

Lung
Salivary gland type tumors
Mucoepidermoid carcinoma
Author: Roseann I. Wu, M.D., M.P.H.
Editor-in-Chief: Debra L. Zynger, M.D.
Last author update: 1 May 2018
Last staff update: 20 December 2023
Copyright: 2003-2024, PathologyOutlines.com, Inc.
PubMed Search: Mucoepidermoid carcinoma [title] lung tumor AND (free full text[sb])

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Clinical images | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Virtual slides | Cytology description | Positive stains | Negative stains | Molecular / cytogenetics description | Molecular / cytogenetics images | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1Cite this page: Wu R. Mucoepidermoid carcinoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/lungtumormucoepidermoid.html. Accessed April 25th, 2024.
Definition / general
- Low grade or high grade salivary gland type tumor with mucous secreting cells, squamous cells and intermediate cells
- Distinguished from other lung cancers by central or peribronchial location, mucous cells, lack of keratinization, expression of p63 and MAML2 rearrangement (Mod Pathol 2014;27:1479)
Essential features
- Most common salivary gland type tumor in the lung, tends to arise centrally
- Similar morphology to mucoepidermoid carcinoma arising in the head and neck with a mixture of mucous cells, squamous cells and intermediate cells; must exclude metastasis
- Strong association with t(11;19)(q21;p13) and MAML2 rearrangement by fluorescence in situ hybridization (FISH)
- Squamous component stains with p63 and p40
Terminology
- Same diagnostic terminology as used in the salivary gland
ICD coding
Epidemiology
- 0.1 - 0.2% of primary lung tumors (J Thorac Cardiovasc Surg 1978;76:431) and 9 - 18% in the pediatric population (J Surg Res 2009;156:224, J Pediatr Surg 2015;50:1004)
- May occur in any age group; many cases reported in pediatric population
- Most common of the primary salivary gland type tumors of the lung but still rare
Sites
- Any lung lobe, usually in relation to large bronchi
Pathophysiology
- Usually considered to have low malignant potential with recurrences; more aggressive when high grade (Int J Clin Exp Pathol 2014;7:6792)
- Most tumors are low stage and low to intermediate grade rather than high grade (J Thorac Oncol 2013;8:1578)
Etiology
- May arise from submucosal bronchial glands
Clinical features
- Large central tumors cause obstructive symptoms such as dyspnea, cough, hemoptysis or pneumonia
- Peripheral lesions may be asymptomatic
Diagnosis
- Bronchoscopy may be used to directly visualize and sample an endobronchial tumor
- Diagnosis may be difficult in small biopsies; may mimic primary non small cell lung carcinoma
Radiology description
- Can be difficult to detect on imaging due to small size of tumor, endobronchial location, association with pneumonia or atelectasis (Arch Pathol Lab Med 2007;131:1400)
- On CT, markedly enhanced homogeneous central bronchial nodule / mass suggests low grade mucoepidermoid carcinoma (MEC); high grade MEC tends to be peripheral with poorly defined margins, lobular, heterogeneous with less enhancement (AJR Am J Roentgenol 2015;205:1160)
- Uncommon findings included cavitation, diffuse thickening or spiculation (Clin Imaging 2012;36:8)
Radiology images
Images hosted on other servers:

Heterogeneously enhancing lesion

Mass shadow measuring 30 mm

Mass in right upper lobe and left hilum
Prognostic factors
- Excellent prognosis after surgical removal (Thorac Cardiovasc Surg 2014;62:140, Asian Cardiovasc Thorac Ann 2016;24:257)
- Age, stage, margin status and pathological grade related to overall survival and disease free survival (J Thorac Oncol 2013;8:1578 , Int J Clin Exp Pathol 2014;7:6792)
Case reports
- 22 year old man with tumor in the medial segment of the right lower lobe (Diagn Pathol 2012;7:137)
- 26 year old man with chronic cough and an endobronchial lesion (Respir Med Case Rep 2013;9:18)
- 38 year old woman with mild fever and dry cough (Oxf Med Case Reports 2015;2015:203)
- 40 year old man with dry cough (Asian Cardiovasc Thorac Ann 2015;23:988)
- 46 year old woman with dyspnea on exertion (Case Rep Oncol Med 2013;2013:625243)
- 58 year old man with shortness of breath, dysphagia and weight loss (Ann Clin Lab Sci 2015;45:219)
- 58 year old woman with mixed adenocarcinoma and mucoepidermoid carcinoma (Ann Thorac Surg 2014;98:695)
Treatment
- Complete surgical excision (Int J Clin Exp Pathol 2014;7:6792)
- High grade tumors may require additional treatment, although chemotherapy and radiation controversial (World J Surg Oncol 2014;12:33)
Clinical images
Images hosted on other servers:

Well circumscribed endobronchial tumor
Gross description
- Polypoid, exophytic growth or sessile tumor in major bronchi, may be > 5 cm
- Generally well circumscribed and smooth with tan to yellow cut surface
- May be solid or cystic and potentially show glistening mucoid material
Gross images
Images hosted on other servers:

Mucoepidermoid carcinoma of airways

Tumor in middle lobe bronchus
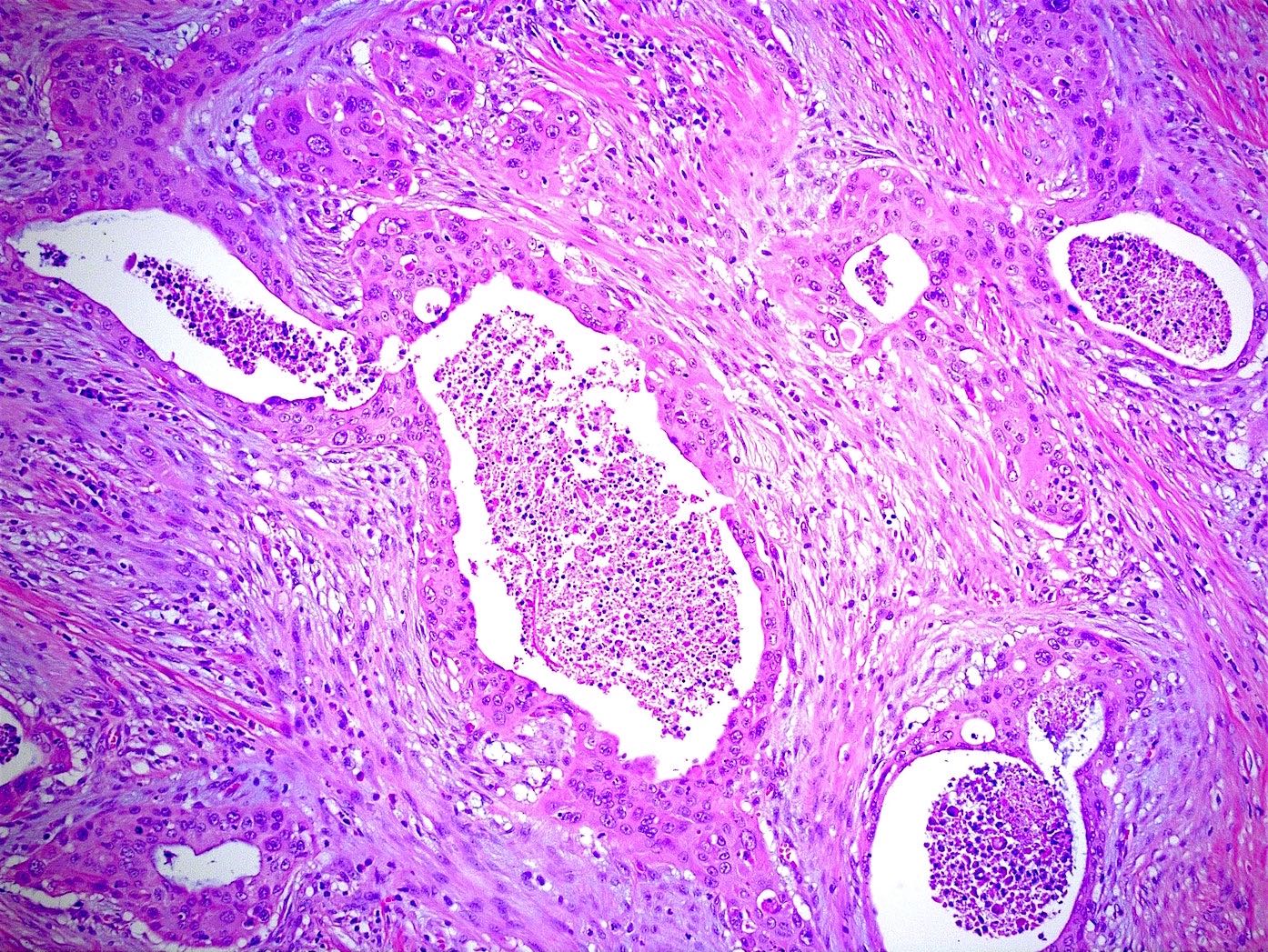
Microscopic (histologic) description
- Low grade has more cysts and mucous cells; high grade has more solid or nested growth, atypia, mitotic activity, necrosis, hemorrhage
- Mucus secreting cells, squamoid cells without significant keratinization, intermediate type cells
- Mucus secreting cells usually large with light blue-gray mucinous cytoplasm; variants include columnar, goblet, cuboidal, clear or oncocytic cells (Arch Pathol Lab Med 2007;131:1400)
- Squamous cells show intercellular bridges but no keratin whorls or pearls; intermediate cells usually polygonal with bland nucleus (Arch Pathol Lab Med 2007;131:1400)
- May show areas of papillary growth or spindled cells
- May have dense lymphoplasmacytic infiltrate (Am J Surg Pathol 2005;29:407)
- Lack in situ carcinoma of overlying epithelium
Microscopic (histologic) images
Contributed by Roseann Wu, M.D., M.P.H. and Yale Rosen, M.D.
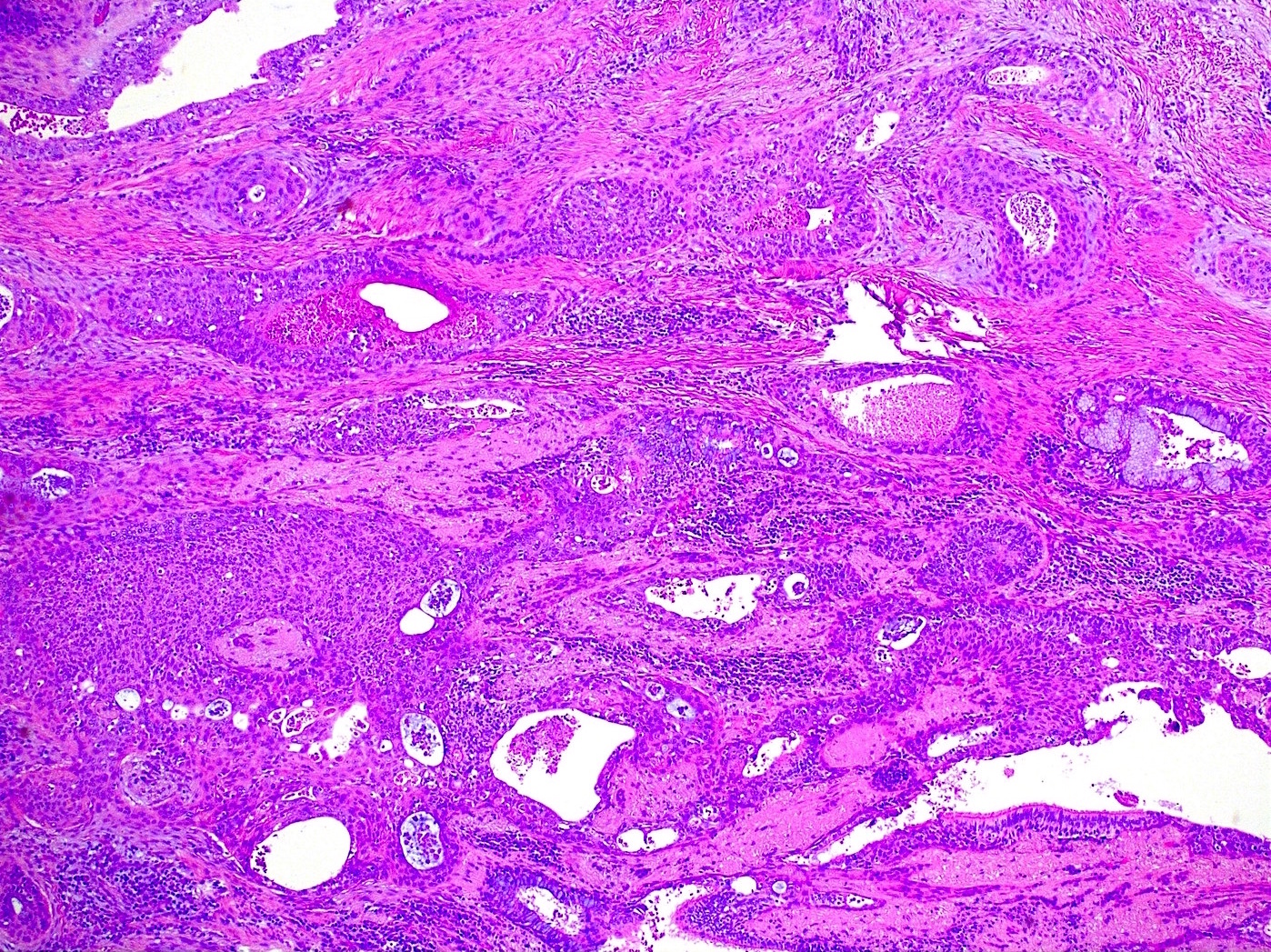
Low grade mucoepidermoid carcinoma
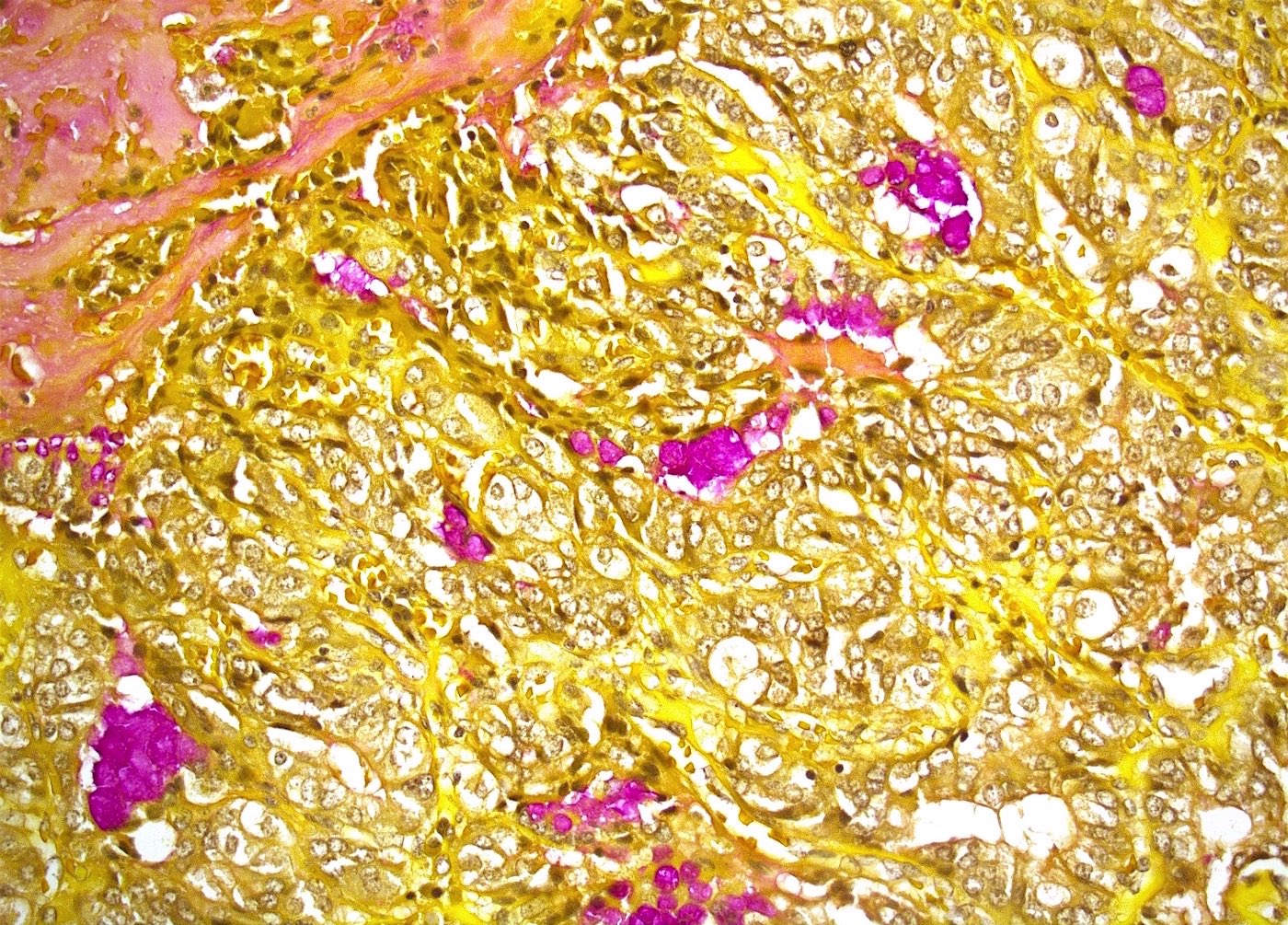
Low grade MEC mucicarmine stain
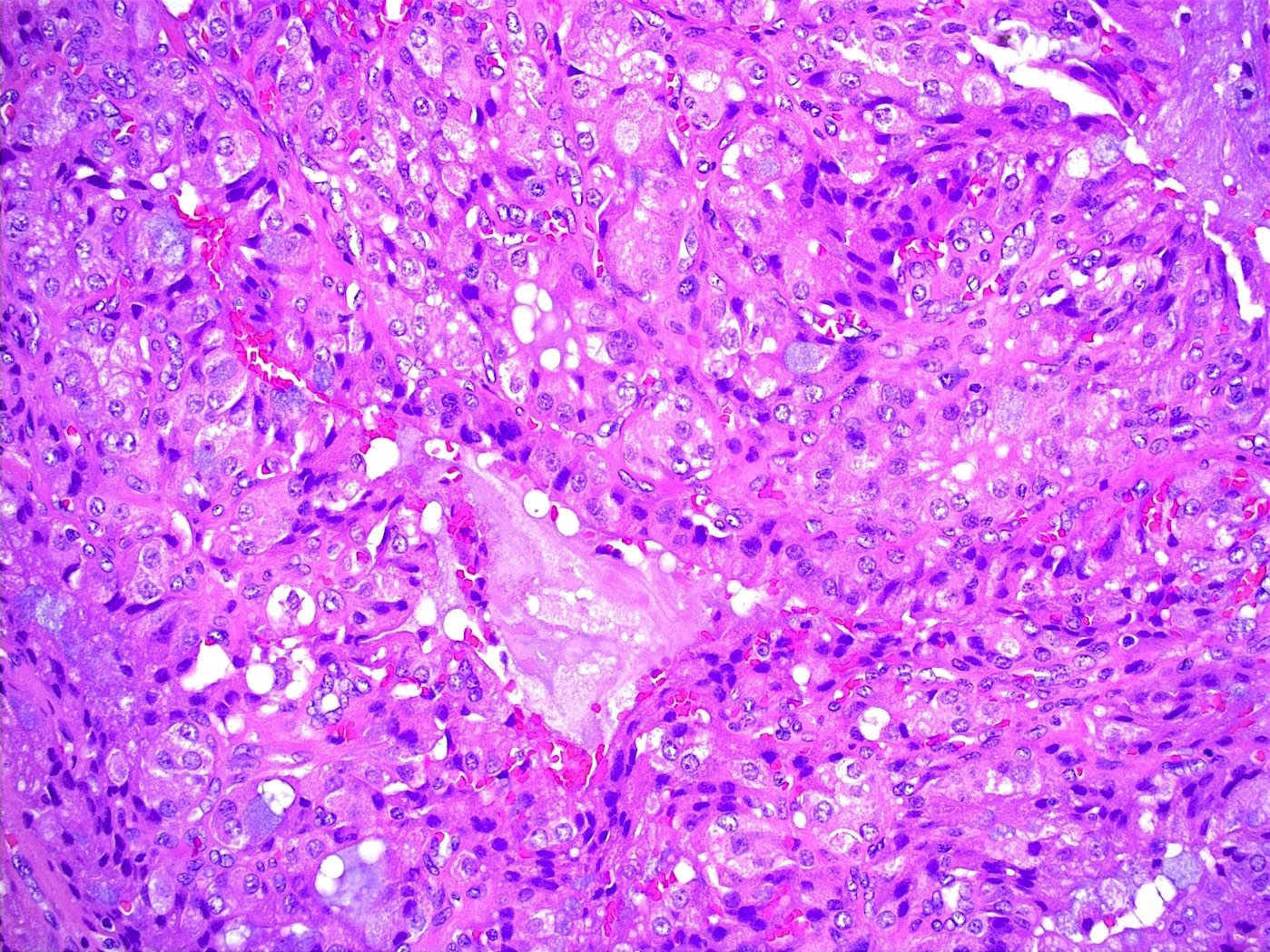
High grade mucoepidermoid carcinoma
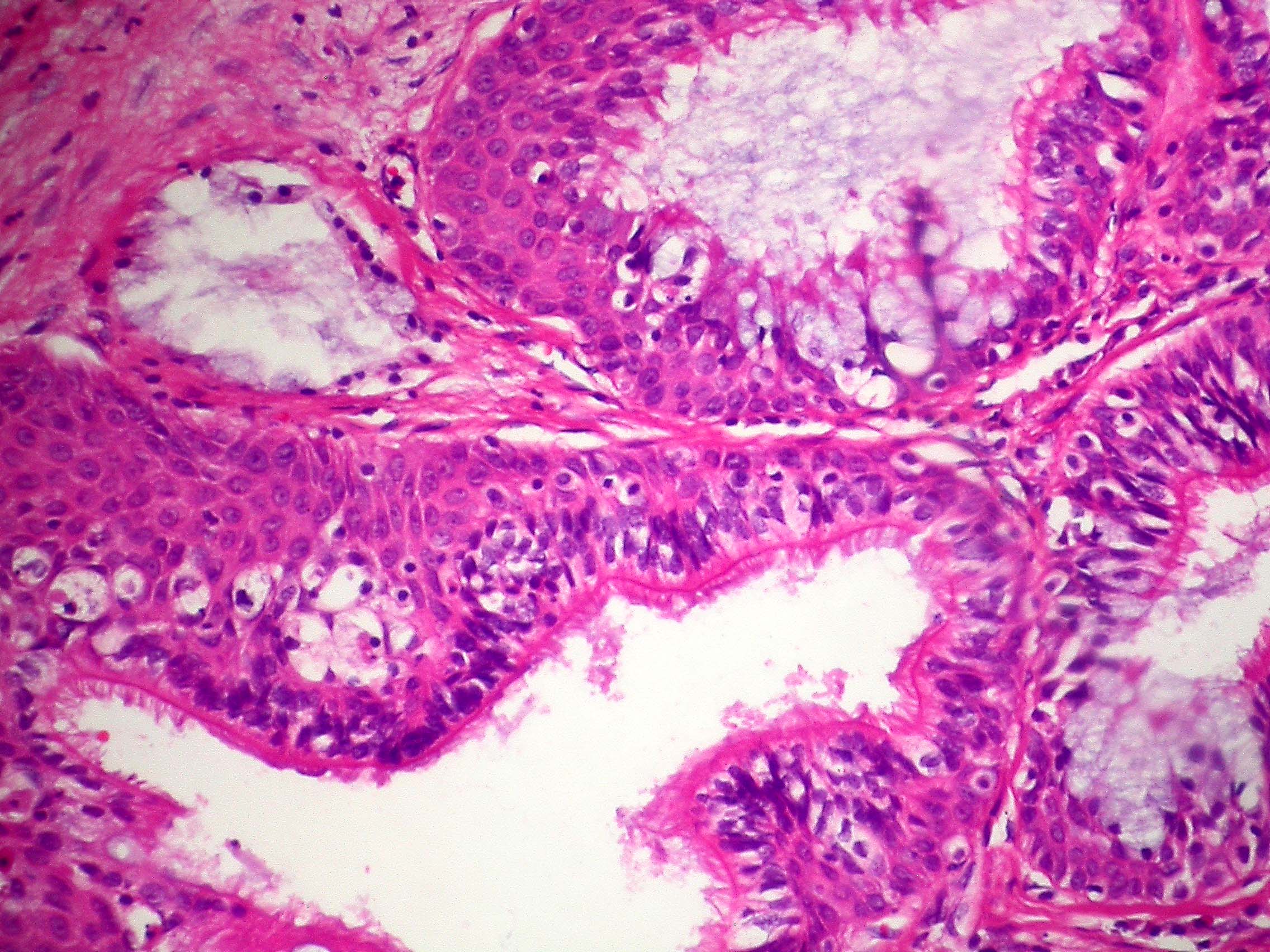
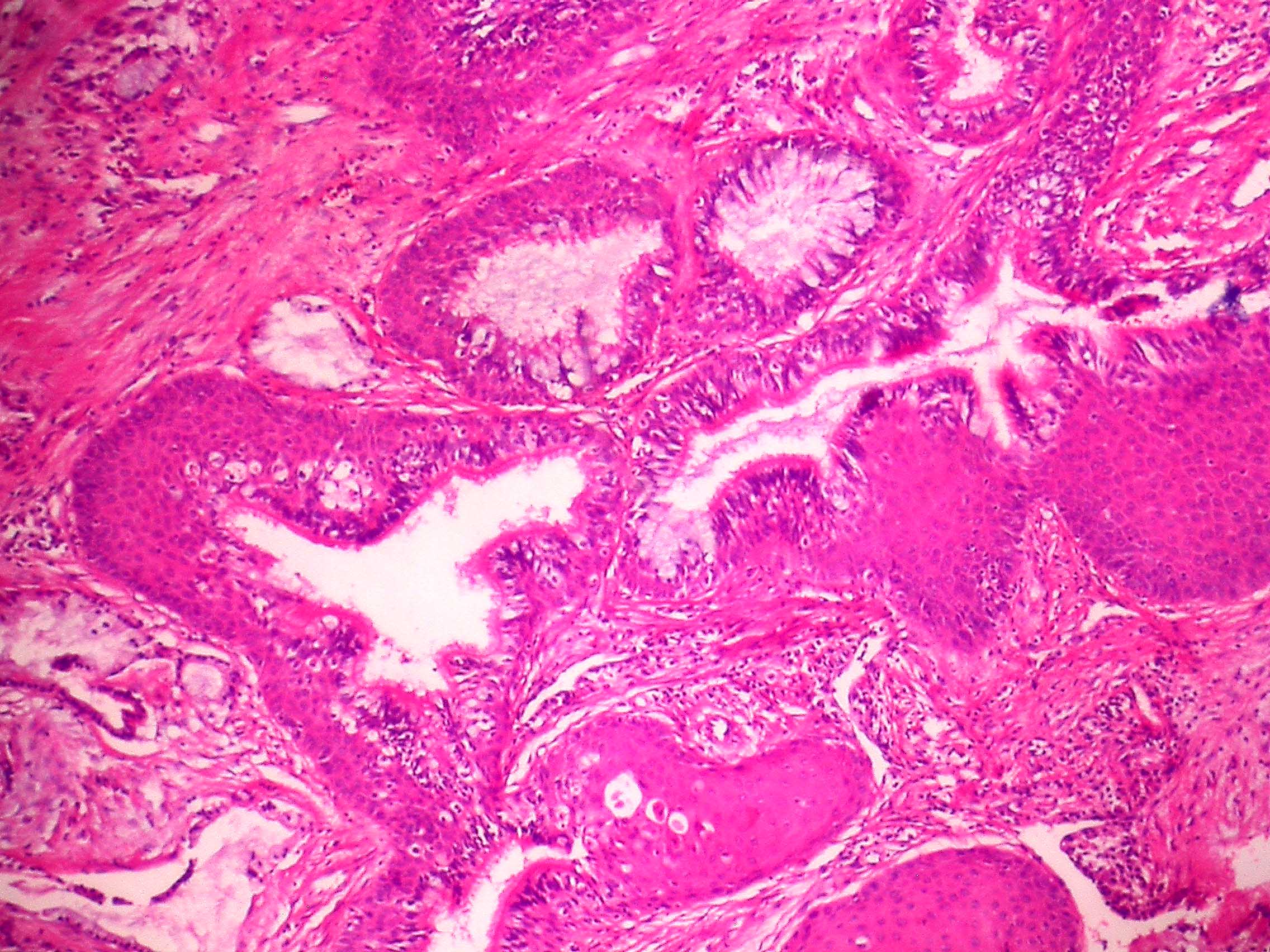
Mucoepidermoid carcinoma, low grade
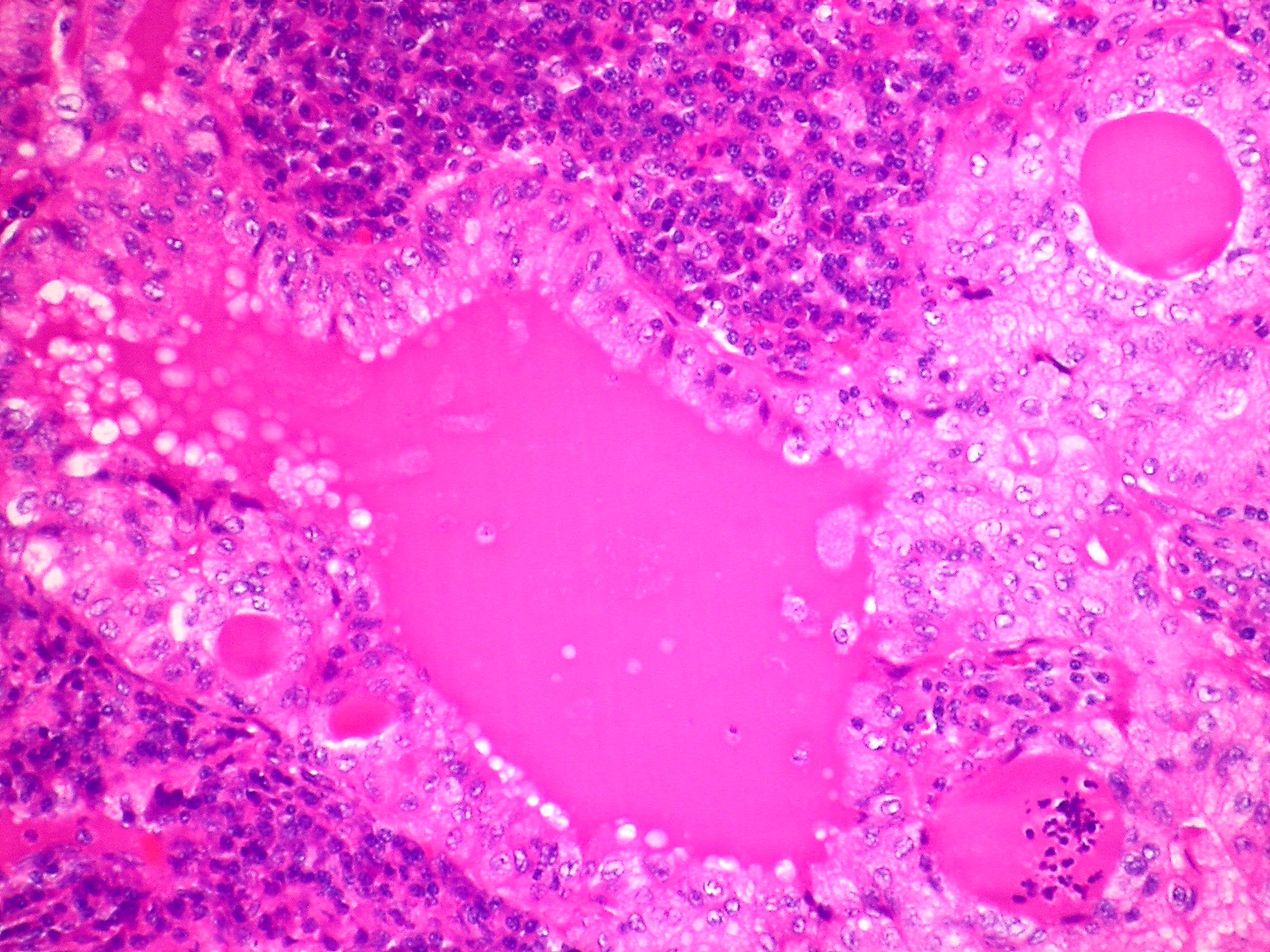
Stroma infiltrated by inflammatory cells
Images hosted on other servers:

MEC of lung

EGFR seen in squamous and intermediate cells



Pulmonary MEC

MEC-like pulmonary carcinoma
Virtual slides
Images hosted on other servers:




Mucoepidermoid carcinoma of the lung, from Juan Rosai’s Collection of Surgical Pathology Seminars
Cytology description
- Mixture of squamoid cells, mucous cells and intermediate cells
- Diff-Quik with numerous tight clusters of relatively small and bland cells with well defined but scant cytoplasm, central round and uniform nuclei with small nucleoli; second population of glandular appearing cells with cytoplasmic vacuoles with mucin, focal extracellular metachromatic mucinous material (Diagn Cytopathol 2013;41:1096)
Molecular / cytogenetics description
- MAML2 rearrangement most common molecular genetic event, found more in low grade tumors (PLoS One 2015;10:e0143169)
- May stain with epidermal growth factor receptor (EGFR) but does not show the mutation or alterations in copy number (Mod Pathol 2008;21:1168)
- Reciprocal translocations, including t(1;11)(p22;q13) with overexpression of cyclin D1, t(11;19)(q14-21;p12) and t(11;19)(q21;p13) which encodes MECT1-MAML2 (MECT1 also known as CRTC1) (Arch Pathol Lab Med 2007;131:1400)
Molecular / cytogenetics images
Images hosted on other servers:

MAML2 rearrangement by FISH
Differential diagnosis
- Adenocarcinoma: lacks squamous and intermediate cells; TTF1+
- Adenosquamous carcinoma: usually peripheral in lung, not centered on bronchi; large tumors, no intermediate cells, contains adenocarcinoma component
- Metastatic renal cell carcinoma: more monotonous with foamy or eosinophilic cytoplasm; CK7-
- Mucous gland adenoma: confined to luminal aspect and not invasive; TTF1+
- PEComa: lacks mucin as well as squamous and intermediate cells; HMB45+
- Squamous cell carcinoma: may show more keratinization and lacks mucin
Additional references
- Cytomorphology of salivary gland type tumors in the lung and mediastinum (Diagn Cytopathol 2012;40:1062)
Board review style question #1
- Rearrangement of which gene would support the diagnosis of mucoepidermoid carcinoma of the lung?
- APC
- BRAF
- MAML2
- PIK3CA
- PLAG1
Board review style answer #1
