

Lung
Infectious
Viral
Influenza
Author: Elliot Weisenberg, M.D.

Last author update: 1 September 2011
Last staff update: 9 August 2022
Copyright: 2003-2024, PathologyOutlines.com, Inc.
PubMed search: influenza pneumonia [title]

Table of Contents
Epidemiology | Case reports | Clinical features | Microscopic (histologic) images | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Weisenberg E. Influenza. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/lungnontumorinfluenza.html. Accessed April 19th, 2024.
Epidemiology
- Most common cause of viral pneumonia
- RNA virus, nucleoprotein determines type of virus: A, B or C (Virol J 2009 Mar 13;6:30)
- Envelope contains the viral hemagglutinin and neuraminidase that establish the viral subtype, e.g., H1N1 (Wikipedia)
- Preexisting antibodies to specific hemagglutinins and neuraminidases prevent or amerliorate future infections
- Type A: causes most severe disease; major cause of epidemics and pandemics; also infects pigs, horses, birds; one subtype predominates at any given time
- Antigenic drift leading to epidemics is caused by small mutations in hemagglutinins and neuraminidases, which allow the virus to evade most host antibodies
- Antigenic shift leads to pandemics, and is caused by recombination of hemagglutinin and neuraminidase RNA with animal influenza RNA, leading to absence of human immunity
- Antigenic drift and shift do NOT occur with influenza types B and C, which usually cause mild, self limited illness in children
- References: World Health Organization Influenza update
Case reports
- 43 year old man in India with with fever for 3 days and sudden onset of shortness of breath (Case of the Week #459)
Clinical features
- Cause mild acute lung injury to necrotizing pneumonia to BOOP-like changes
- May cause bronchiolitis or diffuse alveolar damage
- Viral cytopathic changes do NOT occur
- Airways show mucosal hyperemia with infiltrate of lymphocytes, histiocytes, plasma cells
- Swelling and increased mucus production impair bronchociliary elevator, and may lead to secondary bacterial infection; small airways may become occluded causing focal atelectasis; in severe disease, this is more widespread with distal airways plugged by fibrinopurulent debris
- If process is prolonged, obliterative bronchiolitis with irreversible lung damage may occur
- Histologic findings are nonspecific; the diagnosis can be confirmed with molecular testing, viral culture, DFA, IHC, serology, antigen detection assays
Microscopic (histologic) images
Contributed by Dr. K.V. Vinu Balraam
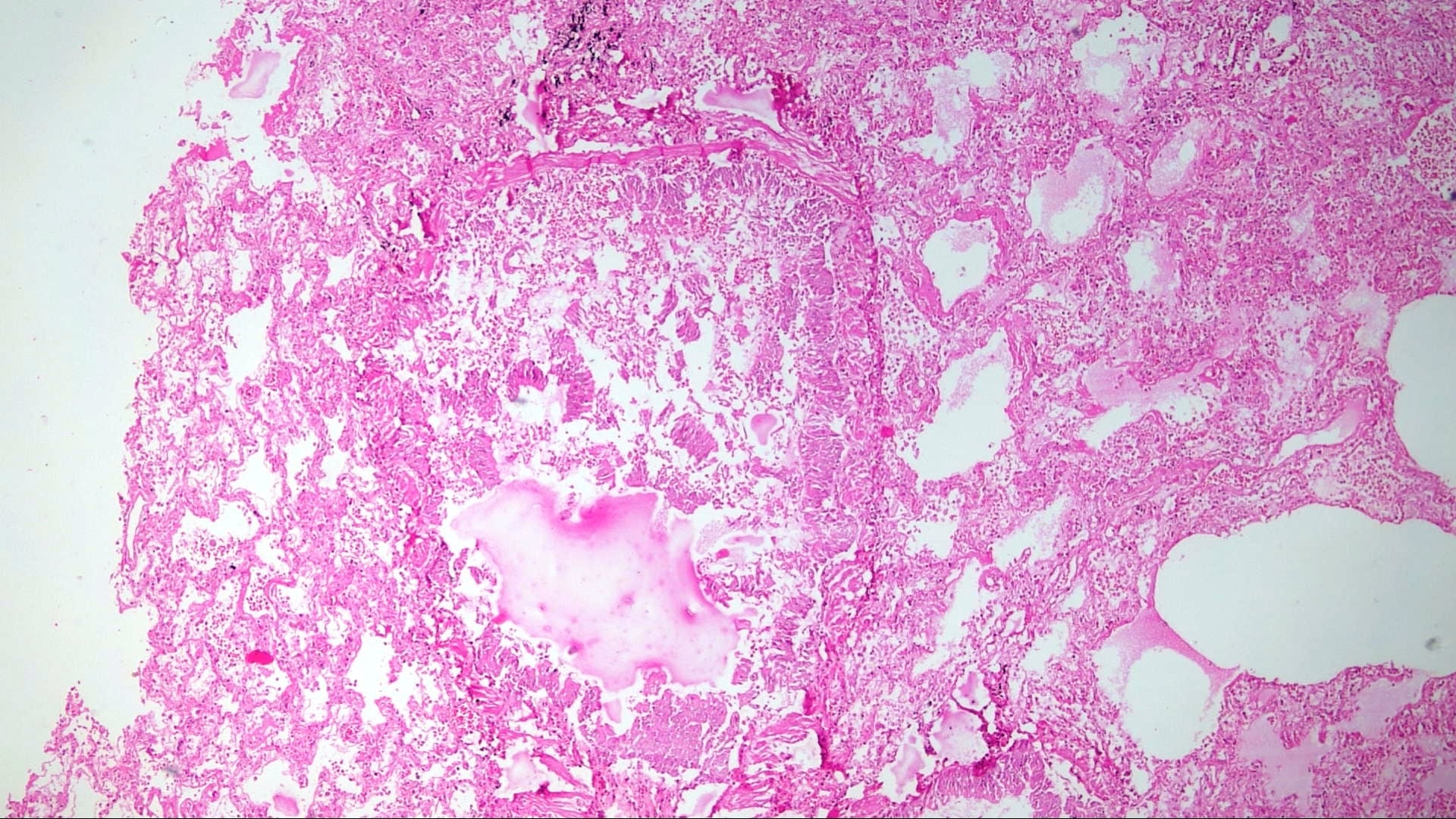
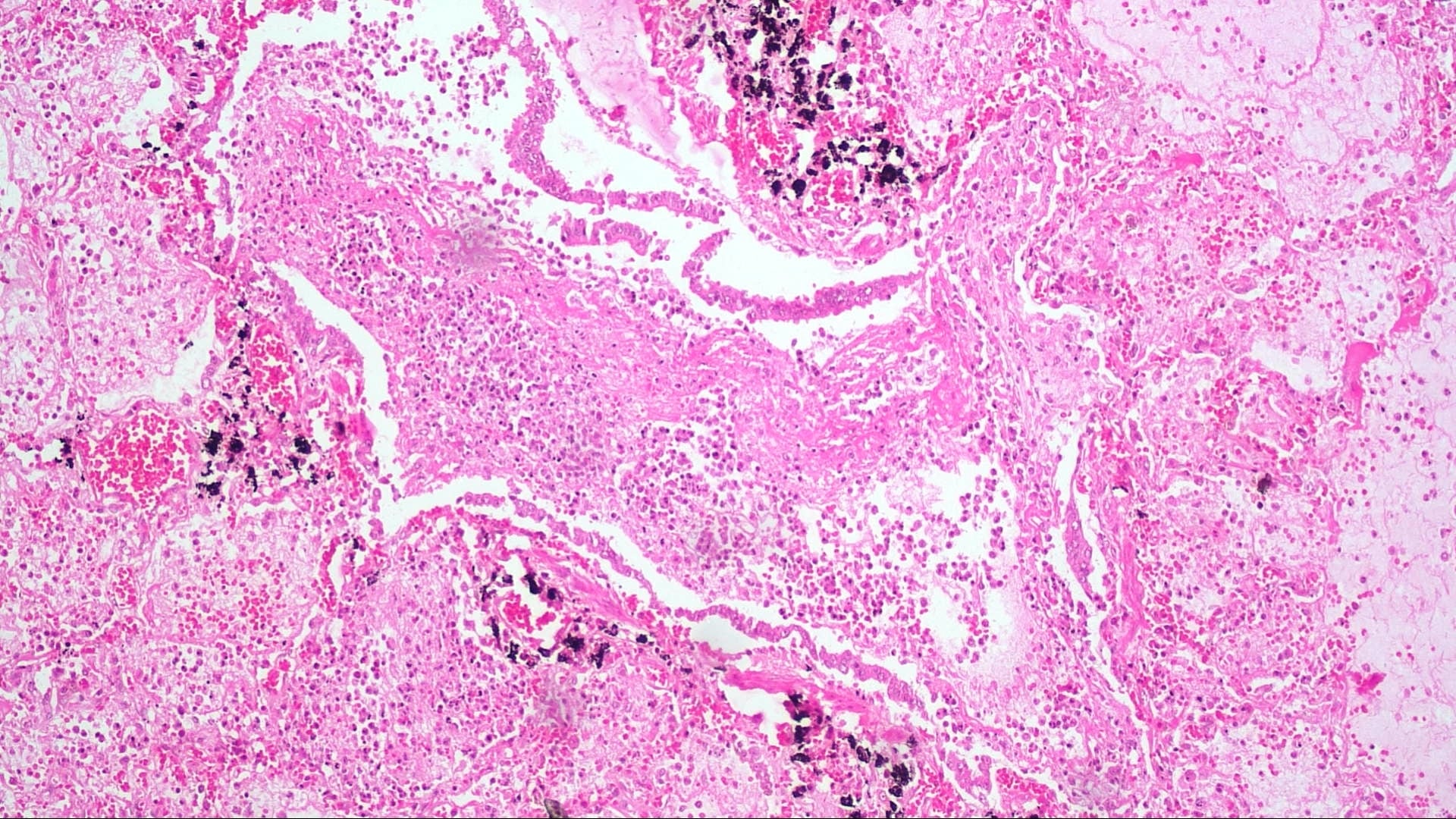
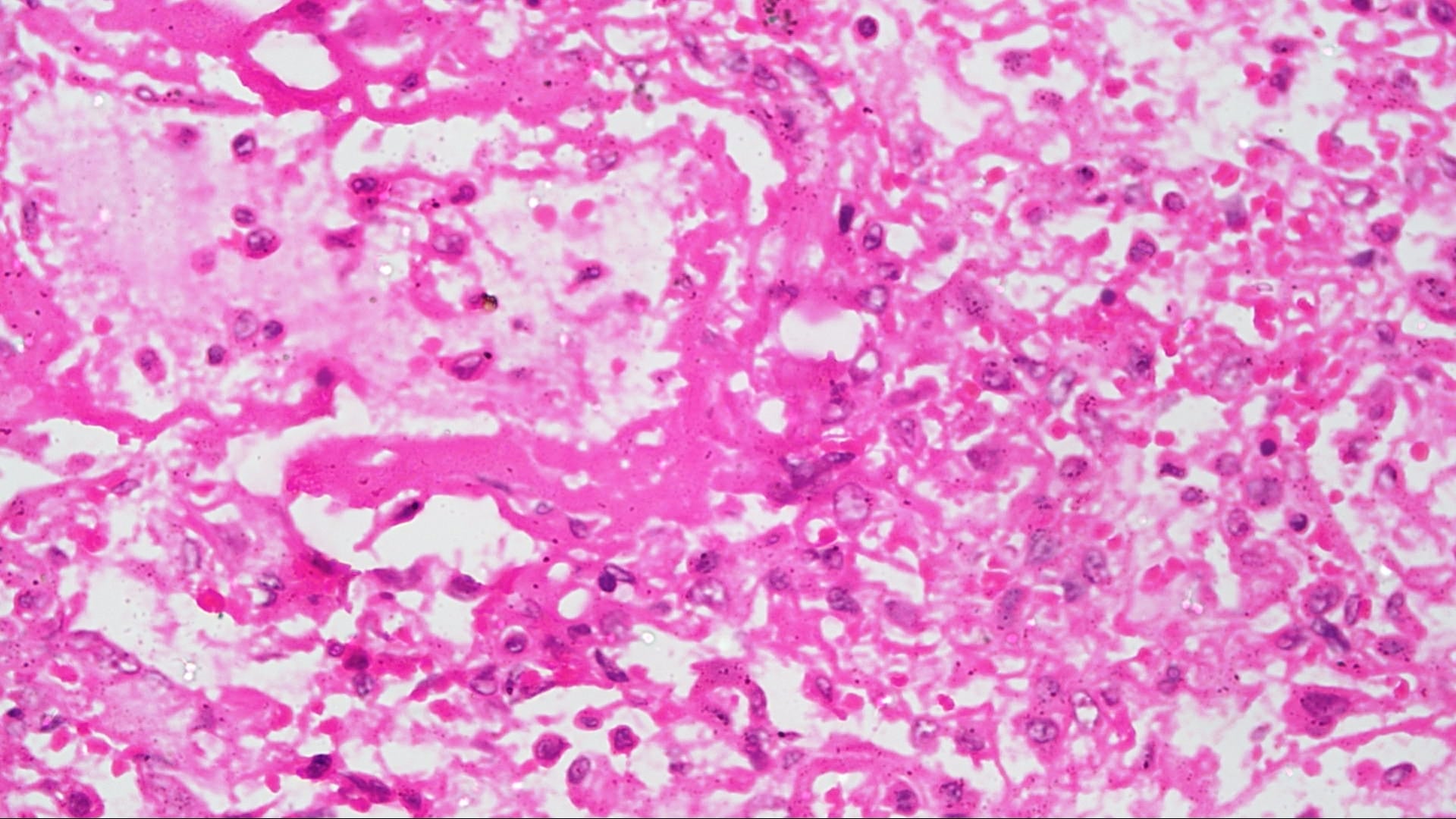
Lung
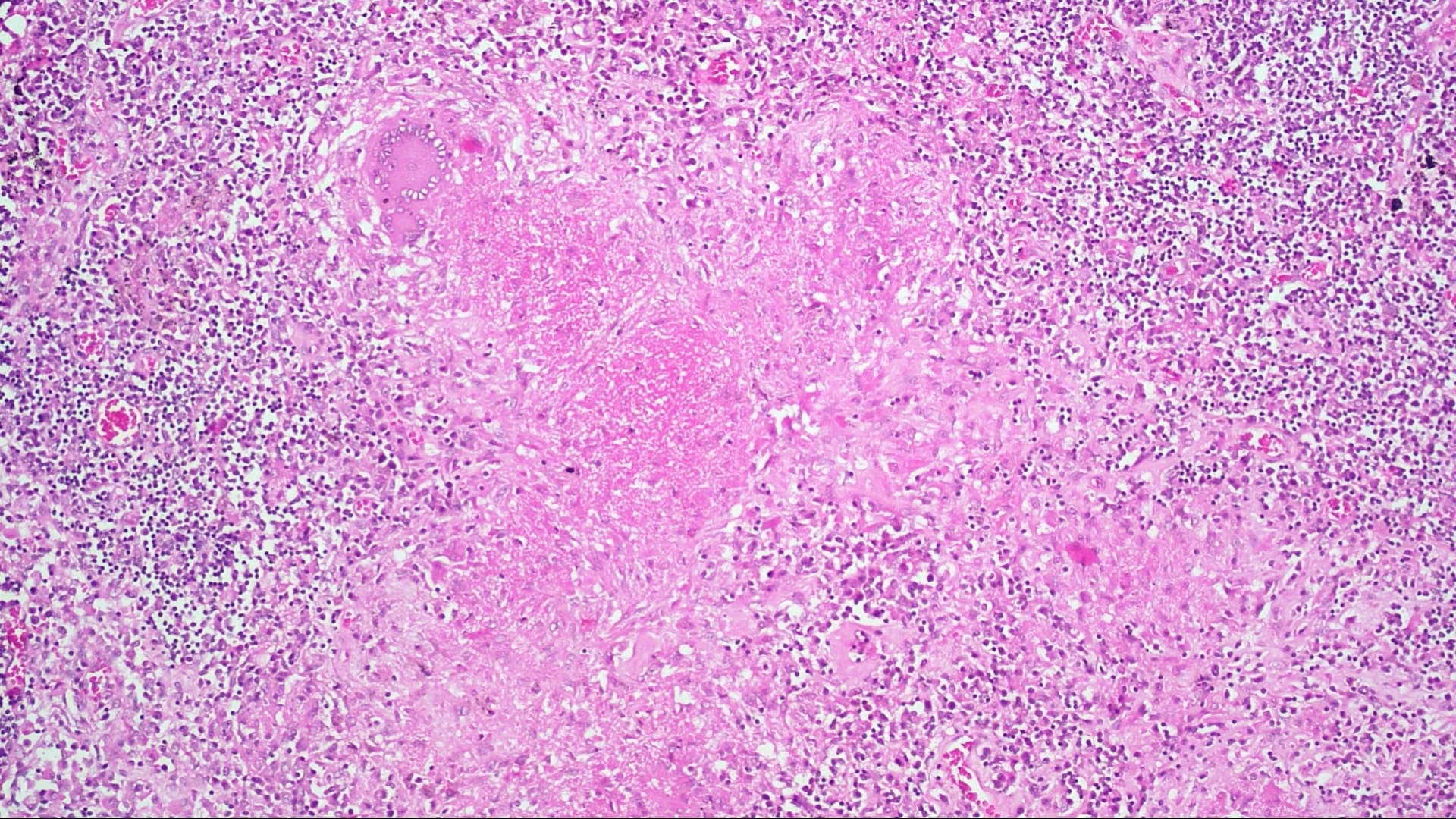
Pulmonary lymph node
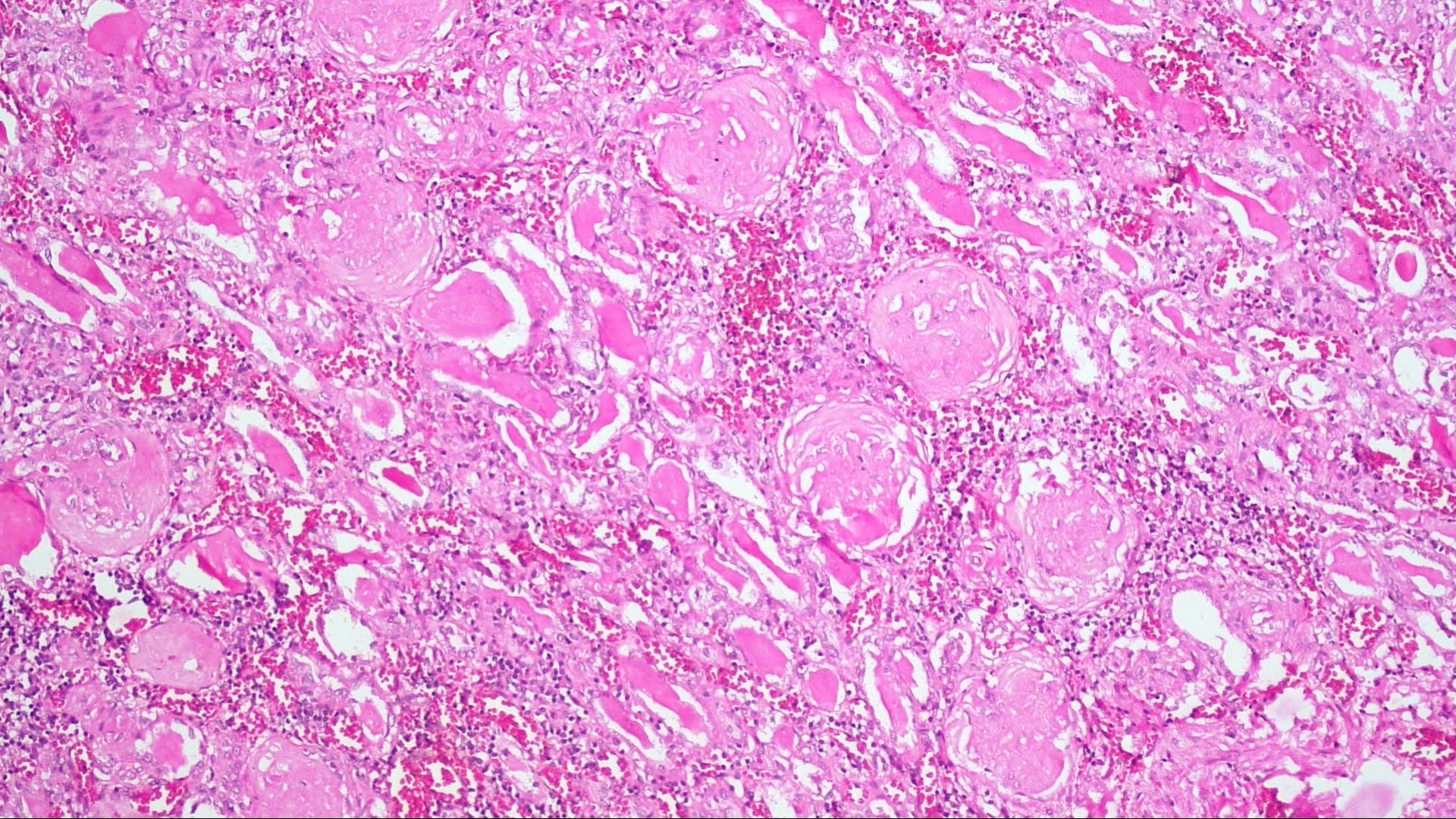
Kidney
Board review style question #1
Which histological feature is highly specific to influenza A/H1N1 infection in diffuse alveolar damage?
- Neutrophilic aggregation
- Organizing pneumonia
- Alveolar hemorrhage
- All of the above
- None of the above
Board review style answer #1
E. No histological finding specific to influenza infection has been identified. The findings in A, B and C are quite common in diffuse alveolar damage of any etiology.
Comment Here
Reference: Influenza
Comment Here
Reference: Influenza
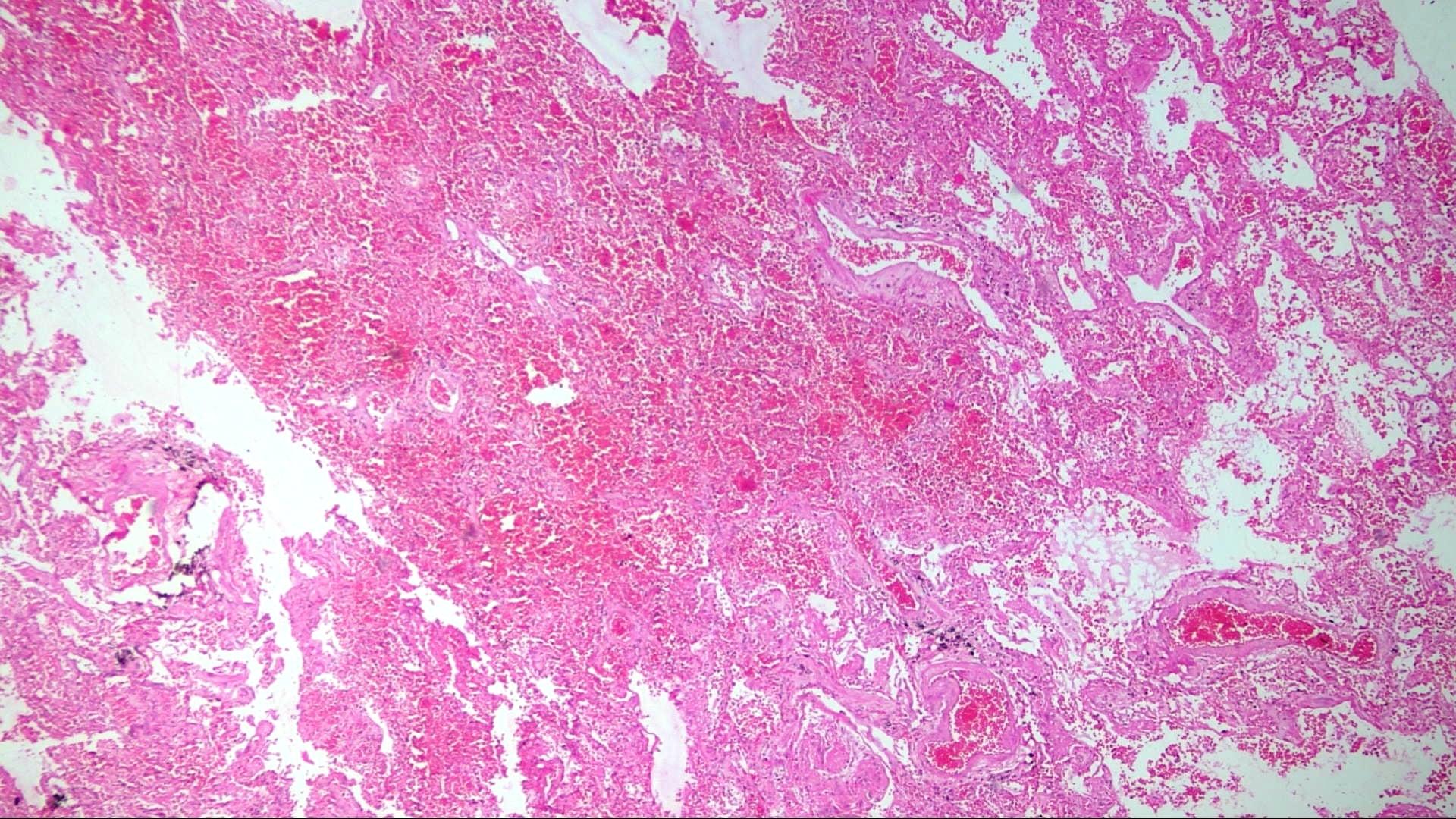
Board review style question #2
This image is from an autopsy of a 43 year old man with influenza A/H1N1 infection. Which histological feature is highly specific to this disease?
- Neutrophilic aggregation
- Organizing pneumonia
- Alveolar hemorrhage
- None of the above
Board review style answer #2
