
Lymph nodes & spleen, nonlymphoma
Lymph nodes-vascular lesions
Angiomyomatous hamartoma
Editorial Board Member: Roberto N. Miranda, M.D.
Deputy Editor-in-Chief: Genevieve M. Crane, M.D., Ph.D.

Last author update: 8 April 2024
Last staff update: 8 April 2024
Copyright: 2003-2024, PathologyOutlines.com, Inc.
PubMed Search: Angiomyomatous hamartoma
Table of Contents
Definition / general | Essential features | ICD coding | Epidemiology | Sites | Etiology | Clinical features | Diagnosis | Radiology description | Case reports | Treatment | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Negative stains | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Nithagon P, Tsang P. Angiomyomatous hamartoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/lymphnodesangiomyomatoushamartoma.html. Accessed April 20th, 2024.
Definition / general
- First described by Chan et al. in 1992 (Am J Surg Pathol 1992;16:335)
- Rare and benign vascular disorder due to proliferation of blood vessels and smooth muscle in mostly the hilar region of lymph nodes, often of long duration
Essential features
- Variably sized, thick walled blood vessels and haphazardly arranged smooth muscles in sclerotic nodal parenchyma
- Benign lesion with no atypia
- Uncommon process, usually asymptomatic and often solitary
- Prominent smooth muscle infiltrate (SMA) with low proliferative fraction
- HMB45 negative (to distinguish from angiomyolipoma)
ICD coding
Epidemiology
- M > F (Blood 2020;136:1794)
- All ages, peaking at sixth decade (Hum Pathol 2017;68:175)
Sites
- Mostly involves inguinal or femoral lymph nodes, usually solitary
- May have associated limb edema; rare case report with a soft tissue mass (JAAD Case Rep 2022;27:117)
- Rare reports of cervical lymph node and popliteal lymph node involvement (Histopathology 1996;29:80, Ann Diagn Pathol 2008;12:372)
- Rarely presents as extensive lymphadenopathy (Blood 2020;136:1794)
Etiology
- Unknown etiology; may represent reparative reaction to previous nodal inflammation or chronic blockage of nodal lymphatic flow (BMC Pediatr 2012;12:172)
Clinical features
- Presents incidentally or as palpable nodule; rare report of lymphadenomegaly in different regions (Blood 2020;136:1794)
- Typically asymptomatic; rarely lymphedema of ipsilateral limb (Fed Pract 2016;33:38)
- Benign clinical course
- No known recurrence or metastasis
Diagnosis
- Excisional biopsy of lymph node usually diagnostic
Radiology description
- Magnetic resonance imaging (MRI): well circumscribed solitary nodule with heterogeneous signal intensity (JAAD Case Rep 2022;27:117)
Case reports
- 33 year old man with postauricular lymph node, clinically masquerading as epidermal inclusion cyst (JAAD Case Rep 2020;7:131)
- 37 year old woman with weight loss and para-aortic lymph node (Prz Menopauzalny 2023;22:111)
- 53 year old woman with multiple neck lymph nodes showing angiomyomatous hamartoma (Int J Surg Pathol 2023 Nov 20 [Epub ahead of print])
- 60 year old man with several year history of lower leg edema (Case #118)
- 63 year old woman with right femoral subcutaneous mass and localized lymphedema (JAAD Case Rep 2022;27:117)
- 75 year old man with incidental extensive lymphadenopathy involving mediastinal, retroperitoneal, pelvic, inguinal and para-aortal lymph nodes (Blood 2020;136:1794)
Treatment
- Surgical excision is curative
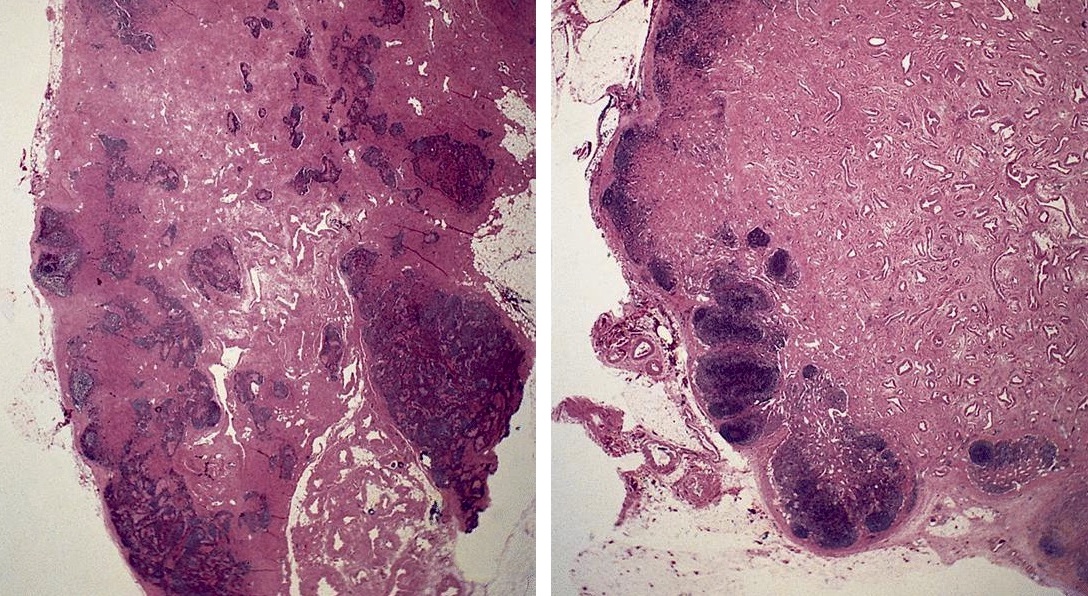
Gross description
- Enlarged lymph node replaced by firm, white tissue
Gross images
AFIP images

Replacement by tan, firm tissue
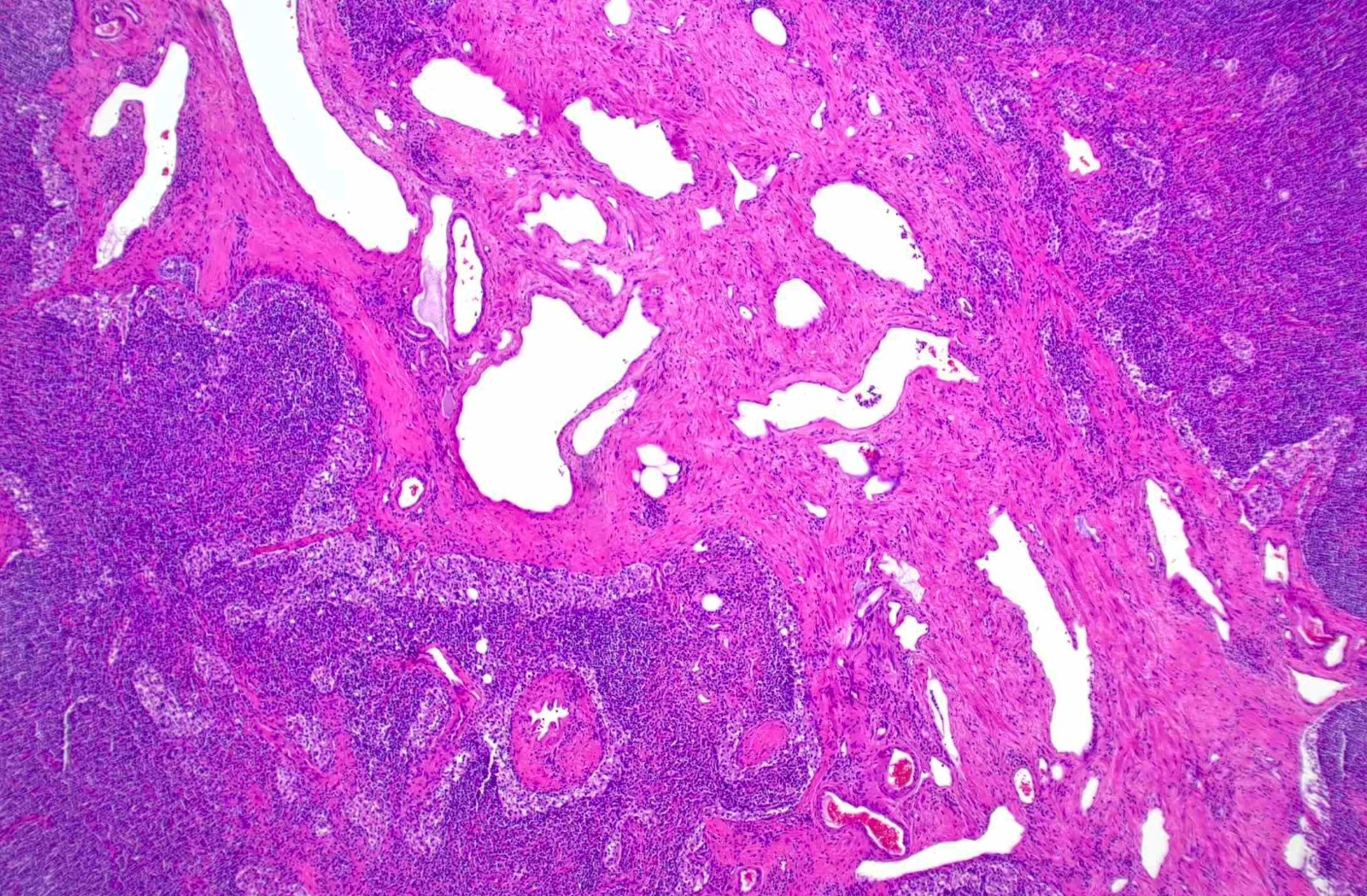
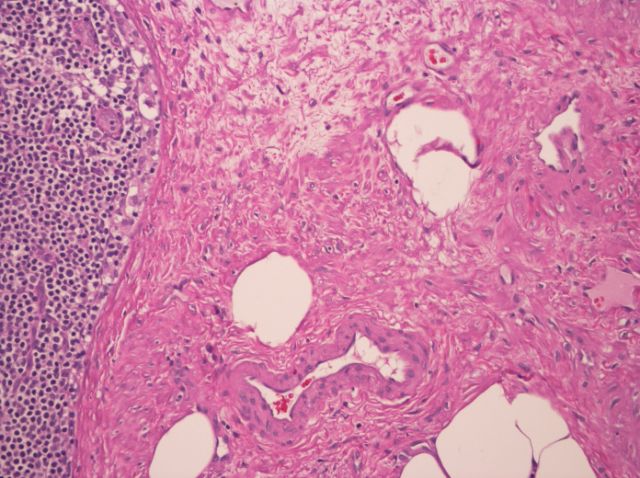
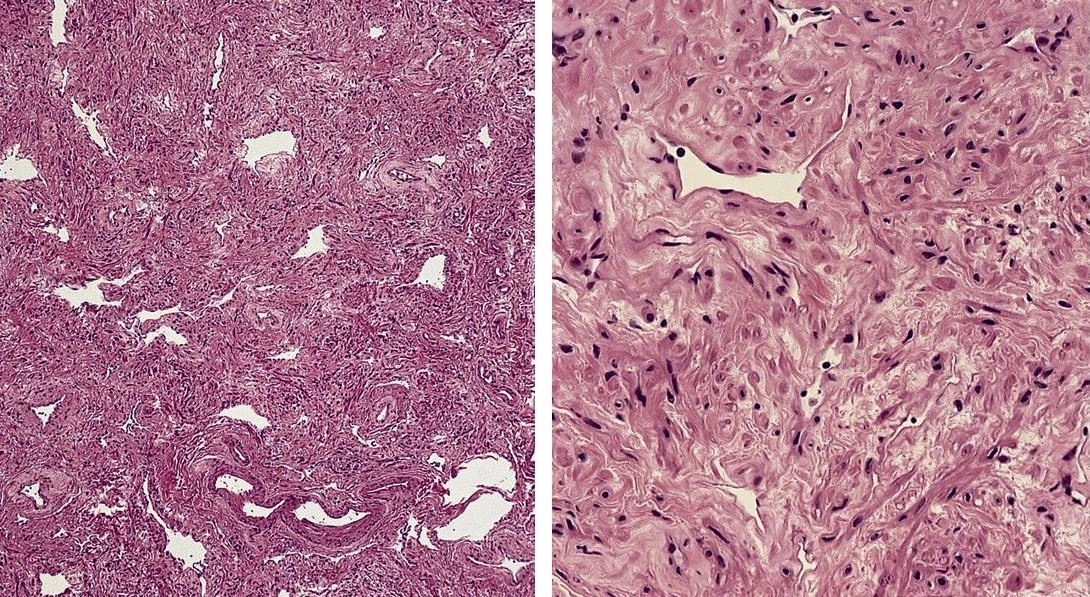
Microscopic (histologic) description
- Extensive and multifocal nodal involvement by thick walled hilar blood vessels, often with increased fibrous tissue
- Nodal parenchyma has haphazard smooth muscle fibers in sclerotic stroma
- Starts in nodal hilum and extends toward cortex
- May have admixed adipose tissue
- No cellular atypia, pleomorphism or necrosis; low mitotic rate (Hum Pathol 2017;68:175)
Microscopic (histologic) images
Contributed by Patricia Tsang, M.D., M.B.A., Vincent A. Graffeo, M.D. and AFIP
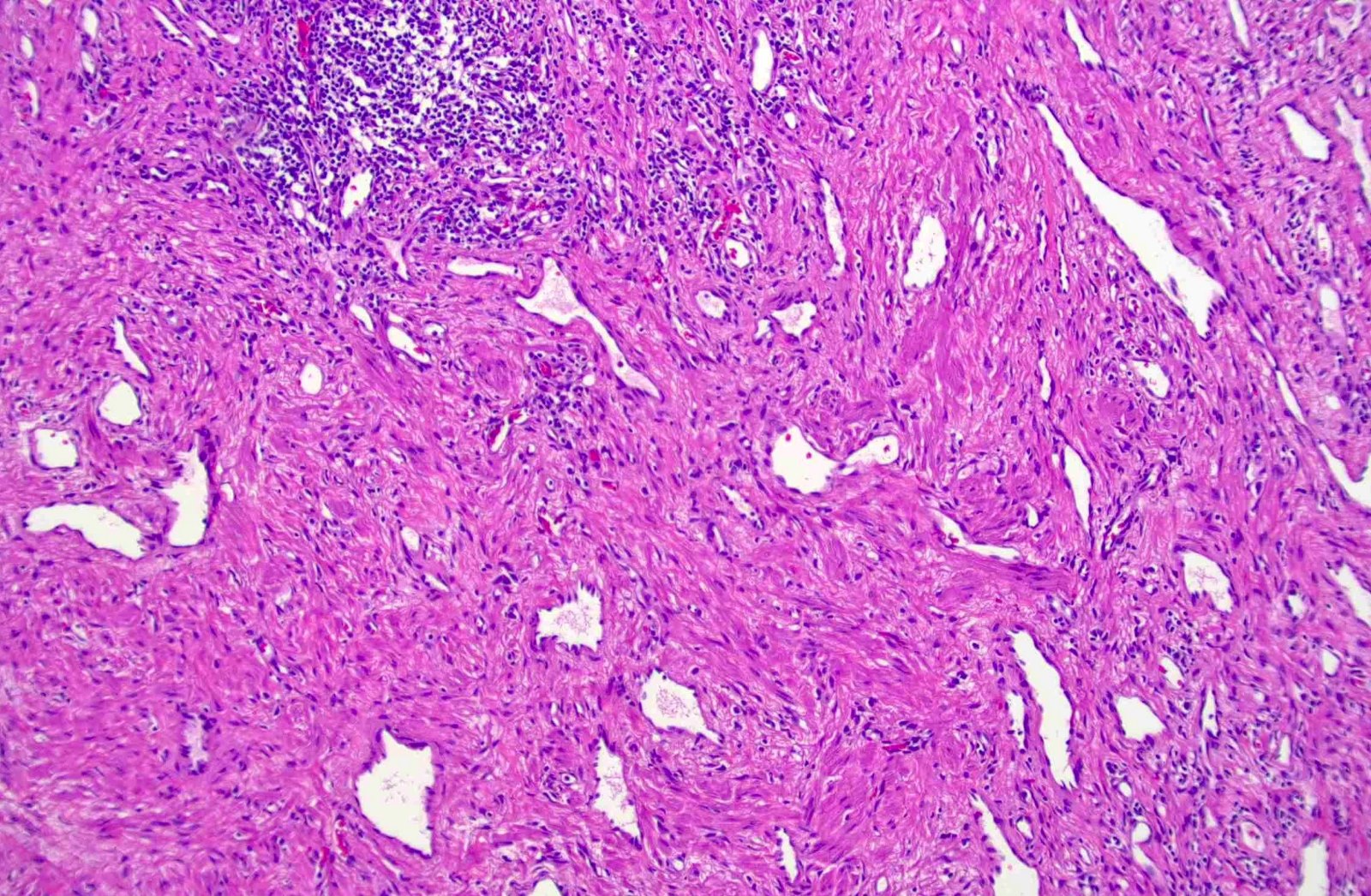
Disarrayed vascular proliferation
Angiomyomatous proliferation
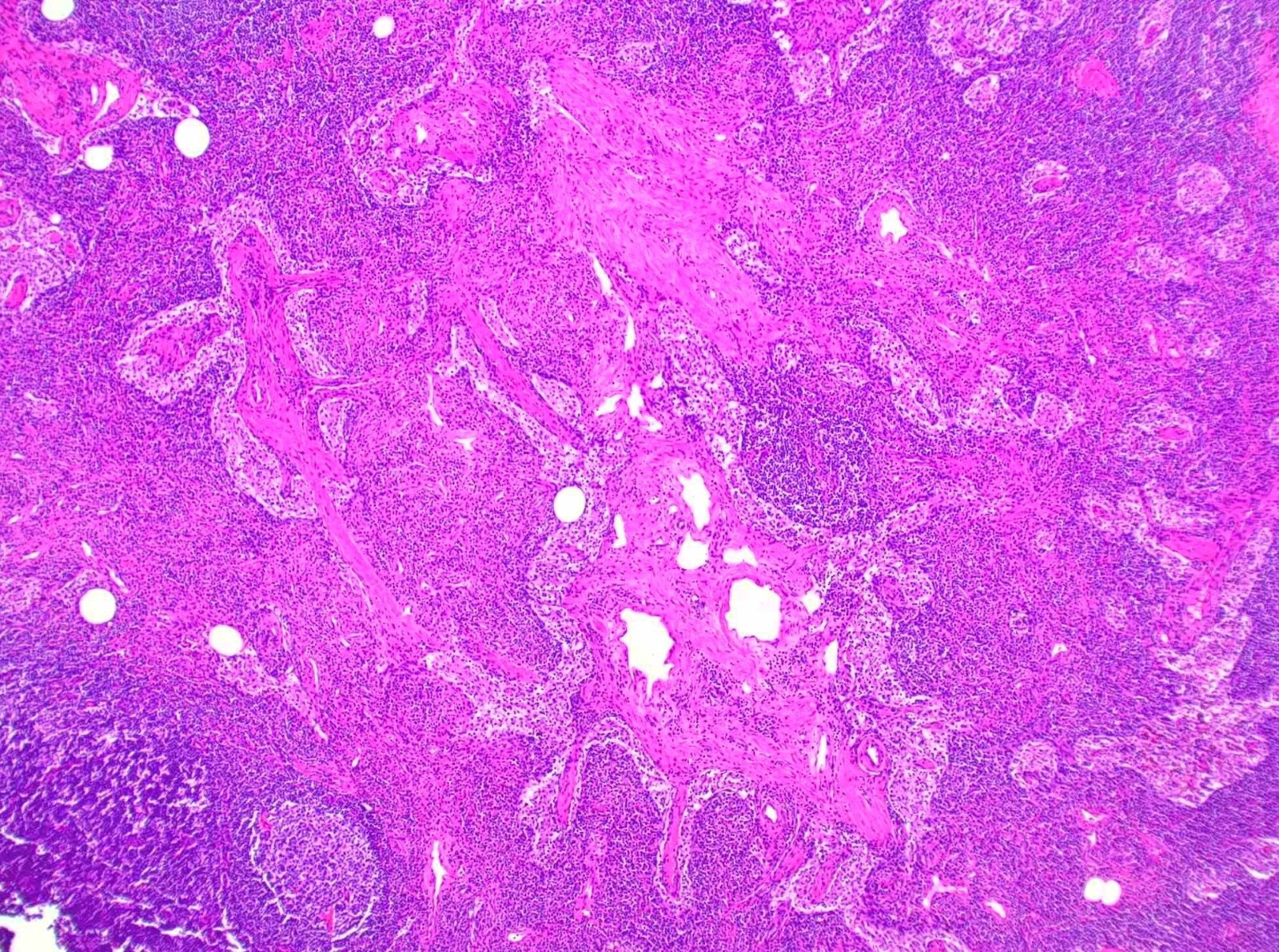
Smooth muscle proliferation
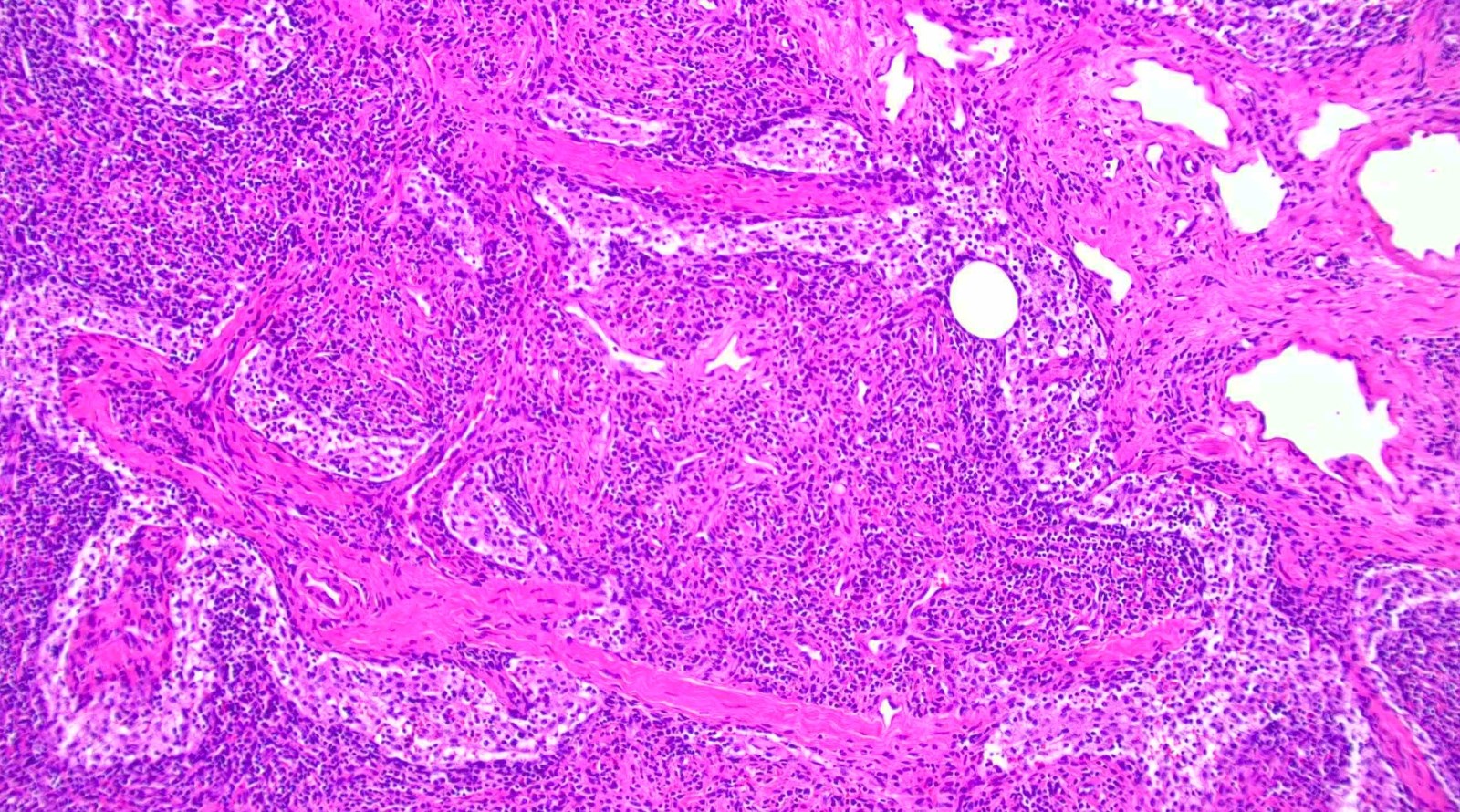
Thick walled vasculature
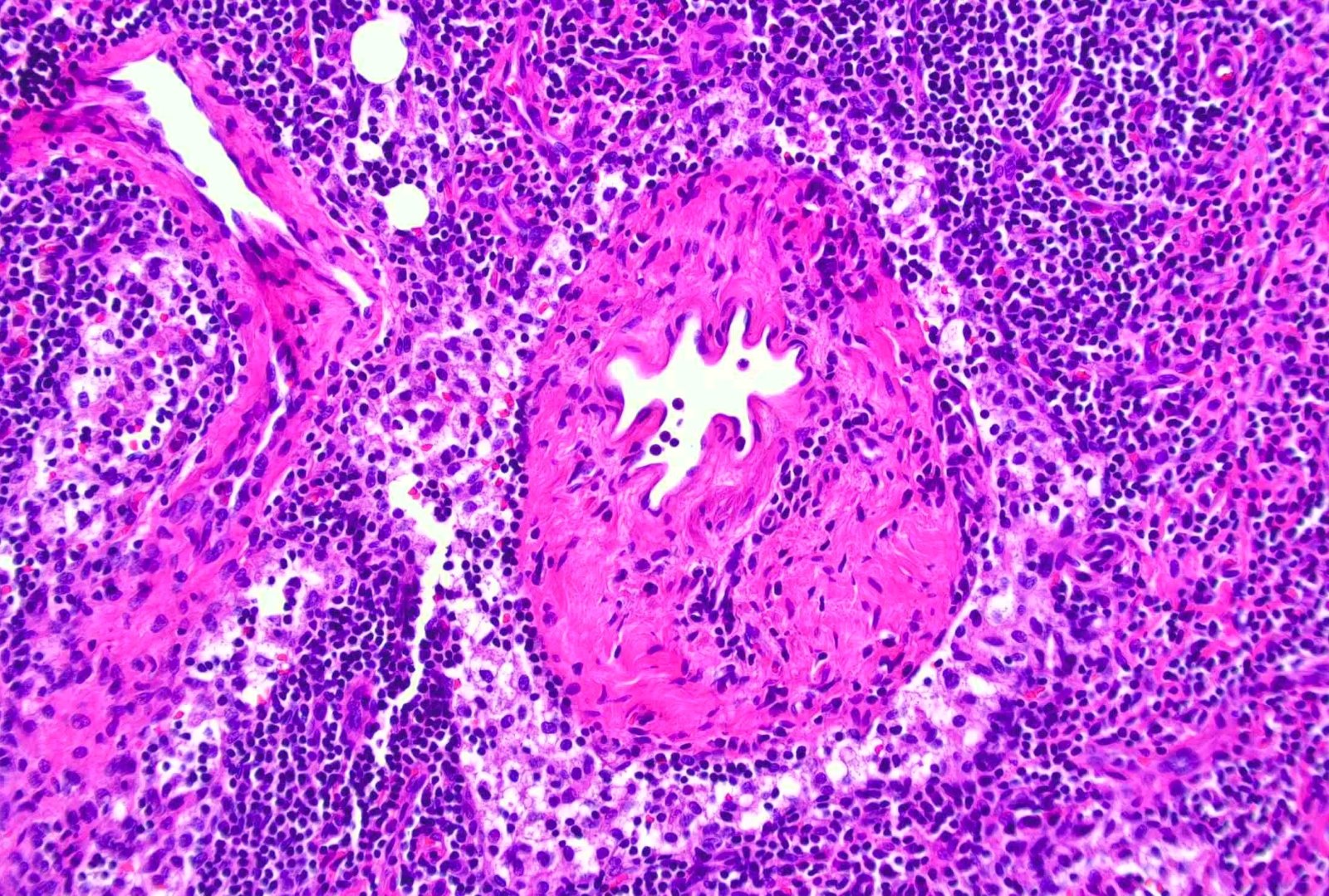
Abnormal blood vessels

Angiomyomatous proliferation

Thick walled vessels

Disarrayed smooth muscles
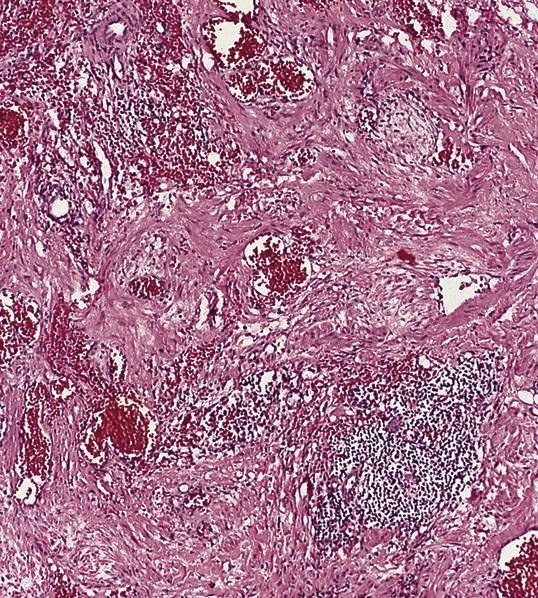
Angiomyomatous hamartoma of lymph node
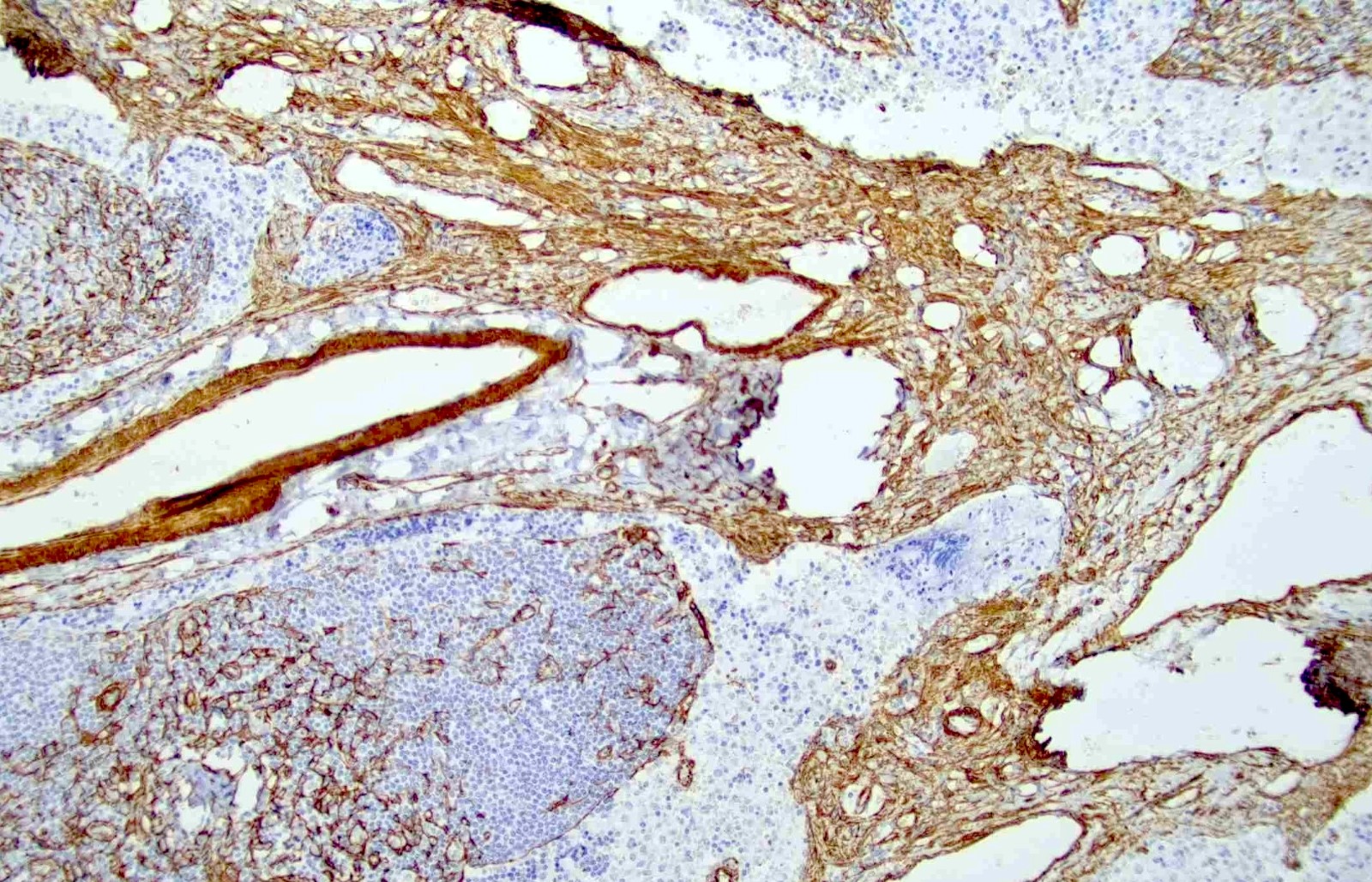
Smooth muscle actin
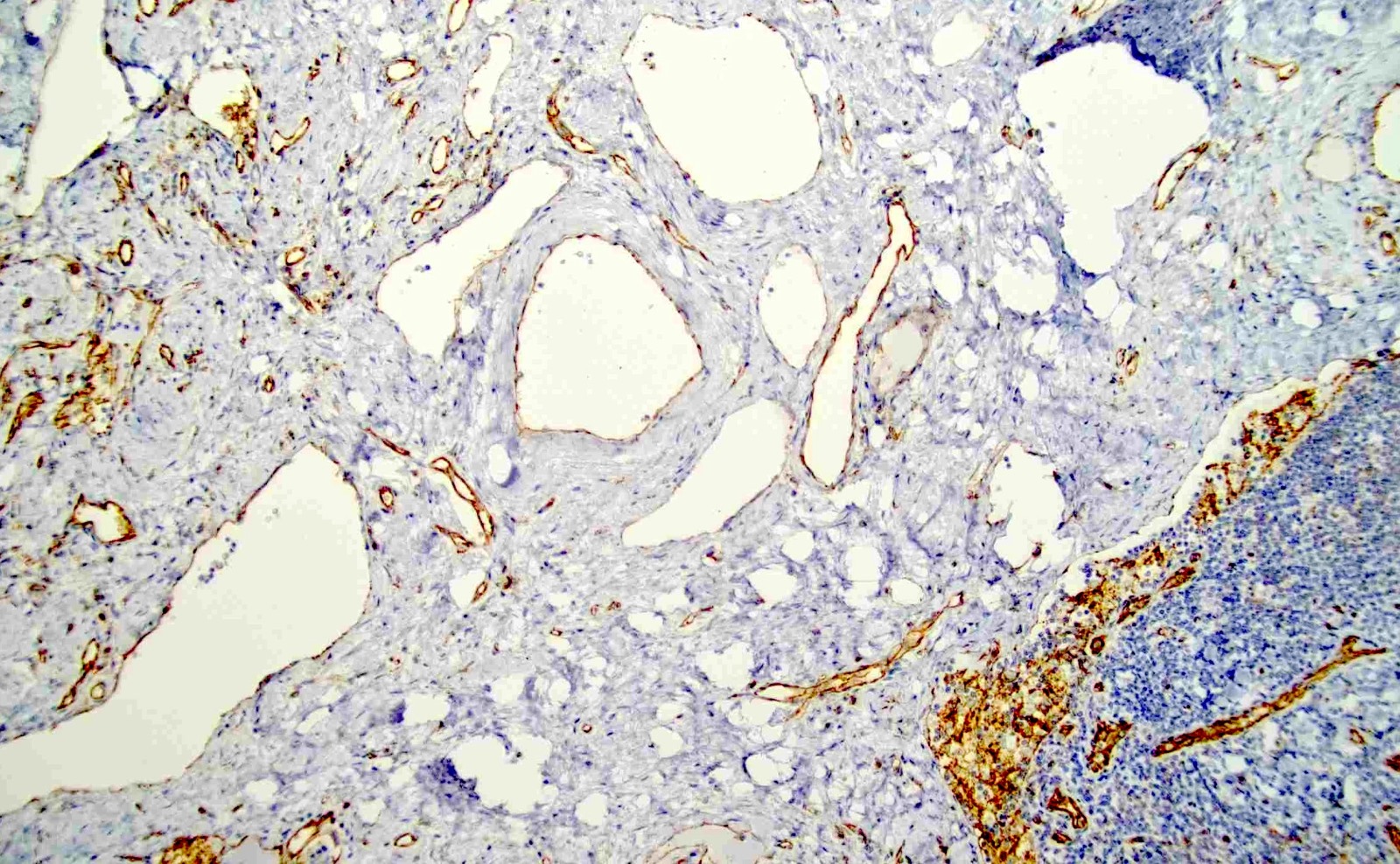
CD31
Positive stains
- Smooth muscle actin, caldesmon and desmin stain smooth muscle fibers
- CD31 and CD34 highlight endothelial cells (Int J Surg Pathol 2023 Nov 20 [Epub ahead of print])
Negative stains
- HMB45 and cathepsin K, in contrast to angiomyolipoma and lymphangioleiomyomatosis
- Ki67 is mostly negative (low proliferation) (Int J Surg Pathol 2023 Nov 20 [Epub ahead of print])
Sample pathology report
- Inguinal lymph node, excision:
- Angiomyomatous hamartoma of lymph node (see comment)
- Comment: The nodal architecture is disrupted by a haphazard proliferation of thick walled vasculature and smooth muscle bundles. Occasional adipocytes are admixed. No cytologic atypia or mitoses are seen. Residual lymphoid tissue with reactive lymphoid follicles is present in the cortex. Immunohistochemistry shows CD31 and SMA highlighting the endothelial cells and smooth muscles, respectively. HMB45 is negative.
Differential diagnosis
- Angiolipomatous hamartoma:
- Various nodal sites, including cervical, mediastinal and retroperitoneal lymph nodes
- Miscellaneous extranodal sites may be involved
- Associated with Castleman disease
- Angiomyolipoma:
- HMB45+
- Typically involves retroperitoneal nodes
- Associated with renal angiomyolipoma
- Lymphangiomatosis (Lymphat Res Biol 2011;9:191):
- Commonly in children and young adults, may be congenital
- Frequently involves lung with pleural effusion and other thoracic locations; also in bone, spleen and liver; primary nodal is rare
- Smooth muscle fascicles around anastomosing dilated vascular spaces lined by flat endothelial cells
- Lymphangioleiomyomatosis:
- Female predominance
- Lungs and occasionally retroperitoneal lymph nodes
- HMB45+ and cathepsin K+
- Thin walled lymphatic channels and spindle cells in a fascicular pattern
- Vascular transformation of lymph node sinuses (Am J Surg Pathol 1991;15:732):
- Small capillary vascular channels replacing nodal subcapsular sinuses
- Reactive process often accompanied by fibrosis; no cytologic atypia
- Involves single or multiple lymph nodes in a diffuse or segmental fashion
Board review style question #1
When differentiating angiomyomatous hamartoma from angiomyolipoma, which of the following immunohistochemical stains is the most helpful?
- CD31
- CD34
- HMB45
- SMA
Board review style answer #1
C. HMB45. Angiomyomatous hamartoma is negative for melanocytic markers (HMB45 and MelanA), while angiomyolipoma is positive for these stains. Answers A and B are incorrect because both lesions contain vascular proliferation which can be highlighted by the endothelial markers, CD31 and CD34. Answer D is incorrect because both lesions show positivity for SMA, which does not help differentiate these entities.
Comment Here
Reference: Angiomyomatous hamartoma
Comment Here
Reference: Angiomyomatous hamartoma
Board review style question #2
Which of the following statements is true of angiomyomatous hamartoma of the lymph node?
- It can present as localized edema of the limb
- It is associated with HHV8 infection
- It is considered a premalignant lesion
- It stains for HMB45
Board review style answer #2
A. It can present as localized edema of the limb. Angiomyomatous hamartoma may be found incidentally or may present with pain or localized edema. It can be present in any location but has a predilection for the inguinal and femoral lymph nodes. Answer C is incorrect because this entity is a benign hamartoma that consists of proliferation of smooth muscles and blood vessels. Answers B and D are incorrect because there is no known association with HHV8 or melanocytic immunostain markers.
Comment Here
Reference: Angiomyomatous hamartoma
Comment Here
Reference: Angiomyomatous hamartoma
