
Liver & intrahepatic bile ducts
Infectious nonviral
Q fever
Editorial Board Members: Claudio Luchini, M.D., Ph.D., Kimberley J. Evason, M.D., Ph.D.


Last author update: 25 May 2023
Last staff update: 25 May 2023
Copyright: 2019-2024, PathologyOutlines.com, Inc.
PubMed Search: Q fever
Table of Contents
Definition / general | Essential features | Terminology | Epidemiology | Sites | Pathophysiology | Clinical features | Diagnosis | Laboratory | Case reports | Treatment | Microscopic (histologic) description | Microscopic (histologic) images | Videos | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Abdalhai A, Gonzalez R. Q fever. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/liverqfever.html. Accessed April 19th, 2024.
Definition / general
- Q fever is a zoonotic infection caused by Coxiella burnetii (obligate intracellular gram negative rods)
- Farm animals (cattle, sheep, goats) and pets are the main source of infection
- Transmission is via airborne aerosols or ingestion of contaminated milk or goat cheese (Korean J Pathol 2012;46:10)
Essential features
- Liver involvement is characterized by acute hepatitis (mild elevation of liver enzymes, hepatomegaly or splenomegaly)
- Fibrin ring granulomas (doughnut granulomas) are characteristic but not specific for Q fever (Korean J Pathol 2012;46:10)
Terminology
- Originally called query fever before the cause was discovered
- Causative organism named after the Australian virologist Frank Macfarlane Burnet
Epidemiology
- M:F = 2.45:1 (Medicine (Baltimore) 2000;79:109)
- More cases of Q fever are reported in older people, especially men
- 36% of cases in the U.S. are reported from 3 states (California, Texas, Iowa) (CDC: Q Fever [Accessed 17 January 2023])
Sites
- Disseminated infection can involve lungs, heart, bone marrow, liver
Pathophysiology
- C. burnetii survives in the environment in spore-like forms
- Genetic variability and virulence depend on lipopolysaccharide expression
- Host defense is mainly through cell mediated immunity with granuloma formation controlled by IFNγ (Clin Microbiol Rev 2017;30:115)
Clinical features
- 60% of patients are asymptomatic in primary infection (Lancet Infect Dis 2005;5:219)
- Infection has acute and chronic forms
- Cases with liver involvement typically present with fever, jaundice, hepatomegaly or splenomegaly and elevated liver enzymes (Korean J Pathol 2012;46:10)
Diagnosis
- Serology, supported by imaging and biopsy sampling
Laboratory
- Serology (Clin Microbiol Rev 2017;30:115):
- Indirect immunofluorescence assay (IFA), complement fixation test (CFT) and enzyme linked immunoassay (ELISA)
- Detection of antiphase I and antiphase II IgM and IgG
- Real time PCR or quantitative PCR (qPCR)
Case reports
- 24 year old man with fever, abdominal pain, fatigue, muscle aches, vomiting and diarrhea (Int J Infect Dis 2020;95:113)
- 35 year old man with 7 day history of fever with chills (BMC Infect Dis 2010;10:193)
- 35 year old man with severe abdominal pain, fever, diaphoresis, weakness and fatigue (Ann Hepatol 2013;12:138)
- 60 year old man with malaise, fever, anorexia and nausea (Acta Gastroenterol Belg 2018;81:441)
- 63 year old woman with fever, rigors and nausea (QJM 2017;110:587)
Treatment
- Antibiotics (doxycycline)
Microscopic (histologic) description
- Granulomatous hepatitis, usually with fibrin ring granulomas
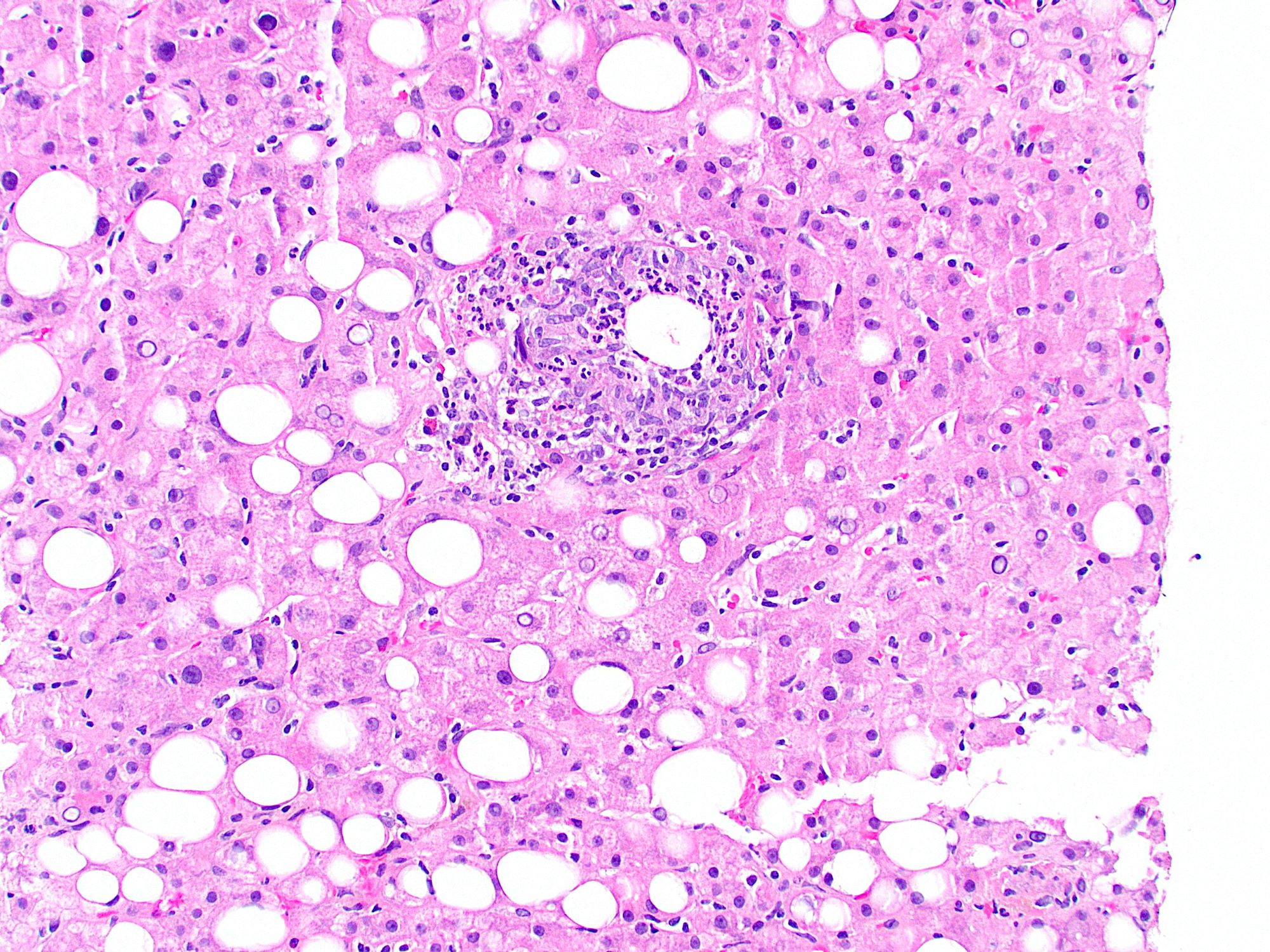
- Typical fibrin ring granulomas (doughnut granulomas) consist of a central fat vacuole, a fibrin ring, activated macrophages and lymphocytes
- Other forms of granulomas: epithelioid with eosinophils and multiple giant cells, lipogranulomas and extensive fibrin deposition without ring configuration, which may mimic necrotizing granuloma (Korean J Pathol 2012;46:10)
- May see acute cholangitis without granuloma formation (Korean J Pathol 2012;46:10)
Microscopic (histologic) images
Contributed by Raul S. Gonzalez, M.D.
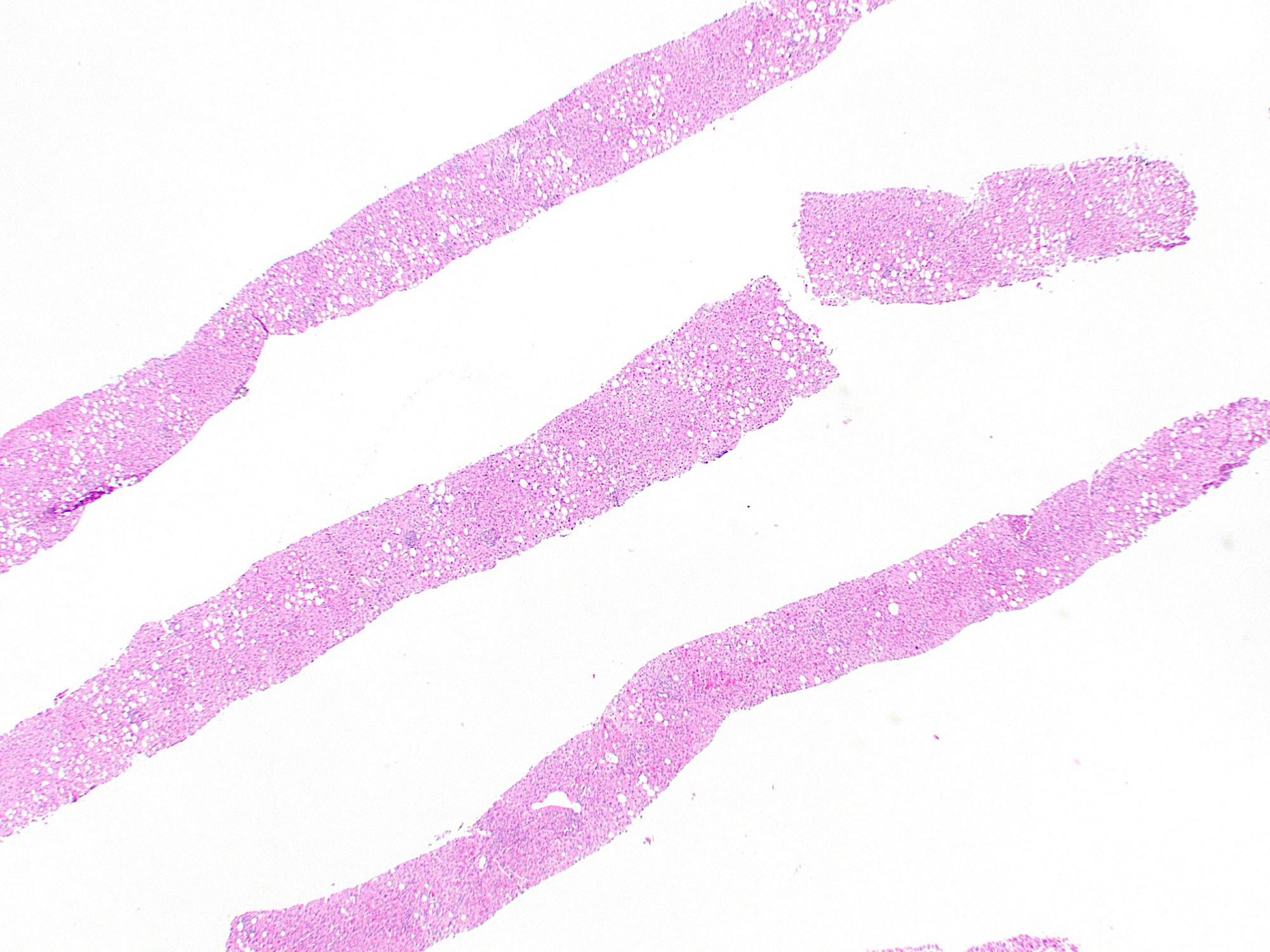
Liver with Q fever

Fibrin ring granulomas
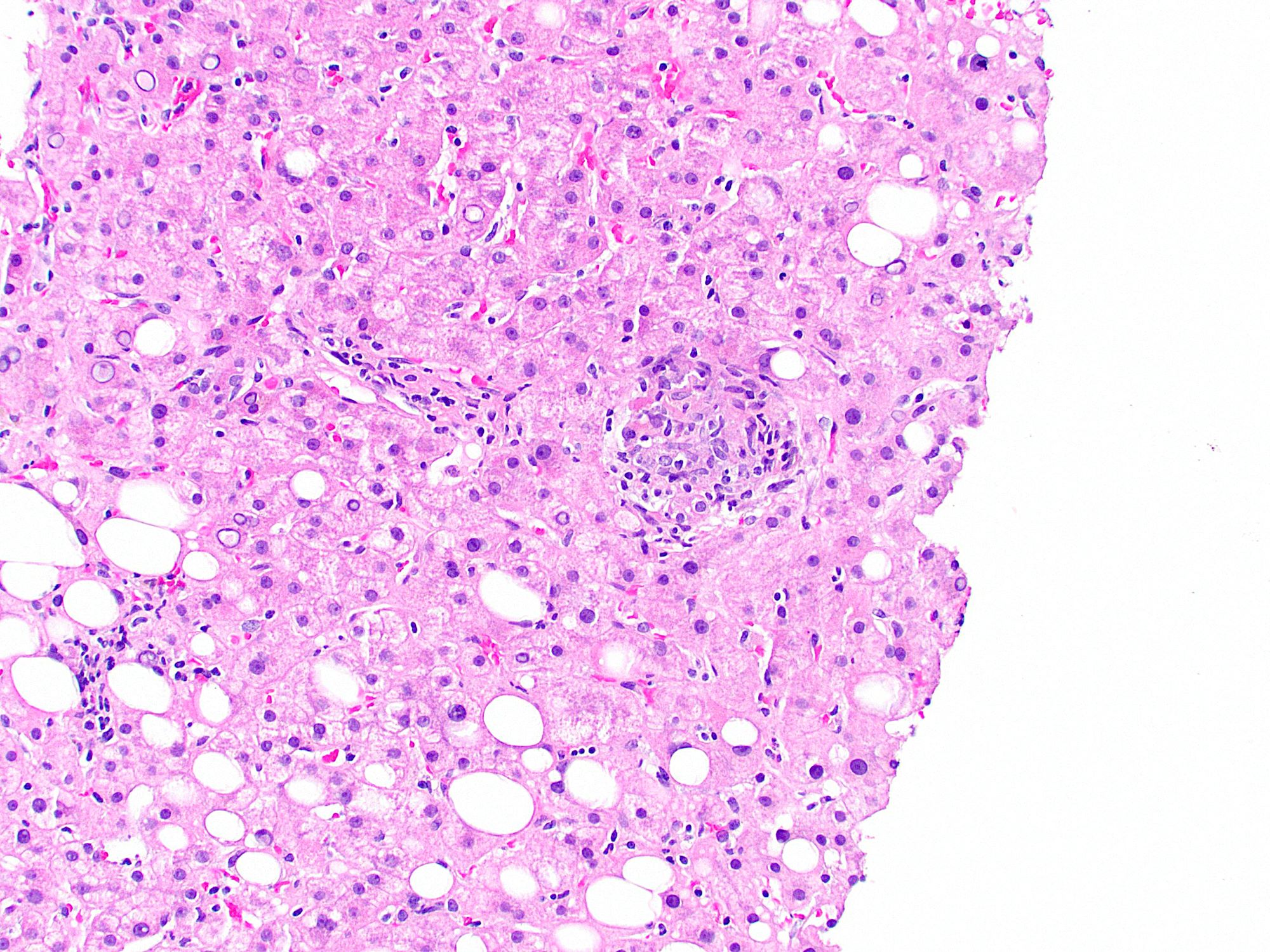
Q fever granulomas
Videos
A summary of Q fever
Sample pathology report
- Liver, biopsy:
- Granulomatous hepatitis (see comment)
- Comment: The biopsy is adequate, consisting of 2 cores containing 15 portal tracts for evaluation. There are fibrin ring granulomas showing a central lipid droplet surrounded by fibrin. In view of liver enzyme elevation and positive serology for Coxiella burnetii, the overall features are compatible with the clinical suspicion of Q fever associated hepatitis.
Differential diagnosis
- EBV hepatitis:
- Diffuse lymphocytic sinusoidal infiltrate in a single file or beads; fibrin ring granulomas are uncommon (Arch Pathol Lab Med 2018;142:1191)
- CMV hepatitis:
- Basophilic intranuclear inclusions (Cowdry bodies) surrounded by a clear halo; fibrin ring granulomas are uncommon
- Other rare causes of fibrin ring granulomas include leishmaniasis, boutonneuse fever, salmonella and toxoplasmosis (Am J Med 2014;127:928)
Additional references
Board review style question #1
A 65 year old farmer presents with fever, fatigue and nausea for 2 weeks. Painful hepatosplenomegaly was noted on abdominal examination. Liver enzymes were elevated. Serological tests were positive for antiphase II IgG and IgM with high titers. Q fever is suspected and a transjugular liver biopsy was obtained. Which of the following microscopic findings would be expected in the patient’s biopsy?
- Acidophilic bodies and intranuclear ground glass inclusions
- Fibrin ring granulomas
- Mixed inflammatory infiltrate with numerous amastigotes
- Necrotizing granulomatous inflammation
Board review style answer #1
B. Fibrin ring granulomas. Fibrin ring granulomas are characteristic of Q fever associated hepatitis. Acidophil bodies and ground glass inclusions are seen in hepatitis B infections. Mixed inflammation with amastigotes is seen in leishmaniasis. Necrotizing granulomas in the liver is suggestive of tuberculosis.
Comment Here
Reference: Q fever
Comment Here
Reference: Q fever
Board review style question #2
A patient presents with fever and hepatomegaly. A liver biopsy is performed (shown above). Clinical workup rules out EBV, CMV and malignancy. Which of the following laboratory tests would help confirm the most likely remaining diagnosis?
- Antismooth muscle antibody testing
- Donor specific antibody assay
- Serology for antiphase I and antiphase II IgM and IgG
- Serology for viral hepatitis E
Board review style answer #2
C. Serology for antiphase I and antiphase II IgM and IgG. The biopsy shows a fibrin ring granuloma, which is characteristic of Q fever associated hepatitis. Serology for antiphase I and antiphase II IgM and IgG is used to establish the diagnosis. The most common remaining causes of fibrin ring granulomas are ruled out in the question stem. Autoimmune hepatitis (choice A), antibody mediated rejection of liver transplant (choice B), and hepatitis E (choice D) are not characterized by fibrin ring granulomas.
Comment Here
Reference: Q fever
Comment Here
Reference: Q fever
