
Oral cavity & oropharynx
Benign epithelial tumors & processes
Verruciform xanthoma
Author: Molly Housley Smith, D.M.D.
Editorial Board Member: Lisa Rooper, M.D.
Deputy Editor-in-Chief: Kelly Magliocca, D.D.S., M.P.H.

Last author update: 12 October 2023
Last staff update: 12 October 2023
Copyright: 2002-2024, PathologyOutlines.com, Inc.
PubMed Search: Verruciform xanthoma
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Case reports | Treatment | Clinical images | Gross description | Microscopic (histologic) description | Microscopic (histologic) images | Videos | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1Cite this page: Smith MH. Verruciform xanthoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/oralcavityverruciformxanthoma.html. Accessed April 23rd, 2024.
Definition / general
- Uncommon, reactive, histiocytic lesion of the oral cavity, first described in 1971 by Dr. Shafer (Oral Surg Oral Med Oral Pathol 1971;31:784)
Essential features
- Often misdiagnosed clinically and presents as a verrucoid or papillary mass, most commonly on the gingiva (Head Neck Pathol 2020;14:742)
- Characterized histologically by aggregates of foamy histiocytes / xanthoma cells within connective tissue papillae of papillary epithelium
- Frequently seen within a background setting of chronic inflammation or trauma
Terminology
- Verruciform xanthoma (VX)
ICD coding
- ICD-10: K13.4 - granuloma and granuloma-like lesions of the oral mucosa (including verruciform xanthoma)
Epidemiology
- Age range: 9 - 94 years, mean of 61 years (Head Neck Pathol 2020;14:742)
- M:F ratio is almost equal
Sites
- ~70% on masticatory mucosa (gingiva and hard palate); less common oral sites: buccal mucosa, tongue, vestibule, lip, floor of mouth (Head Neck Pathol 2020;14:742)
- May also occur on skin or anogenital mucosa
Pathophysiology
- Uncertain pathogenesis; MCP1 / CCR2 mediated recruitment of foamy macrophages in connective tissue papillae and lysosomal engulfment of epithelial lipids by MRS1 bearing macrophages under regulation of T lymphocytes may be essential in formation of VX (Oral Dis 2008;14:150)
- Necrosis of foamy macrophages and macrophage dependent debris may help perpetuate the lesion (Oral Dis 2008;14:150)
- Not related to human papillomavirus (Med Oral Patol Oral Cir Bucal 2018;23:e429)
Etiology
- May be initiated by trauma, inflammation or altered immunological response (Head Neck Pathol 2020;14:742)
- Has been seen in background setting of inflammatory conditions, such as lichen planus, graft versus host disease, oral submucous fibrosis (Case Rep Dent 2018;2018:1615086, Support Care Cancer 2021;29:79, J Oral Maxillofac Pathol 2019;23:43)
- Tobacco, mechanical stimuli, periodontal pathogens, alcohol, food sensitizing or allergic agents, dental materials, medications may trigger epithelial damage (Oral Dis 2008;14:150)
- Also has been seen within epithelial dysplasia / carcinoma in situ (J Oral Maxillofac Surg 1989;47:398)
Clinical features
- Slow growing, asymptomatic, often solitary, well demarcated plaques or masses with papillary, granular or verrucoid surface architecture
- May be white, yellow, pink or red in color (Head Neck Pathol 2020;14:742)
- Often < 1.5 cm
Diagnosis
- Biopsy with histopathological examination
Case reports
- 45 year old patient with VX of floor of mouth clinically mimicking malignancy (BMJ Case Rep 2015;2015:bcr2014209216)
- 47 year old man with chronic graft versus host disease presents with multiple VX lesions of the oral cavity (BMC Res Notes 2017;10:631)
- 52 year old man with oral submucous fibrosis presents with VX of maxillary gingiva (J Oral Maxillofac Pathol 2019;23:43)
- 56 year old woman with oral lichen planus presents with VX of tongue (Case Rep Dent 2018;2018:1615086)
Treatment
- Conservative excision is usually curative
- In a large series of 212 cases, only 3 cases were listed as recurrences (Head Neck Pathol 2020;14:742)
- In another large study of 429 cases, a 12% recurrence rate was noted (Med Oral Patol Oral Cir Bucal 2018;23:e429)
Clinical images
Contributed by Louis Beto, D.D.S., M.D., Hal Levine, D.M.D., M.D., Mark Mintline, D.D.S. and Mark Sutor, D.D.S.

Yellow granular mass of oral vestibule
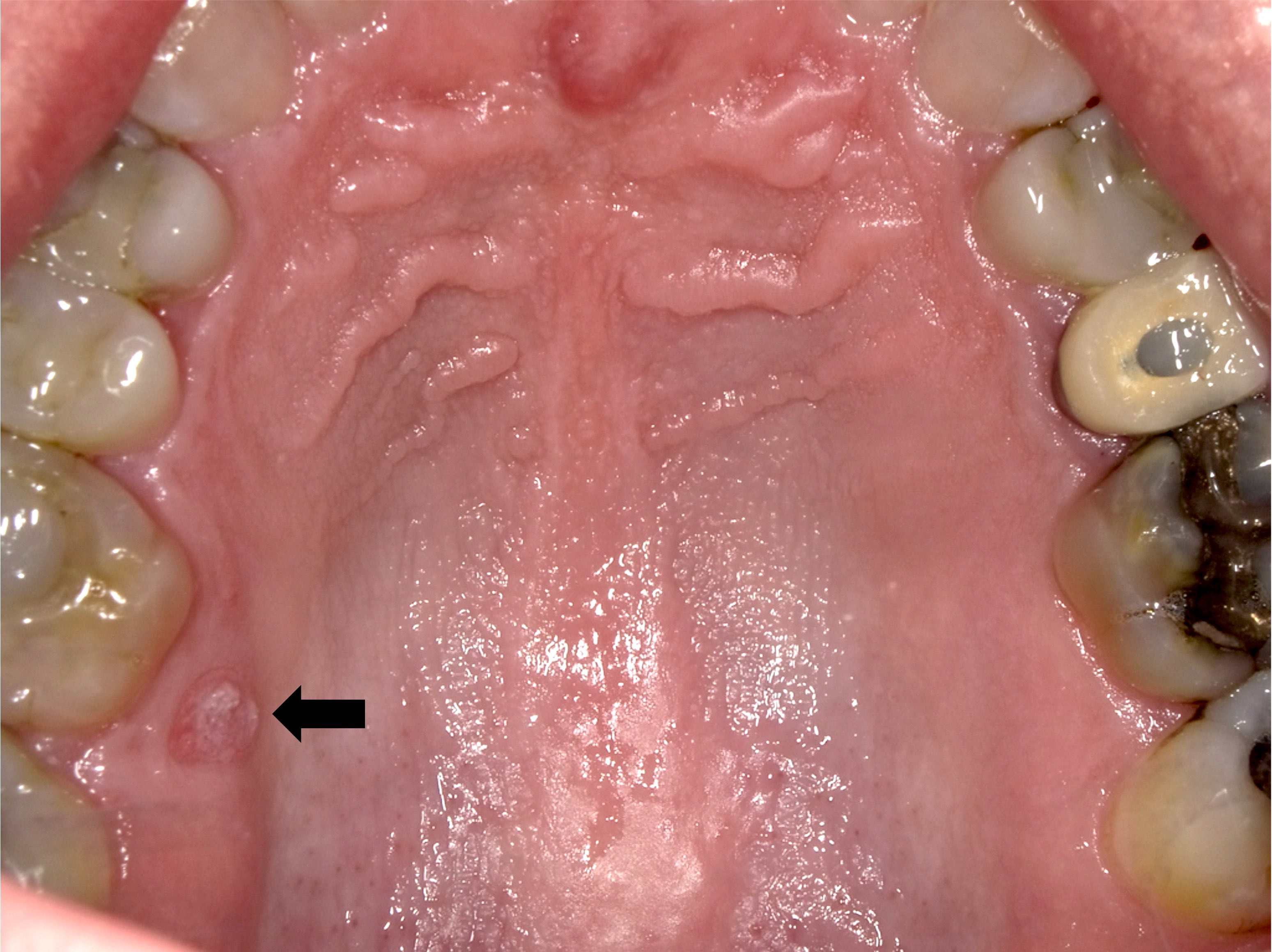
Well circumscribed solitary lesion

Yellow-red pebbly growth

Pink gingival mass
Gross description
- Raised, granular or verrucoid mass
Microscopic (histologic) description
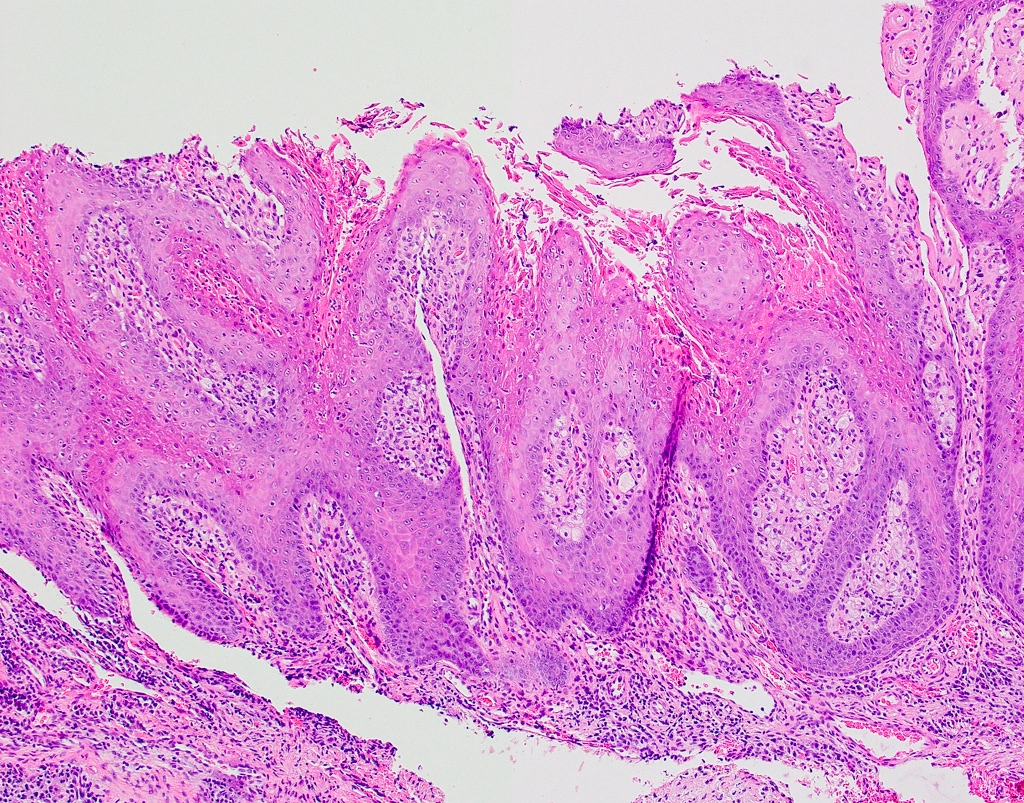
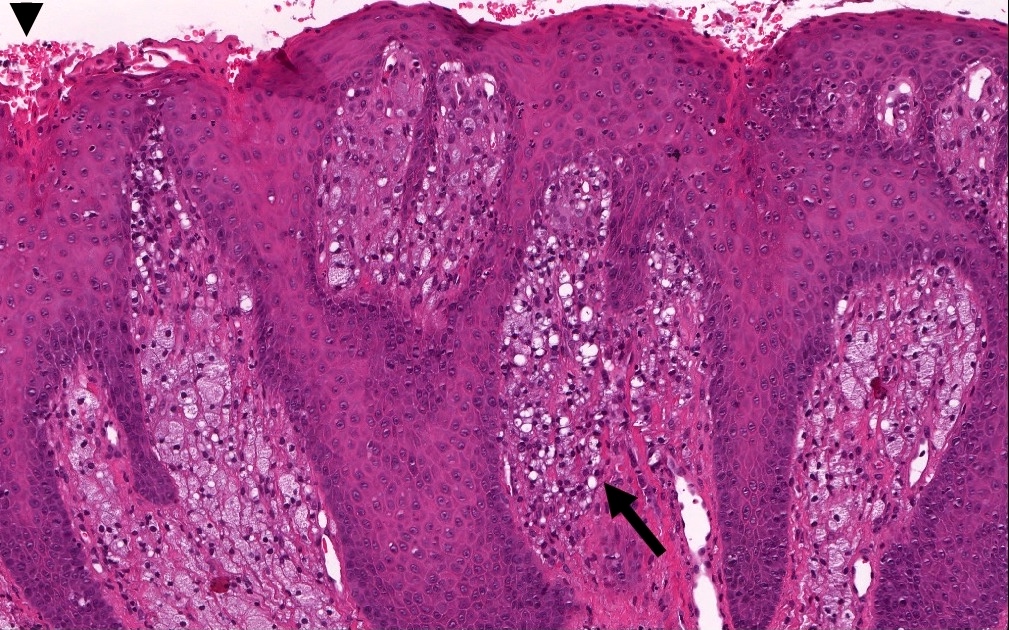
- Accumulations of lipid laden, foamy macrophages within connective tissue papillae of papillary epithelial projections
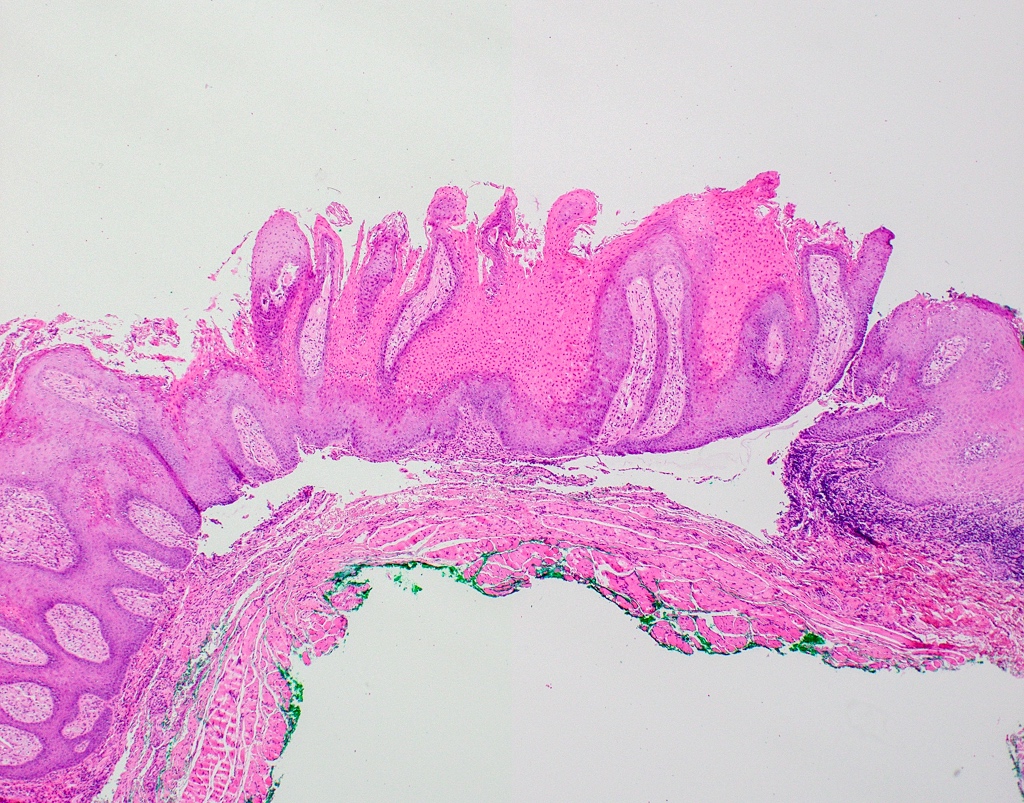
- Papillary or verrucoid surface architecture covered by a thickened layer of orange parakeratin with keratin filled clefts between papillary projections (Med Oral Patol Oral Cir Bucal 2018;23:e429)
- Neutrophilic exocytosis may be present
- Lacks cytologic atypia
- Variable inflammation within the underlying connective tissue
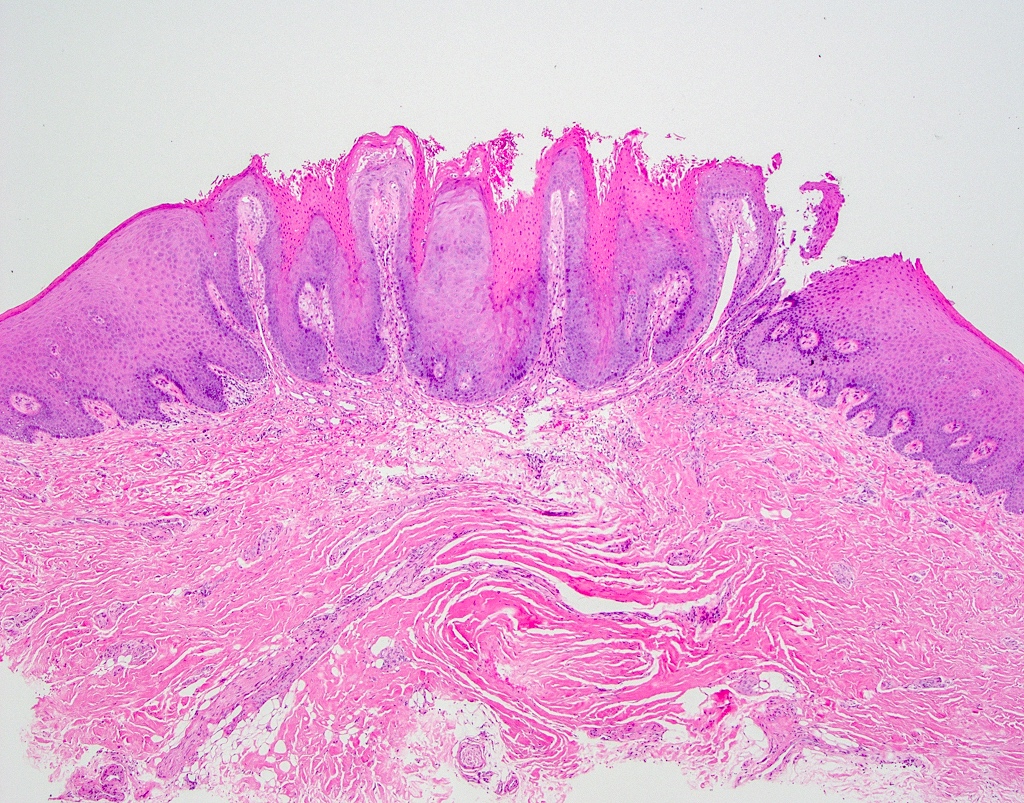
Microscopic (histologic) images
Contributed by Molly Housley Smith, D.M.D. and Kelly Magliocca, D.D.S., M.P.H.
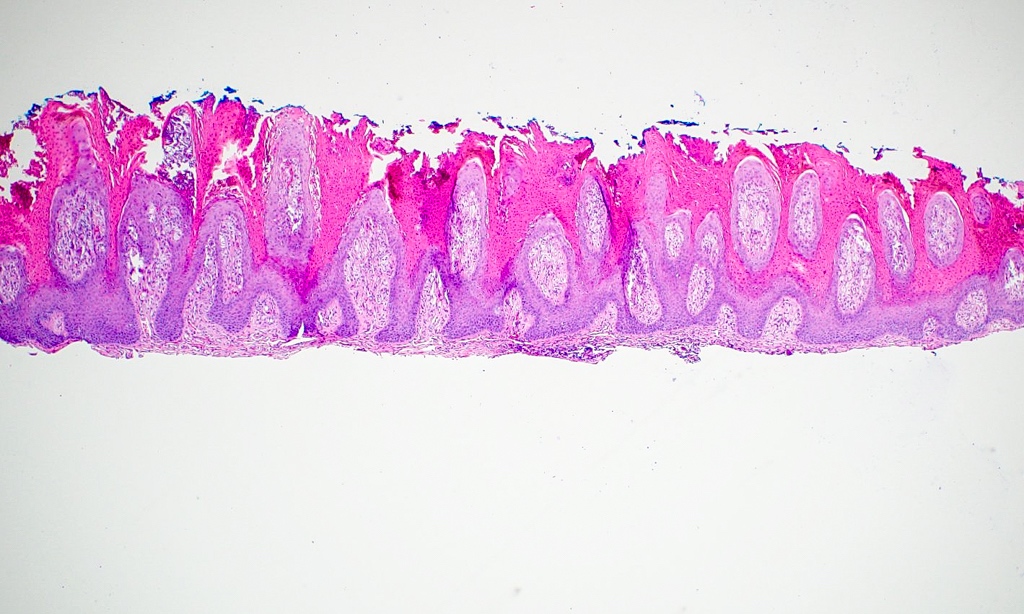
Prominent verrucoid architecture
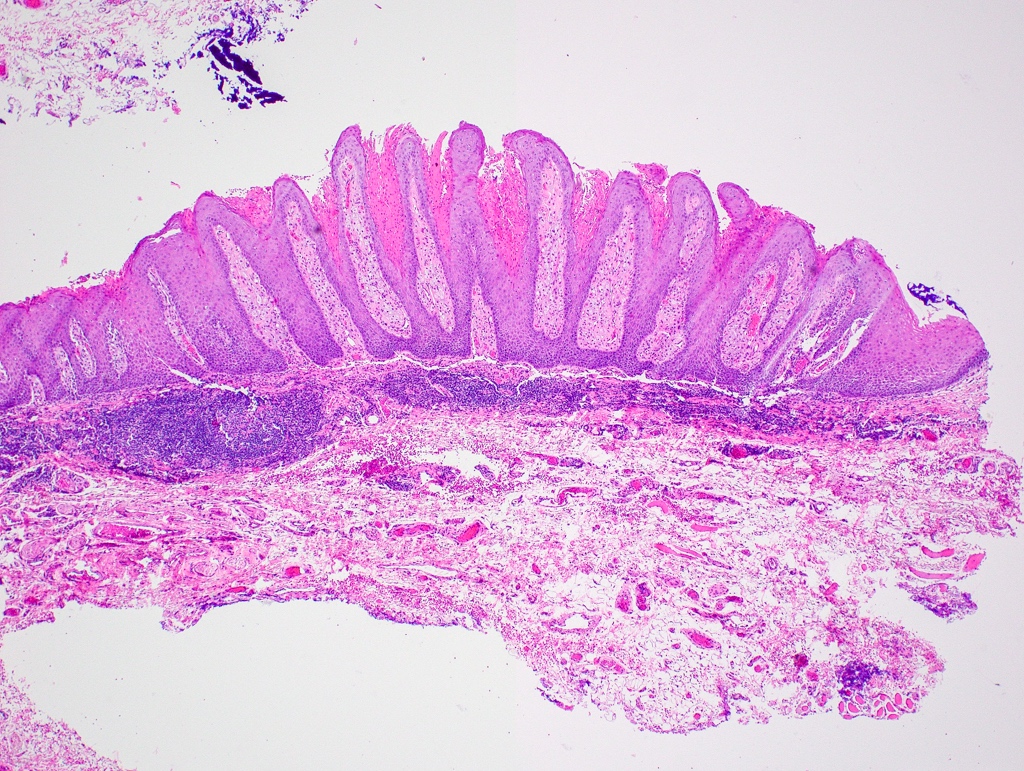
Inflammatory infiltrate
Well circumscribed mass
Keratin filled clefts
Leukocytic exocytosis
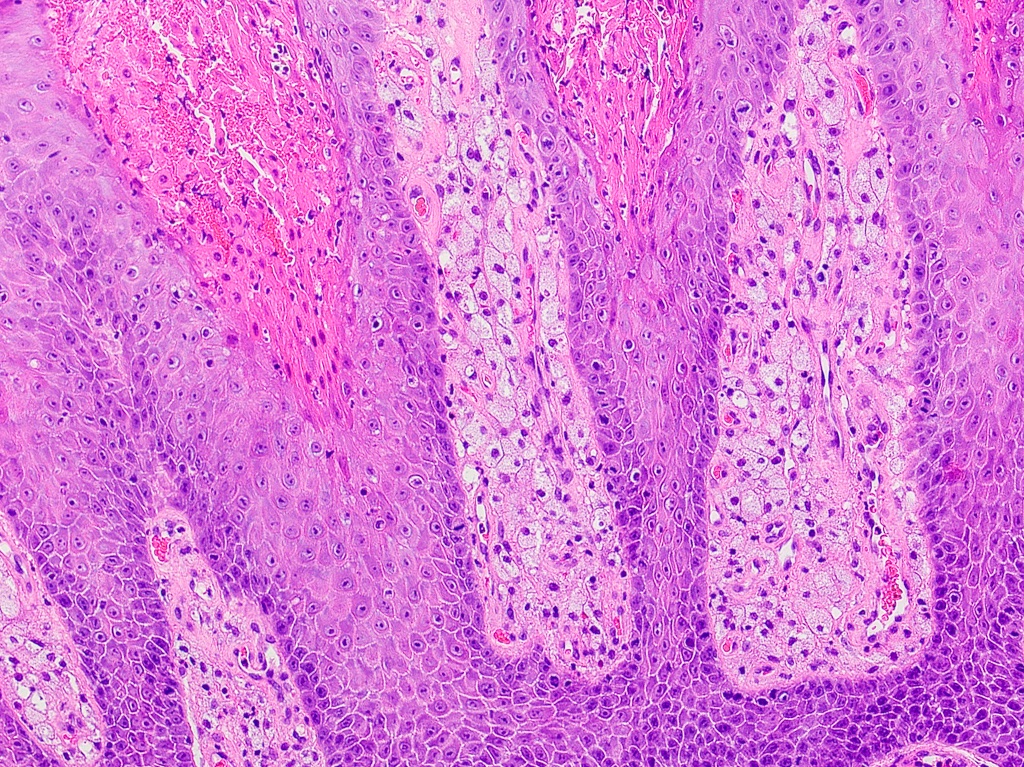
Foamy macrophages
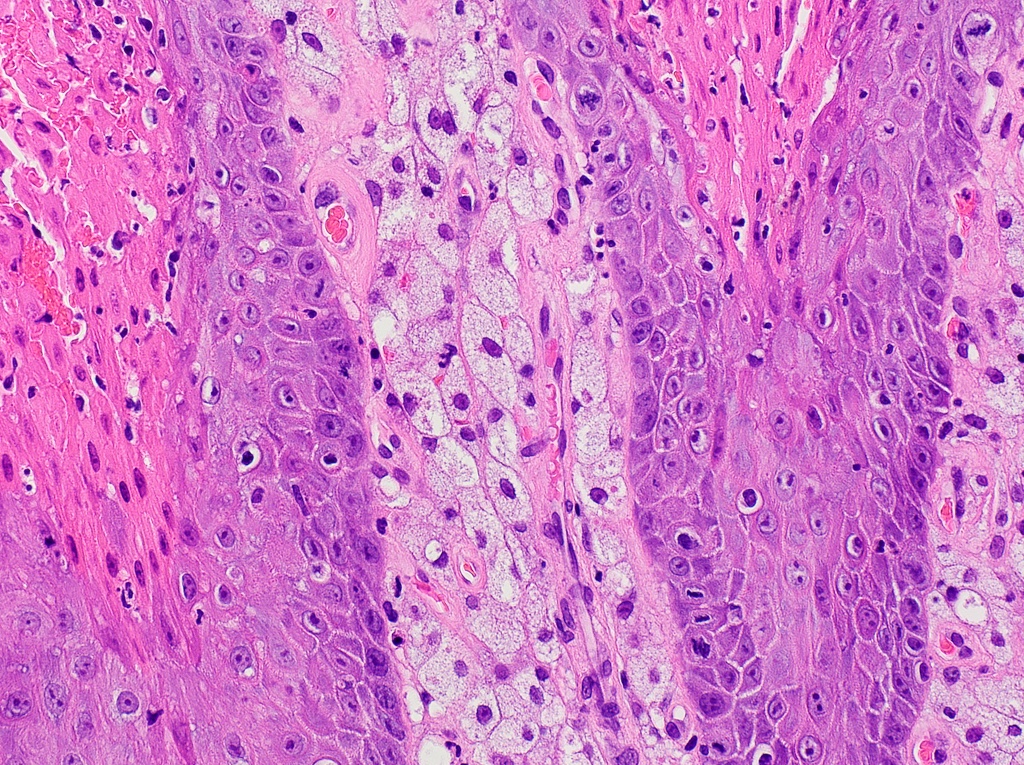
Lipid laden macrophages

Slightly papillary silhouette
Surface parakeratosis and histiocytes

Histiocytes
Videos
VX of skin, histology
Clinical description of VX
Sample pathology report
- Gingiva, excision:
- Verruciform xanthoma (see comment)
- Comment: The microscopic features show a well circumscribed papillary proliferation of epithelium covered by a thickened verrucoid parakeratin exhibiting neutrophilic exocytosis. Notably, the connective tissue papillae in between acanthotic rete ridges contain accumulations of foamy macrophages. Cytologic atypia is not appreciated. A chronic inflammatory cell infiltrate, consisting predominantly of lymphocytes, is appreciated within the superficial lamina propria.
Differential diagnosis
- Squamous papilloma:
- Well circumscribed papillary proliferation of squamous epithelium, often with converging rete ridges
- Lacks collections of lipid laden foamy macrophages in connective tissue papillae (Head Neck Pathol 2020;14:742)
- Associated with HPV (6 and 11 most commonly)
- Verruca vulgaris:
- Well circumscribed papillary / verrucoid proliferation of squamous epithelium, often with converging rete ridges, koilocytes and hypergranulosis
- Associated with HPV (2 and 4 most commonly)
- Lacks collections of lipid laden foamy macrophages in connective tissue papillae
- Proliferative verrucous leukoplakia / verrucous hyperplasia:
- Characterized clinically by multifocal white plaques with well defined margins that often progress
- Often affects marginal gingiva
- Histopathologically demonstrates verrucoid hyperkeratosis, sometimes with keratin plugging / clefting and sharp clonal margins
- Lacks circumscription
- Lacks collections of lipid laden foamy macrophages in connective tissue papillae
- Verrucous carcinoma:
- Atypical verrucoid hyperplasia of squamous epithelium with downward pushing margins and keratin clefting
- Lacks circumscription
- Lacks collections of lipid laden foamy macrophages in connective tissue papillae
Additional references
Board review style question #1
A solitary verrucoid mass was noted on the gingiva. What is the diagnosis?
- Papilloma
- Verruca vulgaris
- Verruciform xanthoma
- Verrucous carcinoma
Board review style answer #1
C. Verruciform xanthoma. Answers A, B and D are incorrect because while papillomas, verrucous carcinomas and verruca vulgaris all may be solitary and show a verrucoid architecture, only verruciform xanthoma shows the characteristic aggregates of lipid laden macrophages within the connective tissue papillae.
Comment Here
Reference: Verruciform xanthoma
Comment Here
Reference: Verruciform xanthoma
