
Liver & intrahepatic bile ducts
Systemic conditions
Pregnancy
Author: Komal Arora, M.D.

Last author update: 1 May 2012
Last staff update: 26 June 2023
Copyright: 2002-2024, PathologyOutlines.com, Inc.
PubMed Search: Pregnancy[TI] liver[TI] free full text[sb]
Table of Contents
Acute fatty liver of pregnancy | Intrahepatic cholestasis of pregnancy | Preeclampsia and eclampsia | Viral hepatitisCite this page: Arora K. Pregnancy. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/liverpregnancy.html. Accessed April 20th, 2024.
Acute fatty liver of pregnancy
Definition / general
Treatment
Gross description
Microscopic (histologic) description
Positive stains (frozen tissue)
Differential diagnosis
Additional references
- Minimal to modest hepatic dysfunction due to defect in mitochondrial fatty acid oxidation that may progress to hepatic failure
- Usually presents in third trimester of primiparas with bleeding, nausea, vomiting, jaundice, coma
- Incidence of 1 case per 15,000 pregnancies
- 20% have coexisting preeclampsia
- Usually mild but may cause death
Treatment
- Terminate pregnancy
Gross description
- Pale, yellow, small liver
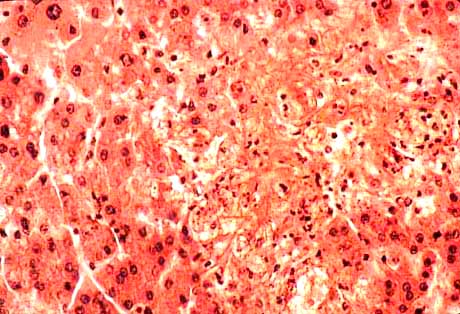
Microscopic (histologic) description
- Microvesicular steatosis in zones 2 or 3 (vacuoles may be very small)
- Also marked ballooning of hepatocytes and macrovesicular fat
- In severe cases, hepatocyte dropout, reticulin collapse, portal tract inflammation
Positive stains (frozen tissue)
- Fat stains (Oil red O, Sudan black)
Differential diagnosis
- Carnitine deficiency
- Jamaican vomiting sickness
- Lábrea hepatitis
- Reye syndrome
- Salicylate intoxication
- Yellow fever
Additional references
Intrahepatic cholestasis of pregnancy
Definition / general
Laboratory
Microscopic (histologic) description
- Second leading cause of gestational jaundice (after viral hepatitis)
- Usually occurs late in pregnancy
- Estrogenic hormones may inhibit hepatocellular bile secretory activity
- Mother at risk for gallstones, malabsorption
- Associated with higher incidence of fetal distress, stillbirths, prematurity
- Symptoms: pruritis in third trimester, dark urine, light stools, jaundice
Laboratory
- Elevated serum bilirubin (< 5 mg/dl), usually conjugated; mildly elevated alkaline phosphatase
Microscopic (histologic) description
- Mild cholestasis without cirrhosis
Preeclampsia and eclampsia
Definition / general
Laboratory
Case reports
Treatment
Gross description
Gross images
Images hosted on other servers:

Microscopic (histologic) description
Microscopic (histologic) images
Images hosted on other servers:


Differential diagnosis
Additional references
- Preeclampsia: complication of pregnancy in third trimester, usually primiparas, with maternal hypertension, proteinuria, peripheral edema, coagulation abnormalities, DIC
- Ecclampsia: preeclampsia, seizures and hyperreflexia; leading cause of maternal death, often due to delay in diagnosis
- Liver disease as part of HELLP syndrome: hemolysis, elevated liver enzymes, low platelets; associated with 4 - 12% of cases of preeclampsia; microangiopathic hemolysis with thrombocytopenia; 10 - 60% infant mortality due to placental abruption, intrauterine ischemia or prematurity
Laboratory
- Early mild increase in liver enzymes, late coagulopathy
Case reports
- Woman in mid 30s with preeclampsia and subcapsular liver hematoma at 23 weeks gestation (Arch Pathol Lab Med 2003;127:1639)
Treatment
- Termination of pregnancy in severe cases
Gross description
- Pale, firm liver with small red hemorrhagic patches (hematoma dissecting under Glisson capsule and causing hepatic rupture)
Gross images
Images hosted on other servers:

Small hemorrhagic infarcts and atrophy
Microscopic (histologic) description
- Periportal fibrin deposits with hemorrhage into space of Disse, causing periportal hepatocellular necrosis
- Less commonly bile inspissation in canaliculi and ductules, steatosis, portal lymphoplasmacytic infiltrate
Microscopic (histologic) images
Images hosted on other servers:
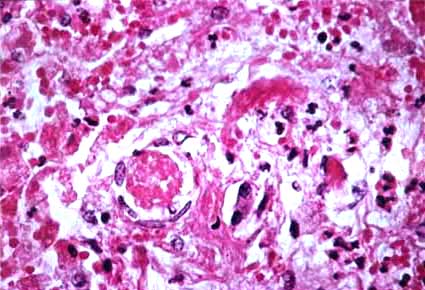
Focal hepatocellular necrosis with fibrin thrombi (image on right)
Differential diagnosis
Additional references
