
Liver & intrahepatic bile ducts
Developmental anomalies / cysts
Congenital hepatic fibrosis
Authors: Irene Y. Chen, M.D., Xiaoyan Liao, M.D., Ph.D.
Editorial Board Member: Monika Vyas, M.D.
Deputy Editor-in-Chief: Catherine E. Hagen, M.D.


Last author update: 6 August 2021
Last staff update: 9 August 2021
Copyright: 2002-2024, PathologyOutlines.com, Inc.
PubMed Search: Congenital hepatic fibrosis[TI] free full text[sb]
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Diagrams / tables | Clinical features | Diagnosis | Laboratory | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Gross description | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Negative stains | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Chen IY, Liao X. Congenital hepatic fibrosis. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/livercongenitalhepaticfibrosis.html. Accessed April 20th, 2024.
Definition / general
- Hereditary form of ductal plate malformation affecting interlobular bile ducts, leading to excessive embryonic bile ducts and fibrosis
- Heterogeneous group of genetic disorders predominantly in an autosomal recessive manner
- Associated with hepatorenal ciliopathies caused by disruption of the physiological functions of cilia
- One of the fibrocystic liver diseases, which include Caroli disease, autosomal dominant polycystic kidney disease, autosomal recessive polycystic kidney disease and choledochal cysts
Essential features
- Commonly presents with portal hypertension and hepatosplenomegaly in children or young adults
- Classic histological triad with evolution
- Abnormal bile duct profile
- Small bile ductal structures lining at the limiting plate or embedded at the center of the portal tracts
- Bile ducts are often dilated, ectatic or have entrapped fibrous stroma
- May or may not contain inspissated bile in the lumen
- Hypoplastic portal vein radicles and prominent portal arteries
- Expansile portal fibrosis progresses to bridging with broad septa separating hepatocytes into islands but lacking the nodular regeneration of hepatocytes seen in cirrhosis
- Abnormal bile duct profile
Terminology
- Ductal plate malformation, fibrocystic liver disease
ICD coding
Epidemiology
- Estimated incidence: 1 in 10,000 - 20,000 live births (J Pak Med Assoc 2016;66:984)
- Age (J Pediatr Gastroenterol Nutr 2012;54:580)
- Predominantly affects infants and children, with median age of onset at 2 years
- Age range: birth to 75 years old
- No apparent sex predilection (J Pediatr Gastroenterol Nutr 2012;54:580)
Sites
- Primary location: liver
- Organs involved in syndromic manifestation: kidney, pancreas, lungs and brain (J Med Genet 2003;40:311)
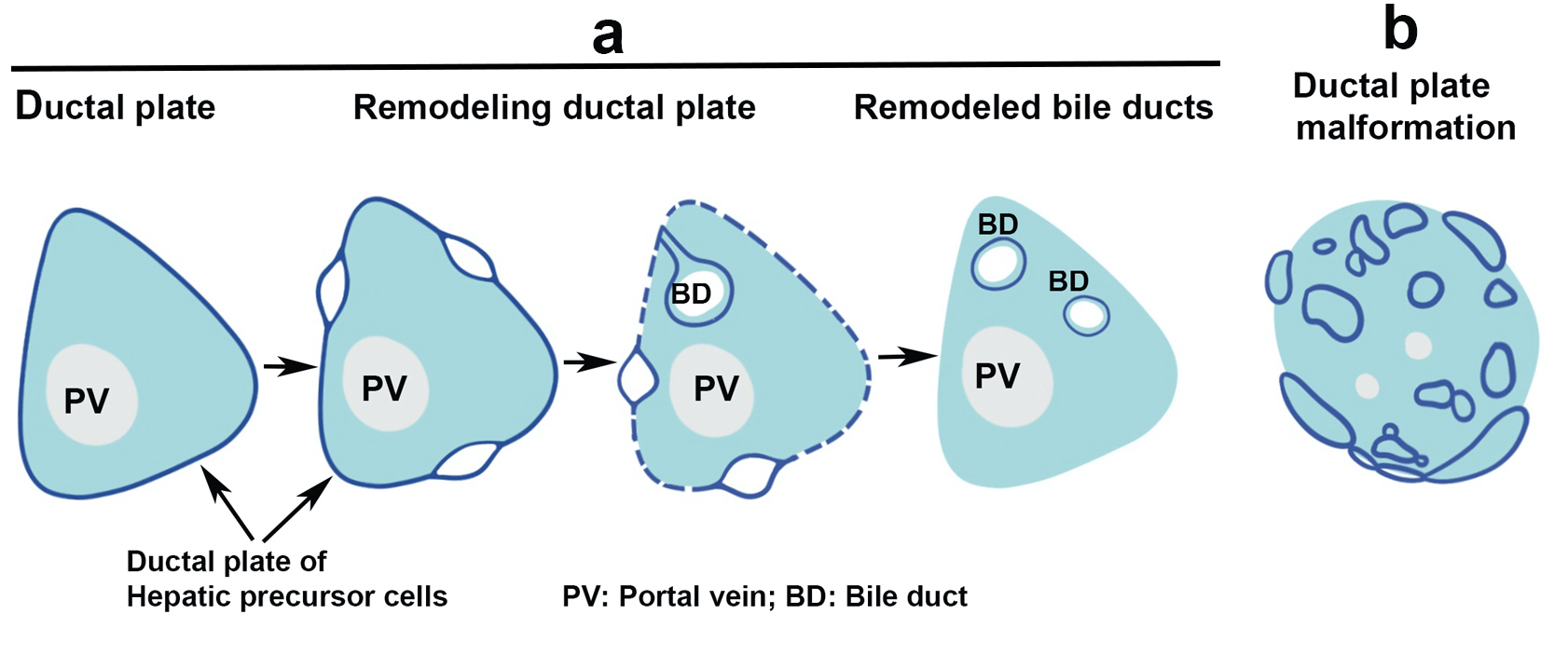
Pathophysiology
- Normal bile duct morphogenesis is a timely regulated process (see Diagrams / tables) (J Med Genet 2003;40:311, Mech Dev 2003;120:81)
- Embryonic day 13.5 - 14.5: precursor cells express biliary specific cytokeratins and migrate closer to the portal mesenchyme
- Embryonic day 15.5: portal vein and the surrounding mesenchyme induce the precursor cells to form a continuous ring called ductal plate
- Embryonic day 16.5: ductal plate becomes partially bilayered
- Embryonic day 17.5: focal dilation between the 2 layers leads to bile duct formation starting from the hilum to the periphery, followed by progressive regression of the remaining ductal plate
- Hereditary / sporadic genetic mutations lead to imbalanced proliferation and apoptosis during ductal plate remodeling, resulting in persistence of embryonic duct profile in ductal plate configuration (J Med Genet 2003;40:311, Hepatology 1992;16:1069, Clin Res Hepatol Gastroenterol 2014;38:407)
- Postnatal pathologic changes
- Variable fibrosis as a consequence of ductal plate malformation or stimulation of the matrix forming cells (Clin Res Hepatol Gastroenterol 2014;38:407)
- Generally, minimal inflammation except when complicated by cholangitis
- Recurrent cholangitis can lead to progressive fibrosis with functional impairment similar to cirrhosis
Etiology
- Genetic disease primarily in autosomal recessive inheritance pattern
- May be associated with Caroli disease (Caroli syndrome) (Cureus 2020;12:e11029)
- Caroli disease
- Rare autosomal recessive disorder
- Prevalence of 1 in 1,000,000 people
- Cystic dilation of large intrahepatic bile ducts
- Caroli syndrome: Caroli disease with congenital hepatic fibrosis
- Caroli disease
- Hepatorenal ciliopathies: mutations in genes encoding proteins on primary cilia (J Med Genet 2003;40:311, Front Pediatr 2018;5:221, Am J Med Genet C Semin Med Genet 2009;151C:296, Mol Cell Pediatr 2015;2:8)
- Autosomal recessive polycystic kidney disease (ARPKD)
- Mutations in fibrocystin / polyductin (PKHD1) on chromosome 6
- Most common ciliopathy of childhood
- Autosomal dominant polycystic kidney disease (ADPKD)
- Mutations in polycystin 1 (PKD1) on chromosome 16
- Mutations in polycystin 2 (PKD2) on chromosome 4
- Nephronophthisis (OMIM: Nephronophthisis 1; NPHP1 [Accessed 23 June 2021])
- Mutations in nephrocystin 1 (NPHP1) on chromosome 2
- Controversial whether the hepatic fibrosis in nephronophthisis is true congenital hepatic fibrosis
- Joubert syndrome (OMIM: Joubert Syndrome 1; JBTS1 [Accessed 23 June 2021])
- Mutations in at least 30 genes
- Heterogeneous disorders characterized by cerebellar dysgenesis
- Meckel-Gruber syndrome (OMIM: Meckel Syndrome, Type 1; MKS1 [Accessed 23 June 2021])
- Lethal mutations in at least 8 genes (MKS)
- Jeune syndrome
- Also known as Jeune asphyxiating thoracic dysplasia
- Mutations in at least 11 genes
- Mutations in dynein 2 (DYNC2H1) and IFT complex B (IFT80) are the most common
- Bardet-Biedl syndrome (OMIM: Bardet-Biedl Syndrome 1; BBS1 [Accessed 23 June 2021])
- Mutations in at least 14 genes (BBS)
- Autosomal recessive polycystic kidney disease (ARPKD)
Clinical features
- Wide range of presentations, depending on age of disease onset and concomitant kidney involvement (J Pak Med Assoc 2016;66:984, Am J Clin Pathol 2020;153:119)
- In children or young adults with early disease onset, disease is progressive and may require liver or kidney transplant
- Portal hypertension and related symptoms
- Hepatosplenomegaly
- Recurrent cholangitis if presents as Caroli syndrome (Cureus 2020;12:e11029)
- Portopulmonary hypertension
- Hepatocellular carcinoma or cholangiocarcinoma, though rare, can be present
- May spontaneously regress or "burn out" in some patients
- Adults may be asymptomatic or with only mild disease
- In children or young adults with early disease onset, disease is progressive and may require liver or kidney transplant
Diagnosis
- Clinical suspicion of concurrent portal hypertension and chronic kidney disease in teenager or young adult
- Imaging: integrated use of ultrasound and abdominal MRI at baseline and follow ups; CT may be helpful (Pediatr Radiol 2009;39:100)
- Diagnostic liver biopsy showing classic histology
Laboratory
- Blood test: normal or elevated liver enzymes
- Thrombocytopenia and leukopenia due to hypersplenism (J Pediatr Gastroenterol Nutr 2012;54:580)
Radiology description
- Ultrasound (Pediatr Radiol 2009;39:100)
- Diffusely increased and coarsened liver echogenicity, splenomegaly and intra and extrahepatic biliary cysts / dilatations
- Periportal thickening
- Macroscopic cystic or fusiform dilatations of the intra and extrahepatic bile ducts
- Magnetic resonance imaging (MRI) (Pediatr Radiol 2009;39:100)
- Enlarged, nodular and misshapen liver with disproportionately hypertrophic left and caudate lobes
- Cystic dilatation of intrahepatic bile ducts; periportal hepatic fibrosis
Radiology images
Contributed by Irene Y. Chen, M.D.
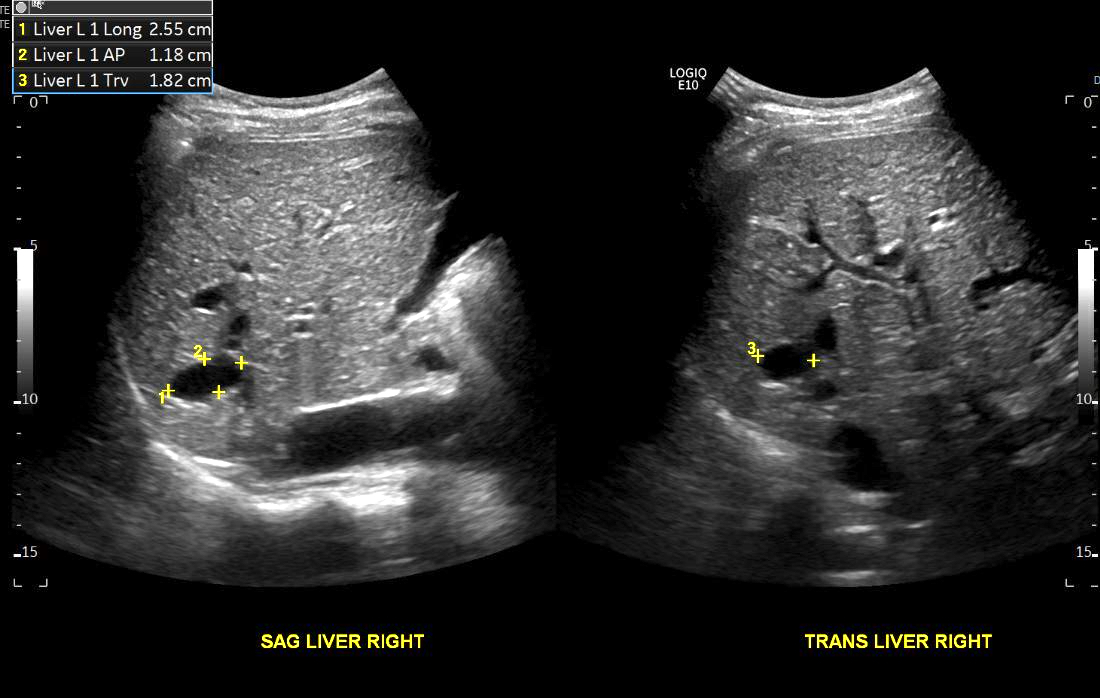
Intrahepatic biliary cysts
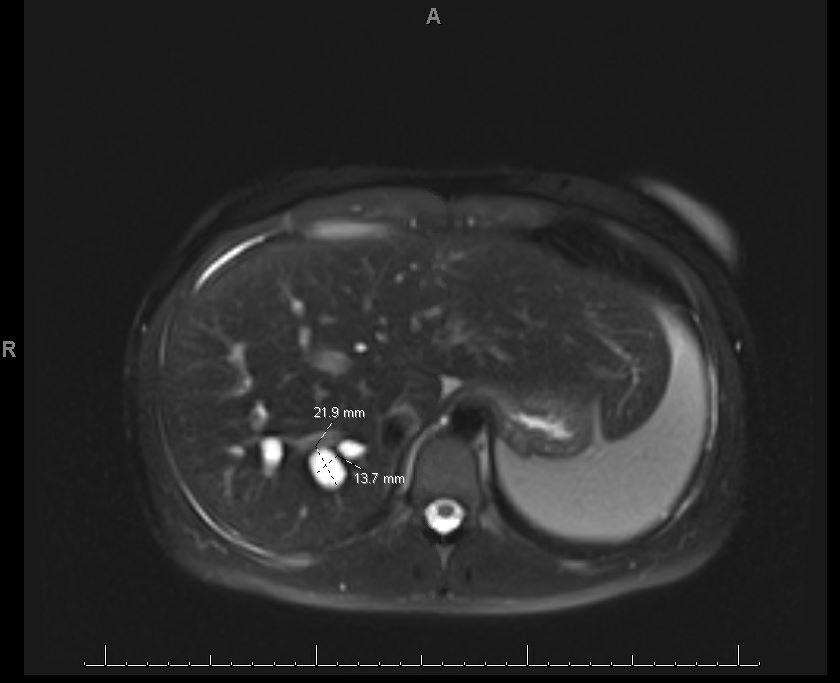
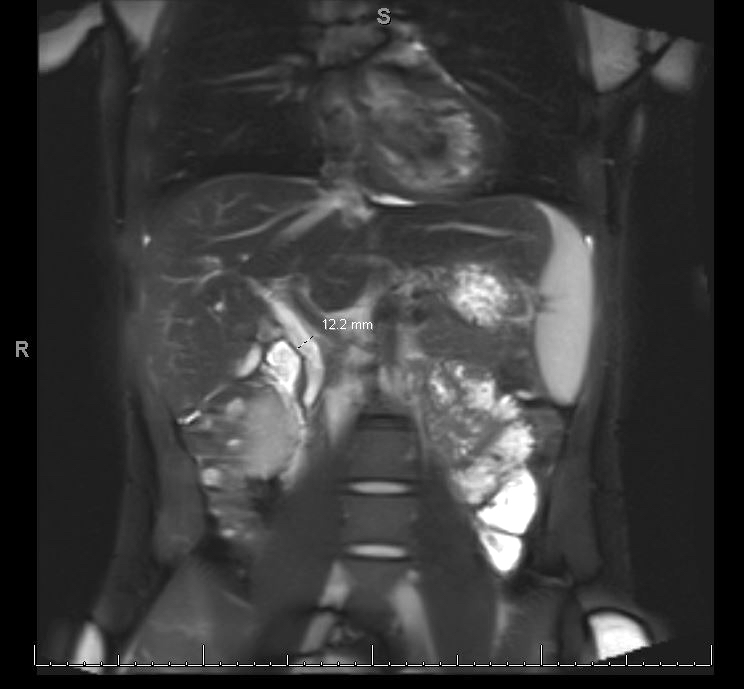

MR abdomen in a patient with Caroli syndrome
Prognostic factors
- Variable; depends on age of onset / degree of involvement
- Children often experience much more severe portal hypertension related symptoms than adults (Gastroenterol Res Pract 2020;2020:8284274)
- Disease onset during neonatal period is a good predictor of the need for transplant (J Pediatr Gastroenterol Nutr 2013;57:161)
- Patients with Caroli syndrome often develop end stage renal disease requiring combined liver and kidney transplant (Cureus 2020;12:e11029)
- Excellent outcome in pediatric and adults patients after transplant (Transpl Int 2021 Apr 20 [Epub ahead of print])
- Rarely associated with hepatobiliary cancer, particularly cholangiocarcinoma (J Pediatr Gastroenterol Nutr 2012;54:580)
Case reports
- 2 year old boy with history of autosomal recessive polycystic kidney disease presented with variceal bleeding secondary to portal hypertension (Cureus 2020;12:e11029)
- 2 year old girl with abdominal distension with persistent hypertransaminasemia and cholestasis and 12 year old boy with hepatomegaly and splenomegaly of 2 years duration (Pan Afr Med J 2021;38:188)
- 5 year old boy with congenital hypothyroidism presented with abnormal liver function tests (World J Clin Cases 2021;9:1475)
- 6 year old girl with recurrent gastrointestinal bleed (World J Gastroenterol 2016;22:9865)
- 25 year old woman with hepatosplenomegaly of 3 months duration presented with abdominal pain and fever (Medicine (Baltimore) 2019;98:e15600)
Treatment
- Manage complications related to portal hypertension (J Pak Med Assoc 2016;66:984)
- Varices: medical management followed by sclerotherapy or band ligation
- Transjugular intrahepatic portosystemic shunts
- Antibiotics for cholangitis
- Liver transplant is the only curative treatment
Gross description
- Enlarged and firm liver with variable nodularity
- Cyst formation and duct dilatation is more common in Caroli syndrome
Microscopic (histologic) description
- Classic histological triad
- Abnormal bile duct profile
- Small ductal structure at the periphery of the fibrous septa
- May or may not contain inspissated bile in the lumen
- Hypoplastic portal vein branches
- Progressive fibrosis: bridging fibrosis with broad septa separating hepatocytes into islands
- Lack of nodular regenerative hepatocytes
- Abnormal bile duct profile
- Evolution of the lesion as patients age
- Infant: circumferential arrangement of ectatic and anastamosing ductal structures surrounding the hypoplastic portal veins
- Ductal structures decrease in size and number with increased fibrosis
- Fully evolved lesion is described in classic histological triad
Microscopic (histologic) images
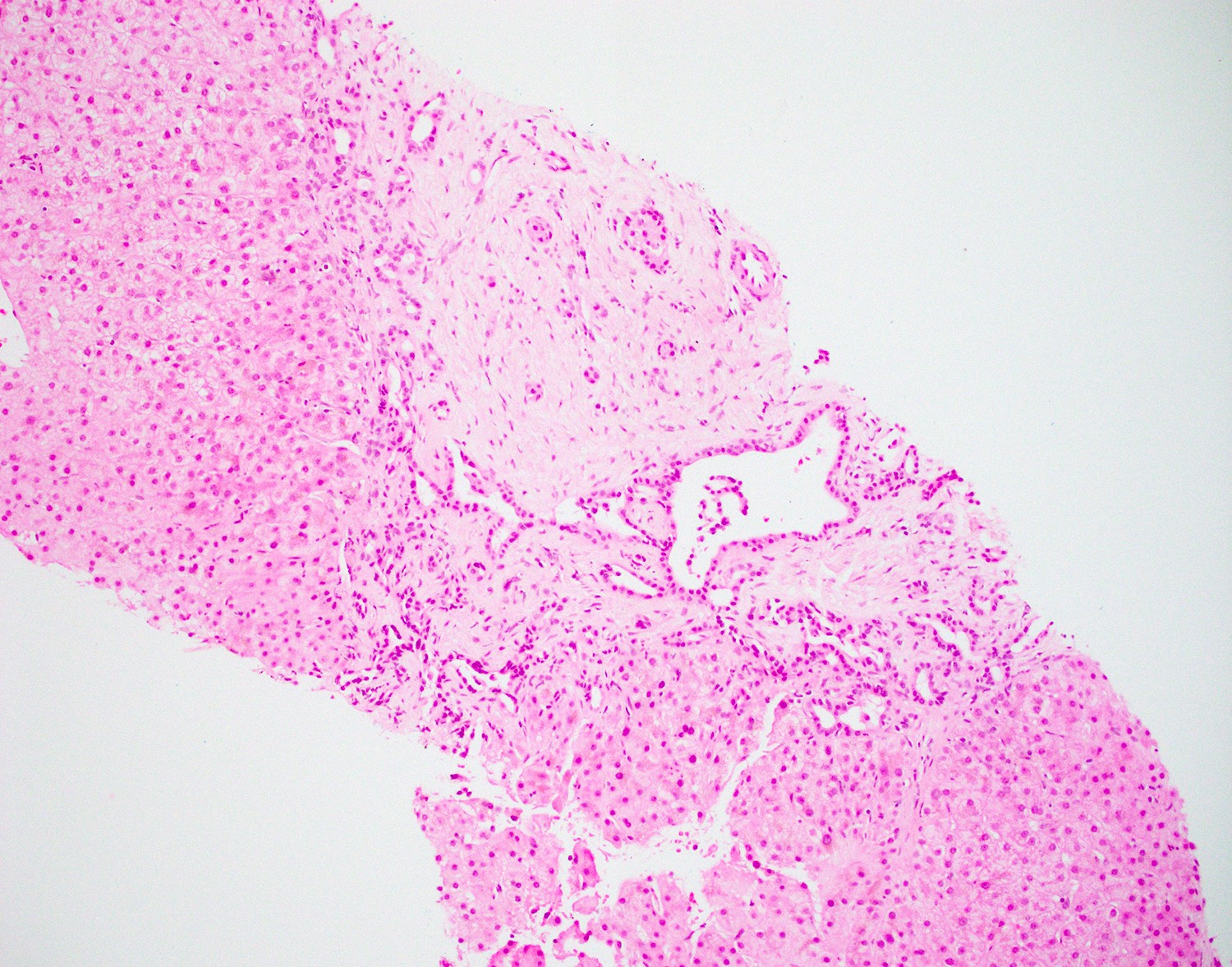
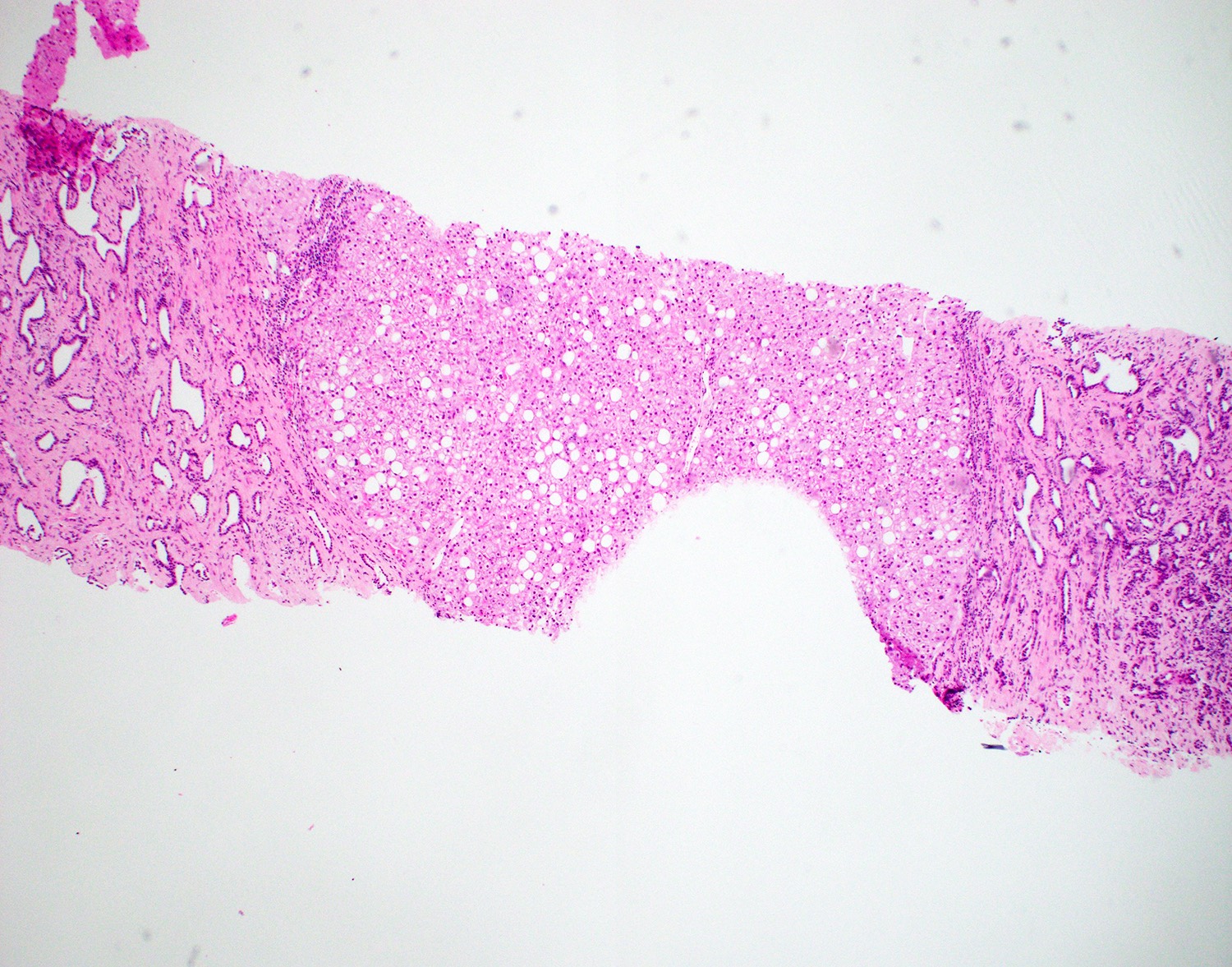
Contributed by Xiaoyan Liao, M.D., Ph.D.
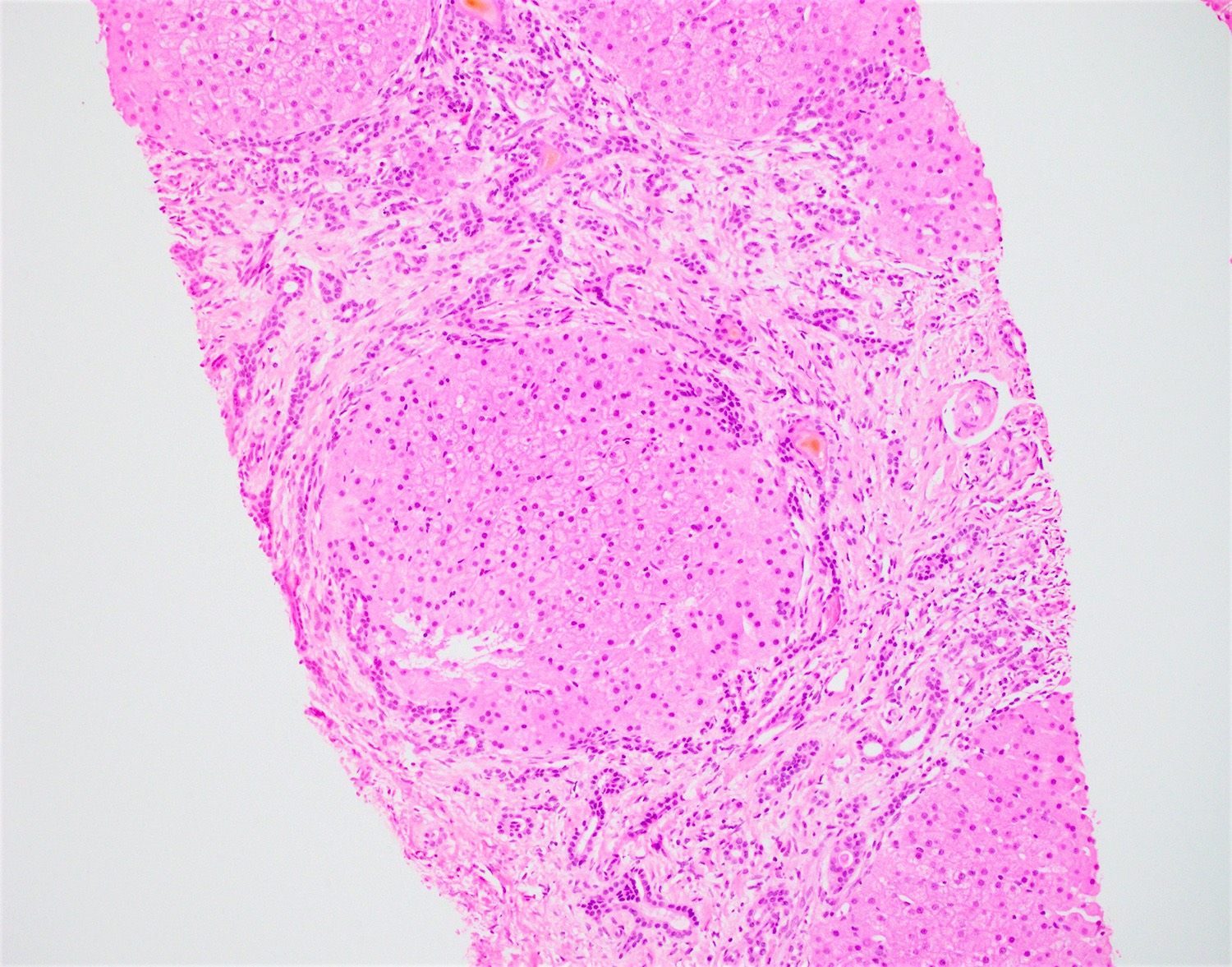
Abnormal duct profile
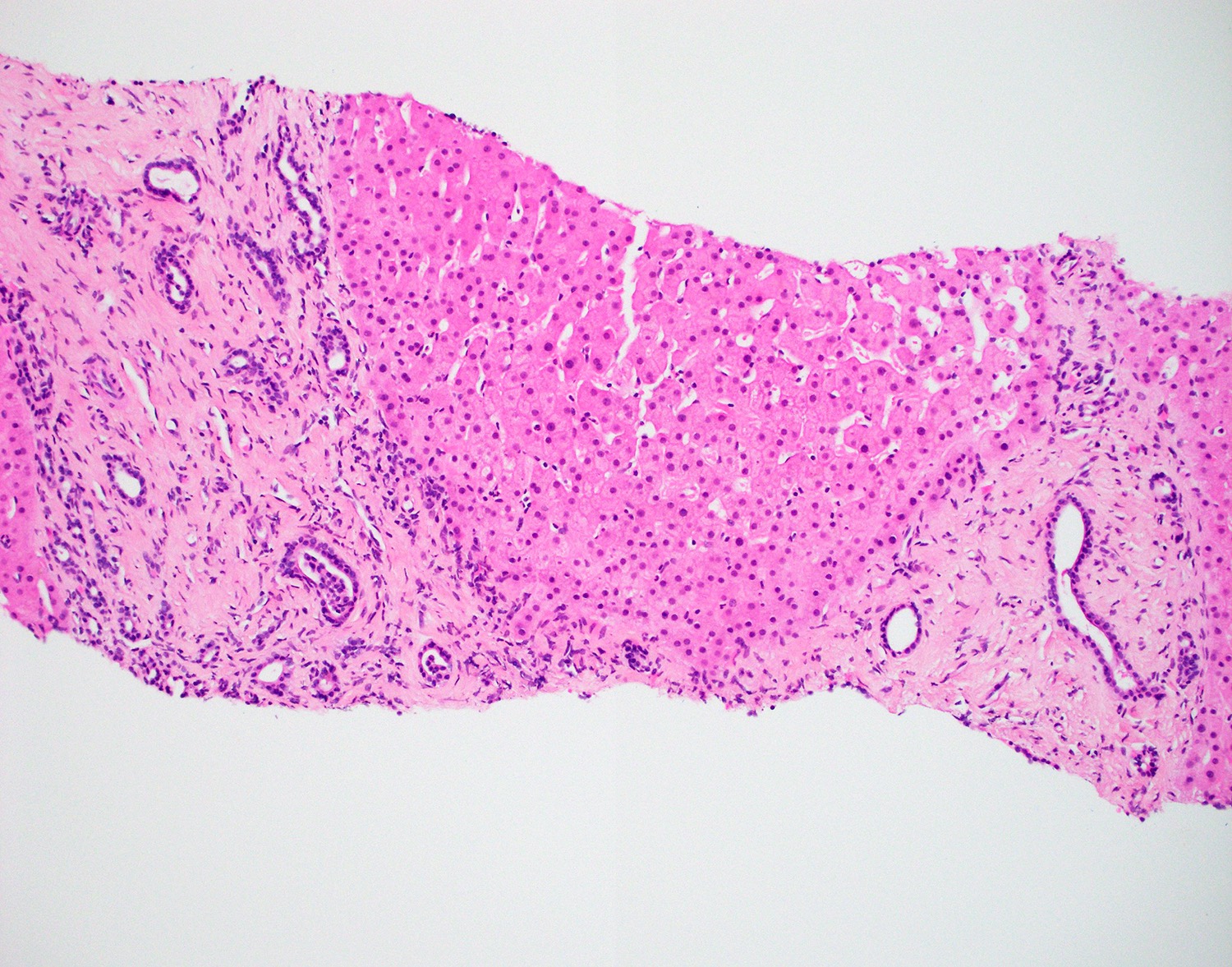
Aberrant bile duct profile
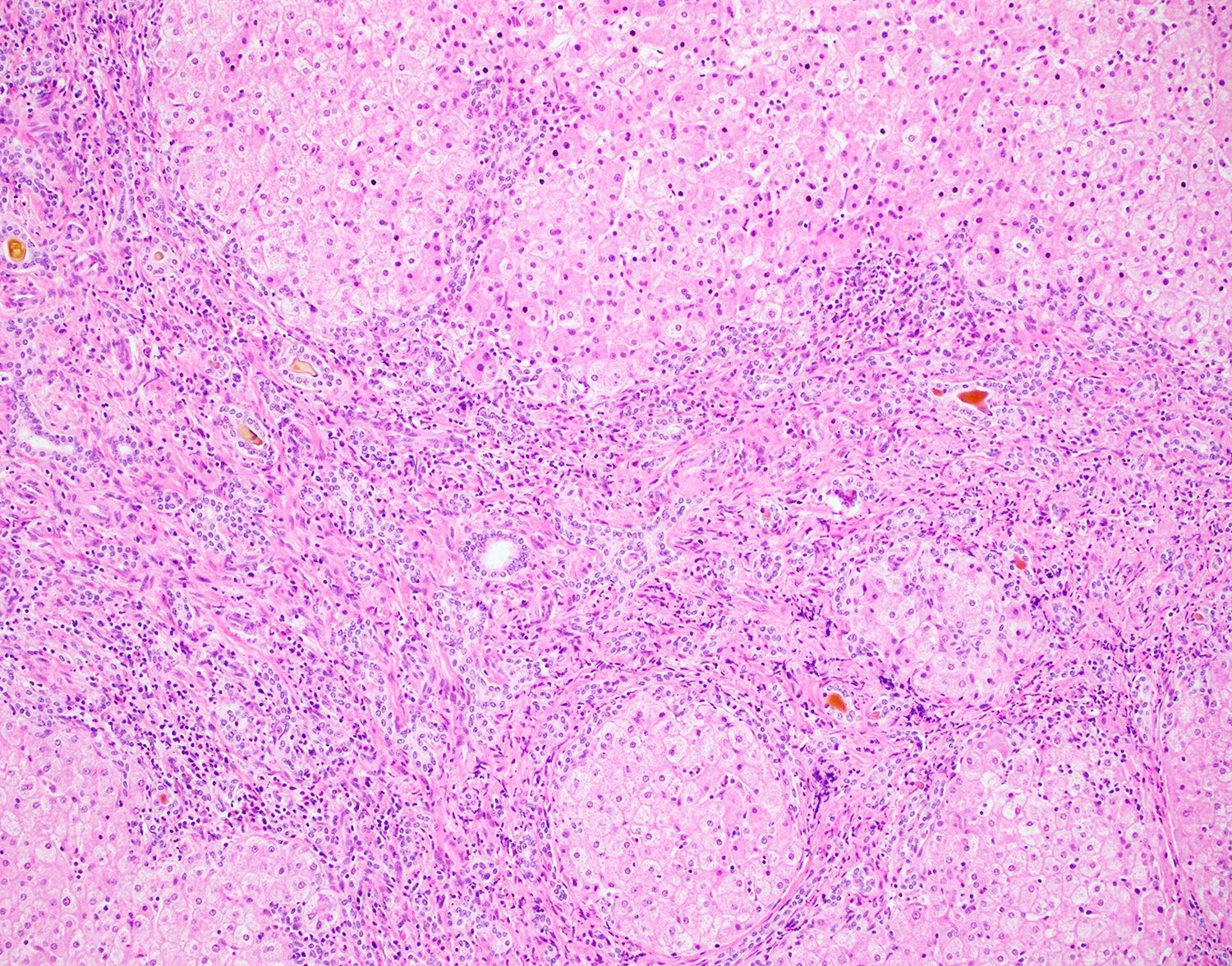
Congenital hepatic fibrosis
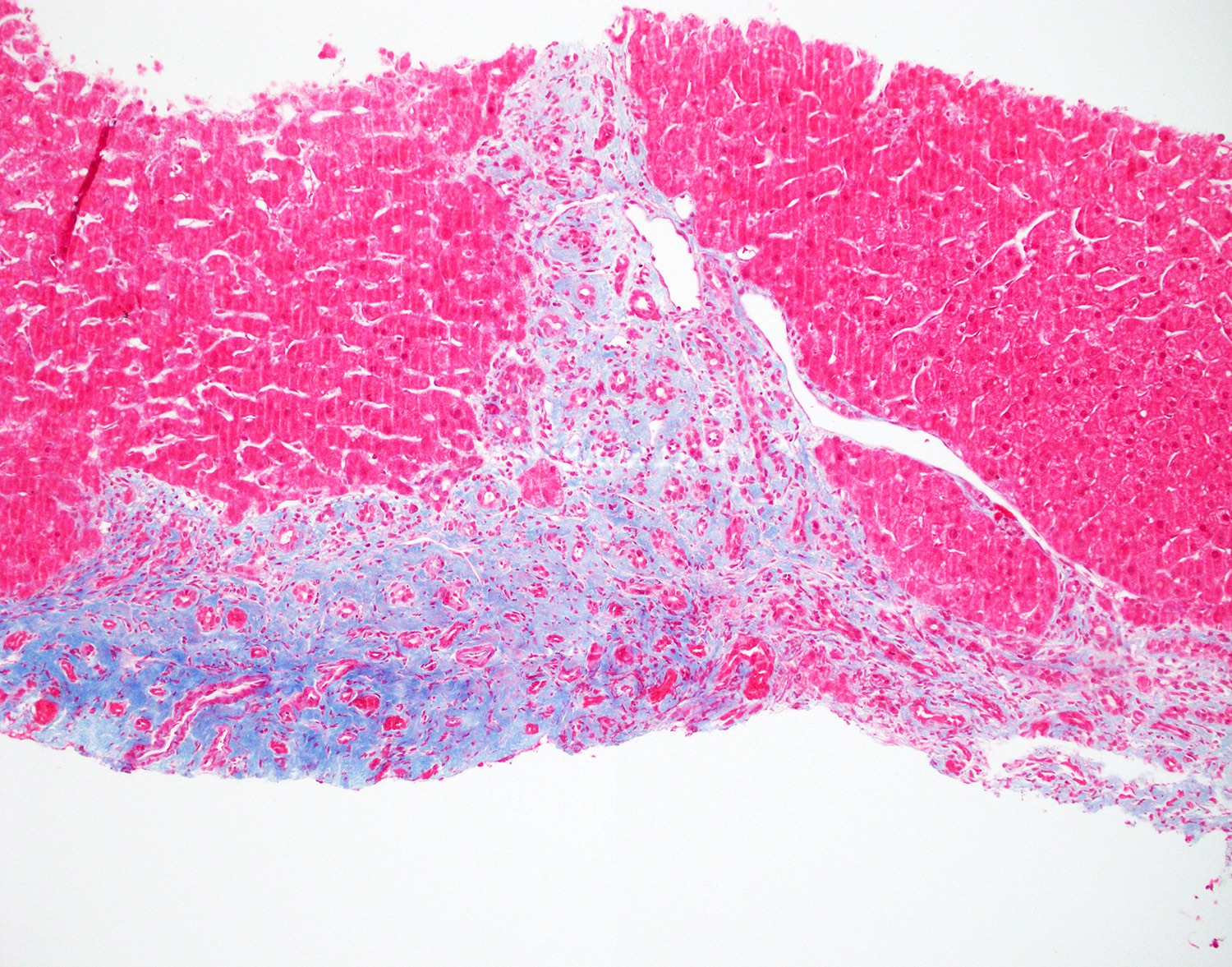
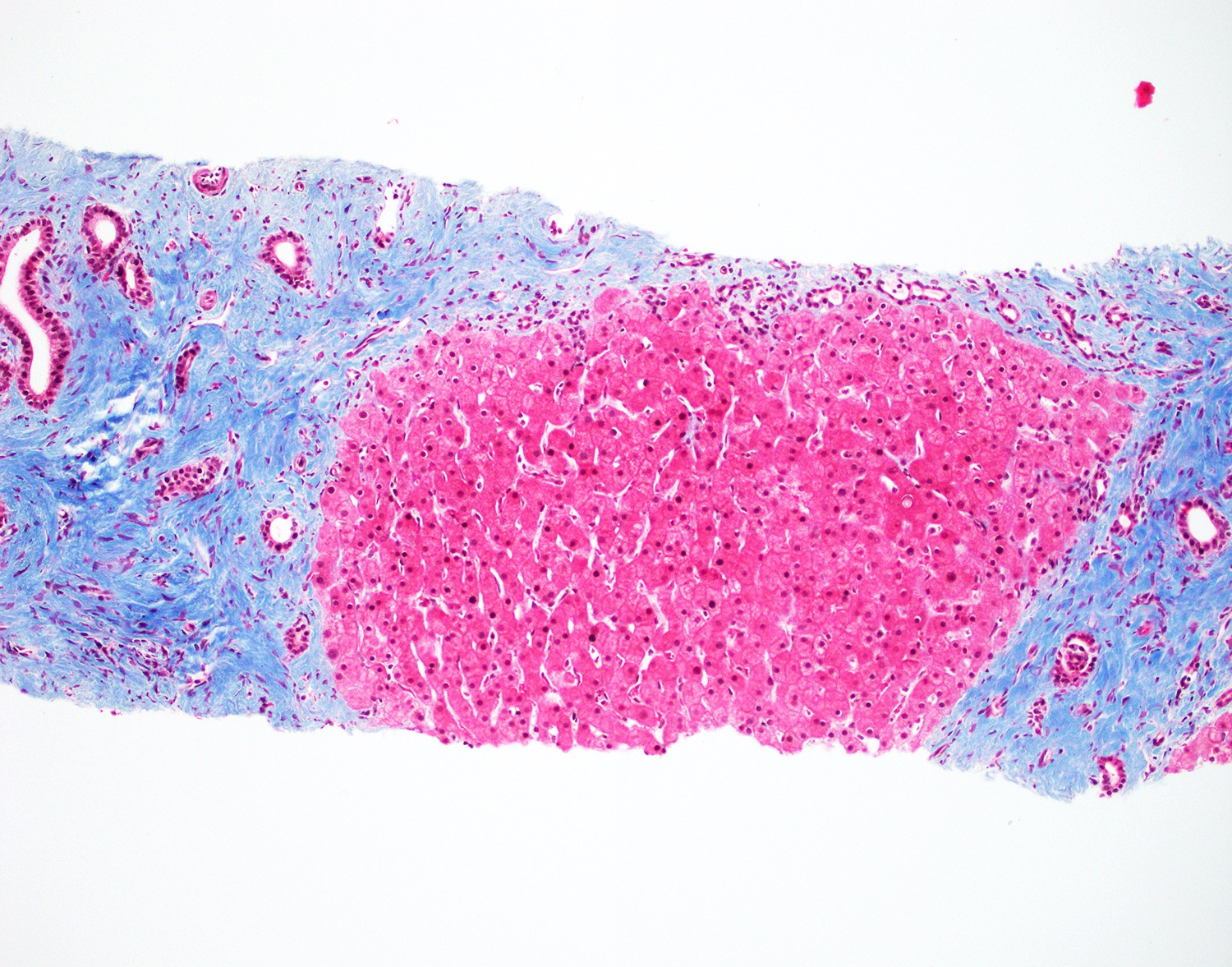
Fibrosis
Positive stains
Negative stains
- Iron: lack of intracytoplasmic iron deposition
- PAS / PASD: lack of intracytoplasmic inclusions
- Reticulin: lack of regenerative nodules
Molecular / cytogenetics description
- PKHD1 gene in autosomal recessive polycystic kidney disease
- PKD1 and PKD2 genes in autosomal dominant polycystic kidney disease
- NPHP1 gene in nephronophthisis (OMIM: Nephronophthisis 1; NPHP1 [Accessed 23 June 2021])
- DYNC2H1, IFT80 and 11 additional genes for Jeune syndrome
- See Etiology for more information
Sample pathology report
- Liver, biopsy:
- Ductal plate malformation consistent with congenital hepatic fibrosis (see comment)
- Comment: The biopsy is adequate for evaluation. Portal tracts diffusely demonstrate ductal plate malformations consisting of bile duct structures with irregular contours and regions of mild dilatation. Portal tracts / fibrous septa are without significant inflammation, interface activity or portal edema. Inspissated bile is noted in small ductal structures at the interface of fibrous septa and hepatic parenchyma. No lobular inflammation or steatosis is noted. Portal expansion by fibrosis is highlighted on trichrome stain. There is no evidence of cirrhosis. Iron and PASD stains show no additional pathologic findings.
- Overall, the histology of this biopsy demonstrates diffuse ductal plate malformation, consistent with congenital hepatic fibrosis (fibrous bands account for 50% of the biopsy volume). Ductal plate malformation disease in the liver is often associated with polycystic renal disease or other cystic abnormalities of tubules. In the present case, the overall features are those of congenital hepatic fibrosis but there may be overlap with other fibropolycystic conditions such as Caroli syndrome. A clinical evaluation to assess the presence or absence of portal hypertension in the setting of these liver biopsy changes warrants consideration.
Differential diagnosis
- Von Meyenburg complex:
- Also known as biliary duct hamartoma or bile duct microhamartoma
- Incidental small nodular lesion consists of mildly dilated ductal structures lined by flat epithelium in hyalinized stroma
- Typically small and may present as multiple lesions
- Autosomal dominant polycystic liver disease:
- Often becomes symptomatic in adulthood because liver cysts increase in number and size with age
- Mutations in hepatocystin (PRKCSH) on chromosome 19
- Mutations in SEC63 protein (SEC63) on chromosome 6
- Mutations in low density lipoprotein receptor related protein 5 (LRP5) on chromosome 11
- Solitary bile duct cyst:
- Incidental solitary unilocular cyst containing clear fluid
- Simple cuboidal / columnar epithelium with bland fibrovascular stroma
- No portal hypertension
- Choledochal cysts:
- Triad of abdominal mass, colicky pain and jaundice
- May present with cirrhosis and portal hypertension due to secondary biliary cirrhosis
- May be associated with colonic or duodenal atresia, anomalies of pancreas or congenital heart defects
- Thick wall cyst with variable inflammation and fibrosis
- Epithelium is usually denuded but can demonstrate metaplastic changes
- Cirrhosis:
- Diffuse nodular regeneration of hepatocyte and remodeling of hepatic architecture
- May show prominent bile ductular proliferation
- Varying degree of inflammation
- Compromised liver function
- No association with polycystic kidney disease
- Hepatoportal sclerosis (Hepat Med 2016;8:81):
- Under the term idiopathic noncirrhotic portal hypertension
- Multifactorial (infection, autoimmune, etc.)
- In young patient with portal hypertension and concurrent kidney disease, clinically mimics congenital hepatic fibrosis
- Portal fibrosis and portal vein with medial hypertrophy and venular dilatation
- Liver biopsy may show nodular regenerative hyperplasia and focal bile duct abnormality
- Recurrent pyogenic cholangitis:
- Associated with liver flukes or bile duct stones
- Dilation and fibrosis of bile ducts with acute inflammation and intraductal abscesses
- Other features include secondary sclerosing cholangitis
- Increased risk of developing cholangiocarcinoma
Additional references
Board review style question #1
A 2 year old boy was found to have portal hypertension while being evaluated in the hospital. A liver biopsy was performed. Which of the following findings is true regarding this disease entity?
- Adults experience much more severe symptom than pediatric patients
- Commonly associated with hepatobiliary cancer
- Liver transplant is the only curative treatment
- Symptoms resolve completely with no intervention
Board review style answer #1
C. Liver transplant is the only curative treatment
Comment Here
Reference: Congenital hepatic fibrosis
Comment Here
Reference: Congenital hepatic fibrosis
Board review style question #2
A 59 year woman with a history of diabetes presented with elevated liver enzymes and positive antimitochondrial antibody concerning for primary biliary cholangitis. A liver biopsy was performed. What is the most appropriate diagnosis?
- Bile duct malformation consistent with congenital hepatic fibrosis
- Primary biliary cholangitis
- Primary sclerosing cholangitis
- Steatosis and steatohepatitis with bridging fibrosis
Board review style answer #2
A. Bile duct malformation consistent with congenital hepatic fibrosis. This patient has undiagnosed congenital hepatic fibrosis. Adult onset congenital hepatic fibrosis may be asymptomatic or experience minor symptoms compared with pediatric patients.
Comment Here
Reference: Congenital hepatic fibrosis
Comment Here
Reference: Congenital hepatic fibrosis
