
Microbiology & infectious diseases
Fungi
Molds
Hyaline molds
Deputy Editor-in-Chief: Patricia Tsang, M.D., M.B.A.


Last author update: 30 August 2022
Last staff update: 30 August 2022
Copyright: 2022, PathologyOutlines.com, Inc.
PubMed Search: Hyaline molds
Table of Contents
Definition / general | Essential features | Epidemiology | Sites | Pathophysiology | Clinical features | Diagnosis | Laboratory | Case reports | Treatment | Clinical images | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Molecular / cytogenetics description | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Larsen N, Perez V, Leal SM. Hyaline molds. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/microbiologyhyalinemolds.html. Accessed April 19th, 2024.
Definition / general
- Hyaline = glass
- Hyaline molds: heterogeneous molds characterized by a lack of pigmentation of hyphae
- Hundreds of species known to cause disease in humans
- Hyalohyphomycosis: invasion of tissue by nonpigmented hyphae
- Mycetoma / fungus ball: intrapulmonary collection of hyphae occupying cavitary lesions
Essential features
- Major risk factors include neutropenia, phagocyte dysfunction, biologic agents (BTK inhibitors)
- Increasing awareness of invasive mold infection following severe viral respiratory infection
- Influenza (Clin Inf Dis 2020;71:1764)
- SARS-CoV-2 (Mycoses 2020;63:528)
- Hyalohyphomycosis
- Aspergillosis: commonly affects lungs, sinuses, systemic, cornea, cystic fibrosis
- Aspergillus fumigatus: most common etiologic agent
- Aspergillus flavus: major cornea pathogen
- Aspergillus terreus: innate resistance to amphotericin B
- Aspergillus niger: fungus balls; ear colonization
- Fusariosis: cornea, skin and lungs
- Fusarium solani
- Fusarium oxysporum
- Scedosporiosis: lungs, association with near drowning, cystic fibrosis
- Scedosporium apiospermum (Pseudallescheria boydii); innate resistance to amphotericin B
- Penicillium sp.: most common contaminant
- Paecilomyces spp.: skin, lungs; important to distinguish from Penicillium sp.
- Aspergillosis: commonly affects lungs, sinuses, systemic, cornea, cystic fibrosis
Epidemiology
- Organisms present in the soil and environment with worldwide distribution (Pathogens 2021;10:643)
- Direct inoculation or spore inhalation
- Hyalohyphomycosis: neutropenia, phagocyte dysfunction, biologic agents (immunosuppressants)
- Mycetoma / fungus ball: occupies cavitary lesions following tuberculosis infection
- Keratitis: trauma, foreign bodies, contact lenses, surgery
- Scedosporiosis: associated with lung infection in near drowning victims
Sites
- Pulmonary
- Subcutaneous
- Ocular
- Sinus
- Systemic
- CNS / brain abscess
Pathophysiology
- Lung:
- Pneumonia: inhaled spores form hyphae which invade tissue and blood vessels (Sci Rep 2018;8:6617)
- Mycetoma / fungus ball: inhaled spores form a thick collection of intertwined hyphae in a preexisting cavity without tissue invasion
- Allergic: IgE antibodies targeting inhaled fungal spores trigger bronchoconstriction
- Skin: airborne inoculation of debrided epithelium (e.g., burn surface) or traumatic inoculation in the setting of immune dysfunction
- Cornea: traumatic inoculation of spores into the paucicellular cornea enables hyphae to form prior to the recruitment of neutrophils
- Sinus: inhaled spores germinate into hyphae forming a fungus ball with or without invasion
- Dissemination: inability to control local infection; hyphal spread through vasculature
- CNS: dissemination of hyphae in blood to vascularized brain tissue
Clinical features
- Lung:
- Pneumonia: progressive dyspnea in immunocompromised individuals that are unresponsive to antibacterial agents
- Mycetoma / fungus ball: chronic cough with or without hemoptysis with compatible radiologic findings
- Allergic: intermittent dyspnea associated with environmental exposure to fungal spores that trigger asthma-like symptoms; bronchoconstriction
- Subcutaneous infection: airborne inoculation of debrided epithelium (e.g., burn surface) or traumatic inoculation in the setting of immune dysfunction
- Keratitis: traumatic inoculation of fungal spores / hyphae with inflammation and ulceration
- Sinusitis: inhaled spores germinate into hyphae forming a fungus ball with or without invasion
- Systemic infection: inability to control local infection; hyphal spread through vasculature (Pathogens 2021;10:643)
- Encephalitis: dissemination of hyphae in blood to vascularized brain tissue
- Reference: Curr Fungal Infect Rep 2013;7:351
Diagnosis
- Updated EORTC / MSG guidelines available to render a diagnosis of invasive mold infection:
- Proven, probable and possible criteria:
- Proven invasive fungal infection (IFI): histopathologic, cytopathologic or direct microscopic examination of a specimen obtained by needle aspiration or biopsy, in which hyphae or melanized yeast-like forms are seen accompanied by evidence of associated tissue damage (Clin Inf Diseases 2020;71:1367)
- Probable IFI: presence of at least 1 host factor, 1 clinical feature and mycologic evidence
- Possible: host factor or clinical feature without mycological evidence
- Proven, probable and possible criteria:
Laboratory
- Antigen tests
- Aspergillus galactomannan can be detected in plasma, serum or bronchoalveolar lavage (BAL)
- Cross reactivity noted with Blastomyces, Nigrospora, Paecilomyces, Penicillium and Trichothecium (Diagn Micro and Inf Dis 2007;59:113)
- Positive serum galactomannan antigen testing has been reported in invasive fusariosis (Int J Antimicrob Agents 2018;51:326)
- Aspergillus galactomannan can be detected in plasma, serum or bronchoalveolar lavage (BAL)
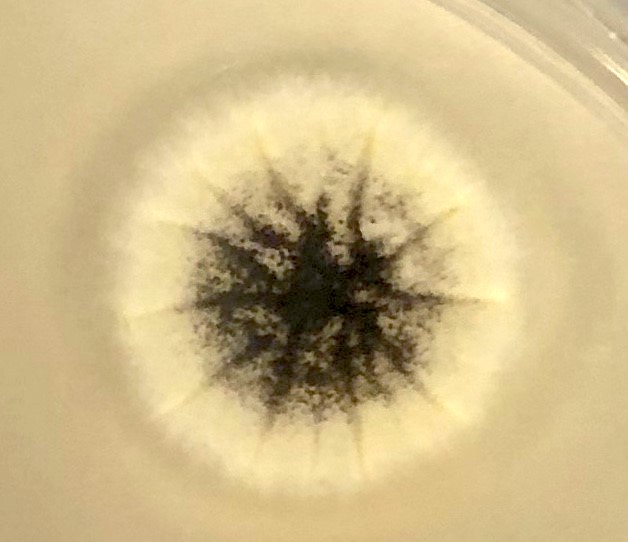
- Colony color / tape prep:
- Spore color is noted on the plate surface; color of hyphae is noted on the reverse of plate (see figure below)
- If reverse is tan / white: hyaline mold
- If brown / black: dematiaceous mold
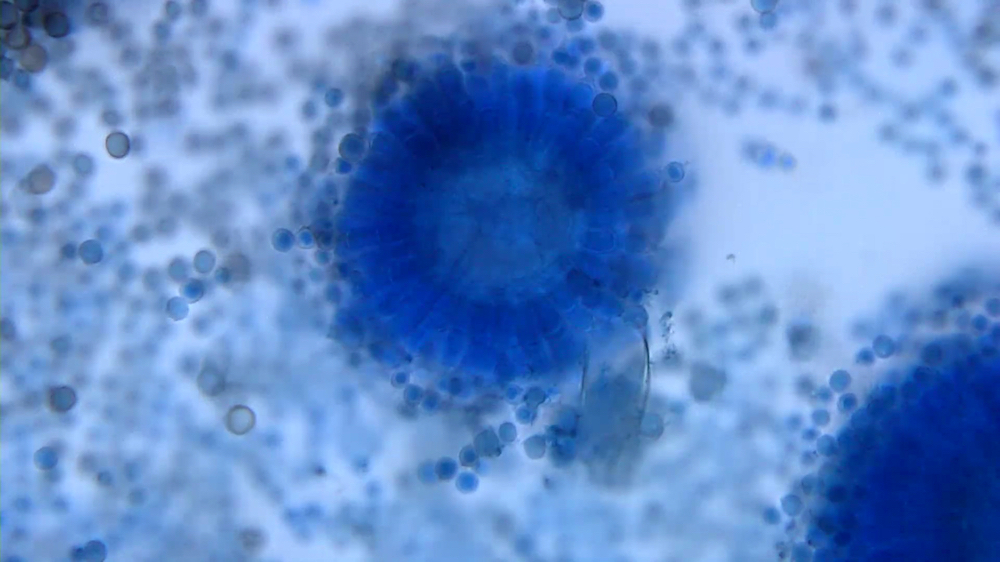
- Lactophenol cotton blue stained slides show characteristic fruiting bodies:
- Aspergillus fumigatus: blue green; columnar, uniseriate
- Aspergillus flavus: yellow green; columnar or circumferential; uniseriate or biseriate; rough conidiophore
- Aspergillus terreus: cinnamon brown, columnar, biseriate
- Aspergillus niger: ochre colored, uniseriate; long conidiophores
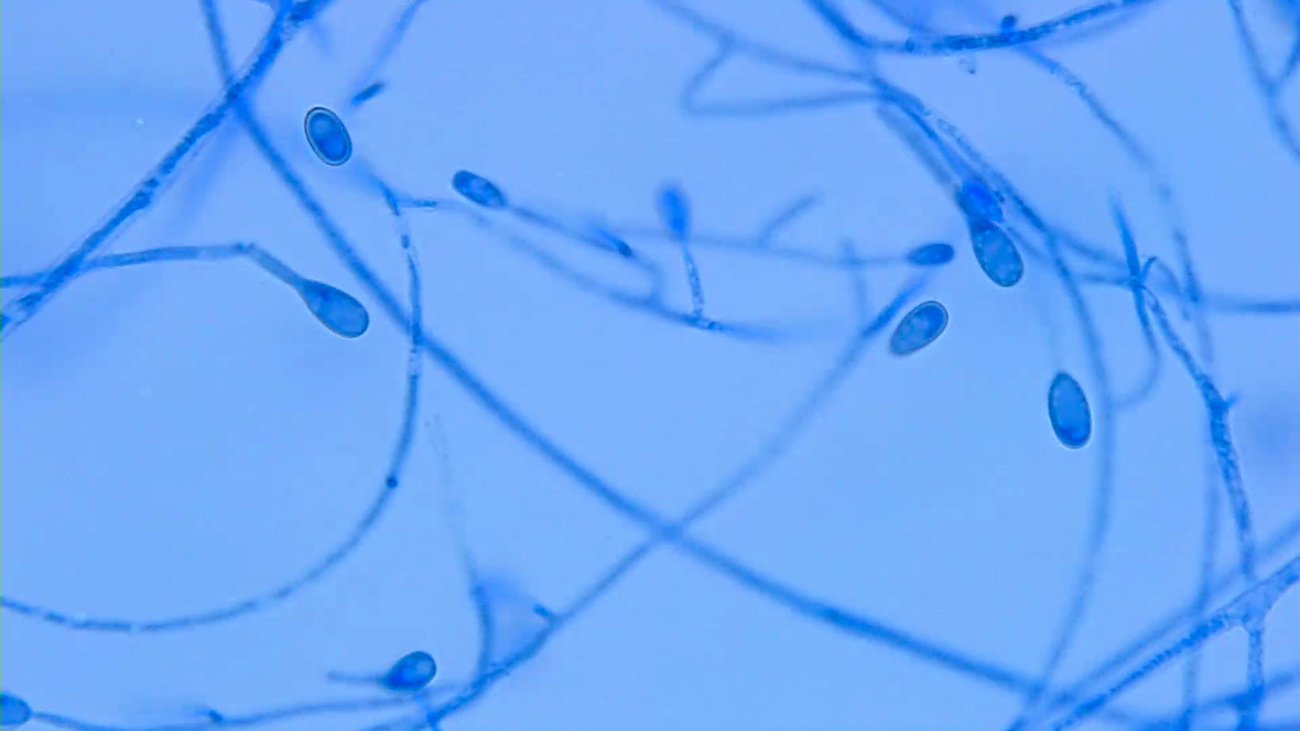
- Fusarium sp.: crescent shaped macroconidia
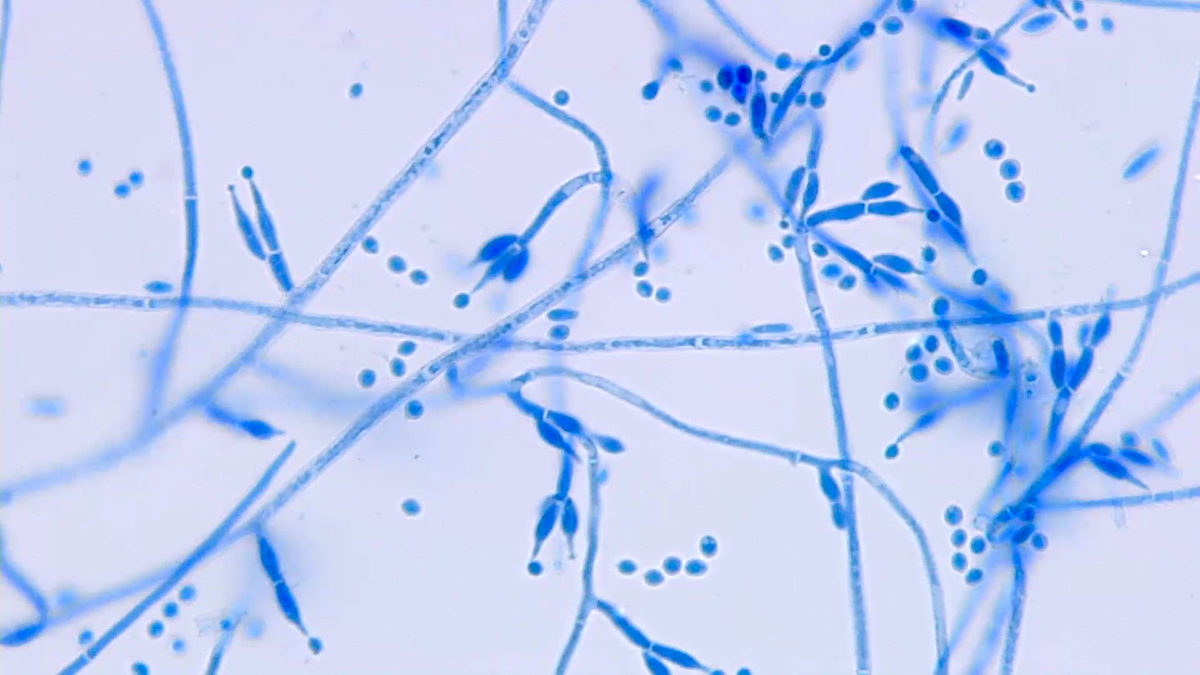
- Scedosporium apiospermum (Pseudallescheria boydii): lollipop-like medium sized oval annelloconidia
- Penicillium sp.: brush-like branched conidiophores with blunt end phialides
- Paecilomyces spp.: branched conidiophores with phialides possessing rounded bases and tapered ends
- Spore color is noted on the plate surface; color of hyphae is noted on the reverse of plate (see figure below)
- Direct exam:
- Gram stain: hyphae stain gram negative; septations visible
- Calcofluor white: a fluorescent blue dye that binds cellulose and chitin in cell walls, used for rapid detection of yeasts and pathogenic fungi
- Molecular:
- Aspergillus PCR with or without detection of azole resistance markers
- Most prevalent azole resistance markers: L98H / TR34 and TR46 / Y121F
- May differentiate A. terreus due to inherent amphotericin B resistance
- Mucormycosis PCR:
- BALs, sinus content, biopsy samples
- 28S rRNA gene sequencing enables species level identification
- Aspergillus PCR with or without detection of azole resistance markers
Case reports
- 18 month old boy with ALL and cerebral aspergillosis (BMC Infect Dis 2020;20:535)
- 7 year old girl with fungal endocarditis (Med Mycol Case Rep 2018;22:48)
- 13 year old girl with ALL and multisystem fusariosis (An Bras Dermatol 2020;95:645)
- 47 year old woman with AIDS, headache and cognitive decline (Open Forum Infect Dis 2016;3:ofw135)
- 60 year old woman with acute abdominal pain and gastric necrosis (JGH Open 2019;4:90)
- 62 year old man decedent with acute fulminant invasive pulmonary aspergillosis in autopsy (Med Mycol Case Rep 2018;20:39)
- Case series of nontraumatic Paecilomyces anterior segment infection (Cornea 2014;33:1031)
- P. boydii in 3 lung transplant recipients (J Comput Assist Tomogr 2009;33:247)
Treatment
- Molds are intrinsically resistant to echinocandins (micafungin)
- Innate resistance to amphotericin B:
- Aspergillus terreus: resistance mechanism not fully understood; thought to be related to reactive oxygen species rather than ergosterol disruption (Antimicrob Agents Chemother 2017;61:e00670)
- Scedosporium apiospermum: voriconazole is the treatment of choice (J Clin Microbiol 2019;57:e02023)
- Azole resistance in Aspergillus species is associated with agricultural azole (J Antimicrob Chemother 2017;72:2443)
- Fusarium sp. and Paecilomyces sp. exhibit variable resistance to voriconazole
Clinical images

Microscopic (histologic) description
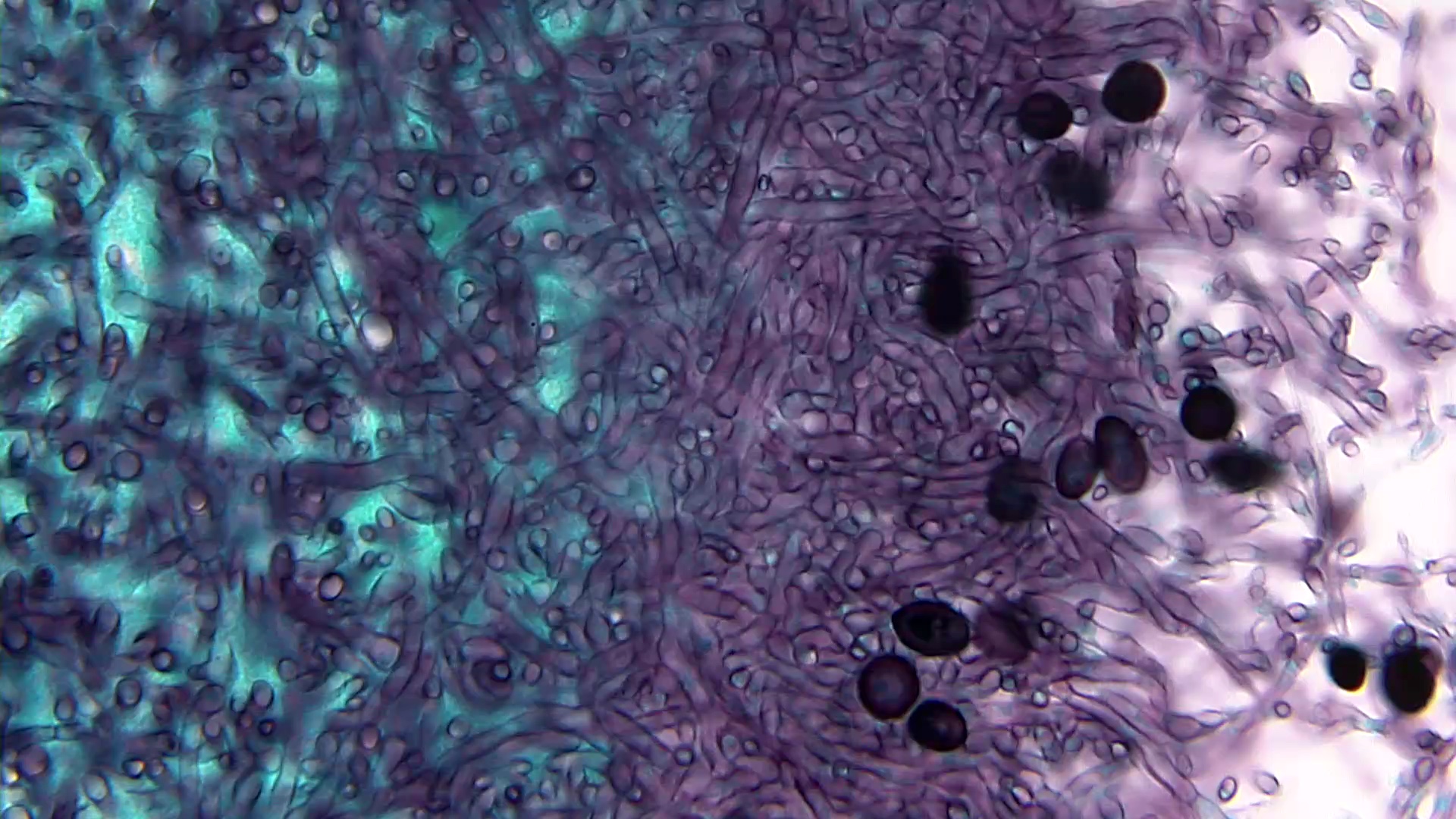
- Gram negative hyphae on H&E; no brown pigmentation; septations present
- GMS and PAS show more precise detail, highlight cell walls, septae, branches, conidial heads (Autops Case Rep 2015;5:9)
- Fruiting bodies and spores vary in color and shape between species
- May occur in areas of the body exposed to air (e.g., lung, sinuses, skin)
Microscopic (histologic) images
Contributed by Sixto M. Leal, Jr., M.D., Ph.D.
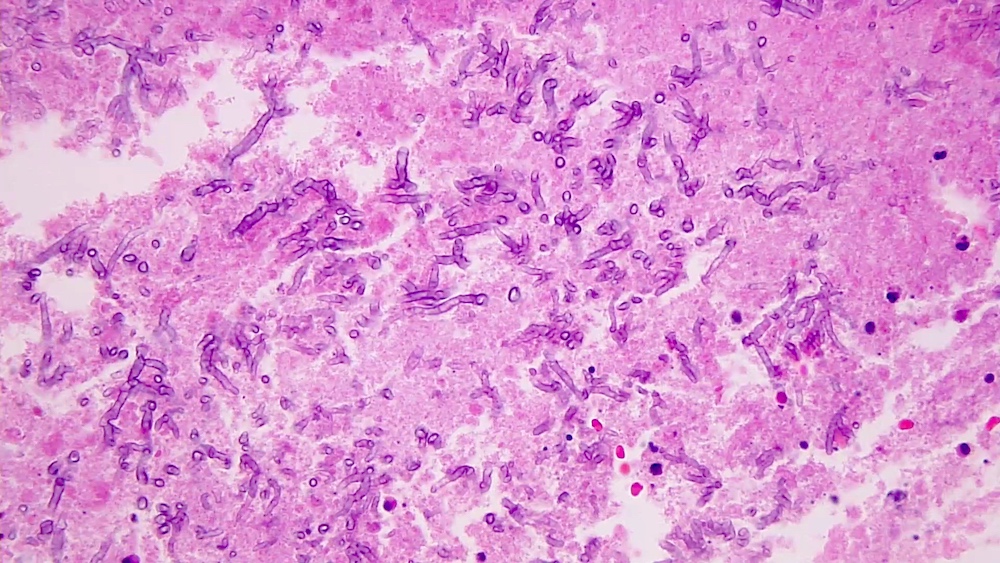
Broad septate hyphae
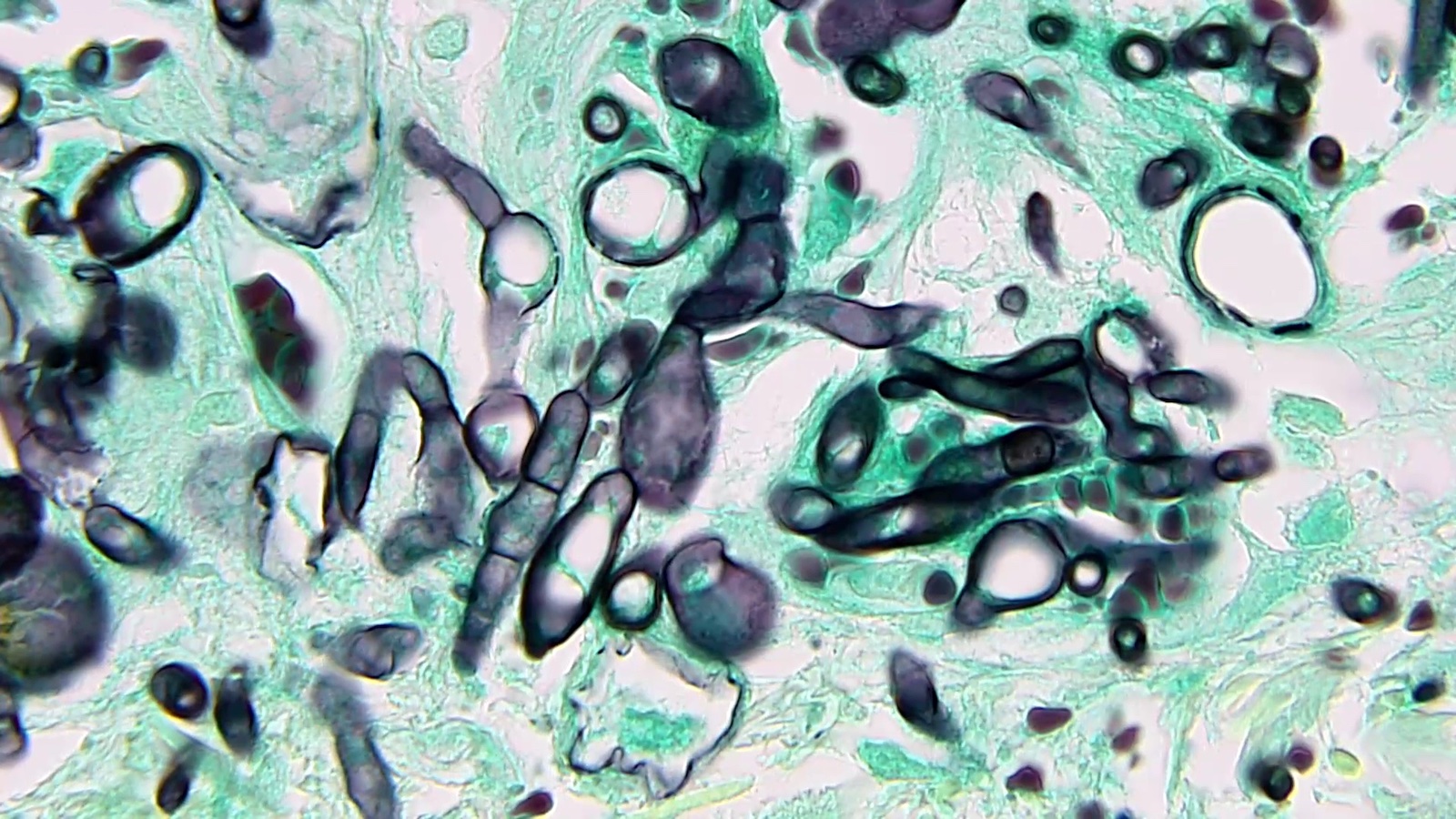
Septate hyphae on GMS
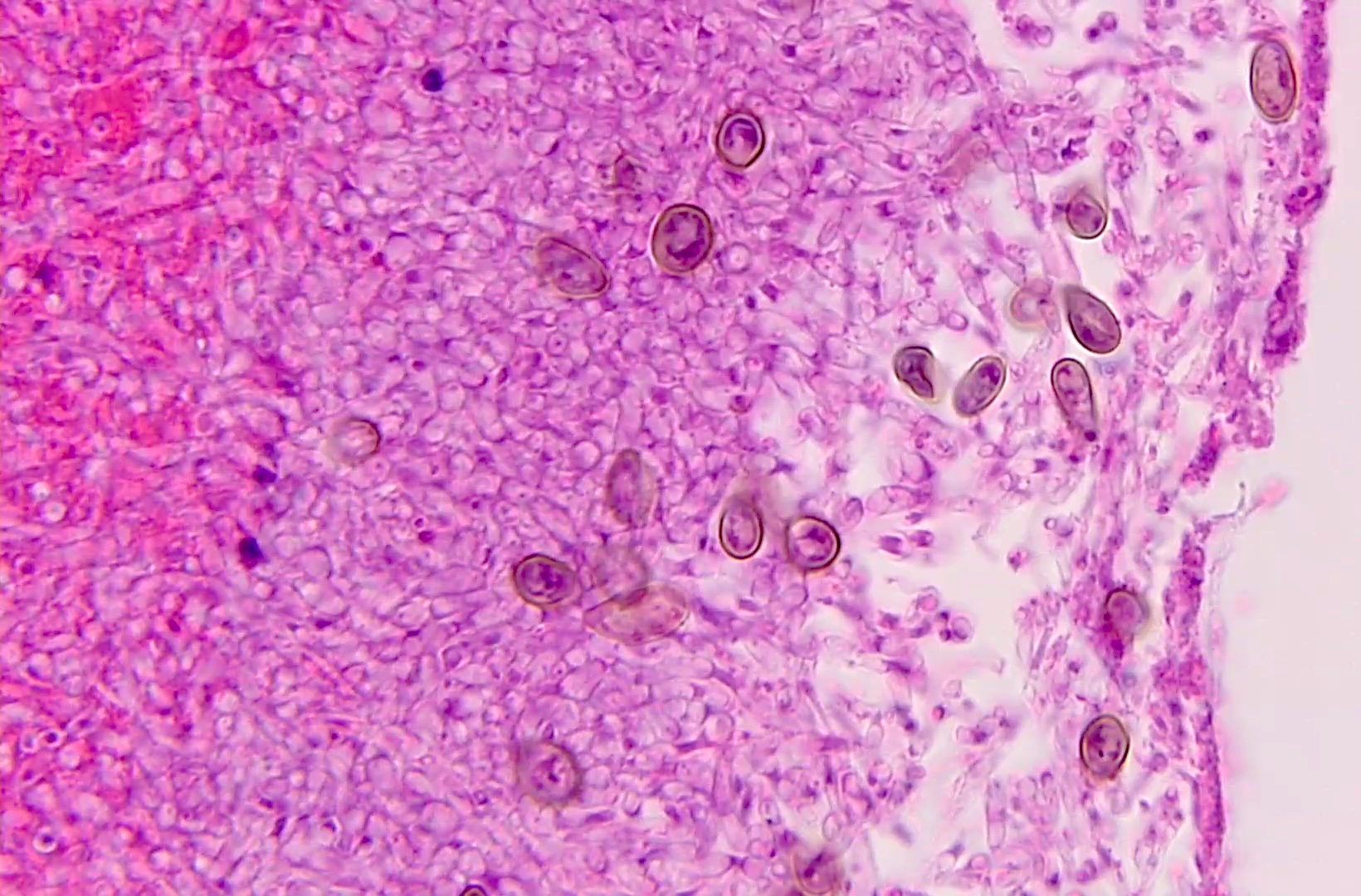
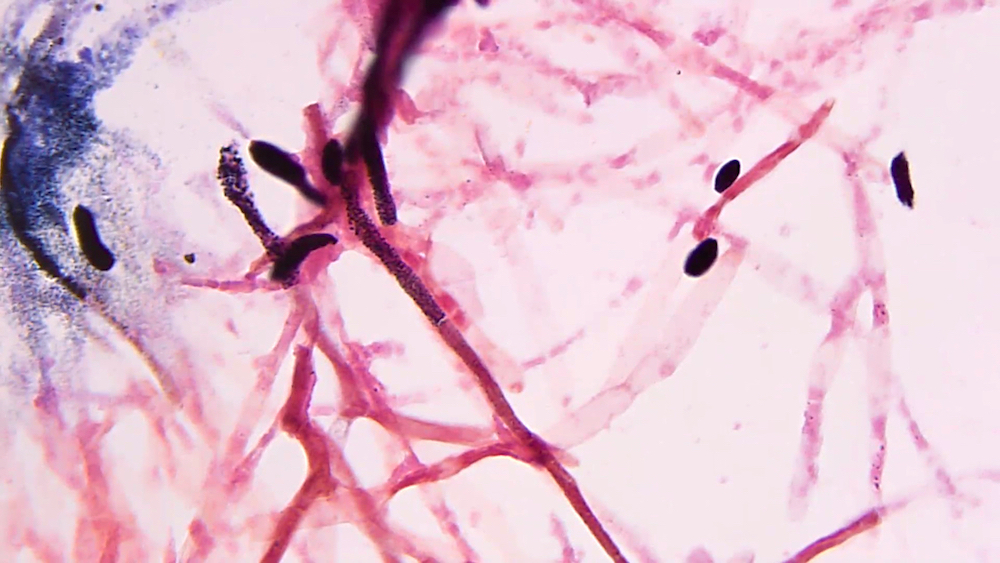
Hyphae with fruiting bodies
Septate hyphae

Fruiting bodies of A. fumigatus

Fruiting bodies of A. terreus

Fruiting bodies of A. flavus
Fruiting bodies of A. niger
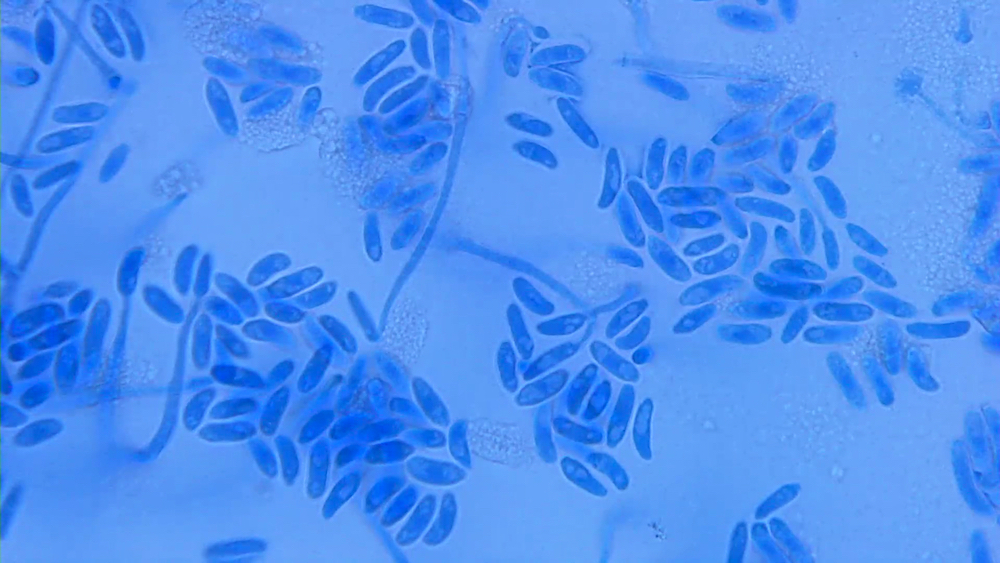
Macroconidia of Fusarium spp.
Spore forming anelloconidia
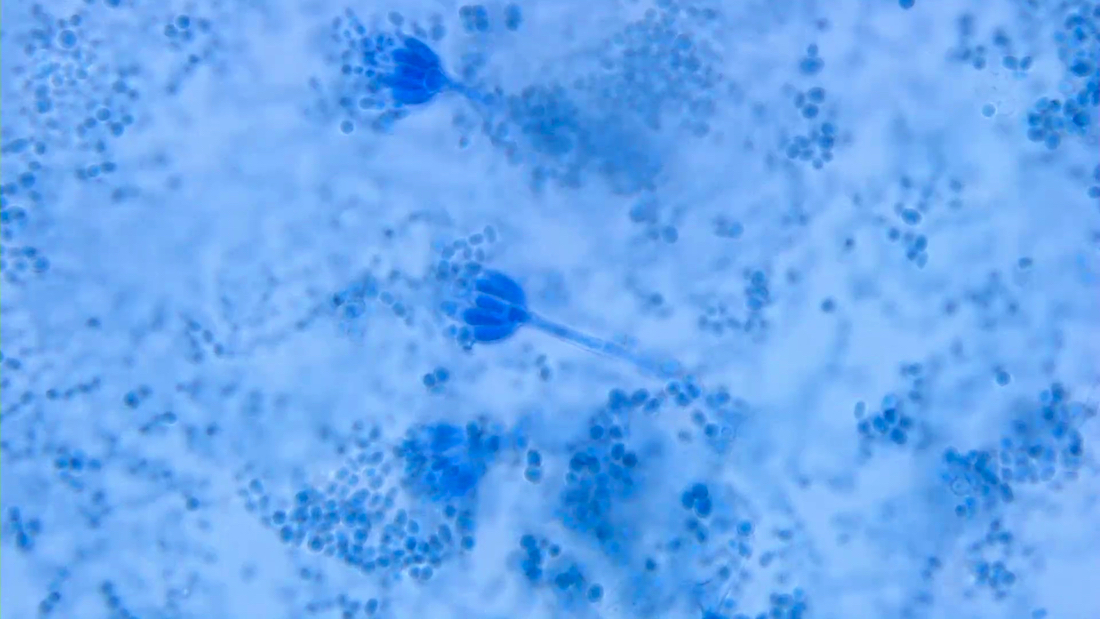
Fruiting bodies of Penicllium spp.
Fruiting bodies of Paecilomyces spp.
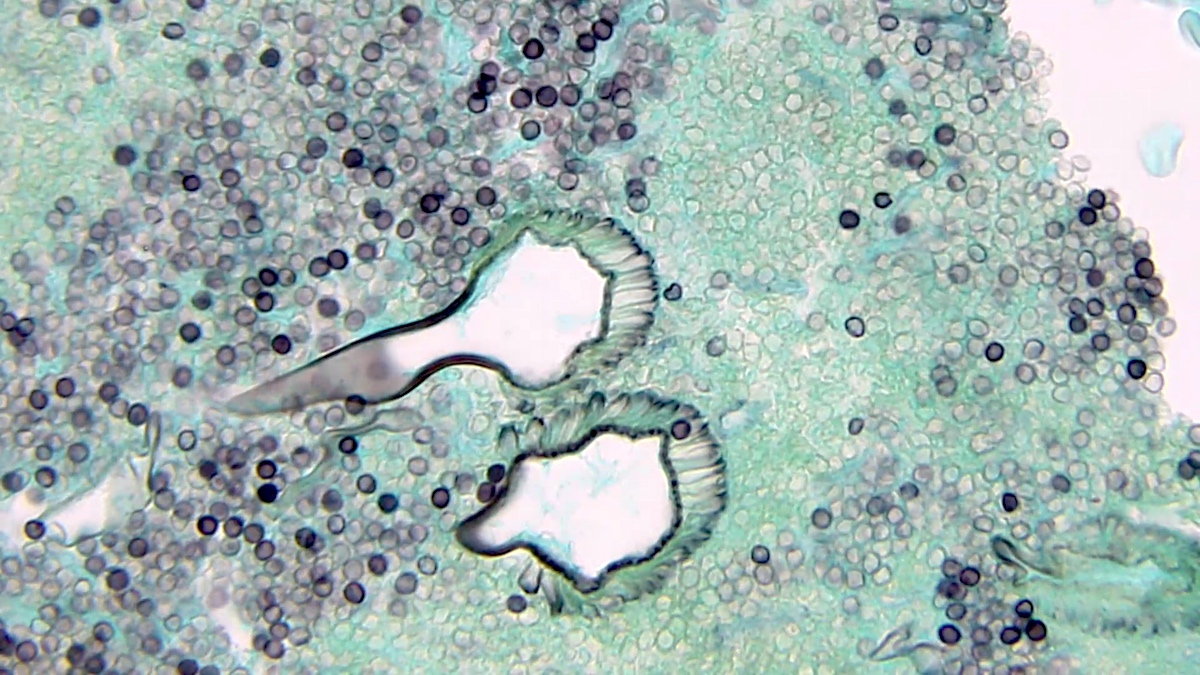
Fruiting bodies on GMS
Positive stains
- Histology:
- H&E: hyaline molds are eosinophilic, whereas dematiaceous molds may have a light to intense brown coloration
- If fruiting bodies are formed, spores and conidiophores often exhibit brownish coloration
- GMS: hyaline molds stain black on a light green background, whereas Mucorales molds tend to stain lightly
- PAS: hyaline molds stain bright magenta
- Fontana-Masson: hyaline molds stain negative given the lack of melanin on hyphae; dematiaceous molds and Cryptococcus stain positive
- H&E: hyaline molds are eosinophilic, whereas dematiaceous molds may have a light to intense brown coloration
- Micro lab stains:
- Gram stain: all molds stain gram negative (pink) on a pink background, whereas yeasts often stain gram positive (purple)
- Lactophenol cotton blue: blue dye used to stain tape preps of mold cultures; all fungi stain blue
- Calcofluor white: fluorescent stain performed on tissues that binds chitin on all fungi yielding blue or green fungal elements, dependent on microscope filters
Molecular / cytogenetics description
- See Laboratory
Differential diagnosis
- Hyalohyphomycosis:
- Caused by other hyaline molds
- Distinction requires culture / sequencing
- Phaeohyphomycosis:
- Direct mycology: pigmented septate hyphae
- Prevalence has increased in immunosuppressed patients (most commonly solid organ transplants) (Int J Dermatol 2017;56:415)
- Mucormycosis (zygomycosis):
- Broad pauciseptate hyphae with irregular branching, occasionally at right angles
- Need culture to diagnose to genus level but 50% of cases yield negative culture
- Organisms very susceptible to tissue grinding due to lack of septation; requires mincing
- Most common: Rhjzopus and Mucor species (CDC: Mucormycosis [Accessed 30 August 2022])
- Nocardiosis:
- Variable colony morphology depending on species
- 1 μm width helps distinguish filamentous bacteria from hyphae
Additional references
Board review style question #1
A 62 year old man with a medical history of diabetes mellitus presents with sinus pain, facial swelling, headache and pain. He admits to not monitoring his blood sugar as stringently as recommended and upon presentation to the emergency department, his serum glucose was 657 mg/dL. After a physical exam and head CT scan were performed, the decision was made to perform an emergent sinus biopsy and send for frozen section diagnosis. What finding on H&E would result in continued surgical exploration and discontinuation of voriconazole?
- Broad pauciseptate ribbon-like hyphae
- Increased neutrophils and necrotic debris
- Morphology consistent with Aspergillus
- Presence of pseudohyphae
Board review style answer #1
A. Broad pauciseptate ribbon-like hyphae. Mucorales molds, which exhibit broad, pauciseptate hyphae with wide angle branching, are resistant to voriconazole and must be treated with amphotericin B or other azole drugs. Aspergillus species display hyaline septate hyphae and are generally susceptible to voriconazole. Pseudohyphae indicate that a yeast, likely a Candida species, is present and require treatment with an echinocandin or fluconazole. Neutrophils and necrosis are not specific for fungal infection.
Comment here
Reference: Hyaline molds
Comment here
Reference: Hyaline molds
Board review style question #2

A 45 year old neutropenic acute myeloid leukemia patient is brought to the emergency department with a fever, tachycardia and altered mental status. A blood sample is sent for culture and turns positive. A Gram stain from the positive blood culture aliquot shows hyaline septate hyphae with rare crescent shaped macroconidia as shown in the photo. Which hyaline septate mold is this most likely to be?
- Aspergillus fumigatus
- Fusarium oxysporum
- Nocardia brasiliensis
- Pseudallescheria boydii
Board review style answer #2
B. Fusarium oxysporum. Fusarium species are the most common pathogenic molds encountered in positive blood culture bottles. Although angioinvasive, Aspergillus fumigatus and P. boydii are rarely isolated in blood culture bottles. Nocardia species are filamentous bacteria. Photo shows Gram stain of a positive blood culture bottle showing hyaline septate hyphae with rare elongated crescent shaped spores consistent with Fusarium sp.
Comment here
Reference: Hyaline molds
Comment here
Reference: Hyaline molds
