
Liver & intrahepatic bile ducts
Dysplasia
Low grade dysplastic nodule
Last author update: 25 January 2021
Last staff update: 26 January 2021
Copyright: 2004-2024, PathologyOutlines.com, Inc.
PubMed search: Low grade "dysplastic nodule" liver


Table of Contents
Definition / general | Essential features | Terminology | Clinical features | Radiology description | Treatment | Gross description | Microscopic (histologic) description | Microscopic (histologic) images | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1Cite this page: Assarzadegan N, Gonzalez RS. Low grade dysplastic nodule. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/livertumorlowgradedysplasticnod.html. Accessed April 19th, 2024.
Definition / general
- Discrete nodules in cirrhotic livers containing mild architectural changes
Essential features
- Dysplastic nodules (both low grade and high grade) are associated with higher risk of development of hepatocellular carcinoma
- Low grade dysplastic nodules have a significantly lower risk to transform into carcinoma than high grade nodules (J Hepatol 2003;39:208)
Terminology
- Also called macroregenerative nodule type I, adenomatous hyperplasia, hepatocellular pseudotumor
Clinical features
- Usually ages 40 and older; 67% arise in males
- May progress to hepatocellular carcinoma but usually stabilize or disappear over time instead
Radiology description
- Usually isovascular or hypovascular compared to surrounding parenchyma, whereas hepatocellular carcinoma appears hypervascular
Treatment
- Follow by imaging
Gross description
- Often distinct nodules (can be vague), separated from the surrounding liver by a rim of thin fibrous scar (not a true capsule)
- Usually multiple, 0.5 to 1.5 cm, occasionally up to 5 cm
- Similar in color and texture to surrounding liver; may be pale or bile stained
- Usually found in cirrhotic livers, rarely in acute liver injury or precirrhotic livers
Microscopic (histologic) description
- Monotonous cell population lacking architectural atypia, with mild increase in cellularity compared to surrounding cirrhotic liver (Hepatology 2009;49:658, Dig Liver Dis 2011;43:S361)
- Portal tracts can be identified within the nodules
- Liver cell plates 1 - 2 cells thick (highlighted on reticulin stain)
- Features of hepatocellular carcinoma (pseudoglands or markedly thickened trabeculae) absent
- May have large cell changes in hepatocytes
- Unpaired arteries, which have no accompanying bile ducts, can be prominent in number and size (unlike cirrhotic nodules)
- May have diffuse iron or copper retention (Arch Pathol Lab Med 2011;135:704)
Microscopic (histologic) images
Contributed by Naziheh Assarzadegan, M.D.
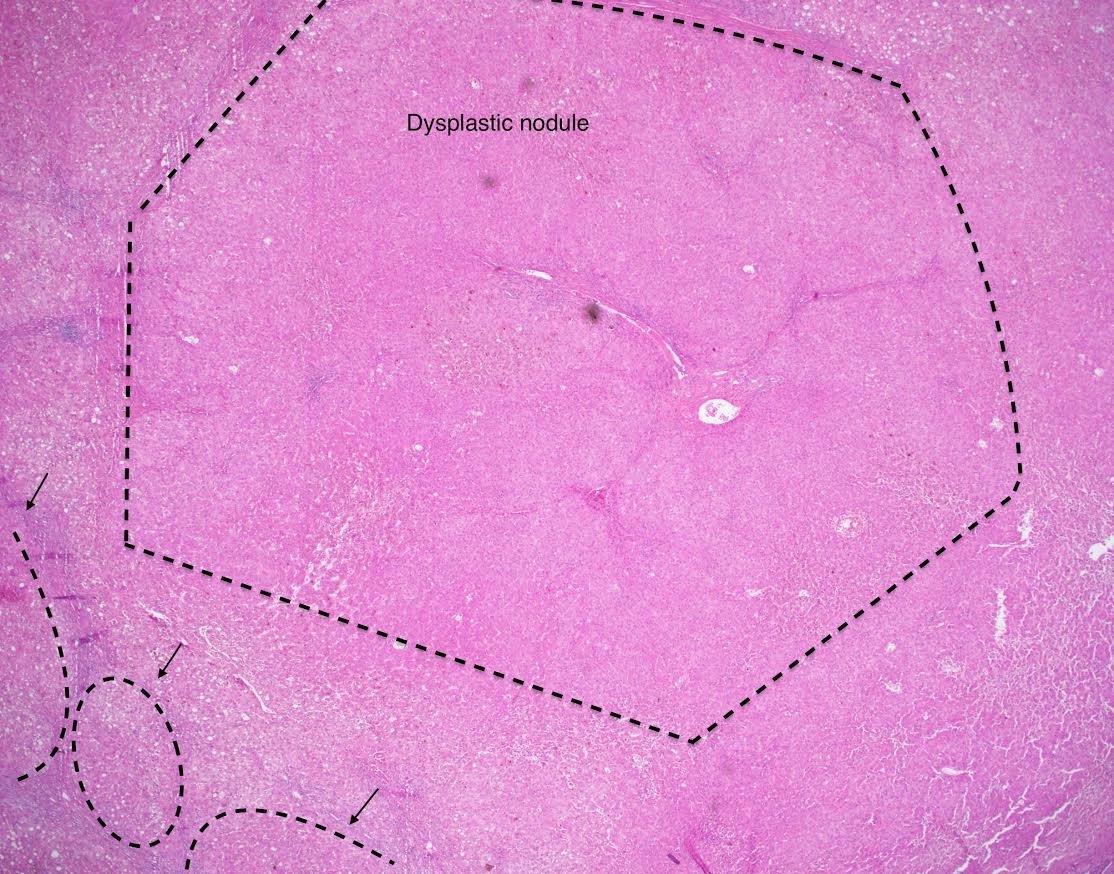
Mild increase in
cellularity compared
to surrounding
cirrhotic liver
Images hosted on other servers:


Low grade dysplastic nodules
Molecular / cytogenetics description
- May be clonal
- Inactivation of p21 checkpoint in contrast to cirrhotic nodules, which show activation
Sample pathology report
- Liver, native, orthotopic transplantation:
- Cirrhosis with mild chronic inflammation and three low grade dysplastic nodules (see comment)
- Negative for high grade dysplasia or malignancy.
- Margins of resection unremarkable.
- Comment: The findings are consistent with the patient’s reported history of chronic hepatitis C infection. A trichrome stain confirms cirrhosis. An iron stain is unremarkable.
Differential diagnosis
- High grade dysplastic nodule:
- Increased hepatocyte density with moderate cytologic or architectural atypia
- Macroregenerative nodule:
- Similar malignant potential
- Distinction by morphology alone can be difficult
- Distinguishing molecular findings include overexpression of semaphorin E, IGFBP3 and caveolin 1 and increased expression of collagen IV
- References: Lab Invest 2002;82:547, Am J Pathol 2003;162:991
Board review style question #1
Which of the following is true about low grade dysplastic nodules in the liver?
- If unresected, they will always progress to hepatocellular carcinoma
- They are grossly distinct from background cirrhotic nodules
- They are hypervascular radiologically
- They have prominent architectural atypia histologically
Board review style answer #1
B. They are grossly distinct from background cirrhotic nodules
Comment Here
Reference: Low grade dysplastic nodule
Comment Here
Reference: Low grade dysplastic nodule
