
Liver & intrahepatic bile ducts
Benign / nonneoplastic
Bile duct adenoma
Authors: Komal Ijaz, M.D., Feng Yin, M.D., Ph.D.
Editorial Board Members: Claudio Luchini, M.D., Ph.D., Monika Vyas, M.D.

Last author update: 16 June 2023
Last staff update: 16 June 2023
Copyright: 2002-2024, PathologyOutlines.com, Inc.
PubMed Search: Bile duct adenoma
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Radiology description | Prognostic factors | Case reports | Gross description | Gross images | Frozen section description | Frozen section images | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Positive stains | Negative stains | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Ijaz K, Yin F. Bile duct adenoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/livertumorbileductadenoma.html. Accessed April 17th, 2024.
Definition / general
- Bile duct adenoma is a benign biliary neoplasm consisting of uniformly distributed small bile ducts in a background of fibrotic stroma
Essential features
- Benign epithelial tumor
- Most commonly a solitary subcapsular nodule (90%)
- Frequently an incidental finding at surgery or autopsy
- Frequently submitted for frozen section to rule out metastatic process
- Can be difficult to distinguish from adenocarcinoma, especially on frozen section
- Uniform distribution of small tubules with no cytological atypia or mitotic figures
- Frequent BRAF V600E mutation supports a neoplastic process
Terminology
- Also known as peribiliary gland hamartoma, cholangioma, cholangioadenoma
ICD coding
- ICD-O: 8160/0 - bile duct adenoma
- ICD-11: 2E92.7 & XH6KR6 - benign neoplasm of liver or intrahepatic bile ducts & bile duct adenoma
Epidemiology
- Usually adults (age > 20), no gender predilection
- Accounts for 1.3% of primary liver tumors and 2.4% in a total of 1,456 resection cases for primary liver tumors and explant for liver cirrhosis (Am J Surg Pathol 1988;12:708, Pathol Int 2014;64:551)
Sites
- Liver, typically subcapsular location
Pathophysiology
- Originally considered to be a reactive ductular proliferation in response to focal injury, a localized biliary healing response equivalent to the function of a peribiliary gland or pyloric gland metaplasia in the foregut or a hamartomatous process (Am J Surg Pathol 1988;12:708, Am J Surg Pathol 2010;34:1312, Am J Surg Pathol 1996;20:858)
- Presence of frequent BRAF V600E mutation supports a neoplastic process (Hepatology 2015;61:403, Histopathology 2015;67:562, Histopathology 2017;70:485)
Etiology
- Unknown; whether focal injury acts as trigger event remains controversial
Clinical features
- Mostly an incidental finding during surgery or autopsy
- Frequently submitted for frozen section to rule out metastatic process
Diagnosis
- Clinical presentation and histopathologic findings
Radiology description
- Hypointense on T1 weighted images, hyperintense on T2 weighted images
- Characteristic arterial phase hyperenhancement that persists into the portal venous and delayed phases on CT and MRI (Diagn Interv Radiol 2018;24:249)
Prognostic factors
- Potential and controversial precursor to intrahepatic cholangiocarcinoma (Histopathology 2021;78:310, Hepatology 2015;61:403, Histopathology 2015;67:562)
Case reports
- 18 month old boy with a large (10 cm) exophytic solid liver tumor (World J Gastrointest Surg 2019;11:414)
- 35 year old woman with resolution of bile duct adenomas after discontinuing oral contraceptive pills (Middle East J Dig Dis 2016;8:327)
- 62, 65 and 76 year old men were identified as having a bile duct adenoma (Endosc Int Open 2018;6:E1312)
- 70 year old man with an incidental finding of intrahepatic bile duct adenoma during laparoscopic distal gastrectomy for gastric cancer (Int Cancer Conf J 2018;8:7)
Gross description
- Usually subcapsular, well circumscribed but nonencapsulated
- Majority are solitary but can be multiple
- Firm, gray-white
- Size ranging from 1 to 20 mm (mean: 5.8 mm) (Am J Surg Pathol 1988;12:708)
Gross images
Images hosted on other servers:

Well circumscribed
nonencapsulated
subcapsular lesion
Frozen section description
- Usually solitary subcapsular lesion, well circumscribed and nonencapsulated
- Bland small tubular proliferation in a background of fibrotic stroma
- Lack of marked nuclear atypia, mitotic figures, necrosis or intraluminal bile
- Potential diagnostic pitfalls: cellular stroma, back to back compact architecture, mucin production, unusual variant (oncocytic, clear cell, etc.), cytologic atypia enhanced by frozen section artifact
Frozen section images
Contributed by Feng Yin, M.D., Ph.D.
Well circumscribed unencapsulated lesion
Lack of atypical features
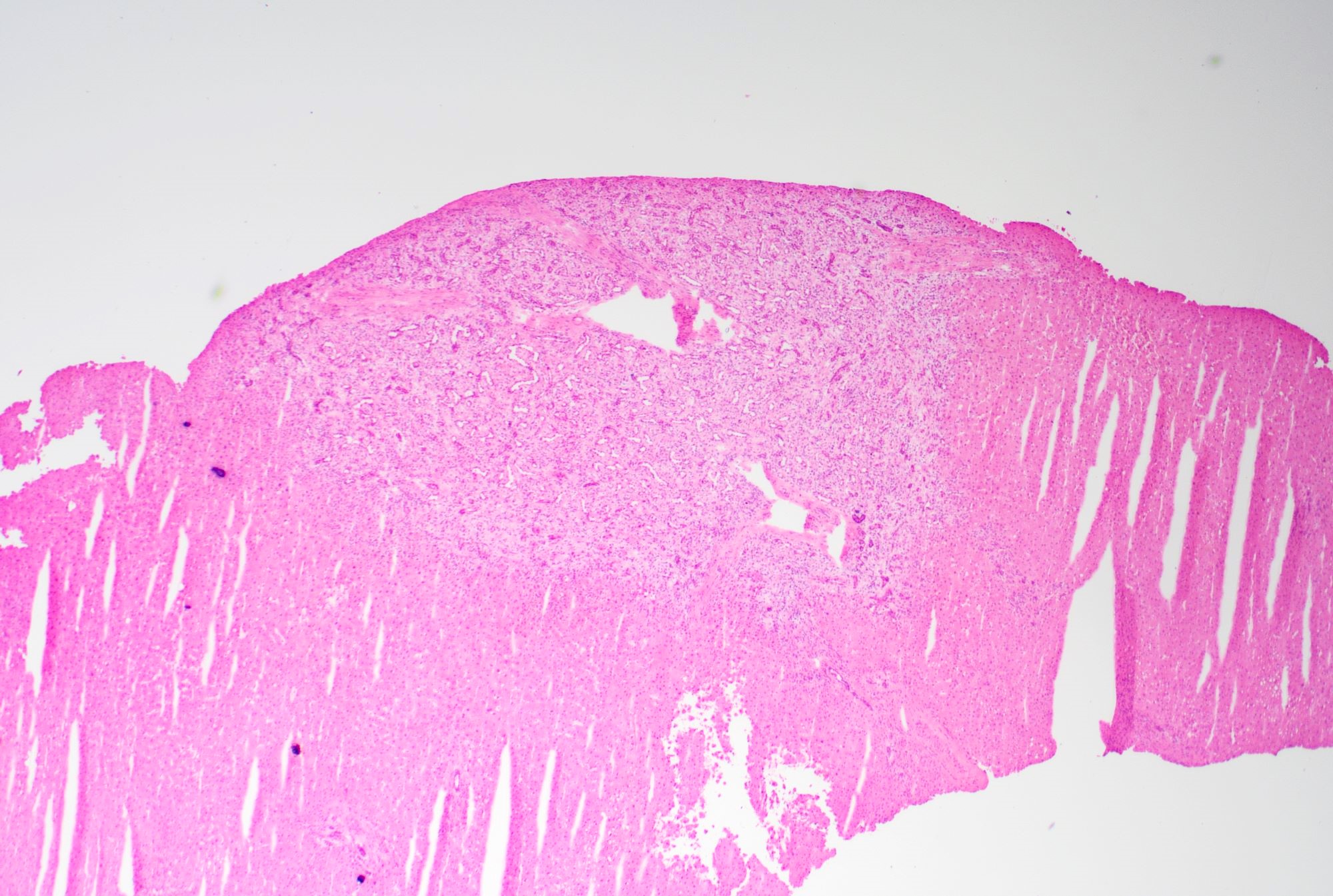
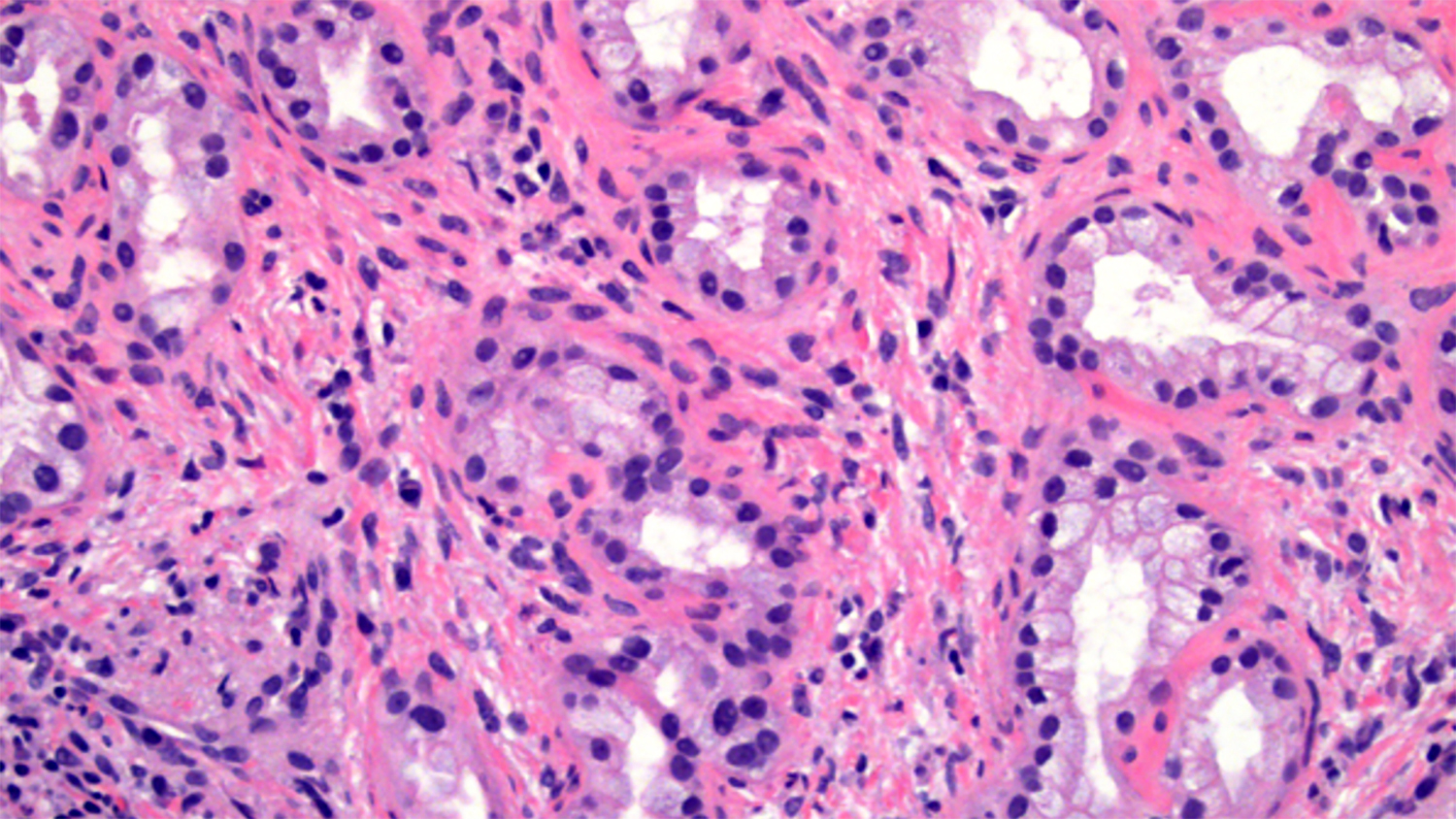
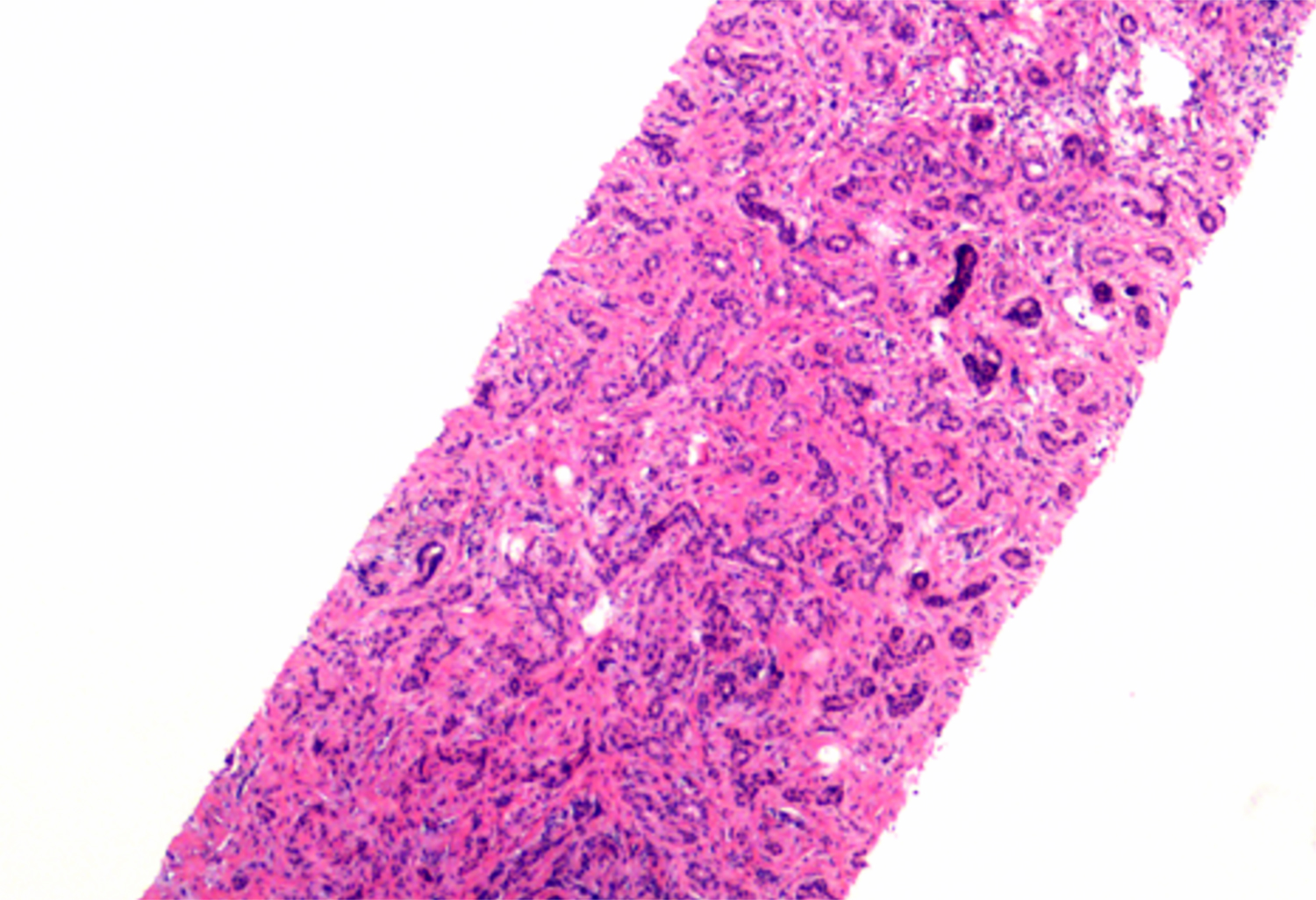
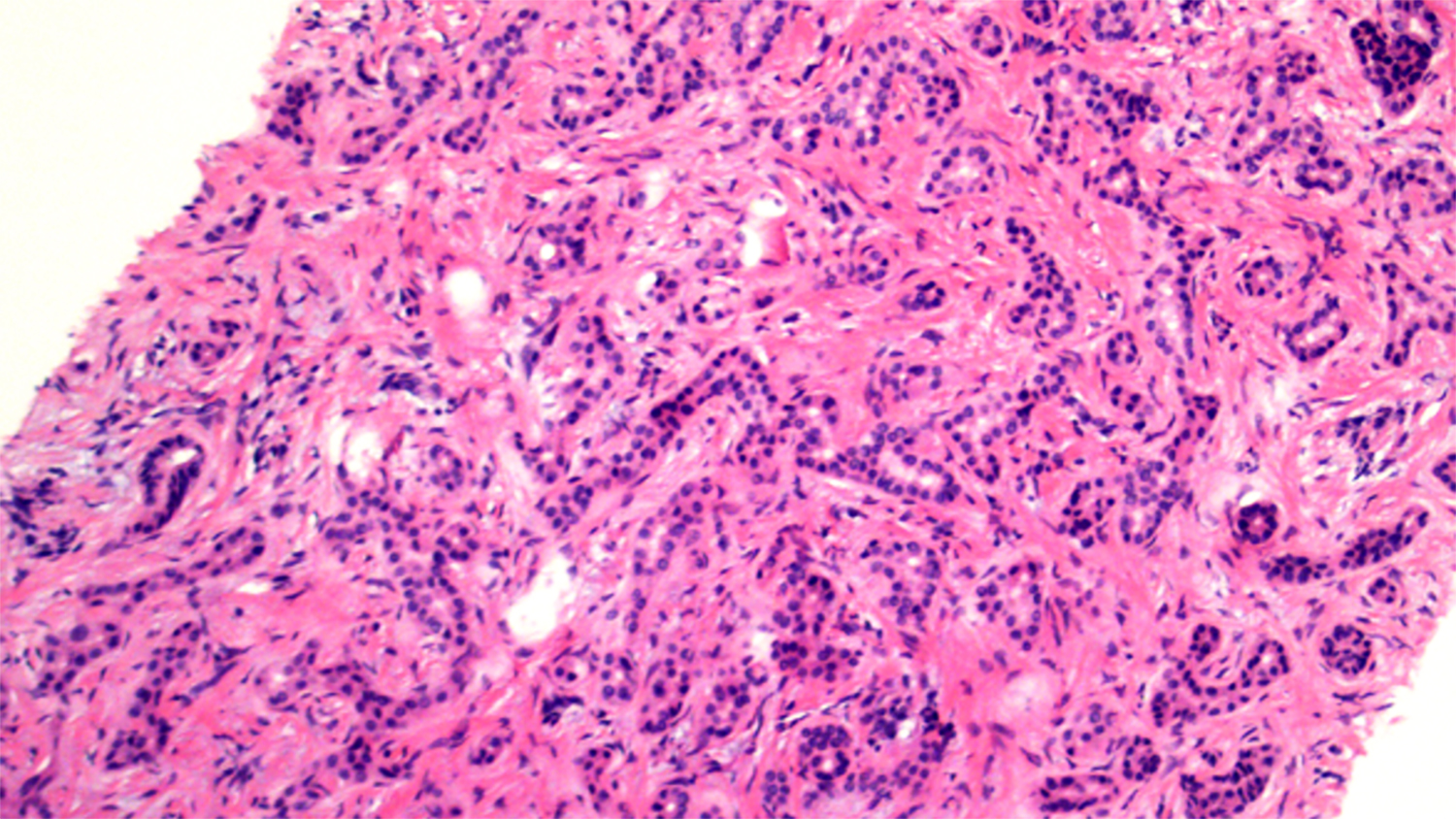
Microscopic (histologic) description
- Relatively uniform distribution of small tubules with little to no lumen
- Lined by single layer of cuboidal cells with no cytological atypia or mitotic figures
- Well circumscribed with fibrotic stroma
- No intraluminal bile; the ducts do not communicate with the biliary tree
- Rarely, variants with clear cell change, oncocytic features, mucin secreting and alpha-1 antitrypsin droplets (Am J Surg Pathol 2001;25:956, Case Rep Pathol 2014;2014:874826, Case Rep Pathol 2014;2014:282010, Dig Surg 2002;19:324, Int J Surg Pathol 2008;16:218)
Microscopic (histologic) images
Contributed by Komal Ijaz, M.D. and Feng Yin, M.D., Ph.D.

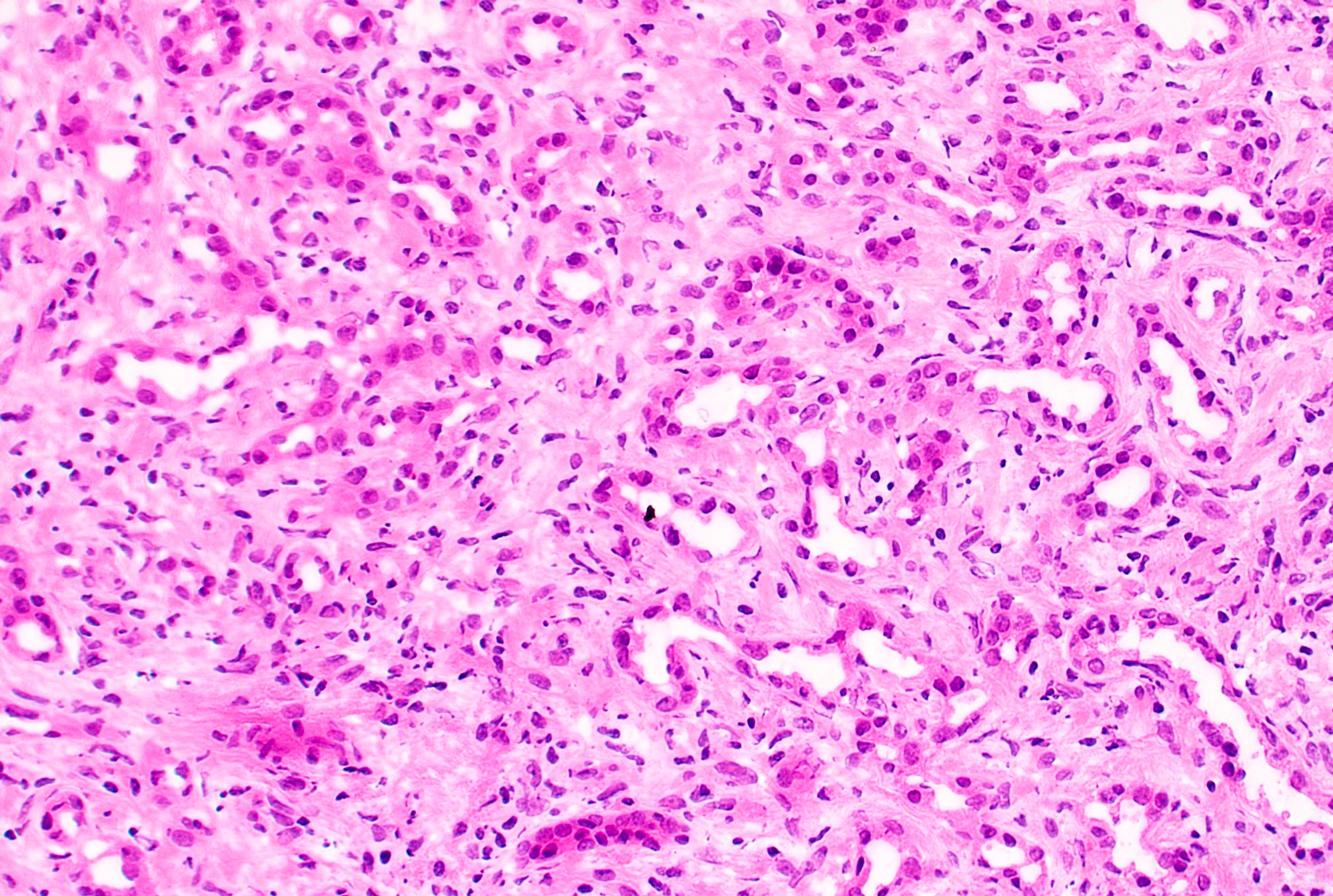
Well circumscribed unencapsulated lesion
Subcapsular well circumscribed lesion
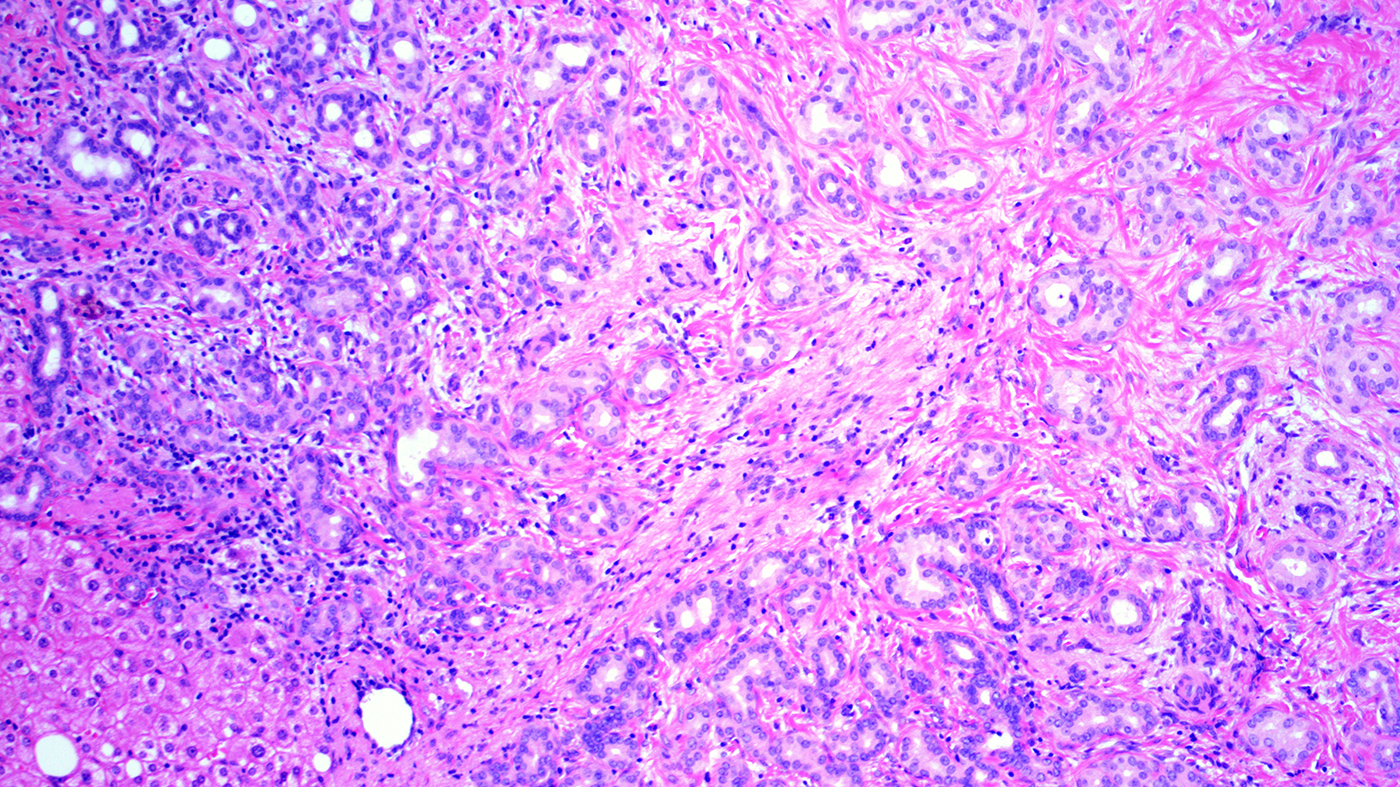
Tubules with fibrous stroma
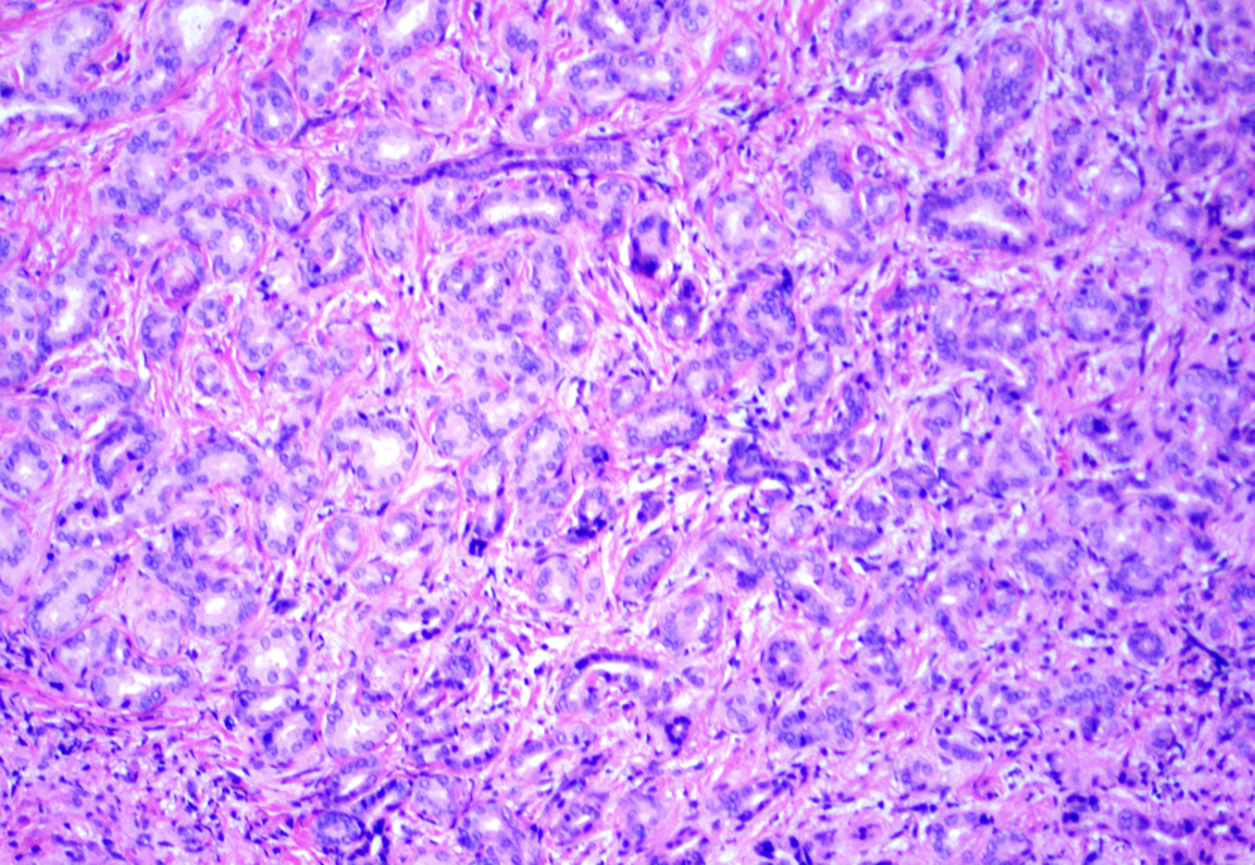
Tubules with focal crowding
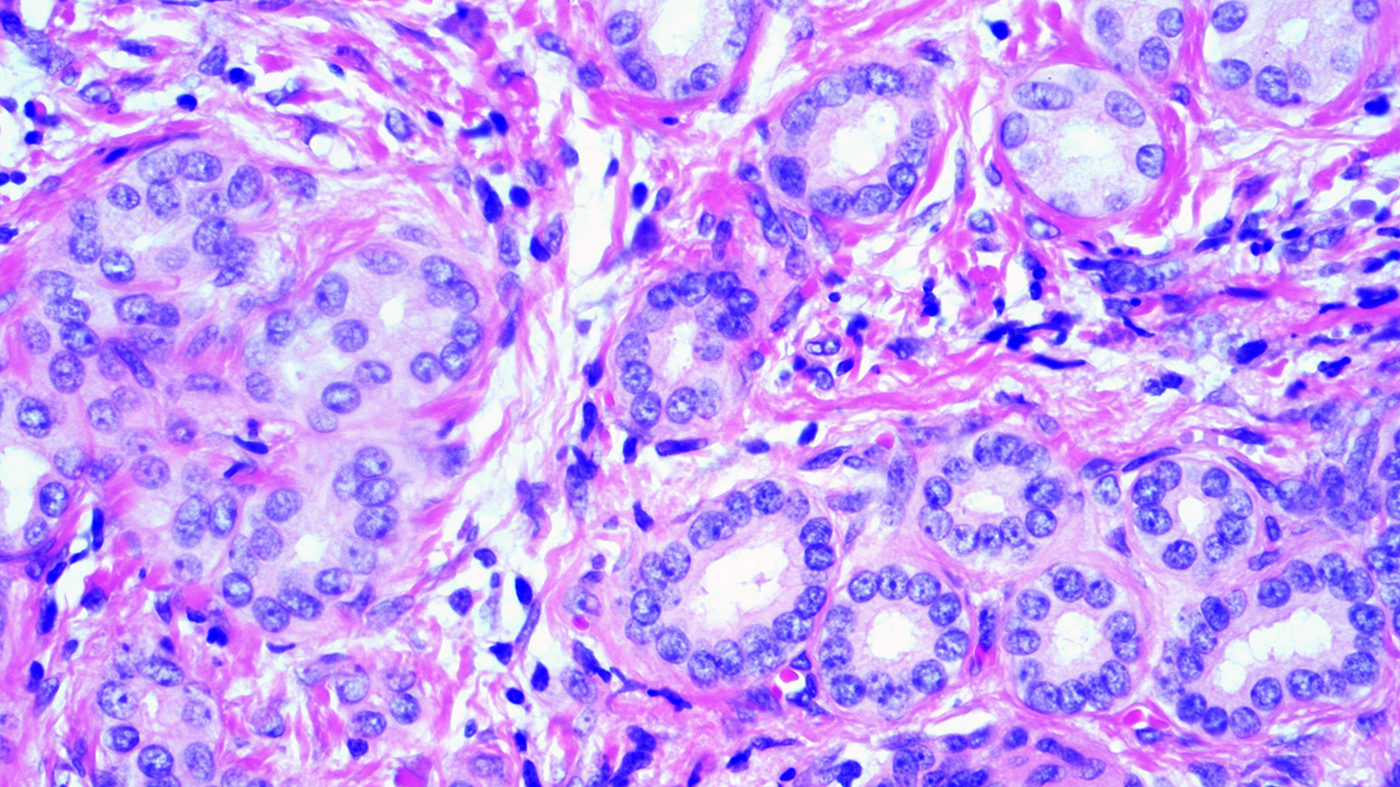
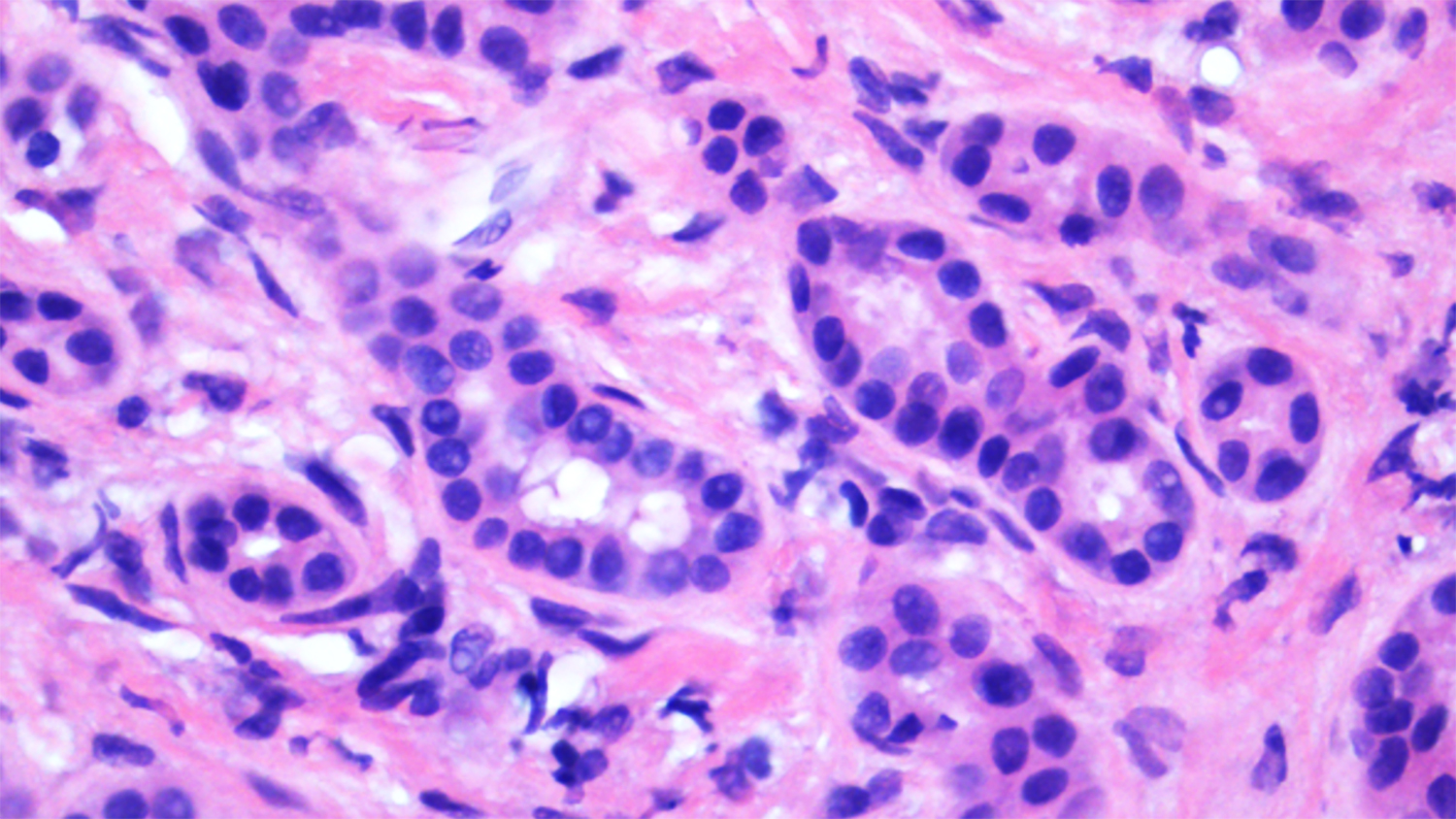
Tubules with bland cytology
Tubules with cytoplastic mucin
Fine needle biopsy
Cytology description
- Abundant normal appearing biliary epithelium
- Often admixed with benign hepatocytes
- Cell block may be useful
- Reference: Sidawy: Fine Needle Aspiration Cytology, 1st Edition, 2007
Positive stains
- Typical biliary immunoprofile (positive for CK7 and CK19)
- Expression of foregut antigens (positive for MUC5AC and MUC6) (Am J Surg Pathol 2010;34:1312)
- Ki67 proliferation rate is low (should not be more than 10%)
- BRAF V600E immunoreactivity in 53% of cases (Histopathology 2015;67:562)
- p16INK4a immunoreactivity in 81% of cases (Am J Surg Pathol 2014;38:364)
Negative stains
Molecular / cytogenetics description
- Majority of bile duct adenomas are positive for albumin in situ hybridization, a feature that distinguishes it from metastatic pancreatic adenocarcinoma (Histopathology 2016;69:423)
Sample pathology report
- Liver, wedge biopsy:
- Intrahepatic bile duct adenoma (see comment)
- Comment: The biopsy demonstrates the proliferation of small tubules with no cytological atypia embedded in the fibrous stroma, consistent with bile duct adenoma.
Differential diagnosis
- Cholangiocarcioma or metastatic adenocarcinoma:
- Cytological atypia, mitosis, size may be > 2 cm
- Infiltrative growth pattern
- Extensive expression of EZH2, no or low expression of p16INK4a (Am J Surg Pathol 2014;38:364)
- Ki67 > 10%
- Lymphovascular or perineural invasion
- Von Meyenburg complex (biliary microhamartoma):
- Angulated, branching and irregularly dilated ducts
- Intraluminal bile plugs
Board review style question #1
A 55 year old man with pancreatic adenocarcinoma was admitted for Whipple procedure. A small liver nodule was noted during surgery and sent for intraoperative consultation. A representative photomicrograph of the frozen section is shown. Which of the following is the most likely diagnosis?
- Bile duct adenoma
- Metastatic pancreatic adenocarcinoma
- Reactive ductular proliferation
- Von Meyenburg complex
Board review style answer #1
A. Bile duct adenoma. The diagnosis of a bile duct adenoma is favored during intraoperative consultation, largely attributed to the presence of uniform distribution of small tubules in a background of fibrous stroma. There are no worrisome morphological features, such as infiltrative growth pattern, desmoplastic stromal reaction, marked cytological atypia, frequent mitosis and necrosis.
Comment Here
Reference: Bile duct adenoma
Comment Here
Reference: Bile duct adenoma
Board review style question #2
Which gene is most frequently mutated in bile duct adenoma?
- BRAF
- KRAS
- p53
- SMAD4
Board review style answer #2
A. BRAF mutations are present in about 53% of bile duct adenomas.
Comment Here
Reference: Bile duct adenoma
Comment Here
Reference: Bile duct adenoma
