
Nasal cavity, paranasal sinuses, nasopharynx
Sinonasal carcinoma
NUT carcinoma
Author: Lisa Rooper, M.D.
Editorial Board Member: Kelly Magliocca, D.D.S., M.P.H.
Editor-in-Chief: Debra L. Zynger, M.D.

Last author update: 29 January 2019
Last staff update: 12 April 2024 (update in progress)
Copyright: 2019-2024, PathologyOutlines.com, Inc.
PubMed Search: NUT carcinoma nasal
See Also: NUTM1
Table of Contents
Definition / general | Essential features | Terminology | Epidemiology | Clinical features | Radiology images | Case reports | Treatment | Clinical images | Gross description | Microscopic (histologic) description | Microscopic (histologic) images | Cytology images | Positive stains | Negative stains | Electron microscopy description | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Rooper L. NUT carcinoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/nasalnutcarcinoma.html. Accessed April 20th, 2024.
Definition / general
- Aggressive carcinoma defined by translocations involving the NUT gene and frequent squamous differentiation
Essential features
- Highly aggressive malignancy with median survival of < 1 year
- Histologically defined by primitive round cells with areas of abrupt keratinization
- Caused by translocations involving the NUT gene (15q14), most commonly with BRD4 (19p13)
- Speckled nuclear positivity for NUT1 immunohistochemistry is sensitive and specific for diagnosis
Terminology
- NUT stands for nuclear protein in testis
- Formerly called NUT midline carcinoma due to proclivity for midline sites
Epidemiology
- Although originally described in children, affects people of all ages (Head Neck Pathol 2013;7:11)
- No sex or geographic predilection (Head Neck Pathol 2013;7:11)
- No clear risk factors established to date (Head Neck Pathol 2013;7:11)
Clinical features
- Aggressive malignancy with median survival of < 1 year (Head Neck Pathol 2013;7:11)
- ~35% involve the head and neck, most commonly in the sinonasal tract (Head Neck Pathol 2013;7:11)
- Although also common in other midline sites such as the mediastinum, can occur anywhere in the body (Head Neck Pathol 2013;7:11)
Radiology images
Images hosted on other servers:

Large nasal mass
Case reports
- 14 year old girl with ethmoid sinus mass (Oncogenesis 2015;4:e174)
- 18 year old woman with undifferentiated sinonasal mass (Pathol Res Pract 2014;210:383)
- 48 year old man with vision changes (Saudi J Ophthalmol 2018;32:62)
- 53 year old man with nasal cavity mass (Head Neck Pathol 2017;11:389)
- 54 year old woman with nasal mass (Arch Pathol Lab Med 2011;135:1494)
Treatment
- Tumors generally show minimal response to radiation and conventional chemotherapy (Head Neck Pathol 2013;7:11)
- In clinical trials, some patients show rapid response to extraterminal bromodomain inhibitors although prognosis remains poor (Cancer Discov 2016;6:492)
Clinical images
Images hosted on other servers:

Lacrimal mass

Nasopharyngeal endoscopy
Gross description
- Highly infiltrative tumor frequently involving multiple anatomic subsites
- Nonspecific white-tan cut surface commonly demonstrating prominent necrosis
Microscopic (histologic) description
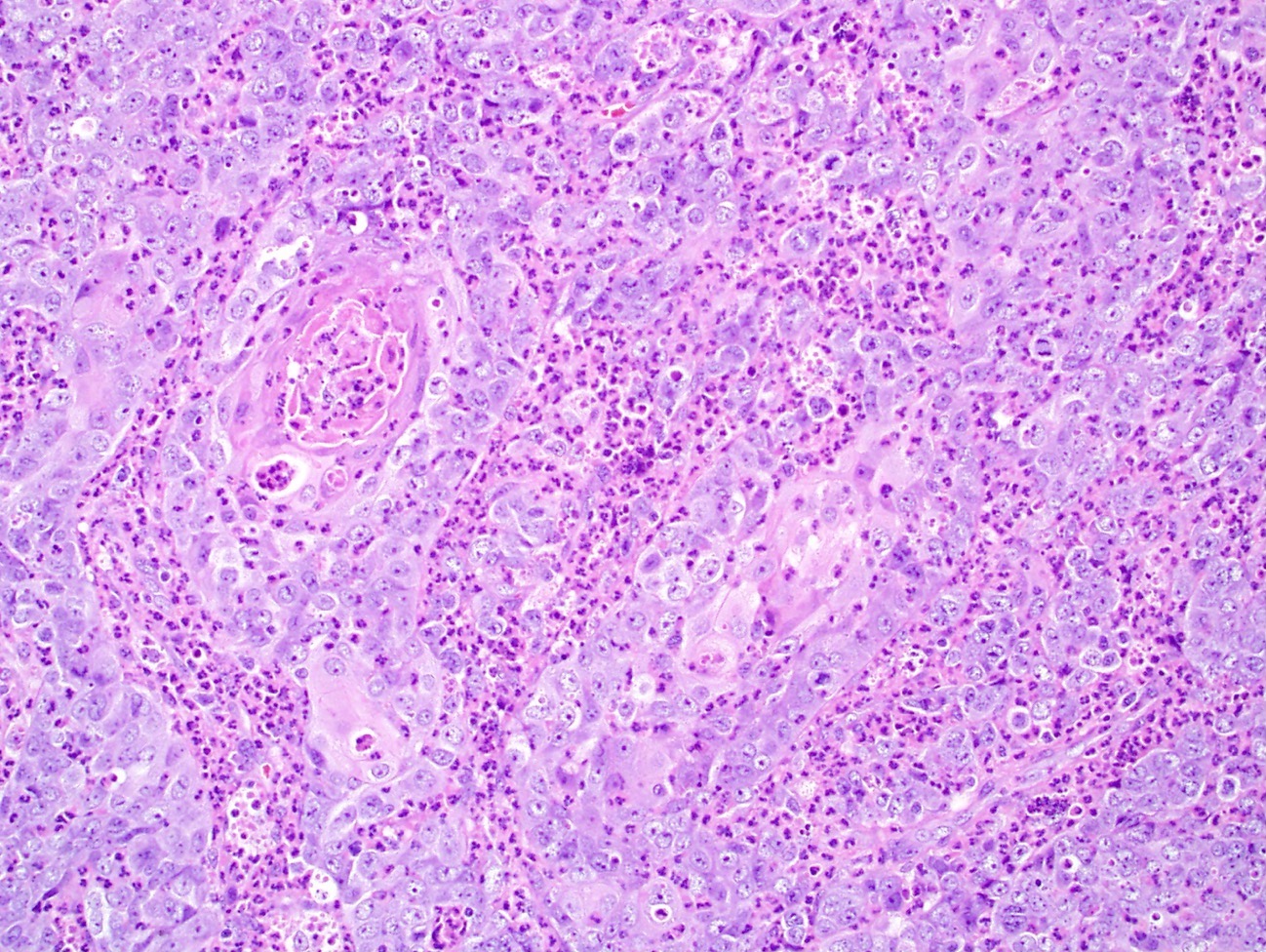
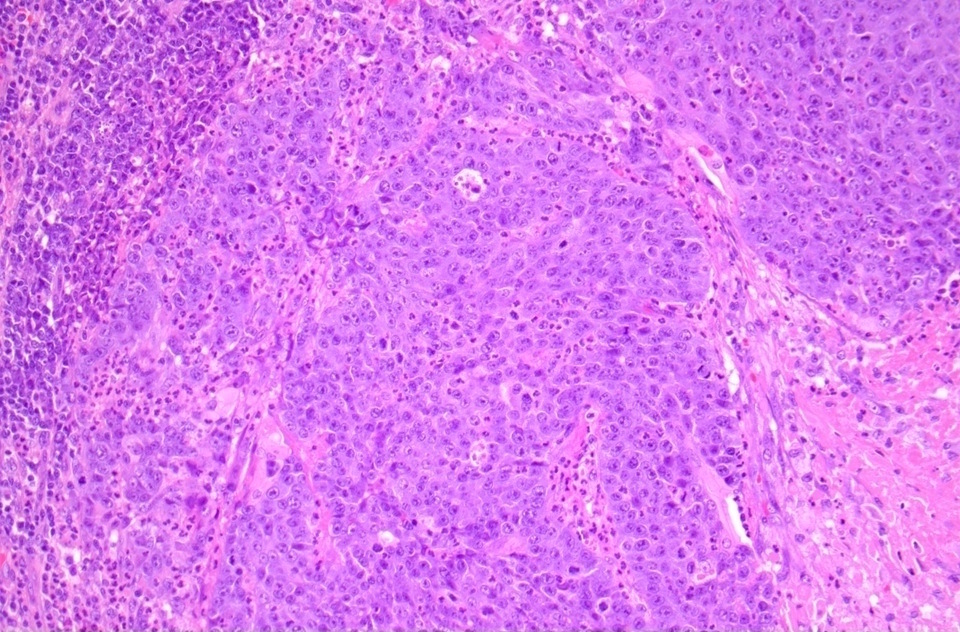
- Primitive small to medium sized cells with minimal indistinct to clear cytoplasm
- Monotonous round to oval nuclei with variably prominent nucleoli
- High mitotic rate with prominent tumor necrosis
- Foci of abrupt squamous differentiation with clear to eosinophilic cytoplasm and keratin pearl formation
- Areas of spindled cells frequently present
- Dense neutrophil infiltrate seen in subset of cases
Microscopic (histologic) images
Contributed by Lisa Rooper, M.D.

Primitive small to medium cells

Highly infiltrative growth
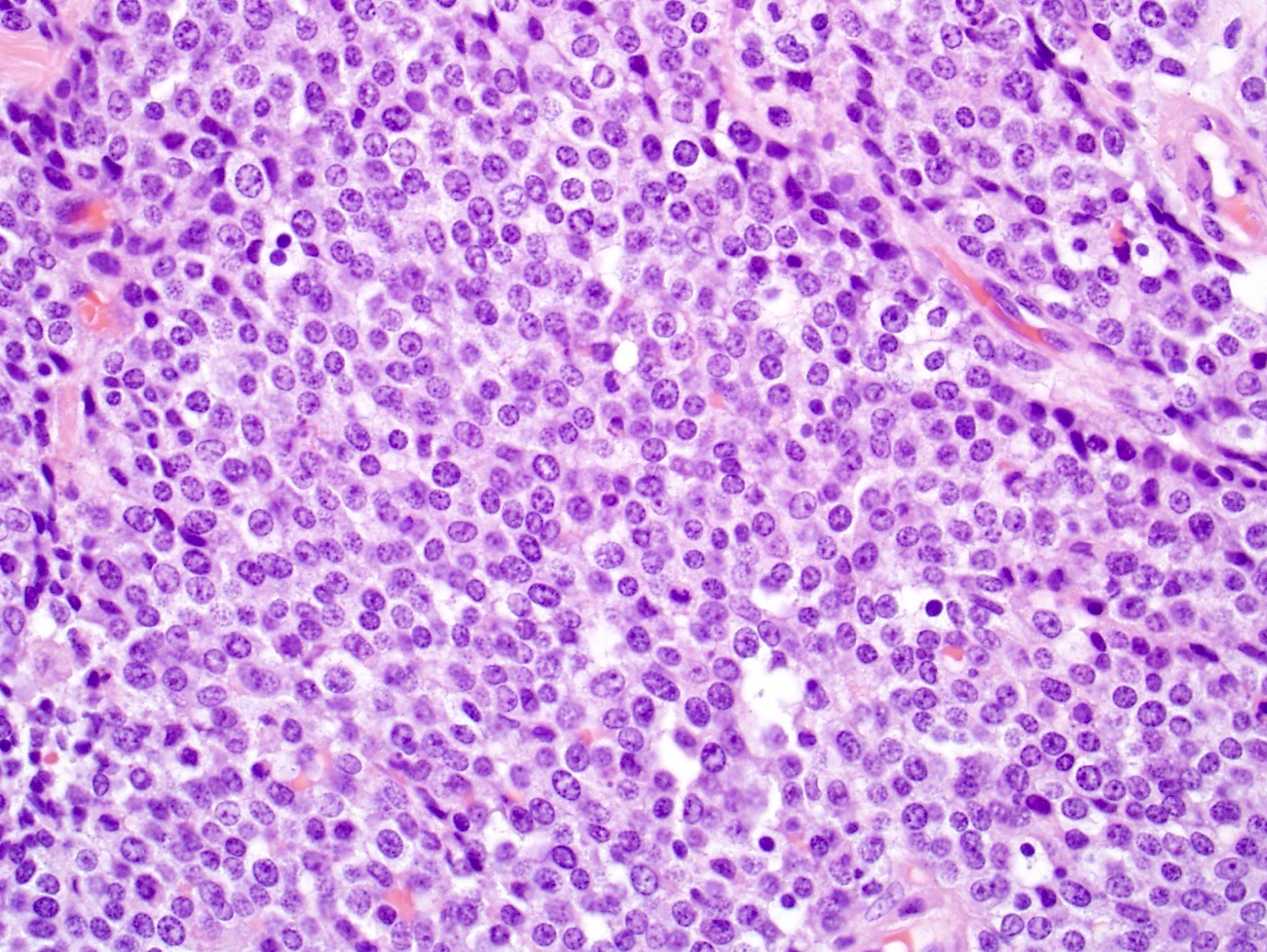
Monotonous nuclei
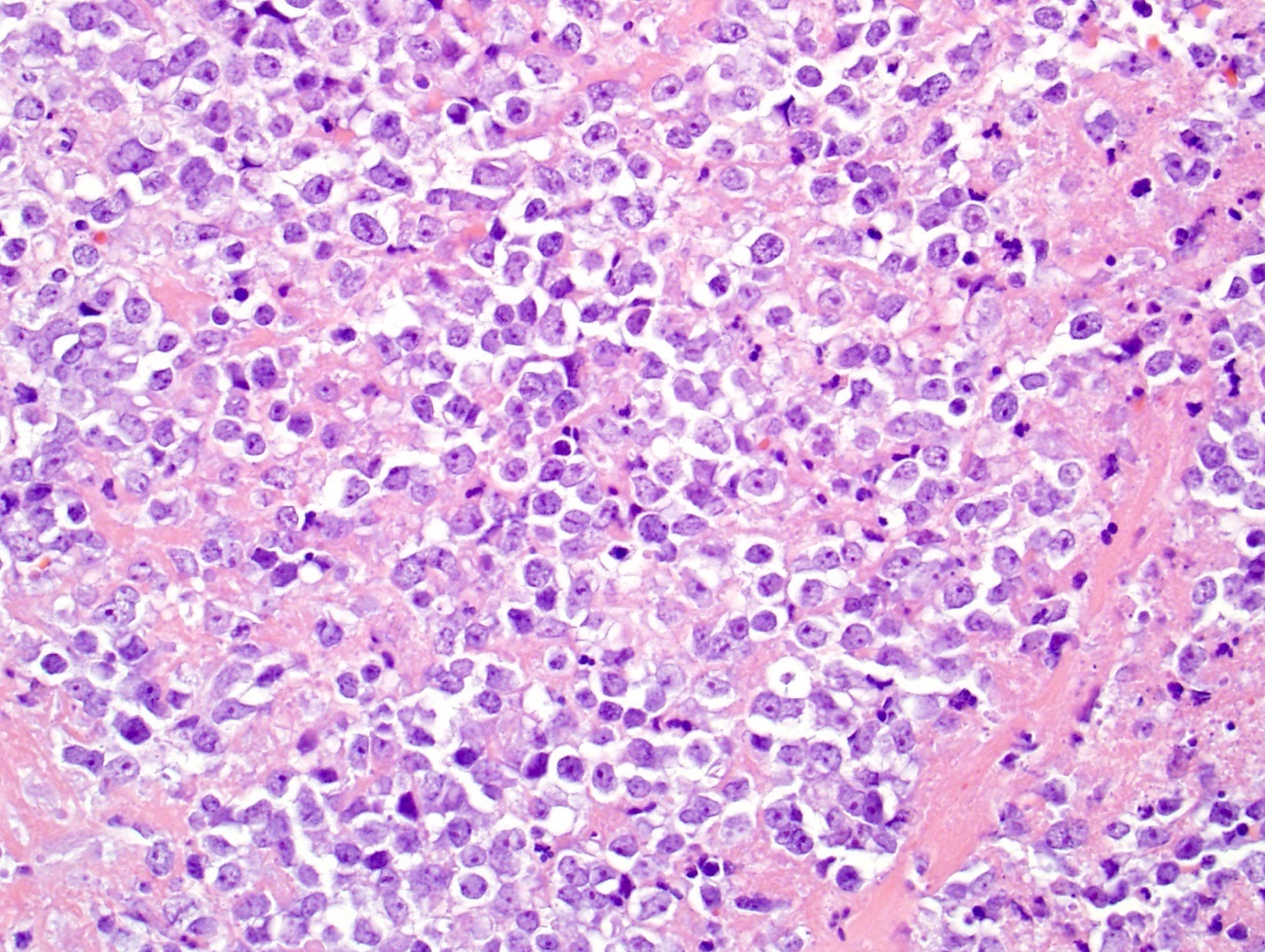
Prominent necrosis
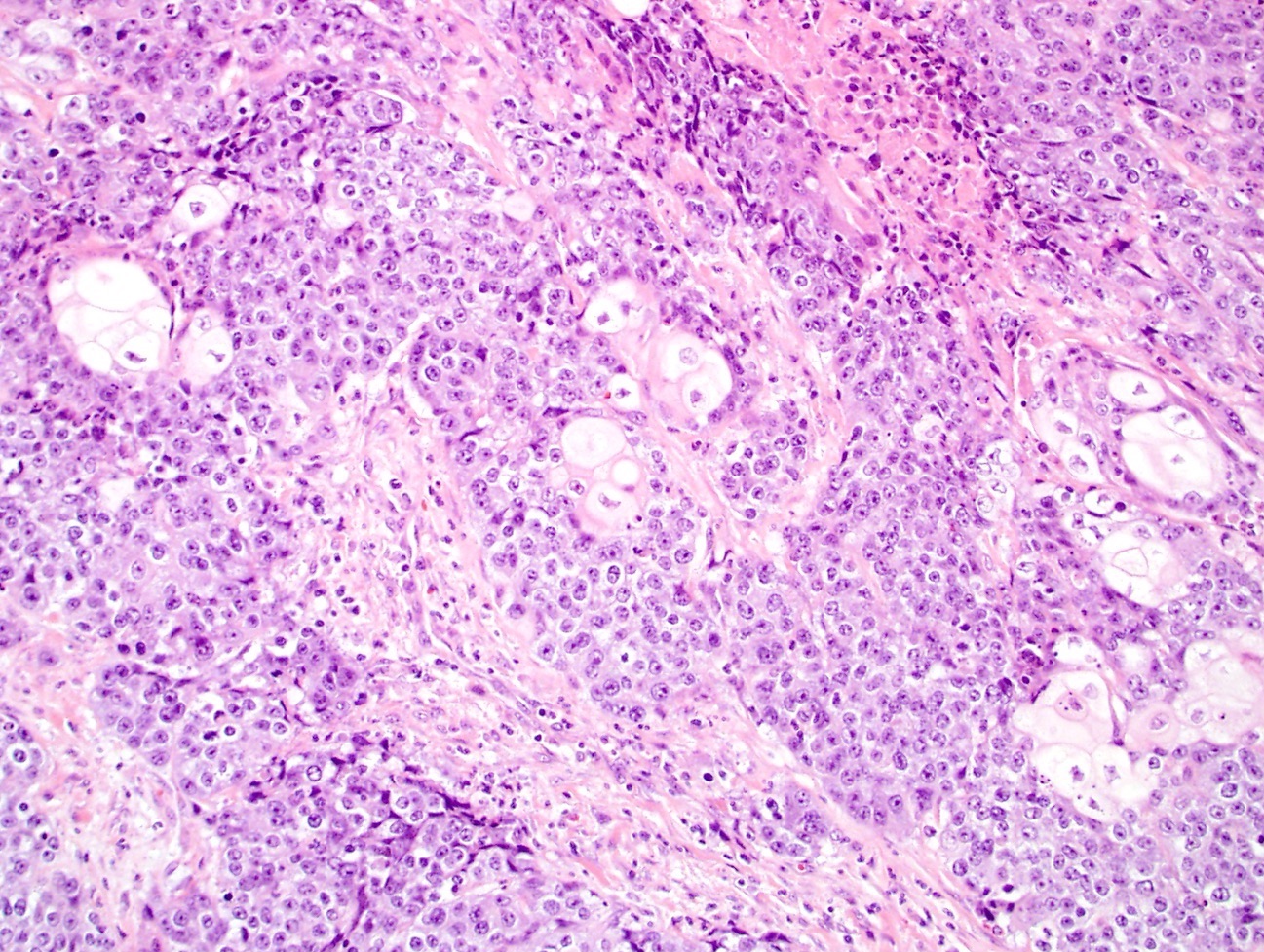
Abrupt keratinization
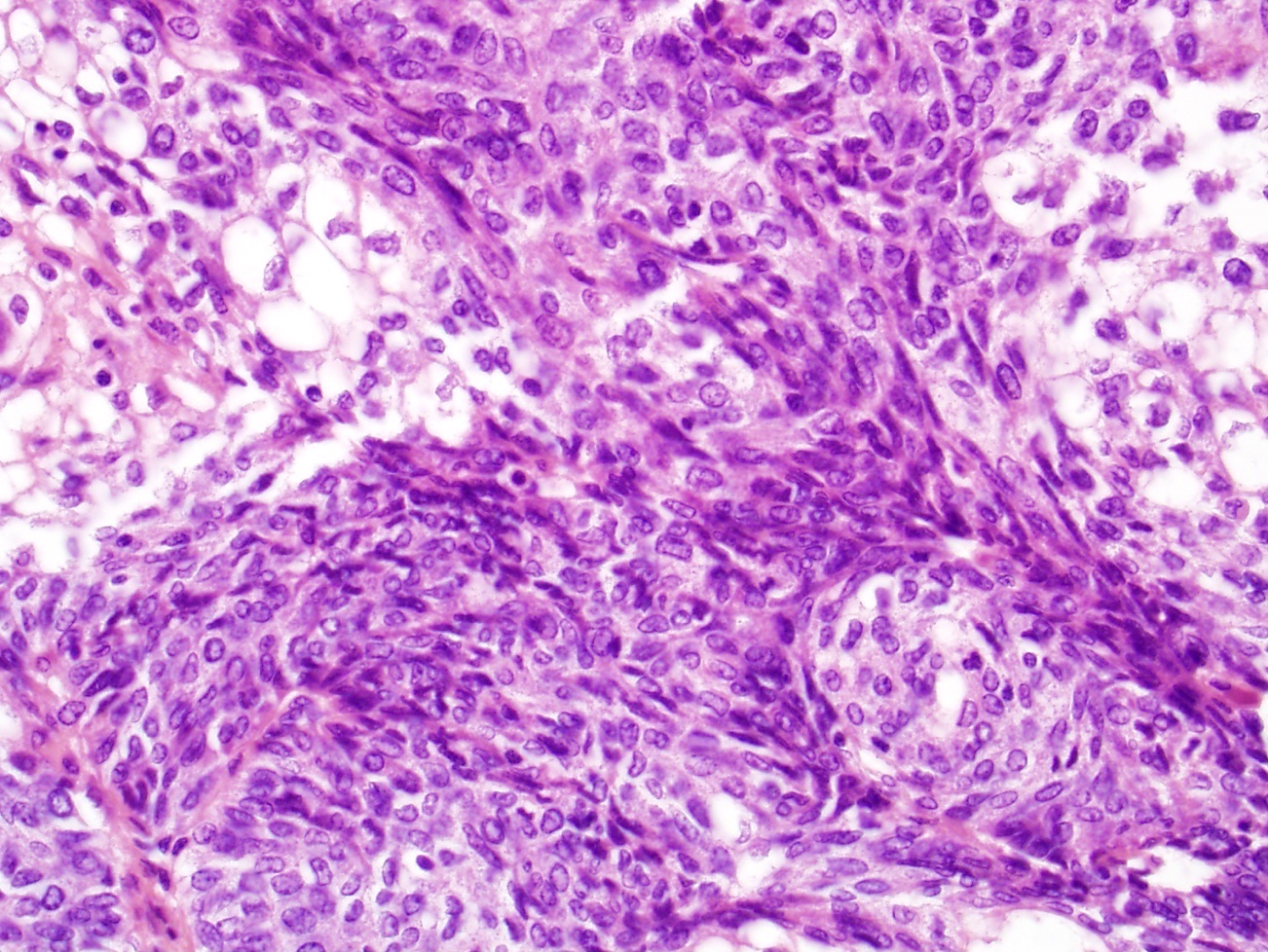
Prominent spindled foci
Infiltrating neutrophils
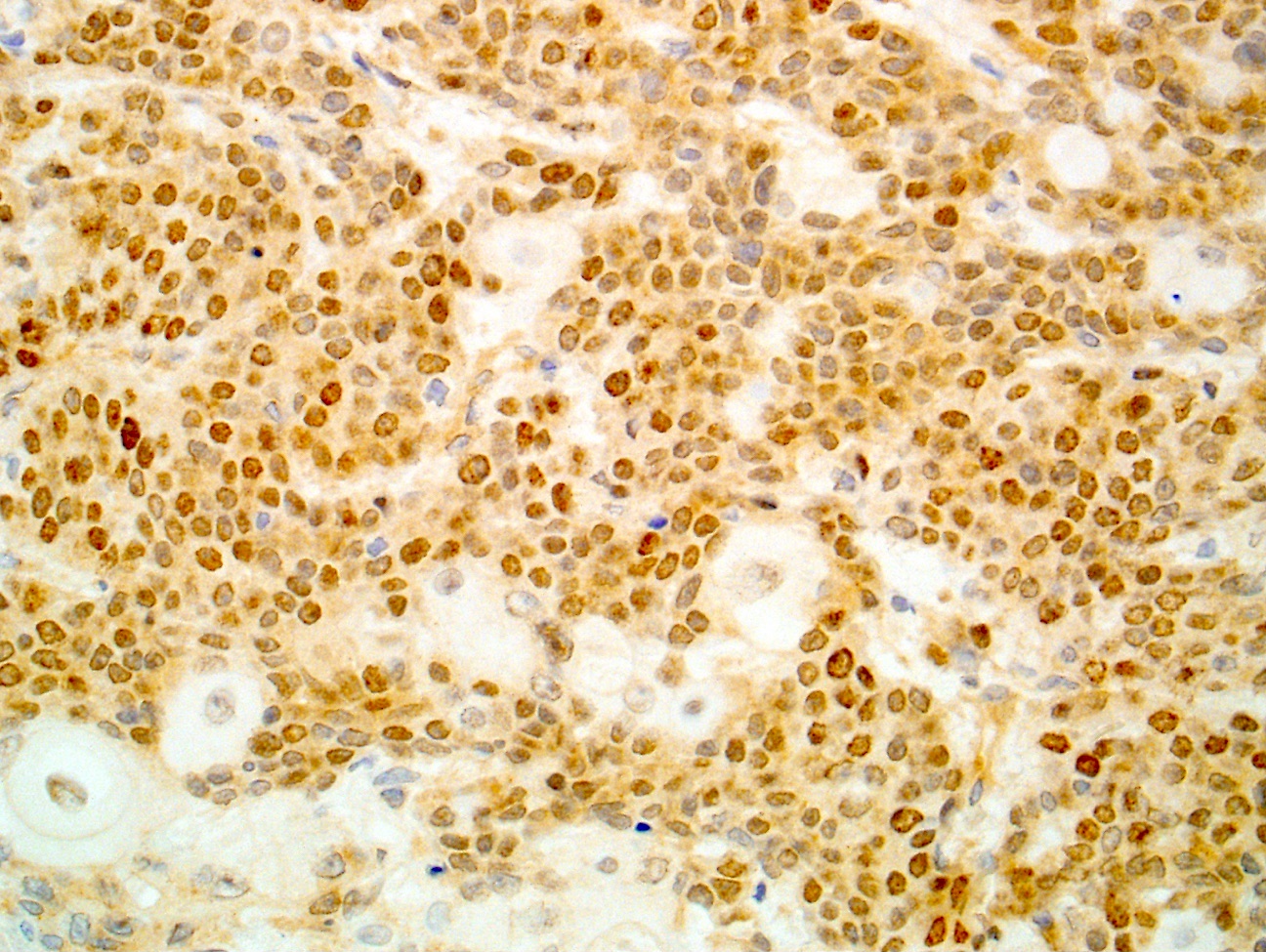
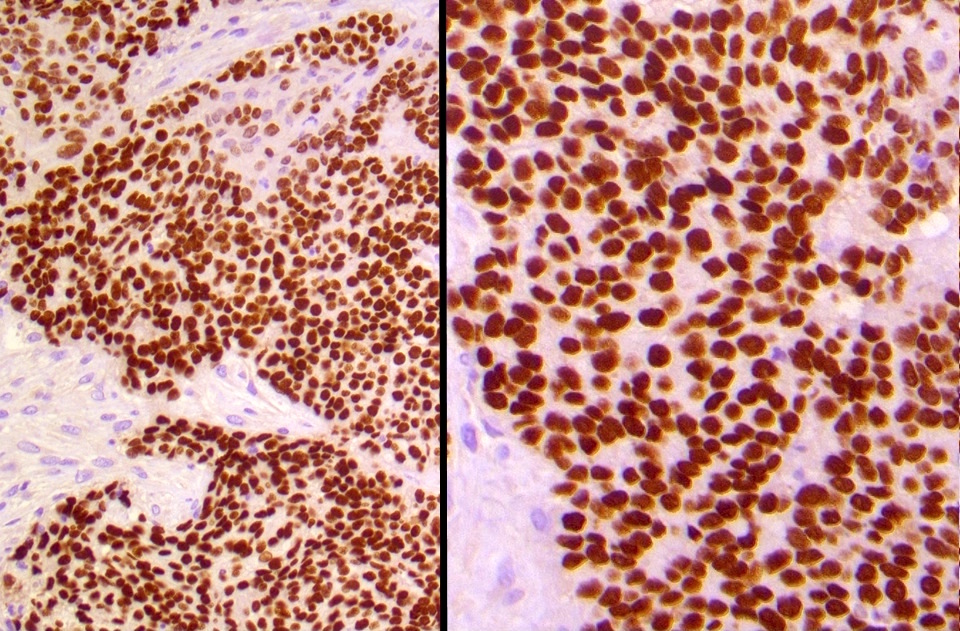
NUT1
Contributed by Brendan Dickson, M.D.

Abrupt keratinization
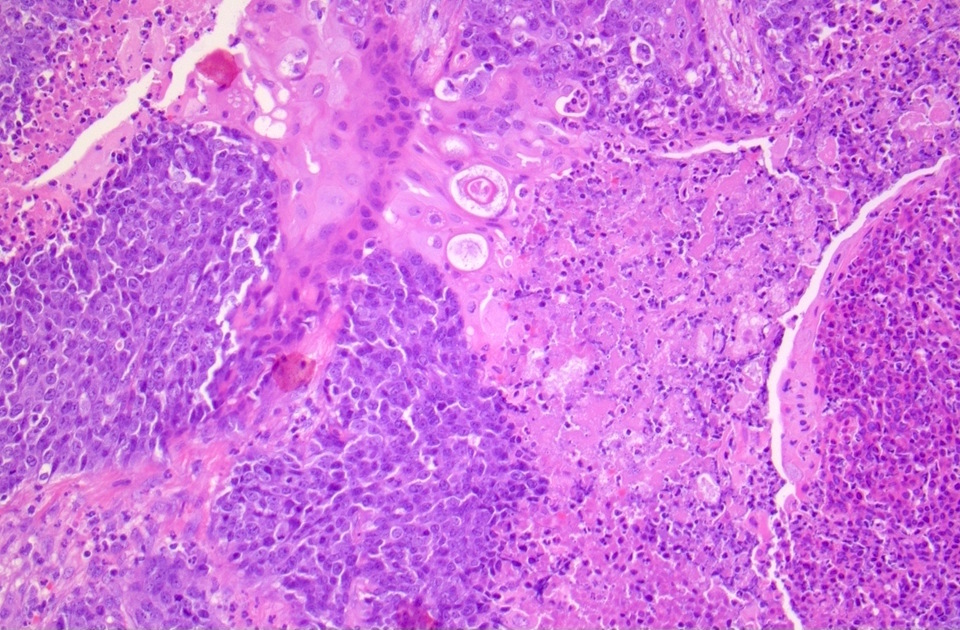
Necrosis
Undifferentiated areas
p63
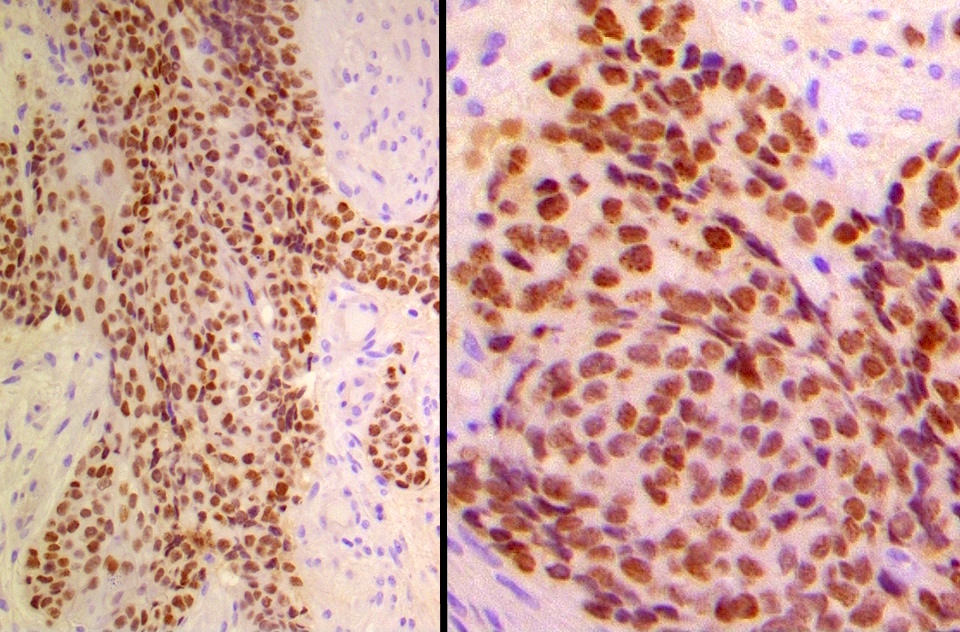
NUT1

AE1 / 3
Cytology images
Images hosted on other servers:

Aspirate of metastasis
Positive stains
- NUT1 diffuse speckled nuclear positivity is 87% sensitive and 100% specific (Am J Surg Pathol 2009;33:984)
- Pancytokeratin, EMA consistently positive (Am J Surg Pathol 2012;36:1216)
- p63 / p40 ~67% (Am J Surg Pathol 2012;36:1216)
- CD34 ~30 - 50% (Am J Surg Pathol 2012;36:1216)
- INI1 retained (Surg Pathol Clin 2017;10:103)
Negative stains
- CD99, NKX2.2
- S100, synaptophysin, chromogranin focal expression in rare cases (Am J Surg Pathol 2012;36:1216)
Electron microscopy description
- Large, irregular nuclei with prominent compact nucleoli (Ultrastruct Pathol 2012;36:280)
- Abundant cytoplasm with prominent tonofilament bundles, scattered pleomorphic granules and numerous desmosomal junctions (Ultrastruct Pathol 2012;36:280)
Molecular / cytogenetics description
- Defined by translocations involving the NUT gene on 15q14 (Cancer Discov 2014;4:928)
- BRD4-NUT (19p13) fusion is present in 67% of cases (Cancer Res 2003;63:304)
- Other cases show BRD3-NUT or NSD3-NUT fusions (Oncogene 2008;27:2237, Cancer Discov 2014;4:928)
- Fusions block epithelial differentiation and maintain proliferation in tumor cells (Oncogene 2008;27:2237)
- In situ hybridization for high risk HPV and EBV is uniformly negative (Int J Surg Pathol 2013;21:102)
Sample pathology report
- NUT carcinoma; see note:
- Note: Immunostains show that the tumor cells are positive for AE1 / AE3, p40 and NUT1 and negative for CD99 and synaptophysin, supporting the above diagnosis. NUT carcinoma is a rare, highly aggressive malignancy that is defined by translocations involving the NUT gene. Please see www.nmcregistry.org for information about enrolling the patient into the International NUT Carcinoma Registry and opportunities for clinical trials.
Differential diagnosis
- Basaloid squamous cell carcinoma: can also show abrupt keratinization and p63 / p40 positivity; negative for NUT1
- Sinonasal undifferentiated carcinoma: also high grade tumor; has more cytologic atypia, lacks keratinization, negative for NUT1 and p63 / p40, frequent IDH2 mutations
- High grade neuroendocrine carcinoma: also high grade tumor; lacks keratinization, negative for NUT1 and p63 / p40 and positive for synaptophysin, chromogranin and INSM1
- Adamantinoma-like Ewing sarcoma: can also show abrupt keratinization and p63 / p40 positivity; negative for NUT1 and positive for CD99 and NKX2.1
- SMARCB1 deficient sinonasal carcinoma: also high grade tumor that can be positive for p63 / p40; lacks keratinization, negative for NUT1 and shows loss of INI1
Board review style question #1
An 18 year old woman presented with a destructive sinonasal tumor; biopsy findings are shown below. What immunohistochemical finding would you expect?

- Cytoplasmic positivity for cytokeratin without significant reactivity for any other markers
- Diffuse strong positivity for synaptophysin and INSM1
- Loss of nuclear INI1 expression
- Speckled nuclear positivity for NUT1
Board review style answer #1
D. Speckled nuclear positivity for NUT1. The picture depicts a NUT carcinoma, diagnosis of which is suggested by the presence of monotonous primitive cells interspersed with areas of abrupt keratinization. The correct immunohistochemical finding for this tumor is speckled nuclear positivity for NUT1, a sensitive and specific marker of this tumor type. The other immunoprofiles listed would be more characteristic of tumors that lack the characteristic keratinization pattern depicted in this photomicrograph, including sinonasal undifferentiated carcinoma (A. Cytoplasmic positivity for cytokeratin without significant reactivity for any other markers), small cell carcinoma (B. Diffuse strong positivity for synaptophysin and INSM1) and SMARCB1 deficient sinonasal carcinoma (C. Loss of nuclear INI1 expression).
Comment Here
Reference: NUT carcinoma
Comment Here
Reference: NUT carcinoma
Board review style question #2
What is the most common genetic abnormality identified in NUT carcinoma?
- BRD3-NUT
- BRD4-NUT
- Deletion of NUT
- NSD3-NUT
Board review style answer #2
B. BRD4-NUT. The most common genetic abnormality identified in NUT carcinoma is BRD4-NUT fusion, which is present in ~67% of cases. The other translocations listed, BRD3-NUT and NSD3-NUT, are less common variant fusions seen in NUT carcinoma; deletion of NUT has not been reported as a cause of this tumor type.
Comment Here
Reference: NUT carcinoma
Comment Here
Reference: NUT carcinoma
