

Lung
Mesenchymal tumors
Pulmonary hamartoma
Last staff update: 29 September 2022 (update in progress)
Copyright: 2002-2024, PathologyOutlines.com, Inc.
PubMed Search: Pulmonary hamartoma[TI] free full text[SB]



Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Clinical images | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Cytology images | Positive stains | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style answer #2 | Board review style answer #2Cite this page: Li HH, Schulte JJ. Pulmonary hamartoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/lungtumorhamartoma.html. Accessed April 24th, 2024.
Definition / general
- Benign neoplasm composed of varying amounts of mesenchymal elements (cartilage, fat, connective tissue, smooth muscle) with entrapped respiratory epithelium
- At least 2 mesenchymal elements should be present for diagnosis
Essential features
- Most common benign pulmonary neoplasm, often incidentally found
- Benign neoplasm composed of varying amounts of at least 2 mesenchymal elements combined with entrapped respiratory epithelium
- Radiographic features often very characteristic
Terminology
- Other names previously used in the literature (chondroid hamartoma, mesenchymoma, chondromatous hamartoma, hamartochondroma) are no longer recommended
ICD coding
- ICD-O: 8992/0 - pulmonary hamartoma
- ICD-11: 2F00.Y & XH3UD9 - other specified benign neoplasm of middle ear or respiratory system & pulmonary hamartoma
Epidemiology
- M > F
- Peak in the sixth decade
- Rare in children
- References: Thorax 1987;42:790, StatPearls: Pulmonary Hamartoma [Accessed 5 November 2021], Mayo Clin Proc 1996;71:14
Sites
- Any lobe can be involved
- Most located in peripheral lung (Thorax 1987;42:790)
- Approximately 10% are endobronchial (Thorax 1987;42:790)
- Can present as multiple lesions, adjacent to lung cancer, as a mediastinal mass or incidentally with another neoplasm (Am J Clin Pathol 2021;155:903, Clin Lab 2021;67:1)
Pathophysiology
- Most hamartomas appear to harbor translocations, often t(3;12) (Genes Chromosomes Cancer 2000;29:363, Cancer Genet Cytogenet 2003;142:153)
- Translocation t(3;12) results in HMGA2-LPP fusion
- Fusion transcripts not universally detected in hamartomas (Cancer Genet Cytogenet 2002;138:160)
- Evidence suggests that HMGA2-LPP fusion protein may promote chondrogenesis and adipogenesis (Biochem Biophys Res Commun 2006;340:476)
Etiology
- Thought to arise from mesenchymal tissue
- Chromosomal aberrations may be a primary event in pulmonary hamartoma but unclear what other genetic events may be necessary to induce tumor development (Cancer Genet Cytogenet 2002;138:160)
Clinical features
- Often incidental finding on imaging
- Usually asymptomatic but endobronchial tumors may cause problems associated with obstruction (Cureus 2021;13:e13717, BMJ Case Rep 2020;13:e235316)
Diagnosis
- Usually incidental finding on imaging
- Biopsy can be performed when lesion lacks characteristic radiographic findings
- Bronchoscopic biopsy (core or fine needle aspiration [FNA]) can be used (see Cytology description below)
- Wedge resection can be used if nonsurgical diagnostic procedures are inconclusive
- Preoperative diagnosis may not be made as hamartoma may be incidentally discovered in a lung removed for another reason
- References: Zhongguo Fei Ai Za Zhi 2020;23:792, Ann Thorac Surg 2008;86:1769, Mayo Clin Proc 1996;71:14
Radiology description
- Small coin lesion, often solitary, characterized by smooth edge, focal fat or fat alternating with calcific foci (Ann Thorac Med 2015;10:231)
- Calcifications often described as popcorn calcification
- Intralesional fat and popcorn-like calcifications allow a confident diagnosis on CT (J Thorac Imaging 2016;31:11)
Radiology images
Contributed by Jeffrey P. Kanne, M.D.
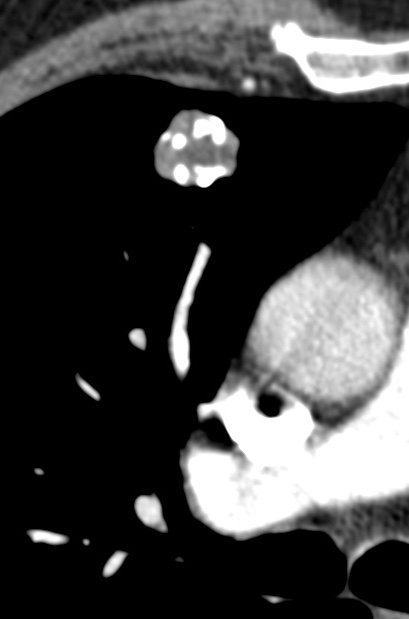
With calcifications
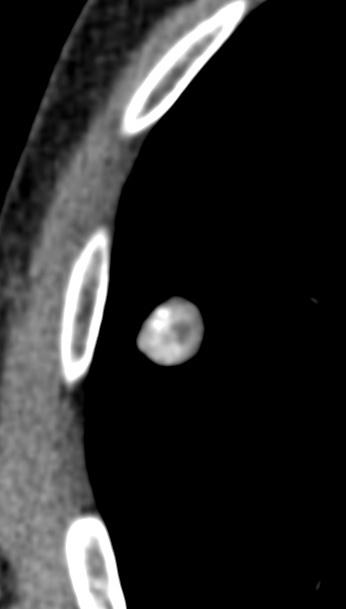
CT scan
Prognostic factors
- Slowly growing with excellent prognosis; most left alone if patient is asymptomatic
- Rapid growth, recurrence and malignant transformation are very rare (Cureus 2020;12:e12150, Thorax 1989;44:232, Case Rep Med 2013;2013:231652)
Case reports
- 30 year old man presenting with hemoptysis and cough (Rare Tumors 2019;11:2036361318823926)
- 49 year old man with recurrent hemoptysis and clinical and radiographic concern for lung cancer (Cureus 2019;11:e5489)
- 54 year old man presenting with hemoptysis and CT scan identified lung nodule (Respirol Case Rep 2020;8:e00553)
- 59 year old woman with pulmonary hamartoma presenting with unusual radiographic features (Respir Med Case Rep 2018;25:133)
- 59 year old woman with incidental hamartoma and tibial enchondroma (BMJ Case Rep 2019;12:e229670)
Treatment
- Surveillance for biopsy proven asymptomatic pulmonary hamartoma
- Surgical resection is the optimal and curative treatment for endobronchial lesions and symptomatic tumors
- Enucleation and wedge resections are the most common surgical choice
- References: Interact Cardiovasc Thorac Surg 2015;21:773, Chin Med Sci J 1998;13:61
Clinical images
Images hosted on other servers:

Bronchoscopy

Large endobronchial mass
Gross description
- Pale, firm, round to multilobulated, well circumscribed nodule (most are < 4 cm in diameter)
- Endobronchial hamartoma manifests as yellow to gray sessile polyps of large airways
- References: Mayo Clin Proc 1996;71:14, Thorax 1987;42:790
Gross images
Contributed by @Andrew_Fltv on Twitter
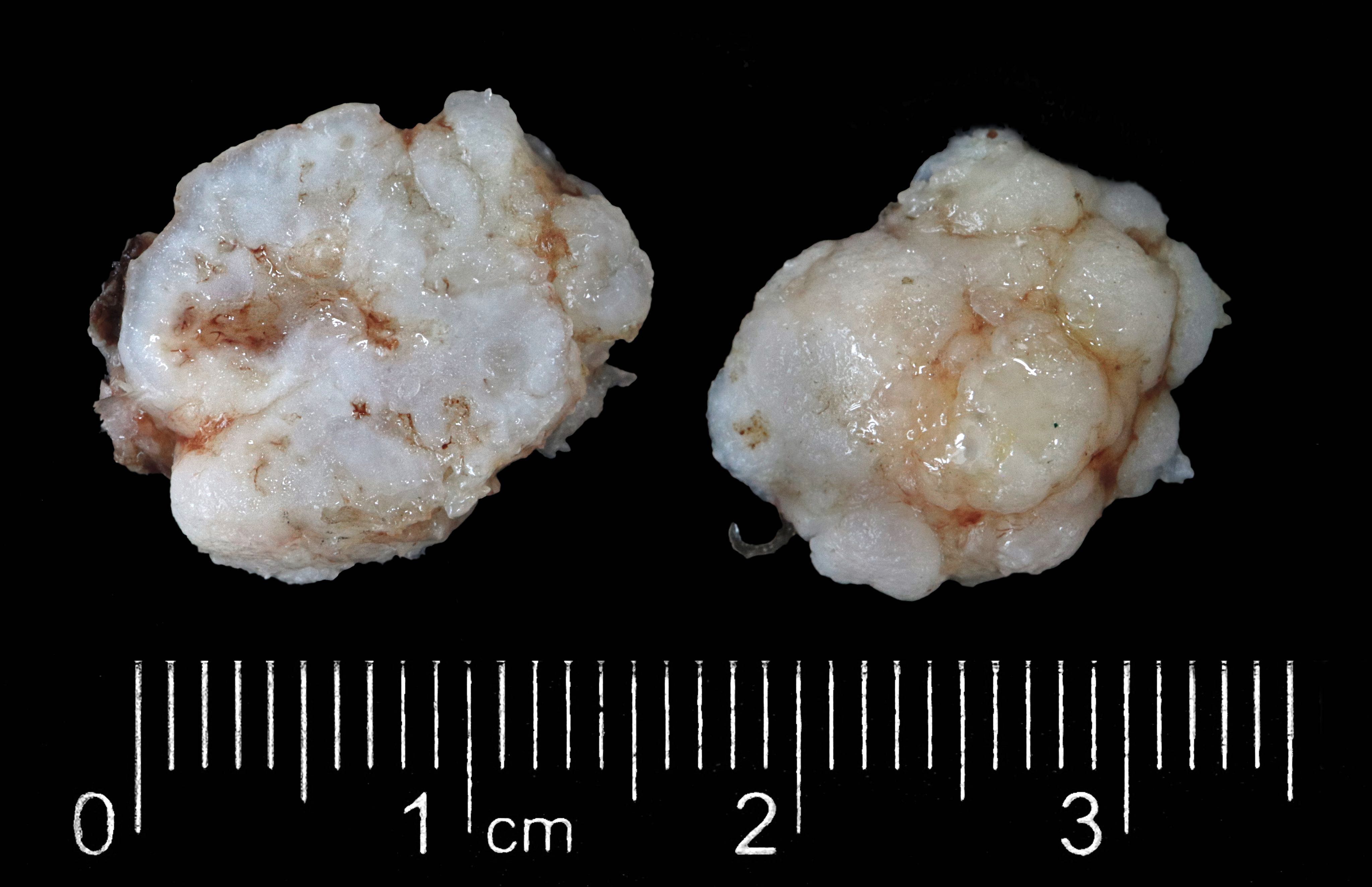


Pulmonary hamartoma
Images hosted on other servers:

Pneumonectomy specimen

Firm and discrete lesions

Resected endobronchial tumor
Microscopic (histologic) description
- Composed predominantly of varying degrees of mesenchymal tissue: hyaline cartilage, fat, smooth muscle and bone
- Other connective tissue elements may be present, represented by bland spindle cells, fibrous tissue or myxoid change
- Variably conspicuous, entrapped benign epithelial cells
- Reference: Thorax 1987;42:790
Microscopic (histologic) images
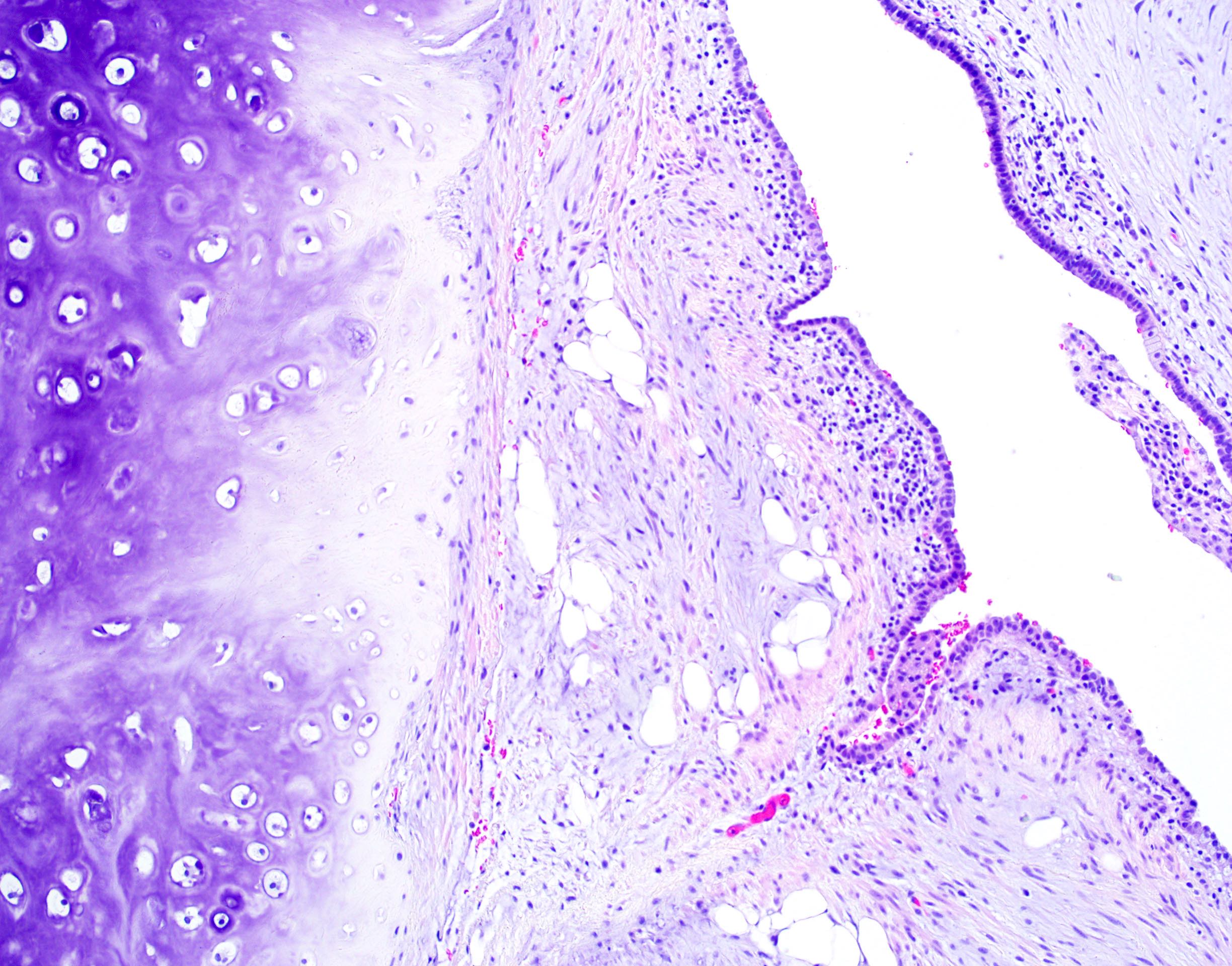
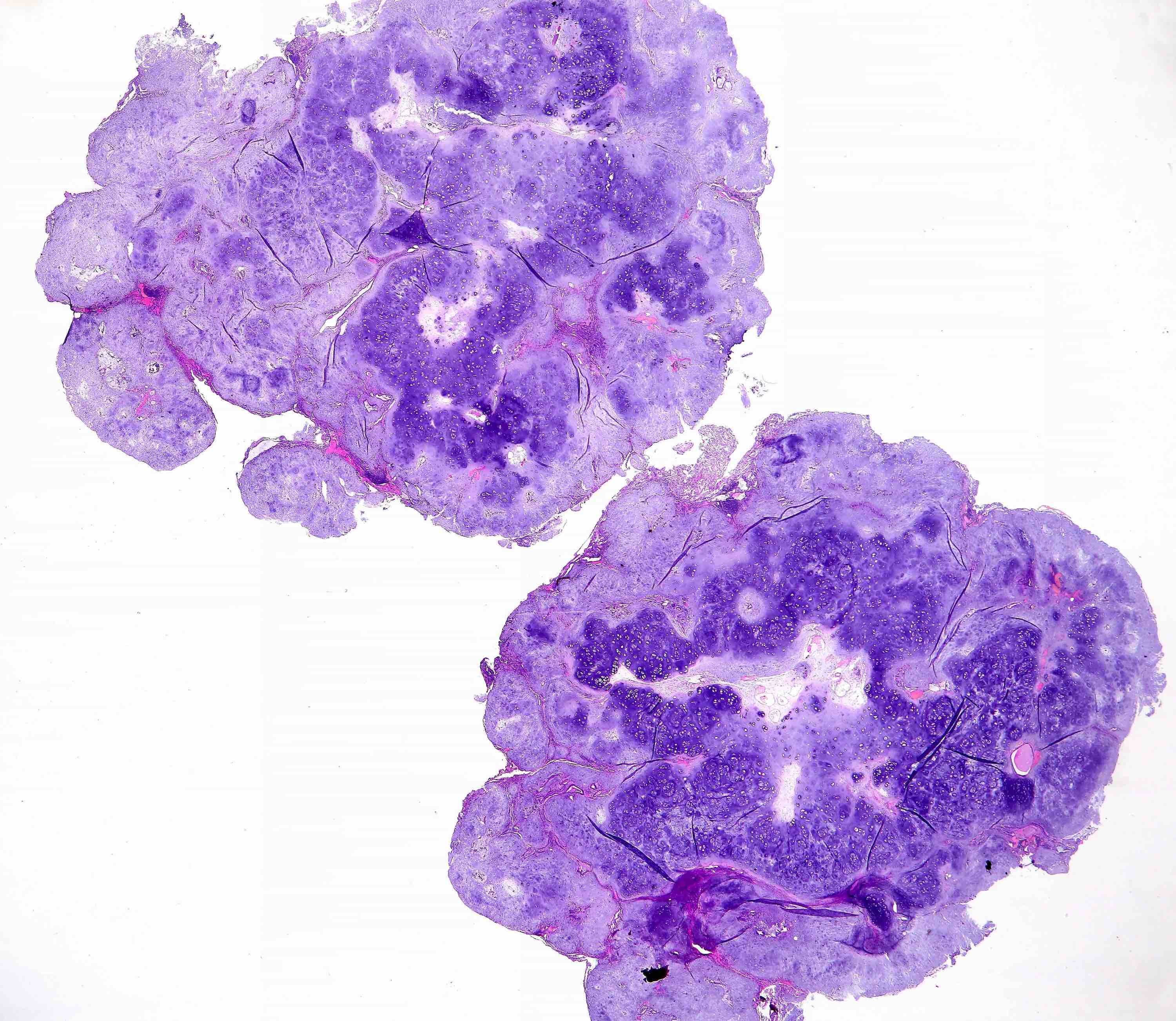
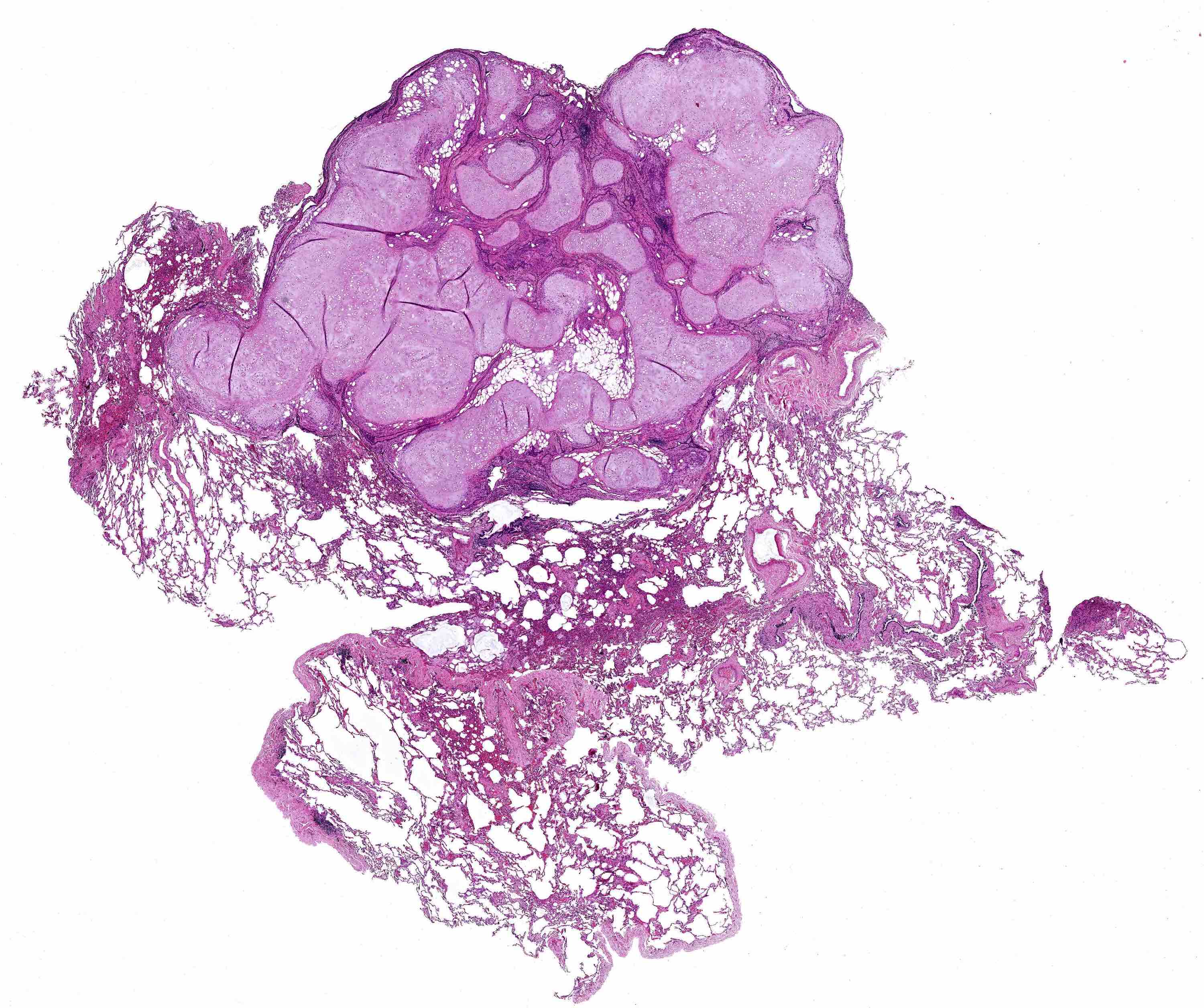
Contributed by Hui-Hua Li, M.D., Ph.D. and Jefree J. Schulte, M.D.
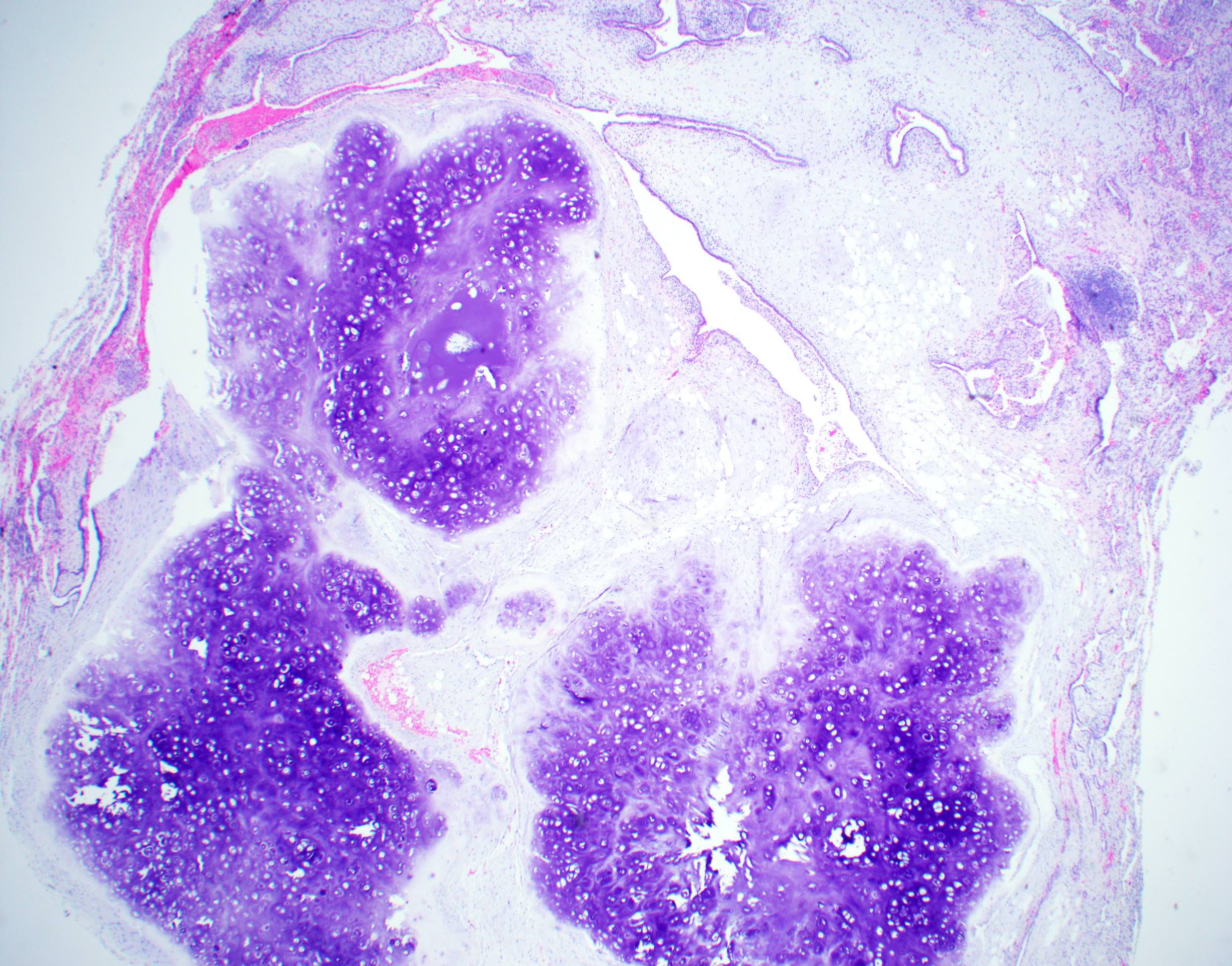
With cartilage
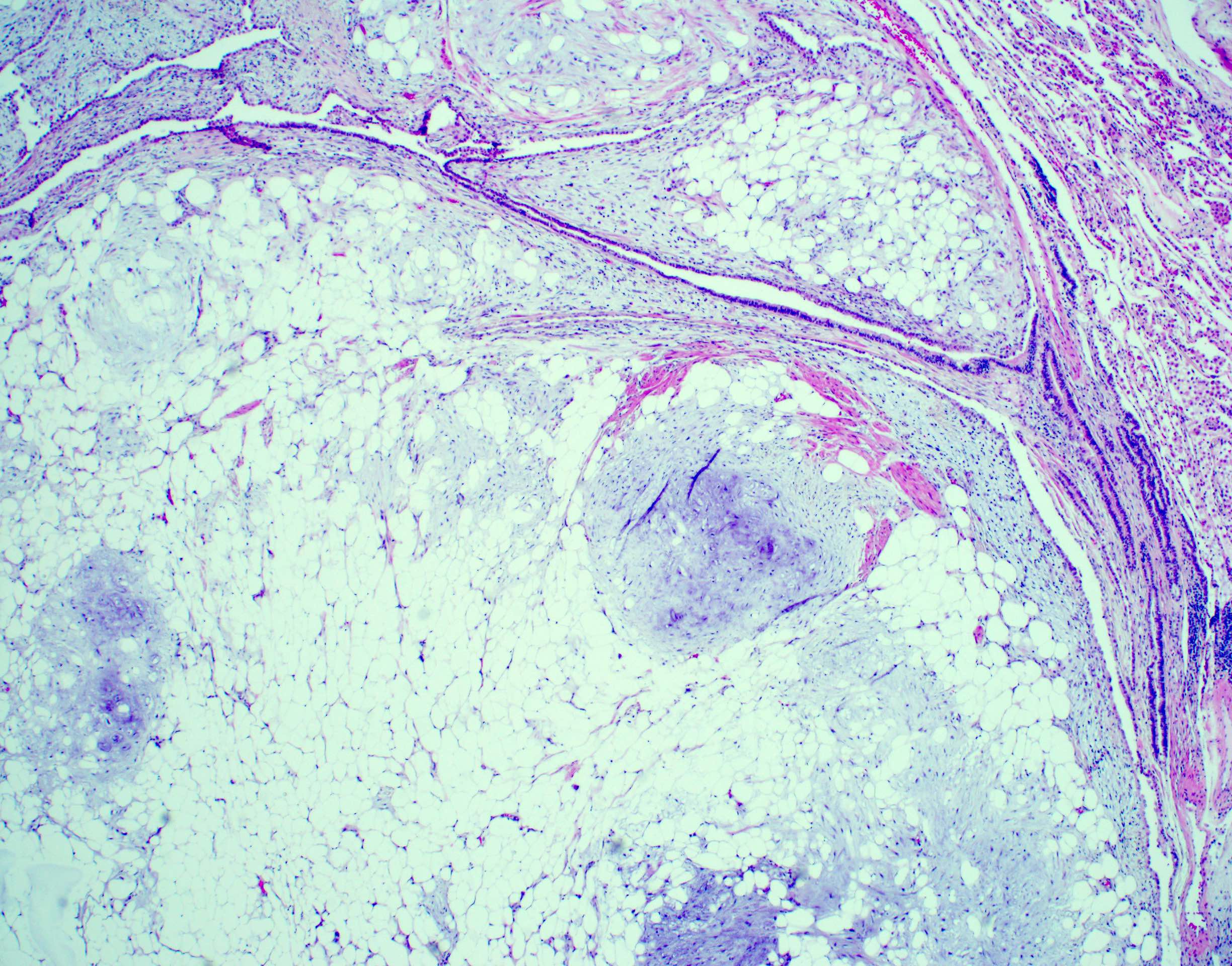
Fat rich
Typical features
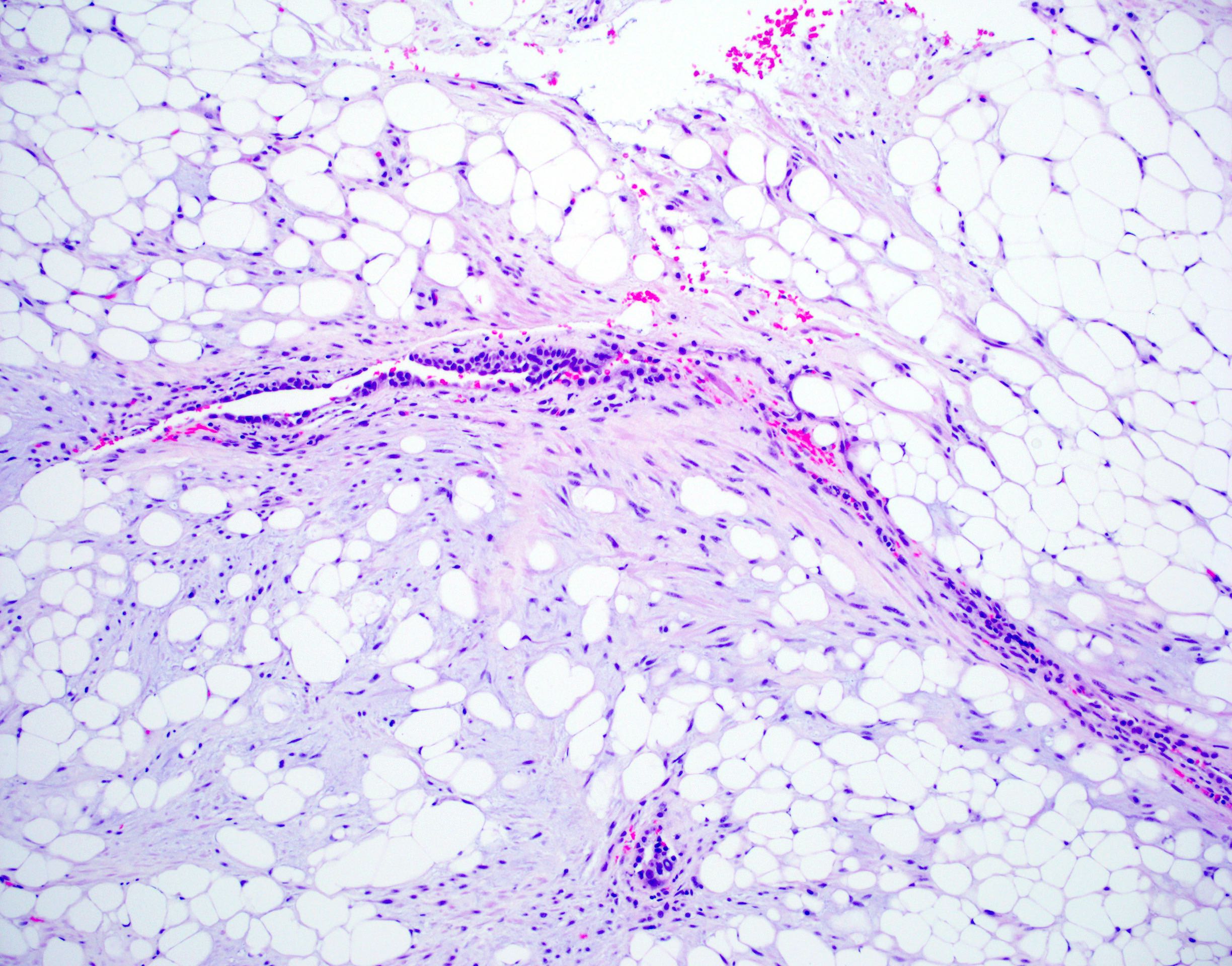
Fat / myxoid stroma
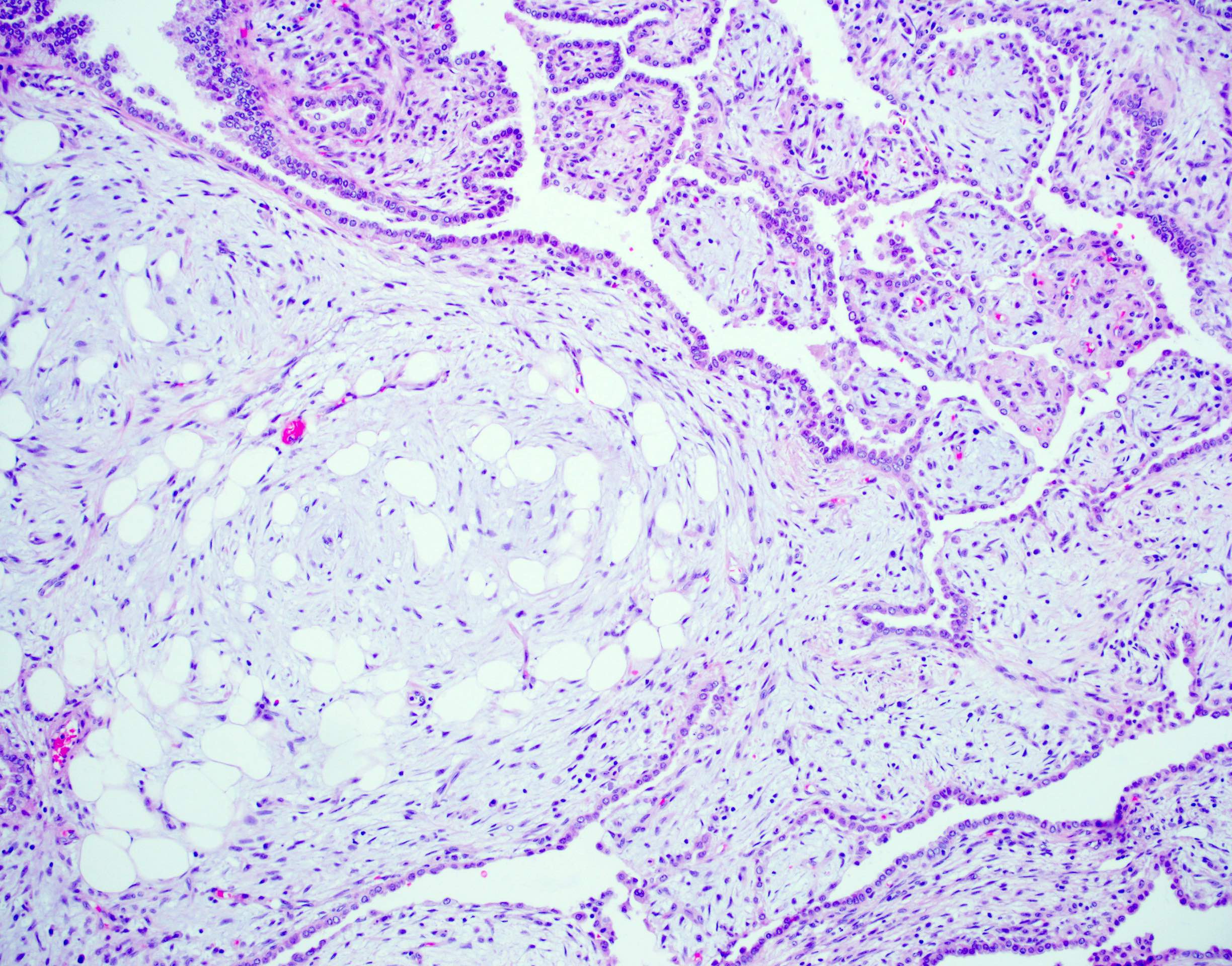
Bland spindle cells
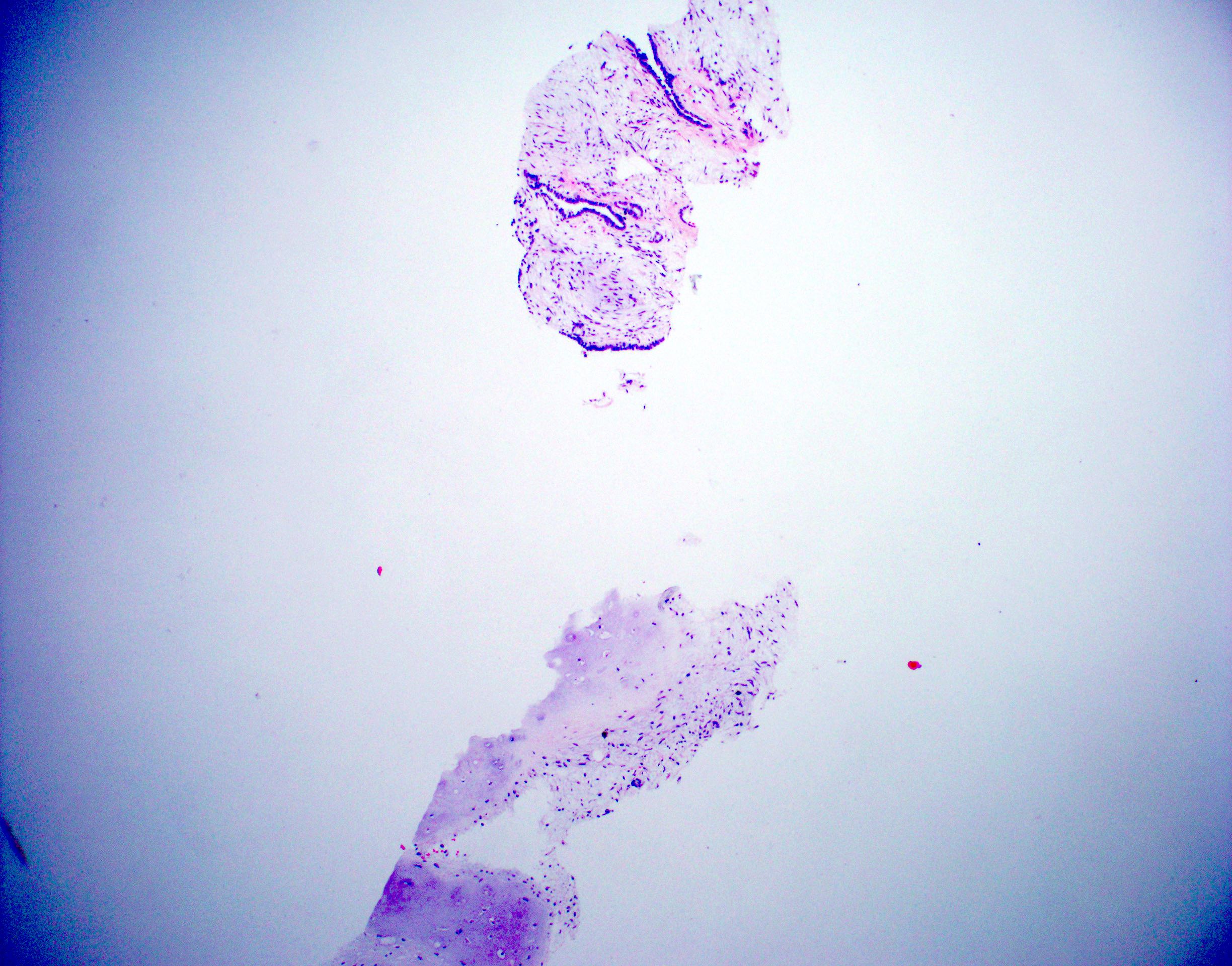
Core biopsy
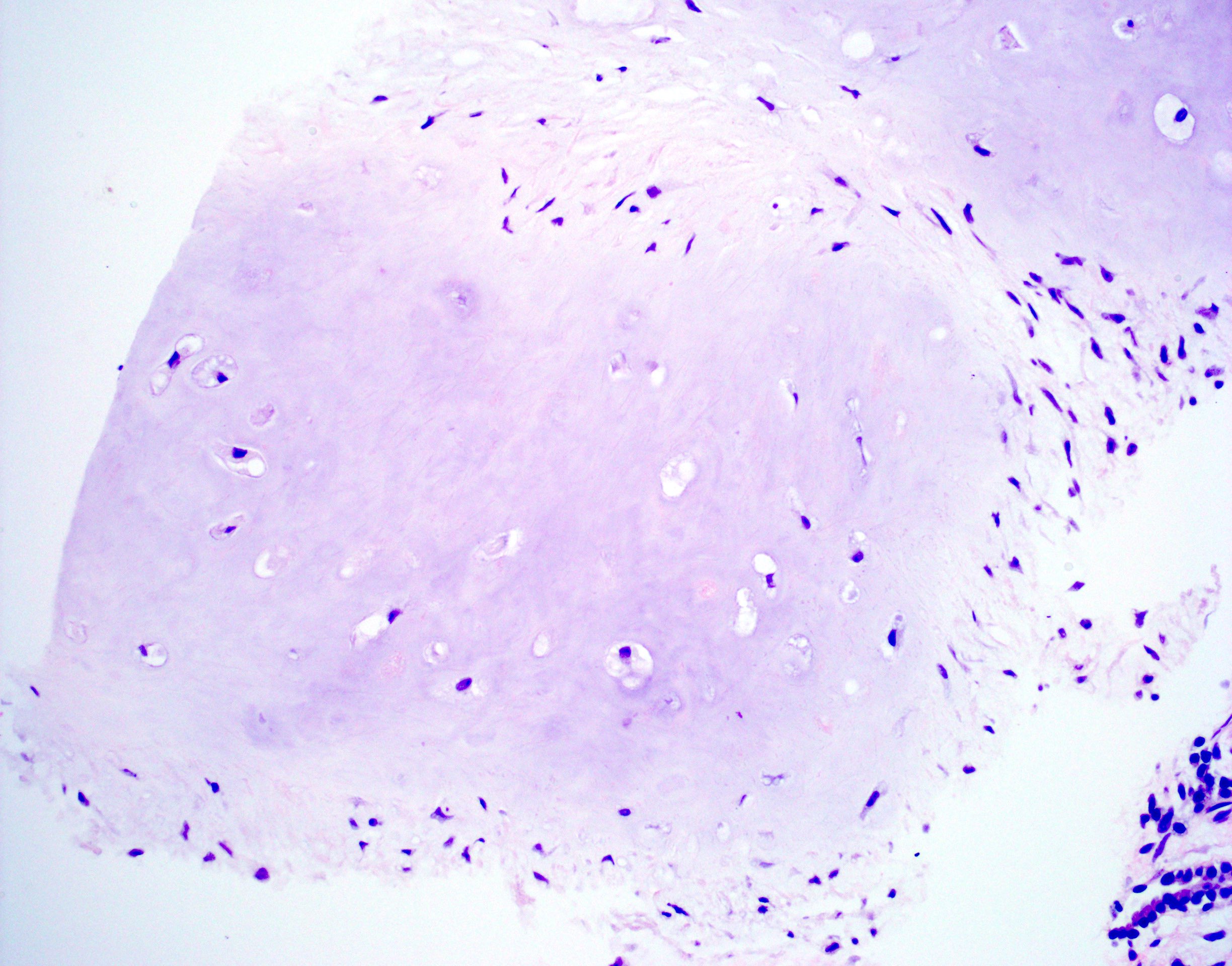
Biopsy, cartilage
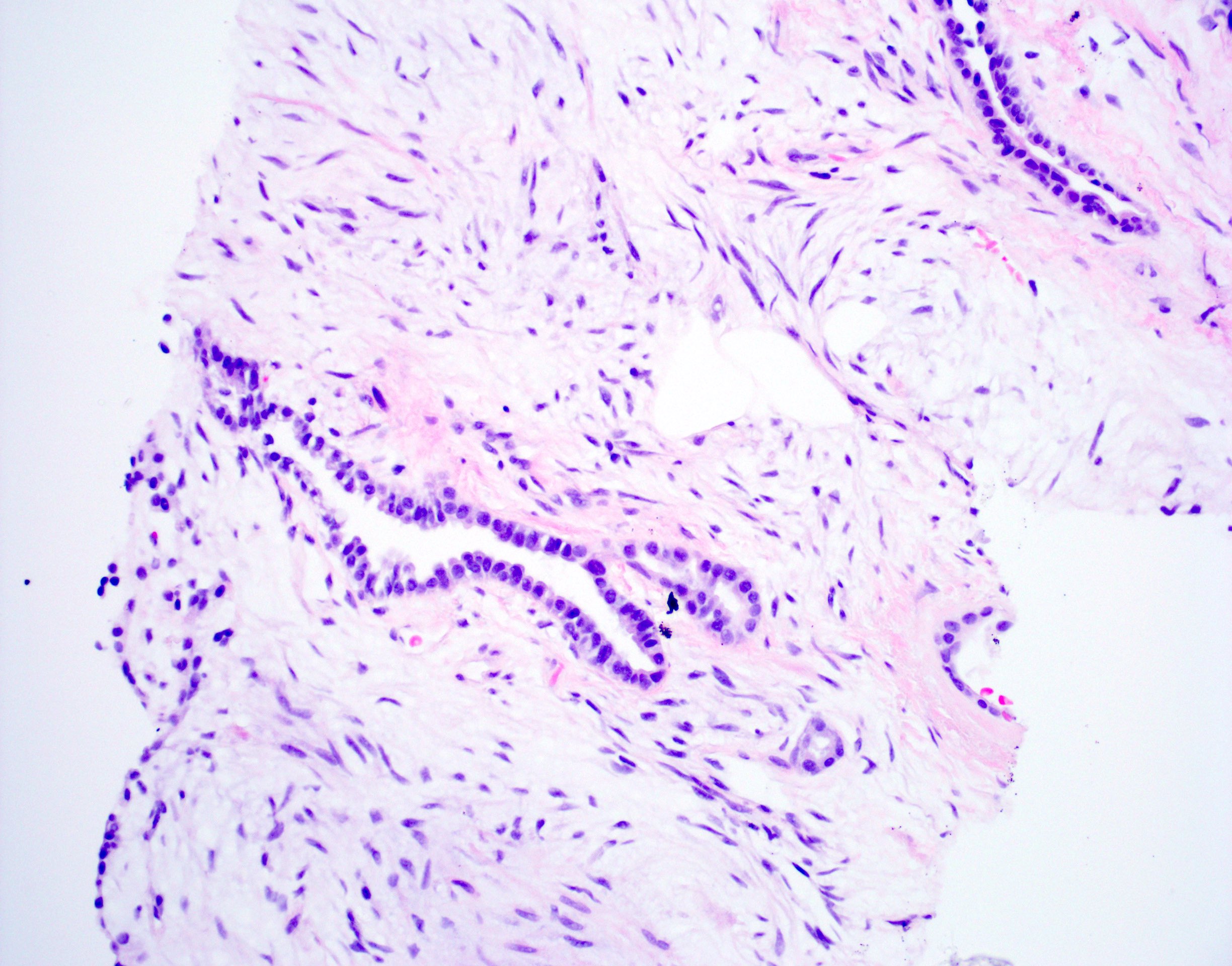
Biopsy, epithelium
Contributed by @Andrew_Fltv on Twitter
Pulmonary hamartoma
Cytology description
- FNA is highly reliable means of diagnosis (Cytopathology 2008;19:185)
- Misclassification as malignancy can occur, especially at the time of immediate adequacy assessment, prior to review of all cytologic preparations (Cytopathology 2008;19:185, BMC Pulm Med 2003;3:2)
- FNA often shows fibromyxoid tissue, fat or cartilage associated with benign reactive epithelial cells
- Lack of cytologic atypia and bland chromatin should point towards a benign diagnosis (Acta Cytol 2009;53:201)
Cytology images
Images hosted on other servers:

FNA smears
Positive stains
- Immunohistochemical markers are not typically needed to confirm diagnosis
- Immunohistochemical profile should be typical for the mesenchymal tissue being stained
- Interestingly, sex steroid receptors (ER, PR, AR) are often expressed (Am J Surg Pathol 2006;30:819)
Molecular / cytogenetics description
- Often not needed for diagnostic purposes
- High frequency of translocation t(3;12)(q27-28;q14-15) resulting in gene fusion of the HMGA2 and LPP genes (see Pathophysiology and Etiology above)
Sample pathology report
- Lung, left, needle core biopsy:
- Pulmonary hamartoma (see comment)
- Comment: The histologic sections reveal the presence of a benign pulmonary lesion composed of hyaline cartilage, fibroadipose tissue, bone and bland spindle cells in myxoid stroma. The mesenchymal elements appear to entrap benign respiratory epithelium. These findings support the above diagnosis.
- Lung, right, wedge resection:
- Pulmonary hamartoma (3.2 cm) (see comment)
- Comment: The histologic sections reveal the presence of a well circumscribed benign pulmonary lesion composed of hyaline cartilage, fibroadipose tissue, smooth muscle and bland spindle cells set in fibromyxoid stroma. The mesenchymal elements appear to entrap benign respiratory epithelium. These findings support the above diagnosis.
Differential diagnosis
- Pulmonary chondroma:
- Lacks entrapped epithelium
- Does not contain secondary mesenchymal elements
- Often seen in patients with Carney triad
- Other soft tissue tumors (including leiomyoma and lipoma):
- Only 1 mesenchymal component may be sampled at the biopsy
- Radiographic (popcorn calcifications and fat) findings may help suggest the diagnosis of hamartoma
- Primary / metastatic sarcoma:
- Cytologic atypia and features of necrosis should be present for diagnosis of sarcoma
Board review style question #1
A 67 year old man died in a work related accident. At autopsy, a 1 cm, circumscribed nodule is identified in the peripheral lung. The cut surface reveals a tan-white rubbery nodule. The histologic findings are seen in the image above. The incidentally discovered tumor is best classified as
- Non small cell carcinoma
- Pulmonary chondroma
- Pulmonary hamartoma
- Pulmonary sequestration
Board review style answer #1
Board review style answer #2
A 60 year old man presents to the emergency department following a motor vehicle accident. A chest CT scan reveals a circumscribed solitary pulmonary nodule containing fibroadipose tissue and calcifications. The patient meets with a thoracic surgeon, who does not immediately recommend excision. The patient is followed by serial CT scans and the nodule shows minimal growth over the next year. The characteristics of this pulmonary nodule are those of
- High grade neuroendocrine carcinoma of the lung
- Metastatic carcinoma to the lung
- Non small cell lung carcinoma
- Pulmonary hamartoma
Board review style answer #2
