
Mandible & maxilla
Benign odontogenic tumors
Dentinogenic ghost cell tumor
Editorial Board Member: Kelly Magliocca, D.D.S., M.P.H.
Editor-in-Chief: Debra L. Zynger, M.D.


Last author update: 5 October 2020
Last staff update: 20 July 2023
Copyright: 2020-2024, PathologyOutlines.com, Inc.
PubMed Search: Dentinogenic ghost cell tumor
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Negative stains | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Jewett FC, Nelson BL. Dentinogenic ghost cell tumor. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/mandiblemaxilladentinogenicghost.html. Accessed April 18th, 2024.
Definition / general
- Benign, locally aggressive odontogenic neoplasm of maxilla and mandible with a predominantly solid pattern of growth
Essential features
- Neoplasm with predominantly solid growth of islands of odontogenic and ameloblastoma-like epithelium
- Ghost cells composed of anucleate epithelial cells with pale cytoplasm
- Focal stellate reticulum-like epithelium
- Varying levels of calcified material to include products of odontogenesis and calcification of the ghost cell
- Locally aggressive with high rates of recurrence
- Histopathologic overlap with calcifying odontogenic cysts
Terminology
- Epithelial odontogenic ghost cell tumor
- Calcifying ghost cell odontogenic tumor
- Previously classified along with calcifying odontogenic cyst (J Periodontol 1985;56:340)
ICD coding
- ICD-10: D16.4 - benign neoplasm of bones of skull and face
Epidemiology
- Broad age range (11 - 79 years old); peak 40 - 60 years old
- M:F = 1.8:1 (J Oral Pathol Med 2018;47:721)
- Rarity may affect demographics
Sites
- Intraosseous sites: posterior maxilla and mandible
- Rarely reported as gingiva or alveolar mucosal tumor
Pathophysiology
- Wnt signaling pathway may have a role in the development similar to calcifying odontogenic cyst since beta catenin gene mutations and beta catenin overexpression are also identified in DGCT (PLoS One 2017;12:e0180224, Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2007;103:97)
Etiology
- Unknown
Clinical features
- Patients frequently present with asymptomatic swelling of the jaw
Diagnosis
- Radiologic and histopathologic correlation required for diagnosis
Radiology description
- Majority present as radiopaque lesions with well defined borders and a mixed radiodensity due to varying levels of calcification
- Rarely associated with odontomas, similar to calcifying odontogenic cyst (Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2006;101:356)
Radiology images
Contributed by Brenda L. Nelson, D.D.S., M.S. and Kelly Magliocca, D.D.S., M.P.H.


Unilocular lesion
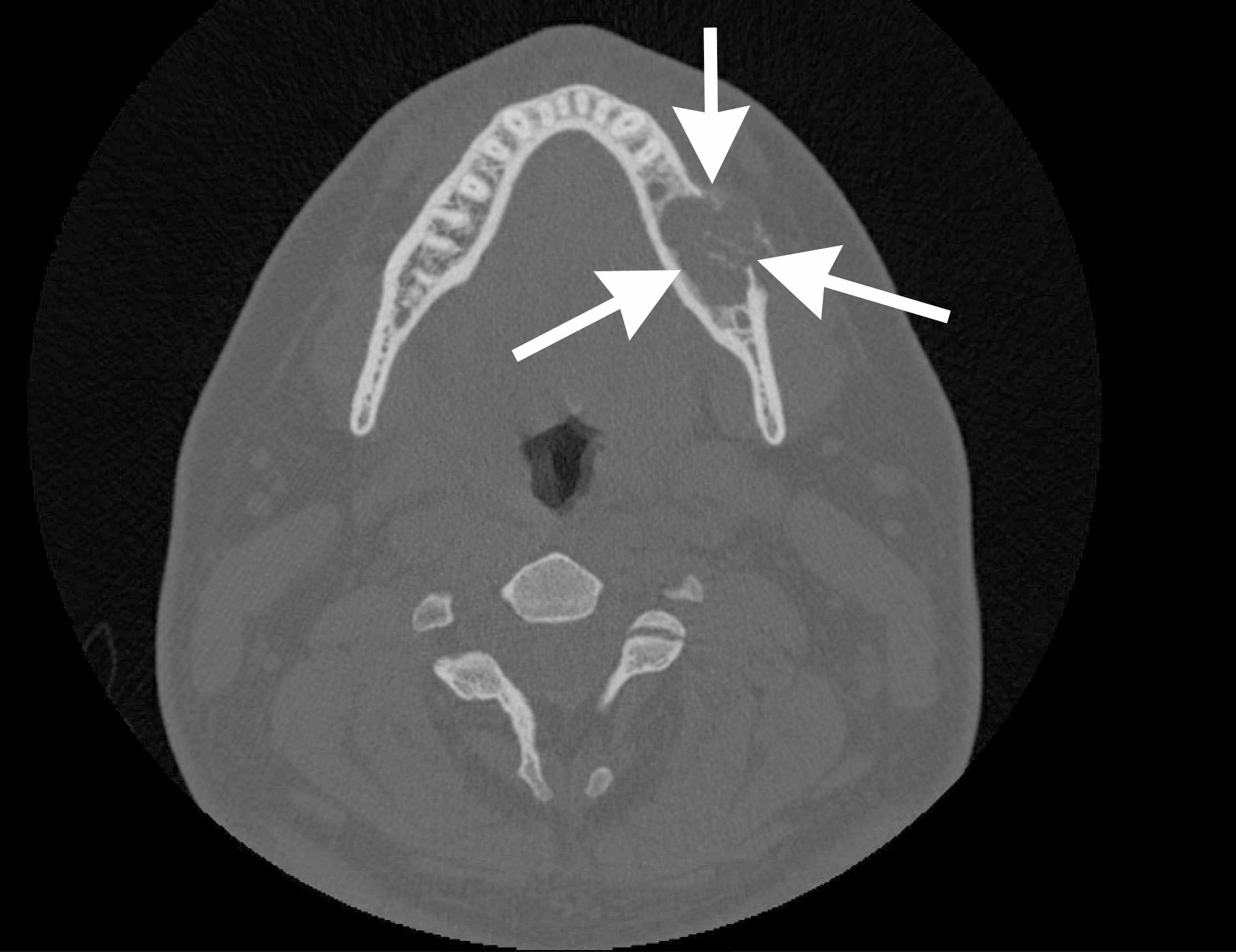
Axial CT
Prognostic factors
- High rates of recurrence with simple enucleation (up to 73%) (J Oral Maxillofac Surg 2016;74:307)
- Lower but still significant rates of recurrence with more extensive procedures (up to 33%) (J Oral Maxillofac Surg 2016;74:307)
- Limited reported cases may affect knowledge of true prognosis
Case reports
- 18 year old man reported with recurrent swelling and pain in upper jaw (World J Clin Oncol 2019;10:192)
- 26 year old man with a growth in the upper left front part of the jaw (J Oral Maxillofac Pathol 2018;22:150)
- 40 year old man with swelling on the right side of the face (J Oral Maxillofac Pathol 2019;23:478)
- 40 year old woman with swelling in the front region of the lower jaw for 2 years (J Oral Maxillofac Pathol 2019;23:66)
- 68 year old man with a soft tissue growth in lower anterior region of the jaw for 3 years (J Oral Maxillofac Pathol 2016;20:163)
Treatment
- Rarity of this tumor limits study of the optimal form of treatment
- Simple enucleation, curettage: recurrence rate of up to 73% after a follow up period of 1 - 20 years
- Recurrence rates vary by surgical approach; recent recommendation includes wide local resection
Gross description
- Predominantly solid tumor; limited macrocystic change
Gross images
Contributed by Kelly Magliocca, D.D.S., M.P.H.
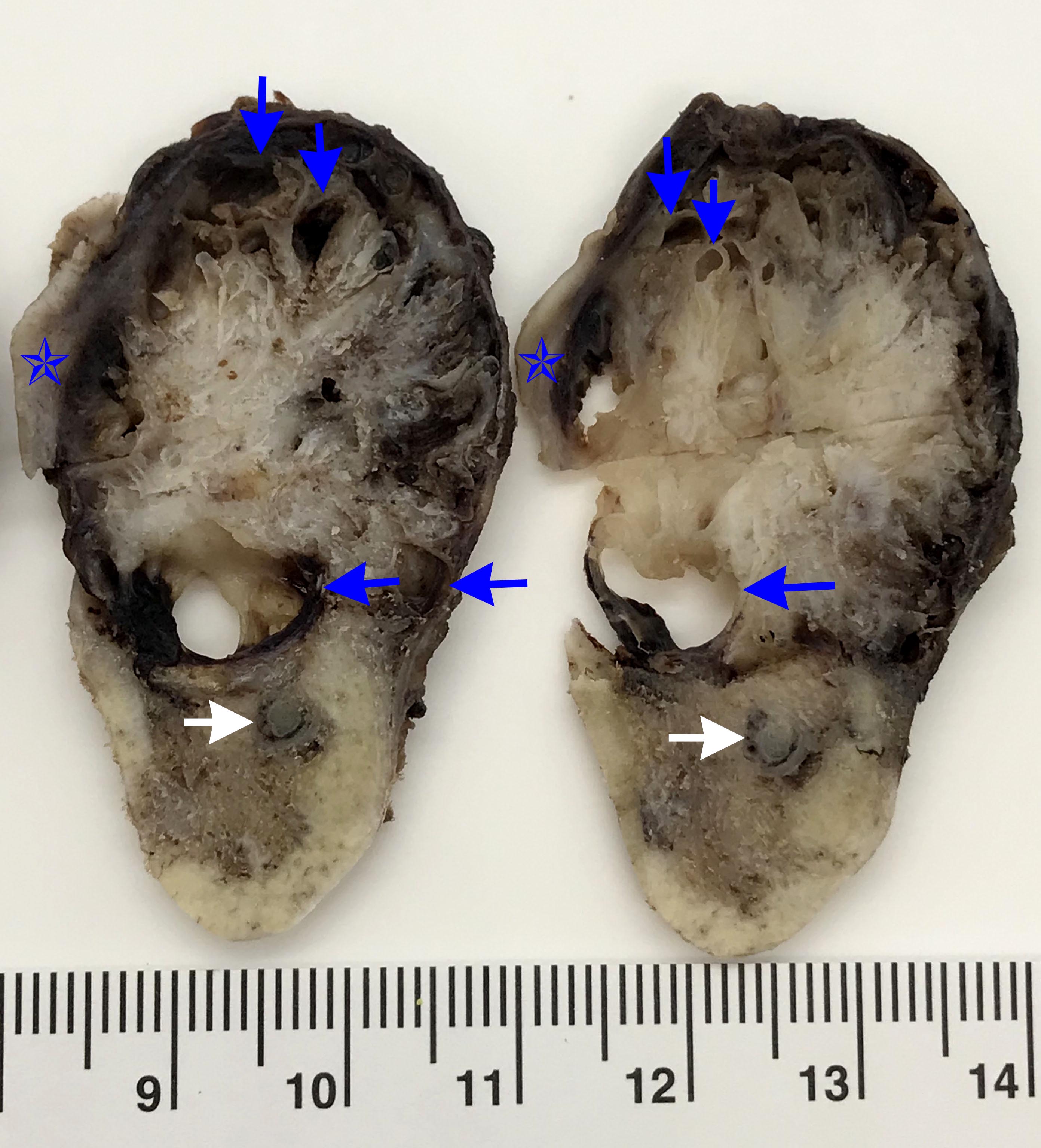
Cross sections of mandible tumor
Microscopic (histologic) description
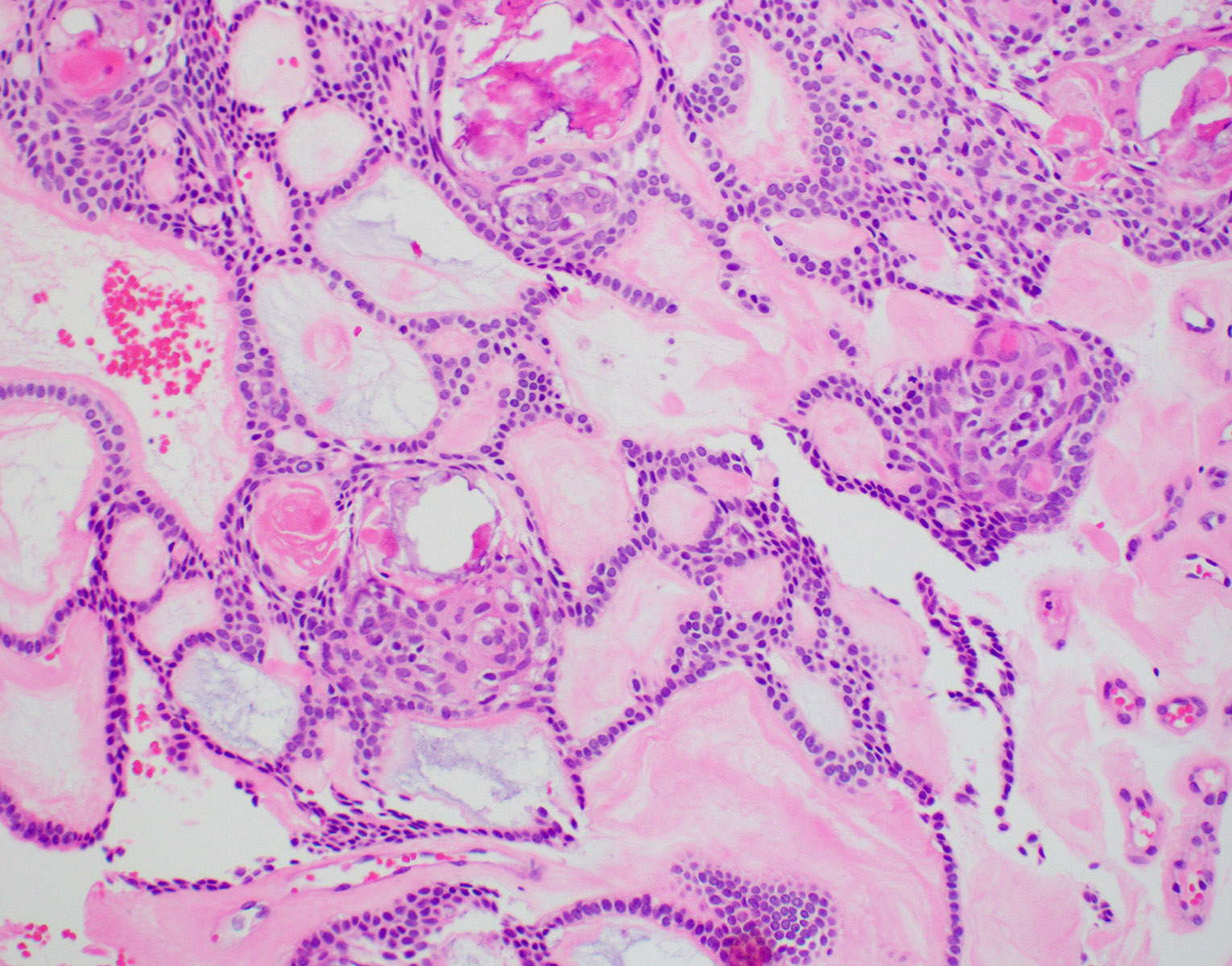
- Predominantly solid mass consisting of sheets of anastomosing cords and strands of odontogenic epithelium; microcystic development possible
- Admixed ghost cells: anucleate epithelial cells with pale cytoplasm containing cytoplasmic clearings representing the location of a previously resorbed nucleus or organelles
- Interspersed with islands of swirling cells with squamous differentiation
- Ameloblastic-like areas with palisading of basaloid cells
- Odontogenic epithelial cells demonstrate round uniform basophilic nuclei and pale eosinophilic to clear cytoplasm
- Background stellate reticulum-like proliferation
- Varying levels of dentinoid and cementum-like calcified collagenous matrix
- Mitosis rare
- Reference: J Oral Maxillofac Surg 2016;74:307
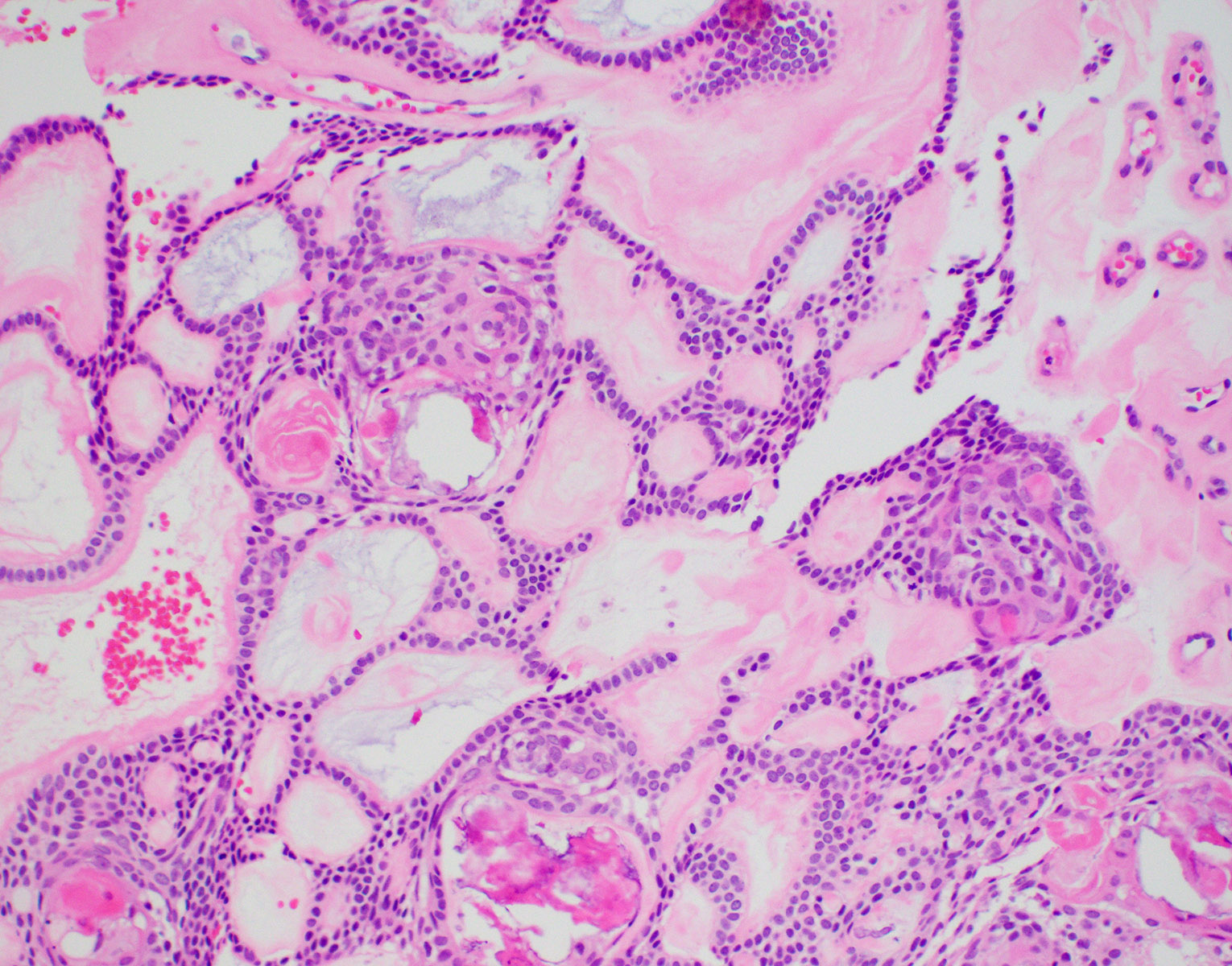
Microscopic (histologic) images
Contributed by Kelly Magliocca, D.D.S., M.P.H., Brenda L. Nelson, D.D.S., M.S. and Anne McLean, D.M.D.
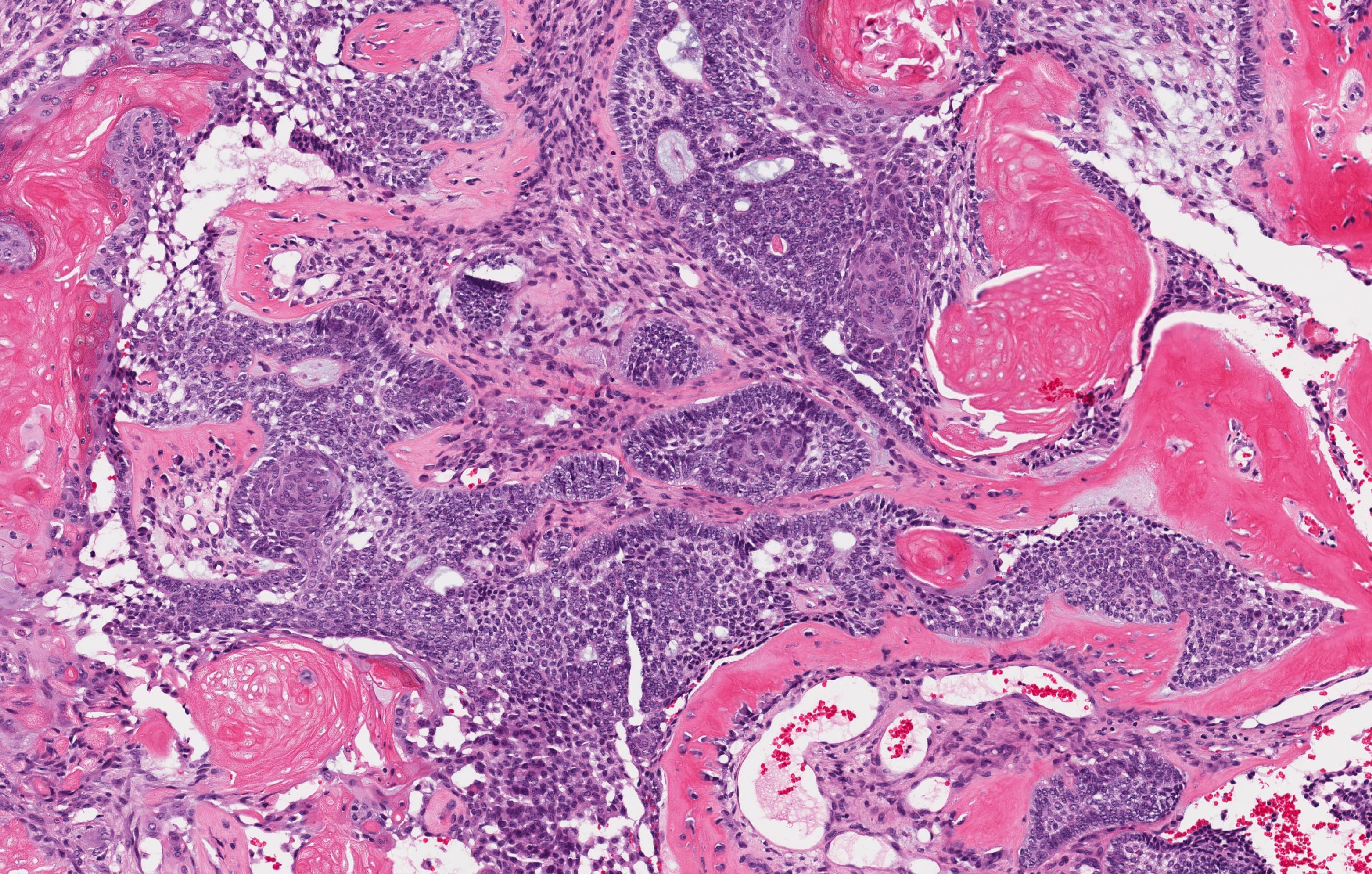
Dentinogenic ghost cell tumor
Calcifications and squamous morules
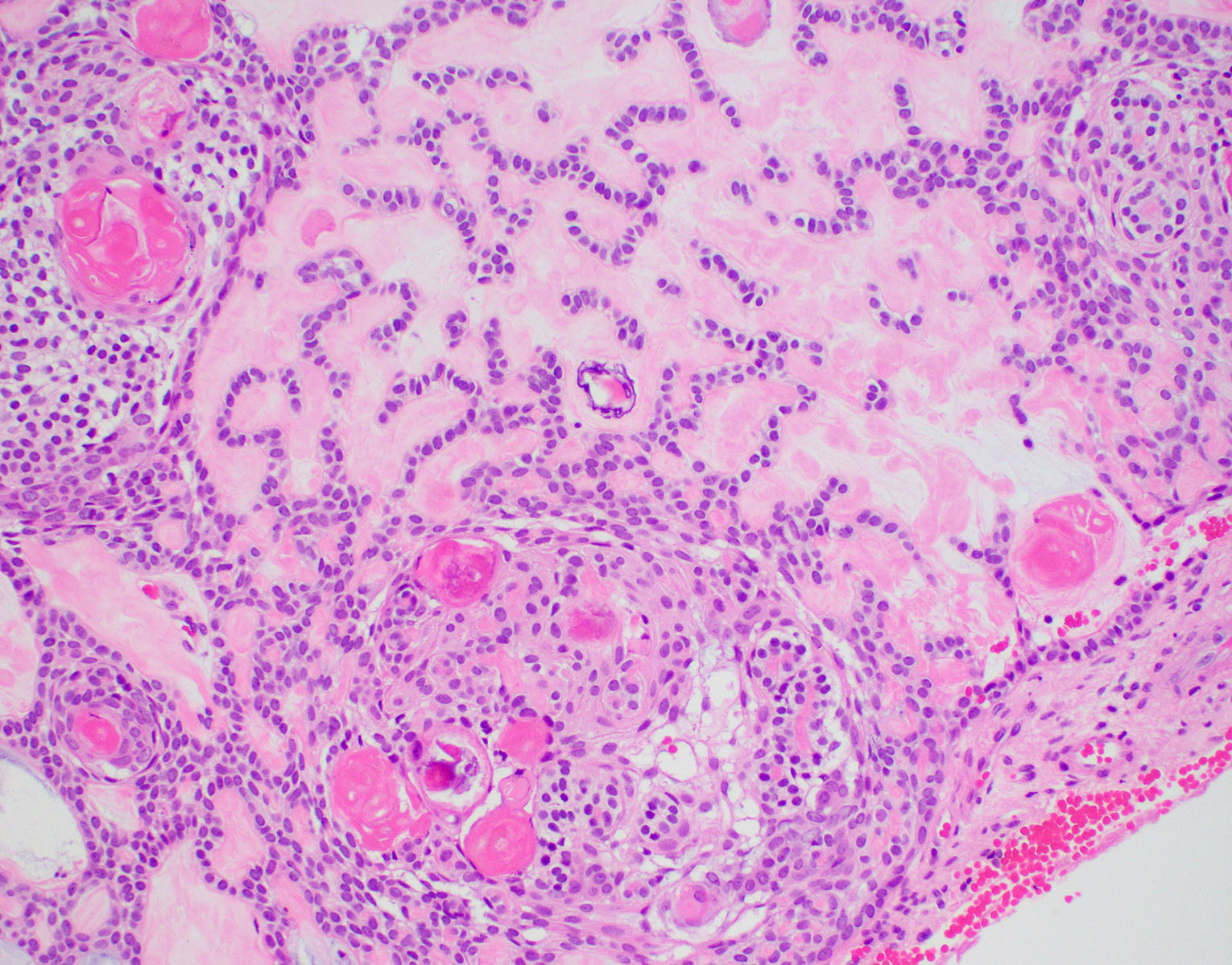
Ghost cells
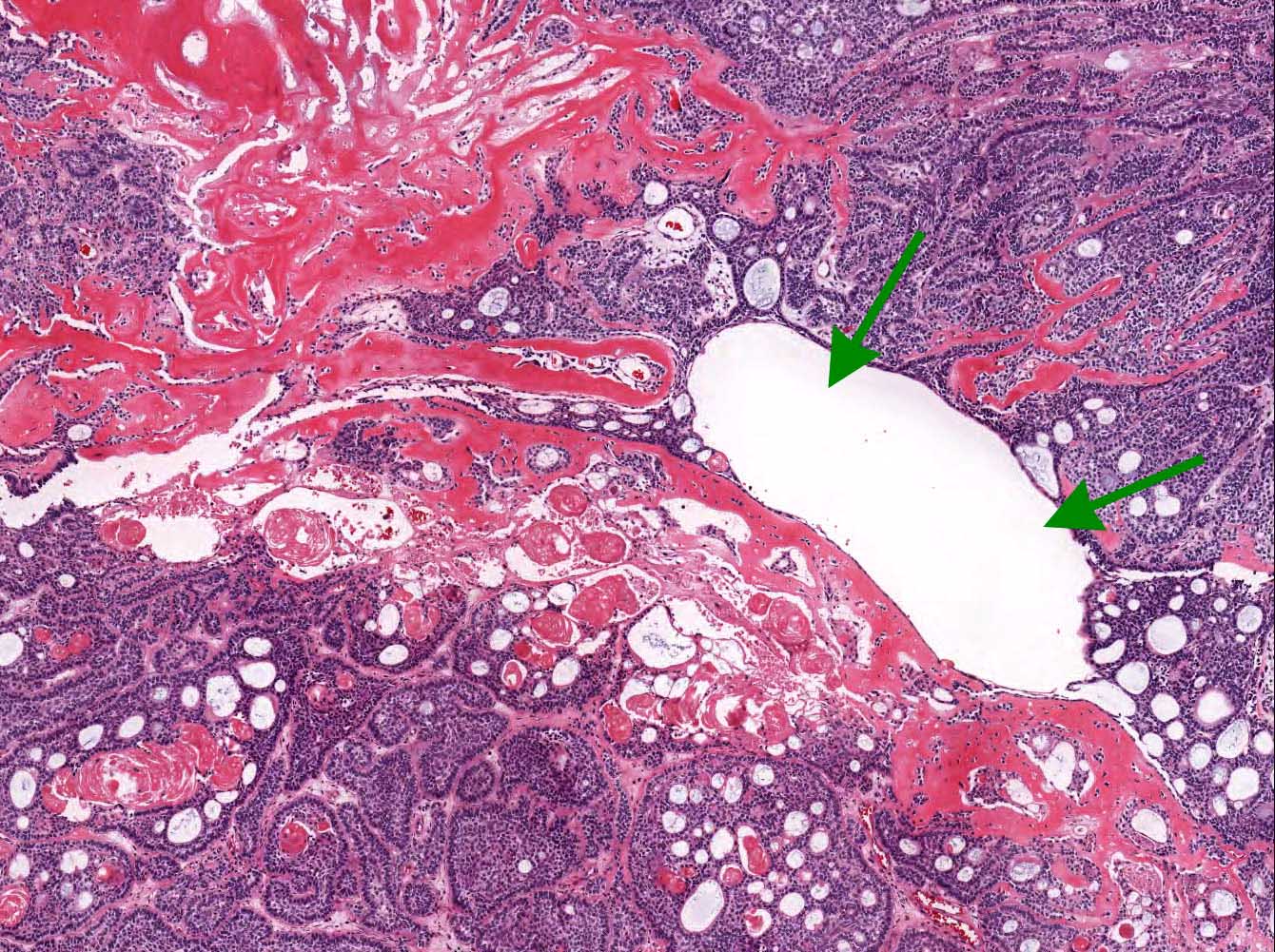

Microcyst formation
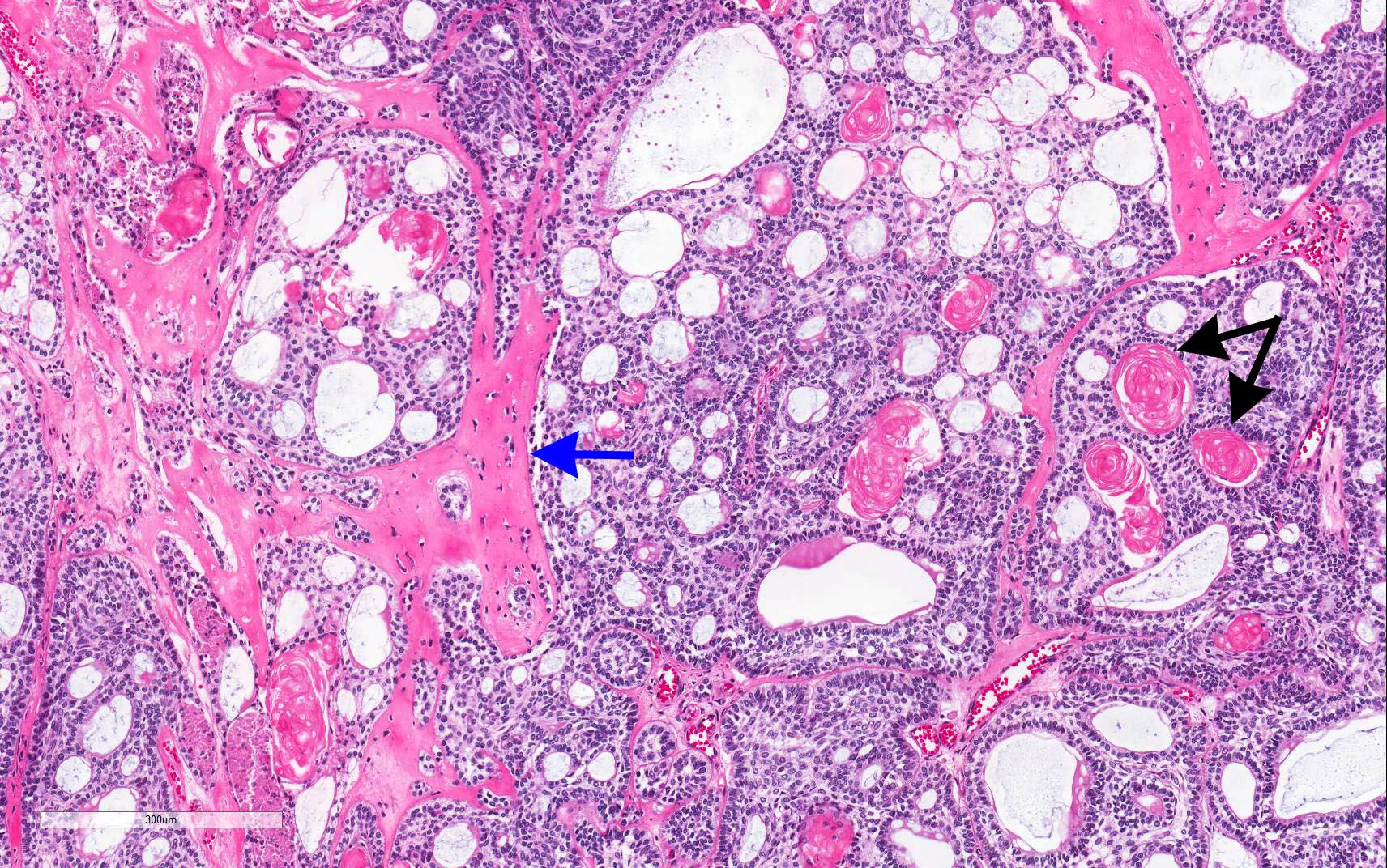
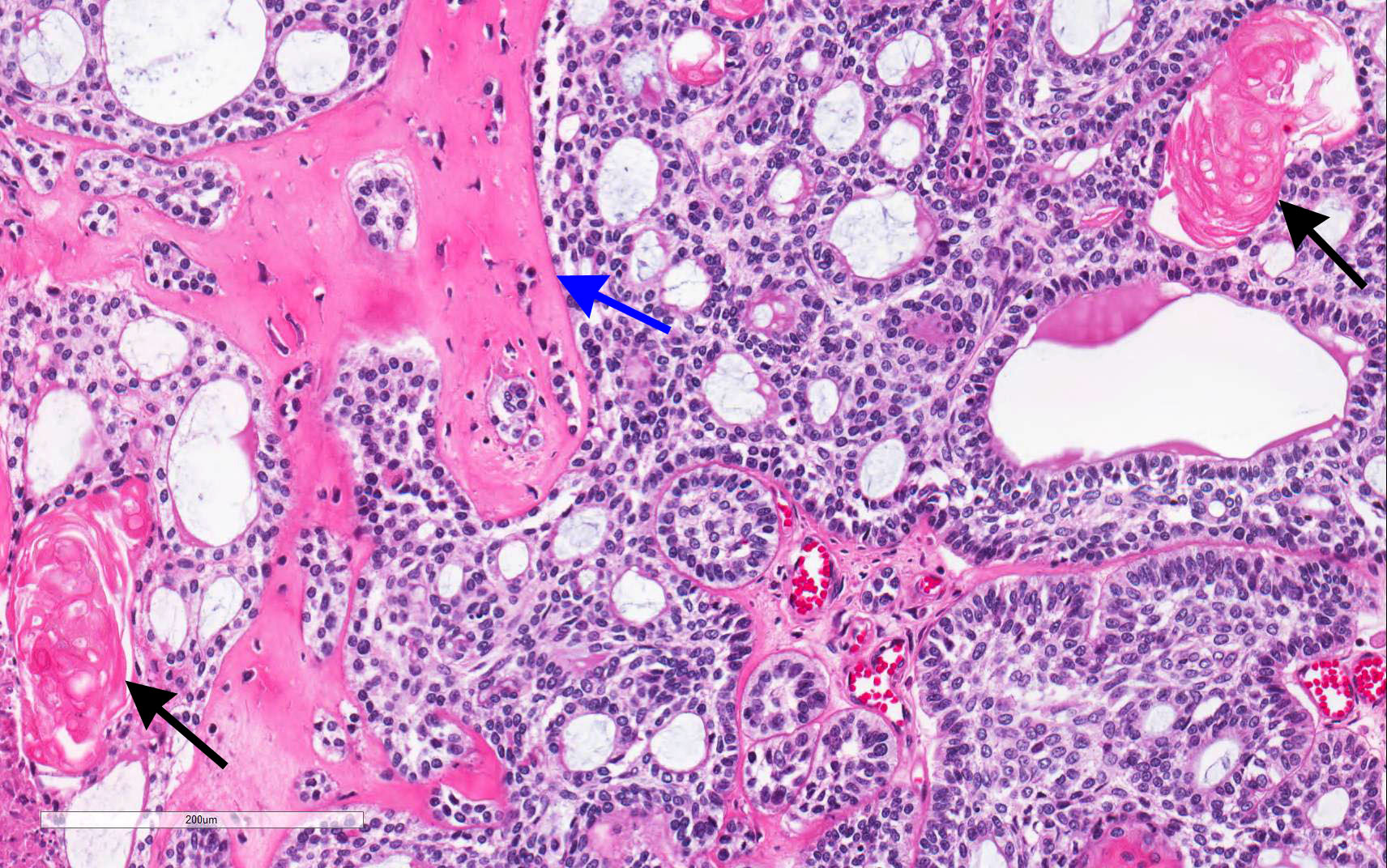
Ghost cells and dentinoid
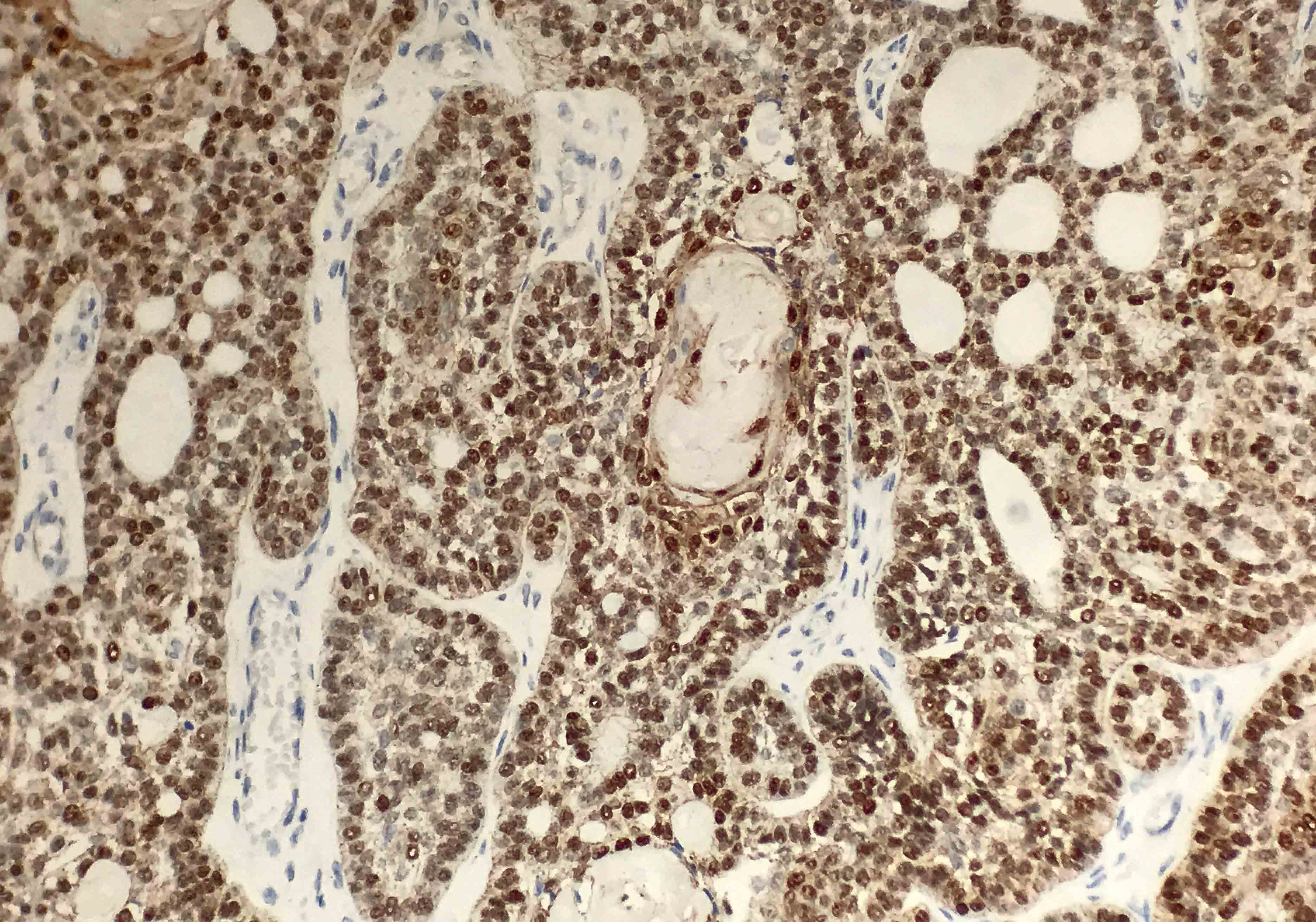
Beta catenin
Positive stains
- Positive but nonspecific:
- Beta catenin (nuclear and cytoplasmic)
- LEF1 (nuclear)
Negative stains
- Negative but nonspecific:
Sample pathology report
- Posterior mandible, right, segmental mandibulectomy:
- Dentinogenic ghost cell tumor (3.2 cm) (see comment)
- Comment: Tumor confined to bone and measures 0.5 cm from anterior and posterior bone margins
- Posterior mandible, right, excision / curettage:
- Dentinogenic ghost cell tumor, in fragments
Differential diagnosis
- Ameloblastoma:
- Second most common odontogenic tumor; however, most clinically significant odontogenic tumor after odontoma
- May have similar basaloid epithelial cells, reverse polarity, stellate reticulum but no ghost cells
- Typically does not have calcifications
- Conventional (nonunicystic), commonly solid and multilocular
- Calcifying odontogenic cyst:
- Similar histology, ameloblast-like epithelium, stellate reticulum-like proliferation, ghost cells, dentinoid and calcifications
- Grossly, predominantly cystic; small satellite cysts, islands of epithelium or ghost cells may be seen in the fibrous capsule
- Likely on a spectrum with dentinogenic ghost cell tumor
- Craniopharyngioma:
- Similar histology, ghost cells and islands of squamous cells present but originates in the sella turcica
- Ghost cell odontogenic carcinoma:
- Extremely rare with only isolated case reports
- Demonstrates pleomorphism and malignant cytology with invasive features
Additional references
Board review style question #1
Which of the following features favors a dentinogenic ghost cell tumor over a calcifying odontogenic cyst?
- Ameloblastic-like epithelium
- Anucleate pink ghost cells
- Islands of squamous differentiation
- Predominantly solid pattern of growth
- Stellate reticulum
Board review style answer #1
D. Predominantly solid pattern of growth. Dentinogenic ghost cell tumor and calcifying odontogenic cyst have significant histopathologic overlap. Both demonstrate amelobastic-like epithelium, ghost cells, stellate reticulum, squamous differentiation and varying levels of dentin and calcification; however, dentinogenic ghost cell tumor is a predominantly solid neoplasm and calcifying odontogenic cyst is a single chamber, unilocular cyst.
Comment Here
Reference: Dentinogenic ghost cell tumor
Comment Here
Reference: Dentinogenic ghost cell tumor
Board review style question #2
Which radiographic features distinguishes an ameloblastoma from a dentinogenic ghost cell tumor?
- Air fluid levels
- Calcifications
- Cystic spaces
- Invasive features
Board review style answer #2
B. Calcifications. Ameloblastoma and dentinogenic ghost cell tumor have significant radiographic and histopathologic overlap; however, radiographically ameloblastoma generally does not have calcifications. Radiographically, ameloblastoma typically demonstrates a multilocular appearance. Ameloblastoma is the most common clinically significant odontogenic tumor and by far more common than dentinogenic ghost cell tumor.
Comment Here
Reference: Dentinogenic ghost cell tumor
Comment Here
Reference: Dentinogenic ghost cell tumor
Back to top
