
Mandible & maxilla
Benign bone tumors
Cemento-osseous dysplasia
Author: Nadim M. Islam, D.D.S., B.D.S.
Editorial Board Member: Kelly Magliocca, D.D.S., M.P.H.
Editor-in-Chief: Debra L. Zynger, M.D.

Last author update: 25 September 2020
Last staff update: 14 September 2023
Copyright: 2003-2024, PathologyOutlines.com, Inc.
PubMed Search: Cemento-osseous dysplasia
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Etiology | Clinical features | Diagnosis | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Clinical images | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2 | Board review style question #3 | Board review style answer #3Cite this page: Islam NM. Cemento-osseous dysplasia. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/mandiblemaxillafloridcemento.html. Accessed April 19th, 2024.
Definition / general
- Cemento-osseous dysplasia is a benign fibro-osseous lesion of the jaws
- Exhibits replacement of mature bone with cementum or immature woven bone surrounded by moderately cellular fibrous connective stroma
- 3 clinicoradiographic subtypes accepted:
- Focal cemento-osseous dysplasia
- Periapical cemento-osseous dysplasia
- Florid cemento-osseous dysplasia
Essential features
- Diagnosis is dependent on clinical, gross description, radiologic and pathologic correlation
- Cemento-osseous dysplasia, ossifying fibroma, fibrous dysplasia and osteoblastoma may exhibit marked histologic, clinical and radiographic overlap
Terminology
- Cemento-osseous dysplasia
- Osseous dysplasia
ICD coding
Epidemiology
- Periapical cemento-osseous dysplasia and florid cemento-osseous dysplasia: middle aged females of African descent
- Focal cemento-osseous dysplasia: middle aged white females
Sites
- Periapical cemento-osseous dysplasia: apices of anterior mandibular teeth
- Focal cemento-osseous dysplasia: apices of posterior mandibular teeth, #19 and #30
- Florid cemento-osseous dysplasia: multiquadrant involvement with more in posterior jaws
Etiology
- Believed to arise from cells of the periodontal ligament
Clinical features
- Most common form of nonexpansile, benign fibro-osseous lesion of the jaws
- Usually asymptomatic, noted as an incidental radiographic finding
- Associated teeth usually test vital, unlike with periapical infections that render teeth nonvital
- Periapical cemento-osseous dysplasia is associated with apices of mandibular anterior teeth
- Focal cemento-osseous dysplasia is a solitary lesion usually associated with apices of teeth #19 and #30
- Florid cemento-osseous dysplasia exhibits multiquadrant involvement of jaws
- Clinical or radiographic expansion does not preclude diagnosis; bone expansion can occur in the setting of a second lesion, for example, inflammation or simple bone cyst formation
- Reference: Dentomaxillofac Radiol 2011;40:230
Diagnosis
- Diagnosis is dependent on clinical, radiologic and pathologic correlation in association with the clinical description and gross findings
Radiology description
- Depends on subtype
- Mixed radiolucent / radiopaque, sclerotic lesion presenting with a lucent halo or rim at apices of teeth
- Mature cemento-osseous dysplasia may be sclerotic, fuse and become completely radiopaque with involvement of apices of anterior mandibular vital teeth, adjacent to the mandibular posterior teeth or may even be multifocal, multiquadrant
- Small isolated lesions often nonexpansile
- Reference: Head Neck Pathol 2020;14:70
Radiology images
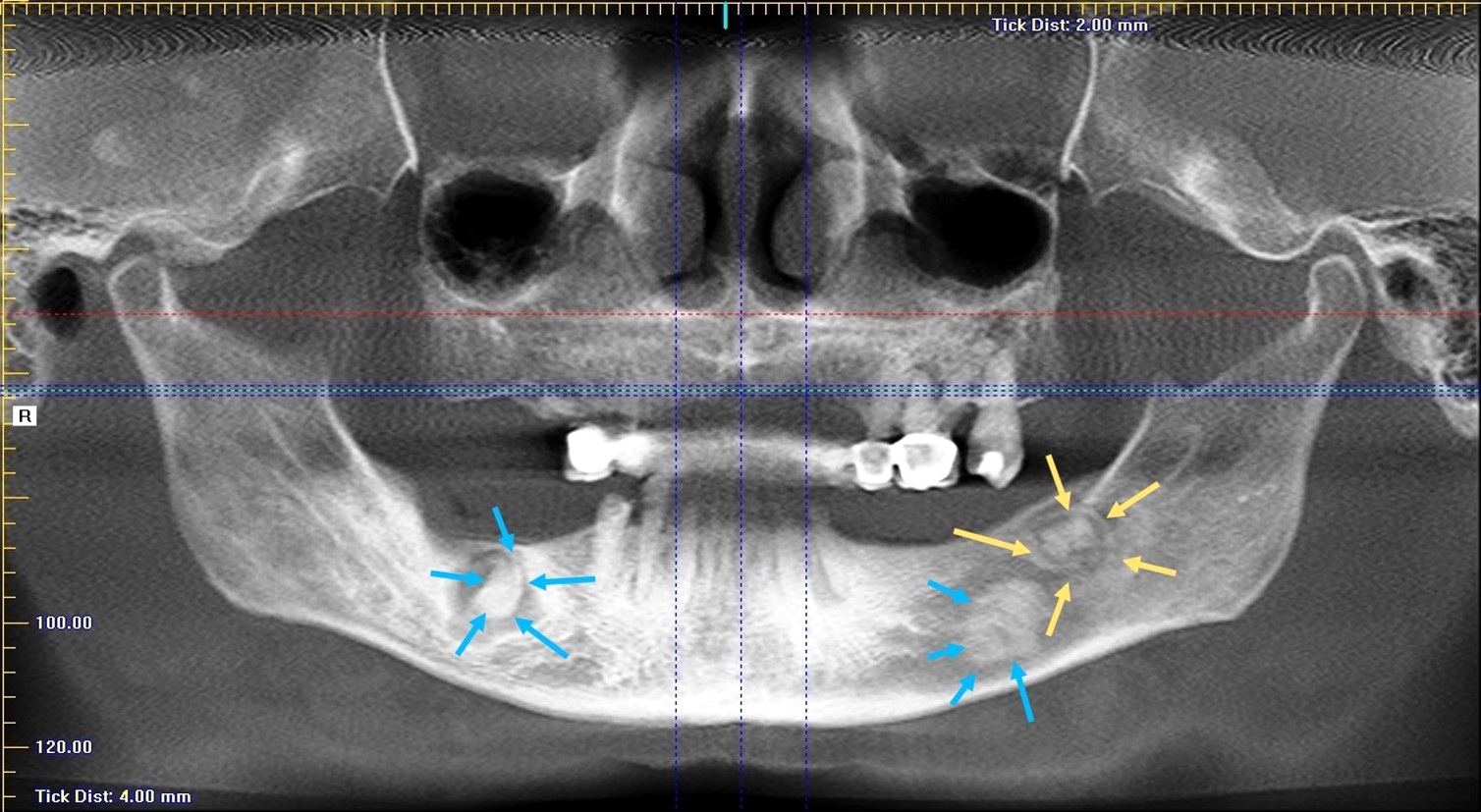
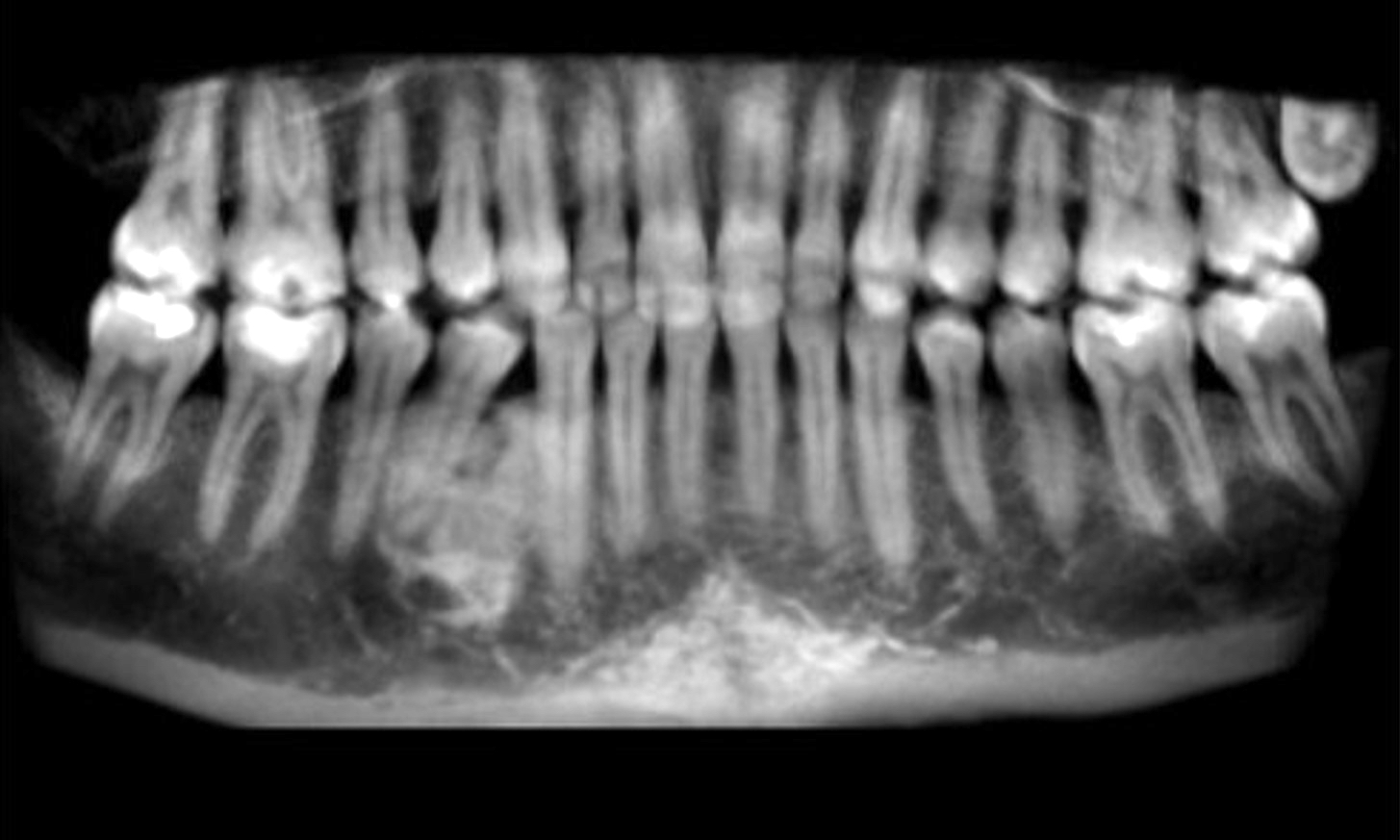
Contributed by Nadim M. Islam, D.D.S., B.D.S.
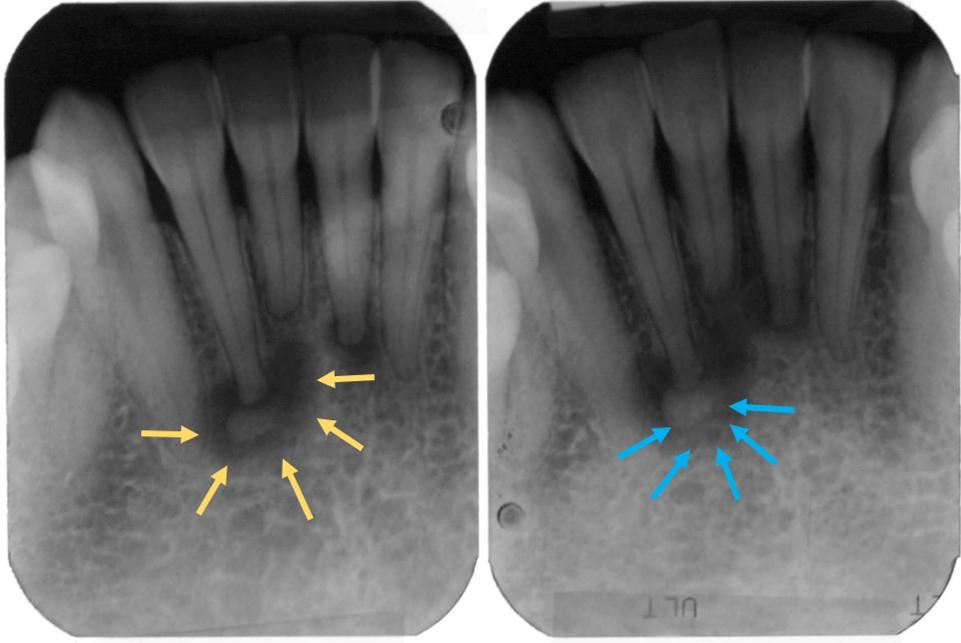
Classic radiolucent rim and central opacity
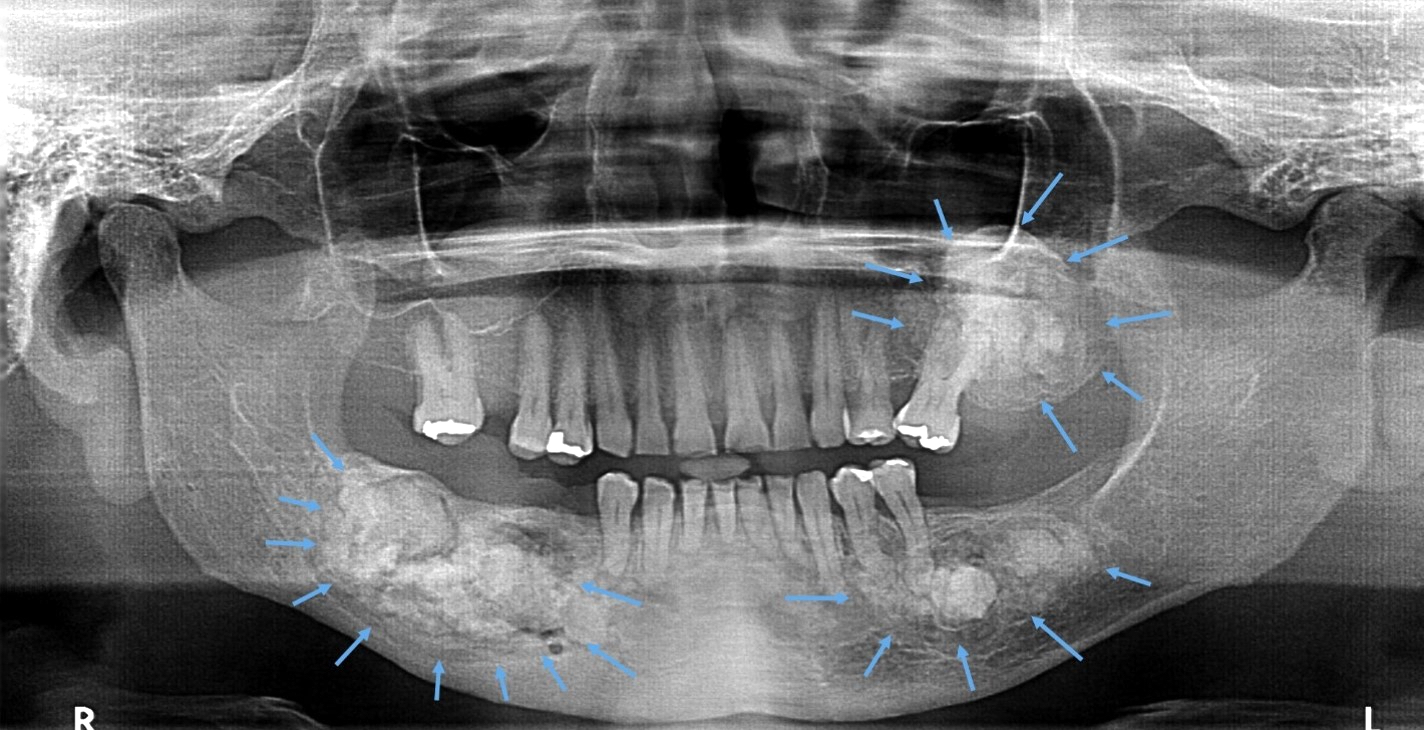
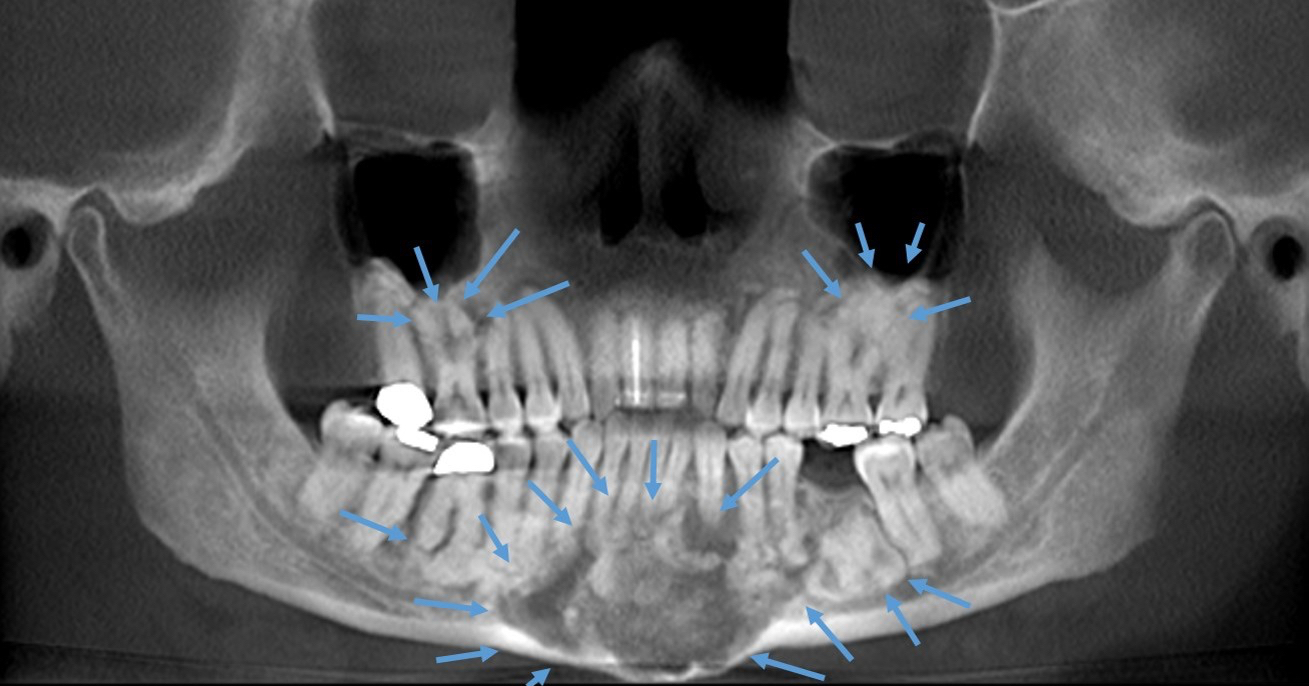
Multiquadrant mixed masses with expansion
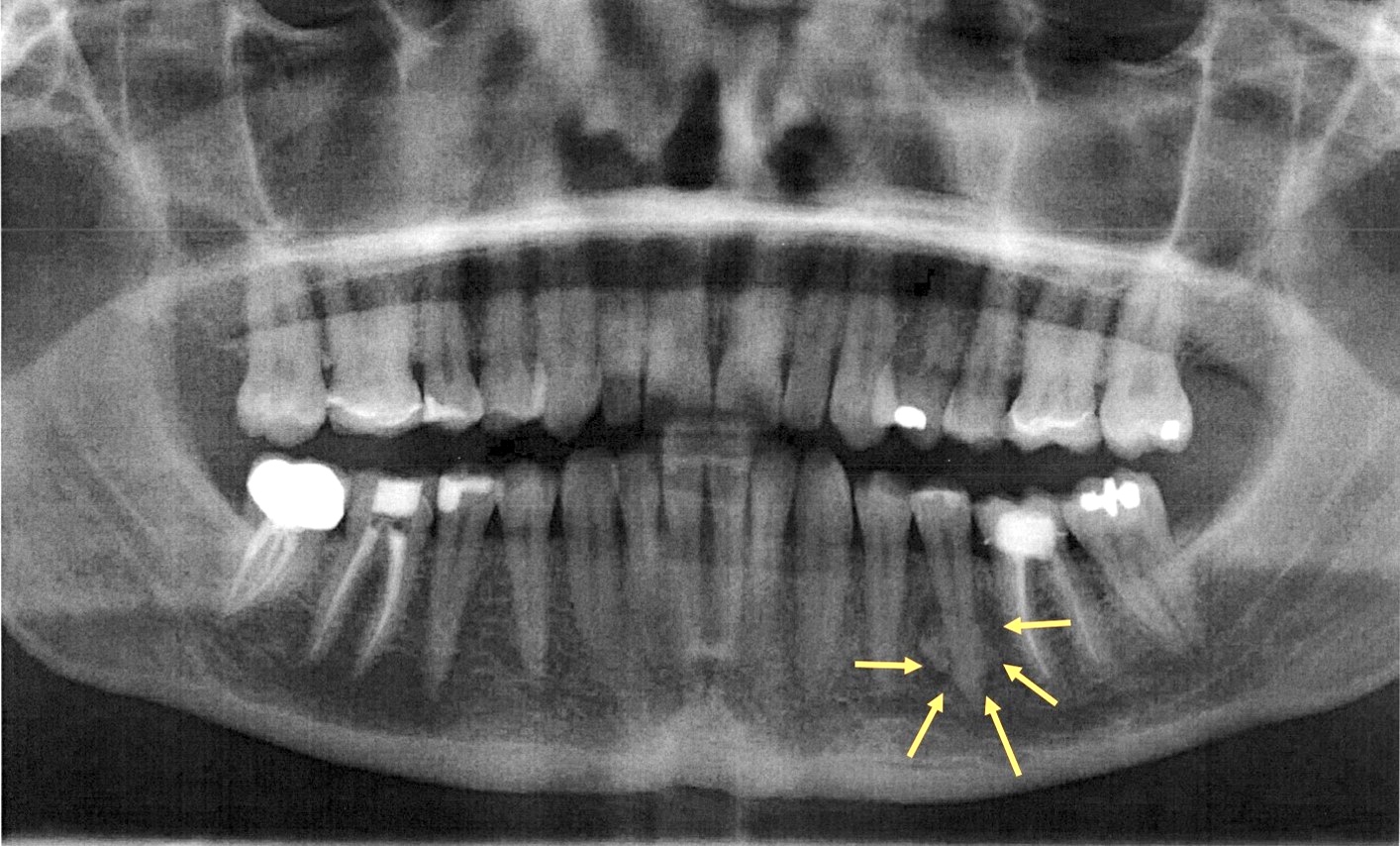
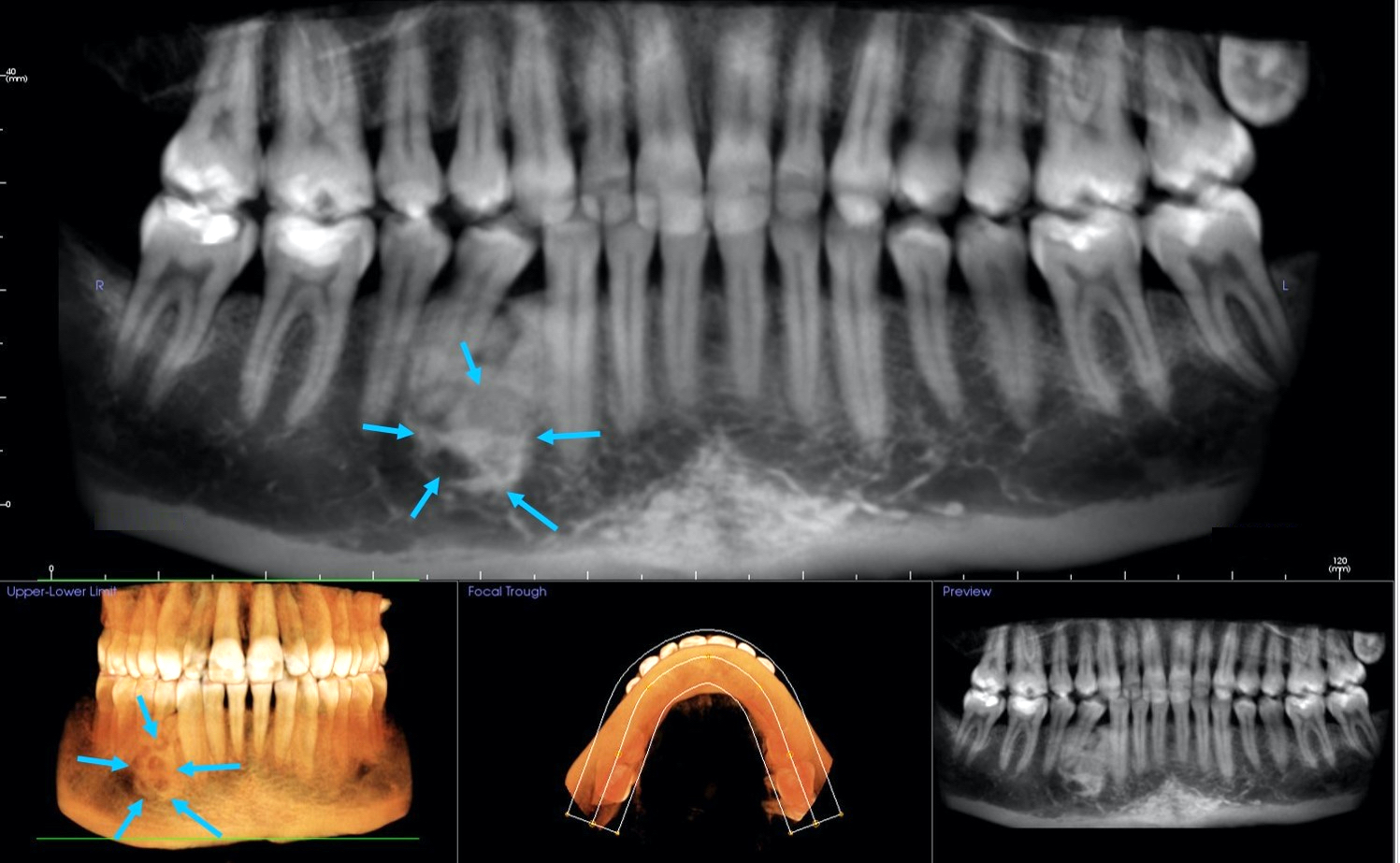
Focal lucent rim with central opacity
Prognostic factors
- In some cases, instrumentation may be associated with local complications
- In cases in which secondary infection occurs, antibiotics and sequestrectomy may be required
- Reference: Regezi: Oral Pathology - Clinical Pathologic Correlations, 7th Edition, 2016
Case reports
- 27 year old man with lower left posterior mandibular lesion (J Oral Maxillofac Pathol 2020;24:S15)
- 37 year old woman with apical radiopaque lesion surrounded by a radiolucent halo and 42 year old woman with mixed radiolucent / opaque lesion of teeth (J Clin Exp Dent 2018;10:e1145)
- 49 year old white woman with several jaw lesions on the apical aspect of teeth (J Clin Exp Dent 2018;10:e291)
Treatment
- Requires no treatment, especially for asymptomatic lesions
- Reference: Regezi: Oral Pathology - Clinical Pathologic Correlations, 7th Edition, 2016
Clinical images
Images hosted on other servers:

Excision
Gross description
- Aggregates of tan-brown, sandy, gritty or granular hard tissue
Gross images
Images hosted on other servers:

Tumor adjacent to tooth
Microscopic (histologic) description
- Fragment of calcified material exhibiting viable cells with numerous smaller calcified masses distributed in a fibrous stroma
- Calcified fragment exhibits a haphazard woven pattern of mineralization with occasional resting and reversal lines with droplets or spherules of cementum-like material and some mature areas exhibiting fused calcified masses resembling ginger root-like formation
- Reference: Head Neck Pathol 2020;14:70
Microscopic (histologic) images
Contributed by Kelly Magliocca, D.D.S., M.P.H. and Nadim M. Islam, D.D.S., B.D.S.
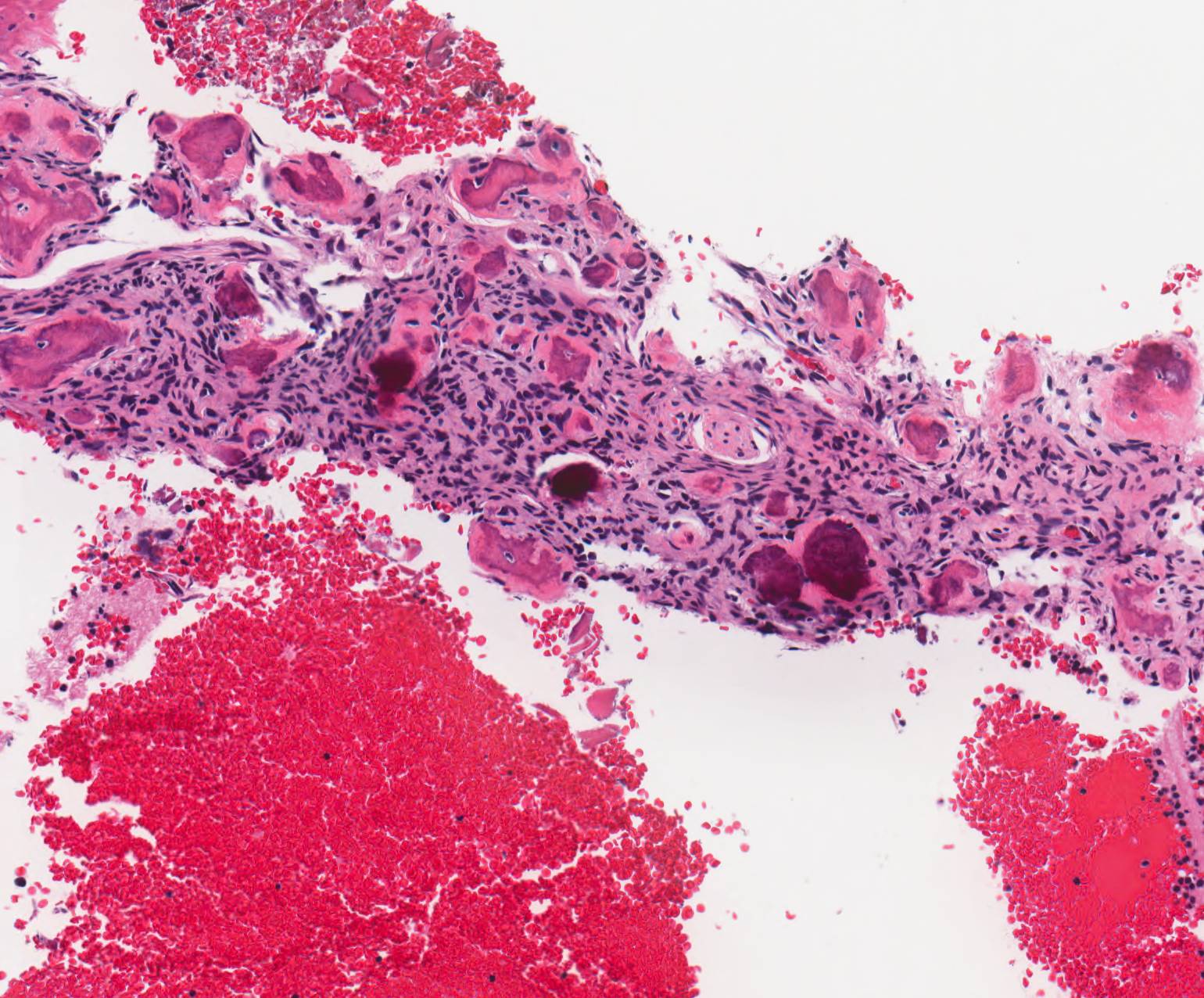
Cemento-osseous dysplasia
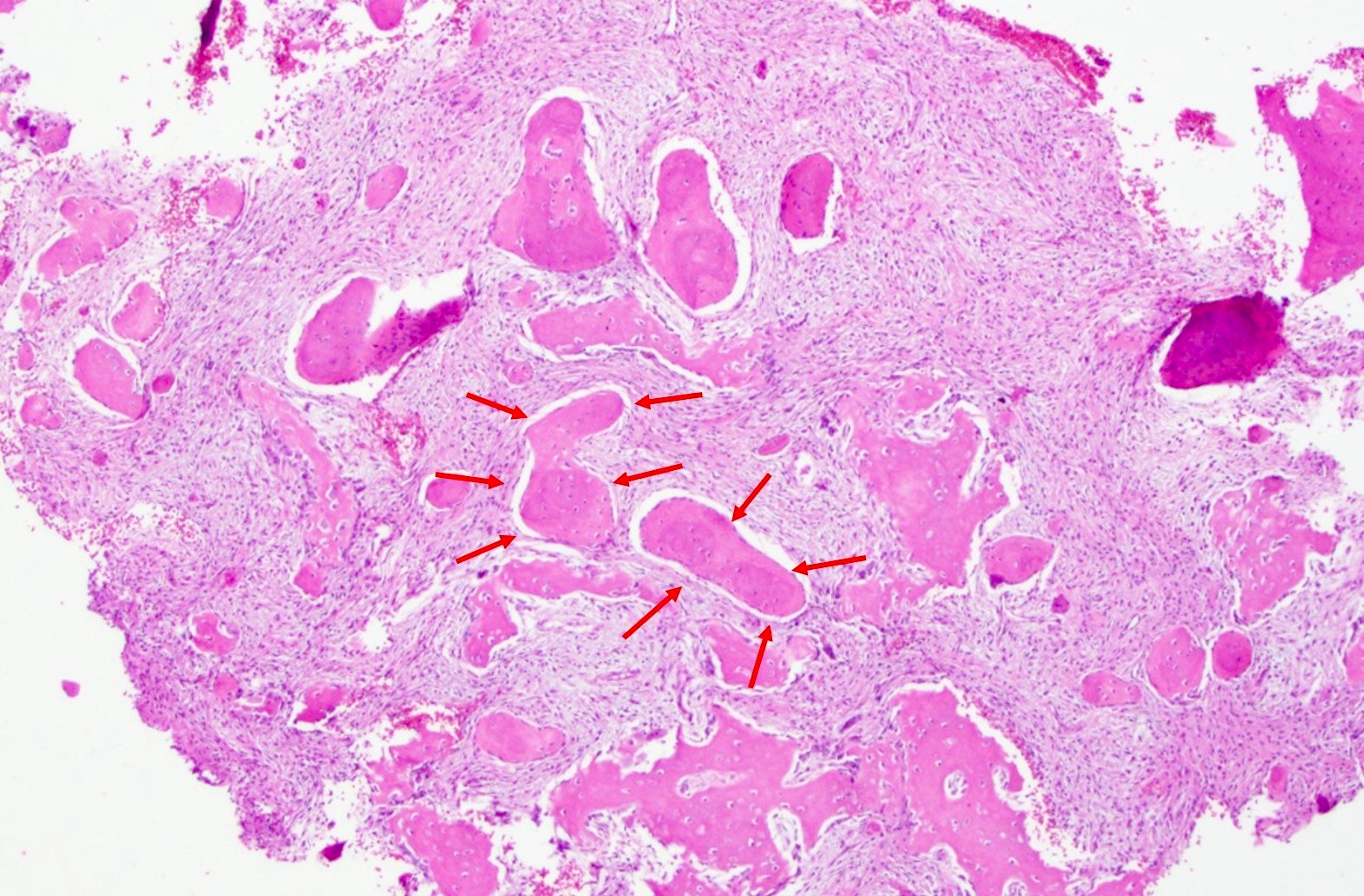
Cemental spherules and modestly cellular stroma
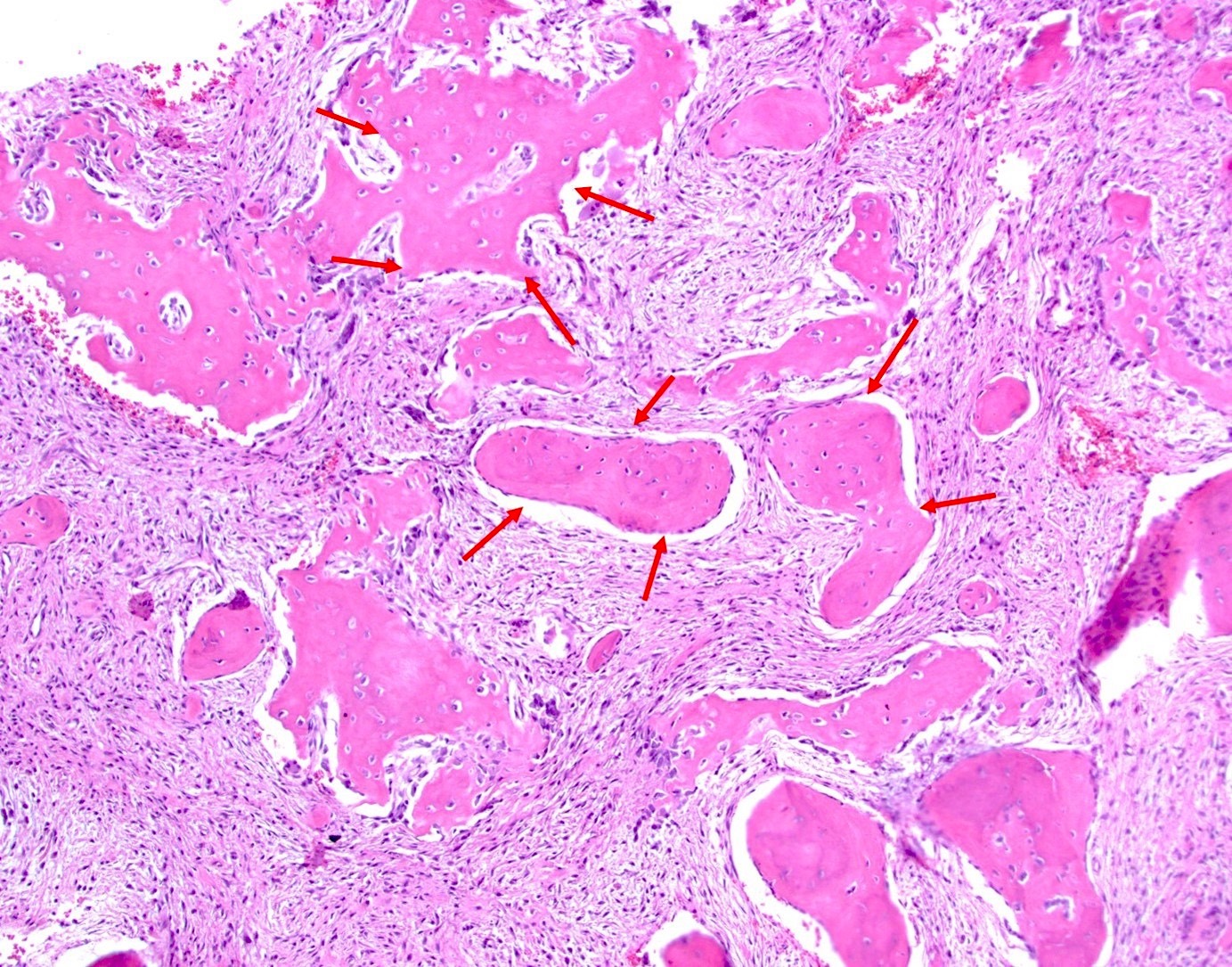
Spherules joining into ginger root-like formations
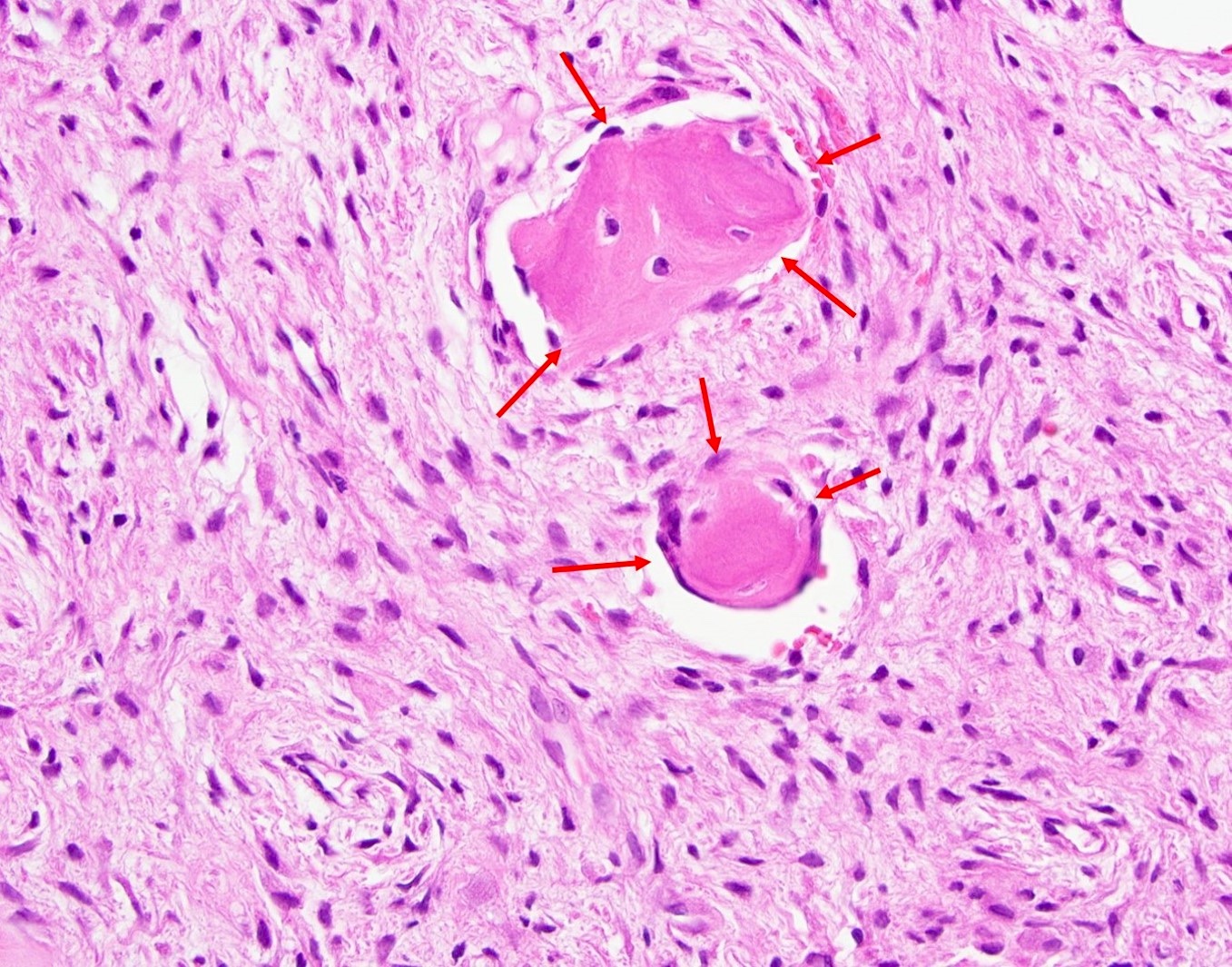
Lack of brush borders helps diagnosis
Sample pathology report
- Right mandible, area of tooth #28, excision:
- Benign fibro-osseous lesion consistent with focal cemento-osseous dysplasia
- Comment: Examination of the decalcified specimen revealed cellular fibrous connective with variably mineralized and calcified bone and cementum-like material. The bony material is variably sized and shaped, ranging from ginger root-like configurations to smaller spherical droplets of material. Dense cortical bone being replaced by cellular fibro-osseous material is also seen. The fibrous tissue exhibits spindle shaped cells that produce osteoid and spherical collections of cementum. The histomorphology combined with the clinical description and radiographic presentation is consistent with focal cemento-osseous dysplasia.
Differential diagnosis
- Ossifying fibroma:
- Cellular stroma, cemento-osseous: lace-like, droplets or spherule with intimate brush borders with the stroma
- Fibrous dysplasia:
- Curvilinear, mature bone dispersed in acellular, dense scar-like fibrous stroma, retraction artifact with absence of osteoblastic rimming and lack of cementum
- Osteoblastoma:
- Highly cellular fibrovascular stroma with reactive boney trabeculae dispersed within vascular, sinusoidal channels, hemorrhage, numerous multinucleated osteoclastic giant cells
Additional references
Board review style question #1
A 39 year old woman presented with an asymptomatic mixed radiolucent / radiopaque lesion at the apical area of vital tooth #28 consistent with cemento-osseous dysplasia. Which of the following is true?
- Antibiotics are often indicated
- Higher recurrence potential
- Lesion best treated by local excision or curettage
- Surgical intervention is required every 2 years
- Treatment is not required but should be observed periodically
Board review style answer #1
E. Treatment is not required but should be observed periodically
Comment Here
Reference: Cemento-osseous dysplasia
Comment Here
Reference: Cemento-osseous dysplasia
Board review style question #2
A 49 year old woman was biopsied for mixed asymptomatic mixed radiolucent / radiopaque lesions at the apices of anterior mandibular teeth. If microscopic features revealed ginger root-like formations as shown in the image, what is your diagnosis?
- Central ossifying fibroma
- Florid cemento-osseous dysplasia
- Focal cemento-osseous dysplasia
- Osteoblastoma
- Periapical cemento-osseous dysplasia
Board review style answer #2
Board review style question #3
Upon diagnosis, cemento-osseous dysplasia is best left untreated with a watchful waiting because
- High risk of severe bleeding during surgical manipulation
- The lesion is an asymptomatic, self limited process
- Teeth in the area must be extracted
- These are difficult to resect and therefore, difficult to treat
- These lesions tend to have a high recurrence rate
Board review style answer #3
B. The lesion is an asymptomatic, self limited process
Comment Here
Reference: Cemento-osseous dysplasia
Comment Here
Reference: Cemento-osseous dysplasia
