
Liver & intrahepatic bile ducts
Biliary tract disease
Ductular reaction
Authors: Shahbaz Khan, M.D., Romil Saxena, M.B.B.S.
Editorial Board Member: Raul S. Gonzalez, M.D.
Deputy Editor-in-Chief: Catherine E. Hagen, M.D.


Last author update: 13 May 2021
Last staff update: 21 July 2022
Copyright: 2021-2024, PathologyOutlines.com, Inc.
PubMed Search: Ductular reaction liver
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Diagrams / tables | Clinical features | Diagnosis | Laboratory | Case reports | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Negative stains | Videos | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Khan S, Saxena R. Ductular reaction. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/liverductularreaction.html. Accessed April 25th, 2024.
Definition / general
- Complex, dynamic and nonspecific reaction to liver injury and disease (acute and chronic), characterized by a ductular phenotype, possibly but not necessarily of ductular origin, at the portal - parenchymal interface
- May arise from:
- Proliferation of preexisting cholangiocytes
- Progenitor cells (local or circulating cells probably bone marrow derived)
- Rarely, biliary metaplasia of hepatocytes
Essential features
- Ductular reactions (DRs) are a response to a wide variety of hepatobiliary injuries that aim to restore compromised physiological function after liver injury
- Variable degree of bile duct profiles, portal edema, fibrosis and an inflammatory infiltrate composed mostly (but not always) of neutrophils
- Ductular reactions are predominantly associated with biliary diseases but can be seen secondary to any liver injury as a response in bipotential hepatic progenitor cells to differentiate into either cholangiocytes (bile ductular profiles) or hepatocytes
- Ductular reactions are characterized by simultaneous expression of biliary antigens (CK7, CK19, OV6) and hepatocyte antigens (e.g. HepPar1, albumin, alpha-1 antitrypsin, alpha fetoprotein) and other markers such as NCAM1 / CD56
- Outcomes of ductular reactions are diverse and include hepatic parenchymal regeneration, fibrogenesis and hepatocarcinogenesis, depending on the duration and severity of underlying pathology
Terminology
- Ductular reaction was coined by Popper et al. in 1957 and has subsequently been used in the hepatology literature, sometimes interchangeably with ductular proliferation
ICD coding
Epidemiology
- Predominantly associated with biliary diseases but can be seen secondary to any liver injury
Sites
- Portal - parenchymal interface in liver
Pathophysiology
- Liver or biliary injury → activation of hepatic progenitor cells, induction of self proliferation of cholangiocytes and transdifferentiation of hepatocytes, resulting in proliferation of bile ductules
- Inflammatory cytokines (IL13, IL6, IL8, etc.) induce proliferation of cholangiocytes and recruitment of inflammatory cellular components, as well as edema and hepatic progenitor cells niche that consists of macrophages, myofibroblasts and matrix and is associated with liver fibrogenesis during liver injury (Hepatology 2019;69:420)
- Mechanisms and associated cellular and tissue components may differ, depending on the underlying pathology / etiology
Etiology
- Any injury / insult to liver / biliary tree induces a response in bipotential hepatic progenitor cells to differentiate into either cholangiocytes (bile ductular profiles) or hepatocytes
- Biliary / cholestatic disorders are more common:
- Primary biliary cholangitis (PBC)
- Primary sclerosing cholangitis (PSC)
- Biliary atresia
- Bile duct obstruction (tumor, stone, stricture)
- Alcoholic and nonalcoholic fatty liver disease
- Chronic viral hepatitis (HBV, HCV)
- Autoimmune hepatitis
- Acute liver failure
- Total parenteral nutrition (TPN)
- Focal nodular hyperplasia
- Hepatocellular adenoma - inflammatory type
- Neoplasms - benign and malignant
- Biliary / cholestatic disorders are more common:
- Reference: Hepatology 2011;54:1853
Diagrams / tables
Images hosted on other servers:

Ductular reaction at the interface
Clinical features
- Depend on the underlying etiology (associations)
Diagnosis
- Liver biopsy
Laboratory
- Nonspecific - could range from normal to abnormal liver function tests
- Cholestatic pattern of liver enzymes - biliary diseases
- Hepatocellular pattern - nonbiliary diseases
Case reports
- 32 week old boy with biliary atresia and total parenteral nutrition associated with ductular reaction (BMC Pediatr 2019;19:72)
- 51 year old man with hepatocellular carcinoma with associated malignant ductular reaction (Int J Clin Exp Pathol 2020;13:1073)
Microscopic (histologic) description
- Traditionally divided into typical and atypical ductular reactions; however, this distinction is subtle, with low reproducibility - no classification with universal consensus
- Typical: ductules have a recognizable lumen lined by cuboidal cells and are the result of proliferation of preexisting ductules
- Atypical: ductules are thin, elongated structures lined by flattened cells that extend irregularly into the lobules, lack easily discernible lumina and are closely related to progenitor cell activation
- Most classifications emphasize on the type of ductules, however the term ductular reaction essentially implies proliferation of cholangiocytes and recruitment of inflammatory cellular components (neutrophils, lymphocytes etc) as well as edema and hepatic progenitor cells niche that consists of macrophages, myofibroblasts and matrix; neutrophils are part of the matrix as a result of chemotactic inflammatory cytokines and do not represent cholangitis / ascending cholangitis - they are mostly confined to the stroma of portal-lobular interface; no bile ductular intraepithelial neutrophils
- Classification systems based on pathobiology and epithelial - mesenchymal differentiation
- Desmet classification (Virchows Arch 2011;458:251)
- DR type 1
- Represents multiplication of preexisting cholangiocytes; immediate rescue mechanism against cholestatic parenchymal damage
- Develops fast, favoring cholehepatic cycling of bile acids
- DR type 2
- Represents activation of hepatic progenitor cells
- Type 2A: develops slowly, creating additional canalicular outlets and a larger cholangiocytic resorbing surface favoring cholehepatic cycling in chronic cholestasis
- Type 2B: creates ductules in hypoxic areas; plays a role in new portal tract induction during liver growth
- DR type 3
- Represents progenitor cell based parenchymal regeneration after liver injury
- DR type 1
- Clerbaux et al. / Jain R et al. classification (Adv Anat Pathol 2021;28:72)
- DR type 1 / noninvasive
- Proliferating ductular profiles are limited to the portal mesenchyme; there is no ductular metaplasia or hepatic progenitor cell proliferation
- Associated with large duct obstruction
- DR type 2 / minimally invasive
- Ductular profiles are largely limited to portal mesenchyme with some extension into lobules; there may be ductular metaplasia
- Nonspecific pattern often seen in chronic cholestatic diseases (PBC, PSC, etc.)
- DR type 3 / invasive
- Extensively proliferating ductules deeply invasive into lobules and accompanied with hepatic progenitor cell proliferation
- Associated with massive hepatic necrosis or parenchymal loss
- DR type 1 / noninvasive
- Desmet classification (Virchows Arch 2011;458:251)
| | ||
| Typical: arising from preexisting ductules and confined to the portal mesenchyme | Type 1: typical ductular reaction | Noninvasive: typical ductular reaction |
| Atypical: characterized by structures extending beyond the portal mesenchyme and associated with progenitor cell activation | Type 2: atypical ductular reaction with ductular metaplasia of hepatocytes | Minimally invasive: ductular reaction that expands 20 - 80 μm beyond portal mesenchyme |
| Type 3: atypical ductular reaction with progenitor cell proliferation | Invasive: ductular reaction that expands > 80 μm beyond portal mesenchyme |
- Reference: Am J Pathol 2019;189:1501
Microscopic (histologic) images
Contributed by Shahbaz Khan, M.D.
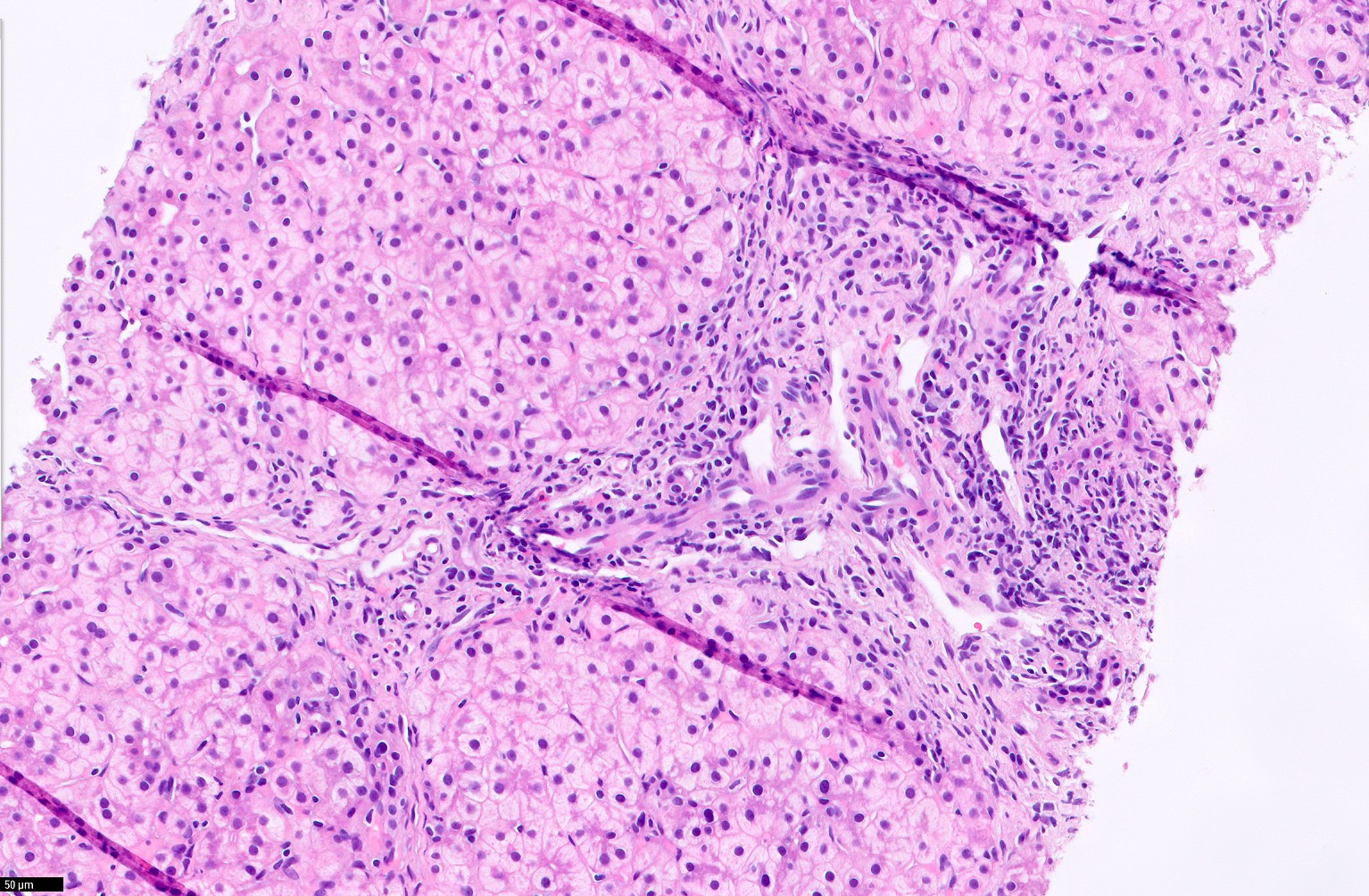
Familial intrahepatic cholestasis
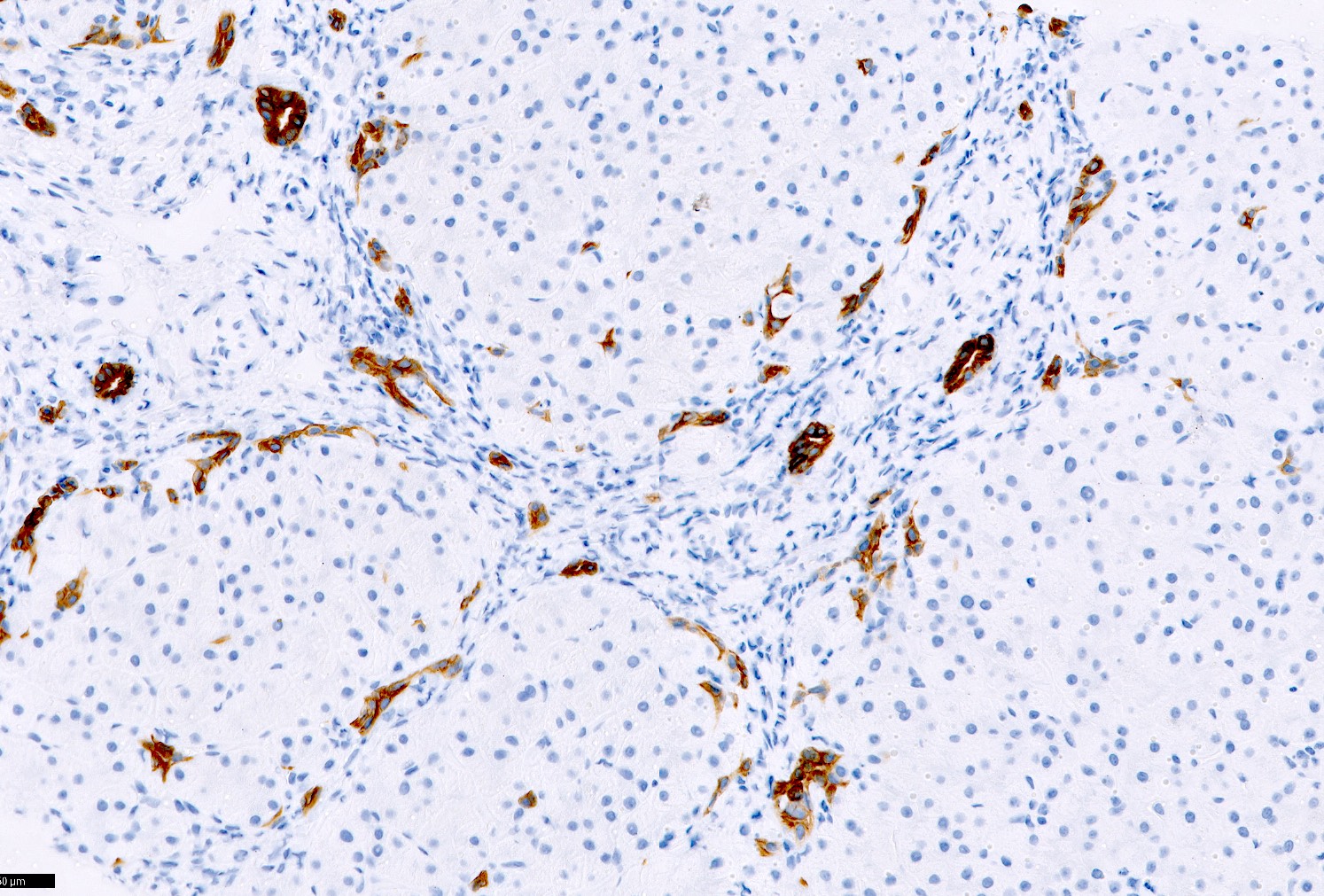
Staining with CK19

Biliary atresia

Prolonged TPN
Positive stains
- Simultaneous expression of biliary antigens (CK7, CK19, OV6) and hepatocyte antigens (HepPar1, albumin, alpha-1 antitrypsin, biliary glycoprotein 1 detected by canalicular staining with polyclonal anti-CEA and occasionally alpha fetoprotein) and other markers, such as NCAM1 / CD56
- Turányi et al. immunohistochemical classification of ductular reactions (Histopathology 2010;57:607):
- Type P (primitive):
- Type D (differentiating):
- Type O (obstruction):
Negative stains
Videos
Ductular reaction in liver disease
Sample pathology report
- Liver, needle core biopsy:
- Severe cholestasis with marked ductular reaction and fibrosis, suggestive of extrahepatic biliary atresia
Differential diagnosis
- Ductal plate malformation:
- Anastomosing, angulated and dilated biliary channels in irregular, bland fibrous stroma, continuous with biliary tree
- Bile ducts often contain inspissated bile
- Bile duct hamartoma / adenoma:
- Compact network of simple noncystic tubular ducts or more complex tortuous arrangement, with small or indistinct lumina
- Epithelium has abundant cytoplasm and pale nuclei compared with interlobular bile ducts in adjacent liver
- Often grossly apparent lesion
- Well differentiated intrahepatic cholangiocarcinoma:
- Larger, infiltrative lesion with desmoplastic stroma and nuclear / cytologic atypia
Additional references
Board review style question #1
The ductular profiles in the ductular reaction at the portal - parenchymal interface are highlighted best by which of the following panels of immunohistochemical stains?
- Alpha-1 antitrypsin, CK19, CK7, EMA
- CD56, glypican 3
- CK7, arginase1
- EMA, albumin, GPC3
- HepPar1, alpha fetoprotein, CK20
Board review style answer #1
Board review style question #2
Which immunohistochemical stain highlights typical ductules in the center of portal tract and atypical ductular profiles at the periphery?
- AFP
- Arginase
- CK19
- HepPar 1
- Glutamine synthetase
Board review style answer #2
