
Liver & intrahepatic bile ducts
Benign / nonneoplastic
Mucinous cystic neoplasm
Author: Kimberley J. Evason, M.D., Ph.D.
Editorial Board Member: Naziheh Assarzadegan, M.D.
Editor-in-Chief: Raul S. Gonzalez, M.D.

Last author update: 5 January 2023
Last staff update: 5 January 2023
Copyright: 2019-2024, PathologyOutlines.com, Inc.
PubMed Search: Mucinous cystic neoplasm
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Laboratory | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Cytology images | Positive stains | Negative stains | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Evason KJ. Mucinous cystic neoplasm. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/livertumorMCN.html. Accessed April 23rd, 2024.
Definition / general
- Cystic hepatic neoplasm with ovarian type stroma and mucinous epithelium that does not communicate with bile ducts
Essential features
- Multiloculated cystic neoplasm lined by biliary type or mucinous epithelial cells overlying ovarian type stroma
- Usually benign (90%) but may be associated with invasive carcinoma (Mod Pathol 2011;24:1079)
- Complete surgical excision with extensive sampling for histology is required to reduce risk of recurrence and determine if associated invasive carcinoma is present
Terminology
- Hepatobiliary cystadenoma
- Hepatobiliary cystadenocarcinoma (if associated invasive carcinoma)
- Biliary cystadenoma
- Cystadenoma with mesenchymal stroma
ICD coding
- ICD-O:
- ICD-11:
- 2E92.6 - benign neoplasm of gallbladder, extrahepatic bile ducts or ampulla of Vater
- XH6NK7 - mucinous cystic neoplasm with low grade intraepithelial neoplasia
- 2E61.Y - carcinoma in situ of other specified digestive organs
- XH81P3 - mucinous cystic tumor with high grade dysplasia
- 2C15.1 - mucinous cystic neoplasm with associated invasive carcinoma of distal bile duct
- 2C18.1 - mucinous cystic neoplasm with associated invasive carcinoma of perihilar bile duct
- 2C17.1 - mucinous cystic neoplasm with associated invasive carcinoma of other or unspecified parts of biliary tract
Epidemiology
- F > M
- Mean age: 45 years (noninvasive) to 59 years (with invasive component) (Am J Surg Pathol 1994;18:1078)
Sites
- Liver parenchyma
- May rarely involve extrahepatic bile ducts or gallbladder
Pathophysiology
- Ovarian type stroma may originate from developing gonads due to their close proximity to the liver during embryologic development (Dig Surg 2010;27:19)
Etiology
- Unknown at this time
Clinical features
- Typically present with abdominal pain and swelling
- May have symptoms of biliary obstruction (jaundice)
Diagnosis
- Fine needle aspiration and imaging studies cannot reliably distinguish mucinous cystic neoplasms (MCN) from other types of liver cysts
- Definitive diagnosis requires histopathologic confirmation of the ovarian type stroma, usually after surgical excision (Am J Surg Pathol 2018;42:95)
Laboratory
- Serum CA19-9 may be elevated, especially if invasive carcinoma is present
Radiology description
- Large, multilocular cyst with internal septations (World J Gastroenterol 2006;12:6062)
- May show calcifications, mural nodules or papillary projections
- Distinction of benign from malignant is usually not possible on imaging studies (Am J Surg Pathol 2018;42:95)
Radiology images
Images hosted on other servers:

CT with cystic mass

CT with large lesion

Cholangiogram

Ultrasound
Prognostic factors
- Complete surgical excision confers a favorable prognosis
- Prognostic significance of invasive component is difficult to determine, as many reported cases with invasive carcinoma lack ovarian type stroma, occur in men and thus may represent intraductal papillary neoplasm rather than mucinous cystic neoplasm (Am J Surg Pathol 1994;18:1078)
Case reports
- 33 year old woman with a rapid progression of a cystic tumor of the liver (Ann Hepatol 2018;17:519)
- 37 year old Tunisian woman who presented with subacute right upper quadrant pain (BMC Gastroenterol 2019;19:103)
- 39 year old woman with complaints of vague abdominal pain and increasing abdominal girth (World J Gastroenterol 2006;12:6062)
- 43 year old woman with an unremarkable previous medical history presented with progressive obstructive jaundice (World J Gastroenterol 2006;12:5735)
- 56 year old woman with a growing solitary unilocular hepatic cyst (Acta Cytol 1993;37:966)
- 60 year old asymptomatic woman with history of echinococcal cyst in the liver (J Surg Case Rep 2012;2012:5)
Treatment
- Complete surgical excision
- Incomplete excision is associated with local recurrence and risk of malignant transformation (World J Surg 2006;30:1560)
Gross description
- Cystic with multiple communicating lobules of varying sizes and a smooth and glistening lining (J Surg Case Rep 2012;2012:5)
- Cystic fluid is usually clear and thin
- Sampling should focus on areas of wall thickening / nodules, potentially submitting the entire lesion
Gross images
Contributed by Justin Smith, M.H.S., PA (ASCP)

Multiloculated cyst
Images hosted on other servers:

Right hepatectomy specimen

Cystic lesion

Thin walled cystic mass
Microscopic (histologic) description
- Multiloculated cysts lined by columnar, cuboidal or flattened biliary type, or mucinous epithelial cells overlying ovarian type stroma (Am J Surg Pathol 2018;42:95)
- Ovarian type stroma consists of densely packed, spindle shaped to oval cells that may be focally luteinized
- Should be sampled extensively to rule out high grade dysplasia (frequent mitotic figures, nuclear pleomorphism, complex tubulopapillary projections, etc.) and invasive carcinoma (usually ductal adenocarcinoma)
- Epithelium of larger lesions can become traumatized, showing ulceration, inflammation with xanthogranulomatous reaction, extravasation of cyst fluid into the wall / stroma or scarring and calcifications
Microscopic (histologic) images
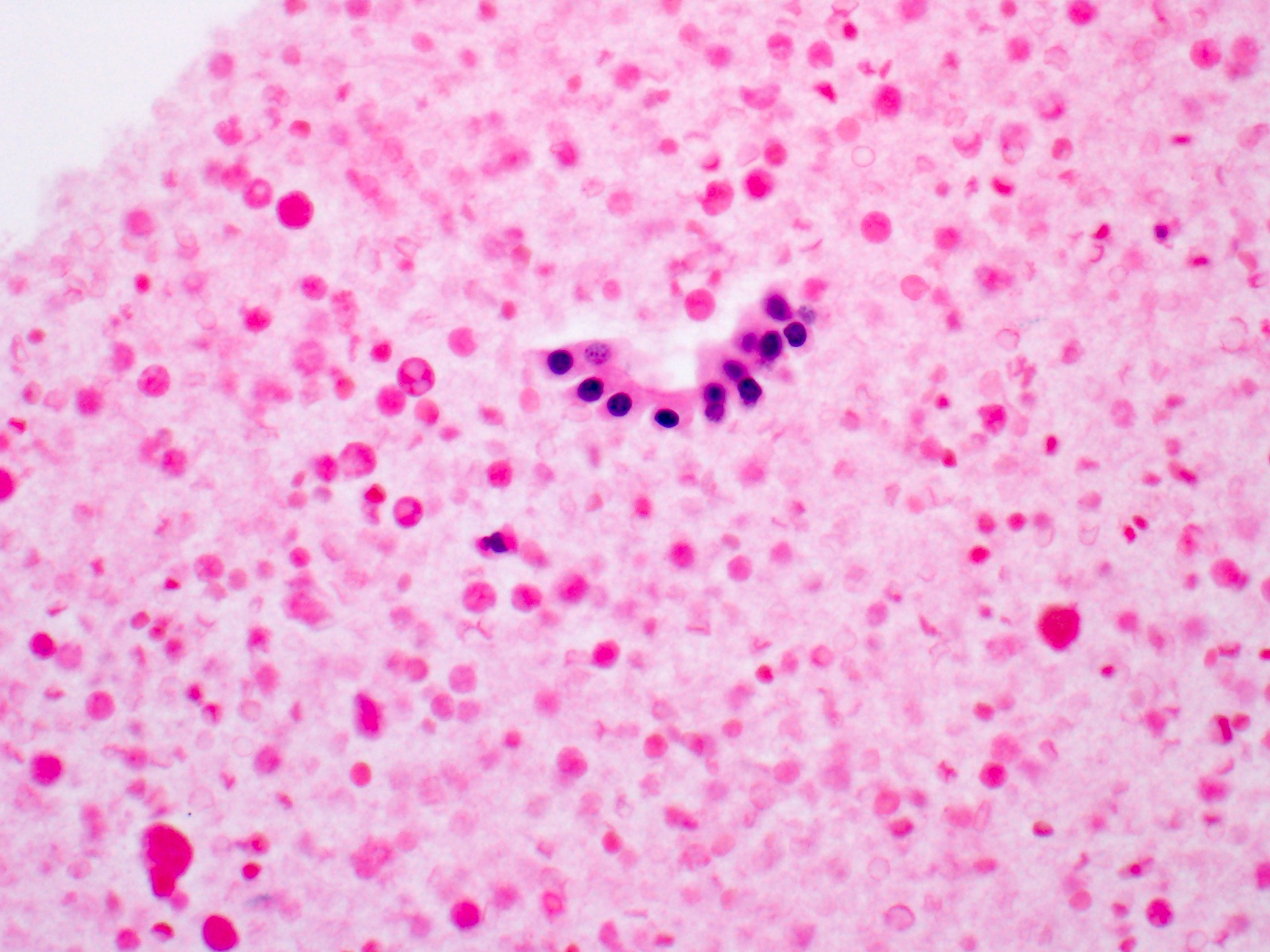
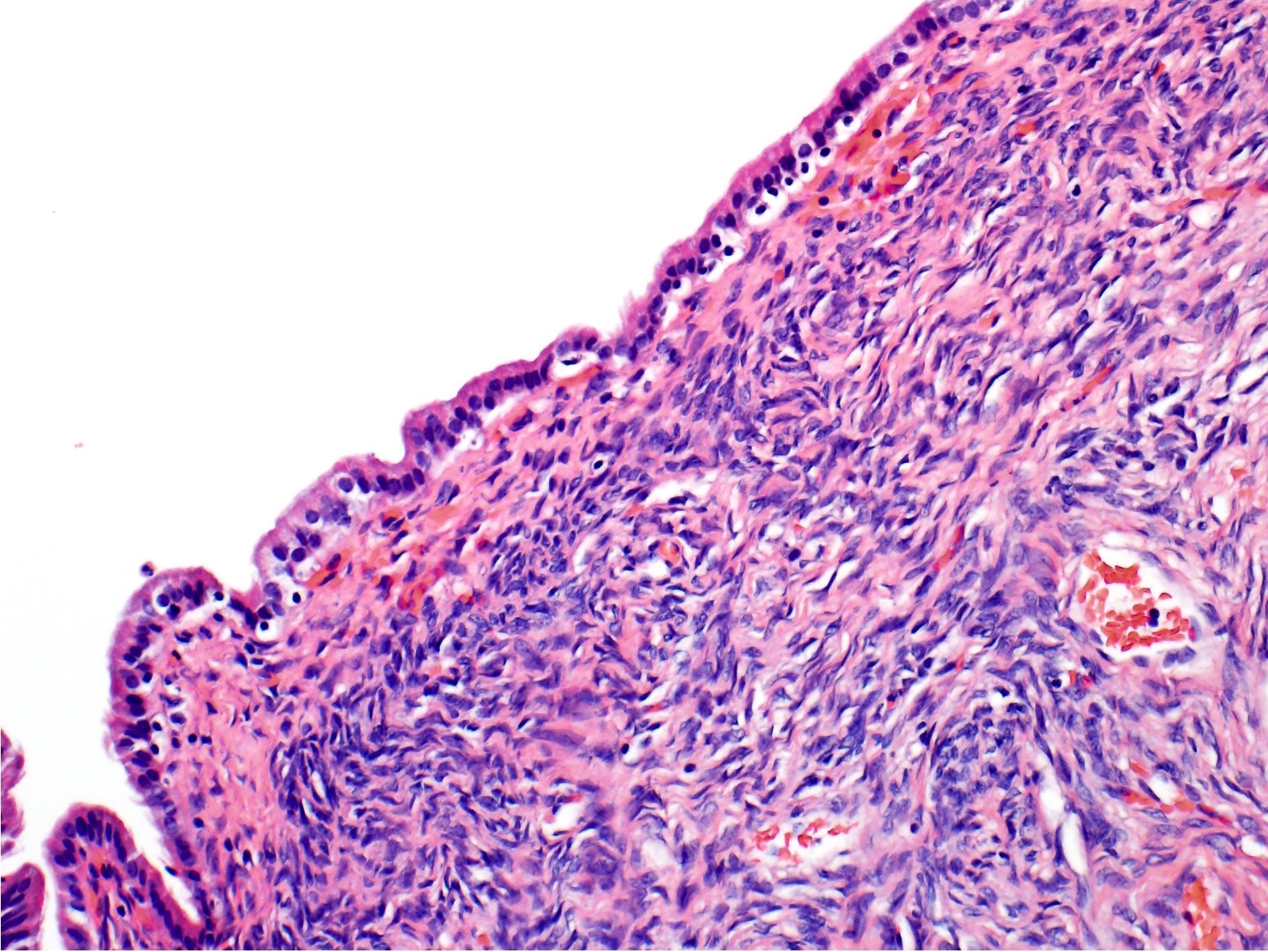
Contributed by Kimberley J. Evason, M.D., Ph.D.
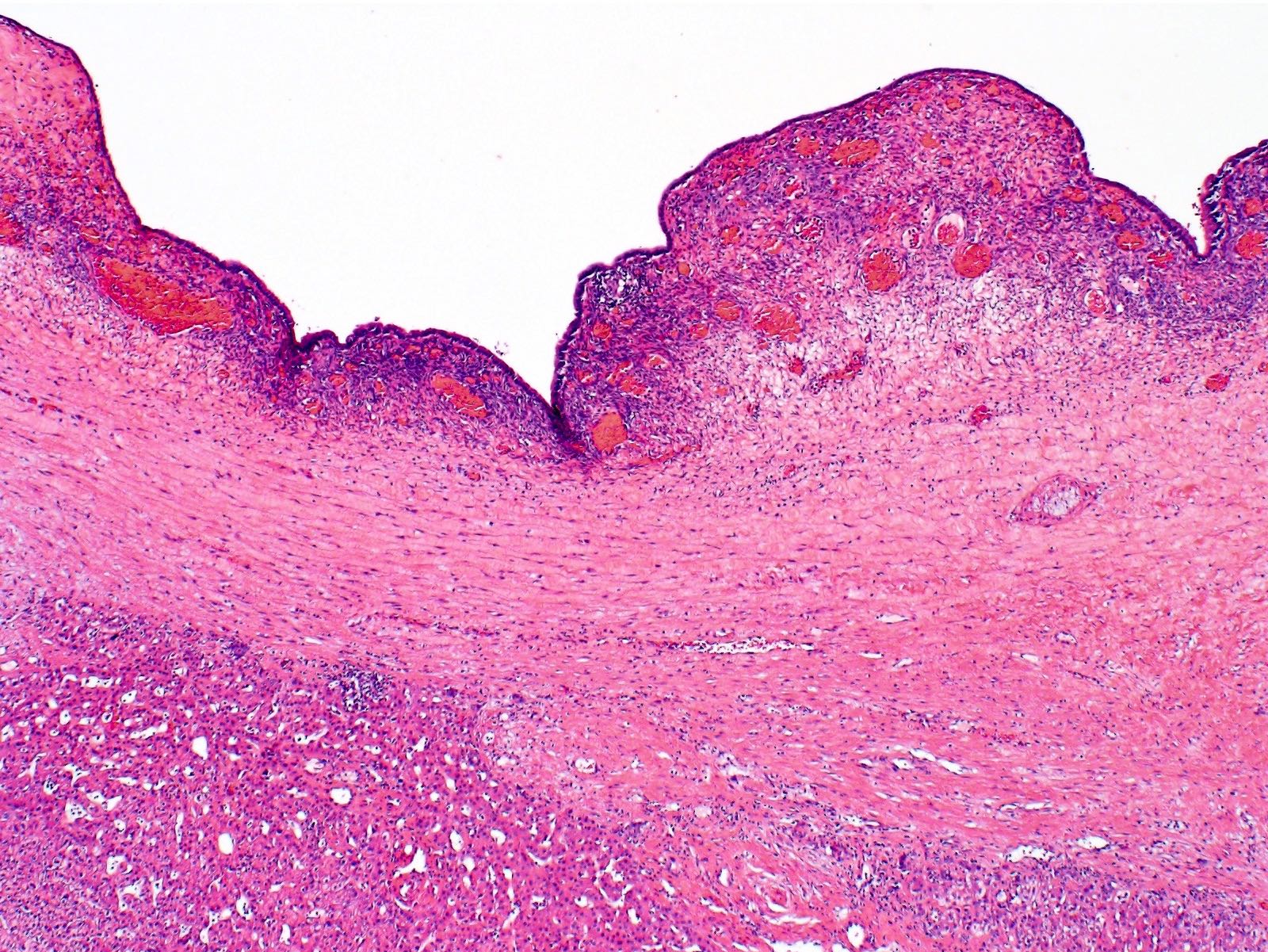
Cystic lesion
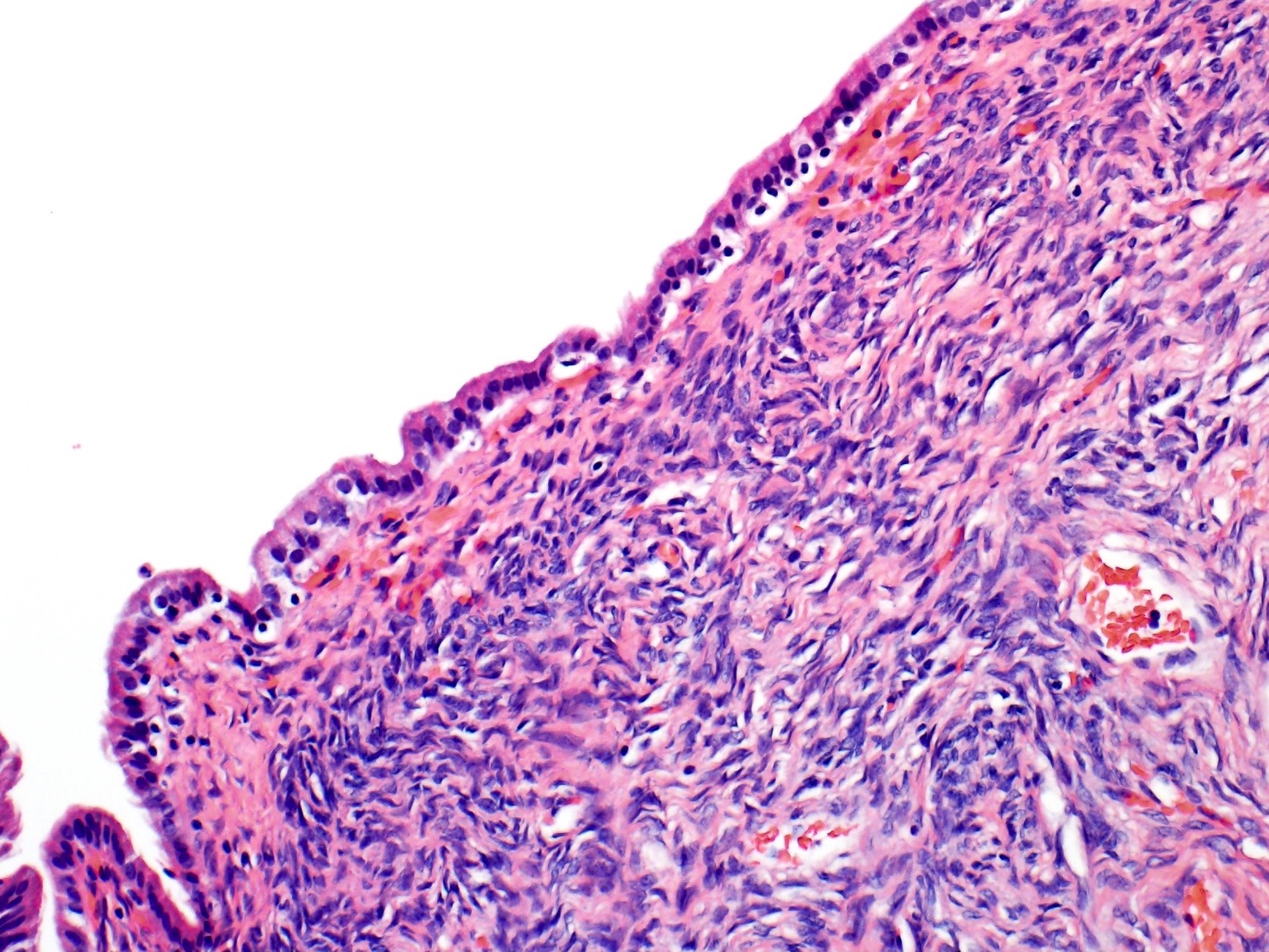
Ovarian stroma
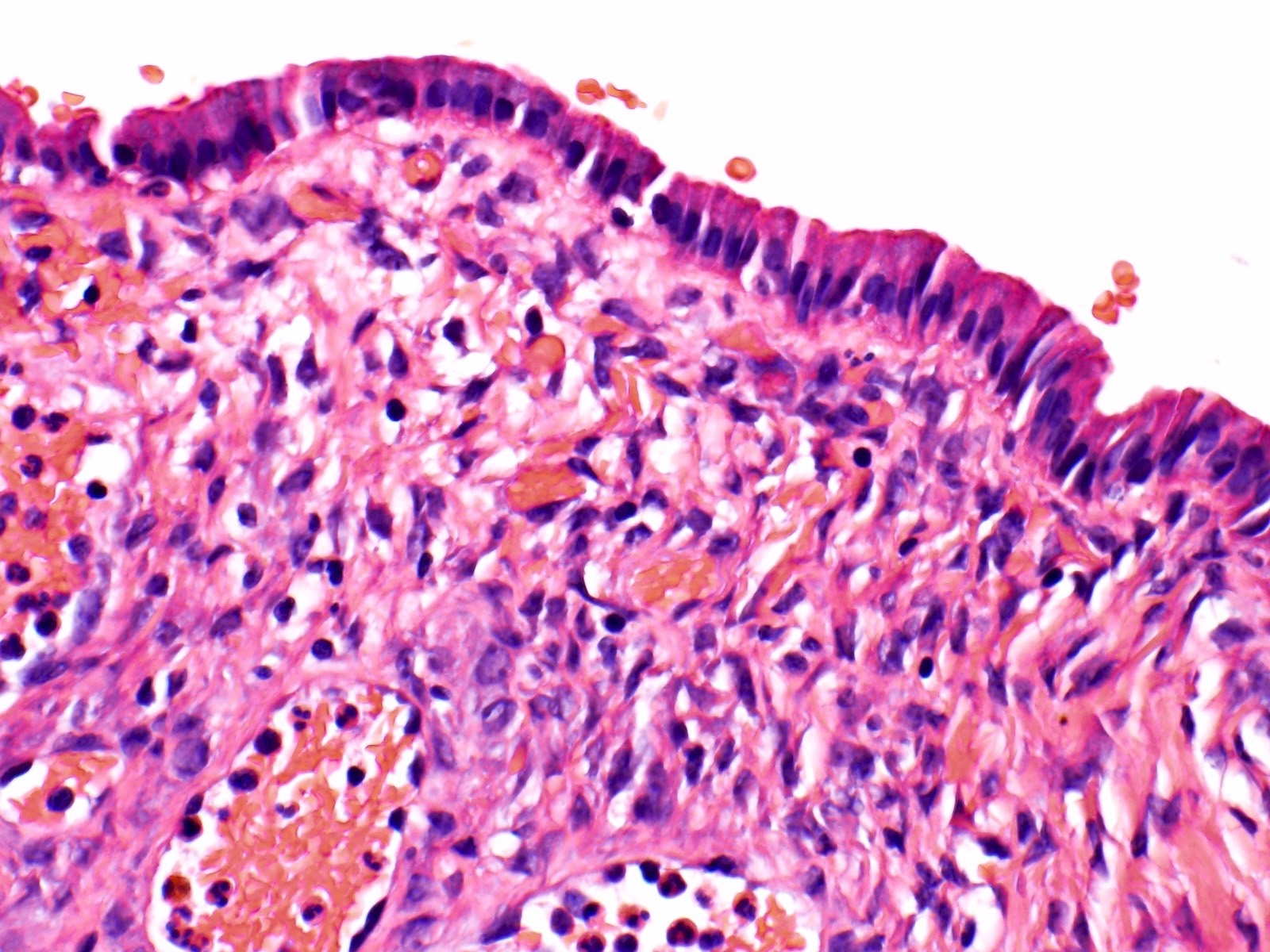
Columnar epithelium
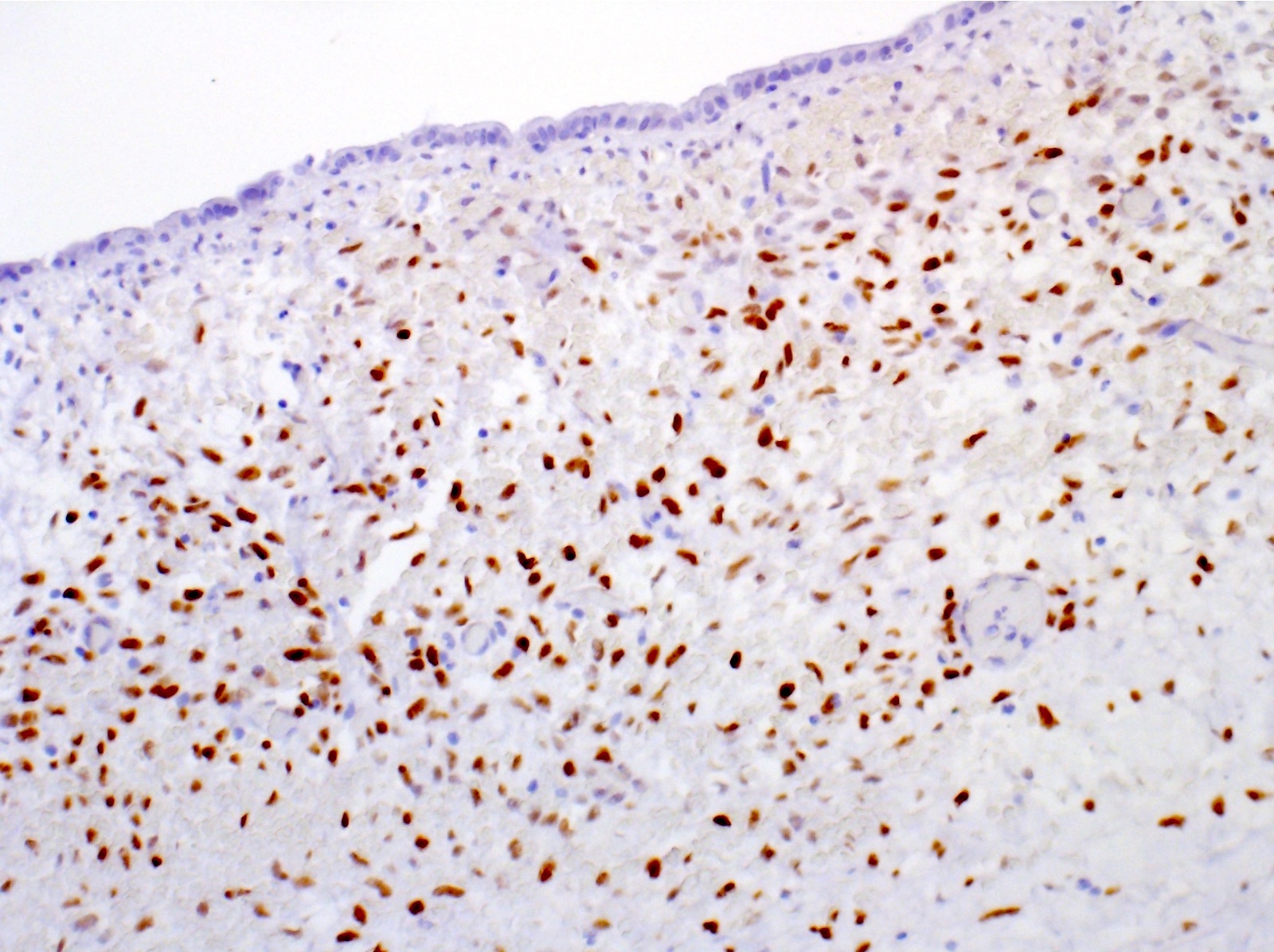
ER / PR
Cytology description
- Few groups of bland, degenerated, columnar or cuboidal epithelial cells (Cancer 2002;96:37)
- Inflammatory background (neutrophils, lymphocytes, macrophages) (Cancer 2002;96:37)
- Stromal components (including ovarian type stroma) are usually absent
- Cyst fluid can be assayed for carcinoembryonic antigen and CA19-9 to help distinguish mucinous neoplasms from nonneoplastic lesions
Cytology images
Contributed by Kimberley J. Evason, M.D., Ph.D.
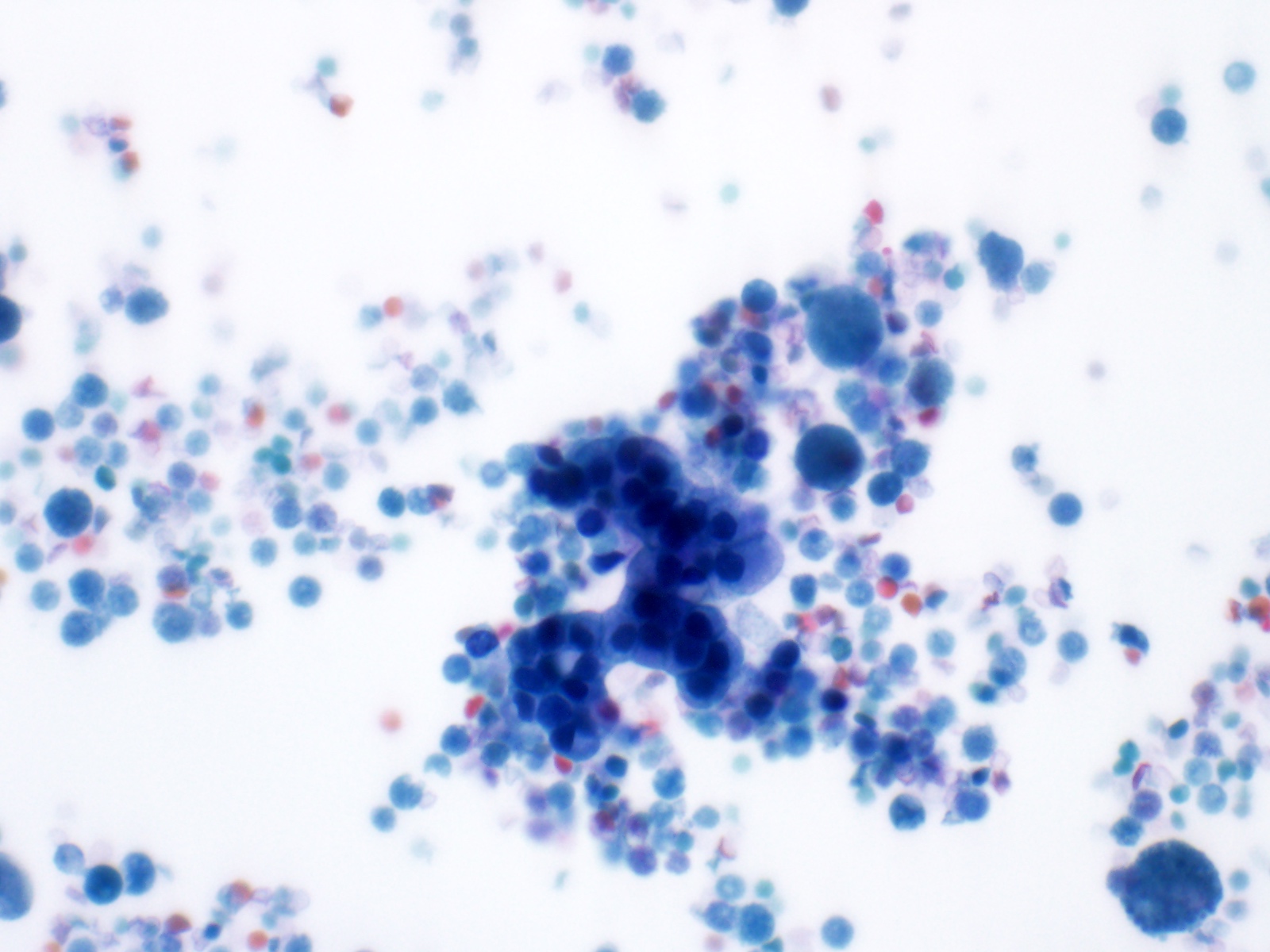
Pap stain of cyst fluid
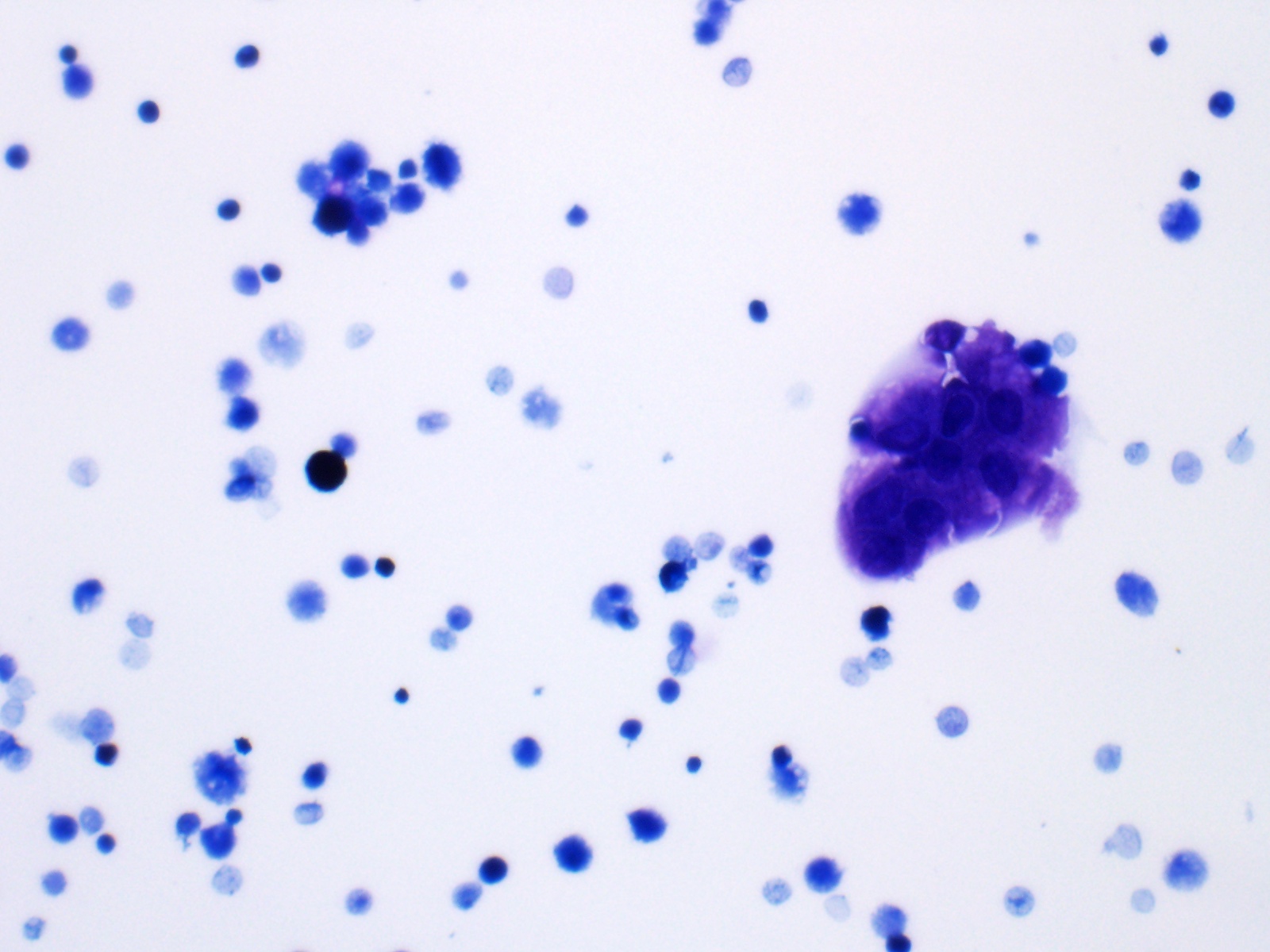
Diff-Quik stain of cyst fluid
Cell block
Positive stains
- Ovarian stroma: ER, PR and inhibin A (Hum Pathol 2014;45:761)
- Epithelium: CK7, CK19, CK8 and CK18 (biliary type) or mucicarmine (mucinous areas)
Sample pathology report
- Liver, left lobe, lobectomy:
- Mucinous cystic neoplasm
- No high grade dysplasia or invasive carcinoma present
Differential diagnosis
- Endometriosis (Hum Pathol 2014;45:761):
- Also may have cystically dilated spaces lined by columnar to cuboidal epithelium and surrounded by spindled cellular stroma
- ER+ in both epithelium and stroma, whereas MCNs are ER+ only in stroma
- Typically has stromal iron laden macrophages and CD10 positivity, whereas the stroma in MCNs is CD10-, inhibin+ and often more cellular
- Intraductal papillary neoplasm (IPN):
- Has dilated bile ducts that may resemble cystic space(s) of MCN
- May be lined by biliary type epithelium, like MCN
- Typically communicates with bile duct, unlike MCN
- Lacks ovarian type stroma
- Simple cyst, simple hepatic cyst, simple biliary cyst, bile duct cyst:
- Lined by biliary type epithelium, like MCN
- Lacks ovarian type stroma
Additional references
Board review style question #1
Which of the following is true about the liver lesion shown above?
- It usually communicates with intrahepatic bile ducts
- The epithelium is usually CK20+
- The stroma is usually ER / PR-
- There is a strong female predominance
- These lesions are most commonly multifocal
Board review style answer #1
D. There is a strong female predominance (this is a mucinous cystic neoplasm)
Comment Here
Reference: Mucinous cystic neoplasm
Comment Here
Reference: Mucinous cystic neoplasm
Board review style question #2
Which of the following describes the conditions under which mucinous cystic neoplasms of the liver most often occur?
- After the sixth decade of life without sex predominance
- In association with invasive carcinoma
- In males before the third decade of life
- Multifocally and associated with bile ducts
- With abdominal pain as the most common presenting symptom
Board review style answer #2
E. With abdominal pain as the most common presenting symptom
Comment Here
Reference: Mucinous cystic neoplasm
Comment Here
Reference: Mucinous cystic neoplasm
