
Lymph nodes & spleen, nonlymphoma
Lymph nodes-inflammatory / reactive disorders
Indolent T lymphoblastic proliferations
Editorial Board Member: Elizabeth Courville, M.D.
Deputy Editor-in-Chief: Genevieve M. Crane, M.D., Ph.D.


Last author update: 19 April 2022
Last staff update: 19 April 2022
Copyright: 2021-2024, PathologyOutlines.com, Inc.
PubMed Search: Indolent T-lymphoblastic proliferations
Table of Contents
Definition / general | Essential features | Terminology | Epidemiology | Sites | Clinical features | Diagnosis | Prognostic factors | Case reports | Treatment | Gross description | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Positive stains | Negative stains | Flow cytometry description | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Singh K, Ohgami R. Indolent T lymphoblastic proliferations. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/lymphnodestlymphoblastic.html. Accessed April 18th, 2024.
Definition / general
- Benign expansion of immature terminal deoxynucleotidyl transferase (TdT) positive T cells in extramedullary and extrathymic tissues
- Can be seen concurrently with other hematologic disorders or epithelial malignancies, such as Castleman disease, follicular dendritic cell sarcomas, angioimmunoblastic T cell lymphoma, hepatocellular carcinoma, acinic cell carcinoma, etc.
Essential features
- Benign proliferation of extrathymic immature T cells that lack significant morphologic atypia but mimic malignant T lymphoblastic lymphoma / leukemia
- Nonclonal process without evidence of TCR γ or β gene rearrangements
- Lack of aberrant immunophenotypic or karyotypic abnormalities
Terminology
- Immature T lymphoblastic proliferation
- iT-LBP
Epidemiology
- Age, gender, ethnicity, incidence / prevalence are undefined at this point
Sites
- Typically presents with localized lymphadenopathy or a discrete mass
- Common anatomical locations: mandible, cervical, supraclavicular, abdominal, retroperitoneal and oropharyngeal regions (Adv Anat Pathol 2013;20:137)
- Rare cases have shown disseminated multinodal involvement (Am J Surg Pathol 2014;38:1298)
- Does not involve mediastinum
- Peripheral blood and bone marrow are not involved
Clinical features
- Clinical presentation varies but patients are generally asymptomatic and healthy
- Can be associated with other underlying neoplastic pathologic conditions, such as carcinomas, Castleman disease, follicular dendritic cell tumors and angioimmunoblastic T cell lymphoma (Am J Surg Pathol 2012;36:1619)
Diagnosis
- Major criteria (Adv Anat Pathol 2013;20:137):
- No aberrant antigen expression (immunophenotype is of normal immature cortical thymocytes)
- Nonclonal TdT+ T cells
- No evidence of T cell gene rearrangements (TCR α and TCR β)
- Clinical evidence of indolence, > 6 months of follow up without progression in the absence of treatment
Prognostic factors
- Clinically indolent
- May persist in the involved tissue
Case reports
- 35 year old man with indolent T lymphoblastic proliferation associated with low grade follicular dendritic cell sarcoma and Castleman disease (Pathology 2018;50:351)
- 37 year old woman with an indolent T lymphoblastic proliferation involving the upper aerodigestive tract (Int J Clin Exp Pathol 2014;7:6350)
- 41 year old woman with pelvic pain found to have localized Castleman disease with concomitant iT-LBP (Ann Pathol 2019;39:29)
Treatment
- Typical lesions show no signs of progression and require no treatment
- Treatment for secondary disease (if present) may be needed
Gross description
- Typically forms a tumor mass, varies in size from ≤ 1 cm to ≥ 9 cm in greatest dimension
- External surface may be firm and fibrous or nonencapsulated
- Displays pink-tan firm fleshy cut surfaces
- Necrotic (yellow) areas may be seen in cases associated with hepatocellular carcinoma (HCC)
- Reference: Adv Anat Pathol 2013;20:137
Microscopic (histologic) description
- Preservation of overall tissue architecture (Adv Anat Pathol 2013;20:137)
- Lymph nodes: benign lymphoblasts localize predominantly to interfollicular / paracortical regions
- Carcinomas: lymphoblasts are interspersed or clustered between malignant epithelial cells without definitive evidence of lymphoepithelial lesions
- Small to intermediate sized lymphoid cells with immature fine / blastoid chromatin lacking significant atypia
- Inconspicuous nucleoli
- Numerous mitotic figures may be present
- Histiocytes are interspersed evenly throughout the proliferation
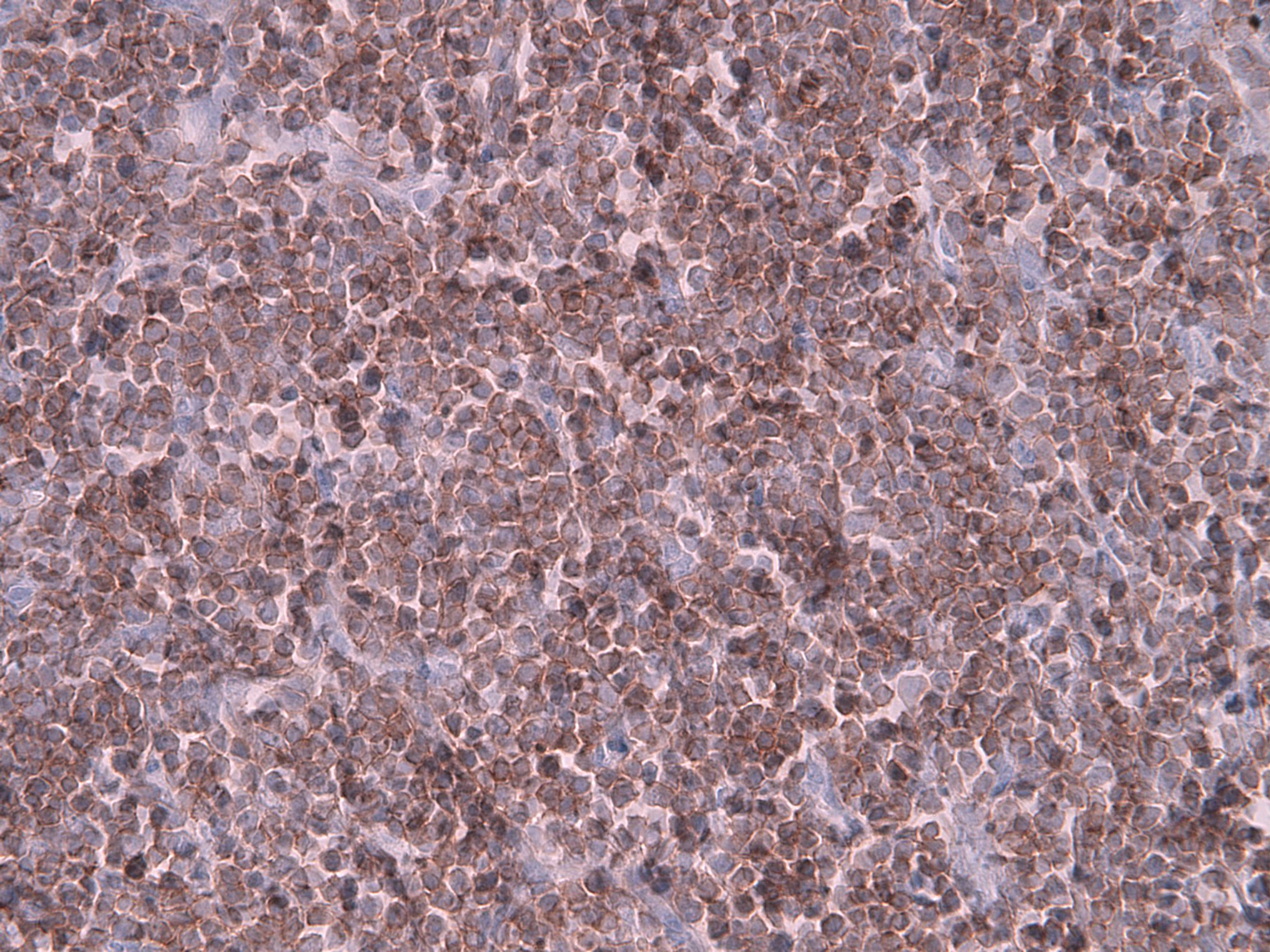
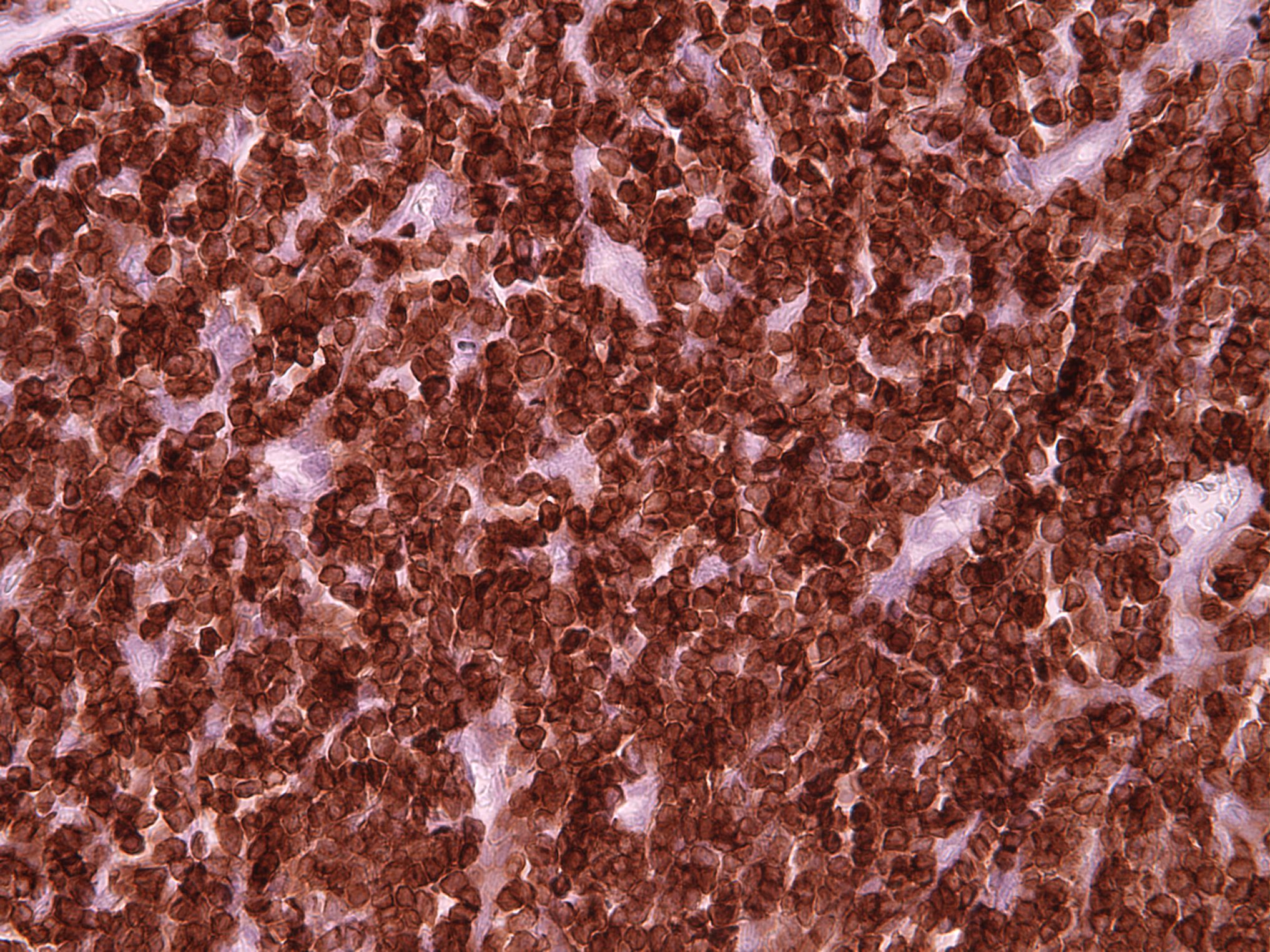
Microscopic (histologic) images
Contributed by Kunwar Singh, M.D. and Robert S. Ohgami, M.D., Ph.D.
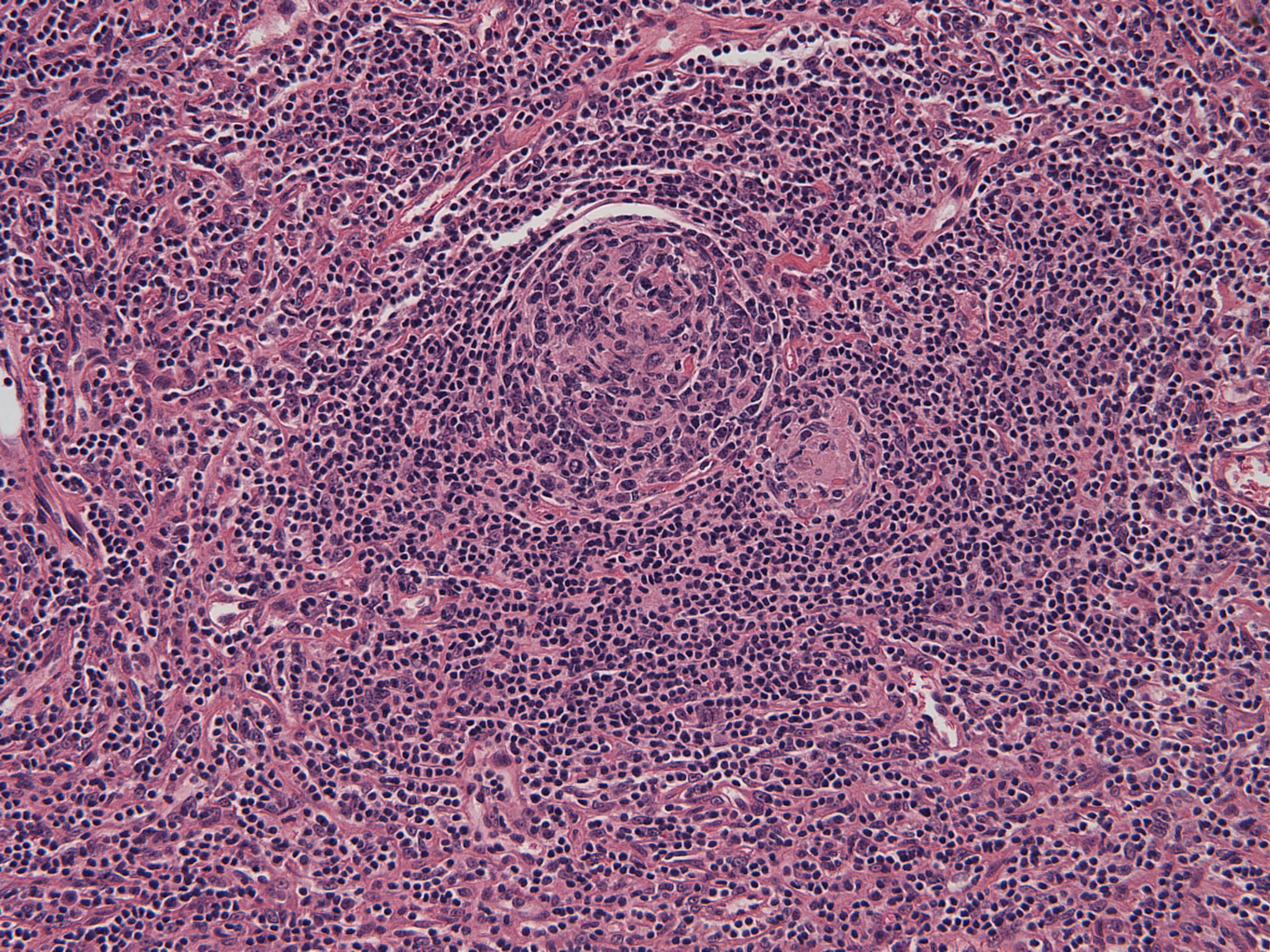
Castleman disease
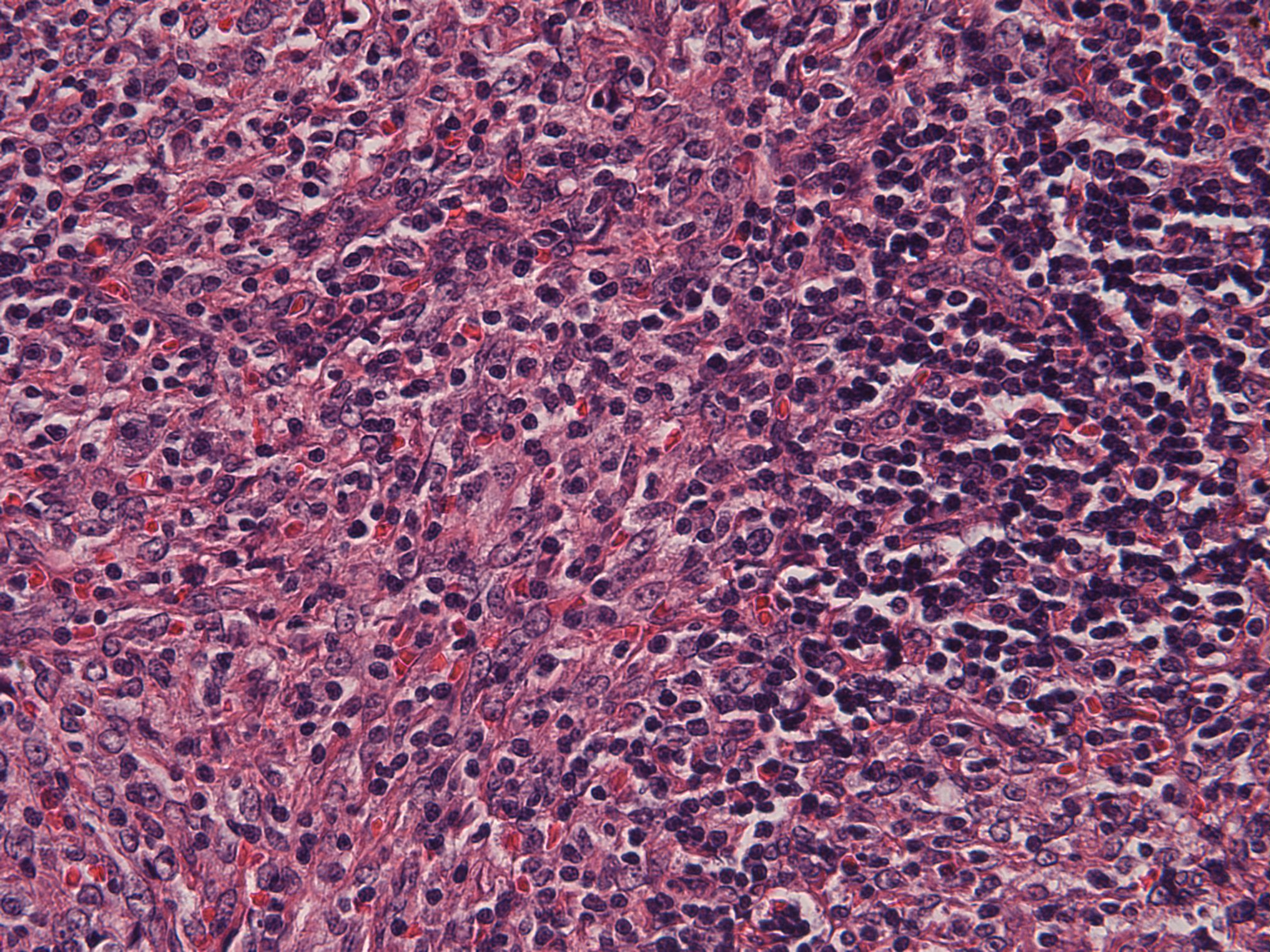
Follicular dendritic cell tumor
CD1a
CD3
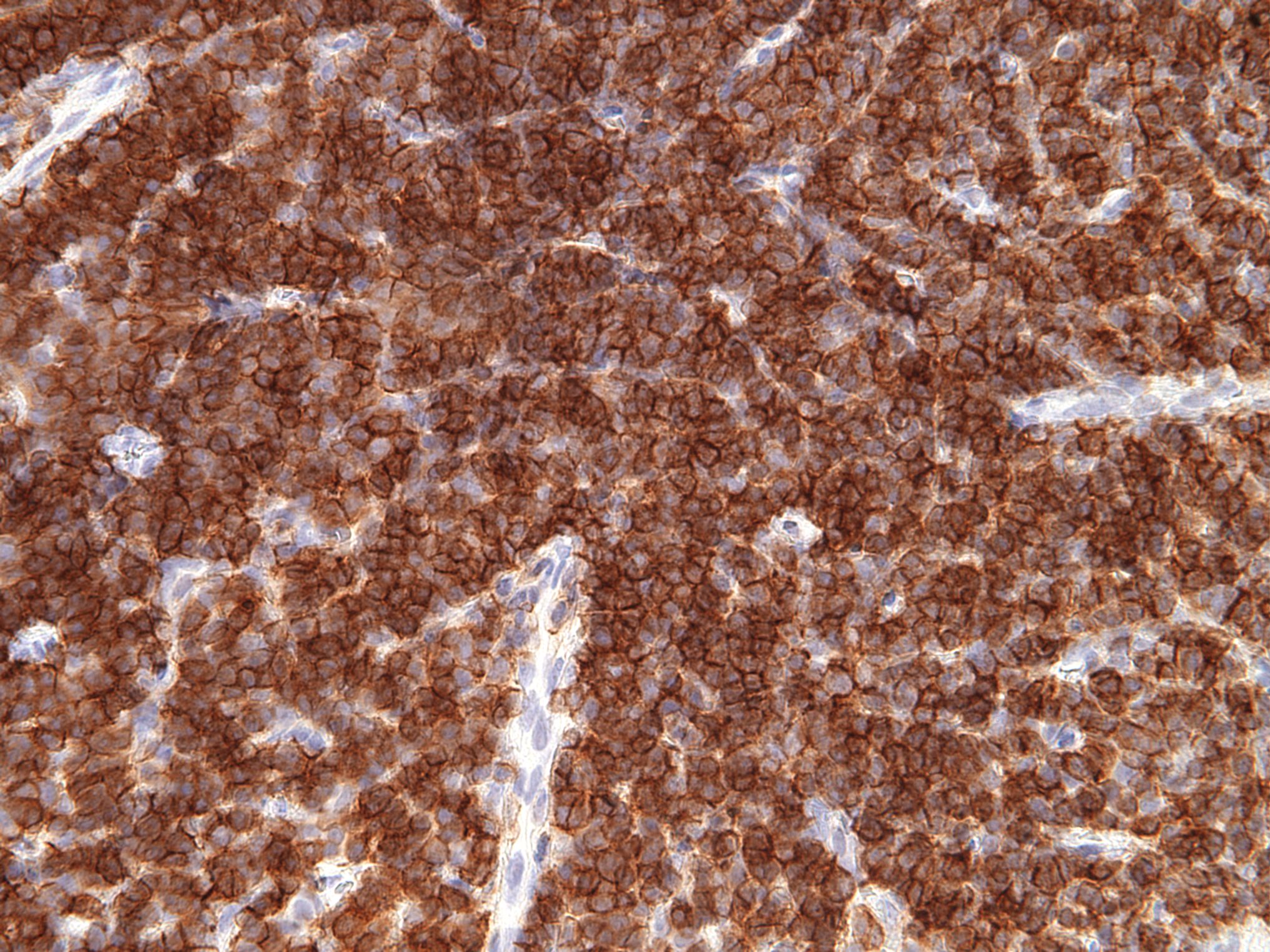
CD4
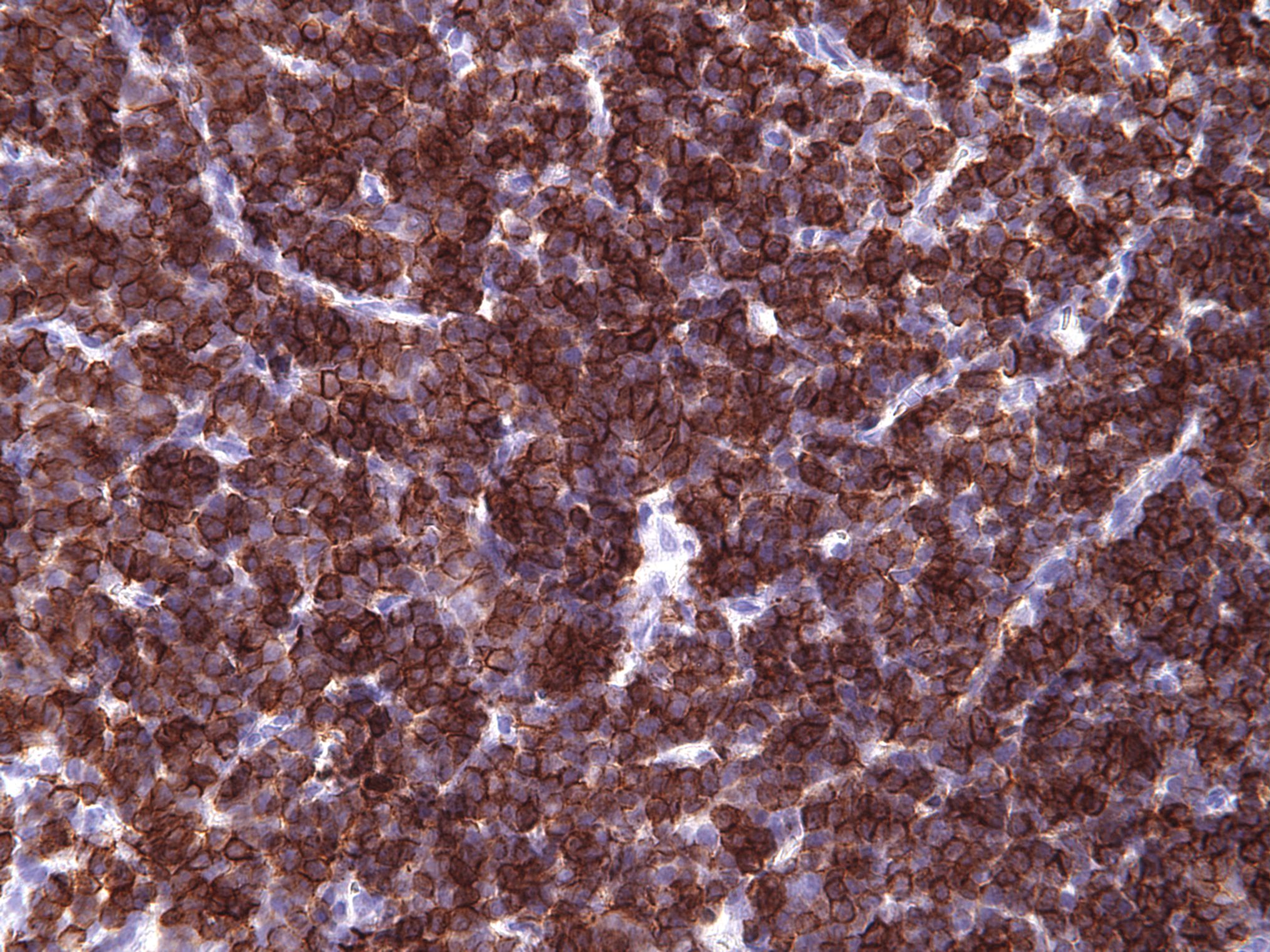
CD8
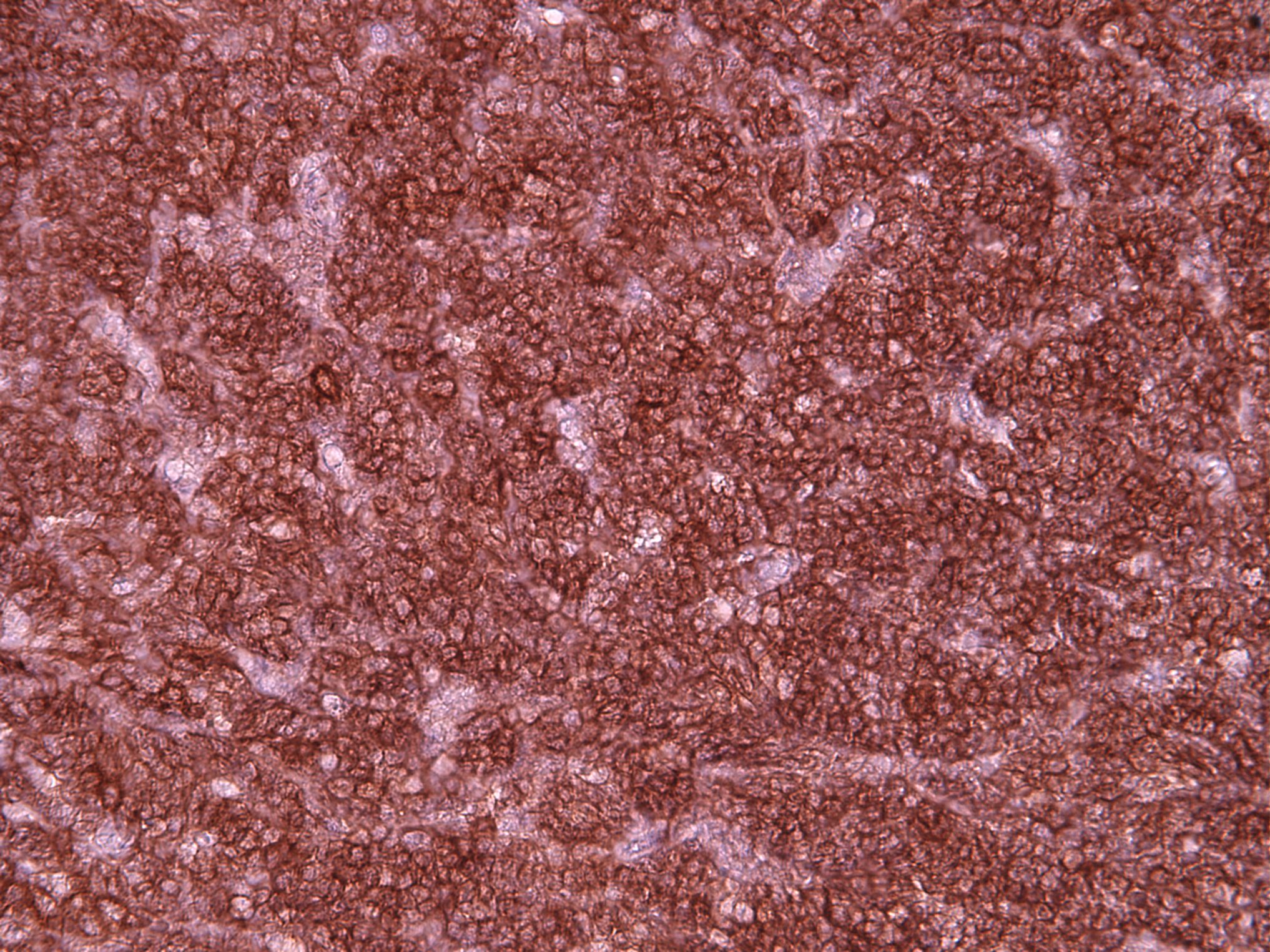
CD99
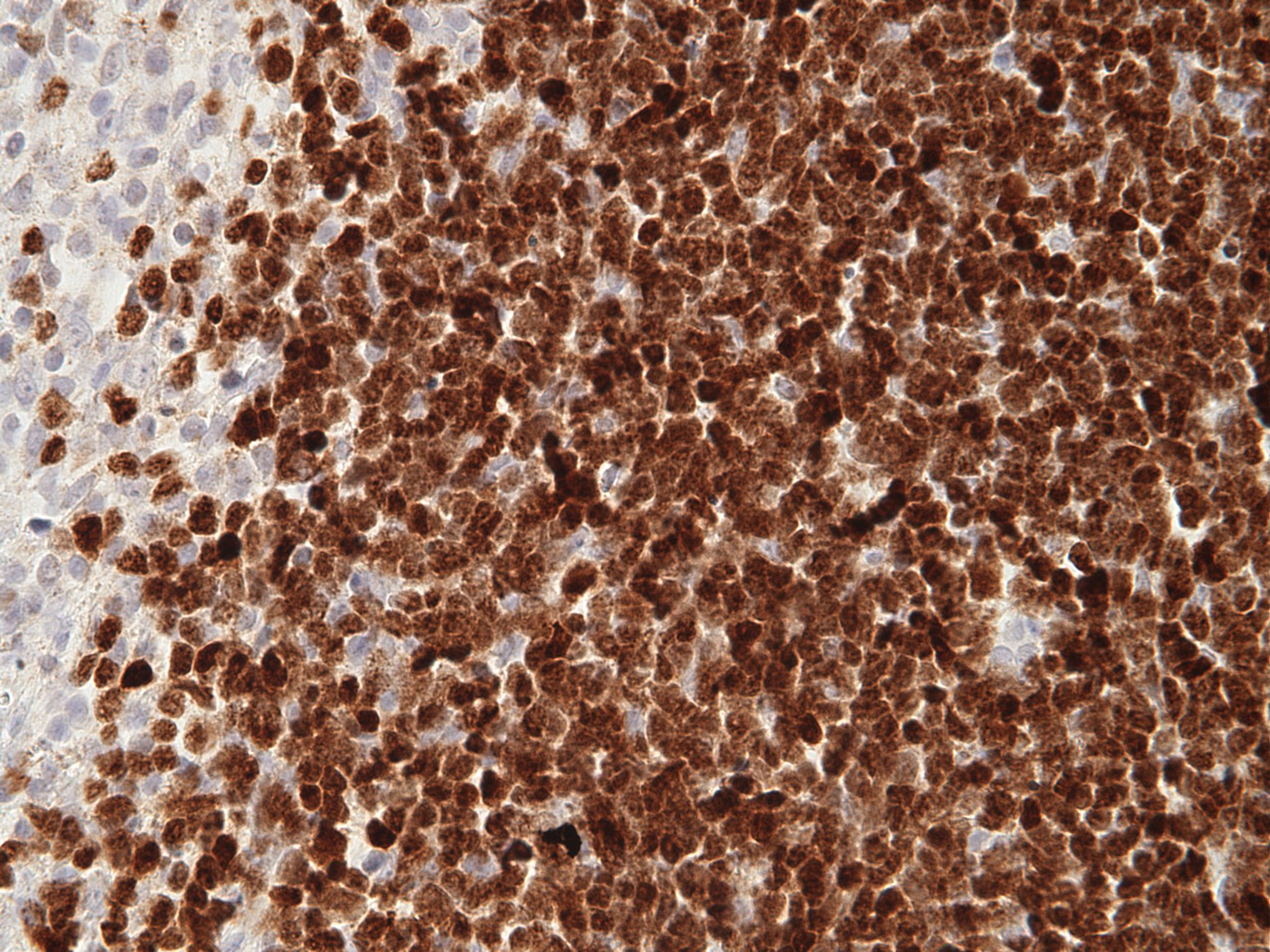
TdT
Cytology description
- Small to intermediate sized monotonous population with fine dispersed chromatin pattern and scant cytoplasm; occasional variably sized nucleoli may be present
Positive stains
Flow cytometry description
- Incidental benign TdT+ T cell populations may be detected by flow cytometry
- Immunophenotype can show the entire range of T cell differentiation from the most immature dual CD4- / CD8- / CD7 bright+ / CD34+ / cytoplasmic CD3+ / surface CD3- forms to surface CD3+ forms with coexpression of CD4 and CD8 (Cytometry B Clin Cytom 2020;98:282)
- Proportion of T lymphoblasts (identified by cytoplasmic CD3 and TdT expression) can vary from < 1% of events to > 50% of events
Molecular / cytogenetics description
- iT-LBP have nonclonal T cell receptor (TCR) gene rearrangement studies (TCR γ or β)
- No definitive chromosomal abnormalities
- Initial reported case reported chromosome 9 inversion of uncertain significance (Am J Surg Pathol 1999;23:977)
Sample pathology report
- Lymph node, inguinal, excision:
- Castleman disease, hyaline vascular variant
- Indolent T lymphoblastic proliferation (see comment)
- Comment: Sections from the inguinal node show predominantly preserved nodal architecture with atretic follicles and increased vascularity with a subset of hyalinized vessels penetrating regressed germinal centers. Interspersed within the paracortical areas are increased CD3+ / TdT+ positive T cells without aberrant antigen expression. The presence of immature T cells in association with hyaline vascular Castleman disease has been reported and typically shows indolent behavior. Clinical correlation is recommended. (Am J Surg Pathol 2012;36:1619)
Differential diagnosis
- T lymphoblastic leukemia / lymphoma:
- Typically effaces nodal architecture or will infiltrate relatively nondiscriminately throughout entire node obliterating residual follicles
- Usually expresses LMO2 on malignant lymphoblasts (Histopathology 2020;77:984)
- Ectopic thymic tissue:
- Thymoma:
- Lobulated architecture
- Presence of thymic epithelial meshworks
- No expression of LMO2 on lymphoblasts
- Presence in the mediastinum
Additional references
Board review style question #1
Which of the following antigens do indolent T lymphoblastic proliferations lack?
- CD3
- CD20
- CD33
- CD45
- TdT
Board review style answer #1
B. CD20. CD20 is a B cell marker which is not expressed by T lymphoblasts. CD3 is incorrect as it is a T cell marker expressed by indolent T lymphoblastic proliferations. CD33 is a myeloid associated marker which has been described as expressed by a subset of indolent T lymphoblastic proliferations. CD45 is a pan-hematopoietic cell marker which is expressed by indolent T lymphoblastic proliferations. TdT is incorrect as it is an immature marker expressed by indolent T lymphoblastic proliferations.
Comment Here
Reference: Indolent T lymphoblastic proliferations
Comment Here
Reference: Indolent T lymphoblastic proliferations
Board review style question #2
Which of the following has been described to concomitantly occur in the disorder seen in the image above?
- Chronic lymphadenitis
- Indolent T lymphoblastic proliferation
- Kikuchi-Fujimoto disease
- Kimura disease
- Rosai-Dorfman disease
Board review style answer #2
B. Indolent T lymphoblastic proliferation. This image shows a lymph node typical of Castleman disease. Indolent T lymphoblastic proliferations have been described in association with Castleman disease. Chronic lymphadenitis is incorrect as it is not a disease well known to occur in association with Castleman disease. Kikuchi-Fujimoto disease is incorrect as this is a necrotizing lymphadenitis of unknown etiology and association. Kimura disease is incorrect as it would show numerous eosinophils and eosinophilic granulomas and is not associated with Castleman disease. Rosai-Dorfman disease is incorrect as it shows large histiocytic cells with round to ovoid nuclei and distinct central nucleoli that exhibit emperipolesis.
Comment Here
Reference: Indolent T lymphoblastic proliferations
Comment Here
Reference: Indolent T lymphoblastic proliferations
