
Oral cavity & oropharynx
Inflammatory / immune mediated (noninfectious)
Pemphigoid
Author: Molly Housley Smith, D.M.D.
Editor-in-Chief: Debra L. Zynger, M.D.

Last author update: 13 January 2020
Last staff update: 3 April 2024
Copyright: 2020-2024, PathologyOutlines.com, Inc.
PubMed Search: Pemphigoid oral pathology
See Also: Bullous pemphigoid, Cicatricial pemphigoid
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology / etiology | Diagrams / tables | Clinical features | Diagnosis | Laboratory | Prognostic factors | Case reports | Treatment | Clinical images | Gross description | Microscopic (histologic) description | Microscopic (histologic) images | Immunofluorescence description | Immunofluorescence images | Videos | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2 | Board review style question #3 | Board review style answer #3Cite this page: Smith MH. Pemphigoid. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/oralcavitypemphigoid.html. Accessed April 25th, 2024.
Definition / general
- Chronic, immune mediated, subepithelial blistering disease that predominantly affects mucous membranes
- Autoantibodies directed at components of the basement membrane zone
Essential features
- Second most common immune mediated, subepithelial blistering disease, after bullous pemphigoid (J Invest Dermatol 2016;136:2495)
- Most often presents in the oral cavity
- Autoimmune (IgG, IgA or C3) attack of hemidesmosomes / basement membrane zone
- May affect the oral cavity, conjunctiva, subglottis, larynx, nose, esophagus, penis, vulva, anal mucosa or skin
Terminology
- Mucous membrane pemphigoid
- Benign mucous membrane pemphigoid (BMMP)
- Cicatricial pemphigoid
- Mucosal pemphigoid
ICD coding
- ICD-10: L12.1 - benign mucous membrane pemphigoid
Epidemiology
- Wide age range; predilection for middle aged to older adults
- Slight female predominance
Sites
- Affects the oral cavity (96.7%), conjunctiva (42.2%), subglottis, larynx, nose, esophagus, skin or anogenital regions (27.9%) (J Eur Acad Dermatol Venereol 2016;30:72)
- Oral cavity is the most commonly affected site
- Gingiva > buccal mucosa > palate > alveolar ridge > tongue > lower lip
Pathophysiology / etiology
- Likely an autoantibody induced and complement mediated sequestration of leukocytes (predominantly neutrophils) with release of cytokines and leukocyte enzymes leading to detachment of epithelium at the basement membrane zone (Br J Oral Maxillofac Surg 2008;46:358)
- Combination of IgG (94.6%), C3 (85.8%) or IgA (16.5%) autoantibodies directed against epithelial basement membrane zone components BP180, BP230, alpha 6 integrin, beta 4 integrin or laminin 332 (laminin-5) (J Eur Acad Dermatol Venereol 2016;30:72, Acta Derm Venereol 2004;84:381)
- BP180 is the most frequently affected target, in ~75% (Br J Dermatol 2006;154:90)
- Oral only subset: α6 integrin target antigen (Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1998;85:37)
- Ocular only subset: β4 integrin (J Invest Dermatol 2006;126:2631)
- Mechanism that links the binding of autoantibodies to the basement membrane zone and the subsequent scarring process is unknown (Clin Dermatol 2012;30:34)
- Association with HLA-DQB1*0301 (Br J Dermatol 2001;145:805, Br J Dermatol 2001;145:406, Br J Oral Maxillofac Surg 2008;46:358)
- Emerging association with anti-PDL1 medications (Front Med (Lausanne) 2018;5:268, J Immunother 2019;42:359, J Eur Acad Dermatol Venereol 2019 Oct 29 [Epub ahead of print], Br J Dermatol 2018;179:993)
Diagrams / tables
Images hosted on other servers:

Epidermal / dermal junction

Table 2 MMPDA Index
Clinical features
- General: erythematous or ulcerated mucous membranes +/- blood blister formation (+ Nikolsky sign); periodic episodes leading to potential scarring (Br J Oral Maxillofac Surg 2008;46:358)
- Ocular: scarring on the conjunctiva may produce a symblepharon or blindness
- Oropharynx: dyspnea, hoarseness
- Esophagus: difficulty swallowing or bleeding; stenosis
- Nose: nosebleeds
- Skin: rare; vesicles / bullae
- Laryngeal involvement can lead to airway loss
Diagnosis
- Diagnosis made on routine H&E histological examination and biopsy for direct immunofluorescence
- Direct immunofluorescence is gold standard for diagnosis
- Cases may be followed with indirect immunofluorescence, immunoblotting or enzyme-linked immunosorbent assay (ELISA) testing
- 2015 consensus group created a disease area index table to standardize diagnosis (J Am Acad Dermatol 2015;72:168)
Laboratory
- IgG autoantibodies against basement membrane zone components (BP180, BP230, alpha 6 integrin, beta 4 integrin or laminin 332) detected
- IgG titers correlate with disease severity (Br J Dermatol 1999;140:645)
- Laminin-332 is detected in up to 20% of patients (J Invest Dermatol 2001;116:348, Br J Dermatol 2019;180:149)
Prognostic factors
- Detection of both IgG and IgA autoantibodies associated with more severe disease (Br J Dermatol 1998;138:602)
- Laminin-332 is associated with more severe disease and solid organ tumors in up to 30% (J Invest Dermatol 2001;116:348, Br J Dermatol 2019;180:149)
Case reports
- 58 year old man presents with painful mouth sores, cutaneous blisters, paronychia and onychomadesis (BMC Dermatol 2019;19:3)
- 83 year old patient presenting with oral blisters and erosions after taking pembrolizumab (Front Med (Lausanne) 2018;5:268)
Treatment
- Mild-to-moderate disease:
- Topical therapies, including betamethasone, fluticasone propionate or clobetasol propionate
- Dapsone (Br J Oral Maxillofac Surg 2008;46:358) or sulfapyridine
- Moderate-to-severe disease:
- Mycophenolate mofetil, azathioprine, sulfa drug or prednisolone
- Severe, recalcitrant disease:
- Pulsed IV cyclophosphamide, IV immunoglobulin and rituximab (Clin Exp Dermatol 2019;44:732)
- Rituximab (anti-CD20 therapy) in combination with conventional immunosuppressive therapy leads to more rapid and sustained disease control with fewer potential adverse events (J Am Acad Dermatol 2016;74:835)
- Encourage excellent oral hygiene habits and regular ophthalmologic examinations
Clinical images
Contributed by Molly Housley Smith, D.M.D. and Sonal Tuli, M.D.

Diffuse gingival involvement

Localized gingival ulceration

Bullae development
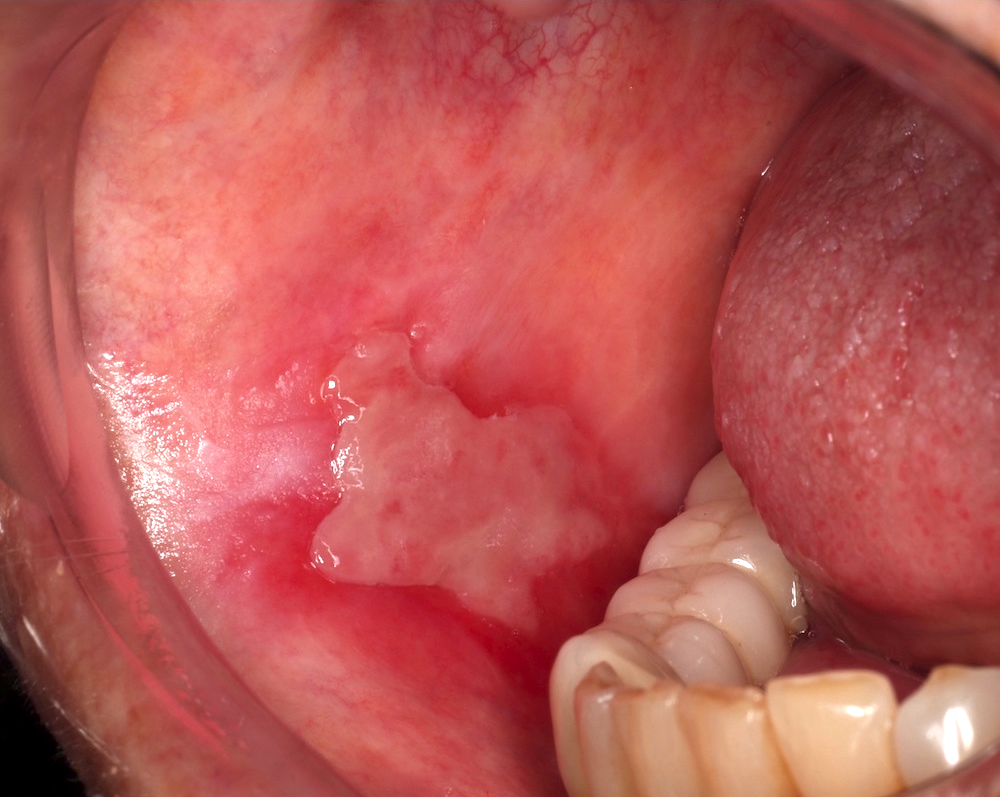
Buccal mucosa involvement
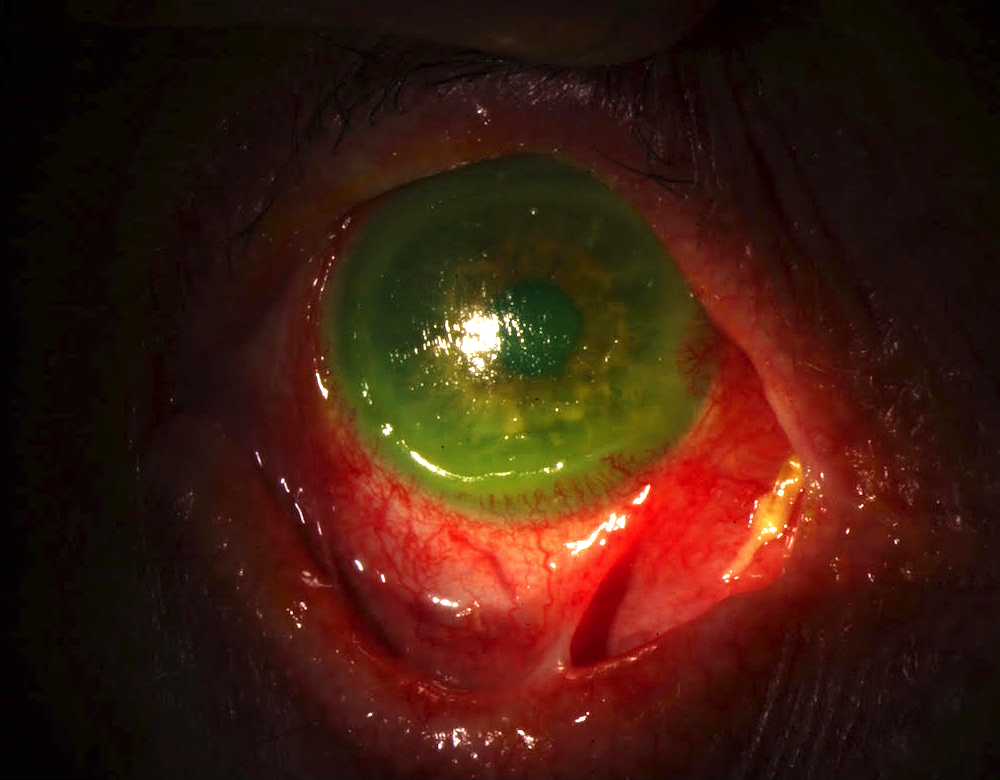
Symblepharon
Gross description
- Thin wedge of white-tan surface epithelium with underlying tan-brown connective tissue
- Epithelium occasionally separated from underlying connective tissue
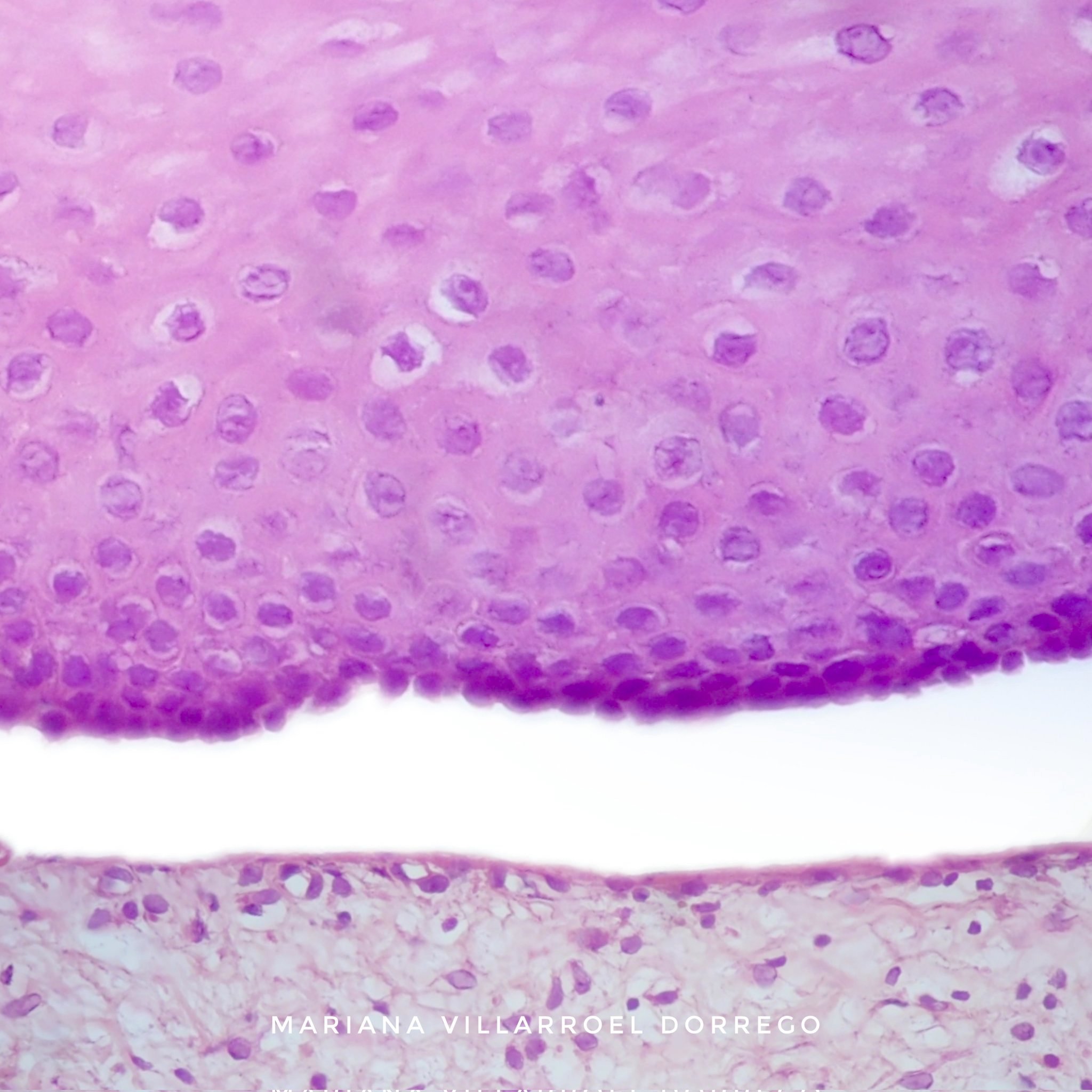
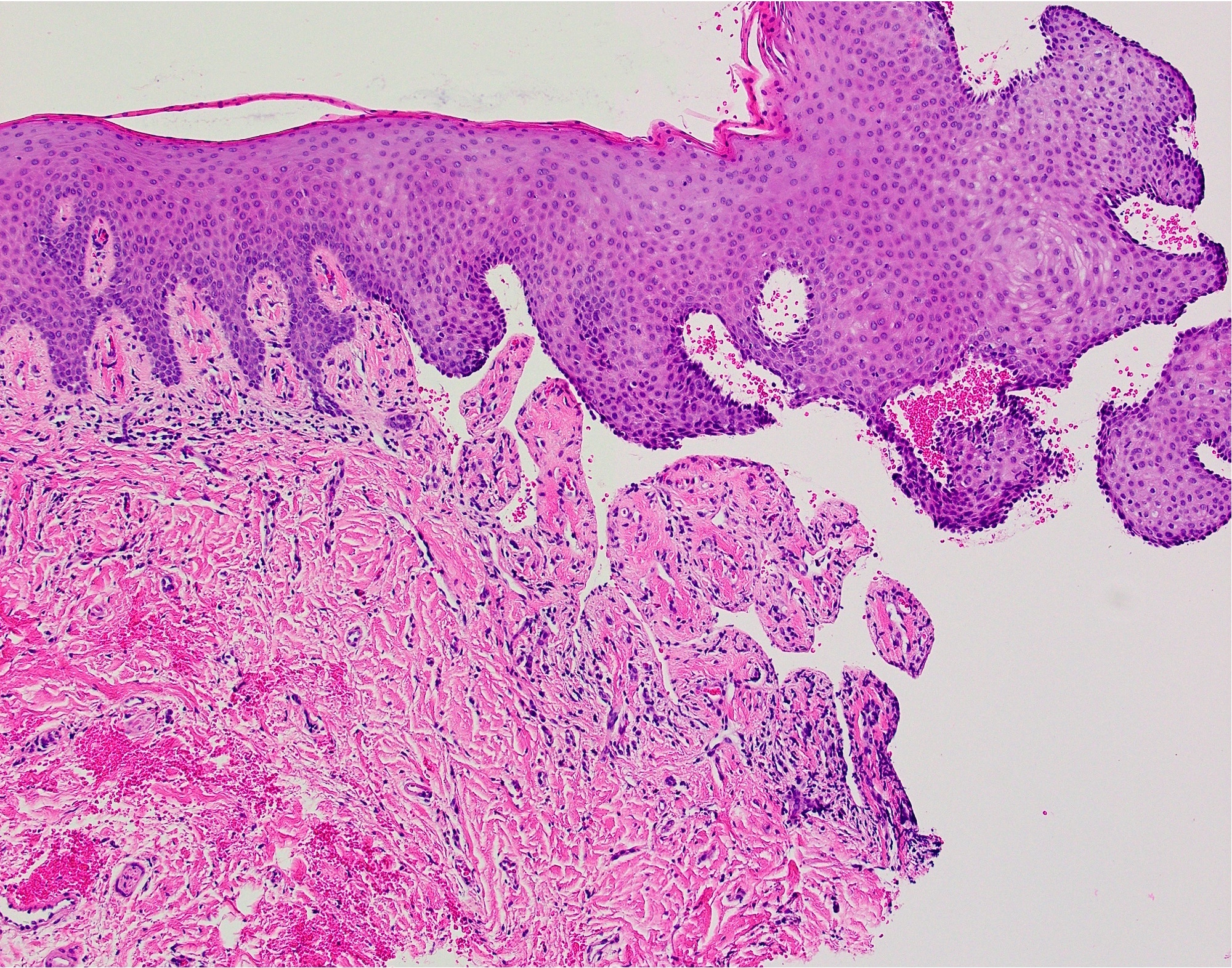
Microscopic (histologic) description
- Surface epithelium cleanly detached from the underlying connective tissue at the point of the basement membrane zone
- Superficial lamina propria contains a variable amount of inflammation that may contain lymphocytes, eosinophils and neutrophils (Br J Oral Maxillofac Surg 2008;46:358)
- Aggregates of erythrocytes may be present in area of bullae formation
Microscopic (histologic) images
Contributed by Molly Housley Smith, D.M.D. and @reportesVilla on Twitter
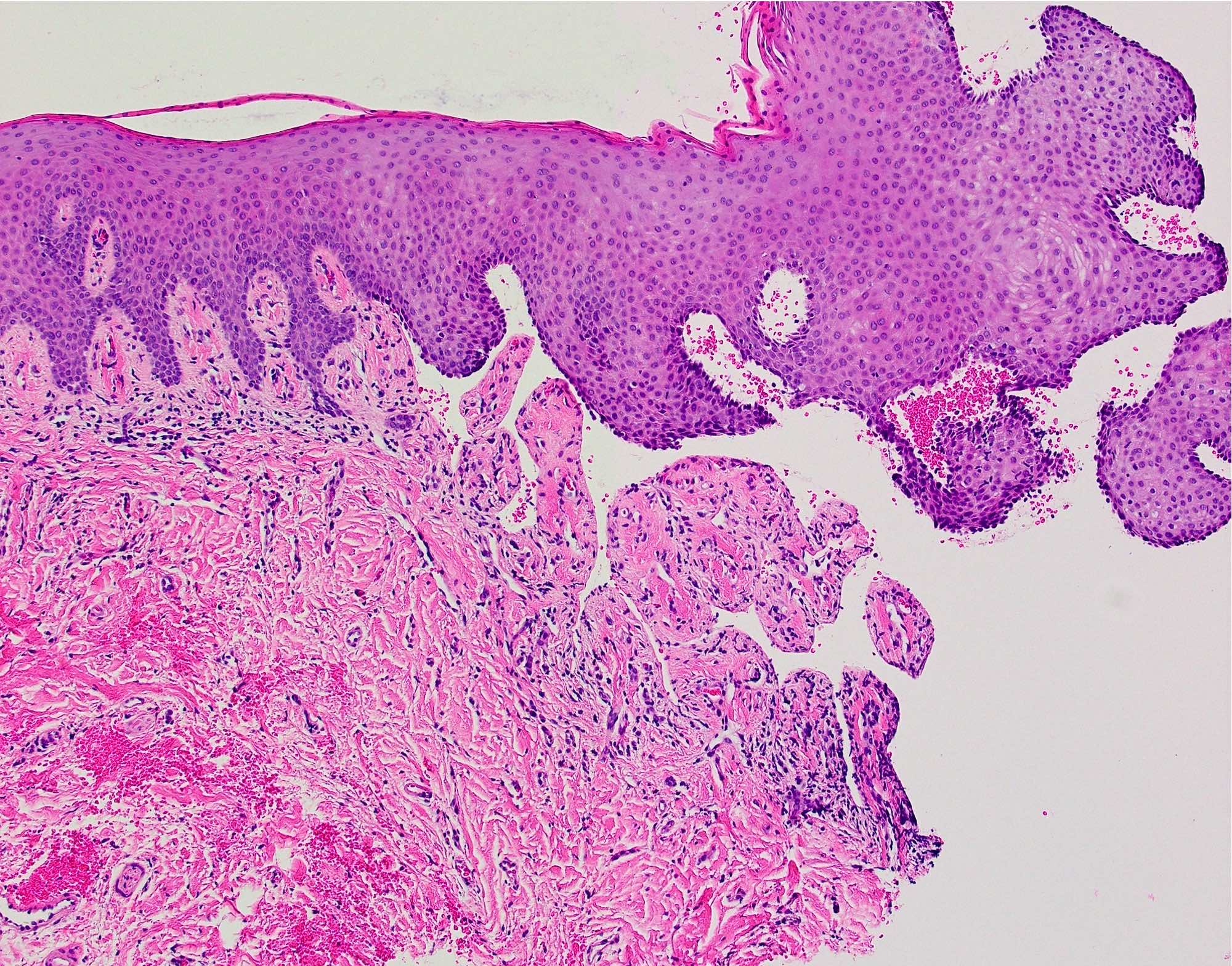
Subepithelial separation
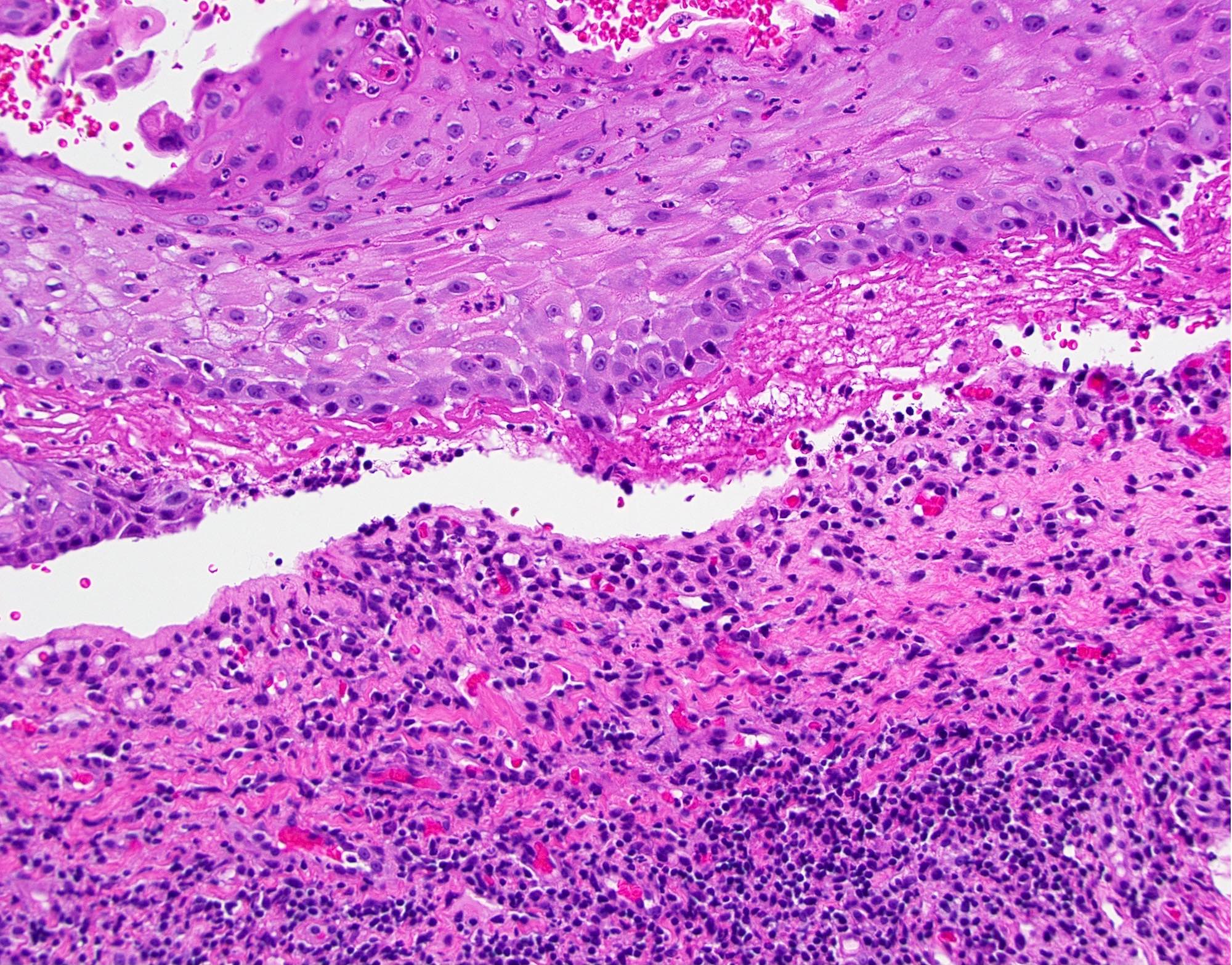
Subepithelial cleft
contains fibrin,
erythrocytes and
inflammatory cells

Subepithelial separation
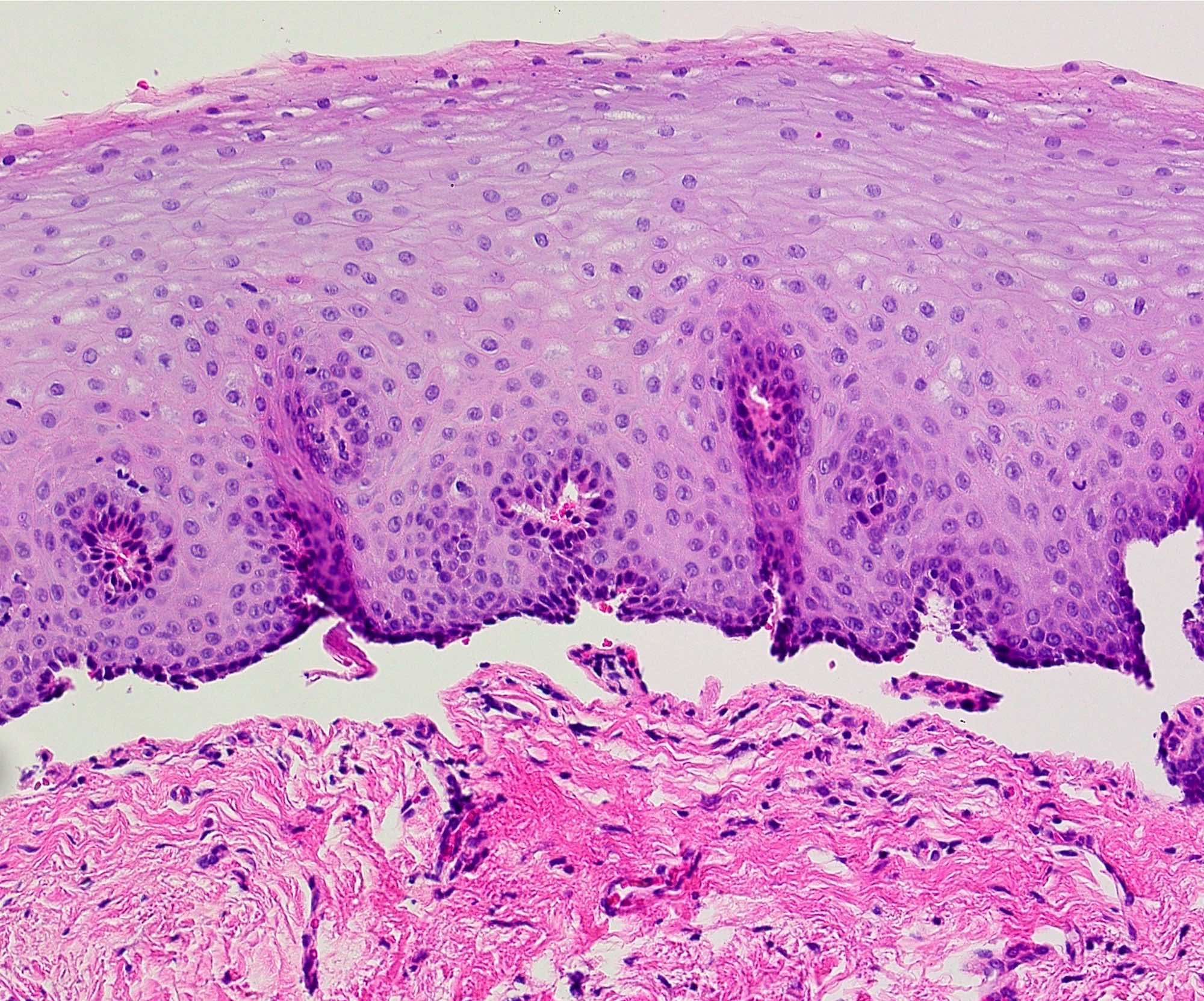
Minimal inflammation
Pemphigoid
Immunofluorescence description
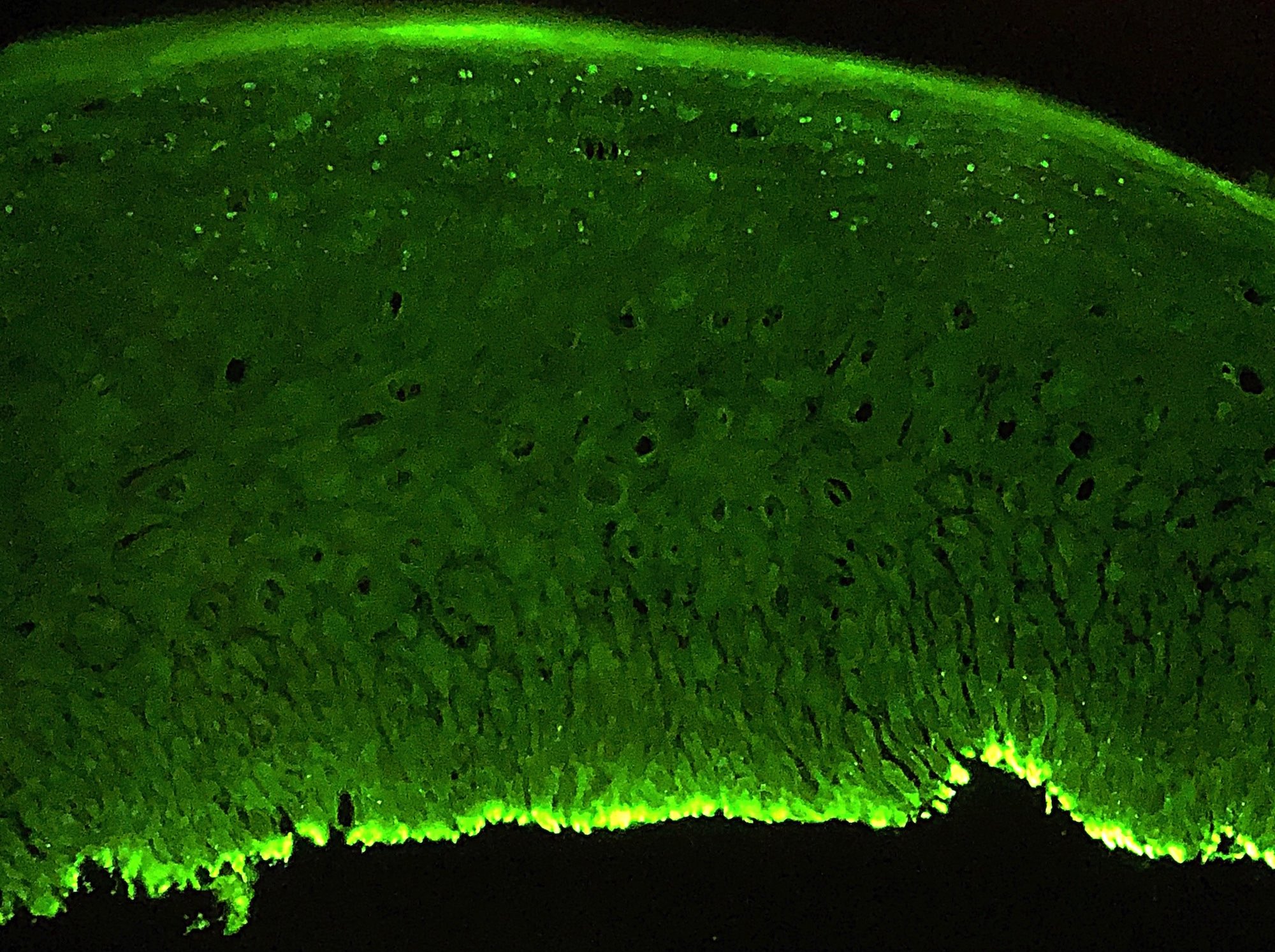
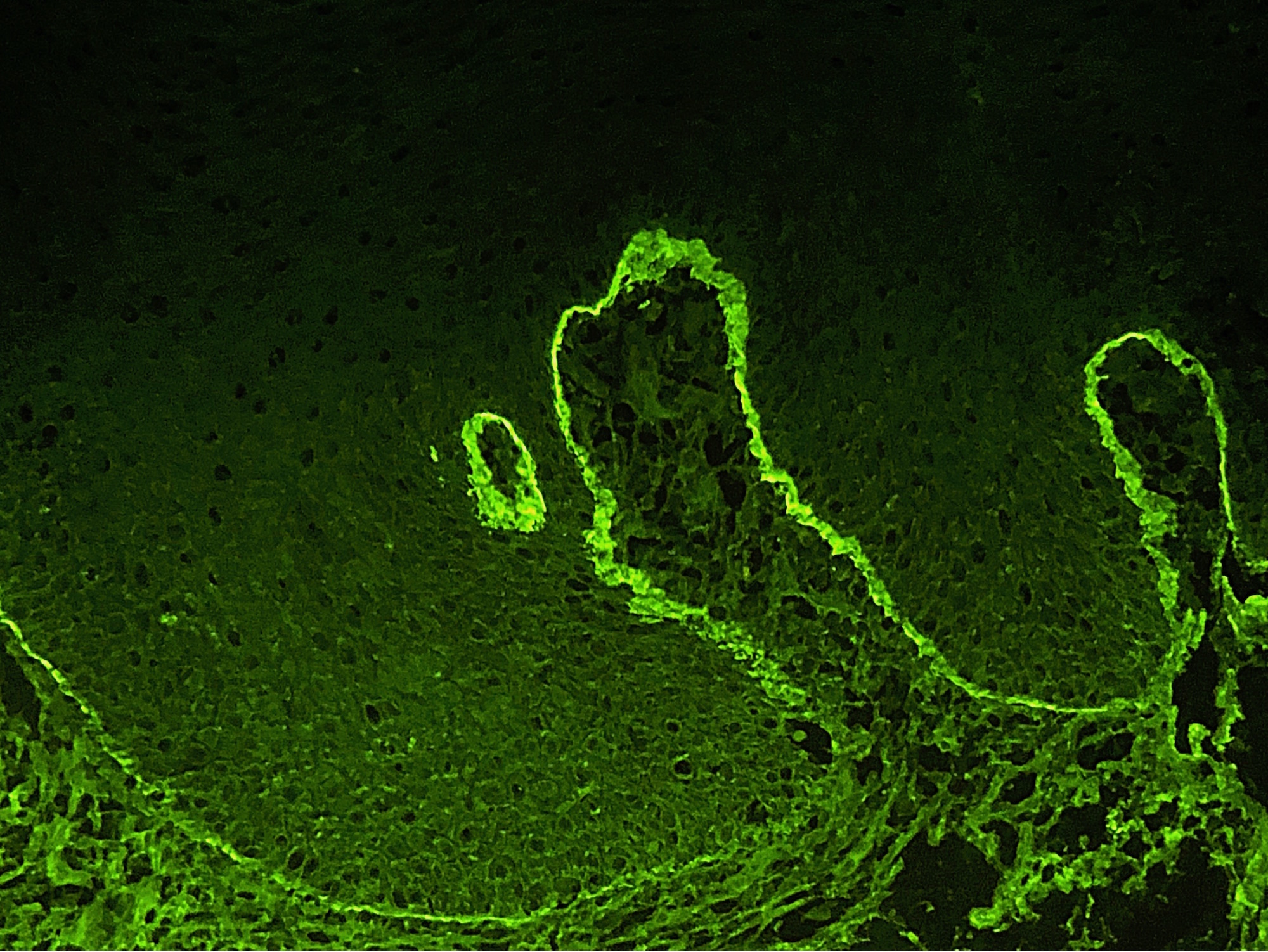
- Direct immunofluorescence (DIF): linear deposits of IgG, IgA or C3 along the basement membrane zone (Br J Oral Maxillofac Surg 2008;46:358)
- Indirect immunofluorescence (IIF): IgG autoantibodies against the basement membrane zone with known target antigens including BP180, BP230, alpha 6 integrin, beta 4 integrin or laminin 332 (laminin-5)
Immunofluorescence images
Contributed by Molly Housley Smith, D.M.D.
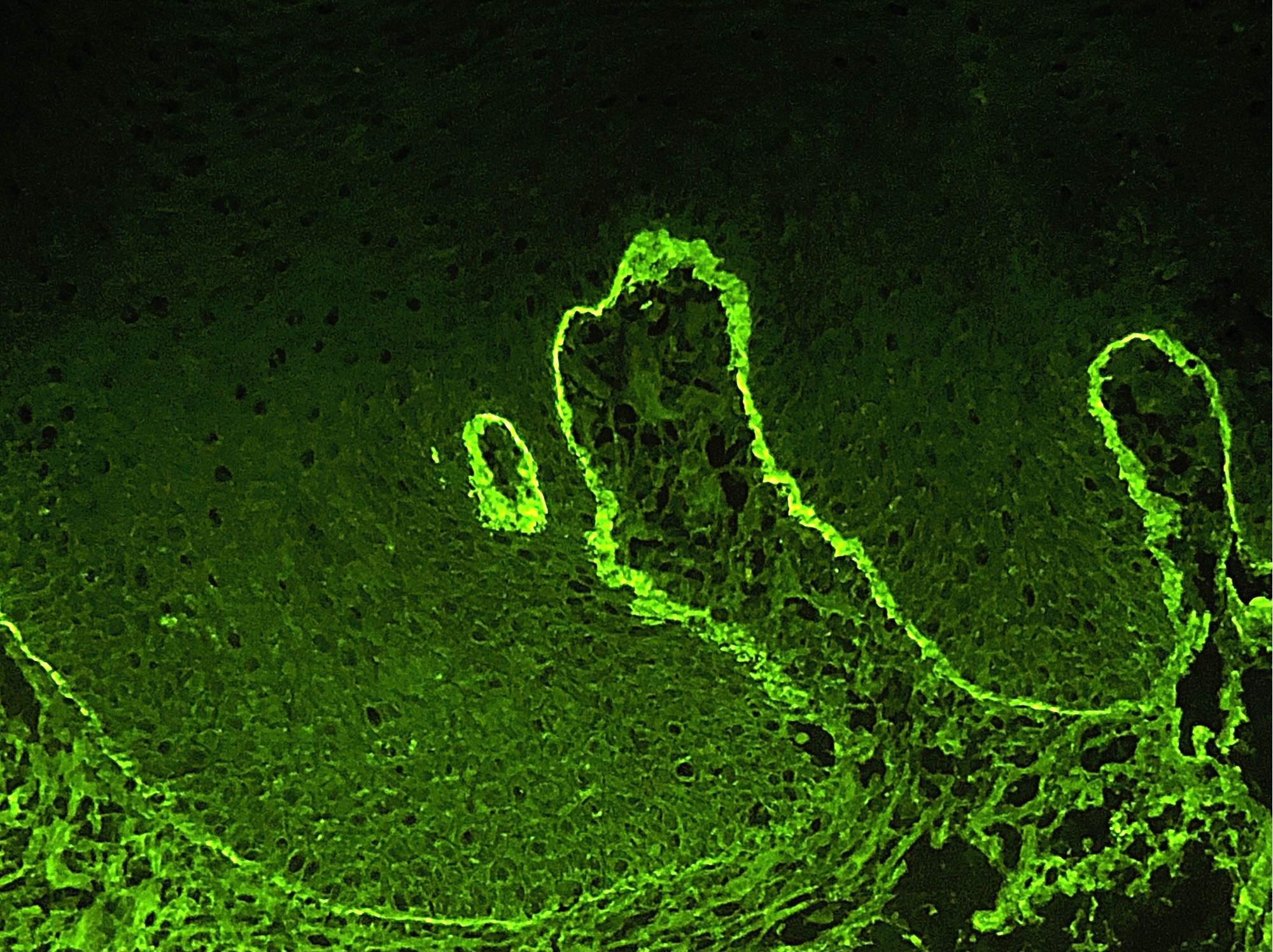
IgG
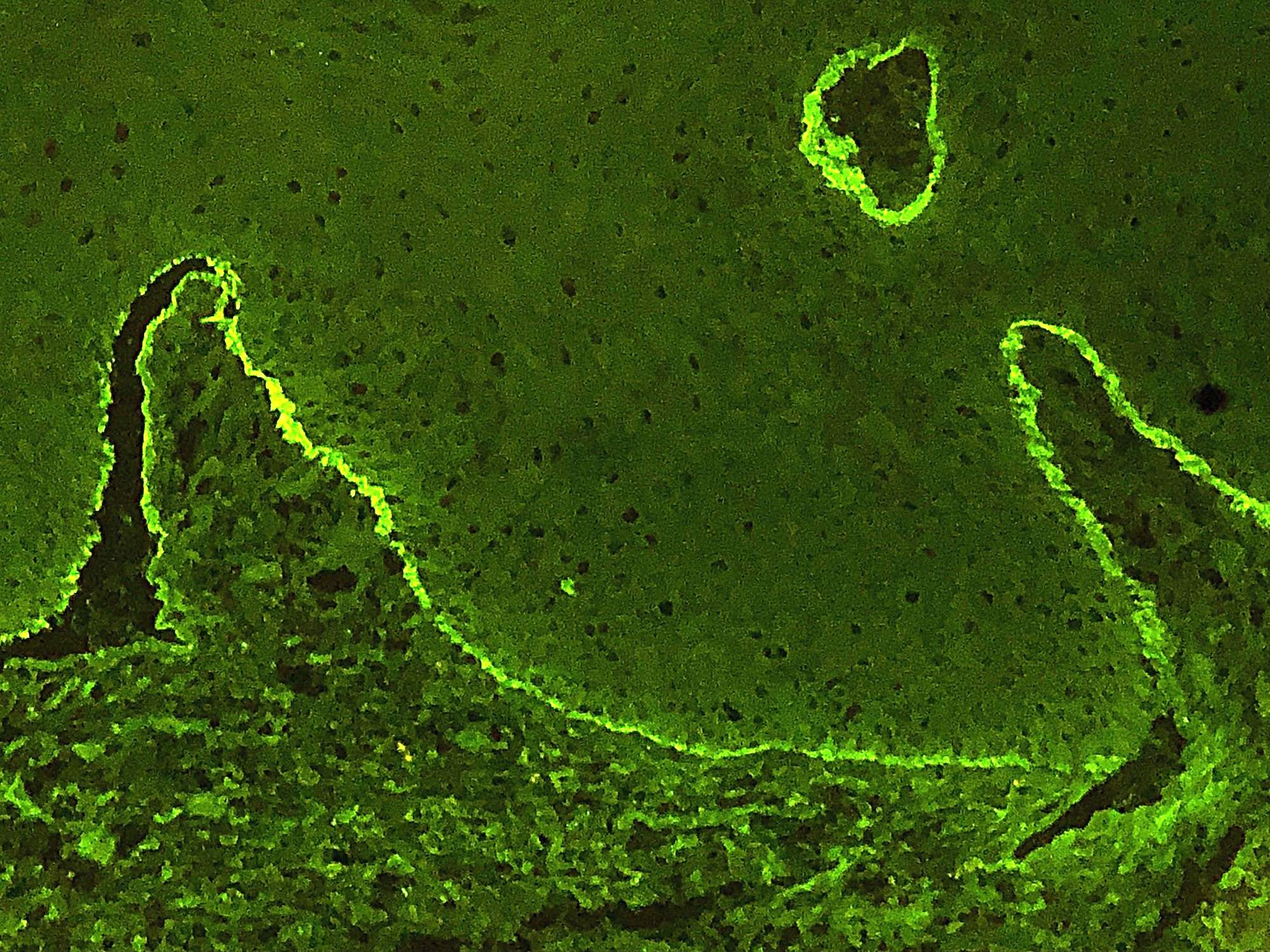
C3
IgA
Videos
Clinical, histology, laboratory findings with discussion on pathophysiology
Sample pathology report
- Buccal gingiva, incisional biopsy:
- Subepithelial vesiculo-erosive condition consistent with benign mucous membrane pemphigoid (see comment)
- Comment: On H&E, there is a clean separation of the superficial stratified squamous epithelium from the underlying connective tissue at the layer of the basement membrane zone. On direct immunofluorescence, a shaggy and linear deposition of IgG, C3 and IgA is present in the basement membrane zone.
Differential diagnosis
- Bullous pemphigoid (BP)
- Most common immune mediated, subepithelial blistering disease
- Widespread skin lesions
- Persistent mucosal lesions are not seen
- Propensity to scar is less frequent
- Infrequent in the oral cavity
- Pemphigus vulgaris
- Autoimmune bullous disease directed against desmosomes
- Skin lesions heal without scarring
- Buccal mucosa > palate > tongue > labial mucosa > gingiva
- Suprabasilar clefting with acantholysis
- Direct immunofluorescence shows intracellular IgG and C3 staining
- Enzyme-linked immunosorbent assay demonstrates antibodies directed against desmoglein 1 and 3
- Paraneoplastic pemphigus
- Autoimmune blistering condition that indicates an underlying benign or malignant disease
- Patient may be unwell at time of diagnosis
- Intraepidermal-acantholytic bullae
- Direct immunofluorescence may demonstrate intracellular or basement membrane zone IgG and C3 staining
- Immunoblotting reveals antibodies to desmoglein 3 (Dsg3), BP230, envoplakin, plectin, periplakin or epiplakin
- Erosive lichen planus
- T-cell mediated autoimmune disease
- Interface mucositis with Civatte bodies
- Subepithelial band of lymphocytes
- Direct immunofluorescence shaggy fibrin deposition at basement membrane zone
- Epidermolysis bullosa acquisita
- Immune mediated, subepithelial blistering condition
- Differentiate using salt split testing or enzyme-linked immunosorbent assay
- Enzyme-linked immunosorbent assay detects antibodies against type VII collagen
- Antibodies bind to the connective tissue floor of the bullae in epidermolysis bullosa acquista rather than the roof of the bullae as seen in metalloproteinases
- Lichen planus pemphigoides
- Generally younger
- Lichenoid lesions along with bullae
- Also has lichenoid characteristics
- Similar direct immunofluorescence with IgG, C3 or IgA+ at basement membrane zone
- Bullous lichen planus
- Least common variant of oral lichen planus
- Extremely rare
- Demonstrates clinical features similar to lichen planus and lichen planus pemphigoides; vesicles or bullae on pre-existing lichen planus lesions
- Histopathologic and immunofluorescent antibody studies are similar to lichen planus
- Angina bullosa hemorrhagica
- Often traumatic in nature
- Blood filled blisters on the soft palate
- Can be a mimicker on H&E
- Direct immunofluorescence is usually negative (Dermatol Reports 2014;6:5282)
- Erythema multiforme
- Self limiting blistering condition
- Lesions typically last 2 - 4 weeks
- Triggers may include infections (HSV, mycoplasma) or medications
- May demonstrate target lesions on the skin
- Lichenoid infiltrate in basement membrane zone
- Epithelium is edematous and spongiotic with necrosis of basal and suprabasal epithelial cells (intraepithelial and subepithelial bullae formation)
- Direct immunofluorescence shows diffuse granular staining of C3 in basement membrane zone
Board review style question #1
- Which is true about this entity (biopsied from the oral cavity)?
- Affected patients are often young, in the second to third decades of life
- Gingiva is the most commonly affected location
- Patients demonstrate significant ulceration and blistering of mucous membranes without subsequent scarring
- This entity mimics erosive lichen planus on direct immunofluorescence
Board review style answer #1
B. Gingiva is the most commonly affected location. This is mucous membrane pemphigoid.
Comment Here
Reference: Mucous membrane pemphigoid
Comment Here
Reference: Mucous membrane pemphigoid
Board review style question #2
- Which of the follow target antigens is not associated with mucous membrane pemphigoid?
- BP180
- BP230
- Desmoglein 1
- Laminin-332
- α6 integrin
Board review style answer #2
Board review style question #3
- Which target antigen is associated with malignancy in up to 30% of mucous membrane pemphigoid cases?
- BP 180
- BP 230
- Desmoglein 3
- Laminin-332
- Type VII collagen
Board review style answer #3
