
Liver & intrahepatic bile ducts
Liver transplantation
Late onset graft injury
Chronic antibody mediated rejection
Author: Mohamed El Hag, M.D., M.S.
Editorial Board Member: Catherine E. Hagen, M.D.
Deputy Editor-in-Chief: Raul S. Gonzalez, M.D.

Last author update: 8 April 2021
Last staff update: 8 April 2021
Copyright: 2020-2024, PathologyOutlines.com, Inc.
PubMed Search: Chronic antibody mediated rejection[title]
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Clinical features | Diagnosis | Laboratory | Radiology description | Case reports | Treatment | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: El Hag M. Chronic antibody mediated rejection. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/liverchronicantibodyrejection.html. Accessed April 25th, 2024.
Definition / general
- Antibody mediated immune injury to liver allografts, resulting in significant fibrosis and persistent inflammation (Am J Transplant 2016;16:2816)
- Consequence of chronic long term immunologic injury (EBioMedicine 2016;9:346)
- Leading cause of retransplantation after 10 years in children (Clin Transplant 2018;32:e13227)
- Second leading cause of retransplantation in adults after disease recurrence (Clin Transplant 2018;32:e13227)
Essential features
- Liver allograft fibrosis
- Unexplained mononuclear, interface or perivenular inflammation / necroinflammatory activity
- Evidence of circulating donor specific antibodies
- C4d deposition
Terminology
- Chronic active antibody mediated rejection (cAMR) (Am J Transplant 2016;16:2816)
- Humoral rejection is considered an old term
ICD coding
- ICD-10: T86.41 - Liver transplant rejection
Epidemiology
- Incidence about 8% at 10 years posttransplantation
- Risk factors:
- Retransplantation (Am J Transplant 2014;14:867)
- Young age (Ann Transplant 2017;22:333)
- Cyclosporine immunosuppression (Am J Transplant 2013;13:1541)
- Low calcineurin inhibitor level (Am J Transplant 2013;13:1541)
Sites
- Liver allografts
- Also occurs in other solid organ allografts such as kidney (Am J Transplant 2017;17:28)
Pathophysiology
- Linked to anti-class II donor specific antibodies (DSA), AT1R and portal inflammation (Transplantation 2017;101:2399, Liver Transpl 2008;14:1582)
- Persistent de novo donor specific antibodies, usually directed at HLA-DQ (Am J Transplant 2013;13:1541, Am J Transplant 2016;16:603)
Clinical features
- Mostly asymptomatic with normal or near normal liver function tests (Liver Transpl 2016;22:1593)
- Mostly detected on protocol biopsies
Diagnosis
- Criteria and categories for the diagnosis of cAMR were defined by the Banff working group (Am J Transplant 2016;16:2816)
| Probable chronic active AMR (all 4 criteria must be met) | |
| 1 | Histopathologic evidence of injury consistent with cAMR (both required):
|
| 2 | Recent evidence of circulating HLA DSA in serum samples |
| 3 | At least focal C4d positive (> 10% portal tract microvascular endothelia); see Acute AMR for C4d scoring |
| 4 | Reasonable exclusion of other insults that might cause a similar pattern of injury |
| Possible chronic active AMR | |
| 1 | As above but C4d staining is negative or minimal (criteria 1, 2 and 4 met) |
- Criteria are intended to be stringent to prevent overdiagnosis and do not include more recently described lesions (see Microscopic description); as more lesions are described, the criteria will likely be updated
- Banff suggests that liver allograft fibrosis scoring be performed in 3 separate compartments (portal, sinusoidal and perivenular) according to Venturi et al. (Am J Transplant 2012;12:2986)
Liver allograft fibrosis semiquantitative scoring system by Venturi et al. (Am J Transplant 2012;12:2986)
| | | | | |
| Portal tracts | No fibrosis | Nonexpanding fibrosis in less than 50% of portal tracts | Fibrosis in more than 50% of portal tracts or expansion into short fibrous septa into periportal parenchyma | Marked expansion of most or all portal tracts with portal to portal or portal to central bridging fibrosis with or without occasional nodules |
| Sinusoids (zones 1 and 2) | No fibrosis | Little fibrosis with thin focal collagen deposits involving less than 50% of sinusoids | Little fibrosis with thin diffuse collagen deposits involving more than 50% of sinusoids or thicker but focal fibrosis in less than 50% of sinusoids | Thick, marked and diffuse sinusoidal fibrosis |
| Centrilobular vein | No fibrosis | Circular perivenular fibrosis involving less than 50% of central veins without invasion into the perivenular parenchyma | Circular perivenular fibrosis in more than 50% of central areas or expansion into short fibrous septa into perivenular parenchyma | Marked centrilobular fibrosis with bridging to other central or portal areas |
- Scores from each compartment are added for a total score out of 9
Laboratory
- Evidence of DSA (HLA or non-HLA); mostly HLA class II DQ
- Negative testing for hepatitis B, C and E (Liver Transpl 2016;22:1593)
- Serum markers of fibrosis have been proposed, including hyaluronic acid and embryonic liver fodrin (Liver Transpl 2016;22:1593)
- No serum markers of inflammation are currently recommended
Radiology description
- Multiple imaging modalities can detect hepatic fibrosis to varying degrees:
- Magnetic resonance elastography (Clin Gastroenterol Hepatol 2015;13:440)
- Acoustic radiation force impulse (J Pediatr Gastroenterol Nutr 2014;58:382, Pediatr Radiol 2013;43:545)
- Transient elastography (J Pediatr Gastroenterol Nutr 2013;56:72, Pediatr Transplant 2013;17:525)
- In general, these modalities are more effective in detecting advanced fibrosis
- Less effective in detecting milder fibrosis when used on split liver allografts and when cholestasis is present
Case reports
- Report of 4 cases with cAMR and obliterative portal venopathy (Pediatr Transplant 2018; 22:e13124)
Treatment
- Retransplantation for failed allografts
Gross description
- Explanted livers show a fibrotic multinodular and rubbery cut surface
- May show a green cholestatic cut surface
Gross images
Contributed by Mohamed El Hag, M.D., M.S.
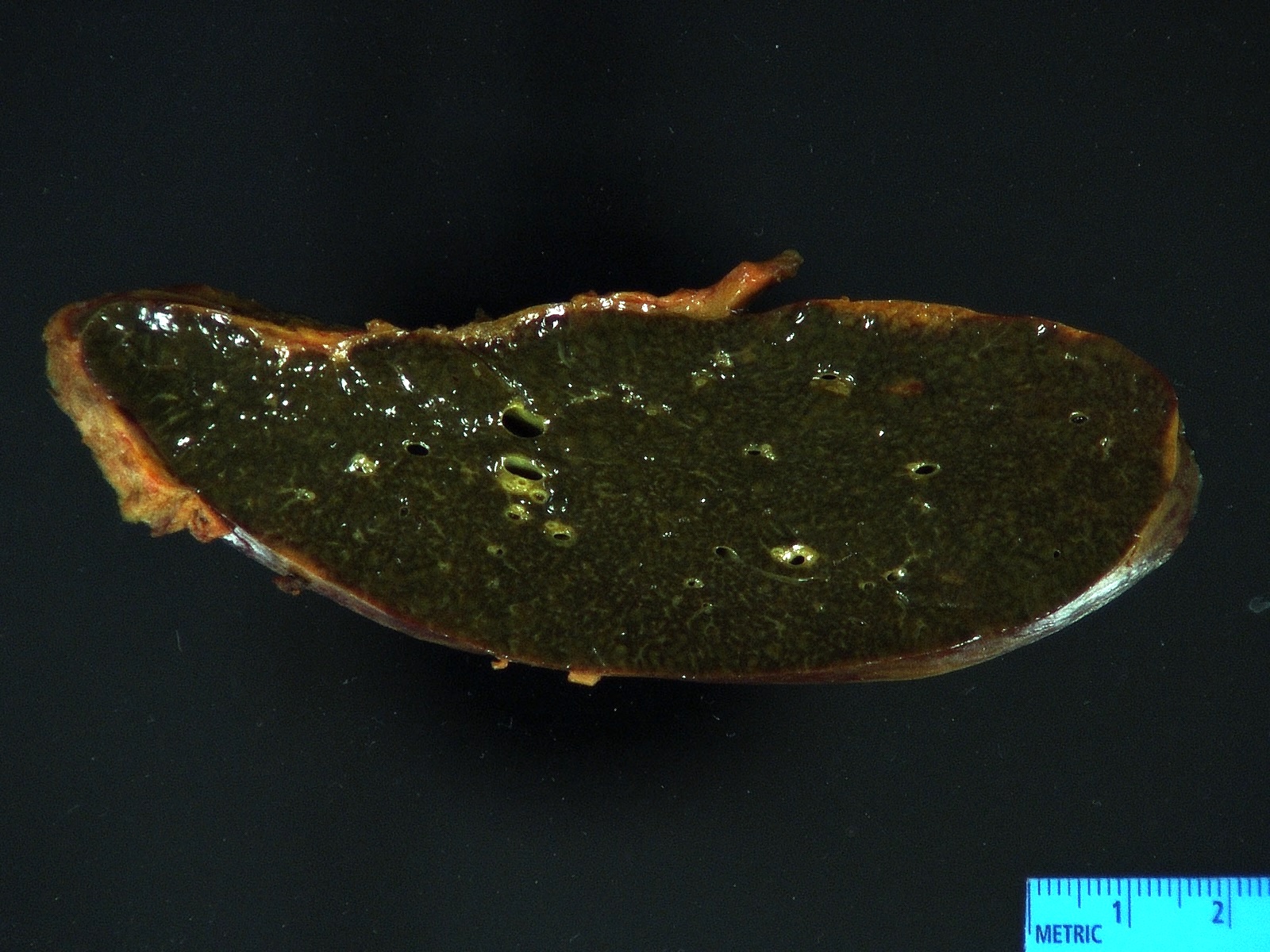
Explanted liver allograft
Microscopic (histologic) description
- Inflammation (Clin Transplant 2018;32:e13227, Liver Transpl 2016;22:1593, Liver Transpl 2018;24:897):
- Chronic hepatitis pattern of mononuclear inflammation with interface hepatitis or lobular and perivenular inflammation
- Perivenulitis
- Vascular changes (Pediatr Transplant 2018; 22:e13124, Am J Transplant 2018;18:1534):
- Obliterative portal venopathy with nodular regenerative hyperplasia-like changes
- Obliterative arteriopathy or isolated arterial "V" lesions (age inappropriate arterial fibrointimal hyperplasia with no T cell mediated rejection) with or without intimal inflammation arterial lesions are associated with subsequent T cell mediated rejection (TCMR), graft failure and C4d positivity; most C4d positive cases show additional histologic features encountered in cAMR such as portal and perivenular inflammation (rejection activity index / RAI 1 - 2) and at least moderate periportal, perivenular or sinusoidal fibrosis (Am J Transplant 2018;18:1534)
- Bile duct changes (Liver Transpl 2018;24:897):
- Biliary epithelial senescence and duct loss may be seen but at lower rates
- Distinct fibrosis patterns (Am J Transplant 2016;16:603, Transplantation 2017;101:2062, Clin Transplant 2018;32:e13227, Liver Transpl 2016;22:1593, Liver Transpl 2018;24:897):
- Dense acellular portal collagen deposition: portal collagenization
- Distinct subsinusoidal and perivenular fibrosis
- Focal nodular hyperplasia-like changes: usually without the map-like glutamine synthetase staining pattern or dystrophic vasculature usually seen in classic focal nodular hyperplasia lesions
Microscopic (histologic) images
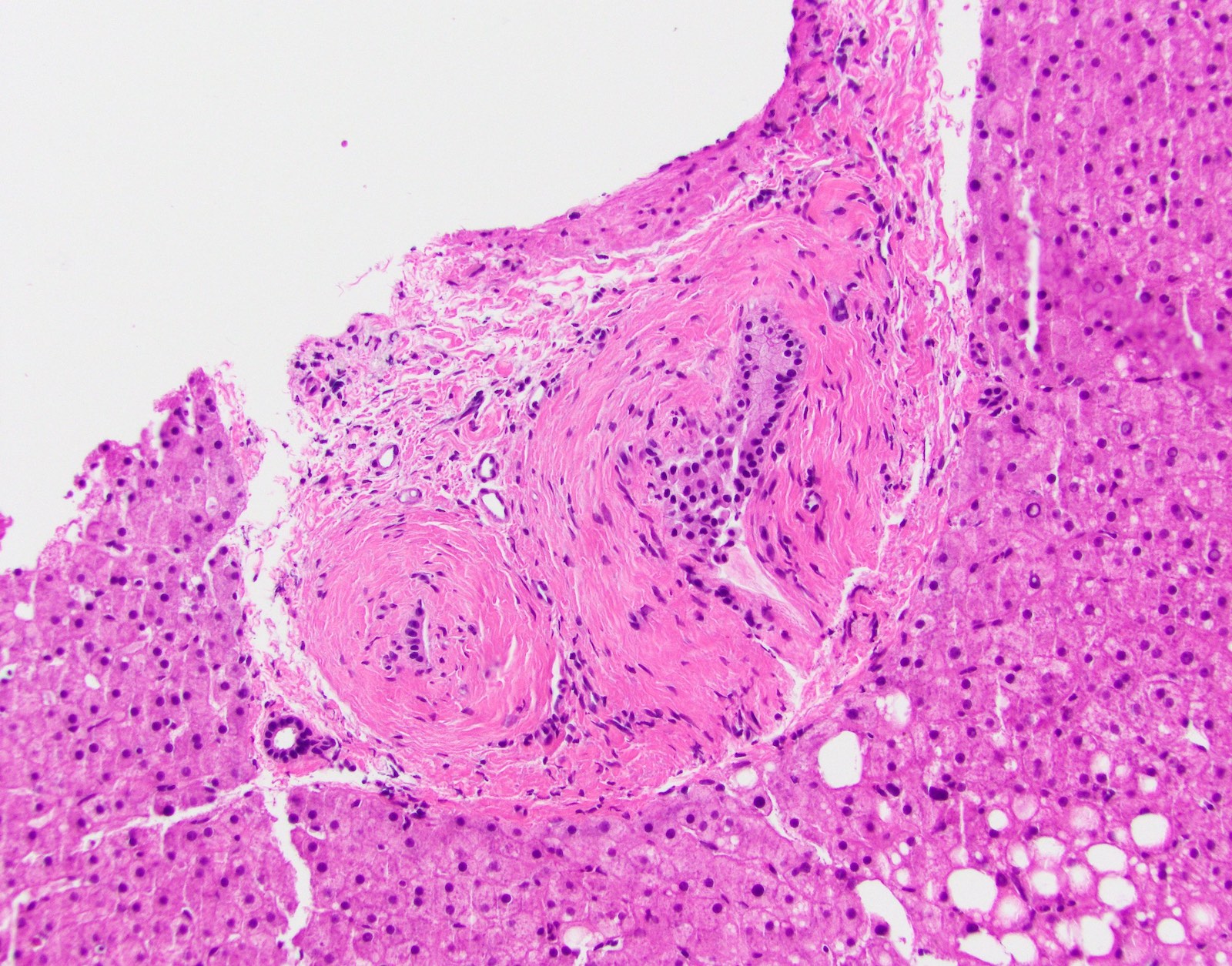
Contributed by Mohamed El Hag, M.D., M.S.
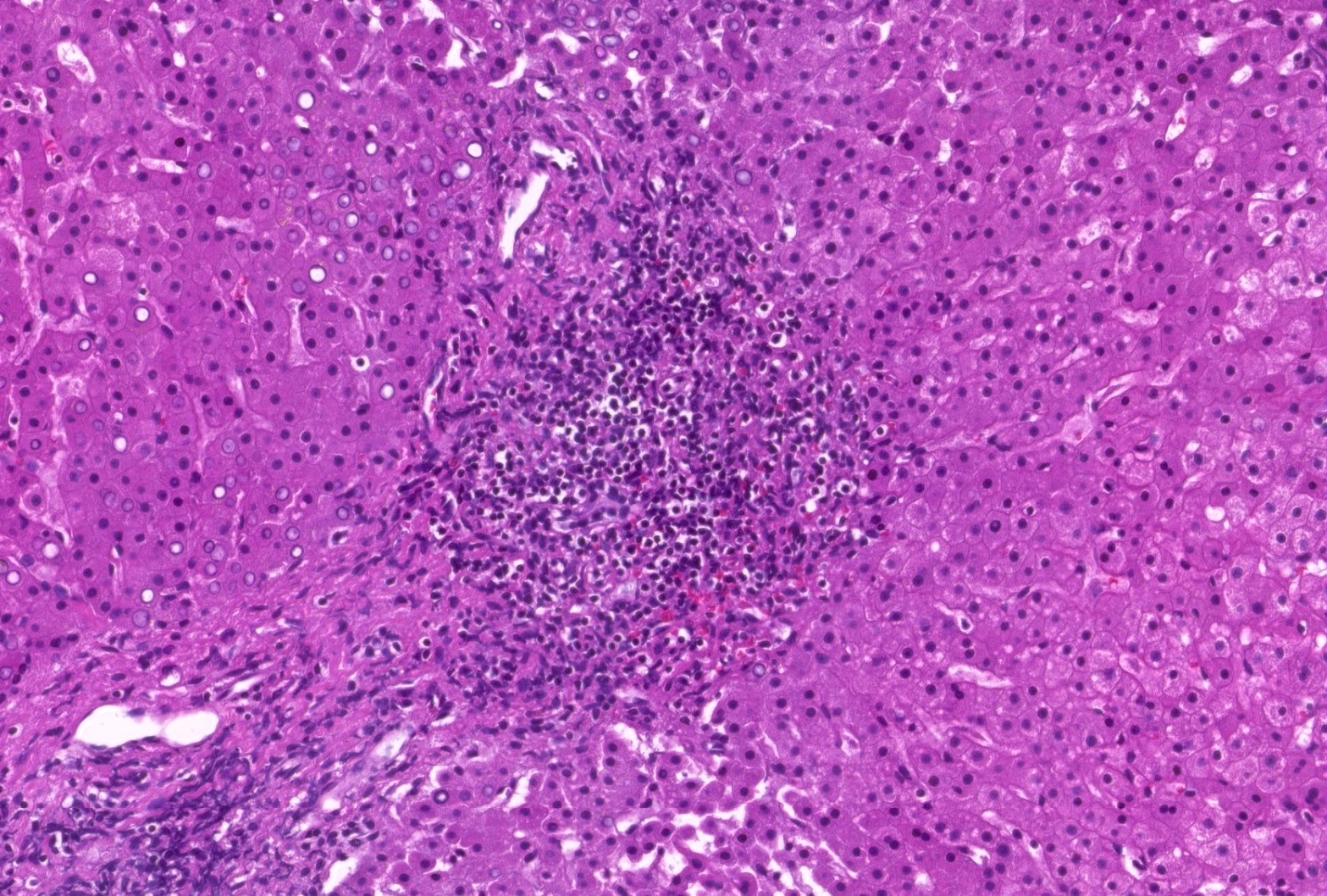
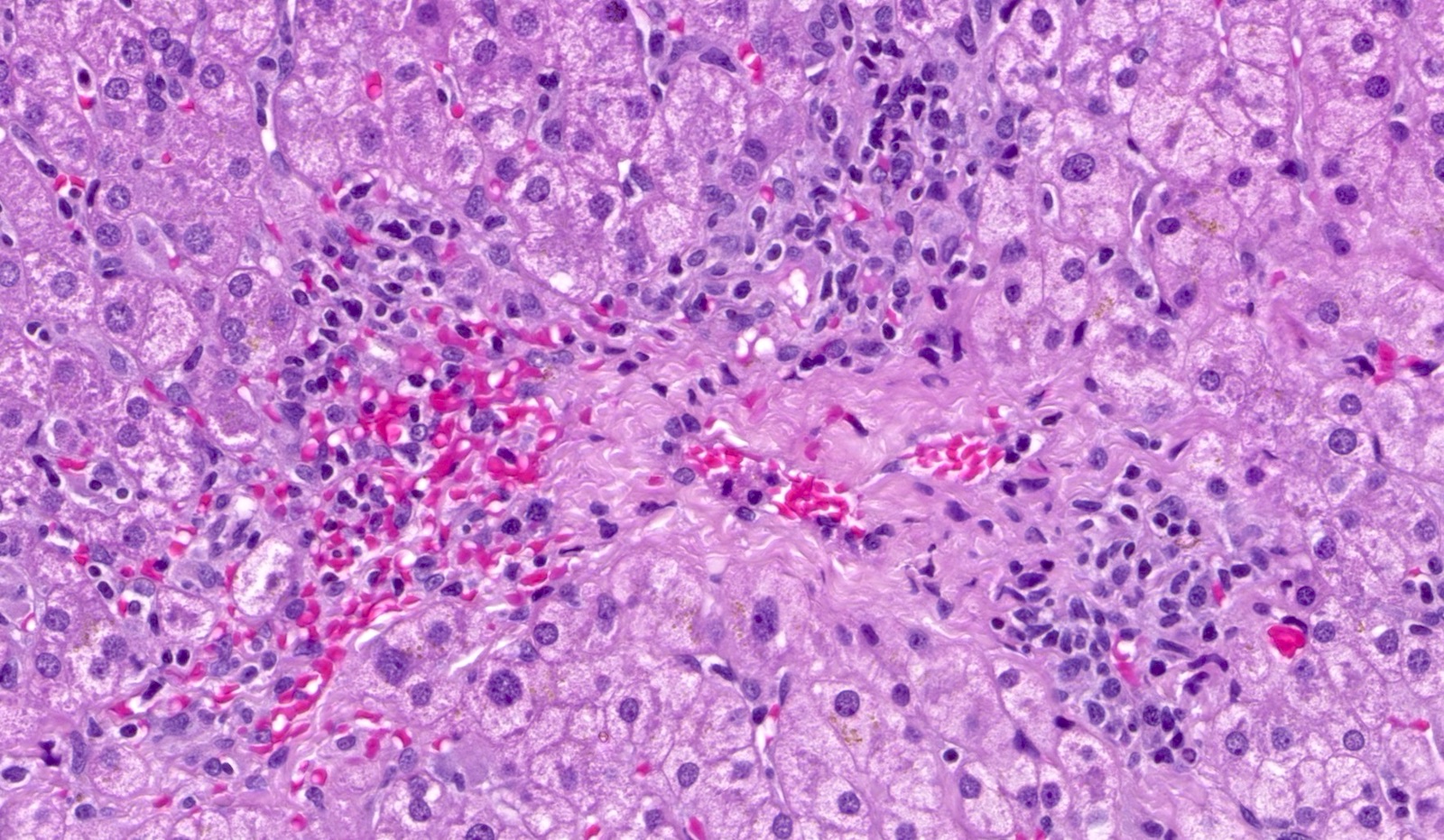
Chronic hepatitis pattern
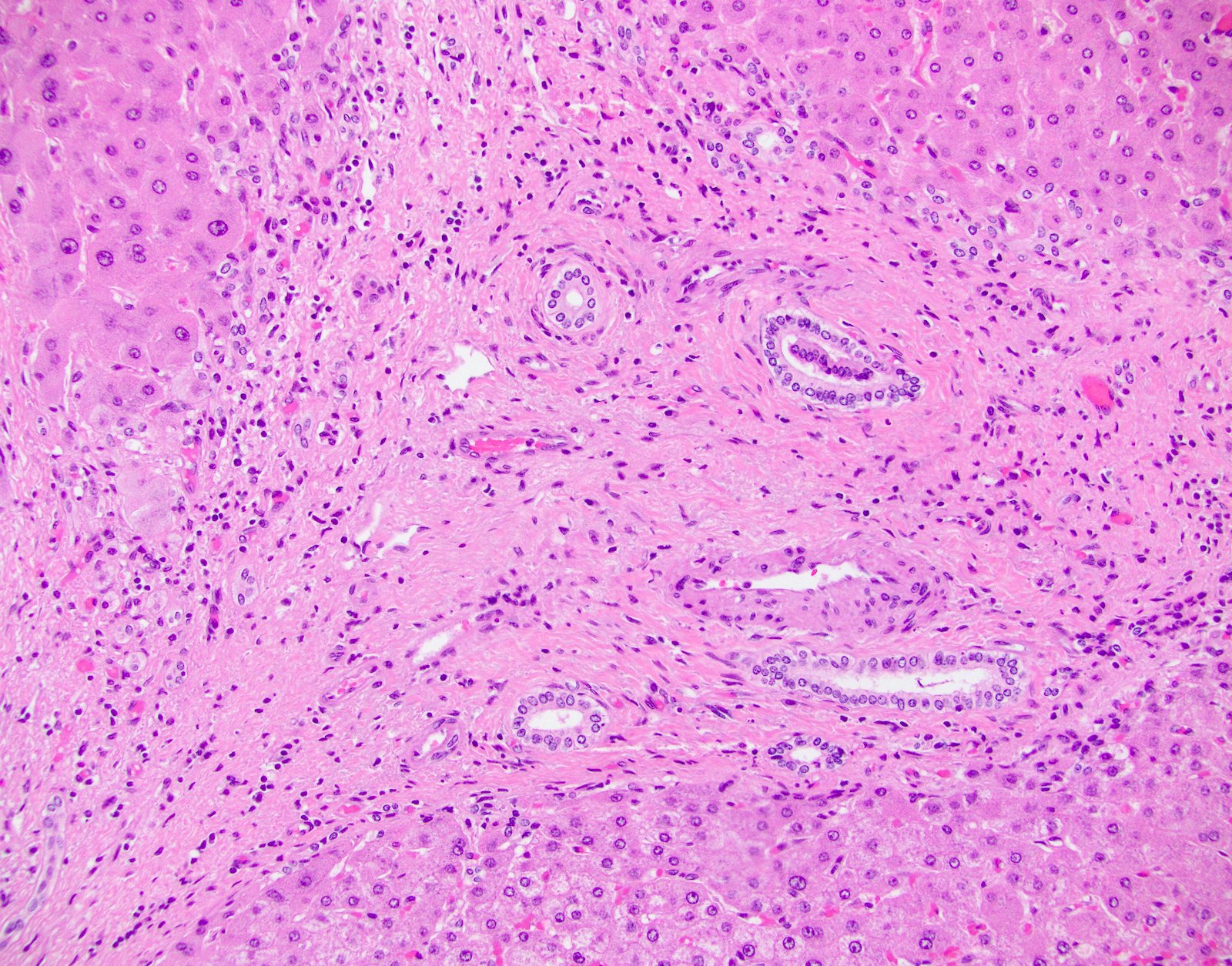
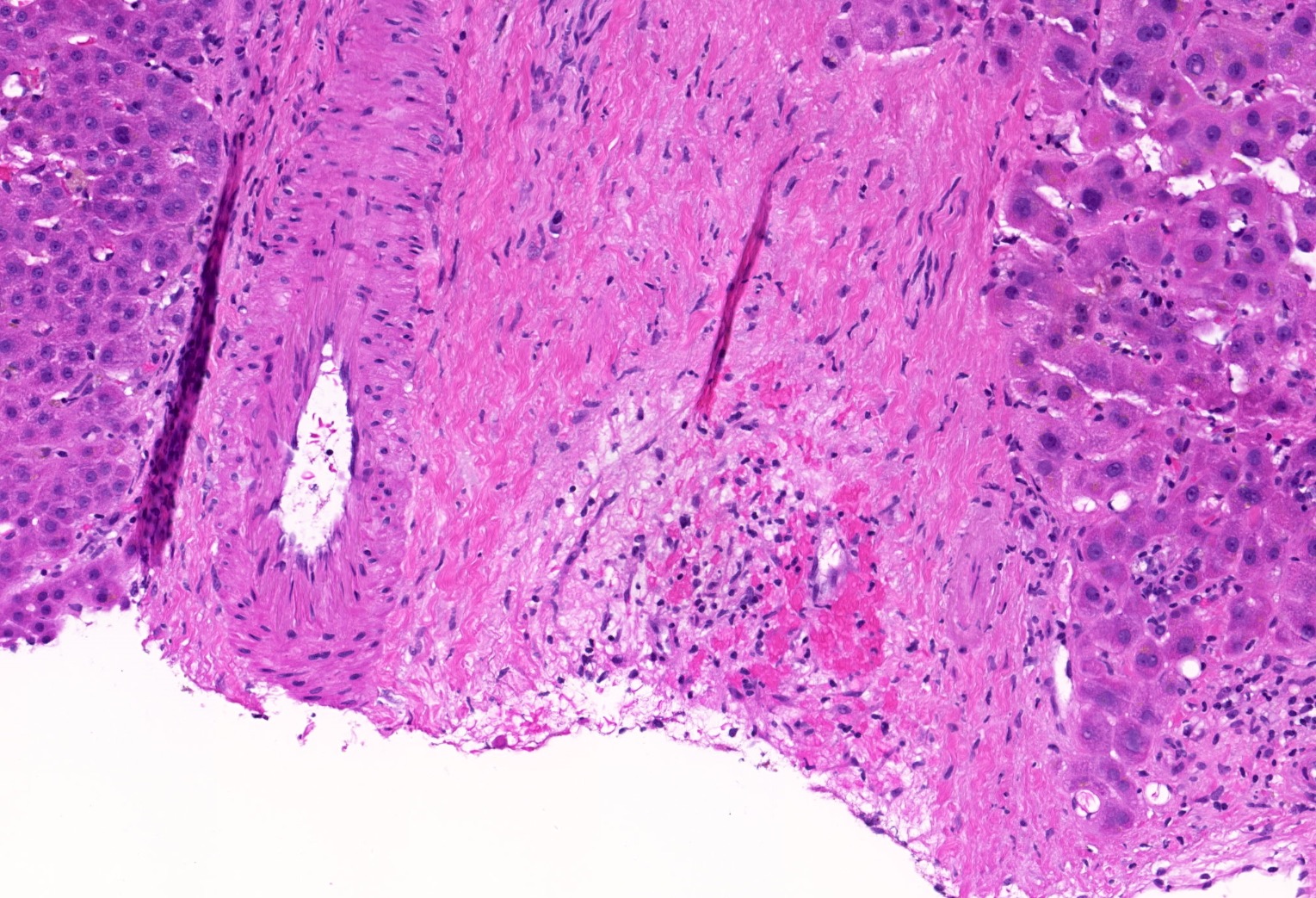
Portal venopathy
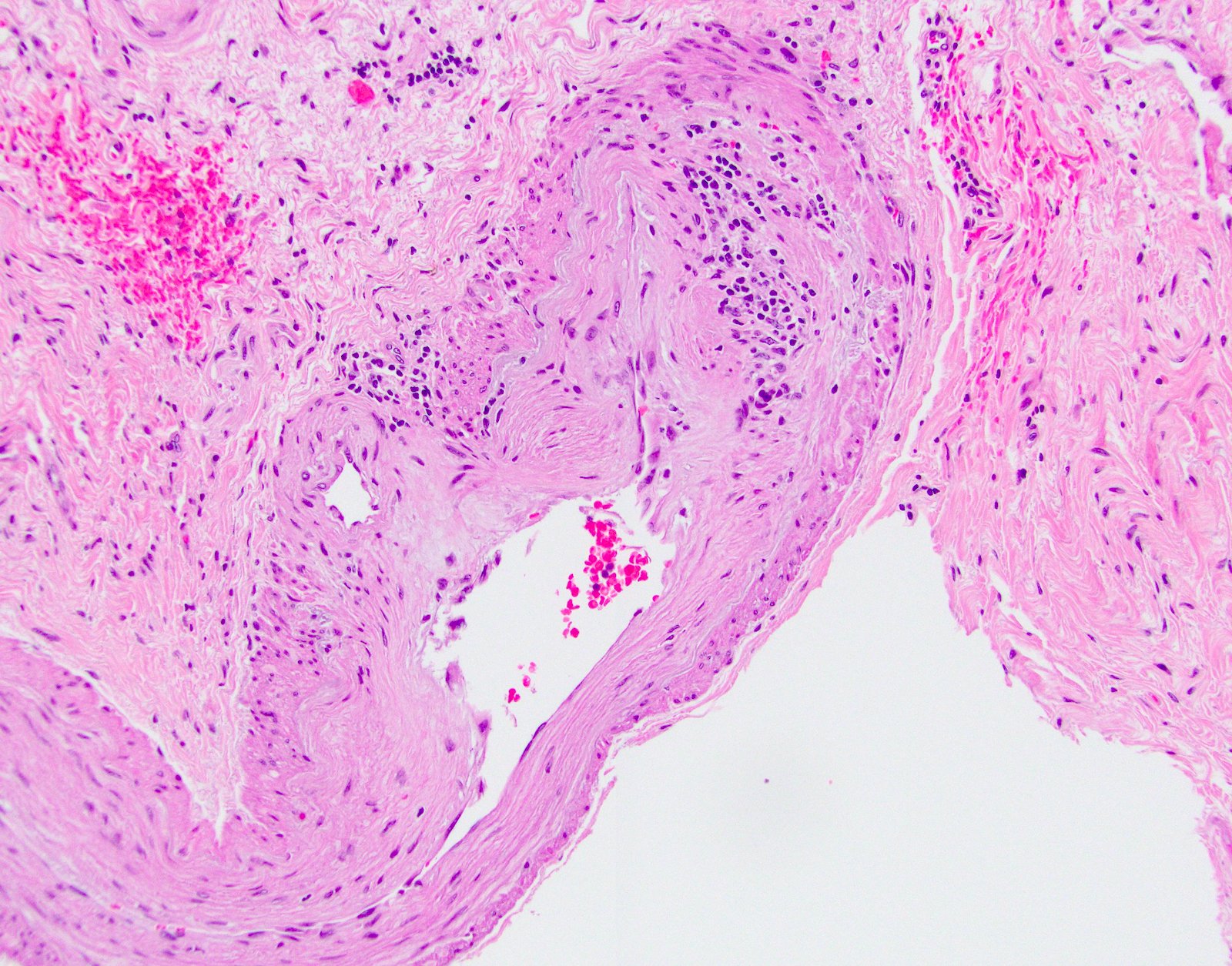
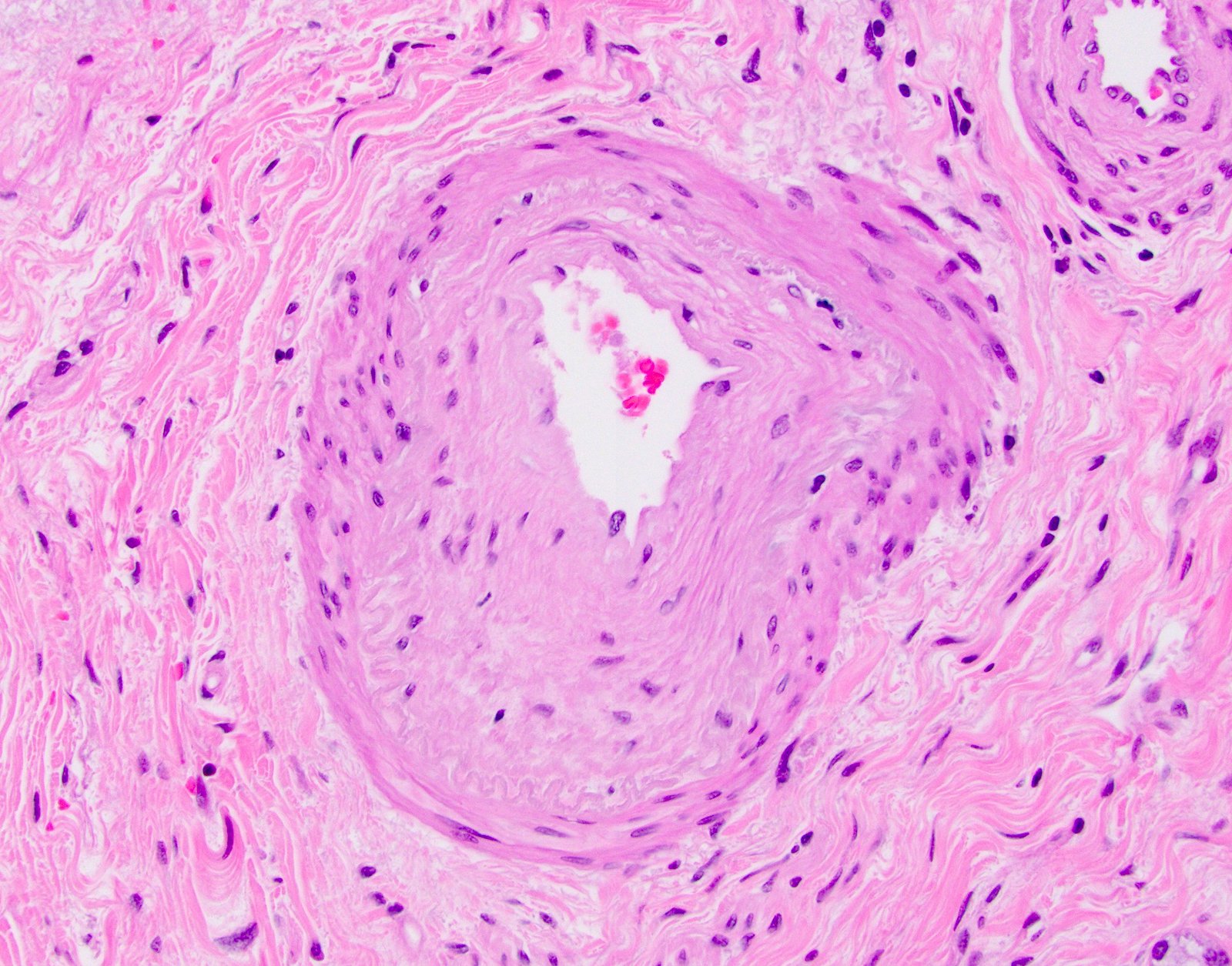
Arterial lesions
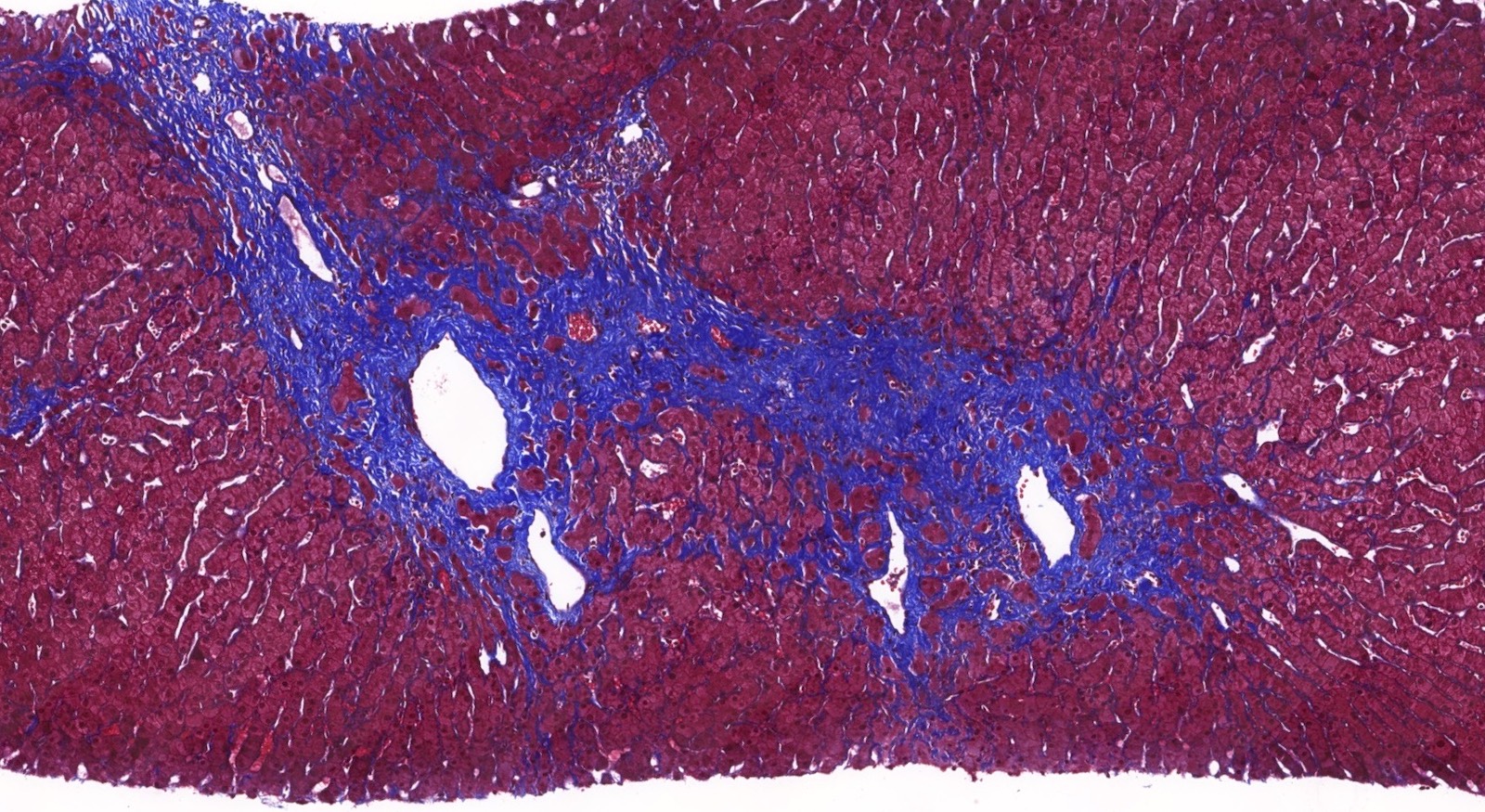
Fibrosis
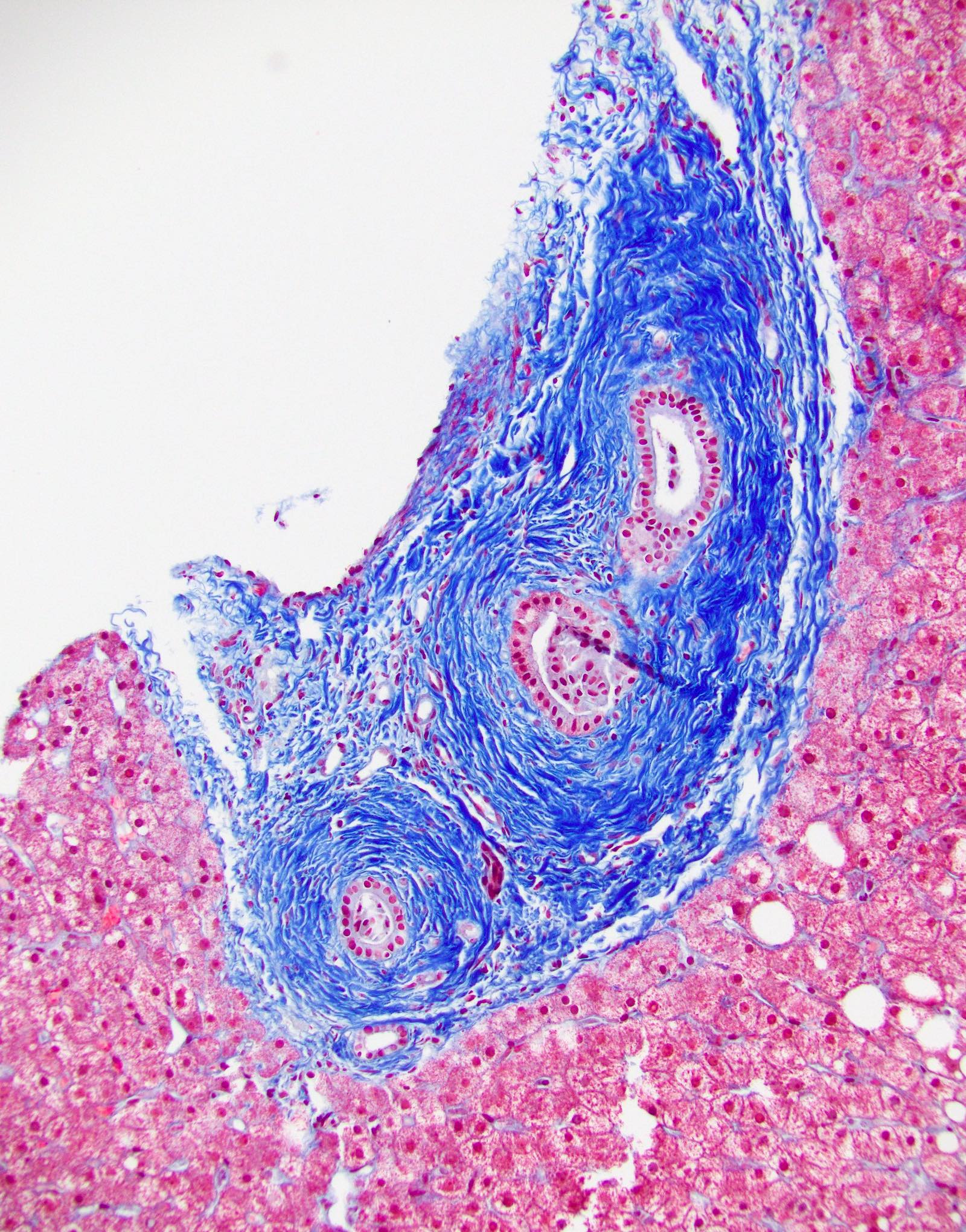
Portal collagenization
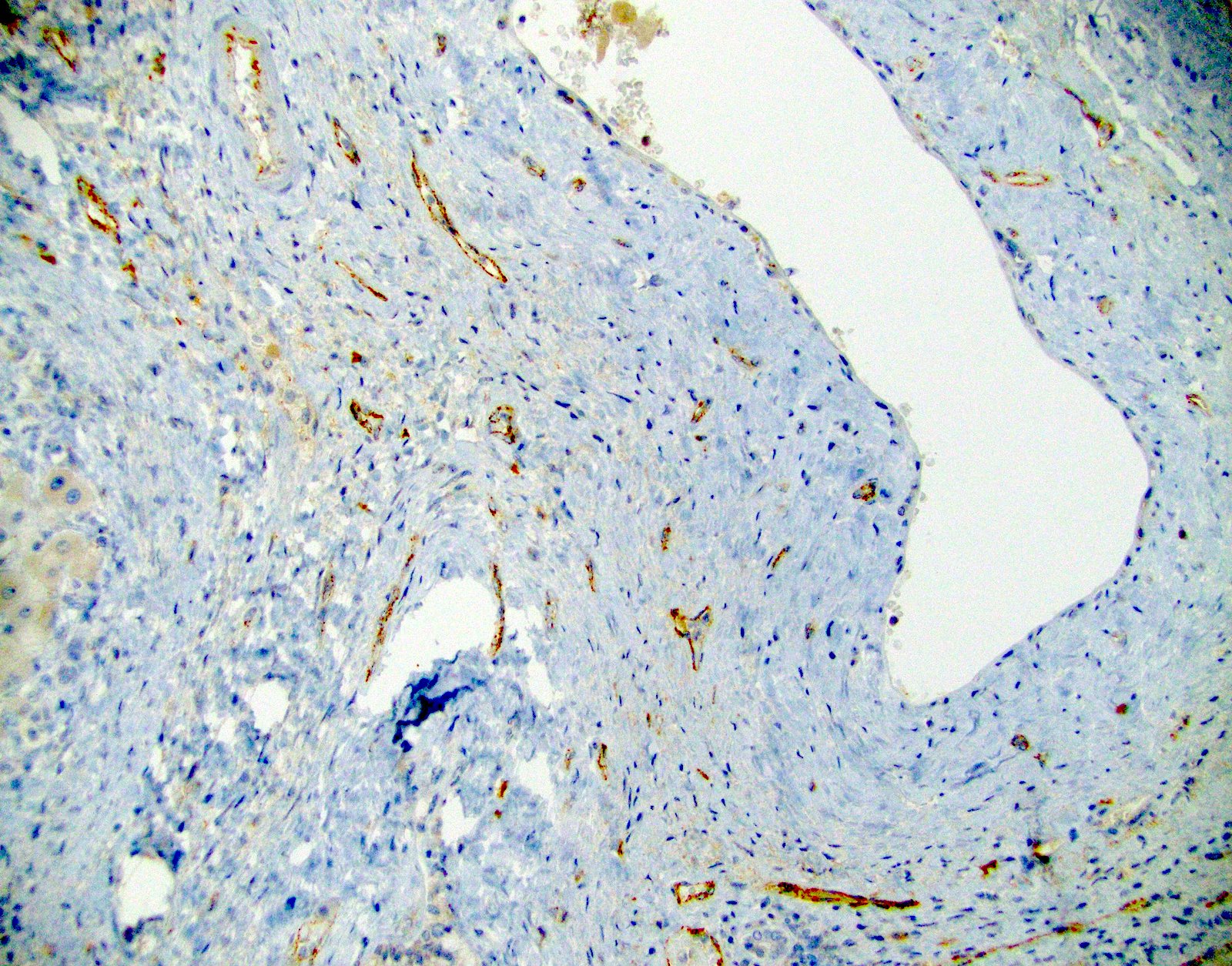
C4d
Positive stains
- Focal to diffuse C4d uptake by portal microvasculature (portal veins and capillaries) that may extend to inlet venules
Sample pathology report
- Allograft liver, explant:
- Chronic hepatitis, favoring chronic active antibody mediated rejection
- C4d on paraffin tissue: diffuse uptake by portal microvasculature (portal vein and capillaries) and inlet venules
- Strong DSA present (antidonor DQ)
- Obliterative arteriopathy
- Portal venopathy
- Allograft fibrosis score (Am J Transplant 2012;12:2986):
- Portal: 3/3
- Central: 3/3
- Sinusoidal: 1/3
- Chronic hepatitis, favoring chronic active antibody mediated rejection
Differential diagnosis
- In general, causes of chronic hepatitis and fibrosis fall in the differential diagnosis
- Idiopathic posttransplantation hepatitis:
- Category that describes otherwise unexplained allograft hepatitis
- Evidence points towards late and chronic rejection (TCMR and cAMR) as causes of this pattern (Liver Transpl 2016;22:1593)
- Recurrent hepatitis C:
- Decreasing cause of liver transplantation and posttransplant liver disease
- Can be ruled out by quantitative PCR
- Hepatitis E virus infection:
- Underdiagnosed in liver allografts (occurs in 1 - 28% of liver allografts)
- Can lead to chronic hepatitis and cirrhosis (Gastroenterology 2011;140:1481, J Hepatol 2014;61:1418)
- Can be excluded by laboratory investigations and immunohistochemical and in situ hybridization techniques
Board review style question #1
Banff criteria for the diagnosis of probable chronic active antibody mediated rejection include
- Cholangitis and bile duct inflammation
- Ductopenia
- Focal to diffuse C4d uptake
- Microvasculitis with dilated portal capillaries and marginating leukocytes
- No to minimal allograft fibrosis
Board review style answer #1
C. Focal to diffuse C4d uptake. Criteria for the diagnosis of chronic active antibody mediated rejection include presence of at least focal C4d uptake in addition to histologic features (at least mild necroinflammatory activity and moderate fibrosis). While microvasculitis with dilated portal capillaries can be seen with chronic active antibody mediated rejection, it is a feature seen with acute antibody mediated rejection. It is important to keep in mind that acute antibody mediated rejection may overlap with chronic active antibody mediated rejection. Cholangitis and bile duct inflammation are components of T cell mediated rejection rather than antibody mediated rejection. Classic chronic rejection is characterized by ductopenia; however, the concept of chronic rejection is evolving as its pathophysiology is further characterized.
Comment Here
Reference: Liver - Chronic antibody mediated rejection
Comment Here
Reference: Liver - Chronic antibody mediated rejection
Board review style question #2
An isolated arterial "V" lesion is defined as age inappropriate arterial fibrointimal hyperplasia with or without associated inflammation without the presence of T cell mediated rejection. What is its significance in liver allografts?
- Almost all are negative for C4d staining
- It is not associated with T cell mediated rejection
- It is only significant in kidney allografts and has no significance in liver allografts
- It suggests underlying chronic active antibody mediated rejection
Board review style answer #2
D.Isolated arterial lesions are rarely encountered in liver allografts and until recently their clinical significance was not known. A recent series of cases showed that isolated arterial "V" lesions are associated with subsequent T cell mediated rejection, graft failure and C4d positivity. The majority of C4d positive cases also showed additional histologic features encountered in chronic active antibody mediated rejection such as portal and perivenular inflammation (rejection activity index / RAI 1 - 2) and at least moderate periportal, perivenular or sinusoidal fibrosis (Am J Transplant 2018;18:1534).
Comment Here
Reference: Liver - Chronic antibody mediated rejection
Comment Here
Reference: Liver - Chronic antibody mediated rejection
