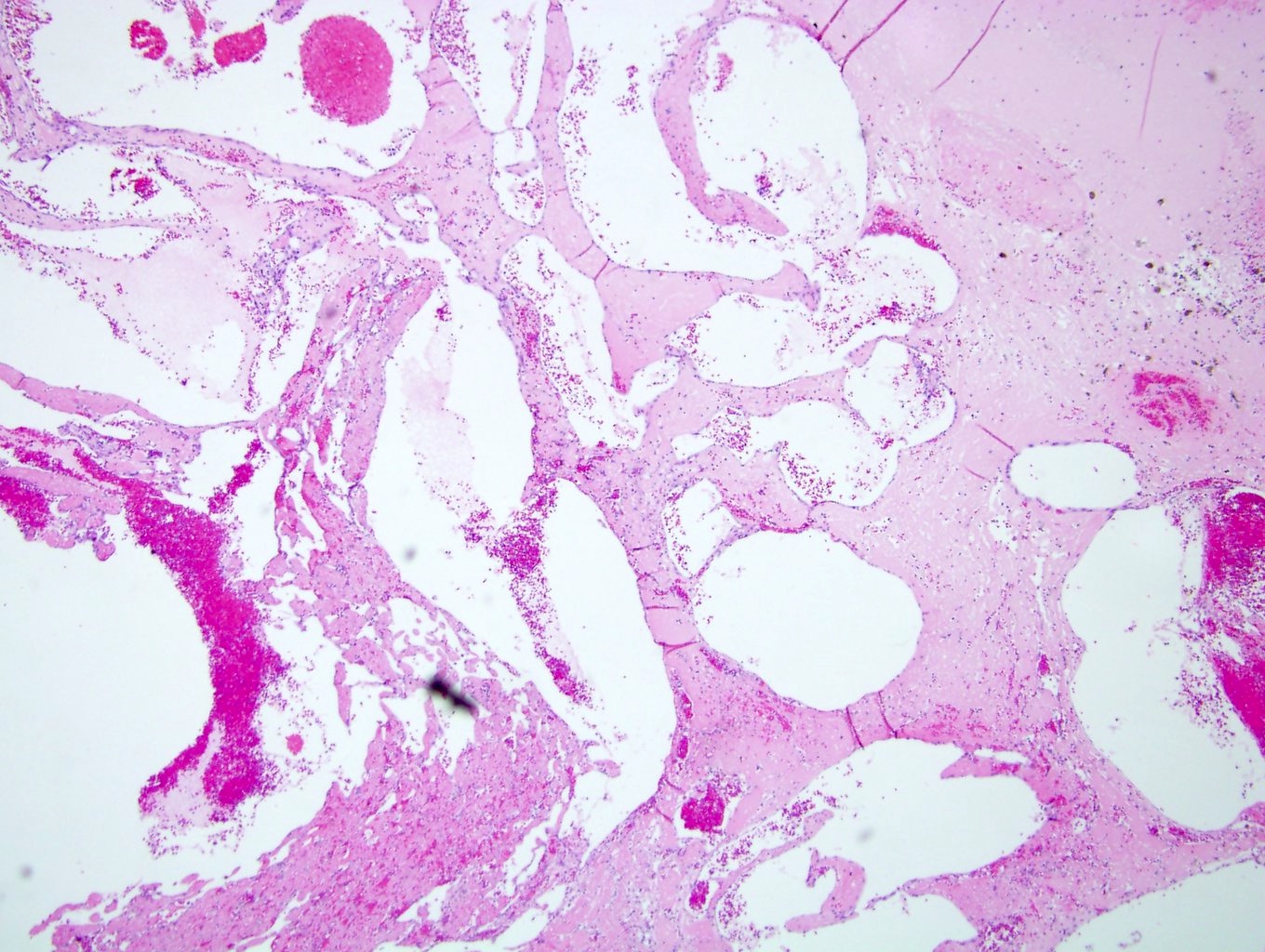
Cavernous hemangioma
Hypocellular AH
Anastomosing hemangioma
Sinusoidal anastomosing pattern
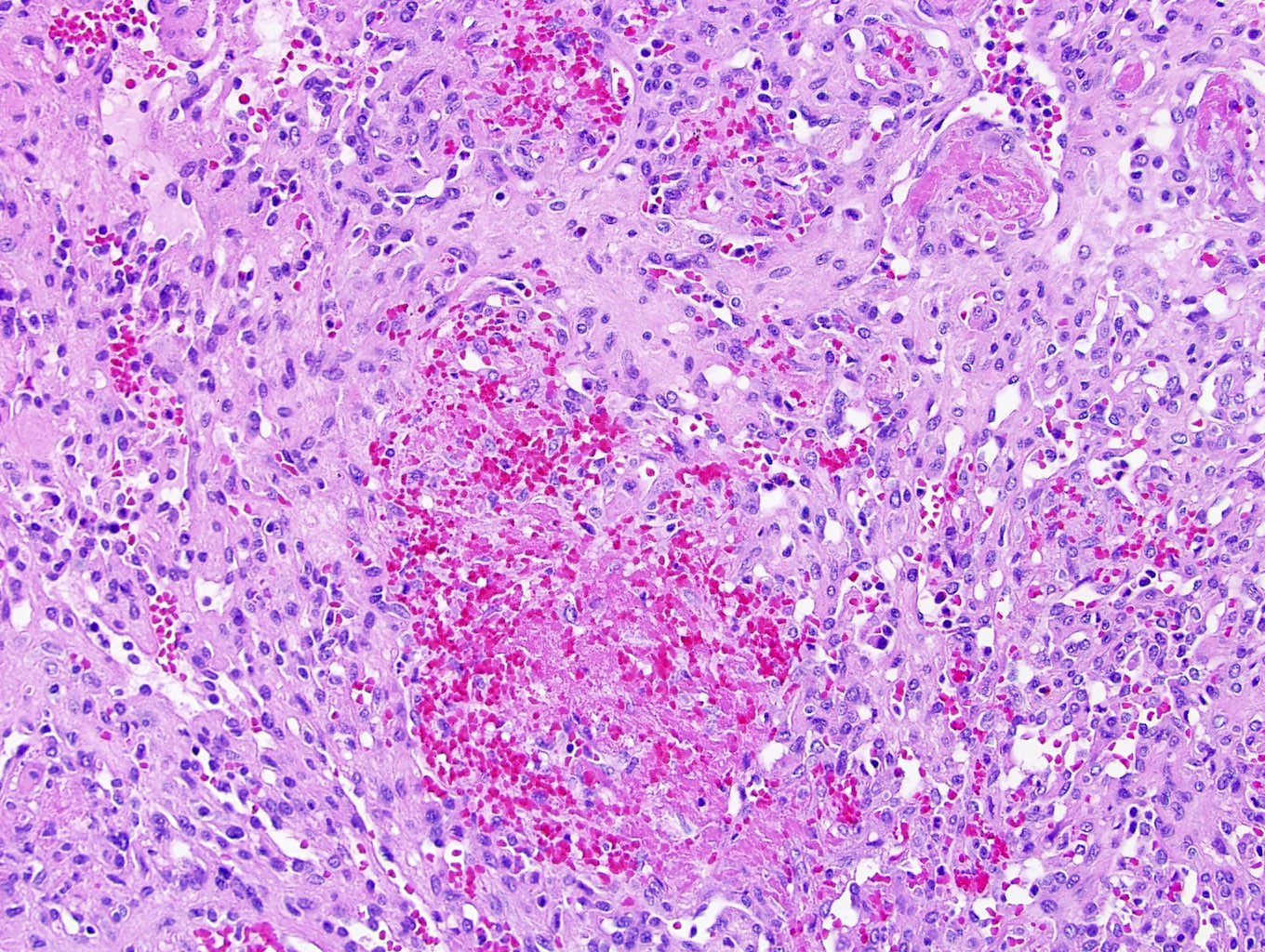
Fibrin thrombi (AH)
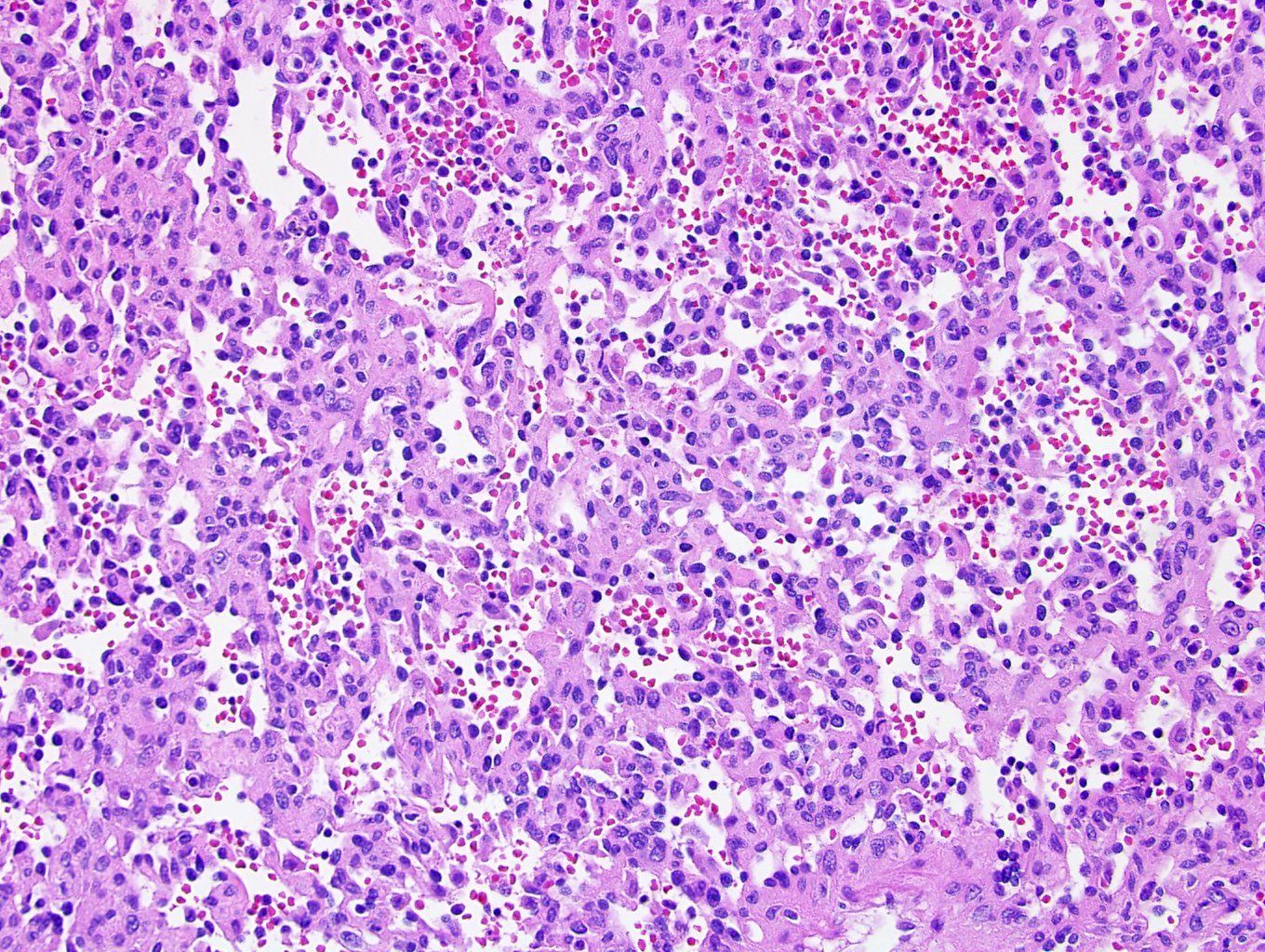
Extramedullary hematopoiesis
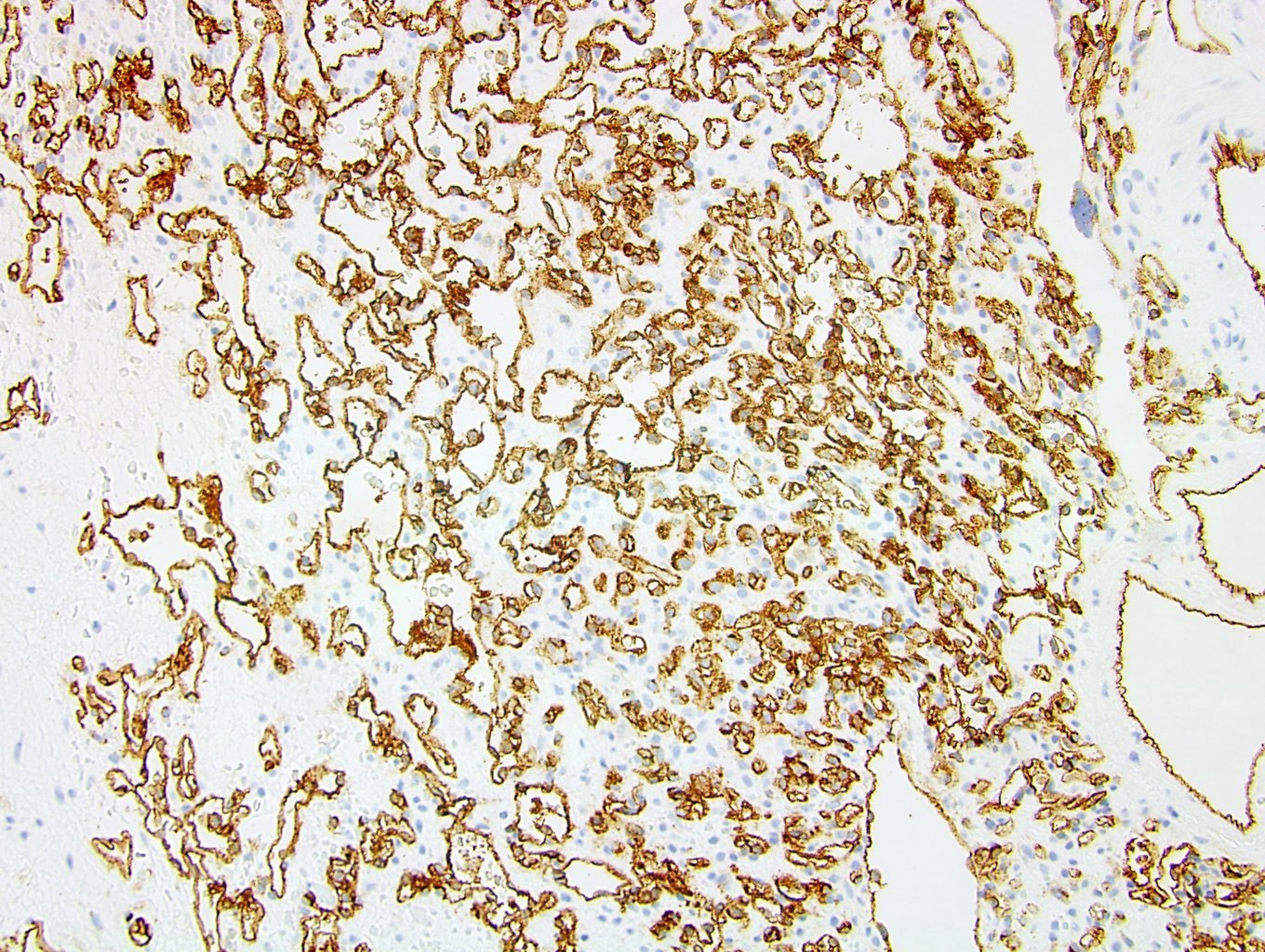
CD31 (AH)

Renal hemangioma
Positive stains
Negative stains
Sample pathology report
- Left kidney, radical nephrectomy:
- Anastomosing hemangioma (1.3 cm) (see comment)
- Comment: The tumor is a well circumscribed, low grade vascular neoplasm composed of small capillary channels in an anastomosing pattern. There is no nuclear atypia or significant mitotic activity. In addition, foci of extramedullary hematopoiesis and fibrin thrombi are present. Immunohistochemistry is positive for CD31, supporting the diagnosis of a vascular neoplasm. The morphologic and immunohistochemical profile of the neoplasm is consistent with anastomosing hemangioma.
Differential diagnosis
- Lymphangioma:
- Thin walled cysts filled with homogenous proteinaceous material and delicate fibrous septae
- Positive for D2-40
- Renal cell carcinoma:
- Epithelial proliferation forming acini, tubules and sheets of renal cells within a vascular rich stroma
- Positive for PAX8, cytokeratins and CD10 (Arch Pathol Lab Med 2020;144:240)
- Angiosarcoma:
- Arteriovenous malformation:
- Mixture of benign, variably sized vessels with abundant thrombi
- Thin and thick walled vessels (Arch Pathol Lab Med 2020;144:240, Am J Surg Pathol 2009;33:1364)
- Glomus tumor / glomangioma:
- Very rare in the kidney
- Positive for smooth muscle actin, vimentin, collagen type IV and CD57 (Int J Surg Pathol 2011;19:393)
- Negative for vascular markers such as CD31, CD34, von Willebrand factor and WT1
Board review style question #1
The tumor in the above image is found in the kidney and is negative for cytokeratins on immunohistochemistry. What is the diagnosis?
- Anastomosing hemangioma
- Kaposi sarcoma
- Renal cell carcinoma
- Well differentiated angiosarcoma
Board review style answer #1
A. Anastomosing hemangioma. Vascular lesion in the kidney with anastomosing sinusoidal-like vascular spaces and absent / minimal atypia of endothelial cells most likely to be anastomosing hemangioma. Kaposi sarcoma more likely to be seen in dermis or subcutaneous tissue. Angiosarcoma would demonstrate more atypial cytologic features and endothelial cell multilayering. Renal cell carcinomas can have vascular rich areas but would stain for cytokeratins.
Comment Here
Reference: Hemangioma
Comment Here
Reference: Hemangioma
Board review style question #2
A 42 year old woman with end stage renal disease presents with a renal mass. Excision of the lesion reveals the above vascular lesion. Which of the following is true concerning this lesion?
- Cytologic atypia and mitotic activity is common
- Extramedullary hematopoiesis, fibrin thrombi and mast cells may be present
- Lesion will be positive for cytokeratins and CD10
- Prognosis is poor
Board review style answer #2
B. Extramedullary hematopoiesis, fibrin thrombi and mast cells may be present. Cytologic atypia and mitotic activity is rare and prognosis after excision is excellent. Cytokeratins and CD10 would be positive in renal cell carcinoma but negative in anastomosing hemangioma.
Comment Here
Reference: Hemangioma
Comment Here
Reference: Hemangioma
